User login
Pulmonary Perspectives: High levels of air pollution in Delhi and adverse health effects
“Nature’s condition, rightly interpreted, reveals a society’s culture and traditions as directly as does a novel or a newspaper or a code of laws.”
– Roderick F. Nash
Adverse effects of air pollution on human health have been known ever since the “Great London Smog” in 1952. Mankind is paying for rapid industrialization by adversely affecting the air that we breathe. The developed world has been able to improve the environmental standards by following stringent norms and practices regarding engines, fuels, and industrial safety. However, the same cannot be said about developing countries. Delhi, the capital of India, has seen high levels of air pollution for the last several decades.
The number of registered vehicles in Delhi has doubled over the last 10 years. This, along with rapidly increasing numbers of small scale industries and inconsistently regulated construction work, has led to ever-increasing levels of air pollution in Delhi. The city has witnessed smog for the last few years.

Smog causing disruption of daily life and health hazards has been reported from Los Angeles, Beijing, and many other major cities around the world. The London Smog of 1952 caused approximately 4,000 deaths within 4 days (Davis D, et al. Environ Health Perspectives. 2002;110[12]:A734) and caused another 8,000 deaths over next few weeks to months (Bell ML, et al. Environ Health Perspectives. 2004;112[1]:6).

Common sources and pollutants with reference to Delhi
As in most cities around the world, rapid industrialization and increases in vehicles using fossil fuels are important contributors to ambient air pollution in Delhi. Additional sources of air pollution unique to Delhi include dust generation during building construction, ash generation from thermal power plants, crop residue burning in neighboring states, and burning of fossil fuels for domestic, as well as small scale, industrial use. Major pollutants include particulate matter (both PM2.5 and PM10), nitrogen oxides (NOx), carbon monoxide (CO), sulfur dioxide (SO2), and ozone (O3).
Delhi is distinct in its geographic location adjoining the Great Indian Desert (Thar) in the west and cool hilly regions in the north and east. This accounts for great seasonal variations in temperature, humidity, and wind speed. Also, being a landlocked territory, there are no moderating effects of sea breeze available to other metropolitan cities (like Mumbai and Chennai).
Dust storms during the summer from the neighboring state of Rajasthan cause an increase in suspended particulate matter (SPM). All these contribute to seasonal and climatic variations in air quality. In addition, the use of fire crackers during the festival of Diwali leads to dangerous levels of air pollution also.
Adverse health effects as witnessed in clinics and community
Many adults, without any prior history of respiratory illness, attended our outpatient department (OPD) with breathlessness, chest congestion, and wheezing requiring inhaled bronchodilators. A significant proportion of patients with previously diagnosed respiratory diseases (including COPD, bronchial asthma, or interstitial lung disease) reported to OPDs or emergency services with worsening cough, wheezing, and breathlessness. A few patients coming from outside Delhi for routine follow-up had exacerbation of COPD after coming to Delhi (personal observations).
We have previously reported increases in asthma, COPD, and acute coronary events (by 21.30%, 24.90%, and 24.30%, respectively) due to higher than acceptable levels of air pollutants in Delhi (Pande JN, et al. Indian J Chest Dis Allied Sci. 2002;44[1]:13). Another concerning development has been the increase in the number of persons being diagnosed with bronchial asthma in middle age, probably related to worsening air quality. Persons at extremes of age (young children and elderly) are particularly affected.
Studies in Delhi assessing ambient air pollution–related morbidity and mortality
Studies have used risk of mortality/morbidity due to air pollution model (Ri–MAP) to assess health impact of various air pollutants in Delhi. According to their estimates, there were 18,229 excess deaths in Delhi in the year 2010, more than 50% of which were due to cardiovascular or respiratory causes. Also, 26,525 excess hospital admissions due to COPD exacerbation could be attributed to ambient air pollution (Nagpure A, et al. Atmospheric Pollution Res. 2014;5[3]:1309).
Interventions: Work in progress
The Central Pollution Control Board convened an Expert Committee (Dr. Khilnani as a member) for formulation and implementation of Air Quality Index (AQI) in major Indian cities (http://cpcb.nic.in/FINAL-REPORT_AQI_.pdf).
Currently reported AQI is calculated by using the following parameters: sulfur dioxide (SO2), nitrogen dioxide (NO2), particulate matter (PM10,PM2.5) averaged over 24 hours, along with ozone (O3) and carbon monoxide (CO), averaged over 1-8 hours. AQI is classified as good (0-50), satisfactory (51-100), moderate (101-200), poor (201-300), very poor (301-400), and severe (greater than 401).
AQI is reported daily in leading newspapers along with public and private news channels. Thanks to the mainstream and social media, smog has become a commonly understood word. Air pollution is a hot topic of discussion among people of all socioeconomic and demographic strata.
Children of almost all schools in Delhi pledged not to use firecrackers this Diwali. People are increasingly sharing taxis or carpooling. Utilization of public transport is gradually increasing.
The Delhi government ordered temporarily shutting off the only working thermal power plant in the megacity (source of 10%-15% of ambient air pollution). The government is also working on an action plan based on air quality, which includes both preventive and prohibitive measures.
Delhi Transport Corporation operates one of the world’s largest fleets of compressed natural gas–operated buses. Delhi Metro Corporation has been lauded by the United Nations for its efforts in reducing the carbon footprint and air pollution.
Yet, a lot needs to be done to improve the air quality in Delhi. Last mile connectivity remains a big hurdle; improving this will go a long way in promoting use of public transport. Implementation of methods to reduce particulate matter generation at construction sites, promoting use of vehicles using electricity or compressed natural gas, increasing parking charges for vehicles, banning the use of diesel-driven heavy vehicles in the city, road cleaning with vacuum cleaners to reduce PM 10 generation, increasing green areas, and promoting carpooling or taxi sharing are some other initiatives that need to be implemented on priority. Delhi and surrounding states need to strengthen awareness drives and norms to discourage crop residue burning on a priority basis.
Conclusion
Delhi’s poor air quality during this winter has indeed affected the respiratory health of the population. Healthy people, as well as those with preexisting respiratory diseases, are adversely affected. A series of actions at the personal and institutional level is required to control this menace.
Dr. Khilnani is Professor, and Dr. Tiwari is Research Officer, Department of Pulmonary Medicine & Sleep Disorders, All India Institute of Medical Sciences, New Delhi, India.
“Nature’s condition, rightly interpreted, reveals a society’s culture and traditions as directly as does a novel or a newspaper or a code of laws.”
– Roderick F. Nash
Adverse effects of air pollution on human health have been known ever since the “Great London Smog” in 1952. Mankind is paying for rapid industrialization by adversely affecting the air that we breathe. The developed world has been able to improve the environmental standards by following stringent norms and practices regarding engines, fuels, and industrial safety. However, the same cannot be said about developing countries. Delhi, the capital of India, has seen high levels of air pollution for the last several decades.
The number of registered vehicles in Delhi has doubled over the last 10 years. This, along with rapidly increasing numbers of small scale industries and inconsistently regulated construction work, has led to ever-increasing levels of air pollution in Delhi. The city has witnessed smog for the last few years.
Smog causing disruption of daily life and health hazards has been reported from Los Angeles, Beijing, and many other major cities around the world. The London Smog of 1952 caused approximately 4,000 deaths within 4 days (Davis D, et al. Environ Health Perspectives. 2002;110[12]:A734) and caused another 8,000 deaths over next few weeks to months (Bell ML, et al. Environ Health Perspectives. 2004;112[1]:6).
Common sources and pollutants with reference to Delhi
As in most cities around the world, rapid industrialization and increases in vehicles using fossil fuels are important contributors to ambient air pollution in Delhi. Additional sources of air pollution unique to Delhi include dust generation during building construction, ash generation from thermal power plants, crop residue burning in neighboring states, and burning of fossil fuels for domestic, as well as small scale, industrial use. Major pollutants include particulate matter (both PM2.5 and PM10), nitrogen oxides (NOx), carbon monoxide (CO), sulfur dioxide (SO2), and ozone (O3).
Delhi is distinct in its geographic location adjoining the Great Indian Desert (Thar) in the west and cool hilly regions in the north and east. This accounts for great seasonal variations in temperature, humidity, and wind speed. Also, being a landlocked territory, there are no moderating effects of sea breeze available to other metropolitan cities (like Mumbai and Chennai).
Dust storms during the summer from the neighboring state of Rajasthan cause an increase in suspended particulate matter (SPM). All these contribute to seasonal and climatic variations in air quality. In addition, the use of fire crackers during the festival of Diwali leads to dangerous levels of air pollution also.
Adverse health effects as witnessed in clinics and community
Many adults, without any prior history of respiratory illness, attended our outpatient department (OPD) with breathlessness, chest congestion, and wheezing requiring inhaled bronchodilators. A significant proportion of patients with previously diagnosed respiratory diseases (including COPD, bronchial asthma, or interstitial lung disease) reported to OPDs or emergency services with worsening cough, wheezing, and breathlessness. A few patients coming from outside Delhi for routine follow-up had exacerbation of COPD after coming to Delhi (personal observations).
We have previously reported increases in asthma, COPD, and acute coronary events (by 21.30%, 24.90%, and 24.30%, respectively) due to higher than acceptable levels of air pollutants in Delhi (Pande JN, et al. Indian J Chest Dis Allied Sci. 2002;44[1]:13). Another concerning development has been the increase in the number of persons being diagnosed with bronchial asthma in middle age, probably related to worsening air quality. Persons at extremes of age (young children and elderly) are particularly affected.
Studies in Delhi assessing ambient air pollution–related morbidity and mortality
Studies have used risk of mortality/morbidity due to air pollution model (Ri–MAP) to assess health impact of various air pollutants in Delhi. According to their estimates, there were 18,229 excess deaths in Delhi in the year 2010, more than 50% of which were due to cardiovascular or respiratory causes. Also, 26,525 excess hospital admissions due to COPD exacerbation could be attributed to ambient air pollution (Nagpure A, et al. Atmospheric Pollution Res. 2014;5[3]:1309).
Interventions: Work in progress
The Central Pollution Control Board convened an Expert Committee (Dr. Khilnani as a member) for formulation and implementation of Air Quality Index (AQI) in major Indian cities (http://cpcb.nic.in/FINAL-REPORT_AQI_.pdf).
Currently reported AQI is calculated by using the following parameters: sulfur dioxide (SO2), nitrogen dioxide (NO2), particulate matter (PM10,PM2.5) averaged over 24 hours, along with ozone (O3) and carbon monoxide (CO), averaged over 1-8 hours. AQI is classified as good (0-50), satisfactory (51-100), moderate (101-200), poor (201-300), very poor (301-400), and severe (greater than 401).
AQI is reported daily in leading newspapers along with public and private news channels. Thanks to the mainstream and social media, smog has become a commonly understood word. Air pollution is a hot topic of discussion among people of all socioeconomic and demographic strata.
Children of almost all schools in Delhi pledged not to use firecrackers this Diwali. People are increasingly sharing taxis or carpooling. Utilization of public transport is gradually increasing.
The Delhi government ordered temporarily shutting off the only working thermal power plant in the megacity (source of 10%-15% of ambient air pollution). The government is also working on an action plan based on air quality, which includes both preventive and prohibitive measures.
Delhi Transport Corporation operates one of the world’s largest fleets of compressed natural gas–operated buses. Delhi Metro Corporation has been lauded by the United Nations for its efforts in reducing the carbon footprint and air pollution.
Yet, a lot needs to be done to improve the air quality in Delhi. Last mile connectivity remains a big hurdle; improving this will go a long way in promoting use of public transport. Implementation of methods to reduce particulate matter generation at construction sites, promoting use of vehicles using electricity or compressed natural gas, increasing parking charges for vehicles, banning the use of diesel-driven heavy vehicles in the city, road cleaning with vacuum cleaners to reduce PM 10 generation, increasing green areas, and promoting carpooling or taxi sharing are some other initiatives that need to be implemented on priority. Delhi and surrounding states need to strengthen awareness drives and norms to discourage crop residue burning on a priority basis.
Conclusion
Delhi’s poor air quality during this winter has indeed affected the respiratory health of the population. Healthy people, as well as those with preexisting respiratory diseases, are adversely affected. A series of actions at the personal and institutional level is required to control this menace.
Dr. Khilnani is Professor, and Dr. Tiwari is Research Officer, Department of Pulmonary Medicine & Sleep Disorders, All India Institute of Medical Sciences, New Delhi, India.
“Nature’s condition, rightly interpreted, reveals a society’s culture and traditions as directly as does a novel or a newspaper or a code of laws.”
– Roderick F. Nash
Adverse effects of air pollution on human health have been known ever since the “Great London Smog” in 1952. Mankind is paying for rapid industrialization by adversely affecting the air that we breathe. The developed world has been able to improve the environmental standards by following stringent norms and practices regarding engines, fuels, and industrial safety. However, the same cannot be said about developing countries. Delhi, the capital of India, has seen high levels of air pollution for the last several decades.
The number of registered vehicles in Delhi has doubled over the last 10 years. This, along with rapidly increasing numbers of small scale industries and inconsistently regulated construction work, has led to ever-increasing levels of air pollution in Delhi. The city has witnessed smog for the last few years.
Smog causing disruption of daily life and health hazards has been reported from Los Angeles, Beijing, and many other major cities around the world. The London Smog of 1952 caused approximately 4,000 deaths within 4 days (Davis D, et al. Environ Health Perspectives. 2002;110[12]:A734) and caused another 8,000 deaths over next few weeks to months (Bell ML, et al. Environ Health Perspectives. 2004;112[1]:6).
Common sources and pollutants with reference to Delhi
As in most cities around the world, rapid industrialization and increases in vehicles using fossil fuels are important contributors to ambient air pollution in Delhi. Additional sources of air pollution unique to Delhi include dust generation during building construction, ash generation from thermal power plants, crop residue burning in neighboring states, and burning of fossil fuels for domestic, as well as small scale, industrial use. Major pollutants include particulate matter (both PM2.5 and PM10), nitrogen oxides (NOx), carbon monoxide (CO), sulfur dioxide (SO2), and ozone (O3).
Delhi is distinct in its geographic location adjoining the Great Indian Desert (Thar) in the west and cool hilly regions in the north and east. This accounts for great seasonal variations in temperature, humidity, and wind speed. Also, being a landlocked territory, there are no moderating effects of sea breeze available to other metropolitan cities (like Mumbai and Chennai).
Dust storms during the summer from the neighboring state of Rajasthan cause an increase in suspended particulate matter (SPM). All these contribute to seasonal and climatic variations in air quality. In addition, the use of fire crackers during the festival of Diwali leads to dangerous levels of air pollution also.
Adverse health effects as witnessed in clinics and community
Many adults, without any prior history of respiratory illness, attended our outpatient department (OPD) with breathlessness, chest congestion, and wheezing requiring inhaled bronchodilators. A significant proportion of patients with previously diagnosed respiratory diseases (including COPD, bronchial asthma, or interstitial lung disease) reported to OPDs or emergency services with worsening cough, wheezing, and breathlessness. A few patients coming from outside Delhi for routine follow-up had exacerbation of COPD after coming to Delhi (personal observations).
We have previously reported increases in asthma, COPD, and acute coronary events (by 21.30%, 24.90%, and 24.30%, respectively) due to higher than acceptable levels of air pollutants in Delhi (Pande JN, et al. Indian J Chest Dis Allied Sci. 2002;44[1]:13). Another concerning development has been the increase in the number of persons being diagnosed with bronchial asthma in middle age, probably related to worsening air quality. Persons at extremes of age (young children and elderly) are particularly affected.
Studies in Delhi assessing ambient air pollution–related morbidity and mortality
Studies have used risk of mortality/morbidity due to air pollution model (Ri–MAP) to assess health impact of various air pollutants in Delhi. According to their estimates, there were 18,229 excess deaths in Delhi in the year 2010, more than 50% of which were due to cardiovascular or respiratory causes. Also, 26,525 excess hospital admissions due to COPD exacerbation could be attributed to ambient air pollution (Nagpure A, et al. Atmospheric Pollution Res. 2014;5[3]:1309).
Interventions: Work in progress
The Central Pollution Control Board convened an Expert Committee (Dr. Khilnani as a member) for formulation and implementation of Air Quality Index (AQI) in major Indian cities (http://cpcb.nic.in/FINAL-REPORT_AQI_.pdf).
Currently reported AQI is calculated by using the following parameters: sulfur dioxide (SO2), nitrogen dioxide (NO2), particulate matter (PM10,PM2.5) averaged over 24 hours, along with ozone (O3) and carbon monoxide (CO), averaged over 1-8 hours. AQI is classified as good (0-50), satisfactory (51-100), moderate (101-200), poor (201-300), very poor (301-400), and severe (greater than 401).
AQI is reported daily in leading newspapers along with public and private news channels. Thanks to the mainstream and social media, smog has become a commonly understood word. Air pollution is a hot topic of discussion among people of all socioeconomic and demographic strata.
Children of almost all schools in Delhi pledged not to use firecrackers this Diwali. People are increasingly sharing taxis or carpooling. Utilization of public transport is gradually increasing.
The Delhi government ordered temporarily shutting off the only working thermal power plant in the megacity (source of 10%-15% of ambient air pollution). The government is also working on an action plan based on air quality, which includes both preventive and prohibitive measures.
Delhi Transport Corporation operates one of the world’s largest fleets of compressed natural gas–operated buses. Delhi Metro Corporation has been lauded by the United Nations for its efforts in reducing the carbon footprint and air pollution.
Yet, a lot needs to be done to improve the air quality in Delhi. Last mile connectivity remains a big hurdle; improving this will go a long way in promoting use of public transport. Implementation of methods to reduce particulate matter generation at construction sites, promoting use of vehicles using electricity or compressed natural gas, increasing parking charges for vehicles, banning the use of diesel-driven heavy vehicles in the city, road cleaning with vacuum cleaners to reduce PM 10 generation, increasing green areas, and promoting carpooling or taxi sharing are some other initiatives that need to be implemented on priority. Delhi and surrounding states need to strengthen awareness drives and norms to discourage crop residue burning on a priority basis.
Conclusion
Delhi’s poor air quality during this winter has indeed affected the respiratory health of the population. Healthy people, as well as those with preexisting respiratory diseases, are adversely affected. A series of actions at the personal and institutional level is required to control this menace.
Dr. Khilnani is Professor, and Dr. Tiwari is Research Officer, Department of Pulmonary Medicine & Sleep Disorders, All India Institute of Medical Sciences, New Delhi, India.

NetWorks: SEALs help physicians, blood storage questions, more. . .
Clinical Research
The unrecognized battlefield in our hospitals: Lessons from the US Navy SEALs
Burnout syndrome (BOS) is a psychological state resulting from prolonged exposure to job stressors. It is characterized by a vicious cycle of emotional exhaustion, detachment from others, and a feeling of decreased accomplishment. Severe BOS is seen in up to 45% of physicians and 33% of nurses who work in ICUs.1
BOS has far-reaching consequences, being associated with an alarmingly high prevalence of posttraumatic stress disorder (PTSD) and substance abuse, almost equivalent to that experienced by veterans returning from war.2 BOS also is associated with self-reported suboptimal patient care practices.3This crisis has long been underrecognized, but now that we have identified the problem, where does that leave us? There are currently no quality studies evaluating how to best treat and prevent BOS/PTSD in health-care professionals. Previous studies have focused on addressing organizational factors to alleviate job stressors, but the psychosocial characteristics of the individual have been largely ignored.
Our medical education has historically focused on an individual’s intelligence quotient (IQ), but developing an individual’s emotional quotient (EQ) is just as valuable. It has long been known that Navy SEALs have the lowest prevalence of PTSD among combat veterans due partially to their specific training in emotional resilience and adaptive psychosocial coping mechanisms.
For this reason, the research team at the University of Texas Health Science Center at San Antonio is collaborating with the US Navy SEAL team to design and validate a tool that teaches critical care staff resilience training similar to what their combat trainees undergo. The goal is to curb these alarming trends in BOS and create a paradigm shift in medical education within medical and nursing schools.
Bravein Amalakuhan, MD
Fellow-in-Training Member
References
1. Embriaco N, Azoulay E, Barrau K, et al. Am J Respir Crit Care Med. 2007;175(7):686.
2. Mealer ML, Shelton A, Berg B, et al. Am J Respir Crit Care Med. 2007;175(7):693.
3. Shanafelt TD, Bradley KA, Wipf JE, et al. Ann Intern Med. 2002;136(5):358.
Critical Care
End of the era for age of blood concerns?
Blood transfusions are common in critically ill patients, with two in five adults admitted to an ICU receiving a transfusion.1,2 Recently, randomized trials have found that more restrictive thresholds for transfusions are associated with improved outcomes.3,4 One theorized explanation for this somewhat counterintuitive association is that the prolonged storage time (i.e., the age of the blood being transfused) might affect outcomes.
There have been three recent publications that help to shed some more light on this. First, Lacroix et al.5 performed a multicenter randomized blinded trial in over 2,400 critically ill patients in 64 centers comparing new blood (mean storage (±SD) of 6.1±4.9 days) vs old blood with storage of 22.0±8.4 days (P less than .001). There was no statistically significant difference in 90-day mortality.5
The second study is a meta-analysis by Alexander et al.6 The investigators looked at 12 trials and 5,229 patients and compared “fresh blood” or blood stored for 3-10 days to “older blood” stored for longer durations. They found that there was no difference in mortality and no difference in adverse events, such as acute transfusion reactions, when comparing the two groups.
Lastly, Heddle et al.7 conducted a randomized trial that compared outcomes in 20,858 hospitalized patients transfused with fresh blood (mean storage time 13.0±7.6 days) to older blood (mean storage time 23.6±8.9 days). They found no differences in mortality when comparing those transfused with fresh vs. old blood (8.7% vs. 9.1%). In addition, there was no difference when examining the predetermined subgroups, including those undergoing cardiovascular surgery, those with cancer, and those admitted to the ICU.
So, is this the end of an era for health-care provider concern about how long blood can be stored to be safe for ICU patients? Possibly.
There may still be high-risk populations (such as patients receiving massive transfusions) for which age of the blood does matter. In addition, it is still unclear based on the present data as to whether blood stored between 35 and 42 days has any significant inherent risk.
However, these publications among others suggest that the age of transfused blood may not matter, even in critically ill patients. Therefore, the present storage practices of many blood banks around the United States and beyond are validated by the present publications regarding the scarce resource of blood.
Christopher L. Carroll, MD, MS, FCCP
Steering Committee Member

Steven Greenberg, MD, FCCP
Steering Committee Member

References
1. Corwin HL, Gettinger A, Pearl RG, et al. Crit Care Med. 2004;32(1):39.
2. Vincent JL, Baron JF, Reinhart K, et al.; ABC (Anemia and Blood Transfusion in Critical Care) Investigators. JAMA. 2002;288(12):1499.
3. Holst LB, Haase N, Wetterslev J, et al.; TRISS Trial Group; Scandinavian Critical Care Trials Group. N Engl J Med. 2014;371(15):1381.
4. Lacroix J, Hebert PC, Hutchison JS, et al.; TRIPICU Investigators; Canadian Critical Care Trials Group; Pediatric Acute Lung Injury and Sepsis Investigators Network. N Engl J Med. 2007;356(16):1609.
5. Lacroix J, Hebert P, Fergusson DA, et al. N Engl J Med. 2015;372:1410.
6. Alexander PE, Barty R, Fei Y, et al. Blood. 2016;127(4):400.
7. Heddle NM, Cook RJ, Arnold DM, et al. N Engl J Med. 2016;375(2):1937.
Airways Disorders
Inhaled corticosteroids in COPD: When to hold and when to fold
The 2017 GOLD guidelines reiterated that inhaled corticosteroids (ICS) be reserved for COPD patients with continued symptoms and exacerbations, despite use of long-acting beta-agonists (LABAs) and long-acting muscarinic agents (LAMAs). ICS are appropriate in approximately 40% of patients; however, prescribing rates can exceed 80% (Yawn et al. 2016; Primary Care Respir J. 26:16068).
Recent literature has begun to define the appropriate use of ICS in COPD. ICS/LABA combinations improve outcomes in patients with moderate to very severe COPD with frequent exacerbations. However, ICS/LABA may not further diminish exacerbation risk compared with those treated with a LABA/LAMA combination (Wedzicha et al., N Engl J Med. 2016;374:2222).
While the addition of LAMA to an ICS/LABA combination (triple therapy) improved lung function and decreased exacerbation risk, the addition of ICS to LABA/LAMA combination did not decrease exacerbations (GOLD Guidelines 2017). It has been suggested that those with asthma-COPD overlap identified by sputum eosinophilia represent ideal candidates for ICS therapy (GINA Guideline 2016).
ICS use in COPD increases pneumonia risk. The risk was highest in the very group for which guidelines recommend its use – those with a FEV1 less than 50% of predicted or with prior COPD exacerbation (Ernst et al. Eur Respir J. 2015;45:525).
ICS may be safely withdrawn in low-risk patients (FEV1 less than 50% predicted and no exacerbations in the previous year [Yawn et al.]).
In a trial comparing patients with severe COPD (FEV1 less than 50%) on continued LAMA/LABA/ICS triple therapy vs LAMA/LABA with ICS withdrawal, the risk of moderate or severe exacerbations at 52 weeks was not increased (Magnussen et al. N Engl J Med. 2014;371:1285).
Conclusions
Based on the 2017 GOLD guidelines:
• Monotherapy with ICS is not recommended in COPD.
• In patients with continued respiratory-related symptoms without exacerbations (GOLD group B), LAMA or LABA or LAMA/LABA combination is recommended. There is no recommendation for ICS in this group.
• In patients with frequent exacerbations (GOLD groups C and D), LAMA/LABA combinations are preferred to LABA/ICS because of superior effectiveness (especially in Group D) and the increased pneumonia risk with ICS. Escalation to triple therapy can be considered if there are continued exacerbations.
Allen Blaivas, DO, FCCP
Steering Committee Member

Navitha Ramesh, MD, MBBS
Fellow-in-Training Member

Home-Based Mechanical Ventilation and Neuromuscular Disease
Advances in neuromuscular disease
Spinal muscular atrophy (SMA) type 1 is the most deadly inherited disease among infants, with most infants dying by 1 to 2 years of age without supportive therapies, such as assisted ventilation. It is caused by homozygous deletions or mutations in the survival motor neuron 1 (SMN1) gene. Disease severity varies in part depending on the number of backup SMN2 gene copies that can produce some functional SMN protein (Arnold et al. Muscle Nerve. 2015;51[2]:157).
Recent developments of disease-modifying agents are giving hope to individuals with SMA and their families. Nusinersen (an antisense oligonucleotide) is an intrathecal medication that increases the production of functional SMN protein by increasing SMN2 exon 7 transcription (Chiriboga et al. Neurology. 2016;86[10]:890).
A recent open-label clinical trial by Finkel et al. (Lancet. 2017;388[10063]:3017) showed a “promising clinical response” that altered the natural history of disease progression. Most infants treated with multiple intrathecal doses of nusinersen had incremental improvement in their motor milestones and motor function (P = .008), as well as improved survival and/or avoidance of ventilation (P = .0014).
Moreover, the study found significant uptake of nusinersen by the motor neuron throughout the spinal cord and other neurons throughout the CNS. It appeared to be well tolerated. Disease-modifying medications may soon become “game changers” in many neuromuscular conditions.
However, a significant concern is the expected prohibitive cost both of a rare-disease-modifying therapy and of administrating intrathecal medications to fragile infants. As such, those obstacles will need to be overcome as neuromuscular clinics, hospitals, and payers start planning for the coming advances that our patients will be expecting.
Ahlam Mazi, MBBS
Fellow-in-Training Member

Interstitial and Diffuse Lung Disease
New advancements in predictive risk factors of IPF
In the last few years, many predictive risk factors were studied in clinical trials monitoring idiopathic pulmonary fibrosis (IPF), such as forced vital capacity and diffuse lung capacity for carbon monoxide (King TE Jr, et al. ASCEND Study Group. N Engl J Med. 2014;18;371[12]:1172; Richeldi L, et al. INPULSIS Trial Investigators. N Engl J Med. 2015;20;373[8]:782; Ley B, et al. Am J Respir Crit Care Med. 2016;15;194[6]:711).
Recent data that have not yet been published by Carbone et al evaluate the prognostic value of the New York Heart Association index (NYHA) compared with high resolution CT scan, somatostatin receptor scintigraphy (octreoscan), and echocardiography in a study population of 128 patients suffering from IPF (61% male subjects), nonspecific interstitial pneumonia, and granulomatous lung diseases (alveolitis, sarcoidosis, granulomatosis with polyangiitis). All patients were confirmed histologically.
The NYHA came out as a reliable prognostic factor in each setting. In fact, the log-rank test showed significant differences among NYHA categories, as cases included with disease showed the worst survival rate while no death cases were observed when NYHA was negative.
Moreover, the prognostic value of NYHA was confirmed by multivariate analysis, where the survival rate results were significantly different among patients with level 7 after adjustment for other variables included in the model.
Furthermore, the prognostic value of the NYHA index was once again confirmed when the analysis was limited to cases with the histological pattern of IPF (usual interstitial pneumonia).
The authors, therefore, strongly recommend utilization of the NYHA index as a prognostic factor of IPF as well as granulomatous lung diseases.
Roberto Carbone, MD, FCCP
Steering Committee Member

A. Monselise, MD, PhD
NetWork Nonmember
Clinical Research
The unrecognized battlefield in our hospitals: Lessons from the US Navy SEALs
Burnout syndrome (BOS) is a psychological state resulting from prolonged exposure to job stressors. It is characterized by a vicious cycle of emotional exhaustion, detachment from others, and a feeling of decreased accomplishment. Severe BOS is seen in up to 45% of physicians and 33% of nurses who work in ICUs.1
BOS has far-reaching consequences, being associated with an alarmingly high prevalence of posttraumatic stress disorder (PTSD) and substance abuse, almost equivalent to that experienced by veterans returning from war.2 BOS also is associated with self-reported suboptimal patient care practices.3This crisis has long been underrecognized, but now that we have identified the problem, where does that leave us? There are currently no quality studies evaluating how to best treat and prevent BOS/PTSD in health-care professionals. Previous studies have focused on addressing organizational factors to alleviate job stressors, but the psychosocial characteristics of the individual have been largely ignored.
Our medical education has historically focused on an individual’s intelligence quotient (IQ), but developing an individual’s emotional quotient (EQ) is just as valuable. It has long been known that Navy SEALs have the lowest prevalence of PTSD among combat veterans due partially to their specific training in emotional resilience and adaptive psychosocial coping mechanisms.
For this reason, the research team at the University of Texas Health Science Center at San Antonio is collaborating with the US Navy SEAL team to design and validate a tool that teaches critical care staff resilience training similar to what their combat trainees undergo. The goal is to curb these alarming trends in BOS and create a paradigm shift in medical education within medical and nursing schools.
Bravein Amalakuhan, MD
Fellow-in-Training Member
References
1. Embriaco N, Azoulay E, Barrau K, et al. Am J Respir Crit Care Med. 2007;175(7):686.
2. Mealer ML, Shelton A, Berg B, et al. Am J Respir Crit Care Med. 2007;175(7):693.
3. Shanafelt TD, Bradley KA, Wipf JE, et al. Ann Intern Med. 2002;136(5):358.
Critical Care
End of the era for age of blood concerns?
Blood transfusions are common in critically ill patients, with two in five adults admitted to an ICU receiving a transfusion.1,2 Recently, randomized trials have found that more restrictive thresholds for transfusions are associated with improved outcomes.3,4 One theorized explanation for this somewhat counterintuitive association is that the prolonged storage time (i.e., the age of the blood being transfused) might affect outcomes.
There have been three recent publications that help to shed some more light on this. First, Lacroix et al.5 performed a multicenter randomized blinded trial in over 2,400 critically ill patients in 64 centers comparing new blood (mean storage (±SD) of 6.1±4.9 days) vs old blood with storage of 22.0±8.4 days (P less than .001). There was no statistically significant difference in 90-day mortality.5
The second study is a meta-analysis by Alexander et al.6 The investigators looked at 12 trials and 5,229 patients and compared “fresh blood” or blood stored for 3-10 days to “older blood” stored for longer durations. They found that there was no difference in mortality and no difference in adverse events, such as acute transfusion reactions, when comparing the two groups.
Lastly, Heddle et al.7 conducted a randomized trial that compared outcomes in 20,858 hospitalized patients transfused with fresh blood (mean storage time 13.0±7.6 days) to older blood (mean storage time 23.6±8.9 days). They found no differences in mortality when comparing those transfused with fresh vs. old blood (8.7% vs. 9.1%). In addition, there was no difference when examining the predetermined subgroups, including those undergoing cardiovascular surgery, those with cancer, and those admitted to the ICU.
So, is this the end of an era for health-care provider concern about how long blood can be stored to be safe for ICU patients? Possibly.
There may still be high-risk populations (such as patients receiving massive transfusions) for which age of the blood does matter. In addition, it is still unclear based on the present data as to whether blood stored between 35 and 42 days has any significant inherent risk.
However, these publications among others suggest that the age of transfused blood may not matter, even in critically ill patients. Therefore, the present storage practices of many blood banks around the United States and beyond are validated by the present publications regarding the scarce resource of blood.
Christopher L. Carroll, MD, MS, FCCP
Steering Committee Member
Steven Greenberg, MD, FCCP
Steering Committee Member
References
1. Corwin HL, Gettinger A, Pearl RG, et al. Crit Care Med. 2004;32(1):39.
2. Vincent JL, Baron JF, Reinhart K, et al.; ABC (Anemia and Blood Transfusion in Critical Care) Investigators. JAMA. 2002;288(12):1499.
3. Holst LB, Haase N, Wetterslev J, et al.; TRISS Trial Group; Scandinavian Critical Care Trials Group. N Engl J Med. 2014;371(15):1381.
4. Lacroix J, Hebert PC, Hutchison JS, et al.; TRIPICU Investigators; Canadian Critical Care Trials Group; Pediatric Acute Lung Injury and Sepsis Investigators Network. N Engl J Med. 2007;356(16):1609.
5. Lacroix J, Hebert P, Fergusson DA, et al. N Engl J Med. 2015;372:1410.
6. Alexander PE, Barty R, Fei Y, et al. Blood. 2016;127(4):400.
7. Heddle NM, Cook RJ, Arnold DM, et al. N Engl J Med. 2016;375(2):1937.
Airways Disorders
Inhaled corticosteroids in COPD: When to hold and when to fold
The 2017 GOLD guidelines reiterated that inhaled corticosteroids (ICS) be reserved for COPD patients with continued symptoms and exacerbations, despite use of long-acting beta-agonists (LABAs) and long-acting muscarinic agents (LAMAs). ICS are appropriate in approximately 40% of patients; however, prescribing rates can exceed 80% (Yawn et al. 2016; Primary Care Respir J. 26:16068).
Recent literature has begun to define the appropriate use of ICS in COPD. ICS/LABA combinations improve outcomes in patients with moderate to very severe COPD with frequent exacerbations. However, ICS/LABA may not further diminish exacerbation risk compared with those treated with a LABA/LAMA combination (Wedzicha et al., N Engl J Med. 2016;374:2222).
While the addition of LAMA to an ICS/LABA combination (triple therapy) improved lung function and decreased exacerbation risk, the addition of ICS to LABA/LAMA combination did not decrease exacerbations (GOLD Guidelines 2017). It has been suggested that those with asthma-COPD overlap identified by sputum eosinophilia represent ideal candidates for ICS therapy (GINA Guideline 2016).
ICS use in COPD increases pneumonia risk. The risk was highest in the very group for which guidelines recommend its use – those with a FEV1 less than 50% of predicted or with prior COPD exacerbation (Ernst et al. Eur Respir J. 2015;45:525).
ICS may be safely withdrawn in low-risk patients (FEV1 less than 50% predicted and no exacerbations in the previous year [Yawn et al.]).
In a trial comparing patients with severe COPD (FEV1 less than 50%) on continued LAMA/LABA/ICS triple therapy vs LAMA/LABA with ICS withdrawal, the risk of moderate or severe exacerbations at 52 weeks was not increased (Magnussen et al. N Engl J Med. 2014;371:1285).
Conclusions
Based on the 2017 GOLD guidelines:
• Monotherapy with ICS is not recommended in COPD.
• In patients with continued respiratory-related symptoms without exacerbations (GOLD group B), LAMA or LABA or LAMA/LABA combination is recommended. There is no recommendation for ICS in this group.
• In patients with frequent exacerbations (GOLD groups C and D), LAMA/LABA combinations are preferred to LABA/ICS because of superior effectiveness (especially in Group D) and the increased pneumonia risk with ICS. Escalation to triple therapy can be considered if there are continued exacerbations.
Allen Blaivas, DO, FCCP
Steering Committee Member
Navitha Ramesh, MD, MBBS
Fellow-in-Training Member
Home-Based Mechanical Ventilation and Neuromuscular Disease
Advances in neuromuscular disease
Spinal muscular atrophy (SMA) type 1 is the most deadly inherited disease among infants, with most infants dying by 1 to 2 years of age without supportive therapies, such as assisted ventilation. It is caused by homozygous deletions or mutations in the survival motor neuron 1 (SMN1) gene. Disease severity varies in part depending on the number of backup SMN2 gene copies that can produce some functional SMN protein (Arnold et al. Muscle Nerve. 2015;51[2]:157).
Recent developments of disease-modifying agents are giving hope to individuals with SMA and their families. Nusinersen (an antisense oligonucleotide) is an intrathecal medication that increases the production of functional SMN protein by increasing SMN2 exon 7 transcription (Chiriboga et al. Neurology. 2016;86[10]:890).
A recent open-label clinical trial by Finkel et al. (Lancet. 2017;388[10063]:3017) showed a “promising clinical response” that altered the natural history of disease progression. Most infants treated with multiple intrathecal doses of nusinersen had incremental improvement in their motor milestones and motor function (P = .008), as well as improved survival and/or avoidance of ventilation (P = .0014).
Moreover, the study found significant uptake of nusinersen by the motor neuron throughout the spinal cord and other neurons throughout the CNS. It appeared to be well tolerated. Disease-modifying medications may soon become “game changers” in many neuromuscular conditions.
However, a significant concern is the expected prohibitive cost both of a rare-disease-modifying therapy and of administrating intrathecal medications to fragile infants. As such, those obstacles will need to be overcome as neuromuscular clinics, hospitals, and payers start planning for the coming advances that our patients will be expecting.
Ahlam Mazi, MBBS
Fellow-in-Training Member
Interstitial and Diffuse Lung Disease
New advancements in predictive risk factors of IPF
In the last few years, many predictive risk factors were studied in clinical trials monitoring idiopathic pulmonary fibrosis (IPF), such as forced vital capacity and diffuse lung capacity for carbon monoxide (King TE Jr, et al. ASCEND Study Group. N Engl J Med. 2014;18;371[12]:1172; Richeldi L, et al. INPULSIS Trial Investigators. N Engl J Med. 2015;20;373[8]:782; Ley B, et al. Am J Respir Crit Care Med. 2016;15;194[6]:711).
Recent data that have not yet been published by Carbone et al evaluate the prognostic value of the New York Heart Association index (NYHA) compared with high resolution CT scan, somatostatin receptor scintigraphy (octreoscan), and echocardiography in a study population of 128 patients suffering from IPF (61% male subjects), nonspecific interstitial pneumonia, and granulomatous lung diseases (alveolitis, sarcoidosis, granulomatosis with polyangiitis). All patients were confirmed histologically.
The NYHA came out as a reliable prognostic factor in each setting. In fact, the log-rank test showed significant differences among NYHA categories, as cases included with disease showed the worst survival rate while no death cases were observed when NYHA was negative.
Moreover, the prognostic value of NYHA was confirmed by multivariate analysis, where the survival rate results were significantly different among patients with level 7 after adjustment for other variables included in the model.
Furthermore, the prognostic value of the NYHA index was once again confirmed when the analysis was limited to cases with the histological pattern of IPF (usual interstitial pneumonia).
The authors, therefore, strongly recommend utilization of the NYHA index as a prognostic factor of IPF as well as granulomatous lung diseases.
Roberto Carbone, MD, FCCP
Steering Committee Member
A. Monselise, MD, PhD
NetWork Nonmember
Clinical Research
The unrecognized battlefield in our hospitals: Lessons from the US Navy SEALs
Burnout syndrome (BOS) is a psychological state resulting from prolonged exposure to job stressors. It is characterized by a vicious cycle of emotional exhaustion, detachment from others, and a feeling of decreased accomplishment. Severe BOS is seen in up to 45% of physicians and 33% of nurses who work in ICUs.1
BOS has far-reaching consequences, being associated with an alarmingly high prevalence of posttraumatic stress disorder (PTSD) and substance abuse, almost equivalent to that experienced by veterans returning from war.2 BOS also is associated with self-reported suboptimal patient care practices.3This crisis has long been underrecognized, but now that we have identified the problem, where does that leave us? There are currently no quality studies evaluating how to best treat and prevent BOS/PTSD in health-care professionals. Previous studies have focused on addressing organizational factors to alleviate job stressors, but the psychosocial characteristics of the individual have been largely ignored.
Our medical education has historically focused on an individual’s intelligence quotient (IQ), but developing an individual’s emotional quotient (EQ) is just as valuable. It has long been known that Navy SEALs have the lowest prevalence of PTSD among combat veterans due partially to their specific training in emotional resilience and adaptive psychosocial coping mechanisms.
For this reason, the research team at the University of Texas Health Science Center at San Antonio is collaborating with the US Navy SEAL team to design and validate a tool that teaches critical care staff resilience training similar to what their combat trainees undergo. The goal is to curb these alarming trends in BOS and create a paradigm shift in medical education within medical and nursing schools.
Bravein Amalakuhan, MD
Fellow-in-Training Member
References
1. Embriaco N, Azoulay E, Barrau K, et al. Am J Respir Crit Care Med. 2007;175(7):686.
2. Mealer ML, Shelton A, Berg B, et al. Am J Respir Crit Care Med. 2007;175(7):693.
3. Shanafelt TD, Bradley KA, Wipf JE, et al. Ann Intern Med. 2002;136(5):358.
Critical Care
End of the era for age of blood concerns?
Blood transfusions are common in critically ill patients, with two in five adults admitted to an ICU receiving a transfusion.1,2 Recently, randomized trials have found that more restrictive thresholds for transfusions are associated with improved outcomes.3,4 One theorized explanation for this somewhat counterintuitive association is that the prolonged storage time (i.e., the age of the blood being transfused) might affect outcomes.
There have been three recent publications that help to shed some more light on this. First, Lacroix et al.5 performed a multicenter randomized blinded trial in over 2,400 critically ill patients in 64 centers comparing new blood (mean storage (±SD) of 6.1±4.9 days) vs old blood with storage of 22.0±8.4 days (P less than .001). There was no statistically significant difference in 90-day mortality.5
The second study is a meta-analysis by Alexander et al.6 The investigators looked at 12 trials and 5,229 patients and compared “fresh blood” or blood stored for 3-10 days to “older blood” stored for longer durations. They found that there was no difference in mortality and no difference in adverse events, such as acute transfusion reactions, when comparing the two groups.
Lastly, Heddle et al.7 conducted a randomized trial that compared outcomes in 20,858 hospitalized patients transfused with fresh blood (mean storage time 13.0±7.6 days) to older blood (mean storage time 23.6±8.9 days). They found no differences in mortality when comparing those transfused with fresh vs. old blood (8.7% vs. 9.1%). In addition, there was no difference when examining the predetermined subgroups, including those undergoing cardiovascular surgery, those with cancer, and those admitted to the ICU.
So, is this the end of an era for health-care provider concern about how long blood can be stored to be safe for ICU patients? Possibly.
There may still be high-risk populations (such as patients receiving massive transfusions) for which age of the blood does matter. In addition, it is still unclear based on the present data as to whether blood stored between 35 and 42 days has any significant inherent risk.
However, these publications among others suggest that the age of transfused blood may not matter, even in critically ill patients. Therefore, the present storage practices of many blood banks around the United States and beyond are validated by the present publications regarding the scarce resource of blood.
Christopher L. Carroll, MD, MS, FCCP
Steering Committee Member
Steven Greenberg, MD, FCCP
Steering Committee Member
References
1. Corwin HL, Gettinger A, Pearl RG, et al. Crit Care Med. 2004;32(1):39.
2. Vincent JL, Baron JF, Reinhart K, et al.; ABC (Anemia and Blood Transfusion in Critical Care) Investigators. JAMA. 2002;288(12):1499.
3. Holst LB, Haase N, Wetterslev J, et al.; TRISS Trial Group; Scandinavian Critical Care Trials Group. N Engl J Med. 2014;371(15):1381.
4. Lacroix J, Hebert PC, Hutchison JS, et al.; TRIPICU Investigators; Canadian Critical Care Trials Group; Pediatric Acute Lung Injury and Sepsis Investigators Network. N Engl J Med. 2007;356(16):1609.
5. Lacroix J, Hebert P, Fergusson DA, et al. N Engl J Med. 2015;372:1410.
6. Alexander PE, Barty R, Fei Y, et al. Blood. 2016;127(4):400.
7. Heddle NM, Cook RJ, Arnold DM, et al. N Engl J Med. 2016;375(2):1937.
Airways Disorders
Inhaled corticosteroids in COPD: When to hold and when to fold
The 2017 GOLD guidelines reiterated that inhaled corticosteroids (ICS) be reserved for COPD patients with continued symptoms and exacerbations, despite use of long-acting beta-agonists (LABAs) and long-acting muscarinic agents (LAMAs). ICS are appropriate in approximately 40% of patients; however, prescribing rates can exceed 80% (Yawn et al. 2016; Primary Care Respir J. 26:16068).
Recent literature has begun to define the appropriate use of ICS in COPD. ICS/LABA combinations improve outcomes in patients with moderate to very severe COPD with frequent exacerbations. However, ICS/LABA may not further diminish exacerbation risk compared with those treated with a LABA/LAMA combination (Wedzicha et al., N Engl J Med. 2016;374:2222).
While the addition of LAMA to an ICS/LABA combination (triple therapy) improved lung function and decreased exacerbation risk, the addition of ICS to LABA/LAMA combination did not decrease exacerbations (GOLD Guidelines 2017). It has been suggested that those with asthma-COPD overlap identified by sputum eosinophilia represent ideal candidates for ICS therapy (GINA Guideline 2016).
ICS use in COPD increases pneumonia risk. The risk was highest in the very group for which guidelines recommend its use – those with a FEV1 less than 50% of predicted or with prior COPD exacerbation (Ernst et al. Eur Respir J. 2015;45:525).
ICS may be safely withdrawn in low-risk patients (FEV1 less than 50% predicted and no exacerbations in the previous year [Yawn et al.]).
In a trial comparing patients with severe COPD (FEV1 less than 50%) on continued LAMA/LABA/ICS triple therapy vs LAMA/LABA with ICS withdrawal, the risk of moderate or severe exacerbations at 52 weeks was not increased (Magnussen et al. N Engl J Med. 2014;371:1285).
Conclusions
Based on the 2017 GOLD guidelines:
• Monotherapy with ICS is not recommended in COPD.
• In patients with continued respiratory-related symptoms without exacerbations (GOLD group B), LAMA or LABA or LAMA/LABA combination is recommended. There is no recommendation for ICS in this group.
• In patients with frequent exacerbations (GOLD groups C and D), LAMA/LABA combinations are preferred to LABA/ICS because of superior effectiveness (especially in Group D) and the increased pneumonia risk with ICS. Escalation to triple therapy can be considered if there are continued exacerbations.
Allen Blaivas, DO, FCCP
Steering Committee Member
Navitha Ramesh, MD, MBBS
Fellow-in-Training Member
Home-Based Mechanical Ventilation and Neuromuscular Disease
Advances in neuromuscular disease
Spinal muscular atrophy (SMA) type 1 is the most deadly inherited disease among infants, with most infants dying by 1 to 2 years of age without supportive therapies, such as assisted ventilation. It is caused by homozygous deletions or mutations in the survival motor neuron 1 (SMN1) gene. Disease severity varies in part depending on the number of backup SMN2 gene copies that can produce some functional SMN protein (Arnold et al. Muscle Nerve. 2015;51[2]:157).
Recent developments of disease-modifying agents are giving hope to individuals with SMA and their families. Nusinersen (an antisense oligonucleotide) is an intrathecal medication that increases the production of functional SMN protein by increasing SMN2 exon 7 transcription (Chiriboga et al. Neurology. 2016;86[10]:890).
A recent open-label clinical trial by Finkel et al. (Lancet. 2017;388[10063]:3017) showed a “promising clinical response” that altered the natural history of disease progression. Most infants treated with multiple intrathecal doses of nusinersen had incremental improvement in their motor milestones and motor function (P = .008), as well as improved survival and/or avoidance of ventilation (P = .0014).
Moreover, the study found significant uptake of nusinersen by the motor neuron throughout the spinal cord and other neurons throughout the CNS. It appeared to be well tolerated. Disease-modifying medications may soon become “game changers” in many neuromuscular conditions.
However, a significant concern is the expected prohibitive cost both of a rare-disease-modifying therapy and of administrating intrathecal medications to fragile infants. As such, those obstacles will need to be overcome as neuromuscular clinics, hospitals, and payers start planning for the coming advances that our patients will be expecting.
Ahlam Mazi, MBBS
Fellow-in-Training Member
Interstitial and Diffuse Lung Disease
New advancements in predictive risk factors of IPF
In the last few years, many predictive risk factors were studied in clinical trials monitoring idiopathic pulmonary fibrosis (IPF), such as forced vital capacity and diffuse lung capacity for carbon monoxide (King TE Jr, et al. ASCEND Study Group. N Engl J Med. 2014;18;371[12]:1172; Richeldi L, et al. INPULSIS Trial Investigators. N Engl J Med. 2015;20;373[8]:782; Ley B, et al. Am J Respir Crit Care Med. 2016;15;194[6]:711).
Recent data that have not yet been published by Carbone et al evaluate the prognostic value of the New York Heart Association index (NYHA) compared with high resolution CT scan, somatostatin receptor scintigraphy (octreoscan), and echocardiography in a study population of 128 patients suffering from IPF (61% male subjects), nonspecific interstitial pneumonia, and granulomatous lung diseases (alveolitis, sarcoidosis, granulomatosis with polyangiitis). All patients were confirmed histologically.
The NYHA came out as a reliable prognostic factor in each setting. In fact, the log-rank test showed significant differences among NYHA categories, as cases included with disease showed the worst survival rate while no death cases were observed when NYHA was negative.
Moreover, the prognostic value of NYHA was confirmed by multivariate analysis, where the survival rate results were significantly different among patients with level 7 after adjustment for other variables included in the model.
Furthermore, the prognostic value of the NYHA index was once again confirmed when the analysis was limited to cases with the histological pattern of IPF (usual interstitial pneumonia).
The authors, therefore, strongly recommend utilization of the NYHA index as a prognostic factor of IPF as well as granulomatous lung diseases.
Roberto Carbone, MD, FCCP
Steering Committee Member
A. Monselise, MD, PhD
NetWork Nonmember
Join Us for COPD: Current Excellence and Future Development May 7-9, 2017 Amsterdam, the Netherlands
The global burden of COPD is increasing and is one of the leading causes of disability worldwide. Attend COPD: Current Excellence and Future Development and join clinicians, experts, and specialists as they convene in Amsterdam to discuss best practices and future directions in diagnosis, treatment, and therapeutic innovations. Plan to discuss the latest cutting-edge findings in COPD with like-minded clinicians.
The conference, taking place at the NH Grand Hotel Krasnapolsky, in the center of Amsterdam, will include these session themes:
- History and burden of COPD.
- Polymorbidity in COPD.
- Infections and exacerbations in COPD.
- Current treatment of COPD.
- The future of COPD.
Don’t Miss These Speakers
- Dirkje Postma (Keynote speaker) – Professor of Pulmonary Medicine at the University of Groningen and the University Medical Center of Groningen. Professor Postma will give a keynote session “From Past to Present, Circle With COPD.”
- David M. Mannino (Conference chair) – Professor and Chair in the Department of Preventive Medicine and Environmental Health at the University of Kentucky (Lexington) College of Public Health. Dr. Mannino’s session topic is “The Natural History of COPD.”
- John Hurst, (Co-chair and speaker) – Senior Lecturer at University College, London, UK, Dr. Hurst’s session topic is “The Importance of Acute Exacerbations.”
- Alberto Papi (Co-chair and speaker) – Professor of Respiratory Medicine and Vice President of the School of Medicine at the University of Ferrara, Italy, and Director of the Respiratory Unit of the Department of Emergency Medicine, S. Anna University Hospital, Ferrara. Professor Papi’s talk will explore “The Role of Infections.”
- Peter J. Barnes (Conference speaker) – Margaret-Turner Warwick Professor of Medicine at the National Heart and Lung Institute, Head of Respiratory Medicine at Imperial College and Honorary Consultant Physician at Royal Brompton Hospital, London. Professor Barnes’ presentation will focus on “Future Novel Therapies.”
- Sally Singh (Conference speaker) - Professor of Pulmonary and Cardiac Rehabilitation at the University Hospitals of Leicester (one of the largest rehabilitation programs in the UK). Professor Singh’s session is on “Pulmonary Rehabilitation.”
- Nicholas Hopkinson (Conference speaker) – Dr. Hopkinson is a Reader in Respiratory Medicine & Honorary Consultant Physician at the National Heart and Lung Institute of Imperial College and the Royal Brompton Hospital. His session focuses on “Cigarette Smoking.”
- Joan Soriano (Conference speaker) - Since 2007, Dr. Soriano has been an Associate Editor of the European Respiratory Journal and since 2013 of the Lancet Respiratory Medicine. His session focuses on “Asthma-COPD Overlap.”
Learn more about what the conference has to offer and how to register at chestcopdconference.com.
The global burden of COPD is increasing and is one of the leading causes of disability worldwide. Attend COPD: Current Excellence and Future Development and join clinicians, experts, and specialists as they convene in Amsterdam to discuss best practices and future directions in diagnosis, treatment, and therapeutic innovations. Plan to discuss the latest cutting-edge findings in COPD with like-minded clinicians.
The conference, taking place at the NH Grand Hotel Krasnapolsky, in the center of Amsterdam, will include these session themes:
- History and burden of COPD.
- Polymorbidity in COPD.
- Infections and exacerbations in COPD.
- Current treatment of COPD.
- The future of COPD.
Don’t Miss These Speakers
- Dirkje Postma (Keynote speaker) – Professor of Pulmonary Medicine at the University of Groningen and the University Medical Center of Groningen. Professor Postma will give a keynote session “From Past to Present, Circle With COPD.”
- David M. Mannino (Conference chair) – Professor and Chair in the Department of Preventive Medicine and Environmental Health at the University of Kentucky (Lexington) College of Public Health. Dr. Mannino’s session topic is “The Natural History of COPD.”
- John Hurst, (Co-chair and speaker) – Senior Lecturer at University College, London, UK, Dr. Hurst’s session topic is “The Importance of Acute Exacerbations.”
- Alberto Papi (Co-chair and speaker) – Professor of Respiratory Medicine and Vice President of the School of Medicine at the University of Ferrara, Italy, and Director of the Respiratory Unit of the Department of Emergency Medicine, S. Anna University Hospital, Ferrara. Professor Papi’s talk will explore “The Role of Infections.”
- Peter J. Barnes (Conference speaker) – Margaret-Turner Warwick Professor of Medicine at the National Heart and Lung Institute, Head of Respiratory Medicine at Imperial College and Honorary Consultant Physician at Royal Brompton Hospital, London. Professor Barnes’ presentation will focus on “Future Novel Therapies.”
- Sally Singh (Conference speaker) - Professor of Pulmonary and Cardiac Rehabilitation at the University Hospitals of Leicester (one of the largest rehabilitation programs in the UK). Professor Singh’s session is on “Pulmonary Rehabilitation.”
- Nicholas Hopkinson (Conference speaker) – Dr. Hopkinson is a Reader in Respiratory Medicine & Honorary Consultant Physician at the National Heart and Lung Institute of Imperial College and the Royal Brompton Hospital. His session focuses on “Cigarette Smoking.”
- Joan Soriano (Conference speaker) - Since 2007, Dr. Soriano has been an Associate Editor of the European Respiratory Journal and since 2013 of the Lancet Respiratory Medicine. His session focuses on “Asthma-COPD Overlap.”
Learn more about what the conference has to offer and how to register at chestcopdconference.com.
The global burden of COPD is increasing and is one of the leading causes of disability worldwide. Attend COPD: Current Excellence and Future Development and join clinicians, experts, and specialists as they convene in Amsterdam to discuss best practices and future directions in diagnosis, treatment, and therapeutic innovations. Plan to discuss the latest cutting-edge findings in COPD with like-minded clinicians.
The conference, taking place at the NH Grand Hotel Krasnapolsky, in the center of Amsterdam, will include these session themes:
- History and burden of COPD.
- Polymorbidity in COPD.
- Infections and exacerbations in COPD.
- Current treatment of COPD.
- The future of COPD.
Don’t Miss These Speakers
- Dirkje Postma (Keynote speaker) – Professor of Pulmonary Medicine at the University of Groningen and the University Medical Center of Groningen. Professor Postma will give a keynote session “From Past to Present, Circle With COPD.”
- David M. Mannino (Conference chair) – Professor and Chair in the Department of Preventive Medicine and Environmental Health at the University of Kentucky (Lexington) College of Public Health. Dr. Mannino’s session topic is “The Natural History of COPD.”
- John Hurst, (Co-chair and speaker) – Senior Lecturer at University College, London, UK, Dr. Hurst’s session topic is “The Importance of Acute Exacerbations.”
- Alberto Papi (Co-chair and speaker) – Professor of Respiratory Medicine and Vice President of the School of Medicine at the University of Ferrara, Italy, and Director of the Respiratory Unit of the Department of Emergency Medicine, S. Anna University Hospital, Ferrara. Professor Papi’s talk will explore “The Role of Infections.”
- Peter J. Barnes (Conference speaker) – Margaret-Turner Warwick Professor of Medicine at the National Heart and Lung Institute, Head of Respiratory Medicine at Imperial College and Honorary Consultant Physician at Royal Brompton Hospital, London. Professor Barnes’ presentation will focus on “Future Novel Therapies.”
- Sally Singh (Conference speaker) - Professor of Pulmonary and Cardiac Rehabilitation at the University Hospitals of Leicester (one of the largest rehabilitation programs in the UK). Professor Singh’s session is on “Pulmonary Rehabilitation.”
- Nicholas Hopkinson (Conference speaker) – Dr. Hopkinson is a Reader in Respiratory Medicine & Honorary Consultant Physician at the National Heart and Lung Institute of Imperial College and the Royal Brompton Hospital. His session focuses on “Cigarette Smoking.”
- Joan Soriano (Conference speaker) - Since 2007, Dr. Soriano has been an Associate Editor of the European Respiratory Journal and since 2013 of the Lancet Respiratory Medicine. His session focuses on “Asthma-COPD Overlap.”
Learn more about what the conference has to offer and how to register at chestcopdconference.com.
PCCM endorsed as pilot subspecialty by the Chinese National Health and Family Planning Commission
On Dec. 23, 2016, the Chinese National Health and Family Planning Commission officially endorsed Pulmonary and Critical Care Medicine (PCCM) as a pilot subspecialty within China. PCCM is one of three subspecialties (together with neurosurgery and cardiology) to pioneer fellowship training education in China. With the official endorsement of PCCM, local efforts will progress within China to administer programs and extend the standards of training throughout medical education in China. PCCM certification will now become a requirement for appointment of pulmonary department chairs and for promotion within the subspecialty.
Since 2012, CHEST has worked closely with partners, such as the Chinese Thoracic Society, the Chinese Association of Chest Physicians, and the Chinese Medical Doctor Association, on the development of China’s first fellowship program offering standardized training in PCCM for Chinese physicians. As a result of these collective efforts, PCCM has now officially earned endorsement as a medical subspecialty – the first of its kind in a country where medical training typically ends after a physician completes residency training. Only a decade ago, physicians in China went directly into practice following medical school. The development of a PCCM subspecialty in China – made possible through the engagement of CHEST’s expert faculty and administration – parallels what has occurred over the past 3 decades in the United States, during which the fields of pulmonary and critical care medicine evolved into the combined subspecialty of PCCM.
The China-CHEST PCCM Fellowship Program was officially launched in 2013 with 12 participating Chinese institutions starting their PCCM training programs. By the end of 2017, 30 programs with 300 fellows and 60 faculty will be participating at institutions throughout China, with the potential to impact the care of thousands of patients. The China-PCCM Fellowship Program proudly graduated its first class of fellows in September 2016.
China-CHEST leaders, including Renli Qiao, MD, PhD, FCCP; Chen Wang, MD, PhD, FCCP; and Jack Buckley, MD, MPH, FCCP; with Steve Welch, CHEST Executive Vice President, recently participated in local site visits to provide ongoing education and support to Chinese PCCM fellowship programs. They also participated in the November 2016 Mingdao Forum in Beijing to highlight the history and achievements of the China-CHEST PCCM program.
The vast reach and clinical exposure of this program highlights how an international professional medical association like CHEST, through innovative education and strategic collaborative partnerships, is able to impact medical training both within and beyond its specialty on a global scale.
Darcy Marciniuk, MD, FCCP
Chair, China–CHEST PCCM Steering Committee
Professor of Medicine, University of Saskatchewan,
Saskatoon, SK, Canada
Renli Qiao, MD, PhD, FCCP
Medical Director, China–CHEST PCCM Program
Professor of Clinical Medicine,
Keck School of Medicine of USC,
Los Angeles, California
Robb Rabito, CHCP
Director, Education Operations CHEST
Glenview, Illinois
On Dec. 23, 2016, the Chinese National Health and Family Planning Commission officially endorsed Pulmonary and Critical Care Medicine (PCCM) as a pilot subspecialty within China. PCCM is one of three subspecialties (together with neurosurgery and cardiology) to pioneer fellowship training education in China. With the official endorsement of PCCM, local efforts will progress within China to administer programs and extend the standards of training throughout medical education in China. PCCM certification will now become a requirement for appointment of pulmonary department chairs and for promotion within the subspecialty.
Since 2012, CHEST has worked closely with partners, such as the Chinese Thoracic Society, the Chinese Association of Chest Physicians, and the Chinese Medical Doctor Association, on the development of China’s first fellowship program offering standardized training in PCCM for Chinese physicians. As a result of these collective efforts, PCCM has now officially earned endorsement as a medical subspecialty – the first of its kind in a country where medical training typically ends after a physician completes residency training. Only a decade ago, physicians in China went directly into practice following medical school. The development of a PCCM subspecialty in China – made possible through the engagement of CHEST’s expert faculty and administration – parallels what has occurred over the past 3 decades in the United States, during which the fields of pulmonary and critical care medicine evolved into the combined subspecialty of PCCM.
The China-CHEST PCCM Fellowship Program was officially launched in 2013 with 12 participating Chinese institutions starting their PCCM training programs. By the end of 2017, 30 programs with 300 fellows and 60 faculty will be participating at institutions throughout China, with the potential to impact the care of thousands of patients. The China-PCCM Fellowship Program proudly graduated its first class of fellows in September 2016.
China-CHEST leaders, including Renli Qiao, MD, PhD, FCCP; Chen Wang, MD, PhD, FCCP; and Jack Buckley, MD, MPH, FCCP; with Steve Welch, CHEST Executive Vice President, recently participated in local site visits to provide ongoing education and support to Chinese PCCM fellowship programs. They also participated in the November 2016 Mingdao Forum in Beijing to highlight the history and achievements of the China-CHEST PCCM program.
The vast reach and clinical exposure of this program highlights how an international professional medical association like CHEST, through innovative education and strategic collaborative partnerships, is able to impact medical training both within and beyond its specialty on a global scale.
Darcy Marciniuk, MD, FCCP
Chair, China–CHEST PCCM Steering Committee
Professor of Medicine, University of Saskatchewan,
Saskatoon, SK, Canada
Renli Qiao, MD, PhD, FCCP
Medical Director, China–CHEST PCCM Program
Professor of Clinical Medicine,
Keck School of Medicine of USC,
Los Angeles, California
Robb Rabito, CHCP
Director, Education Operations CHEST
Glenview, Illinois
On Dec. 23, 2016, the Chinese National Health and Family Planning Commission officially endorsed Pulmonary and Critical Care Medicine (PCCM) as a pilot subspecialty within China. PCCM is one of three subspecialties (together with neurosurgery and cardiology) to pioneer fellowship training education in China. With the official endorsement of PCCM, local efforts will progress within China to administer programs and extend the standards of training throughout medical education in China. PCCM certification will now become a requirement for appointment of pulmonary department chairs and for promotion within the subspecialty.
Since 2012, CHEST has worked closely with partners, such as the Chinese Thoracic Society, the Chinese Association of Chest Physicians, and the Chinese Medical Doctor Association, on the development of China’s first fellowship program offering standardized training in PCCM for Chinese physicians. As a result of these collective efforts, PCCM has now officially earned endorsement as a medical subspecialty – the first of its kind in a country where medical training typically ends after a physician completes residency training. Only a decade ago, physicians in China went directly into practice following medical school. The development of a PCCM subspecialty in China – made possible through the engagement of CHEST’s expert faculty and administration – parallels what has occurred over the past 3 decades in the United States, during which the fields of pulmonary and critical care medicine evolved into the combined subspecialty of PCCM.
The China-CHEST PCCM Fellowship Program was officially launched in 2013 with 12 participating Chinese institutions starting their PCCM training programs. By the end of 2017, 30 programs with 300 fellows and 60 faculty will be participating at institutions throughout China, with the potential to impact the care of thousands of patients. The China-PCCM Fellowship Program proudly graduated its first class of fellows in September 2016.
China-CHEST leaders, including Renli Qiao, MD, PhD, FCCP; Chen Wang, MD, PhD, FCCP; and Jack Buckley, MD, MPH, FCCP; with Steve Welch, CHEST Executive Vice President, recently participated in local site visits to provide ongoing education and support to Chinese PCCM fellowship programs. They also participated in the November 2016 Mingdao Forum in Beijing to highlight the history and achievements of the China-CHEST PCCM program.
The vast reach and clinical exposure of this program highlights how an international professional medical association like CHEST, through innovative education and strategic collaborative partnerships, is able to impact medical training both within and beyond its specialty on a global scale.
Darcy Marciniuk, MD, FCCP
Chair, China–CHEST PCCM Steering Committee
Professor of Medicine, University of Saskatchewan,
Saskatoon, SK, Canada
Renli Qiao, MD, PhD, FCCP
Medical Director, China–CHEST PCCM Program
Professor of Clinical Medicine,
Keck School of Medicine of USC,
Los Angeles, California
Robb Rabito, CHCP
Director, Education Operations CHEST
Glenview, Illinois
CCSC issues five Choosing Wisely recommendations
Overutilization of tests, treatments, and procedures is an important example of low-value care that adds to the high cost of health care and provides little to no benefit for patients. To combat this problem, the American Board of Internal Medicine Foundation developed the Choosing Wisely Campaign, tasking professional societies to develop lists of the top five medical services that patients should question.
The Critical Care Societies Collaborative (CCSC), which comprises the four major U.S. professional and scientific societies – the American Association of Critical-Care Nurses, the American College of Chest Physicians, the American Thoracic Society, and the Society of Critical Care Medicine – participated by creating a task force that addressed this task to focus on critical care delivery.
Five CCSC recommendations were formulated:
1. Don’t order diagnostic tests at regular intervals (such as every day), but rather in response to specific clinical questions.
2. Don’t transfuse red blood cells in hemodynamically stable, nonbleeding patients with a hemoglobin concentration greater than 7 mg/dL.
3. Don’t use parenteral nutrition in adequately nourished critically ill patients within the first 7 days of an ICU stay.
4. Don’t deeply sedate mechanically ventilated patients without a specific indication and without daily attempts to lighten sedation.
5. Don’t continue life support for patients at high risk for death or severely impaired functional recovery without offering patients and their families the alternative of care focused entirely on comfort.
The CCSC is tracking use/implementation of the Choosing Wisely recommendations among its four member organizations. Please complete this short survey at https://redcap.rush.edu/redcap/surveys/?s. Please click submit when finished.
Overutilization of tests, treatments, and procedures is an important example of low-value care that adds to the high cost of health care and provides little to no benefit for patients. To combat this problem, the American Board of Internal Medicine Foundation developed the Choosing Wisely Campaign, tasking professional societies to develop lists of the top five medical services that patients should question.
The Critical Care Societies Collaborative (CCSC), which comprises the four major U.S. professional and scientific societies – the American Association of Critical-Care Nurses, the American College of Chest Physicians, the American Thoracic Society, and the Society of Critical Care Medicine – participated by creating a task force that addressed this task to focus on critical care delivery.
Five CCSC recommendations were formulated:
1. Don’t order diagnostic tests at regular intervals (such as every day), but rather in response to specific clinical questions.
2. Don’t transfuse red blood cells in hemodynamically stable, nonbleeding patients with a hemoglobin concentration greater than 7 mg/dL.
3. Don’t use parenteral nutrition in adequately nourished critically ill patients within the first 7 days of an ICU stay.
4. Don’t deeply sedate mechanically ventilated patients without a specific indication and without daily attempts to lighten sedation.
5. Don’t continue life support for patients at high risk for death or severely impaired functional recovery without offering patients and their families the alternative of care focused entirely on comfort.
The CCSC is tracking use/implementation of the Choosing Wisely recommendations among its four member organizations. Please complete this short survey at https://redcap.rush.edu/redcap/surveys/?s. Please click submit when finished.
Overutilization of tests, treatments, and procedures is an important example of low-value care that adds to the high cost of health care and provides little to no benefit for patients. To combat this problem, the American Board of Internal Medicine Foundation developed the Choosing Wisely Campaign, tasking professional societies to develop lists of the top five medical services that patients should question.
The Critical Care Societies Collaborative (CCSC), which comprises the four major U.S. professional and scientific societies – the American Association of Critical-Care Nurses, the American College of Chest Physicians, the American Thoracic Society, and the Society of Critical Care Medicine – participated by creating a task force that addressed this task to focus on critical care delivery.
Five CCSC recommendations were formulated:
1. Don’t order diagnostic tests at regular intervals (such as every day), but rather in response to specific clinical questions.
2. Don’t transfuse red blood cells in hemodynamically stable, nonbleeding patients with a hemoglobin concentration greater than 7 mg/dL.
3. Don’t use parenteral nutrition in adequately nourished critically ill patients within the first 7 days of an ICU stay.
4. Don’t deeply sedate mechanically ventilated patients without a specific indication and without daily attempts to lighten sedation.
5. Don’t continue life support for patients at high risk for death or severely impaired functional recovery without offering patients and their families the alternative of care focused entirely on comfort.
The CCSC is tracking use/implementation of the Choosing Wisely recommendations among its four member organizations. Please complete this short survey at https://redcap.rush.edu/redcap/surveys/?s. Please click submit when finished.
CHEST Foundation can give more than $500,000 in grants
Every year, the CHEST Foundation awards more than a half-million dollars in grants to the next generation of lung health champions. February 2017 marks the start of the foundation’s next grant cycle, and we are excited to announce a new clinical research grant in Cystic Fibrosis, among many other disease-state topics. In 2016, the foundation awarded 11 CHEST members for their innovative and inspiring research proposals and community service programs.
“I am very proud to have been awarded a CHEST Foundation grant and pleased that clinical research and real-world evidence are a priority to the foundation,” stated Alice Turner, MBChB, PhD. Dr. Turner was awarded the 2016 CHEST Foundation and the Alpha-1 Foundation Clinical Research Grant in Alpha-1 Antitrypsin Deficiency. “This award means that my patients can now see publicly the efforts that are being made to reduce inequities in care and ensure that the best treatments are made available in the UK.”

The award will allow Dr. Turner to compare patients who are being treated in the United States with those who are untreated in the United Kingdom and then analyze the effects on mortality, hospitalization, and quality of life to make inferences about whether or not the treatment should be implemented in the United Kingdom. Currently, the type of treatment used to treat patients with alpha-1 antitrypsin deficiency in the United States is not available in the United Kingdom, and the results of this study will be provided to the National Health Service in England to help overcome the barriers of legalizing the treatment in the United Kingdom.
Sydney Montesi, MD, was awarded the CHEST Foundation Research Grant in Pulmonary Fibrosis for her work on using noninvasive lung imaging to see how contrast agents can be used to measure disease activity and progression.
“As a provider, it can be very difficult when we first meet a patient to know what disease course they will take, but if we had this information, it would help us in determining earlier lung transplant referrals, choosing the best therapies and treatments, and ultimately lowering the mortality rate of idiopathic pulmonary fibrosis,” Dr. Montesi said of her research. “Receiving this grant is essential because it will allow us to test our hypothesis that vascular leakage is increased in patients with pulmonary fibrosis, and we will also be able to look more in depth at the comparison of patients with stable disease and those with progressive disease.”
These grants help advance the work of young investigators all over the globe. Over the last 20 years, thousands of researchers and community service volunteers have received more than $10 million in funding.
Beginning in February 2017, the Foundation will have more than a half-million dollars available in funding toward the next generation of lung health champions.
Learn more about the CHEST Foundation grant application process at chestnet.org/grants or e-mail the foundation at [email protected].
Every year, the CHEST Foundation awards more than a half-million dollars in grants to the next generation of lung health champions. February 2017 marks the start of the foundation’s next grant cycle, and we are excited to announce a new clinical research grant in Cystic Fibrosis, among many other disease-state topics. In 2016, the foundation awarded 11 CHEST members for their innovative and inspiring research proposals and community service programs.
“I am very proud to have been awarded a CHEST Foundation grant and pleased that clinical research and real-world evidence are a priority to the foundation,” stated Alice Turner, MBChB, PhD. Dr. Turner was awarded the 2016 CHEST Foundation and the Alpha-1 Foundation Clinical Research Grant in Alpha-1 Antitrypsin Deficiency. “This award means that my patients can now see publicly the efforts that are being made to reduce inequities in care and ensure that the best treatments are made available in the UK.”
The award will allow Dr. Turner to compare patients who are being treated in the United States with those who are untreated in the United Kingdom and then analyze the effects on mortality, hospitalization, and quality of life to make inferences about whether or not the treatment should be implemented in the United Kingdom. Currently, the type of treatment used to treat patients with alpha-1 antitrypsin deficiency in the United States is not available in the United Kingdom, and the results of this study will be provided to the National Health Service in England to help overcome the barriers of legalizing the treatment in the United Kingdom.
Sydney Montesi, MD, was awarded the CHEST Foundation Research Grant in Pulmonary Fibrosis for her work on using noninvasive lung imaging to see how contrast agents can be used to measure disease activity and progression.
“As a provider, it can be very difficult when we first meet a patient to know what disease course they will take, but if we had this information, it would help us in determining earlier lung transplant referrals, choosing the best therapies and treatments, and ultimately lowering the mortality rate of idiopathic pulmonary fibrosis,” Dr. Montesi said of her research. “Receiving this grant is essential because it will allow us to test our hypothesis that vascular leakage is increased in patients with pulmonary fibrosis, and we will also be able to look more in depth at the comparison of patients with stable disease and those with progressive disease.”
These grants help advance the work of young investigators all over the globe. Over the last 20 years, thousands of researchers and community service volunteers have received more than $10 million in funding.
Beginning in February 2017, the Foundation will have more than a half-million dollars available in funding toward the next generation of lung health champions.
Learn more about the CHEST Foundation grant application process at chestnet.org/grants or e-mail the foundation at [email protected].
Every year, the CHEST Foundation awards more than a half-million dollars in grants to the next generation of lung health champions. February 2017 marks the start of the foundation’s next grant cycle, and we are excited to announce a new clinical research grant in Cystic Fibrosis, among many other disease-state topics. In 2016, the foundation awarded 11 CHEST members for their innovative and inspiring research proposals and community service programs.
“I am very proud to have been awarded a CHEST Foundation grant and pleased that clinical research and real-world evidence are a priority to the foundation,” stated Alice Turner, MBChB, PhD. Dr. Turner was awarded the 2016 CHEST Foundation and the Alpha-1 Foundation Clinical Research Grant in Alpha-1 Antitrypsin Deficiency. “This award means that my patients can now see publicly the efforts that are being made to reduce inequities in care and ensure that the best treatments are made available in the UK.”
The award will allow Dr. Turner to compare patients who are being treated in the United States with those who are untreated in the United Kingdom and then analyze the effects on mortality, hospitalization, and quality of life to make inferences about whether or not the treatment should be implemented in the United Kingdom. Currently, the type of treatment used to treat patients with alpha-1 antitrypsin deficiency in the United States is not available in the United Kingdom, and the results of this study will be provided to the National Health Service in England to help overcome the barriers of legalizing the treatment in the United Kingdom.
Sydney Montesi, MD, was awarded the CHEST Foundation Research Grant in Pulmonary Fibrosis for her work on using noninvasive lung imaging to see how contrast agents can be used to measure disease activity and progression.
“As a provider, it can be very difficult when we first meet a patient to know what disease course they will take, but if we had this information, it would help us in determining earlier lung transplant referrals, choosing the best therapies and treatments, and ultimately lowering the mortality rate of idiopathic pulmonary fibrosis,” Dr. Montesi said of her research. “Receiving this grant is essential because it will allow us to test our hypothesis that vascular leakage is increased in patients with pulmonary fibrosis, and we will also be able to look more in depth at the comparison of patients with stable disease and those with progressive disease.”
These grants help advance the work of young investigators all over the globe. Over the last 20 years, thousands of researchers and community service volunteers have received more than $10 million in funding.
Beginning in February 2017, the Foundation will have more than a half-million dollars available in funding toward the next generation of lung health champions.
Learn more about the CHEST Foundation grant application process at chestnet.org/grants or e-mail the foundation at [email protected].
This Month in CHEST: Editor’s Picks
E
GOLD 2017: A New Report
By Dr. P. J. Barnes
Original Research
Long-term Outcomes of Patients With Ground-Glass Opacities Detected Using CT Scanning. By Dr. S. Sawada, et al.
ICU Telemedicine Program Financial Outcomes. By Dr. C. M. Lilly et al.
Accuracy of Lung Ultrasonography in the Diagnosis of Pneumonia in Adults: Systematic Review and Meta-Analysis. By Dr. A. M. Llamas-Álvarez, et al.
Evidence-based Medicine
Cough in the Athlete: CHEST Guideline and Expert Panel Report. By Dr. L-P Boulet, et al, on behalf of the CHEST Expert Cough Panel.
E
GOLD 2017: A New Report
By Dr. P. J. Barnes
Original Research
Long-term Outcomes of Patients With Ground-Glass Opacities Detected Using CT Scanning. By Dr. S. Sawada, et al.
ICU Telemedicine Program Financial Outcomes. By Dr. C. M. Lilly et al.
Accuracy of Lung Ultrasonography in the Diagnosis of Pneumonia in Adults: Systematic Review and Meta-Analysis. By Dr. A. M. Llamas-Álvarez, et al.
Evidence-based Medicine
Cough in the Athlete: CHEST Guideline and Expert Panel Report. By Dr. L-P Boulet, et al, on behalf of the CHEST Expert Cough Panel.
E
GOLD 2017: A New Report
By Dr. P. J. Barnes
Original Research
Long-term Outcomes of Patients With Ground-Glass Opacities Detected Using CT Scanning. By Dr. S. Sawada, et al.
ICU Telemedicine Program Financial Outcomes. By Dr. C. M. Lilly et al.
Accuracy of Lung Ultrasonography in the Diagnosis of Pneumonia in Adults: Systematic Review and Meta-Analysis. By Dr. A. M. Llamas-Álvarez, et al.
Evidence-based Medicine
Cough in the Athlete: CHEST Guideline and Expert Panel Report. By Dr. L-P Boulet, et al, on behalf of the CHEST Expert Cough Panel.
Meet the CHEST President-Designate
Clayton T. Cowl, MD, FCCP, is the CHEST President-Designate and sits as a member of the Board of Regents. Dr. Cowl’s presidential term will be 2018-2019. He currently is the Chair of the Division of Preventive, Occupational, and Aerospace Medicine with a joint appointment in the Division of Pulmonary and Critical Care Medicine at Mayo Clinic in Rochester, Minnesota.
Dr. Cowl is triple board-certified in Pulmonary and Critical Care Medicine, Occupational Medicine, and Internal Medicine, with an interest in airway disorders, occupational-related respiratory health, toxicology, altitude physiology, and transportation medicine.
His research focus has included projects in altitude physiology at Mayo Clinic’s altitude chamber and testing for the emergency oxygen passenger mask in the Boeing 787 airliner. He has also published in the areas of occupational asthma and toxic inhalations.

He is currently the President of the Civil Aviation Medical Association and is a Senior Aviation Medical Examiner designated by the Federal Aviation Administration.
Dr. Cowl has been a recipient of the Innovation in Education Award from the Mayo School of Continuous Professional Development, and the Laureate Award in the Mayo Clinic Department of Medicine.
Clayton T. Cowl, MD, FCCP, is the CHEST President-Designate and sits as a member of the Board of Regents. Dr. Cowl’s presidential term will be 2018-2019. He currently is the Chair of the Division of Preventive, Occupational, and Aerospace Medicine with a joint appointment in the Division of Pulmonary and Critical Care Medicine at Mayo Clinic in Rochester, Minnesota.
Dr. Cowl is triple board-certified in Pulmonary and Critical Care Medicine, Occupational Medicine, and Internal Medicine, with an interest in airway disorders, occupational-related respiratory health, toxicology, altitude physiology, and transportation medicine.
His research focus has included projects in altitude physiology at Mayo Clinic’s altitude chamber and testing for the emergency oxygen passenger mask in the Boeing 787 airliner. He has also published in the areas of occupational asthma and toxic inhalations.
He is currently the President of the Civil Aviation Medical Association and is a Senior Aviation Medical Examiner designated by the Federal Aviation Administration.
Dr. Cowl has been a recipient of the Innovation in Education Award from the Mayo School of Continuous Professional Development, and the Laureate Award in the Mayo Clinic Department of Medicine.
Clayton T. Cowl, MD, FCCP, is the CHEST President-Designate and sits as a member of the Board of Regents. Dr. Cowl’s presidential term will be 2018-2019. He currently is the Chair of the Division of Preventive, Occupational, and Aerospace Medicine with a joint appointment in the Division of Pulmonary and Critical Care Medicine at Mayo Clinic in Rochester, Minnesota.
Dr. Cowl is triple board-certified in Pulmonary and Critical Care Medicine, Occupational Medicine, and Internal Medicine, with an interest in airway disorders, occupational-related respiratory health, toxicology, altitude physiology, and transportation medicine.
His research focus has included projects in altitude physiology at Mayo Clinic’s altitude chamber and testing for the emergency oxygen passenger mask in the Boeing 787 airliner. He has also published in the areas of occupational asthma and toxic inhalations.
He is currently the President of the Civil Aviation Medical Association and is a Senior Aviation Medical Examiner designated by the Federal Aviation Administration.
Dr. Cowl has been a recipient of the Innovation in Education Award from the Mayo School of Continuous Professional Development, and the Laureate Award in the Mayo Clinic Department of Medicine.
Transgender Patients: Providing Sensitive Care
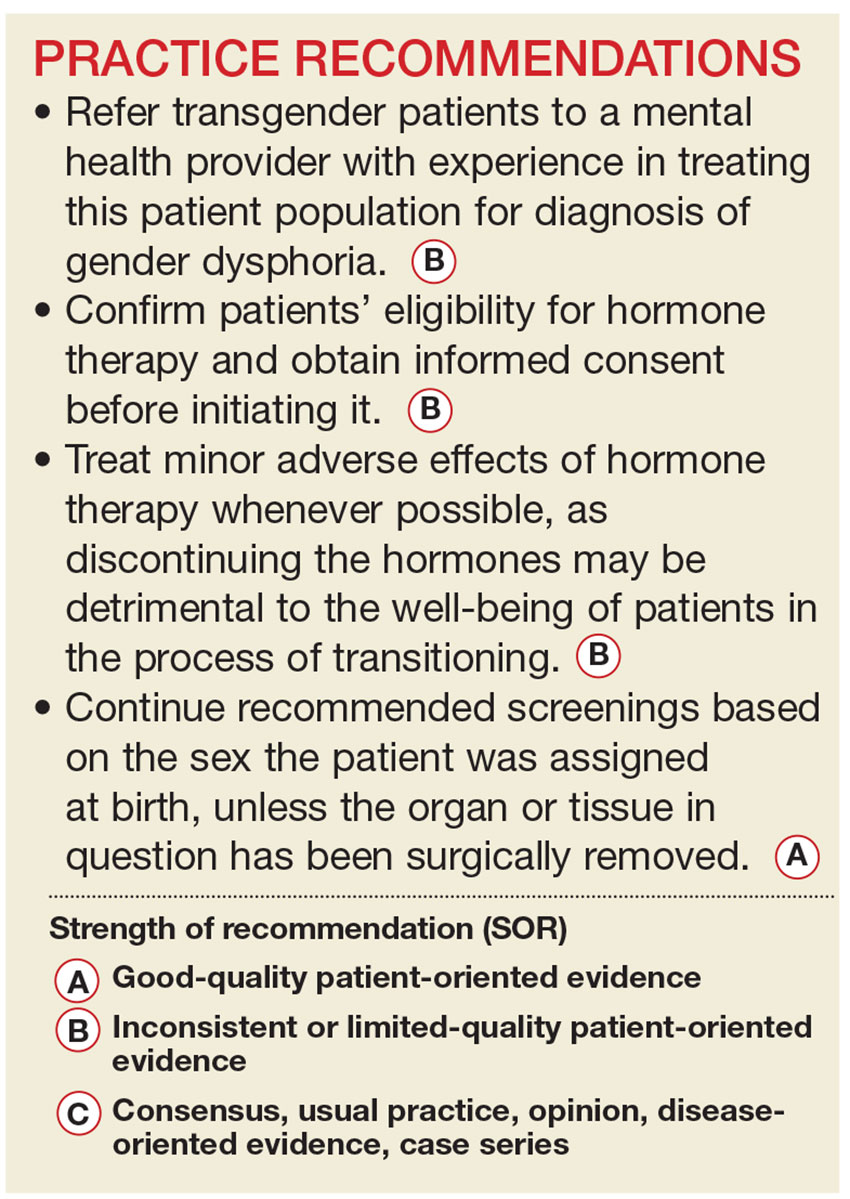
Civil rights for the lesbian, gay, bisexual, and transgender population have advanced markedly in the past decade, and the medical community has gradually begun to address more of their health concerns. More recently, media attention to transgender individuals has encouraged many more to openly seek care.1,2
It is estimated that anywhere from 0.3% to 5% of the US population identifies as transgender.1-3 While awareness of this population has slowly increased, there is a paucity of research on the hormone treatment that is often essential to patients’ well-being. Studies of surgical options for transgender patients have been minimal, as well.
Primary care providers are uniquely positioned to coordinate medical services and ensure continuity of care for transgender patients as they strive to become their authentic selves. Our goal in writing this article is to equip you with the tools to provide this patient population with sensitive, high-quality care (see Table 1).4-7 Our focus is on the diagnosis of gender dysphoria (GD) and its medical and hormonal management—the realm of primary care providers. We briefly discuss surgical management of GD, as well.
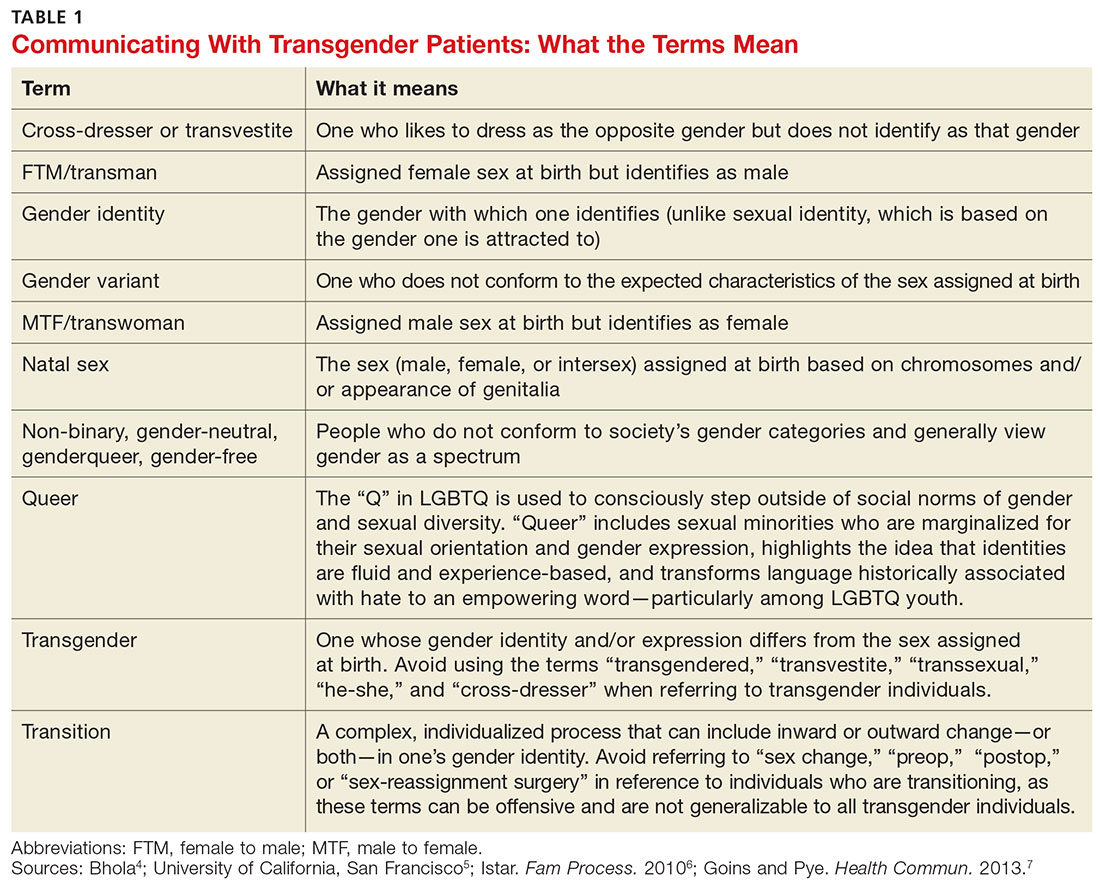
UNDERSTANDING AND DIAGNOSING GENDER DYSPHORIA
Two classification systems are used for diagnoses related to GD: the Diagnostic and Statistical Manual of Mental Disorders, Fifth Ed (DSM-5)8 and the International Classification of Diseases, 10th Rev (ICD-10).9
ICD-10 criteria use the term gender identity disorder; DSM-5 refers to gender dysphoria instead. It is important to emphasize that these classification systems represent an attempt to categorize a group of signs and symptoms that lead to distress for the patient and are not meant to suggest that being transgender is pathological. In fact, in DSM-5—released in 2013—the American Psychiatric Association revised the terminology to emphasize that such individuals are not “disordered” by the nature of their identity, but rather by the distress that being transgender causes.8
For a diagnosis of GD in children, DSM-5 criteria include characteristics perceived to be incongruent between the child’s sex at birth and the self-identified gender based on preferred activities or dislike of his or her own sexual anatomy. The child must meet six or more of the following for at least six months
- A repeatedly stated desire to be, or insistence that he or she is, of the other gender
- In boys, a preference for cross-dressing or simulating female attire; in girls, insistence on wearing only stereotypical masculine clothing
- Strong and persistent preferences for cross-gender roles in make-believe play or fantasy
- A strong rejection of toys/games typically associated with the child’s sex
- Intense desire to participate in stereotypical games and pastimes of the other gender
- Strong preference for playmates of the other gender
- A strong dislike of one’s sexual anatomy
- A strong desire for the primary (eg, penis or vagina) or secondary (eg, menstruation) sex characteristics of the other gender.8
Adolescents and adults must meet two or more of the following for at least six months
- A noticeable incongruence between the gender that the patient sees themselves as and their sex characteristics
- An intense need to do away with (or prevent) his or her primary or secondary sex features
- An intense desire to have the primary and/or secondary sex features of the other gender
- A deep desire to transform into another gender
- A profound need for society to treat them as someone of the other gender
- A powerful assurance of having the characteristic feelings and responses of the other gender.8
For children as well as adolescents and adults, the condition should cause the patient significant distress or significantly affect him or her socially, at work or school, and in other important areas of life.8
Is the patient a candidate for hormone therapy?
Two primary sources—Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7, issued by the World Professional Association for Transgender Health (WPATH)10 and Endocrine Treatment of Transsexual Persons11 by the Endocrine Society—offer clinical practice guidance based on evidence and expert opinion.
WPATH recommends that a mental health professional (MHP) experienced in transgender care diagnose GD to ensure that it is not mistaken for a psychiatric condition manifesting as altered gender identity. However, if no one with such experience is available or accessible in the region, it is reasonable for a primary care provider to make the diagnosis and consider initiating hormone therapy without a mental health referral,12 as the expected benefits outweigh the risks of nontreatment.13
Whether or not an MHP confirms a diagnosis of GD, it is still up to the treating provider to confirm the patient’s eligibility and readiness for hormone therapy: He or she should meet DSM-5 or ICD-10 criteria for GD, have no psychiatric comorbidity (eg, schizophrenia, body dysmorphic disorder, or uncontrolled bipolar disorder) likely to interfere with treatment, understand the expected outcomes and the social benefits and risks, and have indicated a willingness to take the hormones responsibly.
Historically, patients were required to have a documented real-life experience, defined as having fully adopted the new gender role in everyday life for at least three months.10,11 This model has fallen out of favor, however, as it is unsupported by evidence and may place transgender individuals at physical and emotional risk. Instead, readiness is confirmed by obtaining informed consent.12
Puberty may be suppressed with a gonadotropin-releasing hormone (GnRH) agonist in adolescents who have a GD diagnosis and are at Tanner stage 2 to 3 of puberty until age 16. At that point, hormone therapy consistent with their gender identification may be initiated (see “How to Help Transgender Teens”).11

Beginning the transition
The transitioning process is a complex and individualized journey that can include inward or outward change, or both.
For patients interested in medical interventions, possible therapies include cross-sex hormone administration and gender-affirming surgery. Both are aimed at making the physical and the psychologic more congruent. Hormone treatment (see Table 2) is often essential to reduce the distress of individuals with GD and to help them feel comfortable in their own body.10,11,21 Psychologic conditions, such as depression, tend to improve as the transitioning process gets underway.22
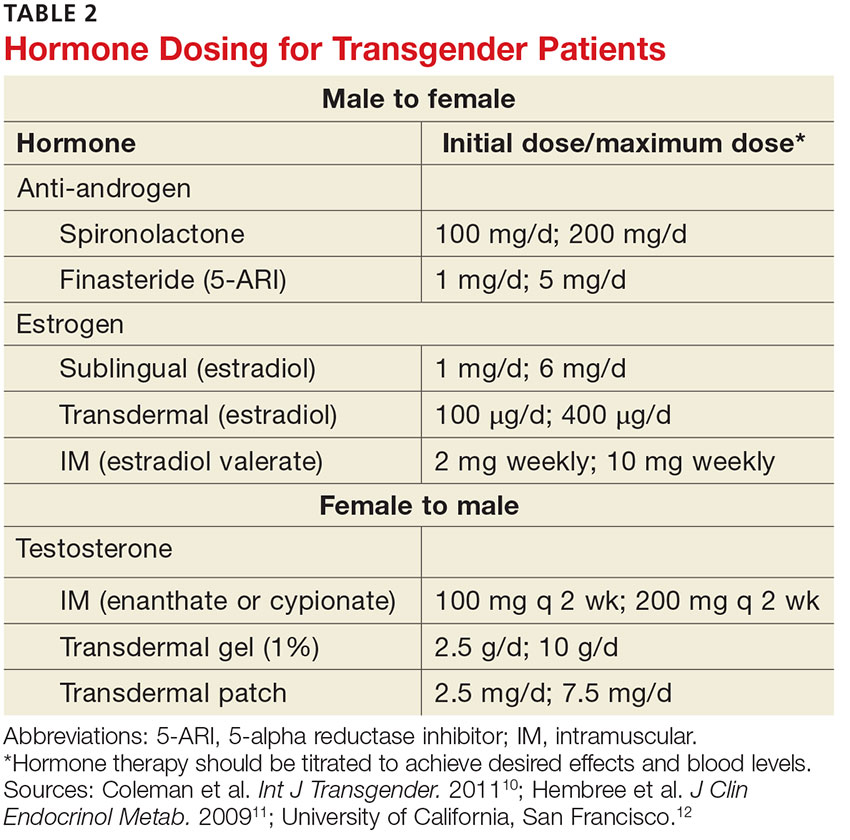
FEMALE-TO-MALE TRANSITION
CASE 1 Jennie R, a 55-year-old postmenopausal patient, comes to your office for an annual exam. Although you’ve been her primary care provider for several years, she confides for the first time that she has never been comfortable as a woman. “I’ve always felt that my body didn’t belong to me,” the patient admits, and goes on to say that for the past several years she has been living as a man. Jennie R says she is ready to start hormone therapy to assist with the gender transition and asks about the process, the benefits and risks, and how quickly she can expect to achieve the desired results.
If Jennie R were your patient, how would you respond?
Masculinizing hormone treatment
As you would explain to a patient like Jennie R, the goal of hormone therapy is to suppress the effects of the sex assigned at birth and replace them with those of the desired gender. In the case of a female transitioning to a male (known as a transman), masculinizing hormones would promote growth of facial and body hair, cessation of menses, increased muscle mass, deepening of the voice, and clitoral enlargement.
Physical changes induced by masculinizing hormone therapy have an expected onset of one to six months and achieve maximum effect in approximately two to five years.10,11 Although there have been no controlled clinical trials evaluating the safety or efficacy of any transitional hormone regimen, WPATH and the Center of Excellence for Transgender Health at the University of California, San Francisco, suggest initiating intramuscular or transdermal testosterone at increasing doses until normal physiologic male testosterone levels between 350 and 700 ng/dL are achieved, or until cessation of menses.13,25-28 The dose at which either, or both, occur should be continued as long-term maintenance therapy. Medroxyprogesterone can be added, if necessary for menstrual cessation, and a GnRH agonist or endometrial ablation can be used for refractory uterine bleeding.29,30
Testosterone is not a contraceptive. It is important to emphasize to transmen like Jennie that they remain at risk for pregnancy if they are having sex with fertile males. Caution patients not to assume that the possibility of pregnancy ends when menses stop.
Treat minor adverse effects. Adverse effects of masculinizing hormones include vaginal atrophy, fat redistribution and weight gain, polycythemia, acne, scalp hair loss, sleep apnea, elevated liver enzymes, hyperlipidemia, cardiovascular disease, diabetes, and bone density loss. Increased risk for cancer of the female organs has not been proven.10,11 It is reasonable to treat minor adverse effects after reviewing the risks/benefits of doing so, as discontinuing hormone therapy could be detrimental to the well-being of transitioning patients.11
There are absolute contraindications to masculinizing hormone therapy, however, including pregnancy, unstable coronary artery disease, and untreated polycythemia with a hematocrit > 55%.10
Monitoring is essential. Patients receiving masculinizing hormone therapy should be monitored every three months during the first year and once or twice a year thereafter, with a focused history (including mood symptoms), physical exam (including weight and blood pressure), and labs (including complete blood count, liver function, renal function, and lipids) at each visit.11,23 Some clinicians also check estradiol levels until they fall below 50 pg/mL,23,27 while others take the cessation of uterine bleeding for > 6 months as an indicator of estrogen suppression.
Preventive health measures continue. Routine screening should continue, based on the patient’s assigned sex at birth. Thus, a transman who has not had a hysterectomy still needs Pap smears, mammograms if the patient has not had a double mastectomy, and bone mineral density (BMD) testing to screen for osteoporosis.31,32 Some experts recommend starting to test BMD at age 50 for patients receiving masculinizing hormones, given the unknown effect of testosterone on bone density.11,31,32
CASE 1 The first question for a transgender patient is about his or her current gender identity, but Jennie R has already reported living as a man. So you start by asking “What name do you prefer to use?” and “Do you prefer to be referred to with male or female pronouns?”
The patient tells you that he sees himself as a man, he wants to be called Jeff, and he prefers male pronouns. You explain that you believe he has gender dysphoria and would benefit from hormone therapy, but it is important to confirm this diagnosis with an MHP. You explain that testosterone can be prescribed for masculinizing effects, and describe the expected effects—more facial and body hair, a deeper voice, and greater muscle mass, among others—and review the likely time frame.
You also discuss the risks of masculinizing hormones (hyperlipidemia, cardiovascular disease, diabetes, and loss of bone density) that will need to be monitored. Before he leaves, you give him the name of an MHP who is experienced in transgender care and tell him to make a follow-up appointment with you after he has seen her. At the conclusion of the visit, you make a note of the patient’s name and gender identity in the chart and inform the staff of the changes.
MALE-TO-FEMALE TRANSITION
CASE 2 Before heading into your office to talk to a new patient named Carl S, you glance at his chart and see that he is a healthy 21-year-old who has come in for a routine physical. When you enter the room, you find Carl wearing a dress, heels, and make-up. After confirming that you have the right patient, you ask, “What is your current gender identity?” “Female,” says Carl, who indicates that she now goes by Carol. The patient has no medical problems, surgical history, or significant family history but reports that she has been taking spironolactone and estrogen for the past three years. Carol also says she has a new female partner and is having unprotected sexual activity.
Feminizing hormone treatment
The desired effects of feminizing hormones include voice change, decreased hair growth, breast growth, body fat redistribution, decreased muscle mass, skin softening, decreased oiliness of skin and hair, and a decrease in spontaneous erections, testicular volume, and sperm production.10,11 The onset of feminizing effects ranges from one month to one year and the expected maximum effect occurs anywhere between three months and five years.10,11 Regimens usually include anti-androgen agents and estrogen.13,26-28
The medications that have been most studied with anti-androgenic effects include spironolactone and 5-α reductase inhibitors (5-ARIs) such as finasteride. Spironolactone inhibits testosterone secretion and inhibits androgen binding to androgen receptors; 5-ARIs block the conversion of testosterone to 5-α-dihydrotestosterone, the more active form.
Estrogen can be administered via oral, sublingual, transdermal, or intramuscular route, but parenteral formulations are preferred to avoid first-pass metabolism. The serum estradiol target is similar to the mean daily level of premenopausal women (< 200 pg/mL) and the level of testosterone should be in the normal female range (< 55 ng/dL).13,26-28
The selection of medications should be individualized for each patient. Comorbidities must be considered, as well as the risk for adverse effects, which include venous thromboembolism, elevated liver enzymes, breast cancer, cardiovascular disease, diabetes, hyperprolactinemia, weight gain, gallstones, cerebrovascular disease, and severe migraine headaches.10,11 Estrogen therapy is not reported to induce hypertrophy or premalignant changes in the prostate.33 As is the case for masculinizing hormones, feminizing hormone therapy should be continued indefinitely for long-term effects.
Frequent monitoring is recommended. Patients taking feminizing hormones (transwomen) should be seen every two to three months in the first year and monitored once or twice a year thereafter. Serum testosterone and estradiol levels should initially be monitored every three months; serum electrolytes, specifically potassium, should be monitored every two to three months in the first year until stable.
CASE 2 You recommend that Carol S be screened annually for sexually transmitted diseases, as you would for any 21-year-old patient. You point out, too, that while estrogen and androgen-suppressing therapy decrease sperm production, there is a possibility that the patient could impregnate a female partner and recommend that contraception be used if the couple is not trying to conceive.
You also discuss the risks and benefits of hormone therapy and reasonable expectations of continued treatment. You ask Carol to schedule a follow-up visit in six months, as her hormone regimen is stable. Finally, if the patient remains on hormone therapy, you mention that the only screening unique to men transitioning to women is for breast cancer, which should begin at age 40 to 50 (as it should for all women).
Gender-affirming surgical options
Surgical management of transgender patients is not within the scope of family medicine. But it is essential to know what procedures are available, as you may have occasion to advocate for patients during the surgical referral process and possibly to provide postoperative care.
For transmen, surgical options include chest reconstruction, hysterectomy/oophorectomy, metoidioplasty (using the clitoris to surgically approximate a penis), phalloplasty, scrotoplasty, urethroplasty, and vaginectomy.10,34 The surgeries available for transwomen are orchiectomy, vaginoplasty, penectomy, breast augmentation, thyroid chondroplasty and voice surgery, and facial feminization.10,34 Keep in mind that not all transgender individuals desire surgery as part of the transitioning process.
The authors would like to acknowledge the assistance of Michelle Forcier, MD, MPH, and Karen S. Bernstein, MD, MPH, in the preparation of this manuscript.
1. Pew Research Center. A survey of LGBT Americans: attitudes, experiences and values in changing times. www.pewsocialtrends.org/2013/06/13/a-survey-of-lgbt-americans. Accessed January 13, 2017.
2. Gates GJ. How many people are lesbian, gay, bisexual and transgender? http://williamsinstitute.law.ucla.edu/wp-content/uploads/Gates-How-Many-People-LGBT-Apr-2011.pdf. Accessed January 13, 2017.
3. van Kesteren PJ, Gooren LJ, Megens JA. An epidemiological and demographic study of transsexuals in The Netherlands. Arch Sex Behav. 1996;25:589-600.
4. Bhola S. An ally’s guide to terminology: talking about LGBT people & equality. www.glaad.org/2011/07/28/an-allys-guide-to-terminology-talking-about-lgbt-people-equality. Accessed January 13, 2017.
5. University of California, San Francisco. Transgender terminology. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/tcoe?page=protocol-terminology. Accessed January 13, 2017.
6. Istar A. How queer! The development of gender identity and sexual orientation in LGBTQ-headed families. Fam Process. 2010;49:268-290.
7. Goins ES, Pye D. Check the box that best describes you: reflexively managing theory and praxis in LGBTQ health communication research. Health Commun. 2013;28:397-407.
8. American Psychiatric Association. Gender dysphoria. Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Washington, DC: American Psychiatric Association; 2013: 451-459.
9. World Health Organization. The International Classification of Diseases, 10th rev. Classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. 1992; Geneva.
10. Coleman E, Bockting W, Botzer M, et al; World Professional Association for Transgender Health. Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7. Int J Transgender. 2011; 13:165-232.
11. Hembree WC, Cohen-Kettenis P, Delemarre-van de Waal HA, et al. Endocrine treatment of transsexual persons: an Endocrine Society clinical practice guideline. J Clin Endo Metabol. 2009;94:3132-3154.
12. University of California, San Francisco. Assessing readiness for hormones. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/tcoe?page=protocol-hormone-ready. Accessed January 13, 2017.
13. Gooren L. Hormone treatment of the adult transsexual patient. Horm Res. 2005;64(suppl 2):S31-S36.
14. Hembree WC. Guidelines for pubertal suspension and gender reassignment for transgender adolescents. Child Adolesc Psychiatr Clin N Am. 2011;20:725-732.
15. Gay, Lesbian, and Straight Education Network (GLSEN). Harsh realities. The experiences of transgender youth in our nation’s schools. www.glsen.org/sites/default/files/Harsh%20Realities.pdf. Accessed January 13, 2017.
16. Berman M, Balingit M. Eleven states sue Obama administration over bathroom guidance for transgender students. May 25, 2016. Washington Post. www.washingtonpost.com/news/post-nation/wp/2016/05/25/texas-governor-says-state-will-sue-obama-administration-over-bathroom-directive/. Accessed January 13, 2017.
17. de Vries AL, Cohen-Kettenis PT, Delemarre-van de Waal H. Clinical management of gender dysphoria in adolescents. 2006. Vancouver Coastal Health - Transgender Health Program. www.amsa.org/wp-content/uploads/2015/04/CaringForTransgenderAdolescents.pdf. Accessed January 13, 2017.
18. TransYouth Family Allies. Empowering transgender youth & families. www.imatyfa.org/. Accessed January 13, 2017.
19. Human Rights Campaign. On our own: a survival guide for independent LGBTQ youth. www.hrc.org/resources/on-our-own-a-survival-guide-for-independent-lgbtq-youth. Accessed January 13, 2017.
20. Gay, Lesbian, Bisexual, and Transgender National Help Center. www.glbthotline.org. Accessed January 13, 2017.
21. University of California, San Francisco. Hormone administration. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/trans?page=protocol-hormones. Accessed January 13, 2017.
22. Gorin-Lazard A, Baumstarck K, Boyer L, et al. Hormonal therapy is associated with better self-esteem, mood, and quality of life in transsexuals. J Nerv Ment Dis. 2013;201:996-1000.
23. Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in adult men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2006;91:1995-2010.
24. Boloña ER, Uraga MV, Haddad RM, et al. Testosterone use in men with sexual dysfunction: a systematic review and meta-analysis of randomized placebo-controlled trials. Mayo Clin Proc. 2007;82:20-28.
25. Gooren LJ, Giltay EJ. Review of studies of androgen treatment of female-to-male transsexuals: effects and risks of administration of androgens to females. J Sex Med. 2008; 5:765-776.
26. Levy A, Crown A, Reid R. Endocrine intervention for transsexuals. Clin Endocrinol (Oxf). 2003;59:409-418.
27. Moore E, Wisniewski A, Dobs A. Endocrine treatment of transsexual people: a review of treatment regimens, outcomes, and adverse effects. J Clin Endocrinol Metab. 2003;88:3467-3473.
28. Tangpricha V, Ducharme SH, Barber TW, et al. Endocrinologic treatment of gender identity disorders. Endocr Pract. 2003;9:12-21.
29. Dickersin K, Munro MG, Clark M, et al. Hysterectomy compared with endometrial ablation for dysfunctional uterine bleeding: a randomized controlled trial. Obstet Gynecol. 2007;110:1279-1289.
30. Prasad P, Powell MC. Prospective observational study of Thermablate Endometrial Ablation System as an outpatient procedure. J Minim Invasive Gynecol. 2008;15:476-479.
31. University of California, San Francisco. General prevention and screening. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/trans?page=protocol-screening. Accessed January 13, 2017.
32. Ganly I, Taylor EW. Breast cancer in a trans-sexual man receiving hormone replacement therapy. Br J Surg. 1995; 82:341.
33. Meriggiola MC, Gava G. Endocrine care of transpeople part II: a review of cross-sex hormonal treatments, outcomes and adverse effects in transwomen. Clin Endocrinol (Oxf). 2015;83:607-615.
34. University of California, San Francisco. Surgical options. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/trans?page=protocol-surgery. Accessed January 13, 2017.
Civil rights for the lesbian, gay, bisexual, and transgender population have advanced markedly in the past decade, and the medical community has gradually begun to address more of their health concerns. More recently, media attention to transgender individuals has encouraged many more to openly seek care.1,2
It is estimated that anywhere from 0.3% to 5% of the US population identifies as transgender.1-3 While awareness of this population has slowly increased, there is a paucity of research on the hormone treatment that is often essential to patients’ well-being. Studies of surgical options for transgender patients have been minimal, as well.
Primary care providers are uniquely positioned to coordinate medical services and ensure continuity of care for transgender patients as they strive to become their authentic selves. Our goal in writing this article is to equip you with the tools to provide this patient population with sensitive, high-quality care (see Table 1).4-7 Our focus is on the diagnosis of gender dysphoria (GD) and its medical and hormonal management—the realm of primary care providers. We briefly discuss surgical management of GD, as well.
UNDERSTANDING AND DIAGNOSING GENDER DYSPHORIA
Two classification systems are used for diagnoses related to GD: the Diagnostic and Statistical Manual of Mental Disorders, Fifth Ed (DSM-5)8 and the International Classification of Diseases, 10th Rev (ICD-10).9
ICD-10 criteria use the term gender identity disorder; DSM-5 refers to gender dysphoria instead. It is important to emphasize that these classification systems represent an attempt to categorize a group of signs and symptoms that lead to distress for the patient and are not meant to suggest that being transgender is pathological. In fact, in DSM-5—released in 2013—the American Psychiatric Association revised the terminology to emphasize that such individuals are not “disordered” by the nature of their identity, but rather by the distress that being transgender causes.8
For a diagnosis of GD in children, DSM-5 criteria include characteristics perceived to be incongruent between the child’s sex at birth and the self-identified gender based on preferred activities or dislike of his or her own sexual anatomy. The child must meet six or more of the following for at least six months
- A repeatedly stated desire to be, or insistence that he or she is, of the other gender
- In boys, a preference for cross-dressing or simulating female attire; in girls, insistence on wearing only stereotypical masculine clothing
- Strong and persistent preferences for cross-gender roles in make-believe play or fantasy
- A strong rejection of toys/games typically associated with the child’s sex
- Intense desire to participate in stereotypical games and pastimes of the other gender
- Strong preference for playmates of the other gender
- A strong dislike of one’s sexual anatomy
- A strong desire for the primary (eg, penis or vagina) or secondary (eg, menstruation) sex characteristics of the other gender.8
Adolescents and adults must meet two or more of the following for at least six months
- A noticeable incongruence between the gender that the patient sees themselves as and their sex characteristics
- An intense need to do away with (or prevent) his or her primary or secondary sex features
- An intense desire to have the primary and/or secondary sex features of the other gender
- A deep desire to transform into another gender
- A profound need for society to treat them as someone of the other gender
- A powerful assurance of having the characteristic feelings and responses of the other gender.8
For children as well as adolescents and adults, the condition should cause the patient significant distress or significantly affect him or her socially, at work or school, and in other important areas of life.8
Is the patient a candidate for hormone therapy?
Two primary sources—Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7, issued by the World Professional Association for Transgender Health (WPATH)10 and Endocrine Treatment of Transsexual Persons11 by the Endocrine Society—offer clinical practice guidance based on evidence and expert opinion.
WPATH recommends that a mental health professional (MHP) experienced in transgender care diagnose GD to ensure that it is not mistaken for a psychiatric condition manifesting as altered gender identity. However, if no one with such experience is available or accessible in the region, it is reasonable for a primary care provider to make the diagnosis and consider initiating hormone therapy without a mental health referral,12 as the expected benefits outweigh the risks of nontreatment.13
Whether or not an MHP confirms a diagnosis of GD, it is still up to the treating provider to confirm the patient’s eligibility and readiness for hormone therapy: He or she should meet DSM-5 or ICD-10 criteria for GD, have no psychiatric comorbidity (eg, schizophrenia, body dysmorphic disorder, or uncontrolled bipolar disorder) likely to interfere with treatment, understand the expected outcomes and the social benefits and risks, and have indicated a willingness to take the hormones responsibly.
Historically, patients were required to have a documented real-life experience, defined as having fully adopted the new gender role in everyday life for at least three months.10,11 This model has fallen out of favor, however, as it is unsupported by evidence and may place transgender individuals at physical and emotional risk. Instead, readiness is confirmed by obtaining informed consent.12
Puberty may be suppressed with a gonadotropin-releasing hormone (GnRH) agonist in adolescents who have a GD diagnosis and are at Tanner stage 2 to 3 of puberty until age 16. At that point, hormone therapy consistent with their gender identification may be initiated (see “How to Help Transgender Teens”).11
Beginning the transition
The transitioning process is a complex and individualized journey that can include inward or outward change, or both.
For patients interested in medical interventions, possible therapies include cross-sex hormone administration and gender-affirming surgery. Both are aimed at making the physical and the psychologic more congruent. Hormone treatment (see Table 2) is often essential to reduce the distress of individuals with GD and to help them feel comfortable in their own body.10,11,21 Psychologic conditions, such as depression, tend to improve as the transitioning process gets underway.22
FEMALE-TO-MALE TRANSITION
CASE 1 Jennie R, a 55-year-old postmenopausal patient, comes to your office for an annual exam. Although you’ve been her primary care provider for several years, she confides for the first time that she has never been comfortable as a woman. “I’ve always felt that my body didn’t belong to me,” the patient admits, and goes on to say that for the past several years she has been living as a man. Jennie R says she is ready to start hormone therapy to assist with the gender transition and asks about the process, the benefits and risks, and how quickly she can expect to achieve the desired results.
If Jennie R were your patient, how would you respond?
Masculinizing hormone treatment
As you would explain to a patient like Jennie R, the goal of hormone therapy is to suppress the effects of the sex assigned at birth and replace them with those of the desired gender. In the case of a female transitioning to a male (known as a transman), masculinizing hormones would promote growth of facial and body hair, cessation of menses, increased muscle mass, deepening of the voice, and clitoral enlargement.
Physical changes induced by masculinizing hormone therapy have an expected onset of one to six months and achieve maximum effect in approximately two to five years.10,11 Although there have been no controlled clinical trials evaluating the safety or efficacy of any transitional hormone regimen, WPATH and the Center of Excellence for Transgender Health at the University of California, San Francisco, suggest initiating intramuscular or transdermal testosterone at increasing doses until normal physiologic male testosterone levels between 350 and 700 ng/dL are achieved, or until cessation of menses.13,25-28 The dose at which either, or both, occur should be continued as long-term maintenance therapy. Medroxyprogesterone can be added, if necessary for menstrual cessation, and a GnRH agonist or endometrial ablation can be used for refractory uterine bleeding.29,30
Testosterone is not a contraceptive. It is important to emphasize to transmen like Jennie that they remain at risk for pregnancy if they are having sex with fertile males. Caution patients not to assume that the possibility of pregnancy ends when menses stop.
Treat minor adverse effects. Adverse effects of masculinizing hormones include vaginal atrophy, fat redistribution and weight gain, polycythemia, acne, scalp hair loss, sleep apnea, elevated liver enzymes, hyperlipidemia, cardiovascular disease, diabetes, and bone density loss. Increased risk for cancer of the female organs has not been proven.10,11 It is reasonable to treat minor adverse effects after reviewing the risks/benefits of doing so, as discontinuing hormone therapy could be detrimental to the well-being of transitioning patients.11
There are absolute contraindications to masculinizing hormone therapy, however, including pregnancy, unstable coronary artery disease, and untreated polycythemia with a hematocrit > 55%.10
Monitoring is essential. Patients receiving masculinizing hormone therapy should be monitored every three months during the first year and once or twice a year thereafter, with a focused history (including mood symptoms), physical exam (including weight and blood pressure), and labs (including complete blood count, liver function, renal function, and lipids) at each visit.11,23 Some clinicians also check estradiol levels until they fall below 50 pg/mL,23,27 while others take the cessation of uterine bleeding for > 6 months as an indicator of estrogen suppression.
Preventive health measures continue. Routine screening should continue, based on the patient’s assigned sex at birth. Thus, a transman who has not had a hysterectomy still needs Pap smears, mammograms if the patient has not had a double mastectomy, and bone mineral density (BMD) testing to screen for osteoporosis.31,32 Some experts recommend starting to test BMD at age 50 for patients receiving masculinizing hormones, given the unknown effect of testosterone on bone density.11,31,32
CASE 1 The first question for a transgender patient is about his or her current gender identity, but Jennie R has already reported living as a man. So you start by asking “What name do you prefer to use?” and “Do you prefer to be referred to with male or female pronouns?”
The patient tells you that he sees himself as a man, he wants to be called Jeff, and he prefers male pronouns. You explain that you believe he has gender dysphoria and would benefit from hormone therapy, but it is important to confirm this diagnosis with an MHP. You explain that testosterone can be prescribed for masculinizing effects, and describe the expected effects—more facial and body hair, a deeper voice, and greater muscle mass, among others—and review the likely time frame.
You also discuss the risks of masculinizing hormones (hyperlipidemia, cardiovascular disease, diabetes, and loss of bone density) that will need to be monitored. Before he leaves, you give him the name of an MHP who is experienced in transgender care and tell him to make a follow-up appointment with you after he has seen her. At the conclusion of the visit, you make a note of the patient’s name and gender identity in the chart and inform the staff of the changes.
MALE-TO-FEMALE TRANSITION
CASE 2 Before heading into your office to talk to a new patient named Carl S, you glance at his chart and see that he is a healthy 21-year-old who has come in for a routine physical. When you enter the room, you find Carl wearing a dress, heels, and make-up. After confirming that you have the right patient, you ask, “What is your current gender identity?” “Female,” says Carl, who indicates that she now goes by Carol. The patient has no medical problems, surgical history, or significant family history but reports that she has been taking spironolactone and estrogen for the past three years. Carol also says she has a new female partner and is having unprotected sexual activity.
Feminizing hormone treatment
The desired effects of feminizing hormones include voice change, decreased hair growth, breast growth, body fat redistribution, decreased muscle mass, skin softening, decreased oiliness of skin and hair, and a decrease in spontaneous erections, testicular volume, and sperm production.10,11 The onset of feminizing effects ranges from one month to one year and the expected maximum effect occurs anywhere between three months and five years.10,11 Regimens usually include anti-androgen agents and estrogen.13,26-28
The medications that have been most studied with anti-androgenic effects include spironolactone and 5-α reductase inhibitors (5-ARIs) such as finasteride. Spironolactone inhibits testosterone secretion and inhibits androgen binding to androgen receptors; 5-ARIs block the conversion of testosterone to 5-α-dihydrotestosterone, the more active form.
Estrogen can be administered via oral, sublingual, transdermal, or intramuscular route, but parenteral formulations are preferred to avoid first-pass metabolism. The serum estradiol target is similar to the mean daily level of premenopausal women (< 200 pg/mL) and the level of testosterone should be in the normal female range (< 55 ng/dL).13,26-28
The selection of medications should be individualized for each patient. Comorbidities must be considered, as well as the risk for adverse effects, which include venous thromboembolism, elevated liver enzymes, breast cancer, cardiovascular disease, diabetes, hyperprolactinemia, weight gain, gallstones, cerebrovascular disease, and severe migraine headaches.10,11 Estrogen therapy is not reported to induce hypertrophy or premalignant changes in the prostate.33 As is the case for masculinizing hormones, feminizing hormone therapy should be continued indefinitely for long-term effects.
Frequent monitoring is recommended. Patients taking feminizing hormones (transwomen) should be seen every two to three months in the first year and monitored once or twice a year thereafter. Serum testosterone and estradiol levels should initially be monitored every three months; serum electrolytes, specifically potassium, should be monitored every two to three months in the first year until stable.
CASE 2 You recommend that Carol S be screened annually for sexually transmitted diseases, as you would for any 21-year-old patient. You point out, too, that while estrogen and androgen-suppressing therapy decrease sperm production, there is a possibility that the patient could impregnate a female partner and recommend that contraception be used if the couple is not trying to conceive.
You also discuss the risks and benefits of hormone therapy and reasonable expectations of continued treatment. You ask Carol to schedule a follow-up visit in six months, as her hormone regimen is stable. Finally, if the patient remains on hormone therapy, you mention that the only screening unique to men transitioning to women is for breast cancer, which should begin at age 40 to 50 (as it should for all women).
Gender-affirming surgical options
Surgical management of transgender patients is not within the scope of family medicine. But it is essential to know what procedures are available, as you may have occasion to advocate for patients during the surgical referral process and possibly to provide postoperative care.
For transmen, surgical options include chest reconstruction, hysterectomy/oophorectomy, metoidioplasty (using the clitoris to surgically approximate a penis), phalloplasty, scrotoplasty, urethroplasty, and vaginectomy.10,34 The surgeries available for transwomen are orchiectomy, vaginoplasty, penectomy, breast augmentation, thyroid chondroplasty and voice surgery, and facial feminization.10,34 Keep in mind that not all transgender individuals desire surgery as part of the transitioning process.
The authors would like to acknowledge the assistance of Michelle Forcier, MD, MPH, and Karen S. Bernstein, MD, MPH, in the preparation of this manuscript.
Civil rights for the lesbian, gay, bisexual, and transgender population have advanced markedly in the past decade, and the medical community has gradually begun to address more of their health concerns. More recently, media attention to transgender individuals has encouraged many more to openly seek care.1,2
It is estimated that anywhere from 0.3% to 5% of the US population identifies as transgender.1-3 While awareness of this population has slowly increased, there is a paucity of research on the hormone treatment that is often essential to patients’ well-being. Studies of surgical options for transgender patients have been minimal, as well.
Primary care providers are uniquely positioned to coordinate medical services and ensure continuity of care for transgender patients as they strive to become their authentic selves. Our goal in writing this article is to equip you with the tools to provide this patient population with sensitive, high-quality care (see Table 1).4-7 Our focus is on the diagnosis of gender dysphoria (GD) and its medical and hormonal management—the realm of primary care providers. We briefly discuss surgical management of GD, as well.
UNDERSTANDING AND DIAGNOSING GENDER DYSPHORIA
Two classification systems are used for diagnoses related to GD: the Diagnostic and Statistical Manual of Mental Disorders, Fifth Ed (DSM-5)8 and the International Classification of Diseases, 10th Rev (ICD-10).9
ICD-10 criteria use the term gender identity disorder; DSM-5 refers to gender dysphoria instead. It is important to emphasize that these classification systems represent an attempt to categorize a group of signs and symptoms that lead to distress for the patient and are not meant to suggest that being transgender is pathological. In fact, in DSM-5—released in 2013—the American Psychiatric Association revised the terminology to emphasize that such individuals are not “disordered” by the nature of their identity, but rather by the distress that being transgender causes.8
For a diagnosis of GD in children, DSM-5 criteria include characteristics perceived to be incongruent between the child’s sex at birth and the self-identified gender based on preferred activities or dislike of his or her own sexual anatomy. The child must meet six or more of the following for at least six months
- A repeatedly stated desire to be, or insistence that he or she is, of the other gender
- In boys, a preference for cross-dressing or simulating female attire; in girls, insistence on wearing only stereotypical masculine clothing
- Strong and persistent preferences for cross-gender roles in make-believe play or fantasy
- A strong rejection of toys/games typically associated with the child’s sex
- Intense desire to participate in stereotypical games and pastimes of the other gender
- Strong preference for playmates of the other gender
- A strong dislike of one’s sexual anatomy
- A strong desire for the primary (eg, penis or vagina) or secondary (eg, menstruation) sex characteristics of the other gender.8
Adolescents and adults must meet two or more of the following for at least six months
- A noticeable incongruence between the gender that the patient sees themselves as and their sex characteristics
- An intense need to do away with (or prevent) his or her primary or secondary sex features
- An intense desire to have the primary and/or secondary sex features of the other gender
- A deep desire to transform into another gender
- A profound need for society to treat them as someone of the other gender
- A powerful assurance of having the characteristic feelings and responses of the other gender.8
For children as well as adolescents and adults, the condition should cause the patient significant distress or significantly affect him or her socially, at work or school, and in other important areas of life.8
Is the patient a candidate for hormone therapy?
Two primary sources—Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7, issued by the World Professional Association for Transgender Health (WPATH)10 and Endocrine Treatment of Transsexual Persons11 by the Endocrine Society—offer clinical practice guidance based on evidence and expert opinion.
WPATH recommends that a mental health professional (MHP) experienced in transgender care diagnose GD to ensure that it is not mistaken for a psychiatric condition manifesting as altered gender identity. However, if no one with such experience is available or accessible in the region, it is reasonable for a primary care provider to make the diagnosis and consider initiating hormone therapy without a mental health referral,12 as the expected benefits outweigh the risks of nontreatment.13
Whether or not an MHP confirms a diagnosis of GD, it is still up to the treating provider to confirm the patient’s eligibility and readiness for hormone therapy: He or she should meet DSM-5 or ICD-10 criteria for GD, have no psychiatric comorbidity (eg, schizophrenia, body dysmorphic disorder, or uncontrolled bipolar disorder) likely to interfere with treatment, understand the expected outcomes and the social benefits and risks, and have indicated a willingness to take the hormones responsibly.
Historically, patients were required to have a documented real-life experience, defined as having fully adopted the new gender role in everyday life for at least three months.10,11 This model has fallen out of favor, however, as it is unsupported by evidence and may place transgender individuals at physical and emotional risk. Instead, readiness is confirmed by obtaining informed consent.12
Puberty may be suppressed with a gonadotropin-releasing hormone (GnRH) agonist in adolescents who have a GD diagnosis and are at Tanner stage 2 to 3 of puberty until age 16. At that point, hormone therapy consistent with their gender identification may be initiated (see “How to Help Transgender Teens”).11
Beginning the transition
The transitioning process is a complex and individualized journey that can include inward or outward change, or both.
For patients interested in medical interventions, possible therapies include cross-sex hormone administration and gender-affirming surgery. Both are aimed at making the physical and the psychologic more congruent. Hormone treatment (see Table 2) is often essential to reduce the distress of individuals with GD and to help them feel comfortable in their own body.10,11,21 Psychologic conditions, such as depression, tend to improve as the transitioning process gets underway.22
FEMALE-TO-MALE TRANSITION
CASE 1 Jennie R, a 55-year-old postmenopausal patient, comes to your office for an annual exam. Although you’ve been her primary care provider for several years, she confides for the first time that she has never been comfortable as a woman. “I’ve always felt that my body didn’t belong to me,” the patient admits, and goes on to say that for the past several years she has been living as a man. Jennie R says she is ready to start hormone therapy to assist with the gender transition and asks about the process, the benefits and risks, and how quickly she can expect to achieve the desired results.
If Jennie R were your patient, how would you respond?
Masculinizing hormone treatment
As you would explain to a patient like Jennie R, the goal of hormone therapy is to suppress the effects of the sex assigned at birth and replace them with those of the desired gender. In the case of a female transitioning to a male (known as a transman), masculinizing hormones would promote growth of facial and body hair, cessation of menses, increased muscle mass, deepening of the voice, and clitoral enlargement.
Physical changes induced by masculinizing hormone therapy have an expected onset of one to six months and achieve maximum effect in approximately two to five years.10,11 Although there have been no controlled clinical trials evaluating the safety or efficacy of any transitional hormone regimen, WPATH and the Center of Excellence for Transgender Health at the University of California, San Francisco, suggest initiating intramuscular or transdermal testosterone at increasing doses until normal physiologic male testosterone levels between 350 and 700 ng/dL are achieved, or until cessation of menses.13,25-28 The dose at which either, or both, occur should be continued as long-term maintenance therapy. Medroxyprogesterone can be added, if necessary for menstrual cessation, and a GnRH agonist or endometrial ablation can be used for refractory uterine bleeding.29,30
Testosterone is not a contraceptive. It is important to emphasize to transmen like Jennie that they remain at risk for pregnancy if they are having sex with fertile males. Caution patients not to assume that the possibility of pregnancy ends when menses stop.
Treat minor adverse effects. Adverse effects of masculinizing hormones include vaginal atrophy, fat redistribution and weight gain, polycythemia, acne, scalp hair loss, sleep apnea, elevated liver enzymes, hyperlipidemia, cardiovascular disease, diabetes, and bone density loss. Increased risk for cancer of the female organs has not been proven.10,11 It is reasonable to treat minor adverse effects after reviewing the risks/benefits of doing so, as discontinuing hormone therapy could be detrimental to the well-being of transitioning patients.11
There are absolute contraindications to masculinizing hormone therapy, however, including pregnancy, unstable coronary artery disease, and untreated polycythemia with a hematocrit > 55%.10
Monitoring is essential. Patients receiving masculinizing hormone therapy should be monitored every three months during the first year and once or twice a year thereafter, with a focused history (including mood symptoms), physical exam (including weight and blood pressure), and labs (including complete blood count, liver function, renal function, and lipids) at each visit.11,23 Some clinicians also check estradiol levels until they fall below 50 pg/mL,23,27 while others take the cessation of uterine bleeding for > 6 months as an indicator of estrogen suppression.
Preventive health measures continue. Routine screening should continue, based on the patient’s assigned sex at birth. Thus, a transman who has not had a hysterectomy still needs Pap smears, mammograms if the patient has not had a double mastectomy, and bone mineral density (BMD) testing to screen for osteoporosis.31,32 Some experts recommend starting to test BMD at age 50 for patients receiving masculinizing hormones, given the unknown effect of testosterone on bone density.11,31,32
CASE 1 The first question for a transgender patient is about his or her current gender identity, but Jennie R has already reported living as a man. So you start by asking “What name do you prefer to use?” and “Do you prefer to be referred to with male or female pronouns?”
The patient tells you that he sees himself as a man, he wants to be called Jeff, and he prefers male pronouns. You explain that you believe he has gender dysphoria and would benefit from hormone therapy, but it is important to confirm this diagnosis with an MHP. You explain that testosterone can be prescribed for masculinizing effects, and describe the expected effects—more facial and body hair, a deeper voice, and greater muscle mass, among others—and review the likely time frame.
You also discuss the risks of masculinizing hormones (hyperlipidemia, cardiovascular disease, diabetes, and loss of bone density) that will need to be monitored. Before he leaves, you give him the name of an MHP who is experienced in transgender care and tell him to make a follow-up appointment with you after he has seen her. At the conclusion of the visit, you make a note of the patient’s name and gender identity in the chart and inform the staff of the changes.
MALE-TO-FEMALE TRANSITION
CASE 2 Before heading into your office to talk to a new patient named Carl S, you glance at his chart and see that he is a healthy 21-year-old who has come in for a routine physical. When you enter the room, you find Carl wearing a dress, heels, and make-up. After confirming that you have the right patient, you ask, “What is your current gender identity?” “Female,” says Carl, who indicates that she now goes by Carol. The patient has no medical problems, surgical history, or significant family history but reports that she has been taking spironolactone and estrogen for the past three years. Carol also says she has a new female partner and is having unprotected sexual activity.
Feminizing hormone treatment
The desired effects of feminizing hormones include voice change, decreased hair growth, breast growth, body fat redistribution, decreased muscle mass, skin softening, decreased oiliness of skin and hair, and a decrease in spontaneous erections, testicular volume, and sperm production.10,11 The onset of feminizing effects ranges from one month to one year and the expected maximum effect occurs anywhere between three months and five years.10,11 Regimens usually include anti-androgen agents and estrogen.13,26-28
The medications that have been most studied with anti-androgenic effects include spironolactone and 5-α reductase inhibitors (5-ARIs) such as finasteride. Spironolactone inhibits testosterone secretion and inhibits androgen binding to androgen receptors; 5-ARIs block the conversion of testosterone to 5-α-dihydrotestosterone, the more active form.
Estrogen can be administered via oral, sublingual, transdermal, or intramuscular route, but parenteral formulations are preferred to avoid first-pass metabolism. The serum estradiol target is similar to the mean daily level of premenopausal women (< 200 pg/mL) and the level of testosterone should be in the normal female range (< 55 ng/dL).13,26-28
The selection of medications should be individualized for each patient. Comorbidities must be considered, as well as the risk for adverse effects, which include venous thromboembolism, elevated liver enzymes, breast cancer, cardiovascular disease, diabetes, hyperprolactinemia, weight gain, gallstones, cerebrovascular disease, and severe migraine headaches.10,11 Estrogen therapy is not reported to induce hypertrophy or premalignant changes in the prostate.33 As is the case for masculinizing hormones, feminizing hormone therapy should be continued indefinitely for long-term effects.
Frequent monitoring is recommended. Patients taking feminizing hormones (transwomen) should be seen every two to three months in the first year and monitored once or twice a year thereafter. Serum testosterone and estradiol levels should initially be monitored every three months; serum electrolytes, specifically potassium, should be monitored every two to three months in the first year until stable.
CASE 2 You recommend that Carol S be screened annually for sexually transmitted diseases, as you would for any 21-year-old patient. You point out, too, that while estrogen and androgen-suppressing therapy decrease sperm production, there is a possibility that the patient could impregnate a female partner and recommend that contraception be used if the couple is not trying to conceive.
You also discuss the risks and benefits of hormone therapy and reasonable expectations of continued treatment. You ask Carol to schedule a follow-up visit in six months, as her hormone regimen is stable. Finally, if the patient remains on hormone therapy, you mention that the only screening unique to men transitioning to women is for breast cancer, which should begin at age 40 to 50 (as it should for all women).
Gender-affirming surgical options
Surgical management of transgender patients is not within the scope of family medicine. But it is essential to know what procedures are available, as you may have occasion to advocate for patients during the surgical referral process and possibly to provide postoperative care.
For transmen, surgical options include chest reconstruction, hysterectomy/oophorectomy, metoidioplasty (using the clitoris to surgically approximate a penis), phalloplasty, scrotoplasty, urethroplasty, and vaginectomy.10,34 The surgeries available for transwomen are orchiectomy, vaginoplasty, penectomy, breast augmentation, thyroid chondroplasty and voice surgery, and facial feminization.10,34 Keep in mind that not all transgender individuals desire surgery as part of the transitioning process.
The authors would like to acknowledge the assistance of Michelle Forcier, MD, MPH, and Karen S. Bernstein, MD, MPH, in the preparation of this manuscript.
1. Pew Research Center. A survey of LGBT Americans: attitudes, experiences and values in changing times. www.pewsocialtrends.org/2013/06/13/a-survey-of-lgbt-americans. Accessed January 13, 2017.
2. Gates GJ. How many people are lesbian, gay, bisexual and transgender? http://williamsinstitute.law.ucla.edu/wp-content/uploads/Gates-How-Many-People-LGBT-Apr-2011.pdf. Accessed January 13, 2017.
3. van Kesteren PJ, Gooren LJ, Megens JA. An epidemiological and demographic study of transsexuals in The Netherlands. Arch Sex Behav. 1996;25:589-600.
4. Bhola S. An ally’s guide to terminology: talking about LGBT people & equality. www.glaad.org/2011/07/28/an-allys-guide-to-terminology-talking-about-lgbt-people-equality. Accessed January 13, 2017.
5. University of California, San Francisco. Transgender terminology. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/tcoe?page=protocol-terminology. Accessed January 13, 2017.
6. Istar A. How queer! The development of gender identity and sexual orientation in LGBTQ-headed families. Fam Process. 2010;49:268-290.
7. Goins ES, Pye D. Check the box that best describes you: reflexively managing theory and praxis in LGBTQ health communication research. Health Commun. 2013;28:397-407.
8. American Psychiatric Association. Gender dysphoria. Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Washington, DC: American Psychiatric Association; 2013: 451-459.
9. World Health Organization. The International Classification of Diseases, 10th rev. Classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. 1992; Geneva.
10. Coleman E, Bockting W, Botzer M, et al; World Professional Association for Transgender Health. Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7. Int J Transgender. 2011; 13:165-232.
11. Hembree WC, Cohen-Kettenis P, Delemarre-van de Waal HA, et al. Endocrine treatment of transsexual persons: an Endocrine Society clinical practice guideline. J Clin Endo Metabol. 2009;94:3132-3154.
12. University of California, San Francisco. Assessing readiness for hormones. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/tcoe?page=protocol-hormone-ready. Accessed January 13, 2017.
13. Gooren L. Hormone treatment of the adult transsexual patient. Horm Res. 2005;64(suppl 2):S31-S36.
14. Hembree WC. Guidelines for pubertal suspension and gender reassignment for transgender adolescents. Child Adolesc Psychiatr Clin N Am. 2011;20:725-732.
15. Gay, Lesbian, and Straight Education Network (GLSEN). Harsh realities. The experiences of transgender youth in our nation’s schools. www.glsen.org/sites/default/files/Harsh%20Realities.pdf. Accessed January 13, 2017.
16. Berman M, Balingit M. Eleven states sue Obama administration over bathroom guidance for transgender students. May 25, 2016. Washington Post. www.washingtonpost.com/news/post-nation/wp/2016/05/25/texas-governor-says-state-will-sue-obama-administration-over-bathroom-directive/. Accessed January 13, 2017.
17. de Vries AL, Cohen-Kettenis PT, Delemarre-van de Waal H. Clinical management of gender dysphoria in adolescents. 2006. Vancouver Coastal Health - Transgender Health Program. www.amsa.org/wp-content/uploads/2015/04/CaringForTransgenderAdolescents.pdf. Accessed January 13, 2017.
18. TransYouth Family Allies. Empowering transgender youth & families. www.imatyfa.org/. Accessed January 13, 2017.
19. Human Rights Campaign. On our own: a survival guide for independent LGBTQ youth. www.hrc.org/resources/on-our-own-a-survival-guide-for-independent-lgbtq-youth. Accessed January 13, 2017.
20. Gay, Lesbian, Bisexual, and Transgender National Help Center. www.glbthotline.org. Accessed January 13, 2017.
21. University of California, San Francisco. Hormone administration. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/trans?page=protocol-hormones. Accessed January 13, 2017.
22. Gorin-Lazard A, Baumstarck K, Boyer L, et al. Hormonal therapy is associated with better self-esteem, mood, and quality of life in transsexuals. J Nerv Ment Dis. 2013;201:996-1000.
23. Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in adult men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2006;91:1995-2010.
24. Boloña ER, Uraga MV, Haddad RM, et al. Testosterone use in men with sexual dysfunction: a systematic review and meta-analysis of randomized placebo-controlled trials. Mayo Clin Proc. 2007;82:20-28.
25. Gooren LJ, Giltay EJ. Review of studies of androgen treatment of female-to-male transsexuals: effects and risks of administration of androgens to females. J Sex Med. 2008; 5:765-776.
26. Levy A, Crown A, Reid R. Endocrine intervention for transsexuals. Clin Endocrinol (Oxf). 2003;59:409-418.
27. Moore E, Wisniewski A, Dobs A. Endocrine treatment of transsexual people: a review of treatment regimens, outcomes, and adverse effects. J Clin Endocrinol Metab. 2003;88:3467-3473.
28. Tangpricha V, Ducharme SH, Barber TW, et al. Endocrinologic treatment of gender identity disorders. Endocr Pract. 2003;9:12-21.
29. Dickersin K, Munro MG, Clark M, et al. Hysterectomy compared with endometrial ablation for dysfunctional uterine bleeding: a randomized controlled trial. Obstet Gynecol. 2007;110:1279-1289.
30. Prasad P, Powell MC. Prospective observational study of Thermablate Endometrial Ablation System as an outpatient procedure. J Minim Invasive Gynecol. 2008;15:476-479.
31. University of California, San Francisco. General prevention and screening. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/trans?page=protocol-screening. Accessed January 13, 2017.
32. Ganly I, Taylor EW. Breast cancer in a trans-sexual man receiving hormone replacement therapy. Br J Surg. 1995; 82:341.
33. Meriggiola MC, Gava G. Endocrine care of transpeople part II: a review of cross-sex hormonal treatments, outcomes and adverse effects in transwomen. Clin Endocrinol (Oxf). 2015;83:607-615.
34. University of California, San Francisco. Surgical options. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/trans?page=protocol-surgery. Accessed January 13, 2017.
1. Pew Research Center. A survey of LGBT Americans: attitudes, experiences and values in changing times. www.pewsocialtrends.org/2013/06/13/a-survey-of-lgbt-americans. Accessed January 13, 2017.
2. Gates GJ. How many people are lesbian, gay, bisexual and transgender? http://williamsinstitute.law.ucla.edu/wp-content/uploads/Gates-How-Many-People-LGBT-Apr-2011.pdf. Accessed January 13, 2017.
3. van Kesteren PJ, Gooren LJ, Megens JA. An epidemiological and demographic study of transsexuals in The Netherlands. Arch Sex Behav. 1996;25:589-600.
4. Bhola S. An ally’s guide to terminology: talking about LGBT people & equality. www.glaad.org/2011/07/28/an-allys-guide-to-terminology-talking-about-lgbt-people-equality. Accessed January 13, 2017.
5. University of California, San Francisco. Transgender terminology. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/tcoe?page=protocol-terminology. Accessed January 13, 2017.
6. Istar A. How queer! The development of gender identity and sexual orientation in LGBTQ-headed families. Fam Process. 2010;49:268-290.
7. Goins ES, Pye D. Check the box that best describes you: reflexively managing theory and praxis in LGBTQ health communication research. Health Commun. 2013;28:397-407.
8. American Psychiatric Association. Gender dysphoria. Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Washington, DC: American Psychiatric Association; 2013: 451-459.
9. World Health Organization. The International Classification of Diseases, 10th rev. Classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. 1992; Geneva.
10. Coleman E, Bockting W, Botzer M, et al; World Professional Association for Transgender Health. Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7. Int J Transgender. 2011; 13:165-232.
11. Hembree WC, Cohen-Kettenis P, Delemarre-van de Waal HA, et al. Endocrine treatment of transsexual persons: an Endocrine Society clinical practice guideline. J Clin Endo Metabol. 2009;94:3132-3154.
12. University of California, San Francisco. Assessing readiness for hormones. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/tcoe?page=protocol-hormone-ready. Accessed January 13, 2017.
13. Gooren L. Hormone treatment of the adult transsexual patient. Horm Res. 2005;64(suppl 2):S31-S36.
14. Hembree WC. Guidelines for pubertal suspension and gender reassignment for transgender adolescents. Child Adolesc Psychiatr Clin N Am. 2011;20:725-732.
15. Gay, Lesbian, and Straight Education Network (GLSEN). Harsh realities. The experiences of transgender youth in our nation’s schools. www.glsen.org/sites/default/files/Harsh%20Realities.pdf. Accessed January 13, 2017.
16. Berman M, Balingit M. Eleven states sue Obama administration over bathroom guidance for transgender students. May 25, 2016. Washington Post. www.washingtonpost.com/news/post-nation/wp/2016/05/25/texas-governor-says-state-will-sue-obama-administration-over-bathroom-directive/. Accessed January 13, 2017.
17. de Vries AL, Cohen-Kettenis PT, Delemarre-van de Waal H. Clinical management of gender dysphoria in adolescents. 2006. Vancouver Coastal Health - Transgender Health Program. www.amsa.org/wp-content/uploads/2015/04/CaringForTransgenderAdolescents.pdf. Accessed January 13, 2017.
18. TransYouth Family Allies. Empowering transgender youth & families. www.imatyfa.org/. Accessed January 13, 2017.
19. Human Rights Campaign. On our own: a survival guide for independent LGBTQ youth. www.hrc.org/resources/on-our-own-a-survival-guide-for-independent-lgbtq-youth. Accessed January 13, 2017.
20. Gay, Lesbian, Bisexual, and Transgender National Help Center. www.glbthotline.org. Accessed January 13, 2017.
21. University of California, San Francisco. Hormone administration. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/trans?page=protocol-hormones. Accessed January 13, 2017.
22. Gorin-Lazard A, Baumstarck K, Boyer L, et al. Hormonal therapy is associated with better self-esteem, mood, and quality of life in transsexuals. J Nerv Ment Dis. 2013;201:996-1000.
23. Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in adult men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2006;91:1995-2010.
24. Boloña ER, Uraga MV, Haddad RM, et al. Testosterone use in men with sexual dysfunction: a systematic review and meta-analysis of randomized placebo-controlled trials. Mayo Clin Proc. 2007;82:20-28.
25. Gooren LJ, Giltay EJ. Review of studies of androgen treatment of female-to-male transsexuals: effects and risks of administration of androgens to females. J Sex Med. 2008; 5:765-776.
26. Levy A, Crown A, Reid R. Endocrine intervention for transsexuals. Clin Endocrinol (Oxf). 2003;59:409-418.
27. Moore E, Wisniewski A, Dobs A. Endocrine treatment of transsexual people: a review of treatment regimens, outcomes, and adverse effects. J Clin Endocrinol Metab. 2003;88:3467-3473.
28. Tangpricha V, Ducharme SH, Barber TW, et al. Endocrinologic treatment of gender identity disorders. Endocr Pract. 2003;9:12-21.
29. Dickersin K, Munro MG, Clark M, et al. Hysterectomy compared with endometrial ablation for dysfunctional uterine bleeding: a randomized controlled trial. Obstet Gynecol. 2007;110:1279-1289.
30. Prasad P, Powell MC. Prospective observational study of Thermablate Endometrial Ablation System as an outpatient procedure. J Minim Invasive Gynecol. 2008;15:476-479.
31. University of California, San Francisco. General prevention and screening. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/trans?page=protocol-screening. Accessed January 13, 2017.
32. Ganly I, Taylor EW. Breast cancer in a trans-sexual man receiving hormone replacement therapy. Br J Surg. 1995; 82:341.
33. Meriggiola MC, Gava G. Endocrine care of transpeople part II: a review of cross-sex hormonal treatments, outcomes and adverse effects in transwomen. Clin Endocrinol (Oxf). 2015;83:607-615.
34. University of California, San Francisco. Surgical options. UCSF Center of Excellence for Transgender Health. http://transhealth.ucsf.edu/trans?page=protocol-surgery. Accessed January 13, 2017.
Critical Care Commentary: Highlights from the 2016 hospital-acquired and ventilator-associated pneumonia guideline
The 2016 hospital-acquired and ventilator-associated pneumonia guidelines, sponsored by the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS), and endorsed by the American College of Chest Physicians (CHEST), Society of Critical Care Medicine (SCCM), and the Society for Healthcare Epidemiology, was published recently (Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016 Sep 1;63[5]:575-82).
This Critical Care Commentary aims to provide the highlights of the new guideline and to motivate readers to read the complete report that best represents the primary intent of the guideline panelists.

The new guideline was written using the Grading of Recommendations Assessment, Development, and Evaluation methodology. This was the framework to address all clinical questions referred to as PICOs (patient; intervention; comparator; outcome), which can be explicitly seen in the published guideline. For every PICO question, the wording “we suggest” was used for a weak recommendation (lack of high confidence; further evidence could change it), and “we recommend” was used for a strong recommendation (high confidence; further evidence is unlikely to change it). Also, part of the panel framework was the requirement to disclose any actual, potential, or perceived conflicts of interest for each panelist to be accepted to participate, as well as to remain in the panel for the duration of the process. The cochairs remained free of any financial conflicts during the entire process.
Choosing an empiric antibiotic regimen for patients with HAP and VAP requires balancing the potentially competing goals of ensuring that likely infecting pathogens are covered while avoiding excess antibiotic use. In order to guide clinicians on empiric antibiotic therapy, the panel performed a comprehensive review of the potential risk factors for HAP and VAP. For VAP, three factors associated with disease severity (septic shock at time of VAP, ARDS preceding VAP, and acute renal replacement prior to VAP onset) and two epidemiologic factors (prior use of IV antibiotic use within 90 days, and 5 or more days of hospitalization prior to the occurrence of VAP) made the final risk factors list. For HAP, only the prior use of IV antibiotics within 90 days was associated with risk for MDR. However, because of the limitations and small number of studies on HAP only, the panel decided to add risk factors for mortality (ventilator support for HAP and septic shock) as surrogates for MDR risk factors in patients with HAP, as these factors presumably increase the risk of poor outcomes if there is initial inadequate empiric therapy.
In conjunction with the bedside evaluation of risk factors for MDR, the guideline recommends the use of local antibiograms not only to guide empiric therapy but also to decide if antibiotic coverage for MDR is needed. Ideally, the antibiogram should be based on the specific ICU, but if this is not feasible, or the hospital is of small size, an institutional antibiogram can also be helpful. The first benefit of local antibiograms is derived from the knowledge gained regarding the prevalence of each microorganism; for example, if only 3% of all VAP or HAP in a given unit or hospital is caused by Pseudomonas aeruginosa, it is likely that an empiric coverage for this microorganism will neither be necessary nor appropriate for most patients. The second benefit is derived from the knowledge concerning the frequency of MDR microorganisms within the unit or hospital: for example, patients with VAP in units where 10%-20% of Staphylococcus aureus isolates are resistant to methicillin, or greater than 10% of gram-negative isolates are resistant to an agent being considered for monotherapy, should receive antibiotics for MDR infections. With these two critical pieces of information, the clinician will have a higher probability of starting the correct empiric antibiotics, and, consequently, improve the survival outcomes of patients with HAP and VAP.
The choice of the empirical treatment of VAP and HAP becomes a natural derivation of the three main factors discussed above: (1) epidemiologic history of antibiotics’ use and prior hospitalization length, (2) local antibiogram for the prevalence and resistance of microorganisms, and (3) disease severity and risk of mortality by the identification of septic shock, ARDS, and acute renal replacement therapy. For example, if 17% of all VAPs in your unit is from P aeruginosa (which is the national prevalence in patients with VAP), and 8% of these strains are resistant to an agent being considered for gram-negative monotherapy, not prescribing double coverage for P aeruginosa would still result in initial appropriate therapy in 98.6% (derived from 1-[0.17 x 0.08]) of cases. The reason why the panelists chose the threshold of 10% for P aeruginosa, and 10%-20% for S aureus, was based on the national prevalence rates reported by the Centers for Disease Control and Prevention, with the goal of limiting the initial inappropriate antibiotic therapy decision to less than 5% of all cases. We strongly believe that this “epidemiologic/antibiogram/disease severity” approach to select the empiric therapy is both clinically intuitive and essential to improve patients’ outcomes. Further, this approach will substantially reduce the unnecessary use of double antibiotic therapy in patients with VAP or HAP.
This guideline suggests that the use of inhaled antibiotic therapy in conjunction with IV antibiotics may benefit patients with VAP or HAP from MDR microorganisms that are sensitive to only polymyxins or aminoglycosides. The panel also suggested that the use of pharmacokinetic and pharmacodynamics should be used to optimize the administration of antibiotic therapy for all patients with HAP or VAP.
Last, after an extensive review and multiple analyses of all available evidence, the panel concluded that the majority of patients with HAP or VAP should be treated with 7 days of therapy, independent of the microorganism causing the pneumonia. In several meta-analyses performed by the panelists to evaluate all patients with VAP, as well as only patients with VAP caused by nonfermenting gram-negative organisms such as Pseudomonas species, Stenotrophomonas species, and Acinetobacter species, the panel did not find differences between short and long courses of antibiotics regarding mortality, clinical cure, pneumonia recurrence, and mechanical ventilation duration. In recognition of the individual needs of each patient, we made a remark that shorter or longer duration of antibiotics may be indicated, depending upon the rate of improvement of clinical, radiologic, and laboratory parameters. Several adjunctive methods of deescalation were assessed, but only procalcitonin was suggested to aid health care providers to shorten the course of antibiotic therapy.
In conclusion, the authors of this 2016 HAP/VAP IDSA/ATS guideline hope to achieve the ultimate goal of improving the treatment and outcomes of patients with HAP and VAP and reducing unnecessary antibiotic use.
Dr. Kalil is with the department of internal medicine, division of infectious diseases, University of Nebraska Medical Center, Omaha; Dr. Metersky is with the division of pulmonary and critical care medicine, University of Connecticut, Farmington.
The 2016 hospital-acquired and ventilator-associated pneumonia guidelines, sponsored by the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS), and endorsed by the American College of Chest Physicians (CHEST), Society of Critical Care Medicine (SCCM), and the Society for Healthcare Epidemiology, was published recently (Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016 Sep 1;63[5]:575-82).
This Critical Care Commentary aims to provide the highlights of the new guideline and to motivate readers to read the complete report that best represents the primary intent of the guideline panelists.
The new guideline was written using the Grading of Recommendations Assessment, Development, and Evaluation methodology. This was the framework to address all clinical questions referred to as PICOs (patient; intervention; comparator; outcome), which can be explicitly seen in the published guideline. For every PICO question, the wording “we suggest” was used for a weak recommendation (lack of high confidence; further evidence could change it), and “we recommend” was used for a strong recommendation (high confidence; further evidence is unlikely to change it). Also, part of the panel framework was the requirement to disclose any actual, potential, or perceived conflicts of interest for each panelist to be accepted to participate, as well as to remain in the panel for the duration of the process. The cochairs remained free of any financial conflicts during the entire process.
Choosing an empiric antibiotic regimen for patients with HAP and VAP requires balancing the potentially competing goals of ensuring that likely infecting pathogens are covered while avoiding excess antibiotic use. In order to guide clinicians on empiric antibiotic therapy, the panel performed a comprehensive review of the potential risk factors for HAP and VAP. For VAP, three factors associated with disease severity (septic shock at time of VAP, ARDS preceding VAP, and acute renal replacement prior to VAP onset) and two epidemiologic factors (prior use of IV antibiotic use within 90 days, and 5 or more days of hospitalization prior to the occurrence of VAP) made the final risk factors list. For HAP, only the prior use of IV antibiotics within 90 days was associated with risk for MDR. However, because of the limitations and small number of studies on HAP only, the panel decided to add risk factors for mortality (ventilator support for HAP and septic shock) as surrogates for MDR risk factors in patients with HAP, as these factors presumably increase the risk of poor outcomes if there is initial inadequate empiric therapy.
In conjunction with the bedside evaluation of risk factors for MDR, the guideline recommends the use of local antibiograms not only to guide empiric therapy but also to decide if antibiotic coverage for MDR is needed. Ideally, the antibiogram should be based on the specific ICU, but if this is not feasible, or the hospital is of small size, an institutional antibiogram can also be helpful. The first benefit of local antibiograms is derived from the knowledge gained regarding the prevalence of each microorganism; for example, if only 3% of all VAP or HAP in a given unit or hospital is caused by Pseudomonas aeruginosa, it is likely that an empiric coverage for this microorganism will neither be necessary nor appropriate for most patients. The second benefit is derived from the knowledge concerning the frequency of MDR microorganisms within the unit or hospital: for example, patients with VAP in units where 10%-20% of Staphylococcus aureus isolates are resistant to methicillin, or greater than 10% of gram-negative isolates are resistant to an agent being considered for monotherapy, should receive antibiotics for MDR infections. With these two critical pieces of information, the clinician will have a higher probability of starting the correct empiric antibiotics, and, consequently, improve the survival outcomes of patients with HAP and VAP.
The choice of the empirical treatment of VAP and HAP becomes a natural derivation of the three main factors discussed above: (1) epidemiologic history of antibiotics’ use and prior hospitalization length, (2) local antibiogram for the prevalence and resistance of microorganisms, and (3) disease severity and risk of mortality by the identification of septic shock, ARDS, and acute renal replacement therapy. For example, if 17% of all VAPs in your unit is from P aeruginosa (which is the national prevalence in patients with VAP), and 8% of these strains are resistant to an agent being considered for gram-negative monotherapy, not prescribing double coverage for P aeruginosa would still result in initial appropriate therapy in 98.6% (derived from 1-[0.17 x 0.08]) of cases. The reason why the panelists chose the threshold of 10% for P aeruginosa, and 10%-20% for S aureus, was based on the national prevalence rates reported by the Centers for Disease Control and Prevention, with the goal of limiting the initial inappropriate antibiotic therapy decision to less than 5% of all cases. We strongly believe that this “epidemiologic/antibiogram/disease severity” approach to select the empiric therapy is both clinically intuitive and essential to improve patients’ outcomes. Further, this approach will substantially reduce the unnecessary use of double antibiotic therapy in patients with VAP or HAP.
This guideline suggests that the use of inhaled antibiotic therapy in conjunction with IV antibiotics may benefit patients with VAP or HAP from MDR microorganisms that are sensitive to only polymyxins or aminoglycosides. The panel also suggested that the use of pharmacokinetic and pharmacodynamics should be used to optimize the administration of antibiotic therapy for all patients with HAP or VAP.
Last, after an extensive review and multiple analyses of all available evidence, the panel concluded that the majority of patients with HAP or VAP should be treated with 7 days of therapy, independent of the microorganism causing the pneumonia. In several meta-analyses performed by the panelists to evaluate all patients with VAP, as well as only patients with VAP caused by nonfermenting gram-negative organisms such as Pseudomonas species, Stenotrophomonas species, and Acinetobacter species, the panel did not find differences between short and long courses of antibiotics regarding mortality, clinical cure, pneumonia recurrence, and mechanical ventilation duration. In recognition of the individual needs of each patient, we made a remark that shorter or longer duration of antibiotics may be indicated, depending upon the rate of improvement of clinical, radiologic, and laboratory parameters. Several adjunctive methods of deescalation were assessed, but only procalcitonin was suggested to aid health care providers to shorten the course of antibiotic therapy.
In conclusion, the authors of this 2016 HAP/VAP IDSA/ATS guideline hope to achieve the ultimate goal of improving the treatment and outcomes of patients with HAP and VAP and reducing unnecessary antibiotic use.
Dr. Kalil is with the department of internal medicine, division of infectious diseases, University of Nebraska Medical Center, Omaha; Dr. Metersky is with the division of pulmonary and critical care medicine, University of Connecticut, Farmington.
The 2016 hospital-acquired and ventilator-associated pneumonia guidelines, sponsored by the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS), and endorsed by the American College of Chest Physicians (CHEST), Society of Critical Care Medicine (SCCM), and the Society for Healthcare Epidemiology, was published recently (Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016 Sep 1;63[5]:575-82).
This Critical Care Commentary aims to provide the highlights of the new guideline and to motivate readers to read the complete report that best represents the primary intent of the guideline panelists.
The new guideline was written using the Grading of Recommendations Assessment, Development, and Evaluation methodology. This was the framework to address all clinical questions referred to as PICOs (patient; intervention; comparator; outcome), which can be explicitly seen in the published guideline. For every PICO question, the wording “we suggest” was used for a weak recommendation (lack of high confidence; further evidence could change it), and “we recommend” was used for a strong recommendation (high confidence; further evidence is unlikely to change it). Also, part of the panel framework was the requirement to disclose any actual, potential, or perceived conflicts of interest for each panelist to be accepted to participate, as well as to remain in the panel for the duration of the process. The cochairs remained free of any financial conflicts during the entire process.
Choosing an empiric antibiotic regimen for patients with HAP and VAP requires balancing the potentially competing goals of ensuring that likely infecting pathogens are covered while avoiding excess antibiotic use. In order to guide clinicians on empiric antibiotic therapy, the panel performed a comprehensive review of the potential risk factors for HAP and VAP. For VAP, three factors associated with disease severity (septic shock at time of VAP, ARDS preceding VAP, and acute renal replacement prior to VAP onset) and two epidemiologic factors (prior use of IV antibiotic use within 90 days, and 5 or more days of hospitalization prior to the occurrence of VAP) made the final risk factors list. For HAP, only the prior use of IV antibiotics within 90 days was associated with risk for MDR. However, because of the limitations and small number of studies on HAP only, the panel decided to add risk factors for mortality (ventilator support for HAP and septic shock) as surrogates for MDR risk factors in patients with HAP, as these factors presumably increase the risk of poor outcomes if there is initial inadequate empiric therapy.
In conjunction with the bedside evaluation of risk factors for MDR, the guideline recommends the use of local antibiograms not only to guide empiric therapy but also to decide if antibiotic coverage for MDR is needed. Ideally, the antibiogram should be based on the specific ICU, but if this is not feasible, or the hospital is of small size, an institutional antibiogram can also be helpful. The first benefit of local antibiograms is derived from the knowledge gained regarding the prevalence of each microorganism; for example, if only 3% of all VAP or HAP in a given unit or hospital is caused by Pseudomonas aeruginosa, it is likely that an empiric coverage for this microorganism will neither be necessary nor appropriate for most patients. The second benefit is derived from the knowledge concerning the frequency of MDR microorganisms within the unit or hospital: for example, patients with VAP in units where 10%-20% of Staphylococcus aureus isolates are resistant to methicillin, or greater than 10% of gram-negative isolates are resistant to an agent being considered for monotherapy, should receive antibiotics for MDR infections. With these two critical pieces of information, the clinician will have a higher probability of starting the correct empiric antibiotics, and, consequently, improve the survival outcomes of patients with HAP and VAP.
The choice of the empirical treatment of VAP and HAP becomes a natural derivation of the three main factors discussed above: (1) epidemiologic history of antibiotics’ use and prior hospitalization length, (2) local antibiogram for the prevalence and resistance of microorganisms, and (3) disease severity and risk of mortality by the identification of septic shock, ARDS, and acute renal replacement therapy. For example, if 17% of all VAPs in your unit is from P aeruginosa (which is the national prevalence in patients with VAP), and 8% of these strains are resistant to an agent being considered for gram-negative monotherapy, not prescribing double coverage for P aeruginosa would still result in initial appropriate therapy in 98.6% (derived from 1-[0.17 x 0.08]) of cases. The reason why the panelists chose the threshold of 10% for P aeruginosa, and 10%-20% for S aureus, was based on the national prevalence rates reported by the Centers for Disease Control and Prevention, with the goal of limiting the initial inappropriate antibiotic therapy decision to less than 5% of all cases. We strongly believe that this “epidemiologic/antibiogram/disease severity” approach to select the empiric therapy is both clinically intuitive and essential to improve patients’ outcomes. Further, this approach will substantially reduce the unnecessary use of double antibiotic therapy in patients with VAP or HAP.
This guideline suggests that the use of inhaled antibiotic therapy in conjunction with IV antibiotics may benefit patients with VAP or HAP from MDR microorganisms that are sensitive to only polymyxins or aminoglycosides. The panel also suggested that the use of pharmacokinetic and pharmacodynamics should be used to optimize the administration of antibiotic therapy for all patients with HAP or VAP.
Last, after an extensive review and multiple analyses of all available evidence, the panel concluded that the majority of patients with HAP or VAP should be treated with 7 days of therapy, independent of the microorganism causing the pneumonia. In several meta-analyses performed by the panelists to evaluate all patients with VAP, as well as only patients with VAP caused by nonfermenting gram-negative organisms such as Pseudomonas species, Stenotrophomonas species, and Acinetobacter species, the panel did not find differences between short and long courses of antibiotics regarding mortality, clinical cure, pneumonia recurrence, and mechanical ventilation duration. In recognition of the individual needs of each patient, we made a remark that shorter or longer duration of antibiotics may be indicated, depending upon the rate of improvement of clinical, radiologic, and laboratory parameters. Several adjunctive methods of deescalation were assessed, but only procalcitonin was suggested to aid health care providers to shorten the course of antibiotic therapy.
In conclusion, the authors of this 2016 HAP/VAP IDSA/ATS guideline hope to achieve the ultimate goal of improving the treatment and outcomes of patients with HAP and VAP and reducing unnecessary antibiotic use.
Dr. Kalil is with the department of internal medicine, division of infectious diseases, University of Nebraska Medical Center, Omaha; Dr. Metersky is with the division of pulmonary and critical care medicine, University of Connecticut, Farmington.