User login
Pulmonary metastasectomy may be useful for soft-tissue sarcoma spread
The rate of soft-tissue sarcoma has nearly doubled over the past two decades, and up to 50% of patients with tissue sarcoma develop lung metastasis. A single-center study of 539 patients who had treatment for soft-tissue sarcoma has revealed disease and treatment characteristics that may aid patient selection and help predict overall and disease-free survival after diagnosis and treatment.
“Histologic subtype and size of the primary tumor were significantly associated with overall survival,” said lead author Neel P. Chudgar, MD, and his coauthors in the July issue of the Journal of Thoracic and Cardiovascular Surgery (2017;154:319-30).
“Patients who underwent pulmonary metastasectomy [PM] for pleomorphic sarcoma/malignant fibrous histocytoma had the shortest median overall survival (23.6 months), whereas those who underwent PM for leiomyosarcoma had a median overall survival of 42 months,” he said.
The study subjects had pulmonary metastasectomies at Memorial Sloan Kettering Cancer Center, New York, during September 1991–June 2014. The median overall survival was 33.2 months, and median disease-free survival was 6.8 months for the entire cohort.
Among the disease characteristics associated with a lower hazard ratio of death shown by multivariable analyses were leiomyosarcoma histologic subtype (HR, 0.57), primary tumor size of 10 cm or less (HR, 1.00 vs. HR, 1.37 for those greater than 10 cm), increasing time from primary tumor resection to development of metastases (HR, 0.4 at less than 24 months vs. 1.0 at less than 6 months), solitary lung metastasis (HR, 1.0 vs. 1.8 for one year or more), and minimally invasive resection (HR, 0.71), all of which were statistically significant differences. Disease-free interval of more than one year and one pulmonary metastasis were significantly associated with lower hazard of disease recurrence.
Of patients, 70% had pulmonary metastasectomy as their primary treatment. The remainder had induction chemotherapy. In addition, 71% had open procedures over the 23-year study period, but minimally invasive operations became more common with time, increasing more than fourfold from the first half of the study period, vs. the last. They accounted for more than half of all procedures in the last five years of the study.
With regard to tumor type, fibrosarcoma was associated with longest median overall survival (65.2 months). Dr. Chudgar and his colleagues noted that 43% of these patients had low-grade primary tumors. Patients with low-grade tumors of all types had a median overall survival of 71.8 months, vs. 30.8 months for those with high-grade tumors.
“Our results indicate that therapeutic-intent pulmonary metastasectomy for soft-tissue sarcoma can be associated with prolonged survival,” Dr. Chudgar and his coauthors said. “The median survivals in our study are comparable with those in previous studies.” However, their analysis went beyond previous studies because they identified positive prognostic factors.
Dr. Chudgar and his coauthors acknowledge that various studies have drawn conflicting conclusions about the validity of histologic subtype as a prognostic factor, but their study differs from previous studies because it is a single-center cohort, “which increases the power to potentially identify significant differences, and we focused on soft-tissue sarcoma exclusively to enhance the homogeneity of the study population.”
Nonetheless, the researchers noted some limitations of their study, namely their collective analysis of the various soft-tissue sarcoma subtypes and the lack of a control group. Soft tissue sarcoma, because of its heterogeneous nature, challenges the adoption of precision medicine for this cancer type, but, until clinicians better understand the underlying mechanism of metastasis in these tumor types, Dr. Chudgar and his coauthors said, pulmonary metastasectomy “remains the best available treatment for soft tissue sarcoma pulmonary metastases.”
Dr. Chudgar and his coauthors had no financial relationships to disclose.
The findings that surgery for pulmonary metastases achieves “relatively good median survival” that Dr. Chudgar and coauthors reported are “especially impressive when considering that more than 25% of these patients with metastatic cancer had five or more pulmonary lesions,” said Mark F. Berry, MD, MHS, of Stanford University in his invited commentary (J Thorac Cardiovasc Surg. 2017;154:117-8).
Dr. Berry also said, however, that surgeons still must consider these results cautiously for several reasons. One, the study is retrospective and uncontrolled. Two, the study does not address whether the researchers selected healthy patients “with favorable disease characteristics” for pulmonary metastasectomy. “The sobering reality is that most patients still had recurrence relatively soon after complete pulmonary resection,” Dr. Berry said.
The study does support the current practice of pulmonary metastasectomy, which many patients may prefer for its invasive nature, compared with systemic chemotherapy treatment, he said. “Overall, surgeons can use this study to aid patient selection [and] to support the clinical decision to pursue resection of soft-tissue sarcoma pulmonary metastases for patients judged to be appropriate surgical candidates,” Dr. Berry concluded.
Dr. Berry had reported no financial disclosures.
The findings that surgery for pulmonary metastases achieves “relatively good median survival” that Dr. Chudgar and coauthors reported are “especially impressive when considering that more than 25% of these patients with metastatic cancer had five or more pulmonary lesions,” said Mark F. Berry, MD, MHS, of Stanford University in his invited commentary (J Thorac Cardiovasc Surg. 2017;154:117-8).
Dr. Berry also said, however, that surgeons still must consider these results cautiously for several reasons. One, the study is retrospective and uncontrolled. Two, the study does not address whether the researchers selected healthy patients “with favorable disease characteristics” for pulmonary metastasectomy. “The sobering reality is that most patients still had recurrence relatively soon after complete pulmonary resection,” Dr. Berry said.
The study does support the current practice of pulmonary metastasectomy, which many patients may prefer for its invasive nature, compared with systemic chemotherapy treatment, he said. “Overall, surgeons can use this study to aid patient selection [and] to support the clinical decision to pursue resection of soft-tissue sarcoma pulmonary metastases for patients judged to be appropriate surgical candidates,” Dr. Berry concluded.
Dr. Berry had reported no financial disclosures.
The findings that surgery for pulmonary metastases achieves “relatively good median survival” that Dr. Chudgar and coauthors reported are “especially impressive when considering that more than 25% of these patients with metastatic cancer had five or more pulmonary lesions,” said Mark F. Berry, MD, MHS, of Stanford University in his invited commentary (J Thorac Cardiovasc Surg. 2017;154:117-8).
Dr. Berry also said, however, that surgeons still must consider these results cautiously for several reasons. One, the study is retrospective and uncontrolled. Two, the study does not address whether the researchers selected healthy patients “with favorable disease characteristics” for pulmonary metastasectomy. “The sobering reality is that most patients still had recurrence relatively soon after complete pulmonary resection,” Dr. Berry said.
The study does support the current practice of pulmonary metastasectomy, which many patients may prefer for its invasive nature, compared with systemic chemotherapy treatment, he said. “Overall, surgeons can use this study to aid patient selection [and] to support the clinical decision to pursue resection of soft-tissue sarcoma pulmonary metastases for patients judged to be appropriate surgical candidates,” Dr. Berry concluded.
Dr. Berry had reported no financial disclosures.
The rate of soft-tissue sarcoma has nearly doubled over the past two decades, and up to 50% of patients with tissue sarcoma develop lung metastasis. A single-center study of 539 patients who had treatment for soft-tissue sarcoma has revealed disease and treatment characteristics that may aid patient selection and help predict overall and disease-free survival after diagnosis and treatment.
“Histologic subtype and size of the primary tumor were significantly associated with overall survival,” said lead author Neel P. Chudgar, MD, and his coauthors in the July issue of the Journal of Thoracic and Cardiovascular Surgery (2017;154:319-30).
“Patients who underwent pulmonary metastasectomy [PM] for pleomorphic sarcoma/malignant fibrous histocytoma had the shortest median overall survival (23.6 months), whereas those who underwent PM for leiomyosarcoma had a median overall survival of 42 months,” he said.
The study subjects had pulmonary metastasectomies at Memorial Sloan Kettering Cancer Center, New York, during September 1991–June 2014. The median overall survival was 33.2 months, and median disease-free survival was 6.8 months for the entire cohort.
Among the disease characteristics associated with a lower hazard ratio of death shown by multivariable analyses were leiomyosarcoma histologic subtype (HR, 0.57), primary tumor size of 10 cm or less (HR, 1.00 vs. HR, 1.37 for those greater than 10 cm), increasing time from primary tumor resection to development of metastases (HR, 0.4 at less than 24 months vs. 1.0 at less than 6 months), solitary lung metastasis (HR, 1.0 vs. 1.8 for one year or more), and minimally invasive resection (HR, 0.71), all of which were statistically significant differences. Disease-free interval of more than one year and one pulmonary metastasis were significantly associated with lower hazard of disease recurrence.
Of patients, 70% had pulmonary metastasectomy as their primary treatment. The remainder had induction chemotherapy. In addition, 71% had open procedures over the 23-year study period, but minimally invasive operations became more common with time, increasing more than fourfold from the first half of the study period, vs. the last. They accounted for more than half of all procedures in the last five years of the study.
With regard to tumor type, fibrosarcoma was associated with longest median overall survival (65.2 months). Dr. Chudgar and his colleagues noted that 43% of these patients had low-grade primary tumors. Patients with low-grade tumors of all types had a median overall survival of 71.8 months, vs. 30.8 months for those with high-grade tumors.
“Our results indicate that therapeutic-intent pulmonary metastasectomy for soft-tissue sarcoma can be associated with prolonged survival,” Dr. Chudgar and his coauthors said. “The median survivals in our study are comparable with those in previous studies.” However, their analysis went beyond previous studies because they identified positive prognostic factors.
Dr. Chudgar and his coauthors acknowledge that various studies have drawn conflicting conclusions about the validity of histologic subtype as a prognostic factor, but their study differs from previous studies because it is a single-center cohort, “which increases the power to potentially identify significant differences, and we focused on soft-tissue sarcoma exclusively to enhance the homogeneity of the study population.”
Nonetheless, the researchers noted some limitations of their study, namely their collective analysis of the various soft-tissue sarcoma subtypes and the lack of a control group. Soft tissue sarcoma, because of its heterogeneous nature, challenges the adoption of precision medicine for this cancer type, but, until clinicians better understand the underlying mechanism of metastasis in these tumor types, Dr. Chudgar and his coauthors said, pulmonary metastasectomy “remains the best available treatment for soft tissue sarcoma pulmonary metastases.”
Dr. Chudgar and his coauthors had no financial relationships to disclose.
The rate of soft-tissue sarcoma has nearly doubled over the past two decades, and up to 50% of patients with tissue sarcoma develop lung metastasis. A single-center study of 539 patients who had treatment for soft-tissue sarcoma has revealed disease and treatment characteristics that may aid patient selection and help predict overall and disease-free survival after diagnosis and treatment.
“Histologic subtype and size of the primary tumor were significantly associated with overall survival,” said lead author Neel P. Chudgar, MD, and his coauthors in the July issue of the Journal of Thoracic and Cardiovascular Surgery (2017;154:319-30).
“Patients who underwent pulmonary metastasectomy [PM] for pleomorphic sarcoma/malignant fibrous histocytoma had the shortest median overall survival (23.6 months), whereas those who underwent PM for leiomyosarcoma had a median overall survival of 42 months,” he said.
The study subjects had pulmonary metastasectomies at Memorial Sloan Kettering Cancer Center, New York, during September 1991–June 2014. The median overall survival was 33.2 months, and median disease-free survival was 6.8 months for the entire cohort.
Among the disease characteristics associated with a lower hazard ratio of death shown by multivariable analyses were leiomyosarcoma histologic subtype (HR, 0.57), primary tumor size of 10 cm or less (HR, 1.00 vs. HR, 1.37 for those greater than 10 cm), increasing time from primary tumor resection to development of metastases (HR, 0.4 at less than 24 months vs. 1.0 at less than 6 months), solitary lung metastasis (HR, 1.0 vs. 1.8 for one year or more), and minimally invasive resection (HR, 0.71), all of which were statistically significant differences. Disease-free interval of more than one year and one pulmonary metastasis were significantly associated with lower hazard of disease recurrence.
Of patients, 70% had pulmonary metastasectomy as their primary treatment. The remainder had induction chemotherapy. In addition, 71% had open procedures over the 23-year study period, but minimally invasive operations became more common with time, increasing more than fourfold from the first half of the study period, vs. the last. They accounted for more than half of all procedures in the last five years of the study.
With regard to tumor type, fibrosarcoma was associated with longest median overall survival (65.2 months). Dr. Chudgar and his colleagues noted that 43% of these patients had low-grade primary tumors. Patients with low-grade tumors of all types had a median overall survival of 71.8 months, vs. 30.8 months for those with high-grade tumors.
“Our results indicate that therapeutic-intent pulmonary metastasectomy for soft-tissue sarcoma can be associated with prolonged survival,” Dr. Chudgar and his coauthors said. “The median survivals in our study are comparable with those in previous studies.” However, their analysis went beyond previous studies because they identified positive prognostic factors.
Dr. Chudgar and his coauthors acknowledge that various studies have drawn conflicting conclusions about the validity of histologic subtype as a prognostic factor, but their study differs from previous studies because it is a single-center cohort, “which increases the power to potentially identify significant differences, and we focused on soft-tissue sarcoma exclusively to enhance the homogeneity of the study population.”
Nonetheless, the researchers noted some limitations of their study, namely their collective analysis of the various soft-tissue sarcoma subtypes and the lack of a control group. Soft tissue sarcoma, because of its heterogeneous nature, challenges the adoption of precision medicine for this cancer type, but, until clinicians better understand the underlying mechanism of metastasis in these tumor types, Dr. Chudgar and his coauthors said, pulmonary metastasectomy “remains the best available treatment for soft tissue sarcoma pulmonary metastases.”
Dr. Chudgar and his coauthors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Characteristics that determine survival in patients with sarcomatous pulmonary metastases are tumor subtype and size, number of and time to metastases, and minimally invasive surgery.
Major finding: Patients with leiomyosarcoma histologic subtype tumor had a hazard ratio of 0.57 (P = .001), and those with a primary tumor size of 10 cm or less had an HR of 1, vs. an HR of 1.37 for those greater than 10 cm (P = .006)
Data source: A single-institution study of 539 patients who had pulmonary mastectomy for metastatic soft tissue sarcoma from September 1991 to June 2014.
Disclosures: Dr. Chudgar and his coauthors had no financial relationships to disclose.
Even a few middle age pounds are dangerous
Gaining just 5-22 pounds in the first half of adulthood significantly increases the risk of chronic disease in the second half, especially the likelihood of type 2 diabetes, gallstones, and hypertension, according to investigators.
They looked at how much 92,837 women in the Nurses’ Health Study remembered weighing when they were 18 years old, and how much 25,303 men in the Health Professionals Follow-Up Study recalled weighing at age 21. The Harvard team matched those weights to how much their subjects actually weighed at age 55, and then followed the women out to a median of 73 years and the men out to a median of 69 years to see how their weight changes in early adulthood affected their health later on (JAMA. 2017;318[3]:255-269. doi: 10.1001/jama.2017.7092).
The investigators found that even a moderate gain of up to 10 kg increased the risk of major chronic diseases and early death. “Maintaining a healthy weight throughout early and middle adulthood is associated with overall health ... These findings may help counsel patients regarding the risks of weight gain,” wrote the investigators, led by Yan Zheng, MD, PhD, of the department of nutrition, Harvard T. H. Chan School of Public Health, Boston.
It’s not news that packing on a few pounds with age isn’t healthy, but quantifying the effects of early adulthood weight gain is novel. “The advantage of focusing on weight gain throughout” the first half of adult life “is that it primarily reflects the accumulation of excess adiposity from early to middle adulthood, which is often ignored by individuals and their physicians because the consequences of modest weight accumulation may not yet be apparent,” the investigators noted.
Specifically, they found that compared to participants who maintained a stable weight – no more than 2.5 kg either way – people who gained up to 10 kg had an increased incidence of not only type 2 diabetes, gallstones, and hypertension, but also cardiovascular disease, cataracts, severe osteoarthritis, and death, and added weight increased health risks in a dose-dependent manner. People who gained more than 10 kg from their high school years fared worse, even if they started out as obese.
The adjusted incidence per 100,000 person-years for type 2 diabetes rose from 110 cases to 207 cases per 100,000 person-years among women 55 years old who weighed up to 22 pounds more than they did in high school; it was similar for men, with a rise from 147 cases to 258 cases per 100,000 person-years. Weight gain up to 10 kg boosted the incidence of hypertension from 2,754 cases to 3,415 cases per 100,000 person-years for women and from 2,366 cases to 2,861 cases for men.
Results were similar for cardiovascular disease and obesity-related cancers, particularly breast cancer among women and colorectal and prostate cancer among men. Higher amounts of weight gain were also associated with a lower likelihood of healthy aging, a composite score of the absence of multiple chronic diseases, cognitive decline, and physical limitations.
However, the investigators noted that “considering that individuals tend to underreport their weight, it is possible that our findings might have exaggerated the true risks associated with the measured weight change from early to middle adulthood.”
Also, “participants were all health professionals and were mostly white ... the results might not be generalizable to all populations,” they said.
The National Institutes of Health and American Diabetes Association funded the work. The researchers reported no conflicts of interest.
The prevalence of obesity emphasizes that it will not be possible to provide effective treatment for all of those affected. Therefore, efforts to prevent and control this widespread disease must be renewed. Reducing and preventing obesity and excessive weight gain in young adults provides a new target, and one that could offer an effective transgenerational approach for prevention.
Broader venues for intervention efforts could include a supplemental nutrition plan for the Women, Infants, and Children program that provides nutritional counseling for pregnant women and women, infants, and children up to the age of 4 years. Sustained productivity and reduced absenteeism among employees with healthy weights might motivate employers with long-term work forces to invest in prevention efforts directed at families. Beyond clinical interventions, identification and implementation of environmental changes that effectively promote weight maintenance are essential for population-based efforts.
William Dietz, MD, PhD, is the director of the Redstone Global Center for Prevention and Wellness at The George Washington University in Washington, D.C. He is an adviser for Weight Watchers and RTI, and has grant support from Bridgespan. Dr. Dietz’s remarks came from an editorial accompanying the research report ( JAMA. 2017;318[3]:241-2 ).
The prevalence of obesity emphasizes that it will not be possible to provide effective treatment for all of those affected. Therefore, efforts to prevent and control this widespread disease must be renewed. Reducing and preventing obesity and excessive weight gain in young adults provides a new target, and one that could offer an effective transgenerational approach for prevention.
Broader venues for intervention efforts could include a supplemental nutrition plan for the Women, Infants, and Children program that provides nutritional counseling for pregnant women and women, infants, and children up to the age of 4 years. Sustained productivity and reduced absenteeism among employees with healthy weights might motivate employers with long-term work forces to invest in prevention efforts directed at families. Beyond clinical interventions, identification and implementation of environmental changes that effectively promote weight maintenance are essential for population-based efforts.
William Dietz, MD, PhD, is the director of the Redstone Global Center for Prevention and Wellness at The George Washington University in Washington, D.C. He is an adviser for Weight Watchers and RTI, and has grant support from Bridgespan. Dr. Dietz’s remarks came from an editorial accompanying the research report ( JAMA. 2017;318[3]:241-2 ).
The prevalence of obesity emphasizes that it will not be possible to provide effective treatment for all of those affected. Therefore, efforts to prevent and control this widespread disease must be renewed. Reducing and preventing obesity and excessive weight gain in young adults provides a new target, and one that could offer an effective transgenerational approach for prevention.
Broader venues for intervention efforts could include a supplemental nutrition plan for the Women, Infants, and Children program that provides nutritional counseling for pregnant women and women, infants, and children up to the age of 4 years. Sustained productivity and reduced absenteeism among employees with healthy weights might motivate employers with long-term work forces to invest in prevention efforts directed at families. Beyond clinical interventions, identification and implementation of environmental changes that effectively promote weight maintenance are essential for population-based efforts.
William Dietz, MD, PhD, is the director of the Redstone Global Center for Prevention and Wellness at The George Washington University in Washington, D.C. He is an adviser for Weight Watchers and RTI, and has grant support from Bridgespan. Dr. Dietz’s remarks came from an editorial accompanying the research report ( JAMA. 2017;318[3]:241-2 ).
Gaining just 5-22 pounds in the first half of adulthood significantly increases the risk of chronic disease in the second half, especially the likelihood of type 2 diabetes, gallstones, and hypertension, according to investigators.
They looked at how much 92,837 women in the Nurses’ Health Study remembered weighing when they were 18 years old, and how much 25,303 men in the Health Professionals Follow-Up Study recalled weighing at age 21. The Harvard team matched those weights to how much their subjects actually weighed at age 55, and then followed the women out to a median of 73 years and the men out to a median of 69 years to see how their weight changes in early adulthood affected their health later on (JAMA. 2017;318[3]:255-269. doi: 10.1001/jama.2017.7092).
The investigators found that even a moderate gain of up to 10 kg increased the risk of major chronic diseases and early death. “Maintaining a healthy weight throughout early and middle adulthood is associated with overall health ... These findings may help counsel patients regarding the risks of weight gain,” wrote the investigators, led by Yan Zheng, MD, PhD, of the department of nutrition, Harvard T. H. Chan School of Public Health, Boston.
It’s not news that packing on a few pounds with age isn’t healthy, but quantifying the effects of early adulthood weight gain is novel. “The advantage of focusing on weight gain throughout” the first half of adult life “is that it primarily reflects the accumulation of excess adiposity from early to middle adulthood, which is often ignored by individuals and their physicians because the consequences of modest weight accumulation may not yet be apparent,” the investigators noted.
Specifically, they found that compared to participants who maintained a stable weight – no more than 2.5 kg either way – people who gained up to 10 kg had an increased incidence of not only type 2 diabetes, gallstones, and hypertension, but also cardiovascular disease, cataracts, severe osteoarthritis, and death, and added weight increased health risks in a dose-dependent manner. People who gained more than 10 kg from their high school years fared worse, even if they started out as obese.
The adjusted incidence per 100,000 person-years for type 2 diabetes rose from 110 cases to 207 cases per 100,000 person-years among women 55 years old who weighed up to 22 pounds more than they did in high school; it was similar for men, with a rise from 147 cases to 258 cases per 100,000 person-years. Weight gain up to 10 kg boosted the incidence of hypertension from 2,754 cases to 3,415 cases per 100,000 person-years for women and from 2,366 cases to 2,861 cases for men.
Results were similar for cardiovascular disease and obesity-related cancers, particularly breast cancer among women and colorectal and prostate cancer among men. Higher amounts of weight gain were also associated with a lower likelihood of healthy aging, a composite score of the absence of multiple chronic diseases, cognitive decline, and physical limitations.
However, the investigators noted that “considering that individuals tend to underreport their weight, it is possible that our findings might have exaggerated the true risks associated with the measured weight change from early to middle adulthood.”
Also, “participants were all health professionals and were mostly white ... the results might not be generalizable to all populations,” they said.
The National Institutes of Health and American Diabetes Association funded the work. The researchers reported no conflicts of interest.
Gaining just 5-22 pounds in the first half of adulthood significantly increases the risk of chronic disease in the second half, especially the likelihood of type 2 diabetes, gallstones, and hypertension, according to investigators.
They looked at how much 92,837 women in the Nurses’ Health Study remembered weighing when they were 18 years old, and how much 25,303 men in the Health Professionals Follow-Up Study recalled weighing at age 21. The Harvard team matched those weights to how much their subjects actually weighed at age 55, and then followed the women out to a median of 73 years and the men out to a median of 69 years to see how their weight changes in early adulthood affected their health later on (JAMA. 2017;318[3]:255-269. doi: 10.1001/jama.2017.7092).
The investigators found that even a moderate gain of up to 10 kg increased the risk of major chronic diseases and early death. “Maintaining a healthy weight throughout early and middle adulthood is associated with overall health ... These findings may help counsel patients regarding the risks of weight gain,” wrote the investigators, led by Yan Zheng, MD, PhD, of the department of nutrition, Harvard T. H. Chan School of Public Health, Boston.
It’s not news that packing on a few pounds with age isn’t healthy, but quantifying the effects of early adulthood weight gain is novel. “The advantage of focusing on weight gain throughout” the first half of adult life “is that it primarily reflects the accumulation of excess adiposity from early to middle adulthood, which is often ignored by individuals and their physicians because the consequences of modest weight accumulation may not yet be apparent,” the investigators noted.
Specifically, they found that compared to participants who maintained a stable weight – no more than 2.5 kg either way – people who gained up to 10 kg had an increased incidence of not only type 2 diabetes, gallstones, and hypertension, but also cardiovascular disease, cataracts, severe osteoarthritis, and death, and added weight increased health risks in a dose-dependent manner. People who gained more than 10 kg from their high school years fared worse, even if they started out as obese.
The adjusted incidence per 100,000 person-years for type 2 diabetes rose from 110 cases to 207 cases per 100,000 person-years among women 55 years old who weighed up to 22 pounds more than they did in high school; it was similar for men, with a rise from 147 cases to 258 cases per 100,000 person-years. Weight gain up to 10 kg boosted the incidence of hypertension from 2,754 cases to 3,415 cases per 100,000 person-years for women and from 2,366 cases to 2,861 cases for men.
Results were similar for cardiovascular disease and obesity-related cancers, particularly breast cancer among women and colorectal and prostate cancer among men. Higher amounts of weight gain were also associated with a lower likelihood of healthy aging, a composite score of the absence of multiple chronic diseases, cognitive decline, and physical limitations.
However, the investigators noted that “considering that individuals tend to underreport their weight, it is possible that our findings might have exaggerated the true risks associated with the measured weight change from early to middle adulthood.”
Also, “participants were all health professionals and were mostly white ... the results might not be generalizable to all populations,” they said.
The National Institutes of Health and American Diabetes Association funded the work. The researchers reported no conflicts of interest.
FROM JAMA
Key clinical point:
Major finding: The adjusted incidence per 100,000 person-years for type 2 diabetes rose from 110 cases to 207 cases per 100,000 person-years among women 55 years old who weighed up to 22 pounds more than they did in high school; it was similar for men, with a rise from 147 cases to 258 cases per 100,000 person-years.
Data source: Review of data on 92,837 women in the Nurses’ Health Study and 25,303 men in the Health Professionals Follow-Up Study.
Disclosures: The National Institutes of Health and American Diabetes Association funded the work. The researchers reported no conflicts of interest.
Study: No increased mortality with ACA-prompted readmission declines
Concerns that efforts to reduce 30-day hospital readmission rates under the Affordable Care Act’s Hospital Readmission Reduction Program might lead to unintended increases in mortality rates appear to be unfounded, according to a review of more than 6.7 million hospitalizations for heart failure, acute myocardial infarction, or pneumonia between 2008 and 2014.
In fact, reductions in 30-day readmission rates among Medicare fee-for-service beneficiaries are weakly but significantly correlated with reductions in hospital 30-day mortality rates after discharge, according to Kumar Dharmarajan, MD, of Yale New Haven (Conn.) Health, and colleagues (JAMA 2017 Jul 18;318[3]:270-8. doi: 10.1001/jama.2017.8444).
From 2008 to 2014, the RARRs declined in aggregate across hospitals (–0.053% for heart failure, –0.044% for acute MI, and –0.033% for pneumonia).
“In contrast, monthly aggregate trends across hospitals in 30-day risk-adjusted mortality rates after discharge varied by admitting condition” the investigators said.
For heart failure, acute MI, and pneumonia, there was an increase of 0.008%, a decrease of 0.003%, and an increase of 0.001%, respectively, they said. However, paired monthly trends in 30-day RARRs and 30-day RAMRs after discharge “identified concomitant reduction in readmission and mortality rates within hospitals.”
Correlation coefficients of the paired monthly trends for heart failure, acute MI, and pneumonia in 2008-2014 were 0.066, 0.067, and 0.108, respectively.
“Paired trends in hospital 30-day risk-adjusted readmission rates and both 90-day risk-adjusted mortality rates after discharge and 90-day risk-adjusted mortality rates after the admission date also identified concomitant reductions in readmission and mortality rates within hospitals,” the authors wrote.
The findings “do not support increasing postdischarge mortality related to reducing hospital readmissions,” they concluded.
The authors work under contract with the Centers for Medicare & Medicaid Services to develop and maintain performance measures. Dr. Dharmarajan reported serving as a consultant and scientific advisory board member for Clover Health at the time this research was performed. He is supported by grants from the National Institute on Aging and the American Federation for Aging Research, and the Yale Claude D. Pepper Older Americans Independence Center.
The findings by Dharmarajan and colleagues are “certainly good news,” Karen E. Joynt Maddox, MD, wrote in an editorial.
The study provides support for strategies that hospitals are using to reduce readmissions, and also underscores the importance of evaluating unintended consequences of policy changes such as the Affordable Care Act’s Hospital Readmissions Reduction Program (HRRP), she said (JAMA. 2017 Jul 18;318[3]:243-4).
The study did not address the possibility that attention to reducing readmissions has taken priority over reducing mortality, which could have the unintended consequence of slowing improvements in mortality, she noted, suggesting that for this and other reasons it may be “time to reexamine and reengineer the HRRP to avoid unintended consequences and to ensure that its incentives are fully aligned with the ultimate goal of improving the health outcomes of patients.
“Only with full knowledge of the advantages and disadvantages of a particular policy decision can policy makers and advocates work to craft statutes and rules that maximize benefits while minimizing harms,” she wrote.
Dr. Joynt Maddox is with Brigham and Women’s Hospital, Boston. She is supported by a grant from the National Heart, Lung, and Blood Institute.
The findings by Dharmarajan and colleagues are “certainly good news,” Karen E. Joynt Maddox, MD, wrote in an editorial.
The study provides support for strategies that hospitals are using to reduce readmissions, and also underscores the importance of evaluating unintended consequences of policy changes such as the Affordable Care Act’s Hospital Readmissions Reduction Program (HRRP), she said (JAMA. 2017 Jul 18;318[3]:243-4).
The study did not address the possibility that attention to reducing readmissions has taken priority over reducing mortality, which could have the unintended consequence of slowing improvements in mortality, she noted, suggesting that for this and other reasons it may be “time to reexamine and reengineer the HRRP to avoid unintended consequences and to ensure that its incentives are fully aligned with the ultimate goal of improving the health outcomes of patients.
“Only with full knowledge of the advantages and disadvantages of a particular policy decision can policy makers and advocates work to craft statutes and rules that maximize benefits while minimizing harms,” she wrote.
Dr. Joynt Maddox is with Brigham and Women’s Hospital, Boston. She is supported by a grant from the National Heart, Lung, and Blood Institute.
The findings by Dharmarajan and colleagues are “certainly good news,” Karen E. Joynt Maddox, MD, wrote in an editorial.
The study provides support for strategies that hospitals are using to reduce readmissions, and also underscores the importance of evaluating unintended consequences of policy changes such as the Affordable Care Act’s Hospital Readmissions Reduction Program (HRRP), she said (JAMA. 2017 Jul 18;318[3]:243-4).
The study did not address the possibility that attention to reducing readmissions has taken priority over reducing mortality, which could have the unintended consequence of slowing improvements in mortality, she noted, suggesting that for this and other reasons it may be “time to reexamine and reengineer the HRRP to avoid unintended consequences and to ensure that its incentives are fully aligned with the ultimate goal of improving the health outcomes of patients.
“Only with full knowledge of the advantages and disadvantages of a particular policy decision can policy makers and advocates work to craft statutes and rules that maximize benefits while minimizing harms,” she wrote.
Dr. Joynt Maddox is with Brigham and Women’s Hospital, Boston. She is supported by a grant from the National Heart, Lung, and Blood Institute.
Concerns that efforts to reduce 30-day hospital readmission rates under the Affordable Care Act’s Hospital Readmission Reduction Program might lead to unintended increases in mortality rates appear to be unfounded, according to a review of more than 6.7 million hospitalizations for heart failure, acute myocardial infarction, or pneumonia between 2008 and 2014.
In fact, reductions in 30-day readmission rates among Medicare fee-for-service beneficiaries are weakly but significantly correlated with reductions in hospital 30-day mortality rates after discharge, according to Kumar Dharmarajan, MD, of Yale New Haven (Conn.) Health, and colleagues (JAMA 2017 Jul 18;318[3]:270-8. doi: 10.1001/jama.2017.8444).
From 2008 to 2014, the RARRs declined in aggregate across hospitals (–0.053% for heart failure, –0.044% for acute MI, and –0.033% for pneumonia).
“In contrast, monthly aggregate trends across hospitals in 30-day risk-adjusted mortality rates after discharge varied by admitting condition” the investigators said.
For heart failure, acute MI, and pneumonia, there was an increase of 0.008%, a decrease of 0.003%, and an increase of 0.001%, respectively, they said. However, paired monthly trends in 30-day RARRs and 30-day RAMRs after discharge “identified concomitant reduction in readmission and mortality rates within hospitals.”
Correlation coefficients of the paired monthly trends for heart failure, acute MI, and pneumonia in 2008-2014 were 0.066, 0.067, and 0.108, respectively.
“Paired trends in hospital 30-day risk-adjusted readmission rates and both 90-day risk-adjusted mortality rates after discharge and 90-day risk-adjusted mortality rates after the admission date also identified concomitant reductions in readmission and mortality rates within hospitals,” the authors wrote.
The findings “do not support increasing postdischarge mortality related to reducing hospital readmissions,” they concluded.
The authors work under contract with the Centers for Medicare & Medicaid Services to develop and maintain performance measures. Dr. Dharmarajan reported serving as a consultant and scientific advisory board member for Clover Health at the time this research was performed. He is supported by grants from the National Institute on Aging and the American Federation for Aging Research, and the Yale Claude D. Pepper Older Americans Independence Center.
Concerns that efforts to reduce 30-day hospital readmission rates under the Affordable Care Act’s Hospital Readmission Reduction Program might lead to unintended increases in mortality rates appear to be unfounded, according to a review of more than 6.7 million hospitalizations for heart failure, acute myocardial infarction, or pneumonia between 2008 and 2014.
In fact, reductions in 30-day readmission rates among Medicare fee-for-service beneficiaries are weakly but significantly correlated with reductions in hospital 30-day mortality rates after discharge, according to Kumar Dharmarajan, MD, of Yale New Haven (Conn.) Health, and colleagues (JAMA 2017 Jul 18;318[3]:270-8. doi: 10.1001/jama.2017.8444).
From 2008 to 2014, the RARRs declined in aggregate across hospitals (–0.053% for heart failure, –0.044% for acute MI, and –0.033% for pneumonia).
“In contrast, monthly aggregate trends across hospitals in 30-day risk-adjusted mortality rates after discharge varied by admitting condition” the investigators said.
For heart failure, acute MI, and pneumonia, there was an increase of 0.008%, a decrease of 0.003%, and an increase of 0.001%, respectively, they said. However, paired monthly trends in 30-day RARRs and 30-day RAMRs after discharge “identified concomitant reduction in readmission and mortality rates within hospitals.”
Correlation coefficients of the paired monthly trends for heart failure, acute MI, and pneumonia in 2008-2014 were 0.066, 0.067, and 0.108, respectively.
“Paired trends in hospital 30-day risk-adjusted readmission rates and both 90-day risk-adjusted mortality rates after discharge and 90-day risk-adjusted mortality rates after the admission date also identified concomitant reductions in readmission and mortality rates within hospitals,” the authors wrote.
The findings “do not support increasing postdischarge mortality related to reducing hospital readmissions,” they concluded.
The authors work under contract with the Centers for Medicare & Medicaid Services to develop and maintain performance measures. Dr. Dharmarajan reported serving as a consultant and scientific advisory board member for Clover Health at the time this research was performed. He is supported by grants from the National Institute on Aging and the American Federation for Aging Research, and the Yale Claude D. Pepper Older Americans Independence Center.
FROM JAMA
Key clinical point:
Major finding: Correlation coefficients of the paired monthly trends for heart failure, acute myocardial infarction, and pneumonia in 2008-2014 were 0.066, 0.067, and 0.108, respectively.
Data source: A retrospective review of more than 6.7 million hospitalized Medicare fee-for-service beneficiaries.
Disclosures: The authors work under contract with the Centers for Medicare & Medicaid Services to develop and maintain performance measures. Dr. Dharmarajan reported serving as a consultant and scientific advisory board member for Clover Health at the time this research was performed. He is supported by grants from the National Institute on Aging and the American Federation for Aging Research, and the Yale Claude D. Pepper Older Americans Independence Center.
This Month in CHEST: Editor’s Picks
Giants in Chest Medicine
John B. West, MD, PhD, DSc
By Dr. F. L. Powell
Original Research
Endothelial Permeability and Hemostasis in Septic Shock: Results From the ProCESS Trial.
By Dr. P. C. Hou, et al.
Maximal Inspiratory Pressure: Does the Choice of Reference Values Actually Matter?
By Dr. A. Rodrigues, et al.
Research Into Childhood Obstructive Sleep-Disordered Breathing:
A Systematic Review
By Dr. R. P. Venekamp, et al.
Topics in Practice Management
Low-Dose CT Scan for Lung Cancer Screening: Clinical and Coding Considerations
By Drs.Y. Shieh and M. Bohnenkamp
Giants in Chest Medicine
John B. West, MD, PhD, DSc
By Dr. F. L. Powell
Original Research
Endothelial Permeability and Hemostasis in Septic Shock: Results From the ProCESS Trial.
By Dr. P. C. Hou, et al.
Maximal Inspiratory Pressure: Does the Choice of Reference Values Actually Matter?
By Dr. A. Rodrigues, et al.
Research Into Childhood Obstructive Sleep-Disordered Breathing:
A Systematic Review
By Dr. R. P. Venekamp, et al.
Topics in Practice Management
Low-Dose CT Scan for Lung Cancer Screening: Clinical and Coding Considerations
By Drs.Y. Shieh and M. Bohnenkamp
Giants in Chest Medicine
John B. West, MD, PhD, DSc
By Dr. F. L. Powell
Original Research
Endothelial Permeability and Hemostasis in Septic Shock: Results From the ProCESS Trial.
By Dr. P. C. Hou, et al.
Maximal Inspiratory Pressure: Does the Choice of Reference Values Actually Matter?
By Dr. A. Rodrigues, et al.
Research Into Childhood Obstructive Sleep-Disordered Breathing:
A Systematic Review
By Dr. R. P. Venekamp, et al.
Topics in Practice Management
Low-Dose CT Scan for Lung Cancer Screening: Clinical and Coding Considerations
By Drs.Y. Shieh and M. Bohnenkamp
SLEEP STRATEGIES: Group 3 pulmonary hypertension linked to sleep-disordered breathing
Pulmonary hypertension (PH) is a progressive disease characterized by an increase in pulmonary arterial pressure and pulmonary vascular resistance (PVR) leading to right ventricular failure. Although substantial progress has been achieved in the treatment of PH, mostly due to improved pharmacotherapy, it remains a life-threatening disease with a poor prognosis. Increased pulmonary arterial pressure is a common feature of many chronic lung diseases, and chronic lung disease is the second most common cause of pulmonary hypertension. PH caused by chronic lung disease, including PH due to sleep-disordered breathing (SDB), is referred to as group 3 PH in the classification of pulmonary hypertension (Simonneau et al. J Am Coll Cardiol. 2013;62:D34 e41). Many reports since have linked pulmonary arterial hypertension to obstructive sleep apnea (OSA). These were validated in animal trials, when rodents were exposed to intermittent hypoxia for several hours over a few weeks, similar to what is seen in patients with OSA; this resulted in pulmonary vascular remodeling, sustained PH, and right ventricular hypertrophy. As with other chronic lung disease, prevalence rates of PH in SDB vary greatly, with some studies suggesting prevalence of pulmonary hypertension in OSA to be as high as 40%, although a lack of large-scale studies with clearly defined patient populations makes it difficult to determine the true prevalence rate. Most studies suggest that about 20% to 30% of patients with OSA have some degree of PH. OSA has been shown to be an independent causal factor for the development of PH (Hurdman et al. Eur Respir J. 2012; 39, 945–955). PH associated with OSA appears to be mild and may be due to a combination of precapillary and postcapillary factors, including pulmonary arteriolar remodeling, hyperreactivity to hypoxia, and left ventricular diastolic dysfunction resulting in left atrial enlargement. Despite differences in reported prevalence rates, most studies consistently reported mild increases in pulmonary arterial pressure with mPAP averaging less than 30 mm Hg. In one of the largest studies to date, the prevalence rate of PH in 220 patients with SDB was 17%, and the mPAP was 26 +/- 6 mm Hg (Chaouat et al. Chest. 1996;109[2]:380).
The other consistent finding in most studies was that PH correlated with the severity of obesity, daytime hypoxia and hypercapnia, obstructive airways disease, and nocturnal oxygen desaturation. PH seems to be more common and more severe in obesity hypoventilation syndrome (OHS) than in “pure” OSA patients (58% vs 9%) (Kessler et al. Chest. 2001;120[2]:369).
The incidence of OSA is rising in parallel with the rising global incide

Patients with OSA who have PH are more likely to be obese, have decreased respiratory function (FEV1, vital capacity, and FEV1/VC ratio), and lower oxygen saturation/higher carbon dioxide content in blood (Chaouat et al. Chest. 1996;109[2]:380). These patients frequently present with shortness of breath and dyspnea on exertion. Echocardiogram remains the main screening tool for evaluation of PH. With that said, right-sided heart catheterization remains the gold standard for the diagnosis of all classes of PH; however, use of right-sided heart catheterization in group 3 pulmonary hypertension is reserved for select patients. This is likely because PH in patients with OSA is accepted as a more benign prognostic marker compared with other group 3 forms. Furthermore, patients with OHS are more prone to developing PH and cor pulmonale compared with patients with isolated OSA. OSA with PH has lower survival rates than OSA without PH. Studies showed that patients with OHS tend to do worse than patients with OSA alone (Aljohara et al. J Thorac Dis. 2017;9[3]:779).
AHI and PH
Various studies have looked at different polysomnographic variables to understand the relationship between PH and OSA. Initial studies showed that the apnea hypopnea index (AHI) does not predict development of PH among patients with OSA. Decrements in nocturnal oxygen saturation, however, is predictive of the development of PH; the only predictor of developing PH among patients with OSA in one study was time spent with oxygen saturation below 70% during sleep (Wong et al. Eur Arch Otorhinolaryngol. 2017;74:2601). In addition, recent data suggest there is no statistically significant association between age, gender, body mass index, or AHI and chance for development of PH (Wong et al. 2017). It was found that the percentage of time during sleep with oxygen saturation below 90% was significant and independently associated with higher PAP. Furthermore, a recent study demonstrated that patients with moderate to severe OSA (AHI over 15/h) who develop PH tend to have worse hemodynamics (higher PVR and mPAP) and subclinical myocardial damage (evaluated by troponin T), as well as increased ventricular wall stress (assessed by proBNP) when compared with patients with mild OSA (AHI less than 15/h).
Treatment
The mainstay treatment for OSA and OHS is positive airway pressure (PAP). This therapy has been shown to improve sleep and respiratory parameters, including sleep quality, overall quality of life, as well as promote reduction in mean pulmonary arterial pressure. The regular use of noninvasive positive-pressure ventilation has also been shown to reverse daytime hypoxia and hypercapnia, as well as influence inflammatory markers: decrease circulating levels of endothelin-1, interleukin-6, and C-reactive protein, thereby improving vascular endothelial function and reducing platelet activation and aggregation (Yokoe et al. Circulation. 2003;107[8]:1129). Indeed, there is a decrease in mean pulmonary arterial pressure in some patients with long-term daily use of PAP, but, in some patients, both pulmonary and right ventricular dysfunction persists, suggesting vascular remodeling and/or endothelial dysfunction. These findings indicate the need for early recognition of OSA and early treatment for patients, thus preventing remodeling and further development of PH and right ventricular dysfunction. Adequate control of OSA/OHS has important long-term effects on overall health, because it significantly reduces the risk of systemic hypertension, congestive heart failure, arrhythmias, and stroke. It is imperative to control underlying SDB before considering PAH-specific medications to treat PH associated with OSA or OHS unless the patient is demonstrating signs of right-sided heart failure; in such cases, concomitant therapy may be considered upfront. It is recommended that

Dr. Singhal is a second-year fellow in Pulmonary/Critical Care and Dr. Minkin is Director, Pulmonary Hypertension Program, New York Presbyterian-Brooklyn Methodist Hospital. Dr. Minkin is also Assistant Professor of Clinical Medicine, Weill Cornell Medical College, New York.
Pulmonary hypertension (PH) is a progressive disease characterized by an increase in pulmonary arterial pressure and pulmonary vascular resistance (PVR) leading to right ventricular failure. Although substantial progress has been achieved in the treatment of PH, mostly due to improved pharmacotherapy, it remains a life-threatening disease with a poor prognosis. Increased pulmonary arterial pressure is a common feature of many chronic lung diseases, and chronic lung disease is the second most common cause of pulmonary hypertension. PH caused by chronic lung disease, including PH due to sleep-disordered breathing (SDB), is referred to as group 3 PH in the classification of pulmonary hypertension (Simonneau et al. J Am Coll Cardiol. 2013;62:D34 e41). Many reports since have linked pulmonary arterial hypertension to obstructive sleep apnea (OSA). These were validated in animal trials, when rodents were exposed to intermittent hypoxia for several hours over a few weeks, similar to what is seen in patients with OSA; this resulted in pulmonary vascular remodeling, sustained PH, and right ventricular hypertrophy. As with other chronic lung disease, prevalence rates of PH in SDB vary greatly, with some studies suggesting prevalence of pulmonary hypertension in OSA to be as high as 40%, although a lack of large-scale studies with clearly defined patient populations makes it difficult to determine the true prevalence rate. Most studies suggest that about 20% to 30% of patients with OSA have some degree of PH. OSA has been shown to be an independent causal factor for the development of PH (Hurdman et al. Eur Respir J. 2012; 39, 945–955). PH associated with OSA appears to be mild and may be due to a combination of precapillary and postcapillary factors, including pulmonary arteriolar remodeling, hyperreactivity to hypoxia, and left ventricular diastolic dysfunction resulting in left atrial enlargement. Despite differences in reported prevalence rates, most studies consistently reported mild increases in pulmonary arterial pressure with mPAP averaging less than 30 mm Hg. In one of the largest studies to date, the prevalence rate of PH in 220 patients with SDB was 17%, and the mPAP was 26 +/- 6 mm Hg (Chaouat et al. Chest. 1996;109[2]:380).
The other consistent finding in most studies was that PH correlated with the severity of obesity, daytime hypoxia and hypercapnia, obstructive airways disease, and nocturnal oxygen desaturation. PH seems to be more common and more severe in obesity hypoventilation syndrome (OHS) than in “pure” OSA patients (58% vs 9%) (Kessler et al. Chest. 2001;120[2]:369).
The incidence of OSA is rising in parallel with the rising global incide
Patients with OSA who have PH are more likely to be obese, have decreased respiratory function (FEV1, vital capacity, and FEV1/VC ratio), and lower oxygen saturation/higher carbon dioxide content in blood (Chaouat et al. Chest. 1996;109[2]:380). These patients frequently present with shortness of breath and dyspnea on exertion. Echocardiogram remains the main screening tool for evaluation of PH. With that said, right-sided heart catheterization remains the gold standard for the diagnosis of all classes of PH; however, use of right-sided heart catheterization in group 3 pulmonary hypertension is reserved for select patients. This is likely because PH in patients with OSA is accepted as a more benign prognostic marker compared with other group 3 forms. Furthermore, patients with OHS are more prone to developing PH and cor pulmonale compared with patients with isolated OSA. OSA with PH has lower survival rates than OSA without PH. Studies showed that patients with OHS tend to do worse than patients with OSA alone (Aljohara et al. J Thorac Dis. 2017;9[3]:779).
AHI and PH
Various studies have looked at different polysomnographic variables to understand the relationship between PH and OSA. Initial studies showed that the apnea hypopnea index (AHI) does not predict development of PH among patients with OSA. Decrements in nocturnal oxygen saturation, however, is predictive of the development of PH; the only predictor of developing PH among patients with OSA in one study was time spent with oxygen saturation below 70% during sleep (Wong et al. Eur Arch Otorhinolaryngol. 2017;74:2601). In addition, recent data suggest there is no statistically significant association between age, gender, body mass index, or AHI and chance for development of PH (Wong et al. 2017). It was found that the percentage of time during sleep with oxygen saturation below 90% was significant and independently associated with higher PAP. Furthermore, a recent study demonstrated that patients with moderate to severe OSA (AHI over 15/h) who develop PH tend to have worse hemodynamics (higher PVR and mPAP) and subclinical myocardial damage (evaluated by troponin T), as well as increased ventricular wall stress (assessed by proBNP) when compared with patients with mild OSA (AHI less than 15/h).
Treatment
The mainstay treatment for OSA and OHS is positive airway pressure (PAP). This therapy has been shown to improve sleep and respiratory parameters, including sleep quality, overall quality of life, as well as promote reduction in mean pulmonary arterial pressure. The regular use of noninvasive positive-pressure ventilation has also been shown to reverse daytime hypoxia and hypercapnia, as well as influence inflammatory markers: decrease circulating levels of endothelin-1, interleukin-6, and C-reactive protein, thereby improving vascular endothelial function and reducing platelet activation and aggregation (Yokoe et al. Circulation. 2003;107[8]:1129). Indeed, there is a decrease in mean pulmonary arterial pressure in some patients with long-term daily use of PAP, but, in some patients, both pulmonary and right ventricular dysfunction persists, suggesting vascular remodeling and/or endothelial dysfunction. These findings indicate the need for early recognition of OSA and early treatment for patients, thus preventing remodeling and further development of PH and right ventricular dysfunction. Adequate control of OSA/OHS has important long-term effects on overall health, because it significantly reduces the risk of systemic hypertension, congestive heart failure, arrhythmias, and stroke. It is imperative to control underlying SDB before considering PAH-specific medications to treat PH associated with OSA or OHS unless the patient is demonstrating signs of right-sided heart failure; in such cases, concomitant therapy may be considered upfront. It is recommended that
Dr. Singhal is a second-year fellow in Pulmonary/Critical Care and Dr. Minkin is Director, Pulmonary Hypertension Program, New York Presbyterian-Brooklyn Methodist Hospital. Dr. Minkin is also Assistant Professor of Clinical Medicine, Weill Cornell Medical College, New York.
Pulmonary hypertension (PH) is a progressive disease characterized by an increase in pulmonary arterial pressure and pulmonary vascular resistance (PVR) leading to right ventricular failure. Although substantial progress has been achieved in the treatment of PH, mostly due to improved pharmacotherapy, it remains a life-threatening disease with a poor prognosis. Increased pulmonary arterial pressure is a common feature of many chronic lung diseases, and chronic lung disease is the second most common cause of pulmonary hypertension. PH caused by chronic lung disease, including PH due to sleep-disordered breathing (SDB), is referred to as group 3 PH in the classification of pulmonary hypertension (Simonneau et al. J Am Coll Cardiol. 2013;62:D34 e41). Many reports since have linked pulmonary arterial hypertension to obstructive sleep apnea (OSA). These were validated in animal trials, when rodents were exposed to intermittent hypoxia for several hours over a few weeks, similar to what is seen in patients with OSA; this resulted in pulmonary vascular remodeling, sustained PH, and right ventricular hypertrophy. As with other chronic lung disease, prevalence rates of PH in SDB vary greatly, with some studies suggesting prevalence of pulmonary hypertension in OSA to be as high as 40%, although a lack of large-scale studies with clearly defined patient populations makes it difficult to determine the true prevalence rate. Most studies suggest that about 20% to 30% of patients with OSA have some degree of PH. OSA has been shown to be an independent causal factor for the development of PH (Hurdman et al. Eur Respir J. 2012; 39, 945–955). PH associated with OSA appears to be mild and may be due to a combination of precapillary and postcapillary factors, including pulmonary arteriolar remodeling, hyperreactivity to hypoxia, and left ventricular diastolic dysfunction resulting in left atrial enlargement. Despite differences in reported prevalence rates, most studies consistently reported mild increases in pulmonary arterial pressure with mPAP averaging less than 30 mm Hg. In one of the largest studies to date, the prevalence rate of PH in 220 patients with SDB was 17%, and the mPAP was 26 +/- 6 mm Hg (Chaouat et al. Chest. 1996;109[2]:380).
The other consistent finding in most studies was that PH correlated with the severity of obesity, daytime hypoxia and hypercapnia, obstructive airways disease, and nocturnal oxygen desaturation. PH seems to be more common and more severe in obesity hypoventilation syndrome (OHS) than in “pure” OSA patients (58% vs 9%) (Kessler et al. Chest. 2001;120[2]:369).
The incidence of OSA is rising in parallel with the rising global incide
Patients with OSA who have PH are more likely to be obese, have decreased respiratory function (FEV1, vital capacity, and FEV1/VC ratio), and lower oxygen saturation/higher carbon dioxide content in blood (Chaouat et al. Chest. 1996;109[2]:380). These patients frequently present with shortness of breath and dyspnea on exertion. Echocardiogram remains the main screening tool for evaluation of PH. With that said, right-sided heart catheterization remains the gold standard for the diagnosis of all classes of PH; however, use of right-sided heart catheterization in group 3 pulmonary hypertension is reserved for select patients. This is likely because PH in patients with OSA is accepted as a more benign prognostic marker compared with other group 3 forms. Furthermore, patients with OHS are more prone to developing PH and cor pulmonale compared with patients with isolated OSA. OSA with PH has lower survival rates than OSA without PH. Studies showed that patients with OHS tend to do worse than patients with OSA alone (Aljohara et al. J Thorac Dis. 2017;9[3]:779).
AHI and PH
Various studies have looked at different polysomnographic variables to understand the relationship between PH and OSA. Initial studies showed that the apnea hypopnea index (AHI) does not predict development of PH among patients with OSA. Decrements in nocturnal oxygen saturation, however, is predictive of the development of PH; the only predictor of developing PH among patients with OSA in one study was time spent with oxygen saturation below 70% during sleep (Wong et al. Eur Arch Otorhinolaryngol. 2017;74:2601). In addition, recent data suggest there is no statistically significant association between age, gender, body mass index, or AHI and chance for development of PH (Wong et al. 2017). It was found that the percentage of time during sleep with oxygen saturation below 90% was significant and independently associated with higher PAP. Furthermore, a recent study demonstrated that patients with moderate to severe OSA (AHI over 15/h) who develop PH tend to have worse hemodynamics (higher PVR and mPAP) and subclinical myocardial damage (evaluated by troponin T), as well as increased ventricular wall stress (assessed by proBNP) when compared with patients with mild OSA (AHI less than 15/h).
Treatment
The mainstay treatment for OSA and OHS is positive airway pressure (PAP). This therapy has been shown to improve sleep and respiratory parameters, including sleep quality, overall quality of life, as well as promote reduction in mean pulmonary arterial pressure. The regular use of noninvasive positive-pressure ventilation has also been shown to reverse daytime hypoxia and hypercapnia, as well as influence inflammatory markers: decrease circulating levels of endothelin-1, interleukin-6, and C-reactive protein, thereby improving vascular endothelial function and reducing platelet activation and aggregation (Yokoe et al. Circulation. 2003;107[8]:1129). Indeed, there is a decrease in mean pulmonary arterial pressure in some patients with long-term daily use of PAP, but, in some patients, both pulmonary and right ventricular dysfunction persists, suggesting vascular remodeling and/or endothelial dysfunction. These findings indicate the need for early recognition of OSA and early treatment for patients, thus preventing remodeling and further development of PH and right ventricular dysfunction. Adequate control of OSA/OHS has important long-term effects on overall health, because it significantly reduces the risk of systemic hypertension, congestive heart failure, arrhythmias, and stroke. It is imperative to control underlying SDB before considering PAH-specific medications to treat PH associated with OSA or OHS unless the patient is demonstrating signs of right-sided heart failure; in such cases, concomitant therapy may be considered upfront. It is recommended that
Dr. Singhal is a second-year fellow in Pulmonary/Critical Care and Dr. Minkin is Director, Pulmonary Hypertension Program, New York Presbyterian-Brooklyn Methodist Hospital. Dr. Minkin is also Assistant Professor of Clinical Medicine, Weill Cornell Medical College, New York.
High-dose vitamin D fails against young children’s upper respiratory infections
A daily dose of 2,000 IU of vitamin D had no impact on reducing wintertime upper respiratory tract infections in young children, compared with a 400 IU dose, based on a study of 703 children aged 1-5 years. The report was published July 18 in JAMA.
“Vitamin D increases the synthesis of the antimicrobial peptide cathelicidin in respiratory epithelium, which has been shown to reduce disease severity and replication of the influenza virus in vitro,” but studies on the effect of vitamin D on upper respiratory infections have been limited, wrote Mary Aglipay of St. Michael’s Hospital, Toronto, and her colleagues.
The average number of laboratory-confirmed cases of upper respiratory tract infections per child was not significantly different between the high-dose and low-dose groups (1.05 vs. 1.03).
The median time to the first laboratory-confirmed infection was similar between the groups: 3.95 months in the high-dose group and 3.29 months in the low-dose group. In addition, the number of parent-reported upper respiratory tract infections was similar between the high-dose and low-dose groups (625 vs. 600).
Serum 25-hydroxyvitamin D levels also remained comparable between the high-dose and low-dose groups at the study’s end (48.7 ng/mL vs. 36.8 ng/mL).
The results were limited by several factors, including the lack of a placebo group and the high baseline vitamin D levels in the children at the end of the summer, the researchers noted.
However, “these findings do not support the routine use of high-dose vitamin D supplementation in children for the prevention of viral upper respiratory tract infection,” they said.
The study was supported by the Canadian Institutes of Health Research, Institute of Human Development, Child and Youth Health, and Institute of Nutrition, Metabolism and Diabetes, and the Thrasher Research Fund. The vitamin D formulations were donated by Ddrops. Ms. Aglipay had no financial conflicts to disclose. One coauthor, Muhammad Mamdani, MPH, had ties to a number of pharmaceutical companies.
A daily dose of 2,000 IU of vitamin D had no impact on reducing wintertime upper respiratory tract infections in young children, compared with a 400 IU dose, based on a study of 703 children aged 1-5 years. The report was published July 18 in JAMA.
“Vitamin D increases the synthesis of the antimicrobial peptide cathelicidin in respiratory epithelium, which has been shown to reduce disease severity and replication of the influenza virus in vitro,” but studies on the effect of vitamin D on upper respiratory infections have been limited, wrote Mary Aglipay of St. Michael’s Hospital, Toronto, and her colleagues.
The average number of laboratory-confirmed cases of upper respiratory tract infections per child was not significantly different between the high-dose and low-dose groups (1.05 vs. 1.03).
The median time to the first laboratory-confirmed infection was similar between the groups: 3.95 months in the high-dose group and 3.29 months in the low-dose group. In addition, the number of parent-reported upper respiratory tract infections was similar between the high-dose and low-dose groups (625 vs. 600).
Serum 25-hydroxyvitamin D levels also remained comparable between the high-dose and low-dose groups at the study’s end (48.7 ng/mL vs. 36.8 ng/mL).
The results were limited by several factors, including the lack of a placebo group and the high baseline vitamin D levels in the children at the end of the summer, the researchers noted.
However, “these findings do not support the routine use of high-dose vitamin D supplementation in children for the prevention of viral upper respiratory tract infection,” they said.
The study was supported by the Canadian Institutes of Health Research, Institute of Human Development, Child and Youth Health, and Institute of Nutrition, Metabolism and Diabetes, and the Thrasher Research Fund. The vitamin D formulations were donated by Ddrops. Ms. Aglipay had no financial conflicts to disclose. One coauthor, Muhammad Mamdani, MPH, had ties to a number of pharmaceutical companies.
A daily dose of 2,000 IU of vitamin D had no impact on reducing wintertime upper respiratory tract infections in young children, compared with a 400 IU dose, based on a study of 703 children aged 1-5 years. The report was published July 18 in JAMA.
“Vitamin D increases the synthesis of the antimicrobial peptide cathelicidin in respiratory epithelium, which has been shown to reduce disease severity and replication of the influenza virus in vitro,” but studies on the effect of vitamin D on upper respiratory infections have been limited, wrote Mary Aglipay of St. Michael’s Hospital, Toronto, and her colleagues.
The average number of laboratory-confirmed cases of upper respiratory tract infections per child was not significantly different between the high-dose and low-dose groups (1.05 vs. 1.03).
The median time to the first laboratory-confirmed infection was similar between the groups: 3.95 months in the high-dose group and 3.29 months in the low-dose group. In addition, the number of parent-reported upper respiratory tract infections was similar between the high-dose and low-dose groups (625 vs. 600).
Serum 25-hydroxyvitamin D levels also remained comparable between the high-dose and low-dose groups at the study’s end (48.7 ng/mL vs. 36.8 ng/mL).
The results were limited by several factors, including the lack of a placebo group and the high baseline vitamin D levels in the children at the end of the summer, the researchers noted.
However, “these findings do not support the routine use of high-dose vitamin D supplementation in children for the prevention of viral upper respiratory tract infection,” they said.
The study was supported by the Canadian Institutes of Health Research, Institute of Human Development, Child and Youth Health, and Institute of Nutrition, Metabolism and Diabetes, and the Thrasher Research Fund. The vitamin D formulations were donated by Ddrops. Ms. Aglipay had no financial conflicts to disclose. One coauthor, Muhammad Mamdani, MPH, had ties to a number of pharmaceutical companies.
FROM JAMA
Key clinical point:
Major finding: The average number of laboratory-confirmed upper respiratory tract infections per child was not significantly different between the high-dose and low-dose groups (1.05 vs. 1.03).
Data source: A study of 703 healthy children aged 1-5 years randomized to 2,000 IU or 400 IU of vitamin D.
Disclosures: The study was supported by the Canadian Institutes of Health Research, Institute of Human Development, Child and Youth Health, and Institute of Nutrition, Metabolism and Diabetes, and the Thrasher Research Fund. The vitamin D formulations were donated by Ddrops. Ms. Aglipay had no financial conflicts to disclose. One coauthor, Muhammad Mamdani, MPH, had ties to a number of pharmaceutical companies.

FDA approves neratinib for extended adjuvant treatment of HER2+ breast cancer
The Food and Drug Administration has approved neratinib, an oral tyrosine kinase inhibitor, for the extended adjuvant treatment of patients with early-stage, HER2-positive breast cancer who have previously been treated with trastuzumab.
Approval was based on improved invasive disease-free survival (iDFS) in the phase 3 ExteNET trial of 2,840 women with early-stage HER2-positive breast cancer who were within 2 years of completing adjuvant trastuzumab. Patients were randomized to receive either neratinib or placebo daily for 1 year. After 2 years of follow-up, iDFS was 94.2% in patients treated with neratinib, compared with 91.9% in those receiving placebo (hazard ratio, 0.66; 95% confidence interval, 0.49, 0.90; P = .008), according to the FDA statement.
The most common adverse reactions to neratinib in ExteNET were diarrhea, nausea, abdominal pain, fatigue, vomiting, rash, stomatitis, decreased appetite, muscle spasms, dyspepsia, AST or ALT increase, nail disorder, dry skin, abdominal distention, weight loss, and urinary tract infection. Diarrhea was observed in 16.8% of neratinib-treated patients.
The recommended dose of of neratinib is 240 mg (six 40 mg tablets) given orally once daily with food, continuously, for 1 year. Patients should be given antidiarrheal prophylaxis for the first 56 days of treatment with neratinib and as needed thereafter to help manage diarrhea, the FDA said.
The Food and Drug Administration has approved neratinib, an oral tyrosine kinase inhibitor, for the extended adjuvant treatment of patients with early-stage, HER2-positive breast cancer who have previously been treated with trastuzumab.
Approval was based on improved invasive disease-free survival (iDFS) in the phase 3 ExteNET trial of 2,840 women with early-stage HER2-positive breast cancer who were within 2 years of completing adjuvant trastuzumab. Patients were randomized to receive either neratinib or placebo daily for 1 year. After 2 years of follow-up, iDFS was 94.2% in patients treated with neratinib, compared with 91.9% in those receiving placebo (hazard ratio, 0.66; 95% confidence interval, 0.49, 0.90; P = .008), according to the FDA statement.
The most common adverse reactions to neratinib in ExteNET were diarrhea, nausea, abdominal pain, fatigue, vomiting, rash, stomatitis, decreased appetite, muscle spasms, dyspepsia, AST or ALT increase, nail disorder, dry skin, abdominal distention, weight loss, and urinary tract infection. Diarrhea was observed in 16.8% of neratinib-treated patients.
The recommended dose of of neratinib is 240 mg (six 40 mg tablets) given orally once daily with food, continuously, for 1 year. Patients should be given antidiarrheal prophylaxis for the first 56 days of treatment with neratinib and as needed thereafter to help manage diarrhea, the FDA said.
The Food and Drug Administration has approved neratinib, an oral tyrosine kinase inhibitor, for the extended adjuvant treatment of patients with early-stage, HER2-positive breast cancer who have previously been treated with trastuzumab.
Approval was based on improved invasive disease-free survival (iDFS) in the phase 3 ExteNET trial of 2,840 women with early-stage HER2-positive breast cancer who were within 2 years of completing adjuvant trastuzumab. Patients were randomized to receive either neratinib or placebo daily for 1 year. After 2 years of follow-up, iDFS was 94.2% in patients treated with neratinib, compared with 91.9% in those receiving placebo (hazard ratio, 0.66; 95% confidence interval, 0.49, 0.90; P = .008), according to the FDA statement.
The most common adverse reactions to neratinib in ExteNET were diarrhea, nausea, abdominal pain, fatigue, vomiting, rash, stomatitis, decreased appetite, muscle spasms, dyspepsia, AST or ALT increase, nail disorder, dry skin, abdominal distention, weight loss, and urinary tract infection. Diarrhea was observed in 16.8% of neratinib-treated patients.
The recommended dose of of neratinib is 240 mg (six 40 mg tablets) given orally once daily with food, continuously, for 1 year. Patients should be given antidiarrheal prophylaxis for the first 56 days of treatment with neratinib and as needed thereafter to help manage diarrhea, the FDA said.
Small brain infarcts’ cognitive impact equals that of large infarcts
LONDON – Small infarct-like brain lesions have long been ignored in both research and clinical settings, but an ongoing analysis of an observational cohort shows that they can be just as cognitively damaging as large infarcts. Having both is a serious one-two punch to thinking and memory.
At less than 3 mm, infarct-like lesions (ILL) may be tiny, but, over 20 years, they exerted exactly the same deleterious effect on cognition as lesions 3 mm or larger, Beverly Gwen Windham, MD, said at the Alzheimer’s Association International Conference.

When neuroradiologists began to look at brain infarcts several decades ago, they used then state-of-the-art 1.5 Tesla MRI. As infarct description and classification evolved, anything measuring smaller than 3 mm was classified as an infarct-like lesion and anything 3 mm or larger as a large infarct. There was some concern that readers would confuse the ILLs with perivascular spaces and flag these normal voids as pathological changes, Dr. Windham said. As a result, research studies have always excluded them. Since they’re usually associated with silent events, without any clinical signs or symptoms, they’ve been clinically disregarded as well, adding to the perception that they have little long-term impact.
However, in 2015, Dr. Windham and her team proved this perception incorrect, at least when it came to stroke and stroke mortality. Using the large Atherosclerosis Risk in Communities (ARIC) Study cohort, they showed that ILLs alone tripled the risk of both a stroke and stroke mortality. Patients who had both ILLs and large infarcts were nine times more likely to have a stroke and seven times more likely to die from a stroke than were patients who had no lesions.
Dr. Windham used the same ARIC cohort in the 20-year cognition study. Begun in 1987, ARIC enrolled 15,800 middle-aged adults who have been followed regularly with physical and neurocognitive testing. Its goals are largely to investigate the natural history and multiple risk factors of cardiovascular and cerebrovascular disease. In 1993, subjects who had not experienced a stroke also had a brain MRI to add more detail to the study. The investigators also have performed cognitive assessments of a large number of participants five times since 1993 on measures of delayed word recall, digit symbol substitution, and word fluency. The outcome was the change in the composite Z-score over time.
The cognition study comprised 1,881 who had brain MRI and the full five cognitive assessments over a 20-year period. The participants were stratified as having no infarcts (1,611), only ILLs (50) or large infarcts (185), or both lesions (35).
At baseline, these subjects had a mean age of 63 years, 17% had diabetes, and 48% had hypertension. About one-third were positive for an ApoE e4 allele. The mean white matter intensity score was 1.4.
“In general, everyone in the cohort had some decline in cognitive function as they got older,” Dr. Windham said. But, a striking observation was that those with ILLs only and those with large lesions only had virtually identical decline slopes over the 20-year follow-up. The change from baseline in global Z-score was 0.18 standard deviations for the ILL-only group and 0.24 standard deviations for the large infarct group. For those with both lesions, the change from baseline was 0.62.
“At the end of 20 years, those with no lesion burden declined 1.3 standard deviations from baseline, those with only ILLs declined 1.5 standard deviations, and those with large infarcts, 1.6 standard deviations,” Dr. Windham said. “But, subjects who had both lesions declined 2.5 standard deviations from baseline. This is equivalent to adding 27 years of aging. The effect of having both was nearly four times greater than [that of] having only large lesions, which, up until now, have been the only ones read on MRI in either clinical practice or in research. Overall, our findings confirm that the relationship of ILLs to cognition is very similar that of large infarcts.
“The presence of midlife ILLs appears to amplify the effect of large infarcts on cognition, and we hypothesize that this process may represent vascular disease at midlife. We may also be able to identify people at high risk of cognitive decline or even dementia at midlife. I also think that we need to be rethinking how we read MRIs. Stopping at the 3-mm threshold may be too conservative. We should be looking at other studies on the consequences of these small lesions,” she said.
Dr. Windham had no financial disclosures.
[email protected]
On Twitter @alz_gal
Virtually every time researchers look for an effect of brain vascular health on cognition, they find it. Not only do these data reveal a surprisingly large effect of a previously ignored type of brain lesion on cognition, they also highlight that poor management of vascular risk factors in midlife may lead to dementia decades later. This suggests we need more research to understand the long-term impact of these small lesions on brain health and the development of Alzheimer’s disease.
Keith Fargo, PhD, is the Alzheimer’s Association’s director of scientific programs and outreach.
Virtually every time researchers look for an effect of brain vascular health on cognition, they find it. Not only do these data reveal a surprisingly large effect of a previously ignored type of brain lesion on cognition, they also highlight that poor management of vascular risk factors in midlife may lead to dementia decades later. This suggests we need more research to understand the long-term impact of these small lesions on brain health and the development of Alzheimer’s disease.
Keith Fargo, PhD, is the Alzheimer’s Association’s director of scientific programs and outreach.
Virtually every time researchers look for an effect of brain vascular health on cognition, they find it. Not only do these data reveal a surprisingly large effect of a previously ignored type of brain lesion on cognition, they also highlight that poor management of vascular risk factors in midlife may lead to dementia decades later. This suggests we need more research to understand the long-term impact of these small lesions on brain health and the development of Alzheimer’s disease.
Keith Fargo, PhD, is the Alzheimer’s Association’s director of scientific programs and outreach.
LONDON – Small infarct-like brain lesions have long been ignored in both research and clinical settings, but an ongoing analysis of an observational cohort shows that they can be just as cognitively damaging as large infarcts. Having both is a serious one-two punch to thinking and memory.
At less than 3 mm, infarct-like lesions (ILL) may be tiny, but, over 20 years, they exerted exactly the same deleterious effect on cognition as lesions 3 mm or larger, Beverly Gwen Windham, MD, said at the Alzheimer’s Association International Conference.
When neuroradiologists began to look at brain infarcts several decades ago, they used then state-of-the-art 1.5 Tesla MRI. As infarct description and classification evolved, anything measuring smaller than 3 mm was classified as an infarct-like lesion and anything 3 mm or larger as a large infarct. There was some concern that readers would confuse the ILLs with perivascular spaces and flag these normal voids as pathological changes, Dr. Windham said. As a result, research studies have always excluded them. Since they’re usually associated with silent events, without any clinical signs or symptoms, they’ve been clinically disregarded as well, adding to the perception that they have little long-term impact.
However, in 2015, Dr. Windham and her team proved this perception incorrect, at least when it came to stroke and stroke mortality. Using the large Atherosclerosis Risk in Communities (ARIC) Study cohort, they showed that ILLs alone tripled the risk of both a stroke and stroke mortality. Patients who had both ILLs and large infarcts were nine times more likely to have a stroke and seven times more likely to die from a stroke than were patients who had no lesions.
Dr. Windham used the same ARIC cohort in the 20-year cognition study. Begun in 1987, ARIC enrolled 15,800 middle-aged adults who have been followed regularly with physical and neurocognitive testing. Its goals are largely to investigate the natural history and multiple risk factors of cardiovascular and cerebrovascular disease. In 1993, subjects who had not experienced a stroke also had a brain MRI to add more detail to the study. The investigators also have performed cognitive assessments of a large number of participants five times since 1993 on measures of delayed word recall, digit symbol substitution, and word fluency. The outcome was the change in the composite Z-score over time.
The cognition study comprised 1,881 who had brain MRI and the full five cognitive assessments over a 20-year period. The participants were stratified as having no infarcts (1,611), only ILLs (50) or large infarcts (185), or both lesions (35).
At baseline, these subjects had a mean age of 63 years, 17% had diabetes, and 48% had hypertension. About one-third were positive for an ApoE e4 allele. The mean white matter intensity score was 1.4.
“In general, everyone in the cohort had some decline in cognitive function as they got older,” Dr. Windham said. But, a striking observation was that those with ILLs only and those with large lesions only had virtually identical decline slopes over the 20-year follow-up. The change from baseline in global Z-score was 0.18 standard deviations for the ILL-only group and 0.24 standard deviations for the large infarct group. For those with both lesions, the change from baseline was 0.62.
“At the end of 20 years, those with no lesion burden declined 1.3 standard deviations from baseline, those with only ILLs declined 1.5 standard deviations, and those with large infarcts, 1.6 standard deviations,” Dr. Windham said. “But, subjects who had both lesions declined 2.5 standard deviations from baseline. This is equivalent to adding 27 years of aging. The effect of having both was nearly four times greater than [that of] having only large lesions, which, up until now, have been the only ones read on MRI in either clinical practice or in research. Overall, our findings confirm that the relationship of ILLs to cognition is very similar that of large infarcts.
“The presence of midlife ILLs appears to amplify the effect of large infarcts on cognition, and we hypothesize that this process may represent vascular disease at midlife. We may also be able to identify people at high risk of cognitive decline or even dementia at midlife. I also think that we need to be rethinking how we read MRIs. Stopping at the 3-mm threshold may be too conservative. We should be looking at other studies on the consequences of these small lesions,” she said.
Dr. Windham had no financial disclosures.
[email protected]
On Twitter @alz_gal
LONDON – Small infarct-like brain lesions have long been ignored in both research and clinical settings, but an ongoing analysis of an observational cohort shows that they can be just as cognitively damaging as large infarcts. Having both is a serious one-two punch to thinking and memory.
At less than 3 mm, infarct-like lesions (ILL) may be tiny, but, over 20 years, they exerted exactly the same deleterious effect on cognition as lesions 3 mm or larger, Beverly Gwen Windham, MD, said at the Alzheimer’s Association International Conference.
When neuroradiologists began to look at brain infarcts several decades ago, they used then state-of-the-art 1.5 Tesla MRI. As infarct description and classification evolved, anything measuring smaller than 3 mm was classified as an infarct-like lesion and anything 3 mm or larger as a large infarct. There was some concern that readers would confuse the ILLs with perivascular spaces and flag these normal voids as pathological changes, Dr. Windham said. As a result, research studies have always excluded them. Since they’re usually associated with silent events, without any clinical signs or symptoms, they’ve been clinically disregarded as well, adding to the perception that they have little long-term impact.
However, in 2015, Dr. Windham and her team proved this perception incorrect, at least when it came to stroke and stroke mortality. Using the large Atherosclerosis Risk in Communities (ARIC) Study cohort, they showed that ILLs alone tripled the risk of both a stroke and stroke mortality. Patients who had both ILLs and large infarcts were nine times more likely to have a stroke and seven times more likely to die from a stroke than were patients who had no lesions.
Dr. Windham used the same ARIC cohort in the 20-year cognition study. Begun in 1987, ARIC enrolled 15,800 middle-aged adults who have been followed regularly with physical and neurocognitive testing. Its goals are largely to investigate the natural history and multiple risk factors of cardiovascular and cerebrovascular disease. In 1993, subjects who had not experienced a stroke also had a brain MRI to add more detail to the study. The investigators also have performed cognitive assessments of a large number of participants five times since 1993 on measures of delayed word recall, digit symbol substitution, and word fluency. The outcome was the change in the composite Z-score over time.
The cognition study comprised 1,881 who had brain MRI and the full five cognitive assessments over a 20-year period. The participants were stratified as having no infarcts (1,611), only ILLs (50) or large infarcts (185), or both lesions (35).
At baseline, these subjects had a mean age of 63 years, 17% had diabetes, and 48% had hypertension. About one-third were positive for an ApoE e4 allele. The mean white matter intensity score was 1.4.
“In general, everyone in the cohort had some decline in cognitive function as they got older,” Dr. Windham said. But, a striking observation was that those with ILLs only and those with large lesions only had virtually identical decline slopes over the 20-year follow-up. The change from baseline in global Z-score was 0.18 standard deviations for the ILL-only group and 0.24 standard deviations for the large infarct group. For those with both lesions, the change from baseline was 0.62.
“At the end of 20 years, those with no lesion burden declined 1.3 standard deviations from baseline, those with only ILLs declined 1.5 standard deviations, and those with large infarcts, 1.6 standard deviations,” Dr. Windham said. “But, subjects who had both lesions declined 2.5 standard deviations from baseline. This is equivalent to adding 27 years of aging. The effect of having both was nearly four times greater than [that of] having only large lesions, which, up until now, have been the only ones read on MRI in either clinical practice or in research. Overall, our findings confirm that the relationship of ILLs to cognition is very similar that of large infarcts.
“The presence of midlife ILLs appears to amplify the effect of large infarcts on cognition, and we hypothesize that this process may represent vascular disease at midlife. We may also be able to identify people at high risk of cognitive decline or even dementia at midlife. I also think that we need to be rethinking how we read MRIs. Stopping at the 3-mm threshold may be too conservative. We should be looking at other studies on the consequences of these small lesions,” she said.
Dr. Windham had no financial disclosures.
[email protected]
On Twitter @alz_gal
AT AAIC 2017
Key clinical point:
Major finding: A composite cognitive measure showed a decline of 1.5 standard deviations from baseline in patients with only infarct-like lesions, 1.6 standard deviations in those with large infarcts, and 2.5 standard deviations in subjects who had both lesions.
Data source: The ARIC substudy comprised 1,881 subjects followed for 20 years.
Disclosures: Dr. Windham had no financial disclosures.
High Value Care curriculum reduced echocardiogram ordering
Study Title
The impact of a High Value Care curriculum on rate of repeat of trans-thoracic echocardiogram ordering among medical residents
Background
There is little data to confirm the impact of a High Value Care curriculum on echocardiogram ordering practices in a residency training program. We sought to evaluate the rate of performance of repeat transthoracic echocardiograms (TTE) before and after implementation of a High Vale Care curriculum.
Methods
A High Value Care curriculum was developed for the medical residents at Griffin Hospital, a community hospital, in 2015. The curriculum included a series of lectures aimed at promoting cost-conscious care while maintaining high quality. It also involved house staff in different quality improvement (QI) projects aimed at promoting high value care.
A group of residents decided to work on an initiative to reduce repeat echocardiograms. Repeat echocardiograms were defined as those performed within 6 months of a previous echocardiogram on the same patient. Only results in our EHR reflecting in-patient echocardiograms were utilized.
We retrospectively examined the rates of repeat echocardiograms performed in a 6 month period in 2014 before the High Vale Care curriculum was initiated. We assessed data from a 5 month period in 2016 to determine the rate of repeat electrocardiograms ordered at our institution.
Results
A total of 1,709 echocardiograms were reviewed in both time periods. Of these, 275 were considered repeat. At baseline, or before the implementation of a High Value Care curriculum, we examined 908 echocardiograms that were ordered, of which 21% were repeats.
After the implementation of a High Vale Care curriculum, 801 echocardiograms were ordered. Only 11% of these were repeats. This corresponds to a 52% reduction in the rate of repeated ordering of echocardiograms.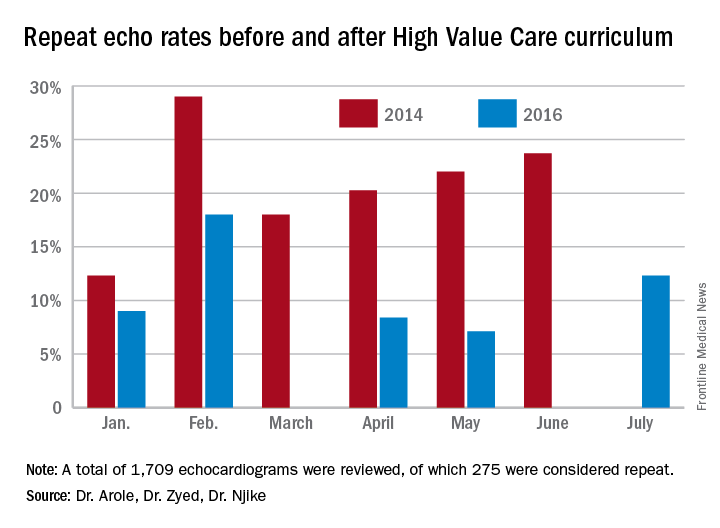
Discussion
The significant improvement in the rate of repeat echocardiograms was noted without any initiative directed specifically at echocardiogram ordering practices. During the planning phases of the proposed QI initiative to reduce repeat echocardiograms, house staff noted that their colleagues were already being more selective in their echocardiogram ordering practices because of the impact of the-cost conscious care lectures they had attended, as well as hospital-wide attention on the first resident-driven QI initiative that was aimed at reducing repetitive daily labs.
As part of the reducing repetitive labs QI, house staff had to provide clear rationale for why they were ordering daily labs. The received regular updates about their lab ordering practices and direct feedback if they consistently did not provide clear rationale for ordering daily labs.

Conclusion
Our study clearly showed a greater than 50% reduction in the ordering of repeat echocardiograms because of a High Value Care curriculum in our residency training program.
The improvement was brought on by increased awareness by house staff regarding provision of high quality care while being cognizant of the costs involved. The reduction in repeat echocardiograms resulted in more efficient use of a limited hospital resource.
Dr. Arole is chief of hospital medicine at Griffin Hospital, Derby, Conn. Dr. Zyed is in the department of internal medicine at Griffin Hospital. Dr. Njike is with the Yale University Prevention Research Center at Griffin Hospital.
Study Title
The impact of a High Value Care curriculum on rate of repeat of trans-thoracic echocardiogram ordering among medical residents
Background
There is little data to confirm the impact of a High Value Care curriculum on echocardiogram ordering practices in a residency training program. We sought to evaluate the rate of performance of repeat transthoracic echocardiograms (TTE) before and after implementation of a High Vale Care curriculum.
Methods
A High Value Care curriculum was developed for the medical residents at Griffin Hospital, a community hospital, in 2015. The curriculum included a series of lectures aimed at promoting cost-conscious care while maintaining high quality. It also involved house staff in different quality improvement (QI) projects aimed at promoting high value care.
A group of residents decided to work on an initiative to reduce repeat echocardiograms. Repeat echocardiograms were defined as those performed within 6 months of a previous echocardiogram on the same patient. Only results in our EHR reflecting in-patient echocardiograms were utilized.
We retrospectively examined the rates of repeat echocardiograms performed in a 6 month period in 2014 before the High Vale Care curriculum was initiated. We assessed data from a 5 month period in 2016 to determine the rate of repeat electrocardiograms ordered at our institution.
Results
A total of 1,709 echocardiograms were reviewed in both time periods. Of these, 275 were considered repeat. At baseline, or before the implementation of a High Value Care curriculum, we examined 908 echocardiograms that were ordered, of which 21% were repeats.
After the implementation of a High Vale Care curriculum, 801 echocardiograms were ordered. Only 11% of these were repeats. This corresponds to a 52% reduction in the rate of repeated ordering of echocardiograms.
Discussion
The significant improvement in the rate of repeat echocardiograms was noted without any initiative directed specifically at echocardiogram ordering practices. During the planning phases of the proposed QI initiative to reduce repeat echocardiograms, house staff noted that their colleagues were already being more selective in their echocardiogram ordering practices because of the impact of the-cost conscious care lectures they had attended, as well as hospital-wide attention on the first resident-driven QI initiative that was aimed at reducing repetitive daily labs.
As part of the reducing repetitive labs QI, house staff had to provide clear rationale for why they were ordering daily labs. The received regular updates about their lab ordering practices and direct feedback if they consistently did not provide clear rationale for ordering daily labs.
Conclusion
Our study clearly showed a greater than 50% reduction in the ordering of repeat echocardiograms because of a High Value Care curriculum in our residency training program.
The improvement was brought on by increased awareness by house staff regarding provision of high quality care while being cognizant of the costs involved. The reduction in repeat echocardiograms resulted in more efficient use of a limited hospital resource.
Dr. Arole is chief of hospital medicine at Griffin Hospital, Derby, Conn. Dr. Zyed is in the department of internal medicine at Griffin Hospital. Dr. Njike is with the Yale University Prevention Research Center at Griffin Hospital.
Study Title
The impact of a High Value Care curriculum on rate of repeat of trans-thoracic echocardiogram ordering among medical residents
Background
There is little data to confirm the impact of a High Value Care curriculum on echocardiogram ordering practices in a residency training program. We sought to evaluate the rate of performance of repeat transthoracic echocardiograms (TTE) before and after implementation of a High Vale Care curriculum.
Methods
A High Value Care curriculum was developed for the medical residents at Griffin Hospital, a community hospital, in 2015. The curriculum included a series of lectures aimed at promoting cost-conscious care while maintaining high quality. It also involved house staff in different quality improvement (QI) projects aimed at promoting high value care.
A group of residents decided to work on an initiative to reduce repeat echocardiograms. Repeat echocardiograms were defined as those performed within 6 months of a previous echocardiogram on the same patient. Only results in our EHR reflecting in-patient echocardiograms were utilized.
We retrospectively examined the rates of repeat echocardiograms performed in a 6 month period in 2014 before the High Vale Care curriculum was initiated. We assessed data from a 5 month period in 2016 to determine the rate of repeat electrocardiograms ordered at our institution.
Results
A total of 1,709 echocardiograms were reviewed in both time periods. Of these, 275 were considered repeat. At baseline, or before the implementation of a High Value Care curriculum, we examined 908 echocardiograms that were ordered, of which 21% were repeats.
After the implementation of a High Vale Care curriculum, 801 echocardiograms were ordered. Only 11% of these were repeats. This corresponds to a 52% reduction in the rate of repeated ordering of echocardiograms.
Discussion
The significant improvement in the rate of repeat echocardiograms was noted without any initiative directed specifically at echocardiogram ordering practices. During the planning phases of the proposed QI initiative to reduce repeat echocardiograms, house staff noted that their colleagues were already being more selective in their echocardiogram ordering practices because of the impact of the-cost conscious care lectures they had attended, as well as hospital-wide attention on the first resident-driven QI initiative that was aimed at reducing repetitive daily labs.
As part of the reducing repetitive labs QI, house staff had to provide clear rationale for why they were ordering daily labs. The received regular updates about their lab ordering practices and direct feedback if they consistently did not provide clear rationale for ordering daily labs.
Conclusion
Our study clearly showed a greater than 50% reduction in the ordering of repeat echocardiograms because of a High Value Care curriculum in our residency training program.
The improvement was brought on by increased awareness by house staff regarding provision of high quality care while being cognizant of the costs involved. The reduction in repeat echocardiograms resulted in more efficient use of a limited hospital resource.
Dr. Arole is chief of hospital medicine at Griffin Hospital, Derby, Conn. Dr. Zyed is in the department of internal medicine at Griffin Hospital. Dr. Njike is with the Yale University Prevention Research Center at Griffin Hospital.
Immune signature shows good prognostic performance in early-stage NSCLC
A new tumor immune-related gene signature may help take the guesswork out of prognostication in patients with early-stage non–small cell lung cancer (NSCLC), according to a retrospective cohort study.
“Various components of the immune system have been shown to be a determining factor during cancer initiation and progression,” note the investigators, who were led by Bailiang Li, PhD, of Stanford (Calif.) University. “Recent immunotherapies targeting specific immune checkpoints such as programmed death 1 or programmed death ligand 1 have demonstrated a remarkable, durable response in NSCLC. Certain histopathologic patterns, such as intratumoral infiltration by cytotoxic lymphocytes, have also been associated with better prognoses in several cancer types, including NSCLC.”
For the study, the investigators developed and validated an immune-related gene signature using frozen tumors from 2,414 patients with stage I or II nonsquamous NSCLC from 19 public cohorts who underwent resection with negative margins and did not receive any neoadjuvant or adjuvant therapy.
The new signature contained 25 gene pairs consisting of 40 unique immune-related genes, Dr. Li and associates report (JAMA Oncol. 2017 Jul 6. doi: 10.1001/jamaoncol.2017.1609).
Processes such as chemotaxis were enriched among the included genes.
The signature significantly stratified patients into groups that have high and low risks of death during follow-up, both across and within subsets with stage I, IA, IB, or II disease. Relative to counterparts falling into the signature-defined low-risk group, those falling into the signature-defined high-risk group had roughly twice the risk of death after adjustment for clinical and pathologic characteristics, with a hazard ratio range of 1.72 (P less than .001) to 2.36 (P less than .001).
Accuracy of the immune signature exceeded that of two commercialized gene signatures for estimating survival in similar validation cohorts (mean concordance index [C-index], 0.64 vs 0.53 and 0.61).
Moreover, the combination of the immune signature with clinical factors outperformed the signature alone (mean C-index, 0.70 vs 0.63) and another commercialized clinical-molecular combination signature (mean C-index, 0.68 vs 0.65).
“The proposed immune-related gene pair–based signature is a promising prognostic biomarker in nonsquamous NSCLC, including early-stage disease,” concluded the investigators. “Prospective studies are needed to further validate its analytical accuracy for estimating prognoses and to test its clinical utility in individualized management of nonsquamous NSCLC.”
M. Patricia Rivera, MD, FCCP, comments: As lung cancer screening implementation increases, it is expected that the prevalence of early-stage non–small cell lung cancer (NSCLC) will increase.

Currently, adjuvant therapy is reserved for patients with tumors greater than 4 cm or those with N1 disease. Having reliable biomarkers to identify patients at a high risk for recurrence after surgical resection is a significant clinical advantage in order to guide adjuvant therapy. The clinical-immune signature described in this study is an exciting and promising biomarker for estimating overall survival in NSCLC.
M. Patricia Rivera, MD, FCCP, comments: As lung cancer screening implementation increases, it is expected that the prevalence of early-stage non–small cell lung cancer (NSCLC) will increase.
Currently, adjuvant therapy is reserved for patients with tumors greater than 4 cm or those with N1 disease. Having reliable biomarkers to identify patients at a high risk for recurrence after surgical resection is a significant clinical advantage in order to guide adjuvant therapy. The clinical-immune signature described in this study is an exciting and promising biomarker for estimating overall survival in NSCLC.
M. Patricia Rivera, MD, FCCP, comments: As lung cancer screening implementation increases, it is expected that the prevalence of early-stage non–small cell lung cancer (NSCLC) will increase.
Currently, adjuvant therapy is reserved for patients with tumors greater than 4 cm or those with N1 disease. Having reliable biomarkers to identify patients at a high risk for recurrence after surgical resection is a significant clinical advantage in order to guide adjuvant therapy. The clinical-immune signature described in this study is an exciting and promising biomarker for estimating overall survival in NSCLC.
A new tumor immune-related gene signature may help take the guesswork out of prognostication in patients with early-stage non–small cell lung cancer (NSCLC), according to a retrospective cohort study.
“Various components of the immune system have been shown to be a determining factor during cancer initiation and progression,” note the investigators, who were led by Bailiang Li, PhD, of Stanford (Calif.) University. “Recent immunotherapies targeting specific immune checkpoints such as programmed death 1 or programmed death ligand 1 have demonstrated a remarkable, durable response in NSCLC. Certain histopathologic patterns, such as intratumoral infiltration by cytotoxic lymphocytes, have also been associated with better prognoses in several cancer types, including NSCLC.”
For the study, the investigators developed and validated an immune-related gene signature using frozen tumors from 2,414 patients with stage I or II nonsquamous NSCLC from 19 public cohorts who underwent resection with negative margins and did not receive any neoadjuvant or adjuvant therapy.
The new signature contained 25 gene pairs consisting of 40 unique immune-related genes, Dr. Li and associates report (JAMA Oncol. 2017 Jul 6. doi: 10.1001/jamaoncol.2017.1609).
Processes such as chemotaxis were enriched among the included genes.
The signature significantly stratified patients into groups that have high and low risks of death during follow-up, both across and within subsets with stage I, IA, IB, or II disease. Relative to counterparts falling into the signature-defined low-risk group, those falling into the signature-defined high-risk group had roughly twice the risk of death after adjustment for clinical and pathologic characteristics, with a hazard ratio range of 1.72 (P less than .001) to 2.36 (P less than .001).
Accuracy of the immune signature exceeded that of two commercialized gene signatures for estimating survival in similar validation cohorts (mean concordance index [C-index], 0.64 vs 0.53 and 0.61).
Moreover, the combination of the immune signature with clinical factors outperformed the signature alone (mean C-index, 0.70 vs 0.63) and another commercialized clinical-molecular combination signature (mean C-index, 0.68 vs 0.65).
“The proposed immune-related gene pair–based signature is a promising prognostic biomarker in nonsquamous NSCLC, including early-stage disease,” concluded the investigators. “Prospective studies are needed to further validate its analytical accuracy for estimating prognoses and to test its clinical utility in individualized management of nonsquamous NSCLC.”
A new tumor immune-related gene signature may help take the guesswork out of prognostication in patients with early-stage non–small cell lung cancer (NSCLC), according to a retrospective cohort study.
“Various components of the immune system have been shown to be a determining factor during cancer initiation and progression,” note the investigators, who were led by Bailiang Li, PhD, of Stanford (Calif.) University. “Recent immunotherapies targeting specific immune checkpoints such as programmed death 1 or programmed death ligand 1 have demonstrated a remarkable, durable response in NSCLC. Certain histopathologic patterns, such as intratumoral infiltration by cytotoxic lymphocytes, have also been associated with better prognoses in several cancer types, including NSCLC.”
For the study, the investigators developed and validated an immune-related gene signature using frozen tumors from 2,414 patients with stage I or II nonsquamous NSCLC from 19 public cohorts who underwent resection with negative margins and did not receive any neoadjuvant or adjuvant therapy.
The new signature contained 25 gene pairs consisting of 40 unique immune-related genes, Dr. Li and associates report (JAMA Oncol. 2017 Jul 6. doi: 10.1001/jamaoncol.2017.1609).
Processes such as chemotaxis were enriched among the included genes.
The signature significantly stratified patients into groups that have high and low risks of death during follow-up, both across and within subsets with stage I, IA, IB, or II disease. Relative to counterparts falling into the signature-defined low-risk group, those falling into the signature-defined high-risk group had roughly twice the risk of death after adjustment for clinical and pathologic characteristics, with a hazard ratio range of 1.72 (P less than .001) to 2.36 (P less than .001).
Accuracy of the immune signature exceeded that of two commercialized gene signatures for estimating survival in similar validation cohorts (mean concordance index [C-index], 0.64 vs 0.53 and 0.61).
Moreover, the combination of the immune signature with clinical factors outperformed the signature alone (mean C-index, 0.70 vs 0.63) and another commercialized clinical-molecular combination signature (mean C-index, 0.68 vs 0.65).
“The proposed immune-related gene pair–based signature is a promising prognostic biomarker in nonsquamous NSCLC, including early-stage disease,” concluded the investigators. “Prospective studies are needed to further validate its analytical accuracy for estimating prognoses and to test its clinical utility in individualized management of nonsquamous NSCLC.”
FROM JAMA ONCOLOGY
Key clinical point:
Major finding: Compared with peers in the signature-defined low-risk group, patients in the signature-defined high-risk group had roughly twice the adjusted risk of death (hazard ratio range, 1.72-2.36).
Data source: A retrospective cohort study using frozen tumors from 2,414 patients with stage I or II nonsquamous NSCLC who underwent complete resection and did not receive adjuvant or neoadjuvant therapy.
Disclosures: The investigators reported that they had no relevant disclosures. The study was supported in part by the National Institutes of Health.