User login
Selim Benbadis, MD

Allele-matching in cord blood transplant yields better survival
Matching down to the allele level in umbilical cord blood transplantation between unrelated donors results in greater overall survival for those with nonmalignant diseases, such as aplastic anemia, researchers found in a retrospective study published in the Lancet Haematology.
The review (Lancet Haematol. 2017 Jul;4[7]:e325-33), the largest published on the topic, indicates that clinicians should change practice from the current standard of antigen-level matching, said Mary Eapen, MD, director of the Center for International Blood and Marrow Transplant Research (CIBMTR) in Wauwatosa, Wisconsin.
“Our findings,” Dr. Eapen wrote, “support a change in clinical practice to prioritization of units on allele-level HLA matching at HLA-A, HLA-B, HLA-C, and HLA-DRB1.”
Data were pulled from cases reported to the Center for International Blood and Marrow Transplant Research or the European Group for Blood and Marrow Transplant. Researchers looked at 1,199 donor-recipient matches of cord blood transplantation for diseases, such as severe combined immunodeficiency (SCID), non-SCID primary immunodeficiency, inborn errors of metabolism, severe aplastic anemia, and Fanconi anemia. Recipients could be as old as age 16, but most were age 5 or younger.
After adjustment for factors, including cytomegalovirus serostatus, the intensity of the conditioning regimen, and the total nucleated cell dose, the 5-year overall survival was 79% for transplants that were matched at all eight alleles at HLA-A, HLA-B, HLA-C and HLA-DRB1. These results compare with 76% after transplants with one mismatch, 70% with two mismatches, 62% with three mismatches, and 49% with 4 or more mismatches.
Mortality risks were significantly higher for patients who received transplants with two (P = .018), three (P = .0001), and four or more mismatches (P less than .0001), compared with those whose transplants were fully matched. There was no difference statistically between full matches and one mismatch, but the findings suggest that the mortality risk might prove significant with a larger sample size.
Researchers cautioned that, because most patients were age 5 or younger, the results might not be generalizable to older children.
Although HLA typing is available at CIBMTR for most blood cord transplants for nonmalignant diseases, full allele matches or just one mismatch are not the norm, Dr. Eapen wrote. Researchers said that they suspect this is because of difficulties finding matches or because a high total nucleated cell count is prioritized above HLA matching. They suggest clinicians change their decision making in this regard.
Matching down to the allele level in umbilical cord blood transplantation between unrelated donors results in greater overall survival for those with nonmalignant diseases, such as aplastic anemia, researchers found in a retrospective study published in the Lancet Haematology.
The review (Lancet Haematol. 2017 Jul;4[7]:e325-33), the largest published on the topic, indicates that clinicians should change practice from the current standard of antigen-level matching, said Mary Eapen, MD, director of the Center for International Blood and Marrow Transplant Research (CIBMTR) in Wauwatosa, Wisconsin.
“Our findings,” Dr. Eapen wrote, “support a change in clinical practice to prioritization of units on allele-level HLA matching at HLA-A, HLA-B, HLA-C, and HLA-DRB1.”
Data were pulled from cases reported to the Center for International Blood and Marrow Transplant Research or the European Group for Blood and Marrow Transplant. Researchers looked at 1,199 donor-recipient matches of cord blood transplantation for diseases, such as severe combined immunodeficiency (SCID), non-SCID primary immunodeficiency, inborn errors of metabolism, severe aplastic anemia, and Fanconi anemia. Recipients could be as old as age 16, but most were age 5 or younger.
After adjustment for factors, including cytomegalovirus serostatus, the intensity of the conditioning regimen, and the total nucleated cell dose, the 5-year overall survival was 79% for transplants that were matched at all eight alleles at HLA-A, HLA-B, HLA-C and HLA-DRB1. These results compare with 76% after transplants with one mismatch, 70% with two mismatches, 62% with three mismatches, and 49% with 4 or more mismatches.
Mortality risks were significantly higher for patients who received transplants with two (P = .018), three (P = .0001), and four or more mismatches (P less than .0001), compared with those whose transplants were fully matched. There was no difference statistically between full matches and one mismatch, but the findings suggest that the mortality risk might prove significant with a larger sample size.
Researchers cautioned that, because most patients were age 5 or younger, the results might not be generalizable to older children.
Although HLA typing is available at CIBMTR for most blood cord transplants for nonmalignant diseases, full allele matches or just one mismatch are not the norm, Dr. Eapen wrote. Researchers said that they suspect this is because of difficulties finding matches or because a high total nucleated cell count is prioritized above HLA matching. They suggest clinicians change their decision making in this regard.
Matching down to the allele level in umbilical cord blood transplantation between unrelated donors results in greater overall survival for those with nonmalignant diseases, such as aplastic anemia, researchers found in a retrospective study published in the Lancet Haematology.
The review (Lancet Haematol. 2017 Jul;4[7]:e325-33), the largest published on the topic, indicates that clinicians should change practice from the current standard of antigen-level matching, said Mary Eapen, MD, director of the Center for International Blood and Marrow Transplant Research (CIBMTR) in Wauwatosa, Wisconsin.
“Our findings,” Dr. Eapen wrote, “support a change in clinical practice to prioritization of units on allele-level HLA matching at HLA-A, HLA-B, HLA-C, and HLA-DRB1.”
Data were pulled from cases reported to the Center for International Blood and Marrow Transplant Research or the European Group for Blood and Marrow Transplant. Researchers looked at 1,199 donor-recipient matches of cord blood transplantation for diseases, such as severe combined immunodeficiency (SCID), non-SCID primary immunodeficiency, inborn errors of metabolism, severe aplastic anemia, and Fanconi anemia. Recipients could be as old as age 16, but most were age 5 or younger.
After adjustment for factors, including cytomegalovirus serostatus, the intensity of the conditioning regimen, and the total nucleated cell dose, the 5-year overall survival was 79% for transplants that were matched at all eight alleles at HLA-A, HLA-B, HLA-C and HLA-DRB1. These results compare with 76% after transplants with one mismatch, 70% with two mismatches, 62% with three mismatches, and 49% with 4 or more mismatches.
Mortality risks were significantly higher for patients who received transplants with two (P = .018), three (P = .0001), and four or more mismatches (P less than .0001), compared with those whose transplants were fully matched. There was no difference statistically between full matches and one mismatch, but the findings suggest that the mortality risk might prove significant with a larger sample size.
Researchers cautioned that, because most patients were age 5 or younger, the results might not be generalizable to older children.
Although HLA typing is available at CIBMTR for most blood cord transplants for nonmalignant diseases, full allele matches or just one mismatch are not the norm, Dr. Eapen wrote. Researchers said that they suspect this is because of difficulties finding matches or because a high total nucleated cell count is prioritized above HLA matching. They suggest clinicians change their decision making in this regard.
FROM THE LANCET HAEMATOLOGY
Key clinical point: HLA matching at the allele-level produces better survival in umbilical cord blood transplantation for nonmalignant diseases.
Major finding: Mortality risks were significantly higher for patients who received transplants with two (P = .018), three (P = .0001), and four or more mismatches (P less than .0001), compared with those whose transplants were fully matched at all eight alleles at HLA-A, HLA-B, HLA-C and HLA-DRB1.
Data source: A retrospective review of 1,199 cases reported to the Center for International Blood and Marrow Transplant Research (CIBMTR) or the European Group for Blood and Marrow Transplant (EGBMT).
Disclosures: The authors reported no conflicts of interest.
Avelumab induces response in Hodgkin lymphoma after failed allo-SCT
LUGANO, SWITZERLAND – The immune checkpoint inhibitor avelumab showed efficacy against classical Hodgkin lymphoma among patients with disease progression following allogeneic stem cell transplants (allo-SCT), based on results of a phase 1 trial.
Two of eight patients with disease progression following an allogeneic transplant (allo-SCT) had complete responses (CR) to the programmed death ligand-1 (PD-L1) inhibitor avelumab (Bavencio), three had partial responses (PRs), and two had stable disease, reported Robert Chen, MD, of City of Hope Medical Center in Duarte, California.
“The overall response rate observed in the postallo population of 62.5% suggests that the PD-L1 blockade inhibitor may potentiate a graft-vs.-lymphoma response,” he said at the 14th International Conference on Malignant Lymphoma.
Amplification of the chromosome 9p24.1 locus is frequent in classical Hodgkin lymphoma, and the amplicon contains the genes encoding for PD-L1 and PD-L2, resulting in the over expression of both ligands, Dr. Chen said.
Both nivolumab (Opdivo) and pembrolizumab (Keytruda) are indicated for the treatment of relapsed/refractory classical Hodgkin lymphoma. Both agents block the interactions between PD-1 and both PD-L1 and PD-L2.
“However, it has not been established whether blockade of the PD-1/PD-L1 interaction is necessary and/or sufficient for the therapeutic effect observed in classical Hodgkin lymphoma,” he said.
Avelumab is an anti–PD-L1, immunoglobulin G1 monoclonal antibody that inhibits PD-1/PD-L1 interactions but leaves PD-1/PD-L2 interactions intact. This agent, which recently received FDA approval for the treatment of Merkel cell carcinoma and locally advanced or metastatic urothelial carcinoma, targets tumor cells rather than the T cells targeted by nivolumab and pembrolizumab.
In the phase 1b JAVELIN Hodgkin study, patients with histologically confirmed relapsed/refractory classical Hodgkin lymphoma who were ineligible for transplant or for whom allogeneic or autologous stem cell transplants had failed were enrolled and were assigned to one of five cohorts to receive avelumab in doses ranging from 70 mg intravenously to 10 mg/kg IV every 2 weeks (or every 3 weeks for the 500 mg dose cohort).
A total of 31 patients were randomized in the dose-finding phase of the study. The median patient age was 38 years, 24 patients were younger than 65, and 7 were 65 or older. Only 1 of the 31 patients had received a single prior line of therapy. Of those, 3 had received two prior therapies, 7 had been treated with three prior lines, and 20 had four or more prior lines of therapy. All patients had received brentuximab vedotin (Adcetris).
The median follow-up was 43.3 weeks. In all, nine patients were continuing on avelumab at the time of the data analysis. Because of disease progression, 10 patients discontinued therapy. Additionally, four discontinued because of adverse events, two chose to withdraw, one was removed from the study by the treating physicians, one did not receive treatment, and four others discontinued because of unspecified reasons.
The median treatment duration was 16.9 weeks. The mean number of cycles was 8.6.
The objective response rate was 42%, including five CRs and eight PRs. Three of the CRs were in patients treated at the 70 mg every 2 week dose, and two were in patients treated at the 500 mg every 3 week level.
In all, 23 patients experienced some degree of tumor shrinkage, and 13 had shrinkage greater than 50%.
In an analysis of best overall response among patients whose disease progressed following SCT, the investigators found that two of eight patients (25%) who had disease progression following allo-SCT had a complete response. Three of these patients had a PR, two had stable disease, and one was not eligible for response evaluation.
In contrast, there was only one objective response, a PR, among five patients who had relapses following autologous SCT.
Grade 3 or 4 treatment-related adverse events occurred in 37% of patients. There were no treatment-related deaths. The incidence of treatment-related adverse events was similar across the five dosing cohorts.
“Based on the observed efficacy and safety profiles and unmet need, this study has recently been amended to focus the expansion of patients who progressed post allo-SCT,” Dr. Chen said.
The study was sponsored by Pfizer in collaboration with Merck KGaA, Germany. Dr. Chen has consulted and served in a speakers’ bureau for Seattle Genetics, Millennium, and Genentech. He has also received research funding from Pharmacyclics, Seattle Genetics, Millennium, and Merck.
LUGANO, SWITZERLAND – The immune checkpoint inhibitor avelumab showed efficacy against classical Hodgkin lymphoma among patients with disease progression following allogeneic stem cell transplants (allo-SCT), based on results of a phase 1 trial.
Two of eight patients with disease progression following an allogeneic transplant (allo-SCT) had complete responses (CR) to the programmed death ligand-1 (PD-L1) inhibitor avelumab (Bavencio), three had partial responses (PRs), and two had stable disease, reported Robert Chen, MD, of City of Hope Medical Center in Duarte, California.
“The overall response rate observed in the postallo population of 62.5% suggests that the PD-L1 blockade inhibitor may potentiate a graft-vs.-lymphoma response,” he said at the 14th International Conference on Malignant Lymphoma.
Amplification of the chromosome 9p24.1 locus is frequent in classical Hodgkin lymphoma, and the amplicon contains the genes encoding for PD-L1 and PD-L2, resulting in the over expression of both ligands, Dr. Chen said.
Both nivolumab (Opdivo) and pembrolizumab (Keytruda) are indicated for the treatment of relapsed/refractory classical Hodgkin lymphoma. Both agents block the interactions between PD-1 and both PD-L1 and PD-L2.
“However, it has not been established whether blockade of the PD-1/PD-L1 interaction is necessary and/or sufficient for the therapeutic effect observed in classical Hodgkin lymphoma,” he said.
Avelumab is an anti–PD-L1, immunoglobulin G1 monoclonal antibody that inhibits PD-1/PD-L1 interactions but leaves PD-1/PD-L2 interactions intact. This agent, which recently received FDA approval for the treatment of Merkel cell carcinoma and locally advanced or metastatic urothelial carcinoma, targets tumor cells rather than the T cells targeted by nivolumab and pembrolizumab.
In the phase 1b JAVELIN Hodgkin study, patients with histologically confirmed relapsed/refractory classical Hodgkin lymphoma who were ineligible for transplant or for whom allogeneic or autologous stem cell transplants had failed were enrolled and were assigned to one of five cohorts to receive avelumab in doses ranging from 70 mg intravenously to 10 mg/kg IV every 2 weeks (or every 3 weeks for the 500 mg dose cohort).
A total of 31 patients were randomized in the dose-finding phase of the study. The median patient age was 38 years, 24 patients were younger than 65, and 7 were 65 or older. Only 1 of the 31 patients had received a single prior line of therapy. Of those, 3 had received two prior therapies, 7 had been treated with three prior lines, and 20 had four or more prior lines of therapy. All patients had received brentuximab vedotin (Adcetris).
The median follow-up was 43.3 weeks. In all, nine patients were continuing on avelumab at the time of the data analysis. Because of disease progression, 10 patients discontinued therapy. Additionally, four discontinued because of adverse events, two chose to withdraw, one was removed from the study by the treating physicians, one did not receive treatment, and four others discontinued because of unspecified reasons.
The median treatment duration was 16.9 weeks. The mean number of cycles was 8.6.
The objective response rate was 42%, including five CRs and eight PRs. Three of the CRs were in patients treated at the 70 mg every 2 week dose, and two were in patients treated at the 500 mg every 3 week level.
In all, 23 patients experienced some degree of tumor shrinkage, and 13 had shrinkage greater than 50%.
In an analysis of best overall response among patients whose disease progressed following SCT, the investigators found that two of eight patients (25%) who had disease progression following allo-SCT had a complete response. Three of these patients had a PR, two had stable disease, and one was not eligible for response evaluation.
In contrast, there was only one objective response, a PR, among five patients who had relapses following autologous SCT.
Grade 3 or 4 treatment-related adverse events occurred in 37% of patients. There were no treatment-related deaths. The incidence of treatment-related adverse events was similar across the five dosing cohorts.
“Based on the observed efficacy and safety profiles and unmet need, this study has recently been amended to focus the expansion of patients who progressed post allo-SCT,” Dr. Chen said.
The study was sponsored by Pfizer in collaboration with Merck KGaA, Germany. Dr. Chen has consulted and served in a speakers’ bureau for Seattle Genetics, Millennium, and Genentech. He has also received research funding from Pharmacyclics, Seattle Genetics, Millennium, and Merck.
LUGANO, SWITZERLAND – The immune checkpoint inhibitor avelumab showed efficacy against classical Hodgkin lymphoma among patients with disease progression following allogeneic stem cell transplants (allo-SCT), based on results of a phase 1 trial.
Two of eight patients with disease progression following an allogeneic transplant (allo-SCT) had complete responses (CR) to the programmed death ligand-1 (PD-L1) inhibitor avelumab (Bavencio), three had partial responses (PRs), and two had stable disease, reported Robert Chen, MD, of City of Hope Medical Center in Duarte, California.
“The overall response rate observed in the postallo population of 62.5% suggests that the PD-L1 blockade inhibitor may potentiate a graft-vs.-lymphoma response,” he said at the 14th International Conference on Malignant Lymphoma.
Amplification of the chromosome 9p24.1 locus is frequent in classical Hodgkin lymphoma, and the amplicon contains the genes encoding for PD-L1 and PD-L2, resulting in the over expression of both ligands, Dr. Chen said.
Both nivolumab (Opdivo) and pembrolizumab (Keytruda) are indicated for the treatment of relapsed/refractory classical Hodgkin lymphoma. Both agents block the interactions between PD-1 and both PD-L1 and PD-L2.
“However, it has not been established whether blockade of the PD-1/PD-L1 interaction is necessary and/or sufficient for the therapeutic effect observed in classical Hodgkin lymphoma,” he said.
Avelumab is an anti–PD-L1, immunoglobulin G1 monoclonal antibody that inhibits PD-1/PD-L1 interactions but leaves PD-1/PD-L2 interactions intact. This agent, which recently received FDA approval for the treatment of Merkel cell carcinoma and locally advanced or metastatic urothelial carcinoma, targets tumor cells rather than the T cells targeted by nivolumab and pembrolizumab.
In the phase 1b JAVELIN Hodgkin study, patients with histologically confirmed relapsed/refractory classical Hodgkin lymphoma who were ineligible for transplant or for whom allogeneic or autologous stem cell transplants had failed were enrolled and were assigned to one of five cohorts to receive avelumab in doses ranging from 70 mg intravenously to 10 mg/kg IV every 2 weeks (or every 3 weeks for the 500 mg dose cohort).
A total of 31 patients were randomized in the dose-finding phase of the study. The median patient age was 38 years, 24 patients were younger than 65, and 7 were 65 or older. Only 1 of the 31 patients had received a single prior line of therapy. Of those, 3 had received two prior therapies, 7 had been treated with three prior lines, and 20 had four or more prior lines of therapy. All patients had received brentuximab vedotin (Adcetris).
The median follow-up was 43.3 weeks. In all, nine patients were continuing on avelumab at the time of the data analysis. Because of disease progression, 10 patients discontinued therapy. Additionally, four discontinued because of adverse events, two chose to withdraw, one was removed from the study by the treating physicians, one did not receive treatment, and four others discontinued because of unspecified reasons.
The median treatment duration was 16.9 weeks. The mean number of cycles was 8.6.
The objective response rate was 42%, including five CRs and eight PRs. Three of the CRs were in patients treated at the 70 mg every 2 week dose, and two were in patients treated at the 500 mg every 3 week level.
In all, 23 patients experienced some degree of tumor shrinkage, and 13 had shrinkage greater than 50%.
In an analysis of best overall response among patients whose disease progressed following SCT, the investigators found that two of eight patients (25%) who had disease progression following allo-SCT had a complete response. Three of these patients had a PR, two had stable disease, and one was not eligible for response evaluation.
In contrast, there was only one objective response, a PR, among five patients who had relapses following autologous SCT.
Grade 3 or 4 treatment-related adverse events occurred in 37% of patients. There were no treatment-related deaths. The incidence of treatment-related adverse events was similar across the five dosing cohorts.
“Based on the observed efficacy and safety profiles and unmet need, this study has recently been amended to focus the expansion of patients who progressed post allo-SCT,” Dr. Chen said.
The study was sponsored by Pfizer in collaboration with Merck KGaA, Germany. Dr. Chen has consulted and served in a speakers’ bureau for Seattle Genetics, Millennium, and Genentech. He has also received research funding from Pharmacyclics, Seattle Genetics, Millennium, and Merck.
AT 14-ICML
Key clinical point: Avelumab showed efficacy in patients with classical Hodgkin lymphoma that relapsed following allogeneic stem cell transplant.
Major finding: The objective response rate among all patients in the study was 41.9%.
Data source: A phase 1 dose-finding and expansion study in 31 patients with relapsed/refractory classical Hodgkin lymphoma who were ineligible for SCT or experienced relapses following SCT.
Disclosures: The study was sponsored by Pfizer in collaboration with Merck KGaA, Germany. Dr. Chen has consulted and served in a speakers’ bureau for Seattle Genetics, Millennium, and Genentech. He has also received research funding from Pharmacyclics, Seattle Genetics, Millennium, and Merck.
TKI dose de-escalation feasible in CML with stable MMR
Tyrosine kinase inhibitor de-escalation is generally safe and may lead to symptom improvement in patients with chronic myeloid leukemia who respond well to the therapy, according to an interim analysis of the nonrandomized phase 2 DESTINY trial.
The findings imply that some patients are unnecessarily overtreated, as responses were sometimes maintained with lower tyrosine kinase inhibitor (TKI) doses, according to Richard E. Clark, MD, of the University of Liverpool, England, and his colleagues (Lancet Haematol. 2017 May 26;4:e310-16).
Of 174 patients with chronic myeloid leukemia (CML) in first chronic phase who had received TKIs for at least 3 years and who were either in stable molecular response 4 logs below the standard arbitrary baseline (MR4, 125 patients) or stable major molecular response (MMR) but not MR4 (49 patients) for at least 12 months at the time of enrollment, 12 (7%) had molecular recurrence during 12 months of half-dose TKI therapy, and all patients who experienced molecular recurrence regained MMR within 4 months of being back on full-dose TKIs, the researchers noted.
The median time to recovery was 77 days.
The recurrence rate was significantly lower in the MR4 cohort than in the MMR cohort (2% vs. 19%; hazard ratio, 0.12), and time to relapse was significantly longer in the MR4 cohort (median, 8.7 vs. 4.4 months), the investigators said.
Recurrence was not associated with age, sex, weight, performance status, BCR-ABL1 transcript type, or duration of TKI therapy, which was a median of 6.9 years overall, they noted.
During the first 3 months of de-escalation, adverse events associated with treatment, including lethargy, diarrhea, rash, and nausea, all improved.
Adverse events during de-escalation occurred in 16 patients, and included one fatality due to worsening of peripheral arterial occlusive disease, but all were deemed unrelated to the TKI or underlying chronic CML, the investigators noted.
Study subjects were adults with positive BCR-ABL1 transcripts, with either e13a2, e14a2, or e19a2 fusion transcript. They were enrolled between December 2013 and April 2015 from 20 hospitals in the United Kingdom; 148 were receiving imatinib, 16 were receiving nilotinib, and 10 were receiving dasatinib. They received half of their standard dose of imatinib (200 mg daily), dasatinib (50 mg daily), or nilotinib (200 mg twice daily) for 12 months. Recurrence during de-escalation was defined as BCR-ABL1:ABL1 ratio greater than 0.1% on two consecutive measurements.
“Although several studies of TKI cessation have been reported, little is known about the feasibility of treatment de-escalation in patients with stable molecular responses,” the investigators wrote, adding that the current study shows that de-escalation is “clearly safe for patients in stable MR4 or deeper remission” and could be a “reasonable option.”
This “practice-changing view” is reinforced by the finding of general improvement of adverse events in both cohorts, they said.
Also of note, de-escalation in this study was associated with savings of almost half the expected TKI costs, they added.
The findings imply that many patients with stable responses might be able to maintain responses on lower TKI doses, they concluded, adding that studies of more ambitious de-escalation are warranted.
Newcastle University and Bloodwise funded the study. Dr. Clark received other grants from Bloodwise during the study, as well as grants and personal fees from Novartis, Bristol-Myers Squibb, and Pfizer, and personal fees from Ariad/Incyte.
The interim DESTINY trial findings indicate the feasibility of a dose reduction approach to minimize adverse events associated with TKI treatment and to improve quality of life, Elisabetta Abruzzese, MD, wrote in an editorial.
De-escalation also appears to provide important cost savings, she noted (Lancet Haematol. 2017 Jul;4:e304-5).
“For patients who are unable to stop therapy, adjustment of the treatment doses without jeopardizing the clinical outcome has important clinical implications. Combination of reduced dosage TKIs with newer (ABL001) or older approaches (immunomodulation) might represent a future answer to that,” she said.
Dr. Abruzzese is with Tor Vergata University, Rome. She reported receiving personal fees from Ariad/Incyte, and serving on the advisory board or as a consultant for Novartis, Pfizer, Ariad/Incyte, and Bristol-Myers Squibb.
The interim DESTINY trial findings indicate the feasibility of a dose reduction approach to minimize adverse events associated with TKI treatment and to improve quality of life, Elisabetta Abruzzese, MD, wrote in an editorial.
De-escalation also appears to provide important cost savings, she noted (Lancet Haematol. 2017 Jul;4:e304-5).
“For patients who are unable to stop therapy, adjustment of the treatment doses without jeopardizing the clinical outcome has important clinical implications. Combination of reduced dosage TKIs with newer (ABL001) or older approaches (immunomodulation) might represent a future answer to that,” she said.
Dr. Abruzzese is with Tor Vergata University, Rome. She reported receiving personal fees from Ariad/Incyte, and serving on the advisory board or as a consultant for Novartis, Pfizer, Ariad/Incyte, and Bristol-Myers Squibb.
The interim DESTINY trial findings indicate the feasibility of a dose reduction approach to minimize adverse events associated with TKI treatment and to improve quality of life, Elisabetta Abruzzese, MD, wrote in an editorial.
De-escalation also appears to provide important cost savings, she noted (Lancet Haematol. 2017 Jul;4:e304-5).
“For patients who are unable to stop therapy, adjustment of the treatment doses without jeopardizing the clinical outcome has important clinical implications. Combination of reduced dosage TKIs with newer (ABL001) or older approaches (immunomodulation) might represent a future answer to that,” she said.
Dr. Abruzzese is with Tor Vergata University, Rome. She reported receiving personal fees from Ariad/Incyte, and serving on the advisory board or as a consultant for Novartis, Pfizer, Ariad/Incyte, and Bristol-Myers Squibb.
Tyrosine kinase inhibitor de-escalation is generally safe and may lead to symptom improvement in patients with chronic myeloid leukemia who respond well to the therapy, according to an interim analysis of the nonrandomized phase 2 DESTINY trial.
The findings imply that some patients are unnecessarily overtreated, as responses were sometimes maintained with lower tyrosine kinase inhibitor (TKI) doses, according to Richard E. Clark, MD, of the University of Liverpool, England, and his colleagues (Lancet Haematol. 2017 May 26;4:e310-16).
Of 174 patients with chronic myeloid leukemia (CML) in first chronic phase who had received TKIs for at least 3 years and who were either in stable molecular response 4 logs below the standard arbitrary baseline (MR4, 125 patients) or stable major molecular response (MMR) but not MR4 (49 patients) for at least 12 months at the time of enrollment, 12 (7%) had molecular recurrence during 12 months of half-dose TKI therapy, and all patients who experienced molecular recurrence regained MMR within 4 months of being back on full-dose TKIs, the researchers noted.
The median time to recovery was 77 days.
The recurrence rate was significantly lower in the MR4 cohort than in the MMR cohort (2% vs. 19%; hazard ratio, 0.12), and time to relapse was significantly longer in the MR4 cohort (median, 8.7 vs. 4.4 months), the investigators said.
Recurrence was not associated with age, sex, weight, performance status, BCR-ABL1 transcript type, or duration of TKI therapy, which was a median of 6.9 years overall, they noted.
During the first 3 months of de-escalation, adverse events associated with treatment, including lethargy, diarrhea, rash, and nausea, all improved.
Adverse events during de-escalation occurred in 16 patients, and included one fatality due to worsening of peripheral arterial occlusive disease, but all were deemed unrelated to the TKI or underlying chronic CML, the investigators noted.
Study subjects were adults with positive BCR-ABL1 transcripts, with either e13a2, e14a2, or e19a2 fusion transcript. They were enrolled between December 2013 and April 2015 from 20 hospitals in the United Kingdom; 148 were receiving imatinib, 16 were receiving nilotinib, and 10 were receiving dasatinib. They received half of their standard dose of imatinib (200 mg daily), dasatinib (50 mg daily), or nilotinib (200 mg twice daily) for 12 months. Recurrence during de-escalation was defined as BCR-ABL1:ABL1 ratio greater than 0.1% on two consecutive measurements.
“Although several studies of TKI cessation have been reported, little is known about the feasibility of treatment de-escalation in patients with stable molecular responses,” the investigators wrote, adding that the current study shows that de-escalation is “clearly safe for patients in stable MR4 or deeper remission” and could be a “reasonable option.”
This “practice-changing view” is reinforced by the finding of general improvement of adverse events in both cohorts, they said.
Also of note, de-escalation in this study was associated with savings of almost half the expected TKI costs, they added.
The findings imply that many patients with stable responses might be able to maintain responses on lower TKI doses, they concluded, adding that studies of more ambitious de-escalation are warranted.
Newcastle University and Bloodwise funded the study. Dr. Clark received other grants from Bloodwise during the study, as well as grants and personal fees from Novartis, Bristol-Myers Squibb, and Pfizer, and personal fees from Ariad/Incyte.
Tyrosine kinase inhibitor de-escalation is generally safe and may lead to symptom improvement in patients with chronic myeloid leukemia who respond well to the therapy, according to an interim analysis of the nonrandomized phase 2 DESTINY trial.
The findings imply that some patients are unnecessarily overtreated, as responses were sometimes maintained with lower tyrosine kinase inhibitor (TKI) doses, according to Richard E. Clark, MD, of the University of Liverpool, England, and his colleagues (Lancet Haematol. 2017 May 26;4:e310-16).
Of 174 patients with chronic myeloid leukemia (CML) in first chronic phase who had received TKIs for at least 3 years and who were either in stable molecular response 4 logs below the standard arbitrary baseline (MR4, 125 patients) or stable major molecular response (MMR) but not MR4 (49 patients) for at least 12 months at the time of enrollment, 12 (7%) had molecular recurrence during 12 months of half-dose TKI therapy, and all patients who experienced molecular recurrence regained MMR within 4 months of being back on full-dose TKIs, the researchers noted.
The median time to recovery was 77 days.
The recurrence rate was significantly lower in the MR4 cohort than in the MMR cohort (2% vs. 19%; hazard ratio, 0.12), and time to relapse was significantly longer in the MR4 cohort (median, 8.7 vs. 4.4 months), the investigators said.
Recurrence was not associated with age, sex, weight, performance status, BCR-ABL1 transcript type, or duration of TKI therapy, which was a median of 6.9 years overall, they noted.
During the first 3 months of de-escalation, adverse events associated with treatment, including lethargy, diarrhea, rash, and nausea, all improved.
Adverse events during de-escalation occurred in 16 patients, and included one fatality due to worsening of peripheral arterial occlusive disease, but all were deemed unrelated to the TKI or underlying chronic CML, the investigators noted.
Study subjects were adults with positive BCR-ABL1 transcripts, with either e13a2, e14a2, or e19a2 fusion transcript. They were enrolled between December 2013 and April 2015 from 20 hospitals in the United Kingdom; 148 were receiving imatinib, 16 were receiving nilotinib, and 10 were receiving dasatinib. They received half of their standard dose of imatinib (200 mg daily), dasatinib (50 mg daily), or nilotinib (200 mg twice daily) for 12 months. Recurrence during de-escalation was defined as BCR-ABL1:ABL1 ratio greater than 0.1% on two consecutive measurements.
“Although several studies of TKI cessation have been reported, little is known about the feasibility of treatment de-escalation in patients with stable molecular responses,” the investigators wrote, adding that the current study shows that de-escalation is “clearly safe for patients in stable MR4 or deeper remission” and could be a “reasonable option.”
This “practice-changing view” is reinforced by the finding of general improvement of adverse events in both cohorts, they said.
Also of note, de-escalation in this study was associated with savings of almost half the expected TKI costs, they added.
The findings imply that many patients with stable responses might be able to maintain responses on lower TKI doses, they concluded, adding that studies of more ambitious de-escalation are warranted.
Newcastle University and Bloodwise funded the study. Dr. Clark received other grants from Bloodwise during the study, as well as grants and personal fees from Novartis, Bristol-Myers Squibb, and Pfizer, and personal fees from Ariad/Incyte.
FROM LANCET HAEMATOLOGY
Key clinical point:
Major finding: Only 12 of 174 CML patients had molecular recurrence during 12 months of half-dose TKI therapy, and all regained MMR within 4 months of being back on full-dose TKIs.
Data source: The nonrandomized phase 2 DESTINY study of 174 adults with CML.
Disclosures: Newcastle University and Bloodwise funded the study. Dr. Clark received other grants from Bloodwise during the study, as well as grants and personal fees from Novartis, Bristol-Myers Squibb, and Pfizer, and personal fees from Ariad/Incyte.
Enhanced antimicrobial prophylaxis cuts advanced HIV mortality
An enhanced antimicrobial prophylaxis regimen administered to patients with advanced HIV infection who were starting antiretroviral therapy for the first time led to significantly reduced mortality after 24 weeks, compared with patients who received standard antimicrobial prophylaxis, in a randomized, multicenter trial with 1,805 patients.
The enhanced prophylaxis regimen tested “is relatively inexpensive, has a low pill burden and an acceptable side effect profile, and would be easy to implement at primary health centers,” according to James Hakim, MD, and his associates. The report was published July 20 (N Engl J Med. 2017 July 20;377[3]:233-45).
The researchers who ran the Reduction of Early Mortality in HIV-Infected Adults and Children Starting Antiretroviral Therapy (REALITY) trial enrolled HIV-infected patients who were at least 5 years old who had not previously received antiretroviral therapy and had a CD4+ T cell count of fewer than 100 cells/mm3 at the time of entry. Enrollment occurred during June 2013–April 2015 at eight centers in Kenya, Malawi, Uganda, or Zimbabwe. All patients started treatment with two nucleoside and one non-nucleoside reverse-transcriptase inhibitors.
After randomization, 906 patients entered the subgroup that received enhanced prophylaxis with a single dose of albendazole, 5 days of azithromycin, 12 weeks of fluconazole, and open-ended prophylaxis with trimethoprim-sulfamethoxazole, isoniazid, and pyridoxine (use of isoniazid and pyridoxine beyond 12 weeks depended on national guidelines in each country). Another 899 patients entered the subgroup that received standard antimicrobial prophylaxis with trimethoprim-sulfamethoxazole and isoniazid only.
All-cause mortality at 24 weeks after entry was the primary endpoint. This occurred in about 9% of patients on enhanced prophylaxis and about 12% of those on standard prophylaxis, which calculated to a statistically significant relative risk reduction of 27% with enhanced prophylaxis, and a number needed to treat of 30 patients with enhanced prophylaxis to prevent one additional death. At 48 weeks after entry, the relative risk reduction for all-cause mortality with enhanced prophylaxis was a statistically significant 24% lower with enhanced prophylaxis.
Enhanced prophylaxis also led to significant gains in life years and quality-adjusted life years. Based on actual drug costs, enhanced prophylaxis cost $613 per life year gained and $761 per quality-adjusted life year gained.
The REALITY trial received no commercial support. Dr. Hakim has been an adviser to Mylan and a consultant to Gilead and Johnson & Johnson.
[email protected]
On Twitter @mitchelzoler
A substantial number of HIV patients, when first diagnosed, continue to have advanced infection, defined by the World Health Organization as a CD4+ T cell count of fewer than 200 cell/mm3. In the REALITY trial, nearly half the patients with a CD4+ T cell count of fewer than 100 cells/mm3 at the time of their initial HIV diagnosis had mild or no symptoms. This finding highlights the limitations of relying on clinical assessment alone to identify people infected with HIV and needing testing and treatment.
In addition to showing the efficacy of enhanced antimicrobial prophylaxis compared with standard prophylaxis in the types of patients studied in REALITY, the results showed that the enhanced prophylaxis regimen had an acceptable side-effect profile, a high level of patient adherence to prophylaxis treatment, and no discernible effect on adherence to antiretroviral therapy. Nevertheless, the regimen used raises some concerns that warrant careful assessment: What is the risk posed by the enhanced regimen tested to producing microbial resistance to fluconazole or azithromycin? And is blanket use of this prophylaxis cost effective in locations where diagnostic testing for microbial infections is available?
The relatively consistent proportion of HIV-infected patients who newly present with a low CD4+ T cell count, as well as the seriously ill patients who return for care after an interruption in their HIV treatment, both call for renewed focus on the needs of patients with advanced HIV infection who have a high risk for illness and death.
Nathan Ford, PhD, and Meg Doherty, MD , are in the department of HIV/AIDS at the World Health Organization in Geneva. They had no disclosures. Their comments appeared in an editorial that accompanied the REALITY trial report ( N Engl J Med. 2017 Jul 20;377[3]:283-4 ).
A substantial number of HIV patients, when first diagnosed, continue to have advanced infection, defined by the World Health Organization as a CD4+ T cell count of fewer than 200 cell/mm3. In the REALITY trial, nearly half the patients with a CD4+ T cell count of fewer than 100 cells/mm3 at the time of their initial HIV diagnosis had mild or no symptoms. This finding highlights the limitations of relying on clinical assessment alone to identify people infected with HIV and needing testing and treatment.
In addition to showing the efficacy of enhanced antimicrobial prophylaxis compared with standard prophylaxis in the types of patients studied in REALITY, the results showed that the enhanced prophylaxis regimen had an acceptable side-effect profile, a high level of patient adherence to prophylaxis treatment, and no discernible effect on adherence to antiretroviral therapy. Nevertheless, the regimen used raises some concerns that warrant careful assessment: What is the risk posed by the enhanced regimen tested to producing microbial resistance to fluconazole or azithromycin? And is blanket use of this prophylaxis cost effective in locations where diagnostic testing for microbial infections is available?
The relatively consistent proportion of HIV-infected patients who newly present with a low CD4+ T cell count, as well as the seriously ill patients who return for care after an interruption in their HIV treatment, both call for renewed focus on the needs of patients with advanced HIV infection who have a high risk for illness and death.
Nathan Ford, PhD, and Meg Doherty, MD , are in the department of HIV/AIDS at the World Health Organization in Geneva. They had no disclosures. Their comments appeared in an editorial that accompanied the REALITY trial report ( N Engl J Med. 2017 Jul 20;377[3]:283-4 ).
A substantial number of HIV patients, when first diagnosed, continue to have advanced infection, defined by the World Health Organization as a CD4+ T cell count of fewer than 200 cell/mm3. In the REALITY trial, nearly half the patients with a CD4+ T cell count of fewer than 100 cells/mm3 at the time of their initial HIV diagnosis had mild or no symptoms. This finding highlights the limitations of relying on clinical assessment alone to identify people infected with HIV and needing testing and treatment.
In addition to showing the efficacy of enhanced antimicrobial prophylaxis compared with standard prophylaxis in the types of patients studied in REALITY, the results showed that the enhanced prophylaxis regimen had an acceptable side-effect profile, a high level of patient adherence to prophylaxis treatment, and no discernible effect on adherence to antiretroviral therapy. Nevertheless, the regimen used raises some concerns that warrant careful assessment: What is the risk posed by the enhanced regimen tested to producing microbial resistance to fluconazole or azithromycin? And is blanket use of this prophylaxis cost effective in locations where diagnostic testing for microbial infections is available?
The relatively consistent proportion of HIV-infected patients who newly present with a low CD4+ T cell count, as well as the seriously ill patients who return for care after an interruption in their HIV treatment, both call for renewed focus on the needs of patients with advanced HIV infection who have a high risk for illness and death.
Nathan Ford, PhD, and Meg Doherty, MD , are in the department of HIV/AIDS at the World Health Organization in Geneva. They had no disclosures. Their comments appeared in an editorial that accompanied the REALITY trial report ( N Engl J Med. 2017 Jul 20;377[3]:283-4 ).
An enhanced antimicrobial prophylaxis regimen administered to patients with advanced HIV infection who were starting antiretroviral therapy for the first time led to significantly reduced mortality after 24 weeks, compared with patients who received standard antimicrobial prophylaxis, in a randomized, multicenter trial with 1,805 patients.
The enhanced prophylaxis regimen tested “is relatively inexpensive, has a low pill burden and an acceptable side effect profile, and would be easy to implement at primary health centers,” according to James Hakim, MD, and his associates. The report was published July 20 (N Engl J Med. 2017 July 20;377[3]:233-45).
The researchers who ran the Reduction of Early Mortality in HIV-Infected Adults and Children Starting Antiretroviral Therapy (REALITY) trial enrolled HIV-infected patients who were at least 5 years old who had not previously received antiretroviral therapy and had a CD4+ T cell count of fewer than 100 cells/mm3 at the time of entry. Enrollment occurred during June 2013–April 2015 at eight centers in Kenya, Malawi, Uganda, or Zimbabwe. All patients started treatment with two nucleoside and one non-nucleoside reverse-transcriptase inhibitors.
After randomization, 906 patients entered the subgroup that received enhanced prophylaxis with a single dose of albendazole, 5 days of azithromycin, 12 weeks of fluconazole, and open-ended prophylaxis with trimethoprim-sulfamethoxazole, isoniazid, and pyridoxine (use of isoniazid and pyridoxine beyond 12 weeks depended on national guidelines in each country). Another 899 patients entered the subgroup that received standard antimicrobial prophylaxis with trimethoprim-sulfamethoxazole and isoniazid only.
All-cause mortality at 24 weeks after entry was the primary endpoint. This occurred in about 9% of patients on enhanced prophylaxis and about 12% of those on standard prophylaxis, which calculated to a statistically significant relative risk reduction of 27% with enhanced prophylaxis, and a number needed to treat of 30 patients with enhanced prophylaxis to prevent one additional death. At 48 weeks after entry, the relative risk reduction for all-cause mortality with enhanced prophylaxis was a statistically significant 24% lower with enhanced prophylaxis.
Enhanced prophylaxis also led to significant gains in life years and quality-adjusted life years. Based on actual drug costs, enhanced prophylaxis cost $613 per life year gained and $761 per quality-adjusted life year gained.
The REALITY trial received no commercial support. Dr. Hakim has been an adviser to Mylan and a consultant to Gilead and Johnson & Johnson.
[email protected]
On Twitter @mitchelzoler
An enhanced antimicrobial prophylaxis regimen administered to patients with advanced HIV infection who were starting antiretroviral therapy for the first time led to significantly reduced mortality after 24 weeks, compared with patients who received standard antimicrobial prophylaxis, in a randomized, multicenter trial with 1,805 patients.
The enhanced prophylaxis regimen tested “is relatively inexpensive, has a low pill burden and an acceptable side effect profile, and would be easy to implement at primary health centers,” according to James Hakim, MD, and his associates. The report was published July 20 (N Engl J Med. 2017 July 20;377[3]:233-45).
The researchers who ran the Reduction of Early Mortality in HIV-Infected Adults and Children Starting Antiretroviral Therapy (REALITY) trial enrolled HIV-infected patients who were at least 5 years old who had not previously received antiretroviral therapy and had a CD4+ T cell count of fewer than 100 cells/mm3 at the time of entry. Enrollment occurred during June 2013–April 2015 at eight centers in Kenya, Malawi, Uganda, or Zimbabwe. All patients started treatment with two nucleoside and one non-nucleoside reverse-transcriptase inhibitors.
After randomization, 906 patients entered the subgroup that received enhanced prophylaxis with a single dose of albendazole, 5 days of azithromycin, 12 weeks of fluconazole, and open-ended prophylaxis with trimethoprim-sulfamethoxazole, isoniazid, and pyridoxine (use of isoniazid and pyridoxine beyond 12 weeks depended on national guidelines in each country). Another 899 patients entered the subgroup that received standard antimicrobial prophylaxis with trimethoprim-sulfamethoxazole and isoniazid only.
All-cause mortality at 24 weeks after entry was the primary endpoint. This occurred in about 9% of patients on enhanced prophylaxis and about 12% of those on standard prophylaxis, which calculated to a statistically significant relative risk reduction of 27% with enhanced prophylaxis, and a number needed to treat of 30 patients with enhanced prophylaxis to prevent one additional death. At 48 weeks after entry, the relative risk reduction for all-cause mortality with enhanced prophylaxis was a statistically significant 24% lower with enhanced prophylaxis.
Enhanced prophylaxis also led to significant gains in life years and quality-adjusted life years. Based on actual drug costs, enhanced prophylaxis cost $613 per life year gained and $761 per quality-adjusted life year gained.
The REALITY trial received no commercial support. Dr. Hakim has been an adviser to Mylan and a consultant to Gilead and Johnson & Johnson.
[email protected]
On Twitter @mitchelzoler
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: Enhanced prophylaxis cut mortality by a relative 27% compared with standard prophylaxis after 24 weeks.
Data source: REALITY, a multicenter randomized trial with 1,805 patients.
Disclosures: REALITY received no commercial support. Dr. Hakim has been an adviser to Mylan and a consultant to Gilead and Johnson & Johnson.
Lower Limb Morel-Lavallée Lesion Treated With Short-Stretch Compression Bandaging
Take-Home Points
- Have a high-index of suspicion for MLLs and initiate treatment early.
- Compression needs to occur through short-stretch bandaging over a conventional Ace wrap in order to be successful.
- Apply the short-stretch compression with care to avoid shearing underlying tissue.
- Nonoperative treatment modalities require high patient compliance.
- MLLs need close monitoring until final healing occurs.
Morel-Lavallée lesions (MLLs) are traumatic degloving injuries resulting from separation of subcutaneous fat from underlying fascia. MLLs occur in association with acetabular fractures and are also associated with low-velocity crush injuries.1,2 Shearing creates a “false” space that is filled with hemorrhaged blood, fat, and lymphatic tissue.3 Disruption of the lymphatics leads to cavity formation and, eventually, a fibrotic pseudocapsule.4The pseudocapsule prevents resorption, leading to a chronic fluid collection, which potentiates the risk of infection or tissue necrosis.3,5,6 Skin necrosis may occur through direct-pressure compromise of the dermal vascular plexus.4 Necrotic skin may require multiple débridements, negative-pressure wound therapy or soft-tissue coverage, and may ultimately result in infection. MLLs classically occur in the greater trochanteric region, lateral thigh, buttocks, and back but also appear in the prepatellar region.1,3 Patients present with soft-tissue swelling, bruising, bulging, decreased cutaneous sensation over the region, and a palpable, fluctuant subcutaneous fluid collection with mobile skin.2,4,7 The mechanism of injury may cause a concomitant fracture. Magnetic resonance imaging (MRI), the preferred imaging modality, shows a discrete fluid collection between subcutaneous fat and underlying fascia. Ultrasonography may reveal a thickened capsule surrounding either a hypoechoic area or an anechoic area but its accuracy is user-dependent.7
Large MLLs may be treated with open serial débridement and healing by secondary intention; infection rates, however, are high. Authors have described several other treatment modalities, including percutaneous débridement with a brush followed by use of a large-bore drain and antibiotics; open débridement with meticulous dead-space closure; elastic compression bandaging; aspiration; and doxycycline sclerodesis.1,5,6,8,9 Modifications of short-stretch compression bandaging were recently described in edema control for hindfoot trauma, ankle trauma, and total ankle arthroplasty, but not for MLLs.10,11 Nickerson and colleagues4 retrospectively reviewed 87 MLLs, found that fluid aspirate of >50 mL predicted recurrence and failure with conservative measures, and recommended operative intervention for any MLL with >50 mL of fluid aspirated.
We report the case of an MLL that occurred in an unusual anatomical region, and we describe a novel application of a conservative treatment, which was selected on the basis of its success in lymphedema management. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 66-year-old man was injured when a parked vehicle began moving, pulled him under, and ran over his lower right leg. In the emergency department, no fractures or major injuries were noted (Figures 1A, 1B), and the patient was discharged.
About 10 days after injury, profuse ecchymosis and swelling were noted running from the distal medial thigh to the proximal medial calf (Figures 2A-2C).
Given the size of the MLL, the fluid collection reaccumulated. The patient was evaluated by an orthopedic traumatologist 3 days after the aspiration (17 days after injury).
Another orthopedic traumatologist confirmed the low likelihood that compression would resolve the MLL, given its size (Figures 4A, 4B). 

After the second orthopedic consultation, the patient saw a physical therapist trained in complete decongestive therapy. The therapist suggested placing short-stretch bandage wraps over the conventional long-stretch Ace bandage currently being used—a treatment common in lymphedema. The patient was wrapped from toe to groin without an initial layer of padding (Figures 6A, 6B), and the response was immediate. 
Nine weeks after injury, the leg was significantly improved, and clinical signs resolved (Figure 7). 
Discussion
Short-stretch bandaging has been performed mainly in lymphedema and ulcer management. 
Compression bandaging reduces volume in lymphedematous limbs by reducing capillary filtration, shifting fluid into noncompressed parts of the body, increasing lymphatic reabsorption and lymphatic transport stimulation, improving venous pumping, and breaking down fibrosclerotic tissue.15 We think containment, improved venous flow, and enhanced muscle contraction contributed to the effectiveness of short-stretch bandaging as treatment for our patient’s MLL. Because MLLs also contain disrupted lymphatics, lymphedema management strategies (eg, short-stretch bandages) can be used. Our patient rapidly improved after conversion to short-stretch bandages.
These bandages are applied with 50% overlap to ensure even pressures throughout.16 Multiple layers are applied using a combination of spiral and figure-of-8 techniques, first clockwise and then counterclockwise, to avoid shearing underlying tissue.17 This method is very important in MLL treatment, given the degloving involved and the highly mobile skin and subcutaneous fat.
In standard lymphedema management, a foam padding layer is applied before the short-stretch bandage in order to reshape the limb and avoid proximal constrictions.13 In our patient’s case, the short-stretch wrap was applied without padding. Because his condition was acute, and the limb contour was preserved, limb reshaping and thus padding were not necessary.
Given the rapid, high-volume reduction that occurs within the first 1 to 2 weeks, bandages are reapplied daily to effectively adjust for the decreased swelling and altered limb shape.17 Most improvement is expected within the first few weeks—consistent with our patient’s case. Bandages usually are applied to the entire limb. For partial cases, the bandaging must extend past the area of swelling and incorporate the knee to prevent displacement of fluid into the joint.17 Feet and ankles are bandaged in dorsiflexion.17Several factors must be considered with short-stretch wraps. For example, pressure may need to be adjusted in patients with peripheral vascular disease. In patients with ankle-brachial indexes >0.5, it is safe to apply pressure up to 40 mm Hg.12 Reduced pressure is recommended for patients with arterial disease, sensory disturbance, lipoedema, poor mobility, frailty, or palliative needs.13The unusual location of our patient’s MLL accounts for the delay in diagnosis. To our knowledge, no other authors have reported such a large MLL in this location. A few series and case reports have listed MLLs in the calf near the gastrocnemius muscle, in the ankle, in the prepatellar area, and in the suprapatellar region, including the thigh,1,3,18-20 but there are no reports of MLLs running from medial thigh to proximal calf. MLLs of this size classically are treated surgically, but our patient selected nonoperative management.
To our knowledge, there are no earlier reports of using this nonoperative technique to treat MLLs. Conservative treatment with compression has been discussed, but no case involved short-stretch bandages. Large MLLs are thought to require surgery plus some type of drainage. The success of using short-stretch bandages in our patient’s case should prompt further investigation of use in adherent patients—which could ultimately result in reduced surgical needs, improved wound care (surgery is avoided), and a maintained low risk of infection. Although more work is needed to come to a more definitive verdict on this treatment method, it is a promising option that warrants consideration.
Am J Orthop. 2017;46(4):E213-E218. Copyright Frontline Medical Communications Inc. 2017. All rights reserved.
1. Tejwani SG, Cohen SB, Bradley JP. Management of Morel-Lavallee lesion of the knee: twenty-seven cases in the National Football League. Am J Sports Med. 2007;35(7):1162-1167.
2. Tsur A, Galin A, Kogan L, Loberant N. Morel-Lavallee syndrome after crush injury [in Hebrew]. Harefuah. 2006;145(2):111-113.
3. Ciaschini M, Sundaram M. Radiologic case study. Prepatellar Morel-Lavallée lesion. Orthopedics. 2008;31(7):626, 719-721.
4. Nickerson TP, Zielinski MD, Jenkins DH, Schiller HJ. The Mayo Clinic experience with Morel-Lavallée lesions: establishment of a practice management guideline. J Trauma Acute Care Surg. 2014;76(2):493-497.
5. Bansal A, Bhatia N, Singh A, Singh AK. Doxycycline sclerodesis as a treatment option for persistent Morel-Lavallée lesions. Injury. 2013;44(1):66-69.
6. Carlson DA, Simmons J, Sando W, Weber T, Clements B. Morel-Lavalée lesions treated with debridement and meticulous dead space closure: surgical technique. J Orthop Trauma. 2007;21(2):140-144.
7. Miller J, Daggett J, Ambay R, Payne WG. Morel-Lavallée lesion. Eplasty. 2014;14:ic12.
8. Tseng S, Tornetta P 3rd. Percutaneous management of Morel-Lavallee lesions. J Bone Joint Surg Am. 2006;88(1):92-96.
9. Harma A, Inan M, Ertem K. The Morel-Lavallée lesion: a conservative approach to closed degloving injuries [in Turkish]. Acta Orthop Traumatol Turc. 2004;38(4):270-273.
10. Hsu A, Franceschina D, Haddad SL. A novel method of postoperative wound care following total ankle arthroplasty. Foot Ankle Int. 2014;35(7):719-724.
11. Rohner-Spengler M, Frotzler A, Honigmann P, Babst R. Effective treatment of posttraumatic and postoperative edema in patients with ankle and hindfoot fractures: a randomized controlled trial comparing multilayer compression therapy and intermittent impulse compression with the standard treatment with ice. J Bone Joint Surg Am. 2014;96(15):1263-1271.
12. Bjork R. The long and short of it: understanding compression bandaging. Wound Care Advisor. 2013;2(6):12-15.
13. Partsch H. Assessing the effectiveness of multilayer inelastic bandaging. J Lymphoedema. 2007;2(2):55-61.
14. Hafner J, Botonakis I, Burg G. A comparison of multilayer bandage systems during rest, exercise, and over 2 days of wear time. Arch Dermatol. 2000;136(7):857-863.
15. Földi E, Jünger M, Partsch H. The science of lymphoedema bandaging. In: Lymphoedema Bandaging in Practice [European Wound Management Association focus document]. London, England: Medical Education Partnership; 2005:2-4.
16. King TI, Droessler JL. Physical properties of short-stretch compression bandages used to treat lymphedema. Am J Occup Ther. 2001;55(5):573-576.
17. Williams AF, Keller M. Practical guidance on lymphoedema bandaging of the upper and lower limbs. In: Lymphoedema Bandaging in Practice [European Wound Management Association focus document]. London, England: Medical Education Partnership; 2005:10-14.
18. Moriarty JM, Borrero CG, Kavanagh EC. A rare cause of calf swelling: the Morel-Lavallee lesion. Ir J Med Sci. 2011;180(1):265-268.
19. Anakwenze OA, Trivedi V, Goodman AM, Ganley TJ. Knee Morel-Lavallee lesion after a football injury in an 11-year-old boy: case report and review of the literature. Univ Pa Orthop J. 2011;21:56-58.
20. Hudson DA, Knottenbelt JD, Krige JE. Closed degloving injuries: results following conservative surgery. Plast Reconstr Surg. 1992;89(5):853-855.
Take-Home Points
- Have a high-index of suspicion for MLLs and initiate treatment early.
- Compression needs to occur through short-stretch bandaging over a conventional Ace wrap in order to be successful.
- Apply the short-stretch compression with care to avoid shearing underlying tissue.
- Nonoperative treatment modalities require high patient compliance.
- MLLs need close monitoring until final healing occurs.
Morel-Lavallée lesions (MLLs) are traumatic degloving injuries resulting from separation of subcutaneous fat from underlying fascia. MLLs occur in association with acetabular fractures and are also associated with low-velocity crush injuries.1,2 Shearing creates a “false” space that is filled with hemorrhaged blood, fat, and lymphatic tissue.3 Disruption of the lymphatics leads to cavity formation and, eventually, a fibrotic pseudocapsule.4The pseudocapsule prevents resorption, leading to a chronic fluid collection, which potentiates the risk of infection or tissue necrosis.3,5,6 Skin necrosis may occur through direct-pressure compromise of the dermal vascular plexus.4 Necrotic skin may require multiple débridements, negative-pressure wound therapy or soft-tissue coverage, and may ultimately result in infection. MLLs classically occur in the greater trochanteric region, lateral thigh, buttocks, and back but also appear in the prepatellar region.1,3 Patients present with soft-tissue swelling, bruising, bulging, decreased cutaneous sensation over the region, and a palpable, fluctuant subcutaneous fluid collection with mobile skin.2,4,7 The mechanism of injury may cause a concomitant fracture. Magnetic resonance imaging (MRI), the preferred imaging modality, shows a discrete fluid collection between subcutaneous fat and underlying fascia. Ultrasonography may reveal a thickened capsule surrounding either a hypoechoic area or an anechoic area but its accuracy is user-dependent.7
Large MLLs may be treated with open serial débridement and healing by secondary intention; infection rates, however, are high. Authors have described several other treatment modalities, including percutaneous débridement with a brush followed by use of a large-bore drain and antibiotics; open débridement with meticulous dead-space closure; elastic compression bandaging; aspiration; and doxycycline sclerodesis.1,5,6,8,9 Modifications of short-stretch compression bandaging were recently described in edema control for hindfoot trauma, ankle trauma, and total ankle arthroplasty, but not for MLLs.10,11 Nickerson and colleagues4 retrospectively reviewed 87 MLLs, found that fluid aspirate of >50 mL predicted recurrence and failure with conservative measures, and recommended operative intervention for any MLL with >50 mL of fluid aspirated.
We report the case of an MLL that occurred in an unusual anatomical region, and we describe a novel application of a conservative treatment, which was selected on the basis of its success in lymphedema management. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 66-year-old man was injured when a parked vehicle began moving, pulled him under, and ran over his lower right leg. In the emergency department, no fractures or major injuries were noted (Figures 1A, 1B), and the patient was discharged.
About 10 days after injury, profuse ecchymosis and swelling were noted running from the distal medial thigh to the proximal medial calf (Figures 2A-2C).
Given the size of the MLL, the fluid collection reaccumulated. The patient was evaluated by an orthopedic traumatologist 3 days after the aspiration (17 days after injury).
Another orthopedic traumatologist confirmed the low likelihood that compression would resolve the MLL, given its size (Figures 4A, 4B).
After the second orthopedic consultation, the patient saw a physical therapist trained in complete decongestive therapy. The therapist suggested placing short-stretch bandage wraps over the conventional long-stretch Ace bandage currently being used—a treatment common in lymphedema. The patient was wrapped from toe to groin without an initial layer of padding (Figures 6A, 6B), and the response was immediate.
Nine weeks after injury, the leg was significantly improved, and clinical signs resolved (Figure 7).
Discussion
Short-stretch bandaging has been performed mainly in lymphedema and ulcer management.
Compression bandaging reduces volume in lymphedematous limbs by reducing capillary filtration, shifting fluid into noncompressed parts of the body, increasing lymphatic reabsorption and lymphatic transport stimulation, improving venous pumping, and breaking down fibrosclerotic tissue.15 We think containment, improved venous flow, and enhanced muscle contraction contributed to the effectiveness of short-stretch bandaging as treatment for our patient’s MLL. Because MLLs also contain disrupted lymphatics, lymphedema management strategies (eg, short-stretch bandages) can be used. Our patient rapidly improved after conversion to short-stretch bandages.
These bandages are applied with 50% overlap to ensure even pressures throughout.16 Multiple layers are applied using a combination of spiral and figure-of-8 techniques, first clockwise and then counterclockwise, to avoid shearing underlying tissue.17 This method is very important in MLL treatment, given the degloving involved and the highly mobile skin and subcutaneous fat.
In standard lymphedema management, a foam padding layer is applied before the short-stretch bandage in order to reshape the limb and avoid proximal constrictions.13 In our patient’s case, the short-stretch wrap was applied without padding. Because his condition was acute, and the limb contour was preserved, limb reshaping and thus padding were not necessary.
Given the rapid, high-volume reduction that occurs within the first 1 to 2 weeks, bandages are reapplied daily to effectively adjust for the decreased swelling and altered limb shape.17 Most improvement is expected within the first few weeks—consistent with our patient’s case. Bandages usually are applied to the entire limb. For partial cases, the bandaging must extend past the area of swelling and incorporate the knee to prevent displacement of fluid into the joint.17 Feet and ankles are bandaged in dorsiflexion.17Several factors must be considered with short-stretch wraps. For example, pressure may need to be adjusted in patients with peripheral vascular disease. In patients with ankle-brachial indexes >0.5, it is safe to apply pressure up to 40 mm Hg.12 Reduced pressure is recommended for patients with arterial disease, sensory disturbance, lipoedema, poor mobility, frailty, or palliative needs.13The unusual location of our patient’s MLL accounts for the delay in diagnosis. To our knowledge, no other authors have reported such a large MLL in this location. A few series and case reports have listed MLLs in the calf near the gastrocnemius muscle, in the ankle, in the prepatellar area, and in the suprapatellar region, including the thigh,1,3,18-20 but there are no reports of MLLs running from medial thigh to proximal calf. MLLs of this size classically are treated surgically, but our patient selected nonoperative management.
To our knowledge, there are no earlier reports of using this nonoperative technique to treat MLLs. Conservative treatment with compression has been discussed, but no case involved short-stretch bandages. Large MLLs are thought to require surgery plus some type of drainage. The success of using short-stretch bandages in our patient’s case should prompt further investigation of use in adherent patients—which could ultimately result in reduced surgical needs, improved wound care (surgery is avoided), and a maintained low risk of infection. Although more work is needed to come to a more definitive verdict on this treatment method, it is a promising option that warrants consideration.
Am J Orthop. 2017;46(4):E213-E218. Copyright Frontline Medical Communications Inc. 2017. All rights reserved.
Take-Home Points
- Have a high-index of suspicion for MLLs and initiate treatment early.
- Compression needs to occur through short-stretch bandaging over a conventional Ace wrap in order to be successful.
- Apply the short-stretch compression with care to avoid shearing underlying tissue.
- Nonoperative treatment modalities require high patient compliance.
- MLLs need close monitoring until final healing occurs.
Morel-Lavallée lesions (MLLs) are traumatic degloving injuries resulting from separation of subcutaneous fat from underlying fascia. MLLs occur in association with acetabular fractures and are also associated with low-velocity crush injuries.1,2 Shearing creates a “false” space that is filled with hemorrhaged blood, fat, and lymphatic tissue.3 Disruption of the lymphatics leads to cavity formation and, eventually, a fibrotic pseudocapsule.4The pseudocapsule prevents resorption, leading to a chronic fluid collection, which potentiates the risk of infection or tissue necrosis.3,5,6 Skin necrosis may occur through direct-pressure compromise of the dermal vascular plexus.4 Necrotic skin may require multiple débridements, negative-pressure wound therapy or soft-tissue coverage, and may ultimately result in infection. MLLs classically occur in the greater trochanteric region, lateral thigh, buttocks, and back but also appear in the prepatellar region.1,3 Patients present with soft-tissue swelling, bruising, bulging, decreased cutaneous sensation over the region, and a palpable, fluctuant subcutaneous fluid collection with mobile skin.2,4,7 The mechanism of injury may cause a concomitant fracture. Magnetic resonance imaging (MRI), the preferred imaging modality, shows a discrete fluid collection between subcutaneous fat and underlying fascia. Ultrasonography may reveal a thickened capsule surrounding either a hypoechoic area or an anechoic area but its accuracy is user-dependent.7
Large MLLs may be treated with open serial débridement and healing by secondary intention; infection rates, however, are high. Authors have described several other treatment modalities, including percutaneous débridement with a brush followed by use of a large-bore drain and antibiotics; open débridement with meticulous dead-space closure; elastic compression bandaging; aspiration; and doxycycline sclerodesis.1,5,6,8,9 Modifications of short-stretch compression bandaging were recently described in edema control for hindfoot trauma, ankle trauma, and total ankle arthroplasty, but not for MLLs.10,11 Nickerson and colleagues4 retrospectively reviewed 87 MLLs, found that fluid aspirate of >50 mL predicted recurrence and failure with conservative measures, and recommended operative intervention for any MLL with >50 mL of fluid aspirated.
We report the case of an MLL that occurred in an unusual anatomical region, and we describe a novel application of a conservative treatment, which was selected on the basis of its success in lymphedema management. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 66-year-old man was injured when a parked vehicle began moving, pulled him under, and ran over his lower right leg. In the emergency department, no fractures or major injuries were noted (Figures 1A, 1B), and the patient was discharged.
About 10 days after injury, profuse ecchymosis and swelling were noted running from the distal medial thigh to the proximal medial calf (Figures 2A-2C).
Given the size of the MLL, the fluid collection reaccumulated. The patient was evaluated by an orthopedic traumatologist 3 days after the aspiration (17 days after injury).
Another orthopedic traumatologist confirmed the low likelihood that compression would resolve the MLL, given its size (Figures 4A, 4B).
After the second orthopedic consultation, the patient saw a physical therapist trained in complete decongestive therapy. The therapist suggested placing short-stretch bandage wraps over the conventional long-stretch Ace bandage currently being used—a treatment common in lymphedema. The patient was wrapped from toe to groin without an initial layer of padding (Figures 6A, 6B), and the response was immediate.
Nine weeks after injury, the leg was significantly improved, and clinical signs resolved (Figure 7).
Discussion
Short-stretch bandaging has been performed mainly in lymphedema and ulcer management.
Compression bandaging reduces volume in lymphedematous limbs by reducing capillary filtration, shifting fluid into noncompressed parts of the body, increasing lymphatic reabsorption and lymphatic transport stimulation, improving venous pumping, and breaking down fibrosclerotic tissue.15 We think containment, improved venous flow, and enhanced muscle contraction contributed to the effectiveness of short-stretch bandaging as treatment for our patient’s MLL. Because MLLs also contain disrupted lymphatics, lymphedema management strategies (eg, short-stretch bandages) can be used. Our patient rapidly improved after conversion to short-stretch bandages.
These bandages are applied with 50% overlap to ensure even pressures throughout.16 Multiple layers are applied using a combination of spiral and figure-of-8 techniques, first clockwise and then counterclockwise, to avoid shearing underlying tissue.17 This method is very important in MLL treatment, given the degloving involved and the highly mobile skin and subcutaneous fat.
In standard lymphedema management, a foam padding layer is applied before the short-stretch bandage in order to reshape the limb and avoid proximal constrictions.13 In our patient’s case, the short-stretch wrap was applied without padding. Because his condition was acute, and the limb contour was preserved, limb reshaping and thus padding were not necessary.
Given the rapid, high-volume reduction that occurs within the first 1 to 2 weeks, bandages are reapplied daily to effectively adjust for the decreased swelling and altered limb shape.17 Most improvement is expected within the first few weeks—consistent with our patient’s case. Bandages usually are applied to the entire limb. For partial cases, the bandaging must extend past the area of swelling and incorporate the knee to prevent displacement of fluid into the joint.17 Feet and ankles are bandaged in dorsiflexion.17Several factors must be considered with short-stretch wraps. For example, pressure may need to be adjusted in patients with peripheral vascular disease. In patients with ankle-brachial indexes >0.5, it is safe to apply pressure up to 40 mm Hg.12 Reduced pressure is recommended for patients with arterial disease, sensory disturbance, lipoedema, poor mobility, frailty, or palliative needs.13The unusual location of our patient’s MLL accounts for the delay in diagnosis. To our knowledge, no other authors have reported such a large MLL in this location. A few series and case reports have listed MLLs in the calf near the gastrocnemius muscle, in the ankle, in the prepatellar area, and in the suprapatellar region, including the thigh,1,3,18-20 but there are no reports of MLLs running from medial thigh to proximal calf. MLLs of this size classically are treated surgically, but our patient selected nonoperative management.
To our knowledge, there are no earlier reports of using this nonoperative technique to treat MLLs. Conservative treatment with compression has been discussed, but no case involved short-stretch bandages. Large MLLs are thought to require surgery plus some type of drainage. The success of using short-stretch bandages in our patient’s case should prompt further investigation of use in adherent patients—which could ultimately result in reduced surgical needs, improved wound care (surgery is avoided), and a maintained low risk of infection. Although more work is needed to come to a more definitive verdict on this treatment method, it is a promising option that warrants consideration.
Am J Orthop. 2017;46(4):E213-E218. Copyright Frontline Medical Communications Inc. 2017. All rights reserved.
1. Tejwani SG, Cohen SB, Bradley JP. Management of Morel-Lavallee lesion of the knee: twenty-seven cases in the National Football League. Am J Sports Med. 2007;35(7):1162-1167.
2. Tsur A, Galin A, Kogan L, Loberant N. Morel-Lavallee syndrome after crush injury [in Hebrew]. Harefuah. 2006;145(2):111-113.
3. Ciaschini M, Sundaram M. Radiologic case study. Prepatellar Morel-Lavallée lesion. Orthopedics. 2008;31(7):626, 719-721.
4. Nickerson TP, Zielinski MD, Jenkins DH, Schiller HJ. The Mayo Clinic experience with Morel-Lavallée lesions: establishment of a practice management guideline. J Trauma Acute Care Surg. 2014;76(2):493-497.
5. Bansal A, Bhatia N, Singh A, Singh AK. Doxycycline sclerodesis as a treatment option for persistent Morel-Lavallée lesions. Injury. 2013;44(1):66-69.
6. Carlson DA, Simmons J, Sando W, Weber T, Clements B. Morel-Lavalée lesions treated with debridement and meticulous dead space closure: surgical technique. J Orthop Trauma. 2007;21(2):140-144.
7. Miller J, Daggett J, Ambay R, Payne WG. Morel-Lavallée lesion. Eplasty. 2014;14:ic12.
8. Tseng S, Tornetta P 3rd. Percutaneous management of Morel-Lavallee lesions. J Bone Joint Surg Am. 2006;88(1):92-96.
9. Harma A, Inan M, Ertem K. The Morel-Lavallée lesion: a conservative approach to closed degloving injuries [in Turkish]. Acta Orthop Traumatol Turc. 2004;38(4):270-273.
10. Hsu A, Franceschina D, Haddad SL. A novel method of postoperative wound care following total ankle arthroplasty. Foot Ankle Int. 2014;35(7):719-724.
11. Rohner-Spengler M, Frotzler A, Honigmann P, Babst R. Effective treatment of posttraumatic and postoperative edema in patients with ankle and hindfoot fractures: a randomized controlled trial comparing multilayer compression therapy and intermittent impulse compression with the standard treatment with ice. J Bone Joint Surg Am. 2014;96(15):1263-1271.
12. Bjork R. The long and short of it: understanding compression bandaging. Wound Care Advisor. 2013;2(6):12-15.
13. Partsch H. Assessing the effectiveness of multilayer inelastic bandaging. J Lymphoedema. 2007;2(2):55-61.
14. Hafner J, Botonakis I, Burg G. A comparison of multilayer bandage systems during rest, exercise, and over 2 days of wear time. Arch Dermatol. 2000;136(7):857-863.
15. Földi E, Jünger M, Partsch H. The science of lymphoedema bandaging. In: Lymphoedema Bandaging in Practice [European Wound Management Association focus document]. London, England: Medical Education Partnership; 2005:2-4.
16. King TI, Droessler JL. Physical properties of short-stretch compression bandages used to treat lymphedema. Am J Occup Ther. 2001;55(5):573-576.
17. Williams AF, Keller M. Practical guidance on lymphoedema bandaging of the upper and lower limbs. In: Lymphoedema Bandaging in Practice [European Wound Management Association focus document]. London, England: Medical Education Partnership; 2005:10-14.
18. Moriarty JM, Borrero CG, Kavanagh EC. A rare cause of calf swelling: the Morel-Lavallee lesion. Ir J Med Sci. 2011;180(1):265-268.
19. Anakwenze OA, Trivedi V, Goodman AM, Ganley TJ. Knee Morel-Lavallee lesion after a football injury in an 11-year-old boy: case report and review of the literature. Univ Pa Orthop J. 2011;21:56-58.
20. Hudson DA, Knottenbelt JD, Krige JE. Closed degloving injuries: results following conservative surgery. Plast Reconstr Surg. 1992;89(5):853-855.
1. Tejwani SG, Cohen SB, Bradley JP. Management of Morel-Lavallee lesion of the knee: twenty-seven cases in the National Football League. Am J Sports Med. 2007;35(7):1162-1167.
2. Tsur A, Galin A, Kogan L, Loberant N. Morel-Lavallee syndrome after crush injury [in Hebrew]. Harefuah. 2006;145(2):111-113.
3. Ciaschini M, Sundaram M. Radiologic case study. Prepatellar Morel-Lavallée lesion. Orthopedics. 2008;31(7):626, 719-721.
4. Nickerson TP, Zielinski MD, Jenkins DH, Schiller HJ. The Mayo Clinic experience with Morel-Lavallée lesions: establishment of a practice management guideline. J Trauma Acute Care Surg. 2014;76(2):493-497.
5. Bansal A, Bhatia N, Singh A, Singh AK. Doxycycline sclerodesis as a treatment option for persistent Morel-Lavallée lesions. Injury. 2013;44(1):66-69.
6. Carlson DA, Simmons J, Sando W, Weber T, Clements B. Morel-Lavalée lesions treated with debridement and meticulous dead space closure: surgical technique. J Orthop Trauma. 2007;21(2):140-144.
7. Miller J, Daggett J, Ambay R, Payne WG. Morel-Lavallée lesion. Eplasty. 2014;14:ic12.
8. Tseng S, Tornetta P 3rd. Percutaneous management of Morel-Lavallee lesions. J Bone Joint Surg Am. 2006;88(1):92-96.
9. Harma A, Inan M, Ertem K. The Morel-Lavallée lesion: a conservative approach to closed degloving injuries [in Turkish]. Acta Orthop Traumatol Turc. 2004;38(4):270-273.
10. Hsu A, Franceschina D, Haddad SL. A novel method of postoperative wound care following total ankle arthroplasty. Foot Ankle Int. 2014;35(7):719-724.
11. Rohner-Spengler M, Frotzler A, Honigmann P, Babst R. Effective treatment of posttraumatic and postoperative edema in patients with ankle and hindfoot fractures: a randomized controlled trial comparing multilayer compression therapy and intermittent impulse compression with the standard treatment with ice. J Bone Joint Surg Am. 2014;96(15):1263-1271.
12. Bjork R. The long and short of it: understanding compression bandaging. Wound Care Advisor. 2013;2(6):12-15.
13. Partsch H. Assessing the effectiveness of multilayer inelastic bandaging. J Lymphoedema. 2007;2(2):55-61.
14. Hafner J, Botonakis I, Burg G. A comparison of multilayer bandage systems during rest, exercise, and over 2 days of wear time. Arch Dermatol. 2000;136(7):857-863.
15. Földi E, Jünger M, Partsch H. The science of lymphoedema bandaging. In: Lymphoedema Bandaging in Practice [European Wound Management Association focus document]. London, England: Medical Education Partnership; 2005:2-4.
16. King TI, Droessler JL. Physical properties of short-stretch compression bandages used to treat lymphedema. Am J Occup Ther. 2001;55(5):573-576.
17. Williams AF, Keller M. Practical guidance on lymphoedema bandaging of the upper and lower limbs. In: Lymphoedema Bandaging in Practice [European Wound Management Association focus document]. London, England: Medical Education Partnership; 2005:10-14.
18. Moriarty JM, Borrero CG, Kavanagh EC. A rare cause of calf swelling: the Morel-Lavallee lesion. Ir J Med Sci. 2011;180(1):265-268.
19. Anakwenze OA, Trivedi V, Goodman AM, Ganley TJ. Knee Morel-Lavallee lesion after a football injury in an 11-year-old boy: case report and review of the literature. Univ Pa Orthop J. 2011;21:56-58.
20. Hudson DA, Knottenbelt JD, Krige JE. Closed degloving injuries: results following conservative surgery. Plast Reconstr Surg. 1992;89(5):853-855.
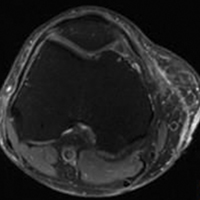
Algorithm-based trunk support system shows potential for recovery of walking ability
A multidirectional gravity-assist device that delivers precise trunk support to stroke and spinal cord injury (SCI) patients via an artificial intelligence algorithm has demonstrated significantly improved locomotor performance beyond treadmill-based systems in a new study.
The harness device used in the study adjusts patients’ balance while they stand still or walk by employing a unique, adaptive multidirectional gravity-assist (MGA) algorithm tailored to the specific needs of the patient, according to Jean-Baptiste Mignardot, PhD, of the Center for Neuroprosthetics and Brain Mind Institute, Swiss Federal Institute of Technology, Lausanne, Switzerland, and fellow investigators.
“The MGA establishes a safe and natural rehabilitation environment wherein individuals with neurological deficits can perform basic and skilled locomotor activities that would not be possible without robotic assistance,” according to the investigators. “The immediate and short-term ameliorations of gait performance during locomotion with MGA illustrate the potential of this environment to augment motor recovery.”
Current gait rehabilitation methods in stroke or SCI patients most commonly involves counterweight mechanisms or force-controlled equipment that apply upward support while walking on a treadmill. However Dr. Mignardot and his colleagues believe these methods are flawed.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“Treadmill-restricted environments markedly differ from the rich repertoire of natural locomotor activities underlying daily living,” the investigators wrote. “Vertically restricted trunk support creates undesired forces that impede gait execution.”
To counteract these negative effects, the MGA adjusts both upward and forward forces on the patient’s body, re-creating a more naturally occurring gait posture, which investigators have likened to an inverted pendulum with a natural forward tilt. In order to create the algorithm, investigators ran through a series of procedures, starting with calibrations based on the gait of healthy subjects and adjusting for necessary upward and forward assistance for stroke and SCI patients.
The artificial neural network within the algorithm analyzes patients’ support needs, a job that therapists currently have to do based on visual observations. This opens a window to faster and more accurate estimations, according to the investigators (Sci Transl Med. 2017 Jul 19. doi: 10.1126/scitranslmed.aah3621).
Investigators tested the algorithm on 15 SCI patients and 12 stroke patients. The stroke patients had an average age of 51 years, with length of time after stroke varying from 8 to 235 months. The SCI patients had an average age of 47 years, with a length of time since injury ranging from 12 to 264 months. Most patients in both groups were male.
When tested, the algorithm showed varying success depending on the severity of the injury, according to the researchers.
“For example, the MGA enabled subjects who could not stand independently to walk overground with or without assistive device.” Subjects who were able to move around only with crutches or a walker progressed without the use of assistive devices and exhibited improved spatiotemporal gait features, according to Dr. Mignardot and fellow investigators. “Individuals with stroke exhibited similar or even superior amelioration of locomotor performance and showed that individuals who could only walk with crutches exhibited improved intralimb coordination.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
After initial efficacy tests, the researchers tested the MGA’s effectiveness in five SCI patients immediately after 1 hour of training with the device and found that their gait speed increased during the training. However, the improvements were not evident in a similar test 1 week later. Similar tests using treadmill-restricted step training without the MGA device did not show any improvement during either week of testing.
Although the study’s small sample size limited the conclusions that could be reached, the investigators were encouraged by the overall effects of the algorithm. They noted that further tests are required to test the potential sensitivity and accuracy of the software.
The study was supported by the European Commission’s Seventh Framework Programme, various foundations, and the Swiss National Science Foundation.
Investigators reported holding patents on the step-by-step procedure and use of the MGA algorithm in this study.
[email protected]
On Twitter @eaztweets
A multidirectional gravity-assist device that delivers precise trunk support to stroke and spinal cord injury (SCI) patients via an artificial intelligence algorithm has demonstrated significantly improved locomotor performance beyond treadmill-based systems in a new study.
The harness device used in the study adjusts patients’ balance while they stand still or walk by employing a unique, adaptive multidirectional gravity-assist (MGA) algorithm tailored to the specific needs of the patient, according to Jean-Baptiste Mignardot, PhD, of the Center for Neuroprosthetics and Brain Mind Institute, Swiss Federal Institute of Technology, Lausanne, Switzerland, and fellow investigators.
“The MGA establishes a safe and natural rehabilitation environment wherein individuals with neurological deficits can perform basic and skilled locomotor activities that would not be possible without robotic assistance,” according to the investigators. “The immediate and short-term ameliorations of gait performance during locomotion with MGA illustrate the potential of this environment to augment motor recovery.”
Current gait rehabilitation methods in stroke or SCI patients most commonly involves counterweight mechanisms or force-controlled equipment that apply upward support while walking on a treadmill. However Dr. Mignardot and his colleagues believe these methods are flawed.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“Treadmill-restricted environments markedly differ from the rich repertoire of natural locomotor activities underlying daily living,” the investigators wrote. “Vertically restricted trunk support creates undesired forces that impede gait execution.”
To counteract these negative effects, the MGA adjusts both upward and forward forces on the patient’s body, re-creating a more naturally occurring gait posture, which investigators have likened to an inverted pendulum with a natural forward tilt. In order to create the algorithm, investigators ran through a series of procedures, starting with calibrations based on the gait of healthy subjects and adjusting for necessary upward and forward assistance for stroke and SCI patients.
The artificial neural network within the algorithm analyzes patients’ support needs, a job that therapists currently have to do based on visual observations. This opens a window to faster and more accurate estimations, according to the investigators (Sci Transl Med. 2017 Jul 19. doi: 10.1126/scitranslmed.aah3621).
Investigators tested the algorithm on 15 SCI patients and 12 stroke patients. The stroke patients had an average age of 51 years, with length of time after stroke varying from 8 to 235 months. The SCI patients had an average age of 47 years, with a length of time since injury ranging from 12 to 264 months. Most patients in both groups were male.
When tested, the algorithm showed varying success depending on the severity of the injury, according to the researchers.
“For example, the MGA enabled subjects who could not stand independently to walk overground with or without assistive device.” Subjects who were able to move around only with crutches or a walker progressed without the use of assistive devices and exhibited improved spatiotemporal gait features, according to Dr. Mignardot and fellow investigators. “Individuals with stroke exhibited similar or even superior amelioration of locomotor performance and showed that individuals who could only walk with crutches exhibited improved intralimb coordination.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
After initial efficacy tests, the researchers tested the MGA’s effectiveness in five SCI patients immediately after 1 hour of training with the device and found that their gait speed increased during the training. However, the improvements were not evident in a similar test 1 week later. Similar tests using treadmill-restricted step training without the MGA device did not show any improvement during either week of testing.
Although the study’s small sample size limited the conclusions that could be reached, the investigators were encouraged by the overall effects of the algorithm. They noted that further tests are required to test the potential sensitivity and accuracy of the software.
The study was supported by the European Commission’s Seventh Framework Programme, various foundations, and the Swiss National Science Foundation.
Investigators reported holding patents on the step-by-step procedure and use of the MGA algorithm in this study.
[email protected]
On Twitter @eaztweets
A multidirectional gravity-assist device that delivers precise trunk support to stroke and spinal cord injury (SCI) patients via an artificial intelligence algorithm has demonstrated significantly improved locomotor performance beyond treadmill-based systems in a new study.
The harness device used in the study adjusts patients’ balance while they stand still or walk by employing a unique, adaptive multidirectional gravity-assist (MGA) algorithm tailored to the specific needs of the patient, according to Jean-Baptiste Mignardot, PhD, of the Center for Neuroprosthetics and Brain Mind Institute, Swiss Federal Institute of Technology, Lausanne, Switzerland, and fellow investigators.
“The MGA establishes a safe and natural rehabilitation environment wherein individuals with neurological deficits can perform basic and skilled locomotor activities that would not be possible without robotic assistance,” according to the investigators. “The immediate and short-term ameliorations of gait performance during locomotion with MGA illustrate the potential of this environment to augment motor recovery.”
Current gait rehabilitation methods in stroke or SCI patients most commonly involves counterweight mechanisms or force-controlled equipment that apply upward support while walking on a treadmill. However Dr. Mignardot and his colleagues believe these methods are flawed.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“Treadmill-restricted environments markedly differ from the rich repertoire of natural locomotor activities underlying daily living,” the investigators wrote. “Vertically restricted trunk support creates undesired forces that impede gait execution.”
To counteract these negative effects, the MGA adjusts both upward and forward forces on the patient’s body, re-creating a more naturally occurring gait posture, which investigators have likened to an inverted pendulum with a natural forward tilt. In order to create the algorithm, investigators ran through a series of procedures, starting with calibrations based on the gait of healthy subjects and adjusting for necessary upward and forward assistance for stroke and SCI patients.
The artificial neural network within the algorithm analyzes patients’ support needs, a job that therapists currently have to do based on visual observations. This opens a window to faster and more accurate estimations, according to the investigators (Sci Transl Med. 2017 Jul 19. doi: 10.1126/scitranslmed.aah3621).
Investigators tested the algorithm on 15 SCI patients and 12 stroke patients. The stroke patients had an average age of 51 years, with length of time after stroke varying from 8 to 235 months. The SCI patients had an average age of 47 years, with a length of time since injury ranging from 12 to 264 months. Most patients in both groups were male.
When tested, the algorithm showed varying success depending on the severity of the injury, according to the researchers.
“For example, the MGA enabled subjects who could not stand independently to walk overground with or without assistive device.” Subjects who were able to move around only with crutches or a walker progressed without the use of assistive devices and exhibited improved spatiotemporal gait features, according to Dr. Mignardot and fellow investigators. “Individuals with stroke exhibited similar or even superior amelioration of locomotor performance and showed that individuals who could only walk with crutches exhibited improved intralimb coordination.”
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
After initial efficacy tests, the researchers tested the MGA’s effectiveness in five SCI patients immediately after 1 hour of training with the device and found that their gait speed increased during the training. However, the improvements were not evident in a similar test 1 week later. Similar tests using treadmill-restricted step training without the MGA device did not show any improvement during either week of testing.
Although the study’s small sample size limited the conclusions that could be reached, the investigators were encouraged by the overall effects of the algorithm. They noted that further tests are required to test the potential sensitivity and accuracy of the software.
The study was supported by the European Commission’s Seventh Framework Programme, various foundations, and the Swiss National Science Foundation.
Investigators reported holding patents on the step-by-step procedure and use of the MGA algorithm in this study.
[email protected]
On Twitter @eaztweets
FROM SCIENCE TRANSLATIONAL MEDICINE
Ibrutinib and bleeding complications in Mohs surgery
Clinically significant bleeding events occurred in two elderly men who were taking ibrutinib and underwent Mohs micrographic surgery for squamous cell carcinomas, Cindy E. Parra and her colleagues reported in JAMA Dermatology.
On day 3 after his Mohs procedure, one 73-year-old man taking ibrutinib for Waldenstrom macroglobulinemia developed extensive bilateral periorbital ecchymosis that extended down to his upper chest. The other patient, an 88-year-old man taking ibrutinib for chronic lymphocytic leukemia, developed ecchymosis down to the chin. The first patient discontinued ibrutinib 3 days before his surgery; the second patient was taking ibrutinib at the time of his surgery.
“The increased incidence of nonmelanoma skin cancer and poorer outcomes in patients with non-Hodgkin lymphoma and CLL is well recognized, as is the importance of aggressive dermatologic management,” the researchers wrote (JAMA Dermatol. 2017 Jul 12. doi: 10.1001/jamadermatol.2017.1877). “It may be prudent to withhold ibrutinib treatment prior to dermatologic surgery to avoid potential bleeding complications.”
The findings argue for close collaboration between the dermatologic surgeon and the patient’s hematologist when scheduling extended-duration dermatologic procedures in patients taking ibrutinib.
Find the full summary here.
Clinically significant bleeding events occurred in two elderly men who were taking ibrutinib and underwent Mohs micrographic surgery for squamous cell carcinomas, Cindy E. Parra and her colleagues reported in JAMA Dermatology.
On day 3 after his Mohs procedure, one 73-year-old man taking ibrutinib for Waldenstrom macroglobulinemia developed extensive bilateral periorbital ecchymosis that extended down to his upper chest. The other patient, an 88-year-old man taking ibrutinib for chronic lymphocytic leukemia, developed ecchymosis down to the chin. The first patient discontinued ibrutinib 3 days before his surgery; the second patient was taking ibrutinib at the time of his surgery.
“The increased incidence of nonmelanoma skin cancer and poorer outcomes in patients with non-Hodgkin lymphoma and CLL is well recognized, as is the importance of aggressive dermatologic management,” the researchers wrote (JAMA Dermatol. 2017 Jul 12. doi: 10.1001/jamadermatol.2017.1877). “It may be prudent to withhold ibrutinib treatment prior to dermatologic surgery to avoid potential bleeding complications.”
The findings argue for close collaboration between the dermatologic surgeon and the patient’s hematologist when scheduling extended-duration dermatologic procedures in patients taking ibrutinib.
Find the full summary here.
Clinically significant bleeding events occurred in two elderly men who were taking ibrutinib and underwent Mohs micrographic surgery for squamous cell carcinomas, Cindy E. Parra and her colleagues reported in JAMA Dermatology.
On day 3 after his Mohs procedure, one 73-year-old man taking ibrutinib for Waldenstrom macroglobulinemia developed extensive bilateral periorbital ecchymosis that extended down to his upper chest. The other patient, an 88-year-old man taking ibrutinib for chronic lymphocytic leukemia, developed ecchymosis down to the chin. The first patient discontinued ibrutinib 3 days before his surgery; the second patient was taking ibrutinib at the time of his surgery.
“The increased incidence of nonmelanoma skin cancer and poorer outcomes in patients with non-Hodgkin lymphoma and CLL is well recognized, as is the importance of aggressive dermatologic management,” the researchers wrote (JAMA Dermatol. 2017 Jul 12. doi: 10.1001/jamadermatol.2017.1877). “It may be prudent to withhold ibrutinib treatment prior to dermatologic surgery to avoid potential bleeding complications.”
The findings argue for close collaboration between the dermatologic surgeon and the patient’s hematologist when scheduling extended-duration dermatologic procedures in patients taking ibrutinib.
Find the full summary here.
FROM JAMA DERMATOLOGY
Getting a Better Picture of Skin Cancer
A handheld detector that offers noninvasive real-time imaging can help dermatologic surgeons get a better idea of skin cancer dimensions before committing to surgery, according to researchers from National Skin Centre and Singapore Bioimaging Consortium, both in Singapore, and Technical University of Munich and iThera Medical GmbH, both in Germany.
Current imaging technologies can lead to excessive or incomplete removal of the cancer, the researchers say. The multispectral optoacoustic tomography (MSOT) allows the user to differentiate tissue chromophores (the chromophore is the part of the molecule responsible for its color) and exogenous contrast agents based on their spectral signatures.
The researchers performed MSOT imaging with 2- and 3-dimensional handheld scanners on 21 patients with nonmelanoma skin cancers. All the skin lesions had recognizable images on MSOT with both detectors, visualizing the shape and thickness of the lesions. The 2D and 3D detectors also offered images with well-resolved tissue chromophores. But the volumetric probe gave more accurate tumor dimensions compared with those from histology analysis.
Aggressive types of skin cancers can involve deeper structures, such as predominant deep blood vessels, the researchers note—another reason the MSOT detector could be useful. In one case, the depth of the basal cell carcinoma, which included its underlying vasculature, reached beyond 3 mm, which might have gone undetected by other imaging modalities, they say.
The fact that the device is also noninvasive and offers real-time imaging, the researchers suggest, makes volumetric MSOT “an ideal modality for longitudinal monitoring of skin diseases and treatment responses.”
Source:
Attia ABE, Chuah SY, Razansky D, et al. Photoacoustics. 2017;7:20-26.
doi: 10.1016/j.pacs.2017.05.003.
A handheld detector that offers noninvasive real-time imaging can help dermatologic surgeons get a better idea of skin cancer dimensions before committing to surgery, according to researchers from National Skin Centre and Singapore Bioimaging Consortium, both in Singapore, and Technical University of Munich and iThera Medical GmbH, both in Germany.
Current imaging technologies can lead to excessive or incomplete removal of the cancer, the researchers say. The multispectral optoacoustic tomography (MSOT) allows the user to differentiate tissue chromophores (the chromophore is the part of the molecule responsible for its color) and exogenous contrast agents based on their spectral signatures.
The researchers performed MSOT imaging with 2- and 3-dimensional handheld scanners on 21 patients with nonmelanoma skin cancers. All the skin lesions had recognizable images on MSOT with both detectors, visualizing the shape and thickness of the lesions. The 2D and 3D detectors also offered images with well-resolved tissue chromophores. But the volumetric probe gave more accurate tumor dimensions compared with those from histology analysis.
Aggressive types of skin cancers can involve deeper structures, such as predominant deep blood vessels, the researchers note—another reason the MSOT detector could be useful. In one case, the depth of the basal cell carcinoma, which included its underlying vasculature, reached beyond 3 mm, which might have gone undetected by other imaging modalities, they say.
The fact that the device is also noninvasive and offers real-time imaging, the researchers suggest, makes volumetric MSOT “an ideal modality for longitudinal monitoring of skin diseases and treatment responses.”
Source:
Attia ABE, Chuah SY, Razansky D, et al. Photoacoustics. 2017;7:20-26.
doi: 10.1016/j.pacs.2017.05.003.
A handheld detector that offers noninvasive real-time imaging can help dermatologic surgeons get a better idea of skin cancer dimensions before committing to surgery, according to researchers from National Skin Centre and Singapore Bioimaging Consortium, both in Singapore, and Technical University of Munich and iThera Medical GmbH, both in Germany.
Current imaging technologies can lead to excessive or incomplete removal of the cancer, the researchers say. The multispectral optoacoustic tomography (MSOT) allows the user to differentiate tissue chromophores (the chromophore is the part of the molecule responsible for its color) and exogenous contrast agents based on their spectral signatures.
The researchers performed MSOT imaging with 2- and 3-dimensional handheld scanners on 21 patients with nonmelanoma skin cancers. All the skin lesions had recognizable images on MSOT with both detectors, visualizing the shape and thickness of the lesions. The 2D and 3D detectors also offered images with well-resolved tissue chromophores. But the volumetric probe gave more accurate tumor dimensions compared with those from histology analysis.
Aggressive types of skin cancers can involve deeper structures, such as predominant deep blood vessels, the researchers note—another reason the MSOT detector could be useful. In one case, the depth of the basal cell carcinoma, which included its underlying vasculature, reached beyond 3 mm, which might have gone undetected by other imaging modalities, they say.
The fact that the device is also noninvasive and offers real-time imaging, the researchers suggest, makes volumetric MSOT “an ideal modality for longitudinal monitoring of skin diseases and treatment responses.”
Source:
Attia ABE, Chuah SY, Razansky D, et al. Photoacoustics. 2017;7:20-26.
doi: 10.1016/j.pacs.2017.05.003.
FDA Approves First New ALS Drug in Years
A new treatment for amyotrophic lateral sclerosis (ALS), Radicava (edaravone), is on the way for U.S. patients.
“After learning about the use of edaravone to treat ALS in Japan, we rapidly engaged with the drug developer about filing a marketing application in the United States,” said Eric Bastings, MD, deputy director of the Division of Neurology Products in the FDA’s Center for Drug Evaluation and Research. “This is the first new treatment approved by the FDA for ALS in many years, and we are pleased that people with ALS will now have an additional option.”
In a 6-month trial, 137 patients were randomly assigned to edaravone or placebo. At week 24, those receiving edaravone had declined less on a clinical assessment of daily functioning.
Edaravon is given intravenously daily for 14 days to start, followed by 14 days drug free. Subsequent treatment cycles consist of dosing on 10 of 14 days, followed by 14 days drug free.
The most common adverse reactions are bruising and gait disturbance. Edaravon also contains sodium bisulfite, which can cause serious allergic reactions in patients with sulfite sensitivity.
A new treatment for amyotrophic lateral sclerosis (ALS), Radicava (edaravone), is on the way for U.S. patients.
“After learning about the use of edaravone to treat ALS in Japan, we rapidly engaged with the drug developer about filing a marketing application in the United States,” said Eric Bastings, MD, deputy director of the Division of Neurology Products in the FDA’s Center for Drug Evaluation and Research. “This is the first new treatment approved by the FDA for ALS in many years, and we are pleased that people with ALS will now have an additional option.”
In a 6-month trial, 137 patients were randomly assigned to edaravone or placebo. At week 24, those receiving edaravone had declined less on a clinical assessment of daily functioning.
Edaravon is given intravenously daily for 14 days to start, followed by 14 days drug free. Subsequent treatment cycles consist of dosing on 10 of 14 days, followed by 14 days drug free.
The most common adverse reactions are bruising and gait disturbance. Edaravon also contains sodium bisulfite, which can cause serious allergic reactions in patients with sulfite sensitivity.
A new treatment for amyotrophic lateral sclerosis (ALS), Radicava (edaravone), is on the way for U.S. patients.
“After learning about the use of edaravone to treat ALS in Japan, we rapidly engaged with the drug developer about filing a marketing application in the United States,” said Eric Bastings, MD, deputy director of the Division of Neurology Products in the FDA’s Center for Drug Evaluation and Research. “This is the first new treatment approved by the FDA for ALS in many years, and we are pleased that people with ALS will now have an additional option.”
In a 6-month trial, 137 patients were randomly assigned to edaravone or placebo. At week 24, those receiving edaravone had declined less on a clinical assessment of daily functioning.
Edaravon is given intravenously daily for 14 days to start, followed by 14 days drug free. Subsequent treatment cycles consist of dosing on 10 of 14 days, followed by 14 days drug free.
The most common adverse reactions are bruising and gait disturbance. Edaravon also contains sodium bisulfite, which can cause serious allergic reactions in patients with sulfite sensitivity.