User login
Caval Interruption Strategies in the Spotlight
Caval interruption, typically by the installation of a filter, traps dislodged blood clots in the inferior vena cava, before they can reach the heart and lungs. The strategy will be the topic of the second half of the Friday afternoon session entitled “Endovascular and Open Solutions for Inferior Vena Cava Tumors and Occlusions, Vena Cava Filtration Strategies, Pitfalls, and Complications and More About Iliac Vein Stenting.”

The first half of the session will focus on the general topic of interventions of the inferior vena cava. This will include everything from percutaneous recanalization for occluded IVC filters to open and robotic vena cava reconstruction for the removal of benign and malignant tumors. The second half will cover the current controversies involving inferior vena cava filter indications for placement, retrieval, and the management of their complications.
“Session attendees will be able to understand current methods and indications for IVC filter placement, follow-up and retrieval. In addition, they will get an update on current research to improve the care of our patients requiring IVC interruption. The session will aid practitioners to better understand the requirements for open and endovascular management of vena cava tumors and obstruction,” said Dr. Gillespie.

Dr. John Rectenwald, the co-moderator, will consider the indications for IVC filters and discuss whether these are being observed in clinical practice. He will be followed by Dr. David Rosenthal of the Medical College of Georgia, who will provide an update on the Sentry bioconvertible non-retrieval IVS filter. The Sentry device is designed to provide protection against pulmonary embolism at the time of highest risk of embolism, followed by bioconversion to leave an unobstructed IVC lumen. The next speaker will be Dr. Gillespie, who will discuss the retrieval of IVC filters and the influence on retrieval rate by the filter design, institutional practice, and the individual surgeon. Dr. Steven Abramowitz of Georgetown University School of Medicine will talk about ulcer healing and quality of life following endovascular iliocaval reconstructive stenting in patients who have both IVC and iliac occlusive disease.
Dr. Rectenwald will discuss the Prevention du Risque d’Embolie Pulmonaire par Interruption Cav (PREPIC) trial of over 400 patients randomized to receive or not receive a filter along with standard anticoagulation treatment. Recommendations regarding IVC filters have been based on the PREPIC trial and follow-up data. The follow-up data showed no survival benefit. Whether the evidence supports the use of IVC filters will be discussed. Continuing this theme, Dr. Gillespie will update the physician-initiated, Investigational Device Exemption vena cava PRESERVE study, a large-scale, multi-specialty, prospective study launched in October 2016, which is assessing the use of IVC filters in the United States. The study involves all commercially available inferior vena cava filters placed in subjects for the prevention of death from fatal or symptomatic pulmonary embolism.
IVC filters are subject to complications. How to deal with these is a major challenge. Complications and how to avoid them will be the topic of a presentation by Dr. Clifford Sales of Mount Sinai School of Medicine, and how best to deal with filters that are difficult to retrieve will be discussed by Dr. Brian DeRubertis of UCLA Division of Vascular Surgery, Los Angeles, Calif. What to do when filters actually fracture and generate embolic fragments will be the topic of a presentation by Dr. Constantino Peña, University of South Florida. Finally, Dr. Nicholas Gargiulo, III, of The Clinch Valley Medical Center will consider prophylactic caval filtration in term of bariatric surgery patients who are the best candidates.
“There are special challenges involved in the open and endovascular management of inferior vena cava problems. These represent opportunities for practitioners to grow their practice. These patients are some of the most complicated patients we care for. Their management requires advanced techniques and dedicated clinicians to their care and management,” said Dr. Gillespie.
Session 91:
Endovascular and Open Solutions for Inferior Vena Cava Tumors and Occusions, Vena Cava Filtration Strategies, Pitfalls, and Complications and More About Iliac Vein Stenting
Caval Interruption
Friday 4:00 p.m. to 4:53 p.m.
Trianon Ballroom, 3rd Floor
Caval interruption, typically by the installation of a filter, traps dislodged blood clots in the inferior vena cava, before they can reach the heart and lungs. The strategy will be the topic of the second half of the Friday afternoon session entitled “Endovascular and Open Solutions for Inferior Vena Cava Tumors and Occlusions, Vena Cava Filtration Strategies, Pitfalls, and Complications and More About Iliac Vein Stenting.”
The first half of the session will focus on the general topic of interventions of the inferior vena cava. This will include everything from percutaneous recanalization for occluded IVC filters to open and robotic vena cava reconstruction for the removal of benign and malignant tumors. The second half will cover the current controversies involving inferior vena cava filter indications for placement, retrieval, and the management of their complications.
“Session attendees will be able to understand current methods and indications for IVC filter placement, follow-up and retrieval. In addition, they will get an update on current research to improve the care of our patients requiring IVC interruption. The session will aid practitioners to better understand the requirements for open and endovascular management of vena cava tumors and obstruction,” said Dr. Gillespie.
Dr. John Rectenwald, the co-moderator, will consider the indications for IVC filters and discuss whether these are being observed in clinical practice. He will be followed by Dr. David Rosenthal of the Medical College of Georgia, who will provide an update on the Sentry bioconvertible non-retrieval IVS filter. The Sentry device is designed to provide protection against pulmonary embolism at the time of highest risk of embolism, followed by bioconversion to leave an unobstructed IVC lumen. The next speaker will be Dr. Gillespie, who will discuss the retrieval of IVC filters and the influence on retrieval rate by the filter design, institutional practice, and the individual surgeon. Dr. Steven Abramowitz of Georgetown University School of Medicine will talk about ulcer healing and quality of life following endovascular iliocaval reconstructive stenting in patients who have both IVC and iliac occlusive disease.
Dr. Rectenwald will discuss the Prevention du Risque d’Embolie Pulmonaire par Interruption Cav (PREPIC) trial of over 400 patients randomized to receive or not receive a filter along with standard anticoagulation treatment. Recommendations regarding IVC filters have been based on the PREPIC trial and follow-up data. The follow-up data showed no survival benefit. Whether the evidence supports the use of IVC filters will be discussed. Continuing this theme, Dr. Gillespie will update the physician-initiated, Investigational Device Exemption vena cava PRESERVE study, a large-scale, multi-specialty, prospective study launched in October 2016, which is assessing the use of IVC filters in the United States. The study involves all commercially available inferior vena cava filters placed in subjects for the prevention of death from fatal or symptomatic pulmonary embolism.
IVC filters are subject to complications. How to deal with these is a major challenge. Complications and how to avoid them will be the topic of a presentation by Dr. Clifford Sales of Mount Sinai School of Medicine, and how best to deal with filters that are difficult to retrieve will be discussed by Dr. Brian DeRubertis of UCLA Division of Vascular Surgery, Los Angeles, Calif. What to do when filters actually fracture and generate embolic fragments will be the topic of a presentation by Dr. Constantino Peña, University of South Florida. Finally, Dr. Nicholas Gargiulo, III, of The Clinch Valley Medical Center will consider prophylactic caval filtration in term of bariatric surgery patients who are the best candidates.
“There are special challenges involved in the open and endovascular management of inferior vena cava problems. These represent opportunities for practitioners to grow their practice. These patients are some of the most complicated patients we care for. Their management requires advanced techniques and dedicated clinicians to their care and management,” said Dr. Gillespie.
Session 91:
Endovascular and Open Solutions for Inferior Vena Cava Tumors and Occusions, Vena Cava Filtration Strategies, Pitfalls, and Complications and More About Iliac Vein Stenting
Caval Interruption
Friday 4:00 p.m. to 4:53 p.m.
Trianon Ballroom, 3rd Floor
Caval interruption, typically by the installation of a filter, traps dislodged blood clots in the inferior vena cava, before they can reach the heart and lungs. The strategy will be the topic of the second half of the Friday afternoon session entitled “Endovascular and Open Solutions for Inferior Vena Cava Tumors and Occlusions, Vena Cava Filtration Strategies, Pitfalls, and Complications and More About Iliac Vein Stenting.”
The first half of the session will focus on the general topic of interventions of the inferior vena cava. This will include everything from percutaneous recanalization for occluded IVC filters to open and robotic vena cava reconstruction for the removal of benign and malignant tumors. The second half will cover the current controversies involving inferior vena cava filter indications for placement, retrieval, and the management of their complications.
“Session attendees will be able to understand current methods and indications for IVC filter placement, follow-up and retrieval. In addition, they will get an update on current research to improve the care of our patients requiring IVC interruption. The session will aid practitioners to better understand the requirements for open and endovascular management of vena cava tumors and obstruction,” said Dr. Gillespie.
Dr. John Rectenwald, the co-moderator, will consider the indications for IVC filters and discuss whether these are being observed in clinical practice. He will be followed by Dr. David Rosenthal of the Medical College of Georgia, who will provide an update on the Sentry bioconvertible non-retrieval IVS filter. The Sentry device is designed to provide protection against pulmonary embolism at the time of highest risk of embolism, followed by bioconversion to leave an unobstructed IVC lumen. The next speaker will be Dr. Gillespie, who will discuss the retrieval of IVC filters and the influence on retrieval rate by the filter design, institutional practice, and the individual surgeon. Dr. Steven Abramowitz of Georgetown University School of Medicine will talk about ulcer healing and quality of life following endovascular iliocaval reconstructive stenting in patients who have both IVC and iliac occlusive disease.
Dr. Rectenwald will discuss the Prevention du Risque d’Embolie Pulmonaire par Interruption Cav (PREPIC) trial of over 400 patients randomized to receive or not receive a filter along with standard anticoagulation treatment. Recommendations regarding IVC filters have been based on the PREPIC trial and follow-up data. The follow-up data showed no survival benefit. Whether the evidence supports the use of IVC filters will be discussed. Continuing this theme, Dr. Gillespie will update the physician-initiated, Investigational Device Exemption vena cava PRESERVE study, a large-scale, multi-specialty, prospective study launched in October 2016, which is assessing the use of IVC filters in the United States. The study involves all commercially available inferior vena cava filters placed in subjects for the prevention of death from fatal or symptomatic pulmonary embolism.
IVC filters are subject to complications. How to deal with these is a major challenge. Complications and how to avoid them will be the topic of a presentation by Dr. Clifford Sales of Mount Sinai School of Medicine, and how best to deal with filters that are difficult to retrieve will be discussed by Dr. Brian DeRubertis of UCLA Division of Vascular Surgery, Los Angeles, Calif. What to do when filters actually fracture and generate embolic fragments will be the topic of a presentation by Dr. Constantino Peña, University of South Florida. Finally, Dr. Nicholas Gargiulo, III, of The Clinch Valley Medical Center will consider prophylactic caval filtration in term of bariatric surgery patients who are the best candidates.
“There are special challenges involved in the open and endovascular management of inferior vena cava problems. These represent opportunities for practitioners to grow their practice. These patients are some of the most complicated patients we care for. Their management requires advanced techniques and dedicated clinicians to their care and management,” said Dr. Gillespie.
Session 91:
Endovascular and Open Solutions for Inferior Vena Cava Tumors and Occusions, Vena Cava Filtration Strategies, Pitfalls, and Complications and More About Iliac Vein Stenting
Caval Interruption
Friday 4:00 p.m. to 4:53 p.m.
Trianon Ballroom, 3rd Floor
Updates Presented on Robotic Vena Cava Surgery
Developments in robotic vena cava surgery will be presented Friday afternoon during the session entitled “Endovascular and Open Solutions for Inferior Vena Cava Tumors and Occusions, Vena Cava Filtration Strategies, Pitfalls, and Complications and More About Iliac Vein Stenting.”

“The selective use of robotic surgery on the vena cava is a tremendous step forward because of its minimal invasiveness and also because of the magnification that the robot gives and the technical advantages the robot gives over open surgery or laparoscopic surgery,” said Dr. Money.
Traditionally, inferior vena cava thrombectomy is done using a large open incision, since it is difficult otherwise to gain access to the vein. The surgery is done most often to address involvement of the inferior vena cava by an adjacent tumor. In addition, surgery may be needed to remove filters inserted to prevent migration of pulmonary emboli when problems develop with the filter.
The open incision approach carries a considerable risk of morbidity with the approach. A minimally invasive treatment option has been needed. Minimally invasive laparoscopy is an option. But drawbacks include the technically challenging nature of the procedure which makes for a steep learning curve.
Within the past decade, the use of robotic surgery has been utilized for interior vena cava thrombectomy. The approach involves multiple but smaller incisions to allow access of robotic tools. The robotic approach provides better visualization with magnification, three-dimensional vision, tremor filtration, and seven degrees of freedom, among other advantages.
“The overall take-home message from my presentation is that robotic vena caval surgery can be done and it should be used. Overall, robotic surgery for the vena cava is a field that is developing. It requires collaboration with other specialties and a realization that minimally invasive procedures are not just endovascular procedures but may be laparoscopic or robotic in nature,” said Dr. Money.
Dr. Money will describe the outcomes of a prospective study undertaken at the Scottsdale Mayo Clinic that evaluated the efficacy of a vena cava surgical system for radical nephrectomy and inferior vena cava tumor thrombectomy and, in a few patients, inferior vena cava filter removal. More recently, the robotic surgery was used to treat compression of the left renal vein between the superior mesenteric artery and aorta.
A focus of the presentation will be the key importance of the collaboration between vascular and robotic surgeons. “As time has developed I have become more aware and more adept at what the robot can do. However, it is not a routine part of my practice. By collaborating with others who use it more frequently, we have developed a practice where vena caval surgery can be done in a minimally invasive fashion with patients going home following a shorter length of stay, with less significant blood loss, and overall an easier recovery,” said Dr. Money.
Session 91:Endovascular and Open Solutions for Inferior Vena Cava Tumors and Occusions, Vena Cava Filtration Strategies, Pitfalls, and Complications and More About Iliac Vein Stenting
Robotic Vena Cava Surgery
Friday, 3:48 p.m. – 3:53 p.m.
Trianon Ballroom, 3rd Floor
Developments in robotic vena cava surgery will be presented Friday afternoon during the session entitled “Endovascular and Open Solutions for Inferior Vena Cava Tumors and Occusions, Vena Cava Filtration Strategies, Pitfalls, and Complications and More About Iliac Vein Stenting.”
“The selective use of robotic surgery on the vena cava is a tremendous step forward because of its minimal invasiveness and also because of the magnification that the robot gives and the technical advantages the robot gives over open surgery or laparoscopic surgery,” said Dr. Money.
Traditionally, inferior vena cava thrombectomy is done using a large open incision, since it is difficult otherwise to gain access to the vein. The surgery is done most often to address involvement of the inferior vena cava by an adjacent tumor. In addition, surgery may be needed to remove filters inserted to prevent migration of pulmonary emboli when problems develop with the filter.
The open incision approach carries a considerable risk of morbidity with the approach. A minimally invasive treatment option has been needed. Minimally invasive laparoscopy is an option. But drawbacks include the technically challenging nature of the procedure which makes for a steep learning curve.
Within the past decade, the use of robotic surgery has been utilized for interior vena cava thrombectomy. The approach involves multiple but smaller incisions to allow access of robotic tools. The robotic approach provides better visualization with magnification, three-dimensional vision, tremor filtration, and seven degrees of freedom, among other advantages.
“The overall take-home message from my presentation is that robotic vena caval surgery can be done and it should be used. Overall, robotic surgery for the vena cava is a field that is developing. It requires collaboration with other specialties and a realization that minimally invasive procedures are not just endovascular procedures but may be laparoscopic or robotic in nature,” said Dr. Money.
Dr. Money will describe the outcomes of a prospective study undertaken at the Scottsdale Mayo Clinic that evaluated the efficacy of a vena cava surgical system for radical nephrectomy and inferior vena cava tumor thrombectomy and, in a few patients, inferior vena cava filter removal. More recently, the robotic surgery was used to treat compression of the left renal vein between the superior mesenteric artery and aorta.
A focus of the presentation will be the key importance of the collaboration between vascular and robotic surgeons. “As time has developed I have become more aware and more adept at what the robot can do. However, it is not a routine part of my practice. By collaborating with others who use it more frequently, we have developed a practice where vena caval surgery can be done in a minimally invasive fashion with patients going home following a shorter length of stay, with less significant blood loss, and overall an easier recovery,” said Dr. Money.
Session 91:Endovascular and Open Solutions for Inferior Vena Cava Tumors and Occusions, Vena Cava Filtration Strategies, Pitfalls, and Complications and More About Iliac Vein Stenting
Robotic Vena Cava Surgery
Friday, 3:48 p.m. – 3:53 p.m.
Trianon Ballroom, 3rd Floor
Developments in robotic vena cava surgery will be presented Friday afternoon during the session entitled “Endovascular and Open Solutions for Inferior Vena Cava Tumors and Occusions, Vena Cava Filtration Strategies, Pitfalls, and Complications and More About Iliac Vein Stenting.”
“The selective use of robotic surgery on the vena cava is a tremendous step forward because of its minimal invasiveness and also because of the magnification that the robot gives and the technical advantages the robot gives over open surgery or laparoscopic surgery,” said Dr. Money.
Traditionally, inferior vena cava thrombectomy is done using a large open incision, since it is difficult otherwise to gain access to the vein. The surgery is done most often to address involvement of the inferior vena cava by an adjacent tumor. In addition, surgery may be needed to remove filters inserted to prevent migration of pulmonary emboli when problems develop with the filter.
The open incision approach carries a considerable risk of morbidity with the approach. A minimally invasive treatment option has been needed. Minimally invasive laparoscopy is an option. But drawbacks include the technically challenging nature of the procedure which makes for a steep learning curve.
Within the past decade, the use of robotic surgery has been utilized for interior vena cava thrombectomy. The approach involves multiple but smaller incisions to allow access of robotic tools. The robotic approach provides better visualization with magnification, three-dimensional vision, tremor filtration, and seven degrees of freedom, among other advantages.
“The overall take-home message from my presentation is that robotic vena caval surgery can be done and it should be used. Overall, robotic surgery for the vena cava is a field that is developing. It requires collaboration with other specialties and a realization that minimally invasive procedures are not just endovascular procedures but may be laparoscopic or robotic in nature,” said Dr. Money.
Dr. Money will describe the outcomes of a prospective study undertaken at the Scottsdale Mayo Clinic that evaluated the efficacy of a vena cava surgical system for radical nephrectomy and inferior vena cava tumor thrombectomy and, in a few patients, inferior vena cava filter removal. More recently, the robotic surgery was used to treat compression of the left renal vein between the superior mesenteric artery and aorta.
A focus of the presentation will be the key importance of the collaboration between vascular and robotic surgeons. “As time has developed I have become more aware and more adept at what the robot can do. However, it is not a routine part of my practice. By collaborating with others who use it more frequently, we have developed a practice where vena caval surgery can be done in a minimally invasive fashion with patients going home following a shorter length of stay, with less significant blood loss, and overall an easier recovery,” said Dr. Money.
Session 91:Endovascular and Open Solutions for Inferior Vena Cava Tumors and Occusions, Vena Cava Filtration Strategies, Pitfalls, and Complications and More About Iliac Vein Stenting
Robotic Vena Cava Surgery
Friday, 3:48 p.m. – 3:53 p.m.
Trianon Ballroom, 3rd Floor
Nutraceutical cocktail protects against postpartum blues
VIENNA – A dietary supplement blend virtually eliminated postpartum blues in a promising proof-of-concept controlled trial, Yekta Dowlati, PhD, reported during the annual congress of the European College of Neuropsychopharmacology.
The nutraceutical cocktail is designed to compensate for the effects of the early postpartum surge in monoamine oxidase A (MAO-A) activity that her research group previously has reported. They found that as estrogen levels plunge by 100-fold in the first 3 days postpartum, brain MAO-A levels rise by 40% in affect-controlling regions, including the prefrontal cortex and anterior cingulate cortex (Arch Gen Psychiatry. 2010 May;67[5]:468-74).
That suggests a potential causal relationship with postpartum blues, since MAO-A is an enzyme whose effects include promotion of oxidative stress, apoptosis, and metabolizing serotonin, norepinephrine, and dopamine, explained Dr. Dowlati of the department of psychiatry at the University of Toronto.
Postpartum blues is a common prodrome for postpartum depression, the most frequent complication of childbearing, which has an estimated incidence of 13%. Severe postpartum blues is a strong predictor of subsequent postpartum depression. Yet, despite the large burden of illness imposed by postpartum depression, there is no proven preventive strategy. The hypothesis being pursued in developing this nutraceutical is that a safe dietary intervention that prevents postpartum blues also may prevent postpartum depression.
The nutraceutical cocktail developed by Dr. Dowlati and her coinvestigators consists of monoamine precursors: 2 g of tryptophan, 10 g of tyrosine, and blueberry juice plus blueberry extract.
She reported on 41 healthy breast-feeding mothers who on day 5 postpartum, when postpartum blues typically peaks, were assigned to drink the dietary supplement or not. Later that day, they underwent a quantified assessment of their severity of postpartum blues based upon change from baseline in depressed mood scores on a 0-100 visual analog scale after undergoing a standardized sad mood induction procedure. This is a simple protocol widely used by psychiatrists and psychologists researching the neurobiology of mood states. Dr. Dowlati and her colleagues used the Velten protocol, in which subjects read depressing sentences while listening to sad music.
Mean scores on the Visual Analog Scale for sadness following the standardized mood induction procedure jumped by 43.8 points in the control group but were unchanged, with a mere 0.5-point increase, in the 21 women in the active treatment arm.
“The results of the present study, albeit in an open-label trial, reflect by far the most robust effects of a dietary supplement ever seen on postpartum blues. Our effect size was 2.9. Previous trials have reported effect sizes of 0.07-0.28,” she noted.
An effect size of 2.9 means that if a postpartum woman did not experience a plunge in mood after the induction protocol, there was statistically a 98%-99% chance that she had consumed the supplement.
“One explanation to account for an active effect is that the supplement is compensating for the effects of monoamine metabolism and increased oxidative stress by elevated postpartum MAO-A levels,” according to Dr. Dowlati. “Given the effect size of 2.9 and minimal effects of tryptophan and tyrosine supplementation on total levels in breast milk, there is excellent reason to pursue this supplement in a randomized, double-blind, placebo-controlled trial to further assess its effects.”
Before conducting this efficacy study, the investigators evaluated the safety of their planned intervention by randomizing 54 healthy breast-feeding women to single larger doses of oral tyrosine or tryptophan than were used in the nutraceutical cocktail or to no supplements. They found no subsequent increase in total tyrosine or total tryptophan levels in the subjects’ breast milk, although dose-dependent increases were found in free tyrosine and free tryptophan in maternal plasma. Free tyrosine was increased in breast milk; however, the level was significantly lower than what the investigators found in laboratory analysis of a dozen popular brands of infant formula.
The safety and open-label efficacy studies were funded by the Canadian Institutes of Health Research, the Ontario Mental Health Foundation, and university research grants. Dr. Dowlati reported having no financial conflicts of interest.
VIENNA – A dietary supplement blend virtually eliminated postpartum blues in a promising proof-of-concept controlled trial, Yekta Dowlati, PhD, reported during the annual congress of the European College of Neuropsychopharmacology.
The nutraceutical cocktail is designed to compensate for the effects of the early postpartum surge in monoamine oxidase A (MAO-A) activity that her research group previously has reported. They found that as estrogen levels plunge by 100-fold in the first 3 days postpartum, brain MAO-A levels rise by 40% in affect-controlling regions, including the prefrontal cortex and anterior cingulate cortex (Arch Gen Psychiatry. 2010 May;67[5]:468-74).
That suggests a potential causal relationship with postpartum blues, since MAO-A is an enzyme whose effects include promotion of oxidative stress, apoptosis, and metabolizing serotonin, norepinephrine, and dopamine, explained Dr. Dowlati of the department of psychiatry at the University of Toronto.
Postpartum blues is a common prodrome for postpartum depression, the most frequent complication of childbearing, which has an estimated incidence of 13%. Severe postpartum blues is a strong predictor of subsequent postpartum depression. Yet, despite the large burden of illness imposed by postpartum depression, there is no proven preventive strategy. The hypothesis being pursued in developing this nutraceutical is that a safe dietary intervention that prevents postpartum blues also may prevent postpartum depression.
The nutraceutical cocktail developed by Dr. Dowlati and her coinvestigators consists of monoamine precursors: 2 g of tryptophan, 10 g of tyrosine, and blueberry juice plus blueberry extract.
She reported on 41 healthy breast-feeding mothers who on day 5 postpartum, when postpartum blues typically peaks, were assigned to drink the dietary supplement or not. Later that day, they underwent a quantified assessment of their severity of postpartum blues based upon change from baseline in depressed mood scores on a 0-100 visual analog scale after undergoing a standardized sad mood induction procedure. This is a simple protocol widely used by psychiatrists and psychologists researching the neurobiology of mood states. Dr. Dowlati and her colleagues used the Velten protocol, in which subjects read depressing sentences while listening to sad music.
Mean scores on the Visual Analog Scale for sadness following the standardized mood induction procedure jumped by 43.8 points in the control group but were unchanged, with a mere 0.5-point increase, in the 21 women in the active treatment arm.
“The results of the present study, albeit in an open-label trial, reflect by far the most robust effects of a dietary supplement ever seen on postpartum blues. Our effect size was 2.9. Previous trials have reported effect sizes of 0.07-0.28,” she noted.
An effect size of 2.9 means that if a postpartum woman did not experience a plunge in mood after the induction protocol, there was statistically a 98%-99% chance that she had consumed the supplement.
“One explanation to account for an active effect is that the supplement is compensating for the effects of monoamine metabolism and increased oxidative stress by elevated postpartum MAO-A levels,” according to Dr. Dowlati. “Given the effect size of 2.9 and minimal effects of tryptophan and tyrosine supplementation on total levels in breast milk, there is excellent reason to pursue this supplement in a randomized, double-blind, placebo-controlled trial to further assess its effects.”
Before conducting this efficacy study, the investigators evaluated the safety of their planned intervention by randomizing 54 healthy breast-feeding women to single larger doses of oral tyrosine or tryptophan than were used in the nutraceutical cocktail or to no supplements. They found no subsequent increase in total tyrosine or total tryptophan levels in the subjects’ breast milk, although dose-dependent increases were found in free tyrosine and free tryptophan in maternal plasma. Free tyrosine was increased in breast milk; however, the level was significantly lower than what the investigators found in laboratory analysis of a dozen popular brands of infant formula.
The safety and open-label efficacy studies were funded by the Canadian Institutes of Health Research, the Ontario Mental Health Foundation, and university research grants. Dr. Dowlati reported having no financial conflicts of interest.
VIENNA – A dietary supplement blend virtually eliminated postpartum blues in a promising proof-of-concept controlled trial, Yekta Dowlati, PhD, reported during the annual congress of the European College of Neuropsychopharmacology.
The nutraceutical cocktail is designed to compensate for the effects of the early postpartum surge in monoamine oxidase A (MAO-A) activity that her research group previously has reported. They found that as estrogen levels plunge by 100-fold in the first 3 days postpartum, brain MAO-A levels rise by 40% in affect-controlling regions, including the prefrontal cortex and anterior cingulate cortex (Arch Gen Psychiatry. 2010 May;67[5]:468-74).
That suggests a potential causal relationship with postpartum blues, since MAO-A is an enzyme whose effects include promotion of oxidative stress, apoptosis, and metabolizing serotonin, norepinephrine, and dopamine, explained Dr. Dowlati of the department of psychiatry at the University of Toronto.
Postpartum blues is a common prodrome for postpartum depression, the most frequent complication of childbearing, which has an estimated incidence of 13%. Severe postpartum blues is a strong predictor of subsequent postpartum depression. Yet, despite the large burden of illness imposed by postpartum depression, there is no proven preventive strategy. The hypothesis being pursued in developing this nutraceutical is that a safe dietary intervention that prevents postpartum blues also may prevent postpartum depression.
The nutraceutical cocktail developed by Dr. Dowlati and her coinvestigators consists of monoamine precursors: 2 g of tryptophan, 10 g of tyrosine, and blueberry juice plus blueberry extract.
She reported on 41 healthy breast-feeding mothers who on day 5 postpartum, when postpartum blues typically peaks, were assigned to drink the dietary supplement or not. Later that day, they underwent a quantified assessment of their severity of postpartum blues based upon change from baseline in depressed mood scores on a 0-100 visual analog scale after undergoing a standardized sad mood induction procedure. This is a simple protocol widely used by psychiatrists and psychologists researching the neurobiology of mood states. Dr. Dowlati and her colleagues used the Velten protocol, in which subjects read depressing sentences while listening to sad music.
Mean scores on the Visual Analog Scale for sadness following the standardized mood induction procedure jumped by 43.8 points in the control group but were unchanged, with a mere 0.5-point increase, in the 21 women in the active treatment arm.
“The results of the present study, albeit in an open-label trial, reflect by far the most robust effects of a dietary supplement ever seen on postpartum blues. Our effect size was 2.9. Previous trials have reported effect sizes of 0.07-0.28,” she noted.
An effect size of 2.9 means that if a postpartum woman did not experience a plunge in mood after the induction protocol, there was statistically a 98%-99% chance that she had consumed the supplement.
“One explanation to account for an active effect is that the supplement is compensating for the effects of monoamine metabolism and increased oxidative stress by elevated postpartum MAO-A levels,” according to Dr. Dowlati. “Given the effect size of 2.9 and minimal effects of tryptophan and tyrosine supplementation on total levels in breast milk, there is excellent reason to pursue this supplement in a randomized, double-blind, placebo-controlled trial to further assess its effects.”
Before conducting this efficacy study, the investigators evaluated the safety of their planned intervention by randomizing 54 healthy breast-feeding women to single larger doses of oral tyrosine or tryptophan than were used in the nutraceutical cocktail or to no supplements. They found no subsequent increase in total tyrosine or total tryptophan levels in the subjects’ breast milk, although dose-dependent increases were found in free tyrosine and free tryptophan in maternal plasma. Free tyrosine was increased in breast milk; however, the level was significantly lower than what the investigators found in laboratory analysis of a dozen popular brands of infant formula.
The safety and open-label efficacy studies were funded by the Canadian Institutes of Health Research, the Ontario Mental Health Foundation, and university research grants. Dr. Dowlati reported having no financial conflicts of interest.
Key clinical point:
Major finding: Postpartum women who consumed a dietary supplement designed to compensate for the effects of a surge in monoamine oxidase A activity did not experience any lowering of mood after completing a standardized sad mood induction protocol, while a control group showed a steep rise in sadness scores.
Data source: An open-label proof-of-concept study in which 41 women undertook a standardized sad mood induction protocol on day 5 postpartum, after 21 of them had consumed a dietary supplement blend designed to ward off postpartum blues.
Disclosures: The safety and open-label efficacy studies were funded by the Canadian Institutes of Health Research, the Ontario Mental Health Foundation, and university research grants. Dr. Dowlati reported having no financial conflicts of interest.
MARIANNE: Same PFS but TDM-1 more tolerable than trastuzumab + chemo
Trastuzumab emtansine (TDM-1) provided similar progression-free survival, compared with trastuzumab plus taxane for first-line treatment of human epidermal growth factor receptor 2–positive advanced breast cancer, but proved more tolerable to patients.
In the phase III MARIANNE study, 1,095 patients with HER2-positive advanced breast cancer were randomized 1:1:1 to trastuzumab plus taxane, T-DM1 plus placebo, or T-DM1 plus pertuzumab. Median duration of follow-up was approximately 35 months.

Incidence of adverse events equal to or greater than grade 3 were 54.1% for trastuzumab plus taxane, 45.4% for T-DM1, and 46.2% for T-DM1 plus pertuzumab, respectively. Adverse events led to discontinuation of treatment by a greater number of patients receiving trastuzumab plus taxane, compared with patients in other arms of the study.
Objective response rate and median response duration in those patients who achieved a response were 67.9% and 12.5 months for trastuzumab plus taxane, 59.7% and 20.7 months for T-DM1, and 64.2% and 21.2 months for T-DM1 plus pertuzumab, respectively.
Subgroup analysis demonstrated a numerical trend for an increased relative treatment effect for patients who, during early breast cancer treatment, had received either HER2-directed therapy or taxanes.
Time to clinically meaningful decrease in health-related quality of life was a median of 3.6 months for trastuzumab plus taxane, 7.7 months for T-DM1, and 9.0 months for T-DM1 plus pertuzumab.
A left ventricular ejection fraction of less than 50% accompanied by a greater than or equal to 15 percentage-point decease from baseline occurred in 0.8% of T-DM1 patients, compared with 4.5% with trastuzumab plus taxane and 2.5% with T-DM1 plus pertuzumab.
The authors note that the breast cancer guidelines of the National Comprehensive Cancer Network include T-DM1 as a first-line treatment option for patients with HER2-positive metastatic breast cancer who are not considered suitable for treatment with the preferred regimen of pertuzumab, trastuzumab, and a taxane.
Trastuzumab emtansine (TDM-1) provided similar progression-free survival, compared with trastuzumab plus taxane for first-line treatment of human epidermal growth factor receptor 2–positive advanced breast cancer, but proved more tolerable to patients.
In the phase III MARIANNE study, 1,095 patients with HER2-positive advanced breast cancer were randomized 1:1:1 to trastuzumab plus taxane, T-DM1 plus placebo, or T-DM1 plus pertuzumab. Median duration of follow-up was approximately 35 months.
Incidence of adverse events equal to or greater than grade 3 were 54.1% for trastuzumab plus taxane, 45.4% for T-DM1, and 46.2% for T-DM1 plus pertuzumab, respectively. Adverse events led to discontinuation of treatment by a greater number of patients receiving trastuzumab plus taxane, compared with patients in other arms of the study.
Objective response rate and median response duration in those patients who achieved a response were 67.9% and 12.5 months for trastuzumab plus taxane, 59.7% and 20.7 months for T-DM1, and 64.2% and 21.2 months for T-DM1 plus pertuzumab, respectively.
Subgroup analysis demonstrated a numerical trend for an increased relative treatment effect for patients who, during early breast cancer treatment, had received either HER2-directed therapy or taxanes.
Time to clinically meaningful decrease in health-related quality of life was a median of 3.6 months for trastuzumab plus taxane, 7.7 months for T-DM1, and 9.0 months for T-DM1 plus pertuzumab.
A left ventricular ejection fraction of less than 50% accompanied by a greater than or equal to 15 percentage-point decease from baseline occurred in 0.8% of T-DM1 patients, compared with 4.5% with trastuzumab plus taxane and 2.5% with T-DM1 plus pertuzumab.
The authors note that the breast cancer guidelines of the National Comprehensive Cancer Network include T-DM1 as a first-line treatment option for patients with HER2-positive metastatic breast cancer who are not considered suitable for treatment with the preferred regimen of pertuzumab, trastuzumab, and a taxane.
Trastuzumab emtansine (TDM-1) provided similar progression-free survival, compared with trastuzumab plus taxane for first-line treatment of human epidermal growth factor receptor 2–positive advanced breast cancer, but proved more tolerable to patients.
In the phase III MARIANNE study, 1,095 patients with HER2-positive advanced breast cancer were randomized 1:1:1 to trastuzumab plus taxane, T-DM1 plus placebo, or T-DM1 plus pertuzumab. Median duration of follow-up was approximately 35 months.
Incidence of adverse events equal to or greater than grade 3 were 54.1% for trastuzumab plus taxane, 45.4% for T-DM1, and 46.2% for T-DM1 plus pertuzumab, respectively. Adverse events led to discontinuation of treatment by a greater number of patients receiving trastuzumab plus taxane, compared with patients in other arms of the study.
Objective response rate and median response duration in those patients who achieved a response were 67.9% and 12.5 months for trastuzumab plus taxane, 59.7% and 20.7 months for T-DM1, and 64.2% and 21.2 months for T-DM1 plus pertuzumab, respectively.
Subgroup analysis demonstrated a numerical trend for an increased relative treatment effect for patients who, during early breast cancer treatment, had received either HER2-directed therapy or taxanes.
Time to clinically meaningful decrease in health-related quality of life was a median of 3.6 months for trastuzumab plus taxane, 7.7 months for T-DM1, and 9.0 months for T-DM1 plus pertuzumab.
A left ventricular ejection fraction of less than 50% accompanied by a greater than or equal to 15 percentage-point decease from baseline occurred in 0.8% of T-DM1 patients, compared with 4.5% with trastuzumab plus taxane and 2.5% with T-DM1 plus pertuzumab.
The authors note that the breast cancer guidelines of the National Comprehensive Cancer Network include T-DM1 as a first-line treatment option for patients with HER2-positive metastatic breast cancer who are not considered suitable for treatment with the preferred regimen of pertuzumab, trastuzumab, and a taxane.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point:
Major finding: Median progression-free survival for trastuzumab plus taxane was 13.7 months; for T-DM1, 14.1 months; and for T-DM1 plus pertuzumab, 15.2 months.
Data source: MARIANNE, a phase III trial of 1,095 patients with HER2-positive advanced breast cancer.
Disclosures: Dr. Perez disclosed employment with Genentech. Several other authors disclosed employment or other relationships with Genentech or Roche. The trial was sponsored by Genentech.
Fragmented readmission after liver transplant linked to adverse outcomes
CORONADO, CALIF. – Postdischarge surgical care fragmentation significantly increases the risk of both 30-day mortality and subsequent readmission in the first year following orthotopic liver transplantation, results from a study of national data showed.
“In an era of regionalization and centers of excellence, the likelihood for postdischarge fragmentation, defined as readmission to any hospital other than the hospital at which the surgery was performed, is an increasing reality,” Anai N. Kothari, MD, said at the annual meeting of the Western Surgical Association. “In many different surgical subspecialties – major vascular operations, bariatric surgery, oncologic resections – it’s known to be a risk factor for adverse events and poor quality. Postdischarge fragmentation is common, [and related to] as often as one in four readmissions. It increases the risk for short- and long-term morbidity and mortality, decreases survival, and increases cost.”

Dr. Kothari reported results from 2,996 patients with 7,485 readmission encounters at 299 hospitals. Of the 7,485 readmissions, 6,249 (83.5%) were nonfragmented, and 1,236 (16.5%) were fragmented. The mean age of patients was 55 years. There were no significant differences in baseline characteristics between patients with nonfragmented and fragmented admissions in terms of patient age, sex, preoperative and postoperative length of stay, Charlson comorbidity index, and comorbidities, with the exception of renal failure, which was more common among patients in the fragmented admission group.
Compared with the patients in the nonfragmented admission group, those in the fragmented admission group had a greater number of average readmissions per patient (3.3 vs. 2.5, respectively; P less than .0001) and a greater number of average days to readmission (168 vs. 105; P less than .0001). Reasons for readmission differed among the two groups. Patients readmitted to the index transplant center were more likely to have a biliary, hematologic, or neurologic complication, while those in the fragmented admissions group were more likely to be readmitted for things like electrolyte disturbances, respiratory issues, gastrointestinal issues, or hematologic-related issues. There was no difference in overall cost of care between the two groups (an average of $11,621.68 vs. $11.585.39, respectively).
After the investigators adjusted for age, sex, reason for readmission, cost of the index liver transplant, readmission length of stay, number of previous readmissions, and time from transplant, postdischarge fragmentation increased the odds of both 30-day mortality (OR, 1.75) and 30-day readmission (OR, 2.14). “It looks like just having a fragmented readmission is an independent predictor for an adverse event,” Dr. Kothari said.
Significant predictors of adverse events following a fragmented readmission included an increased number of previous readmissions (OR, 1.07) and readmission within 90 days of orthotopic liver transplant (OR, 2.19). “These two factors may be important for guiding providers to say, ‘If you have these things, this patient should likely come back to their index transplant center,’” Dr. Kothari said.
He reported having no relevant financial disclosures.
CORONADO, CALIF. – Postdischarge surgical care fragmentation significantly increases the risk of both 30-day mortality and subsequent readmission in the first year following orthotopic liver transplantation, results from a study of national data showed.
“In an era of regionalization and centers of excellence, the likelihood for postdischarge fragmentation, defined as readmission to any hospital other than the hospital at which the surgery was performed, is an increasing reality,” Anai N. Kothari, MD, said at the annual meeting of the Western Surgical Association. “In many different surgical subspecialties – major vascular operations, bariatric surgery, oncologic resections – it’s known to be a risk factor for adverse events and poor quality. Postdischarge fragmentation is common, [and related to] as often as one in four readmissions. It increases the risk for short- and long-term morbidity and mortality, decreases survival, and increases cost.”
Dr. Kothari reported results from 2,996 patients with 7,485 readmission encounters at 299 hospitals. Of the 7,485 readmissions, 6,249 (83.5%) were nonfragmented, and 1,236 (16.5%) were fragmented. The mean age of patients was 55 years. There were no significant differences in baseline characteristics between patients with nonfragmented and fragmented admissions in terms of patient age, sex, preoperative and postoperative length of stay, Charlson comorbidity index, and comorbidities, with the exception of renal failure, which was more common among patients in the fragmented admission group.
Compared with the patients in the nonfragmented admission group, those in the fragmented admission group had a greater number of average readmissions per patient (3.3 vs. 2.5, respectively; P less than .0001) and a greater number of average days to readmission (168 vs. 105; P less than .0001). Reasons for readmission differed among the two groups. Patients readmitted to the index transplant center were more likely to have a biliary, hematologic, or neurologic complication, while those in the fragmented admissions group were more likely to be readmitted for things like electrolyte disturbances, respiratory issues, gastrointestinal issues, or hematologic-related issues. There was no difference in overall cost of care between the two groups (an average of $11,621.68 vs. $11.585.39, respectively).
After the investigators adjusted for age, sex, reason for readmission, cost of the index liver transplant, readmission length of stay, number of previous readmissions, and time from transplant, postdischarge fragmentation increased the odds of both 30-day mortality (OR, 1.75) and 30-day readmission (OR, 2.14). “It looks like just having a fragmented readmission is an independent predictor for an adverse event,” Dr. Kothari said.
Significant predictors of adverse events following a fragmented readmission included an increased number of previous readmissions (OR, 1.07) and readmission within 90 days of orthotopic liver transplant (OR, 2.19). “These two factors may be important for guiding providers to say, ‘If you have these things, this patient should likely come back to their index transplant center,’” Dr. Kothari said.
He reported having no relevant financial disclosures.
CORONADO, CALIF. – Postdischarge surgical care fragmentation significantly increases the risk of both 30-day mortality and subsequent readmission in the first year following orthotopic liver transplantation, results from a study of national data showed.
“In an era of regionalization and centers of excellence, the likelihood for postdischarge fragmentation, defined as readmission to any hospital other than the hospital at which the surgery was performed, is an increasing reality,” Anai N. Kothari, MD, said at the annual meeting of the Western Surgical Association. “In many different surgical subspecialties – major vascular operations, bariatric surgery, oncologic resections – it’s known to be a risk factor for adverse events and poor quality. Postdischarge fragmentation is common, [and related to] as often as one in four readmissions. It increases the risk for short- and long-term morbidity and mortality, decreases survival, and increases cost.”
Dr. Kothari reported results from 2,996 patients with 7,485 readmission encounters at 299 hospitals. Of the 7,485 readmissions, 6,249 (83.5%) were nonfragmented, and 1,236 (16.5%) were fragmented. The mean age of patients was 55 years. There were no significant differences in baseline characteristics between patients with nonfragmented and fragmented admissions in terms of patient age, sex, preoperative and postoperative length of stay, Charlson comorbidity index, and comorbidities, with the exception of renal failure, which was more common among patients in the fragmented admission group.
Compared with the patients in the nonfragmented admission group, those in the fragmented admission group had a greater number of average readmissions per patient (3.3 vs. 2.5, respectively; P less than .0001) and a greater number of average days to readmission (168 vs. 105; P less than .0001). Reasons for readmission differed among the two groups. Patients readmitted to the index transplant center were more likely to have a biliary, hematologic, or neurologic complication, while those in the fragmented admissions group were more likely to be readmitted for things like electrolyte disturbances, respiratory issues, gastrointestinal issues, or hematologic-related issues. There was no difference in overall cost of care between the two groups (an average of $11,621.68 vs. $11.585.39, respectively).
After the investigators adjusted for age, sex, reason for readmission, cost of the index liver transplant, readmission length of stay, number of previous readmissions, and time from transplant, postdischarge fragmentation increased the odds of both 30-day mortality (OR, 1.75) and 30-day readmission (OR, 2.14). “It looks like just having a fragmented readmission is an independent predictor for an adverse event,” Dr. Kothari said.
Significant predictors of adverse events following a fragmented readmission included an increased number of previous readmissions (OR, 1.07) and readmission within 90 days of orthotopic liver transplant (OR, 2.19). “These two factors may be important for guiding providers to say, ‘If you have these things, this patient should likely come back to their index transplant center,’” Dr. Kothari said.
He reported having no relevant financial disclosures.
AT WSA 2016
Key clinical point:
Major finding: After investigators adjusted for numerous variables, postdischarge fragmentation following orthotopic liver transplantation increased the odds of both 30-day mortality (OR, 1.75) and 30-day readmission (OR, 2.14).
Data source: An analysis of data from the Healthcare Cost and Utilization Project State Inpatient Databases for Florida and California between 2006 and 2011 to identify 2,996 patients who underwent orthotopic liver transplantation.
Disclosures: Dr. Kothari reported having no relevant financial disclosures.
Factor VIII microcapsules eyed for eluding neutralizing antibodies
Using platelet microcapsules to deliver factor VIII, a process that is expected to increase factor VIII efficacy and avoid the development of neutralizing antibodies, is being examined via in vitro testing, according to an abstract to be featured during a press conference at the annual meeting of the American Society of Hematology.
Caroline E. Hansen of the Georgia Institute of Technology, Atlanta, and her colleagues performed in vitro experiments that show this technology has the potential to increase factor VIII efficacy for hemophilia A patients with inhibitors.
“Current work evaluating localized thrombin generation due to the factor VIII–loaded microcapsules and the effect of platelet contraction force via pharmacologic agents, such as blebbistatin, ROCK, and myosin inhibitors, [is] ongoing,” the researchers wrote in their abstract.
They fabricated polyelectrolyte layers onto calcium carbonate cores and incorporated fibrinogen into the final layer to facilitate binding with platelets. The microcapsule’s inner core contains factor VIII separated from the polyelectrolyte layers by a dextran core.
In the in vitro model, platelets adhered to the microcapsules, which were incorporated into fibrin networks upon platelet activation. During clot contraction, the microcapsules ruptured only in the vicinity of contracting platelets, ensuring drug delivery was targeted at sites of active clot formation.
The researchers perfused recalcified whole blood and platelet poor plasma into in vitro microfluidic models of vascular injury, which consisted of a collagen/tissue factor patch. The efficacy of systemic and microcapsular factor VIII was quantitatively evaluated by comparing fibrin fluorescence intensity on the patch, which was normalized to platelet number.
Fibrin formation was comparable using microcapsules without dextran, fibrinogen, and loaded factor VIII. Compared with standard systemic infusion of 0.05 U/mL factor VIII, however, microcapsules loaded with 0.01 U/mL factor VIII produced four times as much fibrin.
To mimic hemophilia A blood with inhibitors, a factor VIII inhibitory antibody was introduced into healthy blood samples. Again, significantly more fibrin was produced in samples with microcapsules loaded with 0.01 U/mL factor VIII than with systemic factor VIII infusions at clinically relevant high and low dosages of 0.05 and 0.5 U/mL (P less than .05).
This increased efficacy is likely due to the microcapsule shielding effect on factor VIII, preventing exposure to inhibitory antibodies, the researchers reported.
Ms. Hansen had no relevant financial disclosures. One of her colleagues, Shannon L. Meeks, MD, disclosed adviser relationships with Biogen, Genentech, Bayer Healthcare, Grifols, CSL Behring, and Shire. Another, Wilbur A Lam, MD, PhD, disclosed equity ownership in Sanguina.
Abstract 81: Leveraging the Contractile Force of Platelets for Targeted Factor VIII Delivery in Hemophilia With Inhibitors.
[email protected]
On Twitter @maryjodales
Using platelet microcapsules to deliver factor VIII, a process that is expected to increase factor VIII efficacy and avoid the development of neutralizing antibodies, is being examined via in vitro testing, according to an abstract to be featured during a press conference at the annual meeting of the American Society of Hematology.
Caroline E. Hansen of the Georgia Institute of Technology, Atlanta, and her colleagues performed in vitro experiments that show this technology has the potential to increase factor VIII efficacy for hemophilia A patients with inhibitors.
“Current work evaluating localized thrombin generation due to the factor VIII–loaded microcapsules and the effect of platelet contraction force via pharmacologic agents, such as blebbistatin, ROCK, and myosin inhibitors, [is] ongoing,” the researchers wrote in their abstract.
They fabricated polyelectrolyte layers onto calcium carbonate cores and incorporated fibrinogen into the final layer to facilitate binding with platelets. The microcapsule’s inner core contains factor VIII separated from the polyelectrolyte layers by a dextran core.
In the in vitro model, platelets adhered to the microcapsules, which were incorporated into fibrin networks upon platelet activation. During clot contraction, the microcapsules ruptured only in the vicinity of contracting platelets, ensuring drug delivery was targeted at sites of active clot formation.
The researchers perfused recalcified whole blood and platelet poor plasma into in vitro microfluidic models of vascular injury, which consisted of a collagen/tissue factor patch. The efficacy of systemic and microcapsular factor VIII was quantitatively evaluated by comparing fibrin fluorescence intensity on the patch, which was normalized to platelet number.
Fibrin formation was comparable using microcapsules without dextran, fibrinogen, and loaded factor VIII. Compared with standard systemic infusion of 0.05 U/mL factor VIII, however, microcapsules loaded with 0.01 U/mL factor VIII produced four times as much fibrin.
To mimic hemophilia A blood with inhibitors, a factor VIII inhibitory antibody was introduced into healthy blood samples. Again, significantly more fibrin was produced in samples with microcapsules loaded with 0.01 U/mL factor VIII than with systemic factor VIII infusions at clinically relevant high and low dosages of 0.05 and 0.5 U/mL (P less than .05).
This increased efficacy is likely due to the microcapsule shielding effect on factor VIII, preventing exposure to inhibitory antibodies, the researchers reported.
Ms. Hansen had no relevant financial disclosures. One of her colleagues, Shannon L. Meeks, MD, disclosed adviser relationships with Biogen, Genentech, Bayer Healthcare, Grifols, CSL Behring, and Shire. Another, Wilbur A Lam, MD, PhD, disclosed equity ownership in Sanguina.
Abstract 81: Leveraging the Contractile Force of Platelets for Targeted Factor VIII Delivery in Hemophilia With Inhibitors.
[email protected]
On Twitter @maryjodales
Using platelet microcapsules to deliver factor VIII, a process that is expected to increase factor VIII efficacy and avoid the development of neutralizing antibodies, is being examined via in vitro testing, according to an abstract to be featured during a press conference at the annual meeting of the American Society of Hematology.
Caroline E. Hansen of the Georgia Institute of Technology, Atlanta, and her colleagues performed in vitro experiments that show this technology has the potential to increase factor VIII efficacy for hemophilia A patients with inhibitors.
“Current work evaluating localized thrombin generation due to the factor VIII–loaded microcapsules and the effect of platelet contraction force via pharmacologic agents, such as blebbistatin, ROCK, and myosin inhibitors, [is] ongoing,” the researchers wrote in their abstract.
They fabricated polyelectrolyte layers onto calcium carbonate cores and incorporated fibrinogen into the final layer to facilitate binding with platelets. The microcapsule’s inner core contains factor VIII separated from the polyelectrolyte layers by a dextran core.
In the in vitro model, platelets adhered to the microcapsules, which were incorporated into fibrin networks upon platelet activation. During clot contraction, the microcapsules ruptured only in the vicinity of contracting platelets, ensuring drug delivery was targeted at sites of active clot formation.
The researchers perfused recalcified whole blood and platelet poor plasma into in vitro microfluidic models of vascular injury, which consisted of a collagen/tissue factor patch. The efficacy of systemic and microcapsular factor VIII was quantitatively evaluated by comparing fibrin fluorescence intensity on the patch, which was normalized to platelet number.
Fibrin formation was comparable using microcapsules without dextran, fibrinogen, and loaded factor VIII. Compared with standard systemic infusion of 0.05 U/mL factor VIII, however, microcapsules loaded with 0.01 U/mL factor VIII produced four times as much fibrin.
To mimic hemophilia A blood with inhibitors, a factor VIII inhibitory antibody was introduced into healthy blood samples. Again, significantly more fibrin was produced in samples with microcapsules loaded with 0.01 U/mL factor VIII than with systemic factor VIII infusions at clinically relevant high and low dosages of 0.05 and 0.5 U/mL (P less than .05).
This increased efficacy is likely due to the microcapsule shielding effect on factor VIII, preventing exposure to inhibitory antibodies, the researchers reported.
Ms. Hansen had no relevant financial disclosures. One of her colleagues, Shannon L. Meeks, MD, disclosed adviser relationships with Biogen, Genentech, Bayer Healthcare, Grifols, CSL Behring, and Shire. Another, Wilbur A Lam, MD, PhD, disclosed equity ownership in Sanguina.
Abstract 81: Leveraging the Contractile Force of Platelets for Targeted Factor VIII Delivery in Hemophilia With Inhibitors.
[email protected]
On Twitter @maryjodales
ASH 2016 PREVIEW
FDA approves tenofovir alafenamide for patients with chronic hepatitis B and liver disease
The Food and Drug Administration has approved tenofovir alafenamide (marketed as Vemlidy by Gilead Sciences) for the treatment of adults with chronic hepatitis B virus infection with compensated liver disease.
Tenofovir alafenamide is a novel, targeted prodrug of tenofovir that has demonstrated antiviral efficacy similar to tenofovir disoproxil fumarate (Viread) at significantly lower doses.
Compared with tenofovir disoproxil fumarate, tenofovir alafenamide has “greater plasma stability and more efficiently delivers tenofovir to hepatocytes” which allows tenofovir alafenamide to be administered in daily doses of 25mg while tenofovir disoproxil fumarate requires a dose of 300 mg to be as effective.
In addition, patients treated with tenofovir alafenamide demonstrated “improvements in certain bone and renal laboratory parameters.”
Overall, tenofovir alafenamide was well tolerated. Only 1% of patients discontinued treatment because of adverse events, and the most common adverse events were headache, abdominal pain, fatigue, cough, nausea, and back pain. Vemlidy has a boxed warning in its product label regarding the risks of lactic acidosis/severe hepatomegaly with steatosis and severe acute exacerbation of hepatitis B with discontinuation.
“Vemlidy is the first medication approved to treat this disease in nearly a decade,” said President and Chief Executive Officer of Gilead Sciences John Milligan. “We are excited to offer a new, effective option to help advance long-term care for patients.”
[email protected]
On Twitter @jessnicolecraig
The Food and Drug Administration has approved tenofovir alafenamide (marketed as Vemlidy by Gilead Sciences) for the treatment of adults with chronic hepatitis B virus infection with compensated liver disease.
Tenofovir alafenamide is a novel, targeted prodrug of tenofovir that has demonstrated antiviral efficacy similar to tenofovir disoproxil fumarate (Viread) at significantly lower doses.
Compared with tenofovir disoproxil fumarate, tenofovir alafenamide has “greater plasma stability and more efficiently delivers tenofovir to hepatocytes” which allows tenofovir alafenamide to be administered in daily doses of 25mg while tenofovir disoproxil fumarate requires a dose of 300 mg to be as effective.
In addition, patients treated with tenofovir alafenamide demonstrated “improvements in certain bone and renal laboratory parameters.”
Overall, tenofovir alafenamide was well tolerated. Only 1% of patients discontinued treatment because of adverse events, and the most common adverse events were headache, abdominal pain, fatigue, cough, nausea, and back pain. Vemlidy has a boxed warning in its product label regarding the risks of lactic acidosis/severe hepatomegaly with steatosis and severe acute exacerbation of hepatitis B with discontinuation.
“Vemlidy is the first medication approved to treat this disease in nearly a decade,” said President and Chief Executive Officer of Gilead Sciences John Milligan. “We are excited to offer a new, effective option to help advance long-term care for patients.”
[email protected]
On Twitter @jessnicolecraig
The Food and Drug Administration has approved tenofovir alafenamide (marketed as Vemlidy by Gilead Sciences) for the treatment of adults with chronic hepatitis B virus infection with compensated liver disease.
Tenofovir alafenamide is a novel, targeted prodrug of tenofovir that has demonstrated antiviral efficacy similar to tenofovir disoproxil fumarate (Viread) at significantly lower doses.
Compared with tenofovir disoproxil fumarate, tenofovir alafenamide has “greater plasma stability and more efficiently delivers tenofovir to hepatocytes” which allows tenofovir alafenamide to be administered in daily doses of 25mg while tenofovir disoproxil fumarate requires a dose of 300 mg to be as effective.
In addition, patients treated with tenofovir alafenamide demonstrated “improvements in certain bone and renal laboratory parameters.”
Overall, tenofovir alafenamide was well tolerated. Only 1% of patients discontinued treatment because of adverse events, and the most common adverse events were headache, abdominal pain, fatigue, cough, nausea, and back pain. Vemlidy has a boxed warning in its product label regarding the risks of lactic acidosis/severe hepatomegaly with steatosis and severe acute exacerbation of hepatitis B with discontinuation.
“Vemlidy is the first medication approved to treat this disease in nearly a decade,” said President and Chief Executive Officer of Gilead Sciences John Milligan. “We are excited to offer a new, effective option to help advance long-term care for patients.”
[email protected]
On Twitter @jessnicolecraig
Detecting PH in IPF ‘more art than science’
LOS ANGELES – When it comes to the optimal management of pulmonary hypertension (PH) in patients with idiopathic pulmonary fibrosis (IPF), there are more questions than definitive answers, according to Brett E. Fenster, MD, FACC.
“Is PH in IPF a disease marker, an independent treatment target, or both?” he asked attendees at the annual meeting of the American College of Chest Physicians. “I think we have conflicting information about that.”

The prevalence of PH is estimated to be 10% in patients with mild to moderate IPF and tends to progress slowly. Common features of PH in IPF patients include shortness of breath, a greater degree of exertional desaturation, and an increased mortality rate.
Dr. Fenster described the ability to detect PH in IPF patients as “more art than science. A lot of different work has been done to look at different testing to get at the patients that may have PH that is a comorbid disease to their IPF. But a lot of times it comes down to assessing their level of dyspnea proportional to their level of disease. In those patients where we think there is something else going on besides their IPF, we’ll oftentimes get an echocardiogram and try to look at their right heart to see if they have features of PH. If it looks like they do, we will circle back and look at the amount of lung disease they have as characterized by their chest imaging, by their pulmonary function testing, and getting a blood gas. If this patient has findings of right heart enlargement, systolic dysfunction, et cetera, that clues us more into looking at PH and referring them to a center that has expertise in that version of PH.”
According to the most recent European Society of Cardiology/European Respiratory Society guidelines, the diagnosis of chronic obstructive pulmonary disease (COPD)/IPF/combined pulmonary fibrosis and emphysema (CPFE) without PH can be considered when the mean pulmonary artery pressure (mPAP) on right heart catheterization is less than 25 mm Hg. The diagnosis of COPD/IPF/CPFE with PH, based on these same guidelines, can be considered when the mPAP is 25 mm Hg or more. A patient may have COPD/IPF/CPFE with severe PH when his or her mPAP exceeds 35 mm Hg, or is 25 mm Hg or greater in the presence of a low cardiac output, the guidelines says (Eur Heart J. 2016;37:67-119). “That begins to separate out a group that may potentially benefit from targeted PH therapy,” Dr. Fenster said.
Current treatment approaches include long-term oxygen, diuretics, transplant, and pulmonary rehabilitation, but Dr. Fenster said there is sparse data on the optimal treatment approach. A study of sildenafil in IPF known as STEP-IPF failed to increase 6-minute walking test distance but improved diffusion capacity of carbon monoxide, quality of life, and arterial oxygenation (N Engl J Med. 2010;363:620-8). A study evaluating riociguat for idiopathic interstitial pneumonitis PH was discontinued early because of increased risk of death and adverse events. More recently, the drug ambrisentan was found to be ineffective at reducing the rate of IPF progression and was linked to an increase in disease progression events, including a decline in pulmonary function test values, hospitalization, and death, in the ARTEMIS-IPF trial (Ann Intern Med. 2013;158:641-9).
Randomized, placebo-controlled studies of bosentan in IPF give researchers pause for hope, Dr. Fenster said. BUILD-1 demonstrated a trend toward delayed time to death, delayed disease progression, improved quality of life, and no clear worsening of IPF (Am J Respir Crit Care Med. 2008;177[1]:75-81), while BUILD-3 showed a significant improvement in forced vital capacity (FVC) and carbon monoxide diffusing capacity (Am J Respir Crit Care Med. 2011;184[1]:92-9). A more recent trial evaluated IV treprostinil in 15 patients with interstitial lung disease and PH (Thorax 2014;69[2]:123-9). Eight of the patients had IPF. “After 12 weeks of treprostinil therapy, almost all of them experienced some degree of improvement in their walk distance,” said Dr. Fenster, who was not involved with the study. “Perhaps more importantly there were significant improvements in almost all parameters from their right heart catheterizations. So when we think about how to treat these patients, we have to weigh the risks and benefits of what we make potentially worse with our IPF therapy, such as worsening hypoxia, V/Q mismatch, disease progression, and volume overload. On the flip side, we might be improving right heart hemodynamics and RV function, which are prognostic in this disease. What’s the net balance of these things in terms of how it translates into functional capacity, quality of life, hospitalization, and mortality? We don’t know.”
According to Dr. Fenster, current data suggest that future IPF PH research should focus on prostanoid pathways and not on the estrogen-receptor and riociguat pathways to determine effective treatments. “We have numerous studies showing potential harm with IPF PH therapy, so we need to very much wade cautiously into this arena,” he said. “There is a potential role for PH therapy in IPF, but we will likely need to study patients with severe PH and IPF to show benefit. I think that’s where we’ll have the most success.”
Dr. Fenster reported having no relevant financial disclosures.
LOS ANGELES – When it comes to the optimal management of pulmonary hypertension (PH) in patients with idiopathic pulmonary fibrosis (IPF), there are more questions than definitive answers, according to Brett E. Fenster, MD, FACC.
“Is PH in IPF a disease marker, an independent treatment target, or both?” he asked attendees at the annual meeting of the American College of Chest Physicians. “I think we have conflicting information about that.”
The prevalence of PH is estimated to be 10% in patients with mild to moderate IPF and tends to progress slowly. Common features of PH in IPF patients include shortness of breath, a greater degree of exertional desaturation, and an increased mortality rate.
Dr. Fenster described the ability to detect PH in IPF patients as “more art than science. A lot of different work has been done to look at different testing to get at the patients that may have PH that is a comorbid disease to their IPF. But a lot of times it comes down to assessing their level of dyspnea proportional to their level of disease. In those patients where we think there is something else going on besides their IPF, we’ll oftentimes get an echocardiogram and try to look at their right heart to see if they have features of PH. If it looks like they do, we will circle back and look at the amount of lung disease they have as characterized by their chest imaging, by their pulmonary function testing, and getting a blood gas. If this patient has findings of right heart enlargement, systolic dysfunction, et cetera, that clues us more into looking at PH and referring them to a center that has expertise in that version of PH.”
According to the most recent European Society of Cardiology/European Respiratory Society guidelines, the diagnosis of chronic obstructive pulmonary disease (COPD)/IPF/combined pulmonary fibrosis and emphysema (CPFE) without PH can be considered when the mean pulmonary artery pressure (mPAP) on right heart catheterization is less than 25 mm Hg. The diagnosis of COPD/IPF/CPFE with PH, based on these same guidelines, can be considered when the mPAP is 25 mm Hg or more. A patient may have COPD/IPF/CPFE with severe PH when his or her mPAP exceeds 35 mm Hg, or is 25 mm Hg or greater in the presence of a low cardiac output, the guidelines says (Eur Heart J. 2016;37:67-119). “That begins to separate out a group that may potentially benefit from targeted PH therapy,” Dr. Fenster said.
Current treatment approaches include long-term oxygen, diuretics, transplant, and pulmonary rehabilitation, but Dr. Fenster said there is sparse data on the optimal treatment approach. A study of sildenafil in IPF known as STEP-IPF failed to increase 6-minute walking test distance but improved diffusion capacity of carbon monoxide, quality of life, and arterial oxygenation (N Engl J Med. 2010;363:620-8). A study evaluating riociguat for idiopathic interstitial pneumonitis PH was discontinued early because of increased risk of death and adverse events. More recently, the drug ambrisentan was found to be ineffective at reducing the rate of IPF progression and was linked to an increase in disease progression events, including a decline in pulmonary function test values, hospitalization, and death, in the ARTEMIS-IPF trial (Ann Intern Med. 2013;158:641-9).
Randomized, placebo-controlled studies of bosentan in IPF give researchers pause for hope, Dr. Fenster said. BUILD-1 demonstrated a trend toward delayed time to death, delayed disease progression, improved quality of life, and no clear worsening of IPF (Am J Respir Crit Care Med. 2008;177[1]:75-81), while BUILD-3 showed a significant improvement in forced vital capacity (FVC) and carbon monoxide diffusing capacity (Am J Respir Crit Care Med. 2011;184[1]:92-9). A more recent trial evaluated IV treprostinil in 15 patients with interstitial lung disease and PH (Thorax 2014;69[2]:123-9). Eight of the patients had IPF. “After 12 weeks of treprostinil therapy, almost all of them experienced some degree of improvement in their walk distance,” said Dr. Fenster, who was not involved with the study. “Perhaps more importantly there were significant improvements in almost all parameters from their right heart catheterizations. So when we think about how to treat these patients, we have to weigh the risks and benefits of what we make potentially worse with our IPF therapy, such as worsening hypoxia, V/Q mismatch, disease progression, and volume overload. On the flip side, we might be improving right heart hemodynamics and RV function, which are prognostic in this disease. What’s the net balance of these things in terms of how it translates into functional capacity, quality of life, hospitalization, and mortality? We don’t know.”
According to Dr. Fenster, current data suggest that future IPF PH research should focus on prostanoid pathways and not on the estrogen-receptor and riociguat pathways to determine effective treatments. “We have numerous studies showing potential harm with IPF PH therapy, so we need to very much wade cautiously into this arena,” he said. “There is a potential role for PH therapy in IPF, but we will likely need to study patients with severe PH and IPF to show benefit. I think that’s where we’ll have the most success.”
Dr. Fenster reported having no relevant financial disclosures.
LOS ANGELES – When it comes to the optimal management of pulmonary hypertension (PH) in patients with idiopathic pulmonary fibrosis (IPF), there are more questions than definitive answers, according to Brett E. Fenster, MD, FACC.
“Is PH in IPF a disease marker, an independent treatment target, or both?” he asked attendees at the annual meeting of the American College of Chest Physicians. “I think we have conflicting information about that.”
The prevalence of PH is estimated to be 10% in patients with mild to moderate IPF and tends to progress slowly. Common features of PH in IPF patients include shortness of breath, a greater degree of exertional desaturation, and an increased mortality rate.
Dr. Fenster described the ability to detect PH in IPF patients as “more art than science. A lot of different work has been done to look at different testing to get at the patients that may have PH that is a comorbid disease to their IPF. But a lot of times it comes down to assessing their level of dyspnea proportional to their level of disease. In those patients where we think there is something else going on besides their IPF, we’ll oftentimes get an echocardiogram and try to look at their right heart to see if they have features of PH. If it looks like they do, we will circle back and look at the amount of lung disease they have as characterized by their chest imaging, by their pulmonary function testing, and getting a blood gas. If this patient has findings of right heart enlargement, systolic dysfunction, et cetera, that clues us more into looking at PH and referring them to a center that has expertise in that version of PH.”
According to the most recent European Society of Cardiology/European Respiratory Society guidelines, the diagnosis of chronic obstructive pulmonary disease (COPD)/IPF/combined pulmonary fibrosis and emphysema (CPFE) without PH can be considered when the mean pulmonary artery pressure (mPAP) on right heart catheterization is less than 25 mm Hg. The diagnosis of COPD/IPF/CPFE with PH, based on these same guidelines, can be considered when the mPAP is 25 mm Hg or more. A patient may have COPD/IPF/CPFE with severe PH when his or her mPAP exceeds 35 mm Hg, or is 25 mm Hg or greater in the presence of a low cardiac output, the guidelines says (Eur Heart J. 2016;37:67-119). “That begins to separate out a group that may potentially benefit from targeted PH therapy,” Dr. Fenster said.
Current treatment approaches include long-term oxygen, diuretics, transplant, and pulmonary rehabilitation, but Dr. Fenster said there is sparse data on the optimal treatment approach. A study of sildenafil in IPF known as STEP-IPF failed to increase 6-minute walking test distance but improved diffusion capacity of carbon monoxide, quality of life, and arterial oxygenation (N Engl J Med. 2010;363:620-8). A study evaluating riociguat for idiopathic interstitial pneumonitis PH was discontinued early because of increased risk of death and adverse events. More recently, the drug ambrisentan was found to be ineffective at reducing the rate of IPF progression and was linked to an increase in disease progression events, including a decline in pulmonary function test values, hospitalization, and death, in the ARTEMIS-IPF trial (Ann Intern Med. 2013;158:641-9).
Randomized, placebo-controlled studies of bosentan in IPF give researchers pause for hope, Dr. Fenster said. BUILD-1 demonstrated a trend toward delayed time to death, delayed disease progression, improved quality of life, and no clear worsening of IPF (Am J Respir Crit Care Med. 2008;177[1]:75-81), while BUILD-3 showed a significant improvement in forced vital capacity (FVC) and carbon monoxide diffusing capacity (Am J Respir Crit Care Med. 2011;184[1]:92-9). A more recent trial evaluated IV treprostinil in 15 patients with interstitial lung disease and PH (Thorax 2014;69[2]:123-9). Eight of the patients had IPF. “After 12 weeks of treprostinil therapy, almost all of them experienced some degree of improvement in their walk distance,” said Dr. Fenster, who was not involved with the study. “Perhaps more importantly there were significant improvements in almost all parameters from their right heart catheterizations. So when we think about how to treat these patients, we have to weigh the risks and benefits of what we make potentially worse with our IPF therapy, such as worsening hypoxia, V/Q mismatch, disease progression, and volume overload. On the flip side, we might be improving right heart hemodynamics and RV function, which are prognostic in this disease. What’s the net balance of these things in terms of how it translates into functional capacity, quality of life, hospitalization, and mortality? We don’t know.”
According to Dr. Fenster, current data suggest that future IPF PH research should focus on prostanoid pathways and not on the estrogen-receptor and riociguat pathways to determine effective treatments. “We have numerous studies showing potential harm with IPF PH therapy, so we need to very much wade cautiously into this arena,” he said. “There is a potential role for PH therapy in IPF, but we will likely need to study patients with severe PH and IPF to show benefit. I think that’s where we’ll have the most success.”
Dr. Fenster reported having no relevant financial disclosures.
Toddler gaze patterns heritable, stable over time
NEW YORK – A team of autism researchers has found that patterns of social-visual engagement are markedly more similar among identical twin toddlers than among fraternal twins.
Social-visual engagement (SVE), which can be measured using eye-tracking technology, is how humans give preferential attention to social stimuli – in particular, people’s eyes and mouths, which provide important information for communication.
Lower levels of SVE have been shown to be associated with the later development of autism, even in children just a few months old (Nature. 2013 Dec 19;504:427-31). “But what hasn’t been shown until now is that this measure relates to genetics,” said Natasha Marrus, MD, PhD, of the department of psychiatry at Washington University in St. Louis.
The identical twins, who share 100% of their genes, “showed much more similar levels of social-visual engagement than fraternal twins,” Dr. Marrus said, with an intraclass correlation coefficient (ICC) of 0.91 (95% confidence interval, 0.85-0.95) for time spent looking at eyes, compared with 0.35 (95% CI, 0.07-0.59) for fraternal twins. Similar results were obtained for the caregiver questionnaire, suggesting strong genetic influences on both early reciprocal social behavior and SVE, said Dr. Marrus, also of Washington University.
At 36 months, 69 of the twin pairs were reevaluated. The investigators again found significantly greater SVE concordance for the identical twins: ICC, 0.93 (95% CI, 0.75-0.98), compared with ICC, 0.25 (95% CI, 0.0-0.60) for fraternal twins. They also found SVE patterns strongly correlated between 21 and 36 months for individual twins, indicating traitlike stability of this behavior over time.
“These two measures that are heritable, like autism, can be measured in a general population sample, which means they show good variability – potentially allowing the detection of subtle differences that may correspond to levels of risk for autism,” Dr. Marrus said. “By 18-21 months, the risk markers for later autism are already there – if you use a nuanced enough measure to detect them.”
Dr. Marrus said that while some practitioners have been able to reliably diagnose autism in children younger than 24 months, “it’s usually with the most severe cases,” she said. “But 18 months is a big time for social as well as language development, which becomes easier to measure at that point.”
A future direction for study, she said, “would be to go earlier. If we’re seeing this at 18 months, maybe we’d see it at 12.”
With autism, “early intervention is key, and even 6 months could make a difference,” Dr. Marrus said. “These two measures stand a really good chance of telling us important things about autism – which at early ages means better diagnostic prediction, measurement of severity and risk, and the potential to monitor responses to interventions.”
The National Institutes of Health supported the study through a grant to Dr. Constantino, and Dr. Marrus’s work was supported with a postdoctoral fellowship from the Autism Science Foundation. The investigators declared no relevant financial conflicts.
NEW YORK – A team of autism researchers has found that patterns of social-visual engagement are markedly more similar among identical twin toddlers than among fraternal twins.
Social-visual engagement (SVE), which can be measured using eye-tracking technology, is how humans give preferential attention to social stimuli – in particular, people’s eyes and mouths, which provide important information for communication.
Lower levels of SVE have been shown to be associated with the later development of autism, even in children just a few months old (Nature. 2013 Dec 19;504:427-31). “But what hasn’t been shown until now is that this measure relates to genetics,” said Natasha Marrus, MD, PhD, of the department of psychiatry at Washington University in St. Louis.
The identical twins, who share 100% of their genes, “showed much more similar levels of social-visual engagement than fraternal twins,” Dr. Marrus said, with an intraclass correlation coefficient (ICC) of 0.91 (95% confidence interval, 0.85-0.95) for time spent looking at eyes, compared with 0.35 (95% CI, 0.07-0.59) for fraternal twins. Similar results were obtained for the caregiver questionnaire, suggesting strong genetic influences on both early reciprocal social behavior and SVE, said Dr. Marrus, also of Washington University.
At 36 months, 69 of the twin pairs were reevaluated. The investigators again found significantly greater SVE concordance for the identical twins: ICC, 0.93 (95% CI, 0.75-0.98), compared with ICC, 0.25 (95% CI, 0.0-0.60) for fraternal twins. They also found SVE patterns strongly correlated between 21 and 36 months for individual twins, indicating traitlike stability of this behavior over time.
“These two measures that are heritable, like autism, can be measured in a general population sample, which means they show good variability – potentially allowing the detection of subtle differences that may correspond to levels of risk for autism,” Dr. Marrus said. “By 18-21 months, the risk markers for later autism are already there – if you use a nuanced enough measure to detect them.”
Dr. Marrus said that while some practitioners have been able to reliably diagnose autism in children younger than 24 months, “it’s usually with the most severe cases,” she said. “But 18 months is a big time for social as well as language development, which becomes easier to measure at that point.”
A future direction for study, she said, “would be to go earlier. If we’re seeing this at 18 months, maybe we’d see it at 12.”
With autism, “early intervention is key, and even 6 months could make a difference,” Dr. Marrus said. “These two measures stand a really good chance of telling us important things about autism – which at early ages means better diagnostic prediction, measurement of severity and risk, and the potential to monitor responses to interventions.”
The National Institutes of Health supported the study through a grant to Dr. Constantino, and Dr. Marrus’s work was supported with a postdoctoral fellowship from the Autism Science Foundation. The investigators declared no relevant financial conflicts.
NEW YORK – A team of autism researchers has found that patterns of social-visual engagement are markedly more similar among identical twin toddlers than among fraternal twins.
Social-visual engagement (SVE), which can be measured using eye-tracking technology, is how humans give preferential attention to social stimuli – in particular, people’s eyes and mouths, which provide important information for communication.
Lower levels of SVE have been shown to be associated with the later development of autism, even in children just a few months old (Nature. 2013 Dec 19;504:427-31). “But what hasn’t been shown until now is that this measure relates to genetics,” said Natasha Marrus, MD, PhD, of the department of psychiatry at Washington University in St. Louis.
The identical twins, who share 100% of their genes, “showed much more similar levels of social-visual engagement than fraternal twins,” Dr. Marrus said, with an intraclass correlation coefficient (ICC) of 0.91 (95% confidence interval, 0.85-0.95) for time spent looking at eyes, compared with 0.35 (95% CI, 0.07-0.59) for fraternal twins. Similar results were obtained for the caregiver questionnaire, suggesting strong genetic influences on both early reciprocal social behavior and SVE, said Dr. Marrus, also of Washington University.
At 36 months, 69 of the twin pairs were reevaluated. The investigators again found significantly greater SVE concordance for the identical twins: ICC, 0.93 (95% CI, 0.75-0.98), compared with ICC, 0.25 (95% CI, 0.0-0.60) for fraternal twins. They also found SVE patterns strongly correlated between 21 and 36 months for individual twins, indicating traitlike stability of this behavior over time.
“These two measures that are heritable, like autism, can be measured in a general population sample, which means they show good variability – potentially allowing the detection of subtle differences that may correspond to levels of risk for autism,” Dr. Marrus said. “By 18-21 months, the risk markers for later autism are already there – if you use a nuanced enough measure to detect them.”
Dr. Marrus said that while some practitioners have been able to reliably diagnose autism in children younger than 24 months, “it’s usually with the most severe cases,” she said. “But 18 months is a big time for social as well as language development, which becomes easier to measure at that point.”
A future direction for study, she said, “would be to go earlier. If we’re seeing this at 18 months, maybe we’d see it at 12.”
With autism, “early intervention is key, and even 6 months could make a difference,” Dr. Marrus said. “These two measures stand a really good chance of telling us important things about autism – which at early ages means better diagnostic prediction, measurement of severity and risk, and the potential to monitor responses to interventions.”
The National Institutes of Health supported the study through a grant to Dr. Constantino, and Dr. Marrus’s work was supported with a postdoctoral fellowship from the Autism Science Foundation. The investigators declared no relevant financial conflicts.
AT AACAP 2016
Weekly number of Zika-infected pregnancies drops by half
There were 146 new cases of pregnant women with laboratory evidence of Zika infection reported in the United States for the week ending Nov. 3 – just about half of the 288-case increase reported the week before, according to Centers for Disease Control and Prevention.
For the year so far, there have been 1,057 cases of pregnant women with Zika in the states and the District of Columbia – 52 for the week ending Nov. 3 – and 2,357 cases in the territories, the CDC announced, with 94 reported in the most recent week. The total number of U.S. cases – 3,414 – is up by 4.4% over the previous week.
The CDC also reported one new infant born with Zika-related birth defects for the week ending Nov. 3, bringing the total for the year to 26 in the states/D.C. There were no new Zika-related pregnancy losses reported, so the total remains at five. State-level data are not being reported to protect the privacy of affected women and children.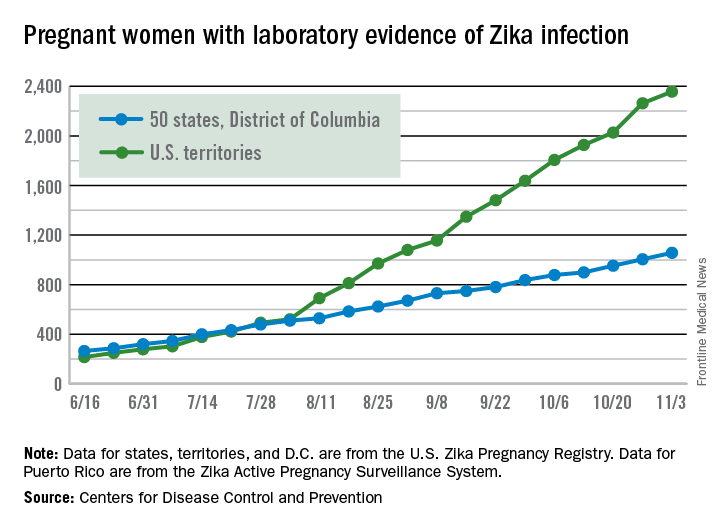
The CDC is no longer reporting adverse pregnancy outcomes for the territories because Puerto Rico is not using the same “inclusion criteria to monitor brain abnormalities and other adverse pregnancy outcomes.” As of Sept. 29 – the date of the last territorial report – there had been one liveborn infant and one pregnancy loss related to Zika.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
There were 146 new cases of pregnant women with laboratory evidence of Zika infection reported in the United States for the week ending Nov. 3 – just about half of the 288-case increase reported the week before, according to Centers for Disease Control and Prevention.
For the year so far, there have been 1,057 cases of pregnant women with Zika in the states and the District of Columbia – 52 for the week ending Nov. 3 – and 2,357 cases in the territories, the CDC announced, with 94 reported in the most recent week. The total number of U.S. cases – 3,414 – is up by 4.4% over the previous week.
The CDC also reported one new infant born with Zika-related birth defects for the week ending Nov. 3, bringing the total for the year to 26 in the states/D.C. There were no new Zika-related pregnancy losses reported, so the total remains at five. State-level data are not being reported to protect the privacy of affected women and children.
The CDC is no longer reporting adverse pregnancy outcomes for the territories because Puerto Rico is not using the same “inclusion criteria to monitor brain abnormalities and other adverse pregnancy outcomes.” As of Sept. 29 – the date of the last territorial report – there had been one liveborn infant and one pregnancy loss related to Zika.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
There were 146 new cases of pregnant women with laboratory evidence of Zika infection reported in the United States for the week ending Nov. 3 – just about half of the 288-case increase reported the week before, according to Centers for Disease Control and Prevention.
For the year so far, there have been 1,057 cases of pregnant women with Zika in the states and the District of Columbia – 52 for the week ending Nov. 3 – and 2,357 cases in the territories, the CDC announced, with 94 reported in the most recent week. The total number of U.S. cases – 3,414 – is up by 4.4% over the previous week.
The CDC also reported one new infant born with Zika-related birth defects for the week ending Nov. 3, bringing the total for the year to 26 in the states/D.C. There were no new Zika-related pregnancy losses reported, so the total remains at five. State-level data are not being reported to protect the privacy of affected women and children.
The CDC is no longer reporting adverse pregnancy outcomes for the territories because Puerto Rico is not using the same “inclusion criteria to monitor brain abnormalities and other adverse pregnancy outcomes.” As of Sept. 29 – the date of the last territorial report – there had been one liveborn infant and one pregnancy loss related to Zika.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.