User login
APAP improves aerophagia symptoms
Switching continuous positive airway pressure–treated patients to autotitrating positive airway pressure (APAP) systems resulted in reduced severity of patient-reported aerophagia symptoms, according to results from a double-blind, randomized study.
Aerophagia, the swallowing of air leading to gastrointestinal distress, is a frequently reported adverse effect among people treated for obstructive sleep apnea with continuous positive airway pressure (CPAP).
The APAP-treated group saw significantly reduced median therapeutic pressure levels compared with the CPAP-treated patients (9.8 vs. 14.0 cm H2O, P less than .001) and slight but statistically significant reductions in self-reported symptoms of bloating, flatulence, and belching. No significant difference was seen in compliance with therapy between the two treatment groups in this study, published in the August 2017 issue of Journal of Clinical Sleep Medicine (J Clin Sleep Med. 2017;13[7]:881-8).
For their research, Teresa Shirlaw and her colleagues in the sleep clinic at Princess Alexandra Hospital in Woolloongabba, Queensland, Australia, analyzed results from 56 adult patients with sleep apnea who had been recently treated with CPAP and reported bloating, flatulence, or belching following therapy.
Patients were randomized 1:1 to in-clinic nighttime CPAP or APAP for 2 weeks and blinded to treatment assignment, while investigators recorded therapy usage hours, pressure, leak, and residual apnea-hypopnea index across the study period. Most of the subjects (n = 39) used full face masks, while others used nasal-only systems.
The researchers considered differences in PAP therapy usage of at least 30 minutes per night to be statistically significant. The APAP group used the assigned therapy a mean 7 hours per night, vs. 6.8 for the CPAP group. Daytime sleepiness outcomes were also similar for the two treatment groups.
Ms. Shirlaw and her colleagues described the compliance findings as a surprise, noting that an earlier meta-analysis had shown slight improvements in compliance associated with APAP (Syst Rev. 2012;1[1]:20). In clinical practice, patients complaining of aerophagia associated with CPAP are frequently switched to APAP based on the belief that doing so “will lead to improved therapy acceptance and … improved compliance,” they wrote.
The investigators described the self-reporting of aerophagia symptoms as one of the study’s limitations. They surmised that the lack of difference seen for compliance measures might be explained in part by the 30-minute usage increments in the study design (compared with 10-minute increments used in some other studies), and the fact that the cohort had relatively high compliance with CPAP at baseline (5.5 hours/night), suggesting a motivated patient population at entry.
The study received some funding from the government of Queensland, and the authors disclosed no conflicts of interest related to their findings.

Switching continuous positive airway pressure–treated patients to autotitrating positive airway pressure (APAP) systems resulted in reduced severity of patient-reported aerophagia symptoms, according to results from a double-blind, randomized study.
Aerophagia, the swallowing of air leading to gastrointestinal distress, is a frequently reported adverse effect among people treated for obstructive sleep apnea with continuous positive airway pressure (CPAP).
The APAP-treated group saw significantly reduced median therapeutic pressure levels compared with the CPAP-treated patients (9.8 vs. 14.0 cm H2O, P less than .001) and slight but statistically significant reductions in self-reported symptoms of bloating, flatulence, and belching. No significant difference was seen in compliance with therapy between the two treatment groups in this study, published in the August 2017 issue of Journal of Clinical Sleep Medicine (J Clin Sleep Med. 2017;13[7]:881-8).
For their research, Teresa Shirlaw and her colleagues in the sleep clinic at Princess Alexandra Hospital in Woolloongabba, Queensland, Australia, analyzed results from 56 adult patients with sleep apnea who had been recently treated with CPAP and reported bloating, flatulence, or belching following therapy.
Patients were randomized 1:1 to in-clinic nighttime CPAP or APAP for 2 weeks and blinded to treatment assignment, while investigators recorded therapy usage hours, pressure, leak, and residual apnea-hypopnea index across the study period. Most of the subjects (n = 39) used full face masks, while others used nasal-only systems.
The researchers considered differences in PAP therapy usage of at least 30 minutes per night to be statistically significant. The APAP group used the assigned therapy a mean 7 hours per night, vs. 6.8 for the CPAP group. Daytime sleepiness outcomes were also similar for the two treatment groups.
Ms. Shirlaw and her colleagues described the compliance findings as a surprise, noting that an earlier meta-analysis had shown slight improvements in compliance associated with APAP (Syst Rev. 2012;1[1]:20). In clinical practice, patients complaining of aerophagia associated with CPAP are frequently switched to APAP based on the belief that doing so “will lead to improved therapy acceptance and … improved compliance,” they wrote.
The investigators described the self-reporting of aerophagia symptoms as one of the study’s limitations. They surmised that the lack of difference seen for compliance measures might be explained in part by the 30-minute usage increments in the study design (compared with 10-minute increments used in some other studies), and the fact that the cohort had relatively high compliance with CPAP at baseline (5.5 hours/night), suggesting a motivated patient population at entry.
The study received some funding from the government of Queensland, and the authors disclosed no conflicts of interest related to their findings.
Switching continuous positive airway pressure–treated patients to autotitrating positive airway pressure (APAP) systems resulted in reduced severity of patient-reported aerophagia symptoms, according to results from a double-blind, randomized study.
Aerophagia, the swallowing of air leading to gastrointestinal distress, is a frequently reported adverse effect among people treated for obstructive sleep apnea with continuous positive airway pressure (CPAP).
The APAP-treated group saw significantly reduced median therapeutic pressure levels compared with the CPAP-treated patients (9.8 vs. 14.0 cm H2O, P less than .001) and slight but statistically significant reductions in self-reported symptoms of bloating, flatulence, and belching. No significant difference was seen in compliance with therapy between the two treatment groups in this study, published in the August 2017 issue of Journal of Clinical Sleep Medicine (J Clin Sleep Med. 2017;13[7]:881-8).
For their research, Teresa Shirlaw and her colleagues in the sleep clinic at Princess Alexandra Hospital in Woolloongabba, Queensland, Australia, analyzed results from 56 adult patients with sleep apnea who had been recently treated with CPAP and reported bloating, flatulence, or belching following therapy.
Patients were randomized 1:1 to in-clinic nighttime CPAP or APAP for 2 weeks and blinded to treatment assignment, while investigators recorded therapy usage hours, pressure, leak, and residual apnea-hypopnea index across the study period. Most of the subjects (n = 39) used full face masks, while others used nasal-only systems.
The researchers considered differences in PAP therapy usage of at least 30 minutes per night to be statistically significant. The APAP group used the assigned therapy a mean 7 hours per night, vs. 6.8 for the CPAP group. Daytime sleepiness outcomes were also similar for the two treatment groups.
Ms. Shirlaw and her colleagues described the compliance findings as a surprise, noting that an earlier meta-analysis had shown slight improvements in compliance associated with APAP (Syst Rev. 2012;1[1]:20). In clinical practice, patients complaining of aerophagia associated with CPAP are frequently switched to APAP based on the belief that doing so “will lead to improved therapy acceptance and … improved compliance,” they wrote.
The investigators described the self-reporting of aerophagia symptoms as one of the study’s limitations. They surmised that the lack of difference seen for compliance measures might be explained in part by the 30-minute usage increments in the study design (compared with 10-minute increments used in some other studies), and the fact that the cohort had relatively high compliance with CPAP at baseline (5.5 hours/night), suggesting a motivated patient population at entry.
The study received some funding from the government of Queensland, and the authors disclosed no conflicts of interest related to their findings.
FROM THE JOURNAL OF CLINICAL SLEEP MEDICINE
Key clinical point: Sleep apnea patients complaining of aerophagia associated with continuous positive airway pressure may find relief using autotitrating positive airway pressure.
Major finding: The APAP-treated group saw significantly reduced median therapeutic pressure levels compared with the CPAP-treated patients (9.8 vs. 14.0 cm H2O, P less than .001) and slight but statistically significant reductions in self-reported symptoms of bloating, flatulence, and belching.
Data source: A randomized, double-blinded trial of 56 adult sleep apnea patients, with previous CPAP and aerophagia, treated at a hospital sleep clinic in Australia.
Disclosures: The government of Queensland helped fund the study. The authors disclosed no conflicts of interest.
Treating women with opioid use disorders poses unique challenges
The opioid epidemic in the United States is reaching a boiling point, with President Trump calling it a “national emergency” and instructing his administration to use all appropriate authority to respond. Experts say that women are disproportionately affected and require unique treatment approaches.
The rate of prescription opioid–related overdoses increased by 471% among women in 2015, compared with an increase of 218% among men. Heroin deaths among women have risen at more than twice the rate among men, according to a report from the Office of Women’s Health (OWH), part of the U.S. Department of Health & Human Services.
The OWH report, released in July, paints a different picture of addiction for women than for men. Women are more likely to experience chronic pain and turn to prescription opioids for longer periods of time and in higher doses. But women also become dependent at smaller doses and in a shorter period of time. Add to this the fact that psychological and emotional distress are risk factors for opioid abuse among women, but not among men, according to the report.
ACOG guidance
In August, the American College of Obstetricians and Gynecologists (ACOG) updated its recommendations for treatments and best practices related to opioid use among pregnant women (Obstet Gynecol. 2017;130:e81-94).
The committee opinion, developed with the American Society of Addiction Medicine, focuses on tearing down stereotypes about women with substance use disorders that could cause patients to slip through the cracks. ACOG recommended universal screening as a part of regular obstetric care, starting with the first prenatal visit.
While screening can involve laboratory testing, the recommendations focus more on creating a comfortable environment for pregnant women to share substance use history and to have a frank conversation about what treatment options are available.
“The document highlights the use of a verbal screening tool which enables the obstetric provider to have a direct conversation with the patient about their answers,” Maria Mascola, MD, an ob.gyn. at the Marshfield (Wis.) Clinic and lead author of the ACOG committee opinion, said in an interview. “It talks about substance use and then provides an opportunity to understand what substances and how much, why these substances might be bad, why this behavior should be changed, and how obstetricians can try to help the person make those changes.”
ACOG continues to recommend medication-assisted treatment (MAT) – typically with methadone or buprenorphine – as the most effective pathway for pregnant women to deal with substance use disorders. However, in cases in which the patient does not accept treatment with an opioid agonist or the treatment is unavailable, medically supervised withdrawal can be considered. ACOG cautions that relapse rates are high (from 59% to more than 90%) and that withdrawal often involves inpatient care and intensive outpatient follow-up. But recent evidence suggests medically supervised withdrawal is not associated with fetal death or preterm delivery.
“There have been some studies looking at smaller groups that have shown pregnant women going through medically supervised withdrawals and there have been some data from those studies that indicate women may be able to successfully go through this withdrawal without harm to the baby,” Dr. Mascola said. “The information we have on medically supervised withdrawal is a small amount of data, and we definitely need more before this is a primary approach.”
Access to care
Regardless of the treatment approach, the larger issue may be accessibility of care. Just 20% of adults with an opioid use disorder get the treatment and care they need each year, according to the OWH, with access and cost cited as the primary barriers to care. This problem is likely worse in rural areas.
“Rural health care is tougher. There is less access; that is an absolute truth, and it’s a burden then for those women to travel long distances to get the care they need,” Dr. Mascola said. “I think ob.gyns. should advocate for more attention in those areas where patients are underserved.”
One potential solution is for ob.gyns. to become certified in providing buprenorphine, which would allow physicians in rural areas to dispense these approved pharmacotherapies to patients who would otherwise be unable to have the proper treatment and follow-up necessary to prevent relapse, Dr. Mascola said.
There is already some federal funding available for this approach. In 2016, the Health Resources and Services Administration awarded $94 million to health centers across the country to expand substance use services, specifically increasing screening for substance use disorders, improving access to medication-assisted treatment, and training clinicians. Similarly, the Substance Abuse and Mental Health Services Administration recently announced it will allocate an additional $485 million to states through the State Targeted Response to the Opioid Crisis Grants to fund medication-assisted treatment and other services.
Unique challenges
Treating women with opioid use disorder isn’t just about identifying the best treatment approach. Social factors appear to play a larger role among women.

“Another difference with women over men is the prevalence of sexual trauma, as well as being in unhealthy relationships where the women are more likely to be enticed into leaving treatment,” she added.
Trauma among women with substance abuse disorders is prevalent, with 55%-99% of women reporting experiencing some form of trauma, compared with 36%-51% of the general population, according to the OWH report.
Beyond exploratory research, there needs to be a major shift in the public perception of opioid substance use, which currently does not approach the disorder as a chronic disease, according to Dr. Jones.
“The treatment process cannot just involve a detoxification program and then send patients off because that will commonly just end in relapse.” Dr. Jones said. “We need to approach substance use disorders with a recovery-oriented system of care in order to create a true safety net they can rely on.”
[email protected]
On Twitter @eaztweets
The opioid epidemic in the United States is reaching a boiling point, with President Trump calling it a “national emergency” and instructing his administration to use all appropriate authority to respond. Experts say that women are disproportionately affected and require unique treatment approaches.
The rate of prescription opioid–related overdoses increased by 471% among women in 2015, compared with an increase of 218% among men. Heroin deaths among women have risen at more than twice the rate among men, according to a report from the Office of Women’s Health (OWH), part of the U.S. Department of Health & Human Services.
The OWH report, released in July, paints a different picture of addiction for women than for men. Women are more likely to experience chronic pain and turn to prescription opioids for longer periods of time and in higher doses. But women also become dependent at smaller doses and in a shorter period of time. Add to this the fact that psychological and emotional distress are risk factors for opioid abuse among women, but not among men, according to the report.
ACOG guidance
In August, the American College of Obstetricians and Gynecologists (ACOG) updated its recommendations for treatments and best practices related to opioid use among pregnant women (Obstet Gynecol. 2017;130:e81-94).
The committee opinion, developed with the American Society of Addiction Medicine, focuses on tearing down stereotypes about women with substance use disorders that could cause patients to slip through the cracks. ACOG recommended universal screening as a part of regular obstetric care, starting with the first prenatal visit.
While screening can involve laboratory testing, the recommendations focus more on creating a comfortable environment for pregnant women to share substance use history and to have a frank conversation about what treatment options are available.
“The document highlights the use of a verbal screening tool which enables the obstetric provider to have a direct conversation with the patient about their answers,” Maria Mascola, MD, an ob.gyn. at the Marshfield (Wis.) Clinic and lead author of the ACOG committee opinion, said in an interview. “It talks about substance use and then provides an opportunity to understand what substances and how much, why these substances might be bad, why this behavior should be changed, and how obstetricians can try to help the person make those changes.”
ACOG continues to recommend medication-assisted treatment (MAT) – typically with methadone or buprenorphine – as the most effective pathway for pregnant women to deal with substance use disorders. However, in cases in which the patient does not accept treatment with an opioid agonist or the treatment is unavailable, medically supervised withdrawal can be considered. ACOG cautions that relapse rates are high (from 59% to more than 90%) and that withdrawal often involves inpatient care and intensive outpatient follow-up. But recent evidence suggests medically supervised withdrawal is not associated with fetal death or preterm delivery.
“There have been some studies looking at smaller groups that have shown pregnant women going through medically supervised withdrawals and there have been some data from those studies that indicate women may be able to successfully go through this withdrawal without harm to the baby,” Dr. Mascola said. “The information we have on medically supervised withdrawal is a small amount of data, and we definitely need more before this is a primary approach.”
Access to care
Regardless of the treatment approach, the larger issue may be accessibility of care. Just 20% of adults with an opioid use disorder get the treatment and care they need each year, according to the OWH, with access and cost cited as the primary barriers to care. This problem is likely worse in rural areas.
“Rural health care is tougher. There is less access; that is an absolute truth, and it’s a burden then for those women to travel long distances to get the care they need,” Dr. Mascola said. “I think ob.gyns. should advocate for more attention in those areas where patients are underserved.”
One potential solution is for ob.gyns. to become certified in providing buprenorphine, which would allow physicians in rural areas to dispense these approved pharmacotherapies to patients who would otherwise be unable to have the proper treatment and follow-up necessary to prevent relapse, Dr. Mascola said.
There is already some federal funding available for this approach. In 2016, the Health Resources and Services Administration awarded $94 million to health centers across the country to expand substance use services, specifically increasing screening for substance use disorders, improving access to medication-assisted treatment, and training clinicians. Similarly, the Substance Abuse and Mental Health Services Administration recently announced it will allocate an additional $485 million to states through the State Targeted Response to the Opioid Crisis Grants to fund medication-assisted treatment and other services.
Unique challenges
Treating women with opioid use disorder isn’t just about identifying the best treatment approach. Social factors appear to play a larger role among women.
“Another difference with women over men is the prevalence of sexual trauma, as well as being in unhealthy relationships where the women are more likely to be enticed into leaving treatment,” she added.
Trauma among women with substance abuse disorders is prevalent, with 55%-99% of women reporting experiencing some form of trauma, compared with 36%-51% of the general population, according to the OWH report.
Beyond exploratory research, there needs to be a major shift in the public perception of opioid substance use, which currently does not approach the disorder as a chronic disease, according to Dr. Jones.
“The treatment process cannot just involve a detoxification program and then send patients off because that will commonly just end in relapse.” Dr. Jones said. “We need to approach substance use disorders with a recovery-oriented system of care in order to create a true safety net they can rely on.”
[email protected]
On Twitter @eaztweets
The opioid epidemic in the United States is reaching a boiling point, with President Trump calling it a “national emergency” and instructing his administration to use all appropriate authority to respond. Experts say that women are disproportionately affected and require unique treatment approaches.
The rate of prescription opioid–related overdoses increased by 471% among women in 2015, compared with an increase of 218% among men. Heroin deaths among women have risen at more than twice the rate among men, according to a report from the Office of Women’s Health (OWH), part of the U.S. Department of Health & Human Services.
The OWH report, released in July, paints a different picture of addiction for women than for men. Women are more likely to experience chronic pain and turn to prescription opioids for longer periods of time and in higher doses. But women also become dependent at smaller doses and in a shorter period of time. Add to this the fact that psychological and emotional distress are risk factors for opioid abuse among women, but not among men, according to the report.
ACOG guidance
In August, the American College of Obstetricians and Gynecologists (ACOG) updated its recommendations for treatments and best practices related to opioid use among pregnant women (Obstet Gynecol. 2017;130:e81-94).
The committee opinion, developed with the American Society of Addiction Medicine, focuses on tearing down stereotypes about women with substance use disorders that could cause patients to slip through the cracks. ACOG recommended universal screening as a part of regular obstetric care, starting with the first prenatal visit.
While screening can involve laboratory testing, the recommendations focus more on creating a comfortable environment for pregnant women to share substance use history and to have a frank conversation about what treatment options are available.
“The document highlights the use of a verbal screening tool which enables the obstetric provider to have a direct conversation with the patient about their answers,” Maria Mascola, MD, an ob.gyn. at the Marshfield (Wis.) Clinic and lead author of the ACOG committee opinion, said in an interview. “It talks about substance use and then provides an opportunity to understand what substances and how much, why these substances might be bad, why this behavior should be changed, and how obstetricians can try to help the person make those changes.”
ACOG continues to recommend medication-assisted treatment (MAT) – typically with methadone or buprenorphine – as the most effective pathway for pregnant women to deal with substance use disorders. However, in cases in which the patient does not accept treatment with an opioid agonist or the treatment is unavailable, medically supervised withdrawal can be considered. ACOG cautions that relapse rates are high (from 59% to more than 90%) and that withdrawal often involves inpatient care and intensive outpatient follow-up. But recent evidence suggests medically supervised withdrawal is not associated with fetal death or preterm delivery.
“There have been some studies looking at smaller groups that have shown pregnant women going through medically supervised withdrawals and there have been some data from those studies that indicate women may be able to successfully go through this withdrawal without harm to the baby,” Dr. Mascola said. “The information we have on medically supervised withdrawal is a small amount of data, and we definitely need more before this is a primary approach.”
Access to care
Regardless of the treatment approach, the larger issue may be accessibility of care. Just 20% of adults with an opioid use disorder get the treatment and care they need each year, according to the OWH, with access and cost cited as the primary barriers to care. This problem is likely worse in rural areas.
“Rural health care is tougher. There is less access; that is an absolute truth, and it’s a burden then for those women to travel long distances to get the care they need,” Dr. Mascola said. “I think ob.gyns. should advocate for more attention in those areas where patients are underserved.”
One potential solution is for ob.gyns. to become certified in providing buprenorphine, which would allow physicians in rural areas to dispense these approved pharmacotherapies to patients who would otherwise be unable to have the proper treatment and follow-up necessary to prevent relapse, Dr. Mascola said.
There is already some federal funding available for this approach. In 2016, the Health Resources and Services Administration awarded $94 million to health centers across the country to expand substance use services, specifically increasing screening for substance use disorders, improving access to medication-assisted treatment, and training clinicians. Similarly, the Substance Abuse and Mental Health Services Administration recently announced it will allocate an additional $485 million to states through the State Targeted Response to the Opioid Crisis Grants to fund medication-assisted treatment and other services.
Unique challenges
Treating women with opioid use disorder isn’t just about identifying the best treatment approach. Social factors appear to play a larger role among women.
“Another difference with women over men is the prevalence of sexual trauma, as well as being in unhealthy relationships where the women are more likely to be enticed into leaving treatment,” she added.
Trauma among women with substance abuse disorders is prevalent, with 55%-99% of women reporting experiencing some form of trauma, compared with 36%-51% of the general population, according to the OWH report.
Beyond exploratory research, there needs to be a major shift in the public perception of opioid substance use, which currently does not approach the disorder as a chronic disease, according to Dr. Jones.
“The treatment process cannot just involve a detoxification program and then send patients off because that will commonly just end in relapse.” Dr. Jones said. “We need to approach substance use disorders with a recovery-oriented system of care in order to create a true safety net they can rely on.”
[email protected]
On Twitter @eaztweets
How to manage submassive pulmonary embolism
The case
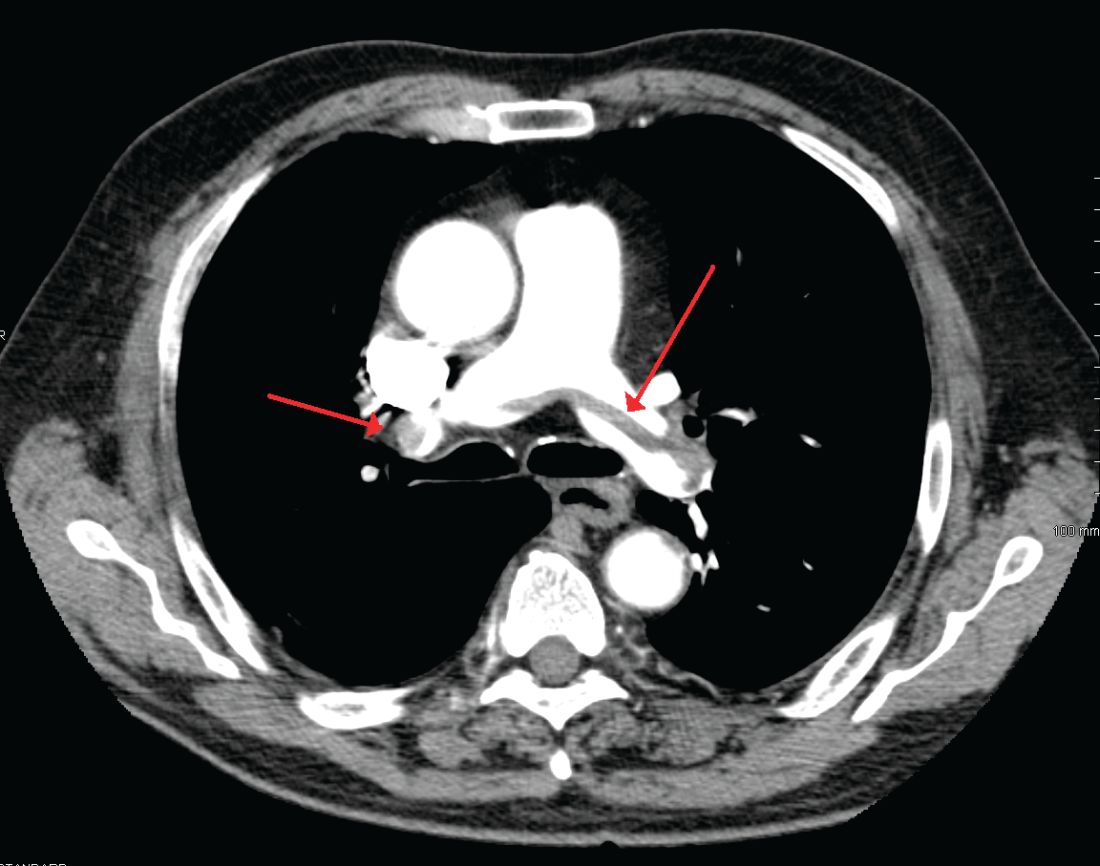
A 49-year-old morbidly obese woman presented to the emergency department with shortness of breath and abdominal distention. On presentation, her blood pressure was 100/60 mm Hg with a heart rate of 110, respiratory rate of 24, and a pulse oximetric saturation (SpO2) of 86% on room air. Troponin T was elevated at 0.3 ng/mL. Computed tomography (CT) of the chest with intravenous contrast showed saddle pulmonary embolism (PE) with dilated right ventricle (RV). CT abdomen/pelvis revealed a very large uterine mass with diffuse lymphadenopathy.
Heparin infusion was started promptly. Echocardiogram demonstrated RV strain. Findings on duplex ultrasound of the lower extremities were consistent with acute deep vein thromboses (DVT) involving the left common femoral vein and the right popliteal vein. Biopsy of a supraclavicular lymph node showed high grade undifferentiated carcinoma most likely of uterine origin.
Clinical questions
What, if any, therapeutic options should be considered beyond standard systemic anticoagulation? Is there a role for:
1. Systemic thrombolysis?
2. Catheter-directed thrombolysis (CDT)?
3. Inferior vena cava (IVC) filter placement?
What is the appropriate management of “submassive” PE?
In the case of massive PE, where the thrombus is located in the central pulmonary vasculature and associated with hypotension due to impaired cardiac output, systemic thrombolysis, embolectomy, and CDT are indicated as potentially life-saving measures. However, the evidence is less clear when the PE is large and has led to RV strain, but without overt hemodynamic instability. This is commonly known as an intermediate risk or “submassive” PE. Submassive PE based on American Heart Association (AHA) guidelines is:1
An acute PE without systemic hypotension (systolic blood pressure less than 90 mm Hg) but with either RV dysfunction or myocardial necrosis. RV dysfunction is defined by the presence of at least one of these following:
• RV dilation (apical 4-chamber RV diameter divided by LV diameter greater than 0.9) or RV systolic dysfunction on echocardiography;
• RV dilation on CT, elevation of BNP (greater than 90 pg/mL), elevation of N-terminal pro-BNP (greater than 500 pg/mL);
• Electrocardiographic changes (new complete or incomplete right bundle branch block, anteroseptal ST elevation or depression, or anteroseptal T-wave inversion).
Myocardial necrosis is defined as elevated troponin I (greater than 0.4 ng/mL) or elevated troponin T (greater than 0.1 ng/mL).
Why is submassive PE of clinical significance?
In 1999, analysis of the International Cooperative Pulmonary Embolism Registry (ICOPER) revealed that RV dysfunction in PE patients was associated with a near doubling of the 3-month mortality risk (hazard ratio 2.0, 1.3-2.9).2 Given this increased risk, one could draw the logical conclusion that we need to treat submassive PE more aggressively than PE without RV strain. But will this necessarily result in a better outcome for the patient given the 3% risk of intracranial hemorrhage associated with thrombolytic therapy?
In the clinical scenario above, the patient did meet the definition of submassive PE. While the patient did not experience systemic hypotension, she did have RV dilation on CT, RV systolic dysfunction on echo as well as an elevated Troponin T level. In addition to starting anticoagulant therapy, what more should be done to increase her probability of a good outcome?
The AHA recommends that systemic thrombolysis and CDT be considered for patients with acute submassive PE if they have clinical evidence of adverse prognosis, including worsening respiratory failure, severe RV dysfunction, or major myocardial necrosis and low risk of bleeding complications (Class IIB; Level of Evidence C).1
The 2016 American College of Chest Physicians (CHEST) guidelines update3 recommends systemically administered thrombolytic therapy over no therapy in selected patients with acute PE who deteriorate after starting anticoagulant therapy but have yet to develop hypotension and who have a low bleeding risk (Grade 2C recommendation).
Systemic thrombolysis
Systemic thrombolysis is administered as an intravenous thrombolytic infusion delivered over a period of time. The Food and Drug Administration–approved thrombolytic drugs currently include tissue plasminogen activator (tPA)/alteplase, streptokinase and urokinase.
Efficacy of low dose thrombolysis was studied in MOPETT 2013,5 a single-center, prospective, randomized, open label study, in which 126 participants found to have submassive PE based on symptoms and CT angiographic or ventilation/perfusion scan data received either 50 mg tPA plus heparin or heparin anticoagulation alone. The composite endpoint of pulmonary hypertension and recurrent PE at 28 months was 16% in the tPA group compared to 63% in the control group (P less than .001). Systemic thrombolysis was associated with lower risk of pulmonary hypertension and recurrent PE, although no mortality benefit was seen in this small study.
In the randomized, double-blind PEITHO trial (n = 1,006) of 20146 comparing tenecteplase plus heparin versus heparin in the submassive PE patients, the primary outcomes of death and hemodynamic decompensation occurred in 2.6% of the tenecteplase group, compared to 5.6% in the placebo group (P = .02). Thrombolytic therapy was associated with 2% rate of hemorrhagic stroke, whereas hemorrhagic stroke in the placebo group was 0.2% (P = .03). In this case, systemic thrombolysis was associated with a 3% lower risk of death and hemodynamic instability, but also a 1.8% increased risk of hemorrhagic stroke.
Catheter-directed thrombolysis (CDT)
CDT was originally developed to treat arterial, dialysis graft and deep vein thromboses, but is now approved by the FDA for the treatment of acute submassive or massive PE.
A wire is passed through the embolus and a multihole infusion catheter is placed, through which a thrombolytic drug is infused over 12-24 hours. The direct delivery of the drug into the thrombus is thought to be as effective as systemic therapy but with a lower risk of bleeding. If more rapid thrombus removal is indicated due to large clot burden and hemodynamic instability, mechanical therapies, such as fragmentation and aspiration, can be used as an adjunct to CDT. However, these mechanical techniques carry the risk of pulmonary artery injury, and therefore should only be used as a last resort. An ultrasound-emitting wire can be added to the multihole infusion catheter to expedite thrombolysis by ultrasonically disrupting the thrombus, a technique known as ultrasound-enhanced thrombolysis (EKOS).7,10
The ULTIMA 2014 trial,8 a small, randomized, open-label study of Ultrasound-Assisted Catheter Directed Thrombolysis (USAT, the term can be used interchangeably with EKOS) versus heparin anticoagulation alone in 59 patients, was designed to study if the former strategy was better at improving the primary outcome measure of RV/LV ratio in submassive PE patients. The mean reduction in RV/LV ratio was 0.30 +/– 0.20 in the USAT group compared to 0.03 +/– 0.16 in the heparin group (P less than .001). However, no significant difference in mortality or bleeding was observed in the groups at 90-day follow up.
The PERFECT 2015 Trial,9 a multicenter registry-based study, prospectively enrolled 101 patients who received CDT as first-line therapy for massive and submassive PE. Among patients with submassive PE, 97.3% were found to have “clinical success” with this treatment, defined as stabilization of hemodynamics, improvement in pulmonary hypertension and right heart strain, and survival to hospital discharge. There was no major bleeding or intracranial hemorrhage. Subgroup analyses in this study comparing USAT against standard CDT did not reveal significant difference in average pulmonary pressure changes, average thrombolytic doses, or average infusion times.
A prospective single-arm multicenter trial, SEATTLE II 2015,10 evaluated the efficacy of EKOS in a sample of 159 patients. Patients with both massive and submassive PE received approximately 24 mg tPA infused via a catheter over 12-24 hours. The primary efficacy outcome was the chest CT-measured RV/LV ratio decrease from the baseline compared to 48 hours post procedure. The pre- and postprocedure ratio was 1.55 versus 1.13 respectively (P less than .001), indicating that EKOS decreased RV dilation. No intracranial hemorrhage was observed and the investigators did not comment on long-term outcomes such as mortality or quality of life. The study was limited by the lack of a comparison group, such as anticoagulation with heparin as monotherapy, or systemic thrombolysis or standard CDT.
Treatment of submassive PE varies between different institutions. There simply are not adequate data comparing low dose systemic thrombolysis, CDT, EKOS, and standard heparin anticoagulation to make firm recommendations. Some investigators feel low-dose systemic thrombolysis is probably as good as the expensive catheter-based thrombolytic therapies.11,12 Low-dose thrombolytic therapy can be followed by use of oral direct factor Xa inhibitors for maintenance of antithrombotic activity.13
Bottom line
In our institution, the interventional radiology team screens patients who meet criteria for submassive PE on a case-by-case basis. We use pulmonary angiographic data (nature and extent of the thrombus), clinical stability, and analysis of other comorbid conditions to decide the best treatment modality for an individual patient. Our team prefers EKOS for submassive PE patients as well as for massive PE patients and as a rescue procedure for patients who have failed systemic thrombolysis.
Until more data are available to support firm guidelines, we feel establishing multidisciplinary teams composed of interventional radiologists, intensivists, cardiologists, and vascular surgeons is prudent to make individualized decisions and to achieve the best outcomes for our patients.14
IVC filter
Since the patient in this case already has a submassive PE, can she tolerate additional clot burden should her remaining DVT embolize again? Is there a role for IVC filter?
The implantation of IVC filters has increased significantly in the past 30 years, without quality evidence justifying their use.15
The 2016 Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report states clearly: In patients with acute DVT of the leg or PE who are treated with anticoagulants, the use of an IVC filter is not recommended (Grade 1B).3 This recommendation is based on findings of the Prevention du Risque d’Embolie Pulmonaire par Interruption Cave (PREPIC) randomized trial,16 and the recently published PREPIC 2 randomized trial,17 both showing that in anticoagulated patients with PE and DVT, concurrent placement of an IVC filter for 3 months did not reduce recurrent PE, including fatal PE.
CHEST guidelines state that an IVC filter should not be routinely placed as an adjunct in patients with PE and DVT. However, what about in the subgroup of patients with submassive or massive PE in whom another PE would be catastrophic? Clinical data are lacking in this area.
Deshpande et al. reported on a series of six patients with massive PE and cardiopulmonary instability; patients all received an IVC filter with anticoagulation. The short-term outcome was excellent, but long-term follow-up was not done.18 Kucher and colleagues reported that from the ICOPER in 2006, out of the 108 massive PE patients with systolic arterial pressure under 90 mm Hg, 11 patients received adjunctive IVC filter placement. None of these 11 patients developed recurrent PE in 90 days and 10 of them survived at least 90 days; IVC filter placement was associated with a reduction in 90-day mortality. In this study, the placement of an IVC filter was entirely decided by the physicians at different sites.19 In a 2012 study examining case fatality rates in 3,770 patients with acute PE who received pulmonary embolectomy, the data showed that in both unstable and stable patients, case fatality rates were lower in those who received an IVC filter.20
Although the above data are favorable for adjunctive IVC filter placement in massive PE patients, at least in short-term outcomes, the small size and lack of randomization preclude establishment of evidence-based guidelines. The 2016 CHEST guidelines point out that as it is uncertain if there is benefit to place an IVC filter adjunctively in anticoagulated patients with severe PE, in this specific subgroup of patients, the recommendation against insertion of an IVC filter in patients with acute PE who are anticoagulated may not apply.3
Bottom line
There is no evidence-based guideline as to whether IVC filters should be placed adjunctively in patients with submassive or massive PE; however, based on expert consensus, it may be appropriate to place an IVC filter as an adjunct to anticoagulation in patients with severe PE. The decision should be individualized based on each patient’s characteristics, preferences, and institutional expertise.
In our case, in hope of preventing further embolic burden, the patient received an IVC filter the day after presentation. Despite the initiation of anticoagulation with heparin, she remained tachycardic and tachypneic, prompting referral for CDT. The interventional radiology team did not feel that she was a good candidate, given her persistent vaginal bleeding and widely metastatic uterine carcinoma. She was switched to therapeutic enoxaparin after no further invasive intervention was deemed appropriate. Her respiratory status did not improve and bilevel positive airway pressure was initiated. Taking into consideration the terminal nature of her cancer, she ultimately elected to pursue comfort care and died shortly afterward.
Acknowledgements
The authors would like to thank Benjamin A. Hohmuth, MD, A. Joseph Layon, MD, and Luis L. Nadal, MD, for their review of the article and invaluable feedback.
Dr. Wenqian Wang, Dr. Vedamurthy, and Dr. Wang are based in the department of hospital medicine at The Medicine Institute, Geisinger Health System, Danville, Penn. Contact Dr. Wenqian Wang at [email protected].
Key Points
• Use pulmonary angiographic data, clinical stability, and analysis of other comorbid conditions to decide the best treatment modality.
• Our team prefers ultrasound-enhanced thrombolysis (EKOS) for submassive PE patients, massive PE patients, and as a rescue procedure for patients who fail systemic thrombolysis.
• Establishing multidisciplinary teams composed of interventional radiologists, intensivists, cardiologists, and vascular surgeons is prudent to make individualized decisions.
• It may be appropriate to place an IVC filter as an adjunct to anticoagulation in patients with severe PE.
References
1. Jaff MR, McMurtry MS, Archer SL, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123:1788-1830.
2. Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet. 1999;353:1386-9.
3. Kearon C, Akl EA, Ornelas J, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149:315-52.
4. Konstantinides S, Geibel A, Heusel G, Heinrich F, Kasper W. Management Strategies and Prognosis of Pulmonary Embolism-3 Trial Investigators. Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. N Engl J Med. 2002;347:1143-50.
5. Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M, “MOPETT” Investigators. Moderate pulmonary embolism treated with thrombolysis (from the “MOPETT” Trial). Am J Cardiol. 2013;111:273-7.
6. Meyer G, Vicaut E, Danays T, et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370:1402-11.
7. Kuo WT. Endovascular therapy for acute pulmonary embolism. J Vasc Interv Radiol 2012;23:167-79. e164
8. Kucher N, Boekstegers P, Muller OJ, et al. Randomized, controlled trial of ultrasound-assisted catheter-directed thrombolysis for acute intermediate-risk pulmonary embolism. Circulation. 2014;129:479-86.
9. Kuo WT, Banerjee A, Kim PS, et al. Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT): Initial Results From a Prospective Multicenter Registry. Chest. 2015;148:667-73.
10. Piazza G, Hohlfelder B, Jaff MR, et al. A Prospective, Single-Arm, Multicenter Trial of Ultrasound-Facilitated, Catheter-Directed, Low-Dose Fibrinolysis for Acute Massive and Submassive Pulmonary Embolism: The SEATTLE II Study. JACC Cardiovasc Interv. 2015;8:1382-92.
11. Sharifi M. Systemic Full Dose, Half Dose, and Catheter Directed Thrombolysis for Pulmonary Embolism. When to Use and How to Choose? Curr Treat Options Cardiovasc Med. 2016;18:31.
12. Wang C, Zhai Z, Yang Y, et al. Efficacy and safety of low dose recombinant tissue-type plasminogen activator for the treatment of acute pulmonary thromboembolism: a randomized, multicenter, controlled trial. Chest. 2010;137:254-62.
13. Sharifi M, Vajo Z, Freeman W, Bay C, Sharifi M, Schwartz F. Transforming and simplifying the treatment of pulmonary embolism: “safe dose” thrombolysis plus new oral anticoagulants. Lung. 2015;193:369-74.
14. Kabrhel C, Rosovsky R, Channick R, et al. A Multidisciplinary Pulmonary Embolism Response Team: Initial 30-Month Experience With a Novel Approach to Delivery of Care to Patients With Submassive and Massive Pulmonary Embolism. Chest. 2016;150:384-93.
15. Lessne ML, Sing RF. Counterpoint: Do the Benefits Outweigh the Risks for Most Patients Under Consideration for inferior vena cava filters? No. Chest. 2016; 150(6):1182-4.
16. The PREPIC Study Group. Eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC (Prevention du Risque d’Embolie Pulmonaire par Interruption Cave) randomized study. Circulation. 2005;112(3):416-22.
17. Mismetti P, Laporte S, Pellerin O, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs. anticoagulation alone on risk of recurrent pulmonary embolism: a randomized clinical trial. JAMA. 2015. 313(16):1627-35.
18. Deshpande KS, Hatem C, Karwa M, et al. The use of inferior vena cava filter as a treatment modality for massive pulmonary embolism. A case series and review of pathophysiology. Respir Med. 2002.96(12):984-9.
19. Kucher N, Rossi E, De Rosa M, et al. Massive Pulmonary embolism. Circulation. 2006;113(4):577-82.
20. Stein P, Matta F. Case Fatality Rate with Pulmonary Embolectomy for Acute Pulmonary Embolism. Am J Med. 2012;125:471-7.
The case
A 49-year-old morbidly obese woman presented to the emergency department with shortness of breath and abdominal distention. On presentation, her blood pressure was 100/60 mm Hg with a heart rate of 110, respiratory rate of 24, and a pulse oximetric saturation (SpO2) of 86% on room air. Troponin T was elevated at 0.3 ng/mL. Computed tomography (CT) of the chest with intravenous contrast showed saddle pulmonary embolism (PE) with dilated right ventricle (RV). CT abdomen/pelvis revealed a very large uterine mass with diffuse lymphadenopathy.
Heparin infusion was started promptly. Echocardiogram demonstrated RV strain. Findings on duplex ultrasound of the lower extremities were consistent with acute deep vein thromboses (DVT) involving the left common femoral vein and the right popliteal vein. Biopsy of a supraclavicular lymph node showed high grade undifferentiated carcinoma most likely of uterine origin.
Clinical questions
What, if any, therapeutic options should be considered beyond standard systemic anticoagulation? Is there a role for:
1. Systemic thrombolysis?
2. Catheter-directed thrombolysis (CDT)?
3. Inferior vena cava (IVC) filter placement?
What is the appropriate management of “submassive” PE?
In the case of massive PE, where the thrombus is located in the central pulmonary vasculature and associated with hypotension due to impaired cardiac output, systemic thrombolysis, embolectomy, and CDT are indicated as potentially life-saving measures. However, the evidence is less clear when the PE is large and has led to RV strain, but without overt hemodynamic instability. This is commonly known as an intermediate risk or “submassive” PE. Submassive PE based on American Heart Association (AHA) guidelines is:1
An acute PE without systemic hypotension (systolic blood pressure less than 90 mm Hg) but with either RV dysfunction or myocardial necrosis. RV dysfunction is defined by the presence of at least one of these following:
• RV dilation (apical 4-chamber RV diameter divided by LV diameter greater than 0.9) or RV systolic dysfunction on echocardiography;
• RV dilation on CT, elevation of BNP (greater than 90 pg/mL), elevation of N-terminal pro-BNP (greater than 500 pg/mL);
• Electrocardiographic changes (new complete or incomplete right bundle branch block, anteroseptal ST elevation or depression, or anteroseptal T-wave inversion).
Myocardial necrosis is defined as elevated troponin I (greater than 0.4 ng/mL) or elevated troponin T (greater than 0.1 ng/mL).
Why is submassive PE of clinical significance?
In 1999, analysis of the International Cooperative Pulmonary Embolism Registry (ICOPER) revealed that RV dysfunction in PE patients was associated with a near doubling of the 3-month mortality risk (hazard ratio 2.0, 1.3-2.9).2 Given this increased risk, one could draw the logical conclusion that we need to treat submassive PE more aggressively than PE without RV strain. But will this necessarily result in a better outcome for the patient given the 3% risk of intracranial hemorrhage associated with thrombolytic therapy?
In the clinical scenario above, the patient did meet the definition of submassive PE. While the patient did not experience systemic hypotension, she did have RV dilation on CT, RV systolic dysfunction on echo as well as an elevated Troponin T level. In addition to starting anticoagulant therapy, what more should be done to increase her probability of a good outcome?
The AHA recommends that systemic thrombolysis and CDT be considered for patients with acute submassive PE if they have clinical evidence of adverse prognosis, including worsening respiratory failure, severe RV dysfunction, or major myocardial necrosis and low risk of bleeding complications (Class IIB; Level of Evidence C).1
The 2016 American College of Chest Physicians (CHEST) guidelines update3 recommends systemically administered thrombolytic therapy over no therapy in selected patients with acute PE who deteriorate after starting anticoagulant therapy but have yet to develop hypotension and who have a low bleeding risk (Grade 2C recommendation).
Systemic thrombolysis
Systemic thrombolysis is administered as an intravenous thrombolytic infusion delivered over a period of time. The Food and Drug Administration–approved thrombolytic drugs currently include tissue plasminogen activator (tPA)/alteplase, streptokinase and urokinase.
Efficacy of low dose thrombolysis was studied in MOPETT 2013,5 a single-center, prospective, randomized, open label study, in which 126 participants found to have submassive PE based on symptoms and CT angiographic or ventilation/perfusion scan data received either 50 mg tPA plus heparin or heparin anticoagulation alone. The composite endpoint of pulmonary hypertension and recurrent PE at 28 months was 16% in the tPA group compared to 63% in the control group (P less than .001). Systemic thrombolysis was associated with lower risk of pulmonary hypertension and recurrent PE, although no mortality benefit was seen in this small study.
In the randomized, double-blind PEITHO trial (n = 1,006) of 20146 comparing tenecteplase plus heparin versus heparin in the submassive PE patients, the primary outcomes of death and hemodynamic decompensation occurred in 2.6% of the tenecteplase group, compared to 5.6% in the placebo group (P = .02). Thrombolytic therapy was associated with 2% rate of hemorrhagic stroke, whereas hemorrhagic stroke in the placebo group was 0.2% (P = .03). In this case, systemic thrombolysis was associated with a 3% lower risk of death and hemodynamic instability, but also a 1.8% increased risk of hemorrhagic stroke.
Catheter-directed thrombolysis (CDT)
CDT was originally developed to treat arterial, dialysis graft and deep vein thromboses, but is now approved by the FDA for the treatment of acute submassive or massive PE.
A wire is passed through the embolus and a multihole infusion catheter is placed, through which a thrombolytic drug is infused over 12-24 hours. The direct delivery of the drug into the thrombus is thought to be as effective as systemic therapy but with a lower risk of bleeding. If more rapid thrombus removal is indicated due to large clot burden and hemodynamic instability, mechanical therapies, such as fragmentation and aspiration, can be used as an adjunct to CDT. However, these mechanical techniques carry the risk of pulmonary artery injury, and therefore should only be used as a last resort. An ultrasound-emitting wire can be added to the multihole infusion catheter to expedite thrombolysis by ultrasonically disrupting the thrombus, a technique known as ultrasound-enhanced thrombolysis (EKOS).7,10
The ULTIMA 2014 trial,8 a small, randomized, open-label study of Ultrasound-Assisted Catheter Directed Thrombolysis (USAT, the term can be used interchangeably with EKOS) versus heparin anticoagulation alone in 59 patients, was designed to study if the former strategy was better at improving the primary outcome measure of RV/LV ratio in submassive PE patients. The mean reduction in RV/LV ratio was 0.30 +/– 0.20 in the USAT group compared to 0.03 +/– 0.16 in the heparin group (P less than .001). However, no significant difference in mortality or bleeding was observed in the groups at 90-day follow up.
The PERFECT 2015 Trial,9 a multicenter registry-based study, prospectively enrolled 101 patients who received CDT as first-line therapy for massive and submassive PE. Among patients with submassive PE, 97.3% were found to have “clinical success” with this treatment, defined as stabilization of hemodynamics, improvement in pulmonary hypertension and right heart strain, and survival to hospital discharge. There was no major bleeding or intracranial hemorrhage. Subgroup analyses in this study comparing USAT against standard CDT did not reveal significant difference in average pulmonary pressure changes, average thrombolytic doses, or average infusion times.
A prospective single-arm multicenter trial, SEATTLE II 2015,10 evaluated the efficacy of EKOS in a sample of 159 patients. Patients with both massive and submassive PE received approximately 24 mg tPA infused via a catheter over 12-24 hours. The primary efficacy outcome was the chest CT-measured RV/LV ratio decrease from the baseline compared to 48 hours post procedure. The pre- and postprocedure ratio was 1.55 versus 1.13 respectively (P less than .001), indicating that EKOS decreased RV dilation. No intracranial hemorrhage was observed and the investigators did not comment on long-term outcomes such as mortality or quality of life. The study was limited by the lack of a comparison group, such as anticoagulation with heparin as monotherapy, or systemic thrombolysis or standard CDT.
Treatment of submassive PE varies between different institutions. There simply are not adequate data comparing low dose systemic thrombolysis, CDT, EKOS, and standard heparin anticoagulation to make firm recommendations. Some investigators feel low-dose systemic thrombolysis is probably as good as the expensive catheter-based thrombolytic therapies.11,12 Low-dose thrombolytic therapy can be followed by use of oral direct factor Xa inhibitors for maintenance of antithrombotic activity.13
Bottom line
In our institution, the interventional radiology team screens patients who meet criteria for submassive PE on a case-by-case basis. We use pulmonary angiographic data (nature and extent of the thrombus), clinical stability, and analysis of other comorbid conditions to decide the best treatment modality for an individual patient. Our team prefers EKOS for submassive PE patients as well as for massive PE patients and as a rescue procedure for patients who have failed systemic thrombolysis.
Until more data are available to support firm guidelines, we feel establishing multidisciplinary teams composed of interventional radiologists, intensivists, cardiologists, and vascular surgeons is prudent to make individualized decisions and to achieve the best outcomes for our patients.14
IVC filter
Since the patient in this case already has a submassive PE, can she tolerate additional clot burden should her remaining DVT embolize again? Is there a role for IVC filter?
The implantation of IVC filters has increased significantly in the past 30 years, without quality evidence justifying their use.15
The 2016 Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report states clearly: In patients with acute DVT of the leg or PE who are treated with anticoagulants, the use of an IVC filter is not recommended (Grade 1B).3 This recommendation is based on findings of the Prevention du Risque d’Embolie Pulmonaire par Interruption Cave (PREPIC) randomized trial,16 and the recently published PREPIC 2 randomized trial,17 both showing that in anticoagulated patients with PE and DVT, concurrent placement of an IVC filter for 3 months did not reduce recurrent PE, including fatal PE.
CHEST guidelines state that an IVC filter should not be routinely placed as an adjunct in patients with PE and DVT. However, what about in the subgroup of patients with submassive or massive PE in whom another PE would be catastrophic? Clinical data are lacking in this area.
Deshpande et al. reported on a series of six patients with massive PE and cardiopulmonary instability; patients all received an IVC filter with anticoagulation. The short-term outcome was excellent, but long-term follow-up was not done.18 Kucher and colleagues reported that from the ICOPER in 2006, out of the 108 massive PE patients with systolic arterial pressure under 90 mm Hg, 11 patients received adjunctive IVC filter placement. None of these 11 patients developed recurrent PE in 90 days and 10 of them survived at least 90 days; IVC filter placement was associated with a reduction in 90-day mortality. In this study, the placement of an IVC filter was entirely decided by the physicians at different sites.19 In a 2012 study examining case fatality rates in 3,770 patients with acute PE who received pulmonary embolectomy, the data showed that in both unstable and stable patients, case fatality rates were lower in those who received an IVC filter.20
Although the above data are favorable for adjunctive IVC filter placement in massive PE patients, at least in short-term outcomes, the small size and lack of randomization preclude establishment of evidence-based guidelines. The 2016 CHEST guidelines point out that as it is uncertain if there is benefit to place an IVC filter adjunctively in anticoagulated patients with severe PE, in this specific subgroup of patients, the recommendation against insertion of an IVC filter in patients with acute PE who are anticoagulated may not apply.3
Bottom line
There is no evidence-based guideline as to whether IVC filters should be placed adjunctively in patients with submassive or massive PE; however, based on expert consensus, it may be appropriate to place an IVC filter as an adjunct to anticoagulation in patients with severe PE. The decision should be individualized based on each patient’s characteristics, preferences, and institutional expertise.
In our case, in hope of preventing further embolic burden, the patient received an IVC filter the day after presentation. Despite the initiation of anticoagulation with heparin, she remained tachycardic and tachypneic, prompting referral for CDT. The interventional radiology team did not feel that she was a good candidate, given her persistent vaginal bleeding and widely metastatic uterine carcinoma. She was switched to therapeutic enoxaparin after no further invasive intervention was deemed appropriate. Her respiratory status did not improve and bilevel positive airway pressure was initiated. Taking into consideration the terminal nature of her cancer, she ultimately elected to pursue comfort care and died shortly afterward.
Acknowledgements
The authors would like to thank Benjamin A. Hohmuth, MD, A. Joseph Layon, MD, and Luis L. Nadal, MD, for their review of the article and invaluable feedback.
Dr. Wenqian Wang, Dr. Vedamurthy, and Dr. Wang are based in the department of hospital medicine at The Medicine Institute, Geisinger Health System, Danville, Penn. Contact Dr. Wenqian Wang at [email protected].
Key Points
• Use pulmonary angiographic data, clinical stability, and analysis of other comorbid conditions to decide the best treatment modality.
• Our team prefers ultrasound-enhanced thrombolysis (EKOS) for submassive PE patients, massive PE patients, and as a rescue procedure for patients who fail systemic thrombolysis.
• Establishing multidisciplinary teams composed of interventional radiologists, intensivists, cardiologists, and vascular surgeons is prudent to make individualized decisions.
• It may be appropriate to place an IVC filter as an adjunct to anticoagulation in patients with severe PE.
References
1. Jaff MR, McMurtry MS, Archer SL, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123:1788-1830.
2. Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet. 1999;353:1386-9.
3. Kearon C, Akl EA, Ornelas J, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149:315-52.
4. Konstantinides S, Geibel A, Heusel G, Heinrich F, Kasper W. Management Strategies and Prognosis of Pulmonary Embolism-3 Trial Investigators. Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. N Engl J Med. 2002;347:1143-50.
5. Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M, “MOPETT” Investigators. Moderate pulmonary embolism treated with thrombolysis (from the “MOPETT” Trial). Am J Cardiol. 2013;111:273-7.
6. Meyer G, Vicaut E, Danays T, et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370:1402-11.
7. Kuo WT. Endovascular therapy for acute pulmonary embolism. J Vasc Interv Radiol 2012;23:167-79. e164
8. Kucher N, Boekstegers P, Muller OJ, et al. Randomized, controlled trial of ultrasound-assisted catheter-directed thrombolysis for acute intermediate-risk pulmonary embolism. Circulation. 2014;129:479-86.
9. Kuo WT, Banerjee A, Kim PS, et al. Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT): Initial Results From a Prospective Multicenter Registry. Chest. 2015;148:667-73.
10. Piazza G, Hohlfelder B, Jaff MR, et al. A Prospective, Single-Arm, Multicenter Trial of Ultrasound-Facilitated, Catheter-Directed, Low-Dose Fibrinolysis for Acute Massive and Submassive Pulmonary Embolism: The SEATTLE II Study. JACC Cardiovasc Interv. 2015;8:1382-92.
11. Sharifi M. Systemic Full Dose, Half Dose, and Catheter Directed Thrombolysis for Pulmonary Embolism. When to Use and How to Choose? Curr Treat Options Cardiovasc Med. 2016;18:31.
12. Wang C, Zhai Z, Yang Y, et al. Efficacy and safety of low dose recombinant tissue-type plasminogen activator for the treatment of acute pulmonary thromboembolism: a randomized, multicenter, controlled trial. Chest. 2010;137:254-62.
13. Sharifi M, Vajo Z, Freeman W, Bay C, Sharifi M, Schwartz F. Transforming and simplifying the treatment of pulmonary embolism: “safe dose” thrombolysis plus new oral anticoagulants. Lung. 2015;193:369-74.
14. Kabrhel C, Rosovsky R, Channick R, et al. A Multidisciplinary Pulmonary Embolism Response Team: Initial 30-Month Experience With a Novel Approach to Delivery of Care to Patients With Submassive and Massive Pulmonary Embolism. Chest. 2016;150:384-93.
15. Lessne ML, Sing RF. Counterpoint: Do the Benefits Outweigh the Risks for Most Patients Under Consideration for inferior vena cava filters? No. Chest. 2016; 150(6):1182-4.
16. The PREPIC Study Group. Eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC (Prevention du Risque d’Embolie Pulmonaire par Interruption Cave) randomized study. Circulation. 2005;112(3):416-22.
17. Mismetti P, Laporte S, Pellerin O, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs. anticoagulation alone on risk of recurrent pulmonary embolism: a randomized clinical trial. JAMA. 2015. 313(16):1627-35.
18. Deshpande KS, Hatem C, Karwa M, et al. The use of inferior vena cava filter as a treatment modality for massive pulmonary embolism. A case series and review of pathophysiology. Respir Med. 2002.96(12):984-9.
19. Kucher N, Rossi E, De Rosa M, et al. Massive Pulmonary embolism. Circulation. 2006;113(4):577-82.
20. Stein P, Matta F. Case Fatality Rate with Pulmonary Embolectomy for Acute Pulmonary Embolism. Am J Med. 2012;125:471-7.
The case
A 49-year-old morbidly obese woman presented to the emergency department with shortness of breath and abdominal distention. On presentation, her blood pressure was 100/60 mm Hg with a heart rate of 110, respiratory rate of 24, and a pulse oximetric saturation (SpO2) of 86% on room air. Troponin T was elevated at 0.3 ng/mL. Computed tomography (CT) of the chest with intravenous contrast showed saddle pulmonary embolism (PE) with dilated right ventricle (RV). CT abdomen/pelvis revealed a very large uterine mass with diffuse lymphadenopathy.
Heparin infusion was started promptly. Echocardiogram demonstrated RV strain. Findings on duplex ultrasound of the lower extremities were consistent with acute deep vein thromboses (DVT) involving the left common femoral vein and the right popliteal vein. Biopsy of a supraclavicular lymph node showed high grade undifferentiated carcinoma most likely of uterine origin.
Clinical questions
What, if any, therapeutic options should be considered beyond standard systemic anticoagulation? Is there a role for:
1. Systemic thrombolysis?
2. Catheter-directed thrombolysis (CDT)?
3. Inferior vena cava (IVC) filter placement?
What is the appropriate management of “submassive” PE?
In the case of massive PE, where the thrombus is located in the central pulmonary vasculature and associated with hypotension due to impaired cardiac output, systemic thrombolysis, embolectomy, and CDT are indicated as potentially life-saving measures. However, the evidence is less clear when the PE is large and has led to RV strain, but without overt hemodynamic instability. This is commonly known as an intermediate risk or “submassive” PE. Submassive PE based on American Heart Association (AHA) guidelines is:1
An acute PE without systemic hypotension (systolic blood pressure less than 90 mm Hg) but with either RV dysfunction or myocardial necrosis. RV dysfunction is defined by the presence of at least one of these following:
• RV dilation (apical 4-chamber RV diameter divided by LV diameter greater than 0.9) or RV systolic dysfunction on echocardiography;
• RV dilation on CT, elevation of BNP (greater than 90 pg/mL), elevation of N-terminal pro-BNP (greater than 500 pg/mL);
• Electrocardiographic changes (new complete or incomplete right bundle branch block, anteroseptal ST elevation or depression, or anteroseptal T-wave inversion).
Myocardial necrosis is defined as elevated troponin I (greater than 0.4 ng/mL) or elevated troponin T (greater than 0.1 ng/mL).
Why is submassive PE of clinical significance?
In 1999, analysis of the International Cooperative Pulmonary Embolism Registry (ICOPER) revealed that RV dysfunction in PE patients was associated with a near doubling of the 3-month mortality risk (hazard ratio 2.0, 1.3-2.9).2 Given this increased risk, one could draw the logical conclusion that we need to treat submassive PE more aggressively than PE without RV strain. But will this necessarily result in a better outcome for the patient given the 3% risk of intracranial hemorrhage associated with thrombolytic therapy?
In the clinical scenario above, the patient did meet the definition of submassive PE. While the patient did not experience systemic hypotension, she did have RV dilation on CT, RV systolic dysfunction on echo as well as an elevated Troponin T level. In addition to starting anticoagulant therapy, what more should be done to increase her probability of a good outcome?
The AHA recommends that systemic thrombolysis and CDT be considered for patients with acute submassive PE if they have clinical evidence of adverse prognosis, including worsening respiratory failure, severe RV dysfunction, or major myocardial necrosis and low risk of bleeding complications (Class IIB; Level of Evidence C).1
The 2016 American College of Chest Physicians (CHEST) guidelines update3 recommends systemically administered thrombolytic therapy over no therapy in selected patients with acute PE who deteriorate after starting anticoagulant therapy but have yet to develop hypotension and who have a low bleeding risk (Grade 2C recommendation).
Systemic thrombolysis
Systemic thrombolysis is administered as an intravenous thrombolytic infusion delivered over a period of time. The Food and Drug Administration–approved thrombolytic drugs currently include tissue plasminogen activator (tPA)/alteplase, streptokinase and urokinase.
Efficacy of low dose thrombolysis was studied in MOPETT 2013,5 a single-center, prospective, randomized, open label study, in which 126 participants found to have submassive PE based on symptoms and CT angiographic or ventilation/perfusion scan data received either 50 mg tPA plus heparin or heparin anticoagulation alone. The composite endpoint of pulmonary hypertension and recurrent PE at 28 months was 16% in the tPA group compared to 63% in the control group (P less than .001). Systemic thrombolysis was associated with lower risk of pulmonary hypertension and recurrent PE, although no mortality benefit was seen in this small study.
In the randomized, double-blind PEITHO trial (n = 1,006) of 20146 comparing tenecteplase plus heparin versus heparin in the submassive PE patients, the primary outcomes of death and hemodynamic decompensation occurred in 2.6% of the tenecteplase group, compared to 5.6% in the placebo group (P = .02). Thrombolytic therapy was associated with 2% rate of hemorrhagic stroke, whereas hemorrhagic stroke in the placebo group was 0.2% (P = .03). In this case, systemic thrombolysis was associated with a 3% lower risk of death and hemodynamic instability, but also a 1.8% increased risk of hemorrhagic stroke.
Catheter-directed thrombolysis (CDT)
CDT was originally developed to treat arterial, dialysis graft and deep vein thromboses, but is now approved by the FDA for the treatment of acute submassive or massive PE.
A wire is passed through the embolus and a multihole infusion catheter is placed, through which a thrombolytic drug is infused over 12-24 hours. The direct delivery of the drug into the thrombus is thought to be as effective as systemic therapy but with a lower risk of bleeding. If more rapid thrombus removal is indicated due to large clot burden and hemodynamic instability, mechanical therapies, such as fragmentation and aspiration, can be used as an adjunct to CDT. However, these mechanical techniques carry the risk of pulmonary artery injury, and therefore should only be used as a last resort. An ultrasound-emitting wire can be added to the multihole infusion catheter to expedite thrombolysis by ultrasonically disrupting the thrombus, a technique known as ultrasound-enhanced thrombolysis (EKOS).7,10
The ULTIMA 2014 trial,8 a small, randomized, open-label study of Ultrasound-Assisted Catheter Directed Thrombolysis (USAT, the term can be used interchangeably with EKOS) versus heparin anticoagulation alone in 59 patients, was designed to study if the former strategy was better at improving the primary outcome measure of RV/LV ratio in submassive PE patients. The mean reduction in RV/LV ratio was 0.30 +/– 0.20 in the USAT group compared to 0.03 +/– 0.16 in the heparin group (P less than .001). However, no significant difference in mortality or bleeding was observed in the groups at 90-day follow up.
The PERFECT 2015 Trial,9 a multicenter registry-based study, prospectively enrolled 101 patients who received CDT as first-line therapy for massive and submassive PE. Among patients with submassive PE, 97.3% were found to have “clinical success” with this treatment, defined as stabilization of hemodynamics, improvement in pulmonary hypertension and right heart strain, and survival to hospital discharge. There was no major bleeding or intracranial hemorrhage. Subgroup analyses in this study comparing USAT against standard CDT did not reveal significant difference in average pulmonary pressure changes, average thrombolytic doses, or average infusion times.
A prospective single-arm multicenter trial, SEATTLE II 2015,10 evaluated the efficacy of EKOS in a sample of 159 patients. Patients with both massive and submassive PE received approximately 24 mg tPA infused via a catheter over 12-24 hours. The primary efficacy outcome was the chest CT-measured RV/LV ratio decrease from the baseline compared to 48 hours post procedure. The pre- and postprocedure ratio was 1.55 versus 1.13 respectively (P less than .001), indicating that EKOS decreased RV dilation. No intracranial hemorrhage was observed and the investigators did not comment on long-term outcomes such as mortality or quality of life. The study was limited by the lack of a comparison group, such as anticoagulation with heparin as monotherapy, or systemic thrombolysis or standard CDT.
Treatment of submassive PE varies between different institutions. There simply are not adequate data comparing low dose systemic thrombolysis, CDT, EKOS, and standard heparin anticoagulation to make firm recommendations. Some investigators feel low-dose systemic thrombolysis is probably as good as the expensive catheter-based thrombolytic therapies.11,12 Low-dose thrombolytic therapy can be followed by use of oral direct factor Xa inhibitors for maintenance of antithrombotic activity.13
Bottom line
In our institution, the interventional radiology team screens patients who meet criteria for submassive PE on a case-by-case basis. We use pulmonary angiographic data (nature and extent of the thrombus), clinical stability, and analysis of other comorbid conditions to decide the best treatment modality for an individual patient. Our team prefers EKOS for submassive PE patients as well as for massive PE patients and as a rescue procedure for patients who have failed systemic thrombolysis.
Until more data are available to support firm guidelines, we feel establishing multidisciplinary teams composed of interventional radiologists, intensivists, cardiologists, and vascular surgeons is prudent to make individualized decisions and to achieve the best outcomes for our patients.14
IVC filter
Since the patient in this case already has a submassive PE, can she tolerate additional clot burden should her remaining DVT embolize again? Is there a role for IVC filter?
The implantation of IVC filters has increased significantly in the past 30 years, without quality evidence justifying their use.15
The 2016 Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report states clearly: In patients with acute DVT of the leg or PE who are treated with anticoagulants, the use of an IVC filter is not recommended (Grade 1B).3 This recommendation is based on findings of the Prevention du Risque d’Embolie Pulmonaire par Interruption Cave (PREPIC) randomized trial,16 and the recently published PREPIC 2 randomized trial,17 both showing that in anticoagulated patients with PE and DVT, concurrent placement of an IVC filter for 3 months did not reduce recurrent PE, including fatal PE.
CHEST guidelines state that an IVC filter should not be routinely placed as an adjunct in patients with PE and DVT. However, what about in the subgroup of patients with submassive or massive PE in whom another PE would be catastrophic? Clinical data are lacking in this area.
Deshpande et al. reported on a series of six patients with massive PE and cardiopulmonary instability; patients all received an IVC filter with anticoagulation. The short-term outcome was excellent, but long-term follow-up was not done.18 Kucher and colleagues reported that from the ICOPER in 2006, out of the 108 massive PE patients with systolic arterial pressure under 90 mm Hg, 11 patients received adjunctive IVC filter placement. None of these 11 patients developed recurrent PE in 90 days and 10 of them survived at least 90 days; IVC filter placement was associated with a reduction in 90-day mortality. In this study, the placement of an IVC filter was entirely decided by the physicians at different sites.19 In a 2012 study examining case fatality rates in 3,770 patients with acute PE who received pulmonary embolectomy, the data showed that in both unstable and stable patients, case fatality rates were lower in those who received an IVC filter.20
Although the above data are favorable for adjunctive IVC filter placement in massive PE patients, at least in short-term outcomes, the small size and lack of randomization preclude establishment of evidence-based guidelines. The 2016 CHEST guidelines point out that as it is uncertain if there is benefit to place an IVC filter adjunctively in anticoagulated patients with severe PE, in this specific subgroup of patients, the recommendation against insertion of an IVC filter in patients with acute PE who are anticoagulated may not apply.3
Bottom line
There is no evidence-based guideline as to whether IVC filters should be placed adjunctively in patients with submassive or massive PE; however, based on expert consensus, it may be appropriate to place an IVC filter as an adjunct to anticoagulation in patients with severe PE. The decision should be individualized based on each patient’s characteristics, preferences, and institutional expertise.
In our case, in hope of preventing further embolic burden, the patient received an IVC filter the day after presentation. Despite the initiation of anticoagulation with heparin, she remained tachycardic and tachypneic, prompting referral for CDT. The interventional radiology team did not feel that she was a good candidate, given her persistent vaginal bleeding and widely metastatic uterine carcinoma. She was switched to therapeutic enoxaparin after no further invasive intervention was deemed appropriate. Her respiratory status did not improve and bilevel positive airway pressure was initiated. Taking into consideration the terminal nature of her cancer, she ultimately elected to pursue comfort care and died shortly afterward.
Acknowledgements
The authors would like to thank Benjamin A. Hohmuth, MD, A. Joseph Layon, MD, and Luis L. Nadal, MD, for their review of the article and invaluable feedback.
Dr. Wenqian Wang, Dr. Vedamurthy, and Dr. Wang are based in the department of hospital medicine at The Medicine Institute, Geisinger Health System, Danville, Penn. Contact Dr. Wenqian Wang at [email protected].
Key Points
• Use pulmonary angiographic data, clinical stability, and analysis of other comorbid conditions to decide the best treatment modality.
• Our team prefers ultrasound-enhanced thrombolysis (EKOS) for submassive PE patients, massive PE patients, and as a rescue procedure for patients who fail systemic thrombolysis.
• Establishing multidisciplinary teams composed of interventional radiologists, intensivists, cardiologists, and vascular surgeons is prudent to make individualized decisions.
• It may be appropriate to place an IVC filter as an adjunct to anticoagulation in patients with severe PE.
References
1. Jaff MR, McMurtry MS, Archer SL, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123:1788-1830.
2. Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet. 1999;353:1386-9.
3. Kearon C, Akl EA, Ornelas J, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149:315-52.
4. Konstantinides S, Geibel A, Heusel G, Heinrich F, Kasper W. Management Strategies and Prognosis of Pulmonary Embolism-3 Trial Investigators. Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. N Engl J Med. 2002;347:1143-50.
5. Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M, “MOPETT” Investigators. Moderate pulmonary embolism treated with thrombolysis (from the “MOPETT” Trial). Am J Cardiol. 2013;111:273-7.
6. Meyer G, Vicaut E, Danays T, et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370:1402-11.
7. Kuo WT. Endovascular therapy for acute pulmonary embolism. J Vasc Interv Radiol 2012;23:167-79. e164
8. Kucher N, Boekstegers P, Muller OJ, et al. Randomized, controlled trial of ultrasound-assisted catheter-directed thrombolysis for acute intermediate-risk pulmonary embolism. Circulation. 2014;129:479-86.
9. Kuo WT, Banerjee A, Kim PS, et al. Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT): Initial Results From a Prospective Multicenter Registry. Chest. 2015;148:667-73.
10. Piazza G, Hohlfelder B, Jaff MR, et al. A Prospective, Single-Arm, Multicenter Trial of Ultrasound-Facilitated, Catheter-Directed, Low-Dose Fibrinolysis for Acute Massive and Submassive Pulmonary Embolism: The SEATTLE II Study. JACC Cardiovasc Interv. 2015;8:1382-92.
11. Sharifi M. Systemic Full Dose, Half Dose, and Catheter Directed Thrombolysis for Pulmonary Embolism. When to Use and How to Choose? Curr Treat Options Cardiovasc Med. 2016;18:31.
12. Wang C, Zhai Z, Yang Y, et al. Efficacy and safety of low dose recombinant tissue-type plasminogen activator for the treatment of acute pulmonary thromboembolism: a randomized, multicenter, controlled trial. Chest. 2010;137:254-62.
13. Sharifi M, Vajo Z, Freeman W, Bay C, Sharifi M, Schwartz F. Transforming and simplifying the treatment of pulmonary embolism: “safe dose” thrombolysis plus new oral anticoagulants. Lung. 2015;193:369-74.
14. Kabrhel C, Rosovsky R, Channick R, et al. A Multidisciplinary Pulmonary Embolism Response Team: Initial 30-Month Experience With a Novel Approach to Delivery of Care to Patients With Submassive and Massive Pulmonary Embolism. Chest. 2016;150:384-93.
15. Lessne ML, Sing RF. Counterpoint: Do the Benefits Outweigh the Risks for Most Patients Under Consideration for inferior vena cava filters? No. Chest. 2016; 150(6):1182-4.
16. The PREPIC Study Group. Eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC (Prevention du Risque d’Embolie Pulmonaire par Interruption Cave) randomized study. Circulation. 2005;112(3):416-22.
17. Mismetti P, Laporte S, Pellerin O, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs. anticoagulation alone on risk of recurrent pulmonary embolism: a randomized clinical trial. JAMA. 2015. 313(16):1627-35.
18. Deshpande KS, Hatem C, Karwa M, et al. The use of inferior vena cava filter as a treatment modality for massive pulmonary embolism. A case series and review of pathophysiology. Respir Med. 2002.96(12):984-9.
19. Kucher N, Rossi E, De Rosa M, et al. Massive Pulmonary embolism. Circulation. 2006;113(4):577-82.
20. Stein P, Matta F. Case Fatality Rate with Pulmonary Embolectomy for Acute Pulmonary Embolism. Am J Med. 2012;125:471-7.
Zika linked to a spectrum of neuroinflammatory diseases
New evidence in support of a link between Zika virus infection and an increase in the incidence of neurological syndromes in adults has come from a prospective, observational study that demonstrates the presence of the infection in both serum and cerebrospinal fluid of patients with new-onset acute neuroinflammatory disease.
From Dec. 5, 2015, to May 10, 2016, 40 patients who were hospitalized for Guillain-Barré syndrome (GBS), meningoencephalitis, or transverse myelitis were evaluated for Zika virus. Of those, 35 (88%) tested positive for Zika, indicating that there is a correlation between the Zika outbreak and recorded increases in neurological syndromes in adults, according to Ivan Rocha Ferreira da Silva, MD, PhD, of the neurology department of Universidade Federal Fluminense in Niteroi, Brazil, and his coauthors (JAMA Neurol. 2017 Aug 14. doi: 10.1001/jamaneurol.2017.1703). Dr. da Silva is now with the department of neurology at Rush University Medical Center, Chicago.
Overall, it appears that Zika virus is associated with the trend for the rapid increase in hospital admissions for certain neurological syndromes, Dr. da Silva and his coauthors said. In addition, “we believe that our method of matching CSF and blood serologic findings offers a substantial aid to minimize [costs and] cross-reactivity in countries with a high prevalence of other concurrent flavivirosis.”
The study cohort was enrolled at a tertiary care, academic hospital in Rio de Janeiro. The median age was 44, and 15 were women. The study was limited by selection of neurological syndromes that have previously been associated with other flaviviruses, the short study period, and the use of patients from only one hospital.
Dr. da Silva reported no financial disclosures. One author reported receiving grants from Conselho Nacional de Desenvolvimento e Pesquisa and Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro. Other study authors reported no financial disclosures.
The 2015 Zika outbreaks in the Americas were notable for the recognition that Zika virus could be associated with neurological conditions. It was found that the overall risk of congenital neurologic abnormalities in fetuses and liveborn children of mothers enrolled in the Centers for Disease Control and Prevention’s Zika Pregnancy Registry with definite laboratory evidence of Zika virus infection during pregnancy was approximately 17 times higher than the expected baseline rate in uninfected mothers. It wasn’t until later, however, that GBS became the first non–pregnancy-related neurological syndrome to be associate with Zika in adults.
It is critically important to understand both the spectrum and frequency of Zika virus–induced neurologic diseases. The article by Dr. da Silva and colleagues in this issue of JAMA Neurology represents an initial approach to this problem. During the reporting period, they found that 93% of the patients with GBS (27 of 29), 71% of the patients with encephalitis (5 of 7), 67% of the patients with transverse myelitis (2 of 3), and the single patient with chronic inflammatory demyelinating polyneuropathy showed evidence of recent Zika virus infection, indicating a link between neurological syndromes and Zika.
However, it should be noted that, because of factors including referral bias, a study such as this cannot determine exact frequencies of Zika virus infection among patients with the syndromes examined, but it may serve to help confirm that Zika can be associated with such syndromes.
Kenneth L. Tyler, MD, is the Louise Baum Endowed Professor and Chair of the department of neurology at the University of Colorado at Denver, Aurora. Karen L. Roos, MD, is the John and Nancy Professor of Neurology at the University of Indiana, Indianapolis. They published these comments in an editorial accompanying the da Silva et al. article in JAMA Neurology (2017 Aug 14. doi: 10.1001/jamaneurol.2017.1471). Neither author reported any financial disclosures.
The 2015 Zika outbreaks in the Americas were notable for the recognition that Zika virus could be associated with neurological conditions. It was found that the overall risk of congenital neurologic abnormalities in fetuses and liveborn children of mothers enrolled in the Centers for Disease Control and Prevention’s Zika Pregnancy Registry with definite laboratory evidence of Zika virus infection during pregnancy was approximately 17 times higher than the expected baseline rate in uninfected mothers. It wasn’t until later, however, that GBS became the first non–pregnancy-related neurological syndrome to be associate with Zika in adults.
It is critically important to understand both the spectrum and frequency of Zika virus–induced neurologic diseases. The article by Dr. da Silva and colleagues in this issue of JAMA Neurology represents an initial approach to this problem. During the reporting period, they found that 93% of the patients with GBS (27 of 29), 71% of the patients with encephalitis (5 of 7), 67% of the patients with transverse myelitis (2 of 3), and the single patient with chronic inflammatory demyelinating polyneuropathy showed evidence of recent Zika virus infection, indicating a link between neurological syndromes and Zika.
However, it should be noted that, because of factors including referral bias, a study such as this cannot determine exact frequencies of Zika virus infection among patients with the syndromes examined, but it may serve to help confirm that Zika can be associated with such syndromes.
Kenneth L. Tyler, MD, is the Louise Baum Endowed Professor and Chair of the department of neurology at the University of Colorado at Denver, Aurora. Karen L. Roos, MD, is the John and Nancy Professor of Neurology at the University of Indiana, Indianapolis. They published these comments in an editorial accompanying the da Silva et al. article in JAMA Neurology (2017 Aug 14. doi: 10.1001/jamaneurol.2017.1471). Neither author reported any financial disclosures.
The 2015 Zika outbreaks in the Americas were notable for the recognition that Zika virus could be associated with neurological conditions. It was found that the overall risk of congenital neurologic abnormalities in fetuses and liveborn children of mothers enrolled in the Centers for Disease Control and Prevention’s Zika Pregnancy Registry with definite laboratory evidence of Zika virus infection during pregnancy was approximately 17 times higher than the expected baseline rate in uninfected mothers. It wasn’t until later, however, that GBS became the first non–pregnancy-related neurological syndrome to be associate with Zika in adults.
It is critically important to understand both the spectrum and frequency of Zika virus–induced neurologic diseases. The article by Dr. da Silva and colleagues in this issue of JAMA Neurology represents an initial approach to this problem. During the reporting period, they found that 93% of the patients with GBS (27 of 29), 71% of the patients with encephalitis (5 of 7), 67% of the patients with transverse myelitis (2 of 3), and the single patient with chronic inflammatory demyelinating polyneuropathy showed evidence of recent Zika virus infection, indicating a link between neurological syndromes and Zika.
However, it should be noted that, because of factors including referral bias, a study such as this cannot determine exact frequencies of Zika virus infection among patients with the syndromes examined, but it may serve to help confirm that Zika can be associated with such syndromes.
Kenneth L. Tyler, MD, is the Louise Baum Endowed Professor and Chair of the department of neurology at the University of Colorado at Denver, Aurora. Karen L. Roos, MD, is the John and Nancy Professor of Neurology at the University of Indiana, Indianapolis. They published these comments in an editorial accompanying the da Silva et al. article in JAMA Neurology (2017 Aug 14. doi: 10.1001/jamaneurol.2017.1471). Neither author reported any financial disclosures.
New evidence in support of a link between Zika virus infection and an increase in the incidence of neurological syndromes in adults has come from a prospective, observational study that demonstrates the presence of the infection in both serum and cerebrospinal fluid of patients with new-onset acute neuroinflammatory disease.
From Dec. 5, 2015, to May 10, 2016, 40 patients who were hospitalized for Guillain-Barré syndrome (GBS), meningoencephalitis, or transverse myelitis were evaluated for Zika virus. Of those, 35 (88%) tested positive for Zika, indicating that there is a correlation between the Zika outbreak and recorded increases in neurological syndromes in adults, according to Ivan Rocha Ferreira da Silva, MD, PhD, of the neurology department of Universidade Federal Fluminense in Niteroi, Brazil, and his coauthors (JAMA Neurol. 2017 Aug 14. doi: 10.1001/jamaneurol.2017.1703). Dr. da Silva is now with the department of neurology at Rush University Medical Center, Chicago.
Overall, it appears that Zika virus is associated with the trend for the rapid increase in hospital admissions for certain neurological syndromes, Dr. da Silva and his coauthors said. In addition, “we believe that our method of matching CSF and blood serologic findings offers a substantial aid to minimize [costs and] cross-reactivity in countries with a high prevalence of other concurrent flavivirosis.”
The study cohort was enrolled at a tertiary care, academic hospital in Rio de Janeiro. The median age was 44, and 15 were women. The study was limited by selection of neurological syndromes that have previously been associated with other flaviviruses, the short study period, and the use of patients from only one hospital.
Dr. da Silva reported no financial disclosures. One author reported receiving grants from Conselho Nacional de Desenvolvimento e Pesquisa and Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro. Other study authors reported no financial disclosures.
New evidence in support of a link between Zika virus infection and an increase in the incidence of neurological syndromes in adults has come from a prospective, observational study that demonstrates the presence of the infection in both serum and cerebrospinal fluid of patients with new-onset acute neuroinflammatory disease.
From Dec. 5, 2015, to May 10, 2016, 40 patients who were hospitalized for Guillain-Barré syndrome (GBS), meningoencephalitis, or transverse myelitis were evaluated for Zika virus. Of those, 35 (88%) tested positive for Zika, indicating that there is a correlation between the Zika outbreak and recorded increases in neurological syndromes in adults, according to Ivan Rocha Ferreira da Silva, MD, PhD, of the neurology department of Universidade Federal Fluminense in Niteroi, Brazil, and his coauthors (JAMA Neurol. 2017 Aug 14. doi: 10.1001/jamaneurol.2017.1703). Dr. da Silva is now with the department of neurology at Rush University Medical Center, Chicago.
Overall, it appears that Zika virus is associated with the trend for the rapid increase in hospital admissions for certain neurological syndromes, Dr. da Silva and his coauthors said. In addition, “we believe that our method of matching CSF and blood serologic findings offers a substantial aid to minimize [costs and] cross-reactivity in countries with a high prevalence of other concurrent flavivirosis.”
The study cohort was enrolled at a tertiary care, academic hospital in Rio de Janeiro. The median age was 44, and 15 were women. The study was limited by selection of neurological syndromes that have previously been associated with other flaviviruses, the short study period, and the use of patients from only one hospital.
Dr. da Silva reported no financial disclosures. One author reported receiving grants from Conselho Nacional de Desenvolvimento e Pesquisa and Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro. Other study authors reported no financial disclosures.
FROM JAMA NEUROLOGY
Key clinical point: Increases in neurological syndromes in adults are associated with the Zika epidemic.
Major finding: Of 40 patients who were hospitalized for Guillain-Barré syndrome (GBS), meningoencephalitis, or transverse myelitis, 35 tested positive for Zika.
Data source: A prospective, observational cohort study of 40 patients who were admitted to a hospital in Brazil for a number of neurological conditions.
Disclosures: Dr. da Silva reported no financial disclosures. One author reported receiving grants from Conselho Nacional de Desenvolvimento e Pesquisa and Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro. Other study authors reported no financial disclosures.
Miss the MIPS Webinar? View it Online
The SVS Patient Safety Organization and M2S, in conjunction with the SVS, presented a webinar last month on getting started in the Medicare reimbursement program, including the Merit-based Incentive Payment System (MIPS).
For those who couldn't attend, it is posted, along with the presentation slides, on the Vascular Quality Initiative website's home page. View it today to get up to speed on MIPS and MACRA (Medicare Access and CHIP Reauthorization Act of 2015).
The SVS Patient Safety Organization and M2S, in conjunction with the SVS, presented a webinar last month on getting started in the Medicare reimbursement program, including the Merit-based Incentive Payment System (MIPS).
For those who couldn't attend, it is posted, along with the presentation slides, on the Vascular Quality Initiative website's home page. View it today to get up to speed on MIPS and MACRA (Medicare Access and CHIP Reauthorization Act of 2015).
The SVS Patient Safety Organization and M2S, in conjunction with the SVS, presented a webinar last month on getting started in the Medicare reimbursement program, including the Merit-based Incentive Payment System (MIPS).
For those who couldn't attend, it is posted, along with the presentation slides, on the Vascular Quality Initiative website's home page. View it today to get up to speed on MIPS and MACRA (Medicare Access and CHIP Reauthorization Act of 2015).
Birth Control Pills for Acne: Tips From Julie Harper at the Summer AAD
Acne treatment options now extend beyond antibiotics, and hormonal therapy, particularly birth control pills (BCPs), may provide clearance of acne in women who may not respond to other therapies. "Challenge [yourselves] to learn how to safely use BCPs," said Dr. Julie Harper, Clinical Associate Professor of Dermatology at the University of Alabama in Birmingham, in the presentation, "Use of Hormonal Therapy for Acne," at the Summer Meeting of the American Academy of Dermatology. The use of BCPs for acne has a strength-of-recommendation grade of A (consistent, good-quality patient-oriented evidence).
According to Dr. Harper, all combination BCPs should work for acne, except progestin-only BCPs, which will make acne worse. Currently, there are 4 BCPs approved by the US Food and Drug Administration for acne: norgestimate-ethinyl estradiol (Ortho Tri-Cyclen); norethindrone acetate-ethinyl estradiol (Estrostep Fe); drospirenone-ethinyl estradiol (Yaz); and drospirenone-ethinyl estradiol-levomefolate calcium (Beyaz). Birth control pills are known to carry risks for venous thromboembolism (VTE), stroke, hypertension, and myocardial infarction; however, they are generally well tolerated in acne patients. "The risk of venous thromboembolism in women who take BCPs is doubled or tripled compared to women who do not take these pills. This sounds scary until you put it into context," said Dr. Harper. She explains the risks to patients using the following 3-6-9-12 model: A woman's baseline risk of having a VTE if she is not on a BCP is approximately 3 in 10,000 women in one year. When she takes a BCP, her risk doubles to 6 per 10,000 women in one year. If she takes a BCP that contains drospirenone, her risk is 9 per 10,000 women in one year. If she gets pregnant, her risk is 12 per 10,000 women in one year.
Dermatologists may be apprehensive to prescribe BCPs, but Dr. Harper provided several important tips on managing patient expectations and monitoring patients. Dr. Harper emphasized that BCPs should be used patiently for acne. "It frequently takes at least 3 cycles of BCPs to see a meaningful change in acne reduction," she advised. She recommended obtaining a thorough medical history and blood pressure measurement prior to prescribing BCPs. However, a Papanicolaou test and bimanual pelvic examination are no longer deemed mandatory prior to initiating a BCP, according to the World Health Organization and the American Congress of Obstetricians and Gynecologists. "While these exams may help to detect cervical cancer and other pelvic diseases, BCPs help to prevent unwanted pregnancies and the risks that accompany those pregnancies," said Dr. Harper. "Remember that BCPs reduce the risk of ovarian, uterine and colorectal cancer and also lessen ovarian cysts and pelvic inflammatory disease." Dermatologists also should inform patients that rifampin and griseofulvin, both anti-infectives, will interact with BCPs, lessening their effectiveness.
A March 2017 study published in Cutis (2017;99:195-201) of US dermatologists' knowledge, comfort, and prescribing practices (N=116) revealed that most dermatologists (95.4%) believe BCPs effectively treat acne; however, only 54% reported prescribing them. The American Academy of Dermatology's guidelines of care for the management of acne vulgaris published in February 2016 (J Am Acad Dermatol. 2016;74:945-973) stated that "estrogen-containing combined oral contraceptives are effective and recommended in the treatment of inflammatory acne in females."
Overall, Dr. Harper's take-home message was that dermatologists should not be afraid to prescribe BCPs, even in teenaged girls (following the onset of menarche). "Birth control pills can be used in younger patients but it is not my first line of treatment," said Dr. Harper. "It is recommended that BCPs not be prescribed for acne until 2 years after the young woman has achieved menarche. When considering whether or not to use a BCP in the early teenage years, keep in mind that these are not short-term treatments. If a BCP does help acne, it will likely need to be maintained for many years." When discussing this treatment in front of parents/guardians, consider referring to it as hormonal therapy and use the term birth control pills only initially.
Acne treatment options now extend beyond antibiotics, and hormonal therapy, particularly birth control pills (BCPs), may provide clearance of acne in women who may not respond to other therapies. "Challenge [yourselves] to learn how to safely use BCPs," said Dr. Julie Harper, Clinical Associate Professor of Dermatology at the University of Alabama in Birmingham, in the presentation, "Use of Hormonal Therapy for Acne," at the Summer Meeting of the American Academy of Dermatology. The use of BCPs for acne has a strength-of-recommendation grade of A (consistent, good-quality patient-oriented evidence).
According to Dr. Harper, all combination BCPs should work for acne, except progestin-only BCPs, which will make acne worse. Currently, there are 4 BCPs approved by the US Food and Drug Administration for acne: norgestimate-ethinyl estradiol (Ortho Tri-Cyclen); norethindrone acetate-ethinyl estradiol (Estrostep Fe); drospirenone-ethinyl estradiol (Yaz); and drospirenone-ethinyl estradiol-levomefolate calcium (Beyaz). Birth control pills are known to carry risks for venous thromboembolism (VTE), stroke, hypertension, and myocardial infarction; however, they are generally well tolerated in acne patients. "The risk of venous thromboembolism in women who take BCPs is doubled or tripled compared to women who do not take these pills. This sounds scary until you put it into context," said Dr. Harper. She explains the risks to patients using the following 3-6-9-12 model: A woman's baseline risk of having a VTE if she is not on a BCP is approximately 3 in 10,000 women in one year. When she takes a BCP, her risk doubles to 6 per 10,000 women in one year. If she takes a BCP that contains drospirenone, her risk is 9 per 10,000 women in one year. If she gets pregnant, her risk is 12 per 10,000 women in one year.
Dermatologists may be apprehensive to prescribe BCPs, but Dr. Harper provided several important tips on managing patient expectations and monitoring patients. Dr. Harper emphasized that BCPs should be used patiently for acne. "It frequently takes at least 3 cycles of BCPs to see a meaningful change in acne reduction," she advised. She recommended obtaining a thorough medical history and blood pressure measurement prior to prescribing BCPs. However, a Papanicolaou test and bimanual pelvic examination are no longer deemed mandatory prior to initiating a BCP, according to the World Health Organization and the American Congress of Obstetricians and Gynecologists. "While these exams may help to detect cervical cancer and other pelvic diseases, BCPs help to prevent unwanted pregnancies and the risks that accompany those pregnancies," said Dr. Harper. "Remember that BCPs reduce the risk of ovarian, uterine and colorectal cancer and also lessen ovarian cysts and pelvic inflammatory disease." Dermatologists also should inform patients that rifampin and griseofulvin, both anti-infectives, will interact with BCPs, lessening their effectiveness.
A March 2017 study published in Cutis (2017;99:195-201) of US dermatologists' knowledge, comfort, and prescribing practices (N=116) revealed that most dermatologists (95.4%) believe BCPs effectively treat acne; however, only 54% reported prescribing them. The American Academy of Dermatology's guidelines of care for the management of acne vulgaris published in February 2016 (J Am Acad Dermatol. 2016;74:945-973) stated that "estrogen-containing combined oral contraceptives are effective and recommended in the treatment of inflammatory acne in females."
Overall, Dr. Harper's take-home message was that dermatologists should not be afraid to prescribe BCPs, even in teenaged girls (following the onset of menarche). "Birth control pills can be used in younger patients but it is not my first line of treatment," said Dr. Harper. "It is recommended that BCPs not be prescribed for acne until 2 years after the young woman has achieved menarche. When considering whether or not to use a BCP in the early teenage years, keep in mind that these are not short-term treatments. If a BCP does help acne, it will likely need to be maintained for many years." When discussing this treatment in front of parents/guardians, consider referring to it as hormonal therapy and use the term birth control pills only initially.
Acne treatment options now extend beyond antibiotics, and hormonal therapy, particularly birth control pills (BCPs), may provide clearance of acne in women who may not respond to other therapies. "Challenge [yourselves] to learn how to safely use BCPs," said Dr. Julie Harper, Clinical Associate Professor of Dermatology at the University of Alabama in Birmingham, in the presentation, "Use of Hormonal Therapy for Acne," at the Summer Meeting of the American Academy of Dermatology. The use of BCPs for acne has a strength-of-recommendation grade of A (consistent, good-quality patient-oriented evidence).
According to Dr. Harper, all combination BCPs should work for acne, except progestin-only BCPs, which will make acne worse. Currently, there are 4 BCPs approved by the US Food and Drug Administration for acne: norgestimate-ethinyl estradiol (Ortho Tri-Cyclen); norethindrone acetate-ethinyl estradiol (Estrostep Fe); drospirenone-ethinyl estradiol (Yaz); and drospirenone-ethinyl estradiol-levomefolate calcium (Beyaz). Birth control pills are known to carry risks for venous thromboembolism (VTE), stroke, hypertension, and myocardial infarction; however, they are generally well tolerated in acne patients. "The risk of venous thromboembolism in women who take BCPs is doubled or tripled compared to women who do not take these pills. This sounds scary until you put it into context," said Dr. Harper. She explains the risks to patients using the following 3-6-9-12 model: A woman's baseline risk of having a VTE if she is not on a BCP is approximately 3 in 10,000 women in one year. When she takes a BCP, her risk doubles to 6 per 10,000 women in one year. If she takes a BCP that contains drospirenone, her risk is 9 per 10,000 women in one year. If she gets pregnant, her risk is 12 per 10,000 women in one year.
Dermatologists may be apprehensive to prescribe BCPs, but Dr. Harper provided several important tips on managing patient expectations and monitoring patients. Dr. Harper emphasized that BCPs should be used patiently for acne. "It frequently takes at least 3 cycles of BCPs to see a meaningful change in acne reduction," she advised. She recommended obtaining a thorough medical history and blood pressure measurement prior to prescribing BCPs. However, a Papanicolaou test and bimanual pelvic examination are no longer deemed mandatory prior to initiating a BCP, according to the World Health Organization and the American Congress of Obstetricians and Gynecologists. "While these exams may help to detect cervical cancer and other pelvic diseases, BCPs help to prevent unwanted pregnancies and the risks that accompany those pregnancies," said Dr. Harper. "Remember that BCPs reduce the risk of ovarian, uterine and colorectal cancer and also lessen ovarian cysts and pelvic inflammatory disease." Dermatologists also should inform patients that rifampin and griseofulvin, both anti-infectives, will interact with BCPs, lessening their effectiveness.
A March 2017 study published in Cutis (2017;99:195-201) of US dermatologists' knowledge, comfort, and prescribing practices (N=116) revealed that most dermatologists (95.4%) believe BCPs effectively treat acne; however, only 54% reported prescribing them. The American Academy of Dermatology's guidelines of care for the management of acne vulgaris published in February 2016 (J Am Acad Dermatol. 2016;74:945-973) stated that "estrogen-containing combined oral contraceptives are effective and recommended in the treatment of inflammatory acne in females."
Overall, Dr. Harper's take-home message was that dermatologists should not be afraid to prescribe BCPs, even in teenaged girls (following the onset of menarche). "Birth control pills can be used in younger patients but it is not my first line of treatment," said Dr. Harper. "It is recommended that BCPs not be prescribed for acne until 2 years after the young woman has achieved menarche. When considering whether or not to use a BCP in the early teenage years, keep in mind that these are not short-term treatments. If a BCP does help acne, it will likely need to be maintained for many years." When discussing this treatment in front of parents/guardians, consider referring to it as hormonal therapy and use the term birth control pills only initially.
‘Motivational pharmacotherapy’ engages Latino patients with depression
MIAMI – Approaching treatment as a partnership between clinician and patient can help improve adherence in underserved members of racial/ethnic groups with depression, according to an expert.
“There is plenty of evidence that clinicians are less likely to engage minorities in a participatory way,” Roberto Lewis-Fernández, MD, said during a plenary session at a meeting of the American Society of Clinical Psychopharmacology, formerly the New Clinical Drug Evaluation Unit meeting. “They tend to ask fewer questions [of patients]. They tend to engage [patients] less in clinical decision making.”
This can lead to nonadherence or even discontinuation of therapy, said Dr. Lewis-Fernández, director of the New York State (NYS) Center of Excellence for Cultural Competence, as well as the Anxiety Disorders Clinic and the Hispanic Treatment Program at NYS Psychiatric Institute.

One solution for bridging what Dr. Lewis-Fernández calls the “power differential” between therapist and patient, and improving adherence rates, is to use “motivational pharmacotherapy,” a derivative of motivational interviewing, created by Dr. Lewis-Fernández and his colleagues. With motivational pharmacotherapy, patients are viewed as the experts in their challenges when meeting the needs of their treatment plan. The clinician is the expert partner in the technical aspects of care.
In a 12-week, open-trial pilot study for this intervention in 50 first-generation Latino patients diagnosed with major depressive disorder, Dr. Lewis-Fernández and his colleagues found that 20% of patients discontinued treatment, with a mean therapy duration of 74.2 out of 84 days (Psychiatry. 2013 Fall;76[3]:210-22).This was in comparison to reports in the literature of discontinuation rates among Latino patients ranging from 32% to 53%, and to rates between 36% and 46% in previous studies conducted at Dr. Lewis-Fernández’s own clinic, using similar medications and methods.
They also found that responder and remitter rates were 82% and 68%. The average length of the first clinical visit was 36.7 minutes, and 24.3 minutes for subsequent visits, which Dr. Lewis-Fernández said was compatible with community clinics.
Motivational pharmacotherapy relies on the psychotherapy components of motivational interviewing that address the need for behavioral change and for helping patients reduce their ambivalence about taking antidepressants. Those components are combined with manualized pharmacotherapy, said Dr. Lewis-Fernández, professor of clinical psychiatry at Columbia University, New York.
The language and tone of this kind of intervention must be empathetic and nonconfrontational, he said. “You can’t say to people who are ambivalent, ‘No, you’re wrong. Take your medication.’ Instead, [focus on] the discrepancy between the current situation and the desired state. Then medication can serve as the solution.”
This allows the patient to “roll with their resistance,” he said, rather than meet it head on. In turn, this approach emphasizes the patient’s capacity to advocate for himself or herself.
“You can’t do the treatment without the patient,” Dr. Lewis-Fernández said. “It’s essentially psychoeducation.”
Among some of the tips for conducting this intervention cited by Dr. Lewis-Fernández:
- Ask questions to elicit the patients’ cultural understanding about their illness and what troubles them most about their condition.
- Ask patients’ permission to show them the supportive data for the intervention.
- Ask them about their thoughts and feelings in response to learning the data.
- Use their understanding of the pros and cons of the medication to “negotiate” their engagement.
In previous studies, Dr. Lewis-Fernández said, he and his colleagues analyzed the reasons for nonadherence, which he said often were tied to the “chaos of their lives.” However, he said, there were improvements after the patients engaged in this psychoeducation-enriched intervention.
Not blaming minority patients for poor adherence is important, he said, since their ambivalence takes place in the context of having less access to quality care. Among the many obstacles these patients face in getting the care they need, insufficient clinician training in how to engage them should not have to be one of them, Dr. Lewis-Fernández said. “We should be doing something about this as a profession.”
Dr. Lewis-Fernández said he had no relevant disclosures. The study on motivational pharmacotherapy was sponsored by Pfizer and the National Institute of Mental Health.
On Twitter @whitneymcknight
MIAMI – Approaching treatment as a partnership between clinician and patient can help improve adherence in underserved members of racial/ethnic groups with depression, according to an expert.
“There is plenty of evidence that clinicians are less likely to engage minorities in a participatory way,” Roberto Lewis-Fernández, MD, said during a plenary session at a meeting of the American Society of Clinical Psychopharmacology, formerly the New Clinical Drug Evaluation Unit meeting. “They tend to ask fewer questions [of patients]. They tend to engage [patients] less in clinical decision making.”
This can lead to nonadherence or even discontinuation of therapy, said Dr. Lewis-Fernández, director of the New York State (NYS) Center of Excellence for Cultural Competence, as well as the Anxiety Disorders Clinic and the Hispanic Treatment Program at NYS Psychiatric Institute.
One solution for bridging what Dr. Lewis-Fernández calls the “power differential” between therapist and patient, and improving adherence rates, is to use “motivational pharmacotherapy,” a derivative of motivational interviewing, created by Dr. Lewis-Fernández and his colleagues. With motivational pharmacotherapy, patients are viewed as the experts in their challenges when meeting the needs of their treatment plan. The clinician is the expert partner in the technical aspects of care.
In a 12-week, open-trial pilot study for this intervention in 50 first-generation Latino patients diagnosed with major depressive disorder, Dr. Lewis-Fernández and his colleagues found that 20% of patients discontinued treatment, with a mean therapy duration of 74.2 out of 84 days (Psychiatry. 2013 Fall;76[3]:210-22).This was in comparison to reports in the literature of discontinuation rates among Latino patients ranging from 32% to 53%, and to rates between 36% and 46% in previous studies conducted at Dr. Lewis-Fernández’s own clinic, using similar medications and methods.
They also found that responder and remitter rates were 82% and 68%. The average length of the first clinical visit was 36.7 minutes, and 24.3 minutes for subsequent visits, which Dr. Lewis-Fernández said was compatible with community clinics.
Motivational pharmacotherapy relies on the psychotherapy components of motivational interviewing that address the need for behavioral change and for helping patients reduce their ambivalence about taking antidepressants. Those components are combined with manualized pharmacotherapy, said Dr. Lewis-Fernández, professor of clinical psychiatry at Columbia University, New York.
The language and tone of this kind of intervention must be empathetic and nonconfrontational, he said. “You can’t say to people who are ambivalent, ‘No, you’re wrong. Take your medication.’ Instead, [focus on] the discrepancy between the current situation and the desired state. Then medication can serve as the solution.”
This allows the patient to “roll with their resistance,” he said, rather than meet it head on. In turn, this approach emphasizes the patient’s capacity to advocate for himself or herself.
“You can’t do the treatment without the patient,” Dr. Lewis-Fernández said. “It’s essentially psychoeducation.”
Among some of the tips for conducting this intervention cited by Dr. Lewis-Fernández:
- Ask questions to elicit the patients’ cultural understanding about their illness and what troubles them most about their condition.
- Ask patients’ permission to show them the supportive data for the intervention.
- Ask them about their thoughts and feelings in response to learning the data.
- Use their understanding of the pros and cons of the medication to “negotiate” their engagement.
In previous studies, Dr. Lewis-Fernández said, he and his colleagues analyzed the reasons for nonadherence, which he said often were tied to the “chaos of their lives.” However, he said, there were improvements after the patients engaged in this psychoeducation-enriched intervention.
Not blaming minority patients for poor adherence is important, he said, since their ambivalence takes place in the context of having less access to quality care. Among the many obstacles these patients face in getting the care they need, insufficient clinician training in how to engage them should not have to be one of them, Dr. Lewis-Fernández said. “We should be doing something about this as a profession.”
Dr. Lewis-Fernández said he had no relevant disclosures. The study on motivational pharmacotherapy was sponsored by Pfizer and the National Institute of Mental Health.
On Twitter @whitneymcknight
MIAMI – Approaching treatment as a partnership between clinician and patient can help improve adherence in underserved members of racial/ethnic groups with depression, according to an expert.
“There is plenty of evidence that clinicians are less likely to engage minorities in a participatory way,” Roberto Lewis-Fernández, MD, said during a plenary session at a meeting of the American Society of Clinical Psychopharmacology, formerly the New Clinical Drug Evaluation Unit meeting. “They tend to ask fewer questions [of patients]. They tend to engage [patients] less in clinical decision making.”
This can lead to nonadherence or even discontinuation of therapy, said Dr. Lewis-Fernández, director of the New York State (NYS) Center of Excellence for Cultural Competence, as well as the Anxiety Disorders Clinic and the Hispanic Treatment Program at NYS Psychiatric Institute.
One solution for bridging what Dr. Lewis-Fernández calls the “power differential” between therapist and patient, and improving adherence rates, is to use “motivational pharmacotherapy,” a derivative of motivational interviewing, created by Dr. Lewis-Fernández and his colleagues. With motivational pharmacotherapy, patients are viewed as the experts in their challenges when meeting the needs of their treatment plan. The clinician is the expert partner in the technical aspects of care.
In a 12-week, open-trial pilot study for this intervention in 50 first-generation Latino patients diagnosed with major depressive disorder, Dr. Lewis-Fernández and his colleagues found that 20% of patients discontinued treatment, with a mean therapy duration of 74.2 out of 84 days (Psychiatry. 2013 Fall;76[3]:210-22).This was in comparison to reports in the literature of discontinuation rates among Latino patients ranging from 32% to 53%, and to rates between 36% and 46% in previous studies conducted at Dr. Lewis-Fernández’s own clinic, using similar medications and methods.
They also found that responder and remitter rates were 82% and 68%. The average length of the first clinical visit was 36.7 minutes, and 24.3 minutes for subsequent visits, which Dr. Lewis-Fernández said was compatible with community clinics.
Motivational pharmacotherapy relies on the psychotherapy components of motivational interviewing that address the need for behavioral change and for helping patients reduce their ambivalence about taking antidepressants. Those components are combined with manualized pharmacotherapy, said Dr. Lewis-Fernández, professor of clinical psychiatry at Columbia University, New York.
The language and tone of this kind of intervention must be empathetic and nonconfrontational, he said. “You can’t say to people who are ambivalent, ‘No, you’re wrong. Take your medication.’ Instead, [focus on] the discrepancy between the current situation and the desired state. Then medication can serve as the solution.”
This allows the patient to “roll with their resistance,” he said, rather than meet it head on. In turn, this approach emphasizes the patient’s capacity to advocate for himself or herself.
“You can’t do the treatment without the patient,” Dr. Lewis-Fernández said. “It’s essentially psychoeducation.”
Among some of the tips for conducting this intervention cited by Dr. Lewis-Fernández:
- Ask questions to elicit the patients’ cultural understanding about their illness and what troubles them most about their condition.
- Ask patients’ permission to show them the supportive data for the intervention.
- Ask them about their thoughts and feelings in response to learning the data.
- Use their understanding of the pros and cons of the medication to “negotiate” their engagement.
In previous studies, Dr. Lewis-Fernández said, he and his colleagues analyzed the reasons for nonadherence, which he said often were tied to the “chaos of their lives.” However, he said, there were improvements after the patients engaged in this psychoeducation-enriched intervention.
Not blaming minority patients for poor adherence is important, he said, since their ambivalence takes place in the context of having less access to quality care. Among the many obstacles these patients face in getting the care they need, insufficient clinician training in how to engage them should not have to be one of them, Dr. Lewis-Fernández said. “We should be doing something about this as a profession.”
Dr. Lewis-Fernández said he had no relevant disclosures. The study on motivational pharmacotherapy was sponsored by Pfizer and the National Institute of Mental Health.
On Twitter @whitneymcknight
EXPERT ANALYSIS FROM THE ASCP ANNUAL MEETING
ACA lawsuits progress through the courts
While Republican efforts to repeal and/or replace the Affordable Care Act are likely to resurface after the congressional summer recess, lawsuits challenging the health law continue to wind their way through the courts.
Judges recently ruled in three ACA cases regarding the contraceptive mandate, risk corridors program, and cost-sharing reduction payments.
Real Alternatives Inc. v. HHS
Secular groups are not entitled to a religious exemption to the ACA’s contraceptive mandate and must offer plans to employees that cover birth control, the United States Court of Appeals for the Third Circuit ruled in an Aug. 4 opinion.

But a majority of appeal judges disagreed, concluding that Real Alternatives is not similar to a religious denomination or one of its nontheistic counterparts, “not in structure, not in aim, not in purpose, and not in function.”
“We do not doubt that Real Alternative’s stance on contraceptives is grounded in sincerely-held moral values, but religion is not generally confined to one question or one moral teaching, it has a broader scope,” Judge Marjorie O. Rendell wrote in the majority opinion. “Real Alternatives is functionally similar not to a church, but to the countless nonreligious nonprofit organizations that take morally informed positions on some discrete set of issues ... While commitment to an anti-abortion platform may be important to the people who hold them, that commitment is not a religion in any legally or theologically accepted sense; and organizations do not become quasi-churches for equal-protection purposes merely by espousing a commitment of that sort.”
Molina Healthcare v. HHS
The federal Heath & Human Services department may have to dish out millions to marketplace insurers after a recent decision by the U.S. Court of Federal Claims. In an Aug. 4 opinion, a federal claims judge ruled the federal government owes Long Beach, Calif.–based insurer Molina Healthcare $52 million in risk corridor payments under the ACA.
The decision stems from a lawsuit by Molina and dozens of other insurers against HHS over the ACA’s risk corridor program. The program requires HHS to collect funds from excessively profitable insurers that offer qualified health plans (QHP) under the exchanges, while paying out funds to QHP insurers with excessive losses. Collections from profitable insurers under the program fell short in 2014 and again in 2015, resulting in HHS paying about 12 cents on the dollar in payments to insurers.
Insurers allege they’ve been shortchanged and that the government must reimburse them full payments for 2014 and 2015. Under the Obama administration, the Department of Justice requested to dismiss the cases, arguing that riders attached to appropriations bills in 2015 and 2016 barred it from making full risk corridor payments.
In his decision, Judge Thomas Wheeler said the ACA mandates that HHS pay insurers what they are owed under the risk corridor program, regardless of the riders.
“The undisputed facts show the government entered into an implied-in-fact contract with Molina and subsequently breached the contract when it failed to make full risk corridor payments,” Judge Wheeler wrote. “Importantly, Molina prevails on its argument of breach of an implied-in-fact contract regardless of the government’s appropriation law defenses – later appropriation restrictions cannot erase a previously created contractual obligation ...The government is liable for its breach of a statutory and contractual obligation to make full annual payments to insurers who participated in the risk corridor program.”
Judge Wheeler ruled similarly in February when he concluded the federal government owes Portland, Ore.–based Moda Health $214 million in risk corridor payments.
The issue is far from over. More than 25 lawsuits have been filed in the Court of Federal Claims by insurers seeking risk corridor money. Several of the cases have moved onto federal appeals courts, while other cases have been dismissed. Analysts say the issue is likely to reach the U.S. Supreme Court. It’s unclear where the Trump administration would get the funds to reimburse insurers if the payback rulings stand. About $19.3 billion in risk corridor payments are at stake for 2014 and 2015 and an estimated $3 billion is in play for 2016, the final risk corridor year.
House v. Price
A U.S. appeals court has allowed 16 states to intervene in a lawsuit over whether subsidy payments made to insurers under the ACA are legal. The decision comes as President Trump recently threatened to cut off the cost sharing reduction (CSR) payments to marketplace insurers, calling them a “bailout.”
On Aug. 1, the U.S. Court of Appeals for the District of Columbia Circuit granted a motion by 18 attorneys general to enter the lawsuit. The attorneys general represent California, New York, Connecticut, Delaware, Hawaii, Illinois, Iowa, Kentucky, Maryland, Massachusetts, Minnesota, New Mexico, North Carolina, Pennsylvania, Vermont, Virginia, Washington, and the District of Columbia.
Under the ACA, the federal government provides CSR payments to insurers to offset the costs for providing discount plans to patients who earn up to 200% of the federal poverty level. Plans on the individual exchanges are required to cover a package of essential benefits with pricing limitations to ensure that out-of-pocket costs are low enough for low-income patients.
Republican members of the House of Representatives sued the HHS over the CSR payments under the Obama administration, claiming the funding was illegal because it was never appropriated by Congress. A court ruled in favor of the House in 2016, but an appeal filed by the Obama administration allowed the CSR payments to continue. President Trump has not indicated whether he plans to drop the appeal or carry on the case. But if he fails to continue the suit, the move would immediately end the CSR payments.
On July 29, President Trump tweeted, “If a new HealthCare Bill is not approved quickly, BAILOUTS for Insurance Companies and BAILOUTS for Members of Congress will end very soon!”
The state attorneys general are ready to defend the ACA and the cost sharing reduction payments, California Attorney General Xavier Becerra said in a statement.
“If Donald Trump won’t defend these vital subsidies for American families, then we will,” Mr. Becerra said in the statement. “This ruling gives my fellow attorneys general and me the ability to stand up for the millions of families who otherwise would lack access to affordable health care. It’s time Americans knew we were working for them, not against them.”
[email protected]
On Twitter @legal_med
While Republican efforts to repeal and/or replace the Affordable Care Act are likely to resurface after the congressional summer recess, lawsuits challenging the health law continue to wind their way through the courts.
Judges recently ruled in three ACA cases regarding the contraceptive mandate, risk corridors program, and cost-sharing reduction payments.
Real Alternatives Inc. v. HHS
Secular groups are not entitled to a religious exemption to the ACA’s contraceptive mandate and must offer plans to employees that cover birth control, the United States Court of Appeals for the Third Circuit ruled in an Aug. 4 opinion.
But a majority of appeal judges disagreed, concluding that Real Alternatives is not similar to a religious denomination or one of its nontheistic counterparts, “not in structure, not in aim, not in purpose, and not in function.”
“We do not doubt that Real Alternative’s stance on contraceptives is grounded in sincerely-held moral values, but religion is not generally confined to one question or one moral teaching, it has a broader scope,” Judge Marjorie O. Rendell wrote in the majority opinion. “Real Alternatives is functionally similar not to a church, but to the countless nonreligious nonprofit organizations that take morally informed positions on some discrete set of issues ... While commitment to an anti-abortion platform may be important to the people who hold them, that commitment is not a religion in any legally or theologically accepted sense; and organizations do not become quasi-churches for equal-protection purposes merely by espousing a commitment of that sort.”
Molina Healthcare v. HHS
The federal Heath & Human Services department may have to dish out millions to marketplace insurers after a recent decision by the U.S. Court of Federal Claims. In an Aug. 4 opinion, a federal claims judge ruled the federal government owes Long Beach, Calif.–based insurer Molina Healthcare $52 million in risk corridor payments under the ACA.
The decision stems from a lawsuit by Molina and dozens of other insurers against HHS over the ACA’s risk corridor program. The program requires HHS to collect funds from excessively profitable insurers that offer qualified health plans (QHP) under the exchanges, while paying out funds to QHP insurers with excessive losses. Collections from profitable insurers under the program fell short in 2014 and again in 2015, resulting in HHS paying about 12 cents on the dollar in payments to insurers.
Insurers allege they’ve been shortchanged and that the government must reimburse them full payments for 2014 and 2015. Under the Obama administration, the Department of Justice requested to dismiss the cases, arguing that riders attached to appropriations bills in 2015 and 2016 barred it from making full risk corridor payments.
In his decision, Judge Thomas Wheeler said the ACA mandates that HHS pay insurers what they are owed under the risk corridor program, regardless of the riders.
“The undisputed facts show the government entered into an implied-in-fact contract with Molina and subsequently breached the contract when it failed to make full risk corridor payments,” Judge Wheeler wrote. “Importantly, Molina prevails on its argument of breach of an implied-in-fact contract regardless of the government’s appropriation law defenses – later appropriation restrictions cannot erase a previously created contractual obligation ...The government is liable for its breach of a statutory and contractual obligation to make full annual payments to insurers who participated in the risk corridor program.”
Judge Wheeler ruled similarly in February when he concluded the federal government owes Portland, Ore.–based Moda Health $214 million in risk corridor payments.
The issue is far from over. More than 25 lawsuits have been filed in the Court of Federal Claims by insurers seeking risk corridor money. Several of the cases have moved onto federal appeals courts, while other cases have been dismissed. Analysts say the issue is likely to reach the U.S. Supreme Court. It’s unclear where the Trump administration would get the funds to reimburse insurers if the payback rulings stand. About $19.3 billion in risk corridor payments are at stake for 2014 and 2015 and an estimated $3 billion is in play for 2016, the final risk corridor year.
House v. Price
A U.S. appeals court has allowed 16 states to intervene in a lawsuit over whether subsidy payments made to insurers under the ACA are legal. The decision comes as President Trump recently threatened to cut off the cost sharing reduction (CSR) payments to marketplace insurers, calling them a “bailout.”
On Aug. 1, the U.S. Court of Appeals for the District of Columbia Circuit granted a motion by 18 attorneys general to enter the lawsuit. The attorneys general represent California, New York, Connecticut, Delaware, Hawaii, Illinois, Iowa, Kentucky, Maryland, Massachusetts, Minnesota, New Mexico, North Carolina, Pennsylvania, Vermont, Virginia, Washington, and the District of Columbia.
Under the ACA, the federal government provides CSR payments to insurers to offset the costs for providing discount plans to patients who earn up to 200% of the federal poverty level. Plans on the individual exchanges are required to cover a package of essential benefits with pricing limitations to ensure that out-of-pocket costs are low enough for low-income patients.
Republican members of the House of Representatives sued the HHS over the CSR payments under the Obama administration, claiming the funding was illegal because it was never appropriated by Congress. A court ruled in favor of the House in 2016, but an appeal filed by the Obama administration allowed the CSR payments to continue. President Trump has not indicated whether he plans to drop the appeal or carry on the case. But if he fails to continue the suit, the move would immediately end the CSR payments.
On July 29, President Trump tweeted, “If a new HealthCare Bill is not approved quickly, BAILOUTS for Insurance Companies and BAILOUTS for Members of Congress will end very soon!”
The state attorneys general are ready to defend the ACA and the cost sharing reduction payments, California Attorney General Xavier Becerra said in a statement.
“If Donald Trump won’t defend these vital subsidies for American families, then we will,” Mr. Becerra said in the statement. “This ruling gives my fellow attorneys general and me the ability to stand up for the millions of families who otherwise would lack access to affordable health care. It’s time Americans knew we were working for them, not against them.”
[email protected]
On Twitter @legal_med
While Republican efforts to repeal and/or replace the Affordable Care Act are likely to resurface after the congressional summer recess, lawsuits challenging the health law continue to wind their way through the courts.
Judges recently ruled in three ACA cases regarding the contraceptive mandate, risk corridors program, and cost-sharing reduction payments.
Real Alternatives Inc. v. HHS
Secular groups are not entitled to a religious exemption to the ACA’s contraceptive mandate and must offer plans to employees that cover birth control, the United States Court of Appeals for the Third Circuit ruled in an Aug. 4 opinion.
But a majority of appeal judges disagreed, concluding that Real Alternatives is not similar to a religious denomination or one of its nontheistic counterparts, “not in structure, not in aim, not in purpose, and not in function.”
“We do not doubt that Real Alternative’s stance on contraceptives is grounded in sincerely-held moral values, but religion is not generally confined to one question or one moral teaching, it has a broader scope,” Judge Marjorie O. Rendell wrote in the majority opinion. “Real Alternatives is functionally similar not to a church, but to the countless nonreligious nonprofit organizations that take morally informed positions on some discrete set of issues ... While commitment to an anti-abortion platform may be important to the people who hold them, that commitment is not a religion in any legally or theologically accepted sense; and organizations do not become quasi-churches for equal-protection purposes merely by espousing a commitment of that sort.”
Molina Healthcare v. HHS
The federal Heath & Human Services department may have to dish out millions to marketplace insurers after a recent decision by the U.S. Court of Federal Claims. In an Aug. 4 opinion, a federal claims judge ruled the federal government owes Long Beach, Calif.–based insurer Molina Healthcare $52 million in risk corridor payments under the ACA.
The decision stems from a lawsuit by Molina and dozens of other insurers against HHS over the ACA’s risk corridor program. The program requires HHS to collect funds from excessively profitable insurers that offer qualified health plans (QHP) under the exchanges, while paying out funds to QHP insurers with excessive losses. Collections from profitable insurers under the program fell short in 2014 and again in 2015, resulting in HHS paying about 12 cents on the dollar in payments to insurers.
Insurers allege they’ve been shortchanged and that the government must reimburse them full payments for 2014 and 2015. Under the Obama administration, the Department of Justice requested to dismiss the cases, arguing that riders attached to appropriations bills in 2015 and 2016 barred it from making full risk corridor payments.
In his decision, Judge Thomas Wheeler said the ACA mandates that HHS pay insurers what they are owed under the risk corridor program, regardless of the riders.
“The undisputed facts show the government entered into an implied-in-fact contract with Molina and subsequently breached the contract when it failed to make full risk corridor payments,” Judge Wheeler wrote. “Importantly, Molina prevails on its argument of breach of an implied-in-fact contract regardless of the government’s appropriation law defenses – later appropriation restrictions cannot erase a previously created contractual obligation ...The government is liable for its breach of a statutory and contractual obligation to make full annual payments to insurers who participated in the risk corridor program.”
Judge Wheeler ruled similarly in February when he concluded the federal government owes Portland, Ore.–based Moda Health $214 million in risk corridor payments.
The issue is far from over. More than 25 lawsuits have been filed in the Court of Federal Claims by insurers seeking risk corridor money. Several of the cases have moved onto federal appeals courts, while other cases have been dismissed. Analysts say the issue is likely to reach the U.S. Supreme Court. It’s unclear where the Trump administration would get the funds to reimburse insurers if the payback rulings stand. About $19.3 billion in risk corridor payments are at stake for 2014 and 2015 and an estimated $3 billion is in play for 2016, the final risk corridor year.
House v. Price
A U.S. appeals court has allowed 16 states to intervene in a lawsuit over whether subsidy payments made to insurers under the ACA are legal. The decision comes as President Trump recently threatened to cut off the cost sharing reduction (CSR) payments to marketplace insurers, calling them a “bailout.”
On Aug. 1, the U.S. Court of Appeals for the District of Columbia Circuit granted a motion by 18 attorneys general to enter the lawsuit. The attorneys general represent California, New York, Connecticut, Delaware, Hawaii, Illinois, Iowa, Kentucky, Maryland, Massachusetts, Minnesota, New Mexico, North Carolina, Pennsylvania, Vermont, Virginia, Washington, and the District of Columbia.
Under the ACA, the federal government provides CSR payments to insurers to offset the costs for providing discount plans to patients who earn up to 200% of the federal poverty level. Plans on the individual exchanges are required to cover a package of essential benefits with pricing limitations to ensure that out-of-pocket costs are low enough for low-income patients.
Republican members of the House of Representatives sued the HHS over the CSR payments under the Obama administration, claiming the funding was illegal because it was never appropriated by Congress. A court ruled in favor of the House in 2016, but an appeal filed by the Obama administration allowed the CSR payments to continue. President Trump has not indicated whether he plans to drop the appeal or carry on the case. But if he fails to continue the suit, the move would immediately end the CSR payments.
On July 29, President Trump tweeted, “If a new HealthCare Bill is not approved quickly, BAILOUTS for Insurance Companies and BAILOUTS for Members of Congress will end very soon!”
The state attorneys general are ready to defend the ACA and the cost sharing reduction payments, California Attorney General Xavier Becerra said in a statement.
“If Donald Trump won’t defend these vital subsidies for American families, then we will,” Mr. Becerra said in the statement. “This ruling gives my fellow attorneys general and me the ability to stand up for the millions of families who otherwise would lack access to affordable health care. It’s time Americans knew we were working for them, not against them.”
[email protected]
On Twitter @legal_med

Practitioner Cognitive Reframing: Working More Effectively in Addictions
I am a behavioral health-licensed clinical social worker, an approved motivational enhancement therapy provider, and the point of contact for substance use disorders at the Berks CBOC of the Lebanon VAMC in Wyomissing, Pennsylvania. Recently, an exasperated primary care provider at the Berks CBOC approached me about working with patients with substance use disorders and asked “How do you work with this challenging population?”
The question was cause for some introspection. When I started working in addictions, I had to modify my approach to work effectively with this population. I experienced a paradigm shift in which I no longer assigned myself credit or blame for a veteran’s continued sobriety or relapse: Each patient is responsible for his or her progress in the recovery journey. When a patient has a relapse, I remind myself that statistically relapse is a probability for the majority of those in recovery; even multiple relapses are common. Therefore, another way of viewing relapse is that the relapse itself may bring the veteran a step closer to permanent abstinence.
Cognitive Reframing
Consider a toddler learning to walk. Parents and caregivers of the child expect the child to fall quite a few times before he or she has mastered walking. The parents and caregivers don’t get angry, take the situation personally, or feel manipulated by the child’s “failure.” Instead, the parents offer the child emotional support and encouragement.
Arguably, the practitioner should take a similar stance—emotionally supportive and encouraging—in combination with dialogue guided by motivational interviewing to support change and help the veteran get back on track. Although not inevitable, relapse is a normal part of recovery.
Practitioners should avoid either scolding or praising patients. Scolding doesn’t help in the recovery journey, and if the veteran learns that the practitioner reacts by scolding after learning of the relapse, then it is less likely that he or she will be open about future missteps. In fact, the veteran may not return at all. The goal is to have the patient come back when relapse occurs to help him or her progress to recovery.
Too much praise can cause similar problems. A veteran accustomed to praise when he or she is doing well, may be too embarrassed or ashamed to return to ask for help after a relapse. Instead the practitioner should use affirmations, which are widely discussed in motivational interviewing (MI) literature.
“I want to be clean and sober” or “I want to stop drinking” are vague statements that should raise a red flag for experienced practitioners. Is this patient just telling me what he or she thinks I want to hear to respond? That may be the case but also may be an assumption. Instead these assertions could be regarded as global treatment goals, and the task of the practitioner is to help the veteran develop objectives and interventions in relation to this goal. These broad statements can be a starting point in MI. These words can sound just as foreign to a patient who isn’t sure whether becoming clean and sober is a possibility. The veteran may not have the confidence to reach the goal of being clean and sober, and these statements may seem awkward and out of sync with his or her facial expression and body language.
Showing disbelief in a veteran also can have negative consequences. The veteran might feel that “even my therapist/health care provider doesn’t believe I can become clean and sober.” Instead, I remind myself that we all must manipulate our environment for survival. I find it more valuable to think of the veteran as being resourceful rather than manipulative.
This point may seem self-evident, but it took me a while to catch on: Most of the change in the recovery journey transpires outside the practitioner’s office. I had to embrace this truism and be prepared when the veteran returned for the next session. The task, then, is to determine at this moment where the veteran is in his or her recovery journey instead of continuing the conversation from the previous session. The previous session may be irrelevant. Thinking this way was an adjustment for me. One of my favorite therapy approaches was to consciously continue a conversation from the previous session to demonstrate that I remembered what the patient had said, thereby showing that I care.
In addition, get to know the patient underneath, behind, and before the substance use disorder. Knowing and liking the veteran helps me avoid burnout, bringing me back to my values and the reason I became a therapist. I make efforts in my thinking process to convert “alcoholic” or “drug abuser” into a more helpful “client addicted to alcohol” or “client with a substance use disorder.” The veteran should not be labeled.
Motivational Interviewing
Oftentimes what propels veterans forward in their recovery is the cognitive dissonance created between who they were and how they acted before substance addiction and how they act now. Conversation steered in this direction, fueled by MI, can enhance a veteran’s motivation to change and ready the veteran to change behaviors. Listen to the veteran’s account of loved ones and remember the names of these important family members and friends. Weave into the conversation the names of these loved ones when the veteran makes statements about becoming a better son/father/grandfather or daughter/mother/grandmother. These references make the goal concrete . A loved one can even be a pet; and for some, the desire to be a more competent and reliable pet owner can be a strong motivation. Give the veteran an opportunity to describe his or her strengths and bask in a self-description. In recovery, it is critical to identify strengths that can be built on to sustain recovery.
Veterans who are confronting a substance use disorder may approach the practitioner with a “fix it for me” attitude as a mental inventory is being taken of all of the negative consequences (eg, homelessness, legal issues, or unemployment). Getting the veteran to take ownership of the problem and the solution is key.
I don’t promise to fix things, instead I engage the veteran in problem-solving. I offer to team up with the veteran in this process, and I promise my best efforts but not outcomes. I avoid giving advice and work to empower the veteran to make sound decisions. Veterans who make their own decisions feel as though they have more control over their lives.
Working with the substance use disorder population is challenging but rewarding when a practitioner can embrace some of the paradigms described in this article. Practitioners may need to do some cognitive reframing within their own thinking, as I described in this article, to become more effective in the field and to help avoid burnout.
I am a behavioral health-licensed clinical social worker, an approved motivational enhancement therapy provider, and the point of contact for substance use disorders at the Berks CBOC of the Lebanon VAMC in Wyomissing, Pennsylvania. Recently, an exasperated primary care provider at the Berks CBOC approached me about working with patients with substance use disorders and asked “How do you work with this challenging population?”
The question was cause for some introspection. When I started working in addictions, I had to modify my approach to work effectively with this population. I experienced a paradigm shift in which I no longer assigned myself credit or blame for a veteran’s continued sobriety or relapse: Each patient is responsible for his or her progress in the recovery journey. When a patient has a relapse, I remind myself that statistically relapse is a probability for the majority of those in recovery; even multiple relapses are common. Therefore, another way of viewing relapse is that the relapse itself may bring the veteran a step closer to permanent abstinence.
Cognitive Reframing
Consider a toddler learning to walk. Parents and caregivers of the child expect the child to fall quite a few times before he or she has mastered walking. The parents and caregivers don’t get angry, take the situation personally, or feel manipulated by the child’s “failure.” Instead, the parents offer the child emotional support and encouragement.
Arguably, the practitioner should take a similar stance—emotionally supportive and encouraging—in combination with dialogue guided by motivational interviewing to support change and help the veteran get back on track. Although not inevitable, relapse is a normal part of recovery.
Practitioners should avoid either scolding or praising patients. Scolding doesn’t help in the recovery journey, and if the veteran learns that the practitioner reacts by scolding after learning of the relapse, then it is less likely that he or she will be open about future missteps. In fact, the veteran may not return at all. The goal is to have the patient come back when relapse occurs to help him or her progress to recovery.
Too much praise can cause similar problems. A veteran accustomed to praise when he or she is doing well, may be too embarrassed or ashamed to return to ask for help after a relapse. Instead the practitioner should use affirmations, which are widely discussed in motivational interviewing (MI) literature.
“I want to be clean and sober” or “I want to stop drinking” are vague statements that should raise a red flag for experienced practitioners. Is this patient just telling me what he or she thinks I want to hear to respond? That may be the case but also may be an assumption. Instead these assertions could be regarded as global treatment goals, and the task of the practitioner is to help the veteran develop objectives and interventions in relation to this goal. These broad statements can be a starting point in MI. These words can sound just as foreign to a patient who isn’t sure whether becoming clean and sober is a possibility. The veteran may not have the confidence to reach the goal of being clean and sober, and these statements may seem awkward and out of sync with his or her facial expression and body language.
Showing disbelief in a veteran also can have negative consequences. The veteran might feel that “even my therapist/health care provider doesn’t believe I can become clean and sober.” Instead, I remind myself that we all must manipulate our environment for survival. I find it more valuable to think of the veteran as being resourceful rather than manipulative.
This point may seem self-evident, but it took me a while to catch on: Most of the change in the recovery journey transpires outside the practitioner’s office. I had to embrace this truism and be prepared when the veteran returned for the next session. The task, then, is to determine at this moment where the veteran is in his or her recovery journey instead of continuing the conversation from the previous session. The previous session may be irrelevant. Thinking this way was an adjustment for me. One of my favorite therapy approaches was to consciously continue a conversation from the previous session to demonstrate that I remembered what the patient had said, thereby showing that I care.
In addition, get to know the patient underneath, behind, and before the substance use disorder. Knowing and liking the veteran helps me avoid burnout, bringing me back to my values and the reason I became a therapist. I make efforts in my thinking process to convert “alcoholic” or “drug abuser” into a more helpful “client addicted to alcohol” or “client with a substance use disorder.” The veteran should not be labeled.
Motivational Interviewing
Oftentimes what propels veterans forward in their recovery is the cognitive dissonance created between who they were and how they acted before substance addiction and how they act now. Conversation steered in this direction, fueled by MI, can enhance a veteran’s motivation to change and ready the veteran to change behaviors. Listen to the veteran’s account of loved ones and remember the names of these important family members and friends. Weave into the conversation the names of these loved ones when the veteran makes statements about becoming a better son/father/grandfather or daughter/mother/grandmother. These references make the goal concrete . A loved one can even be a pet; and for some, the desire to be a more competent and reliable pet owner can be a strong motivation. Give the veteran an opportunity to describe his or her strengths and bask in a self-description. In recovery, it is critical to identify strengths that can be built on to sustain recovery.
Veterans who are confronting a substance use disorder may approach the practitioner with a “fix it for me” attitude as a mental inventory is being taken of all of the negative consequences (eg, homelessness, legal issues, or unemployment). Getting the veteran to take ownership of the problem and the solution is key.
I don’t promise to fix things, instead I engage the veteran in problem-solving. I offer to team up with the veteran in this process, and I promise my best efforts but not outcomes. I avoid giving advice and work to empower the veteran to make sound decisions. Veterans who make their own decisions feel as though they have more control over their lives.
Working with the substance use disorder population is challenging but rewarding when a practitioner can embrace some of the paradigms described in this article. Practitioners may need to do some cognitive reframing within their own thinking, as I described in this article, to become more effective in the field and to help avoid burnout.
I am a behavioral health-licensed clinical social worker, an approved motivational enhancement therapy provider, and the point of contact for substance use disorders at the Berks CBOC of the Lebanon VAMC in Wyomissing, Pennsylvania. Recently, an exasperated primary care provider at the Berks CBOC approached me about working with patients with substance use disorders and asked “How do you work with this challenging population?”
The question was cause for some introspection. When I started working in addictions, I had to modify my approach to work effectively with this population. I experienced a paradigm shift in which I no longer assigned myself credit or blame for a veteran’s continued sobriety or relapse: Each patient is responsible for his or her progress in the recovery journey. When a patient has a relapse, I remind myself that statistically relapse is a probability for the majority of those in recovery; even multiple relapses are common. Therefore, another way of viewing relapse is that the relapse itself may bring the veteran a step closer to permanent abstinence.
Cognitive Reframing
Consider a toddler learning to walk. Parents and caregivers of the child expect the child to fall quite a few times before he or she has mastered walking. The parents and caregivers don’t get angry, take the situation personally, or feel manipulated by the child’s “failure.” Instead, the parents offer the child emotional support and encouragement.
Arguably, the practitioner should take a similar stance—emotionally supportive and encouraging—in combination with dialogue guided by motivational interviewing to support change and help the veteran get back on track. Although not inevitable, relapse is a normal part of recovery.
Practitioners should avoid either scolding or praising patients. Scolding doesn’t help in the recovery journey, and if the veteran learns that the practitioner reacts by scolding after learning of the relapse, then it is less likely that he or she will be open about future missteps. In fact, the veteran may not return at all. The goal is to have the patient come back when relapse occurs to help him or her progress to recovery.
Too much praise can cause similar problems. A veteran accustomed to praise when he or she is doing well, may be too embarrassed or ashamed to return to ask for help after a relapse. Instead the practitioner should use affirmations, which are widely discussed in motivational interviewing (MI) literature.
“I want to be clean and sober” or “I want to stop drinking” are vague statements that should raise a red flag for experienced practitioners. Is this patient just telling me what he or she thinks I want to hear to respond? That may be the case but also may be an assumption. Instead these assertions could be regarded as global treatment goals, and the task of the practitioner is to help the veteran develop objectives and interventions in relation to this goal. These broad statements can be a starting point in MI. These words can sound just as foreign to a patient who isn’t sure whether becoming clean and sober is a possibility. The veteran may not have the confidence to reach the goal of being clean and sober, and these statements may seem awkward and out of sync with his or her facial expression and body language.
Showing disbelief in a veteran also can have negative consequences. The veteran might feel that “even my therapist/health care provider doesn’t believe I can become clean and sober.” Instead, I remind myself that we all must manipulate our environment for survival. I find it more valuable to think of the veteran as being resourceful rather than manipulative.
This point may seem self-evident, but it took me a while to catch on: Most of the change in the recovery journey transpires outside the practitioner’s office. I had to embrace this truism and be prepared when the veteran returned for the next session. The task, then, is to determine at this moment where the veteran is in his or her recovery journey instead of continuing the conversation from the previous session. The previous session may be irrelevant. Thinking this way was an adjustment for me. One of my favorite therapy approaches was to consciously continue a conversation from the previous session to demonstrate that I remembered what the patient had said, thereby showing that I care.
In addition, get to know the patient underneath, behind, and before the substance use disorder. Knowing and liking the veteran helps me avoid burnout, bringing me back to my values and the reason I became a therapist. I make efforts in my thinking process to convert “alcoholic” or “drug abuser” into a more helpful “client addicted to alcohol” or “client with a substance use disorder.” The veteran should not be labeled.
Motivational Interviewing
Oftentimes what propels veterans forward in their recovery is the cognitive dissonance created between who they were and how they acted before substance addiction and how they act now. Conversation steered in this direction, fueled by MI, can enhance a veteran’s motivation to change and ready the veteran to change behaviors. Listen to the veteran’s account of loved ones and remember the names of these important family members and friends. Weave into the conversation the names of these loved ones when the veteran makes statements about becoming a better son/father/grandfather or daughter/mother/grandmother. These references make the goal concrete . A loved one can even be a pet; and for some, the desire to be a more competent and reliable pet owner can be a strong motivation. Give the veteran an opportunity to describe his or her strengths and bask in a self-description. In recovery, it is critical to identify strengths that can be built on to sustain recovery.
Veterans who are confronting a substance use disorder may approach the practitioner with a “fix it for me” attitude as a mental inventory is being taken of all of the negative consequences (eg, homelessness, legal issues, or unemployment). Getting the veteran to take ownership of the problem and the solution is key.
I don’t promise to fix things, instead I engage the veteran in problem-solving. I offer to team up with the veteran in this process, and I promise my best efforts but not outcomes. I avoid giving advice and work to empower the veteran to make sound decisions. Veterans who make their own decisions feel as though they have more control over their lives.
Working with the substance use disorder population is challenging but rewarding when a practitioner can embrace some of the paradigms described in this article. Practitioners may need to do some cognitive reframing within their own thinking, as I described in this article, to become more effective in the field and to help avoid burnout.
Preop atrial fib in CABG patients spells trouble
COLORADO SPRINGS – Preoperative atrial fibrillation is present in more than 10% of patients undergoing isolated coronary artery bypass graft (CABG) surgery, and if not subjected to concomitant surgical ablation it’s associated with increased perioperative and long-term major morbidity and mortality, S. Chris Malaisrie, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
The increased early and late risks posed by preoperative atrial fibrillation (AF) that go unaddressed remain significant even after adjusting for the numerous comorbid conditions more prevalent in CABG patients with preoperative AF than in those without the arrhythmia, added Dr. Malaisrie, a cardiac surgeon at Northwestern University in Chicago.

The unadjusted operative mortality rate was 1.8% in the no-AF group and 4.0% in patients with preoperative AF. Unadjusted in-hospital rates of permanent stroke, prolonged ventilation, reoperation, and new renal failure were also significantly higher in the preoperative AF group.
Not surprisingly, the preoperative AF group was older. They also had significantly higher baseline rates of numerous comorbid conditions, including diabetes, peripheral vascular disease, renal failure, and prior stroke, as well as a lower mean left ventricular ejection fraction. However, after adjustment for the many comorbidities in multivariate regression analysis, the risks of all in-hospital adverse outcomes remained significantly higher in the preoperative AF group. For example, their adjusted risk of operative mortality was 1.5-fold greater than in the no-AF patients.
In the long-term follow-up analysis, the unadjusted risk of mortality in the first 5 years after CABG was 2.5-fold greater in the preoperative AF group. Their 5-year risk of stroke or systemic embolization was 1.5-fold greater, too. Upon adjustment for potentially confounding comorbid conditions, preoperative AF was associated with a 1.5-fold increased 5-year risk of mortality and a 1.2-fold increase in stroke or systemic embolism.
In an effort to identify a particularly high-risk group of CABG patients with preoperative AF, Dr. Malaisrie and his coinvestigators stratified the group’s long-term stroke and mortality risks by their CHA2DS2-VASc score at the time of surgery. The results were revealing: the unadjusted 5-year risk of stroke or systemic embolization was 7.9% in those with a CHA2DS2-VASc score of 1-3, 12.2% with a score of 4-6, and 15.4% with a score of 7-9. The 5-year survival rate was 74.8% with a score of 1-3, 56.5% with a score of 4-6, and 41.2% with a score of 7-9.
“That’s really a striking finding,” Dr. Malaisrie observed. “When you consider a patient who’s, say, 72-75 years old, who is undergoing isolated CABG with preoperative atrial fibrillation and who has a high CHA2DS2-VASc score of 7-9, 5-year survival is only 41%, with a 15% risk of stroke or systemic embolization.”
Discussant William T. Caine, MD, found the study results unsettling.
“I was surprised to see that in this day and age, fully two-thirds of the patients who had preoperative atrial fibrillation had no attempt at any ablation procedure to treat their atrial fibrillation,” declared Dr. Caine of Intermountain Medical Center in Salt Lake City.
In reply, Dr. Malaisrie noted that other, smaller studies have also found that only about 30% of CABG patients with preoperative AF undergo surgical AF ablation through a maze procedure or some other method.
“Probably most of us in this room would go ahead and perform surgical ablation, but the STS database represents all isolated CABG procedures done throughout the United States,” Dr. Malaisrie said. “I think this dataset should help convince the other 70% of surgeons out there that there is a high cost for preoperative AF – in particular, in patients with very high CHA2DS2-VASc scores. If you can identify a group of patients at increased risk for stroke and mortality, you’d certainly want to bend their survival curve.”
The maze procedure has been convincingly shown to be very safe, with no associated increased risk of perioperative morbidity and mortality. The downside is cost. But while it’s true that adding surgical ablation to an isolated CABG procedure boosts OR time and procedural costs, a successful ablation is likely to pay dividends through reduced downstream rates of major morbidity and mortality.
“I look forward to the second part of our analysis, where we’ll look at the comparative data for the patients who did in fact have surgical ablation. That dataset is pending from the Duke Clinical Research Institute,” according to Dr. Malaisrie.
He cited as study limitations the inability to complete linkage to the Medicare database in about 37% of CABG patients in the STS database, or more than 200,000 people. Also, the Medicare database is an administrative dataset reliant upon medical record coding. The mortality data are probably quite accurate, but the stroke and systemic embolization rates cited in this analysis likely underestimate the true rates.
He reported serving as a consultant to Edwards Lifesciences, Abbott Vascular, and Baxter, and serving on speakers’ bureaus for Bolton and Abiomed. However, the STS analysis was funded exclusively by philanthropy.
COLORADO SPRINGS – Preoperative atrial fibrillation is present in more than 10% of patients undergoing isolated coronary artery bypass graft (CABG) surgery, and if not subjected to concomitant surgical ablation it’s associated with increased perioperative and long-term major morbidity and mortality, S. Chris Malaisrie, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
The increased early and late risks posed by preoperative atrial fibrillation (AF) that go unaddressed remain significant even after adjusting for the numerous comorbid conditions more prevalent in CABG patients with preoperative AF than in those without the arrhythmia, added Dr. Malaisrie, a cardiac surgeon at Northwestern University in Chicago.
The unadjusted operative mortality rate was 1.8% in the no-AF group and 4.0% in patients with preoperative AF. Unadjusted in-hospital rates of permanent stroke, prolonged ventilation, reoperation, and new renal failure were also significantly higher in the preoperative AF group.
Not surprisingly, the preoperative AF group was older. They also had significantly higher baseline rates of numerous comorbid conditions, including diabetes, peripheral vascular disease, renal failure, and prior stroke, as well as a lower mean left ventricular ejection fraction. However, after adjustment for the many comorbidities in multivariate regression analysis, the risks of all in-hospital adverse outcomes remained significantly higher in the preoperative AF group. For example, their adjusted risk of operative mortality was 1.5-fold greater than in the no-AF patients.
In the long-term follow-up analysis, the unadjusted risk of mortality in the first 5 years after CABG was 2.5-fold greater in the preoperative AF group. Their 5-year risk of stroke or systemic embolization was 1.5-fold greater, too. Upon adjustment for potentially confounding comorbid conditions, preoperative AF was associated with a 1.5-fold increased 5-year risk of mortality and a 1.2-fold increase in stroke or systemic embolism.
In an effort to identify a particularly high-risk group of CABG patients with preoperative AF, Dr. Malaisrie and his coinvestigators stratified the group’s long-term stroke and mortality risks by their CHA2DS2-VASc score at the time of surgery. The results were revealing: the unadjusted 5-year risk of stroke or systemic embolization was 7.9% in those with a CHA2DS2-VASc score of 1-3, 12.2% with a score of 4-6, and 15.4% with a score of 7-9. The 5-year survival rate was 74.8% with a score of 1-3, 56.5% with a score of 4-6, and 41.2% with a score of 7-9.
“That’s really a striking finding,” Dr. Malaisrie observed. “When you consider a patient who’s, say, 72-75 years old, who is undergoing isolated CABG with preoperative atrial fibrillation and who has a high CHA2DS2-VASc score of 7-9, 5-year survival is only 41%, with a 15% risk of stroke or systemic embolization.”
Discussant William T. Caine, MD, found the study results unsettling.
“I was surprised to see that in this day and age, fully two-thirds of the patients who had preoperative atrial fibrillation had no attempt at any ablation procedure to treat their atrial fibrillation,” declared Dr. Caine of Intermountain Medical Center in Salt Lake City.
In reply, Dr. Malaisrie noted that other, smaller studies have also found that only about 30% of CABG patients with preoperative AF undergo surgical AF ablation through a maze procedure or some other method.
“Probably most of us in this room would go ahead and perform surgical ablation, but the STS database represents all isolated CABG procedures done throughout the United States,” Dr. Malaisrie said. “I think this dataset should help convince the other 70% of surgeons out there that there is a high cost for preoperative AF – in particular, in patients with very high CHA2DS2-VASc scores. If you can identify a group of patients at increased risk for stroke and mortality, you’d certainly want to bend their survival curve.”
The maze procedure has been convincingly shown to be very safe, with no associated increased risk of perioperative morbidity and mortality. The downside is cost. But while it’s true that adding surgical ablation to an isolated CABG procedure boosts OR time and procedural costs, a successful ablation is likely to pay dividends through reduced downstream rates of major morbidity and mortality.
“I look forward to the second part of our analysis, where we’ll look at the comparative data for the patients who did in fact have surgical ablation. That dataset is pending from the Duke Clinical Research Institute,” according to Dr. Malaisrie.
He cited as study limitations the inability to complete linkage to the Medicare database in about 37% of CABG patients in the STS database, or more than 200,000 people. Also, the Medicare database is an administrative dataset reliant upon medical record coding. The mortality data are probably quite accurate, but the stroke and systemic embolization rates cited in this analysis likely underestimate the true rates.
He reported serving as a consultant to Edwards Lifesciences, Abbott Vascular, and Baxter, and serving on speakers’ bureaus for Bolton and Abiomed. However, the STS analysis was funded exclusively by philanthropy.
COLORADO SPRINGS – Preoperative atrial fibrillation is present in more than 10% of patients undergoing isolated coronary artery bypass graft (CABG) surgery, and if not subjected to concomitant surgical ablation it’s associated with increased perioperative and long-term major morbidity and mortality, S. Chris Malaisrie, MD, reported at the annual meeting of the Western Thoracic Surgical Association.
The increased early and late risks posed by preoperative atrial fibrillation (AF) that go unaddressed remain significant even after adjusting for the numerous comorbid conditions more prevalent in CABG patients with preoperative AF than in those without the arrhythmia, added Dr. Malaisrie, a cardiac surgeon at Northwestern University in Chicago.
The unadjusted operative mortality rate was 1.8% in the no-AF group and 4.0% in patients with preoperative AF. Unadjusted in-hospital rates of permanent stroke, prolonged ventilation, reoperation, and new renal failure were also significantly higher in the preoperative AF group.
Not surprisingly, the preoperative AF group was older. They also had significantly higher baseline rates of numerous comorbid conditions, including diabetes, peripheral vascular disease, renal failure, and prior stroke, as well as a lower mean left ventricular ejection fraction. However, after adjustment for the many comorbidities in multivariate regression analysis, the risks of all in-hospital adverse outcomes remained significantly higher in the preoperative AF group. For example, their adjusted risk of operative mortality was 1.5-fold greater than in the no-AF patients.
In the long-term follow-up analysis, the unadjusted risk of mortality in the first 5 years after CABG was 2.5-fold greater in the preoperative AF group. Their 5-year risk of stroke or systemic embolization was 1.5-fold greater, too. Upon adjustment for potentially confounding comorbid conditions, preoperative AF was associated with a 1.5-fold increased 5-year risk of mortality and a 1.2-fold increase in stroke or systemic embolism.
In an effort to identify a particularly high-risk group of CABG patients with preoperative AF, Dr. Malaisrie and his coinvestigators stratified the group’s long-term stroke and mortality risks by their CHA2DS2-VASc score at the time of surgery. The results were revealing: the unadjusted 5-year risk of stroke or systemic embolization was 7.9% in those with a CHA2DS2-VASc score of 1-3, 12.2% with a score of 4-6, and 15.4% with a score of 7-9. The 5-year survival rate was 74.8% with a score of 1-3, 56.5% with a score of 4-6, and 41.2% with a score of 7-9.
“That’s really a striking finding,” Dr. Malaisrie observed. “When you consider a patient who’s, say, 72-75 years old, who is undergoing isolated CABG with preoperative atrial fibrillation and who has a high CHA2DS2-VASc score of 7-9, 5-year survival is only 41%, with a 15% risk of stroke or systemic embolization.”
Discussant William T. Caine, MD, found the study results unsettling.
“I was surprised to see that in this day and age, fully two-thirds of the patients who had preoperative atrial fibrillation had no attempt at any ablation procedure to treat their atrial fibrillation,” declared Dr. Caine of Intermountain Medical Center in Salt Lake City.
In reply, Dr. Malaisrie noted that other, smaller studies have also found that only about 30% of CABG patients with preoperative AF undergo surgical AF ablation through a maze procedure or some other method.
“Probably most of us in this room would go ahead and perform surgical ablation, but the STS database represents all isolated CABG procedures done throughout the United States,” Dr. Malaisrie said. “I think this dataset should help convince the other 70% of surgeons out there that there is a high cost for preoperative AF – in particular, in patients with very high CHA2DS2-VASc scores. If you can identify a group of patients at increased risk for stroke and mortality, you’d certainly want to bend their survival curve.”
The maze procedure has been convincingly shown to be very safe, with no associated increased risk of perioperative morbidity and mortality. The downside is cost. But while it’s true that adding surgical ablation to an isolated CABG procedure boosts OR time and procedural costs, a successful ablation is likely to pay dividends through reduced downstream rates of major morbidity and mortality.
“I look forward to the second part of our analysis, where we’ll look at the comparative data for the patients who did in fact have surgical ablation. That dataset is pending from the Duke Clinical Research Institute,” according to Dr. Malaisrie.
He cited as study limitations the inability to complete linkage to the Medicare database in about 37% of CABG patients in the STS database, or more than 200,000 people. Also, the Medicare database is an administrative dataset reliant upon medical record coding. The mortality data are probably quite accurate, but the stroke and systemic embolization rates cited in this analysis likely underestimate the true rates.
He reported serving as a consultant to Edwards Lifesciences, Abbott Vascular, and Baxter, and serving on speakers’ bureaus for Bolton and Abiomed. However, the STS analysis was funded exclusively by philanthropy.
AT THE WTSA ANNUAL MEETING
Key clinical point:
Major finding: Preoperative AF in patients undergoing isolated CABG was tied to an adjusted 45% greater 5-year mortality and 25% increase in stroke and systemic embolization risk, compared with CABG patients without the preoperative arrhythmia.
Data source: This retrospective study compared perioperative and long-term morbidity and mortality in nearly 350,000 patients in the Society of Thoracic Surgeons database who underwent isolated CABG, including more than 24,000 who had preoperative atrial fibrillation that wasn’t addressed surgically.
Disclosures: The study presenter reported serving as a consultant to Edwards Lifesciences, Abbott Vascular, and Baxter, and serving on speakers’ bureaus for Bolton and Abiomed. However, the STS analysis was funded exclusively by philanthropy.