User login
Fat shaming interferes with patients’ medical care, experts say
WASHINGTON – Stereotypical views held by physicians, psychologists, nurses, and other medical professionals about overweight and obese patients need to change, panelists said at the annual convention of the American Psychological Association.
“We have a lot of negative attitudes toward heavy-weight people. Judging patients as too big or too fat produces physical and mental health effects,” said Joan C. Chrisler, PhD, the Class of ’43 Professor of Psychology at Connecticut College, New London. “Shame and disrespectful treatment can lead to delay in seeking health care, reluctance to return visits, or lower trust in the providers and their recommendations.”
A study of more than 300 autopsy reports showed that obese patients were 1.65 times more likely than normal weight and underweight groups combined were to have medical conditions such as endocarditis, ischemic bowel disease, and lung cancer that were not diagnosed, Dr. Chrisler said in a press release (Am J Clin Pathol. 2006 Jan;125[1]:127-31).
In addition to preventing patients from seeking care, Dr. Chrisler said in the release, unfamiliarity with the dosing adjustments sometimes required on medications based on the body mass index of patients affects the quality of care. She cited a retrospective study showing that emergency physicians frequently underdose common antibiotics in the emergency department (Am J Emerg Med. 2012 Sep;30[7]:1212-4).

“People aren’t born repulsed by fat people,” said Dr. McHugh, professor of psychology at Indiana University of Pennsylvania. “Fat hate is learned within the family.”
They encouraged more sensitivity from medical professionals when it comes to treating overweight and obese patients, such as providing changing gowns of different sizes in examination rooms and weighing patients in private areas of the medical office.
Dr. Chrisler and Dr. McHugh said weight stigma should be addressed in medicine and psychology through training and research, and in working with patients who are obese. “Treatments should focus on mental and physical health as the desired outcomes for therapy rather than weight,” Dr. McHugh said.
Dr. Chrisler, coauthor of a recent article on sizeism (Fat Studies. 2017 Aug;6[1]:38-53), had no disclosures. Dr. McHugh also had no disclosures.
Obesity is a major modifiable cause of diseases of the digestive tract that routinely goes unaddressed. The AGA Obesity Practice Guide was created to support gastroenterologists leading a care team to help patients with obesity achieve a healthy weight. The AGA Obesity Practice Guide provides a comprehensive, multi-disciplinary process to personalize innovative obesity care for safe and effective weight management. Learn more at www.gastro.org/obesity.
[email protected]
On Twitter @ginalhenderson
WASHINGTON – Stereotypical views held by physicians, psychologists, nurses, and other medical professionals about overweight and obese patients need to change, panelists said at the annual convention of the American Psychological Association.
“We have a lot of negative attitudes toward heavy-weight people. Judging patients as too big or too fat produces physical and mental health effects,” said Joan C. Chrisler, PhD, the Class of ’43 Professor of Psychology at Connecticut College, New London. “Shame and disrespectful treatment can lead to delay in seeking health care, reluctance to return visits, or lower trust in the providers and their recommendations.”
A study of more than 300 autopsy reports showed that obese patients were 1.65 times more likely than normal weight and underweight groups combined were to have medical conditions such as endocarditis, ischemic bowel disease, and lung cancer that were not diagnosed, Dr. Chrisler said in a press release (Am J Clin Pathol. 2006 Jan;125[1]:127-31).
In addition to preventing patients from seeking care, Dr. Chrisler said in the release, unfamiliarity with the dosing adjustments sometimes required on medications based on the body mass index of patients affects the quality of care. She cited a retrospective study showing that emergency physicians frequently underdose common antibiotics in the emergency department (Am J Emerg Med. 2012 Sep;30[7]:1212-4).
“People aren’t born repulsed by fat people,” said Dr. McHugh, professor of psychology at Indiana University of Pennsylvania. “Fat hate is learned within the family.”
They encouraged more sensitivity from medical professionals when it comes to treating overweight and obese patients, such as providing changing gowns of different sizes in examination rooms and weighing patients in private areas of the medical office.
Dr. Chrisler and Dr. McHugh said weight stigma should be addressed in medicine and psychology through training and research, and in working with patients who are obese. “Treatments should focus on mental and physical health as the desired outcomes for therapy rather than weight,” Dr. McHugh said.
Dr. Chrisler, coauthor of a recent article on sizeism (Fat Studies. 2017 Aug;6[1]:38-53), had no disclosures. Dr. McHugh also had no disclosures.
Obesity is a major modifiable cause of diseases of the digestive tract that routinely goes unaddressed. The AGA Obesity Practice Guide was created to support gastroenterologists leading a care team to help patients with obesity achieve a healthy weight. The AGA Obesity Practice Guide provides a comprehensive, multi-disciplinary process to personalize innovative obesity care for safe and effective weight management. Learn more at www.gastro.org/obesity.
[email protected]
On Twitter @ginalhenderson
WASHINGTON – Stereotypical views held by physicians, psychologists, nurses, and other medical professionals about overweight and obese patients need to change, panelists said at the annual convention of the American Psychological Association.
“We have a lot of negative attitudes toward heavy-weight people. Judging patients as too big or too fat produces physical and mental health effects,” said Joan C. Chrisler, PhD, the Class of ’43 Professor of Psychology at Connecticut College, New London. “Shame and disrespectful treatment can lead to delay in seeking health care, reluctance to return visits, or lower trust in the providers and their recommendations.”
A study of more than 300 autopsy reports showed that obese patients were 1.65 times more likely than normal weight and underweight groups combined were to have medical conditions such as endocarditis, ischemic bowel disease, and lung cancer that were not diagnosed, Dr. Chrisler said in a press release (Am J Clin Pathol. 2006 Jan;125[1]:127-31).
In addition to preventing patients from seeking care, Dr. Chrisler said in the release, unfamiliarity with the dosing adjustments sometimes required on medications based on the body mass index of patients affects the quality of care. She cited a retrospective study showing that emergency physicians frequently underdose common antibiotics in the emergency department (Am J Emerg Med. 2012 Sep;30[7]:1212-4).
“People aren’t born repulsed by fat people,” said Dr. McHugh, professor of psychology at Indiana University of Pennsylvania. “Fat hate is learned within the family.”
They encouraged more sensitivity from medical professionals when it comes to treating overweight and obese patients, such as providing changing gowns of different sizes in examination rooms and weighing patients in private areas of the medical office.
Dr. Chrisler and Dr. McHugh said weight stigma should be addressed in medicine and psychology through training and research, and in working with patients who are obese. “Treatments should focus on mental and physical health as the desired outcomes for therapy rather than weight,” Dr. McHugh said.
Dr. Chrisler, coauthor of a recent article on sizeism (Fat Studies. 2017 Aug;6[1]:38-53), had no disclosures. Dr. McHugh also had no disclosures.
Obesity is a major modifiable cause of diseases of the digestive tract that routinely goes unaddressed. The AGA Obesity Practice Guide was created to support gastroenterologists leading a care team to help patients with obesity achieve a healthy weight. The AGA Obesity Practice Guide provides a comprehensive, multi-disciplinary process to personalize innovative obesity care for safe and effective weight management. Learn more at www.gastro.org/obesity.
[email protected]
On Twitter @ginalhenderson
EXPERT ANALYSIS FROM THE 2017 APA CONVENTION
Radiographic progression in axial spondyloarthritis moves slowly in first 5 years
Sacroiliac joint radiographic progression during the first 5 years of the onset of axial spondyloarthritis occurs to an extent related to the degree of inflammation seen on MRI at baseline, according to new findings from 416 French patients in the DESIR cohort.
Maxime Dougados, MD, of Paris Descartes University, and his colleagues found that 15% of patients at baseline met modified New York (mNY) criteria – and therefore had radiographic axial spondyloarthritis (r-axSpA) – and this increased to 20% at 5 years. During the 5-year follow-up, the net percentage of patients who progressed was 5% (those who went from nonradiographic axial spondyloarthritis [nr-axSpA] to r-axSpA minus those who regressed from r-axSpA to nr-axSpA). Overall, 13% changed at least one grade on mNY criteria, and if an mNY criteria grade change from zero to one was not considered, only 10% experienced a change in at least one grade. These patients overall had a mean age of 34 years and had inflammatory back pain that had lasted at least 3 months but less than 3 years.

“The association between baseline MRI inflammation and 5-year SIJ damage was consistently found, regardless of the analytical method and the definition of SIJ progression,” the investigators wrote.
The estimated risk for progression by at least one mNY criteria grade varied from as high as 18% in HLA-B27–positive individuals with baseline SIJ inflammation on MRI and elevated C-reactive protein to just 1% in those who were negative for those three variables.
Read the full report online (Ann Rheum Dis. 2017 Jul 6. doi: 10.1136/annrheumdis-2017-211596).
Sacroiliac joint radiographic progression during the first 5 years of the onset of axial spondyloarthritis occurs to an extent related to the degree of inflammation seen on MRI at baseline, according to new findings from 416 French patients in the DESIR cohort.
Maxime Dougados, MD, of Paris Descartes University, and his colleagues found that 15% of patients at baseline met modified New York (mNY) criteria – and therefore had radiographic axial spondyloarthritis (r-axSpA) – and this increased to 20% at 5 years. During the 5-year follow-up, the net percentage of patients who progressed was 5% (those who went from nonradiographic axial spondyloarthritis [nr-axSpA] to r-axSpA minus those who regressed from r-axSpA to nr-axSpA). Overall, 13% changed at least one grade on mNY criteria, and if an mNY criteria grade change from zero to one was not considered, only 10% experienced a change in at least one grade. These patients overall had a mean age of 34 years and had inflammatory back pain that had lasted at least 3 months but less than 3 years.
“The association between baseline MRI inflammation and 5-year SIJ damage was consistently found, regardless of the analytical method and the definition of SIJ progression,” the investigators wrote.
The estimated risk for progression by at least one mNY criteria grade varied from as high as 18% in HLA-B27–positive individuals with baseline SIJ inflammation on MRI and elevated C-reactive protein to just 1% in those who were negative for those three variables.
Read the full report online (Ann Rheum Dis. 2017 Jul 6. doi: 10.1136/annrheumdis-2017-211596).
Sacroiliac joint radiographic progression during the first 5 years of the onset of axial spondyloarthritis occurs to an extent related to the degree of inflammation seen on MRI at baseline, according to new findings from 416 French patients in the DESIR cohort.
Maxime Dougados, MD, of Paris Descartes University, and his colleagues found that 15% of patients at baseline met modified New York (mNY) criteria – and therefore had radiographic axial spondyloarthritis (r-axSpA) – and this increased to 20% at 5 years. During the 5-year follow-up, the net percentage of patients who progressed was 5% (those who went from nonradiographic axial spondyloarthritis [nr-axSpA] to r-axSpA minus those who regressed from r-axSpA to nr-axSpA). Overall, 13% changed at least one grade on mNY criteria, and if an mNY criteria grade change from zero to one was not considered, only 10% experienced a change in at least one grade. These patients overall had a mean age of 34 years and had inflammatory back pain that had lasted at least 3 months but less than 3 years.
“The association between baseline MRI inflammation and 5-year SIJ damage was consistently found, regardless of the analytical method and the definition of SIJ progression,” the investigators wrote.
The estimated risk for progression by at least one mNY criteria grade varied from as high as 18% in HLA-B27–positive individuals with baseline SIJ inflammation on MRI and elevated C-reactive protein to just 1% in those who were negative for those three variables.
Read the full report online (Ann Rheum Dis. 2017 Jul 6. doi: 10.1136/annrheumdis-2017-211596).
FROM ANNALS OF THE RHEUMATIC DISEASES
New genetic causes of ichthyoses likely to emerge
CHICAGO– The way Keith Choate, MD, PhD, sees it, he and other clinicians are only beginning to scratch the surface on their understanding of the genetic causes of ichthyosis and ichthyosis syndromes.
“Despite the fact that we now understand that there are about 21,000 genes in the genome, we have very superficial understanding and functions known for only about 4,000 genes,” Dr. Choate of the departments of dermatology and genetics at Yale University, New Haven, Conn., said at the World Congress of Pediatric Dermatology. “Clinical insight is what’s driving all of the discovery. We continue to find new disorders, and these next-generation technologies really permit us to find the genetic basis for those disorders. I like to say that it’s the disorders that we don’t read about in the textbook that end up being the ones that are most interesting.”
Ichthyoses are cardinal disorders that occur when the normal pattern of epidermal differentiation is disrupted and leads to compensatory hyperproliferation. Clinically, ichthyoses present in a variety of ways, and more than 50 genes can cause them.

Dr. Choate is the principal investigator of the National Registry for Ichthyosis and Related Skin Types, which has been recruiting kindreds of ichthyosis patients within the United States and internationally. To date, they have provided genetic diagnoses for 674 of the 880 cases enrolled. The process involves phenotyping with a clinical history and photography, obtaining DNA from blood or saliva, and prescreening the DNA samples for mutations in 51 genes currently implicated in ichthyosis. Subjects without known mutations undergo whole exome or genome sequencing.
“We have created a unique resource in doing this,” he said. “Genotyped/phenotyped patients provide a resource for clinical and translational studies in disorders of keratinization.”
When the researchers examined patients from the registry who have epidermolytic presentations, 100% had mutations in the known genes, “so the biopsy is diagnostic,” Dr. Choate said. “About 80% have mutations in keratin 10, about 13% have mutations in keratin 1, and another 6% have mutations in keratin 2.”
About 85% of patients with recessive and syndromic disorders have mutations in this same 51-gene panel; 15% of cases don’t have mutations in those genes. “This is a similar fraction to what my colleagues have found at a variety of institutions around the world,” Dr. Choate said. “What’s fascinating is that this 15% has been the source of remarkable discovery.”
He then discussed three cases of a novel erythrokeratoderma phenotype that were referred to the registry. In one case, a boy had pervasive intellectual disability, congenital alopecia, and absence of the eyebrows. “Within the first days of life, he developed a significant erythroderma with copious scaling of the skin that persisted throughout life and that was unresponsive to a variety of different therapeutic interventions, including immunosuppressant medications,” Dr. Choate said. “He had nail dystrophy and progressive enamel decay with severe caries, leading to loss of all of his teeth by the age of 6.”
Another case was a child who died of cardiomyopathy at about 3 years of age. He had congenital absence of the eyebrows and eyelashes, nail dystrophy, and scaling. “About 2 weeks before his death, he had a skin biopsy that we would ultimately repurpose to identify a new genetic cause of what we would call the erythrokeratodermia-cardiomyopathy syndrome,” Dr. Choate said. “It included features of congenital erythroderma, defective dental enamel, abnormal nails, and progressive and lethal cardiomyopathy. When we did exome sequencing, we found that all three of these patients showed tightly clustered de novo mutations in a gene called desmoplakin (DSP). Other DSP mutations do not cause erythrokeratoderma.”
Electron microscopy showed aggregates of desmosomes, normal corneodesmosomes, widening of intercellular spaces, and abnormal lipid secretion. The finding led the researchers to conclude that clustered DSP mutations cause a novel cutaneous phenotype with erythrokeratoderma and progressive cardiomyopathy. “The next time an insurer refuses to do genetic testing for you in a patient who has erythrokeratoderma, this is the disorder that you want to cite as the reason why you need to do genetic testing,” he said.
In a recent study, Dr. Choate and his associates identified the genetic cause for a rare subtype of progressive symmetric erythrokeratoderma (PSEK), a disorder that features thick facial plaques and thickened palms and soles (Am J Hum Genet. 2017 Jun 1;100[6]:978-84). Histology reveals a thickened epidermis, loss of granular layer, and retention of nuclei in the stratum corneum. They discovered that PSEK was caused by mutations in 3-ketodihydrosphingosine reductase (KDSR), an enzyme that is central to de novo ceramides in skin.
“Ceramides are secreted by keratinocytes with cholesterol and free fatty acids to form the cutaneous lipid barrier,” he explained. “They also regulate cutaneous proliferation and differentiation. One of the things this story in particular told us was, when you find just one mutation and a compelling candidate gene and can’t find the other, it’s often because of how you’re approaching detection. In two of our cases, genome sequencing was necessary to find a large inversion, which disrupted the encoded protein. Finally, the challenge of studying ceramides is that it’s hard to get cells in culture to produce them. Therefore, we had to work with collaborators in yeast biology to prove pathogenesis.”
Dr. Choate cited other recent developments, including the discovery that familial pityriasis rubra pilaris is caused by mutations in CARD14, which is a known activator of nuclear factor kappa B signaling (Am J Hum Genet. 2012 Jul 13;91[1]:163-70). This led to the subsequent use of ustekinumab for patients with familial pityriasis rubra pilaris. Another group of researchers found that SULT2B1 encodes sulfotransferase family 2B member 1 and is central to epidermal cholesterol metabolism (Am J Hum Genet. 2017 Jun 1;100[6]:926-39).
“There are still new genetic causes of ichthyosis to be found, particularly cases that don’t meet the textbook criteria for the disorder,” he concluded. “Severe, dominant disorders primarily due to de novo mutations are fertile ground for discovery. Genetic investigation is critical to our understanding of disease biology and biology of the skin. It’s also potentially relevant to outcomes of therapy. [Erythrokeratodermia-cardiomyopathy syndrome] highlights the potential for comorbidities, and the efficacy of ustekinumab in familial [pityriasis rubra pilaris] highlights the therapeutic importance of understanding the pathway underlying the disease.”
Dr. Choate reported having no financial disclosures.
CHICAGO– The way Keith Choate, MD, PhD, sees it, he and other clinicians are only beginning to scratch the surface on their understanding of the genetic causes of ichthyosis and ichthyosis syndromes.
“Despite the fact that we now understand that there are about 21,000 genes in the genome, we have very superficial understanding and functions known for only about 4,000 genes,” Dr. Choate of the departments of dermatology and genetics at Yale University, New Haven, Conn., said at the World Congress of Pediatric Dermatology. “Clinical insight is what’s driving all of the discovery. We continue to find new disorders, and these next-generation technologies really permit us to find the genetic basis for those disorders. I like to say that it’s the disorders that we don’t read about in the textbook that end up being the ones that are most interesting.”
Ichthyoses are cardinal disorders that occur when the normal pattern of epidermal differentiation is disrupted and leads to compensatory hyperproliferation. Clinically, ichthyoses present in a variety of ways, and more than 50 genes can cause them.
Dr. Choate is the principal investigator of the National Registry for Ichthyosis and Related Skin Types, which has been recruiting kindreds of ichthyosis patients within the United States and internationally. To date, they have provided genetic diagnoses for 674 of the 880 cases enrolled. The process involves phenotyping with a clinical history and photography, obtaining DNA from blood or saliva, and prescreening the DNA samples for mutations in 51 genes currently implicated in ichthyosis. Subjects without known mutations undergo whole exome or genome sequencing.
“We have created a unique resource in doing this,” he said. “Genotyped/phenotyped patients provide a resource for clinical and translational studies in disorders of keratinization.”
When the researchers examined patients from the registry who have epidermolytic presentations, 100% had mutations in the known genes, “so the biopsy is diagnostic,” Dr. Choate said. “About 80% have mutations in keratin 10, about 13% have mutations in keratin 1, and another 6% have mutations in keratin 2.”
About 85% of patients with recessive and syndromic disorders have mutations in this same 51-gene panel; 15% of cases don’t have mutations in those genes. “This is a similar fraction to what my colleagues have found at a variety of institutions around the world,” Dr. Choate said. “What’s fascinating is that this 15% has been the source of remarkable discovery.”
He then discussed three cases of a novel erythrokeratoderma phenotype that were referred to the registry. In one case, a boy had pervasive intellectual disability, congenital alopecia, and absence of the eyebrows. “Within the first days of life, he developed a significant erythroderma with copious scaling of the skin that persisted throughout life and that was unresponsive to a variety of different therapeutic interventions, including immunosuppressant medications,” Dr. Choate said. “He had nail dystrophy and progressive enamel decay with severe caries, leading to loss of all of his teeth by the age of 6.”
Another case was a child who died of cardiomyopathy at about 3 years of age. He had congenital absence of the eyebrows and eyelashes, nail dystrophy, and scaling. “About 2 weeks before his death, he had a skin biopsy that we would ultimately repurpose to identify a new genetic cause of what we would call the erythrokeratodermia-cardiomyopathy syndrome,” Dr. Choate said. “It included features of congenital erythroderma, defective dental enamel, abnormal nails, and progressive and lethal cardiomyopathy. When we did exome sequencing, we found that all three of these patients showed tightly clustered de novo mutations in a gene called desmoplakin (DSP). Other DSP mutations do not cause erythrokeratoderma.”
Electron microscopy showed aggregates of desmosomes, normal corneodesmosomes, widening of intercellular spaces, and abnormal lipid secretion. The finding led the researchers to conclude that clustered DSP mutations cause a novel cutaneous phenotype with erythrokeratoderma and progressive cardiomyopathy. “The next time an insurer refuses to do genetic testing for you in a patient who has erythrokeratoderma, this is the disorder that you want to cite as the reason why you need to do genetic testing,” he said.
In a recent study, Dr. Choate and his associates identified the genetic cause for a rare subtype of progressive symmetric erythrokeratoderma (PSEK), a disorder that features thick facial plaques and thickened palms and soles (Am J Hum Genet. 2017 Jun 1;100[6]:978-84). Histology reveals a thickened epidermis, loss of granular layer, and retention of nuclei in the stratum corneum. They discovered that PSEK was caused by mutations in 3-ketodihydrosphingosine reductase (KDSR), an enzyme that is central to de novo ceramides in skin.
“Ceramides are secreted by keratinocytes with cholesterol and free fatty acids to form the cutaneous lipid barrier,” he explained. “They also regulate cutaneous proliferation and differentiation. One of the things this story in particular told us was, when you find just one mutation and a compelling candidate gene and can’t find the other, it’s often because of how you’re approaching detection. In two of our cases, genome sequencing was necessary to find a large inversion, which disrupted the encoded protein. Finally, the challenge of studying ceramides is that it’s hard to get cells in culture to produce them. Therefore, we had to work with collaborators in yeast biology to prove pathogenesis.”
Dr. Choate cited other recent developments, including the discovery that familial pityriasis rubra pilaris is caused by mutations in CARD14, which is a known activator of nuclear factor kappa B signaling (Am J Hum Genet. 2012 Jul 13;91[1]:163-70). This led to the subsequent use of ustekinumab for patients with familial pityriasis rubra pilaris. Another group of researchers found that SULT2B1 encodes sulfotransferase family 2B member 1 and is central to epidermal cholesterol metabolism (Am J Hum Genet. 2017 Jun 1;100[6]:926-39).
“There are still new genetic causes of ichthyosis to be found, particularly cases that don’t meet the textbook criteria for the disorder,” he concluded. “Severe, dominant disorders primarily due to de novo mutations are fertile ground for discovery. Genetic investigation is critical to our understanding of disease biology and biology of the skin. It’s also potentially relevant to outcomes of therapy. [Erythrokeratodermia-cardiomyopathy syndrome] highlights the potential for comorbidities, and the efficacy of ustekinumab in familial [pityriasis rubra pilaris] highlights the therapeutic importance of understanding the pathway underlying the disease.”
Dr. Choate reported having no financial disclosures.
CHICAGO– The way Keith Choate, MD, PhD, sees it, he and other clinicians are only beginning to scratch the surface on their understanding of the genetic causes of ichthyosis and ichthyosis syndromes.
“Despite the fact that we now understand that there are about 21,000 genes in the genome, we have very superficial understanding and functions known for only about 4,000 genes,” Dr. Choate of the departments of dermatology and genetics at Yale University, New Haven, Conn., said at the World Congress of Pediatric Dermatology. “Clinical insight is what’s driving all of the discovery. We continue to find new disorders, and these next-generation technologies really permit us to find the genetic basis for those disorders. I like to say that it’s the disorders that we don’t read about in the textbook that end up being the ones that are most interesting.”
Ichthyoses are cardinal disorders that occur when the normal pattern of epidermal differentiation is disrupted and leads to compensatory hyperproliferation. Clinically, ichthyoses present in a variety of ways, and more than 50 genes can cause them.
Dr. Choate is the principal investigator of the National Registry for Ichthyosis and Related Skin Types, which has been recruiting kindreds of ichthyosis patients within the United States and internationally. To date, they have provided genetic diagnoses for 674 of the 880 cases enrolled. The process involves phenotyping with a clinical history and photography, obtaining DNA from blood or saliva, and prescreening the DNA samples for mutations in 51 genes currently implicated in ichthyosis. Subjects without known mutations undergo whole exome or genome sequencing.
“We have created a unique resource in doing this,” he said. “Genotyped/phenotyped patients provide a resource for clinical and translational studies in disorders of keratinization.”
When the researchers examined patients from the registry who have epidermolytic presentations, 100% had mutations in the known genes, “so the biopsy is diagnostic,” Dr. Choate said. “About 80% have mutations in keratin 10, about 13% have mutations in keratin 1, and another 6% have mutations in keratin 2.”
About 85% of patients with recessive and syndromic disorders have mutations in this same 51-gene panel; 15% of cases don’t have mutations in those genes. “This is a similar fraction to what my colleagues have found at a variety of institutions around the world,” Dr. Choate said. “What’s fascinating is that this 15% has been the source of remarkable discovery.”
He then discussed three cases of a novel erythrokeratoderma phenotype that were referred to the registry. In one case, a boy had pervasive intellectual disability, congenital alopecia, and absence of the eyebrows. “Within the first days of life, he developed a significant erythroderma with copious scaling of the skin that persisted throughout life and that was unresponsive to a variety of different therapeutic interventions, including immunosuppressant medications,” Dr. Choate said. “He had nail dystrophy and progressive enamel decay with severe caries, leading to loss of all of his teeth by the age of 6.”
Another case was a child who died of cardiomyopathy at about 3 years of age. He had congenital absence of the eyebrows and eyelashes, nail dystrophy, and scaling. “About 2 weeks before his death, he had a skin biopsy that we would ultimately repurpose to identify a new genetic cause of what we would call the erythrokeratodermia-cardiomyopathy syndrome,” Dr. Choate said. “It included features of congenital erythroderma, defective dental enamel, abnormal nails, and progressive and lethal cardiomyopathy. When we did exome sequencing, we found that all three of these patients showed tightly clustered de novo mutations in a gene called desmoplakin (DSP). Other DSP mutations do not cause erythrokeratoderma.”
Electron microscopy showed aggregates of desmosomes, normal corneodesmosomes, widening of intercellular spaces, and abnormal lipid secretion. The finding led the researchers to conclude that clustered DSP mutations cause a novel cutaneous phenotype with erythrokeratoderma and progressive cardiomyopathy. “The next time an insurer refuses to do genetic testing for you in a patient who has erythrokeratoderma, this is the disorder that you want to cite as the reason why you need to do genetic testing,” he said.
In a recent study, Dr. Choate and his associates identified the genetic cause for a rare subtype of progressive symmetric erythrokeratoderma (PSEK), a disorder that features thick facial plaques and thickened palms and soles (Am J Hum Genet. 2017 Jun 1;100[6]:978-84). Histology reveals a thickened epidermis, loss of granular layer, and retention of nuclei in the stratum corneum. They discovered that PSEK was caused by mutations in 3-ketodihydrosphingosine reductase (KDSR), an enzyme that is central to de novo ceramides in skin.
“Ceramides are secreted by keratinocytes with cholesterol and free fatty acids to form the cutaneous lipid barrier,” he explained. “They also regulate cutaneous proliferation and differentiation. One of the things this story in particular told us was, when you find just one mutation and a compelling candidate gene and can’t find the other, it’s often because of how you’re approaching detection. In two of our cases, genome sequencing was necessary to find a large inversion, which disrupted the encoded protein. Finally, the challenge of studying ceramides is that it’s hard to get cells in culture to produce them. Therefore, we had to work with collaborators in yeast biology to prove pathogenesis.”
Dr. Choate cited other recent developments, including the discovery that familial pityriasis rubra pilaris is caused by mutations in CARD14, which is a known activator of nuclear factor kappa B signaling (Am J Hum Genet. 2012 Jul 13;91[1]:163-70). This led to the subsequent use of ustekinumab for patients with familial pityriasis rubra pilaris. Another group of researchers found that SULT2B1 encodes sulfotransferase family 2B member 1 and is central to epidermal cholesterol metabolism (Am J Hum Genet. 2017 Jun 1;100[6]:926-39).
“There are still new genetic causes of ichthyosis to be found, particularly cases that don’t meet the textbook criteria for the disorder,” he concluded. “Severe, dominant disorders primarily due to de novo mutations are fertile ground for discovery. Genetic investigation is critical to our understanding of disease biology and biology of the skin. It’s also potentially relevant to outcomes of therapy. [Erythrokeratodermia-cardiomyopathy syndrome] highlights the potential for comorbidities, and the efficacy of ustekinumab in familial [pityriasis rubra pilaris] highlights the therapeutic importance of understanding the pathway underlying the disease.”
Dr. Choate reported having no financial disclosures.
AT WCPD 2017
Hair and Scalp Disorders in Patients With Skin of Color


Best Practices: Umbilical Cord Blood and Tissue Preservation

Topics include:
- Background on Umbilical Cord Blood and Cord Tissue
- Scientific Education for Parents
- Family and Public Banking Options
- Cost and the Collection Process
Faculty/Faculty Disclosure:
Madelyn Butler, MD
Obstetrics & Gynecology
St. Joseph’s Hospital
Florida Hospital
Tampa, Florida
Click here to access a Cord Blood and Cord Tissue Preservation handout for your patients.
Topics include:
- Background on Umbilical Cord Blood and Cord Tissue
- Scientific Education for Parents
- Family and Public Banking Options
- Cost and the Collection Process
Faculty/Faculty Disclosure:
Madelyn Butler, MD
Obstetrics & Gynecology
St. Joseph’s Hospital
Florida Hospital
Tampa, Florida
Click here to access a Cord Blood and Cord Tissue Preservation handout for your patients.
Topics include:
- Background on Umbilical Cord Blood and Cord Tissue
- Scientific Education for Parents
- Family and Public Banking Options
- Cost and the Collection Process
Faculty/Faculty Disclosure:
Madelyn Butler, MD
Obstetrics & Gynecology
St. Joseph’s Hospital
Florida Hospital
Tampa, Florida
Click here to access a Cord Blood and Cord Tissue Preservation handout for your patients.

Repeat blood cultures not useful in treating Gram-negative bacteremia
Follow-up blood cultures rarely provide useful clinical information in patients who are being treated for Gram-negative bacteremia, according to a study by Gabriel M. Aisenberg, MD, and his colleagues.
In a review of 140 Gram-negative bacteremia episodes, 17 follow-up blood cultures (FUBC) were required to identify one positive result, wrote Dr. Aisenberg of McGovern Medical School at the University of Texas Health Science Center in Houston. This was in stark contest to the test’s utility in patients with Gram-positive infections, which identified one positive result for every five cultures. (Clin Infect Dis. 2017 July 26. doi: 10.1093/cid/cix648)
Dr. Aisenberg and his colleagues reviewed 500 bacteremias treated at a single center during 2015. The mean duration of bacteremia was about 3 days, with a mean follow-up time of 4.5 days. Most of the cases (206) were caused by Gram-positive cocci; 140 were due to Gram-negative bacilli, and 30 were polymicrobial.
Most patients (383; 77%) had at least one FUBC. Patients had an average of 2.3 FUBC, but the range was wide: Up to 12 cultures were performed for Gram-positive infections and up to six for Gram-negative infections.
Only 14% of the FUBC were positive, and most of these (78%) were for Gram-positive infections. Only eight cultures (15%) returned positive results for Gram-negative infections.
The mean duration of bacteremia was 3 days, and did not vary between Gram-positive, Gram-negative, or polymicrobial infections. The use of antibiotics wasn’t associated with a positive FUBC, although fever on the day of the test was. Urinary tract and severe skin infections were negatively associated with a positive FUBC, while IV catheter infections increased the risk. There were no associations between positive FUBC and mortality or ICU placement.
There are no guidelines describing the best use of FUBC in Gram-negative bacteremia, which are usually managed clinically, Dr. Aisenberg said.
“Even in Gram-negative bacteremia infections most prone to seeding the bloodstream, the bacteremia usually resolves within a short time after the institution of appropriate antibiotic therapy and/or source control,” he wrote. “Currently the management of [such infections] is determined by clinical judgment, allowing some clinicians to utilize blood cultures in an unrestricted way. Unrestrained use of blood cultures has serious implications for patient safety and health care costs,” driven by the strong likelihood of false positive results, which grows even stronger with repeat tests.
“As many as 90% of all blood cultures grow no organisms,” Dr. Aisenberg said. “Of the 10% that do, almost half are considered contaminants. Assuming a constant rate of contamination, the more FUBC performed, the higher the chance of encountering contamination, which may result in increased costs, longer hospital stays, unnecessary consultations, and inappropriate use of antibiotics.”
Neither Dr. Aisenberg nor his colleagues had any financial disclosures.
Follow-up blood cultures rarely provide useful clinical information in patients who are being treated for Gram-negative bacteremia, according to a study by Gabriel M. Aisenberg, MD, and his colleagues.
In a review of 140 Gram-negative bacteremia episodes, 17 follow-up blood cultures (FUBC) were required to identify one positive result, wrote Dr. Aisenberg of McGovern Medical School at the University of Texas Health Science Center in Houston. This was in stark contest to the test’s utility in patients with Gram-positive infections, which identified one positive result for every five cultures. (Clin Infect Dis. 2017 July 26. doi: 10.1093/cid/cix648)
Dr. Aisenberg and his colleagues reviewed 500 bacteremias treated at a single center during 2015. The mean duration of bacteremia was about 3 days, with a mean follow-up time of 4.5 days. Most of the cases (206) were caused by Gram-positive cocci; 140 were due to Gram-negative bacilli, and 30 were polymicrobial.
Most patients (383; 77%) had at least one FUBC. Patients had an average of 2.3 FUBC, but the range was wide: Up to 12 cultures were performed for Gram-positive infections and up to six for Gram-negative infections.
Only 14% of the FUBC were positive, and most of these (78%) were for Gram-positive infections. Only eight cultures (15%) returned positive results for Gram-negative infections.
The mean duration of bacteremia was 3 days, and did not vary between Gram-positive, Gram-negative, or polymicrobial infections. The use of antibiotics wasn’t associated with a positive FUBC, although fever on the day of the test was. Urinary tract and severe skin infections were negatively associated with a positive FUBC, while IV catheter infections increased the risk. There were no associations between positive FUBC and mortality or ICU placement.
There are no guidelines describing the best use of FUBC in Gram-negative bacteremia, which are usually managed clinically, Dr. Aisenberg said.
“Even in Gram-negative bacteremia infections most prone to seeding the bloodstream, the bacteremia usually resolves within a short time after the institution of appropriate antibiotic therapy and/or source control,” he wrote. “Currently the management of [such infections] is determined by clinical judgment, allowing some clinicians to utilize blood cultures in an unrestricted way. Unrestrained use of blood cultures has serious implications for patient safety and health care costs,” driven by the strong likelihood of false positive results, which grows even stronger with repeat tests.
“As many as 90% of all blood cultures grow no organisms,” Dr. Aisenberg said. “Of the 10% that do, almost half are considered contaminants. Assuming a constant rate of contamination, the more FUBC performed, the higher the chance of encountering contamination, which may result in increased costs, longer hospital stays, unnecessary consultations, and inappropriate use of antibiotics.”
Neither Dr. Aisenberg nor his colleagues had any financial disclosures.
Follow-up blood cultures rarely provide useful clinical information in patients who are being treated for Gram-negative bacteremia, according to a study by Gabriel M. Aisenberg, MD, and his colleagues.
In a review of 140 Gram-negative bacteremia episodes, 17 follow-up blood cultures (FUBC) were required to identify one positive result, wrote Dr. Aisenberg of McGovern Medical School at the University of Texas Health Science Center in Houston. This was in stark contest to the test’s utility in patients with Gram-positive infections, which identified one positive result for every five cultures. (Clin Infect Dis. 2017 July 26. doi: 10.1093/cid/cix648)
Dr. Aisenberg and his colleagues reviewed 500 bacteremias treated at a single center during 2015. The mean duration of bacteremia was about 3 days, with a mean follow-up time of 4.5 days. Most of the cases (206) were caused by Gram-positive cocci; 140 were due to Gram-negative bacilli, and 30 were polymicrobial.
Most patients (383; 77%) had at least one FUBC. Patients had an average of 2.3 FUBC, but the range was wide: Up to 12 cultures were performed for Gram-positive infections and up to six for Gram-negative infections.
Only 14% of the FUBC were positive, and most of these (78%) were for Gram-positive infections. Only eight cultures (15%) returned positive results for Gram-negative infections.
The mean duration of bacteremia was 3 days, and did not vary between Gram-positive, Gram-negative, or polymicrobial infections. The use of antibiotics wasn’t associated with a positive FUBC, although fever on the day of the test was. Urinary tract and severe skin infections were negatively associated with a positive FUBC, while IV catheter infections increased the risk. There were no associations between positive FUBC and mortality or ICU placement.
There are no guidelines describing the best use of FUBC in Gram-negative bacteremia, which are usually managed clinically, Dr. Aisenberg said.
“Even in Gram-negative bacteremia infections most prone to seeding the bloodstream, the bacteremia usually resolves within a short time after the institution of appropriate antibiotic therapy and/or source control,” he wrote. “Currently the management of [such infections] is determined by clinical judgment, allowing some clinicians to utilize blood cultures in an unrestricted way. Unrestrained use of blood cultures has serious implications for patient safety and health care costs,” driven by the strong likelihood of false positive results, which grows even stronger with repeat tests.
“As many as 90% of all blood cultures grow no organisms,” Dr. Aisenberg said. “Of the 10% that do, almost half are considered contaminants. Assuming a constant rate of contamination, the more FUBC performed, the higher the chance of encountering contamination, which may result in increased costs, longer hospital stays, unnecessary consultations, and inappropriate use of antibiotics.”
Neither Dr. Aisenberg nor his colleagues had any financial disclosures.
FROM CLINICAL INFECTIOUS DISEASES
Key clinical point:
Major finding: Among 140 cases of Gram-negative bacteremia, 17 follow-up blood cultures were necessary to return one positive result.
Data source: A retrospective study comprising 500 infections.
Disclosures: None of the study authors reported financial disclosures.
VIDEO: Triple therapy study and new recommendations provide guidance on CAPS
MADRID – Catastrophic antiphospholipid syndrome (CAPS) is associated with a high mortality rate, but new research presented at the European Congress of Rheumatology shows that patient survival can be significantly improved by a triple therapy treatment approach.
Researchers at the Congress also presented clinical practice guidelines for the diagnosis and management of the rare disease, which accounts for just 1% of patients with antiphospholipid syndrome (APS).
CAPS is characterized by a fast onset of widespread thrombosis, mainly in the small vessels, and, often, microangiopathic hemolytic anemia is seen in the laboratory. If undiagnosed or left untreated, patients may present with multiorgan failure needing intensive care treatment, which can be fatal in up to 50% of cases.
At the Congress, Ignasi Rodríguez-Pintó, MD, presented new data from the CAPS Registry that looks at the combined effect of anticoagulation, corticosteroids, and plasma exchange or intravenous immunoglobulins on the survival of patients with CAPS as well as the new clinical practice guidelines.
CAPS Registry study
The aim of the study Dr. Rodríguez-Pintó presented on behalf of the CAPS Registry Project Group was to determine what, if any, survival benefit would be incurred from a triple therapy approach when compared with other different combinations of anticoagulation, corticosteroids, and plasma exchange or intravenous immunoglobulins, or none of these treatments.
Although the triple therapy treatment approach is already being used in practice, its use is largely empirical, Dr. Rodríguez-Pintó of the department of autoimmune disease at the Hospital Clinic, Barcelona, explained in a video interview.
The investigators derived their data from episodes of CAPS occurring in patients in the CAPS Registry from the European Forum on Antiphospholipid Antibodies. This international registry was set up in 2000 and has been assembling the clinical, laboratory, and therapeutic findings of patients with CAPS for almost 20 years.
“We observed 525 episodes of CAPS in 502 patients. That means that some patients had two to three episodes of CAPS,” Dr. Rodríguez-Pintó said. Data on 38 episodes of CAPS had to be excluded from the analysis because of missing information, which left 487 episodes occurring in 471 patients.
The mean age of the 471 patients included in the analysis was 38 years. The majority (67.9%) were female and had primary (68.8%) APS. Triple therapy was given to about 40% of patients who experienced CAPS, with about 57% receiving other combinations of drugs and 2.5% receiving no treatment for CAPS.
Overall, 177 of the 487 (36.3%) episodes of CAPS were fatal.
“Triple therapy was associated with a higher chance of survival when compared to other combinations or to none of these treatments,” Dr. Rodríguez-Pintó said.
While 28% of patients with CAPS died in the triple therapy group, mortality was 41% with other combinations of treatments and 75% with none of these treatments.
All-cause mortality was reduced by 47% with triple therapy, compared with none of these treatments. The adjusted odds ratio (aOR) when comparing survival between triple therapy and no treatment was 7.7, with a 95% confidence interval of 2.0 to 29.7. The aOR comparing other drug combinations versus none of these treatments was 6.8 (95% CI, 1.7-29.6).
“For a long time, we have been saying that triple therapy would probably be the best approach, but we had no firm evidence,” Dr. Rodríguez-Pintó said.
“So, this is the first time that we have clear clinical evidence of the benefit of these approaches, and I think that these results are important because they will give us more confidence in how we treat patients and help develop guidance on [the treatment’s] use in the future.”
Guidelines
A steering committee composed of representatives from the European Commission–funded RARE-BestPractices project and McMaster University in Hamilton, Ont., used GRADE methodology to develop the guidelines for CAPS diagnosis and management. The committee answered three diagnostic and seven treatment questions that originated from a panel of 19 international stakeholders, including Dr. Rodríguez-Pintó, through systematic reviews of the literature that used Cochrane criteria.
Although the review of studies did not include the study of CAPS Registry data that Dr. Rodríguez-Pintó and his colleagues conducted, he said that the recommendations still confirm the value of using a triple therapy approach to treatment.
The panel created three diagnostic recommendations for patients suspected of having CAPS, all of which were conditional and based on very low certainty of evidence: use preliminary CAPS classification criteria to diagnose CAPS; use or nonuse of biopsy, depending on the circumstances, because of its high specificity but possibly low sensitivity for thrombotic microangiopathy; and test for antiphospholipid antibodies, which should not delay initiation of treatment.
All seven first-line treatment recommendations that the panel developed relied on a very low certainty of evidence, and most were conditional:
- Triple therapy combination treatment with corticosteroids, heparin, and plasma exchange or intravenous immunoglobulins instead of a single agent or other combination treatments.
- Therapeutic dose anticoagulation was one of only two treatment recommendations to be considered “strong,” but use of direct oral anticoagulants is not advised.
- Therapeutic plasma exchange is recommended for use with other therapies and should be strongly considered for patients with microangiopathic hemolytic anemia.
- Intravenous immunoglobulin is advised for use in conjunction with other therapies and should be given special consideration for patients with immune thrombocytopenia or renal insufficiency.
- Antiplatelet agents are conditionally recommended as an add-on therapy, but their potential mortality benefit is tempered by increased risk of bleeding when used with anticoagulants. Strong consideration should be given to their use as an alternative therapy to anticoagulation when anticoagulation is contraindicated for a reason other than bleeding.
- Rituximab (Rituxan) should not be used because of little available data on its use, uncertainty regarding long-term consequences, and its expense – except for refractory cases where other therapies have been insufficient.
- Corticosteroids should not be used because of their lack of efficacy in CAPS when used alone and potential for adverse effects, except for certain circumstances where they may be indicated.
The authors of the guidelines emphasized that these recommendations are not meant to apply to every CAPS patient. They also noted that the available evidence did not allow for temporal analysis of treatments and that conclusions could not be drawn regarding “first-line” versus “second-line” therapies.
None of the authors of the registry study or the guidelines had relevant conflicts of interest to declare.
MADRID – Catastrophic antiphospholipid syndrome (CAPS) is associated with a high mortality rate, but new research presented at the European Congress of Rheumatology shows that patient survival can be significantly improved by a triple therapy treatment approach.
Researchers at the Congress also presented clinical practice guidelines for the diagnosis and management of the rare disease, which accounts for just 1% of patients with antiphospholipid syndrome (APS).
CAPS is characterized by a fast onset of widespread thrombosis, mainly in the small vessels, and, often, microangiopathic hemolytic anemia is seen in the laboratory. If undiagnosed or left untreated, patients may present with multiorgan failure needing intensive care treatment, which can be fatal in up to 50% of cases.
At the Congress, Ignasi Rodríguez-Pintó, MD, presented new data from the CAPS Registry that looks at the combined effect of anticoagulation, corticosteroids, and plasma exchange or intravenous immunoglobulins on the survival of patients with CAPS as well as the new clinical practice guidelines.
CAPS Registry study
The aim of the study Dr. Rodríguez-Pintó presented on behalf of the CAPS Registry Project Group was to determine what, if any, survival benefit would be incurred from a triple therapy approach when compared with other different combinations of anticoagulation, corticosteroids, and plasma exchange or intravenous immunoglobulins, or none of these treatments.
Although the triple therapy treatment approach is already being used in practice, its use is largely empirical, Dr. Rodríguez-Pintó of the department of autoimmune disease at the Hospital Clinic, Barcelona, explained in a video interview.
The investigators derived their data from episodes of CAPS occurring in patients in the CAPS Registry from the European Forum on Antiphospholipid Antibodies. This international registry was set up in 2000 and has been assembling the clinical, laboratory, and therapeutic findings of patients with CAPS for almost 20 years.
“We observed 525 episodes of CAPS in 502 patients. That means that some patients had two to three episodes of CAPS,” Dr. Rodríguez-Pintó said. Data on 38 episodes of CAPS had to be excluded from the analysis because of missing information, which left 487 episodes occurring in 471 patients.
The mean age of the 471 patients included in the analysis was 38 years. The majority (67.9%) were female and had primary (68.8%) APS. Triple therapy was given to about 40% of patients who experienced CAPS, with about 57% receiving other combinations of drugs and 2.5% receiving no treatment for CAPS.
Overall, 177 of the 487 (36.3%) episodes of CAPS were fatal.
“Triple therapy was associated with a higher chance of survival when compared to other combinations or to none of these treatments,” Dr. Rodríguez-Pintó said.
While 28% of patients with CAPS died in the triple therapy group, mortality was 41% with other combinations of treatments and 75% with none of these treatments.
All-cause mortality was reduced by 47% with triple therapy, compared with none of these treatments. The adjusted odds ratio (aOR) when comparing survival between triple therapy and no treatment was 7.7, with a 95% confidence interval of 2.0 to 29.7. The aOR comparing other drug combinations versus none of these treatments was 6.8 (95% CI, 1.7-29.6).
“For a long time, we have been saying that triple therapy would probably be the best approach, but we had no firm evidence,” Dr. Rodríguez-Pintó said.
“So, this is the first time that we have clear clinical evidence of the benefit of these approaches, and I think that these results are important because they will give us more confidence in how we treat patients and help develop guidance on [the treatment’s] use in the future.”
Guidelines
A steering committee composed of representatives from the European Commission–funded RARE-BestPractices project and McMaster University in Hamilton, Ont., used GRADE methodology to develop the guidelines for CAPS diagnosis and management. The committee answered three diagnostic and seven treatment questions that originated from a panel of 19 international stakeholders, including Dr. Rodríguez-Pintó, through systematic reviews of the literature that used Cochrane criteria.
Although the review of studies did not include the study of CAPS Registry data that Dr. Rodríguez-Pintó and his colleagues conducted, he said that the recommendations still confirm the value of using a triple therapy approach to treatment.
The panel created three diagnostic recommendations for patients suspected of having CAPS, all of which were conditional and based on very low certainty of evidence: use preliminary CAPS classification criteria to diagnose CAPS; use or nonuse of biopsy, depending on the circumstances, because of its high specificity but possibly low sensitivity for thrombotic microangiopathy; and test for antiphospholipid antibodies, which should not delay initiation of treatment.
All seven first-line treatment recommendations that the panel developed relied on a very low certainty of evidence, and most were conditional:
- Triple therapy combination treatment with corticosteroids, heparin, and plasma exchange or intravenous immunoglobulins instead of a single agent or other combination treatments.
- Therapeutic dose anticoagulation was one of only two treatment recommendations to be considered “strong,” but use of direct oral anticoagulants is not advised.
- Therapeutic plasma exchange is recommended for use with other therapies and should be strongly considered for patients with microangiopathic hemolytic anemia.
- Intravenous immunoglobulin is advised for use in conjunction with other therapies and should be given special consideration for patients with immune thrombocytopenia or renal insufficiency.
- Antiplatelet agents are conditionally recommended as an add-on therapy, but their potential mortality benefit is tempered by increased risk of bleeding when used with anticoagulants. Strong consideration should be given to their use as an alternative therapy to anticoagulation when anticoagulation is contraindicated for a reason other than bleeding.
- Rituximab (Rituxan) should not be used because of little available data on its use, uncertainty regarding long-term consequences, and its expense – except for refractory cases where other therapies have been insufficient.
- Corticosteroids should not be used because of their lack of efficacy in CAPS when used alone and potential for adverse effects, except for certain circumstances where they may be indicated.
The authors of the guidelines emphasized that these recommendations are not meant to apply to every CAPS patient. They also noted that the available evidence did not allow for temporal analysis of treatments and that conclusions could not be drawn regarding “first-line” versus “second-line” therapies.
None of the authors of the registry study or the guidelines had relevant conflicts of interest to declare.
MADRID – Catastrophic antiphospholipid syndrome (CAPS) is associated with a high mortality rate, but new research presented at the European Congress of Rheumatology shows that patient survival can be significantly improved by a triple therapy treatment approach.
Researchers at the Congress also presented clinical practice guidelines for the diagnosis and management of the rare disease, which accounts for just 1% of patients with antiphospholipid syndrome (APS).
CAPS is characterized by a fast onset of widespread thrombosis, mainly in the small vessels, and, often, microangiopathic hemolytic anemia is seen in the laboratory. If undiagnosed or left untreated, patients may present with multiorgan failure needing intensive care treatment, which can be fatal in up to 50% of cases.
At the Congress, Ignasi Rodríguez-Pintó, MD, presented new data from the CAPS Registry that looks at the combined effect of anticoagulation, corticosteroids, and plasma exchange or intravenous immunoglobulins on the survival of patients with CAPS as well as the new clinical practice guidelines.
CAPS Registry study
The aim of the study Dr. Rodríguez-Pintó presented on behalf of the CAPS Registry Project Group was to determine what, if any, survival benefit would be incurred from a triple therapy approach when compared with other different combinations of anticoagulation, corticosteroids, and plasma exchange or intravenous immunoglobulins, or none of these treatments.
Although the triple therapy treatment approach is already being used in practice, its use is largely empirical, Dr. Rodríguez-Pintó of the department of autoimmune disease at the Hospital Clinic, Barcelona, explained in a video interview.
The investigators derived their data from episodes of CAPS occurring in patients in the CAPS Registry from the European Forum on Antiphospholipid Antibodies. This international registry was set up in 2000 and has been assembling the clinical, laboratory, and therapeutic findings of patients with CAPS for almost 20 years.
“We observed 525 episodes of CAPS in 502 patients. That means that some patients had two to three episodes of CAPS,” Dr. Rodríguez-Pintó said. Data on 38 episodes of CAPS had to be excluded from the analysis because of missing information, which left 487 episodes occurring in 471 patients.
The mean age of the 471 patients included in the analysis was 38 years. The majority (67.9%) were female and had primary (68.8%) APS. Triple therapy was given to about 40% of patients who experienced CAPS, with about 57% receiving other combinations of drugs and 2.5% receiving no treatment for CAPS.
Overall, 177 of the 487 (36.3%) episodes of CAPS were fatal.
“Triple therapy was associated with a higher chance of survival when compared to other combinations or to none of these treatments,” Dr. Rodríguez-Pintó said.
While 28% of patients with CAPS died in the triple therapy group, mortality was 41% with other combinations of treatments and 75% with none of these treatments.
All-cause mortality was reduced by 47% with triple therapy, compared with none of these treatments. The adjusted odds ratio (aOR) when comparing survival between triple therapy and no treatment was 7.7, with a 95% confidence interval of 2.0 to 29.7. The aOR comparing other drug combinations versus none of these treatments was 6.8 (95% CI, 1.7-29.6).
“For a long time, we have been saying that triple therapy would probably be the best approach, but we had no firm evidence,” Dr. Rodríguez-Pintó said.
“So, this is the first time that we have clear clinical evidence of the benefit of these approaches, and I think that these results are important because they will give us more confidence in how we treat patients and help develop guidance on [the treatment’s] use in the future.”
Guidelines
A steering committee composed of representatives from the European Commission–funded RARE-BestPractices project and McMaster University in Hamilton, Ont., used GRADE methodology to develop the guidelines for CAPS diagnosis and management. The committee answered three diagnostic and seven treatment questions that originated from a panel of 19 international stakeholders, including Dr. Rodríguez-Pintó, through systematic reviews of the literature that used Cochrane criteria.
Although the review of studies did not include the study of CAPS Registry data that Dr. Rodríguez-Pintó and his colleagues conducted, he said that the recommendations still confirm the value of using a triple therapy approach to treatment.
The panel created three diagnostic recommendations for patients suspected of having CAPS, all of which were conditional and based on very low certainty of evidence: use preliminary CAPS classification criteria to diagnose CAPS; use or nonuse of biopsy, depending on the circumstances, because of its high specificity but possibly low sensitivity for thrombotic microangiopathy; and test for antiphospholipid antibodies, which should not delay initiation of treatment.
All seven first-line treatment recommendations that the panel developed relied on a very low certainty of evidence, and most were conditional:
- Triple therapy combination treatment with corticosteroids, heparin, and plasma exchange or intravenous immunoglobulins instead of a single agent or other combination treatments.
- Therapeutic dose anticoagulation was one of only two treatment recommendations to be considered “strong,” but use of direct oral anticoagulants is not advised.
- Therapeutic plasma exchange is recommended for use with other therapies and should be strongly considered for patients with microangiopathic hemolytic anemia.
- Intravenous immunoglobulin is advised for use in conjunction with other therapies and should be given special consideration for patients with immune thrombocytopenia or renal insufficiency.
- Antiplatelet agents are conditionally recommended as an add-on therapy, but their potential mortality benefit is tempered by increased risk of bleeding when used with anticoagulants. Strong consideration should be given to their use as an alternative therapy to anticoagulation when anticoagulation is contraindicated for a reason other than bleeding.
- Rituximab (Rituxan) should not be used because of little available data on its use, uncertainty regarding long-term consequences, and its expense – except for refractory cases where other therapies have been insufficient.
- Corticosteroids should not be used because of their lack of efficacy in CAPS when used alone and potential for adverse effects, except for certain circumstances where they may be indicated.
The authors of the guidelines emphasized that these recommendations are not meant to apply to every CAPS patient. They also noted that the available evidence did not allow for temporal analysis of treatments and that conclusions could not be drawn regarding “first-line” versus “second-line” therapies.
None of the authors of the registry study or the guidelines had relevant conflicts of interest to declare.
AT THE EULAR 2017 CONGRESS
Key clinical point:
Major finding: Mortality was 28% with triple therapy, 41% with other combinations of treatments, and 75% with none of these treatments.
Data source: A registry study of 471 CAPS patients and clinical practice guidelines for CAPS.
Disclosures: None of the authors of the registry study or the guidelines had relevant conflicts of interest to declare.
Pregnancy not a barrier to providing cutaneous surgery
NEW YORK – For some dermatologists, surgical care of the pregnant patient represents an area of uncertainty. But with few exceptions, dermatologists can continue with business as usual for their pregnant patients, according to Keith Harrigill, MD.
Dr. Harrigill, a dermatologist who previously was a practicing obstetrician-gynecologist, delineated the safe zones of dermatologic surgery in these patients at the summer meeting of the American Academy of Dermatology.
About 2% of pregnant women will require nonobstetric surgery and about 75,000 pregnant women in the United States will have surgery annually, he said. Appendectomies and other emergent abdominal surgery account for a large proportion of these cases; dermatologic surgeries are not included in these figures, and cutaneous procedures in pregnant women are not usually tracked. The literature on dermatologic treatments during pregnancy is “scant,” said Dr. Harrigill, a dermatologist in private practice in Birmingham, Ala.
However, it’s known that one-third of women with melanoma are of childbearing age, and melanoma accounts for 8% of the malignancies diagnosed during pregnancy, with a rate estimated at 0.14 to 2.8 per 1,000 live births, he said.
Since some women will have to address potentially serious skin issues during pregnancy, what’s safe, and what isn’t? Dr. Harrigill said that the American College of Obstetrics and Gynecology has provided guidance with an April 2017 opinion, prepared in conjunction with the American Society for Anesthesia, on nonobstetric surgery during pregnancy (Obstet Gynecol. 2017;129:777-8).
The opinion primarily focuses on major surgery. “What we do – cutaneous surgeries – they consider to be minor surgery,” he said. But even with major procedures, the good news is that “there’s no increase in birth defects in fetal exposure to anesthesia at any age,” he noted.
Dr. Harrigill’s approach, which conforms to the general guidance provided by the opinion, is to think of dermatologic procedures in three categories: urgent, nonurgent, and elective. Urgent procedures might include biopsying and treating a lesion suspicious for melanoma or an aggressive nonmelanoma skin cancer, or controlling a friable, bleeding pyogenic granuloma. “Do these right away,” he said.
Nonurgent procedures, such as treatment of a nodular basal cell carcinoma, should be done during the second trimester, when possible. Elective procedures, such as a scar excision, should be deferred until after delivery.
Dermatologists can almost always achieve adequate pain control with local anesthesia alone, said Dr. Harrigill, pointing out that local anesthesia is “the safest known way to give anesthesia during pregnancy.”
However, when thinking about even a remote risk of teratogenesis, it’s important to understand that fetal organogenesis occurs from day 15 to day 56, and that before 15 days, adverse events are limited to spontaneous abortion. So it’s particularly important to avoid teratogenic medications during the first 2 months of gestation, Dr. Harrigill said.
Part of the concern, he noted, is that it’s ethically problematic to perform large randomized trials in pregnant women, so the guidelines regarding surgery and medication safety are drawn from retrospective studies, registries, meta-analyses, and expert consensus.
Still, according to the ACOG guidelines, “a pregnant woman should never be denied indicated surgery, regardless of trimester.”
There’s no reason to risk delaying a diagnosis of malignancy in a pregnant patient, Dr. Harrigill said. “My dermatologic surgery approach is to biopsy anything that is clinically suspicious for malignancy, at any gestational age.”
When performing biopsies in pregnant patients, he uses the same protocol as he uses with any other patient. Skin preparation can be done with either isopropyl alcohol or chlorhexidine. Some practitioners avoid using povidone iodine because of a theoretical risk of fetal hypothyroidism.
For anesthesia, Dr. Harrigill noted that lidocaine is generally considered safe in pregnancy. He is also comfortable using epinephrine, despite the theoretical concern of uterine artery spasm, for which “studies are lacking.” The relatively minute amount of epinephrine used in dermatologic anesthesia, he said, is not likely to have an impact on such a large vessel.
Prilocaine is generally safe, and combination creams with prilocaine are fine to use, he said. Diphenhydramine is also safe to use. However, he advised avoiding long-acting anesthetic agents, such as mepivacaine and bupivacaine.
His advice regarding sedation? “Don’t do it.” Dr. Harrigill said he doesn’t use sedation in the office for his nonpregnant patients, either.
Before about 20 weeks of pregnancy, Dr. Harrigill said not to worry about how the patient is positioned. But after that, the lateral decubitus position is best because it keeps the gravid uterus from compressing the great vessels.
“Pregnant women are prone to fainting due to progesterone-mediated vasodilation,” he said. Dermatologists can work with their office staff to keep these patients well hydrated, and make sure they get in and out of chairs and off exam tables slowly.
No changes are needed in excision or suturing techniques. Because cicatrization is delayed in pregnant women, Dr. Harrigill uses longer-lasting absorbable sutures with high tensile strength, especially when performing procedures on the trunk or abdomen. This means that his closures will use delayed-absorption epidermal sutures with running nylon pull-through subcuticular sutures as well. He will leave these in for 5-7 days longer than usual.
Pregnant women are not at a higher risk of infection than the general population, so he follows the standard procedures here as well. If an antibiotic is indicated, penicillin, a cephalosporin, azithromycin, and erythromycin base are all logical choices.
To be avoided are sulfamethoxazole/trimethoprim, which carries a risk of feta hyperbilirubinemia, especially when given in the second trimester; doxycycline and tetracycline, which can cause permanent brown discoloration of the teeth; and fluoroquinolones, which have been associated with cartilage defects.
For analgesia, acetaminophen is an option. Ibuprofen and salicylates should be avoided, especially at the end of pregnancy when their administration is associated with premature closure of the ductus arteriosus, and, possibly, placental abruption, Dr. Harrigill noted.
However, short-term use of opioids is generally considered safe for the fetus. If larger doses are given just before delivery, the neonate may experience respiratory depression. This scenario is unlikely to be faced by the dermatologist, noted Dr. Harrigill. “I use these without reservation” in terms of fetal risk, he said.
Collaboration is key when caring for pregnant patients, said Dr. Harrigill, who recommends consulting the obstetrician of record for any procedures other than a simple biopsy or shave removal.
Dr. Harrigill reported that he had no conflicts of interest.
[email protected]
On Twitter @karioakes
NEW YORK – For some dermatologists, surgical care of the pregnant patient represents an area of uncertainty. But with few exceptions, dermatologists can continue with business as usual for their pregnant patients, according to Keith Harrigill, MD.
Dr. Harrigill, a dermatologist who previously was a practicing obstetrician-gynecologist, delineated the safe zones of dermatologic surgery in these patients at the summer meeting of the American Academy of Dermatology.
About 2% of pregnant women will require nonobstetric surgery and about 75,000 pregnant women in the United States will have surgery annually, he said. Appendectomies and other emergent abdominal surgery account for a large proportion of these cases; dermatologic surgeries are not included in these figures, and cutaneous procedures in pregnant women are not usually tracked. The literature on dermatologic treatments during pregnancy is “scant,” said Dr. Harrigill, a dermatologist in private practice in Birmingham, Ala.
However, it’s known that one-third of women with melanoma are of childbearing age, and melanoma accounts for 8% of the malignancies diagnosed during pregnancy, with a rate estimated at 0.14 to 2.8 per 1,000 live births, he said.
Since some women will have to address potentially serious skin issues during pregnancy, what’s safe, and what isn’t? Dr. Harrigill said that the American College of Obstetrics and Gynecology has provided guidance with an April 2017 opinion, prepared in conjunction with the American Society for Anesthesia, on nonobstetric surgery during pregnancy (Obstet Gynecol. 2017;129:777-8).
The opinion primarily focuses on major surgery. “What we do – cutaneous surgeries – they consider to be minor surgery,” he said. But even with major procedures, the good news is that “there’s no increase in birth defects in fetal exposure to anesthesia at any age,” he noted.
Dr. Harrigill’s approach, which conforms to the general guidance provided by the opinion, is to think of dermatologic procedures in three categories: urgent, nonurgent, and elective. Urgent procedures might include biopsying and treating a lesion suspicious for melanoma or an aggressive nonmelanoma skin cancer, or controlling a friable, bleeding pyogenic granuloma. “Do these right away,” he said.
Nonurgent procedures, such as treatment of a nodular basal cell carcinoma, should be done during the second trimester, when possible. Elective procedures, such as a scar excision, should be deferred until after delivery.
Dermatologists can almost always achieve adequate pain control with local anesthesia alone, said Dr. Harrigill, pointing out that local anesthesia is “the safest known way to give anesthesia during pregnancy.”
However, when thinking about even a remote risk of teratogenesis, it’s important to understand that fetal organogenesis occurs from day 15 to day 56, and that before 15 days, adverse events are limited to spontaneous abortion. So it’s particularly important to avoid teratogenic medications during the first 2 months of gestation, Dr. Harrigill said.
Part of the concern, he noted, is that it’s ethically problematic to perform large randomized trials in pregnant women, so the guidelines regarding surgery and medication safety are drawn from retrospective studies, registries, meta-analyses, and expert consensus.
Still, according to the ACOG guidelines, “a pregnant woman should never be denied indicated surgery, regardless of trimester.”
There’s no reason to risk delaying a diagnosis of malignancy in a pregnant patient, Dr. Harrigill said. “My dermatologic surgery approach is to biopsy anything that is clinically suspicious for malignancy, at any gestational age.”
When performing biopsies in pregnant patients, he uses the same protocol as he uses with any other patient. Skin preparation can be done with either isopropyl alcohol or chlorhexidine. Some practitioners avoid using povidone iodine because of a theoretical risk of fetal hypothyroidism.
For anesthesia, Dr. Harrigill noted that lidocaine is generally considered safe in pregnancy. He is also comfortable using epinephrine, despite the theoretical concern of uterine artery spasm, for which “studies are lacking.” The relatively minute amount of epinephrine used in dermatologic anesthesia, he said, is not likely to have an impact on such a large vessel.
Prilocaine is generally safe, and combination creams with prilocaine are fine to use, he said. Diphenhydramine is also safe to use. However, he advised avoiding long-acting anesthetic agents, such as mepivacaine and bupivacaine.
His advice regarding sedation? “Don’t do it.” Dr. Harrigill said he doesn’t use sedation in the office for his nonpregnant patients, either.
Before about 20 weeks of pregnancy, Dr. Harrigill said not to worry about how the patient is positioned. But after that, the lateral decubitus position is best because it keeps the gravid uterus from compressing the great vessels.
“Pregnant women are prone to fainting due to progesterone-mediated vasodilation,” he said. Dermatologists can work with their office staff to keep these patients well hydrated, and make sure they get in and out of chairs and off exam tables slowly.
No changes are needed in excision or suturing techniques. Because cicatrization is delayed in pregnant women, Dr. Harrigill uses longer-lasting absorbable sutures with high tensile strength, especially when performing procedures on the trunk or abdomen. This means that his closures will use delayed-absorption epidermal sutures with running nylon pull-through subcuticular sutures as well. He will leave these in for 5-7 days longer than usual.
Pregnant women are not at a higher risk of infection than the general population, so he follows the standard procedures here as well. If an antibiotic is indicated, penicillin, a cephalosporin, azithromycin, and erythromycin base are all logical choices.
To be avoided are sulfamethoxazole/trimethoprim, which carries a risk of feta hyperbilirubinemia, especially when given in the second trimester; doxycycline and tetracycline, which can cause permanent brown discoloration of the teeth; and fluoroquinolones, which have been associated with cartilage defects.
For analgesia, acetaminophen is an option. Ibuprofen and salicylates should be avoided, especially at the end of pregnancy when their administration is associated with premature closure of the ductus arteriosus, and, possibly, placental abruption, Dr. Harrigill noted.
However, short-term use of opioids is generally considered safe for the fetus. If larger doses are given just before delivery, the neonate may experience respiratory depression. This scenario is unlikely to be faced by the dermatologist, noted Dr. Harrigill. “I use these without reservation” in terms of fetal risk, he said.
Collaboration is key when caring for pregnant patients, said Dr. Harrigill, who recommends consulting the obstetrician of record for any procedures other than a simple biopsy or shave removal.
Dr. Harrigill reported that he had no conflicts of interest.
[email protected]
On Twitter @karioakes
NEW YORK – For some dermatologists, surgical care of the pregnant patient represents an area of uncertainty. But with few exceptions, dermatologists can continue with business as usual for their pregnant patients, according to Keith Harrigill, MD.
Dr. Harrigill, a dermatologist who previously was a practicing obstetrician-gynecologist, delineated the safe zones of dermatologic surgery in these patients at the summer meeting of the American Academy of Dermatology.
About 2% of pregnant women will require nonobstetric surgery and about 75,000 pregnant women in the United States will have surgery annually, he said. Appendectomies and other emergent abdominal surgery account for a large proportion of these cases; dermatologic surgeries are not included in these figures, and cutaneous procedures in pregnant women are not usually tracked. The literature on dermatologic treatments during pregnancy is “scant,” said Dr. Harrigill, a dermatologist in private practice in Birmingham, Ala.
However, it’s known that one-third of women with melanoma are of childbearing age, and melanoma accounts for 8% of the malignancies diagnosed during pregnancy, with a rate estimated at 0.14 to 2.8 per 1,000 live births, he said.
Since some women will have to address potentially serious skin issues during pregnancy, what’s safe, and what isn’t? Dr. Harrigill said that the American College of Obstetrics and Gynecology has provided guidance with an April 2017 opinion, prepared in conjunction with the American Society for Anesthesia, on nonobstetric surgery during pregnancy (Obstet Gynecol. 2017;129:777-8).
The opinion primarily focuses on major surgery. “What we do – cutaneous surgeries – they consider to be minor surgery,” he said. But even with major procedures, the good news is that “there’s no increase in birth defects in fetal exposure to anesthesia at any age,” he noted.
Dr. Harrigill’s approach, which conforms to the general guidance provided by the opinion, is to think of dermatologic procedures in three categories: urgent, nonurgent, and elective. Urgent procedures might include biopsying and treating a lesion suspicious for melanoma or an aggressive nonmelanoma skin cancer, or controlling a friable, bleeding pyogenic granuloma. “Do these right away,” he said.
Nonurgent procedures, such as treatment of a nodular basal cell carcinoma, should be done during the second trimester, when possible. Elective procedures, such as a scar excision, should be deferred until after delivery.
Dermatologists can almost always achieve adequate pain control with local anesthesia alone, said Dr. Harrigill, pointing out that local anesthesia is “the safest known way to give anesthesia during pregnancy.”
However, when thinking about even a remote risk of teratogenesis, it’s important to understand that fetal organogenesis occurs from day 15 to day 56, and that before 15 days, adverse events are limited to spontaneous abortion. So it’s particularly important to avoid teratogenic medications during the first 2 months of gestation, Dr. Harrigill said.
Part of the concern, he noted, is that it’s ethically problematic to perform large randomized trials in pregnant women, so the guidelines regarding surgery and medication safety are drawn from retrospective studies, registries, meta-analyses, and expert consensus.
Still, according to the ACOG guidelines, “a pregnant woman should never be denied indicated surgery, regardless of trimester.”
There’s no reason to risk delaying a diagnosis of malignancy in a pregnant patient, Dr. Harrigill said. “My dermatologic surgery approach is to biopsy anything that is clinically suspicious for malignancy, at any gestational age.”
When performing biopsies in pregnant patients, he uses the same protocol as he uses with any other patient. Skin preparation can be done with either isopropyl alcohol or chlorhexidine. Some practitioners avoid using povidone iodine because of a theoretical risk of fetal hypothyroidism.
For anesthesia, Dr. Harrigill noted that lidocaine is generally considered safe in pregnancy. He is also comfortable using epinephrine, despite the theoretical concern of uterine artery spasm, for which “studies are lacking.” The relatively minute amount of epinephrine used in dermatologic anesthesia, he said, is not likely to have an impact on such a large vessel.
Prilocaine is generally safe, and combination creams with prilocaine are fine to use, he said. Diphenhydramine is also safe to use. However, he advised avoiding long-acting anesthetic agents, such as mepivacaine and bupivacaine.
His advice regarding sedation? “Don’t do it.” Dr. Harrigill said he doesn’t use sedation in the office for his nonpregnant patients, either.
Before about 20 weeks of pregnancy, Dr. Harrigill said not to worry about how the patient is positioned. But after that, the lateral decubitus position is best because it keeps the gravid uterus from compressing the great vessels.
“Pregnant women are prone to fainting due to progesterone-mediated vasodilation,” he said. Dermatologists can work with their office staff to keep these patients well hydrated, and make sure they get in and out of chairs and off exam tables slowly.
No changes are needed in excision or suturing techniques. Because cicatrization is delayed in pregnant women, Dr. Harrigill uses longer-lasting absorbable sutures with high tensile strength, especially when performing procedures on the trunk or abdomen. This means that his closures will use delayed-absorption epidermal sutures with running nylon pull-through subcuticular sutures as well. He will leave these in for 5-7 days longer than usual.
Pregnant women are not at a higher risk of infection than the general population, so he follows the standard procedures here as well. If an antibiotic is indicated, penicillin, a cephalosporin, azithromycin, and erythromycin base are all logical choices.
To be avoided are sulfamethoxazole/trimethoprim, which carries a risk of feta hyperbilirubinemia, especially when given in the second trimester; doxycycline and tetracycline, which can cause permanent brown discoloration of the teeth; and fluoroquinolones, which have been associated with cartilage defects.
For analgesia, acetaminophen is an option. Ibuprofen and salicylates should be avoided, especially at the end of pregnancy when their administration is associated with premature closure of the ductus arteriosus, and, possibly, placental abruption, Dr. Harrigill noted.
However, short-term use of opioids is generally considered safe for the fetus. If larger doses are given just before delivery, the neonate may experience respiratory depression. This scenario is unlikely to be faced by the dermatologist, noted Dr. Harrigill. “I use these without reservation” in terms of fetal risk, he said.
Collaboration is key when caring for pregnant patients, said Dr. Harrigill, who recommends consulting the obstetrician of record for any procedures other than a simple biopsy or shave removal.
Dr. Harrigill reported that he had no conflicts of interest.
[email protected]
On Twitter @karioakes
EXPERT ANALYSIS FROM THE 2017 AAD SUMMER MEETING
Right Paraduodenal Hernia
Paraduodenal hernia, also called mesocolic hernia, is a type of internal hernia that is thought to be caused by a congenital defect involving abnormal retroperitoneal fixation of the mesentery due to abnormal rotation of the midgut.1 Internal hernias account for only 1% of all hernias, and paraduodenal hernias make up 50% of those.2
Paraduodenal hernias can be classified as left or right with left being far more common than right, 75% and 25%, respectively.2 Due to the fixation abnormalities in the midgut, fossae are formed that help to classify left vs right paraduodenal hernias. Herniation through Landzert fossae results in a left paraduodenal hernia with the primary constituents of the hernia sac being the inferior mesenteric artery and vein.1 This result is due to an in utero defect of the small intestine herniated between the inferior mesenteric vein and posterior parietal attachments of the descending mesocolon to the retroperitoneal.3
In a right paraduodenal hernia, herniation occurs through Waldeyer fossae with the main contents of the hernia sac being the iliocolic, right colic, and middle colic vessels within the anterior wall and the superior mesenteric artery along the medial border of the hernia.1 Since there is a failure of rotation around the superior mesenteric artery, the majority of the small intestine remains to the right of the superior mesenteric artery, resulting in the small intestine being trapped between the posteriolateral peritoneum.3 Regardless of the type of paraduodenal hernia, patients usually will present with symptoms of small bowel obstruction. In these types of hernias, a computed tomography (CT) scan with IV contrast may suggest evidence of obstruction between the duodenum and jejunum, but this may be unclear. Although rare, clinical suspicion of paraduodenal hernia is necessary to prevent ensuing complications and mortality.
Case Presentation
A 43-year-old man presented to the emergency department with symptoms that included nausea, vomiting, intermittent epigastric abdominal pain, and obstipation, which were suggestive of a small bowel obstruction. The patient reported similar intermittent episodes over the past 10 years that had resolved without surgery. The patient had no history of abdominal surgeries. A nasogastric tube was inserted and immediately drew out a significant amount of bilious contents. A CT scan indicated an obstruction at the proximal jejunum with suspicion of an internal hernia.
The patient underwent exploratory laparotomy soon after, which confirmed a right paraduodenal hernia (Figure). The surgery began laproscopically by retracting the omentum and transverse colon cranially to expose the ligament of Treitz. The hernia defect was identified on the mesentery where the proximal jejunum twisted on itself in a loop. The hernia was untwisted, and adhesions were removed. The posterior attachment of the hernia sac was freed with harmonic cautery and blunt dissection along with its attachment to the ligament of Treitz. In the process of freeing the herniation, a 1-cm enterotomy ensued, which did not contain succus or spillage of luminal contents at that time. Due to difficulties in visualizing the remainder of the small bowel, the procedure was converted to a laparotomy. This allowed complete freeing of the twisted loop of bowel.
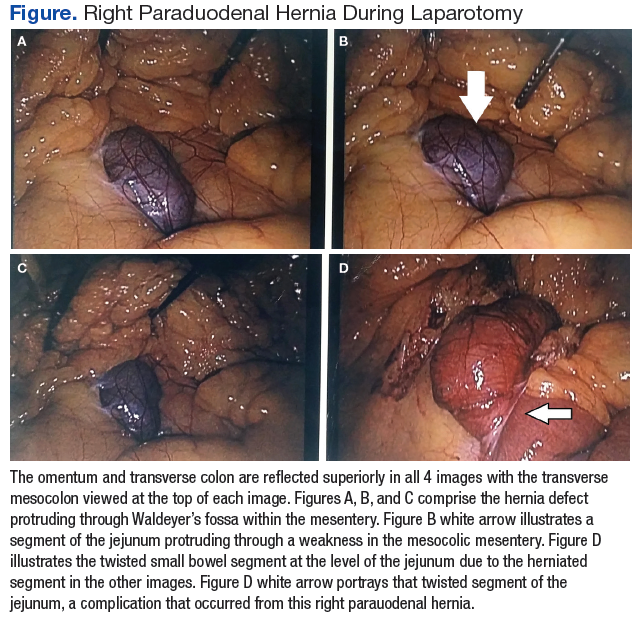
Afterward, there was succus and bile draining from the enterotomy, so it was closed transversely in 2 layers, making sure there was a lumen between the layers. The first and second parts of the duodenum were examined followed by palpitation of the duodenal sweep. The remainder of the small bowel was visualized to the cecum, and the retroperitoneal space was dissected out of the hernia sac space. The abdomen was irrigated, and the omentum was draped back over the intestines. The fascia was closed followed by skin reapproximation with staples. The patient experienced an uneventful recovery and was discharged on day 6 with resolution of his symptoms.
Discussion
Paraduodenal hernias are a type of internal hernia and a rare cause of intestinal obstruction accounting for about 0.5% of all hernias. Right paraduodenal hernias are far less common than left paraduodenal hernias and occur due to a defect in the jejunum mesentery called Waldeyer fossae.4 This is located at the third part of the duodenum and behind the superior mesenteric artery.4 Symptoms of paraduodenal hernias are nonspecific and may include nausea, vomiting, and intermittent cramping. Symptoms of obstruction can be intermittent due to the small bowel herniating through the fossae and then retracting.1 Computed tomography has good specificity and aides in the diagnosis of an internal hernia, but physicians must have a high index of suspicion as well.5
Definitive diagnosis and treatment of paraduodenal hernias involves laparoscopy or exploratory laparotomy to visualize the internal hernia and its surrounding sac.4,5 All hernias should be repaired to prevent strangulation of the bowel, but internal hernias are even more important to fix because these hernias may not present until there is severe injury to the bowel.5 On identification of the paraduodenal hernia, it is important to release the bowel from the hernia sac, free up adhesions, and place small bowel segments back into the correct anatomical position.4,5
In the event of bowel injury, resection with reanastomosis is indicated. Careful dissection is important to prevent injury to the superior mesenteric artery, which supplies most of the small bowel and ascending colon.4,5 Injury to the superior mesenteric artery could lead to ischemia and gangrenous bowel.2 Immediate detection and early surgery intervention of these congenital hernias can prevent such complications.2 The literature includes reports of paraduodenal hernias with complications of gangrenous bowel that required small bowel resection.2 These complications further emphasize the need to proceed immediately with surgery if a paraduodenal hernia is suspected.
Conclusion
This rare cause of bowel obstruction was documented in order to emphasize the importance of having a high clinical suspicion for a paraduodenal hernia. This particular patient with no history of abdominal surgeries had previously dealt with bowel obstruction and would likely have this complication again without surgical intervention. Patients with paraduodenal hernias also are at risk for bowel ischemia, other high-risk complications, and even death.5 Although a CT scan provided information about an approximate location of the obstruction, laparoscopy confirmed the diagnosis. Going into the operation with paraduodenal hernia in the differential allowed the surgeon to be prepared for the appropriate anatomy involved with this procedure to minimize damage to important structures, such as the superior mesenteric artery and its branches.
1. Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 19th ed. Philadelphia, PA: Saunders; 2012.
2. Fukada T, Mukai H, Shimamura F, Furukawa T, Miyazaki M. A causal relationship between right paraduodenal hernia and superior mesenteric artery syndrome: a case report. J Med Case Rep. 2010;4:159.
3. Skandalakis JE. Peritoneum, omenta, and internal hernias. In: Skandalakis JE, Colborn GL, eds. Skandalakis Surgical Anatomy: The Embryologic and Anatomic Basis of Modern Surgery. 1st ed. Athens, Greece: Paschalidis Medical Publications; 2004:chap 10.
4. Papaziogas B, Souparis A, Makris J, Alexandrakis A, Papaziogas T. Surgical images: soft tissue. Right paraduodenal hernia. Can J Surg. 2004;47(3):195-196.
5. Manfredelli S, Andrea Z, Stefano P, et al. Rare small bowel obstruction: right paraduodenal hernia. Case report. Int J Surg Case Rep. 2013;4(4):412-415.
Paraduodenal hernia, also called mesocolic hernia, is a type of internal hernia that is thought to be caused by a congenital defect involving abnormal retroperitoneal fixation of the mesentery due to abnormal rotation of the midgut.1 Internal hernias account for only 1% of all hernias, and paraduodenal hernias make up 50% of those.2
Paraduodenal hernias can be classified as left or right with left being far more common than right, 75% and 25%, respectively.2 Due to the fixation abnormalities in the midgut, fossae are formed that help to classify left vs right paraduodenal hernias. Herniation through Landzert fossae results in a left paraduodenal hernia with the primary constituents of the hernia sac being the inferior mesenteric artery and vein.1 This result is due to an in utero defect of the small intestine herniated between the inferior mesenteric vein and posterior parietal attachments of the descending mesocolon to the retroperitoneal.3
In a right paraduodenal hernia, herniation occurs through Waldeyer fossae with the main contents of the hernia sac being the iliocolic, right colic, and middle colic vessels within the anterior wall and the superior mesenteric artery along the medial border of the hernia.1 Since there is a failure of rotation around the superior mesenteric artery, the majority of the small intestine remains to the right of the superior mesenteric artery, resulting in the small intestine being trapped between the posteriolateral peritoneum.3 Regardless of the type of paraduodenal hernia, patients usually will present with symptoms of small bowel obstruction. In these types of hernias, a computed tomography (CT) scan with IV contrast may suggest evidence of obstruction between the duodenum and jejunum, but this may be unclear. Although rare, clinical suspicion of paraduodenal hernia is necessary to prevent ensuing complications and mortality.
Case Presentation
A 43-year-old man presented to the emergency department with symptoms that included nausea, vomiting, intermittent epigastric abdominal pain, and obstipation, which were suggestive of a small bowel obstruction. The patient reported similar intermittent episodes over the past 10 years that had resolved without surgery. The patient had no history of abdominal surgeries. A nasogastric tube was inserted and immediately drew out a significant amount of bilious contents. A CT scan indicated an obstruction at the proximal jejunum with suspicion of an internal hernia.
The patient underwent exploratory laparotomy soon after, which confirmed a right paraduodenal hernia (Figure). The surgery began laproscopically by retracting the omentum and transverse colon cranially to expose the ligament of Treitz. The hernia defect was identified on the mesentery where the proximal jejunum twisted on itself in a loop. The hernia was untwisted, and adhesions were removed. The posterior attachment of the hernia sac was freed with harmonic cautery and blunt dissection along with its attachment to the ligament of Treitz. In the process of freeing the herniation, a 1-cm enterotomy ensued, which did not contain succus or spillage of luminal contents at that time. Due to difficulties in visualizing the remainder of the small bowel, the procedure was converted to a laparotomy. This allowed complete freeing of the twisted loop of bowel.
Afterward, there was succus and bile draining from the enterotomy, so it was closed transversely in 2 layers, making sure there was a lumen between the layers. The first and second parts of the duodenum were examined followed by palpitation of the duodenal sweep. The remainder of the small bowel was visualized to the cecum, and the retroperitoneal space was dissected out of the hernia sac space. The abdomen was irrigated, and the omentum was draped back over the intestines. The fascia was closed followed by skin reapproximation with staples. The patient experienced an uneventful recovery and was discharged on day 6 with resolution of his symptoms.
Discussion
Paraduodenal hernias are a type of internal hernia and a rare cause of intestinal obstruction accounting for about 0.5% of all hernias. Right paraduodenal hernias are far less common than left paraduodenal hernias and occur due to a defect in the jejunum mesentery called Waldeyer fossae.4 This is located at the third part of the duodenum and behind the superior mesenteric artery.4 Symptoms of paraduodenal hernias are nonspecific and may include nausea, vomiting, and intermittent cramping. Symptoms of obstruction can be intermittent due to the small bowel herniating through the fossae and then retracting.1 Computed tomography has good specificity and aides in the diagnosis of an internal hernia, but physicians must have a high index of suspicion as well.5
Definitive diagnosis and treatment of paraduodenal hernias involves laparoscopy or exploratory laparotomy to visualize the internal hernia and its surrounding sac.4,5 All hernias should be repaired to prevent strangulation of the bowel, but internal hernias are even more important to fix because these hernias may not present until there is severe injury to the bowel.5 On identification of the paraduodenal hernia, it is important to release the bowel from the hernia sac, free up adhesions, and place small bowel segments back into the correct anatomical position.4,5
In the event of bowel injury, resection with reanastomosis is indicated. Careful dissection is important to prevent injury to the superior mesenteric artery, which supplies most of the small bowel and ascending colon.4,5 Injury to the superior mesenteric artery could lead to ischemia and gangrenous bowel.2 Immediate detection and early surgery intervention of these congenital hernias can prevent such complications.2 The literature includes reports of paraduodenal hernias with complications of gangrenous bowel that required small bowel resection.2 These complications further emphasize the need to proceed immediately with surgery if a paraduodenal hernia is suspected.
Conclusion
This rare cause of bowel obstruction was documented in order to emphasize the importance of having a high clinical suspicion for a paraduodenal hernia. This particular patient with no history of abdominal surgeries had previously dealt with bowel obstruction and would likely have this complication again without surgical intervention. Patients with paraduodenal hernias also are at risk for bowel ischemia, other high-risk complications, and even death.5 Although a CT scan provided information about an approximate location of the obstruction, laparoscopy confirmed the diagnosis. Going into the operation with paraduodenal hernia in the differential allowed the surgeon to be prepared for the appropriate anatomy involved with this procedure to minimize damage to important structures, such as the superior mesenteric artery and its branches.
Paraduodenal hernia, also called mesocolic hernia, is a type of internal hernia that is thought to be caused by a congenital defect involving abnormal retroperitoneal fixation of the mesentery due to abnormal rotation of the midgut.1 Internal hernias account for only 1% of all hernias, and paraduodenal hernias make up 50% of those.2
Paraduodenal hernias can be classified as left or right with left being far more common than right, 75% and 25%, respectively.2 Due to the fixation abnormalities in the midgut, fossae are formed that help to classify left vs right paraduodenal hernias. Herniation through Landzert fossae results in a left paraduodenal hernia with the primary constituents of the hernia sac being the inferior mesenteric artery and vein.1 This result is due to an in utero defect of the small intestine herniated between the inferior mesenteric vein and posterior parietal attachments of the descending mesocolon to the retroperitoneal.3
In a right paraduodenal hernia, herniation occurs through Waldeyer fossae with the main contents of the hernia sac being the iliocolic, right colic, and middle colic vessels within the anterior wall and the superior mesenteric artery along the medial border of the hernia.1 Since there is a failure of rotation around the superior mesenteric artery, the majority of the small intestine remains to the right of the superior mesenteric artery, resulting in the small intestine being trapped between the posteriolateral peritoneum.3 Regardless of the type of paraduodenal hernia, patients usually will present with symptoms of small bowel obstruction. In these types of hernias, a computed tomography (CT) scan with IV contrast may suggest evidence of obstruction between the duodenum and jejunum, but this may be unclear. Although rare, clinical suspicion of paraduodenal hernia is necessary to prevent ensuing complications and mortality.
Case Presentation
A 43-year-old man presented to the emergency department with symptoms that included nausea, vomiting, intermittent epigastric abdominal pain, and obstipation, which were suggestive of a small bowel obstruction. The patient reported similar intermittent episodes over the past 10 years that had resolved without surgery. The patient had no history of abdominal surgeries. A nasogastric tube was inserted and immediately drew out a significant amount of bilious contents. A CT scan indicated an obstruction at the proximal jejunum with suspicion of an internal hernia.
The patient underwent exploratory laparotomy soon after, which confirmed a right paraduodenal hernia (Figure). The surgery began laproscopically by retracting the omentum and transverse colon cranially to expose the ligament of Treitz. The hernia defect was identified on the mesentery where the proximal jejunum twisted on itself in a loop. The hernia was untwisted, and adhesions were removed. The posterior attachment of the hernia sac was freed with harmonic cautery and blunt dissection along with its attachment to the ligament of Treitz. In the process of freeing the herniation, a 1-cm enterotomy ensued, which did not contain succus or spillage of luminal contents at that time. Due to difficulties in visualizing the remainder of the small bowel, the procedure was converted to a laparotomy. This allowed complete freeing of the twisted loop of bowel.
Afterward, there was succus and bile draining from the enterotomy, so it was closed transversely in 2 layers, making sure there was a lumen between the layers. The first and second parts of the duodenum were examined followed by palpitation of the duodenal sweep. The remainder of the small bowel was visualized to the cecum, and the retroperitoneal space was dissected out of the hernia sac space. The abdomen was irrigated, and the omentum was draped back over the intestines. The fascia was closed followed by skin reapproximation with staples. The patient experienced an uneventful recovery and was discharged on day 6 with resolution of his symptoms.
Discussion
Paraduodenal hernias are a type of internal hernia and a rare cause of intestinal obstruction accounting for about 0.5% of all hernias. Right paraduodenal hernias are far less common than left paraduodenal hernias and occur due to a defect in the jejunum mesentery called Waldeyer fossae.4 This is located at the third part of the duodenum and behind the superior mesenteric artery.4 Symptoms of paraduodenal hernias are nonspecific and may include nausea, vomiting, and intermittent cramping. Symptoms of obstruction can be intermittent due to the small bowel herniating through the fossae and then retracting.1 Computed tomography has good specificity and aides in the diagnosis of an internal hernia, but physicians must have a high index of suspicion as well.5
Definitive diagnosis and treatment of paraduodenal hernias involves laparoscopy or exploratory laparotomy to visualize the internal hernia and its surrounding sac.4,5 All hernias should be repaired to prevent strangulation of the bowel, but internal hernias are even more important to fix because these hernias may not present until there is severe injury to the bowel.5 On identification of the paraduodenal hernia, it is important to release the bowel from the hernia sac, free up adhesions, and place small bowel segments back into the correct anatomical position.4,5
In the event of bowel injury, resection with reanastomosis is indicated. Careful dissection is important to prevent injury to the superior mesenteric artery, which supplies most of the small bowel and ascending colon.4,5 Injury to the superior mesenteric artery could lead to ischemia and gangrenous bowel.2 Immediate detection and early surgery intervention of these congenital hernias can prevent such complications.2 The literature includes reports of paraduodenal hernias with complications of gangrenous bowel that required small bowel resection.2 These complications further emphasize the need to proceed immediately with surgery if a paraduodenal hernia is suspected.
Conclusion
This rare cause of bowel obstruction was documented in order to emphasize the importance of having a high clinical suspicion for a paraduodenal hernia. This particular patient with no history of abdominal surgeries had previously dealt with bowel obstruction and would likely have this complication again without surgical intervention. Patients with paraduodenal hernias also are at risk for bowel ischemia, other high-risk complications, and even death.5 Although a CT scan provided information about an approximate location of the obstruction, laparoscopy confirmed the diagnosis. Going into the operation with paraduodenal hernia in the differential allowed the surgeon to be prepared for the appropriate anatomy involved with this procedure to minimize damage to important structures, such as the superior mesenteric artery and its branches.
1. Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 19th ed. Philadelphia, PA: Saunders; 2012.
2. Fukada T, Mukai H, Shimamura F, Furukawa T, Miyazaki M. A causal relationship between right paraduodenal hernia and superior mesenteric artery syndrome: a case report. J Med Case Rep. 2010;4:159.
3. Skandalakis JE. Peritoneum, omenta, and internal hernias. In: Skandalakis JE, Colborn GL, eds. Skandalakis Surgical Anatomy: The Embryologic and Anatomic Basis of Modern Surgery. 1st ed. Athens, Greece: Paschalidis Medical Publications; 2004:chap 10.
4. Papaziogas B, Souparis A, Makris J, Alexandrakis A, Papaziogas T. Surgical images: soft tissue. Right paraduodenal hernia. Can J Surg. 2004;47(3):195-196.
5. Manfredelli S, Andrea Z, Stefano P, et al. Rare small bowel obstruction: right paraduodenal hernia. Case report. Int J Surg Case Rep. 2013;4(4):412-415.
1. Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 19th ed. Philadelphia, PA: Saunders; 2012.
2. Fukada T, Mukai H, Shimamura F, Furukawa T, Miyazaki M. A causal relationship between right paraduodenal hernia and superior mesenteric artery syndrome: a case report. J Med Case Rep. 2010;4:159.
3. Skandalakis JE. Peritoneum, omenta, and internal hernias. In: Skandalakis JE, Colborn GL, eds. Skandalakis Surgical Anatomy: The Embryologic and Anatomic Basis of Modern Surgery. 1st ed. Athens, Greece: Paschalidis Medical Publications; 2004:chap 10.
4. Papaziogas B, Souparis A, Makris J, Alexandrakis A, Papaziogas T. Surgical images: soft tissue. Right paraduodenal hernia. Can J Surg. 2004;47(3):195-196.
5. Manfredelli S, Andrea Z, Stefano P, et al. Rare small bowel obstruction: right paraduodenal hernia. Case report. Int J Surg Case Rep. 2013;4(4):412-415.
New telehealth legislation would provide for testing, expansion
A bipartisan bill introduced in the U.S. Senate in late March 2017 would authorize the Center for Medicare & Medicaid Innovation (CMMI) to test expanded telehealth services provided to Medicare beneficiaries.
The Telehealth Innovation and Improvement Act (S.787), currently in the Senate Finance Committee, was introduced by Sen. Gary Peters (D-Mich.) and Sen. Cory Gardner (R-Colo.). A similar bill they introduced in 2015 was never enacted.
However, there are physicians hoping to see this bill or others like it granted consideration. Currently, the Centers for Medicare & Medicaid Services reimburses only for certain telemedicine services provided in rural or underserved geographic areas, but the new bill would apply in suburban and urban areas as well, based on pilot testing of models and evaluating them for cost, quality, and effectiveness. Successful models would be covered by Medicare.
“Medicare has made some provisions for specific rural sites and niche areas, but writ large, there’s no prescribed way for people to just open a telemedicine shop and begin to bill,” said Bradley Flansbaum, DO, MPH, MHM, a member of the SHM Public Policy Committee.
With the exception of telestroke and critical care, “evidence is needed for the type of setting and type of clinical problems addressed by telemedicine. It’s not been tested enough,” added Dr. Flansbaum, who holds a dual appointment in hospital medicine and population health at Geisinger Medical Center in Danville, Penn. “How does it work for routine inpatient problems and how do hospitalists use it? We haven’t seen data there and that’s where a pilot comes in.”

Dr. Mac believes it inconsistent that, in many circumstances, physicians providing services via telemedicine technology are not reimbursed by Medicare and other payers.
“The expansion and ability to provide care in more unique ways – more specialties and in more environments – has expanded more quickly than the systems of reimbursement for professional fees have and it really is a bit of a hodgepodge now,” he said. “We certainly are pleased that this is getting attention and that we have leaders pushing for this in Congress. We don’t know for sure how the final legislation (on this bill) may look but hopefully there will be some form of this that will come to fruition.”
Whether telemedicine can reduce costs while improving outcomes, or improve outcomes without increasing costs, remains unsettled. A study published in Health Affairs in March 2017 indicates that while telehealth can improve access to care, it results in greater utilization, thereby increasing costs.1
The study relied on claims data for more than 300,000 patients in the California Public Employees’ Retirement System during 2011-2013. It looked at utilization of direct-to-consumer telehealth and spending for acute respiratory illness, one of the most common reasons patients seek telehealth services. While, per episode, telehealth visits cost 50% less than did an outpatient visit and less than 5% of an emergency department visit, annual spending per individual for acute respiratory illness went up $45 because, as the authors estimated, 88% of direct-to-consumer telehealth visits represented new utilization.
Whether this would be the case for hospitalist patients remains to be tested.
“It gets back to whether or not you’re adding a necessary service or substituting a less expensive one for a more expensive one,” said Dr. Flansbaum. “Are physicians providing a needed service or adding unnecessary visits to the system?”
Jayne Lee, MD, has been a hospitalist with Eagle for nearly a decade. Before making the transition from an in-hospital physician to one treating patients from behind a robot – with assistance at the point of service from a nurse – she was working 10 shifts in a row at her home in the United States before traveling to her home in Paris. Dr. Mac offered her the opportunity to practice full time as a telehospitalist from overseas. Today, she is also the company’s chief medical officer and estimates she’s had more than 7,000 patient encounters using telemedicine technology.

Dr. Lee is licensed in multiple states – a barrier that plagues many would-be telehealth providers, but which Eagle has solved with its licensing and credentialing staff – and because she is often providing services at night to urban and rural areas, she sees a broad range of patients.
“We see things from coronary artery disease, COPD [chronic obstructive pulmonary disease] exacerbations, and diabetes-related conditions to drug overdoses and alcohol abuse,” she said. “I enjoy seeing the variety of patients I encounter every night.”
Dr. Lee has to navigate each health system’s electronic medical records and triage systems but, she says, patient care has remained the same. And she’s providing services for hospitals that may not have another hospitalist to assign.
“Our practices keep growing, a sign that hospitals are needing our services now more than ever, given that there is a physician shortage and given the financial constraints we’re seeing in the healthcare system.” she said.
References
1. Ashwood JS, Mehrota A, Cowling D, et al. Direct-to-consumer telehealth may increase access to care but does not decrease spending. Health Affairs. 2017; 36(3):485-491. doi: 10.1377/hlthaff.2016.1130.
A bipartisan bill introduced in the U.S. Senate in late March 2017 would authorize the Center for Medicare & Medicaid Innovation (CMMI) to test expanded telehealth services provided to Medicare beneficiaries.
The Telehealth Innovation and Improvement Act (S.787), currently in the Senate Finance Committee, was introduced by Sen. Gary Peters (D-Mich.) and Sen. Cory Gardner (R-Colo.). A similar bill they introduced in 2015 was never enacted.
However, there are physicians hoping to see this bill or others like it granted consideration. Currently, the Centers for Medicare & Medicaid Services reimburses only for certain telemedicine services provided in rural or underserved geographic areas, but the new bill would apply in suburban and urban areas as well, based on pilot testing of models and evaluating them for cost, quality, and effectiveness. Successful models would be covered by Medicare.
“Medicare has made some provisions for specific rural sites and niche areas, but writ large, there’s no prescribed way for people to just open a telemedicine shop and begin to bill,” said Bradley Flansbaum, DO, MPH, MHM, a member of the SHM Public Policy Committee.
With the exception of telestroke and critical care, “evidence is needed for the type of setting and type of clinical problems addressed by telemedicine. It’s not been tested enough,” added Dr. Flansbaum, who holds a dual appointment in hospital medicine and population health at Geisinger Medical Center in Danville, Penn. “How does it work for routine inpatient problems and how do hospitalists use it? We haven’t seen data there and that’s where a pilot comes in.”
Dr. Mac believes it inconsistent that, in many circumstances, physicians providing services via telemedicine technology are not reimbursed by Medicare and other payers.
“The expansion and ability to provide care in more unique ways – more specialties and in more environments – has expanded more quickly than the systems of reimbursement for professional fees have and it really is a bit of a hodgepodge now,” he said. “We certainly are pleased that this is getting attention and that we have leaders pushing for this in Congress. We don’t know for sure how the final legislation (on this bill) may look but hopefully there will be some form of this that will come to fruition.”
Whether telemedicine can reduce costs while improving outcomes, or improve outcomes without increasing costs, remains unsettled. A study published in Health Affairs in March 2017 indicates that while telehealth can improve access to care, it results in greater utilization, thereby increasing costs.1
The study relied on claims data for more than 300,000 patients in the California Public Employees’ Retirement System during 2011-2013. It looked at utilization of direct-to-consumer telehealth and spending for acute respiratory illness, one of the most common reasons patients seek telehealth services. While, per episode, telehealth visits cost 50% less than did an outpatient visit and less than 5% of an emergency department visit, annual spending per individual for acute respiratory illness went up $45 because, as the authors estimated, 88% of direct-to-consumer telehealth visits represented new utilization.
Whether this would be the case for hospitalist patients remains to be tested.
“It gets back to whether or not you’re adding a necessary service or substituting a less expensive one for a more expensive one,” said Dr. Flansbaum. “Are physicians providing a needed service or adding unnecessary visits to the system?”
Jayne Lee, MD, has been a hospitalist with Eagle for nearly a decade. Before making the transition from an in-hospital physician to one treating patients from behind a robot – with assistance at the point of service from a nurse – she was working 10 shifts in a row at her home in the United States before traveling to her home in Paris. Dr. Mac offered her the opportunity to practice full time as a telehospitalist from overseas. Today, she is also the company’s chief medical officer and estimates she’s had more than 7,000 patient encounters using telemedicine technology.
Dr. Lee is licensed in multiple states – a barrier that plagues many would-be telehealth providers, but which Eagle has solved with its licensing and credentialing staff – and because she is often providing services at night to urban and rural areas, she sees a broad range of patients.
“We see things from coronary artery disease, COPD [chronic obstructive pulmonary disease] exacerbations, and diabetes-related conditions to drug overdoses and alcohol abuse,” she said. “I enjoy seeing the variety of patients I encounter every night.”
Dr. Lee has to navigate each health system’s electronic medical records and triage systems but, she says, patient care has remained the same. And she’s providing services for hospitals that may not have another hospitalist to assign.
“Our practices keep growing, a sign that hospitals are needing our services now more than ever, given that there is a physician shortage and given the financial constraints we’re seeing in the healthcare system.” she said.
References
1. Ashwood JS, Mehrota A, Cowling D, et al. Direct-to-consumer telehealth may increase access to care but does not decrease spending. Health Affairs. 2017; 36(3):485-491. doi: 10.1377/hlthaff.2016.1130.
A bipartisan bill introduced in the U.S. Senate in late March 2017 would authorize the Center for Medicare & Medicaid Innovation (CMMI) to test expanded telehealth services provided to Medicare beneficiaries.
The Telehealth Innovation and Improvement Act (S.787), currently in the Senate Finance Committee, was introduced by Sen. Gary Peters (D-Mich.) and Sen. Cory Gardner (R-Colo.). A similar bill they introduced in 2015 was never enacted.
However, there are physicians hoping to see this bill or others like it granted consideration. Currently, the Centers for Medicare & Medicaid Services reimburses only for certain telemedicine services provided in rural or underserved geographic areas, but the new bill would apply in suburban and urban areas as well, based on pilot testing of models and evaluating them for cost, quality, and effectiveness. Successful models would be covered by Medicare.
“Medicare has made some provisions for specific rural sites and niche areas, but writ large, there’s no prescribed way for people to just open a telemedicine shop and begin to bill,” said Bradley Flansbaum, DO, MPH, MHM, a member of the SHM Public Policy Committee.
With the exception of telestroke and critical care, “evidence is needed for the type of setting and type of clinical problems addressed by telemedicine. It’s not been tested enough,” added Dr. Flansbaum, who holds a dual appointment in hospital medicine and population health at Geisinger Medical Center in Danville, Penn. “How does it work for routine inpatient problems and how do hospitalists use it? We haven’t seen data there and that’s where a pilot comes in.”
Dr. Mac believes it inconsistent that, in many circumstances, physicians providing services via telemedicine technology are not reimbursed by Medicare and other payers.
“The expansion and ability to provide care in more unique ways – more specialties and in more environments – has expanded more quickly than the systems of reimbursement for professional fees have and it really is a bit of a hodgepodge now,” he said. “We certainly are pleased that this is getting attention and that we have leaders pushing for this in Congress. We don’t know for sure how the final legislation (on this bill) may look but hopefully there will be some form of this that will come to fruition.”
Whether telemedicine can reduce costs while improving outcomes, or improve outcomes without increasing costs, remains unsettled. A study published in Health Affairs in March 2017 indicates that while telehealth can improve access to care, it results in greater utilization, thereby increasing costs.1
The study relied on claims data for more than 300,000 patients in the California Public Employees’ Retirement System during 2011-2013. It looked at utilization of direct-to-consumer telehealth and spending for acute respiratory illness, one of the most common reasons patients seek telehealth services. While, per episode, telehealth visits cost 50% less than did an outpatient visit and less than 5% of an emergency department visit, annual spending per individual for acute respiratory illness went up $45 because, as the authors estimated, 88% of direct-to-consumer telehealth visits represented new utilization.
Whether this would be the case for hospitalist patients remains to be tested.
“It gets back to whether or not you’re adding a necessary service or substituting a less expensive one for a more expensive one,” said Dr. Flansbaum. “Are physicians providing a needed service or adding unnecessary visits to the system?”
Jayne Lee, MD, has been a hospitalist with Eagle for nearly a decade. Before making the transition from an in-hospital physician to one treating patients from behind a robot – with assistance at the point of service from a nurse – she was working 10 shifts in a row at her home in the United States before traveling to her home in Paris. Dr. Mac offered her the opportunity to practice full time as a telehospitalist from overseas. Today, she is also the company’s chief medical officer and estimates she’s had more than 7,000 patient encounters using telemedicine technology.
Dr. Lee is licensed in multiple states – a barrier that plagues many would-be telehealth providers, but which Eagle has solved with its licensing and credentialing staff – and because she is often providing services at night to urban and rural areas, she sees a broad range of patients.
“We see things from coronary artery disease, COPD [chronic obstructive pulmonary disease] exacerbations, and diabetes-related conditions to drug overdoses and alcohol abuse,” she said. “I enjoy seeing the variety of patients I encounter every night.”
Dr. Lee has to navigate each health system’s electronic medical records and triage systems but, she says, patient care has remained the same. And she’s providing services for hospitals that may not have another hospitalist to assign.
“Our practices keep growing, a sign that hospitals are needing our services now more than ever, given that there is a physician shortage and given the financial constraints we’re seeing in the healthcare system.” she said.
References
1. Ashwood JS, Mehrota A, Cowling D, et al. Direct-to-consumer telehealth may increase access to care but does not decrease spending. Health Affairs. 2017; 36(3):485-491. doi: 10.1377/hlthaff.2016.1130.