User login
Tips for Working with Difficult Doctors
As a hospitalist, caring for critically ill or injured patients can be stressful and demanding. Working with difficult doctors, those who exhibit intimidating and disruptive behaviors such as verbal outbursts and physical threats as well as passive activities such as refusing to perform assigned tasks, can make the work environment even more challenging.1 Some docs are routinely reluctant—or refuse—to answer questions or return phone calls or pages. Some communicate in condescending language or voice intonation; some are brutally impatient.1

The most difficult doctors to work with are those who are not aligned with the hospital’s or treatment team’s goals and those who aren’t open to feedback and coaching, says Rob Zipper, MD, MMM, SFHM, regional chief medical officer of Sound Physicians, based in Tacoma, Wash.
“If physicians are aware of a practice’s guidelines and goals but simply won’t comply with them, it makes it harder on everyone else who is pulling the ship in the same direction,” he says.
Unruly physicians don’t just annoy their coworkers. According to a sentinel event alert from The Joint Commission, they can:
- foster medical errors;
- contribute to poor patient satisfaction;
- contribute to preventable adverse outcomes;
- increase the cost of care;
- undermine team effectiveness; and
- cause qualified clinicians, administrators, and managers to seek new positions in more professional environments.1
“These issues are all connected,” says Stephen R. Nichols, MD, chief of clinical operations performance at the Schumacher Group in Brownwood, Texas. “Disruptive behaviors create mitigated communications and dissatisfaction among staff, which bleeds over into other aspects that are involved secondarily.”
Stephen M. Paskoff, Esq., president and CEO of ELI in Atlanta, can attest to the most severe consequences of bad behavior on patient care.
At one institution, a surgeon’s disruptive behavior lead to a coworker forgetting to perform a procedure and a patient dying.2 In another incident, the emergency department stopped calling on a medical subspecialist who was predictably abusive. The subspecialist knew how to treat a specific patient with an unusual intervention. Since the specialist was not consulted initially, the patient ended up in the intensive care unit.2
One bad hospitalist can bring down the reputation of an entire team.
“Many programs are incentivized based on medical staff and primary-care physicians’ perceptions of their care, so there are direct and indirect consequences,” Dr. Zipper says.
The bottom line, says Felix Aguirre, MD, SFHM, vice president of medical affairs at IPC Healthcare in North Hollywood, Calif., is that it only takes one bad experience to tarnish a group, but it takes many positive experiences to erase the damage.
The Roots of Evil
Intimidating and disruptive behavior stems from both individual and systemic factors. Care providers who exhibit characteristics such as self-centeredness, immaturity, or defensiveness can be more prone to unprofessional behavior. They can lack interpersonal, coping, or conflict-management skills.1
Systemic factors are marked by pressures related to increased productivity demands, cost-containment requirements, embedded hierarchies, and fear of litigation in the healthcare environment. These pressures can be further exacerbated by changes to or differences in the authority, autonomy, empowerment, and roles or values of professionals on the healthcare team as well as by the continual daily changes in shifts, rotations, and interdepartmental support staff. This dynamic creates challenges for interprofessional communication and development of trust among team members.1
According to The Joint Commission, intimidating and disruptive behaviors are often manifested by healthcare professionals in positions of power.1 But other members of the care team can be problematic as well.
“In my experience, conflicts usually revolve around different perspectives and objectives, even if both parties are acting respectfully,” Dr. Zipper says. “Sometimes, however, providers or other care team members are tired or stressed and don’t behave professionally.”
Paskoff, who has more than 40 years of experience in healthcare-related workplace issues, including serving as an investigator for the U.S. Equal Employment Opportunity Commission, says some doctors learn bad behaviors from their mentors and that behaviors can be passed down through generations because they are tolerated.
“When I asked one physician who had outstanding training and an outstanding technical reputation how he became abusive, he said, ‘I learned from the best.’” Paskoff was actually able to track the doctor’s training to the late 1800s and physicians who were known for similar behaviors.
Confronting Those Who Misbehave
Dr. Zipper says physicians should confront behavioral issues directly.
“I will typically discuss a complaint with a doctor privately, and ask him or her what happened without being accusatory,” he says. “I try to provide as much concrete and objective information as I can. The doctor needs to know that you are trying to help him or her succeed. That said, if something is clearly bad behavior, feedback should be direct and include a statement such as, ‘This is not how we behave in this practice.’”
At times, it may not be possible to discuss an emergent matter, such as during a code blue.
“However, I will often ask if anyone on the code team has any ideas or concerns before ending the code,” Dr. Nichols says. “Then after the critical time has passed, it is important to debrief and reconnect with the team, especially the less-experienced members who may have lingering concerns.”
For many employees, however, it is difficult to report disruptive behaviors. This is due to a fear of retaliation and the stigma associated with “blowing the whistle” on a colleague as well as a general reluctance to confront an intimidator.1
If an employee cannot muster the courage to confront a disruptive coworker or if the issue isn’t resolved by talking with the difficult individual, an employee should be a good citizen and report bad behavior to the appropriate hospital authority in a timely manner, says A. Kevin Troutman, Esq., a partner at Fisher Phillips in Houston and a former healthcare human resources executive.
Hospitals accredited by The Joint Commission are required to create a code of conduct that defines disruptive and inappropriate behaviors. In addition, leaders must create and implement a process for managing these behaviors.1
Helping Difficult Doctors
After a physician or another employee has been called out for bad behavior, steps need to be taken to correct the problem. Robert Fuller, Esq., an attorney with Nelson Hardiman, LLP, in Los Angeles, has found a positive-oriented intervention called “the 3-Ds”—which stands for diagnose, design, and do—that has been a successful tool for achieving positive change. The strategy involves a supervisor and employee mutually developing a worksheet to diagnose the problem. Next, they design a remediation and improvement plan. Finally, they implement the plan and specify dates to achieve certain milestones. Coworkers should be informed of the plan and be urged to support it.
“Make it clear that the positive aspect of this plan turns to progressive discipline, including termination, if the employee doesn’t improve or abandons the plan of action,” Fuller says. In most cases, troublemakers will make a sincere effort to control disruptive tendencies.
Troutman suggests enlisting the assistance of a respected peer.
“Have a senior-level doctor help the noncompliant physician understand why his or her behavior creates problems for everyone, including the doctor himself,” he says. “Also, consider connecting compensation and other rewards to job performance, which encompasses good behavior and good citizenship within the organization. Make expectations and consequences clear.”
If an employee has a recent change in behavior, ask if there is a reason.
“It is my experience that sudden changes in behaviors are often the result of a personal or clinical issue, so it is important and humane to make certain that there is not some other cause for the change before assuming someone is simply being disruptive or difficult,” Dr. Nichols says.
Many healthcare institutions are now setting up centers of professionalism. Paskoff reports that The Center for Professionalism and Peer Support (CPPS) was created in 2008 at Brigham and Women’s Hospital in Boston to educate the hospital community regarding professionalism and manage unprofessional behavior.3 CPPS has established standards of behavior and a framework to deal with difficult behaviors.
“An employee is told what he or she is doing wrong, receives counseling, and is given resources to improve,” he explains. “If an employee doesn’t improve, he or she is told that the behavior won’t be tolerated.”
Dismissing Bad Employees
After addressing the specifics of unacceptable behavior and explaining the consequences of repeating it, leadership should monitor subsequent conduct and provide feedback.
“If the employee commits other violations or behaves badly, promptly address the misconduct again and make it clear that further such actions will not be tolerated,” Troutman says. “Expect immediate and sustained improvement and compliance. Be consistent, and if bad conduct continues after an opportunity to improve, do not prolong anyone’s suffering. Instead, terminate the disruptive employee. When you do, make the reasons clear.”
Karen Appold is a medical writer in Pennsylvania.
References
- Behaviors that undermine a culture of safety. The Joint Commission website. Accessed April 17, 2015.
- Whittemore AD, New England Society for Vascular Surgery. The impact of professionalism on safe surgical care. J Vasc Surg. 2007;45(2):415-419.
- Shapiro J, Whittemore A, Tsen LC. Instituting a culture of professionalism: the establishment of a center for professionalism and peer support. Jt Comm J Qual Patient Saf. 2014;40(4):168-177.
Are Behaviors Getting Better or Worse?
The Joint Commission issued a sentinel event alert1 on July 9, 2008, as a result of continuous reports to the commission’s Office of Quality and Patient Safety about disruptive behavior. Despite efforts to prevent employees from behaving badly, Ronald Wyatt, MD, MHA, medical director of the Division of Healthcare Improvement, says there is no evidence that the number of instances of bad behavior is decreasing.
According to a 2013 Institute for Safe Medication Practices survey with 4,884 respondents:2
- 73% reported encountering negative comments about colleagues or leaders during the previous year.
- 68% reported condescending language or demeaning comments or insults.
- 77% said they had encountered reluctance or refusal to answer questions or return calls.
- 69% reported they had encountered impatience with questions or hanging up the phone.
In addition, in a 2011 survey of more than 500 physician leaders and more than 300 staff physicians, 71 percent of respondents stated they had witnessed some type of disruptive behavior within the previous month, while 26 percent stated that they had been disruptive at one point in their career.3
Despite the gloomy news, Dr. Wyatt says, “There is increased awareness of disruptive behaviors, and they are being reported more often than in the past.”
As a former chief of medicine at a hospital, Dr. Wyatt says the lack of improvement could be due to hospital leadership.
“This is a critical piece to having a sound patient safety system,” he says.
In order for bad behaviors to improve, hospital leadership needs to be committed to creating a culture of safety. This would involve answering “yes” to the following questions:
- Does staff feel safe to report disruptive behaviors, and will leadership act on those reports?
- Is leadership committed to decreasing these types of behaviors?
- Is there a reporting system in place, and is it being used, monitored, and acted on?
- Can leadership step in and enforce the process if physicians aren’t complying?
- Is a model in place if intervention is necessary?
According to Dr. Wyatt, data show that one intervention is usually enough for most physicians to cease bad behaviors, but a small portion will persist.4
Hospitals accredited by The Joint Commission can contact the organization for a template regarding a policy for disruptive behaviors. Some consultants can also provide this.
—Karen Appold
References
- Behaviors that undermine a culture of safety. The Joint Commission website. Accessed April 17, 2015.
- Patient safety systems. Comprehensive Accreditation Manual for Hospitals. The Joint Commission. January 1, 2015:7-8.
- MacDonald O. Disruptive physician behavior. Quantia Communications, Inc.: Waltham, MA. May 15, 2011.
- Pichert JW, Moore IN, Karrass J, et al. An intervention model that promotes accountability: peer messengers and patient/family complaints. Jt Comm J Qual Patient Saf. 2013;39(10):435-446.
Proceed with Caution When Hiring Staff

Ideally, an institution won’t hire someone with intimidating and disruptive behavior in the first place. But this is always easier said than done.
In an effort to select and hire the best employees, it is important during the interview process to ask many questions about a candidate’s prior experiences and previous bosses as well as what the employee perceives to be good behavior and reasonable expectations.
“Listen for victim-like responses and criticisms of prior supervisors or employers,” says A. Kevin Troutman, Esq., a partner at Fisher Phillips in Houston and a former healthcare human resources executive. “Such responses are red flags that may help predict how the applicant will work out in your organization.”
Stephen M. Paskoff, Esq., president and CEO of ELI in Atlanta, says it’s best for the candidate to have interviews with multiple staff members in different ranks.
“Sometimes people will show a different side if he or she perceives someone as unimportant or someone that he or she could boss around,” he says. “The interview can be very telling if the applicant is a cultural fit or not.”
Carefully check a candidate’s previous training and employment records. It can be difficult, however, to decipher whether a potential employee will indeed be a good choice because prior employers almost uniformly refuse to provide more than someone’s position and dates of employment when references are checked, says Robert Fuller, Esq., an attorney with Nelson Hardiman, LLP, in Los Angeles.
Consequently, Fuller recommends that hospitals have very specific probation policies, allowing for termination for any reason within the first 90 days of employment and active supervision of new employees to ensure that no red flags are raised within that time frame.
If someone was fired from a previous job, use extra caution in making a hiring decision. Paskoff advises considering the facts: What was the person fired for? What do his or her records look like?
“Just because someone was fired, you shouldn’t dismiss him or her, but know what he or she was fired for and how well the firing was documented and investigated,” he says.
Fuller advises differently.
“If proper policies were followed and the employee failed to comport with improvement recommendations, he or she is not going to be any different the second time around,” he says.
Although the job interview process can be lengthy, “don’t take any shortcuts,” Paskoff says. You may end up costing an organization a lot more than time if you do.
—Karen Appold
As a hospitalist, caring for critically ill or injured patients can be stressful and demanding. Working with difficult doctors, those who exhibit intimidating and disruptive behaviors such as verbal outbursts and physical threats as well as passive activities such as refusing to perform assigned tasks, can make the work environment even more challenging.1 Some docs are routinely reluctant—or refuse—to answer questions or return phone calls or pages. Some communicate in condescending language or voice intonation; some are brutally impatient.1
The most difficult doctors to work with are those who are not aligned with the hospital’s or treatment team’s goals and those who aren’t open to feedback and coaching, says Rob Zipper, MD, MMM, SFHM, regional chief medical officer of Sound Physicians, based in Tacoma, Wash.
“If physicians are aware of a practice’s guidelines and goals but simply won’t comply with them, it makes it harder on everyone else who is pulling the ship in the same direction,” he says.
Unruly physicians don’t just annoy their coworkers. According to a sentinel event alert from The Joint Commission, they can:
- foster medical errors;
- contribute to poor patient satisfaction;
- contribute to preventable adverse outcomes;
- increase the cost of care;
- undermine team effectiveness; and
- cause qualified clinicians, administrators, and managers to seek new positions in more professional environments.1
“These issues are all connected,” says Stephen R. Nichols, MD, chief of clinical operations performance at the Schumacher Group in Brownwood, Texas. “Disruptive behaviors create mitigated communications and dissatisfaction among staff, which bleeds over into other aspects that are involved secondarily.”
Stephen M. Paskoff, Esq., president and CEO of ELI in Atlanta, can attest to the most severe consequences of bad behavior on patient care.
At one institution, a surgeon’s disruptive behavior lead to a coworker forgetting to perform a procedure and a patient dying.2 In another incident, the emergency department stopped calling on a medical subspecialist who was predictably abusive. The subspecialist knew how to treat a specific patient with an unusual intervention. Since the specialist was not consulted initially, the patient ended up in the intensive care unit.2
One bad hospitalist can bring down the reputation of an entire team.
“Many programs are incentivized based on medical staff and primary-care physicians’ perceptions of their care, so there are direct and indirect consequences,” Dr. Zipper says.
The bottom line, says Felix Aguirre, MD, SFHM, vice president of medical affairs at IPC Healthcare in North Hollywood, Calif., is that it only takes one bad experience to tarnish a group, but it takes many positive experiences to erase the damage.
The Roots of Evil
Intimidating and disruptive behavior stems from both individual and systemic factors. Care providers who exhibit characteristics such as self-centeredness, immaturity, or defensiveness can be more prone to unprofessional behavior. They can lack interpersonal, coping, or conflict-management skills.1
Systemic factors are marked by pressures related to increased productivity demands, cost-containment requirements, embedded hierarchies, and fear of litigation in the healthcare environment. These pressures can be further exacerbated by changes to or differences in the authority, autonomy, empowerment, and roles or values of professionals on the healthcare team as well as by the continual daily changes in shifts, rotations, and interdepartmental support staff. This dynamic creates challenges for interprofessional communication and development of trust among team members.1
According to The Joint Commission, intimidating and disruptive behaviors are often manifested by healthcare professionals in positions of power.1 But other members of the care team can be problematic as well.
“In my experience, conflicts usually revolve around different perspectives and objectives, even if both parties are acting respectfully,” Dr. Zipper says. “Sometimes, however, providers or other care team members are tired or stressed and don’t behave professionally.”
Paskoff, who has more than 40 years of experience in healthcare-related workplace issues, including serving as an investigator for the U.S. Equal Employment Opportunity Commission, says some doctors learn bad behaviors from their mentors and that behaviors can be passed down through generations because they are tolerated.
“When I asked one physician who had outstanding training and an outstanding technical reputation how he became abusive, he said, ‘I learned from the best.’” Paskoff was actually able to track the doctor’s training to the late 1800s and physicians who were known for similar behaviors.
Confronting Those Who Misbehave
Dr. Zipper says physicians should confront behavioral issues directly.
“I will typically discuss a complaint with a doctor privately, and ask him or her what happened without being accusatory,” he says. “I try to provide as much concrete and objective information as I can. The doctor needs to know that you are trying to help him or her succeed. That said, if something is clearly bad behavior, feedback should be direct and include a statement such as, ‘This is not how we behave in this practice.’”
At times, it may not be possible to discuss an emergent matter, such as during a code blue.
“However, I will often ask if anyone on the code team has any ideas or concerns before ending the code,” Dr. Nichols says. “Then after the critical time has passed, it is important to debrief and reconnect with the team, especially the less-experienced members who may have lingering concerns.”
For many employees, however, it is difficult to report disruptive behaviors. This is due to a fear of retaliation and the stigma associated with “blowing the whistle” on a colleague as well as a general reluctance to confront an intimidator.1
If an employee cannot muster the courage to confront a disruptive coworker or if the issue isn’t resolved by talking with the difficult individual, an employee should be a good citizen and report bad behavior to the appropriate hospital authority in a timely manner, says A. Kevin Troutman, Esq., a partner at Fisher Phillips in Houston and a former healthcare human resources executive.
Hospitals accredited by The Joint Commission are required to create a code of conduct that defines disruptive and inappropriate behaviors. In addition, leaders must create and implement a process for managing these behaviors.1
Helping Difficult Doctors
After a physician or another employee has been called out for bad behavior, steps need to be taken to correct the problem. Robert Fuller, Esq., an attorney with Nelson Hardiman, LLP, in Los Angeles, has found a positive-oriented intervention called “the 3-Ds”—which stands for diagnose, design, and do—that has been a successful tool for achieving positive change. The strategy involves a supervisor and employee mutually developing a worksheet to diagnose the problem. Next, they design a remediation and improvement plan. Finally, they implement the plan and specify dates to achieve certain milestones. Coworkers should be informed of the plan and be urged to support it.
“Make it clear that the positive aspect of this plan turns to progressive discipline, including termination, if the employee doesn’t improve or abandons the plan of action,” Fuller says. In most cases, troublemakers will make a sincere effort to control disruptive tendencies.
Troutman suggests enlisting the assistance of a respected peer.
“Have a senior-level doctor help the noncompliant physician understand why his or her behavior creates problems for everyone, including the doctor himself,” he says. “Also, consider connecting compensation and other rewards to job performance, which encompasses good behavior and good citizenship within the organization. Make expectations and consequences clear.”
If an employee has a recent change in behavior, ask if there is a reason.
“It is my experience that sudden changes in behaviors are often the result of a personal or clinical issue, so it is important and humane to make certain that there is not some other cause for the change before assuming someone is simply being disruptive or difficult,” Dr. Nichols says.
Many healthcare institutions are now setting up centers of professionalism. Paskoff reports that The Center for Professionalism and Peer Support (CPPS) was created in 2008 at Brigham and Women’s Hospital in Boston to educate the hospital community regarding professionalism and manage unprofessional behavior.3 CPPS has established standards of behavior and a framework to deal with difficult behaviors.
“An employee is told what he or she is doing wrong, receives counseling, and is given resources to improve,” he explains. “If an employee doesn’t improve, he or she is told that the behavior won’t be tolerated.”
Dismissing Bad Employees
After addressing the specifics of unacceptable behavior and explaining the consequences of repeating it, leadership should monitor subsequent conduct and provide feedback.
“If the employee commits other violations or behaves badly, promptly address the misconduct again and make it clear that further such actions will not be tolerated,” Troutman says. “Expect immediate and sustained improvement and compliance. Be consistent, and if bad conduct continues after an opportunity to improve, do not prolong anyone’s suffering. Instead, terminate the disruptive employee. When you do, make the reasons clear.”
Karen Appold is a medical writer in Pennsylvania.
References
- Behaviors that undermine a culture of safety. The Joint Commission website. Accessed April 17, 2015.
- Whittemore AD, New England Society for Vascular Surgery. The impact of professionalism on safe surgical care. J Vasc Surg. 2007;45(2):415-419.
- Shapiro J, Whittemore A, Tsen LC. Instituting a culture of professionalism: the establishment of a center for professionalism and peer support. Jt Comm J Qual Patient Saf. 2014;40(4):168-177.
Are Behaviors Getting Better or Worse?
The Joint Commission issued a sentinel event alert1 on July 9, 2008, as a result of continuous reports to the commission’s Office of Quality and Patient Safety about disruptive behavior. Despite efforts to prevent employees from behaving badly, Ronald Wyatt, MD, MHA, medical director of the Division of Healthcare Improvement, says there is no evidence that the number of instances of bad behavior is decreasing.
According to a 2013 Institute for Safe Medication Practices survey with 4,884 respondents:2
- 73% reported encountering negative comments about colleagues or leaders during the previous year.
- 68% reported condescending language or demeaning comments or insults.
- 77% said they had encountered reluctance or refusal to answer questions or return calls.
- 69% reported they had encountered impatience with questions or hanging up the phone.
In addition, in a 2011 survey of more than 500 physician leaders and more than 300 staff physicians, 71 percent of respondents stated they had witnessed some type of disruptive behavior within the previous month, while 26 percent stated that they had been disruptive at one point in their career.3
Despite the gloomy news, Dr. Wyatt says, “There is increased awareness of disruptive behaviors, and they are being reported more often than in the past.”
As a former chief of medicine at a hospital, Dr. Wyatt says the lack of improvement could be due to hospital leadership.
“This is a critical piece to having a sound patient safety system,” he says.
In order for bad behaviors to improve, hospital leadership needs to be committed to creating a culture of safety. This would involve answering “yes” to the following questions:
- Does staff feel safe to report disruptive behaviors, and will leadership act on those reports?
- Is leadership committed to decreasing these types of behaviors?
- Is there a reporting system in place, and is it being used, monitored, and acted on?
- Can leadership step in and enforce the process if physicians aren’t complying?
- Is a model in place if intervention is necessary?
According to Dr. Wyatt, data show that one intervention is usually enough for most physicians to cease bad behaviors, but a small portion will persist.4
Hospitals accredited by The Joint Commission can contact the organization for a template regarding a policy for disruptive behaviors. Some consultants can also provide this.
—Karen Appold
References
- Behaviors that undermine a culture of safety. The Joint Commission website. Accessed April 17, 2015.
- Patient safety systems. Comprehensive Accreditation Manual for Hospitals. The Joint Commission. January 1, 2015:7-8.
- MacDonald O. Disruptive physician behavior. Quantia Communications, Inc.: Waltham, MA. May 15, 2011.
- Pichert JW, Moore IN, Karrass J, et al. An intervention model that promotes accountability: peer messengers and patient/family complaints. Jt Comm J Qual Patient Saf. 2013;39(10):435-446.
Proceed with Caution When Hiring Staff
Ideally, an institution won’t hire someone with intimidating and disruptive behavior in the first place. But this is always easier said than done.
In an effort to select and hire the best employees, it is important during the interview process to ask many questions about a candidate’s prior experiences and previous bosses as well as what the employee perceives to be good behavior and reasonable expectations.
“Listen for victim-like responses and criticisms of prior supervisors or employers,” says A. Kevin Troutman, Esq., a partner at Fisher Phillips in Houston and a former healthcare human resources executive. “Such responses are red flags that may help predict how the applicant will work out in your organization.”
Stephen M. Paskoff, Esq., president and CEO of ELI in Atlanta, says it’s best for the candidate to have interviews with multiple staff members in different ranks.
“Sometimes people will show a different side if he or she perceives someone as unimportant or someone that he or she could boss around,” he says. “The interview can be very telling if the applicant is a cultural fit or not.”
Carefully check a candidate’s previous training and employment records. It can be difficult, however, to decipher whether a potential employee will indeed be a good choice because prior employers almost uniformly refuse to provide more than someone’s position and dates of employment when references are checked, says Robert Fuller, Esq., an attorney with Nelson Hardiman, LLP, in Los Angeles.
Consequently, Fuller recommends that hospitals have very specific probation policies, allowing for termination for any reason within the first 90 days of employment and active supervision of new employees to ensure that no red flags are raised within that time frame.
If someone was fired from a previous job, use extra caution in making a hiring decision. Paskoff advises considering the facts: What was the person fired for? What do his or her records look like?
“Just because someone was fired, you shouldn’t dismiss him or her, but know what he or she was fired for and how well the firing was documented and investigated,” he says.
Fuller advises differently.
“If proper policies were followed and the employee failed to comport with improvement recommendations, he or she is not going to be any different the second time around,” he says.
Although the job interview process can be lengthy, “don’t take any shortcuts,” Paskoff says. You may end up costing an organization a lot more than time if you do.
—Karen Appold
As a hospitalist, caring for critically ill or injured patients can be stressful and demanding. Working with difficult doctors, those who exhibit intimidating and disruptive behaviors such as verbal outbursts and physical threats as well as passive activities such as refusing to perform assigned tasks, can make the work environment even more challenging.1 Some docs are routinely reluctant—or refuse—to answer questions or return phone calls or pages. Some communicate in condescending language or voice intonation; some are brutally impatient.1
The most difficult doctors to work with are those who are not aligned with the hospital’s or treatment team’s goals and those who aren’t open to feedback and coaching, says Rob Zipper, MD, MMM, SFHM, regional chief medical officer of Sound Physicians, based in Tacoma, Wash.
“If physicians are aware of a practice’s guidelines and goals but simply won’t comply with them, it makes it harder on everyone else who is pulling the ship in the same direction,” he says.
Unruly physicians don’t just annoy their coworkers. According to a sentinel event alert from The Joint Commission, they can:
- foster medical errors;
- contribute to poor patient satisfaction;
- contribute to preventable adverse outcomes;
- increase the cost of care;
- undermine team effectiveness; and
- cause qualified clinicians, administrators, and managers to seek new positions in more professional environments.1
“These issues are all connected,” says Stephen R. Nichols, MD, chief of clinical operations performance at the Schumacher Group in Brownwood, Texas. “Disruptive behaviors create mitigated communications and dissatisfaction among staff, which bleeds over into other aspects that are involved secondarily.”
Stephen M. Paskoff, Esq., president and CEO of ELI in Atlanta, can attest to the most severe consequences of bad behavior on patient care.
At one institution, a surgeon’s disruptive behavior lead to a coworker forgetting to perform a procedure and a patient dying.2 In another incident, the emergency department stopped calling on a medical subspecialist who was predictably abusive. The subspecialist knew how to treat a specific patient with an unusual intervention. Since the specialist was not consulted initially, the patient ended up in the intensive care unit.2
One bad hospitalist can bring down the reputation of an entire team.
“Many programs are incentivized based on medical staff and primary-care physicians’ perceptions of their care, so there are direct and indirect consequences,” Dr. Zipper says.
The bottom line, says Felix Aguirre, MD, SFHM, vice president of medical affairs at IPC Healthcare in North Hollywood, Calif., is that it only takes one bad experience to tarnish a group, but it takes many positive experiences to erase the damage.
The Roots of Evil
Intimidating and disruptive behavior stems from both individual and systemic factors. Care providers who exhibit characteristics such as self-centeredness, immaturity, or defensiveness can be more prone to unprofessional behavior. They can lack interpersonal, coping, or conflict-management skills.1
Systemic factors are marked by pressures related to increased productivity demands, cost-containment requirements, embedded hierarchies, and fear of litigation in the healthcare environment. These pressures can be further exacerbated by changes to or differences in the authority, autonomy, empowerment, and roles or values of professionals on the healthcare team as well as by the continual daily changes in shifts, rotations, and interdepartmental support staff. This dynamic creates challenges for interprofessional communication and development of trust among team members.1
According to The Joint Commission, intimidating and disruptive behaviors are often manifested by healthcare professionals in positions of power.1 But other members of the care team can be problematic as well.
“In my experience, conflicts usually revolve around different perspectives and objectives, even if both parties are acting respectfully,” Dr. Zipper says. “Sometimes, however, providers or other care team members are tired or stressed and don’t behave professionally.”
Paskoff, who has more than 40 years of experience in healthcare-related workplace issues, including serving as an investigator for the U.S. Equal Employment Opportunity Commission, says some doctors learn bad behaviors from their mentors and that behaviors can be passed down through generations because they are tolerated.
“When I asked one physician who had outstanding training and an outstanding technical reputation how he became abusive, he said, ‘I learned from the best.’” Paskoff was actually able to track the doctor’s training to the late 1800s and physicians who were known for similar behaviors.
Confronting Those Who Misbehave
Dr. Zipper says physicians should confront behavioral issues directly.
“I will typically discuss a complaint with a doctor privately, and ask him or her what happened without being accusatory,” he says. “I try to provide as much concrete and objective information as I can. The doctor needs to know that you are trying to help him or her succeed. That said, if something is clearly bad behavior, feedback should be direct and include a statement such as, ‘This is not how we behave in this practice.’”
At times, it may not be possible to discuss an emergent matter, such as during a code blue.
“However, I will often ask if anyone on the code team has any ideas or concerns before ending the code,” Dr. Nichols says. “Then after the critical time has passed, it is important to debrief and reconnect with the team, especially the less-experienced members who may have lingering concerns.”
For many employees, however, it is difficult to report disruptive behaviors. This is due to a fear of retaliation and the stigma associated with “blowing the whistle” on a colleague as well as a general reluctance to confront an intimidator.1
If an employee cannot muster the courage to confront a disruptive coworker or if the issue isn’t resolved by talking with the difficult individual, an employee should be a good citizen and report bad behavior to the appropriate hospital authority in a timely manner, says A. Kevin Troutman, Esq., a partner at Fisher Phillips in Houston and a former healthcare human resources executive.
Hospitals accredited by The Joint Commission are required to create a code of conduct that defines disruptive and inappropriate behaviors. In addition, leaders must create and implement a process for managing these behaviors.1
Helping Difficult Doctors
After a physician or another employee has been called out for bad behavior, steps need to be taken to correct the problem. Robert Fuller, Esq., an attorney with Nelson Hardiman, LLP, in Los Angeles, has found a positive-oriented intervention called “the 3-Ds”—which stands for diagnose, design, and do—that has been a successful tool for achieving positive change. The strategy involves a supervisor and employee mutually developing a worksheet to diagnose the problem. Next, they design a remediation and improvement plan. Finally, they implement the plan and specify dates to achieve certain milestones. Coworkers should be informed of the plan and be urged to support it.
“Make it clear that the positive aspect of this plan turns to progressive discipline, including termination, if the employee doesn’t improve or abandons the plan of action,” Fuller says. In most cases, troublemakers will make a sincere effort to control disruptive tendencies.
Troutman suggests enlisting the assistance of a respected peer.
“Have a senior-level doctor help the noncompliant physician understand why his or her behavior creates problems for everyone, including the doctor himself,” he says. “Also, consider connecting compensation and other rewards to job performance, which encompasses good behavior and good citizenship within the organization. Make expectations and consequences clear.”
If an employee has a recent change in behavior, ask if there is a reason.
“It is my experience that sudden changes in behaviors are often the result of a personal or clinical issue, so it is important and humane to make certain that there is not some other cause for the change before assuming someone is simply being disruptive or difficult,” Dr. Nichols says.
Many healthcare institutions are now setting up centers of professionalism. Paskoff reports that The Center for Professionalism and Peer Support (CPPS) was created in 2008 at Brigham and Women’s Hospital in Boston to educate the hospital community regarding professionalism and manage unprofessional behavior.3 CPPS has established standards of behavior and a framework to deal with difficult behaviors.
“An employee is told what he or she is doing wrong, receives counseling, and is given resources to improve,” he explains. “If an employee doesn’t improve, he or she is told that the behavior won’t be tolerated.”
Dismissing Bad Employees
After addressing the specifics of unacceptable behavior and explaining the consequences of repeating it, leadership should monitor subsequent conduct and provide feedback.
“If the employee commits other violations or behaves badly, promptly address the misconduct again and make it clear that further such actions will not be tolerated,” Troutman says. “Expect immediate and sustained improvement and compliance. Be consistent, and if bad conduct continues after an opportunity to improve, do not prolong anyone’s suffering. Instead, terminate the disruptive employee. When you do, make the reasons clear.”
Karen Appold is a medical writer in Pennsylvania.
References
- Behaviors that undermine a culture of safety. The Joint Commission website. Accessed April 17, 2015.
- Whittemore AD, New England Society for Vascular Surgery. The impact of professionalism on safe surgical care. J Vasc Surg. 2007;45(2):415-419.
- Shapiro J, Whittemore A, Tsen LC. Instituting a culture of professionalism: the establishment of a center for professionalism and peer support. Jt Comm J Qual Patient Saf. 2014;40(4):168-177.
Are Behaviors Getting Better or Worse?
The Joint Commission issued a sentinel event alert1 on July 9, 2008, as a result of continuous reports to the commission’s Office of Quality and Patient Safety about disruptive behavior. Despite efforts to prevent employees from behaving badly, Ronald Wyatt, MD, MHA, medical director of the Division of Healthcare Improvement, says there is no evidence that the number of instances of bad behavior is decreasing.
According to a 2013 Institute for Safe Medication Practices survey with 4,884 respondents:2
- 73% reported encountering negative comments about colleagues or leaders during the previous year.
- 68% reported condescending language or demeaning comments or insults.
- 77% said they had encountered reluctance or refusal to answer questions or return calls.
- 69% reported they had encountered impatience with questions or hanging up the phone.
In addition, in a 2011 survey of more than 500 physician leaders and more than 300 staff physicians, 71 percent of respondents stated they had witnessed some type of disruptive behavior within the previous month, while 26 percent stated that they had been disruptive at one point in their career.3
Despite the gloomy news, Dr. Wyatt says, “There is increased awareness of disruptive behaviors, and they are being reported more often than in the past.”
As a former chief of medicine at a hospital, Dr. Wyatt says the lack of improvement could be due to hospital leadership.
“This is a critical piece to having a sound patient safety system,” he says.
In order for bad behaviors to improve, hospital leadership needs to be committed to creating a culture of safety. This would involve answering “yes” to the following questions:
- Does staff feel safe to report disruptive behaviors, and will leadership act on those reports?
- Is leadership committed to decreasing these types of behaviors?
- Is there a reporting system in place, and is it being used, monitored, and acted on?
- Can leadership step in and enforce the process if physicians aren’t complying?
- Is a model in place if intervention is necessary?
According to Dr. Wyatt, data show that one intervention is usually enough for most physicians to cease bad behaviors, but a small portion will persist.4
Hospitals accredited by The Joint Commission can contact the organization for a template regarding a policy for disruptive behaviors. Some consultants can also provide this.
—Karen Appold
References
- Behaviors that undermine a culture of safety. The Joint Commission website. Accessed April 17, 2015.
- Patient safety systems. Comprehensive Accreditation Manual for Hospitals. The Joint Commission. January 1, 2015:7-8.
- MacDonald O. Disruptive physician behavior. Quantia Communications, Inc.: Waltham, MA. May 15, 2011.
- Pichert JW, Moore IN, Karrass J, et al. An intervention model that promotes accountability: peer messengers and patient/family complaints. Jt Comm J Qual Patient Saf. 2013;39(10):435-446.
Proceed with Caution When Hiring Staff
Ideally, an institution won’t hire someone with intimidating and disruptive behavior in the first place. But this is always easier said than done.
In an effort to select and hire the best employees, it is important during the interview process to ask many questions about a candidate’s prior experiences and previous bosses as well as what the employee perceives to be good behavior and reasonable expectations.
“Listen for victim-like responses and criticisms of prior supervisors or employers,” says A. Kevin Troutman, Esq., a partner at Fisher Phillips in Houston and a former healthcare human resources executive. “Such responses are red flags that may help predict how the applicant will work out in your organization.”
Stephen M. Paskoff, Esq., president and CEO of ELI in Atlanta, says it’s best for the candidate to have interviews with multiple staff members in different ranks.
“Sometimes people will show a different side if he or she perceives someone as unimportant or someone that he or she could boss around,” he says. “The interview can be very telling if the applicant is a cultural fit or not.”
Carefully check a candidate’s previous training and employment records. It can be difficult, however, to decipher whether a potential employee will indeed be a good choice because prior employers almost uniformly refuse to provide more than someone’s position and dates of employment when references are checked, says Robert Fuller, Esq., an attorney with Nelson Hardiman, LLP, in Los Angeles.
Consequently, Fuller recommends that hospitals have very specific probation policies, allowing for termination for any reason within the first 90 days of employment and active supervision of new employees to ensure that no red flags are raised within that time frame.
If someone was fired from a previous job, use extra caution in making a hiring decision. Paskoff advises considering the facts: What was the person fired for? What do his or her records look like?
“Just because someone was fired, you shouldn’t dismiss him or her, but know what he or she was fired for and how well the firing was documented and investigated,” he says.
Fuller advises differently.
“If proper policies were followed and the employee failed to comport with improvement recommendations, he or she is not going to be any different the second time around,” he says.
Although the job interview process can be lengthy, “don’t take any shortcuts,” Paskoff says. You may end up costing an organization a lot more than time if you do.
—Karen Appold
Pacritinib bests BAT despite study truncation
SAN DIEGO—The JAK2/FLT3 inhibitor pacritinib significantly reduces spleen volume and symptoms in patients with myelofibrosis and low platelet counts,
compared to best available therapy (BAT), according to results of the PERSIST-2 trial.
In this phase 3 trial, BAT included the JAK1/2 inhibitor ruxolitinib. And pacritinib demonstrated benefits over BAT despite a truncated trial.
The US Food and Drug Administration (FDA) placed PERSIST-2 on clinical hold in February 2016 due to concerns over interim survival results, bleeding, and cardiovascular events.
Patients randomized at least 22 weeks prior to the clinical hold contributed data to the week 24 endpoint, the results of which were presented at the 2016 ASH Annual Meeting.
John Mascarenhas, MD, of Icahn School of Medicine at Mount Sinai in New York, New York, delivered the results as a late-breaking abstract (LBA-5).
Ruxolitinib is FDA-approved to treat myelofibrosis, but it is associated with dose-limiting cytopenias and is not indicated for patients with platelet counts less than 50,000/μL.
The earlier PERSIST-1 trial demonstrated sustained spleen volume reduction (SVR) and symptom control with pacritinib therapy regardless of baseline platelet count, but it did not include ruxolitinib in the BAT arm.
PERSIST-2 study design
Patients were randomized on a 1:1:1 basis to pacritinib at 400 mg once daily (PAC QD), pacritinib at 200 mg twice daily (PAC BID), or BAT, including ruxolitinib.
Patients had to have primary or secondary myelofibrosis and platelet counts of 100,000/μL or less. Patients were allowed to have had prior JAK2 inhibitors.
Crossover from BAT was allowed after progression at any time or at week 24.
The study had 2 primary endpoints: percent of patients achieving a 35% or greater SVR and the percent of patients achieving a 50% or more reduction in total symptom score (TSS) by MPN-SAF TSS 2.0.
The primary study objective was the efficacy of pooled QD and BID pacritinib compared to BAT. The secondary objective was the efficacy of QD or BD separately compared to BAT.
Patient demographics
The study randomized 311 patients, and 221 were included in the intent-to-treat efficacy population.
The efficacy population consisted of all patients randomized prior to September 7, 2015, which allowed their data to be included in the week 24 endpoint analysis prior to the clinical hold.
The PAC QD arm consisted of 75 patients with a median age of 69 (range, 39-85). Seventy-one percent were 65 or older, and about half were male.
About three-quarters had an ECOG performance status of 0-1, 61% had primary myelofibrosis, 21% had primary polycythemia vera (PPV), and 17% had primary essential thrombocythemia (PET). About half were DIPSS Intermediate-2 risk, 80% were JAK2V617F positive, and 51% had a platelet count less than 50,000/μL.
The PAC BID arm consisted of 74 patients with a median age of 67 (range, 39-85). Sixty-two percent were 65 or older, and 65% were male.
Eighty-eight percent had an ECOG performance status of 0-1, 74% had primary myelofibrosis, 19% had PPV, and 7% had PET. About half were DIPSS Intermediate-2 risk, 80% were JAK2V617F positive, and 42% had a platelet count less than 50,000/μL.
The BAT arm consisted of 72 patients with a median age of 69 (range, 32-83). Seventy-one percent were 65 or older, and about half were male.
Three-quarters had an ECOG performance status of 0-1, 60% had primary myelofibrosis, 22% had PPV, and 18% had PET. About half were DIPSS Intermediate-2 risk, 71% were JAK2V617F positive, and 44% had a platelet count less than 50,000/µL.
Prior ruxolitinib therapy was consistent across the arms—41.3% (PAC QD), 42% (PAC BID), and 46% (BAT).
“Now, it’s important to note,” Dr Mascarenhas said, “that the most common BAT was ruxolitinib, 45%, and hydroxyurea, 19%. And 19% of BAT patients actually had no treatment, watch and wait. This highlights the fact that this is an area where there is really no other viable therapeutic option for these patients.”
Efficacy
Pacritinib-treated patients had significantly greater spleen reduction from baseline to week 24 than BAT-treated patients, with 18% (QD+BID), 15% (QD), and 22% (BID) achieving 35% or more SVR compared to 3% in the BAT arm.
Pacritinib-treated patients also experienced greater TSS reduction, with 25% (QD+BID), 17% (QD), and 32% (BID) reporting 50% or more reduction in TSS compared to 14% in the BAT arm. However, only the PAC BID arm was significantly different from BAT.
SVR in all subgroups—age, gender, JAK2 mutation status, prior treatment, platelet count, hemoglobin, peripheral blasts, and white blood cell count—demonstrated superiority for pacritinib.
Median changes in individual symptom scores were also better in the pacritinib arms than in the BAT arm in almost every category—tiredness, early satiety, abdominal discomfort, inactivity, night sweats, bone pain, and pain under ribs on the left side.
Pruritus was the only category in which BAT was superior, and that was compared to the QD arm and not the BID arm.
The majority of patients who stopped pacritinib therapy were taken off due to the clinical hold.
There were no significant differences between the groups in overall survival. Hazard ratios for overall survival (95% confidence intervals) were 0.68 (0.30, 1.53) for PAC BID vs BAT, 1.18 (0.57, 2.44) for PAC QD vs BAT, and 0.61 (0.27, 1.35) for PAC BID vs QD.
PAC BID maintained this survival advantage compared with BAT across nearly all demographic and myelofibrosis-associated risk factors.
Patients who were red blood cell transfusion-dependent at baseline experienced a statistically significant decrease in transfusion frequency from baseline to week 24 in both the QD and BID pacritinib arms compared with BAT.
And thrombocytopenia was not a significant factor for patients who were receiving pacritinib and had platelet counts less than 50,000/μL.
Toxicity
The most common treatment-emergent adverse events (AEs) associated with pacritinib were diarrhea, nausea, vomiting, anemia, and thrombocytopenia. They were generally less frequent for BID compared with QD administration.
The most common serious adverse events (SAEs)—occurring in 5% of patients or more in any arms—were anemia (5%, 8%, and 3%), thrombocytopenia (2%, 6%, and 2%), pneumonia (5%, 6%, and 4%), and acute renal failure (5%, 2%, and 2%) in the QD, BID, and BAT arms, respectively.
SAEs of interest included congestive heart failure, atrial fibrillation, cardiac arrest, epistaxis, and subdural hematoma, which occurred in 3% or fewer patients in any arm.
“They [the SAEs] were relatively infrequent, and there was not a clear signal of toxicity,” Dr Mascarenhas said.
Deaths
Deaths in the intent-to-treat evaluable population were censored at the time of full clinical hold.
For the entire enrolled population, 15/104 deaths occurred in the QD arm, 10/107 in the BID arm, and 14/100 in the BAT arm.
After the full clinical hold, 7, 10, and 6 deaths occurred in the QD, BID, and BAT arms, respectively.
Seven of 20 patients died after crossover to pacritinib. Five were due to AEs—3 cardiac, 1 bleeding, and 1 other.
“It’s important to note that progression of disease was the leading cause of death in the PAC BID arm,” Dr Mascarenhas noted. “This is after the patients stopped the drug [when the trial was on clinical hold].”
Conclusions
Despite study truncation, pacritinib (QD+BID) was significantly more effective than BAT for SVR (P=0.001) and trended toward improved TSS (P=0.079).
Pacritinib BID appeared more effective than QD versus BAT for SVR and TSS, and pacritinib BID appeared to have a better benefit/risk profile than BAT.
“This is a well-tolerated drug in many respects,” Dr Mascarenhas said. “This is a patient population that is quite ill, low platelets, poor outcome, and they did pretty well.”
When asked about the future of pacritinib, Dr Mascarenhas said he believes the benefit-to-risk ratio is in favor of the drug.
“Pacritinib offers patients in this vulnerable situation an opportunity for symptom relief, basically spleen and symptoms,” he said. “So I think this is a drug that will hopefully move forward.”
Dr Mascarenhas disclosed research funding from CTI Biopharma, the sponsor of the trial. ![]()
SAN DIEGO—The JAK2/FLT3 inhibitor pacritinib significantly reduces spleen volume and symptoms in patients with myelofibrosis and low platelet counts,
compared to best available therapy (BAT), according to results of the PERSIST-2 trial.
In this phase 3 trial, BAT included the JAK1/2 inhibitor ruxolitinib. And pacritinib demonstrated benefits over BAT despite a truncated trial.
The US Food and Drug Administration (FDA) placed PERSIST-2 on clinical hold in February 2016 due to concerns over interim survival results, bleeding, and cardiovascular events.
Patients randomized at least 22 weeks prior to the clinical hold contributed data to the week 24 endpoint, the results of which were presented at the 2016 ASH Annual Meeting.
John Mascarenhas, MD, of Icahn School of Medicine at Mount Sinai in New York, New York, delivered the results as a late-breaking abstract (LBA-5).
Ruxolitinib is FDA-approved to treat myelofibrosis, but it is associated with dose-limiting cytopenias and is not indicated for patients with platelet counts less than 50,000/μL.
The earlier PERSIST-1 trial demonstrated sustained spleen volume reduction (SVR) and symptom control with pacritinib therapy regardless of baseline platelet count, but it did not include ruxolitinib in the BAT arm.
PERSIST-2 study design
Patients were randomized on a 1:1:1 basis to pacritinib at 400 mg once daily (PAC QD), pacritinib at 200 mg twice daily (PAC BID), or BAT, including ruxolitinib.
Patients had to have primary or secondary myelofibrosis and platelet counts of 100,000/μL or less. Patients were allowed to have had prior JAK2 inhibitors.
Crossover from BAT was allowed after progression at any time or at week 24.
The study had 2 primary endpoints: percent of patients achieving a 35% or greater SVR and the percent of patients achieving a 50% or more reduction in total symptom score (TSS) by MPN-SAF TSS 2.0.
The primary study objective was the efficacy of pooled QD and BID pacritinib compared to BAT. The secondary objective was the efficacy of QD or BD separately compared to BAT.
Patient demographics
The study randomized 311 patients, and 221 were included in the intent-to-treat efficacy population.
The efficacy population consisted of all patients randomized prior to September 7, 2015, which allowed their data to be included in the week 24 endpoint analysis prior to the clinical hold.
The PAC QD arm consisted of 75 patients with a median age of 69 (range, 39-85). Seventy-one percent were 65 or older, and about half were male.
About three-quarters had an ECOG performance status of 0-1, 61% had primary myelofibrosis, 21% had primary polycythemia vera (PPV), and 17% had primary essential thrombocythemia (PET). About half were DIPSS Intermediate-2 risk, 80% were JAK2V617F positive, and 51% had a platelet count less than 50,000/μL.
The PAC BID arm consisted of 74 patients with a median age of 67 (range, 39-85). Sixty-two percent were 65 or older, and 65% were male.
Eighty-eight percent had an ECOG performance status of 0-1, 74% had primary myelofibrosis, 19% had PPV, and 7% had PET. About half were DIPSS Intermediate-2 risk, 80% were JAK2V617F positive, and 42% had a platelet count less than 50,000/μL.
The BAT arm consisted of 72 patients with a median age of 69 (range, 32-83). Seventy-one percent were 65 or older, and about half were male.
Three-quarters had an ECOG performance status of 0-1, 60% had primary myelofibrosis, 22% had PPV, and 18% had PET. About half were DIPSS Intermediate-2 risk, 71% were JAK2V617F positive, and 44% had a platelet count less than 50,000/µL.
Prior ruxolitinib therapy was consistent across the arms—41.3% (PAC QD), 42% (PAC BID), and 46% (BAT).
“Now, it’s important to note,” Dr Mascarenhas said, “that the most common BAT was ruxolitinib, 45%, and hydroxyurea, 19%. And 19% of BAT patients actually had no treatment, watch and wait. This highlights the fact that this is an area where there is really no other viable therapeutic option for these patients.”
Efficacy
Pacritinib-treated patients had significantly greater spleen reduction from baseline to week 24 than BAT-treated patients, with 18% (QD+BID), 15% (QD), and 22% (BID) achieving 35% or more SVR compared to 3% in the BAT arm.
Pacritinib-treated patients also experienced greater TSS reduction, with 25% (QD+BID), 17% (QD), and 32% (BID) reporting 50% or more reduction in TSS compared to 14% in the BAT arm. However, only the PAC BID arm was significantly different from BAT.
SVR in all subgroups—age, gender, JAK2 mutation status, prior treatment, platelet count, hemoglobin, peripheral blasts, and white blood cell count—demonstrated superiority for pacritinib.
Median changes in individual symptom scores were also better in the pacritinib arms than in the BAT arm in almost every category—tiredness, early satiety, abdominal discomfort, inactivity, night sweats, bone pain, and pain under ribs on the left side.
Pruritus was the only category in which BAT was superior, and that was compared to the QD arm and not the BID arm.
The majority of patients who stopped pacritinib therapy were taken off due to the clinical hold.
There were no significant differences between the groups in overall survival. Hazard ratios for overall survival (95% confidence intervals) were 0.68 (0.30, 1.53) for PAC BID vs BAT, 1.18 (0.57, 2.44) for PAC QD vs BAT, and 0.61 (0.27, 1.35) for PAC BID vs QD.
PAC BID maintained this survival advantage compared with BAT across nearly all demographic and myelofibrosis-associated risk factors.
Patients who were red blood cell transfusion-dependent at baseline experienced a statistically significant decrease in transfusion frequency from baseline to week 24 in both the QD and BID pacritinib arms compared with BAT.
And thrombocytopenia was not a significant factor for patients who were receiving pacritinib and had platelet counts less than 50,000/μL.
Toxicity
The most common treatment-emergent adverse events (AEs) associated with pacritinib were diarrhea, nausea, vomiting, anemia, and thrombocytopenia. They were generally less frequent for BID compared with QD administration.
The most common serious adverse events (SAEs)—occurring in 5% of patients or more in any arms—were anemia (5%, 8%, and 3%), thrombocytopenia (2%, 6%, and 2%), pneumonia (5%, 6%, and 4%), and acute renal failure (5%, 2%, and 2%) in the QD, BID, and BAT arms, respectively.
SAEs of interest included congestive heart failure, atrial fibrillation, cardiac arrest, epistaxis, and subdural hematoma, which occurred in 3% or fewer patients in any arm.
“They [the SAEs] were relatively infrequent, and there was not a clear signal of toxicity,” Dr Mascarenhas said.
Deaths
Deaths in the intent-to-treat evaluable population were censored at the time of full clinical hold.
For the entire enrolled population, 15/104 deaths occurred in the QD arm, 10/107 in the BID arm, and 14/100 in the BAT arm.
After the full clinical hold, 7, 10, and 6 deaths occurred in the QD, BID, and BAT arms, respectively.
Seven of 20 patients died after crossover to pacritinib. Five were due to AEs—3 cardiac, 1 bleeding, and 1 other.
“It’s important to note that progression of disease was the leading cause of death in the PAC BID arm,” Dr Mascarenhas noted. “This is after the patients stopped the drug [when the trial was on clinical hold].”
Conclusions
Despite study truncation, pacritinib (QD+BID) was significantly more effective than BAT for SVR (P=0.001) and trended toward improved TSS (P=0.079).
Pacritinib BID appeared more effective than QD versus BAT for SVR and TSS, and pacritinib BID appeared to have a better benefit/risk profile than BAT.
“This is a well-tolerated drug in many respects,” Dr Mascarenhas said. “This is a patient population that is quite ill, low platelets, poor outcome, and they did pretty well.”
When asked about the future of pacritinib, Dr Mascarenhas said he believes the benefit-to-risk ratio is in favor of the drug.
“Pacritinib offers patients in this vulnerable situation an opportunity for symptom relief, basically spleen and symptoms,” he said. “So I think this is a drug that will hopefully move forward.”
Dr Mascarenhas disclosed research funding from CTI Biopharma, the sponsor of the trial. ![]()
SAN DIEGO—The JAK2/FLT3 inhibitor pacritinib significantly reduces spleen volume and symptoms in patients with myelofibrosis and low platelet counts,
compared to best available therapy (BAT), according to results of the PERSIST-2 trial.
In this phase 3 trial, BAT included the JAK1/2 inhibitor ruxolitinib. And pacritinib demonstrated benefits over BAT despite a truncated trial.
The US Food and Drug Administration (FDA) placed PERSIST-2 on clinical hold in February 2016 due to concerns over interim survival results, bleeding, and cardiovascular events.
Patients randomized at least 22 weeks prior to the clinical hold contributed data to the week 24 endpoint, the results of which were presented at the 2016 ASH Annual Meeting.
John Mascarenhas, MD, of Icahn School of Medicine at Mount Sinai in New York, New York, delivered the results as a late-breaking abstract (LBA-5).
Ruxolitinib is FDA-approved to treat myelofibrosis, but it is associated with dose-limiting cytopenias and is not indicated for patients with platelet counts less than 50,000/μL.
The earlier PERSIST-1 trial demonstrated sustained spleen volume reduction (SVR) and symptom control with pacritinib therapy regardless of baseline platelet count, but it did not include ruxolitinib in the BAT arm.
PERSIST-2 study design
Patients were randomized on a 1:1:1 basis to pacritinib at 400 mg once daily (PAC QD), pacritinib at 200 mg twice daily (PAC BID), or BAT, including ruxolitinib.
Patients had to have primary or secondary myelofibrosis and platelet counts of 100,000/μL or less. Patients were allowed to have had prior JAK2 inhibitors.
Crossover from BAT was allowed after progression at any time or at week 24.
The study had 2 primary endpoints: percent of patients achieving a 35% or greater SVR and the percent of patients achieving a 50% or more reduction in total symptom score (TSS) by MPN-SAF TSS 2.0.
The primary study objective was the efficacy of pooled QD and BID pacritinib compared to BAT. The secondary objective was the efficacy of QD or BD separately compared to BAT.
Patient demographics
The study randomized 311 patients, and 221 were included in the intent-to-treat efficacy population.
The efficacy population consisted of all patients randomized prior to September 7, 2015, which allowed their data to be included in the week 24 endpoint analysis prior to the clinical hold.
The PAC QD arm consisted of 75 patients with a median age of 69 (range, 39-85). Seventy-one percent were 65 or older, and about half were male.
About three-quarters had an ECOG performance status of 0-1, 61% had primary myelofibrosis, 21% had primary polycythemia vera (PPV), and 17% had primary essential thrombocythemia (PET). About half were DIPSS Intermediate-2 risk, 80% were JAK2V617F positive, and 51% had a platelet count less than 50,000/μL.
The PAC BID arm consisted of 74 patients with a median age of 67 (range, 39-85). Sixty-two percent were 65 or older, and 65% were male.
Eighty-eight percent had an ECOG performance status of 0-1, 74% had primary myelofibrosis, 19% had PPV, and 7% had PET. About half were DIPSS Intermediate-2 risk, 80% were JAK2V617F positive, and 42% had a platelet count less than 50,000/μL.
The BAT arm consisted of 72 patients with a median age of 69 (range, 32-83). Seventy-one percent were 65 or older, and about half were male.
Three-quarters had an ECOG performance status of 0-1, 60% had primary myelofibrosis, 22% had PPV, and 18% had PET. About half were DIPSS Intermediate-2 risk, 71% were JAK2V617F positive, and 44% had a platelet count less than 50,000/µL.
Prior ruxolitinib therapy was consistent across the arms—41.3% (PAC QD), 42% (PAC BID), and 46% (BAT).
“Now, it’s important to note,” Dr Mascarenhas said, “that the most common BAT was ruxolitinib, 45%, and hydroxyurea, 19%. And 19% of BAT patients actually had no treatment, watch and wait. This highlights the fact that this is an area where there is really no other viable therapeutic option for these patients.”
Efficacy
Pacritinib-treated patients had significantly greater spleen reduction from baseline to week 24 than BAT-treated patients, with 18% (QD+BID), 15% (QD), and 22% (BID) achieving 35% or more SVR compared to 3% in the BAT arm.
Pacritinib-treated patients also experienced greater TSS reduction, with 25% (QD+BID), 17% (QD), and 32% (BID) reporting 50% or more reduction in TSS compared to 14% in the BAT arm. However, only the PAC BID arm was significantly different from BAT.
SVR in all subgroups—age, gender, JAK2 mutation status, prior treatment, platelet count, hemoglobin, peripheral blasts, and white blood cell count—demonstrated superiority for pacritinib.
Median changes in individual symptom scores were also better in the pacritinib arms than in the BAT arm in almost every category—tiredness, early satiety, abdominal discomfort, inactivity, night sweats, bone pain, and pain under ribs on the left side.
Pruritus was the only category in which BAT was superior, and that was compared to the QD arm and not the BID arm.
The majority of patients who stopped pacritinib therapy were taken off due to the clinical hold.
There were no significant differences between the groups in overall survival. Hazard ratios for overall survival (95% confidence intervals) were 0.68 (0.30, 1.53) for PAC BID vs BAT, 1.18 (0.57, 2.44) for PAC QD vs BAT, and 0.61 (0.27, 1.35) for PAC BID vs QD.
PAC BID maintained this survival advantage compared with BAT across nearly all demographic and myelofibrosis-associated risk factors.
Patients who were red blood cell transfusion-dependent at baseline experienced a statistically significant decrease in transfusion frequency from baseline to week 24 in both the QD and BID pacritinib arms compared with BAT.
And thrombocytopenia was not a significant factor for patients who were receiving pacritinib and had platelet counts less than 50,000/μL.
Toxicity
The most common treatment-emergent adverse events (AEs) associated with pacritinib were diarrhea, nausea, vomiting, anemia, and thrombocytopenia. They were generally less frequent for BID compared with QD administration.
The most common serious adverse events (SAEs)—occurring in 5% of patients or more in any arms—were anemia (5%, 8%, and 3%), thrombocytopenia (2%, 6%, and 2%), pneumonia (5%, 6%, and 4%), and acute renal failure (5%, 2%, and 2%) in the QD, BID, and BAT arms, respectively.
SAEs of interest included congestive heart failure, atrial fibrillation, cardiac arrest, epistaxis, and subdural hematoma, which occurred in 3% or fewer patients in any arm.
“They [the SAEs] were relatively infrequent, and there was not a clear signal of toxicity,” Dr Mascarenhas said.
Deaths
Deaths in the intent-to-treat evaluable population were censored at the time of full clinical hold.
For the entire enrolled population, 15/104 deaths occurred in the QD arm, 10/107 in the BID arm, and 14/100 in the BAT arm.
After the full clinical hold, 7, 10, and 6 deaths occurred in the QD, BID, and BAT arms, respectively.
Seven of 20 patients died after crossover to pacritinib. Five were due to AEs—3 cardiac, 1 bleeding, and 1 other.
“It’s important to note that progression of disease was the leading cause of death in the PAC BID arm,” Dr Mascarenhas noted. “This is after the patients stopped the drug [when the trial was on clinical hold].”
Conclusions
Despite study truncation, pacritinib (QD+BID) was significantly more effective than BAT for SVR (P=0.001) and trended toward improved TSS (P=0.079).
Pacritinib BID appeared more effective than QD versus BAT for SVR and TSS, and pacritinib BID appeared to have a better benefit/risk profile than BAT.
“This is a well-tolerated drug in many respects,” Dr Mascarenhas said. “This is a patient population that is quite ill, low platelets, poor outcome, and they did pretty well.”
When asked about the future of pacritinib, Dr Mascarenhas said he believes the benefit-to-risk ratio is in favor of the drug.
“Pacritinib offers patients in this vulnerable situation an opportunity for symptom relief, basically spleen and symptoms,” he said. “So I think this is a drug that will hopefully move forward.”
Dr Mascarenhas disclosed research funding from CTI Biopharma, the sponsor of the trial. ![]()
Blood products unharmed by drone trips

products attached to a
S900-model drone.
Photo courtesy of
Johns Hopkins Medicine
A proof-of-concept study suggests that large bags of blood products can maintain temperature and cellular integrity when transported by drones.
Researchers say these findings, published in Transfusion, add to evidence that remotely piloted drones are an effective, safe, and timely way to quickly get blood products to remote accident or natural catastrophe sites, or other time-sensitive destinations.
“For rural areas that lack access to nearby clinics, or that may lack the infrastructure for collecting blood products or transporting them on their own, drones can provide that access,” said study author Timothy Amukele, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
Drones also can help in urban centers to improve distribution of blood products and the quality of care, he added.
Dr Amukele and his colleagues previously studied the impact of drone transportation on the chemical, hematological, and microbial makeup of drone-flown blood samples and found that none were negatively affected.
Study design, methods
In the new study, the team examined the effects of drone transportation on larger amounts of blood products used for transfusion, which have significantly more complex handling, transport, and storage requirements compared to blood samples for laboratory testing.
The researchers purchased 6 units of red blood cells (RBCs), 6 units of platelets, and 6 units of unthawed plasma from the American Red Cross. They then packed the units into a 5-quart cooler, 2 to 3 units at a time, in keeping with weight restrictions for the transport drone.
The cooler was then attached to a commercial S900-model drone. This particular drone model comes equipped with a camera mount, which the team removed and replaced with the cooler.
For each test, the drone was flown by remote control a distance of approximately 13 to 20 kilometers (8 to 12 miles) while 100 meters (328 feet) above ground. This flight took up to 26.5 minutes.
The researchers designed the test to maintain temperature for the RBCs, platelets, and plasma units. They used wet ice, pre-calibrated thermal packs, and dry ice for each type of blood product, respectively.
Temperature monitoring was constant, keeping with transport and storage requirements for blood components.
The team conducted the tests in an unpopulated area, and a certified, ground-based pilot flew the drone.
Following flight, all units were transported to The Johns Hopkins Hospital and compared to blood products that had not taken a drone trip.
Results
Dr Amukele and his colleagues checked the RBCs for signs of hemolysis. They checked the platelets for changes in pH, the number of platelets, and mean platelet volume. And they checked the plasma units for evidence of air bubbles, which would indicate thawing.
The researchers found no evidence of hemolysis in the control RBCs or the RBCs that had taken the drone flight.
There was no significant difference in pH, platelet counts, or mean platelet volume between control and drone-flown platelets.
And there was no apparent change in the size or shape of air bubbles in the plasma units before and after drone flight.
However, the researchers did find that, for all flown units, there was a decrease in temperature of between 1.5°C and 4°C during the course of the flight. They said the cause of this decrease was probably the ambient temperature in the case of the platelet units, the wet ice in the case of the RBCs, and the dry ice in the case of the plasma.
The team also found an up to 2°C difference between individual flights for both the RBCs and the plasma units. They said this difference is likely due to the differences in the amounts of wet and dry ice placed in the cooler.
The researchers are planning further and larger studies in the US and overseas, and they hope to test methods of active cooling, such as programming a cooler to maintain a specific temperature.
“My vision is that, in the future, when a first responder arrives to the scene of an accident, he or she can test the victim’s blood type right on the spot and send for a drone to bring the correct blood product,” Dr Amukele said.
Funding for this study was provided by Peter Kovler of the Blum-Kovler Foundation. ![]()
products attached to a
S900-model drone.
Photo courtesy of
Johns Hopkins Medicine
A proof-of-concept study suggests that large bags of blood products can maintain temperature and cellular integrity when transported by drones.
Researchers say these findings, published in Transfusion, add to evidence that remotely piloted drones are an effective, safe, and timely way to quickly get blood products to remote accident or natural catastrophe sites, or other time-sensitive destinations.
“For rural areas that lack access to nearby clinics, or that may lack the infrastructure for collecting blood products or transporting them on their own, drones can provide that access,” said study author Timothy Amukele, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
Drones also can help in urban centers to improve distribution of blood products and the quality of care, he added.
Dr Amukele and his colleagues previously studied the impact of drone transportation on the chemical, hematological, and microbial makeup of drone-flown blood samples and found that none were negatively affected.
Study design, methods
In the new study, the team examined the effects of drone transportation on larger amounts of blood products used for transfusion, which have significantly more complex handling, transport, and storage requirements compared to blood samples for laboratory testing.
The researchers purchased 6 units of red blood cells (RBCs), 6 units of platelets, and 6 units of unthawed plasma from the American Red Cross. They then packed the units into a 5-quart cooler, 2 to 3 units at a time, in keeping with weight restrictions for the transport drone.
The cooler was then attached to a commercial S900-model drone. This particular drone model comes equipped with a camera mount, which the team removed and replaced with the cooler.
For each test, the drone was flown by remote control a distance of approximately 13 to 20 kilometers (8 to 12 miles) while 100 meters (328 feet) above ground. This flight took up to 26.5 minutes.
The researchers designed the test to maintain temperature for the RBCs, platelets, and plasma units. They used wet ice, pre-calibrated thermal packs, and dry ice for each type of blood product, respectively.
Temperature monitoring was constant, keeping with transport and storage requirements for blood components.
The team conducted the tests in an unpopulated area, and a certified, ground-based pilot flew the drone.
Following flight, all units were transported to The Johns Hopkins Hospital and compared to blood products that had not taken a drone trip.
Results
Dr Amukele and his colleagues checked the RBCs for signs of hemolysis. They checked the platelets for changes in pH, the number of platelets, and mean platelet volume. And they checked the plasma units for evidence of air bubbles, which would indicate thawing.
The researchers found no evidence of hemolysis in the control RBCs or the RBCs that had taken the drone flight.
There was no significant difference in pH, platelet counts, or mean platelet volume between control and drone-flown platelets.
And there was no apparent change in the size or shape of air bubbles in the plasma units before and after drone flight.
However, the researchers did find that, for all flown units, there was a decrease in temperature of between 1.5°C and 4°C during the course of the flight. They said the cause of this decrease was probably the ambient temperature in the case of the platelet units, the wet ice in the case of the RBCs, and the dry ice in the case of the plasma.
The team also found an up to 2°C difference between individual flights for both the RBCs and the plasma units. They said this difference is likely due to the differences in the amounts of wet and dry ice placed in the cooler.
The researchers are planning further and larger studies in the US and overseas, and they hope to test methods of active cooling, such as programming a cooler to maintain a specific temperature.
“My vision is that, in the future, when a first responder arrives to the scene of an accident, he or she can test the victim’s blood type right on the spot and send for a drone to bring the correct blood product,” Dr Amukele said.
Funding for this study was provided by Peter Kovler of the Blum-Kovler Foundation. ![]()
products attached to a
S900-model drone.
Photo courtesy of
Johns Hopkins Medicine
A proof-of-concept study suggests that large bags of blood products can maintain temperature and cellular integrity when transported by drones.
Researchers say these findings, published in Transfusion, add to evidence that remotely piloted drones are an effective, safe, and timely way to quickly get blood products to remote accident or natural catastrophe sites, or other time-sensitive destinations.
“For rural areas that lack access to nearby clinics, or that may lack the infrastructure for collecting blood products or transporting them on their own, drones can provide that access,” said study author Timothy Amukele, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
Drones also can help in urban centers to improve distribution of blood products and the quality of care, he added.
Dr Amukele and his colleagues previously studied the impact of drone transportation on the chemical, hematological, and microbial makeup of drone-flown blood samples and found that none were negatively affected.
Study design, methods
In the new study, the team examined the effects of drone transportation on larger amounts of blood products used for transfusion, which have significantly more complex handling, transport, and storage requirements compared to blood samples for laboratory testing.
The researchers purchased 6 units of red blood cells (RBCs), 6 units of platelets, and 6 units of unthawed plasma from the American Red Cross. They then packed the units into a 5-quart cooler, 2 to 3 units at a time, in keeping with weight restrictions for the transport drone.
The cooler was then attached to a commercial S900-model drone. This particular drone model comes equipped with a camera mount, which the team removed and replaced with the cooler.
For each test, the drone was flown by remote control a distance of approximately 13 to 20 kilometers (8 to 12 miles) while 100 meters (328 feet) above ground. This flight took up to 26.5 minutes.
The researchers designed the test to maintain temperature for the RBCs, platelets, and plasma units. They used wet ice, pre-calibrated thermal packs, and dry ice for each type of blood product, respectively.
Temperature monitoring was constant, keeping with transport and storage requirements for blood components.
The team conducted the tests in an unpopulated area, and a certified, ground-based pilot flew the drone.
Following flight, all units were transported to The Johns Hopkins Hospital and compared to blood products that had not taken a drone trip.
Results
Dr Amukele and his colleagues checked the RBCs for signs of hemolysis. They checked the platelets for changes in pH, the number of platelets, and mean platelet volume. And they checked the plasma units for evidence of air bubbles, which would indicate thawing.
The researchers found no evidence of hemolysis in the control RBCs or the RBCs that had taken the drone flight.
There was no significant difference in pH, platelet counts, or mean platelet volume between control and drone-flown platelets.
And there was no apparent change in the size or shape of air bubbles in the plasma units before and after drone flight.
However, the researchers did find that, for all flown units, there was a decrease in temperature of between 1.5°C and 4°C during the course of the flight. They said the cause of this decrease was probably the ambient temperature in the case of the platelet units, the wet ice in the case of the RBCs, and the dry ice in the case of the plasma.
The team also found an up to 2°C difference between individual flights for both the RBCs and the plasma units. They said this difference is likely due to the differences in the amounts of wet and dry ice placed in the cooler.
The researchers are planning further and larger studies in the US and overseas, and they hope to test methods of active cooling, such as programming a cooler to maintain a specific temperature.
“My vision is that, in the future, when a first responder arrives to the scene of an accident, he or she can test the victim’s blood type right on the spot and send for a drone to bring the correct blood product,” Dr Amukele said.
Funding for this study was provided by Peter Kovler of the Blum-Kovler Foundation. ![]()
EC grants venetoclax conditional approval for CLL

(US version, Venclexta)
Photo courtesy of Abbvie
The European Commission (EC) has granted conditional marketing authorization for the oral BCL-2 inhibitor venetoclax (Venclyxto™) to treat certain patients with chronic lymphocytic leukemia (CLL).
The drug is now approved as monotherapy to treat adults with CLL who have 17p deletion or TP53 mutation and are unsuitable for or have failed a B-cell receptor pathway inhibitor.
Venetoclax is also approved as monotherapy to treat CLL in the absence of 17p deletion or TP53 mutation in adults who have failed both chemoimmunotherapy and a B-cell receptor pathway inhibitor.
Venetoclax is the first BCL-2 inhibitor authorized for use in Europe.
Conditional marketing authorization represents an expedited path for approval. The EC grants conditional marketing authorization to products whose benefits are thought to outweigh their risks, products that address unmet needs, and products that are expected to provide a significant public health benefit.
Conditional marketing authorization is granted before pivotal registration studies of a product are completed, but the company developing the product is required to complete post-marketing studies showing that the product provides a clinical benefit.
Venetoclax is being developed by AbbVie and Genentech, a member of the Roche Group. The drug is jointly commercialized by the companies in the US and by AbbVie outside of the US.
Phase 2 trials
Venetoclax has produced high objective response rates (ORR) in two phase 2 trials of CLL patients.
In one of these trials, researchers tested venetoclax in 107 patients with previously treated CLL and 17p deletion. The results were published in The Lancet Oncology in June.
The ORR in this trial was 79%. At the time of analysis, the median duration of response had not been reached. The same was true for progression-free survival and overall survival.
The progression-free survival estimate for 12 months was 72%, and the overall survival estimate was 87%.
The incidence of treatment-emergent adverse events was 96%, and the incidence of serious adverse events was 55%.
Grade 3 laboratory tumor lysis syndrome (TLS) was reported in 5 patients. Three of these patients continued on venetoclax, but 2 patients required a dose interruption of 1 day each.
In the second trial, researchers tested venetoclax in 64 patients with CLL who had failed treatment with ibrutinib and/or idelalisib. Results from this trial were presented at the 2016 ASH Annual Meeting.
The ORR was 67%. At 11.8 months of follow-up, the median duration of response, progression-free survival, and overall survival had not been reached. The estimated 12-month progression-free survival was 80%.
The incidence of adverse events was 100%, and the incidence of serious adverse events was 53%. No clinical TLS was observed, but 1 patient met Howard criteria for laboratory TLS. ![]()
(US version, Venclexta)
Photo courtesy of Abbvie
The European Commission (EC) has granted conditional marketing authorization for the oral BCL-2 inhibitor venetoclax (Venclyxto™) to treat certain patients with chronic lymphocytic leukemia (CLL).
The drug is now approved as monotherapy to treat adults with CLL who have 17p deletion or TP53 mutation and are unsuitable for or have failed a B-cell receptor pathway inhibitor.
Venetoclax is also approved as monotherapy to treat CLL in the absence of 17p deletion or TP53 mutation in adults who have failed both chemoimmunotherapy and a B-cell receptor pathway inhibitor.
Venetoclax is the first BCL-2 inhibitor authorized for use in Europe.
Conditional marketing authorization represents an expedited path for approval. The EC grants conditional marketing authorization to products whose benefits are thought to outweigh their risks, products that address unmet needs, and products that are expected to provide a significant public health benefit.
Conditional marketing authorization is granted before pivotal registration studies of a product are completed, but the company developing the product is required to complete post-marketing studies showing that the product provides a clinical benefit.
Venetoclax is being developed by AbbVie and Genentech, a member of the Roche Group. The drug is jointly commercialized by the companies in the US and by AbbVie outside of the US.
Phase 2 trials
Venetoclax has produced high objective response rates (ORR) in two phase 2 trials of CLL patients.
In one of these trials, researchers tested venetoclax in 107 patients with previously treated CLL and 17p deletion. The results were published in The Lancet Oncology in June.
The ORR in this trial was 79%. At the time of analysis, the median duration of response had not been reached. The same was true for progression-free survival and overall survival.
The progression-free survival estimate for 12 months was 72%, and the overall survival estimate was 87%.
The incidence of treatment-emergent adverse events was 96%, and the incidence of serious adverse events was 55%.
Grade 3 laboratory tumor lysis syndrome (TLS) was reported in 5 patients. Three of these patients continued on venetoclax, but 2 patients required a dose interruption of 1 day each.
In the second trial, researchers tested venetoclax in 64 patients with CLL who had failed treatment with ibrutinib and/or idelalisib. Results from this trial were presented at the 2016 ASH Annual Meeting.
The ORR was 67%. At 11.8 months of follow-up, the median duration of response, progression-free survival, and overall survival had not been reached. The estimated 12-month progression-free survival was 80%.
The incidence of adverse events was 100%, and the incidence of serious adverse events was 53%. No clinical TLS was observed, but 1 patient met Howard criteria for laboratory TLS. ![]()
(US version, Venclexta)
Photo courtesy of Abbvie
The European Commission (EC) has granted conditional marketing authorization for the oral BCL-2 inhibitor venetoclax (Venclyxto™) to treat certain patients with chronic lymphocytic leukemia (CLL).
The drug is now approved as monotherapy to treat adults with CLL who have 17p deletion or TP53 mutation and are unsuitable for or have failed a B-cell receptor pathway inhibitor.
Venetoclax is also approved as monotherapy to treat CLL in the absence of 17p deletion or TP53 mutation in adults who have failed both chemoimmunotherapy and a B-cell receptor pathway inhibitor.
Venetoclax is the first BCL-2 inhibitor authorized for use in Europe.
Conditional marketing authorization represents an expedited path for approval. The EC grants conditional marketing authorization to products whose benefits are thought to outweigh their risks, products that address unmet needs, and products that are expected to provide a significant public health benefit.
Conditional marketing authorization is granted before pivotal registration studies of a product are completed, but the company developing the product is required to complete post-marketing studies showing that the product provides a clinical benefit.
Venetoclax is being developed by AbbVie and Genentech, a member of the Roche Group. The drug is jointly commercialized by the companies in the US and by AbbVie outside of the US.
Phase 2 trials
Venetoclax has produced high objective response rates (ORR) in two phase 2 trials of CLL patients.
In one of these trials, researchers tested venetoclax in 107 patients with previously treated CLL and 17p deletion. The results were published in The Lancet Oncology in June.
The ORR in this trial was 79%. At the time of analysis, the median duration of response had not been reached. The same was true for progression-free survival and overall survival.
The progression-free survival estimate for 12 months was 72%, and the overall survival estimate was 87%.
The incidence of treatment-emergent adverse events was 96%, and the incidence of serious adverse events was 55%.
Grade 3 laboratory tumor lysis syndrome (TLS) was reported in 5 patients. Three of these patients continued on venetoclax, but 2 patients required a dose interruption of 1 day each.
In the second trial, researchers tested venetoclax in 64 patients with CLL who had failed treatment with ibrutinib and/or idelalisib. Results from this trial were presented at the 2016 ASH Annual Meeting.
The ORR was 67%. At 11.8 months of follow-up, the median duration of response, progression-free survival, and overall survival had not been reached. The estimated 12-month progression-free survival was 80%.
The incidence of adverse events was 100%, and the incidence of serious adverse events was 53%. No clinical TLS was observed, but 1 patient met Howard criteria for laboratory TLS. ![]()
Drug produces responses in ‘challenging’ patients

© Todd Buchanan 2016
SAN DIEGO—The oral BCL-2 inhibitor venetoclax can produce high objective response rates (ORRs) in chronic lymphocytic leukemia (CLL) patients who have failed treatment with at least one B-cell receptor inhibitor, according to investigators.
In a phase 2 study, venetoclax produced an ORR of 67% among all patients enrolled.
The drug produced a 70% ORR among patients who had failed treatment with ibrutinib and a 62% ORR among patients who had failed idelalisib.
“This represents the first prospective study in this patient population and does demonstrate high rates of durable responses, certainly making [venetoclax] a very viable option for a challenging group of patients to treat,” said study investigator Jeffrey Jones, MD, of The Ohio State University in Columbus.
Dr Jones presented results from this trial at the 2016 ASH Annual Meeting (abstract 637*). This study is sponsored by AbbVie in collaboration with Genentech/Roche.
The trial enrolled patients with CLL who relapsed after or were refractory to ibrutinib (arm A) or idelalisib (arm B). At the time of the data cut-off, 64 patients had been enrolled and treated with venetoclax, including 43 patients in arm A and 21 in arm B.
Patients received venetoclax via a recommended dose-titration schedule—20 mg once daily in week 1, 50 mg daily in week 2, 100 mg daily in week 3, 200 mg daily in week 4, and 400 mg daily from week 5 onward. Patients continued to receive the drug until disease progression or unacceptable toxicity.
To mitigate the risk of tumor lysis syndrome (TLS), patients received prophylaxis with uric acid lowering agents and hydration starting at least 72 hours before the first dose of venetoclax.
Patients with a high tumor burden were hospitalized for the first 20 mg dose and the first 50 mg dose, and they received intravenous hydration and rasburicase. Laboratory values were monitored at the first dose and all dose increases.
Patient characteristics: Arm A
Among patients who had failed ibrutinib, the median age was 66 (range, 48-80). Forty-nine percent of the patients had del(17p), and 35% had bulky nodal disease (5 cm or greater).
The median number of prior treatments was 4 (range, 1-12). All patients had received ibrutinib, but 9% had also received idelalisib. Ninety-one percent of patients were refractory to ibrutinib, and 5% were refractory to idelalisib.
The median time on ibrutinib was 17 months (range, 1-56), and the median time on idelalisib was 10 months (range, 2-31).
Patient characteristics: Arm B
Among patients who had failed idelalisib, the median age was 68 (range, 56-85). Ten percent of patients had del(17p), and 52% had bulky nodal disease (5 cm or greater).
The median number of prior treatments was 3 (range, 1-11). All patients had received idelalisib, but 24% had also received ibrutinib. Sixty-seven percent of patients were refractory to idelalisib, and 10% were refractory to ibrutinib.
The median time on idelalisib was 8 months (range, 1-27), and the median time on ibrutinib was 6 months (range, 2-11).
Results: Arm A
The median time on study in arm A was 13 months (range, 0.1-18). Eighteen patients in this arm discontinued the study—12 due to disease progression, 3 due to adverse events (AEs), 2 due to stem cell transplant, and 1 patient withdrew consent.
The ORR was 70% according to an independent review committee (IRC) and 67% according to investigators.
The rate of complete response (CR) was 0%, and the rate of CR with incomplete bone marrow recovery (CRi) was 2% according to the IRC. According to investigators, the CR rate was 5%, and the CRi rate was 2%.
Sixty-seven percent of patients had a partial response (PR) according to the IRC, and 56% had a PR according to investigators.
Results: Arm B
The median time on study in arm B was 9 months (range, 1.3-16). Four patients in this arm discontinued the study—3 related to disease progression and 1 for an “other” reason.
The ORR was 62% according to the IRC and 57% according to investigators.
The rate of CR/CRi was 0% according to the IRC. According to investigators, the CR rate was 10%, and the CRi rate was 5%.
Sixty-two percent of patients had a PR according to the IRC, and 43% had a PR according to investigators.
Results: Overall
The ORR was 67% according to the IRC and 64% according to investigators.
Forty-five percent of patient samples analyzed (14/31) demonstrated minimal residual disease (MRD) negativity in the peripheral blood between weeks 24 and 48. Five patients with sustained MRD negativity had bone marrow evaluations, and 1 was MRD negative.
At 11.8 months of follow-up, the median duration of response, progression-free survival, and overall survival had not been reached. The estimated 12-month progression-free survival for all patients was 80%.
“Venetoclax has been well-tolerated,” Dr Jones noted. “The toxicity profile in this study is consistent with previous reports. Most of the toxicity has been cytopenias, which can be managed with dose adjustments or supportive care interventions, such as G-CSF.”
All 64 patients experienced an AE. Common AEs were neutropenia (58%), thrombocytopenia (44%), diarrhea (42%), nausea (41%), anemia (36%), fatigue (31%), decreased white blood cell count (22%), and hyperphosphatemia (22%).
Eighty-three percent of patients had grade 3/4 AEs, including neutropenia (45%), thrombocytopenia (28%), anemia (22%), decreased white blood cell count (13%), febrile neutropenia (11%), and pneumonia (11%).
Fifty-three percent of patients had serious AEs, including febrile neutropenia (9%), pneumonia (8%), multi-organ failure (3%), septic shock (3%), and increased potassium (3%).
There were no cases of clinical TLS. However, 1 patient with high tumor burden met Howard criteria for laboratory TLS. ![]()
*Information presented at the meeting differs from the abstract.
© Todd Buchanan 2016
SAN DIEGO—The oral BCL-2 inhibitor venetoclax can produce high objective response rates (ORRs) in chronic lymphocytic leukemia (CLL) patients who have failed treatment with at least one B-cell receptor inhibitor, according to investigators.
In a phase 2 study, venetoclax produced an ORR of 67% among all patients enrolled.
The drug produced a 70% ORR among patients who had failed treatment with ibrutinib and a 62% ORR among patients who had failed idelalisib.
“This represents the first prospective study in this patient population and does demonstrate high rates of durable responses, certainly making [venetoclax] a very viable option for a challenging group of patients to treat,” said study investigator Jeffrey Jones, MD, of The Ohio State University in Columbus.
Dr Jones presented results from this trial at the 2016 ASH Annual Meeting (abstract 637*). This study is sponsored by AbbVie in collaboration with Genentech/Roche.
The trial enrolled patients with CLL who relapsed after or were refractory to ibrutinib (arm A) or idelalisib (arm B). At the time of the data cut-off, 64 patients had been enrolled and treated with venetoclax, including 43 patients in arm A and 21 in arm B.
Patients received venetoclax via a recommended dose-titration schedule—20 mg once daily in week 1, 50 mg daily in week 2, 100 mg daily in week 3, 200 mg daily in week 4, and 400 mg daily from week 5 onward. Patients continued to receive the drug until disease progression or unacceptable toxicity.
To mitigate the risk of tumor lysis syndrome (TLS), patients received prophylaxis with uric acid lowering agents and hydration starting at least 72 hours before the first dose of venetoclax.
Patients with a high tumor burden were hospitalized for the first 20 mg dose and the first 50 mg dose, and they received intravenous hydration and rasburicase. Laboratory values were monitored at the first dose and all dose increases.
Patient characteristics: Arm A
Among patients who had failed ibrutinib, the median age was 66 (range, 48-80). Forty-nine percent of the patients had del(17p), and 35% had bulky nodal disease (5 cm or greater).
The median number of prior treatments was 4 (range, 1-12). All patients had received ibrutinib, but 9% had also received idelalisib. Ninety-one percent of patients were refractory to ibrutinib, and 5% were refractory to idelalisib.
The median time on ibrutinib was 17 months (range, 1-56), and the median time on idelalisib was 10 months (range, 2-31).
Patient characteristics: Arm B
Among patients who had failed idelalisib, the median age was 68 (range, 56-85). Ten percent of patients had del(17p), and 52% had bulky nodal disease (5 cm or greater).
The median number of prior treatments was 3 (range, 1-11). All patients had received idelalisib, but 24% had also received ibrutinib. Sixty-seven percent of patients were refractory to idelalisib, and 10% were refractory to ibrutinib.
The median time on idelalisib was 8 months (range, 1-27), and the median time on ibrutinib was 6 months (range, 2-11).
Results: Arm A
The median time on study in arm A was 13 months (range, 0.1-18). Eighteen patients in this arm discontinued the study—12 due to disease progression, 3 due to adverse events (AEs), 2 due to stem cell transplant, and 1 patient withdrew consent.
The ORR was 70% according to an independent review committee (IRC) and 67% according to investigators.
The rate of complete response (CR) was 0%, and the rate of CR with incomplete bone marrow recovery (CRi) was 2% according to the IRC. According to investigators, the CR rate was 5%, and the CRi rate was 2%.
Sixty-seven percent of patients had a partial response (PR) according to the IRC, and 56% had a PR according to investigators.
Results: Arm B
The median time on study in arm B was 9 months (range, 1.3-16). Four patients in this arm discontinued the study—3 related to disease progression and 1 for an “other” reason.
The ORR was 62% according to the IRC and 57% according to investigators.
The rate of CR/CRi was 0% according to the IRC. According to investigators, the CR rate was 10%, and the CRi rate was 5%.
Sixty-two percent of patients had a PR according to the IRC, and 43% had a PR according to investigators.
Results: Overall
The ORR was 67% according to the IRC and 64% according to investigators.
Forty-five percent of patient samples analyzed (14/31) demonstrated minimal residual disease (MRD) negativity in the peripheral blood between weeks 24 and 48. Five patients with sustained MRD negativity had bone marrow evaluations, and 1 was MRD negative.
At 11.8 months of follow-up, the median duration of response, progression-free survival, and overall survival had not been reached. The estimated 12-month progression-free survival for all patients was 80%.
“Venetoclax has been well-tolerated,” Dr Jones noted. “The toxicity profile in this study is consistent with previous reports. Most of the toxicity has been cytopenias, which can be managed with dose adjustments or supportive care interventions, such as G-CSF.”
All 64 patients experienced an AE. Common AEs were neutropenia (58%), thrombocytopenia (44%), diarrhea (42%), nausea (41%), anemia (36%), fatigue (31%), decreased white blood cell count (22%), and hyperphosphatemia (22%).
Eighty-three percent of patients had grade 3/4 AEs, including neutropenia (45%), thrombocytopenia (28%), anemia (22%), decreased white blood cell count (13%), febrile neutropenia (11%), and pneumonia (11%).
Fifty-three percent of patients had serious AEs, including febrile neutropenia (9%), pneumonia (8%), multi-organ failure (3%), septic shock (3%), and increased potassium (3%).
There were no cases of clinical TLS. However, 1 patient with high tumor burden met Howard criteria for laboratory TLS. ![]()
*Information presented at the meeting differs from the abstract.
© Todd Buchanan 2016
SAN DIEGO—The oral BCL-2 inhibitor venetoclax can produce high objective response rates (ORRs) in chronic lymphocytic leukemia (CLL) patients who have failed treatment with at least one B-cell receptor inhibitor, according to investigators.
In a phase 2 study, venetoclax produced an ORR of 67% among all patients enrolled.
The drug produced a 70% ORR among patients who had failed treatment with ibrutinib and a 62% ORR among patients who had failed idelalisib.
“This represents the first prospective study in this patient population and does demonstrate high rates of durable responses, certainly making [venetoclax] a very viable option for a challenging group of patients to treat,” said study investigator Jeffrey Jones, MD, of The Ohio State University in Columbus.
Dr Jones presented results from this trial at the 2016 ASH Annual Meeting (abstract 637*). This study is sponsored by AbbVie in collaboration with Genentech/Roche.
The trial enrolled patients with CLL who relapsed after or were refractory to ibrutinib (arm A) or idelalisib (arm B). At the time of the data cut-off, 64 patients had been enrolled and treated with venetoclax, including 43 patients in arm A and 21 in arm B.
Patients received venetoclax via a recommended dose-titration schedule—20 mg once daily in week 1, 50 mg daily in week 2, 100 mg daily in week 3, 200 mg daily in week 4, and 400 mg daily from week 5 onward. Patients continued to receive the drug until disease progression or unacceptable toxicity.
To mitigate the risk of tumor lysis syndrome (TLS), patients received prophylaxis with uric acid lowering agents and hydration starting at least 72 hours before the first dose of venetoclax.
Patients with a high tumor burden were hospitalized for the first 20 mg dose and the first 50 mg dose, and they received intravenous hydration and rasburicase. Laboratory values were monitored at the first dose and all dose increases.
Patient characteristics: Arm A
Among patients who had failed ibrutinib, the median age was 66 (range, 48-80). Forty-nine percent of the patients had del(17p), and 35% had bulky nodal disease (5 cm or greater).
The median number of prior treatments was 4 (range, 1-12). All patients had received ibrutinib, but 9% had also received idelalisib. Ninety-one percent of patients were refractory to ibrutinib, and 5% were refractory to idelalisib.
The median time on ibrutinib was 17 months (range, 1-56), and the median time on idelalisib was 10 months (range, 2-31).
Patient characteristics: Arm B
Among patients who had failed idelalisib, the median age was 68 (range, 56-85). Ten percent of patients had del(17p), and 52% had bulky nodal disease (5 cm or greater).
The median number of prior treatments was 3 (range, 1-11). All patients had received idelalisib, but 24% had also received ibrutinib. Sixty-seven percent of patients were refractory to idelalisib, and 10% were refractory to ibrutinib.
The median time on idelalisib was 8 months (range, 1-27), and the median time on ibrutinib was 6 months (range, 2-11).
Results: Arm A
The median time on study in arm A was 13 months (range, 0.1-18). Eighteen patients in this arm discontinued the study—12 due to disease progression, 3 due to adverse events (AEs), 2 due to stem cell transplant, and 1 patient withdrew consent.
The ORR was 70% according to an independent review committee (IRC) and 67% according to investigators.
The rate of complete response (CR) was 0%, and the rate of CR with incomplete bone marrow recovery (CRi) was 2% according to the IRC. According to investigators, the CR rate was 5%, and the CRi rate was 2%.
Sixty-seven percent of patients had a partial response (PR) according to the IRC, and 56% had a PR according to investigators.
Results: Arm B
The median time on study in arm B was 9 months (range, 1.3-16). Four patients in this arm discontinued the study—3 related to disease progression and 1 for an “other” reason.
The ORR was 62% according to the IRC and 57% according to investigators.
The rate of CR/CRi was 0% according to the IRC. According to investigators, the CR rate was 10%, and the CRi rate was 5%.
Sixty-two percent of patients had a PR according to the IRC, and 43% had a PR according to investigators.
Results: Overall
The ORR was 67% according to the IRC and 64% according to investigators.
Forty-five percent of patient samples analyzed (14/31) demonstrated minimal residual disease (MRD) negativity in the peripheral blood between weeks 24 and 48. Five patients with sustained MRD negativity had bone marrow evaluations, and 1 was MRD negative.
At 11.8 months of follow-up, the median duration of response, progression-free survival, and overall survival had not been reached. The estimated 12-month progression-free survival for all patients was 80%.
“Venetoclax has been well-tolerated,” Dr Jones noted. “The toxicity profile in this study is consistent with previous reports. Most of the toxicity has been cytopenias, which can be managed with dose adjustments or supportive care interventions, such as G-CSF.”
All 64 patients experienced an AE. Common AEs were neutropenia (58%), thrombocytopenia (44%), diarrhea (42%), nausea (41%), anemia (36%), fatigue (31%), decreased white blood cell count (22%), and hyperphosphatemia (22%).
Eighty-three percent of patients had grade 3/4 AEs, including neutropenia (45%), thrombocytopenia (28%), anemia (22%), decreased white blood cell count (13%), febrile neutropenia (11%), and pneumonia (11%).
Fifty-three percent of patients had serious AEs, including febrile neutropenia (9%), pneumonia (8%), multi-organ failure (3%), septic shock (3%), and increased potassium (3%).
There were no cases of clinical TLS. However, 1 patient with high tumor burden met Howard criteria for laboratory TLS. ![]()
*Information presented at the meeting differs from the abstract.
New Zika cases in pregnant women continue to drop
There were 136 new cases of pregnant women with laboratory evidence of Zika infection reported during the 2-week period ending Nov. 30, along with four liveborn infants with Zika-related birth defects, according to the Centers for Disease Control and Prevention.
The CDC did not report new totals for pregnant women and pregnancy outcomes for the week ending Nov. 23, so the most recent data release covers the 2-week period from Nov. 17-30. That 2-week total was barely more than the 124 reported for the week ending Nov. 10.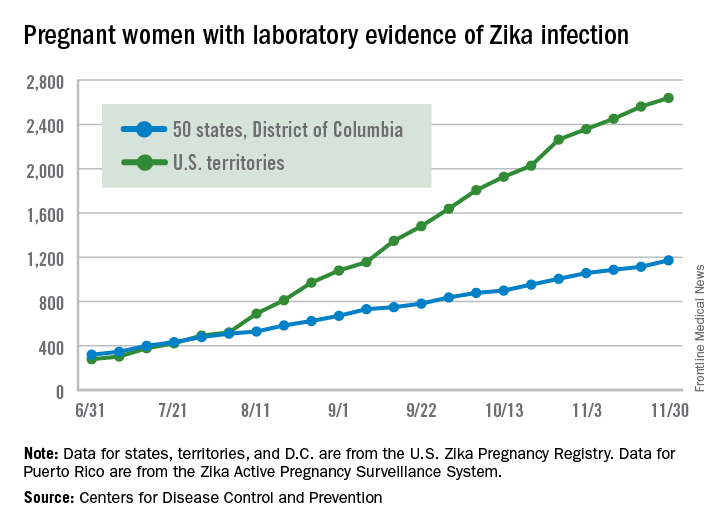
The four infants born with Zika-related birth defects were all born in the 50 states and D.C., as the CDC is no longer reporting adverse pregnancy outcomes for the territories because Puerto Rico is not using the same “inclusion criteria to monitor brain abnormalities and other adverse pregnancy outcomes.” As of Sept. 29 – the date of the last territorial report – there had been one liveborn infant and one pregnancy loss related to Zika. There were no new pregnancy losses with Zika-related birth defects in the states/D.C., so that number remains at five, while the total number of liveborn infants with Zika-related birth defects is now 32, the CDC reported.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
There were 136 new cases of pregnant women with laboratory evidence of Zika infection reported during the 2-week period ending Nov. 30, along with four liveborn infants with Zika-related birth defects, according to the Centers for Disease Control and Prevention.
The CDC did not report new totals for pregnant women and pregnancy outcomes for the week ending Nov. 23, so the most recent data release covers the 2-week period from Nov. 17-30. That 2-week total was barely more than the 124 reported for the week ending Nov. 10.
The four infants born with Zika-related birth defects were all born in the 50 states and D.C., as the CDC is no longer reporting adverse pregnancy outcomes for the territories because Puerto Rico is not using the same “inclusion criteria to monitor brain abnormalities and other adverse pregnancy outcomes.” As of Sept. 29 – the date of the last territorial report – there had been one liveborn infant and one pregnancy loss related to Zika. There were no new pregnancy losses with Zika-related birth defects in the states/D.C., so that number remains at five, while the total number of liveborn infants with Zika-related birth defects is now 32, the CDC reported.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
There were 136 new cases of pregnant women with laboratory evidence of Zika infection reported during the 2-week period ending Nov. 30, along with four liveborn infants with Zika-related birth defects, according to the Centers for Disease Control and Prevention.
The CDC did not report new totals for pregnant women and pregnancy outcomes for the week ending Nov. 23, so the most recent data release covers the 2-week period from Nov. 17-30. That 2-week total was barely more than the 124 reported for the week ending Nov. 10.
The four infants born with Zika-related birth defects were all born in the 50 states and D.C., as the CDC is no longer reporting adverse pregnancy outcomes for the territories because Puerto Rico is not using the same “inclusion criteria to monitor brain abnormalities and other adverse pregnancy outcomes.” As of Sept. 29 – the date of the last territorial report – there had been one liveborn infant and one pregnancy loss related to Zika. There were no new pregnancy losses with Zika-related birth defects in the states/D.C., so that number remains at five, while the total number of liveborn infants with Zika-related birth defects is now 32, the CDC reported.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
VIDEO: No improvement in pCR with dual ER and HER2 inhibition
SAN ANTONIO – Breast cancers that are positive for the estrogen receptor (ER) and human epidermal growth factor receptor–2 (HER2) are less likely than ER-negative/HER2-positive tumors to respond to dual anti-HER2 therapy, suggesting that the estrogen receptor may act as a pathway of resistance to anti-HER2 treatment.
The National Surgical Adjuvant Breast and Bowel Project (NSABP) B-52 trial was designed to test the hypothesis that concurrent inhibition of both ER and HER2 added to chemotherapy with a platinum compound and a taxane will overcome resistance to treatment and improve pathologic complete response (pCR) rates in patients with ER-positive/HER2-positive breast cancer.
In a video interview at the San Antonio Breast Cancer Symposium, Mothaffar F. Rimawi, MD, discusses the trial results, which failed to show a significant difference in pCR rates between women who received chemotherapy with estrogen deprivation or chemotherapy alone. However, the trial still provided important information about the interplay between hormonal and HER2 receptors, and may inform future clinical trials examining reduction in tumor burden as a prognostic measure, says Dr. Rimawi from the Breast Center at Baylor College of Medicine, Houston.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – Breast cancers that are positive for the estrogen receptor (ER) and human epidermal growth factor receptor–2 (HER2) are less likely than ER-negative/HER2-positive tumors to respond to dual anti-HER2 therapy, suggesting that the estrogen receptor may act as a pathway of resistance to anti-HER2 treatment.
The National Surgical Adjuvant Breast and Bowel Project (NSABP) B-52 trial was designed to test the hypothesis that concurrent inhibition of both ER and HER2 added to chemotherapy with a platinum compound and a taxane will overcome resistance to treatment and improve pathologic complete response (pCR) rates in patients with ER-positive/HER2-positive breast cancer.
In a video interview at the San Antonio Breast Cancer Symposium, Mothaffar F. Rimawi, MD, discusses the trial results, which failed to show a significant difference in pCR rates between women who received chemotherapy with estrogen deprivation or chemotherapy alone. However, the trial still provided important information about the interplay between hormonal and HER2 receptors, and may inform future clinical trials examining reduction in tumor burden as a prognostic measure, says Dr. Rimawi from the Breast Center at Baylor College of Medicine, Houston.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN ANTONIO – Breast cancers that are positive for the estrogen receptor (ER) and human epidermal growth factor receptor–2 (HER2) are less likely than ER-negative/HER2-positive tumors to respond to dual anti-HER2 therapy, suggesting that the estrogen receptor may act as a pathway of resistance to anti-HER2 treatment.
The National Surgical Adjuvant Breast and Bowel Project (NSABP) B-52 trial was designed to test the hypothesis that concurrent inhibition of both ER and HER2 added to chemotherapy with a platinum compound and a taxane will overcome resistance to treatment and improve pathologic complete response (pCR) rates in patients with ER-positive/HER2-positive breast cancer.
In a video interview at the San Antonio Breast Cancer Symposium, Mothaffar F. Rimawi, MD, discusses the trial results, which failed to show a significant difference in pCR rates between women who received chemotherapy with estrogen deprivation or chemotherapy alone. However, the trial still provided important information about the interplay between hormonal and HER2 receptors, and may inform future clinical trials examining reduction in tumor burden as a prognostic measure, says Dr. Rimawi from the Breast Center at Baylor College of Medicine, Houston.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT SABCS 2016

VIDEO: Tips & Strategies for the Hospital Medicine Job Search
Dr. Thomas Frederickson, Dr. Benjamin Frizner, and Dr. Darlene Tad-y are all experienced at hiring and mentoring hospitalists at all career stages. They offer tips and strategies for assessing opportunity and negotiating your ideal HM job.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Thomas Frederickson, Dr. Benjamin Frizner, and Dr. Darlene Tad-y are all experienced at hiring and mentoring hospitalists at all career stages. They offer tips and strategies for assessing opportunity and negotiating your ideal HM job.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Thomas Frederickson, Dr. Benjamin Frizner, and Dr. Darlene Tad-y are all experienced at hiring and mentoring hospitalists at all career stages. They offer tips and strategies for assessing opportunity and negotiating your ideal HM job.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
1967 at a glance
• The Early and Periodic Screening, Diagnostic and Treatment (EPSDT) program was enacted as the child health component of Medicaid. Children under 21 years enrolled in Medicaid are entitled to EPSDT benefits, and states must cover a “broad array of preventive and treatment services.”
• By 1967, all states had laws requiring that physicians report child abuse.
• Field trials of experimental respiratory syncytial virus vaccines were performed but stalled. Currently, 65 RSV vaccines are being studied, and 13 are in phase III trials.

• The World Health Association declared a war on smallpox with a worldwide vaccination campaign. Twelve years later the disease was eradicated.
• The Public Health Service issued the second Surgeon General’s report on the health consequences of smoking.
• The first heart transplant was performed by Christian Barnard.
• The Early and Periodic Screening, Diagnostic and Treatment (EPSDT) program was enacted as the child health component of Medicaid. Children under 21 years enrolled in Medicaid are entitled to EPSDT benefits, and states must cover a “broad array of preventive and treatment services.”
• By 1967, all states had laws requiring that physicians report child abuse.
• Field trials of experimental respiratory syncytial virus vaccines were performed but stalled. Currently, 65 RSV vaccines are being studied, and 13 are in phase III trials.
• The World Health Association declared a war on smallpox with a worldwide vaccination campaign. Twelve years later the disease was eradicated.
• The Public Health Service issued the second Surgeon General’s report on the health consequences of smoking.
• The first heart transplant was performed by Christian Barnard.
• The Early and Periodic Screening, Diagnostic and Treatment (EPSDT) program was enacted as the child health component of Medicaid. Children under 21 years enrolled in Medicaid are entitled to EPSDT benefits, and states must cover a “broad array of preventive and treatment services.”
• By 1967, all states had laws requiring that physicians report child abuse.
• Field trials of experimental respiratory syncytial virus vaccines were performed but stalled. Currently, 65 RSV vaccines are being studied, and 13 are in phase III trials.
• The World Health Association declared a war on smallpox with a worldwide vaccination campaign. Twelve years later the disease was eradicated.
• The Public Health Service issued the second Surgeon General’s report on the health consequences of smoking.
• The first heart transplant was performed by Christian Barnard.
A look back at 1967
As Pediatric News celebrates 50 years of publication, we’re taking a look back at our first year: 1967.
A review of the 1967 issues of the journal Pediatrics offers a snapshot of the state of the science and some surprising similarities with pediatric medicine today.
A commentary in the November issue entitled “Pediatrics at a Crossroad” described an accelerating trend toward pediatric group practice and noted that full-time hospital employment of pediatricians was an emerging pattern of pediatric practice. The author, Richard Smith, MD, of the University of Florida, Gainesville, expressed concern about certain practices, such as the wide employment of antibiotics for uncomplicated respiratory infections and “routine use of gamma globulin in community hospital nurseries supposedly to treat sepsis or its regular injection in putatively allergic children.” He also was concerned about a quality gap in pediatric specialty education (Pediatrics. 1967 Nov;40[5]:783-7).
Articles of interest in the infectious disease area included an article demonstrating the response of infants to trivalent polio vaccine (Dec;40[6]:980-5); a new antibody test for rubella (Dec;40[5]:787-8, 789-97); and a live attenuated mumps vaccine (Dec;40[5]:798-803). And as we deal with emerging infectious diseases on a large scale, a fatal case of dengue hemorrhagic fever was reported in an American child (Dec;40[5]:804-7).
In a commentary, Starkey D. Davis, MD, and Ralph J. Wedgwood, MD, of the University of Washington, Seattle, said that the annual tuberculosis infection rate was low and falling, and that new cases were decreasing. Sufficient beds were available to isolate infectious cases, and effective chemotherapy made most cases noninfectious quickly. Isoniazid was cheap and effective, and it decreased complications of asymptomatic primary tuberculosis in children by 85%. “Pediatricians can expect to see tuberculosis in children become a medical curiosity in this country as infection rates continue to fall, if isoniazid prophylaxis is energetically used,” they predicted (Jun;39[6]:809-10).
D. Holdaway of the Royal Victoria Infirmary in Newcastle Upon Tyne, England, and associates reported on 211 children with acute bronchiolitis and 295 controls with nonrespiratory illness. Of the children with bronchiolitis, 59% had respiratory syncytial virus (RSV), compared with 1% of the controls, which confirmed the etiological significance of RSV in bronchiolitis, the researchers said. They also maintained that “oxygen is vitally important in bronchiolitis and there is little conclusive evidence that any other therapy is consistently or even occasionally useful” (Jun;39[6]:924-8).
In a commentary, Leon Eisenberg, MD, of the division of child psychiatry at the Johns Hopkins Hospital, Baltimore, called for more training in child development for pediatricians (May;39[5];645-7). Today, pediatricians are calling for more training in child psychiatry.
A report by the American Academy of Pediatrics Committee on Nutrition on obesity in childhood was prescient. They said, despite much research, that “our ignorance concerning the etiology, pathogenesis, and treatment is remarkable” (Sep;40[3]:455-67). The committee acknowledged that morbidity and mortality for diabetes and cardiovascular disease were higher in obese adults than in those of average weight, and that obese children tended to remain obese as adults. The committee also wrote that no treatments had achieved more than minor success of weight reduction. It suggested prevention of weight gain as the likely best approach, with initiation by the pediatrician in high-risk families – advice that still holds true today 50 years later.
Throughout 2017, Pediatric News will celebrate its 50th anniversary with exclusive articles looking at the evolution of the specialty, including changes in child psychiatry, pediatric dermatology, and infectious disease medicine, changes in residency training, and the transformation of the well-child visit. Look for these articles and more special features on the pages of Pediatric News and here online.
As Pediatric News celebrates 50 years of publication, we’re taking a look back at our first year: 1967.
A review of the 1967 issues of the journal Pediatrics offers a snapshot of the state of the science and some surprising similarities with pediatric medicine today.
A commentary in the November issue entitled “Pediatrics at a Crossroad” described an accelerating trend toward pediatric group practice and noted that full-time hospital employment of pediatricians was an emerging pattern of pediatric practice. The author, Richard Smith, MD, of the University of Florida, Gainesville, expressed concern about certain practices, such as the wide employment of antibiotics for uncomplicated respiratory infections and “routine use of gamma globulin in community hospital nurseries supposedly to treat sepsis or its regular injection in putatively allergic children.” He also was concerned about a quality gap in pediatric specialty education (Pediatrics. 1967 Nov;40[5]:783-7).
Articles of interest in the infectious disease area included an article demonstrating the response of infants to trivalent polio vaccine (Dec;40[6]:980-5); a new antibody test for rubella (Dec;40[5]:787-8, 789-97); and a live attenuated mumps vaccine (Dec;40[5]:798-803). And as we deal with emerging infectious diseases on a large scale, a fatal case of dengue hemorrhagic fever was reported in an American child (Dec;40[5]:804-7).
In a commentary, Starkey D. Davis, MD, and Ralph J. Wedgwood, MD, of the University of Washington, Seattle, said that the annual tuberculosis infection rate was low and falling, and that new cases were decreasing. Sufficient beds were available to isolate infectious cases, and effective chemotherapy made most cases noninfectious quickly. Isoniazid was cheap and effective, and it decreased complications of asymptomatic primary tuberculosis in children by 85%. “Pediatricians can expect to see tuberculosis in children become a medical curiosity in this country as infection rates continue to fall, if isoniazid prophylaxis is energetically used,” they predicted (Jun;39[6]:809-10).
D. Holdaway of the Royal Victoria Infirmary in Newcastle Upon Tyne, England, and associates reported on 211 children with acute bronchiolitis and 295 controls with nonrespiratory illness. Of the children with bronchiolitis, 59% had respiratory syncytial virus (RSV), compared with 1% of the controls, which confirmed the etiological significance of RSV in bronchiolitis, the researchers said. They also maintained that “oxygen is vitally important in bronchiolitis and there is little conclusive evidence that any other therapy is consistently or even occasionally useful” (Jun;39[6]:924-8).
In a commentary, Leon Eisenberg, MD, of the division of child psychiatry at the Johns Hopkins Hospital, Baltimore, called for more training in child development for pediatricians (May;39[5];645-7). Today, pediatricians are calling for more training in child psychiatry.
A report by the American Academy of Pediatrics Committee on Nutrition on obesity in childhood was prescient. They said, despite much research, that “our ignorance concerning the etiology, pathogenesis, and treatment is remarkable” (Sep;40[3]:455-67). The committee acknowledged that morbidity and mortality for diabetes and cardiovascular disease were higher in obese adults than in those of average weight, and that obese children tended to remain obese as adults. The committee also wrote that no treatments had achieved more than minor success of weight reduction. It suggested prevention of weight gain as the likely best approach, with initiation by the pediatrician in high-risk families – advice that still holds true today 50 years later.
Throughout 2017, Pediatric News will celebrate its 50th anniversary with exclusive articles looking at the evolution of the specialty, including changes in child psychiatry, pediatric dermatology, and infectious disease medicine, changes in residency training, and the transformation of the well-child visit. Look for these articles and more special features on the pages of Pediatric News and here online.
As Pediatric News celebrates 50 years of publication, we’re taking a look back at our first year: 1967.
A review of the 1967 issues of the journal Pediatrics offers a snapshot of the state of the science and some surprising similarities with pediatric medicine today.
A commentary in the November issue entitled “Pediatrics at a Crossroad” described an accelerating trend toward pediatric group practice and noted that full-time hospital employment of pediatricians was an emerging pattern of pediatric practice. The author, Richard Smith, MD, of the University of Florida, Gainesville, expressed concern about certain practices, such as the wide employment of antibiotics for uncomplicated respiratory infections and “routine use of gamma globulin in community hospital nurseries supposedly to treat sepsis or its regular injection in putatively allergic children.” He also was concerned about a quality gap in pediatric specialty education (Pediatrics. 1967 Nov;40[5]:783-7).
Articles of interest in the infectious disease area included an article demonstrating the response of infants to trivalent polio vaccine (Dec;40[6]:980-5); a new antibody test for rubella (Dec;40[5]:787-8, 789-97); and a live attenuated mumps vaccine (Dec;40[5]:798-803). And as we deal with emerging infectious diseases on a large scale, a fatal case of dengue hemorrhagic fever was reported in an American child (Dec;40[5]:804-7).
In a commentary, Starkey D. Davis, MD, and Ralph J. Wedgwood, MD, of the University of Washington, Seattle, said that the annual tuberculosis infection rate was low and falling, and that new cases were decreasing. Sufficient beds were available to isolate infectious cases, and effective chemotherapy made most cases noninfectious quickly. Isoniazid was cheap and effective, and it decreased complications of asymptomatic primary tuberculosis in children by 85%. “Pediatricians can expect to see tuberculosis in children become a medical curiosity in this country as infection rates continue to fall, if isoniazid prophylaxis is energetically used,” they predicted (Jun;39[6]:809-10).
D. Holdaway of the Royal Victoria Infirmary in Newcastle Upon Tyne, England, and associates reported on 211 children with acute bronchiolitis and 295 controls with nonrespiratory illness. Of the children with bronchiolitis, 59% had respiratory syncytial virus (RSV), compared with 1% of the controls, which confirmed the etiological significance of RSV in bronchiolitis, the researchers said. They also maintained that “oxygen is vitally important in bronchiolitis and there is little conclusive evidence that any other therapy is consistently or even occasionally useful” (Jun;39[6]:924-8).
In a commentary, Leon Eisenberg, MD, of the division of child psychiatry at the Johns Hopkins Hospital, Baltimore, called for more training in child development for pediatricians (May;39[5];645-7). Today, pediatricians are calling for more training in child psychiatry.
A report by the American Academy of Pediatrics Committee on Nutrition on obesity in childhood was prescient. They said, despite much research, that “our ignorance concerning the etiology, pathogenesis, and treatment is remarkable” (Sep;40[3]:455-67). The committee acknowledged that morbidity and mortality for diabetes and cardiovascular disease were higher in obese adults than in those of average weight, and that obese children tended to remain obese as adults. The committee also wrote that no treatments had achieved more than minor success of weight reduction. It suggested prevention of weight gain as the likely best approach, with initiation by the pediatrician in high-risk families – advice that still holds true today 50 years later.
Throughout 2017, Pediatric News will celebrate its 50th anniversary with exclusive articles looking at the evolution of the specialty, including changes in child psychiatry, pediatric dermatology, and infectious disease medicine, changes in residency training, and the transformation of the well-child visit. Look for these articles and more special features on the pages of Pediatric News and here online.