User login
Honoring a physician who led by example
In July, mostly unnoticed by Americans, a remarkable physician died in Japan.
Dr. Shigeaki Hinohara was a young 105 years old at the end, still practicing medicine.
When he was born in 1911, the average Japanese lifespan was 40. Due in part to him, it’s now one of the longest on Earth.
No stranger to medical disasters, he cared for those injured in the 1945 firebombing of Tokyo. Fifty years later, still working, he treated 640 victims of the 1995 nerve gas terror attack on the city’s subway. Between them, he survived being taken hostage in a 4-day plane hijacking in 1970.

He didn’t believe in retirement, since keeping busy is good. At the same time he advocated for finding fun in what you were doing.
A staunch opponent of obesity, he advocated a spartan lifestyle. For breakfast he had coffee, milk, and orange juice (the last with a spoonful of olive oil mixed in). For lunch (if he didn’t skip it) hard biscuits and milk. Dinner was vegetables, rice, and a small amount of either beef or fish.
He believed in exercise, even if it was limited to your daily routine. Always take stairs. Carry your own bags and packages. Even in his last months, using a cane, he walked 2,000 steps per day.
At the end, unable to eat, he still led by example. He refused a feeding tube and opted to leave quietly, passing on at home.
Medicine today, including my own field, is full of gadgets. Amazing tests and treatments. I believe in them 100%, and use them, as we all do, to help alleviate suffering and help people live longer and better lives.
But at the same time, we need to keep in mind that prevention is the best treatment. Keeping your mind active is good. Palliative care doesn’t mean you gave up.
In a world of increasing obesity, diabetes, and vascular disease, his simple advice on exercise and eating modestly is a lesson for many, including myself.
Never underestimate the benefits of music and pets.
And always have fun.
Good night, good doctor.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
In July, mostly unnoticed by Americans, a remarkable physician died in Japan.
Dr. Shigeaki Hinohara was a young 105 years old at the end, still practicing medicine.
When he was born in 1911, the average Japanese lifespan was 40. Due in part to him, it’s now one of the longest on Earth.
No stranger to medical disasters, he cared for those injured in the 1945 firebombing of Tokyo. Fifty years later, still working, he treated 640 victims of the 1995 nerve gas terror attack on the city’s subway. Between them, he survived being taken hostage in a 4-day plane hijacking in 1970.
He didn’t believe in retirement, since keeping busy is good. At the same time he advocated for finding fun in what you were doing.
A staunch opponent of obesity, he advocated a spartan lifestyle. For breakfast he had coffee, milk, and orange juice (the last with a spoonful of olive oil mixed in). For lunch (if he didn’t skip it) hard biscuits and milk. Dinner was vegetables, rice, and a small amount of either beef or fish.
He believed in exercise, even if it was limited to your daily routine. Always take stairs. Carry your own bags and packages. Even in his last months, using a cane, he walked 2,000 steps per day.
At the end, unable to eat, he still led by example. He refused a feeding tube and opted to leave quietly, passing on at home.
Medicine today, including my own field, is full of gadgets. Amazing tests and treatments. I believe in them 100%, and use them, as we all do, to help alleviate suffering and help people live longer and better lives.
But at the same time, we need to keep in mind that prevention is the best treatment. Keeping your mind active is good. Palliative care doesn’t mean you gave up.
In a world of increasing obesity, diabetes, and vascular disease, his simple advice on exercise and eating modestly is a lesson for many, including myself.
Never underestimate the benefits of music and pets.
And always have fun.
Good night, good doctor.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
In July, mostly unnoticed by Americans, a remarkable physician died in Japan.
Dr. Shigeaki Hinohara was a young 105 years old at the end, still practicing medicine.
When he was born in 1911, the average Japanese lifespan was 40. Due in part to him, it’s now one of the longest on Earth.
No stranger to medical disasters, he cared for those injured in the 1945 firebombing of Tokyo. Fifty years later, still working, he treated 640 victims of the 1995 nerve gas terror attack on the city’s subway. Between them, he survived being taken hostage in a 4-day plane hijacking in 1970.
He didn’t believe in retirement, since keeping busy is good. At the same time he advocated for finding fun in what you were doing.
A staunch opponent of obesity, he advocated a spartan lifestyle. For breakfast he had coffee, milk, and orange juice (the last with a spoonful of olive oil mixed in). For lunch (if he didn’t skip it) hard biscuits and milk. Dinner was vegetables, rice, and a small amount of either beef or fish.
He believed in exercise, even if it was limited to your daily routine. Always take stairs. Carry your own bags and packages. Even in his last months, using a cane, he walked 2,000 steps per day.
At the end, unable to eat, he still led by example. He refused a feeding tube and opted to leave quietly, passing on at home.
Medicine today, including my own field, is full of gadgets. Amazing tests and treatments. I believe in them 100%, and use them, as we all do, to help alleviate suffering and help people live longer and better lives.
But at the same time, we need to keep in mind that prevention is the best treatment. Keeping your mind active is good. Palliative care doesn’t mean you gave up.
In a world of increasing obesity, diabetes, and vascular disease, his simple advice on exercise and eating modestly is a lesson for many, including myself.
Never underestimate the benefits of music and pets.
And always have fun.
Good night, good doctor.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
New AML approvals changing the treatment landscape
With a recent flurry of new drug approvals, the treatment landscape for acute myeloid leukemia has expanded, raising new questions about how to incorporate those drugs into patient care.
Until about a decade ago, advances in AML therapy centered mainly around iterations of daunorubicin and cytarabine. Now, novel and targeted agents, many specifically going after mutational byproducts, are yielding some great results and raising hopes for better survival outcomes, Jeffrey Lancet, MD, said in an interview.
“When I go to sleep at night, I often dream about ... 10-year survival rates in the 80% range. And then I wake up ... and I realize this is actually [the survival curve for chronic myeloid leukemia]. This is where we’d like to be [with AML].” Those outcomes are a long way off, but appreciable incremental gains may lie ahead with the recent advances in AML therapy, said Dr. Lancet, chair of the department of malignant hematology at Moffitt Cancer Center in Tampa.
In addition to the new approvals, 16 drugs are in late stage clinical development and will likely contribute to an AML market that is expected to surpass $1.5 billion by 2026, according to projections by the market intelligence company GlobalData.
Vyxeos
The liposome-encapsulated combination of daunorubicin and cytarabine (Vyxeos) was approved in August by the Food and Drug Administration for the treatment of therapy-related AML and AML with myelodysplasia-related changes.
In a phase 3 randomized trial, the fixed-dose combination product was associated with median overall survival of 9.6 months, compared with 5.9 months with a standard combination of cytarabine and daunorubicin (7+3).
“I would envision that Vyxeos will hold and become the primary standard of care for fit chemotherapy-suitable older patients, or any patients for that matter, who are dealing with secondary-like AML or high-risk AML, based on the phase 3 results that we demonstrated,” Dr. Lancet, the principal investigator for the trial, said in an interview.
Asked whether the improved survival with Vyxeos is primarily related to more patients becoming transplant eligible or to significant reductions in disease burden, Dr. Lancet remarked that it’s likely a mixture of both.
The high remission rate with Vyxeos vs. standard 7+3 therapy means Vyxeos has the ability to stand on its own, and “the potential to send more patients to transplant and to get better results.”
“Transplant is part of the continuum of care of AML, including in older patients, and Vyxeos is going to become a standard part of that care,” he remarked. But transplant outcomes were not a predesignated component of the phase 3 trial, and further study will be needed to determine Vyxeos’ role as a bridge to transplant. “At this stage I can reasonably state that it has a role in the upfront therapy of secondary and high-risk AML, regardless of whether the patient is being considered for transplant.”
The early stages of working Vyxeos into the therapeutic mix come with some challenges, however, according to Donna Capozzi, PharmD.

Vyxeos is a fixed-dose combination that comes in vials containing 44 mg daunorubicin and 100 mg cytarabine encapsulated in liposomes. Patient dosing is based on the daunorubicin component and calculated based on body surface area (mg/m2), meaning the cytarabine dose does not need to be calculated. There are both pros and cons to this approach, she explained.
Benefits include a longer half-life with Vyxeos vs. standard 7+3, and the fact that during induction the drug is delivered on days 1, 3, and 5 for 90 minutes rather than continuously for 7 days as with 7+3, Dr. Capozzi said.
The main concern relates to ensuring that the dosing is calculated based on the proper component, she said.
“We had our first patient last week. It was very time consuming, with double and triple checking to make sure everything was correct,” she said. Preparing the drug is also time-consuming, as it involves multiple steps, such as warming, which is not required with standard 7+3; the additional labor factors will have to be built into workflow, she noted.
“The other piece not fully in place right now is building [the use of Vyxeos] into electronic health records,” she said, adding that safeguards put into place through EHRs will also help to streamline the administration process.
For example, cardiac toxicity is a known effect of daunorubicin; the EHR will help track lifetime cumulative dosing of that component, which is otherwise challenging, especially when using a combination product, she said.
The process will get easier over time, as use of Vyxeos becomes more prevalent in practice, she added. “None of these are insurmountable issues.”
Cost is another matter. Based on average wholesale prices, the cost per cycle is approximately $40,000 with Vyxeos vs. about $4,300 for conventional 7+3 therapy, Dr. Capozzi said. Given the differential, there will be a great deal of debate as to which patients will derive the most benefit from Vyxeos, she said.
Also, it will take time to figure out the extent of adverse events. “For liposomal products in general, rash-type side effects can be really significant. Hand-foot syndrome was not reported in the initial trials, but we’ll keep our eyes open to see how that plays out,” she said noting that the one patient treated so far at the University of Pennsylvania is doing very well. “We will learn more with real world experience.”
Oral targeted therapies
Enasidenib (Idhifa) was approved under priority review in August in conjunction with a companion diagnostic IDH2 assay for patients with relapsed or refractory disease and specific mutations in the IDH2 gene. Midostaurin (Rydapt) was approved in April for use in conjunction with standard daunorubicin and cytarabine induction and cytarabine consolidation in adults with FLT3 mutation-positive AML.
In a phase 1 dose escalation study reported at the annual meeting of the European Hematology Association, enasidenib was associated with an overall response rate of 37% in patients with relapsed/refractory AML, including 20.1% complete responses and 7.9% complete responses with incomplete recovery of platelets or incomplete hematologic recovery, 3.7% with partial responses, and 5.1% with a morphologic leukemia-free state. Patients who had a CR had a median overall survival of 22.9 months. For patients with responses other than CR, the median OS was 15.1 months. For patients with no response to the drug, the median OS was 5.6 months, Dr. Eytan M. Stein, of Memorial Sloan Kettering Cancer Center in New York, reported.
Additionally, need for transfusions was reduced in 34% of 157 patients who required transfusions at study entry.
“In a relapsed or refractory group of patients where there’s no true standard of care, this drug definitely represents a major breakthrough and has a lot of utility as a single agent, as a potential bridge to a transplant, and in combination with new or even old drugs – including regular old induction chemotherapy as a way to improve responses and outcomes in the future,” Dr. Lancet said, adding that as an oral agent it has potential for development as a maintenance strategy.
This agent could have a large impact, he said, adding: “I think this sets the paradigm for novel targeted therapies.”
Midostaurin has also emerged as a new standard of care, particularly for younger patients, Dr. Lancet said.
The approval of the multitargeted kinase inhibitor was based on the results of the randomized, placebo-controlled phase 3 RATIFY trial, which demonstrated significantly longer overall and event-free survival vs. placebo and standard chemotherapy in newly diagnosed AML patients with FLT3 gene mutations.
“I think this will be the new comparator for future studies, whatever they may be, for this patient population,” he said.
Dr. Capozzi noted that she has had some difficulty obtaining prior authorization for enasidenib due to its high cost (about $1,000/day).
The drug is taken orally on days 8-21 of a 28-day treatment cycle. In RATIFY, patients who achieved complete remission after induction therapy received four 28-day cycles of consolidation therapy.
Dr. Capozzi noted that the dosing regimen can be confusing, as it changes depending on whether it is used for induction or consolidation. It remains to be seen how these agents will fit into the treatment setting, she said.
Targeted therapies in development
Other targeted therapies in development for AML include an IDH1 inhibitor, the BCL2 inhibitor venetoclax, and several second-generation FLT3 inhibitors such as gilteritinib, Dr. Lancet said.
Venetoclax, which is currently approved for chronic lymphocytic leukemia, has shown single agent activity, but is even more promising in combination with low-dose cytarabine or aza-nucleosides, he noted.
For example, in one recent study reported at the annual congress of the European Hematology Association, response rates in older, newly diagnosed AML patients were as high as 72% for azacitidine plus venetoclax, and 76% for decitabine plus venetoclax.
“So there’s a lot of interest and promise,” Dr. Lancet said, adding that venetoclax may have broad application in AML. “We’ll be seeing a lot more data in the next year or two.”
An unusual aspect of venetoclax, which is used often for CLL, is the need for observation during dose escalation, Dr. Capozzi noted. Patients tend to question the need for admission for observation with the use of an oral agent, thus efforts are underway to develop criteria for outpatient observation.
Otherwise, venetoclax is fairly easy to access and use, and is well tolerated, she said.
“I expect as we learn more about where (venetoclax) fits in, it will be a much more commonplace agent” as part of AML therapy, she said.
Gilteritinib, as well as the second generation FLT3 inhibitors quizartinib and crenolanib, are also of interest in AML. With midostaurin already on the market, however, different strategies are being pursued, Dr. Lancet said.
“I believe gilteritinib is entering the fray in relapsed/refractory disease, and crenolanib is being looked at in the upfront FLT3 AML-positive setting and ultimately will be compared to midostaurin in combination with chemotherapy in that setting,” he added, noting that these drugs have the advantage of being more potent and selective inhibitors of FLT3, and some appear to have the ability to target resistance-conferring mutations.
“It still remains to be determined what the ultimate role will be, especially now that midostaurin is approved as frontline therapy and, in my opinion, will likely be entrenched there for awhile,” he said. “It’s a fairly competitive field right now, but certainly one where there’s a lot of excitement. The encouraging part is the second generation inhibitors, especially crenolanib and gilteritinib, are able to rescue some patients who may have failed primary therapy with an FLT3 inhibitor.”
Future direction and outcomes
So how should one go about selecting therapies, in the absence of data on combining therapies, for patients with multiple mutations?
Ideally, that means teasing out which of the AML patient’s mutations is clonal and the driver of their disease, and which one is subclonal. There are no guarantees, but that seems like a rational way to begin and move the field forward to studies of combination therapies, Dr. Lancet said.
“I think with the right combinations that target leukemias that are mutationally driven, there is potential to treat subsets of patient with very targeted therapies that will lead to prolonged survival. Right now, for the most part, we don’t have drugs for many of the targets that are very important in AML, and we don’t always know which target is driving the disease ... these are considerations that remain to be discovered,” he said. “But I do think that in 10 years we will have the ability with novel drugs and increased understanding of the clinical relevance of these targets to really personalize the approach more so than we are today, and to increase response rates significantly and improve survival as a result.”
Dr. Lancet is a consultant for Jazz Pharmaceuticals, Daiichi Sankyo, and Celgene. Dr. Capozzi reported having no disclosures.
With a recent flurry of new drug approvals, the treatment landscape for acute myeloid leukemia has expanded, raising new questions about how to incorporate those drugs into patient care.
Until about a decade ago, advances in AML therapy centered mainly around iterations of daunorubicin and cytarabine. Now, novel and targeted agents, many specifically going after mutational byproducts, are yielding some great results and raising hopes for better survival outcomes, Jeffrey Lancet, MD, said in an interview.
“When I go to sleep at night, I often dream about ... 10-year survival rates in the 80% range. And then I wake up ... and I realize this is actually [the survival curve for chronic myeloid leukemia]. This is where we’d like to be [with AML].” Those outcomes are a long way off, but appreciable incremental gains may lie ahead with the recent advances in AML therapy, said Dr. Lancet, chair of the department of malignant hematology at Moffitt Cancer Center in Tampa.
In addition to the new approvals, 16 drugs are in late stage clinical development and will likely contribute to an AML market that is expected to surpass $1.5 billion by 2026, according to projections by the market intelligence company GlobalData.
Vyxeos
The liposome-encapsulated combination of daunorubicin and cytarabine (Vyxeos) was approved in August by the Food and Drug Administration for the treatment of therapy-related AML and AML with myelodysplasia-related changes.
In a phase 3 randomized trial, the fixed-dose combination product was associated with median overall survival of 9.6 months, compared with 5.9 months with a standard combination of cytarabine and daunorubicin (7+3).
“I would envision that Vyxeos will hold and become the primary standard of care for fit chemotherapy-suitable older patients, or any patients for that matter, who are dealing with secondary-like AML or high-risk AML, based on the phase 3 results that we demonstrated,” Dr. Lancet, the principal investigator for the trial, said in an interview.
Asked whether the improved survival with Vyxeos is primarily related to more patients becoming transplant eligible or to significant reductions in disease burden, Dr. Lancet remarked that it’s likely a mixture of both.
The high remission rate with Vyxeos vs. standard 7+3 therapy means Vyxeos has the ability to stand on its own, and “the potential to send more patients to transplant and to get better results.”
“Transplant is part of the continuum of care of AML, including in older patients, and Vyxeos is going to become a standard part of that care,” he remarked. But transplant outcomes were not a predesignated component of the phase 3 trial, and further study will be needed to determine Vyxeos’ role as a bridge to transplant. “At this stage I can reasonably state that it has a role in the upfront therapy of secondary and high-risk AML, regardless of whether the patient is being considered for transplant.”
The early stages of working Vyxeos into the therapeutic mix come with some challenges, however, according to Donna Capozzi, PharmD.
Vyxeos is a fixed-dose combination that comes in vials containing 44 mg daunorubicin and 100 mg cytarabine encapsulated in liposomes. Patient dosing is based on the daunorubicin component and calculated based on body surface area (mg/m2), meaning the cytarabine dose does not need to be calculated. There are both pros and cons to this approach, she explained.
Benefits include a longer half-life with Vyxeos vs. standard 7+3, and the fact that during induction the drug is delivered on days 1, 3, and 5 for 90 minutes rather than continuously for 7 days as with 7+3, Dr. Capozzi said.
The main concern relates to ensuring that the dosing is calculated based on the proper component, she said.
“We had our first patient last week. It was very time consuming, with double and triple checking to make sure everything was correct,” she said. Preparing the drug is also time-consuming, as it involves multiple steps, such as warming, which is not required with standard 7+3; the additional labor factors will have to be built into workflow, she noted.
“The other piece not fully in place right now is building [the use of Vyxeos] into electronic health records,” she said, adding that safeguards put into place through EHRs will also help to streamline the administration process.
For example, cardiac toxicity is a known effect of daunorubicin; the EHR will help track lifetime cumulative dosing of that component, which is otherwise challenging, especially when using a combination product, she said.
The process will get easier over time, as use of Vyxeos becomes more prevalent in practice, she added. “None of these are insurmountable issues.”
Cost is another matter. Based on average wholesale prices, the cost per cycle is approximately $40,000 with Vyxeos vs. about $4,300 for conventional 7+3 therapy, Dr. Capozzi said. Given the differential, there will be a great deal of debate as to which patients will derive the most benefit from Vyxeos, she said.
Also, it will take time to figure out the extent of adverse events. “For liposomal products in general, rash-type side effects can be really significant. Hand-foot syndrome was not reported in the initial trials, but we’ll keep our eyes open to see how that plays out,” she said noting that the one patient treated so far at the University of Pennsylvania is doing very well. “We will learn more with real world experience.”
Oral targeted therapies
Enasidenib (Idhifa) was approved under priority review in August in conjunction with a companion diagnostic IDH2 assay for patients with relapsed or refractory disease and specific mutations in the IDH2 gene. Midostaurin (Rydapt) was approved in April for use in conjunction with standard daunorubicin and cytarabine induction and cytarabine consolidation in adults with FLT3 mutation-positive AML.
In a phase 1 dose escalation study reported at the annual meeting of the European Hematology Association, enasidenib was associated with an overall response rate of 37% in patients with relapsed/refractory AML, including 20.1% complete responses and 7.9% complete responses with incomplete recovery of platelets or incomplete hematologic recovery, 3.7% with partial responses, and 5.1% with a morphologic leukemia-free state. Patients who had a CR had a median overall survival of 22.9 months. For patients with responses other than CR, the median OS was 15.1 months. For patients with no response to the drug, the median OS was 5.6 months, Dr. Eytan M. Stein, of Memorial Sloan Kettering Cancer Center in New York, reported.
Additionally, need for transfusions was reduced in 34% of 157 patients who required transfusions at study entry.
“In a relapsed or refractory group of patients where there’s no true standard of care, this drug definitely represents a major breakthrough and has a lot of utility as a single agent, as a potential bridge to a transplant, and in combination with new or even old drugs – including regular old induction chemotherapy as a way to improve responses and outcomes in the future,” Dr. Lancet said, adding that as an oral agent it has potential for development as a maintenance strategy.
This agent could have a large impact, he said, adding: “I think this sets the paradigm for novel targeted therapies.”
Midostaurin has also emerged as a new standard of care, particularly for younger patients, Dr. Lancet said.
The approval of the multitargeted kinase inhibitor was based on the results of the randomized, placebo-controlled phase 3 RATIFY trial, which demonstrated significantly longer overall and event-free survival vs. placebo and standard chemotherapy in newly diagnosed AML patients with FLT3 gene mutations.
“I think this will be the new comparator for future studies, whatever they may be, for this patient population,” he said.
Dr. Capozzi noted that she has had some difficulty obtaining prior authorization for enasidenib due to its high cost (about $1,000/day).
The drug is taken orally on days 8-21 of a 28-day treatment cycle. In RATIFY, patients who achieved complete remission after induction therapy received four 28-day cycles of consolidation therapy.
Dr. Capozzi noted that the dosing regimen can be confusing, as it changes depending on whether it is used for induction or consolidation. It remains to be seen how these agents will fit into the treatment setting, she said.
Targeted therapies in development
Other targeted therapies in development for AML include an IDH1 inhibitor, the BCL2 inhibitor venetoclax, and several second-generation FLT3 inhibitors such as gilteritinib, Dr. Lancet said.
Venetoclax, which is currently approved for chronic lymphocytic leukemia, has shown single agent activity, but is even more promising in combination with low-dose cytarabine or aza-nucleosides, he noted.
For example, in one recent study reported at the annual congress of the European Hematology Association, response rates in older, newly diagnosed AML patients were as high as 72% for azacitidine plus venetoclax, and 76% for decitabine plus venetoclax.
“So there’s a lot of interest and promise,” Dr. Lancet said, adding that venetoclax may have broad application in AML. “We’ll be seeing a lot more data in the next year or two.”
An unusual aspect of venetoclax, which is used often for CLL, is the need for observation during dose escalation, Dr. Capozzi noted. Patients tend to question the need for admission for observation with the use of an oral agent, thus efforts are underway to develop criteria for outpatient observation.
Otherwise, venetoclax is fairly easy to access and use, and is well tolerated, she said.
“I expect as we learn more about where (venetoclax) fits in, it will be a much more commonplace agent” as part of AML therapy, she said.
Gilteritinib, as well as the second generation FLT3 inhibitors quizartinib and crenolanib, are also of interest in AML. With midostaurin already on the market, however, different strategies are being pursued, Dr. Lancet said.
“I believe gilteritinib is entering the fray in relapsed/refractory disease, and crenolanib is being looked at in the upfront FLT3 AML-positive setting and ultimately will be compared to midostaurin in combination with chemotherapy in that setting,” he added, noting that these drugs have the advantage of being more potent and selective inhibitors of FLT3, and some appear to have the ability to target resistance-conferring mutations.
“It still remains to be determined what the ultimate role will be, especially now that midostaurin is approved as frontline therapy and, in my opinion, will likely be entrenched there for awhile,” he said. “It’s a fairly competitive field right now, but certainly one where there’s a lot of excitement. The encouraging part is the second generation inhibitors, especially crenolanib and gilteritinib, are able to rescue some patients who may have failed primary therapy with an FLT3 inhibitor.”
Future direction and outcomes
So how should one go about selecting therapies, in the absence of data on combining therapies, for patients with multiple mutations?
Ideally, that means teasing out which of the AML patient’s mutations is clonal and the driver of their disease, and which one is subclonal. There are no guarantees, but that seems like a rational way to begin and move the field forward to studies of combination therapies, Dr. Lancet said.
“I think with the right combinations that target leukemias that are mutationally driven, there is potential to treat subsets of patient with very targeted therapies that will lead to prolonged survival. Right now, for the most part, we don’t have drugs for many of the targets that are very important in AML, and we don’t always know which target is driving the disease ... these are considerations that remain to be discovered,” he said. “But I do think that in 10 years we will have the ability with novel drugs and increased understanding of the clinical relevance of these targets to really personalize the approach more so than we are today, and to increase response rates significantly and improve survival as a result.”
Dr. Lancet is a consultant for Jazz Pharmaceuticals, Daiichi Sankyo, and Celgene. Dr. Capozzi reported having no disclosures.
With a recent flurry of new drug approvals, the treatment landscape for acute myeloid leukemia has expanded, raising new questions about how to incorporate those drugs into patient care.
Until about a decade ago, advances in AML therapy centered mainly around iterations of daunorubicin and cytarabine. Now, novel and targeted agents, many specifically going after mutational byproducts, are yielding some great results and raising hopes for better survival outcomes, Jeffrey Lancet, MD, said in an interview.
“When I go to sleep at night, I often dream about ... 10-year survival rates in the 80% range. And then I wake up ... and I realize this is actually [the survival curve for chronic myeloid leukemia]. This is where we’d like to be [with AML].” Those outcomes are a long way off, but appreciable incremental gains may lie ahead with the recent advances in AML therapy, said Dr. Lancet, chair of the department of malignant hematology at Moffitt Cancer Center in Tampa.
In addition to the new approvals, 16 drugs are in late stage clinical development and will likely contribute to an AML market that is expected to surpass $1.5 billion by 2026, according to projections by the market intelligence company GlobalData.
Vyxeos
The liposome-encapsulated combination of daunorubicin and cytarabine (Vyxeos) was approved in August by the Food and Drug Administration for the treatment of therapy-related AML and AML with myelodysplasia-related changes.
In a phase 3 randomized trial, the fixed-dose combination product was associated with median overall survival of 9.6 months, compared with 5.9 months with a standard combination of cytarabine and daunorubicin (7+3).
“I would envision that Vyxeos will hold and become the primary standard of care for fit chemotherapy-suitable older patients, or any patients for that matter, who are dealing with secondary-like AML or high-risk AML, based on the phase 3 results that we demonstrated,” Dr. Lancet, the principal investigator for the trial, said in an interview.
Asked whether the improved survival with Vyxeos is primarily related to more patients becoming transplant eligible or to significant reductions in disease burden, Dr. Lancet remarked that it’s likely a mixture of both.
The high remission rate with Vyxeos vs. standard 7+3 therapy means Vyxeos has the ability to stand on its own, and “the potential to send more patients to transplant and to get better results.”
“Transplant is part of the continuum of care of AML, including in older patients, and Vyxeos is going to become a standard part of that care,” he remarked. But transplant outcomes were not a predesignated component of the phase 3 trial, and further study will be needed to determine Vyxeos’ role as a bridge to transplant. “At this stage I can reasonably state that it has a role in the upfront therapy of secondary and high-risk AML, regardless of whether the patient is being considered for transplant.”
The early stages of working Vyxeos into the therapeutic mix come with some challenges, however, according to Donna Capozzi, PharmD.
Vyxeos is a fixed-dose combination that comes in vials containing 44 mg daunorubicin and 100 mg cytarabine encapsulated in liposomes. Patient dosing is based on the daunorubicin component and calculated based on body surface area (mg/m2), meaning the cytarabine dose does not need to be calculated. There are both pros and cons to this approach, she explained.
Benefits include a longer half-life with Vyxeos vs. standard 7+3, and the fact that during induction the drug is delivered on days 1, 3, and 5 for 90 minutes rather than continuously for 7 days as with 7+3, Dr. Capozzi said.
The main concern relates to ensuring that the dosing is calculated based on the proper component, she said.
“We had our first patient last week. It was very time consuming, with double and triple checking to make sure everything was correct,” she said. Preparing the drug is also time-consuming, as it involves multiple steps, such as warming, which is not required with standard 7+3; the additional labor factors will have to be built into workflow, she noted.
“The other piece not fully in place right now is building [the use of Vyxeos] into electronic health records,” she said, adding that safeguards put into place through EHRs will also help to streamline the administration process.
For example, cardiac toxicity is a known effect of daunorubicin; the EHR will help track lifetime cumulative dosing of that component, which is otherwise challenging, especially when using a combination product, she said.
The process will get easier over time, as use of Vyxeos becomes more prevalent in practice, she added. “None of these are insurmountable issues.”
Cost is another matter. Based on average wholesale prices, the cost per cycle is approximately $40,000 with Vyxeos vs. about $4,300 for conventional 7+3 therapy, Dr. Capozzi said. Given the differential, there will be a great deal of debate as to which patients will derive the most benefit from Vyxeos, she said.
Also, it will take time to figure out the extent of adverse events. “For liposomal products in general, rash-type side effects can be really significant. Hand-foot syndrome was not reported in the initial trials, but we’ll keep our eyes open to see how that plays out,” she said noting that the one patient treated so far at the University of Pennsylvania is doing very well. “We will learn more with real world experience.”
Oral targeted therapies
Enasidenib (Idhifa) was approved under priority review in August in conjunction with a companion diagnostic IDH2 assay for patients with relapsed or refractory disease and specific mutations in the IDH2 gene. Midostaurin (Rydapt) was approved in April for use in conjunction with standard daunorubicin and cytarabine induction and cytarabine consolidation in adults with FLT3 mutation-positive AML.
In a phase 1 dose escalation study reported at the annual meeting of the European Hematology Association, enasidenib was associated with an overall response rate of 37% in patients with relapsed/refractory AML, including 20.1% complete responses and 7.9% complete responses with incomplete recovery of platelets or incomplete hematologic recovery, 3.7% with partial responses, and 5.1% with a morphologic leukemia-free state. Patients who had a CR had a median overall survival of 22.9 months. For patients with responses other than CR, the median OS was 15.1 months. For patients with no response to the drug, the median OS was 5.6 months, Dr. Eytan M. Stein, of Memorial Sloan Kettering Cancer Center in New York, reported.
Additionally, need for transfusions was reduced in 34% of 157 patients who required transfusions at study entry.
“In a relapsed or refractory group of patients where there’s no true standard of care, this drug definitely represents a major breakthrough and has a lot of utility as a single agent, as a potential bridge to a transplant, and in combination with new or even old drugs – including regular old induction chemotherapy as a way to improve responses and outcomes in the future,” Dr. Lancet said, adding that as an oral agent it has potential for development as a maintenance strategy.
This agent could have a large impact, he said, adding: “I think this sets the paradigm for novel targeted therapies.”
Midostaurin has also emerged as a new standard of care, particularly for younger patients, Dr. Lancet said.
The approval of the multitargeted kinase inhibitor was based on the results of the randomized, placebo-controlled phase 3 RATIFY trial, which demonstrated significantly longer overall and event-free survival vs. placebo and standard chemotherapy in newly diagnosed AML patients with FLT3 gene mutations.
“I think this will be the new comparator for future studies, whatever they may be, for this patient population,” he said.
Dr. Capozzi noted that she has had some difficulty obtaining prior authorization for enasidenib due to its high cost (about $1,000/day).
The drug is taken orally on days 8-21 of a 28-day treatment cycle. In RATIFY, patients who achieved complete remission after induction therapy received four 28-day cycles of consolidation therapy.
Dr. Capozzi noted that the dosing regimen can be confusing, as it changes depending on whether it is used for induction or consolidation. It remains to be seen how these agents will fit into the treatment setting, she said.
Targeted therapies in development
Other targeted therapies in development for AML include an IDH1 inhibitor, the BCL2 inhibitor venetoclax, and several second-generation FLT3 inhibitors such as gilteritinib, Dr. Lancet said.
Venetoclax, which is currently approved for chronic lymphocytic leukemia, has shown single agent activity, but is even more promising in combination with low-dose cytarabine or aza-nucleosides, he noted.
For example, in one recent study reported at the annual congress of the European Hematology Association, response rates in older, newly diagnosed AML patients were as high as 72% for azacitidine plus venetoclax, and 76% for decitabine plus venetoclax.
“So there’s a lot of interest and promise,” Dr. Lancet said, adding that venetoclax may have broad application in AML. “We’ll be seeing a lot more data in the next year or two.”
An unusual aspect of venetoclax, which is used often for CLL, is the need for observation during dose escalation, Dr. Capozzi noted. Patients tend to question the need for admission for observation with the use of an oral agent, thus efforts are underway to develop criteria for outpatient observation.
Otherwise, venetoclax is fairly easy to access and use, and is well tolerated, she said.
“I expect as we learn more about where (venetoclax) fits in, it will be a much more commonplace agent” as part of AML therapy, she said.
Gilteritinib, as well as the second generation FLT3 inhibitors quizartinib and crenolanib, are also of interest in AML. With midostaurin already on the market, however, different strategies are being pursued, Dr. Lancet said.
“I believe gilteritinib is entering the fray in relapsed/refractory disease, and crenolanib is being looked at in the upfront FLT3 AML-positive setting and ultimately will be compared to midostaurin in combination with chemotherapy in that setting,” he added, noting that these drugs have the advantage of being more potent and selective inhibitors of FLT3, and some appear to have the ability to target resistance-conferring mutations.
“It still remains to be determined what the ultimate role will be, especially now that midostaurin is approved as frontline therapy and, in my opinion, will likely be entrenched there for awhile,” he said. “It’s a fairly competitive field right now, but certainly one where there’s a lot of excitement. The encouraging part is the second generation inhibitors, especially crenolanib and gilteritinib, are able to rescue some patients who may have failed primary therapy with an FLT3 inhibitor.”
Future direction and outcomes
So how should one go about selecting therapies, in the absence of data on combining therapies, for patients with multiple mutations?
Ideally, that means teasing out which of the AML patient’s mutations is clonal and the driver of their disease, and which one is subclonal. There are no guarantees, but that seems like a rational way to begin and move the field forward to studies of combination therapies, Dr. Lancet said.
“I think with the right combinations that target leukemias that are mutationally driven, there is potential to treat subsets of patient with very targeted therapies that will lead to prolonged survival. Right now, for the most part, we don’t have drugs for many of the targets that are very important in AML, and we don’t always know which target is driving the disease ... these are considerations that remain to be discovered,” he said. “But I do think that in 10 years we will have the ability with novel drugs and increased understanding of the clinical relevance of these targets to really personalize the approach more so than we are today, and to increase response rates significantly and improve survival as a result.”
Dr. Lancet is a consultant for Jazz Pharmaceuticals, Daiichi Sankyo, and Celgene. Dr. Capozzi reported having no disclosures.

Tender Edematous Nodules on the Hand
The Diagnosis: Ecthyma Contagiosum (Orf)
Orf, or ecthyma contagiosum, is a zoonotic cutaneous infection caused by the orf DNA virus of the genus Parapoxvirus of the family Poxviridae. It is transmitted to humans through direct contact with infected animals, namely sheep and goats, and as such is most commonly seen in patients with occupational exposure to these animals such as butchers, farmers, veterinarians, and shepherds.1,2 Human-to-human transmission is exceedingly rare in immunocompetent patients.2,3 In affected animals, lesions usually are found around the mouth, muzzle, and eyes. In humans, hands are the most commonly affected site, and lesions occur 3 to 10 days after contact. Clinically, the lesions are nonspecific, and our patient presented with tender, erythematous, edematous nodules on the left hand. The differential diagnosis is broad and includes a milker's nodule, pyogenic granuloma, tularemia, anthrax, atypical mycobacterial infection, and sporotrichosis.1,4,5
The diagnosis usually is made with a thorough history and examination, but in cases of uncertainty, routine pathology with hematoxylin and eosin staining, electron microscopy, or real-time polymerase chain reaction may be used.2-4 Histopathologically, lesions demonstrate intraepidermal vesicles, vacuolization of keratinocytes of the upper epidermis with characteristic cytoplasmic inclusion bodies, rete ridge elongation, and dilated vessels in the intervening dermal papillae. Central necrosis may occur in well-developed lesions.2,6 Interestingly, our patient's biopsy exhibited all of these findings (Figure). Immunostains for cytomegalovirus and herpes simplex virus were negative, and Grocott-Gomori methenamine-silver and acid-fast bacillus stains also were negative.

Our patient also developed lymphangitic streaking suggestive of a bacterial superinfection and was treated with a course of intravenous antibiotics. She eventually was discharged with reassurance, wound care instructions, and outpatient antibiotics. She returned to an outside institution's emergency department for further evaluation, and she was admitted for workup. A lesional swab was sent for real-time polymerase chain reaction, which confirmed the diagnosis as orf. When the patient was contacted for follow-up 1 week after biopsy, the hand lesions had notably improved.
Orf is self-limited and typically resolves within 4 to 8 weeks after undergoing evolution through 5 described stages. The maculopapular stage is denoted by enlarging erythematous macule. The targetoid stage is described by a red center within a white halo surrounded by a broader red halo. The nodular stage is self-descriptive. The regenerative and regression stages describe the progressively improving, drier, and crusted nodules.3
Because orf is self-limited, no treatment is required, and patients should be counseled that their lesions should resolve within weeks. Complications include lymphangitis, secondary bacterial infection, and erythema multiforme.1,2,4,5 Immunocompromised patients may develop recalcitrant, giant, or multiple lesions that may be treated with topical imiquimod, topical cidofovir, intralesional interferon alfa, or surgical excision.1,2,4,7
We present a case of orf to remind practitioners of this rare entity. Although the disease is endemic worldwide, it likely is underreported due to its self-limited nature.2,4 A careful history may reveal the diagnosis, and overtreatment with antibiotics, many of which have their own significant side-effect profile, can then be avoided.
Acknowledgment
We thank Eric Behling, MD (Camden, New Jersey), for his contributions in obtaining the histologic images.
- Veraldi S, Nazzaro G, Vaira F, et al. Presentation of orf (ecthyma contagiosum) after sheep slaughtering for religious feasts. Infection. 2014;42:767-769.
- Al-Salam S, Nowotny N, Sohail MR, et al. Ecthyma contagiosum (orf)--report of a human case from the United Arab Emirates and review of the literature. J Cutan Pathol. 2008;35:603-607.
- Thurman RJ, Fitch RW. Images in clinical medicine. contagious ecthyma. N Engl J Med. 2015;372:E12.
- Meier R, Sommacal A, Stahel A, et al. Orf--an orphan disease? JRSM Open. 2015;6:2054270415593718.
- Joseph RH, Haddad FA, Matthews AL, et al. Erythema multiforme after orf virus infection: a report of two cases and literature review. Epidemiol Infect. 2015;143:385-390.
- Xu X, Yun SJ, Erikson L, et al. Diseases caused by viruses. In: Elder DE, Elenitsas R, Rosenbach M, eds. Lever's Histopathology of the Skin. 11th ed. Philadelphia, PA: Wolters Kluwer; 2015:781-815.
- Koufakis T, Katsaitis P, Gabranis I. Orf disease: a report of a case. Braz J Infect Dis. 2014;18:568-569.
The Diagnosis: Ecthyma Contagiosum (Orf)
Orf, or ecthyma contagiosum, is a zoonotic cutaneous infection caused by the orf DNA virus of the genus Parapoxvirus of the family Poxviridae. It is transmitted to humans through direct contact with infected animals, namely sheep and goats, and as such is most commonly seen in patients with occupational exposure to these animals such as butchers, farmers, veterinarians, and shepherds.1,2 Human-to-human transmission is exceedingly rare in immunocompetent patients.2,3 In affected animals, lesions usually are found around the mouth, muzzle, and eyes. In humans, hands are the most commonly affected site, and lesions occur 3 to 10 days after contact. Clinically, the lesions are nonspecific, and our patient presented with tender, erythematous, edematous nodules on the left hand. The differential diagnosis is broad and includes a milker's nodule, pyogenic granuloma, tularemia, anthrax, atypical mycobacterial infection, and sporotrichosis.1,4,5
The diagnosis usually is made with a thorough history and examination, but in cases of uncertainty, routine pathology with hematoxylin and eosin staining, electron microscopy, or real-time polymerase chain reaction may be used.2-4 Histopathologically, lesions demonstrate intraepidermal vesicles, vacuolization of keratinocytes of the upper epidermis with characteristic cytoplasmic inclusion bodies, rete ridge elongation, and dilated vessels in the intervening dermal papillae. Central necrosis may occur in well-developed lesions.2,6 Interestingly, our patient's biopsy exhibited all of these findings (Figure). Immunostains for cytomegalovirus and herpes simplex virus were negative, and Grocott-Gomori methenamine-silver and acid-fast bacillus stains also were negative.
Our patient also developed lymphangitic streaking suggestive of a bacterial superinfection and was treated with a course of intravenous antibiotics. She eventually was discharged with reassurance, wound care instructions, and outpatient antibiotics. She returned to an outside institution's emergency department for further evaluation, and she was admitted for workup. A lesional swab was sent for real-time polymerase chain reaction, which confirmed the diagnosis as orf. When the patient was contacted for follow-up 1 week after biopsy, the hand lesions had notably improved.
Orf is self-limited and typically resolves within 4 to 8 weeks after undergoing evolution through 5 described stages. The maculopapular stage is denoted by enlarging erythematous macule. The targetoid stage is described by a red center within a white halo surrounded by a broader red halo. The nodular stage is self-descriptive. The regenerative and regression stages describe the progressively improving, drier, and crusted nodules.3
Because orf is self-limited, no treatment is required, and patients should be counseled that their lesions should resolve within weeks. Complications include lymphangitis, secondary bacterial infection, and erythema multiforme.1,2,4,5 Immunocompromised patients may develop recalcitrant, giant, or multiple lesions that may be treated with topical imiquimod, topical cidofovir, intralesional interferon alfa, or surgical excision.1,2,4,7
We present a case of orf to remind practitioners of this rare entity. Although the disease is endemic worldwide, it likely is underreported due to its self-limited nature.2,4 A careful history may reveal the diagnosis, and overtreatment with antibiotics, many of which have their own significant side-effect profile, can then be avoided.
Acknowledgment
We thank Eric Behling, MD (Camden, New Jersey), for his contributions in obtaining the histologic images.
The Diagnosis: Ecthyma Contagiosum (Orf)
Orf, or ecthyma contagiosum, is a zoonotic cutaneous infection caused by the orf DNA virus of the genus Parapoxvirus of the family Poxviridae. It is transmitted to humans through direct contact with infected animals, namely sheep and goats, and as such is most commonly seen in patients with occupational exposure to these animals such as butchers, farmers, veterinarians, and shepherds.1,2 Human-to-human transmission is exceedingly rare in immunocompetent patients.2,3 In affected animals, lesions usually are found around the mouth, muzzle, and eyes. In humans, hands are the most commonly affected site, and lesions occur 3 to 10 days after contact. Clinically, the lesions are nonspecific, and our patient presented with tender, erythematous, edematous nodules on the left hand. The differential diagnosis is broad and includes a milker's nodule, pyogenic granuloma, tularemia, anthrax, atypical mycobacterial infection, and sporotrichosis.1,4,5
The diagnosis usually is made with a thorough history and examination, but in cases of uncertainty, routine pathology with hematoxylin and eosin staining, electron microscopy, or real-time polymerase chain reaction may be used.2-4 Histopathologically, lesions demonstrate intraepidermal vesicles, vacuolization of keratinocytes of the upper epidermis with characteristic cytoplasmic inclusion bodies, rete ridge elongation, and dilated vessels in the intervening dermal papillae. Central necrosis may occur in well-developed lesions.2,6 Interestingly, our patient's biopsy exhibited all of these findings (Figure). Immunostains for cytomegalovirus and herpes simplex virus were negative, and Grocott-Gomori methenamine-silver and acid-fast bacillus stains also were negative.
Our patient also developed lymphangitic streaking suggestive of a bacterial superinfection and was treated with a course of intravenous antibiotics. She eventually was discharged with reassurance, wound care instructions, and outpatient antibiotics. She returned to an outside institution's emergency department for further evaluation, and she was admitted for workup. A lesional swab was sent for real-time polymerase chain reaction, which confirmed the diagnosis as orf. When the patient was contacted for follow-up 1 week after biopsy, the hand lesions had notably improved.
Orf is self-limited and typically resolves within 4 to 8 weeks after undergoing evolution through 5 described stages. The maculopapular stage is denoted by enlarging erythematous macule. The targetoid stage is described by a red center within a white halo surrounded by a broader red halo. The nodular stage is self-descriptive. The regenerative and regression stages describe the progressively improving, drier, and crusted nodules.3
Because orf is self-limited, no treatment is required, and patients should be counseled that their lesions should resolve within weeks. Complications include lymphangitis, secondary bacterial infection, and erythema multiforme.1,2,4,5 Immunocompromised patients may develop recalcitrant, giant, or multiple lesions that may be treated with topical imiquimod, topical cidofovir, intralesional interferon alfa, or surgical excision.1,2,4,7
We present a case of orf to remind practitioners of this rare entity. Although the disease is endemic worldwide, it likely is underreported due to its self-limited nature.2,4 A careful history may reveal the diagnosis, and overtreatment with antibiotics, many of which have their own significant side-effect profile, can then be avoided.
Acknowledgment
We thank Eric Behling, MD (Camden, New Jersey), for his contributions in obtaining the histologic images.
- Veraldi S, Nazzaro G, Vaira F, et al. Presentation of orf (ecthyma contagiosum) after sheep slaughtering for religious feasts. Infection. 2014;42:767-769.
- Al-Salam S, Nowotny N, Sohail MR, et al. Ecthyma contagiosum (orf)--report of a human case from the United Arab Emirates and review of the literature. J Cutan Pathol. 2008;35:603-607.
- Thurman RJ, Fitch RW. Images in clinical medicine. contagious ecthyma. N Engl J Med. 2015;372:E12.
- Meier R, Sommacal A, Stahel A, et al. Orf--an orphan disease? JRSM Open. 2015;6:2054270415593718.
- Joseph RH, Haddad FA, Matthews AL, et al. Erythema multiforme after orf virus infection: a report of two cases and literature review. Epidemiol Infect. 2015;143:385-390.
- Xu X, Yun SJ, Erikson L, et al. Diseases caused by viruses. In: Elder DE, Elenitsas R, Rosenbach M, eds. Lever's Histopathology of the Skin. 11th ed. Philadelphia, PA: Wolters Kluwer; 2015:781-815.
- Koufakis T, Katsaitis P, Gabranis I. Orf disease: a report of a case. Braz J Infect Dis. 2014;18:568-569.
- Veraldi S, Nazzaro G, Vaira F, et al. Presentation of orf (ecthyma contagiosum) after sheep slaughtering for religious feasts. Infection. 2014;42:767-769.
- Al-Salam S, Nowotny N, Sohail MR, et al. Ecthyma contagiosum (orf)--report of a human case from the United Arab Emirates and review of the literature. J Cutan Pathol. 2008;35:603-607.
- Thurman RJ, Fitch RW. Images in clinical medicine. contagious ecthyma. N Engl J Med. 2015;372:E12.
- Meier R, Sommacal A, Stahel A, et al. Orf--an orphan disease? JRSM Open. 2015;6:2054270415593718.
- Joseph RH, Haddad FA, Matthews AL, et al. Erythema multiforme after orf virus infection: a report of two cases and literature review. Epidemiol Infect. 2015;143:385-390.
- Xu X, Yun SJ, Erikson L, et al. Diseases caused by viruses. In: Elder DE, Elenitsas R, Rosenbach M, eds. Lever's Histopathology of the Skin. 11th ed. Philadelphia, PA: Wolters Kluwer; 2015:781-815.
- Koufakis T, Katsaitis P, Gabranis I. Orf disease: a report of a case. Braz J Infect Dis. 2014;18:568-569.

A 57-year-old woman presented to the emergency department (ED) for evaluation of a rash on the left hand of 2 weeks' duration. She described pinpoint red lesions on the left palm, as well as the third, fourth, and fifth fingers, which gradually enlarged and became painful. She denied any specific trauma but recalled cutting her hand on a piece of metal in the ground prior to the onset of the rash. She worked on a farm and bottle-fed sheep and chickens. Physical examination revealed tender edematous nodules with central gray pustules, and the left axillary lymph node was enlarged and tender. Ulceration was not appreciated. Various antibiotics including cephalexin, trimethoprim-sulfamethoxazole, and clindamycin were prescribed during prior ED visits, but she reported no improvement with these medications. She remained afebrile throughout the course of the hand rash, and laboratory workup was consistently unremarkable. Two sets of herpes simplex virus cultures from the ED visits showed no growth, and a hand radiograph also was normal. Medical history included coronary artery disease, myocardial infarction, mitral regurgitation, and hyperlipidemia.

Hospitalist movers and shakers – Sept. 2017
Robert Harrington, MD, recently was tabbed as chief medical officer of SurveyVitals, a health care analytics company specializing in digital patient-experience surveys. Dr. Harrington has 20 years experience, including CMO roles with Reliant Post–Acute Care Solutions and Locum Leaders, a hospitalist staffing firm.

Dr. Harrington is a senior fellow in Hospital Medicine and is past president and member of the board of directors with the Society of Hospital Medicine.
David Northington, DO, has been named the new chief medical officer at Stone County Hospital in Wiggins, Miss. The former hospitalist comes to Stone County after working as chief of staff and chief medical information officer at Memorial Hospital in Gulfport, Miss., where he was also medical director of the hospitalist program.
In addition to his new role, Dr. Northington will serve as medical director of the Woodland Village Nursing Center in Diamondhead, Miss., and the Stone County Nursing and Rehabilitation Center in Wiggins.
Schuyler K. Geller, MD, has been recognized by Continental Who’s Who as a Pinnacle Lifetime Member in the medical field. Dr. Geller works as a full-time hospitalist and a principal consultant for The CopperRidge Group, which provides guidance to patients in health, wellness, and fitness services and products.
In addition to his work at the CopperRidge Group, Dr. Geller is a member of Civil Vision International’s board of directors. He has extensive civilian and military-based experience in the United States, Africa, the Middle East, and South Asia.
A physician leader in the U.S. Air Force, Dr. Geller earned White House Medical Unit commendations for planning and leading the surgical and intensive care unit teams to support President Clinton’s trips to Vietnam and Africa in 2000.
Nikhil Sharma, MD, recently was selected by the International Association of HealthCare Professionals to be part of the Leading Physicians of the World. Dr. Sharma is a hospitalist serving at the Ochsner Health System in New Orleans.
Dr. Sharma, a member of the Southern Hospital Association and the Louisiana Medical Association, began his medical career in 2009 with a residency and fellowship at Ochsner, where he has remained ever since. He specializes in internal medicine and transplants.
I. Carol Nwelue, MD, a longtime hospitalist and the medical director of the Sparrow Medical Group Adult Hospitalist Service, recently received the Sparrow Physician Leadership Award. The award goes to an emerging leader who provides outstanding work in areas such as safety, clinical or service excellence, research, teaching, publishing, teamwork, and innovation.
Dr. Nwelue completed the Sparrow Physician Leadership Academy program, earning recognition for innovation in leadership, as well as practice management.
Laura Jin, MD, recently was promoted to medical director for utilization management at the University of Maryland Shore Regional Health. In her new role, Dr. Jin will identify and facilitate the resolution of utilization issues; in so doing, she will serve as a consultant leader to the health care system, its physicians, its advance practice providers, and the care management team.
Dr. Jin will remain as a hospitalist at Digestive Health Associates while fulfilling the duties in her new position at Shore Regional. She will guide the center on issues such as compliance, level of care, length of stay, resource management, reimbursement, emergency department throughput, and more.
Business Moves
The Mount Sinai Health System and The New Jewish Home, both based in New York City, have extended their relationship to improve care of hospitalized patients who require specialized post-acute or long-term care at a skilled nursing facility. Through the Mount Sinai-New Jewish Home Hospitalist Program, Mount Sinai hospitalists will be charged with providing a seamless transition to The New Jewish Home for patients who need nursing care.
This model will buoy communication and ensure the sharing of vital information between the two venues, reducing the risk of rehospitalization.
Gryphon Investors, based in San Francisco, recently announced it will acquire OB Hospitalist Group, one of the nation’s leading providers of obstetric hospital medicine. The deal with OBHG’s current partner, Ares Management, was finalized in late July.
OBHG, based out of Mauldin, S.C., has a national network of more than 550 OB hospitalists, covering more than 120 hospitals in 28 states. OBHG’s hospitalist program features an obstetric emergency department, providing expectant mothers at partner hospitals with 24/7/365 access to medical care.
Envision Healthcare, based in Nashville, Tenn., and Greenwood Village, Colo., a provider of physician-led services and ambulatory surgery services, has acquired Milwaukee-based Infinity Healthcare. Infinity’s group-physician practice includes more than 340 physicians and providers delivering emergency and hospital medicine, anesthesia, and radiology services.
Robert Harrington, MD, recently was tabbed as chief medical officer of SurveyVitals, a health care analytics company specializing in digital patient-experience surveys. Dr. Harrington has 20 years experience, including CMO roles with Reliant Post–Acute Care Solutions and Locum Leaders, a hospitalist staffing firm.
Dr. Harrington is a senior fellow in Hospital Medicine and is past president and member of the board of directors with the Society of Hospital Medicine.
David Northington, DO, has been named the new chief medical officer at Stone County Hospital in Wiggins, Miss. The former hospitalist comes to Stone County after working as chief of staff and chief medical information officer at Memorial Hospital in Gulfport, Miss., where he was also medical director of the hospitalist program.
In addition to his new role, Dr. Northington will serve as medical director of the Woodland Village Nursing Center in Diamondhead, Miss., and the Stone County Nursing and Rehabilitation Center in Wiggins.
Schuyler K. Geller, MD, has been recognized by Continental Who’s Who as a Pinnacle Lifetime Member in the medical field. Dr. Geller works as a full-time hospitalist and a principal consultant for The CopperRidge Group, which provides guidance to patients in health, wellness, and fitness services and products.
In addition to his work at the CopperRidge Group, Dr. Geller is a member of Civil Vision International’s board of directors. He has extensive civilian and military-based experience in the United States, Africa, the Middle East, and South Asia.
A physician leader in the U.S. Air Force, Dr. Geller earned White House Medical Unit commendations for planning and leading the surgical and intensive care unit teams to support President Clinton’s trips to Vietnam and Africa in 2000.
Nikhil Sharma, MD, recently was selected by the International Association of HealthCare Professionals to be part of the Leading Physicians of the World. Dr. Sharma is a hospitalist serving at the Ochsner Health System in New Orleans.
Dr. Sharma, a member of the Southern Hospital Association and the Louisiana Medical Association, began his medical career in 2009 with a residency and fellowship at Ochsner, where he has remained ever since. He specializes in internal medicine and transplants.
I. Carol Nwelue, MD, a longtime hospitalist and the medical director of the Sparrow Medical Group Adult Hospitalist Service, recently received the Sparrow Physician Leadership Award. The award goes to an emerging leader who provides outstanding work in areas such as safety, clinical or service excellence, research, teaching, publishing, teamwork, and innovation.
Dr. Nwelue completed the Sparrow Physician Leadership Academy program, earning recognition for innovation in leadership, as well as practice management.
Laura Jin, MD, recently was promoted to medical director for utilization management at the University of Maryland Shore Regional Health. In her new role, Dr. Jin will identify and facilitate the resolution of utilization issues; in so doing, she will serve as a consultant leader to the health care system, its physicians, its advance practice providers, and the care management team.
Dr. Jin will remain as a hospitalist at Digestive Health Associates while fulfilling the duties in her new position at Shore Regional. She will guide the center on issues such as compliance, level of care, length of stay, resource management, reimbursement, emergency department throughput, and more.
Business Moves
The Mount Sinai Health System and The New Jewish Home, both based in New York City, have extended their relationship to improve care of hospitalized patients who require specialized post-acute or long-term care at a skilled nursing facility. Through the Mount Sinai-New Jewish Home Hospitalist Program, Mount Sinai hospitalists will be charged with providing a seamless transition to The New Jewish Home for patients who need nursing care.
This model will buoy communication and ensure the sharing of vital information between the two venues, reducing the risk of rehospitalization.
Gryphon Investors, based in San Francisco, recently announced it will acquire OB Hospitalist Group, one of the nation’s leading providers of obstetric hospital medicine. The deal with OBHG’s current partner, Ares Management, was finalized in late July.
OBHG, based out of Mauldin, S.C., has a national network of more than 550 OB hospitalists, covering more than 120 hospitals in 28 states. OBHG’s hospitalist program features an obstetric emergency department, providing expectant mothers at partner hospitals with 24/7/365 access to medical care.
Envision Healthcare, based in Nashville, Tenn., and Greenwood Village, Colo., a provider of physician-led services and ambulatory surgery services, has acquired Milwaukee-based Infinity Healthcare. Infinity’s group-physician practice includes more than 340 physicians and providers delivering emergency and hospital medicine, anesthesia, and radiology services.
Robert Harrington, MD, recently was tabbed as chief medical officer of SurveyVitals, a health care analytics company specializing in digital patient-experience surveys. Dr. Harrington has 20 years experience, including CMO roles with Reliant Post–Acute Care Solutions and Locum Leaders, a hospitalist staffing firm.
Dr. Harrington is a senior fellow in Hospital Medicine and is past president and member of the board of directors with the Society of Hospital Medicine.
David Northington, DO, has been named the new chief medical officer at Stone County Hospital in Wiggins, Miss. The former hospitalist comes to Stone County after working as chief of staff and chief medical information officer at Memorial Hospital in Gulfport, Miss., where he was also medical director of the hospitalist program.
In addition to his new role, Dr. Northington will serve as medical director of the Woodland Village Nursing Center in Diamondhead, Miss., and the Stone County Nursing and Rehabilitation Center in Wiggins.
Schuyler K. Geller, MD, has been recognized by Continental Who’s Who as a Pinnacle Lifetime Member in the medical field. Dr. Geller works as a full-time hospitalist and a principal consultant for The CopperRidge Group, which provides guidance to patients in health, wellness, and fitness services and products.
In addition to his work at the CopperRidge Group, Dr. Geller is a member of Civil Vision International’s board of directors. He has extensive civilian and military-based experience in the United States, Africa, the Middle East, and South Asia.
A physician leader in the U.S. Air Force, Dr. Geller earned White House Medical Unit commendations for planning and leading the surgical and intensive care unit teams to support President Clinton’s trips to Vietnam and Africa in 2000.
Nikhil Sharma, MD, recently was selected by the International Association of HealthCare Professionals to be part of the Leading Physicians of the World. Dr. Sharma is a hospitalist serving at the Ochsner Health System in New Orleans.
Dr. Sharma, a member of the Southern Hospital Association and the Louisiana Medical Association, began his medical career in 2009 with a residency and fellowship at Ochsner, where he has remained ever since. He specializes in internal medicine and transplants.
I. Carol Nwelue, MD, a longtime hospitalist and the medical director of the Sparrow Medical Group Adult Hospitalist Service, recently received the Sparrow Physician Leadership Award. The award goes to an emerging leader who provides outstanding work in areas such as safety, clinical or service excellence, research, teaching, publishing, teamwork, and innovation.
Dr. Nwelue completed the Sparrow Physician Leadership Academy program, earning recognition for innovation in leadership, as well as practice management.
Laura Jin, MD, recently was promoted to medical director for utilization management at the University of Maryland Shore Regional Health. In her new role, Dr. Jin will identify and facilitate the resolution of utilization issues; in so doing, she will serve as a consultant leader to the health care system, its physicians, its advance practice providers, and the care management team.
Dr. Jin will remain as a hospitalist at Digestive Health Associates while fulfilling the duties in her new position at Shore Regional. She will guide the center on issues such as compliance, level of care, length of stay, resource management, reimbursement, emergency department throughput, and more.
Business Moves
The Mount Sinai Health System and The New Jewish Home, both based in New York City, have extended their relationship to improve care of hospitalized patients who require specialized post-acute or long-term care at a skilled nursing facility. Through the Mount Sinai-New Jewish Home Hospitalist Program, Mount Sinai hospitalists will be charged with providing a seamless transition to The New Jewish Home for patients who need nursing care.
This model will buoy communication and ensure the sharing of vital information between the two venues, reducing the risk of rehospitalization.
Gryphon Investors, based in San Francisco, recently announced it will acquire OB Hospitalist Group, one of the nation’s leading providers of obstetric hospital medicine. The deal with OBHG’s current partner, Ares Management, was finalized in late July.
OBHG, based out of Mauldin, S.C., has a national network of more than 550 OB hospitalists, covering more than 120 hospitals in 28 states. OBHG’s hospitalist program features an obstetric emergency department, providing expectant mothers at partner hospitals with 24/7/365 access to medical care.
Envision Healthcare, based in Nashville, Tenn., and Greenwood Village, Colo., a provider of physician-led services and ambulatory surgery services, has acquired Milwaukee-based Infinity Healthcare. Infinity’s group-physician practice includes more than 340 physicians and providers delivering emergency and hospital medicine, anesthesia, and radiology services.
Identifying Pediatric Skull Fracture Using Point-of-Care Ultrasound
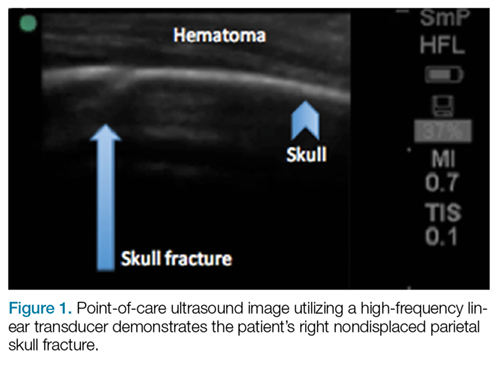
Evaluating pediatric patients presenting to the ED with head trauma can be a challenging task for emergency physicians (EPs). Specifically, identifying a nondisplaced skull fracture is not always possible through physical examination alone.1 However, point-of-care (POC) ultrasound permits rapid identification of skull fractures, which in turn assists the EP to determine if advanced imaging studies such as computed tomography (CT) are necessary.
Case
A previously healthy 10-month-old male infant presented to the ED with his mother for evaluation of rhinorrhea, cough, and fever, the onset of which began 24 hours prior to presentation. The patient’s mother reported that the infant continually tugged at his right ear throughout the previous evening and was increasingly irritable, but not inconsolable.
Initial vital signs at presentation were: blood pressure, 95/54 mm Hg; heart rate, 146 beats/min; respiratory rate, 36 beats/min, and temperature, 101.8°F. Oxygen saturation was 96% on room air. The physical examination was notable for an alert well-appearing infant who had a tender nonecchymotic scalp hematoma superior to the right pinna, clear tympanic membranes, crusted mucous bilaterally at the nares, nonlabored respirations, and wheezing throughout the lung fields.
Imaging Technique
To evaluate for skull fractures using POC ultrasound, the area of localized trauma must first be identified.2,3 Evidence of trauma includes an area of focal tenderness, abrasion, soft-tissue swelling, and hematoma.2,3 The presence of any depressed and open cranial injuries are contraindications to ultrasound. In which case, a physician should consult a neurosurgical specialist and obtain a CT scan of the head.
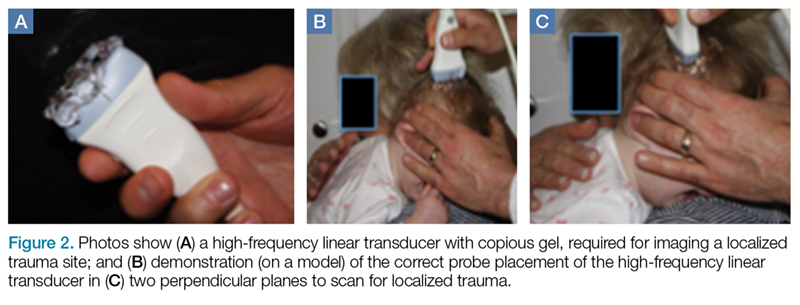
A high-frequency linear probe (5-10 MHz) is used to scan the area of localized trauma; this should be performed in two perpendicular planes using copious gel and light pressure (Figures 2a-2c).
Discussion
Closed head trauma is one of the most common pediatric injuries, accounting for roughly 1.4 million ED visits annually in the United States.5 Four to 12% percent of these minor traumas result in an intracranial injury,2 and the presence of a skull fracture is associated with a 4- to 20-fold increase in risk of underlying intracranial hemorrhage.3
Clinical assessment alone is not always reliable in predicting skull fracture and intracranial injury, especially in children younger than 2 years of age.2,3 Ultrasound is safe, noninvasive, expedient, cost-effective, and well tolerated in the pediatric population for identifying skull fractures,3 and can obviate the need for skull radiographs4 or procedural sedation. Moreover, POC ultrasound can serve as an adjunct to the Pediatric Emergency Care Applied Research Network head injury algorithm for head CT use decision rules if the fracture is not palpable on examination.
Several prospective studies and case reports have demonstrated the usefulness of POC ultrasound in diagnosing pediatric skull fractures in the ED.1-4 Two of the four cases published represented cases in which the EP identified an undisclosed nonaccidental trauma through POC ultrasound. Rabiner et al,3 estimates a combined sensitivity and specificity of 94% and 96%, respectively. It is important to remember that intracranial injury can still occur without an associated skull fracture. As our case demonstrates, POC ultrasound is a useful tool in risk-stratifying minor head trauma in children.
Case Conclusion
The head CT study confirmed a nondisplaced, oblique, and acute-appearing linear fracture of the right parietal bone extending from the squamosal to the lambdoid suture. There was no associated intracranial hemorrhage. The patient was admitted to the hospital for a nonaccidental trauma evaluation. The Department of Children and Family Services was contacted and the patient was discharged in the temporary custody of his maternal grandmother.
Summary
Point-of-care ultrasound is a useful diagnostic tool to rapidly evaluate for, and diagnose skull fractures in pediatric patients. Given its high sensitivity and specificity, ultrasound can help EPs identify occult nondisplaced skull fractures in children.
1. Riera A, Chen L. Ultrasound evaluation of skull fractures in children: a feasibility study. Pediatr Emerg Care. 2012;28(5):420-425. doi:10.1097/PEC.0b013e318252da3b.
2. Parri N, Crosby BJ, Glass C, et al. Ability of emergency ultrasonography to detect pediatric skull fractures: a prospective, observational study. J Emerg Med. 2013;44(1)135-141.
3. Rabiner JE, Friedman LM, Khine H, Avner JR, Tsung JW. Accuracy of point-of-care ultrasound for diagnosis of skull fractures in children. Pediatrics. 2013;131(6):e1757-1764. doi:10.1542/peds.2012-3921.
4. Ramirez-Schrempp D, Vinci RJ, Liteplo AS. Bedside ultrasound in the diagnosis of skull fractures in the pediatric emergency department. Pediatr Emerg Care. 2011;27(4):312-314. doi:10.1097/PEC.0b013e3182131579.
5. Coronado VG, Xu L, Basavaraju SV, et al; Centers for Disease Control and Prevention (CDC). Surveillance for traumatic brain injury-related deaths--United States, 1997-2007. MMWR Surveill Summ. 2011;60(5):1-32.
Evaluating pediatric patients presenting to the ED with head trauma can be a challenging task for emergency physicians (EPs). Specifically, identifying a nondisplaced skull fracture is not always possible through physical examination alone.1 However, point-of-care (POC) ultrasound permits rapid identification of skull fractures, which in turn assists the EP to determine if advanced imaging studies such as computed tomography (CT) are necessary.
Case
A previously healthy 10-month-old male infant presented to the ED with his mother for evaluation of rhinorrhea, cough, and fever, the onset of which began 24 hours prior to presentation. The patient’s mother reported that the infant continually tugged at his right ear throughout the previous evening and was increasingly irritable, but not inconsolable.
Initial vital signs at presentation were: blood pressure, 95/54 mm Hg; heart rate, 146 beats/min; respiratory rate, 36 beats/min, and temperature, 101.8°F. Oxygen saturation was 96% on room air. The physical examination was notable for an alert well-appearing infant who had a tender nonecchymotic scalp hematoma superior to the right pinna, clear tympanic membranes, crusted mucous bilaterally at the nares, nonlabored respirations, and wheezing throughout the lung fields.
Imaging Technique
To evaluate for skull fractures using POC ultrasound, the area of localized trauma must first be identified.2,3 Evidence of trauma includes an area of focal tenderness, abrasion, soft-tissue swelling, and hematoma.2,3 The presence of any depressed and open cranial injuries are contraindications to ultrasound. In which case, a physician should consult a neurosurgical specialist and obtain a CT scan of the head.
A high-frequency linear probe (5-10 MHz) is used to scan the area of localized trauma; this should be performed in two perpendicular planes using copious gel and light pressure (Figures 2a-2c).
Discussion
Closed head trauma is one of the most common pediatric injuries, accounting for roughly 1.4 million ED visits annually in the United States.5 Four to 12% percent of these minor traumas result in an intracranial injury,2 and the presence of a skull fracture is associated with a 4- to 20-fold increase in risk of underlying intracranial hemorrhage.3
Clinical assessment alone is not always reliable in predicting skull fracture and intracranial injury, especially in children younger than 2 years of age.2,3 Ultrasound is safe, noninvasive, expedient, cost-effective, and well tolerated in the pediatric population for identifying skull fractures,3 and can obviate the need for skull radiographs4 or procedural sedation. Moreover, POC ultrasound can serve as an adjunct to the Pediatric Emergency Care Applied Research Network head injury algorithm for head CT use decision rules if the fracture is not palpable on examination.
Several prospective studies and case reports have demonstrated the usefulness of POC ultrasound in diagnosing pediatric skull fractures in the ED.1-4 Two of the four cases published represented cases in which the EP identified an undisclosed nonaccidental trauma through POC ultrasound. Rabiner et al,3 estimates a combined sensitivity and specificity of 94% and 96%, respectively. It is important to remember that intracranial injury can still occur without an associated skull fracture. As our case demonstrates, POC ultrasound is a useful tool in risk-stratifying minor head trauma in children.
Case Conclusion
The head CT study confirmed a nondisplaced, oblique, and acute-appearing linear fracture of the right parietal bone extending from the squamosal to the lambdoid suture. There was no associated intracranial hemorrhage. The patient was admitted to the hospital for a nonaccidental trauma evaluation. The Department of Children and Family Services was contacted and the patient was discharged in the temporary custody of his maternal grandmother.
Summary
Point-of-care ultrasound is a useful diagnostic tool to rapidly evaluate for, and diagnose skull fractures in pediatric patients. Given its high sensitivity and specificity, ultrasound can help EPs identify occult nondisplaced skull fractures in children.
Evaluating pediatric patients presenting to the ED with head trauma can be a challenging task for emergency physicians (EPs). Specifically, identifying a nondisplaced skull fracture is not always possible through physical examination alone.1 However, point-of-care (POC) ultrasound permits rapid identification of skull fractures, which in turn assists the EP to determine if advanced imaging studies such as computed tomography (CT) are necessary.
Case
A previously healthy 10-month-old male infant presented to the ED with his mother for evaluation of rhinorrhea, cough, and fever, the onset of which began 24 hours prior to presentation. The patient’s mother reported that the infant continually tugged at his right ear throughout the previous evening and was increasingly irritable, but not inconsolable.
Initial vital signs at presentation were: blood pressure, 95/54 mm Hg; heart rate, 146 beats/min; respiratory rate, 36 beats/min, and temperature, 101.8°F. Oxygen saturation was 96% on room air. The physical examination was notable for an alert well-appearing infant who had a tender nonecchymotic scalp hematoma superior to the right pinna, clear tympanic membranes, crusted mucous bilaterally at the nares, nonlabored respirations, and wheezing throughout the lung fields.
Imaging Technique
To evaluate for skull fractures using POC ultrasound, the area of localized trauma must first be identified.2,3 Evidence of trauma includes an area of focal tenderness, abrasion, soft-tissue swelling, and hematoma.2,3 The presence of any depressed and open cranial injuries are contraindications to ultrasound. In which case, a physician should consult a neurosurgical specialist and obtain a CT scan of the head.
A high-frequency linear probe (5-10 MHz) is used to scan the area of localized trauma; this should be performed in two perpendicular planes using copious gel and light pressure (Figures 2a-2c).
Discussion
Closed head trauma is one of the most common pediatric injuries, accounting for roughly 1.4 million ED visits annually in the United States.5 Four to 12% percent of these minor traumas result in an intracranial injury,2 and the presence of a skull fracture is associated with a 4- to 20-fold increase in risk of underlying intracranial hemorrhage.3
Clinical assessment alone is not always reliable in predicting skull fracture and intracranial injury, especially in children younger than 2 years of age.2,3 Ultrasound is safe, noninvasive, expedient, cost-effective, and well tolerated in the pediatric population for identifying skull fractures,3 and can obviate the need for skull radiographs4 or procedural sedation. Moreover, POC ultrasound can serve as an adjunct to the Pediatric Emergency Care Applied Research Network head injury algorithm for head CT use decision rules if the fracture is not palpable on examination.
Several prospective studies and case reports have demonstrated the usefulness of POC ultrasound in diagnosing pediatric skull fractures in the ED.1-4 Two of the four cases published represented cases in which the EP identified an undisclosed nonaccidental trauma through POC ultrasound. Rabiner et al,3 estimates a combined sensitivity and specificity of 94% and 96%, respectively. It is important to remember that intracranial injury can still occur without an associated skull fracture. As our case demonstrates, POC ultrasound is a useful tool in risk-stratifying minor head trauma in children.
Case Conclusion
The head CT study confirmed a nondisplaced, oblique, and acute-appearing linear fracture of the right parietal bone extending from the squamosal to the lambdoid suture. There was no associated intracranial hemorrhage. The patient was admitted to the hospital for a nonaccidental trauma evaluation. The Department of Children and Family Services was contacted and the patient was discharged in the temporary custody of his maternal grandmother.
Summary
Point-of-care ultrasound is a useful diagnostic tool to rapidly evaluate for, and diagnose skull fractures in pediatric patients. Given its high sensitivity and specificity, ultrasound can help EPs identify occult nondisplaced skull fractures in children.
1. Riera A, Chen L. Ultrasound evaluation of skull fractures in children: a feasibility study. Pediatr Emerg Care. 2012;28(5):420-425. doi:10.1097/PEC.0b013e318252da3b.
2. Parri N, Crosby BJ, Glass C, et al. Ability of emergency ultrasonography to detect pediatric skull fractures: a prospective, observational study. J Emerg Med. 2013;44(1)135-141.
3. Rabiner JE, Friedman LM, Khine H, Avner JR, Tsung JW. Accuracy of point-of-care ultrasound for diagnosis of skull fractures in children. Pediatrics. 2013;131(6):e1757-1764. doi:10.1542/peds.2012-3921.
4. Ramirez-Schrempp D, Vinci RJ, Liteplo AS. Bedside ultrasound in the diagnosis of skull fractures in the pediatric emergency department. Pediatr Emerg Care. 2011;27(4):312-314. doi:10.1097/PEC.0b013e3182131579.
5. Coronado VG, Xu L, Basavaraju SV, et al; Centers for Disease Control and Prevention (CDC). Surveillance for traumatic brain injury-related deaths--United States, 1997-2007. MMWR Surveill Summ. 2011;60(5):1-32.
1. Riera A, Chen L. Ultrasound evaluation of skull fractures in children: a feasibility study. Pediatr Emerg Care. 2012;28(5):420-425. doi:10.1097/PEC.0b013e318252da3b.
2. Parri N, Crosby BJ, Glass C, et al. Ability of emergency ultrasonography to detect pediatric skull fractures: a prospective, observational study. J Emerg Med. 2013;44(1)135-141.
3. Rabiner JE, Friedman LM, Khine H, Avner JR, Tsung JW. Accuracy of point-of-care ultrasound for diagnosis of skull fractures in children. Pediatrics. 2013;131(6):e1757-1764. doi:10.1542/peds.2012-3921.
4. Ramirez-Schrempp D, Vinci RJ, Liteplo AS. Bedside ultrasound in the diagnosis of skull fractures in the pediatric emergency department. Pediatr Emerg Care. 2011;27(4):312-314. doi:10.1097/PEC.0b013e3182131579.
5. Coronado VG, Xu L, Basavaraju SV, et al; Centers for Disease Control and Prevention (CDC). Surveillance for traumatic brain injury-related deaths--United States, 1997-2007. MMWR Surveill Summ. 2011;60(5):1-32.
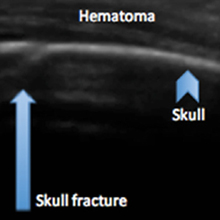
Thyroid Cartilage Fracture in Context of Noncompetitive "Horseplay" Wrestling
An isolated thyroid cartilage fracture is very rare.1-5 More interestingly, an isolated thyroid cartilage fracture from a wrestling injury, especially in a non-sports competition context, such as horseplay, has not been previously reported in the literature. Sports-related injuries to the larynx and related structures are uncommon.6,7
Case
A 38-year-old man presented with a complaint of throat pain after wrestling at home, in horseplay, with his 15-year-old son. He reported that when his son placed a choke hold on him, he felt a "crack" in the area of his neck, and soon afterwards felt throat pain with swallowing, along with discomfort with breathing. He also felt a sensation of "fluid building up in his throat." There were no changes noted with his voice and the patient was speaking in full sentences. There was no wheezing or stridor. He denied shortness of breath or any other complaints. He denied pain over the posterior elements of his cervical spine. At the time of the incident, there was no loss of consciousness. Palpation of the neck and chest did not elicit any crepitance to suggest subcutaneous emphysema. The trachea was midline. There was no pain overlying the carotids bilaterally, and the patient had no bruits. The neck examination did not show any surface abnormalities to suggest trauma, such as ecchymosis or swelling. He did have slight tenderness to palpation over the thyroid cartilage.
The patient was sent for a computed tomography (CT) scan of the soft-tissue neck with intravenous (IV) contrast, and a CT scan of the cervical spine. The results showed no cervical spine fracture. However, there was a minimally displaced fracture of the left thyroid cartilage, with soft-tissue swelling that was noted, along with minimal narrowing of the subglottic trachea. There were no abnormal enhancements or fluid collections. No evidence of vocal cord abnormality or asymmetry was seen, and there was no evidence of airway compromise (Figure).
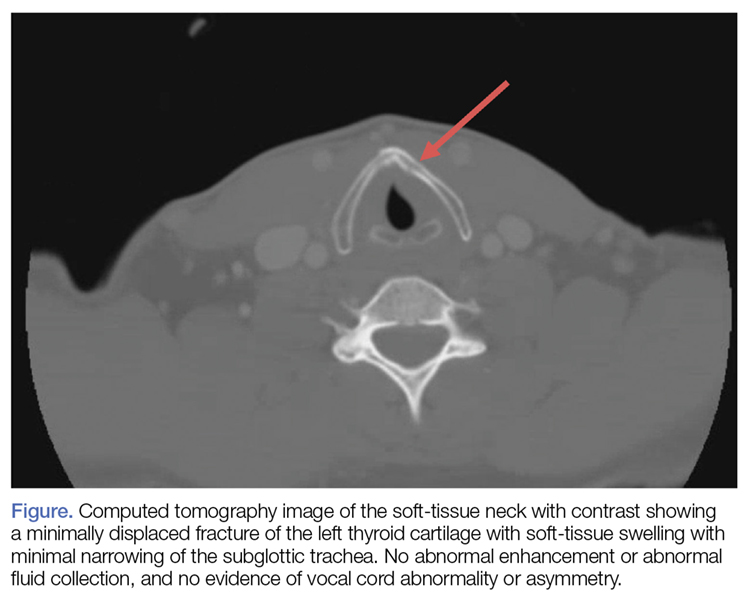
Discussion
Our patient sustained an isolated thyroid cartilage fracture. A thyroid cartilage fracture is a type of laryngeal fracture. Using an anatomic system in which such injuries are classified by location (supraglottic, glottis, or infraglottic), a thyroid cartilage fracture is classified as a supraglottic laryngeal injury.1,2 In our case, the fracture was due to a blunt force mechanism. Most blunt force laryngeal fractures are associated with multiple trauma.8 An isolated thyroid cartilage fracture is very rare.1-5 More interestingly, an isolated thyroid cartilage fracture from a wrestling injury, especially in a non-sports competition context, such as horseplay, has not been previously reported in the literature.
Sports-related injuries to the larynx and related structures are uncommon.6,7 When reported, significant force is usually involved. For example, Tasca et al6 reported a thyroid cartilage fracture from direct blunt trauma (rugby, opponent stamped on patient’s throat) in which the patient presented with pain with swallowing and a lowering of the pitch of his voice. Rejali et al9 reported the case of a midair collision in a soccer match, resulting in an obvious mandibular fracture, but with an arytenoid cartilage fracture that was not initially identified. A football struck a 17-year-old boy with a resulting fracture of the superior cornu of the larynx and a puncture of the laryngeal mucosal wall in a case reported by Saab and Birkinshaw.10 The patient presented with neck pain and dysphagia, as well as subcutaneous air.10 A 21-year-old collegiate basketball player was struck in the neck by a teammate’s head while jumping for a rebound. He sustained a fracture of the thyroid cartilage and a fracture of the anterior cricoid ring.3 Patients with such injuries "may appear deceptively normal when seeking medical attention."8 Kragha2 refers to such injuries as "rare but potentially deadly."
Symptoms can include neck pain, voice changes, pain with swallowing, and shortness of breath. Signs can include tenderness, ecchymosis, and even subcutaneous emphysema. There may be loss of prominence of the thyroid cartilage.3 Tracheal deviation and stridor can occur.10,11 Computed tomography scan and laryngoscopy can be helpful in the diagnostic process; 3-dimensional (3-D) reconstructions may be needed.
Various classification systems have been proposed with related treatment strategies. Percevik et al11 summarized a five-part clinical classification. Group 1 (hematoma, no fracture) and Group 2 (non-displaced fracture) may be treated conservatively. Group 3 (stable, displaced fracture), Group 4 (unstable, displaced fracture), and Group 5 (laryngotracheal disinsertion) are more likely to be treated with surgery.11 Surgical techniques vary and have been refined over time.12
In this case, the patient sustained a thyroid cartilage fracture without the energy and force involved in a motor vehicle collision and without significant sports-related force. It is possible that this injury may have involved neck hyperflexion, rather than direct compressive force. Lin et al,1 described a case of neck hyperflexion in an unrestrained driver, with a resulting isolated thyroid cartilage fracture without direct impact to the neck. Walsh and Trotter5 presented a case of a motorcyclist with a blow to the back of the head, with resulting neck hyperflexion, which resulted in a fracture of the thyroid cartilage. Beato-Martínez et al,13 reported a case of thyroid cartilage fracture following a sneezing episode. The patient presented with odynophagia, dysphonia and neck pain.13 In our review of the literature, we found that only one other similar case has been reported. In that case, a patient experienced a feeling of a neck click, followed by neck pain and hoarseness. He sustained a fracture of the thyroid cartilage.14
In reviewing the hyperflexion mechanism, Lin et al1 noted that isolated thyroid cartilage fractures are rare and that "most of these are caused by direct injury to the neck, except for two patients reported in the literature who sustained isolated thyroid cartilage fractures after sneezing." Lin et al1 proposed an interesting hypothesis—that "the mechanism causing thyroid cartilage fracture during impaction may be the same with sneezing." Sneezing can be associated with sudden and forceful flexion of the neck.
It is certainly possible that this hyperflexion mechanism was involved in our case, given there was no history of significant blunt force to the neck, as in the sports-related injuries discussed. Wrestling holds can produce hyperflexion. The patient described a feeling of a "crack", which is similar to the clicking sound described in one of the sneezing-related cases. An isolated thyroid cartilage fracture is rare in the absence of major trauma. However, as noted by Rejali et al,9 this can create a potential management pitfall. "In the context of non-contact sports, the attendant doctor may not realize the significance of apparently minor head and neck trauma."9
There are no series data to provide us with an exact incidence of airway compromise. However, seemingly minor insults to the anterior neck can cause posterior compression of the larynx and can result in airway compromise.9-11
The CT scan is described as an important imaging modality to rule out cervical spine fracture. Although there was no significant blunt force, the cervical spine was exposed to hyperflexion forces. Another important potential consequence is long-term injury to the vocal cords, with subsequent speech difficulties.11 Computed tomography can visualize the thyroid fracture, but many authors point out that visualization of the vocal cords, with nasopharyngeal laryngoscopy or other modality, is an important adjunct to the CT scan.9-11
Otolaryngologist consultation should be strongly considered. This patient was transferred to a tertiary care center with expertise in thyroid fractures, and planned nasopharyngeal laryngoscopy to be performed at the receiving institution.
Conclusion
Our patient sustained an isolated thyroid cartilage fracture. Most blunt force laryngeal fractures are associated with multiple trauma. An isolated thyroid cartilage fracture is very rare. An isolated thyroid cartilage fracture from a wrestling injury, especially in a non-sports competition context, such as horseplay, has not been previously reported in the literature. Symptoms can include neck pain, voice changes, pain with swallowing, and shortness of breath. Signs can include tenderness, ecchymosis, or even subcutaneous emphysema. There may be loss of the prominence of the thyroid cartilage, tracheal deviation, and stridor. Computed tomography scan imaging with 3-D reconstructions and laryngoscopy can be helpful in the diagnostic process. In our case, the patient sustained a thyroid cartilage fracture without the energy and force involved in a motor vehicle collision and without significant sports-related force. It is possible this injury may have involved neck hyperflexion, rather than direct compressive forces, similar to that described by Lin et al.1 Certainly, there was no history of significant blunt force to the neck on the level of the sports-related injuries discussed.
1. Lin HL, Kuo LC, Chen CW, Cheng YC, Lee WC. Neck hyperflexion causing isolated thyroid cartilage fracture--a case report. Am J Emerg Med. 2008;26(9):1064.e1-e3. doi:10.1016/j.ajem.2008.02.030
2. Kragha KO. Acute traumatic injury of the larynx. Case Reports in Otolaryngology. Volume 2015. Article ID393978. http://dx.doi.org/10.1155/2015/393978
3. Kim JD, Shuler FD, Mo B, Gibbs SR, Belmaggio T, Giangarra CE. Traumatic laryngeal fracture in a collegiate basketball player. Sports Health. 2013;5(3):
273-275.
4. Knopke S, Todt I, Ernst A, Seidl RO. Pseudarthroses of the cornu of the thyroid cartilage. Otolaryngol Head Neck Surg. 2010;143(2):186-189. doi:10.1016/5.otohns.2010.04.011.
5. Walsh PV, Trotter GA. Fracture of the thyroid cartilage associated with full face integral crash helmet. Injury. 1979;11(1):47-48.
6. Tasca RA, Sherman IW, Wood GD. Thyroid cartilage fracture: treatment with biodegradable plates. Br J Oral Maxillofac Surg. 2008;46(2):159-160.
7. Mitrović SM. Blunt external laryngeal trauma. Two case reports. Med Pregl. 2007;60(9-10):489-492.
8. O'Keefe LJ, Maw AR. The dangers of minor blunt laryngeal trauma. J. Laryngol Otol. 1992;106(4):372-373.
9. Rejali SD, Bennett JD, Upile T, Rothera MP. Diagnostic pitfalls in sports related laryngeal injury. Br J Sports Med. 1998;32(2):180-181.
10. Saab M, Birkinshaw R. Blunt laryngeal trauma: an unusual case. Int J Clin Pract. 1997;51(8):527.
11. Pekcevik Y, Ibrahim C, Ülker C. Cricoid and thyroid cartilage fracture, cricothyroid joint dislocation,pseudofracture appearance of the hyoid bone: CT, MRI and laryngoscopic findings. JAEM. 2013;12:170-173.
12. Bent JP 3rd, Porubsky ES. The management of blunt fractures of the thyroid cartilage. Otolaryngol Head Neck Surg. 1994;110(2):195-202. doi: 10:.1177/019459989411000209.
13. Beato Martínez A, Moreno Juara A, López Moya JJ. Fracture of thyroid cartilage after a sneezing episode. Acta Otorrinolaringol Esp. 2007;58(2):73-74.
14. Quinlan PT. Fracture of thyroid cartilage during a sneezing attack. Br Med J. 1950;1(4661):1052.
An isolated thyroid cartilage fracture is very rare.1-5 More interestingly, an isolated thyroid cartilage fracture from a wrestling injury, especially in a non-sports competition context, such as horseplay, has not been previously reported in the literature. Sports-related injuries to the larynx and related structures are uncommon.6,7
Case
A 38-year-old man presented with a complaint of throat pain after wrestling at home, in horseplay, with his 15-year-old son. He reported that when his son placed a choke hold on him, he felt a "crack" in the area of his neck, and soon afterwards felt throat pain with swallowing, along with discomfort with breathing. He also felt a sensation of "fluid building up in his throat." There were no changes noted with his voice and the patient was speaking in full sentences. There was no wheezing or stridor. He denied shortness of breath or any other complaints. He denied pain over the posterior elements of his cervical spine. At the time of the incident, there was no loss of consciousness. Palpation of the neck and chest did not elicit any crepitance to suggest subcutaneous emphysema. The trachea was midline. There was no pain overlying the carotids bilaterally, and the patient had no bruits. The neck examination did not show any surface abnormalities to suggest trauma, such as ecchymosis or swelling. He did have slight tenderness to palpation over the thyroid cartilage.
The patient was sent for a computed tomography (CT) scan of the soft-tissue neck with intravenous (IV) contrast, and a CT scan of the cervical spine. The results showed no cervical spine fracture. However, there was a minimally displaced fracture of the left thyroid cartilage, with soft-tissue swelling that was noted, along with minimal narrowing of the subglottic trachea. There were no abnormal enhancements or fluid collections. No evidence of vocal cord abnormality or asymmetry was seen, and there was no evidence of airway compromise (Figure).
Discussion
Our patient sustained an isolated thyroid cartilage fracture. A thyroid cartilage fracture is a type of laryngeal fracture. Using an anatomic system in which such injuries are classified by location (supraglottic, glottis, or infraglottic), a thyroid cartilage fracture is classified as a supraglottic laryngeal injury.1,2 In our case, the fracture was due to a blunt force mechanism. Most blunt force laryngeal fractures are associated with multiple trauma.8 An isolated thyroid cartilage fracture is very rare.1-5 More interestingly, an isolated thyroid cartilage fracture from a wrestling injury, especially in a non-sports competition context, such as horseplay, has not been previously reported in the literature.
Sports-related injuries to the larynx and related structures are uncommon.6,7 When reported, significant force is usually involved. For example, Tasca et al6 reported a thyroid cartilage fracture from direct blunt trauma (rugby, opponent stamped on patient’s throat) in which the patient presented with pain with swallowing and a lowering of the pitch of his voice. Rejali et al9 reported the case of a midair collision in a soccer match, resulting in an obvious mandibular fracture, but with an arytenoid cartilage fracture that was not initially identified. A football struck a 17-year-old boy with a resulting fracture of the superior cornu of the larynx and a puncture of the laryngeal mucosal wall in a case reported by Saab and Birkinshaw.10 The patient presented with neck pain and dysphagia, as well as subcutaneous air.10 A 21-year-old collegiate basketball player was struck in the neck by a teammate’s head while jumping for a rebound. He sustained a fracture of the thyroid cartilage and a fracture of the anterior cricoid ring.3 Patients with such injuries "may appear deceptively normal when seeking medical attention."8 Kragha2 refers to such injuries as "rare but potentially deadly."
Symptoms can include neck pain, voice changes, pain with swallowing, and shortness of breath. Signs can include tenderness, ecchymosis, and even subcutaneous emphysema. There may be loss of prominence of the thyroid cartilage.3 Tracheal deviation and stridor can occur.10,11 Computed tomography scan and laryngoscopy can be helpful in the diagnostic process; 3-dimensional (3-D) reconstructions may be needed.
Various classification systems have been proposed with related treatment strategies. Percevik et al11 summarized a five-part clinical classification. Group 1 (hematoma, no fracture) and Group 2 (non-displaced fracture) may be treated conservatively. Group 3 (stable, displaced fracture), Group 4 (unstable, displaced fracture), and Group 5 (laryngotracheal disinsertion) are more likely to be treated with surgery.11 Surgical techniques vary and have been refined over time.12
In this case, the patient sustained a thyroid cartilage fracture without the energy and force involved in a motor vehicle collision and without significant sports-related force. It is possible that this injury may have involved neck hyperflexion, rather than direct compressive force. Lin et al,1 described a case of neck hyperflexion in an unrestrained driver, with a resulting isolated thyroid cartilage fracture without direct impact to the neck. Walsh and Trotter5 presented a case of a motorcyclist with a blow to the back of the head, with resulting neck hyperflexion, which resulted in a fracture of the thyroid cartilage. Beato-Martínez et al,13 reported a case of thyroid cartilage fracture following a sneezing episode. The patient presented with odynophagia, dysphonia and neck pain.13 In our review of the literature, we found that only one other similar case has been reported. In that case, a patient experienced a feeling of a neck click, followed by neck pain and hoarseness. He sustained a fracture of the thyroid cartilage.14
In reviewing the hyperflexion mechanism, Lin et al1 noted that isolated thyroid cartilage fractures are rare and that "most of these are caused by direct injury to the neck, except for two patients reported in the literature who sustained isolated thyroid cartilage fractures after sneezing." Lin et al1 proposed an interesting hypothesis—that "the mechanism causing thyroid cartilage fracture during impaction may be the same with sneezing." Sneezing can be associated with sudden and forceful flexion of the neck.
It is certainly possible that this hyperflexion mechanism was involved in our case, given there was no history of significant blunt force to the neck, as in the sports-related injuries discussed. Wrestling holds can produce hyperflexion. The patient described a feeling of a "crack", which is similar to the clicking sound described in one of the sneezing-related cases. An isolated thyroid cartilage fracture is rare in the absence of major trauma. However, as noted by Rejali et al,9 this can create a potential management pitfall. "In the context of non-contact sports, the attendant doctor may not realize the significance of apparently minor head and neck trauma."9
There are no series data to provide us with an exact incidence of airway compromise. However, seemingly minor insults to the anterior neck can cause posterior compression of the larynx and can result in airway compromise.9-11
The CT scan is described as an important imaging modality to rule out cervical spine fracture. Although there was no significant blunt force, the cervical spine was exposed to hyperflexion forces. Another important potential consequence is long-term injury to the vocal cords, with subsequent speech difficulties.11 Computed tomography can visualize the thyroid fracture, but many authors point out that visualization of the vocal cords, with nasopharyngeal laryngoscopy or other modality, is an important adjunct to the CT scan.9-11
Otolaryngologist consultation should be strongly considered. This patient was transferred to a tertiary care center with expertise in thyroid fractures, and planned nasopharyngeal laryngoscopy to be performed at the receiving institution.
Conclusion
Our patient sustained an isolated thyroid cartilage fracture. Most blunt force laryngeal fractures are associated with multiple trauma. An isolated thyroid cartilage fracture is very rare. An isolated thyroid cartilage fracture from a wrestling injury, especially in a non-sports competition context, such as horseplay, has not been previously reported in the literature. Symptoms can include neck pain, voice changes, pain with swallowing, and shortness of breath. Signs can include tenderness, ecchymosis, or even subcutaneous emphysema. There may be loss of the prominence of the thyroid cartilage, tracheal deviation, and stridor. Computed tomography scan imaging with 3-D reconstructions and laryngoscopy can be helpful in the diagnostic process. In our case, the patient sustained a thyroid cartilage fracture without the energy and force involved in a motor vehicle collision and without significant sports-related force. It is possible this injury may have involved neck hyperflexion, rather than direct compressive forces, similar to that described by Lin et al.1 Certainly, there was no history of significant blunt force to the neck on the level of the sports-related injuries discussed.
An isolated thyroid cartilage fracture is very rare.1-5 More interestingly, an isolated thyroid cartilage fracture from a wrestling injury, especially in a non-sports competition context, such as horseplay, has not been previously reported in the literature. Sports-related injuries to the larynx and related structures are uncommon.6,7
Case
A 38-year-old man presented with a complaint of throat pain after wrestling at home, in horseplay, with his 15-year-old son. He reported that when his son placed a choke hold on him, he felt a "crack" in the area of his neck, and soon afterwards felt throat pain with swallowing, along with discomfort with breathing. He also felt a sensation of "fluid building up in his throat." There were no changes noted with his voice and the patient was speaking in full sentences. There was no wheezing or stridor. He denied shortness of breath or any other complaints. He denied pain over the posterior elements of his cervical spine. At the time of the incident, there was no loss of consciousness. Palpation of the neck and chest did not elicit any crepitance to suggest subcutaneous emphysema. The trachea was midline. There was no pain overlying the carotids bilaterally, and the patient had no bruits. The neck examination did not show any surface abnormalities to suggest trauma, such as ecchymosis or swelling. He did have slight tenderness to palpation over the thyroid cartilage.
The patient was sent for a computed tomography (CT) scan of the soft-tissue neck with intravenous (IV) contrast, and a CT scan of the cervical spine. The results showed no cervical spine fracture. However, there was a minimally displaced fracture of the left thyroid cartilage, with soft-tissue swelling that was noted, along with minimal narrowing of the subglottic trachea. There were no abnormal enhancements or fluid collections. No evidence of vocal cord abnormality or asymmetry was seen, and there was no evidence of airway compromise (Figure).
Discussion
Our patient sustained an isolated thyroid cartilage fracture. A thyroid cartilage fracture is a type of laryngeal fracture. Using an anatomic system in which such injuries are classified by location (supraglottic, glottis, or infraglottic), a thyroid cartilage fracture is classified as a supraglottic laryngeal injury.1,2 In our case, the fracture was due to a blunt force mechanism. Most blunt force laryngeal fractures are associated with multiple trauma.8 An isolated thyroid cartilage fracture is very rare.1-5 More interestingly, an isolated thyroid cartilage fracture from a wrestling injury, especially in a non-sports competition context, such as horseplay, has not been previously reported in the literature.
Sports-related injuries to the larynx and related structures are uncommon.6,7 When reported, significant force is usually involved. For example, Tasca et al6 reported a thyroid cartilage fracture from direct blunt trauma (rugby, opponent stamped on patient’s throat) in which the patient presented with pain with swallowing and a lowering of the pitch of his voice. Rejali et al9 reported the case of a midair collision in a soccer match, resulting in an obvious mandibular fracture, but with an arytenoid cartilage fracture that was not initially identified. A football struck a 17-year-old boy with a resulting fracture of the superior cornu of the larynx and a puncture of the laryngeal mucosal wall in a case reported by Saab and Birkinshaw.10 The patient presented with neck pain and dysphagia, as well as subcutaneous air.10 A 21-year-old collegiate basketball player was struck in the neck by a teammate’s head while jumping for a rebound. He sustained a fracture of the thyroid cartilage and a fracture of the anterior cricoid ring.3 Patients with such injuries "may appear deceptively normal when seeking medical attention."8 Kragha2 refers to such injuries as "rare but potentially deadly."
Symptoms can include neck pain, voice changes, pain with swallowing, and shortness of breath. Signs can include tenderness, ecchymosis, and even subcutaneous emphysema. There may be loss of prominence of the thyroid cartilage.3 Tracheal deviation and stridor can occur.10,11 Computed tomography scan and laryngoscopy can be helpful in the diagnostic process; 3-dimensional (3-D) reconstructions may be needed.
Various classification systems have been proposed with related treatment strategies. Percevik et al11 summarized a five-part clinical classification. Group 1 (hematoma, no fracture) and Group 2 (non-displaced fracture) may be treated conservatively. Group 3 (stable, displaced fracture), Group 4 (unstable, displaced fracture), and Group 5 (laryngotracheal disinsertion) are more likely to be treated with surgery.11 Surgical techniques vary and have been refined over time.12
In this case, the patient sustained a thyroid cartilage fracture without the energy and force involved in a motor vehicle collision and without significant sports-related force. It is possible that this injury may have involved neck hyperflexion, rather than direct compressive force. Lin et al,1 described a case of neck hyperflexion in an unrestrained driver, with a resulting isolated thyroid cartilage fracture without direct impact to the neck. Walsh and Trotter5 presented a case of a motorcyclist with a blow to the back of the head, with resulting neck hyperflexion, which resulted in a fracture of the thyroid cartilage. Beato-Martínez et al,13 reported a case of thyroid cartilage fracture following a sneezing episode. The patient presented with odynophagia, dysphonia and neck pain.13 In our review of the literature, we found that only one other similar case has been reported. In that case, a patient experienced a feeling of a neck click, followed by neck pain and hoarseness. He sustained a fracture of the thyroid cartilage.14
In reviewing the hyperflexion mechanism, Lin et al1 noted that isolated thyroid cartilage fractures are rare and that "most of these are caused by direct injury to the neck, except for two patients reported in the literature who sustained isolated thyroid cartilage fractures after sneezing." Lin et al1 proposed an interesting hypothesis—that "the mechanism causing thyroid cartilage fracture during impaction may be the same with sneezing." Sneezing can be associated with sudden and forceful flexion of the neck.
It is certainly possible that this hyperflexion mechanism was involved in our case, given there was no history of significant blunt force to the neck, as in the sports-related injuries discussed. Wrestling holds can produce hyperflexion. The patient described a feeling of a "crack", which is similar to the clicking sound described in one of the sneezing-related cases. An isolated thyroid cartilage fracture is rare in the absence of major trauma. However, as noted by Rejali et al,9 this can create a potential management pitfall. "In the context of non-contact sports, the attendant doctor may not realize the significance of apparently minor head and neck trauma."9
There are no series data to provide us with an exact incidence of airway compromise. However, seemingly minor insults to the anterior neck can cause posterior compression of the larynx and can result in airway compromise.9-11
The CT scan is described as an important imaging modality to rule out cervical spine fracture. Although there was no significant blunt force, the cervical spine was exposed to hyperflexion forces. Another important potential consequence is long-term injury to the vocal cords, with subsequent speech difficulties.11 Computed tomography can visualize the thyroid fracture, but many authors point out that visualization of the vocal cords, with nasopharyngeal laryngoscopy or other modality, is an important adjunct to the CT scan.9-11
Otolaryngologist consultation should be strongly considered. This patient was transferred to a tertiary care center with expertise in thyroid fractures, and planned nasopharyngeal laryngoscopy to be performed at the receiving institution.
Conclusion
Our patient sustained an isolated thyroid cartilage fracture. Most blunt force laryngeal fractures are associated with multiple trauma. An isolated thyroid cartilage fracture is very rare. An isolated thyroid cartilage fracture from a wrestling injury, especially in a non-sports competition context, such as horseplay, has not been previously reported in the literature. Symptoms can include neck pain, voice changes, pain with swallowing, and shortness of breath. Signs can include tenderness, ecchymosis, or even subcutaneous emphysema. There may be loss of the prominence of the thyroid cartilage, tracheal deviation, and stridor. Computed tomography scan imaging with 3-D reconstructions and laryngoscopy can be helpful in the diagnostic process. In our case, the patient sustained a thyroid cartilage fracture without the energy and force involved in a motor vehicle collision and without significant sports-related force. It is possible this injury may have involved neck hyperflexion, rather than direct compressive forces, similar to that described by Lin et al.1 Certainly, there was no history of significant blunt force to the neck on the level of the sports-related injuries discussed.
1. Lin HL, Kuo LC, Chen CW, Cheng YC, Lee WC. Neck hyperflexion causing isolated thyroid cartilage fracture--a case report. Am J Emerg Med. 2008;26(9):1064.e1-e3. doi:10.1016/j.ajem.2008.02.030
2. Kragha KO. Acute traumatic injury of the larynx. Case Reports in Otolaryngology. Volume 2015. Article ID393978. http://dx.doi.org/10.1155/2015/393978
3. Kim JD, Shuler FD, Mo B, Gibbs SR, Belmaggio T, Giangarra CE. Traumatic laryngeal fracture in a collegiate basketball player. Sports Health. 2013;5(3):
273-275.
4. Knopke S, Todt I, Ernst A, Seidl RO. Pseudarthroses of the cornu of the thyroid cartilage. Otolaryngol Head Neck Surg. 2010;143(2):186-189. doi:10.1016/5.otohns.2010.04.011.
5. Walsh PV, Trotter GA. Fracture of the thyroid cartilage associated with full face integral crash helmet. Injury. 1979;11(1):47-48.
6. Tasca RA, Sherman IW, Wood GD. Thyroid cartilage fracture: treatment with biodegradable plates. Br J Oral Maxillofac Surg. 2008;46(2):159-160.
7. Mitrović SM. Blunt external laryngeal trauma. Two case reports. Med Pregl. 2007;60(9-10):489-492.
8. O'Keefe LJ, Maw AR. The dangers of minor blunt laryngeal trauma. J. Laryngol Otol. 1992;106(4):372-373.
9. Rejali SD, Bennett JD, Upile T, Rothera MP. Diagnostic pitfalls in sports related laryngeal injury. Br J Sports Med. 1998;32(2):180-181.
10. Saab M, Birkinshaw R. Blunt laryngeal trauma: an unusual case. Int J Clin Pract. 1997;51(8):527.
11. Pekcevik Y, Ibrahim C, Ülker C. Cricoid and thyroid cartilage fracture, cricothyroid joint dislocation,pseudofracture appearance of the hyoid bone: CT, MRI and laryngoscopic findings. JAEM. 2013;12:170-173.
12. Bent JP 3rd, Porubsky ES. The management of blunt fractures of the thyroid cartilage. Otolaryngol Head Neck Surg. 1994;110(2):195-202. doi: 10:.1177/019459989411000209.
13. Beato Martínez A, Moreno Juara A, López Moya JJ. Fracture of thyroid cartilage after a sneezing episode. Acta Otorrinolaringol Esp. 2007;58(2):73-74.
14. Quinlan PT. Fracture of thyroid cartilage during a sneezing attack. Br Med J. 1950;1(4661):1052.
1. Lin HL, Kuo LC, Chen CW, Cheng YC, Lee WC. Neck hyperflexion causing isolated thyroid cartilage fracture--a case report. Am J Emerg Med. 2008;26(9):1064.e1-e3. doi:10.1016/j.ajem.2008.02.030
2. Kragha KO. Acute traumatic injury of the larynx. Case Reports in Otolaryngology. Volume 2015. Article ID393978. http://dx.doi.org/10.1155/2015/393978
3. Kim JD, Shuler FD, Mo B, Gibbs SR, Belmaggio T, Giangarra CE. Traumatic laryngeal fracture in a collegiate basketball player. Sports Health. 2013;5(3):
273-275.
4. Knopke S, Todt I, Ernst A, Seidl RO. Pseudarthroses of the cornu of the thyroid cartilage. Otolaryngol Head Neck Surg. 2010;143(2):186-189. doi:10.1016/5.otohns.2010.04.011.
5. Walsh PV, Trotter GA. Fracture of the thyroid cartilage associated with full face integral crash helmet. Injury. 1979;11(1):47-48.
6. Tasca RA, Sherman IW, Wood GD. Thyroid cartilage fracture: treatment with biodegradable plates. Br J Oral Maxillofac Surg. 2008;46(2):159-160.
7. Mitrović SM. Blunt external laryngeal trauma. Two case reports. Med Pregl. 2007;60(9-10):489-492.
8. O'Keefe LJ, Maw AR. The dangers of minor blunt laryngeal trauma. J. Laryngol Otol. 1992;106(4):372-373.
9. Rejali SD, Bennett JD, Upile T, Rothera MP. Diagnostic pitfalls in sports related laryngeal injury. Br J Sports Med. 1998;32(2):180-181.
10. Saab M, Birkinshaw R. Blunt laryngeal trauma: an unusual case. Int J Clin Pract. 1997;51(8):527.
11. Pekcevik Y, Ibrahim C, Ülker C. Cricoid and thyroid cartilage fracture, cricothyroid joint dislocation,pseudofracture appearance of the hyoid bone: CT, MRI and laryngoscopic findings. JAEM. 2013;12:170-173.
12. Bent JP 3rd, Porubsky ES. The management of blunt fractures of the thyroid cartilage. Otolaryngol Head Neck Surg. 1994;110(2):195-202. doi: 10:.1177/019459989411000209.
13. Beato Martínez A, Moreno Juara A, López Moya JJ. Fracture of thyroid cartilage after a sneezing episode. Acta Otorrinolaringol Esp. 2007;58(2):73-74.
14. Quinlan PT. Fracture of thyroid cartilage during a sneezing attack. Br Med J. 1950;1(4661):1052.

Retropharyngeal Hematoma in a 90-Year-Old Woman
Case
A 90-year-old woman with chronic obstructive pulmonary disease; hypertension; chronic kidney disease; diastolic dysfunction; severe tricuspid regurgitation; and atrial fibrillation (AF), for which she was taking rivaroxaban, presented to the ED for evaluation of injuries she sustained during a fall. The patient’s family stated that she fell while walking with the assistance of a walker and landed on her face. There was no reported loss of consciousness. Upon arrival at the ED, the patient’s vital signs were: blood pressure, 188/105 mm Hg; heart rate, 91 beats/min; respiratory rate, 20 breaths/min; and temperature, 97.88°F (36.6°C). Oxygen (O2) saturation was 90% on room air, but increased to 98% after the patient received 10 L/min of O2 through a non-rebreather mask.
On physical examination, the patient was awake, alert, and oriented to person, place, and time, with a Glasgow Coma Scale score of 15. She was able to move all four extremities and had 4/5 motor strength in the upper extremities bilaterally, and 3/5 motor strength in the bilateral lower limbs, which her family reported was the same as her baseline. On pulmonary examination, the lungs were clear to auscultation bilaterally and had no stridor. On auscultation she had a regular rate, with no murmurs or rubs.
The patient had nasal bone tenderness with epistaxis that resolved spontaneously and did not require packing; she had no other facial tenderness. The oropharynx was clear. There was mild posterior midline tenderness over C5 and C6, but no skin ecchymosis or neck swelling. Along with the non-rebreather mask, the patient was placed in a neck collar while she awaited transport to radiology for computed tomography (CT) studies.
The CT scan of the cervical spine demonstrated a minimally displaced fracture of the right anterior arch, both sides of the posterior arch of C1, and a comminuted minimally displaced fracture involving the posterior arch and spinous process of C5, with mild retrolisthesis of C5 over C6.

Based on the CT findings, the patient was taken to the operating room (OR) where she underwent awake fiberoptic laryngoscopy. During transfer to the OR, the patient’s O2 dropped to 87%; however, after successful intubation without complication, O2 saturation improved to 95%. After intubation, the patient was admitted to the intensive care unit for observation, and rivaroxaban therapy was discontinued.
A CT scan of the neck postintubation showed a mild interval decrease in the retropharyngeal hematoma, but an increase in the anterior disc space at C5-C6 with mild retrolisthesis, which raised suspicion for an anterior longitudinal ligamentous injury. A repeat CT scan on hospital day 4 revealed a new bleed within the old retropharyngeal hematoma, with no increase in thickness or size of the initial hematoma. The head and neck surgical team kept the patient intubated while awaiting resolution of the hematoma, with no plan of surgery.
On hospital day 6, the patient was transferred to another facility for continued long-term care. She was transitioned to a tracheostomy 4 days later. Follow-up approximately 2 weeks after presentation confirmed complete resolution of the hematoma, and no surgical intervention was required.
Discussion
Overview
Retropharyngeal hematomas are infrequent, but potentially life-threatening complications of cervical fractures, foreign body trauma, infection, violent coughing, and anticoagulation therapy.1 Although retropharyngeal hematomas associated with warfarin have been well described, to our knowledge, there are no reported cases associated with a direct oral anticoagulant (DOAC).2
Though multiple studies have supported the effectiveness and safety of DOACs for prevention of stroke and systemic embolism in patients with AF, the risk of hemorrhage still exists.3 Postmarketing surveillance studies of DOACs report an overall risk of bleeding comparable to warfarin. Gastrointestinal bleeding was found to be slightly higher in patients taking a DOAC compared to those on warfarin, but the risk of intracranial bleeding from DOACs was notably lower.3 With limited effective reversal agents, DOACs present a tremendous challenge in managing acute life-threatening hemorrhage.4
Signs and Symptoms
Patients with retropharyngeal hematomas can present with dyspnea, sore throat, dysphagia, or odynophagia. Neck tenderness and swelling can suggest a retropharyngeal hematoma.5 The diagnosis of a retropharyngeal hemorrhage is of clinical importance because of the possible threat of airway obstruction—which may not be initially detectable clinically, and depends on how quickly the blood fills the retropharyngeal space.1,6
Diagnosis
Computed tomography with intravenous contrast is the imaging study of choice for diagnosing retropharyngeal hematomas in the emergent care setting, and can detect the presence of any associated vertebral facture.5,7,8 Lateral neck X-ray imaging can detect prevertebral swelling, but is not as sensitive as CT and may underestimate the extent of spinal injury; moreover, lesions or early bleeding may be missed.9 In the absence of vertebral fracture on CT imaging, magnetic resonance imaging should be considered to evaluate for possible associated ligamentous injury.9
Treatment and Management
Airway Management. Given the risk of progression to complete airway obstruction, the first step in managing retropharyngeal hematomas is to secure the patient’s airway. Even though the published literature recommends either endotracheal intubation or tracheostomy, the latter should only be considered as a last resort for patients on DOACs because of the increased risk of bleeding.
The fiberoptic approach to endotracheal intubation minimizes the risk of further trauma and rupture of the hematoma.1,10 Once the patient’s airway is secure, the hematoma can be managed conservatively with spinal immobilization and observation for resolution, which may take 2 to 3 weeks.6,11
Surgical Intervention. Some clinicians believe early surgical intervention leads to early recovery and a shorter hospitalization.12 Surgical intervention using a transoral or anterior cervical approach is recommended for large hematomas that fail to regress.6 Surgical intervention may be considered for patients taking warfarin after successful anticoagulation reversal is achieved using fresh frozen plasma (FFP) and vitamin K. However, due to the increased bleeding potential and limited reversal options, there is an increased risk of surgical complications in patients on DOACs.5
Direct Oral Anticoagulation Reversal
The anticoagulation effect of DOACs resolves after five half-lives from the last administered dose, which in the case of rivaroxaban, is between 1 to 2 days.13 Therefore, when emergent surgical intervention is required for a retropharyngeal hematoma, understanding the options and limitations of reversal agents is necessary.
Idarucizumab. Currently the only DOAC anticoagulation reversal agent approved by the US Food and Drug Administration, idarucizumab is only effective for reversing the anticoagulation effects of dabigatran.4,14
Prothrombin Complex Concentrate. Also referred to as factor IX complex, prothrombin complex concentrate (PCC) has been shown to correct prolonged prothrombin time in experimental models of bleeding. Although there is no clinical evidence for its use in DOAC-associated bleeding, PCC should be considered in life-threatening cases, including large or expanding prevertebral hematoma, or other cases in which the potential benefit outweighs the potential risk of thrombosis associated with PCC.4
Fresh Frozen Plasma. In the absence of PCC, FFP may be considered, though there are no data supporting its use as a reversal agent for rivaroxaban.15
Conclusion
Although a rare entity, retropharyngeal hematoma should be suspected in patients with cervical fractures or trauma, especially in the setting of anticoagulation. Early airway management should be considered in a patient with a retropharyngeal hematoma, as symptoms of airway obstruction may be insidious. In patients on DOACs, the potential benefit of earlier resolution with surgical intervention must be strongly weighed against the increased risk of bleeding.
1. Duvillard C, Ballester M, Romanet P. Traumatic retropharyngeal hematoma: a rare and critical pathology needed for early diagnosis. Eur Arch Otorhinolaryngol. 2005;262(9):713-715. doi:10.1007/s00405-004-0767-3.
2. Karmacharya P, Pathak R, Ghimire S, et al. Upper airway hematoma secondary to warfarin therapy: a systematic review of reported cases. N Am J Med Sci. 2015;7(11):494-502. doi:10.4103/1947-2714.170606.
3. Villines TC, Peacock WF. Safety of direct oral anticoagulants: insights from postmarketing studies. Am J Emerg Med. 2016;34(11S):9-13. doi:10.1016/j.ajem.2016.09.047.
4. Levi M. Management of bleeding in patients treated with direct oral anticoagulants. Crit Care. 2016;20:249. doi:10.1186/s13054-016-1413-3.
5. Toker I, Duman Atilla O, Yesilaras M, Ursavas B. Retropharyngeal hematoma due to oral warfarin usage. Turk J Emerg Med. 2014;14(4):182-184. doi:10.5505/1304.7361.2014.25594.
6. Senel AC, Gunduz AK. Retropharyngeal hematoma secondary to minor blunt neck trauma: case report. Rev Bras Anestesiol. 2012;62(5):731-735. doi:10.1016/S0034-7094(12)70171-X.
7. Koulouris G, Pianta M, Stuckey S. The ‘sentinel clot’ sign in spontaneous retropharyngeal hematoma secondary to parathyroid apoplexy. Ear Nose Throat J. 2006;85(9):606-608.
8. Ryan MF, Meurer D, Tyndall JA. Expanding prevertebral soft tissue swelling subsequent to a motor vehicle collision. Case Rep Emerg Med. 2014;2014:870580. doi:10.1155/2014/870580.
9. Parizel PM, van der Zijden T, Gaudino S, et al. Trauma of the spine and spinal cord: imaging strategies. Eur Spine J. 2010;19(suppl 1):S8-S17. doi:10.1007/s00586-009-1123-5.
10. Shaw CB, Bawa R, Snider G, Wax MK. Traumatic retropharyngeal hematoma: a case report. Otolaryngol Head Neck Surg. 1995;113(4):485-488. doi:10.1016/S0194-59989570091-9.
11. Mackenzie JW, Jellicoe JA. Acute upper airway obstruction. Spontaneous retropharyngeal haematoma in a patient with polycythaemia rubra vera. Anaesthesia. 1986;41(1):57-60.
12. Park JH, Jeong EK, Kang DH, Jeon SR. Surgical treatment of a life-threatening large retropharyngeal hematoma after minor trauma: two case reports and a literature review. J Korean Neurosurg Soc. 2015;58(3):304-307. doi:10.3340/jkns.2015.58.3.304.
13. Scaglione F. New oral anticoagulants: comparative pharmacology with vitamin K antagonists. Clin Pharmacokinet. 2013;52(2):69-82. doi:10.1007/s40262-012-0030-9.
14. Christos S, Naples R. Anticoagulation reversal and treatment strategies in major bleeding: update 2016. West J Emerg Med. 2016;17(3):264-270. doi:10.5811/westjem.2016.3.29294. Erratum in: West J Emerg Med. 2016;17(5):669-670.
15. Chai-Adisaksopha C, Hillis C, Lim W, Boonyawat K, Moffat K, Crowther M. Hemodialysis for the treatment of dabigatran-associated bleeding: a case report and systematic review. J Thromb Haemost. 2015;13(10):1790-1798. doi:10.1111/jth.13117.
Case
A 90-year-old woman with chronic obstructive pulmonary disease; hypertension; chronic kidney disease; diastolic dysfunction; severe tricuspid regurgitation; and atrial fibrillation (AF), for which she was taking rivaroxaban, presented to the ED for evaluation of injuries she sustained during a fall. The patient’s family stated that she fell while walking with the assistance of a walker and landed on her face. There was no reported loss of consciousness. Upon arrival at the ED, the patient’s vital signs were: blood pressure, 188/105 mm Hg; heart rate, 91 beats/min; respiratory rate, 20 breaths/min; and temperature, 97.88°F (36.6°C). Oxygen (O2) saturation was 90% on room air, but increased to 98% after the patient received 10 L/min of O2 through a non-rebreather mask.
On physical examination, the patient was awake, alert, and oriented to person, place, and time, with a Glasgow Coma Scale score of 15. She was able to move all four extremities and had 4/5 motor strength in the upper extremities bilaterally, and 3/5 motor strength in the bilateral lower limbs, which her family reported was the same as her baseline. On pulmonary examination, the lungs were clear to auscultation bilaterally and had no stridor. On auscultation she had a regular rate, with no murmurs or rubs.
The patient had nasal bone tenderness with epistaxis that resolved spontaneously and did not require packing; she had no other facial tenderness. The oropharynx was clear. There was mild posterior midline tenderness over C5 and C6, but no skin ecchymosis or neck swelling. Along with the non-rebreather mask, the patient was placed in a neck collar while she awaited transport to radiology for computed tomography (CT) studies.
The CT scan of the cervical spine demonstrated a minimally displaced fracture of the right anterior arch, both sides of the posterior arch of C1, and a comminuted minimally displaced fracture involving the posterior arch and spinous process of C5, with mild retrolisthesis of C5 over C6.
Based on the CT findings, the patient was taken to the operating room (OR) where she underwent awake fiberoptic laryngoscopy. During transfer to the OR, the patient’s O2 dropped to 87%; however, after successful intubation without complication, O2 saturation improved to 95%. After intubation, the patient was admitted to the intensive care unit for observation, and rivaroxaban therapy was discontinued.
A CT scan of the neck postintubation showed a mild interval decrease in the retropharyngeal hematoma, but an increase in the anterior disc space at C5-C6 with mild retrolisthesis, which raised suspicion for an anterior longitudinal ligamentous injury. A repeat CT scan on hospital day 4 revealed a new bleed within the old retropharyngeal hematoma, with no increase in thickness or size of the initial hematoma. The head and neck surgical team kept the patient intubated while awaiting resolution of the hematoma, with no plan of surgery.
On hospital day 6, the patient was transferred to another facility for continued long-term care. She was transitioned to a tracheostomy 4 days later. Follow-up approximately 2 weeks after presentation confirmed complete resolution of the hematoma, and no surgical intervention was required.
Discussion
Overview
Retropharyngeal hematomas are infrequent, but potentially life-threatening complications of cervical fractures, foreign body trauma, infection, violent coughing, and anticoagulation therapy.1 Although retropharyngeal hematomas associated with warfarin have been well described, to our knowledge, there are no reported cases associated with a direct oral anticoagulant (DOAC).2
Though multiple studies have supported the effectiveness and safety of DOACs for prevention of stroke and systemic embolism in patients with AF, the risk of hemorrhage still exists.3 Postmarketing surveillance studies of DOACs report an overall risk of bleeding comparable to warfarin. Gastrointestinal bleeding was found to be slightly higher in patients taking a DOAC compared to those on warfarin, but the risk of intracranial bleeding from DOACs was notably lower.3 With limited effective reversal agents, DOACs present a tremendous challenge in managing acute life-threatening hemorrhage.4
Signs and Symptoms
Patients with retropharyngeal hematomas can present with dyspnea, sore throat, dysphagia, or odynophagia. Neck tenderness and swelling can suggest a retropharyngeal hematoma.5 The diagnosis of a retropharyngeal hemorrhage is of clinical importance because of the possible threat of airway obstruction—which may not be initially detectable clinically, and depends on how quickly the blood fills the retropharyngeal space.1,6
Diagnosis
Computed tomography with intravenous contrast is the imaging study of choice for diagnosing retropharyngeal hematomas in the emergent care setting, and can detect the presence of any associated vertebral facture.5,7,8 Lateral neck X-ray imaging can detect prevertebral swelling, but is not as sensitive as CT and may underestimate the extent of spinal injury; moreover, lesions or early bleeding may be missed.9 In the absence of vertebral fracture on CT imaging, magnetic resonance imaging should be considered to evaluate for possible associated ligamentous injury.9
Treatment and Management
Airway Management. Given the risk of progression to complete airway obstruction, the first step in managing retropharyngeal hematomas is to secure the patient’s airway. Even though the published literature recommends either endotracheal intubation or tracheostomy, the latter should only be considered as a last resort for patients on DOACs because of the increased risk of bleeding.
The fiberoptic approach to endotracheal intubation minimizes the risk of further trauma and rupture of the hematoma.1,10 Once the patient’s airway is secure, the hematoma can be managed conservatively with spinal immobilization and observation for resolution, which may take 2 to 3 weeks.6,11
Surgical Intervention. Some clinicians believe early surgical intervention leads to early recovery and a shorter hospitalization.12 Surgical intervention using a transoral or anterior cervical approach is recommended for large hematomas that fail to regress.6 Surgical intervention may be considered for patients taking warfarin after successful anticoagulation reversal is achieved using fresh frozen plasma (FFP) and vitamin K. However, due to the increased bleeding potential and limited reversal options, there is an increased risk of surgical complications in patients on DOACs.5
Direct Oral Anticoagulation Reversal
The anticoagulation effect of DOACs resolves after five half-lives from the last administered dose, which in the case of rivaroxaban, is between 1 to 2 days.13 Therefore, when emergent surgical intervention is required for a retropharyngeal hematoma, understanding the options and limitations of reversal agents is necessary.
Idarucizumab. Currently the only DOAC anticoagulation reversal agent approved by the US Food and Drug Administration, idarucizumab is only effective for reversing the anticoagulation effects of dabigatran.4,14
Prothrombin Complex Concentrate. Also referred to as factor IX complex, prothrombin complex concentrate (PCC) has been shown to correct prolonged prothrombin time in experimental models of bleeding. Although there is no clinical evidence for its use in DOAC-associated bleeding, PCC should be considered in life-threatening cases, including large or expanding prevertebral hematoma, or other cases in which the potential benefit outweighs the potential risk of thrombosis associated with PCC.4
Fresh Frozen Plasma. In the absence of PCC, FFP may be considered, though there are no data supporting its use as a reversal agent for rivaroxaban.15
Conclusion
Although a rare entity, retropharyngeal hematoma should be suspected in patients with cervical fractures or trauma, especially in the setting of anticoagulation. Early airway management should be considered in a patient with a retropharyngeal hematoma, as symptoms of airway obstruction may be insidious. In patients on DOACs, the potential benefit of earlier resolution with surgical intervention must be strongly weighed against the increased risk of bleeding.
Case
A 90-year-old woman with chronic obstructive pulmonary disease; hypertension; chronic kidney disease; diastolic dysfunction; severe tricuspid regurgitation; and atrial fibrillation (AF), for which she was taking rivaroxaban, presented to the ED for evaluation of injuries she sustained during a fall. The patient’s family stated that she fell while walking with the assistance of a walker and landed on her face. There was no reported loss of consciousness. Upon arrival at the ED, the patient’s vital signs were: blood pressure, 188/105 mm Hg; heart rate, 91 beats/min; respiratory rate, 20 breaths/min; and temperature, 97.88°F (36.6°C). Oxygen (O2) saturation was 90% on room air, but increased to 98% after the patient received 10 L/min of O2 through a non-rebreather mask.
On physical examination, the patient was awake, alert, and oriented to person, place, and time, with a Glasgow Coma Scale score of 15. She was able to move all four extremities and had 4/5 motor strength in the upper extremities bilaterally, and 3/5 motor strength in the bilateral lower limbs, which her family reported was the same as her baseline. On pulmonary examination, the lungs were clear to auscultation bilaterally and had no stridor. On auscultation she had a regular rate, with no murmurs or rubs.
The patient had nasal bone tenderness with epistaxis that resolved spontaneously and did not require packing; she had no other facial tenderness. The oropharynx was clear. There was mild posterior midline tenderness over C5 and C6, but no skin ecchymosis or neck swelling. Along with the non-rebreather mask, the patient was placed in a neck collar while she awaited transport to radiology for computed tomography (CT) studies.
The CT scan of the cervical spine demonstrated a minimally displaced fracture of the right anterior arch, both sides of the posterior arch of C1, and a comminuted minimally displaced fracture involving the posterior arch and spinous process of C5, with mild retrolisthesis of C5 over C6.
Based on the CT findings, the patient was taken to the operating room (OR) where she underwent awake fiberoptic laryngoscopy. During transfer to the OR, the patient’s O2 dropped to 87%; however, after successful intubation without complication, O2 saturation improved to 95%. After intubation, the patient was admitted to the intensive care unit for observation, and rivaroxaban therapy was discontinued.
A CT scan of the neck postintubation showed a mild interval decrease in the retropharyngeal hematoma, but an increase in the anterior disc space at C5-C6 with mild retrolisthesis, which raised suspicion for an anterior longitudinal ligamentous injury. A repeat CT scan on hospital day 4 revealed a new bleed within the old retropharyngeal hematoma, with no increase in thickness or size of the initial hematoma. The head and neck surgical team kept the patient intubated while awaiting resolution of the hematoma, with no plan of surgery.
On hospital day 6, the patient was transferred to another facility for continued long-term care. She was transitioned to a tracheostomy 4 days later. Follow-up approximately 2 weeks after presentation confirmed complete resolution of the hematoma, and no surgical intervention was required.
Discussion
Overview
Retropharyngeal hematomas are infrequent, but potentially life-threatening complications of cervical fractures, foreign body trauma, infection, violent coughing, and anticoagulation therapy.1 Although retropharyngeal hematomas associated with warfarin have been well described, to our knowledge, there are no reported cases associated with a direct oral anticoagulant (DOAC).2
Though multiple studies have supported the effectiveness and safety of DOACs for prevention of stroke and systemic embolism in patients with AF, the risk of hemorrhage still exists.3 Postmarketing surveillance studies of DOACs report an overall risk of bleeding comparable to warfarin. Gastrointestinal bleeding was found to be slightly higher in patients taking a DOAC compared to those on warfarin, but the risk of intracranial bleeding from DOACs was notably lower.3 With limited effective reversal agents, DOACs present a tremendous challenge in managing acute life-threatening hemorrhage.4
Signs and Symptoms
Patients with retropharyngeal hematomas can present with dyspnea, sore throat, dysphagia, or odynophagia. Neck tenderness and swelling can suggest a retropharyngeal hematoma.5 The diagnosis of a retropharyngeal hemorrhage is of clinical importance because of the possible threat of airway obstruction—which may not be initially detectable clinically, and depends on how quickly the blood fills the retropharyngeal space.1,6
Diagnosis
Computed tomography with intravenous contrast is the imaging study of choice for diagnosing retropharyngeal hematomas in the emergent care setting, and can detect the presence of any associated vertebral facture.5,7,8 Lateral neck X-ray imaging can detect prevertebral swelling, but is not as sensitive as CT and may underestimate the extent of spinal injury; moreover, lesions or early bleeding may be missed.9 In the absence of vertebral fracture on CT imaging, magnetic resonance imaging should be considered to evaluate for possible associated ligamentous injury.9
Treatment and Management
Airway Management. Given the risk of progression to complete airway obstruction, the first step in managing retropharyngeal hematomas is to secure the patient’s airway. Even though the published literature recommends either endotracheal intubation or tracheostomy, the latter should only be considered as a last resort for patients on DOACs because of the increased risk of bleeding.
The fiberoptic approach to endotracheal intubation minimizes the risk of further trauma and rupture of the hematoma.1,10 Once the patient’s airway is secure, the hematoma can be managed conservatively with spinal immobilization and observation for resolution, which may take 2 to 3 weeks.6,11
Surgical Intervention. Some clinicians believe early surgical intervention leads to early recovery and a shorter hospitalization.12 Surgical intervention using a transoral or anterior cervical approach is recommended for large hematomas that fail to regress.6 Surgical intervention may be considered for patients taking warfarin after successful anticoagulation reversal is achieved using fresh frozen plasma (FFP) and vitamin K. However, due to the increased bleeding potential and limited reversal options, there is an increased risk of surgical complications in patients on DOACs.5
Direct Oral Anticoagulation Reversal
The anticoagulation effect of DOACs resolves after five half-lives from the last administered dose, which in the case of rivaroxaban, is between 1 to 2 days.13 Therefore, when emergent surgical intervention is required for a retropharyngeal hematoma, understanding the options and limitations of reversal agents is necessary.
Idarucizumab. Currently the only DOAC anticoagulation reversal agent approved by the US Food and Drug Administration, idarucizumab is only effective for reversing the anticoagulation effects of dabigatran.4,14
Prothrombin Complex Concentrate. Also referred to as factor IX complex, prothrombin complex concentrate (PCC) has been shown to correct prolonged prothrombin time in experimental models of bleeding. Although there is no clinical evidence for its use in DOAC-associated bleeding, PCC should be considered in life-threatening cases, including large or expanding prevertebral hematoma, or other cases in which the potential benefit outweighs the potential risk of thrombosis associated with PCC.4
Fresh Frozen Plasma. In the absence of PCC, FFP may be considered, though there are no data supporting its use as a reversal agent for rivaroxaban.15
Conclusion
Although a rare entity, retropharyngeal hematoma should be suspected in patients with cervical fractures or trauma, especially in the setting of anticoagulation. Early airway management should be considered in a patient with a retropharyngeal hematoma, as symptoms of airway obstruction may be insidious. In patients on DOACs, the potential benefit of earlier resolution with surgical intervention must be strongly weighed against the increased risk of bleeding.
1. Duvillard C, Ballester M, Romanet P. Traumatic retropharyngeal hematoma: a rare and critical pathology needed for early diagnosis. Eur Arch Otorhinolaryngol. 2005;262(9):713-715. doi:10.1007/s00405-004-0767-3.
2. Karmacharya P, Pathak R, Ghimire S, et al. Upper airway hematoma secondary to warfarin therapy: a systematic review of reported cases. N Am J Med Sci. 2015;7(11):494-502. doi:10.4103/1947-2714.170606.
3. Villines TC, Peacock WF. Safety of direct oral anticoagulants: insights from postmarketing studies. Am J Emerg Med. 2016;34(11S):9-13. doi:10.1016/j.ajem.2016.09.047.
4. Levi M. Management of bleeding in patients treated with direct oral anticoagulants. Crit Care. 2016;20:249. doi:10.1186/s13054-016-1413-3.
5. Toker I, Duman Atilla O, Yesilaras M, Ursavas B. Retropharyngeal hematoma due to oral warfarin usage. Turk J Emerg Med. 2014;14(4):182-184. doi:10.5505/1304.7361.2014.25594.
6. Senel AC, Gunduz AK. Retropharyngeal hematoma secondary to minor blunt neck trauma: case report. Rev Bras Anestesiol. 2012;62(5):731-735. doi:10.1016/S0034-7094(12)70171-X.
7. Koulouris G, Pianta M, Stuckey S. The ‘sentinel clot’ sign in spontaneous retropharyngeal hematoma secondary to parathyroid apoplexy. Ear Nose Throat J. 2006;85(9):606-608.
8. Ryan MF, Meurer D, Tyndall JA. Expanding prevertebral soft tissue swelling subsequent to a motor vehicle collision. Case Rep Emerg Med. 2014;2014:870580. doi:10.1155/2014/870580.
9. Parizel PM, van der Zijden T, Gaudino S, et al. Trauma of the spine and spinal cord: imaging strategies. Eur Spine J. 2010;19(suppl 1):S8-S17. doi:10.1007/s00586-009-1123-5.
10. Shaw CB, Bawa R, Snider G, Wax MK. Traumatic retropharyngeal hematoma: a case report. Otolaryngol Head Neck Surg. 1995;113(4):485-488. doi:10.1016/S0194-59989570091-9.
11. Mackenzie JW, Jellicoe JA. Acute upper airway obstruction. Spontaneous retropharyngeal haematoma in a patient with polycythaemia rubra vera. Anaesthesia. 1986;41(1):57-60.
12. Park JH, Jeong EK, Kang DH, Jeon SR. Surgical treatment of a life-threatening large retropharyngeal hematoma after minor trauma: two case reports and a literature review. J Korean Neurosurg Soc. 2015;58(3):304-307. doi:10.3340/jkns.2015.58.3.304.
13. Scaglione F. New oral anticoagulants: comparative pharmacology with vitamin K antagonists. Clin Pharmacokinet. 2013;52(2):69-82. doi:10.1007/s40262-012-0030-9.
14. Christos S, Naples R. Anticoagulation reversal and treatment strategies in major bleeding: update 2016. West J Emerg Med. 2016;17(3):264-270. doi:10.5811/westjem.2016.3.29294. Erratum in: West J Emerg Med. 2016;17(5):669-670.
15. Chai-Adisaksopha C, Hillis C, Lim W, Boonyawat K, Moffat K, Crowther M. Hemodialysis for the treatment of dabigatran-associated bleeding: a case report and systematic review. J Thromb Haemost. 2015;13(10):1790-1798. doi:10.1111/jth.13117.
1. Duvillard C, Ballester M, Romanet P. Traumatic retropharyngeal hematoma: a rare and critical pathology needed for early diagnosis. Eur Arch Otorhinolaryngol. 2005;262(9):713-715. doi:10.1007/s00405-004-0767-3.
2. Karmacharya P, Pathak R, Ghimire S, et al. Upper airway hematoma secondary to warfarin therapy: a systematic review of reported cases. N Am J Med Sci. 2015;7(11):494-502. doi:10.4103/1947-2714.170606.
3. Villines TC, Peacock WF. Safety of direct oral anticoagulants: insights from postmarketing studies. Am J Emerg Med. 2016;34(11S):9-13. doi:10.1016/j.ajem.2016.09.047.
4. Levi M. Management of bleeding in patients treated with direct oral anticoagulants. Crit Care. 2016;20:249. doi:10.1186/s13054-016-1413-3.
5. Toker I, Duman Atilla O, Yesilaras M, Ursavas B. Retropharyngeal hematoma due to oral warfarin usage. Turk J Emerg Med. 2014;14(4):182-184. doi:10.5505/1304.7361.2014.25594.
6. Senel AC, Gunduz AK. Retropharyngeal hematoma secondary to minor blunt neck trauma: case report. Rev Bras Anestesiol. 2012;62(5):731-735. doi:10.1016/S0034-7094(12)70171-X.
7. Koulouris G, Pianta M, Stuckey S. The ‘sentinel clot’ sign in spontaneous retropharyngeal hematoma secondary to parathyroid apoplexy. Ear Nose Throat J. 2006;85(9):606-608.
8. Ryan MF, Meurer D, Tyndall JA. Expanding prevertebral soft tissue swelling subsequent to a motor vehicle collision. Case Rep Emerg Med. 2014;2014:870580. doi:10.1155/2014/870580.
9. Parizel PM, van der Zijden T, Gaudino S, et al. Trauma of the spine and spinal cord: imaging strategies. Eur Spine J. 2010;19(suppl 1):S8-S17. doi:10.1007/s00586-009-1123-5.
10. Shaw CB, Bawa R, Snider G, Wax MK. Traumatic retropharyngeal hematoma: a case report. Otolaryngol Head Neck Surg. 1995;113(4):485-488. doi:10.1016/S0194-59989570091-9.
11. Mackenzie JW, Jellicoe JA. Acute upper airway obstruction. Spontaneous retropharyngeal haematoma in a patient with polycythaemia rubra vera. Anaesthesia. 1986;41(1):57-60.
12. Park JH, Jeong EK, Kang DH, Jeon SR. Surgical treatment of a life-threatening large retropharyngeal hematoma after minor trauma: two case reports and a literature review. J Korean Neurosurg Soc. 2015;58(3):304-307. doi:10.3340/jkns.2015.58.3.304.
13. Scaglione F. New oral anticoagulants: comparative pharmacology with vitamin K antagonists. Clin Pharmacokinet. 2013;52(2):69-82. doi:10.1007/s40262-012-0030-9.
14. Christos S, Naples R. Anticoagulation reversal and treatment strategies in major bleeding: update 2016. West J Emerg Med. 2016;17(3):264-270. doi:10.5811/westjem.2016.3.29294. Erratum in: West J Emerg Med. 2016;17(5):669-670.
15. Chai-Adisaksopha C, Hillis C, Lim W, Boonyawat K, Moffat K, Crowther M. Hemodialysis for the treatment of dabigatran-associated bleeding: a case report and systematic review. J Thromb Haemost. 2015;13(10):1790-1798. doi:10.1111/jth.13117.

Nontraumatic Disc Herniation as a Cause of Unusual Cervical Spondylotic Myelopathy
Case
A 55-year-old previously healthy woman with an insignificant medical history presented to the ED for evaluation of right-sided numbness, tingling, and inability to sense temperature. The patient stated the numbness and tingling first began in her right leg and thigh 2 months earlier, and had progressively worsened to her entire right-side. She said she first experienced the thermoanesthesia while taking a shower the morning of presentation. While showering, the patient noted that she could not feel any hot or cold sensation on the right side of her body, including her right leg and arm. She also reported decreased sensation to her extremities on the right side.
She denied any new weakness, headache, chest pain, shortness of breath, fever, chills, nausea, vomiting, back pain, neck pain, or any other symptoms. In addition, she denied any difficulty swallowing, speaking, blurry vision, or double vision. Regarding her social history, the patient denied a history of sexually transmitted diseases, including syphilis; or any tobacco, alcohol, or illicit drug use. The patient confirmed that she had never experienced any of the presenting symptoms prior to 2 months ago. There was no history of trauma or falls. A review of systems was otherwise negative.
Vital signs at presentation were: blood pressure, 129/88 mm Hg; heart rate, 99 beats/min; respiratory rate, 18 breaths/min; and temperature, 98.5°F. Oxygen saturation was 98% on room air. Physical examination revealed a middle-aged woman who was awake, alert, and oriented. Her head was normocephalic and atraumatic, and her pupils were 5 mm, equal, round, and reactive to light bilaterally. Her cranial nerves II through XII were intact. She had normal 5/5 strength in both her upper and lower extremities bilaterally, and had 2+ and equal bilateral patella and Achilles deep tendon reflexes. The patient had no truncal ataxia, and she had a normal gait on ambulation. She was unable to sense temperature (assessed by touching a cold metal tray with her right hand). There was no neck or back midline tenderness to palpation of her spine.
Initial laboratory studies included a complete blood count (CBC); basic metabolic panel (BMP), including blood urea nitrogen; and urine drug screen (UDS). The CBC and BMP were within normal limits, except for an elevated creatine kinase of 249 U/L. The UDS was positive for cocaine. A head computed tomography (CT) scan without contrast was unremarkable.
The patient was admitted to the hospital for further evaluation. Additional laboratory workup during the inpatient stay included nonreactive treponemal immunoglobulin G/immunoglobulin M; nonreactive HIV antigen antibody assay; normal thyroid stimulating hormone; normal free thyroxine, folate, and vitamin B12 levels; normal erythrocyte sedimentation rate, and C-reactive protein levels. The patient’s hemoglobin A1C was also within normal range.
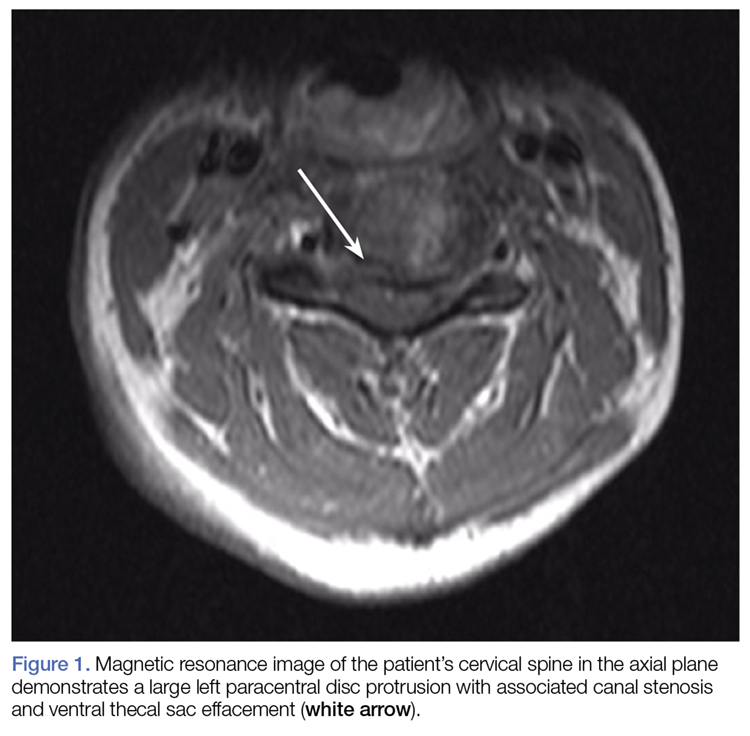
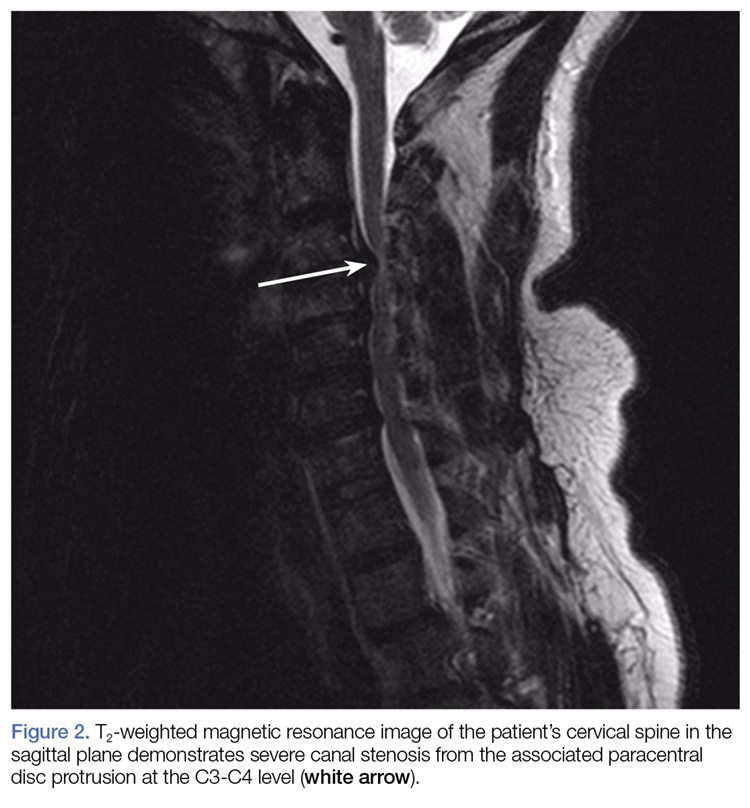
Other imaging studies, which included MR angiography (MRA) of the head and neck, and MRI of the thoracic and lumbar spine, were unremarkable, with the exception of some chronic spondylitic changes.
Due to the significant C3-C4 stenosis, orthopedic surgery services were consulted for a spinal surgery workup. The orthopedic examination identified a few beats of clonus, intact proprioception, and no dysmetria. The patient had decreased sensation to fine touch in the distribution of C7 at the level of the triceps, midphalangeal joints to distal fingertips on the right, fourth, and fifth fingers on the left and right lateral lower extremity. A Hoffmann sign was positive bilaterally. A CT scan of the cervical spine showed severe canal stenosis at the C3-C4 level secondary to a large C3-C4 left paracentral disc protrusion with AP dimensions of the canal measured at 4 to 5 mm. There was no evidence of acute cervical spine fracture or subluxation.
The patient was offered operative and nonoperative management options, including anterior cervical discectomy and fusion vs conservative management with corticosteroid therapy. She agreed to conservative management and received intravenous (IV) dexamethasone with subjective improvement in her symptoms. The patient was discharged home on hospital day 3, with instructions to follow-up with a spine surgeon in 2 weeks. She was also counseled on abstaining from further cocaine or other illicit drug use.
The patient eventually returned for an elective anterior cervical discectomy and fusion 2 months later, after several outpatient visits and progression of symptoms. She was discharged home on postoperative day 1 with pain well-controlled and was able to ambulate without assistance. On follow-up, she reported 15% improvement in her symptoms.
Discussion
Cervical spondylotic myelopathy (CSM) is the most common myelopathy in patients aged 55 years and older. Immediate neuroimaging studies followed by spinal surgery consultation are recommended for patients presenting with acute symptoms suggestive of cord compression.1,2
Diagnosis and Differential Diagnosis
Diagnosis of CSM can be made with a thorough patient history, neurological examination, and MRI/MRA. However, because cases of cervical disc herniation (CDH) are often atraumatic, the patient history may not always be contributory to the diagnosis and severity of the offending cause.
During our patient’s hospital course, there was initially a concern for Brown-Séquard syndrome (BSS) due to the lateralizing symptoms and radiographic findings. This is a rare condition that can occur in the setting of spinal trauma, unilateral disc herniation, tumors, epidural hematomas, and spinal cord ischemia.3,4 In one retrospective case review by Sayer et al,4 the incidence of CDH causing BSS was only 0.21% (5 per 2,350 patients), and 67% of the cases involved C5-C6 or C6-C7.
Although disc herniation usually presents with symptoms on the ipsilateral side in patients with BSS, there are rare case reports of patients with contralateral symptoms in the form of complete or incomplete BSS manifesting as ipsilateral motor deficit and/or loss of contralateral pain and temperature due to an incomplete spinal cord compression.5-7 We were able to rule-out BSS in our patient due to the absence of motor symptoms.
Treatment
Corticosteroid Therapy. High-dose IV corticosteroids should be given to all patients with CSM prior to surgery to reduce cord edema caused by spinal cord injury. In one randomized control trial by Bracken et al,8 patients given methylprednisolone within 8 hours of spinal cord injury had improvement in motor function, sensation to pinprick, and touch at 6 months when compared to placebo. When the aforementioned steps are taken in the emergent care setting, they may significantly improve patient outcomes.
Surgical Intervention. All cases of CSM in the review literature were treated surgically with laminectomy or hemilaminectomy, anterior discectomy with or without fusion, or corpectomy followed by interbody fusion, with the goal of achieving cord decompression. A large majority of patients underwent anterior discectomy with interbody fusion, and all of the cases recommend early surgical intervention in severe CSM to prevent rapidly worsening symptoms, including permanent hemiparesis.
Early surgical intervention is positively correlated with better outcomes, most often resulting in significant improvement of symptoms to full recovery.3,4,6,7,9-12 In one case report, surgical intervention did not result in a significant improvement, and the patient had been suffering from progressive symptoms for 7 years prior to diagnosis and treatment.11
Conservative Management. Conservative management of CSM includes immobilization, activity modification, pain management, and/or corticosteroids therapy.13 However, for patients undergoing surgical decompression, 50% to 80% reported symptom improvement.14,15 This evidence strongly supports management of CSM with early diagnosis and surgical intervention. Despite delays in diagnosis and treatment, surgical intervention can still offer significant relief of weakness and sensory deficits associated with severe CSM.11
Conclusion
Cervical spondylotic myelopathy is the most common myelopathy in patients aged 55 years and older. Common symptoms involve upper extremity sensation, gait disturbances, and deterioration of hand use16; however, there is a large differential for patients presenting to the ED with these symptoms, including mass effect, infection, vascular conditions, metabolic disorders, inflammatory conditions, and trauma.
Our patient with CSM presented with signs of an incomplete cord syndrome with lateralizing features caused by asymmetric disc herniation. This case is unique in that though our patient had some symptom resolution with corticosteroids therapy alone, she ultimately returned for definitive surgical decompression after symptom progression.
1. Chen TY, Dickman CA, Eleraky M, Sonntag VK. The role of decompression for acute incomplete cervical spinal cord injury in cervical spondylosis. Spine (Phila Pa 1976). 1998;23(22):2398-2403.
2. Ishida Y, Tominaga T. Predictors of neurologic recovery in acute central cervical cord injury with only upper extremity impairment. Spine (Phila Pa 1976). 2002;27(15):1652-1658. discussion 1658.
3. Porto GB, Tan LA, Kasliwal MK, Traynelis VC. Progressive Brown-Séquard syndrome: a rare manifestation of cervical disc herniation. J Clin Neurosci. 2016;29:196-198. doi:10.1016/j.jocn.2015.12.021
4. Sayer FT, Vitali AM, Low HL, Paquette S, Honey CR. Brown-Sèquard syndrome produced by C3-C4 cervical disc herniation: a case report and review of the literature. Spine (Phila Pa 1976). 2008;33(9):E279-E282. doi:10.1097/BRS.0b013e31816c835d.
5. Urrutia J, Fadic R. Cervical disc herniation producing acute Brown-Sequard syndrome: dynamic changes documented by intraoperative neuromonitoring. Eur Spine J. 2012;21 Suppl 4:S418-S421. doi:10.1007/s00586-011-1881-8.
6. Choi KB, Lee CD, Chung DJ, Lee SH. Cervical disc herniation as a cause of Brown-Séquard syndrome. J Korean Neurosurg Soc. 2009;46(5):505-510. doi:10.3340/jkns.2009.46.5.505. doi:10.3340/jkns.2009.46.5.505.
7. Kobayashi N, Asamoto S, Doi H, Sugiyama H. Brown-Sèquard syndrome produced by cervical disc herniation: report of two cases and review of the literature. Spine J. 2003;3(6):530-533.
8. Bracken MB, Shepard MJ, Collins WF, et al. A randomized, controlled trial of methylprednisolone or naloxone in the treatment of acute spinal-cord injury. Results of the Second National Acute Spinal Cord Injury Study. N Engl J Med. 1990; 322(20):1405-1411. doi:10.1056/NEJM199005173222001.
9. Stookey B. Compression of the spinal cord due to ventral extradural cervical chondromas: diagnosis and surgical treatment. Arch Neurol Psychiatry. 1928;20:275-291.
10. Antich PA, Sanjuan AC, Girvent FM, Simó JD. High cervical disc herniation and Brown-Sequard syndrome. A case report and review of the literature. J Bone Joint Surg Br. 1999;81(3):462-463.
11. Guan D, Wang G, Claire M, Kuang Z. Brown-Sequard syndrome produced by calcified herniated cervical disc and posterior vertebral osteophyte: case report.
J Orthop. 2015;12(Suppl 2):S260-S263. doi:10.1016/j.jor.2015.10.007.
12. Abouhashem S, Ammar M, Barakat M, Abdelhameed E. Management of Brown-Sequard syndrome in cervical disc diseases. Turk Neurosurg. 2013;23(4):470-475. doi:10.5137/1019-5149.JTN.7433-12.0.
13. Mazanec D, Reddy A. Medical management of cervical spondylosis. Neurosurgery. 2007;60(1 Suppl 1):S43-S50. doi:10.1227/01.NEU.0000215386.05760.6D.
14. Chagas H, Domingues F, Aversa A, Vidal Fonseca AL, de Souza JM. Cervical spondylotic myelopathy: 10 years of prospective outcome analysis of anterior decompression and fusion. Surg Neurol. 2005;64(Suppl 1):S1:30-S1:35; discussion S1:35-S1:36. doi:10.1016/j.surneu.2005.02.016.
15. Cheung WY, Arvinte D, Wong YW, Luk KD, Cheung KM. Neurological recovery after surgical decompression in patients with cervical spondylotic myelopathy - a prospective study. Int Orthop. 2008;32(2):273-378. doi:10.1007/s00264-006-0315-4.
16. Chiles BW 3rd, Leonard MA, Choudhri HF, Cooper PR. Cervical spondylotic myelopathy: patterns of neurological deficit and recovery after anterior cervical decompression. Neurosurgery. 1999;44(4):762-769; discussion 769-770
Case
A 55-year-old previously healthy woman with an insignificant medical history presented to the ED for evaluation of right-sided numbness, tingling, and inability to sense temperature. The patient stated the numbness and tingling first began in her right leg and thigh 2 months earlier, and had progressively worsened to her entire right-side. She said she first experienced the thermoanesthesia while taking a shower the morning of presentation. While showering, the patient noted that she could not feel any hot or cold sensation on the right side of her body, including her right leg and arm. She also reported decreased sensation to her extremities on the right side.
She denied any new weakness, headache, chest pain, shortness of breath, fever, chills, nausea, vomiting, back pain, neck pain, or any other symptoms. In addition, she denied any difficulty swallowing, speaking, blurry vision, or double vision. Regarding her social history, the patient denied a history of sexually transmitted diseases, including syphilis; or any tobacco, alcohol, or illicit drug use. The patient confirmed that she had never experienced any of the presenting symptoms prior to 2 months ago. There was no history of trauma or falls. A review of systems was otherwise negative.
Vital signs at presentation were: blood pressure, 129/88 mm Hg; heart rate, 99 beats/min; respiratory rate, 18 breaths/min; and temperature, 98.5°F. Oxygen saturation was 98% on room air. Physical examination revealed a middle-aged woman who was awake, alert, and oriented. Her head was normocephalic and atraumatic, and her pupils were 5 mm, equal, round, and reactive to light bilaterally. Her cranial nerves II through XII were intact. She had normal 5/5 strength in both her upper and lower extremities bilaterally, and had 2+ and equal bilateral patella and Achilles deep tendon reflexes. The patient had no truncal ataxia, and she had a normal gait on ambulation. She was unable to sense temperature (assessed by touching a cold metal tray with her right hand). There was no neck or back midline tenderness to palpation of her spine.
Initial laboratory studies included a complete blood count (CBC); basic metabolic panel (BMP), including blood urea nitrogen; and urine drug screen (UDS). The CBC and BMP were within normal limits, except for an elevated creatine kinase of 249 U/L. The UDS was positive for cocaine. A head computed tomography (CT) scan without contrast was unremarkable.
The patient was admitted to the hospital for further evaluation. Additional laboratory workup during the inpatient stay included nonreactive treponemal immunoglobulin G/immunoglobulin M; nonreactive HIV antigen antibody assay; normal thyroid stimulating hormone; normal free thyroxine, folate, and vitamin B12 levels; normal erythrocyte sedimentation rate, and C-reactive protein levels. The patient’s hemoglobin A1C was also within normal range.
Other imaging studies, which included MR angiography (MRA) of the head and neck, and MRI of the thoracic and lumbar spine, were unremarkable, with the exception of some chronic spondylitic changes.
Due to the significant C3-C4 stenosis, orthopedic surgery services were consulted for a spinal surgery workup. The orthopedic examination identified a few beats of clonus, intact proprioception, and no dysmetria. The patient had decreased sensation to fine touch in the distribution of C7 at the level of the triceps, midphalangeal joints to distal fingertips on the right, fourth, and fifth fingers on the left and right lateral lower extremity. A Hoffmann sign was positive bilaterally. A CT scan of the cervical spine showed severe canal stenosis at the C3-C4 level secondary to a large C3-C4 left paracentral disc protrusion with AP dimensions of the canal measured at 4 to 5 mm. There was no evidence of acute cervical spine fracture or subluxation.
The patient was offered operative and nonoperative management options, including anterior cervical discectomy and fusion vs conservative management with corticosteroid therapy. She agreed to conservative management and received intravenous (IV) dexamethasone with subjective improvement in her symptoms. The patient was discharged home on hospital day 3, with instructions to follow-up with a spine surgeon in 2 weeks. She was also counseled on abstaining from further cocaine or other illicit drug use.
The patient eventually returned for an elective anterior cervical discectomy and fusion 2 months later, after several outpatient visits and progression of symptoms. She was discharged home on postoperative day 1 with pain well-controlled and was able to ambulate without assistance. On follow-up, she reported 15% improvement in her symptoms.
Discussion
Cervical spondylotic myelopathy (CSM) is the most common myelopathy in patients aged 55 years and older. Immediate neuroimaging studies followed by spinal surgery consultation are recommended for patients presenting with acute symptoms suggestive of cord compression.1,2
Diagnosis and Differential Diagnosis
Diagnosis of CSM can be made with a thorough patient history, neurological examination, and MRI/MRA. However, because cases of cervical disc herniation (CDH) are often atraumatic, the patient history may not always be contributory to the diagnosis and severity of the offending cause.
During our patient’s hospital course, there was initially a concern for Brown-Séquard syndrome (BSS) due to the lateralizing symptoms and radiographic findings. This is a rare condition that can occur in the setting of spinal trauma, unilateral disc herniation, tumors, epidural hematomas, and spinal cord ischemia.3,4 In one retrospective case review by Sayer et al,4 the incidence of CDH causing BSS was only 0.21% (5 per 2,350 patients), and 67% of the cases involved C5-C6 or C6-C7.
Although disc herniation usually presents with symptoms on the ipsilateral side in patients with BSS, there are rare case reports of patients with contralateral symptoms in the form of complete or incomplete BSS manifesting as ipsilateral motor deficit and/or loss of contralateral pain and temperature due to an incomplete spinal cord compression.5-7 We were able to rule-out BSS in our patient due to the absence of motor symptoms.
Treatment
Corticosteroid Therapy. High-dose IV corticosteroids should be given to all patients with CSM prior to surgery to reduce cord edema caused by spinal cord injury. In one randomized control trial by Bracken et al,8 patients given methylprednisolone within 8 hours of spinal cord injury had improvement in motor function, sensation to pinprick, and touch at 6 months when compared to placebo. When the aforementioned steps are taken in the emergent care setting, they may significantly improve patient outcomes.
Surgical Intervention. All cases of CSM in the review literature were treated surgically with laminectomy or hemilaminectomy, anterior discectomy with or without fusion, or corpectomy followed by interbody fusion, with the goal of achieving cord decompression. A large majority of patients underwent anterior discectomy with interbody fusion, and all of the cases recommend early surgical intervention in severe CSM to prevent rapidly worsening symptoms, including permanent hemiparesis.
Early surgical intervention is positively correlated with better outcomes, most often resulting in significant improvement of symptoms to full recovery.3,4,6,7,9-12 In one case report, surgical intervention did not result in a significant improvement, and the patient had been suffering from progressive symptoms for 7 years prior to diagnosis and treatment.11
Conservative Management. Conservative management of CSM includes immobilization, activity modification, pain management, and/or corticosteroids therapy.13 However, for patients undergoing surgical decompression, 50% to 80% reported symptom improvement.14,15 This evidence strongly supports management of CSM with early diagnosis and surgical intervention. Despite delays in diagnosis and treatment, surgical intervention can still offer significant relief of weakness and sensory deficits associated with severe CSM.11
Conclusion
Cervical spondylotic myelopathy is the most common myelopathy in patients aged 55 years and older. Common symptoms involve upper extremity sensation, gait disturbances, and deterioration of hand use16; however, there is a large differential for patients presenting to the ED with these symptoms, including mass effect, infection, vascular conditions, metabolic disorders, inflammatory conditions, and trauma.
Our patient with CSM presented with signs of an incomplete cord syndrome with lateralizing features caused by asymmetric disc herniation. This case is unique in that though our patient had some symptom resolution with corticosteroids therapy alone, she ultimately returned for definitive surgical decompression after symptom progression.
Case
A 55-year-old previously healthy woman with an insignificant medical history presented to the ED for evaluation of right-sided numbness, tingling, and inability to sense temperature. The patient stated the numbness and tingling first began in her right leg and thigh 2 months earlier, and had progressively worsened to her entire right-side. She said she first experienced the thermoanesthesia while taking a shower the morning of presentation. While showering, the patient noted that she could not feel any hot or cold sensation on the right side of her body, including her right leg and arm. She also reported decreased sensation to her extremities on the right side.
She denied any new weakness, headache, chest pain, shortness of breath, fever, chills, nausea, vomiting, back pain, neck pain, or any other symptoms. In addition, she denied any difficulty swallowing, speaking, blurry vision, or double vision. Regarding her social history, the patient denied a history of sexually transmitted diseases, including syphilis; or any tobacco, alcohol, or illicit drug use. The patient confirmed that she had never experienced any of the presenting symptoms prior to 2 months ago. There was no history of trauma or falls. A review of systems was otherwise negative.
Vital signs at presentation were: blood pressure, 129/88 mm Hg; heart rate, 99 beats/min; respiratory rate, 18 breaths/min; and temperature, 98.5°F. Oxygen saturation was 98% on room air. Physical examination revealed a middle-aged woman who was awake, alert, and oriented. Her head was normocephalic and atraumatic, and her pupils were 5 mm, equal, round, and reactive to light bilaterally. Her cranial nerves II through XII were intact. She had normal 5/5 strength in both her upper and lower extremities bilaterally, and had 2+ and equal bilateral patella and Achilles deep tendon reflexes. The patient had no truncal ataxia, and she had a normal gait on ambulation. She was unable to sense temperature (assessed by touching a cold metal tray with her right hand). There was no neck or back midline tenderness to palpation of her spine.
Initial laboratory studies included a complete blood count (CBC); basic metabolic panel (BMP), including blood urea nitrogen; and urine drug screen (UDS). The CBC and BMP were within normal limits, except for an elevated creatine kinase of 249 U/L. The UDS was positive for cocaine. A head computed tomography (CT) scan without contrast was unremarkable.
The patient was admitted to the hospital for further evaluation. Additional laboratory workup during the inpatient stay included nonreactive treponemal immunoglobulin G/immunoglobulin M; nonreactive HIV antigen antibody assay; normal thyroid stimulating hormone; normal free thyroxine, folate, and vitamin B12 levels; normal erythrocyte sedimentation rate, and C-reactive protein levels. The patient’s hemoglobin A1C was also within normal range.
Other imaging studies, which included MR angiography (MRA) of the head and neck, and MRI of the thoracic and lumbar spine, were unremarkable, with the exception of some chronic spondylitic changes.
Due to the significant C3-C4 stenosis, orthopedic surgery services were consulted for a spinal surgery workup. The orthopedic examination identified a few beats of clonus, intact proprioception, and no dysmetria. The patient had decreased sensation to fine touch in the distribution of C7 at the level of the triceps, midphalangeal joints to distal fingertips on the right, fourth, and fifth fingers on the left and right lateral lower extremity. A Hoffmann sign was positive bilaterally. A CT scan of the cervical spine showed severe canal stenosis at the C3-C4 level secondary to a large C3-C4 left paracentral disc protrusion with AP dimensions of the canal measured at 4 to 5 mm. There was no evidence of acute cervical spine fracture or subluxation.
The patient was offered operative and nonoperative management options, including anterior cervical discectomy and fusion vs conservative management with corticosteroid therapy. She agreed to conservative management and received intravenous (IV) dexamethasone with subjective improvement in her symptoms. The patient was discharged home on hospital day 3, with instructions to follow-up with a spine surgeon in 2 weeks. She was also counseled on abstaining from further cocaine or other illicit drug use.
The patient eventually returned for an elective anterior cervical discectomy and fusion 2 months later, after several outpatient visits and progression of symptoms. She was discharged home on postoperative day 1 with pain well-controlled and was able to ambulate without assistance. On follow-up, she reported 15% improvement in her symptoms.
Discussion
Cervical spondylotic myelopathy (CSM) is the most common myelopathy in patients aged 55 years and older. Immediate neuroimaging studies followed by spinal surgery consultation are recommended for patients presenting with acute symptoms suggestive of cord compression.1,2
Diagnosis and Differential Diagnosis
Diagnosis of CSM can be made with a thorough patient history, neurological examination, and MRI/MRA. However, because cases of cervical disc herniation (CDH) are often atraumatic, the patient history may not always be contributory to the diagnosis and severity of the offending cause.
During our patient’s hospital course, there was initially a concern for Brown-Séquard syndrome (BSS) due to the lateralizing symptoms and radiographic findings. This is a rare condition that can occur in the setting of spinal trauma, unilateral disc herniation, tumors, epidural hematomas, and spinal cord ischemia.3,4 In one retrospective case review by Sayer et al,4 the incidence of CDH causing BSS was only 0.21% (5 per 2,350 patients), and 67% of the cases involved C5-C6 or C6-C7.
Although disc herniation usually presents with symptoms on the ipsilateral side in patients with BSS, there are rare case reports of patients with contralateral symptoms in the form of complete or incomplete BSS manifesting as ipsilateral motor deficit and/or loss of contralateral pain and temperature due to an incomplete spinal cord compression.5-7 We were able to rule-out BSS in our patient due to the absence of motor symptoms.
Treatment
Corticosteroid Therapy. High-dose IV corticosteroids should be given to all patients with CSM prior to surgery to reduce cord edema caused by spinal cord injury. In one randomized control trial by Bracken et al,8 patients given methylprednisolone within 8 hours of spinal cord injury had improvement in motor function, sensation to pinprick, and touch at 6 months when compared to placebo. When the aforementioned steps are taken in the emergent care setting, they may significantly improve patient outcomes.
Surgical Intervention. All cases of CSM in the review literature were treated surgically with laminectomy or hemilaminectomy, anterior discectomy with or without fusion, or corpectomy followed by interbody fusion, with the goal of achieving cord decompression. A large majority of patients underwent anterior discectomy with interbody fusion, and all of the cases recommend early surgical intervention in severe CSM to prevent rapidly worsening symptoms, including permanent hemiparesis.
Early surgical intervention is positively correlated with better outcomes, most often resulting in significant improvement of symptoms to full recovery.3,4,6,7,9-12 In one case report, surgical intervention did not result in a significant improvement, and the patient had been suffering from progressive symptoms for 7 years prior to diagnosis and treatment.11
Conservative Management. Conservative management of CSM includes immobilization, activity modification, pain management, and/or corticosteroids therapy.13 However, for patients undergoing surgical decompression, 50% to 80% reported symptom improvement.14,15 This evidence strongly supports management of CSM with early diagnosis and surgical intervention. Despite delays in diagnosis and treatment, surgical intervention can still offer significant relief of weakness and sensory deficits associated with severe CSM.11
Conclusion
Cervical spondylotic myelopathy is the most common myelopathy in patients aged 55 years and older. Common symptoms involve upper extremity sensation, gait disturbances, and deterioration of hand use16; however, there is a large differential for patients presenting to the ED with these symptoms, including mass effect, infection, vascular conditions, metabolic disorders, inflammatory conditions, and trauma.
Our patient with CSM presented with signs of an incomplete cord syndrome with lateralizing features caused by asymmetric disc herniation. This case is unique in that though our patient had some symptom resolution with corticosteroids therapy alone, she ultimately returned for definitive surgical decompression after symptom progression.
1. Chen TY, Dickman CA, Eleraky M, Sonntag VK. The role of decompression for acute incomplete cervical spinal cord injury in cervical spondylosis. Spine (Phila Pa 1976). 1998;23(22):2398-2403.
2. Ishida Y, Tominaga T. Predictors of neurologic recovery in acute central cervical cord injury with only upper extremity impairment. Spine (Phila Pa 1976). 2002;27(15):1652-1658. discussion 1658.
3. Porto GB, Tan LA, Kasliwal MK, Traynelis VC. Progressive Brown-Séquard syndrome: a rare manifestation of cervical disc herniation. J Clin Neurosci. 2016;29:196-198. doi:10.1016/j.jocn.2015.12.021
4. Sayer FT, Vitali AM, Low HL, Paquette S, Honey CR. Brown-Sèquard syndrome produced by C3-C4 cervical disc herniation: a case report and review of the literature. Spine (Phila Pa 1976). 2008;33(9):E279-E282. doi:10.1097/BRS.0b013e31816c835d.
5. Urrutia J, Fadic R. Cervical disc herniation producing acute Brown-Sequard syndrome: dynamic changes documented by intraoperative neuromonitoring. Eur Spine J. 2012;21 Suppl 4:S418-S421. doi:10.1007/s00586-011-1881-8.
6. Choi KB, Lee CD, Chung DJ, Lee SH. Cervical disc herniation as a cause of Brown-Séquard syndrome. J Korean Neurosurg Soc. 2009;46(5):505-510. doi:10.3340/jkns.2009.46.5.505. doi:10.3340/jkns.2009.46.5.505.
7. Kobayashi N, Asamoto S, Doi H, Sugiyama H. Brown-Sèquard syndrome produced by cervical disc herniation: report of two cases and review of the literature. Spine J. 2003;3(6):530-533.
8. Bracken MB, Shepard MJ, Collins WF, et al. A randomized, controlled trial of methylprednisolone or naloxone in the treatment of acute spinal-cord injury. Results of the Second National Acute Spinal Cord Injury Study. N Engl J Med. 1990; 322(20):1405-1411. doi:10.1056/NEJM199005173222001.
9. Stookey B. Compression of the spinal cord due to ventral extradural cervical chondromas: diagnosis and surgical treatment. Arch Neurol Psychiatry. 1928;20:275-291.
10. Antich PA, Sanjuan AC, Girvent FM, Simó JD. High cervical disc herniation and Brown-Sequard syndrome. A case report and review of the literature. J Bone Joint Surg Br. 1999;81(3):462-463.
11. Guan D, Wang G, Claire M, Kuang Z. Brown-Sequard syndrome produced by calcified herniated cervical disc and posterior vertebral osteophyte: case report.
J Orthop. 2015;12(Suppl 2):S260-S263. doi:10.1016/j.jor.2015.10.007.
12. Abouhashem S, Ammar M, Barakat M, Abdelhameed E. Management of Brown-Sequard syndrome in cervical disc diseases. Turk Neurosurg. 2013;23(4):470-475. doi:10.5137/1019-5149.JTN.7433-12.0.
13. Mazanec D, Reddy A. Medical management of cervical spondylosis. Neurosurgery. 2007;60(1 Suppl 1):S43-S50. doi:10.1227/01.NEU.0000215386.05760.6D.
14. Chagas H, Domingues F, Aversa A, Vidal Fonseca AL, de Souza JM. Cervical spondylotic myelopathy: 10 years of prospective outcome analysis of anterior decompression and fusion. Surg Neurol. 2005;64(Suppl 1):S1:30-S1:35; discussion S1:35-S1:36. doi:10.1016/j.surneu.2005.02.016.
15. Cheung WY, Arvinte D, Wong YW, Luk KD, Cheung KM. Neurological recovery after surgical decompression in patients with cervical spondylotic myelopathy - a prospective study. Int Orthop. 2008;32(2):273-378. doi:10.1007/s00264-006-0315-4.
16. Chiles BW 3rd, Leonard MA, Choudhri HF, Cooper PR. Cervical spondylotic myelopathy: patterns of neurological deficit and recovery after anterior cervical decompression. Neurosurgery. 1999;44(4):762-769; discussion 769-770
1. Chen TY, Dickman CA, Eleraky M, Sonntag VK. The role of decompression for acute incomplete cervical spinal cord injury in cervical spondylosis. Spine (Phila Pa 1976). 1998;23(22):2398-2403.
2. Ishida Y, Tominaga T. Predictors of neurologic recovery in acute central cervical cord injury with only upper extremity impairment. Spine (Phila Pa 1976). 2002;27(15):1652-1658. discussion 1658.
3. Porto GB, Tan LA, Kasliwal MK, Traynelis VC. Progressive Brown-Séquard syndrome: a rare manifestation of cervical disc herniation. J Clin Neurosci. 2016;29:196-198. doi:10.1016/j.jocn.2015.12.021
4. Sayer FT, Vitali AM, Low HL, Paquette S, Honey CR. Brown-Sèquard syndrome produced by C3-C4 cervical disc herniation: a case report and review of the literature. Spine (Phila Pa 1976). 2008;33(9):E279-E282. doi:10.1097/BRS.0b013e31816c835d.
5. Urrutia J, Fadic R. Cervical disc herniation producing acute Brown-Sequard syndrome: dynamic changes documented by intraoperative neuromonitoring. Eur Spine J. 2012;21 Suppl 4:S418-S421. doi:10.1007/s00586-011-1881-8.
6. Choi KB, Lee CD, Chung DJ, Lee SH. Cervical disc herniation as a cause of Brown-Séquard syndrome. J Korean Neurosurg Soc. 2009;46(5):505-510. doi:10.3340/jkns.2009.46.5.505. doi:10.3340/jkns.2009.46.5.505.
7. Kobayashi N, Asamoto S, Doi H, Sugiyama H. Brown-Sèquard syndrome produced by cervical disc herniation: report of two cases and review of the literature. Spine J. 2003;3(6):530-533.
8. Bracken MB, Shepard MJ, Collins WF, et al. A randomized, controlled trial of methylprednisolone or naloxone in the treatment of acute spinal-cord injury. Results of the Second National Acute Spinal Cord Injury Study. N Engl J Med. 1990; 322(20):1405-1411. doi:10.1056/NEJM199005173222001.
9. Stookey B. Compression of the spinal cord due to ventral extradural cervical chondromas: diagnosis and surgical treatment. Arch Neurol Psychiatry. 1928;20:275-291.
10. Antich PA, Sanjuan AC, Girvent FM, Simó JD. High cervical disc herniation and Brown-Sequard syndrome. A case report and review of the literature. J Bone Joint Surg Br. 1999;81(3):462-463.
11. Guan D, Wang G, Claire M, Kuang Z. Brown-Sequard syndrome produced by calcified herniated cervical disc and posterior vertebral osteophyte: case report.
J Orthop. 2015;12(Suppl 2):S260-S263. doi:10.1016/j.jor.2015.10.007.
12. Abouhashem S, Ammar M, Barakat M, Abdelhameed E. Management of Brown-Sequard syndrome in cervical disc diseases. Turk Neurosurg. 2013;23(4):470-475. doi:10.5137/1019-5149.JTN.7433-12.0.
13. Mazanec D, Reddy A. Medical management of cervical spondylosis. Neurosurgery. 2007;60(1 Suppl 1):S43-S50. doi:10.1227/01.NEU.0000215386.05760.6D.
14. Chagas H, Domingues F, Aversa A, Vidal Fonseca AL, de Souza JM. Cervical spondylotic myelopathy: 10 years of prospective outcome analysis of anterior decompression and fusion. Surg Neurol. 2005;64(Suppl 1):S1:30-S1:35; discussion S1:35-S1:36. doi:10.1016/j.surneu.2005.02.016.
15. Cheung WY, Arvinte D, Wong YW, Luk KD, Cheung KM. Neurological recovery after surgical decompression in patients with cervical spondylotic myelopathy - a prospective study. Int Orthop. 2008;32(2):273-378. doi:10.1007/s00264-006-0315-4.
16. Chiles BW 3rd, Leonard MA, Choudhri HF, Cooper PR. Cervical spondylotic myelopathy: patterns of neurological deficit and recovery after anterior cervical decompression. Neurosurgery. 1999;44(4):762-769; discussion 769-770

Don’t Always Rush to Rally Renal
Case
An otherwise healthy 20-month-old boy presented to the ED for evaluation after his father witnessed the child ingest a model race car fuel additive. According to the patient’s father, the boy was playing with several closed bottles that were stored in the garage, when he witnessed the boy open up and take a sip of a pink-colored fuel additive, which the father believed to contain 100% methanol. The patient’s father further noted that immediately after drinking the fluid, the patient spat and drooled, and had one episode of nonbloody emesis prior to arrival at the ED.
Initial vital signs at presentation were: blood pressure, 84/54 mm Hg; heart rate, 97 beats/min; respiratory rate, 24 breaths/min; and temperature 98°F. Oxygen saturation was 99% on room air. Physical examination was notable for mild erythema in the posterior oropharynx. Otherwise, the patient was acting appropriately for his age and in no acute distress. Laboratory studies were within normal limits, except for the following: serum anion gap, 18 mEq/L (reference range for children < 3 years old, 10-14 mEq/L); serum bicarbonate, 19 mmol/L (reference range for children 12-24 months, 17-25 mmol/L); and serum creatinine, 2.8 mg/dL (reference range for children 12 to 24 months, 0.2-0.5 mg/dL). A repeat creatinine test taken after bolus of fluid administration was 2.4 mg/dL. A renal ultrasound, performed to investigate the cause of the renal failure, was unremarkable.
What toxic exposures are of concern based on the clinical history?
The history of exposure to a liquid stored in a garage raises the likelihood of exposure to an automobile-related item such as diethylene glycol, ethylene glycol (EG), and methanol.
Diethylene Glycol. Diethylene glycol is an ingredient in brake and power steering fluids, and has toxic properties qualitatively similar to EG.
Ethylene Glycol. A clear, colorless, odorless fluid with a sweet taste, EG is an ingredient in radiator antifreeze, refrigerant fluid, coolants, and pesticides. Like methylene, EG reaches peak plasma concentration within 1 to 4 hours, but toxic clinical findings do not occur for 3 to 6 hours.1
Methanol. Methanol is a clear, colorless, alcohol found in antifreeze, windshield washer fluid, and race car fuel.2 Although methanol reaches peak plasma concentration in about 30 to 60 minutes, signs of systemic toxicity (ie, metabolic acidosis) typically take 6 to 12 hours to manifest.1
In both EG and methanol, there is a delay in toxic clinical findings because the parent compounds are not toxic in their initial form; rather, major toxicity is derived from their metabolites: formic acid and oxalic acid, respectively.
Other Toxins. Many other potentially toxic liquids are associated with a homeowner’s occupation or avocational interests. These include painting supplies (eg, industrial paints containing lead), gardening materials (eg, pesticides containing organophosphates), fuels (eg, gasoline, polychlorinated biphenyls in coolant, and lubricants), and cleaning supplies (eg, caustics, detergents, and air freshener).
Case Continuation
Since the patient’s elevated anion gap raised concerns for methanol or EG exposure, he was given fomepizole and transferred to a tertiary care children’s hospital for further management and possible hemodialysis. Upon arrival at the receiving hospital, the patient’s vital signs and physical examination remained unchanged. Repeat laboratory studies were notable for a creatinine level of 0.3 mg/dL. The patient’s father was instructed to retrieve the implicated bottle from home. An inspection of the bottle’s ingredients was notable for nitromethane, castor oil, and methanol.
What is nitromethane and what are its uses?
Nitromethane, the simplest nitro compound, is a colorless, viscous, lipid-soluble fluid.3 The polarity of nitromethane permits its use as a stabilizer in a number of chemical solvents, such as dry cleaning fluid, degreasers, and "super glue."4,5 Nitromethane is also commonly added to model-engine and drag-race fuels, which also contain methanol and castor oil.3 In this capacity, nitromethane functions as an oxygen carrier, allowing more efficient fuel use in combustion cylinders (compared to gasoline), thereby increasing the horsepower of the vehicle.6 It is therefore commonly added to fuel for drag racers, radio-controlled cars, and model aircrafts.4 In the small concentrations typically inadvertently ingested, the clinical effects of nitromethane itself are inconsequential.
What is the differential for creatinine elevation?
Creatinine itself is a normal breakdown product of muscle metabolism produced by spontaneous conversion from creatine and is found at a fairly constant serum level in proportion to muscle mass.7 Thus, as people age and muscle mass decreases, their baseline creatinine levels decrease proportionally.
Elimination. The majority of creatinine (85%-90%) is filtered and excreted by the kidneys, with the remaining 10% to 15% secreted by the tubules, allowing creatinine to be a surrogate measure of the glomerular filtration rate.7 Exogenous sources of creatine or creatinine include meat and creatine supplements, the latter of which are used as an "energy source" to enhance athletic performance.
Etiology. The etiology for an elevated serum creatinine concentration includes renal failure, both acute and chronic; volume depletion; hemorrhage (low blood volume); and medications, including diuretics, angiotensin converting enzyme inhibitors, angiotensin-receptor blockers, nonsteroidal anti-inflammatory drugs, and certain antibiotics. These etiologies can also be categorized as processes that increase creatinine production, decrease elimination (H2 antagonist and trimethoprim both inhibit the cation secretory pump in the tubules), or interfere with the creatinine assay (ketones, keto acids, lipemia, hemolysis, cephalosporins).7
Because creatinine is filtered so efficiently by the kidney, neither exogenous nor endogenous creatinine sources are expected to increase serum creatinine in the absence of renal dysfunction. However, transient elevation may occur in body builders who use extreme doses of creatine. Patients with rhabdomyolysis often develop elevated creatinine concentrations, but nearly always in the setting of myoglobinuric renal failure.
Jaffe Reaction and Enzymatic Methods. Serum creatinine can be measured using either the Jaffe reaction or the enzymatic method. In the Jaffe reaction, creatinine reacts with alkaline sodium picrate to form a red-orange chromophore, which absorbs light in the range of 470 to 550 nanometers on spectroscopy.6,8,9 The active methylene group on nitromethane also reacts with alkaline sodium picrate to form a chromophore which absorbs light in the same wavelength range.10 Thus, serum creatinine measurements via the Jaffe reaction are falsely elevated due to the cross-reactivity between nitromethane and alkaline sodium picrate. In some reported cases, there is a 20-fold increase in the measured serum creatinine in the presence of nitromethane; renal function, however, remains normal.5
This false reading seen in the Jaffe reaction can be avoided by utilizing the enzymatic method of creatinine measurement, a three-step process that ultimately produces hydrogen peroxide, which is measured and accurately correlates with serum creatinine—even in the presence of nitromethane.8 This distinction explains the dramatically different creatinine concentrations measured at the two institutions in this case.
Case Conclusion
The patient was monitored overnight at the children’s hospital. Repeat laboratory studies in the morning showed a normal creatinine level of 0.3 mg/dL and a negative methanol level. The patient was discharged home in the care of his father, who was instructed to follow-up with his son’s pediatrician. The father also received counseling on safe storage practices for dangerous chemicals.
1. Kruse JA. Methanol and ethylene glycol intoxication. Crit Care Clin. 2012;28(4):661-711. doi:10.1016/j.ccc.2012.07.002.
2. McMahon DM, Winstead S, Weant KA. Toxic alcohol ingestions: focus on ethylene glycol and methanol. Adv Emerg Nurs J. 2009;31(3):206-213. doi:10.1097/TME.0b013e3181ad8be8.
3. Cook MD, Clark RF. Creatinine elevation associated with nitromethane exposure: a marker of potential methanol toxicity. J Emerg Med. 2007;33(3):249-253. doi:10.1016/j.jemermed.2007.02.015.
4. Markofsky SB. Nitro compounds, aliphatic. In: Elvers B, ed. Ullmann’s Encyclopedia of Industrial Chemistry. Wiley-VCH Verlag GmbH & Co. KGaA; 2000. doi:10.1002/14356007.a17_401. [digital]
5. Mullins ME, Hammett-Stabler CA. Intoxication with nitromethane-containing fuels: don’t be "fueled" by the creatinine. J Toxicol Clin Toxicol. 1998;36(4):
315-320.
6. Ngo AS, Rowley F, Olson KR. Case files of the California poison control system, San Francisco division: blue thunder ingestion: methanol, nitromethane, and elevated creatinine. J Med Toxicol. 2010;6(1):67-71. doi:10.1007/s13181-010-0042-5.
7. Samra M, Abcar AC. False estimates of elevated creatinine. Perm J. 2012;16(2):51-52.
8. Booth C, Naidoo D, Rosenberg A, Kainer G. Elevated creatinine after ingestion of model aviation fuel: interference with the Jaffe reaction by nitromethane. J Paediatr Child Health. 1999;35(5):503-504.
9. de Lelis Medeiros de Morais C, Gomes de Lima KM. Determination and analytical validation of creatinine content in serum using image analysis by multivariate transfer calibration procedures. Anal Meth. 2015;7:6904-6910. doi:10.1039/C5AY01369K.
10. Killorn E, Lim RK, Rieder M. Apparent elevated creatinine after ingestion of nitromethane: interference with the Jaffe reaction. Ther Drug Monit. 2011;33(1):1-2. doi:10.1097/FTD.0b013e3181fe7e52.
Case
An otherwise healthy 20-month-old boy presented to the ED for evaluation after his father witnessed the child ingest a model race car fuel additive. According to the patient’s father, the boy was playing with several closed bottles that were stored in the garage, when he witnessed the boy open up and take a sip of a pink-colored fuel additive, which the father believed to contain 100% methanol. The patient’s father further noted that immediately after drinking the fluid, the patient spat and drooled, and had one episode of nonbloody emesis prior to arrival at the ED.
Initial vital signs at presentation were: blood pressure, 84/54 mm Hg; heart rate, 97 beats/min; respiratory rate, 24 breaths/min; and temperature 98°F. Oxygen saturation was 99% on room air. Physical examination was notable for mild erythema in the posterior oropharynx. Otherwise, the patient was acting appropriately for his age and in no acute distress. Laboratory studies were within normal limits, except for the following: serum anion gap, 18 mEq/L (reference range for children < 3 years old, 10-14 mEq/L); serum bicarbonate, 19 mmol/L (reference range for children 12-24 months, 17-25 mmol/L); and serum creatinine, 2.8 mg/dL (reference range for children 12 to 24 months, 0.2-0.5 mg/dL). A repeat creatinine test taken after bolus of fluid administration was 2.4 mg/dL. A renal ultrasound, performed to investigate the cause of the renal failure, was unremarkable.
What toxic exposures are of concern based on the clinical history?
The history of exposure to a liquid stored in a garage raises the likelihood of exposure to an automobile-related item such as diethylene glycol, ethylene glycol (EG), and methanol.
Diethylene Glycol. Diethylene glycol is an ingredient in brake and power steering fluids, and has toxic properties qualitatively similar to EG.
Ethylene Glycol. A clear, colorless, odorless fluid with a sweet taste, EG is an ingredient in radiator antifreeze, refrigerant fluid, coolants, and pesticides. Like methylene, EG reaches peak plasma concentration within 1 to 4 hours, but toxic clinical findings do not occur for 3 to 6 hours.1
Methanol. Methanol is a clear, colorless, alcohol found in antifreeze, windshield washer fluid, and race car fuel.2 Although methanol reaches peak plasma concentration in about 30 to 60 minutes, signs of systemic toxicity (ie, metabolic acidosis) typically take 6 to 12 hours to manifest.1
In both EG and methanol, there is a delay in toxic clinical findings because the parent compounds are not toxic in their initial form; rather, major toxicity is derived from their metabolites: formic acid and oxalic acid, respectively.
Other Toxins. Many other potentially toxic liquids are associated with a homeowner’s occupation or avocational interests. These include painting supplies (eg, industrial paints containing lead), gardening materials (eg, pesticides containing organophosphates), fuels (eg, gasoline, polychlorinated biphenyls in coolant, and lubricants), and cleaning supplies (eg, caustics, detergents, and air freshener).
Case Continuation
Since the patient’s elevated anion gap raised concerns for methanol or EG exposure, he was given fomepizole and transferred to a tertiary care children’s hospital for further management and possible hemodialysis. Upon arrival at the receiving hospital, the patient’s vital signs and physical examination remained unchanged. Repeat laboratory studies were notable for a creatinine level of 0.3 mg/dL. The patient’s father was instructed to retrieve the implicated bottle from home. An inspection of the bottle’s ingredients was notable for nitromethane, castor oil, and methanol.
What is nitromethane and what are its uses?
Nitromethane, the simplest nitro compound, is a colorless, viscous, lipid-soluble fluid.3 The polarity of nitromethane permits its use as a stabilizer in a number of chemical solvents, such as dry cleaning fluid, degreasers, and "super glue."4,5 Nitromethane is also commonly added to model-engine and drag-race fuels, which also contain methanol and castor oil.3 In this capacity, nitromethane functions as an oxygen carrier, allowing more efficient fuel use in combustion cylinders (compared to gasoline), thereby increasing the horsepower of the vehicle.6 It is therefore commonly added to fuel for drag racers, radio-controlled cars, and model aircrafts.4 In the small concentrations typically inadvertently ingested, the clinical effects of nitromethane itself are inconsequential.
What is the differential for creatinine elevation?
Creatinine itself is a normal breakdown product of muscle metabolism produced by spontaneous conversion from creatine and is found at a fairly constant serum level in proportion to muscle mass.7 Thus, as people age and muscle mass decreases, their baseline creatinine levels decrease proportionally.
Elimination. The majority of creatinine (85%-90%) is filtered and excreted by the kidneys, with the remaining 10% to 15% secreted by the tubules, allowing creatinine to be a surrogate measure of the glomerular filtration rate.7 Exogenous sources of creatine or creatinine include meat and creatine supplements, the latter of which are used as an "energy source" to enhance athletic performance.
Etiology. The etiology for an elevated serum creatinine concentration includes renal failure, both acute and chronic; volume depletion; hemorrhage (low blood volume); and medications, including diuretics, angiotensin converting enzyme inhibitors, angiotensin-receptor blockers, nonsteroidal anti-inflammatory drugs, and certain antibiotics. These etiologies can also be categorized as processes that increase creatinine production, decrease elimination (H2 antagonist and trimethoprim both inhibit the cation secretory pump in the tubules), or interfere with the creatinine assay (ketones, keto acids, lipemia, hemolysis, cephalosporins).7
Because creatinine is filtered so efficiently by the kidney, neither exogenous nor endogenous creatinine sources are expected to increase serum creatinine in the absence of renal dysfunction. However, transient elevation may occur in body builders who use extreme doses of creatine. Patients with rhabdomyolysis often develop elevated creatinine concentrations, but nearly always in the setting of myoglobinuric renal failure.
Jaffe Reaction and Enzymatic Methods. Serum creatinine can be measured using either the Jaffe reaction or the enzymatic method. In the Jaffe reaction, creatinine reacts with alkaline sodium picrate to form a red-orange chromophore, which absorbs light in the range of 470 to 550 nanometers on spectroscopy.6,8,9 The active methylene group on nitromethane also reacts with alkaline sodium picrate to form a chromophore which absorbs light in the same wavelength range.10 Thus, serum creatinine measurements via the Jaffe reaction are falsely elevated due to the cross-reactivity between nitromethane and alkaline sodium picrate. In some reported cases, there is a 20-fold increase in the measured serum creatinine in the presence of nitromethane; renal function, however, remains normal.5
This false reading seen in the Jaffe reaction can be avoided by utilizing the enzymatic method of creatinine measurement, a three-step process that ultimately produces hydrogen peroxide, which is measured and accurately correlates with serum creatinine—even in the presence of nitromethane.8 This distinction explains the dramatically different creatinine concentrations measured at the two institutions in this case.
Case Conclusion
The patient was monitored overnight at the children’s hospital. Repeat laboratory studies in the morning showed a normal creatinine level of 0.3 mg/dL and a negative methanol level. The patient was discharged home in the care of his father, who was instructed to follow-up with his son’s pediatrician. The father also received counseling on safe storage practices for dangerous chemicals.
Case
An otherwise healthy 20-month-old boy presented to the ED for evaluation after his father witnessed the child ingest a model race car fuel additive. According to the patient’s father, the boy was playing with several closed bottles that were stored in the garage, when he witnessed the boy open up and take a sip of a pink-colored fuel additive, which the father believed to contain 100% methanol. The patient’s father further noted that immediately after drinking the fluid, the patient spat and drooled, and had one episode of nonbloody emesis prior to arrival at the ED.
Initial vital signs at presentation were: blood pressure, 84/54 mm Hg; heart rate, 97 beats/min; respiratory rate, 24 breaths/min; and temperature 98°F. Oxygen saturation was 99% on room air. Physical examination was notable for mild erythema in the posterior oropharynx. Otherwise, the patient was acting appropriately for his age and in no acute distress. Laboratory studies were within normal limits, except for the following: serum anion gap, 18 mEq/L (reference range for children < 3 years old, 10-14 mEq/L); serum bicarbonate, 19 mmol/L (reference range for children 12-24 months, 17-25 mmol/L); and serum creatinine, 2.8 mg/dL (reference range for children 12 to 24 months, 0.2-0.5 mg/dL). A repeat creatinine test taken after bolus of fluid administration was 2.4 mg/dL. A renal ultrasound, performed to investigate the cause of the renal failure, was unremarkable.
What toxic exposures are of concern based on the clinical history?
The history of exposure to a liquid stored in a garage raises the likelihood of exposure to an automobile-related item such as diethylene glycol, ethylene glycol (EG), and methanol.
Diethylene Glycol. Diethylene glycol is an ingredient in brake and power steering fluids, and has toxic properties qualitatively similar to EG.
Ethylene Glycol. A clear, colorless, odorless fluid with a sweet taste, EG is an ingredient in radiator antifreeze, refrigerant fluid, coolants, and pesticides. Like methylene, EG reaches peak plasma concentration within 1 to 4 hours, but toxic clinical findings do not occur for 3 to 6 hours.1
Methanol. Methanol is a clear, colorless, alcohol found in antifreeze, windshield washer fluid, and race car fuel.2 Although methanol reaches peak plasma concentration in about 30 to 60 minutes, signs of systemic toxicity (ie, metabolic acidosis) typically take 6 to 12 hours to manifest.1
In both EG and methanol, there is a delay in toxic clinical findings because the parent compounds are not toxic in their initial form; rather, major toxicity is derived from their metabolites: formic acid and oxalic acid, respectively.
Other Toxins. Many other potentially toxic liquids are associated with a homeowner’s occupation or avocational interests. These include painting supplies (eg, industrial paints containing lead), gardening materials (eg, pesticides containing organophosphates), fuels (eg, gasoline, polychlorinated biphenyls in coolant, and lubricants), and cleaning supplies (eg, caustics, detergents, and air freshener).
Case Continuation
Since the patient’s elevated anion gap raised concerns for methanol or EG exposure, he was given fomepizole and transferred to a tertiary care children’s hospital for further management and possible hemodialysis. Upon arrival at the receiving hospital, the patient’s vital signs and physical examination remained unchanged. Repeat laboratory studies were notable for a creatinine level of 0.3 mg/dL. The patient’s father was instructed to retrieve the implicated bottle from home. An inspection of the bottle’s ingredients was notable for nitromethane, castor oil, and methanol.
What is nitromethane and what are its uses?
Nitromethane, the simplest nitro compound, is a colorless, viscous, lipid-soluble fluid.3 The polarity of nitromethane permits its use as a stabilizer in a number of chemical solvents, such as dry cleaning fluid, degreasers, and "super glue."4,5 Nitromethane is also commonly added to model-engine and drag-race fuels, which also contain methanol and castor oil.3 In this capacity, nitromethane functions as an oxygen carrier, allowing more efficient fuel use in combustion cylinders (compared to gasoline), thereby increasing the horsepower of the vehicle.6 It is therefore commonly added to fuel for drag racers, radio-controlled cars, and model aircrafts.4 In the small concentrations typically inadvertently ingested, the clinical effects of nitromethane itself are inconsequential.
What is the differential for creatinine elevation?
Creatinine itself is a normal breakdown product of muscle metabolism produced by spontaneous conversion from creatine and is found at a fairly constant serum level in proportion to muscle mass.7 Thus, as people age and muscle mass decreases, their baseline creatinine levels decrease proportionally.
Elimination. The majority of creatinine (85%-90%) is filtered and excreted by the kidneys, with the remaining 10% to 15% secreted by the tubules, allowing creatinine to be a surrogate measure of the glomerular filtration rate.7 Exogenous sources of creatine or creatinine include meat and creatine supplements, the latter of which are used as an "energy source" to enhance athletic performance.
Etiology. The etiology for an elevated serum creatinine concentration includes renal failure, both acute and chronic; volume depletion; hemorrhage (low blood volume); and medications, including diuretics, angiotensin converting enzyme inhibitors, angiotensin-receptor blockers, nonsteroidal anti-inflammatory drugs, and certain antibiotics. These etiologies can also be categorized as processes that increase creatinine production, decrease elimination (H2 antagonist and trimethoprim both inhibit the cation secretory pump in the tubules), or interfere with the creatinine assay (ketones, keto acids, lipemia, hemolysis, cephalosporins).7
Because creatinine is filtered so efficiently by the kidney, neither exogenous nor endogenous creatinine sources are expected to increase serum creatinine in the absence of renal dysfunction. However, transient elevation may occur in body builders who use extreme doses of creatine. Patients with rhabdomyolysis often develop elevated creatinine concentrations, but nearly always in the setting of myoglobinuric renal failure.
Jaffe Reaction and Enzymatic Methods. Serum creatinine can be measured using either the Jaffe reaction or the enzymatic method. In the Jaffe reaction, creatinine reacts with alkaline sodium picrate to form a red-orange chromophore, which absorbs light in the range of 470 to 550 nanometers on spectroscopy.6,8,9 The active methylene group on nitromethane also reacts with alkaline sodium picrate to form a chromophore which absorbs light in the same wavelength range.10 Thus, serum creatinine measurements via the Jaffe reaction are falsely elevated due to the cross-reactivity between nitromethane and alkaline sodium picrate. In some reported cases, there is a 20-fold increase in the measured serum creatinine in the presence of nitromethane; renal function, however, remains normal.5
This false reading seen in the Jaffe reaction can be avoided by utilizing the enzymatic method of creatinine measurement, a three-step process that ultimately produces hydrogen peroxide, which is measured and accurately correlates with serum creatinine—even in the presence of nitromethane.8 This distinction explains the dramatically different creatinine concentrations measured at the two institutions in this case.
Case Conclusion
The patient was monitored overnight at the children’s hospital. Repeat laboratory studies in the morning showed a normal creatinine level of 0.3 mg/dL and a negative methanol level. The patient was discharged home in the care of his father, who was instructed to follow-up with his son’s pediatrician. The father also received counseling on safe storage practices for dangerous chemicals.
1. Kruse JA. Methanol and ethylene glycol intoxication. Crit Care Clin. 2012;28(4):661-711. doi:10.1016/j.ccc.2012.07.002.
2. McMahon DM, Winstead S, Weant KA. Toxic alcohol ingestions: focus on ethylene glycol and methanol. Adv Emerg Nurs J. 2009;31(3):206-213. doi:10.1097/TME.0b013e3181ad8be8.
3. Cook MD, Clark RF. Creatinine elevation associated with nitromethane exposure: a marker of potential methanol toxicity. J Emerg Med. 2007;33(3):249-253. doi:10.1016/j.jemermed.2007.02.015.
4. Markofsky SB. Nitro compounds, aliphatic. In: Elvers B, ed. Ullmann’s Encyclopedia of Industrial Chemistry. Wiley-VCH Verlag GmbH & Co. KGaA; 2000. doi:10.1002/14356007.a17_401. [digital]
5. Mullins ME, Hammett-Stabler CA. Intoxication with nitromethane-containing fuels: don’t be "fueled" by the creatinine. J Toxicol Clin Toxicol. 1998;36(4):
315-320.
6. Ngo AS, Rowley F, Olson KR. Case files of the California poison control system, San Francisco division: blue thunder ingestion: methanol, nitromethane, and elevated creatinine. J Med Toxicol. 2010;6(1):67-71. doi:10.1007/s13181-010-0042-5.
7. Samra M, Abcar AC. False estimates of elevated creatinine. Perm J. 2012;16(2):51-52.
8. Booth C, Naidoo D, Rosenberg A, Kainer G. Elevated creatinine after ingestion of model aviation fuel: interference with the Jaffe reaction by nitromethane. J Paediatr Child Health. 1999;35(5):503-504.
9. de Lelis Medeiros de Morais C, Gomes de Lima KM. Determination and analytical validation of creatinine content in serum using image analysis by multivariate transfer calibration procedures. Anal Meth. 2015;7:6904-6910. doi:10.1039/C5AY01369K.
10. Killorn E, Lim RK, Rieder M. Apparent elevated creatinine after ingestion of nitromethane: interference with the Jaffe reaction. Ther Drug Monit. 2011;33(1):1-2. doi:10.1097/FTD.0b013e3181fe7e52.
1. Kruse JA. Methanol and ethylene glycol intoxication. Crit Care Clin. 2012;28(4):661-711. doi:10.1016/j.ccc.2012.07.002.
2. McMahon DM, Winstead S, Weant KA. Toxic alcohol ingestions: focus on ethylene glycol and methanol. Adv Emerg Nurs J. 2009;31(3):206-213. doi:10.1097/TME.0b013e3181ad8be8.
3. Cook MD, Clark RF. Creatinine elevation associated with nitromethane exposure: a marker of potential methanol toxicity. J Emerg Med. 2007;33(3):249-253. doi:10.1016/j.jemermed.2007.02.015.
4. Markofsky SB. Nitro compounds, aliphatic. In: Elvers B, ed. Ullmann’s Encyclopedia of Industrial Chemistry. Wiley-VCH Verlag GmbH & Co. KGaA; 2000. doi:10.1002/14356007.a17_401. [digital]
5. Mullins ME, Hammett-Stabler CA. Intoxication with nitromethane-containing fuels: don’t be "fueled" by the creatinine. J Toxicol Clin Toxicol. 1998;36(4):
315-320.
6. Ngo AS, Rowley F, Olson KR. Case files of the California poison control system, San Francisco division: blue thunder ingestion: methanol, nitromethane, and elevated creatinine. J Med Toxicol. 2010;6(1):67-71. doi:10.1007/s13181-010-0042-5.
7. Samra M, Abcar AC. False estimates of elevated creatinine. Perm J. 2012;16(2):51-52.
8. Booth C, Naidoo D, Rosenberg A, Kainer G. Elevated creatinine after ingestion of model aviation fuel: interference with the Jaffe reaction by nitromethane. J Paediatr Child Health. 1999;35(5):503-504.
9. de Lelis Medeiros de Morais C, Gomes de Lima KM. Determination and analytical validation of creatinine content in serum using image analysis by multivariate transfer calibration procedures. Anal Meth. 2015;7:6904-6910. doi:10.1039/C5AY01369K.
10. Killorn E, Lim RK, Rieder M. Apparent elevated creatinine after ingestion of nitromethane: interference with the Jaffe reaction. Ther Drug Monit. 2011;33(1):1-2. doi:10.1097/FTD.0b013e3181fe7e52.

Vascular Access Emergencies in the Dialysis Patient
According to the National Institute of Diabetes and Digestive and Kidney Diseases, approximately 468,000 persons in the United States are on dialysis—a number that continues to grow annually.1 The 1-year rate for hemorrhagic complications from arteriovenous fistulas (AVFs) is estimated to be 0.4%.2 One study by Ellingson et al3 reported 1,654 deaths secondary to fatal vascular access hemorrhage over a 6-year period, accounting for 0.4% of all deaths of hemodialysis (HD) patients in that study.3
Nonhemorrhagic vascular access-related complications also contribute to the morbidity and mortality associated with AVFs and arteriovenous grafts (AVGs). Venous stenosis resulting in thrombosis has been estimated to occur in 24.7% of AVGs and 9.0% of AVFs, both of which are common causes of access failure.
Infection is reported to be the second leading cause of death in dialysis patients, and vascular access-related infection rates are reported to occur in 9.5% of AVGs vs 0.4% to 0.9% of AVFs.2,4 Pseudoaneurysms and aneurysms range from 30% to 60% for AVFs,2,5 and contribute to morbidity by limiting available areas to cannulate for dialysis, occasionally requiring surgical revision to restore access function or prevent access rupture.
Steal phenomena, including dialysis access-induced steal syndrome (DASS) and ischemic monomelic neuropathy, as well as heart failure secondary to high output are additional contributors to morbidity and mortality.
With the growing rate of end-stage renal disease (ESRD) in the United States and the contribution to morbidity and mortality by bleeding and other complications, it is essential to understand how to evaluate and treat these patients in the ED. This article reviews the evaluation and treatment of vascular access emergencies, as well as risk factors that contribute to complications in the ESRD patient population.
Hemorrhagic Complications of Vascular Access
Risk Factors
Many patients with ESRD have multiple comorbidities such as coronary artery disease and atrial fibrillation that require anticoagulation, antiplatelet medications, or both. Studies have shown that ESRD patients taking warfarin have an increase in major bleeding episodes of 3.1% per person-year and 4.4% per person-year for those taking aspirin alone, while those taking both medications have an increased bleeding risk of 6.3% per person-year.6 A recent systematic review by Elliott et al7 has suggested a 2-fold increase in bleeding rates in HD patients anticoagulated with warfarin as compared to HD patients not on warfarin.
While uremia secondary to chronic kidney disease (CKD) is a well-known facilitator of bleeding complications, the underlying pathophysiology is not yet completely delineated. However, there are some general underlying principles that may help in understanding the best treatment modalities available at this time. As the kidneys fail, uremic toxins accumulate in the bloodstream. These toxins include urea, creatinine, and phenolic acids, which are believed to interfere with primary hemostasis by effecting platelet adherence to endothelium, platelet activation, and aggregation.8 Functional defects are created in the interactions between the glycoprotein Ib (GPIb) receptor and von Willebrand factor (vWF), which are essential to endothelial adhesion of platelets.9 Additionally, these toxins impair the up regulation of the GPIIbIIIa receptor which is integral to platelet aggregation.10 Platelet activation normally leads to platelet aggregation by increasing production of thromboxane A2 (TXA2) and serotonin that are released from storage granules.10 Some toxins may increase nitric oxide (NO) synthesis, effectively reducing aggregation by decreasing TXA2 and adenosine diphosphate (ADP) levels.11 In addition, elevated levels of fibrinogen fragments have also recently been shown to inhibit platelet function by competing with fibrinogen for the GPIIbIIIa receptor with decreasing levels demonstrated after HD.12
Finally, increased pressure in the venous outflow segment also increases persistent bleeding from puncture sites. These pressures may be exaggerated secondary to venous thrombosis, venous stenosis, pseudoaneurysm, aneurysm, or infection.13 The following sections further describe the evaluation and treatment of these complications.
Clinical Presentation
Patients presenting with bleeding from the vascular access site may present with slow continuous oozing from the needle puncture-site itself or with life-threatening hemorrhage secondary to AVF or AVG rupture.14 The incidence of vascular access rupture is unknown, but it appears the majority of ruptures occur in patients with AVG vs AVF.3 However, several case reports have also described hemorrhagic complications of AVF ruptures.15-17 The risk of rupture may be associated with the development of aneurysms or pseudoaneuryms.18 Possible impending perforation may be signaled by skin thinning or a shiny appearance overlying the aneurysm, or evidence of infection overlying the access site.3 Many patients were shown to have complications such as stenosis, thrombosis, or infection within 6 months prior to rupture.3 Education of patients is also important as most hemorrhages occur prior to hospital arrival.3,19
Evaluation in the ED
As with any patient presenting to the ED, the initial evaluation of an unstable patient experiencing bleeding from a vascular access site includes assessing the airway, breathing, and circulation as a first priority—paying special attention to the area of bleeding while simultaneously preparing for possible intervention. It is also important to determine when the patient last underwent dialysis and if he or she was able to complete HD. This information will identify patients who are candidates for reversing the heparin load likely given during dialysis.
It is also important to note that some patients undergoing HD who have already been identified as having an increased risk of bleeding may not receive heparin or may undergo local heparinization, minimal heparinization, or regional citrate anticoagulation during dialysis, in which case protamine is not indicated.14 The emergency physician (EP) must also determine if the patient is on any antiplatelet or anticoagulation agents.
The vascular access site should be inspected for evidence of aneurysmal changes, infection, and skin thinning as these factors increase the risk of bleeding and vascular rupture. Additionally auscultation and palpation of the vascular access site should be performed to evaluate for other potential complications such as stenosis and thrombosis. Lastly, the EP should anticipate the patient’s need for HD in the setting of a potentially unavailable AVG or AVF to determine whether the patient may need an alternative access.
Treatment and Management
The primary responsibility during the initial treatment of a bleeding access site is to stop further blood loss by utilizing methods that employ direct pressure or, in extreme cases, application of a tourniquet, followed by other interventions such as fluid and blood-product resuscitation; coagulopathy reversal; consideration of desmopressin, cryoprecipitate, tranexamic acid (TXA); HD; and vascular repair.
Control of a bleeding dialysis access-site is a balancing act of adequately controlling the bleeding while maintaining the integrity of the fistula. Overly aggressive management may cause thrombosis in the vascular access site, which is associated with morbidity—eg, site revisions, potential for the need to create a new access site. On the opposite end of the spectrum, failing to adequately control bleeding can lead to significant anemia ranging from minimal symptoms to hemodynamic compromise and death.
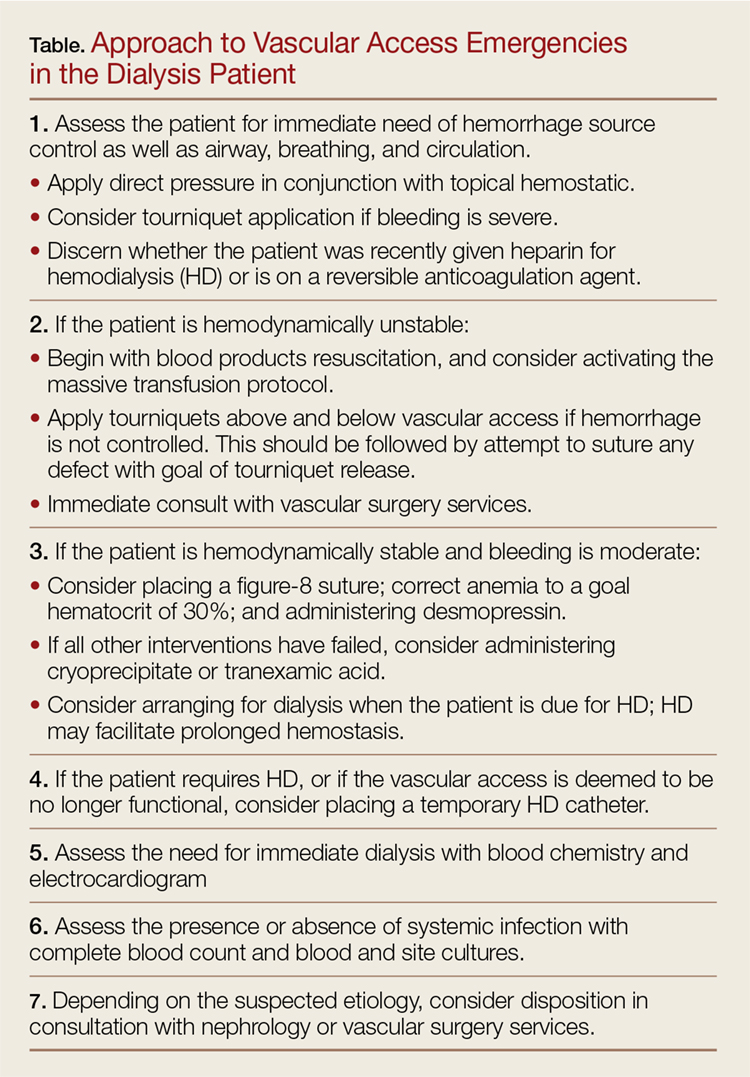
Peripheral Venous Access
While peripheral venous access is notoriously difficult in patients with ESRD, it is essential for the resuscitation of hemorrhaging patients. Ideally, two large bore peripheral intravenous (IV) lines should be placed in the proximal upper extremities. If peripheral venous access is not achieved, central venous access or interosseous access placement is indicated (Figure).
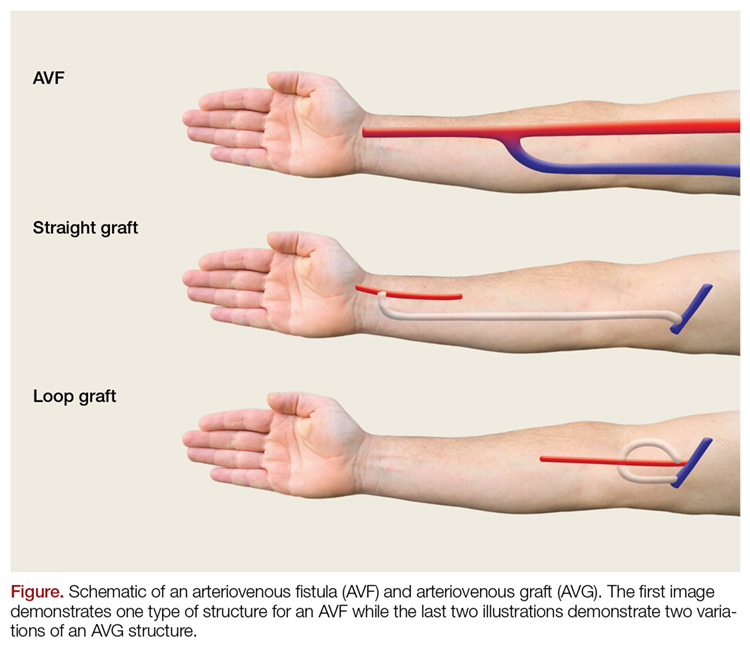
Direct Pressure
With low-volume bleeding, the first attempt to control the bleeding is simple direct pressure. Except in the instance of trauma or self-inflicted injury, bleeding usually occurs at the site of cannulation of the vascular access post-HD. Direct pressure should be light and limited to as small of an area as possible to prevent thrombosis; the force and area encompassed by direct pressure can be expanded as needed for bleeding that is more difficult to control. In cases of higher volume bleeding, pressure should be placed both proximally and distally to the shunt due to its bidirectional flow. Another possible temporizing measure is to place an upright gallipot or cup over the bleeding site on top of a folded piece of gauze and then securing it with tape.21
Topical Hemostatic Agents
Second simple direct pressure, topical hemostatic agents may be a good adjunct to help obtain hemostasis. There is a wide range of products available, from procoagulants (eg, Combat Gauze, topical thrombin) to factor concentrators (eg, QuikClot). These can be used directly on the bleeding site and only in conjunction with direct pressure.
In addition to topical hemostatic agents, another option is skin glue, which should be applied generously after bleeding has been temporized, with pressure both proximally and distally to the site.
Anticoagulation Reversal
As previously mentioned, it is important to determine when the patient’s last HD was. Heparin is used during dialysis to prevent clotting within the circuit, and although clotting times are monitored during dialysis to guide anticoagulation, it is possible that a patient bleeding after dialysis could still have therapeutic levels of heparin requiring reversal with protamine.
The recommended dose of protamine is 1 mg for every 100 U of heparin given during dialysis; protamine should be administered over 10 minutes. Alternatively, a 10- to 20-mg dose of protamine can be given if the amount of heparin administered during HD is unknown. Additionally, the patient’s medication list, as with any ED presentation, should be carefully reviewed as many dialysis patients have comorbidities requiring anticoagulation with potentially reversible agents.
Hemodialysis to Improve Platelet Dysfunction
It is thought that long-term exposure of platelets to the dialysis membrane can lead to chronic platelet activation leading to platelet dysfunction. There is conflicting data regarding the effects of HD on improving bleeding in renal patients.9,22,23 Hemodialysis is thought to be beneficial, at least partially, through reversing uremia, thus improving platelet function.24 Therefore, in the stable bleeding patient who missed a scheduled dialysis, initiating HD in the ED setting could be beneficial. If the vascular access site is deemed unsafe for HD, another access site must be obtained, for example, by placing a temporary central venous catheter that will allow for successful HD.
Desmopressin
Desmopressin acetate has been shown to reduce bleeding time in uremic patients by releasing vWF and factor VIII into plasma, taking effect within 1 hour and lasting 4 to 8 hours.25-27 Desmopressin has also been shown to reduce blood loss and bleeding times in patients with platelet dysfunction undergoing cardiac surgery.28 While the underlying mechanism is unclear, desmopressin acetate is thought to help with platelet adhesion to the endothelial wall.
Alternatively, one study by Soslau et al29 has suggested that desmopressin may increase serotonin uptake by platelets and increase adenosine triphosphate release, thereby facilitating platelet aggregation. The dosing of desmopressin is 0.2 to 0.3 mcg/kg IV.30 Adverse effects include facial flushing, mild headache, and transient small decrease in blood pressure (BP) with increase in heart rate. Historically, it was thought that desmopressin could lead to water retention, volume overload, congestive heart failure, and hyponatremia; however, these adverse effects have not been seen in uremic patients.30 Tachyphylaxis may occur after just a few doses of desmopressin are given.31 Additionally, hyponatremia and seizures have been seen after repeated administration in children.31
Anemia and Low Hematocrit
As mentioned earlier, anemia and low hematocrit (HCT) may actually exacerbate bleeding tendencies by decreasing the number of platelets exposed to the vessel wall. Red blood cells (RBCs) also produce TXA2 and ADP, both of which play vital roles in normal platelet aggregation. Secondly, RBCs have been shown to increase NO uptake. Nitric oxide is a potent vasodilator and inhibitor of platelet aggregation. The degree of uptake appears to be augmented by increasing HCT levels.32 A goal HCT of greater than 30% has been suggested and demonstrated benefit.33
Cryoprecipitate
Cryoprecipitate is rich in fibrinogen and vWF. Its mechanism is thought to be secondary to increasing functional vWF levels and possibly fibrinogen levels. While the overall effects appear to be variable, studies suggest 10 U of cryoprecipitate is adequate to reverse significant bleeding with resolution of effect at 24 hours.34,35 Given the risks of adverse reactions, variable responses, and risks of hepatitis C and HIV transmission, this therapy must be used cautiously with risk-benefit analysis.
Tranexamic Acid
Tranexamic acid is an antifibrinolytic agent that binds to fibrinogen as a competitive inhibitor of plasmin, inhibiting plasminogen activation. The trauma literature has shown TXA to significantly reduce all-cause mortality.36 It has also been shown to be beneficial in the bleeding uremic patient.37-39
However, it is important to keep in mind that the clearance of TXA in patients with renal disease is unclear. One study by Andersson et al40 demonstrated that TXA has increased plasma concentrations in patients with renal impairment, and a generally accepted practice is to renal-dose this medication. This study recommended a dose of 10 mg/kg IV at varying intervals, such as once daily, twice daily, or every 48 hours depending on the creatinine value, compared to patients with no renal impairment.40 Another study by Sabovic et al39 that evaluated the effects of TXA on gastrointestinal bleeding in patients with renal impairment used a 20-mg IV loading dose of TXA followed by 10 mg/kg orally every 48 hours. Though no adverse events occurred in this study, the study group was small. Other studies have not shown an increase in thromboembolic risk in patients who have no renal disease.36,41
At this time, there is no consensus on the exact dosing of TXA in this patient population. Therefore, this therapy should only be considered if others have failed and the patient continues to have significant blood loss.
Life-threatening Hemorrhage
If a patient is experiencing life-threatening blood loss, more aggressive measures must be employed regardless of risk of damage to the access. In such cases, a consultation with vascular surgery services should be obtained as early as possible. If none of the previously discussed measures are ineffective, the EP may be required to place sutures in the vascular access itself or apply a tourniquet. Again, these interventions may cause permanent damage to the access; however, in the setting of life-threatening hemorrhage such interventions clearly outweigh the risks associated with continued blood loss.
As blood can flow bidirectionally within a fistula, a tourniquet should be placed both proximally and distally to the fistula to obtain adequate hemostasis. Once the tourniquets are in place, if there is no immediate surgical consultation available, the EP may need to temporarily repair the defect to allow minimal tourniquet time. There are a few considerations when placing sutures. Ideally, a noncutting needle should be used to minimize damage. An adequate-sized suture, such as a 3-0 nylon suture, should be used to maintain strength in the high-pressure system. A figure-8 suture or purse-string suture may be placed around the defect. Adequate repair should allow for tourniquet removal.
Hemodynamic Status
The EP must remain aware of the patient’s hemodynamic status. Massive transfusion protocols may need to be initiated. Best current evidence dictates that this should be done in a 1:1:1 ratio of packed red blood cells, platelets, and fresh frozen plasma respectively.42 In our experience, the EP should consider permissive hypotension as aggressive resuscitation and increasing BP can compromise the vascular repair.
Lastly, transfer for definitive management should be arranged if not available at the EP’s institution. The patient should travel with tourniquets in place (although not tightened) in the event of further bleeding.
Nonhemorrhagic Complications of AVF or AVG
Stenosis/Thrombosis
Prolonged bleeding from the cannulation site may suggest outflow stenosis.43 Stenosis with or without subsequent thrombosis is a common cause of vascular access failure. Access failure has also been implicated secondary to poor vascular mapping, resulting in undetected pre-existing stenosis of the inflow artery, outflow vein, or juxta-anastomosis. However, development of stenosis may occur at any time throughout the life of the vascular access. One study by Schild et al4 reported thrombosis rates of 24.7% for grafts and 9.0% for fistula. Additionally, AVGs have a higher reported stenosis rate than AVFs, which is a risk factor for thrombosis.44,45
There has been much debate regarding routine surveillance to prevent clinically significant stenosis with subsequent thrombosis. Surveillance includes a clinical examination, Doppler imaging studies, and flow measurements during dialysis. A recent systematic review from 2016 by Ravani et al,46 demonstrated no difference in risk of access loss in preemptive stenosis correction in AVF or AVG without evidence of access dysfunction. However, on subgroup analysis this review did demonstrate a small benefit regarding risk of thrombosis and access loss in the AVF group.46
The physical examination may indicate evidence of vascular access stenosis or thrombosis. Evidence of stenosis may be indicated by failure of the outflow vein to collapse on arm raise test (distal stenosis), hyperpulsatility or hypopulsatility, loss of the diastolic component of the normal continuous thrill and bruit with only systolic components appreciated, and arm edema (central vein stenosis).43,47 Thrombosis of the vein may be evidenced by complete loss of the thrill and pulsatility on palpation. Sensitivity and specificity of the physical examination for inflow or outflow stenosis has been reported to be between 70% to 92% and 71% to 100%, respectively.48-50
While evidence may or may not support preemptive correction of stenosis, interventions are usually required when the stenosis is more than 50% and interferes with dialysis, decreased flow, abnormal physical examination, or elevated venous pressures.51 If stenosis is associated with interference of effective dialysis or thrombosis is suspected, ultrasound imaging and consultation with a vascular surgeon or interventional radiologist are indicated. Treatment of AVF or AVG stenosis and thrombosis includes percutaneous and surgical interventions.52
A systematic review by Tanner and da Silva53 evaluating adjuvant medical treatments for increasing patency rates of AVF and AVG found no therapy had any improvement in patency rates at 1 month. Another review from 2015 by Palmer et al54 suggested antiplatelet therapy may be protective for stenosis and thrombosis in AVF, but not AVG.
Infection
Infection in patients with ESRD is a major cause of morbidity and mortality, and 24% of these infections may be attributed to the vascular access itself, including central venous catheters (CVC).55 Central venous catheters are associated with the highest rate of infection, followed by AVGs, then AVFs.4,54 Studies have reported 9.5% vs 0.4% to 0.9% infection rates for AVG and AVF, respectively.2,4 These infections are usually due to gram-positive organisms, with the Staphylococcus species being the most common organism involved.55-57 However, infections caused by gram-negative organisms are possible, and broad-spectrum antibiotics should be initiated in the ED if infection is suspected. Patients may present with localized infection with increased risk of rupture of access to profound sepsis. Definitive treatment of an infected graft or fistula usually requires removal of the infected access or at least partial excision with possible interposition of additional graft material.58
Pseudoaneurysm/Aneurysm
Pseudoaneuryms are usually caused by hematoma development after needle puncture or in juxta-anastomic segments postoperatively. Pseudoaneurysms do not have a true wall and may secondarily become infected.59 Pseudoaneurysms occur more frequently in AVG, and are usually reported along with true aneurysms. One study by Al-Thani et al60 detected pseudoaneurysms in 15% of clinically significant aneurysms.
Approximately 30% to 60% of patients with AVFs will develop an aneurysm.2,5 One study by Al-Thani et al60 reported the need for surgical intervention in 31% of patients with an AVF in whom an aneurysm was detected. The risk for developing an aneurysm is highest for those patients on high flux membrane type HD and polycystic kidney disease.5 As discussed earlier in this article, cannulation sites and techniques may also influence aneurysmal changes in the fistula. Aneurysm formation at the site of previous cannulation site should not be re-cannulated.18 Aneurysmal changes can contribute to other complications including high-output heart failure, thrombosis with fistula or graft failure, increased risk of bleeding, ineffective HD when associated with thrombosis or stenosis, pain and peripheral neuropathies secondary to compression of nearby nerves, and interference with functional HD.
Many asymptomatic aneurysmal changes to vascular access may not compromise access function. If a patient is identified with a vascular access pseudoaneurysm or aneurysmal changes with high-risk features, early referral to vascular surgeon for surgical interventions is imperative. High-risk features include any of the complications previously discussed—infection, threatened overlying skin, or shiny appearance. The EP should consider duplex imaging to assist with evaluation. Treatment may include ligation of the AVF, partial resection, stenting, or grafting of the aneurysm with hopes of salvaging the vascular access.61,62
Ischemic Monomelic Neuropathy
Ischemic monomelic neuropathy may result secondary to a type of steal phenomenon, thereby inducing ischemia to supplied nerves. Ischemic monomelic neuropathy has been described in many case reports and narrative reviews.63-67 It has been described as ischemia or infarction of the blood supply to the nerves (vasa nervosa) in the lower arm.68 Ischemic monomelic neuropathy typically occurs immediately after the vascular access creation in the postoperative period. Therefore, it is unlikely to be seen in the ED but as patients may have sequelae of this complication, EPs should be aware of its existence. Patients with ischemic monomelic neuropathy will have severe pain, paresthesia, and weakness immediately after placement of a vascular access. Patients also typically have sensorimotor deficits in the radial, ulnar, and median nerves. Pulses should be preserved. Severe neuropathic pain will develop and may limit the examination. Clinical diagnosis may be difficult immediately after surgery because patients will often have minor deficits secondary to the surgical procedure itself or secondary to the regional block provided by anesthesia, but nerve-conduction studies usually reveal the diagnosis. The treatment is ligation of the access immediately and prognosis is variable, depending on the severity and duration of ischemia, and may result in complete loss of function of the hand.
Steal Syndrome
Dialysis access-associated steal syndrome is a type of distal ischemia secondary to the vascular access site with a reported incidence of 6.2%, and appears to occur more frequently in AVF than AVGs.69,70 Diabetes appears to be a strong risk factor for developing DASS.71 Patients with DASS can present with classic ischemic symptoms such as pain, paresthesia, claudication, pallor, and diminished or absent arterial pulse. Pain may be present only while undergoing dialysis or exercising, or symptoms may be persistent.68,72 There are several possible causes of DASS, including arterial occlusion or insufficiency proximal or distal to the anastomosis, increased flow through the conduit (true steal), or increased flow diverted through collateral vessels.73,74 One clue to the diagnosis is a diminished or absent radial pulse that should improve with compression of the access site.
Once DASS is suspected, diagnosis should be confirmed using venous duplex scanning with finger pressure waveform analysis or arteriogram. Definitive management is surgical intervention with ligation of the access or banding.
High-Output Heart Failure
Changes in cardiac output (CO) are a well-documented effect of AVF placement, with one small study by Korsheed et al75 demonstrating an average increase in CO of 17% only 2 weeks after AVF placement. The increase in CO is thought to be secondary to alterations in systemic vascular resistance and sympathetic activity. While an increase in CO can ultimately lead to high-output heart failure, this is typically only seen in patients with pre-existing cardiac dysfunction.76 Patients are at an increased risk of high-output heart failure when flow through the AVF exceeds 2 L/min; flows below this rate are typically not associated with adverse cardiac effects.77 Another objective measurement for identifying patients at risk of high-output heart failure is the ratio of flow in the fistula (Qa) to cardiac output ratio. Patients with a Qa:CO ratio greater than 0.3 have a significantly increased risk of high-output heart failure.78 There is thought to be no difference in risk of heart failure between AVF and AVG.79
Once overt heart failure has developed, it should be treated in the usual fashion, with IV fluid management and standard pharmacological therapies. If standard conservative heart failure treatment is ineffective, several surgical options are available, including banding, changing the location of the anastomosis, and ultimately closing the fistula.80
Conclusion
While life-threatening bleeding and vascular access rupture are uncommon complications of AVFs and AVGs, it is essential for the EP to rapidly treat the potentially catastrophic hemorrhagic vascular access complications. Depending on the severity and stability of the patient, it is reasonable to begin in a stepwise fashion as presented in this article for patients with minor bleeding, while more severe or persistent bleeding may require several interventions simultaneously to gain control of the bleeding.
Patients with hemodynamic instability requiring transfusion will need a vascular surgery consult and admission. Disposition for stable patients, without evidence of impending aneurysmal related rupture and concern for overlying infection or other complication requiring immediate intervention, will depend on clinical judgment, patient-specific factors and family support, follow-up, and proximity of the patient to medical care.
1. National Institute of Diabetes and Digestive and Kidney Diseases. Kidney disease statistics for the United States. https://www.niddk.nih.gov/health-information/health-statistics/Pages/kidney-disease-statistics-united-states.aspx. Accessed August 24, 2017.
2. Salahi H, Fazelzadeh A, Mehdizadeh A, Razmkon A, Malek-Hosseini SA. Complications of arteriovenous fistula in dialysis patients. Transplant Proc. 2006;38(5):1261-1264. doi:10.1016/j.transproceed.2006.02.066.
3. Ellingson KD, Palekar RS, Lucero CA, et al. Vascular access hemorrhages contribute to deaths among hemodialysis patients. Kidney Int. 2012;82(6):686-692. doi:10.1038/ki.2012.185.
4. Schild AF, Perez E, Gillaspie E, Seaver C, Livingstone J, Thibonnier A. Arteriovenous fistulae vs. arteriovenous grafts: a retrospective review of 1,700 consecutive vascular access cases. J Vasc Access. 2008;9(4):231-235.
5. Jankovic A, Donfrid B, Adam J, et al. Arteriovenous fistula aneurysm in patients on regular hemodialysis: prevalence and risk factors. Nephron Clin Pract. 2013;124(1-2):94-98. doi:10.1159/000355548.
6. Holden RM, Harman GJ, Wang M, Holland D, Day AG. Major bleeding in hemodialysis patients. Clin J Am Soc Nephrol. 2008 Jan;3(1):105-110. doi:10.2215/CJN.01810407.
7. Elliott MJ, Zimmerman D, Holden RM. Warfarin anticoagulation in hemodialysis patients: a systematic review of bleeding rates. Am J Kidney Dis. 2007;50(3):433-440. doi:10.1053/j.ajkd.2007.06.017.
8. Jubelirer SJ. Hemostatic abnormalities in renal disease. Am J Kidney Dis. 1985;5(5):219-225.
9. Salvati F, Liani M. Role of platelet surface receptor abnormalities in the bleeding and thrombotic diathesis of uremic patients on hemodialysis and peritoneal dialysis. Int J Artif Organs. 2001;24(3):131-135.
10. Kaw D, Malhotra D. Platelet dysfunction and end-stage renal disease. Semin Dial. 2006;19(4):317-322. doi:10.1111/j.1525-139X.2006.00179.x.
11. Hedges SJ, Dehoney SB, Hooper JS, Amanzadeh J, Busti AJ. Evidence-based treatment recommendations for uremic bleeding. Nat Clin Pract Nephrol. 2007;3(3):138-153. doi:10.1038/ncpneph0421.
12. Thekkedath UR, Chirananthavat T, Leypoldt JK, Cheung AK, Mohammad SF. Elevated fibrinogen fragment levels in uremic plasma inhibit platelet function and expression of glycoprotein IIb-IIIa. Am J Hematol. 2006;81(12):915-926. doi:10.1002/ajh.20720.
13. Padberg FT, Calligaro KD, Sidawy AN. Complications of arteriovenous hemodialysis access: recognition and management. J Vasc Surg. 2008;48(5 Suppl):S55-S80. doi:10.1016/j.jvs.2008.08.067.
14. Lohr JW, Schwab SJ. Minimizing hemorrhagic complications in dialysis patients. J Am Soc Nephrol. 1991;2(5):961-975.
15. Yang TH, Lee CH, Tsai CS, Tsai YT. Successful surgical treatment of a rupture to an arteriovenous fistula aneurysm. Cardiovasc J Afr. 2009;20(3):196-197.
16. Caksen HH, Odabaş D, Arslan S, Kaya A. Spontaneous rupture of arteriovenous fistula in a chronic dialysis patient. J Emerg Med. 2003;24(2):224-225. doi:10.1016/S0736-4679(02)00744-8.
17. Saeed F, Kousar N, Sinnakirouchenan R, Ramalingam VS, Johnson PB, Holley JL. Blood loss through AV fistula: a case report and literature review. Int J Nephrol. 2011;2011:350870. doi:10.4061/2011/350870.
18. NKF KDOQI Guidelines. Clinical practice guidelines for vascular access. Guideline 5. Treatment of fistula complications. Available at http://www2.kidney.org/professionals/kdoqi/guideline_uphd_pd_va/va_guide5.htm. Accessed August 24, 2017.
19. Gill JR, Storck K, Kelly S. Fatal exsanguination from hemodialysis vascular access sites. Forensic Sci Med Pathol. 2012;8(3):259-262. doi:10.1007/s12024-011-9303-0.
20. Manning MA. Use of dialysis access in emergent situations. J Emerg Nurs. 2008;34(1):37-40. doi:10.1016/j.jen.2007.03.018.
21. Reddy VM, Bagul A, Qureshi AA, Nicholson ML. A simple technique to control a bleeding arteriovenous fistula. Ann R Coll Surg Engl. 2006;88(6):592-593. doi:10.1308/003588406X130714f.
22. Oudemans-van Straaten HM. Hemostasis and thrombosis in continuous renal replacement treatment. Semin Thromb Hemost. 2015;41(1):91-98. doi:10.1055/s-0034-1398384.
23. Casserly LF, Dember LM. Thrombosis in end-stage renal disease. Semin Dial. 2003;16(3):245-256. doi:10.1046/j.1525-139X.2003.16048.x.
24. Boccardo P, Remuzzi G, Galbusera M. Platelet dysfunction in renal failure. Semin Thromb Hemost. 2004;30(5):579-589. doi:10.1055/s-2004-835678.
25. Mannucci PM, Remuzzi G, Pusineri F, et al. Deamino-8-D-arginine vasopressin shortens the bleeding time in uremia. N Engl J Med. 1983;308(1):8-12. doi:10.1056/NEJM198301063080102.
26. Ho SJ, Gemmell R, Brighton TA. Platelet function testing in uraemic patients. Hematology. 2008;13(1):49-58. doi:10.1179/102453308X315834.
27. Showalter J, Nguyen ND, Baba S, et al. Platelet aggregometry cannot identify uremic platelet dysfunction in heart failure patients prior to cardiac surgery. J Clin Lab Anal. 2016:1-5. doi:10.1002/jcla.22084.1308/003588406X130714f.
28. Wademan BH, Galvin SD. Desmopressin for reducing postoperative blood loss and transfusion requirements following cardiac surgery in adults. Interact Cardiovasc Thorac Surg. 2014;18(3):360-370. doi:10.1093/icvts/ivt491.
29. Soslau G, Schwartz AB, Putatunda B, et al. Desmopressin-induced improvement in bleeding times in chronic renal failure patients correlates with platelet serotonin uptake and ATP release. Am J Med Sci. 1990;300(6):372-379. http://www.ncbi.nlm.nih.gov/pubmed/2264575. Accessed January 31, 2017.
30. Lethagen S. Desmopressin (DDAVP) and hemostasis. Ann Hematol. 1994;69(4):173-180.
31. Mannucci PM. Hemostatic drugs. N Engl J Med. 1998;339(4):245-253. doi:10.1056/NEJM199807233390407.
32. Azarov I, Huang KT, Basu S, Gladwin MT, Hogg N, Kim-Shapiro DB. Nitric oxide scavenging by red blood cells as a function of hematocrit and oxygenation. J Biol Chem. 2005;280(47):39024-39032. doi:10.1074/jbc.M509045200.
33. Livio M, Marchesi D, Remuzzi G, Gotti E, Mecca G, De Gaetano G. Uraemic bleeding: role of anaemia and beneficial effect of red cell transfusions. Lancet. 1982;320(8306):1013-1015. doi:10.1016/S0140-6736(82)90050-2.
34. Janson PA, Jubelirer SJ, Weinstein MJ, Deykin D. Treatment of the bleeding tendency in uremia with cryoprecipitate. N Engl J Med. 1980;303(23):1318-1322. doi:10.1056/NEJM198012043032302.
35. Triulzi DJ, Blumberg N. Variability in response to cryoprecipitate treatment for hemostatic defects in uremia. Yale J Biol Med. 1990;63(1):1-7.
36. Roberts I, Shakur H, Coats T, et al. The CRASH-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Heal Technol Assess. 2013;17(10):1-79. doi:10.3310/hta17100.
37. Mezzano D, Panes O, Muñoz B, et al. Tranexamic acid inhibits fibrinolysis, shortens the bleeding time and improves platelet function in patients with chronic renal failure.Thromb Haemost. 1999;82(4):1250-1254.
38. Mezzano D, Muñoz B, Pais E, Downey P, Pereira J. Fast decrease of bleeding time by tranexamic acid in uremia. Thromb Haemost. 2000;83(5):785.
39. Sabovic M, Lavre J, Vujkovac B. Tranexamic acid is beneficial as adjunctive therapy in treating major upper gastrointestinal bleeding in dialysis patients. Nephrol Dial Transplant. 2003;18(7):1388-1391. doi:10.1093/ndt/gfg117.
40. Andersson L, Eriksson O, Hedlund PO, Kjellman H, Lindqvist B. Special considerations with regard to the dosage of tranexamic acid in patients with chronic renal diseases. Urol Res. 1978;6(2):83-88.
41. Bennett C, Klingenberg SL, Langholz E, Gluud LL. Tranexamic acid for upper gastrointestinal bleeding. Cochrane Database Syst Rev. 2014;(11):CD006640. doi: 10.1002/14651858.CD006640.pub3.
42. Holcomb JB, Tilley BC, Baraniuk S, et al; PROPPR Study Group. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313(5):471-482. doi:10.1001/jama.2015.12.
43. Salman L, Beathard G. Interventional nephrology: physical examination as a tool for surveillance for the hemodialysis arteriovenous access. Clin J Am Soc Nephrol. 2013;8(7):1220-1227. doi:10.2215/CJN.00740113.
44. Maya ID, Oser R, Saddekni S, Barker J, Allon M. Vascular access stenosis: comparison of arteriovenous grafts and fistulas. Am J Kidney Dis. 2004;44(5):859-865.
45. Ocak G, Verduijn M, Vossen CY, et al. Chronic kidney disease stages 1-3 increase the risk of venous thrombosis. J Thromb Haemost. 2010;8(11):2428-2435. doi:10.1111/j.1538-7836.2010.04048.x.
46. Ravani P, Quinn RR, Oliver MJ, et al. Pre-emptive correction for haemodialysis arteriovenous access stenosis. Cochrane Database Syst Rev. 2016;(1):CD010709. doi:10.1002/14651858.CD010709.pub2.
47. Pietryga JA, Little MD, Robbin ML. Sonography of arteriovenous fistulas and grafts. Semin Dial. 2017;30(4):309-318. doi:10.1111/sdi.12599.
48. Asif A, Leon C, Orozco-Vargas LC, et al. Accuracy of physical examination in the detection of arteriovenous fistula stenosis. Clin J Am Soc Nephrol. 2007;2(6):1191-1194. doi:10.2215/CJN.02400607.
49. Tessitore N, Bedogna V, Melilli E, et al. In search of an optimal bedside screening program for arteriovenous fistula stenosis. Clin J Am Soc Nephrol. 2011;6(4):819-826. doi:10.2215/CJN.06220710.
50. Dhamija R, Nash SK, Nguyen SV, Slack K, Tadeo J. Monitoring and surveillance of hemodialysis vascular access using StenTec and physical exam. Semin Dial. 2015;28(3):299-304. doi:10.1111/sdi.12311.
51. NKF KDOQI Guidelines. Clinical practice guidelines for hemodialysis adequacy, update 2006. Available at http://kidneyfoundation.cachefly.net/professionals/KDOQI/guideline_upHD_PD_VA/index.htm. Accessed August 12, 2017.
52. Gelbfish GA. Surgical versus percutaneous care of arteriovenous access. Semin Vasc Surg. 2007;20(3):167-174. doi:10.1053/j.semvascsurg.2007.07.011.
53. Tanner NC, da Silva AF. Medical adjuvant treatment to improve the patency of arteriovenous fistulae and grafts: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2016;52(2):243-252. doi:10.1016/j.ejvs.2016.04.016.
54. Palmer SC, Di Micco L, Razavian M, et al. Antiplatelet therapy to prevent hemodialysis vascular access failure: systematic review and meta-analysis. Am J Kidney Dis. 2013;61(1):112-122. doi:10.1053/j.ajkd.2012.08.031.
55. Lafrance JP, Rahme E, Lelorier J, Iqbal S. Vascular access-related infections: definitions, incidence rates, and risk factors. Am J Kidney Dis. 2008;52(5):982-993. doi:10.1053/j.ajkd.2008.06.014.
56. Piraino B. Staphylococcus aureus infections in dialysis patients: focus on prevention. ASAIO J. 46(6):S13-S17.
57. Minga TE, Flanagan KH, Allon M. Clinical consequences of infected arteriovenous grafts in hemodialysis patients. Am J Kidney Dis. 2001;38(5):975-978. doi:10.1053/ajkd.2001.28583.
58. Benrashid E, Youngwirth LM, Mureebe L, Lawson JH. Operative and perioperative management of infected arteriovenous grafts. J Vasc Access. 2017;18(1):13-21. doi:10.5301/jva.5000613.
59. Lazarides MK, Georgiadis GS, Argyriou C. Aneurysm formation and infection in AV prosthesis. J Vasc Access. 2014;15 Suppl 7(Suppl. 7):S120-S124. doi:10.5301/jva.5000228.
60. Al-Thani H, El-Menyar A, Al-Thani N, et al. Characteristics, management, and outcomes of surgically treated arteriovenous fistula aneurysm in patients on regular hemodialysis. Ann Vasc Surg. 2017;41:46-55. doi:10.1016/j.avsg.2016.08.046.
61. Mudoni A, Cornacchiari M, Gallieni M, et al. Aneurysms and pseudoaneurysms in dialysis access. Clin Kidney J. 2015;8(4):363-367. doi:10.1093/ckj/sfv042.
62. Georgiadis GS, Lazarides MK, Panagoutsos SA, et al. Surgical revision of complicated false and true vascular access–related aneurysms. J Vasc Surg. 2008;47(6):1284-1291. doi:10.1016/j.jvs.2008.01.051.
63. Singh V, Qaisar H, Masud A, et al. Ischemic monomelic neuropathy: a long-term follow-up of two cases. J Vasc Access. 2017:0. [Epub ahead of print] doi:10.5301/jva.5000743.
64. Sheetal S, Byju P, Manoj P. Ischemic monomelic neuropathy. J Postgrad Med. 2017;63(1):42-43. doi:10.4103/0022-3859.194221.
65. Rabbani MA, Ahmad B, Shah SM, Ahmad A. Ischemic monomelic neuropathy: a complication of vascular access procedure. J Pak Med Assoc. 2005;55(9):400-401.
66. Hye RJ, Wolf YG. Ischemic monomelic neuropathy: an under-recognized complication of hemodialysis access. Ann Vasc Surg. 1994;8(6):578-582. doi:10.1007/BF02017415.
67. Thimmisetty RK, Pedavally S, Rossi NF, Fernandes JAM, Fixley J. Ischemic monomelic neuropathy: diagnosis, pathophysiology, and management. Kidney Int Reports. 2017;2(1):76-79. doi:10.1016/j.ekir.2016.08.013.
68. MacRae JM, Dipchand C, Oliver M, et al. Arteriovenous access: infection, neuropathy, and other complications. Can J Kidney Heal Dis. 2016;3:2054358116669127. doi:10.1177/2054358116669127.
69. Davidson D, Louridas G, Guzman R, et al. Steal syndrome complicating upper extremity hemoaccess procedures: incidence and risk factors. Can J Surg. 2003;46(6):408-412.
70. Kokkosis AA, Abramowitz SD, Schwitzer J, Nowakowski S, Teodorescu VJ, Schanzer H. Inflow stenosis as a contributing factor in the etiology of AV access-induced ischemic steal. J Vasc Access. 2014;15(4):286-290. doi:10.5301/jva.5000205.
71. Rocha A, Silva F, Queirós J, Malheiro J, Cabrita A. Predictors of steal syndrome in hemodialysis patients. Hemodial Int. 2012;16(4):539-544. doi:10.1111/j.1542-4758.2012.00684.x.
72. Mwipatayi BP, Bowles T, Balakrishnan S, Callaghan J, Haluszkiewicz E, Sieunarine K. Ischemic steal syndrome: a case series and review of current management. Curr Surg. 2006;63(2):130-135. doi:10.1016/j.cursur.2005.04.017.
73. Raml NM. Irreversible sequela in an arterial venous fistula with steal syndrome: A case study. J Vasc Nurs. 2012;30(3):94-97. doi:10.1016/j.jvn.2012.02.001.
74. Malik J, Tuka V, Kasalova Z, et al. Understanding the dialysis access steal syndrome. A review of the etiologies, diagnosis, prevention and treatment strategies. J Vasc Access. 2008;9(3):155-166.
75. Korsheed S, Eldehni MT, John SG, Fluck RJ, McIntyre CW. Effects of arteriovenous fistula formation on arterial stiffness and cardiovascular performance and function. Nephrol Dial Transplant. 2011;26(10):3296-3302. doi:10.1093/ndt/gfq851.
76. Lazarides MK, Staramos DN, Panagopoulos GN, Tzilalis VD, Eleftheriou GJ, Dayantas JN. Indications for surgical treatment of angioaccess-induced arterial "steal". J Am Coll Surg. 1998;187(4):422-426.
77. Basile C, Lomonte C, Vernaglione L, Casucci F, Antonelli M, Losurdo N. The relationship between the flow of arteriovenous fistula and cardiac output in haemodialysis patients. Nephrol Dial Transplant. 2008;23(1):282-287. doi:10.1093/ndt/gfm549.
78. Wijnen E, Keuter XH, Planken NR, et al. The relation between vascular access flow and different types of vascular access with systemic hemodynamics in hemodialysis patients. Artif Organs. 2005;29(12):960-964. doi:10.1111/j.1525-1594.2005.00165.x.
79. Keuter XH, Kooman JP, Habets J, et al. Effect of upper arm brachial basilic and prosthetic forearm arteriovenous fistula on left ventricular hypertrophy. J Vasc Access. 2007;8(4):296-301.
80. Miller GA, Hwang WW. Challenges and management of high-flow arteriovenous fistulae. Semin Nephrol. 2012;32(6):545-550. doi:10.1016/j.semnephrol.2012.10.005.
According to the National Institute of Diabetes and Digestive and Kidney Diseases, approximately 468,000 persons in the United States are on dialysis—a number that continues to grow annually.1 The 1-year rate for hemorrhagic complications from arteriovenous fistulas (AVFs) is estimated to be 0.4%.2 One study by Ellingson et al3 reported 1,654 deaths secondary to fatal vascular access hemorrhage over a 6-year period, accounting for 0.4% of all deaths of hemodialysis (HD) patients in that study.3
Nonhemorrhagic vascular access-related complications also contribute to the morbidity and mortality associated with AVFs and arteriovenous grafts (AVGs). Venous stenosis resulting in thrombosis has been estimated to occur in 24.7% of AVGs and 9.0% of AVFs, both of which are common causes of access failure.
Infection is reported to be the second leading cause of death in dialysis patients, and vascular access-related infection rates are reported to occur in 9.5% of AVGs vs 0.4% to 0.9% of AVFs.2,4 Pseudoaneurysms and aneurysms range from 30% to 60% for AVFs,2,5 and contribute to morbidity by limiting available areas to cannulate for dialysis, occasionally requiring surgical revision to restore access function or prevent access rupture.
Steal phenomena, including dialysis access-induced steal syndrome (DASS) and ischemic monomelic neuropathy, as well as heart failure secondary to high output are additional contributors to morbidity and mortality.
With the growing rate of end-stage renal disease (ESRD) in the United States and the contribution to morbidity and mortality by bleeding and other complications, it is essential to understand how to evaluate and treat these patients in the ED. This article reviews the evaluation and treatment of vascular access emergencies, as well as risk factors that contribute to complications in the ESRD patient population.
Hemorrhagic Complications of Vascular Access
Risk Factors
Many patients with ESRD have multiple comorbidities such as coronary artery disease and atrial fibrillation that require anticoagulation, antiplatelet medications, or both. Studies have shown that ESRD patients taking warfarin have an increase in major bleeding episodes of 3.1% per person-year and 4.4% per person-year for those taking aspirin alone, while those taking both medications have an increased bleeding risk of 6.3% per person-year.6 A recent systematic review by Elliott et al7 has suggested a 2-fold increase in bleeding rates in HD patients anticoagulated with warfarin as compared to HD patients not on warfarin.
While uremia secondary to chronic kidney disease (CKD) is a well-known facilitator of bleeding complications, the underlying pathophysiology is not yet completely delineated. However, there are some general underlying principles that may help in understanding the best treatment modalities available at this time. As the kidneys fail, uremic toxins accumulate in the bloodstream. These toxins include urea, creatinine, and phenolic acids, which are believed to interfere with primary hemostasis by effecting platelet adherence to endothelium, platelet activation, and aggregation.8 Functional defects are created in the interactions between the glycoprotein Ib (GPIb) receptor and von Willebrand factor (vWF), which are essential to endothelial adhesion of platelets.9 Additionally, these toxins impair the up regulation of the GPIIbIIIa receptor which is integral to platelet aggregation.10 Platelet activation normally leads to platelet aggregation by increasing production of thromboxane A2 (TXA2) and serotonin that are released from storage granules.10 Some toxins may increase nitric oxide (NO) synthesis, effectively reducing aggregation by decreasing TXA2 and adenosine diphosphate (ADP) levels.11 In addition, elevated levels of fibrinogen fragments have also recently been shown to inhibit platelet function by competing with fibrinogen for the GPIIbIIIa receptor with decreasing levels demonstrated after HD.12
Finally, increased pressure in the venous outflow segment also increases persistent bleeding from puncture sites. These pressures may be exaggerated secondary to venous thrombosis, venous stenosis, pseudoaneurysm, aneurysm, or infection.13 The following sections further describe the evaluation and treatment of these complications.
Clinical Presentation
Patients presenting with bleeding from the vascular access site may present with slow continuous oozing from the needle puncture-site itself or with life-threatening hemorrhage secondary to AVF or AVG rupture.14 The incidence of vascular access rupture is unknown, but it appears the majority of ruptures occur in patients with AVG vs AVF.3 However, several case reports have also described hemorrhagic complications of AVF ruptures.15-17 The risk of rupture may be associated with the development of aneurysms or pseudoaneuryms.18 Possible impending perforation may be signaled by skin thinning or a shiny appearance overlying the aneurysm, or evidence of infection overlying the access site.3 Many patients were shown to have complications such as stenosis, thrombosis, or infection within 6 months prior to rupture.3 Education of patients is also important as most hemorrhages occur prior to hospital arrival.3,19
Evaluation in the ED
As with any patient presenting to the ED, the initial evaluation of an unstable patient experiencing bleeding from a vascular access site includes assessing the airway, breathing, and circulation as a first priority—paying special attention to the area of bleeding while simultaneously preparing for possible intervention. It is also important to determine when the patient last underwent dialysis and if he or she was able to complete HD. This information will identify patients who are candidates for reversing the heparin load likely given during dialysis.
It is also important to note that some patients undergoing HD who have already been identified as having an increased risk of bleeding may not receive heparin or may undergo local heparinization, minimal heparinization, or regional citrate anticoagulation during dialysis, in which case protamine is not indicated.14 The emergency physician (EP) must also determine if the patient is on any antiplatelet or anticoagulation agents.
The vascular access site should be inspected for evidence of aneurysmal changes, infection, and skin thinning as these factors increase the risk of bleeding and vascular rupture. Additionally auscultation and palpation of the vascular access site should be performed to evaluate for other potential complications such as stenosis and thrombosis. Lastly, the EP should anticipate the patient’s need for HD in the setting of a potentially unavailable AVG or AVF to determine whether the patient may need an alternative access.
Treatment and Management
The primary responsibility during the initial treatment of a bleeding access site is to stop further blood loss by utilizing methods that employ direct pressure or, in extreme cases, application of a tourniquet, followed by other interventions such as fluid and blood-product resuscitation; coagulopathy reversal; consideration of desmopressin, cryoprecipitate, tranexamic acid (TXA); HD; and vascular repair.
Control of a bleeding dialysis access-site is a balancing act of adequately controlling the bleeding while maintaining the integrity of the fistula. Overly aggressive management may cause thrombosis in the vascular access site, which is associated with morbidity—eg, site revisions, potential for the need to create a new access site. On the opposite end of the spectrum, failing to adequately control bleeding can lead to significant anemia ranging from minimal symptoms to hemodynamic compromise and death.
Peripheral Venous Access
While peripheral venous access is notoriously difficult in patients with ESRD, it is essential for the resuscitation of hemorrhaging patients. Ideally, two large bore peripheral intravenous (IV) lines should be placed in the proximal upper extremities. If peripheral venous access is not achieved, central venous access or interosseous access placement is indicated (Figure).
Direct Pressure
With low-volume bleeding, the first attempt to control the bleeding is simple direct pressure. Except in the instance of trauma or self-inflicted injury, bleeding usually occurs at the site of cannulation of the vascular access post-HD. Direct pressure should be light and limited to as small of an area as possible to prevent thrombosis; the force and area encompassed by direct pressure can be expanded as needed for bleeding that is more difficult to control. In cases of higher volume bleeding, pressure should be placed both proximally and distally to the shunt due to its bidirectional flow. Another possible temporizing measure is to place an upright gallipot or cup over the bleeding site on top of a folded piece of gauze and then securing it with tape.21
Topical Hemostatic Agents
Second simple direct pressure, topical hemostatic agents may be a good adjunct to help obtain hemostasis. There is a wide range of products available, from procoagulants (eg, Combat Gauze, topical thrombin) to factor concentrators (eg, QuikClot). These can be used directly on the bleeding site and only in conjunction with direct pressure.
In addition to topical hemostatic agents, another option is skin glue, which should be applied generously after bleeding has been temporized, with pressure both proximally and distally to the site.
Anticoagulation Reversal
As previously mentioned, it is important to determine when the patient’s last HD was. Heparin is used during dialysis to prevent clotting within the circuit, and although clotting times are monitored during dialysis to guide anticoagulation, it is possible that a patient bleeding after dialysis could still have therapeutic levels of heparin requiring reversal with protamine.
The recommended dose of protamine is 1 mg for every 100 U of heparin given during dialysis; protamine should be administered over 10 minutes. Alternatively, a 10- to 20-mg dose of protamine can be given if the amount of heparin administered during HD is unknown. Additionally, the patient’s medication list, as with any ED presentation, should be carefully reviewed as many dialysis patients have comorbidities requiring anticoagulation with potentially reversible agents.
Hemodialysis to Improve Platelet Dysfunction
It is thought that long-term exposure of platelets to the dialysis membrane can lead to chronic platelet activation leading to platelet dysfunction. There is conflicting data regarding the effects of HD on improving bleeding in renal patients.9,22,23 Hemodialysis is thought to be beneficial, at least partially, through reversing uremia, thus improving platelet function.24 Therefore, in the stable bleeding patient who missed a scheduled dialysis, initiating HD in the ED setting could be beneficial. If the vascular access site is deemed unsafe for HD, another access site must be obtained, for example, by placing a temporary central venous catheter that will allow for successful HD.
Desmopressin
Desmopressin acetate has been shown to reduce bleeding time in uremic patients by releasing vWF and factor VIII into plasma, taking effect within 1 hour and lasting 4 to 8 hours.25-27 Desmopressin has also been shown to reduce blood loss and bleeding times in patients with platelet dysfunction undergoing cardiac surgery.28 While the underlying mechanism is unclear, desmopressin acetate is thought to help with platelet adhesion to the endothelial wall.
Alternatively, one study by Soslau et al29 has suggested that desmopressin may increase serotonin uptake by platelets and increase adenosine triphosphate release, thereby facilitating platelet aggregation. The dosing of desmopressin is 0.2 to 0.3 mcg/kg IV.30 Adverse effects include facial flushing, mild headache, and transient small decrease in blood pressure (BP) with increase in heart rate. Historically, it was thought that desmopressin could lead to water retention, volume overload, congestive heart failure, and hyponatremia; however, these adverse effects have not been seen in uremic patients.30 Tachyphylaxis may occur after just a few doses of desmopressin are given.31 Additionally, hyponatremia and seizures have been seen after repeated administration in children.31
Anemia and Low Hematocrit
As mentioned earlier, anemia and low hematocrit (HCT) may actually exacerbate bleeding tendencies by decreasing the number of platelets exposed to the vessel wall. Red blood cells (RBCs) also produce TXA2 and ADP, both of which play vital roles in normal platelet aggregation. Secondly, RBCs have been shown to increase NO uptake. Nitric oxide is a potent vasodilator and inhibitor of platelet aggregation. The degree of uptake appears to be augmented by increasing HCT levels.32 A goal HCT of greater than 30% has been suggested and demonstrated benefit.33
Cryoprecipitate
Cryoprecipitate is rich in fibrinogen and vWF. Its mechanism is thought to be secondary to increasing functional vWF levels and possibly fibrinogen levels. While the overall effects appear to be variable, studies suggest 10 U of cryoprecipitate is adequate to reverse significant bleeding with resolution of effect at 24 hours.34,35 Given the risks of adverse reactions, variable responses, and risks of hepatitis C and HIV transmission, this therapy must be used cautiously with risk-benefit analysis.
Tranexamic Acid
Tranexamic acid is an antifibrinolytic agent that binds to fibrinogen as a competitive inhibitor of plasmin, inhibiting plasminogen activation. The trauma literature has shown TXA to significantly reduce all-cause mortality.36 It has also been shown to be beneficial in the bleeding uremic patient.37-39
However, it is important to keep in mind that the clearance of TXA in patients with renal disease is unclear. One study by Andersson et al40 demonstrated that TXA has increased plasma concentrations in patients with renal impairment, and a generally accepted practice is to renal-dose this medication. This study recommended a dose of 10 mg/kg IV at varying intervals, such as once daily, twice daily, or every 48 hours depending on the creatinine value, compared to patients with no renal impairment.40 Another study by Sabovic et al39 that evaluated the effects of TXA on gastrointestinal bleeding in patients with renal impairment used a 20-mg IV loading dose of TXA followed by 10 mg/kg orally every 48 hours. Though no adverse events occurred in this study, the study group was small. Other studies have not shown an increase in thromboembolic risk in patients who have no renal disease.36,41
At this time, there is no consensus on the exact dosing of TXA in this patient population. Therefore, this therapy should only be considered if others have failed and the patient continues to have significant blood loss.
Life-threatening Hemorrhage
If a patient is experiencing life-threatening blood loss, more aggressive measures must be employed regardless of risk of damage to the access. In such cases, a consultation with vascular surgery services should be obtained as early as possible. If none of the previously discussed measures are ineffective, the EP may be required to place sutures in the vascular access itself or apply a tourniquet. Again, these interventions may cause permanent damage to the access; however, in the setting of life-threatening hemorrhage such interventions clearly outweigh the risks associated with continued blood loss.
As blood can flow bidirectionally within a fistula, a tourniquet should be placed both proximally and distally to the fistula to obtain adequate hemostasis. Once the tourniquets are in place, if there is no immediate surgical consultation available, the EP may need to temporarily repair the defect to allow minimal tourniquet time. There are a few considerations when placing sutures. Ideally, a noncutting needle should be used to minimize damage. An adequate-sized suture, such as a 3-0 nylon suture, should be used to maintain strength in the high-pressure system. A figure-8 suture or purse-string suture may be placed around the defect. Adequate repair should allow for tourniquet removal.
Hemodynamic Status
The EP must remain aware of the patient’s hemodynamic status. Massive transfusion protocols may need to be initiated. Best current evidence dictates that this should be done in a 1:1:1 ratio of packed red blood cells, platelets, and fresh frozen plasma respectively.42 In our experience, the EP should consider permissive hypotension as aggressive resuscitation and increasing BP can compromise the vascular repair.
Lastly, transfer for definitive management should be arranged if not available at the EP’s institution. The patient should travel with tourniquets in place (although not tightened) in the event of further bleeding.
Nonhemorrhagic Complications of AVF or AVG
Stenosis/Thrombosis
Prolonged bleeding from the cannulation site may suggest outflow stenosis.43 Stenosis with or without subsequent thrombosis is a common cause of vascular access failure. Access failure has also been implicated secondary to poor vascular mapping, resulting in undetected pre-existing stenosis of the inflow artery, outflow vein, or juxta-anastomosis. However, development of stenosis may occur at any time throughout the life of the vascular access. One study by Schild et al4 reported thrombosis rates of 24.7% for grafts and 9.0% for fistula. Additionally, AVGs have a higher reported stenosis rate than AVFs, which is a risk factor for thrombosis.44,45
There has been much debate regarding routine surveillance to prevent clinically significant stenosis with subsequent thrombosis. Surveillance includes a clinical examination, Doppler imaging studies, and flow measurements during dialysis. A recent systematic review from 2016 by Ravani et al,46 demonstrated no difference in risk of access loss in preemptive stenosis correction in AVF or AVG without evidence of access dysfunction. However, on subgroup analysis this review did demonstrate a small benefit regarding risk of thrombosis and access loss in the AVF group.46
The physical examination may indicate evidence of vascular access stenosis or thrombosis. Evidence of stenosis may be indicated by failure of the outflow vein to collapse on arm raise test (distal stenosis), hyperpulsatility or hypopulsatility, loss of the diastolic component of the normal continuous thrill and bruit with only systolic components appreciated, and arm edema (central vein stenosis).43,47 Thrombosis of the vein may be evidenced by complete loss of the thrill and pulsatility on palpation. Sensitivity and specificity of the physical examination for inflow or outflow stenosis has been reported to be between 70% to 92% and 71% to 100%, respectively.48-50
While evidence may or may not support preemptive correction of stenosis, interventions are usually required when the stenosis is more than 50% and interferes with dialysis, decreased flow, abnormal physical examination, or elevated venous pressures.51 If stenosis is associated with interference of effective dialysis or thrombosis is suspected, ultrasound imaging and consultation with a vascular surgeon or interventional radiologist are indicated. Treatment of AVF or AVG stenosis and thrombosis includes percutaneous and surgical interventions.52
A systematic review by Tanner and da Silva53 evaluating adjuvant medical treatments for increasing patency rates of AVF and AVG found no therapy had any improvement in patency rates at 1 month. Another review from 2015 by Palmer et al54 suggested antiplatelet therapy may be protective for stenosis and thrombosis in AVF, but not AVG.
Infection
Infection in patients with ESRD is a major cause of morbidity and mortality, and 24% of these infections may be attributed to the vascular access itself, including central venous catheters (CVC).55 Central venous catheters are associated with the highest rate of infection, followed by AVGs, then AVFs.4,54 Studies have reported 9.5% vs 0.4% to 0.9% infection rates for AVG and AVF, respectively.2,4 These infections are usually due to gram-positive organisms, with the Staphylococcus species being the most common organism involved.55-57 However, infections caused by gram-negative organisms are possible, and broad-spectrum antibiotics should be initiated in the ED if infection is suspected. Patients may present with localized infection with increased risk of rupture of access to profound sepsis. Definitive treatment of an infected graft or fistula usually requires removal of the infected access or at least partial excision with possible interposition of additional graft material.58
Pseudoaneurysm/Aneurysm
Pseudoaneuryms are usually caused by hematoma development after needle puncture or in juxta-anastomic segments postoperatively. Pseudoaneurysms do not have a true wall and may secondarily become infected.59 Pseudoaneurysms occur more frequently in AVG, and are usually reported along with true aneurysms. One study by Al-Thani et al60 detected pseudoaneurysms in 15% of clinically significant aneurysms.
Approximately 30% to 60% of patients with AVFs will develop an aneurysm.2,5 One study by Al-Thani et al60 reported the need for surgical intervention in 31% of patients with an AVF in whom an aneurysm was detected. The risk for developing an aneurysm is highest for those patients on high flux membrane type HD and polycystic kidney disease.5 As discussed earlier in this article, cannulation sites and techniques may also influence aneurysmal changes in the fistula. Aneurysm formation at the site of previous cannulation site should not be re-cannulated.18 Aneurysmal changes can contribute to other complications including high-output heart failure, thrombosis with fistula or graft failure, increased risk of bleeding, ineffective HD when associated with thrombosis or stenosis, pain and peripheral neuropathies secondary to compression of nearby nerves, and interference with functional HD.
Many asymptomatic aneurysmal changes to vascular access may not compromise access function. If a patient is identified with a vascular access pseudoaneurysm or aneurysmal changes with high-risk features, early referral to vascular surgeon for surgical interventions is imperative. High-risk features include any of the complications previously discussed—infection, threatened overlying skin, or shiny appearance. The EP should consider duplex imaging to assist with evaluation. Treatment may include ligation of the AVF, partial resection, stenting, or grafting of the aneurysm with hopes of salvaging the vascular access.61,62
Ischemic Monomelic Neuropathy
Ischemic monomelic neuropathy may result secondary to a type of steal phenomenon, thereby inducing ischemia to supplied nerves. Ischemic monomelic neuropathy has been described in many case reports and narrative reviews.63-67 It has been described as ischemia or infarction of the blood supply to the nerves (vasa nervosa) in the lower arm.68 Ischemic monomelic neuropathy typically occurs immediately after the vascular access creation in the postoperative period. Therefore, it is unlikely to be seen in the ED but as patients may have sequelae of this complication, EPs should be aware of its existence. Patients with ischemic monomelic neuropathy will have severe pain, paresthesia, and weakness immediately after placement of a vascular access. Patients also typically have sensorimotor deficits in the radial, ulnar, and median nerves. Pulses should be preserved. Severe neuropathic pain will develop and may limit the examination. Clinical diagnosis may be difficult immediately after surgery because patients will often have minor deficits secondary to the surgical procedure itself or secondary to the regional block provided by anesthesia, but nerve-conduction studies usually reveal the diagnosis. The treatment is ligation of the access immediately and prognosis is variable, depending on the severity and duration of ischemia, and may result in complete loss of function of the hand.
Steal Syndrome
Dialysis access-associated steal syndrome is a type of distal ischemia secondary to the vascular access site with a reported incidence of 6.2%, and appears to occur more frequently in AVF than AVGs.69,70 Diabetes appears to be a strong risk factor for developing DASS.71 Patients with DASS can present with classic ischemic symptoms such as pain, paresthesia, claudication, pallor, and diminished or absent arterial pulse. Pain may be present only while undergoing dialysis or exercising, or symptoms may be persistent.68,72 There are several possible causes of DASS, including arterial occlusion or insufficiency proximal or distal to the anastomosis, increased flow through the conduit (true steal), or increased flow diverted through collateral vessels.73,74 One clue to the diagnosis is a diminished or absent radial pulse that should improve with compression of the access site.
Once DASS is suspected, diagnosis should be confirmed using venous duplex scanning with finger pressure waveform analysis or arteriogram. Definitive management is surgical intervention with ligation of the access or banding.
High-Output Heart Failure
Changes in cardiac output (CO) are a well-documented effect of AVF placement, with one small study by Korsheed et al75 demonstrating an average increase in CO of 17% only 2 weeks after AVF placement. The increase in CO is thought to be secondary to alterations in systemic vascular resistance and sympathetic activity. While an increase in CO can ultimately lead to high-output heart failure, this is typically only seen in patients with pre-existing cardiac dysfunction.76 Patients are at an increased risk of high-output heart failure when flow through the AVF exceeds 2 L/min; flows below this rate are typically not associated with adverse cardiac effects.77 Another objective measurement for identifying patients at risk of high-output heart failure is the ratio of flow in the fistula (Qa) to cardiac output ratio. Patients with a Qa:CO ratio greater than 0.3 have a significantly increased risk of high-output heart failure.78 There is thought to be no difference in risk of heart failure between AVF and AVG.79
Once overt heart failure has developed, it should be treated in the usual fashion, with IV fluid management and standard pharmacological therapies. If standard conservative heart failure treatment is ineffective, several surgical options are available, including banding, changing the location of the anastomosis, and ultimately closing the fistula.80
Conclusion
While life-threatening bleeding and vascular access rupture are uncommon complications of AVFs and AVGs, it is essential for the EP to rapidly treat the potentially catastrophic hemorrhagic vascular access complications. Depending on the severity and stability of the patient, it is reasonable to begin in a stepwise fashion as presented in this article for patients with minor bleeding, while more severe or persistent bleeding may require several interventions simultaneously to gain control of the bleeding.
Patients with hemodynamic instability requiring transfusion will need a vascular surgery consult and admission. Disposition for stable patients, without evidence of impending aneurysmal related rupture and concern for overlying infection or other complication requiring immediate intervention, will depend on clinical judgment, patient-specific factors and family support, follow-up, and proximity of the patient to medical care.
According to the National Institute of Diabetes and Digestive and Kidney Diseases, approximately 468,000 persons in the United States are on dialysis—a number that continues to grow annually.1 The 1-year rate for hemorrhagic complications from arteriovenous fistulas (AVFs) is estimated to be 0.4%.2 One study by Ellingson et al3 reported 1,654 deaths secondary to fatal vascular access hemorrhage over a 6-year period, accounting for 0.4% of all deaths of hemodialysis (HD) patients in that study.3
Nonhemorrhagic vascular access-related complications also contribute to the morbidity and mortality associated with AVFs and arteriovenous grafts (AVGs). Venous stenosis resulting in thrombosis has been estimated to occur in 24.7% of AVGs and 9.0% of AVFs, both of which are common causes of access failure.
Infection is reported to be the second leading cause of death in dialysis patients, and vascular access-related infection rates are reported to occur in 9.5% of AVGs vs 0.4% to 0.9% of AVFs.2,4 Pseudoaneurysms and aneurysms range from 30% to 60% for AVFs,2,5 and contribute to morbidity by limiting available areas to cannulate for dialysis, occasionally requiring surgical revision to restore access function or prevent access rupture.
Steal phenomena, including dialysis access-induced steal syndrome (DASS) and ischemic monomelic neuropathy, as well as heart failure secondary to high output are additional contributors to morbidity and mortality.
With the growing rate of end-stage renal disease (ESRD) in the United States and the contribution to morbidity and mortality by bleeding and other complications, it is essential to understand how to evaluate and treat these patients in the ED. This article reviews the evaluation and treatment of vascular access emergencies, as well as risk factors that contribute to complications in the ESRD patient population.
Hemorrhagic Complications of Vascular Access
Risk Factors
Many patients with ESRD have multiple comorbidities such as coronary artery disease and atrial fibrillation that require anticoagulation, antiplatelet medications, or both. Studies have shown that ESRD patients taking warfarin have an increase in major bleeding episodes of 3.1% per person-year and 4.4% per person-year for those taking aspirin alone, while those taking both medications have an increased bleeding risk of 6.3% per person-year.6 A recent systematic review by Elliott et al7 has suggested a 2-fold increase in bleeding rates in HD patients anticoagulated with warfarin as compared to HD patients not on warfarin.
While uremia secondary to chronic kidney disease (CKD) is a well-known facilitator of bleeding complications, the underlying pathophysiology is not yet completely delineated. However, there are some general underlying principles that may help in understanding the best treatment modalities available at this time. As the kidneys fail, uremic toxins accumulate in the bloodstream. These toxins include urea, creatinine, and phenolic acids, which are believed to interfere with primary hemostasis by effecting platelet adherence to endothelium, platelet activation, and aggregation.8 Functional defects are created in the interactions between the glycoprotein Ib (GPIb) receptor and von Willebrand factor (vWF), which are essential to endothelial adhesion of platelets.9 Additionally, these toxins impair the up regulation of the GPIIbIIIa receptor which is integral to platelet aggregation.10 Platelet activation normally leads to platelet aggregation by increasing production of thromboxane A2 (TXA2) and serotonin that are released from storage granules.10 Some toxins may increase nitric oxide (NO) synthesis, effectively reducing aggregation by decreasing TXA2 and adenosine diphosphate (ADP) levels.11 In addition, elevated levels of fibrinogen fragments have also recently been shown to inhibit platelet function by competing with fibrinogen for the GPIIbIIIa receptor with decreasing levels demonstrated after HD.12
Finally, increased pressure in the venous outflow segment also increases persistent bleeding from puncture sites. These pressures may be exaggerated secondary to venous thrombosis, venous stenosis, pseudoaneurysm, aneurysm, or infection.13 The following sections further describe the evaluation and treatment of these complications.
Clinical Presentation
Patients presenting with bleeding from the vascular access site may present with slow continuous oozing from the needle puncture-site itself or with life-threatening hemorrhage secondary to AVF or AVG rupture.14 The incidence of vascular access rupture is unknown, but it appears the majority of ruptures occur in patients with AVG vs AVF.3 However, several case reports have also described hemorrhagic complications of AVF ruptures.15-17 The risk of rupture may be associated with the development of aneurysms or pseudoaneuryms.18 Possible impending perforation may be signaled by skin thinning or a shiny appearance overlying the aneurysm, or evidence of infection overlying the access site.3 Many patients were shown to have complications such as stenosis, thrombosis, or infection within 6 months prior to rupture.3 Education of patients is also important as most hemorrhages occur prior to hospital arrival.3,19
Evaluation in the ED
As with any patient presenting to the ED, the initial evaluation of an unstable patient experiencing bleeding from a vascular access site includes assessing the airway, breathing, and circulation as a first priority—paying special attention to the area of bleeding while simultaneously preparing for possible intervention. It is also important to determine when the patient last underwent dialysis and if he or she was able to complete HD. This information will identify patients who are candidates for reversing the heparin load likely given during dialysis.
It is also important to note that some patients undergoing HD who have already been identified as having an increased risk of bleeding may not receive heparin or may undergo local heparinization, minimal heparinization, or regional citrate anticoagulation during dialysis, in which case protamine is not indicated.14 The emergency physician (EP) must also determine if the patient is on any antiplatelet or anticoagulation agents.
The vascular access site should be inspected for evidence of aneurysmal changes, infection, and skin thinning as these factors increase the risk of bleeding and vascular rupture. Additionally auscultation and palpation of the vascular access site should be performed to evaluate for other potential complications such as stenosis and thrombosis. Lastly, the EP should anticipate the patient’s need for HD in the setting of a potentially unavailable AVG or AVF to determine whether the patient may need an alternative access.
Treatment and Management
The primary responsibility during the initial treatment of a bleeding access site is to stop further blood loss by utilizing methods that employ direct pressure or, in extreme cases, application of a tourniquet, followed by other interventions such as fluid and blood-product resuscitation; coagulopathy reversal; consideration of desmopressin, cryoprecipitate, tranexamic acid (TXA); HD; and vascular repair.
Control of a bleeding dialysis access-site is a balancing act of adequately controlling the bleeding while maintaining the integrity of the fistula. Overly aggressive management may cause thrombosis in the vascular access site, which is associated with morbidity—eg, site revisions, potential for the need to create a new access site. On the opposite end of the spectrum, failing to adequately control bleeding can lead to significant anemia ranging from minimal symptoms to hemodynamic compromise and death.
Peripheral Venous Access
While peripheral venous access is notoriously difficult in patients with ESRD, it is essential for the resuscitation of hemorrhaging patients. Ideally, two large bore peripheral intravenous (IV) lines should be placed in the proximal upper extremities. If peripheral venous access is not achieved, central venous access or interosseous access placement is indicated (Figure).
Direct Pressure
With low-volume bleeding, the first attempt to control the bleeding is simple direct pressure. Except in the instance of trauma or self-inflicted injury, bleeding usually occurs at the site of cannulation of the vascular access post-HD. Direct pressure should be light and limited to as small of an area as possible to prevent thrombosis; the force and area encompassed by direct pressure can be expanded as needed for bleeding that is more difficult to control. In cases of higher volume bleeding, pressure should be placed both proximally and distally to the shunt due to its bidirectional flow. Another possible temporizing measure is to place an upright gallipot or cup over the bleeding site on top of a folded piece of gauze and then securing it with tape.21
Topical Hemostatic Agents
Second simple direct pressure, topical hemostatic agents may be a good adjunct to help obtain hemostasis. There is a wide range of products available, from procoagulants (eg, Combat Gauze, topical thrombin) to factor concentrators (eg, QuikClot). These can be used directly on the bleeding site and only in conjunction with direct pressure.
In addition to topical hemostatic agents, another option is skin glue, which should be applied generously after bleeding has been temporized, with pressure both proximally and distally to the site.
Anticoagulation Reversal
As previously mentioned, it is important to determine when the patient’s last HD was. Heparin is used during dialysis to prevent clotting within the circuit, and although clotting times are monitored during dialysis to guide anticoagulation, it is possible that a patient bleeding after dialysis could still have therapeutic levels of heparin requiring reversal with protamine.
The recommended dose of protamine is 1 mg for every 100 U of heparin given during dialysis; protamine should be administered over 10 minutes. Alternatively, a 10- to 20-mg dose of protamine can be given if the amount of heparin administered during HD is unknown. Additionally, the patient’s medication list, as with any ED presentation, should be carefully reviewed as many dialysis patients have comorbidities requiring anticoagulation with potentially reversible agents.
Hemodialysis to Improve Platelet Dysfunction
It is thought that long-term exposure of platelets to the dialysis membrane can lead to chronic platelet activation leading to platelet dysfunction. There is conflicting data regarding the effects of HD on improving bleeding in renal patients.9,22,23 Hemodialysis is thought to be beneficial, at least partially, through reversing uremia, thus improving platelet function.24 Therefore, in the stable bleeding patient who missed a scheduled dialysis, initiating HD in the ED setting could be beneficial. If the vascular access site is deemed unsafe for HD, another access site must be obtained, for example, by placing a temporary central venous catheter that will allow for successful HD.
Desmopressin
Desmopressin acetate has been shown to reduce bleeding time in uremic patients by releasing vWF and factor VIII into plasma, taking effect within 1 hour and lasting 4 to 8 hours.25-27 Desmopressin has also been shown to reduce blood loss and bleeding times in patients with platelet dysfunction undergoing cardiac surgery.28 While the underlying mechanism is unclear, desmopressin acetate is thought to help with platelet adhesion to the endothelial wall.
Alternatively, one study by Soslau et al29 has suggested that desmopressin may increase serotonin uptake by platelets and increase adenosine triphosphate release, thereby facilitating platelet aggregation. The dosing of desmopressin is 0.2 to 0.3 mcg/kg IV.30 Adverse effects include facial flushing, mild headache, and transient small decrease in blood pressure (BP) with increase in heart rate. Historically, it was thought that desmopressin could lead to water retention, volume overload, congestive heart failure, and hyponatremia; however, these adverse effects have not been seen in uremic patients.30 Tachyphylaxis may occur after just a few doses of desmopressin are given.31 Additionally, hyponatremia and seizures have been seen after repeated administration in children.31
Anemia and Low Hematocrit
As mentioned earlier, anemia and low hematocrit (HCT) may actually exacerbate bleeding tendencies by decreasing the number of platelets exposed to the vessel wall. Red blood cells (RBCs) also produce TXA2 and ADP, both of which play vital roles in normal platelet aggregation. Secondly, RBCs have been shown to increase NO uptake. Nitric oxide is a potent vasodilator and inhibitor of platelet aggregation. The degree of uptake appears to be augmented by increasing HCT levels.32 A goal HCT of greater than 30% has been suggested and demonstrated benefit.33
Cryoprecipitate
Cryoprecipitate is rich in fibrinogen and vWF. Its mechanism is thought to be secondary to increasing functional vWF levels and possibly fibrinogen levels. While the overall effects appear to be variable, studies suggest 10 U of cryoprecipitate is adequate to reverse significant bleeding with resolution of effect at 24 hours.34,35 Given the risks of adverse reactions, variable responses, and risks of hepatitis C and HIV transmission, this therapy must be used cautiously with risk-benefit analysis.
Tranexamic Acid
Tranexamic acid is an antifibrinolytic agent that binds to fibrinogen as a competitive inhibitor of plasmin, inhibiting plasminogen activation. The trauma literature has shown TXA to significantly reduce all-cause mortality.36 It has also been shown to be beneficial in the bleeding uremic patient.37-39
However, it is important to keep in mind that the clearance of TXA in patients with renal disease is unclear. One study by Andersson et al40 demonstrated that TXA has increased plasma concentrations in patients with renal impairment, and a generally accepted practice is to renal-dose this medication. This study recommended a dose of 10 mg/kg IV at varying intervals, such as once daily, twice daily, or every 48 hours depending on the creatinine value, compared to patients with no renal impairment.40 Another study by Sabovic et al39 that evaluated the effects of TXA on gastrointestinal bleeding in patients with renal impairment used a 20-mg IV loading dose of TXA followed by 10 mg/kg orally every 48 hours. Though no adverse events occurred in this study, the study group was small. Other studies have not shown an increase in thromboembolic risk in patients who have no renal disease.36,41
At this time, there is no consensus on the exact dosing of TXA in this patient population. Therefore, this therapy should only be considered if others have failed and the patient continues to have significant blood loss.
Life-threatening Hemorrhage
If a patient is experiencing life-threatening blood loss, more aggressive measures must be employed regardless of risk of damage to the access. In such cases, a consultation with vascular surgery services should be obtained as early as possible. If none of the previously discussed measures are ineffective, the EP may be required to place sutures in the vascular access itself or apply a tourniquet. Again, these interventions may cause permanent damage to the access; however, in the setting of life-threatening hemorrhage such interventions clearly outweigh the risks associated with continued blood loss.
As blood can flow bidirectionally within a fistula, a tourniquet should be placed both proximally and distally to the fistula to obtain adequate hemostasis. Once the tourniquets are in place, if there is no immediate surgical consultation available, the EP may need to temporarily repair the defect to allow minimal tourniquet time. There are a few considerations when placing sutures. Ideally, a noncutting needle should be used to minimize damage. An adequate-sized suture, such as a 3-0 nylon suture, should be used to maintain strength in the high-pressure system. A figure-8 suture or purse-string suture may be placed around the defect. Adequate repair should allow for tourniquet removal.
Hemodynamic Status
The EP must remain aware of the patient’s hemodynamic status. Massive transfusion protocols may need to be initiated. Best current evidence dictates that this should be done in a 1:1:1 ratio of packed red blood cells, platelets, and fresh frozen plasma respectively.42 In our experience, the EP should consider permissive hypotension as aggressive resuscitation and increasing BP can compromise the vascular repair.
Lastly, transfer for definitive management should be arranged if not available at the EP’s institution. The patient should travel with tourniquets in place (although not tightened) in the event of further bleeding.
Nonhemorrhagic Complications of AVF or AVG
Stenosis/Thrombosis
Prolonged bleeding from the cannulation site may suggest outflow stenosis.43 Stenosis with or without subsequent thrombosis is a common cause of vascular access failure. Access failure has also been implicated secondary to poor vascular mapping, resulting in undetected pre-existing stenosis of the inflow artery, outflow vein, or juxta-anastomosis. However, development of stenosis may occur at any time throughout the life of the vascular access. One study by Schild et al4 reported thrombosis rates of 24.7% for grafts and 9.0% for fistula. Additionally, AVGs have a higher reported stenosis rate than AVFs, which is a risk factor for thrombosis.44,45
There has been much debate regarding routine surveillance to prevent clinically significant stenosis with subsequent thrombosis. Surveillance includes a clinical examination, Doppler imaging studies, and flow measurements during dialysis. A recent systematic review from 2016 by Ravani et al,46 demonstrated no difference in risk of access loss in preemptive stenosis correction in AVF or AVG without evidence of access dysfunction. However, on subgroup analysis this review did demonstrate a small benefit regarding risk of thrombosis and access loss in the AVF group.46
The physical examination may indicate evidence of vascular access stenosis or thrombosis. Evidence of stenosis may be indicated by failure of the outflow vein to collapse on arm raise test (distal stenosis), hyperpulsatility or hypopulsatility, loss of the diastolic component of the normal continuous thrill and bruit with only systolic components appreciated, and arm edema (central vein stenosis).43,47 Thrombosis of the vein may be evidenced by complete loss of the thrill and pulsatility on palpation. Sensitivity and specificity of the physical examination for inflow or outflow stenosis has been reported to be between 70% to 92% and 71% to 100%, respectively.48-50
While evidence may or may not support preemptive correction of stenosis, interventions are usually required when the stenosis is more than 50% and interferes with dialysis, decreased flow, abnormal physical examination, or elevated venous pressures.51 If stenosis is associated with interference of effective dialysis or thrombosis is suspected, ultrasound imaging and consultation with a vascular surgeon or interventional radiologist are indicated. Treatment of AVF or AVG stenosis and thrombosis includes percutaneous and surgical interventions.52
A systematic review by Tanner and da Silva53 evaluating adjuvant medical treatments for increasing patency rates of AVF and AVG found no therapy had any improvement in patency rates at 1 month. Another review from 2015 by Palmer et al54 suggested antiplatelet therapy may be protective for stenosis and thrombosis in AVF, but not AVG.
Infection
Infection in patients with ESRD is a major cause of morbidity and mortality, and 24% of these infections may be attributed to the vascular access itself, including central venous catheters (CVC).55 Central venous catheters are associated with the highest rate of infection, followed by AVGs, then AVFs.4,54 Studies have reported 9.5% vs 0.4% to 0.9% infection rates for AVG and AVF, respectively.2,4 These infections are usually due to gram-positive organisms, with the Staphylococcus species being the most common organism involved.55-57 However, infections caused by gram-negative organisms are possible, and broad-spectrum antibiotics should be initiated in the ED if infection is suspected. Patients may present with localized infection with increased risk of rupture of access to profound sepsis. Definitive treatment of an infected graft or fistula usually requires removal of the infected access or at least partial excision with possible interposition of additional graft material.58
Pseudoaneurysm/Aneurysm
Pseudoaneuryms are usually caused by hematoma development after needle puncture or in juxta-anastomic segments postoperatively. Pseudoaneurysms do not have a true wall and may secondarily become infected.59 Pseudoaneurysms occur more frequently in AVG, and are usually reported along with true aneurysms. One study by Al-Thani et al60 detected pseudoaneurysms in 15% of clinically significant aneurysms.
Approximately 30% to 60% of patients with AVFs will develop an aneurysm.2,5 One study by Al-Thani et al60 reported the need for surgical intervention in 31% of patients with an AVF in whom an aneurysm was detected. The risk for developing an aneurysm is highest for those patients on high flux membrane type HD and polycystic kidney disease.5 As discussed earlier in this article, cannulation sites and techniques may also influence aneurysmal changes in the fistula. Aneurysm formation at the site of previous cannulation site should not be re-cannulated.18 Aneurysmal changes can contribute to other complications including high-output heart failure, thrombosis with fistula or graft failure, increased risk of bleeding, ineffective HD when associated with thrombosis or stenosis, pain and peripheral neuropathies secondary to compression of nearby nerves, and interference with functional HD.
Many asymptomatic aneurysmal changes to vascular access may not compromise access function. If a patient is identified with a vascular access pseudoaneurysm or aneurysmal changes with high-risk features, early referral to vascular surgeon for surgical interventions is imperative. High-risk features include any of the complications previously discussed—infection, threatened overlying skin, or shiny appearance. The EP should consider duplex imaging to assist with evaluation. Treatment may include ligation of the AVF, partial resection, stenting, or grafting of the aneurysm with hopes of salvaging the vascular access.61,62
Ischemic Monomelic Neuropathy
Ischemic monomelic neuropathy may result secondary to a type of steal phenomenon, thereby inducing ischemia to supplied nerves. Ischemic monomelic neuropathy has been described in many case reports and narrative reviews.63-67 It has been described as ischemia or infarction of the blood supply to the nerves (vasa nervosa) in the lower arm.68 Ischemic monomelic neuropathy typically occurs immediately after the vascular access creation in the postoperative period. Therefore, it is unlikely to be seen in the ED but as patients may have sequelae of this complication, EPs should be aware of its existence. Patients with ischemic monomelic neuropathy will have severe pain, paresthesia, and weakness immediately after placement of a vascular access. Patients also typically have sensorimotor deficits in the radial, ulnar, and median nerves. Pulses should be preserved. Severe neuropathic pain will develop and may limit the examination. Clinical diagnosis may be difficult immediately after surgery because patients will often have minor deficits secondary to the surgical procedure itself or secondary to the regional block provided by anesthesia, but nerve-conduction studies usually reveal the diagnosis. The treatment is ligation of the access immediately and prognosis is variable, depending on the severity and duration of ischemia, and may result in complete loss of function of the hand.
Steal Syndrome
Dialysis access-associated steal syndrome is a type of distal ischemia secondary to the vascular access site with a reported incidence of 6.2%, and appears to occur more frequently in AVF than AVGs.69,70 Diabetes appears to be a strong risk factor for developing DASS.71 Patients with DASS can present with classic ischemic symptoms such as pain, paresthesia, claudication, pallor, and diminished or absent arterial pulse. Pain may be present only while undergoing dialysis or exercising, or symptoms may be persistent.68,72 There are several possible causes of DASS, including arterial occlusion or insufficiency proximal or distal to the anastomosis, increased flow through the conduit (true steal), or increased flow diverted through collateral vessels.73,74 One clue to the diagnosis is a diminished or absent radial pulse that should improve with compression of the access site.
Once DASS is suspected, diagnosis should be confirmed using venous duplex scanning with finger pressure waveform analysis or arteriogram. Definitive management is surgical intervention with ligation of the access or banding.
High-Output Heart Failure
Changes in cardiac output (CO) are a well-documented effect of AVF placement, with one small study by Korsheed et al75 demonstrating an average increase in CO of 17% only 2 weeks after AVF placement. The increase in CO is thought to be secondary to alterations in systemic vascular resistance and sympathetic activity. While an increase in CO can ultimately lead to high-output heart failure, this is typically only seen in patients with pre-existing cardiac dysfunction.76 Patients are at an increased risk of high-output heart failure when flow through the AVF exceeds 2 L/min; flows below this rate are typically not associated with adverse cardiac effects.77 Another objective measurement for identifying patients at risk of high-output heart failure is the ratio of flow in the fistula (Qa) to cardiac output ratio. Patients with a Qa:CO ratio greater than 0.3 have a significantly increased risk of high-output heart failure.78 There is thought to be no difference in risk of heart failure between AVF and AVG.79
Once overt heart failure has developed, it should be treated in the usual fashion, with IV fluid management and standard pharmacological therapies. If standard conservative heart failure treatment is ineffective, several surgical options are available, including banding, changing the location of the anastomosis, and ultimately closing the fistula.80
Conclusion
While life-threatening bleeding and vascular access rupture are uncommon complications of AVFs and AVGs, it is essential for the EP to rapidly treat the potentially catastrophic hemorrhagic vascular access complications. Depending on the severity and stability of the patient, it is reasonable to begin in a stepwise fashion as presented in this article for patients with minor bleeding, while more severe or persistent bleeding may require several interventions simultaneously to gain control of the bleeding.
Patients with hemodynamic instability requiring transfusion will need a vascular surgery consult and admission. Disposition for stable patients, without evidence of impending aneurysmal related rupture and concern for overlying infection or other complication requiring immediate intervention, will depend on clinical judgment, patient-specific factors and family support, follow-up, and proximity of the patient to medical care.
1. National Institute of Diabetes and Digestive and Kidney Diseases. Kidney disease statistics for the United States. https://www.niddk.nih.gov/health-information/health-statistics/Pages/kidney-disease-statistics-united-states.aspx. Accessed August 24, 2017.
2. Salahi H, Fazelzadeh A, Mehdizadeh A, Razmkon A, Malek-Hosseini SA. Complications of arteriovenous fistula in dialysis patients. Transplant Proc. 2006;38(5):1261-1264. doi:10.1016/j.transproceed.2006.02.066.
3. Ellingson KD, Palekar RS, Lucero CA, et al. Vascular access hemorrhages contribute to deaths among hemodialysis patients. Kidney Int. 2012;82(6):686-692. doi:10.1038/ki.2012.185.
4. Schild AF, Perez E, Gillaspie E, Seaver C, Livingstone J, Thibonnier A. Arteriovenous fistulae vs. arteriovenous grafts: a retrospective review of 1,700 consecutive vascular access cases. J Vasc Access. 2008;9(4):231-235.
5. Jankovic A, Donfrid B, Adam J, et al. Arteriovenous fistula aneurysm in patients on regular hemodialysis: prevalence and risk factors. Nephron Clin Pract. 2013;124(1-2):94-98. doi:10.1159/000355548.
6. Holden RM, Harman GJ, Wang M, Holland D, Day AG. Major bleeding in hemodialysis patients. Clin J Am Soc Nephrol. 2008 Jan;3(1):105-110. doi:10.2215/CJN.01810407.
7. Elliott MJ, Zimmerman D, Holden RM. Warfarin anticoagulation in hemodialysis patients: a systematic review of bleeding rates. Am J Kidney Dis. 2007;50(3):433-440. doi:10.1053/j.ajkd.2007.06.017.
8. Jubelirer SJ. Hemostatic abnormalities in renal disease. Am J Kidney Dis. 1985;5(5):219-225.
9. Salvati F, Liani M. Role of platelet surface receptor abnormalities in the bleeding and thrombotic diathesis of uremic patients on hemodialysis and peritoneal dialysis. Int J Artif Organs. 2001;24(3):131-135.
10. Kaw D, Malhotra D. Platelet dysfunction and end-stage renal disease. Semin Dial. 2006;19(4):317-322. doi:10.1111/j.1525-139X.2006.00179.x.
11. Hedges SJ, Dehoney SB, Hooper JS, Amanzadeh J, Busti AJ. Evidence-based treatment recommendations for uremic bleeding. Nat Clin Pract Nephrol. 2007;3(3):138-153. doi:10.1038/ncpneph0421.
12. Thekkedath UR, Chirananthavat T, Leypoldt JK, Cheung AK, Mohammad SF. Elevated fibrinogen fragment levels in uremic plasma inhibit platelet function and expression of glycoprotein IIb-IIIa. Am J Hematol. 2006;81(12):915-926. doi:10.1002/ajh.20720.
13. Padberg FT, Calligaro KD, Sidawy AN. Complications of arteriovenous hemodialysis access: recognition and management. J Vasc Surg. 2008;48(5 Suppl):S55-S80. doi:10.1016/j.jvs.2008.08.067.
14. Lohr JW, Schwab SJ. Minimizing hemorrhagic complications in dialysis patients. J Am Soc Nephrol. 1991;2(5):961-975.
15. Yang TH, Lee CH, Tsai CS, Tsai YT. Successful surgical treatment of a rupture to an arteriovenous fistula aneurysm. Cardiovasc J Afr. 2009;20(3):196-197.
16. Caksen HH, Odabaş D, Arslan S, Kaya A. Spontaneous rupture of arteriovenous fistula in a chronic dialysis patient. J Emerg Med. 2003;24(2):224-225. doi:10.1016/S0736-4679(02)00744-8.
17. Saeed F, Kousar N, Sinnakirouchenan R, Ramalingam VS, Johnson PB, Holley JL. Blood loss through AV fistula: a case report and literature review. Int J Nephrol. 2011;2011:350870. doi:10.4061/2011/350870.
18. NKF KDOQI Guidelines. Clinical practice guidelines for vascular access. Guideline 5. Treatment of fistula complications. Available at http://www2.kidney.org/professionals/kdoqi/guideline_uphd_pd_va/va_guide5.htm. Accessed August 24, 2017.
19. Gill JR, Storck K, Kelly S. Fatal exsanguination from hemodialysis vascular access sites. Forensic Sci Med Pathol. 2012;8(3):259-262. doi:10.1007/s12024-011-9303-0.
20. Manning MA. Use of dialysis access in emergent situations. J Emerg Nurs. 2008;34(1):37-40. doi:10.1016/j.jen.2007.03.018.
21. Reddy VM, Bagul A, Qureshi AA, Nicholson ML. A simple technique to control a bleeding arteriovenous fistula. Ann R Coll Surg Engl. 2006;88(6):592-593. doi:10.1308/003588406X130714f.
22. Oudemans-van Straaten HM. Hemostasis and thrombosis in continuous renal replacement treatment. Semin Thromb Hemost. 2015;41(1):91-98. doi:10.1055/s-0034-1398384.
23. Casserly LF, Dember LM. Thrombosis in end-stage renal disease. Semin Dial. 2003;16(3):245-256. doi:10.1046/j.1525-139X.2003.16048.x.
24. Boccardo P, Remuzzi G, Galbusera M. Platelet dysfunction in renal failure. Semin Thromb Hemost. 2004;30(5):579-589. doi:10.1055/s-2004-835678.
25. Mannucci PM, Remuzzi G, Pusineri F, et al. Deamino-8-D-arginine vasopressin shortens the bleeding time in uremia. N Engl J Med. 1983;308(1):8-12. doi:10.1056/NEJM198301063080102.
26. Ho SJ, Gemmell R, Brighton TA. Platelet function testing in uraemic patients. Hematology. 2008;13(1):49-58. doi:10.1179/102453308X315834.
27. Showalter J, Nguyen ND, Baba S, et al. Platelet aggregometry cannot identify uremic platelet dysfunction in heart failure patients prior to cardiac surgery. J Clin Lab Anal. 2016:1-5. doi:10.1002/jcla.22084.1308/003588406X130714f.
28. Wademan BH, Galvin SD. Desmopressin for reducing postoperative blood loss and transfusion requirements following cardiac surgery in adults. Interact Cardiovasc Thorac Surg. 2014;18(3):360-370. doi:10.1093/icvts/ivt491.
29. Soslau G, Schwartz AB, Putatunda B, et al. Desmopressin-induced improvement in bleeding times in chronic renal failure patients correlates with platelet serotonin uptake and ATP release. Am J Med Sci. 1990;300(6):372-379. http://www.ncbi.nlm.nih.gov/pubmed/2264575. Accessed January 31, 2017.
30. Lethagen S. Desmopressin (DDAVP) and hemostasis. Ann Hematol. 1994;69(4):173-180.
31. Mannucci PM. Hemostatic drugs. N Engl J Med. 1998;339(4):245-253. doi:10.1056/NEJM199807233390407.
32. Azarov I, Huang KT, Basu S, Gladwin MT, Hogg N, Kim-Shapiro DB. Nitric oxide scavenging by red blood cells as a function of hematocrit and oxygenation. J Biol Chem. 2005;280(47):39024-39032. doi:10.1074/jbc.M509045200.
33. Livio M, Marchesi D, Remuzzi G, Gotti E, Mecca G, De Gaetano G. Uraemic bleeding: role of anaemia and beneficial effect of red cell transfusions. Lancet. 1982;320(8306):1013-1015. doi:10.1016/S0140-6736(82)90050-2.
34. Janson PA, Jubelirer SJ, Weinstein MJ, Deykin D. Treatment of the bleeding tendency in uremia with cryoprecipitate. N Engl J Med. 1980;303(23):1318-1322. doi:10.1056/NEJM198012043032302.
35. Triulzi DJ, Blumberg N. Variability in response to cryoprecipitate treatment for hemostatic defects in uremia. Yale J Biol Med. 1990;63(1):1-7.
36. Roberts I, Shakur H, Coats T, et al. The CRASH-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Heal Technol Assess. 2013;17(10):1-79. doi:10.3310/hta17100.
37. Mezzano D, Panes O, Muñoz B, et al. Tranexamic acid inhibits fibrinolysis, shortens the bleeding time and improves platelet function in patients with chronic renal failure.Thromb Haemost. 1999;82(4):1250-1254.
38. Mezzano D, Muñoz B, Pais E, Downey P, Pereira J. Fast decrease of bleeding time by tranexamic acid in uremia. Thromb Haemost. 2000;83(5):785.
39. Sabovic M, Lavre J, Vujkovac B. Tranexamic acid is beneficial as adjunctive therapy in treating major upper gastrointestinal bleeding in dialysis patients. Nephrol Dial Transplant. 2003;18(7):1388-1391. doi:10.1093/ndt/gfg117.
40. Andersson L, Eriksson O, Hedlund PO, Kjellman H, Lindqvist B. Special considerations with regard to the dosage of tranexamic acid in patients with chronic renal diseases. Urol Res. 1978;6(2):83-88.
41. Bennett C, Klingenberg SL, Langholz E, Gluud LL. Tranexamic acid for upper gastrointestinal bleeding. Cochrane Database Syst Rev. 2014;(11):CD006640. doi: 10.1002/14651858.CD006640.pub3.
42. Holcomb JB, Tilley BC, Baraniuk S, et al; PROPPR Study Group. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313(5):471-482. doi:10.1001/jama.2015.12.
43. Salman L, Beathard G. Interventional nephrology: physical examination as a tool for surveillance for the hemodialysis arteriovenous access. Clin J Am Soc Nephrol. 2013;8(7):1220-1227. doi:10.2215/CJN.00740113.
44. Maya ID, Oser R, Saddekni S, Barker J, Allon M. Vascular access stenosis: comparison of arteriovenous grafts and fistulas. Am J Kidney Dis. 2004;44(5):859-865.
45. Ocak G, Verduijn M, Vossen CY, et al. Chronic kidney disease stages 1-3 increase the risk of venous thrombosis. J Thromb Haemost. 2010;8(11):2428-2435. doi:10.1111/j.1538-7836.2010.04048.x.
46. Ravani P, Quinn RR, Oliver MJ, et al. Pre-emptive correction for haemodialysis arteriovenous access stenosis. Cochrane Database Syst Rev. 2016;(1):CD010709. doi:10.1002/14651858.CD010709.pub2.
47. Pietryga JA, Little MD, Robbin ML. Sonography of arteriovenous fistulas and grafts. Semin Dial. 2017;30(4):309-318. doi:10.1111/sdi.12599.
48. Asif A, Leon C, Orozco-Vargas LC, et al. Accuracy of physical examination in the detection of arteriovenous fistula stenosis. Clin J Am Soc Nephrol. 2007;2(6):1191-1194. doi:10.2215/CJN.02400607.
49. Tessitore N, Bedogna V, Melilli E, et al. In search of an optimal bedside screening program for arteriovenous fistula stenosis. Clin J Am Soc Nephrol. 2011;6(4):819-826. doi:10.2215/CJN.06220710.
50. Dhamija R, Nash SK, Nguyen SV, Slack K, Tadeo J. Monitoring and surveillance of hemodialysis vascular access using StenTec and physical exam. Semin Dial. 2015;28(3):299-304. doi:10.1111/sdi.12311.
51. NKF KDOQI Guidelines. Clinical practice guidelines for hemodialysis adequacy, update 2006. Available at http://kidneyfoundation.cachefly.net/professionals/KDOQI/guideline_upHD_PD_VA/index.htm. Accessed August 12, 2017.
52. Gelbfish GA. Surgical versus percutaneous care of arteriovenous access. Semin Vasc Surg. 2007;20(3):167-174. doi:10.1053/j.semvascsurg.2007.07.011.
53. Tanner NC, da Silva AF. Medical adjuvant treatment to improve the patency of arteriovenous fistulae and grafts: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2016;52(2):243-252. doi:10.1016/j.ejvs.2016.04.016.
54. Palmer SC, Di Micco L, Razavian M, et al. Antiplatelet therapy to prevent hemodialysis vascular access failure: systematic review and meta-analysis. Am J Kidney Dis. 2013;61(1):112-122. doi:10.1053/j.ajkd.2012.08.031.
55. Lafrance JP, Rahme E, Lelorier J, Iqbal S. Vascular access-related infections: definitions, incidence rates, and risk factors. Am J Kidney Dis. 2008;52(5):982-993. doi:10.1053/j.ajkd.2008.06.014.
56. Piraino B. Staphylococcus aureus infections in dialysis patients: focus on prevention. ASAIO J. 46(6):S13-S17.
57. Minga TE, Flanagan KH, Allon M. Clinical consequences of infected arteriovenous grafts in hemodialysis patients. Am J Kidney Dis. 2001;38(5):975-978. doi:10.1053/ajkd.2001.28583.
58. Benrashid E, Youngwirth LM, Mureebe L, Lawson JH. Operative and perioperative management of infected arteriovenous grafts. J Vasc Access. 2017;18(1):13-21. doi:10.5301/jva.5000613.
59. Lazarides MK, Georgiadis GS, Argyriou C. Aneurysm formation and infection in AV prosthesis. J Vasc Access. 2014;15 Suppl 7(Suppl. 7):S120-S124. doi:10.5301/jva.5000228.
60. Al-Thani H, El-Menyar A, Al-Thani N, et al. Characteristics, management, and outcomes of surgically treated arteriovenous fistula aneurysm in patients on regular hemodialysis. Ann Vasc Surg. 2017;41:46-55. doi:10.1016/j.avsg.2016.08.046.
61. Mudoni A, Cornacchiari M, Gallieni M, et al. Aneurysms and pseudoaneurysms in dialysis access. Clin Kidney J. 2015;8(4):363-367. doi:10.1093/ckj/sfv042.
62. Georgiadis GS, Lazarides MK, Panagoutsos SA, et al. Surgical revision of complicated false and true vascular access–related aneurysms. J Vasc Surg. 2008;47(6):1284-1291. doi:10.1016/j.jvs.2008.01.051.
63. Singh V, Qaisar H, Masud A, et al. Ischemic monomelic neuropathy: a long-term follow-up of two cases. J Vasc Access. 2017:0. [Epub ahead of print] doi:10.5301/jva.5000743.
64. Sheetal S, Byju P, Manoj P. Ischemic monomelic neuropathy. J Postgrad Med. 2017;63(1):42-43. doi:10.4103/0022-3859.194221.
65. Rabbani MA, Ahmad B, Shah SM, Ahmad A. Ischemic monomelic neuropathy: a complication of vascular access procedure. J Pak Med Assoc. 2005;55(9):400-401.
66. Hye RJ, Wolf YG. Ischemic monomelic neuropathy: an under-recognized complication of hemodialysis access. Ann Vasc Surg. 1994;8(6):578-582. doi:10.1007/BF02017415.
67. Thimmisetty RK, Pedavally S, Rossi NF, Fernandes JAM, Fixley J. Ischemic monomelic neuropathy: diagnosis, pathophysiology, and management. Kidney Int Reports. 2017;2(1):76-79. doi:10.1016/j.ekir.2016.08.013.
68. MacRae JM, Dipchand C, Oliver M, et al. Arteriovenous access: infection, neuropathy, and other complications. Can J Kidney Heal Dis. 2016;3:2054358116669127. doi:10.1177/2054358116669127.
69. Davidson D, Louridas G, Guzman R, et al. Steal syndrome complicating upper extremity hemoaccess procedures: incidence and risk factors. Can J Surg. 2003;46(6):408-412.
70. Kokkosis AA, Abramowitz SD, Schwitzer J, Nowakowski S, Teodorescu VJ, Schanzer H. Inflow stenosis as a contributing factor in the etiology of AV access-induced ischemic steal. J Vasc Access. 2014;15(4):286-290. doi:10.5301/jva.5000205.
71. Rocha A, Silva F, Queirós J, Malheiro J, Cabrita A. Predictors of steal syndrome in hemodialysis patients. Hemodial Int. 2012;16(4):539-544. doi:10.1111/j.1542-4758.2012.00684.x.
72. Mwipatayi BP, Bowles T, Balakrishnan S, Callaghan J, Haluszkiewicz E, Sieunarine K. Ischemic steal syndrome: a case series and review of current management. Curr Surg. 2006;63(2):130-135. doi:10.1016/j.cursur.2005.04.017.
73. Raml NM. Irreversible sequela in an arterial venous fistula with steal syndrome: A case study. J Vasc Nurs. 2012;30(3):94-97. doi:10.1016/j.jvn.2012.02.001.
74. Malik J, Tuka V, Kasalova Z, et al. Understanding the dialysis access steal syndrome. A review of the etiologies, diagnosis, prevention and treatment strategies. J Vasc Access. 2008;9(3):155-166.
75. Korsheed S, Eldehni MT, John SG, Fluck RJ, McIntyre CW. Effects of arteriovenous fistula formation on arterial stiffness and cardiovascular performance and function. Nephrol Dial Transplant. 2011;26(10):3296-3302. doi:10.1093/ndt/gfq851.
76. Lazarides MK, Staramos DN, Panagopoulos GN, Tzilalis VD, Eleftheriou GJ, Dayantas JN. Indications for surgical treatment of angioaccess-induced arterial "steal". J Am Coll Surg. 1998;187(4):422-426.
77. Basile C, Lomonte C, Vernaglione L, Casucci F, Antonelli M, Losurdo N. The relationship between the flow of arteriovenous fistula and cardiac output in haemodialysis patients. Nephrol Dial Transplant. 2008;23(1):282-287. doi:10.1093/ndt/gfm549.
78. Wijnen E, Keuter XH, Planken NR, et al. The relation between vascular access flow and different types of vascular access with systemic hemodynamics in hemodialysis patients. Artif Organs. 2005;29(12):960-964. doi:10.1111/j.1525-1594.2005.00165.x.
79. Keuter XH, Kooman JP, Habets J, et al. Effect of upper arm brachial basilic and prosthetic forearm arteriovenous fistula on left ventricular hypertrophy. J Vasc Access. 2007;8(4):296-301.
80. Miller GA, Hwang WW. Challenges and management of high-flow arteriovenous fistulae. Semin Nephrol. 2012;32(6):545-550. doi:10.1016/j.semnephrol.2012.10.005.
1. National Institute of Diabetes and Digestive and Kidney Diseases. Kidney disease statistics for the United States. https://www.niddk.nih.gov/health-information/health-statistics/Pages/kidney-disease-statistics-united-states.aspx. Accessed August 24, 2017.
2. Salahi H, Fazelzadeh A, Mehdizadeh A, Razmkon A, Malek-Hosseini SA. Complications of arteriovenous fistula in dialysis patients. Transplant Proc. 2006;38(5):1261-1264. doi:10.1016/j.transproceed.2006.02.066.
3. Ellingson KD, Palekar RS, Lucero CA, et al. Vascular access hemorrhages contribute to deaths among hemodialysis patients. Kidney Int. 2012;82(6):686-692. doi:10.1038/ki.2012.185.
4. Schild AF, Perez E, Gillaspie E, Seaver C, Livingstone J, Thibonnier A. Arteriovenous fistulae vs. arteriovenous grafts: a retrospective review of 1,700 consecutive vascular access cases. J Vasc Access. 2008;9(4):231-235.
5. Jankovic A, Donfrid B, Adam J, et al. Arteriovenous fistula aneurysm in patients on regular hemodialysis: prevalence and risk factors. Nephron Clin Pract. 2013;124(1-2):94-98. doi:10.1159/000355548.
6. Holden RM, Harman GJ, Wang M, Holland D, Day AG. Major bleeding in hemodialysis patients. Clin J Am Soc Nephrol. 2008 Jan;3(1):105-110. doi:10.2215/CJN.01810407.
7. Elliott MJ, Zimmerman D, Holden RM. Warfarin anticoagulation in hemodialysis patients: a systematic review of bleeding rates. Am J Kidney Dis. 2007;50(3):433-440. doi:10.1053/j.ajkd.2007.06.017.
8. Jubelirer SJ. Hemostatic abnormalities in renal disease. Am J Kidney Dis. 1985;5(5):219-225.
9. Salvati F, Liani M. Role of platelet surface receptor abnormalities in the bleeding and thrombotic diathesis of uremic patients on hemodialysis and peritoneal dialysis. Int J Artif Organs. 2001;24(3):131-135.
10. Kaw D, Malhotra D. Platelet dysfunction and end-stage renal disease. Semin Dial. 2006;19(4):317-322. doi:10.1111/j.1525-139X.2006.00179.x.
11. Hedges SJ, Dehoney SB, Hooper JS, Amanzadeh J, Busti AJ. Evidence-based treatment recommendations for uremic bleeding. Nat Clin Pract Nephrol. 2007;3(3):138-153. doi:10.1038/ncpneph0421.
12. Thekkedath UR, Chirananthavat T, Leypoldt JK, Cheung AK, Mohammad SF. Elevated fibrinogen fragment levels in uremic plasma inhibit platelet function and expression of glycoprotein IIb-IIIa. Am J Hematol. 2006;81(12):915-926. doi:10.1002/ajh.20720.
13. Padberg FT, Calligaro KD, Sidawy AN. Complications of arteriovenous hemodialysis access: recognition and management. J Vasc Surg. 2008;48(5 Suppl):S55-S80. doi:10.1016/j.jvs.2008.08.067.
14. Lohr JW, Schwab SJ. Minimizing hemorrhagic complications in dialysis patients. J Am Soc Nephrol. 1991;2(5):961-975.
15. Yang TH, Lee CH, Tsai CS, Tsai YT. Successful surgical treatment of a rupture to an arteriovenous fistula aneurysm. Cardiovasc J Afr. 2009;20(3):196-197.
16. Caksen HH, Odabaş D, Arslan S, Kaya A. Spontaneous rupture of arteriovenous fistula in a chronic dialysis patient. J Emerg Med. 2003;24(2):224-225. doi:10.1016/S0736-4679(02)00744-8.
17. Saeed F, Kousar N, Sinnakirouchenan R, Ramalingam VS, Johnson PB, Holley JL. Blood loss through AV fistula: a case report and literature review. Int J Nephrol. 2011;2011:350870. doi:10.4061/2011/350870.
18. NKF KDOQI Guidelines. Clinical practice guidelines for vascular access. Guideline 5. Treatment of fistula complications. Available at http://www2.kidney.org/professionals/kdoqi/guideline_uphd_pd_va/va_guide5.htm. Accessed August 24, 2017.
19. Gill JR, Storck K, Kelly S. Fatal exsanguination from hemodialysis vascular access sites. Forensic Sci Med Pathol. 2012;8(3):259-262. doi:10.1007/s12024-011-9303-0.
20. Manning MA. Use of dialysis access in emergent situations. J Emerg Nurs. 2008;34(1):37-40. doi:10.1016/j.jen.2007.03.018.
21. Reddy VM, Bagul A, Qureshi AA, Nicholson ML. A simple technique to control a bleeding arteriovenous fistula. Ann R Coll Surg Engl. 2006;88(6):592-593. doi:10.1308/003588406X130714f.
22. Oudemans-van Straaten HM. Hemostasis and thrombosis in continuous renal replacement treatment. Semin Thromb Hemost. 2015;41(1):91-98. doi:10.1055/s-0034-1398384.
23. Casserly LF, Dember LM. Thrombosis in end-stage renal disease. Semin Dial. 2003;16(3):245-256. doi:10.1046/j.1525-139X.2003.16048.x.
24. Boccardo P, Remuzzi G, Galbusera M. Platelet dysfunction in renal failure. Semin Thromb Hemost. 2004;30(5):579-589. doi:10.1055/s-2004-835678.
25. Mannucci PM, Remuzzi G, Pusineri F, et al. Deamino-8-D-arginine vasopressin shortens the bleeding time in uremia. N Engl J Med. 1983;308(1):8-12. doi:10.1056/NEJM198301063080102.
26. Ho SJ, Gemmell R, Brighton TA. Platelet function testing in uraemic patients. Hematology. 2008;13(1):49-58. doi:10.1179/102453308X315834.
27. Showalter J, Nguyen ND, Baba S, et al. Platelet aggregometry cannot identify uremic platelet dysfunction in heart failure patients prior to cardiac surgery. J Clin Lab Anal. 2016:1-5. doi:10.1002/jcla.22084.1308/003588406X130714f.
28. Wademan BH, Galvin SD. Desmopressin for reducing postoperative blood loss and transfusion requirements following cardiac surgery in adults. Interact Cardiovasc Thorac Surg. 2014;18(3):360-370. doi:10.1093/icvts/ivt491.
29. Soslau G, Schwartz AB, Putatunda B, et al. Desmopressin-induced improvement in bleeding times in chronic renal failure patients correlates with platelet serotonin uptake and ATP release. Am J Med Sci. 1990;300(6):372-379. http://www.ncbi.nlm.nih.gov/pubmed/2264575. Accessed January 31, 2017.
30. Lethagen S. Desmopressin (DDAVP) and hemostasis. Ann Hematol. 1994;69(4):173-180.
31. Mannucci PM. Hemostatic drugs. N Engl J Med. 1998;339(4):245-253. doi:10.1056/NEJM199807233390407.
32. Azarov I, Huang KT, Basu S, Gladwin MT, Hogg N, Kim-Shapiro DB. Nitric oxide scavenging by red blood cells as a function of hematocrit and oxygenation. J Biol Chem. 2005;280(47):39024-39032. doi:10.1074/jbc.M509045200.
33. Livio M, Marchesi D, Remuzzi G, Gotti E, Mecca G, De Gaetano G. Uraemic bleeding: role of anaemia and beneficial effect of red cell transfusions. Lancet. 1982;320(8306):1013-1015. doi:10.1016/S0140-6736(82)90050-2.
34. Janson PA, Jubelirer SJ, Weinstein MJ, Deykin D. Treatment of the bleeding tendency in uremia with cryoprecipitate. N Engl J Med. 1980;303(23):1318-1322. doi:10.1056/NEJM198012043032302.
35. Triulzi DJ, Blumberg N. Variability in response to cryoprecipitate treatment for hemostatic defects in uremia. Yale J Biol Med. 1990;63(1):1-7.
36. Roberts I, Shakur H, Coats T, et al. The CRASH-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Heal Technol Assess. 2013;17(10):1-79. doi:10.3310/hta17100.
37. Mezzano D, Panes O, Muñoz B, et al. Tranexamic acid inhibits fibrinolysis, shortens the bleeding time and improves platelet function in patients with chronic renal failure.Thromb Haemost. 1999;82(4):1250-1254.
38. Mezzano D, Muñoz B, Pais E, Downey P, Pereira J. Fast decrease of bleeding time by tranexamic acid in uremia. Thromb Haemost. 2000;83(5):785.
39. Sabovic M, Lavre J, Vujkovac B. Tranexamic acid is beneficial as adjunctive therapy in treating major upper gastrointestinal bleeding in dialysis patients. Nephrol Dial Transplant. 2003;18(7):1388-1391. doi:10.1093/ndt/gfg117.
40. Andersson L, Eriksson O, Hedlund PO, Kjellman H, Lindqvist B. Special considerations with regard to the dosage of tranexamic acid in patients with chronic renal diseases. Urol Res. 1978;6(2):83-88.
41. Bennett C, Klingenberg SL, Langholz E, Gluud LL. Tranexamic acid for upper gastrointestinal bleeding. Cochrane Database Syst Rev. 2014;(11):CD006640. doi: 10.1002/14651858.CD006640.pub3.
42. Holcomb JB, Tilley BC, Baraniuk S, et al; PROPPR Study Group. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313(5):471-482. doi:10.1001/jama.2015.12.
43. Salman L, Beathard G. Interventional nephrology: physical examination as a tool for surveillance for the hemodialysis arteriovenous access. Clin J Am Soc Nephrol. 2013;8(7):1220-1227. doi:10.2215/CJN.00740113.
44. Maya ID, Oser R, Saddekni S, Barker J, Allon M. Vascular access stenosis: comparison of arteriovenous grafts and fistulas. Am J Kidney Dis. 2004;44(5):859-865.
45. Ocak G, Verduijn M, Vossen CY, et al. Chronic kidney disease stages 1-3 increase the risk of venous thrombosis. J Thromb Haemost. 2010;8(11):2428-2435. doi:10.1111/j.1538-7836.2010.04048.x.
46. Ravani P, Quinn RR, Oliver MJ, et al. Pre-emptive correction for haemodialysis arteriovenous access stenosis. Cochrane Database Syst Rev. 2016;(1):CD010709. doi:10.1002/14651858.CD010709.pub2.
47. Pietryga JA, Little MD, Robbin ML. Sonography of arteriovenous fistulas and grafts. Semin Dial. 2017;30(4):309-318. doi:10.1111/sdi.12599.
48. Asif A, Leon C, Orozco-Vargas LC, et al. Accuracy of physical examination in the detection of arteriovenous fistula stenosis. Clin J Am Soc Nephrol. 2007;2(6):1191-1194. doi:10.2215/CJN.02400607.
49. Tessitore N, Bedogna V, Melilli E, et al. In search of an optimal bedside screening program for arteriovenous fistula stenosis. Clin J Am Soc Nephrol. 2011;6(4):819-826. doi:10.2215/CJN.06220710.
50. Dhamija R, Nash SK, Nguyen SV, Slack K, Tadeo J. Monitoring and surveillance of hemodialysis vascular access using StenTec and physical exam. Semin Dial. 2015;28(3):299-304. doi:10.1111/sdi.12311.
51. NKF KDOQI Guidelines. Clinical practice guidelines for hemodialysis adequacy, update 2006. Available at http://kidneyfoundation.cachefly.net/professionals/KDOQI/guideline_upHD_PD_VA/index.htm. Accessed August 12, 2017.
52. Gelbfish GA. Surgical versus percutaneous care of arteriovenous access. Semin Vasc Surg. 2007;20(3):167-174. doi:10.1053/j.semvascsurg.2007.07.011.
53. Tanner NC, da Silva AF. Medical adjuvant treatment to improve the patency of arteriovenous fistulae and grafts: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2016;52(2):243-252. doi:10.1016/j.ejvs.2016.04.016.
54. Palmer SC, Di Micco L, Razavian M, et al. Antiplatelet therapy to prevent hemodialysis vascular access failure: systematic review and meta-analysis. Am J Kidney Dis. 2013;61(1):112-122. doi:10.1053/j.ajkd.2012.08.031.
55. Lafrance JP, Rahme E, Lelorier J, Iqbal S. Vascular access-related infections: definitions, incidence rates, and risk factors. Am J Kidney Dis. 2008;52(5):982-993. doi:10.1053/j.ajkd.2008.06.014.
56. Piraino B. Staphylococcus aureus infections in dialysis patients: focus on prevention. ASAIO J. 46(6):S13-S17.
57. Minga TE, Flanagan KH, Allon M. Clinical consequences of infected arteriovenous grafts in hemodialysis patients. Am J Kidney Dis. 2001;38(5):975-978. doi:10.1053/ajkd.2001.28583.
58. Benrashid E, Youngwirth LM, Mureebe L, Lawson JH. Operative and perioperative management of infected arteriovenous grafts. J Vasc Access. 2017;18(1):13-21. doi:10.5301/jva.5000613.
59. Lazarides MK, Georgiadis GS, Argyriou C. Aneurysm formation and infection in AV prosthesis. J Vasc Access. 2014;15 Suppl 7(Suppl. 7):S120-S124. doi:10.5301/jva.5000228.
60. Al-Thani H, El-Menyar A, Al-Thani N, et al. Characteristics, management, and outcomes of surgically treated arteriovenous fistula aneurysm in patients on regular hemodialysis. Ann Vasc Surg. 2017;41:46-55. doi:10.1016/j.avsg.2016.08.046.
61. Mudoni A, Cornacchiari M, Gallieni M, et al. Aneurysms and pseudoaneurysms in dialysis access. Clin Kidney J. 2015;8(4):363-367. doi:10.1093/ckj/sfv042.
62. Georgiadis GS, Lazarides MK, Panagoutsos SA, et al. Surgical revision of complicated false and true vascular access–related aneurysms. J Vasc Surg. 2008;47(6):1284-1291. doi:10.1016/j.jvs.2008.01.051.
63. Singh V, Qaisar H, Masud A, et al. Ischemic monomelic neuropathy: a long-term follow-up of two cases. J Vasc Access. 2017:0. [Epub ahead of print] doi:10.5301/jva.5000743.
64. Sheetal S, Byju P, Manoj P. Ischemic monomelic neuropathy. J Postgrad Med. 2017;63(1):42-43. doi:10.4103/0022-3859.194221.
65. Rabbani MA, Ahmad B, Shah SM, Ahmad A. Ischemic monomelic neuropathy: a complication of vascular access procedure. J Pak Med Assoc. 2005;55(9):400-401.
66. Hye RJ, Wolf YG. Ischemic monomelic neuropathy: an under-recognized complication of hemodialysis access. Ann Vasc Surg. 1994;8(6):578-582. doi:10.1007/BF02017415.
67. Thimmisetty RK, Pedavally S, Rossi NF, Fernandes JAM, Fixley J. Ischemic monomelic neuropathy: diagnosis, pathophysiology, and management. Kidney Int Reports. 2017;2(1):76-79. doi:10.1016/j.ekir.2016.08.013.
68. MacRae JM, Dipchand C, Oliver M, et al. Arteriovenous access: infection, neuropathy, and other complications. Can J Kidney Heal Dis. 2016;3:2054358116669127. doi:10.1177/2054358116669127.
69. Davidson D, Louridas G, Guzman R, et al. Steal syndrome complicating upper extremity hemoaccess procedures: incidence and risk factors. Can J Surg. 2003;46(6):408-412.
70. Kokkosis AA, Abramowitz SD, Schwitzer J, Nowakowski S, Teodorescu VJ, Schanzer H. Inflow stenosis as a contributing factor in the etiology of AV access-induced ischemic steal. J Vasc Access. 2014;15(4):286-290. doi:10.5301/jva.5000205.
71. Rocha A, Silva F, Queirós J, Malheiro J, Cabrita A. Predictors of steal syndrome in hemodialysis patients. Hemodial Int. 2012;16(4):539-544. doi:10.1111/j.1542-4758.2012.00684.x.
72. Mwipatayi BP, Bowles T, Balakrishnan S, Callaghan J, Haluszkiewicz E, Sieunarine K. Ischemic steal syndrome: a case series and review of current management. Curr Surg. 2006;63(2):130-135. doi:10.1016/j.cursur.2005.04.017.
73. Raml NM. Irreversible sequela in an arterial venous fistula with steal syndrome: A case study. J Vasc Nurs. 2012;30(3):94-97. doi:10.1016/j.jvn.2012.02.001.
74. Malik J, Tuka V, Kasalova Z, et al. Understanding the dialysis access steal syndrome. A review of the etiologies, diagnosis, prevention and treatment strategies. J Vasc Access. 2008;9(3):155-166.
75. Korsheed S, Eldehni MT, John SG, Fluck RJ, McIntyre CW. Effects of arteriovenous fistula formation on arterial stiffness and cardiovascular performance and function. Nephrol Dial Transplant. 2011;26(10):3296-3302. doi:10.1093/ndt/gfq851.
76. Lazarides MK, Staramos DN, Panagopoulos GN, Tzilalis VD, Eleftheriou GJ, Dayantas JN. Indications for surgical treatment of angioaccess-induced arterial "steal". J Am Coll Surg. 1998;187(4):422-426.
77. Basile C, Lomonte C, Vernaglione L, Casucci F, Antonelli M, Losurdo N. The relationship between the flow of arteriovenous fistula and cardiac output in haemodialysis patients. Nephrol Dial Transplant. 2008;23(1):282-287. doi:10.1093/ndt/gfm549.
78. Wijnen E, Keuter XH, Planken NR, et al. The relation between vascular access flow and different types of vascular access with systemic hemodynamics in hemodialysis patients. Artif Organs. 2005;29(12):960-964. doi:10.1111/j.1525-1594.2005.00165.x.
79. Keuter XH, Kooman JP, Habets J, et al. Effect of upper arm brachial basilic and prosthetic forearm arteriovenous fistula on left ventricular hypertrophy. J Vasc Access. 2007;8(4):296-301.
80. Miller GA, Hwang WW. Challenges and management of high-flow arteriovenous fistulae. Semin Nephrol. 2012;32(6):545-550. doi:10.1016/j.semnephrol.2012.10.005.
