User login
Pediatric Dermatology Consult - June 2017
BY CATALINA MATIZ, MD, AND ANDREA WALDMAN, MD
Serum sickness
How does serum sickness–like reaction present?
At the time of initial evaluation, the patient presented with a recent history of fever, edema of the hands and feet, limited gait, and a diffuse, persistent serpiginous and annular dermatitis for 48 hours. Of note, the patient was prescribed a 10-day course of amoxicillin for otitis media 8 days prior to initial presentation.
The distribution and morphology of our patient’s cutaneous eruption, in combination with the systemic symptoms, facial and acral edema, lymphadenopathy, and arthralgia, were highly suggestive of serum sickness–like reaction (SSLR). SSLR is an allergic reaction characterized by a cutaneous eruption, arthralgias, fever, lymphadenopathy, facial edema, and malaise. True serum sickness was originally distinguished in 1905 as a self-limited illness that occurred in several patients after administration of equine diphtheria antitoxin.1 Today this reaction is rarely noted in the pediatric population.
Pathogenically, true serum sickness represents a type III arthus hypersensitivity reaction to proteins in toxins or drugs, mediated by circulating antigen-antibody complexes. In contrast, SSLR is not associated with circulating immune complexes or hypocomplementemia.2 Histopathology frequently resembles the findings of urticaria, including a perivascular and dermal inflammatory infiltrate with associated neutrophils, eosinophils, and lymphocytes.2 Several hypotheses concerning the etiology of SSLR have been suggested in the literature, most commonly including an inflammatory response to defective drug metabolism. However, definitive pathology remains unknown.3
Initially, an urticarial rash and low-grade fever typically develop 7-21 days after exposure to the offending agent or sooner in individuals previously sensitized to the drug. The lesions quickly evolve to the classic purpuric lesions of SSLR over the following 24-48 hours. These dermatologic findings include pink to red oval and/or polycyclic lesions with large central areas of purple discoloration, classically involving the trunk, extremities, and/or face. The lesions may be discrete, scattered, or confluent.2
Several medications are associated with SSLR, but cefaclor is most frequently implicated, occurring in 0.2% of treated children.4,5 Other common culprits include penicillins, tetracycline, sulfonamides, macrolides, ciprofloxacin, rifampin, griseofulvin, bupropion, and fluoxetine.6-10 More recently, biologic agents have been implicated in SSLR, including rituximab, efalizumab, and infliximab.11,12 SSLR also has been described in association with immunizations (hepatitis B, tetanus, and rabies) and active infections with hepatitis B or C.13,14
The diagnosis of SSLR is primarily clinical, formulated based on the constellation of characteristic lesions, fever, adenopathy, facial edema, and/or arthralgia in conjunction with recent history (within 7-21 days) of offending medications or agents. Supporting laboratory findings include normal or mildly low complement C3 and C4 levels and mild proteinuria. Abnormalities in liver and renal function test results are rare, in contrast to true serum sickness. Biopsy and histopathology may be utilized to exclude other diagnoses.2
An extensive variety of cutaneous conditions bearing a resemblance to SSLR were considered in the differential, including urticaria multiforme, Kawasaki disease, erythema multiforme, and urticarial vasculitis. A common challenge for practitioners is distinguishing SSLR from similar dermatoses, particularly urticarial multiforme (UM), which some experts consider clinically related to SSLR. Despite the cutaneous similarities of UM and SSLR, including urticarial plaques with an associated central duskiness, SSLR tends to have a more delayed onset following offending agent exposure and more extracutaneous symptoms, especially arthralgias and/or arthritis, lymphadenopathy, and higher fevers.15 The rash of UM classically presents 1-3 days following agent exposure or illness, whereas SSLR presentation is delayed 1-3 weeks. Further distinguishing UM is the transient nature of the individual lesions, each lasting less than 24 hours.
Urticarial vasculitis (UV), morphologically similar to SSLR and UM, causes persistent urticarial-like plaques that last longer than 24-48 hours and resolve with bruising. Biopsy results revealing leukocytoclastic vasculitis distinguish UV, but case reports exist reporting leukocytoclastic vasculitis in association with SSLR.
Erythema multiforme (EM), a hypersensitivity reaction usually triggered by infections (most commonly herpes simplex virus), also may appear morphologically similar to SSLR. These lesions also persist for longer than 24-48 hours and often have a target appearance with central duskiness that sometimes can blister. Patients may have mucosal involvement with vesicles and erosions, compared with patients with SSLR in whom mucosal lesions are rarely seen. Medications are an uncommon trigger for EM, occurring in less than 10% of cases, and alternative drug eruptions including SSLR should be excluded prior to diagnosis.
Other disorders commonly presenting with similar extracutaneous manifestations to SSLR and concomitant dermatitis were further excluded based on the morphologic appearance of the lesions and other clinical dissimilarities. Henoch-Schönlein purpura, which also may present with arthralgia, fever, GI symptoms, and extremity edema, was unlikely given the urticarial appearance of the lesions, rather than palpable purpura. Furthermore, the arthritis/arthralgia of Henoch-Schönlein purpura is typically oligoarticular, affecting the large joints of the lower extremities most frequently.
If the patient presents with persistent fever for more than 5 days, Kawasaki disease may be considered in the differential and ruled out with clinical and laboratory assessment. The presence of fever, lymphadenopathy, and acute rash similarly should prompt consideration of a clinical and laboratory work-up for drug reaction with eosinophilia and systemic symptoms. Morphologically, this drug reaction is characterized by a maculopapular eruption more than 3 weeks after exposure to an offending agent. Patients with SSLR respond favorably to cessation of the causative drug and supportive care with antipyretics, NSAIDs, and antihistamines. The cutaneous and extracutaneous manifestations of this drug reaction typically disappear within 2-3 weeks after discontinuation of the offending agent. If symptoms are severe, a short systemic corticosteroid course may be warranted. Our patient’s symptoms completely resolved within 2-3 weeks of discontinuing amoxicillin therapy.
Dr. Matiz is assistant professor of dermatology at Rady Children’s Hospital–San Diego, University of California, San Diego. Dr. Waldman is a clinical research fellow at the hospital. Email them at [email protected].
References
1. von Pirquet, C. Frh, and Bela Schick. “Serum Sickness.” Translated by B. Schick. (London: Bailliere, Tindall and Cox, 1951).
2. Cutis. 2002 May;69(5):395-7.
3. J Pediatr. 1994 Nov;125(5 Pt 1):805-11.
4. J Am Acad Dermatol. 1991 Nov;25(5 Pt 1):805-8.
5. J Paediatr Child Health. 2003 Dec;39(9):677-81.
6. Ann Pharmacother. 1996 May;30(5):481-3.
7. J Hosp Med. 2011 Apr;6(4):231-2.
8. Allergy Asthma Immunol Res. 2014 Mar;6(2):183-5.
9. Ann Pharmacother. 2004 Apr;38(4):609-11.
10. Ann Pharmacother. 2000 Apr;34(4):471-3.
11. J Clin Rheumatol. 2013 Sep;19(6):360.
12. Int J Rheum Dis. 2012 Feb;15(1):e6-7.
13. Am J Med Sci. 2013 May;345(5):412-3.
14. Semin Cutan Med Surg. 2007 Sep;26(3):179-87.
15. J Clin Aesthet Dermatol. 2013 Mar;6(3):34-9.
BY CATALINA MATIZ, MD, AND ANDREA WALDMAN, MD
Serum sickness
How does serum sickness–like reaction present?
At the time of initial evaluation, the patient presented with a recent history of fever, edema of the hands and feet, limited gait, and a diffuse, persistent serpiginous and annular dermatitis for 48 hours. Of note, the patient was prescribed a 10-day course of amoxicillin for otitis media 8 days prior to initial presentation.
The distribution and morphology of our patient’s cutaneous eruption, in combination with the systemic symptoms, facial and acral edema, lymphadenopathy, and arthralgia, were highly suggestive of serum sickness–like reaction (SSLR). SSLR is an allergic reaction characterized by a cutaneous eruption, arthralgias, fever, lymphadenopathy, facial edema, and malaise. True serum sickness was originally distinguished in 1905 as a self-limited illness that occurred in several patients after administration of equine diphtheria antitoxin.1 Today this reaction is rarely noted in the pediatric population.
Pathogenically, true serum sickness represents a type III arthus hypersensitivity reaction to proteins in toxins or drugs, mediated by circulating antigen-antibody complexes. In contrast, SSLR is not associated with circulating immune complexes or hypocomplementemia.2 Histopathology frequently resembles the findings of urticaria, including a perivascular and dermal inflammatory infiltrate with associated neutrophils, eosinophils, and lymphocytes.2 Several hypotheses concerning the etiology of SSLR have been suggested in the literature, most commonly including an inflammatory response to defective drug metabolism. However, definitive pathology remains unknown.3
Initially, an urticarial rash and low-grade fever typically develop 7-21 days after exposure to the offending agent or sooner in individuals previously sensitized to the drug. The lesions quickly evolve to the classic purpuric lesions of SSLR over the following 24-48 hours. These dermatologic findings include pink to red oval and/or polycyclic lesions with large central areas of purple discoloration, classically involving the trunk, extremities, and/or face. The lesions may be discrete, scattered, or confluent.2
Several medications are associated with SSLR, but cefaclor is most frequently implicated, occurring in 0.2% of treated children.4,5 Other common culprits include penicillins, tetracycline, sulfonamides, macrolides, ciprofloxacin, rifampin, griseofulvin, bupropion, and fluoxetine.6-10 More recently, biologic agents have been implicated in SSLR, including rituximab, efalizumab, and infliximab.11,12 SSLR also has been described in association with immunizations (hepatitis B, tetanus, and rabies) and active infections with hepatitis B or C.13,14
The diagnosis of SSLR is primarily clinical, formulated based on the constellation of characteristic lesions, fever, adenopathy, facial edema, and/or arthralgia in conjunction with recent history (within 7-21 days) of offending medications or agents. Supporting laboratory findings include normal or mildly low complement C3 and C4 levels and mild proteinuria. Abnormalities in liver and renal function test results are rare, in contrast to true serum sickness. Biopsy and histopathology may be utilized to exclude other diagnoses.2
An extensive variety of cutaneous conditions bearing a resemblance to SSLR were considered in the differential, including urticaria multiforme, Kawasaki disease, erythema multiforme, and urticarial vasculitis. A common challenge for practitioners is distinguishing SSLR from similar dermatoses, particularly urticarial multiforme (UM), which some experts consider clinically related to SSLR. Despite the cutaneous similarities of UM and SSLR, including urticarial plaques with an associated central duskiness, SSLR tends to have a more delayed onset following offending agent exposure and more extracutaneous symptoms, especially arthralgias and/or arthritis, lymphadenopathy, and higher fevers.15 The rash of UM classically presents 1-3 days following agent exposure or illness, whereas SSLR presentation is delayed 1-3 weeks. Further distinguishing UM is the transient nature of the individual lesions, each lasting less than 24 hours.
Urticarial vasculitis (UV), morphologically similar to SSLR and UM, causes persistent urticarial-like plaques that last longer than 24-48 hours and resolve with bruising. Biopsy results revealing leukocytoclastic vasculitis distinguish UV, but case reports exist reporting leukocytoclastic vasculitis in association with SSLR.
Erythema multiforme (EM), a hypersensitivity reaction usually triggered by infections (most commonly herpes simplex virus), also may appear morphologically similar to SSLR. These lesions also persist for longer than 24-48 hours and often have a target appearance with central duskiness that sometimes can blister. Patients may have mucosal involvement with vesicles and erosions, compared with patients with SSLR in whom mucosal lesions are rarely seen. Medications are an uncommon trigger for EM, occurring in less than 10% of cases, and alternative drug eruptions including SSLR should be excluded prior to diagnosis.
Other disorders commonly presenting with similar extracutaneous manifestations to SSLR and concomitant dermatitis were further excluded based on the morphologic appearance of the lesions and other clinical dissimilarities. Henoch-Schönlein purpura, which also may present with arthralgia, fever, GI symptoms, and extremity edema, was unlikely given the urticarial appearance of the lesions, rather than palpable purpura. Furthermore, the arthritis/arthralgia of Henoch-Schönlein purpura is typically oligoarticular, affecting the large joints of the lower extremities most frequently.
If the patient presents with persistent fever for more than 5 days, Kawasaki disease may be considered in the differential and ruled out with clinical and laboratory assessment. The presence of fever, lymphadenopathy, and acute rash similarly should prompt consideration of a clinical and laboratory work-up for drug reaction with eosinophilia and systemic symptoms. Morphologically, this drug reaction is characterized by a maculopapular eruption more than 3 weeks after exposure to an offending agent. Patients with SSLR respond favorably to cessation of the causative drug and supportive care with antipyretics, NSAIDs, and antihistamines. The cutaneous and extracutaneous manifestations of this drug reaction typically disappear within 2-3 weeks after discontinuation of the offending agent. If symptoms are severe, a short systemic corticosteroid course may be warranted. Our patient’s symptoms completely resolved within 2-3 weeks of discontinuing amoxicillin therapy.
Dr. Matiz is assistant professor of dermatology at Rady Children’s Hospital–San Diego, University of California, San Diego. Dr. Waldman is a clinical research fellow at the hospital. Email them at [email protected].
References
1. von Pirquet, C. Frh, and Bela Schick. “Serum Sickness.” Translated by B. Schick. (London: Bailliere, Tindall and Cox, 1951).
2. Cutis. 2002 May;69(5):395-7.
3. J Pediatr. 1994 Nov;125(5 Pt 1):805-11.
4. J Am Acad Dermatol. 1991 Nov;25(5 Pt 1):805-8.
5. J Paediatr Child Health. 2003 Dec;39(9):677-81.
6. Ann Pharmacother. 1996 May;30(5):481-3.
7. J Hosp Med. 2011 Apr;6(4):231-2.
8. Allergy Asthma Immunol Res. 2014 Mar;6(2):183-5.
9. Ann Pharmacother. 2004 Apr;38(4):609-11.
10. Ann Pharmacother. 2000 Apr;34(4):471-3.
11. J Clin Rheumatol. 2013 Sep;19(6):360.
12. Int J Rheum Dis. 2012 Feb;15(1):e6-7.
13. Am J Med Sci. 2013 May;345(5):412-3.
14. Semin Cutan Med Surg. 2007 Sep;26(3):179-87.
15. J Clin Aesthet Dermatol. 2013 Mar;6(3):34-9.
BY CATALINA MATIZ, MD, AND ANDREA WALDMAN, MD
Serum sickness
How does serum sickness–like reaction present?
At the time of initial evaluation, the patient presented with a recent history of fever, edema of the hands and feet, limited gait, and a diffuse, persistent serpiginous and annular dermatitis for 48 hours. Of note, the patient was prescribed a 10-day course of amoxicillin for otitis media 8 days prior to initial presentation.
The distribution and morphology of our patient’s cutaneous eruption, in combination with the systemic symptoms, facial and acral edema, lymphadenopathy, and arthralgia, were highly suggestive of serum sickness–like reaction (SSLR). SSLR is an allergic reaction characterized by a cutaneous eruption, arthralgias, fever, lymphadenopathy, facial edema, and malaise. True serum sickness was originally distinguished in 1905 as a self-limited illness that occurred in several patients after administration of equine diphtheria antitoxin.1 Today this reaction is rarely noted in the pediatric population.
Pathogenically, true serum sickness represents a type III arthus hypersensitivity reaction to proteins in toxins or drugs, mediated by circulating antigen-antibody complexes. In contrast, SSLR is not associated with circulating immune complexes or hypocomplementemia.2 Histopathology frequently resembles the findings of urticaria, including a perivascular and dermal inflammatory infiltrate with associated neutrophils, eosinophils, and lymphocytes.2 Several hypotheses concerning the etiology of SSLR have been suggested in the literature, most commonly including an inflammatory response to defective drug metabolism. However, definitive pathology remains unknown.3
Initially, an urticarial rash and low-grade fever typically develop 7-21 days after exposure to the offending agent or sooner in individuals previously sensitized to the drug. The lesions quickly evolve to the classic purpuric lesions of SSLR over the following 24-48 hours. These dermatologic findings include pink to red oval and/or polycyclic lesions with large central areas of purple discoloration, classically involving the trunk, extremities, and/or face. The lesions may be discrete, scattered, or confluent.2
Several medications are associated with SSLR, but cefaclor is most frequently implicated, occurring in 0.2% of treated children.4,5 Other common culprits include penicillins, tetracycline, sulfonamides, macrolides, ciprofloxacin, rifampin, griseofulvin, bupropion, and fluoxetine.6-10 More recently, biologic agents have been implicated in SSLR, including rituximab, efalizumab, and infliximab.11,12 SSLR also has been described in association with immunizations (hepatitis B, tetanus, and rabies) and active infections with hepatitis B or C.13,14
The diagnosis of SSLR is primarily clinical, formulated based on the constellation of characteristic lesions, fever, adenopathy, facial edema, and/or arthralgia in conjunction with recent history (within 7-21 days) of offending medications or agents. Supporting laboratory findings include normal or mildly low complement C3 and C4 levels and mild proteinuria. Abnormalities in liver and renal function test results are rare, in contrast to true serum sickness. Biopsy and histopathology may be utilized to exclude other diagnoses.2
An extensive variety of cutaneous conditions bearing a resemblance to SSLR were considered in the differential, including urticaria multiforme, Kawasaki disease, erythema multiforme, and urticarial vasculitis. A common challenge for practitioners is distinguishing SSLR from similar dermatoses, particularly urticarial multiforme (UM), which some experts consider clinically related to SSLR. Despite the cutaneous similarities of UM and SSLR, including urticarial plaques with an associated central duskiness, SSLR tends to have a more delayed onset following offending agent exposure and more extracutaneous symptoms, especially arthralgias and/or arthritis, lymphadenopathy, and higher fevers.15 The rash of UM classically presents 1-3 days following agent exposure or illness, whereas SSLR presentation is delayed 1-3 weeks. Further distinguishing UM is the transient nature of the individual lesions, each lasting less than 24 hours.
Urticarial vasculitis (UV), morphologically similar to SSLR and UM, causes persistent urticarial-like plaques that last longer than 24-48 hours and resolve with bruising. Biopsy results revealing leukocytoclastic vasculitis distinguish UV, but case reports exist reporting leukocytoclastic vasculitis in association with SSLR.
Erythema multiforme (EM), a hypersensitivity reaction usually triggered by infections (most commonly herpes simplex virus), also may appear morphologically similar to SSLR. These lesions also persist for longer than 24-48 hours and often have a target appearance with central duskiness that sometimes can blister. Patients may have mucosal involvement with vesicles and erosions, compared with patients with SSLR in whom mucosal lesions are rarely seen. Medications are an uncommon trigger for EM, occurring in less than 10% of cases, and alternative drug eruptions including SSLR should be excluded prior to diagnosis.
Other disorders commonly presenting with similar extracutaneous manifestations to SSLR and concomitant dermatitis were further excluded based on the morphologic appearance of the lesions and other clinical dissimilarities. Henoch-Schönlein purpura, which also may present with arthralgia, fever, GI symptoms, and extremity edema, was unlikely given the urticarial appearance of the lesions, rather than palpable purpura. Furthermore, the arthritis/arthralgia of Henoch-Schönlein purpura is typically oligoarticular, affecting the large joints of the lower extremities most frequently.
If the patient presents with persistent fever for more than 5 days, Kawasaki disease may be considered in the differential and ruled out with clinical and laboratory assessment. The presence of fever, lymphadenopathy, and acute rash similarly should prompt consideration of a clinical and laboratory work-up for drug reaction with eosinophilia and systemic symptoms. Morphologically, this drug reaction is characterized by a maculopapular eruption more than 3 weeks after exposure to an offending agent. Patients with SSLR respond favorably to cessation of the causative drug and supportive care with antipyretics, NSAIDs, and antihistamines. The cutaneous and extracutaneous manifestations of this drug reaction typically disappear within 2-3 weeks after discontinuation of the offending agent. If symptoms are severe, a short systemic corticosteroid course may be warranted. Our patient’s symptoms completely resolved within 2-3 weeks of discontinuing amoxicillin therapy.
Dr. Matiz is assistant professor of dermatology at Rady Children’s Hospital–San Diego, University of California, San Diego. Dr. Waldman is a clinical research fellow at the hospital. Email them at [email protected].
References
1. von Pirquet, C. Frh, and Bela Schick. “Serum Sickness.” Translated by B. Schick. (London: Bailliere, Tindall and Cox, 1951).
2. Cutis. 2002 May;69(5):395-7.
3. J Pediatr. 1994 Nov;125(5 Pt 1):805-11.
4. J Am Acad Dermatol. 1991 Nov;25(5 Pt 1):805-8.
5. J Paediatr Child Health. 2003 Dec;39(9):677-81.
6. Ann Pharmacother. 1996 May;30(5):481-3.
7. J Hosp Med. 2011 Apr;6(4):231-2.
8. Allergy Asthma Immunol Res. 2014 Mar;6(2):183-5.
9. Ann Pharmacother. 2004 Apr;38(4):609-11.
10. Ann Pharmacother. 2000 Apr;34(4):471-3.
11. J Clin Rheumatol. 2013 Sep;19(6):360.
12. Int J Rheum Dis. 2012 Feb;15(1):e6-7.
13. Am J Med Sci. 2013 May;345(5):412-3.
14. Semin Cutan Med Surg. 2007 Sep;26(3):179-87.
15. J Clin Aesthet Dermatol. 2013 Mar;6(3):34-9.
Make the diagnosis

The day prior to presentation, the family took the patient to the ED for evaluation of the lesions and concomitant swelling of the face, eyelids, hands, and feet, as well as fever and irritability. The ED discharged the patient after comprehensive examination and arranged follow-up in the dermatology clinic the following day. Review of systems further revealed limited gait. Parents denied any recent travel or pets residing in the home. Family history is noncontributory.
Physical exam
The patient is a well-appearing toddler, who is in no acute distress but is irritable. Patient is afebrile, with a temperature of 99.5°F, and vital signs are within normal limits. On skin examination, there are serpiginous and annular confluent erythematous urticarial plaques with a central ecchymotic discoloration over the eyes, peripheral malar distribution, neck, chest, abdomen, back, buttock, extremities, hands, and feet. There is notable eyelid, hand, and feet edema. There was no mucosal involvement. The patient has posterior cervical lymphadenopathy but no hepatomegaly or splenomegaly. The patient refused to walk.
Effect of Non–Insulin-Based Glucose-Lowering Therapies on Cardiovascular Outcomes in Patients With Type 2 Diabetes
While type 2 diabetes (T2D) is commonly seen in primary care, it is difficult to control successfully over time. This series offers brief eNewsletters written by clinical experts that are designed to assist in the clinical management of patients with T2D.
This fourth eNewsletter in the series, entitled Effect of Non–Insulin-Based Glucose-Lowering Therapies on Cardiovascular Outcomes in Patients With Type 2 Diabetes, was written by Szymon L. Wiernek, MD, PhD, and Matthew A. Cavender, MD, MPH. It presents an overview of commonly used non–insulin-based glucose-lowering drugs in the context of cardiovascular disease risk. The basic mechanisms of action for each pharmacotherapeutic class and the effects of these medications on cardiovascular events are discussed so that physicians can make informed treatment decisions
Click here to read the supplement

Department of Medicine University of North Carolina-Chapel Hill
Chapel Hill, NC

Department of Medicine University of North Carolina-Chapel Hill
Chapel Hill, NC
While type 2 diabetes (T2D) is commonly seen in primary care, it is difficult to control successfully over time. This series offers brief eNewsletters written by clinical experts that are designed to assist in the clinical management of patients with T2D.
This fourth eNewsletter in the series, entitled Effect of Non–Insulin-Based Glucose-Lowering Therapies on Cardiovascular Outcomes in Patients With Type 2 Diabetes, was written by Szymon L. Wiernek, MD, PhD, and Matthew A. Cavender, MD, MPH. It presents an overview of commonly used non–insulin-based glucose-lowering drugs in the context of cardiovascular disease risk. The basic mechanisms of action for each pharmacotherapeutic class and the effects of these medications on cardiovascular events are discussed so that physicians can make informed treatment decisions
Click here to read the supplement
Department of Medicine University of North Carolina-Chapel Hill
Chapel Hill, NC
Department of Medicine University of North Carolina-Chapel Hill
Chapel Hill, NC
While type 2 diabetes (T2D) is commonly seen in primary care, it is difficult to control successfully over time. This series offers brief eNewsletters written by clinical experts that are designed to assist in the clinical management of patients with T2D.
This fourth eNewsletter in the series, entitled Effect of Non–Insulin-Based Glucose-Lowering Therapies on Cardiovascular Outcomes in Patients With Type 2 Diabetes, was written by Szymon L. Wiernek, MD, PhD, and Matthew A. Cavender, MD, MPH. It presents an overview of commonly used non–insulin-based glucose-lowering drugs in the context of cardiovascular disease risk. The basic mechanisms of action for each pharmacotherapeutic class and the effects of these medications on cardiovascular events are discussed so that physicians can make informed treatment decisions
Click here to read the supplement
Department of Medicine University of North Carolina-Chapel Hill
Chapel Hill, NC
Department of Medicine University of North Carolina-Chapel Hill
Chapel Hill, NC

When Should Neurologists Discontinue Disease-Modifying Treatments in Patients With MS?
NEW ORLEANS—Discontinuation of disease-modifying treatments (DMTs) may be considered for patients with secondary progressive multiple sclerosis (SPMS) age 55 or older with ongoing progression and no clinical relapses or new MRI lesions consistent with MS in the previous five years, according to research presented at the 31st Annual Meeting of the Consortium of MS Centers. Data from the study also suggest that it is reasonable to consider discontinuing DMTs for patients in the same age range with stable relapsing remitting (RR) MS who have had no clinical relapses or new MRI lesions consistent with MS in the previous five years.
Although DMTs can reduce relapse rates and progression of disability early in the course of RRMS, it remains unknown whether these treatments maintain efficacy late in the course of RRMS, in SPMS, or in older patients. Considerations for discontinuing treatment include potential inefficacy of DMTs and adverse effects in this cohort, said the authors.
Devyn Parsons, a medical student at the University of British Columbia in Vancouver, Canada, working with Anthony Traboulsee, MD, and colleagues, conducted a systematic search to examine literature relevant to the discontinuation of DMTs and to provide guidance about when DMTs may be discontinued. The investigators used the keywords “multiple sclerosis,” “disease modifying treatments,” “treatment withdrawal,” “stopping medication,” and “medication withdrawal” to search PubMed, Embase, and the Cochrane Database of Systematic Reviews. The search included articles up to June 2016 and was limited to English-language publications.
The review yielded what Ms. Parsons described as a “paucity of information.” The investigators found evidence that disease activity in RRMS declined with increasing age and longer disease duration. Some observational studies suggested that older patients who continuously receive DMT and are free of disease activity for several years might be good candidates for discontinuation of DMTs. Since DMTs are associated with adverse events that may affect quality of life or pose serious safety risks, it is important to consider patient preference, said the authors.
Safety monitoring following discontinuation of DMTs should include annual clinical assessment and annual brain MRIs for two to five years, with consideration of reinitiation of DMTs if evidence of new clinical relapse emerges or more than two new MRI lesions consistent with MS appear, said the researchers.
This study was supported by Sanofi Genzyme.
NEW ORLEANS—Discontinuation of disease-modifying treatments (DMTs) may be considered for patients with secondary progressive multiple sclerosis (SPMS) age 55 or older with ongoing progression and no clinical relapses or new MRI lesions consistent with MS in the previous five years, according to research presented at the 31st Annual Meeting of the Consortium of MS Centers. Data from the study also suggest that it is reasonable to consider discontinuing DMTs for patients in the same age range with stable relapsing remitting (RR) MS who have had no clinical relapses or new MRI lesions consistent with MS in the previous five years.
Although DMTs can reduce relapse rates and progression of disability early in the course of RRMS, it remains unknown whether these treatments maintain efficacy late in the course of RRMS, in SPMS, or in older patients. Considerations for discontinuing treatment include potential inefficacy of DMTs and adverse effects in this cohort, said the authors.
Devyn Parsons, a medical student at the University of British Columbia in Vancouver, Canada, working with Anthony Traboulsee, MD, and colleagues, conducted a systematic search to examine literature relevant to the discontinuation of DMTs and to provide guidance about when DMTs may be discontinued. The investigators used the keywords “multiple sclerosis,” “disease modifying treatments,” “treatment withdrawal,” “stopping medication,” and “medication withdrawal” to search PubMed, Embase, and the Cochrane Database of Systematic Reviews. The search included articles up to June 2016 and was limited to English-language publications.
The review yielded what Ms. Parsons described as a “paucity of information.” The investigators found evidence that disease activity in RRMS declined with increasing age and longer disease duration. Some observational studies suggested that older patients who continuously receive DMT and are free of disease activity for several years might be good candidates for discontinuation of DMTs. Since DMTs are associated with adverse events that may affect quality of life or pose serious safety risks, it is important to consider patient preference, said the authors.
Safety monitoring following discontinuation of DMTs should include annual clinical assessment and annual brain MRIs for two to five years, with consideration of reinitiation of DMTs if evidence of new clinical relapse emerges or more than two new MRI lesions consistent with MS appear, said the researchers.
This study was supported by Sanofi Genzyme.
NEW ORLEANS—Discontinuation of disease-modifying treatments (DMTs) may be considered for patients with secondary progressive multiple sclerosis (SPMS) age 55 or older with ongoing progression and no clinical relapses or new MRI lesions consistent with MS in the previous five years, according to research presented at the 31st Annual Meeting of the Consortium of MS Centers. Data from the study also suggest that it is reasonable to consider discontinuing DMTs for patients in the same age range with stable relapsing remitting (RR) MS who have had no clinical relapses or new MRI lesions consistent with MS in the previous five years.
Although DMTs can reduce relapse rates and progression of disability early in the course of RRMS, it remains unknown whether these treatments maintain efficacy late in the course of RRMS, in SPMS, or in older patients. Considerations for discontinuing treatment include potential inefficacy of DMTs and adverse effects in this cohort, said the authors.
Devyn Parsons, a medical student at the University of British Columbia in Vancouver, Canada, working with Anthony Traboulsee, MD, and colleagues, conducted a systematic search to examine literature relevant to the discontinuation of DMTs and to provide guidance about when DMTs may be discontinued. The investigators used the keywords “multiple sclerosis,” “disease modifying treatments,” “treatment withdrawal,” “stopping medication,” and “medication withdrawal” to search PubMed, Embase, and the Cochrane Database of Systematic Reviews. The search included articles up to June 2016 and was limited to English-language publications.
The review yielded what Ms. Parsons described as a “paucity of information.” The investigators found evidence that disease activity in RRMS declined with increasing age and longer disease duration. Some observational studies suggested that older patients who continuously receive DMT and are free of disease activity for several years might be good candidates for discontinuation of DMTs. Since DMTs are associated with adverse events that may affect quality of life or pose serious safety risks, it is important to consider patient preference, said the authors.
Safety monitoring following discontinuation of DMTs should include annual clinical assessment and annual brain MRIs for two to five years, with consideration of reinitiation of DMTs if evidence of new clinical relapse emerges or more than two new MRI lesions consistent with MS appear, said the researchers.
This study was supported by Sanofi Genzyme.
Arab Americans reluctant to seek depression care from psychiatrists
SAN DIEGO – A new study, the first of its kind, finds that Arab Americans in a Michigan community are among least likely ethnic groups to seek help for depression from a mental health specialist. But they’re especially likely to look for assistance from a primary care physician.
Researchers aren’t sure why the discrepancy exists. “This may be because of the stigma associated with mental health in the community,” study lead author Florence J. Dallo, PhD, said in an interview. Whatever the case, she said, the finding points to the importance of paying close attention to the diagnosis and treatment of depression in Arab Americans.
Dr. Dallo presented her findings in an oral presentation at the annual meeting of the American Psychiatric Association. She told colleagues that Arab Americans are “largely invisible in health research.”
According to her, the sparse studies that do exist look at depression and posttraumatic stress disorder among Arab American refugees. But simply being Arab in the United States has its own challenges. “Let’s not forget the political climate in which we live, with a lot of discrimination, stress, and marginalization for this group,” Dr. Dallo said.
For the new study, she and her colleagues tracked a sample of patients who sought care at a large metropolitan hospital in southeast Michigan. This region of the country has a high Arab American population.
The researchers found that Arab Americans were less likely to complete a depression screening questionnaire than were whites, Asian Americans, African Americans, and Latinos.
Of those who did complete the questionnaire, 6.3% of Arab Americans screened positive for depression, compared with 5.6% of whites, 6.3% of African Americans, 7.7% of Latinos and 2.1% of Asian Americans.
Compared with the other ethnic groups, Arab Americans were especially likely to seek help from primary care physicians but especially unlikely to look to mental health specialists.
Why does this gap exist? In addition to the stigma surrounding mental illness in the community, Dr. Dallo said, religion might play a factor. “Arab Americans may feel their mental health condition is the will of God and that God will take care of them,” she said. “They may feel they do not need a psychiatrist or medication to help them manage their mental health condition.”
In an interview, Hikmet Jamil, MD, PhD, professor in the department of family medicine at Michigan State University, East Lansing, said there is a stigma surrounding mental health among Arab immigrants. “They don’t want to hear about psychiatry or psychology, because back home, if a person goes to a psychologist, he is a mad man,” he said. “They find it very hard to take advice from psychiatrists.”
But they still have a need for care, he said, because many suffer from PTSD and anxiety.
In some cases, this is tied to trauma suffered before they came to the United States, he said. However, “when they come here, they face another kind of trauma. They feel that there is discrimination against them, especially in terms of finding a job.”
According to Dr. Jamil, highly educated Arabs often face special challenges in finding jobs because their educational background does not always open doors in the United States – where they must take exams to get licenses. If they can’t get jobs in their chosen fields, he said, “they’ll take any kind of work to get money.”
How can clinicians serve this population? One approach is to cloak the fact that a patient is getting care for a mental issue. “They may go for primary health care but not mention depression or psychiatry,” Dr. Jamil said. “The physician can pick up on that and sometimes give them psychiatric advice without making it clear that they have some depression or psychiatric disorder.”
Dr. Dallo suggests a focus on primary care. “Given that Arab Americans are more likely to follow up with a primary care doctor rather than a behavioral specialist, perhaps the relationship with the primary care doctor can be encouraged and become regular,” she said. “The more comfortable the patient becomes with his or her primary care doctor, the more they may be more likely to see a behavioral specialist in the future.”
The study was funded by a grant from the Blue Cross Blue Shield of Michigan Foundation. Dr. Dallo and Dr. Jamil report no relevant disclosures.
SAN DIEGO – A new study, the first of its kind, finds that Arab Americans in a Michigan community are among least likely ethnic groups to seek help for depression from a mental health specialist. But they’re especially likely to look for assistance from a primary care physician.
Researchers aren’t sure why the discrepancy exists. “This may be because of the stigma associated with mental health in the community,” study lead author Florence J. Dallo, PhD, said in an interview. Whatever the case, she said, the finding points to the importance of paying close attention to the diagnosis and treatment of depression in Arab Americans.
Dr. Dallo presented her findings in an oral presentation at the annual meeting of the American Psychiatric Association. She told colleagues that Arab Americans are “largely invisible in health research.”
According to her, the sparse studies that do exist look at depression and posttraumatic stress disorder among Arab American refugees. But simply being Arab in the United States has its own challenges. “Let’s not forget the political climate in which we live, with a lot of discrimination, stress, and marginalization for this group,” Dr. Dallo said.
For the new study, she and her colleagues tracked a sample of patients who sought care at a large metropolitan hospital in southeast Michigan. This region of the country has a high Arab American population.
The researchers found that Arab Americans were less likely to complete a depression screening questionnaire than were whites, Asian Americans, African Americans, and Latinos.
Of those who did complete the questionnaire, 6.3% of Arab Americans screened positive for depression, compared with 5.6% of whites, 6.3% of African Americans, 7.7% of Latinos and 2.1% of Asian Americans.
Compared with the other ethnic groups, Arab Americans were especially likely to seek help from primary care physicians but especially unlikely to look to mental health specialists.
Why does this gap exist? In addition to the stigma surrounding mental illness in the community, Dr. Dallo said, religion might play a factor. “Arab Americans may feel their mental health condition is the will of God and that God will take care of them,” she said. “They may feel they do not need a psychiatrist or medication to help them manage their mental health condition.”
In an interview, Hikmet Jamil, MD, PhD, professor in the department of family medicine at Michigan State University, East Lansing, said there is a stigma surrounding mental health among Arab immigrants. “They don’t want to hear about psychiatry or psychology, because back home, if a person goes to a psychologist, he is a mad man,” he said. “They find it very hard to take advice from psychiatrists.”
But they still have a need for care, he said, because many suffer from PTSD and anxiety.
In some cases, this is tied to trauma suffered before they came to the United States, he said. However, “when they come here, they face another kind of trauma. They feel that there is discrimination against them, especially in terms of finding a job.”
According to Dr. Jamil, highly educated Arabs often face special challenges in finding jobs because their educational background does not always open doors in the United States – where they must take exams to get licenses. If they can’t get jobs in their chosen fields, he said, “they’ll take any kind of work to get money.”
How can clinicians serve this population? One approach is to cloak the fact that a patient is getting care for a mental issue. “They may go for primary health care but not mention depression or psychiatry,” Dr. Jamil said. “The physician can pick up on that and sometimes give them psychiatric advice without making it clear that they have some depression or psychiatric disorder.”
Dr. Dallo suggests a focus on primary care. “Given that Arab Americans are more likely to follow up with a primary care doctor rather than a behavioral specialist, perhaps the relationship with the primary care doctor can be encouraged and become regular,” she said. “The more comfortable the patient becomes with his or her primary care doctor, the more they may be more likely to see a behavioral specialist in the future.”
The study was funded by a grant from the Blue Cross Blue Shield of Michigan Foundation. Dr. Dallo and Dr. Jamil report no relevant disclosures.
SAN DIEGO – A new study, the first of its kind, finds that Arab Americans in a Michigan community are among least likely ethnic groups to seek help for depression from a mental health specialist. But they’re especially likely to look for assistance from a primary care physician.
Researchers aren’t sure why the discrepancy exists. “This may be because of the stigma associated with mental health in the community,” study lead author Florence J. Dallo, PhD, said in an interview. Whatever the case, she said, the finding points to the importance of paying close attention to the diagnosis and treatment of depression in Arab Americans.
Dr. Dallo presented her findings in an oral presentation at the annual meeting of the American Psychiatric Association. She told colleagues that Arab Americans are “largely invisible in health research.”
According to her, the sparse studies that do exist look at depression and posttraumatic stress disorder among Arab American refugees. But simply being Arab in the United States has its own challenges. “Let’s not forget the political climate in which we live, with a lot of discrimination, stress, and marginalization for this group,” Dr. Dallo said.
For the new study, she and her colleagues tracked a sample of patients who sought care at a large metropolitan hospital in southeast Michigan. This region of the country has a high Arab American population.
The researchers found that Arab Americans were less likely to complete a depression screening questionnaire than were whites, Asian Americans, African Americans, and Latinos.
Of those who did complete the questionnaire, 6.3% of Arab Americans screened positive for depression, compared with 5.6% of whites, 6.3% of African Americans, 7.7% of Latinos and 2.1% of Asian Americans.
Compared with the other ethnic groups, Arab Americans were especially likely to seek help from primary care physicians but especially unlikely to look to mental health specialists.
Why does this gap exist? In addition to the stigma surrounding mental illness in the community, Dr. Dallo said, religion might play a factor. “Arab Americans may feel their mental health condition is the will of God and that God will take care of them,” she said. “They may feel they do not need a psychiatrist or medication to help them manage their mental health condition.”
In an interview, Hikmet Jamil, MD, PhD, professor in the department of family medicine at Michigan State University, East Lansing, said there is a stigma surrounding mental health among Arab immigrants. “They don’t want to hear about psychiatry or psychology, because back home, if a person goes to a psychologist, he is a mad man,” he said. “They find it very hard to take advice from psychiatrists.”
But they still have a need for care, he said, because many suffer from PTSD and anxiety.
In some cases, this is tied to trauma suffered before they came to the United States, he said. However, “when they come here, they face another kind of trauma. They feel that there is discrimination against them, especially in terms of finding a job.”
According to Dr. Jamil, highly educated Arabs often face special challenges in finding jobs because their educational background does not always open doors in the United States – where they must take exams to get licenses. If they can’t get jobs in their chosen fields, he said, “they’ll take any kind of work to get money.”
How can clinicians serve this population? One approach is to cloak the fact that a patient is getting care for a mental issue. “They may go for primary health care but not mention depression or psychiatry,” Dr. Jamil said. “The physician can pick up on that and sometimes give them psychiatric advice without making it clear that they have some depression or psychiatric disorder.”
Dr. Dallo suggests a focus on primary care. “Given that Arab Americans are more likely to follow up with a primary care doctor rather than a behavioral specialist, perhaps the relationship with the primary care doctor can be encouraged and become regular,” she said. “The more comfortable the patient becomes with his or her primary care doctor, the more they may be more likely to see a behavioral specialist in the future.”
The study was funded by a grant from the Blue Cross Blue Shield of Michigan Foundation. Dr. Dallo and Dr. Jamil report no relevant disclosures.
EXPERT ANALYSIS FROM APA
Dietary carbohydrate and glycemic load linked to acne
A cross-sectional study of 64 adults in New York City with and without moderate/severe acne found a significant association between dietary carbohydrate consumption and acne, which the authors said merited further study.
“Epidemiologic studies typically report a low incidence of acne in non-developed nations, suggesting that environmental factors, such as diet, can play a role in acne pathogenesis,” wrote Jennifer Burris, PhD, of the department of nutrition and food studies, at Steinhardt School of Culture, Education, and Human Development, New York University, and her coauthors.
The study participants either had no acne (32) or had moderate or severe acne (32); those with mild or shorter-term acne (less than 6 months) were excluded. They made a 5-day food record and took a questionnaire, and had blood drawn and anthropometric measurements taken during two visits.
Moderate and severe acne was associated with significantly greater total carbohydrate consumption (P = .003), available carbohydrate (total carbohydrate minus dietary fiber), percent energy from carbohydrate, and glycemic load (all P less than .001), compared with those who did not have acne.
The patients with moderate or severe acne also had greater insulin and insulin growth factor–1 concentrations, and lower sex hormone–binding globulin concentrations, (P = .002, .009, and .015, respectively); and greater insulin resistance (P = .001), compared with those who did not have acne.
“Although the results from our study cannot determine causation, these preliminary results suggest a relationship between dietary [glycemic load] and acne,” Dr. Burris and her coauthors wrote. “In addition to replicating our findings, future research is necessary to elucidate the mechanisms linking diet and acne and to evaluate the effectiveness of [medical nutrition therapy] on biological factors associated with acne and conceivably acne-specific quality of life,” they added (J Acad Nutr Diet. 2017 Jun 9. doi: 10.1016/j.jand.2017.03.024).
[email protected]
A cross-sectional study of 64 adults in New York City with and without moderate/severe acne found a significant association between dietary carbohydrate consumption and acne, which the authors said merited further study.
“Epidemiologic studies typically report a low incidence of acne in non-developed nations, suggesting that environmental factors, such as diet, can play a role in acne pathogenesis,” wrote Jennifer Burris, PhD, of the department of nutrition and food studies, at Steinhardt School of Culture, Education, and Human Development, New York University, and her coauthors.
The study participants either had no acne (32) or had moderate or severe acne (32); those with mild or shorter-term acne (less than 6 months) were excluded. They made a 5-day food record and took a questionnaire, and had blood drawn and anthropometric measurements taken during two visits.
Moderate and severe acne was associated with significantly greater total carbohydrate consumption (P = .003), available carbohydrate (total carbohydrate minus dietary fiber), percent energy from carbohydrate, and glycemic load (all P less than .001), compared with those who did not have acne.
The patients with moderate or severe acne also had greater insulin and insulin growth factor–1 concentrations, and lower sex hormone–binding globulin concentrations, (P = .002, .009, and .015, respectively); and greater insulin resistance (P = .001), compared with those who did not have acne.
“Although the results from our study cannot determine causation, these preliminary results suggest a relationship between dietary [glycemic load] and acne,” Dr. Burris and her coauthors wrote. “In addition to replicating our findings, future research is necessary to elucidate the mechanisms linking diet and acne and to evaluate the effectiveness of [medical nutrition therapy] on biological factors associated with acne and conceivably acne-specific quality of life,” they added (J Acad Nutr Diet. 2017 Jun 9. doi: 10.1016/j.jand.2017.03.024).
[email protected]
A cross-sectional study of 64 adults in New York City with and without moderate/severe acne found a significant association between dietary carbohydrate consumption and acne, which the authors said merited further study.
“Epidemiologic studies typically report a low incidence of acne in non-developed nations, suggesting that environmental factors, such as diet, can play a role in acne pathogenesis,” wrote Jennifer Burris, PhD, of the department of nutrition and food studies, at Steinhardt School of Culture, Education, and Human Development, New York University, and her coauthors.
The study participants either had no acne (32) or had moderate or severe acne (32); those with mild or shorter-term acne (less than 6 months) were excluded. They made a 5-day food record and took a questionnaire, and had blood drawn and anthropometric measurements taken during two visits.
Moderate and severe acne was associated with significantly greater total carbohydrate consumption (P = .003), available carbohydrate (total carbohydrate minus dietary fiber), percent energy from carbohydrate, and glycemic load (all P less than .001), compared with those who did not have acne.
The patients with moderate or severe acne also had greater insulin and insulin growth factor–1 concentrations, and lower sex hormone–binding globulin concentrations, (P = .002, .009, and .015, respectively); and greater insulin resistance (P = .001), compared with those who did not have acne.
“Although the results from our study cannot determine causation, these preliminary results suggest a relationship between dietary [glycemic load] and acne,” Dr. Burris and her coauthors wrote. “In addition to replicating our findings, future research is necessary to elucidate the mechanisms linking diet and acne and to evaluate the effectiveness of [medical nutrition therapy] on biological factors associated with acne and conceivably acne-specific quality of life,” they added (J Acad Nutr Diet. 2017 Jun 9. doi: 10.1016/j.jand.2017.03.024).
[email protected]
FROM THE JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS
Weekly buprenorphine depot effective for opioid use disorder
A weekly subcutaneous buprenorphine depot could improve adherence and reduce the potential for misuse, according to a study presented at the annual meeting of the College on Problems of Drug Dependence and published simultaneously June 22 in JAMA Psychiatry.
In a phase II, double-blind, randomized study, 47 adults with moderate to severe opioid use disorder were randomized to a weekly dose of the subcutaneous buprenorphine depot CAM2038 – either 24 mg or 32 mg – for 2 weeks. They also underwent five 3-day test sessions to evaluate their response to 6 mg and 18 mg doses of intramuscular hydromorphone and a 0 mg control. One qualification session was held before randomization and the remaining four sessions after.
The primary outcome of the study was drug liking, and both doses of CAM2038 were associated with immediate, sustained, and dose-related suppression of participants’ response to hydromorphone (JAMA Psychiatry. 2017 June 22. doi:10.1001/jamapsychiatry.2017.1874).
The depot also appeared to block the dose-dependent increase in drowsiness that was seen in response to hydromorphone in the qualification session.
However, there was a reversal of the dose-dependent response in participants’ desire to use opioids, with greater suppression seen at the lower depot dose.
Buprenorphine is known to be safer than methadone for the treatment of opioid use disorders, but Sharon L. Walsh, PhD, of the Center on Drug and Alcohol Research at the University of Kentucky, Lexington, and her coauthors said sublingual buprenorphine itself has become an abuse liability in some countries.
“Sublingual formulations of buprenorphine can be injected or snorted to enhance euphoric effects,” they wrote. “Unintentional overdose with buprenorphine has been reported, leading to toxicity and fatality in children and those who coingest buprenorphine with benzodiazepines or alcohol.”
The results mean the formulation meets the U.S. Food and Drug Administration criteria for complete opioid blockade.
CAM2038 achieved complete suppression of opioid withdrawal at both doses, and Clinical Opiate Withdrawal Scale (COWS) remained suppressed for the entire duration of the study.
“During treatment initiation, it is important that withdrawal symptoms are well-controlled,” the authors wrote. “The COWS and [Objective Opioid Withdrawal Scale] scores were reduced to near zero on the first dosing day with suppression thereafter.”
The mean COWS preinjection score was 11, which did not include five participants who accidentally were inducted with CAM2038 before they had achieved the prespecified criteria of a COWS score of 8 or above.
They also noted that the pharmacokinetic profile of CAM2038 showed gradually increasing buprenorphine concentrations, reaching maximum at around 24 hours after the dose was given. Perhaps because of this effect – which they likened to a de factor induction procedure mimicking the recommended induction with sublingual buprenorphine – the authors suggested that patients using CAM2038 could likely be inducted directly using the depot.
Researchers also looked at some key physiological outcomes before and after treatment with the depot. They found that, while patients showed significant dose-dependent reductions in oxygen saturation with hydromorphone before receiving depot treatment, these were significantly attenuated after treatment with CAM2038.
One subject withdrew from the study because of ventricular extrasystoles, and one showed abnormal liver function at discharge that was later attributed a hepatitis C diagnosis. Neither event was linked to the study drug.
However, 81% of patients experienced at least one adverse event, with significantly more events reported in the higher dose group. The most common reported events that were possibly related to the study drug were constipation, injection site pain and erythema, and headache. Most were rated as mild.
The College on Problems of Drug Dependence, a nonprofit corporation, is holding its annual meeting in Montreal. The study was supported by research contracts from Braeburn Pharmaceuticals, with additional support from the National Institute on Drug Abuse, the National Center for Research Resources, and the National Center for Advancing of Translational Sciences. Two authors are employees of study sponsor Braeburn Pharmaceuticals, and one is an employee of Camurus – a partner to the sponsor. Three authors also received research contract support from Braeburn, four research consultant fees from Braeburn, and two received consulting fees or partial salary support from Camurus, and other pharmaceutical companies.
A weekly subcutaneous buprenorphine depot could improve adherence and reduce the potential for misuse, according to a study presented at the annual meeting of the College on Problems of Drug Dependence and published simultaneously June 22 in JAMA Psychiatry.
In a phase II, double-blind, randomized study, 47 adults with moderate to severe opioid use disorder were randomized to a weekly dose of the subcutaneous buprenorphine depot CAM2038 – either 24 mg or 32 mg – for 2 weeks. They also underwent five 3-day test sessions to evaluate their response to 6 mg and 18 mg doses of intramuscular hydromorphone and a 0 mg control. One qualification session was held before randomization and the remaining four sessions after.
The primary outcome of the study was drug liking, and both doses of CAM2038 were associated with immediate, sustained, and dose-related suppression of participants’ response to hydromorphone (JAMA Psychiatry. 2017 June 22. doi:10.1001/jamapsychiatry.2017.1874).
The depot also appeared to block the dose-dependent increase in drowsiness that was seen in response to hydromorphone in the qualification session.
However, there was a reversal of the dose-dependent response in participants’ desire to use opioids, with greater suppression seen at the lower depot dose.
Buprenorphine is known to be safer than methadone for the treatment of opioid use disorders, but Sharon L. Walsh, PhD, of the Center on Drug and Alcohol Research at the University of Kentucky, Lexington, and her coauthors said sublingual buprenorphine itself has become an abuse liability in some countries.
“Sublingual formulations of buprenorphine can be injected or snorted to enhance euphoric effects,” they wrote. “Unintentional overdose with buprenorphine has been reported, leading to toxicity and fatality in children and those who coingest buprenorphine with benzodiazepines or alcohol.”
The results mean the formulation meets the U.S. Food and Drug Administration criteria for complete opioid blockade.
CAM2038 achieved complete suppression of opioid withdrawal at both doses, and Clinical Opiate Withdrawal Scale (COWS) remained suppressed for the entire duration of the study.
“During treatment initiation, it is important that withdrawal symptoms are well-controlled,” the authors wrote. “The COWS and [Objective Opioid Withdrawal Scale] scores were reduced to near zero on the first dosing day with suppression thereafter.”
The mean COWS preinjection score was 11, which did not include five participants who accidentally were inducted with CAM2038 before they had achieved the prespecified criteria of a COWS score of 8 or above.
They also noted that the pharmacokinetic profile of CAM2038 showed gradually increasing buprenorphine concentrations, reaching maximum at around 24 hours after the dose was given. Perhaps because of this effect – which they likened to a de factor induction procedure mimicking the recommended induction with sublingual buprenorphine – the authors suggested that patients using CAM2038 could likely be inducted directly using the depot.
Researchers also looked at some key physiological outcomes before and after treatment with the depot. They found that, while patients showed significant dose-dependent reductions in oxygen saturation with hydromorphone before receiving depot treatment, these were significantly attenuated after treatment with CAM2038.
One subject withdrew from the study because of ventricular extrasystoles, and one showed abnormal liver function at discharge that was later attributed a hepatitis C diagnosis. Neither event was linked to the study drug.
However, 81% of patients experienced at least one adverse event, with significantly more events reported in the higher dose group. The most common reported events that were possibly related to the study drug were constipation, injection site pain and erythema, and headache. Most were rated as mild.
The College on Problems of Drug Dependence, a nonprofit corporation, is holding its annual meeting in Montreal. The study was supported by research contracts from Braeburn Pharmaceuticals, with additional support from the National Institute on Drug Abuse, the National Center for Research Resources, and the National Center for Advancing of Translational Sciences. Two authors are employees of study sponsor Braeburn Pharmaceuticals, and one is an employee of Camurus – a partner to the sponsor. Three authors also received research contract support from Braeburn, four research consultant fees from Braeburn, and two received consulting fees or partial salary support from Camurus, and other pharmaceutical companies.
A weekly subcutaneous buprenorphine depot could improve adherence and reduce the potential for misuse, according to a study presented at the annual meeting of the College on Problems of Drug Dependence and published simultaneously June 22 in JAMA Psychiatry.
In a phase II, double-blind, randomized study, 47 adults with moderate to severe opioid use disorder were randomized to a weekly dose of the subcutaneous buprenorphine depot CAM2038 – either 24 mg or 32 mg – for 2 weeks. They also underwent five 3-day test sessions to evaluate their response to 6 mg and 18 mg doses of intramuscular hydromorphone and a 0 mg control. One qualification session was held before randomization and the remaining four sessions after.
The primary outcome of the study was drug liking, and both doses of CAM2038 were associated with immediate, sustained, and dose-related suppression of participants’ response to hydromorphone (JAMA Psychiatry. 2017 June 22. doi:10.1001/jamapsychiatry.2017.1874).
The depot also appeared to block the dose-dependent increase in drowsiness that was seen in response to hydromorphone in the qualification session.
However, there was a reversal of the dose-dependent response in participants’ desire to use opioids, with greater suppression seen at the lower depot dose.
Buprenorphine is known to be safer than methadone for the treatment of opioid use disorders, but Sharon L. Walsh, PhD, of the Center on Drug and Alcohol Research at the University of Kentucky, Lexington, and her coauthors said sublingual buprenorphine itself has become an abuse liability in some countries.
“Sublingual formulations of buprenorphine can be injected or snorted to enhance euphoric effects,” they wrote. “Unintentional overdose with buprenorphine has been reported, leading to toxicity and fatality in children and those who coingest buprenorphine with benzodiazepines or alcohol.”
The results mean the formulation meets the U.S. Food and Drug Administration criteria for complete opioid blockade.
CAM2038 achieved complete suppression of opioid withdrawal at both doses, and Clinical Opiate Withdrawal Scale (COWS) remained suppressed for the entire duration of the study.
“During treatment initiation, it is important that withdrawal symptoms are well-controlled,” the authors wrote. “The COWS and [Objective Opioid Withdrawal Scale] scores were reduced to near zero on the first dosing day with suppression thereafter.”
The mean COWS preinjection score was 11, which did not include five participants who accidentally were inducted with CAM2038 before they had achieved the prespecified criteria of a COWS score of 8 or above.
They also noted that the pharmacokinetic profile of CAM2038 showed gradually increasing buprenorphine concentrations, reaching maximum at around 24 hours after the dose was given. Perhaps because of this effect – which they likened to a de factor induction procedure mimicking the recommended induction with sublingual buprenorphine – the authors suggested that patients using CAM2038 could likely be inducted directly using the depot.
Researchers also looked at some key physiological outcomes before and after treatment with the depot. They found that, while patients showed significant dose-dependent reductions in oxygen saturation with hydromorphone before receiving depot treatment, these were significantly attenuated after treatment with CAM2038.
One subject withdrew from the study because of ventricular extrasystoles, and one showed abnormal liver function at discharge that was later attributed a hepatitis C diagnosis. Neither event was linked to the study drug.
However, 81% of patients experienced at least one adverse event, with significantly more events reported in the higher dose group. The most common reported events that were possibly related to the study drug were constipation, injection site pain and erythema, and headache. Most were rated as mild.
The College on Problems of Drug Dependence, a nonprofit corporation, is holding its annual meeting in Montreal. The study was supported by research contracts from Braeburn Pharmaceuticals, with additional support from the National Institute on Drug Abuse, the National Center for Research Resources, and the National Center for Advancing of Translational Sciences. Two authors are employees of study sponsor Braeburn Pharmaceuticals, and one is an employee of Camurus – a partner to the sponsor. Three authors also received research contract support from Braeburn, four research consultant fees from Braeburn, and two received consulting fees or partial salary support from Camurus, and other pharmaceutical companies.
FROM JAMA Psychiatry
Key clinical point: A weekly subcutaneous buprenorphine depot is effective and could reduce the potential for misuse of buprenorphine in patients with opioid use disorder.
Major finding: Buprenorphine depot CAM2038 achieves immediate and sustained opioid blockade and suppression of opioid withdrawal.
Data source: A double-blind, randomized phase II study in 47 patients with opioid use disorder.
Disclosures: The study was supported by research contracts from Braeburn Pharmaceuticals, with additional support from the National Institute on Drug Abuse, the National Center for Research Resources, and the National Center for Advancing of Translational Sciences. Two authors are employees of study sponsor Braeburn Pharmaceuticals, and one is an employee of Camurus – a partner to the sponsor. Three authors also received research contract support from Braeburn, four recieved research consultant fees from Braeburn, and two received consulting fees or partial salary support from Camurus and other pharmaceutical companies.
If doctors recommend it, teens are more likely to get HPV vaccine
, Brandon Brown, PhD, at the University of California, Riverside, and his associates said.
In a year-long survey of 200 parents’ reasons for agreeing or refusing initial HPV vaccination following practitioner recommendation in a California pediatric practice of six pediatricians, 82% of parents accepted initiation of the HPV series. A significantly higher percentage of parents of male teens did so, compared with parents of female teens (89% vs. 71%; P less than .01), but there were more male children (61.5%) among offspring of the study participants.
Among parents who refused initiation of the HPV vaccine for their adolescents, the most common reason for refusing (53%) and most influential reason (49%) was “I want to learn more about this vaccine,” while 25% said their child was too young to get the vaccine. Some in this latter group said they would vaccinate their child when they were older.
Of the 195 parents who answered a question regarding whether they had a friend or family member diagnosed with cervical cancer, 13% said yes. Of these parents, 92% agreed to have their child get the HPV vaccine.
Read more at Papillomavirus Research (2017 Jan 17. doi: 10.1016/j.pvr.2017.01.002).
, Brandon Brown, PhD, at the University of California, Riverside, and his associates said.
In a year-long survey of 200 parents’ reasons for agreeing or refusing initial HPV vaccination following practitioner recommendation in a California pediatric practice of six pediatricians, 82% of parents accepted initiation of the HPV series. A significantly higher percentage of parents of male teens did so, compared with parents of female teens (89% vs. 71%; P less than .01), but there were more male children (61.5%) among offspring of the study participants.
Among parents who refused initiation of the HPV vaccine for their adolescents, the most common reason for refusing (53%) and most influential reason (49%) was “I want to learn more about this vaccine,” while 25% said their child was too young to get the vaccine. Some in this latter group said they would vaccinate their child when they were older.
Of the 195 parents who answered a question regarding whether they had a friend or family member diagnosed with cervical cancer, 13% said yes. Of these parents, 92% agreed to have their child get the HPV vaccine.
Read more at Papillomavirus Research (2017 Jan 17. doi: 10.1016/j.pvr.2017.01.002).
, Brandon Brown, PhD, at the University of California, Riverside, and his associates said.
In a year-long survey of 200 parents’ reasons for agreeing or refusing initial HPV vaccination following practitioner recommendation in a California pediatric practice of six pediatricians, 82% of parents accepted initiation of the HPV series. A significantly higher percentage of parents of male teens did so, compared with parents of female teens (89% vs. 71%; P less than .01), but there were more male children (61.5%) among offspring of the study participants.
Among parents who refused initiation of the HPV vaccine for their adolescents, the most common reason for refusing (53%) and most influential reason (49%) was “I want to learn more about this vaccine,” while 25% said their child was too young to get the vaccine. Some in this latter group said they would vaccinate their child when they were older.
Of the 195 parents who answered a question regarding whether they had a friend or family member diagnosed with cervical cancer, 13% said yes. Of these parents, 92% agreed to have their child get the HPV vaccine.
Read more at Papillomavirus Research (2017 Jan 17. doi: 10.1016/j.pvr.2017.01.002).
FROM PAPILLOMAVIRUS RESEARCH
Proper catheter removal promotes colorectal surgery recovery
Adherence to guidelines for urinary catheter removal significantly reduced rates of urinary tract infection and length of hospital stay, based on data from almost 3,000 patients.
UTIs occurred in 0.8% of colonic surgery patients who were guideline compliant, compared with 4.1% of noncompliant patients. Similarly, UTIs were significantly less likely in rectal surgery patients who complied with guidelines, compared with those who did not (3.5% vs. 9.6%).
The Implementation of the Enhanced Recovery After Surgery (iERAS) program involved 15 academic hospitals in Ontario, Canada. The guidelines include prompt removal of catheters from colonic and rectal surgery patients. Recommended removal times ranged from 24 hours to 72 hours, depending on the procedure.
“Although numerous reports have documented the overall effectiveness of bundled ERAS interventions improving outcome, the contribution of individual components of the pathway in the context of an ERAS implementation program is uncertain,” wrote Allan Okrainec, MD, of the University of Toronto, and his colleagues.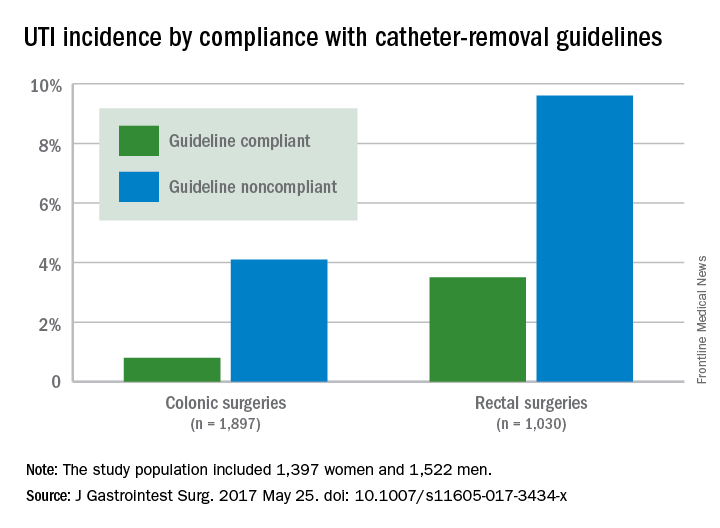
Overall, 53% of patients had catheters removed in compliance with the guidelines, including 47.2% of those with colonic resections and 69.5% of those with rectal resections.
The average length of hospital stay for colonic surgery patients who complied with the urinary catheter guideline was 4 days, compared with 5 days for noncompliant patients, a statistically significant difference. Similarly, the average length of stay was significantly shorter for compliant rectal surgery patients, compared with noncompliant patients (5 days vs. 8 days, respectively).
Reinsertion of the urinary catheter was needed for 6% of the patients, including 122 patients with suspected or confirmed urinary retention and 36 patients who had other indications for reinsertion.
“One of the concerns about early removal of catheters is that it might lead to an increased need for reinsertion,” the researchers noted. “In our study, guideline compliance was associated with an increased rate of catheter reinsertion, but [it] only increased the risk by 2%-3% in patients having rectal or colonic procedures,” the investigators said.
The study results were limited by a lack of information about reasons for noncompliance with the guidelines, the researchers added. However, the data support the value of early catheter removal for surgical patients. “It is noteworthy that, in our study, as well as others, urinary retention rates are relatively low,” they said.
The Council of Academic Hospitals of Ontario funded the study. The researchers had no financial conflicts to disclose.
Adherence to guidelines for urinary catheter removal significantly reduced rates of urinary tract infection and length of hospital stay, based on data from almost 3,000 patients.
UTIs occurred in 0.8% of colonic surgery patients who were guideline compliant, compared with 4.1% of noncompliant patients. Similarly, UTIs were significantly less likely in rectal surgery patients who complied with guidelines, compared with those who did not (3.5% vs. 9.6%).
The Implementation of the Enhanced Recovery After Surgery (iERAS) program involved 15 academic hospitals in Ontario, Canada. The guidelines include prompt removal of catheters from colonic and rectal surgery patients. Recommended removal times ranged from 24 hours to 72 hours, depending on the procedure.
“Although numerous reports have documented the overall effectiveness of bundled ERAS interventions improving outcome, the contribution of individual components of the pathway in the context of an ERAS implementation program is uncertain,” wrote Allan Okrainec, MD, of the University of Toronto, and his colleagues.
Overall, 53% of patients had catheters removed in compliance with the guidelines, including 47.2% of those with colonic resections and 69.5% of those with rectal resections.
The average length of hospital stay for colonic surgery patients who complied with the urinary catheter guideline was 4 days, compared with 5 days for noncompliant patients, a statistically significant difference. Similarly, the average length of stay was significantly shorter for compliant rectal surgery patients, compared with noncompliant patients (5 days vs. 8 days, respectively).
Reinsertion of the urinary catheter was needed for 6% of the patients, including 122 patients with suspected or confirmed urinary retention and 36 patients who had other indications for reinsertion.
“One of the concerns about early removal of catheters is that it might lead to an increased need for reinsertion,” the researchers noted. “In our study, guideline compliance was associated with an increased rate of catheter reinsertion, but [it] only increased the risk by 2%-3% in patients having rectal or colonic procedures,” the investigators said.
The study results were limited by a lack of information about reasons for noncompliance with the guidelines, the researchers added. However, the data support the value of early catheter removal for surgical patients. “It is noteworthy that, in our study, as well as others, urinary retention rates are relatively low,” they said.
The Council of Academic Hospitals of Ontario funded the study. The researchers had no financial conflicts to disclose.
Adherence to guidelines for urinary catheter removal significantly reduced rates of urinary tract infection and length of hospital stay, based on data from almost 3,000 patients.
UTIs occurred in 0.8% of colonic surgery patients who were guideline compliant, compared with 4.1% of noncompliant patients. Similarly, UTIs were significantly less likely in rectal surgery patients who complied with guidelines, compared with those who did not (3.5% vs. 9.6%).
The Implementation of the Enhanced Recovery After Surgery (iERAS) program involved 15 academic hospitals in Ontario, Canada. The guidelines include prompt removal of catheters from colonic and rectal surgery patients. Recommended removal times ranged from 24 hours to 72 hours, depending on the procedure.
“Although numerous reports have documented the overall effectiveness of bundled ERAS interventions improving outcome, the contribution of individual components of the pathway in the context of an ERAS implementation program is uncertain,” wrote Allan Okrainec, MD, of the University of Toronto, and his colleagues.
Overall, 53% of patients had catheters removed in compliance with the guidelines, including 47.2% of those with colonic resections and 69.5% of those with rectal resections.
The average length of hospital stay for colonic surgery patients who complied with the urinary catheter guideline was 4 days, compared with 5 days for noncompliant patients, a statistically significant difference. Similarly, the average length of stay was significantly shorter for compliant rectal surgery patients, compared with noncompliant patients (5 days vs. 8 days, respectively).
Reinsertion of the urinary catheter was needed for 6% of the patients, including 122 patients with suspected or confirmed urinary retention and 36 patients who had other indications for reinsertion.
“One of the concerns about early removal of catheters is that it might lead to an increased need for reinsertion,” the researchers noted. “In our study, guideline compliance was associated with an increased rate of catheter reinsertion, but [it] only increased the risk by 2%-3% in patients having rectal or colonic procedures,” the investigators said.
The study results were limited by a lack of information about reasons for noncompliance with the guidelines, the researchers added. However, the data support the value of early catheter removal for surgical patients. “It is noteworthy that, in our study, as well as others, urinary retention rates are relatively low,” they said.
The Council of Academic Hospitals of Ontario funded the study. The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF GASTROINTESTINAL SURGERY
Key clinical point: Compliance with guidelines for urinary catheter removal significantly reduced hospital stay and UTI rates in colon and rectal surgery patients.
Major finding: UTI rates in colonic surgery patients were 0.8% and 4.1%, respectively, for those who were compliant and noncompliant with the guidelines. Rates were 3.5% and 9.6%, respectively, for compliant and noncompliant rectal surgery patients.
Data source: A prospective study of 2,927 adults who underwent colonic or rectal surgery between September 2012 and April 2015.
Disclosures: The Council of Academic Hospitals of Ontario funded the study. The researchers had no financial conflicts to disclose.
ACIP approves new hepatitis A vaccine draft recommendations
, including a focus on catch-up vaccines for adolescents and those over age 40 years.
While hepatitis A cases have dropped significantly since the vaccine’s debut – with the number of reported cases in 2015 dropping to 1,390, compared with 9,606 in 1971 – previous recommendations regarding catch-up vaccinations suggested patients should consider treatment, as opposed to catch-up vaccination.
Adult catch-up vaccines now are recommended to be considered in areas with increasing disease risks, an addition that was not part of the current recommendations but has been changed because of evidence that patients over 40 years old are more vulnerable to the virus and more likely to be hospitalized if infected, said Noele Nelson, MD, PhD, of the Division of Viral Hepatitis at the CDC.
“Increasing proportions of adults in the United States are susceptible to hepatitis A ... due to reduced exposure to virus early in life and significant serum prevalence in older adults greater and equal to 40 years,” said Dr. Nelson. “In addition, there is low two-dose vaccination coverage among adults, including high risk adults, and morbidity and mortality increases with age.”
Recommendations for pregnant women also have been updated with a more definitive message. Previous recommendations advised pregnant women to weigh the options of acquiring hepatitis A against possible adverse effects of the vaccine. But, new evidence was presented at the meeting: in a study of 139 pregnant women vaccinated between 1996 and 2015 who experienced adverse effects, only seven of the effects were considered serious, and no maternal or infant deaths were apparent. In light of this, the ACIP approved the recommendation change to advise all pregnant women to be vaccinated, if they have not already been so before pregnancy.
Updates also included recommendations for patients with chronic liver disease, who are considered to be members of a high-risk population. Newly approved recommendations include a section on epidemiology, which states that, while those with chronic liver disease are not at increased risk for hepatitis A virus infection unless they experience fecal-oral exposure to the virus, those with acute hepatitis A may be more at risk to develop more severe liver disease. Recommendations for those with chronic liver disease also include a statement advising patients to seek immunoglobulin, as well as a hepatitis A, vaccination as soon as possible after exposure.
The ACIP also approved a change in recommendations to advise all residents and caretakers of those living in a group home, specifically those caring for developmentally disabled patients, to be vaccinated because of the historically high endemic nature of such institutions.
Committee members hope these new recommendations will help the United States reach its goal of a national hepatitis A case ratio of 0.3/100,000 people and a hepatitis A vaccination rate of 85%.
If these recommendations are approved by the director of the CDC and the U.S. Health Department, as they usually are, they will be published in the CDC’s Weekly Morbidity and Mortality Report.
Members of the committee reported no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
, including a focus on catch-up vaccines for adolescents and those over age 40 years.
While hepatitis A cases have dropped significantly since the vaccine’s debut – with the number of reported cases in 2015 dropping to 1,390, compared with 9,606 in 1971 – previous recommendations regarding catch-up vaccinations suggested patients should consider treatment, as opposed to catch-up vaccination.
Adult catch-up vaccines now are recommended to be considered in areas with increasing disease risks, an addition that was not part of the current recommendations but has been changed because of evidence that patients over 40 years old are more vulnerable to the virus and more likely to be hospitalized if infected, said Noele Nelson, MD, PhD, of the Division of Viral Hepatitis at the CDC.
“Increasing proportions of adults in the United States are susceptible to hepatitis A ... due to reduced exposure to virus early in life and significant serum prevalence in older adults greater and equal to 40 years,” said Dr. Nelson. “In addition, there is low two-dose vaccination coverage among adults, including high risk adults, and morbidity and mortality increases with age.”
Recommendations for pregnant women also have been updated with a more definitive message. Previous recommendations advised pregnant women to weigh the options of acquiring hepatitis A against possible adverse effects of the vaccine. But, new evidence was presented at the meeting: in a study of 139 pregnant women vaccinated between 1996 and 2015 who experienced adverse effects, only seven of the effects were considered serious, and no maternal or infant deaths were apparent. In light of this, the ACIP approved the recommendation change to advise all pregnant women to be vaccinated, if they have not already been so before pregnancy.
Updates also included recommendations for patients with chronic liver disease, who are considered to be members of a high-risk population. Newly approved recommendations include a section on epidemiology, which states that, while those with chronic liver disease are not at increased risk for hepatitis A virus infection unless they experience fecal-oral exposure to the virus, those with acute hepatitis A may be more at risk to develop more severe liver disease. Recommendations for those with chronic liver disease also include a statement advising patients to seek immunoglobulin, as well as a hepatitis A, vaccination as soon as possible after exposure.
The ACIP also approved a change in recommendations to advise all residents and caretakers of those living in a group home, specifically those caring for developmentally disabled patients, to be vaccinated because of the historically high endemic nature of such institutions.
Committee members hope these new recommendations will help the United States reach its goal of a national hepatitis A case ratio of 0.3/100,000 people and a hepatitis A vaccination rate of 85%.
If these recommendations are approved by the director of the CDC and the U.S. Health Department, as they usually are, they will be published in the CDC’s Weekly Morbidity and Mortality Report.
Members of the committee reported no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
, including a focus on catch-up vaccines for adolescents and those over age 40 years.
While hepatitis A cases have dropped significantly since the vaccine’s debut – with the number of reported cases in 2015 dropping to 1,390, compared with 9,606 in 1971 – previous recommendations regarding catch-up vaccinations suggested patients should consider treatment, as opposed to catch-up vaccination.
Adult catch-up vaccines now are recommended to be considered in areas with increasing disease risks, an addition that was not part of the current recommendations but has been changed because of evidence that patients over 40 years old are more vulnerable to the virus and more likely to be hospitalized if infected, said Noele Nelson, MD, PhD, of the Division of Viral Hepatitis at the CDC.
“Increasing proportions of adults in the United States are susceptible to hepatitis A ... due to reduced exposure to virus early in life and significant serum prevalence in older adults greater and equal to 40 years,” said Dr. Nelson. “In addition, there is low two-dose vaccination coverage among adults, including high risk adults, and morbidity and mortality increases with age.”
Recommendations for pregnant women also have been updated with a more definitive message. Previous recommendations advised pregnant women to weigh the options of acquiring hepatitis A against possible adverse effects of the vaccine. But, new evidence was presented at the meeting: in a study of 139 pregnant women vaccinated between 1996 and 2015 who experienced adverse effects, only seven of the effects were considered serious, and no maternal or infant deaths were apparent. In light of this, the ACIP approved the recommendation change to advise all pregnant women to be vaccinated, if they have not already been so before pregnancy.
Updates also included recommendations for patients with chronic liver disease, who are considered to be members of a high-risk population. Newly approved recommendations include a section on epidemiology, which states that, while those with chronic liver disease are not at increased risk for hepatitis A virus infection unless they experience fecal-oral exposure to the virus, those with acute hepatitis A may be more at risk to develop more severe liver disease. Recommendations for those with chronic liver disease also include a statement advising patients to seek immunoglobulin, as well as a hepatitis A, vaccination as soon as possible after exposure.
The ACIP also approved a change in recommendations to advise all residents and caretakers of those living in a group home, specifically those caring for developmentally disabled patients, to be vaccinated because of the historically high endemic nature of such institutions.
Committee members hope these new recommendations will help the United States reach its goal of a national hepatitis A case ratio of 0.3/100,000 people and a hepatitis A vaccination rate of 85%.
If these recommendations are approved by the director of the CDC and the U.S. Health Department, as they usually are, they will be published in the CDC’s Weekly Morbidity and Mortality Report.
Members of the committee reported no relevant financial disclosures.
[email protected]
On Twitter @eaztweets
FROM ACIP MEETING