User login
Diagnostic testing in AKI: Let’s move the field forward
In this issue of the Journal of Hospital Medicine, Lusica et al.1 discuss the utility of urine eosinophils (UEs) in evaluating for acute interstitial nephritis (AIN) in patients with acute kidney injury (AKI), an important and oft-confused concern in medicine. I can’t think of a more appropriate topic for the “Things We Do for No Reason” (TWDFNR) series. Numerous tests are ordered in the evaluation of AKI.2 Many, such as batteries of serological tests, are unnecessary and add little diagnostic information. Some, such as UEs and fractional excretion of sodium (FENa), provide misinformation. And others, such as contrast-enhanced computed tomography scans, are potentially harmful.2 In a previous TWDFNR article, the limitations of FENa in the evaluation of AKI were reviewed.3 There are common threads linking the shortcomings of UEs and FENa and even new diagnostic tests. What are the lessons from these studies, and how might clinicians best apply them in their practice?
As reviewed in this issue, UE testing is employed in AKI to evaluate for hospital-acquired AIN. Small initial studies led to widespread use of this test, despite methodological flaws.4 A later, definitive study involving 566 patients who had both UEs and kidney biopsies performed within the same week demonstrated that UEs offered no diagnostic value in AKI.5 The same pattern occurred in the increased use of FENa to distinguish prerenal azotemia from acute tubular necrosis in AKI patients.3 Small studies in highly select patients supported its use for this purpose.6 Subsequently, larger studies in more diverse populations noted that FENa was associated with many false positive and negative results,6 likely due to more widespread use of this test in disease states such as cirrhosis, congestive heart failure, chronic kidney disease, and diabetes, which were not included in initial studies.
It is apparent that clinicians have been led astray by small, flawed positive studies employed in highly selected populations. These initial positive studies based on excessively large effect size estimates were subsequently shown to be negative in larger studies with more plausible effect sizes. Examples of this error are seen in publications involving prophylactic measures to reduce contrast nephrotoxicity.7 Early studies on N-acetylcysteine administration prior to radiocontrast exposure showed positive results. Examination of these studies, however, demonstrates 2 key problems: 1) inclusion of small numbers of patients due to power calculations based on excessively large effect sizes, and 2) use of clinically unimportant endpoints such as serum creatinine changes.7 The same issue complicates studies evaluating isotonic sodium bicarbonate vs. normal saline for contrast prophylaxis.7
The past 10-plus years have seen a proliferation of studies evaluating the utility of novel biomarkers for early diagnosis and prognosis in AKI. Have we fallen down the same rabbit hole in evaluating these new diagnostic tests for AKI? There is reason for concern if we examine published studies of novel biomarkers in other areas of medicine. To this point, many highly cited novel biomarker studies used for various diagnostic purposes (eg, cancer, infection, cardiovascular disease) employed excessively large effect size estimates for postulated associations that resulted in small, underpowered studies with initially positive results.8 Subsequent large studies and meta-analyses reported negative or modestly positive test results when examining these same associations.8 But we may be moving in the right direction. An early urine biomarker publication from a small, single center study9 revealed overly optimistic results (area under the curve [AUC], 0.998; sensitivity, 100%; specificity, 98%) for AKI prediction. Subsequent large, multicenter biomarker studies showed only modest improvement in their discriminative value when compared with traditional clinical models.10 These results precluded U.S. Food and Drug Administration (FDA) approval of most novel biomarkers for clinical practice and they were not adopted. In 2014, the FDA approved the point-of-care urinary biomarker TIMP-2/IGFBP7 (NephroCheck®) for predicting risk of AKI based on fairly rigorous testing using larger numbers of patients, heterogeneous populations, and important clinical endpoints.11 In a 522-patient discovery cohort, this biomarker had an AUC of 0.80 for AKI prediction, which was validated in a 722-patient cohort and subsequently followed by a 420-patient multicenter cohort study revealing similar test characteristics (AUC, 0.82; sensitivity, 92%; specificity, 46%).11 A study involving 382 critically ill AKI patients noted that this biomarker had a hazard ratio of 2.16 (95% confidence interval [CI] 1.32 to 3.53) for predict
In summary, clinicians should be aware of the strengths and limitations of diagnostic tests ordered in AKI patients, as seen with the overly optimistic results in small, flawed UE and FENa studies. While we have taken a step in the right direction with diagnostic and prognostic biomarkers for AKI, we must apply rigorous study design to diagnostic tests under evaluation before adopting them into clinical practice. Only then can we move the field forward and improve patient care.
Disclosure
Nothing to report.
1. Lusica M, Rondon-Berrios H, Feldman L. Urine eosinophils for acute interstitial nephritis. J Hosp Med. 2017;12(5):343-345. PubMed
2. Leaf DE, Srivastava A, Zeng X, et al. Excessive diagnostic testing in acute kidney injury. BMC Nephrol. 2016;17:9. PubMed
3. Pahwa AK, Sperati CJ. Urinary fractional excretion indices in the evaluation of acute kidney injury. J Hosp Med. 2016;11(1):77-80. PubMed
4. Perazella MA, Bomback AS. Urinary eosinophils in AIN: farewell to an old biomarker? Clin J Am Soc Nephrol. 2013;8(11):1841-1843. PubMed
5. Muriithi AK, Nasr SH, Leung N. Utility of urine eosinophils in the diagnosis of acute interstitial nephritis. Clin J Am Soc Nephrol. 2013;8(11):1857-1862. PubMed
6. Perazella MA, Coca SG. Traditional urinary biomarkers in the assessment of hospital-acquired AKI. Clin J Am Soc Nephrol. 2012;7(1):167-174. PubMed
7. Weisbord SD, Palevsky PM. Strategies for the prevention of contrast-induced acute kidney injury. Curr Opin Nephrol Hypertens. 2010;19(6):539-549. PubMed
8. Ioannidis JP, Panagiotou OA. Comparison of effect sizes associated with biomarkers reported in highly cited individual articles and in subsequent meta-analyses. JAMA. 2011;305(21):2200-2210. PubMed
9. Mishra J, Dent C, Tarabishi R, et al. Neutrophil gelatinase-associated lipocalin as a biomarker for acute renal injury after cardiac surgery. Lancet. 2005;365(9466):1231-1238. PubMed
10. Schaub JA, Parikh CR. Biomarkers of acute kidney injury and associations with short- and long-term outcomes. F1000Res. 2016;5(F1000 Faculty Rev.):986. PubMed
11. McMahon BA, Koyner JL. Risk stratification for acute kidney injury: Are biomarkers enough? Adv Chronic Kidney Dis. 2016;23(3):167-178. PubMed
In this issue of the Journal of Hospital Medicine, Lusica et al.1 discuss the utility of urine eosinophils (UEs) in evaluating for acute interstitial nephritis (AIN) in patients with acute kidney injury (AKI), an important and oft-confused concern in medicine. I can’t think of a more appropriate topic for the “Things We Do for No Reason” (TWDFNR) series. Numerous tests are ordered in the evaluation of AKI.2 Many, such as batteries of serological tests, are unnecessary and add little diagnostic information. Some, such as UEs and fractional excretion of sodium (FENa), provide misinformation. And others, such as contrast-enhanced computed tomography scans, are potentially harmful.2 In a previous TWDFNR article, the limitations of FENa in the evaluation of AKI were reviewed.3 There are common threads linking the shortcomings of UEs and FENa and even new diagnostic tests. What are the lessons from these studies, and how might clinicians best apply them in their practice?
As reviewed in this issue, UE testing is employed in AKI to evaluate for hospital-acquired AIN. Small initial studies led to widespread use of this test, despite methodological flaws.4 A later, definitive study involving 566 patients who had both UEs and kidney biopsies performed within the same week demonstrated that UEs offered no diagnostic value in AKI.5 The same pattern occurred in the increased use of FENa to distinguish prerenal azotemia from acute tubular necrosis in AKI patients.3 Small studies in highly select patients supported its use for this purpose.6 Subsequently, larger studies in more diverse populations noted that FENa was associated with many false positive and negative results,6 likely due to more widespread use of this test in disease states such as cirrhosis, congestive heart failure, chronic kidney disease, and diabetes, which were not included in initial studies.
It is apparent that clinicians have been led astray by small, flawed positive studies employed in highly selected populations. These initial positive studies based on excessively large effect size estimates were subsequently shown to be negative in larger studies with more plausible effect sizes. Examples of this error are seen in publications involving prophylactic measures to reduce contrast nephrotoxicity.7 Early studies on N-acetylcysteine administration prior to radiocontrast exposure showed positive results. Examination of these studies, however, demonstrates 2 key problems: 1) inclusion of small numbers of patients due to power calculations based on excessively large effect sizes, and 2) use of clinically unimportant endpoints such as serum creatinine changes.7 The same issue complicates studies evaluating isotonic sodium bicarbonate vs. normal saline for contrast prophylaxis.7
The past 10-plus years have seen a proliferation of studies evaluating the utility of novel biomarkers for early diagnosis and prognosis in AKI. Have we fallen down the same rabbit hole in evaluating these new diagnostic tests for AKI? There is reason for concern if we examine published studies of novel biomarkers in other areas of medicine. To this point, many highly cited novel biomarker studies used for various diagnostic purposes (eg, cancer, infection, cardiovascular disease) employed excessively large effect size estimates for postulated associations that resulted in small, underpowered studies with initially positive results.8 Subsequent large studies and meta-analyses reported negative or modestly positive test results when examining these same associations.8 But we may be moving in the right direction. An early urine biomarker publication from a small, single center study9 revealed overly optimistic results (area under the curve [AUC], 0.998; sensitivity, 100%; specificity, 98%) for AKI prediction. Subsequent large, multicenter biomarker studies showed only modest improvement in their discriminative value when compared with traditional clinical models.10 These results precluded U.S. Food and Drug Administration (FDA) approval of most novel biomarkers for clinical practice and they were not adopted. In 2014, the FDA approved the point-of-care urinary biomarker TIMP-2/IGFBP7 (NephroCheck®) for predicting risk of AKI based on fairly rigorous testing using larger numbers of patients, heterogeneous populations, and important clinical endpoints.11 In a 522-patient discovery cohort, this biomarker had an AUC of 0.80 for AKI prediction, which was validated in a 722-patient cohort and subsequently followed by a 420-patient multicenter cohort study revealing similar test characteristics (AUC, 0.82; sensitivity, 92%; specificity, 46%).11 A study involving 382 critically ill AKI patients noted that this biomarker had a hazard ratio of 2.16 (95% confidence interval [CI] 1.32 to 3.53) for predict
In summary, clinicians should be aware of the strengths and limitations of diagnostic tests ordered in AKI patients, as seen with the overly optimistic results in small, flawed UE and FENa studies. While we have taken a step in the right direction with diagnostic and prognostic biomarkers for AKI, we must apply rigorous study design to diagnostic tests under evaluation before adopting them into clinical practice. Only then can we move the field forward and improve patient care.
Disclosure
Nothing to report.
In this issue of the Journal of Hospital Medicine, Lusica et al.1 discuss the utility of urine eosinophils (UEs) in evaluating for acute interstitial nephritis (AIN) in patients with acute kidney injury (AKI), an important and oft-confused concern in medicine. I can’t think of a more appropriate topic for the “Things We Do for No Reason” (TWDFNR) series. Numerous tests are ordered in the evaluation of AKI.2 Many, such as batteries of serological tests, are unnecessary and add little diagnostic information. Some, such as UEs and fractional excretion of sodium (FENa), provide misinformation. And others, such as contrast-enhanced computed tomography scans, are potentially harmful.2 In a previous TWDFNR article, the limitations of FENa in the evaluation of AKI were reviewed.3 There are common threads linking the shortcomings of UEs and FENa and even new diagnostic tests. What are the lessons from these studies, and how might clinicians best apply them in their practice?
As reviewed in this issue, UE testing is employed in AKI to evaluate for hospital-acquired AIN. Small initial studies led to widespread use of this test, despite methodological flaws.4 A later, definitive study involving 566 patients who had both UEs and kidney biopsies performed within the same week demonstrated that UEs offered no diagnostic value in AKI.5 The same pattern occurred in the increased use of FENa to distinguish prerenal azotemia from acute tubular necrosis in AKI patients.3 Small studies in highly select patients supported its use for this purpose.6 Subsequently, larger studies in more diverse populations noted that FENa was associated with many false positive and negative results,6 likely due to more widespread use of this test in disease states such as cirrhosis, congestive heart failure, chronic kidney disease, and diabetes, which were not included in initial studies.
It is apparent that clinicians have been led astray by small, flawed positive studies employed in highly selected populations. These initial positive studies based on excessively large effect size estimates were subsequently shown to be negative in larger studies with more plausible effect sizes. Examples of this error are seen in publications involving prophylactic measures to reduce contrast nephrotoxicity.7 Early studies on N-acetylcysteine administration prior to radiocontrast exposure showed positive results. Examination of these studies, however, demonstrates 2 key problems: 1) inclusion of small numbers of patients due to power calculations based on excessively large effect sizes, and 2) use of clinically unimportant endpoints such as serum creatinine changes.7 The same issue complicates studies evaluating isotonic sodium bicarbonate vs. normal saline for contrast prophylaxis.7
The past 10-plus years have seen a proliferation of studies evaluating the utility of novel biomarkers for early diagnosis and prognosis in AKI. Have we fallen down the same rabbit hole in evaluating these new diagnostic tests for AKI? There is reason for concern if we examine published studies of novel biomarkers in other areas of medicine. To this point, many highly cited novel biomarker studies used for various diagnostic purposes (eg, cancer, infection, cardiovascular disease) employed excessively large effect size estimates for postulated associations that resulted in small, underpowered studies with initially positive results.8 Subsequent large studies and meta-analyses reported negative or modestly positive test results when examining these same associations.8 But we may be moving in the right direction. An early urine biomarker publication from a small, single center study9 revealed overly optimistic results (area under the curve [AUC], 0.998; sensitivity, 100%; specificity, 98%) for AKI prediction. Subsequent large, multicenter biomarker studies showed only modest improvement in their discriminative value when compared with traditional clinical models.10 These results precluded U.S. Food and Drug Administration (FDA) approval of most novel biomarkers for clinical practice and they were not adopted. In 2014, the FDA approved the point-of-care urinary biomarker TIMP-2/IGFBP7 (NephroCheck®) for predicting risk of AKI based on fairly rigorous testing using larger numbers of patients, heterogeneous populations, and important clinical endpoints.11 In a 522-patient discovery cohort, this biomarker had an AUC of 0.80 for AKI prediction, which was validated in a 722-patient cohort and subsequently followed by a 420-patient multicenter cohort study revealing similar test characteristics (AUC, 0.82; sensitivity, 92%; specificity, 46%).11 A study involving 382 critically ill AKI patients noted that this biomarker had a hazard ratio of 2.16 (95% confidence interval [CI] 1.32 to 3.53) for predict
In summary, clinicians should be aware of the strengths and limitations of diagnostic tests ordered in AKI patients, as seen with the overly optimistic results in small, flawed UE and FENa studies. While we have taken a step in the right direction with diagnostic and prognostic biomarkers for AKI, we must apply rigorous study design to diagnostic tests under evaluation before adopting them into clinical practice. Only then can we move the field forward and improve patient care.
Disclosure
Nothing to report.
1. Lusica M, Rondon-Berrios H, Feldman L. Urine eosinophils for acute interstitial nephritis. J Hosp Med. 2017;12(5):343-345. PubMed
2. Leaf DE, Srivastava A, Zeng X, et al. Excessive diagnostic testing in acute kidney injury. BMC Nephrol. 2016;17:9. PubMed
3. Pahwa AK, Sperati CJ. Urinary fractional excretion indices in the evaluation of acute kidney injury. J Hosp Med. 2016;11(1):77-80. PubMed
4. Perazella MA, Bomback AS. Urinary eosinophils in AIN: farewell to an old biomarker? Clin J Am Soc Nephrol. 2013;8(11):1841-1843. PubMed
5. Muriithi AK, Nasr SH, Leung N. Utility of urine eosinophils in the diagnosis of acute interstitial nephritis. Clin J Am Soc Nephrol. 2013;8(11):1857-1862. PubMed
6. Perazella MA, Coca SG. Traditional urinary biomarkers in the assessment of hospital-acquired AKI. Clin J Am Soc Nephrol. 2012;7(1):167-174. PubMed
7. Weisbord SD, Palevsky PM. Strategies for the prevention of contrast-induced acute kidney injury. Curr Opin Nephrol Hypertens. 2010;19(6):539-549. PubMed
8. Ioannidis JP, Panagiotou OA. Comparison of effect sizes associated with biomarkers reported in highly cited individual articles and in subsequent meta-analyses. JAMA. 2011;305(21):2200-2210. PubMed
9. Mishra J, Dent C, Tarabishi R, et al. Neutrophil gelatinase-associated lipocalin as a biomarker for acute renal injury after cardiac surgery. Lancet. 2005;365(9466):1231-1238. PubMed
10. Schaub JA, Parikh CR. Biomarkers of acute kidney injury and associations with short- and long-term outcomes. F1000Res. 2016;5(F1000 Faculty Rev.):986. PubMed
11. McMahon BA, Koyner JL. Risk stratification for acute kidney injury: Are biomarkers enough? Adv Chronic Kidney Dis. 2016;23(3):167-178. PubMed
1. Lusica M, Rondon-Berrios H, Feldman L. Urine eosinophils for acute interstitial nephritis. J Hosp Med. 2017;12(5):343-345. PubMed
2. Leaf DE, Srivastava A, Zeng X, et al. Excessive diagnostic testing in acute kidney injury. BMC Nephrol. 2016;17:9. PubMed
3. Pahwa AK, Sperati CJ. Urinary fractional excretion indices in the evaluation of acute kidney injury. J Hosp Med. 2016;11(1):77-80. PubMed
4. Perazella MA, Bomback AS. Urinary eosinophils in AIN: farewell to an old biomarker? Clin J Am Soc Nephrol. 2013;8(11):1841-1843. PubMed
5. Muriithi AK, Nasr SH, Leung N. Utility of urine eosinophils in the diagnosis of acute interstitial nephritis. Clin J Am Soc Nephrol. 2013;8(11):1857-1862. PubMed
6. Perazella MA, Coca SG. Traditional urinary biomarkers in the assessment of hospital-acquired AKI. Clin J Am Soc Nephrol. 2012;7(1):167-174. PubMed
7. Weisbord SD, Palevsky PM. Strategies for the prevention of contrast-induced acute kidney injury. Curr Opin Nephrol Hypertens. 2010;19(6):539-549. PubMed
8. Ioannidis JP, Panagiotou OA. Comparison of effect sizes associated with biomarkers reported in highly cited individual articles and in subsequent meta-analyses. JAMA. 2011;305(21):2200-2210. PubMed
9. Mishra J, Dent C, Tarabishi R, et al. Neutrophil gelatinase-associated lipocalin as a biomarker for acute renal injury after cardiac surgery. Lancet. 2005;365(9466):1231-1238. PubMed
10. Schaub JA, Parikh CR. Biomarkers of acute kidney injury and associations with short- and long-term outcomes. F1000Res. 2016;5(F1000 Faculty Rev.):986. PubMed
11. McMahon BA, Koyner JL. Risk stratification for acute kidney injury: Are biomarkers enough? Adv Chronic Kidney Dis. 2016;23(3):167-178. PubMed
© 2017 Society of Hospital Medicine
Moving antibiotic stewardship from theory to practice
We both attend on the Infectious Disease consult team in Veterans Affairs (VA) Hospitals, and predictably the conversation on afternoon rounds often revolves around antibiotics. When we have those discussions, our focus is not on a need to “preserve antibiotics” so they might be available to some unknown patient in the future. Rather, we are working with the primary team to provide the very best treatment for the patient entrusted to our care in the bed right in front of us. We believe it is in this context—providing optimal patient care—that the current efforts in the United States to improve antibiotic use should be viewed.
The growing challenges posed by antibiotic-resistant infections and the related threat of Clostridium difficile infection combine to sicken more than 2 million people each year and contribute to the deaths of more than 25,000 patients.1 Improving antibiotic use through antibiotic stewardship is often proposed to hospitalists as an important part of stemming this tide. While this is true, even as infectious disease specialists with strong interests in antimicrobial stewardship we do not find that pitch compelling when we are on clinical service.
What motivates us to optimize antibiotic use for our patients is the evidence that doing so will have direct and immediate benefits to the patients under our care. Improving antibiotic use has been proven to decrease a patient’s risk of acquiring C. difficile infection or an antibiotic-resistant infection not at some ill-defined time in the future, but during their current hospital stay.2,3 Even more important, support from antibiotic stewardship programs has been proven to improve infection cure rates and reduce the risk of treatment failure for hospitalized patients.4 The bottom line of antibiotic stewardship is better patient care. Sometimes that means narrowing or stopping antibiotics to reduce the risks of adverse events. In other cases, like in the treatment of suspected sepsis, it means ensuring patients get broad spectrum antibiotics quickly.
The patient care benefits of improving antibiotic use led the Centers for Disease Control and Prevention (CDC) to issue a call in 2014 for all hospitals to have antibiotic stewardship programs, and to the development of The Core Elements of Hospital Antibiotic Stewardship Programs to support that effort. As of January 1, 2017, antibiotic stewardship programs that incorporate all the CDC core elements became an accreditation requirement of The Joint Commission, and the Centers for Medicare and Medicaid Services has proposed making the same requirement of all hospitals that participate in their payment programs.
STEWARDSHIP IN PRACTICE: PNEUMONIA
The literature on treatment of pneumonia is increasingly demonstrating that shorter use of antibiotics is often better.7 Even though current guidelines recommend 5 to 7 days of antibiotics for uncomplicated community-acquired pneumonia, average durations of therapy are often longer.8 Previous work published in the Journal of Hospital Medicine focused on improving antimicrobial documentation as well as access to local clinical guidelines and implementing a 72-hour antimicrobial “time out” by hospitalists.9 When these multimodal interventions tailored for hospitalists were in place, utilization of antibiotics improved. Graber et al.5 also found that facility educational programs for prudent antimicrobial use and frequency of de-escalation review were associated with decreased overall antimicrobial use. Providing vague recommendations on antibiotic course, or none at all, at discharge or sign-out can lead to unnecessary antibiotics or an extended course of them. Pneumonia-specific interventions could target duration by outlining antibiotic course in hospitalist progress notes and at hand-off.
STEWARDSHIP IN PRACTICE: UTI
Misuse of antibiotics in UTI often stems from overtreatment of asymptomatic bacteriuria or unneeded diagnostic testing. Often, the pivotal step in avoiding unnecessary treatment lies in the ordering of the urine culture.10 Graber et al.5 showed that order sets were associated with decreased antimicrobial use. In the case of UTI, hospitalists could work with the stewardship team to design order sets that guide providers to appropriate reasons for ordering a urine culture. Order sets could also help providers recognize important patient-specific risks for certain antibiotics, such as the risk of C. difficile with fluoroquinolones in an elderly patient. Targeting different steps in overutilization of antibiotics would encompass more prescribers and could lead to reducing other unnecessary testing, which is a current focus for many hospitalists.
STEWARDSHIP IN PRACTICE: SSTI
Skin and soft tissue infections (SSTI) also offer a specific disease state to use order sets and education to improve duration of antibiotics, decrease overuse of broad spectrum antibiotics, and reduce unnecessary diagnostic studies. For example, gram negative and/or anaerobic coverage are rarely indicated in treating SSTIs but are often used. SSTI-specific order sets and guidelines have already been shown to improve both diagnostic work-up and antibiotic treatment.11 As the providers who manage most of these infections in hospitals, hospitalists are ideally positioned to inform the development of SSTI order sets and pathways. The work by Graber et al.5 provides some important insights into how we can effectively implement interventions to improve antibiotic use. These insights have never been more important as more hospitals move toward starting or expanding antibiotic stewardship programs. As leaders in patient safety and quality, and as the most important antibiotic prescribers in hospitals, hospitalists must play a central role in stewardship if we are to make meaningful progress.
Disclosure
Nothing to report.
1. Centers for Disease Control and Prevention. Antibiotic Resistance Threats in the United States, 2013. https://www.cdc.gov/drugresistance/pdf/ar-threats-2013-508.pdf. Accessed April 12, 2017.
2. Feazel LM, Malhotra A, Perencevich EN, Kaboli P, Diekema DJ, Schweizer ML. Effect of antibiotic stewardship programmes on Clostridium difficile incidence: a systematic review and meta-analysis. J Antimicrob Chemother. 2014;69(7):1748-1754. PubMed
3. Singh N, Rogers P, Atwood CW, Wagener MM, Yu VL. Short-course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription. Am J Respir Crit Care Med. 2000;162(2 Pt 1):505-511. PubMed
4. Fishman N. Antimicrobial stewardship. Am J Med. 2006;119(6 Suppl 1):S53-S61; discussion S62-S70. PubMed
5. Graber CJ, Jones MM, Chou AF, et al. Association of inpatient antimicrobial utilization measures with antimicrobial stewardship activities and facility characteristics of Veterans Affairs medical centers. J Hosp Med. 2017;12:301-309. PubMed
6. Magill SS, Edwards JR, Beldavs ZG, et al. Prevalence of antimicrobial use in US acute care hospitals, May-September 2011. JAMA. 2014;312(14):1438-1446. PubMed
7. Viasus D, Vecino-Moreno M, De La Hoz JM, Carratala J. Antibiotic stewardship in community-acquired pneumonia. Expert Rev Anti Infect Ther. 2016:1-2019. PubMed
8. Avdic E, Cushinotto LA, Hughes AH, et al. Impact of an antimicrobial stewardship intervention on shortening the duration of therapy for community-acquired pneumonia. Clin Infect Dis. 2012;54(11):1581-1587. PubMed
9. Mack MR, Rohde JM, Jacobsen D, et al. Engaging hospitalists in antimicrobial stewardship: Lessons from a multihospital collaborative. J Hosp Med. 2016;11(8):576-580. PubMed
10. Trautner BW, Grigoryan L, Petersen NJ, et al. Effectiveness of an Antimicrobial Stewardship Approach for Urinary Catheter-Associated Asymptomatic Bacteriuria. JAMA Intern Med. 2015;175(7):1120-1127. PubMed
11. Jenkins TC, Knepper BC, Sabel AL, et al. Decreased antibiotic utilization after implementation of a guideline for inpatient cellulitis and cutaneous abscess. Arch Intern Med. 2011;171(12):1072-1079. PubMed
We both attend on the Infectious Disease consult team in Veterans Affairs (VA) Hospitals, and predictably the conversation on afternoon rounds often revolves around antibiotics. When we have those discussions, our focus is not on a need to “preserve antibiotics” so they might be available to some unknown patient in the future. Rather, we are working with the primary team to provide the very best treatment for the patient entrusted to our care in the bed right in front of us. We believe it is in this context—providing optimal patient care—that the current efforts in the United States to improve antibiotic use should be viewed.
The growing challenges posed by antibiotic-resistant infections and the related threat of Clostridium difficile infection combine to sicken more than 2 million people each year and contribute to the deaths of more than 25,000 patients.1 Improving antibiotic use through antibiotic stewardship is often proposed to hospitalists as an important part of stemming this tide. While this is true, even as infectious disease specialists with strong interests in antimicrobial stewardship we do not find that pitch compelling when we are on clinical service.
What motivates us to optimize antibiotic use for our patients is the evidence that doing so will have direct and immediate benefits to the patients under our care. Improving antibiotic use has been proven to decrease a patient’s risk of acquiring C. difficile infection or an antibiotic-resistant infection not at some ill-defined time in the future, but during their current hospital stay.2,3 Even more important, support from antibiotic stewardship programs has been proven to improve infection cure rates and reduce the risk of treatment failure for hospitalized patients.4 The bottom line of antibiotic stewardship is better patient care. Sometimes that means narrowing or stopping antibiotics to reduce the risks of adverse events. In other cases, like in the treatment of suspected sepsis, it means ensuring patients get broad spectrum antibiotics quickly.
The patient care benefits of improving antibiotic use led the Centers for Disease Control and Prevention (CDC) to issue a call in 2014 for all hospitals to have antibiotic stewardship programs, and to the development of The Core Elements of Hospital Antibiotic Stewardship Programs to support that effort. As of January 1, 2017, antibiotic stewardship programs that incorporate all the CDC core elements became an accreditation requirement of The Joint Commission, and the Centers for Medicare and Medicaid Services has proposed making the same requirement of all hospitals that participate in their payment programs.
STEWARDSHIP IN PRACTICE: PNEUMONIA
The literature on treatment of pneumonia is increasingly demonstrating that shorter use of antibiotics is often better.7 Even though current guidelines recommend 5 to 7 days of antibiotics for uncomplicated community-acquired pneumonia, average durations of therapy are often longer.8 Previous work published in the Journal of Hospital Medicine focused on improving antimicrobial documentation as well as access to local clinical guidelines and implementing a 72-hour antimicrobial “time out” by hospitalists.9 When these multimodal interventions tailored for hospitalists were in place, utilization of antibiotics improved. Graber et al.5 also found that facility educational programs for prudent antimicrobial use and frequency of de-escalation review were associated with decreased overall antimicrobial use. Providing vague recommendations on antibiotic course, or none at all, at discharge or sign-out can lead to unnecessary antibiotics or an extended course of them. Pneumonia-specific interventions could target duration by outlining antibiotic course in hospitalist progress notes and at hand-off.
STEWARDSHIP IN PRACTICE: UTI
Misuse of antibiotics in UTI often stems from overtreatment of asymptomatic bacteriuria or unneeded diagnostic testing. Often, the pivotal step in avoiding unnecessary treatment lies in the ordering of the urine culture.10 Graber et al.5 showed that order sets were associated with decreased antimicrobial use. In the case of UTI, hospitalists could work with the stewardship team to design order sets that guide providers to appropriate reasons for ordering a urine culture. Order sets could also help providers recognize important patient-specific risks for certain antibiotics, such as the risk of C. difficile with fluoroquinolones in an elderly patient. Targeting different steps in overutilization of antibiotics would encompass more prescribers and could lead to reducing other unnecessary testing, which is a current focus for many hospitalists.
STEWARDSHIP IN PRACTICE: SSTI
Skin and soft tissue infections (SSTI) also offer a specific disease state to use order sets and education to improve duration of antibiotics, decrease overuse of broad spectrum antibiotics, and reduce unnecessary diagnostic studies. For example, gram negative and/or anaerobic coverage are rarely indicated in treating SSTIs but are often used. SSTI-specific order sets and guidelines have already been shown to improve both diagnostic work-up and antibiotic treatment.11 As the providers who manage most of these infections in hospitals, hospitalists are ideally positioned to inform the development of SSTI order sets and pathways. The work by Graber et al.5 provides some important insights into how we can effectively implement interventions to improve antibiotic use. These insights have never been more important as more hospitals move toward starting or expanding antibiotic stewardship programs. As leaders in patient safety and quality, and as the most important antibiotic prescribers in hospitals, hospitalists must play a central role in stewardship if we are to make meaningful progress.
Disclosure
Nothing to report.
We both attend on the Infectious Disease consult team in Veterans Affairs (VA) Hospitals, and predictably the conversation on afternoon rounds often revolves around antibiotics. When we have those discussions, our focus is not on a need to “preserve antibiotics” so they might be available to some unknown patient in the future. Rather, we are working with the primary team to provide the very best treatment for the patient entrusted to our care in the bed right in front of us. We believe it is in this context—providing optimal patient care—that the current efforts in the United States to improve antibiotic use should be viewed.
The growing challenges posed by antibiotic-resistant infections and the related threat of Clostridium difficile infection combine to sicken more than 2 million people each year and contribute to the deaths of more than 25,000 patients.1 Improving antibiotic use through antibiotic stewardship is often proposed to hospitalists as an important part of stemming this tide. While this is true, even as infectious disease specialists with strong interests in antimicrobial stewardship we do not find that pitch compelling when we are on clinical service.
What motivates us to optimize antibiotic use for our patients is the evidence that doing so will have direct and immediate benefits to the patients under our care. Improving antibiotic use has been proven to decrease a patient’s risk of acquiring C. difficile infection or an antibiotic-resistant infection not at some ill-defined time in the future, but during their current hospital stay.2,3 Even more important, support from antibiotic stewardship programs has been proven to improve infection cure rates and reduce the risk of treatment failure for hospitalized patients.4 The bottom line of antibiotic stewardship is better patient care. Sometimes that means narrowing or stopping antibiotics to reduce the risks of adverse events. In other cases, like in the treatment of suspected sepsis, it means ensuring patients get broad spectrum antibiotics quickly.
The patient care benefits of improving antibiotic use led the Centers for Disease Control and Prevention (CDC) to issue a call in 2014 for all hospitals to have antibiotic stewardship programs, and to the development of The Core Elements of Hospital Antibiotic Stewardship Programs to support that effort. As of January 1, 2017, antibiotic stewardship programs that incorporate all the CDC core elements became an accreditation requirement of The Joint Commission, and the Centers for Medicare and Medicaid Services has proposed making the same requirement of all hospitals that participate in their payment programs.
STEWARDSHIP IN PRACTICE: PNEUMONIA
The literature on treatment of pneumonia is increasingly demonstrating that shorter use of antibiotics is often better.7 Even though current guidelines recommend 5 to 7 days of antibiotics for uncomplicated community-acquired pneumonia, average durations of therapy are often longer.8 Previous work published in the Journal of Hospital Medicine focused on improving antimicrobial documentation as well as access to local clinical guidelines and implementing a 72-hour antimicrobial “time out” by hospitalists.9 When these multimodal interventions tailored for hospitalists were in place, utilization of antibiotics improved. Graber et al.5 also found that facility educational programs for prudent antimicrobial use and frequency of de-escalation review were associated with decreased overall antimicrobial use. Providing vague recommendations on antibiotic course, or none at all, at discharge or sign-out can lead to unnecessary antibiotics or an extended course of them. Pneumonia-specific interventions could target duration by outlining antibiotic course in hospitalist progress notes and at hand-off.
STEWARDSHIP IN PRACTICE: UTI
Misuse of antibiotics in UTI often stems from overtreatment of asymptomatic bacteriuria or unneeded diagnostic testing. Often, the pivotal step in avoiding unnecessary treatment lies in the ordering of the urine culture.10 Graber et al.5 showed that order sets were associated with decreased antimicrobial use. In the case of UTI, hospitalists could work with the stewardship team to design order sets that guide providers to appropriate reasons for ordering a urine culture. Order sets could also help providers recognize important patient-specific risks for certain antibiotics, such as the risk of C. difficile with fluoroquinolones in an elderly patient. Targeting different steps in overutilization of antibiotics would encompass more prescribers and could lead to reducing other unnecessary testing, which is a current focus for many hospitalists.
STEWARDSHIP IN PRACTICE: SSTI
Skin and soft tissue infections (SSTI) also offer a specific disease state to use order sets and education to improve duration of antibiotics, decrease overuse of broad spectrum antibiotics, and reduce unnecessary diagnostic studies. For example, gram negative and/or anaerobic coverage are rarely indicated in treating SSTIs but are often used. SSTI-specific order sets and guidelines have already been shown to improve both diagnostic work-up and antibiotic treatment.11 As the providers who manage most of these infections in hospitals, hospitalists are ideally positioned to inform the development of SSTI order sets and pathways. The work by Graber et al.5 provides some important insights into how we can effectively implement interventions to improve antibiotic use. These insights have never been more important as more hospitals move toward starting or expanding antibiotic stewardship programs. As leaders in patient safety and quality, and as the most important antibiotic prescribers in hospitals, hospitalists must play a central role in stewardship if we are to make meaningful progress.
Disclosure
Nothing to report.
1. Centers for Disease Control and Prevention. Antibiotic Resistance Threats in the United States, 2013. https://www.cdc.gov/drugresistance/pdf/ar-threats-2013-508.pdf. Accessed April 12, 2017.
2. Feazel LM, Malhotra A, Perencevich EN, Kaboli P, Diekema DJ, Schweizer ML. Effect of antibiotic stewardship programmes on Clostridium difficile incidence: a systematic review and meta-analysis. J Antimicrob Chemother. 2014;69(7):1748-1754. PubMed
3. Singh N, Rogers P, Atwood CW, Wagener MM, Yu VL. Short-course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription. Am J Respir Crit Care Med. 2000;162(2 Pt 1):505-511. PubMed
4. Fishman N. Antimicrobial stewardship. Am J Med. 2006;119(6 Suppl 1):S53-S61; discussion S62-S70. PubMed
5. Graber CJ, Jones MM, Chou AF, et al. Association of inpatient antimicrobial utilization measures with antimicrobial stewardship activities and facility characteristics of Veterans Affairs medical centers. J Hosp Med. 2017;12:301-309. PubMed
6. Magill SS, Edwards JR, Beldavs ZG, et al. Prevalence of antimicrobial use in US acute care hospitals, May-September 2011. JAMA. 2014;312(14):1438-1446. PubMed
7. Viasus D, Vecino-Moreno M, De La Hoz JM, Carratala J. Antibiotic stewardship in community-acquired pneumonia. Expert Rev Anti Infect Ther. 2016:1-2019. PubMed
8. Avdic E, Cushinotto LA, Hughes AH, et al. Impact of an antimicrobial stewardship intervention on shortening the duration of therapy for community-acquired pneumonia. Clin Infect Dis. 2012;54(11):1581-1587. PubMed
9. Mack MR, Rohde JM, Jacobsen D, et al. Engaging hospitalists in antimicrobial stewardship: Lessons from a multihospital collaborative. J Hosp Med. 2016;11(8):576-580. PubMed
10. Trautner BW, Grigoryan L, Petersen NJ, et al. Effectiveness of an Antimicrobial Stewardship Approach for Urinary Catheter-Associated Asymptomatic Bacteriuria. JAMA Intern Med. 2015;175(7):1120-1127. PubMed
11. Jenkins TC, Knepper BC, Sabel AL, et al. Decreased antibiotic utilization after implementation of a guideline for inpatient cellulitis and cutaneous abscess. Arch Intern Med. 2011;171(12):1072-1079. PubMed
1. Centers for Disease Control and Prevention. Antibiotic Resistance Threats in the United States, 2013. https://www.cdc.gov/drugresistance/pdf/ar-threats-2013-508.pdf. Accessed April 12, 2017.
2. Feazel LM, Malhotra A, Perencevich EN, Kaboli P, Diekema DJ, Schweizer ML. Effect of antibiotic stewardship programmes on Clostridium difficile incidence: a systematic review and meta-analysis. J Antimicrob Chemother. 2014;69(7):1748-1754. PubMed
3. Singh N, Rogers P, Atwood CW, Wagener MM, Yu VL. Short-course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription. Am J Respir Crit Care Med. 2000;162(2 Pt 1):505-511. PubMed
4. Fishman N. Antimicrobial stewardship. Am J Med. 2006;119(6 Suppl 1):S53-S61; discussion S62-S70. PubMed
5. Graber CJ, Jones MM, Chou AF, et al. Association of inpatient antimicrobial utilization measures with antimicrobial stewardship activities and facility characteristics of Veterans Affairs medical centers. J Hosp Med. 2017;12:301-309. PubMed
6. Magill SS, Edwards JR, Beldavs ZG, et al. Prevalence of antimicrobial use in US acute care hospitals, May-September 2011. JAMA. 2014;312(14):1438-1446. PubMed
7. Viasus D, Vecino-Moreno M, De La Hoz JM, Carratala J. Antibiotic stewardship in community-acquired pneumonia. Expert Rev Anti Infect Ther. 2016:1-2019. PubMed
8. Avdic E, Cushinotto LA, Hughes AH, et al. Impact of an antimicrobial stewardship intervention on shortening the duration of therapy for community-acquired pneumonia. Clin Infect Dis. 2012;54(11):1581-1587. PubMed
9. Mack MR, Rohde JM, Jacobsen D, et al. Engaging hospitalists in antimicrobial stewardship: Lessons from a multihospital collaborative. J Hosp Med. 2016;11(8):576-580. PubMed
10. Trautner BW, Grigoryan L, Petersen NJ, et al. Effectiveness of an Antimicrobial Stewardship Approach for Urinary Catheter-Associated Asymptomatic Bacteriuria. JAMA Intern Med. 2015;175(7):1120-1127. PubMed
11. Jenkins TC, Knepper BC, Sabel AL, et al. Decreased antibiotic utilization after implementation of a guideline for inpatient cellulitis and cutaneous abscess. Arch Intern Med. 2011;171(12):1072-1079. PubMed
© 2017 Society of Hospital Medicine
Hospitalist movers and shakers
Andrew Auerbach, MD, MPH, SFHM, and Vineet Arora, MD, MPP, MHM, recently were elected to the new member class of American Society for Clinical Investigation (ASCI) for 2017. Members must have “accomplished meritorious, original, creative, and independent investigations in the clinical or allied sciences of medicine and enjoy an unimpeachable moral standing in the medical profession.”
Dr. Auerbach and Dr. Arora are just the third and fourth hospitalists to become ASCI members. Dr. Auerbach is the professor of medicine in residence and director of the research division of hospital medicine at the University of California, San Francisco. Dr. Aurora is associate professor of medicine, assistant dean for scholarship and discovery, and director of graduate medical education’s clinical learning environment innovation at the University of Chicago.

Mark V. Williams, MD, FACP, MHM, director of the University of Kentucky’s Center for Health Services Research (CHSR), recently presented at the International Conference of Hospital Medicine held in Taiwan.
Olevia M. Pitts, MD, SFHM, made history at Research Medical Center in Kansas City, becoming the first woman and the first person of color to be named the facility’s chief medical officer. Dr. Pitts assumed her role at the 131-year-old RMC on January 30.

Greta Boynton, MD, SFHM, was promoted to the role of associate chief medical officer of Sound Physicians’ northeast region. She was elevated from her position as regional medical director for Sound Physicians, a health care organization that serves as a provider practice in 225 hospitals in 38 states.
Dr. Boynton will be charged with overseeing clinical operation of 13 programs, 120 providers, and a team of regional medical directors. She joined Sound Physicians in 2013 as chief hospitalist and divisional chief at Baystate Medical Center in Springfield, Mass. She was, previously, chief of hospital medicine for Eastern Connecticut Health Network, Manchester, from 2008-2013.
Business Moves
Sound Physicians, Tacoma, Wash., added to its list of partners on March 1, when Eagle Hospital Medicine Practices, Atlanta, joined the Sound group’s organization. Eagle’s 150 providers in 16 hospitals across the United States raises Sound’s resume to more than 2,500 providers.
Eagle will continue to run its own Locum Connections and Telemedicine divisions.
The Society of Hospital Medicine’s Center for Quality Improvement recently was recognized and honored by the Centers for Medicare & Medicaid Services (CMS) for its patient-safety partnership with CMS. The two entities have maintained a relationship since August 2016.
SHM’s Center for QI has participated in weekly CMS webinars to generate strategies intended to limit opioid use, including SHM’s pilot RADEO – Reducing Adverse Drug Events Related to Opioids – program. In January 2017, CMS contacted SHM to provide best practices for patients receiving opioids and better use data to monitor those patients.
University of Iowa Health Care, Iowa City, and Van Buren County Hospital, Keosauqua, Iowa, have created a partnership, allowing patients at VBCH access to UI hospitalists through a telemedicine connection. The relationship will allow VBCH patients to remain at their local hospital – located 90 minutes from Iowa City – while getting care and treatment advice from UI hospitalists through videoconferencing and a shared electronic health record.
With their VBCH provider bedside, patients meet face-to–virtual face with the UI hospitalist during twice-daily virtual rounding.
Unity Medical Center, Manchester, Tenn., recently partnered with physician-owned and -operated Concord Medical Group, Knoxville, Tenn., to provide hospitalist services at its facility in Manchester. Unity now will have hospitalists on duty 24 hours per day thanks to the relationship with Concord, a hospital management and staffing specialist group.
Andrew Auerbach, MD, MPH, SFHM, and Vineet Arora, MD, MPP, MHM, recently were elected to the new member class of American Society for Clinical Investigation (ASCI) for 2017. Members must have “accomplished meritorious, original, creative, and independent investigations in the clinical or allied sciences of medicine and enjoy an unimpeachable moral standing in the medical profession.”
Dr. Auerbach and Dr. Arora are just the third and fourth hospitalists to become ASCI members. Dr. Auerbach is the professor of medicine in residence and director of the research division of hospital medicine at the University of California, San Francisco. Dr. Aurora is associate professor of medicine, assistant dean for scholarship and discovery, and director of graduate medical education’s clinical learning environment innovation at the University of Chicago.
Mark V. Williams, MD, FACP, MHM, director of the University of Kentucky’s Center for Health Services Research (CHSR), recently presented at the International Conference of Hospital Medicine held in Taiwan.
Olevia M. Pitts, MD, SFHM, made history at Research Medical Center in Kansas City, becoming the first woman and the first person of color to be named the facility’s chief medical officer. Dr. Pitts assumed her role at the 131-year-old RMC on January 30.
Greta Boynton, MD, SFHM, was promoted to the role of associate chief medical officer of Sound Physicians’ northeast region. She was elevated from her position as regional medical director for Sound Physicians, a health care organization that serves as a provider practice in 225 hospitals in 38 states.
Dr. Boynton will be charged with overseeing clinical operation of 13 programs, 120 providers, and a team of regional medical directors. She joined Sound Physicians in 2013 as chief hospitalist and divisional chief at Baystate Medical Center in Springfield, Mass. She was, previously, chief of hospital medicine for Eastern Connecticut Health Network, Manchester, from 2008-2013.
Business Moves
Sound Physicians, Tacoma, Wash., added to its list of partners on March 1, when Eagle Hospital Medicine Practices, Atlanta, joined the Sound group’s organization. Eagle’s 150 providers in 16 hospitals across the United States raises Sound’s resume to more than 2,500 providers.
Eagle will continue to run its own Locum Connections and Telemedicine divisions.
The Society of Hospital Medicine’s Center for Quality Improvement recently was recognized and honored by the Centers for Medicare & Medicaid Services (CMS) for its patient-safety partnership with CMS. The two entities have maintained a relationship since August 2016.
SHM’s Center for QI has participated in weekly CMS webinars to generate strategies intended to limit opioid use, including SHM’s pilot RADEO – Reducing Adverse Drug Events Related to Opioids – program. In January 2017, CMS contacted SHM to provide best practices for patients receiving opioids and better use data to monitor those patients.
University of Iowa Health Care, Iowa City, and Van Buren County Hospital, Keosauqua, Iowa, have created a partnership, allowing patients at VBCH access to UI hospitalists through a telemedicine connection. The relationship will allow VBCH patients to remain at their local hospital – located 90 minutes from Iowa City – while getting care and treatment advice from UI hospitalists through videoconferencing and a shared electronic health record.
With their VBCH provider bedside, patients meet face-to–virtual face with the UI hospitalist during twice-daily virtual rounding.
Unity Medical Center, Manchester, Tenn., recently partnered with physician-owned and -operated Concord Medical Group, Knoxville, Tenn., to provide hospitalist services at its facility in Manchester. Unity now will have hospitalists on duty 24 hours per day thanks to the relationship with Concord, a hospital management and staffing specialist group.
Andrew Auerbach, MD, MPH, SFHM, and Vineet Arora, MD, MPP, MHM, recently were elected to the new member class of American Society for Clinical Investigation (ASCI) for 2017. Members must have “accomplished meritorious, original, creative, and independent investigations in the clinical or allied sciences of medicine and enjoy an unimpeachable moral standing in the medical profession.”
Dr. Auerbach and Dr. Arora are just the third and fourth hospitalists to become ASCI members. Dr. Auerbach is the professor of medicine in residence and director of the research division of hospital medicine at the University of California, San Francisco. Dr. Aurora is associate professor of medicine, assistant dean for scholarship and discovery, and director of graduate medical education’s clinical learning environment innovation at the University of Chicago.
Mark V. Williams, MD, FACP, MHM, director of the University of Kentucky’s Center for Health Services Research (CHSR), recently presented at the International Conference of Hospital Medicine held in Taiwan.
Olevia M. Pitts, MD, SFHM, made history at Research Medical Center in Kansas City, becoming the first woman and the first person of color to be named the facility’s chief medical officer. Dr. Pitts assumed her role at the 131-year-old RMC on January 30.
Greta Boynton, MD, SFHM, was promoted to the role of associate chief medical officer of Sound Physicians’ northeast region. She was elevated from her position as regional medical director for Sound Physicians, a health care organization that serves as a provider practice in 225 hospitals in 38 states.
Dr. Boynton will be charged with overseeing clinical operation of 13 programs, 120 providers, and a team of regional medical directors. She joined Sound Physicians in 2013 as chief hospitalist and divisional chief at Baystate Medical Center in Springfield, Mass. She was, previously, chief of hospital medicine for Eastern Connecticut Health Network, Manchester, from 2008-2013.
Business Moves
Sound Physicians, Tacoma, Wash., added to its list of partners on March 1, when Eagle Hospital Medicine Practices, Atlanta, joined the Sound group’s organization. Eagle’s 150 providers in 16 hospitals across the United States raises Sound’s resume to more than 2,500 providers.
Eagle will continue to run its own Locum Connections and Telemedicine divisions.
The Society of Hospital Medicine’s Center for Quality Improvement recently was recognized and honored by the Centers for Medicare & Medicaid Services (CMS) for its patient-safety partnership with CMS. The two entities have maintained a relationship since August 2016.
SHM’s Center for QI has participated in weekly CMS webinars to generate strategies intended to limit opioid use, including SHM’s pilot RADEO – Reducing Adverse Drug Events Related to Opioids – program. In January 2017, CMS contacted SHM to provide best practices for patients receiving opioids and better use data to monitor those patients.
University of Iowa Health Care, Iowa City, and Van Buren County Hospital, Keosauqua, Iowa, have created a partnership, allowing patients at VBCH access to UI hospitalists through a telemedicine connection. The relationship will allow VBCH patients to remain at their local hospital – located 90 minutes from Iowa City – while getting care and treatment advice from UI hospitalists through videoconferencing and a shared electronic health record.
With their VBCH provider bedside, patients meet face-to–virtual face with the UI hospitalist during twice-daily virtual rounding.
Unity Medical Center, Manchester, Tenn., recently partnered with physician-owned and -operated Concord Medical Group, Knoxville, Tenn., to provide hospitalist services at its facility in Manchester. Unity now will have hospitalists on duty 24 hours per day thanks to the relationship with Concord, a hospital management and staffing specialist group.
Digoxin and heart failure mortality: The Swedes weigh in
WASHINGTON – The use of digoxin by Swedish Heart Failure Registry participants with heart failure with reduced ejection fraction was associated with significantly increased risk of all-cause mortality if they had concomitant paroxysmal atrial fibrillation or were in normal sinus rhythm, Gianluigi Savarese, MD, reported at the annual meeting of the American College of Cardiology.
In contrast, digoxin in Swedish patients with heart failure with reduced ejection fraction (HFrEF) and permanent atrial fibrillation (AF) was associated with a reduced risk of heart failure hospitalization but had no impact on mortality, added Dr. Savarese of the Karolinska Institute in Stockholm.
The Swedish Heart Failure Registry includes the majority of heart failure patients in that country. Data on 80 variables gets collected for each participant.
Dr. Savarese reported on 23,708 Swedes with HFrEF, 18% of whom were on digoxin. In a multivariate Cox regression analysis adjusted for numerous potential confounders, the use of digoxin was associated with an 8% increased risk of all-cause mortality and a 10% lower risk of heart failure hospitalizations during up to 11 years of follow-up.
In the 12,162 patients with HFrEF and comorbid AF, 30% of whom were on digoxin, the drug was associated with a 12% reduction in heart failure hospitalizations and had no effect on all-cause mortality.
In contrast, among patients with HFrEF without AF, 5% of whom were taking digoxin, use of the drug was associated with an adjusted 31% increase in mortality risk. But digoxin didn’t affect the risk of heart failure hospitalization one way or the other in this group.
Stratifying subjects by their type of AF, the use of digoxin in patients with HFrEF and permanent AF was associated with a 16% reduction in risk of heart failure hospitalization with no impact on mortality. In contrast, among the 2,723 patients with HFrEF and paroxysmal AF, digoxin was associated with a 29% increase in the risk of mortality and no effect on hospitalization.
Current ACC/American Heart Association heart failure guidelines give digoxin a strong Class IIa recommendation for reducing heart failure hospitalizations in patients with HFrEF. European Society of Cardiology guidelines provide a Class IIb recommendation for digoxin to reduce the risk of hospitalization in patients with symptomatic HFrEF in normal sinus rhythm.
Dr. Savarese said he and his coinvestigators decided to examine the impact of digoxin in the Swedish Heart Failure Registry because despite the guideline support for the drug’s use, recent years have brought conflicting data regarding digoxin’s impact on mortality. For example, a meta-analysis of nine studies in more than 235,000 AF patients, seven studies in patients with heart failure, and three in patients with both disorders showed that digoxin was associated with a 29% increased mortality risk in AF patients and a 14% increase in those with heart failure (Eur Heart J. 2015 Jul 21;36[28]:1831-8).
Moreover, at a late-breaking clinical trial session elsewhere at ACC 17, a secondary analysis of the roughly 18,000-patient ARISTOTLE trial came down emphatically on the side of avoiding the venerable drug in patients with AF, where it was found to be associated with a fourfold increased risk of sudden death.
Session comoderator Lee R. Goldberg, MD, medical director of the University of Pennsylvania Heart Failure and Transplantation Program in Philadelphia, observed that the use of digoxin has become quite controversial. He posed a question to Dr. Savarese: “Every few months someone writes the last paper on digoxin as they look at thousands of patients, and then there’s always a new paper. If you were to rewrite the guidelines now, what would you recommend for digoxin?”
Dr. Savarese replied that the current guidelines rely heavily upon the results of a 20-year-old randomized, double-blind, placebo-controlled trial of digoxin in heart failure (N Engl J Med. 1997 Feb 20;336[8]:525-33). Those study participants look nothing at all like the heart failure patients physicians see today in clinical practice. Hardly any of them were on what today is guideline-directed medical therapy with a beta-blocker or mineralocorticoid receptor antagonist. So the trial’s applicability is dubious.
“Our Swedish data are observational. They are hypothesis-generating. They should drive trialists to design a new trial of digoxin. But I think we all know that’s not going to happen. So actually I don’t think there is still space for a IIb or IIa recommendation for digoxin in the guidelines,” Dr. Savarese said.
He reported having no financial conflicts.
WASHINGTON – The use of digoxin by Swedish Heart Failure Registry participants with heart failure with reduced ejection fraction was associated with significantly increased risk of all-cause mortality if they had concomitant paroxysmal atrial fibrillation or were in normal sinus rhythm, Gianluigi Savarese, MD, reported at the annual meeting of the American College of Cardiology.
In contrast, digoxin in Swedish patients with heart failure with reduced ejection fraction (HFrEF) and permanent atrial fibrillation (AF) was associated with a reduced risk of heart failure hospitalization but had no impact on mortality, added Dr. Savarese of the Karolinska Institute in Stockholm.
The Swedish Heart Failure Registry includes the majority of heart failure patients in that country. Data on 80 variables gets collected for each participant.
Dr. Savarese reported on 23,708 Swedes with HFrEF, 18% of whom were on digoxin. In a multivariate Cox regression analysis adjusted for numerous potential confounders, the use of digoxin was associated with an 8% increased risk of all-cause mortality and a 10% lower risk of heart failure hospitalizations during up to 11 years of follow-up.
In the 12,162 patients with HFrEF and comorbid AF, 30% of whom were on digoxin, the drug was associated with a 12% reduction in heart failure hospitalizations and had no effect on all-cause mortality.
In contrast, among patients with HFrEF without AF, 5% of whom were taking digoxin, use of the drug was associated with an adjusted 31% increase in mortality risk. But digoxin didn’t affect the risk of heart failure hospitalization one way or the other in this group.
Stratifying subjects by their type of AF, the use of digoxin in patients with HFrEF and permanent AF was associated with a 16% reduction in risk of heart failure hospitalization with no impact on mortality. In contrast, among the 2,723 patients with HFrEF and paroxysmal AF, digoxin was associated with a 29% increase in the risk of mortality and no effect on hospitalization.
Current ACC/American Heart Association heart failure guidelines give digoxin a strong Class IIa recommendation for reducing heart failure hospitalizations in patients with HFrEF. European Society of Cardiology guidelines provide a Class IIb recommendation for digoxin to reduce the risk of hospitalization in patients with symptomatic HFrEF in normal sinus rhythm.
Dr. Savarese said he and his coinvestigators decided to examine the impact of digoxin in the Swedish Heart Failure Registry because despite the guideline support for the drug’s use, recent years have brought conflicting data regarding digoxin’s impact on mortality. For example, a meta-analysis of nine studies in more than 235,000 AF patients, seven studies in patients with heart failure, and three in patients with both disorders showed that digoxin was associated with a 29% increased mortality risk in AF patients and a 14% increase in those with heart failure (Eur Heart J. 2015 Jul 21;36[28]:1831-8).
Moreover, at a late-breaking clinical trial session elsewhere at ACC 17, a secondary analysis of the roughly 18,000-patient ARISTOTLE trial came down emphatically on the side of avoiding the venerable drug in patients with AF, where it was found to be associated with a fourfold increased risk of sudden death.
Session comoderator Lee R. Goldberg, MD, medical director of the University of Pennsylvania Heart Failure and Transplantation Program in Philadelphia, observed that the use of digoxin has become quite controversial. He posed a question to Dr. Savarese: “Every few months someone writes the last paper on digoxin as they look at thousands of patients, and then there’s always a new paper. If you were to rewrite the guidelines now, what would you recommend for digoxin?”
Dr. Savarese replied that the current guidelines rely heavily upon the results of a 20-year-old randomized, double-blind, placebo-controlled trial of digoxin in heart failure (N Engl J Med. 1997 Feb 20;336[8]:525-33). Those study participants look nothing at all like the heart failure patients physicians see today in clinical practice. Hardly any of them were on what today is guideline-directed medical therapy with a beta-blocker or mineralocorticoid receptor antagonist. So the trial’s applicability is dubious.
“Our Swedish data are observational. They are hypothesis-generating. They should drive trialists to design a new trial of digoxin. But I think we all know that’s not going to happen. So actually I don’t think there is still space for a IIb or IIa recommendation for digoxin in the guidelines,” Dr. Savarese said.
He reported having no financial conflicts.
WASHINGTON – The use of digoxin by Swedish Heart Failure Registry participants with heart failure with reduced ejection fraction was associated with significantly increased risk of all-cause mortality if they had concomitant paroxysmal atrial fibrillation or were in normal sinus rhythm, Gianluigi Savarese, MD, reported at the annual meeting of the American College of Cardiology.
In contrast, digoxin in Swedish patients with heart failure with reduced ejection fraction (HFrEF) and permanent atrial fibrillation (AF) was associated with a reduced risk of heart failure hospitalization but had no impact on mortality, added Dr. Savarese of the Karolinska Institute in Stockholm.
The Swedish Heart Failure Registry includes the majority of heart failure patients in that country. Data on 80 variables gets collected for each participant.
Dr. Savarese reported on 23,708 Swedes with HFrEF, 18% of whom were on digoxin. In a multivariate Cox regression analysis adjusted for numerous potential confounders, the use of digoxin was associated with an 8% increased risk of all-cause mortality and a 10% lower risk of heart failure hospitalizations during up to 11 years of follow-up.
In the 12,162 patients with HFrEF and comorbid AF, 30% of whom were on digoxin, the drug was associated with a 12% reduction in heart failure hospitalizations and had no effect on all-cause mortality.
In contrast, among patients with HFrEF without AF, 5% of whom were taking digoxin, use of the drug was associated with an adjusted 31% increase in mortality risk. But digoxin didn’t affect the risk of heart failure hospitalization one way or the other in this group.
Stratifying subjects by their type of AF, the use of digoxin in patients with HFrEF and permanent AF was associated with a 16% reduction in risk of heart failure hospitalization with no impact on mortality. In contrast, among the 2,723 patients with HFrEF and paroxysmal AF, digoxin was associated with a 29% increase in the risk of mortality and no effect on hospitalization.
Current ACC/American Heart Association heart failure guidelines give digoxin a strong Class IIa recommendation for reducing heart failure hospitalizations in patients with HFrEF. European Society of Cardiology guidelines provide a Class IIb recommendation for digoxin to reduce the risk of hospitalization in patients with symptomatic HFrEF in normal sinus rhythm.
Dr. Savarese said he and his coinvestigators decided to examine the impact of digoxin in the Swedish Heart Failure Registry because despite the guideline support for the drug’s use, recent years have brought conflicting data regarding digoxin’s impact on mortality. For example, a meta-analysis of nine studies in more than 235,000 AF patients, seven studies in patients with heart failure, and three in patients with both disorders showed that digoxin was associated with a 29% increased mortality risk in AF patients and a 14% increase in those with heart failure (Eur Heart J. 2015 Jul 21;36[28]:1831-8).
Moreover, at a late-breaking clinical trial session elsewhere at ACC 17, a secondary analysis of the roughly 18,000-patient ARISTOTLE trial came down emphatically on the side of avoiding the venerable drug in patients with AF, where it was found to be associated with a fourfold increased risk of sudden death.
Session comoderator Lee R. Goldberg, MD, medical director of the University of Pennsylvania Heart Failure and Transplantation Program in Philadelphia, observed that the use of digoxin has become quite controversial. He posed a question to Dr. Savarese: “Every few months someone writes the last paper on digoxin as they look at thousands of patients, and then there’s always a new paper. If you were to rewrite the guidelines now, what would you recommend for digoxin?”
Dr. Savarese replied that the current guidelines rely heavily upon the results of a 20-year-old randomized, double-blind, placebo-controlled trial of digoxin in heart failure (N Engl J Med. 1997 Feb 20;336[8]:525-33). Those study participants look nothing at all like the heart failure patients physicians see today in clinical practice. Hardly any of them were on what today is guideline-directed medical therapy with a beta-blocker or mineralocorticoid receptor antagonist. So the trial’s applicability is dubious.
“Our Swedish data are observational. They are hypothesis-generating. They should drive trialists to design a new trial of digoxin. But I think we all know that’s not going to happen. So actually I don’t think there is still space for a IIb or IIa recommendation for digoxin in the guidelines,” Dr. Savarese said.
He reported having no financial conflicts.
AT ACC 17
Key clinical point:
Major finding: The use of digoxin in patients with heart failure with reduced ejection fraction was associated with significantly increased risk of all-cause mortality if they had concomitant paroxysmal atrial fibrillation or were in normal sinus rhythm.
Data source: An observational study of nearly 24,000 patients enrolled in the Swedish Heart Failure Registry, 18% of whom were on digoxin.
Disclosures: The study presenter reported having no financial conflicts.
Just over half of FPs accept Medicaid
Medicaid acceptance was 55% among family physicians in the 2017 edition of an ongoing survey conducted in 15 large cities by physician recruitment firm Merritt Hawkins.
That was up from almost 52% in the previous survey, conducted in 2014, but lower than the average of 64% for FPs in 15 midsized cities that were included for the first time in 2017, the company reported.
There was one large city with a Medicaid acceptance rate of 100% – Minneapolis (up from 35% in 2014) – along with three midsized cities – Billings, Mt.; Dayton, Ohio; and Fargo, N.D. The lowest rate among the large cities was in Denver (20%), with the midsized basement occupied by Lafayette, La., at 20%, Merritt Hawkins reported.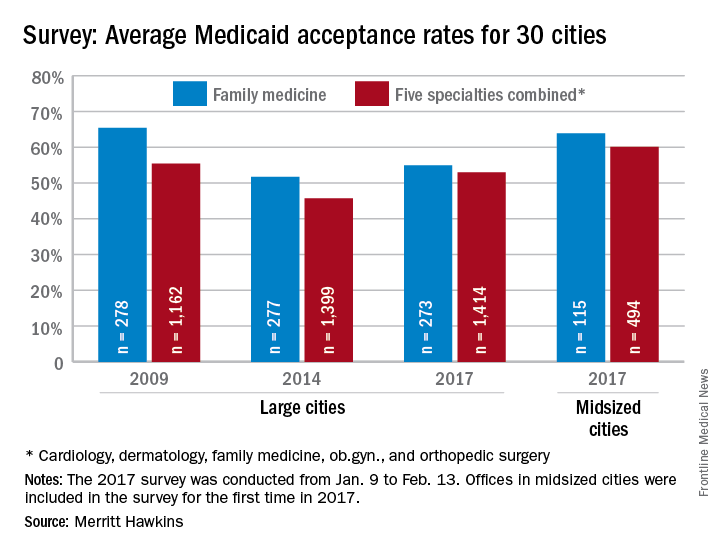
Investigators called 273 randomly selected family physicians in the large cities and 115 FPs in the midsized cities in January and February. It was the fourth such survey the company has conducted since 2004.
The survey included four other specialties – cardiology, dermatology, ob.gyn., and orthopedic surgery. The Medicaid acceptance rate for all 1,414 physicians in all five specialties in the 15 large cities was 53%, and the average rate for all specialties in the midsized cities was 60% for the 494 offices surveyed, the company noted.
Cardiology had the highest rates by specialty and dermatology the lowest in both the large and midsized cities. For all five specialties combined, Minneapolis (97%) and Fargo (100%) had the highest acceptance rates, with the lowest rates coming from Dallas (17%) for large cities and Lafayette (11%) for midsized cities, the Merritt Hawkins data show.
Medicaid acceptance was 55% among family physicians in the 2017 edition of an ongoing survey conducted in 15 large cities by physician recruitment firm Merritt Hawkins.
That was up from almost 52% in the previous survey, conducted in 2014, but lower than the average of 64% for FPs in 15 midsized cities that were included for the first time in 2017, the company reported.
There was one large city with a Medicaid acceptance rate of 100% – Minneapolis (up from 35% in 2014) – along with three midsized cities – Billings, Mt.; Dayton, Ohio; and Fargo, N.D. The lowest rate among the large cities was in Denver (20%), with the midsized basement occupied by Lafayette, La., at 20%, Merritt Hawkins reported.
Investigators called 273 randomly selected family physicians in the large cities and 115 FPs in the midsized cities in January and February. It was the fourth such survey the company has conducted since 2004.
The survey included four other specialties – cardiology, dermatology, ob.gyn., and orthopedic surgery. The Medicaid acceptance rate for all 1,414 physicians in all five specialties in the 15 large cities was 53%, and the average rate for all specialties in the midsized cities was 60% for the 494 offices surveyed, the company noted.
Cardiology had the highest rates by specialty and dermatology the lowest in both the large and midsized cities. For all five specialties combined, Minneapolis (97%) and Fargo (100%) had the highest acceptance rates, with the lowest rates coming from Dallas (17%) for large cities and Lafayette (11%) for midsized cities, the Merritt Hawkins data show.
Medicaid acceptance was 55% among family physicians in the 2017 edition of an ongoing survey conducted in 15 large cities by physician recruitment firm Merritt Hawkins.
That was up from almost 52% in the previous survey, conducted in 2014, but lower than the average of 64% for FPs in 15 midsized cities that were included for the first time in 2017, the company reported.
There was one large city with a Medicaid acceptance rate of 100% – Minneapolis (up from 35% in 2014) – along with three midsized cities – Billings, Mt.; Dayton, Ohio; and Fargo, N.D. The lowest rate among the large cities was in Denver (20%), with the midsized basement occupied by Lafayette, La., at 20%, Merritt Hawkins reported.
Investigators called 273 randomly selected family physicians in the large cities and 115 FPs in the midsized cities in January and February. It was the fourth such survey the company has conducted since 2004.
The survey included four other specialties – cardiology, dermatology, ob.gyn., and orthopedic surgery. The Medicaid acceptance rate for all 1,414 physicians in all five specialties in the 15 large cities was 53%, and the average rate for all specialties in the midsized cities was 60% for the 494 offices surveyed, the company noted.
Cardiology had the highest rates by specialty and dermatology the lowest in both the large and midsized cities. For all five specialties combined, Minneapolis (97%) and Fargo (100%) had the highest acceptance rates, with the lowest rates coming from Dallas (17%) for large cities and Lafayette (11%) for midsized cities, the Merritt Hawkins data show.
Address procrastination, disorganization in hoarding disorder
SAN FRANCISCO – Procrastination, disorganization, indecisiveness, and perfectionism each are significant independent predictors of hoarding severity, even though none of these associated factors is included in the DSM-5 diagnostic criteria for hoarding disorder, according to Sanjaya Saxena, MD.
Of these four associated factors, disorganization and procrastination had the strongest correlation with hoarding severity in his study. Patients meeting the DSM-5 criteria for hoarding disorder scored significantly higher on measures of disorganization and procrastination than did patients with nonhoarding obsessive-compulsive disorder or anxiety disorders, said Dr. Saxena, professor of psychiatry and director of the obsessive-compulsive disorders program at the University of California, San Diego.

The DSM-5 lists as the core symptoms of hoarding disorder difficulty in discarding possessions; perceived need to save items; excessive acquisition, clutter, and resultant distress; and impaired functioning. But while procrastination, disorganization, perfectionism, and indecisiveness aren’t included in the diagnostic criteria, Dr. Saxena said he and some other experts have considered those features to be characteristic of affected individuals. So he decided to formally test the strength of the associations.
He reported on 21 patients with hoarding disorder and 13 controls with nonhoarding OCD or an anxiety disorder. All subjects completed a battery of assessment tools, including the Beck Depression Inventory, the Beck Anxiety Inventory, the Frost Multidimensional Perfectionism Scale, the Frost Indecisiveness Scale, the Adult Inventory of Procrastination Scale, and three different measures of hoarding severity. Participants also completed a disorganization index based on their answers to three questions drawn from the Swanson, Nolan, and Pelham (SNAP-IV) Rating Scale: How often did you have difficulty organizing tasks and activities as a child? How disorganized are you in your thinking, planning, and time management? And how disorganized are your belongings at home?
Neither disorganization, procrastination, perfectionism, nor indecisiveness turned out to be associated with severity of nonhoarding OCD or anxiety disorder symptoms. Surprisingly, no significant differences were found between hoarding disorder patients and controls on the measures of indecisiveness or perfectionism, Dr. Saxena said. And the two groups did not differ in their levels of anxiety and depression.
However, levels of procrastination and disorganization were strongly correlated with hoarding severity as assessed via the Saving Inventory – Revised, the UCLA Hoarding Severity Scale, and the Hoarding Rating Scale. The hoarding disorder group’s average score on the disorganization index was 5.67, more than twice that of the 2.67 in the control group. And patients with hoarding disorder had an average Adult Inventory of Procrastination score of 50.9 out of a possible maximum of 75 points, compared with 41 in controls.
In a multivariate regression analysis, age and level of depression collectively explained 23.5% of the variance in hoarding severity scores in the study population. Disorganization independently explained an additional 29.9% of the variance, and procrastination accounted for another 19.1%, Dr. Saxena reported.
He reported having no financial conflicts regarding his study, which was funded by the university’s department of psychiatry.
SAN FRANCISCO – Procrastination, disorganization, indecisiveness, and perfectionism each are significant independent predictors of hoarding severity, even though none of these associated factors is included in the DSM-5 diagnostic criteria for hoarding disorder, according to Sanjaya Saxena, MD.
Of these four associated factors, disorganization and procrastination had the strongest correlation with hoarding severity in his study. Patients meeting the DSM-5 criteria for hoarding disorder scored significantly higher on measures of disorganization and procrastination than did patients with nonhoarding obsessive-compulsive disorder or anxiety disorders, said Dr. Saxena, professor of psychiatry and director of the obsessive-compulsive disorders program at the University of California, San Diego.
The DSM-5 lists as the core symptoms of hoarding disorder difficulty in discarding possessions; perceived need to save items; excessive acquisition, clutter, and resultant distress; and impaired functioning. But while procrastination, disorganization, perfectionism, and indecisiveness aren’t included in the diagnostic criteria, Dr. Saxena said he and some other experts have considered those features to be characteristic of affected individuals. So he decided to formally test the strength of the associations.
He reported on 21 patients with hoarding disorder and 13 controls with nonhoarding OCD or an anxiety disorder. All subjects completed a battery of assessment tools, including the Beck Depression Inventory, the Beck Anxiety Inventory, the Frost Multidimensional Perfectionism Scale, the Frost Indecisiveness Scale, the Adult Inventory of Procrastination Scale, and three different measures of hoarding severity. Participants also completed a disorganization index based on their answers to three questions drawn from the Swanson, Nolan, and Pelham (SNAP-IV) Rating Scale: How often did you have difficulty organizing tasks and activities as a child? How disorganized are you in your thinking, planning, and time management? And how disorganized are your belongings at home?
Neither disorganization, procrastination, perfectionism, nor indecisiveness turned out to be associated with severity of nonhoarding OCD or anxiety disorder symptoms. Surprisingly, no significant differences were found between hoarding disorder patients and controls on the measures of indecisiveness or perfectionism, Dr. Saxena said. And the two groups did not differ in their levels of anxiety and depression.
However, levels of procrastination and disorganization were strongly correlated with hoarding severity as assessed via the Saving Inventory – Revised, the UCLA Hoarding Severity Scale, and the Hoarding Rating Scale. The hoarding disorder group’s average score on the disorganization index was 5.67, more than twice that of the 2.67 in the control group. And patients with hoarding disorder had an average Adult Inventory of Procrastination score of 50.9 out of a possible maximum of 75 points, compared with 41 in controls.
In a multivariate regression analysis, age and level of depression collectively explained 23.5% of the variance in hoarding severity scores in the study population. Disorganization independently explained an additional 29.9% of the variance, and procrastination accounted for another 19.1%, Dr. Saxena reported.
He reported having no financial conflicts regarding his study, which was funded by the university’s department of psychiatry.
SAN FRANCISCO – Procrastination, disorganization, indecisiveness, and perfectionism each are significant independent predictors of hoarding severity, even though none of these associated factors is included in the DSM-5 diagnostic criteria for hoarding disorder, according to Sanjaya Saxena, MD.
Of these four associated factors, disorganization and procrastination had the strongest correlation with hoarding severity in his study. Patients meeting the DSM-5 criteria for hoarding disorder scored significantly higher on measures of disorganization and procrastination than did patients with nonhoarding obsessive-compulsive disorder or anxiety disorders, said Dr. Saxena, professor of psychiatry and director of the obsessive-compulsive disorders program at the University of California, San Diego.
The DSM-5 lists as the core symptoms of hoarding disorder difficulty in discarding possessions; perceived need to save items; excessive acquisition, clutter, and resultant distress; and impaired functioning. But while procrastination, disorganization, perfectionism, and indecisiveness aren’t included in the diagnostic criteria, Dr. Saxena said he and some other experts have considered those features to be characteristic of affected individuals. So he decided to formally test the strength of the associations.
He reported on 21 patients with hoarding disorder and 13 controls with nonhoarding OCD or an anxiety disorder. All subjects completed a battery of assessment tools, including the Beck Depression Inventory, the Beck Anxiety Inventory, the Frost Multidimensional Perfectionism Scale, the Frost Indecisiveness Scale, the Adult Inventory of Procrastination Scale, and three different measures of hoarding severity. Participants also completed a disorganization index based on their answers to three questions drawn from the Swanson, Nolan, and Pelham (SNAP-IV) Rating Scale: How often did you have difficulty organizing tasks and activities as a child? How disorganized are you in your thinking, planning, and time management? And how disorganized are your belongings at home?
Neither disorganization, procrastination, perfectionism, nor indecisiveness turned out to be associated with severity of nonhoarding OCD or anxiety disorder symptoms. Surprisingly, no significant differences were found between hoarding disorder patients and controls on the measures of indecisiveness or perfectionism, Dr. Saxena said. And the two groups did not differ in their levels of anxiety and depression.
However, levels of procrastination and disorganization were strongly correlated with hoarding severity as assessed via the Saving Inventory – Revised, the UCLA Hoarding Severity Scale, and the Hoarding Rating Scale. The hoarding disorder group’s average score on the disorganization index was 5.67, more than twice that of the 2.67 in the control group. And patients with hoarding disorder had an average Adult Inventory of Procrastination score of 50.9 out of a possible maximum of 75 points, compared with 41 in controls.
In a multivariate regression analysis, age and level of depression collectively explained 23.5% of the variance in hoarding severity scores in the study population. Disorganization independently explained an additional 29.9% of the variance, and procrastination accounted for another 19.1%, Dr. Saxena reported.
He reported having no financial conflicts regarding his study, which was funded by the university’s department of psychiatry.
AT THE ANXIETY AND DEPRESSION CONFERENCE 2017
Key clinical point:
Major finding: Severity of procrastination explained 30% of the variance in hoarding severity scores between patients with hoarding disorder and controls with nonhoarding obsessive-compulsive disorder or an anxiety disorder.
Data source: A cross-sectional study involving 21 patients with hoarding disorder and 13 controls, all of whom completed a battery of tests assessing anxiety, depression, hoarding severity, disorganization, procrastination, indecisiveness, and perfectionism.
Disclosures: The presenter reported having no financial conflicts regarding the study, which was funded by a university psychiatry department.
Target self-medication of mood and anxiety symptoms
SAN FRANCISCO – Drinking to alleviate mood or anxiety symptoms is responsible for 12%-16% of cases of new-onset alcohol use disorder in affected individuals, Jitender Sareen, MD, said at the annual conference of the Anxiety and Depression Association of America.
Similarly, the use of prescription or nonprescription drugs to self-medicate mood or anxiety symptoms accounts for 20% of new-onset drug use disorders in this population, added Dr. Sareen, professor and head of the department of psychiatry at the University of Manitoba in Winnipeg.

He was a coauthor of two landmark longitudinal epidemiologic studies that support the concept of self-medication as a direct causal mechanism that explains a phenomenon often observed in clinical practice: namely, the high rate of comorbid mood or anxiety disorders accompanied by an alcohol or substance use disorder.
“The clinical implication is that questions about self-medication with alcohol or drugs should be included in the assessment of patients with anxiety and mood symptoms, because self-medication is a marker of higher likelihood of psychopathology. And psychologic therapies like cognitive-behavioral therapy and dialectical behavior therapy could prevent onset of substance use disorders by teaching patients emotion regulation skills to manage their mood and anxiety symptoms without self-medication,” Dr. Sareen said.
The first longitudinal study of the role of self-medication in the development of comorbid anxiety and substance use disorders included 34,653 nationally representative adults who completed both the initial face-to-face National Epidemiologic Survey on Alcohol and Related Conditions in 2001-2002 and a follow-up survey conducted 3 years later.
During the 3-year follow-up period, 9.7% of subjects developed a new-onset anxiety disorder, 5.9% of participants newly met DSM-IV diagnostic criteria for alcohol use disorder, and 2% developed a new-onset drug use disorder.
Among subjects who met the criteria for an anxiety disorder at baseline and at that time also reported self-medication with alcohol, 12.6% developed an incident alcohol use disorder during follow-up. Among those who self-medicated with drugs, 10.4% developed a drug use disorder.
In contrast, only 4.7% of subjects with a baseline anxiety disorder who did not self-medicate with alcohol at baseline developed an incident alcohol use disorder. And an incident drug use disorder occurred in 1.7% of patients with a baseline anxiety disorder who did not self-medicate with drugs.
Among patients with a baseline alcohol or other substance use disorder, self-medication with alcohol was associated with an adjusted 2.13-fold increased likelihood of developing social phobia during 3 years of follow-up, while self-medication with other drugs was independently associated with a 3.27-fold increased likelihood of subsequently developing social phobia.
In a multivariate logistic regression analysis, Dr. Sareen and his coinvestigators determined that self-medication with alcohol by patients with an anxiety disorder at baseline was associated with a 2.63-fold increased risk of incident alcohol use disorder during follow-up. Self-medication with drugs in patients with a baseline anxiety disorder was associated with a 4.99-fold risk of a new-onset substance use disorder during the 3 years of follow-up (Arch Gen Psychiatry. 2011;68[8]:800-7).
In a subsequent analysis of the same prospectively studied population, Dr. Sareen and his colleagues focused specifically on drinking to self-medicate mood symptoms. They found that self-medication with alcohol was associated with an adjusted 3.1-fold increased likelihood of new-onset alcohol dependence during the 3-year follow-up, as well as with a 3.45-fold increased risk of persistence of alcohol dependence. Roughly 12% of all cases of incident alcohol dependence arising during follow-up of patients with baseline mood symptoms were attributed to self-medication with alcohol. The increased risk of new-onset alcohol dependence was observed not only in subjects who met DSM-IV criteria for an affective disorder, but in those with subthreshold mood symptoms as well (JAMA Psychiatry. 2013 Jul;70[7]:718-26).
Again, this points to drinking as a behavior employed to self-medicate mood symptoms as a potential target for preventive interventions aimed at reducing the occurrence of alcohol dependence. As yet, however, no formal studies have been done to confirm the effectiveness of this strategy, the psychiatrist continued.
Dr. Sareen was not involved in the third iteration of the National Epidemiologic Survey on Alcohol and Related Conditions, in which a different group of 36,309 nationally representative adults was interviewed during 2011-2013 to assess the impact of the DSM-5 criteria for alcohol use disorder. Using DSM-5, 13.9% of the population met criteria for an alcohol use disorder during the past 12 months, and the lifetime prevalence of alcohol use disorder was 29.1%. Fewer than one in five subjects with a lifetime DSM-5 alcohol use disorder had ever been treated.
In the first national survey, which used DSM-IV criteria, the 12-month and lifetime prevalences of alcohol abuse and/or dependence were 8.5% and 30.3%, respectively.
DSM-5 alcohol use disorder was highly comorbid. Both lifetime and 12-month alcohol use disorder were associated with significantly increased likelihood of other substance use disorders, major depression, bipolar I disorder, borderline personality disorder, and antisocial personality disorder.
These data indicate “an urgent need to educate the public and policy makers about alcohol use disorder and its treatment alternatives, to destigmatize the disorder, and to encourage those who cannot reduce their alcohol consumption on their own, despite substantial harm to themselves and others, to seek treatment,” the investigators wrote (JAMA Psychiatry. 2015 Aug;72[8]:757-66).
The surveys were supported by the National Institute on Alcohol Abuse and Alcoholism. Dr. Sareen reported having no financial conflicts of interest.
SAN FRANCISCO – Drinking to alleviate mood or anxiety symptoms is responsible for 12%-16% of cases of new-onset alcohol use disorder in affected individuals, Jitender Sareen, MD, said at the annual conference of the Anxiety and Depression Association of America.
Similarly, the use of prescription or nonprescription drugs to self-medicate mood or anxiety symptoms accounts for 20% of new-onset drug use disorders in this population, added Dr. Sareen, professor and head of the department of psychiatry at the University of Manitoba in Winnipeg.
He was a coauthor of two landmark longitudinal epidemiologic studies that support the concept of self-medication as a direct causal mechanism that explains a phenomenon often observed in clinical practice: namely, the high rate of comorbid mood or anxiety disorders accompanied by an alcohol or substance use disorder.
“The clinical implication is that questions about self-medication with alcohol or drugs should be included in the assessment of patients with anxiety and mood symptoms, because self-medication is a marker of higher likelihood of psychopathology. And psychologic therapies like cognitive-behavioral therapy and dialectical behavior therapy could prevent onset of substance use disorders by teaching patients emotion regulation skills to manage their mood and anxiety symptoms without self-medication,” Dr. Sareen said.
The first longitudinal study of the role of self-medication in the development of comorbid anxiety and substance use disorders included 34,653 nationally representative adults who completed both the initial face-to-face National Epidemiologic Survey on Alcohol and Related Conditions in 2001-2002 and a follow-up survey conducted 3 years later.
During the 3-year follow-up period, 9.7% of subjects developed a new-onset anxiety disorder, 5.9% of participants newly met DSM-IV diagnostic criteria for alcohol use disorder, and 2% developed a new-onset drug use disorder.
Among subjects who met the criteria for an anxiety disorder at baseline and at that time also reported self-medication with alcohol, 12.6% developed an incident alcohol use disorder during follow-up. Among those who self-medicated with drugs, 10.4% developed a drug use disorder.
In contrast, only 4.7% of subjects with a baseline anxiety disorder who did not self-medicate with alcohol at baseline developed an incident alcohol use disorder. And an incident drug use disorder occurred in 1.7% of patients with a baseline anxiety disorder who did not self-medicate with drugs.
Among patients with a baseline alcohol or other substance use disorder, self-medication with alcohol was associated with an adjusted 2.13-fold increased likelihood of developing social phobia during 3 years of follow-up, while self-medication with other drugs was independently associated with a 3.27-fold increased likelihood of subsequently developing social phobia.
In a multivariate logistic regression analysis, Dr. Sareen and his coinvestigators determined that self-medication with alcohol by patients with an anxiety disorder at baseline was associated with a 2.63-fold increased risk of incident alcohol use disorder during follow-up. Self-medication with drugs in patients with a baseline anxiety disorder was associated with a 4.99-fold risk of a new-onset substance use disorder during the 3 years of follow-up (Arch Gen Psychiatry. 2011;68[8]:800-7).
In a subsequent analysis of the same prospectively studied population, Dr. Sareen and his colleagues focused specifically on drinking to self-medicate mood symptoms. They found that self-medication with alcohol was associated with an adjusted 3.1-fold increased likelihood of new-onset alcohol dependence during the 3-year follow-up, as well as with a 3.45-fold increased risk of persistence of alcohol dependence. Roughly 12% of all cases of incident alcohol dependence arising during follow-up of patients with baseline mood symptoms were attributed to self-medication with alcohol. The increased risk of new-onset alcohol dependence was observed not only in subjects who met DSM-IV criteria for an affective disorder, but in those with subthreshold mood symptoms as well (JAMA Psychiatry. 2013 Jul;70[7]:718-26).
Again, this points to drinking as a behavior employed to self-medicate mood symptoms as a potential target for preventive interventions aimed at reducing the occurrence of alcohol dependence. As yet, however, no formal studies have been done to confirm the effectiveness of this strategy, the psychiatrist continued.
Dr. Sareen was not involved in the third iteration of the National Epidemiologic Survey on Alcohol and Related Conditions, in which a different group of 36,309 nationally representative adults was interviewed during 2011-2013 to assess the impact of the DSM-5 criteria for alcohol use disorder. Using DSM-5, 13.9% of the population met criteria for an alcohol use disorder during the past 12 months, and the lifetime prevalence of alcohol use disorder was 29.1%. Fewer than one in five subjects with a lifetime DSM-5 alcohol use disorder had ever been treated.
In the first national survey, which used DSM-IV criteria, the 12-month and lifetime prevalences of alcohol abuse and/or dependence were 8.5% and 30.3%, respectively.
DSM-5 alcohol use disorder was highly comorbid. Both lifetime and 12-month alcohol use disorder were associated with significantly increased likelihood of other substance use disorders, major depression, bipolar I disorder, borderline personality disorder, and antisocial personality disorder.
These data indicate “an urgent need to educate the public and policy makers about alcohol use disorder and its treatment alternatives, to destigmatize the disorder, and to encourage those who cannot reduce their alcohol consumption on their own, despite substantial harm to themselves and others, to seek treatment,” the investigators wrote (JAMA Psychiatry. 2015 Aug;72[8]:757-66).
The surveys were supported by the National Institute on Alcohol Abuse and Alcoholism. Dr. Sareen reported having no financial conflicts of interest.
SAN FRANCISCO – Drinking to alleviate mood or anxiety symptoms is responsible for 12%-16% of cases of new-onset alcohol use disorder in affected individuals, Jitender Sareen, MD, said at the annual conference of the Anxiety and Depression Association of America.
Similarly, the use of prescription or nonprescription drugs to self-medicate mood or anxiety symptoms accounts for 20% of new-onset drug use disorders in this population, added Dr. Sareen, professor and head of the department of psychiatry at the University of Manitoba in Winnipeg.
He was a coauthor of two landmark longitudinal epidemiologic studies that support the concept of self-medication as a direct causal mechanism that explains a phenomenon often observed in clinical practice: namely, the high rate of comorbid mood or anxiety disorders accompanied by an alcohol or substance use disorder.
“The clinical implication is that questions about self-medication with alcohol or drugs should be included in the assessment of patients with anxiety and mood symptoms, because self-medication is a marker of higher likelihood of psychopathology. And psychologic therapies like cognitive-behavioral therapy and dialectical behavior therapy could prevent onset of substance use disorders by teaching patients emotion regulation skills to manage their mood and anxiety symptoms without self-medication,” Dr. Sareen said.
The first longitudinal study of the role of self-medication in the development of comorbid anxiety and substance use disorders included 34,653 nationally representative adults who completed both the initial face-to-face National Epidemiologic Survey on Alcohol and Related Conditions in 2001-2002 and a follow-up survey conducted 3 years later.
During the 3-year follow-up period, 9.7% of subjects developed a new-onset anxiety disorder, 5.9% of participants newly met DSM-IV diagnostic criteria for alcohol use disorder, and 2% developed a new-onset drug use disorder.
Among subjects who met the criteria for an anxiety disorder at baseline and at that time also reported self-medication with alcohol, 12.6% developed an incident alcohol use disorder during follow-up. Among those who self-medicated with drugs, 10.4% developed a drug use disorder.
In contrast, only 4.7% of subjects with a baseline anxiety disorder who did not self-medicate with alcohol at baseline developed an incident alcohol use disorder. And an incident drug use disorder occurred in 1.7% of patients with a baseline anxiety disorder who did not self-medicate with drugs.
Among patients with a baseline alcohol or other substance use disorder, self-medication with alcohol was associated with an adjusted 2.13-fold increased likelihood of developing social phobia during 3 years of follow-up, while self-medication with other drugs was independently associated with a 3.27-fold increased likelihood of subsequently developing social phobia.
In a multivariate logistic regression analysis, Dr. Sareen and his coinvestigators determined that self-medication with alcohol by patients with an anxiety disorder at baseline was associated with a 2.63-fold increased risk of incident alcohol use disorder during follow-up. Self-medication with drugs in patients with a baseline anxiety disorder was associated with a 4.99-fold risk of a new-onset substance use disorder during the 3 years of follow-up (Arch Gen Psychiatry. 2011;68[8]:800-7).
In a subsequent analysis of the same prospectively studied population, Dr. Sareen and his colleagues focused specifically on drinking to self-medicate mood symptoms. They found that self-medication with alcohol was associated with an adjusted 3.1-fold increased likelihood of new-onset alcohol dependence during the 3-year follow-up, as well as with a 3.45-fold increased risk of persistence of alcohol dependence. Roughly 12% of all cases of incident alcohol dependence arising during follow-up of patients with baseline mood symptoms were attributed to self-medication with alcohol. The increased risk of new-onset alcohol dependence was observed not only in subjects who met DSM-IV criteria for an affective disorder, but in those with subthreshold mood symptoms as well (JAMA Psychiatry. 2013 Jul;70[7]:718-26).
Again, this points to drinking as a behavior employed to self-medicate mood symptoms as a potential target for preventive interventions aimed at reducing the occurrence of alcohol dependence. As yet, however, no formal studies have been done to confirm the effectiveness of this strategy, the psychiatrist continued.
Dr. Sareen was not involved in the third iteration of the National Epidemiologic Survey on Alcohol and Related Conditions, in which a different group of 36,309 nationally representative adults was interviewed during 2011-2013 to assess the impact of the DSM-5 criteria for alcohol use disorder. Using DSM-5, 13.9% of the population met criteria for an alcohol use disorder during the past 12 months, and the lifetime prevalence of alcohol use disorder was 29.1%. Fewer than one in five subjects with a lifetime DSM-5 alcohol use disorder had ever been treated.
In the first national survey, which used DSM-IV criteria, the 12-month and lifetime prevalences of alcohol abuse and/or dependence were 8.5% and 30.3%, respectively.
DSM-5 alcohol use disorder was highly comorbid. Both lifetime and 12-month alcohol use disorder were associated with significantly increased likelihood of other substance use disorders, major depression, bipolar I disorder, borderline personality disorder, and antisocial personality disorder.
These data indicate “an urgent need to educate the public and policy makers about alcohol use disorder and its treatment alternatives, to destigmatize the disorder, and to encourage those who cannot reduce their alcohol consumption on their own, despite substantial harm to themselves and others, to seek treatment,” the investigators wrote (JAMA Psychiatry. 2015 Aug;72[8]:757-66).
The surveys were supported by the National Institute on Alcohol Abuse and Alcoholism. Dr. Sareen reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM THE ANXIETY AND DEPRESSION CONFERENCE 2017
Sarilumab showed sustained effect on RA progression at 3 years
BIRMINGHAM, ENGLAND – A “durable clinical response and stabilization of structural damage” was observed at 3 years of follow-up in the Long Term Evaluation of Sarilumab in Rheumatoid Arthritis Patients (SARIL-RA-EXTEND) study.
Désirée van der Heijde, MD, PhD, who reported the findings of the EXTEND study at the British Society for Rheumatology annual conference, noted that the benefit was seen regardless of the initial treatment that had been given at baseline.

The aim of the EXTEND trial was to examine the continuity of response to sarilumab seen in the MOBILITY trial, said Dr. van der Heijde, professor of rheumatology at Leiden (The Netherlands) University Medical Center.
Sarilumab is a fully human (IgG1) monoclonal antibody that binds to interleukin (IL)-6 receptors, both soluble and membrane-bound, and thus inhibits IL-6-mediated signaling through the soluble IL-6R alpha and membrane-bound IL-6R alpha receptors. It is undergoing regulatory approval in the United States, European Union, and Japan, but was recently approved in Canada for treatment of adult patients with moderate to severe rheumatoid arthritis (RA) who have had an inadequate response to one or more biologic or nonbiologic disease-modifying antirheumatic drugs (DMARDs) (Drugs. 2017;77:705-12).
In the MOBILITY trial, 1,197 patients who were being treated with methotrexate but who had an inadequate response were randomized to receive placebo (n = 398) or sarilumab given subcutaneously every 2 weeks at one of two doses: 150 mg (n = 400) or 200 mg (n = 399).
EXTEND allowed patients completing this trial who still had active disease to continue or start (if they had been given placebo) treatment with sarilumab at a dose of 200 mg given every 2 weeks, with dose reduction to 150 mg every 2 weeks if needed, in addition to methotrexate. A total of 901 patients participated in the extension study.
“In the MOBILITY trial, all three groups were very balanced, and if you then take the patients who entered the EXTEND trial, they are very similar to the patients who also were randomized into MOBILITY,” Dr. van der Heijde said.
This was a fairly typical RA population, she observed: About 80% were female, the mean age was 50 years, and the mean duration of RA was 9 years. About 20%-25% had prior treatment with a DMARD, more than 80% were rheumatoid factor or anti-CCP antibody positive. There were similar mean C-reactive protein (CRP) levels between the groups, and the 28-joint disease activity score (DAS28) with CRP was around 6, and Clinical Disease Activity Index (CDAI) score around 40.
Radiographs that were taken at baseline, at the end of year 2, and at the end of year 3 were reread by two independent readers and scored together in one session. Data had to be extrapolated for 29 patients who did not have a radiographs taken at year 3 but who had been seen during the third year of treatment.
The significant radiographic inhibition seen at the end of the MOBILITY trial in both the 150-mg and 200-mg active treatment groups was sustained in the EXTEND study.
“There is a small progression between year 2 and 3, and this progression is quite similar in all the three treatment arms,” Dr. van der Heijde reported, nothing that all patients were taking 200 mg of sarilumab at this point.
The mean change in the modified total Sharp score (mTSS) from year 2 to 3 was 0.35 in the patients who had originally been randomized to the placebo arm, 0.64 in patients originally randomized to 150 mg sarilumab every 2 weeks, and 0.44 in those originally taking 200 mg sarilumab every 2 weeks.
From baseline to year 3, the mean change in mTSS were a respective 3.3, 1.9, and 0.8.
“If you present the data in a different way, like the percentage of patients showing no progression, you see the differentiation between the patients who started on placebo versus those who were started on sarilumab 150 mg or 200 mg,” said Dr. van der Heijde.
At year 2, 67%, 59%, and 48% of patients treated with sarilumab 200 mg, sarilumab 150 mg, or placebo, respectively had no progression in mTSS (signified by a change from baseline of 0.5 points or more).
At year 3, corresponding rates were a respective 75%, 55%, and 49%.
DAS-28-CRP response at year 3 was similar across the initial treatment groups, Dr. van der Heijde observed. Reductions seen in the MOBILITY trial were clearly continued, she said. The percentage of patients achieving DAS-28-CRP of less than 2.6 was 22%, 34%, and 36% of placebo, sarilumab 150-mg, and sarilumab 200-mg treated patients at the end of the MOBILITY study. At the end of year 2, the corresponding numbers were 60%, 62%, and 62%, and by year 3, not much had changed in the percentage of patients achieving DAS-28-CRP of less than 2.6: 58% for placebo, 62% for sarilumab 150 mg, and 68% for sarilumab 200 mg.
Similar results were seen for patients achieving a CDAI of 2.8 or lower at years 2 and 3 in the extension study.
Treatment-emergent adverse events (TEAEs) occurred in 89.7% of patients over 3 years. One in five (20%) patients experienced serious adverse events, with 23% of patients discontinuing treatment because of TEAEs. There were 9 (0.8%) deaths during the trial.
TEAEs that occurred at rates of 5% or higher in any treatment group were neutropenia in 19.4%, increased alanine aminotransferase in 13.0%, and upper respiratory tract infections in 12.7%.
There were some changes in laboratory values, Dr. van der Heijde said, but “most of the changes were very small” and in line with the effects expected with IL-6 inhibition.
The study was sponsored by Sanofi Genzyme and Regeneron Pharmaceuticals. Dr. van der Heijde and coauthors disclosed receiving consulting fees, research grants, or both from multiple pharmaceutical companies, including the sponsors of the study. Dr. van der Heijde is director of Imaging Rheumatology.
BIRMINGHAM, ENGLAND – A “durable clinical response and stabilization of structural damage” was observed at 3 years of follow-up in the Long Term Evaluation of Sarilumab in Rheumatoid Arthritis Patients (SARIL-RA-EXTEND) study.
Désirée van der Heijde, MD, PhD, who reported the findings of the EXTEND study at the British Society for Rheumatology annual conference, noted that the benefit was seen regardless of the initial treatment that had been given at baseline.
The aim of the EXTEND trial was to examine the continuity of response to sarilumab seen in the MOBILITY trial, said Dr. van der Heijde, professor of rheumatology at Leiden (The Netherlands) University Medical Center.
Sarilumab is a fully human (IgG1) monoclonal antibody that binds to interleukin (IL)-6 receptors, both soluble and membrane-bound, and thus inhibits IL-6-mediated signaling through the soluble IL-6R alpha and membrane-bound IL-6R alpha receptors. It is undergoing regulatory approval in the United States, European Union, and Japan, but was recently approved in Canada for treatment of adult patients with moderate to severe rheumatoid arthritis (RA) who have had an inadequate response to one or more biologic or nonbiologic disease-modifying antirheumatic drugs (DMARDs) (Drugs. 2017;77:705-12).
In the MOBILITY trial, 1,197 patients who were being treated with methotrexate but who had an inadequate response were randomized to receive placebo (n = 398) or sarilumab given subcutaneously every 2 weeks at one of two doses: 150 mg (n = 400) or 200 mg (n = 399).
EXTEND allowed patients completing this trial who still had active disease to continue or start (if they had been given placebo) treatment with sarilumab at a dose of 200 mg given every 2 weeks, with dose reduction to 150 mg every 2 weeks if needed, in addition to methotrexate. A total of 901 patients participated in the extension study.
“In the MOBILITY trial, all three groups were very balanced, and if you then take the patients who entered the EXTEND trial, they are very similar to the patients who also were randomized into MOBILITY,” Dr. van der Heijde said.
This was a fairly typical RA population, she observed: About 80% were female, the mean age was 50 years, and the mean duration of RA was 9 years. About 20%-25% had prior treatment with a DMARD, more than 80% were rheumatoid factor or anti-CCP antibody positive. There were similar mean C-reactive protein (CRP) levels between the groups, and the 28-joint disease activity score (DAS28) with CRP was around 6, and Clinical Disease Activity Index (CDAI) score around 40.
Radiographs that were taken at baseline, at the end of year 2, and at the end of year 3 were reread by two independent readers and scored together in one session. Data had to be extrapolated for 29 patients who did not have a radiographs taken at year 3 but who had been seen during the third year of treatment.
The significant radiographic inhibition seen at the end of the MOBILITY trial in both the 150-mg and 200-mg active treatment groups was sustained in the EXTEND study.
“There is a small progression between year 2 and 3, and this progression is quite similar in all the three treatment arms,” Dr. van der Heijde reported, nothing that all patients were taking 200 mg of sarilumab at this point.
The mean change in the modified total Sharp score (mTSS) from year 2 to 3 was 0.35 in the patients who had originally been randomized to the placebo arm, 0.64 in patients originally randomized to 150 mg sarilumab every 2 weeks, and 0.44 in those originally taking 200 mg sarilumab every 2 weeks.
From baseline to year 3, the mean change in mTSS were a respective 3.3, 1.9, and 0.8.
“If you present the data in a different way, like the percentage of patients showing no progression, you see the differentiation between the patients who started on placebo versus those who were started on sarilumab 150 mg or 200 mg,” said Dr. van der Heijde.
At year 2, 67%, 59%, and 48% of patients treated with sarilumab 200 mg, sarilumab 150 mg, or placebo, respectively had no progression in mTSS (signified by a change from baseline of 0.5 points or more).
At year 3, corresponding rates were a respective 75%, 55%, and 49%.
DAS-28-CRP response at year 3 was similar across the initial treatment groups, Dr. van der Heijde observed. Reductions seen in the MOBILITY trial were clearly continued, she said. The percentage of patients achieving DAS-28-CRP of less than 2.6 was 22%, 34%, and 36% of placebo, sarilumab 150-mg, and sarilumab 200-mg treated patients at the end of the MOBILITY study. At the end of year 2, the corresponding numbers were 60%, 62%, and 62%, and by year 3, not much had changed in the percentage of patients achieving DAS-28-CRP of less than 2.6: 58% for placebo, 62% for sarilumab 150 mg, and 68% for sarilumab 200 mg.
Similar results were seen for patients achieving a CDAI of 2.8 or lower at years 2 and 3 in the extension study.
Treatment-emergent adverse events (TEAEs) occurred in 89.7% of patients over 3 years. One in five (20%) patients experienced serious adverse events, with 23% of patients discontinuing treatment because of TEAEs. There were 9 (0.8%) deaths during the trial.
TEAEs that occurred at rates of 5% or higher in any treatment group were neutropenia in 19.4%, increased alanine aminotransferase in 13.0%, and upper respiratory tract infections in 12.7%.
There were some changes in laboratory values, Dr. van der Heijde said, but “most of the changes were very small” and in line with the effects expected with IL-6 inhibition.
The study was sponsored by Sanofi Genzyme and Regeneron Pharmaceuticals. Dr. van der Heijde and coauthors disclosed receiving consulting fees, research grants, or both from multiple pharmaceutical companies, including the sponsors of the study. Dr. van der Heijde is director of Imaging Rheumatology.
BIRMINGHAM, ENGLAND – A “durable clinical response and stabilization of structural damage” was observed at 3 years of follow-up in the Long Term Evaluation of Sarilumab in Rheumatoid Arthritis Patients (SARIL-RA-EXTEND) study.
Désirée van der Heijde, MD, PhD, who reported the findings of the EXTEND study at the British Society for Rheumatology annual conference, noted that the benefit was seen regardless of the initial treatment that had been given at baseline.
The aim of the EXTEND trial was to examine the continuity of response to sarilumab seen in the MOBILITY trial, said Dr. van der Heijde, professor of rheumatology at Leiden (The Netherlands) University Medical Center.
Sarilumab is a fully human (IgG1) monoclonal antibody that binds to interleukin (IL)-6 receptors, both soluble and membrane-bound, and thus inhibits IL-6-mediated signaling through the soluble IL-6R alpha and membrane-bound IL-6R alpha receptors. It is undergoing regulatory approval in the United States, European Union, and Japan, but was recently approved in Canada for treatment of adult patients with moderate to severe rheumatoid arthritis (RA) who have had an inadequate response to one or more biologic or nonbiologic disease-modifying antirheumatic drugs (DMARDs) (Drugs. 2017;77:705-12).
In the MOBILITY trial, 1,197 patients who were being treated with methotrexate but who had an inadequate response were randomized to receive placebo (n = 398) or sarilumab given subcutaneously every 2 weeks at one of two doses: 150 mg (n = 400) or 200 mg (n = 399).
EXTEND allowed patients completing this trial who still had active disease to continue or start (if they had been given placebo) treatment with sarilumab at a dose of 200 mg given every 2 weeks, with dose reduction to 150 mg every 2 weeks if needed, in addition to methotrexate. A total of 901 patients participated in the extension study.
“In the MOBILITY trial, all three groups were very balanced, and if you then take the patients who entered the EXTEND trial, they are very similar to the patients who also were randomized into MOBILITY,” Dr. van der Heijde said.
This was a fairly typical RA population, she observed: About 80% were female, the mean age was 50 years, and the mean duration of RA was 9 years. About 20%-25% had prior treatment with a DMARD, more than 80% were rheumatoid factor or anti-CCP antibody positive. There were similar mean C-reactive protein (CRP) levels between the groups, and the 28-joint disease activity score (DAS28) with CRP was around 6, and Clinical Disease Activity Index (CDAI) score around 40.
Radiographs that were taken at baseline, at the end of year 2, and at the end of year 3 were reread by two independent readers and scored together in one session. Data had to be extrapolated for 29 patients who did not have a radiographs taken at year 3 but who had been seen during the third year of treatment.
The significant radiographic inhibition seen at the end of the MOBILITY trial in both the 150-mg and 200-mg active treatment groups was sustained in the EXTEND study.
“There is a small progression between year 2 and 3, and this progression is quite similar in all the three treatment arms,” Dr. van der Heijde reported, nothing that all patients were taking 200 mg of sarilumab at this point.
The mean change in the modified total Sharp score (mTSS) from year 2 to 3 was 0.35 in the patients who had originally been randomized to the placebo arm, 0.64 in patients originally randomized to 150 mg sarilumab every 2 weeks, and 0.44 in those originally taking 200 mg sarilumab every 2 weeks.
From baseline to year 3, the mean change in mTSS were a respective 3.3, 1.9, and 0.8.
“If you present the data in a different way, like the percentage of patients showing no progression, you see the differentiation between the patients who started on placebo versus those who were started on sarilumab 150 mg or 200 mg,” said Dr. van der Heijde.
At year 2, 67%, 59%, and 48% of patients treated with sarilumab 200 mg, sarilumab 150 mg, or placebo, respectively had no progression in mTSS (signified by a change from baseline of 0.5 points or more).
At year 3, corresponding rates were a respective 75%, 55%, and 49%.
DAS-28-CRP response at year 3 was similar across the initial treatment groups, Dr. van der Heijde observed. Reductions seen in the MOBILITY trial were clearly continued, she said. The percentage of patients achieving DAS-28-CRP of less than 2.6 was 22%, 34%, and 36% of placebo, sarilumab 150-mg, and sarilumab 200-mg treated patients at the end of the MOBILITY study. At the end of year 2, the corresponding numbers were 60%, 62%, and 62%, and by year 3, not much had changed in the percentage of patients achieving DAS-28-CRP of less than 2.6: 58% for placebo, 62% for sarilumab 150 mg, and 68% for sarilumab 200 mg.
Similar results were seen for patients achieving a CDAI of 2.8 or lower at years 2 and 3 in the extension study.
Treatment-emergent adverse events (TEAEs) occurred in 89.7% of patients over 3 years. One in five (20%) patients experienced serious adverse events, with 23% of patients discontinuing treatment because of TEAEs. There were 9 (0.8%) deaths during the trial.
TEAEs that occurred at rates of 5% or higher in any treatment group were neutropenia in 19.4%, increased alanine aminotransferase in 13.0%, and upper respiratory tract infections in 12.7%.
There were some changes in laboratory values, Dr. van der Heijde said, but “most of the changes were very small” and in line with the effects expected with IL-6 inhibition.
The study was sponsored by Sanofi Genzyme and Regeneron Pharmaceuticals. Dr. van der Heijde and coauthors disclosed receiving consulting fees, research grants, or both from multiple pharmaceutical companies, including the sponsors of the study. Dr. van der Heijde is director of Imaging Rheumatology.
AT RHEUMATOLOGY 2017
Key clinical point:
Major finding: The mean change in the modified total Sharp score (mTSS) from year 2 to 3 was 0.35 in the patients who had originally been randomized to the placebo arm, 0.64 in patients originally randomized to 150 mg sarilumab every 2 weeks, and 0.44 in those originally taking 200 mg sarilumab every 2 weeks.
Data source: SARIL-RA-EXTEND: a multicenter, uncontrolled extension study involving 1,197 patients who had participated in the phase III SARIL-RA-MOBILITY trial.
Disclosures: The study was sponsored by Sanofi Genzyme and Regeneron Pharmaceuticals. Dr. van der Heijde and her coauthors disclosed receiving consulting fees, research grants, or both from multiple pharmaceutical companies, including the sponsors of the study. Dr. van der Heijde is director of Imaging Rheumatology.

Here’s what’s trending at SHM
SHM gives QI a new look
SHM is proud to announce that its Center for Hospital Innovation & Improvement has a fresh look and name: SHM’s Center for Quality Improvement. While the name may have changed, SHM’s Center for QI will remain your partner in quality and patient safety.
“SHM’s Center for QI provides a comprehensive set of resources and programs to support hospitalists and other hospital clinicians as they work to improve quality and safety in their hospitals,” says Eric E. Howell, MD, MHM, senior physician advisor for SHM’s Center for QI.
SHM’s Center for QI’s mentored implementation programs are deployed in hundreds of hospitals and have been recognized with the John M. Eisenberg Award. More recently, its opioid-safety program (RADEO) was recognized by the CMS for its efforts to enhance patient safety.
Visit http://www.hospitalmedicine.org/QI to learn more about SHM’s Center for QI and about opportunities for partnerships, solutions, and tools to address your QI needs.
PHM 2017 is coming! Book your ticket to Nashville today
Pediatric Hospital Medicine (PHM) 2017 is the largest, leading educational event for health care professionals who specialize in the care of hospitalized children. This year’s meeting will be held July 20-23 at the Omni Nashville in Tennessee.
Attendees will have the opportunity to network with colleagues from across the nation, learn from renowned faculty from throughout the discipline, and acquire skills, tools, and resources to directly benefit their patients and practice.
PHM 2017 has been designed to provide participants with tools to improve clinical skills and practice, address management issues, lead change and innovation within their institutions, and network with thought leaders to collaborate and learn about new innovations.
View the full meeting schedule, educational objectives, and more at www.peds2017.org.![]()
Benchmark your HMG appropriately with the State of Hospital Medicine Report
The State of Hospital Medicine Report continues to be the best source of detail regarding the configuration and operation of hospital medicine groups. The biennial report provides current data on hospitalist compensation and production, in addition to cutting-edge knowledge covering practice demographics, staffing levels, turnover, staff growth, compensation methods, and financial support for solid, evidence-based management decisions.
“We’ve used data from the report to hold more informed discussions with the group that provides our note-coding services and to determine how to benchmark our nocturnists’ workloads and pay,” said Andrew White, MD, SFHM, director of the Hospital Medicine Service at the University of Washington in Seattle. “The results are broken into region and academic practice type, which gives me the confidence that I’m looking at results from groups like mine, rather than comparing to the country-wide average.”
The report is designed for hospital medicine leaders (both physician leaders and nonphysician practice administrators and executives), as well as frontline hospitalists, nurse practitioners, physician assistants, pediatricians, and internal and family medicine physicians.
In addition to the print version, the 2016 State of Hospital Medicine Report is also available in an enhanced, fully searchable digital version. To order your copy in either print or digital, visit www.hospitalmedicine.org/survey.
Learn how to drive change as a leader in hospital medicine
A successful hospitalist program requires strong leadership from the floor to the C-suite. SHM’s Leadership Academy prepares clinical and academic leaders with vital skills that, traditionally, are not taught in medical school or typical residency programs. This year’s meeting will be held October 23-26 at the JW Marriott Camelback Inn in Scottsdale, Ariz.
New for Leadership Academy 2017, Strategic Essentials (formerly Leadership Foundations), Influential Management, and Mastering Teamwork will be available to all attendees, regardless of previous attendance. SHM provides recommendations for interested registrants so they can determine which course fits them best in their leadership journey.
Take the Strategic Essentials course to evaluate your personal leadership strengths and weaknesses, understand key hospital drivers, and more.
If you are looking to learn skills needed to drive culture change through specific leadership behaviors as well as financial storytelling, then Leadership: Influential Management would be a great course for you.
The third course, Leadership: Mastering Teamwork, will help attendees learn to critically assess program growth opportunities, lead and motivate teams, and design effective communication strategies. Learn more at www.shmleadershipacademy.org.![]()
Stay ahead of the MACRA curve with SHM
The Medicare Access and CHIP Reauthorization Act (MACRA) put into motion the new Quality Payment Program, which replaces past pay-for-performance programs, such as the Physician Quality Reporting System and physician value-based modifier. The new program has many complicated requirements, and hospitalists will be impacted.
The first year of the program has flexible participation, yet hospitalists need to do at least one thing (report one quality measure, attest to one improvement activity) in the program in order to avoid a 4% penalty to Medicare payments. 2017 is the first reporting year, so now is the time for providers to familiarize themselves with the requirements.
To support hospitalists who are looking for hospital medicine–specific ways to participate and avoid penalties, SHM hosted a webinar that is now available at www.macraforhm.org under “Resources.” SHM’s policy staff broke down the program requirements and went into detail on ways in which hospitalists can and should participate in the new program. Updates and other resources are also available at www.macraforhm.org.
Looking to be a speaker at Hospital Medicine 2018?
The Society of Hospital Medicine reminds you to submit your workshop proposal for the 2018 Annual Meeting to be held April 8-11, 2018, at the Orlando World Center Marriott. Workshops should involve topics in one of ten categories: clinical, career development, research, academic, patient experience/communication, perioperative, information technology, practice management, quality and patient safety, and evidence‐based medicine/high‐value care. Each workshop should last 90 minutes.
Proposals that are the most likely to be accepted will be innovative as well as highly interactive, utilizing small groups and limiting didactic/lecture content. Workshops previously presented at national or regional meetings will be considered. Four faculty members from each workshop that is accepted will receive 50% off their annual meeting registration, although workshops may include a maximum of six additional facilitators.
The submission deadline is Friday, May 12, 2017 at 8:00 a.m. EST. Visit www.hospitalmedicine2018.org for more information.
Brett Radler is SHM’s communications specialist.
SHM gives QI a new look
SHM is proud to announce that its Center for Hospital Innovation & Improvement has a fresh look and name: SHM’s Center for Quality Improvement. While the name may have changed, SHM’s Center for QI will remain your partner in quality and patient safety.
“SHM’s Center for QI provides a comprehensive set of resources and programs to support hospitalists and other hospital clinicians as they work to improve quality and safety in their hospitals,” says Eric E. Howell, MD, MHM, senior physician advisor for SHM’s Center for QI.
SHM’s Center for QI’s mentored implementation programs are deployed in hundreds of hospitals and have been recognized with the John M. Eisenberg Award. More recently, its opioid-safety program (RADEO) was recognized by the CMS for its efforts to enhance patient safety.
Visit http://www.hospitalmedicine.org/QI to learn more about SHM’s Center for QI and about opportunities for partnerships, solutions, and tools to address your QI needs.
PHM 2017 is coming! Book your ticket to Nashville today
Pediatric Hospital Medicine (PHM) 2017 is the largest, leading educational event for health care professionals who specialize in the care of hospitalized children. This year’s meeting will be held July 20-23 at the Omni Nashville in Tennessee.
Attendees will have the opportunity to network with colleagues from across the nation, learn from renowned faculty from throughout the discipline, and acquire skills, tools, and resources to directly benefit their patients and practice.
PHM 2017 has been designed to provide participants with tools to improve clinical skills and practice, address management issues, lead change and innovation within their institutions, and network with thought leaders to collaborate and learn about new innovations.
View the full meeting schedule, educational objectives, and more at www.peds2017.org.![]()
Benchmark your HMG appropriately with the State of Hospital Medicine Report
The State of Hospital Medicine Report continues to be the best source of detail regarding the configuration and operation of hospital medicine groups. The biennial report provides current data on hospitalist compensation and production, in addition to cutting-edge knowledge covering practice demographics, staffing levels, turnover, staff growth, compensation methods, and financial support for solid, evidence-based management decisions.
“We’ve used data from the report to hold more informed discussions with the group that provides our note-coding services and to determine how to benchmark our nocturnists’ workloads and pay,” said Andrew White, MD, SFHM, director of the Hospital Medicine Service at the University of Washington in Seattle. “The results are broken into region and academic practice type, which gives me the confidence that I’m looking at results from groups like mine, rather than comparing to the country-wide average.”
The report is designed for hospital medicine leaders (both physician leaders and nonphysician practice administrators and executives), as well as frontline hospitalists, nurse practitioners, physician assistants, pediatricians, and internal and family medicine physicians.
In addition to the print version, the 2016 State of Hospital Medicine Report is also available in an enhanced, fully searchable digital version. To order your copy in either print or digital, visit www.hospitalmedicine.org/survey.
Learn how to drive change as a leader in hospital medicine
A successful hospitalist program requires strong leadership from the floor to the C-suite. SHM’s Leadership Academy prepares clinical and academic leaders with vital skills that, traditionally, are not taught in medical school or typical residency programs. This year’s meeting will be held October 23-26 at the JW Marriott Camelback Inn in Scottsdale, Ariz.
New for Leadership Academy 2017, Strategic Essentials (formerly Leadership Foundations), Influential Management, and Mastering Teamwork will be available to all attendees, regardless of previous attendance. SHM provides recommendations for interested registrants so they can determine which course fits them best in their leadership journey.
Take the Strategic Essentials course to evaluate your personal leadership strengths and weaknesses, understand key hospital drivers, and more.
If you are looking to learn skills needed to drive culture change through specific leadership behaviors as well as financial storytelling, then Leadership: Influential Management would be a great course for you.
The third course, Leadership: Mastering Teamwork, will help attendees learn to critically assess program growth opportunities, lead and motivate teams, and design effective communication strategies. Learn more at www.shmleadershipacademy.org.![]()
Stay ahead of the MACRA curve with SHM
The Medicare Access and CHIP Reauthorization Act (MACRA) put into motion the new Quality Payment Program, which replaces past pay-for-performance programs, such as the Physician Quality Reporting System and physician value-based modifier. The new program has many complicated requirements, and hospitalists will be impacted.
The first year of the program has flexible participation, yet hospitalists need to do at least one thing (report one quality measure, attest to one improvement activity) in the program in order to avoid a 4% penalty to Medicare payments. 2017 is the first reporting year, so now is the time for providers to familiarize themselves with the requirements.
To support hospitalists who are looking for hospital medicine–specific ways to participate and avoid penalties, SHM hosted a webinar that is now available at www.macraforhm.org under “Resources.” SHM’s policy staff broke down the program requirements and went into detail on ways in which hospitalists can and should participate in the new program. Updates and other resources are also available at www.macraforhm.org.
Looking to be a speaker at Hospital Medicine 2018?
The Society of Hospital Medicine reminds you to submit your workshop proposal for the 2018 Annual Meeting to be held April 8-11, 2018, at the Orlando World Center Marriott. Workshops should involve topics in one of ten categories: clinical, career development, research, academic, patient experience/communication, perioperative, information technology, practice management, quality and patient safety, and evidence‐based medicine/high‐value care. Each workshop should last 90 minutes.
Proposals that are the most likely to be accepted will be innovative as well as highly interactive, utilizing small groups and limiting didactic/lecture content. Workshops previously presented at national or regional meetings will be considered. Four faculty members from each workshop that is accepted will receive 50% off their annual meeting registration, although workshops may include a maximum of six additional facilitators.
The submission deadline is Friday, May 12, 2017 at 8:00 a.m. EST. Visit www.hospitalmedicine2018.org for more information.
Brett Radler is SHM’s communications specialist.
SHM gives QI a new look
SHM is proud to announce that its Center for Hospital Innovation & Improvement has a fresh look and name: SHM’s Center for Quality Improvement. While the name may have changed, SHM’s Center for QI will remain your partner in quality and patient safety.
“SHM’s Center for QI provides a comprehensive set of resources and programs to support hospitalists and other hospital clinicians as they work to improve quality and safety in their hospitals,” says Eric E. Howell, MD, MHM, senior physician advisor for SHM’s Center for QI.
SHM’s Center for QI’s mentored implementation programs are deployed in hundreds of hospitals and have been recognized with the John M. Eisenberg Award. More recently, its opioid-safety program (RADEO) was recognized by the CMS for its efforts to enhance patient safety.
Visit http://www.hospitalmedicine.org/QI to learn more about SHM’s Center for QI and about opportunities for partnerships, solutions, and tools to address your QI needs.
PHM 2017 is coming! Book your ticket to Nashville today
Pediatric Hospital Medicine (PHM) 2017 is the largest, leading educational event for health care professionals who specialize in the care of hospitalized children. This year’s meeting will be held July 20-23 at the Omni Nashville in Tennessee.
Attendees will have the opportunity to network with colleagues from across the nation, learn from renowned faculty from throughout the discipline, and acquire skills, tools, and resources to directly benefit their patients and practice.
PHM 2017 has been designed to provide participants with tools to improve clinical skills and practice, address management issues, lead change and innovation within their institutions, and network with thought leaders to collaborate and learn about new innovations.
View the full meeting schedule, educational objectives, and more at www.peds2017.org.![]()
Benchmark your HMG appropriately with the State of Hospital Medicine Report
The State of Hospital Medicine Report continues to be the best source of detail regarding the configuration and operation of hospital medicine groups. The biennial report provides current data on hospitalist compensation and production, in addition to cutting-edge knowledge covering practice demographics, staffing levels, turnover, staff growth, compensation methods, and financial support for solid, evidence-based management decisions.
“We’ve used data from the report to hold more informed discussions with the group that provides our note-coding services and to determine how to benchmark our nocturnists’ workloads and pay,” said Andrew White, MD, SFHM, director of the Hospital Medicine Service at the University of Washington in Seattle. “The results are broken into region and academic practice type, which gives me the confidence that I’m looking at results from groups like mine, rather than comparing to the country-wide average.”
The report is designed for hospital medicine leaders (both physician leaders and nonphysician practice administrators and executives), as well as frontline hospitalists, nurse practitioners, physician assistants, pediatricians, and internal and family medicine physicians.
In addition to the print version, the 2016 State of Hospital Medicine Report is also available in an enhanced, fully searchable digital version. To order your copy in either print or digital, visit www.hospitalmedicine.org/survey.
Learn how to drive change as a leader in hospital medicine
A successful hospitalist program requires strong leadership from the floor to the C-suite. SHM’s Leadership Academy prepares clinical and academic leaders with vital skills that, traditionally, are not taught in medical school or typical residency programs. This year’s meeting will be held October 23-26 at the JW Marriott Camelback Inn in Scottsdale, Ariz.
New for Leadership Academy 2017, Strategic Essentials (formerly Leadership Foundations), Influential Management, and Mastering Teamwork will be available to all attendees, regardless of previous attendance. SHM provides recommendations for interested registrants so they can determine which course fits them best in their leadership journey.
Take the Strategic Essentials course to evaluate your personal leadership strengths and weaknesses, understand key hospital drivers, and more.
If you are looking to learn skills needed to drive culture change through specific leadership behaviors as well as financial storytelling, then Leadership: Influential Management would be a great course for you.
The third course, Leadership: Mastering Teamwork, will help attendees learn to critically assess program growth opportunities, lead and motivate teams, and design effective communication strategies. Learn more at www.shmleadershipacademy.org.![]()
Stay ahead of the MACRA curve with SHM
The Medicare Access and CHIP Reauthorization Act (MACRA) put into motion the new Quality Payment Program, which replaces past pay-for-performance programs, such as the Physician Quality Reporting System and physician value-based modifier. The new program has many complicated requirements, and hospitalists will be impacted.
The first year of the program has flexible participation, yet hospitalists need to do at least one thing (report one quality measure, attest to one improvement activity) in the program in order to avoid a 4% penalty to Medicare payments. 2017 is the first reporting year, so now is the time for providers to familiarize themselves with the requirements.
To support hospitalists who are looking for hospital medicine–specific ways to participate and avoid penalties, SHM hosted a webinar that is now available at www.macraforhm.org under “Resources.” SHM’s policy staff broke down the program requirements and went into detail on ways in which hospitalists can and should participate in the new program. Updates and other resources are also available at www.macraforhm.org.
Looking to be a speaker at Hospital Medicine 2018?
The Society of Hospital Medicine reminds you to submit your workshop proposal for the 2018 Annual Meeting to be held April 8-11, 2018, at the Orlando World Center Marriott. Workshops should involve topics in one of ten categories: clinical, career development, research, academic, patient experience/communication, perioperative, information technology, practice management, quality and patient safety, and evidence‐based medicine/high‐value care. Each workshop should last 90 minutes.
Proposals that are the most likely to be accepted will be innovative as well as highly interactive, utilizing small groups and limiting didactic/lecture content. Workshops previously presented at national or regional meetings will be considered. Four faculty members from each workshop that is accepted will receive 50% off their annual meeting registration, although workshops may include a maximum of six additional facilitators.
The submission deadline is Friday, May 12, 2017 at 8:00 a.m. EST. Visit www.hospitalmedicine2018.org for more information.
Brett Radler is SHM’s communications specialist.
Scientists create online database to aid CML research

A newly launched online database provides researchers with access to data on gene expression in chronic myeloid leukemia (CML).
The LEUKomics database includes datasets relating to clinical parameters in CML, normal and leukemic stem cells, CML disease stages, treatments for the disease, and mouse models of CML.
The database is free for researchers to use and share.
The scientists who developed the database hope it will increase our understanding of CML and lead to new treatments for the disease.
“LEUKomics is a very valuable resource and could help us to reveal new underlying mechanisms that drive CML,” said Jeff Evans, Director of the Institute of Cancer Sciences at the University of Glasgow in Scotland.
“It has the potential to transform CML research on a global level, as the findings can be downloaded and shared with other researchers across the world. We also hope it inspires new research ideas and ultimately fuels a global search into finding cures for CML.”
The LEUKomics database includes datasets with information on gene expression related to:
- Clinical parameters in CML, such as disease aggressiveness and response to treatment
- Stem and progenitor cells from CML patients and healthy individuals
- Chronic, accelerated, and blast phases of CML
- CML treatment (currently only tyrosine kinase inhibitors)
- Stem and progenitor cells from mouse models of CML.
The LEUKomics database was launched by scientists at the University of Glasgow and the University of Melbourne.
The website has been built as part of the stem cell database Stemformatics, with funding from the Scottish Cancer Foundation and Bloodwise.
“Thanks to research, most patients with CML will now live a normal life by taking a single pill,” said Alasdair Rankin, Director of Research at Bloodwise in London, England.
“But treatment is life-long, and not everyone can tolerate the side effects from their treatment or may not respond and see their CML return. There remains a need to develop a permanent cure for all people with this blood cancer. LEUKomics is a highly innovative way to speed up this search for a cure and should be a valuable asset for the global blood cancer research community. We look forward to seeing its impact in the months to come.”
The LEUKomics database can be accessed at: www.stemformatics.org/leukomics. ![]()
A newly launched online database provides researchers with access to data on gene expression in chronic myeloid leukemia (CML).
The LEUKomics database includes datasets relating to clinical parameters in CML, normal and leukemic stem cells, CML disease stages, treatments for the disease, and mouse models of CML.
The database is free for researchers to use and share.
The scientists who developed the database hope it will increase our understanding of CML and lead to new treatments for the disease.
“LEUKomics is a very valuable resource and could help us to reveal new underlying mechanisms that drive CML,” said Jeff Evans, Director of the Institute of Cancer Sciences at the University of Glasgow in Scotland.
“It has the potential to transform CML research on a global level, as the findings can be downloaded and shared with other researchers across the world. We also hope it inspires new research ideas and ultimately fuels a global search into finding cures for CML.”
The LEUKomics database includes datasets with information on gene expression related to:
- Clinical parameters in CML, such as disease aggressiveness and response to treatment
- Stem and progenitor cells from CML patients and healthy individuals
- Chronic, accelerated, and blast phases of CML
- CML treatment (currently only tyrosine kinase inhibitors)
- Stem and progenitor cells from mouse models of CML.
The LEUKomics database was launched by scientists at the University of Glasgow and the University of Melbourne.
The website has been built as part of the stem cell database Stemformatics, with funding from the Scottish Cancer Foundation and Bloodwise.
“Thanks to research, most patients with CML will now live a normal life by taking a single pill,” said Alasdair Rankin, Director of Research at Bloodwise in London, England.
“But treatment is life-long, and not everyone can tolerate the side effects from their treatment or may not respond and see their CML return. There remains a need to develop a permanent cure for all people with this blood cancer. LEUKomics is a highly innovative way to speed up this search for a cure and should be a valuable asset for the global blood cancer research community. We look forward to seeing its impact in the months to come.”
The LEUKomics database can be accessed at: www.stemformatics.org/leukomics. ![]()
A newly launched online database provides researchers with access to data on gene expression in chronic myeloid leukemia (CML).
The LEUKomics database includes datasets relating to clinical parameters in CML, normal and leukemic stem cells, CML disease stages, treatments for the disease, and mouse models of CML.
The database is free for researchers to use and share.
The scientists who developed the database hope it will increase our understanding of CML and lead to new treatments for the disease.
“LEUKomics is a very valuable resource and could help us to reveal new underlying mechanisms that drive CML,” said Jeff Evans, Director of the Institute of Cancer Sciences at the University of Glasgow in Scotland.
“It has the potential to transform CML research on a global level, as the findings can be downloaded and shared with other researchers across the world. We also hope it inspires new research ideas and ultimately fuels a global search into finding cures for CML.”
The LEUKomics database includes datasets with information on gene expression related to:
- Clinical parameters in CML, such as disease aggressiveness and response to treatment
- Stem and progenitor cells from CML patients and healthy individuals
- Chronic, accelerated, and blast phases of CML
- CML treatment (currently only tyrosine kinase inhibitors)
- Stem and progenitor cells from mouse models of CML.
The LEUKomics database was launched by scientists at the University of Glasgow and the University of Melbourne.
The website has been built as part of the stem cell database Stemformatics, with funding from the Scottish Cancer Foundation and Bloodwise.
“Thanks to research, most patients with CML will now live a normal life by taking a single pill,” said Alasdair Rankin, Director of Research at Bloodwise in London, England.
“But treatment is life-long, and not everyone can tolerate the side effects from their treatment or may not respond and see their CML return. There remains a need to develop a permanent cure for all people with this blood cancer. LEUKomics is a highly innovative way to speed up this search for a cure and should be a valuable asset for the global blood cancer research community. We look forward to seeing its impact in the months to come.”
The LEUKomics database can be accessed at: www.stemformatics.org/leukomics. ![]()