User login
How Well Does the Braden Nutrition Subscale Agree With the VA Nutrition Classification Scheme Related to Pressure Ulcer Risk?
A pressure ulcer (PrU) is a localized injury to the skin and/or deep tissues that is due to pressure, friction, or shearing forces. Pressure ulcers are strongly associated with serious comorbidities, particularly inadequate nutrition and immobility.1,2 Pressure ulcers increase hospital costs significantly. In the U.S., PrU care is about $11 billion annually and a cost of between $2,000 and $21,410 per individual PrU.3-5
The impact of nosocomial PrUs remains a key health and economic concern of acute care facilities worldwide. In the U.S., about 2.5 million inpatients annually develop some degree of a PrU during their hospital stay. The reported incidence rates range from 0.4% to 38%.3,6 Each year about 60,000 people die of complications of a PrU.3,6,7 Inadequate nutrition is a critical factor that contributes to the incidence of PrUs.8-12 Consequences of inadequate nutrition have included alterations in skin integrity resulting in PrUs, longer hospital stays, increased costs of care, and higher rates of mortality.9 As a patient’s nutritional status becomes compromised, the likelihood of developing a PrU increases, especially if an individual is immobilized.7,9-11,13
Braden Scale History
The Braden Scale for Predicting Pressure Sore Risk was developed by Barbara Braden, PhD, RN, and Nancy Bergstrom, PhD, RN, in 1987.
The scale is composed of 6 factors: sensory perception, moisture, activity, mobility, friction and shear, and nutrition.14 Each factor is scored on a scale of 1 to 4 points (friction and shear are scored on a point scale of only 1 to 3) for a total possible score of 6 to 23 points (the lower the score, the greater the assumed PrU risk).
The Braden nutrition subscale relies heavily on recording observed or patient self-reported eating habits. It is typically documented by nurses who assess the daily intake of meals: recording a score of 4 if the patient’s meal intake is excellent (eats most of every meal), 3 if the patient’s intake is adequate (eats more than half of most meals), 2 if the patient’s intake is probably inadequate (rarely eats a complete meal), and 1 if a patient’s intake is very poor (never eats a complete meal) (Table 1).14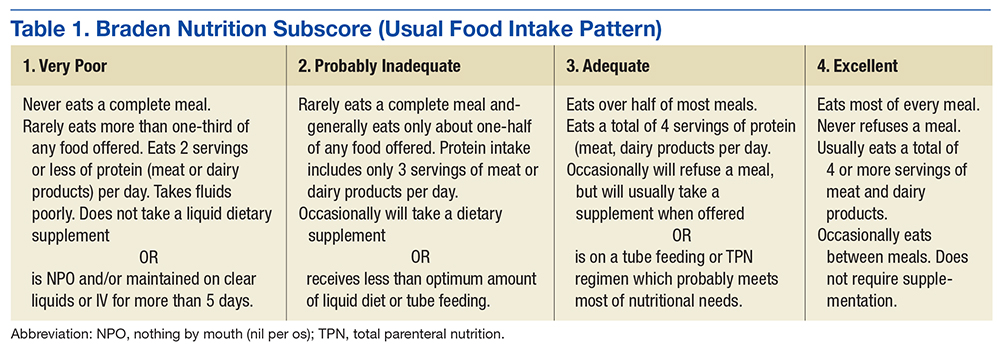
Historically, the Braden scale is reported to have good reliability when used by registered nurses as a risk prediction tool.14,16 A recent review also reported high interrater reliability of the Braden scale total score among nurses, nursing assistants, and graduate assistants.17 However, other studies suggest certain subscales (such as sensory and nutrition) may have very low interrater reliability among nurses and poor PrU predictability.18,19 To date, there are no known studies evaluating the agreement of the Braden nutrition subscale primarily used by nurses and the VA Nutrition Classification Scheme (VANCS) used by dietitians.
The VA standard of care recommends that PrU risk assessments are documented for all hospitalized veterans within 24 hours of admission, daily, with transfers or discharges, and when there is a status change in the patient. In addition, nutritional assessments by dietitians (using the VANCS) are encouraged within 24 hours of acute care hospitalization.20
The VANCS performed by dietitians consists of 4 classifications: no nutritional compromise, mild nutritional compromise, moderate nutritional compromise, and severenutritional compromise. These classifications are based on well-documented “comprehensive approaches to defining nutritional status that uses multiple parameters” including nutrition history, weight (body mass index and weight loss), diagnoses, diet (and diet orders), brief physical assessment, and preliminary laboratory data (serum albumin/pre-albumin and total lymphocyte count).20,21
The predictive ability of a risk assessment tool is critical to its clinical effectiveness in determining a clinical outcome.17 The Braden scale has been used for more than 30 years in various settings without any significant change to the scale or subscales. In a 2012 study, 4 medical factors were found to be more predictive of PrUs than the Braden scale total score in a sample of 213 acutely ill adult veterans.8 By performing a retrospective study using logistic regression predictive models, severe nutritional compromise (as identified by a dietitian), pneumonia, candidiasis, and surgery were identified as stronger predictors of PrU risk than was the Braden total score.8
With malnutrition as one of the most significant predictive factors in PrU risk, it is critical to determine whether discrepancies exist between the Braden nutrition subscale used primarily by nurses and the VANCS used by dietitians. Hence, the overall purpose of this study was to determine the level of agreement between the Braden nutrition subscale scores documented by nurses and the VANCS used by dietitians and examine the relationship of these assessments with PrU development.
Methods
The parent study was approved by the University of Florida Institutional Review Board before data collection. This secondary analysis of the parent study examined data already collected by Cowan and colleagues, which demonstrated the significance of nutritional compromise in PrU risk.
The de-identified data subset consisted of general demographics, hospital length of stay, specific diagnoses, Braden scores, PrU status, and registered dietician nutritional classification data from 213 acutely ill veterans admitted to North Florida/South Georgia Veterans Health System (NF/SGVHS) in Florida for more than 3 days between January and July 2008.8 The sample consisted of 100 veterans with nosocomial PrUs and 113 veterans without PrUs during their admission.
Scoring
Using the de-identified dataset, the variables of interest (VANCS, Braden nutrition subscale score, and the presence/absence of PrU) were coded. The VANCS was given a corresponding score ranging from 1 to 4 (1, severe nutritional compromise; 2, moderate nutritional compromise; 3, mild nutritional compromise; and 4, no nutritional compromise). The Braden nutrition subscale ranged from 1 to 4 (1 very poor nutrition; 2, probably inadequate nutrition; 3, adequate nutrition; and 4, excellent nutrition). PrU development was coded as 0, no PrU development and 1, PrU development. All nutritional assessments had been recorded in the electronic health record before any PrU reported in the parent study.
Statistical Analysis
After coding the variables of interest, the data were transferred into SAS v 9.4 (Cary, NC). The data collected compared VANCS and Braden nutrition subscale results. In addition, the authors examined the agreement between the score assigned to the VANCS and Braden nutrition subscale results with a weighted
Additionally, the authors computed sensitivity and specificity of the Braden nutrition subscale using the VANCS as the gold standard. The severe and moderately compromised categories of the VANCS combined to form the high-risk category, and the mild-to-no compromise categories were combined to form the low-risk category. The Braden nutrition subscale was similarly dichotomized with the very poor and probably inadequate intake forming the high-risk category and the adequate and excellent intake forming the low-risk category. Sensitivity and specificity of the Braden were then calculated.
Results
Nursing assessments using the Braden nutrition subscale were completed on 213 patients whose mean age (SD) was 71.0 (10.6) years. The VANCS documented by dietitians was completed on 205 patients. For 7 patients, a nutrition assessment was documented only by the Braden nutrition subscale and not the VANCS. Most of the patients were male (97%, n = 206), and white (81.4%, n = 171). The weighted
Landis and colleagues suggest that a 
Figure 2 shows the percentage of patients who developed a PrU during hospitalization among different measures of Braden nutrition subscale vs VANCS. In Figure 2, nutritional categories 1, 2, and 3 correspond to very poor intake (Braden)/severe compromise (VANCS), probably inadequate intake (Braden)/moderate compromise (VANCS), and adequate intake (Braden)/mild compromise (VANCS), respectively. There were 3 patients who had a no compromise VANCS; none of these had a PrU, so their data are not represented in Figure 2.
Discussion
Findings from this study indicate that the VANCS documented by dietitians is superior in assessing nutritional risk and predicting the development of PrUs in acutely ill hospitalized veterans compared with the Braden nutrition subscale. This study also shows that the Braden nutrition subscale did not accurately predict PrU development in acutely ill veterans. This finding concurs with the Serpa and Santos study in which the Braden nutrition subscale scores were not predictive for PrU development in hospitalized patients.
One possible explanation for the findings in this study is that the nutrition subscale of the Braden tool asks the assessing clinician to evaluate the amount of food intake the patient is currently taking in for their usual meals. This assessment is highly subjective and speculative and does not account for recent intake fluctuations or weight loss. By comparison, the VANCS is more comprehensive in its ability to assess nutritional compromise based on multiple factors, such as recent weight loss, laboratory indices, body habitus, dentition, and swallowing ability.20 The National Pressure Ulcer Advisory Panel suggests that following an acute care admission, a patient receive a consult from a dietitian if the health care provider suspects that the patient may be nutritionally compromised.1 The study findings demonstrate the utility of the VANCS as predictive of PrU risk.
Unfortunately, the authors have learned that the VANCS may be phased out soon, and many VA facilities are no longer using it. Findings from this study and other recent scientific literature suggest that all inpatients may benefit from nutritional assessments by dietitians. When performed, dietitian assessments provide the basis for more accurate nursing assessment of nutritional risk and targeted interventions. Nursing professionals should be encouraged to review the dietitian assessment and consultation notes and to incorporate this information into a more comprehensive PrU prevention and treatment plan.
Interestingly, in spite of those assessed to have severe nutritional compromise by dietitian assessment (n = 39), very few of these patients (n = 4) had an ICD-9 diagnosis related to malnutrition (ICD-9 codes, 262, 273.8, 269.9, 263.9) entered in their chart for that hospitalization. This observation suggests that 88% of patients with severe nutritional compromise were not appropriately coded at discharge. Improper coding has implications for researchers using ICD-9 diagnosis codes at discharge for accurate analysis of risk factors as well as for health care providers who may look at coded diagnoses information in the charts when considering comorbid conditions for health management.
This study highlights the importance of nutritional status as a risk factor for PrU development. Reasons suggested for nutritional status seeming to be the most significant correlate to PrUs in the acute care setting include the following: decreased protein alters oncotic pressure, making tissue prone to edema; decreases in subcutaneous fat reduce protection from pressure effects; nutritional compromise alters cellular transport of nutrients and waste and makes tissue cells more vulnerable to deformation and physical stresses; and lactate (a by-product of anaerobic glycolysis) or any other metabolic by-product of malnutrition could cause biochemical stress, and tissue cells can die faster as a result of the increased plasma membrane permeability.7,24-26
Limitations
This study was limited to 1 sample of veterans hospitalized in the 2 acute care facilities of NF/SGVHS and the use of a retrospective chart review. As a result, further research is necessary to establish generalizability to other acute care settings and high-risk populations. In spite of these limitations, this and other studies highlight the need for revision of the Braden scale, specifically the nutritional subscale, to lessen the ambiguity seen between dietitian and nursing assessments while also increasing the accuracy in determining a patient’s nutrition risk of PrU development during hospitalization.
Conclusion
These findings provide evidence that dietitians’ documentation of the VANCS related to nutritional compromise are superior to current nutritional risk assessments using the Braden nutrition subscale in predicting PrU risk.
Acknowledgments
The authors acknowledge that this work was supported by the resources of the North Florida/South Georgia Veterans Health System in Gainesville, Florida, and in part by a Small Project Award from the VA Office of Nursing Services.
1. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. http://www.npuap.org/resources/educational-and-clinical -resources/prevention-and-treatment-of-pressure -ulcers-clinical-practice-guideline. Updated 2014. Accessed November 7, 2016.
2. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, Pan Pacific Pressure Injury Alliance. Prevention and treatment of pressure ulcers: quick reference guide. http://www .npuap.org/wp-content/uploads/2014/08/Updated -10-16-14-Quick-Reference-Guide-DIGITAL-NPUAP-EPUAP-PPPIA-16Oct2014.pdf. Updated October 16, 2014. Accessed October 21, 2016.
3. Sullivan N. Preventing in-facility pressure ulcers. In: Agency for Healthcare Research and Quality. Making Health Care Safer II. An Updated Critical Analysis of the Evidence for Patient Safety Practices. Evidence Reports/Technology Assessments. http://www.ahrq.gov/sites/default/files/wysiwyg/research/findings/evidence-based-reports/services/quality/ptsafetyII-full.pdf:212-232. Published March 2013. Accessed October 21, 2016.
4. Russo CA, Steiner C, Spector W. Hospitalizations related to pressure ulcers among adults 18 years and older, 2006. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. http://www.ncbi .nlm.nih.gov/books/NBK54557. Published December 2008. Accessed October 21, 2016.
5. Spetz J, Brown DS, Aydin C, Donaldson N. The value of reducing hospital-acquired pressure ulcer prevalence: an illustrative analysis. J Nurs Adm. 2013;43(4):235-241.
6. Whittington KT, Briones R. National prevalence and incidence study: 6-year sequential acute care data. Adv Skin Wound Care. 2004;17(9):490-494.
7. Dorner B, Posthauer ME, Thomas D; National Pressure Ulcer Advisory Panel. The role of nutrition in pressure ulcer prevention and treatment: National Pressure Ulcer Advisory Panel white paper. http://www.npuap.org/wp-content/uploads/2012/03/Nutrition-White-Paper-Website-Version.pdf. Published 2009. Accessed November 7, 2016.
8. Cowan LJ, Stechmiller JK, Rowe M, Kairalla JA. Enhancing Braden pressure ulcer risk assessment in acutely ill adult veterans. Wound Repair Regen. 2012;20(2):137-148.
9. Correia MI, Hegazi RA, Higashiguchi T, et al. Evidence-based recommendations for addressing malnutrition in health care: an updated strategy from the feedM.E. Global Study Group. J Am Med Dir Assoc. 2014;15(8):544-550.
10. Malafarina V, Úriz-Otano F, Fernández-Catalán C, Tejedo-Flors D. Nutritional status and pressure ulcers. Risk assessment and estimation in older adults. J Am Geriatr Soc. 2014;62(6):1209-1210.
11. Posthauer ME, Banks M, Dorner B, Schols JM. The role of nutrition for pressure ulcer management: national pressure ulcer advisory panel, European pressure ulcer advisory panel, and pan pacific pressure injury alliance white paper. Adv Skin Wound Care. 2015;28(4):175-188.
12. Brito PA, de Vasconcelos Generoso S, Correia MI. Prevalence of pressure ulcers in hospitals in Brazil and association with nutritional status—a multicenter, cross-sectional study. Nutrition. 2013;29(4):646-649.
13. Coleman S, Gorecki C, Nelson EA, et al. Patient risk factors for pressure ulcer development: systematic review. Int J Nurs Stud. 2013;50(7):974-1003.
14. Bergstrom N, Braden BJ, Laguzza A, Holman V. The Braden Scale for predicting pressure sore risk. Nurs Res. 1987;36(4):205-210.
15. Ayello EA, Braden B. How and why to do pressure ulcer risk assessment. Adv Skin Wound Care. 2002;15(3):125-131.
16. Wang LH, Chen HL, Yan HY, et al. Inter-rater reliability of three most commonly used pressure ulcer risk assessment scales in clinical practice. Int Wound J. 2015;12(5):590-594.
17. Wilchesky M, Lungu O. Predictive and concurrent validity of the Braden scale in long-term care: a meta-analysis. Wound Repair Regen. 2015;23(1):44-56.
18. Kottner J, Dassen T. An interrater reliability study of the Braden scale in two nursing homes. Int J Nurs Stud. 2008;45(10):1501-1511.
19. Yatabe MS, Taguchi F, Ishida I, et al. Mini nutritional assessment as a useful method of predicting the development of pressure ulcers in elderly inpatients. J Am Geriatr Soc. 2013;61(10):1698-1704.
20. Hiller L, Lowery JC, Davis JA, Shore CJ, Striplin DT. Nutritional status classification in the Department of Veterans Affairs. J Am Diet Assoc. 2001;101(7):786-792.
21. U.S. Department of Veterans Affairs. VHA Handbook 1109.02. Clinical nutrition management. http://www.va.gov/vhapublications/ViewPublica tion.asp?pub_ID=2493. Published February 2012. Accessed October 21, 2016.
22. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174.
23. Serpa LF, Santos VL. Validity of the Braden Nutrition Subscale in predicting pressure ulcer development. J Wound Ostomy Continence Nurs. 2014;41(5):436-443.
24. Reddy M, Gill SS, Rochon PA. Preventing pressure ulcers: a systematic review. JAMA. 2006;296(8):974-984.
25. Cooper KL. Evidence-based prevention of pressure ulcers in the intensive care unit. Crit Care Nurse. 2013;33(6):57-66.
26. Leopold E, Gefen A. Changes in permeability of the plasma membrane of myoblasts to fluorescent dyes with different molecular masses under sustained uniaxial stretching. Med Eng Phys. 2013;35(5):601-607.
A pressure ulcer (PrU) is a localized injury to the skin and/or deep tissues that is due to pressure, friction, or shearing forces. Pressure ulcers are strongly associated with serious comorbidities, particularly inadequate nutrition and immobility.1,2 Pressure ulcers increase hospital costs significantly. In the U.S., PrU care is about $11 billion annually and a cost of between $2,000 and $21,410 per individual PrU.3-5
The impact of nosocomial PrUs remains a key health and economic concern of acute care facilities worldwide. In the U.S., about 2.5 million inpatients annually develop some degree of a PrU during their hospital stay. The reported incidence rates range from 0.4% to 38%.3,6 Each year about 60,000 people die of complications of a PrU.3,6,7 Inadequate nutrition is a critical factor that contributes to the incidence of PrUs.8-12 Consequences of inadequate nutrition have included alterations in skin integrity resulting in PrUs, longer hospital stays, increased costs of care, and higher rates of mortality.9 As a patient’s nutritional status becomes compromised, the likelihood of developing a PrU increases, especially if an individual is immobilized.7,9-11,13
Braden Scale History
The Braden Scale for Predicting Pressure Sore Risk was developed by Barbara Braden, PhD, RN, and Nancy Bergstrom, PhD, RN, in 1987.
The scale is composed of 6 factors: sensory perception, moisture, activity, mobility, friction and shear, and nutrition.14 Each factor is scored on a scale of 1 to 4 points (friction and shear are scored on a point scale of only 1 to 3) for a total possible score of 6 to 23 points (the lower the score, the greater the assumed PrU risk).
The Braden nutrition subscale relies heavily on recording observed or patient self-reported eating habits. It is typically documented by nurses who assess the daily intake of meals: recording a score of 4 if the patient’s meal intake is excellent (eats most of every meal), 3 if the patient’s intake is adequate (eats more than half of most meals), 2 if the patient’s intake is probably inadequate (rarely eats a complete meal), and 1 if a patient’s intake is very poor (never eats a complete meal) (Table 1).14
Historically, the Braden scale is reported to have good reliability when used by registered nurses as a risk prediction tool.14,16 A recent review also reported high interrater reliability of the Braden scale total score among nurses, nursing assistants, and graduate assistants.17 However, other studies suggest certain subscales (such as sensory and nutrition) may have very low interrater reliability among nurses and poor PrU predictability.18,19 To date, there are no known studies evaluating the agreement of the Braden nutrition subscale primarily used by nurses and the VA Nutrition Classification Scheme (VANCS) used by dietitians.
The VA standard of care recommends that PrU risk assessments are documented for all hospitalized veterans within 24 hours of admission, daily, with transfers or discharges, and when there is a status change in the patient. In addition, nutritional assessments by dietitians (using the VANCS) are encouraged within 24 hours of acute care hospitalization.20
The VANCS performed by dietitians consists of 4 classifications: no nutritional compromise, mild nutritional compromise, moderate nutritional compromise, and severenutritional compromise. These classifications are based on well-documented “comprehensive approaches to defining nutritional status that uses multiple parameters” including nutrition history, weight (body mass index and weight loss), diagnoses, diet (and diet orders), brief physical assessment, and preliminary laboratory data (serum albumin/pre-albumin and total lymphocyte count).20,21
The predictive ability of a risk assessment tool is critical to its clinical effectiveness in determining a clinical outcome.17 The Braden scale has been used for more than 30 years in various settings without any significant change to the scale or subscales. In a 2012 study, 4 medical factors were found to be more predictive of PrUs than the Braden scale total score in a sample of 213 acutely ill adult veterans.8 By performing a retrospective study using logistic regression predictive models, severe nutritional compromise (as identified by a dietitian), pneumonia, candidiasis, and surgery were identified as stronger predictors of PrU risk than was the Braden total score.8
With malnutrition as one of the most significant predictive factors in PrU risk, it is critical to determine whether discrepancies exist between the Braden nutrition subscale used primarily by nurses and the VANCS used by dietitians. Hence, the overall purpose of this study was to determine the level of agreement between the Braden nutrition subscale scores documented by nurses and the VANCS used by dietitians and examine the relationship of these assessments with PrU development.
Methods
The parent study was approved by the University of Florida Institutional Review Board before data collection. This secondary analysis of the parent study examined data already collected by Cowan and colleagues, which demonstrated the significance of nutritional compromise in PrU risk.
The de-identified data subset consisted of general demographics, hospital length of stay, specific diagnoses, Braden scores, PrU status, and registered dietician nutritional classification data from 213 acutely ill veterans admitted to North Florida/South Georgia Veterans Health System (NF/SGVHS) in Florida for more than 3 days between January and July 2008.8 The sample consisted of 100 veterans with nosocomial PrUs and 113 veterans without PrUs during their admission.
Scoring
Using the de-identified dataset, the variables of interest (VANCS, Braden nutrition subscale score, and the presence/absence of PrU) were coded. The VANCS was given a corresponding score ranging from 1 to 4 (1, severe nutritional compromise; 2, moderate nutritional compromise; 3, mild nutritional compromise; and 4, no nutritional compromise). The Braden nutrition subscale ranged from 1 to 4 (1 very poor nutrition; 2, probably inadequate nutrition; 3, adequate nutrition; and 4, excellent nutrition). PrU development was coded as 0, no PrU development and 1, PrU development. All nutritional assessments had been recorded in the electronic health record before any PrU reported in the parent study.
Statistical Analysis
After coding the variables of interest, the data were transferred into SAS v 9.4 (Cary, NC). The data collected compared VANCS and Braden nutrition subscale results. In addition, the authors examined the agreement between the score assigned to the VANCS and Braden nutrition subscale results with a weighted
Additionally, the authors computed sensitivity and specificity of the Braden nutrition subscale using the VANCS as the gold standard. The severe and moderately compromised categories of the VANCS combined to form the high-risk category, and the mild-to-no compromise categories were combined to form the low-risk category. The Braden nutrition subscale was similarly dichotomized with the very poor and probably inadequate intake forming the high-risk category and the adequate and excellent intake forming the low-risk category. Sensitivity and specificity of the Braden were then calculated.
Results
Nursing assessments using the Braden nutrition subscale were completed on 213 patients whose mean age (SD) was 71.0 (10.6) years. The VANCS documented by dietitians was completed on 205 patients. For 7 patients, a nutrition assessment was documented only by the Braden nutrition subscale and not the VANCS. Most of the patients were male (97%, n = 206), and white (81.4%, n = 171). The weighted
Landis and colleagues suggest that a
Figure 2 shows the percentage of patients who developed a PrU during hospitalization among different measures of Braden nutrition subscale vs VANCS. In Figure 2, nutritional categories 1, 2, and 3 correspond to very poor intake (Braden)/severe compromise (VANCS), probably inadequate intake (Braden)/moderate compromise (VANCS), and adequate intake (Braden)/mild compromise (VANCS), respectively. There were 3 patients who had a no compromise VANCS; none of these had a PrU, so their data are not represented in Figure 2.
Discussion
Findings from this study indicate that the VANCS documented by dietitians is superior in assessing nutritional risk and predicting the development of PrUs in acutely ill hospitalized veterans compared with the Braden nutrition subscale. This study also shows that the Braden nutrition subscale did not accurately predict PrU development in acutely ill veterans. This finding concurs with the Serpa and Santos study in which the Braden nutrition subscale scores were not predictive for PrU development in hospitalized patients.
One possible explanation for the findings in this study is that the nutrition subscale of the Braden tool asks the assessing clinician to evaluate the amount of food intake the patient is currently taking in for their usual meals. This assessment is highly subjective and speculative and does not account for recent intake fluctuations or weight loss. By comparison, the VANCS is more comprehensive in its ability to assess nutritional compromise based on multiple factors, such as recent weight loss, laboratory indices, body habitus, dentition, and swallowing ability.20 The National Pressure Ulcer Advisory Panel suggests that following an acute care admission, a patient receive a consult from a dietitian if the health care provider suspects that the patient may be nutritionally compromised.1 The study findings demonstrate the utility of the VANCS as predictive of PrU risk.
Unfortunately, the authors have learned that the VANCS may be phased out soon, and many VA facilities are no longer using it. Findings from this study and other recent scientific literature suggest that all inpatients may benefit from nutritional assessments by dietitians. When performed, dietitian assessments provide the basis for more accurate nursing assessment of nutritional risk and targeted interventions. Nursing professionals should be encouraged to review the dietitian assessment and consultation notes and to incorporate this information into a more comprehensive PrU prevention and treatment plan.
Interestingly, in spite of those assessed to have severe nutritional compromise by dietitian assessment (n = 39), very few of these patients (n = 4) had an ICD-9 diagnosis related to malnutrition (ICD-9 codes, 262, 273.8, 269.9, 263.9) entered in their chart for that hospitalization. This observation suggests that 88% of patients with severe nutritional compromise were not appropriately coded at discharge. Improper coding has implications for researchers using ICD-9 diagnosis codes at discharge for accurate analysis of risk factors as well as for health care providers who may look at coded diagnoses information in the charts when considering comorbid conditions for health management.
This study highlights the importance of nutritional status as a risk factor for PrU development. Reasons suggested for nutritional status seeming to be the most significant correlate to PrUs in the acute care setting include the following: decreased protein alters oncotic pressure, making tissue prone to edema; decreases in subcutaneous fat reduce protection from pressure effects; nutritional compromise alters cellular transport of nutrients and waste and makes tissue cells more vulnerable to deformation and physical stresses; and lactate (a by-product of anaerobic glycolysis) or any other metabolic by-product of malnutrition could cause biochemical stress, and tissue cells can die faster as a result of the increased plasma membrane permeability.7,24-26
Limitations
This study was limited to 1 sample of veterans hospitalized in the 2 acute care facilities of NF/SGVHS and the use of a retrospective chart review. As a result, further research is necessary to establish generalizability to other acute care settings and high-risk populations. In spite of these limitations, this and other studies highlight the need for revision of the Braden scale, specifically the nutritional subscale, to lessen the ambiguity seen between dietitian and nursing assessments while also increasing the accuracy in determining a patient’s nutrition risk of PrU development during hospitalization.
Conclusion
These findings provide evidence that dietitians’ documentation of the VANCS related to nutritional compromise are superior to current nutritional risk assessments using the Braden nutrition subscale in predicting PrU risk.
Acknowledgments
The authors acknowledge that this work was supported by the resources of the North Florida/South Georgia Veterans Health System in Gainesville, Florida, and in part by a Small Project Award from the VA Office of Nursing Services.
A pressure ulcer (PrU) is a localized injury to the skin and/or deep tissues that is due to pressure, friction, or shearing forces. Pressure ulcers are strongly associated with serious comorbidities, particularly inadequate nutrition and immobility.1,2 Pressure ulcers increase hospital costs significantly. In the U.S., PrU care is about $11 billion annually and a cost of between $2,000 and $21,410 per individual PrU.3-5
The impact of nosocomial PrUs remains a key health and economic concern of acute care facilities worldwide. In the U.S., about 2.5 million inpatients annually develop some degree of a PrU during their hospital stay. The reported incidence rates range from 0.4% to 38%.3,6 Each year about 60,000 people die of complications of a PrU.3,6,7 Inadequate nutrition is a critical factor that contributes to the incidence of PrUs.8-12 Consequences of inadequate nutrition have included alterations in skin integrity resulting in PrUs, longer hospital stays, increased costs of care, and higher rates of mortality.9 As a patient’s nutritional status becomes compromised, the likelihood of developing a PrU increases, especially if an individual is immobilized.7,9-11,13
Braden Scale History
The Braden Scale for Predicting Pressure Sore Risk was developed by Barbara Braden, PhD, RN, and Nancy Bergstrom, PhD, RN, in 1987.
The scale is composed of 6 factors: sensory perception, moisture, activity, mobility, friction and shear, and nutrition.14 Each factor is scored on a scale of 1 to 4 points (friction and shear are scored on a point scale of only 1 to 3) for a total possible score of 6 to 23 points (the lower the score, the greater the assumed PrU risk).
The Braden nutrition subscale relies heavily on recording observed or patient self-reported eating habits. It is typically documented by nurses who assess the daily intake of meals: recording a score of 4 if the patient’s meal intake is excellent (eats most of every meal), 3 if the patient’s intake is adequate (eats more than half of most meals), 2 if the patient’s intake is probably inadequate (rarely eats a complete meal), and 1 if a patient’s intake is very poor (never eats a complete meal) (Table 1).14
Historically, the Braden scale is reported to have good reliability when used by registered nurses as a risk prediction tool.14,16 A recent review also reported high interrater reliability of the Braden scale total score among nurses, nursing assistants, and graduate assistants.17 However, other studies suggest certain subscales (such as sensory and nutrition) may have very low interrater reliability among nurses and poor PrU predictability.18,19 To date, there are no known studies evaluating the agreement of the Braden nutrition subscale primarily used by nurses and the VA Nutrition Classification Scheme (VANCS) used by dietitians.
The VA standard of care recommends that PrU risk assessments are documented for all hospitalized veterans within 24 hours of admission, daily, with transfers or discharges, and when there is a status change in the patient. In addition, nutritional assessments by dietitians (using the VANCS) are encouraged within 24 hours of acute care hospitalization.20
The VANCS performed by dietitians consists of 4 classifications: no nutritional compromise, mild nutritional compromise, moderate nutritional compromise, and severenutritional compromise. These classifications are based on well-documented “comprehensive approaches to defining nutritional status that uses multiple parameters” including nutrition history, weight (body mass index and weight loss), diagnoses, diet (and diet orders), brief physical assessment, and preliminary laboratory data (serum albumin/pre-albumin and total lymphocyte count).20,21
The predictive ability of a risk assessment tool is critical to its clinical effectiveness in determining a clinical outcome.17 The Braden scale has been used for more than 30 years in various settings without any significant change to the scale or subscales. In a 2012 study, 4 medical factors were found to be more predictive of PrUs than the Braden scale total score in a sample of 213 acutely ill adult veterans.8 By performing a retrospective study using logistic regression predictive models, severe nutritional compromise (as identified by a dietitian), pneumonia, candidiasis, and surgery were identified as stronger predictors of PrU risk than was the Braden total score.8
With malnutrition as one of the most significant predictive factors in PrU risk, it is critical to determine whether discrepancies exist between the Braden nutrition subscale used primarily by nurses and the VANCS used by dietitians. Hence, the overall purpose of this study was to determine the level of agreement between the Braden nutrition subscale scores documented by nurses and the VANCS used by dietitians and examine the relationship of these assessments with PrU development.
Methods
The parent study was approved by the University of Florida Institutional Review Board before data collection. This secondary analysis of the parent study examined data already collected by Cowan and colleagues, which demonstrated the significance of nutritional compromise in PrU risk.
The de-identified data subset consisted of general demographics, hospital length of stay, specific diagnoses, Braden scores, PrU status, and registered dietician nutritional classification data from 213 acutely ill veterans admitted to North Florida/South Georgia Veterans Health System (NF/SGVHS) in Florida for more than 3 days between January and July 2008.8 The sample consisted of 100 veterans with nosocomial PrUs and 113 veterans without PrUs during their admission.
Scoring
Using the de-identified dataset, the variables of interest (VANCS, Braden nutrition subscale score, and the presence/absence of PrU) were coded. The VANCS was given a corresponding score ranging from 1 to 4 (1, severe nutritional compromise; 2, moderate nutritional compromise; 3, mild nutritional compromise; and 4, no nutritional compromise). The Braden nutrition subscale ranged from 1 to 4 (1 very poor nutrition; 2, probably inadequate nutrition; 3, adequate nutrition; and 4, excellent nutrition). PrU development was coded as 0, no PrU development and 1, PrU development. All nutritional assessments had been recorded in the electronic health record before any PrU reported in the parent study.
Statistical Analysis
After coding the variables of interest, the data were transferred into SAS v 9.4 (Cary, NC). The data collected compared VANCS and Braden nutrition subscale results. In addition, the authors examined the agreement between the score assigned to the VANCS and Braden nutrition subscale results with a weighted
Additionally, the authors computed sensitivity and specificity of the Braden nutrition subscale using the VANCS as the gold standard. The severe and moderately compromised categories of the VANCS combined to form the high-risk category, and the mild-to-no compromise categories were combined to form the low-risk category. The Braden nutrition subscale was similarly dichotomized with the very poor and probably inadequate intake forming the high-risk category and the adequate and excellent intake forming the low-risk category. Sensitivity and specificity of the Braden were then calculated.
Results
Nursing assessments using the Braden nutrition subscale were completed on 213 patients whose mean age (SD) was 71.0 (10.6) years. The VANCS documented by dietitians was completed on 205 patients. For 7 patients, a nutrition assessment was documented only by the Braden nutrition subscale and not the VANCS. Most of the patients were male (97%, n = 206), and white (81.4%, n = 171). The weighted
Landis and colleagues suggest that a
Figure 2 shows the percentage of patients who developed a PrU during hospitalization among different measures of Braden nutrition subscale vs VANCS. In Figure 2, nutritional categories 1, 2, and 3 correspond to very poor intake (Braden)/severe compromise (VANCS), probably inadequate intake (Braden)/moderate compromise (VANCS), and adequate intake (Braden)/mild compromise (VANCS), respectively. There were 3 patients who had a no compromise VANCS; none of these had a PrU, so their data are not represented in Figure 2.
Discussion
Findings from this study indicate that the VANCS documented by dietitians is superior in assessing nutritional risk and predicting the development of PrUs in acutely ill hospitalized veterans compared with the Braden nutrition subscale. This study also shows that the Braden nutrition subscale did not accurately predict PrU development in acutely ill veterans. This finding concurs with the Serpa and Santos study in which the Braden nutrition subscale scores were not predictive for PrU development in hospitalized patients.
One possible explanation for the findings in this study is that the nutrition subscale of the Braden tool asks the assessing clinician to evaluate the amount of food intake the patient is currently taking in for their usual meals. This assessment is highly subjective and speculative and does not account for recent intake fluctuations or weight loss. By comparison, the VANCS is more comprehensive in its ability to assess nutritional compromise based on multiple factors, such as recent weight loss, laboratory indices, body habitus, dentition, and swallowing ability.20 The National Pressure Ulcer Advisory Panel suggests that following an acute care admission, a patient receive a consult from a dietitian if the health care provider suspects that the patient may be nutritionally compromised.1 The study findings demonstrate the utility of the VANCS as predictive of PrU risk.
Unfortunately, the authors have learned that the VANCS may be phased out soon, and many VA facilities are no longer using it. Findings from this study and other recent scientific literature suggest that all inpatients may benefit from nutritional assessments by dietitians. When performed, dietitian assessments provide the basis for more accurate nursing assessment of nutritional risk and targeted interventions. Nursing professionals should be encouraged to review the dietitian assessment and consultation notes and to incorporate this information into a more comprehensive PrU prevention and treatment plan.
Interestingly, in spite of those assessed to have severe nutritional compromise by dietitian assessment (n = 39), very few of these patients (n = 4) had an ICD-9 diagnosis related to malnutrition (ICD-9 codes, 262, 273.8, 269.9, 263.9) entered in their chart for that hospitalization. This observation suggests that 88% of patients with severe nutritional compromise were not appropriately coded at discharge. Improper coding has implications for researchers using ICD-9 diagnosis codes at discharge for accurate analysis of risk factors as well as for health care providers who may look at coded diagnoses information in the charts when considering comorbid conditions for health management.
This study highlights the importance of nutritional status as a risk factor for PrU development. Reasons suggested for nutritional status seeming to be the most significant correlate to PrUs in the acute care setting include the following: decreased protein alters oncotic pressure, making tissue prone to edema; decreases in subcutaneous fat reduce protection from pressure effects; nutritional compromise alters cellular transport of nutrients and waste and makes tissue cells more vulnerable to deformation and physical stresses; and lactate (a by-product of anaerobic glycolysis) or any other metabolic by-product of malnutrition could cause biochemical stress, and tissue cells can die faster as a result of the increased plasma membrane permeability.7,24-26
Limitations
This study was limited to 1 sample of veterans hospitalized in the 2 acute care facilities of NF/SGVHS and the use of a retrospective chart review. As a result, further research is necessary to establish generalizability to other acute care settings and high-risk populations. In spite of these limitations, this and other studies highlight the need for revision of the Braden scale, specifically the nutritional subscale, to lessen the ambiguity seen between dietitian and nursing assessments while also increasing the accuracy in determining a patient’s nutrition risk of PrU development during hospitalization.
Conclusion
These findings provide evidence that dietitians’ documentation of the VANCS related to nutritional compromise are superior to current nutritional risk assessments using the Braden nutrition subscale in predicting PrU risk.
Acknowledgments
The authors acknowledge that this work was supported by the resources of the North Florida/South Georgia Veterans Health System in Gainesville, Florida, and in part by a Small Project Award from the VA Office of Nursing Services.
1. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. http://www.npuap.org/resources/educational-and-clinical -resources/prevention-and-treatment-of-pressure -ulcers-clinical-practice-guideline. Updated 2014. Accessed November 7, 2016.
2. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, Pan Pacific Pressure Injury Alliance. Prevention and treatment of pressure ulcers: quick reference guide. http://www .npuap.org/wp-content/uploads/2014/08/Updated -10-16-14-Quick-Reference-Guide-DIGITAL-NPUAP-EPUAP-PPPIA-16Oct2014.pdf. Updated October 16, 2014. Accessed October 21, 2016.
3. Sullivan N. Preventing in-facility pressure ulcers. In: Agency for Healthcare Research and Quality. Making Health Care Safer II. An Updated Critical Analysis of the Evidence for Patient Safety Practices. Evidence Reports/Technology Assessments. http://www.ahrq.gov/sites/default/files/wysiwyg/research/findings/evidence-based-reports/services/quality/ptsafetyII-full.pdf:212-232. Published March 2013. Accessed October 21, 2016.
4. Russo CA, Steiner C, Spector W. Hospitalizations related to pressure ulcers among adults 18 years and older, 2006. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. http://www.ncbi .nlm.nih.gov/books/NBK54557. Published December 2008. Accessed October 21, 2016.
5. Spetz J, Brown DS, Aydin C, Donaldson N. The value of reducing hospital-acquired pressure ulcer prevalence: an illustrative analysis. J Nurs Adm. 2013;43(4):235-241.
6. Whittington KT, Briones R. National prevalence and incidence study: 6-year sequential acute care data. Adv Skin Wound Care. 2004;17(9):490-494.
7. Dorner B, Posthauer ME, Thomas D; National Pressure Ulcer Advisory Panel. The role of nutrition in pressure ulcer prevention and treatment: National Pressure Ulcer Advisory Panel white paper. http://www.npuap.org/wp-content/uploads/2012/03/Nutrition-White-Paper-Website-Version.pdf. Published 2009. Accessed November 7, 2016.
8. Cowan LJ, Stechmiller JK, Rowe M, Kairalla JA. Enhancing Braden pressure ulcer risk assessment in acutely ill adult veterans. Wound Repair Regen. 2012;20(2):137-148.
9. Correia MI, Hegazi RA, Higashiguchi T, et al. Evidence-based recommendations for addressing malnutrition in health care: an updated strategy from the feedM.E. Global Study Group. J Am Med Dir Assoc. 2014;15(8):544-550.
10. Malafarina V, Úriz-Otano F, Fernández-Catalán C, Tejedo-Flors D. Nutritional status and pressure ulcers. Risk assessment and estimation in older adults. J Am Geriatr Soc. 2014;62(6):1209-1210.
11. Posthauer ME, Banks M, Dorner B, Schols JM. The role of nutrition for pressure ulcer management: national pressure ulcer advisory panel, European pressure ulcer advisory panel, and pan pacific pressure injury alliance white paper. Adv Skin Wound Care. 2015;28(4):175-188.
12. Brito PA, de Vasconcelos Generoso S, Correia MI. Prevalence of pressure ulcers in hospitals in Brazil and association with nutritional status—a multicenter, cross-sectional study. Nutrition. 2013;29(4):646-649.
13. Coleman S, Gorecki C, Nelson EA, et al. Patient risk factors for pressure ulcer development: systematic review. Int J Nurs Stud. 2013;50(7):974-1003.
14. Bergstrom N, Braden BJ, Laguzza A, Holman V. The Braden Scale for predicting pressure sore risk. Nurs Res. 1987;36(4):205-210.
15. Ayello EA, Braden B. How and why to do pressure ulcer risk assessment. Adv Skin Wound Care. 2002;15(3):125-131.
16. Wang LH, Chen HL, Yan HY, et al. Inter-rater reliability of three most commonly used pressure ulcer risk assessment scales in clinical practice. Int Wound J. 2015;12(5):590-594.
17. Wilchesky M, Lungu O. Predictive and concurrent validity of the Braden scale in long-term care: a meta-analysis. Wound Repair Regen. 2015;23(1):44-56.
18. Kottner J, Dassen T. An interrater reliability study of the Braden scale in two nursing homes. Int J Nurs Stud. 2008;45(10):1501-1511.
19. Yatabe MS, Taguchi F, Ishida I, et al. Mini nutritional assessment as a useful method of predicting the development of pressure ulcers in elderly inpatients. J Am Geriatr Soc. 2013;61(10):1698-1704.
20. Hiller L, Lowery JC, Davis JA, Shore CJ, Striplin DT. Nutritional status classification in the Department of Veterans Affairs. J Am Diet Assoc. 2001;101(7):786-792.
21. U.S. Department of Veterans Affairs. VHA Handbook 1109.02. Clinical nutrition management. http://www.va.gov/vhapublications/ViewPublica tion.asp?pub_ID=2493. Published February 2012. Accessed October 21, 2016.
22. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174.
23. Serpa LF, Santos VL. Validity of the Braden Nutrition Subscale in predicting pressure ulcer development. J Wound Ostomy Continence Nurs. 2014;41(5):436-443.
24. Reddy M, Gill SS, Rochon PA. Preventing pressure ulcers: a systematic review. JAMA. 2006;296(8):974-984.
25. Cooper KL. Evidence-based prevention of pressure ulcers in the intensive care unit. Crit Care Nurse. 2013;33(6):57-66.
26. Leopold E, Gefen A. Changes in permeability of the plasma membrane of myoblasts to fluorescent dyes with different molecular masses under sustained uniaxial stretching. Med Eng Phys. 2013;35(5):601-607.
1. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. http://www.npuap.org/resources/educational-and-clinical -resources/prevention-and-treatment-of-pressure -ulcers-clinical-practice-guideline. Updated 2014. Accessed November 7, 2016.
2. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, Pan Pacific Pressure Injury Alliance. Prevention and treatment of pressure ulcers: quick reference guide. http://www .npuap.org/wp-content/uploads/2014/08/Updated -10-16-14-Quick-Reference-Guide-DIGITAL-NPUAP-EPUAP-PPPIA-16Oct2014.pdf. Updated October 16, 2014. Accessed October 21, 2016.
3. Sullivan N. Preventing in-facility pressure ulcers. In: Agency for Healthcare Research and Quality. Making Health Care Safer II. An Updated Critical Analysis of the Evidence for Patient Safety Practices. Evidence Reports/Technology Assessments. http://www.ahrq.gov/sites/default/files/wysiwyg/research/findings/evidence-based-reports/services/quality/ptsafetyII-full.pdf:212-232. Published March 2013. Accessed October 21, 2016.
4. Russo CA, Steiner C, Spector W. Hospitalizations related to pressure ulcers among adults 18 years and older, 2006. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. http://www.ncbi .nlm.nih.gov/books/NBK54557. Published December 2008. Accessed October 21, 2016.
5. Spetz J, Brown DS, Aydin C, Donaldson N. The value of reducing hospital-acquired pressure ulcer prevalence: an illustrative analysis. J Nurs Adm. 2013;43(4):235-241.
6. Whittington KT, Briones R. National prevalence and incidence study: 6-year sequential acute care data. Adv Skin Wound Care. 2004;17(9):490-494.
7. Dorner B, Posthauer ME, Thomas D; National Pressure Ulcer Advisory Panel. The role of nutrition in pressure ulcer prevention and treatment: National Pressure Ulcer Advisory Panel white paper. http://www.npuap.org/wp-content/uploads/2012/03/Nutrition-White-Paper-Website-Version.pdf. Published 2009. Accessed November 7, 2016.
8. Cowan LJ, Stechmiller JK, Rowe M, Kairalla JA. Enhancing Braden pressure ulcer risk assessment in acutely ill adult veterans. Wound Repair Regen. 2012;20(2):137-148.
9. Correia MI, Hegazi RA, Higashiguchi T, et al. Evidence-based recommendations for addressing malnutrition in health care: an updated strategy from the feedM.E. Global Study Group. J Am Med Dir Assoc. 2014;15(8):544-550.
10. Malafarina V, Úriz-Otano F, Fernández-Catalán C, Tejedo-Flors D. Nutritional status and pressure ulcers. Risk assessment and estimation in older adults. J Am Geriatr Soc. 2014;62(6):1209-1210.
11. Posthauer ME, Banks M, Dorner B, Schols JM. The role of nutrition for pressure ulcer management: national pressure ulcer advisory panel, European pressure ulcer advisory panel, and pan pacific pressure injury alliance white paper. Adv Skin Wound Care. 2015;28(4):175-188.
12. Brito PA, de Vasconcelos Generoso S, Correia MI. Prevalence of pressure ulcers in hospitals in Brazil and association with nutritional status—a multicenter, cross-sectional study. Nutrition. 2013;29(4):646-649.
13. Coleman S, Gorecki C, Nelson EA, et al. Patient risk factors for pressure ulcer development: systematic review. Int J Nurs Stud. 2013;50(7):974-1003.
14. Bergstrom N, Braden BJ, Laguzza A, Holman V. The Braden Scale for predicting pressure sore risk. Nurs Res. 1987;36(4):205-210.
15. Ayello EA, Braden B. How and why to do pressure ulcer risk assessment. Adv Skin Wound Care. 2002;15(3):125-131.
16. Wang LH, Chen HL, Yan HY, et al. Inter-rater reliability of three most commonly used pressure ulcer risk assessment scales in clinical practice. Int Wound J. 2015;12(5):590-594.
17. Wilchesky M, Lungu O. Predictive and concurrent validity of the Braden scale in long-term care: a meta-analysis. Wound Repair Regen. 2015;23(1):44-56.
18. Kottner J, Dassen T. An interrater reliability study of the Braden scale in two nursing homes. Int J Nurs Stud. 2008;45(10):1501-1511.
19. Yatabe MS, Taguchi F, Ishida I, et al. Mini nutritional assessment as a useful method of predicting the development of pressure ulcers in elderly inpatients. J Am Geriatr Soc. 2013;61(10):1698-1704.
20. Hiller L, Lowery JC, Davis JA, Shore CJ, Striplin DT. Nutritional status classification in the Department of Veterans Affairs. J Am Diet Assoc. 2001;101(7):786-792.
21. U.S. Department of Veterans Affairs. VHA Handbook 1109.02. Clinical nutrition management. http://www.va.gov/vhapublications/ViewPublica tion.asp?pub_ID=2493. Published February 2012. Accessed October 21, 2016.
22. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174.
23. Serpa LF, Santos VL. Validity of the Braden Nutrition Subscale in predicting pressure ulcer development. J Wound Ostomy Continence Nurs. 2014;41(5):436-443.
24. Reddy M, Gill SS, Rochon PA. Preventing pressure ulcers: a systematic review. JAMA. 2006;296(8):974-984.
25. Cooper KL. Evidence-based prevention of pressure ulcers in the intensive care unit. Crit Care Nurse. 2013;33(6):57-66.
26. Leopold E, Gefen A. Changes in permeability of the plasma membrane of myoblasts to fluorescent dyes with different molecular masses under sustained uniaxial stretching. Med Eng Phys. 2013;35(5):601-607.
Rinse could provide short-term treatment of oral cGVHD

Photo courtesy of NIH
SAN DIEGO—Results of a phase 2 study suggest an oral mouth rinse formulation of the steroid clobetasol could provide short-term treatment of oral chronic graft-vs-host disease (cGVHD).
A majority of patients had a greater than 25% improvement in their cGVHD after using the clobetasol rinse, and patients reported improvements in oral health-related quality of life.
The rinse even proved effective in patients who had failed prior treatment with clobetasol ointment.
However, researchers found evidence to suggest the clobetasol rinse is not suitable for unmonitored, long-term use, as some patients experienced adrenal suppression.
Jacqueline W. Mays, DDS, PhD, of the National Institutes of Health (NIH) in Bethesda, Maryland, presented these findings at the 2016 ASH Annual Meeting (abstract 826).
Dr Mays noted that topical therapy for oral cGVHD is intended to spare patients from exposure to systemic immunosuppressive agents.
According to NIH consensus criteria, dexamethasone is recommended as the first-line topical therapy for these patients. However, clinical trial data suggest only 29% to 58% of patients respond to this therapy.
Second-line treatment is not well-established, but it typically consists of topical steroids in a gel or ointment formulation. Unfortunately, patient compliance is an issue with this type of treatment.
“If you can imagine trying to apply something in a petrolatum base to the inside of your very wet wall cavity, you can imagine that’s a challenge for a healthy individual, much less for a chronic graft-vs-host disease patient who often will have joint mobility and fine motor issues,” Dr Mays said.
“So this leads to frequent treatment failures of topical regimens, not only due to the drug agents but also due to patient compliance.”
Dr Mays noted that clobetasol is a superpotent synthetic glucocorticoid that has been used off-label in ointment form to treat refractory oral GVHD.
In an attempt to overcome the application challenges with this ointment and improve patient adherence to oral cGVHD treatment, Dr Mays and her colleagues decided to investigate a clobetasol 0.05% solution formulated as an oral rinse in an aqueous base.
The team tested the rinse in a phase 2 trial with an initial 2-week randomized, double-blind, placebo-controlled period.
Patient population
The trial enrolled and randomized 36 patients with oral cGVHD. The patients had an Oral Mucositis Rating Scale (OMRS) score of ≥20 with moderate erythema and/or ulceration. They also had stable or tapering systemic therapy during the 2 weeks prior to starting the study and for the duration of the blinded period.
The patients’ median age was 42 (range, 18-68), and 20 were male. Thirty-five patients received ablative conditioning, 18 received a related-donor transplant, 34 received a matched-donor transplant, and 30 received a peripheral blood stem cell graft.
The median time from cGVHD diagnosis to trial enrollment was 257 days (range, 15-3013). Thirty-six patients had mouth cGVHD, 21 had skin cGVHD, 26 had eye cGVHD, 14 had gastrointestinal cGVHD, 16 had liver cGVHD, 11 had lung cGVHD, and 10 had cGVHD of the joints and fascia.
Six patients had not received any prior oral topical therapy. The other 30 patients had a median of 2 prior oral topical therapies. Eleven patients had received prior clobetasol ointment.
Treatment
The patients were randomized to receive clobetasol or placebo rinse for 2 weeks (blinded period). After that, all patients received clobetasol rinse until they completed 28 days of treatment.
The patients were required to perform a 2-minute swish with 10 ml of clobetasol rinse 3 times daily and a once-daily swish with nystatin (100,000 u/ml) rinse for antifungal prophylaxis. The patients continued on systemic pneumocystis, antiviral, and antifungal prophylaxis, per NIH cGVHD guidelines.
Thirty-two of the patients completed treatment, using the clobetasol rinse for the full 28 days.
Four patients went off study before completing 28 days of treatment. One of these patients could not tolerate the rinse. This patient had gastrointestinal issues that were attributed (by the patient and the physician) to use of the study drug.
Two patients went off study because they could not make it to the NIH for follow-up visits, and 1 patient died. The death was unrelated to the study drug.
Safety
Dr Mays noted that small amounts of clobetasol were detectable in the bloodstream, but she and her colleagues found this was not directly correlated to patient serum cortisol levels.
However, the researchers did observe a significant drop in serum cortisol levels from baseline to day 28, suggesting the rinse has an adrenal impact.
On the other hand, the peripheral lymphocyte profile was unchanged by the use of clobetasol rinse, which suggests there were no significant systemic immunosuppressive effects.
Adverse events considered possibly or probably related to clobetasol rinse included herpes simplex virus reactivation (n=3, grade 2-3), oral candidiasis (n=3, grade 2), other oral viral infection (n=1, grade 2), facial edema (n=3, grade 1), and adrenal suppression (6 grade 1 and 1 grade 2).
Dr Mays noted that many of the patients came on the study with adrenal suppression, but the clobetasol rinse had an additional impact.
Efficacy
The study’s primary endpoint was change in oral cGVHD severity scale at day 28 compared to baseline. Complete response was defined as a score of 0 on the erythema and ulceration components. Partial response was defined as a 25% decrease in score.
Progression was defined as a 25% increase in initial score. Stable disease was defined as a status that does not meet the criteria for progression or response.
Ninety-one percent of patients had a greater than 25% improvement in oral cGVHD severity scale. Nineteen percent of patients had a complete response, 72% of patients had a partial response, and 9% had stable disease. None of the patients progressed.
Dr Mays noted that patients who failed treatment with prior clobetasol ointment responded similarly to the clobetasol rinse when compared with the full study cohort.
Among the 11 patients with prior clobetasol ointment, 18% had a complete response, 73% had a partial response, 9% had stable disease, and none progressed.
Clobetasol rinse significantly decreased the clinical OMRS score (P<0.0001) and improved cGVHD pathology diagnosis (P=0.0001).
Patients reported a significant improvement in oral health-based quality of life (P=0.0008) after completing treatment, as well as significant improvements in oral pain (P=0.017) and oral sensitivity (P=0.0081).
Though saliva production did not change significantly from baseline to day 28, patients reported a significant improvement in oral dryness (P=0.014).
The blinded period of the study showed that placebo treatment was not effective. There was a significant difference between the placebo and clobetasol groups with regard to improvement in OMRS score from baseline to day 14 (P=0.0031).
“We found clobetasol oral rinse to be both effective and safe for short-term treatment of oral mucosal cGVHD and hope that it will improve sparing of systemic immunosuppressants in this patient population,” Dr Mays said. “Its risk profile is generally not suitable for unmonitored, long-term use.” ![]()
Photo courtesy of NIH
SAN DIEGO—Results of a phase 2 study suggest an oral mouth rinse formulation of the steroid clobetasol could provide short-term treatment of oral chronic graft-vs-host disease (cGVHD).
A majority of patients had a greater than 25% improvement in their cGVHD after using the clobetasol rinse, and patients reported improvements in oral health-related quality of life.
The rinse even proved effective in patients who had failed prior treatment with clobetasol ointment.
However, researchers found evidence to suggest the clobetasol rinse is not suitable for unmonitored, long-term use, as some patients experienced adrenal suppression.
Jacqueline W. Mays, DDS, PhD, of the National Institutes of Health (NIH) in Bethesda, Maryland, presented these findings at the 2016 ASH Annual Meeting (abstract 826).
Dr Mays noted that topical therapy for oral cGVHD is intended to spare patients from exposure to systemic immunosuppressive agents.
According to NIH consensus criteria, dexamethasone is recommended as the first-line topical therapy for these patients. However, clinical trial data suggest only 29% to 58% of patients respond to this therapy.
Second-line treatment is not well-established, but it typically consists of topical steroids in a gel or ointment formulation. Unfortunately, patient compliance is an issue with this type of treatment.
“If you can imagine trying to apply something in a petrolatum base to the inside of your very wet wall cavity, you can imagine that’s a challenge for a healthy individual, much less for a chronic graft-vs-host disease patient who often will have joint mobility and fine motor issues,” Dr Mays said.
“So this leads to frequent treatment failures of topical regimens, not only due to the drug agents but also due to patient compliance.”
Dr Mays noted that clobetasol is a superpotent synthetic glucocorticoid that has been used off-label in ointment form to treat refractory oral GVHD.
In an attempt to overcome the application challenges with this ointment and improve patient adherence to oral cGVHD treatment, Dr Mays and her colleagues decided to investigate a clobetasol 0.05% solution formulated as an oral rinse in an aqueous base.
The team tested the rinse in a phase 2 trial with an initial 2-week randomized, double-blind, placebo-controlled period.
Patient population
The trial enrolled and randomized 36 patients with oral cGVHD. The patients had an Oral Mucositis Rating Scale (OMRS) score of ≥20 with moderate erythema and/or ulceration. They also had stable or tapering systemic therapy during the 2 weeks prior to starting the study and for the duration of the blinded period.
The patients’ median age was 42 (range, 18-68), and 20 were male. Thirty-five patients received ablative conditioning, 18 received a related-donor transplant, 34 received a matched-donor transplant, and 30 received a peripheral blood stem cell graft.
The median time from cGVHD diagnosis to trial enrollment was 257 days (range, 15-3013). Thirty-six patients had mouth cGVHD, 21 had skin cGVHD, 26 had eye cGVHD, 14 had gastrointestinal cGVHD, 16 had liver cGVHD, 11 had lung cGVHD, and 10 had cGVHD of the joints and fascia.
Six patients had not received any prior oral topical therapy. The other 30 patients had a median of 2 prior oral topical therapies. Eleven patients had received prior clobetasol ointment.
Treatment
The patients were randomized to receive clobetasol or placebo rinse for 2 weeks (blinded period). After that, all patients received clobetasol rinse until they completed 28 days of treatment.
The patients were required to perform a 2-minute swish with 10 ml of clobetasol rinse 3 times daily and a once-daily swish with nystatin (100,000 u/ml) rinse for antifungal prophylaxis. The patients continued on systemic pneumocystis, antiviral, and antifungal prophylaxis, per NIH cGVHD guidelines.
Thirty-two of the patients completed treatment, using the clobetasol rinse for the full 28 days.
Four patients went off study before completing 28 days of treatment. One of these patients could not tolerate the rinse. This patient had gastrointestinal issues that were attributed (by the patient and the physician) to use of the study drug.
Two patients went off study because they could not make it to the NIH for follow-up visits, and 1 patient died. The death was unrelated to the study drug.
Safety
Dr Mays noted that small amounts of clobetasol were detectable in the bloodstream, but she and her colleagues found this was not directly correlated to patient serum cortisol levels.
However, the researchers did observe a significant drop in serum cortisol levels from baseline to day 28, suggesting the rinse has an adrenal impact.
On the other hand, the peripheral lymphocyte profile was unchanged by the use of clobetasol rinse, which suggests there were no significant systemic immunosuppressive effects.
Adverse events considered possibly or probably related to clobetasol rinse included herpes simplex virus reactivation (n=3, grade 2-3), oral candidiasis (n=3, grade 2), other oral viral infection (n=1, grade 2), facial edema (n=3, grade 1), and adrenal suppression (6 grade 1 and 1 grade 2).
Dr Mays noted that many of the patients came on the study with adrenal suppression, but the clobetasol rinse had an additional impact.
Efficacy
The study’s primary endpoint was change in oral cGVHD severity scale at day 28 compared to baseline. Complete response was defined as a score of 0 on the erythema and ulceration components. Partial response was defined as a 25% decrease in score.
Progression was defined as a 25% increase in initial score. Stable disease was defined as a status that does not meet the criteria for progression or response.
Ninety-one percent of patients had a greater than 25% improvement in oral cGVHD severity scale. Nineteen percent of patients had a complete response, 72% of patients had a partial response, and 9% had stable disease. None of the patients progressed.
Dr Mays noted that patients who failed treatment with prior clobetasol ointment responded similarly to the clobetasol rinse when compared with the full study cohort.
Among the 11 patients with prior clobetasol ointment, 18% had a complete response, 73% had a partial response, 9% had stable disease, and none progressed.
Clobetasol rinse significantly decreased the clinical OMRS score (P<0.0001) and improved cGVHD pathology diagnosis (P=0.0001).
Patients reported a significant improvement in oral health-based quality of life (P=0.0008) after completing treatment, as well as significant improvements in oral pain (P=0.017) and oral sensitivity (P=0.0081).
Though saliva production did not change significantly from baseline to day 28, patients reported a significant improvement in oral dryness (P=0.014).
The blinded period of the study showed that placebo treatment was not effective. There was a significant difference between the placebo and clobetasol groups with regard to improvement in OMRS score from baseline to day 14 (P=0.0031).
“We found clobetasol oral rinse to be both effective and safe for short-term treatment of oral mucosal cGVHD and hope that it will improve sparing of systemic immunosuppressants in this patient population,” Dr Mays said. “Its risk profile is generally not suitable for unmonitored, long-term use.” ![]()
Photo courtesy of NIH
SAN DIEGO—Results of a phase 2 study suggest an oral mouth rinse formulation of the steroid clobetasol could provide short-term treatment of oral chronic graft-vs-host disease (cGVHD).
A majority of patients had a greater than 25% improvement in their cGVHD after using the clobetasol rinse, and patients reported improvements in oral health-related quality of life.
The rinse even proved effective in patients who had failed prior treatment with clobetasol ointment.
However, researchers found evidence to suggest the clobetasol rinse is not suitable for unmonitored, long-term use, as some patients experienced adrenal suppression.
Jacqueline W. Mays, DDS, PhD, of the National Institutes of Health (NIH) in Bethesda, Maryland, presented these findings at the 2016 ASH Annual Meeting (abstract 826).
Dr Mays noted that topical therapy for oral cGVHD is intended to spare patients from exposure to systemic immunosuppressive agents.
According to NIH consensus criteria, dexamethasone is recommended as the first-line topical therapy for these patients. However, clinical trial data suggest only 29% to 58% of patients respond to this therapy.
Second-line treatment is not well-established, but it typically consists of topical steroids in a gel or ointment formulation. Unfortunately, patient compliance is an issue with this type of treatment.
“If you can imagine trying to apply something in a petrolatum base to the inside of your very wet wall cavity, you can imagine that’s a challenge for a healthy individual, much less for a chronic graft-vs-host disease patient who often will have joint mobility and fine motor issues,” Dr Mays said.
“So this leads to frequent treatment failures of topical regimens, not only due to the drug agents but also due to patient compliance.”
Dr Mays noted that clobetasol is a superpotent synthetic glucocorticoid that has been used off-label in ointment form to treat refractory oral GVHD.
In an attempt to overcome the application challenges with this ointment and improve patient adherence to oral cGVHD treatment, Dr Mays and her colleagues decided to investigate a clobetasol 0.05% solution formulated as an oral rinse in an aqueous base.
The team tested the rinse in a phase 2 trial with an initial 2-week randomized, double-blind, placebo-controlled period.
Patient population
The trial enrolled and randomized 36 patients with oral cGVHD. The patients had an Oral Mucositis Rating Scale (OMRS) score of ≥20 with moderate erythema and/or ulceration. They also had stable or tapering systemic therapy during the 2 weeks prior to starting the study and for the duration of the blinded period.
The patients’ median age was 42 (range, 18-68), and 20 were male. Thirty-five patients received ablative conditioning, 18 received a related-donor transplant, 34 received a matched-donor transplant, and 30 received a peripheral blood stem cell graft.
The median time from cGVHD diagnosis to trial enrollment was 257 days (range, 15-3013). Thirty-six patients had mouth cGVHD, 21 had skin cGVHD, 26 had eye cGVHD, 14 had gastrointestinal cGVHD, 16 had liver cGVHD, 11 had lung cGVHD, and 10 had cGVHD of the joints and fascia.
Six patients had not received any prior oral topical therapy. The other 30 patients had a median of 2 prior oral topical therapies. Eleven patients had received prior clobetasol ointment.
Treatment
The patients were randomized to receive clobetasol or placebo rinse for 2 weeks (blinded period). After that, all patients received clobetasol rinse until they completed 28 days of treatment.
The patients were required to perform a 2-minute swish with 10 ml of clobetasol rinse 3 times daily and a once-daily swish with nystatin (100,000 u/ml) rinse for antifungal prophylaxis. The patients continued on systemic pneumocystis, antiviral, and antifungal prophylaxis, per NIH cGVHD guidelines.
Thirty-two of the patients completed treatment, using the clobetasol rinse for the full 28 days.
Four patients went off study before completing 28 days of treatment. One of these patients could not tolerate the rinse. This patient had gastrointestinal issues that were attributed (by the patient and the physician) to use of the study drug.
Two patients went off study because they could not make it to the NIH for follow-up visits, and 1 patient died. The death was unrelated to the study drug.
Safety
Dr Mays noted that small amounts of clobetasol were detectable in the bloodstream, but she and her colleagues found this was not directly correlated to patient serum cortisol levels.
However, the researchers did observe a significant drop in serum cortisol levels from baseline to day 28, suggesting the rinse has an adrenal impact.
On the other hand, the peripheral lymphocyte profile was unchanged by the use of clobetasol rinse, which suggests there were no significant systemic immunosuppressive effects.
Adverse events considered possibly or probably related to clobetasol rinse included herpes simplex virus reactivation (n=3, grade 2-3), oral candidiasis (n=3, grade 2), other oral viral infection (n=1, grade 2), facial edema (n=3, grade 1), and adrenal suppression (6 grade 1 and 1 grade 2).
Dr Mays noted that many of the patients came on the study with adrenal suppression, but the clobetasol rinse had an additional impact.
Efficacy
The study’s primary endpoint was change in oral cGVHD severity scale at day 28 compared to baseline. Complete response was defined as a score of 0 on the erythema and ulceration components. Partial response was defined as a 25% decrease in score.
Progression was defined as a 25% increase in initial score. Stable disease was defined as a status that does not meet the criteria for progression or response.
Ninety-one percent of patients had a greater than 25% improvement in oral cGVHD severity scale. Nineteen percent of patients had a complete response, 72% of patients had a partial response, and 9% had stable disease. None of the patients progressed.
Dr Mays noted that patients who failed treatment with prior clobetasol ointment responded similarly to the clobetasol rinse when compared with the full study cohort.
Among the 11 patients with prior clobetasol ointment, 18% had a complete response, 73% had a partial response, 9% had stable disease, and none progressed.
Clobetasol rinse significantly decreased the clinical OMRS score (P<0.0001) and improved cGVHD pathology diagnosis (P=0.0001).
Patients reported a significant improvement in oral health-based quality of life (P=0.0008) after completing treatment, as well as significant improvements in oral pain (P=0.017) and oral sensitivity (P=0.0081).
Though saliva production did not change significantly from baseline to day 28, patients reported a significant improvement in oral dryness (P=0.014).
The blinded period of the study showed that placebo treatment was not effective. There was a significant difference between the placebo and clobetasol groups with regard to improvement in OMRS score from baseline to day 14 (P=0.0031).
“We found clobetasol oral rinse to be both effective and safe for short-term treatment of oral mucosal cGVHD and hope that it will improve sparing of systemic immunosuppressants in this patient population,” Dr Mays said. “Its risk profile is generally not suitable for unmonitored, long-term use.” ![]()
P falciparum malaria existed 2000 years ago, team says
individual from Velia, Italy
Photo courtesy of Luca
Bandioli, Pigorini Museum
An analysis of 2000-year-old human remains from several regions across the Italian peninsula has confirmed the presence of Plasmodium falciparum malaria during the Roman Empire, according to researchers.
The team found mitochondrial genomic evidence of P falciparum malaria, coaxed from the teeth of bodies buried in 3 Italian cemeteries, dating back to the Imperial period.
The researchers said these finding provide a key reference point for when and where the malaria parasite existed in humans, as well as more information about the evolution of human disease.
The team reported these findings in Current Biology.
“There is extensive written evidence describing fevers that sound like malaria in ancient Greece and Rome, but the specific malaria species responsible is unknown,” said study author Stephanie Marciniak, PhD, of Pennsylvania State University in University Park.
“Our data confirm that the species was likely Plasmodium falciparum and that it affected people in different ecological and cultural environments. These results open up new questions to explore, particularly how widespread this parasite was and what burden it placed upon communities in Imperial Roman Italy.”
Dr Marciniak and her colleagues sampled teeth taken from 58 adults interred at 3 Imperial period Italian cemeteries: Isola Sacra, Velia, and Vagnari.
Located on the coast, Velia and Isola Sacra were known as important port cities and trading centers. Vagnari is located further inland and believed to be the burial site of laborers who would have worked on a Roman rural estate.
The researchers mined tiny DNA fragments from dental pulp. They were able to extract, purify, and enrich specifically for the Plasmodium species known to infect humans.
The team noted that usable DNA is challenging to extract because the parasites primarily dwell within the bloodstream and organs, which decompose and break down over time—in this instance, over the course of 2 millennia.
However, the researchers recovered more than half of the P falciparum mitochondrial genome from 2 individuals from Velia and Vagnari. ![]()
individual from Velia, Italy
Photo courtesy of Luca
Bandioli, Pigorini Museum
An analysis of 2000-year-old human remains from several regions across the Italian peninsula has confirmed the presence of Plasmodium falciparum malaria during the Roman Empire, according to researchers.
The team found mitochondrial genomic evidence of P falciparum malaria, coaxed from the teeth of bodies buried in 3 Italian cemeteries, dating back to the Imperial period.
The researchers said these finding provide a key reference point for when and where the malaria parasite existed in humans, as well as more information about the evolution of human disease.
The team reported these findings in Current Biology.
“There is extensive written evidence describing fevers that sound like malaria in ancient Greece and Rome, but the specific malaria species responsible is unknown,” said study author Stephanie Marciniak, PhD, of Pennsylvania State University in University Park.
“Our data confirm that the species was likely Plasmodium falciparum and that it affected people in different ecological and cultural environments. These results open up new questions to explore, particularly how widespread this parasite was and what burden it placed upon communities in Imperial Roman Italy.”
Dr Marciniak and her colleagues sampled teeth taken from 58 adults interred at 3 Imperial period Italian cemeteries: Isola Sacra, Velia, and Vagnari.
Located on the coast, Velia and Isola Sacra were known as important port cities and trading centers. Vagnari is located further inland and believed to be the burial site of laborers who would have worked on a Roman rural estate.
The researchers mined tiny DNA fragments from dental pulp. They were able to extract, purify, and enrich specifically for the Plasmodium species known to infect humans.
The team noted that usable DNA is challenging to extract because the parasites primarily dwell within the bloodstream and organs, which decompose and break down over time—in this instance, over the course of 2 millennia.
However, the researchers recovered more than half of the P falciparum mitochondrial genome from 2 individuals from Velia and Vagnari. ![]()
individual from Velia, Italy
Photo courtesy of Luca
Bandioli, Pigorini Museum
An analysis of 2000-year-old human remains from several regions across the Italian peninsula has confirmed the presence of Plasmodium falciparum malaria during the Roman Empire, according to researchers.
The team found mitochondrial genomic evidence of P falciparum malaria, coaxed from the teeth of bodies buried in 3 Italian cemeteries, dating back to the Imperial period.
The researchers said these finding provide a key reference point for when and where the malaria parasite existed in humans, as well as more information about the evolution of human disease.
The team reported these findings in Current Biology.
“There is extensive written evidence describing fevers that sound like malaria in ancient Greece and Rome, but the specific malaria species responsible is unknown,” said study author Stephanie Marciniak, PhD, of Pennsylvania State University in University Park.
“Our data confirm that the species was likely Plasmodium falciparum and that it affected people in different ecological and cultural environments. These results open up new questions to explore, particularly how widespread this parasite was and what burden it placed upon communities in Imperial Roman Italy.”
Dr Marciniak and her colleagues sampled teeth taken from 58 adults interred at 3 Imperial period Italian cemeteries: Isola Sacra, Velia, and Vagnari.
Located on the coast, Velia and Isola Sacra were known as important port cities and trading centers. Vagnari is located further inland and believed to be the burial site of laborers who would have worked on a Roman rural estate.
The researchers mined tiny DNA fragments from dental pulp. They were able to extract, purify, and enrich specifically for the Plasmodium species known to infect humans.
The team noted that usable DNA is challenging to extract because the parasites primarily dwell within the bloodstream and organs, which decompose and break down over time—in this instance, over the course of 2 millennia.
However, the researchers recovered more than half of the P falciparum mitochondrial genome from 2 individuals from Velia and Vagnari. ![]()
Partnerships with pediatric tertiary care centers improve community ED asthma treatment
Partnerships between community emergency departments and pediatric tertiary care centers are feasible and improve care of pediatric asthma, according to Theresa A. Walls, MD, of the Children’s National Health Systems, Washington, D.C., and her associates.
A total of 724 asthma patients aged 2-17 years were included in the study. Of this group, 289 (40%) were treated at the community ED before the pediatric tertiary care center intervention and 435 (60%) were treated after the intervention. Treatment with steroids was significantly increased post intervention, with 76% of patients receiving steroids, compared with 60% of patients before the intervention.
“Because the overwhelming majority of pediatric emergency visits occur in community EDs, partnerships with these EDs can broaden the impact of quality improvement activities and should be part of future quality improvement efforts,” the investigators concluded.
Find the full study in Pediatrics (2016. doi: 10.1542/peds.2016-0088).
Dr. Walls and her group developed a quality improvement (QI) initiative with a community emergency department. One important part of the study was the use of an asthma score, which helped determine steps for ED therapy.

Dr. Walls and her group developed a quality improvement (QI) initiative with a community emergency department. One important part of the study was the use of an asthma score, which helped determine steps for ED therapy.
Dr. Walls and her group developed a quality improvement (QI) initiative with a community emergency department. One important part of the study was the use of an asthma score, which helped determine steps for ED therapy.
Partnerships between community emergency departments and pediatric tertiary care centers are feasible and improve care of pediatric asthma, according to Theresa A. Walls, MD, of the Children’s National Health Systems, Washington, D.C., and her associates.
A total of 724 asthma patients aged 2-17 years were included in the study. Of this group, 289 (40%) were treated at the community ED before the pediatric tertiary care center intervention and 435 (60%) were treated after the intervention. Treatment with steroids was significantly increased post intervention, with 76% of patients receiving steroids, compared with 60% of patients before the intervention.
“Because the overwhelming majority of pediatric emergency visits occur in community EDs, partnerships with these EDs can broaden the impact of quality improvement activities and should be part of future quality improvement efforts,” the investigators concluded.
Find the full study in Pediatrics (2016. doi: 10.1542/peds.2016-0088).
Partnerships between community emergency departments and pediatric tertiary care centers are feasible and improve care of pediatric asthma, according to Theresa A. Walls, MD, of the Children’s National Health Systems, Washington, D.C., and her associates.
A total of 724 asthma patients aged 2-17 years were included in the study. Of this group, 289 (40%) were treated at the community ED before the pediatric tertiary care center intervention and 435 (60%) were treated after the intervention. Treatment with steroids was significantly increased post intervention, with 76% of patients receiving steroids, compared with 60% of patients before the intervention.
“Because the overwhelming majority of pediatric emergency visits occur in community EDs, partnerships with these EDs can broaden the impact of quality improvement activities and should be part of future quality improvement efforts,” the investigators concluded.
Find the full study in Pediatrics (2016. doi: 10.1542/peds.2016-0088).
FROM PEDIATRICS
Itchy blisters on feet

The patient was given a diagnosis of vesicular (vesiculobullous) tinea pedis, based on the vesicles and bullae over the arch region of the foot. The arch is a typical location for vesiculobullous tinea pedis. There are 3 main types of tinea pedis: interdigital, moccasin distribution, and vesiculobullous (which is the least common type). Interdigital tinea pedis is the most common type and is typically seen between the fourth and fifth digits. The moccasin distribution tends to involve more erythema and scale—especially on the sides of the feet—giving the appearance of moccasins.
In general, tinea pedis is most commonly caused by Trichophyton rubrum. Other causative organisms include Trichophyton mentagrophytes and Epidermophyton floccosum. The vesiculobullous type of tinea pedis is usually caused by T mentagrophytes. The FP made this diagnosis clinically and did not perform a potassium hydroxide (KOH) preparation, as this type of tinea pedis has minimal scale and the dermatophyte may be harder to identify with the superficial scraping.
The FP prescribed 2 weeks of oral terbinafine 250 mg/d instead of relying on topical antifungal medicine because a better response can be expected with it. One month later, the vesiculobullous tinea pedis was fully resolved.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Reppa R. Tinea pedis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:799-804.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The patient was given a diagnosis of vesicular (vesiculobullous) tinea pedis, based on the vesicles and bullae over the arch region of the foot. The arch is a typical location for vesiculobullous tinea pedis. There are 3 main types of tinea pedis: interdigital, moccasin distribution, and vesiculobullous (which is the least common type). Interdigital tinea pedis is the most common type and is typically seen between the fourth and fifth digits. The moccasin distribution tends to involve more erythema and scale—especially on the sides of the feet—giving the appearance of moccasins.
In general, tinea pedis is most commonly caused by Trichophyton rubrum. Other causative organisms include Trichophyton mentagrophytes and Epidermophyton floccosum. The vesiculobullous type of tinea pedis is usually caused by T mentagrophytes. The FP made this diagnosis clinically and did not perform a potassium hydroxide (KOH) preparation, as this type of tinea pedis has minimal scale and the dermatophyte may be harder to identify with the superficial scraping.
The FP prescribed 2 weeks of oral terbinafine 250 mg/d instead of relying on topical antifungal medicine because a better response can be expected with it. One month later, the vesiculobullous tinea pedis was fully resolved.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Reppa R. Tinea pedis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:799-804.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The patient was given a diagnosis of vesicular (vesiculobullous) tinea pedis, based on the vesicles and bullae over the arch region of the foot. The arch is a typical location for vesiculobullous tinea pedis. There are 3 main types of tinea pedis: interdigital, moccasin distribution, and vesiculobullous (which is the least common type). Interdigital tinea pedis is the most common type and is typically seen between the fourth and fifth digits. The moccasin distribution tends to involve more erythema and scale—especially on the sides of the feet—giving the appearance of moccasins.
In general, tinea pedis is most commonly caused by Trichophyton rubrum. Other causative organisms include Trichophyton mentagrophytes and Epidermophyton floccosum. The vesiculobullous type of tinea pedis is usually caused by T mentagrophytes. The FP made this diagnosis clinically and did not perform a potassium hydroxide (KOH) preparation, as this type of tinea pedis has minimal scale and the dermatophyte may be harder to identify with the superficial scraping.
The FP prescribed 2 weeks of oral terbinafine 250 mg/d instead of relying on topical antifungal medicine because a better response can be expected with it. One month later, the vesiculobullous tinea pedis was fully resolved.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Reppa R. Tinea pedis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:799-804.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

15 and Going Gray
ANSWER
The correct answer is seborrheic dermatitis (choice “d”).
Psoriasis (choice “a”) can manifest in a similar fashion but would also appear elsewhere (eg, the elbows, knees, or nails). The scaling seen with psoriasis is usually white on a salmon-colored base and much coarser.
Vitiligo (choice “b”) presents with total, porcelain-white depigmentation and is not scaly at all; this patient’s loss of pigment was only partial.
Rashes like this are often thought to be fungal, but a fungal infection (choice “c”) is rarely seen on the face and would not demonstrate this exact pattern.
DISCUSSION
Seborrheic dermatitis (SD) is an extremely common papulosquamous skin condition that manifests primarily in oil-rich areas, such as the central face, scalp (dandruff), and in and behind the ears. On white skin, it yields a pinkish-brown scaly rash, but on darker skin, SD causes partial depigmentation—sometimes to an alarming extent. The distribution in this case is typical, with nasolabial, glabellar, ear, and brow involvement.
SD might be caused by a number of factors, some related to climate or genetics. One prevailing theory is that it involves an inflammatory reaction resulting from commensal yeast organisms (Malassezia furfur) feeding on sebum. In this case, the contribution of stress was clear.
TREATMENT/PROGNOSIS
Treatment comprised daily use of ketoconazole shampoo on the scalp and face and a topical ketoconazole cream. The condition cleared within two weeks. Although the chances of a recurrence are quite high, the patient is now armed with information and products to avoid the worst effects.
ANSWER
The correct answer is seborrheic dermatitis (choice “d”).
Psoriasis (choice “a”) can manifest in a similar fashion but would also appear elsewhere (eg, the elbows, knees, or nails). The scaling seen with psoriasis is usually white on a salmon-colored base and much coarser.
Vitiligo (choice “b”) presents with total, porcelain-white depigmentation and is not scaly at all; this patient’s loss of pigment was only partial.
Rashes like this are often thought to be fungal, but a fungal infection (choice “c”) is rarely seen on the face and would not demonstrate this exact pattern.
DISCUSSION
Seborrheic dermatitis (SD) is an extremely common papulosquamous skin condition that manifests primarily in oil-rich areas, such as the central face, scalp (dandruff), and in and behind the ears. On white skin, it yields a pinkish-brown scaly rash, but on darker skin, SD causes partial depigmentation—sometimes to an alarming extent. The distribution in this case is typical, with nasolabial, glabellar, ear, and brow involvement.
SD might be caused by a number of factors, some related to climate or genetics. One prevailing theory is that it involves an inflammatory reaction resulting from commensal yeast organisms (Malassezia furfur) feeding on sebum. In this case, the contribution of stress was clear.
TREATMENT/PROGNOSIS
Treatment comprised daily use of ketoconazole shampoo on the scalp and face and a topical ketoconazole cream. The condition cleared within two weeks. Although the chances of a recurrence are quite high, the patient is now armed with information and products to avoid the worst effects.
ANSWER
The correct answer is seborrheic dermatitis (choice “d”).
Psoriasis (choice “a”) can manifest in a similar fashion but would also appear elsewhere (eg, the elbows, knees, or nails). The scaling seen with psoriasis is usually white on a salmon-colored base and much coarser.
Vitiligo (choice “b”) presents with total, porcelain-white depigmentation and is not scaly at all; this patient’s loss of pigment was only partial.
Rashes like this are often thought to be fungal, but a fungal infection (choice “c”) is rarely seen on the face and would not demonstrate this exact pattern.
DISCUSSION
Seborrheic dermatitis (SD) is an extremely common papulosquamous skin condition that manifests primarily in oil-rich areas, such as the central face, scalp (dandruff), and in and behind the ears. On white skin, it yields a pinkish-brown scaly rash, but on darker skin, SD causes partial depigmentation—sometimes to an alarming extent. The distribution in this case is typical, with nasolabial, glabellar, ear, and brow involvement.
SD might be caused by a number of factors, some related to climate or genetics. One prevailing theory is that it involves an inflammatory reaction resulting from commensal yeast organisms (Malassezia furfur) feeding on sebum. In this case, the contribution of stress was clear.
TREATMENT/PROGNOSIS
Treatment comprised daily use of ketoconazole shampoo on the scalp and face and a topical ketoconazole cream. The condition cleared within two weeks. Although the chances of a recurrence are quite high, the patient is now armed with information and products to avoid the worst effects.

A 15-year-old African-American boy is brought in by his family for evaluation of a condition that began several months ago. Despite multiple attempts at treatment, the uniform but partial depigmentation of the skin around his nose persists. It is made obvious by his type V skin, extending up into the glabellar area and into both eyebrows.
Fine but definite scaling is confined to the depigmented areas. There is heavier white to gray scaling on his frontal scalp, and light scaling in and behind both ears. His elbows, knees, and nails appear normal. He is asymptomatic and in excellent health otherwise, but he considers his condition “unsightly and embarrassing.”
More history-taking reveals that around the time this problem manifested, he was facing the threat of a one-year suspension from school for disciplinary reasons.

Group estimates global cancer cases, deaths in 2015

receiving chemotherapy
Photo by Rhoda Baer
Researchers have estimated the global incidence of 32 cancer types and deaths related to these malignancies in 2015.
The group’s data, published in JAMA Oncology, suggest there were 17.5 million cancer cases and 8.7 million cancer deaths last year.
There were 78,000 cases of Hodgkin lymphoma and 24,000 deaths from the disease, as well as 666,000 cases of non-Hodgkin lymphoma (NHL) and 231,000 NHL deaths.
There were 154,000 cases of multiple myeloma and 101,000 deaths from the disease.
And there were 606,000 cases of leukemia, with 353,000 leukemia deaths. This included 161,000 cases of acute lymphoid leukemia (110,000 deaths), 191,000 cases of chronic lymphoid leukemia (61,000 deaths), 190,000 cases of acute myeloid leukemia (147,000 deaths), and 64,000 cases of chronic myeloid leukemia (35,000 deaths).
The data also show that, between 2005 and 2015, cancer cases increased by 33%, mostly due to population aging and growth, plus changes in age-specific cancer rates.
Globally, the odds of developing cancer during a lifetime were 1 in 3 for men and 1 in 4 for women in 2015.
Prostate cancer was the most common cancer in men (1.6 million cases), although tracheal, bronchus, and lung cancer was the leading cause of cancer deaths for men.
Breast cancer was the most common cancer for women (2.4 million cases) and the leading cause of cancer deaths in women.
The most common childhood cancers were leukemia, “other neoplasms,” NHL, and brain and nervous system cancers. ![]()
receiving chemotherapy
Photo by Rhoda Baer
Researchers have estimated the global incidence of 32 cancer types and deaths related to these malignancies in 2015.
The group’s data, published in JAMA Oncology, suggest there were 17.5 million cancer cases and 8.7 million cancer deaths last year.
There were 78,000 cases of Hodgkin lymphoma and 24,000 deaths from the disease, as well as 666,000 cases of non-Hodgkin lymphoma (NHL) and 231,000 NHL deaths.
There were 154,000 cases of multiple myeloma and 101,000 deaths from the disease.
And there were 606,000 cases of leukemia, with 353,000 leukemia deaths. This included 161,000 cases of acute lymphoid leukemia (110,000 deaths), 191,000 cases of chronic lymphoid leukemia (61,000 deaths), 190,000 cases of acute myeloid leukemia (147,000 deaths), and 64,000 cases of chronic myeloid leukemia (35,000 deaths).
The data also show that, between 2005 and 2015, cancer cases increased by 33%, mostly due to population aging and growth, plus changes in age-specific cancer rates.
Globally, the odds of developing cancer during a lifetime were 1 in 3 for men and 1 in 4 for women in 2015.
Prostate cancer was the most common cancer in men (1.6 million cases), although tracheal, bronchus, and lung cancer was the leading cause of cancer deaths for men.
Breast cancer was the most common cancer for women (2.4 million cases) and the leading cause of cancer deaths in women.
The most common childhood cancers were leukemia, “other neoplasms,” NHL, and brain and nervous system cancers. ![]()
receiving chemotherapy
Photo by Rhoda Baer
Researchers have estimated the global incidence of 32 cancer types and deaths related to these malignancies in 2015.
The group’s data, published in JAMA Oncology, suggest there were 17.5 million cancer cases and 8.7 million cancer deaths last year.
There were 78,000 cases of Hodgkin lymphoma and 24,000 deaths from the disease, as well as 666,000 cases of non-Hodgkin lymphoma (NHL) and 231,000 NHL deaths.
There were 154,000 cases of multiple myeloma and 101,000 deaths from the disease.
And there were 606,000 cases of leukemia, with 353,000 leukemia deaths. This included 161,000 cases of acute lymphoid leukemia (110,000 deaths), 191,000 cases of chronic lymphoid leukemia (61,000 deaths), 190,000 cases of acute myeloid leukemia (147,000 deaths), and 64,000 cases of chronic myeloid leukemia (35,000 deaths).
The data also show that, between 2005 and 2015, cancer cases increased by 33%, mostly due to population aging and growth, plus changes in age-specific cancer rates.
Globally, the odds of developing cancer during a lifetime were 1 in 3 for men and 1 in 4 for women in 2015.
Prostate cancer was the most common cancer in men (1.6 million cases), although tracheal, bronchus, and lung cancer was the leading cause of cancer deaths for men.
Breast cancer was the most common cancer for women (2.4 million cases) and the leading cause of cancer deaths in women.
The most common childhood cancers were leukemia, “other neoplasms,” NHL, and brain and nervous system cancers. ![]()
Data suggest one BTK inhibitor could replace another

ASH Annual Meeting
SAN DIEGO—When patients with chronic lymphocytic leukemia (CLL) cannot tolerate one Bruton’s tyrosine kinase (BTK) inhibitor, they may do well on another, according to a presentation at the 2016 ASH Annual Meeting.
Researchers conducting a phase 1/2 study found that acalabrutinib was “well-tolerated” and demonstrated “promising activity” in patients intolerant to ibrutinib.
Seventy-nine percent of patients responded to acalabrutinib.
And although 36% of patients had a recurrence of an adverse event (AE) they experienced while on ibrutinib, none of the patients discontinued acalabrutinib due to AE recurrence.
Farrukh T. Awan, MD, of The Ohio State University in Columbus, Ohio, presented these results at the meeting as abstract 638.*
Dr Awan noted that integrating ibrutinib into standard CLL therapy has improved patient outcomes, but a lack of tolerability observed in some patients suggests that more selective BTK inhibition may be desirable.
“We know that around 10% to 20% of patients who are treated with ibrutinib would have to stop therapy because of an adverse event,” Dr Awan said. “Acalabrutinib is a highly selective, potent BTK inhibitor that has shown promising efficacy, and that [research] was published last year.”
In this ongoing, phase 1/2 study, Dr Awan and his colleagues are testing acalabrutinib in patients with CLL/small lymphocytic leukemia. The study has enrolled multiple cohorts of patients—relapsed/refractory, treatment-naïve, Richter’s transformation/prolymphocytic leukemia, and ibrutinib intolerant.
At this year’s ASH meeting, Dr Awan presented data on the 33 CLL patients who were ibrutinib intolerant. The patients’ median age was 64 (range, 50-82), 61% were male, 97% had an ECOG performance status of 0-1, 52% had Rai stage III-IV, and 31% had bulky disease.
The median number of prior therapies was 4 (range, 2-13), and 91% of patients had ibrutinib as their last therapy. The median duration of prior ibrutinib treatment was 11.5 months (range, 1-62), and the median time from ending ibrutinib to starting acalabrutinib was 47 days (range, 3-331 days).
Treatment and safety
Patients received acalabrutinib at 100 mg twice daily (n=30) or 200 mg daily (n=3) until disease progression or discontinuation for another reason. The patients’ median time on therapy was 12.2 months (range, 0.2-23.6 months).
Nine patients discontinued treatment—3 due to disease progression, 3 due to AEs, 2 due to an increase in BTK C481S mutation frequency in the peripheral blood and central nervous system involvement, and 1 due to physician decision (because the patient had concurrent hemophilia).
The 3 AEs that led to treatment discontinuation were fatal hemorrhagic stroke, fatal fungal infection, and metastatic endometrial cancer. All 3 events were considered unrelated to acalabrutinib.
Serious AEs occurred in 11 patients (33%). A serious AE that occurred in more than 1 patient was pneumonia (n=2).
The most common AEs were diarrhea (52%, grade 1-2), headache (39%, grade 1-2), cough (24%, grade 1-2), increased weight (24%, grade 1-2), nausea (21%, grade 1-2), contusion (18%, grade 1-2), ecchymosis (18%, grade 1-2), fatigue (18%, grade 1-2), hypertension (18% overall, 6% ≥ grade 3), pyrexia (18% overall, 3% ≥ grade 3), vomiting (18%, grade 1-2), myalgia (15% overall, 3% ≥ grade 3), rash (15%, grade 1-2), stomatitis (15%, grade 1-2), upper respiratory tract infection (15%, grade 1-2), and urinary tract infection (15%, grade 1-2).
AE recurrence
Twelve patients (36%) had a recurrence of ibrutinib-related AEs—a total of 16 events. Fourteen of these events either decreased in severity or were unchanged with acalabrutinib treatment.
The events without a change in severity were atrial fibrillation (n=1), fatigue (n=1), muscle spasms (n=1), myalgia (n=1), peripheral edema (n=1), panniculitis (n=1), and rash (n=1).
The events that decreased in severity were diarrhea (n=2), arthralgia (n=1), ecchymosis (n=1), fatigue (n=1), panniculitis (n=1), and rash (n=1).
The events that increased in severity were contusion (n=1, grade 1 to 2) and fatigue (n=1, grade 1 to 2).
None of the patients discontinued acalabrutinib due to AE recurrence.
Efficacy
Twenty-nine patients were evaluable for efficacy.
The overall response rate was 79% (n=23). One patient had a complete response (3%), 15 had a partial response (52%), and 7 had a partial response with lymphocytosis (24%). Six patients had stable disease (21%).
The median time to response was 1.9 months. Eighty-one percent of responding patients have a response duration of 12 months or longer.
The median progression-free survival has not been reached.
The research is sponsored by Acerta Pharma.![]()
*Information presented at the meeting differs from the abstract.
ASH Annual Meeting
SAN DIEGO—When patients with chronic lymphocytic leukemia (CLL) cannot tolerate one Bruton’s tyrosine kinase (BTK) inhibitor, they may do well on another, according to a presentation at the 2016 ASH Annual Meeting.
Researchers conducting a phase 1/2 study found that acalabrutinib was “well-tolerated” and demonstrated “promising activity” in patients intolerant to ibrutinib.
Seventy-nine percent of patients responded to acalabrutinib.
And although 36% of patients had a recurrence of an adverse event (AE) they experienced while on ibrutinib, none of the patients discontinued acalabrutinib due to AE recurrence.
Farrukh T. Awan, MD, of The Ohio State University in Columbus, Ohio, presented these results at the meeting as abstract 638.*
Dr Awan noted that integrating ibrutinib into standard CLL therapy has improved patient outcomes, but a lack of tolerability observed in some patients suggests that more selective BTK inhibition may be desirable.
“We know that around 10% to 20% of patients who are treated with ibrutinib would have to stop therapy because of an adverse event,” Dr Awan said. “Acalabrutinib is a highly selective, potent BTK inhibitor that has shown promising efficacy, and that [research] was published last year.”
In this ongoing, phase 1/2 study, Dr Awan and his colleagues are testing acalabrutinib in patients with CLL/small lymphocytic leukemia. The study has enrolled multiple cohorts of patients—relapsed/refractory, treatment-naïve, Richter’s transformation/prolymphocytic leukemia, and ibrutinib intolerant.
At this year’s ASH meeting, Dr Awan presented data on the 33 CLL patients who were ibrutinib intolerant. The patients’ median age was 64 (range, 50-82), 61% were male, 97% had an ECOG performance status of 0-1, 52% had Rai stage III-IV, and 31% had bulky disease.
The median number of prior therapies was 4 (range, 2-13), and 91% of patients had ibrutinib as their last therapy. The median duration of prior ibrutinib treatment was 11.5 months (range, 1-62), and the median time from ending ibrutinib to starting acalabrutinib was 47 days (range, 3-331 days).
Treatment and safety
Patients received acalabrutinib at 100 mg twice daily (n=30) or 200 mg daily (n=3) until disease progression or discontinuation for another reason. The patients’ median time on therapy was 12.2 months (range, 0.2-23.6 months).
Nine patients discontinued treatment—3 due to disease progression, 3 due to AEs, 2 due to an increase in BTK C481S mutation frequency in the peripheral blood and central nervous system involvement, and 1 due to physician decision (because the patient had concurrent hemophilia).
The 3 AEs that led to treatment discontinuation were fatal hemorrhagic stroke, fatal fungal infection, and metastatic endometrial cancer. All 3 events were considered unrelated to acalabrutinib.
Serious AEs occurred in 11 patients (33%). A serious AE that occurred in more than 1 patient was pneumonia (n=2).
The most common AEs were diarrhea (52%, grade 1-2), headache (39%, grade 1-2), cough (24%, grade 1-2), increased weight (24%, grade 1-2), nausea (21%, grade 1-2), contusion (18%, grade 1-2), ecchymosis (18%, grade 1-2), fatigue (18%, grade 1-2), hypertension (18% overall, 6% ≥ grade 3), pyrexia (18% overall, 3% ≥ grade 3), vomiting (18%, grade 1-2), myalgia (15% overall, 3% ≥ grade 3), rash (15%, grade 1-2), stomatitis (15%, grade 1-2), upper respiratory tract infection (15%, grade 1-2), and urinary tract infection (15%, grade 1-2).
AE recurrence
Twelve patients (36%) had a recurrence of ibrutinib-related AEs—a total of 16 events. Fourteen of these events either decreased in severity or were unchanged with acalabrutinib treatment.
The events without a change in severity were atrial fibrillation (n=1), fatigue (n=1), muscle spasms (n=1), myalgia (n=1), peripheral edema (n=1), panniculitis (n=1), and rash (n=1).
The events that decreased in severity were diarrhea (n=2), arthralgia (n=1), ecchymosis (n=1), fatigue (n=1), panniculitis (n=1), and rash (n=1).
The events that increased in severity were contusion (n=1, grade 1 to 2) and fatigue (n=1, grade 1 to 2).
None of the patients discontinued acalabrutinib due to AE recurrence.
Efficacy
Twenty-nine patients were evaluable for efficacy.
The overall response rate was 79% (n=23). One patient had a complete response (3%), 15 had a partial response (52%), and 7 had a partial response with lymphocytosis (24%). Six patients had stable disease (21%).
The median time to response was 1.9 months. Eighty-one percent of responding patients have a response duration of 12 months or longer.
The median progression-free survival has not been reached.
The research is sponsored by Acerta Pharma.![]()
*Information presented at the meeting differs from the abstract.
ASH Annual Meeting
SAN DIEGO—When patients with chronic lymphocytic leukemia (CLL) cannot tolerate one Bruton’s tyrosine kinase (BTK) inhibitor, they may do well on another, according to a presentation at the 2016 ASH Annual Meeting.
Researchers conducting a phase 1/2 study found that acalabrutinib was “well-tolerated” and demonstrated “promising activity” in patients intolerant to ibrutinib.
Seventy-nine percent of patients responded to acalabrutinib.
And although 36% of patients had a recurrence of an adverse event (AE) they experienced while on ibrutinib, none of the patients discontinued acalabrutinib due to AE recurrence.
Farrukh T. Awan, MD, of The Ohio State University in Columbus, Ohio, presented these results at the meeting as abstract 638.*
Dr Awan noted that integrating ibrutinib into standard CLL therapy has improved patient outcomes, but a lack of tolerability observed in some patients suggests that more selective BTK inhibition may be desirable.
“We know that around 10% to 20% of patients who are treated with ibrutinib would have to stop therapy because of an adverse event,” Dr Awan said. “Acalabrutinib is a highly selective, potent BTK inhibitor that has shown promising efficacy, and that [research] was published last year.”
In this ongoing, phase 1/2 study, Dr Awan and his colleagues are testing acalabrutinib in patients with CLL/small lymphocytic leukemia. The study has enrolled multiple cohorts of patients—relapsed/refractory, treatment-naïve, Richter’s transformation/prolymphocytic leukemia, and ibrutinib intolerant.
At this year’s ASH meeting, Dr Awan presented data on the 33 CLL patients who were ibrutinib intolerant. The patients’ median age was 64 (range, 50-82), 61% were male, 97% had an ECOG performance status of 0-1, 52% had Rai stage III-IV, and 31% had bulky disease.
The median number of prior therapies was 4 (range, 2-13), and 91% of patients had ibrutinib as their last therapy. The median duration of prior ibrutinib treatment was 11.5 months (range, 1-62), and the median time from ending ibrutinib to starting acalabrutinib was 47 days (range, 3-331 days).
Treatment and safety
Patients received acalabrutinib at 100 mg twice daily (n=30) or 200 mg daily (n=3) until disease progression or discontinuation for another reason. The patients’ median time on therapy was 12.2 months (range, 0.2-23.6 months).
Nine patients discontinued treatment—3 due to disease progression, 3 due to AEs, 2 due to an increase in BTK C481S mutation frequency in the peripheral blood and central nervous system involvement, and 1 due to physician decision (because the patient had concurrent hemophilia).
The 3 AEs that led to treatment discontinuation were fatal hemorrhagic stroke, fatal fungal infection, and metastatic endometrial cancer. All 3 events were considered unrelated to acalabrutinib.
Serious AEs occurred in 11 patients (33%). A serious AE that occurred in more than 1 patient was pneumonia (n=2).
The most common AEs were diarrhea (52%, grade 1-2), headache (39%, grade 1-2), cough (24%, grade 1-2), increased weight (24%, grade 1-2), nausea (21%, grade 1-2), contusion (18%, grade 1-2), ecchymosis (18%, grade 1-2), fatigue (18%, grade 1-2), hypertension (18% overall, 6% ≥ grade 3), pyrexia (18% overall, 3% ≥ grade 3), vomiting (18%, grade 1-2), myalgia (15% overall, 3% ≥ grade 3), rash (15%, grade 1-2), stomatitis (15%, grade 1-2), upper respiratory tract infection (15%, grade 1-2), and urinary tract infection (15%, grade 1-2).
AE recurrence
Twelve patients (36%) had a recurrence of ibrutinib-related AEs—a total of 16 events. Fourteen of these events either decreased in severity or were unchanged with acalabrutinib treatment.
The events without a change in severity were atrial fibrillation (n=1), fatigue (n=1), muscle spasms (n=1), myalgia (n=1), peripheral edema (n=1), panniculitis (n=1), and rash (n=1).
The events that decreased in severity were diarrhea (n=2), arthralgia (n=1), ecchymosis (n=1), fatigue (n=1), panniculitis (n=1), and rash (n=1).
The events that increased in severity were contusion (n=1, grade 1 to 2) and fatigue (n=1, grade 1 to 2).
None of the patients discontinued acalabrutinib due to AE recurrence.
Efficacy
Twenty-nine patients were evaluable for efficacy.
The overall response rate was 79% (n=23). One patient had a complete response (3%), 15 had a partial response (52%), and 7 had a partial response with lymphocytosis (24%). Six patients had stable disease (21%).
The median time to response was 1.9 months. Eighty-one percent of responding patients have a response duration of 12 months or longer.
The median progression-free survival has not been reached.
The research is sponsored by Acerta Pharma.![]()
*Information presented at the meeting differs from the abstract.
Serious mental illness gets serious attention in 21st Century Cures Act
WASHINGTON – Bipartisan legislation to improve care of patients with serious mental illness is just a pen stroke from passage, now that the 21st Century Cures Act is headed for the President’s desk.
While the mental health care reform provisions in the legislation (H.R. 34) will impact mental health services broadly, the bulk of the reform language comes from H.R. 2646, a bill sponsored by Rep. Tim Murphy (R-Penn.), which was intended to reverse decades of fragmented – and at times nonexistent – care for persons with serious mental illness.
The legislation calls for the expanded use of assisted outpatient treatment, federal guidance on how states can be reimbursed for offering inpatient psychiatric services, better data collection on mental health services paid for with state and federal dollars, new oversight of the federal agency in charge of mental health, and clarification of HIPAA laws, among other provisions.
“This is big,” Rep. Murphy said at a press conference Dec. 5. “After all the tears and suffering … know that those times when you felt no one was willing to listen, and you were ready to give up, now there is hope.”
Treatment vs. incarceration
Currently, states and communities can draw from $80 million dollars in federal grants for assisted outpatient treatment for patients with serious mental illness. The new legislation adds another $20 million and extends availability of the funding until 2022. It also allows state criminal justice systems to use assisted outpatient treatment grants to treat convicted criminals with serious mental illness instead of incarcerating them.
“[In prison], their illness gets worse, not better, creating a turnstile through which they will return time and again through our criminal justice system,” Senate Majority Whip John Cornyn (R.-Tex.) said during the press conference.

Paying for inpatient psychiatric care
The Cures Act also strengthens momentum for overhauling the Medicaid Institutions of Mental Diseases (IMD) exclusion, long a focus of mental health care advocates who view it as a governor on the number of psychiatric beds available nationally.
The exclusion prohibits any medical facility with more than 16 beds from using federal funds to pay for inpatient mental health care for adults under age 65 years. The Cures Act requires the Centers for Medicare & Medicaid Services to offer guidance on how states can use Medicaid demonstration projects to provide innovative inpatient psychiatric services using these waivers.
This follows an April 2016 CMS final rule that matches state funding dollar-per-dollar for up to 15 days of inpatient psychiatric treatment given to Medicaid managed care patients.
Although Rep. Murphy’s original bill called for abolishing the exclusion, he and other advocates are not disappointed in the progress made so far. “We didn’t get everything we wanted, but we needed everything we got,” he said.
“That 15 days was a massive win,” Frankie Berger, advocacy director of the Treatment Advocacy Center in Arlington, Va., said in an interview. “Now we have this legislation that requires CMS to tell state Medicaid directors what their wiggle room is when solving the problem on how to get care to these patients. If you read between the lines, this is care that is going to be provided by an IMD.”
The legislation also calls for more data collection and evaluation of IMDs, something that until now has been missing, Ms. Berger said. “A lot of us who work on this issue have found there is absolutely no data on where IMDs are, or who the folks are that are getting treatment in them. We need that information to make good choices,” she said.
“I think we will find savings as we expand the number of psychiatric beds … [and persons with serious mental illness] do not end up in jail cells, homeless, or in the morgue,” Sen. Bill Cassidy (R-La.) said at the press conference. He predicted that for each additional psychiatric bed introduced, savings would amount to between $30,000 and $50,000.

Restructuring, clarifying
The Cures Act reforms also restructure the Substance Abuse and Mental Health Services Administration, putting it under the authority of a new assistant secretary of Health and Human Services and giving it a chief medical officer. The law calls for the new CMO to have “real-world” experience treating patients with serious mental illness. The reformed SAMHSA will have responsibility for centralizing data collection to be used in creating best practices in mental health care. These reforms are particular victories for Rep. Murphy who has railed against the agency for years, citing its lack of medically trained leadership and lack of evidence-based approaches to care.
HIPAA requirements in serious mental illness are also clarified.
“Existing HIPAA laws are badly misunderstood,” said Sen. Chris Murphy (D-Conn.) at the briefing. “Many physicians think there is an outright ban on sharing [patient health] information.”
The legislation calls for the U.S. Department of Health and Human Services secretary to clarify when providers can disclose protected health information related to the treatment of an adult with a mental illness or substance use disorder.
“I would argue that [HIPAA] may be an area we will have to work on down the line, if the education campaign doesn’t work, but we will give this a try,” said Sen. Murphy, who has cosponsored legislation to do so.

As passed, the mental health provisions of the 21st Century Cures Act are an amalgamation of several bills introduced during the 114th Congress and are unique in that they largely were written by health care professionals with direct, relevant experience. Rep. Murphy is a clinical psychologist, while Rep. Cassidy is a physician with experience treating uninsured and incarcerated patients. Rep. Eddie Bernice Johnson (D-Tex.), who cosponsored Rep. Murphy’s bill, previously served as chief psychiatric nurse at the Dallas Veterans Affairs Medical Center.
[email protected]
On Twitter @whitneymcknight
WASHINGTON – Bipartisan legislation to improve care of patients with serious mental illness is just a pen stroke from passage, now that the 21st Century Cures Act is headed for the President’s desk.
While the mental health care reform provisions in the legislation (H.R. 34) will impact mental health services broadly, the bulk of the reform language comes from H.R. 2646, a bill sponsored by Rep. Tim Murphy (R-Penn.), which was intended to reverse decades of fragmented – and at times nonexistent – care for persons with serious mental illness.
The legislation calls for the expanded use of assisted outpatient treatment, federal guidance on how states can be reimbursed for offering inpatient psychiatric services, better data collection on mental health services paid for with state and federal dollars, new oversight of the federal agency in charge of mental health, and clarification of HIPAA laws, among other provisions.
“This is big,” Rep. Murphy said at a press conference Dec. 5. “After all the tears and suffering … know that those times when you felt no one was willing to listen, and you were ready to give up, now there is hope.”
Treatment vs. incarceration
Currently, states and communities can draw from $80 million dollars in federal grants for assisted outpatient treatment for patients with serious mental illness. The new legislation adds another $20 million and extends availability of the funding until 2022. It also allows state criminal justice systems to use assisted outpatient treatment grants to treat convicted criminals with serious mental illness instead of incarcerating them.
“[In prison], their illness gets worse, not better, creating a turnstile through which they will return time and again through our criminal justice system,” Senate Majority Whip John Cornyn (R.-Tex.) said during the press conference.
Paying for inpatient psychiatric care
The Cures Act also strengthens momentum for overhauling the Medicaid Institutions of Mental Diseases (IMD) exclusion, long a focus of mental health care advocates who view it as a governor on the number of psychiatric beds available nationally.
The exclusion prohibits any medical facility with more than 16 beds from using federal funds to pay for inpatient mental health care for adults under age 65 years. The Cures Act requires the Centers for Medicare & Medicaid Services to offer guidance on how states can use Medicaid demonstration projects to provide innovative inpatient psychiatric services using these waivers.
This follows an April 2016 CMS final rule that matches state funding dollar-per-dollar for up to 15 days of inpatient psychiatric treatment given to Medicaid managed care patients.
Although Rep. Murphy’s original bill called for abolishing the exclusion, he and other advocates are not disappointed in the progress made so far. “We didn’t get everything we wanted, but we needed everything we got,” he said.
“That 15 days was a massive win,” Frankie Berger, advocacy director of the Treatment Advocacy Center in Arlington, Va., said in an interview. “Now we have this legislation that requires CMS to tell state Medicaid directors what their wiggle room is when solving the problem on how to get care to these patients. If you read between the lines, this is care that is going to be provided by an IMD.”
The legislation also calls for more data collection and evaluation of IMDs, something that until now has been missing, Ms. Berger said. “A lot of us who work on this issue have found there is absolutely no data on where IMDs are, or who the folks are that are getting treatment in them. We need that information to make good choices,” she said.
“I think we will find savings as we expand the number of psychiatric beds … [and persons with serious mental illness] do not end up in jail cells, homeless, or in the morgue,” Sen. Bill Cassidy (R-La.) said at the press conference. He predicted that for each additional psychiatric bed introduced, savings would amount to between $30,000 and $50,000.
Restructuring, clarifying
The Cures Act reforms also restructure the Substance Abuse and Mental Health Services Administration, putting it under the authority of a new assistant secretary of Health and Human Services and giving it a chief medical officer. The law calls for the new CMO to have “real-world” experience treating patients with serious mental illness. The reformed SAMHSA will have responsibility for centralizing data collection to be used in creating best practices in mental health care. These reforms are particular victories for Rep. Murphy who has railed against the agency for years, citing its lack of medically trained leadership and lack of evidence-based approaches to care.
HIPAA requirements in serious mental illness are also clarified.
“Existing HIPAA laws are badly misunderstood,” said Sen. Chris Murphy (D-Conn.) at the briefing. “Many physicians think there is an outright ban on sharing [patient health] information.”
The legislation calls for the U.S. Department of Health and Human Services secretary to clarify when providers can disclose protected health information related to the treatment of an adult with a mental illness or substance use disorder.
“I would argue that [HIPAA] may be an area we will have to work on down the line, if the education campaign doesn’t work, but we will give this a try,” said Sen. Murphy, who has cosponsored legislation to do so.
As passed, the mental health provisions of the 21st Century Cures Act are an amalgamation of several bills introduced during the 114th Congress and are unique in that they largely were written by health care professionals with direct, relevant experience. Rep. Murphy is a clinical psychologist, while Rep. Cassidy is a physician with experience treating uninsured and incarcerated patients. Rep. Eddie Bernice Johnson (D-Tex.), who cosponsored Rep. Murphy’s bill, previously served as chief psychiatric nurse at the Dallas Veterans Affairs Medical Center.
[email protected]
On Twitter @whitneymcknight
WASHINGTON – Bipartisan legislation to improve care of patients with serious mental illness is just a pen stroke from passage, now that the 21st Century Cures Act is headed for the President’s desk.
While the mental health care reform provisions in the legislation (H.R. 34) will impact mental health services broadly, the bulk of the reform language comes from H.R. 2646, a bill sponsored by Rep. Tim Murphy (R-Penn.), which was intended to reverse decades of fragmented – and at times nonexistent – care for persons with serious mental illness.
The legislation calls for the expanded use of assisted outpatient treatment, federal guidance on how states can be reimbursed for offering inpatient psychiatric services, better data collection on mental health services paid for with state and federal dollars, new oversight of the federal agency in charge of mental health, and clarification of HIPAA laws, among other provisions.
“This is big,” Rep. Murphy said at a press conference Dec. 5. “After all the tears and suffering … know that those times when you felt no one was willing to listen, and you were ready to give up, now there is hope.”
Treatment vs. incarceration
Currently, states and communities can draw from $80 million dollars in federal grants for assisted outpatient treatment for patients with serious mental illness. The new legislation adds another $20 million and extends availability of the funding until 2022. It also allows state criminal justice systems to use assisted outpatient treatment grants to treat convicted criminals with serious mental illness instead of incarcerating them.
“[In prison], their illness gets worse, not better, creating a turnstile through which they will return time and again through our criminal justice system,” Senate Majority Whip John Cornyn (R.-Tex.) said during the press conference.
Paying for inpatient psychiatric care
The Cures Act also strengthens momentum for overhauling the Medicaid Institutions of Mental Diseases (IMD) exclusion, long a focus of mental health care advocates who view it as a governor on the number of psychiatric beds available nationally.
The exclusion prohibits any medical facility with more than 16 beds from using federal funds to pay for inpatient mental health care for adults under age 65 years. The Cures Act requires the Centers for Medicare & Medicaid Services to offer guidance on how states can use Medicaid demonstration projects to provide innovative inpatient psychiatric services using these waivers.
This follows an April 2016 CMS final rule that matches state funding dollar-per-dollar for up to 15 days of inpatient psychiatric treatment given to Medicaid managed care patients.
Although Rep. Murphy’s original bill called for abolishing the exclusion, he and other advocates are not disappointed in the progress made so far. “We didn’t get everything we wanted, but we needed everything we got,” he said.
“That 15 days was a massive win,” Frankie Berger, advocacy director of the Treatment Advocacy Center in Arlington, Va., said in an interview. “Now we have this legislation that requires CMS to tell state Medicaid directors what their wiggle room is when solving the problem on how to get care to these patients. If you read between the lines, this is care that is going to be provided by an IMD.”
The legislation also calls for more data collection and evaluation of IMDs, something that until now has been missing, Ms. Berger said. “A lot of us who work on this issue have found there is absolutely no data on where IMDs are, or who the folks are that are getting treatment in them. We need that information to make good choices,” she said.
“I think we will find savings as we expand the number of psychiatric beds … [and persons with serious mental illness] do not end up in jail cells, homeless, or in the morgue,” Sen. Bill Cassidy (R-La.) said at the press conference. He predicted that for each additional psychiatric bed introduced, savings would amount to between $30,000 and $50,000.
Restructuring, clarifying
The Cures Act reforms also restructure the Substance Abuse and Mental Health Services Administration, putting it under the authority of a new assistant secretary of Health and Human Services and giving it a chief medical officer. The law calls for the new CMO to have “real-world” experience treating patients with serious mental illness. The reformed SAMHSA will have responsibility for centralizing data collection to be used in creating best practices in mental health care. These reforms are particular victories for Rep. Murphy who has railed against the agency for years, citing its lack of medically trained leadership and lack of evidence-based approaches to care.
HIPAA requirements in serious mental illness are also clarified.
“Existing HIPAA laws are badly misunderstood,” said Sen. Chris Murphy (D-Conn.) at the briefing. “Many physicians think there is an outright ban on sharing [patient health] information.”
The legislation calls for the U.S. Department of Health and Human Services secretary to clarify when providers can disclose protected health information related to the treatment of an adult with a mental illness or substance use disorder.
“I would argue that [HIPAA] may be an area we will have to work on down the line, if the education campaign doesn’t work, but we will give this a try,” said Sen. Murphy, who has cosponsored legislation to do so.
As passed, the mental health provisions of the 21st Century Cures Act are an amalgamation of several bills introduced during the 114th Congress and are unique in that they largely were written by health care professionals with direct, relevant experience. Rep. Murphy is a clinical psychologist, while Rep. Cassidy is a physician with experience treating uninsured and incarcerated patients. Rep. Eddie Bernice Johnson (D-Tex.), who cosponsored Rep. Murphy’s bill, previously served as chief psychiatric nurse at the Dallas Veterans Affairs Medical Center.
[email protected]
On Twitter @whitneymcknight
KRAS-targeted T-cell therapy derails metastatic cancer
Adoptive transfer of cytotoxic T cells targeting a specific KRAS mutation (KRAS G12D) expressed by a metastatic colorectal cancer induced the regression of all seven lung metastases in a single patient, investigators report in the New England Journal of Medicine.
Mutations of the KRAS oncogene are frequent and drive the formation and progression of many human cancers. “The high incidence of KRAS G12D expression in [colorectal, pancreatic, and multiple other] cancers means that in the United States alone, thousands of patients per year would be potentially eligible for T-cell–based immunotherapy targeting KRAS G12D,” said Eric Tran, PhD, and his associates in the surgery branch, National Cancer Institute, Bethesda, Md.
They described the case of a 50-year-old woman participating in an ongoing phase II clinical trial assessing adoptive transfer of tumor-infiltrating lymphocytes targeting personalized cancer neoepitopes (individualized T-cell therapy). This patient was the only participant to date in whom the treatment induced tumor regression.
A total of 3 of her 10 lung metastases were resected to identify mutations expressed by the tumors, and these were found to express mutant KRAS G12D and HLA-C*08:02. The lymphocyte cultures that reacted most strongly against these antigens were expanded and made into a single infusion, which was administered after the patient had undergone nonmyeloablative conditioning using cyclophosphamide and fludarabine. The patient then received five doses of interleukin-2, which produced the only adverse effect of the entire regimen, fatigue.
At 40-day follow-up, all seven remaining lung metastases showed marked regression. One lesion showed progression at 9-month follow-up and was resected, and the patient has remained cancer free for the subsequent 4 months (N Engl J Med. 2016 Dec 8. doi:10.1056/NEJMoa1609279).
Laboratory analysis of the one metastasis that progressed showed that it had mutated further, losing heterozygosity of the copy of chromosome 6 that encoded HLA-C*08:02. “The presence of this molecule is required for direct tumor recognition by the transferred KRAS G12D-specific T cells. ... [Such a loss] has been observed in human cancers and may represent a hurdle that needs to be overcome to enhance immunotherapeutic efficacy in some patients,” Dr. Tran and his associates wrote.
“In such cases, targeting antigens that are presented by the remaining HLA class I alleles or exploiting the CD4+ T-cell response or the innate immune system against cancer may be necessary to induce a durable clinical response,” they added.
Adoptive transfer of cytotoxic T cells targeting a specific KRAS mutation (KRAS G12D) expressed by a metastatic colorectal cancer induced the regression of all seven lung metastases in a single patient, investigators report in the New England Journal of Medicine.
Mutations of the KRAS oncogene are frequent and drive the formation and progression of many human cancers. “The high incidence of KRAS G12D expression in [colorectal, pancreatic, and multiple other] cancers means that in the United States alone, thousands of patients per year would be potentially eligible for T-cell–based immunotherapy targeting KRAS G12D,” said Eric Tran, PhD, and his associates in the surgery branch, National Cancer Institute, Bethesda, Md.
They described the case of a 50-year-old woman participating in an ongoing phase II clinical trial assessing adoptive transfer of tumor-infiltrating lymphocytes targeting personalized cancer neoepitopes (individualized T-cell therapy). This patient was the only participant to date in whom the treatment induced tumor regression.
A total of 3 of her 10 lung metastases were resected to identify mutations expressed by the tumors, and these were found to express mutant KRAS G12D and HLA-C*08:02. The lymphocyte cultures that reacted most strongly against these antigens were expanded and made into a single infusion, which was administered after the patient had undergone nonmyeloablative conditioning using cyclophosphamide and fludarabine. The patient then received five doses of interleukin-2, which produced the only adverse effect of the entire regimen, fatigue.
At 40-day follow-up, all seven remaining lung metastases showed marked regression. One lesion showed progression at 9-month follow-up and was resected, and the patient has remained cancer free for the subsequent 4 months (N Engl J Med. 2016 Dec 8. doi:10.1056/NEJMoa1609279).
Laboratory analysis of the one metastasis that progressed showed that it had mutated further, losing heterozygosity of the copy of chromosome 6 that encoded HLA-C*08:02. “The presence of this molecule is required for direct tumor recognition by the transferred KRAS G12D-specific T cells. ... [Such a loss] has been observed in human cancers and may represent a hurdle that needs to be overcome to enhance immunotherapeutic efficacy in some patients,” Dr. Tran and his associates wrote.
“In such cases, targeting antigens that are presented by the remaining HLA class I alleles or exploiting the CD4+ T-cell response or the innate immune system against cancer may be necessary to induce a durable clinical response,” they added.
Adoptive transfer of cytotoxic T cells targeting a specific KRAS mutation (KRAS G12D) expressed by a metastatic colorectal cancer induced the regression of all seven lung metastases in a single patient, investigators report in the New England Journal of Medicine.
Mutations of the KRAS oncogene are frequent and drive the formation and progression of many human cancers. “The high incidence of KRAS G12D expression in [colorectal, pancreatic, and multiple other] cancers means that in the United States alone, thousands of patients per year would be potentially eligible for T-cell–based immunotherapy targeting KRAS G12D,” said Eric Tran, PhD, and his associates in the surgery branch, National Cancer Institute, Bethesda, Md.
They described the case of a 50-year-old woman participating in an ongoing phase II clinical trial assessing adoptive transfer of tumor-infiltrating lymphocytes targeting personalized cancer neoepitopes (individualized T-cell therapy). This patient was the only participant to date in whom the treatment induced tumor regression.
A total of 3 of her 10 lung metastases were resected to identify mutations expressed by the tumors, and these were found to express mutant KRAS G12D and HLA-C*08:02. The lymphocyte cultures that reacted most strongly against these antigens were expanded and made into a single infusion, which was administered after the patient had undergone nonmyeloablative conditioning using cyclophosphamide and fludarabine. The patient then received five doses of interleukin-2, which produced the only adverse effect of the entire regimen, fatigue.
At 40-day follow-up, all seven remaining lung metastases showed marked regression. One lesion showed progression at 9-month follow-up and was resected, and the patient has remained cancer free for the subsequent 4 months (N Engl J Med. 2016 Dec 8. doi:10.1056/NEJMoa1609279).
Laboratory analysis of the one metastasis that progressed showed that it had mutated further, losing heterozygosity of the copy of chromosome 6 that encoded HLA-C*08:02. “The presence of this molecule is required for direct tumor recognition by the transferred KRAS G12D-specific T cells. ... [Such a loss] has been observed in human cancers and may represent a hurdle that needs to be overcome to enhance immunotherapeutic efficacy in some patients,” Dr. Tran and his associates wrote.
“In such cases, targeting antigens that are presented by the remaining HLA class I alleles or exploiting the CD4+ T-cell response or the innate immune system against cancer may be necessary to induce a durable clinical response,” they added.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Adoptive transfer of cytotoxic T cells targeting a specific KRAS mutation expressed by a metastatic colorectal cancer induced the regression of all seven lung metastases in a single patient.
Major finding: At 40-day follow-up, all seven lung metastases showed marked regression; the single metastasis that showed progression at 9-month follow-up was resected, and the patient has remained cancer free for the subsequent 4 months.
Data source: A single case study involving a woman with metastatic colorectal cancer treated with a experimental immunotherapy and followed for 13 months.
Disclosures: This work was supported by the National Cancer Institute. Dr. Tran and some of his associates reported holding a pending patent related to anti-KRAS G12D T-cell receptors.