User login
Ecofriendly surfactant is allergen of the year
ORLANDO – Alkyl glucosides, mild surfactants derived from natural, sustainable sources, have been named allergen of the year by the American Contact Dermatitis Society.
The ecofriendly nature of these compounds has led to their inclusion in more personal care products in the last decade and a half. Alkyl glucosides are derived from coconut, palm, or rapeseed oil with glucose supplied by corn, wheat starch, or potatoes. They can be found in rinse-off products such as shampoos, shower gels, and liquid cleansers but also in leave-on products such as deodorants, sunscreens, and moisturizers, investigators said at the annual meeting of the American Contact Dermatitis Society, held just prior to the start of the American Academy of Dermatology’s annual meeting.
Camille Loranger, MD, of the department of dermatology, McGill University Health Center, Montreal, presented her institution’s experience with allergic contact dermatitis caused by alkyl glucosides. A total of 3,095 patients were patch tested at the clinic between January 2009 and June 2016. Researchers used the North American Contact Dermatitis Group 65-allergen series, which includes decyl glucoside (5% in petrolatum). Slightly more than half of patients (1,628) also were tested for reactions to lauryl glucoside (3% in petrolatum) as part of an additional cosmetic series. Twenty patients in the larger series reacted to decyl glucoside, while 15 of those who tested for lauryl glucoside reacted. Of those 15 patients, 6 were found to be allergic to decyl glucoside as well (Dermatitis. 2017 Jan/Feb;28[1]:5-13).
Allergy to alkyl glucosides became more common over time in the McGill series. The rate of positivity was low in the early years of the series, but increased from 1.37% of 437 patients in 2014 to 2.2% of 227 patients tested in the first half of 2016, Dr. Loranger said.
“Most of our patients were women with an average age of 48 years,” she added. “Body sites most commonly affected were the head and the hands. Only one case could be attributed to occupational exposure.”
Most patients – 86% – also were atopic (asthma, eczema, and rhinitis).
Products identified as most commonly causing a positive reaction were leave-on moisturizers and hand creams.
Donald V. Belsito, MD, professor of dermatology at Columbia University, N.Y., introduced the allergen of the year, pointing out that the compounds selected are not necessarily “bad actors.”
“The allergen of the year is really chosen to educate dermatologists about allergens that may be of low prevalence but a high relevance,” Dr. Belsito said. The allergens selected “are difficult to test for because they are tested for at irritant concentrations. It doesn’t mean they are these horrible substances that are damaging the world necessarily.”
The ACDS has been naming an allergen of the year since 2004.
[email protected]
On Twitter @denisefulton
ORLANDO – Alkyl glucosides, mild surfactants derived from natural, sustainable sources, have been named allergen of the year by the American Contact Dermatitis Society.
The ecofriendly nature of these compounds has led to their inclusion in more personal care products in the last decade and a half. Alkyl glucosides are derived from coconut, palm, or rapeseed oil with glucose supplied by corn, wheat starch, or potatoes. They can be found in rinse-off products such as shampoos, shower gels, and liquid cleansers but also in leave-on products such as deodorants, sunscreens, and moisturizers, investigators said at the annual meeting of the American Contact Dermatitis Society, held just prior to the start of the American Academy of Dermatology’s annual meeting.
Camille Loranger, MD, of the department of dermatology, McGill University Health Center, Montreal, presented her institution’s experience with allergic contact dermatitis caused by alkyl glucosides. A total of 3,095 patients were patch tested at the clinic between January 2009 and June 2016. Researchers used the North American Contact Dermatitis Group 65-allergen series, which includes decyl glucoside (5% in petrolatum). Slightly more than half of patients (1,628) also were tested for reactions to lauryl glucoside (3% in petrolatum) as part of an additional cosmetic series. Twenty patients in the larger series reacted to decyl glucoside, while 15 of those who tested for lauryl glucoside reacted. Of those 15 patients, 6 were found to be allergic to decyl glucoside as well (Dermatitis. 2017 Jan/Feb;28[1]:5-13).
Allergy to alkyl glucosides became more common over time in the McGill series. The rate of positivity was low in the early years of the series, but increased from 1.37% of 437 patients in 2014 to 2.2% of 227 patients tested in the first half of 2016, Dr. Loranger said.
“Most of our patients were women with an average age of 48 years,” she added. “Body sites most commonly affected were the head and the hands. Only one case could be attributed to occupational exposure.”
Most patients – 86% – also were atopic (asthma, eczema, and rhinitis).
Products identified as most commonly causing a positive reaction were leave-on moisturizers and hand creams.
Donald V. Belsito, MD, professor of dermatology at Columbia University, N.Y., introduced the allergen of the year, pointing out that the compounds selected are not necessarily “bad actors.”
“The allergen of the year is really chosen to educate dermatologists about allergens that may be of low prevalence but a high relevance,” Dr. Belsito said. The allergens selected “are difficult to test for because they are tested for at irritant concentrations. It doesn’t mean they are these horrible substances that are damaging the world necessarily.”
The ACDS has been naming an allergen of the year since 2004.
[email protected]
On Twitter @denisefulton
ORLANDO – Alkyl glucosides, mild surfactants derived from natural, sustainable sources, have been named allergen of the year by the American Contact Dermatitis Society.
The ecofriendly nature of these compounds has led to their inclusion in more personal care products in the last decade and a half. Alkyl glucosides are derived from coconut, palm, or rapeseed oil with glucose supplied by corn, wheat starch, or potatoes. They can be found in rinse-off products such as shampoos, shower gels, and liquid cleansers but also in leave-on products such as deodorants, sunscreens, and moisturizers, investigators said at the annual meeting of the American Contact Dermatitis Society, held just prior to the start of the American Academy of Dermatology’s annual meeting.
Camille Loranger, MD, of the department of dermatology, McGill University Health Center, Montreal, presented her institution’s experience with allergic contact dermatitis caused by alkyl glucosides. A total of 3,095 patients were patch tested at the clinic between January 2009 and June 2016. Researchers used the North American Contact Dermatitis Group 65-allergen series, which includes decyl glucoside (5% in petrolatum). Slightly more than half of patients (1,628) also were tested for reactions to lauryl glucoside (3% in petrolatum) as part of an additional cosmetic series. Twenty patients in the larger series reacted to decyl glucoside, while 15 of those who tested for lauryl glucoside reacted. Of those 15 patients, 6 were found to be allergic to decyl glucoside as well (Dermatitis. 2017 Jan/Feb;28[1]:5-13).
Allergy to alkyl glucosides became more common over time in the McGill series. The rate of positivity was low in the early years of the series, but increased from 1.37% of 437 patients in 2014 to 2.2% of 227 patients tested in the first half of 2016, Dr. Loranger said.
“Most of our patients were women with an average age of 48 years,” she added. “Body sites most commonly affected were the head and the hands. Only one case could be attributed to occupational exposure.”
Most patients – 86% – also were atopic (asthma, eczema, and rhinitis).
Products identified as most commonly causing a positive reaction were leave-on moisturizers and hand creams.
Donald V. Belsito, MD, professor of dermatology at Columbia University, N.Y., introduced the allergen of the year, pointing out that the compounds selected are not necessarily “bad actors.”
“The allergen of the year is really chosen to educate dermatologists about allergens that may be of low prevalence but a high relevance,” Dr. Belsito said. The allergens selected “are difficult to test for because they are tested for at irritant concentrations. It doesn’t mean they are these horrible substances that are damaging the world necessarily.”
The ACDS has been naming an allergen of the year since 2004.
[email protected]
On Twitter @denisefulton
CAR designers report high B-cell cancer response rates
ORLANDO – Patients with advanced hematologic malignancies of B-cell lineage had robust immune responses following infusion of a chimeric antigen receptor (CAR)–T-cell construct designed to deliver a specific balance of antigens, investigators reported.
Adults with relapsed or refractory B-lineage acute myeloid leukemia (ALL), non–Hodgkin lymphoma (NHL), and chronic lymphocytic leukemia (CLL) who received a CAR-T cell construct consisting of autologous CD4-positive and CD-8-positive T cells that were transduced separately, recombined, and then delivered in a single infusion had comparatively high overall response and complete response rates, reported Cameron Turtle, MBBS, PhD, from the Fred Hutchinson Cancer Research Center in Seattle.
“We know that patients have a highly variable CD4 to CD8 ratio, so by actually controlling this and separately transducing, expanding, and then reformulating in this defined composition, we’re able to eliminate one source of variability in CAR-T cell products,” Dr. Turtle said at the ASCO-SITC Clinical Immuno-Oncology Symposium.
In preclinical studies, an even balance of CD4-positive and CD8-positive central memory T cells or naive T cells evoked more potent immune responses against B-cell malignancies in mice than CD19-positive cells, he explained
To see whether this would also hold true in humans, the investigators enrolled into a phase I/II trial adults with relapsed/refractory B-cell malignancies, including ALL (36 patients), NHL (41), and CLL (24). No patients were excluded on the basis of either absolute lymphocyte, circulating tumors cells, history of stem cell transplant, or results of in vitro test expansions.
All patients underwent leukapheresis for harvesting of T-cells, and populations of CD4- and CD8-positive cells were separated and transduced with a lentiviral vector to express a CD19 CAR and a truncated human epidermal growth factor receptor that allowed tracing of the transduced cells via flow cytometry. The patients underwent lymphodepleting chemotherapy with cyclophosphamide (for the earliest patients), or cyclophosphamide plus fludarabine. Fifteen days after leukapheresis, the separated, transduced, and expanded cells were combined and delivered back to patients in a single infusion at one of three dose levels: 2 x 105, 2 x 106, or 2 x 107 CAR-T cells/kg.
ALL results
Two of the 36 patients with ALL died from complications of the CAR-T cell infusion process prior to evaluation. The 34 remaining patients all had morphologic bone marrow complete responses (CR). Of this group, 32 also had bone marrow CR on flow cytometry.
Using immunoglobulin H (IgH) deep sequencing in a subset of 20 patients 3 weeks after CAR-T cell infusion, the investigators could not detect the malignant IgH index clone in 13 of the patients, and found fewer than 10 copies in the bone marrow of 5 patients.
Six of seven patients with extramedullary disease at baseline had a complete response. The remaining patient in this group had an equivocal PET scan result, and experienced a relapse 2 months after assessment.
The investigators also determined that the lymphodepletion regimen may affect overall results, based on the finding that 10 of 12 patients who received cyclophosphamide alone achieved a CR, but seven of these 10 patients had a relapse within a few months. Of these seven patients. five received a second T-cell infusion, but none had significant T-cell expansion. The investigators traced the failure of the second attempt to a CD8-mediated transgene immune response to a murine single-chain variable fragment used in the construct.
For subsequent patients, they altered the lymphodepletion regimen to include fludarabine to prevent priming of the anti-CAR transgenic immune response. This modification resulted in improved progression-free survival and overall survival for subsequent patients receiving a second infusion, Dr. Turtle said.
NHL results
Of the 41 patients with NHL, 30 (73%) had aggressive histologies, including diffuse large B-cell lymphoma, primary mediastinal large B-cell lymphoma, T-cell/histiocyte-rich large B-cell, and Burkitt lymphomas, and 11 (27%) had indolent histologies, including mantle cell and follicular lymphomas. Most of the patients had received multiple prior lines of therapy, and 19 (46%) had undergone either an autologous or allogeneic stem cell transplant.
Of the 39 evaluable patients who completed therapy, the overall response rate was 67%, including 13 (39%) with CR. Dr. Turtle noted that the CR rate was substantially higher among patients who received cyclophosphamide and fludarabine lymphodepletion, compared with cyclophosphamide alone.
There were also a few responses, including two CRs, among patients with indolent histologies, he said.
CLL, safety results
All 24 patients with CLL had previously received ibrutinib (Imbruvica). Of this group, 19 either had no significant responses to the drug, inactivating mutations, or intolerable toxicities. All but 1 of the 24 patients also had high-risk cytogenetics.
Of the 16 ibrutinib-refractory patients who were evaluable for restaging, 14 had no evidence of disease in bone marrow by flow cytometry at 4 weeks. The overall response rate in this group was 69%, which included four CRs.
Among a majority of all patients, toxicity with the CAR-T cell therapy was mild to moderate. Early cytokine changes appeared to be predictive of serious adverse events such as the cytokine release syndrome, a finding that may allow clinicians to intervene early to prevent complications, Dr. Turtle said.
In the CAR-T cell therapy, “multiple things affect the response and toxicity, including CAR T-cell dose, disease burden, the anti-CAR transgene immune response and the lymphodepletion regimen, not to mention other patient factors that we’re still sorting out,” he commented.
The trial was funded by the National Institutes of Health, Life Science Development Fund, Juno Therapeutics and the Bezos Family Foundation. Dr. Turtle disclosed consultancy, honoraria, and/or research funding from Juno Therapeutics and Seattle Genetics.
ORLANDO – Patients with advanced hematologic malignancies of B-cell lineage had robust immune responses following infusion of a chimeric antigen receptor (CAR)–T-cell construct designed to deliver a specific balance of antigens, investigators reported.
Adults with relapsed or refractory B-lineage acute myeloid leukemia (ALL), non–Hodgkin lymphoma (NHL), and chronic lymphocytic leukemia (CLL) who received a CAR-T cell construct consisting of autologous CD4-positive and CD-8-positive T cells that were transduced separately, recombined, and then delivered in a single infusion had comparatively high overall response and complete response rates, reported Cameron Turtle, MBBS, PhD, from the Fred Hutchinson Cancer Research Center in Seattle.
“We know that patients have a highly variable CD4 to CD8 ratio, so by actually controlling this and separately transducing, expanding, and then reformulating in this defined composition, we’re able to eliminate one source of variability in CAR-T cell products,” Dr. Turtle said at the ASCO-SITC Clinical Immuno-Oncology Symposium.
In preclinical studies, an even balance of CD4-positive and CD8-positive central memory T cells or naive T cells evoked more potent immune responses against B-cell malignancies in mice than CD19-positive cells, he explained
To see whether this would also hold true in humans, the investigators enrolled into a phase I/II trial adults with relapsed/refractory B-cell malignancies, including ALL (36 patients), NHL (41), and CLL (24). No patients were excluded on the basis of either absolute lymphocyte, circulating tumors cells, history of stem cell transplant, or results of in vitro test expansions.
All patients underwent leukapheresis for harvesting of T-cells, and populations of CD4- and CD8-positive cells were separated and transduced with a lentiviral vector to express a CD19 CAR and a truncated human epidermal growth factor receptor that allowed tracing of the transduced cells via flow cytometry. The patients underwent lymphodepleting chemotherapy with cyclophosphamide (for the earliest patients), or cyclophosphamide plus fludarabine. Fifteen days after leukapheresis, the separated, transduced, and expanded cells were combined and delivered back to patients in a single infusion at one of three dose levels: 2 x 105, 2 x 106, or 2 x 107 CAR-T cells/kg.
ALL results
Two of the 36 patients with ALL died from complications of the CAR-T cell infusion process prior to evaluation. The 34 remaining patients all had morphologic bone marrow complete responses (CR). Of this group, 32 also had bone marrow CR on flow cytometry.
Using immunoglobulin H (IgH) deep sequencing in a subset of 20 patients 3 weeks after CAR-T cell infusion, the investigators could not detect the malignant IgH index clone in 13 of the patients, and found fewer than 10 copies in the bone marrow of 5 patients.
Six of seven patients with extramedullary disease at baseline had a complete response. The remaining patient in this group had an equivocal PET scan result, and experienced a relapse 2 months after assessment.
The investigators also determined that the lymphodepletion regimen may affect overall results, based on the finding that 10 of 12 patients who received cyclophosphamide alone achieved a CR, but seven of these 10 patients had a relapse within a few months. Of these seven patients. five received a second T-cell infusion, but none had significant T-cell expansion. The investigators traced the failure of the second attempt to a CD8-mediated transgene immune response to a murine single-chain variable fragment used in the construct.
For subsequent patients, they altered the lymphodepletion regimen to include fludarabine to prevent priming of the anti-CAR transgenic immune response. This modification resulted in improved progression-free survival and overall survival for subsequent patients receiving a second infusion, Dr. Turtle said.
NHL results
Of the 41 patients with NHL, 30 (73%) had aggressive histologies, including diffuse large B-cell lymphoma, primary mediastinal large B-cell lymphoma, T-cell/histiocyte-rich large B-cell, and Burkitt lymphomas, and 11 (27%) had indolent histologies, including mantle cell and follicular lymphomas. Most of the patients had received multiple prior lines of therapy, and 19 (46%) had undergone either an autologous or allogeneic stem cell transplant.
Of the 39 evaluable patients who completed therapy, the overall response rate was 67%, including 13 (39%) with CR. Dr. Turtle noted that the CR rate was substantially higher among patients who received cyclophosphamide and fludarabine lymphodepletion, compared with cyclophosphamide alone.
There were also a few responses, including two CRs, among patients with indolent histologies, he said.
CLL, safety results
All 24 patients with CLL had previously received ibrutinib (Imbruvica). Of this group, 19 either had no significant responses to the drug, inactivating mutations, or intolerable toxicities. All but 1 of the 24 patients also had high-risk cytogenetics.
Of the 16 ibrutinib-refractory patients who were evaluable for restaging, 14 had no evidence of disease in bone marrow by flow cytometry at 4 weeks. The overall response rate in this group was 69%, which included four CRs.
Among a majority of all patients, toxicity with the CAR-T cell therapy was mild to moderate. Early cytokine changes appeared to be predictive of serious adverse events such as the cytokine release syndrome, a finding that may allow clinicians to intervene early to prevent complications, Dr. Turtle said.
In the CAR-T cell therapy, “multiple things affect the response and toxicity, including CAR T-cell dose, disease burden, the anti-CAR transgene immune response and the lymphodepletion regimen, not to mention other patient factors that we’re still sorting out,” he commented.
The trial was funded by the National Institutes of Health, Life Science Development Fund, Juno Therapeutics and the Bezos Family Foundation. Dr. Turtle disclosed consultancy, honoraria, and/or research funding from Juno Therapeutics and Seattle Genetics.
ORLANDO – Patients with advanced hematologic malignancies of B-cell lineage had robust immune responses following infusion of a chimeric antigen receptor (CAR)–T-cell construct designed to deliver a specific balance of antigens, investigators reported.
Adults with relapsed or refractory B-lineage acute myeloid leukemia (ALL), non–Hodgkin lymphoma (NHL), and chronic lymphocytic leukemia (CLL) who received a CAR-T cell construct consisting of autologous CD4-positive and CD-8-positive T cells that were transduced separately, recombined, and then delivered in a single infusion had comparatively high overall response and complete response rates, reported Cameron Turtle, MBBS, PhD, from the Fred Hutchinson Cancer Research Center in Seattle.
“We know that patients have a highly variable CD4 to CD8 ratio, so by actually controlling this and separately transducing, expanding, and then reformulating in this defined composition, we’re able to eliminate one source of variability in CAR-T cell products,” Dr. Turtle said at the ASCO-SITC Clinical Immuno-Oncology Symposium.
In preclinical studies, an even balance of CD4-positive and CD8-positive central memory T cells or naive T cells evoked more potent immune responses against B-cell malignancies in mice than CD19-positive cells, he explained
To see whether this would also hold true in humans, the investigators enrolled into a phase I/II trial adults with relapsed/refractory B-cell malignancies, including ALL (36 patients), NHL (41), and CLL (24). No patients were excluded on the basis of either absolute lymphocyte, circulating tumors cells, history of stem cell transplant, or results of in vitro test expansions.
All patients underwent leukapheresis for harvesting of T-cells, and populations of CD4- and CD8-positive cells were separated and transduced with a lentiviral vector to express a CD19 CAR and a truncated human epidermal growth factor receptor that allowed tracing of the transduced cells via flow cytometry. The patients underwent lymphodepleting chemotherapy with cyclophosphamide (for the earliest patients), or cyclophosphamide plus fludarabine. Fifteen days after leukapheresis, the separated, transduced, and expanded cells were combined and delivered back to patients in a single infusion at one of three dose levels: 2 x 105, 2 x 106, or 2 x 107 CAR-T cells/kg.
ALL results
Two of the 36 patients with ALL died from complications of the CAR-T cell infusion process prior to evaluation. The 34 remaining patients all had morphologic bone marrow complete responses (CR). Of this group, 32 also had bone marrow CR on flow cytometry.
Using immunoglobulin H (IgH) deep sequencing in a subset of 20 patients 3 weeks after CAR-T cell infusion, the investigators could not detect the malignant IgH index clone in 13 of the patients, and found fewer than 10 copies in the bone marrow of 5 patients.
Six of seven patients with extramedullary disease at baseline had a complete response. The remaining patient in this group had an equivocal PET scan result, and experienced a relapse 2 months after assessment.
The investigators also determined that the lymphodepletion regimen may affect overall results, based on the finding that 10 of 12 patients who received cyclophosphamide alone achieved a CR, but seven of these 10 patients had a relapse within a few months. Of these seven patients. five received a second T-cell infusion, but none had significant T-cell expansion. The investigators traced the failure of the second attempt to a CD8-mediated transgene immune response to a murine single-chain variable fragment used in the construct.
For subsequent patients, they altered the lymphodepletion regimen to include fludarabine to prevent priming of the anti-CAR transgenic immune response. This modification resulted in improved progression-free survival and overall survival for subsequent patients receiving a second infusion, Dr. Turtle said.
NHL results
Of the 41 patients with NHL, 30 (73%) had aggressive histologies, including diffuse large B-cell lymphoma, primary mediastinal large B-cell lymphoma, T-cell/histiocyte-rich large B-cell, and Burkitt lymphomas, and 11 (27%) had indolent histologies, including mantle cell and follicular lymphomas. Most of the patients had received multiple prior lines of therapy, and 19 (46%) had undergone either an autologous or allogeneic stem cell transplant.
Of the 39 evaluable patients who completed therapy, the overall response rate was 67%, including 13 (39%) with CR. Dr. Turtle noted that the CR rate was substantially higher among patients who received cyclophosphamide and fludarabine lymphodepletion, compared with cyclophosphamide alone.
There were also a few responses, including two CRs, among patients with indolent histologies, he said.
CLL, safety results
All 24 patients with CLL had previously received ibrutinib (Imbruvica). Of this group, 19 either had no significant responses to the drug, inactivating mutations, or intolerable toxicities. All but 1 of the 24 patients also had high-risk cytogenetics.
Of the 16 ibrutinib-refractory patients who were evaluable for restaging, 14 had no evidence of disease in bone marrow by flow cytometry at 4 weeks. The overall response rate in this group was 69%, which included four CRs.
Among a majority of all patients, toxicity with the CAR-T cell therapy was mild to moderate. Early cytokine changes appeared to be predictive of serious adverse events such as the cytokine release syndrome, a finding that may allow clinicians to intervene early to prevent complications, Dr. Turtle said.
In the CAR-T cell therapy, “multiple things affect the response and toxicity, including CAR T-cell dose, disease burden, the anti-CAR transgene immune response and the lymphodepletion regimen, not to mention other patient factors that we’re still sorting out,” he commented.
The trial was funded by the National Institutes of Health, Life Science Development Fund, Juno Therapeutics and the Bezos Family Foundation. Dr. Turtle disclosed consultancy, honoraria, and/or research funding from Juno Therapeutics and Seattle Genetics.
AT THE CLINICAL IMMUNO-ONCOLOGY SYMPOSIUM
Key clinical point: A defined CAR-T cell construct was associated with high response rates in patients with B-cell malignancies.
Major finding: The overall response rate among patients with ibrutinib-refractory chronic lymphocytic leukemia was 69%, including four complete responses.
Data source: Phase I/II dose-finding, safety and efficacy study in patients with B-lineage hematologic malignancies
Disclosures: The trial was funded by the National Institutes of Health, Life Science Development Fund, Juno Therapeutics and the Bezos Family Foundation. Dr. Turtle disclosed consultancy, honoraria, and/or research funding from Juno Therapeutics and Seattle Genetics.
CMS nominee Verma clears Senate Finance hurdle
Seema Verma has moved one step closer to becoming the administrator of the Centers for Medicare & Medicaid Services.
The Senate Finance Committee voted 13-12 on March 2 to approve Ms. Verma’s nomination after a delayed vote the day before. The vote, conducted during a meeting off the floor, was a straight party-line vote, with 13 Republicans voting for Ms. Verma and 12 Democrats voting against. One proxy vote was not counted into the final tally per Senate rules.
Her nomination will now be considered by the full Senate.
Senate Finance Committee Chairman Orrin Hatch (R-Utah) praised Ms. Verma as a qualified leader who will help improve CMS.
Senate Finance Committee Ranking Member Ron Wyden, (D-Ore.) denounced Ms. Verma, stressing that she failed to adequately answer questions during her nomination hearing and has presented no clear vision of her plans as the next CMS administrator.

During her nomination hearing on Feb. 16, Ms. Verma came under fire for past consulting agreements with states while working for Hewlett Packard, a company that had financial interests in the health programs she designed. The issue was raised again during a preliminary vote by the Finance Committee on March 1.
“Ms. Verma was on both sides of the deal, helping manage the state’s health programs while being paid by vendors to those same programs,” Sen. Wyden said during the hearing. “I am concerned that if Ms. Verma is confirmed to lead CMS, where many of the companies she worked for are major vendors, there will not be adequate scrutiny of her past relationships with them, just as there wasn’t in Indiana.”
Ms. Verma previously said she never negotiated on behalf of Hewlett Packard and that the work she conducted for the states did not overlap with work she completed for HP.
“I hold honesty and integrity and adherence to a high ethical standard as part of my personal philosophy. That’s for me, I demand that from my employees, and I set that example for my own children,” she said during the Feb. 16 hearing. “We were never in a position where we were negotiating on behalf of HP or any other contractor with the state that we had a relationship with. If there was the potential [for a conflict], we would recuse ourselves.”
Ms. Verma’s nomination will now move to the full Senate. No date has yet been set for the vote.
[email protected]
On Twitter @legal_med
Seema Verma has moved one step closer to becoming the administrator of the Centers for Medicare & Medicaid Services.
The Senate Finance Committee voted 13-12 on March 2 to approve Ms. Verma’s nomination after a delayed vote the day before. The vote, conducted during a meeting off the floor, was a straight party-line vote, with 13 Republicans voting for Ms. Verma and 12 Democrats voting against. One proxy vote was not counted into the final tally per Senate rules.
Her nomination will now be considered by the full Senate.
Senate Finance Committee Chairman Orrin Hatch (R-Utah) praised Ms. Verma as a qualified leader who will help improve CMS.
Senate Finance Committee Ranking Member Ron Wyden, (D-Ore.) denounced Ms. Verma, stressing that she failed to adequately answer questions during her nomination hearing and has presented no clear vision of her plans as the next CMS administrator.
During her nomination hearing on Feb. 16, Ms. Verma came under fire for past consulting agreements with states while working for Hewlett Packard, a company that had financial interests in the health programs she designed. The issue was raised again during a preliminary vote by the Finance Committee on March 1.
“Ms. Verma was on both sides of the deal, helping manage the state’s health programs while being paid by vendors to those same programs,” Sen. Wyden said during the hearing. “I am concerned that if Ms. Verma is confirmed to lead CMS, where many of the companies she worked for are major vendors, there will not be adequate scrutiny of her past relationships with them, just as there wasn’t in Indiana.”
Ms. Verma previously said she never negotiated on behalf of Hewlett Packard and that the work she conducted for the states did not overlap with work she completed for HP.
“I hold honesty and integrity and adherence to a high ethical standard as part of my personal philosophy. That’s for me, I demand that from my employees, and I set that example for my own children,” she said during the Feb. 16 hearing. “We were never in a position where we were negotiating on behalf of HP or any other contractor with the state that we had a relationship with. If there was the potential [for a conflict], we would recuse ourselves.”
Ms. Verma’s nomination will now move to the full Senate. No date has yet been set for the vote.
[email protected]
On Twitter @legal_med
Seema Verma has moved one step closer to becoming the administrator of the Centers for Medicare & Medicaid Services.
The Senate Finance Committee voted 13-12 on March 2 to approve Ms. Verma’s nomination after a delayed vote the day before. The vote, conducted during a meeting off the floor, was a straight party-line vote, with 13 Republicans voting for Ms. Verma and 12 Democrats voting against. One proxy vote was not counted into the final tally per Senate rules.
Her nomination will now be considered by the full Senate.
Senate Finance Committee Chairman Orrin Hatch (R-Utah) praised Ms. Verma as a qualified leader who will help improve CMS.
Senate Finance Committee Ranking Member Ron Wyden, (D-Ore.) denounced Ms. Verma, stressing that she failed to adequately answer questions during her nomination hearing and has presented no clear vision of her plans as the next CMS administrator.
During her nomination hearing on Feb. 16, Ms. Verma came under fire for past consulting agreements with states while working for Hewlett Packard, a company that had financial interests in the health programs she designed. The issue was raised again during a preliminary vote by the Finance Committee on March 1.
“Ms. Verma was on both sides of the deal, helping manage the state’s health programs while being paid by vendors to those same programs,” Sen. Wyden said during the hearing. “I am concerned that if Ms. Verma is confirmed to lead CMS, where many of the companies she worked for are major vendors, there will not be adequate scrutiny of her past relationships with them, just as there wasn’t in Indiana.”
Ms. Verma previously said she never negotiated on behalf of Hewlett Packard and that the work she conducted for the states did not overlap with work she completed for HP.
“I hold honesty and integrity and adherence to a high ethical standard as part of my personal philosophy. That’s for me, I demand that from my employees, and I set that example for my own children,” she said during the Feb. 16 hearing. “We were never in a position where we were negotiating on behalf of HP or any other contractor with the state that we had a relationship with. If there was the potential [for a conflict], we would recuse ourselves.”
Ms. Verma’s nomination will now move to the full Senate. No date has yet been set for the vote.
[email protected]
On Twitter @legal_med
Children with chronic conditions have poor influenza vaccination coverage
Poor influenza vaccination rates in children with chronic diseases is primarily due to poor parental understanding of influenza risk and vaccination benefits, according to Janita Pak Chun Chau, PhD, of the Chinese University of Hong Kong, and associates.
Studies show that children with chronic conditions “are at a disproportionately higher risk for severe influenza-associated complications, causing increased visits to outpatient or emergency departments, longer hospital stays, and higher mortality,” the researchers said.
A total of 623 parents of children with chronic conditions in Hong Kong were included in the study. The most common chronic condition was asthma, followed by chronic respiratory disease and cardiomyopathy. Only 33% of children had received an influenza vaccination in the previous 12 months, and 57% of children had ever received one.
Just under 40% of parents indicated intent to have their children vaccinated in the next 12 months. Parents who had their children vaccinated were more aware of vaccination benefits and considered vaccination a social norm, compared with parents who had not had their children vaccinated. Television was by far the most common source of information about influenza, followed by health professionals, and newspapers and magazines.
“Development of community-based influenza vaccination programs by health care professionals targeted to promote awareness and communicate the benefits and effectiveness of the vaccines in children with chronic conditions, as well as clarifying safety issues concerning the vaccination, may be able to promote the uptake of influenza vaccination,” the investigators wrote.
Find the study in the Pediatric Infectious Disease Journal (doi: INF.0000000000001550).
Poor influenza vaccination rates in children with chronic diseases is primarily due to poor parental understanding of influenza risk and vaccination benefits, according to Janita Pak Chun Chau, PhD, of the Chinese University of Hong Kong, and associates.
Studies show that children with chronic conditions “are at a disproportionately higher risk for severe influenza-associated complications, causing increased visits to outpatient or emergency departments, longer hospital stays, and higher mortality,” the researchers said.
A total of 623 parents of children with chronic conditions in Hong Kong were included in the study. The most common chronic condition was asthma, followed by chronic respiratory disease and cardiomyopathy. Only 33% of children had received an influenza vaccination in the previous 12 months, and 57% of children had ever received one.
Just under 40% of parents indicated intent to have their children vaccinated in the next 12 months. Parents who had their children vaccinated were more aware of vaccination benefits and considered vaccination a social norm, compared with parents who had not had their children vaccinated. Television was by far the most common source of information about influenza, followed by health professionals, and newspapers and magazines.
“Development of community-based influenza vaccination programs by health care professionals targeted to promote awareness and communicate the benefits and effectiveness of the vaccines in children with chronic conditions, as well as clarifying safety issues concerning the vaccination, may be able to promote the uptake of influenza vaccination,” the investigators wrote.
Find the study in the Pediatric Infectious Disease Journal (doi: INF.0000000000001550).
Poor influenza vaccination rates in children with chronic diseases is primarily due to poor parental understanding of influenza risk and vaccination benefits, according to Janita Pak Chun Chau, PhD, of the Chinese University of Hong Kong, and associates.
Studies show that children with chronic conditions “are at a disproportionately higher risk for severe influenza-associated complications, causing increased visits to outpatient or emergency departments, longer hospital stays, and higher mortality,” the researchers said.
A total of 623 parents of children with chronic conditions in Hong Kong were included in the study. The most common chronic condition was asthma, followed by chronic respiratory disease and cardiomyopathy. Only 33% of children had received an influenza vaccination in the previous 12 months, and 57% of children had ever received one.
Just under 40% of parents indicated intent to have their children vaccinated in the next 12 months. Parents who had their children vaccinated were more aware of vaccination benefits and considered vaccination a social norm, compared with parents who had not had their children vaccinated. Television was by far the most common source of information about influenza, followed by health professionals, and newspapers and magazines.
“Development of community-based influenza vaccination programs by health care professionals targeted to promote awareness and communicate the benefits and effectiveness of the vaccines in children with chronic conditions, as well as clarifying safety issues concerning the vaccination, may be able to promote the uptake of influenza vaccination,” the investigators wrote.
Find the study in the Pediatric Infectious Disease Journal (doi: INF.0000000000001550).
FROM THE PEDIATRIC INFECTIOUS DISEASE JOURNAL
Pigmented skin lesions lightened during melanoma immunotherapy
Treatment with pembrolizumab, a humanized antibody used in cancer immunotherapy, may affect the pigmentation of some benign skin lesions, according to a case study in British Journal of Dermatology.
Pembrolizumab works by targeting the programmed cell death-1 (PD-1) receptor and is used in the treatment of metastatic melanoma and some other cancers.
The case report, by Zachary J. Wolner, MD, of Memorial Sloan Kettering Cancer Center in New York, and his colleagues, describes a male patient in his 60s with HRAS mutant metastatic melanoma who was treated with pembrolizumab 2 mg/kg every 3 weeks for 13 months, and had received no previous systematic treatment. At 4 months after starting pembrolizumab, the patient experienced whitening of eyebrows and eyelashes, along with scalp and body hair, followed by lighter overall skin pigmentation and the fading of pigmented skin lesions. Baseline (pre-pembrolizumab) and 1-year follow-up skin photography confirmed lightening or disappearance of solar lentigines, seborrheic keratoses, and melanocytic nevi along with overall lightening of the skin (Br J. Dermatol. 2017 doi: 10.1111/bjd.15354).
Dr. Wolner and his colleagues noted that while changing skin lesions have not been reported in clinical trials of anti-PD-1 therapies, one study in patients treated with an anti-PD-1 therapy for metastatic melanoma found changes to nevi in 6 of 34 (18%) patients. Patients using a melanoma website also have self-reported disappearing nevi after immunotherapy treatment, the authors noted.
Expression of the coinhibitory molecule PD-L1 “is not limited to malignant tumors,” the researchers wrote, adding that previous studies have identified PD-L1 expression in melanocytes of benign melanocytic nevi. “Therefore it is biologically plausible that PD-1 inhibition may affect the natural history of benign melanocytic neoplasms.”
Also, they wrote, “the co-occurrence of vitiligo and poliosis in our patient suggests a role for autoimmunity in the fading/disappearance of his pigmented lesions.” The investigators cited a recent study in 67 patients with metastatic melanoma receiving pembrolizumab, which found that 25% developed vitiligo. Response to treatment also was significantly associated with occurrence of vitiligo (JAMA Dermatol. 2016;152[1]:45-51).
Dr. Wolner and his colleagues cautioned that their findings were limited to a single case report, and also by “lack of histological sampling and molecular characterization of fading/disappearing nevi.” An alternative explanation for the observed changes “includes fading/disappearance not related to PD-1 inhibition or due to chance alone.”
A National Institutes of Health/National Cancer Institute Cancer Center grant was used to help fund the study. Two of Dr. Wolner’s coauthors disclosed consultant or advisory board relationships with Merck and other pharmaceutical manufacturers.
Treatment with pembrolizumab, a humanized antibody used in cancer immunotherapy, may affect the pigmentation of some benign skin lesions, according to a case study in British Journal of Dermatology.
Pembrolizumab works by targeting the programmed cell death-1 (PD-1) receptor and is used in the treatment of metastatic melanoma and some other cancers.
The case report, by Zachary J. Wolner, MD, of Memorial Sloan Kettering Cancer Center in New York, and his colleagues, describes a male patient in his 60s with HRAS mutant metastatic melanoma who was treated with pembrolizumab 2 mg/kg every 3 weeks for 13 months, and had received no previous systematic treatment. At 4 months after starting pembrolizumab, the patient experienced whitening of eyebrows and eyelashes, along with scalp and body hair, followed by lighter overall skin pigmentation and the fading of pigmented skin lesions. Baseline (pre-pembrolizumab) and 1-year follow-up skin photography confirmed lightening or disappearance of solar lentigines, seborrheic keratoses, and melanocytic nevi along with overall lightening of the skin (Br J. Dermatol. 2017 doi: 10.1111/bjd.15354).
Dr. Wolner and his colleagues noted that while changing skin lesions have not been reported in clinical trials of anti-PD-1 therapies, one study in patients treated with an anti-PD-1 therapy for metastatic melanoma found changes to nevi in 6 of 34 (18%) patients. Patients using a melanoma website also have self-reported disappearing nevi after immunotherapy treatment, the authors noted.
Expression of the coinhibitory molecule PD-L1 “is not limited to malignant tumors,” the researchers wrote, adding that previous studies have identified PD-L1 expression in melanocytes of benign melanocytic nevi. “Therefore it is biologically plausible that PD-1 inhibition may affect the natural history of benign melanocytic neoplasms.”
Also, they wrote, “the co-occurrence of vitiligo and poliosis in our patient suggests a role for autoimmunity in the fading/disappearance of his pigmented lesions.” The investigators cited a recent study in 67 patients with metastatic melanoma receiving pembrolizumab, which found that 25% developed vitiligo. Response to treatment also was significantly associated with occurrence of vitiligo (JAMA Dermatol. 2016;152[1]:45-51).
Dr. Wolner and his colleagues cautioned that their findings were limited to a single case report, and also by “lack of histological sampling and molecular characterization of fading/disappearing nevi.” An alternative explanation for the observed changes “includes fading/disappearance not related to PD-1 inhibition or due to chance alone.”
A National Institutes of Health/National Cancer Institute Cancer Center grant was used to help fund the study. Two of Dr. Wolner’s coauthors disclosed consultant or advisory board relationships with Merck and other pharmaceutical manufacturers.
Treatment with pembrolizumab, a humanized antibody used in cancer immunotherapy, may affect the pigmentation of some benign skin lesions, according to a case study in British Journal of Dermatology.
Pembrolizumab works by targeting the programmed cell death-1 (PD-1) receptor and is used in the treatment of metastatic melanoma and some other cancers.
The case report, by Zachary J. Wolner, MD, of Memorial Sloan Kettering Cancer Center in New York, and his colleagues, describes a male patient in his 60s with HRAS mutant metastatic melanoma who was treated with pembrolizumab 2 mg/kg every 3 weeks for 13 months, and had received no previous systematic treatment. At 4 months after starting pembrolizumab, the patient experienced whitening of eyebrows and eyelashes, along with scalp and body hair, followed by lighter overall skin pigmentation and the fading of pigmented skin lesions. Baseline (pre-pembrolizumab) and 1-year follow-up skin photography confirmed lightening or disappearance of solar lentigines, seborrheic keratoses, and melanocytic nevi along with overall lightening of the skin (Br J. Dermatol. 2017 doi: 10.1111/bjd.15354).
Dr. Wolner and his colleagues noted that while changing skin lesions have not been reported in clinical trials of anti-PD-1 therapies, one study in patients treated with an anti-PD-1 therapy for metastatic melanoma found changes to nevi in 6 of 34 (18%) patients. Patients using a melanoma website also have self-reported disappearing nevi after immunotherapy treatment, the authors noted.
Expression of the coinhibitory molecule PD-L1 “is not limited to malignant tumors,” the researchers wrote, adding that previous studies have identified PD-L1 expression in melanocytes of benign melanocytic nevi. “Therefore it is biologically plausible that PD-1 inhibition may affect the natural history of benign melanocytic neoplasms.”
Also, they wrote, “the co-occurrence of vitiligo and poliosis in our patient suggests a role for autoimmunity in the fading/disappearance of his pigmented lesions.” The investigators cited a recent study in 67 patients with metastatic melanoma receiving pembrolizumab, which found that 25% developed vitiligo. Response to treatment also was significantly associated with occurrence of vitiligo (JAMA Dermatol. 2016;152[1]:45-51).
Dr. Wolner and his colleagues cautioned that their findings were limited to a single case report, and also by “lack of histological sampling and molecular characterization of fading/disappearing nevi.” An alternative explanation for the observed changes “includes fading/disappearance not related to PD-1 inhibition or due to chance alone.”
A National Institutes of Health/National Cancer Institute Cancer Center grant was used to help fund the study. Two of Dr. Wolner’s coauthors disclosed consultant or advisory board relationships with Merck and other pharmaceutical manufacturers.
Key clinical point:
Major finding: Pembrolizumab and other PD-1 inhibitors may affect benign pigmented lesions.
Data source: A single-center, single-patient case report.
Disclosures: A National Institutes of Health/National Cancer Institute Cancer Center grant was used to help fund the study. Two of Dr. Wolner’s coauthors disclosed consultant or advisory board relationships with Merck and other pharmaceutical manufacturers.
How Can Neurologists Manage Pediatric Migraine?
OJAI, CA—Migraine headaches can be debilitating in children and adolescents and result in more missed days of school and poorer performance in the classroom, compared with children without migraine, according to an overview presented at the 10th Annual Winter Conference of the Headache Cooperative of the Pacific.

Understanding Pediatric Migraine
Pediatric migraine is defined as at least five attacks that fulfill the following criteria: headache attack lasting for two to 72 hours (untreated or unsuccessfully treated), headache with at least two of four characteristics (ie, unilateral location [though in children it is often bilateral], pulsating quality, moderate or severe intensity, and aggravation by or causing avoidance of routine physical activity), and headache accompanied by either nausea and vomiting or phonophobia and photophobia. It affects approximately 5% of children by age 10, making migraine five to 10 times more common than epilepsy in children. Chronic migraine, which entails headache on at least 15 days per month for at least three months, affects 0.6% of children between ages 5 and 12.
Pediatric migraine can have a different phenotype than adult migraine. The shortest duration for untreated or unsuccessfully treated attacks in adults is four hours, compared with two hours in children. In addition, migraines in children and adolescents tend to be bilateral.
Following puberty, there is a higher prevalence of migraine among young women and girls than among boys and young men, said Dr. Gelfand. Also, children with low socioeconomic status are nearly fourfold more likely to have chronic migraine than children from affluent backgrounds.
How to Take a Pediatric Headache History
A systematic approach to taking a headache history can be helpful, said Dr. Gelfand. When neurologists take a headache history, seating the child or adolescent in a central position near the clinican can help signal that the patient is going to be the primary person to provide the history. In addition, neurologists should set expectations for pediatric patients by explaining the questions they are going to ask about the child’s headaches.
Children are encouraged to share additional information about their headaches and to ask parents for help when necessary. Also, neurologists should hesitate to consider “not really” an answer to questions about the presence of symptoms such as nausea or movement sensitivity, because it often means “yes, but it is mild, and I can handle it and do not want to complain.”
Finally, when querying for sensitivity to light or sound, neurologists are advised to ask the following questions: During your headaches, do lights ever bother you? Do lights ever seem brighter than usual? Do lights ever make the headache worse? “For younger kids who might not be able to articulate sensitivity to light or sensitivity to sound, we may be able to infer those sensitivity symptoms from their behavior. Are they pulling the blankets up over their head or are they asking for the TV to be turned off? These are behaviors that their caregivers can report,” said Dr. Gelfand.
Acute Migraine Treatment
Acetaminophen and ibuprofen have been examined in randomized controlled trials that included children as young as 4. These drugs appear to be efficacious. In addition, the FDA has approved four triptans for acute treatment of pediatric migraine. Almotriptan was approved in 2009 for adolescents ages 12 to 17. In 2012, the FDA approved rizatriptan for children and adolescents ages 6 to 17. Finally, in 2015, zolmitriptan, a nasal spray, was approved for adolescents ages 12 to 17, as was a combination including naproxen and sumatriptan. Children with a history of peripheral vascular disease, stroke, and uncontrolled hypertension should not use triptans for the treatment of pediatric migraine.
In addition, Powers et al observed that amitriptyline and topiramate were no different from placebo for reducing headache frequency; approximately 60% of participants in all three study arms improved. The 361 children and adolescents involved in the study received a lot of headache education and counseling about medication overuse, and also received optimally dosed acute migraine medications, which may have contributed to the high rate of excellent outcomes, said Dr. Gelfand.
Preventative Strategies and Diet
A key component to preventive care in pediatric migraine is maintaining a healthy lifestyle. Neurologists should encourage patients to eat regular meals, get regular exercise and sleep, and stay consistently hydrated. Additionally, daily preventive treatment may include medications or supplements that are well tolerated. Cognitive behavioral therapy can also be beneficial.
Children and adolescents with migraine should avoid fasting, alcohol, or nitrate-containing meats such as hot dogs, some lunch meats, salami, and beef jerky. Chocolate, cheese, citrus, gluten, sugar, or dairy might not need to be avoided. Also, proper hydration can help control or prevent migraines. Pilot studies have shown that increased water intake decreases headache hours and severity. Spigt et al found that greater water intake resulted in a statically significant improvement in quality of life.
The Future of Pediatric Migraine Research
Sixty percent of patients will improve following treatment, but 40% of patients do not get better. In addition, “children who have continous headache and medication overuse have not been well studied, so we do not know what treatments might be most effective for them,
—Erica Tricarico
Suggested Reading
Qubty W, Gelfand AA. Psychological and behavioral issues in the management of migraine in children and adolescents. Curr Pain Headache Rep. 2016;20(12):69.
Spigt MG, Kuijper EC, Schayck CP, et al. Increasing the daily water intake for the prophylactic treatment of headache: a pilot trial. Eur J Neurol. 2005;12(9):715-718.
OJAI, CA—Migraine headaches can be debilitating in children and adolescents and result in more missed days of school and poorer performance in the classroom, compared with children without migraine, according to an overview presented at the 10th Annual Winter Conference of the Headache Cooperative of the Pacific.
Understanding Pediatric Migraine
Pediatric migraine is defined as at least five attacks that fulfill the following criteria: headache attack lasting for two to 72 hours (untreated or unsuccessfully treated), headache with at least two of four characteristics (ie, unilateral location [though in children it is often bilateral], pulsating quality, moderate or severe intensity, and aggravation by or causing avoidance of routine physical activity), and headache accompanied by either nausea and vomiting or phonophobia and photophobia. It affects approximately 5% of children by age 10, making migraine five to 10 times more common than epilepsy in children. Chronic migraine, which entails headache on at least 15 days per month for at least three months, affects 0.6% of children between ages 5 and 12.
Pediatric migraine can have a different phenotype than adult migraine. The shortest duration for untreated or unsuccessfully treated attacks in adults is four hours, compared with two hours in children. In addition, migraines in children and adolescents tend to be bilateral.
Following puberty, there is a higher prevalence of migraine among young women and girls than among boys and young men, said Dr. Gelfand. Also, children with low socioeconomic status are nearly fourfold more likely to have chronic migraine than children from affluent backgrounds.
How to Take a Pediatric Headache History
A systematic approach to taking a headache history can be helpful, said Dr. Gelfand. When neurologists take a headache history, seating the child or adolescent in a central position near the clinican can help signal that the patient is going to be the primary person to provide the history. In addition, neurologists should set expectations for pediatric patients by explaining the questions they are going to ask about the child’s headaches.
Children are encouraged to share additional information about their headaches and to ask parents for help when necessary. Also, neurologists should hesitate to consider “not really” an answer to questions about the presence of symptoms such as nausea or movement sensitivity, because it often means “yes, but it is mild, and I can handle it and do not want to complain.”
Finally, when querying for sensitivity to light or sound, neurologists are advised to ask the following questions: During your headaches, do lights ever bother you? Do lights ever seem brighter than usual? Do lights ever make the headache worse? “For younger kids who might not be able to articulate sensitivity to light or sensitivity to sound, we may be able to infer those sensitivity symptoms from their behavior. Are they pulling the blankets up over their head or are they asking for the TV to be turned off? These are behaviors that their caregivers can report,” said Dr. Gelfand.
Acute Migraine Treatment
Acetaminophen and ibuprofen have been examined in randomized controlled trials that included children as young as 4. These drugs appear to be efficacious. In addition, the FDA has approved four triptans for acute treatment of pediatric migraine. Almotriptan was approved in 2009 for adolescents ages 12 to 17. In 2012, the FDA approved rizatriptan for children and adolescents ages 6 to 17. Finally, in 2015, zolmitriptan, a nasal spray, was approved for adolescents ages 12 to 17, as was a combination including naproxen and sumatriptan. Children with a history of peripheral vascular disease, stroke, and uncontrolled hypertension should not use triptans for the treatment of pediatric migraine.
In addition, Powers et al observed that amitriptyline and topiramate were no different from placebo for reducing headache frequency; approximately 60% of participants in all three study arms improved. The 361 children and adolescents involved in the study received a lot of headache education and counseling about medication overuse, and also received optimally dosed acute migraine medications, which may have contributed to the high rate of excellent outcomes, said Dr. Gelfand.
Preventative Strategies and Diet
A key component to preventive care in pediatric migraine is maintaining a healthy lifestyle. Neurologists should encourage patients to eat regular meals, get regular exercise and sleep, and stay consistently hydrated. Additionally, daily preventive treatment may include medications or supplements that are well tolerated. Cognitive behavioral therapy can also be beneficial.
Children and adolescents with migraine should avoid fasting, alcohol, or nitrate-containing meats such as hot dogs, some lunch meats, salami, and beef jerky. Chocolate, cheese, citrus, gluten, sugar, or dairy might not need to be avoided. Also, proper hydration can help control or prevent migraines. Pilot studies have shown that increased water intake decreases headache hours and severity. Spigt et al found that greater water intake resulted in a statically significant improvement in quality of life.
The Future of Pediatric Migraine Research
Sixty percent of patients will improve following treatment, but 40% of patients do not get better. In addition, “children who have continous headache and medication overuse have not been well studied, so we do not know what treatments might be most effective for them,
—Erica Tricarico
Suggested Reading
Qubty W, Gelfand AA. Psychological and behavioral issues in the management of migraine in children and adolescents. Curr Pain Headache Rep. 2016;20(12):69.
Spigt MG, Kuijper EC, Schayck CP, et al. Increasing the daily water intake for the prophylactic treatment of headache: a pilot trial. Eur J Neurol. 2005;12(9):715-718.
OJAI, CA—Migraine headaches can be debilitating in children and adolescents and result in more missed days of school and poorer performance in the classroom, compared with children without migraine, according to an overview presented at the 10th Annual Winter Conference of the Headache Cooperative of the Pacific.
Understanding Pediatric Migraine
Pediatric migraine is defined as at least five attacks that fulfill the following criteria: headache attack lasting for two to 72 hours (untreated or unsuccessfully treated), headache with at least two of four characteristics (ie, unilateral location [though in children it is often bilateral], pulsating quality, moderate or severe intensity, and aggravation by or causing avoidance of routine physical activity), and headache accompanied by either nausea and vomiting or phonophobia and photophobia. It affects approximately 5% of children by age 10, making migraine five to 10 times more common than epilepsy in children. Chronic migraine, which entails headache on at least 15 days per month for at least three months, affects 0.6% of children between ages 5 and 12.
Pediatric migraine can have a different phenotype than adult migraine. The shortest duration for untreated or unsuccessfully treated attacks in adults is four hours, compared with two hours in children. In addition, migraines in children and adolescents tend to be bilateral.
Following puberty, there is a higher prevalence of migraine among young women and girls than among boys and young men, said Dr. Gelfand. Also, children with low socioeconomic status are nearly fourfold more likely to have chronic migraine than children from affluent backgrounds.
How to Take a Pediatric Headache History
A systematic approach to taking a headache history can be helpful, said Dr. Gelfand. When neurologists take a headache history, seating the child or adolescent in a central position near the clinican can help signal that the patient is going to be the primary person to provide the history. In addition, neurologists should set expectations for pediatric patients by explaining the questions they are going to ask about the child’s headaches.
Children are encouraged to share additional information about their headaches and to ask parents for help when necessary. Also, neurologists should hesitate to consider “not really” an answer to questions about the presence of symptoms such as nausea or movement sensitivity, because it often means “yes, but it is mild, and I can handle it and do not want to complain.”
Finally, when querying for sensitivity to light or sound, neurologists are advised to ask the following questions: During your headaches, do lights ever bother you? Do lights ever seem brighter than usual? Do lights ever make the headache worse? “For younger kids who might not be able to articulate sensitivity to light or sensitivity to sound, we may be able to infer those sensitivity symptoms from their behavior. Are they pulling the blankets up over their head or are they asking for the TV to be turned off? These are behaviors that their caregivers can report,” said Dr. Gelfand.
Acute Migraine Treatment
Acetaminophen and ibuprofen have been examined in randomized controlled trials that included children as young as 4. These drugs appear to be efficacious. In addition, the FDA has approved four triptans for acute treatment of pediatric migraine. Almotriptan was approved in 2009 for adolescents ages 12 to 17. In 2012, the FDA approved rizatriptan for children and adolescents ages 6 to 17. Finally, in 2015, zolmitriptan, a nasal spray, was approved for adolescents ages 12 to 17, as was a combination including naproxen and sumatriptan. Children with a history of peripheral vascular disease, stroke, and uncontrolled hypertension should not use triptans for the treatment of pediatric migraine.
In addition, Powers et al observed that amitriptyline and topiramate were no different from placebo for reducing headache frequency; approximately 60% of participants in all three study arms improved. The 361 children and adolescents involved in the study received a lot of headache education and counseling about medication overuse, and also received optimally dosed acute migraine medications, which may have contributed to the high rate of excellent outcomes, said Dr. Gelfand.
Preventative Strategies and Diet
A key component to preventive care in pediatric migraine is maintaining a healthy lifestyle. Neurologists should encourage patients to eat regular meals, get regular exercise and sleep, and stay consistently hydrated. Additionally, daily preventive treatment may include medications or supplements that are well tolerated. Cognitive behavioral therapy can also be beneficial.
Children and adolescents with migraine should avoid fasting, alcohol, or nitrate-containing meats such as hot dogs, some lunch meats, salami, and beef jerky. Chocolate, cheese, citrus, gluten, sugar, or dairy might not need to be avoided. Also, proper hydration can help control or prevent migraines. Pilot studies have shown that increased water intake decreases headache hours and severity. Spigt et al found that greater water intake resulted in a statically significant improvement in quality of life.
The Future of Pediatric Migraine Research
Sixty percent of patients will improve following treatment, but 40% of patients do not get better. In addition, “children who have continous headache and medication overuse have not been well studied, so we do not know what treatments might be most effective for them,
—Erica Tricarico
Suggested Reading
Qubty W, Gelfand AA. Psychological and behavioral issues in the management of migraine in children and adolescents. Curr Pain Headache Rep. 2016;20(12):69.
Spigt MG, Kuijper EC, Schayck CP, et al. Increasing the daily water intake for the prophylactic treatment of headache: a pilot trial. Eur J Neurol. 2005;12(9):715-718.
FDA approves sublingual immunotherapy for dust mite allergies
Odactra (Merck, Sharp & Dohme) had been approved in adults aged 18-65 years, with allergic rhinitis with or without conjunctivitis. The tablets offer an alternative to subcutaneous injections, the FDA said in a statement issued March 1. 
The sublingual tablets are intended to be taken daily, year-round, and the first dose must be taken under physician supervision to monitor for adverse reactions, according to the FDA. As with other sublingual immunotherapies, patients using the tablets should be simultaneously prescribed autoinjectable epinephrine.
The approval was based on results from randomized trials enrolling about 2,500 patients in Europe and the United States, according to the FDA. Patients taking the tablets saw a 16%-18% reduction in symptoms across studies, compared with placebo. Clinical benefit may be delayed by 8-14 weeks after starting the therapy, the agency said. Common adverse reactions reported in the studies included nausea, itching of the ears and mouth, and swelling of the lips and tongue.
Odactra is the fourth sublingual immunotherapy to be approved in the United States since 2014. Other approved therapies target grass and ragweed allergies.
Odactra (Merck, Sharp & Dohme) had been approved in adults aged 18-65 years, with allergic rhinitis with or without conjunctivitis. The tablets offer an alternative to subcutaneous injections, the FDA said in a statement issued March 1.
The sublingual tablets are intended to be taken daily, year-round, and the first dose must be taken under physician supervision to monitor for adverse reactions, according to the FDA. As with other sublingual immunotherapies, patients using the tablets should be simultaneously prescribed autoinjectable epinephrine.
The approval was based on results from randomized trials enrolling about 2,500 patients in Europe and the United States, according to the FDA. Patients taking the tablets saw a 16%-18% reduction in symptoms across studies, compared with placebo. Clinical benefit may be delayed by 8-14 weeks after starting the therapy, the agency said. Common adverse reactions reported in the studies included nausea, itching of the ears and mouth, and swelling of the lips and tongue.
Odactra is the fourth sublingual immunotherapy to be approved in the United States since 2014. Other approved therapies target grass and ragweed allergies.
Odactra (Merck, Sharp & Dohme) had been approved in adults aged 18-65 years, with allergic rhinitis with or without conjunctivitis. The tablets offer an alternative to subcutaneous injections, the FDA said in a statement issued March 1.
The sublingual tablets are intended to be taken daily, year-round, and the first dose must be taken under physician supervision to monitor for adverse reactions, according to the FDA. As with other sublingual immunotherapies, patients using the tablets should be simultaneously prescribed autoinjectable epinephrine.
The approval was based on results from randomized trials enrolling about 2,500 patients in Europe and the United States, according to the FDA. Patients taking the tablets saw a 16%-18% reduction in symptoms across studies, compared with placebo. Clinical benefit may be delayed by 8-14 weeks after starting the therapy, the agency said. Common adverse reactions reported in the studies included nausea, itching of the ears and mouth, and swelling of the lips and tongue.
Odactra is the fourth sublingual immunotherapy to be approved in the United States since 2014. Other approved therapies target grass and ragweed allergies.
Use of IHC stains on rise in melanoma diagnosis
While there is little consensus on the ideal role of immunohistochemical (IHC) stains in the diagnosis of melanoma, their use increased dramatically over a 15-year period, according to results from a study.
Randie H. Kim, MD, PhD, and Shane A. Meehan, MD, of New York University, reviewed nearly 6,300 pathology reports from patients with melanomas, all referred (along with tissue samples) to their center from other institutions during 2001-2015. One or more IHC stains were used diagnostically in 871 cases during the study period, with use increasing from 5% of patients in 2001 to 25% in 2015 (P less than .0001). Usage increased gradually over time, although the number of stains used per case did not increase significantly (J Cutan Pathol. 2017 Mar;44[3]:221-7).
IHC stain use was associated with melanomas occurring on the head or neck (odds ratio = 1.6; 95% confidence interval, 1.4-1.9), acral melanomas (OR = 1.5; 95% CI 1.1-2.0) and melanomas thicker than 4 mm (OR = 2.5; 95% CI 1.7-3.6). The most common stain used in the study was Melan-A/MART-1 (melanoma antigen recognized by T cells), the most specific of the IHC markers available and the one “largely responsible for the increased incidence in overall immunostain use in our study,” the researchers wrote. “The perception that melanocytic markers, such as Melan-A, can more accurately stage melanomas, is a potential explanation for its increased usage over the duration of the study period.”
The higher use of immunostains in thicker melanomas may be because these “exhibit greater morphological heterogeneity, such as nodular, spindled and desmoplastic subtypes, that lead to additional confirmational testing,” Dr. Kim and Dr. Meehan noted. However, they cautioned that extrinsic factors, including reimbursement fees and concerns about malpractice claims, could also influence the use of IHC stains in the diagnosis of melanomas.
“While Melan-A/MART-1 is a useful adjunct for determining melanocytic density or the presence of invasion in difficult cases, its routine use on melanomas has not been validated,” the researchers wrote in their analysis. “A consensus conference delineating the appropriate use of IHC in the diagnosis of melanoma may be of value in this regard.”
Dr. Kim and Dr. Meehan also noted that while a greater proportion of the melanomas seen in the study were thick (greater than 4 mm) compared with most population-based studies, this may reflect patient management practices in which thinner melanomas are treated in outpatient centers while thicker ones get referred to tertiary care centers such as theirs.
The researchers disclosed no outside funding or conflicts of interest.
While there is little consensus on the ideal role of immunohistochemical (IHC) stains in the diagnosis of melanoma, their use increased dramatically over a 15-year period, according to results from a study.
Randie H. Kim, MD, PhD, and Shane A. Meehan, MD, of New York University, reviewed nearly 6,300 pathology reports from patients with melanomas, all referred (along with tissue samples) to their center from other institutions during 2001-2015. One or more IHC stains were used diagnostically in 871 cases during the study period, with use increasing from 5% of patients in 2001 to 25% in 2015 (P less than .0001). Usage increased gradually over time, although the number of stains used per case did not increase significantly (J Cutan Pathol. 2017 Mar;44[3]:221-7).
IHC stain use was associated with melanomas occurring on the head or neck (odds ratio = 1.6; 95% confidence interval, 1.4-1.9), acral melanomas (OR = 1.5; 95% CI 1.1-2.0) and melanomas thicker than 4 mm (OR = 2.5; 95% CI 1.7-3.6). The most common stain used in the study was Melan-A/MART-1 (melanoma antigen recognized by T cells), the most specific of the IHC markers available and the one “largely responsible for the increased incidence in overall immunostain use in our study,” the researchers wrote. “The perception that melanocytic markers, such as Melan-A, can more accurately stage melanomas, is a potential explanation for its increased usage over the duration of the study period.”
The higher use of immunostains in thicker melanomas may be because these “exhibit greater morphological heterogeneity, such as nodular, spindled and desmoplastic subtypes, that lead to additional confirmational testing,” Dr. Kim and Dr. Meehan noted. However, they cautioned that extrinsic factors, including reimbursement fees and concerns about malpractice claims, could also influence the use of IHC stains in the diagnosis of melanomas.
“While Melan-A/MART-1 is a useful adjunct for determining melanocytic density or the presence of invasion in difficult cases, its routine use on melanomas has not been validated,” the researchers wrote in their analysis. “A consensus conference delineating the appropriate use of IHC in the diagnosis of melanoma may be of value in this regard.”
Dr. Kim and Dr. Meehan also noted that while a greater proportion of the melanomas seen in the study were thick (greater than 4 mm) compared with most population-based studies, this may reflect patient management practices in which thinner melanomas are treated in outpatient centers while thicker ones get referred to tertiary care centers such as theirs.
The researchers disclosed no outside funding or conflicts of interest.
While there is little consensus on the ideal role of immunohistochemical (IHC) stains in the diagnosis of melanoma, their use increased dramatically over a 15-year period, according to results from a study.
Randie H. Kim, MD, PhD, and Shane A. Meehan, MD, of New York University, reviewed nearly 6,300 pathology reports from patients with melanomas, all referred (along with tissue samples) to their center from other institutions during 2001-2015. One or more IHC stains were used diagnostically in 871 cases during the study period, with use increasing from 5% of patients in 2001 to 25% in 2015 (P less than .0001). Usage increased gradually over time, although the number of stains used per case did not increase significantly (J Cutan Pathol. 2017 Mar;44[3]:221-7).
IHC stain use was associated with melanomas occurring on the head or neck (odds ratio = 1.6; 95% confidence interval, 1.4-1.9), acral melanomas (OR = 1.5; 95% CI 1.1-2.0) and melanomas thicker than 4 mm (OR = 2.5; 95% CI 1.7-3.6). The most common stain used in the study was Melan-A/MART-1 (melanoma antigen recognized by T cells), the most specific of the IHC markers available and the one “largely responsible for the increased incidence in overall immunostain use in our study,” the researchers wrote. “The perception that melanocytic markers, such as Melan-A, can more accurately stage melanomas, is a potential explanation for its increased usage over the duration of the study period.”
The higher use of immunostains in thicker melanomas may be because these “exhibit greater morphological heterogeneity, such as nodular, spindled and desmoplastic subtypes, that lead to additional confirmational testing,” Dr. Kim and Dr. Meehan noted. However, they cautioned that extrinsic factors, including reimbursement fees and concerns about malpractice claims, could also influence the use of IHC stains in the diagnosis of melanomas.
“While Melan-A/MART-1 is a useful adjunct for determining melanocytic density or the presence of invasion in difficult cases, its routine use on melanomas has not been validated,” the researchers wrote in their analysis. “A consensus conference delineating the appropriate use of IHC in the diagnosis of melanoma may be of value in this regard.”
Dr. Kim and Dr. Meehan also noted that while a greater proportion of the melanomas seen in the study were thick (greater than 4 mm) compared with most population-based studies, this may reflect patient management practices in which thinner melanomas are treated in outpatient centers while thicker ones get referred to tertiary care centers such as theirs.
The researchers disclosed no outside funding or conflicts of interest.
FROM THE JOURNAL OF CUTANEOUS PATHOLOGY
Key clinical point:
Major finding: One or more stains was used diagnostically in 5% of melanoma cases in 2001, compared with 25% in 2015 (P less than .0001).
Data source: A retrospective review of more than 6,000 case records referred after diagnosis to a tertiary care center during 2001-2015.
Disclosures: The researchers disclosed no outside funding or conflicts of interest.
Colorectal cancer mortality highest in W.Va., lowest in Utah
Mortality from cancers of the colon and rectum is expected to be about 15.6 per 100,000 in 2017, with the highest rate in West Virginia and the lowest in Utah.
Approximately 50,260 colorectal cancer deaths are predicted for the year in the United States by the American Cancer Society in its Cancer Facts & Figures 2017, based on 2000-2014 data from the National Center for Health Statistics. With the population currently around 321 million, that works out to an expected death rate of 15.6 per 100,000 population. Doing a little more math produces death rates of 23.4 for West Virginia and 8.7 for Utah.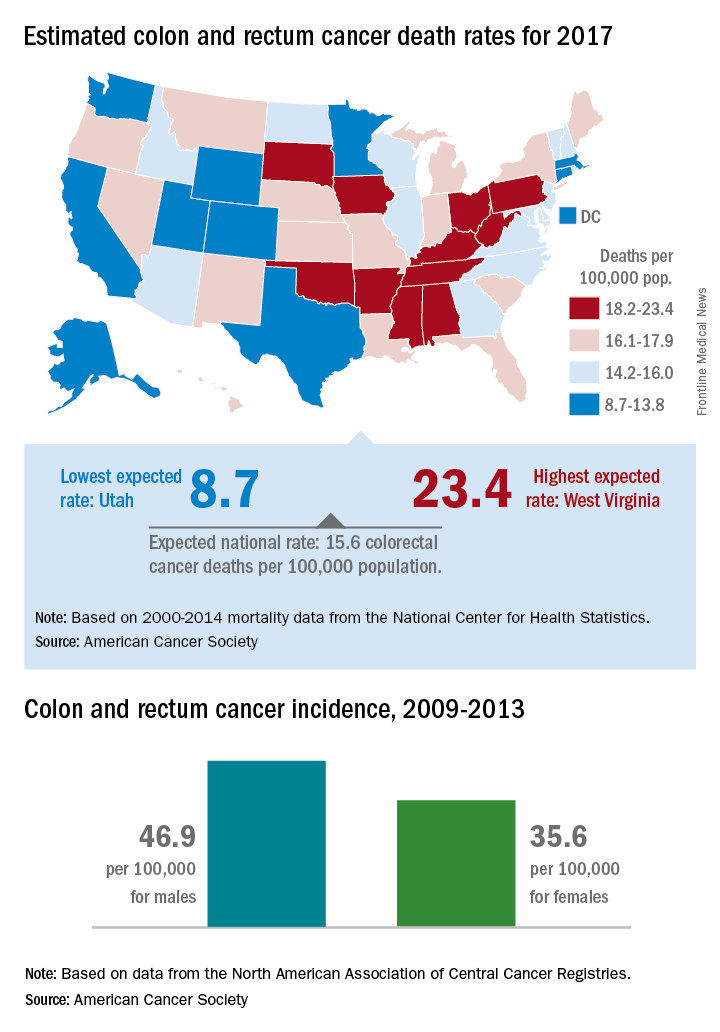
Utah had the lowest incidence rate over that time period for both men (36.1 per 100,000) and women (28.2 per 100,000), and Kentucky had the highest for both, with rates of 59.6 for men and 43.7 for women, the ACS said.
Mortality from cancers of the colon and rectum is expected to be about 15.6 per 100,000 in 2017, with the highest rate in West Virginia and the lowest in Utah.
Approximately 50,260 colorectal cancer deaths are predicted for the year in the United States by the American Cancer Society in its Cancer Facts & Figures 2017, based on 2000-2014 data from the National Center for Health Statistics. With the population currently around 321 million, that works out to an expected death rate of 15.6 per 100,000 population. Doing a little more math produces death rates of 23.4 for West Virginia and 8.7 for Utah.
Utah had the lowest incidence rate over that time period for both men (36.1 per 100,000) and women (28.2 per 100,000), and Kentucky had the highest for both, with rates of 59.6 for men and 43.7 for women, the ACS said.
Mortality from cancers of the colon and rectum is expected to be about 15.6 per 100,000 in 2017, with the highest rate in West Virginia and the lowest in Utah.
Approximately 50,260 colorectal cancer deaths are predicted for the year in the United States by the American Cancer Society in its Cancer Facts & Figures 2017, based on 2000-2014 data from the National Center for Health Statistics. With the population currently around 321 million, that works out to an expected death rate of 15.6 per 100,000 population. Doing a little more math produces death rates of 23.4 for West Virginia and 8.7 for Utah.
Utah had the lowest incidence rate over that time period for both men (36.1 per 100,000) and women (28.2 per 100,000), and Kentucky had the highest for both, with rates of 59.6 for men and 43.7 for women, the ACS said.
Standardize opioid prescribing after endocrine neck surgery, researchers say
Twenty oral morphine equivalents is the best option for pain relief medication with which to discharge outpatients after thyroidectomy or parathyroidectomy surgery, according to researchers. The report was published online in Annals of Surgical Oncology.
Irene Lou, MD, of the department of surgery at the University of Wisconsin–Madison, and her coauthors conducted a prospective observational cohort study collecting data on pain scores and the oral morphine equivalents used by 313 adult patients undergoing thyroidectomy or parathyroidectomy at two large endocrine surgery centers.

While patients were prescribed a median of 30 oral morphine equivalents at discharge – with a range from 0 to 120 – the median number of equivalents taken was 3 (with a range of 0-60).
Overall, 68.4% of patients took at least one oral morphine equivalent. The majority of patients (83%) took 10 or fewer oral morphine equivalents, and only 7% of patients took more than 20 oral morphine equivalents (Ann Surg Oncol. 2017 Feb 3. doi: 10.1245/s10434-017-5781-y).
Among the patients who took more than 10 oral morphine equivalents, 85% said it was for incisional pain, 4% said it was for sore throat, and 11% said it was for some other pain.
While the overall mean pain score after surgery was 2, the study found that mean pain scores in the patients who took more than 10 oral morphine equivalents were significantly higher than in patients who took 10 or fewer. Among patients who used narcotic pain relief, 1% said they did so because they were instructed to despite having reported no pain.
Other factors predicting higher oral morphine equivalent use were age – patients tended to be younger than 45 years – total thyroidectomy, or a history of previous narcotic use.
“Based on our results, we have changed our practices to discharge all patients undergoing parathyroid or thyroid surgery and to request an oral narcotic prescription with no more than 20 equivalents, which translates to 20 tablets of hydrocodone/acetaminophen 5/325” the authors wrote.
Noting that the abuse and misuse of prescription opioids is the leading cause of overdose deaths in the United States, they argued that standardized prescribing practices are a way to not only reduce waste but also to improve patient safety.
“We also discovered that even between our two institutions, there was no standard prescribing pattern, with a wide range of prescriptions and number of equivalents dispensed.”
The authors also examined alternative and adjunctive methods of pain relief, pointing to previous studies suggesting benefits from preoperative gabapentin, postoperative music therapy, postoperative ice packs, and nonopioid analgesics.
They noted that because their study covered the breadth of endocrine neck operations, it did include patients who had minimally invasive surgery through to those who underwent total thyroidectomy with neck dissections. They also pointed out that the data pain scores and oral morphine equivalent use was based on patient recollection.
“Notwithstanding these limitations, our study is the first to examine outpatient narcotic pain medication use after thyroid and parathyroid surgery,” they said. “A standardized practice of prescribing stands to increase patient safety and minimize the risks of dependence and overdose.”
Two authors were supported by National Institutes of Health grants. No other conflicts of interest were declared.
Twenty oral morphine equivalents is the best option for pain relief medication with which to discharge outpatients after thyroidectomy or parathyroidectomy surgery, according to researchers. The report was published online in Annals of Surgical Oncology.
Irene Lou, MD, of the department of surgery at the University of Wisconsin–Madison, and her coauthors conducted a prospective observational cohort study collecting data on pain scores and the oral morphine equivalents used by 313 adult patients undergoing thyroidectomy or parathyroidectomy at two large endocrine surgery centers.
While patients were prescribed a median of 30 oral morphine equivalents at discharge – with a range from 0 to 120 – the median number of equivalents taken was 3 (with a range of 0-60).
Overall, 68.4% of patients took at least one oral morphine equivalent. The majority of patients (83%) took 10 or fewer oral morphine equivalents, and only 7% of patients took more than 20 oral morphine equivalents (Ann Surg Oncol. 2017 Feb 3. doi: 10.1245/s10434-017-5781-y).
Among the patients who took more than 10 oral morphine equivalents, 85% said it was for incisional pain, 4% said it was for sore throat, and 11% said it was for some other pain.
While the overall mean pain score after surgery was 2, the study found that mean pain scores in the patients who took more than 10 oral morphine equivalents were significantly higher than in patients who took 10 or fewer. Among patients who used narcotic pain relief, 1% said they did so because they were instructed to despite having reported no pain.
Other factors predicting higher oral morphine equivalent use were age – patients tended to be younger than 45 years – total thyroidectomy, or a history of previous narcotic use.
“Based on our results, we have changed our practices to discharge all patients undergoing parathyroid or thyroid surgery and to request an oral narcotic prescription with no more than 20 equivalents, which translates to 20 tablets of hydrocodone/acetaminophen 5/325” the authors wrote.
Noting that the abuse and misuse of prescription opioids is the leading cause of overdose deaths in the United States, they argued that standardized prescribing practices are a way to not only reduce waste but also to improve patient safety.
“We also discovered that even between our two institutions, there was no standard prescribing pattern, with a wide range of prescriptions and number of equivalents dispensed.”
The authors also examined alternative and adjunctive methods of pain relief, pointing to previous studies suggesting benefits from preoperative gabapentin, postoperative music therapy, postoperative ice packs, and nonopioid analgesics.
They noted that because their study covered the breadth of endocrine neck operations, it did include patients who had minimally invasive surgery through to those who underwent total thyroidectomy with neck dissections. They also pointed out that the data pain scores and oral morphine equivalent use was based on patient recollection.
“Notwithstanding these limitations, our study is the first to examine outpatient narcotic pain medication use after thyroid and parathyroid surgery,” they said. “A standardized practice of prescribing stands to increase patient safety and minimize the risks of dependence and overdose.”
Two authors were supported by National Institutes of Health grants. No other conflicts of interest were declared.
Twenty oral morphine equivalents is the best option for pain relief medication with which to discharge outpatients after thyroidectomy or parathyroidectomy surgery, according to researchers. The report was published online in Annals of Surgical Oncology.
Irene Lou, MD, of the department of surgery at the University of Wisconsin–Madison, and her coauthors conducted a prospective observational cohort study collecting data on pain scores and the oral morphine equivalents used by 313 adult patients undergoing thyroidectomy or parathyroidectomy at two large endocrine surgery centers.
While patients were prescribed a median of 30 oral morphine equivalents at discharge – with a range from 0 to 120 – the median number of equivalents taken was 3 (with a range of 0-60).
Overall, 68.4% of patients took at least one oral morphine equivalent. The majority of patients (83%) took 10 or fewer oral morphine equivalents, and only 7% of patients took more than 20 oral morphine equivalents (Ann Surg Oncol. 2017 Feb 3. doi: 10.1245/s10434-017-5781-y).
Among the patients who took more than 10 oral morphine equivalents, 85% said it was for incisional pain, 4% said it was for sore throat, and 11% said it was for some other pain.
While the overall mean pain score after surgery was 2, the study found that mean pain scores in the patients who took more than 10 oral morphine equivalents were significantly higher than in patients who took 10 or fewer. Among patients who used narcotic pain relief, 1% said they did so because they were instructed to despite having reported no pain.
Other factors predicting higher oral morphine equivalent use were age – patients tended to be younger than 45 years – total thyroidectomy, or a history of previous narcotic use.
“Based on our results, we have changed our practices to discharge all patients undergoing parathyroid or thyroid surgery and to request an oral narcotic prescription with no more than 20 equivalents, which translates to 20 tablets of hydrocodone/acetaminophen 5/325” the authors wrote.
Noting that the abuse and misuse of prescription opioids is the leading cause of overdose deaths in the United States, they argued that standardized prescribing practices are a way to not only reduce waste but also to improve patient safety.
“We also discovered that even between our two institutions, there was no standard prescribing pattern, with a wide range of prescriptions and number of equivalents dispensed.”
The authors also examined alternative and adjunctive methods of pain relief, pointing to previous studies suggesting benefits from preoperative gabapentin, postoperative music therapy, postoperative ice packs, and nonopioid analgesics.
They noted that because their study covered the breadth of endocrine neck operations, it did include patients who had minimally invasive surgery through to those who underwent total thyroidectomy with neck dissections. They also pointed out that the data pain scores and oral morphine equivalent use was based on patient recollection.
“Notwithstanding these limitations, our study is the first to examine outpatient narcotic pain medication use after thyroid and parathyroid surgery,” they said. “A standardized practice of prescribing stands to increase patient safety and minimize the risks of dependence and overdose.”
Two authors were supported by National Institutes of Health grants. No other conflicts of interest were declared.
FROM ANNALS OF SURGICAL ONCOLOGY
Key clinical point: Twenty oral morphine equivalents is the ideal amount of pain relief medication with which to discharge outpatients after thyroidectomy or parathyroidectomy surgery.
Major finding: Only 7% of patients who undergo thyroidectomy or parathyroidectomy use more than 20 oral morphine equivalents for postoperative pain relief.
Data source: Observational cohort study of 313 adult patients undergoing thyroidectomy or parathyroidectomy.
Disclosures: Two authors were supported by National Institutes of Health grants. No other conflicts of interest were declared.