User login
Patient transfer before thrombectomy worsens stroke outcomes
HOUSTON – Drip and ship may not be the most time-effective way to treat acute ischemic stroke patients who are candidates for endovascular thrombectomy.
Results from two separate real-world, observational studies showed that acute ischemic stroke patients with large vessel occlusions amenable to mechanical thrombectomy had significantly worse clinical outcomes when their management path included a stop at a primary stroke center followed by transfer to a comprehensive stroke center that had the capacity to perform thrombectomy, compared with going straight to the thrombectomy site.

The findings show “the system of care has room for improvement. Patients with large vessel occlusions clearly do better when we get them to mechanical thrombectomy as quickly as possible,” said Dr. Froehler, a vascular neurologist at Vanderbilt University in Nashville, Tenn. Thrombectomy “has a more powerful treatment effect than TPA [tissue plasminogen activator] and we need to adjust our standard of care to best deliver” thrombectomy, he said in an interview.

The study run by Dr. Froehler used data collected in the Systematic Evaluation of Patients Treated With Stroke Devices for Acute Ischemic Stroke (STRATIS) registry, which began in 2014 and has data for 984 acute ischemic stroke patients with large vessel occlusions treated by mechanical thrombectomy seen at any of 55 U.S. centers. The series included 445 (45%) patients first seen as a primary stroke center and then transferred to a comprehensive center and 539 (55%) who went directly to a comprehensive stroke center (direct patients). Prior to thrombectomy, 628 of all patients (64%) received TPA, with a roughly similar percentage in both the transferred and direct patients.
The data showed that the median time from symptom onset to revascularization was 202 minutes among the direct patients and 312 minutes among those first seen at a primary stroke center and then transferred, a statistically significant difference. The average time difference per patient between the two subgroups was 100 minutes, Dr. Froehler reported.
This difference in time to reperfusion led directly to significant differences in functional outcomes after 90 days measured on the modified Rankin Scale (mRS). The percentage of patients with a mRS score of 0 or 1 (an excellent functional outcome) was 38% for the patients first seen at primary stroke centers and 47% in direct patients, a 47% relative rise in excellent outcomes among the direct patients. The percentage of patients with a mRS score of 0-2, which identifies functional independence post stroke, was 52% among transferred patients and 60% in direct patients, a 38% relative improvement for this outcome among direct patients.
The second study of stroke transfer times and outcomes used data from 562 acute ischemic stroke patients with large vessel occlusions treated in the Providence Health & Services system in five western U.S. states during 2012-2016. Nearly half the patients required a transfer and the other half went directly to a center able to perform thrombectomy. The analysis used clinical outcomes scored on the mRS at the time of hospital discharge.

“Right now, the big delay at primary stroke centers is the door-in door-out time,” commented Ryan A. McTaggart, MD, an interventional neuroradiologist at Rhode Island Hospital in Providence, the only comprehensive stroke center in Rhode Island. He helped organize a partnership with 14 primary stroke centers in Rhode Island that uses a streamlined imaging, treatment (with TPA), and transfer protocol that hacked dozens of minutes off transfer times and produced a median time from onset of symptoms to revascularization by thrombectomy of 184 minutes in patients first seen at a primary stroke center. This clocking blows past the 202 minute median for stroke onset to revascularization in the direct patients from Dr. Froehler’s study.

Stroke transport and treatment networks are now undergoing refinement in Tennessee, said Dr. Froehler, based in part on the data he reported. Considerations in Tennessee include how EMS workers assess possible stroke patients, decisions by EMS on where to take patients, and how quality of care is measured at primary and comprehensive stroke centers.
The STRATIS registry is sponsored by Medtronic. Dr. Froehler is a consultant to Medtronic, Blockade, Stryker, and Control Medical. Dr. Smith, Dr. Tarpley, and Dr. McTaggart had no disclosures.
[email protected]
On Twitter @mitchelzoler
HOUSTON – Drip and ship may not be the most time-effective way to treat acute ischemic stroke patients who are candidates for endovascular thrombectomy.
Results from two separate real-world, observational studies showed that acute ischemic stroke patients with large vessel occlusions amenable to mechanical thrombectomy had significantly worse clinical outcomes when their management path included a stop at a primary stroke center followed by transfer to a comprehensive stroke center that had the capacity to perform thrombectomy, compared with going straight to the thrombectomy site.
The findings show “the system of care has room for improvement. Patients with large vessel occlusions clearly do better when we get them to mechanical thrombectomy as quickly as possible,” said Dr. Froehler, a vascular neurologist at Vanderbilt University in Nashville, Tenn. Thrombectomy “has a more powerful treatment effect than TPA [tissue plasminogen activator] and we need to adjust our standard of care to best deliver” thrombectomy, he said in an interview.
The study run by Dr. Froehler used data collected in the Systematic Evaluation of Patients Treated With Stroke Devices for Acute Ischemic Stroke (STRATIS) registry, which began in 2014 and has data for 984 acute ischemic stroke patients with large vessel occlusions treated by mechanical thrombectomy seen at any of 55 U.S. centers. The series included 445 (45%) patients first seen as a primary stroke center and then transferred to a comprehensive center and 539 (55%) who went directly to a comprehensive stroke center (direct patients). Prior to thrombectomy, 628 of all patients (64%) received TPA, with a roughly similar percentage in both the transferred and direct patients.
The data showed that the median time from symptom onset to revascularization was 202 minutes among the direct patients and 312 minutes among those first seen at a primary stroke center and then transferred, a statistically significant difference. The average time difference per patient between the two subgroups was 100 minutes, Dr. Froehler reported.
This difference in time to reperfusion led directly to significant differences in functional outcomes after 90 days measured on the modified Rankin Scale (mRS). The percentage of patients with a mRS score of 0 or 1 (an excellent functional outcome) was 38% for the patients first seen at primary stroke centers and 47% in direct patients, a 47% relative rise in excellent outcomes among the direct patients. The percentage of patients with a mRS score of 0-2, which identifies functional independence post stroke, was 52% among transferred patients and 60% in direct patients, a 38% relative improvement for this outcome among direct patients.
The second study of stroke transfer times and outcomes used data from 562 acute ischemic stroke patients with large vessel occlusions treated in the Providence Health & Services system in five western U.S. states during 2012-2016. Nearly half the patients required a transfer and the other half went directly to a center able to perform thrombectomy. The analysis used clinical outcomes scored on the mRS at the time of hospital discharge.
“Right now, the big delay at primary stroke centers is the door-in door-out time,” commented Ryan A. McTaggart, MD, an interventional neuroradiologist at Rhode Island Hospital in Providence, the only comprehensive stroke center in Rhode Island. He helped organize a partnership with 14 primary stroke centers in Rhode Island that uses a streamlined imaging, treatment (with TPA), and transfer protocol that hacked dozens of minutes off transfer times and produced a median time from onset of symptoms to revascularization by thrombectomy of 184 minutes in patients first seen at a primary stroke center. This clocking blows past the 202 minute median for stroke onset to revascularization in the direct patients from Dr. Froehler’s study.
Stroke transport and treatment networks are now undergoing refinement in Tennessee, said Dr. Froehler, based in part on the data he reported. Considerations in Tennessee include how EMS workers assess possible stroke patients, decisions by EMS on where to take patients, and how quality of care is measured at primary and comprehensive stroke centers.
The STRATIS registry is sponsored by Medtronic. Dr. Froehler is a consultant to Medtronic, Blockade, Stryker, and Control Medical. Dr. Smith, Dr. Tarpley, and Dr. McTaggart had no disclosures.
[email protected]
On Twitter @mitchelzoler
HOUSTON – Drip and ship may not be the most time-effective way to treat acute ischemic stroke patients who are candidates for endovascular thrombectomy.
Results from two separate real-world, observational studies showed that acute ischemic stroke patients with large vessel occlusions amenable to mechanical thrombectomy had significantly worse clinical outcomes when their management path included a stop at a primary stroke center followed by transfer to a comprehensive stroke center that had the capacity to perform thrombectomy, compared with going straight to the thrombectomy site.
The findings show “the system of care has room for improvement. Patients with large vessel occlusions clearly do better when we get them to mechanical thrombectomy as quickly as possible,” said Dr. Froehler, a vascular neurologist at Vanderbilt University in Nashville, Tenn. Thrombectomy “has a more powerful treatment effect than TPA [tissue plasminogen activator] and we need to adjust our standard of care to best deliver” thrombectomy, he said in an interview.
The study run by Dr. Froehler used data collected in the Systematic Evaluation of Patients Treated With Stroke Devices for Acute Ischemic Stroke (STRATIS) registry, which began in 2014 and has data for 984 acute ischemic stroke patients with large vessel occlusions treated by mechanical thrombectomy seen at any of 55 U.S. centers. The series included 445 (45%) patients first seen as a primary stroke center and then transferred to a comprehensive center and 539 (55%) who went directly to a comprehensive stroke center (direct patients). Prior to thrombectomy, 628 of all patients (64%) received TPA, with a roughly similar percentage in both the transferred and direct patients.
The data showed that the median time from symptom onset to revascularization was 202 minutes among the direct patients and 312 minutes among those first seen at a primary stroke center and then transferred, a statistically significant difference. The average time difference per patient between the two subgroups was 100 minutes, Dr. Froehler reported.
This difference in time to reperfusion led directly to significant differences in functional outcomes after 90 days measured on the modified Rankin Scale (mRS). The percentage of patients with a mRS score of 0 or 1 (an excellent functional outcome) was 38% for the patients first seen at primary stroke centers and 47% in direct patients, a 47% relative rise in excellent outcomes among the direct patients. The percentage of patients with a mRS score of 0-2, which identifies functional independence post stroke, was 52% among transferred patients and 60% in direct patients, a 38% relative improvement for this outcome among direct patients.
The second study of stroke transfer times and outcomes used data from 562 acute ischemic stroke patients with large vessel occlusions treated in the Providence Health & Services system in five western U.S. states during 2012-2016. Nearly half the patients required a transfer and the other half went directly to a center able to perform thrombectomy. The analysis used clinical outcomes scored on the mRS at the time of hospital discharge.
“Right now, the big delay at primary stroke centers is the door-in door-out time,” commented Ryan A. McTaggart, MD, an interventional neuroradiologist at Rhode Island Hospital in Providence, the only comprehensive stroke center in Rhode Island. He helped organize a partnership with 14 primary stroke centers in Rhode Island that uses a streamlined imaging, treatment (with TPA), and transfer protocol that hacked dozens of minutes off transfer times and produced a median time from onset of symptoms to revascularization by thrombectomy of 184 minutes in patients first seen at a primary stroke center. This clocking blows past the 202 minute median for stroke onset to revascularization in the direct patients from Dr. Froehler’s study.
Stroke transport and treatment networks are now undergoing refinement in Tennessee, said Dr. Froehler, based in part on the data he reported. Considerations in Tennessee include how EMS workers assess possible stroke patients, decisions by EMS on where to take patients, and how quality of care is measured at primary and comprehensive stroke centers.
The STRATIS registry is sponsored by Medtronic. Dr. Froehler is a consultant to Medtronic, Blockade, Stryker, and Control Medical. Dr. Smith, Dr. Tarpley, and Dr. McTaggart had no disclosures.
[email protected]
On Twitter @mitchelzoler
AT THE INTERNATIONAL STROKE CONFERENCE
Key clinical point:
Major finding: In STRATIS, excellent outcomes occurred in 47% of patients sent directly to a thrombectomy hospital and in 38% of transferred patients.
Data source: The STRATIS registry, with 984 U.S. acute ischemic stroke patients, and 562 U.S. acute ischemic stroke patients from the Providence Health & Services network.
Disclosures: The STRATIS registry is sponsored by Medtronic. Dr. Froehler is a consultant to Medtronic, Blockade, Stryker, and Control Medical. Dr. Smith, Dr. Tarpley, and Dr. McTaggart had no disclosures.
Maternal vitamin E isoform levels possible marker for infant wheezing risk
ATLANTA – Increasing maternal postpartum–plasma alpha-tocopherol isoform concentration was associated with a decreased likelihood of wheezing at age 2 years, defined as wheezing in the past 12 months, use of asthma medications in the past 12 months, or diagnosis of asthma, results from a large analysis showed.
“For now, this is an association and not causation,” study author Cosby Stone, MD, MPH, said in an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology. “We need a clinical trial to evaluate the effect of giving more alpha-tocopherol to mothers during pregnancy before anyone should jump to giving supplements.”

The median age of children at the time of maternal sample collection was 50 days. 47% were female, and 61% were white. Of the 652 children, 167 (26%) met criteria for wheezing at age 2 years. These children had mothers with significantly lower postpartum concentrations of plasma alpha-tocopherol, compared with those who did not meet criteria for wheezing at 2 years (a mean of 69 micromol/L vs. 75 micromol/L, respectively; P = .02). In multivariable regression analysis, the researchers detected a significant interaction between gamma-tocopherol and alpha-tocopherol, where the highest amounts of maternal gamma-tocopherol modified and mitigated the protective association of maternal alpha-tocopherol with risk of wheezing at 2 years (P = .05).
Dr. Stone cautioned that, what is currently labeled as vitamin E or alpha-tocopherol in foods and supplements, “could be any of eight different isoforms, and alpha-tocopherol may not actually be the dominant isoform being provided. In addition, the oils that we eat are the main sources of tocopherols in our diet, and they vary widely in terms of their tocopherol isoforms. Sunflower and safflower oil, for example, provide predominantly alpha-tocopherol as their isoform of vitamin E, while corn and soy oil provide predominantly gamma-tocopherol.”
For now, he continued, correcting maternal alpha-tocopherol deficiency, currently defined by a serum alpha-tocopherol concentration less than 11.6 micromol/L, is certainly reasonable. Down the road, modification of maternal alpha-tocopherol or gamma-tocopherol concentrations through dietary counseling may provide clinicians with a tool to prevent wheezing or asthma in affected children. “In the future there may be a role for checking tocopherol isoforms in pregnant women and then modifying dietary oil consumption to protect the health of their children,” he said.
He acknowledged certain limitations of the study, including that researchers obtained maternal vitamin E isoform measurements at enrollment, when the infants were, on average, 6 weeks post partum, and not during pregnancy. “However, the literature has shown that postpartum vitamin E levels at this time point are very similar to those during the second trimester of pregnancy,” Dr. Stone said. “The literature has also shown that plasma vitamin E isoform concentrations are tightly tied to diet and body stores and do not change very rapidly (such that a woman would not be likely to go from the highest quartile to the lowest, or vice versa). People’s diets don’t tend to change that much, in general.”
INSPIRE is funded by the National Institutes of Health. Dr. Stone is funded by an NIH training grant through Vanderbilt University. He reported having no relevant financial disclosures.
ATLANTA – Increasing maternal postpartum–plasma alpha-tocopherol isoform concentration was associated with a decreased likelihood of wheezing at age 2 years, defined as wheezing in the past 12 months, use of asthma medications in the past 12 months, or diagnosis of asthma, results from a large analysis showed.
“For now, this is an association and not causation,” study author Cosby Stone, MD, MPH, said in an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology. “We need a clinical trial to evaluate the effect of giving more alpha-tocopherol to mothers during pregnancy before anyone should jump to giving supplements.”
The median age of children at the time of maternal sample collection was 50 days. 47% were female, and 61% were white. Of the 652 children, 167 (26%) met criteria for wheezing at age 2 years. These children had mothers with significantly lower postpartum concentrations of plasma alpha-tocopherol, compared with those who did not meet criteria for wheezing at 2 years (a mean of 69 micromol/L vs. 75 micromol/L, respectively; P = .02). In multivariable regression analysis, the researchers detected a significant interaction between gamma-tocopherol and alpha-tocopherol, where the highest amounts of maternal gamma-tocopherol modified and mitigated the protective association of maternal alpha-tocopherol with risk of wheezing at 2 years (P = .05).
Dr. Stone cautioned that, what is currently labeled as vitamin E or alpha-tocopherol in foods and supplements, “could be any of eight different isoforms, and alpha-tocopherol may not actually be the dominant isoform being provided. In addition, the oils that we eat are the main sources of tocopherols in our diet, and they vary widely in terms of their tocopherol isoforms. Sunflower and safflower oil, for example, provide predominantly alpha-tocopherol as their isoform of vitamin E, while corn and soy oil provide predominantly gamma-tocopherol.”
For now, he continued, correcting maternal alpha-tocopherol deficiency, currently defined by a serum alpha-tocopherol concentration less than 11.6 micromol/L, is certainly reasonable. Down the road, modification of maternal alpha-tocopherol or gamma-tocopherol concentrations through dietary counseling may provide clinicians with a tool to prevent wheezing or asthma in affected children. “In the future there may be a role for checking tocopherol isoforms in pregnant women and then modifying dietary oil consumption to protect the health of their children,” he said.
He acknowledged certain limitations of the study, including that researchers obtained maternal vitamin E isoform measurements at enrollment, when the infants were, on average, 6 weeks post partum, and not during pregnancy. “However, the literature has shown that postpartum vitamin E levels at this time point are very similar to those during the second trimester of pregnancy,” Dr. Stone said. “The literature has also shown that plasma vitamin E isoform concentrations are tightly tied to diet and body stores and do not change very rapidly (such that a woman would not be likely to go from the highest quartile to the lowest, or vice versa). People’s diets don’t tend to change that much, in general.”
INSPIRE is funded by the National Institutes of Health. Dr. Stone is funded by an NIH training grant through Vanderbilt University. He reported having no relevant financial disclosures.
ATLANTA – Increasing maternal postpartum–plasma alpha-tocopherol isoform concentration was associated with a decreased likelihood of wheezing at age 2 years, defined as wheezing in the past 12 months, use of asthma medications in the past 12 months, or diagnosis of asthma, results from a large analysis showed.
“For now, this is an association and not causation,” study author Cosby Stone, MD, MPH, said in an interview in advance of the annual meeting of the American Academy of Allergy, Asthma, and Immunology. “We need a clinical trial to evaluate the effect of giving more alpha-tocopherol to mothers during pregnancy before anyone should jump to giving supplements.”
The median age of children at the time of maternal sample collection was 50 days. 47% were female, and 61% were white. Of the 652 children, 167 (26%) met criteria for wheezing at age 2 years. These children had mothers with significantly lower postpartum concentrations of plasma alpha-tocopherol, compared with those who did not meet criteria for wheezing at 2 years (a mean of 69 micromol/L vs. 75 micromol/L, respectively; P = .02). In multivariable regression analysis, the researchers detected a significant interaction between gamma-tocopherol and alpha-tocopherol, where the highest amounts of maternal gamma-tocopherol modified and mitigated the protective association of maternal alpha-tocopherol with risk of wheezing at 2 years (P = .05).
Dr. Stone cautioned that, what is currently labeled as vitamin E or alpha-tocopherol in foods and supplements, “could be any of eight different isoforms, and alpha-tocopherol may not actually be the dominant isoform being provided. In addition, the oils that we eat are the main sources of tocopherols in our diet, and they vary widely in terms of their tocopherol isoforms. Sunflower and safflower oil, for example, provide predominantly alpha-tocopherol as their isoform of vitamin E, while corn and soy oil provide predominantly gamma-tocopherol.”
For now, he continued, correcting maternal alpha-tocopherol deficiency, currently defined by a serum alpha-tocopherol concentration less than 11.6 micromol/L, is certainly reasonable. Down the road, modification of maternal alpha-tocopherol or gamma-tocopherol concentrations through dietary counseling may provide clinicians with a tool to prevent wheezing or asthma in affected children. “In the future there may be a role for checking tocopherol isoforms in pregnant women and then modifying dietary oil consumption to protect the health of their children,” he said.
He acknowledged certain limitations of the study, including that researchers obtained maternal vitamin E isoform measurements at enrollment, when the infants were, on average, 6 weeks post partum, and not during pregnancy. “However, the literature has shown that postpartum vitamin E levels at this time point are very similar to those during the second trimester of pregnancy,” Dr. Stone said. “The literature has also shown that plasma vitamin E isoform concentrations are tightly tied to diet and body stores and do not change very rapidly (such that a woman would not be likely to go from the highest quartile to the lowest, or vice versa). People’s diets don’t tend to change that much, in general.”
INSPIRE is funded by the National Institutes of Health. Dr. Stone is funded by an NIH training grant through Vanderbilt University. He reported having no relevant financial disclosures.
AT THE 2017 AAAAI ANNUAL MEETING
Key clinical point:
Major finding: Increasing maternal postpartum–plasma alpha-tocopherol concentration was associated with a decreased likelihood of wheezing requiring asthma medications at 2 years (P = .02).
Data source: A prospective evaluation of 652 children with maternal postpartum–plasma vitamin E isoforms measured at study enrollment.
Disclosures: INSPIRE is funded by the National Institutes of Health. Dr. Stone is funded by an NIH training grant through Vanderbilt University. He reported having no relevant financial disclosures.
Study advances precision opioid dosing for mucositis

ORLANDO, FL—A pilot study to determine the burden of mucositis in pediatric patients undergoing hematopoietic stem cell transplant (HSCT) showed that more than 50% of patients required a change in their opioids either for toxicity or lack of efficacy.
Investigators also observed that patients’ genotypes were associated with time to optimal pain control, although this needs to be defined more clearly in larger prospective studies.
“Pain from mucositis is a major problem during the early post-transplant period in pediatric patients,” said M. Christa Krupski, DO, of Cincinnati Children’s Hospital Medical Center in Ohio.
The pain frequently requires intravenous (IV) pain medication, but adequate pain management is often delayed by the trial and error of finding the right agent or the right dose, Dr Krupski added.
She and her colleagues tried to find predictors of mucositis that would help optimize pain control and minimize adverse effects of pain medication.
Dr Krupski presented the group’s findings at the 2017 BMT Tandem Meetings as abstract 50*.
Based on the investigators’ previous experience using a pain chip, they hypothesized that host genetic polymorphisms would predict perception of mucositis pain, opioid efficacy, and opioid-induced adverse effects in pediatric patients undergoing HSCT.
The pain chip was comprised of a panel of 46 single-nucleotide polymorphisms (SNPs) in a set of candidate genes known to influence opioid effect.
Study design
In this single-institution, retrospective pilot study, investigators genotyped 100 consecutive HSCT patients using pre-transplant samples.
The team collected demographic and transplant data, information on the utilization of pain medication, and mucositis data according to the standard CTCAE guidelines.
“And it must be noted,” Dr Krupski said, “that many of our patients required total parenteral nutrition during the transplant process, which automatically made them a grade 3 for mucositis.”
The investigators assessed pain using 2 scales, the Face, Legs, Activity, Cry, Consolability (FLACC) Scale, which is an objective measurement, and the more subjective Numeric Rating Scores (NRS).
Demographics
Patients were a median age of 9.9 years (range, 0.5–32.8), 65% were male, 87% were Caucasian, and 13% non-Caucasian.
The main indications for transplant were malignancy (45%), immune deficiency/dysregulation (30%), and bone marrow failure syndrome (19%).
More than two-thirds (68%) of patients had received a myeloablative conditioning regimen.
Results—mucositis
Seventy-six patients experienced mucositis, three-quarters of whom (78%) had received a myeloablative conditioning regimen.
The majority of patients (57%) had severe mucositis, which developed a median of 3 days after transplant (range, -2 to 17).
Regarding treatment, 13 (17%) had medication as needed or no medication, 5 (7%) had scheduled IV opioid, and 58 (76%) had patient-controlled analgesia (PCA).
For analysis purposes, the investigators grouped together the scheduled IV opioid and PCA treatment groups.
Results—opioid efficacy
The opioid efficacy analysis was based on 63 patients.
Time to optimal pain control was a median of 7 days (range, 0–22), and the morphine dose at the time of optimal pain control was a median of 1.5 mg/kg (range, 0.2–15.7).
“You will note, though, the wide inter-patient variability,” Dr Krupski pointed out, “with some of our patients immediately achieving optimal pain control the day the medication was started and others taking over 3 weeks to reach optimal pain control.”
Investigators observed similar inter-patient variability in morphine equivalent use at the time of optimal pain control and total morphine equivalent use.
The total time patients were on PCA was a median of 16 days (range, 1–32), and the median total morphine equivalent use was 0.99 mg/kg/day (range, 0.10–8.07).
“Most interesting, though, was that 18 patients, or nearly one-third of the patients requiring IV opioids, required a change in this opioid due to poor efficacy,” Dr Krupski said.
Results—opioid toxicity
Thirty-two (51%) patients experienced at least 1 adverse effect from their pain medication.
Specific toxicities, based on 32 patients, included pruritus (53%), sedation (16%), and nausea/vomiting (9%). Six patients (19%) had more than one adverse event.
“Similar to what we observed with respect to opioid efficacy,” Dr Krupski said, “another one-third of our patients with mucositis required a change in opioid due to toxicity.”
Results—impact of race
Non-Caucasians patients (n=13) had a significantly higher incidence of mucositis (100%) than Caucasians (n=87, 72%, P=0.03).
Non-Caucasian patients also experienced significantly more pain with mucositis (P=0.03), even though the severity of mucositis did not differ between the 2 groups.
The total equivalent dose of morphine used also did not differ between the groups.
“This raises the question of whether there are factors other than race that may be contributing to this difference,” Dr Krupski said.
Genetic findings
The UGT2B7 gene encodes the main enzyme metabolizer of morphine, and SNPs of this gene (rs7668258 and rs7439366) vary by race.
Non-Caucasian patients had significantly more wild-type SNPs than Caucasian patients (P=0.001). And patients with the wild-type UGT2B7 genotype spent more total days on IV opioids than patients with variant alleles (P=0.03).
On examination of rs4633, a SNP of the COMT gene, which is a key regulator of pain perception, the investigators observed some different findings from what had previously been reported.
There was no difference in mucositis severity between patients with the wild-type and variant allele (P=0.3).
However, patients with the variant allele required more days to optimal pain control than patients with the wild-type allele (P=0.04). This finding confirmed increased pain sensitivity associated with the genotype, irrespective of race.
“[I]f this association holds true in future studies,” Dr Krupski explained, “one may be more aggressive in the initial opioid titration to optimize pain control.”
Despite limitations of sample size, especially with respect to non-Caucasian patients, the pilot study showed association, but not causation, with respect to genetic variants.
“Racial differences affect mucositis pain perception and opioid requirement,” Dr Krupski said. “If genotyping is not feasible, it is important to pay particular attention to this difference while managing patients’ pain from mucositis.”
“We have an opportunity here to improve our care. Therefore, our plan is to validate these findings in additional patients before we use them to achieve our ultimate goal: precision dosing of opioids to individual patients.” ![]()
*Data in the abstract differ slightly from the presentation.
ORLANDO, FL—A pilot study to determine the burden of mucositis in pediatric patients undergoing hematopoietic stem cell transplant (HSCT) showed that more than 50% of patients required a change in their opioids either for toxicity or lack of efficacy.
Investigators also observed that patients’ genotypes were associated with time to optimal pain control, although this needs to be defined more clearly in larger prospective studies.
“Pain from mucositis is a major problem during the early post-transplant period in pediatric patients,” said M. Christa Krupski, DO, of Cincinnati Children’s Hospital Medical Center in Ohio.
The pain frequently requires intravenous (IV) pain medication, but adequate pain management is often delayed by the trial and error of finding the right agent or the right dose, Dr Krupski added.
She and her colleagues tried to find predictors of mucositis that would help optimize pain control and minimize adverse effects of pain medication.
Dr Krupski presented the group’s findings at the 2017 BMT Tandem Meetings as abstract 50*.
Based on the investigators’ previous experience using a pain chip, they hypothesized that host genetic polymorphisms would predict perception of mucositis pain, opioid efficacy, and opioid-induced adverse effects in pediatric patients undergoing HSCT.
The pain chip was comprised of a panel of 46 single-nucleotide polymorphisms (SNPs) in a set of candidate genes known to influence opioid effect.
Study design
In this single-institution, retrospective pilot study, investigators genotyped 100 consecutive HSCT patients using pre-transplant samples.
The team collected demographic and transplant data, information on the utilization of pain medication, and mucositis data according to the standard CTCAE guidelines.
“And it must be noted,” Dr Krupski said, “that many of our patients required total parenteral nutrition during the transplant process, which automatically made them a grade 3 for mucositis.”
The investigators assessed pain using 2 scales, the Face, Legs, Activity, Cry, Consolability (FLACC) Scale, which is an objective measurement, and the more subjective Numeric Rating Scores (NRS).
Demographics
Patients were a median age of 9.9 years (range, 0.5–32.8), 65% were male, 87% were Caucasian, and 13% non-Caucasian.
The main indications for transplant were malignancy (45%), immune deficiency/dysregulation (30%), and bone marrow failure syndrome (19%).
More than two-thirds (68%) of patients had received a myeloablative conditioning regimen.
Results—mucositis
Seventy-six patients experienced mucositis, three-quarters of whom (78%) had received a myeloablative conditioning regimen.
The majority of patients (57%) had severe mucositis, which developed a median of 3 days after transplant (range, -2 to 17).
Regarding treatment, 13 (17%) had medication as needed or no medication, 5 (7%) had scheduled IV opioid, and 58 (76%) had patient-controlled analgesia (PCA).
For analysis purposes, the investigators grouped together the scheduled IV opioid and PCA treatment groups.
Results—opioid efficacy
The opioid efficacy analysis was based on 63 patients.
Time to optimal pain control was a median of 7 days (range, 0–22), and the morphine dose at the time of optimal pain control was a median of 1.5 mg/kg (range, 0.2–15.7).
“You will note, though, the wide inter-patient variability,” Dr Krupski pointed out, “with some of our patients immediately achieving optimal pain control the day the medication was started and others taking over 3 weeks to reach optimal pain control.”
Investigators observed similar inter-patient variability in morphine equivalent use at the time of optimal pain control and total morphine equivalent use.
The total time patients were on PCA was a median of 16 days (range, 1–32), and the median total morphine equivalent use was 0.99 mg/kg/day (range, 0.10–8.07).
“Most interesting, though, was that 18 patients, or nearly one-third of the patients requiring IV opioids, required a change in this opioid due to poor efficacy,” Dr Krupski said.
Results—opioid toxicity
Thirty-two (51%) patients experienced at least 1 adverse effect from their pain medication.
Specific toxicities, based on 32 patients, included pruritus (53%), sedation (16%), and nausea/vomiting (9%). Six patients (19%) had more than one adverse event.
“Similar to what we observed with respect to opioid efficacy,” Dr Krupski said, “another one-third of our patients with mucositis required a change in opioid due to toxicity.”
Results—impact of race
Non-Caucasians patients (n=13) had a significantly higher incidence of mucositis (100%) than Caucasians (n=87, 72%, P=0.03).
Non-Caucasian patients also experienced significantly more pain with mucositis (P=0.03), even though the severity of mucositis did not differ between the 2 groups.
The total equivalent dose of morphine used also did not differ between the groups.
“This raises the question of whether there are factors other than race that may be contributing to this difference,” Dr Krupski said.
Genetic findings
The UGT2B7 gene encodes the main enzyme metabolizer of morphine, and SNPs of this gene (rs7668258 and rs7439366) vary by race.
Non-Caucasian patients had significantly more wild-type SNPs than Caucasian patients (P=0.001). And patients with the wild-type UGT2B7 genotype spent more total days on IV opioids than patients with variant alleles (P=0.03).
On examination of rs4633, a SNP of the COMT gene, which is a key regulator of pain perception, the investigators observed some different findings from what had previously been reported.
There was no difference in mucositis severity between patients with the wild-type and variant allele (P=0.3).
However, patients with the variant allele required more days to optimal pain control than patients with the wild-type allele (P=0.04). This finding confirmed increased pain sensitivity associated with the genotype, irrespective of race.
“[I]f this association holds true in future studies,” Dr Krupski explained, “one may be more aggressive in the initial opioid titration to optimize pain control.”
Despite limitations of sample size, especially with respect to non-Caucasian patients, the pilot study showed association, but not causation, with respect to genetic variants.
“Racial differences affect mucositis pain perception and opioid requirement,” Dr Krupski said. “If genotyping is not feasible, it is important to pay particular attention to this difference while managing patients’ pain from mucositis.”
“We have an opportunity here to improve our care. Therefore, our plan is to validate these findings in additional patients before we use them to achieve our ultimate goal: precision dosing of opioids to individual patients.” ![]()
*Data in the abstract differ slightly from the presentation.
ORLANDO, FL—A pilot study to determine the burden of mucositis in pediatric patients undergoing hematopoietic stem cell transplant (HSCT) showed that more than 50% of patients required a change in their opioids either for toxicity or lack of efficacy.
Investigators also observed that patients’ genotypes were associated with time to optimal pain control, although this needs to be defined more clearly in larger prospective studies.
“Pain from mucositis is a major problem during the early post-transplant period in pediatric patients,” said M. Christa Krupski, DO, of Cincinnati Children’s Hospital Medical Center in Ohio.
The pain frequently requires intravenous (IV) pain medication, but adequate pain management is often delayed by the trial and error of finding the right agent or the right dose, Dr Krupski added.
She and her colleagues tried to find predictors of mucositis that would help optimize pain control and minimize adverse effects of pain medication.
Dr Krupski presented the group’s findings at the 2017 BMT Tandem Meetings as abstract 50*.
Based on the investigators’ previous experience using a pain chip, they hypothesized that host genetic polymorphisms would predict perception of mucositis pain, opioid efficacy, and opioid-induced adverse effects in pediatric patients undergoing HSCT.
The pain chip was comprised of a panel of 46 single-nucleotide polymorphisms (SNPs) in a set of candidate genes known to influence opioid effect.
Study design
In this single-institution, retrospective pilot study, investigators genotyped 100 consecutive HSCT patients using pre-transplant samples.
The team collected demographic and transplant data, information on the utilization of pain medication, and mucositis data according to the standard CTCAE guidelines.
“And it must be noted,” Dr Krupski said, “that many of our patients required total parenteral nutrition during the transplant process, which automatically made them a grade 3 for mucositis.”
The investigators assessed pain using 2 scales, the Face, Legs, Activity, Cry, Consolability (FLACC) Scale, which is an objective measurement, and the more subjective Numeric Rating Scores (NRS).
Demographics
Patients were a median age of 9.9 years (range, 0.5–32.8), 65% were male, 87% were Caucasian, and 13% non-Caucasian.
The main indications for transplant were malignancy (45%), immune deficiency/dysregulation (30%), and bone marrow failure syndrome (19%).
More than two-thirds (68%) of patients had received a myeloablative conditioning regimen.
Results—mucositis
Seventy-six patients experienced mucositis, three-quarters of whom (78%) had received a myeloablative conditioning regimen.
The majority of patients (57%) had severe mucositis, which developed a median of 3 days after transplant (range, -2 to 17).
Regarding treatment, 13 (17%) had medication as needed or no medication, 5 (7%) had scheduled IV opioid, and 58 (76%) had patient-controlled analgesia (PCA).
For analysis purposes, the investigators grouped together the scheduled IV opioid and PCA treatment groups.
Results—opioid efficacy
The opioid efficacy analysis was based on 63 patients.
Time to optimal pain control was a median of 7 days (range, 0–22), and the morphine dose at the time of optimal pain control was a median of 1.5 mg/kg (range, 0.2–15.7).
“You will note, though, the wide inter-patient variability,” Dr Krupski pointed out, “with some of our patients immediately achieving optimal pain control the day the medication was started and others taking over 3 weeks to reach optimal pain control.”
Investigators observed similar inter-patient variability in morphine equivalent use at the time of optimal pain control and total morphine equivalent use.
The total time patients were on PCA was a median of 16 days (range, 1–32), and the median total morphine equivalent use was 0.99 mg/kg/day (range, 0.10–8.07).
“Most interesting, though, was that 18 patients, or nearly one-third of the patients requiring IV opioids, required a change in this opioid due to poor efficacy,” Dr Krupski said.
Results—opioid toxicity
Thirty-two (51%) patients experienced at least 1 adverse effect from their pain medication.
Specific toxicities, based on 32 patients, included pruritus (53%), sedation (16%), and nausea/vomiting (9%). Six patients (19%) had more than one adverse event.
“Similar to what we observed with respect to opioid efficacy,” Dr Krupski said, “another one-third of our patients with mucositis required a change in opioid due to toxicity.”
Results—impact of race
Non-Caucasians patients (n=13) had a significantly higher incidence of mucositis (100%) than Caucasians (n=87, 72%, P=0.03).
Non-Caucasian patients also experienced significantly more pain with mucositis (P=0.03), even though the severity of mucositis did not differ between the 2 groups.
The total equivalent dose of morphine used also did not differ between the groups.
“This raises the question of whether there are factors other than race that may be contributing to this difference,” Dr Krupski said.
Genetic findings
The UGT2B7 gene encodes the main enzyme metabolizer of morphine, and SNPs of this gene (rs7668258 and rs7439366) vary by race.
Non-Caucasian patients had significantly more wild-type SNPs than Caucasian patients (P=0.001). And patients with the wild-type UGT2B7 genotype spent more total days on IV opioids than patients with variant alleles (P=0.03).
On examination of rs4633, a SNP of the COMT gene, which is a key regulator of pain perception, the investigators observed some different findings from what had previously been reported.
There was no difference in mucositis severity between patients with the wild-type and variant allele (P=0.3).
However, patients with the variant allele required more days to optimal pain control than patients with the wild-type allele (P=0.04). This finding confirmed increased pain sensitivity associated with the genotype, irrespective of race.
“[I]f this association holds true in future studies,” Dr Krupski explained, “one may be more aggressive in the initial opioid titration to optimize pain control.”
Despite limitations of sample size, especially with respect to non-Caucasian patients, the pilot study showed association, but not causation, with respect to genetic variants.
“Racial differences affect mucositis pain perception and opioid requirement,” Dr Krupski said. “If genotyping is not feasible, it is important to pay particular attention to this difference while managing patients’ pain from mucositis.”
“We have an opportunity here to improve our care. Therefore, our plan is to validate these findings in additional patients before we use them to achieve our ultimate goal: precision dosing of opioids to individual patients.” ![]()
*Data in the abstract differ slightly from the presentation.
FDA approves new unit for clot-dissolving device

The US Food and Drug Administration (FDA) has granted 510(k) clearance for the EKOS® Control Unit 4.0, a new unit that can control the EKOS® System.
The EKOS System includes an ultrasonic device that uses acoustic pulses to enhance the effects of thrombolytic drugs and dissolve blood clots in patients with deep vein thrombosis, pulmonary embolism, and peripheral arterial occlusions.
With this system, acoustic pulses unwind and thin fibrin to expose drug receptor sites.
This allows thrombolytic drugs to reach deeper into clots, accelerating absorption and helping to dissolve clots faster and with less drug, according to BTG International LTD, the company that markets the EKOS System.
The EKOS Control Unit 4.0 replaces the EKOS System’s old control unit. The new unit can support 2 EKOS devices, allowing physicians to use a single control unit to treat both pulmonary arteries, with the goal of simplifying bilateral pulmonary embolism treatment.
The EKOS System (formerly known as the EkoSonic Endovascular System) was approved by the FDA in 2014.
In clinical studies, the system has been shown to speed time to clot dissolution, increase clot removal, and enhance clinical improvement compared to either standard catheter-directed drug therapy or thrombectomy.1,2
Research has also shown that the EKOS System requires significantly shorter treatment times and less thrombolytic compared to standard catheter-directed drug therapy3, 4,5, lowering the risk of bleeding and other complications.1,5,6 ![]()
1. Lin, P, et al, “Comparison of Percutaneous Ultrasound-Accelerated Thrombolysis versus Catheter-Directed Thrombolysis in Patients with Acute Massive Pulmonary Embolism.” Vascular, Vol. 17, Suppl. 3, 2009, S137–S147.
2. Schrijver, AM, et al, “Dutch Randomized Trial Comparing Standard Catheter-Directed Thrombolysis and Ultrasound-Accelerated Thrombolysis for Arterial Thromboembolic Infrainguinal Disease (DUET)." Journal of Endovascular Therapy 2015, Vol. 22(1):87-95.
3. Litzendorf, ME, et al, “Ultrasound-accelerated thrombolysis is superior to catheter-directed thrombolysis for the treatment of acute limb ischemia.” Journal of Vascular Surgery, Jun 2011; 53(Suppl S), p106S-107S.
4. Lin, P, et al, “Catheter-Directed Thrombectomy and Thrombolysis for Symptomatic Lower-Extremity Deep Vein Thrombosis: Review of Current Interventional Treatment Strategies.” Perspectives in Vascular Surgery and Endovascular Therapy, 2010, 22(3): 152–163.
5. Parikh, S, et al, “Ultrasound-Accelerated Thrombolysis for the Treatment of Deep Vein Thrombosis: Initial Clinical Experience.” Journal of Vascular and Interventional Radiology, Vol. 19, Issue 4, April 2008, 521–528.
6. Kucher, N, et al, “Randomized, Controlled Trial of Ultrasound-Assisted Catheter-Directed Thrombolysis for Acute Intermediate-Risk Pulmonary Embolism.” Circulation, Vol. 129, No. 4, 2014, 479–486.
The US Food and Drug Administration (FDA) has granted 510(k) clearance for the EKOS® Control Unit 4.0, a new unit that can control the EKOS® System.
The EKOS System includes an ultrasonic device that uses acoustic pulses to enhance the effects of thrombolytic drugs and dissolve blood clots in patients with deep vein thrombosis, pulmonary embolism, and peripheral arterial occlusions.
With this system, acoustic pulses unwind and thin fibrin to expose drug receptor sites.
This allows thrombolytic drugs to reach deeper into clots, accelerating absorption and helping to dissolve clots faster and with less drug, according to BTG International LTD, the company that markets the EKOS System.
The EKOS Control Unit 4.0 replaces the EKOS System’s old control unit. The new unit can support 2 EKOS devices, allowing physicians to use a single control unit to treat both pulmonary arteries, with the goal of simplifying bilateral pulmonary embolism treatment.
The EKOS System (formerly known as the EkoSonic Endovascular System) was approved by the FDA in 2014.
In clinical studies, the system has been shown to speed time to clot dissolution, increase clot removal, and enhance clinical improvement compared to either standard catheter-directed drug therapy or thrombectomy.1,2
Research has also shown that the EKOS System requires significantly shorter treatment times and less thrombolytic compared to standard catheter-directed drug therapy3, 4,5, lowering the risk of bleeding and other complications.1,5,6 ![]()
1. Lin, P, et al, “Comparison of Percutaneous Ultrasound-Accelerated Thrombolysis versus Catheter-Directed Thrombolysis in Patients with Acute Massive Pulmonary Embolism.” Vascular, Vol. 17, Suppl. 3, 2009, S137–S147.
2. Schrijver, AM, et al, “Dutch Randomized Trial Comparing Standard Catheter-Directed Thrombolysis and Ultrasound-Accelerated Thrombolysis for Arterial Thromboembolic Infrainguinal Disease (DUET)." Journal of Endovascular Therapy 2015, Vol. 22(1):87-95.
3. Litzendorf, ME, et al, “Ultrasound-accelerated thrombolysis is superior to catheter-directed thrombolysis for the treatment of acute limb ischemia.” Journal of Vascular Surgery, Jun 2011; 53(Suppl S), p106S-107S.
4. Lin, P, et al, “Catheter-Directed Thrombectomy and Thrombolysis for Symptomatic Lower-Extremity Deep Vein Thrombosis: Review of Current Interventional Treatment Strategies.” Perspectives in Vascular Surgery and Endovascular Therapy, 2010, 22(3): 152–163.
5. Parikh, S, et al, “Ultrasound-Accelerated Thrombolysis for the Treatment of Deep Vein Thrombosis: Initial Clinical Experience.” Journal of Vascular and Interventional Radiology, Vol. 19, Issue 4, April 2008, 521–528.
6. Kucher, N, et al, “Randomized, Controlled Trial of Ultrasound-Assisted Catheter-Directed Thrombolysis for Acute Intermediate-Risk Pulmonary Embolism.” Circulation, Vol. 129, No. 4, 2014, 479–486.
The US Food and Drug Administration (FDA) has granted 510(k) clearance for the EKOS® Control Unit 4.0, a new unit that can control the EKOS® System.
The EKOS System includes an ultrasonic device that uses acoustic pulses to enhance the effects of thrombolytic drugs and dissolve blood clots in patients with deep vein thrombosis, pulmonary embolism, and peripheral arterial occlusions.
With this system, acoustic pulses unwind and thin fibrin to expose drug receptor sites.
This allows thrombolytic drugs to reach deeper into clots, accelerating absorption and helping to dissolve clots faster and with less drug, according to BTG International LTD, the company that markets the EKOS System.
The EKOS Control Unit 4.0 replaces the EKOS System’s old control unit. The new unit can support 2 EKOS devices, allowing physicians to use a single control unit to treat both pulmonary arteries, with the goal of simplifying bilateral pulmonary embolism treatment.
The EKOS System (formerly known as the EkoSonic Endovascular System) was approved by the FDA in 2014.
In clinical studies, the system has been shown to speed time to clot dissolution, increase clot removal, and enhance clinical improvement compared to either standard catheter-directed drug therapy or thrombectomy.1,2
Research has also shown that the EKOS System requires significantly shorter treatment times and less thrombolytic compared to standard catheter-directed drug therapy3, 4,5, lowering the risk of bleeding and other complications.1,5,6 ![]()
1. Lin, P, et al, “Comparison of Percutaneous Ultrasound-Accelerated Thrombolysis versus Catheter-Directed Thrombolysis in Patients with Acute Massive Pulmonary Embolism.” Vascular, Vol. 17, Suppl. 3, 2009, S137–S147.
2. Schrijver, AM, et al, “Dutch Randomized Trial Comparing Standard Catheter-Directed Thrombolysis and Ultrasound-Accelerated Thrombolysis for Arterial Thromboembolic Infrainguinal Disease (DUET)." Journal of Endovascular Therapy 2015, Vol. 22(1):87-95.
3. Litzendorf, ME, et al, “Ultrasound-accelerated thrombolysis is superior to catheter-directed thrombolysis for the treatment of acute limb ischemia.” Journal of Vascular Surgery, Jun 2011; 53(Suppl S), p106S-107S.
4. Lin, P, et al, “Catheter-Directed Thrombectomy and Thrombolysis for Symptomatic Lower-Extremity Deep Vein Thrombosis: Review of Current Interventional Treatment Strategies.” Perspectives in Vascular Surgery and Endovascular Therapy, 2010, 22(3): 152–163.
5. Parikh, S, et al, “Ultrasound-Accelerated Thrombolysis for the Treatment of Deep Vein Thrombosis: Initial Clinical Experience.” Journal of Vascular and Interventional Radiology, Vol. 19, Issue 4, April 2008, 521–528.
6. Kucher, N, et al, “Randomized, Controlled Trial of Ultrasound-Assisted Catheter-Directed Thrombolysis for Acute Intermediate-Risk Pulmonary Embolism.” Circulation, Vol. 129, No. 4, 2014, 479–486.
Large, intermittent vitamin D doses may increase fracture, fall risk in elderly
ORLANDO – The vitamin that keeps bones strong and protects against colon cancer also can, in large doses, increase the risk of falls and fractures.
Studies of high-dose vitamin D keep turning up the same concerns, Dr. Martin Weinstock said at the annual meeting of the American Academy of Dermatology. The most striking of these findings are the significantly increased risks of falls and fractures associated with vitamin D megadoses, said Dr. Weinstock of Brown University, Providence, R.I. These trials examined very-large intermittent doses of the vitamin given to elderly patients.
That amount of vitamin D, taken all at once, may seem like a therapeutic outlier to clinicians who are used to giving 2,000-4,000 IU/day, as recommended by the 2011 Institute of Medicine report.
Not so fast, said Dr. Weinstock.
“If you do the math, if you’re taking 2,000 IU every day, that’s 60,000 IU per month. That’s a high dose,” he said. However, he noted, daily supplements in that range appear safe. “It seems that this intermittent dosing in these studies might be the problem.”
The IOM report, an exhaustive, 1,000-page article summarizing the extant data on vitamin D – is considered the optimal dosing guide. For healthy patients, it recommends the following as minimum effective and maximum safe doses:
- 400-1,000 IU/day for infants younger than 6 month.
- 400-1,500 IU/day for infants aged 6-12 months.
- 600-2,000 IU/day for children aged 1-3 years.
- 600-3,000 IU/day for children aged 4-8 years.
- 600-4,000 IU/day for everyone aged 9 years and older.
But dosing of this fat-soluble vitamin should, in some cases, be individualized. For example, obese patients may have persistently low levels despite supplementation, as fat can sequester the vitamin. Patients with fat-metabolizing disorders may not absorb it well. And patients who have had gastric bypass may face the same issues of malabsorption, but from a mechanical, not a metabolic, standpoint.
Elderly people are particularly susceptible to vitamin D deficiency for a couple of reasons, Dr. Weinstock said. They may be less mobile, so lack exposure to sunlight. Age also can decrease the ability to convert 25-hydroxyvitamin D to the biologically active vitamin.
Mega-dosing has been an attractive method of raising and maintaining levels in this population. But several studies illustrate the risks that come along with this strategy, he noted.
A 2007 study randomized 9,440 men and women 75 years or older to placebo or to a single, 300,000 IU vitamin D intramuscular injection for 3 years. At the end of that time, the rate of falls had not significantly changed, but the rate of hip fractures had increased by 49% (Rheumatology [Oxford] 2007;46:1852-7).
Fractures occurred in 585 subjects, including 110 hip fractures, 116 wrist fractures, and 37 ankle fractures. This represented a 49% increase in any hip fracture and a 22% increase in wrist fracture over the placebo group.
A similar study, published in 2010, randomized 2,225 elderly women to placebo or a single 500,000 oral dose of vitamin D for 4 years. There were 171 fractures in the active group and 135 in the placebo group – a 26% increased risk (JAMA. 2010;303[18]:1815-22).
The fall rate in the active group was 83.4/100 person-years, compared with 72.7/100 person-years in the placebo group. This represented a significant 26% increased fracture risk and 15% increased fall risk.
Interestingly, most of these incidents occurred within the first 3 months after each dose,” Dr. Weinstock said. Those taking vitamin D were 31% more likely to fall in that time period, but no more likely to fall in the subsequent 9 months after each dose.
In 2016, a third study looked at functional status among 200 elderly men and women in a three-armed randomization: a low-dose control group receiving 24,000 IU of vitamin D; 60,000 IU vitamin D3; or 24,000 IU of vitamin plus 300 mcg calcifediol.
Functional status didn’t differ between the groups at the end of 1 year. But the incidence of falls did differ, with falls occurring in 67% of the 60,000 IU group, 54% of the 24,000 IU/calcifediol group, and 48% of the 24,000 IU control group (JAMA Intern Med. 2016;176[2]:175-83).
This represented a 47% increased fall risk in the high dose group, compared with the two low-dose groups.
Dr. Weinstein had no financial disclosures relevant to his lecture.
[email protected]
On Twitter @Alz_Gal
ORLANDO – The vitamin that keeps bones strong and protects against colon cancer also can, in large doses, increase the risk of falls and fractures.
Studies of high-dose vitamin D keep turning up the same concerns, Dr. Martin Weinstock said at the annual meeting of the American Academy of Dermatology. The most striking of these findings are the significantly increased risks of falls and fractures associated with vitamin D megadoses, said Dr. Weinstock of Brown University, Providence, R.I. These trials examined very-large intermittent doses of the vitamin given to elderly patients.
That amount of vitamin D, taken all at once, may seem like a therapeutic outlier to clinicians who are used to giving 2,000-4,000 IU/day, as recommended by the 2011 Institute of Medicine report.
Not so fast, said Dr. Weinstock.
“If you do the math, if you’re taking 2,000 IU every day, that’s 60,000 IU per month. That’s a high dose,” he said. However, he noted, daily supplements in that range appear safe. “It seems that this intermittent dosing in these studies might be the problem.”
The IOM report, an exhaustive, 1,000-page article summarizing the extant data on vitamin D – is considered the optimal dosing guide. For healthy patients, it recommends the following as minimum effective and maximum safe doses:
- 400-1,000 IU/day for infants younger than 6 month.
- 400-1,500 IU/day for infants aged 6-12 months.
- 600-2,000 IU/day for children aged 1-3 years.
- 600-3,000 IU/day for children aged 4-8 years.
- 600-4,000 IU/day for everyone aged 9 years and older.
But dosing of this fat-soluble vitamin should, in some cases, be individualized. For example, obese patients may have persistently low levels despite supplementation, as fat can sequester the vitamin. Patients with fat-metabolizing disorders may not absorb it well. And patients who have had gastric bypass may face the same issues of malabsorption, but from a mechanical, not a metabolic, standpoint.
Elderly people are particularly susceptible to vitamin D deficiency for a couple of reasons, Dr. Weinstock said. They may be less mobile, so lack exposure to sunlight. Age also can decrease the ability to convert 25-hydroxyvitamin D to the biologically active vitamin.
Mega-dosing has been an attractive method of raising and maintaining levels in this population. But several studies illustrate the risks that come along with this strategy, he noted.
A 2007 study randomized 9,440 men and women 75 years or older to placebo or to a single, 300,000 IU vitamin D intramuscular injection for 3 years. At the end of that time, the rate of falls had not significantly changed, but the rate of hip fractures had increased by 49% (Rheumatology [Oxford] 2007;46:1852-7).
Fractures occurred in 585 subjects, including 110 hip fractures, 116 wrist fractures, and 37 ankle fractures. This represented a 49% increase in any hip fracture and a 22% increase in wrist fracture over the placebo group.
A similar study, published in 2010, randomized 2,225 elderly women to placebo or a single 500,000 oral dose of vitamin D for 4 years. There were 171 fractures in the active group and 135 in the placebo group – a 26% increased risk (JAMA. 2010;303[18]:1815-22).
The fall rate in the active group was 83.4/100 person-years, compared with 72.7/100 person-years in the placebo group. This represented a significant 26% increased fracture risk and 15% increased fall risk.
Interestingly, most of these incidents occurred within the first 3 months after each dose,” Dr. Weinstock said. Those taking vitamin D were 31% more likely to fall in that time period, but no more likely to fall in the subsequent 9 months after each dose.
In 2016, a third study looked at functional status among 200 elderly men and women in a three-armed randomization: a low-dose control group receiving 24,000 IU of vitamin D; 60,000 IU vitamin D3; or 24,000 IU of vitamin plus 300 mcg calcifediol.
Functional status didn’t differ between the groups at the end of 1 year. But the incidence of falls did differ, with falls occurring in 67% of the 60,000 IU group, 54% of the 24,000 IU/calcifediol group, and 48% of the 24,000 IU control group (JAMA Intern Med. 2016;176[2]:175-83).
This represented a 47% increased fall risk in the high dose group, compared with the two low-dose groups.
Dr. Weinstein had no financial disclosures relevant to his lecture.
[email protected]
On Twitter @Alz_Gal
ORLANDO – The vitamin that keeps bones strong and protects against colon cancer also can, in large doses, increase the risk of falls and fractures.
Studies of high-dose vitamin D keep turning up the same concerns, Dr. Martin Weinstock said at the annual meeting of the American Academy of Dermatology. The most striking of these findings are the significantly increased risks of falls and fractures associated with vitamin D megadoses, said Dr. Weinstock of Brown University, Providence, R.I. These trials examined very-large intermittent doses of the vitamin given to elderly patients.
That amount of vitamin D, taken all at once, may seem like a therapeutic outlier to clinicians who are used to giving 2,000-4,000 IU/day, as recommended by the 2011 Institute of Medicine report.
Not so fast, said Dr. Weinstock.
“If you do the math, if you’re taking 2,000 IU every day, that’s 60,000 IU per month. That’s a high dose,” he said. However, he noted, daily supplements in that range appear safe. “It seems that this intermittent dosing in these studies might be the problem.”
The IOM report, an exhaustive, 1,000-page article summarizing the extant data on vitamin D – is considered the optimal dosing guide. For healthy patients, it recommends the following as minimum effective and maximum safe doses:
- 400-1,000 IU/day for infants younger than 6 month.
- 400-1,500 IU/day for infants aged 6-12 months.
- 600-2,000 IU/day for children aged 1-3 years.
- 600-3,000 IU/day for children aged 4-8 years.
- 600-4,000 IU/day for everyone aged 9 years and older.
But dosing of this fat-soluble vitamin should, in some cases, be individualized. For example, obese patients may have persistently low levels despite supplementation, as fat can sequester the vitamin. Patients with fat-metabolizing disorders may not absorb it well. And patients who have had gastric bypass may face the same issues of malabsorption, but from a mechanical, not a metabolic, standpoint.
Elderly people are particularly susceptible to vitamin D deficiency for a couple of reasons, Dr. Weinstock said. They may be less mobile, so lack exposure to sunlight. Age also can decrease the ability to convert 25-hydroxyvitamin D to the biologically active vitamin.
Mega-dosing has been an attractive method of raising and maintaining levels in this population. But several studies illustrate the risks that come along with this strategy, he noted.
A 2007 study randomized 9,440 men and women 75 years or older to placebo or to a single, 300,000 IU vitamin D intramuscular injection for 3 years. At the end of that time, the rate of falls had not significantly changed, but the rate of hip fractures had increased by 49% (Rheumatology [Oxford] 2007;46:1852-7).
Fractures occurred in 585 subjects, including 110 hip fractures, 116 wrist fractures, and 37 ankle fractures. This represented a 49% increase in any hip fracture and a 22% increase in wrist fracture over the placebo group.
A similar study, published in 2010, randomized 2,225 elderly women to placebo or a single 500,000 oral dose of vitamin D for 4 years. There were 171 fractures in the active group and 135 in the placebo group – a 26% increased risk (JAMA. 2010;303[18]:1815-22).
The fall rate in the active group was 83.4/100 person-years, compared with 72.7/100 person-years in the placebo group. This represented a significant 26% increased fracture risk and 15% increased fall risk.
Interestingly, most of these incidents occurred within the first 3 months after each dose,” Dr. Weinstock said. Those taking vitamin D were 31% more likely to fall in that time period, but no more likely to fall in the subsequent 9 months after each dose.
In 2016, a third study looked at functional status among 200 elderly men and women in a three-armed randomization: a low-dose control group receiving 24,000 IU of vitamin D; 60,000 IU vitamin D3; or 24,000 IU of vitamin plus 300 mcg calcifediol.
Functional status didn’t differ between the groups at the end of 1 year. But the incidence of falls did differ, with falls occurring in 67% of the 60,000 IU group, 54% of the 24,000 IU/calcifediol group, and 48% of the 24,000 IU control group (JAMA Intern Med. 2016;176[2]:175-83).
This represented a 47% increased fall risk in the high dose group, compared with the two low-dose groups.
Dr. Weinstein had no financial disclosures relevant to his lecture.
[email protected]
On Twitter @Alz_Gal
Mixed leukemias can benefit from allo-HST
ORLANDO – Allogeneic hematopoietic stem cell transplantation using a matched donor is a valid treatment option – and potential cure – for leukemias with markers of both myeloid and lymphoid lineages, or mixed phenotype acute leukemias, according to findings from the Acute Leukemia Working Party of the European Group for Blood and Marrow Transplantation (ALWP-EBMT) database.
Treatment outcomes at 3 years in 519 patients from the database who received an allogeneic transplant (allo-HCT) for mixed-phenotype acute leukemia (MPAL) between 2000 and 2014 and were transplanted in complete remission (CR1) included an overall survival of 56.3%, a leukemia-free survival of 46.5%, a relapse incidence of 31.4%, a nonrelapse mortality of 22.1%, and an incidence of chronic graft-versus-host disease (GVHD) of 37.5%, Reinhold Munker, MD, reported at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
“The outcome in this large adult study is pretty favorable based upon 519 patients; 45%-65% can expect overall survival at 5 years,” he said.
The median age of the study subjects was 38.1 years (range, 18-75). Transplants were from a matched sibling donor in 54.5% of cases, and from a matched unrelated donor in 45.5% of cases. Myeloablative conditioning was used in 400 patients and included only chemotherapy in 140 patients and chemotherapy with total body irradiation in 260 patients. The remaining patients received nonmyeloablative conditioning, said Dr. Munker of Tulane University, New Orleans.
The source of stem cells was bone marrow in 26% of patients, and peripheral blood in 73%. Grade II-IV acute GVHD developed in 32.5% of patients. Median follow-up was 32 months, he noted.
In univariate analysis, age at transplant was strongly associated with leukemia-free survival, nonrelapse mortality, relapse incidence, and overall survival. The best outcomes were among those aged 18-35 years. The nonrelapse mortality rate and overall survival rate were lower for transplants done in 2005-2014 vs. 2000-2004 (20% vs 33.2% and 58.3 vs 44.7%, respectively). No differences in outcomes were found between related and unrelated donors, but chronic GVHD was more common with female donors and male recipients, with no in vivo T-cell depletion, and with use of peripheral blood stem cells – findings which are not unexpected, Dr. Munker noted.
Use of myeloablative conditioning with total-body irradiation correlated with a lower relapse incidence and with better leukemia-free survival vs. both myeloablative conditioning with only chemotherapy and reduced-intensity conditioning, he said.
In multivariate analysis, younger age and more recent year of transplant were associated with a better leukemia-free survival and overall survival, and use of myeloablative conditioning with total-body irradiation was associated with better leukemia-free survival and with a trend for higher overall survival.
MPALs are rare, accounting for only 2%-5% of all acute leukemias, Dr. Munker said, noting that prognosis is considered to be intermediate in children and unfavorable in adults.
The diagnostic criteria for MPAL were revised by the World Health Organization (WHO) in 2008 and accepted by most centers, but until recently data were lacking with respect to the recommended treatment strategy of induction regimens similar to those used in acute lymphoblastic leukemia, and consolidation by allogeneic transplant, he explained.
However, the Center for International Blood and Marrow Transplant Research last year published a series of 95 cases showing encouraging long-term survival with allo-HCT in MPAL patients with a median age of 20 years.
The current findings confirm and extend those prior findings, Dr. Munker said.
Dr. Munker reported having no disclosures.
ORLANDO – Allogeneic hematopoietic stem cell transplantation using a matched donor is a valid treatment option – and potential cure – for leukemias with markers of both myeloid and lymphoid lineages, or mixed phenotype acute leukemias, according to findings from the Acute Leukemia Working Party of the European Group for Blood and Marrow Transplantation (ALWP-EBMT) database.
Treatment outcomes at 3 years in 519 patients from the database who received an allogeneic transplant (allo-HCT) for mixed-phenotype acute leukemia (MPAL) between 2000 and 2014 and were transplanted in complete remission (CR1) included an overall survival of 56.3%, a leukemia-free survival of 46.5%, a relapse incidence of 31.4%, a nonrelapse mortality of 22.1%, and an incidence of chronic graft-versus-host disease (GVHD) of 37.5%, Reinhold Munker, MD, reported at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
“The outcome in this large adult study is pretty favorable based upon 519 patients; 45%-65% can expect overall survival at 5 years,” he said.
The median age of the study subjects was 38.1 years (range, 18-75). Transplants were from a matched sibling donor in 54.5% of cases, and from a matched unrelated donor in 45.5% of cases. Myeloablative conditioning was used in 400 patients and included only chemotherapy in 140 patients and chemotherapy with total body irradiation in 260 patients. The remaining patients received nonmyeloablative conditioning, said Dr. Munker of Tulane University, New Orleans.
The source of stem cells was bone marrow in 26% of patients, and peripheral blood in 73%. Grade II-IV acute GVHD developed in 32.5% of patients. Median follow-up was 32 months, he noted.
In univariate analysis, age at transplant was strongly associated with leukemia-free survival, nonrelapse mortality, relapse incidence, and overall survival. The best outcomes were among those aged 18-35 years. The nonrelapse mortality rate and overall survival rate were lower for transplants done in 2005-2014 vs. 2000-2004 (20% vs 33.2% and 58.3 vs 44.7%, respectively). No differences in outcomes were found between related and unrelated donors, but chronic GVHD was more common with female donors and male recipients, with no in vivo T-cell depletion, and with use of peripheral blood stem cells – findings which are not unexpected, Dr. Munker noted.
Use of myeloablative conditioning with total-body irradiation correlated with a lower relapse incidence and with better leukemia-free survival vs. both myeloablative conditioning with only chemotherapy and reduced-intensity conditioning, he said.
In multivariate analysis, younger age and more recent year of transplant were associated with a better leukemia-free survival and overall survival, and use of myeloablative conditioning with total-body irradiation was associated with better leukemia-free survival and with a trend for higher overall survival.
MPALs are rare, accounting for only 2%-5% of all acute leukemias, Dr. Munker said, noting that prognosis is considered to be intermediate in children and unfavorable in adults.
The diagnostic criteria for MPAL were revised by the World Health Organization (WHO) in 2008 and accepted by most centers, but until recently data were lacking with respect to the recommended treatment strategy of induction regimens similar to those used in acute lymphoblastic leukemia, and consolidation by allogeneic transplant, he explained.
However, the Center for International Blood and Marrow Transplant Research last year published a series of 95 cases showing encouraging long-term survival with allo-HCT in MPAL patients with a median age of 20 years.
The current findings confirm and extend those prior findings, Dr. Munker said.
Dr. Munker reported having no disclosures.
ORLANDO – Allogeneic hematopoietic stem cell transplantation using a matched donor is a valid treatment option – and potential cure – for leukemias with markers of both myeloid and lymphoid lineages, or mixed phenotype acute leukemias, according to findings from the Acute Leukemia Working Party of the European Group for Blood and Marrow Transplantation (ALWP-EBMT) database.
Treatment outcomes at 3 years in 519 patients from the database who received an allogeneic transplant (allo-HCT) for mixed-phenotype acute leukemia (MPAL) between 2000 and 2014 and were transplanted in complete remission (CR1) included an overall survival of 56.3%, a leukemia-free survival of 46.5%, a relapse incidence of 31.4%, a nonrelapse mortality of 22.1%, and an incidence of chronic graft-versus-host disease (GVHD) of 37.5%, Reinhold Munker, MD, reported at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
“The outcome in this large adult study is pretty favorable based upon 519 patients; 45%-65% can expect overall survival at 5 years,” he said.
The median age of the study subjects was 38.1 years (range, 18-75). Transplants were from a matched sibling donor in 54.5% of cases, and from a matched unrelated donor in 45.5% of cases. Myeloablative conditioning was used in 400 patients and included only chemotherapy in 140 patients and chemotherapy with total body irradiation in 260 patients. The remaining patients received nonmyeloablative conditioning, said Dr. Munker of Tulane University, New Orleans.
The source of stem cells was bone marrow in 26% of patients, and peripheral blood in 73%. Grade II-IV acute GVHD developed in 32.5% of patients. Median follow-up was 32 months, he noted.
In univariate analysis, age at transplant was strongly associated with leukemia-free survival, nonrelapse mortality, relapse incidence, and overall survival. The best outcomes were among those aged 18-35 years. The nonrelapse mortality rate and overall survival rate were lower for transplants done in 2005-2014 vs. 2000-2004 (20% vs 33.2% and 58.3 vs 44.7%, respectively). No differences in outcomes were found between related and unrelated donors, but chronic GVHD was more common with female donors and male recipients, with no in vivo T-cell depletion, and with use of peripheral blood stem cells – findings which are not unexpected, Dr. Munker noted.
Use of myeloablative conditioning with total-body irradiation correlated with a lower relapse incidence and with better leukemia-free survival vs. both myeloablative conditioning with only chemotherapy and reduced-intensity conditioning, he said.
In multivariate analysis, younger age and more recent year of transplant were associated with a better leukemia-free survival and overall survival, and use of myeloablative conditioning with total-body irradiation was associated with better leukemia-free survival and with a trend for higher overall survival.
MPALs are rare, accounting for only 2%-5% of all acute leukemias, Dr. Munker said, noting that prognosis is considered to be intermediate in children and unfavorable in adults.
The diagnostic criteria for MPAL were revised by the World Health Organization (WHO) in 2008 and accepted by most centers, but until recently data were lacking with respect to the recommended treatment strategy of induction regimens similar to those used in acute lymphoblastic leukemia, and consolidation by allogeneic transplant, he explained.
However, the Center for International Blood and Marrow Transplant Research last year published a series of 95 cases showing encouraging long-term survival with allo-HCT in MPAL patients with a median age of 20 years.
The current findings confirm and extend those prior findings, Dr. Munker said.
Dr. Munker reported having no disclosures.
Key clinical point:
Major finding: Treatment outcomes at 3 years included overall survival of 56.3%, leukemia-free survival of 46.5%, relapse incidence of 31.4%, nonrelapse mortality of 22.1%, and incidence of chronic graft-versus-host disease of 37.5%.
Data source: A review of 519 cases from the ALWP-EBMT database.
Disclosures: Dr. Munker reported having no disclosures.
Pre- and post-HCT MRD levels predict ALL survival
ORLANDO – Minimal residual disease (MRD) measured before and after allogeneic hematopoietic stem cell transplantation (HCT) is a powerful predictor of survival in children with acute lymphoblastic leukemia (ALL), according to a review of hundreds of cases from around the world.
The findings could have implications for using minimal residual disease measures to guide posttransplant interventions, Michael A. Pulsipher, MD, reported at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
“MRD pretransplant was a very powerful predictor of outcomes. MRD posttransplant highlights individual patients at risk,” Dr. Pulsipher said. Results comparing reverse transcriptase–polymerase chain reaction with flow cytometry require validation by direct comparison in the same patient cohort, but “the new risk scores ... very nicely predict outcomes both pre- and post-transplant and can guide study planning and patient counseling.”
A total of 2,960 bone marrow MRD measurements were performed in the 747 patients included in the study. MRD was assessed prior to HCT and on or near days 30, 60, 100, 180, and 365 and beyond after HCT.
Patients were grouped for analysis according to MRD level: Group 1 had no detectable MRD, group 2 had low detectable MRD levels (less than 10E-4, or 0.01% by flow cytometry), and group 3 had high detectable MRD levels (10E-4 or higher). A second analysis compared findings in those tested by flow cytometry and those tested by real-time quantitative PCR (RQ-PCR), said Dr. Pulsipher of Children’s Hospital Los Angeles.
In 648 patients with pre-HCT MRD measurements available, the 4-year probability of event-free survival was 62%, 67%, and 37% for groups 1, 2, and 3, respectively. Group 3 – the high MRD level group – had 2.47 times the increased hazard ratio for relapse and 1.67 times the increased risk of treatment-related mortality, Dr. Pulsipher said, adding that pre-HCT MRD and remission status both significantly influenced survival, while age, sex, relapse site, cytogenetics, donor type, and stem cell source did not influence outcome.
Post-HCT MRD values were analyzed as time-dependent covariates.
“As time went by more and more, any detectable level of MRD led to a very poor prognosis, whereas patients arriving at day 365 with no detectable MRD had exceptional prognosis with survival approaching 90%,” he said.
Specifically, the 4-year probability of event-free survival for groups 1, 2, and 3, respectively, were 59%, 65%, and 43% at day 30; 64%, 47%, and 36% at day 60; 65%, 69%, and 44% at day 90; 79%, 40%, and 12% at day 180; and 87%, 36%, and 25% at day 365.
Of note, a very significant interaction was seen between acute graft-versus-host disease (GVHD) and MRD, Dr. Pulsipher said, explaining that patients who were MRD positive and had developed GVHD had a significant decrease in the cumulative incidence of relapse, compared with those with no GVHD.
“This translated into improved event-free survival with patients post transplant, who were MRD-positive [and] developing GVHD, still having a reasonable chance of survival, whereas patients post transplant who had MRD measured who did not develop GVHD had a very poor chance of survival,” he added.
Additionally, based on detailed multivariate analysis including a number of clinical factors, risk predictive scores were developed for event-free survival risk at 18 months or cumulative incidence of relapse at 18 months. Multiple scores were developed for each, but, as an example of factors that had an important effect on outcomes, patients with very early pretransplant relapse (those who went into remission but relapsed within 18 months) or with greater than 2nd relapse had a high risk for poor event-free survival. Mismatched donors and unrelated cord-blood stem cell transplant recipients also had high risk, he said, noting that, “of course, MRD had a significant effect” and was the most important factor prior to transplant.
These patients, who had a 4-point or greater risk score, were the poorest risk group, with survival that was less than 50%, as opposed to better risk groups that exceeded 90%, he said.
“A score of greater than 5 could identify 80% of patients who were going to relapse after transplant, and of course, event-free and overall survival in those patients were very poor,” he added.
As time went by, the early risk of GVHD diminished somewhat, as did the risk of mismatched donors.
“Most of the risk was associated with any MRD detection,” he said.
Flow cytometry and RQ-PCR levels of at least 10-4 were highly predictive of relapse at all pre- and post-HCT time points; however, RQ-PCR values between 10-4 and 10-3, in cases where adequate numbers were available for comparison, better predicted relapse as compared with flow cytometry results.
For example, before HCT, hazard ratios were 1.26 and 2.41 with flow cytometry vs. RQ-PCR. At day 30, the hazard ratios were 1.33 and 2.53, and at day 365, they were 3.54 and 31.84, Dr. Pulsipher reported.
The findings provide important information for improving outcomes in children with high-risk ALL undergoing HCT, he said.
“Older prognostic models for relapsed and refractory high-risk ALL have focused on timing and location of relapse, as well as disease phenotype. But it is clear that, in order to treat children with very high risk ALL with transplantation, MRD has become the most important thing to look at in the pretreatment setting. The challenges that we face in assessing MRD, however, have been hampered by the fact that we have differing MRD measurements,” he said, noting that RQ-PCR is often used in Europe, while flow cytometry is more often used in the United States. As such, direct comparisons are lacking, as are T-cell and posttransplant data.
The current study represents a “tremendous effort” by international collaborators to address these shortcoming, he said.
“This is a great opportunity, as our goal, of course, is to avoid futility in transplantation, but, more importantly, to find opportunities to identify groups for which we can improve our outcomes,” he added.
Patients included in the study were treated in Europe, North America, and Australia and were transplanted during Sept. 1999-May 2016. Most were in first or second remission, and most (586) had pre-B ALL. A notable 145 had T-cell ALL – “more than ever has been analyzed previously” – and 16 had B-lineage or biphenotypic ALL. About half were under age 10 years, 62% were boys, and stem cell sources were typical, although 20% received a cord blood transplant.
Dr. Pulsipher reported serving as an advisor and/or consultant for Chimerix, Novartis, Jazz Pharmaceutical, and receiving housing support from Medac Pharma for an educational meeting.
ORLANDO – Minimal residual disease (MRD) measured before and after allogeneic hematopoietic stem cell transplantation (HCT) is a powerful predictor of survival in children with acute lymphoblastic leukemia (ALL), according to a review of hundreds of cases from around the world.
The findings could have implications for using minimal residual disease measures to guide posttransplant interventions, Michael A. Pulsipher, MD, reported at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
“MRD pretransplant was a very powerful predictor of outcomes. MRD posttransplant highlights individual patients at risk,” Dr. Pulsipher said. Results comparing reverse transcriptase–polymerase chain reaction with flow cytometry require validation by direct comparison in the same patient cohort, but “the new risk scores ... very nicely predict outcomes both pre- and post-transplant and can guide study planning and patient counseling.”
A total of 2,960 bone marrow MRD measurements were performed in the 747 patients included in the study. MRD was assessed prior to HCT and on or near days 30, 60, 100, 180, and 365 and beyond after HCT.
Patients were grouped for analysis according to MRD level: Group 1 had no detectable MRD, group 2 had low detectable MRD levels (less than 10E-4, or 0.01% by flow cytometry), and group 3 had high detectable MRD levels (10E-4 or higher). A second analysis compared findings in those tested by flow cytometry and those tested by real-time quantitative PCR (RQ-PCR), said Dr. Pulsipher of Children’s Hospital Los Angeles.
In 648 patients with pre-HCT MRD measurements available, the 4-year probability of event-free survival was 62%, 67%, and 37% for groups 1, 2, and 3, respectively. Group 3 – the high MRD level group – had 2.47 times the increased hazard ratio for relapse and 1.67 times the increased risk of treatment-related mortality, Dr. Pulsipher said, adding that pre-HCT MRD and remission status both significantly influenced survival, while age, sex, relapse site, cytogenetics, donor type, and stem cell source did not influence outcome.
Post-HCT MRD values were analyzed as time-dependent covariates.
“As time went by more and more, any detectable level of MRD led to a very poor prognosis, whereas patients arriving at day 365 with no detectable MRD had exceptional prognosis with survival approaching 90%,” he said.
Specifically, the 4-year probability of event-free survival for groups 1, 2, and 3, respectively, were 59%, 65%, and 43% at day 30; 64%, 47%, and 36% at day 60; 65%, 69%, and 44% at day 90; 79%, 40%, and 12% at day 180; and 87%, 36%, and 25% at day 365.
Of note, a very significant interaction was seen between acute graft-versus-host disease (GVHD) and MRD, Dr. Pulsipher said, explaining that patients who were MRD positive and had developed GVHD had a significant decrease in the cumulative incidence of relapse, compared with those with no GVHD.
“This translated into improved event-free survival with patients post transplant, who were MRD-positive [and] developing GVHD, still having a reasonable chance of survival, whereas patients post transplant who had MRD measured who did not develop GVHD had a very poor chance of survival,” he added.
Additionally, based on detailed multivariate analysis including a number of clinical factors, risk predictive scores were developed for event-free survival risk at 18 months or cumulative incidence of relapse at 18 months. Multiple scores were developed for each, but, as an example of factors that had an important effect on outcomes, patients with very early pretransplant relapse (those who went into remission but relapsed within 18 months) or with greater than 2nd relapse had a high risk for poor event-free survival. Mismatched donors and unrelated cord-blood stem cell transplant recipients also had high risk, he said, noting that, “of course, MRD had a significant effect” and was the most important factor prior to transplant.
These patients, who had a 4-point or greater risk score, were the poorest risk group, with survival that was less than 50%, as opposed to better risk groups that exceeded 90%, he said.
“A score of greater than 5 could identify 80% of patients who were going to relapse after transplant, and of course, event-free and overall survival in those patients were very poor,” he added.
As time went by, the early risk of GVHD diminished somewhat, as did the risk of mismatched donors.
“Most of the risk was associated with any MRD detection,” he said.
Flow cytometry and RQ-PCR levels of at least 10-4 were highly predictive of relapse at all pre- and post-HCT time points; however, RQ-PCR values between 10-4 and 10-3, in cases where adequate numbers were available for comparison, better predicted relapse as compared with flow cytometry results.
For example, before HCT, hazard ratios were 1.26 and 2.41 with flow cytometry vs. RQ-PCR. At day 30, the hazard ratios were 1.33 and 2.53, and at day 365, they were 3.54 and 31.84, Dr. Pulsipher reported.
The findings provide important information for improving outcomes in children with high-risk ALL undergoing HCT, he said.
“Older prognostic models for relapsed and refractory high-risk ALL have focused on timing and location of relapse, as well as disease phenotype. But it is clear that, in order to treat children with very high risk ALL with transplantation, MRD has become the most important thing to look at in the pretreatment setting. The challenges that we face in assessing MRD, however, have been hampered by the fact that we have differing MRD measurements,” he said, noting that RQ-PCR is often used in Europe, while flow cytometry is more often used in the United States. As such, direct comparisons are lacking, as are T-cell and posttransplant data.
The current study represents a “tremendous effort” by international collaborators to address these shortcoming, he said.
“This is a great opportunity, as our goal, of course, is to avoid futility in transplantation, but, more importantly, to find opportunities to identify groups for which we can improve our outcomes,” he added.
Patients included in the study were treated in Europe, North America, and Australia and were transplanted during Sept. 1999-May 2016. Most were in first or second remission, and most (586) had pre-B ALL. A notable 145 had T-cell ALL – “more than ever has been analyzed previously” – and 16 had B-lineage or biphenotypic ALL. About half were under age 10 years, 62% were boys, and stem cell sources were typical, although 20% received a cord blood transplant.
Dr. Pulsipher reported serving as an advisor and/or consultant for Chimerix, Novartis, Jazz Pharmaceutical, and receiving housing support from Medac Pharma for an educational meeting.
ORLANDO – Minimal residual disease (MRD) measured before and after allogeneic hematopoietic stem cell transplantation (HCT) is a powerful predictor of survival in children with acute lymphoblastic leukemia (ALL), according to a review of hundreds of cases from around the world.
The findings could have implications for using minimal residual disease measures to guide posttransplant interventions, Michael A. Pulsipher, MD, reported at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
“MRD pretransplant was a very powerful predictor of outcomes. MRD posttransplant highlights individual patients at risk,” Dr. Pulsipher said. Results comparing reverse transcriptase–polymerase chain reaction with flow cytometry require validation by direct comparison in the same patient cohort, but “the new risk scores ... very nicely predict outcomes both pre- and post-transplant and can guide study planning and patient counseling.”
A total of 2,960 bone marrow MRD measurements were performed in the 747 patients included in the study. MRD was assessed prior to HCT and on or near days 30, 60, 100, 180, and 365 and beyond after HCT.
Patients were grouped for analysis according to MRD level: Group 1 had no detectable MRD, group 2 had low detectable MRD levels (less than 10E-4, or 0.01% by flow cytometry), and group 3 had high detectable MRD levels (10E-4 or higher). A second analysis compared findings in those tested by flow cytometry and those tested by real-time quantitative PCR (RQ-PCR), said Dr. Pulsipher of Children’s Hospital Los Angeles.
In 648 patients with pre-HCT MRD measurements available, the 4-year probability of event-free survival was 62%, 67%, and 37% for groups 1, 2, and 3, respectively. Group 3 – the high MRD level group – had 2.47 times the increased hazard ratio for relapse and 1.67 times the increased risk of treatment-related mortality, Dr. Pulsipher said, adding that pre-HCT MRD and remission status both significantly influenced survival, while age, sex, relapse site, cytogenetics, donor type, and stem cell source did not influence outcome.
Post-HCT MRD values were analyzed as time-dependent covariates.
“As time went by more and more, any detectable level of MRD led to a very poor prognosis, whereas patients arriving at day 365 with no detectable MRD had exceptional prognosis with survival approaching 90%,” he said.
Specifically, the 4-year probability of event-free survival for groups 1, 2, and 3, respectively, were 59%, 65%, and 43% at day 30; 64%, 47%, and 36% at day 60; 65%, 69%, and 44% at day 90; 79%, 40%, and 12% at day 180; and 87%, 36%, and 25% at day 365.
Of note, a very significant interaction was seen between acute graft-versus-host disease (GVHD) and MRD, Dr. Pulsipher said, explaining that patients who were MRD positive and had developed GVHD had a significant decrease in the cumulative incidence of relapse, compared with those with no GVHD.
“This translated into improved event-free survival with patients post transplant, who were MRD-positive [and] developing GVHD, still having a reasonable chance of survival, whereas patients post transplant who had MRD measured who did not develop GVHD had a very poor chance of survival,” he added.
Additionally, based on detailed multivariate analysis including a number of clinical factors, risk predictive scores were developed for event-free survival risk at 18 months or cumulative incidence of relapse at 18 months. Multiple scores were developed for each, but, as an example of factors that had an important effect on outcomes, patients with very early pretransplant relapse (those who went into remission but relapsed within 18 months) or with greater than 2nd relapse had a high risk for poor event-free survival. Mismatched donors and unrelated cord-blood stem cell transplant recipients also had high risk, he said, noting that, “of course, MRD had a significant effect” and was the most important factor prior to transplant.
These patients, who had a 4-point or greater risk score, were the poorest risk group, with survival that was less than 50%, as opposed to better risk groups that exceeded 90%, he said.
“A score of greater than 5 could identify 80% of patients who were going to relapse after transplant, and of course, event-free and overall survival in those patients were very poor,” he added.
As time went by, the early risk of GVHD diminished somewhat, as did the risk of mismatched donors.
“Most of the risk was associated with any MRD detection,” he said.
Flow cytometry and RQ-PCR levels of at least 10-4 were highly predictive of relapse at all pre- and post-HCT time points; however, RQ-PCR values between 10-4 and 10-3, in cases where adequate numbers were available for comparison, better predicted relapse as compared with flow cytometry results.
For example, before HCT, hazard ratios were 1.26 and 2.41 with flow cytometry vs. RQ-PCR. At day 30, the hazard ratios were 1.33 and 2.53, and at day 365, they were 3.54 and 31.84, Dr. Pulsipher reported.
The findings provide important information for improving outcomes in children with high-risk ALL undergoing HCT, he said.
“Older prognostic models for relapsed and refractory high-risk ALL have focused on timing and location of relapse, as well as disease phenotype. But it is clear that, in order to treat children with very high risk ALL with transplantation, MRD has become the most important thing to look at in the pretreatment setting. The challenges that we face in assessing MRD, however, have been hampered by the fact that we have differing MRD measurements,” he said, noting that RQ-PCR is often used in Europe, while flow cytometry is more often used in the United States. As such, direct comparisons are lacking, as are T-cell and posttransplant data.
The current study represents a “tremendous effort” by international collaborators to address these shortcoming, he said.
“This is a great opportunity, as our goal, of course, is to avoid futility in transplantation, but, more importantly, to find opportunities to identify groups for which we can improve our outcomes,” he added.
Patients included in the study were treated in Europe, North America, and Australia and were transplanted during Sept. 1999-May 2016. Most were in first or second remission, and most (586) had pre-B ALL. A notable 145 had T-cell ALL – “more than ever has been analyzed previously” – and 16 had B-lineage or biphenotypic ALL. About half were under age 10 years, 62% were boys, and stem cell sources were typical, although 20% received a cord blood transplant.
Dr. Pulsipher reported serving as an advisor and/or consultant for Chimerix, Novartis, Jazz Pharmaceutical, and receiving housing support from Medac Pharma for an educational meeting.
Key clinical point:
Major finding: Patients with high pretransplant MRD levels had a 2.47-fold increased hazard ratio for relapse and a 1.67-fold increased risk of treatment-related mortality.
Data source: A review of data from 747 pediatric high-risk ALL cases.
Disclosures: Dr. Pulsipher reported serving as an adviser and/or consultant for Chimerix, Novartis, and Jazz Pharmaceuticals and receiving housing support from Medac Pharma for an educational meeting.
The percutaneous mitral valve replacement pipe dream
SNOWMASS, COLO. – Percutaneous mitral valve replacement is unlikely to ever catch on in any way remotely approaching that of transcatheter aortic valve replacement for the treatment of aortic stenosis, Blase A. Carabello, MD, predicted at the Annual Cardiovascular Conference at Snowmass.
“We’ve spent $2 billion looking for methods of percutaneous mitral valve replacement, and yet, I have to wonder if that makes any sense,” said Dr. Carabello, professor of medicine and chief of cardiology at East Carolina University in Greenville, N.C.
“If repair is superior to replacement in primary MR [mitral regurgitation], which I think we all agree is true, and you don’t need to get rid of every last molecule of blood going backward across the mitral valve when you’ve got a good left ventricle, then a percutaneous replacement in primary MR would have only the niche of patients who are inoperable and whose leaflets can’t be grabbed by the MitraClip or some new percutaneous device down the road. And, in secondary MR, it doesn’t seem to matter whether you replace or repair the valve, so why not just repair it with a clip?” he argued.
Numerous nonrandomized studies have invariably demonstrated superior survival for surgical repair versus replacement in patients with primary MR.
“There’s never going to be a randomized controlled trial of repair versus replacement; there’s no equipoise there. We all believe that, in primary MR, repair is superior to replacement. There are no data anywhere to suggest the opposite. It’s essentially sacrosanct,” according to the cardiologist.
In contrast, a major randomized trial of surgical repair versus replacement has been conducted in patients with severe secondary MR. This NIH-funded study conducted by the Cardiothoracic Surgical Trials Network found no difference in survival between the two groups (N Engl J Med. 2016 Jan 28; 374[4]:344-53). That’s not a surprising result, Dr. Carabello said, since the underlying cause of this type of valve disease is a sick left ventricle. But, since surgical repair entails less morbidity than replacement – and a percutaneous repair with a leaflet-grasping device such as the MitraClip is simpler and safer than a surgical repair – it seems likely that the future treatment for secondary MR will be a percutaneous device, he said.
That future could depend upon the results of the ongoing COAPT trial (Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy), in which the MitraClip is being studied as an alternative to surgical repair for significant secondary MR. The MitraClip, which doesn’t entail a concomitant annuloplasty, is currently approved by the Food and Drug Administration only for patients with primary, degenerative mitral regurgitation not amenable to surgical repair. But, if COAPT yields positive results, the role of the MitraClip will greatly expand.
An intriguing and poorly understood difference exists in the significance of residual mitral regurgitation following surgical repair as opposed to percutaneous MitraClip repair, Dr. Carabello observed.
“I go to the OR a lot, and I know of no surgeon [who] will leave 2+ MR behind. Most surgeons won’t leave 1+ MR behind. They’ll put the patient back on the pump to repair even mild residual MR, accepting only trace MR or zero before they leave the OR because they know that the best predictor of a failed mitral repair is the presence of residual MR in the OR,” he said.
In contrast, following successful deployment of the MitraClip most patients are left with 1-2+ MR. Yet, as was demonstrated in the 5-year results of the randomized EVEREST II trial (Endovascular Valve Edge-to-Edge Repair Study), this residual MR wasn’t a harbinger of poor outcomes long-term (J Am Coll Cardiol. 2015 Dec 29;66[25]:2844-54).
“You would have expected, with that much residual MR, there would be a perpetually increasing failure rate over time, but that didn’t happen. In Everest II, there was an early failure rate for percutaneous repair, where the MitraClip didn’t work and those patients required surgical mitral valve repair. But, after the first 6 months, the failure rate for the clip was exactly the same as the surgical failure rate, even though, with the clip, you start with more MR to begin with,” the cardiologist noted.
The MitraClip procedure is modeled after the surgical Alfieri double-orifice end-to-end stitch technique, which has been shown to have durable results when performed in conjunction with an annuloplasty ring for primary MR.
“The MitraClip essentially joins the valve in the middle the way the Alfieri stitch does, but it doesn’t appear to behave the same way. Why is that? Maybe the clip does something different than the Alfieri stitch on which it was modeled. Maybe that bar in the middle of the mitral valve does something in terms of scarring or stabilization that we don’t know about yet,” he speculated.
As for the prospects for percutaneous mitral valve replacement, Dr. Carabello said that this type of procedure “is a very difficult thing to do, and so far, has been met with a fair amount of failure. It’ll be very interesting to see what percentage of market share it gets 10 years down the road. My prediction is that, for mitral regurgitation, repair is always going to be it.”
Dr. Carabello reported serving on a data safety monitoring board for Edwards Lifesciences.
The author provides valuable insight into how the definition of “success” of a procedure can change depending on the approach to the problem. While the gold standard of open mitral valve repair is 1+ regurgitation or less, those promoting percutaneous valve replacement are willing to accept long term 1+ to 2+ regurgitation. New technology and innovation is critical in medicine, provided the results are at least equivalent or superior to the standard techniques.

The author provides valuable insight into how the definition of “success” of a procedure can change depending on the approach to the problem. While the gold standard of open mitral valve repair is 1+ regurgitation or less, those promoting percutaneous valve replacement are willing to accept long term 1+ to 2+ regurgitation. New technology and innovation is critical in medicine, provided the results are at least equivalent or superior to the standard techniques.
The author provides valuable insight into how the definition of “success” of a procedure can change depending on the approach to the problem. While the gold standard of open mitral valve repair is 1+ regurgitation or less, those promoting percutaneous valve replacement are willing to accept long term 1+ to 2+ regurgitation. New technology and innovation is critical in medicine, provided the results are at least equivalent or superior to the standard techniques.
SNOWMASS, COLO. – Percutaneous mitral valve replacement is unlikely to ever catch on in any way remotely approaching that of transcatheter aortic valve replacement for the treatment of aortic stenosis, Blase A. Carabello, MD, predicted at the Annual Cardiovascular Conference at Snowmass.
“We’ve spent $2 billion looking for methods of percutaneous mitral valve replacement, and yet, I have to wonder if that makes any sense,” said Dr. Carabello, professor of medicine and chief of cardiology at East Carolina University in Greenville, N.C.
“If repair is superior to replacement in primary MR [mitral regurgitation], which I think we all agree is true, and you don’t need to get rid of every last molecule of blood going backward across the mitral valve when you’ve got a good left ventricle, then a percutaneous replacement in primary MR would have only the niche of patients who are inoperable and whose leaflets can’t be grabbed by the MitraClip or some new percutaneous device down the road. And, in secondary MR, it doesn’t seem to matter whether you replace or repair the valve, so why not just repair it with a clip?” he argued.
Numerous nonrandomized studies have invariably demonstrated superior survival for surgical repair versus replacement in patients with primary MR.
“There’s never going to be a randomized controlled trial of repair versus replacement; there’s no equipoise there. We all believe that, in primary MR, repair is superior to replacement. There are no data anywhere to suggest the opposite. It’s essentially sacrosanct,” according to the cardiologist.
In contrast, a major randomized trial of surgical repair versus replacement has been conducted in patients with severe secondary MR. This NIH-funded study conducted by the Cardiothoracic Surgical Trials Network found no difference in survival between the two groups (N Engl J Med. 2016 Jan 28; 374[4]:344-53). That’s not a surprising result, Dr. Carabello said, since the underlying cause of this type of valve disease is a sick left ventricle. But, since surgical repair entails less morbidity than replacement – and a percutaneous repair with a leaflet-grasping device such as the MitraClip is simpler and safer than a surgical repair – it seems likely that the future treatment for secondary MR will be a percutaneous device, he said.
That future could depend upon the results of the ongoing COAPT trial (Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy), in which the MitraClip is being studied as an alternative to surgical repair for significant secondary MR. The MitraClip, which doesn’t entail a concomitant annuloplasty, is currently approved by the Food and Drug Administration only for patients with primary, degenerative mitral regurgitation not amenable to surgical repair. But, if COAPT yields positive results, the role of the MitraClip will greatly expand.
An intriguing and poorly understood difference exists in the significance of residual mitral regurgitation following surgical repair as opposed to percutaneous MitraClip repair, Dr. Carabello observed.
“I go to the OR a lot, and I know of no surgeon [who] will leave 2+ MR behind. Most surgeons won’t leave 1+ MR behind. They’ll put the patient back on the pump to repair even mild residual MR, accepting only trace MR or zero before they leave the OR because they know that the best predictor of a failed mitral repair is the presence of residual MR in the OR,” he said.
In contrast, following successful deployment of the MitraClip most patients are left with 1-2+ MR. Yet, as was demonstrated in the 5-year results of the randomized EVEREST II trial (Endovascular Valve Edge-to-Edge Repair Study), this residual MR wasn’t a harbinger of poor outcomes long-term (J Am Coll Cardiol. 2015 Dec 29;66[25]:2844-54).
“You would have expected, with that much residual MR, there would be a perpetually increasing failure rate over time, but that didn’t happen. In Everest II, there was an early failure rate for percutaneous repair, where the MitraClip didn’t work and those patients required surgical mitral valve repair. But, after the first 6 months, the failure rate for the clip was exactly the same as the surgical failure rate, even though, with the clip, you start with more MR to begin with,” the cardiologist noted.
The MitraClip procedure is modeled after the surgical Alfieri double-orifice end-to-end stitch technique, which has been shown to have durable results when performed in conjunction with an annuloplasty ring for primary MR.
“The MitraClip essentially joins the valve in the middle the way the Alfieri stitch does, but it doesn’t appear to behave the same way. Why is that? Maybe the clip does something different than the Alfieri stitch on which it was modeled. Maybe that bar in the middle of the mitral valve does something in terms of scarring or stabilization that we don’t know about yet,” he speculated.
As for the prospects for percutaneous mitral valve replacement, Dr. Carabello said that this type of procedure “is a very difficult thing to do, and so far, has been met with a fair amount of failure. It’ll be very interesting to see what percentage of market share it gets 10 years down the road. My prediction is that, for mitral regurgitation, repair is always going to be it.”
Dr. Carabello reported serving on a data safety monitoring board for Edwards Lifesciences.
SNOWMASS, COLO. – Percutaneous mitral valve replacement is unlikely to ever catch on in any way remotely approaching that of transcatheter aortic valve replacement for the treatment of aortic stenosis, Blase A. Carabello, MD, predicted at the Annual Cardiovascular Conference at Snowmass.
“We’ve spent $2 billion looking for methods of percutaneous mitral valve replacement, and yet, I have to wonder if that makes any sense,” said Dr. Carabello, professor of medicine and chief of cardiology at East Carolina University in Greenville, N.C.
“If repair is superior to replacement in primary MR [mitral regurgitation], which I think we all agree is true, and you don’t need to get rid of every last molecule of blood going backward across the mitral valve when you’ve got a good left ventricle, then a percutaneous replacement in primary MR would have only the niche of patients who are inoperable and whose leaflets can’t be grabbed by the MitraClip or some new percutaneous device down the road. And, in secondary MR, it doesn’t seem to matter whether you replace or repair the valve, so why not just repair it with a clip?” he argued.
Numerous nonrandomized studies have invariably demonstrated superior survival for surgical repair versus replacement in patients with primary MR.
“There’s never going to be a randomized controlled trial of repair versus replacement; there’s no equipoise there. We all believe that, in primary MR, repair is superior to replacement. There are no data anywhere to suggest the opposite. It’s essentially sacrosanct,” according to the cardiologist.
In contrast, a major randomized trial of surgical repair versus replacement has been conducted in patients with severe secondary MR. This NIH-funded study conducted by the Cardiothoracic Surgical Trials Network found no difference in survival between the two groups (N Engl J Med. 2016 Jan 28; 374[4]:344-53). That’s not a surprising result, Dr. Carabello said, since the underlying cause of this type of valve disease is a sick left ventricle. But, since surgical repair entails less morbidity than replacement – and a percutaneous repair with a leaflet-grasping device such as the MitraClip is simpler and safer than a surgical repair – it seems likely that the future treatment for secondary MR will be a percutaneous device, he said.
That future could depend upon the results of the ongoing COAPT trial (Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy), in which the MitraClip is being studied as an alternative to surgical repair for significant secondary MR. The MitraClip, which doesn’t entail a concomitant annuloplasty, is currently approved by the Food and Drug Administration only for patients with primary, degenerative mitral regurgitation not amenable to surgical repair. But, if COAPT yields positive results, the role of the MitraClip will greatly expand.
An intriguing and poorly understood difference exists in the significance of residual mitral regurgitation following surgical repair as opposed to percutaneous MitraClip repair, Dr. Carabello observed.
“I go to the OR a lot, and I know of no surgeon [who] will leave 2+ MR behind. Most surgeons won’t leave 1+ MR behind. They’ll put the patient back on the pump to repair even mild residual MR, accepting only trace MR or zero before they leave the OR because they know that the best predictor of a failed mitral repair is the presence of residual MR in the OR,” he said.
In contrast, following successful deployment of the MitraClip most patients are left with 1-2+ MR. Yet, as was demonstrated in the 5-year results of the randomized EVEREST II trial (Endovascular Valve Edge-to-Edge Repair Study), this residual MR wasn’t a harbinger of poor outcomes long-term (J Am Coll Cardiol. 2015 Dec 29;66[25]:2844-54).
“You would have expected, with that much residual MR, there would be a perpetually increasing failure rate over time, but that didn’t happen. In Everest II, there was an early failure rate for percutaneous repair, where the MitraClip didn’t work and those patients required surgical mitral valve repair. But, after the first 6 months, the failure rate for the clip was exactly the same as the surgical failure rate, even though, with the clip, you start with more MR to begin with,” the cardiologist noted.
The MitraClip procedure is modeled after the surgical Alfieri double-orifice end-to-end stitch technique, which has been shown to have durable results when performed in conjunction with an annuloplasty ring for primary MR.
“The MitraClip essentially joins the valve in the middle the way the Alfieri stitch does, but it doesn’t appear to behave the same way. Why is that? Maybe the clip does something different than the Alfieri stitch on which it was modeled. Maybe that bar in the middle of the mitral valve does something in terms of scarring or stabilization that we don’t know about yet,” he speculated.
As for the prospects for percutaneous mitral valve replacement, Dr. Carabello said that this type of procedure “is a very difficult thing to do, and so far, has been met with a fair amount of failure. It’ll be very interesting to see what percentage of market share it gets 10 years down the road. My prediction is that, for mitral regurgitation, repair is always going to be it.”
Dr. Carabello reported serving on a data safety monitoring board for Edwards Lifesciences.
Connective tissue diseases reported in patients receiving immune checkpoint inhibitors
For the first time, new-onset connective tissue disease has been reported in patients who were treated with anti-PD1/PDL-1 agents, according to findings published in the Annals of the Rheumatic Diseases.
In a cohort of 447 cancer patients who received therapy with immune checkpoint inhibitors (ICIs), Sébastien Le Burel, MD, of the Bicêtre Hospital in Le Kremlin-Bicêtre, France, and his colleagues described four patients who developed a connective tissue disease (CTD). There were two cases of Sjögren’s syndrome in patients taking an anti–programmed cell death 1 (anti-PD1) drug, one case of cryoglobulinemic vasculitis as a complication of suspected Sjögren’s syndrome in a patient taking an anti–programmed cell death ligand 1 (PDL-1) agent, and a case of a patient with antinuclear antibody positive myositis who was taking an anti-PDL-1 drug (Ann Rheum Dis. 2017 Feb 27. doi: 10.1136/annrheumdis-2016-210820).
“While the onset of systemic autoimmune disease after ICI treatment remains uncommon, greater awareness of these conditions should enable physicians to provide more effective patient care,” the investigators wrote. “This underlines the need for close collaboration within a network of oncologists and other specialist physicians in the new era of immunotherapy.”
The investigators discovered the cases by screening the French prospective, multicenter, academic REISAMIC registry for reports of CTD among patients being treated with anti-PD1 or anti-PDL-1 agents.
All four of the patients who developed a CTD had metastatic cancer, and their mean age was 62 years. Two patients had been treated with anti-PD1 agents and two with anti-PDL-1 agents. None of the four patients had presented with symptoms of CTD before they began treatment.
The mean time interval between the first treatment dose and the first symptom of CTD was 60 days (range, 24-72), and the mean time interval between the first symptom and subsequent diagnosis of CTD was 40 days (range, 10-74).
Three patients discontinued the ICI agent, and two patients were treated with steroids (1 mg/kg/day).
The estimated prevalence of CTD was 0.7% in the REISAMIC registry, and the authors emphasize that the high proportion of cases of Sjögren’s syndrome is noteworthy, with two of the patients fulfilling the recent American College of Rheumatology/European League Against Rheumatism criteria for Sjögren’s syndrome.
A limitation of the study is that some patients presenting with milder symptoms might not have been investigated by their oncologist.
The findings raise the question of whether asymptomatic patients taking ICIs who are at risk for immune-related adverse events should be screened and monitored closely, the authors explained.
One of the study authors received research funding from Novartis and Pfizer for the current paper. Several authors report relationships with industry.
For the first time, new-onset connective tissue disease has been reported in patients who were treated with anti-PD1/PDL-1 agents, according to findings published in the Annals of the Rheumatic Diseases.
In a cohort of 447 cancer patients who received therapy with immune checkpoint inhibitors (ICIs), Sébastien Le Burel, MD, of the Bicêtre Hospital in Le Kremlin-Bicêtre, France, and his colleagues described four patients who developed a connective tissue disease (CTD). There were two cases of Sjögren’s syndrome in patients taking an anti–programmed cell death 1 (anti-PD1) drug, one case of cryoglobulinemic vasculitis as a complication of suspected Sjögren’s syndrome in a patient taking an anti–programmed cell death ligand 1 (PDL-1) agent, and a case of a patient with antinuclear antibody positive myositis who was taking an anti-PDL-1 drug (Ann Rheum Dis. 2017 Feb 27. doi: 10.1136/annrheumdis-2016-210820).
“While the onset of systemic autoimmune disease after ICI treatment remains uncommon, greater awareness of these conditions should enable physicians to provide more effective patient care,” the investigators wrote. “This underlines the need for close collaboration within a network of oncologists and other specialist physicians in the new era of immunotherapy.”
The investigators discovered the cases by screening the French prospective, multicenter, academic REISAMIC registry for reports of CTD among patients being treated with anti-PD1 or anti-PDL-1 agents.
All four of the patients who developed a CTD had metastatic cancer, and their mean age was 62 years. Two patients had been treated with anti-PD1 agents and two with anti-PDL-1 agents. None of the four patients had presented with symptoms of CTD before they began treatment.
The mean time interval between the first treatment dose and the first symptom of CTD was 60 days (range, 24-72), and the mean time interval between the first symptom and subsequent diagnosis of CTD was 40 days (range, 10-74).
Three patients discontinued the ICI agent, and two patients were treated with steroids (1 mg/kg/day).
The estimated prevalence of CTD was 0.7% in the REISAMIC registry, and the authors emphasize that the high proportion of cases of Sjögren’s syndrome is noteworthy, with two of the patients fulfilling the recent American College of Rheumatology/European League Against Rheumatism criteria for Sjögren’s syndrome.
A limitation of the study is that some patients presenting with milder symptoms might not have been investigated by their oncologist.
The findings raise the question of whether asymptomatic patients taking ICIs who are at risk for immune-related adverse events should be screened and monitored closely, the authors explained.
One of the study authors received research funding from Novartis and Pfizer for the current paper. Several authors report relationships with industry.
For the first time, new-onset connective tissue disease has been reported in patients who were treated with anti-PD1/PDL-1 agents, according to findings published in the Annals of the Rheumatic Diseases.
In a cohort of 447 cancer patients who received therapy with immune checkpoint inhibitors (ICIs), Sébastien Le Burel, MD, of the Bicêtre Hospital in Le Kremlin-Bicêtre, France, and his colleagues described four patients who developed a connective tissue disease (CTD). There were two cases of Sjögren’s syndrome in patients taking an anti–programmed cell death 1 (anti-PD1) drug, one case of cryoglobulinemic vasculitis as a complication of suspected Sjögren’s syndrome in a patient taking an anti–programmed cell death ligand 1 (PDL-1) agent, and a case of a patient with antinuclear antibody positive myositis who was taking an anti-PDL-1 drug (Ann Rheum Dis. 2017 Feb 27. doi: 10.1136/annrheumdis-2016-210820).
“While the onset of systemic autoimmune disease after ICI treatment remains uncommon, greater awareness of these conditions should enable physicians to provide more effective patient care,” the investigators wrote. “This underlines the need for close collaboration within a network of oncologists and other specialist physicians in the new era of immunotherapy.”
The investigators discovered the cases by screening the French prospective, multicenter, academic REISAMIC registry for reports of CTD among patients being treated with anti-PD1 or anti-PDL-1 agents.
All four of the patients who developed a CTD had metastatic cancer, and their mean age was 62 years. Two patients had been treated with anti-PD1 agents and two with anti-PDL-1 agents. None of the four patients had presented with symptoms of CTD before they began treatment.
The mean time interval between the first treatment dose and the first symptom of CTD was 60 days (range, 24-72), and the mean time interval between the first symptom and subsequent diagnosis of CTD was 40 days (range, 10-74).
Three patients discontinued the ICI agent, and two patients were treated with steroids (1 mg/kg/day).
The estimated prevalence of CTD was 0.7% in the REISAMIC registry, and the authors emphasize that the high proportion of cases of Sjögren’s syndrome is noteworthy, with two of the patients fulfilling the recent American College of Rheumatology/European League Against Rheumatism criteria for Sjögren’s syndrome.
A limitation of the study is that some patients presenting with milder symptoms might not have been investigated by their oncologist.
The findings raise the question of whether asymptomatic patients taking ICIs who are at risk for immune-related adverse events should be screened and monitored closely, the authors explained.
One of the study authors received research funding from Novartis and Pfizer for the current paper. Several authors report relationships with industry.
Key clinical point:
Major finding: In a cohort of 447 patients, 4 with metastatic cancer developed connective tissue disease following anti-PD-1/PDL-1 treatment.
Data source: A prospective, multicenter, academic registry was screened for reports of CTD among patients being treated with anti-PD1/PDL-1 agents.
Disclosures: One of the study authors received research funding from Novartis and Pfizer for the current paper. Several authors report relationships with industry.
Skin disease costs $75 billion a year
The direct cost of treating skin diseases in the United States was almost $75 billion in 2013, according to a report on the burden of skin disease from the American Academy of Dermatology.
For the nearly 85 million Americans who were seen by a physician for a skin disease in 2013, about $45.9 billion was spent on medical costs such as office visits, procedures, and tests; $15 billion was spent on prescription drugs; and $4.1 billion went for vaccines and skin cancer screening. Another $10 billion was spent on OTC products, the AAD’s Burden of Skin Disease Work Group reported (J Am Acad Dermatol. 2017 Feb 24. doi: 10.1016/j.jaad.2016.12.043).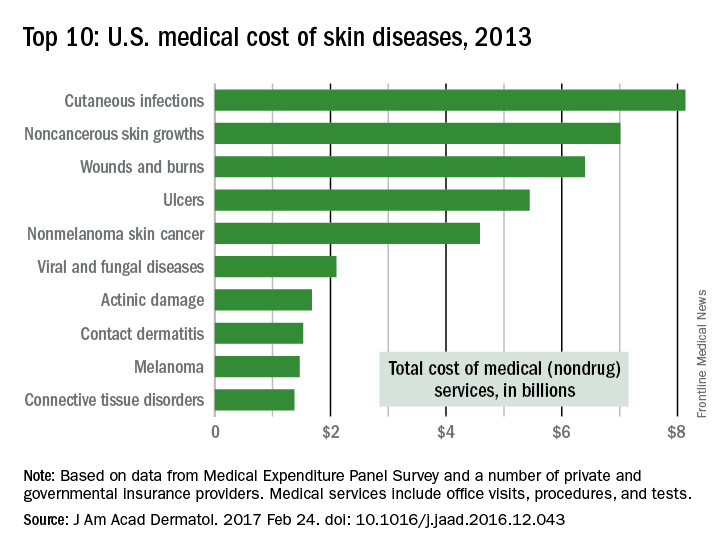
The per-capita cost of skin disease in 2013 was $213, compared with $950 per person for cardiovascular disease, $785 for diabetes, and $147 for end-stage renal disease, they noted.
In discussing the future burden of skin disease, the work group noted that the aging U.S. population and “the increased costs of currently in-use and newly developed dermatologic treatment options [need] to be addressed by an appropriate increase in dermatologic care providers.”
The direct cost of treating skin diseases in the United States was almost $75 billion in 2013, according to a report on the burden of skin disease from the American Academy of Dermatology.
For the nearly 85 million Americans who were seen by a physician for a skin disease in 2013, about $45.9 billion was spent on medical costs such as office visits, procedures, and tests; $15 billion was spent on prescription drugs; and $4.1 billion went for vaccines and skin cancer screening. Another $10 billion was spent on OTC products, the AAD’s Burden of Skin Disease Work Group reported (J Am Acad Dermatol. 2017 Feb 24. doi: 10.1016/j.jaad.2016.12.043).
The per-capita cost of skin disease in 2013 was $213, compared with $950 per person for cardiovascular disease, $785 for diabetes, and $147 for end-stage renal disease, they noted.
In discussing the future burden of skin disease, the work group noted that the aging U.S. population and “the increased costs of currently in-use and newly developed dermatologic treatment options [need] to be addressed by an appropriate increase in dermatologic care providers.”
The direct cost of treating skin diseases in the United States was almost $75 billion in 2013, according to a report on the burden of skin disease from the American Academy of Dermatology.
For the nearly 85 million Americans who were seen by a physician for a skin disease in 2013, about $45.9 billion was spent on medical costs such as office visits, procedures, and tests; $15 billion was spent on prescription drugs; and $4.1 billion went for vaccines and skin cancer screening. Another $10 billion was spent on OTC products, the AAD’s Burden of Skin Disease Work Group reported (J Am Acad Dermatol. 2017 Feb 24. doi: 10.1016/j.jaad.2016.12.043).
The per-capita cost of skin disease in 2013 was $213, compared with $950 per person for cardiovascular disease, $785 for diabetes, and $147 for end-stage renal disease, they noted.
In discussing the future burden of skin disease, the work group noted that the aging U.S. population and “the increased costs of currently in-use and newly developed dermatologic treatment options [need] to be addressed by an appropriate increase in dermatologic care providers.”