User login
EUS beats MRCP on sensitivity for bile duct stones
Endoscopic ultrasound (EUS) beat magnetic resonance cholangiopancreatography (MRCP) on diagnostic accuracy for choledocholithiasis, but both provided similar specificity, according to data from a meta-analysis of head-to-head comparisons. The findings were published in Gastrointestinal Endoscopy.
EUS and MRCP can provide accurate diagnosis of choledocholithiasis with lower adverse event rates than the clinical standards of endoscopic retrograde cholangiopancreatography and intraoperative cholangiography, but a meta-analysis of the diagnostic test accuracy (DTA) of the two methods was lacking, wrote Mohammad Yaghoobi, MD, of McMaster University, Hamilton, Ont., and his colleagues (Gastrointest Endosc. 2017. doi: 10.1016/j.gie.2017.06.009).
“The methodology of a meta-analysis of DTA is different from a conventional meta-analysis in several aspects, including statistical analysis and quality assessment of the included trials,” the researchers wrote.
They reviewed data from studies conducted between 1980 and January 2017 and identified five studies of head-to-head comparisons of EUS and MRCP. Studies involving children, and those with insufficient data, no reference standards, and a gap of more than 48 hours between two index tests were excluded.
Overall, the diagnostic odds ratio was significantly higher for EUS than MRCP (P = .008). This difference was mainly a factor of the significantly higher sensitivity of EUS vs. MRCP (P = .006). Specificity was not significantly different between the two tests.
The results were limited by several factors, including inadequate data for a subgroup analysis based on stone size and the relatively small number of studies included in the analysis, but the strict inclusion criteria add to the strength of the findings, the researchers noted.
“EUS should be incorporated in the diagnostic algorithm in patients suspected for choledocholithiasis, whenever appropriate, given its reasonable safety profile,” the researchers said. “This might specially apply to the patients who need an esophagogastroduodenoscopy for investigating other alternative causes of abdominal pain,” they added. The researchers had no financial conflicts to disclose.
Endoscopic ultrasound (EUS) beat magnetic resonance cholangiopancreatography (MRCP) on diagnostic accuracy for choledocholithiasis, but both provided similar specificity, according to data from a meta-analysis of head-to-head comparisons. The findings were published in Gastrointestinal Endoscopy.
EUS and MRCP can provide accurate diagnosis of choledocholithiasis with lower adverse event rates than the clinical standards of endoscopic retrograde cholangiopancreatography and intraoperative cholangiography, but a meta-analysis of the diagnostic test accuracy (DTA) of the two methods was lacking, wrote Mohammad Yaghoobi, MD, of McMaster University, Hamilton, Ont., and his colleagues (Gastrointest Endosc. 2017. doi: 10.1016/j.gie.2017.06.009).
“The methodology of a meta-analysis of DTA is different from a conventional meta-analysis in several aspects, including statistical analysis and quality assessment of the included trials,” the researchers wrote.
They reviewed data from studies conducted between 1980 and January 2017 and identified five studies of head-to-head comparisons of EUS and MRCP. Studies involving children, and those with insufficient data, no reference standards, and a gap of more than 48 hours between two index tests were excluded.
Overall, the diagnostic odds ratio was significantly higher for EUS than MRCP (P = .008). This difference was mainly a factor of the significantly higher sensitivity of EUS vs. MRCP (P = .006). Specificity was not significantly different between the two tests.
The results were limited by several factors, including inadequate data for a subgroup analysis based on stone size and the relatively small number of studies included in the analysis, but the strict inclusion criteria add to the strength of the findings, the researchers noted.
“EUS should be incorporated in the diagnostic algorithm in patients suspected for choledocholithiasis, whenever appropriate, given its reasonable safety profile,” the researchers said. “This might specially apply to the patients who need an esophagogastroduodenoscopy for investigating other alternative causes of abdominal pain,” they added. The researchers had no financial conflicts to disclose.
Endoscopic ultrasound (EUS) beat magnetic resonance cholangiopancreatography (MRCP) on diagnostic accuracy for choledocholithiasis, but both provided similar specificity, according to data from a meta-analysis of head-to-head comparisons. The findings were published in Gastrointestinal Endoscopy.
EUS and MRCP can provide accurate diagnosis of choledocholithiasis with lower adverse event rates than the clinical standards of endoscopic retrograde cholangiopancreatography and intraoperative cholangiography, but a meta-analysis of the diagnostic test accuracy (DTA) of the two methods was lacking, wrote Mohammad Yaghoobi, MD, of McMaster University, Hamilton, Ont., and his colleagues (Gastrointest Endosc. 2017. doi: 10.1016/j.gie.2017.06.009).
“The methodology of a meta-analysis of DTA is different from a conventional meta-analysis in several aspects, including statistical analysis and quality assessment of the included trials,” the researchers wrote.
They reviewed data from studies conducted between 1980 and January 2017 and identified five studies of head-to-head comparisons of EUS and MRCP. Studies involving children, and those with insufficient data, no reference standards, and a gap of more than 48 hours between two index tests were excluded.
Overall, the diagnostic odds ratio was significantly higher for EUS than MRCP (P = .008). This difference was mainly a factor of the significantly higher sensitivity of EUS vs. MRCP (P = .006). Specificity was not significantly different between the two tests.
The results were limited by several factors, including inadequate data for a subgroup analysis based on stone size and the relatively small number of studies included in the analysis, but the strict inclusion criteria add to the strength of the findings, the researchers noted.
“EUS should be incorporated in the diagnostic algorithm in patients suspected for choledocholithiasis, whenever appropriate, given its reasonable safety profile,” the researchers said. “This might specially apply to the patients who need an esophagogastroduodenoscopy for investigating other alternative causes of abdominal pain,” they added. The researchers had no financial conflicts to disclose.
FROM GASTROINTESTINAL ENDOSCOPY
Key clinical point: EUS offers greater sensitivity and similar specificity compared with MRCP in detecting choledocholithiasis.
Major finding: The diagnostic odds ratio was significantly higher for EUS than MRCP (P = .008).
Data source: A meta-analysis of diagnostic test accuracy including five head-to-head studies.
Disclosures: The researchers had no financial conflicts to disclose.
Study finds family history, chocolate intake increases acne risk
Having two parents with a history of acne was associated with an eightfold higher risk of acne during adolescence and young adulthood, in a European study that surveyed people aged 15-24 years in seven European countries.
Researchers conducted an online population-based survey of 10,521 individuals aged 15-24 years in Belgium, Czech and Slovak republics, France, Italy, Poland, and Spain, with questions about the presence or absence of acne, sociodemographic characteristics, and lifestyle factors (such as diet, tobacco, cannabis or alcohol use, and family history). The results were published online on July 14.
The overall prevalence of self-reported acne was 57.8%, with the highest prevalence – 65.8% – found in the 15- to 17-years age group, and the lowest being 52.6% in the 21- to 24-years age group. Individuals who reported having one parent with a history of acne had a threefold greater incidence of acne compared to those without a history of paternal or maternal acne (P less than .0001 for both). Individuals whose parents both had acne had a nearly eightfold higher risk, which the authors noted was consistent with other studies showing a strong hereditary component of acne (J Eur Acad Dermatol Venereol. 2017 Jul 14. doi: 10.1111/jdv.14475).
“Previous studies have demonstrated an association between high glycemic index foods and acne, although in our study, only chocolate, and not pasta or sweets, was independently associated in multivariate analysis,” wrote Pierre Wolkenstein, MD, of the department of dermatology, Hôpital Henri Mondor, Créteil, France, and his coauthors.
“The relationship between smoking and acne is not clear. Some observational studies have found that smoking increases the prevalence of acne, others have found a negative association, and some have found no relationship,” they added.
The study also showed significant variation in the incidence of acne across different countries. Using Spain, which had a median prevalence of acne, as a reference point, the researchers found that respondents in the Czech and Slovak republics had a 96% higher incidence of acne, while those in Poland had a 55% lower incidence.
The authors cautioned that their results were based on self-report, rather than a physician diagnosis, but they noted that since acne is so common, false positive or false negative reports were unlikely. “An association between self-reported acne and chocolate consumption, and an apparent inverse relationship with smoking, need to be confirmed by additional studies,” they noted.
The survey was funded and supported by Pierre Fabre Dermatologie. Five authors declared fees as members of the European Severe Acne Board, supported by Pierre Fabre Dermatologie, and one author is an employee of the company.
Having two parents with a history of acne was associated with an eightfold higher risk of acne during adolescence and young adulthood, in a European study that surveyed people aged 15-24 years in seven European countries.
Researchers conducted an online population-based survey of 10,521 individuals aged 15-24 years in Belgium, Czech and Slovak republics, France, Italy, Poland, and Spain, with questions about the presence or absence of acne, sociodemographic characteristics, and lifestyle factors (such as diet, tobacco, cannabis or alcohol use, and family history). The results were published online on July 14.
The overall prevalence of self-reported acne was 57.8%, with the highest prevalence – 65.8% – found in the 15- to 17-years age group, and the lowest being 52.6% in the 21- to 24-years age group. Individuals who reported having one parent with a history of acne had a threefold greater incidence of acne compared to those without a history of paternal or maternal acne (P less than .0001 for both). Individuals whose parents both had acne had a nearly eightfold higher risk, which the authors noted was consistent with other studies showing a strong hereditary component of acne (J Eur Acad Dermatol Venereol. 2017 Jul 14. doi: 10.1111/jdv.14475).
“Previous studies have demonstrated an association between high glycemic index foods and acne, although in our study, only chocolate, and not pasta or sweets, was independently associated in multivariate analysis,” wrote Pierre Wolkenstein, MD, of the department of dermatology, Hôpital Henri Mondor, Créteil, France, and his coauthors.
“The relationship between smoking and acne is not clear. Some observational studies have found that smoking increases the prevalence of acne, others have found a negative association, and some have found no relationship,” they added.
The study also showed significant variation in the incidence of acne across different countries. Using Spain, which had a median prevalence of acne, as a reference point, the researchers found that respondents in the Czech and Slovak republics had a 96% higher incidence of acne, while those in Poland had a 55% lower incidence.
The authors cautioned that their results were based on self-report, rather than a physician diagnosis, but they noted that since acne is so common, false positive or false negative reports were unlikely. “An association between self-reported acne and chocolate consumption, and an apparent inverse relationship with smoking, need to be confirmed by additional studies,” they noted.
The survey was funded and supported by Pierre Fabre Dermatologie. Five authors declared fees as members of the European Severe Acne Board, supported by Pierre Fabre Dermatologie, and one author is an employee of the company.
Having two parents with a history of acne was associated with an eightfold higher risk of acne during adolescence and young adulthood, in a European study that surveyed people aged 15-24 years in seven European countries.
Researchers conducted an online population-based survey of 10,521 individuals aged 15-24 years in Belgium, Czech and Slovak republics, France, Italy, Poland, and Spain, with questions about the presence or absence of acne, sociodemographic characteristics, and lifestyle factors (such as diet, tobacco, cannabis or alcohol use, and family history). The results were published online on July 14.
The overall prevalence of self-reported acne was 57.8%, with the highest prevalence – 65.8% – found in the 15- to 17-years age group, and the lowest being 52.6% in the 21- to 24-years age group. Individuals who reported having one parent with a history of acne had a threefold greater incidence of acne compared to those without a history of paternal or maternal acne (P less than .0001 for both). Individuals whose parents both had acne had a nearly eightfold higher risk, which the authors noted was consistent with other studies showing a strong hereditary component of acne (J Eur Acad Dermatol Venereol. 2017 Jul 14. doi: 10.1111/jdv.14475).
“Previous studies have demonstrated an association between high glycemic index foods and acne, although in our study, only chocolate, and not pasta or sweets, was independently associated in multivariate analysis,” wrote Pierre Wolkenstein, MD, of the department of dermatology, Hôpital Henri Mondor, Créteil, France, and his coauthors.
“The relationship between smoking and acne is not clear. Some observational studies have found that smoking increases the prevalence of acne, others have found a negative association, and some have found no relationship,” they added.
The study also showed significant variation in the incidence of acne across different countries. Using Spain, which had a median prevalence of acne, as a reference point, the researchers found that respondents in the Czech and Slovak republics had a 96% higher incidence of acne, while those in Poland had a 55% lower incidence.
The authors cautioned that their results were based on self-report, rather than a physician diagnosis, but they noted that since acne is so common, false positive or false negative reports were unlikely. “An association between self-reported acne and chocolate consumption, and an apparent inverse relationship with smoking, need to be confirmed by additional studies,” they noted.
The survey was funded and supported by Pierre Fabre Dermatologie. Five authors declared fees as members of the European Severe Acne Board, supported by Pierre Fabre Dermatologie, and one author is an employee of the company.
FROM THE JOURNAL OF THE EUROPEAN ACADEMY OF DERMATOLOGY AND VENEREOLOGY
Key clinical point: A parental history of acne, higher levels of personal chocolate consumption, and younger age were significantly associated with an increased risk of acne.
Major finding: Adolescents and young adults with two parents with a history of acne have a nearly eightfold higher risk of the condition.
Data source: A population-based survey of 10,521 individuals aged 15-24 years in seven European countries.
Disclosures: Five authors declared fees as members of the European Severe Acne Board – supported by Pierre Fabre Dermatologie, which funded the survey – and one author is an employee of the company.
Get involved with AGA
We’re soliciting members to serve in AGA leadership positions – as committee and center members, as well as on the AGA Institute Governing Board. This is an opportunity to network with other physicians and scientists, pursue a special interest, and make an impact in an area that is important to you.
Join a committee or center
AGA and AGA Institute are seeking members to serve on several committees and centers that recommend and oversee new and existing policies and programs. Terms will start in June 2018; nominations must be received by Nov. 1, 2017. Members can either nominate themselves or other members. For more information on the positions available, take a look at the AGA Committee page, http://www.gastro.org/about/people/committees.
Serve in a leadership position
The AGA Nominating Committee is in the midst of identifying candidates to join the governing board – in the offices of vice president, clinical research councillor, and practice councillor – as well as 10 nominees for the 2018-2019 AGA Nominating Committee. To learn more, or to nominate yourself or a colleague, email [email protected]. Nominations are due by Oct. 1, 2017; earlier submissions are encouraged.
We’re soliciting members to serve in AGA leadership positions – as committee and center members, as well as on the AGA Institute Governing Board. This is an opportunity to network with other physicians and scientists, pursue a special interest, and make an impact in an area that is important to you.
Join a committee or center
AGA and AGA Institute are seeking members to serve on several committees and centers that recommend and oversee new and existing policies and programs. Terms will start in June 2018; nominations must be received by Nov. 1, 2017. Members can either nominate themselves or other members. For more information on the positions available, take a look at the AGA Committee page, http://www.gastro.org/about/people/committees.
Serve in a leadership position
The AGA Nominating Committee is in the midst of identifying candidates to join the governing board – in the offices of vice president, clinical research councillor, and practice councillor – as well as 10 nominees for the 2018-2019 AGA Nominating Committee. To learn more, or to nominate yourself or a colleague, email [email protected]. Nominations are due by Oct. 1, 2017; earlier submissions are encouraged.
We’re soliciting members to serve in AGA leadership positions – as committee and center members, as well as on the AGA Institute Governing Board. This is an opportunity to network with other physicians and scientists, pursue a special interest, and make an impact in an area that is important to you.
Join a committee or center
AGA and AGA Institute are seeking members to serve on several committees and centers that recommend and oversee new and existing policies and programs. Terms will start in June 2018; nominations must be received by Nov. 1, 2017. Members can either nominate themselves or other members. For more information on the positions available, take a look at the AGA Committee page, http://www.gastro.org/about/people/committees.
Serve in a leadership position
The AGA Nominating Committee is in the midst of identifying candidates to join the governing board – in the offices of vice president, clinical research councillor, and practice councillor – as well as 10 nominees for the 2018-2019 AGA Nominating Committee. To learn more, or to nominate yourself or a colleague, email [email protected]. Nominations are due by Oct. 1, 2017; earlier submissions are encouraged.
Mark your calendar: 2018 AGA grants cycle announced
The AGA Research Foundation is excited to announce the start of its 2018 Research Grants cycle. This year the foundation will be awarding over $2 million in funding to support researchers within gastroenterology and hepatology. Now is your chance to view upcoming opportunities and plan your applications. Learn more below about the first application due in August, and visit the AGA Research Funding website (www.gastro.org/research-funding) for the full list. Contact [email protected] with any questions.
Applications due: Aug. 4, 2017
AGA-R. Robert & Sally Funderburg Research Award in Gastric Cancer
This award provides $50,000 per year for 2 years to an established investigator working on novel approaches in gastric cancer research. For the past 25 years, this $100,000 award has enhanced the fundamental understanding of gastric cancer pathobiology toward ultimately developing a cure for the disease.
The AGA Research Foundation is excited to announce the start of its 2018 Research Grants cycle. This year the foundation will be awarding over $2 million in funding to support researchers within gastroenterology and hepatology. Now is your chance to view upcoming opportunities and plan your applications. Learn more below about the first application due in August, and visit the AGA Research Funding website (www.gastro.org/research-funding) for the full list. Contact [email protected] with any questions.
Applications due: Aug. 4, 2017
AGA-R. Robert & Sally Funderburg Research Award in Gastric Cancer
This award provides $50,000 per year for 2 years to an established investigator working on novel approaches in gastric cancer research. For the past 25 years, this $100,000 award has enhanced the fundamental understanding of gastric cancer pathobiology toward ultimately developing a cure for the disease.
The AGA Research Foundation is excited to announce the start of its 2018 Research Grants cycle. This year the foundation will be awarding over $2 million in funding to support researchers within gastroenterology and hepatology. Now is your chance to view upcoming opportunities and plan your applications. Learn more below about the first application due in August, and visit the AGA Research Funding website (www.gastro.org/research-funding) for the full list. Contact [email protected] with any questions.
Applications due: Aug. 4, 2017
AGA-R. Robert & Sally Funderburg Research Award in Gastric Cancer
This award provides $50,000 per year for 2 years to an established investigator working on novel approaches in gastric cancer research. For the past 25 years, this $100,000 award has enhanced the fundamental understanding of gastric cancer pathobiology toward ultimately developing a cure for the disease.
Physician compensation growing but at a slightly slower pace
Physicians working in large multispecialty groups saw their compensation increase in 2016, albeit at a slower pace than in 2015, according to survey results reported by AMGA.
The 2017 Medical Group Compensation and Productivity Survey shows that the overall weighted average increase in physician compensation for the calendar year 2016 was 2.9%, slightly lower than the 3.1% increase seen in 2015. Doctors in more than three-quarters (77%) of specialties saw increases in 2016.
Opthalmologic surgery saw the largest compensation increase at 7.7%, followed by cardiothoracic surgery (7.0%), hematology and medical oncology (6.7%), allergy/immunology (5.9%) and pulmonary disease (5.6%). Emergency medicine saw a decrease in compensation of 2.0% in 2016 after experiencing a 9.6% increase in 2015.
Value-based payment is beginning to factor into the growth in payment by specialty. Overall, about 8% of compensation is being linked to value-based pay, and that number is expected to rise, with some medical practice groups linking 15% or more of compensation to value-based metrics.
“In almost all of the groups that I have worked with in the last few years on [compensation] design, that has been one of the drivers of decision to do the compensation redesign is to allocate to the value-based metrics,” Wayne Hartley, vice president of AMGA Consulting, said in an interview. 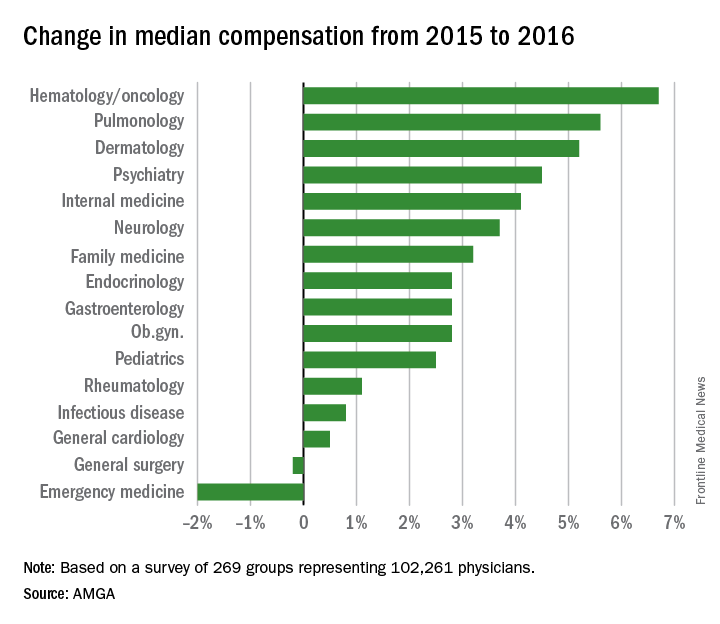
AMGA said that the data covers responses from 269 medical groups covering more than 102,000 providers and is representative of large multispecialty groups and integrated health systems that average 380 providers per group.
Physicians working in large multispecialty groups saw their compensation increase in 2016, albeit at a slower pace than in 2015, according to survey results reported by AMGA.
The 2017 Medical Group Compensation and Productivity Survey shows that the overall weighted average increase in physician compensation for the calendar year 2016 was 2.9%, slightly lower than the 3.1% increase seen in 2015. Doctors in more than three-quarters (77%) of specialties saw increases in 2016.
Opthalmologic surgery saw the largest compensation increase at 7.7%, followed by cardiothoracic surgery (7.0%), hematology and medical oncology (6.7%), allergy/immunology (5.9%) and pulmonary disease (5.6%). Emergency medicine saw a decrease in compensation of 2.0% in 2016 after experiencing a 9.6% increase in 2015.
Value-based payment is beginning to factor into the growth in payment by specialty. Overall, about 8% of compensation is being linked to value-based pay, and that number is expected to rise, with some medical practice groups linking 15% or more of compensation to value-based metrics.
“In almost all of the groups that I have worked with in the last few years on [compensation] design, that has been one of the drivers of decision to do the compensation redesign is to allocate to the value-based metrics,” Wayne Hartley, vice president of AMGA Consulting, said in an interview.
AMGA said that the data covers responses from 269 medical groups covering more than 102,000 providers and is representative of large multispecialty groups and integrated health systems that average 380 providers per group.
Physicians working in large multispecialty groups saw their compensation increase in 2016, albeit at a slower pace than in 2015, according to survey results reported by AMGA.
The 2017 Medical Group Compensation and Productivity Survey shows that the overall weighted average increase in physician compensation for the calendar year 2016 was 2.9%, slightly lower than the 3.1% increase seen in 2015. Doctors in more than three-quarters (77%) of specialties saw increases in 2016.
Opthalmologic surgery saw the largest compensation increase at 7.7%, followed by cardiothoracic surgery (7.0%), hematology and medical oncology (6.7%), allergy/immunology (5.9%) and pulmonary disease (5.6%). Emergency medicine saw a decrease in compensation of 2.0% in 2016 after experiencing a 9.6% increase in 2015.
Value-based payment is beginning to factor into the growth in payment by specialty. Overall, about 8% of compensation is being linked to value-based pay, and that number is expected to rise, with some medical practice groups linking 15% or more of compensation to value-based metrics.
“In almost all of the groups that I have worked with in the last few years on [compensation] design, that has been one of the drivers of decision to do the compensation redesign is to allocate to the value-based metrics,” Wayne Hartley, vice president of AMGA Consulting, said in an interview.
AMGA said that the data covers responses from 269 medical groups covering more than 102,000 providers and is representative of large multispecialty groups and integrated health systems that average 380 providers per group.
HHS eliminates funding for teen pregnancy prevention programs
The Trump administration’s sudden funding cut to the Teen Pregnancy Prevention Program will not only halt research and programming efforts at more than 80 institutions across the country, but also will likely unravel recent progress made in reducing teen pregnancies, physicians and program advocates say.
In early July, officials at the U.S. Department of Health & Human Services notified program grantees that the administration would be eliminating funding for the Teen Pregnancy Prevention Program (TPP Program) and that 5-year grants awarded under the Obama administration would be ending in June 2018, 2 years earlier than planned.
The TPP Program is a national, evidence-based initiative established in 2010 to fund medically accurate and age-appropriate programs that work to prevent teen pregnancy in the United States.

“Those programs serve many youth across the country, so of course the individuals in the programs are going to be impacted,” Dr. Oelschlager said in an interview. “It’s demoralizing for the educators, [and] the researchers, who are looking at innovative methods, to have their funding cut in the middle of evaluating whether their programs are effective.”
An HHS spokeswoman confirmed that on July 1, the agency informed TPP Program grantees that funding for the program would be eliminated as detailed in President Trump’s fiscal 2018 budget proposal. The HHS awarded 81 continuations for TPP Program Tier 1 and Tier 2 grant awards for a total of $89 million through June 30, 2018, according to the spokeswoman. The HHS informed the grantees of their June 30, 2018, end date “to give them an opportunity to adjust their programs and plan for an orderly closeout,” she said.
The University of Southern California, Los Angeles, is one of many institutions impacted by the funding cut. The primary objectives of the Keeping it Real Together project are to implement evidence-based sexual health education programs for youth in middle and alternative high schools and provide an education program for parents of middle school–aged youth, said Luanne Rohrbach, PhD, associate professor of clinical preventive medicine at the university’s Institute for Health Promotion & Disease Prevention and principal investigator for the program.

Dr. Rohrbach said she anticipated pushback from the new administration as far as receiving the full 5-year funding, but the sudden program elimination was unexpected.
In March, when President Trump announced his budget priorities for fiscal 2016 and 2017, it was clear that the TPP Program was on the chopping block, Dr. Rohrbach said. However, when Congress passed a continuing resolution for the remainder of fiscal 2016 and 2017, the program remained intact. In his budget recommendations for fiscal 2017 and 2018, the President proposed that the TPP Program be eliminated.
“Despite this recommendation, it was our understanding that the program would be debated in Congress as they developed their recommendations for FY 2017-18 funding,” she said. “That is, we expected there would at least be discussion about it in Congressional budget committees. We did not expect that the program would be eliminated by the Office of the Secretary of HHS.”
Haywood L. Brown, MD, president of the American Congress of Obstetricians and Gynecologists (ACOG) called the administration’s decision “highly unusual” and said it is a step backward for ensuring healthy moms and healthy babies.
“This program and others provide vital research and programming that successfully brought our nation to an all-time low rate of teen pregnancies – progress we cannot afford to jeopardize,” Dr. Brown said in a statement.
Federal data show that the teen pregnancy rate has steadily declined over the last decade. In 2015, the birth rate for girls and young women aged 15-19 years fell by nearly 8% from 2014, according to data from the National Center for Health Statistics. Since 1991, the rate has fallen by 64%. The rate for the younger half of the age group, girls aged 15-17 years, was down 9% from 2014.
Researchers attribute the decline to a combination of economic, cultural, and social factors, as well as a lower prevalence of sexual activity among youth, the use of more effective contraception, and the provision of more information about pregnancy prevention, Dr. Rohrbach said.
“The [TPP Program] has been focused on implementation of evidence-based, comprehensive sexual health education,” she said. “Elimination of these efforts endangers the progress that has been made in reducing teen pregnancies.”
Dr. Oelschlager noted that between 2008 and 2015, the teen birth rate in King County, Washington, declined by 55%. She attributed the reduction to multiple drivers, including a program called Flash, that incorporates a sexual health education curriculum in Seattle-area public schools. Some TPP programs in Northwest Seattle are using the FLASH curriculum, she said.
“This is a very comprehensive program, which includes discussion about reproductive health, sexual violence, prevention of teen pregnancy, sexually transmitted infections, [and] harm reduction,” she said. “That’s been a very effective method of educating our teens about these issues.”
[email protected]
On Twitter @legal_med
The Trump administration’s sudden funding cut to the Teen Pregnancy Prevention Program will not only halt research and programming efforts at more than 80 institutions across the country, but also will likely unravel recent progress made in reducing teen pregnancies, physicians and program advocates say.
In early July, officials at the U.S. Department of Health & Human Services notified program grantees that the administration would be eliminating funding for the Teen Pregnancy Prevention Program (TPP Program) and that 5-year grants awarded under the Obama administration would be ending in June 2018, 2 years earlier than planned.
The TPP Program is a national, evidence-based initiative established in 2010 to fund medically accurate and age-appropriate programs that work to prevent teen pregnancy in the United States.
“Those programs serve many youth across the country, so of course the individuals in the programs are going to be impacted,” Dr. Oelschlager said in an interview. “It’s demoralizing for the educators, [and] the researchers, who are looking at innovative methods, to have their funding cut in the middle of evaluating whether their programs are effective.”
An HHS spokeswoman confirmed that on July 1, the agency informed TPP Program grantees that funding for the program would be eliminated as detailed in President Trump’s fiscal 2018 budget proposal. The HHS awarded 81 continuations for TPP Program Tier 1 and Tier 2 grant awards for a total of $89 million through June 30, 2018, according to the spokeswoman. The HHS informed the grantees of their June 30, 2018, end date “to give them an opportunity to adjust their programs and plan for an orderly closeout,” she said.
The University of Southern California, Los Angeles, is one of many institutions impacted by the funding cut. The primary objectives of the Keeping it Real Together project are to implement evidence-based sexual health education programs for youth in middle and alternative high schools and provide an education program for parents of middle school–aged youth, said Luanne Rohrbach, PhD, associate professor of clinical preventive medicine at the university’s Institute for Health Promotion & Disease Prevention and principal investigator for the program.
Dr. Rohrbach said she anticipated pushback from the new administration as far as receiving the full 5-year funding, but the sudden program elimination was unexpected.
In March, when President Trump announced his budget priorities for fiscal 2016 and 2017, it was clear that the TPP Program was on the chopping block, Dr. Rohrbach said. However, when Congress passed a continuing resolution for the remainder of fiscal 2016 and 2017, the program remained intact. In his budget recommendations for fiscal 2017 and 2018, the President proposed that the TPP Program be eliminated.
“Despite this recommendation, it was our understanding that the program would be debated in Congress as they developed their recommendations for FY 2017-18 funding,” she said. “That is, we expected there would at least be discussion about it in Congressional budget committees. We did not expect that the program would be eliminated by the Office of the Secretary of HHS.”
Haywood L. Brown, MD, president of the American Congress of Obstetricians and Gynecologists (ACOG) called the administration’s decision “highly unusual” and said it is a step backward for ensuring healthy moms and healthy babies.
“This program and others provide vital research and programming that successfully brought our nation to an all-time low rate of teen pregnancies – progress we cannot afford to jeopardize,” Dr. Brown said in a statement.
Federal data show that the teen pregnancy rate has steadily declined over the last decade. In 2015, the birth rate for girls and young women aged 15-19 years fell by nearly 8% from 2014, according to data from the National Center for Health Statistics. Since 1991, the rate has fallen by 64%. The rate for the younger half of the age group, girls aged 15-17 years, was down 9% from 2014.
Researchers attribute the decline to a combination of economic, cultural, and social factors, as well as a lower prevalence of sexual activity among youth, the use of more effective contraception, and the provision of more information about pregnancy prevention, Dr. Rohrbach said.
“The [TPP Program] has been focused on implementation of evidence-based, comprehensive sexual health education,” she said. “Elimination of these efforts endangers the progress that has been made in reducing teen pregnancies.”
Dr. Oelschlager noted that between 2008 and 2015, the teen birth rate in King County, Washington, declined by 55%. She attributed the reduction to multiple drivers, including a program called Flash, that incorporates a sexual health education curriculum in Seattle-area public schools. Some TPP programs in Northwest Seattle are using the FLASH curriculum, she said.
“This is a very comprehensive program, which includes discussion about reproductive health, sexual violence, prevention of teen pregnancy, sexually transmitted infections, [and] harm reduction,” she said. “That’s been a very effective method of educating our teens about these issues.”
[email protected]
On Twitter @legal_med
The Trump administration’s sudden funding cut to the Teen Pregnancy Prevention Program will not only halt research and programming efforts at more than 80 institutions across the country, but also will likely unravel recent progress made in reducing teen pregnancies, physicians and program advocates say.
In early July, officials at the U.S. Department of Health & Human Services notified program grantees that the administration would be eliminating funding for the Teen Pregnancy Prevention Program (TPP Program) and that 5-year grants awarded under the Obama administration would be ending in June 2018, 2 years earlier than planned.
The TPP Program is a national, evidence-based initiative established in 2010 to fund medically accurate and age-appropriate programs that work to prevent teen pregnancy in the United States.
“Those programs serve many youth across the country, so of course the individuals in the programs are going to be impacted,” Dr. Oelschlager said in an interview. “It’s demoralizing for the educators, [and] the researchers, who are looking at innovative methods, to have their funding cut in the middle of evaluating whether their programs are effective.”
An HHS spokeswoman confirmed that on July 1, the agency informed TPP Program grantees that funding for the program would be eliminated as detailed in President Trump’s fiscal 2018 budget proposal. The HHS awarded 81 continuations for TPP Program Tier 1 and Tier 2 grant awards for a total of $89 million through June 30, 2018, according to the spokeswoman. The HHS informed the grantees of their June 30, 2018, end date “to give them an opportunity to adjust their programs and plan for an orderly closeout,” she said.
The University of Southern California, Los Angeles, is one of many institutions impacted by the funding cut. The primary objectives of the Keeping it Real Together project are to implement evidence-based sexual health education programs for youth in middle and alternative high schools and provide an education program for parents of middle school–aged youth, said Luanne Rohrbach, PhD, associate professor of clinical preventive medicine at the university’s Institute for Health Promotion & Disease Prevention and principal investigator for the program.
Dr. Rohrbach said she anticipated pushback from the new administration as far as receiving the full 5-year funding, but the sudden program elimination was unexpected.
In March, when President Trump announced his budget priorities for fiscal 2016 and 2017, it was clear that the TPP Program was on the chopping block, Dr. Rohrbach said. However, when Congress passed a continuing resolution for the remainder of fiscal 2016 and 2017, the program remained intact. In his budget recommendations for fiscal 2017 and 2018, the President proposed that the TPP Program be eliminated.
“Despite this recommendation, it was our understanding that the program would be debated in Congress as they developed their recommendations for FY 2017-18 funding,” she said. “That is, we expected there would at least be discussion about it in Congressional budget committees. We did not expect that the program would be eliminated by the Office of the Secretary of HHS.”
Haywood L. Brown, MD, president of the American Congress of Obstetricians and Gynecologists (ACOG) called the administration’s decision “highly unusual” and said it is a step backward for ensuring healthy moms and healthy babies.
“This program and others provide vital research and programming that successfully brought our nation to an all-time low rate of teen pregnancies – progress we cannot afford to jeopardize,” Dr. Brown said in a statement.
Federal data show that the teen pregnancy rate has steadily declined over the last decade. In 2015, the birth rate for girls and young women aged 15-19 years fell by nearly 8% from 2014, according to data from the National Center for Health Statistics. Since 1991, the rate has fallen by 64%. The rate for the younger half of the age group, girls aged 15-17 years, was down 9% from 2014.
Researchers attribute the decline to a combination of economic, cultural, and social factors, as well as a lower prevalence of sexual activity among youth, the use of more effective contraception, and the provision of more information about pregnancy prevention, Dr. Rohrbach said.
“The [TPP Program] has been focused on implementation of evidence-based, comprehensive sexual health education,” she said. “Elimination of these efforts endangers the progress that has been made in reducing teen pregnancies.”
Dr. Oelschlager noted that between 2008 and 2015, the teen birth rate in King County, Washington, declined by 55%. She attributed the reduction to multiple drivers, including a program called Flash, that incorporates a sexual health education curriculum in Seattle-area public schools. Some TPP programs in Northwest Seattle are using the FLASH curriculum, she said.
“This is a very comprehensive program, which includes discussion about reproductive health, sexual violence, prevention of teen pregnancy, sexually transmitted infections, [and] harm reduction,” she said. “That’s been a very effective method of educating our teens about these issues.”
[email protected]
On Twitter @legal_med

Blocking a lipoprotein lipase inhibitor improves lipid profiles
Two different approaches to shutting down the function of a human liver protein that inhibits lipoprotein lipase showed preliminary evidence of safely producing favorable lipid changes in healthy volunteers in two separate, phase 1 studies.
These findings, coupled with promising observational data from people who carry loss-of-function mutations in the gene for this protein, angiopoietin-like 3 (ANGPTL3), have raised hopes that interventions that interfere with the function of the ANGPTL3 protein may provide new and effective ways to improve lipid levels and cut the incidence of cardiovascular disease events.
“There is now a growing body of epidemiologic, genetic, and genomewide association studies supporting the hypothesis that lowering levels of ANGPTL3 in plasma by inhibiting hepatic ANGPTL3 synthesis will be beneficial in terms of reducing plasma levels of atherogenic apolipoprotein B and in improving metabolic measures associated with dyslipidemia,” wrote Mark J. Graham and his associates in a recently published article (N Engl J Med. 2017 Jul 20;377[3]:222-32).
The phase 1 study results reported by this group came from 44 healthy adults aged 18-65 years who received varying doses of a commercially developed antisense drug, ANGPTL3-LRX, as either single or serial subcutaneous injections. ANGPTL3-LRX is an oligonucleotide designed to inhibit production of messenger RNA for the ANGPTL3 protein.
Six people received the highest ANGPTL3-LRX dosage administered, 60 mg given as a weekly injection for 6 weeks, and after this regimen they showed an average 50% cut in triglycerides levels, compared with baseline, and an average 33% drop in their low LDL cholesterol levels from baseline. None of the 33 people treated with ANGPTL3-LRX in the trial had a documented serious adverse event, and the only treatment dropout was a patient who was lost to follow-up during the treatment phase, reported Mr. Graham, a researcher at Ionis Pharmaceuticals, the sponsor of the study and the company developing the antisense drug, and his associates.
The second phase 1 study examined a different way to block ANGPTL3 activity, with a human monoclonal antibody to this protein. The study involved 83 healthy adults aged 18-65 years with fasting triglyceride levels of 150-450 mg/dL and fasting LDL cholesterol levels of at least 100 mg/dL. Each participant received a single subcutaneous injection or intravenous dose of the antibody, evinacumab, at varying amounts or placebo. The maximum observed lipid changes seen was a drop in triglycerides of 76% and a fall in LDL cholesterol by 23%. Treatment also produced a maximum drop in HDL cholesterol of 18%. No person left the study because of an adverse event. The most common adverse event was headache, in seven people (11% of evinacumab recipients), reported Frederick E. Dewey, MD, a researcher at Regeneron Pharmaceuticals, the company developing evinacumab, and his associates (N Engl J Med. 2017 Jul 20;377[3]:211-21).
The Regeneron report also included results from population studies they ran. They reported performing genome sequencing on specimens from 58,335 adults enrolled in the DiscovEHR study, and identified 13 distinct loss-of-function variants in the ANGPTL3 genes that occurred individually in a small number of these people.
They then ran analyses of lipid levels and coronary artery disease prevalence rates in people who carry one of these 13 loss-of-function genetic signatures in one of their ANGTPL3 genes. Among 45,226 of the people in DiscovEHR those with a variant had on average a 27% lower triglyceride level, a 9% lower LDL cholesterol level, and a 4% lower HDL cholesterol level than noncarriers, after adjustment for covariates. Analysis of coronary artery disease prevalence showed that, after adjusting for age, sex, and ancestry, carrying a loss-of-function variant was linked with a statistically significant 41% lower prevalence of all coronary artery disease, and a 34% lower prevalence of myocardial infarction that fell short of statistical significance.
A second population study looked at links between loss-of-function variants and coronary artery disease in more than 130,000 Danish people. This showed a nonsignificant 37% lower prevalence of coronary artery disease in people with a variant. Two different types of meta-analyses of the data from both the DiscovEHR and Danish studies showed coronary disease rates reduced by either 31% or 39% in variant carriers depending on which meta-analysis approach the researchers used, both statistically significant reductions.
[email protected]
On Twitter @mitchelzoler
The findings from these two studies together with other recent study results open a new therapeutic window for reducing elevated levels of triglyceride-rich lipoproteins by activating lipoprotein lipase.
The findings also suggest that inhibition of the ANGPTL3 gene or protein is potentially an effective way to treat patients with familial hypercholesterolemia because of a deficiency in the receptor for low density lipoprotein. It is likely that lowering triglyceride levels with an agent that boosts the activity of lipoprotein lipase will result in a different spectrum of benefits and adverse effects, compared with agents that boost the number of LDL receptors.
New approaches to boost lipoprotein lipase activity, such as inhibiting ANGPTL3 function as was done in these two reports, represents a fresh frontier for treatment of hypertriglyceridemia and coronary artery disease.
Alan R. Tall, MD , professor of medicine at Columbia University, New York, made these comments in an editorial ( N Engl J Med. 2017 Jul 20;377[3]:280-3 ).
The findings from these two studies together with other recent study results open a new therapeutic window for reducing elevated levels of triglyceride-rich lipoproteins by activating lipoprotein lipase.
The findings also suggest that inhibition of the ANGPTL3 gene or protein is potentially an effective way to treat patients with familial hypercholesterolemia because of a deficiency in the receptor for low density lipoprotein. It is likely that lowering triglyceride levels with an agent that boosts the activity of lipoprotein lipase will result in a different spectrum of benefits and adverse effects, compared with agents that boost the number of LDL receptors.
New approaches to boost lipoprotein lipase activity, such as inhibiting ANGPTL3 function as was done in these two reports, represents a fresh frontier for treatment of hypertriglyceridemia and coronary artery disease.
Alan R. Tall, MD , professor of medicine at Columbia University, New York, made these comments in an editorial ( N Engl J Med. 2017 Jul 20;377[3]:280-3 ).
The findings from these two studies together with other recent study results open a new therapeutic window for reducing elevated levels of triglyceride-rich lipoproteins by activating lipoprotein lipase.
The findings also suggest that inhibition of the ANGPTL3 gene or protein is potentially an effective way to treat patients with familial hypercholesterolemia because of a deficiency in the receptor for low density lipoprotein. It is likely that lowering triglyceride levels with an agent that boosts the activity of lipoprotein lipase will result in a different spectrum of benefits and adverse effects, compared with agents that boost the number of LDL receptors.
New approaches to boost lipoprotein lipase activity, such as inhibiting ANGPTL3 function as was done in these two reports, represents a fresh frontier for treatment of hypertriglyceridemia and coronary artery disease.
Alan R. Tall, MD , professor of medicine at Columbia University, New York, made these comments in an editorial ( N Engl J Med. 2017 Jul 20;377[3]:280-3 ).
Two different approaches to shutting down the function of a human liver protein that inhibits lipoprotein lipase showed preliminary evidence of safely producing favorable lipid changes in healthy volunteers in two separate, phase 1 studies.
These findings, coupled with promising observational data from people who carry loss-of-function mutations in the gene for this protein, angiopoietin-like 3 (ANGPTL3), have raised hopes that interventions that interfere with the function of the ANGPTL3 protein may provide new and effective ways to improve lipid levels and cut the incidence of cardiovascular disease events.
“There is now a growing body of epidemiologic, genetic, and genomewide association studies supporting the hypothesis that lowering levels of ANGPTL3 in plasma by inhibiting hepatic ANGPTL3 synthesis will be beneficial in terms of reducing plasma levels of atherogenic apolipoprotein B and in improving metabolic measures associated with dyslipidemia,” wrote Mark J. Graham and his associates in a recently published article (N Engl J Med. 2017 Jul 20;377[3]:222-32).
The phase 1 study results reported by this group came from 44 healthy adults aged 18-65 years who received varying doses of a commercially developed antisense drug, ANGPTL3-LRX, as either single or serial subcutaneous injections. ANGPTL3-LRX is an oligonucleotide designed to inhibit production of messenger RNA for the ANGPTL3 protein.
Six people received the highest ANGPTL3-LRX dosage administered, 60 mg given as a weekly injection for 6 weeks, and after this regimen they showed an average 50% cut in triglycerides levels, compared with baseline, and an average 33% drop in their low LDL cholesterol levels from baseline. None of the 33 people treated with ANGPTL3-LRX in the trial had a documented serious adverse event, and the only treatment dropout was a patient who was lost to follow-up during the treatment phase, reported Mr. Graham, a researcher at Ionis Pharmaceuticals, the sponsor of the study and the company developing the antisense drug, and his associates.
The second phase 1 study examined a different way to block ANGPTL3 activity, with a human monoclonal antibody to this protein. The study involved 83 healthy adults aged 18-65 years with fasting triglyceride levels of 150-450 mg/dL and fasting LDL cholesterol levels of at least 100 mg/dL. Each participant received a single subcutaneous injection or intravenous dose of the antibody, evinacumab, at varying amounts or placebo. The maximum observed lipid changes seen was a drop in triglycerides of 76% and a fall in LDL cholesterol by 23%. Treatment also produced a maximum drop in HDL cholesterol of 18%. No person left the study because of an adverse event. The most common adverse event was headache, in seven people (11% of evinacumab recipients), reported Frederick E. Dewey, MD, a researcher at Regeneron Pharmaceuticals, the company developing evinacumab, and his associates (N Engl J Med. 2017 Jul 20;377[3]:211-21).
The Regeneron report also included results from population studies they ran. They reported performing genome sequencing on specimens from 58,335 adults enrolled in the DiscovEHR study, and identified 13 distinct loss-of-function variants in the ANGPTL3 genes that occurred individually in a small number of these people.
They then ran analyses of lipid levels and coronary artery disease prevalence rates in people who carry one of these 13 loss-of-function genetic signatures in one of their ANGTPL3 genes. Among 45,226 of the people in DiscovEHR those with a variant had on average a 27% lower triglyceride level, a 9% lower LDL cholesterol level, and a 4% lower HDL cholesterol level than noncarriers, after adjustment for covariates. Analysis of coronary artery disease prevalence showed that, after adjusting for age, sex, and ancestry, carrying a loss-of-function variant was linked with a statistically significant 41% lower prevalence of all coronary artery disease, and a 34% lower prevalence of myocardial infarction that fell short of statistical significance.
A second population study looked at links between loss-of-function variants and coronary artery disease in more than 130,000 Danish people. This showed a nonsignificant 37% lower prevalence of coronary artery disease in people with a variant. Two different types of meta-analyses of the data from both the DiscovEHR and Danish studies showed coronary disease rates reduced by either 31% or 39% in variant carriers depending on which meta-analysis approach the researchers used, both statistically significant reductions.
[email protected]
On Twitter @mitchelzoler
Two different approaches to shutting down the function of a human liver protein that inhibits lipoprotein lipase showed preliminary evidence of safely producing favorable lipid changes in healthy volunteers in two separate, phase 1 studies.
These findings, coupled with promising observational data from people who carry loss-of-function mutations in the gene for this protein, angiopoietin-like 3 (ANGPTL3), have raised hopes that interventions that interfere with the function of the ANGPTL3 protein may provide new and effective ways to improve lipid levels and cut the incidence of cardiovascular disease events.
“There is now a growing body of epidemiologic, genetic, and genomewide association studies supporting the hypothesis that lowering levels of ANGPTL3 in plasma by inhibiting hepatic ANGPTL3 synthesis will be beneficial in terms of reducing plasma levels of atherogenic apolipoprotein B and in improving metabolic measures associated with dyslipidemia,” wrote Mark J. Graham and his associates in a recently published article (N Engl J Med. 2017 Jul 20;377[3]:222-32).
The phase 1 study results reported by this group came from 44 healthy adults aged 18-65 years who received varying doses of a commercially developed antisense drug, ANGPTL3-LRX, as either single or serial subcutaneous injections. ANGPTL3-LRX is an oligonucleotide designed to inhibit production of messenger RNA for the ANGPTL3 protein.
Six people received the highest ANGPTL3-LRX dosage administered, 60 mg given as a weekly injection for 6 weeks, and after this regimen they showed an average 50% cut in triglycerides levels, compared with baseline, and an average 33% drop in their low LDL cholesterol levels from baseline. None of the 33 people treated with ANGPTL3-LRX in the trial had a documented serious adverse event, and the only treatment dropout was a patient who was lost to follow-up during the treatment phase, reported Mr. Graham, a researcher at Ionis Pharmaceuticals, the sponsor of the study and the company developing the antisense drug, and his associates.
The second phase 1 study examined a different way to block ANGPTL3 activity, with a human monoclonal antibody to this protein. The study involved 83 healthy adults aged 18-65 years with fasting triglyceride levels of 150-450 mg/dL and fasting LDL cholesterol levels of at least 100 mg/dL. Each participant received a single subcutaneous injection or intravenous dose of the antibody, evinacumab, at varying amounts or placebo. The maximum observed lipid changes seen was a drop in triglycerides of 76% and a fall in LDL cholesterol by 23%. Treatment also produced a maximum drop in HDL cholesterol of 18%. No person left the study because of an adverse event. The most common adverse event was headache, in seven people (11% of evinacumab recipients), reported Frederick E. Dewey, MD, a researcher at Regeneron Pharmaceuticals, the company developing evinacumab, and his associates (N Engl J Med. 2017 Jul 20;377[3]:211-21).
The Regeneron report also included results from population studies they ran. They reported performing genome sequencing on specimens from 58,335 adults enrolled in the DiscovEHR study, and identified 13 distinct loss-of-function variants in the ANGPTL3 genes that occurred individually in a small number of these people.
They then ran analyses of lipid levels and coronary artery disease prevalence rates in people who carry one of these 13 loss-of-function genetic signatures in one of their ANGTPL3 genes. Among 45,226 of the people in DiscovEHR those with a variant had on average a 27% lower triglyceride level, a 9% lower LDL cholesterol level, and a 4% lower HDL cholesterol level than noncarriers, after adjustment for covariates. Analysis of coronary artery disease prevalence showed that, after adjusting for age, sex, and ancestry, carrying a loss-of-function variant was linked with a statistically significant 41% lower prevalence of all coronary artery disease, and a 34% lower prevalence of myocardial infarction that fell short of statistical significance.
A second population study looked at links between loss-of-function variants and coronary artery disease in more than 130,000 Danish people. This showed a nonsignificant 37% lower prevalence of coronary artery disease in people with a variant. Two different types of meta-analyses of the data from both the DiscovEHR and Danish studies showed coronary disease rates reduced by either 31% or 39% in variant carriers depending on which meta-analysis approach the researchers used, both statistically significant reductions.
[email protected]
On Twitter @mitchelzoler
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: Serial doses of the antisense oligonucleotide ANGPTL3-LRX produced an average 50% cut in triglycerides and 33% cut in LDL cholesterol.
Data source: The ANGPTL3-LRX phase 1 trial enrolled 44 healthy adults. The evinacumab phase 1 trial enrolled 83 healthy adults.
Disclosures: The ANGPTL3-LRX study was funded by Ionis. Mr. Graham is an employee of Ionis. The evinacumab study was funded by Regeneron. Dr. Dewey is an employee of Regeneron.
Cord Blood and Cord Tissue Preservation Information for Your Patients

Your patients may be overwhelmed with so many decisions as they prepare for their newborn to arrive. We want to help make one decision easier. The Cord Blood and Cord Tissue Preservation Patient Handout provides simple and clear education about their cord blood and cord tissue preservation options.
Access and print the handout now and give it to your patients so they can review the information at their own pace.
Your patients may be overwhelmed with so many decisions as they prepare for their newborn to arrive. We want to help make one decision easier. The Cord Blood and Cord Tissue Preservation Patient Handout provides simple and clear education about their cord blood and cord tissue preservation options.
Access and print the handout now and give it to your patients so they can review the information at their own pace.
Your patients may be overwhelmed with so many decisions as they prepare for their newborn to arrive. We want to help make one decision easier. The Cord Blood and Cord Tissue Preservation Patient Handout provides simple and clear education about their cord blood and cord tissue preservation options.
Access and print the handout now and give it to your patients so they can review the information at their own pace.

Ventricular assist devices linked to sepsis
NEW ORLEANS – Back in 2008, there was only one case.
Since then, however, the number of patients with ventricular assist devices who developed sepsis while being treated in the cardiac unit at Queen Elizabeth Hospital in Birmingham, England, appeared to be noticeably growing. So, investigators launched a study to confirm their suspicions and to learn more about the underlying causes.
“Bloodstream infection is a serious infection, so I thought, ‘Let’s see what’s happening,’ ” explained Ira Das, MD, a consultant microbiologist at Queen Elizabeth Hospital.
Coagulase-negative staphylococci were the most common cause, present in 32% of the 25 cases. Sepsis was caused by Enterococcus faecium in 12%, Candida parapsilosis in 8%, and Staphylococcus aureus in 2%. Another 4% were either Enterococcus faecalis, Serratia marcescens, Pseudomonas aeruginosa, C. guilliermondii, or C. orthopsilosis. The remaining 16% of bloodstream infections were polymicrobial.
Less certain was the source of these infections.
“In the majority of cases, we didn’t know where it was coming from,” Dr. Das said at the annual meeting of the American Society for Microbiology. In 6 of the 25 cases, VAD was confirmed to be the focus of infection, either through imaging or because a failing component of the explanted device was examined later. An intravascular catheter was the source in another 5 patients, and in 14 cases, the source remained a mystery.
“Some of these infections just might have been hard to see,” Dr. Das said. “If the infection is inside the device, it’s not always easy to visualize.”
The study supports earlier findings from a review article that points to a significant infection risk associated with the implantation of VADs (Expert Rev Med Devices. 2011 Sep;8[5]:627-34). That article’s authors noted, “Despite recent improvements in outcomes, device-related infections remain a significant complication of LVAD [left ventricular assist device] therapy.”
In a previous study of people with end-stage heart failure, other investigators noted that, “despite the substantial survival benefit, the morbidity and mortality associated with the use of the left ventricular assist device were considerable. In particular, infection and mechanical failure of the device were major factors in the 2-year survival rate of only 23%” (N Engl J Med. 2001 Nov 15;345[20]:1435-43).
Similarly, in the current study, mortality was higher among those with sepsis and a VAD. Mortality was 39% – including eight patients who died with a VAD in situ and one following cardiac transplantation. However, Dr. Das cautioned, “It’s a small number, and there are other factors that could have contributed. They all go on anticoagulants so they have bleeding tendencies, and many of the patients are in the ICU with multiorgan failure.”
Infection prevention remains paramount to minimize mortality and other adverse events associated with a patient’s having a VAD. “We have to make sure that infection control procedures and our treatments are up to the optimal standard,” Dr. Das said. “It’s not easy to remove the device.”
Of the 129 VADs implanted, 68 were long-term LVADs, 11 were short-term LVADs, 15 were right ventricular devices, and 35 were biventricular devices.
The study is ongoing. The data presented at the meeting were collected up until December 2016.
“Since then, I’ve seen two more cases, and – very interestingly – one was Haemophilus influenzae,” Dr. Das said. “The patient was on the device, he was at home, and he came in with bacteremia.” Again, the source of infection proved elusive. “With H. influenzae, you would think it was coming from his chest, but the chest x-ray was normal.”
The second case, a patient with a coagulase-negative staphylococci bloodstream infection, was scheduled for a PET scan at the time of Dr. Das’ presentation to try to identify the source of infection.
Dr. Das had no relevant disclosures.

Modern technology saves our patients' lives, but there is always another side to the coin. Reports that LVAD devices are associated with a high incidence of bloodstream infections is important for future clinical practice. The fact that the causes and risk factors for these infections are unknown make this phenomena one of high interest.
Modern technology saves our patients' lives, but there is always another side to the coin. Reports that LVAD devices are associated with a high incidence of bloodstream infections is important for future clinical practice. The fact that the causes and risk factors for these infections are unknown make this phenomena one of high interest.
Modern technology saves our patients' lives, but there is always another side to the coin. Reports that LVAD devices are associated with a high incidence of bloodstream infections is important for future clinical practice. The fact that the causes and risk factors for these infections are unknown make this phenomena one of high interest.
NEW ORLEANS – Back in 2008, there was only one case.
Since then, however, the number of patients with ventricular assist devices who developed sepsis while being treated in the cardiac unit at Queen Elizabeth Hospital in Birmingham, England, appeared to be noticeably growing. So, investigators launched a study to confirm their suspicions and to learn more about the underlying causes.
“Bloodstream infection is a serious infection, so I thought, ‘Let’s see what’s happening,’ ” explained Ira Das, MD, a consultant microbiologist at Queen Elizabeth Hospital.
Coagulase-negative staphylococci were the most common cause, present in 32% of the 25 cases. Sepsis was caused by Enterococcus faecium in 12%, Candida parapsilosis in 8%, and Staphylococcus aureus in 2%. Another 4% were either Enterococcus faecalis, Serratia marcescens, Pseudomonas aeruginosa, C. guilliermondii, or C. orthopsilosis. The remaining 16% of bloodstream infections were polymicrobial.
Less certain was the source of these infections.
“In the majority of cases, we didn’t know where it was coming from,” Dr. Das said at the annual meeting of the American Society for Microbiology. In 6 of the 25 cases, VAD was confirmed to be the focus of infection, either through imaging or because a failing component of the explanted device was examined later. An intravascular catheter was the source in another 5 patients, and in 14 cases, the source remained a mystery.
“Some of these infections just might have been hard to see,” Dr. Das said. “If the infection is inside the device, it’s not always easy to visualize.”
The study supports earlier findings from a review article that points to a significant infection risk associated with the implantation of VADs (Expert Rev Med Devices. 2011 Sep;8[5]:627-34). That article’s authors noted, “Despite recent improvements in outcomes, device-related infections remain a significant complication of LVAD [left ventricular assist device] therapy.”
In a previous study of people with end-stage heart failure, other investigators noted that, “despite the substantial survival benefit, the morbidity and mortality associated with the use of the left ventricular assist device were considerable. In particular, infection and mechanical failure of the device were major factors in the 2-year survival rate of only 23%” (N Engl J Med. 2001 Nov 15;345[20]:1435-43).
Similarly, in the current study, mortality was higher among those with sepsis and a VAD. Mortality was 39% – including eight patients who died with a VAD in situ and one following cardiac transplantation. However, Dr. Das cautioned, “It’s a small number, and there are other factors that could have contributed. They all go on anticoagulants so they have bleeding tendencies, and many of the patients are in the ICU with multiorgan failure.”
Infection prevention remains paramount to minimize mortality and other adverse events associated with a patient’s having a VAD. “We have to make sure that infection control procedures and our treatments are up to the optimal standard,” Dr. Das said. “It’s not easy to remove the device.”
Of the 129 VADs implanted, 68 were long-term LVADs, 11 were short-term LVADs, 15 were right ventricular devices, and 35 were biventricular devices.
The study is ongoing. The data presented at the meeting were collected up until December 2016.
“Since then, I’ve seen two more cases, and – very interestingly – one was Haemophilus influenzae,” Dr. Das said. “The patient was on the device, he was at home, and he came in with bacteremia.” Again, the source of infection proved elusive. “With H. influenzae, you would think it was coming from his chest, but the chest x-ray was normal.”
The second case, a patient with a coagulase-negative staphylococci bloodstream infection, was scheduled for a PET scan at the time of Dr. Das’ presentation to try to identify the source of infection.
Dr. Das had no relevant disclosures.
NEW ORLEANS – Back in 2008, there was only one case.
Since then, however, the number of patients with ventricular assist devices who developed sepsis while being treated in the cardiac unit at Queen Elizabeth Hospital in Birmingham, England, appeared to be noticeably growing. So, investigators launched a study to confirm their suspicions and to learn more about the underlying causes.
“Bloodstream infection is a serious infection, so I thought, ‘Let’s see what’s happening,’ ” explained Ira Das, MD, a consultant microbiologist at Queen Elizabeth Hospital.
Coagulase-negative staphylococci were the most common cause, present in 32% of the 25 cases. Sepsis was caused by Enterococcus faecium in 12%, Candida parapsilosis in 8%, and Staphylococcus aureus in 2%. Another 4% were either Enterococcus faecalis, Serratia marcescens, Pseudomonas aeruginosa, C. guilliermondii, or C. orthopsilosis. The remaining 16% of bloodstream infections were polymicrobial.
Less certain was the source of these infections.
“In the majority of cases, we didn’t know where it was coming from,” Dr. Das said at the annual meeting of the American Society for Microbiology. In 6 of the 25 cases, VAD was confirmed to be the focus of infection, either through imaging or because a failing component of the explanted device was examined later. An intravascular catheter was the source in another 5 patients, and in 14 cases, the source remained a mystery.
“Some of these infections just might have been hard to see,” Dr. Das said. “If the infection is inside the device, it’s not always easy to visualize.”
The study supports earlier findings from a review article that points to a significant infection risk associated with the implantation of VADs (Expert Rev Med Devices. 2011 Sep;8[5]:627-34). That article’s authors noted, “Despite recent improvements in outcomes, device-related infections remain a significant complication of LVAD [left ventricular assist device] therapy.”
In a previous study of people with end-stage heart failure, other investigators noted that, “despite the substantial survival benefit, the morbidity and mortality associated with the use of the left ventricular assist device were considerable. In particular, infection and mechanical failure of the device were major factors in the 2-year survival rate of only 23%” (N Engl J Med. 2001 Nov 15;345[20]:1435-43).
Similarly, in the current study, mortality was higher among those with sepsis and a VAD. Mortality was 39% – including eight patients who died with a VAD in situ and one following cardiac transplantation. However, Dr. Das cautioned, “It’s a small number, and there are other factors that could have contributed. They all go on anticoagulants so they have bleeding tendencies, and many of the patients are in the ICU with multiorgan failure.”
Infection prevention remains paramount to minimize mortality and other adverse events associated with a patient’s having a VAD. “We have to make sure that infection control procedures and our treatments are up to the optimal standard,” Dr. Das said. “It’s not easy to remove the device.”
Of the 129 VADs implanted, 68 were long-term LVADs, 11 were short-term LVADs, 15 were right ventricular devices, and 35 were biventricular devices.
The study is ongoing. The data presented at the meeting were collected up until December 2016.
“Since then, I’ve seen two more cases, and – very interestingly – one was Haemophilus influenzae,” Dr. Das said. “The patient was on the device, he was at home, and he came in with bacteremia.” Again, the source of infection proved elusive. “With H. influenzae, you would think it was coming from his chest, but the chest x-ray was normal.”
The second case, a patient with a coagulase-negative staphylococci bloodstream infection, was scheduled for a PET scan at the time of Dr. Das’ presentation to try to identify the source of infection.
Dr. Das had no relevant disclosures.
AT ASM MICROBE 2017
Key clinical point: There may be a significant rate of bloodstream infections among people with a ventricular assist device.
Major finding: A total of 20% of the 118 people with a VAD had a bloodstream infection.
Data source: A retrospective study of 129 ventricular assist devices placed in 118 people between 2008 and 2016.
Disclosures: Dr. Das had no relevant disclosures.
Online intervention aims to prevent teen depression
AT PAS 17
SAN FRANCISCO – One in eight teenagers experienced at least one major depressive episode in 2015, according to the National Institute for Mental Health. Yet the recent uptick in teen suicide rates suggests that U.S. mental health care services are not meeting their needs.
A team at the University of Illinois in Chicago, led by Benjamin Van Voorhees, MD, MPH, hopes so, and they have spent the past several years developing and testing such a program with a National Institute of Mental Health (NIMH) grant.
“Adolescents are in a really plastic moment in their psychobehavioral repertoire and brain development as they program themselves to adapt to adult life,” Dr. Van Voorhees said in an interview. “Right now we have nothing to offer those individuals other than an occasional referral to an overtaxed mental health system. The only rational strategy is a mass dissemination model, which is going to have to be technology.”
The CATCH-IT program is aimed at teens showing early signs of depression or predepressive symptoms as determined through screening during well checks or other visits for acute or chronic concerns. The study uses multiple screening tools in selecting participants, but Dr. Van Voorhees estimates that screening in practice would require about 1-2 minutes of a medical assistant’s or nurse’s time, followed by 1-2 minutes of the practitioner’s time for positive screens – “and one in five of those screens is going to be positive,” he said.
“The thing we want to convey to primary care practitioners is that these individuals are coming through your office every day, we’re doing nothing for them, and in some ways we are ignoring their enormous future potential adverse trajectory toward mental disorders,” he said.
The program includes 14 modules drawing on cognitive behavioral therapy, behavioral activation, interpersonal psychotherapy, and community resiliency. Six archetypal teens – such as teen living with a single mom or one whose parents are divorcing – are featured in each of the modules to demonstrate six ways of applying the strategies taught in that module. The archetypal teens are around 14-15 years old, but the program is aimed at teens aged 13-18 years, with a reading level at about grade 6, Dr. Van Voorhees said.

Two and a half years after those teens used the CATCH-IT intervention, they showed “a sustained reduction in automatic negative thoughts and educational impairment,” but no difference in their perceptions of support from family or friends. The lack of a control group in that pilot limits what conclusions can be drawn about the program’s effectiveness, but the researchers did learn that motivational interviewing led to greater engagement with the program, compared with teens who received a brief recommendation of it.
Therefore, in the subsequent – and still ongoing – study, physicians used motivational interviewing when offering teens the opportunity to join the program. That study does include a control group, in which participants are assigned a generic health education program online instead of CATCH-IT, and the randomized participants have been stratified by site, gender, and depression risk level.
The researchers first assessed the baseline characteristics of the population, recruited from 38 clinics in two cities. The study enrolled 369 teens aged 13-18 years – 248 in Chicago and 121 in Boston. All were identified as high risk for depression based on elevated scores on the Center for Epidemiological Studies Depression (CES-D) scale or the Kiddie Schedule for Affective Disorders Scale (K-SADS). Two thirds (68%) of participants are female, and most (63%) are in high school. About a third (34%) are in middle school. The racial/ethnic breakdown of the sample is 21% Hispanic, 26% black, 43% white, 4% Asian, 6% multiracial, and 1% other (which adds up to 101% due to rounding). More than half of the participants’ mothers (60%) and fathers (53%) were college graduates.
The teens completed the CES-D, the Screen for Child Related Anxiety Disorders (SCARED), the Beck Hopelessness Scale (BHS), the CRAFFT screening for adolescent substance misuse and the Disruptive Behaviors Disorder Scale (DBD-A). A parent of each teen also filled out the CES-D and DBD-A.
The baseline results did not suggest any concerns about substance use, hopelessness, or disruptive behaviors such as ADHD or conduct disorder. But the average scores on the CES-D and SCARED sat just at the threshold for a potential depressive or anxiety disorders. A CES-D score of at least 16 suggests a possible depressive disorder, and a SCARED score of at least 25 suggests a possible anxiety disorder. The mean scores on the teens’ CES-D were 17.7 in the Chicago cohort, 15.4 in the Boston cohort and 16.9 for the whole group. Similarly, the SCARED mean scores were 26.3 in the Chicago cohort, 23.5 in the Boston cohort and 25.3 overall.
Scores from K-SADS showed subthreshold levels of depressed mood in 36% of teens in both cities, and a nearly identical subthreshold level of irritability. Subthreshold anhedonia was identified in 20% of the overall population. One percent of the overall population had current suicidal ideation.
The next steps are to analyze outcomes among the participants, as the team is doing currently. They have just passed the 1-year anniversary of the trial and are analyzing the data they collected over the past year. The study will run an additional year for longer-term data collection.
One of the abstracts presented at PAS explored the economic implications of incorporating CATCH-IT in primary care.
“The cost for implementation is where the challenge is,” Dr. Van Voorhees said. “Screening takes time, and calling people takes time.” But when spread across a practice’s overall clientele in a year, the costs drop considerably, he said, and savings from effective identification and depression prevention may outweigh costs. The researchers have not yet conducted a cost-effectiveness study because they still are analyzing data on outcomes.
But Dr. Van Voorhees is optimistic about the possibilities of the program.
“What this entire model is about is, how do we understand what’s going on in the environment of the primary care clinic to find these people, identify them, and motivate them, and how can we give them something relevant enough to actually complete,” Dr. Van Voorhees said in the interview. “Then, let’s actually see if it changes their behavioral trajectory.”
The National Institute of Mental Health funded the research. Dr. Van Voorhees has consulted for Prevail Health Solutions, Mevident, Social Kinetics, and Hong Kong University on development of Internet-based interventions.
AT PAS 17
SAN FRANCISCO – One in eight teenagers experienced at least one major depressive episode in 2015, according to the National Institute for Mental Health. Yet the recent uptick in teen suicide rates suggests that U.S. mental health care services are not meeting their needs.
A team at the University of Illinois in Chicago, led by Benjamin Van Voorhees, MD, MPH, hopes so, and they have spent the past several years developing and testing such a program with a National Institute of Mental Health (NIMH) grant.
“Adolescents are in a really plastic moment in their psychobehavioral repertoire and brain development as they program themselves to adapt to adult life,” Dr. Van Voorhees said in an interview. “Right now we have nothing to offer those individuals other than an occasional referral to an overtaxed mental health system. The only rational strategy is a mass dissemination model, which is going to have to be technology.”
The CATCH-IT program is aimed at teens showing early signs of depression or predepressive symptoms as determined through screening during well checks or other visits for acute or chronic concerns. The study uses multiple screening tools in selecting participants, but Dr. Van Voorhees estimates that screening in practice would require about 1-2 minutes of a medical assistant’s or nurse’s time, followed by 1-2 minutes of the practitioner’s time for positive screens – “and one in five of those screens is going to be positive,” he said.
“The thing we want to convey to primary care practitioners is that these individuals are coming through your office every day, we’re doing nothing for them, and in some ways we are ignoring their enormous future potential adverse trajectory toward mental disorders,” he said.
The program includes 14 modules drawing on cognitive behavioral therapy, behavioral activation, interpersonal psychotherapy, and community resiliency. Six archetypal teens – such as teen living with a single mom or one whose parents are divorcing – are featured in each of the modules to demonstrate six ways of applying the strategies taught in that module. The archetypal teens are around 14-15 years old, but the program is aimed at teens aged 13-18 years, with a reading level at about grade 6, Dr. Van Voorhees said.
Two and a half years after those teens used the CATCH-IT intervention, they showed “a sustained reduction in automatic negative thoughts and educational impairment,” but no difference in their perceptions of support from family or friends. The lack of a control group in that pilot limits what conclusions can be drawn about the program’s effectiveness, but the researchers did learn that motivational interviewing led to greater engagement with the program, compared with teens who received a brief recommendation of it.
Therefore, in the subsequent – and still ongoing – study, physicians used motivational interviewing when offering teens the opportunity to join the program. That study does include a control group, in which participants are assigned a generic health education program online instead of CATCH-IT, and the randomized participants have been stratified by site, gender, and depression risk level.
The researchers first assessed the baseline characteristics of the population, recruited from 38 clinics in two cities. The study enrolled 369 teens aged 13-18 years – 248 in Chicago and 121 in Boston. All were identified as high risk for depression based on elevated scores on the Center for Epidemiological Studies Depression (CES-D) scale or the Kiddie Schedule for Affective Disorders Scale (K-SADS). Two thirds (68%) of participants are female, and most (63%) are in high school. About a third (34%) are in middle school. The racial/ethnic breakdown of the sample is 21% Hispanic, 26% black, 43% white, 4% Asian, 6% multiracial, and 1% other (which adds up to 101% due to rounding). More than half of the participants’ mothers (60%) and fathers (53%) were college graduates.
The teens completed the CES-D, the Screen for Child Related Anxiety Disorders (SCARED), the Beck Hopelessness Scale (BHS), the CRAFFT screening for adolescent substance misuse and the Disruptive Behaviors Disorder Scale (DBD-A). A parent of each teen also filled out the CES-D and DBD-A.
The baseline results did not suggest any concerns about substance use, hopelessness, or disruptive behaviors such as ADHD or conduct disorder. But the average scores on the CES-D and SCARED sat just at the threshold for a potential depressive or anxiety disorders. A CES-D score of at least 16 suggests a possible depressive disorder, and a SCARED score of at least 25 suggests a possible anxiety disorder. The mean scores on the teens’ CES-D were 17.7 in the Chicago cohort, 15.4 in the Boston cohort and 16.9 for the whole group. Similarly, the SCARED mean scores were 26.3 in the Chicago cohort, 23.5 in the Boston cohort and 25.3 overall.
Scores from K-SADS showed subthreshold levels of depressed mood in 36% of teens in both cities, and a nearly identical subthreshold level of irritability. Subthreshold anhedonia was identified in 20% of the overall population. One percent of the overall population had current suicidal ideation.
The next steps are to analyze outcomes among the participants, as the team is doing currently. They have just passed the 1-year anniversary of the trial and are analyzing the data they collected over the past year. The study will run an additional year for longer-term data collection.
One of the abstracts presented at PAS explored the economic implications of incorporating CATCH-IT in primary care.
“The cost for implementation is where the challenge is,” Dr. Van Voorhees said. “Screening takes time, and calling people takes time.” But when spread across a practice’s overall clientele in a year, the costs drop considerably, he said, and savings from effective identification and depression prevention may outweigh costs. The researchers have not yet conducted a cost-effectiveness study because they still are analyzing data on outcomes.
But Dr. Van Voorhees is optimistic about the possibilities of the program.
“What this entire model is about is, how do we understand what’s going on in the environment of the primary care clinic to find these people, identify them, and motivate them, and how can we give them something relevant enough to actually complete,” Dr. Van Voorhees said in the interview. “Then, let’s actually see if it changes their behavioral trajectory.”
The National Institute of Mental Health funded the research. Dr. Van Voorhees has consulted for Prevail Health Solutions, Mevident, Social Kinetics, and Hong Kong University on development of Internet-based interventions.
AT PAS 17
SAN FRANCISCO – One in eight teenagers experienced at least one major depressive episode in 2015, according to the National Institute for Mental Health. Yet the recent uptick in teen suicide rates suggests that U.S. mental health care services are not meeting their needs.
A team at the University of Illinois in Chicago, led by Benjamin Van Voorhees, MD, MPH, hopes so, and they have spent the past several years developing and testing such a program with a National Institute of Mental Health (NIMH) grant.
“Adolescents are in a really plastic moment in their psychobehavioral repertoire and brain development as they program themselves to adapt to adult life,” Dr. Van Voorhees said in an interview. “Right now we have nothing to offer those individuals other than an occasional referral to an overtaxed mental health system. The only rational strategy is a mass dissemination model, which is going to have to be technology.”
The CATCH-IT program is aimed at teens showing early signs of depression or predepressive symptoms as determined through screening during well checks or other visits for acute or chronic concerns. The study uses multiple screening tools in selecting participants, but Dr. Van Voorhees estimates that screening in practice would require about 1-2 minutes of a medical assistant’s or nurse’s time, followed by 1-2 minutes of the practitioner’s time for positive screens – “and one in five of those screens is going to be positive,” he said.
“The thing we want to convey to primary care practitioners is that these individuals are coming through your office every day, we’re doing nothing for them, and in some ways we are ignoring their enormous future potential adverse trajectory toward mental disorders,” he said.
The program includes 14 modules drawing on cognitive behavioral therapy, behavioral activation, interpersonal psychotherapy, and community resiliency. Six archetypal teens – such as teen living with a single mom or one whose parents are divorcing – are featured in each of the modules to demonstrate six ways of applying the strategies taught in that module. The archetypal teens are around 14-15 years old, but the program is aimed at teens aged 13-18 years, with a reading level at about grade 6, Dr. Van Voorhees said.
Two and a half years after those teens used the CATCH-IT intervention, they showed “a sustained reduction in automatic negative thoughts and educational impairment,” but no difference in their perceptions of support from family or friends. The lack of a control group in that pilot limits what conclusions can be drawn about the program’s effectiveness, but the researchers did learn that motivational interviewing led to greater engagement with the program, compared with teens who received a brief recommendation of it.
Therefore, in the subsequent – and still ongoing – study, physicians used motivational interviewing when offering teens the opportunity to join the program. That study does include a control group, in which participants are assigned a generic health education program online instead of CATCH-IT, and the randomized participants have been stratified by site, gender, and depression risk level.
The researchers first assessed the baseline characteristics of the population, recruited from 38 clinics in two cities. The study enrolled 369 teens aged 13-18 years – 248 in Chicago and 121 in Boston. All were identified as high risk for depression based on elevated scores on the Center for Epidemiological Studies Depression (CES-D) scale or the Kiddie Schedule for Affective Disorders Scale (K-SADS). Two thirds (68%) of participants are female, and most (63%) are in high school. About a third (34%) are in middle school. The racial/ethnic breakdown of the sample is 21% Hispanic, 26% black, 43% white, 4% Asian, 6% multiracial, and 1% other (which adds up to 101% due to rounding). More than half of the participants’ mothers (60%) and fathers (53%) were college graduates.
The teens completed the CES-D, the Screen for Child Related Anxiety Disorders (SCARED), the Beck Hopelessness Scale (BHS), the CRAFFT screening for adolescent substance misuse and the Disruptive Behaviors Disorder Scale (DBD-A). A parent of each teen also filled out the CES-D and DBD-A.
The baseline results did not suggest any concerns about substance use, hopelessness, or disruptive behaviors such as ADHD or conduct disorder. But the average scores on the CES-D and SCARED sat just at the threshold for a potential depressive or anxiety disorders. A CES-D score of at least 16 suggests a possible depressive disorder, and a SCARED score of at least 25 suggests a possible anxiety disorder. The mean scores on the teens’ CES-D were 17.7 in the Chicago cohort, 15.4 in the Boston cohort and 16.9 for the whole group. Similarly, the SCARED mean scores were 26.3 in the Chicago cohort, 23.5 in the Boston cohort and 25.3 overall.
Scores from K-SADS showed subthreshold levels of depressed mood in 36% of teens in both cities, and a nearly identical subthreshold level of irritability. Subthreshold anhedonia was identified in 20% of the overall population. One percent of the overall population had current suicidal ideation.
The next steps are to analyze outcomes among the participants, as the team is doing currently. They have just passed the 1-year anniversary of the trial and are analyzing the data they collected over the past year. The study will run an additional year for longer-term data collection.
One of the abstracts presented at PAS explored the economic implications of incorporating CATCH-IT in primary care.
“The cost for implementation is where the challenge is,” Dr. Van Voorhees said. “Screening takes time, and calling people takes time.” But when spread across a practice’s overall clientele in a year, the costs drop considerably, he said, and savings from effective identification and depression prevention may outweigh costs. The researchers have not yet conducted a cost-effectiveness study because they still are analyzing data on outcomes.
But Dr. Van Voorhees is optimistic about the possibilities of the program.
“What this entire model is about is, how do we understand what’s going on in the environment of the primary care clinic to find these people, identify them, and motivate them, and how can we give them something relevant enough to actually complete,” Dr. Van Voorhees said in the interview. “Then, let’s actually see if it changes their behavioral trajectory.”
The National Institute of Mental Health funded the research. Dr. Van Voorhees has consulted for Prevail Health Solutions, Mevident, Social Kinetics, and Hong Kong University on development of Internet-based interventions.