User login
Headache after drinking red wine? This could be why
This transcript has been edited for clarity.
Robert Louis Stevenson famously said, “Wine is bottled poetry.” And I think it works quite well. I’ve had wines that are simple, elegant, and unpretentious like Emily Dickinson, and passionate and mysterious like Pablo Neruda. And I’ve had wines that are more analogous to the limerick you might read scrawled on a rest-stop bathroom wall. Those ones give me headaches.
– and apparently it’s not just the alcohol.
Headaches are common, and headaches after drinking alcohol are particularly common. An interesting epidemiologic phenomenon, not yet adequately explained, is why red wine is associated with more headache than other forms of alcohol. There have been many studies fingering many suspects, from sulfites to tannins to various phenolic compounds, but none have really provided a concrete explanation for what might be going on.
A new hypothesis came to the fore on Nov. 20 in the journal Scientific Reports:
To understand the idea, first a reminder of what happens when you drink alcohol, physiologically.
Alcohol is metabolized by the enzyme alcohol dehydrogenase in the gut and then in the liver. That turns it into acetaldehyde, a toxic metabolite. In most of us, aldehyde dehydrogenase (ALDH) quickly metabolizes acetaldehyde to the inert acetate, which can be safely excreted.
I say “most of us” because some populations, particularly those with East Asian ancestry, have a mutation in the ALDH gene which can lead to accumulation of toxic acetaldehyde with alcohol consumption – leading to facial flushing, nausea, and headache.
We can also inhibit the enzyme medically. That’s what the drug disulfiram, also known as Antabuse, does. It doesn’t prevent you from wanting to drink; it makes the consequences of drinking incredibly aversive.
The researchers focused in on the aldehyde dehydrogenase enzyme and conducted a screening study. Are there any compounds in red wine that naturally inhibit ALDH?
The results pointed squarely at quercetin, and particularly its metabolite quercetin glucuronide, which, at 20 micromolar concentrations, inhibited about 80% of ALDH activity.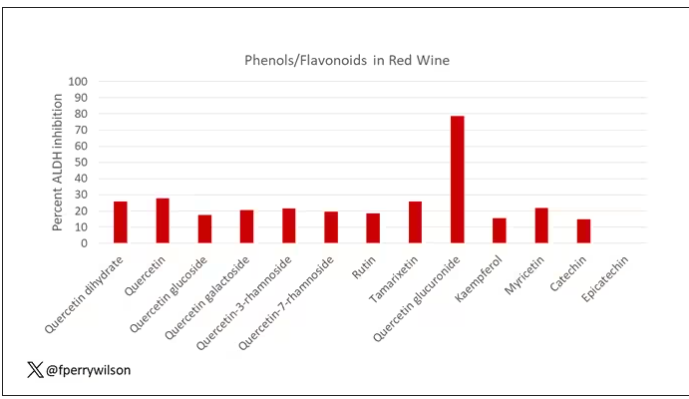
Quercetin is a flavonoid – a compound that gives color to a variety of vegetables and fruits, including grapes. In a test tube, it is an antioxidant, which is enough evidence to spawn a small quercetin-as-supplement industry, but there is no convincing evidence that it is medically useful. The authors then examined the concentration of quercetin glucuronide to achieve various inhibitions of ALDH, as you can see in this graph here.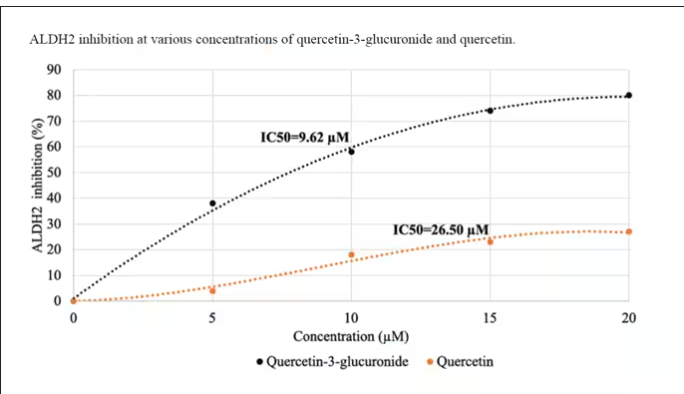
By about 10 micromolar, we see a decent amount of inhibition. Disulfiram is about 10 times more potent than that, but then again, you don’t drink three glasses of disulfiram with Thanksgiving dinner.
This is where this study stops. But it obviously tells us very little about what might be happening in the human body. For that, we need to ask the question: Can we get our quercetin levels to 10 micromolar? Is that remotely achievable?
Let’s start with how much quercetin there is in red wine. Like all things wine, it varies, but this study examining Australian wines found mean concentrations of 11 mg/L. The highest value I saw was close to 50 mg/L.
So let’s do some math. To make the numbers easy, let’s say you drank a liter of Australian wine, taking in 50 mg of quercetin glucuronide.
How much of that gets into your bloodstream? Some studies suggest a bioavailability of less than 1%, which basically means none and should probably put the quercetin hypothesis to bed. But there is some variation here too; it seems to depend on the form of quercetin you ingest.
Let’s say all 50 mg gets into your bloodstream. What blood concentration would that lead to? Well, I’ll keep the stoichiometry in the graphics and just say that if we assume that the volume of distribution of the compound is restricted to plasma alone, then you could achieve similar concentrations to what was done in petri dishes during this study.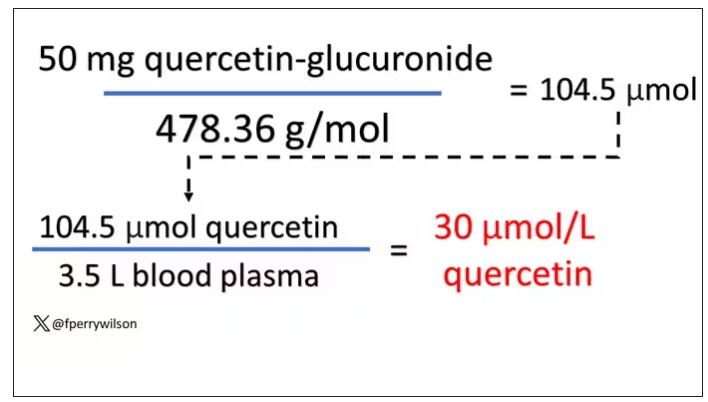
Of course, if quercetin is really the culprit behind red wine headache, I have some questions: Why aren’t the Amazon reviews of quercetin supplements chock full of warnings not to take them with alcohol? And other foods have way higher quercetin concentration than wine, but you don’t hear people warning not to take your red onions with alcohol, or your capers, or lingonberries.
There’s some more work to be done here – most importantly, some human studies. Let’s give people wine with different amounts of quercetin and see what happens. Sign me up. Seriously.
As for Thanksgiving, it’s worth noting that cranberries have a lot of quercetin in them. So between the cranberry sauce, the Beaujolais, and your uncle ranting about the contrails again, the probability of headache is pretty darn high. Stay safe out there, and Happy Thanksgiving.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Robert Louis Stevenson famously said, “Wine is bottled poetry.” And I think it works quite well. I’ve had wines that are simple, elegant, and unpretentious like Emily Dickinson, and passionate and mysterious like Pablo Neruda. And I’ve had wines that are more analogous to the limerick you might read scrawled on a rest-stop bathroom wall. Those ones give me headaches.
– and apparently it’s not just the alcohol.
Headaches are common, and headaches after drinking alcohol are particularly common. An interesting epidemiologic phenomenon, not yet adequately explained, is why red wine is associated with more headache than other forms of alcohol. There have been many studies fingering many suspects, from sulfites to tannins to various phenolic compounds, but none have really provided a concrete explanation for what might be going on.
A new hypothesis came to the fore on Nov. 20 in the journal Scientific Reports:
To understand the idea, first a reminder of what happens when you drink alcohol, physiologically.
Alcohol is metabolized by the enzyme alcohol dehydrogenase in the gut and then in the liver. That turns it into acetaldehyde, a toxic metabolite. In most of us, aldehyde dehydrogenase (ALDH) quickly metabolizes acetaldehyde to the inert acetate, which can be safely excreted.
I say “most of us” because some populations, particularly those with East Asian ancestry, have a mutation in the ALDH gene which can lead to accumulation of toxic acetaldehyde with alcohol consumption – leading to facial flushing, nausea, and headache.
We can also inhibit the enzyme medically. That’s what the drug disulfiram, also known as Antabuse, does. It doesn’t prevent you from wanting to drink; it makes the consequences of drinking incredibly aversive.
The researchers focused in on the aldehyde dehydrogenase enzyme and conducted a screening study. Are there any compounds in red wine that naturally inhibit ALDH?
The results pointed squarely at quercetin, and particularly its metabolite quercetin glucuronide, which, at 20 micromolar concentrations, inhibited about 80% of ALDH activity.
Quercetin is a flavonoid – a compound that gives color to a variety of vegetables and fruits, including grapes. In a test tube, it is an antioxidant, which is enough evidence to spawn a small quercetin-as-supplement industry, but there is no convincing evidence that it is medically useful. The authors then examined the concentration of quercetin glucuronide to achieve various inhibitions of ALDH, as you can see in this graph here.
By about 10 micromolar, we see a decent amount of inhibition. Disulfiram is about 10 times more potent than that, but then again, you don’t drink three glasses of disulfiram with Thanksgiving dinner.
This is where this study stops. But it obviously tells us very little about what might be happening in the human body. For that, we need to ask the question: Can we get our quercetin levels to 10 micromolar? Is that remotely achievable?
Let’s start with how much quercetin there is in red wine. Like all things wine, it varies, but this study examining Australian wines found mean concentrations of 11 mg/L. The highest value I saw was close to 50 mg/L.
So let’s do some math. To make the numbers easy, let’s say you drank a liter of Australian wine, taking in 50 mg of quercetin glucuronide.
How much of that gets into your bloodstream? Some studies suggest a bioavailability of less than 1%, which basically means none and should probably put the quercetin hypothesis to bed. But there is some variation here too; it seems to depend on the form of quercetin you ingest.
Let’s say all 50 mg gets into your bloodstream. What blood concentration would that lead to? Well, I’ll keep the stoichiometry in the graphics and just say that if we assume that the volume of distribution of the compound is restricted to plasma alone, then you could achieve similar concentrations to what was done in petri dishes during this study.
Of course, if quercetin is really the culprit behind red wine headache, I have some questions: Why aren’t the Amazon reviews of quercetin supplements chock full of warnings not to take them with alcohol? And other foods have way higher quercetin concentration than wine, but you don’t hear people warning not to take your red onions with alcohol, or your capers, or lingonberries.
There’s some more work to be done here – most importantly, some human studies. Let’s give people wine with different amounts of quercetin and see what happens. Sign me up. Seriously.
As for Thanksgiving, it’s worth noting that cranberries have a lot of quercetin in them. So between the cranberry sauce, the Beaujolais, and your uncle ranting about the contrails again, the probability of headache is pretty darn high. Stay safe out there, and Happy Thanksgiving.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Robert Louis Stevenson famously said, “Wine is bottled poetry.” And I think it works quite well. I’ve had wines that are simple, elegant, and unpretentious like Emily Dickinson, and passionate and mysterious like Pablo Neruda. And I’ve had wines that are more analogous to the limerick you might read scrawled on a rest-stop bathroom wall. Those ones give me headaches.
– and apparently it’s not just the alcohol.
Headaches are common, and headaches after drinking alcohol are particularly common. An interesting epidemiologic phenomenon, not yet adequately explained, is why red wine is associated with more headache than other forms of alcohol. There have been many studies fingering many suspects, from sulfites to tannins to various phenolic compounds, but none have really provided a concrete explanation for what might be going on.
A new hypothesis came to the fore on Nov. 20 in the journal Scientific Reports:
To understand the idea, first a reminder of what happens when you drink alcohol, physiologically.
Alcohol is metabolized by the enzyme alcohol dehydrogenase in the gut and then in the liver. That turns it into acetaldehyde, a toxic metabolite. In most of us, aldehyde dehydrogenase (ALDH) quickly metabolizes acetaldehyde to the inert acetate, which can be safely excreted.
I say “most of us” because some populations, particularly those with East Asian ancestry, have a mutation in the ALDH gene which can lead to accumulation of toxic acetaldehyde with alcohol consumption – leading to facial flushing, nausea, and headache.
We can also inhibit the enzyme medically. That’s what the drug disulfiram, also known as Antabuse, does. It doesn’t prevent you from wanting to drink; it makes the consequences of drinking incredibly aversive.
The researchers focused in on the aldehyde dehydrogenase enzyme and conducted a screening study. Are there any compounds in red wine that naturally inhibit ALDH?
The results pointed squarely at quercetin, and particularly its metabolite quercetin glucuronide, which, at 20 micromolar concentrations, inhibited about 80% of ALDH activity.
Quercetin is a flavonoid – a compound that gives color to a variety of vegetables and fruits, including grapes. In a test tube, it is an antioxidant, which is enough evidence to spawn a small quercetin-as-supplement industry, but there is no convincing evidence that it is medically useful. The authors then examined the concentration of quercetin glucuronide to achieve various inhibitions of ALDH, as you can see in this graph here.
By about 10 micromolar, we see a decent amount of inhibition. Disulfiram is about 10 times more potent than that, but then again, you don’t drink three glasses of disulfiram with Thanksgiving dinner.
This is where this study stops. But it obviously tells us very little about what might be happening in the human body. For that, we need to ask the question: Can we get our quercetin levels to 10 micromolar? Is that remotely achievable?
Let’s start with how much quercetin there is in red wine. Like all things wine, it varies, but this study examining Australian wines found mean concentrations of 11 mg/L. The highest value I saw was close to 50 mg/L.
So let’s do some math. To make the numbers easy, let’s say you drank a liter of Australian wine, taking in 50 mg of quercetin glucuronide.
How much of that gets into your bloodstream? Some studies suggest a bioavailability of less than 1%, which basically means none and should probably put the quercetin hypothesis to bed. But there is some variation here too; it seems to depend on the form of quercetin you ingest.
Let’s say all 50 mg gets into your bloodstream. What blood concentration would that lead to? Well, I’ll keep the stoichiometry in the graphics and just say that if we assume that the volume of distribution of the compound is restricted to plasma alone, then you could achieve similar concentrations to what was done in petri dishes during this study.
Of course, if quercetin is really the culprit behind red wine headache, I have some questions: Why aren’t the Amazon reviews of quercetin supplements chock full of warnings not to take them with alcohol? And other foods have way higher quercetin concentration than wine, but you don’t hear people warning not to take your red onions with alcohol, or your capers, or lingonberries.
There’s some more work to be done here – most importantly, some human studies. Let’s give people wine with different amounts of quercetin and see what happens. Sign me up. Seriously.
As for Thanksgiving, it’s worth noting that cranberries have a lot of quercetin in them. So between the cranberry sauce, the Beaujolais, and your uncle ranting about the contrails again, the probability of headache is pretty darn high. Stay safe out there, and Happy Thanksgiving.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
New insights into how omega-3 fatty acids improve NASH
TOPLINE:
that contributes to liver fibrosis and progression to cirrhosis and liver cancer, new data suggest.
METHODOLOGY:
- Because omega-3 polyunsaturated fatty acids have been shown to reduce hepatic dysfunction in NASH, but the molecular underpinnings of this action were elusive, researchers conducted a multiomic network analysis applied to a mouse model of Western diet–induced NASH to identify the key mechanisms involved.
- They also performed a meta-analysis of human liver cancer transcriptome data to evaluate which aspects of NASH pathogenesis leading to cancer are reversed by omega-3 polyunsaturated fatty acids.
TAKEAWAY:
- BTC, an epidermal growth factor–binding protein, was consistently upregulated in liver cancer and downregulated by omega-3 polyunsaturated fatty acids in mice and humans with NASH.
- BTC promotes NASH fibrosis by activating dormant hepatic stellate cells to produce transforming growth factor beta-2 and increase collagen production. It also exacerbates toll-like receptor-dependent inflammatory processes in NASH.
- By downregulating BTC, omega-3 polyunsaturated fatty acids have therapeutic potential in NASH and could serve as a novel drug target.
IN PRACTICE:
“BTC represents a candidate master regulator inducing two most important factors (collagens and integrins) contributing to liver fibrosis and consequently promoting liver cancer,” the researchers write. “Future studies should investigate if BTC-triggered gene expression signatures can serve as biomarkers guiding personalized [omega-3 polyunsaturated fatty acid] therapy, as targets of new NAFLD/NASH drugs, and finally as a predictors of hepatic cancer risk in humans.”
SOURCE:
The study, with lead first author Jyothi Padiadpu, PhD, Oregon State University College of Pharmacy, Corvallis, was published online in EMBO Molecular Medicine (2023. doi: 10.15252/emmm.202318367).
LIMITATIONS:
The study authors report no limitations. However, the findings are based on mouse model and human transcriptome data.
DISCLOSURES:
This research was supported by the National Institute of Diabetes and Digestive Kidney Diseases and the U.S. Department of Agriculture. The authors report no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
that contributes to liver fibrosis and progression to cirrhosis and liver cancer, new data suggest.
METHODOLOGY:
- Because omega-3 polyunsaturated fatty acids have been shown to reduce hepatic dysfunction in NASH, but the molecular underpinnings of this action were elusive, researchers conducted a multiomic network analysis applied to a mouse model of Western diet–induced NASH to identify the key mechanisms involved.
- They also performed a meta-analysis of human liver cancer transcriptome data to evaluate which aspects of NASH pathogenesis leading to cancer are reversed by omega-3 polyunsaturated fatty acids.
TAKEAWAY:
- BTC, an epidermal growth factor–binding protein, was consistently upregulated in liver cancer and downregulated by omega-3 polyunsaturated fatty acids in mice and humans with NASH.
- BTC promotes NASH fibrosis by activating dormant hepatic stellate cells to produce transforming growth factor beta-2 and increase collagen production. It also exacerbates toll-like receptor-dependent inflammatory processes in NASH.
- By downregulating BTC, omega-3 polyunsaturated fatty acids have therapeutic potential in NASH and could serve as a novel drug target.
IN PRACTICE:
“BTC represents a candidate master regulator inducing two most important factors (collagens and integrins) contributing to liver fibrosis and consequently promoting liver cancer,” the researchers write. “Future studies should investigate if BTC-triggered gene expression signatures can serve as biomarkers guiding personalized [omega-3 polyunsaturated fatty acid] therapy, as targets of new NAFLD/NASH drugs, and finally as a predictors of hepatic cancer risk in humans.”
SOURCE:
The study, with lead first author Jyothi Padiadpu, PhD, Oregon State University College of Pharmacy, Corvallis, was published online in EMBO Molecular Medicine (2023. doi: 10.15252/emmm.202318367).
LIMITATIONS:
The study authors report no limitations. However, the findings are based on mouse model and human transcriptome data.
DISCLOSURES:
This research was supported by the National Institute of Diabetes and Digestive Kidney Diseases and the U.S. Department of Agriculture. The authors report no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
that contributes to liver fibrosis and progression to cirrhosis and liver cancer, new data suggest.
METHODOLOGY:
- Because omega-3 polyunsaturated fatty acids have been shown to reduce hepatic dysfunction in NASH, but the molecular underpinnings of this action were elusive, researchers conducted a multiomic network analysis applied to a mouse model of Western diet–induced NASH to identify the key mechanisms involved.
- They also performed a meta-analysis of human liver cancer transcriptome data to evaluate which aspects of NASH pathogenesis leading to cancer are reversed by omega-3 polyunsaturated fatty acids.
TAKEAWAY:
- BTC, an epidermal growth factor–binding protein, was consistently upregulated in liver cancer and downregulated by omega-3 polyunsaturated fatty acids in mice and humans with NASH.
- BTC promotes NASH fibrosis by activating dormant hepatic stellate cells to produce transforming growth factor beta-2 and increase collagen production. It also exacerbates toll-like receptor-dependent inflammatory processes in NASH.
- By downregulating BTC, omega-3 polyunsaturated fatty acids have therapeutic potential in NASH and could serve as a novel drug target.
IN PRACTICE:
“BTC represents a candidate master regulator inducing two most important factors (collagens and integrins) contributing to liver fibrosis and consequently promoting liver cancer,” the researchers write. “Future studies should investigate if BTC-triggered gene expression signatures can serve as biomarkers guiding personalized [omega-3 polyunsaturated fatty acid] therapy, as targets of new NAFLD/NASH drugs, and finally as a predictors of hepatic cancer risk in humans.”
SOURCE:
The study, with lead first author Jyothi Padiadpu, PhD, Oregon State University College of Pharmacy, Corvallis, was published online in EMBO Molecular Medicine (2023. doi: 10.15252/emmm.202318367).
LIMITATIONS:
The study authors report no limitations. However, the findings are based on mouse model and human transcriptome data.
DISCLOSURES:
This research was supported by the National Institute of Diabetes and Digestive Kidney Diseases and the U.S. Department of Agriculture. The authors report no conflicts of interest.
A version of this article appeared on Medscape.com.
UHC accused of using AI to skirt doctors’ orders, deny claims
.
In a class action suit filed in Minnesota district court, the attorneys for the families of two deceased UHC Medicare Advantage plan policyholders say that the company uses the technology to systematically deny skilled nursing facility (SNF) claims and shirk its responsibility to adhere to Medicare’s coverage determination standards.
The case raises ethical and legal questions about whether AI can replace or supplement human tasks and interactions, particularly in a field as complex as health care. California-based public advocacy firm Clarkson Law filed a similar complaint against Cigna earlier this year and has previously sued tech giants Google and ChatGPT creator OpenAI for harvesting Internet users’ data to train their AI systems.
Clarkson Law represents the plaintiffs and says that the policyholders had to pay thousands in out-of-pocket costs or forgo the recommended postacute care owing to UHC’s faulty AI model, nH Predict. The tool has a 90% error rate, says the lawsuit, as evidenced by the number of claims that are reversed following review by a medical professional. Still, just 0.2% of policyholders appeal the denials.
nH Predict was created by naviHealth and was acquired by UnitedHealth Group, UHC’s parent company, in 2020. In a statement to Bloomberg Law, a spokesperson for naviHealth said that the lawsuit has no merit and the model was not used for making coverage determinations.
According to the complaint, nH Predict determines the appropriate amount of SNF, home health, or rehabilitation services a patient requires on the basis of the diagnosis, age, and living situation. The model compares the patient with its database of 6 million patients and estimates the ideal length of stay and target discharge date, “pinpointing the precise moment when [UHC] will cut off payment for a patient’s treatment.”
The lawsuit says that employees are instructed to strictly adhere to the AI model’s predictions, and those who do not are disciplined and terminated, even when additional care for the patient is warranted. Employees are told that the generated reports contain proprietary information and that they cannot share them with physicians and patients who inquire about extending care.
“Every patient is entitled to a nuanced evaluation of their health care needs,” Zarrina Ozari, senior associate at Clarkson Law, said in a prepared statement. “By replacing licensed practitioners with unchecked AI, UHC is telling its patients that they are completely interchangeable with one another and undervaluing the expertise of the physicians devoted to key elements of care.”
According to the complaint, Gene Lokken fell in May 2022 and fractured his leg and ankle. After a 1-month SNF stay, the 91-year-old man’s doctor ordered physical therapy. However, the insurer said Mr. Lokken was safe to be discharged home two and a half weeks later, conflicting with a physical therapist’s notes that indicated he still had paralyzed and weak muscles. The insurer denied Mr. Lokken’s appeal. He remained in the facility for another year until his death, paying about $150,000 in out-of-pocket expenses, according to the lawsuit.
Another patient, Dale H. Tetzloff, initially spent just 20 days in a SNF for stroke rehabilitation before UHC denied coverage. An appeal later extended the stay to 40 days, short of the 100 days recommended by his physician. Requests for further extensions were unsuccessful, and Mr. Tetzloff ultimately paid about $70,000 in out-of-pocket expenses over the next 10 months, according to the complaint.
New federal rules prohibit Medicare Advantage plans from relying on an algorithm or software to make medically necessary determinations instead of an individual’s specific circumstances. Any medical necessity denial must be “reviewed by a physician or other appropriate health care professional with expertise in the field of medicine or health care that is appropriate for the service at issue.”
Clarkson is demanding a jury trial and has asked the court to certify the case as a federal class action, which could open the suit to any U.S. resident who purchased a UHC Medicare Advantage plan in the past 4 years.
A version of this article appeared on Medscape.com.
.
In a class action suit filed in Minnesota district court, the attorneys for the families of two deceased UHC Medicare Advantage plan policyholders say that the company uses the technology to systematically deny skilled nursing facility (SNF) claims and shirk its responsibility to adhere to Medicare’s coverage determination standards.
The case raises ethical and legal questions about whether AI can replace or supplement human tasks and interactions, particularly in a field as complex as health care. California-based public advocacy firm Clarkson Law filed a similar complaint against Cigna earlier this year and has previously sued tech giants Google and ChatGPT creator OpenAI for harvesting Internet users’ data to train their AI systems.
Clarkson Law represents the plaintiffs and says that the policyholders had to pay thousands in out-of-pocket costs or forgo the recommended postacute care owing to UHC’s faulty AI model, nH Predict. The tool has a 90% error rate, says the lawsuit, as evidenced by the number of claims that are reversed following review by a medical professional. Still, just 0.2% of policyholders appeal the denials.
nH Predict was created by naviHealth and was acquired by UnitedHealth Group, UHC’s parent company, in 2020. In a statement to Bloomberg Law, a spokesperson for naviHealth said that the lawsuit has no merit and the model was not used for making coverage determinations.
According to the complaint, nH Predict determines the appropriate amount of SNF, home health, or rehabilitation services a patient requires on the basis of the diagnosis, age, and living situation. The model compares the patient with its database of 6 million patients and estimates the ideal length of stay and target discharge date, “pinpointing the precise moment when [UHC] will cut off payment for a patient’s treatment.”
The lawsuit says that employees are instructed to strictly adhere to the AI model’s predictions, and those who do not are disciplined and terminated, even when additional care for the patient is warranted. Employees are told that the generated reports contain proprietary information and that they cannot share them with physicians and patients who inquire about extending care.
“Every patient is entitled to a nuanced evaluation of their health care needs,” Zarrina Ozari, senior associate at Clarkson Law, said in a prepared statement. “By replacing licensed practitioners with unchecked AI, UHC is telling its patients that they are completely interchangeable with one another and undervaluing the expertise of the physicians devoted to key elements of care.”
According to the complaint, Gene Lokken fell in May 2022 and fractured his leg and ankle. After a 1-month SNF stay, the 91-year-old man’s doctor ordered physical therapy. However, the insurer said Mr. Lokken was safe to be discharged home two and a half weeks later, conflicting with a physical therapist’s notes that indicated he still had paralyzed and weak muscles. The insurer denied Mr. Lokken’s appeal. He remained in the facility for another year until his death, paying about $150,000 in out-of-pocket expenses, according to the lawsuit.
Another patient, Dale H. Tetzloff, initially spent just 20 days in a SNF for stroke rehabilitation before UHC denied coverage. An appeal later extended the stay to 40 days, short of the 100 days recommended by his physician. Requests for further extensions were unsuccessful, and Mr. Tetzloff ultimately paid about $70,000 in out-of-pocket expenses over the next 10 months, according to the complaint.
New federal rules prohibit Medicare Advantage plans from relying on an algorithm or software to make medically necessary determinations instead of an individual’s specific circumstances. Any medical necessity denial must be “reviewed by a physician or other appropriate health care professional with expertise in the field of medicine or health care that is appropriate for the service at issue.”
Clarkson is demanding a jury trial and has asked the court to certify the case as a federal class action, which could open the suit to any U.S. resident who purchased a UHC Medicare Advantage plan in the past 4 years.
A version of this article appeared on Medscape.com.
.
In a class action suit filed in Minnesota district court, the attorneys for the families of two deceased UHC Medicare Advantage plan policyholders say that the company uses the technology to systematically deny skilled nursing facility (SNF) claims and shirk its responsibility to adhere to Medicare’s coverage determination standards.
The case raises ethical and legal questions about whether AI can replace or supplement human tasks and interactions, particularly in a field as complex as health care. California-based public advocacy firm Clarkson Law filed a similar complaint against Cigna earlier this year and has previously sued tech giants Google and ChatGPT creator OpenAI for harvesting Internet users’ data to train their AI systems.
Clarkson Law represents the plaintiffs and says that the policyholders had to pay thousands in out-of-pocket costs or forgo the recommended postacute care owing to UHC’s faulty AI model, nH Predict. The tool has a 90% error rate, says the lawsuit, as evidenced by the number of claims that are reversed following review by a medical professional. Still, just 0.2% of policyholders appeal the denials.
nH Predict was created by naviHealth and was acquired by UnitedHealth Group, UHC’s parent company, in 2020. In a statement to Bloomberg Law, a spokesperson for naviHealth said that the lawsuit has no merit and the model was not used for making coverage determinations.
According to the complaint, nH Predict determines the appropriate amount of SNF, home health, or rehabilitation services a patient requires on the basis of the diagnosis, age, and living situation. The model compares the patient with its database of 6 million patients and estimates the ideal length of stay and target discharge date, “pinpointing the precise moment when [UHC] will cut off payment for a patient’s treatment.”
The lawsuit says that employees are instructed to strictly adhere to the AI model’s predictions, and those who do not are disciplined and terminated, even when additional care for the patient is warranted. Employees are told that the generated reports contain proprietary information and that they cannot share them with physicians and patients who inquire about extending care.
“Every patient is entitled to a nuanced evaluation of their health care needs,” Zarrina Ozari, senior associate at Clarkson Law, said in a prepared statement. “By replacing licensed practitioners with unchecked AI, UHC is telling its patients that they are completely interchangeable with one another and undervaluing the expertise of the physicians devoted to key elements of care.”
According to the complaint, Gene Lokken fell in May 2022 and fractured his leg and ankle. After a 1-month SNF stay, the 91-year-old man’s doctor ordered physical therapy. However, the insurer said Mr. Lokken was safe to be discharged home two and a half weeks later, conflicting with a physical therapist’s notes that indicated he still had paralyzed and weak muscles. The insurer denied Mr. Lokken’s appeal. He remained in the facility for another year until his death, paying about $150,000 in out-of-pocket expenses, according to the lawsuit.
Another patient, Dale H. Tetzloff, initially spent just 20 days in a SNF for stroke rehabilitation before UHC denied coverage. An appeal later extended the stay to 40 days, short of the 100 days recommended by his physician. Requests for further extensions were unsuccessful, and Mr. Tetzloff ultimately paid about $70,000 in out-of-pocket expenses over the next 10 months, according to the complaint.
New federal rules prohibit Medicare Advantage plans from relying on an algorithm or software to make medically necessary determinations instead of an individual’s specific circumstances. Any medical necessity denial must be “reviewed by a physician or other appropriate health care professional with expertise in the field of medicine or health care that is appropriate for the service at issue.”
Clarkson is demanding a jury trial and has asked the court to certify the case as a federal class action, which could open the suit to any U.S. resident who purchased a UHC Medicare Advantage plan in the past 4 years.
A version of this article appeared on Medscape.com.
Before signing an offer letter: Read this
You’ve just received an offer letter from that job you interviewed for. Sometimes you want to let the employer know right away how interested you are. The verbiage says the letter isn’t “binding.” So you eagerly sign on the dotted line. Everything looks great ... until it isn’t.
Attorney Ericka Adler, JD, LLM, a partner at Roetzel & Andress, a Chicago-based law firm that represents physicians and health care professionals nationwide, described her client who was in this predicament. The physician, a dermatologist, left a practice where she had been employed because she had received an “amazing” offer letter that included promises about her new work location, staffing, equipment, and hours. She signed and immediately gave notice to her previous employer.
“When she received the actual employment contract, none of those details from the offer letter – which is also called a letter of intent [LOI] – were included,” Ms. Adler told this news organization. The physician wanted to have the details from the LOI formally spelled out in the contract, but the employer refused.
“Basically, they said, ‘This is our standard contract and you’ll just have to trust us that we’ll keep our word. We meant what we said in the LOI, but we cannot include those details in the actual agreement because everyone has the same form of agreement.’ “ The physician decided to sign the contract and accept the position.
She contacted Ms. Adler after she had been at her new position for a month. “She had received none of the things they had promised her in the LOI,” Ms. Adler reported. “She lacked the NP and PA support, she lacked the equipment, she didn’t have enough exam rooms. As soon as she started, someone with whom she was sharing call coverage left, and she was expected to take over. The LOI had a cap on the amount of call she would be required to take, but that verbiage didn’t make it into the contract.”
Ms. Adler tried to address this issue with the employer. “We couldn’t say they had literally breached the agreement, but we did list the things that were mentioned in the LOI but on which they hadn’t delivered. We asked them to fix the issue within 10 days.”
The employer argued “that they didn’t have to fulfill anything that wasn’t spelled out in the contract, even if it was in the LOI. In fact, the contract specified clearly that the signed employment agreement was the only agreement and replaced any previous written or oral agreements between the parties.”
The dermatologist ultimately left the new position. “She might have been able to have a legal claim against the employer for breach or perhaps ‘detrimental reliance’ – meaning, she might have argued that she had been financially harmed due to the false promises made to her. But it would have been difficult and expensive for her to litigate the issue,” said Ms. Adler.
“It also didn’t seem like the physician could remain in the job and develop a positive work relationship with the employer, given that she felt betrayed and misled, and didn’t like the terms of employment, which didn’t match her needs or expectations,” said Ms. Adler.
She added that “most employers are not as unscrupulous and dishonest as this one was. But some employers do play on the fact that younger doctors – especially residents and fellows – tend to be trusting or feel they don’t have negotiation power. They’re often excited to get an offer and sign it without a second thought.”
That’s why she advises physicians to “review the terms of the LOI carefully and make sure you’re comfortable with them before signing it; but know that the real contract to negotiate will be the actual Employment Agreement.”
She also advises physicians not to give notice at their current place of employment until they’ve signed the final contract with the new employer.
On the same page?
Anu Murthy, JD, an attorney and associate contract review specialist at Contract Diagnostics, explained that the LOI is a document that the candidate receives after an interview but before a full contract. Sometimes, the LOI is preceded by a verbal or e-mailed offer, which is less formal.
“An LOI is sometimes called a Term Sheet or Memorandum of Understanding,“ Ms. Murthy told this news organization. “Typically, it lays out key provisions, such as compensation, initial term of the contract, location, and recruitment incentives.” Sometimes it includes mention of staffing, call schedule, malpractice, noncompete covenants, and other components of the position.
Justin Nabity, founder and CEO of Physicians Thrive, a physician financial advisory group, said that LOIs are “a way for employers to gauge a prospective employee’s level of interest.”
The employer “doesn’t want to send a contract with a lot of details before determining whether the candidate is really serious about the position, so the offer letter doesn’t show the whole picture,” Mr. Nabity told this news organization.
Dennis Hursh, managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, agreed.
“Another way of putting it is that the employer wants to see whether the prospective employee is on the same page. The LOI will typically include some key components that will later appear in a more complete and formal contract, together with other topics and details. Agreeing to those key components signals that indeed you and the employer are in accord,” said Mr. Hursh.
But are you really on the same page with your prospective employer? And if you seem to be on the same page, and you sign the LOI, is that a guarantee that the employer will honor its terms?
Not necessarily, according to the experts. In fact, many LOIs contain some verbiage stating that the letter isn’t binding, which can be confusing. Others suggest that it is binding, but the candidate doesn’t realize that the letter isn’t a formal contract and that the contract may contain details not included in the LOI or may omit details mentioned in the LOI, as happened to Ms. Adler’s unfortunate client.
“One of the pitfalls I see is that doctors sign the LOI without recognizing whether it’s binding or nonbinding,” Ms. Murthy said. “If it’s binding, it creates a legal obligation on your part and could preclude you from further negotiation once you see the contract and feel you’d like to negotiate some of its terms.”
Binding letters are typically offered to candidates after some back-and-forth between the parties, and important terms have been agreed to, which can happen either verbally or via e-mail. Once these agreements have been reached, they’re summarized in a “binding” letter before being extended into a full contract.
“But even if you’ve agreed on the terms verbally, it’s still important to have someone more experienced review the offer letter before signing it,” Ms. Murthy said. “It’s important to understand the ‘legalese’ and what your rights and obligations are before agreeing to anything.”
And certainly, if you receive a binding LOI, you shouldn’t sign anything until you’re sure you’re comfortable with its contents and have more details.
Are “nonbinding” LOIs really not binding?
Even if the LOI is nonbinding, that doesn’t necessarily mean you can sign it and expect to negotiate later. “I see people tripped up when they sign the LOI, thinking they’ll negotiate later,” said Mr. Hursh. “They may not like the terms – for example, they think the compensation is too low – and they figure they’ll work it out at the contract stage, because the LOI is ‘not legally binding.’ “
But because the candidate signed the LOI, “the employer is under the impression that the compensation was acceptable, so now you’ve tied your hands – and the hands of any attorney you may consult down the road – to negotiate those terms.”
Mr. Hursh said he is often consulted by physicians who signed the contract “to get the ball rolling,” thinking that the LOI was “just a meaningless bureaucratic paper.” They need to understand “that the employer wants to make sure they’re in agreement on the basic points before getting into the details,” he said. “Large hospitals with in-house counsel may not want to use their legal department’s valuable time in redrafting terms they thought were acceptable to the candidate, and most practices don’t want to pay a lawyer to draft an LOI and then come back and say, ‘Actually, the physician wants more compensation.’ “
Mr. Nabity summarized: “The LOI is essentially a negotiation tactic to take some of the cards out of the hands of the doctor and commit him or her to something they’re not ready to commit to.” Employers may be playing on the sense of pressure and candidate’s fear that the job will slip through their fingers if they wait too long to sign. “But it’s better to wait longer at this stage before signing even a nonbinding LOI,” he said.
What to do before signing
So how should physicians relate to the LOI? Mr. Nabity advises “working through the details of the offer letter first, going through it carefully and identifying areas of concern, bearing in mind that employers never begin with their best offer.”
He pointed out that physicians “rarely know their value and usually don’t know how to work through the dynamics of compensation, call schedules, additional incentives, bonuses, and productivity,” so they need to be informed about these areas before signing anything.
Ms. Murthy recommended “going back and saying [to the prospective employer], ‘Thank you, but I need time to consider and evaluate this offer.’ Then, do some due diligence.”
At that point, you can hire an attorney to go over the offer, educate yourself about compensation benchmarks and what your worth actually is, or consult another trained professional or more experienced individual who can review the LOI before you sign it.
That’s what Dominique Cleveland, MD, a Texas-based ob.gyn., did when she received an LOI 5 years ago.
“The offer letter from the group practice contained a statement that the group wanted me to come on board, what the salary would be, and the time frame that would be covered in the contract,” she told this news organization. “It mentioned benefits and incentives and relocation, but it was only a short document – maybe one or two pages long.”
At the time that she received her LOI, Dr. Cleveland was completing her residency. She consulted experienced faculty members from her institution to find out whether the terms laid out in the LOI “were the norm and were reasonable.” She was “fairly certain” that the salary was low and this was confirmed by the faculty members she talked to. “So I felt comfortable asking for more [compensation],” she said.
The employer was receptive to her proposed changes, which were included in the more detailed contract that followed. “I can’t say there were any surprises per se in the contract because I had negotiated my salary after receiving the offer letter,” she said. She accepted the position and has been working there ever since.
Dr. Cleveland advises physicians “not to make a decision without speaking to someone who’s experienced and can help you compare what’s out there.”
She also encourages physicians to ask for what they want, whether it’s compensation or something else, such as call schedule or vacation time, without being afraid. “I’m a firm believer that you won’t know what you can get if you don’t ask for it,” she said.
Negotiation tips
Mr. Nabity recommended not agreeing to any terms until you are ready to enter into negotiation, recognizing that negotiation is an “art” that requires skill and training. “Either get trained in negotiation, perhaps taking courses to advocate for yourself – which is rare, and most doctors aren’t likely to do this – or go to a trained advocate, such as a lawyer, who can do so on your behalf.”
You might share your concerns with the person who interviewed you, with the person whose name is on the LOI, or with the recruiter who can advocate on your behalf, Ms. Murthy said. “You can reach out to the recruiter and say, ‘I really appreciate the opportunity, but there are some things in the offer letter I’d like to continue discussing.’ “
When you’re ready to negotiate, be sure to assemble all of your “asks” in a single document rather than going back to the prospective employer with “multiple individual questions multiple times,” Ms. Murthy advised. It’s more efficient and the employer or recruiter will appreciate that.
She also advised couching your request in language that expresses your appreciation for the offer and stating that you would like the agreement to serve the best interests of both parties. “Use open-ended language like that, and ask if it’s all right for you to send back some questions, ask for clarification, or share concerns.”
Most employers “will be fine with that,” Ms. Murthy said. “Most won’t say, ‘This is it, take it or leave it.’ If they do, that’s a red flag for you to reconsider whether you really want to work for this particular employer.”
Mr. Hursh suggested that if you choose to sign the LOI immediately, so as to rapidly let the prospective employer know of your interest, “you should add some type of qualification such as, ‘I’m signing this to express my interest, but accepting the position will be dependent upon a more thorough review of compensation benchmarks,’ for example.”
Mr. Nabity agreed: “You can add a handwritten note to the signed LOI expressing that you’re eager to move forward and proceed with the position, but it shouldn’t be construed as accepting the terms of the LOI until you’ve seen the full contract.
“Remember, health care can’t exist without doctors,” Mr. Nabity said. “Doctors are the star players and should go into the negotiation process recognizing their true worth.”
A version of this article appeared on Medscape.com.
You’ve just received an offer letter from that job you interviewed for. Sometimes you want to let the employer know right away how interested you are. The verbiage says the letter isn’t “binding.” So you eagerly sign on the dotted line. Everything looks great ... until it isn’t.
Attorney Ericka Adler, JD, LLM, a partner at Roetzel & Andress, a Chicago-based law firm that represents physicians and health care professionals nationwide, described her client who was in this predicament. The physician, a dermatologist, left a practice where she had been employed because she had received an “amazing” offer letter that included promises about her new work location, staffing, equipment, and hours. She signed and immediately gave notice to her previous employer.
“When she received the actual employment contract, none of those details from the offer letter – which is also called a letter of intent [LOI] – were included,” Ms. Adler told this news organization. The physician wanted to have the details from the LOI formally spelled out in the contract, but the employer refused.
“Basically, they said, ‘This is our standard contract and you’ll just have to trust us that we’ll keep our word. We meant what we said in the LOI, but we cannot include those details in the actual agreement because everyone has the same form of agreement.’ “ The physician decided to sign the contract and accept the position.
She contacted Ms. Adler after she had been at her new position for a month. “She had received none of the things they had promised her in the LOI,” Ms. Adler reported. “She lacked the NP and PA support, she lacked the equipment, she didn’t have enough exam rooms. As soon as she started, someone with whom she was sharing call coverage left, and she was expected to take over. The LOI had a cap on the amount of call she would be required to take, but that verbiage didn’t make it into the contract.”
Ms. Adler tried to address this issue with the employer. “We couldn’t say they had literally breached the agreement, but we did list the things that were mentioned in the LOI but on which they hadn’t delivered. We asked them to fix the issue within 10 days.”
The employer argued “that they didn’t have to fulfill anything that wasn’t spelled out in the contract, even if it was in the LOI. In fact, the contract specified clearly that the signed employment agreement was the only agreement and replaced any previous written or oral agreements between the parties.”
The dermatologist ultimately left the new position. “She might have been able to have a legal claim against the employer for breach or perhaps ‘detrimental reliance’ – meaning, she might have argued that she had been financially harmed due to the false promises made to her. But it would have been difficult and expensive for her to litigate the issue,” said Ms. Adler.
“It also didn’t seem like the physician could remain in the job and develop a positive work relationship with the employer, given that she felt betrayed and misled, and didn’t like the terms of employment, which didn’t match her needs or expectations,” said Ms. Adler.
She added that “most employers are not as unscrupulous and dishonest as this one was. But some employers do play on the fact that younger doctors – especially residents and fellows – tend to be trusting or feel they don’t have negotiation power. They’re often excited to get an offer and sign it without a second thought.”
That’s why she advises physicians to “review the terms of the LOI carefully and make sure you’re comfortable with them before signing it; but know that the real contract to negotiate will be the actual Employment Agreement.”
She also advises physicians not to give notice at their current place of employment until they’ve signed the final contract with the new employer.
On the same page?
Anu Murthy, JD, an attorney and associate contract review specialist at Contract Diagnostics, explained that the LOI is a document that the candidate receives after an interview but before a full contract. Sometimes, the LOI is preceded by a verbal or e-mailed offer, which is less formal.
“An LOI is sometimes called a Term Sheet or Memorandum of Understanding,“ Ms. Murthy told this news organization. “Typically, it lays out key provisions, such as compensation, initial term of the contract, location, and recruitment incentives.” Sometimes it includes mention of staffing, call schedule, malpractice, noncompete covenants, and other components of the position.
Justin Nabity, founder and CEO of Physicians Thrive, a physician financial advisory group, said that LOIs are “a way for employers to gauge a prospective employee’s level of interest.”
The employer “doesn’t want to send a contract with a lot of details before determining whether the candidate is really serious about the position, so the offer letter doesn’t show the whole picture,” Mr. Nabity told this news organization.
Dennis Hursh, managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, agreed.
“Another way of putting it is that the employer wants to see whether the prospective employee is on the same page. The LOI will typically include some key components that will later appear in a more complete and formal contract, together with other topics and details. Agreeing to those key components signals that indeed you and the employer are in accord,” said Mr. Hursh.
But are you really on the same page with your prospective employer? And if you seem to be on the same page, and you sign the LOI, is that a guarantee that the employer will honor its terms?
Not necessarily, according to the experts. In fact, many LOIs contain some verbiage stating that the letter isn’t binding, which can be confusing. Others suggest that it is binding, but the candidate doesn’t realize that the letter isn’t a formal contract and that the contract may contain details not included in the LOI or may omit details mentioned in the LOI, as happened to Ms. Adler’s unfortunate client.
“One of the pitfalls I see is that doctors sign the LOI without recognizing whether it’s binding or nonbinding,” Ms. Murthy said. “If it’s binding, it creates a legal obligation on your part and could preclude you from further negotiation once you see the contract and feel you’d like to negotiate some of its terms.”
Binding letters are typically offered to candidates after some back-and-forth between the parties, and important terms have been agreed to, which can happen either verbally or via e-mail. Once these agreements have been reached, they’re summarized in a “binding” letter before being extended into a full contract.
“But even if you’ve agreed on the terms verbally, it’s still important to have someone more experienced review the offer letter before signing it,” Ms. Murthy said. “It’s important to understand the ‘legalese’ and what your rights and obligations are before agreeing to anything.”
And certainly, if you receive a binding LOI, you shouldn’t sign anything until you’re sure you’re comfortable with its contents and have more details.
Are “nonbinding” LOIs really not binding?
Even if the LOI is nonbinding, that doesn’t necessarily mean you can sign it and expect to negotiate later. “I see people tripped up when they sign the LOI, thinking they’ll negotiate later,” said Mr. Hursh. “They may not like the terms – for example, they think the compensation is too low – and they figure they’ll work it out at the contract stage, because the LOI is ‘not legally binding.’ “
But because the candidate signed the LOI, “the employer is under the impression that the compensation was acceptable, so now you’ve tied your hands – and the hands of any attorney you may consult down the road – to negotiate those terms.”
Mr. Hursh said he is often consulted by physicians who signed the contract “to get the ball rolling,” thinking that the LOI was “just a meaningless bureaucratic paper.” They need to understand “that the employer wants to make sure they’re in agreement on the basic points before getting into the details,” he said. “Large hospitals with in-house counsel may not want to use their legal department’s valuable time in redrafting terms they thought were acceptable to the candidate, and most practices don’t want to pay a lawyer to draft an LOI and then come back and say, ‘Actually, the physician wants more compensation.’ “
Mr. Nabity summarized: “The LOI is essentially a negotiation tactic to take some of the cards out of the hands of the doctor and commit him or her to something they’re not ready to commit to.” Employers may be playing on the sense of pressure and candidate’s fear that the job will slip through their fingers if they wait too long to sign. “But it’s better to wait longer at this stage before signing even a nonbinding LOI,” he said.
What to do before signing
So how should physicians relate to the LOI? Mr. Nabity advises “working through the details of the offer letter first, going through it carefully and identifying areas of concern, bearing in mind that employers never begin with their best offer.”
He pointed out that physicians “rarely know their value and usually don’t know how to work through the dynamics of compensation, call schedules, additional incentives, bonuses, and productivity,” so they need to be informed about these areas before signing anything.
Ms. Murthy recommended “going back and saying [to the prospective employer], ‘Thank you, but I need time to consider and evaluate this offer.’ Then, do some due diligence.”
At that point, you can hire an attorney to go over the offer, educate yourself about compensation benchmarks and what your worth actually is, or consult another trained professional or more experienced individual who can review the LOI before you sign it.
That’s what Dominique Cleveland, MD, a Texas-based ob.gyn., did when she received an LOI 5 years ago.
“The offer letter from the group practice contained a statement that the group wanted me to come on board, what the salary would be, and the time frame that would be covered in the contract,” she told this news organization. “It mentioned benefits and incentives and relocation, but it was only a short document – maybe one or two pages long.”
At the time that she received her LOI, Dr. Cleveland was completing her residency. She consulted experienced faculty members from her institution to find out whether the terms laid out in the LOI “were the norm and were reasonable.” She was “fairly certain” that the salary was low and this was confirmed by the faculty members she talked to. “So I felt comfortable asking for more [compensation],” she said.
The employer was receptive to her proposed changes, which were included in the more detailed contract that followed. “I can’t say there were any surprises per se in the contract because I had negotiated my salary after receiving the offer letter,” she said. She accepted the position and has been working there ever since.
Dr. Cleveland advises physicians “not to make a decision without speaking to someone who’s experienced and can help you compare what’s out there.”
She also encourages physicians to ask for what they want, whether it’s compensation or something else, such as call schedule or vacation time, without being afraid. “I’m a firm believer that you won’t know what you can get if you don’t ask for it,” she said.
Negotiation tips
Mr. Nabity recommended not agreeing to any terms until you are ready to enter into negotiation, recognizing that negotiation is an “art” that requires skill and training. “Either get trained in negotiation, perhaps taking courses to advocate for yourself – which is rare, and most doctors aren’t likely to do this – or go to a trained advocate, such as a lawyer, who can do so on your behalf.”
You might share your concerns with the person who interviewed you, with the person whose name is on the LOI, or with the recruiter who can advocate on your behalf, Ms. Murthy said. “You can reach out to the recruiter and say, ‘I really appreciate the opportunity, but there are some things in the offer letter I’d like to continue discussing.’ “
When you’re ready to negotiate, be sure to assemble all of your “asks” in a single document rather than going back to the prospective employer with “multiple individual questions multiple times,” Ms. Murthy advised. It’s more efficient and the employer or recruiter will appreciate that.
She also advised couching your request in language that expresses your appreciation for the offer and stating that you would like the agreement to serve the best interests of both parties. “Use open-ended language like that, and ask if it’s all right for you to send back some questions, ask for clarification, or share concerns.”
Most employers “will be fine with that,” Ms. Murthy said. “Most won’t say, ‘This is it, take it or leave it.’ If they do, that’s a red flag for you to reconsider whether you really want to work for this particular employer.”
Mr. Hursh suggested that if you choose to sign the LOI immediately, so as to rapidly let the prospective employer know of your interest, “you should add some type of qualification such as, ‘I’m signing this to express my interest, but accepting the position will be dependent upon a more thorough review of compensation benchmarks,’ for example.”
Mr. Nabity agreed: “You can add a handwritten note to the signed LOI expressing that you’re eager to move forward and proceed with the position, but it shouldn’t be construed as accepting the terms of the LOI until you’ve seen the full contract.
“Remember, health care can’t exist without doctors,” Mr. Nabity said. “Doctors are the star players and should go into the negotiation process recognizing their true worth.”
A version of this article appeared on Medscape.com.
You’ve just received an offer letter from that job you interviewed for. Sometimes you want to let the employer know right away how interested you are. The verbiage says the letter isn’t “binding.” So you eagerly sign on the dotted line. Everything looks great ... until it isn’t.
Attorney Ericka Adler, JD, LLM, a partner at Roetzel & Andress, a Chicago-based law firm that represents physicians and health care professionals nationwide, described her client who was in this predicament. The physician, a dermatologist, left a practice where she had been employed because she had received an “amazing” offer letter that included promises about her new work location, staffing, equipment, and hours. She signed and immediately gave notice to her previous employer.
“When she received the actual employment contract, none of those details from the offer letter – which is also called a letter of intent [LOI] – were included,” Ms. Adler told this news organization. The physician wanted to have the details from the LOI formally spelled out in the contract, but the employer refused.
“Basically, they said, ‘This is our standard contract and you’ll just have to trust us that we’ll keep our word. We meant what we said in the LOI, but we cannot include those details in the actual agreement because everyone has the same form of agreement.’ “ The physician decided to sign the contract and accept the position.
She contacted Ms. Adler after she had been at her new position for a month. “She had received none of the things they had promised her in the LOI,” Ms. Adler reported. “She lacked the NP and PA support, she lacked the equipment, she didn’t have enough exam rooms. As soon as she started, someone with whom she was sharing call coverage left, and she was expected to take over. The LOI had a cap on the amount of call she would be required to take, but that verbiage didn’t make it into the contract.”
Ms. Adler tried to address this issue with the employer. “We couldn’t say they had literally breached the agreement, but we did list the things that were mentioned in the LOI but on which they hadn’t delivered. We asked them to fix the issue within 10 days.”
The employer argued “that they didn’t have to fulfill anything that wasn’t spelled out in the contract, even if it was in the LOI. In fact, the contract specified clearly that the signed employment agreement was the only agreement and replaced any previous written or oral agreements between the parties.”
The dermatologist ultimately left the new position. “She might have been able to have a legal claim against the employer for breach or perhaps ‘detrimental reliance’ – meaning, she might have argued that she had been financially harmed due to the false promises made to her. But it would have been difficult and expensive for her to litigate the issue,” said Ms. Adler.
“It also didn’t seem like the physician could remain in the job and develop a positive work relationship with the employer, given that she felt betrayed and misled, and didn’t like the terms of employment, which didn’t match her needs or expectations,” said Ms. Adler.
She added that “most employers are not as unscrupulous and dishonest as this one was. But some employers do play on the fact that younger doctors – especially residents and fellows – tend to be trusting or feel they don’t have negotiation power. They’re often excited to get an offer and sign it without a second thought.”
That’s why she advises physicians to “review the terms of the LOI carefully and make sure you’re comfortable with them before signing it; but know that the real contract to negotiate will be the actual Employment Agreement.”
She also advises physicians not to give notice at their current place of employment until they’ve signed the final contract with the new employer.
On the same page?
Anu Murthy, JD, an attorney and associate contract review specialist at Contract Diagnostics, explained that the LOI is a document that the candidate receives after an interview but before a full contract. Sometimes, the LOI is preceded by a verbal or e-mailed offer, which is less formal.
“An LOI is sometimes called a Term Sheet or Memorandum of Understanding,“ Ms. Murthy told this news organization. “Typically, it lays out key provisions, such as compensation, initial term of the contract, location, and recruitment incentives.” Sometimes it includes mention of staffing, call schedule, malpractice, noncompete covenants, and other components of the position.
Justin Nabity, founder and CEO of Physicians Thrive, a physician financial advisory group, said that LOIs are “a way for employers to gauge a prospective employee’s level of interest.”
The employer “doesn’t want to send a contract with a lot of details before determining whether the candidate is really serious about the position, so the offer letter doesn’t show the whole picture,” Mr. Nabity told this news organization.
Dennis Hursh, managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, agreed.
“Another way of putting it is that the employer wants to see whether the prospective employee is on the same page. The LOI will typically include some key components that will later appear in a more complete and formal contract, together with other topics and details. Agreeing to those key components signals that indeed you and the employer are in accord,” said Mr. Hursh.
But are you really on the same page with your prospective employer? And if you seem to be on the same page, and you sign the LOI, is that a guarantee that the employer will honor its terms?
Not necessarily, according to the experts. In fact, many LOIs contain some verbiage stating that the letter isn’t binding, which can be confusing. Others suggest that it is binding, but the candidate doesn’t realize that the letter isn’t a formal contract and that the contract may contain details not included in the LOI or may omit details mentioned in the LOI, as happened to Ms. Adler’s unfortunate client.
“One of the pitfalls I see is that doctors sign the LOI without recognizing whether it’s binding or nonbinding,” Ms. Murthy said. “If it’s binding, it creates a legal obligation on your part and could preclude you from further negotiation once you see the contract and feel you’d like to negotiate some of its terms.”
Binding letters are typically offered to candidates after some back-and-forth between the parties, and important terms have been agreed to, which can happen either verbally or via e-mail. Once these agreements have been reached, they’re summarized in a “binding” letter before being extended into a full contract.
“But even if you’ve agreed on the terms verbally, it’s still important to have someone more experienced review the offer letter before signing it,” Ms. Murthy said. “It’s important to understand the ‘legalese’ and what your rights and obligations are before agreeing to anything.”
And certainly, if you receive a binding LOI, you shouldn’t sign anything until you’re sure you’re comfortable with its contents and have more details.
Are “nonbinding” LOIs really not binding?
Even if the LOI is nonbinding, that doesn’t necessarily mean you can sign it and expect to negotiate later. “I see people tripped up when they sign the LOI, thinking they’ll negotiate later,” said Mr. Hursh. “They may not like the terms – for example, they think the compensation is too low – and they figure they’ll work it out at the contract stage, because the LOI is ‘not legally binding.’ “
But because the candidate signed the LOI, “the employer is under the impression that the compensation was acceptable, so now you’ve tied your hands – and the hands of any attorney you may consult down the road – to negotiate those terms.”
Mr. Hursh said he is often consulted by physicians who signed the contract “to get the ball rolling,” thinking that the LOI was “just a meaningless bureaucratic paper.” They need to understand “that the employer wants to make sure they’re in agreement on the basic points before getting into the details,” he said. “Large hospitals with in-house counsel may not want to use their legal department’s valuable time in redrafting terms they thought were acceptable to the candidate, and most practices don’t want to pay a lawyer to draft an LOI and then come back and say, ‘Actually, the physician wants more compensation.’ “
Mr. Nabity summarized: “The LOI is essentially a negotiation tactic to take some of the cards out of the hands of the doctor and commit him or her to something they’re not ready to commit to.” Employers may be playing on the sense of pressure and candidate’s fear that the job will slip through their fingers if they wait too long to sign. “But it’s better to wait longer at this stage before signing even a nonbinding LOI,” he said.
What to do before signing
So how should physicians relate to the LOI? Mr. Nabity advises “working through the details of the offer letter first, going through it carefully and identifying areas of concern, bearing in mind that employers never begin with their best offer.”
He pointed out that physicians “rarely know their value and usually don’t know how to work through the dynamics of compensation, call schedules, additional incentives, bonuses, and productivity,” so they need to be informed about these areas before signing anything.
Ms. Murthy recommended “going back and saying [to the prospective employer], ‘Thank you, but I need time to consider and evaluate this offer.’ Then, do some due diligence.”
At that point, you can hire an attorney to go over the offer, educate yourself about compensation benchmarks and what your worth actually is, or consult another trained professional or more experienced individual who can review the LOI before you sign it.
That’s what Dominique Cleveland, MD, a Texas-based ob.gyn., did when she received an LOI 5 years ago.
“The offer letter from the group practice contained a statement that the group wanted me to come on board, what the salary would be, and the time frame that would be covered in the contract,” she told this news organization. “It mentioned benefits and incentives and relocation, but it was only a short document – maybe one or two pages long.”
At the time that she received her LOI, Dr. Cleveland was completing her residency. She consulted experienced faculty members from her institution to find out whether the terms laid out in the LOI “were the norm and were reasonable.” She was “fairly certain” that the salary was low and this was confirmed by the faculty members she talked to. “So I felt comfortable asking for more [compensation],” she said.
The employer was receptive to her proposed changes, which were included in the more detailed contract that followed. “I can’t say there were any surprises per se in the contract because I had negotiated my salary after receiving the offer letter,” she said. She accepted the position and has been working there ever since.
Dr. Cleveland advises physicians “not to make a decision without speaking to someone who’s experienced and can help you compare what’s out there.”
She also encourages physicians to ask for what they want, whether it’s compensation or something else, such as call schedule or vacation time, without being afraid. “I’m a firm believer that you won’t know what you can get if you don’t ask for it,” she said.
Negotiation tips
Mr. Nabity recommended not agreeing to any terms until you are ready to enter into negotiation, recognizing that negotiation is an “art” that requires skill and training. “Either get trained in negotiation, perhaps taking courses to advocate for yourself – which is rare, and most doctors aren’t likely to do this – or go to a trained advocate, such as a lawyer, who can do so on your behalf.”
You might share your concerns with the person who interviewed you, with the person whose name is on the LOI, or with the recruiter who can advocate on your behalf, Ms. Murthy said. “You can reach out to the recruiter and say, ‘I really appreciate the opportunity, but there are some things in the offer letter I’d like to continue discussing.’ “
When you’re ready to negotiate, be sure to assemble all of your “asks” in a single document rather than going back to the prospective employer with “multiple individual questions multiple times,” Ms. Murthy advised. It’s more efficient and the employer or recruiter will appreciate that.
She also advised couching your request in language that expresses your appreciation for the offer and stating that you would like the agreement to serve the best interests of both parties. “Use open-ended language like that, and ask if it’s all right for you to send back some questions, ask for clarification, or share concerns.”
Most employers “will be fine with that,” Ms. Murthy said. “Most won’t say, ‘This is it, take it or leave it.’ If they do, that’s a red flag for you to reconsider whether you really want to work for this particular employer.”
Mr. Hursh suggested that if you choose to sign the LOI immediately, so as to rapidly let the prospective employer know of your interest, “you should add some type of qualification such as, ‘I’m signing this to express my interest, but accepting the position will be dependent upon a more thorough review of compensation benchmarks,’ for example.”
Mr. Nabity agreed: “You can add a handwritten note to the signed LOI expressing that you’re eager to move forward and proceed with the position, but it shouldn’t be construed as accepting the terms of the LOI until you’ve seen the full contract.
“Remember, health care can’t exist without doctors,” Mr. Nabity said. “Doctors are the star players and should go into the negotiation process recognizing their true worth.”
A version of this article appeared on Medscape.com.
Surgery is falling out of favor in rectal cancer
TOPLINE:
METHODOLOGY:
- The National Comprehensive Cancer Network endorses watchful waiting, instead of surgery, when patients with rectal cancer have a complete clinical response to neoadjuvant therapy, but it’s unclear how often patients and providers opt for this organ preservation approach.
- To find out, investigators reviewed 175,545 adults in the National Cancer Database treated for rectal adenocarcinoma from 2006 to 2020.
- The research team assessed changes in the proportion of patients who were treated with chemotherapy and/or radiation without tumor resection, transanal local excision, or removal of the rectum.
- Patients had a mean age of 63 years, 39.7% were women, 17.4% had stage 1 disease, 24.7% had stage 2A-C disease, and 32.1% had stage 3A-C tumors; tumor stage was unknown in just over a quarter of patients.
TAKEAWAY:
- The absolute annual proportion of organ preservation increased by more than 50% from 18.4% in 2006 to 28.2% in 2020.
- In that time frame, organ preservation increased from 19.5% to 32.5% – a percent increase of about 67% – for patients with stage 2A-C disease, 16.2% to 29.1% – a percent increase of about 80% – for patients with stage 3A-C disease, and 16.5% to 26.6% – a percent increase of about 60% – for those with unknown stages.
- However, the rate of proctectomies increased by 6.1 percentage points, or by about 30%, among patients with stage I rectal cancer – from 20.3% to 26.4%.
- Among patients who did have surgery, the proportion who had complete pathologic responses to neoadjuvant therapy nearly tripled, increasing from 6.5% to 18.8%.
IN PRACTICE:
“This case series shows that rectal cancer is increasingly being managed medically, especially among patients whose treatment historically relied on proctectomy,” the authors concluded. However, protocols to standardize the approach are lacking, which is why “establishing quality standards for organ preservation is a pressing issue that should involve all relevant stakeholders, including patients.”
SOURCE:
The study, led by Anthony Loria, MD, MSCI, of the University of Rochester (N.Y.), was published online in JAMA Oncology.
LIMITATIONS:
The percentage of people who needed surgery for recurrence, patient and facility factors associated with organ preservation, and overall survival outcomes were not addressed.
DISCLOSURES:
No external funding was reported, and the investigators reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The National Comprehensive Cancer Network endorses watchful waiting, instead of surgery, when patients with rectal cancer have a complete clinical response to neoadjuvant therapy, but it’s unclear how often patients and providers opt for this organ preservation approach.
- To find out, investigators reviewed 175,545 adults in the National Cancer Database treated for rectal adenocarcinoma from 2006 to 2020.
- The research team assessed changes in the proportion of patients who were treated with chemotherapy and/or radiation without tumor resection, transanal local excision, or removal of the rectum.
- Patients had a mean age of 63 years, 39.7% were women, 17.4% had stage 1 disease, 24.7% had stage 2A-C disease, and 32.1% had stage 3A-C tumors; tumor stage was unknown in just over a quarter of patients.
TAKEAWAY:
- The absolute annual proportion of organ preservation increased by more than 50% from 18.4% in 2006 to 28.2% in 2020.
- In that time frame, organ preservation increased from 19.5% to 32.5% – a percent increase of about 67% – for patients with stage 2A-C disease, 16.2% to 29.1% – a percent increase of about 80% – for patients with stage 3A-C disease, and 16.5% to 26.6% – a percent increase of about 60% – for those with unknown stages.
- However, the rate of proctectomies increased by 6.1 percentage points, or by about 30%, among patients with stage I rectal cancer – from 20.3% to 26.4%.
- Among patients who did have surgery, the proportion who had complete pathologic responses to neoadjuvant therapy nearly tripled, increasing from 6.5% to 18.8%.
IN PRACTICE:
“This case series shows that rectal cancer is increasingly being managed medically, especially among patients whose treatment historically relied on proctectomy,” the authors concluded. However, protocols to standardize the approach are lacking, which is why “establishing quality standards for organ preservation is a pressing issue that should involve all relevant stakeholders, including patients.”
SOURCE:
The study, led by Anthony Loria, MD, MSCI, of the University of Rochester (N.Y.), was published online in JAMA Oncology.
LIMITATIONS:
The percentage of people who needed surgery for recurrence, patient and facility factors associated with organ preservation, and overall survival outcomes were not addressed.
DISCLOSURES:
No external funding was reported, and the investigators reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The National Comprehensive Cancer Network endorses watchful waiting, instead of surgery, when patients with rectal cancer have a complete clinical response to neoadjuvant therapy, but it’s unclear how often patients and providers opt for this organ preservation approach.
- To find out, investigators reviewed 175,545 adults in the National Cancer Database treated for rectal adenocarcinoma from 2006 to 2020.
- The research team assessed changes in the proportion of patients who were treated with chemotherapy and/or radiation without tumor resection, transanal local excision, or removal of the rectum.
- Patients had a mean age of 63 years, 39.7% were women, 17.4% had stage 1 disease, 24.7% had stage 2A-C disease, and 32.1% had stage 3A-C tumors; tumor stage was unknown in just over a quarter of patients.
TAKEAWAY:
- The absolute annual proportion of organ preservation increased by more than 50% from 18.4% in 2006 to 28.2% in 2020.
- In that time frame, organ preservation increased from 19.5% to 32.5% – a percent increase of about 67% – for patients with stage 2A-C disease, 16.2% to 29.1% – a percent increase of about 80% – for patients with stage 3A-C disease, and 16.5% to 26.6% – a percent increase of about 60% – for those with unknown stages.
- However, the rate of proctectomies increased by 6.1 percentage points, or by about 30%, among patients with stage I rectal cancer – from 20.3% to 26.4%.
- Among patients who did have surgery, the proportion who had complete pathologic responses to neoadjuvant therapy nearly tripled, increasing from 6.5% to 18.8%.
IN PRACTICE:
“This case series shows that rectal cancer is increasingly being managed medically, especially among patients whose treatment historically relied on proctectomy,” the authors concluded. However, protocols to standardize the approach are lacking, which is why “establishing quality standards for organ preservation is a pressing issue that should involve all relevant stakeholders, including patients.”
SOURCE:
The study, led by Anthony Loria, MD, MSCI, of the University of Rochester (N.Y.), was published online in JAMA Oncology.
LIMITATIONS:
The percentage of people who needed surgery for recurrence, patient and facility factors associated with organ preservation, and overall survival outcomes were not addressed.
DISCLOSURES:
No external funding was reported, and the investigators reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FDA OKs symplicity renal denervation system for hypertension
the company has announced.
The Symplicity Spyral system, also known as the Symplicity blood pressure procedure, provides a catheter-based approach to denervate the renal arteries using radiofrequency energy.
Back in August, the FDA’s Circulatory System Devices Panel unanimously agreed that the Symplicity Spyral system is safe, but the panel was split on its efficacy and whether the benefits outweighed the risks associated with its use.
As part of the Medtronic SPYRAL HTN Global Clinical Program, more than 25,000 patients have been treated worldwide, both in the presence and absence of medication, and in patients with high baseline cardiovascular risk.
The SPYRAL HTN-OFF study enrolled patients with hypertension whose medications could be stopped at the start of the trial.
The primary effectiveness endpoint was the mean difference in the baseline adjusted 24-hour ambulatory systolic blood pressure (ASBP) from baseline to 3 months after renal denervation or sham procedure. The study showed a statistically significant reduction of 3.9 mm Hg ASBP in patients who received the device, compared with sham-control patients.
The SPYRAL HTN-ON study evaluated patients with uncontrolled hypertension who continued taking their BP medications during treatment with either the Spyral renal denervation device or a sham device.
The primary endpoint was the mean difference in the baseline adjusted 24-hour ambulatory systolic blood pressure at 6 months. The study showed a nonsignificant 24-hour 0.03 mm Hg reduction in ASBP in active-treatment patients, compared with sham-control patients.
“The Symplicity blood pressure procedure is safe and effective, providing significant ‘always-on’ blood pressure reductions for patients,” David Kandzari, MD, chief, Piedmont Heart Institute, Atlanta, and co–principal investigator of the SPYRAL clinical program, said in the news release.
“This approval paves the way for a transformation in hypertension treatment, offering a solution that complements medication and lifestyle changes,” added co–principal investigator Raymond Townsend, MD, with University of Pennsylvania, Philadelphia.
Medtronic notes that patient preference and shared decision-making are key components when considering the Symplicity blood pressure procedure.
In a patient preference study led by Medtronic, when presented with an interventional treatment with BP reduction and potential risks in line with those of the Symplicity blood pressure procedure, approximately one-third of patients were likely to choose the interventional treatment.
Earlier in November, the FDA also approved the Paradise Ultrasound Renal Denervation system (Recor Medical, Otsuka Medical Devices) for the treatment of hypertension.
A version of this article first appeared on Medscape.com.
the company has announced.
The Symplicity Spyral system, also known as the Symplicity blood pressure procedure, provides a catheter-based approach to denervate the renal arteries using radiofrequency energy.
Back in August, the FDA’s Circulatory System Devices Panel unanimously agreed that the Symplicity Spyral system is safe, but the panel was split on its efficacy and whether the benefits outweighed the risks associated with its use.
As part of the Medtronic SPYRAL HTN Global Clinical Program, more than 25,000 patients have been treated worldwide, both in the presence and absence of medication, and in patients with high baseline cardiovascular risk.
The SPYRAL HTN-OFF study enrolled patients with hypertension whose medications could be stopped at the start of the trial.
The primary effectiveness endpoint was the mean difference in the baseline adjusted 24-hour ambulatory systolic blood pressure (ASBP) from baseline to 3 months after renal denervation or sham procedure. The study showed a statistically significant reduction of 3.9 mm Hg ASBP in patients who received the device, compared with sham-control patients.
The SPYRAL HTN-ON study evaluated patients with uncontrolled hypertension who continued taking their BP medications during treatment with either the Spyral renal denervation device or a sham device.
The primary endpoint was the mean difference in the baseline adjusted 24-hour ambulatory systolic blood pressure at 6 months. The study showed a nonsignificant 24-hour 0.03 mm Hg reduction in ASBP in active-treatment patients, compared with sham-control patients.
“The Symplicity blood pressure procedure is safe and effective, providing significant ‘always-on’ blood pressure reductions for patients,” David Kandzari, MD, chief, Piedmont Heart Institute, Atlanta, and co–principal investigator of the SPYRAL clinical program, said in the news release.
“This approval paves the way for a transformation in hypertension treatment, offering a solution that complements medication and lifestyle changes,” added co–principal investigator Raymond Townsend, MD, with University of Pennsylvania, Philadelphia.
Medtronic notes that patient preference and shared decision-making are key components when considering the Symplicity blood pressure procedure.
In a patient preference study led by Medtronic, when presented with an interventional treatment with BP reduction and potential risks in line with those of the Symplicity blood pressure procedure, approximately one-third of patients were likely to choose the interventional treatment.
Earlier in November, the FDA also approved the Paradise Ultrasound Renal Denervation system (Recor Medical, Otsuka Medical Devices) for the treatment of hypertension.
A version of this article first appeared on Medscape.com.
the company has announced.
The Symplicity Spyral system, also known as the Symplicity blood pressure procedure, provides a catheter-based approach to denervate the renal arteries using radiofrequency energy.
Back in August, the FDA’s Circulatory System Devices Panel unanimously agreed that the Symplicity Spyral system is safe, but the panel was split on its efficacy and whether the benefits outweighed the risks associated with its use.
As part of the Medtronic SPYRAL HTN Global Clinical Program, more than 25,000 patients have been treated worldwide, both in the presence and absence of medication, and in patients with high baseline cardiovascular risk.
The SPYRAL HTN-OFF study enrolled patients with hypertension whose medications could be stopped at the start of the trial.
The primary effectiveness endpoint was the mean difference in the baseline adjusted 24-hour ambulatory systolic blood pressure (ASBP) from baseline to 3 months after renal denervation or sham procedure. The study showed a statistically significant reduction of 3.9 mm Hg ASBP in patients who received the device, compared with sham-control patients.
The SPYRAL HTN-ON study evaluated patients with uncontrolled hypertension who continued taking their BP medications during treatment with either the Spyral renal denervation device or a sham device.
The primary endpoint was the mean difference in the baseline adjusted 24-hour ambulatory systolic blood pressure at 6 months. The study showed a nonsignificant 24-hour 0.03 mm Hg reduction in ASBP in active-treatment patients, compared with sham-control patients.
“The Symplicity blood pressure procedure is safe and effective, providing significant ‘always-on’ blood pressure reductions for patients,” David Kandzari, MD, chief, Piedmont Heart Institute, Atlanta, and co–principal investigator of the SPYRAL clinical program, said in the news release.
“This approval paves the way for a transformation in hypertension treatment, offering a solution that complements medication and lifestyle changes,” added co–principal investigator Raymond Townsend, MD, with University of Pennsylvania, Philadelphia.
Medtronic notes that patient preference and shared decision-making are key components when considering the Symplicity blood pressure procedure.
In a patient preference study led by Medtronic, when presented with an interventional treatment with BP reduction and potential risks in line with those of the Symplicity blood pressure procedure, approximately one-third of patients were likely to choose the interventional treatment.
Earlier in November, the FDA also approved the Paradise Ultrasound Renal Denervation system (Recor Medical, Otsuka Medical Devices) for the treatment of hypertension.
A version of this article first appeared on Medscape.com.
Adolescents with migraine need smooth handoff to adult care
, according to a headache specialist who treats adults and children and spoke at the 2023 Scottsdale Headache Symposium.
“I would start at about the age of 15 or 16,” said Hope L. O’Brien, MD, Headache Center of Hope, University of Cincinnati.
Describing the steps that she thinks should be included in an effective transition, Dr. O’Brien maintained, “you will have a greater chance of successful transition and lessen the likelihood of the chronicity and the poor outcomes that we see in adults.”
Dr. O’Brien, who developed a headache clinic that serves individuals between the ages of 15 and 27, has substantial experience with headache patients in this age range. She acknowledged that there are no guideline recommendations for how best to guide the transition from pediatric to adult care, but she has developed some strategies at her own institution, including a tool for determining when the transition should be considered.
“Transition readiness is something that you need to think about,” she said. “You don’t just do it [automatically] at the age of 18.”
TRAQ questionnaire is helpful
The Transition Readiness Assessment Questionnaire (TRAQ) is one tool that can be helpful, according to Dr. O’Brien, This tool, which can be used to evaluate whether young patients feel prepared to describe their own health status and needs and advocate on their own behalf, is not specific to headache, but the principle is particularly important in headache because of the importance of the patient’s history. Dr. O’Brien said that a fellow in her program, Allyson Bazarsky, MD, who is now affiliated with the University of Vermont Medical Center, Burlington, validated TRAQ for headache about 6 years ago.
“TRAQ is available online. It’s free. You can download it as a PDF,” Dr. O’Brien said. In fact, several age-specific versions can now be found readily on a web search for TRAQ questionnaire.
Ultimately, TRAQ helps the clinician to gauge what patients know about their disease, the medications they are taking, and the relevance of any comorbidities, such as mood disorders. It also provides insight about the ability to understand their health issues and to communicate well with caregivers.
Dr. O’Brien sees this as a process over time, rather than something to be implemented a few months before the transition.
“It is important to start making the shift during childhood and talking directly to the child,” Dr. O’Brien said. If education about the disease and its triggers are started relatively early in adolescence, the transition will not only be easier, but patients might have a chance to understand and control their disease at an earlier age.
With this kind of approach, most children are at least in the preparation stage by age 18 years. However, the age at which patients are suitable for transition varies substantially. Many patients 18 years of age or older are in the “action phase,” meaning it is time to take steps to transition.
Again, based on the interrelationship between headache and comorbidities, particularly mood disorders, such as depression and anxiety, the goal should not be limited to headache. Young adults should be educated about taking responsibility for their overall health.
In addition to educating the patient, Dr. O’Brien recommended preparing a transfer packet, such as the one described in an article published in Headache. Geared for communicating with the clinician who will take over care, the contents should include a detailed medical history along with the current treatment plan and list of medications that have been effective and those that have failed, according to Dr. O’Brien.
“An emergency plan in the form of an emergency department letter in case the patient needs to seek emergent care at an outside facility” is also appropriate, Dr. O’Brien said.
The patient should be aware of what is in the transfer pack in order to participate in an informed discussion of health care with the adult neurologist.
Poor transition linked to poor outcomes
A substantial proportion of adolescents with migraine continue to experience episodes as an adult, particularly those with a delayed diagnosis of migraine, those with a first degree relative who has migraine, and those with poor health habits, but this is not inevitable. Dr. O’Brien noted that “unsuccessful transition of care” into adulthood is a factor associated with poorer outcomes, making it an appropriate target for optimizing outcomes.
“Have that discussion on transfer of care with an action plan and do that early, especially in those with chronic or persistent disability headaches,” Dr. O’Brien emphasized.
This is pertinent advice, according to Amy A. Gelfand, MD, director of the child and adolescent headache program at Benioff Children’s Hospitals, University of California, San Francisco. Senior author of a comprehensive review article on pediatric migraine in Neurologic Clinics, Dr. Gelfand said the practical value of young adults learning what medications they are taking, and why, can place them in a better position to monitor their disease and to understand when a clinical visit is appropriate.
“I agree that it is important to help young adults (i.e., 18- or 19-year-olds) to prepare for the transition from the pediatric health care environment to the adult one,” said Dr. Gelfand, who has written frequently on this and related topics, such as the impact of comorbidities on outcome.
Dr. O’Brien reports financial relationships with AbbVie, Eli Lilly, Guidepoint, Pfizer, and Vector Psychometric Group. Dr. Gelfand reports financial relationships with Allergan, Eli Lilly, EMKinetics, eNeura, Teva and Zosano.
, according to a headache specialist who treats adults and children and spoke at the 2023 Scottsdale Headache Symposium.
“I would start at about the age of 15 or 16,” said Hope L. O’Brien, MD, Headache Center of Hope, University of Cincinnati.
Describing the steps that she thinks should be included in an effective transition, Dr. O’Brien maintained, “you will have a greater chance of successful transition and lessen the likelihood of the chronicity and the poor outcomes that we see in adults.”
Dr. O’Brien, who developed a headache clinic that serves individuals between the ages of 15 and 27, has substantial experience with headache patients in this age range. She acknowledged that there are no guideline recommendations for how best to guide the transition from pediatric to adult care, but she has developed some strategies at her own institution, including a tool for determining when the transition should be considered.
“Transition readiness is something that you need to think about,” she said. “You don’t just do it [automatically] at the age of 18.”
TRAQ questionnaire is helpful
The Transition Readiness Assessment Questionnaire (TRAQ) is one tool that can be helpful, according to Dr. O’Brien, This tool, which can be used to evaluate whether young patients feel prepared to describe their own health status and needs and advocate on their own behalf, is not specific to headache, but the principle is particularly important in headache because of the importance of the patient’s history. Dr. O’Brien said that a fellow in her program, Allyson Bazarsky, MD, who is now affiliated with the University of Vermont Medical Center, Burlington, validated TRAQ for headache about 6 years ago.
“TRAQ is available online. It’s free. You can download it as a PDF,” Dr. O’Brien said. In fact, several age-specific versions can now be found readily on a web search for TRAQ questionnaire.
Ultimately, TRAQ helps the clinician to gauge what patients know about their disease, the medications they are taking, and the relevance of any comorbidities, such as mood disorders. It also provides insight about the ability to understand their health issues and to communicate well with caregivers.
Dr. O’Brien sees this as a process over time, rather than something to be implemented a few months before the transition.
“It is important to start making the shift during childhood and talking directly to the child,” Dr. O’Brien said. If education about the disease and its triggers are started relatively early in adolescence, the transition will not only be easier, but patients might have a chance to understand and control their disease at an earlier age.
With this kind of approach, most children are at least in the preparation stage by age 18 years. However, the age at which patients are suitable for transition varies substantially. Many patients 18 years of age or older are in the “action phase,” meaning it is time to take steps to transition.
Again, based on the interrelationship between headache and comorbidities, particularly mood disorders, such as depression and anxiety, the goal should not be limited to headache. Young adults should be educated about taking responsibility for their overall health.
In addition to educating the patient, Dr. O’Brien recommended preparing a transfer packet, such as the one described in an article published in Headache. Geared for communicating with the clinician who will take over care, the contents should include a detailed medical history along with the current treatment plan and list of medications that have been effective and those that have failed, according to Dr. O’Brien.
“An emergency plan in the form of an emergency department letter in case the patient needs to seek emergent care at an outside facility” is also appropriate, Dr. O’Brien said.
The patient should be aware of what is in the transfer pack in order to participate in an informed discussion of health care with the adult neurologist.
Poor transition linked to poor outcomes
A substantial proportion of adolescents with migraine continue to experience episodes as an adult, particularly those with a delayed diagnosis of migraine, those with a first degree relative who has migraine, and those with poor health habits, but this is not inevitable. Dr. O’Brien noted that “unsuccessful transition of care” into adulthood is a factor associated with poorer outcomes, making it an appropriate target for optimizing outcomes.
“Have that discussion on transfer of care with an action plan and do that early, especially in those with chronic or persistent disability headaches,” Dr. O’Brien emphasized.
This is pertinent advice, according to Amy A. Gelfand, MD, director of the child and adolescent headache program at Benioff Children’s Hospitals, University of California, San Francisco. Senior author of a comprehensive review article on pediatric migraine in Neurologic Clinics, Dr. Gelfand said the practical value of young adults learning what medications they are taking, and why, can place them in a better position to monitor their disease and to understand when a clinical visit is appropriate.
“I agree that it is important to help young adults (i.e., 18- or 19-year-olds) to prepare for the transition from the pediatric health care environment to the adult one,” said Dr. Gelfand, who has written frequently on this and related topics, such as the impact of comorbidities on outcome.
Dr. O’Brien reports financial relationships with AbbVie, Eli Lilly, Guidepoint, Pfizer, and Vector Psychometric Group. Dr. Gelfand reports financial relationships with Allergan, Eli Lilly, EMKinetics, eNeura, Teva and Zosano.
, according to a headache specialist who treats adults and children and spoke at the 2023 Scottsdale Headache Symposium.
“I would start at about the age of 15 or 16,” said Hope L. O’Brien, MD, Headache Center of Hope, University of Cincinnati.
Describing the steps that she thinks should be included in an effective transition, Dr. O’Brien maintained, “you will have a greater chance of successful transition and lessen the likelihood of the chronicity and the poor outcomes that we see in adults.”
Dr. O’Brien, who developed a headache clinic that serves individuals between the ages of 15 and 27, has substantial experience with headache patients in this age range. She acknowledged that there are no guideline recommendations for how best to guide the transition from pediatric to adult care, but she has developed some strategies at her own institution, including a tool for determining when the transition should be considered.
“Transition readiness is something that you need to think about,” she said. “You don’t just do it [automatically] at the age of 18.”
TRAQ questionnaire is helpful
The Transition Readiness Assessment Questionnaire (TRAQ) is one tool that can be helpful, according to Dr. O’Brien, This tool, which can be used to evaluate whether young patients feel prepared to describe their own health status and needs and advocate on their own behalf, is not specific to headache, but the principle is particularly important in headache because of the importance of the patient’s history. Dr. O’Brien said that a fellow in her program, Allyson Bazarsky, MD, who is now affiliated with the University of Vermont Medical Center, Burlington, validated TRAQ for headache about 6 years ago.
“TRAQ is available online. It’s free. You can download it as a PDF,” Dr. O’Brien said. In fact, several age-specific versions can now be found readily on a web search for TRAQ questionnaire.
Ultimately, TRAQ helps the clinician to gauge what patients know about their disease, the medications they are taking, and the relevance of any comorbidities, such as mood disorders. It also provides insight about the ability to understand their health issues and to communicate well with caregivers.
Dr. O’Brien sees this as a process over time, rather than something to be implemented a few months before the transition.
“It is important to start making the shift during childhood and talking directly to the child,” Dr. O’Brien said. If education about the disease and its triggers are started relatively early in adolescence, the transition will not only be easier, but patients might have a chance to understand and control their disease at an earlier age.
With this kind of approach, most children are at least in the preparation stage by age 18 years. However, the age at which patients are suitable for transition varies substantially. Many patients 18 years of age or older are in the “action phase,” meaning it is time to take steps to transition.
Again, based on the interrelationship between headache and comorbidities, particularly mood disorders, such as depression and anxiety, the goal should not be limited to headache. Young adults should be educated about taking responsibility for their overall health.
In addition to educating the patient, Dr. O’Brien recommended preparing a transfer packet, such as the one described in an article published in Headache. Geared for communicating with the clinician who will take over care, the contents should include a detailed medical history along with the current treatment plan and list of medications that have been effective and those that have failed, according to Dr. O’Brien.
“An emergency plan in the form of an emergency department letter in case the patient needs to seek emergent care at an outside facility” is also appropriate, Dr. O’Brien said.
The patient should be aware of what is in the transfer pack in order to participate in an informed discussion of health care with the adult neurologist.
Poor transition linked to poor outcomes
A substantial proportion of adolescents with migraine continue to experience episodes as an adult, particularly those with a delayed diagnosis of migraine, those with a first degree relative who has migraine, and those with poor health habits, but this is not inevitable. Dr. O’Brien noted that “unsuccessful transition of care” into adulthood is a factor associated with poorer outcomes, making it an appropriate target for optimizing outcomes.
“Have that discussion on transfer of care with an action plan and do that early, especially in those with chronic or persistent disability headaches,” Dr. O’Brien emphasized.
This is pertinent advice, according to Amy A. Gelfand, MD, director of the child and adolescent headache program at Benioff Children’s Hospitals, University of California, San Francisco. Senior author of a comprehensive review article on pediatric migraine in Neurologic Clinics, Dr. Gelfand said the practical value of young adults learning what medications they are taking, and why, can place them in a better position to monitor their disease and to understand when a clinical visit is appropriate.
“I agree that it is important to help young adults (i.e., 18- or 19-year-olds) to prepare for the transition from the pediatric health care environment to the adult one,” said Dr. Gelfand, who has written frequently on this and related topics, such as the impact of comorbidities on outcome.
Dr. O’Brien reports financial relationships with AbbVie, Eli Lilly, Guidepoint, Pfizer, and Vector Psychometric Group. Dr. Gelfand reports financial relationships with Allergan, Eli Lilly, EMKinetics, eNeura, Teva and Zosano.
FROM THE 2023 SCOTTSDALE HEADACHE SYMPOSIUM
Single injection reduces blood pressure for 6 months: KARDIA-1
with what appeared to be an encouraging side-effect profile, in the phase 2 dose-ranging KARDIA-1 study.
“Our study demonstrates that either quarterly or biannual doses of zilebesiran can effectively and safely lower blood pressure in patients with uncontrolled hypertension,” said senior study investigator George Bakris, MD.
“Based on these results, zilebesiran has the potential to improve medication adherence, which will, in turn, reduce cardiovascular risk in people with hypertension,” added Dr. Bakris, who is professor of medicine and director of the Comprehensive Hypertension Center at the University of Chicago Medicine.
The KARDIA-1 study was presented at the American Heart Association scientific sessions.
Dr. Bakris noted that uncontrolled hypertension is a leading cause of morbidity and mortality, and despite availability of effective antihypertensives, many adults with hypertension are untreated, and up to 80% have uncontrolled disease, both globally and in the United States.
Zilebesiran is a subcutaneous RNA interference therapeutic that binds with high affinity to the hepatic asialoglycoprotein receptor, bringing about a reduction in the synthesis of angiotensinogen, the sole precursor of all angiotensin peptides. It is hoped that its hepatocyte-targeted delivery may allow extrahepatic angiotensinogen expression to be preserved, which could limit off-target effects in the kidney and other tissues.
The KARDIA-1 trial investigated the safety and efficacy of different doses of zilebesiran in patients with mild to moderate hypertension (systolic BP of 135-160 mm Hg), who are untreated or on stable therapy with up to two antihypertensive medications.
The study included 394 such patients (average baseline systolic BP was 142 mm Hg) who were randomly assigned to receive one of four different zilebesiran doses (150 mg, 300 mg, or 600 mg once every 6 months or 300 mg once every 2 months) or a placebo. The final analysis included 377 patients (56% men, 25% Black).
Results showed sustained reductions in serum angiotensinogen (between 88% and 98%) over the 6-month follow-up period.
Ambulatory systolic BP measured over 24 hours was significantly decreased with all zilebesiran regimens, with a mean reduction from baseline to month 6 of around 10 mm Hg in the three top doses studied and by around 14 mm Hg compared with placebo.
Patients receiving zilebesiran were more likely to achieve 24-hour average systolic BP measurements of 130 mm Hg or less at 6 months.
In addition, participants in all four zilebesiran groups consistently experienced significantly greater reductions in both daytime and nighttime systolic BP.
There were four nonserious adverse reactions leading to discontinuation in the zilebesiran groups: two instances of orthostatic hypotension, one of BP elevation, and one of injection site reaction.
Most hyperkalemia adverse events, which occurred in 6% of patients, were mild, did not require intervention, and generally resolved with repeat measurement; none were associated with acute kidney injury or led to study drug discontinuation. The incidence of hypotension events was low, and no clinically relevant changes in renal or hepatic function were observed, Dr. Bakris reported.
There was one death caused by cardiopulmonary arrest in a patient receiving zilebesiran 300 mg every 3 months, but this was not classified as drug related.
Zilebesiran is being further evaluated as an add-on therapy for treatment of hypertension in the ongoing KARDIA-2 phase 2 study.
Moderator of an AHA press conference at which the study was discussed, Sandra Taler, MD, professor of medicine at the Mayo Clinic, Rochester, Minn., said that “to have an injectable medicine that gives long-term blood pressure lowering is extremely exciting.”
Dr. Taler raised the point that some patients may not return for subsequent doses, but added that with subcutaneous dosing, administration at home may be a possibility.
Also commenting at the press conference, Keith Ferdinand, MD, professor of clinical medicine at Tulane University, New Orleans, said that this study “suggests we can now target the first step in the renin-angiotensin system – angiotensinogen – which then appears to lead to robust and continued blood pressure lowering for up to 6 months, which should improve adherence.”
Noting that only 50% of patients continue to take antihypertensive drugs after 1 year, Dr. Ferdinand added: “If we can increase adherence, we will increase efficacy and perhaps protect against some of the target organ damage.”
Designated discussant of the KARDIA-1 study at the AHA late-breaking clinical trial session, Anna Dominiczak, MD, University of Glasgow, noted that hypertension affects one in three adults worldwide, but only around 20% of people have it under control.
“An increase in the number of patients effectively treated for hypertension to levels observed in high-performing countries could prevent 76 million deaths, 120 million strokes, 79 million heart attacks, and 17 million cases of heart failure between now and 2050,” she said.
Dr. Bakris has received consulting fees from Alnylam Pharmaceuticals.
A version of this article first appeared on Medscape.com.
with what appeared to be an encouraging side-effect profile, in the phase 2 dose-ranging KARDIA-1 study.
“Our study demonstrates that either quarterly or biannual doses of zilebesiran can effectively and safely lower blood pressure in patients with uncontrolled hypertension,” said senior study investigator George Bakris, MD.
“Based on these results, zilebesiran has the potential to improve medication adherence, which will, in turn, reduce cardiovascular risk in people with hypertension,” added Dr. Bakris, who is professor of medicine and director of the Comprehensive Hypertension Center at the University of Chicago Medicine.
The KARDIA-1 study was presented at the American Heart Association scientific sessions.
Dr. Bakris noted that uncontrolled hypertension is a leading cause of morbidity and mortality, and despite availability of effective antihypertensives, many adults with hypertension are untreated, and up to 80% have uncontrolled disease, both globally and in the United States.
Zilebesiran is a subcutaneous RNA interference therapeutic that binds with high affinity to the hepatic asialoglycoprotein receptor, bringing about a reduction in the synthesis of angiotensinogen, the sole precursor of all angiotensin peptides. It is hoped that its hepatocyte-targeted delivery may allow extrahepatic angiotensinogen expression to be preserved, which could limit off-target effects in the kidney and other tissues.
The KARDIA-1 trial investigated the safety and efficacy of different doses of zilebesiran in patients with mild to moderate hypertension (systolic BP of 135-160 mm Hg), who are untreated or on stable therapy with up to two antihypertensive medications.
The study included 394 such patients (average baseline systolic BP was 142 mm Hg) who were randomly assigned to receive one of four different zilebesiran doses (150 mg, 300 mg, or 600 mg once every 6 months or 300 mg once every 2 months) or a placebo. The final analysis included 377 patients (56% men, 25% Black).
Results showed sustained reductions in serum angiotensinogen (between 88% and 98%) over the 6-month follow-up period.
Ambulatory systolic BP measured over 24 hours was significantly decreased with all zilebesiran regimens, with a mean reduction from baseline to month 6 of around 10 mm Hg in the three top doses studied and by around 14 mm Hg compared with placebo.
Patients receiving zilebesiran were more likely to achieve 24-hour average systolic BP measurements of 130 mm Hg or less at 6 months.
In addition, participants in all four zilebesiran groups consistently experienced significantly greater reductions in both daytime and nighttime systolic BP.
There were four nonserious adverse reactions leading to discontinuation in the zilebesiran groups: two instances of orthostatic hypotension, one of BP elevation, and one of injection site reaction.
Most hyperkalemia adverse events, which occurred in 6% of patients, were mild, did not require intervention, and generally resolved with repeat measurement; none were associated with acute kidney injury or led to study drug discontinuation. The incidence of hypotension events was low, and no clinically relevant changes in renal or hepatic function were observed, Dr. Bakris reported.
There was one death caused by cardiopulmonary arrest in a patient receiving zilebesiran 300 mg every 3 months, but this was not classified as drug related.
Zilebesiran is being further evaluated as an add-on therapy for treatment of hypertension in the ongoing KARDIA-2 phase 2 study.
Moderator of an AHA press conference at which the study was discussed, Sandra Taler, MD, professor of medicine at the Mayo Clinic, Rochester, Minn., said that “to have an injectable medicine that gives long-term blood pressure lowering is extremely exciting.”
Dr. Taler raised the point that some patients may not return for subsequent doses, but added that with subcutaneous dosing, administration at home may be a possibility.
Also commenting at the press conference, Keith Ferdinand, MD, professor of clinical medicine at Tulane University, New Orleans, said that this study “suggests we can now target the first step in the renin-angiotensin system – angiotensinogen – which then appears to lead to robust and continued blood pressure lowering for up to 6 months, which should improve adherence.”
Noting that only 50% of patients continue to take antihypertensive drugs after 1 year, Dr. Ferdinand added: “If we can increase adherence, we will increase efficacy and perhaps protect against some of the target organ damage.”
Designated discussant of the KARDIA-1 study at the AHA late-breaking clinical trial session, Anna Dominiczak, MD, University of Glasgow, noted that hypertension affects one in three adults worldwide, but only around 20% of people have it under control.
“An increase in the number of patients effectively treated for hypertension to levels observed in high-performing countries could prevent 76 million deaths, 120 million strokes, 79 million heart attacks, and 17 million cases of heart failure between now and 2050,” she said.
Dr. Bakris has received consulting fees from Alnylam Pharmaceuticals.
A version of this article first appeared on Medscape.com.
with what appeared to be an encouraging side-effect profile, in the phase 2 dose-ranging KARDIA-1 study.
“Our study demonstrates that either quarterly or biannual doses of zilebesiran can effectively and safely lower blood pressure in patients with uncontrolled hypertension,” said senior study investigator George Bakris, MD.
“Based on these results, zilebesiran has the potential to improve medication adherence, which will, in turn, reduce cardiovascular risk in people with hypertension,” added Dr. Bakris, who is professor of medicine and director of the Comprehensive Hypertension Center at the University of Chicago Medicine.
The KARDIA-1 study was presented at the American Heart Association scientific sessions.
Dr. Bakris noted that uncontrolled hypertension is a leading cause of morbidity and mortality, and despite availability of effective antihypertensives, many adults with hypertension are untreated, and up to 80% have uncontrolled disease, both globally and in the United States.
Zilebesiran is a subcutaneous RNA interference therapeutic that binds with high affinity to the hepatic asialoglycoprotein receptor, bringing about a reduction in the synthesis of angiotensinogen, the sole precursor of all angiotensin peptides. It is hoped that its hepatocyte-targeted delivery may allow extrahepatic angiotensinogen expression to be preserved, which could limit off-target effects in the kidney and other tissues.
The KARDIA-1 trial investigated the safety and efficacy of different doses of zilebesiran in patients with mild to moderate hypertension (systolic BP of 135-160 mm Hg), who are untreated or on stable therapy with up to two antihypertensive medications.
The study included 394 such patients (average baseline systolic BP was 142 mm Hg) who were randomly assigned to receive one of four different zilebesiran doses (150 mg, 300 mg, or 600 mg once every 6 months or 300 mg once every 2 months) or a placebo. The final analysis included 377 patients (56% men, 25% Black).
Results showed sustained reductions in serum angiotensinogen (between 88% and 98%) over the 6-month follow-up period.
Ambulatory systolic BP measured over 24 hours was significantly decreased with all zilebesiran regimens, with a mean reduction from baseline to month 6 of around 10 mm Hg in the three top doses studied and by around 14 mm Hg compared with placebo.
Patients receiving zilebesiran were more likely to achieve 24-hour average systolic BP measurements of 130 mm Hg or less at 6 months.
In addition, participants in all four zilebesiran groups consistently experienced significantly greater reductions in both daytime and nighttime systolic BP.
There were four nonserious adverse reactions leading to discontinuation in the zilebesiran groups: two instances of orthostatic hypotension, one of BP elevation, and one of injection site reaction.
Most hyperkalemia adverse events, which occurred in 6% of patients, were mild, did not require intervention, and generally resolved with repeat measurement; none were associated with acute kidney injury or led to study drug discontinuation. The incidence of hypotension events was low, and no clinically relevant changes in renal or hepatic function were observed, Dr. Bakris reported.
There was one death caused by cardiopulmonary arrest in a patient receiving zilebesiran 300 mg every 3 months, but this was not classified as drug related.
Zilebesiran is being further evaluated as an add-on therapy for treatment of hypertension in the ongoing KARDIA-2 phase 2 study.
Moderator of an AHA press conference at which the study was discussed, Sandra Taler, MD, professor of medicine at the Mayo Clinic, Rochester, Minn., said that “to have an injectable medicine that gives long-term blood pressure lowering is extremely exciting.”
Dr. Taler raised the point that some patients may not return for subsequent doses, but added that with subcutaneous dosing, administration at home may be a possibility.
Also commenting at the press conference, Keith Ferdinand, MD, professor of clinical medicine at Tulane University, New Orleans, said that this study “suggests we can now target the first step in the renin-angiotensin system – angiotensinogen – which then appears to lead to robust and continued blood pressure lowering for up to 6 months, which should improve adherence.”
Noting that only 50% of patients continue to take antihypertensive drugs after 1 year, Dr. Ferdinand added: “If we can increase adherence, we will increase efficacy and perhaps protect against some of the target organ damage.”
Designated discussant of the KARDIA-1 study at the AHA late-breaking clinical trial session, Anna Dominiczak, MD, University of Glasgow, noted that hypertension affects one in three adults worldwide, but only around 20% of people have it under control.
“An increase in the number of patients effectively treated for hypertension to levels observed in high-performing countries could prevent 76 million deaths, 120 million strokes, 79 million heart attacks, and 17 million cases of heart failure between now and 2050,” she said.
Dr. Bakris has received consulting fees from Alnylam Pharmaceuticals.
A version of this article first appeared on Medscape.com.
FROM AHA 2023
Novel myasthenia gravis therapies bring opportunities, challenges
PHOENIX – , according to Pushpa Narayanaswami, MD, who discussed the topic at the 2023 annual meeting of the American Association for Neuromuscular & Electrodiagnostic Medicine (AANEM).
The first Food and Drug Administration–approved drug was pyridostigmine in 1955, and it was more than 60 years before the second drug, eculizumab, gained FDA approval in 2017. Activity in more recent years has been much more brisk with the approvals of efgartigimod in 2021; ravulizumab in 2022; and efgartigimod SQ, rozanolixizumab, and zilucoplan (Japan) in 2023. Eculizumab, efgartigimod, efgartigimod SQ, ravulizumab, and rozanolixizumab are approved for patients who are anti–acetylcholine receptor (AchR) positive. Rozanolixizumab is also approved for patients who are anti–muscle-specific tyrosine kinase (MuSK) antibody positive.
The new drugs have novel mechanisms of action, giving physicians more tools to treat the condition. The mechanisms fall into two general groups: C5-complement inhibitors and neonatal Fc receptor (FcRn) agonists. Dr. Narayanaswami sought to provide guidance in thinking about how to prescribe the new drugs. “How do we really use these drugs? It’s sort of confusing in terms of where they fit in in the algorithm. I don’t pretend to have the answers, but I’m going to sort of give you a general overview of how I look at these based on the trial data and based on what we’ve done in the past,” she said during her talk.
Assessing the risk/benefit ratio
Myasthenia gravis treatment strategies should take into account both disease control and minimization of the adverse effects of treatment, which can include both short- and long-term concerns such as hematologic issues, changes in mood and sleep, diarrhea, infection risk, detriments to bone health, hypertension, diabetes mellitus, glaucoma, and cancer.
Disease control can be subjective. “Each patient may have a different approach to what their disease control means, so we don’t quite understand what the definition of disease control is,” said Dr. Narayanaswami. For example, “[a physician] may think of a sleep disturbance as mild, but [the patient] may not. They may not be able to function, so a lot of conversations [are needed] there,” she added.
The international consensus guidance for myasthenia gravis, first published in 2016 and updated a few years later, which Dr. Narayanaswami coauthored, suggested that minimal manifestation of disease is achievable and is relevant to patients. “These are patients who are doing well, they come to your office and say, ‘I’m doing well, I really don’t have any problem [though they may have some weakness],’ ” said Dr. Narayanaswami. In such patients, mild, grade 1 side effects from medications are acceptable.
Dr. Narayanaswami discussed the efficacy of older drugs, including evidence from a 2022 study of 367 patients, that found that 72% of patients achieved MGFA-PIS (postintervention status) of minimal manifestations within 2 years of treatment. That rose to 76% within 3 years and 84% within 5 years. “The incremental benefit [after the first 2] years was not huge, and I think that’s something to pay attention to,” said Dr. Narayanaswami. The study also found that disease duration at first visit was shorter among patients who achieved minimal manifestation at 12 months versus at 16 months. That finding follows a trend in current thinking about treatment of myasthenia gravis. “Chip (James) Howard [of Duke University], who’s my sort of guru, says you’ve got to address this like MS. You’ve got to hit them early and hit them hard. And I think we’re seeing more and more of this. If you think about it even in your clinical practice, patients who did well tended to do well early on,” said Dr. Narayanaswami. She noted an important limitation in that the study did not adjust for confounders or covariates.
In addition, the PROMISE-MG study, which Dr. Narayanaswami coauthored, found that 57%-89% of patients treated with azathioprine or mycophenolate achieved clinically meaningful improvement in a variety of different outcome measures. “More than half to two-thirds of patients do well in clinical practice with the older drugs,” said Dr. Narayanaswami. In terms of time to outcomes, the study found that it took 2-6 months of azathioprine treatment and 2-3 months of mycophenolate mofetil (MMF) treatment for 25% of patients to experience clinically meaningful improvements. It took 14-22 months and 13-18 months, respectively, for 75% of patients to achieve this benchmark.
Regarding when to consider switching to newer therapies, Dr. Narayanaswami pointed out that there is no FDA requirement that patients fail previous therapies, but insurance companies often require it before reimbursement.
Dr. Narayanaswami said that the benefits of these drugs are well known, so she focused instead on their safety profiles in clinical practice. C-5 complement inhibitors carry a risk of meningococcal infection, which has been addressed in various postmarketing studies. “I will say that data is difficult to interpret for various reasons … but the point is that there is a risk for meningococcal infections. The risk appears to be low, but it’s not zero, even if you immunize patients, and I think that’s the conversation we need to have [with patients],” she said. Other issues with C5-complement inhibitors can include headache, nasopharyngitis, diarrhea, abdominal pain, back pain, nausea, and other infections.
FcRn antagonists have a range of potential side effects, but Dr. Narayanaswami emphasized timing of vaccinations, since the drugs antagonize recycling of IgG. She said vaccines should be given before the first dose of the cycle. There are no data on their use in pregnancy, but the agents could potentially reduce the passive transfer of IgG antibodies to the fetus.
Treatment strategies
In clinical practice, Dr. Narayanaswami employs the newer drugs in patients who have failed older drugs, or who experience intolerable side effects. An important consideration is how long to wait before determining a failure on previous therapies. Her current inclination is to treat earlier, which leads her to consider newer drugs at 2 years after disease onset, or after 1 year if the patient has had no improvement at all. She would consider the therapies as first-line therapies in patients for whom she doesn’t feel comfortable prescribing older medications, often older or more frail patients, or patients at any age when comorbidities might contraindicate glucocorticoids.
During the Q&A session after the talk, an attendee asked Dr. Narayanaswami what she does when payers balk at paying for new drugs. She noted that payers don’t necessarily have a specific number of months in mind for patients who are quite sick. “They just want somebody to try something. That has been my experience,” she said. She also goes peer-to-peer when disputing coverage. “Sometimes you can convince them on a peer-to-peer [basis] because they don’t really know myasthenia gravis.”
Another questioner wondered if clinical trials have been done or are in progress to demonstrate that earlier treatment can lead to better results. Dr. Narayanaswami responded that several observational trials are looking at the question. “It’s challenging because sometimes we don’t know the time from diagnosis. We know the first time they came in, which is not necessarily the same as the time from diagnosis, and sometimes that can be hard to get. And, again, it’s observational data, which can be dirty,” she said.
Dr. Narayanaswami disclosed ties with Alexion, Argenx, Dianthus, GSK, Janssen, Patient Centered Outcomes Research Institute, Sanofi, and UCB.
PHOENIX – , according to Pushpa Narayanaswami, MD, who discussed the topic at the 2023 annual meeting of the American Association for Neuromuscular & Electrodiagnostic Medicine (AANEM).
The first Food and Drug Administration–approved drug was pyridostigmine in 1955, and it was more than 60 years before the second drug, eculizumab, gained FDA approval in 2017. Activity in more recent years has been much more brisk with the approvals of efgartigimod in 2021; ravulizumab in 2022; and efgartigimod SQ, rozanolixizumab, and zilucoplan (Japan) in 2023. Eculizumab, efgartigimod, efgartigimod SQ, ravulizumab, and rozanolixizumab are approved for patients who are anti–acetylcholine receptor (AchR) positive. Rozanolixizumab is also approved for patients who are anti–muscle-specific tyrosine kinase (MuSK) antibody positive.
The new drugs have novel mechanisms of action, giving physicians more tools to treat the condition. The mechanisms fall into two general groups: C5-complement inhibitors and neonatal Fc receptor (FcRn) agonists. Dr. Narayanaswami sought to provide guidance in thinking about how to prescribe the new drugs. “How do we really use these drugs? It’s sort of confusing in terms of where they fit in in the algorithm. I don’t pretend to have the answers, but I’m going to sort of give you a general overview of how I look at these based on the trial data and based on what we’ve done in the past,” she said during her talk.
Assessing the risk/benefit ratio
Myasthenia gravis treatment strategies should take into account both disease control and minimization of the adverse effects of treatment, which can include both short- and long-term concerns such as hematologic issues, changes in mood and sleep, diarrhea, infection risk, detriments to bone health, hypertension, diabetes mellitus, glaucoma, and cancer.
Disease control can be subjective. “Each patient may have a different approach to what their disease control means, so we don’t quite understand what the definition of disease control is,” said Dr. Narayanaswami. For example, “[a physician] may think of a sleep disturbance as mild, but [the patient] may not. They may not be able to function, so a lot of conversations [are needed] there,” she added.
The international consensus guidance for myasthenia gravis, first published in 2016 and updated a few years later, which Dr. Narayanaswami coauthored, suggested that minimal manifestation of disease is achievable and is relevant to patients. “These are patients who are doing well, they come to your office and say, ‘I’m doing well, I really don’t have any problem [though they may have some weakness],’ ” said Dr. Narayanaswami. In such patients, mild, grade 1 side effects from medications are acceptable.
Dr. Narayanaswami discussed the efficacy of older drugs, including evidence from a 2022 study of 367 patients, that found that 72% of patients achieved MGFA-PIS (postintervention status) of minimal manifestations within 2 years of treatment. That rose to 76% within 3 years and 84% within 5 years. “The incremental benefit [after the first 2] years was not huge, and I think that’s something to pay attention to,” said Dr. Narayanaswami. The study also found that disease duration at first visit was shorter among patients who achieved minimal manifestation at 12 months versus at 16 months. That finding follows a trend in current thinking about treatment of myasthenia gravis. “Chip (James) Howard [of Duke University], who’s my sort of guru, says you’ve got to address this like MS. You’ve got to hit them early and hit them hard. And I think we’re seeing more and more of this. If you think about it even in your clinical practice, patients who did well tended to do well early on,” said Dr. Narayanaswami. She noted an important limitation in that the study did not adjust for confounders or covariates.
In addition, the PROMISE-MG study, which Dr. Narayanaswami coauthored, found that 57%-89% of patients treated with azathioprine or mycophenolate achieved clinically meaningful improvement in a variety of different outcome measures. “More than half to two-thirds of patients do well in clinical practice with the older drugs,” said Dr. Narayanaswami. In terms of time to outcomes, the study found that it took 2-6 months of azathioprine treatment and 2-3 months of mycophenolate mofetil (MMF) treatment for 25% of patients to experience clinically meaningful improvements. It took 14-22 months and 13-18 months, respectively, for 75% of patients to achieve this benchmark.
Regarding when to consider switching to newer therapies, Dr. Narayanaswami pointed out that there is no FDA requirement that patients fail previous therapies, but insurance companies often require it before reimbursement.
Dr. Narayanaswami said that the benefits of these drugs are well known, so she focused instead on their safety profiles in clinical practice. C-5 complement inhibitors carry a risk of meningococcal infection, which has been addressed in various postmarketing studies. “I will say that data is difficult to interpret for various reasons … but the point is that there is a risk for meningococcal infections. The risk appears to be low, but it’s not zero, even if you immunize patients, and I think that’s the conversation we need to have [with patients],” she said. Other issues with C5-complement inhibitors can include headache, nasopharyngitis, diarrhea, abdominal pain, back pain, nausea, and other infections.
FcRn antagonists have a range of potential side effects, but Dr. Narayanaswami emphasized timing of vaccinations, since the drugs antagonize recycling of IgG. She said vaccines should be given before the first dose of the cycle. There are no data on their use in pregnancy, but the agents could potentially reduce the passive transfer of IgG antibodies to the fetus.
Treatment strategies
In clinical practice, Dr. Narayanaswami employs the newer drugs in patients who have failed older drugs, or who experience intolerable side effects. An important consideration is how long to wait before determining a failure on previous therapies. Her current inclination is to treat earlier, which leads her to consider newer drugs at 2 years after disease onset, or after 1 year if the patient has had no improvement at all. She would consider the therapies as first-line therapies in patients for whom she doesn’t feel comfortable prescribing older medications, often older or more frail patients, or patients at any age when comorbidities might contraindicate glucocorticoids.
During the Q&A session after the talk, an attendee asked Dr. Narayanaswami what she does when payers balk at paying for new drugs. She noted that payers don’t necessarily have a specific number of months in mind for patients who are quite sick. “They just want somebody to try something. That has been my experience,” she said. She also goes peer-to-peer when disputing coverage. “Sometimes you can convince them on a peer-to-peer [basis] because they don’t really know myasthenia gravis.”
Another questioner wondered if clinical trials have been done or are in progress to demonstrate that earlier treatment can lead to better results. Dr. Narayanaswami responded that several observational trials are looking at the question. “It’s challenging because sometimes we don’t know the time from diagnosis. We know the first time they came in, which is not necessarily the same as the time from diagnosis, and sometimes that can be hard to get. And, again, it’s observational data, which can be dirty,” she said.
Dr. Narayanaswami disclosed ties with Alexion, Argenx, Dianthus, GSK, Janssen, Patient Centered Outcomes Research Institute, Sanofi, and UCB.
PHOENIX – , according to Pushpa Narayanaswami, MD, who discussed the topic at the 2023 annual meeting of the American Association for Neuromuscular & Electrodiagnostic Medicine (AANEM).
The first Food and Drug Administration–approved drug was pyridostigmine in 1955, and it was more than 60 years before the second drug, eculizumab, gained FDA approval in 2017. Activity in more recent years has been much more brisk with the approvals of efgartigimod in 2021; ravulizumab in 2022; and efgartigimod SQ, rozanolixizumab, and zilucoplan (Japan) in 2023. Eculizumab, efgartigimod, efgartigimod SQ, ravulizumab, and rozanolixizumab are approved for patients who are anti–acetylcholine receptor (AchR) positive. Rozanolixizumab is also approved for patients who are anti–muscle-specific tyrosine kinase (MuSK) antibody positive.
The new drugs have novel mechanisms of action, giving physicians more tools to treat the condition. The mechanisms fall into two general groups: C5-complement inhibitors and neonatal Fc receptor (FcRn) agonists. Dr. Narayanaswami sought to provide guidance in thinking about how to prescribe the new drugs. “How do we really use these drugs? It’s sort of confusing in terms of where they fit in in the algorithm. I don’t pretend to have the answers, but I’m going to sort of give you a general overview of how I look at these based on the trial data and based on what we’ve done in the past,” she said during her talk.
Assessing the risk/benefit ratio
Myasthenia gravis treatment strategies should take into account both disease control and minimization of the adverse effects of treatment, which can include both short- and long-term concerns such as hematologic issues, changes in mood and sleep, diarrhea, infection risk, detriments to bone health, hypertension, diabetes mellitus, glaucoma, and cancer.
Disease control can be subjective. “Each patient may have a different approach to what their disease control means, so we don’t quite understand what the definition of disease control is,” said Dr. Narayanaswami. For example, “[a physician] may think of a sleep disturbance as mild, but [the patient] may not. They may not be able to function, so a lot of conversations [are needed] there,” she added.
The international consensus guidance for myasthenia gravis, first published in 2016 and updated a few years later, which Dr. Narayanaswami coauthored, suggested that minimal manifestation of disease is achievable and is relevant to patients. “These are patients who are doing well, they come to your office and say, ‘I’m doing well, I really don’t have any problem [though they may have some weakness],’ ” said Dr. Narayanaswami. In such patients, mild, grade 1 side effects from medications are acceptable.
Dr. Narayanaswami discussed the efficacy of older drugs, including evidence from a 2022 study of 367 patients, that found that 72% of patients achieved MGFA-PIS (postintervention status) of minimal manifestations within 2 years of treatment. That rose to 76% within 3 years and 84% within 5 years. “The incremental benefit [after the first 2] years was not huge, and I think that’s something to pay attention to,” said Dr. Narayanaswami. The study also found that disease duration at first visit was shorter among patients who achieved minimal manifestation at 12 months versus at 16 months. That finding follows a trend in current thinking about treatment of myasthenia gravis. “Chip (James) Howard [of Duke University], who’s my sort of guru, says you’ve got to address this like MS. You’ve got to hit them early and hit them hard. And I think we’re seeing more and more of this. If you think about it even in your clinical practice, patients who did well tended to do well early on,” said Dr. Narayanaswami. She noted an important limitation in that the study did not adjust for confounders or covariates.
In addition, the PROMISE-MG study, which Dr. Narayanaswami coauthored, found that 57%-89% of patients treated with azathioprine or mycophenolate achieved clinically meaningful improvement in a variety of different outcome measures. “More than half to two-thirds of patients do well in clinical practice with the older drugs,” said Dr. Narayanaswami. In terms of time to outcomes, the study found that it took 2-6 months of azathioprine treatment and 2-3 months of mycophenolate mofetil (MMF) treatment for 25% of patients to experience clinically meaningful improvements. It took 14-22 months and 13-18 months, respectively, for 75% of patients to achieve this benchmark.
Regarding when to consider switching to newer therapies, Dr. Narayanaswami pointed out that there is no FDA requirement that patients fail previous therapies, but insurance companies often require it before reimbursement.
Dr. Narayanaswami said that the benefits of these drugs are well known, so she focused instead on their safety profiles in clinical practice. C-5 complement inhibitors carry a risk of meningococcal infection, which has been addressed in various postmarketing studies. “I will say that data is difficult to interpret for various reasons … but the point is that there is a risk for meningococcal infections. The risk appears to be low, but it’s not zero, even if you immunize patients, and I think that’s the conversation we need to have [with patients],” she said. Other issues with C5-complement inhibitors can include headache, nasopharyngitis, diarrhea, abdominal pain, back pain, nausea, and other infections.
FcRn antagonists have a range of potential side effects, but Dr. Narayanaswami emphasized timing of vaccinations, since the drugs antagonize recycling of IgG. She said vaccines should be given before the first dose of the cycle. There are no data on their use in pregnancy, but the agents could potentially reduce the passive transfer of IgG antibodies to the fetus.
Treatment strategies
In clinical practice, Dr. Narayanaswami employs the newer drugs in patients who have failed older drugs, or who experience intolerable side effects. An important consideration is how long to wait before determining a failure on previous therapies. Her current inclination is to treat earlier, which leads her to consider newer drugs at 2 years after disease onset, or after 1 year if the patient has had no improvement at all. She would consider the therapies as first-line therapies in patients for whom she doesn’t feel comfortable prescribing older medications, often older or more frail patients, or patients at any age when comorbidities might contraindicate glucocorticoids.
During the Q&A session after the talk, an attendee asked Dr. Narayanaswami what she does when payers balk at paying for new drugs. She noted that payers don’t necessarily have a specific number of months in mind for patients who are quite sick. “They just want somebody to try something. That has been my experience,” she said. She also goes peer-to-peer when disputing coverage. “Sometimes you can convince them on a peer-to-peer [basis] because they don’t really know myasthenia gravis.”
Another questioner wondered if clinical trials have been done or are in progress to demonstrate that earlier treatment can lead to better results. Dr. Narayanaswami responded that several observational trials are looking at the question. “It’s challenging because sometimes we don’t know the time from diagnosis. We know the first time they came in, which is not necessarily the same as the time from diagnosis, and sometimes that can be hard to get. And, again, it’s observational data, which can be dirty,” she said.
Dr. Narayanaswami disclosed ties with Alexion, Argenx, Dianthus, GSK, Janssen, Patient Centered Outcomes Research Institute, Sanofi, and UCB.
AT AANEM 2023
PREVENT: AHA’s new risk calculator incorporates CKM health
.
The new Predicting Risk of CVD Events (PREVENT) calculator is the first risk calculator that combines measures of cardiovascular, kidney, and metabolic health to estimate risk for CVD.
It follows an AHA presidential advisory and scientific statement published in October, formally defining cardiovascular-kidney-metabolic (CKM) syndrome.
The PREVENT calculator also “starts earlier and goes longer” than the pooled cohort equations (PCE), Sadiya Khan, MD, MSc, chair of the statement writing committee, told this news organization.
PREVENT is for use in adults aged 30-79 years and estimates the 10- and 30-year risk of total CVD including, for the first time, heart failure. The PCE were designed to assess 10-year risk of only myocardial infarction and stroke and only in adults aged 40-79 years.
“The new PREVENT equations are important for doctors because they allow us to start conversations earlier and more comprehensively and accurately calculate risk for our patients,” said Dr. Khan, preventive cardiologist at Northwestern Medicine and associate professor at Northwestern University in Chicago.
“We want to support clinicians in starting these conversations around optimizing CKM health earlier and begin to engage in discussions on ways to optimize health,” Dr. Khan added.
The AHA scientific statement on the PREVENT calculator, with Dr. Khan as lead author, was published online in Circulation, with an accompanying article that describes development and validation of the tool.
Going beyond the PCE
The new calculator was developed using health information from more than 6 million adults from diverse racial and ethnic, socioeconomic, and geographic backgrounds.
In addition to blood pressure and cholesterol levels, the PREVENT equations allow for inclusion of hemoglobin A1c, if necessary, to monitor metabolic health.
It also includes estimated glomerular filtration rate (eGFR), a measure of kidney function, and allows for use of albumin excretion to monitor kidney disease to further individualize risk assessment and help inform personalized treatment options.
The new calculator also asks about tobacco use and use of medications for CVD risk factors and factors in age and sex, and it removes race from the risk calculations.
“The inclusion of race in risk prediction may imply that differences by race are not modifiable and may reify race as a biological construct, which may worsen health disparities. Therefore, it was decided a priori not to include race as a predictor in the development of PREVENT,” the writing group said.
They emphasized that the PREVENT calculator has similar accuracy among varied racial and ethnic groups.
The equations include an option to use the Social Deprivation Index, which incorporates measures of adverse social determinants of health such as education, poverty, unemployment, and factors based on a person’s environment.
The PREVENT equations are a “critical first step” toward including CKM health and social factors in risk prediction for CVD, Dr. Khan said in a news release.
“We are working on finalizing the online tool and it should be available soon – hopefully in a few weeks,” Dr. Khan told this news organization.
Knowledge gaps
The scientific statement lists several knowledge gaps and areas for more research. These include:
- Incorporating “net benefit” to identify the expected benefit of treatment recommendations based on an individual’s level of risk.
- Collecting more data from people of diverse race and ethnic backgrounds to better represent the increasing diversity in the United States. The number of Hispanic and Asian people included in the PREVENT datasets is lower than national estimates in the general U.S. population, so risk estimations in these populations may be less precise.
- Expanding the collection, reporting, and standardization of social determinants of health data, such as individual information rather than neighborhood information.
- Expanding risk assessment and prevention to earlier in life (childhood and/or adolescence) and in key life periods, such as during the peripartum period, since adverse pregnancy outcomes are associated with increased CVD risk.
- Investigating whether predicting adverse kidney outcomes, particularly among people with and without type 2 diabetes, may further optimize cardiovascular risk prediction.
The scientific statement was prepared by the volunteer writing group on behalf of the AHA. Dr. Khan reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
.
The new Predicting Risk of CVD Events (PREVENT) calculator is the first risk calculator that combines measures of cardiovascular, kidney, and metabolic health to estimate risk for CVD.
It follows an AHA presidential advisory and scientific statement published in October, formally defining cardiovascular-kidney-metabolic (CKM) syndrome.
The PREVENT calculator also “starts earlier and goes longer” than the pooled cohort equations (PCE), Sadiya Khan, MD, MSc, chair of the statement writing committee, told this news organization.
PREVENT is for use in adults aged 30-79 years and estimates the 10- and 30-year risk of total CVD including, for the first time, heart failure. The PCE were designed to assess 10-year risk of only myocardial infarction and stroke and only in adults aged 40-79 years.
“The new PREVENT equations are important for doctors because they allow us to start conversations earlier and more comprehensively and accurately calculate risk for our patients,” said Dr. Khan, preventive cardiologist at Northwestern Medicine and associate professor at Northwestern University in Chicago.
“We want to support clinicians in starting these conversations around optimizing CKM health earlier and begin to engage in discussions on ways to optimize health,” Dr. Khan added.
The AHA scientific statement on the PREVENT calculator, with Dr. Khan as lead author, was published online in Circulation, with an accompanying article that describes development and validation of the tool.
Going beyond the PCE
The new calculator was developed using health information from more than 6 million adults from diverse racial and ethnic, socioeconomic, and geographic backgrounds.
In addition to blood pressure and cholesterol levels, the PREVENT equations allow for inclusion of hemoglobin A1c, if necessary, to monitor metabolic health.
It also includes estimated glomerular filtration rate (eGFR), a measure of kidney function, and allows for use of albumin excretion to monitor kidney disease to further individualize risk assessment and help inform personalized treatment options.
The new calculator also asks about tobacco use and use of medications for CVD risk factors and factors in age and sex, and it removes race from the risk calculations.
“The inclusion of race in risk prediction may imply that differences by race are not modifiable and may reify race as a biological construct, which may worsen health disparities. Therefore, it was decided a priori not to include race as a predictor in the development of PREVENT,” the writing group said.
They emphasized that the PREVENT calculator has similar accuracy among varied racial and ethnic groups.
The equations include an option to use the Social Deprivation Index, which incorporates measures of adverse social determinants of health such as education, poverty, unemployment, and factors based on a person’s environment.
The PREVENT equations are a “critical first step” toward including CKM health and social factors in risk prediction for CVD, Dr. Khan said in a news release.
“We are working on finalizing the online tool and it should be available soon – hopefully in a few weeks,” Dr. Khan told this news organization.
Knowledge gaps
The scientific statement lists several knowledge gaps and areas for more research. These include:
- Incorporating “net benefit” to identify the expected benefit of treatment recommendations based on an individual’s level of risk.
- Collecting more data from people of diverse race and ethnic backgrounds to better represent the increasing diversity in the United States. The number of Hispanic and Asian people included in the PREVENT datasets is lower than national estimates in the general U.S. population, so risk estimations in these populations may be less precise.
- Expanding the collection, reporting, and standardization of social determinants of health data, such as individual information rather than neighborhood information.
- Expanding risk assessment and prevention to earlier in life (childhood and/or adolescence) and in key life periods, such as during the peripartum period, since adverse pregnancy outcomes are associated with increased CVD risk.
- Investigating whether predicting adverse kidney outcomes, particularly among people with and without type 2 diabetes, may further optimize cardiovascular risk prediction.
The scientific statement was prepared by the volunteer writing group on behalf of the AHA. Dr. Khan reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
.
The new Predicting Risk of CVD Events (PREVENT) calculator is the first risk calculator that combines measures of cardiovascular, kidney, and metabolic health to estimate risk for CVD.
It follows an AHA presidential advisory and scientific statement published in October, formally defining cardiovascular-kidney-metabolic (CKM) syndrome.
The PREVENT calculator also “starts earlier and goes longer” than the pooled cohort equations (PCE), Sadiya Khan, MD, MSc, chair of the statement writing committee, told this news organization.
PREVENT is for use in adults aged 30-79 years and estimates the 10- and 30-year risk of total CVD including, for the first time, heart failure. The PCE were designed to assess 10-year risk of only myocardial infarction and stroke and only in adults aged 40-79 years.
“The new PREVENT equations are important for doctors because they allow us to start conversations earlier and more comprehensively and accurately calculate risk for our patients,” said Dr. Khan, preventive cardiologist at Northwestern Medicine and associate professor at Northwestern University in Chicago.
“We want to support clinicians in starting these conversations around optimizing CKM health earlier and begin to engage in discussions on ways to optimize health,” Dr. Khan added.
The AHA scientific statement on the PREVENT calculator, with Dr. Khan as lead author, was published online in Circulation, with an accompanying article that describes development and validation of the tool.
Going beyond the PCE
The new calculator was developed using health information from more than 6 million adults from diverse racial and ethnic, socioeconomic, and geographic backgrounds.
In addition to blood pressure and cholesterol levels, the PREVENT equations allow for inclusion of hemoglobin A1c, if necessary, to monitor metabolic health.
It also includes estimated glomerular filtration rate (eGFR), a measure of kidney function, and allows for use of albumin excretion to monitor kidney disease to further individualize risk assessment and help inform personalized treatment options.
The new calculator also asks about tobacco use and use of medications for CVD risk factors and factors in age and sex, and it removes race from the risk calculations.
“The inclusion of race in risk prediction may imply that differences by race are not modifiable and may reify race as a biological construct, which may worsen health disparities. Therefore, it was decided a priori not to include race as a predictor in the development of PREVENT,” the writing group said.
They emphasized that the PREVENT calculator has similar accuracy among varied racial and ethnic groups.
The equations include an option to use the Social Deprivation Index, which incorporates measures of adverse social determinants of health such as education, poverty, unemployment, and factors based on a person’s environment.
The PREVENT equations are a “critical first step” toward including CKM health and social factors in risk prediction for CVD, Dr. Khan said in a news release.
“We are working on finalizing the online tool and it should be available soon – hopefully in a few weeks,” Dr. Khan told this news organization.
Knowledge gaps
The scientific statement lists several knowledge gaps and areas for more research. These include:
- Incorporating “net benefit” to identify the expected benefit of treatment recommendations based on an individual’s level of risk.
- Collecting more data from people of diverse race and ethnic backgrounds to better represent the increasing diversity in the United States. The number of Hispanic and Asian people included in the PREVENT datasets is lower than national estimates in the general U.S. population, so risk estimations in these populations may be less precise.
- Expanding the collection, reporting, and standardization of social determinants of health data, such as individual information rather than neighborhood information.
- Expanding risk assessment and prevention to earlier in life (childhood and/or adolescence) and in key life periods, such as during the peripartum period, since adverse pregnancy outcomes are associated with increased CVD risk.
- Investigating whether predicting adverse kidney outcomes, particularly among people with and without type 2 diabetes, may further optimize cardiovascular risk prediction.
The scientific statement was prepared by the volunteer writing group on behalf of the AHA. Dr. Khan reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CIRCULATION