User login
For girls with Turner syndrome, experimental fertility preservation may offer the hope of a baby of their own
ORLANDO – Fertility preservation techniques pioneered in young cancer patients may someday allow some women with Turner syndrome to give birth to their own children, without relying on donated eggs.
Spontaneous conception and live birth are exceedingly rare among women with the genetic disorder. Until very recently, adoption was the only practical way for most to grow a family. In the last decade, however, fertility specialists in Europe and the United States have had good success with in vitro fertilization using donated eggs. Now, those clinicians are aiming for a higher goal: babies born from a patient’s own eggs, cryopreserved either individually or within whole ovarian tissue.
These are not pipe dreams, according to experts interviewed for this story. Autologous oocyte freezing is well established in healthy women and is now coming of age in cancer patients, with recent reports of live births. Ovarian tissue freezing and reimplantation is a much newer technique, also pioneered in cancer patients. To date, more than 70 live births have occurred from ovarian cortical tissue conservation and later transplantation in adults. Last December brought the first report of a live birth to a childhood cancer survivor who had prepubertal ovarian tissue frozen before chemotherapy. And a 2015 report detailed the case of a girl with primary ovarian failure secondary to sickle cell anemia treatment. At 25, she gave birth to a healthy child conceived from ovarian tissue removed when she was 14 years old.
Not all clinicians so enthusiastically embrace this future, however. A new set of consensus guidelines for the management of girls and women with Turner syndrome is in the works and will recommend a more conservative clinical approach, according to Nelly Mauras, MD, chief of endocrinology, diabetes, and metabolism at the Nemours Children’s Health System in Jacksonville, Fla.
A group of academic and patient advocacy stakeholders is cooperatively honing the document based on a meeting last summer in Cincinnati. These groups include the European Society of Endocrinology, the Endocrine Society, the U.S. Pediatric Endocrine Society, the European Society for Pediatric Endocrinology, Cardiology, and Reproductive Endocrinology, as well as Turner syndrome patient advocacy groups.
Dr. Mauras said the guideline will be “less discouraging” than the existing one issued in 2012 by the American Society of Reproductive Medicine. In its 2012 guidelines, the society identified Turner syndrome as a relative contraindication to pregnancy and an absolute contraindication in those with documented cardiac anomalies. However, greater experience has since been accrued in reproductive techniques of oocyte donation in Turner, with better outcomes.
The upcoming guidelines, however, will still recommend strongly against ovarian stimulation for fertility preservation for girls younger than 12, Dr. Mauras said, and will not recommend ovarian tissue conservation. “We just do not have the safety data and pregnancy outcomes that we need to give strong recommendations for these treatments,” she said. “These are still considered experimental treatments for girls with Turner syndrome.”
Turner syndrome, caused by a deletion of one X chromosome, throws a unique curve into the game – very early ovarian failure. Those with a complete deletion (45,X) begin losing their primordial ovarian follicles even before birth. Most will never experience spontaneous puberty; even if they do, their egg reserve is virtually gone soon after. Ovarian reserve may not be completely lost in girls with mosaicism, however, who have the X deletion in only a portion of their cells (46,XX/45,X). Some will enter puberty, and about 5% may even conceive spontaneously in younger years. But of the majority of Turner girls eventually experience complete ovarian failure.
This means that fertility preservation can’t be a wait-and-see issue, according to Kutluk Oktay, MD, PhD, a fertility specialist on the leading edge of this issue in the United States.
“We have to be proactive,” said Dr. Oktay, professor of obstetrics and gynecology at New York Medical College, Valhalla. “If we wait until girls are 12 or 13 to address this, a majority will have totally depleted their ovarian reserve by then. They will have no option other than an egg donor or adoption. We are suggesting that they should be screened as soon as they are diagnosed, and if they and their parents wish it, something should be done before it’s too late.”
Dr. Oktay is also the founder of fertilitypreservation.org, which specializes in advanced fertility treatments for cancer patients. He is one of a handful of physicians in the United States who advocate early oocyte harvesting in peripubertal girls and ovarian tissue harvesting in prepubertal girls with Turner syndrome. Last year, in conjunction with the Turner Syndrome Foundation, he and his colleagues published a set of guidelines for preserving fertility in these patients.
The paper recommends fertility assessment pathways for pre- and postpubertal girls. For both groups, Dr. Oktay employs serial assessments of ovarian reserve by monitoring several hormones, including follicle-stimulating hormone, luteinizing hormone, and antimüllerian hormone (AMH). Produced by primordial follicles, AMH declines as egg reserve declines over a lifetime, and is considered an accurate marker of ovarian reserve. When a girl experiences two consecutive AMH declines, egg depletion is probably accelerating. “This is the time to consider fertility preservation,” he said.
If a girl is peri- or postpubertal, the choice would probably be ovarian stimulation with the goal of retrieving mature oocytes. For prepubertal girls, the best choice is probably ovarian tissue cryopreservation. But because the egg reserve may already be spotty inside the ovary, he recommended freezing it en bloc, rather than preserving just cortical sections.
Because these techniques are only beginning to be used in young Turner patients, neither has been tested yet to see if it would result in a pregnancy. However, Dr. Oktay said, more than 80 babies have been born to women with other disorders who had ovaries frozen as adults. And European women with Turner syndrome have been successfully bearing children with donated oocytes for years.
“I don’t differentiate Europe from the U.S.,” he said. “We have no reason to believe Turner syndrome girls would be any different here than they are there.”
Pregnancy rates by egg donation in Turner syndrome patients are about half that typically seen in an otherwise healthy infertile woman, according to numerous sources; with a take-home baby rate of about 18%. There are numerous reasons for this. The miscarriage rate in Turner patients is about 44%. Women with Turner tend to have smaller uteri, with thinner endometrium, mostly because of the lack of estrogen.
But with careful management, those who do conceive can safely deliver a healthy baby, said Outi Hovatta, MD, a Finnish fertility specialist who has done extensive work in the area. “In Europe, we have been doing this quite liberally for years, and haven’t had a bad experience,” she said in an interview.
A 2013 review summarized both the success and the risks of these pregnancies. It examined obstetric and neonatal outcomes among 106 women with Turner syndrome who gave birth via egg donation from 1992 to 2011 in Sweden, Finland, and Denmark.
Most (70%) had a single embryo transferred, as virtually all guidelines recommend. Women with Turner are prone to cardiac and aortic defects that can worsen under the strain of pregnancy, or even present for the first time during gestation. Aortic dissection is a real threat; up to a third of patients with Turner experience it during adulthood, and it’s a major cause of death among them. In the Nordic series, 10 women (9%) had a known cardiac anomaly.
The multiple birth rate was 7%. More than a third (35%) developed a hypertensive disorder, including preeclampsia (20%). Four women had potentially life-threatening complications, including one with aortic dissection, one who developed mild regurgitation of the tricuspid and mitral valve, one with a mechanical heart valve who developed HELLP syndrome (hemolysis, elevated liver enzymes, low platelets), and one who underwent a postpartum hysterectomy because of severe hemorrhaging.
The infants, nevertheless, did well. The preterm birth rate was 8%, with 9% of the singleton infants having a low birth weight. About 4% had a major birth defect. Of the 131 born, three died (2.3%), including a set of extremely preterm twins.
Close follow-up and cross-specialty cooperation are what make these positive outcomes possible, said Dr. Hovatta, who is now a professor emeritus at the Karolinska Institute, Sweden.
“We do everything we can to exclude things that could cause bad outcomes.” That includes extremely rigorous cardiac testing before pregnancy and continuous monitoring during it. “If a woman has any sign of cardiac anomaly, she is advised not to become pregnant. If she shows any signs of aortic dilation, we follow her extremely carefully with experienced cardiologists.”
Like Dr. Oktay, Dr. Hovatta and her European colleagues make fertility preservation an early topic of conversation. Unlike in the United States, where many girls aren’t diagnosed with the disorder until they fail to enter puberty, almost all Turner girls in Europe are identified very early in childhood. They receive early growth hormone treatment, and there is frequent consultation with interdisciplinary specialists. Fertility is spoken of early and often.
Early oocyte retrieval is common, Dr. Hovatta said. “Yes, it’s possible to wait until puberty, but for so many girls, most of the eggs have disappeared by then, so we typically don’t wait. We start looking at that option around 11 years, which is the same time we think about cryopreserving ovarian tissue.”
However, she added, as in the United States, the outcomes of these procedures are still unknown. But the existing data in other populations, the ability to carefully shepherd women through a successful pregnancy, and the willingness of families to provide the option all support further exploring them. Dr. Hovatta was at the Cincinnati gathering last summer and said she did not agree with the conservative tone she heard. Dr. Oktay also does not agree.
“This evidence we have so far is good evidence,” he said. “Look, where we are right now with Turner girls is where we were 15 years ago with cancer patients. People thought, ‘They have cancer. They should just be worrying about surviving cancer, not about their fertility.’ Now fertility counseling is a very important part of cancer care. We have all these tools available to us for cancer patients who don’t want to lose their fertility. This accumulated experience that has already been applied in other medical conditions … why not use that for Turner syndrome? This is my point: With all the data out there about the potential benefits and the ways to manage the risks, we shouldn’t have to tell girls, ‘Well, you have to become menopausal, and maybe you can adopt someday.’ That doesn’t sit well with parents any more. We want these girls to thrive. Not just to survive, but to have as close to a normal quality of life as possible.”
ORLANDO – Fertility preservation techniques pioneered in young cancer patients may someday allow some women with Turner syndrome to give birth to their own children, without relying on donated eggs.
Spontaneous conception and live birth are exceedingly rare among women with the genetic disorder. Until very recently, adoption was the only practical way for most to grow a family. In the last decade, however, fertility specialists in Europe and the United States have had good success with in vitro fertilization using donated eggs. Now, those clinicians are aiming for a higher goal: babies born from a patient’s own eggs, cryopreserved either individually or within whole ovarian tissue.
These are not pipe dreams, according to experts interviewed for this story. Autologous oocyte freezing is well established in healthy women and is now coming of age in cancer patients, with recent reports of live births. Ovarian tissue freezing and reimplantation is a much newer technique, also pioneered in cancer patients. To date, more than 70 live births have occurred from ovarian cortical tissue conservation and later transplantation in adults. Last December brought the first report of a live birth to a childhood cancer survivor who had prepubertal ovarian tissue frozen before chemotherapy. And a 2015 report detailed the case of a girl with primary ovarian failure secondary to sickle cell anemia treatment. At 25, she gave birth to a healthy child conceived from ovarian tissue removed when she was 14 years old.
Not all clinicians so enthusiastically embrace this future, however. A new set of consensus guidelines for the management of girls and women with Turner syndrome is in the works and will recommend a more conservative clinical approach, according to Nelly Mauras, MD, chief of endocrinology, diabetes, and metabolism at the Nemours Children’s Health System in Jacksonville, Fla.
A group of academic and patient advocacy stakeholders is cooperatively honing the document based on a meeting last summer in Cincinnati. These groups include the European Society of Endocrinology, the Endocrine Society, the U.S. Pediatric Endocrine Society, the European Society for Pediatric Endocrinology, Cardiology, and Reproductive Endocrinology, as well as Turner syndrome patient advocacy groups.
Dr. Mauras said the guideline will be “less discouraging” than the existing one issued in 2012 by the American Society of Reproductive Medicine. In its 2012 guidelines, the society identified Turner syndrome as a relative contraindication to pregnancy and an absolute contraindication in those with documented cardiac anomalies. However, greater experience has since been accrued in reproductive techniques of oocyte donation in Turner, with better outcomes.
The upcoming guidelines, however, will still recommend strongly against ovarian stimulation for fertility preservation for girls younger than 12, Dr. Mauras said, and will not recommend ovarian tissue conservation. “We just do not have the safety data and pregnancy outcomes that we need to give strong recommendations for these treatments,” she said. “These are still considered experimental treatments for girls with Turner syndrome.”
Turner syndrome, caused by a deletion of one X chromosome, throws a unique curve into the game – very early ovarian failure. Those with a complete deletion (45,X) begin losing their primordial ovarian follicles even before birth. Most will never experience spontaneous puberty; even if they do, their egg reserve is virtually gone soon after. Ovarian reserve may not be completely lost in girls with mosaicism, however, who have the X deletion in only a portion of their cells (46,XX/45,X). Some will enter puberty, and about 5% may even conceive spontaneously in younger years. But of the majority of Turner girls eventually experience complete ovarian failure.
This means that fertility preservation can’t be a wait-and-see issue, according to Kutluk Oktay, MD, PhD, a fertility specialist on the leading edge of this issue in the United States.
“We have to be proactive,” said Dr. Oktay, professor of obstetrics and gynecology at New York Medical College, Valhalla. “If we wait until girls are 12 or 13 to address this, a majority will have totally depleted their ovarian reserve by then. They will have no option other than an egg donor or adoption. We are suggesting that they should be screened as soon as they are diagnosed, and if they and their parents wish it, something should be done before it’s too late.”
Dr. Oktay is also the founder of fertilitypreservation.org, which specializes in advanced fertility treatments for cancer patients. He is one of a handful of physicians in the United States who advocate early oocyte harvesting in peripubertal girls and ovarian tissue harvesting in prepubertal girls with Turner syndrome. Last year, in conjunction with the Turner Syndrome Foundation, he and his colleagues published a set of guidelines for preserving fertility in these patients.
The paper recommends fertility assessment pathways for pre- and postpubertal girls. For both groups, Dr. Oktay employs serial assessments of ovarian reserve by monitoring several hormones, including follicle-stimulating hormone, luteinizing hormone, and antimüllerian hormone (AMH). Produced by primordial follicles, AMH declines as egg reserve declines over a lifetime, and is considered an accurate marker of ovarian reserve. When a girl experiences two consecutive AMH declines, egg depletion is probably accelerating. “This is the time to consider fertility preservation,” he said.
If a girl is peri- or postpubertal, the choice would probably be ovarian stimulation with the goal of retrieving mature oocytes. For prepubertal girls, the best choice is probably ovarian tissue cryopreservation. But because the egg reserve may already be spotty inside the ovary, he recommended freezing it en bloc, rather than preserving just cortical sections.
Because these techniques are only beginning to be used in young Turner patients, neither has been tested yet to see if it would result in a pregnancy. However, Dr. Oktay said, more than 80 babies have been born to women with other disorders who had ovaries frozen as adults. And European women with Turner syndrome have been successfully bearing children with donated oocytes for years.
“I don’t differentiate Europe from the U.S.,” he said. “We have no reason to believe Turner syndrome girls would be any different here than they are there.”
Pregnancy rates by egg donation in Turner syndrome patients are about half that typically seen in an otherwise healthy infertile woman, according to numerous sources; with a take-home baby rate of about 18%. There are numerous reasons for this. The miscarriage rate in Turner patients is about 44%. Women with Turner tend to have smaller uteri, with thinner endometrium, mostly because of the lack of estrogen.
But with careful management, those who do conceive can safely deliver a healthy baby, said Outi Hovatta, MD, a Finnish fertility specialist who has done extensive work in the area. “In Europe, we have been doing this quite liberally for years, and haven’t had a bad experience,” she said in an interview.
A 2013 review summarized both the success and the risks of these pregnancies. It examined obstetric and neonatal outcomes among 106 women with Turner syndrome who gave birth via egg donation from 1992 to 2011 in Sweden, Finland, and Denmark.
Most (70%) had a single embryo transferred, as virtually all guidelines recommend. Women with Turner are prone to cardiac and aortic defects that can worsen under the strain of pregnancy, or even present for the first time during gestation. Aortic dissection is a real threat; up to a third of patients with Turner experience it during adulthood, and it’s a major cause of death among them. In the Nordic series, 10 women (9%) had a known cardiac anomaly.
The multiple birth rate was 7%. More than a third (35%) developed a hypertensive disorder, including preeclampsia (20%). Four women had potentially life-threatening complications, including one with aortic dissection, one who developed mild regurgitation of the tricuspid and mitral valve, one with a mechanical heart valve who developed HELLP syndrome (hemolysis, elevated liver enzymes, low platelets), and one who underwent a postpartum hysterectomy because of severe hemorrhaging.
The infants, nevertheless, did well. The preterm birth rate was 8%, with 9% of the singleton infants having a low birth weight. About 4% had a major birth defect. Of the 131 born, three died (2.3%), including a set of extremely preterm twins.
Close follow-up and cross-specialty cooperation are what make these positive outcomes possible, said Dr. Hovatta, who is now a professor emeritus at the Karolinska Institute, Sweden.
“We do everything we can to exclude things that could cause bad outcomes.” That includes extremely rigorous cardiac testing before pregnancy and continuous monitoring during it. “If a woman has any sign of cardiac anomaly, she is advised not to become pregnant. If she shows any signs of aortic dilation, we follow her extremely carefully with experienced cardiologists.”
Like Dr. Oktay, Dr. Hovatta and her European colleagues make fertility preservation an early topic of conversation. Unlike in the United States, where many girls aren’t diagnosed with the disorder until they fail to enter puberty, almost all Turner girls in Europe are identified very early in childhood. They receive early growth hormone treatment, and there is frequent consultation with interdisciplinary specialists. Fertility is spoken of early and often.
Early oocyte retrieval is common, Dr. Hovatta said. “Yes, it’s possible to wait until puberty, but for so many girls, most of the eggs have disappeared by then, so we typically don’t wait. We start looking at that option around 11 years, which is the same time we think about cryopreserving ovarian tissue.”
However, she added, as in the United States, the outcomes of these procedures are still unknown. But the existing data in other populations, the ability to carefully shepherd women through a successful pregnancy, and the willingness of families to provide the option all support further exploring them. Dr. Hovatta was at the Cincinnati gathering last summer and said she did not agree with the conservative tone she heard. Dr. Oktay also does not agree.
“This evidence we have so far is good evidence,” he said. “Look, where we are right now with Turner girls is where we were 15 years ago with cancer patients. People thought, ‘They have cancer. They should just be worrying about surviving cancer, not about their fertility.’ Now fertility counseling is a very important part of cancer care. We have all these tools available to us for cancer patients who don’t want to lose their fertility. This accumulated experience that has already been applied in other medical conditions … why not use that for Turner syndrome? This is my point: With all the data out there about the potential benefits and the ways to manage the risks, we shouldn’t have to tell girls, ‘Well, you have to become menopausal, and maybe you can adopt someday.’ That doesn’t sit well with parents any more. We want these girls to thrive. Not just to survive, but to have as close to a normal quality of life as possible.”
ORLANDO – Fertility preservation techniques pioneered in young cancer patients may someday allow some women with Turner syndrome to give birth to their own children, without relying on donated eggs.
Spontaneous conception and live birth are exceedingly rare among women with the genetic disorder. Until very recently, adoption was the only practical way for most to grow a family. In the last decade, however, fertility specialists in Europe and the United States have had good success with in vitro fertilization using donated eggs. Now, those clinicians are aiming for a higher goal: babies born from a patient’s own eggs, cryopreserved either individually or within whole ovarian tissue.
These are not pipe dreams, according to experts interviewed for this story. Autologous oocyte freezing is well established in healthy women and is now coming of age in cancer patients, with recent reports of live births. Ovarian tissue freezing and reimplantation is a much newer technique, also pioneered in cancer patients. To date, more than 70 live births have occurred from ovarian cortical tissue conservation and later transplantation in adults. Last December brought the first report of a live birth to a childhood cancer survivor who had prepubertal ovarian tissue frozen before chemotherapy. And a 2015 report detailed the case of a girl with primary ovarian failure secondary to sickle cell anemia treatment. At 25, she gave birth to a healthy child conceived from ovarian tissue removed when she was 14 years old.
Not all clinicians so enthusiastically embrace this future, however. A new set of consensus guidelines for the management of girls and women with Turner syndrome is in the works and will recommend a more conservative clinical approach, according to Nelly Mauras, MD, chief of endocrinology, diabetes, and metabolism at the Nemours Children’s Health System in Jacksonville, Fla.
A group of academic and patient advocacy stakeholders is cooperatively honing the document based on a meeting last summer in Cincinnati. These groups include the European Society of Endocrinology, the Endocrine Society, the U.S. Pediatric Endocrine Society, the European Society for Pediatric Endocrinology, Cardiology, and Reproductive Endocrinology, as well as Turner syndrome patient advocacy groups.
Dr. Mauras said the guideline will be “less discouraging” than the existing one issued in 2012 by the American Society of Reproductive Medicine. In its 2012 guidelines, the society identified Turner syndrome as a relative contraindication to pregnancy and an absolute contraindication in those with documented cardiac anomalies. However, greater experience has since been accrued in reproductive techniques of oocyte donation in Turner, with better outcomes.
The upcoming guidelines, however, will still recommend strongly against ovarian stimulation for fertility preservation for girls younger than 12, Dr. Mauras said, and will not recommend ovarian tissue conservation. “We just do not have the safety data and pregnancy outcomes that we need to give strong recommendations for these treatments,” she said. “These are still considered experimental treatments for girls with Turner syndrome.”
Turner syndrome, caused by a deletion of one X chromosome, throws a unique curve into the game – very early ovarian failure. Those with a complete deletion (45,X) begin losing their primordial ovarian follicles even before birth. Most will never experience spontaneous puberty; even if they do, their egg reserve is virtually gone soon after. Ovarian reserve may not be completely lost in girls with mosaicism, however, who have the X deletion in only a portion of their cells (46,XX/45,X). Some will enter puberty, and about 5% may even conceive spontaneously in younger years. But of the majority of Turner girls eventually experience complete ovarian failure.
This means that fertility preservation can’t be a wait-and-see issue, according to Kutluk Oktay, MD, PhD, a fertility specialist on the leading edge of this issue in the United States.
“We have to be proactive,” said Dr. Oktay, professor of obstetrics and gynecology at New York Medical College, Valhalla. “If we wait until girls are 12 or 13 to address this, a majority will have totally depleted their ovarian reserve by then. They will have no option other than an egg donor or adoption. We are suggesting that they should be screened as soon as they are diagnosed, and if they and their parents wish it, something should be done before it’s too late.”
Dr. Oktay is also the founder of fertilitypreservation.org, which specializes in advanced fertility treatments for cancer patients. He is one of a handful of physicians in the United States who advocate early oocyte harvesting in peripubertal girls and ovarian tissue harvesting in prepubertal girls with Turner syndrome. Last year, in conjunction with the Turner Syndrome Foundation, he and his colleagues published a set of guidelines for preserving fertility in these patients.
The paper recommends fertility assessment pathways for pre- and postpubertal girls. For both groups, Dr. Oktay employs serial assessments of ovarian reserve by monitoring several hormones, including follicle-stimulating hormone, luteinizing hormone, and antimüllerian hormone (AMH). Produced by primordial follicles, AMH declines as egg reserve declines over a lifetime, and is considered an accurate marker of ovarian reserve. When a girl experiences two consecutive AMH declines, egg depletion is probably accelerating. “This is the time to consider fertility preservation,” he said.
If a girl is peri- or postpubertal, the choice would probably be ovarian stimulation with the goal of retrieving mature oocytes. For prepubertal girls, the best choice is probably ovarian tissue cryopreservation. But because the egg reserve may already be spotty inside the ovary, he recommended freezing it en bloc, rather than preserving just cortical sections.
Because these techniques are only beginning to be used in young Turner patients, neither has been tested yet to see if it would result in a pregnancy. However, Dr. Oktay said, more than 80 babies have been born to women with other disorders who had ovaries frozen as adults. And European women with Turner syndrome have been successfully bearing children with donated oocytes for years.
“I don’t differentiate Europe from the U.S.,” he said. “We have no reason to believe Turner syndrome girls would be any different here than they are there.”
Pregnancy rates by egg donation in Turner syndrome patients are about half that typically seen in an otherwise healthy infertile woman, according to numerous sources; with a take-home baby rate of about 18%. There are numerous reasons for this. The miscarriage rate in Turner patients is about 44%. Women with Turner tend to have smaller uteri, with thinner endometrium, mostly because of the lack of estrogen.
But with careful management, those who do conceive can safely deliver a healthy baby, said Outi Hovatta, MD, a Finnish fertility specialist who has done extensive work in the area. “In Europe, we have been doing this quite liberally for years, and haven’t had a bad experience,” she said in an interview.
A 2013 review summarized both the success and the risks of these pregnancies. It examined obstetric and neonatal outcomes among 106 women with Turner syndrome who gave birth via egg donation from 1992 to 2011 in Sweden, Finland, and Denmark.
Most (70%) had a single embryo transferred, as virtually all guidelines recommend. Women with Turner are prone to cardiac and aortic defects that can worsen under the strain of pregnancy, or even present for the first time during gestation. Aortic dissection is a real threat; up to a third of patients with Turner experience it during adulthood, and it’s a major cause of death among them. In the Nordic series, 10 women (9%) had a known cardiac anomaly.
The multiple birth rate was 7%. More than a third (35%) developed a hypertensive disorder, including preeclampsia (20%). Four women had potentially life-threatening complications, including one with aortic dissection, one who developed mild regurgitation of the tricuspid and mitral valve, one with a mechanical heart valve who developed HELLP syndrome (hemolysis, elevated liver enzymes, low platelets), and one who underwent a postpartum hysterectomy because of severe hemorrhaging.
The infants, nevertheless, did well. The preterm birth rate was 8%, with 9% of the singleton infants having a low birth weight. About 4% had a major birth defect. Of the 131 born, three died (2.3%), including a set of extremely preterm twins.
Close follow-up and cross-specialty cooperation are what make these positive outcomes possible, said Dr. Hovatta, who is now a professor emeritus at the Karolinska Institute, Sweden.
“We do everything we can to exclude things that could cause bad outcomes.” That includes extremely rigorous cardiac testing before pregnancy and continuous monitoring during it. “If a woman has any sign of cardiac anomaly, she is advised not to become pregnant. If she shows any signs of aortic dilation, we follow her extremely carefully with experienced cardiologists.”
Like Dr. Oktay, Dr. Hovatta and her European colleagues make fertility preservation an early topic of conversation. Unlike in the United States, where many girls aren’t diagnosed with the disorder until they fail to enter puberty, almost all Turner girls in Europe are identified very early in childhood. They receive early growth hormone treatment, and there is frequent consultation with interdisciplinary specialists. Fertility is spoken of early and often.
Early oocyte retrieval is common, Dr. Hovatta said. “Yes, it’s possible to wait until puberty, but for so many girls, most of the eggs have disappeared by then, so we typically don’t wait. We start looking at that option around 11 years, which is the same time we think about cryopreserving ovarian tissue.”
However, she added, as in the United States, the outcomes of these procedures are still unknown. But the existing data in other populations, the ability to carefully shepherd women through a successful pregnancy, and the willingness of families to provide the option all support further exploring them. Dr. Hovatta was at the Cincinnati gathering last summer and said she did not agree with the conservative tone she heard. Dr. Oktay also does not agree.
“This evidence we have so far is good evidence,” he said. “Look, where we are right now with Turner girls is where we were 15 years ago with cancer patients. People thought, ‘They have cancer. They should just be worrying about surviving cancer, not about their fertility.’ Now fertility counseling is a very important part of cancer care. We have all these tools available to us for cancer patients who don’t want to lose their fertility. This accumulated experience that has already been applied in other medical conditions … why not use that for Turner syndrome? This is my point: With all the data out there about the potential benefits and the ways to manage the risks, we shouldn’t have to tell girls, ‘Well, you have to become menopausal, and maybe you can adopt someday.’ That doesn’t sit well with parents any more. We want these girls to thrive. Not just to survive, but to have as close to a normal quality of life as possible.”
Failed expectations: When cultural similarities do not favor a therapeutic bond
The importance of establishing a bond with a patient early in treatment is instilled in psychiatry trainees during their first year of residency. It is well-known that a strong therapeutic connection is correlated with successful treatment and favorable outcomes.
We present a case in which sharing my cultural background with a patient was detrimental to the therapeutic relationship and forced me to look beyond superficial similarities to forge a meaningful connection.
A shared language, a shared connection?
When I, a psychiatry intern who emigrated from Honduras 11 years ago, met Ms. M, a middle-age, Spanish-speaking Honduran immigrant with schizoaffective disorder, I was curious to hear the story of how her immigration intermingled with her mental illness. As a budding psychiatrist, I was certain our common culture would intensify our interactions. It did, although in ways I did not expect.
Despite my enthusiasm and best intentions, our first meeting was less than ideal. Ms. M believed she not only was God’s wife and my attending physician’s wife, but that I was her rival for my attending’s affections. “I heard you are from Honduras. I am from Honduras, too. What part are you from?” I asked her. She became angry. “I am not from there. I am from Israel,” she said. For many days, we had the same hostile and disappointing conversations, during which I would try to tease out the basis for her delusions and understand our lack of connection. I felt hurt and puzzled. If I could not connect with someone with whom I shared a common background, then to whom could I connect with? I had to re-evaluate my approach. Should I alter my attire to seem less feminine? Should I tell her I am happily married? Should I not speak Spanish? Would these changes make our interactions feel less threatening to her?
“You are focused too much on you and not enough on her,” my attending retorted. I came to realize that, in my crusade to have Ms. M perceive me a certain way, I had lost sight of who she was and what lay at the core of her delusions. I stepped back and considered Ms. M: a patient, yes, but also a woman who was unable to communicate freely with others because she did not speak English. Because of her perpetual paranoia and psychosis, she was emotionally isolated, lacked necessary social support from her family, and had no sense of community. However, in her delusions she was a prophet, a herald for God’s news, with a vital role in His plans. In her mind, she was a mother and had the support of a life-long partner.
As I considered her struggles, I thought about myself. When I first came to the United States, it was difficult to develop relationships with my peers because I worried about my accent and idioms. In Honduras, my friends and family knew me as a gregarious, quick-witted individual. In acculturating to my new home, I became reclusive and insecure. It took years to regain a semblance of identity.
In my attending’s office, I found that it was not our shared heritage that was the path to engaging Ms. M, but rather our shared isolation, which I had not been validating. This helped me reframe the way I viewed the therapeutic relationship and changed the focus of my attempts to engage her. I stopped taking her rejection personally and focused on providing her support and solace. By tapping into her isolation, she opened up and eventually agreed to medication changes, which slowly reduced—but did not eliminate—her delusions, hallucinations, and hostility toward others. Because of her intractable psychotic symptoms, she required a long-term structured care setting and was transferred to the state hospital.
Culture is only ‘skin deep’
I assumed our shared background would have effortlessly led to a trustworthy relationship, but her resistance challenged that notion. My own desires to have a deep connection with a fellow immigrant contributed to my internalization of her rejection. Our physical and cultural similarities acted as a hindrance because she subconsciously projected her idealized image of a woman onto me. Nevertheless, she helped me recognize the importance of unexamined projective identification and countertransference, evidenced by wanting to change my appearance and behavior and my increased willingness for self-disclosure.
As I start my second year of residency and reflect on my experiences as an intern, Ms. M always comes to mind. She taught me that culture may be only “skin deep” and similarities between therapist and patient do not guarantee a successful bond. Searching for deeper, fundamental connections and validating these bonds can open the doors to connecting with those from all walks of life, from whichever road they come.
1. Krupnick JL, Sotsky SM, Simmens S, et al. The role of the therapeutic alliance in psychotherapy and pharmacotherapy outcome: findings in the National Institute of Mental Health Treatment of Depression Collaborative Research Program. J Consult Clin Psychol. 1996;64(3):532-539.
The importance of establishing a bond with a patient early in treatment is instilled in psychiatry trainees during their first year of residency. It is well-known that a strong therapeutic connection is correlated with successful treatment and favorable outcomes.
We present a case in which sharing my cultural background with a patient was detrimental to the therapeutic relationship and forced me to look beyond superficial similarities to forge a meaningful connection.
A shared language, a shared connection?
When I, a psychiatry intern who emigrated from Honduras 11 years ago, met Ms. M, a middle-age, Spanish-speaking Honduran immigrant with schizoaffective disorder, I was curious to hear the story of how her immigration intermingled with her mental illness. As a budding psychiatrist, I was certain our common culture would intensify our interactions. It did, although in ways I did not expect.
Despite my enthusiasm and best intentions, our first meeting was less than ideal. Ms. M believed she not only was God’s wife and my attending physician’s wife, but that I was her rival for my attending’s affections. “I heard you are from Honduras. I am from Honduras, too. What part are you from?” I asked her. She became angry. “I am not from there. I am from Israel,” she said. For many days, we had the same hostile and disappointing conversations, during which I would try to tease out the basis for her delusions and understand our lack of connection. I felt hurt and puzzled. If I could not connect with someone with whom I shared a common background, then to whom could I connect with? I had to re-evaluate my approach. Should I alter my attire to seem less feminine? Should I tell her I am happily married? Should I not speak Spanish? Would these changes make our interactions feel less threatening to her?
“You are focused too much on you and not enough on her,” my attending retorted. I came to realize that, in my crusade to have Ms. M perceive me a certain way, I had lost sight of who she was and what lay at the core of her delusions. I stepped back and considered Ms. M: a patient, yes, but also a woman who was unable to communicate freely with others because she did not speak English. Because of her perpetual paranoia and psychosis, she was emotionally isolated, lacked necessary social support from her family, and had no sense of community. However, in her delusions she was a prophet, a herald for God’s news, with a vital role in His plans. In her mind, she was a mother and had the support of a life-long partner.
As I considered her struggles, I thought about myself. When I first came to the United States, it was difficult to develop relationships with my peers because I worried about my accent and idioms. In Honduras, my friends and family knew me as a gregarious, quick-witted individual. In acculturating to my new home, I became reclusive and insecure. It took years to regain a semblance of identity.
In my attending’s office, I found that it was not our shared heritage that was the path to engaging Ms. M, but rather our shared isolation, which I had not been validating. This helped me reframe the way I viewed the therapeutic relationship and changed the focus of my attempts to engage her. I stopped taking her rejection personally and focused on providing her support and solace. By tapping into her isolation, she opened up and eventually agreed to medication changes, which slowly reduced—but did not eliminate—her delusions, hallucinations, and hostility toward others. Because of her intractable psychotic symptoms, she required a long-term structured care setting and was transferred to the state hospital.
Culture is only ‘skin deep’
I assumed our shared background would have effortlessly led to a trustworthy relationship, but her resistance challenged that notion. My own desires to have a deep connection with a fellow immigrant contributed to my internalization of her rejection. Our physical and cultural similarities acted as a hindrance because she subconsciously projected her idealized image of a woman onto me. Nevertheless, she helped me recognize the importance of unexamined projective identification and countertransference, evidenced by wanting to change my appearance and behavior and my increased willingness for self-disclosure.
As I start my second year of residency and reflect on my experiences as an intern, Ms. M always comes to mind. She taught me that culture may be only “skin deep” and similarities between therapist and patient do not guarantee a successful bond. Searching for deeper, fundamental connections and validating these bonds can open the doors to connecting with those from all walks of life, from whichever road they come.
The importance of establishing a bond with a patient early in treatment is instilled in psychiatry trainees during their first year of residency. It is well-known that a strong therapeutic connection is correlated with successful treatment and favorable outcomes.
We present a case in which sharing my cultural background with a patient was detrimental to the therapeutic relationship and forced me to look beyond superficial similarities to forge a meaningful connection.
A shared language, a shared connection?
When I, a psychiatry intern who emigrated from Honduras 11 years ago, met Ms. M, a middle-age, Spanish-speaking Honduran immigrant with schizoaffective disorder, I was curious to hear the story of how her immigration intermingled with her mental illness. As a budding psychiatrist, I was certain our common culture would intensify our interactions. It did, although in ways I did not expect.
Despite my enthusiasm and best intentions, our first meeting was less than ideal. Ms. M believed she not only was God’s wife and my attending physician’s wife, but that I was her rival for my attending’s affections. “I heard you are from Honduras. I am from Honduras, too. What part are you from?” I asked her. She became angry. “I am not from there. I am from Israel,” she said. For many days, we had the same hostile and disappointing conversations, during which I would try to tease out the basis for her delusions and understand our lack of connection. I felt hurt and puzzled. If I could not connect with someone with whom I shared a common background, then to whom could I connect with? I had to re-evaluate my approach. Should I alter my attire to seem less feminine? Should I tell her I am happily married? Should I not speak Spanish? Would these changes make our interactions feel less threatening to her?
“You are focused too much on you and not enough on her,” my attending retorted. I came to realize that, in my crusade to have Ms. M perceive me a certain way, I had lost sight of who she was and what lay at the core of her delusions. I stepped back and considered Ms. M: a patient, yes, but also a woman who was unable to communicate freely with others because she did not speak English. Because of her perpetual paranoia and psychosis, she was emotionally isolated, lacked necessary social support from her family, and had no sense of community. However, in her delusions she was a prophet, a herald for God’s news, with a vital role in His plans. In her mind, she was a mother and had the support of a life-long partner.
As I considered her struggles, I thought about myself. When I first came to the United States, it was difficult to develop relationships with my peers because I worried about my accent and idioms. In Honduras, my friends and family knew me as a gregarious, quick-witted individual. In acculturating to my new home, I became reclusive and insecure. It took years to regain a semblance of identity.
In my attending’s office, I found that it was not our shared heritage that was the path to engaging Ms. M, but rather our shared isolation, which I had not been validating. This helped me reframe the way I viewed the therapeutic relationship and changed the focus of my attempts to engage her. I stopped taking her rejection personally and focused on providing her support and solace. By tapping into her isolation, she opened up and eventually agreed to medication changes, which slowly reduced—but did not eliminate—her delusions, hallucinations, and hostility toward others. Because of her intractable psychotic symptoms, she required a long-term structured care setting and was transferred to the state hospital.
Culture is only ‘skin deep’
I assumed our shared background would have effortlessly led to a trustworthy relationship, but her resistance challenged that notion. My own desires to have a deep connection with a fellow immigrant contributed to my internalization of her rejection. Our physical and cultural similarities acted as a hindrance because she subconsciously projected her idealized image of a woman onto me. Nevertheless, she helped me recognize the importance of unexamined projective identification and countertransference, evidenced by wanting to change my appearance and behavior and my increased willingness for self-disclosure.
As I start my second year of residency and reflect on my experiences as an intern, Ms. M always comes to mind. She taught me that culture may be only “skin deep” and similarities between therapist and patient do not guarantee a successful bond. Searching for deeper, fundamental connections and validating these bonds can open the doors to connecting with those from all walks of life, from whichever road they come.
1. Krupnick JL, Sotsky SM, Simmens S, et al. The role of the therapeutic alliance in psychotherapy and pharmacotherapy outcome: findings in the National Institute of Mental Health Treatment of Depression Collaborative Research Program. J Consult Clin Psychol. 1996;64(3):532-539.
1. Krupnick JL, Sotsky SM, Simmens S, et al. The role of the therapeutic alliance in psychotherapy and pharmacotherapy outcome: findings in the National Institute of Mental Health Treatment of Depression Collaborative Research Program. J Consult Clin Psychol. 1996;64(3):532-539.

Truncal vagotomy might help delay Parkinson’s disease
Patients who were followed for more than 5 years after truncal vagotomy had about a 40% lower risk of being diagnosed with Parkinson’s disease, compared with matched population controls, according to the results of a cohort registry study.
Selective vagotomy did not decrease the risk of Parkinson’s disease (PD), however, reported Bojing Liu of Karolinska Institutet, Stockholm, and her associates. The findings, which reflect those from a prior Danish study, “provide preliminary and indirect support” for the idea that Lewy pathology in PD begins in peripheral nerves and spreads to the central nervous system through “prion-like mechanisms,” they added.
The findings reflect a prior registry study that found a 15% decrease in the risk of PD compared with the general population more than 5 years after truncal vagotomy (Ann Neurol. 2015 Oct. 78[4];522-9). “This Danish study, however, did not differentiate truncal from selective vagotomy and thus might have underestimated the association of truncal vagotomy with PD,” the researchers said.
Another study found that truncal vagotomy exhibited a nonsignificant protective effect overall and an insignificantly increased risk of PD more than 20 years after surgery (Neurology Today 2015 Dec 3;15[23]:27-30). Likewise, the current study yielded “stronger evidence for PD risk reduction more than 5 or 10 years after truncal vagotomy,” and the protective effect appeared to weaken with longer follow-up, the investigators noted. If PD started at multiple sites within the peripheral nervous system, “even truncal vagotomy may delay, rather than eliminate, the risk for PD,” they emphasized. “Indeed, abnormal alpha-synuclein accumulation has been found throughout the digestive tract of patients with PD with descending pattern of density, and even in the submandibular gland in patients with preclinical PD.”
The study was funded by the Swedish Research Council for Health, Working Life and Welfare, the Parkinson Research Foundation in Sweden, the Karolinska Institutet, the Swedish Society for Medical Research, the Stockholm County Council, and Karolinska Institutet–NIH Doctoral Partnership Program in Neuroscience. The investigators had no relevant disclosures.
The current study provides an independent dataset suggesting that truncal vagotomy may be protective in Parkinson’s disease. Therefore, the time has come to seriously consider the implications of these findings.
Could it be true that alpha-synuclein misfolding in PD may originate in the autonomic nerve terminals of the gastrointestinal tract? For the moment, more research is needed. One may consider studying the effects of vagotomy in patients with mutations in the leucine-rich repeat kinase-2 gene (LRRK2), which dramatically increases the risk of developing neurodegenerative parkinsonism. Some of these mutations have a penetrance of up to 80% in the very elderly. However, it is largely unknown whether alpha-synuclein aggregates are present in gastrointestinal nerve endings of these patients. At this stage, we have insufficient knowledge to propose vagotomy as a putative treatment for PD. Although vagotomy will likely never become a widespread treatment for PD, strategies to prevent alpha-synuclein misfolding in the gastrointestinal tract may be proposed, because nerve terminals are reachable by oral therapeutic interventions.
Per Borghammer, MD, PhD, is in the department of nuclear medicine and PET Centre, Aarhus University Hospital, Denmark. Clement Hamani, MD, PhD, is at the division of neurosurgery, Toronto Western Hospital, University of Toronto, and the department of neuroimaging, Centre for Addiction and Mental Health, Campbell Family Mental Health Research Institute, Toronto. They reported no conflicts of interest. These comments are excerpted from their editorial (Neurology. 2017 Apr 26. doi: 10.1212/WNL.0000000000003969).
The current study provides an independent dataset suggesting that truncal vagotomy may be protective in Parkinson’s disease. Therefore, the time has come to seriously consider the implications of these findings.
Could it be true that alpha-synuclein misfolding in PD may originate in the autonomic nerve terminals of the gastrointestinal tract? For the moment, more research is needed. One may consider studying the effects of vagotomy in patients with mutations in the leucine-rich repeat kinase-2 gene (LRRK2), which dramatically increases the risk of developing neurodegenerative parkinsonism. Some of these mutations have a penetrance of up to 80% in the very elderly. However, it is largely unknown whether alpha-synuclein aggregates are present in gastrointestinal nerve endings of these patients. At this stage, we have insufficient knowledge to propose vagotomy as a putative treatment for PD. Although vagotomy will likely never become a widespread treatment for PD, strategies to prevent alpha-synuclein misfolding in the gastrointestinal tract may be proposed, because nerve terminals are reachable by oral therapeutic interventions.
Per Borghammer, MD, PhD, is in the department of nuclear medicine and PET Centre, Aarhus University Hospital, Denmark. Clement Hamani, MD, PhD, is at the division of neurosurgery, Toronto Western Hospital, University of Toronto, and the department of neuroimaging, Centre for Addiction and Mental Health, Campbell Family Mental Health Research Institute, Toronto. They reported no conflicts of interest. These comments are excerpted from their editorial (Neurology. 2017 Apr 26. doi: 10.1212/WNL.0000000000003969).
The current study provides an independent dataset suggesting that truncal vagotomy may be protective in Parkinson’s disease. Therefore, the time has come to seriously consider the implications of these findings.
Could it be true that alpha-synuclein misfolding in PD may originate in the autonomic nerve terminals of the gastrointestinal tract? For the moment, more research is needed. One may consider studying the effects of vagotomy in patients with mutations in the leucine-rich repeat kinase-2 gene (LRRK2), which dramatically increases the risk of developing neurodegenerative parkinsonism. Some of these mutations have a penetrance of up to 80% in the very elderly. However, it is largely unknown whether alpha-synuclein aggregates are present in gastrointestinal nerve endings of these patients. At this stage, we have insufficient knowledge to propose vagotomy as a putative treatment for PD. Although vagotomy will likely never become a widespread treatment for PD, strategies to prevent alpha-synuclein misfolding in the gastrointestinal tract may be proposed, because nerve terminals are reachable by oral therapeutic interventions.
Per Borghammer, MD, PhD, is in the department of nuclear medicine and PET Centre, Aarhus University Hospital, Denmark. Clement Hamani, MD, PhD, is at the division of neurosurgery, Toronto Western Hospital, University of Toronto, and the department of neuroimaging, Centre for Addiction and Mental Health, Campbell Family Mental Health Research Institute, Toronto. They reported no conflicts of interest. These comments are excerpted from their editorial (Neurology. 2017 Apr 26. doi: 10.1212/WNL.0000000000003969).
Patients who were followed for more than 5 years after truncal vagotomy had about a 40% lower risk of being diagnosed with Parkinson’s disease, compared with matched population controls, according to the results of a cohort registry study.
Selective vagotomy did not decrease the risk of Parkinson’s disease (PD), however, reported Bojing Liu of Karolinska Institutet, Stockholm, and her associates. The findings, which reflect those from a prior Danish study, “provide preliminary and indirect support” for the idea that Lewy pathology in PD begins in peripheral nerves and spreads to the central nervous system through “prion-like mechanisms,” they added.
The findings reflect a prior registry study that found a 15% decrease in the risk of PD compared with the general population more than 5 years after truncal vagotomy (Ann Neurol. 2015 Oct. 78[4];522-9). “This Danish study, however, did not differentiate truncal from selective vagotomy and thus might have underestimated the association of truncal vagotomy with PD,” the researchers said.
Another study found that truncal vagotomy exhibited a nonsignificant protective effect overall and an insignificantly increased risk of PD more than 20 years after surgery (Neurology Today 2015 Dec 3;15[23]:27-30). Likewise, the current study yielded “stronger evidence for PD risk reduction more than 5 or 10 years after truncal vagotomy,” and the protective effect appeared to weaken with longer follow-up, the investigators noted. If PD started at multiple sites within the peripheral nervous system, “even truncal vagotomy may delay, rather than eliminate, the risk for PD,” they emphasized. “Indeed, abnormal alpha-synuclein accumulation has been found throughout the digestive tract of patients with PD with descending pattern of density, and even in the submandibular gland in patients with preclinical PD.”
The study was funded by the Swedish Research Council for Health, Working Life and Welfare, the Parkinson Research Foundation in Sweden, the Karolinska Institutet, the Swedish Society for Medical Research, the Stockholm County Council, and Karolinska Institutet–NIH Doctoral Partnership Program in Neuroscience. The investigators had no relevant disclosures.
Patients who were followed for more than 5 years after truncal vagotomy had about a 40% lower risk of being diagnosed with Parkinson’s disease, compared with matched population controls, according to the results of a cohort registry study.
Selective vagotomy did not decrease the risk of Parkinson’s disease (PD), however, reported Bojing Liu of Karolinska Institutet, Stockholm, and her associates. The findings, which reflect those from a prior Danish study, “provide preliminary and indirect support” for the idea that Lewy pathology in PD begins in peripheral nerves and spreads to the central nervous system through “prion-like mechanisms,” they added.
The findings reflect a prior registry study that found a 15% decrease in the risk of PD compared with the general population more than 5 years after truncal vagotomy (Ann Neurol. 2015 Oct. 78[4];522-9). “This Danish study, however, did not differentiate truncal from selective vagotomy and thus might have underestimated the association of truncal vagotomy with PD,” the researchers said.
Another study found that truncal vagotomy exhibited a nonsignificant protective effect overall and an insignificantly increased risk of PD more than 20 years after surgery (Neurology Today 2015 Dec 3;15[23]:27-30). Likewise, the current study yielded “stronger evidence for PD risk reduction more than 5 or 10 years after truncal vagotomy,” and the protective effect appeared to weaken with longer follow-up, the investigators noted. If PD started at multiple sites within the peripheral nervous system, “even truncal vagotomy may delay, rather than eliminate, the risk for PD,” they emphasized. “Indeed, abnormal alpha-synuclein accumulation has been found throughout the digestive tract of patients with PD with descending pattern of density, and even in the submandibular gland in patients with preclinical PD.”
The study was funded by the Swedish Research Council for Health, Working Life and Welfare, the Parkinson Research Foundation in Sweden, the Karolinska Institutet, the Swedish Society for Medical Research, the Stockholm County Council, and Karolinska Institutet–NIH Doctoral Partnership Program in Neuroscience. The investigators had no relevant disclosures.
Key clinical point:
Major finding: Compared with controls, patients who underwent truncal vagotomy were at decreased risk of Parkinson’s disease after more than 5 years (hazard ratio, 0.59, 95% confidence interval, 0.37-0.93). Selective vagotomy did not show this association.
Data source: A matched cohort study of 9,430 vagotomized patients (3,445 truncal, 5,978 selective, 7 unknown) between 1970 and 2010, and 377,200 population controls matched by age and sex.
Disclosures: The Swedish Research Council for Health, Working Life and Welfare, the Parkinson Research Foundation in Sweden, the Karolinska Institutet, the Swedish Society for Medical Research, the Stockholm County Council, and Karolinska Institutet–NIH Doctoral Partnership Program in Neuroscience funded the study. The investigators had no relevant disclosures.
RIV poster contest a meeting highlight
Look back at the history of SHM’s annual Research, Innovations and Clinical Vignettes poster competition – better known as the RIV – and it may seem inevitable that it’s grown into one of the main highlights of the conference. The RIV has become so popular that the number of submissions has nearly tripled from 634 in 2010 to 1,712 this year.

“Certainly, there is some natural evolution,” said Dr. Fang, a hospitalist, researcher, and anticoagulation clinic director at the University of California San Francisco. “But not all specialty societies embrace research or encourage its growth, so I would give a lot of credit to the Society of Hospital Medicine for being very deliberate in trying to strengthen its research program, highlight the research that hospitalists do, and make research a core pillar of what SHM stands for.”
The efforts have clearly worked, as RIV is a major driver for annual meeting attendance. The poster competition draws massive crowds that snake their way through the accepted posters.
For those interested in a deeper dive, SHM chooses a dozen or so top abstracts for oral presentations that are, in Dr. Fang’s words, “the creme de la creme of all the research and innovations for the given year.”
The growth of the abstracts competition comes, of course, as the specialty itself has seen its ranks skyrocket. Hospitalists now number an estimated 52,000 nationally, and in addition to providing direct clinical care, have taken ownership of key health care drivers like patient safety, quality improvement, and systems change.
“We do what we do for the good of health care and, ultimately, for the good of our patients,” Dr. Fang said. “Sometimes that’s rounding and taking care of patients in a clinical fashion, and sometimes it’s contributing to the medical literature. It could have been really easy for a specialty to say, ‘Not our problem,’ or ‘No, we’re just rounding.’ ”
HM17 course director Lenny Feldman, MD, FACP, FAAP, SFHM, believes that the commitment of SHM’s founding generation to do research for the past decade has created a group of mentors that push younger hospitalists to do more of the same.
“If we didn’t have the research engine part of hospital medicine, if we didn’t have the folks who are getting into administration and other important leadership areas, we wouldn’t see the maturation of this specialty and we would, in many ways, be stuck at the point at which we started,” Dr. Feldman said. “The only way for us to move forward is to do the research, to be in position to make sure that hospital medicine continues to grow in a direction that is good for our patients, for us, and for the entire system.”
That perspective is what motivates hospitalists to make the RIV bigger each year, said Dr. Fang.
“Having your abstract accepted as a poster or an oral presentation showcases all the work that you’ve put into it,” Dr. Fang said. “There’s a huge amount of pride in showing what you’ve been able to achieve. The driving force is the desire to see what other people are doing, and network to share ideas. That’s the really wonderful part of the RIV competition.”
Look back at the history of SHM’s annual Research, Innovations and Clinical Vignettes poster competition – better known as the RIV – and it may seem inevitable that it’s grown into one of the main highlights of the conference. The RIV has become so popular that the number of submissions has nearly tripled from 634 in 2010 to 1,712 this year.
“Certainly, there is some natural evolution,” said Dr. Fang, a hospitalist, researcher, and anticoagulation clinic director at the University of California San Francisco. “But not all specialty societies embrace research or encourage its growth, so I would give a lot of credit to the Society of Hospital Medicine for being very deliberate in trying to strengthen its research program, highlight the research that hospitalists do, and make research a core pillar of what SHM stands for.”
The efforts have clearly worked, as RIV is a major driver for annual meeting attendance. The poster competition draws massive crowds that snake their way through the accepted posters.
For those interested in a deeper dive, SHM chooses a dozen or so top abstracts for oral presentations that are, in Dr. Fang’s words, “the creme de la creme of all the research and innovations for the given year.”
The growth of the abstracts competition comes, of course, as the specialty itself has seen its ranks skyrocket. Hospitalists now number an estimated 52,000 nationally, and in addition to providing direct clinical care, have taken ownership of key health care drivers like patient safety, quality improvement, and systems change.
“We do what we do for the good of health care and, ultimately, for the good of our patients,” Dr. Fang said. “Sometimes that’s rounding and taking care of patients in a clinical fashion, and sometimes it’s contributing to the medical literature. It could have been really easy for a specialty to say, ‘Not our problem,’ or ‘No, we’re just rounding.’ ”
HM17 course director Lenny Feldman, MD, FACP, FAAP, SFHM, believes that the commitment of SHM’s founding generation to do research for the past decade has created a group of mentors that push younger hospitalists to do more of the same.
“If we didn’t have the research engine part of hospital medicine, if we didn’t have the folks who are getting into administration and other important leadership areas, we wouldn’t see the maturation of this specialty and we would, in many ways, be stuck at the point at which we started,” Dr. Feldman said. “The only way for us to move forward is to do the research, to be in position to make sure that hospital medicine continues to grow in a direction that is good for our patients, for us, and for the entire system.”
That perspective is what motivates hospitalists to make the RIV bigger each year, said Dr. Fang.
“Having your abstract accepted as a poster or an oral presentation showcases all the work that you’ve put into it,” Dr. Fang said. “There’s a huge amount of pride in showing what you’ve been able to achieve. The driving force is the desire to see what other people are doing, and network to share ideas. That’s the really wonderful part of the RIV competition.”
Look back at the history of SHM’s annual Research, Innovations and Clinical Vignettes poster competition – better known as the RIV – and it may seem inevitable that it’s grown into one of the main highlights of the conference. The RIV has become so popular that the number of submissions has nearly tripled from 634 in 2010 to 1,712 this year.
“Certainly, there is some natural evolution,” said Dr. Fang, a hospitalist, researcher, and anticoagulation clinic director at the University of California San Francisco. “But not all specialty societies embrace research or encourage its growth, so I would give a lot of credit to the Society of Hospital Medicine for being very deliberate in trying to strengthen its research program, highlight the research that hospitalists do, and make research a core pillar of what SHM stands for.”
The efforts have clearly worked, as RIV is a major driver for annual meeting attendance. The poster competition draws massive crowds that snake their way through the accepted posters.
For those interested in a deeper dive, SHM chooses a dozen or so top abstracts for oral presentations that are, in Dr. Fang’s words, “the creme de la creme of all the research and innovations for the given year.”
The growth of the abstracts competition comes, of course, as the specialty itself has seen its ranks skyrocket. Hospitalists now number an estimated 52,000 nationally, and in addition to providing direct clinical care, have taken ownership of key health care drivers like patient safety, quality improvement, and systems change.
“We do what we do for the good of health care and, ultimately, for the good of our patients,” Dr. Fang said. “Sometimes that’s rounding and taking care of patients in a clinical fashion, and sometimes it’s contributing to the medical literature. It could have been really easy for a specialty to say, ‘Not our problem,’ or ‘No, we’re just rounding.’ ”
HM17 course director Lenny Feldman, MD, FACP, FAAP, SFHM, believes that the commitment of SHM’s founding generation to do research for the past decade has created a group of mentors that push younger hospitalists to do more of the same.
“If we didn’t have the research engine part of hospital medicine, if we didn’t have the folks who are getting into administration and other important leadership areas, we wouldn’t see the maturation of this specialty and we would, in many ways, be stuck at the point at which we started,” Dr. Feldman said. “The only way for us to move forward is to do the research, to be in position to make sure that hospital medicine continues to grow in a direction that is good for our patients, for us, and for the entire system.”
That perspective is what motivates hospitalists to make the RIV bigger each year, said Dr. Fang.
“Having your abstract accepted as a poster or an oral presentation showcases all the work that you’ve put into it,” Dr. Fang said. “There’s a huge amount of pride in showing what you’ve been able to achieve. The driving force is the desire to see what other people are doing, and network to share ideas. That’s the really wonderful part of the RIV competition.”

Postmenopausal hot flashes cut by 93% with novel nonhormonal treatment
AT ENDO 2017
ORLANDO –
After 12 weeks of treatment with the oral small molecule, women had a 93% reduction in moderate to severe hot flashes, compared with a 23% reduction for those taking placebo (P less than .0001). The effects of fezolinetant were seen earlier as well, with an 88% reduction in hot flashes at 4 weeks into the trial, compared with a 12% reduction for the placebo group (P less than .001).

The eight-site study enrolled 87 patients in a double-blind, randomized, placebo-controlled trial that assessed hot flash frequency and severity at study weeks 4 and 12. Postmenopausal women had to have frequent, moderate to severe hot flashes to qualify for enrollment, and they had to be otherwise healthy.
To capture data for a secondary endpoint, participants also completed a quality of life questionnaire. Dr. Fraser and his coinvestigators tracked safety and pharmacokinetic data by measuring levels of luteinizing hormone, follicle-stimulating hormone, estradiol, and sex hormone–binding globulin at baseline and 12 weeks, as well.
Evenly divided between study arms, 80 patients completed the trial. Two patients withdrew because of adverse events, one patient violated inclusion criteria, and the others withdrew for a variety of reasons. Mean age was similar between the two groups, at 53.7 years for those on placebo and 53.3 years for the fezolinetant group. Other anthropometric characteristics were similar, as well.
At baseline, patients taking placebo experienced a mean 10.3 moderate to severe hot flashes daily, compared with the fezolinetant group at a mean of 11.5. By study week 4, 14 of the 40 patients in the active arm had zero hot flashes, compared with 2 of 40 in the in the placebo arm, when the intention-to-treat population was examined. Hot flash severity dropped by 70% (P less than .0001).
Quality of life was assessed with the Hot Flash Related Daily Interference Scale (HFRDIS). When the two groups were compared, a significant (P less than .001) reduction in HFRDIS score was seen by week 4 and continued through to week 12 in the group on active treatment. Lower HFRDIS scores mean improved hot flash–related quality of life.
Using the Leeds Sleep Evaluation Questionnaire allowed Dr. Fraser and his colleagues to ask about how long it took patients to get to sleep while they were participating in the study, compared with their normal sleep latency. Patients taking fezolinetant reported getting to sleep significantly more quickly (P less than .01) than the placebo group. They also reported better quality of sleep (P less than .001) and a better awakening experience (P less than .05). However, they did not report feeling better after awakening (P = .08).
Women taking fezolinetant also showed significant improvement, compared with the placebo group, on other quality of life questionnaires, the Greene Climacteric Scale and the Sheehan Disability Scale. By week 8, a significant (P less than .001) improvement was seen on both scales and specifically at week 4 on the Sheehan Disability Scale.
Among the hormone biomarkers that were followed in the study, only plasma luteinizing-hormone levels dropped, compared with patients’ baseline levels. These were reduced 20% 12 hours after one of the two daily 60-mg oral doses, and 50% at 3 hours post dose, a point at which maximum serum fezolinetant concentration would be seen. These were all statistically significant reductions and expected effects of the drug’s mechanism of action.
Further pharmacokinetic analysis, said Dr. Fraser, “supports testing of once-daily dosing for vasomotor symptoms,” given that, when the drug was tested in premenopausal women in phase I clinical trials, there was no difference in peak and trough drug concentration.
The safety profile was good overall, said Dr. Fraser. No patients in the fezolinetant group reported serious treatment-emergent adverse events. “More patients reported treatment-emergent adverse events in the placebo group than in the fezolinetant group,” he said.
The NK3R antagonist is also under investigation for use in the treatment of polycystic ovary syndrome and uterine fibroids.
The study was funded by Ogeda, which employs Dr. Fraser. Another author reported serving as a clinical adviser for Ogeda.
[email protected]
On Twitter @karioakes
AT ENDO 2017
ORLANDO –
After 12 weeks of treatment with the oral small molecule, women had a 93% reduction in moderate to severe hot flashes, compared with a 23% reduction for those taking placebo (P less than .0001). The effects of fezolinetant were seen earlier as well, with an 88% reduction in hot flashes at 4 weeks into the trial, compared with a 12% reduction for the placebo group (P less than .001).
The eight-site study enrolled 87 patients in a double-blind, randomized, placebo-controlled trial that assessed hot flash frequency and severity at study weeks 4 and 12. Postmenopausal women had to have frequent, moderate to severe hot flashes to qualify for enrollment, and they had to be otherwise healthy.
To capture data for a secondary endpoint, participants also completed a quality of life questionnaire. Dr. Fraser and his coinvestigators tracked safety and pharmacokinetic data by measuring levels of luteinizing hormone, follicle-stimulating hormone, estradiol, and sex hormone–binding globulin at baseline and 12 weeks, as well.
Evenly divided between study arms, 80 patients completed the trial. Two patients withdrew because of adverse events, one patient violated inclusion criteria, and the others withdrew for a variety of reasons. Mean age was similar between the two groups, at 53.7 years for those on placebo and 53.3 years for the fezolinetant group. Other anthropometric characteristics were similar, as well.
At baseline, patients taking placebo experienced a mean 10.3 moderate to severe hot flashes daily, compared with the fezolinetant group at a mean of 11.5. By study week 4, 14 of the 40 patients in the active arm had zero hot flashes, compared with 2 of 40 in the in the placebo arm, when the intention-to-treat population was examined. Hot flash severity dropped by 70% (P less than .0001).
Quality of life was assessed with the Hot Flash Related Daily Interference Scale (HFRDIS). When the two groups were compared, a significant (P less than .001) reduction in HFRDIS score was seen by week 4 and continued through to week 12 in the group on active treatment. Lower HFRDIS scores mean improved hot flash–related quality of life.
Using the Leeds Sleep Evaluation Questionnaire allowed Dr. Fraser and his colleagues to ask about how long it took patients to get to sleep while they were participating in the study, compared with their normal sleep latency. Patients taking fezolinetant reported getting to sleep significantly more quickly (P less than .01) than the placebo group. They also reported better quality of sleep (P less than .001) and a better awakening experience (P less than .05). However, they did not report feeling better after awakening (P = .08).
Women taking fezolinetant also showed significant improvement, compared with the placebo group, on other quality of life questionnaires, the Greene Climacteric Scale and the Sheehan Disability Scale. By week 8, a significant (P less than .001) improvement was seen on both scales and specifically at week 4 on the Sheehan Disability Scale.
Among the hormone biomarkers that were followed in the study, only plasma luteinizing-hormone levels dropped, compared with patients’ baseline levels. These were reduced 20% 12 hours after one of the two daily 60-mg oral doses, and 50% at 3 hours post dose, a point at which maximum serum fezolinetant concentration would be seen. These were all statistically significant reductions and expected effects of the drug’s mechanism of action.
Further pharmacokinetic analysis, said Dr. Fraser, “supports testing of once-daily dosing for vasomotor symptoms,” given that, when the drug was tested in premenopausal women in phase I clinical trials, there was no difference in peak and trough drug concentration.
The safety profile was good overall, said Dr. Fraser. No patients in the fezolinetant group reported serious treatment-emergent adverse events. “More patients reported treatment-emergent adverse events in the placebo group than in the fezolinetant group,” he said.
The NK3R antagonist is also under investigation for use in the treatment of polycystic ovary syndrome and uterine fibroids.
The study was funded by Ogeda, which employs Dr. Fraser. Another author reported serving as a clinical adviser for Ogeda.
[email protected]
On Twitter @karioakes
AT ENDO 2017
ORLANDO –
After 12 weeks of treatment with the oral small molecule, women had a 93% reduction in moderate to severe hot flashes, compared with a 23% reduction for those taking placebo (P less than .0001). The effects of fezolinetant were seen earlier as well, with an 88% reduction in hot flashes at 4 weeks into the trial, compared with a 12% reduction for the placebo group (P less than .001).
The eight-site study enrolled 87 patients in a double-blind, randomized, placebo-controlled trial that assessed hot flash frequency and severity at study weeks 4 and 12. Postmenopausal women had to have frequent, moderate to severe hot flashes to qualify for enrollment, and they had to be otherwise healthy.
To capture data for a secondary endpoint, participants also completed a quality of life questionnaire. Dr. Fraser and his coinvestigators tracked safety and pharmacokinetic data by measuring levels of luteinizing hormone, follicle-stimulating hormone, estradiol, and sex hormone–binding globulin at baseline and 12 weeks, as well.
Evenly divided between study arms, 80 patients completed the trial. Two patients withdrew because of adverse events, one patient violated inclusion criteria, and the others withdrew for a variety of reasons. Mean age was similar between the two groups, at 53.7 years for those on placebo and 53.3 years for the fezolinetant group. Other anthropometric characteristics were similar, as well.
At baseline, patients taking placebo experienced a mean 10.3 moderate to severe hot flashes daily, compared with the fezolinetant group at a mean of 11.5. By study week 4, 14 of the 40 patients in the active arm had zero hot flashes, compared with 2 of 40 in the in the placebo arm, when the intention-to-treat population was examined. Hot flash severity dropped by 70% (P less than .0001).
Quality of life was assessed with the Hot Flash Related Daily Interference Scale (HFRDIS). When the two groups were compared, a significant (P less than .001) reduction in HFRDIS score was seen by week 4 and continued through to week 12 in the group on active treatment. Lower HFRDIS scores mean improved hot flash–related quality of life.
Using the Leeds Sleep Evaluation Questionnaire allowed Dr. Fraser and his colleagues to ask about how long it took patients to get to sleep while they were participating in the study, compared with their normal sleep latency. Patients taking fezolinetant reported getting to sleep significantly more quickly (P less than .01) than the placebo group. They also reported better quality of sleep (P less than .001) and a better awakening experience (P less than .05). However, they did not report feeling better after awakening (P = .08).
Women taking fezolinetant also showed significant improvement, compared with the placebo group, on other quality of life questionnaires, the Greene Climacteric Scale and the Sheehan Disability Scale. By week 8, a significant (P less than .001) improvement was seen on both scales and specifically at week 4 on the Sheehan Disability Scale.
Among the hormone biomarkers that were followed in the study, only plasma luteinizing-hormone levels dropped, compared with patients’ baseline levels. These were reduced 20% 12 hours after one of the two daily 60-mg oral doses, and 50% at 3 hours post dose, a point at which maximum serum fezolinetant concentration would be seen. These were all statistically significant reductions and expected effects of the drug’s mechanism of action.
Further pharmacokinetic analysis, said Dr. Fraser, “supports testing of once-daily dosing for vasomotor symptoms,” given that, when the drug was tested in premenopausal women in phase I clinical trials, there was no difference in peak and trough drug concentration.
The safety profile was good overall, said Dr. Fraser. No patients in the fezolinetant group reported serious treatment-emergent adverse events. “More patients reported treatment-emergent adverse events in the placebo group than in the fezolinetant group,” he said.
The NK3R antagonist is also under investigation for use in the treatment of polycystic ovary syndrome and uterine fibroids.
The study was funded by Ogeda, which employs Dr. Fraser. Another author reported serving as a clinical adviser for Ogeda.
[email protected]
On Twitter @karioakes
Key clinical point: .
Major finding: Women on fezolinetant had a 93% drop in hot flash frequency, compared with a 23% reduction for those on placebo (P less than .0001).
Data source: A phase II randomized, double-blind, placebo-controlled clinical trial of 87 postmenopausal women with moderate to severe hot flashes.
Disclosures: The study was funded by Ogeda, which employs Dr. Fraser. Another author reported serving as a clinical adviser for Ogeda.
Multiple miscarriages in a 29-year-old woman
A) Didelphys uterus INCORRECT
A didelphys uterus occurs as a result of complete nonfusion of the Müllerian duct, resulting in duplicated uterine horns, duplicated cervices, and occasionally the proximal vagina, which is often associated with a transverse or longitudinal vaginal septum.1,2 Fusion anomalies (didelphys and bicornuate) can be differentiated from resorption anomalies (septate and arcuate) on ultrasonography (US) by a deep fundal cleft (>1 cm).1 3D US is highly accurate in identifying Müllerian duct anomalies (MDAs), it correlates well with magnetic resonance imaging (MRI), and it is more cost effective and accessible.3 For the didelphys uterus, 3D US obtained coronal to the uterine fundus often demonstrates widely divergent uterine horns separated by a deep serosal fundal cleft (>1 cm) and noncommunicating endometrial cavities with 2 cervices.1 Identifying a duplicated vaginal canal can help differentiate a didelphys uterus from a bicornuate bicollis uterus.1

B) Unicornuate uterus INCORRECT
A unicornuate uterus results from arrested development of one Müllerian duct and normal development of the other. There are 4 different subtypes: no rudimentary horn, rudimentary horn without endometrial cavity, rudimentary horn with communicating endometrial cavity, and rudimentary horn with noncommunicating uterine cavity.1 Renal anomalies, especially renal agenesis when present, are usually ipsilateral to the rudimentary horn.1 On US, unicornuate uterus appears as a lobular oblong (banana-shaped) structure away from the midline. The rudimentary horn is often difficult to identify and, when seen, the presence or absence of endometrium is an important finding.1
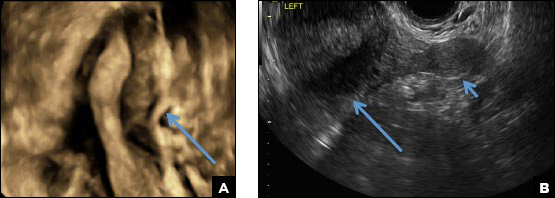
C) Partial septate uterus CORRECT
A septate uterus is a result of a resorption anomaly. The septum may be partial (subseptate) or complete secondary to failure of resorption of the uterovaginal septum. A complete septum extends to the external cervical os and occasionally to the vagina.1 US demonstrates interruption of the myometrium by a hypoechoic fibrous septum and/or a muscular septum which is isoechoic to the myometrium and arises midline from the fundus.1 3D US often clearly delineates the septum and improves visualization of the external fundal contour.2 The external fundal contour in septate uterus is convex (little or no serosal fundal cleft) and the apex is greater than 5 mm above the interostial line compared with a bicornuate or didelphys uterus, where the apex is less than 5 mm from the interostial line.1,2 Additionally, the intercornual distance is less than 4 cm.4 A septate uterus with duplicated cervix can appear similar to a bicornuate bicollis uterus and can be correctly diagnosed by evaluating the external fundal contour.1
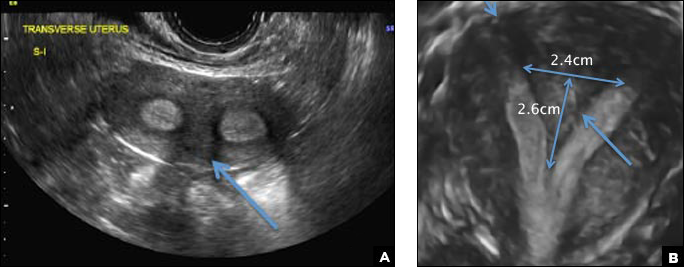
D) Arcuate uterus INCORRECT
The arcuate uterus also represents a resorption anomaly as a sequela of near-complete resorption of the uterovaginal septum.1 On 3D US, the fundal indentation in an arcuate uterus is well delineated and appears broad based with an obtuse angle at the most central point, which can help differentiate it from a septate uterus that has an acute angle.2,3 Both an arcuate and a septate uterus have a normal external (serosal) fundal contour.2,3 With an arcuate uterus, the length of the vertical measurement from the tubal ostia line, which is drawn horizontally between the tubal ostia to the fundal midline component of the endometrial cavity, is 1 cm or less. With a septate uterus, this vertical distance is greater than 1 cm.
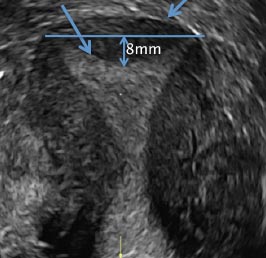
- CambriaBehr SC, Courtier JL, Qayyum A. Imaging of MMS PGothicüCambriallerian duct anomalies. RadioGraphics. 2012;32(6):e23.
- Bermejo C, Martinez Ten P, Diaz D, et al. Three-dimensional ultrasound in the diagnosis of MMS PGothicüCambriallerian duct anomaly and concordance with MRI. Ultrasound Obstet Gynecol.Cambria 2010;35(5):593–601.
- Deutch TD, Abuhamed AZ. The role of 3-dimensional ultrasonography and magnetic resonance imaging in the diagnosis of MMS PGothicüCambriallerian duct anomalies. J Ultrasound Med. 2008;27(3):413–423.
- CambriaChandler TM, Machan LS, Cooperberg PL, Harris AC, Chang SD. MMS PGothicüCambriallerian duct anomalies: from diagnosis to intervention.Cambria Br J Radiol. 2009;82(984):1034–1042.

Dr. Kanmaniraja is Assistant Professor and Chief, Division of Abdominal Imaging, Department of Radiology, University of Florida College of Medicine–Jacksonville.

Dr. Kaunitz is University of Florida Research Foundation Professor and Associate Chairman, Department of Obstetrics and Gynecology, University of Florida College of Medicine–Jacksonville. He is Medical Director and Director of Menopause and Gynecologic Ultrasound Services at UF Women’s Health Specialists–Emerson. He also serves on the OBG Management Board of Editors.
The authors report no financial relationships relevant to this quiz.
The authors wish to acknowledge Leeber S. Cohen, MD, Professor of Obstetrics and Gynecology in the Division of Diagnostic Ultrasound at Feinberg School of Medicine, Northwestern University, Chicago, Illinois.
Dr. Kanmaniraja is Assistant Professor and Chief, Division of Abdominal Imaging, Department of Radiology, University of Florida College of Medicine–Jacksonville.
Dr. Kaunitz is University of Florida Research Foundation Professor and Associate Chairman, Department of Obstetrics and Gynecology, University of Florida College of Medicine–Jacksonville. He is Medical Director and Director of Menopause and Gynecologic Ultrasound Services at UF Women’s Health Specialists–Emerson. He also serves on the OBG Management Board of Editors.
The authors report no financial relationships relevant to this quiz.
The authors wish to acknowledge Leeber S. Cohen, MD, Professor of Obstetrics and Gynecology in the Division of Diagnostic Ultrasound at Feinberg School of Medicine, Northwestern University, Chicago, Illinois.
Dr. Kanmaniraja is Assistant Professor and Chief, Division of Abdominal Imaging, Department of Radiology, University of Florida College of Medicine–Jacksonville.
Dr. Kaunitz is University of Florida Research Foundation Professor and Associate Chairman, Department of Obstetrics and Gynecology, University of Florida College of Medicine–Jacksonville. He is Medical Director and Director of Menopause and Gynecologic Ultrasound Services at UF Women’s Health Specialists–Emerson. He also serves on the OBG Management Board of Editors.
The authors report no financial relationships relevant to this quiz.
The authors wish to acknowledge Leeber S. Cohen, MD, Professor of Obstetrics and Gynecology in the Division of Diagnostic Ultrasound at Feinberg School of Medicine, Northwestern University, Chicago, Illinois.
A) Didelphys uterus INCORRECT
A didelphys uterus occurs as a result of complete nonfusion of the Müllerian duct, resulting in duplicated uterine horns, duplicated cervices, and occasionally the proximal vagina, which is often associated with a transverse or longitudinal vaginal septum.1,2 Fusion anomalies (didelphys and bicornuate) can be differentiated from resorption anomalies (septate and arcuate) on ultrasonography (US) by a deep fundal cleft (>1 cm).1 3D US is highly accurate in identifying Müllerian duct anomalies (MDAs), it correlates well with magnetic resonance imaging (MRI), and it is more cost effective and accessible.3 For the didelphys uterus, 3D US obtained coronal to the uterine fundus often demonstrates widely divergent uterine horns separated by a deep serosal fundal cleft (>1 cm) and noncommunicating endometrial cavities with 2 cervices.1 Identifying a duplicated vaginal canal can help differentiate a didelphys uterus from a bicornuate bicollis uterus.1
B) Unicornuate uterus INCORRECT
A unicornuate uterus results from arrested development of one Müllerian duct and normal development of the other. There are 4 different subtypes: no rudimentary horn, rudimentary horn without endometrial cavity, rudimentary horn with communicating endometrial cavity, and rudimentary horn with noncommunicating uterine cavity.1 Renal anomalies, especially renal agenesis when present, are usually ipsilateral to the rudimentary horn.1 On US, unicornuate uterus appears as a lobular oblong (banana-shaped) structure away from the midline. The rudimentary horn is often difficult to identify and, when seen, the presence or absence of endometrium is an important finding.1
C) Partial septate uterus CORRECT
A septate uterus is a result of a resorption anomaly. The septum may be partial (subseptate) or complete secondary to failure of resorption of the uterovaginal septum. A complete septum extends to the external cervical os and occasionally to the vagina.1 US demonstrates interruption of the myometrium by a hypoechoic fibrous septum and/or a muscular septum which is isoechoic to the myometrium and arises midline from the fundus.1 3D US often clearly delineates the septum and improves visualization of the external fundal contour.2 The external fundal contour in septate uterus is convex (little or no serosal fundal cleft) and the apex is greater than 5 mm above the interostial line compared with a bicornuate or didelphys uterus, where the apex is less than 5 mm from the interostial line.1,2 Additionally, the intercornual distance is less than 4 cm.4 A septate uterus with duplicated cervix can appear similar to a bicornuate bicollis uterus and can be correctly diagnosed by evaluating the external fundal contour.1
D) Arcuate uterus INCORRECT
The arcuate uterus also represents a resorption anomaly as a sequela of near-complete resorption of the uterovaginal septum.1 On 3D US, the fundal indentation in an arcuate uterus is well delineated and appears broad based with an obtuse angle at the most central point, which can help differentiate it from a septate uterus that has an acute angle.2,3 Both an arcuate and a septate uterus have a normal external (serosal) fundal contour.2,3 With an arcuate uterus, the length of the vertical measurement from the tubal ostia line, which is drawn horizontally between the tubal ostia to the fundal midline component of the endometrial cavity, is 1 cm or less. With a septate uterus, this vertical distance is greater than 1 cm.
A) Didelphys uterus INCORRECT
A didelphys uterus occurs as a result of complete nonfusion of the Müllerian duct, resulting in duplicated uterine horns, duplicated cervices, and occasionally the proximal vagina, which is often associated with a transverse or longitudinal vaginal septum.1,2 Fusion anomalies (didelphys and bicornuate) can be differentiated from resorption anomalies (septate and arcuate) on ultrasonography (US) by a deep fundal cleft (>1 cm).1 3D US is highly accurate in identifying Müllerian duct anomalies (MDAs), it correlates well with magnetic resonance imaging (MRI), and it is more cost effective and accessible.3 For the didelphys uterus, 3D US obtained coronal to the uterine fundus often demonstrates widely divergent uterine horns separated by a deep serosal fundal cleft (>1 cm) and noncommunicating endometrial cavities with 2 cervices.1 Identifying a duplicated vaginal canal can help differentiate a didelphys uterus from a bicornuate bicollis uterus.1
B) Unicornuate uterus INCORRECT
A unicornuate uterus results from arrested development of one Müllerian duct and normal development of the other. There are 4 different subtypes: no rudimentary horn, rudimentary horn without endometrial cavity, rudimentary horn with communicating endometrial cavity, and rudimentary horn with noncommunicating uterine cavity.1 Renal anomalies, especially renal agenesis when present, are usually ipsilateral to the rudimentary horn.1 On US, unicornuate uterus appears as a lobular oblong (banana-shaped) structure away from the midline. The rudimentary horn is often difficult to identify and, when seen, the presence or absence of endometrium is an important finding.1
C) Partial septate uterus CORRECT
A septate uterus is a result of a resorption anomaly. The septum may be partial (subseptate) or complete secondary to failure of resorption of the uterovaginal septum. A complete septum extends to the external cervical os and occasionally to the vagina.1 US demonstrates interruption of the myometrium by a hypoechoic fibrous septum and/or a muscular septum which is isoechoic to the myometrium and arises midline from the fundus.1 3D US often clearly delineates the septum and improves visualization of the external fundal contour.2 The external fundal contour in septate uterus is convex (little or no serosal fundal cleft) and the apex is greater than 5 mm above the interostial line compared with a bicornuate or didelphys uterus, where the apex is less than 5 mm from the interostial line.1,2 Additionally, the intercornual distance is less than 4 cm.4 A septate uterus with duplicated cervix can appear similar to a bicornuate bicollis uterus and can be correctly diagnosed by evaluating the external fundal contour.1
D) Arcuate uterus INCORRECT
The arcuate uterus also represents a resorption anomaly as a sequela of near-complete resorption of the uterovaginal septum.1 On 3D US, the fundal indentation in an arcuate uterus is well delineated and appears broad based with an obtuse angle at the most central point, which can help differentiate it from a septate uterus that has an acute angle.2,3 Both an arcuate and a septate uterus have a normal external (serosal) fundal contour.2,3 With an arcuate uterus, the length of the vertical measurement from the tubal ostia line, which is drawn horizontally between the tubal ostia to the fundal midline component of the endometrial cavity, is 1 cm or less. With a septate uterus, this vertical distance is greater than 1 cm.
- CambriaBehr SC, Courtier JL, Qayyum A. Imaging of MMS PGothicüCambriallerian duct anomalies. RadioGraphics. 2012;32(6):e23.
- Bermejo C, Martinez Ten P, Diaz D, et al. Three-dimensional ultrasound in the diagnosis of MMS PGothicüCambriallerian duct anomaly and concordance with MRI. Ultrasound Obstet Gynecol.Cambria 2010;35(5):593–601.
- Deutch TD, Abuhamed AZ. The role of 3-dimensional ultrasonography and magnetic resonance imaging in the diagnosis of MMS PGothicüCambriallerian duct anomalies. J Ultrasound Med. 2008;27(3):413–423.
- CambriaChandler TM, Machan LS, Cooperberg PL, Harris AC, Chang SD. MMS PGothicüCambriallerian duct anomalies: from diagnosis to intervention.Cambria Br J Radiol. 2009;82(984):1034–1042.
- CambriaBehr SC, Courtier JL, Qayyum A. Imaging of MMS PGothicüCambriallerian duct anomalies. RadioGraphics. 2012;32(6):e23.
- Bermejo C, Martinez Ten P, Diaz D, et al. Three-dimensional ultrasound in the diagnosis of MMS PGothicüCambriallerian duct anomaly and concordance with MRI. Ultrasound Obstet Gynecol.Cambria 2010;35(5):593–601.
- Deutch TD, Abuhamed AZ. The role of 3-dimensional ultrasonography and magnetic resonance imaging in the diagnosis of MMS PGothicüCambriallerian duct anomalies. J Ultrasound Med. 2008;27(3):413–423.
- CambriaChandler TM, Machan LS, Cooperberg PL, Harris AC, Chang SD. MMS PGothicüCambriallerian duct anomalies: from diagnosis to intervention.Cambria Br J Radiol. 2009;82(984):1034–1042.
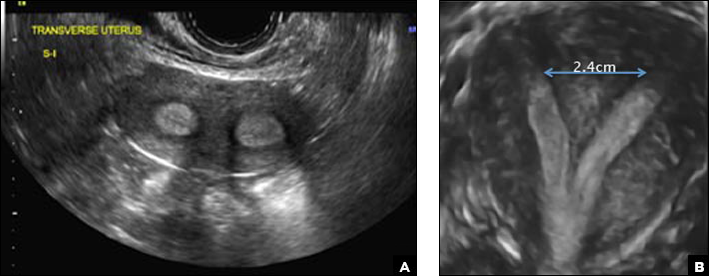
A 29-year-old woman presents to her ObGyn’s office with a history of multiple miscarriages. Transverse pelvic 2D ultrasonography of the uterus (A) and coronal 3D imaging (B) are performed.

GOP health reform: Essential health benefits, community rating under fire
Republicans are targeting two key consumer protections in their latest attempt to gain enough votes to pass the American Health Care Act, phase 1 of their Affordable Care Act repeal and replace plan.
On the chopping block are the essential health care benefits package and so-called community rating provisions – which prevent insurers from charging significantly more for older patients and those with preexisting conditions.
“Obamacare is already in a race to the bottom in terms of quality coverage for the sick and that’s because of the law’s community rating provisions, which penalize high-quality coverage for the sick,” Michael F. Cannon, director of health policy studies at the Cato Institute, said in an interview. “The [AHCA] would arguably accelerate that race to the bottom. The waiver provision in this amendment definitely would and it would because the bill would allow states to waive the community rating provisions, but only for people who were not previously insured.”
The waiver provisions would “increase premiums for the previously uninsured and discourage them from enrolling,” Mr. Cannon predicted.
David Anderson, research associate at the Margolis Center for Health Policy at Duke University, Durham, N.C., said that, if a state elects to take a waiver, so-called high-cost patients “such as individuals with cancer, individuals with cystic fibrosis, individuals with coagulation disorders, [would be] shrugged to the side into a high-cost risk pool or some kind of risk sharing ... with their own premium pool.” This could lower premium costs for healthy patients, he added.
This could be enhanced by narrowing the essential health benefits. For example, Mr. Anderson said that a state could keep the drug benefit, but apply for a waiver to narrow its coverage for all generics plus a limited list of brand names.
“Someone with cystic fibrosis with a $300,000-a-year medication will not have that covered and will be put in the high-cost risk pool,” Mr. Anderson said. “What it does is that it makes insurance cheaper for individuals who are highly unlikely to be high cost, and it makes it much more expensive for any individuals with known high-cost conditions.”
The draft amendment also would make it easier a whole lot easier to get such waivers approved: If enacted, the legislation would give default approval of such waivers and allow just 60 days for the Department of Health & Human Services to deny waiver request.
States would be able to apply for a waiver from the essential health benefits requirements for the 2020 plan year and a waiver to charge higher premiums to certain individuals for the 2019 plan year.
Waivers to change the essential health benefits package would need to meet one or more of the following conditions:
- Reduce average premiums.
- Increase enrollment.
- Stabilize the health insurance market.
- Stabilize premiums for individuals with preexisting conditions.
- Increase consumer choice.
For a state to change community rating provisions, its waiver also would need to create a mechanism, such as high-risk pools, to help those patients. Funding for these pools is provided for in the AHCA, but has been criticized as being inadequate on a national level.
Mr. Cannon of the Cato Institute predicted that such waivers ultimately would lead to more adverse selections for people needing comprehensive coverage and could force more people to lose coverage than to gain access to affordable, high-quality plans.
“If you waive essential health benefits in a community-rated market, you get even more adverse selection against comprehensive plans that sick people want, so those plans disappear,” Mr. Cannon said. “They either disappear because the insurers stop offering them or they disappear because insurers try to make the coverage worse, because Obamacare penalizes them if they don’t make coverage worse.”
He said these waivers provide little incentive for health insurers to stay in the individual markets and they could, as they are already, flee the individual markets.
The AHCA is phase 1 of the GOP repeal and replace plan. Congressional Republicans want to use the budget reconciliation process for the AHCA, so that they need only a simple majority to change revenue-generating provisions of the ACA. Phase 2 is a comprehensive review of all federal health care regulations and phase 3 is slated to be new legislation to replace the ACA with a new health care reform plan, which will require a two-thirds majority in the Senate to pass.
Republicans are targeting two key consumer protections in their latest attempt to gain enough votes to pass the American Health Care Act, phase 1 of their Affordable Care Act repeal and replace plan.
On the chopping block are the essential health care benefits package and so-called community rating provisions – which prevent insurers from charging significantly more for older patients and those with preexisting conditions.
“Obamacare is already in a race to the bottom in terms of quality coverage for the sick and that’s because of the law’s community rating provisions, which penalize high-quality coverage for the sick,” Michael F. Cannon, director of health policy studies at the Cato Institute, said in an interview. “The [AHCA] would arguably accelerate that race to the bottom. The waiver provision in this amendment definitely would and it would because the bill would allow states to waive the community rating provisions, but only for people who were not previously insured.”
The waiver provisions would “increase premiums for the previously uninsured and discourage them from enrolling,” Mr. Cannon predicted.
David Anderson, research associate at the Margolis Center for Health Policy at Duke University, Durham, N.C., said that, if a state elects to take a waiver, so-called high-cost patients “such as individuals with cancer, individuals with cystic fibrosis, individuals with coagulation disorders, [would be] shrugged to the side into a high-cost risk pool or some kind of risk sharing ... with their own premium pool.” This could lower premium costs for healthy patients, he added.
This could be enhanced by narrowing the essential health benefits. For example, Mr. Anderson said that a state could keep the drug benefit, but apply for a waiver to narrow its coverage for all generics plus a limited list of brand names.
“Someone with cystic fibrosis with a $300,000-a-year medication will not have that covered and will be put in the high-cost risk pool,” Mr. Anderson said. “What it does is that it makes insurance cheaper for individuals who are highly unlikely to be high cost, and it makes it much more expensive for any individuals with known high-cost conditions.”
The draft amendment also would make it easier a whole lot easier to get such waivers approved: If enacted, the legislation would give default approval of such waivers and allow just 60 days for the Department of Health & Human Services to deny waiver request.
States would be able to apply for a waiver from the essential health benefits requirements for the 2020 plan year and a waiver to charge higher premiums to certain individuals for the 2019 plan year.
Waivers to change the essential health benefits package would need to meet one or more of the following conditions:
- Reduce average premiums.
- Increase enrollment.
- Stabilize the health insurance market.
- Stabilize premiums for individuals with preexisting conditions.
- Increase consumer choice.
For a state to change community rating provisions, its waiver also would need to create a mechanism, such as high-risk pools, to help those patients. Funding for these pools is provided for in the AHCA, but has been criticized as being inadequate on a national level.
Mr. Cannon of the Cato Institute predicted that such waivers ultimately would lead to more adverse selections for people needing comprehensive coverage and could force more people to lose coverage than to gain access to affordable, high-quality plans.
“If you waive essential health benefits in a community-rated market, you get even more adverse selection against comprehensive plans that sick people want, so those plans disappear,” Mr. Cannon said. “They either disappear because the insurers stop offering them or they disappear because insurers try to make the coverage worse, because Obamacare penalizes them if they don’t make coverage worse.”
He said these waivers provide little incentive for health insurers to stay in the individual markets and they could, as they are already, flee the individual markets.
The AHCA is phase 1 of the GOP repeal and replace plan. Congressional Republicans want to use the budget reconciliation process for the AHCA, so that they need only a simple majority to change revenue-generating provisions of the ACA. Phase 2 is a comprehensive review of all federal health care regulations and phase 3 is slated to be new legislation to replace the ACA with a new health care reform plan, which will require a two-thirds majority in the Senate to pass.
Republicans are targeting two key consumer protections in their latest attempt to gain enough votes to pass the American Health Care Act, phase 1 of their Affordable Care Act repeal and replace plan.
On the chopping block are the essential health care benefits package and so-called community rating provisions – which prevent insurers from charging significantly more for older patients and those with preexisting conditions.
“Obamacare is already in a race to the bottom in terms of quality coverage for the sick and that’s because of the law’s community rating provisions, which penalize high-quality coverage for the sick,” Michael F. Cannon, director of health policy studies at the Cato Institute, said in an interview. “The [AHCA] would arguably accelerate that race to the bottom. The waiver provision in this amendment definitely would and it would because the bill would allow states to waive the community rating provisions, but only for people who were not previously insured.”
The waiver provisions would “increase premiums for the previously uninsured and discourage them from enrolling,” Mr. Cannon predicted.
David Anderson, research associate at the Margolis Center for Health Policy at Duke University, Durham, N.C., said that, if a state elects to take a waiver, so-called high-cost patients “such as individuals with cancer, individuals with cystic fibrosis, individuals with coagulation disorders, [would be] shrugged to the side into a high-cost risk pool or some kind of risk sharing ... with their own premium pool.” This could lower premium costs for healthy patients, he added.
This could be enhanced by narrowing the essential health benefits. For example, Mr. Anderson said that a state could keep the drug benefit, but apply for a waiver to narrow its coverage for all generics plus a limited list of brand names.
“Someone with cystic fibrosis with a $300,000-a-year medication will not have that covered and will be put in the high-cost risk pool,” Mr. Anderson said. “What it does is that it makes insurance cheaper for individuals who are highly unlikely to be high cost, and it makes it much more expensive for any individuals with known high-cost conditions.”
The draft amendment also would make it easier a whole lot easier to get such waivers approved: If enacted, the legislation would give default approval of such waivers and allow just 60 days for the Department of Health & Human Services to deny waiver request.
States would be able to apply for a waiver from the essential health benefits requirements for the 2020 plan year and a waiver to charge higher premiums to certain individuals for the 2019 plan year.
Waivers to change the essential health benefits package would need to meet one or more of the following conditions:
- Reduce average premiums.
- Increase enrollment.
- Stabilize the health insurance market.
- Stabilize premiums for individuals with preexisting conditions.
- Increase consumer choice.
For a state to change community rating provisions, its waiver also would need to create a mechanism, such as high-risk pools, to help those patients. Funding for these pools is provided for in the AHCA, but has been criticized as being inadequate on a national level.
Mr. Cannon of the Cato Institute predicted that such waivers ultimately would lead to more adverse selections for people needing comprehensive coverage and could force more people to lose coverage than to gain access to affordable, high-quality plans.
“If you waive essential health benefits in a community-rated market, you get even more adverse selection against comprehensive plans that sick people want, so those plans disappear,” Mr. Cannon said. “They either disappear because the insurers stop offering them or they disappear because insurers try to make the coverage worse, because Obamacare penalizes them if they don’t make coverage worse.”
He said these waivers provide little incentive for health insurers to stay in the individual markets and they could, as they are already, flee the individual markets.
The AHCA is phase 1 of the GOP repeal and replace plan. Congressional Republicans want to use the budget reconciliation process for the AHCA, so that they need only a simple majority to change revenue-generating provisions of the ACA. Phase 2 is a comprehensive review of all federal health care regulations and phase 3 is slated to be new legislation to replace the ACA with a new health care reform plan, which will require a two-thirds majority in the Senate to pass.
VIDEO: Cannabidiol reduces convulsive seizures in Dravet syndrome
BOSTON – Adjunctive treatment with cannabidiol significantly reduced convulsive seizure frequency in Dravet syndrome patients in a randomized, double-blind, placebo-controlled trial.
Over a 14-week treatment period, including 2 weeks of titration and 12 weeks of maintenance, convulsive seizure frequency in 61 treated children and adolescents decreased from a median of 12.4 to 5.9 per month (median reduction of 39%), compared with a decrease from a median of 14.9 to 14.1 per month (median reduction of 13%) in 59 patients who received placebo, J. Helen Cross, MD, reported at the annual meeting of the American Academy of Neurology.
The proportion of patients with at least a 50% reduction in convulsive seizures was 42.6% with cannabidiol vs. 27.1% with placebo (odds ratio, 2.0), but this difference did not reach statistical significance, said Dr. Cross of the University College London Great Ormond Street Institute of Child Health and the Great Ormond Street Hospital for Children NHS Trust, London.
In a video interview, Dr. Cross discussed the findings and the importance of improving seizure control in patients with Dravet syndrome, a rare infantile-onset developmental and epileptic encephalopathy with very poor prognosis for long-term seizure control and neurodevelopmental outcomes.
Participants in the study (GWPCARE1) had a mean age of 10 years, but nearly a third were younger than 6 years. All had Dravet syndrome and drug-resistant seizures; the median number of antiepilepsy drugs previously tried was four, and the median number being used was three. Those randomized to the treatment group received cannabidiol oral solution up to 20 mg/kg per day.
Adverse events were common, occurring in 93.4% and 74.6% of treatment group and placebo group patients, respectively. But adverse events reported in the treatment group were mild or moderate in 84% of patients, and treatment was generally well tolerated.
“These are very complex patients with a high seizure burden... and therefore, to have another medication that looks as if it can be of benefit is really very exciting for this population,” Dr. Cross said, noting that cannabidiol was also shown in other studies presented at the AAN meeting (GWPCARE3 and GWPCARE4) to reduce seizure frequency in patients with Lennox-Gastaut syndrome.
GW Research sponsored the study. Dr. Cross is a member of the advisory boards for Eisai, GW Pharmaceuticals, Shire, and Zogenix.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
BOSTON – Adjunctive treatment with cannabidiol significantly reduced convulsive seizure frequency in Dravet syndrome patients in a randomized, double-blind, placebo-controlled trial.
Over a 14-week treatment period, including 2 weeks of titration and 12 weeks of maintenance, convulsive seizure frequency in 61 treated children and adolescents decreased from a median of 12.4 to 5.9 per month (median reduction of 39%), compared with a decrease from a median of 14.9 to 14.1 per month (median reduction of 13%) in 59 patients who received placebo, J. Helen Cross, MD, reported at the annual meeting of the American Academy of Neurology.
The proportion of patients with at least a 50% reduction in convulsive seizures was 42.6% with cannabidiol vs. 27.1% with placebo (odds ratio, 2.0), but this difference did not reach statistical significance, said Dr. Cross of the University College London Great Ormond Street Institute of Child Health and the Great Ormond Street Hospital for Children NHS Trust, London.
In a video interview, Dr. Cross discussed the findings and the importance of improving seizure control in patients with Dravet syndrome, a rare infantile-onset developmental and epileptic encephalopathy with very poor prognosis for long-term seizure control and neurodevelopmental outcomes.
Participants in the study (GWPCARE1) had a mean age of 10 years, but nearly a third were younger than 6 years. All had Dravet syndrome and drug-resistant seizures; the median number of antiepilepsy drugs previously tried was four, and the median number being used was three. Those randomized to the treatment group received cannabidiol oral solution up to 20 mg/kg per day.
Adverse events were common, occurring in 93.4% and 74.6% of treatment group and placebo group patients, respectively. But adverse events reported in the treatment group were mild or moderate in 84% of patients, and treatment was generally well tolerated.
“These are very complex patients with a high seizure burden... and therefore, to have another medication that looks as if it can be of benefit is really very exciting for this population,” Dr. Cross said, noting that cannabidiol was also shown in other studies presented at the AAN meeting (GWPCARE3 and GWPCARE4) to reduce seizure frequency in patients with Lennox-Gastaut syndrome.
GW Research sponsored the study. Dr. Cross is a member of the advisory boards for Eisai, GW Pharmaceuticals, Shire, and Zogenix.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
BOSTON – Adjunctive treatment with cannabidiol significantly reduced convulsive seizure frequency in Dravet syndrome patients in a randomized, double-blind, placebo-controlled trial.
Over a 14-week treatment period, including 2 weeks of titration and 12 weeks of maintenance, convulsive seizure frequency in 61 treated children and adolescents decreased from a median of 12.4 to 5.9 per month (median reduction of 39%), compared with a decrease from a median of 14.9 to 14.1 per month (median reduction of 13%) in 59 patients who received placebo, J. Helen Cross, MD, reported at the annual meeting of the American Academy of Neurology.
The proportion of patients with at least a 50% reduction in convulsive seizures was 42.6% with cannabidiol vs. 27.1% with placebo (odds ratio, 2.0), but this difference did not reach statistical significance, said Dr. Cross of the University College London Great Ormond Street Institute of Child Health and the Great Ormond Street Hospital for Children NHS Trust, London.
In a video interview, Dr. Cross discussed the findings and the importance of improving seizure control in patients with Dravet syndrome, a rare infantile-onset developmental and epileptic encephalopathy with very poor prognosis for long-term seizure control and neurodevelopmental outcomes.
Participants in the study (GWPCARE1) had a mean age of 10 years, but nearly a third were younger than 6 years. All had Dravet syndrome and drug-resistant seizures; the median number of antiepilepsy drugs previously tried was four, and the median number being used was three. Those randomized to the treatment group received cannabidiol oral solution up to 20 mg/kg per day.
Adverse events were common, occurring in 93.4% and 74.6% of treatment group and placebo group patients, respectively. But adverse events reported in the treatment group were mild or moderate in 84% of patients, and treatment was generally well tolerated.
“These are very complex patients with a high seizure burden... and therefore, to have another medication that looks as if it can be of benefit is really very exciting for this population,” Dr. Cross said, noting that cannabidiol was also shown in other studies presented at the AAN meeting (GWPCARE3 and GWPCARE4) to reduce seizure frequency in patients with Lennox-Gastaut syndrome.
GW Research sponsored the study. Dr. Cross is a member of the advisory boards for Eisai, GW Pharmaceuticals, Shire, and Zogenix.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
At ANN 2017
Key clinical point:
Major finding: Children and adolescents treated with cannabidiol had a decline in convulsive seizure frequency, from a median of 12.4 to 5.9 per month (median reduction of 39%), compared with a decrease from a median of 14.9 to 14.1 per month with placebo (median reduction of 13%).
Data source: A randomized, double-blind, placebo-controlled trial of adjunctive treatment with cannabidiol in 120 children and adolescents with Dravet syndrome.
Disclosures: GW Research sponsored the study. Dr. Cross is a member of the advisory boards for Eisai, GW Pharmaceuticals, Shire, and Zogenix.

Kids with MS face higher risk of mental disorders
BOSTON – Children with multiple sclerosis (MS) and related conditions are as much as 10 times more likely than the general population to need to be hospitalized for various psychiatric conditions, a study showed.
“The true prevalence of morbidity is almost certainly higher than suggested by our data,” said study lead author Julia Pakpoor, BM BCh, who presented data from her research at the annual meeting of the American Academy of Neurology.
While several studies have examined links between MS and mental illness in adults, there’s been little research into the topic in children. The number of children with the disease is far from tiny, however. According to the National MS Society, an estimated 8,000-10,000 children have the condition in the United States.
The researchers tracked future psychiatric visits by these patients and compared them with a reference cohort of more than 1.1 million children.
The risks of mental conditions in children with MS, compared with the reference cohort, were as follows: psychotic disorders (relative risk [RR] = 10.76; 95% confidence interval [CI], 2.93-27.63; P less than .001), mood disorders (RR = 2.57; 95% CI, 1.03-5.31; P = .022), and intellectual disability (RR = 6.08; 95% CI, 1.25-17.80; P = .004).
The children with other CNS demyelinating diseases also had higher risk levels, compared with the reference cohort: psychotic disorders (RR = 5.77; 95% CI, 2.48-11.41; P less than .001), anxiety, stress-related, and somatoform disorders that cause symptoms like pain (RR = 2.38; 95% CI, 1.39-3.81; P less than .001); intellectual disability (RR = 6.56; 95% CI, 3.66-10.84; P less than .001), and other behavioral disorders (RR = 8.99; 95% CI, 5.13-14.62; P less than .001).
The researchers also reported evidence of a reverse trend. Children with several mental conditions had greater risk than did the reference cohort to go on to develop CNS demyelinating diseases, specifically anxiety, stress-related, and somatoform disorders (RR = 3.15; 95% CI, 1.70-5.39; P less than .001), ADHD (RR = 3.88; 95% CI, 1.75-7.48; P less than .001), autism (RR = 3.80; 95% CI, 2.05-6.50; P less than .001), intellectual disability (RR = 6.33; 95% CI, 2.86-12.21; P less than .001), and other behavioral disorders (RR = 8.30; 95% CI, 5.17-12.75; P less than .001).
“We detected strong associations, and further associations likely exist,” Dr. Pakpoor said.
She acknowledged that the research is limited because it includes information only about patients admitted to a hospital. “There may be many more with psychiatric conditions that are mild,” she said. “We’re probably detecting cases that are more severe.”
In an interview, Flavia M. Nelson, MD, interim chief of the multiple sclerosis division at the University of Texas Health Science Center at Houston, said she often sees psychiatric conditions in her pediatric patients.
Conditions such as depression and anxiety disorders are common, she said, and the pediatric patients often suffer from isolation. “There’s a lot of fear about what this will do to their lives,” she said. Some patients have even refused to go to college because they fear that “they’ll have a disabling attack and everyone will know.”
As for the link between psychiatric illness and MS, Dr. Nelson said the disorders may develop because stress, fear, and anxiety push young people to their limits. “I had one patient who developed tics and rage,” she said. “That was his way of coping with the disease.”
Dr. Nelson suggested doing cognitive testing on young patients and referring them to counseling, especially in light of the fact that teens often put up walls when they don’t know how to express their feelings. Simply asking questions may not be enough to draw them out, she said, so professional counseling can be helpful.
No specific funding was reported. Dr. Pakpoor reported no relevant disclosures. Dr. Nelson has received personal compensation for activities with Bayer, Sanofi-Genzyme, Genentech, Novartis, Teva, and the Consortium of Multiple Sclerosis Centers. She has received research support from the National Institutes of Health, the National MS Society, and Novartis.
BOSTON – Children with multiple sclerosis (MS) and related conditions are as much as 10 times more likely than the general population to need to be hospitalized for various psychiatric conditions, a study showed.
“The true prevalence of morbidity is almost certainly higher than suggested by our data,” said study lead author Julia Pakpoor, BM BCh, who presented data from her research at the annual meeting of the American Academy of Neurology.
While several studies have examined links between MS and mental illness in adults, there’s been little research into the topic in children. The number of children with the disease is far from tiny, however. According to the National MS Society, an estimated 8,000-10,000 children have the condition in the United States.
The researchers tracked future psychiatric visits by these patients and compared them with a reference cohort of more than 1.1 million children.
The risks of mental conditions in children with MS, compared with the reference cohort, were as follows: psychotic disorders (relative risk [RR] = 10.76; 95% confidence interval [CI], 2.93-27.63; P less than .001), mood disorders (RR = 2.57; 95% CI, 1.03-5.31; P = .022), and intellectual disability (RR = 6.08; 95% CI, 1.25-17.80; P = .004).
The children with other CNS demyelinating diseases also had higher risk levels, compared with the reference cohort: psychotic disorders (RR = 5.77; 95% CI, 2.48-11.41; P less than .001), anxiety, stress-related, and somatoform disorders that cause symptoms like pain (RR = 2.38; 95% CI, 1.39-3.81; P less than .001); intellectual disability (RR = 6.56; 95% CI, 3.66-10.84; P less than .001), and other behavioral disorders (RR = 8.99; 95% CI, 5.13-14.62; P less than .001).
The researchers also reported evidence of a reverse trend. Children with several mental conditions had greater risk than did the reference cohort to go on to develop CNS demyelinating diseases, specifically anxiety, stress-related, and somatoform disorders (RR = 3.15; 95% CI, 1.70-5.39; P less than .001), ADHD (RR = 3.88; 95% CI, 1.75-7.48; P less than .001), autism (RR = 3.80; 95% CI, 2.05-6.50; P less than .001), intellectual disability (RR = 6.33; 95% CI, 2.86-12.21; P less than .001), and other behavioral disorders (RR = 8.30; 95% CI, 5.17-12.75; P less than .001).
“We detected strong associations, and further associations likely exist,” Dr. Pakpoor said.
She acknowledged that the research is limited because it includes information only about patients admitted to a hospital. “There may be many more with psychiatric conditions that are mild,” she said. “We’re probably detecting cases that are more severe.”
In an interview, Flavia M. Nelson, MD, interim chief of the multiple sclerosis division at the University of Texas Health Science Center at Houston, said she often sees psychiatric conditions in her pediatric patients.
Conditions such as depression and anxiety disorders are common, she said, and the pediatric patients often suffer from isolation. “There’s a lot of fear about what this will do to their lives,” she said. Some patients have even refused to go to college because they fear that “they’ll have a disabling attack and everyone will know.”
As for the link between psychiatric illness and MS, Dr. Nelson said the disorders may develop because stress, fear, and anxiety push young people to their limits. “I had one patient who developed tics and rage,” she said. “That was his way of coping with the disease.”
Dr. Nelson suggested doing cognitive testing on young patients and referring them to counseling, especially in light of the fact that teens often put up walls when they don’t know how to express their feelings. Simply asking questions may not be enough to draw them out, she said, so professional counseling can be helpful.
No specific funding was reported. Dr. Pakpoor reported no relevant disclosures. Dr. Nelson has received personal compensation for activities with Bayer, Sanofi-Genzyme, Genentech, Novartis, Teva, and the Consortium of Multiple Sclerosis Centers. She has received research support from the National Institutes of Health, the National MS Society, and Novartis.
BOSTON – Children with multiple sclerosis (MS) and related conditions are as much as 10 times more likely than the general population to need to be hospitalized for various psychiatric conditions, a study showed.
“The true prevalence of morbidity is almost certainly higher than suggested by our data,” said study lead author Julia Pakpoor, BM BCh, who presented data from her research at the annual meeting of the American Academy of Neurology.
While several studies have examined links between MS and mental illness in adults, there’s been little research into the topic in children. The number of children with the disease is far from tiny, however. According to the National MS Society, an estimated 8,000-10,000 children have the condition in the United States.
The researchers tracked future psychiatric visits by these patients and compared them with a reference cohort of more than 1.1 million children.
The risks of mental conditions in children with MS, compared with the reference cohort, were as follows: psychotic disorders (relative risk [RR] = 10.76; 95% confidence interval [CI], 2.93-27.63; P less than .001), mood disorders (RR = 2.57; 95% CI, 1.03-5.31; P = .022), and intellectual disability (RR = 6.08; 95% CI, 1.25-17.80; P = .004).
The children with other CNS demyelinating diseases also had higher risk levels, compared with the reference cohort: psychotic disorders (RR = 5.77; 95% CI, 2.48-11.41; P less than .001), anxiety, stress-related, and somatoform disorders that cause symptoms like pain (RR = 2.38; 95% CI, 1.39-3.81; P less than .001); intellectual disability (RR = 6.56; 95% CI, 3.66-10.84; P less than .001), and other behavioral disorders (RR = 8.99; 95% CI, 5.13-14.62; P less than .001).
The researchers also reported evidence of a reverse trend. Children with several mental conditions had greater risk than did the reference cohort to go on to develop CNS demyelinating diseases, specifically anxiety, stress-related, and somatoform disorders (RR = 3.15; 95% CI, 1.70-5.39; P less than .001), ADHD (RR = 3.88; 95% CI, 1.75-7.48; P less than .001), autism (RR = 3.80; 95% CI, 2.05-6.50; P less than .001), intellectual disability (RR = 6.33; 95% CI, 2.86-12.21; P less than .001), and other behavioral disorders (RR = 8.30; 95% CI, 5.17-12.75; P less than .001).
“We detected strong associations, and further associations likely exist,” Dr. Pakpoor said.
She acknowledged that the research is limited because it includes information only about patients admitted to a hospital. “There may be many more with psychiatric conditions that are mild,” she said. “We’re probably detecting cases that are more severe.”
In an interview, Flavia M. Nelson, MD, interim chief of the multiple sclerosis division at the University of Texas Health Science Center at Houston, said she often sees psychiatric conditions in her pediatric patients.
Conditions such as depression and anxiety disorders are common, she said, and the pediatric patients often suffer from isolation. “There’s a lot of fear about what this will do to their lives,” she said. Some patients have even refused to go to college because they fear that “they’ll have a disabling attack and everyone will know.”
As for the link between psychiatric illness and MS, Dr. Nelson said the disorders may develop because stress, fear, and anxiety push young people to their limits. “I had one patient who developed tics and rage,” she said. “That was his way of coping with the disease.”
Dr. Nelson suggested doing cognitive testing on young patients and referring them to counseling, especially in light of the fact that teens often put up walls when they don’t know how to express their feelings. Simply asking questions may not be enough to draw them out, she said, so professional counseling can be helpful.
No specific funding was reported. Dr. Pakpoor reported no relevant disclosures. Dr. Nelson has received personal compensation for activities with Bayer, Sanofi-Genzyme, Genentech, Novartis, Teva, and the Consortium of Multiple Sclerosis Centers. She has received research support from the National Institutes of Health, the National MS Society, and Novartis.
Key clinical point: Children with MS and similar conditions are at higher risk of a long list of psychiatric disorders.
Major finding:
Data source: An analysis of children admitted to hospitals in England from 1999 to 2011 with MS (n = 201) and other CNS demyelinating diseases (n = 1,097) plus a reference cohort of more than 1.1 million.
Disclosures: No specific funding or disclosures were reported.
Study reveals crazy quilt of laser laws across the United States
SAN DIEGO – Laser hair removal isn’t typically in an office cleaner’s job description. So it’s no wonder that Virginia legislators were spooked when they heard from a constituent who was treated by a spa worker who turned out to be a janitor.
Earlier this year, legislators in the Old Dominion passed a bill limiting laser hair removal procedures to a “properly trained” medical doctor, physician assistant, or nurse practitioner – or a “properly trained” person who is supervised by one of these professionals. Therefore, it’s still possible for a “properly trained” person without a degree of any kind to operate a laser in Virginia.
To the north in New Jersey, the rules are much stricter: Only physicians can perform laser procedures. But in New York, it appears that anyone can fire up a laser and go to work on unwanted hair. And in Florida, nonphysicians can perform laser procedures only if they’re physician assistants or nurse practitioners. But they’re only allowed to remove hair with lasers at a clinic that just performs laser hair removal.
Such is the chaotic state of laser law in the United States, a new study finds. The rules, which vary widely from state to state, are often vague and confusing. And, as Virginia’s new law shows, they’re still evolving. (The study is current as of March 2016.)

She and study coauthor Mathew M. Avram, MD, JD, director of the Laser and Cosmetic Center at Massachusetts General, analyzed regulations in the 50 states regarding the operation of lasers. They reported their findings at the annual meeting of the American Society for Laser Medicine and Surgery.
Dr. DiGiorgio said that laser operator laws address three issues:
1. Who can operate a laser?
At other clinics across the country, nonphysician employees — such as nurse practitioners and registered nurses – often operate lasers. Whether they can legally actually do so isn’t always obvious.
New Jersey is the only state that requires laser operators to be physicians. At the other extreme, 11 states, including Massachusetts, Colorado, Florida, Missouri, New York, and Pennsylvania, have “no” limits on who can perform laser procedures. (At Massachusetts General Hospital, physicians perform all laser procedures.)
So does that mean anyone can perform a laser procedure? It’s not clear. “The laws are a lot more vague than they should be,” Dr. DiGiorgio said in an interview.
Eighteen states allow people to perform laser procedures as part of the “practice of medicine,” although legislation can be vague on what that means. Those states include Illinois, Michigan, Minnesota, North Carolina, and Texas.
Another 19 states, including California, Ohio, Washington, Wisconsin, and now Virginia, have specific limits on who can perform laser procedures. In California, for example, physician assistants and registered nurses – but not licensed vocational nurses – are allowed to use lasers to remove hair, spider veins, and tattoos. Unlicensed medical assistants, cosmetologists, electrologists, and estheticians are not allowed to perform the procedures
2. Can someone delegate laser procedures to someone else?
In nine states, including Iowa and New Hampshire, there’s no oversight of delegation or nonphysicians can delegate procedures to someone else.
In another nine states, certain procedures can be delegated with no physician oversight, such as laser hair removal in Alaska and ablative procedures (to advanced practice registered nurses only) in Utah.
3. Is supervision required of nonphysicians?
Physicians don’t need to supervise certain laser procedures in 11 states, including Hawaii, Oregon, and Vermont, where they can be performed by a nonphysician with no supervision or under supervision by a non-physician.
In 17 states, supervision isn’t always required or it’s under the discretion of the supervising physician. These states include California, Michigan, Pennsylvania, and Wisconsin.
In 11 states, including Illinois and Massachusetts, only certain procedures require on-site supervision. Six states, including Connecticut and Maryland, require on-site physician supervision for all laser procedures, but Dr. DiGiorgio said the requirements can be vague about what “on site” actually means.
Idaho requires the physician to be on site or immediately available, and South Carolina allows registered nurses to perform laser hair and leg vein removal if a physician is on site and can respond within 5 minutes.
“We don’t know what the ideal regulation is,” Dr. DiGiorgio said. But she believes laser regulations are crucial to safety, especially as fields such as plastic surgery, ophthalmology, and gynecology embrace cosmetic laser procedures.
Information about state-by-state laser operator laws is available on the American Med Spa Association website.
Dr. DiGiorgio reported no relevant disclosures.
SAN DIEGO – Laser hair removal isn’t typically in an office cleaner’s job description. So it’s no wonder that Virginia legislators were spooked when they heard from a constituent who was treated by a spa worker who turned out to be a janitor.
Earlier this year, legislators in the Old Dominion passed a bill limiting laser hair removal procedures to a “properly trained” medical doctor, physician assistant, or nurse practitioner – or a “properly trained” person who is supervised by one of these professionals. Therefore, it’s still possible for a “properly trained” person without a degree of any kind to operate a laser in Virginia.
To the north in New Jersey, the rules are much stricter: Only physicians can perform laser procedures. But in New York, it appears that anyone can fire up a laser and go to work on unwanted hair. And in Florida, nonphysicians can perform laser procedures only if they’re physician assistants or nurse practitioners. But they’re only allowed to remove hair with lasers at a clinic that just performs laser hair removal.
Such is the chaotic state of laser law in the United States, a new study finds. The rules, which vary widely from state to state, are often vague and confusing. And, as Virginia’s new law shows, they’re still evolving. (The study is current as of March 2016.)
She and study coauthor Mathew M. Avram, MD, JD, director of the Laser and Cosmetic Center at Massachusetts General, analyzed regulations in the 50 states regarding the operation of lasers. They reported their findings at the annual meeting of the American Society for Laser Medicine and Surgery.
Dr. DiGiorgio said that laser operator laws address three issues:
1. Who can operate a laser?
At other clinics across the country, nonphysician employees — such as nurse practitioners and registered nurses – often operate lasers. Whether they can legally actually do so isn’t always obvious.
New Jersey is the only state that requires laser operators to be physicians. At the other extreme, 11 states, including Massachusetts, Colorado, Florida, Missouri, New York, and Pennsylvania, have “no” limits on who can perform laser procedures. (At Massachusetts General Hospital, physicians perform all laser procedures.)
So does that mean anyone can perform a laser procedure? It’s not clear. “The laws are a lot more vague than they should be,” Dr. DiGiorgio said in an interview.
Eighteen states allow people to perform laser procedures as part of the “practice of medicine,” although legislation can be vague on what that means. Those states include Illinois, Michigan, Minnesota, North Carolina, and Texas.
Another 19 states, including California, Ohio, Washington, Wisconsin, and now Virginia, have specific limits on who can perform laser procedures. In California, for example, physician assistants and registered nurses – but not licensed vocational nurses – are allowed to use lasers to remove hair, spider veins, and tattoos. Unlicensed medical assistants, cosmetologists, electrologists, and estheticians are not allowed to perform the procedures
2. Can someone delegate laser procedures to someone else?
In nine states, including Iowa and New Hampshire, there’s no oversight of delegation or nonphysicians can delegate procedures to someone else.
In another nine states, certain procedures can be delegated with no physician oversight, such as laser hair removal in Alaska and ablative procedures (to advanced practice registered nurses only) in Utah.
3. Is supervision required of nonphysicians?
Physicians don’t need to supervise certain laser procedures in 11 states, including Hawaii, Oregon, and Vermont, where they can be performed by a nonphysician with no supervision or under supervision by a non-physician.
In 17 states, supervision isn’t always required or it’s under the discretion of the supervising physician. These states include California, Michigan, Pennsylvania, and Wisconsin.
In 11 states, including Illinois and Massachusetts, only certain procedures require on-site supervision. Six states, including Connecticut and Maryland, require on-site physician supervision for all laser procedures, but Dr. DiGiorgio said the requirements can be vague about what “on site” actually means.
Idaho requires the physician to be on site or immediately available, and South Carolina allows registered nurses to perform laser hair and leg vein removal if a physician is on site and can respond within 5 minutes.
“We don’t know what the ideal regulation is,” Dr. DiGiorgio said. But she believes laser regulations are crucial to safety, especially as fields such as plastic surgery, ophthalmology, and gynecology embrace cosmetic laser procedures.
Information about state-by-state laser operator laws is available on the American Med Spa Association website.
Dr. DiGiorgio reported no relevant disclosures.
SAN DIEGO – Laser hair removal isn’t typically in an office cleaner’s job description. So it’s no wonder that Virginia legislators were spooked when they heard from a constituent who was treated by a spa worker who turned out to be a janitor.
Earlier this year, legislators in the Old Dominion passed a bill limiting laser hair removal procedures to a “properly trained” medical doctor, physician assistant, or nurse practitioner – or a “properly trained” person who is supervised by one of these professionals. Therefore, it’s still possible for a “properly trained” person without a degree of any kind to operate a laser in Virginia.
To the north in New Jersey, the rules are much stricter: Only physicians can perform laser procedures. But in New York, it appears that anyone can fire up a laser and go to work on unwanted hair. And in Florida, nonphysicians can perform laser procedures only if they’re physician assistants or nurse practitioners. But they’re only allowed to remove hair with lasers at a clinic that just performs laser hair removal.
Such is the chaotic state of laser law in the United States, a new study finds. The rules, which vary widely from state to state, are often vague and confusing. And, as Virginia’s new law shows, they’re still evolving. (The study is current as of March 2016.)
She and study coauthor Mathew M. Avram, MD, JD, director of the Laser and Cosmetic Center at Massachusetts General, analyzed regulations in the 50 states regarding the operation of lasers. They reported their findings at the annual meeting of the American Society for Laser Medicine and Surgery.
Dr. DiGiorgio said that laser operator laws address three issues:
1. Who can operate a laser?
At other clinics across the country, nonphysician employees — such as nurse practitioners and registered nurses – often operate lasers. Whether they can legally actually do so isn’t always obvious.
New Jersey is the only state that requires laser operators to be physicians. At the other extreme, 11 states, including Massachusetts, Colorado, Florida, Missouri, New York, and Pennsylvania, have “no” limits on who can perform laser procedures. (At Massachusetts General Hospital, physicians perform all laser procedures.)
So does that mean anyone can perform a laser procedure? It’s not clear. “The laws are a lot more vague than they should be,” Dr. DiGiorgio said in an interview.
Eighteen states allow people to perform laser procedures as part of the “practice of medicine,” although legislation can be vague on what that means. Those states include Illinois, Michigan, Minnesota, North Carolina, and Texas.
Another 19 states, including California, Ohio, Washington, Wisconsin, and now Virginia, have specific limits on who can perform laser procedures. In California, for example, physician assistants and registered nurses – but not licensed vocational nurses – are allowed to use lasers to remove hair, spider veins, and tattoos. Unlicensed medical assistants, cosmetologists, electrologists, and estheticians are not allowed to perform the procedures
2. Can someone delegate laser procedures to someone else?
In nine states, including Iowa and New Hampshire, there’s no oversight of delegation or nonphysicians can delegate procedures to someone else.
In another nine states, certain procedures can be delegated with no physician oversight, such as laser hair removal in Alaska and ablative procedures (to advanced practice registered nurses only) in Utah.
3. Is supervision required of nonphysicians?
Physicians don’t need to supervise certain laser procedures in 11 states, including Hawaii, Oregon, and Vermont, where they can be performed by a nonphysician with no supervision or under supervision by a non-physician.
In 17 states, supervision isn’t always required or it’s under the discretion of the supervising physician. These states include California, Michigan, Pennsylvania, and Wisconsin.
In 11 states, including Illinois and Massachusetts, only certain procedures require on-site supervision. Six states, including Connecticut and Maryland, require on-site physician supervision for all laser procedures, but Dr. DiGiorgio said the requirements can be vague about what “on site” actually means.
Idaho requires the physician to be on site or immediately available, and South Carolina allows registered nurses to perform laser hair and leg vein removal if a physician is on site and can respond within 5 minutes.
“We don’t know what the ideal regulation is,” Dr. DiGiorgio said. But she believes laser regulations are crucial to safety, especially as fields such as plastic surgery, ophthalmology, and gynecology embrace cosmetic laser procedures.
Information about state-by-state laser operator laws is available on the American Med Spa Association website.
Dr. DiGiorgio reported no relevant disclosures.
AT LASER 2017
Key clinical point:
Major finding: The study found wide variations in who can operate lasers, and in regulations regarding the delegation and supervision of laser treatments in the different states.
Data source: Analysis of regulations in the 50 states regarding the operation of lasers.
Disclosures: Dr. DiGiorgio reported no relevant disclosures