User login
Climate change expected to impose major burden on mental health
NEW YORK – Of the broad range of direct and indirect threats to public health anticipated from climate change, those involving mental health will place psychiatrists on the front lines of efforts to mitigate the impact, a member of the Climate Psychiatry Alliance said at the annual meeting of the American Psychiatric Association.
“One thing climate changes mean for us in psychiatry is more work,” reported Janet L. Lewis, MD, an assistant clinical professor of psychiatry at the University of Rochester (N.Y.).
Mental health is sensitive to climate. “Psychiatric patients can be particularly vulnerable to the medical effects of climate change,” Dr. Lewis said. “People with schizophrenia exhibit impaired thermoregulatory functioning, and many of our medications can impair the body’s normal heat regulation.”
The evidence of increased death rates among schizophrenia patients during heat waves has been attributed to this phenomenon as well as to the failure of patients with mental disorders to seek or obtain relief from heat, according to Dr. Lewis, but she noted that These links are true for the individual, and they affect trends in communities.
As a cause of societal stresses, such as food and water insecurity, climate change also has the very real potential of producing traumatic disruptions commensurate with disasters such as hurricanes or earthquakes. Noting that the rate of PTSD after such natural disasters typically runs at around 30%, Dr. Lewis suggested that psychiatrists might face large challenges from major upheavals induced by climate change.
However, even in the absence of catastrophic consequences, significant psychiatric morbidity may be generated by climate change in the form of “ecoanxieties” or “solastalgia,” a term coined about 10 years ago to describe psychic anxiety induced by environmental change. While many individuals continue to function normally despite fear or anxiety about climate change, Dr. Lewis said that there are many reports in the literature now show that psychoterratic illness, another term for this phenomenon, is associated with degraded or threatened environments linked to climate change.
The Climate Psychiatry Alliance is one of several professional psychiatry groups that is engaged in evaluating how psychiatry as a profession should react to climate change. The Climate Psychiatry committee of the Group for the Advancement of Psychiatry is another. Dr. Lewis, addressing the potential criticism that climate is a political issue, said that “we bring some very particular things to this 21st-century disaster … hopefully, everything I have said about the mental effects of climate change convinces you that it is not just a political problem.”
It is, however, a problem that is complex. Differentiating complex problems from complicated problems – which can be solved eventually with sufficient information – Dr. Lewis explained that complex problems are dynamic with an interplay between components that make solutions uncertain without experimentation and continual reassessment. She believes both mitigation of the problem and adaption to the inevitability of rising temperatures will be necessary.
This is relevant for psychiatrists who also must adapt to the environmental changes and develop resilience that will help them deal objectively with the mental health consequences of climate change. She noted that environmentalists recognize two traps in approaching solutions to climate change. The first is proposing overly simplistic solutions that fail to address the profound implications of climate change. The second is being rendered inactive by the overwhelming complexity of this growing problem.
Ultimately, Dr. Lewis called for psychiatrists to be proactive in dealing the mental health consequences of climate change. She noted that the APA issued a position statement in 2017, which emphasized that individuals with mental health disorders are disproportionately affected by climate change.
“We as psychiatrists know what it is to deal with complex systems, and we understand through our own work with traumatized patients how to manage patients with trauma responses and how to get empowered and engaged in the rebuilding of realistic lives,” Dr. Lewis said. She believes those skills will be important as the impact of climate change on mental health unfolds.
NEW YORK – Of the broad range of direct and indirect threats to public health anticipated from climate change, those involving mental health will place psychiatrists on the front lines of efforts to mitigate the impact, a member of the Climate Psychiatry Alliance said at the annual meeting of the American Psychiatric Association.
“One thing climate changes mean for us in psychiatry is more work,” reported Janet L. Lewis, MD, an assistant clinical professor of psychiatry at the University of Rochester (N.Y.).
Mental health is sensitive to climate. “Psychiatric patients can be particularly vulnerable to the medical effects of climate change,” Dr. Lewis said. “People with schizophrenia exhibit impaired thermoregulatory functioning, and many of our medications can impair the body’s normal heat regulation.”
The evidence of increased death rates among schizophrenia patients during heat waves has been attributed to this phenomenon as well as to the failure of patients with mental disorders to seek or obtain relief from heat, according to Dr. Lewis, but she noted that These links are true for the individual, and they affect trends in communities.
As a cause of societal stresses, such as food and water insecurity, climate change also has the very real potential of producing traumatic disruptions commensurate with disasters such as hurricanes or earthquakes. Noting that the rate of PTSD after such natural disasters typically runs at around 30%, Dr. Lewis suggested that psychiatrists might face large challenges from major upheavals induced by climate change.
However, even in the absence of catastrophic consequences, significant psychiatric morbidity may be generated by climate change in the form of “ecoanxieties” or “solastalgia,” a term coined about 10 years ago to describe psychic anxiety induced by environmental change. While many individuals continue to function normally despite fear or anxiety about climate change, Dr. Lewis said that there are many reports in the literature now show that psychoterratic illness, another term for this phenomenon, is associated with degraded or threatened environments linked to climate change.
The Climate Psychiatry Alliance is one of several professional psychiatry groups that is engaged in evaluating how psychiatry as a profession should react to climate change. The Climate Psychiatry committee of the Group for the Advancement of Psychiatry is another. Dr. Lewis, addressing the potential criticism that climate is a political issue, said that “we bring some very particular things to this 21st-century disaster … hopefully, everything I have said about the mental effects of climate change convinces you that it is not just a political problem.”
It is, however, a problem that is complex. Differentiating complex problems from complicated problems – which can be solved eventually with sufficient information – Dr. Lewis explained that complex problems are dynamic with an interplay between components that make solutions uncertain without experimentation and continual reassessment. She believes both mitigation of the problem and adaption to the inevitability of rising temperatures will be necessary.
This is relevant for psychiatrists who also must adapt to the environmental changes and develop resilience that will help them deal objectively with the mental health consequences of climate change. She noted that environmentalists recognize two traps in approaching solutions to climate change. The first is proposing overly simplistic solutions that fail to address the profound implications of climate change. The second is being rendered inactive by the overwhelming complexity of this growing problem.
Ultimately, Dr. Lewis called for psychiatrists to be proactive in dealing the mental health consequences of climate change. She noted that the APA issued a position statement in 2017, which emphasized that individuals with mental health disorders are disproportionately affected by climate change.
“We as psychiatrists know what it is to deal with complex systems, and we understand through our own work with traumatized patients how to manage patients with trauma responses and how to get empowered and engaged in the rebuilding of realistic lives,” Dr. Lewis said. She believes those skills will be important as the impact of climate change on mental health unfolds.
NEW YORK – Of the broad range of direct and indirect threats to public health anticipated from climate change, those involving mental health will place psychiatrists on the front lines of efforts to mitigate the impact, a member of the Climate Psychiatry Alliance said at the annual meeting of the American Psychiatric Association.
“One thing climate changes mean for us in psychiatry is more work,” reported Janet L. Lewis, MD, an assistant clinical professor of psychiatry at the University of Rochester (N.Y.).
Mental health is sensitive to climate. “Psychiatric patients can be particularly vulnerable to the medical effects of climate change,” Dr. Lewis said. “People with schizophrenia exhibit impaired thermoregulatory functioning, and many of our medications can impair the body’s normal heat regulation.”
The evidence of increased death rates among schizophrenia patients during heat waves has been attributed to this phenomenon as well as to the failure of patients with mental disorders to seek or obtain relief from heat, according to Dr. Lewis, but she noted that These links are true for the individual, and they affect trends in communities.
As a cause of societal stresses, such as food and water insecurity, climate change also has the very real potential of producing traumatic disruptions commensurate with disasters such as hurricanes or earthquakes. Noting that the rate of PTSD after such natural disasters typically runs at around 30%, Dr. Lewis suggested that psychiatrists might face large challenges from major upheavals induced by climate change.
However, even in the absence of catastrophic consequences, significant psychiatric morbidity may be generated by climate change in the form of “ecoanxieties” or “solastalgia,” a term coined about 10 years ago to describe psychic anxiety induced by environmental change. While many individuals continue to function normally despite fear or anxiety about climate change, Dr. Lewis said that there are many reports in the literature now show that psychoterratic illness, another term for this phenomenon, is associated with degraded or threatened environments linked to climate change.
The Climate Psychiatry Alliance is one of several professional psychiatry groups that is engaged in evaluating how psychiatry as a profession should react to climate change. The Climate Psychiatry committee of the Group for the Advancement of Psychiatry is another. Dr. Lewis, addressing the potential criticism that climate is a political issue, said that “we bring some very particular things to this 21st-century disaster … hopefully, everything I have said about the mental effects of climate change convinces you that it is not just a political problem.”
It is, however, a problem that is complex. Differentiating complex problems from complicated problems – which can be solved eventually with sufficient information – Dr. Lewis explained that complex problems are dynamic with an interplay between components that make solutions uncertain without experimentation and continual reassessment. She believes both mitigation of the problem and adaption to the inevitability of rising temperatures will be necessary.
This is relevant for psychiatrists who also must adapt to the environmental changes and develop resilience that will help them deal objectively with the mental health consequences of climate change. She noted that environmentalists recognize two traps in approaching solutions to climate change. The first is proposing overly simplistic solutions that fail to address the profound implications of climate change. The second is being rendered inactive by the overwhelming complexity of this growing problem.
Ultimately, Dr. Lewis called for psychiatrists to be proactive in dealing the mental health consequences of climate change. She noted that the APA issued a position statement in 2017, which emphasized that individuals with mental health disorders are disproportionately affected by climate change.
“We as psychiatrists know what it is to deal with complex systems, and we understand through our own work with traumatized patients how to manage patients with trauma responses and how to get empowered and engaged in the rebuilding of realistic lives,” Dr. Lewis said. She believes those skills will be important as the impact of climate change on mental health unfolds.
VIDEO: Consider unique stressors when treating members of peacekeeping operations
NEW YORK – Sustained peacekeeping operations are associated with unique psychological stressors, and understanding of these stressors on the part of both community and military psychiatrists can help make a difference at each stage of a deployment cycle, according to Elspeth Cameron Ritchie, MD.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
During a workshop at the annual meeting of the American Psychiatric Association entitled “War and Peace: Understanding the Psychological Stressors Associated with Sustained Peacekeeping Operations (PKOs),” chaired by Dr. Ritchie of the Uniformed Services University of the Health Sciences, Bethesda, Md., various dimensions of salient psychological stress were discussed, as were approaches for minimizing any resultant impact on the psychological health of peacekeepers.
In this video interview, Dr. Ritchie discussed the differences and similarities between peacekeeping operations and military operations with respect to stressors and their effects, and the risk of posttraumatic stress disorder among peacekeepers.
Although treatment for PTSD is “pretty much the same,” it is important to “tailor the treatment for the situation,” she said.
“Lay out the different options, explain them to the patient, and partner with the patient in terms of what is the best option for them,” she said.
Dr. Ritchie reported having no relevant disclosures.
SOURCE: Ritchie EC et al. APA Workshop
NEW YORK – Sustained peacekeeping operations are associated with unique psychological stressors, and understanding of these stressors on the part of both community and military psychiatrists can help make a difference at each stage of a deployment cycle, according to Elspeth Cameron Ritchie, MD.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
During a workshop at the annual meeting of the American Psychiatric Association entitled “War and Peace: Understanding the Psychological Stressors Associated with Sustained Peacekeeping Operations (PKOs),” chaired by Dr. Ritchie of the Uniformed Services University of the Health Sciences, Bethesda, Md., various dimensions of salient psychological stress were discussed, as were approaches for minimizing any resultant impact on the psychological health of peacekeepers.
In this video interview, Dr. Ritchie discussed the differences and similarities between peacekeeping operations and military operations with respect to stressors and their effects, and the risk of posttraumatic stress disorder among peacekeepers.
Although treatment for PTSD is “pretty much the same,” it is important to “tailor the treatment for the situation,” she said.
“Lay out the different options, explain them to the patient, and partner with the patient in terms of what is the best option for them,” she said.
Dr. Ritchie reported having no relevant disclosures.
SOURCE: Ritchie EC et al. APA Workshop
NEW YORK – Sustained peacekeeping operations are associated with unique psychological stressors, and understanding of these stressors on the part of both community and military psychiatrists can help make a difference at each stage of a deployment cycle, according to Elspeth Cameron Ritchie, MD.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
During a workshop at the annual meeting of the American Psychiatric Association entitled “War and Peace: Understanding the Psychological Stressors Associated with Sustained Peacekeeping Operations (PKOs),” chaired by Dr. Ritchie of the Uniformed Services University of the Health Sciences, Bethesda, Md., various dimensions of salient psychological stress were discussed, as were approaches for minimizing any resultant impact on the psychological health of peacekeepers.
In this video interview, Dr. Ritchie discussed the differences and similarities between peacekeeping operations and military operations with respect to stressors and their effects, and the risk of posttraumatic stress disorder among peacekeepers.
Although treatment for PTSD is “pretty much the same,” it is important to “tailor the treatment for the situation,” she said.
“Lay out the different options, explain them to the patient, and partner with the patient in terms of what is the best option for them,” she said.
Dr. Ritchie reported having no relevant disclosures.
SOURCE: Ritchie EC et al. APA Workshop

Experts explore issues, controversies around medical marijuana use
I live and work in Maryland, where medical marijuana dispensaries are just beginning to open. So far, my patients have been content to smoke illegal marijuana, even after my admonishments. Last week, however, a patient who suffers from chronic pain told me that one of her doctors suggested she try medical marijuana. What did I think? The patient is in her 70s, and she has not tolerated opiates. She lives an active life, and she drives. I didn’t know what to think and was left to tell her that I had no experience and would not object if she wanted to try it. The timing was right for “Issues and Controversies Around Marijuana Use: What’s the Buzz?” at the American Psychiatric Association’s annual meeting in New York this week.

William Iacono, PhD, a professor of psychiatry at the University of Minnesota, Minneapolis, started with a session called “Does Adolescent Marijuana Use Cause Cognitive Decline?” Dr. Iacono and all the speakers who followed him pointed out how difficult it is to research these issues. The research is largely retrospective, and the questions are complex. The degree of use is determined by self-report, and there are questions about acute versus chronic use, whether cognitive decline is temporary or permanent, whether the age of initiating drug use is important, and finally, which tests are used to measure cognitive abilities. Dr. Iacono noted that results are inconsistent and mentioned a large population study done in Dunedin, New Zealand, which measured a decrease in verbal IQ and vocabulary measures at age 38 years if the user began smoking cannabis as an adolescent. Dr. Iacono’s twin studies showed that marijuana users scored lower on these measures in childhood, well before they began smoking, and poor academic performance predisposes to marijuana use.
“Adolescents who use cannabis are not the same as those who don’t,” Dr. Iacono said, “and heavy or daily use does not cause cognitive decline in those who begin smoking as adults.”
Dr. Pearlson introduced the second speaker by saying, “It’s easier to get funding to show the ill effects of cannabis than to show medicinal effects.” Sue Sisley, MD, director of Midtown Roots, a medical marijuana dispensary in Phoenix, conducts cannabis trials for the treatment of PTSD in veterans and noted that she has had a long and difficult road with marijuana research, and hers is the only controlled trial on cannabis for PTSD. When her Schedule I license was approved by the Food and Drug Administration, she was able to receive marijuana from the National Institute on Drug Abuse that was grown by the University of Mississippi in Oxford – the only federal growing facility. The marijuana was delivered by FedEx, and the drug was the consistency of talcum powder. It was a challenge to find a lab that could verify the components of the test drug, and when she did, she found the tetrahydrocannabinol content was considerably lower than marijuana sold on the black market. Also, the product contained both mold and lead. “As a physician, how do you hand out mold weed to our veterans?”
Her trials are still in progress, and more veterans are needed. Anecdotally, she says, a decrease has been seen in the use of both opiates and Viagra by the research subjects.
Michael Stevens, PhD, adjunct professor of psychiatry at Yale University, New Haven, Conn., discussed the risk of motor vehicle accidents in marijuana smokers and the logistical issues enforcement poses for law enforcement officials. “There is evidence that marijuana increases the risk for accidents.” Dr. Stevens went on to say that the elevated risk is notably less than that associated with the use of alcohol or stimulants. Studying the effects of marijuana on driving is difficult, as driving simulators do not necessarily reflect on-road experiences, and cognitive testing does not always translate into impairment. “We can’t give marijuana to teens and test them, and you can’t tell people who smoke every day that you’ll check in with them in a few years and check their driving records.”
In terms of law enforcement issues, roadside sobriety tests have not been validated for marijuana use, and plasma levels of the drug drop within minutes of use. “The alcohol model works well with alcohol, but cannabis is not alcohol.”
Deborah Hasin, PhD, professor of epidemiology (psychiatry) at Columbia University, New York, talked about trends of cannabis use in the United States. “Looking at states before and after legalization, we see that there is an increase in both cannabis use and cannabis disorders in adults.” Adolescents, however, are not smoking more, and “Kids are just not socializing; they are in their bedrooms with their smartphones. Depression is increasing in teens, but substance abuse is not.”
The last speaker was Deepak Cyril D’Souza, MD, a professor of psychiatry at Yale University, who talked about cannabis and psychosis. He defined three distinct relationships: acute transient psychosis that resolves fairly quickly, acute persistent psychosis that takes days or weeks to resolve, and psychotic reactions that are associated with recurrent psychotic symptoms. Studies suggest that those who have a psychotic reaction to marijuana are at elevated risk of being diagnosed with schizophrenia later, and that timing of exposure to marijuana may be important.

With regard to the important question of whether marijuana causes schizophrenia, Dr. D’Souza noted that “it’s neither a necessary nor sufficient component, but it does appear it hastens psychosis in schizophrenia and earlier symptoms are associated with a worse prognosis.”
I’ll see what happens with my patient. A Canadian physician in the audience noted that he has treated thousands of patients, and most find medical marijuana to be helpful. In our country, marijuana continues to be a controversial topic with strong opinions about its usefulness and a conversation that is limited by our lack of research.
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care,” (Baltimore: Johns Hopkins University Press, 2016). She practices in Baltimore.
I live and work in Maryland, where medical marijuana dispensaries are just beginning to open. So far, my patients have been content to smoke illegal marijuana, even after my admonishments. Last week, however, a patient who suffers from chronic pain told me that one of her doctors suggested she try medical marijuana. What did I think? The patient is in her 70s, and she has not tolerated opiates. She lives an active life, and she drives. I didn’t know what to think and was left to tell her that I had no experience and would not object if she wanted to try it. The timing was right for “Issues and Controversies Around Marijuana Use: What’s the Buzz?” at the American Psychiatric Association’s annual meeting in New York this week.
William Iacono, PhD, a professor of psychiatry at the University of Minnesota, Minneapolis, started with a session called “Does Adolescent Marijuana Use Cause Cognitive Decline?” Dr. Iacono and all the speakers who followed him pointed out how difficult it is to research these issues. The research is largely retrospective, and the questions are complex. The degree of use is determined by self-report, and there are questions about acute versus chronic use, whether cognitive decline is temporary or permanent, whether the age of initiating drug use is important, and finally, which tests are used to measure cognitive abilities. Dr. Iacono noted that results are inconsistent and mentioned a large population study done in Dunedin, New Zealand, which measured a decrease in verbal IQ and vocabulary measures at age 38 years if the user began smoking cannabis as an adolescent. Dr. Iacono’s twin studies showed that marijuana users scored lower on these measures in childhood, well before they began smoking, and poor academic performance predisposes to marijuana use.
“Adolescents who use cannabis are not the same as those who don’t,” Dr. Iacono said, “and heavy or daily use does not cause cognitive decline in those who begin smoking as adults.”
Dr. Pearlson introduced the second speaker by saying, “It’s easier to get funding to show the ill effects of cannabis than to show medicinal effects.” Sue Sisley, MD, director of Midtown Roots, a medical marijuana dispensary in Phoenix, conducts cannabis trials for the treatment of PTSD in veterans and noted that she has had a long and difficult road with marijuana research, and hers is the only controlled trial on cannabis for PTSD. When her Schedule I license was approved by the Food and Drug Administration, she was able to receive marijuana from the National Institute on Drug Abuse that was grown by the University of Mississippi in Oxford – the only federal growing facility. The marijuana was delivered by FedEx, and the drug was the consistency of talcum powder. It was a challenge to find a lab that could verify the components of the test drug, and when she did, she found the tetrahydrocannabinol content was considerably lower than marijuana sold on the black market. Also, the product contained both mold and lead. “As a physician, how do you hand out mold weed to our veterans?”
Her trials are still in progress, and more veterans are needed. Anecdotally, she says, a decrease has been seen in the use of both opiates and Viagra by the research subjects.
Michael Stevens, PhD, adjunct professor of psychiatry at Yale University, New Haven, Conn., discussed the risk of motor vehicle accidents in marijuana smokers and the logistical issues enforcement poses for law enforcement officials. “There is evidence that marijuana increases the risk for accidents.” Dr. Stevens went on to say that the elevated risk is notably less than that associated with the use of alcohol or stimulants. Studying the effects of marijuana on driving is difficult, as driving simulators do not necessarily reflect on-road experiences, and cognitive testing does not always translate into impairment. “We can’t give marijuana to teens and test them, and you can’t tell people who smoke every day that you’ll check in with them in a few years and check their driving records.”
In terms of law enforcement issues, roadside sobriety tests have not been validated for marijuana use, and plasma levels of the drug drop within minutes of use. “The alcohol model works well with alcohol, but cannabis is not alcohol.”
Deborah Hasin, PhD, professor of epidemiology (psychiatry) at Columbia University, New York, talked about trends of cannabis use in the United States. “Looking at states before and after legalization, we see that there is an increase in both cannabis use and cannabis disorders in adults.” Adolescents, however, are not smoking more, and “Kids are just not socializing; they are in their bedrooms with their smartphones. Depression is increasing in teens, but substance abuse is not.”
The last speaker was Deepak Cyril D’Souza, MD, a professor of psychiatry at Yale University, who talked about cannabis and psychosis. He defined three distinct relationships: acute transient psychosis that resolves fairly quickly, acute persistent psychosis that takes days or weeks to resolve, and psychotic reactions that are associated with recurrent psychotic symptoms. Studies suggest that those who have a psychotic reaction to marijuana are at elevated risk of being diagnosed with schizophrenia later, and that timing of exposure to marijuana may be important.
With regard to the important question of whether marijuana causes schizophrenia, Dr. D’Souza noted that “it’s neither a necessary nor sufficient component, but it does appear it hastens psychosis in schizophrenia and earlier symptoms are associated with a worse prognosis.”
I’ll see what happens with my patient. A Canadian physician in the audience noted that he has treated thousands of patients, and most find medical marijuana to be helpful. In our country, marijuana continues to be a controversial topic with strong opinions about its usefulness and a conversation that is limited by our lack of research.
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care,” (Baltimore: Johns Hopkins University Press, 2016). She practices in Baltimore.
I live and work in Maryland, where medical marijuana dispensaries are just beginning to open. So far, my patients have been content to smoke illegal marijuana, even after my admonishments. Last week, however, a patient who suffers from chronic pain told me that one of her doctors suggested she try medical marijuana. What did I think? The patient is in her 70s, and she has not tolerated opiates. She lives an active life, and she drives. I didn’t know what to think and was left to tell her that I had no experience and would not object if she wanted to try it. The timing was right for “Issues and Controversies Around Marijuana Use: What’s the Buzz?” at the American Psychiatric Association’s annual meeting in New York this week.
William Iacono, PhD, a professor of psychiatry at the University of Minnesota, Minneapolis, started with a session called “Does Adolescent Marijuana Use Cause Cognitive Decline?” Dr. Iacono and all the speakers who followed him pointed out how difficult it is to research these issues. The research is largely retrospective, and the questions are complex. The degree of use is determined by self-report, and there are questions about acute versus chronic use, whether cognitive decline is temporary or permanent, whether the age of initiating drug use is important, and finally, which tests are used to measure cognitive abilities. Dr. Iacono noted that results are inconsistent and mentioned a large population study done in Dunedin, New Zealand, which measured a decrease in verbal IQ and vocabulary measures at age 38 years if the user began smoking cannabis as an adolescent. Dr. Iacono’s twin studies showed that marijuana users scored lower on these measures in childhood, well before they began smoking, and poor academic performance predisposes to marijuana use.
“Adolescents who use cannabis are not the same as those who don’t,” Dr. Iacono said, “and heavy or daily use does not cause cognitive decline in those who begin smoking as adults.”
Dr. Pearlson introduced the second speaker by saying, “It’s easier to get funding to show the ill effects of cannabis than to show medicinal effects.” Sue Sisley, MD, director of Midtown Roots, a medical marijuana dispensary in Phoenix, conducts cannabis trials for the treatment of PTSD in veterans and noted that she has had a long and difficult road with marijuana research, and hers is the only controlled trial on cannabis for PTSD. When her Schedule I license was approved by the Food and Drug Administration, she was able to receive marijuana from the National Institute on Drug Abuse that was grown by the University of Mississippi in Oxford – the only federal growing facility. The marijuana was delivered by FedEx, and the drug was the consistency of talcum powder. It was a challenge to find a lab that could verify the components of the test drug, and when she did, she found the tetrahydrocannabinol content was considerably lower than marijuana sold on the black market. Also, the product contained both mold and lead. “As a physician, how do you hand out mold weed to our veterans?”
Her trials are still in progress, and more veterans are needed. Anecdotally, she says, a decrease has been seen in the use of both opiates and Viagra by the research subjects.
Michael Stevens, PhD, adjunct professor of psychiatry at Yale University, New Haven, Conn., discussed the risk of motor vehicle accidents in marijuana smokers and the logistical issues enforcement poses for law enforcement officials. “There is evidence that marijuana increases the risk for accidents.” Dr. Stevens went on to say that the elevated risk is notably less than that associated with the use of alcohol or stimulants. Studying the effects of marijuana on driving is difficult, as driving simulators do not necessarily reflect on-road experiences, and cognitive testing does not always translate into impairment. “We can’t give marijuana to teens and test them, and you can’t tell people who smoke every day that you’ll check in with them in a few years and check their driving records.”
In terms of law enforcement issues, roadside sobriety tests have not been validated for marijuana use, and plasma levels of the drug drop within minutes of use. “The alcohol model works well with alcohol, but cannabis is not alcohol.”
Deborah Hasin, PhD, professor of epidemiology (psychiatry) at Columbia University, New York, talked about trends of cannabis use in the United States. “Looking at states before and after legalization, we see that there is an increase in both cannabis use and cannabis disorders in adults.” Adolescents, however, are not smoking more, and “Kids are just not socializing; they are in their bedrooms with their smartphones. Depression is increasing in teens, but substance abuse is not.”
The last speaker was Deepak Cyril D’Souza, MD, a professor of psychiatry at Yale University, who talked about cannabis and psychosis. He defined three distinct relationships: acute transient psychosis that resolves fairly quickly, acute persistent psychosis that takes days or weeks to resolve, and psychotic reactions that are associated with recurrent psychotic symptoms. Studies suggest that those who have a psychotic reaction to marijuana are at elevated risk of being diagnosed with schizophrenia later, and that timing of exposure to marijuana may be important.
With regard to the important question of whether marijuana causes schizophrenia, Dr. D’Souza noted that “it’s neither a necessary nor sufficient component, but it does appear it hastens psychosis in schizophrenia and earlier symptoms are associated with a worse prognosis.”
I’ll see what happens with my patient. A Canadian physician in the audience noted that he has treated thousands of patients, and most find medical marijuana to be helpful. In our country, marijuana continues to be a controversial topic with strong opinions about its usefulness and a conversation that is limited by our lack of research.
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care,” (Baltimore: Johns Hopkins University Press, 2016). She practices in Baltimore.
Off-label prescribing of SGAs in children varies by diagnosis
TORONTO – On-label prescribing of second-generation antipsychotics in hospitalized pediatric patients with bipolar disorder and schizophrenia was greater than off-label prescribing, but not for patients with autism spectrum disorder, results from a single-center study showed.
“There is an increasing trend for using second-generation antipsychotics (SGAs) in children,” lead study author Debra V. McQuade, MD, PhD, said in an interview in advance of the Pediatric Academic Societies meeting. “This trend has already been widely acknowledged as concerning, due to the relatively high adverse event burden associated with them. Also, and perhaps more concerning, the great majority of these prescriptions are prescribed as ‘off-label’ (without Food and Drug Administration approval or indication). This is true in all settings, whether outpatient or inpatient. And, this off-label use is really high – usually reported as 60%-95% of all SGA prescriptions to children. We wanted to understand more about this practice of off-label prescribing of SGAs to children – to understand what drives it, to see if there were any organizing principles that might help to better explain it.”
Dr. McQuade and her associates found that for the three diagnostic groups overall, on-label prescribing of SGAs was greater than off-label prescribing (65% vs. 35%, respectively; P less than .001). Prescriptions for patients with bipolar disorder and schizophrenia followed this pattern, with on-label and off-label prescribing rates of 73% vs. 27%, for bipolar disorder, and 85% vs. 14% for schizophrenia. However, this prescription pattern was reversed for patients with autism spectrum disorder (35% vs. 64%; P less than .001), a finding that the researchers did not expect.

She said that while off-label prescribing of SGAs to pediatric patients remains widespread and is a concerning trend, the study findings suggested that prescribers “do select and prescribe SGAs in ways that are directly or indirectly influenced by FDA guidelines, mitigating risk to their pediatric patients.” Dr. McQuade acknowledged certain weaknesses of the study, including the fact that it was limited to one hospital setting and by the small number of prescribers who contributed to the overall pool of data.
She reported having no relevant financial disclosures.
TORONTO – On-label prescribing of second-generation antipsychotics in hospitalized pediatric patients with bipolar disorder and schizophrenia was greater than off-label prescribing, but not for patients with autism spectrum disorder, results from a single-center study showed.
“There is an increasing trend for using second-generation antipsychotics (SGAs) in children,” lead study author Debra V. McQuade, MD, PhD, said in an interview in advance of the Pediatric Academic Societies meeting. “This trend has already been widely acknowledged as concerning, due to the relatively high adverse event burden associated with them. Also, and perhaps more concerning, the great majority of these prescriptions are prescribed as ‘off-label’ (without Food and Drug Administration approval or indication). This is true in all settings, whether outpatient or inpatient. And, this off-label use is really high – usually reported as 60%-95% of all SGA prescriptions to children. We wanted to understand more about this practice of off-label prescribing of SGAs to children – to understand what drives it, to see if there were any organizing principles that might help to better explain it.”
Dr. McQuade and her associates found that for the three diagnostic groups overall, on-label prescribing of SGAs was greater than off-label prescribing (65% vs. 35%, respectively; P less than .001). Prescriptions for patients with bipolar disorder and schizophrenia followed this pattern, with on-label and off-label prescribing rates of 73% vs. 27%, for bipolar disorder, and 85% vs. 14% for schizophrenia. However, this prescription pattern was reversed for patients with autism spectrum disorder (35% vs. 64%; P less than .001), a finding that the researchers did not expect.
She said that while off-label prescribing of SGAs to pediatric patients remains widespread and is a concerning trend, the study findings suggested that prescribers “do select and prescribe SGAs in ways that are directly or indirectly influenced by FDA guidelines, mitigating risk to their pediatric patients.” Dr. McQuade acknowledged certain weaknesses of the study, including the fact that it was limited to one hospital setting and by the small number of prescribers who contributed to the overall pool of data.
She reported having no relevant financial disclosures.
TORONTO – On-label prescribing of second-generation antipsychotics in hospitalized pediatric patients with bipolar disorder and schizophrenia was greater than off-label prescribing, but not for patients with autism spectrum disorder, results from a single-center study showed.
“There is an increasing trend for using second-generation antipsychotics (SGAs) in children,” lead study author Debra V. McQuade, MD, PhD, said in an interview in advance of the Pediatric Academic Societies meeting. “This trend has already been widely acknowledged as concerning, due to the relatively high adverse event burden associated with them. Also, and perhaps more concerning, the great majority of these prescriptions are prescribed as ‘off-label’ (without Food and Drug Administration approval or indication). This is true in all settings, whether outpatient or inpatient. And, this off-label use is really high – usually reported as 60%-95% of all SGA prescriptions to children. We wanted to understand more about this practice of off-label prescribing of SGAs to children – to understand what drives it, to see if there were any organizing principles that might help to better explain it.”
Dr. McQuade and her associates found that for the three diagnostic groups overall, on-label prescribing of SGAs was greater than off-label prescribing (65% vs. 35%, respectively; P less than .001). Prescriptions for patients with bipolar disorder and schizophrenia followed this pattern, with on-label and off-label prescribing rates of 73% vs. 27%, for bipolar disorder, and 85% vs. 14% for schizophrenia. However, this prescription pattern was reversed for patients with autism spectrum disorder (35% vs. 64%; P less than .001), a finding that the researchers did not expect.
She said that while off-label prescribing of SGAs to pediatric patients remains widespread and is a concerning trend, the study findings suggested that prescribers “do select and prescribe SGAs in ways that are directly or indirectly influenced by FDA guidelines, mitigating risk to their pediatric patients.” Dr. McQuade acknowledged certain weaknesses of the study, including the fact that it was limited to one hospital setting and by the small number of prescribers who contributed to the overall pool of data.
She reported having no relevant financial disclosures.
Key clinical point:
Major finding: Overall, on-label prescribing of SGAs was greater than off-label prescribing (65% vs. 35%, respectively; P less than .001), but this prescription pattern did not hold true for patients with autism spectrum disorder.
Study details: A retrospective review of 86 hospitalized pediatric inpatients with a diagnosis of autism spectrum disorder, bipolar disorder, or schizophrenia.
Disclosures: Dr. McQuade reported having no financial disclosures.
Celiac disease: Can biopsy be avoided?
LAS VEGAS – It may be only a matter of time before the “gold standard” small biopsy is no longer considered mandatory to make a diagnosis of celiac disease in adults, according to Joseph A. Murray, MD, consultant in the division of gastroenterology and hepatology and department of immunology, Mayo Clinic, Rochester, Minn.
“Right now, none of the adult societies support biopsy avoidance, but I predict that it will come to be,” Dr. Murray said at the inaugural Perspectives in Digestive Diseases meeting held by Global Academy for Medical Education.
Biopsy, already a tarnished standard because of issues such as interpretation, according to Dr. Murray, is being challenged in studies that examine alternate ways of making the diagnosis.
In one recently reported study, investigators at Royal Derby Hospital, England, suggested that clinicians could make a reliable diagnosis of celiac disease by looking at serum IgA-tissue transglutaminase antibody levels.
Those investigators retrospectively analyzed an unselected series of 270 adult patients and found that an IgA-tissue transglutaminase antibody cut-off of 45 U/mL, or 8 times the upper limit of normal, had a positive predictive value of 100%.
Biopsy avoidance remains controversial, however. In a published letter to the editor commenting on the Derby study, authors took issue with some of the statistical analysis and remarked that the study included some patients with Marsh 1 histology.
“Studies suggest that the majority of seropositive patients with Marsh 1 histology do not progress to develop villous atrophy while on a gluten-containing diet, raising the question whether all of them are truly celiac,” they wrote.
The first society to endorse skipping the biopsy was the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition.
In guidelines for the diagnosis of celiac disease, that group said a celiac diagnosis could be made based on symptoms, antibodies, and HLA in children with symptoms suggestive of the disease and high antibody levels (IgA anti-tissue transglutaminase type 2 antibody titers greater than 10 times the upper limit of normal).

“The data [are] now pretty good to support that approach in symptomatic children,” Dr. Murray said. “If we apply these to adult patients, it’s not bad, actually, partly because our biopsies aren’t perfect.”
However, not all adult gastroenterology specialists agreed with the recommendations of the pediatric society. Guidelines from the British Society of Gastroenterology have stated that serology cannot replace biopsy, which “remains essential” for celiac disease diagnosis.
Global Academy and this news organization are owned by the same parent company.Dr. Murray reported disclosures related to Ardent Mills, DBV Technologies, Evelo, GlaxoSmithKline, Johnson & Johnson, Immunogenix, Innovate, National Center for Complementary and Integrative Health, Takeda, Torax Medical, and UCB.
AGA offers celiac disease information for your patients in the GI Patient Center at http://ow.ly/VwJ130jN7Sx.
LAS VEGAS – It may be only a matter of time before the “gold standard” small biopsy is no longer considered mandatory to make a diagnosis of celiac disease in adults, according to Joseph A. Murray, MD, consultant in the division of gastroenterology and hepatology and department of immunology, Mayo Clinic, Rochester, Minn.
“Right now, none of the adult societies support biopsy avoidance, but I predict that it will come to be,” Dr. Murray said at the inaugural Perspectives in Digestive Diseases meeting held by Global Academy for Medical Education.
Biopsy, already a tarnished standard because of issues such as interpretation, according to Dr. Murray, is being challenged in studies that examine alternate ways of making the diagnosis.
In one recently reported study, investigators at Royal Derby Hospital, England, suggested that clinicians could make a reliable diagnosis of celiac disease by looking at serum IgA-tissue transglutaminase antibody levels.
Those investigators retrospectively analyzed an unselected series of 270 adult patients and found that an IgA-tissue transglutaminase antibody cut-off of 45 U/mL, or 8 times the upper limit of normal, had a positive predictive value of 100%.
Biopsy avoidance remains controversial, however. In a published letter to the editor commenting on the Derby study, authors took issue with some of the statistical analysis and remarked that the study included some patients with Marsh 1 histology.
“Studies suggest that the majority of seropositive patients with Marsh 1 histology do not progress to develop villous atrophy while on a gluten-containing diet, raising the question whether all of them are truly celiac,” they wrote.
The first society to endorse skipping the biopsy was the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition.
In guidelines for the diagnosis of celiac disease, that group said a celiac diagnosis could be made based on symptoms, antibodies, and HLA in children with symptoms suggestive of the disease and high antibody levels (IgA anti-tissue transglutaminase type 2 antibody titers greater than 10 times the upper limit of normal).
“The data [are] now pretty good to support that approach in symptomatic children,” Dr. Murray said. “If we apply these to adult patients, it’s not bad, actually, partly because our biopsies aren’t perfect.”
However, not all adult gastroenterology specialists agreed with the recommendations of the pediatric society. Guidelines from the British Society of Gastroenterology have stated that serology cannot replace biopsy, which “remains essential” for celiac disease diagnosis.
Global Academy and this news organization are owned by the same parent company.Dr. Murray reported disclosures related to Ardent Mills, DBV Technologies, Evelo, GlaxoSmithKline, Johnson & Johnson, Immunogenix, Innovate, National Center for Complementary and Integrative Health, Takeda, Torax Medical, and UCB.
AGA offers celiac disease information for your patients in the GI Patient Center at http://ow.ly/VwJ130jN7Sx.
LAS VEGAS – It may be only a matter of time before the “gold standard” small biopsy is no longer considered mandatory to make a diagnosis of celiac disease in adults, according to Joseph A. Murray, MD, consultant in the division of gastroenterology and hepatology and department of immunology, Mayo Clinic, Rochester, Minn.
“Right now, none of the adult societies support biopsy avoidance, but I predict that it will come to be,” Dr. Murray said at the inaugural Perspectives in Digestive Diseases meeting held by Global Academy for Medical Education.
Biopsy, already a tarnished standard because of issues such as interpretation, according to Dr. Murray, is being challenged in studies that examine alternate ways of making the diagnosis.
In one recently reported study, investigators at Royal Derby Hospital, England, suggested that clinicians could make a reliable diagnosis of celiac disease by looking at serum IgA-tissue transglutaminase antibody levels.
Those investigators retrospectively analyzed an unselected series of 270 adult patients and found that an IgA-tissue transglutaminase antibody cut-off of 45 U/mL, or 8 times the upper limit of normal, had a positive predictive value of 100%.
Biopsy avoidance remains controversial, however. In a published letter to the editor commenting on the Derby study, authors took issue with some of the statistical analysis and remarked that the study included some patients with Marsh 1 histology.
“Studies suggest that the majority of seropositive patients with Marsh 1 histology do not progress to develop villous atrophy while on a gluten-containing diet, raising the question whether all of them are truly celiac,” they wrote.
The first society to endorse skipping the biopsy was the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition.
In guidelines for the diagnosis of celiac disease, that group said a celiac diagnosis could be made based on symptoms, antibodies, and HLA in children with symptoms suggestive of the disease and high antibody levels (IgA anti-tissue transglutaminase type 2 antibody titers greater than 10 times the upper limit of normal).
“The data [are] now pretty good to support that approach in symptomatic children,” Dr. Murray said. “If we apply these to adult patients, it’s not bad, actually, partly because our biopsies aren’t perfect.”
However, not all adult gastroenterology specialists agreed with the recommendations of the pediatric society. Guidelines from the British Society of Gastroenterology have stated that serology cannot replace biopsy, which “remains essential” for celiac disease diagnosis.
Global Academy and this news organization are owned by the same parent company.Dr. Murray reported disclosures related to Ardent Mills, DBV Technologies, Evelo, GlaxoSmithKline, Johnson & Johnson, Immunogenix, Innovate, National Center for Complementary and Integrative Health, Takeda, Torax Medical, and UCB.
AGA offers celiac disease information for your patients in the GI Patient Center at http://ow.ly/VwJ130jN7Sx.
VIDEO: Research underscores murky relationship between mental illness, gun violence
NEW YORK – Legislation enacted in some states in the wake of mass shootings seeks to limit access to firearms for people with mental illness, but research presented at the annual meeting of the American Psychiatric Association raises questions about the value of that approach.
During a workshop entitled “The ‘Crazed Gunman’ Myth: Examining Mental Illness and Firearm Violence,” researchers from the Yale University in New Haven, Conn., presented new findings that support existing data calling into question whether laws considered to be “common-sense approaches” to stopping gun violence really can reduce the likelihood of mass shootings.
It appears, based on the frequency and context of firearm use in more than 400 crimes that resulted in an insanity acquittal in Connecticut, for example, that individuals with mental illness are less likely than others to misuse firearms.
In this video, workshop chair Reena Kapoor, MD, also of Yale University, discusses the findings and notes that she and her colleagues seek to move past politics and ideology to focus on science that can guide policy and legislative efforts in a potentially more effective direction.
“We’ve also found that in spite of the media narrative, there has also been a slight decrease in how often [mentally ill offenders] use guns, over the years in the study,” she said. “Although the data are preliminary, it doesn’t support this idea that mentally ill people are more dangerous than ever, that they’re using guns more often in their violence; it actually says quite the opposite.”
Dr. Kapoor reported having no disclosures.
SOURCE: Kapoor R et al. APA 2018 Workshop.
NEW YORK – Legislation enacted in some states in the wake of mass shootings seeks to limit access to firearms for people with mental illness, but research presented at the annual meeting of the American Psychiatric Association raises questions about the value of that approach.
During a workshop entitled “The ‘Crazed Gunman’ Myth: Examining Mental Illness and Firearm Violence,” researchers from the Yale University in New Haven, Conn., presented new findings that support existing data calling into question whether laws considered to be “common-sense approaches” to stopping gun violence really can reduce the likelihood of mass shootings.
It appears, based on the frequency and context of firearm use in more than 400 crimes that resulted in an insanity acquittal in Connecticut, for example, that individuals with mental illness are less likely than others to misuse firearms.
In this video, workshop chair Reena Kapoor, MD, also of Yale University, discusses the findings and notes that she and her colleagues seek to move past politics and ideology to focus on science that can guide policy and legislative efforts in a potentially more effective direction.
“We’ve also found that in spite of the media narrative, there has also been a slight decrease in how often [mentally ill offenders] use guns, over the years in the study,” she said. “Although the data are preliminary, it doesn’t support this idea that mentally ill people are more dangerous than ever, that they’re using guns more often in their violence; it actually says quite the opposite.”
Dr. Kapoor reported having no disclosures.
SOURCE: Kapoor R et al. APA 2018 Workshop.
NEW YORK – Legislation enacted in some states in the wake of mass shootings seeks to limit access to firearms for people with mental illness, but research presented at the annual meeting of the American Psychiatric Association raises questions about the value of that approach.
During a workshop entitled “The ‘Crazed Gunman’ Myth: Examining Mental Illness and Firearm Violence,” researchers from the Yale University in New Haven, Conn., presented new findings that support existing data calling into question whether laws considered to be “common-sense approaches” to stopping gun violence really can reduce the likelihood of mass shootings.
It appears, based on the frequency and context of firearm use in more than 400 crimes that resulted in an insanity acquittal in Connecticut, for example, that individuals with mental illness are less likely than others to misuse firearms.
In this video, workshop chair Reena Kapoor, MD, also of Yale University, discusses the findings and notes that she and her colleagues seek to move past politics and ideology to focus on science that can guide policy and legislative efforts in a potentially more effective direction.
“We’ve also found that in spite of the media narrative, there has also been a slight decrease in how often [mentally ill offenders] use guns, over the years in the study,” she said. “Although the data are preliminary, it doesn’t support this idea that mentally ill people are more dangerous than ever, that they’re using guns more often in their violence; it actually says quite the opposite.”
Dr. Kapoor reported having no disclosures.
SOURCE: Kapoor R et al. APA 2018 Workshop.
REPORTING FROM APA

New BP guidelines synergize with transformed primary care
In mid-November, the American College of Cardiology, the American Heart Association, and nine other collaborating societies released a new and long-anticipated guideline for diagnosing and managing hypertension. The top-line, seismic change that the new guidelines called for – treating many patients with hypertension to a blood pressure below 130/80 mm Hg – rubbed the primary care community the wrong way, as described in Part 1 of this feature.
But the novel steps the guideline calls for, from including more careful and methodical measurement of BP, both in and out of the office, to increased reliance on lifestyle interventions, running a formal calculation to identify patients who warrant drug treatment, to a team approach to management, seem to dovetail nicely with the broader goals of primary care.
Part 2 of this feature explores how the approach to diagnosis and management of hypertension spelled out in the ACC/AHA guidelines fits into the protocol-driven, data-monitored, team-delivered primary care model that has come to dominate U.S. primary care in the decade following passage of the Affordable Care Act.
The importance of performance metrics
Regardless of what individual primary care physicians (PCPs) and other physicians and clinicians decide about the appropriate BP treatment target for hypertensive patients, their decisions these days are often strongly influenced by the standards set for population levels of BP control by the Centers for Medicare & Medicaid Services and other payers. In a trend traced by experts to the Affordable Care Act of 2009, many payers now emphasize value-based reimbursements and incentives based on health care organizations meeting performance-metric goals. One of the most common goals measured today in primary care is the percentage of patients with hypertension treated to a particular BP target that today is most commonly set as less than 140/90 mm Hg.
The “vast majority” of PCPs now work in practices that are subject to performance targets including levels of BP control, said Romsai T. Boonyasai, MD, an internist at Johns Hopkins Medicine in Baltimore who specializes in quality improvement research in hypertension and other chronic diseases and also works as a PCP.

Adoption of BP control to less than 130/80 mm Hg by groups such as the National Quality Forum (NQF), National Committee for Quality Assurance (NCQA), and America’s Health Insurance Plans (AHIP) “would add more pressure to comply, especially in an environment where there already is division of opinion between the ACC/AHA and American Association of Family Physicians,” agreed John P.A. Ioannidis, MD, professor of medicine and a preventive medicine specialist at Stanford (Calif.) University.
“The AHA is looking for endorsement from the metric groups,” noted Brent M. Egan, MD, vice president for research at the Care Coordination Institute in Greenville, S.C., and a consultant to the AHA.
But a new performance metric that reflects the ACC/AHA BP target won’t appear immediately. Step one is crafting performance measures based on the ACC/AHA guideline to submit to the NQF and similar groups, a process that will soon start, said Donald E. Casey Jr., MD, a member of the guideline-writing panel and chief clinical affairs officer at Medecision in Wayne, Pa.. He will chair a committee that will review existing hypertension management performance measures and as needed also write new measures based on the guideline, a process he expects to have completed by the end of 2018. After that comes field testing the measures, and if they prove effective and workable, the next step is to submit them to the performance metric groups for review and potential adoption, steps that may take another year. In short, performance metrics for hypertension management that call for a large segment of U.S. patients to be treated to a BP below 130/80 mm Hg likely won’t be in place until the end of 2019 or sometime in 2020 at the earliest, and of course only if the metric-setting groups decide to adopt the new measures as part of their standards.
“It takes a while for guidelines to go from publication to practice. Once [the new guideline] is systematized into performance measures it will help” adoption of what the new guideline recommends, Dr. Casey said in an interview.
Target:BP
Performance metrics are not the only path that could take U.S. medicine toward lower BP targets. Another active player is the Target:BP program, a voluntary quality-improvement program for increased U.S. hypertension awareness and better management launched in late 2015 as a collaboration between the AHA and the American Medical Association.
Given that both the new guideline and Target:BP were developed through partnerships involving the AHA, “it’s logical to connect [the guideline] to Target:BP, said Dr. Egan, an AHA spokesman for Target:BP and professor of medicine at the Medical University of South Carolina in Charleston.

Target:BP’s participants are health care organizations, including health systems, medical groups, community health centers, and physician practices. The program has two primary threads.
First, it functions as a recognition program that cites participating organizations if they achieve a prespecified level of BP control.
In 2017, the program released its initial list of successful participants, organizations that maintained at least 70% of their patients diagnosed with hypertension at a BP of less than 140/90 mm Hg. According to data reported by Willie E. Lawrence Jr., MD, during the AHA scientific sessions in November in Anaheim, Calif., 191 participating programs reached this level and won a “gold” designation from the program for their level of BP control during 2016, out of 310 participating organizations that submitted 2016 data to the program.
Dr. Lawrence also reported that nearly 1,200 total health care organizations were participating in Target:BP as of his presentation, and that the 310 programs that reported 2016 data cared for roughly 12 million people, numbers that extrapolate to more than 45 million Americans cared for in all 1,200 organizations now participating in Target:BP. Among all 310 organizations reporting 2016 data, the average level of hypertension control (patients with BPs maintained at less than 140/90 mm Hg) was 66%, said Dr. Lawrence, chief of cardiology at Research Medical Center in Kansas City, Mo. The cited “gold” programs averaged 76% of their hypertensive patients treated to less than 140/90 mm Hg.
The second thread of Target:BP’s program is to supply participating organizations with training and practice tools aimed at improving hypertension diagnosis and management. The core element of the tools the program currently promotes is the MAP checklists, which stands for Measure accurately, Act rapidly, and Partner with patients, families, and communities (J Clin Hypertens. 2017 Jul;19[7]:684-94).
Target:BP’s focus on a recognition program for organizational success in BP management is very reminiscent of the Get With the Guidelines programs that the AHA previously launched for the management of various cardiovascular diseases such as ischemic stroke. Get With the Guidelines–Stroke, begun in the early 2000s, helped achieve recent success in improving the rates at which U.S. stroke patients receive timely intervention with tissue plasminogen activator, demonstrating the power a recognition program can have for improving patient care.
Target:BP moved quickly to embrace the new ACC/AHA guideline BP targets, posting a treatment target of less than 130/80 mm Hg on its website by December 2017, scant weeks after the guideline’s release in mid-November. But for the time being, Target:BP will continue to use the NQF BP quality metric as the basis for its recognition program, according to an AMA spokesperson for the program. “While the AHA and AMA will keep our joint recognition program in accordance with the NQF measure, we will simultaneously build resources, including an updated treatment algorithm, that align with the new blood pressure guideline,” according to an AMA statement.
Part of the thinking about the timing for revising the BP recognition goal in Target:BP is that it would be too confusing and challenging for participating organizations to attend to two different treatment goals at once, one for Target:BP recognition and a different one for NQF compliance, Dr. Egan explained.
Development of the MAP checklists and several other tools promoted by Target:BP came into existence through a research program sponsored by the AMA in collaboration with researchers at Johns Hopkins Medicine (led by Dr. Boonyasai), and with Dr. Egan and the Care Coordination Institute. Some of these tools also received endorsement in the ACC/AHA guideline, such as the call for more accurate BP measurement. This link means that the experiences physicians have had implementing the Target:BP program provides a degree of foreshadowing for what U.S. physicians might face if they attempt to follow what the ACC/AHA guideline calls for.
Dr. Amofah and his colleagues at Community Health of South Florida, which serves about 76,000 patients with some 90 practitioners, started implementing Target:BP in the Spring of 2016. “Step one was adopting our own, customized algorithm that our entire staff could accept. Many of our clinicians practiced differently, so developing an algorithm yielded a lot of results. We gave clinicians a flow sheet for a hypertension visit,” Dr. Amofah said in an interview.
“We also pushed a program to measure BP accurately. Target:BP provided the training. Patient self-measurement of blood pressure is another key part of Target:BP. We pushed patient self-measurement, accurate measurement, and nurse-run blood pressure clinics. All these made a big difference in our success. Having a structured approach to blood pressure measurement was a major change for us.” Other “major changes” were quickly responding to uncontrolled BP, and empowering patients, he said. All of these also appear as practice recommendations in the new guideline.
When Community Health began participating in Target:BP, it had a 59% hypertension control rate (less than 140/90 mm Hg). By September 2017, roughly 18 months after starting with Target:BP, this had risen to 65%: a significant improvement, but still short of the program’s goal of 70%. Community Health had hoped to reach 70% by the end of 2017 – though as of January 2018 it remained unclear whether this had been achieved – and 80% control by the end of 2018. Reaching these goals is not completely unrealistic, but it’s challenging, Dr. Amofah said, because many of the patients at Community Health of South Florida are underserved, have poor access to medicine, have other survival priorities in their life, and have comorbidities that require attention and complicate their lives.
Dr. Amofah also serves as medical director for Health Choice Network, which includes 44 health organizations in 21 states with about 1 million patients. Of these 44 organizations, 16 have decided to participate in Target:BP, he said. The nonparticipating organizations decided to not be part of a structured program such as Target:BP and many also lacked the infrastructure that implementing Target:BP requires. But he has still tried to sell his colleagues at the nonparticipating organizations on the Target:BP approach, even if they don’t formally participate.
“Not having the support that Target:BP provides can prevent an organization from achieving its best potential,” he said. With Target:BP you get support and reinforcement. “It makes a difference; it creates a focus” Dr. Amofah said.
“Target:BP provides a lot of important guidance and tools that can help providers implement necessary changes” to aid BP control, said Jordana B. Cohen, MD, a nephrologist and hypertension researcher at the University of Pennsylvania in Philadelphia. Her practice does not participate in Target:BP, but she said that she is planning to look into joining.
Systematizing blood pressure management
“Hypertension is a microcosm of the changes that are already happening in U.S. medicine. A lot of what is now going on [in U.S. medicine] is reflected in the guideline,” said Dr. Casey. “Population medicine is now a big deal.”

Several experts trace the start of systematized U.S. primary care medicine to the advent of patient-centered medical homes, which date to 2007 (JAMA. 2009 May 20;301[19]:2038-40) and rapidly expanded with the quality demands of the Affordable Care Act (Health Aff [Millwood]. 2014 Oct;33[10]:1823-31).
These days, the systematization of U.S. primary care transcends the patient-centered medical home model and appears in several forms. Some of the unifying themes are health care organizations that monitor care through quality metrics, apply quality improvement methods, and provide integrated care through multidisciplinary teams of PCPs, various physician specialists, and an array of nonphysician clinicians, The new ACC/AHA guideline, with its call for new methods of BP measurement, home measurement, lifestyle interventions, team-based care, and use of telemedicine when needed both fits into the patient-centered medical home model and provides an added impetus for primary care medicine to move further down this road.
“The patient-centered medical home has been focused on managing diabetes, so I believe that a patient-centered medical home could be easily designed to deliver better hypertension care,” Dr. Casey noted.
When Paul K. Whelton, MD, chair of the ACC/AHA guideline panel, introduced the guideline during the AHA scientific sessions in November, he cited Kaiser Permanente Northern California and the VA Health System as examples of health care organizations that have already achieved high levels of BP control (at the less than 140/90 mm Hg level) in hypertensive patients. Clinicians at Kaiser Permanente Northern California reported that by 2013 they had reached 90% control in their hypertensive patients (J Clin Hypertens. 2016 Apr;18[4]:260-1).
“Primary care systems like Kaiser Permanente and Geisinger have had the most success in controlling hypertension due to their underlying infrastructures and multidisciplinary, team-based approach to blood pressure measurement and management,” noted Dr. Cohen of the University of Pennsylvania. “I am not certain that these [ACC/AHA] guidelines are enough to drive PCPs into different health systems from where they are now established to achieve these measures. Such a shift in practice would potentially leave certain high-risk populations with a greater dearth of care providers that already exists. Ideally, there needs to be more support from Medicare and Medicaid and for those who care for uninsured patients to aid them in implementing these changes broadly into practice.”
But other experts envision the guidelines either promoting further tweaks to existing systems, or providing a further push on PCP practices into more organized systems that can marshal greater resources.
“At the most recent meeting of the clinical practice committee of the Johns Hopkins Community Physicians [which includes about 200 PCPs], I presented the new guideline, and I expected some pushback. I was shocked” by the uniform acceptance the guideline received, said Dr. Boonyasai. “The consensus of our physicians was that the only way to do this is to keep building out our team-based care models, because we can’t do it all ourselves.
“The physicians were brainstorming ways to do it. The guidelines are a discussion point around this general trend toward team-based care that has been going on for a while. We’re trying to figure out how to make it work, at Hopkins and at primary care practices everywhere. The principles of team care also work for diabetes, chronic kidney disease, etc. What we struggle to figure out is how to engage patients so that they take an active role. We can prescribe medications, but if patients don’t take them their blood pressure won’t change. They also need to eat a DASH diet and lose weight. But we need to do more than just tell patients to lose weight. We need to help them do it and we’re looking for ways to help them do this, and that means involving our medical systems with education, follow-up, and patient involvement,” Dr. Boonyasai explained.
“The question is, how does a small practice do team care with their staffing? Where do you get the staff and how do you train them? The guideline spurs us to think more creatively about how we can take better care of more patients,” he said.
“A transition is occurring in U.S. medicine,” noted Dr. Egan. “What we are generally seeing is integration of small practices into larger groups. Larger groups have quality improvement specialists who help redesign the practice to have more efficient delivery of integrated care. Recognition that our health care system was not optimal for a lot of people in terms of results led us to a different model in which the health care system pays attention to a lot of social determinant of health. Not every practice has all the people to deliver this care, but collectively a system does,” noted Dr. Egan.
“Health care systems are reimbursed for quality; that provides some of the money to ensure that extra resources exist” to improve the quality and breadth of care, he said. Introduction of new technologies means “it does not require face-to-face visits to assist in lifestyle changes. The transition in health care is making it easier to do this. Succeeding in managing patients with multiple chronic diseases requires better integration of support services. Part of the barrier to success in implementing evidence-based guidelines is they involve too much work for one person to do. Even practices in remote locations are combining into groups so that their ability to get these resources through scaling is improving.”
Dr. Egan described his own experience consulting with variously sized local practices. “I’ve worked with practices in South Carolina for 18 years, and I’ve seen the majority now become part of health care systems. When a small practice is in a rural area, it shares electronic health records with a larger group, and they get access to a network of specialists and a broader range of resources. That’s the advantage to larger networks. They get access to treatment for medical and behavioral problems in pretty close to real time. The technology is spreading rapidly and is being used. I’ve seen groups with 20 practices that have the resources to hire three PharmDs, who then rotate to meet with patients [from all the practices] to do drug reconciliation and education. An individual practice couldn’t afford something like this. This is happening to treat things like depression and opioid addiction.”
“Hypertension management is no longer a patient going to see a doctor for 15 minutes, getting their blood pressure checked, and then leaving with a prescription,” said Dr. Casey. “We are not doing a good enough job measuring, diagnosing, and treating high blood pressure. We have to come up with better ways to do it. We think that the guideline provides the pathway forward for this.”
Just after the ACC/AHA guidelines had their introduction in November, Target:BP in collaboration with TEDMED organized a panel discussion of the new guideline that included Thomas H. Lee, MD, chief medical officer of Press Ganey in Boston and a practicing internal medicine physician at Brigham and Women’s Hospital in Boston.
During the webcast discussion, Dr. Lee delivered this message to U.S. PCPs and other physicians and health care providers about the future of U.S. hypertension management:
“Physicians and other providers will need to adapt, even those in systems. If we don’t adapt, someone else will fill the space. Patients will find someone else who can help them.
“If providers really are about the health of their patients, then they have a responsibility to try to do better. We need to measure our outcomes and put it out there.” If a health care provider responds, ‘I can’t do it in my current practice model,’ then they should think about how their model must change.”
Dr. Egan has been a consultant to AstraZeneca, Medtronic, and Valencia, has received honoraria from Merck Serono and Emcore, received royalties from UpToDate, and received research support from Medtronic and Quintiles. Dr. Lawrence has an ownership interest in Heka Health. Dr. Casey, Dr. Cohen, Dr. Ioannidis, Dr. Boonyasai, and Dr. Amofah had no disclosures.
In mid-November, the American College of Cardiology, the American Heart Association, and nine other collaborating societies released a new and long-anticipated guideline for diagnosing and managing hypertension. The top-line, seismic change that the new guidelines called for – treating many patients with hypertension to a blood pressure below 130/80 mm Hg – rubbed the primary care community the wrong way, as described in Part 1 of this feature.
But the novel steps the guideline calls for, from including more careful and methodical measurement of BP, both in and out of the office, to increased reliance on lifestyle interventions, running a formal calculation to identify patients who warrant drug treatment, to a team approach to management, seem to dovetail nicely with the broader goals of primary care.
Part 2 of this feature explores how the approach to diagnosis and management of hypertension spelled out in the ACC/AHA guidelines fits into the protocol-driven, data-monitored, team-delivered primary care model that has come to dominate U.S. primary care in the decade following passage of the Affordable Care Act.
The importance of performance metrics
Regardless of what individual primary care physicians (PCPs) and other physicians and clinicians decide about the appropriate BP treatment target for hypertensive patients, their decisions these days are often strongly influenced by the standards set for population levels of BP control by the Centers for Medicare & Medicaid Services and other payers. In a trend traced by experts to the Affordable Care Act of 2009, many payers now emphasize value-based reimbursements and incentives based on health care organizations meeting performance-metric goals. One of the most common goals measured today in primary care is the percentage of patients with hypertension treated to a particular BP target that today is most commonly set as less than 140/90 mm Hg.
The “vast majority” of PCPs now work in practices that are subject to performance targets including levels of BP control, said Romsai T. Boonyasai, MD, an internist at Johns Hopkins Medicine in Baltimore who specializes in quality improvement research in hypertension and other chronic diseases and also works as a PCP.
Adoption of BP control to less than 130/80 mm Hg by groups such as the National Quality Forum (NQF), National Committee for Quality Assurance (NCQA), and America’s Health Insurance Plans (AHIP) “would add more pressure to comply, especially in an environment where there already is division of opinion between the ACC/AHA and American Association of Family Physicians,” agreed John P.A. Ioannidis, MD, professor of medicine and a preventive medicine specialist at Stanford (Calif.) University.
“The AHA is looking for endorsement from the metric groups,” noted Brent M. Egan, MD, vice president for research at the Care Coordination Institute in Greenville, S.C., and a consultant to the AHA.
But a new performance metric that reflects the ACC/AHA BP target won’t appear immediately. Step one is crafting performance measures based on the ACC/AHA guideline to submit to the NQF and similar groups, a process that will soon start, said Donald E. Casey Jr., MD, a member of the guideline-writing panel and chief clinical affairs officer at Medecision in Wayne, Pa.. He will chair a committee that will review existing hypertension management performance measures and as needed also write new measures based on the guideline, a process he expects to have completed by the end of 2018. After that comes field testing the measures, and if they prove effective and workable, the next step is to submit them to the performance metric groups for review and potential adoption, steps that may take another year. In short, performance metrics for hypertension management that call for a large segment of U.S. patients to be treated to a BP below 130/80 mm Hg likely won’t be in place until the end of 2019 or sometime in 2020 at the earliest, and of course only if the metric-setting groups decide to adopt the new measures as part of their standards.
“It takes a while for guidelines to go from publication to practice. Once [the new guideline] is systematized into performance measures it will help” adoption of what the new guideline recommends, Dr. Casey said in an interview.
Target:BP
Performance metrics are not the only path that could take U.S. medicine toward lower BP targets. Another active player is the Target:BP program, a voluntary quality-improvement program for increased U.S. hypertension awareness and better management launched in late 2015 as a collaboration between the AHA and the American Medical Association.
Given that both the new guideline and Target:BP were developed through partnerships involving the AHA, “it’s logical to connect [the guideline] to Target:BP, said Dr. Egan, an AHA spokesman for Target:BP and professor of medicine at the Medical University of South Carolina in Charleston.
Target:BP’s participants are health care organizations, including health systems, medical groups, community health centers, and physician practices. The program has two primary threads.
First, it functions as a recognition program that cites participating organizations if they achieve a prespecified level of BP control.
In 2017, the program released its initial list of successful participants, organizations that maintained at least 70% of their patients diagnosed with hypertension at a BP of less than 140/90 mm Hg. According to data reported by Willie E. Lawrence Jr., MD, during the AHA scientific sessions in November in Anaheim, Calif., 191 participating programs reached this level and won a “gold” designation from the program for their level of BP control during 2016, out of 310 participating organizations that submitted 2016 data to the program.
Dr. Lawrence also reported that nearly 1,200 total health care organizations were participating in Target:BP as of his presentation, and that the 310 programs that reported 2016 data cared for roughly 12 million people, numbers that extrapolate to more than 45 million Americans cared for in all 1,200 organizations now participating in Target:BP. Among all 310 organizations reporting 2016 data, the average level of hypertension control (patients with BPs maintained at less than 140/90 mm Hg) was 66%, said Dr. Lawrence, chief of cardiology at Research Medical Center in Kansas City, Mo. The cited “gold” programs averaged 76% of their hypertensive patients treated to less than 140/90 mm Hg.
The second thread of Target:BP’s program is to supply participating organizations with training and practice tools aimed at improving hypertension diagnosis and management. The core element of the tools the program currently promotes is the MAP checklists, which stands for Measure accurately, Act rapidly, and Partner with patients, families, and communities (J Clin Hypertens. 2017 Jul;19[7]:684-94).
Target:BP’s focus on a recognition program for organizational success in BP management is very reminiscent of the Get With the Guidelines programs that the AHA previously launched for the management of various cardiovascular diseases such as ischemic stroke. Get With the Guidelines–Stroke, begun in the early 2000s, helped achieve recent success in improving the rates at which U.S. stroke patients receive timely intervention with tissue plasminogen activator, demonstrating the power a recognition program can have for improving patient care.
Target:BP moved quickly to embrace the new ACC/AHA guideline BP targets, posting a treatment target of less than 130/80 mm Hg on its website by December 2017, scant weeks after the guideline’s release in mid-November. But for the time being, Target:BP will continue to use the NQF BP quality metric as the basis for its recognition program, according to an AMA spokesperson for the program. “While the AHA and AMA will keep our joint recognition program in accordance with the NQF measure, we will simultaneously build resources, including an updated treatment algorithm, that align with the new blood pressure guideline,” according to an AMA statement.
Part of the thinking about the timing for revising the BP recognition goal in Target:BP is that it would be too confusing and challenging for participating organizations to attend to two different treatment goals at once, one for Target:BP recognition and a different one for NQF compliance, Dr. Egan explained.
Development of the MAP checklists and several other tools promoted by Target:BP came into existence through a research program sponsored by the AMA in collaboration with researchers at Johns Hopkins Medicine (led by Dr. Boonyasai), and with Dr. Egan and the Care Coordination Institute. Some of these tools also received endorsement in the ACC/AHA guideline, such as the call for more accurate BP measurement. This link means that the experiences physicians have had implementing the Target:BP program provides a degree of foreshadowing for what U.S. physicians might face if they attempt to follow what the ACC/AHA guideline calls for.
Dr. Amofah and his colleagues at Community Health of South Florida, which serves about 76,000 patients with some 90 practitioners, started implementing Target:BP in the Spring of 2016. “Step one was adopting our own, customized algorithm that our entire staff could accept. Many of our clinicians practiced differently, so developing an algorithm yielded a lot of results. We gave clinicians a flow sheet for a hypertension visit,” Dr. Amofah said in an interview.
“We also pushed a program to measure BP accurately. Target:BP provided the training. Patient self-measurement of blood pressure is another key part of Target:BP. We pushed patient self-measurement, accurate measurement, and nurse-run blood pressure clinics. All these made a big difference in our success. Having a structured approach to blood pressure measurement was a major change for us.” Other “major changes” were quickly responding to uncontrolled BP, and empowering patients, he said. All of these also appear as practice recommendations in the new guideline.
When Community Health began participating in Target:BP, it had a 59% hypertension control rate (less than 140/90 mm Hg). By September 2017, roughly 18 months after starting with Target:BP, this had risen to 65%: a significant improvement, but still short of the program’s goal of 70%. Community Health had hoped to reach 70% by the end of 2017 – though as of January 2018 it remained unclear whether this had been achieved – and 80% control by the end of 2018. Reaching these goals is not completely unrealistic, but it’s challenging, Dr. Amofah said, because many of the patients at Community Health of South Florida are underserved, have poor access to medicine, have other survival priorities in their life, and have comorbidities that require attention and complicate their lives.
Dr. Amofah also serves as medical director for Health Choice Network, which includes 44 health organizations in 21 states with about 1 million patients. Of these 44 organizations, 16 have decided to participate in Target:BP, he said. The nonparticipating organizations decided to not be part of a structured program such as Target:BP and many also lacked the infrastructure that implementing Target:BP requires. But he has still tried to sell his colleagues at the nonparticipating organizations on the Target:BP approach, even if they don’t formally participate.
“Not having the support that Target:BP provides can prevent an organization from achieving its best potential,” he said. With Target:BP you get support and reinforcement. “It makes a difference; it creates a focus” Dr. Amofah said.
“Target:BP provides a lot of important guidance and tools that can help providers implement necessary changes” to aid BP control, said Jordana B. Cohen, MD, a nephrologist and hypertension researcher at the University of Pennsylvania in Philadelphia. Her practice does not participate in Target:BP, but she said that she is planning to look into joining.
Systematizing blood pressure management
“Hypertension is a microcosm of the changes that are already happening in U.S. medicine. A lot of what is now going on [in U.S. medicine] is reflected in the guideline,” said Dr. Casey. “Population medicine is now a big deal.”
Several experts trace the start of systematized U.S. primary care medicine to the advent of patient-centered medical homes, which date to 2007 (JAMA. 2009 May 20;301[19]:2038-40) and rapidly expanded with the quality demands of the Affordable Care Act (Health Aff [Millwood]. 2014 Oct;33[10]:1823-31).
These days, the systematization of U.S. primary care transcends the patient-centered medical home model and appears in several forms. Some of the unifying themes are health care organizations that monitor care through quality metrics, apply quality improvement methods, and provide integrated care through multidisciplinary teams of PCPs, various physician specialists, and an array of nonphysician clinicians, The new ACC/AHA guideline, with its call for new methods of BP measurement, home measurement, lifestyle interventions, team-based care, and use of telemedicine when needed both fits into the patient-centered medical home model and provides an added impetus for primary care medicine to move further down this road.
“The patient-centered medical home has been focused on managing diabetes, so I believe that a patient-centered medical home could be easily designed to deliver better hypertension care,” Dr. Casey noted.
When Paul K. Whelton, MD, chair of the ACC/AHA guideline panel, introduced the guideline during the AHA scientific sessions in November, he cited Kaiser Permanente Northern California and the VA Health System as examples of health care organizations that have already achieved high levels of BP control (at the less than 140/90 mm Hg level) in hypertensive patients. Clinicians at Kaiser Permanente Northern California reported that by 2013 they had reached 90% control in their hypertensive patients (J Clin Hypertens. 2016 Apr;18[4]:260-1).
“Primary care systems like Kaiser Permanente and Geisinger have had the most success in controlling hypertension due to their underlying infrastructures and multidisciplinary, team-based approach to blood pressure measurement and management,” noted Dr. Cohen of the University of Pennsylvania. “I am not certain that these [ACC/AHA] guidelines are enough to drive PCPs into different health systems from where they are now established to achieve these measures. Such a shift in practice would potentially leave certain high-risk populations with a greater dearth of care providers that already exists. Ideally, there needs to be more support from Medicare and Medicaid and for those who care for uninsured patients to aid them in implementing these changes broadly into practice.”
But other experts envision the guidelines either promoting further tweaks to existing systems, or providing a further push on PCP practices into more organized systems that can marshal greater resources.
“At the most recent meeting of the clinical practice committee of the Johns Hopkins Community Physicians [which includes about 200 PCPs], I presented the new guideline, and I expected some pushback. I was shocked” by the uniform acceptance the guideline received, said Dr. Boonyasai. “The consensus of our physicians was that the only way to do this is to keep building out our team-based care models, because we can’t do it all ourselves.
“The physicians were brainstorming ways to do it. The guidelines are a discussion point around this general trend toward team-based care that has been going on for a while. We’re trying to figure out how to make it work, at Hopkins and at primary care practices everywhere. The principles of team care also work for diabetes, chronic kidney disease, etc. What we struggle to figure out is how to engage patients so that they take an active role. We can prescribe medications, but if patients don’t take them their blood pressure won’t change. They also need to eat a DASH diet and lose weight. But we need to do more than just tell patients to lose weight. We need to help them do it and we’re looking for ways to help them do this, and that means involving our medical systems with education, follow-up, and patient involvement,” Dr. Boonyasai explained.
“The question is, how does a small practice do team care with their staffing? Where do you get the staff and how do you train them? The guideline spurs us to think more creatively about how we can take better care of more patients,” he said.
“A transition is occurring in U.S. medicine,” noted Dr. Egan. “What we are generally seeing is integration of small practices into larger groups. Larger groups have quality improvement specialists who help redesign the practice to have more efficient delivery of integrated care. Recognition that our health care system was not optimal for a lot of people in terms of results led us to a different model in which the health care system pays attention to a lot of social determinant of health. Not every practice has all the people to deliver this care, but collectively a system does,” noted Dr. Egan.
“Health care systems are reimbursed for quality; that provides some of the money to ensure that extra resources exist” to improve the quality and breadth of care, he said. Introduction of new technologies means “it does not require face-to-face visits to assist in lifestyle changes. The transition in health care is making it easier to do this. Succeeding in managing patients with multiple chronic diseases requires better integration of support services. Part of the barrier to success in implementing evidence-based guidelines is they involve too much work for one person to do. Even practices in remote locations are combining into groups so that their ability to get these resources through scaling is improving.”
Dr. Egan described his own experience consulting with variously sized local practices. “I’ve worked with practices in South Carolina for 18 years, and I’ve seen the majority now become part of health care systems. When a small practice is in a rural area, it shares electronic health records with a larger group, and they get access to a network of specialists and a broader range of resources. That’s the advantage to larger networks. They get access to treatment for medical and behavioral problems in pretty close to real time. The technology is spreading rapidly and is being used. I’ve seen groups with 20 practices that have the resources to hire three PharmDs, who then rotate to meet with patients [from all the practices] to do drug reconciliation and education. An individual practice couldn’t afford something like this. This is happening to treat things like depression and opioid addiction.”
“Hypertension management is no longer a patient going to see a doctor for 15 minutes, getting their blood pressure checked, and then leaving with a prescription,” said Dr. Casey. “We are not doing a good enough job measuring, diagnosing, and treating high blood pressure. We have to come up with better ways to do it. We think that the guideline provides the pathway forward for this.”
Just after the ACC/AHA guidelines had their introduction in November, Target:BP in collaboration with TEDMED organized a panel discussion of the new guideline that included Thomas H. Lee, MD, chief medical officer of Press Ganey in Boston and a practicing internal medicine physician at Brigham and Women’s Hospital in Boston.
During the webcast discussion, Dr. Lee delivered this message to U.S. PCPs and other physicians and health care providers about the future of U.S. hypertension management:
“Physicians and other providers will need to adapt, even those in systems. If we don’t adapt, someone else will fill the space. Patients will find someone else who can help them.
“If providers really are about the health of their patients, then they have a responsibility to try to do better. We need to measure our outcomes and put it out there.” If a health care provider responds, ‘I can’t do it in my current practice model,’ then they should think about how their model must change.”
Dr. Egan has been a consultant to AstraZeneca, Medtronic, and Valencia, has received honoraria from Merck Serono and Emcore, received royalties from UpToDate, and received research support from Medtronic and Quintiles. Dr. Lawrence has an ownership interest in Heka Health. Dr. Casey, Dr. Cohen, Dr. Ioannidis, Dr. Boonyasai, and Dr. Amofah had no disclosures.
In mid-November, the American College of Cardiology, the American Heart Association, and nine other collaborating societies released a new and long-anticipated guideline for diagnosing and managing hypertension. The top-line, seismic change that the new guidelines called for – treating many patients with hypertension to a blood pressure below 130/80 mm Hg – rubbed the primary care community the wrong way, as described in Part 1 of this feature.
But the novel steps the guideline calls for, from including more careful and methodical measurement of BP, both in and out of the office, to increased reliance on lifestyle interventions, running a formal calculation to identify patients who warrant drug treatment, to a team approach to management, seem to dovetail nicely with the broader goals of primary care.
Part 2 of this feature explores how the approach to diagnosis and management of hypertension spelled out in the ACC/AHA guidelines fits into the protocol-driven, data-monitored, team-delivered primary care model that has come to dominate U.S. primary care in the decade following passage of the Affordable Care Act.
The importance of performance metrics
Regardless of what individual primary care physicians (PCPs) and other physicians and clinicians decide about the appropriate BP treatment target for hypertensive patients, their decisions these days are often strongly influenced by the standards set for population levels of BP control by the Centers for Medicare & Medicaid Services and other payers. In a trend traced by experts to the Affordable Care Act of 2009, many payers now emphasize value-based reimbursements and incentives based on health care organizations meeting performance-metric goals. One of the most common goals measured today in primary care is the percentage of patients with hypertension treated to a particular BP target that today is most commonly set as less than 140/90 mm Hg.
The “vast majority” of PCPs now work in practices that are subject to performance targets including levels of BP control, said Romsai T. Boonyasai, MD, an internist at Johns Hopkins Medicine in Baltimore who specializes in quality improvement research in hypertension and other chronic diseases and also works as a PCP.
Adoption of BP control to less than 130/80 mm Hg by groups such as the National Quality Forum (NQF), National Committee for Quality Assurance (NCQA), and America’s Health Insurance Plans (AHIP) “would add more pressure to comply, especially in an environment where there already is division of opinion between the ACC/AHA and American Association of Family Physicians,” agreed John P.A. Ioannidis, MD, professor of medicine and a preventive medicine specialist at Stanford (Calif.) University.
“The AHA is looking for endorsement from the metric groups,” noted Brent M. Egan, MD, vice president for research at the Care Coordination Institute in Greenville, S.C., and a consultant to the AHA.
But a new performance metric that reflects the ACC/AHA BP target won’t appear immediately. Step one is crafting performance measures based on the ACC/AHA guideline to submit to the NQF and similar groups, a process that will soon start, said Donald E. Casey Jr., MD, a member of the guideline-writing panel and chief clinical affairs officer at Medecision in Wayne, Pa.. He will chair a committee that will review existing hypertension management performance measures and as needed also write new measures based on the guideline, a process he expects to have completed by the end of 2018. After that comes field testing the measures, and if they prove effective and workable, the next step is to submit them to the performance metric groups for review and potential adoption, steps that may take another year. In short, performance metrics for hypertension management that call for a large segment of U.S. patients to be treated to a BP below 130/80 mm Hg likely won’t be in place until the end of 2019 or sometime in 2020 at the earliest, and of course only if the metric-setting groups decide to adopt the new measures as part of their standards.
“It takes a while for guidelines to go from publication to practice. Once [the new guideline] is systematized into performance measures it will help” adoption of what the new guideline recommends, Dr. Casey said in an interview.
Target:BP
Performance metrics are not the only path that could take U.S. medicine toward lower BP targets. Another active player is the Target:BP program, a voluntary quality-improvement program for increased U.S. hypertension awareness and better management launched in late 2015 as a collaboration between the AHA and the American Medical Association.
Given that both the new guideline and Target:BP were developed through partnerships involving the AHA, “it’s logical to connect [the guideline] to Target:BP, said Dr. Egan, an AHA spokesman for Target:BP and professor of medicine at the Medical University of South Carolina in Charleston.
Target:BP’s participants are health care organizations, including health systems, medical groups, community health centers, and physician practices. The program has two primary threads.
First, it functions as a recognition program that cites participating organizations if they achieve a prespecified level of BP control.
In 2017, the program released its initial list of successful participants, organizations that maintained at least 70% of their patients diagnosed with hypertension at a BP of less than 140/90 mm Hg. According to data reported by Willie E. Lawrence Jr., MD, during the AHA scientific sessions in November in Anaheim, Calif., 191 participating programs reached this level and won a “gold” designation from the program for their level of BP control during 2016, out of 310 participating organizations that submitted 2016 data to the program.
Dr. Lawrence also reported that nearly 1,200 total health care organizations were participating in Target:BP as of his presentation, and that the 310 programs that reported 2016 data cared for roughly 12 million people, numbers that extrapolate to more than 45 million Americans cared for in all 1,200 organizations now participating in Target:BP. Among all 310 organizations reporting 2016 data, the average level of hypertension control (patients with BPs maintained at less than 140/90 mm Hg) was 66%, said Dr. Lawrence, chief of cardiology at Research Medical Center in Kansas City, Mo. The cited “gold” programs averaged 76% of their hypertensive patients treated to less than 140/90 mm Hg.
The second thread of Target:BP’s program is to supply participating organizations with training and practice tools aimed at improving hypertension diagnosis and management. The core element of the tools the program currently promotes is the MAP checklists, which stands for Measure accurately, Act rapidly, and Partner with patients, families, and communities (J Clin Hypertens. 2017 Jul;19[7]:684-94).
Target:BP’s focus on a recognition program for organizational success in BP management is very reminiscent of the Get With the Guidelines programs that the AHA previously launched for the management of various cardiovascular diseases such as ischemic stroke. Get With the Guidelines–Stroke, begun in the early 2000s, helped achieve recent success in improving the rates at which U.S. stroke patients receive timely intervention with tissue plasminogen activator, demonstrating the power a recognition program can have for improving patient care.
Target:BP moved quickly to embrace the new ACC/AHA guideline BP targets, posting a treatment target of less than 130/80 mm Hg on its website by December 2017, scant weeks after the guideline’s release in mid-November. But for the time being, Target:BP will continue to use the NQF BP quality metric as the basis for its recognition program, according to an AMA spokesperson for the program. “While the AHA and AMA will keep our joint recognition program in accordance with the NQF measure, we will simultaneously build resources, including an updated treatment algorithm, that align with the new blood pressure guideline,” according to an AMA statement.
Part of the thinking about the timing for revising the BP recognition goal in Target:BP is that it would be too confusing and challenging for participating organizations to attend to two different treatment goals at once, one for Target:BP recognition and a different one for NQF compliance, Dr. Egan explained.
Development of the MAP checklists and several other tools promoted by Target:BP came into existence through a research program sponsored by the AMA in collaboration with researchers at Johns Hopkins Medicine (led by Dr. Boonyasai), and with Dr. Egan and the Care Coordination Institute. Some of these tools also received endorsement in the ACC/AHA guideline, such as the call for more accurate BP measurement. This link means that the experiences physicians have had implementing the Target:BP program provides a degree of foreshadowing for what U.S. physicians might face if they attempt to follow what the ACC/AHA guideline calls for.
Dr. Amofah and his colleagues at Community Health of South Florida, which serves about 76,000 patients with some 90 practitioners, started implementing Target:BP in the Spring of 2016. “Step one was adopting our own, customized algorithm that our entire staff could accept. Many of our clinicians practiced differently, so developing an algorithm yielded a lot of results. We gave clinicians a flow sheet for a hypertension visit,” Dr. Amofah said in an interview.
“We also pushed a program to measure BP accurately. Target:BP provided the training. Patient self-measurement of blood pressure is another key part of Target:BP. We pushed patient self-measurement, accurate measurement, and nurse-run blood pressure clinics. All these made a big difference in our success. Having a structured approach to blood pressure measurement was a major change for us.” Other “major changes” were quickly responding to uncontrolled BP, and empowering patients, he said. All of these also appear as practice recommendations in the new guideline.
When Community Health began participating in Target:BP, it had a 59% hypertension control rate (less than 140/90 mm Hg). By September 2017, roughly 18 months after starting with Target:BP, this had risen to 65%: a significant improvement, but still short of the program’s goal of 70%. Community Health had hoped to reach 70% by the end of 2017 – though as of January 2018 it remained unclear whether this had been achieved – and 80% control by the end of 2018. Reaching these goals is not completely unrealistic, but it’s challenging, Dr. Amofah said, because many of the patients at Community Health of South Florida are underserved, have poor access to medicine, have other survival priorities in their life, and have comorbidities that require attention and complicate their lives.
Dr. Amofah also serves as medical director for Health Choice Network, which includes 44 health organizations in 21 states with about 1 million patients. Of these 44 organizations, 16 have decided to participate in Target:BP, he said. The nonparticipating organizations decided to not be part of a structured program such as Target:BP and many also lacked the infrastructure that implementing Target:BP requires. But he has still tried to sell his colleagues at the nonparticipating organizations on the Target:BP approach, even if they don’t formally participate.
“Not having the support that Target:BP provides can prevent an organization from achieving its best potential,” he said. With Target:BP you get support and reinforcement. “It makes a difference; it creates a focus” Dr. Amofah said.
“Target:BP provides a lot of important guidance and tools that can help providers implement necessary changes” to aid BP control, said Jordana B. Cohen, MD, a nephrologist and hypertension researcher at the University of Pennsylvania in Philadelphia. Her practice does not participate in Target:BP, but she said that she is planning to look into joining.
Systematizing blood pressure management
“Hypertension is a microcosm of the changes that are already happening in U.S. medicine. A lot of what is now going on [in U.S. medicine] is reflected in the guideline,” said Dr. Casey. “Population medicine is now a big deal.”
Several experts trace the start of systematized U.S. primary care medicine to the advent of patient-centered medical homes, which date to 2007 (JAMA. 2009 May 20;301[19]:2038-40) and rapidly expanded with the quality demands of the Affordable Care Act (Health Aff [Millwood]. 2014 Oct;33[10]:1823-31).
These days, the systematization of U.S. primary care transcends the patient-centered medical home model and appears in several forms. Some of the unifying themes are health care organizations that monitor care through quality metrics, apply quality improvement methods, and provide integrated care through multidisciplinary teams of PCPs, various physician specialists, and an array of nonphysician clinicians, The new ACC/AHA guideline, with its call for new methods of BP measurement, home measurement, lifestyle interventions, team-based care, and use of telemedicine when needed both fits into the patient-centered medical home model and provides an added impetus for primary care medicine to move further down this road.
“The patient-centered medical home has been focused on managing diabetes, so I believe that a patient-centered medical home could be easily designed to deliver better hypertension care,” Dr. Casey noted.
When Paul K. Whelton, MD, chair of the ACC/AHA guideline panel, introduced the guideline during the AHA scientific sessions in November, he cited Kaiser Permanente Northern California and the VA Health System as examples of health care organizations that have already achieved high levels of BP control (at the less than 140/90 mm Hg level) in hypertensive patients. Clinicians at Kaiser Permanente Northern California reported that by 2013 they had reached 90% control in their hypertensive patients (J Clin Hypertens. 2016 Apr;18[4]:260-1).
“Primary care systems like Kaiser Permanente and Geisinger have had the most success in controlling hypertension due to their underlying infrastructures and multidisciplinary, team-based approach to blood pressure measurement and management,” noted Dr. Cohen of the University of Pennsylvania. “I am not certain that these [ACC/AHA] guidelines are enough to drive PCPs into different health systems from where they are now established to achieve these measures. Such a shift in practice would potentially leave certain high-risk populations with a greater dearth of care providers that already exists. Ideally, there needs to be more support from Medicare and Medicaid and for those who care for uninsured patients to aid them in implementing these changes broadly into practice.”
But other experts envision the guidelines either promoting further tweaks to existing systems, or providing a further push on PCP practices into more organized systems that can marshal greater resources.
“At the most recent meeting of the clinical practice committee of the Johns Hopkins Community Physicians [which includes about 200 PCPs], I presented the new guideline, and I expected some pushback. I was shocked” by the uniform acceptance the guideline received, said Dr. Boonyasai. “The consensus of our physicians was that the only way to do this is to keep building out our team-based care models, because we can’t do it all ourselves.
“The physicians were brainstorming ways to do it. The guidelines are a discussion point around this general trend toward team-based care that has been going on for a while. We’re trying to figure out how to make it work, at Hopkins and at primary care practices everywhere. The principles of team care also work for diabetes, chronic kidney disease, etc. What we struggle to figure out is how to engage patients so that they take an active role. We can prescribe medications, but if patients don’t take them their blood pressure won’t change. They also need to eat a DASH diet and lose weight. But we need to do more than just tell patients to lose weight. We need to help them do it and we’re looking for ways to help them do this, and that means involving our medical systems with education, follow-up, and patient involvement,” Dr. Boonyasai explained.
“The question is, how does a small practice do team care with their staffing? Where do you get the staff and how do you train them? The guideline spurs us to think more creatively about how we can take better care of more patients,” he said.
“A transition is occurring in U.S. medicine,” noted Dr. Egan. “What we are generally seeing is integration of small practices into larger groups. Larger groups have quality improvement specialists who help redesign the practice to have more efficient delivery of integrated care. Recognition that our health care system was not optimal for a lot of people in terms of results led us to a different model in which the health care system pays attention to a lot of social determinant of health. Not every practice has all the people to deliver this care, but collectively a system does,” noted Dr. Egan.
“Health care systems are reimbursed for quality; that provides some of the money to ensure that extra resources exist” to improve the quality and breadth of care, he said. Introduction of new technologies means “it does not require face-to-face visits to assist in lifestyle changes. The transition in health care is making it easier to do this. Succeeding in managing patients with multiple chronic diseases requires better integration of support services. Part of the barrier to success in implementing evidence-based guidelines is they involve too much work for one person to do. Even practices in remote locations are combining into groups so that their ability to get these resources through scaling is improving.”
Dr. Egan described his own experience consulting with variously sized local practices. “I’ve worked with practices in South Carolina for 18 years, and I’ve seen the majority now become part of health care systems. When a small practice is in a rural area, it shares electronic health records with a larger group, and they get access to a network of specialists and a broader range of resources. That’s the advantage to larger networks. They get access to treatment for medical and behavioral problems in pretty close to real time. The technology is spreading rapidly and is being used. I’ve seen groups with 20 practices that have the resources to hire three PharmDs, who then rotate to meet with patients [from all the practices] to do drug reconciliation and education. An individual practice couldn’t afford something like this. This is happening to treat things like depression and opioid addiction.”
“Hypertension management is no longer a patient going to see a doctor for 15 minutes, getting their blood pressure checked, and then leaving with a prescription,” said Dr. Casey. “We are not doing a good enough job measuring, diagnosing, and treating high blood pressure. We have to come up with better ways to do it. We think that the guideline provides the pathway forward for this.”
Just after the ACC/AHA guidelines had their introduction in November, Target:BP in collaboration with TEDMED organized a panel discussion of the new guideline that included Thomas H. Lee, MD, chief medical officer of Press Ganey in Boston and a practicing internal medicine physician at Brigham and Women’s Hospital in Boston.
During the webcast discussion, Dr. Lee delivered this message to U.S. PCPs and other physicians and health care providers about the future of U.S. hypertension management:
“Physicians and other providers will need to adapt, even those in systems. If we don’t adapt, someone else will fill the space. Patients will find someone else who can help them.
“If providers really are about the health of their patients, then they have a responsibility to try to do better. We need to measure our outcomes and put it out there.” If a health care provider responds, ‘I can’t do it in my current practice model,’ then they should think about how their model must change.”
Dr. Egan has been a consultant to AstraZeneca, Medtronic, and Valencia, has received honoraria from Merck Serono and Emcore, received royalties from UpToDate, and received research support from Medtronic and Quintiles. Dr. Lawrence has an ownership interest in Heka Health. Dr. Casey, Dr. Cohen, Dr. Ioannidis, Dr. Boonyasai, and Dr. Amofah had no disclosures.
The Effects of Ranolazine on Hemoglobin A1c in a Veteran Population
Diabetes mellitus (DM) is a risk factor for cardiovascular disease(CVD).1-4 Death rates from heart disease are 2- to 4-times higher among adults with DM compared with those of adults without DM. In the US, it is estimated that 21.1 million adults have diagnosed DM, 8.1 million adults have undiagnosed DM, and 80.8 million adults have prediabetes.3 The American Heart Association has identified an untreated fasting blood glucose level < 100 mg/dL as a component of ideal cardiovascular health.3
Although the use of antidiabetic agents has been shown to reduce the risks of microvascular complications among patients with DM, a cardiovascular benefit has not been consistently demonstrated with all available agents, and some used in the treatment of DM are associated with cardiovascular harm.5 In addition, some cardiovascular medications may contribute to the development of DM or may mask the symptoms of hypoglycemia.6 Given the risk for CVD among patients with DM, a medication with utility in both DM and CVD could be beneficial.
Evidence for Use of Ranolazine
Ranolazine is indicated for the treatment of chronic angina.7 In clinical trials, ranolazine also was found to decrease hemoglobin A1c (HbA1c).8-15 The possible mechanisms for lowering HbA1c with ranolazine include preservation of pancreatic β-cells and an increase in glucose-dependent insulin secretion.6 The most common adverse effects associated with ranolazine include dizziness, headache, constipation, and nausea.7
Ranolazine has been shown to be efficacious and safe in the reduction of angina symptoms among patients with and without DM.8-12 In addition to improving symptoms of angina, studies have demonstrated a reduction in HbA1c among patients taking ranolazine.9,13-15 In an open-label extension of the Combination Assessment of Ranolazine in Stable Angina (CARISA) trial, ranolazine 750 mg twice daily and 1,000 mg twice daily led to a greater reduction in HbA1c when each was compared with placebo (-0.48% HbA1c, P = .008; and -0.70% HbA1c, P = .001, respectively).9
Among the 5,576 patients enrolled in the Metabolic Efficiency With Ranolazine for Less Ischemia in Non-ST-Elevation Acute Coronary Syndromes—Thrombolysis in Myocardial Infarction 36 (MERLIN-TIMI 36) trial with a baseline HbA1c, ranolazine significantly reduced HbA1c at 4 months when compared with placebo among patients with and without DM.13 In addition, patients with DM who were treated with ranolazine were more likely to achieve a HbA1c < 7% at 4 months when compared with placebo (59% vs 49%; P < .001). Ranolazine was not found to increase the incidence of hypoglycemia.
A subgroup analysis of MERLIN-TIMI 36 evaluated the effects of ranolazine compared with those of placebo on fasting plasma glucose and HbA1c in patients with moderate DM (HbA1c ≥ 6% but < 8%, fasting plasma glucose < 250 mg/dL) and severe DM (A1c ≥ 8%, fasting plasma glucose 150-400 mg/dL).14 A significant reduction in HbA1c with ranolazine in addition to standard of care antidiabetes treatment was observed among both groups. The placebo-corrected decrease in HbA1c in the moderate DM group was 0.28% (95% confidence interval [CI] -0.55 to 0; P = .045) and in the severe DM group was 0.59% (95% CI -0.99 to -0.20; P < .001).
In a trial designed to evaluate change in HbA1c in patients taking ranolazine 1,000 mg twice daily compared with that of placebo, ranolazine led to a greater decrease in HbA1c compared with that of placebo (placebo corrected change in HbA1c -0.56%, P = .001).15 In addition, a higher percentage of patients achieved HbA1c < 7% at 24 weeks in the ranolazine group compared with that of placebo (41.2% vs 25.7%; P = .001). No patient experienced severe hypoglycemia or had documented hypoglycemia in this study.
These trials suggest that ranolazine, in addition to decreasing anginal events, is potentially beneficial in achieving better control of DM. However, more studies are needed to determine this benefit. In addition, no trials have examined the 500-mg twice daily dose of ranolazine in HbA1c reduction.
The purpose of this study was to evaluate the change in HbA1c among veterans with DM after the initiation of ranolazine. The study compared the percentage of veterans achieving HbA1c < 7% or < 8% after initiation of ranolazine with the baseline, to determine whether there is a dose-related change in HbA1c among different ranolazine regimens and to determine whether there is a change in the incidence of hypoglycemia after the initiation of ranolazine.
Methods
This was a multicenter, retrospective study. The institutional review board and research and development committee for 3 Veterans Affairs medical centers (VAMCs) approved this study and waived informed consent. Additionally, this study was approved for access to national patient information through the Corporate Data Warehouse (CDW).
Subjects were eligible for inclusion in this study if they were aged ≥ 18 years, had a diagnosis of type 2 DM, and received their first prescription of ranolazine at a VAMC from January 1, 2008 through March 31, 2015. Exclusion criteria included subjects with no baseline HbA1c (defined as the HbA1c result closest to the ranolazine initiation date and within 90 days before to 14 days after ranolazine initiation), no follow-up HbA1c (defined as the first HbA1c result within 60 to 180 days after the ranolazine initiation date), any change to their DM medication regimen during the follow-up period, or who discontinued ranolazine prior to collection of the follow-up HbA1c.
Data were collected from the electronic health record (EHR) for each subject from 6 months prior to the ranolazine initiation date through 6 months after the ranolazine initiation date. The ranolazine initiation date was defined as the date ranolazine was picked up in person at a VAMC pharmacy or 7 days after the date filled for medications sent by mail. 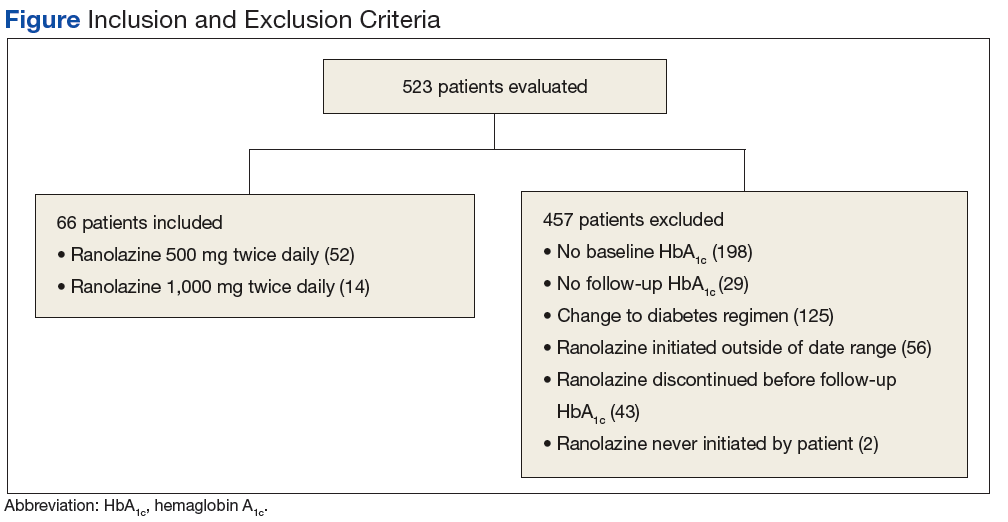
The primary endpoint of this study was the change in HbA1c after ranolazine initiation. The secondary endpoint was the percentage of study subjects achieving HbA1c < 7% and < 8% before and after the initiation of ranolazine.
To achieve 80% power to detect a change in HbA1c of 0.4%, a sample size of 52 patients was required. For the primary endpoint, a paired t test was used to test for statistical significance. The McNemar test was used to evaluate for a significant change in subjects achieving an HbA1c < 7% and HbA1c < 8% with the initiation of ranolazine.
Results
A total of 523 patients were evaluated for study inclusion, of which 66 patients were included (Figure). The most common reasons for exclusion included no HbA1c at baseline and changes to the DM medication regimen during follow-up. 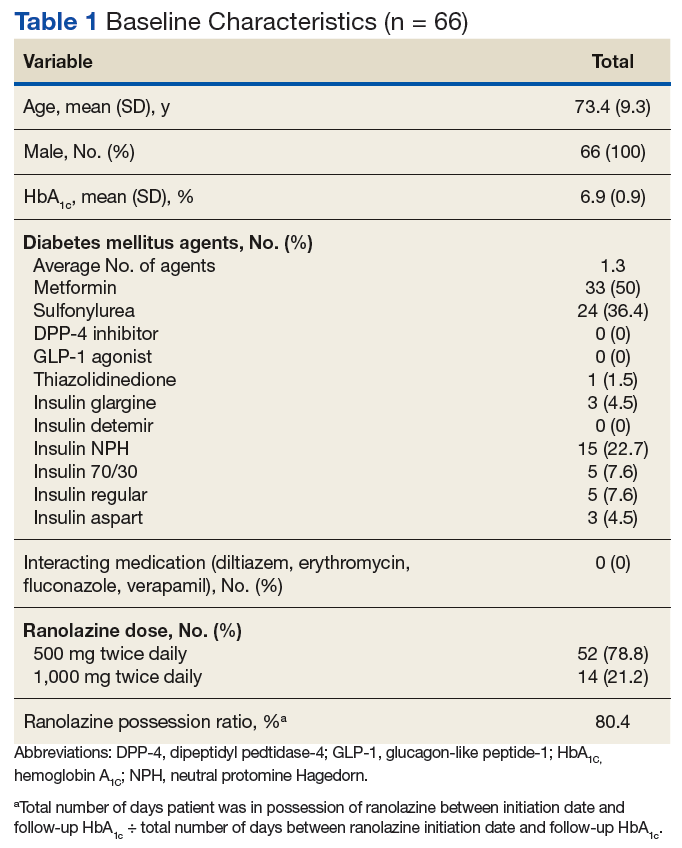
Ranolazine at any dose was associated with a change in HbA1c of -0.3% (P < .001). 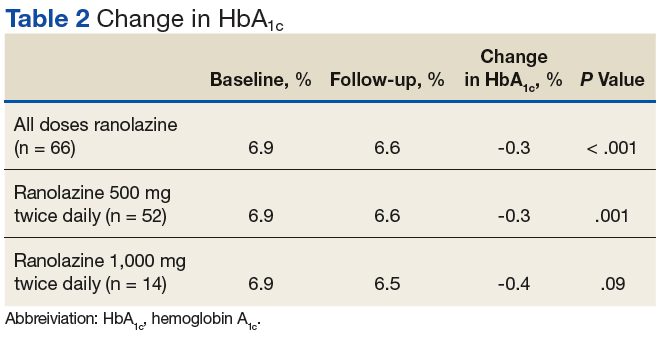
A dose of 500 mg ranolazine twice daily also was associated with a significant decrease in HbA1c by 0.3% (P = .001). A significant increase in veterans achieving HbA1c < 7% after ranolazine initiation was observed (42.3% before ranolazine initiation vs 73.1% after ranolazine initiation; P = .001), and a nonsignificant increase in veterans achieving HbA1c < 8% was observed (82.7% before ranolazine initiation vs 90.4% after ranolazine initiation, P = .37).
At a dose of 1,000 mg twice daily, a 0.4% decrease in HbA1c was observed. However, this result was not found to be statistically significant (P = .09), and the study was underpowered to detect a significant change in HbA1c at this dose. 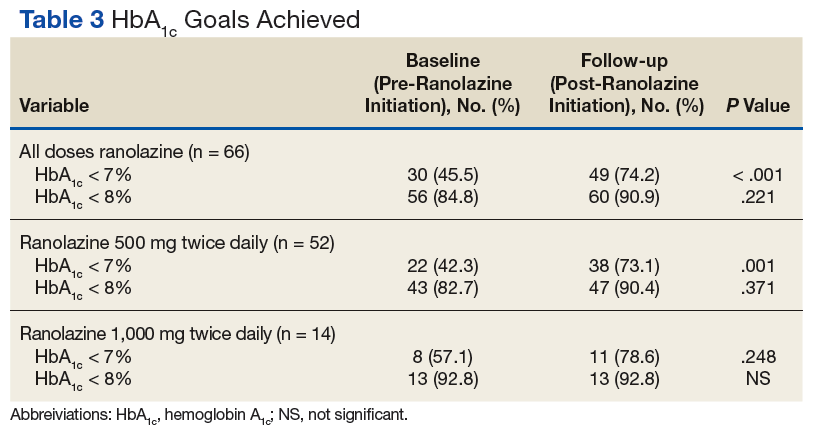
Hypoglycemia was not reported in a majority of study patient progress notes; thus, it was not evaluated further.
Discussion
In this study of a veteran population, ranolazine was associated with an HbA1c decrease of 0.3%. This change is less than that observed in previous studies, which may be related to a lower baseline HbA1c for the patients in this study. In addition, a greater percentage of veterans achieved an HbA1c < 7% after initiation of ranolazine compared with that of the baseline.
To the authors’ knowledge, this is the first study evaluating ranolazine and HbA1c in a veteran population. It also is the first study to demonstrate an association between HbA1c lowering and ranolazine at a dose of 500 mg twice daily. These results suggest that in patients with chronic angina and type 2 DM, ranolazine could potentially play a dual role in therapy.
Limitations
The authors recognize several limitations in this study. Given its observational design, it cannot be definitively concluded that the decrease in HbA1c was due to the initiation of ranolazine. While excluding patients with changes to their antidiabetic medication regimen was done in an effort to minimize confounding factors, it is possible that other factors, such as lifestyle, also could explain changes in HbA1c. It is possible that changes to the DM medication regimen were made but not documented in the EHR. In addition, information on hypoglycemia was not readily available; thus, the safety of ranolazine among patients with DM could not be evaluated fully. Finally, the patient population characteristics may limit external validity.
Conclusion
In this observational study, ranolazine was associated with a statistically significant decrease in HbA1c among veterans with DM, which supports previously published literature.9, 13-15 However, no randomized controlled trials have been performed specifically studying the impact of ranolazine on HbA1c among patient with DM. Ideally, future prospective, randomized placebo-controlled studies will take place to further evaluate the association between ranolazine use and HbA1c lowering.
1. Kannel WB, McGee DL. Diabetes and cardiovascular disease—the Framingham study. JAMA. 1979;241(19): 2035-2038.
2. Selvin E, Coresh J, Golden SH, Boland LL, Brancati FL, Steffes MW; Atherosclerosis risk in communities study. Glycemic control, atherosclerosis, and risk factors for cardiovascular disease in individuals with diabetes: the atherosclerosis risk in communities study. Diabetes Care. 2005;28(8):1965-1973.
3. Writing Group Members, Mozaffarian D, Benjamion EJ, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133(4):e38-e360.
4. Conaway DG, O’Keefe JH, Reid KJ, Spertus J. Frequency of undiagnosed diabetes mellitus in patients with acute coronary syndrome. Am J Cardiol. 2005;96(3):363-365.
5. Hiatt WR, Kaul S, Smith RJ. The cardiovascular safety of diabetes drugs—insights from the rosiglitazone experience. N Engl J Med. 2013;369(14):1285-1287.
6. Ning Y, Zhen W, Fu Z, et al. Ranolazine increases β-cell survival and improves glucose homeostasis in low-dose streptozotocin-induced diabetes in mice. J Pharmacol Exp Ther. 2011;337(1):50-58.
7. Ranexa [package insert]. Foster City, CA: Gilead Sciences Inc; 2016.
8. Chaitman BR, Pepine CJ, Parker JO, et al; Combination Assessment of Ranolazine In Stable Angina (CARISA) Investigators. Effects of ranolazine with atenolol, amlodipine, or diltiazem on exercise tolerance and angina frequency in patients with severe chronic angina: a randomized controlled trial. JAMA. 2004;291(3):309-316.
9. Timmis AD, Chaitman BR, Crager M. Effects of ranolazine on exercise tolerance and HbA1c in patients with chronic angina and diabetes. Eur Heart J. 2006;27(1):42-48.
10. Morrow DA, Scirica BM, Karwatowska-Prokopczuk E, et al; MERLIN-TIMI 36 Trial Investigators. Effects of ranolazine on recurrent cardiovascular events in patients with non-ST-elevation acute coronary syndromes: the MERLIN-TIMI 36 randomized trial. JAMA. 2007;297(16):1775-1783.
11. Kosiborod M, Arnold SV, Spertus JA, et al. Evaluation of ranolazine in patients with type 2 diabetes mellitus and chronic stable angina: results from the TERISA randomized clinical trial (Type 2 Diabetes Evaluation of Ranolazine in Subjects With Chronic Stable Angina). J Am Coll Cardiol. 2013;61(20):2038-2045.
12. Arnold SV, McGuire DK, Spertus JA, et al. Effectiveness of ranolazine in patients with type 2 diabetes mellitus and chronic stable angina according to baseline hemoglobin A1c. Am Heart J. 2014;168(4):457-465.e2.
13. Morrow DA, Scirica BM, Chaitman BR, et al; MERLIN-TIMI 36 Trial Investigators. Evaluation of the glycometabolic effects of ranolazine patients with and without diabetes mellitus in the MERLIN-TIMI 36 randomized controlled trial. Circulation. 2009;119(15):2032-2039.
14. Chisholm JW, Goldfine AB, Dhalla AK, et al. Effect of ranolazine on A1c and glucose levels in hyperglycemic patients with non-ST elevation acute coronary syndrome. Diabetes Care. 2010;33(6):1163-1168.
15. Eckel RH, Henry RR, Yue P, et al. Effect of ranolazine monotherapy on glycemic control in subjects with type 2 diabetes. Diabetes Care. 2015;38(7):1189-1196.
Diabetes mellitus (DM) is a risk factor for cardiovascular disease(CVD).1-4 Death rates from heart disease are 2- to 4-times higher among adults with DM compared with those of adults without DM. In the US, it is estimated that 21.1 million adults have diagnosed DM, 8.1 million adults have undiagnosed DM, and 80.8 million adults have prediabetes.3 The American Heart Association has identified an untreated fasting blood glucose level < 100 mg/dL as a component of ideal cardiovascular health.3
Although the use of antidiabetic agents has been shown to reduce the risks of microvascular complications among patients with DM, a cardiovascular benefit has not been consistently demonstrated with all available agents, and some used in the treatment of DM are associated with cardiovascular harm.5 In addition, some cardiovascular medications may contribute to the development of DM or may mask the symptoms of hypoglycemia.6 Given the risk for CVD among patients with DM, a medication with utility in both DM and CVD could be beneficial.
Evidence for Use of Ranolazine
Ranolazine is indicated for the treatment of chronic angina.7 In clinical trials, ranolazine also was found to decrease hemoglobin A1c (HbA1c).8-15 The possible mechanisms for lowering HbA1c with ranolazine include preservation of pancreatic β-cells and an increase in glucose-dependent insulin secretion.6 The most common adverse effects associated with ranolazine include dizziness, headache, constipation, and nausea.7
Ranolazine has been shown to be efficacious and safe in the reduction of angina symptoms among patients with and without DM.8-12 In addition to improving symptoms of angina, studies have demonstrated a reduction in HbA1c among patients taking ranolazine.9,13-15 In an open-label extension of the Combination Assessment of Ranolazine in Stable Angina (CARISA) trial, ranolazine 750 mg twice daily and 1,000 mg twice daily led to a greater reduction in HbA1c when each was compared with placebo (-0.48% HbA1c, P = .008; and -0.70% HbA1c, P = .001, respectively).9
Among the 5,576 patients enrolled in the Metabolic Efficiency With Ranolazine for Less Ischemia in Non-ST-Elevation Acute Coronary Syndromes—Thrombolysis in Myocardial Infarction 36 (MERLIN-TIMI 36) trial with a baseline HbA1c, ranolazine significantly reduced HbA1c at 4 months when compared with placebo among patients with and without DM.13 In addition, patients with DM who were treated with ranolazine were more likely to achieve a HbA1c < 7% at 4 months when compared with placebo (59% vs 49%; P < .001). Ranolazine was not found to increase the incidence of hypoglycemia.
A subgroup analysis of MERLIN-TIMI 36 evaluated the effects of ranolazine compared with those of placebo on fasting plasma glucose and HbA1c in patients with moderate DM (HbA1c ≥ 6% but < 8%, fasting plasma glucose < 250 mg/dL) and severe DM (A1c ≥ 8%, fasting plasma glucose 150-400 mg/dL).14 A significant reduction in HbA1c with ranolazine in addition to standard of care antidiabetes treatment was observed among both groups. The placebo-corrected decrease in HbA1c in the moderate DM group was 0.28% (95% confidence interval [CI] -0.55 to 0; P = .045) and in the severe DM group was 0.59% (95% CI -0.99 to -0.20; P < .001).
In a trial designed to evaluate change in HbA1c in patients taking ranolazine 1,000 mg twice daily compared with that of placebo, ranolazine led to a greater decrease in HbA1c compared with that of placebo (placebo corrected change in HbA1c -0.56%, P = .001).15 In addition, a higher percentage of patients achieved HbA1c < 7% at 24 weeks in the ranolazine group compared with that of placebo (41.2% vs 25.7%; P = .001). No patient experienced severe hypoglycemia or had documented hypoglycemia in this study.
These trials suggest that ranolazine, in addition to decreasing anginal events, is potentially beneficial in achieving better control of DM. However, more studies are needed to determine this benefit. In addition, no trials have examined the 500-mg twice daily dose of ranolazine in HbA1c reduction.
The purpose of this study was to evaluate the change in HbA1c among veterans with DM after the initiation of ranolazine. The study compared the percentage of veterans achieving HbA1c < 7% or < 8% after initiation of ranolazine with the baseline, to determine whether there is a dose-related change in HbA1c among different ranolazine regimens and to determine whether there is a change in the incidence of hypoglycemia after the initiation of ranolazine.
Methods
This was a multicenter, retrospective study. The institutional review board and research and development committee for 3 Veterans Affairs medical centers (VAMCs) approved this study and waived informed consent. Additionally, this study was approved for access to national patient information through the Corporate Data Warehouse (CDW).
Subjects were eligible for inclusion in this study if they were aged ≥ 18 years, had a diagnosis of type 2 DM, and received their first prescription of ranolazine at a VAMC from January 1, 2008 through March 31, 2015. Exclusion criteria included subjects with no baseline HbA1c (defined as the HbA1c result closest to the ranolazine initiation date and within 90 days before to 14 days after ranolazine initiation), no follow-up HbA1c (defined as the first HbA1c result within 60 to 180 days after the ranolazine initiation date), any change to their DM medication regimen during the follow-up period, or who discontinued ranolazine prior to collection of the follow-up HbA1c.
Data were collected from the electronic health record (EHR) for each subject from 6 months prior to the ranolazine initiation date through 6 months after the ranolazine initiation date. The ranolazine initiation date was defined as the date ranolazine was picked up in person at a VAMC pharmacy or 7 days after the date filled for medications sent by mail.
The primary endpoint of this study was the change in HbA1c after ranolazine initiation. The secondary endpoint was the percentage of study subjects achieving HbA1c < 7% and < 8% before and after the initiation of ranolazine.
To achieve 80% power to detect a change in HbA1c of 0.4%, a sample size of 52 patients was required. For the primary endpoint, a paired t test was used to test for statistical significance. The McNemar test was used to evaluate for a significant change in subjects achieving an HbA1c < 7% and HbA1c < 8% with the initiation of ranolazine.
Results
A total of 523 patients were evaluated for study inclusion, of which 66 patients were included (Figure). The most common reasons for exclusion included no HbA1c at baseline and changes to the DM medication regimen during follow-up.
Ranolazine at any dose was associated with a change in HbA1c of -0.3% (P < .001).
A dose of 500 mg ranolazine twice daily also was associated with a significant decrease in HbA1c by 0.3% (P = .001). A significant increase in veterans achieving HbA1c < 7% after ranolazine initiation was observed (42.3% before ranolazine initiation vs 73.1% after ranolazine initiation; P = .001), and a nonsignificant increase in veterans achieving HbA1c < 8% was observed (82.7% before ranolazine initiation vs 90.4% after ranolazine initiation, P = .37).
At a dose of 1,000 mg twice daily, a 0.4% decrease in HbA1c was observed. However, this result was not found to be statistically significant (P = .09), and the study was underpowered to detect a significant change in HbA1c at this dose.
Hypoglycemia was not reported in a majority of study patient progress notes; thus, it was not evaluated further.
Discussion
In this study of a veteran population, ranolazine was associated with an HbA1c decrease of 0.3%. This change is less than that observed in previous studies, which may be related to a lower baseline HbA1c for the patients in this study. In addition, a greater percentage of veterans achieved an HbA1c < 7% after initiation of ranolazine compared with that of the baseline.
To the authors’ knowledge, this is the first study evaluating ranolazine and HbA1c in a veteran population. It also is the first study to demonstrate an association between HbA1c lowering and ranolazine at a dose of 500 mg twice daily. These results suggest that in patients with chronic angina and type 2 DM, ranolazine could potentially play a dual role in therapy.
Limitations
The authors recognize several limitations in this study. Given its observational design, it cannot be definitively concluded that the decrease in HbA1c was due to the initiation of ranolazine. While excluding patients with changes to their antidiabetic medication regimen was done in an effort to minimize confounding factors, it is possible that other factors, such as lifestyle, also could explain changes in HbA1c. It is possible that changes to the DM medication regimen were made but not documented in the EHR. In addition, information on hypoglycemia was not readily available; thus, the safety of ranolazine among patients with DM could not be evaluated fully. Finally, the patient population characteristics may limit external validity.
Conclusion
In this observational study, ranolazine was associated with a statistically significant decrease in HbA1c among veterans with DM, which supports previously published literature.9, 13-15 However, no randomized controlled trials have been performed specifically studying the impact of ranolazine on HbA1c among patient with DM. Ideally, future prospective, randomized placebo-controlled studies will take place to further evaluate the association between ranolazine use and HbA1c lowering.
Diabetes mellitus (DM) is a risk factor for cardiovascular disease(CVD).1-4 Death rates from heart disease are 2- to 4-times higher among adults with DM compared with those of adults without DM. In the US, it is estimated that 21.1 million adults have diagnosed DM, 8.1 million adults have undiagnosed DM, and 80.8 million adults have prediabetes.3 The American Heart Association has identified an untreated fasting blood glucose level < 100 mg/dL as a component of ideal cardiovascular health.3
Although the use of antidiabetic agents has been shown to reduce the risks of microvascular complications among patients with DM, a cardiovascular benefit has not been consistently demonstrated with all available agents, and some used in the treatment of DM are associated with cardiovascular harm.5 In addition, some cardiovascular medications may contribute to the development of DM or may mask the symptoms of hypoglycemia.6 Given the risk for CVD among patients with DM, a medication with utility in both DM and CVD could be beneficial.
Evidence for Use of Ranolazine
Ranolazine is indicated for the treatment of chronic angina.7 In clinical trials, ranolazine also was found to decrease hemoglobin A1c (HbA1c).8-15 The possible mechanisms for lowering HbA1c with ranolazine include preservation of pancreatic β-cells and an increase in glucose-dependent insulin secretion.6 The most common adverse effects associated with ranolazine include dizziness, headache, constipation, and nausea.7
Ranolazine has been shown to be efficacious and safe in the reduction of angina symptoms among patients with and without DM.8-12 In addition to improving symptoms of angina, studies have demonstrated a reduction in HbA1c among patients taking ranolazine.9,13-15 In an open-label extension of the Combination Assessment of Ranolazine in Stable Angina (CARISA) trial, ranolazine 750 mg twice daily and 1,000 mg twice daily led to a greater reduction in HbA1c when each was compared with placebo (-0.48% HbA1c, P = .008; and -0.70% HbA1c, P = .001, respectively).9
Among the 5,576 patients enrolled in the Metabolic Efficiency With Ranolazine for Less Ischemia in Non-ST-Elevation Acute Coronary Syndromes—Thrombolysis in Myocardial Infarction 36 (MERLIN-TIMI 36) trial with a baseline HbA1c, ranolazine significantly reduced HbA1c at 4 months when compared with placebo among patients with and without DM.13 In addition, patients with DM who were treated with ranolazine were more likely to achieve a HbA1c < 7% at 4 months when compared with placebo (59% vs 49%; P < .001). Ranolazine was not found to increase the incidence of hypoglycemia.
A subgroup analysis of MERLIN-TIMI 36 evaluated the effects of ranolazine compared with those of placebo on fasting plasma glucose and HbA1c in patients with moderate DM (HbA1c ≥ 6% but < 8%, fasting plasma glucose < 250 mg/dL) and severe DM (A1c ≥ 8%, fasting plasma glucose 150-400 mg/dL).14 A significant reduction in HbA1c with ranolazine in addition to standard of care antidiabetes treatment was observed among both groups. The placebo-corrected decrease in HbA1c in the moderate DM group was 0.28% (95% confidence interval [CI] -0.55 to 0; P = .045) and in the severe DM group was 0.59% (95% CI -0.99 to -0.20; P < .001).
In a trial designed to evaluate change in HbA1c in patients taking ranolazine 1,000 mg twice daily compared with that of placebo, ranolazine led to a greater decrease in HbA1c compared with that of placebo (placebo corrected change in HbA1c -0.56%, P = .001).15 In addition, a higher percentage of patients achieved HbA1c < 7% at 24 weeks in the ranolazine group compared with that of placebo (41.2% vs 25.7%; P = .001). No patient experienced severe hypoglycemia or had documented hypoglycemia in this study.
These trials suggest that ranolazine, in addition to decreasing anginal events, is potentially beneficial in achieving better control of DM. However, more studies are needed to determine this benefit. In addition, no trials have examined the 500-mg twice daily dose of ranolazine in HbA1c reduction.
The purpose of this study was to evaluate the change in HbA1c among veterans with DM after the initiation of ranolazine. The study compared the percentage of veterans achieving HbA1c < 7% or < 8% after initiation of ranolazine with the baseline, to determine whether there is a dose-related change in HbA1c among different ranolazine regimens and to determine whether there is a change in the incidence of hypoglycemia after the initiation of ranolazine.
Methods
This was a multicenter, retrospective study. The institutional review board and research and development committee for 3 Veterans Affairs medical centers (VAMCs) approved this study and waived informed consent. Additionally, this study was approved for access to national patient information through the Corporate Data Warehouse (CDW).
Subjects were eligible for inclusion in this study if they were aged ≥ 18 years, had a diagnosis of type 2 DM, and received their first prescription of ranolazine at a VAMC from January 1, 2008 through March 31, 2015. Exclusion criteria included subjects with no baseline HbA1c (defined as the HbA1c result closest to the ranolazine initiation date and within 90 days before to 14 days after ranolazine initiation), no follow-up HbA1c (defined as the first HbA1c result within 60 to 180 days after the ranolazine initiation date), any change to their DM medication regimen during the follow-up period, or who discontinued ranolazine prior to collection of the follow-up HbA1c.
Data were collected from the electronic health record (EHR) for each subject from 6 months prior to the ranolazine initiation date through 6 months after the ranolazine initiation date. The ranolazine initiation date was defined as the date ranolazine was picked up in person at a VAMC pharmacy or 7 days after the date filled for medications sent by mail.
The primary endpoint of this study was the change in HbA1c after ranolazine initiation. The secondary endpoint was the percentage of study subjects achieving HbA1c < 7% and < 8% before and after the initiation of ranolazine.
To achieve 80% power to detect a change in HbA1c of 0.4%, a sample size of 52 patients was required. For the primary endpoint, a paired t test was used to test for statistical significance. The McNemar test was used to evaluate for a significant change in subjects achieving an HbA1c < 7% and HbA1c < 8% with the initiation of ranolazine.
Results
A total of 523 patients were evaluated for study inclusion, of which 66 patients were included (Figure). The most common reasons for exclusion included no HbA1c at baseline and changes to the DM medication regimen during follow-up.
Ranolazine at any dose was associated with a change in HbA1c of -0.3% (P < .001).
A dose of 500 mg ranolazine twice daily also was associated with a significant decrease in HbA1c by 0.3% (P = .001). A significant increase in veterans achieving HbA1c < 7% after ranolazine initiation was observed (42.3% before ranolazine initiation vs 73.1% after ranolazine initiation; P = .001), and a nonsignificant increase in veterans achieving HbA1c < 8% was observed (82.7% before ranolazine initiation vs 90.4% after ranolazine initiation, P = .37).
At a dose of 1,000 mg twice daily, a 0.4% decrease in HbA1c was observed. However, this result was not found to be statistically significant (P = .09), and the study was underpowered to detect a significant change in HbA1c at this dose.
Hypoglycemia was not reported in a majority of study patient progress notes; thus, it was not evaluated further.
Discussion
In this study of a veteran population, ranolazine was associated with an HbA1c decrease of 0.3%. This change is less than that observed in previous studies, which may be related to a lower baseline HbA1c for the patients in this study. In addition, a greater percentage of veterans achieved an HbA1c < 7% after initiation of ranolazine compared with that of the baseline.
To the authors’ knowledge, this is the first study evaluating ranolazine and HbA1c in a veteran population. It also is the first study to demonstrate an association between HbA1c lowering and ranolazine at a dose of 500 mg twice daily. These results suggest that in patients with chronic angina and type 2 DM, ranolazine could potentially play a dual role in therapy.
Limitations
The authors recognize several limitations in this study. Given its observational design, it cannot be definitively concluded that the decrease in HbA1c was due to the initiation of ranolazine. While excluding patients with changes to their antidiabetic medication regimen was done in an effort to minimize confounding factors, it is possible that other factors, such as lifestyle, also could explain changes in HbA1c. It is possible that changes to the DM medication regimen were made but not documented in the EHR. In addition, information on hypoglycemia was not readily available; thus, the safety of ranolazine among patients with DM could not be evaluated fully. Finally, the patient population characteristics may limit external validity.
Conclusion
In this observational study, ranolazine was associated with a statistically significant decrease in HbA1c among veterans with DM, which supports previously published literature.9, 13-15 However, no randomized controlled trials have been performed specifically studying the impact of ranolazine on HbA1c among patient with DM. Ideally, future prospective, randomized placebo-controlled studies will take place to further evaluate the association between ranolazine use and HbA1c lowering.
1. Kannel WB, McGee DL. Diabetes and cardiovascular disease—the Framingham study. JAMA. 1979;241(19): 2035-2038.
2. Selvin E, Coresh J, Golden SH, Boland LL, Brancati FL, Steffes MW; Atherosclerosis risk in communities study. Glycemic control, atherosclerosis, and risk factors for cardiovascular disease in individuals with diabetes: the atherosclerosis risk in communities study. Diabetes Care. 2005;28(8):1965-1973.
3. Writing Group Members, Mozaffarian D, Benjamion EJ, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133(4):e38-e360.
4. Conaway DG, O’Keefe JH, Reid KJ, Spertus J. Frequency of undiagnosed diabetes mellitus in patients with acute coronary syndrome. Am J Cardiol. 2005;96(3):363-365.
5. Hiatt WR, Kaul S, Smith RJ. The cardiovascular safety of diabetes drugs—insights from the rosiglitazone experience. N Engl J Med. 2013;369(14):1285-1287.
6. Ning Y, Zhen W, Fu Z, et al. Ranolazine increases β-cell survival and improves glucose homeostasis in low-dose streptozotocin-induced diabetes in mice. J Pharmacol Exp Ther. 2011;337(1):50-58.
7. Ranexa [package insert]. Foster City, CA: Gilead Sciences Inc; 2016.
8. Chaitman BR, Pepine CJ, Parker JO, et al; Combination Assessment of Ranolazine In Stable Angina (CARISA) Investigators. Effects of ranolazine with atenolol, amlodipine, or diltiazem on exercise tolerance and angina frequency in patients with severe chronic angina: a randomized controlled trial. JAMA. 2004;291(3):309-316.
9. Timmis AD, Chaitman BR, Crager M. Effects of ranolazine on exercise tolerance and HbA1c in patients with chronic angina and diabetes. Eur Heart J. 2006;27(1):42-48.
10. Morrow DA, Scirica BM, Karwatowska-Prokopczuk E, et al; MERLIN-TIMI 36 Trial Investigators. Effects of ranolazine on recurrent cardiovascular events in patients with non-ST-elevation acute coronary syndromes: the MERLIN-TIMI 36 randomized trial. JAMA. 2007;297(16):1775-1783.
11. Kosiborod M, Arnold SV, Spertus JA, et al. Evaluation of ranolazine in patients with type 2 diabetes mellitus and chronic stable angina: results from the TERISA randomized clinical trial (Type 2 Diabetes Evaluation of Ranolazine in Subjects With Chronic Stable Angina). J Am Coll Cardiol. 2013;61(20):2038-2045.
12. Arnold SV, McGuire DK, Spertus JA, et al. Effectiveness of ranolazine in patients with type 2 diabetes mellitus and chronic stable angina according to baseline hemoglobin A1c. Am Heart J. 2014;168(4):457-465.e2.
13. Morrow DA, Scirica BM, Chaitman BR, et al; MERLIN-TIMI 36 Trial Investigators. Evaluation of the glycometabolic effects of ranolazine patients with and without diabetes mellitus in the MERLIN-TIMI 36 randomized controlled trial. Circulation. 2009;119(15):2032-2039.
14. Chisholm JW, Goldfine AB, Dhalla AK, et al. Effect of ranolazine on A1c and glucose levels in hyperglycemic patients with non-ST elevation acute coronary syndrome. Diabetes Care. 2010;33(6):1163-1168.
15. Eckel RH, Henry RR, Yue P, et al. Effect of ranolazine monotherapy on glycemic control in subjects with type 2 diabetes. Diabetes Care. 2015;38(7):1189-1196.
1. Kannel WB, McGee DL. Diabetes and cardiovascular disease—the Framingham study. JAMA. 1979;241(19): 2035-2038.
2. Selvin E, Coresh J, Golden SH, Boland LL, Brancati FL, Steffes MW; Atherosclerosis risk in communities study. Glycemic control, atherosclerosis, and risk factors for cardiovascular disease in individuals with diabetes: the atherosclerosis risk in communities study. Diabetes Care. 2005;28(8):1965-1973.
3. Writing Group Members, Mozaffarian D, Benjamion EJ, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133(4):e38-e360.
4. Conaway DG, O’Keefe JH, Reid KJ, Spertus J. Frequency of undiagnosed diabetes mellitus in patients with acute coronary syndrome. Am J Cardiol. 2005;96(3):363-365.
5. Hiatt WR, Kaul S, Smith RJ. The cardiovascular safety of diabetes drugs—insights from the rosiglitazone experience. N Engl J Med. 2013;369(14):1285-1287.
6. Ning Y, Zhen W, Fu Z, et al. Ranolazine increases β-cell survival and improves glucose homeostasis in low-dose streptozotocin-induced diabetes in mice. J Pharmacol Exp Ther. 2011;337(1):50-58.
7. Ranexa [package insert]. Foster City, CA: Gilead Sciences Inc; 2016.
8. Chaitman BR, Pepine CJ, Parker JO, et al; Combination Assessment of Ranolazine In Stable Angina (CARISA) Investigators. Effects of ranolazine with atenolol, amlodipine, or diltiazem on exercise tolerance and angina frequency in patients with severe chronic angina: a randomized controlled trial. JAMA. 2004;291(3):309-316.
9. Timmis AD, Chaitman BR, Crager M. Effects of ranolazine on exercise tolerance and HbA1c in patients with chronic angina and diabetes. Eur Heart J. 2006;27(1):42-48.
10. Morrow DA, Scirica BM, Karwatowska-Prokopczuk E, et al; MERLIN-TIMI 36 Trial Investigators. Effects of ranolazine on recurrent cardiovascular events in patients with non-ST-elevation acute coronary syndromes: the MERLIN-TIMI 36 randomized trial. JAMA. 2007;297(16):1775-1783.
11. Kosiborod M, Arnold SV, Spertus JA, et al. Evaluation of ranolazine in patients with type 2 diabetes mellitus and chronic stable angina: results from the TERISA randomized clinical trial (Type 2 Diabetes Evaluation of Ranolazine in Subjects With Chronic Stable Angina). J Am Coll Cardiol. 2013;61(20):2038-2045.
12. Arnold SV, McGuire DK, Spertus JA, et al. Effectiveness of ranolazine in patients with type 2 diabetes mellitus and chronic stable angina according to baseline hemoglobin A1c. Am Heart J. 2014;168(4):457-465.e2.
13. Morrow DA, Scirica BM, Chaitman BR, et al; MERLIN-TIMI 36 Trial Investigators. Evaluation of the glycometabolic effects of ranolazine patients with and without diabetes mellitus in the MERLIN-TIMI 36 randomized controlled trial. Circulation. 2009;119(15):2032-2039.
14. Chisholm JW, Goldfine AB, Dhalla AK, et al. Effect of ranolazine on A1c and glucose levels in hyperglycemic patients with non-ST elevation acute coronary syndrome. Diabetes Care. 2010;33(6):1163-1168.
15. Eckel RH, Henry RR, Yue P, et al. Effect of ranolazine monotherapy on glycemic control in subjects with type 2 diabetes. Diabetes Care. 2015;38(7):1189-1196.
Reduce referrals: Skip eye chart with automated vision checker for kids
TORONTO – Using an automated photorefractor-based vision screening in preschool-age children reduced referrals to ophthalmologists and optometrists by one-third, compared with standard chart-based screening, according to a nonrandomized trial conducted in Boston. The handheld device that was used requires minimal cooperation from the child and also checks ocular alignment.
“This device requires almost zero cooperation from the child. The nurse or assistant holds the device and the child has to look at it for about two seconds, as opposed to several minutes to do a chart-based test,” reported Louis Vernacchio, MD, at the 2018 Pediatric Academic Societies meeting.

They found a 33.7% decline in initial ophthalmology and optometry visits after practices switched from chart-based vision screening to the hand-held screening device.
“Optometry and ophthalmology is the No. 1 specialist to whom our patients of all ages are referred to in our pediatric network, and the No. 1 diagnosis was normal vision, so in most cases, there’s nothing wrong, and they’re clogging up the system.”
Instrument-based vision screening has been shown to have high sensitivity and specificity, compared with ophthalmic vision screening, and has much better testability in young children than traditional eye chart–based screening.
In previously reported data, Dr. Vernacchio’s group showed that, with instrument-based vision screening, completed screening rates among children aged 3-5 years improved. The most marked improvement was in the 3-year-olds, among whom completed screening rates increased from 39% with chart-based screening to 87% with instrument screening. (Modest JR et al. Pediatrics. 2017 Jul;140[1]. pii: e20163745.) Family satisfaction is also improved with the automated method.
The automated vision screening device used in the study was the Spot Vision Screener produced by Welch Allyn.
“Our nurses are in heaven with these devices, so besides the billing that you can do, you can save staff time and easily justify the cost of the device. My office now has 4 or 5 of these devices because it just saves so much time to have them readily available.”
Professional societies endorse automated vision screening
Amblyopia is seen in 2 or 3 children per 100 in the United States, reported Dr. Vernacchio. Chart-based vision screening is notoriously difficult to accomplish in young children and there is both a risk of missing amblyopia in those who do not cooperate and a risk of overreferral because of poor performance on the test.
Recently, the American Academy of Pediatrics, the U.S. Preventive Services Task Force, and others have endorsed the use of instrument-based vision screening in place of chart-based screening for children aged 3-5 years based on evidence of improved testability and acceptable sensitivity and specificity.
The Spot Vision Screener has a retail cost between $6000 and $7000, according to Dr. Vernacchio. “Many” insurance companies will pay a separate fee for vision screening using an instrument, but others bundle the screening into a well visit, he noted.
“So, you can actually calculate the time to recover the cost of the device based on your payer practices,” he said. Another option is a smart phone app that uses a subscription model, in which the test results are interpreted by the company within a few minutes with a per test charge of about .99 cents.
“The Holy Grail is whether this process will reduce the incidence of amblyopia,” said Dr. Vernacchio. That study is next on his to-do list, he said, but “it’s going to take longer to answer that question.”
The authors reported no conflicts of interest. There was no external funding.
TORONTO – Using an automated photorefractor-based vision screening in preschool-age children reduced referrals to ophthalmologists and optometrists by one-third, compared with standard chart-based screening, according to a nonrandomized trial conducted in Boston. The handheld device that was used requires minimal cooperation from the child and also checks ocular alignment.
“This device requires almost zero cooperation from the child. The nurse or assistant holds the device and the child has to look at it for about two seconds, as opposed to several minutes to do a chart-based test,” reported Louis Vernacchio, MD, at the 2018 Pediatric Academic Societies meeting.
They found a 33.7% decline in initial ophthalmology and optometry visits after practices switched from chart-based vision screening to the hand-held screening device.
“Optometry and ophthalmology is the No. 1 specialist to whom our patients of all ages are referred to in our pediatric network, and the No. 1 diagnosis was normal vision, so in most cases, there’s nothing wrong, and they’re clogging up the system.”
Instrument-based vision screening has been shown to have high sensitivity and specificity, compared with ophthalmic vision screening, and has much better testability in young children than traditional eye chart–based screening.
In previously reported data, Dr. Vernacchio’s group showed that, with instrument-based vision screening, completed screening rates among children aged 3-5 years improved. The most marked improvement was in the 3-year-olds, among whom completed screening rates increased from 39% with chart-based screening to 87% with instrument screening. (Modest JR et al. Pediatrics. 2017 Jul;140[1]. pii: e20163745.) Family satisfaction is also improved with the automated method.
The automated vision screening device used in the study was the Spot Vision Screener produced by Welch Allyn.
“Our nurses are in heaven with these devices, so besides the billing that you can do, you can save staff time and easily justify the cost of the device. My office now has 4 or 5 of these devices because it just saves so much time to have them readily available.”
Professional societies endorse automated vision screening
Amblyopia is seen in 2 or 3 children per 100 in the United States, reported Dr. Vernacchio. Chart-based vision screening is notoriously difficult to accomplish in young children and there is both a risk of missing amblyopia in those who do not cooperate and a risk of overreferral because of poor performance on the test.
Recently, the American Academy of Pediatrics, the U.S. Preventive Services Task Force, and others have endorsed the use of instrument-based vision screening in place of chart-based screening for children aged 3-5 years based on evidence of improved testability and acceptable sensitivity and specificity.
The Spot Vision Screener has a retail cost between $6000 and $7000, according to Dr. Vernacchio. “Many” insurance companies will pay a separate fee for vision screening using an instrument, but others bundle the screening into a well visit, he noted.
“So, you can actually calculate the time to recover the cost of the device based on your payer practices,” he said. Another option is a smart phone app that uses a subscription model, in which the test results are interpreted by the company within a few minutes with a per test charge of about .99 cents.
“The Holy Grail is whether this process will reduce the incidence of amblyopia,” said Dr. Vernacchio. That study is next on his to-do list, he said, but “it’s going to take longer to answer that question.”
The authors reported no conflicts of interest. There was no external funding.
TORONTO – Using an automated photorefractor-based vision screening in preschool-age children reduced referrals to ophthalmologists and optometrists by one-third, compared with standard chart-based screening, according to a nonrandomized trial conducted in Boston. The handheld device that was used requires minimal cooperation from the child and also checks ocular alignment.
“This device requires almost zero cooperation from the child. The nurse or assistant holds the device and the child has to look at it for about two seconds, as opposed to several minutes to do a chart-based test,” reported Louis Vernacchio, MD, at the 2018 Pediatric Academic Societies meeting.
They found a 33.7% decline in initial ophthalmology and optometry visits after practices switched from chart-based vision screening to the hand-held screening device.
“Optometry and ophthalmology is the No. 1 specialist to whom our patients of all ages are referred to in our pediatric network, and the No. 1 diagnosis was normal vision, so in most cases, there’s nothing wrong, and they’re clogging up the system.”
Instrument-based vision screening has been shown to have high sensitivity and specificity, compared with ophthalmic vision screening, and has much better testability in young children than traditional eye chart–based screening.
In previously reported data, Dr. Vernacchio’s group showed that, with instrument-based vision screening, completed screening rates among children aged 3-5 years improved. The most marked improvement was in the 3-year-olds, among whom completed screening rates increased from 39% with chart-based screening to 87% with instrument screening. (Modest JR et al. Pediatrics. 2017 Jul;140[1]. pii: e20163745.) Family satisfaction is also improved with the automated method.
The automated vision screening device used in the study was the Spot Vision Screener produced by Welch Allyn.
“Our nurses are in heaven with these devices, so besides the billing that you can do, you can save staff time and easily justify the cost of the device. My office now has 4 or 5 of these devices because it just saves so much time to have them readily available.”
Professional societies endorse automated vision screening
Amblyopia is seen in 2 or 3 children per 100 in the United States, reported Dr. Vernacchio. Chart-based vision screening is notoriously difficult to accomplish in young children and there is both a risk of missing amblyopia in those who do not cooperate and a risk of overreferral because of poor performance on the test.
Recently, the American Academy of Pediatrics, the U.S. Preventive Services Task Force, and others have endorsed the use of instrument-based vision screening in place of chart-based screening for children aged 3-5 years based on evidence of improved testability and acceptable sensitivity and specificity.
The Spot Vision Screener has a retail cost between $6000 and $7000, according to Dr. Vernacchio. “Many” insurance companies will pay a separate fee for vision screening using an instrument, but others bundle the screening into a well visit, he noted.
“So, you can actually calculate the time to recover the cost of the device based on your payer practices,” he said. Another option is a smart phone app that uses a subscription model, in which the test results are interpreted by the company within a few minutes with a per test charge of about .99 cents.
“The Holy Grail is whether this process will reduce the incidence of amblyopia,” said Dr. Vernacchio. That study is next on his to-do list, he said, but “it’s going to take longer to answer that question.”
The authors reported no conflicts of interest. There was no external funding.
Key clinical point: Switching from a chart-based to an instrument-based vision screening reduced unnecessary pediatric eye care referrals.
Major finding: Use of an automated vision screening system reduced referrals for pediatric eye care by 33.7%.
Study details: A nonrandomized analysis of referral patterns from January 2015 to June 2015 from 12 pediatric primary care practices, with findings compared with a prior time period before the vision screening device was used.
Disclosures: The authors reported no conflicts of interest. There was no external funding
Research Opportunities Page Updated
Looking for a research opportunity? Check our website for current programs in your area. If your institution has an opportunity to promote, let us know at [email protected]
Looking for a research opportunity? Check our website for current programs in your area. If your institution has an opportunity to promote, let us know at [email protected]
Looking for a research opportunity? Check our website for current programs in your area. If your institution has an opportunity to promote, let us know at [email protected]