User login
Managing stress in children, parents can reduce obesity risk
SAN FRANCISCO – Obesity is a multifactorial problem, influenced by factors ranging from genetics to lifestyle to the environment. Yet stress can play an outsize role in obesity as well, Elizabeth Prout Parks, MD, said at the annual meeting of the American Academy of Pediatrics.
Although the calorie-in/calorie-out model of energy balance has driven much of the thought about obesity, it’s not that simple, suggested Dr. Parks, the medical director of the Healthy Weight Adolescent Bariatrics Program at the Children’s Hospital of Philadelphia. Physical activity accounts for an estimated 15%-30% of energy expenditure, and thermogenesis accounts for an estimated 10%. But the energy expenditure required for basal metabolism can range from 60% to 75%, a sufficiently wide range for significant variation across different individuals.
The psychosocial effects can lead to anxiety, depression, disordered eating behaviors such as emotional eating, a sedentary lifestyle, poor sleep, and low maintenance with self-care activities. Further, poor sleep on its own is additionally associated with childhood obesity. The combination of these physiologic and psychosocial effects can increase the risk of metabolic syndrome, type 2 diabetes, and cardiovascular disease or events. While acute stress and chronic stress follow similar pathways in the brain, it’s chronic stress that carries the greater risk of behavioral and physical conditions.
Measuring and understanding child and parental stress
Several clinical assessments can measure stress in children, including the Daily Hassles Scale, which looks at everyday interactions in the environment and factors such as children’s school, family, neighborhood, peers, and lack of resources. The Multidimensional Life Events Rating Questionnaire and Adolescent Stress Questionnaire both are more appropriate for middle school and older adolescents.
In children, the primary biologic indicators of stress are cortisol levels, heart rate, and blood pressure, but it is perceived stress that has been most clearly linked to emotional eating and other disordered eating behaviors, Dr. Parks said. One 2008 study found perceived stress to be associated with emotional eating among middle school students both with and without obesity. A high level of perceived stress in adolescents was associated with a greater waist circumference and body mass index in a 2009 study.
The findings are somewhat more mixed, however, when it comes to parental stress and child weight. A 2012 study identified a link between parents’ perception of their stress and increased fast food consumption in their children, and a 2008 study identified a link between parenting stress and both overweight and underweight children. Yet a different study in 2008 found no association between child obesity and parenting stress. Research in 2011 found a relationship between children’s consumption of fruits and vegetables and their family’s overall functioning, as well as parental psychological stress and child behavior. Within a family, stress can come from financial strain (such as poverty or changes in employment or insurance), the family’s structure, and changes in physical or mental health of one or more family members.
Addressing the effects of stress on diet
Clinicians can help families manage the ways stress can lead to obesity by helping them with ideas for increasing fruit and vegetable intake, and planning ahead for on-the-go eating. For example, to ensure children get in their recommended five servings of fruit and vegetables each day, parents can serve fruit with breakfast every day and offer vegetables and/or fruit as a snack. Including side salads and a frozen vegetable with dinner will add two more servings, and children can munch on chopped veggies while parents prepare dinner. Offering fruit as a dessert provides another opportunity to bump up kids’ fruit and veggie intake, Dr. Parks said.
To manage the risk of unhealthy eating when out and about, Dr. Parks recommends planning ahead by packing a snack such as yogurt, fruit and vegetables, a sandwich or wrap, and water.
She described the “apple test” for determining whether someone is eating because of boredom or stress or because of actual hunger.“The next time you are thinking about a mini meal or second helpings at a meal, ask yourself, ‘Would I eat an apple instead?’ ” Dr. Parks said. “If the answer is no, then you probably are not really hungry and just need to get away from food.”
Other things people can consider when about to eat something are whether they are actually hungry and whether a distraction such as the television is contributing to distracted eating. “People may eat when they’re happy, sad, or bored,” Dr. Parks said, noting that outside messages such as commercials, advertisements, and passing restaurants may make someone feel like eating even if they don’t need sustenance at that moment. “Consider whether you really are hungry before you eat,” she said.
Avoiding emotional eating and using mindfulness
Additionally, parents and children can avoid emotional eating by skipping the food when they feel angry, tired, nervous, bored, or sad, instead choosing activities such as journaling, taking a walk, listening to music, reading a book, or taking deep breaths while thinking pleasant thoughts. It’s only time to eat if you physically feel hungry, your stomach is rumbling, you are not craving some specific sweet or salty food, or it’s a meal or snack time (or at least 2.5-4 hours since the last time you ate).
Dr. Parks also reviewed ways that mindfulness may help reduce the risk of obesity by reducing stress, enhancing a person’s ability to regulate their everyday behaviors, and teaching individuals to accept discomfort. Another stress reduction strategy is repeated use of “4-7-8 breathing,” which begins with exhalation while the mouth is closed. Then, inhale through the nose for 4 seconds, hold the breath for 7 seconds and slowly exhale out the mouth for 8 seconds.
Reducing the risk of obesity from stress comes from learning to manage stress. Clinicians can play a role in helping both parents and children learn strategies to manage and cope with stress in the short term while developing resilience over the longer term and reducing the likelihood of poor eating and emotional eating.
Dr. Parks reported no disclosures.
SAN FRANCISCO – Obesity is a multifactorial problem, influenced by factors ranging from genetics to lifestyle to the environment. Yet stress can play an outsize role in obesity as well, Elizabeth Prout Parks, MD, said at the annual meeting of the American Academy of Pediatrics.
Although the calorie-in/calorie-out model of energy balance has driven much of the thought about obesity, it’s not that simple, suggested Dr. Parks, the medical director of the Healthy Weight Adolescent Bariatrics Program at the Children’s Hospital of Philadelphia. Physical activity accounts for an estimated 15%-30% of energy expenditure, and thermogenesis accounts for an estimated 10%. But the energy expenditure required for basal metabolism can range from 60% to 75%, a sufficiently wide range for significant variation across different individuals.
The psychosocial effects can lead to anxiety, depression, disordered eating behaviors such as emotional eating, a sedentary lifestyle, poor sleep, and low maintenance with self-care activities. Further, poor sleep on its own is additionally associated with childhood obesity. The combination of these physiologic and psychosocial effects can increase the risk of metabolic syndrome, type 2 diabetes, and cardiovascular disease or events. While acute stress and chronic stress follow similar pathways in the brain, it’s chronic stress that carries the greater risk of behavioral and physical conditions.
Measuring and understanding child and parental stress
Several clinical assessments can measure stress in children, including the Daily Hassles Scale, which looks at everyday interactions in the environment and factors such as children’s school, family, neighborhood, peers, and lack of resources. The Multidimensional Life Events Rating Questionnaire and Adolescent Stress Questionnaire both are more appropriate for middle school and older adolescents.
In children, the primary biologic indicators of stress are cortisol levels, heart rate, and blood pressure, but it is perceived stress that has been most clearly linked to emotional eating and other disordered eating behaviors, Dr. Parks said. One 2008 study found perceived stress to be associated with emotional eating among middle school students both with and without obesity. A high level of perceived stress in adolescents was associated with a greater waist circumference and body mass index in a 2009 study.
The findings are somewhat more mixed, however, when it comes to parental stress and child weight. A 2012 study identified a link between parents’ perception of their stress and increased fast food consumption in their children, and a 2008 study identified a link between parenting stress and both overweight and underweight children. Yet a different study in 2008 found no association between child obesity and parenting stress. Research in 2011 found a relationship between children’s consumption of fruits and vegetables and their family’s overall functioning, as well as parental psychological stress and child behavior. Within a family, stress can come from financial strain (such as poverty or changes in employment or insurance), the family’s structure, and changes in physical or mental health of one or more family members.
Addressing the effects of stress on diet
Clinicians can help families manage the ways stress can lead to obesity by helping them with ideas for increasing fruit and vegetable intake, and planning ahead for on-the-go eating. For example, to ensure children get in their recommended five servings of fruit and vegetables each day, parents can serve fruit with breakfast every day and offer vegetables and/or fruit as a snack. Including side salads and a frozen vegetable with dinner will add two more servings, and children can munch on chopped veggies while parents prepare dinner. Offering fruit as a dessert provides another opportunity to bump up kids’ fruit and veggie intake, Dr. Parks said.
To manage the risk of unhealthy eating when out and about, Dr. Parks recommends planning ahead by packing a snack such as yogurt, fruit and vegetables, a sandwich or wrap, and water.
She described the “apple test” for determining whether someone is eating because of boredom or stress or because of actual hunger.“The next time you are thinking about a mini meal or second helpings at a meal, ask yourself, ‘Would I eat an apple instead?’ ” Dr. Parks said. “If the answer is no, then you probably are not really hungry and just need to get away from food.”
Other things people can consider when about to eat something are whether they are actually hungry and whether a distraction such as the television is contributing to distracted eating. “People may eat when they’re happy, sad, or bored,” Dr. Parks said, noting that outside messages such as commercials, advertisements, and passing restaurants may make someone feel like eating even if they don’t need sustenance at that moment. “Consider whether you really are hungry before you eat,” she said.
Avoiding emotional eating and using mindfulness
Additionally, parents and children can avoid emotional eating by skipping the food when they feel angry, tired, nervous, bored, or sad, instead choosing activities such as journaling, taking a walk, listening to music, reading a book, or taking deep breaths while thinking pleasant thoughts. It’s only time to eat if you physically feel hungry, your stomach is rumbling, you are not craving some specific sweet or salty food, or it’s a meal or snack time (or at least 2.5-4 hours since the last time you ate).
Dr. Parks also reviewed ways that mindfulness may help reduce the risk of obesity by reducing stress, enhancing a person’s ability to regulate their everyday behaviors, and teaching individuals to accept discomfort. Another stress reduction strategy is repeated use of “4-7-8 breathing,” which begins with exhalation while the mouth is closed. Then, inhale through the nose for 4 seconds, hold the breath for 7 seconds and slowly exhale out the mouth for 8 seconds.
Reducing the risk of obesity from stress comes from learning to manage stress. Clinicians can play a role in helping both parents and children learn strategies to manage and cope with stress in the short term while developing resilience over the longer term and reducing the likelihood of poor eating and emotional eating.
Dr. Parks reported no disclosures.
SAN FRANCISCO – Obesity is a multifactorial problem, influenced by factors ranging from genetics to lifestyle to the environment. Yet stress can play an outsize role in obesity as well, Elizabeth Prout Parks, MD, said at the annual meeting of the American Academy of Pediatrics.
Although the calorie-in/calorie-out model of energy balance has driven much of the thought about obesity, it’s not that simple, suggested Dr. Parks, the medical director of the Healthy Weight Adolescent Bariatrics Program at the Children’s Hospital of Philadelphia. Physical activity accounts for an estimated 15%-30% of energy expenditure, and thermogenesis accounts for an estimated 10%. But the energy expenditure required for basal metabolism can range from 60% to 75%, a sufficiently wide range for significant variation across different individuals.
The psychosocial effects can lead to anxiety, depression, disordered eating behaviors such as emotional eating, a sedentary lifestyle, poor sleep, and low maintenance with self-care activities. Further, poor sleep on its own is additionally associated with childhood obesity. The combination of these physiologic and psychosocial effects can increase the risk of metabolic syndrome, type 2 diabetes, and cardiovascular disease or events. While acute stress and chronic stress follow similar pathways in the brain, it’s chronic stress that carries the greater risk of behavioral and physical conditions.
Measuring and understanding child and parental stress
Several clinical assessments can measure stress in children, including the Daily Hassles Scale, which looks at everyday interactions in the environment and factors such as children’s school, family, neighborhood, peers, and lack of resources. The Multidimensional Life Events Rating Questionnaire and Adolescent Stress Questionnaire both are more appropriate for middle school and older adolescents.
In children, the primary biologic indicators of stress are cortisol levels, heart rate, and blood pressure, but it is perceived stress that has been most clearly linked to emotional eating and other disordered eating behaviors, Dr. Parks said. One 2008 study found perceived stress to be associated with emotional eating among middle school students both with and without obesity. A high level of perceived stress in adolescents was associated with a greater waist circumference and body mass index in a 2009 study.
The findings are somewhat more mixed, however, when it comes to parental stress and child weight. A 2012 study identified a link between parents’ perception of their stress and increased fast food consumption in their children, and a 2008 study identified a link between parenting stress and both overweight and underweight children. Yet a different study in 2008 found no association between child obesity and parenting stress. Research in 2011 found a relationship between children’s consumption of fruits and vegetables and their family’s overall functioning, as well as parental psychological stress and child behavior. Within a family, stress can come from financial strain (such as poverty or changes in employment or insurance), the family’s structure, and changes in physical or mental health of one or more family members.
Addressing the effects of stress on diet
Clinicians can help families manage the ways stress can lead to obesity by helping them with ideas for increasing fruit and vegetable intake, and planning ahead for on-the-go eating. For example, to ensure children get in their recommended five servings of fruit and vegetables each day, parents can serve fruit with breakfast every day and offer vegetables and/or fruit as a snack. Including side salads and a frozen vegetable with dinner will add two more servings, and children can munch on chopped veggies while parents prepare dinner. Offering fruit as a dessert provides another opportunity to bump up kids’ fruit and veggie intake, Dr. Parks said.
To manage the risk of unhealthy eating when out and about, Dr. Parks recommends planning ahead by packing a snack such as yogurt, fruit and vegetables, a sandwich or wrap, and water.
She described the “apple test” for determining whether someone is eating because of boredom or stress or because of actual hunger.“The next time you are thinking about a mini meal or second helpings at a meal, ask yourself, ‘Would I eat an apple instead?’ ” Dr. Parks said. “If the answer is no, then you probably are not really hungry and just need to get away from food.”
Other things people can consider when about to eat something are whether they are actually hungry and whether a distraction such as the television is contributing to distracted eating. “People may eat when they’re happy, sad, or bored,” Dr. Parks said, noting that outside messages such as commercials, advertisements, and passing restaurants may make someone feel like eating even if they don’t need sustenance at that moment. “Consider whether you really are hungry before you eat,” she said.
Avoiding emotional eating and using mindfulness
Additionally, parents and children can avoid emotional eating by skipping the food when they feel angry, tired, nervous, bored, or sad, instead choosing activities such as journaling, taking a walk, listening to music, reading a book, or taking deep breaths while thinking pleasant thoughts. It’s only time to eat if you physically feel hungry, your stomach is rumbling, you are not craving some specific sweet or salty food, or it’s a meal or snack time (or at least 2.5-4 hours since the last time you ate).
Dr. Parks also reviewed ways that mindfulness may help reduce the risk of obesity by reducing stress, enhancing a person’s ability to regulate their everyday behaviors, and teaching individuals to accept discomfort. Another stress reduction strategy is repeated use of “4-7-8 breathing,” which begins with exhalation while the mouth is closed. Then, inhale through the nose for 4 seconds, hold the breath for 7 seconds and slowly exhale out the mouth for 8 seconds.
Reducing the risk of obesity from stress comes from learning to manage stress. Clinicians can play a role in helping both parents and children learn strategies to manage and cope with stress in the short term while developing resilience over the longer term and reducing the likelihood of poor eating and emotional eating.
Dr. Parks reported no disclosures.
Survey: More than half of gynecologic oncologists altered morcellation practices
ORLANDO – Following the Food and Drug Administration’s 2014 warning against use of laparoscopic uterine power morcellation, 13% of gynecologic oncologists decreased their use of the technique and another 39% discontinued it altogether, according to survey responses from 199 members of the Society of Gynecologic Oncology.
“This really gives a snapshot about how gynecologic oncologists feel about power morcellation in light of the FDA warning,” said Kerac N. Falk, MD, a resident at the Icahn School of Medicine at Mount Sinai, New York.
About 41% of gynecologic oncologists changed their surgical technique to minimally invasive without power morcellation. Another 20% of respondents who previously used power morcellation have switched to laparotomy.
A more rigorous informed consent process, better attention to patient selection, and enhanced protocols are positive effects emerging since the FDA Safety Communication was issued in April 2014, Dr. Falk said at the meeting sponsored by AAGL.
The 34-item survey included questions about demographics, institutional policies, and attitudes before and after the FDA warning. Among the respondents, 65% were men. Both “early” and “very seasoned” surgeons participated in the survey. The majority of the respondents were moderate- to high-volume surgeons.
Men were significantly more likely to decrease or discontinue use of power morcellation, compared with women (P = .0015). Region of practice, years in practice, or institution type did not significantly influence changes in practice. “Most said it was not a personal choice, but more about patient choice or an institutional policy change,” Dr. Falk said.
There is still a role for power morcellation in carefully selected patients, Dr. Falk added.
In July 2014, AAGL issued a statement in response to the FDA warning, stating that “we should improve but not abandon power morcellation, and that power morcellation with appropriate informed consent should remain available to appropriately screened, low-risk women.” In addition, the American College of Obstetricians and Gynecologists stated, “Although the worsening of an occult malignancy as a result of power morcellation is, of course, tragic, we believe that an approach that combines deliberate patient selection criteria with robust informed consent will help protect women from a negative outcome, while maintaining access to morcellation for women who would benefit from it.”
Dr. Falk is not a coauthor on the study. He presented the findings on behalf of a colleague unable to attend the meeting. Dr. Falk reported having no relevant financial disclosures.
ORLANDO – Following the Food and Drug Administration’s 2014 warning against use of laparoscopic uterine power morcellation, 13% of gynecologic oncologists decreased their use of the technique and another 39% discontinued it altogether, according to survey responses from 199 members of the Society of Gynecologic Oncology.
“This really gives a snapshot about how gynecologic oncologists feel about power morcellation in light of the FDA warning,” said Kerac N. Falk, MD, a resident at the Icahn School of Medicine at Mount Sinai, New York.
About 41% of gynecologic oncologists changed their surgical technique to minimally invasive without power morcellation. Another 20% of respondents who previously used power morcellation have switched to laparotomy.
A more rigorous informed consent process, better attention to patient selection, and enhanced protocols are positive effects emerging since the FDA Safety Communication was issued in April 2014, Dr. Falk said at the meeting sponsored by AAGL.
The 34-item survey included questions about demographics, institutional policies, and attitudes before and after the FDA warning. Among the respondents, 65% were men. Both “early” and “very seasoned” surgeons participated in the survey. The majority of the respondents were moderate- to high-volume surgeons.
Men were significantly more likely to decrease or discontinue use of power morcellation, compared with women (P = .0015). Region of practice, years in practice, or institution type did not significantly influence changes in practice. “Most said it was not a personal choice, but more about patient choice or an institutional policy change,” Dr. Falk said.
There is still a role for power morcellation in carefully selected patients, Dr. Falk added.
In July 2014, AAGL issued a statement in response to the FDA warning, stating that “we should improve but not abandon power morcellation, and that power morcellation with appropriate informed consent should remain available to appropriately screened, low-risk women.” In addition, the American College of Obstetricians and Gynecologists stated, “Although the worsening of an occult malignancy as a result of power morcellation is, of course, tragic, we believe that an approach that combines deliberate patient selection criteria with robust informed consent will help protect women from a negative outcome, while maintaining access to morcellation for women who would benefit from it.”
Dr. Falk is not a coauthor on the study. He presented the findings on behalf of a colleague unable to attend the meeting. Dr. Falk reported having no relevant financial disclosures.
ORLANDO – Following the Food and Drug Administration’s 2014 warning against use of laparoscopic uterine power morcellation, 13% of gynecologic oncologists decreased their use of the technique and another 39% discontinued it altogether, according to survey responses from 199 members of the Society of Gynecologic Oncology.
“This really gives a snapshot about how gynecologic oncologists feel about power morcellation in light of the FDA warning,” said Kerac N. Falk, MD, a resident at the Icahn School of Medicine at Mount Sinai, New York.
About 41% of gynecologic oncologists changed their surgical technique to minimally invasive without power morcellation. Another 20% of respondents who previously used power morcellation have switched to laparotomy.
A more rigorous informed consent process, better attention to patient selection, and enhanced protocols are positive effects emerging since the FDA Safety Communication was issued in April 2014, Dr. Falk said at the meeting sponsored by AAGL.
The 34-item survey included questions about demographics, institutional policies, and attitudes before and after the FDA warning. Among the respondents, 65% were men. Both “early” and “very seasoned” surgeons participated in the survey. The majority of the respondents were moderate- to high-volume surgeons.
Men were significantly more likely to decrease or discontinue use of power morcellation, compared with women (P = .0015). Region of practice, years in practice, or institution type did not significantly influence changes in practice. “Most said it was not a personal choice, but more about patient choice or an institutional policy change,” Dr. Falk said.
There is still a role for power morcellation in carefully selected patients, Dr. Falk added.
In July 2014, AAGL issued a statement in response to the FDA warning, stating that “we should improve but not abandon power morcellation, and that power morcellation with appropriate informed consent should remain available to appropriately screened, low-risk women.” In addition, the American College of Obstetricians and Gynecologists stated, “Although the worsening of an occult malignancy as a result of power morcellation is, of course, tragic, we believe that an approach that combines deliberate patient selection criteria with robust informed consent will help protect women from a negative outcome, while maintaining access to morcellation for women who would benefit from it.”
Dr. Falk is not a coauthor on the study. He presented the findings on behalf of a colleague unable to attend the meeting. Dr. Falk reported having no relevant financial disclosures.
AT THE AAGL GLOBAL CONGRESS
Key clinical point:
Major finding: Among 199 members of the Society of Gynecologic Oncology, 39% said they suspended use of power morcellation, and 13% decreased their use of the technique.
Data source: A survey sent to all members of the Society of Gynecologic Oncology with responses from 199 members.
Disclosures: Dr. Falk reported having no relevant financial disclosures.
Evaluating Fontan failure risk after arrhythmia
People who have undergone the Fontan procedure have been known to be prone to developing arrhythmias, but few studies have evaluated their prognosis, so researchers from Australia and New Zealand analyzed results of more than 1,000 patients with Fontan circulation and found that two-thirds did not have any arrhythmia at 20 years, and that, among those who did have arrhythmias, almost three-quarters survived 10 years.
“After the first onset of an arrhythmia, close surveillance of ventricular function is required,” Thomas A. Carins, MD, and his colleagues reported (J Thorac Cardiovasc Surg. 2016;152:1355-63). They analyzed data from 1,034 patients who had Fontan procedures from 1975 to 2014 in the Australia and New Zealand Fontan Registry. “The development of an arrhythmia is associated with a heightened risk of subsequent failure of the Fontan circulation,” they wrote.
The study aimed to determine the type of arrhythmias Fontan patients had and what impact that had on long-term outcomes. The most common Fontan approach used in study patients was the extracardiac conduit (555), followed by the lateral tunnel approach (269) and atriopulmonary (210). Those who had the extracardiac Fontan were least likely to develop an arrhythmia, with a hazard ratio of 0.23 (P less than .001), which Dr. Carins and his coauthors noted was in line with previous reports of arrhythmias occurring in patients who had undergone the atriopulmonary connection (Circulation. 2004;109:2319-25; J Thorac Cardiovasc Surg. 1998;115:499-505).
Overall, 195 patients in the study developed arrhythmia, with 162 having tachyarrhythmia, 74 having bradyarrhythmia and 41 having both. “At 20 years, freedom from any arrhythmia, tachyarrhythmia, and bradyarrhythmia was 66%, 69%, and 85%, respectively,” the researchers said.
The following outcomes occurred after the first onset of arrhythmia – tachyarrhythmia in 153 patients and bradyarrhythmia in 42: Thirty-three died; 12 had heart transplants, 30 had a Fontan correction to an extracardiac conduit, three had a Fontan takedown, 12 developed enteropathy, and 25 developed New York Heart Association class III or IV symptoms. Eighty-four patients reached the composite endpoint of Fontan failure.
After they developed arrhythmias, most patients in all three Fontan procedure groups remained free from Fontan failure at 10 years: 67% in the extracardiac conduit group; 54% in the lateral tunnel group; and 51% in the atriopulmonary group.
Medical management of up to four medications was the preferred initial treatment for those with tachyarrhythmias (86%); 101 patients had a single episode of tachyarrhythmia at follow-up intervals of four to 13 years (7.6 year median). “Those who experienced a single versus multiple episodes of tachyarrhythmia showed comparable freedom from Fontan failure at 15 years,” noted Dr. Carins and his coauthors – with rates of 34% and 33%, respectively. Of the 74 patients with bradyarrhythmias, 66 received pacemakers.
“Survival after the onset of an arrhythmia was surprisingly good with 67% and 84% of patients alive at 10 years after the onset of a tachyarrhythmia and bradyarrhythmia, respectively,” the study authors said. “There was no association between occurrence of arrhythmia and survival.”
About 40% of the patients with a tachyarrhythmia or bradyarrhythmia in the study had reduced ventricular function at 10 years after onset, the researchers wrote. “Although the assessment of ventricular function in this study was clearly subjective, we nonetheless believe that these findings suggest that the onset of an arrhythmia is associated with a progressive deterioration in cardiac function,”they noted.
Coauthor Andrew Bullock, MBBS, disclosed receiving consulting fees from Actelion. Dr. Cairns and other coauthors had no financial relationships to disclose.
When interpreting the data that the Australian and New Zealand researchers analyzed, one must be cautious about viewing arrhythmia as an early indicator for Fontan revision, Mark E. Alexander, MD, of Boston Children’s Hospital and Harvard Medical School, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:1364-5).
The outcome of a Fontan revision after an arrhythmia “becomes self-fulfilling,” Dr. Alexander said. He questioned what the revision procedure would be when the initial operation was an extracardiac Fontan. “The complex risks of that procedure continue to keep decisions regarding Fontan revisions challenging,” he said. He also noted the study did not analyze the association of ventricular function and arrhythmias “in a substantive way.”
And Dr. Alexander did not interpret the study results as an endorsement of the extracardiac Fontan or a rejection of the lateral tunnel approach. The early adoption of the extracardiac Fontan by the groups the authors represented is itself a limitation of the study, he said. Challenges with follow-up of extracardiac techniques in this and other studies “limit our ability to declare a ‘victor’ in that debate,” he said. “It does remind the electrophysiologist that he or she needs to master the techniques of entering the pulmonary venous atrium in these patients.”
The precision of calculating risk after an operation grows weaker with time, he said, and at 15-20 years morbidity starts to increase and follow-up becomes “more diffuse,” Dr. Alexander said. “That reality means we look forward to this group continuing to enhance our understanding of how our changing management decisions can aid our patients.”
Dr. Alexander had no financial relationships to disclose.
When interpreting the data that the Australian and New Zealand researchers analyzed, one must be cautious about viewing arrhythmia as an early indicator for Fontan revision, Mark E. Alexander, MD, of Boston Children’s Hospital and Harvard Medical School, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:1364-5).
The outcome of a Fontan revision after an arrhythmia “becomes self-fulfilling,” Dr. Alexander said. He questioned what the revision procedure would be when the initial operation was an extracardiac Fontan. “The complex risks of that procedure continue to keep decisions regarding Fontan revisions challenging,” he said. He also noted the study did not analyze the association of ventricular function and arrhythmias “in a substantive way.”
And Dr. Alexander did not interpret the study results as an endorsement of the extracardiac Fontan or a rejection of the lateral tunnel approach. The early adoption of the extracardiac Fontan by the groups the authors represented is itself a limitation of the study, he said. Challenges with follow-up of extracardiac techniques in this and other studies “limit our ability to declare a ‘victor’ in that debate,” he said. “It does remind the electrophysiologist that he or she needs to master the techniques of entering the pulmonary venous atrium in these patients.”
The precision of calculating risk after an operation grows weaker with time, he said, and at 15-20 years morbidity starts to increase and follow-up becomes “more diffuse,” Dr. Alexander said. “That reality means we look forward to this group continuing to enhance our understanding of how our changing management decisions can aid our patients.”
Dr. Alexander had no financial relationships to disclose.
When interpreting the data that the Australian and New Zealand researchers analyzed, one must be cautious about viewing arrhythmia as an early indicator for Fontan revision, Mark E. Alexander, MD, of Boston Children’s Hospital and Harvard Medical School, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:1364-5).
The outcome of a Fontan revision after an arrhythmia “becomes self-fulfilling,” Dr. Alexander said. He questioned what the revision procedure would be when the initial operation was an extracardiac Fontan. “The complex risks of that procedure continue to keep decisions regarding Fontan revisions challenging,” he said. He also noted the study did not analyze the association of ventricular function and arrhythmias “in a substantive way.”
And Dr. Alexander did not interpret the study results as an endorsement of the extracardiac Fontan or a rejection of the lateral tunnel approach. The early adoption of the extracardiac Fontan by the groups the authors represented is itself a limitation of the study, he said. Challenges with follow-up of extracardiac techniques in this and other studies “limit our ability to declare a ‘victor’ in that debate,” he said. “It does remind the electrophysiologist that he or she needs to master the techniques of entering the pulmonary venous atrium in these patients.”
The precision of calculating risk after an operation grows weaker with time, he said, and at 15-20 years morbidity starts to increase and follow-up becomes “more diffuse,” Dr. Alexander said. “That reality means we look forward to this group continuing to enhance our understanding of how our changing management decisions can aid our patients.”
Dr. Alexander had no financial relationships to disclose.
People who have undergone the Fontan procedure have been known to be prone to developing arrhythmias, but few studies have evaluated their prognosis, so researchers from Australia and New Zealand analyzed results of more than 1,000 patients with Fontan circulation and found that two-thirds did not have any arrhythmia at 20 years, and that, among those who did have arrhythmias, almost three-quarters survived 10 years.
“After the first onset of an arrhythmia, close surveillance of ventricular function is required,” Thomas A. Carins, MD, and his colleagues reported (J Thorac Cardiovasc Surg. 2016;152:1355-63). They analyzed data from 1,034 patients who had Fontan procedures from 1975 to 2014 in the Australia and New Zealand Fontan Registry. “The development of an arrhythmia is associated with a heightened risk of subsequent failure of the Fontan circulation,” they wrote.
The study aimed to determine the type of arrhythmias Fontan patients had and what impact that had on long-term outcomes. The most common Fontan approach used in study patients was the extracardiac conduit (555), followed by the lateral tunnel approach (269) and atriopulmonary (210). Those who had the extracardiac Fontan were least likely to develop an arrhythmia, with a hazard ratio of 0.23 (P less than .001), which Dr. Carins and his coauthors noted was in line with previous reports of arrhythmias occurring in patients who had undergone the atriopulmonary connection (Circulation. 2004;109:2319-25; J Thorac Cardiovasc Surg. 1998;115:499-505).
Overall, 195 patients in the study developed arrhythmia, with 162 having tachyarrhythmia, 74 having bradyarrhythmia and 41 having both. “At 20 years, freedom from any arrhythmia, tachyarrhythmia, and bradyarrhythmia was 66%, 69%, and 85%, respectively,” the researchers said.
The following outcomes occurred after the first onset of arrhythmia – tachyarrhythmia in 153 patients and bradyarrhythmia in 42: Thirty-three died; 12 had heart transplants, 30 had a Fontan correction to an extracardiac conduit, three had a Fontan takedown, 12 developed enteropathy, and 25 developed New York Heart Association class III or IV symptoms. Eighty-four patients reached the composite endpoint of Fontan failure.
After they developed arrhythmias, most patients in all three Fontan procedure groups remained free from Fontan failure at 10 years: 67% in the extracardiac conduit group; 54% in the lateral tunnel group; and 51% in the atriopulmonary group.
Medical management of up to four medications was the preferred initial treatment for those with tachyarrhythmias (86%); 101 patients had a single episode of tachyarrhythmia at follow-up intervals of four to 13 years (7.6 year median). “Those who experienced a single versus multiple episodes of tachyarrhythmia showed comparable freedom from Fontan failure at 15 years,” noted Dr. Carins and his coauthors – with rates of 34% and 33%, respectively. Of the 74 patients with bradyarrhythmias, 66 received pacemakers.
“Survival after the onset of an arrhythmia was surprisingly good with 67% and 84% of patients alive at 10 years after the onset of a tachyarrhythmia and bradyarrhythmia, respectively,” the study authors said. “There was no association between occurrence of arrhythmia and survival.”
About 40% of the patients with a tachyarrhythmia or bradyarrhythmia in the study had reduced ventricular function at 10 years after onset, the researchers wrote. “Although the assessment of ventricular function in this study was clearly subjective, we nonetheless believe that these findings suggest that the onset of an arrhythmia is associated with a progressive deterioration in cardiac function,”they noted.
Coauthor Andrew Bullock, MBBS, disclosed receiving consulting fees from Actelion. Dr. Cairns and other coauthors had no financial relationships to disclose.
People who have undergone the Fontan procedure have been known to be prone to developing arrhythmias, but few studies have evaluated their prognosis, so researchers from Australia and New Zealand analyzed results of more than 1,000 patients with Fontan circulation and found that two-thirds did not have any arrhythmia at 20 years, and that, among those who did have arrhythmias, almost three-quarters survived 10 years.
“After the first onset of an arrhythmia, close surveillance of ventricular function is required,” Thomas A. Carins, MD, and his colleagues reported (J Thorac Cardiovasc Surg. 2016;152:1355-63). They analyzed data from 1,034 patients who had Fontan procedures from 1975 to 2014 in the Australia and New Zealand Fontan Registry. “The development of an arrhythmia is associated with a heightened risk of subsequent failure of the Fontan circulation,” they wrote.
The study aimed to determine the type of arrhythmias Fontan patients had and what impact that had on long-term outcomes. The most common Fontan approach used in study patients was the extracardiac conduit (555), followed by the lateral tunnel approach (269) and atriopulmonary (210). Those who had the extracardiac Fontan were least likely to develop an arrhythmia, with a hazard ratio of 0.23 (P less than .001), which Dr. Carins and his coauthors noted was in line with previous reports of arrhythmias occurring in patients who had undergone the atriopulmonary connection (Circulation. 2004;109:2319-25; J Thorac Cardiovasc Surg. 1998;115:499-505).
Overall, 195 patients in the study developed arrhythmia, with 162 having tachyarrhythmia, 74 having bradyarrhythmia and 41 having both. “At 20 years, freedom from any arrhythmia, tachyarrhythmia, and bradyarrhythmia was 66%, 69%, and 85%, respectively,” the researchers said.
The following outcomes occurred after the first onset of arrhythmia – tachyarrhythmia in 153 patients and bradyarrhythmia in 42: Thirty-three died; 12 had heart transplants, 30 had a Fontan correction to an extracardiac conduit, three had a Fontan takedown, 12 developed enteropathy, and 25 developed New York Heart Association class III or IV symptoms. Eighty-four patients reached the composite endpoint of Fontan failure.
After they developed arrhythmias, most patients in all three Fontan procedure groups remained free from Fontan failure at 10 years: 67% in the extracardiac conduit group; 54% in the lateral tunnel group; and 51% in the atriopulmonary group.
Medical management of up to four medications was the preferred initial treatment for those with tachyarrhythmias (86%); 101 patients had a single episode of tachyarrhythmia at follow-up intervals of four to 13 years (7.6 year median). “Those who experienced a single versus multiple episodes of tachyarrhythmia showed comparable freedom from Fontan failure at 15 years,” noted Dr. Carins and his coauthors – with rates of 34% and 33%, respectively. Of the 74 patients with bradyarrhythmias, 66 received pacemakers.
“Survival after the onset of an arrhythmia was surprisingly good with 67% and 84% of patients alive at 10 years after the onset of a tachyarrhythmia and bradyarrhythmia, respectively,” the study authors said. “There was no association between occurrence of arrhythmia and survival.”
About 40% of the patients with a tachyarrhythmia or bradyarrhythmia in the study had reduced ventricular function at 10 years after onset, the researchers wrote. “Although the assessment of ventricular function in this study was clearly subjective, we nonetheless believe that these findings suggest that the onset of an arrhythmia is associated with a progressive deterioration in cardiac function,”they noted.
Coauthor Andrew Bullock, MBBS, disclosed receiving consulting fees from Actelion. Dr. Cairns and other coauthors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: The development of arrhythmia is associated with a heightened risk of failure of Fontan circulation after a Fontan procedure.
Major finding: At 20 years, freedom from any arrhythmia was 66%, and after the onset of any arrhythmia freedom from Fontan failure was 55%.
Data source: 1,034 patients who had undergone a Fontan procedure from 1975 to 2014 as recorded in the Australian and New Zealand Fontan Registry.
Disclosures: Coauthor Andrew Bullock, MBBS, reported receiving consulting fees from Actelion. All other others have no financial relationships to disclose.
Tinea Capitis Caused by Trichophyton rubrum Mimicking Favus
In 1909, Sabouraud1 published a report delineating the clinical subsets of a chronic fungal infection of the scalp known as favus. The rarest subset was termed favus papyroide and consisted of a thin, dry, gray, parchmentlike crust up to 5 cm in diameter. Hair shafts were described as piercing the crust, with the underlying skin exhibiting erythema, moisture, and erosions. Children were reported to be affected more often than adults.1 Subsequent descriptions of patients with similar presentations have not appeared in the medical literature. In this case, an elderly woman with tinea capitis (TC) due to Trichophyton rubrum exhibited features of favus papyroide.
Case Report
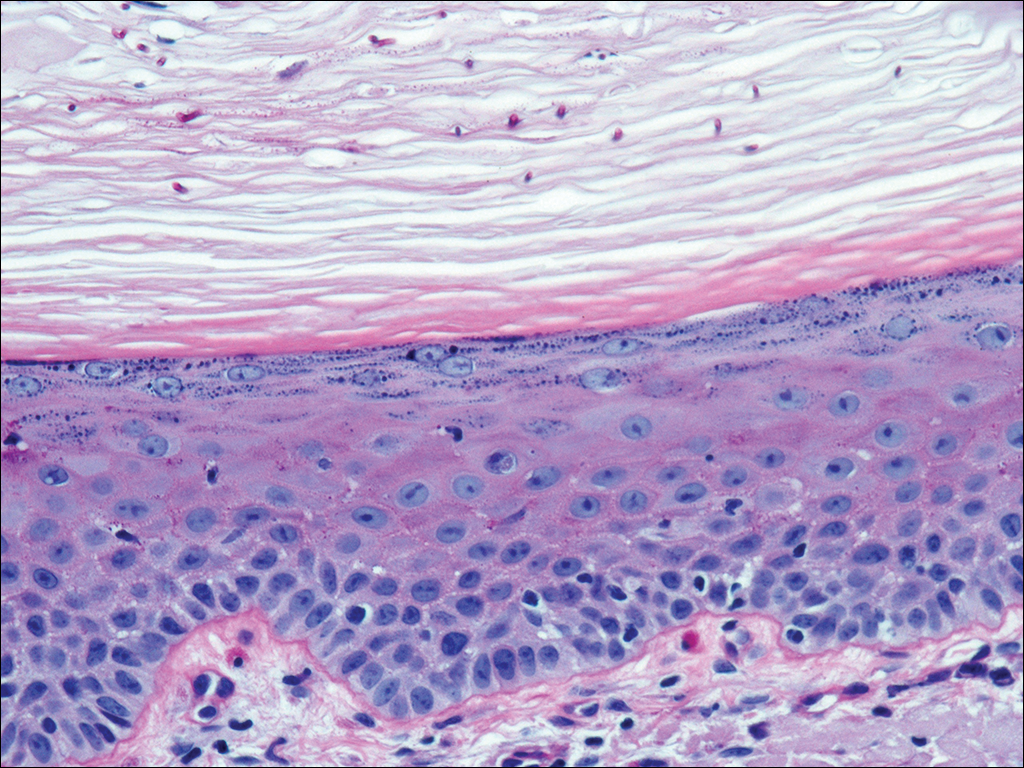
An 87-year-old woman with a long history of actinic keratoses and nonmelanoma skin cancers presented to our dermatology clinic with numerous growths on the head, neck, and arms. The patient resided in a nursing home and had a history of hypertension, osteoarthritis, and mild to moderate dementia. Physical examination revealed a frail elderly woman in a wheelchair. Numerous actinic keratoses were noted on the arms and face. Examination of the scalp revealed a large, white-gray, palm-sized plaque on the crown (Figure 1) with 2 yellow, quarter-sized, hyperkeratotic nodules on the left temple and left parietal scalp. The differential diagnosis for the nodules on the temple and scalp included squamous cell carcinoma and hyperkeratotic actinic keratosis, and both lesions were biopsied. Histologically, they demonstrated pronounced hyperkeratosis and parakeratosis with numerous infiltrating neutrophils. The stratum malpighii exhibited focal atypia consistent with an actinic keratosis with areas of spongiosis and pustular folliculitis but no evidence of an invasive cutaneous malignancy. Periodic acid–Schiff stains were performed on both specimens and revealed numerous fungal hyphae within the stratum corneum (Figure 2) as well as evidence of a fungal folliculitis.

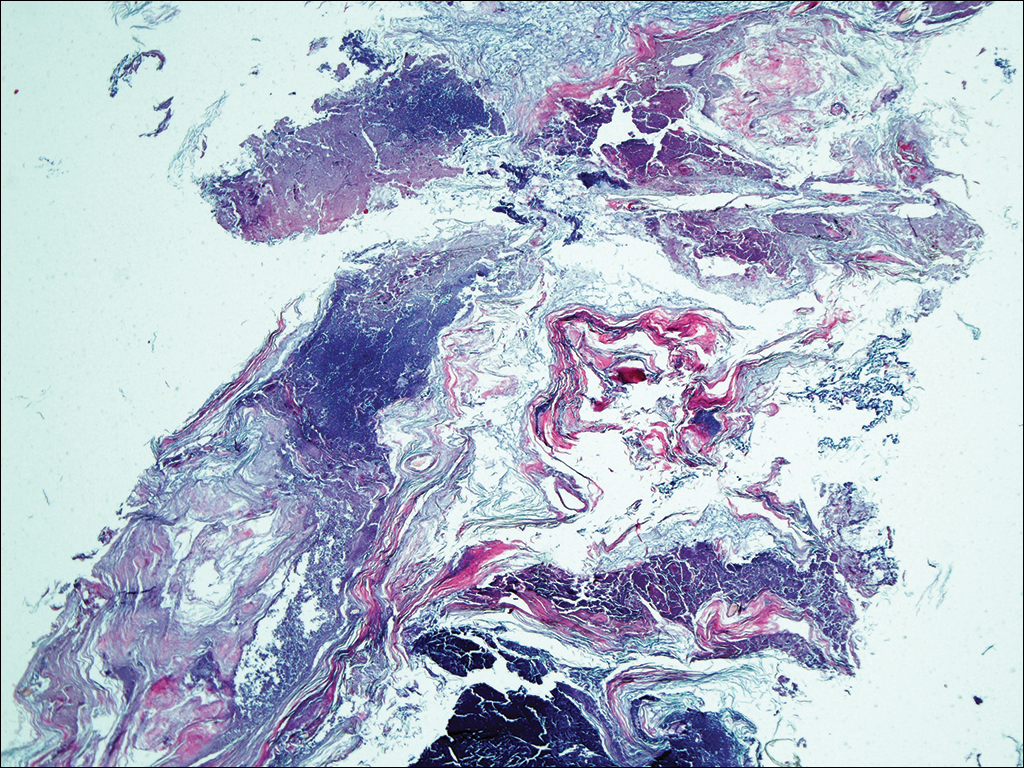
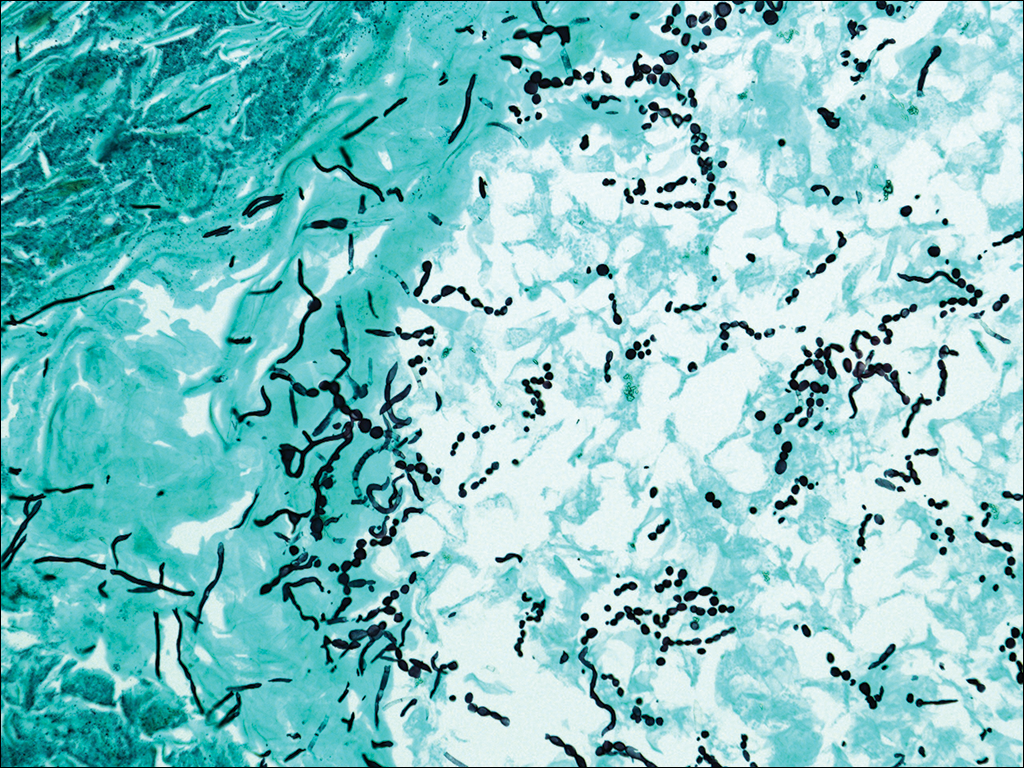
At a follow-up visit 2 weeks later, a portion of the hyperkeratotic material on the crown of the scalp was lifted free from the skin surface, removed with scissors, and submitted for histologic analysis and culture. The underlying skin exhibited substantial erythema and diffuse alopecia. The specimen consisted entirely of masses of hyperkeratotic and parakeratotic stratum corneum with numerous infiltrating neutrophils, cellular debris, and focal secondary bacterial colonization (Figure 3). Fungal hyphae and spores were readily demonstrated on Gomori methenamine-silver stain (Figure 4). A fungal culture from this material failed to demonstrate growth at 28 days. The organism was molecularly identified as T rubrum using the Sanger sequencing assay. The patient was treated with fluconazole 150 mg once daily for 3 weeks with eventual resolution of the plaque. The patient died approximately 3 months later (unrelated to her scalp infection).
Comment
Favus, or tinea favosa, is a chronic inflammatory dermatophyte infection of the scalp, less commonly involving the skin and nails.2 The classic lesion is termed a scutulum or godet consisting of concave, cup-shaped, yellow crusts typically pierced by a single hair shaft.1 With an increase in size, the scutula may become confluent. Alopecia commonly results and infected patients may exude a “cheesy” or “mousy” odor from the lesions.3 Sabouraud1 delineated 3 clinical presentations of favus: (1) favus pityroide, the most common type consisting of a seborrheic dermatitis–like picture and scutula; (2) favus impetigoide, exhibiting honey-colored crusts reminiscent of impetigo but without appreciable scutula; and (3) favus papyroide, the rarest variant, demonstrating a dry, gray, parchmentlike crust pierced by hair shafts overlying an eroded erythematous scalp.
Favus usually is acquired in childhood or adolescence and often persists into adulthood.3 It is transmitted directly by hairs, infected keratinocytes, and fomites. Child-to-child transmission is much less common than other forms of TC.4 The responsible organism is almost always Trichophyton schoenleinii, with rare cases of Trichophyton violaceum, Trichophyton verrucosum, Trichophyton mentagrophytes var quinckeanum, Microsporum canis, and Microsporum gypseum having been reported.2,5,6 This anthropophilic dermatophyte infects only humans, is capable of surviving in the same dwelling space for generations, and is believed to require prolonged exposure for transmission. Trichophyton schoenleinii was the predominant infectious cause of TC in eastern Europe in the 19th and early 20th centuries, but its incidence has dramatically declined in the last 50 years.7 A survey conducted in 1997 and published in 2001 of TC that was culture-positive for T schoenleinii in 19 European countries found only 3 cases among 3671 isolates (0.08%).8 Between 1980 and 2005, no cases were reported in the British Isles.9 Currently, favus generally is found in impoverished geographic regions with poor hygiene, malnutrition, and limited access to health care; however, endemic foci in Kentucky, Quebec, and Montreal have been reported in North America.10 Although favus rarely resolves spontaneously, T schoenleinii was eradicated in most of the world with the introduction of griseofulvin in 1958.7 Terbinafine and itraconazole are currently the drugs of choice for therapy.10
Tinea capitis is the most common fungal infection in children, with 1 in 20 US children displaying evidence of overt infection.11 Infection in adults is rare and most affected patients typically display serious illnesses with concomitant immune compromise.12 Only 3% to 5% of cases arise in patients older than 20 years.13 Adult hair appears to be relatively resistant to dermatophyte infection, probably from the fungistatic properties of long-chain fatty acids found in sebum.13 Tinea capitis in adults usually occurs in postmenopausal women, presumably from involution of sebaceous glands associated with declining estrogen levels. Patients typically exhibit erythematous scaly patches with central clearing, alopecia, varying degrees of inflammation, and few pustules, though exudative and heavily inflammatory lesions also have been described.14
In the current case, TC was not raised in the differential diagnosis. Regardless, given that scaly red patches and papules of the scalp may represent a dermatophyte infection in this patient population, clinicians are encouraged to consider this possibility. Transmission is by direct human-to-human contact and contact with objects containing fomites including brushes, combs, bedding, clothing, toys, furniture, and telephones.15 It is frequently spread among family members and classmates.16
Prior to World War II, most cases of TC in the United States were due to M canis, with Microsporum audouinii becoming more prevalent until the 1960s and 1970s when Trichophyton tonsurans began surging in incidence.12,17 Currently, the latter organism is responsible for more than 95% of TC cases in the United States.18Microsporum canis is the main causative species in Europe but varies widely by country. In the Middle East and Africa, T violaceum is responsible for many infections.
Trichophyton rubrum–associated TC appears to be a rare occurrence. A global study in 1995 noted that less than 1% of TC cases were due to T rubrum infection, most having been described in emerging nations.12 A meta-analysis of 9 studies from developed countries found only 9 of 10,145 cases of TC with a culture positive for T rubrum.14 In adults, infected patients typically exhibit either evidence of a concomitant fungal infection of the skin and/or nails or health conditions with impaired immunity, whereas in children, interfamilial spread appears more common.11
- Sabouraud R. Les favus atypiques, clinique. Paris. 1909;4:296-299.
- Olkit M. Favus of the scalp: an overview and update. Mycopathologia. 2010;170:143-154.
- Elewski BE. Tinea capitis: a current perspective. J Am Acad Dermatol. 2000;42:1-20.
- Aly R, Hay RJ, del Palacio A, et al. Epidemiology of tinea capitis. Med Mycol. 2000;38(suppl 1):183-188.
- Joly J, Delage G, Auger P, et al. Favus: twenty indigenous cases in the province of Quebec. Arch Dermatol. 1978;114:1647-1648.
- Garcia-Sanchez MS, Pereira M, Pereira MM, et al. Favus due to Trichophyton mentagrophytes var. quinckeanum. Dermatology. 1997;194:177-179.
- Seebacher C, Bouchara JP, Mignon B. Updates on the epidemiology of dermatophyte infections. Mycopathologia. 2008;166:335-352.
- Hay RJ, Robles W, Midgley MK, et al. Tinea capitis in Europe: new perspective on an old problem. J Eur Acad Dermatol Venereol. 2001;15:229-233.
- Borman AM, Campbell CK, Fraser M, et al. Analysis of the dermatophyte species isolated in the British Isles between 1980 and 2005 and review of worldwide dermatophyte trends over the last three decades. Med Mycol. 2007;45:131-141.
- Rippon JW. Dermatophytosis and dermatomycosis. In: Rippon JW. Medical Mycology: The Pathogenic Fungi and the Pathogenic Actinomycetes. 3rd ed. Philadelphia, PA: WB Saunders; 1988:197-199.
- Abdel-Rahman SM, Penny J, Alander SW. Trichophyton rubrum tinea capitis in a young child. Ped Dermatol. 2004;21:63-65.
- Schwinn A, Ebert J, Brocker EB. Frequency of Trichophyton rubrum in tinea capitis. Mycoses. 1995;38:1-7.
- Ziemer A, Kohl K, Schroder G. Trichophyton rubrum induced inflammatory tinea capitis in a 63-year-old man. Mycoses. 2005;48:76-79.
- Anstey A, Lucke TW, Philpot C. Tinea capitis caused by Trichophyton rubrum. Br J Dermatol. 1996;135:113-115.
- Schwinn A, Ebert J, Muller I, et al. Trichophyton rubrum as the causative agent of tinea capitis in three children. Mycoses. 1995;38:9-11.
- Chang SE, Kang SK, Choi JH, et al. Tinea capitis due to Trichophyton rubrum in a neonate. Ped Dermatol. 2002;19:356-358.
- Stiller MJ, Rosenthal SA, Weinstein AS. Tinea capitis caused by Trichophyton rubrum in a 67-year-old woman with systemic lupus erythematosus. J Am Acad Dermatol. 1993;29:257-258.
- Foster KW, Ghannoum MA, Elewski BE. Epidemiologic surveillance of cutaneous fungal infection in the United States from 1999 to 2002. J Am Acad Dermatol. 2004;50:748-752.
In 1909, Sabouraud1 published a report delineating the clinical subsets of a chronic fungal infection of the scalp known as favus. The rarest subset was termed favus papyroide and consisted of a thin, dry, gray, parchmentlike crust up to 5 cm in diameter. Hair shafts were described as piercing the crust, with the underlying skin exhibiting erythema, moisture, and erosions. Children were reported to be affected more often than adults.1 Subsequent descriptions of patients with similar presentations have not appeared in the medical literature. In this case, an elderly woman with tinea capitis (TC) due to Trichophyton rubrum exhibited features of favus papyroide.
Case Report
An 87-year-old woman with a long history of actinic keratoses and nonmelanoma skin cancers presented to our dermatology clinic with numerous growths on the head, neck, and arms. The patient resided in a nursing home and had a history of hypertension, osteoarthritis, and mild to moderate dementia. Physical examination revealed a frail elderly woman in a wheelchair. Numerous actinic keratoses were noted on the arms and face. Examination of the scalp revealed a large, white-gray, palm-sized plaque on the crown (Figure 1) with 2 yellow, quarter-sized, hyperkeratotic nodules on the left temple and left parietal scalp. The differential diagnosis for the nodules on the temple and scalp included squamous cell carcinoma and hyperkeratotic actinic keratosis, and both lesions were biopsied. Histologically, they demonstrated pronounced hyperkeratosis and parakeratosis with numerous infiltrating neutrophils. The stratum malpighii exhibited focal atypia consistent with an actinic keratosis with areas of spongiosis and pustular folliculitis but no evidence of an invasive cutaneous malignancy. Periodic acid–Schiff stains were performed on both specimens and revealed numerous fungal hyphae within the stratum corneum (Figure 2) as well as evidence of a fungal folliculitis.
At a follow-up visit 2 weeks later, a portion of the hyperkeratotic material on the crown of the scalp was lifted free from the skin surface, removed with scissors, and submitted for histologic analysis and culture. The underlying skin exhibited substantial erythema and diffuse alopecia. The specimen consisted entirely of masses of hyperkeratotic and parakeratotic stratum corneum with numerous infiltrating neutrophils, cellular debris, and focal secondary bacterial colonization (Figure 3). Fungal hyphae and spores were readily demonstrated on Gomori methenamine-silver stain (Figure 4). A fungal culture from this material failed to demonstrate growth at 28 days. The organism was molecularly identified as T rubrum using the Sanger sequencing assay. The patient was treated with fluconazole 150 mg once daily for 3 weeks with eventual resolution of the plaque. The patient died approximately 3 months later (unrelated to her scalp infection).
Comment
Favus, or tinea favosa, is a chronic inflammatory dermatophyte infection of the scalp, less commonly involving the skin and nails.2 The classic lesion is termed a scutulum or godet consisting of concave, cup-shaped, yellow crusts typically pierced by a single hair shaft.1 With an increase in size, the scutula may become confluent. Alopecia commonly results and infected patients may exude a “cheesy” or “mousy” odor from the lesions.3 Sabouraud1 delineated 3 clinical presentations of favus: (1) favus pityroide, the most common type consisting of a seborrheic dermatitis–like picture and scutula; (2) favus impetigoide, exhibiting honey-colored crusts reminiscent of impetigo but without appreciable scutula; and (3) favus papyroide, the rarest variant, demonstrating a dry, gray, parchmentlike crust pierced by hair shafts overlying an eroded erythematous scalp.
Favus usually is acquired in childhood or adolescence and often persists into adulthood.3 It is transmitted directly by hairs, infected keratinocytes, and fomites. Child-to-child transmission is much less common than other forms of TC.4 The responsible organism is almost always Trichophyton schoenleinii, with rare cases of Trichophyton violaceum, Trichophyton verrucosum, Trichophyton mentagrophytes var quinckeanum, Microsporum canis, and Microsporum gypseum having been reported.2,5,6 This anthropophilic dermatophyte infects only humans, is capable of surviving in the same dwelling space for generations, and is believed to require prolonged exposure for transmission. Trichophyton schoenleinii was the predominant infectious cause of TC in eastern Europe in the 19th and early 20th centuries, but its incidence has dramatically declined in the last 50 years.7 A survey conducted in 1997 and published in 2001 of TC that was culture-positive for T schoenleinii in 19 European countries found only 3 cases among 3671 isolates (0.08%).8 Between 1980 and 2005, no cases were reported in the British Isles.9 Currently, favus generally is found in impoverished geographic regions with poor hygiene, malnutrition, and limited access to health care; however, endemic foci in Kentucky, Quebec, and Montreal have been reported in North America.10 Although favus rarely resolves spontaneously, T schoenleinii was eradicated in most of the world with the introduction of griseofulvin in 1958.7 Terbinafine and itraconazole are currently the drugs of choice for therapy.10
Tinea capitis is the most common fungal infection in children, with 1 in 20 US children displaying evidence of overt infection.11 Infection in adults is rare and most affected patients typically display serious illnesses with concomitant immune compromise.12 Only 3% to 5% of cases arise in patients older than 20 years.13 Adult hair appears to be relatively resistant to dermatophyte infection, probably from the fungistatic properties of long-chain fatty acids found in sebum.13 Tinea capitis in adults usually occurs in postmenopausal women, presumably from involution of sebaceous glands associated with declining estrogen levels. Patients typically exhibit erythematous scaly patches with central clearing, alopecia, varying degrees of inflammation, and few pustules, though exudative and heavily inflammatory lesions also have been described.14
In the current case, TC was not raised in the differential diagnosis. Regardless, given that scaly red patches and papules of the scalp may represent a dermatophyte infection in this patient population, clinicians are encouraged to consider this possibility. Transmission is by direct human-to-human contact and contact with objects containing fomites including brushes, combs, bedding, clothing, toys, furniture, and telephones.15 It is frequently spread among family members and classmates.16
Prior to World War II, most cases of TC in the United States were due to M canis, with Microsporum audouinii becoming more prevalent until the 1960s and 1970s when Trichophyton tonsurans began surging in incidence.12,17 Currently, the latter organism is responsible for more than 95% of TC cases in the United States.18Microsporum canis is the main causative species in Europe but varies widely by country. In the Middle East and Africa, T violaceum is responsible for many infections.
Trichophyton rubrum–associated TC appears to be a rare occurrence. A global study in 1995 noted that less than 1% of TC cases were due to T rubrum infection, most having been described in emerging nations.12 A meta-analysis of 9 studies from developed countries found only 9 of 10,145 cases of TC with a culture positive for T rubrum.14 In adults, infected patients typically exhibit either evidence of a concomitant fungal infection of the skin and/or nails or health conditions with impaired immunity, whereas in children, interfamilial spread appears more common.11
In 1909, Sabouraud1 published a report delineating the clinical subsets of a chronic fungal infection of the scalp known as favus. The rarest subset was termed favus papyroide and consisted of a thin, dry, gray, parchmentlike crust up to 5 cm in diameter. Hair shafts were described as piercing the crust, with the underlying skin exhibiting erythema, moisture, and erosions. Children were reported to be affected more often than adults.1 Subsequent descriptions of patients with similar presentations have not appeared in the medical literature. In this case, an elderly woman with tinea capitis (TC) due to Trichophyton rubrum exhibited features of favus papyroide.
Case Report
An 87-year-old woman with a long history of actinic keratoses and nonmelanoma skin cancers presented to our dermatology clinic with numerous growths on the head, neck, and arms. The patient resided in a nursing home and had a history of hypertension, osteoarthritis, and mild to moderate dementia. Physical examination revealed a frail elderly woman in a wheelchair. Numerous actinic keratoses were noted on the arms and face. Examination of the scalp revealed a large, white-gray, palm-sized plaque on the crown (Figure 1) with 2 yellow, quarter-sized, hyperkeratotic nodules on the left temple and left parietal scalp. The differential diagnosis for the nodules on the temple and scalp included squamous cell carcinoma and hyperkeratotic actinic keratosis, and both lesions were biopsied. Histologically, they demonstrated pronounced hyperkeratosis and parakeratosis with numerous infiltrating neutrophils. The stratum malpighii exhibited focal atypia consistent with an actinic keratosis with areas of spongiosis and pustular folliculitis but no evidence of an invasive cutaneous malignancy. Periodic acid–Schiff stains were performed on both specimens and revealed numerous fungal hyphae within the stratum corneum (Figure 2) as well as evidence of a fungal folliculitis.
At a follow-up visit 2 weeks later, a portion of the hyperkeratotic material on the crown of the scalp was lifted free from the skin surface, removed with scissors, and submitted for histologic analysis and culture. The underlying skin exhibited substantial erythema and diffuse alopecia. The specimen consisted entirely of masses of hyperkeratotic and parakeratotic stratum corneum with numerous infiltrating neutrophils, cellular debris, and focal secondary bacterial colonization (Figure 3). Fungal hyphae and spores were readily demonstrated on Gomori methenamine-silver stain (Figure 4). A fungal culture from this material failed to demonstrate growth at 28 days. The organism was molecularly identified as T rubrum using the Sanger sequencing assay. The patient was treated with fluconazole 150 mg once daily for 3 weeks with eventual resolution of the plaque. The patient died approximately 3 months later (unrelated to her scalp infection).
Comment
Favus, or tinea favosa, is a chronic inflammatory dermatophyte infection of the scalp, less commonly involving the skin and nails.2 The classic lesion is termed a scutulum or godet consisting of concave, cup-shaped, yellow crusts typically pierced by a single hair shaft.1 With an increase in size, the scutula may become confluent. Alopecia commonly results and infected patients may exude a “cheesy” or “mousy” odor from the lesions.3 Sabouraud1 delineated 3 clinical presentations of favus: (1) favus pityroide, the most common type consisting of a seborrheic dermatitis–like picture and scutula; (2) favus impetigoide, exhibiting honey-colored crusts reminiscent of impetigo but without appreciable scutula; and (3) favus papyroide, the rarest variant, demonstrating a dry, gray, parchmentlike crust pierced by hair shafts overlying an eroded erythematous scalp.
Favus usually is acquired in childhood or adolescence and often persists into adulthood.3 It is transmitted directly by hairs, infected keratinocytes, and fomites. Child-to-child transmission is much less common than other forms of TC.4 The responsible organism is almost always Trichophyton schoenleinii, with rare cases of Trichophyton violaceum, Trichophyton verrucosum, Trichophyton mentagrophytes var quinckeanum, Microsporum canis, and Microsporum gypseum having been reported.2,5,6 This anthropophilic dermatophyte infects only humans, is capable of surviving in the same dwelling space for generations, and is believed to require prolonged exposure for transmission. Trichophyton schoenleinii was the predominant infectious cause of TC in eastern Europe in the 19th and early 20th centuries, but its incidence has dramatically declined in the last 50 years.7 A survey conducted in 1997 and published in 2001 of TC that was culture-positive for T schoenleinii in 19 European countries found only 3 cases among 3671 isolates (0.08%).8 Between 1980 and 2005, no cases were reported in the British Isles.9 Currently, favus generally is found in impoverished geographic regions with poor hygiene, malnutrition, and limited access to health care; however, endemic foci in Kentucky, Quebec, and Montreal have been reported in North America.10 Although favus rarely resolves spontaneously, T schoenleinii was eradicated in most of the world with the introduction of griseofulvin in 1958.7 Terbinafine and itraconazole are currently the drugs of choice for therapy.10
Tinea capitis is the most common fungal infection in children, with 1 in 20 US children displaying evidence of overt infection.11 Infection in adults is rare and most affected patients typically display serious illnesses with concomitant immune compromise.12 Only 3% to 5% of cases arise in patients older than 20 years.13 Adult hair appears to be relatively resistant to dermatophyte infection, probably from the fungistatic properties of long-chain fatty acids found in sebum.13 Tinea capitis in adults usually occurs in postmenopausal women, presumably from involution of sebaceous glands associated with declining estrogen levels. Patients typically exhibit erythematous scaly patches with central clearing, alopecia, varying degrees of inflammation, and few pustules, though exudative and heavily inflammatory lesions also have been described.14
In the current case, TC was not raised in the differential diagnosis. Regardless, given that scaly red patches and papules of the scalp may represent a dermatophyte infection in this patient population, clinicians are encouraged to consider this possibility. Transmission is by direct human-to-human contact and contact with objects containing fomites including brushes, combs, bedding, clothing, toys, furniture, and telephones.15 It is frequently spread among family members and classmates.16
Prior to World War II, most cases of TC in the United States were due to M canis, with Microsporum audouinii becoming more prevalent until the 1960s and 1970s when Trichophyton tonsurans began surging in incidence.12,17 Currently, the latter organism is responsible for more than 95% of TC cases in the United States.18Microsporum canis is the main causative species in Europe but varies widely by country. In the Middle East and Africa, T violaceum is responsible for many infections.
Trichophyton rubrum–associated TC appears to be a rare occurrence. A global study in 1995 noted that less than 1% of TC cases were due to T rubrum infection, most having been described in emerging nations.12 A meta-analysis of 9 studies from developed countries found only 9 of 10,145 cases of TC with a culture positive for T rubrum.14 In adults, infected patients typically exhibit either evidence of a concomitant fungal infection of the skin and/or nails or health conditions with impaired immunity, whereas in children, interfamilial spread appears more common.11
- Sabouraud R. Les favus atypiques, clinique. Paris. 1909;4:296-299.
- Olkit M. Favus of the scalp: an overview and update. Mycopathologia. 2010;170:143-154.
- Elewski BE. Tinea capitis: a current perspective. J Am Acad Dermatol. 2000;42:1-20.
- Aly R, Hay RJ, del Palacio A, et al. Epidemiology of tinea capitis. Med Mycol. 2000;38(suppl 1):183-188.
- Joly J, Delage G, Auger P, et al. Favus: twenty indigenous cases in the province of Quebec. Arch Dermatol. 1978;114:1647-1648.
- Garcia-Sanchez MS, Pereira M, Pereira MM, et al. Favus due to Trichophyton mentagrophytes var. quinckeanum. Dermatology. 1997;194:177-179.
- Seebacher C, Bouchara JP, Mignon B. Updates on the epidemiology of dermatophyte infections. Mycopathologia. 2008;166:335-352.
- Hay RJ, Robles W, Midgley MK, et al. Tinea capitis in Europe: new perspective on an old problem. J Eur Acad Dermatol Venereol. 2001;15:229-233.
- Borman AM, Campbell CK, Fraser M, et al. Analysis of the dermatophyte species isolated in the British Isles between 1980 and 2005 and review of worldwide dermatophyte trends over the last three decades. Med Mycol. 2007;45:131-141.
- Rippon JW. Dermatophytosis and dermatomycosis. In: Rippon JW. Medical Mycology: The Pathogenic Fungi and the Pathogenic Actinomycetes. 3rd ed. Philadelphia, PA: WB Saunders; 1988:197-199.
- Abdel-Rahman SM, Penny J, Alander SW. Trichophyton rubrum tinea capitis in a young child. Ped Dermatol. 2004;21:63-65.
- Schwinn A, Ebert J, Brocker EB. Frequency of Trichophyton rubrum in tinea capitis. Mycoses. 1995;38:1-7.
- Ziemer A, Kohl K, Schroder G. Trichophyton rubrum induced inflammatory tinea capitis in a 63-year-old man. Mycoses. 2005;48:76-79.
- Anstey A, Lucke TW, Philpot C. Tinea capitis caused by Trichophyton rubrum. Br J Dermatol. 1996;135:113-115.
- Schwinn A, Ebert J, Muller I, et al. Trichophyton rubrum as the causative agent of tinea capitis in three children. Mycoses. 1995;38:9-11.
- Chang SE, Kang SK, Choi JH, et al. Tinea capitis due to Trichophyton rubrum in a neonate. Ped Dermatol. 2002;19:356-358.
- Stiller MJ, Rosenthal SA, Weinstein AS. Tinea capitis caused by Trichophyton rubrum in a 67-year-old woman with systemic lupus erythematosus. J Am Acad Dermatol. 1993;29:257-258.
- Foster KW, Ghannoum MA, Elewski BE. Epidemiologic surveillance of cutaneous fungal infection in the United States from 1999 to 2002. J Am Acad Dermatol. 2004;50:748-752.
- Sabouraud R. Les favus atypiques, clinique. Paris. 1909;4:296-299.
- Olkit M. Favus of the scalp: an overview and update. Mycopathologia. 2010;170:143-154.
- Elewski BE. Tinea capitis: a current perspective. J Am Acad Dermatol. 2000;42:1-20.
- Aly R, Hay RJ, del Palacio A, et al. Epidemiology of tinea capitis. Med Mycol. 2000;38(suppl 1):183-188.
- Joly J, Delage G, Auger P, et al. Favus: twenty indigenous cases in the province of Quebec. Arch Dermatol. 1978;114:1647-1648.
- Garcia-Sanchez MS, Pereira M, Pereira MM, et al. Favus due to Trichophyton mentagrophytes var. quinckeanum. Dermatology. 1997;194:177-179.
- Seebacher C, Bouchara JP, Mignon B. Updates on the epidemiology of dermatophyte infections. Mycopathologia. 2008;166:335-352.
- Hay RJ, Robles W, Midgley MK, et al. Tinea capitis in Europe: new perspective on an old problem. J Eur Acad Dermatol Venereol. 2001;15:229-233.
- Borman AM, Campbell CK, Fraser M, et al. Analysis of the dermatophyte species isolated in the British Isles between 1980 and 2005 and review of worldwide dermatophyte trends over the last three decades. Med Mycol. 2007;45:131-141.
- Rippon JW. Dermatophytosis and dermatomycosis. In: Rippon JW. Medical Mycology: The Pathogenic Fungi and the Pathogenic Actinomycetes. 3rd ed. Philadelphia, PA: WB Saunders; 1988:197-199.
- Abdel-Rahman SM, Penny J, Alander SW. Trichophyton rubrum tinea capitis in a young child. Ped Dermatol. 2004;21:63-65.
- Schwinn A, Ebert J, Brocker EB. Frequency of Trichophyton rubrum in tinea capitis. Mycoses. 1995;38:1-7.
- Ziemer A, Kohl K, Schroder G. Trichophyton rubrum induced inflammatory tinea capitis in a 63-year-old man. Mycoses. 2005;48:76-79.
- Anstey A, Lucke TW, Philpot C. Tinea capitis caused by Trichophyton rubrum. Br J Dermatol. 1996;135:113-115.
- Schwinn A, Ebert J, Muller I, et al. Trichophyton rubrum as the causative agent of tinea capitis in three children. Mycoses. 1995;38:9-11.
- Chang SE, Kang SK, Choi JH, et al. Tinea capitis due to Trichophyton rubrum in a neonate. Ped Dermatol. 2002;19:356-358.
- Stiller MJ, Rosenthal SA, Weinstein AS. Tinea capitis caused by Trichophyton rubrum in a 67-year-old woman with systemic lupus erythematosus. J Am Acad Dermatol. 1993;29:257-258.
- Foster KW, Ghannoum MA, Elewski BE. Epidemiologic surveillance of cutaneous fungal infection in the United States from 1999 to 2002. J Am Acad Dermatol. 2004;50:748-752.
Practice Points
- Although favus is uncommonly seen in developed countries, it still exists and can mimick other conditions, notably cutaneous malignancies.
- Favus may affect the skin and nails in addition to the hair.
- The lesions of favus may persist for many years.
Differentiating ADHD and bipolar disorder

FDA sunscreen guidance calls for maximal use trials
The Food and Drug Administration has released final industry guidance for nonclinical sunscreen manufacturers, but comments from a top agency official bring into question the pace of progress for getting the products to market.
A 2014 law, the Sunscreen Innovation Act, was intended to speed approval of new sunscreen active ingredients; one impetus for its passage was that no new sunscreen active ingredient has been approved since the late 1990s.
During that time, eight applications for new sunscreen active ingredients languished at the agency, even though many, such as UV filters bisoctrizole and bemotrizinol, are widely available across Europe and elsewhere. The law gave the FDA 1 year to review the backlog of applications for the ingredients and gave the agency 18 months to act on any sunscreen ingredient application submitted after the law went into effect.
“The FDA has issued proposed sunscreen orders identifying data we believe is necessary for the agency to make a positive [generally regarded as safe and effective] determination on those within the [law’s] required time frame, but has yet to receive the additional data we requested” from sunscreen ingredient manufacturers, Theresa M. Michele, MD, director of the FDA’s Division of Nonprescription Drug Products, wrote in a blog post.
To help, the agency has just released the final two of four industry guidance documents. The first addresses the agency’s current thinking on what constitutes a generally safe and effective sunscreen ingredient, while the second outlines data submission procedures. Previous guidance addressed procedural matters.
Specifically, the FDA wants to see evidence that these ingredients aren’t toxic over time, something that requires clinical trials in humans.

“The FDA and industry are essentially at a standstill because industry feels that there is a significant amount of resources they have to [invest] in order to comply with these testing regulations,” Dr. Lim said in an interview. “Industry is not willing to do it.”
In Europe and many other countries, sunscreens are considered cosmetics. The FDA considers them over-the-counter drugs and holds them to a higher approval standard. Although the 2014 law allows the FDA to review 5 years or more of marketing history for ingredients that are in use outside the United States, current approval standards require human absorption data derived from maximal usage trials to determine the risk of chronic exposure to products applied over large areas of the body, Dr. Michele said in a statement. “It is the same standard used by the FDA for all topically applied drugs, and especially for drugs that are used routinely over the course of one’s life.”
Dr. Lim said that the AAD is working as a neutral party to help both sides arrive at a compromise, and that a meeting between FDA and industry officials is scheduled for early 2017. However, he said that he thinks it is “not likely” that the FDA would ever relax its approval process to view sunscreens at the level of cosmetics as is done abroad, since that would mean different sets of standards for the same class of product. “Knowing how the FDA works, this is not going to happen,” Dr. Lim said.
“The FDA is committed to helping ensure that sunscreens are safe and effective for U.S. consumers, but we need data to move forward,” Dr. Michele wrote.
Dr. Lim disclosed that he is a consultant for Pierre Fabre and an investigator for Allergan, Estee Lauder, and Ferndale.
[email protected]
On Twitter @whitneymcknight
The Food and Drug Administration has released final industry guidance for nonclinical sunscreen manufacturers, but comments from a top agency official bring into question the pace of progress for getting the products to market.
A 2014 law, the Sunscreen Innovation Act, was intended to speed approval of new sunscreen active ingredients; one impetus for its passage was that no new sunscreen active ingredient has been approved since the late 1990s.
During that time, eight applications for new sunscreen active ingredients languished at the agency, even though many, such as UV filters bisoctrizole and bemotrizinol, are widely available across Europe and elsewhere. The law gave the FDA 1 year to review the backlog of applications for the ingredients and gave the agency 18 months to act on any sunscreen ingredient application submitted after the law went into effect.
“The FDA has issued proposed sunscreen orders identifying data we believe is necessary for the agency to make a positive [generally regarded as safe and effective] determination on those within the [law’s] required time frame, but has yet to receive the additional data we requested” from sunscreen ingredient manufacturers, Theresa M. Michele, MD, director of the FDA’s Division of Nonprescription Drug Products, wrote in a blog post.
To help, the agency has just released the final two of four industry guidance documents. The first addresses the agency’s current thinking on what constitutes a generally safe and effective sunscreen ingredient, while the second outlines data submission procedures. Previous guidance addressed procedural matters.
Specifically, the FDA wants to see evidence that these ingredients aren’t toxic over time, something that requires clinical trials in humans.
“The FDA and industry are essentially at a standstill because industry feels that there is a significant amount of resources they have to [invest] in order to comply with these testing regulations,” Dr. Lim said in an interview. “Industry is not willing to do it.”
In Europe and many other countries, sunscreens are considered cosmetics. The FDA considers them over-the-counter drugs and holds them to a higher approval standard. Although the 2014 law allows the FDA to review 5 years or more of marketing history for ingredients that are in use outside the United States, current approval standards require human absorption data derived from maximal usage trials to determine the risk of chronic exposure to products applied over large areas of the body, Dr. Michele said in a statement. “It is the same standard used by the FDA for all topically applied drugs, and especially for drugs that are used routinely over the course of one’s life.”
Dr. Lim said that the AAD is working as a neutral party to help both sides arrive at a compromise, and that a meeting between FDA and industry officials is scheduled for early 2017. However, he said that he thinks it is “not likely” that the FDA would ever relax its approval process to view sunscreens at the level of cosmetics as is done abroad, since that would mean different sets of standards for the same class of product. “Knowing how the FDA works, this is not going to happen,” Dr. Lim said.
“The FDA is committed to helping ensure that sunscreens are safe and effective for U.S. consumers, but we need data to move forward,” Dr. Michele wrote.
Dr. Lim disclosed that he is a consultant for Pierre Fabre and an investigator for Allergan, Estee Lauder, and Ferndale.
[email protected]
On Twitter @whitneymcknight
The Food and Drug Administration has released final industry guidance for nonclinical sunscreen manufacturers, but comments from a top agency official bring into question the pace of progress for getting the products to market.
A 2014 law, the Sunscreen Innovation Act, was intended to speed approval of new sunscreen active ingredients; one impetus for its passage was that no new sunscreen active ingredient has been approved since the late 1990s.
During that time, eight applications for new sunscreen active ingredients languished at the agency, even though many, such as UV filters bisoctrizole and bemotrizinol, are widely available across Europe and elsewhere. The law gave the FDA 1 year to review the backlog of applications for the ingredients and gave the agency 18 months to act on any sunscreen ingredient application submitted after the law went into effect.
“The FDA has issued proposed sunscreen orders identifying data we believe is necessary for the agency to make a positive [generally regarded as safe and effective] determination on those within the [law’s] required time frame, but has yet to receive the additional data we requested” from sunscreen ingredient manufacturers, Theresa M. Michele, MD, director of the FDA’s Division of Nonprescription Drug Products, wrote in a blog post.
To help, the agency has just released the final two of four industry guidance documents. The first addresses the agency’s current thinking on what constitutes a generally safe and effective sunscreen ingredient, while the second outlines data submission procedures. Previous guidance addressed procedural matters.
Specifically, the FDA wants to see evidence that these ingredients aren’t toxic over time, something that requires clinical trials in humans.
“The FDA and industry are essentially at a standstill because industry feels that there is a significant amount of resources they have to [invest] in order to comply with these testing regulations,” Dr. Lim said in an interview. “Industry is not willing to do it.”
In Europe and many other countries, sunscreens are considered cosmetics. The FDA considers them over-the-counter drugs and holds them to a higher approval standard. Although the 2014 law allows the FDA to review 5 years or more of marketing history for ingredients that are in use outside the United States, current approval standards require human absorption data derived from maximal usage trials to determine the risk of chronic exposure to products applied over large areas of the body, Dr. Michele said in a statement. “It is the same standard used by the FDA for all topically applied drugs, and especially for drugs that are used routinely over the course of one’s life.”
Dr. Lim said that the AAD is working as a neutral party to help both sides arrive at a compromise, and that a meeting between FDA and industry officials is scheduled for early 2017. However, he said that he thinks it is “not likely” that the FDA would ever relax its approval process to view sunscreens at the level of cosmetics as is done abroad, since that would mean different sets of standards for the same class of product. “Knowing how the FDA works, this is not going to happen,” Dr. Lim said.
“The FDA is committed to helping ensure that sunscreens are safe and effective for U.S. consumers, but we need data to move forward,” Dr. Michele wrote.
Dr. Lim disclosed that he is a consultant for Pierre Fabre and an investigator for Allergan, Estee Lauder, and Ferndale.
[email protected]
On Twitter @whitneymcknight
Proton Pump Inhibitor-Associated Hypomagnesemia: A Retrospective Case-Control Study
In the U.S., proton pump inhibitors (PPIs) are one of the best-selling drug classes—more than $9 billion were spent on PPIs in 2012.1 These medications, available both by prescription and over-the-counter (OTC), are used to treat a variety of gastrointestinal conditions, including heartburn, gastroesophageal reflux disease, and peptic ulcer disease.1
Proton pump inhibitors are generally recognized as safe and effective. In 2011, however, the FDA reviewed Adverse Event Reporting System (AERS) reports, medical literature, and periodic safety updates and issued a safety communication outlining the risk for hypomagnesemia with prolonged PPI use.2 The FDA focused on 53 cases: 30 AERS cases, 15 in the literature, and 8 reported both through AERS and in the literature. The majority involved PPI use that continued for 1 year or longer, but in some cases hypomagnesemia developed after only 3 months. Labeling for prescription PPIs was updated with information about the hypomagnesemia risk, but labeling for the OTC drugs was not affected, as the FDA stated there is little risk with OTC use, and the label already indicated that use should be limited to 14 days at a time and up to 3 courses within 1 year.
Magnesium is an important intracellular cation that plays a role in multiple cellular activities. Low levels of magnesium can lead to a wide variety of adverse events (AEs), including vomiting, diarrhea, cramps, convulsions, bradycardia, and even death.3,4 The mechanism of PPI-associated hypomagnesemia is yet to be established but could be related to, as has been proposed, altered intestinal absorption of magnesium with long-term PPI use.4
Results from investigations of PPI-associated hypomagnesemia have been inconclusive. In a study of PPI-associated AEs reported to the FDA, Luk and colleagues estimated that 1% of patients who experienced an AE reported hypomagnesemia and concluded that all PPIs are associated with hypomagnesemia, but the risk varies. Of the 6 PPIs that have been FDA approved, esomeprazole was associated with the lowest risk, pantoprazole with the most. Results also suggested that the risk was higher for elderly and male patients.
In another study of prior PPI use and its effects on magnesium levels among 11,490 intensive care unit admissions, Danziger and colleagues found that the association of PPI use and hypomagnesemia was limited to patients who concomitantly received a diuretic, and use of a histamine 2 receptor antagonist was not associated with hypomagnesemia.3 A third cross-sectional study of 402 adults with hypomagnesemia on hospital admission found no association between outpatient PPI regimens and hypomagnesemia.5 Other studies designed to investigate PPI-associated hypomagnesemia were limited by short-term PPI use, small samples, concurrent diseases, and confounding variables (eg, history of alcoholism).6,7
Need for Present Study
The evidence needed to establish the incidence of PPI-associated hypomagnesemia is limited. Hypomagnesemia can lead to serious AEs, as just outlined, and is a common indication for hospitalization.8 The hypomagnesemia rate is about 12% in hospitalized patients and sharply higher (60%-65%) in those who are critically ill. Proton pump inhibitor-associated hypomagnesemia is preventable, and monitoring parameters can be recommended to patients undergoing long-term therapy.
Ajumobi and colleagues found that 13,713 (23.4%) of 58,605 patients treated at a VA center over a 12-month period were receiving a PPI.9 Gawron and colleagues found that many veterans had been prescribed a PPI and were receiving high total daily doses for the treatment of gastroesophageal reflux disease.10 The majority of patients received a 90-day or longer supply and showed minimal evidence of step-down therapy or cessation of PPI therapy.
In the present study, the authors investigated the rate of PPI-associated hypomagnesemia in a veteran population at a facility where the majority of PPIs were by prescription, not OTC. The Captain James A. Lovell Federal Health Care Center (FHCC) is a combined DoD and VA facility where veterans and active military members and their dependents receive medical care and prescription drugs.
This study’s primary objective was to determine the rate of PPI-induced hypomagnesemia. The secondary objective was to identify any clinical factors (eg, PPI dose and therapy duration, concomitant use of a diuretic) that might further increase the risk of hypomagnesemia.
Methods
After the study protocol was approved by the Lovell FHCC institutional review board, the authors retrospectively compared patients with a low magnesium level (case group) with patients with a normal magnesium level (control group). In each group, the authors identified patients who underwent PPI therapy and those who did not (Figure).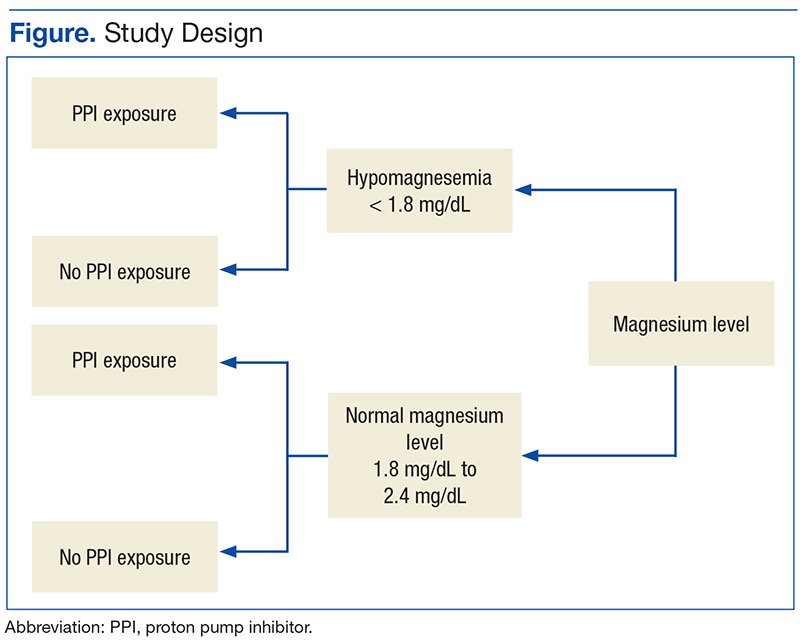
Study inclusion criteria were low magnesium level (< 1.8 mg/dL) within the past 5 years for veterans in the case group and normal magnesium level (1.8-2.4 mg/dL) within the past 5 years for veterans in the control group. Exclusion criteria were nonveterans and no prior magnesium level for a veteran.
Patients were assigned in a ratio of 1 (case group) to 4 (control group) and were added only after confirmation that multiple magnesium levels had been recorded (January 2008-January 2013).
Patients who met the inclusion criteria were enrolled in the study. Patient’s Computerized Patient Record System charts were reviewed for demographics (sex, age, race); magnesium level; active order for PPI during same period magnesium level was drawn; PPI name, dose, and therapy duration; and concomitant use of a diuretic (yes or no) and, if yes, type of diuretic.
To assess a significance criterion (α) of 0.05 and a power of 80% 1,375 patients in a 1:4 ratio (275 cases, 1,100 controls) were required in order to detect a difference in rates of hypomagnesemia between patients who received a PPI and those who did not. Primary outcome data are reported as percentages and calculated odds ratios (ORs). Significance of ORs was determined with 95% confidence intervals (CIs). Secondary outcomes were PPI dose and therapy duration and concomitant use of a diuretic. Descriptive statistics were used for secondary outcomes.
Results
Five hundred thirty charts (106 cases, 424 controls) were included and reviewed. Table 1 lists the baseline demographics. There were no statistically significant differences in age, sex, or race between the case and control groups. Mean (SD) magnesium level was 1.6 (0.15) 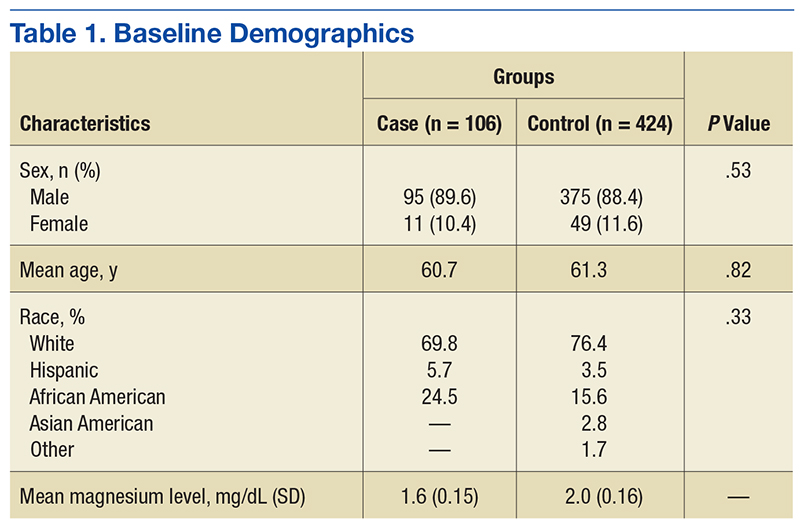
The authors assessed for other clinical factors that might concurrently or 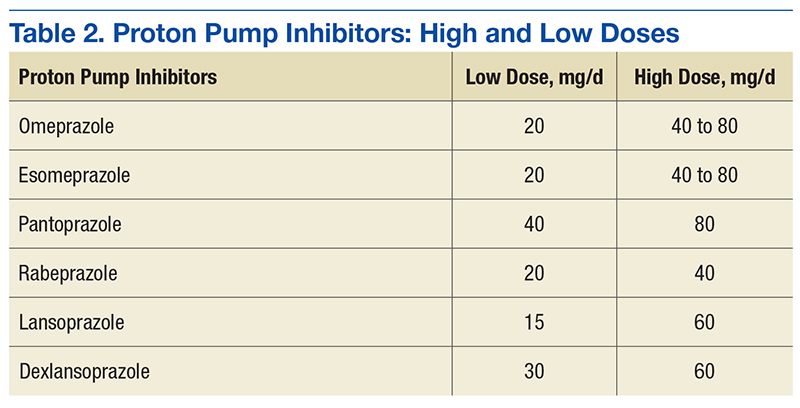
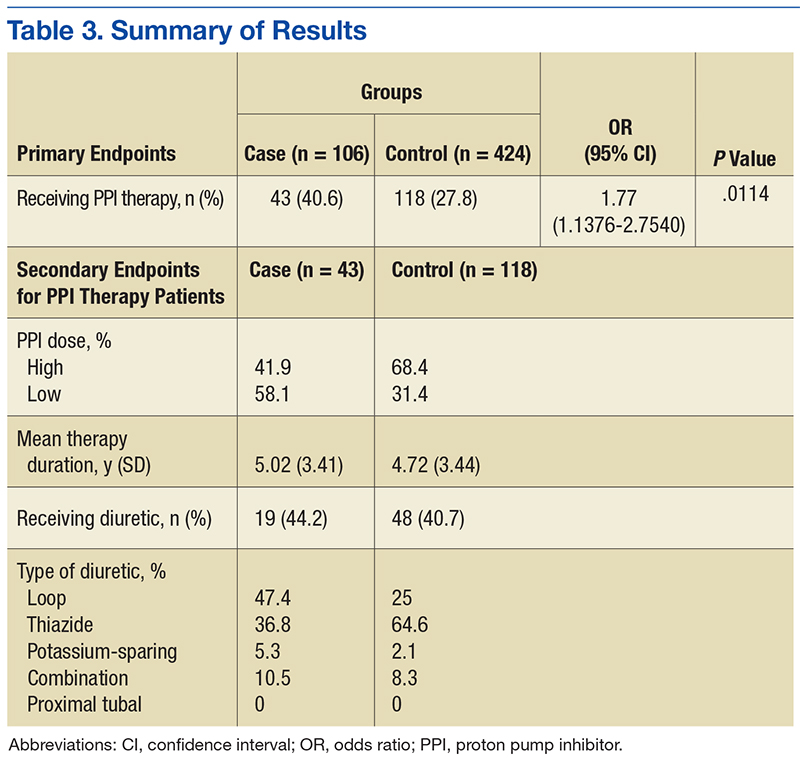
Discussion
One of the most widely prescribed classes of medications, PPIs are often regarded as safe and effective and therefore continued as long-term therapy. Results of this study showed an association of PPI use and hypomagnesemia—thereby adding to the literature. Results for the secondary objective suggest that the association does not necessarily depend on PPI dose, but, given that a statistical analysis of the difference between the case and control groups was not conducted, the statistical significance is unknown.
Although the hypomagnesemia rate remains undetermined, the results of this NNH study suggest a rate higher than previously proposed. Other investigators have estimated the rate of PPI-associated hypomagnesemia at 1%, which does not correlate well with the NNH often calculated in this study. For 2 possible reasons, the poor correlation may be attributable to underreporting of hypomagnesemia: Magnesium levels are not commonly checked with a basic metabolic panel, and many patients who are mildly hypomagnesemic remain asymptomatic.
Future research directions include determining whether the risk for hypomagnesemia is related to patient status (eg, inpatient vs outpatient) and performing statistical analyses on the secondary objective to determine the clinical significance of potential risk factors. Other research directions might involve assessing PPI discontinuation rates in a hypomagnesemic population and assessing outcomes such as hospitalizations and AEs (eg, seizure, tetany, arrhythmia).
Limitations
This study had several limitations. First was the overall design. Study results described only a potential association of PPI use and hypomagnesemia, not definitive cause and effect. Results also depended on an assumed, previously reported rate of PPI-associated hypomagnesemia and a rate of exposure to PPIs, as these data were taken into account in the overall study design. In addition, patient adherence to prescribed therapy and accuracy of medication history were assumed from the medication and dispensing history, as not all medications obtained outside the Lovell FHCC were accurately documented. There also was an external validity limitation in that older men make up the typical FHCC patient population. Last, as inherent to all studies that use objective measures, there was the potential for laboratory magnesium level reporting errors.
Conclusion
The study results identified an association of PPI use and hypomagnesemia in a VA patient population of older men. More studies need to be conducted with non-VA patient populations to further assess the incidence of PPI-associated hypomagnesemia.
1. Consumers Union. Consumer Reports Best Buy Drugs: Using the proton pump inhibitors to treat heartburn and stomach acid reflux, comparing effectiveness, safety, and price. http://www.consumer reports.org/health/resources/pdf/best-buy-drugs/PPIsUpdate-FINAL.pdf. Updated July 2013. Accessed November 4, 2016.
2. U.S. Food and Drug Administration. FDA drug safety communication: low magnesium levels can be associated with long-term use of proton pump inhibitor drugs (PPIs). http://www.fda.gov/Drugs /DrugSafety/ucm245011.htm. Updated April 7, 2016. Accessed November 4, 2016.
3. Danziger J, William JH, Scott DJ, et al. Proton-pump inhibitor use is associated with low serum magnesium concentrations. Kidney Int. 2013;83(4):692-699.
4. Luk CP, Parsons R, Lee YP, Hughes JD. Proton pump inhibitor-associated hypomagnesemia: what do FDA data tell us? Ann Pharmacother. 2013;47(6):773-780.
5. Koulouridis I, Alfayez M, Tighiouart H, et al. Out-of-hospital use of proton pump inhibitors and hypomagnesemia at hospital admission: a nested case-control study. Am J Kidney Dis. 2013;62(4):730-737.
6. Mackay JD, Bladon PT. Hypomagnesaemia due to proton-pump inhibitor therapy: a clinical case series. QJM. 2010;103(6):387-395.
7. Faulhaber GA, Ascoli BA, Lubina A, et al. Serum magnesium and proton-pump inhibitors use: a cross-sectional study. Rev Assoc Med Bras (1992). 2013;59(3):276-279.
8. Yu ASL. Causes of hypomagnesemia. UpToDate. http://www.uptodate.com/contents/causes-of-hypomagnesemia. Updated February 4, 2016. Accessed November 4, 2016.
9. Ajumobi AB, Vuong R, Ahaneku H. Analysis of nonformulary use of PPIs and excess drug cost in a Veterans Affairs population. J Manag Care Pharm. 2012;18(1):63-67.
10. Gawron AJ, Pandolfino JE, Miskevics S, Lavela SL. Proton pump inhibitor prescriptions and subsequent use in US veterans diagnosed with gastroesophageal reflux disease. J Gen Intern Med. 2013;28(7):930-937.
In the U.S., proton pump inhibitors (PPIs) are one of the best-selling drug classes—more than $9 billion were spent on PPIs in 2012.1 These medications, available both by prescription and over-the-counter (OTC), are used to treat a variety of gastrointestinal conditions, including heartburn, gastroesophageal reflux disease, and peptic ulcer disease.1
Proton pump inhibitors are generally recognized as safe and effective. In 2011, however, the FDA reviewed Adverse Event Reporting System (AERS) reports, medical literature, and periodic safety updates and issued a safety communication outlining the risk for hypomagnesemia with prolonged PPI use.2 The FDA focused on 53 cases: 30 AERS cases, 15 in the literature, and 8 reported both through AERS and in the literature. The majority involved PPI use that continued for 1 year or longer, but in some cases hypomagnesemia developed after only 3 months. Labeling for prescription PPIs was updated with information about the hypomagnesemia risk, but labeling for the OTC drugs was not affected, as the FDA stated there is little risk with OTC use, and the label already indicated that use should be limited to 14 days at a time and up to 3 courses within 1 year.
Magnesium is an important intracellular cation that plays a role in multiple cellular activities. Low levels of magnesium can lead to a wide variety of adverse events (AEs), including vomiting, diarrhea, cramps, convulsions, bradycardia, and even death.3,4 The mechanism of PPI-associated hypomagnesemia is yet to be established but could be related to, as has been proposed, altered intestinal absorption of magnesium with long-term PPI use.4
Results from investigations of PPI-associated hypomagnesemia have been inconclusive. In a study of PPI-associated AEs reported to the FDA, Luk and colleagues estimated that 1% of patients who experienced an AE reported hypomagnesemia and concluded that all PPIs are associated with hypomagnesemia, but the risk varies. Of the 6 PPIs that have been FDA approved, esomeprazole was associated with the lowest risk, pantoprazole with the most. Results also suggested that the risk was higher for elderly and male patients.
In another study of prior PPI use and its effects on magnesium levels among 11,490 intensive care unit admissions, Danziger and colleagues found that the association of PPI use and hypomagnesemia was limited to patients who concomitantly received a diuretic, and use of a histamine 2 receptor antagonist was not associated with hypomagnesemia.3 A third cross-sectional study of 402 adults with hypomagnesemia on hospital admission found no association between outpatient PPI regimens and hypomagnesemia.5 Other studies designed to investigate PPI-associated hypomagnesemia were limited by short-term PPI use, small samples, concurrent diseases, and confounding variables (eg, history of alcoholism).6,7
Need for Present Study
The evidence needed to establish the incidence of PPI-associated hypomagnesemia is limited. Hypomagnesemia can lead to serious AEs, as just outlined, and is a common indication for hospitalization.8 The hypomagnesemia rate is about 12% in hospitalized patients and sharply higher (60%-65%) in those who are critically ill. Proton pump inhibitor-associated hypomagnesemia is preventable, and monitoring parameters can be recommended to patients undergoing long-term therapy.
Ajumobi and colleagues found that 13,713 (23.4%) of 58,605 patients treated at a VA center over a 12-month period were receiving a PPI.9 Gawron and colleagues found that many veterans had been prescribed a PPI and were receiving high total daily doses for the treatment of gastroesophageal reflux disease.10 The majority of patients received a 90-day or longer supply and showed minimal evidence of step-down therapy or cessation of PPI therapy.
In the present study, the authors investigated the rate of PPI-associated hypomagnesemia in a veteran population at a facility where the majority of PPIs were by prescription, not OTC. The Captain James A. Lovell Federal Health Care Center (FHCC) is a combined DoD and VA facility where veterans and active military members and their dependents receive medical care and prescription drugs.
This study’s primary objective was to determine the rate of PPI-induced hypomagnesemia. The secondary objective was to identify any clinical factors (eg, PPI dose and therapy duration, concomitant use of a diuretic) that might further increase the risk of hypomagnesemia.
Methods
After the study protocol was approved by the Lovell FHCC institutional review board, the authors retrospectively compared patients with a low magnesium level (case group) with patients with a normal magnesium level (control group). In each group, the authors identified patients who underwent PPI therapy and those who did not (Figure).
Study inclusion criteria were low magnesium level (< 1.8 mg/dL) within the past 5 years for veterans in the case group and normal magnesium level (1.8-2.4 mg/dL) within the past 5 years for veterans in the control group. Exclusion criteria were nonveterans and no prior magnesium level for a veteran.
Patients were assigned in a ratio of 1 (case group) to 4 (control group) and were added only after confirmation that multiple magnesium levels had been recorded (January 2008-January 2013).
Patients who met the inclusion criteria were enrolled in the study. Patient’s Computerized Patient Record System charts were reviewed for demographics (sex, age, race); magnesium level; active order for PPI during same period magnesium level was drawn; PPI name, dose, and therapy duration; and concomitant use of a diuretic (yes or no) and, if yes, type of diuretic.
To assess a significance criterion (α) of 0.05 and a power of 80% 1,375 patients in a 1:4 ratio (275 cases, 1,100 controls) were required in order to detect a difference in rates of hypomagnesemia between patients who received a PPI and those who did not. Primary outcome data are reported as percentages and calculated odds ratios (ORs). Significance of ORs was determined with 95% confidence intervals (CIs). Secondary outcomes were PPI dose and therapy duration and concomitant use of a diuretic. Descriptive statistics were used for secondary outcomes.
Results
Five hundred thirty charts (106 cases, 424 controls) were included and reviewed. Table 1 lists the baseline demographics. There were no statistically significant differences in age, sex, or race between the case and control groups. Mean (SD) magnesium level was 1.6 (0.15)
The authors assessed for other clinical factors that might concurrently or
Discussion
One of the most widely prescribed classes of medications, PPIs are often regarded as safe and effective and therefore continued as long-term therapy. Results of this study showed an association of PPI use and hypomagnesemia—thereby adding to the literature. Results for the secondary objective suggest that the association does not necessarily depend on PPI dose, but, given that a statistical analysis of the difference between the case and control groups was not conducted, the statistical significance is unknown.
Although the hypomagnesemia rate remains undetermined, the results of this NNH study suggest a rate higher than previously proposed. Other investigators have estimated the rate of PPI-associated hypomagnesemia at 1%, which does not correlate well with the NNH often calculated in this study. For 2 possible reasons, the poor correlation may be attributable to underreporting of hypomagnesemia: Magnesium levels are not commonly checked with a basic metabolic panel, and many patients who are mildly hypomagnesemic remain asymptomatic.
Future research directions include determining whether the risk for hypomagnesemia is related to patient status (eg, inpatient vs outpatient) and performing statistical analyses on the secondary objective to determine the clinical significance of potential risk factors. Other research directions might involve assessing PPI discontinuation rates in a hypomagnesemic population and assessing outcomes such as hospitalizations and AEs (eg, seizure, tetany, arrhythmia).
Limitations
This study had several limitations. First was the overall design. Study results described only a potential association of PPI use and hypomagnesemia, not definitive cause and effect. Results also depended on an assumed, previously reported rate of PPI-associated hypomagnesemia and a rate of exposure to PPIs, as these data were taken into account in the overall study design. In addition, patient adherence to prescribed therapy and accuracy of medication history were assumed from the medication and dispensing history, as not all medications obtained outside the Lovell FHCC were accurately documented. There also was an external validity limitation in that older men make up the typical FHCC patient population. Last, as inherent to all studies that use objective measures, there was the potential for laboratory magnesium level reporting errors.
Conclusion
The study results identified an association of PPI use and hypomagnesemia in a VA patient population of older men. More studies need to be conducted with non-VA patient populations to further assess the incidence of PPI-associated hypomagnesemia.
In the U.S., proton pump inhibitors (PPIs) are one of the best-selling drug classes—more than $9 billion were spent on PPIs in 2012.1 These medications, available both by prescription and over-the-counter (OTC), are used to treat a variety of gastrointestinal conditions, including heartburn, gastroesophageal reflux disease, and peptic ulcer disease.1
Proton pump inhibitors are generally recognized as safe and effective. In 2011, however, the FDA reviewed Adverse Event Reporting System (AERS) reports, medical literature, and periodic safety updates and issued a safety communication outlining the risk for hypomagnesemia with prolonged PPI use.2 The FDA focused on 53 cases: 30 AERS cases, 15 in the literature, and 8 reported both through AERS and in the literature. The majority involved PPI use that continued for 1 year or longer, but in some cases hypomagnesemia developed after only 3 months. Labeling for prescription PPIs was updated with information about the hypomagnesemia risk, but labeling for the OTC drugs was not affected, as the FDA stated there is little risk with OTC use, and the label already indicated that use should be limited to 14 days at a time and up to 3 courses within 1 year.
Magnesium is an important intracellular cation that plays a role in multiple cellular activities. Low levels of magnesium can lead to a wide variety of adverse events (AEs), including vomiting, diarrhea, cramps, convulsions, bradycardia, and even death.3,4 The mechanism of PPI-associated hypomagnesemia is yet to be established but could be related to, as has been proposed, altered intestinal absorption of magnesium with long-term PPI use.4
Results from investigations of PPI-associated hypomagnesemia have been inconclusive. In a study of PPI-associated AEs reported to the FDA, Luk and colleagues estimated that 1% of patients who experienced an AE reported hypomagnesemia and concluded that all PPIs are associated with hypomagnesemia, but the risk varies. Of the 6 PPIs that have been FDA approved, esomeprazole was associated with the lowest risk, pantoprazole with the most. Results also suggested that the risk was higher for elderly and male patients.
In another study of prior PPI use and its effects on magnesium levels among 11,490 intensive care unit admissions, Danziger and colleagues found that the association of PPI use and hypomagnesemia was limited to patients who concomitantly received a diuretic, and use of a histamine 2 receptor antagonist was not associated with hypomagnesemia.3 A third cross-sectional study of 402 adults with hypomagnesemia on hospital admission found no association between outpatient PPI regimens and hypomagnesemia.5 Other studies designed to investigate PPI-associated hypomagnesemia were limited by short-term PPI use, small samples, concurrent diseases, and confounding variables (eg, history of alcoholism).6,7
Need for Present Study
The evidence needed to establish the incidence of PPI-associated hypomagnesemia is limited. Hypomagnesemia can lead to serious AEs, as just outlined, and is a common indication for hospitalization.8 The hypomagnesemia rate is about 12% in hospitalized patients and sharply higher (60%-65%) in those who are critically ill. Proton pump inhibitor-associated hypomagnesemia is preventable, and monitoring parameters can be recommended to patients undergoing long-term therapy.
Ajumobi and colleagues found that 13,713 (23.4%) of 58,605 patients treated at a VA center over a 12-month period were receiving a PPI.9 Gawron and colleagues found that many veterans had been prescribed a PPI and were receiving high total daily doses for the treatment of gastroesophageal reflux disease.10 The majority of patients received a 90-day or longer supply and showed minimal evidence of step-down therapy or cessation of PPI therapy.
In the present study, the authors investigated the rate of PPI-associated hypomagnesemia in a veteran population at a facility where the majority of PPIs were by prescription, not OTC. The Captain James A. Lovell Federal Health Care Center (FHCC) is a combined DoD and VA facility where veterans and active military members and their dependents receive medical care and prescription drugs.
This study’s primary objective was to determine the rate of PPI-induced hypomagnesemia. The secondary objective was to identify any clinical factors (eg, PPI dose and therapy duration, concomitant use of a diuretic) that might further increase the risk of hypomagnesemia.
Methods
After the study protocol was approved by the Lovell FHCC institutional review board, the authors retrospectively compared patients with a low magnesium level (case group) with patients with a normal magnesium level (control group). In each group, the authors identified patients who underwent PPI therapy and those who did not (Figure).
Study inclusion criteria were low magnesium level (< 1.8 mg/dL) within the past 5 years for veterans in the case group and normal magnesium level (1.8-2.4 mg/dL) within the past 5 years for veterans in the control group. Exclusion criteria were nonveterans and no prior magnesium level for a veteran.
Patients were assigned in a ratio of 1 (case group) to 4 (control group) and were added only after confirmation that multiple magnesium levels had been recorded (January 2008-January 2013).
Patients who met the inclusion criteria were enrolled in the study. Patient’s Computerized Patient Record System charts were reviewed for demographics (sex, age, race); magnesium level; active order for PPI during same period magnesium level was drawn; PPI name, dose, and therapy duration; and concomitant use of a diuretic (yes or no) and, if yes, type of diuretic.
To assess a significance criterion (α) of 0.05 and a power of 80% 1,375 patients in a 1:4 ratio (275 cases, 1,100 controls) were required in order to detect a difference in rates of hypomagnesemia between patients who received a PPI and those who did not. Primary outcome data are reported as percentages and calculated odds ratios (ORs). Significance of ORs was determined with 95% confidence intervals (CIs). Secondary outcomes were PPI dose and therapy duration and concomitant use of a diuretic. Descriptive statistics were used for secondary outcomes.
Results
Five hundred thirty charts (106 cases, 424 controls) were included and reviewed. Table 1 lists the baseline demographics. There were no statistically significant differences in age, sex, or race between the case and control groups. Mean (SD) magnesium level was 1.6 (0.15)
The authors assessed for other clinical factors that might concurrently or
Discussion
One of the most widely prescribed classes of medications, PPIs are often regarded as safe and effective and therefore continued as long-term therapy. Results of this study showed an association of PPI use and hypomagnesemia—thereby adding to the literature. Results for the secondary objective suggest that the association does not necessarily depend on PPI dose, but, given that a statistical analysis of the difference between the case and control groups was not conducted, the statistical significance is unknown.
Although the hypomagnesemia rate remains undetermined, the results of this NNH study suggest a rate higher than previously proposed. Other investigators have estimated the rate of PPI-associated hypomagnesemia at 1%, which does not correlate well with the NNH often calculated in this study. For 2 possible reasons, the poor correlation may be attributable to underreporting of hypomagnesemia: Magnesium levels are not commonly checked with a basic metabolic panel, and many patients who are mildly hypomagnesemic remain asymptomatic.
Future research directions include determining whether the risk for hypomagnesemia is related to patient status (eg, inpatient vs outpatient) and performing statistical analyses on the secondary objective to determine the clinical significance of potential risk factors. Other research directions might involve assessing PPI discontinuation rates in a hypomagnesemic population and assessing outcomes such as hospitalizations and AEs (eg, seizure, tetany, arrhythmia).
Limitations
This study had several limitations. First was the overall design. Study results described only a potential association of PPI use and hypomagnesemia, not definitive cause and effect. Results also depended on an assumed, previously reported rate of PPI-associated hypomagnesemia and a rate of exposure to PPIs, as these data were taken into account in the overall study design. In addition, patient adherence to prescribed therapy and accuracy of medication history were assumed from the medication and dispensing history, as not all medications obtained outside the Lovell FHCC were accurately documented. There also was an external validity limitation in that older men make up the typical FHCC patient population. Last, as inherent to all studies that use objective measures, there was the potential for laboratory magnesium level reporting errors.
Conclusion
The study results identified an association of PPI use and hypomagnesemia in a VA patient population of older men. More studies need to be conducted with non-VA patient populations to further assess the incidence of PPI-associated hypomagnesemia.
1. Consumers Union. Consumer Reports Best Buy Drugs: Using the proton pump inhibitors to treat heartburn and stomach acid reflux, comparing effectiveness, safety, and price. http://www.consumer reports.org/health/resources/pdf/best-buy-drugs/PPIsUpdate-FINAL.pdf. Updated July 2013. Accessed November 4, 2016.
2. U.S. Food and Drug Administration. FDA drug safety communication: low magnesium levels can be associated with long-term use of proton pump inhibitor drugs (PPIs). http://www.fda.gov/Drugs /DrugSafety/ucm245011.htm. Updated April 7, 2016. Accessed November 4, 2016.
3. Danziger J, William JH, Scott DJ, et al. Proton-pump inhibitor use is associated with low serum magnesium concentrations. Kidney Int. 2013;83(4):692-699.
4. Luk CP, Parsons R, Lee YP, Hughes JD. Proton pump inhibitor-associated hypomagnesemia: what do FDA data tell us? Ann Pharmacother. 2013;47(6):773-780.
5. Koulouridis I, Alfayez M, Tighiouart H, et al. Out-of-hospital use of proton pump inhibitors and hypomagnesemia at hospital admission: a nested case-control study. Am J Kidney Dis. 2013;62(4):730-737.
6. Mackay JD, Bladon PT. Hypomagnesaemia due to proton-pump inhibitor therapy: a clinical case series. QJM. 2010;103(6):387-395.
7. Faulhaber GA, Ascoli BA, Lubina A, et al. Serum magnesium and proton-pump inhibitors use: a cross-sectional study. Rev Assoc Med Bras (1992). 2013;59(3):276-279.
8. Yu ASL. Causes of hypomagnesemia. UpToDate. http://www.uptodate.com/contents/causes-of-hypomagnesemia. Updated February 4, 2016. Accessed November 4, 2016.
9. Ajumobi AB, Vuong R, Ahaneku H. Analysis of nonformulary use of PPIs and excess drug cost in a Veterans Affairs population. J Manag Care Pharm. 2012;18(1):63-67.
10. Gawron AJ, Pandolfino JE, Miskevics S, Lavela SL. Proton pump inhibitor prescriptions and subsequent use in US veterans diagnosed with gastroesophageal reflux disease. J Gen Intern Med. 2013;28(7):930-937.
1. Consumers Union. Consumer Reports Best Buy Drugs: Using the proton pump inhibitors to treat heartburn and stomach acid reflux, comparing effectiveness, safety, and price. http://www.consumer reports.org/health/resources/pdf/best-buy-drugs/PPIsUpdate-FINAL.pdf. Updated July 2013. Accessed November 4, 2016.
2. U.S. Food and Drug Administration. FDA drug safety communication: low magnesium levels can be associated with long-term use of proton pump inhibitor drugs (PPIs). http://www.fda.gov/Drugs /DrugSafety/ucm245011.htm. Updated April 7, 2016. Accessed November 4, 2016.
3. Danziger J, William JH, Scott DJ, et al. Proton-pump inhibitor use is associated with low serum magnesium concentrations. Kidney Int. 2013;83(4):692-699.
4. Luk CP, Parsons R, Lee YP, Hughes JD. Proton pump inhibitor-associated hypomagnesemia: what do FDA data tell us? Ann Pharmacother. 2013;47(6):773-780.
5. Koulouridis I, Alfayez M, Tighiouart H, et al. Out-of-hospital use of proton pump inhibitors and hypomagnesemia at hospital admission: a nested case-control study. Am J Kidney Dis. 2013;62(4):730-737.
6. Mackay JD, Bladon PT. Hypomagnesaemia due to proton-pump inhibitor therapy: a clinical case series. QJM. 2010;103(6):387-395.
7. Faulhaber GA, Ascoli BA, Lubina A, et al. Serum magnesium and proton-pump inhibitors use: a cross-sectional study. Rev Assoc Med Bras (1992). 2013;59(3):276-279.
8. Yu ASL. Causes of hypomagnesemia. UpToDate. http://www.uptodate.com/contents/causes-of-hypomagnesemia. Updated February 4, 2016. Accessed November 4, 2016.
9. Ajumobi AB, Vuong R, Ahaneku H. Analysis of nonformulary use of PPIs and excess drug cost in a Veterans Affairs population. J Manag Care Pharm. 2012;18(1):63-67.
10. Gawron AJ, Pandolfino JE, Miskevics S, Lavela SL. Proton pump inhibitor prescriptions and subsequent use in US veterans diagnosed with gastroesophageal reflux disease. J Gen Intern Med. 2013;28(7):930-937.
Exploring the function of self-criticism
A Stroke of Bad (Pot)luck
ANSWER
The correct interpretation includes normal sinus rhythm, acute ST elevation anterior myocardial infarction (STEMI), and inferolateral injury. Sinus rhythm is signified by a P wave for every QRS complex and a QRS complex for every P wave at a rate between 60 and 100 beats/min.
A STEMI is defined as new ST elevations at the J point in at least two contiguous leads—in women, 1.5 mm in leads V2 and V3 and 1 mm in all other leads; in men, 2 mm (those 40 and older) or 2.5 mm (those younger than 40) in leads V2 and V3 and 1 mm in all other leads. The anterior location is evidenced by the significant Q waves in leads I, V2, V3, and V4. T-wave inversions in these leads are absent due to the STEMI.
Inferolateral injury is identified by the Q waves in leads I, aVL, V5, and V6. Pseudo Q waves are seen in leads II, III, and aVF.
Troponin levels were significant for an acute myocardial infarction (MI). Cardiac cauterization confirmed an occlusion of the proximal left anterior descending coronary artery, and significant stenosis of the first obtuse marginal branch of the circumflex coronary artery. The patient’s lack of chest pain represents a common presentation of an MI in women, particularly those with a history of diabetes.
ANSWER
The correct interpretation includes normal sinus rhythm, acute ST elevation anterior myocardial infarction (STEMI), and inferolateral injury. Sinus rhythm is signified by a P wave for every QRS complex and a QRS complex for every P wave at a rate between 60 and 100 beats/min.
A STEMI is defined as new ST elevations at the J point in at least two contiguous leads—in women, 1.5 mm in leads V2 and V3 and 1 mm in all other leads; in men, 2 mm (those 40 and older) or 2.5 mm (those younger than 40) in leads V2 and V3 and 1 mm in all other leads. The anterior location is evidenced by the significant Q waves in leads I, V2, V3, and V4. T-wave inversions in these leads are absent due to the STEMI.
Inferolateral injury is identified by the Q waves in leads I, aVL, V5, and V6. Pseudo Q waves are seen in leads II, III, and aVF.
Troponin levels were significant for an acute myocardial infarction (MI). Cardiac cauterization confirmed an occlusion of the proximal left anterior descending coronary artery, and significant stenosis of the first obtuse marginal branch of the circumflex coronary artery. The patient’s lack of chest pain represents a common presentation of an MI in women, particularly those with a history of diabetes.
ANSWER
The correct interpretation includes normal sinus rhythm, acute ST elevation anterior myocardial infarction (STEMI), and inferolateral injury. Sinus rhythm is signified by a P wave for every QRS complex and a QRS complex for every P wave at a rate between 60 and 100 beats/min.
A STEMI is defined as new ST elevations at the J point in at least two contiguous leads—in women, 1.5 mm in leads V2 and V3 and 1 mm in all other leads; in men, 2 mm (those 40 and older) or 2.5 mm (those younger than 40) in leads V2 and V3 and 1 mm in all other leads. The anterior location is evidenced by the significant Q waves in leads I, V2, V3, and V4. T-wave inversions in these leads are absent due to the STEMI.
Inferolateral injury is identified by the Q waves in leads I, aVL, V5, and V6. Pseudo Q waves are seen in leads II, III, and aVF.
Troponin levels were significant for an acute myocardial infarction (MI). Cardiac cauterization confirmed an occlusion of the proximal left anterior descending coronary artery, and significant stenosis of the first obtuse marginal branch of the circumflex coronary artery. The patient’s lack of chest pain represents a common presentation of an MI in women, particularly those with a history of diabetes.
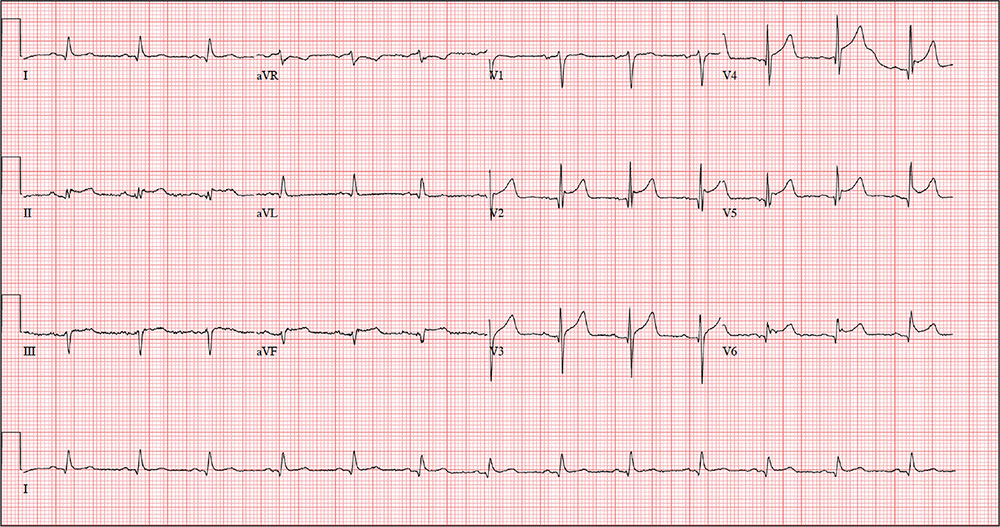
An active 74-year-old woman becomes nauseated and diaphoretic while cleaning up her church’s Sunday evening potluck. She shrugs it off, attributing it to something she ate, but while preparing to go home, she abruptly becomes short of breath and complains she can’t catch her breath. Two coworkers describe her appearance as pale with “complete loss of color” and insist on driving her to the local emergency department (ED).
When she arrives 10 minutes later, her shortness of breath is resolving. She denies chest pain, vomiting, and diarrhea. Despite receiving oxygen via nasal cannula, she still appears pale. An ECG and laboratory tests are ordered.
The patient’s medical history is remarkable for type 2 diabetes, hypothyroidism, obesity, and hypertension. Her surgical history is remarkable for a cholecystectomy and a hysterectomy 40 years ago, following the delivery of her third child.
The patient is a retired elementary school principal. She drinks alcohol socially and has never smoked. She lost her husband to colon cancer several years ago and now lives by herself in her home. She has three adult children who are all alive and well. Her mother died of heart failure, and her father was killed in an automobile accident.
Her current medication list includes metformin, levothyroxine, and hydrochlorothiazide. She states she has tried other medications for her diabetes and hypertension but prefers her current regimen. She is allergic to radiographic contrast media, with a documented near-anaphylactic reaction in the past.
Physical exam reveals a pleasant, cooperative, but apprehensive woman who appears her stated age. She wears corrective lenses and bilateral hearing aids. Her neck veins are not distended, and there is no evidence of thyromegaly. Respirations are rapid and shallow, with few crackles in both bases bilaterally but no rhonchi or rales. Her cardiac exam reveals a regular rate and rhythm with a soft, grade II, mid-systolic murmur at the left upper sternal border without radiation. There are no extra heart sounds or rubs. The abdomen is soft and nontender with well-healed surgical scars. The peripheral pulses are full and equal in both upper and lower extremities. The neurologic exam is grossly intact.
The review of systems shows that she has gained 14 pounds over the past four months, has been less physically active, and feels like she is “slowing down.” She also says her hearing and eyesight aren’t what they used to be, and she has chronic constipation. The remainder of her review of systems is unremarkable.
The patient’s weight is 218 lb and her height, 64 in. Vital signs include a blood pressure of 148/
110 mm Hg; pulse, 80 beats/min and regular; O2 saturation, 98% on 4 L O2 via nasal prongs; and respiratory rate, 20 breaths/min-1.
An ECG is obtained, and blood specimens for labwork—including a complete chemistry profile, complete blood count, thyroid function studies, and troponin levels—are collected. The ECG shows a ventricular rate of 80 beats/min; PR interval, 162 ms; QRS duration, 106 ms; QT/QTc intervals, 370/426 ms; P axis, 51°; R axis, –20°; and T axis, 70°. What is your interpretation of this ECG?
The Liver Meeting 2016 debrief – key abstracts
BOSTON – Amid a plethora of quality research, several abstracts stood out at the annual meeting of the American Association for the Study of Liver Diseases, Arun J. Sanyal, MD, said during the final debrief.
He focused first on nonalcoholic fatty liver disease (NAFLD), which has lacked rigorous studies of disease evolution. Consequently, “current therapeutic development is based on small retrospective data sets with heterogenous populations,” Dr. Sanyal said. Therefore, he and his associates correlated serial biopsies with clinical data (abstract 37). The results confirmed the waxing and waning nature of NAFLD and linked regressing or progressive fibrosis to several factors, including NAFLD Disease Activity score (NAS). NAFLD and nonalcoholic steatohepatitis (NASH) are “not two different diseases, it’s the same disease,” Dr. Sanyal said. “Establishing disease activity as a driver of disease progression is highly relevant for development of noninvasive biomarkers, and also gives us a foundation for the development of clinical trials in this space.”

Several studies of NASH biomarkers yielded notable results at the meeting. In the largest study to date of circulating microRNAs as markers of NASH, (LB2) the miRNAs 34a, 122a, and 200a distinguished patients with and without NAS scores of at least 4 and at least stage 2 fibrosis with areas under the receiver operating characteristic curve (AUROC) between 0.59 and 0.80. “MicroRNAs appear promising, but likely need to be combined with additional biomarkers,” Dr. Sanyal said.
He also noted a study (abstract 40) in which metabolomics of liquid biopsies comprehensively evaluated NAFLD, including fibrosis stage, with AUROCs up to 0.95. Metabolomics “holds promise as a diagnostic tool that can be operationalized for point-of-care testing,” he said.
When it comes to NAFLD, hepatologists “often struggle with what to tell our patients about alcohol,” Dr. Sanyal said. To help clarify the issue, abstract 31 compared NAFLD patients who did or did not report habitually consuming up to two drinks a day in formal prospective questionnaires. After adjustment for baseline histology, abstainers and modest drinkers did not differ on any measure of histologic change, except that abstainers had a greater decrease in steatosis on follow-up biopsy. These findings negate several retrospective studies by suggesting that alcohol consumption does not positively affect the trajectory of NAFLD, Dr. Sanyal concluded.
Many new compounds for treating NASH are in early development, he noted. Among those further along the pipeline, the immunomodulator and CCR2/CCR5 inhibitor cenicriviroc (CVC) missed its primary endpoint (improved NAS and no worsening of fibrosis) but was associated with significantly improved fibrosis without worsening of NASH in the phase 2b CENTAUR study (LB1).
“We also saw highly promising evidence for the effects of ASK1 [apoptosis signal regulating kinase] inhibition on hepatic fibrosis and disease activity in NASH,” Dr. Sanyal added. In a randomized phase II trial (LB3), the ASK1 inhibitor GS-4997 was associated with significant improvement in fibrosis without worsening of NASH when given in combination with simtuzumab, and also improved liver stiffness and magnetic resonance imaging–estimated proton density fat fraction (MRI-PDFF). “These very promising and exciting results need confirmation in more advanced, placebo-controlled trials,” Dr. Sanyal said.
Studies of alcohol use disorders of the liver confirmed that prednisolone has marginal benefits, that the benefits of steroids in general are offset by sepsis, and that pentoxifylline produced no mortality benefit, Dr. Sanyal noted. In studies of primary biliary cirrhosis, the farnesoid-X receptor agonist obeticholic acid (OCA), which was approved by the Food and Drug Administration in 2016, was associated with significantly improved AST to Platelet Ratio Index (APRI) and liver stiffness measures by transient elastography at doses of 10 mg or titrated from 5 mg to 10 mg, with or without ursodeoxycholic acid (abstract 209). In another study, patients with PBC who received norUDCA, a side chain–shortened version of UDCA, experienced decreases in serum ALP levels that were dose dependent and differed significantly from trends in the placebo group (abstract 210).
In another study, the investigational ileal bile acid transporter inhibitor GSK2330672 was associated with significant reductions in itch, compared with placebo, and with lower serum bile acids among pruritic PBC patients (abstract 205). Treatment was associated with diarrhea, but it was usually mild and transient.
Dr. Sanyal concluded by reviewing several studies of cirrhosis and hepatic encephalopathy. In a prospective randomized controlled trial (abstract 247), lactulose with albumin significantly outperformed lactulose monotherapy for reversing hepatic encephalopathy, reducing hospital stays, and preventing mortality, especially sepsis-related death.
In another multicenter, 24-week, phase IV open-label study (abstract 248), 25% of patients experienced breakthrough hepatic encephalopathy when treated with rifaximin monotherapy, compared with only 14% of patients who received both rifaximin and lactulose.
Finally, in a phase II trial (abstract 2064), rifaximin immediate-release (40 mg) significantly outperformed placebo in terms of cirrhosis-related mortality, hospitalizations for cirrhosis, and breakthrough hepatic encephalopathy. The takeaways? “Use albumin with lactulose for acute hepatic encephalopathy,” Dr. Sanyal said. “Rifaximin with lactulose is better than rifaximin alone for secondary prophylaxis, and rifaximin immediate-release may decrease the need for hospitalization and the first bout of hepatic encephalopathy.”
The Liver Meeting next convenes October 20-24, 2017, in Washington, D.C.
Dr. Sanyal disclosed ties to Genfit, NewCo, Akarna, Elsevier, UptoDate, Novartis, Pfizer, Lilly, Astra Zeneca, and a number of other companies.
BOSTON – Amid a plethora of quality research, several abstracts stood out at the annual meeting of the American Association for the Study of Liver Diseases, Arun J. Sanyal, MD, said during the final debrief.
He focused first on nonalcoholic fatty liver disease (NAFLD), which has lacked rigorous studies of disease evolution. Consequently, “current therapeutic development is based on small retrospective data sets with heterogenous populations,” Dr. Sanyal said. Therefore, he and his associates correlated serial biopsies with clinical data (abstract 37). The results confirmed the waxing and waning nature of NAFLD and linked regressing or progressive fibrosis to several factors, including NAFLD Disease Activity score (NAS). NAFLD and nonalcoholic steatohepatitis (NASH) are “not two different diseases, it’s the same disease,” Dr. Sanyal said. “Establishing disease activity as a driver of disease progression is highly relevant for development of noninvasive biomarkers, and also gives us a foundation for the development of clinical trials in this space.”
Several studies of NASH biomarkers yielded notable results at the meeting. In the largest study to date of circulating microRNAs as markers of NASH, (LB2) the miRNAs 34a, 122a, and 200a distinguished patients with and without NAS scores of at least 4 and at least stage 2 fibrosis with areas under the receiver operating characteristic curve (AUROC) between 0.59 and 0.80. “MicroRNAs appear promising, but likely need to be combined with additional biomarkers,” Dr. Sanyal said.
He also noted a study (abstract 40) in which metabolomics of liquid biopsies comprehensively evaluated NAFLD, including fibrosis stage, with AUROCs up to 0.95. Metabolomics “holds promise as a diagnostic tool that can be operationalized for point-of-care testing,” he said.
When it comes to NAFLD, hepatologists “often struggle with what to tell our patients about alcohol,” Dr. Sanyal said. To help clarify the issue, abstract 31 compared NAFLD patients who did or did not report habitually consuming up to two drinks a day in formal prospective questionnaires. After adjustment for baseline histology, abstainers and modest drinkers did not differ on any measure of histologic change, except that abstainers had a greater decrease in steatosis on follow-up biopsy. These findings negate several retrospective studies by suggesting that alcohol consumption does not positively affect the trajectory of NAFLD, Dr. Sanyal concluded.
Many new compounds for treating NASH are in early development, he noted. Among those further along the pipeline, the immunomodulator and CCR2/CCR5 inhibitor cenicriviroc (CVC) missed its primary endpoint (improved NAS and no worsening of fibrosis) but was associated with significantly improved fibrosis without worsening of NASH in the phase 2b CENTAUR study (LB1).
“We also saw highly promising evidence for the effects of ASK1 [apoptosis signal regulating kinase] inhibition on hepatic fibrosis and disease activity in NASH,” Dr. Sanyal added. In a randomized phase II trial (LB3), the ASK1 inhibitor GS-4997 was associated with significant improvement in fibrosis without worsening of NASH when given in combination with simtuzumab, and also improved liver stiffness and magnetic resonance imaging–estimated proton density fat fraction (MRI-PDFF). “These very promising and exciting results need confirmation in more advanced, placebo-controlled trials,” Dr. Sanyal said.
Studies of alcohol use disorders of the liver confirmed that prednisolone has marginal benefits, that the benefits of steroids in general are offset by sepsis, and that pentoxifylline produced no mortality benefit, Dr. Sanyal noted. In studies of primary biliary cirrhosis, the farnesoid-X receptor agonist obeticholic acid (OCA), which was approved by the Food and Drug Administration in 2016, was associated with significantly improved AST to Platelet Ratio Index (APRI) and liver stiffness measures by transient elastography at doses of 10 mg or titrated from 5 mg to 10 mg, with or without ursodeoxycholic acid (abstract 209). In another study, patients with PBC who received norUDCA, a side chain–shortened version of UDCA, experienced decreases in serum ALP levels that were dose dependent and differed significantly from trends in the placebo group (abstract 210).
In another study, the investigational ileal bile acid transporter inhibitor GSK2330672 was associated with significant reductions in itch, compared with placebo, and with lower serum bile acids among pruritic PBC patients (abstract 205). Treatment was associated with diarrhea, but it was usually mild and transient.
Dr. Sanyal concluded by reviewing several studies of cirrhosis and hepatic encephalopathy. In a prospective randomized controlled trial (abstract 247), lactulose with albumin significantly outperformed lactulose monotherapy for reversing hepatic encephalopathy, reducing hospital stays, and preventing mortality, especially sepsis-related death.
In another multicenter, 24-week, phase IV open-label study (abstract 248), 25% of patients experienced breakthrough hepatic encephalopathy when treated with rifaximin monotherapy, compared with only 14% of patients who received both rifaximin and lactulose.
Finally, in a phase II trial (abstract 2064), rifaximin immediate-release (40 mg) significantly outperformed placebo in terms of cirrhosis-related mortality, hospitalizations for cirrhosis, and breakthrough hepatic encephalopathy. The takeaways? “Use albumin with lactulose for acute hepatic encephalopathy,” Dr. Sanyal said. “Rifaximin with lactulose is better than rifaximin alone for secondary prophylaxis, and rifaximin immediate-release may decrease the need for hospitalization and the first bout of hepatic encephalopathy.”
The Liver Meeting next convenes October 20-24, 2017, in Washington, D.C.
Dr. Sanyal disclosed ties to Genfit, NewCo, Akarna, Elsevier, UptoDate, Novartis, Pfizer, Lilly, Astra Zeneca, and a number of other companies.
BOSTON – Amid a plethora of quality research, several abstracts stood out at the annual meeting of the American Association for the Study of Liver Diseases, Arun J. Sanyal, MD, said during the final debrief.
He focused first on nonalcoholic fatty liver disease (NAFLD), which has lacked rigorous studies of disease evolution. Consequently, “current therapeutic development is based on small retrospective data sets with heterogenous populations,” Dr. Sanyal said. Therefore, he and his associates correlated serial biopsies with clinical data (abstract 37). The results confirmed the waxing and waning nature of NAFLD and linked regressing or progressive fibrosis to several factors, including NAFLD Disease Activity score (NAS). NAFLD and nonalcoholic steatohepatitis (NASH) are “not two different diseases, it’s the same disease,” Dr. Sanyal said. “Establishing disease activity as a driver of disease progression is highly relevant for development of noninvasive biomarkers, and also gives us a foundation for the development of clinical trials in this space.”
Several studies of NASH biomarkers yielded notable results at the meeting. In the largest study to date of circulating microRNAs as markers of NASH, (LB2) the miRNAs 34a, 122a, and 200a distinguished patients with and without NAS scores of at least 4 and at least stage 2 fibrosis with areas under the receiver operating characteristic curve (AUROC) between 0.59 and 0.80. “MicroRNAs appear promising, but likely need to be combined with additional biomarkers,” Dr. Sanyal said.
He also noted a study (abstract 40) in which metabolomics of liquid biopsies comprehensively evaluated NAFLD, including fibrosis stage, with AUROCs up to 0.95. Metabolomics “holds promise as a diagnostic tool that can be operationalized for point-of-care testing,” he said.
When it comes to NAFLD, hepatologists “often struggle with what to tell our patients about alcohol,” Dr. Sanyal said. To help clarify the issue, abstract 31 compared NAFLD patients who did or did not report habitually consuming up to two drinks a day in formal prospective questionnaires. After adjustment for baseline histology, abstainers and modest drinkers did not differ on any measure of histologic change, except that abstainers had a greater decrease in steatosis on follow-up biopsy. These findings negate several retrospective studies by suggesting that alcohol consumption does not positively affect the trajectory of NAFLD, Dr. Sanyal concluded.
Many new compounds for treating NASH are in early development, he noted. Among those further along the pipeline, the immunomodulator and CCR2/CCR5 inhibitor cenicriviroc (CVC) missed its primary endpoint (improved NAS and no worsening of fibrosis) but was associated with significantly improved fibrosis without worsening of NASH in the phase 2b CENTAUR study (LB1).
“We also saw highly promising evidence for the effects of ASK1 [apoptosis signal regulating kinase] inhibition on hepatic fibrosis and disease activity in NASH,” Dr. Sanyal added. In a randomized phase II trial (LB3), the ASK1 inhibitor GS-4997 was associated with significant improvement in fibrosis without worsening of NASH when given in combination with simtuzumab, and also improved liver stiffness and magnetic resonance imaging–estimated proton density fat fraction (MRI-PDFF). “These very promising and exciting results need confirmation in more advanced, placebo-controlled trials,” Dr. Sanyal said.
Studies of alcohol use disorders of the liver confirmed that prednisolone has marginal benefits, that the benefits of steroids in general are offset by sepsis, and that pentoxifylline produced no mortality benefit, Dr. Sanyal noted. In studies of primary biliary cirrhosis, the farnesoid-X receptor agonist obeticholic acid (OCA), which was approved by the Food and Drug Administration in 2016, was associated with significantly improved AST to Platelet Ratio Index (APRI) and liver stiffness measures by transient elastography at doses of 10 mg or titrated from 5 mg to 10 mg, with or without ursodeoxycholic acid (abstract 209). In another study, patients with PBC who received norUDCA, a side chain–shortened version of UDCA, experienced decreases in serum ALP levels that were dose dependent and differed significantly from trends in the placebo group (abstract 210).
In another study, the investigational ileal bile acid transporter inhibitor GSK2330672 was associated with significant reductions in itch, compared with placebo, and with lower serum bile acids among pruritic PBC patients (abstract 205). Treatment was associated with diarrhea, but it was usually mild and transient.
Dr. Sanyal concluded by reviewing several studies of cirrhosis and hepatic encephalopathy. In a prospective randomized controlled trial (abstract 247), lactulose with albumin significantly outperformed lactulose monotherapy for reversing hepatic encephalopathy, reducing hospital stays, and preventing mortality, especially sepsis-related death.
In another multicenter, 24-week, phase IV open-label study (abstract 248), 25% of patients experienced breakthrough hepatic encephalopathy when treated with rifaximin monotherapy, compared with only 14% of patients who received both rifaximin and lactulose.
Finally, in a phase II trial (abstract 2064), rifaximin immediate-release (40 mg) significantly outperformed placebo in terms of cirrhosis-related mortality, hospitalizations for cirrhosis, and breakthrough hepatic encephalopathy. The takeaways? “Use albumin with lactulose for acute hepatic encephalopathy,” Dr. Sanyal said. “Rifaximin with lactulose is better than rifaximin alone for secondary prophylaxis, and rifaximin immediate-release may decrease the need for hospitalization and the first bout of hepatic encephalopathy.”
The Liver Meeting next convenes October 20-24, 2017, in Washington, D.C.
Dr. Sanyal disclosed ties to Genfit, NewCo, Akarna, Elsevier, UptoDate, Novartis, Pfizer, Lilly, Astra Zeneca, and a number of other companies.
AT THE LIVER MEETING 2016