User login
Panel revises spondyloarthritis treat-to-target recommendations
MADRID – The newly revised recommendations from an unaffiliated, international expert panel on a treat-to-target approach for axial spondyloarthritis and psoriatic arthritis has one conspicuous feature that the prior recommendations lacked: evidence.
The first treat-to-target recommendations for spondyloarthritis (SpA) and psoriatic arthritis (PsA) from 2013 were based entirely on expert opinion (Ann Rheum Dis. 2014 Jan;73[1]:6-16), but in the new update 4 of the 11 recommendations now have an evidence base as well as a fifth recommendation for the part that pertains to PsA, Désirée van der Heijde, MD, said at the European Congress of Rheumatology.

Among the evidence-based recommendations, the most striking was a new formulation for how to measure disease activity. The new recommendations call the ASDAS (Ankylosing Spondylitis Disease Activity Score) the “preferred” disease activity measure for patients with axial SpA and cite both the DAPSA (Disease Activity Index for Psoriatic Arthritis) as well as minimal disease activity as “considered to define the target” when treating PsA.
“This recommendation just made it,” squeaking onto the list with a 52% vote of approval from the task force members, said Dr. van der Heijde. “It had the longest discussion,” with a significant minority of panelists taking a different view.
ASDAS shook out as the preferred measure for axial SpA because of evidence linking a patient’s ASDAS with syndesmophyte formation. “The idea is that by targeting ASDAS you should have better outcomes,” she explained.
“Applying a treat-to-target approach in axial SpA is feasible but requires systematic collection of outcome parameters in daily practice,” such as ASDAS, said Dr. Dougados, professor of rheumatology at Cochin Hospital in Paris. Another piece currently lacking in the case for treat-to-target is demonstration of the clinical benefit from this approach in a trial, he added.
According to Dr. van der Heijde, the other four recommendations that now have evidence backup are:
- Define clinical remission or minimal disease as the absence of clinical and laboratory evidence of significant disease activity.
- An alternative treatment target for PsA may be low or minimal disease activity.
- Measure disease activity by clinical signs and symptoms and by acute phase reactants.
- Once a treatment target is reached it should be maintained.
The task force also outlined “an extensive research agenda” where evidence is needed, specifying close to 50 individual research topics. Among them Dr. van der Heijde particularly called out the role of the Health Assessment Questionnaire (HAQ), validation of PsA target outcomes, and better parsing of the differences using remission or low disease activity as the treatment target.
Dr. van der Heijde, Dr. Dougados, and Dr. Braun are all consultants for several drug companies.
[email protected]
On Twitter @mitchelzoler
The evidence we now have is the difference between the new recommendations and the prior version. We have evidence from trials in patients with psoriatic arthritis using minimal disease activity as a target. And we have indirect evidence from observational studies in patients with SpA that suggest the higher the ASDAS, the more progression occurs. In addition, results reported at the EULAR 2017 Congress showed that reductions in the ASDAS appeared to correlate with the effect of a tumor necrosis factor inhibitor on reduced radiographic progression in patients with ankylosing spondylitis. But this is just an association; data from a randomized, prospective trial should be available next year.

The recommendations say to manage patients with axial SpA or psoriatic arthritis by treating them to a target. To do that a clinician needs a standardized assessment of a patient’s disease and to perform follow-up measurements to see if the target is met. The data Dr. Dougados cited from Paris document that assessments such as an ASDAS are rarely made. Getting an ASDAS means knowing either a patient’s C-reactive protein level or erythrocyte sedimentation rate. That requires blood work before a clinic visit, something patients often don’t want.
Will these recommendations change practice and make the ASDAS more widely used? That depends to some extent on whether any benefits or penalties linked to ASDAS use go into place.
Next year, we expect to see results from trials that are testing whether the treat-to-target approach produces better outcomes. Evidence like that will be important to further spur adoption.
Lianne S. Gensler, MD , is director of the ankylosing spondylitis clinic at the University of California, San Francisco. She has been a consultant to Novartis and Janssen and has received research support from AbbVie and UCB. Dr. Gensler was a member of the task force that issued the revised recommendations. She made these comments in an interview.
The evidence we now have is the difference between the new recommendations and the prior version. We have evidence from trials in patients with psoriatic arthritis using minimal disease activity as a target. And we have indirect evidence from observational studies in patients with SpA that suggest the higher the ASDAS, the more progression occurs. In addition, results reported at the EULAR 2017 Congress showed that reductions in the ASDAS appeared to correlate with the effect of a tumor necrosis factor inhibitor on reduced radiographic progression in patients with ankylosing spondylitis. But this is just an association; data from a randomized, prospective trial should be available next year.
The recommendations say to manage patients with axial SpA or psoriatic arthritis by treating them to a target. To do that a clinician needs a standardized assessment of a patient’s disease and to perform follow-up measurements to see if the target is met. The data Dr. Dougados cited from Paris document that assessments such as an ASDAS are rarely made. Getting an ASDAS means knowing either a patient’s C-reactive protein level or erythrocyte sedimentation rate. That requires blood work before a clinic visit, something patients often don’t want.
Will these recommendations change practice and make the ASDAS more widely used? That depends to some extent on whether any benefits or penalties linked to ASDAS use go into place.
Next year, we expect to see results from trials that are testing whether the treat-to-target approach produces better outcomes. Evidence like that will be important to further spur adoption.
Lianne S. Gensler, MD , is director of the ankylosing spondylitis clinic at the University of California, San Francisco. She has been a consultant to Novartis and Janssen and has received research support from AbbVie and UCB. Dr. Gensler was a member of the task force that issued the revised recommendations. She made these comments in an interview.
The evidence we now have is the difference between the new recommendations and the prior version. We have evidence from trials in patients with psoriatic arthritis using minimal disease activity as a target. And we have indirect evidence from observational studies in patients with SpA that suggest the higher the ASDAS, the more progression occurs. In addition, results reported at the EULAR 2017 Congress showed that reductions in the ASDAS appeared to correlate with the effect of a tumor necrosis factor inhibitor on reduced radiographic progression in patients with ankylosing spondylitis. But this is just an association; data from a randomized, prospective trial should be available next year.
The recommendations say to manage patients with axial SpA or psoriatic arthritis by treating them to a target. To do that a clinician needs a standardized assessment of a patient’s disease and to perform follow-up measurements to see if the target is met. The data Dr. Dougados cited from Paris document that assessments such as an ASDAS are rarely made. Getting an ASDAS means knowing either a patient’s C-reactive protein level or erythrocyte sedimentation rate. That requires blood work before a clinic visit, something patients often don’t want.
Will these recommendations change practice and make the ASDAS more widely used? That depends to some extent on whether any benefits or penalties linked to ASDAS use go into place.
Next year, we expect to see results from trials that are testing whether the treat-to-target approach produces better outcomes. Evidence like that will be important to further spur adoption.
Lianne S. Gensler, MD , is director of the ankylosing spondylitis clinic at the University of California, San Francisco. She has been a consultant to Novartis and Janssen and has received research support from AbbVie and UCB. Dr. Gensler was a member of the task force that issued the revised recommendations. She made these comments in an interview.
MADRID – The newly revised recommendations from an unaffiliated, international expert panel on a treat-to-target approach for axial spondyloarthritis and psoriatic arthritis has one conspicuous feature that the prior recommendations lacked: evidence.
The first treat-to-target recommendations for spondyloarthritis (SpA) and psoriatic arthritis (PsA) from 2013 were based entirely on expert opinion (Ann Rheum Dis. 2014 Jan;73[1]:6-16), but in the new update 4 of the 11 recommendations now have an evidence base as well as a fifth recommendation for the part that pertains to PsA, Désirée van der Heijde, MD, said at the European Congress of Rheumatology.
Among the evidence-based recommendations, the most striking was a new formulation for how to measure disease activity. The new recommendations call the ASDAS (Ankylosing Spondylitis Disease Activity Score) the “preferred” disease activity measure for patients with axial SpA and cite both the DAPSA (Disease Activity Index for Psoriatic Arthritis) as well as minimal disease activity as “considered to define the target” when treating PsA.
“This recommendation just made it,” squeaking onto the list with a 52% vote of approval from the task force members, said Dr. van der Heijde. “It had the longest discussion,” with a significant minority of panelists taking a different view.
ASDAS shook out as the preferred measure for axial SpA because of evidence linking a patient’s ASDAS with syndesmophyte formation. “The idea is that by targeting ASDAS you should have better outcomes,” she explained.
“Applying a treat-to-target approach in axial SpA is feasible but requires systematic collection of outcome parameters in daily practice,” such as ASDAS, said Dr. Dougados, professor of rheumatology at Cochin Hospital in Paris. Another piece currently lacking in the case for treat-to-target is demonstration of the clinical benefit from this approach in a trial, he added.
According to Dr. van der Heijde, the other four recommendations that now have evidence backup are:
- Define clinical remission or minimal disease as the absence of clinical and laboratory evidence of significant disease activity.
- An alternative treatment target for PsA may be low or minimal disease activity.
- Measure disease activity by clinical signs and symptoms and by acute phase reactants.
- Once a treatment target is reached it should be maintained.
The task force also outlined “an extensive research agenda” where evidence is needed, specifying close to 50 individual research topics. Among them Dr. van der Heijde particularly called out the role of the Health Assessment Questionnaire (HAQ), validation of PsA target outcomes, and better parsing of the differences using remission or low disease activity as the treatment target.
Dr. van der Heijde, Dr. Dougados, and Dr. Braun are all consultants for several drug companies.
[email protected]
On Twitter @mitchelzoler
MADRID – The newly revised recommendations from an unaffiliated, international expert panel on a treat-to-target approach for axial spondyloarthritis and psoriatic arthritis has one conspicuous feature that the prior recommendations lacked: evidence.
The first treat-to-target recommendations for spondyloarthritis (SpA) and psoriatic arthritis (PsA) from 2013 were based entirely on expert opinion (Ann Rheum Dis. 2014 Jan;73[1]:6-16), but in the new update 4 of the 11 recommendations now have an evidence base as well as a fifth recommendation for the part that pertains to PsA, Désirée van der Heijde, MD, said at the European Congress of Rheumatology.
Among the evidence-based recommendations, the most striking was a new formulation for how to measure disease activity. The new recommendations call the ASDAS (Ankylosing Spondylitis Disease Activity Score) the “preferred” disease activity measure for patients with axial SpA and cite both the DAPSA (Disease Activity Index for Psoriatic Arthritis) as well as minimal disease activity as “considered to define the target” when treating PsA.
“This recommendation just made it,” squeaking onto the list with a 52% vote of approval from the task force members, said Dr. van der Heijde. “It had the longest discussion,” with a significant minority of panelists taking a different view.
ASDAS shook out as the preferred measure for axial SpA because of evidence linking a patient’s ASDAS with syndesmophyte formation. “The idea is that by targeting ASDAS you should have better outcomes,” she explained.
“Applying a treat-to-target approach in axial SpA is feasible but requires systematic collection of outcome parameters in daily practice,” such as ASDAS, said Dr. Dougados, professor of rheumatology at Cochin Hospital in Paris. Another piece currently lacking in the case for treat-to-target is demonstration of the clinical benefit from this approach in a trial, he added.
According to Dr. van der Heijde, the other four recommendations that now have evidence backup are:
- Define clinical remission or minimal disease as the absence of clinical and laboratory evidence of significant disease activity.
- An alternative treatment target for PsA may be low or minimal disease activity.
- Measure disease activity by clinical signs and symptoms and by acute phase reactants.
- Once a treatment target is reached it should be maintained.
The task force also outlined “an extensive research agenda” where evidence is needed, specifying close to 50 individual research topics. Among them Dr. van der Heijde particularly called out the role of the Health Assessment Questionnaire (HAQ), validation of PsA target outcomes, and better parsing of the differences using remission or low disease activity as the treatment target.
Dr. van der Heijde, Dr. Dougados, and Dr. Braun are all consultants for several drug companies.
[email protected]
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE EULAR 2017 CONGRESS
Chemo-free triplet produces ‘favorable’ results in advanced disease

LUGANO, SWITZERLAND—A chemotherapy-free combination regimen has demonstrated “favorable” safety and efficacy in patients with advanced chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and non-Hodgkin lymphoma (NHL), according to researchers.
They found that treatment with ublituximab, umbralisib, and ibrutinib produced responses in patients with CLL/SLL, marginal zone lymphoma (MZL), mantle cell lymphoma (MCL), follicular lymphoma (FL), and diffuse large B-cell lymphoma (DLBCL).
Many of these patients are still receiving the combination, some of them beyond 1 year, said Lorretta Nastoupil, MD, of MD Anderson Cancer Center in Houston, Texas.
She presented results with the treatment at the 14th International Conference on Malignant Lymphoma (ICML).
The research was sponsored by TG Therapeutics, the company developing ublituximab (TG-1101) and umbralisib (TGR-1202).
Patients and treatment
Dr Nastoupil presented data on 38 patients—20 with CLL/SLL, and 18 with NHL. Three of the CLL/SLL patients were treatment-naïve. The rest had relapsed/refractory disease.
All NHL patients had relapsed/refractory disease—6 with DLBCL, 6 with FL, 4 with MCL, and 2 with MZL.
For the entire cohort, the median age was 65 (range, 32-85), and most patients (n=29) were male. They had received a median of 3 prior treatment regimens (range, 0-6).
In this trial, the patients received:
- Ublituximab at 900 mg
- Ibrutinib at 420 mg (CLL/SLL) or 560 mg (NHL)
- Umbralisib at 400 mg, 600 mg, or 800 mg.
Eighty-one percent of patients have been on study for more than 6 months. The median time on study is 11.1 months (range, 0.4 to 30+ months).
Safety
There was 1 dose-limiting toxicity in the CLL cohort (umbralisib at 400 mg)—reactivated varicella zoster. And 2 patients discontinued treatment due to an adverse event (AE)—1 due to sepsis and 1 due to pneumonia.
Neutropenia (18%) and pneumonia (11%) were the only grade 3/4 AEs that occurred in more than 10% of patients. Other grade 3/4 AEs included thrombocytopenia (8%), diarrhea (3%), dizziness (3%), pyrexia (3%), rash (3%), anemia (3%), dyspnea (3%), and stomatitis (3%).
The most common AEs of any grade were diarrhea (47%), fatigue (47%), dizziness (37%), insomnia (34%), nausea (34%), neutropenia (32%), cough (32%), and infusion-related reactions (32%).
Efficacy
Thirty-six patients were evaluable for efficacy—19 with CLL/SLL and 17 with NHL patients. Two patients discontinued treatment before the first efficacy assessment—1 due to pneumonia and 1 at investigator discretion.
For the entire cohort, the overall response rate (ORR) was 83%.
In the CLL/SLL cohort, the ORR was 100% (19/19), and the complete response (CR) rate was 32% (n=6). However, 4 of the 6 CRs are pending bone marrow confirmation.
Dr Nastoupil noted that 8 of the CLL patients had a 17p and/or 11q deletion, and 3 had previously received treatment with a BTK and/or PI3Kδ inhibitor.
One patient who was refractory to both idelalisib and ibrutinib achieved a CR with the triplet regimen, and this response has been ongoing for more than 1.5 years.
Among patients with NHL, the ORR was 100% in patients with MZL (2/2) and MCL (4/4). The ORR was 80% (4/5) in FL patients, and 17% (1/6) in DLBCL patients.
The CR rate was 50% in patients with MZL (1/2) and MCL (2/4) and 20% in patients with FL (1/5).
Dr Nastoupil pointed out that the FL patients were heavily pretreated. Two of them had received an autologous stem cell transplant, 1 was refractory to prior ibrutinib treatment, and 1 had received 5 prior lines of rituximab-based therapy.
She also noted that the DLBCL patients had a median of 4 prior therapies, and 4 of these patients had non-GCB DLBCL, including the only patient who responded to the triplet.
“[T]he combination of ublituximab, umbralisib, and ibrutinib in advanced CLL and NHL demonstrated a favorable toxicity profile as well as favorable efficacy,” Dr Nastoupil said in closing.
“[This] suggests umbralisib may be safely combined with other targeted agents to overcome mechanisms of resistance.” ![]()
LUGANO, SWITZERLAND—A chemotherapy-free combination regimen has demonstrated “favorable” safety and efficacy in patients with advanced chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and non-Hodgkin lymphoma (NHL), according to researchers.
They found that treatment with ublituximab, umbralisib, and ibrutinib produced responses in patients with CLL/SLL, marginal zone lymphoma (MZL), mantle cell lymphoma (MCL), follicular lymphoma (FL), and diffuse large B-cell lymphoma (DLBCL).
Many of these patients are still receiving the combination, some of them beyond 1 year, said Lorretta Nastoupil, MD, of MD Anderson Cancer Center in Houston, Texas.
She presented results with the treatment at the 14th International Conference on Malignant Lymphoma (ICML).
The research was sponsored by TG Therapeutics, the company developing ublituximab (TG-1101) and umbralisib (TGR-1202).
Patients and treatment
Dr Nastoupil presented data on 38 patients—20 with CLL/SLL, and 18 with NHL. Three of the CLL/SLL patients were treatment-naïve. The rest had relapsed/refractory disease.
All NHL patients had relapsed/refractory disease—6 with DLBCL, 6 with FL, 4 with MCL, and 2 with MZL.
For the entire cohort, the median age was 65 (range, 32-85), and most patients (n=29) were male. They had received a median of 3 prior treatment regimens (range, 0-6).
In this trial, the patients received:
- Ublituximab at 900 mg
- Ibrutinib at 420 mg (CLL/SLL) or 560 mg (NHL)
- Umbralisib at 400 mg, 600 mg, or 800 mg.
Eighty-one percent of patients have been on study for more than 6 months. The median time on study is 11.1 months (range, 0.4 to 30+ months).
Safety
There was 1 dose-limiting toxicity in the CLL cohort (umbralisib at 400 mg)—reactivated varicella zoster. And 2 patients discontinued treatment due to an adverse event (AE)—1 due to sepsis and 1 due to pneumonia.
Neutropenia (18%) and pneumonia (11%) were the only grade 3/4 AEs that occurred in more than 10% of patients. Other grade 3/4 AEs included thrombocytopenia (8%), diarrhea (3%), dizziness (3%), pyrexia (3%), rash (3%), anemia (3%), dyspnea (3%), and stomatitis (3%).
The most common AEs of any grade were diarrhea (47%), fatigue (47%), dizziness (37%), insomnia (34%), nausea (34%), neutropenia (32%), cough (32%), and infusion-related reactions (32%).
Efficacy
Thirty-six patients were evaluable for efficacy—19 with CLL/SLL and 17 with NHL patients. Two patients discontinued treatment before the first efficacy assessment—1 due to pneumonia and 1 at investigator discretion.
For the entire cohort, the overall response rate (ORR) was 83%.
In the CLL/SLL cohort, the ORR was 100% (19/19), and the complete response (CR) rate was 32% (n=6). However, 4 of the 6 CRs are pending bone marrow confirmation.
Dr Nastoupil noted that 8 of the CLL patients had a 17p and/or 11q deletion, and 3 had previously received treatment with a BTK and/or PI3Kδ inhibitor.
One patient who was refractory to both idelalisib and ibrutinib achieved a CR with the triplet regimen, and this response has been ongoing for more than 1.5 years.
Among patients with NHL, the ORR was 100% in patients with MZL (2/2) and MCL (4/4). The ORR was 80% (4/5) in FL patients, and 17% (1/6) in DLBCL patients.
The CR rate was 50% in patients with MZL (1/2) and MCL (2/4) and 20% in patients with FL (1/5).
Dr Nastoupil pointed out that the FL patients were heavily pretreated. Two of them had received an autologous stem cell transplant, 1 was refractory to prior ibrutinib treatment, and 1 had received 5 prior lines of rituximab-based therapy.
She also noted that the DLBCL patients had a median of 4 prior therapies, and 4 of these patients had non-GCB DLBCL, including the only patient who responded to the triplet.
“[T]he combination of ublituximab, umbralisib, and ibrutinib in advanced CLL and NHL demonstrated a favorable toxicity profile as well as favorable efficacy,” Dr Nastoupil said in closing.
“[This] suggests umbralisib may be safely combined with other targeted agents to overcome mechanisms of resistance.” ![]()
LUGANO, SWITZERLAND—A chemotherapy-free combination regimen has demonstrated “favorable” safety and efficacy in patients with advanced chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and non-Hodgkin lymphoma (NHL), according to researchers.
They found that treatment with ublituximab, umbralisib, and ibrutinib produced responses in patients with CLL/SLL, marginal zone lymphoma (MZL), mantle cell lymphoma (MCL), follicular lymphoma (FL), and diffuse large B-cell lymphoma (DLBCL).
Many of these patients are still receiving the combination, some of them beyond 1 year, said Lorretta Nastoupil, MD, of MD Anderson Cancer Center in Houston, Texas.
She presented results with the treatment at the 14th International Conference on Malignant Lymphoma (ICML).
The research was sponsored by TG Therapeutics, the company developing ublituximab (TG-1101) and umbralisib (TGR-1202).
Patients and treatment
Dr Nastoupil presented data on 38 patients—20 with CLL/SLL, and 18 with NHL. Three of the CLL/SLL patients were treatment-naïve. The rest had relapsed/refractory disease.
All NHL patients had relapsed/refractory disease—6 with DLBCL, 6 with FL, 4 with MCL, and 2 with MZL.
For the entire cohort, the median age was 65 (range, 32-85), and most patients (n=29) were male. They had received a median of 3 prior treatment regimens (range, 0-6).
In this trial, the patients received:
- Ublituximab at 900 mg
- Ibrutinib at 420 mg (CLL/SLL) or 560 mg (NHL)
- Umbralisib at 400 mg, 600 mg, or 800 mg.
Eighty-one percent of patients have been on study for more than 6 months. The median time on study is 11.1 months (range, 0.4 to 30+ months).
Safety
There was 1 dose-limiting toxicity in the CLL cohort (umbralisib at 400 mg)—reactivated varicella zoster. And 2 patients discontinued treatment due to an adverse event (AE)—1 due to sepsis and 1 due to pneumonia.
Neutropenia (18%) and pneumonia (11%) were the only grade 3/4 AEs that occurred in more than 10% of patients. Other grade 3/4 AEs included thrombocytopenia (8%), diarrhea (3%), dizziness (3%), pyrexia (3%), rash (3%), anemia (3%), dyspnea (3%), and stomatitis (3%).
The most common AEs of any grade were diarrhea (47%), fatigue (47%), dizziness (37%), insomnia (34%), nausea (34%), neutropenia (32%), cough (32%), and infusion-related reactions (32%).
Efficacy
Thirty-six patients were evaluable for efficacy—19 with CLL/SLL and 17 with NHL patients. Two patients discontinued treatment before the first efficacy assessment—1 due to pneumonia and 1 at investigator discretion.
For the entire cohort, the overall response rate (ORR) was 83%.
In the CLL/SLL cohort, the ORR was 100% (19/19), and the complete response (CR) rate was 32% (n=6). However, 4 of the 6 CRs are pending bone marrow confirmation.
Dr Nastoupil noted that 8 of the CLL patients had a 17p and/or 11q deletion, and 3 had previously received treatment with a BTK and/or PI3Kδ inhibitor.
One patient who was refractory to both idelalisib and ibrutinib achieved a CR with the triplet regimen, and this response has been ongoing for more than 1.5 years.
Among patients with NHL, the ORR was 100% in patients with MZL (2/2) and MCL (4/4). The ORR was 80% (4/5) in FL patients, and 17% (1/6) in DLBCL patients.
The CR rate was 50% in patients with MZL (1/2) and MCL (2/4) and 20% in patients with FL (1/5).
Dr Nastoupil pointed out that the FL patients were heavily pretreated. Two of them had received an autologous stem cell transplant, 1 was refractory to prior ibrutinib treatment, and 1 had received 5 prior lines of rituximab-based therapy.
She also noted that the DLBCL patients had a median of 4 prior therapies, and 4 of these patients had non-GCB DLBCL, including the only patient who responded to the triplet.
“[T]he combination of ublituximab, umbralisib, and ibrutinib in advanced CLL and NHL demonstrated a favorable toxicity profile as well as favorable efficacy,” Dr Nastoupil said in closing.
“[This] suggests umbralisib may be safely combined with other targeted agents to overcome mechanisms of resistance.” ![]()
Senate health care proposal already facing uphill battle
Senate Republican leaders are facing pushback from almost every side on their Affordable Care Act repeal/replace proposal – so much so that the current plan is unlikely to gain enough support to pass.
“For a variety of reasons, we are not ready to vote for this bill, but we are open to negotiation and obtaining more information before it is brought to the floor,” Sen. Rand Paul (R-Ky.), Sen. Ted Cruz (R-Texas), Sen. Ron Johnson (R-Wis.), and Sen. Mike Lee (R-Utah) said in a joint statement issued June 22, the day the plan was published. “There are provisions in this draft that represent an improvement to our current health care system, but it does not appear this draft as written will accomplish the most important promise that we made to Americans to repeal Obamacare and lower their health care costs.”
Like the House-passed American Health Care Act (H.R. 1628), the proposed BCRA would reduce Medicaid spending and would address rising premiums in the individual health insurance marketplace; however, BCRA would take a slightly different path to the same destination.
Like the House bill, BCRA also targets funding for Planned Parenthood, although because of Senate procedural rules, it is a more indirect funding ban.
A key difference between BCRA and the House bill is how insurance premium support is calculated. The AHCA would base tax credits on age, providing a lesser benefit for older, but pre–Medicare-age adults. In contrast, BCRA would base tax credits on income while limiting eligibility to households at 350% of the federal poverty line. Further, credits would cover only 58% of the actuarial value of health insurance under BCRA.
The draft Senate plan would not allow states to request a waiver from the ACA’s so-called community waiver provisions – the portion of the law that requires health insurance premiums to be the same regardless of age or preexisting condition; the House-passed AHCA would allow those waivers.
Medicaid expansion would be rolled back under the Senate plan, but at a slower pace than the AHCA would require – by 2023 under BCRA vs. 2020 under AHCA.
The BCRA would establish a per capita funding mechanism for Medicaid going forward, which would base funding on historic Medicaid expenditures and uses an economic index to track inflation and adjust payments accordingly.
To address the needs of people with greater health care needs, the Senate proposal would provide $57 billion over the first 4 years, then another $57 billion over the next 8. The funds would be available for programs such as premium support or high-risk pools to help individuals who are expected to be high users of health care. States would be required to match funds starting in 2022.
Experts were quick to weigh in on the Senate plan.
The BCRA needs to do three things, according to Grace-Marie Turner, president of the Galen Institute: Provide a safety net for those covered through the ACA so that they do not lose coverage in the transition, modernize Medicaid, and give states more authority and options to reform their own health insurance markets.
“We have learned that the federal government is not able to regulate something as local as health insurance,” Ms. Turner said. “They cannot create policies and legislation that works for people in downtown Manhattan and rural Montana and southern New Mexico and the panhandle of Florida. There are too many different populations. The states need to do that, and this bill also would give the states more authority to begin to oversee their health insurance markets but with new funding to provide extra help for the people who have difficulty buying progress.”
She said it could be much better if the Senate did not use the reconciliation process, “but within the confines of that, both the House and Senate bills do the same thing.”
Ms. Turner also stressed that there are more reforms coming later, as the Senate and House address other portions of ACA repeal/replacement.
“I hope that [senators] would see moving this forward as beneficial so that then they can move additional pieces of legislation, hopefully, with 60 votes to go through the regular process, to have additional follow-up bills. This is not the end of the story. This is just rescuing us from Obamacare,” she said. “Then we need to go forward and think about what do we need to do to make our health sector work better in the future by putting doctors and patients, rather than government, in charge of choices.”
Doctors, however, did not agree.
“This bill significantly decreases patients’ ability to access high-quality health care, and affordable coverage for millions of Americans will be in jeopardy if the legislation is passed,” Boyd Buser, MD, a doctor of osteopathy and president of the American Osteopathic Association, said in a statement.
He noted that the Medicaid cuts will have a “devastating impact, especially in areas of our country hardest hit by the ongoing opioid epidemic. ... The Senate bill should have prioritized prevention and care coordination, two measures proven to reduce overall health costs by eliminating waste and addressing health problems at the most treatable stage. Decreasing the number of Americans with coverage as it intends does will not lower costs.”
A vote on the proposal could come as early as June 29 before the Senate breaks for the 4th of July recess.
Republican lawmakers and the Trump administration have vowed to address the ACA in other ways as well, by reviewing and possibly changing all relevant regulations, then using the regular legislative process, which would need 60 votes, to address issues that cannot be handled by the budget reconciliation process.
Senate Republican leaders are facing pushback from almost every side on their Affordable Care Act repeal/replace proposal – so much so that the current plan is unlikely to gain enough support to pass.
“For a variety of reasons, we are not ready to vote for this bill, but we are open to negotiation and obtaining more information before it is brought to the floor,” Sen. Rand Paul (R-Ky.), Sen. Ted Cruz (R-Texas), Sen. Ron Johnson (R-Wis.), and Sen. Mike Lee (R-Utah) said in a joint statement issued June 22, the day the plan was published. “There are provisions in this draft that represent an improvement to our current health care system, but it does not appear this draft as written will accomplish the most important promise that we made to Americans to repeal Obamacare and lower their health care costs.”
Like the House-passed American Health Care Act (H.R. 1628), the proposed BCRA would reduce Medicaid spending and would address rising premiums in the individual health insurance marketplace; however, BCRA would take a slightly different path to the same destination.
Like the House bill, BCRA also targets funding for Planned Parenthood, although because of Senate procedural rules, it is a more indirect funding ban.
A key difference between BCRA and the House bill is how insurance premium support is calculated. The AHCA would base tax credits on age, providing a lesser benefit for older, but pre–Medicare-age adults. In contrast, BCRA would base tax credits on income while limiting eligibility to households at 350% of the federal poverty line. Further, credits would cover only 58% of the actuarial value of health insurance under BCRA.
The draft Senate plan would not allow states to request a waiver from the ACA’s so-called community waiver provisions – the portion of the law that requires health insurance premiums to be the same regardless of age or preexisting condition; the House-passed AHCA would allow those waivers.
Medicaid expansion would be rolled back under the Senate plan, but at a slower pace than the AHCA would require – by 2023 under BCRA vs. 2020 under AHCA.
The BCRA would establish a per capita funding mechanism for Medicaid going forward, which would base funding on historic Medicaid expenditures and uses an economic index to track inflation and adjust payments accordingly.
To address the needs of people with greater health care needs, the Senate proposal would provide $57 billion over the first 4 years, then another $57 billion over the next 8. The funds would be available for programs such as premium support or high-risk pools to help individuals who are expected to be high users of health care. States would be required to match funds starting in 2022.
Experts were quick to weigh in on the Senate plan.
The BCRA needs to do three things, according to Grace-Marie Turner, president of the Galen Institute: Provide a safety net for those covered through the ACA so that they do not lose coverage in the transition, modernize Medicaid, and give states more authority and options to reform their own health insurance markets.
“We have learned that the federal government is not able to regulate something as local as health insurance,” Ms. Turner said. “They cannot create policies and legislation that works for people in downtown Manhattan and rural Montana and southern New Mexico and the panhandle of Florida. There are too many different populations. The states need to do that, and this bill also would give the states more authority to begin to oversee their health insurance markets but with new funding to provide extra help for the people who have difficulty buying progress.”
She said it could be much better if the Senate did not use the reconciliation process, “but within the confines of that, both the House and Senate bills do the same thing.”
Ms. Turner also stressed that there are more reforms coming later, as the Senate and House address other portions of ACA repeal/replacement.
“I hope that [senators] would see moving this forward as beneficial so that then they can move additional pieces of legislation, hopefully, with 60 votes to go through the regular process, to have additional follow-up bills. This is not the end of the story. This is just rescuing us from Obamacare,” she said. “Then we need to go forward and think about what do we need to do to make our health sector work better in the future by putting doctors and patients, rather than government, in charge of choices.”
Doctors, however, did not agree.
“This bill significantly decreases patients’ ability to access high-quality health care, and affordable coverage for millions of Americans will be in jeopardy if the legislation is passed,” Boyd Buser, MD, a doctor of osteopathy and president of the American Osteopathic Association, said in a statement.
He noted that the Medicaid cuts will have a “devastating impact, especially in areas of our country hardest hit by the ongoing opioid epidemic. ... The Senate bill should have prioritized prevention and care coordination, two measures proven to reduce overall health costs by eliminating waste and addressing health problems at the most treatable stage. Decreasing the number of Americans with coverage as it intends does will not lower costs.”
A vote on the proposal could come as early as June 29 before the Senate breaks for the 4th of July recess.
Republican lawmakers and the Trump administration have vowed to address the ACA in other ways as well, by reviewing and possibly changing all relevant regulations, then using the regular legislative process, which would need 60 votes, to address issues that cannot be handled by the budget reconciliation process.
Senate Republican leaders are facing pushback from almost every side on their Affordable Care Act repeal/replace proposal – so much so that the current plan is unlikely to gain enough support to pass.
“For a variety of reasons, we are not ready to vote for this bill, but we are open to negotiation and obtaining more information before it is brought to the floor,” Sen. Rand Paul (R-Ky.), Sen. Ted Cruz (R-Texas), Sen. Ron Johnson (R-Wis.), and Sen. Mike Lee (R-Utah) said in a joint statement issued June 22, the day the plan was published. “There are provisions in this draft that represent an improvement to our current health care system, but it does not appear this draft as written will accomplish the most important promise that we made to Americans to repeal Obamacare and lower their health care costs.”
Like the House-passed American Health Care Act (H.R. 1628), the proposed BCRA would reduce Medicaid spending and would address rising premiums in the individual health insurance marketplace; however, BCRA would take a slightly different path to the same destination.
Like the House bill, BCRA also targets funding for Planned Parenthood, although because of Senate procedural rules, it is a more indirect funding ban.
A key difference between BCRA and the House bill is how insurance premium support is calculated. The AHCA would base tax credits on age, providing a lesser benefit for older, but pre–Medicare-age adults. In contrast, BCRA would base tax credits on income while limiting eligibility to households at 350% of the federal poverty line. Further, credits would cover only 58% of the actuarial value of health insurance under BCRA.
The draft Senate plan would not allow states to request a waiver from the ACA’s so-called community waiver provisions – the portion of the law that requires health insurance premiums to be the same regardless of age or preexisting condition; the House-passed AHCA would allow those waivers.
Medicaid expansion would be rolled back under the Senate plan, but at a slower pace than the AHCA would require – by 2023 under BCRA vs. 2020 under AHCA.
The BCRA would establish a per capita funding mechanism for Medicaid going forward, which would base funding on historic Medicaid expenditures and uses an economic index to track inflation and adjust payments accordingly.
To address the needs of people with greater health care needs, the Senate proposal would provide $57 billion over the first 4 years, then another $57 billion over the next 8. The funds would be available for programs such as premium support or high-risk pools to help individuals who are expected to be high users of health care. States would be required to match funds starting in 2022.
Experts were quick to weigh in on the Senate plan.
The BCRA needs to do three things, according to Grace-Marie Turner, president of the Galen Institute: Provide a safety net for those covered through the ACA so that they do not lose coverage in the transition, modernize Medicaid, and give states more authority and options to reform their own health insurance markets.
“We have learned that the federal government is not able to regulate something as local as health insurance,” Ms. Turner said. “They cannot create policies and legislation that works for people in downtown Manhattan and rural Montana and southern New Mexico and the panhandle of Florida. There are too many different populations. The states need to do that, and this bill also would give the states more authority to begin to oversee their health insurance markets but with new funding to provide extra help for the people who have difficulty buying progress.”
She said it could be much better if the Senate did not use the reconciliation process, “but within the confines of that, both the House and Senate bills do the same thing.”
Ms. Turner also stressed that there are more reforms coming later, as the Senate and House address other portions of ACA repeal/replacement.
“I hope that [senators] would see moving this forward as beneficial so that then they can move additional pieces of legislation, hopefully, with 60 votes to go through the regular process, to have additional follow-up bills. This is not the end of the story. This is just rescuing us from Obamacare,” she said. “Then we need to go forward and think about what do we need to do to make our health sector work better in the future by putting doctors and patients, rather than government, in charge of choices.”
Doctors, however, did not agree.
“This bill significantly decreases patients’ ability to access high-quality health care, and affordable coverage for millions of Americans will be in jeopardy if the legislation is passed,” Boyd Buser, MD, a doctor of osteopathy and president of the American Osteopathic Association, said in a statement.
He noted that the Medicaid cuts will have a “devastating impact, especially in areas of our country hardest hit by the ongoing opioid epidemic. ... The Senate bill should have prioritized prevention and care coordination, two measures proven to reduce overall health costs by eliminating waste and addressing health problems at the most treatable stage. Decreasing the number of Americans with coverage as it intends does will not lower costs.”
A vote on the proposal could come as early as June 29 before the Senate breaks for the 4th of July recess.
Republican lawmakers and the Trump administration have vowed to address the ACA in other ways as well, by reviewing and possibly changing all relevant regulations, then using the regular legislative process, which would need 60 votes, to address issues that cannot be handled by the budget reconciliation process.
FDA approves rituximab + hyaluronidase human for FL, DLBCL, and CLL
The Food and Drug Administration has approved rituximab plus hyaluronidase human for adult patients with follicular lymphoma (FL), diffuse large B-cell lymphoma (DLBCL), and chronic lymphocytic leukemia (CLL).
The combination product, to be marketed as Rituxan Hycela, is administered subcutaneously, shortening administration time to 5 to 7 minutes as compared with the several hours needed for intravenous infusion, the FDA said in a statement.
Approval was based on noninferior rituximab trough concentrations for the subcutaneously administered combination, compared with intravenous rituximab, and comparable efficacy and safety results as shown in multiple randomized clinical trials.
The most common adverse events seen with the combination in patients with FL included infections, neutropenia, nausea, constipation, cough, and fatigue. In patients with DLBCL, the most common adverse events were infections, neutropenia, alopecia, nausea, and anemia; in CLL patients, infections, neutropenia, nausea, thrombocytopenia, pyrexia, vomiting, and injection site erythema occurred most commonly.
The combination is indicated for the following previously approved indications for rituximab:
- Relapsed or refractory FL as a single agent.
- Previously untreated FL in combination with first line chemotherapy and, in patients achieving a complete or partial response to rituximab in combination with chemotherapy, as single-agent maintenance therapy.
- Nonprogressing (including stable disease) FL as a single agent after first-line cyclophosphamide, vincristine, and prednisone chemotherapy.
- Previously untreated DLBCL in combination with cyclophosphamide, doxorubicin, vincristine, prednisone or other anthracycline-based chemotherapy regimens.
- Previously untreated and previously treated CLL in combination with fludarabine and cyclophosphamide.
The recommended doses are 1,400 mg rituximab and 23,400 units hyaluronidase human for FL and DLBCL and 1,600 mg rituximab and 26,800 units hyaluronidase human for CLL. The combination treatment should be initiated only after patients have received at least one full dose of a rituximab product by intravenous infusion, according to the prescribing information.
Rituxan Hycela is marketed by Genentech.
The Food and Drug Administration has approved rituximab plus hyaluronidase human for adult patients with follicular lymphoma (FL), diffuse large B-cell lymphoma (DLBCL), and chronic lymphocytic leukemia (CLL).
The combination product, to be marketed as Rituxan Hycela, is administered subcutaneously, shortening administration time to 5 to 7 minutes as compared with the several hours needed for intravenous infusion, the FDA said in a statement.
Approval was based on noninferior rituximab trough concentrations for the subcutaneously administered combination, compared with intravenous rituximab, and comparable efficacy and safety results as shown in multiple randomized clinical trials.
The most common adverse events seen with the combination in patients with FL included infections, neutropenia, nausea, constipation, cough, and fatigue. In patients with DLBCL, the most common adverse events were infections, neutropenia, alopecia, nausea, and anemia; in CLL patients, infections, neutropenia, nausea, thrombocytopenia, pyrexia, vomiting, and injection site erythema occurred most commonly.
The combination is indicated for the following previously approved indications for rituximab:
- Relapsed or refractory FL as a single agent.
- Previously untreated FL in combination with first line chemotherapy and, in patients achieving a complete or partial response to rituximab in combination with chemotherapy, as single-agent maintenance therapy.
- Nonprogressing (including stable disease) FL as a single agent after first-line cyclophosphamide, vincristine, and prednisone chemotherapy.
- Previously untreated DLBCL in combination with cyclophosphamide, doxorubicin, vincristine, prednisone or other anthracycline-based chemotherapy regimens.
- Previously untreated and previously treated CLL in combination with fludarabine and cyclophosphamide.
The recommended doses are 1,400 mg rituximab and 23,400 units hyaluronidase human for FL and DLBCL and 1,600 mg rituximab and 26,800 units hyaluronidase human for CLL. The combination treatment should be initiated only after patients have received at least one full dose of a rituximab product by intravenous infusion, according to the prescribing information.
Rituxan Hycela is marketed by Genentech.
The Food and Drug Administration has approved rituximab plus hyaluronidase human for adult patients with follicular lymphoma (FL), diffuse large B-cell lymphoma (DLBCL), and chronic lymphocytic leukemia (CLL).
The combination product, to be marketed as Rituxan Hycela, is administered subcutaneously, shortening administration time to 5 to 7 minutes as compared with the several hours needed for intravenous infusion, the FDA said in a statement.
Approval was based on noninferior rituximab trough concentrations for the subcutaneously administered combination, compared with intravenous rituximab, and comparable efficacy and safety results as shown in multiple randomized clinical trials.
The most common adverse events seen with the combination in patients with FL included infections, neutropenia, nausea, constipation, cough, and fatigue. In patients with DLBCL, the most common adverse events were infections, neutropenia, alopecia, nausea, and anemia; in CLL patients, infections, neutropenia, nausea, thrombocytopenia, pyrexia, vomiting, and injection site erythema occurred most commonly.
The combination is indicated for the following previously approved indications for rituximab:
- Relapsed or refractory FL as a single agent.
- Previously untreated FL in combination with first line chemotherapy and, in patients achieving a complete or partial response to rituximab in combination with chemotherapy, as single-agent maintenance therapy.
- Nonprogressing (including stable disease) FL as a single agent after first-line cyclophosphamide, vincristine, and prednisone chemotherapy.
- Previously untreated DLBCL in combination with cyclophosphamide, doxorubicin, vincristine, prednisone or other anthracycline-based chemotherapy regimens.
- Previously untreated and previously treated CLL in combination with fludarabine and cyclophosphamide.
The recommended doses are 1,400 mg rituximab and 23,400 units hyaluronidase human for FL and DLBCL and 1,600 mg rituximab and 26,800 units hyaluronidase human for CLL. The combination treatment should be initiated only after patients have received at least one full dose of a rituximab product by intravenous infusion, according to the prescribing information.
Rituxan Hycela is marketed by Genentech.
ACOG recommends women start mammography between ages 40 and 50 years
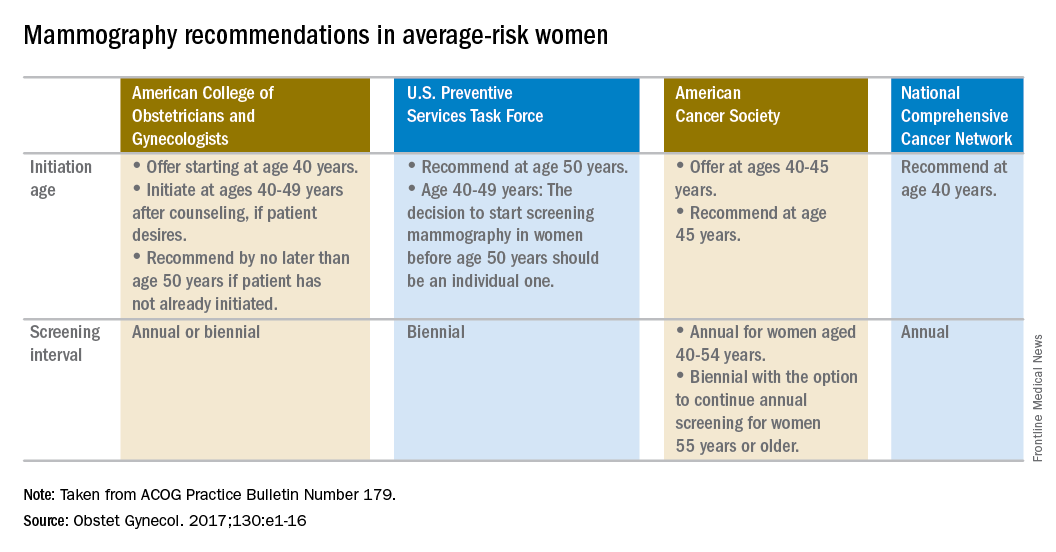
Woman at average risk for breast cancer should be offered their first screening mammogram at age 40, with initiation of screening beginning no later than age 50, according to new recommendations from the American College of Obstetricians and Gynecologists.
ACOG suggested a screening interval of 1-2 years based on patient values and preferences.

Screening should continue until at least age 75 years. Past that age, continuation should be considered in terms of the patient’s overall health and expected lifespan, according to the Practice Bulletin.

That’s a welcome approach, according to Ritu Salani, MD, a gynecologic oncologist at the Ohio State University, Columbus. “I do believe the ACOG guidelines have the most flexibility and are probably the most comprehensive for average-risk patients,” said Dr. Salani, MD, who was not involved in the drafting of the guidelines.
The recommendations are based in part on a review of existing recommendations from the U.S. Preventive Services Task Force, the American Cancer Society, and the National Comprehensive Cancer Network.
“For patients anxious about developing cancer, maybe every year would be appropriate. When you talk to patients, you have a sense of what would be beneficial for them,” said Dr. Salani, who applauded the flexibility built into the new ACOG guidelines, which says the screening interval can be annual or biennial. “It caters to shared decision-making, and that’s a nice way to frame it.”
The ACOG guidelines recommend against breast self examination because this practice carries the risk of false positives and lacks supporting evidence of benefit. But, ACOG encourages “breast self-awareness,” which means being “attuned to noticing a change or potential problem with her breasts” but without the routine examination.
Women who are asymptomatic and at average risk can be offered clinical breast examination as a screening tool, but clinicians should explain the “uncertainty of additional benefits and the possibility of adverse consequences of clinical breast examination beyond screening mammography.” If performed, ACOG recommends intervals of 1-3 years for women aged 25-39 years and annually for women aged 40 years and over.
The recommendations apply to average-risk women. To help determine risk, the Practice Bulletin also lays out a series of breast cancer risk factors that should be considered, including family history of cancer, known germline mutations, prior biopsy findings, early menarche, late menopause, breast density, and a range of lifestyle and other factors.
Woman at average risk for breast cancer should be offered their first screening mammogram at age 40, with initiation of screening beginning no later than age 50, according to new recommendations from the American College of Obstetricians and Gynecologists.
ACOG suggested a screening interval of 1-2 years based on patient values and preferences.
Screening should continue until at least age 75 years. Past that age, continuation should be considered in terms of the patient’s overall health and expected lifespan, according to the Practice Bulletin.
That’s a welcome approach, according to Ritu Salani, MD, a gynecologic oncologist at the Ohio State University, Columbus. “I do believe the ACOG guidelines have the most flexibility and are probably the most comprehensive for average-risk patients,” said Dr. Salani, MD, who was not involved in the drafting of the guidelines.
The recommendations are based in part on a review of existing recommendations from the U.S. Preventive Services Task Force, the American Cancer Society, and the National Comprehensive Cancer Network.
“For patients anxious about developing cancer, maybe every year would be appropriate. When you talk to patients, you have a sense of what would be beneficial for them,” said Dr. Salani, who applauded the flexibility built into the new ACOG guidelines, which says the screening interval can be annual or biennial. “It caters to shared decision-making, and that’s a nice way to frame it.”
The ACOG guidelines recommend against breast self examination because this practice carries the risk of false positives and lacks supporting evidence of benefit. But, ACOG encourages “breast self-awareness,” which means being “attuned to noticing a change or potential problem with her breasts” but without the routine examination.
Women who are asymptomatic and at average risk can be offered clinical breast examination as a screening tool, but clinicians should explain the “uncertainty of additional benefits and the possibility of adverse consequences of clinical breast examination beyond screening mammography.” If performed, ACOG recommends intervals of 1-3 years for women aged 25-39 years and annually for women aged 40 years and over.
The recommendations apply to average-risk women. To help determine risk, the Practice Bulletin also lays out a series of breast cancer risk factors that should be considered, including family history of cancer, known germline mutations, prior biopsy findings, early menarche, late menopause, breast density, and a range of lifestyle and other factors.
Woman at average risk for breast cancer should be offered their first screening mammogram at age 40, with initiation of screening beginning no later than age 50, according to new recommendations from the American College of Obstetricians and Gynecologists.
ACOG suggested a screening interval of 1-2 years based on patient values and preferences.
Screening should continue until at least age 75 years. Past that age, continuation should be considered in terms of the patient’s overall health and expected lifespan, according to the Practice Bulletin.
That’s a welcome approach, according to Ritu Salani, MD, a gynecologic oncologist at the Ohio State University, Columbus. “I do believe the ACOG guidelines have the most flexibility and are probably the most comprehensive for average-risk patients,” said Dr. Salani, MD, who was not involved in the drafting of the guidelines.
The recommendations are based in part on a review of existing recommendations from the U.S. Preventive Services Task Force, the American Cancer Society, and the National Comprehensive Cancer Network.
“For patients anxious about developing cancer, maybe every year would be appropriate. When you talk to patients, you have a sense of what would be beneficial for them,” said Dr. Salani, who applauded the flexibility built into the new ACOG guidelines, which says the screening interval can be annual or biennial. “It caters to shared decision-making, and that’s a nice way to frame it.”
The ACOG guidelines recommend against breast self examination because this practice carries the risk of false positives and lacks supporting evidence of benefit. But, ACOG encourages “breast self-awareness,” which means being “attuned to noticing a change or potential problem with her breasts” but without the routine examination.
Women who are asymptomatic and at average risk can be offered clinical breast examination as a screening tool, but clinicians should explain the “uncertainty of additional benefits and the possibility of adverse consequences of clinical breast examination beyond screening mammography.” If performed, ACOG recommends intervals of 1-3 years for women aged 25-39 years and annually for women aged 40 years and over.
The recommendations apply to average-risk women. To help determine risk, the Practice Bulletin also lays out a series of breast cancer risk factors that should be considered, including family history of cancer, known germline mutations, prior biopsy findings, early menarche, late menopause, breast density, and a range of lifestyle and other factors.
Lenalidomide consolidation linked to extended overall survival in non-del(11q) CLL
CHICAGO – Lenalidomide consolidation therapy was associated with an extended survival plateau for patients with non-del(11q) chronic lymphocytic leukemia (CLL), based on results from the phase 2 CALGB 10404 trial.
This unique survival plateau indicates future studies should continue to examine the role of lenalidomide, compared with fludarabine plus rituximab therapy, as well as the incorporation of lenalidomide into other novel treatment regimens, Amy Ruppert, MAS, said at the annual meeting of the American Society of Clinical Oncology.

All patients received 6 months of FR or FCR therapy, then patients underwent full staging. At 10 months, patients who had been randomized to the FR + lenalidomide group received lenalidomide 5 mg on days 1-21 of the first 28 day cycle and lenalidomide 10 mg on days 1-21 of the subsequent 5 cycles. At 18 months, patients in the FR+L group underwent full staging, and all patients underwent full staging at 24 months.
Based on pretreatment central interphase cytogenetic screening, patients who had del(11q22.3) in at least 20% of their cells were excluded from the primary analysis of 2-year progression-free survival.
Median progression-free survival was significantly shorter with FR, compared with FR+L (P = .03) and FCR (P less than .01), at 43 months (95% CI, 33-50), 66 months (95% CI, 45-not reached), and 78 months (95% CI, 58-not reached), respectively.
Median overall survival has not been reached for any arm of the study. While overall survival was similar across all arms at 1, 2, and 3 years of follow-up, there was a plateau in overall survival with no events seen beyond 41 months in the FR+L arm. Events continued to occur in the FR and FCR arms, reported Ms. Ruppert of the Comprehensive Cancer Center at Ohio State University, Columbus. At 48 months, the hazard ratio for overall survival in FR+L vs. FR was 0.27 (95% CI, 0.10-0.70; P = .01).
Ms. Ruppert had no financial disclosures. The study is sponsored by the National Cancer Institute and Celgene.
[email protected]
On Twitter @maryjodales
CHICAGO – Lenalidomide consolidation therapy was associated with an extended survival plateau for patients with non-del(11q) chronic lymphocytic leukemia (CLL), based on results from the phase 2 CALGB 10404 trial.
This unique survival plateau indicates future studies should continue to examine the role of lenalidomide, compared with fludarabine plus rituximab therapy, as well as the incorporation of lenalidomide into other novel treatment regimens, Amy Ruppert, MAS, said at the annual meeting of the American Society of Clinical Oncology.
All patients received 6 months of FR or FCR therapy, then patients underwent full staging. At 10 months, patients who had been randomized to the FR + lenalidomide group received lenalidomide 5 mg on days 1-21 of the first 28 day cycle and lenalidomide 10 mg on days 1-21 of the subsequent 5 cycles. At 18 months, patients in the FR+L group underwent full staging, and all patients underwent full staging at 24 months.
Based on pretreatment central interphase cytogenetic screening, patients who had del(11q22.3) in at least 20% of their cells were excluded from the primary analysis of 2-year progression-free survival.
Median progression-free survival was significantly shorter with FR, compared with FR+L (P = .03) and FCR (P less than .01), at 43 months (95% CI, 33-50), 66 months (95% CI, 45-not reached), and 78 months (95% CI, 58-not reached), respectively.
Median overall survival has not been reached for any arm of the study. While overall survival was similar across all arms at 1, 2, and 3 years of follow-up, there was a plateau in overall survival with no events seen beyond 41 months in the FR+L arm. Events continued to occur in the FR and FCR arms, reported Ms. Ruppert of the Comprehensive Cancer Center at Ohio State University, Columbus. At 48 months, the hazard ratio for overall survival in FR+L vs. FR was 0.27 (95% CI, 0.10-0.70; P = .01).
Ms. Ruppert had no financial disclosures. The study is sponsored by the National Cancer Institute and Celgene.
[email protected]
On Twitter @maryjodales
CHICAGO – Lenalidomide consolidation therapy was associated with an extended survival plateau for patients with non-del(11q) chronic lymphocytic leukemia (CLL), based on results from the phase 2 CALGB 10404 trial.
This unique survival plateau indicates future studies should continue to examine the role of lenalidomide, compared with fludarabine plus rituximab therapy, as well as the incorporation of lenalidomide into other novel treatment regimens, Amy Ruppert, MAS, said at the annual meeting of the American Society of Clinical Oncology.
All patients received 6 months of FR or FCR therapy, then patients underwent full staging. At 10 months, patients who had been randomized to the FR + lenalidomide group received lenalidomide 5 mg on days 1-21 of the first 28 day cycle and lenalidomide 10 mg on days 1-21 of the subsequent 5 cycles. At 18 months, patients in the FR+L group underwent full staging, and all patients underwent full staging at 24 months.
Based on pretreatment central interphase cytogenetic screening, patients who had del(11q22.3) in at least 20% of their cells were excluded from the primary analysis of 2-year progression-free survival.
Median progression-free survival was significantly shorter with FR, compared with FR+L (P = .03) and FCR (P less than .01), at 43 months (95% CI, 33-50), 66 months (95% CI, 45-not reached), and 78 months (95% CI, 58-not reached), respectively.
Median overall survival has not been reached for any arm of the study. While overall survival was similar across all arms at 1, 2, and 3 years of follow-up, there was a plateau in overall survival with no events seen beyond 41 months in the FR+L arm. Events continued to occur in the FR and FCR arms, reported Ms. Ruppert of the Comprehensive Cancer Center at Ohio State University, Columbus. At 48 months, the hazard ratio for overall survival in FR+L vs. FR was 0.27 (95% CI, 0.10-0.70; P = .01).
Ms. Ruppert had no financial disclosures. The study is sponsored by the National Cancer Institute and Celgene.
[email protected]
On Twitter @maryjodales
AT ASCO 2017
Key clinical point:
Major finding: At 48 months, the hazard ratio for overall survival in FR+L vs. FR was 0.27 (95% CI, 0.10-0.70; P = .01).
Data source: Results from 342 patients in the phase 2 CALGB 10404 trial.
Disclosures: Ms. Ruppert had no financial disclosures. The study is sponsored by the National Cancer Institute and Celgene.
For opioid-related hospitalizations, men and women are equal
Equality is not always a good thing, particularly with opioids.
In 2005, the rate of opioid-related inpatient hospital stays was 145.6 per 100,000 population for males of all ages and 127.8 for females of all ages. By 2014, however, equality had arrived: Females had a rate of 224.1 per 100,000, compared with 225 for males, according to the Agency for Healthcare Research and Quality. Those increases in hospital admissions work out to 75% for females and 55% for males.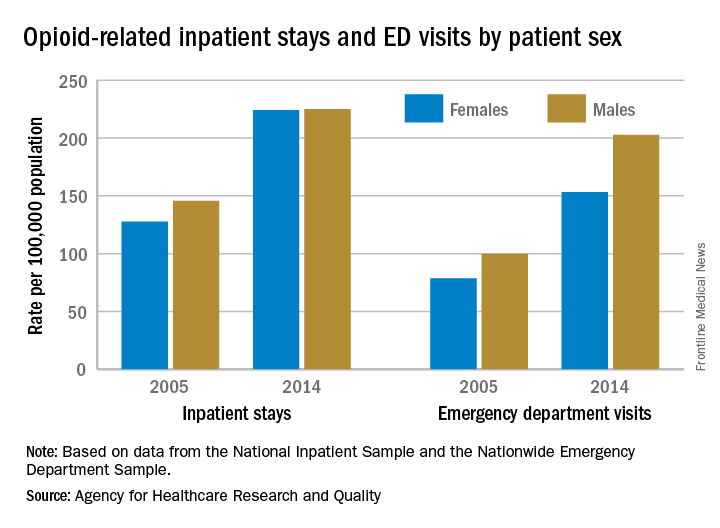
The states tell a similarly unequal story for opioid-related ED visits. In 2014, males had the higher rate in 23 states, and females had the higher rate in 7 states. (Washington, D.C., and 20 states do not participate in the State Emergency Department Databases and were not included in this analysis.)
Among the 30 participating states, Massachusetts had the highest visit rates for both males (598.8) and females (310.4), and Iowa had the lowest at 37 for males and 53.1 for females, AHRQ said.
The roles were reversed for opioid-related hospital admissions in the states in 2014: Females had the higher rate in 33 of the states participating in the State Inpatient Databases, compared with 11 states and the District of Columbia for males.
West Virginia had the highest rate for females at 371.2, and Washington, D.C., had the highest rate for males at 472. The lowest rates for both females (82.3) and males (63) were found in Iowa, according to the report.
Equality is not always a good thing, particularly with opioids.
In 2005, the rate of opioid-related inpatient hospital stays was 145.6 per 100,000 population for males of all ages and 127.8 for females of all ages. By 2014, however, equality had arrived: Females had a rate of 224.1 per 100,000, compared with 225 for males, according to the Agency for Healthcare Research and Quality. Those increases in hospital admissions work out to 75% for females and 55% for males.
The states tell a similarly unequal story for opioid-related ED visits. In 2014, males had the higher rate in 23 states, and females had the higher rate in 7 states. (Washington, D.C., and 20 states do not participate in the State Emergency Department Databases and were not included in this analysis.)
Among the 30 participating states, Massachusetts had the highest visit rates for both males (598.8) and females (310.4), and Iowa had the lowest at 37 for males and 53.1 for females, AHRQ said.
The roles were reversed for opioid-related hospital admissions in the states in 2014: Females had the higher rate in 33 of the states participating in the State Inpatient Databases, compared with 11 states and the District of Columbia for males.
West Virginia had the highest rate for females at 371.2, and Washington, D.C., had the highest rate for males at 472. The lowest rates for both females (82.3) and males (63) were found in Iowa, according to the report.
Equality is not always a good thing, particularly with opioids.
In 2005, the rate of opioid-related inpatient hospital stays was 145.6 per 100,000 population for males of all ages and 127.8 for females of all ages. By 2014, however, equality had arrived: Females had a rate of 224.1 per 100,000, compared with 225 for males, according to the Agency for Healthcare Research and Quality. Those increases in hospital admissions work out to 75% for females and 55% for males.
The states tell a similarly unequal story for opioid-related ED visits. In 2014, males had the higher rate in 23 states, and females had the higher rate in 7 states. (Washington, D.C., and 20 states do not participate in the State Emergency Department Databases and were not included in this analysis.)
Among the 30 participating states, Massachusetts had the highest visit rates for both males (598.8) and females (310.4), and Iowa had the lowest at 37 for males and 53.1 for females, AHRQ said.
The roles were reversed for opioid-related hospital admissions in the states in 2014: Females had the higher rate in 33 of the states participating in the State Inpatient Databases, compared with 11 states and the District of Columbia for males.
West Virginia had the highest rate for females at 371.2, and Washington, D.C., had the highest rate for males at 472. The lowest rates for both females (82.3) and males (63) were found in Iowa, according to the report.
Consortium Develops New Guideline for Dementia With Lewy Bodies
The international Dementia With Lewy Bodies Consortium has updated its guideline for diagnosing and treating this disease. “The updated clinical criteria and associated biomarkers hopefully will lead to earlier and more accurate diagnosis, and that is key to helping patients confront this challenging illness and maximize their quality of life,” said Bradley Boeve, MD, Professor of Neurology at Mayo Clinic in Rochester, Minnesota, and a coauthor. The guideline was published online ahead of print June 7 in Neurology.

The new guideline is a refinement of the consortium’s previous guideline, which was published in December 2005. To develop the new document, the consortium solicited and reviewed reports from four multidisciplinary expert working groups. The consortium also held a meeting in which patients and caregivers participated.
The revised consensus criteria distinguish between the clinical features and diagnostic biomarkers of the disease. The core clinical features are fluctuation in cognition, attention, and arousal; visual hallucinations (eg, of people, children, or animals); parkinsonism; and REM sleep behavior disorder, according to the authors. The criteria now list hypersomnia and hyposmia as supportive clinical features.
Direct biomarker evidence of Lewy body pathology is not available, said the authors. Indicative indirect biomarkers include reduced dopamine transporter uptake in basal ganglia demonstrated by single-photon emission computerized tomography or PET imaging, reduced uptake on metaiodobenzylguanidine (MIBG) myocardial scintigraphy, and polysomnographic confirmation of REM sleep without atonia.
A neurologist can diagnose probable dementia with Lewy bodies if two or more of its core clinical features are present, with or without the presence of indicative biomarkers. This diagnosis also is warranted if only one core clinical feature is present, but one or more indicative biomarkers are present.
The document incorporates new information about previously reported aspects of dementia with Lewy bodies and gives greater diagnostic weight to REM sleep behavior disorder and 123iodine-MIBG myocardial scintigraphy. The authors describe the diagnostic role of other neuroimaging, electrophysiologic, and laboratory investigations. They recommend minor modifications to pathologic methods and criteria to take account of Alzheimer’s disease neuropathologic change, to add previously omitted Lewy-related pathology categories, and to include assessments for substantia nigra neuronal loss.
Because the literature contains few randomized controlled trials, the guideline’s recommendations about clinical management are based on expert opinion. Cholinesterase inhibitors can improve cognition, global function, activities of living, and neuropsychiatric symptoms, according to the authors. Nonpharmacologic management strategies should be developed and tested, they added.
“There remains a pressing need to understand the underlying neurobiology and pathophysiology of dementia with Lewy bodies, to develop and deliver clinical trials with both symptomatic and disease-modifying agents, and to help patients and carers worldwide to inform themselves about the disease, its prognosis, best available treatments, ongoing research, and how to get adequate support,” the authors concluded.
—Erik Greb
Suggested Reading
McKeith IG, Boeve BF, Dickson DW, et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology. 2017 Jun 7 [Epub ahead of print].
The international Dementia With Lewy Bodies Consortium has updated its guideline for diagnosing and treating this disease. “The updated clinical criteria and associated biomarkers hopefully will lead to earlier and more accurate diagnosis, and that is key to helping patients confront this challenging illness and maximize their quality of life,” said Bradley Boeve, MD, Professor of Neurology at Mayo Clinic in Rochester, Minnesota, and a coauthor. The guideline was published online ahead of print June 7 in Neurology.
The new guideline is a refinement of the consortium’s previous guideline, which was published in December 2005. To develop the new document, the consortium solicited and reviewed reports from four multidisciplinary expert working groups. The consortium also held a meeting in which patients and caregivers participated.
The revised consensus criteria distinguish between the clinical features and diagnostic biomarkers of the disease. The core clinical features are fluctuation in cognition, attention, and arousal; visual hallucinations (eg, of people, children, or animals); parkinsonism; and REM sleep behavior disorder, according to the authors. The criteria now list hypersomnia and hyposmia as supportive clinical features.
Direct biomarker evidence of Lewy body pathology is not available, said the authors. Indicative indirect biomarkers include reduced dopamine transporter uptake in basal ganglia demonstrated by single-photon emission computerized tomography or PET imaging, reduced uptake on metaiodobenzylguanidine (MIBG) myocardial scintigraphy, and polysomnographic confirmation of REM sleep without atonia.
A neurologist can diagnose probable dementia with Lewy bodies if two or more of its core clinical features are present, with or without the presence of indicative biomarkers. This diagnosis also is warranted if only one core clinical feature is present, but one or more indicative biomarkers are present.
The document incorporates new information about previously reported aspects of dementia with Lewy bodies and gives greater diagnostic weight to REM sleep behavior disorder and 123iodine-MIBG myocardial scintigraphy. The authors describe the diagnostic role of other neuroimaging, electrophysiologic, and laboratory investigations. They recommend minor modifications to pathologic methods and criteria to take account of Alzheimer’s disease neuropathologic change, to add previously omitted Lewy-related pathology categories, and to include assessments for substantia nigra neuronal loss.
Because the literature contains few randomized controlled trials, the guideline’s recommendations about clinical management are based on expert opinion. Cholinesterase inhibitors can improve cognition, global function, activities of living, and neuropsychiatric symptoms, according to the authors. Nonpharmacologic management strategies should be developed and tested, they added.
“There remains a pressing need to understand the underlying neurobiology and pathophysiology of dementia with Lewy bodies, to develop and deliver clinical trials with both symptomatic and disease-modifying agents, and to help patients and carers worldwide to inform themselves about the disease, its prognosis, best available treatments, ongoing research, and how to get adequate support,” the authors concluded.
—Erik Greb
Suggested Reading
McKeith IG, Boeve BF, Dickson DW, et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology. 2017 Jun 7 [Epub ahead of print].
The international Dementia With Lewy Bodies Consortium has updated its guideline for diagnosing and treating this disease. “The updated clinical criteria and associated biomarkers hopefully will lead to earlier and more accurate diagnosis, and that is key to helping patients confront this challenging illness and maximize their quality of life,” said Bradley Boeve, MD, Professor of Neurology at Mayo Clinic in Rochester, Minnesota, and a coauthor. The guideline was published online ahead of print June 7 in Neurology.
The new guideline is a refinement of the consortium’s previous guideline, which was published in December 2005. To develop the new document, the consortium solicited and reviewed reports from four multidisciplinary expert working groups. The consortium also held a meeting in which patients and caregivers participated.
The revised consensus criteria distinguish between the clinical features and diagnostic biomarkers of the disease. The core clinical features are fluctuation in cognition, attention, and arousal; visual hallucinations (eg, of people, children, or animals); parkinsonism; and REM sleep behavior disorder, according to the authors. The criteria now list hypersomnia and hyposmia as supportive clinical features.
Direct biomarker evidence of Lewy body pathology is not available, said the authors. Indicative indirect biomarkers include reduced dopamine transporter uptake in basal ganglia demonstrated by single-photon emission computerized tomography or PET imaging, reduced uptake on metaiodobenzylguanidine (MIBG) myocardial scintigraphy, and polysomnographic confirmation of REM sleep without atonia.
A neurologist can diagnose probable dementia with Lewy bodies if two or more of its core clinical features are present, with or without the presence of indicative biomarkers. This diagnosis also is warranted if only one core clinical feature is present, but one or more indicative biomarkers are present.
The document incorporates new information about previously reported aspects of dementia with Lewy bodies and gives greater diagnostic weight to REM sleep behavior disorder and 123iodine-MIBG myocardial scintigraphy. The authors describe the diagnostic role of other neuroimaging, electrophysiologic, and laboratory investigations. They recommend minor modifications to pathologic methods and criteria to take account of Alzheimer’s disease neuropathologic change, to add previously omitted Lewy-related pathology categories, and to include assessments for substantia nigra neuronal loss.
Because the literature contains few randomized controlled trials, the guideline’s recommendations about clinical management are based on expert opinion. Cholinesterase inhibitors can improve cognition, global function, activities of living, and neuropsychiatric symptoms, according to the authors. Nonpharmacologic management strategies should be developed and tested, they added.
“There remains a pressing need to understand the underlying neurobiology and pathophysiology of dementia with Lewy bodies, to develop and deliver clinical trials with both symptomatic and disease-modifying agents, and to help patients and carers worldwide to inform themselves about the disease, its prognosis, best available treatments, ongoing research, and how to get adequate support,” the authors concluded.
—Erik Greb
Suggested Reading
McKeith IG, Boeve BF, Dickson DW, et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology. 2017 Jun 7 [Epub ahead of print].
Can Cannabis Help Patients With Parkinson’s Disease?
VANCOUVER—Anecdotal reports, patient surveys, and studies have suggested that cannabis may help treat motor and nonmotor symptoms of Parkinson’s disease. Two studies presented at the 21st International Congress of Parkinson’s Disease and Movement Disorders further explored this possibility and assessed the effects of oral cannabidiol (CBD) and inhaled cannabis in patients with Parkinson’s disease.
Cannabidiol
Maureen A. Leehey, MD, Professor of Neurology and Chief of the Movement Disorders Division at the University of Colorado in Aurora, and colleagues conducted a phase II, open-label, dose-escalation study to evaluate the safety and tolerability of CBD (Epidiolex) in Parkinson’s disease. In addition, the researchers looked at secondary efficacy measures, including change in tremor, cognition, anxiety, psychosis, sleep, daytime sleepiness, mood, fatigue, and pain.

The researchers enrolled 13 patients who had a rest tremor amplitude score of 2 or greater on item 3.17 of the Unified Parkinson’s Disease Rating Scale (UPDRS). They excluded patients who had taken cannabinoids in the previous 30 days or had a history of drug or alcohol dependence.
Over a 31-day treatment period, patients received 5-, 7.5-, 10-, 15-, and 20-mg/kg/day doses of CBD. They received the highest dose on days 17–31. Patients had clinic visits at screening, baseline, and after the 31-day treatment period. Of the 13 patients enrolled, one failed the screening visit, another patient did not start the study drug, and another patient was on the study drug for two days. The 10 remaining patients were included in the adverse events analysis. Adverse events were mostly mild to moderate and included fatigue, diarrhea, somnolence, elevated liver enzymes, and dizziness. Three of the 10 patients dropped out of the study due to intolerance. One of the three patients had an allergic reaction and two had abdominal pain. There were no serious adverse events.
Among the seven patients who completed the treatment period and were included in the efficacy analysis, mean total UPDRS score significantly decreased from 45.9 at baseline to 36.4 at the final visit. UPDRS motor score significantly decreased from 27.3 to 20.3. Mean rigidity subscore significantly decreased from 9.14 to 6.29. In addition, data hinted that CBD treatment might have reduced pain and irritability, the researchers said.
These preliminary results indicate that CBD is tolerated, safe, and has beneficial effects in Parkinson’s disease, Dr. Leehey and colleagues said. The investigators next plan to conduct a crossover, double-blind, randomized controlled trial with 50 subjects.
Inhaled Cannabis
Laurie K. Mischley, ND, PhD, MPH, Associate Clinical Investigator at Bastyr University Research Institute in Kenmore, Washington, and colleagues evaluated the effect of inhaled cannabis on Parkinson’s disease tremor using motion sensors and qualitative interviews.
The study included patients with Parkinson’s disease who used cannabis in the state of Washington. Patients wore a movement monitor for two weeks and logged their cannabis use in a journal. Sensors recorded the frequency and amplitude of tremor during waking hours, and participants pressed a button on the motion sensor every time they used cannabis. The researchers compared tremor duration and magnitude in the hour before and after inhaled cannabis use. After two weeks, interviewers asked participants standardized, open-ended, nonleading questions about their perception of the effects of cannabis on their symptoms.
The 10 patients for whom they had data had a mean age of 60 (range, 40 to 74) and a mean time since diagnosis of 6.3 years. Among four participants who had more than 10 cannabis exposures and a measurable tremor more than 2% of the time in the hour before cannabis use during the study, the percent of the time with detected tremor significantly decreased in the hour after use. Sensor data suggested that tremor reduction may have been sustained for three hours after exposure to cannabis, the researchers said. “In those with a persistent tremor, there was a consistent decrease in the tremor persistence and in detected tremor magnitude following cannabis use,” the investigators said.
During the follow-up interview, nine of the 10 participants thought that cannabis helped their symptoms, and one patient thought it worsened symptoms. “The one participant who reported cannabis worsening symptoms specifically described, ‘sometimes it speeds up the tremor at the start’ but ‘then it relaxes it,’” the researchers said.
Side effects reported by patients included sleepiness, sluggishness, concerns about social stigma and driving, short-term memory, and dry throat.
“Improved sleep was an unsolicited theme during the qualitative interviews, with 60% of individuals reporting improvements,” Dr. Mischley and colleagues said. “The qualitative interviews suggest patients perceive cannabis to have therapeutic potential for Parkinson’s disease symptom management. These data suggest further investigation of cannabis for impaired sleep is warranted.”
The researchers noted that most subjects had a mild, intermittent tremor that was not reliably detected by the motion sensors. Future studies should enroll subjects with more pronounced tremor and use consistent cannabis strains, doses, and delivery systems, they said.
—Jake Remaly
Suggested Reading
Chagas MH, Zuardi AW, Tumas V, et al. Effects of cannabidiol in the treatment of patients with Parkinson’s disease: an exploratory double-blind trial. J Psychopharmacol. 2014;28(11):1088-1098.
Finseth TA, Hedeman JL, Brown RP 2nd, et al. Self-reported efficacy of cannabis and other complementary medicine modalities by Parkinson’s disease patients in Colorado. Evid Based Complement Alternat Med. 2015;2015:874849.
Koppel BS, Brust JC, Fife T, et al. Systematic review: efficacy and safety of medical marijuana in selected neurologic disorders: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2014; 82(17):1556-1563.
Lotan I, Treves TA, Roditi Y, Djaldetti R. Cannabis (medical marijuana) treatment for motor and non-motor symptoms of Parkinson disease: an open-label observational study. Clin Neuropharmacol. 2014;37(2):41-44.
Venderová K, Ruzicka E, Vorísek V, Visnovský P. Survey on cannabis use in Parkinson’s disease: subjective improvement of motor symptoms. Mov Disord. 2004;19(9):1102-1106.
Zuardi AW, Crippa JA, Hallak JE, et al. Cannabidiol for the treatment of psychosis in Parkinson’s disease. J Psychopharmacol. 2009;23(8):979-983.
VANCOUVER—Anecdotal reports, patient surveys, and studies have suggested that cannabis may help treat motor and nonmotor symptoms of Parkinson’s disease. Two studies presented at the 21st International Congress of Parkinson’s Disease and Movement Disorders further explored this possibility and assessed the effects of oral cannabidiol (CBD) and inhaled cannabis in patients with Parkinson’s disease.
Cannabidiol
Maureen A. Leehey, MD, Professor of Neurology and Chief of the Movement Disorders Division at the University of Colorado in Aurora, and colleagues conducted a phase II, open-label, dose-escalation study to evaluate the safety and tolerability of CBD (Epidiolex) in Parkinson’s disease. In addition, the researchers looked at secondary efficacy measures, including change in tremor, cognition, anxiety, psychosis, sleep, daytime sleepiness, mood, fatigue, and pain.
The researchers enrolled 13 patients who had a rest tremor amplitude score of 2 or greater on item 3.17 of the Unified Parkinson’s Disease Rating Scale (UPDRS). They excluded patients who had taken cannabinoids in the previous 30 days or had a history of drug or alcohol dependence.
Over a 31-day treatment period, patients received 5-, 7.5-, 10-, 15-, and 20-mg/kg/day doses of CBD. They received the highest dose on days 17–31. Patients had clinic visits at screening, baseline, and after the 31-day treatment period. Of the 13 patients enrolled, one failed the screening visit, another patient did not start the study drug, and another patient was on the study drug for two days. The 10 remaining patients were included in the adverse events analysis. Adverse events were mostly mild to moderate and included fatigue, diarrhea, somnolence, elevated liver enzymes, and dizziness. Three of the 10 patients dropped out of the study due to intolerance. One of the three patients had an allergic reaction and two had abdominal pain. There were no serious adverse events.
Among the seven patients who completed the treatment period and were included in the efficacy analysis, mean total UPDRS score significantly decreased from 45.9 at baseline to 36.4 at the final visit. UPDRS motor score significantly decreased from 27.3 to 20.3. Mean rigidity subscore significantly decreased from 9.14 to 6.29. In addition, data hinted that CBD treatment might have reduced pain and irritability, the researchers said.
These preliminary results indicate that CBD is tolerated, safe, and has beneficial effects in Parkinson’s disease, Dr. Leehey and colleagues said. The investigators next plan to conduct a crossover, double-blind, randomized controlled trial with 50 subjects.
Inhaled Cannabis
Laurie K. Mischley, ND, PhD, MPH, Associate Clinical Investigator at Bastyr University Research Institute in Kenmore, Washington, and colleagues evaluated the effect of inhaled cannabis on Parkinson’s disease tremor using motion sensors and qualitative interviews.
The study included patients with Parkinson’s disease who used cannabis in the state of Washington. Patients wore a movement monitor for two weeks and logged their cannabis use in a journal. Sensors recorded the frequency and amplitude of tremor during waking hours, and participants pressed a button on the motion sensor every time they used cannabis. The researchers compared tremor duration and magnitude in the hour before and after inhaled cannabis use. After two weeks, interviewers asked participants standardized, open-ended, nonleading questions about their perception of the effects of cannabis on their symptoms.
The 10 patients for whom they had data had a mean age of 60 (range, 40 to 74) and a mean time since diagnosis of 6.3 years. Among four participants who had more than 10 cannabis exposures and a measurable tremor more than 2% of the time in the hour before cannabis use during the study, the percent of the time with detected tremor significantly decreased in the hour after use. Sensor data suggested that tremor reduction may have been sustained for three hours after exposure to cannabis, the researchers said. “In those with a persistent tremor, there was a consistent decrease in the tremor persistence and in detected tremor magnitude following cannabis use,” the investigators said.
During the follow-up interview, nine of the 10 participants thought that cannabis helped their symptoms, and one patient thought it worsened symptoms. “The one participant who reported cannabis worsening symptoms specifically described, ‘sometimes it speeds up the tremor at the start’ but ‘then it relaxes it,’” the researchers said.
Side effects reported by patients included sleepiness, sluggishness, concerns about social stigma and driving, short-term memory, and dry throat.
“Improved sleep was an unsolicited theme during the qualitative interviews, with 60% of individuals reporting improvements,” Dr. Mischley and colleagues said. “The qualitative interviews suggest patients perceive cannabis to have therapeutic potential for Parkinson’s disease symptom management. These data suggest further investigation of cannabis for impaired sleep is warranted.”
The researchers noted that most subjects had a mild, intermittent tremor that was not reliably detected by the motion sensors. Future studies should enroll subjects with more pronounced tremor and use consistent cannabis strains, doses, and delivery systems, they said.
—Jake Remaly
Suggested Reading
Chagas MH, Zuardi AW, Tumas V, et al. Effects of cannabidiol in the treatment of patients with Parkinson’s disease: an exploratory double-blind trial. J Psychopharmacol. 2014;28(11):1088-1098.
Finseth TA, Hedeman JL, Brown RP 2nd, et al. Self-reported efficacy of cannabis and other complementary medicine modalities by Parkinson’s disease patients in Colorado. Evid Based Complement Alternat Med. 2015;2015:874849.
Koppel BS, Brust JC, Fife T, et al. Systematic review: efficacy and safety of medical marijuana in selected neurologic disorders: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2014; 82(17):1556-1563.
Lotan I, Treves TA, Roditi Y, Djaldetti R. Cannabis (medical marijuana) treatment for motor and non-motor symptoms of Parkinson disease: an open-label observational study. Clin Neuropharmacol. 2014;37(2):41-44.
Venderová K, Ruzicka E, Vorísek V, Visnovský P. Survey on cannabis use in Parkinson’s disease: subjective improvement of motor symptoms. Mov Disord. 2004;19(9):1102-1106.
Zuardi AW, Crippa JA, Hallak JE, et al. Cannabidiol for the treatment of psychosis in Parkinson’s disease. J Psychopharmacol. 2009;23(8):979-983.
VANCOUVER—Anecdotal reports, patient surveys, and studies have suggested that cannabis may help treat motor and nonmotor symptoms of Parkinson’s disease. Two studies presented at the 21st International Congress of Parkinson’s Disease and Movement Disorders further explored this possibility and assessed the effects of oral cannabidiol (CBD) and inhaled cannabis in patients with Parkinson’s disease.
Cannabidiol
Maureen A. Leehey, MD, Professor of Neurology and Chief of the Movement Disorders Division at the University of Colorado in Aurora, and colleagues conducted a phase II, open-label, dose-escalation study to evaluate the safety and tolerability of CBD (Epidiolex) in Parkinson’s disease. In addition, the researchers looked at secondary efficacy measures, including change in tremor, cognition, anxiety, psychosis, sleep, daytime sleepiness, mood, fatigue, and pain.
The researchers enrolled 13 patients who had a rest tremor amplitude score of 2 or greater on item 3.17 of the Unified Parkinson’s Disease Rating Scale (UPDRS). They excluded patients who had taken cannabinoids in the previous 30 days or had a history of drug or alcohol dependence.
Over a 31-day treatment period, patients received 5-, 7.5-, 10-, 15-, and 20-mg/kg/day doses of CBD. They received the highest dose on days 17–31. Patients had clinic visits at screening, baseline, and after the 31-day treatment period. Of the 13 patients enrolled, one failed the screening visit, another patient did not start the study drug, and another patient was on the study drug for two days. The 10 remaining patients were included in the adverse events analysis. Adverse events were mostly mild to moderate and included fatigue, diarrhea, somnolence, elevated liver enzymes, and dizziness. Three of the 10 patients dropped out of the study due to intolerance. One of the three patients had an allergic reaction and two had abdominal pain. There were no serious adverse events.
Among the seven patients who completed the treatment period and were included in the efficacy analysis, mean total UPDRS score significantly decreased from 45.9 at baseline to 36.4 at the final visit. UPDRS motor score significantly decreased from 27.3 to 20.3. Mean rigidity subscore significantly decreased from 9.14 to 6.29. In addition, data hinted that CBD treatment might have reduced pain and irritability, the researchers said.
These preliminary results indicate that CBD is tolerated, safe, and has beneficial effects in Parkinson’s disease, Dr. Leehey and colleagues said. The investigators next plan to conduct a crossover, double-blind, randomized controlled trial with 50 subjects.
Inhaled Cannabis
Laurie K. Mischley, ND, PhD, MPH, Associate Clinical Investigator at Bastyr University Research Institute in Kenmore, Washington, and colleagues evaluated the effect of inhaled cannabis on Parkinson’s disease tremor using motion sensors and qualitative interviews.
The study included patients with Parkinson’s disease who used cannabis in the state of Washington. Patients wore a movement monitor for two weeks and logged their cannabis use in a journal. Sensors recorded the frequency and amplitude of tremor during waking hours, and participants pressed a button on the motion sensor every time they used cannabis. The researchers compared tremor duration and magnitude in the hour before and after inhaled cannabis use. After two weeks, interviewers asked participants standardized, open-ended, nonleading questions about their perception of the effects of cannabis on their symptoms.
The 10 patients for whom they had data had a mean age of 60 (range, 40 to 74) and a mean time since diagnosis of 6.3 years. Among four participants who had more than 10 cannabis exposures and a measurable tremor more than 2% of the time in the hour before cannabis use during the study, the percent of the time with detected tremor significantly decreased in the hour after use. Sensor data suggested that tremor reduction may have been sustained for three hours after exposure to cannabis, the researchers said. “In those with a persistent tremor, there was a consistent decrease in the tremor persistence and in detected tremor magnitude following cannabis use,” the investigators said.
During the follow-up interview, nine of the 10 participants thought that cannabis helped their symptoms, and one patient thought it worsened symptoms. “The one participant who reported cannabis worsening symptoms specifically described, ‘sometimes it speeds up the tremor at the start’ but ‘then it relaxes it,’” the researchers said.
Side effects reported by patients included sleepiness, sluggishness, concerns about social stigma and driving, short-term memory, and dry throat.
“Improved sleep was an unsolicited theme during the qualitative interviews, with 60% of individuals reporting improvements,” Dr. Mischley and colleagues said. “The qualitative interviews suggest patients perceive cannabis to have therapeutic potential for Parkinson’s disease symptom management. These data suggest further investigation of cannabis for impaired sleep is warranted.”
The researchers noted that most subjects had a mild, intermittent tremor that was not reliably detected by the motion sensors. Future studies should enroll subjects with more pronounced tremor and use consistent cannabis strains, doses, and delivery systems, they said.
—Jake Remaly
Suggested Reading
Chagas MH, Zuardi AW, Tumas V, et al. Effects of cannabidiol in the treatment of patients with Parkinson’s disease: an exploratory double-blind trial. J Psychopharmacol. 2014;28(11):1088-1098.
Finseth TA, Hedeman JL, Brown RP 2nd, et al. Self-reported efficacy of cannabis and other complementary medicine modalities by Parkinson’s disease patients in Colorado. Evid Based Complement Alternat Med. 2015;2015:874849.
Koppel BS, Brust JC, Fife T, et al. Systematic review: efficacy and safety of medical marijuana in selected neurologic disorders: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2014; 82(17):1556-1563.
Lotan I, Treves TA, Roditi Y, Djaldetti R. Cannabis (medical marijuana) treatment for motor and non-motor symptoms of Parkinson disease: an open-label observational study. Clin Neuropharmacol. 2014;37(2):41-44.
Venderová K, Ruzicka E, Vorísek V, Visnovský P. Survey on cannabis use in Parkinson’s disease: subjective improvement of motor symptoms. Mov Disord. 2004;19(9):1102-1106.
Zuardi AW, Crippa JA, Hallak JE, et al. Cannabidiol for the treatment of psychosis in Parkinson’s disease. J Psychopharmacol. 2009;23(8):979-983.
Benign Epilepsy With Centrotemporal Spikes Entails a Risk of SUDEP
Benign epilepsy with centrotemporal spikes (BECTS) is associated with a low risk of sudden unexpected death in epilepsy (SUDEP), according to a study published in the June 1 JAMA Neurology. Clinicians should consider discussing this rare outcome with patients and their families and factoring this risk into treatment decisions, according to the authors.
“Our data suggest that even children with BECTS who have only focal motor or infrequent seizures are at risk for SUDEP,” said Kyra Doumlele, of New York University School of Medicine’s Department of Neurology, and colleagues.
BECTS is the most common focal epilepsy syndrome among children. This form of epilepsy typically has a good prognosis and tends to resolve before age 16. As a result, many neurologists do not prescribe antiseizure medications for patients with BECTS. However, patients with this disease have predominantly nocturnal seizures and some generalized tonic-clonic seizures, which could put them at risk for SUDEP.
SUDEP in well-characterized patients with BECTS has not been documented. Ms. Doumlele and colleagues sought to determine whether cases of BECTS were present in the North American SUDEP Registry (NASR), a clinical and biospecimen repository established to investigate the risk factors and mechanisms for SUDEP.
Researchers searched records of 189 decedents enrolled in the NASR from June 3, 2011, to June 3, 2016. Investigators identified cases based on a diagnosis of BECTS by parental report during the intake interview and confirmation from treating physicians. Diagnostic criteria for BECTS included the onset of epilepsy at age 3 to age 13, normal cognition and development before onset of seizures, no symptomatic cause of epilepsy, and EEG results reporting discharges consistent with BECTS.
Investigators identified three boys who had received a diagnosis of BECTS. The first patient and third patient met all clinical and EEG features for a diagnosis of BECTS. The second patient had limited EEG data, but had classic clinical features of BECTS.
The first patient (age 9) had seizure onset at age 5. He experienced an increase in focal motor and secondary generalized tonic-clonic seizures in the six months before his death.
The second patient (age 12) developed epilepsy at age 11. Four months prior to death, he experienced at least three nocturnal generalized tonic-clonic seizures. The autopsy report listed his cause of death as “cardiac dysrhythmia associated with lymphocytic myocarditis, left anterior descending coronary artery intramuscular tunneling, and possible hypertrophic cardiomyopathy.”
The third patient (age 13) developed epilepsy at age 3. His severe postictal state indicated that he might have had two generalized tonic-clonic seizures in the year before he died. His death was unwitnessed, and no autopsy was performed. None of these patients had received antiseizure medications or counseling with their families about the risk of SUDEP.
“These cases illustrate that SUDEP is a rare complication of BECTS, and this information should be shared with families at or soon after diagnosis,” said Ms. Doumlele and colleagues.
—Erica Tricarico
Suggested Reading
Doumlele K, Friedman D, Buchhalter J, et al. Sudden unexpected death in epilepsy among patients with benign childhood epilepsy with centrotemporal spikes. JAMA Neurol. 2017;74(6):645-649.
Benign epilepsy with centrotemporal spikes (BECTS) is associated with a low risk of sudden unexpected death in epilepsy (SUDEP), according to a study published in the June 1 JAMA Neurology. Clinicians should consider discussing this rare outcome with patients and their families and factoring this risk into treatment decisions, according to the authors.
“Our data suggest that even children with BECTS who have only focal motor or infrequent seizures are at risk for SUDEP,” said Kyra Doumlele, of New York University School of Medicine’s Department of Neurology, and colleagues.
BECTS is the most common focal epilepsy syndrome among children. This form of epilepsy typically has a good prognosis and tends to resolve before age 16. As a result, many neurologists do not prescribe antiseizure medications for patients with BECTS. However, patients with this disease have predominantly nocturnal seizures and some generalized tonic-clonic seizures, which could put them at risk for SUDEP.
SUDEP in well-characterized patients with BECTS has not been documented. Ms. Doumlele and colleagues sought to determine whether cases of BECTS were present in the North American SUDEP Registry (NASR), a clinical and biospecimen repository established to investigate the risk factors and mechanisms for SUDEP.
Researchers searched records of 189 decedents enrolled in the NASR from June 3, 2011, to June 3, 2016. Investigators identified cases based on a diagnosis of BECTS by parental report during the intake interview and confirmation from treating physicians. Diagnostic criteria for BECTS included the onset of epilepsy at age 3 to age 13, normal cognition and development before onset of seizures, no symptomatic cause of epilepsy, and EEG results reporting discharges consistent with BECTS.
Investigators identified three boys who had received a diagnosis of BECTS. The first patient and third patient met all clinical and EEG features for a diagnosis of BECTS. The second patient had limited EEG data, but had classic clinical features of BECTS.
The first patient (age 9) had seizure onset at age 5. He experienced an increase in focal motor and secondary generalized tonic-clonic seizures in the six months before his death.
The second patient (age 12) developed epilepsy at age 11. Four months prior to death, he experienced at least three nocturnal generalized tonic-clonic seizures. The autopsy report listed his cause of death as “cardiac dysrhythmia associated with lymphocytic myocarditis, left anterior descending coronary artery intramuscular tunneling, and possible hypertrophic cardiomyopathy.”
The third patient (age 13) developed epilepsy at age 3. His severe postictal state indicated that he might have had two generalized tonic-clonic seizures in the year before he died. His death was unwitnessed, and no autopsy was performed. None of these patients had received antiseizure medications or counseling with their families about the risk of SUDEP.
“These cases illustrate that SUDEP is a rare complication of BECTS, and this information should be shared with families at or soon after diagnosis,” said Ms. Doumlele and colleagues.
—Erica Tricarico
Suggested Reading
Doumlele K, Friedman D, Buchhalter J, et al. Sudden unexpected death in epilepsy among patients with benign childhood epilepsy with centrotemporal spikes. JAMA Neurol. 2017;74(6):645-649.
Benign epilepsy with centrotemporal spikes (BECTS) is associated with a low risk of sudden unexpected death in epilepsy (SUDEP), according to a study published in the June 1 JAMA Neurology. Clinicians should consider discussing this rare outcome with patients and their families and factoring this risk into treatment decisions, according to the authors.
“Our data suggest that even children with BECTS who have only focal motor or infrequent seizures are at risk for SUDEP,” said Kyra Doumlele, of New York University School of Medicine’s Department of Neurology, and colleagues.
BECTS is the most common focal epilepsy syndrome among children. This form of epilepsy typically has a good prognosis and tends to resolve before age 16. As a result, many neurologists do not prescribe antiseizure medications for patients with BECTS. However, patients with this disease have predominantly nocturnal seizures and some generalized tonic-clonic seizures, which could put them at risk for SUDEP.
SUDEP in well-characterized patients with BECTS has not been documented. Ms. Doumlele and colleagues sought to determine whether cases of BECTS were present in the North American SUDEP Registry (NASR), a clinical and biospecimen repository established to investigate the risk factors and mechanisms for SUDEP.
Researchers searched records of 189 decedents enrolled in the NASR from June 3, 2011, to June 3, 2016. Investigators identified cases based on a diagnosis of BECTS by parental report during the intake interview and confirmation from treating physicians. Diagnostic criteria for BECTS included the onset of epilepsy at age 3 to age 13, normal cognition and development before onset of seizures, no symptomatic cause of epilepsy, and EEG results reporting discharges consistent with BECTS.
Investigators identified three boys who had received a diagnosis of BECTS. The first patient and third patient met all clinical and EEG features for a diagnosis of BECTS. The second patient had limited EEG data, but had classic clinical features of BECTS.
The first patient (age 9) had seizure onset at age 5. He experienced an increase in focal motor and secondary generalized tonic-clonic seizures in the six months before his death.
The second patient (age 12) developed epilepsy at age 11. Four months prior to death, he experienced at least three nocturnal generalized tonic-clonic seizures. The autopsy report listed his cause of death as “cardiac dysrhythmia associated with lymphocytic myocarditis, left anterior descending coronary artery intramuscular tunneling, and possible hypertrophic cardiomyopathy.”
The third patient (age 13) developed epilepsy at age 3. His severe postictal state indicated that he might have had two generalized tonic-clonic seizures in the year before he died. His death was unwitnessed, and no autopsy was performed. None of these patients had received antiseizure medications or counseling with their families about the risk of SUDEP.
“These cases illustrate that SUDEP is a rare complication of BECTS, and this information should be shared with families at or soon after diagnosis,” said Ms. Doumlele and colleagues.
—Erica Tricarico
Suggested Reading
Doumlele K, Friedman D, Buchhalter J, et al. Sudden unexpected death in epilepsy among patients with benign childhood epilepsy with centrotemporal spikes. JAMA Neurol. 2017;74(6):645-649.