User login
HIV hospitalizations continue to decline
The total number of HIV hospitalizations fell by a third during 2000-2013, even though the number of people living with HIV increased by more than 50%, according to an investigation by the Agency for Healthcare Research and Quality.
“To some extent, the considerable reduction in hospital utilization by persons with HIV disease may be attributed to the diffusion of new antiretroviral medications and the enhanced ability of clinicians to control viral replication,” wrote investigator Fred Hellinger, PhD, of AHRQ’s Center for Delivery, Organization, and Markets (Med Care. 2016 Jun;54[6]:639-44).
Dr. Hellinger used his agency’s State Inpatient Database to collect data on all HIV-related hospital admissions from California, Florida, New Jersey, New York, and South Carolina during 2000-2013. Overall, people with HIV were 64% less likely to be hospitalized in 2013 than they were in 2000; there was also a slight drop in length of stay.
Meanwhile, the average age of hospitalized HIV patients has risen from 41 to 49 years, and the average number of diagnoses from 6 to more than 12. That’s in part because HIV patients are living longer, and “older patients are generally sicker and have more chronic illnesses ... As HIV patients age, they are being hospitalized for conditions that are not closely related to HIV infection,” Dr. Hellinger said.
“Indeed, the principal diagnosis for almost two-thirds of the HIV patients hospitalized in 2013 in our sample was not HIV infection, and as time passes, the mix of diagnoses recorded for hospitalized patients with HIV is likely to resemble the mix of diagnoses found in the general population of hospitalized patients,” he wrote.
U.S. HIV spending continues to go up, but while the number of patients covered by Medicaid has fallen, the number treated by Medicare has risen 50%, reflecting the increase in average life span.
There has not been much demographic change among HIV inpatients. About half are black, a quarter white, and slightly less than one-fifth Hispanic. One-third are women. More than 1.1 million Americans are living with HIV, and 50,000 are newly infected each year.
Dr. Hellinger had no conflicts of interest.
The total number of HIV hospitalizations fell by a third during 2000-2013, even though the number of people living with HIV increased by more than 50%, according to an investigation by the Agency for Healthcare Research and Quality.
“To some extent, the considerable reduction in hospital utilization by persons with HIV disease may be attributed to the diffusion of new antiretroviral medications and the enhanced ability of clinicians to control viral replication,” wrote investigator Fred Hellinger, PhD, of AHRQ’s Center for Delivery, Organization, and Markets (Med Care. 2016 Jun;54[6]:639-44).
Dr. Hellinger used his agency’s State Inpatient Database to collect data on all HIV-related hospital admissions from California, Florida, New Jersey, New York, and South Carolina during 2000-2013. Overall, people with HIV were 64% less likely to be hospitalized in 2013 than they were in 2000; there was also a slight drop in length of stay.
Meanwhile, the average age of hospitalized HIV patients has risen from 41 to 49 years, and the average number of diagnoses from 6 to more than 12. That’s in part because HIV patients are living longer, and “older patients are generally sicker and have more chronic illnesses ... As HIV patients age, they are being hospitalized for conditions that are not closely related to HIV infection,” Dr. Hellinger said.
“Indeed, the principal diagnosis for almost two-thirds of the HIV patients hospitalized in 2013 in our sample was not HIV infection, and as time passes, the mix of diagnoses recorded for hospitalized patients with HIV is likely to resemble the mix of diagnoses found in the general population of hospitalized patients,” he wrote.
U.S. HIV spending continues to go up, but while the number of patients covered by Medicaid has fallen, the number treated by Medicare has risen 50%, reflecting the increase in average life span.
There has not been much demographic change among HIV inpatients. About half are black, a quarter white, and slightly less than one-fifth Hispanic. One-third are women. More than 1.1 million Americans are living with HIV, and 50,000 are newly infected each year.
Dr. Hellinger had no conflicts of interest.
The total number of HIV hospitalizations fell by a third during 2000-2013, even though the number of people living with HIV increased by more than 50%, according to an investigation by the Agency for Healthcare Research and Quality.
“To some extent, the considerable reduction in hospital utilization by persons with HIV disease may be attributed to the diffusion of new antiretroviral medications and the enhanced ability of clinicians to control viral replication,” wrote investigator Fred Hellinger, PhD, of AHRQ’s Center for Delivery, Organization, and Markets (Med Care. 2016 Jun;54[6]:639-44).
Dr. Hellinger used his agency’s State Inpatient Database to collect data on all HIV-related hospital admissions from California, Florida, New Jersey, New York, and South Carolina during 2000-2013. Overall, people with HIV were 64% less likely to be hospitalized in 2013 than they were in 2000; there was also a slight drop in length of stay.
Meanwhile, the average age of hospitalized HIV patients has risen from 41 to 49 years, and the average number of diagnoses from 6 to more than 12. That’s in part because HIV patients are living longer, and “older patients are generally sicker and have more chronic illnesses ... As HIV patients age, they are being hospitalized for conditions that are not closely related to HIV infection,” Dr. Hellinger said.
“Indeed, the principal diagnosis for almost two-thirds of the HIV patients hospitalized in 2013 in our sample was not HIV infection, and as time passes, the mix of diagnoses recorded for hospitalized patients with HIV is likely to resemble the mix of diagnoses found in the general population of hospitalized patients,” he wrote.
U.S. HIV spending continues to go up, but while the number of patients covered by Medicaid has fallen, the number treated by Medicare has risen 50%, reflecting the increase in average life span.
There has not been much demographic change among HIV inpatients. About half are black, a quarter white, and slightly less than one-fifth Hispanic. One-third are women. More than 1.1 million Americans are living with HIV, and 50,000 are newly infected each year.
Dr. Hellinger had no conflicts of interest.
FROM MEDICAL CARE
Key clinical point:
Major finding: People with HIV were 64% less likely to be hospitalized in 2013 than they were in 2000.
Data source: Review of HIV-related hospitalizations in five U.S. states.
Disclosures: The Agency for Healthcare Research and Quality funded the work. The investigator had no disclosures.
Speaker says use the best regimen ASAP in MM

NEW YORK—It’s important to use the best possible regimen as soon as possible when treating patients with multiple myeloma (MM), according to a speaker at Lymphoma & Myeloma 2016.
Antonio Palumbo, MD, of the University of Torino in Italy, explained that the urgency, from a biological point of view, is because myeloma accumulates genetic mutations that change the disease in a “dramatic way.”
“At diagnosis, you might have 5000 mutations, and, at first relapse, there are 12,000 mutations,” he said. “They are completely different tumors. So the first thing that we have to recognize is that, with time, myeloma is not the same. It’s becoming different tumors.”
Dr Palumbo noted that early intervention is important because genetic and epigenetic abnormalities increase as the disease progresses and becomes more resistant.
For example, if 100 patients receive first-line treatment, 40 of them will not reach the second line. Only 60 patients will receive second-line therapy, and only 35 patients will receive third-line treatment. By the fifth line, only 10 patients, or 10%, will receive it.
“If you have very good genomic stability, you can become sensitive to different treatments,” Dr Palumbo said. “But if you become a different disease, you will not be able to receive the next therapy. That’s why it’s so important . . . to use the best possible regimen as soon as possible.”
Best regimens
The triplet bortezomib-lenalidomide-dexamethasone is the “best possible regimen today,” Dr Palumbo said, “followed by continuous therapy.”
The 2-drug combination of lenalidomide and dexamethasone is probably more suitable for the elderly and the frail.
Alternative regimens include carfilzomib-cyclophosphamide-dexamethasone and ixazomib-lenalidomide-dexamethasone.
Continuous therapy
Continuous therapy has been “one of the major achievements” in the treatment of MM, Dr Palumbo said. Without continuous therapy, patients in complete response remain so for about 1 year when treated with conventional chemotherapy.
Investigators found that maintenance therapy significantly prolongs progression-free survival and overall survival (P=0.02). They recommend intensification with maintenance to optimize treatment efficacy and prolong survival.
Immunomodulatory drugs such as lenalidomide are the backbone of continuous therapy today.
However, ixazomib represents another option. Ixazomib maintenance has been shown to produce durable responses for a median of more than 2 years in previously untreated patients not undergoing autologous stem cell transplant.
Salvage therapy
Seven combinations are now available for salvage therapy, including those with proteasome inhibitors, monoclonal antibodies, pomalidomide, and histone deacetylase inhibitors.
Included in some of these combinations are the newer agents ixazomib, elotuzumab, and daratumumab, “which many might consider the new rituximab,” Dr Palumbo said.
Risk stratification
Dr Palumbo stressed the importance of risk stratification—both in clinical trials and in practice.
“[T]he moment you under-treat a patient, you transform a good-risk patient into a high-risk patient . . . ,” he said.
And if trials comparing treatments are not conducted within risk categories, researchers are comparing apples to oranges—good risk with high risk
The Revised International Staging System (R-ISS) for MM effectively stratifies newly diagnosed patients by combining the original ISS, chromosomal abnormalities, and serum lactate dehydrogenase levels to evaluate prognosis.
The R-ISS defines 3 new, distinct categories that researchers believe effectively define patients’ relative risk with respect to their survival.
Age and frailty
MM patients generally fall into 3 age categories: 25-64, 65-74, and 75-101.
The youngest group can receive autologous transplant, the fit patients ages 65 to 74 can receive full-dose chemotherapy, and the oldest, frailer patients should receive reduced-dose chemotherapy.
“It’s important to differentiate fit from frail,” Dr Palumbo said, “because we cannot give the same treatment schema to a 55-year-old versus 65 or 85. At 85, that schema would create a lot of toxicities.”
In frail patients, it’s always important to check which comorbidities are present using the Charlson comorbidity scale, Dr Palumbo said.
“Remember, when we put together age, chromosome abnormalities, and frailty, frailty is the most relevant prognostic factor when you add everything together,” he said.
“Two drugs versus 3 drugs doesn’t make much difference when you are starting to introduce treatment to these very frail patients with comorbidities.”
Minimal residual disease
Dr Palumbo indicated that a combination of MRI and PET-CT should be used for a more accurate indication of minimal residual disease.
“[W]e hope to have cure, [but] I don’t think, today, myeloma is a curable disease,” he said.
He clarified this by saying that patients who are in complete response and minimal residual disease-negative at 3 years do well, but, by 7 years, “something is happening.”
And at 10 years, progression-free survival has dropped off significantly, “telling us that cure is probably not yet there.” ![]()
NEW YORK—It’s important to use the best possible regimen as soon as possible when treating patients with multiple myeloma (MM), according to a speaker at Lymphoma & Myeloma 2016.
Antonio Palumbo, MD, of the University of Torino in Italy, explained that the urgency, from a biological point of view, is because myeloma accumulates genetic mutations that change the disease in a “dramatic way.”
“At diagnosis, you might have 5000 mutations, and, at first relapse, there are 12,000 mutations,” he said. “They are completely different tumors. So the first thing that we have to recognize is that, with time, myeloma is not the same. It’s becoming different tumors.”
Dr Palumbo noted that early intervention is important because genetic and epigenetic abnormalities increase as the disease progresses and becomes more resistant.
For example, if 100 patients receive first-line treatment, 40 of them will not reach the second line. Only 60 patients will receive second-line therapy, and only 35 patients will receive third-line treatment. By the fifth line, only 10 patients, or 10%, will receive it.
“If you have very good genomic stability, you can become sensitive to different treatments,” Dr Palumbo said. “But if you become a different disease, you will not be able to receive the next therapy. That’s why it’s so important . . . to use the best possible regimen as soon as possible.”
Best regimens
The triplet bortezomib-lenalidomide-dexamethasone is the “best possible regimen today,” Dr Palumbo said, “followed by continuous therapy.”
The 2-drug combination of lenalidomide and dexamethasone is probably more suitable for the elderly and the frail.
Alternative regimens include carfilzomib-cyclophosphamide-dexamethasone and ixazomib-lenalidomide-dexamethasone.
Continuous therapy
Continuous therapy has been “one of the major achievements” in the treatment of MM, Dr Palumbo said. Without continuous therapy, patients in complete response remain so for about 1 year when treated with conventional chemotherapy.
Investigators found that maintenance therapy significantly prolongs progression-free survival and overall survival (P=0.02). They recommend intensification with maintenance to optimize treatment efficacy and prolong survival.
Immunomodulatory drugs such as lenalidomide are the backbone of continuous therapy today.
However, ixazomib represents another option. Ixazomib maintenance has been shown to produce durable responses for a median of more than 2 years in previously untreated patients not undergoing autologous stem cell transplant.
Salvage therapy
Seven combinations are now available for salvage therapy, including those with proteasome inhibitors, monoclonal antibodies, pomalidomide, and histone deacetylase inhibitors.
Included in some of these combinations are the newer agents ixazomib, elotuzumab, and daratumumab, “which many might consider the new rituximab,” Dr Palumbo said.
Risk stratification
Dr Palumbo stressed the importance of risk stratification—both in clinical trials and in practice.
“[T]he moment you under-treat a patient, you transform a good-risk patient into a high-risk patient . . . ,” he said.
And if trials comparing treatments are not conducted within risk categories, researchers are comparing apples to oranges—good risk with high risk
The Revised International Staging System (R-ISS) for MM effectively stratifies newly diagnosed patients by combining the original ISS, chromosomal abnormalities, and serum lactate dehydrogenase levels to evaluate prognosis.
The R-ISS defines 3 new, distinct categories that researchers believe effectively define patients’ relative risk with respect to their survival.
Age and frailty
MM patients generally fall into 3 age categories: 25-64, 65-74, and 75-101.
The youngest group can receive autologous transplant, the fit patients ages 65 to 74 can receive full-dose chemotherapy, and the oldest, frailer patients should receive reduced-dose chemotherapy.
“It’s important to differentiate fit from frail,” Dr Palumbo said, “because we cannot give the same treatment schema to a 55-year-old versus 65 or 85. At 85, that schema would create a lot of toxicities.”
In frail patients, it’s always important to check which comorbidities are present using the Charlson comorbidity scale, Dr Palumbo said.
“Remember, when we put together age, chromosome abnormalities, and frailty, frailty is the most relevant prognostic factor when you add everything together,” he said.
“Two drugs versus 3 drugs doesn’t make much difference when you are starting to introduce treatment to these very frail patients with comorbidities.”
Minimal residual disease
Dr Palumbo indicated that a combination of MRI and PET-CT should be used for a more accurate indication of minimal residual disease.
“[W]e hope to have cure, [but] I don’t think, today, myeloma is a curable disease,” he said.
He clarified this by saying that patients who are in complete response and minimal residual disease-negative at 3 years do well, but, by 7 years, “something is happening.”
And at 10 years, progression-free survival has dropped off significantly, “telling us that cure is probably not yet there.” ![]()
NEW YORK—It’s important to use the best possible regimen as soon as possible when treating patients with multiple myeloma (MM), according to a speaker at Lymphoma & Myeloma 2016.
Antonio Palumbo, MD, of the University of Torino in Italy, explained that the urgency, from a biological point of view, is because myeloma accumulates genetic mutations that change the disease in a “dramatic way.”
“At diagnosis, you might have 5000 mutations, and, at first relapse, there are 12,000 mutations,” he said. “They are completely different tumors. So the first thing that we have to recognize is that, with time, myeloma is not the same. It’s becoming different tumors.”
Dr Palumbo noted that early intervention is important because genetic and epigenetic abnormalities increase as the disease progresses and becomes more resistant.
For example, if 100 patients receive first-line treatment, 40 of them will not reach the second line. Only 60 patients will receive second-line therapy, and only 35 patients will receive third-line treatment. By the fifth line, only 10 patients, or 10%, will receive it.
“If you have very good genomic stability, you can become sensitive to different treatments,” Dr Palumbo said. “But if you become a different disease, you will not be able to receive the next therapy. That’s why it’s so important . . . to use the best possible regimen as soon as possible.”
Best regimens
The triplet bortezomib-lenalidomide-dexamethasone is the “best possible regimen today,” Dr Palumbo said, “followed by continuous therapy.”
The 2-drug combination of lenalidomide and dexamethasone is probably more suitable for the elderly and the frail.
Alternative regimens include carfilzomib-cyclophosphamide-dexamethasone and ixazomib-lenalidomide-dexamethasone.
Continuous therapy
Continuous therapy has been “one of the major achievements” in the treatment of MM, Dr Palumbo said. Without continuous therapy, patients in complete response remain so for about 1 year when treated with conventional chemotherapy.
Investigators found that maintenance therapy significantly prolongs progression-free survival and overall survival (P=0.02). They recommend intensification with maintenance to optimize treatment efficacy and prolong survival.
Immunomodulatory drugs such as lenalidomide are the backbone of continuous therapy today.
However, ixazomib represents another option. Ixazomib maintenance has been shown to produce durable responses for a median of more than 2 years in previously untreated patients not undergoing autologous stem cell transplant.
Salvage therapy
Seven combinations are now available for salvage therapy, including those with proteasome inhibitors, monoclonal antibodies, pomalidomide, and histone deacetylase inhibitors.
Included in some of these combinations are the newer agents ixazomib, elotuzumab, and daratumumab, “which many might consider the new rituximab,” Dr Palumbo said.
Risk stratification
Dr Palumbo stressed the importance of risk stratification—both in clinical trials and in practice.
“[T]he moment you under-treat a patient, you transform a good-risk patient into a high-risk patient . . . ,” he said.
And if trials comparing treatments are not conducted within risk categories, researchers are comparing apples to oranges—good risk with high risk
The Revised International Staging System (R-ISS) for MM effectively stratifies newly diagnosed patients by combining the original ISS, chromosomal abnormalities, and serum lactate dehydrogenase levels to evaluate prognosis.
The R-ISS defines 3 new, distinct categories that researchers believe effectively define patients’ relative risk with respect to their survival.
Age and frailty
MM patients generally fall into 3 age categories: 25-64, 65-74, and 75-101.
The youngest group can receive autologous transplant, the fit patients ages 65 to 74 can receive full-dose chemotherapy, and the oldest, frailer patients should receive reduced-dose chemotherapy.
“It’s important to differentiate fit from frail,” Dr Palumbo said, “because we cannot give the same treatment schema to a 55-year-old versus 65 or 85. At 85, that schema would create a lot of toxicities.”
In frail patients, it’s always important to check which comorbidities are present using the Charlson comorbidity scale, Dr Palumbo said.
“Remember, when we put together age, chromosome abnormalities, and frailty, frailty is the most relevant prognostic factor when you add everything together,” he said.
“Two drugs versus 3 drugs doesn’t make much difference when you are starting to introduce treatment to these very frail patients with comorbidities.”
Minimal residual disease
Dr Palumbo indicated that a combination of MRI and PET-CT should be used for a more accurate indication of minimal residual disease.
“[W]e hope to have cure, [but] I don’t think, today, myeloma is a curable disease,” he said.
He clarified this by saying that patients who are in complete response and minimal residual disease-negative at 3 years do well, but, by 7 years, “something is happening.”
And at 10 years, progression-free survival has dropped off significantly, “telling us that cure is probably not yet there.” ![]()
ACIP approves changes to HPV, Tdap, DTaP, MenB vaccination guidance
The Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices approved a series of minor changes to the current guidance for meningococcal, Tdap, DTaP, and human papillomavirus vaccination schedules.
Regarding meningococcal vaccinations, the committee voted to change the recommendations to state that individuals who are at an increased risk of contracting the disease should receive a three-dose regimen of Trumenba at 0 months, 1-2 months, and 6 months. The same regimen also should apply during any outbreaks of serogroup B meningococcal virus. In addition, a two-dose regimen at 0 and 6 months should be given to adolescents who are not considered high risk, and if the second dose is given fewer than 6 months following the first, then a third dose must be given within 6 months of the initial dose. 
“This new recommendation enables flexible vaccination dosing intervals depending on one’s risk of exposure to meningococcal group B disease, also known as MenB, which makes it easier for health care providers to help protect adolescents and young adults from this uncommon but life-threatening disease,” the CDC announced in a statement.
For Tdap and DTaP vaccines, changes to the language of the recommendations were approved unanimously by the committee. These changes will contain the routine recommendations for DTaP, Tdap, and TB, which previously were published as separate statements, along with Tdap recommendations made after the 2005 recommendations and published in Morbidity and Mortality Weekly Report policy notes.
“This statement also contains updates, such as DTaP vaccines that became available after the 1997 DTaP statement, and updates to the label indications on various DTaP and Tdap products,” Jennifer Liang, DVM, of the CDC’s National Center for Immunization and Respiratory Diseases, explained at the ACIP meeting. “Also included in the statement are the following updates: mention of the discontinuation of monovalent tetanus toxoid vaccine, the contraindications and precautions for DTaP are now consistent with the [American Academy of Pediatrics’] Red Book, and for persons aged 7-10 years who received a dose of Tdap as part of the catchup series, an adolescent Tdap dose may be given at age 11-12 years.”
Dr. Liang added that these updated changes would bring the guidance in line with the recommendations for children who are administered Tdap inadvertently.
With one recusal, changes to the HPV vaccination guidance also were unanimously approved. No changes were proposed to the routine and catch-up age groups for HPV vaccination, and for contraindications and precautions. Major additions were made, however, to the sections on dosing schedules, and people with prior vaccination. Clarifying language was added for the sections on interrupted schedules, special populations, and medical conditions.
For individuals initiating vaccination before the 15th birthday, the recommended immunization schedule is two doses of HPV vaccine. The second dose should be administered 6-12 months after the first dose (0 months, 6-12 months schedule). For people initiating vaccination on or after the 15th birthday, the recommendations remain the same as before: three doses of HPV vaccine, with the second dose administered 1-2 months after the first dose, and the third dose administered within 6 months of the first dose.
Those with prior vaccinations who initiated with 9-valent HPV, 4-valent HPV, or 2-valent HPV before their 15th birthday and received either two or three doses at the recommended dosing schedule should be considered adequately vaccinated. Those who initiated any of those three HPV vaccinations on or after their 15th birthday and received three doses at the currently recommended dosing schedule should be considered adequately vaccinated, too.
With regard to the minimum intervals, the proposed change was to add a footnote defining minimum intervals: in a two-dose series of HPV vaccines, the minimum interval is 5 months between the first and second dose, and in a three-dose series, 5 months between the first and third dose. All other language remains as is. Special population language also was changed to “gay, bisexual, and other” men rather than simply men who have sex with men, to broaden the scope of the language. Language also will be amended to include transgender patients.
Finally, for those with other medical conditions, ACIP still recommends that all immunocompromised males and females aged 9-26 years get a three-dose HPV vaccination at 0, 1-2, and 6 months, but now the language change will read that “Persons who should receive three doses are those with primary or secondary immunocompromising conditions that might reduce cell-mediated or humoral immunity, such as B lymphocyte antibody deficiencies, T lymphocyte complete or partial defects, HIV infection, malignant neoplasm, transplantation, autoimmune disease, or immunosuppressive therapy, since response to vaccination may be attenuated.”
In addition, there will be a footnote stating that these recommendations for a three-dose schedule do not apply to children under the age of 15 years with asplenia, asthma, chronic granulomatous disease, chronic heart/liver/lung/renal disease, central nervous system anatomic barrier defects, complement deficiency, diabetes, or sickle cell disease.”
The recommendations agreed upon will be submitted for approval to CDC Director Tom Frieden, MD. If approved, the recommendations will be published by Jan. 1, 2017, at which point, they will go into effect.
The Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices approved a series of minor changes to the current guidance for meningococcal, Tdap, DTaP, and human papillomavirus vaccination schedules.
Regarding meningococcal vaccinations, the committee voted to change the recommendations to state that individuals who are at an increased risk of contracting the disease should receive a three-dose regimen of Trumenba at 0 months, 1-2 months, and 6 months. The same regimen also should apply during any outbreaks of serogroup B meningococcal virus. In addition, a two-dose regimen at 0 and 6 months should be given to adolescents who are not considered high risk, and if the second dose is given fewer than 6 months following the first, then a third dose must be given within 6 months of the initial dose.
“This new recommendation enables flexible vaccination dosing intervals depending on one’s risk of exposure to meningococcal group B disease, also known as MenB, which makes it easier for health care providers to help protect adolescents and young adults from this uncommon but life-threatening disease,” the CDC announced in a statement.
For Tdap and DTaP vaccines, changes to the language of the recommendations were approved unanimously by the committee. These changes will contain the routine recommendations for DTaP, Tdap, and TB, which previously were published as separate statements, along with Tdap recommendations made after the 2005 recommendations and published in Morbidity and Mortality Weekly Report policy notes.
“This statement also contains updates, such as DTaP vaccines that became available after the 1997 DTaP statement, and updates to the label indications on various DTaP and Tdap products,” Jennifer Liang, DVM, of the CDC’s National Center for Immunization and Respiratory Diseases, explained at the ACIP meeting. “Also included in the statement are the following updates: mention of the discontinuation of monovalent tetanus toxoid vaccine, the contraindications and precautions for DTaP are now consistent with the [American Academy of Pediatrics’] Red Book, and for persons aged 7-10 years who received a dose of Tdap as part of the catchup series, an adolescent Tdap dose may be given at age 11-12 years.”
Dr. Liang added that these updated changes would bring the guidance in line with the recommendations for children who are administered Tdap inadvertently.
With one recusal, changes to the HPV vaccination guidance also were unanimously approved. No changes were proposed to the routine and catch-up age groups for HPV vaccination, and for contraindications and precautions. Major additions were made, however, to the sections on dosing schedules, and people with prior vaccination. Clarifying language was added for the sections on interrupted schedules, special populations, and medical conditions.
For individuals initiating vaccination before the 15th birthday, the recommended immunization schedule is two doses of HPV vaccine. The second dose should be administered 6-12 months after the first dose (0 months, 6-12 months schedule). For people initiating vaccination on or after the 15th birthday, the recommendations remain the same as before: three doses of HPV vaccine, with the second dose administered 1-2 months after the first dose, and the third dose administered within 6 months of the first dose.
Those with prior vaccinations who initiated with 9-valent HPV, 4-valent HPV, or 2-valent HPV before their 15th birthday and received either two or three doses at the recommended dosing schedule should be considered adequately vaccinated. Those who initiated any of those three HPV vaccinations on or after their 15th birthday and received three doses at the currently recommended dosing schedule should be considered adequately vaccinated, too.
With regard to the minimum intervals, the proposed change was to add a footnote defining minimum intervals: in a two-dose series of HPV vaccines, the minimum interval is 5 months between the first and second dose, and in a three-dose series, 5 months between the first and third dose. All other language remains as is. Special population language also was changed to “gay, bisexual, and other” men rather than simply men who have sex with men, to broaden the scope of the language. Language also will be amended to include transgender patients.
Finally, for those with other medical conditions, ACIP still recommends that all immunocompromised males and females aged 9-26 years get a three-dose HPV vaccination at 0, 1-2, and 6 months, but now the language change will read that “Persons who should receive three doses are those with primary or secondary immunocompromising conditions that might reduce cell-mediated or humoral immunity, such as B lymphocyte antibody deficiencies, T lymphocyte complete or partial defects, HIV infection, malignant neoplasm, transplantation, autoimmune disease, or immunosuppressive therapy, since response to vaccination may be attenuated.”
In addition, there will be a footnote stating that these recommendations for a three-dose schedule do not apply to children under the age of 15 years with asplenia, asthma, chronic granulomatous disease, chronic heart/liver/lung/renal disease, central nervous system anatomic barrier defects, complement deficiency, diabetes, or sickle cell disease.”
The recommendations agreed upon will be submitted for approval to CDC Director Tom Frieden, MD. If approved, the recommendations will be published by Jan. 1, 2017, at which point, they will go into effect.
The Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices approved a series of minor changes to the current guidance for meningococcal, Tdap, DTaP, and human papillomavirus vaccination schedules.
Regarding meningococcal vaccinations, the committee voted to change the recommendations to state that individuals who are at an increased risk of contracting the disease should receive a three-dose regimen of Trumenba at 0 months, 1-2 months, and 6 months. The same regimen also should apply during any outbreaks of serogroup B meningococcal virus. In addition, a two-dose regimen at 0 and 6 months should be given to adolescents who are not considered high risk, and if the second dose is given fewer than 6 months following the first, then a third dose must be given within 6 months of the initial dose.
“This new recommendation enables flexible vaccination dosing intervals depending on one’s risk of exposure to meningococcal group B disease, also known as MenB, which makes it easier for health care providers to help protect adolescents and young adults from this uncommon but life-threatening disease,” the CDC announced in a statement.
For Tdap and DTaP vaccines, changes to the language of the recommendations were approved unanimously by the committee. These changes will contain the routine recommendations for DTaP, Tdap, and TB, which previously were published as separate statements, along with Tdap recommendations made after the 2005 recommendations and published in Morbidity and Mortality Weekly Report policy notes.
“This statement also contains updates, such as DTaP vaccines that became available after the 1997 DTaP statement, and updates to the label indications on various DTaP and Tdap products,” Jennifer Liang, DVM, of the CDC’s National Center for Immunization and Respiratory Diseases, explained at the ACIP meeting. “Also included in the statement are the following updates: mention of the discontinuation of monovalent tetanus toxoid vaccine, the contraindications and precautions for DTaP are now consistent with the [American Academy of Pediatrics’] Red Book, and for persons aged 7-10 years who received a dose of Tdap as part of the catchup series, an adolescent Tdap dose may be given at age 11-12 years.”
Dr. Liang added that these updated changes would bring the guidance in line with the recommendations for children who are administered Tdap inadvertently.
With one recusal, changes to the HPV vaccination guidance also were unanimously approved. No changes were proposed to the routine and catch-up age groups for HPV vaccination, and for contraindications and precautions. Major additions were made, however, to the sections on dosing schedules, and people with prior vaccination. Clarifying language was added for the sections on interrupted schedules, special populations, and medical conditions.
For individuals initiating vaccination before the 15th birthday, the recommended immunization schedule is two doses of HPV vaccine. The second dose should be administered 6-12 months after the first dose (0 months, 6-12 months schedule). For people initiating vaccination on or after the 15th birthday, the recommendations remain the same as before: three doses of HPV vaccine, with the second dose administered 1-2 months after the first dose, and the third dose administered within 6 months of the first dose.
Those with prior vaccinations who initiated with 9-valent HPV, 4-valent HPV, or 2-valent HPV before their 15th birthday and received either two or three doses at the recommended dosing schedule should be considered adequately vaccinated. Those who initiated any of those three HPV vaccinations on or after their 15th birthday and received three doses at the currently recommended dosing schedule should be considered adequately vaccinated, too.
With regard to the minimum intervals, the proposed change was to add a footnote defining minimum intervals: in a two-dose series of HPV vaccines, the minimum interval is 5 months between the first and second dose, and in a three-dose series, 5 months between the first and third dose. All other language remains as is. Special population language also was changed to “gay, bisexual, and other” men rather than simply men who have sex with men, to broaden the scope of the language. Language also will be amended to include transgender patients.
Finally, for those with other medical conditions, ACIP still recommends that all immunocompromised males and females aged 9-26 years get a three-dose HPV vaccination at 0, 1-2, and 6 months, but now the language change will read that “Persons who should receive three doses are those with primary or secondary immunocompromising conditions that might reduce cell-mediated or humoral immunity, such as B lymphocyte antibody deficiencies, T lymphocyte complete or partial defects, HIV infection, malignant neoplasm, transplantation, autoimmune disease, or immunosuppressive therapy, since response to vaccination may be attenuated.”
In addition, there will be a footnote stating that these recommendations for a three-dose schedule do not apply to children under the age of 15 years with asplenia, asthma, chronic granulomatous disease, chronic heart/liver/lung/renal disease, central nervous system anatomic barrier defects, complement deficiency, diabetes, or sickle cell disease.”
The recommendations agreed upon will be submitted for approval to CDC Director Tom Frieden, MD. If approved, the recommendations will be published by Jan. 1, 2017, at which point, they will go into effect.
FROM AN ACIP MEETING
Resveratrol cut androgen levels in small PCOS trial
SALT LAKE CITY – Resveratrol significantly decreased androgen levels and insulin resistance among women with polycystic ovary syndrome (PCOS), according to a first-in-kind randomized, double-blind placebo-controlled trial of 30 patients.
After 3 months of daily oral treatment with 1.5 g of the antioxidant polyphenol, testosterone levels fell an average of 23%, dehydroepiandrosterone sulfate (DHEAS) levels dropped 22%, fasting insulin levels decreased by 32%, and insulin sensitivity improved by 66%, Antoni Duleba, MD, said at the annual meeting of the American Society for Reproductive Medicine. No such improvements occurred in the placebo group, he and his coinvestigators reported simultaneously in the Journal of Clinical Endocrinology & Metabolism (doi: 10.1210/jc.2016-1858).

Past work has found that resveratrol inhibits mRNA expression of Cyp17a1 and reduces androgen production by ovarian theca-interstitial cells. To build on those findings, Dr. Duleba worked with researchers at Poznan (Poland) University of Medical Sciences to enroll 30 women with PCOS based on the Rotterdam criteria. Treatment and placebo groups resembled each other at baseline in terms of age, body mass index, androgen levels, lipid profiles, and levels of follicle-stimulating hormone, luteinizing hormone, prolactin, sex hormone–binding globulin, fasting glucose, and insulin, as well as scores on an insulin sensitivity index.
For the primary outcome measure – total testosterone level – the resveratrol group averaged 0.53 ng/mL at baseline and 0.41 ng/mL at 3-month follow-up, a statistically significant decrease (P = .01). In contrast, testosterone levels in the placebo group remained essentially unchanged, averaging 0.48 ng/mL at baseline and 0.49 ng/mL at follow-up. The difference in effect between the resveratrol and placebo groups was statistically significant (P = .04).
Similarly, average DHEAS levels dropped from 8.1 to 6.3 micromol/L in the resveratrol group (a 22% decline), but increased by 10% in the placebo group.
Resveratrol did not significantly affect progesterone levels, which is consistent with prior findings, Dr. Duleba said. Nor was resveratrol associated with significant changes in body mass index, lipid profile, markers of inflammation or endothelial function, ovarian volume, or gonadotropins.
“We were disappointed that we didn’t see gross changes in ovarian morphology on ultrasound,” he added. Whether those changes might occur with longer treatment is unknown, but for now, “we can only be sure of declining androgen and insulin levels, and improvements in insulin sensitivity.”
The study won a Scientific Congress Prize from ASRM.
RevGenetics provided the resveratrol for the study. Dr. Duleba reported having no relevant financial disclosures.
SALT LAKE CITY – Resveratrol significantly decreased androgen levels and insulin resistance among women with polycystic ovary syndrome (PCOS), according to a first-in-kind randomized, double-blind placebo-controlled trial of 30 patients.
After 3 months of daily oral treatment with 1.5 g of the antioxidant polyphenol, testosterone levels fell an average of 23%, dehydroepiandrosterone sulfate (DHEAS) levels dropped 22%, fasting insulin levels decreased by 32%, and insulin sensitivity improved by 66%, Antoni Duleba, MD, said at the annual meeting of the American Society for Reproductive Medicine. No such improvements occurred in the placebo group, he and his coinvestigators reported simultaneously in the Journal of Clinical Endocrinology & Metabolism (doi: 10.1210/jc.2016-1858).
Past work has found that resveratrol inhibits mRNA expression of Cyp17a1 and reduces androgen production by ovarian theca-interstitial cells. To build on those findings, Dr. Duleba worked with researchers at Poznan (Poland) University of Medical Sciences to enroll 30 women with PCOS based on the Rotterdam criteria. Treatment and placebo groups resembled each other at baseline in terms of age, body mass index, androgen levels, lipid profiles, and levels of follicle-stimulating hormone, luteinizing hormone, prolactin, sex hormone–binding globulin, fasting glucose, and insulin, as well as scores on an insulin sensitivity index.
For the primary outcome measure – total testosterone level – the resveratrol group averaged 0.53 ng/mL at baseline and 0.41 ng/mL at 3-month follow-up, a statistically significant decrease (P = .01). In contrast, testosterone levels in the placebo group remained essentially unchanged, averaging 0.48 ng/mL at baseline and 0.49 ng/mL at follow-up. The difference in effect between the resveratrol and placebo groups was statistically significant (P = .04).
Similarly, average DHEAS levels dropped from 8.1 to 6.3 micromol/L in the resveratrol group (a 22% decline), but increased by 10% in the placebo group.
Resveratrol did not significantly affect progesterone levels, which is consistent with prior findings, Dr. Duleba said. Nor was resveratrol associated with significant changes in body mass index, lipid profile, markers of inflammation or endothelial function, ovarian volume, or gonadotropins.
“We were disappointed that we didn’t see gross changes in ovarian morphology on ultrasound,” he added. Whether those changes might occur with longer treatment is unknown, but for now, “we can only be sure of declining androgen and insulin levels, and improvements in insulin sensitivity.”
The study won a Scientific Congress Prize from ASRM.
RevGenetics provided the resveratrol for the study. Dr. Duleba reported having no relevant financial disclosures.
SALT LAKE CITY – Resveratrol significantly decreased androgen levels and insulin resistance among women with polycystic ovary syndrome (PCOS), according to a first-in-kind randomized, double-blind placebo-controlled trial of 30 patients.
After 3 months of daily oral treatment with 1.5 g of the antioxidant polyphenol, testosterone levels fell an average of 23%, dehydroepiandrosterone sulfate (DHEAS) levels dropped 22%, fasting insulin levels decreased by 32%, and insulin sensitivity improved by 66%, Antoni Duleba, MD, said at the annual meeting of the American Society for Reproductive Medicine. No such improvements occurred in the placebo group, he and his coinvestigators reported simultaneously in the Journal of Clinical Endocrinology & Metabolism (doi: 10.1210/jc.2016-1858).
Past work has found that resveratrol inhibits mRNA expression of Cyp17a1 and reduces androgen production by ovarian theca-interstitial cells. To build on those findings, Dr. Duleba worked with researchers at Poznan (Poland) University of Medical Sciences to enroll 30 women with PCOS based on the Rotterdam criteria. Treatment and placebo groups resembled each other at baseline in terms of age, body mass index, androgen levels, lipid profiles, and levels of follicle-stimulating hormone, luteinizing hormone, prolactin, sex hormone–binding globulin, fasting glucose, and insulin, as well as scores on an insulin sensitivity index.
For the primary outcome measure – total testosterone level – the resveratrol group averaged 0.53 ng/mL at baseline and 0.41 ng/mL at 3-month follow-up, a statistically significant decrease (P = .01). In contrast, testosterone levels in the placebo group remained essentially unchanged, averaging 0.48 ng/mL at baseline and 0.49 ng/mL at follow-up. The difference in effect between the resveratrol and placebo groups was statistically significant (P = .04).
Similarly, average DHEAS levels dropped from 8.1 to 6.3 micromol/L in the resveratrol group (a 22% decline), but increased by 10% in the placebo group.
Resveratrol did not significantly affect progesterone levels, which is consistent with prior findings, Dr. Duleba said. Nor was resveratrol associated with significant changes in body mass index, lipid profile, markers of inflammation or endothelial function, ovarian volume, or gonadotropins.
“We were disappointed that we didn’t see gross changes in ovarian morphology on ultrasound,” he added. Whether those changes might occur with longer treatment is unknown, but for now, “we can only be sure of declining androgen and insulin levels, and improvements in insulin sensitivity.”
The study won a Scientific Congress Prize from ASRM.
RevGenetics provided the resveratrol for the study. Dr. Duleba reported having no relevant financial disclosures.
AT 2016 ASRM
Key clinical point:
Major finding: Average total testosterone levels dropped 23% in the treatment group and remained unchanged in the placebo group (P = .04).
Data source: A single-center, double-blind, randomized controlled trial of 30 women with polycystic ovary syndrome.
Disclosures: RevGenetics provided the resveratrol for the study. Dr. Duleba reported having no relevant financial disclosures.
Ketamine augmentation doesn’t boost ECT outcomes
VIENNA – Low-dose ketamine provided no benefit as adjunctive anesthesia for severely depressed patients undergoing electroconvulsive therapy in the randomized, multicenter U.K. Ketamine-ECT Study, Ian Anderson, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
The hope was that ketamine would lessen the cognitive impairment that is a prominent side effect of ECT. It’s thought that this cognitive impairment results from treatment-induced excessive stimulation of glutamate receptors, and ketamine is a glutamate antagonist, explained Dr. Anderson of the University of Manchester (England).
He and his coinvestigators had also hypothesized that ketamine might result in more rapid improvement in depression in patients undergoing ECT, since a single intravenous infusion of the drug has been shown to produce an extremely rapid, albeit temporary, antidepressant effect. But this was not borne out in the Ketamine-ECT Study.
Dr. Anderson reported on 70 severely depressed patients who were randomized to ketamine at 0.5 mg/kg or saline as an adjunct to standard propofol anesthesia for their course of weekly ECT sessions at seven U.K. mental health centers.
The primary study endpoint was the delayed verbal recall score on the Hopkins Verbal Learning Test–Revised after four ECT sessions, which was midway through the full course of treatment. Blinded assessors found no significant difference between the ketamine and placebo groups then. Nor were significant differences evident at prespecified further assessments 1 and 4 months after conclusion of the treatment program.
Secondary outcomes comprised of cognitive measures of verbal fluency, and autobiographical, working, and visual memory also proved similar in the two study arms, as did assessments of quality of life, safety, and tolerability.
At the end of the full course of ECT, 39% of the ketamine group were categorized as being in remission based upon at least a 50% drop from their baseline score on the Montgomery-Åsberg Depression Rating Scale (MADRS) with a final score of 10 or less, as were 35% of controls. Forty-nine percent of the ketamine group and 60% of controls were categorized as treatment responders, meaning their MADRS score dropped by at least 50% but their final score was greater than 10.
No serious adverse reactions to ketamine occurred.
The study was funded by the United Kingdom's National Institute for Health Research and the Medical Research Council. Dr. Anderson reported having no relevant financial conflicts.
VIENNA – Low-dose ketamine provided no benefit as adjunctive anesthesia for severely depressed patients undergoing electroconvulsive therapy in the randomized, multicenter U.K. Ketamine-ECT Study, Ian Anderson, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
The hope was that ketamine would lessen the cognitive impairment that is a prominent side effect of ECT. It’s thought that this cognitive impairment results from treatment-induced excessive stimulation of glutamate receptors, and ketamine is a glutamate antagonist, explained Dr. Anderson of the University of Manchester (England).
He and his coinvestigators had also hypothesized that ketamine might result in more rapid improvement in depression in patients undergoing ECT, since a single intravenous infusion of the drug has been shown to produce an extremely rapid, albeit temporary, antidepressant effect. But this was not borne out in the Ketamine-ECT Study.
Dr. Anderson reported on 70 severely depressed patients who were randomized to ketamine at 0.5 mg/kg or saline as an adjunct to standard propofol anesthesia for their course of weekly ECT sessions at seven U.K. mental health centers.
The primary study endpoint was the delayed verbal recall score on the Hopkins Verbal Learning Test–Revised after four ECT sessions, which was midway through the full course of treatment. Blinded assessors found no significant difference between the ketamine and placebo groups then. Nor were significant differences evident at prespecified further assessments 1 and 4 months after conclusion of the treatment program.
Secondary outcomes comprised of cognitive measures of verbal fluency, and autobiographical, working, and visual memory also proved similar in the two study arms, as did assessments of quality of life, safety, and tolerability.
At the end of the full course of ECT, 39% of the ketamine group were categorized as being in remission based upon at least a 50% drop from their baseline score on the Montgomery-Åsberg Depression Rating Scale (MADRS) with a final score of 10 or less, as were 35% of controls. Forty-nine percent of the ketamine group and 60% of controls were categorized as treatment responders, meaning their MADRS score dropped by at least 50% but their final score was greater than 10.
No serious adverse reactions to ketamine occurred.
The study was funded by the United Kingdom's National Institute for Health Research and the Medical Research Council. Dr. Anderson reported having no relevant financial conflicts.
VIENNA – Low-dose ketamine provided no benefit as adjunctive anesthesia for severely depressed patients undergoing electroconvulsive therapy in the randomized, multicenter U.K. Ketamine-ECT Study, Ian Anderson, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
The hope was that ketamine would lessen the cognitive impairment that is a prominent side effect of ECT. It’s thought that this cognitive impairment results from treatment-induced excessive stimulation of glutamate receptors, and ketamine is a glutamate antagonist, explained Dr. Anderson of the University of Manchester (England).
He and his coinvestigators had also hypothesized that ketamine might result in more rapid improvement in depression in patients undergoing ECT, since a single intravenous infusion of the drug has been shown to produce an extremely rapid, albeit temporary, antidepressant effect. But this was not borne out in the Ketamine-ECT Study.
Dr. Anderson reported on 70 severely depressed patients who were randomized to ketamine at 0.5 mg/kg or saline as an adjunct to standard propofol anesthesia for their course of weekly ECT sessions at seven U.K. mental health centers.
The primary study endpoint was the delayed verbal recall score on the Hopkins Verbal Learning Test–Revised after four ECT sessions, which was midway through the full course of treatment. Blinded assessors found no significant difference between the ketamine and placebo groups then. Nor were significant differences evident at prespecified further assessments 1 and 4 months after conclusion of the treatment program.
Secondary outcomes comprised of cognitive measures of verbal fluency, and autobiographical, working, and visual memory also proved similar in the two study arms, as did assessments of quality of life, safety, and tolerability.
At the end of the full course of ECT, 39% of the ketamine group were categorized as being in remission based upon at least a 50% drop from their baseline score on the Montgomery-Åsberg Depression Rating Scale (MADRS) with a final score of 10 or less, as were 35% of controls. Forty-nine percent of the ketamine group and 60% of controls were categorized as treatment responders, meaning their MADRS score dropped by at least 50% but their final score was greater than 10.
No serious adverse reactions to ketamine occurred.
The study was funded by the United Kingdom's National Institute for Health Research and the Medical Research Council. Dr. Anderson reported having no relevant financial conflicts.
AT THE ECNP CONGRESS
Key clinical point:
Major finding: Cognitive impairment as measured by delayed verbal recall on the Hopkins Verbal Learning Task–Revised was not reduced by the use of ketamine as an adjunctive anesthetic agent for ECT.
Data source: This randomized, multicenter trial featuring blinded assessments included 70 severely depressed patients who received either ketamine or saline in addition to standard anesthesia during their ECT sessions.
Disclosures: The Ketamine-ECT Study was funded by the U.K. National Institute for Health Research and the Medical Research Council. The presenter reported having no conflicts of interest.
Zika increase slows slightly in pregnant women
The total number of pregnant women in the United States and its territories with laboratory evidence of Zika infection rose by 142 for the week ending Oct. 13 – the smallest increase since early September, according to the Centers for Disease Control and Prevention.
There were 121 new cases of Zika virus infection in pregnant women reported in the U.S. territories and 21 new cases in the states and the District of Columbia, bringing the corresponding totals for the year to 1,927 cases in the territories and 899 in the states/D.C. – a total of 2,826 pregnant women with Zika in the United States, the CDC reported Oct. 20.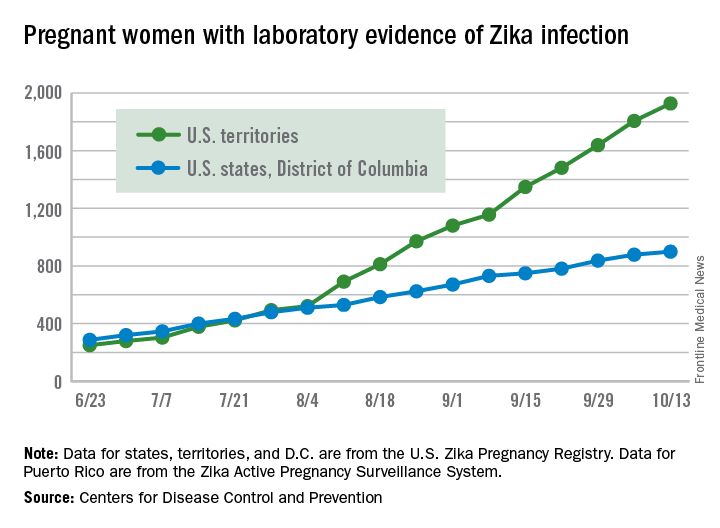
The Zika caseload among all Americans was 31,418 as of Oct. 19. An additional 80 cases reported from Oct. 14 through Oct. 19 brought the state/D.C. total to 4,016, and 1,447 new cases for the week brings the territorial total to 27,402 for 2015-2016, the CDC reported.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
The total number of pregnant women in the United States and its territories with laboratory evidence of Zika infection rose by 142 for the week ending Oct. 13 – the smallest increase since early September, according to the Centers for Disease Control and Prevention.
There were 121 new cases of Zika virus infection in pregnant women reported in the U.S. territories and 21 new cases in the states and the District of Columbia, bringing the corresponding totals for the year to 1,927 cases in the territories and 899 in the states/D.C. – a total of 2,826 pregnant women with Zika in the United States, the CDC reported Oct. 20.
The Zika caseload among all Americans was 31,418 as of Oct. 19. An additional 80 cases reported from Oct. 14 through Oct. 19 brought the state/D.C. total to 4,016, and 1,447 new cases for the week brings the territorial total to 27,402 for 2015-2016, the CDC reported.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
The total number of pregnant women in the United States and its territories with laboratory evidence of Zika infection rose by 142 for the week ending Oct. 13 – the smallest increase since early September, according to the Centers for Disease Control and Prevention.
There were 121 new cases of Zika virus infection in pregnant women reported in the U.S. territories and 21 new cases in the states and the District of Columbia, bringing the corresponding totals for the year to 1,927 cases in the territories and 899 in the states/D.C. – a total of 2,826 pregnant women with Zika in the United States, the CDC reported Oct. 20.
The Zika caseload among all Americans was 31,418 as of Oct. 19. An additional 80 cases reported from Oct. 14 through Oct. 19 brought the state/D.C. total to 4,016, and 1,447 new cases for the week brings the territorial total to 27,402 for 2015-2016, the CDC reported.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Webcast: Contraceptive considerations for women with headache and migraine
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Access Dr. Burkman's Webcasts on contraception:
- Hormonal contraception and risk of venous thromboembolism
- Oral contraceptives and breast cancer: What’s the risk?
- Factors that contribute to overall contraceptive efficacy and risks
- Obesity and contraceptive efficacy and risks
- How to use the CDC's online tools to manage complex cases in contraception
Helpful resources for your practice:
- Book recommendation: Allen RH, Cwiak CA, eds. Contraception for the medically challenging patient. New York, New York: Springer New York; 2014.
- United States Medical Eligibility Criteria for Contraceptive Use, 2016
- United States Medical Eligibility Criteria (US MEC) for Contraceptive Use, 2010
- Summary Chart of US Medical Eligibility for Contraceptive Use
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Access Dr. Burkman's Webcasts on contraception:
- Hormonal contraception and risk of venous thromboembolism
- Oral contraceptives and breast cancer: What’s the risk?
- Factors that contribute to overall contraceptive efficacy and risks
- Obesity and contraceptive efficacy and risks
- How to use the CDC's online tools to manage complex cases in contraception
Helpful resources for your practice:
- Book recommendation: Allen RH, Cwiak CA, eds. Contraception for the medically challenging patient. New York, New York: Springer New York; 2014.
- United States Medical Eligibility Criteria for Contraceptive Use, 2016
- United States Medical Eligibility Criteria (US MEC) for Contraceptive Use, 2010
- Summary Chart of US Medical Eligibility for Contraceptive Use
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Access Dr. Burkman's Webcasts on contraception:
- Hormonal contraception and risk of venous thromboembolism
- Oral contraceptives and breast cancer: What’s the risk?
- Factors that contribute to overall contraceptive efficacy and risks
- Obesity and contraceptive efficacy and risks
- How to use the CDC's online tools to manage complex cases in contraception
Helpful resources for your practice:
- Book recommendation: Allen RH, Cwiak CA, eds. Contraception for the medically challenging patient. New York, New York: Springer New York; 2014.
- United States Medical Eligibility Criteria for Contraceptive Use, 2016
- United States Medical Eligibility Criteria (US MEC) for Contraceptive Use, 2010
- Summary Chart of US Medical Eligibility for Contraceptive Use

Voice recognition software errors: Often silly, sometimes serious
How much is 15%?
Not that much, on paper. With any drug, at least 15% of people will get some kind of side effect. Usually they all list dizziness and headaches at the top.
Could the same be true of a seemingly harmless technology?
Voice recognition software has become pretty commonplace in modern medicine but is far from perfect. I try to be pretty careful about proofreading my dictations, but many docs, especially those in emergency room, don’t have the time to. So VR errors slip by, persisting in 71% of notes.
Most of these errors are just silly and obvious for what they are. But a recent study at a level I ER found that 15% of dictations contained one or more errors deemed as “critical,” with the potential to adversely affect patient care (Int J Med Inform. 2016 Sep;93:70-3).
Communication among doctors, nurses, and all the other key players in the hospital environment is one of the most critical areas in modern medicine. So many people often rely on the initial dictation for an idea of what’s going on that a critical error can affect the way they think about the case from the get-go.
Another issue, sadly, in today’s hospital is that no one takes (or has) the time to get a patient’s past medical history. It’s commonplace to pull the history out of previous admission notes. (Admittedly, sometimes in a demented or unconscious patient you don’t have a choice.) As a result, errors of this sort tend to propagate down the line, from an admission, to the consults, to the discharge summary, and into the next admission.
So let’s get back to that 15%.
I have to assume that 15% of people being admitted aren’t having catastrophic events from medical errors, hopefully because the doctors and nurses handling patient care are thinking for themselves, recognizing dictation errors, and addressing them appropriately.
But even if we dial it down to a tenth of that, say 1.5%, it’s still a serious concern. Bad outcomes in medicine are never entirely avoidable. That’s the nature of the job.
But bad outcomes caused by too much trust in a still-faulty technology are avoidable.
If 15% of people had a serious outcome from a medication, you’d be very cautious about using it. We need to treat these technological gadgets with the same concerns we extend to drugs and procedures. Avoidable bad outcomes, regardless of cause, are never good.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
How much is 15%?
Not that much, on paper. With any drug, at least 15% of people will get some kind of side effect. Usually they all list dizziness and headaches at the top.
Could the same be true of a seemingly harmless technology?
Voice recognition software has become pretty commonplace in modern medicine but is far from perfect. I try to be pretty careful about proofreading my dictations, but many docs, especially those in emergency room, don’t have the time to. So VR errors slip by, persisting in 71% of notes.
Most of these errors are just silly and obvious for what they are. But a recent study at a level I ER found that 15% of dictations contained one or more errors deemed as “critical,” with the potential to adversely affect patient care (Int J Med Inform. 2016 Sep;93:70-3).
Communication among doctors, nurses, and all the other key players in the hospital environment is one of the most critical areas in modern medicine. So many people often rely on the initial dictation for an idea of what’s going on that a critical error can affect the way they think about the case from the get-go.
Another issue, sadly, in today’s hospital is that no one takes (or has) the time to get a patient’s past medical history. It’s commonplace to pull the history out of previous admission notes. (Admittedly, sometimes in a demented or unconscious patient you don’t have a choice.) As a result, errors of this sort tend to propagate down the line, from an admission, to the consults, to the discharge summary, and into the next admission.
So let’s get back to that 15%.
I have to assume that 15% of people being admitted aren’t having catastrophic events from medical errors, hopefully because the doctors and nurses handling patient care are thinking for themselves, recognizing dictation errors, and addressing them appropriately.
But even if we dial it down to a tenth of that, say 1.5%, it’s still a serious concern. Bad outcomes in medicine are never entirely avoidable. That’s the nature of the job.
But bad outcomes caused by too much trust in a still-faulty technology are avoidable.
If 15% of people had a serious outcome from a medication, you’d be very cautious about using it. We need to treat these technological gadgets with the same concerns we extend to drugs and procedures. Avoidable bad outcomes, regardless of cause, are never good.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
How much is 15%?
Not that much, on paper. With any drug, at least 15% of people will get some kind of side effect. Usually they all list dizziness and headaches at the top.
Could the same be true of a seemingly harmless technology?
Voice recognition software has become pretty commonplace in modern medicine but is far from perfect. I try to be pretty careful about proofreading my dictations, but many docs, especially those in emergency room, don’t have the time to. So VR errors slip by, persisting in 71% of notes.
Most of these errors are just silly and obvious for what they are. But a recent study at a level I ER found that 15% of dictations contained one or more errors deemed as “critical,” with the potential to adversely affect patient care (Int J Med Inform. 2016 Sep;93:70-3).
Communication among doctors, nurses, and all the other key players in the hospital environment is one of the most critical areas in modern medicine. So many people often rely on the initial dictation for an idea of what’s going on that a critical error can affect the way they think about the case from the get-go.
Another issue, sadly, in today’s hospital is that no one takes (or has) the time to get a patient’s past medical history. It’s commonplace to pull the history out of previous admission notes. (Admittedly, sometimes in a demented or unconscious patient you don’t have a choice.) As a result, errors of this sort tend to propagate down the line, from an admission, to the consults, to the discharge summary, and into the next admission.
So let’s get back to that 15%.
I have to assume that 15% of people being admitted aren’t having catastrophic events from medical errors, hopefully because the doctors and nurses handling patient care are thinking for themselves, recognizing dictation errors, and addressing them appropriately.
But even if we dial it down to a tenth of that, say 1.5%, it’s still a serious concern. Bad outcomes in medicine are never entirely avoidable. That’s the nature of the job.
But bad outcomes caused by too much trust in a still-faulty technology are avoidable.
If 15% of people had a serious outcome from a medication, you’d be very cautious about using it. We need to treat these technological gadgets with the same concerns we extend to drugs and procedures. Avoidable bad outcomes, regardless of cause, are never good.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
NAMS hormone therapy guidelines stress individualized treatment
An update from the society’s 2012 recommendations, the new statement will also give targeted recommendations for special populations of women to help guide clinicians in individualized treatment.

Highlights from the new position statement were released at the NAMS 2016 annual meeting, and the full document is expected to be published later this year. Among the highlights is the assertion that the clearest benefit for hormone therapy (HT) for treating hot flashes and preventing bone loss is in the early postmenopausal group.
The position statement also represents something of a shift away from the old mantra of “the lowest dose for the shortest period of time,” said Dr. Pinkerton, professor of obstetrics and gynecology at the University of Virginia Health System, Charlottesville.
As a practical matter, clinicians should budget time for these individualized discussions, Cynthia Stuenkel, MD, another member of the guidelines committee, said in an interview.

Currently, HT is approved by the Food and Drug administration as first-line therapy for menopausal vasomotor symptoms (VMS) for women without contraindications. For prevention of bone loss and fractures in postmenopausal women at higher risk, HT may be considered, especially for women younger than 60 years old and less than 10 years post menopause, according to the position statement.
When the predominant symptom pattern involves genitourinary syndrome of menopause (GSM, also known as vulvovaginal atrophy), the position statement recommends starting with low-dose vaginal estrogen as first-line treatment. These are all level I recommendations.

The use of HT in early menopause both provides the most effective treatment for symptoms and the greatest skeletal benefits, according to Michael R. McClung, MD, founding director of the Oregon Osteoporosis Center in Portland. “The benefit far outweighs the risk,” he said, especially in women at risk for bone density loss without contraindication for HT.
Special populations
Several special populations are addressed in the updated position statement. These include those who have reached early menopause because of primary ovarian insufficiency or because of oophorectomy. For these women, NAMS recommends hormone therapy until at least the median age of menopause. Making a level II recommendation, the NAMS committee wrote, “Observational studies suggest that benefits appear to outweigh the risks for effects on bone, heart, cognition, GSM, sexual function, and mood.”
Other special populations for whom HT may be considered include women with a family history of breast cancer and women who are positive for the BRCA gene. Again turning to observational evidence, the NAMS committee makes a level II recommendation that “use of HT does not alter the risk for breast cancer in women with family history of breast cancer, although family history is one risk, among many, that should be assessed.”
BRCA-positive women who do not have breast cancer are at higher risk for primarily estrogen receptor–negative breast cancer. BRCA-positive women may have opted for elective oophorectomy, though, and the committee recommends considering the potential negative effects of estrogen depletion at a premenopausal age when weighing risks and benefits in surgically menopausal BRCA-positive patients. It’s appropriate to offer systemic HT until the median age of menopause in this population, if there are no contraindications, and after appropriate counseling, according to the position statement.
Individualized discussions about continuing HT beyond the median age of menopause are recommended, said Dr. Pinkerton. “We reviewed the literature and found no increased risk in observational studies of women with BRCA genes after oophorectomy who receive hormone therapy,” she said. “These decisions are best taken on an individual basis.” The recommendations for the BRCA population are also a level II recommendation.
Duration of use
Regarding extended use of HT, the NAMS statement breaks with the Beers criteria, saying that routine discontinuation of HT after the age of 65 years “is not supported by data.” These decisions, according to the new recommendations, should be individualized. This is a level III recommendation. Still, said Dr. Kaunitz, “many women grow out of their vasomotor symptoms,” and so an individualized approach might include indefinite use of low-dose vaginal estrogen therapy for GSM, he said.
The overall benefit-risk ratio for HT is also addressed in the position statement, which emphasizes an individualized approach that includes periodic reassessment of risk and benefit for particular patients. However, for patients younger than 60 years of age, or who are within 10 years of menopause, NAMS endorses an overall favorable risk-benefit profile for HT in two particular areas, barring contraindications. For this younger postmenopausal population, hormone therapy is beneficial for bothersome vasomotor symptoms, according to the position statement, and women with an increased risk of osteoporosis or fracture may also benefit from HT.
The benefit-risk profile may tip against HT for women who are starting hormone therapy more than 10 years after menopause, or when they are 60 years old or older, according to the statement. The authors cite elevated risks of coronary heart disease, stroke, venous thromboembolism, and dementia.

The recommendations embodied in the new position statement take into account the “substantial benefit” of estrogen for many women, and provide an updated view of the safety of HT, Dr. McClung said. It’s important for physicians to talk to their patients, because “that information has not made it back to the Internet,” he said.
Dr. Pinkerton, Dr. McClung, and Dr. Kaunitz all reported financial relationships with several pharmaceutical companies. Dr. Kaunitz reported receiving royalties from UpToDate. Dr. Stuenkel reported no relevant financial disclosures.
[email protected]
On Twitter @karioakes
An update from the society’s 2012 recommendations, the new statement will also give targeted recommendations for special populations of women to help guide clinicians in individualized treatment.
Highlights from the new position statement were released at the NAMS 2016 annual meeting, and the full document is expected to be published later this year. Among the highlights is the assertion that the clearest benefit for hormone therapy (HT) for treating hot flashes and preventing bone loss is in the early postmenopausal group.
The position statement also represents something of a shift away from the old mantra of “the lowest dose for the shortest period of time,” said Dr. Pinkerton, professor of obstetrics and gynecology at the University of Virginia Health System, Charlottesville.
As a practical matter, clinicians should budget time for these individualized discussions, Cynthia Stuenkel, MD, another member of the guidelines committee, said in an interview.
Currently, HT is approved by the Food and Drug administration as first-line therapy for menopausal vasomotor symptoms (VMS) for women without contraindications. For prevention of bone loss and fractures in postmenopausal women at higher risk, HT may be considered, especially for women younger than 60 years old and less than 10 years post menopause, according to the position statement.
When the predominant symptom pattern involves genitourinary syndrome of menopause (GSM, also known as vulvovaginal atrophy), the position statement recommends starting with low-dose vaginal estrogen as first-line treatment. These are all level I recommendations.
The use of HT in early menopause both provides the most effective treatment for symptoms and the greatest skeletal benefits, according to Michael R. McClung, MD, founding director of the Oregon Osteoporosis Center in Portland. “The benefit far outweighs the risk,” he said, especially in women at risk for bone density loss without contraindication for HT.
Special populations
Several special populations are addressed in the updated position statement. These include those who have reached early menopause because of primary ovarian insufficiency or because of oophorectomy. For these women, NAMS recommends hormone therapy until at least the median age of menopause. Making a level II recommendation, the NAMS committee wrote, “Observational studies suggest that benefits appear to outweigh the risks for effects on bone, heart, cognition, GSM, sexual function, and mood.”
Other special populations for whom HT may be considered include women with a family history of breast cancer and women who are positive for the BRCA gene. Again turning to observational evidence, the NAMS committee makes a level II recommendation that “use of HT does not alter the risk for breast cancer in women with family history of breast cancer, although family history is one risk, among many, that should be assessed.”
BRCA-positive women who do not have breast cancer are at higher risk for primarily estrogen receptor–negative breast cancer. BRCA-positive women may have opted for elective oophorectomy, though, and the committee recommends considering the potential negative effects of estrogen depletion at a premenopausal age when weighing risks and benefits in surgically menopausal BRCA-positive patients. It’s appropriate to offer systemic HT until the median age of menopause in this population, if there are no contraindications, and after appropriate counseling, according to the position statement.
Individualized discussions about continuing HT beyond the median age of menopause are recommended, said Dr. Pinkerton. “We reviewed the literature and found no increased risk in observational studies of women with BRCA genes after oophorectomy who receive hormone therapy,” she said. “These decisions are best taken on an individual basis.” The recommendations for the BRCA population are also a level II recommendation.
Duration of use
Regarding extended use of HT, the NAMS statement breaks with the Beers criteria, saying that routine discontinuation of HT after the age of 65 years “is not supported by data.” These decisions, according to the new recommendations, should be individualized. This is a level III recommendation. Still, said Dr. Kaunitz, “many women grow out of their vasomotor symptoms,” and so an individualized approach might include indefinite use of low-dose vaginal estrogen therapy for GSM, he said.
The overall benefit-risk ratio for HT is also addressed in the position statement, which emphasizes an individualized approach that includes periodic reassessment of risk and benefit for particular patients. However, for patients younger than 60 years of age, or who are within 10 years of menopause, NAMS endorses an overall favorable risk-benefit profile for HT in two particular areas, barring contraindications. For this younger postmenopausal population, hormone therapy is beneficial for bothersome vasomotor symptoms, according to the position statement, and women with an increased risk of osteoporosis or fracture may also benefit from HT.
The benefit-risk profile may tip against HT for women who are starting hormone therapy more than 10 years after menopause, or when they are 60 years old or older, according to the statement. The authors cite elevated risks of coronary heart disease, stroke, venous thromboembolism, and dementia.
The recommendations embodied in the new position statement take into account the “substantial benefit” of estrogen for many women, and provide an updated view of the safety of HT, Dr. McClung said. It’s important for physicians to talk to their patients, because “that information has not made it back to the Internet,” he said.
Dr. Pinkerton, Dr. McClung, and Dr. Kaunitz all reported financial relationships with several pharmaceutical companies. Dr. Kaunitz reported receiving royalties from UpToDate. Dr. Stuenkel reported no relevant financial disclosures.
[email protected]
On Twitter @karioakes
An update from the society’s 2012 recommendations, the new statement will also give targeted recommendations for special populations of women to help guide clinicians in individualized treatment.
Highlights from the new position statement were released at the NAMS 2016 annual meeting, and the full document is expected to be published later this year. Among the highlights is the assertion that the clearest benefit for hormone therapy (HT) for treating hot flashes and preventing bone loss is in the early postmenopausal group.
The position statement also represents something of a shift away from the old mantra of “the lowest dose for the shortest period of time,” said Dr. Pinkerton, professor of obstetrics and gynecology at the University of Virginia Health System, Charlottesville.
As a practical matter, clinicians should budget time for these individualized discussions, Cynthia Stuenkel, MD, another member of the guidelines committee, said in an interview.
Currently, HT is approved by the Food and Drug administration as first-line therapy for menopausal vasomotor symptoms (VMS) for women without contraindications. For prevention of bone loss and fractures in postmenopausal women at higher risk, HT may be considered, especially for women younger than 60 years old and less than 10 years post menopause, according to the position statement.
When the predominant symptom pattern involves genitourinary syndrome of menopause (GSM, also known as vulvovaginal atrophy), the position statement recommends starting with low-dose vaginal estrogen as first-line treatment. These are all level I recommendations.
The use of HT in early menopause both provides the most effective treatment for symptoms and the greatest skeletal benefits, according to Michael R. McClung, MD, founding director of the Oregon Osteoporosis Center in Portland. “The benefit far outweighs the risk,” he said, especially in women at risk for bone density loss without contraindication for HT.
Special populations
Several special populations are addressed in the updated position statement. These include those who have reached early menopause because of primary ovarian insufficiency or because of oophorectomy. For these women, NAMS recommends hormone therapy until at least the median age of menopause. Making a level II recommendation, the NAMS committee wrote, “Observational studies suggest that benefits appear to outweigh the risks for effects on bone, heart, cognition, GSM, sexual function, and mood.”
Other special populations for whom HT may be considered include women with a family history of breast cancer and women who are positive for the BRCA gene. Again turning to observational evidence, the NAMS committee makes a level II recommendation that “use of HT does not alter the risk for breast cancer in women with family history of breast cancer, although family history is one risk, among many, that should be assessed.”
BRCA-positive women who do not have breast cancer are at higher risk for primarily estrogen receptor–negative breast cancer. BRCA-positive women may have opted for elective oophorectomy, though, and the committee recommends considering the potential negative effects of estrogen depletion at a premenopausal age when weighing risks and benefits in surgically menopausal BRCA-positive patients. It’s appropriate to offer systemic HT until the median age of menopause in this population, if there are no contraindications, and after appropriate counseling, according to the position statement.
Individualized discussions about continuing HT beyond the median age of menopause are recommended, said Dr. Pinkerton. “We reviewed the literature and found no increased risk in observational studies of women with BRCA genes after oophorectomy who receive hormone therapy,” she said. “These decisions are best taken on an individual basis.” The recommendations for the BRCA population are also a level II recommendation.
Duration of use
Regarding extended use of HT, the NAMS statement breaks with the Beers criteria, saying that routine discontinuation of HT after the age of 65 years “is not supported by data.” These decisions, according to the new recommendations, should be individualized. This is a level III recommendation. Still, said Dr. Kaunitz, “many women grow out of their vasomotor symptoms,” and so an individualized approach might include indefinite use of low-dose vaginal estrogen therapy for GSM, he said.
The overall benefit-risk ratio for HT is also addressed in the position statement, which emphasizes an individualized approach that includes periodic reassessment of risk and benefit for particular patients. However, for patients younger than 60 years of age, or who are within 10 years of menopause, NAMS endorses an overall favorable risk-benefit profile for HT in two particular areas, barring contraindications. For this younger postmenopausal population, hormone therapy is beneficial for bothersome vasomotor symptoms, according to the position statement, and women with an increased risk of osteoporosis or fracture may also benefit from HT.
The benefit-risk profile may tip against HT for women who are starting hormone therapy more than 10 years after menopause, or when they are 60 years old or older, according to the statement. The authors cite elevated risks of coronary heart disease, stroke, venous thromboembolism, and dementia.
The recommendations embodied in the new position statement take into account the “substantial benefit” of estrogen for many women, and provide an updated view of the safety of HT, Dr. McClung said. It’s important for physicians to talk to their patients, because “that information has not made it back to the Internet,” he said.
Dr. Pinkerton, Dr. McClung, and Dr. Kaunitz all reported financial relationships with several pharmaceutical companies. Dr. Kaunitz reported receiving royalties from UpToDate. Dr. Stuenkel reported no relevant financial disclosures.
[email protected]
On Twitter @karioakes
Experts outline phenotype approach to rosacea
A phenotype approach should be used to diagnose and manage rosacea, according to an expert panel that included 17 dermatologists from North America, Europe, Asia, Africa, and South America.
“As individual treatments do not address multiple features simultaneously, consideration of specific phenotypical issues facilitates individualized optimization of rosacea,” the panel concluded. As individual presentations of rosacea can span more than one of the currently defined disease subtypes, and vary widely in severity, dermatologists have long expressed a need to move to a phenotype-based system for diagnosis and classification.
The goal of the panel was “to establish international consensus on diagnosis and severity determination to improve outcomes” for people with rosacea (Br J Dermatol. 2016 Oct 8. doi: 10.1111/bjd.15122).
Jerry L. Tan, MD, of the University of Western Ontario, Windsor, and coauthors, explained why they considered a transition to the phenotype-based approach important: “Subtype classification may not fully cover the range of clinical presentations and is likely to confound severity assessment, whereas a phenotype-based approach could improve patient outcomes by addressing an individual patient’s clinical presentation and concerns.”
The panel identified two phenotypes as independently diagnostic of rosacea: persistent, centrofacial erythema associated with periodic intensification, and phymatous changes. Flushing or transient erythema, telangiectasia, inflammatory lesions, and ocular manifestations – the other phenotypes identified in the study – were not considered individually diagnostic.
Severity measurements for each phenotype were defined with a high degree of consensus, and the panel agreed that the severity of each feature should be rated independently and not grouped into subtype. For flushing or transient erythema, for example, the panel recommended that clinicians consider the intensity and frequency of episodes along with the area of involvement. For phymatous changes, inflammation, skin thickening, and deformation were identified as the key severity measures.
Although the investigators acknowledged that their expert consensus was the product of clinical opinion in the absence of extensive evidence, they cited as one of the study’s strengths its broad expert representation across geographical regions, where rosacea presentations may differ. Erythema and telangiectasia, Dr. Tan and colleagues wrote, “may not be visible in skin phototypes V and VI, an issue that may be overcome with experience and appropriate history taking.” They added that “other techniques, including skin biopsy, can also be considered for diagnostic support.” They recommended the development of new validated scales to be used in darker-skinned patients.
The panel also identified the psychosocial impact of rosacea as one severely understudied area of rosacea, and advocated the development of a new research tool that would assess psychological comorbidities. The proposed tool, they wrote, “should go beyond those currently available and assess the psychosocial impact for all major phenotypes.” The only rosacea-specific quality of life scoring measure, RosaQoL, contains notable deficiencies, they noted, including a lack of a measure for phymatous changes.
“Since clinicians and patients often have disparate views of disease,” the researchers wrote, “objective and practical tools based on individual presenting features are likely to be of value in setting treatment targets and monitoring treatment progress for patients with rosacea.”
The panel included three ophthalmologists from Germany and the United States; their recommendations were considered exploratory.
The study, which consisted of both electronic surveys and in-person meetings, was funded by Galderma. Twelve of its coauthors, including Dr. Tan, disclosed financial relationships with manufacturers.
A phenotype approach should be used to diagnose and manage rosacea, according to an expert panel that included 17 dermatologists from North America, Europe, Asia, Africa, and South America.
“As individual treatments do not address multiple features simultaneously, consideration of specific phenotypical issues facilitates individualized optimization of rosacea,” the panel concluded. As individual presentations of rosacea can span more than one of the currently defined disease subtypes, and vary widely in severity, dermatologists have long expressed a need to move to a phenotype-based system for diagnosis and classification.
The goal of the panel was “to establish international consensus on diagnosis and severity determination to improve outcomes” for people with rosacea (Br J Dermatol. 2016 Oct 8. doi: 10.1111/bjd.15122).
Jerry L. Tan, MD, of the University of Western Ontario, Windsor, and coauthors, explained why they considered a transition to the phenotype-based approach important: “Subtype classification may not fully cover the range of clinical presentations and is likely to confound severity assessment, whereas a phenotype-based approach could improve patient outcomes by addressing an individual patient’s clinical presentation and concerns.”
The panel identified two phenotypes as independently diagnostic of rosacea: persistent, centrofacial erythema associated with periodic intensification, and phymatous changes. Flushing or transient erythema, telangiectasia, inflammatory lesions, and ocular manifestations – the other phenotypes identified in the study – were not considered individually diagnostic.
Severity measurements for each phenotype were defined with a high degree of consensus, and the panel agreed that the severity of each feature should be rated independently and not grouped into subtype. For flushing or transient erythema, for example, the panel recommended that clinicians consider the intensity and frequency of episodes along with the area of involvement. For phymatous changes, inflammation, skin thickening, and deformation were identified as the key severity measures.
Although the investigators acknowledged that their expert consensus was the product of clinical opinion in the absence of extensive evidence, they cited as one of the study’s strengths its broad expert representation across geographical regions, where rosacea presentations may differ. Erythema and telangiectasia, Dr. Tan and colleagues wrote, “may not be visible in skin phototypes V and VI, an issue that may be overcome with experience and appropriate history taking.” They added that “other techniques, including skin biopsy, can also be considered for diagnostic support.” They recommended the development of new validated scales to be used in darker-skinned patients.
The panel also identified the psychosocial impact of rosacea as one severely understudied area of rosacea, and advocated the development of a new research tool that would assess psychological comorbidities. The proposed tool, they wrote, “should go beyond those currently available and assess the psychosocial impact for all major phenotypes.” The only rosacea-specific quality of life scoring measure, RosaQoL, contains notable deficiencies, they noted, including a lack of a measure for phymatous changes.
“Since clinicians and patients often have disparate views of disease,” the researchers wrote, “objective and practical tools based on individual presenting features are likely to be of value in setting treatment targets and monitoring treatment progress for patients with rosacea.”
The panel included three ophthalmologists from Germany and the United States; their recommendations were considered exploratory.
The study, which consisted of both electronic surveys and in-person meetings, was funded by Galderma. Twelve of its coauthors, including Dr. Tan, disclosed financial relationships with manufacturers.
A phenotype approach should be used to diagnose and manage rosacea, according to an expert panel that included 17 dermatologists from North America, Europe, Asia, Africa, and South America.
“As individual treatments do not address multiple features simultaneously, consideration of specific phenotypical issues facilitates individualized optimization of rosacea,” the panel concluded. As individual presentations of rosacea can span more than one of the currently defined disease subtypes, and vary widely in severity, dermatologists have long expressed a need to move to a phenotype-based system for diagnosis and classification.
The goal of the panel was “to establish international consensus on diagnosis and severity determination to improve outcomes” for people with rosacea (Br J Dermatol. 2016 Oct 8. doi: 10.1111/bjd.15122).
Jerry L. Tan, MD, of the University of Western Ontario, Windsor, and coauthors, explained why they considered a transition to the phenotype-based approach important: “Subtype classification may not fully cover the range of clinical presentations and is likely to confound severity assessment, whereas a phenotype-based approach could improve patient outcomes by addressing an individual patient’s clinical presentation and concerns.”
The panel identified two phenotypes as independently diagnostic of rosacea: persistent, centrofacial erythema associated with periodic intensification, and phymatous changes. Flushing or transient erythema, telangiectasia, inflammatory lesions, and ocular manifestations – the other phenotypes identified in the study – were not considered individually diagnostic.
Severity measurements for each phenotype were defined with a high degree of consensus, and the panel agreed that the severity of each feature should be rated independently and not grouped into subtype. For flushing or transient erythema, for example, the panel recommended that clinicians consider the intensity and frequency of episodes along with the area of involvement. For phymatous changes, inflammation, skin thickening, and deformation were identified as the key severity measures.
Although the investigators acknowledged that their expert consensus was the product of clinical opinion in the absence of extensive evidence, they cited as one of the study’s strengths its broad expert representation across geographical regions, where rosacea presentations may differ. Erythema and telangiectasia, Dr. Tan and colleagues wrote, “may not be visible in skin phototypes V and VI, an issue that may be overcome with experience and appropriate history taking.” They added that “other techniques, including skin biopsy, can also be considered for diagnostic support.” They recommended the development of new validated scales to be used in darker-skinned patients.
The panel also identified the psychosocial impact of rosacea as one severely understudied area of rosacea, and advocated the development of a new research tool that would assess psychological comorbidities. The proposed tool, they wrote, “should go beyond those currently available and assess the psychosocial impact for all major phenotypes.” The only rosacea-specific quality of life scoring measure, RosaQoL, contains notable deficiencies, they noted, including a lack of a measure for phymatous changes.
“Since clinicians and patients often have disparate views of disease,” the researchers wrote, “objective and practical tools based on individual presenting features are likely to be of value in setting treatment targets and monitoring treatment progress for patients with rosacea.”
The panel included three ophthalmologists from Germany and the United States; their recommendations were considered exploratory.
The study, which consisted of both electronic surveys and in-person meetings, was funded by Galderma. Twelve of its coauthors, including Dr. Tan, disclosed financial relationships with manufacturers.
FROM THE BRITISH JOURNAL OF DERMATOLOGY
Key clinical point: Rosacea diagnosis, severity grading, and management should be based on disease phenotypes, which can span more than one of the currently recognized subtypes.
Major finding: Persistent centrofacial erythema with periodic intensification, and phymatous changes, are two phenotypes independently diagnostic of rosacea
Data source: An expert panel of 17 dermatologists from North America, Europe, Asia, Africa, and South America.
Disclosures: Galderma sponsored the study, for which all authors received honoraria; 12 disclosed additional funding from Galderma or other manufacturers.