User login
After initial rivaroxaban, aspirin is noninferior to rivaroxaban for thromboprophylaxis following joint arthroplasty
Background: While there is a consensus on the need for chemoprophylaxis to reduce the rates of postoperative VTE, there is wide variation in choice of agents recommended. Aspirin, while cheap and widely available, has never been directly compared with a direct oral anticoagulant in randomized, controlled trials.
Study design: Multicenter, double-blind, randomized, controlled noninferiority trial.
Setting: 15 university-affiliated health centers in Canada from January 2013 through April 2016.
Synopsis: 3,224 patients who received daily rivaroxaban for 5 days following joint arthroplasty were randomized to either receive aspirin 81 mg daily or continue daily rivaroxaban. Duration of therapy was determined by type of surgery (9 days for knee, 17 days for hip). The primary effectiveness outcome was defined as symptomatic pulmonary embolism or proximal deep venous thrombosis diagnosed in the 90-day follow-up period. The primary outcome results met the predetermined criterion for noninferiority with similar rates of symptomatic VTE in the aspirin and rivaroxaban group (0.64% vs. 0.7%; P less than .001). There was no significant difference in bleeding rates between the groups. Given that patients with prior VTE, morbid obesity, or cancer were not well represented in this study, these results should not be extrapolated to those populations felt to be at highest risk for VTE.
Bottom line: For thromboprophylaxis after joint arthroplasty, rivaroxaban followed by aspirin may be noninferior to extended rivaroxaban.
Citation: Anderson D et al. Aspirin or rivaroxaban for VTE prophylaxis after hip or knee arthroplasty. N Eng J Med. 2018 Feb 22;378(8):699-707.

Dr. Abdallah is a hospitalist at Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, Boston.
Background: While there is a consensus on the need for chemoprophylaxis to reduce the rates of postoperative VTE, there is wide variation in choice of agents recommended. Aspirin, while cheap and widely available, has never been directly compared with a direct oral anticoagulant in randomized, controlled trials.
Study design: Multicenter, double-blind, randomized, controlled noninferiority trial.
Setting: 15 university-affiliated health centers in Canada from January 2013 through April 2016.
Synopsis: 3,224 patients who received daily rivaroxaban for 5 days following joint arthroplasty were randomized to either receive aspirin 81 mg daily or continue daily rivaroxaban. Duration of therapy was determined by type of surgery (9 days for knee, 17 days for hip). The primary effectiveness outcome was defined as symptomatic pulmonary embolism or proximal deep venous thrombosis diagnosed in the 90-day follow-up period. The primary outcome results met the predetermined criterion for noninferiority with similar rates of symptomatic VTE in the aspirin and rivaroxaban group (0.64% vs. 0.7%; P less than .001). There was no significant difference in bleeding rates between the groups. Given that patients with prior VTE, morbid obesity, or cancer were not well represented in this study, these results should not be extrapolated to those populations felt to be at highest risk for VTE.
Bottom line: For thromboprophylaxis after joint arthroplasty, rivaroxaban followed by aspirin may be noninferior to extended rivaroxaban.
Citation: Anderson D et al. Aspirin or rivaroxaban for VTE prophylaxis after hip or knee arthroplasty. N Eng J Med. 2018 Feb 22;378(8):699-707.
Dr. Abdallah is a hospitalist at Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, Boston.
Background: While there is a consensus on the need for chemoprophylaxis to reduce the rates of postoperative VTE, there is wide variation in choice of agents recommended. Aspirin, while cheap and widely available, has never been directly compared with a direct oral anticoagulant in randomized, controlled trials.
Study design: Multicenter, double-blind, randomized, controlled noninferiority trial.
Setting: 15 university-affiliated health centers in Canada from January 2013 through April 2016.
Synopsis: 3,224 patients who received daily rivaroxaban for 5 days following joint arthroplasty were randomized to either receive aspirin 81 mg daily or continue daily rivaroxaban. Duration of therapy was determined by type of surgery (9 days for knee, 17 days for hip). The primary effectiveness outcome was defined as symptomatic pulmonary embolism or proximal deep venous thrombosis diagnosed in the 90-day follow-up period. The primary outcome results met the predetermined criterion for noninferiority with similar rates of symptomatic VTE in the aspirin and rivaroxaban group (0.64% vs. 0.7%; P less than .001). There was no significant difference in bleeding rates between the groups. Given that patients with prior VTE, morbid obesity, or cancer were not well represented in this study, these results should not be extrapolated to those populations felt to be at highest risk for VTE.
Bottom line: For thromboprophylaxis after joint arthroplasty, rivaroxaban followed by aspirin may be noninferior to extended rivaroxaban.
Citation: Anderson D et al. Aspirin or rivaroxaban for VTE prophylaxis after hip or knee arthroplasty. N Eng J Med. 2018 Feb 22;378(8):699-707.
Dr. Abdallah is a hospitalist at Beth Israel Deaconess Medical Center, and instructor in medicine, Harvard Medical School, Boston.
Short-course IV antibiotics okay for newborn bacteremic UTI
ATLANTA – A short course of IV antibiotics – 7 days or less – is fine for most infants with uncomplicated bacteremic urinary tract infections, according to a review of 116 children younger than 60 days.
How long to treat bacteremic UTIs in the very young has been debated in pediatrics for a while, with some centers opting for a few days and others for 2 weeks or more. Shorter courses reduce length of stay, costs, and complications, but there hasn’t been much research to see whether they work as well.

The new investigation has suggested they do. “Young infants with bacteremic UTI who received less than or equal to 7 days of IV antibiotic therapy did not have more recurrent UTIs,” compared “to infants who received longer courses. Short course IV therapy with early conversion to oral antibiotics may be considered in this population,” said lead investigator Sanyukta Desai, MD, at the Pediatric Hospital Medicine meeting.
The team compared outcomes of 58 infants treated for 7 days or less to outcomes of 58 infants treated for more than 7 days at 11 children’s hospitals scattered across the United States.
Urine was collected by catheter, and each child grew the same organism in their blood and urine cultures, confirming the diagnosis of bacteremic UTI. Children with bacterial meningitis, or suspected of having it, were excluded. The subjects had all been admitted through the ED.
There was quite a bit of variation among the 11 hospitals, with the proportion of children treated with short courses ranging from 10% to 81%.
As for the results, two patients in the short-course group (3%) and four in the long-course group (7%) had recurrent UTIs within 30 days. None of them developed meningitis, and none required ICU admission. Propensity-score matching revealed an odds ratio for recurrence that favored shorter treatment, but it wasn’t statistically significant.
The mean length of stay was 5 days in the short-course arm and 11 days in the long-course arm. There were no serious adverse events within 30 days of the index admission in either group.
Among the recurrences, the two children in the short-course arm were initially treated for 3 and 5 days. Both were older than 28 days at their initial presentation, and both had vesicoureteral reflux of at least grade 2, which was not diagnosed in one child until after the recurrence. The other child had been on prophylactic trimethoprim/sulfamethoxazole before the recurrence.
The four recurrent cases in the long arm initially received either 10 or 14 days of IV antibiotics. Two children had grade 4 vesicoureteral reflux and had been on prophylactic amoxicillin.
Infants treated with longer antibiotic courses were more likely to be under 28 days old, appear ill at presentation, have had bacteremia for more than 24 hours, and have and grow out pathogens other than Escherichia coli. The two groups were otherwise balanced for sex, prematurity, complex chronic conditions, and known genitourinary anomalies.
With such low event rates, the study wasn’t powered to detect small but potentially meaningful differences in outcomes, and further work is needed to define which children would benefit from longer treatment courses. Even so, “it was reassuring that patients did well in both arms,” said Dr. Desai, a clinical fellow in the division of hospital medicine at Cincinnati Children’s Hospital.
“At our institution with uncomplicated UTI, we wait to see what the culture grows.” If there’s an oral antibiotic that will work, “we send [infants] home in 3-4 days. We haven’t had any poor outcomes, even when they’re bacteremic,” she said.
The work was funded by the National Institutes of Health. The investigators didn’t have any disclosures.
ATLANTA – A short course of IV antibiotics – 7 days or less – is fine for most infants with uncomplicated bacteremic urinary tract infections, according to a review of 116 children younger than 60 days.
How long to treat bacteremic UTIs in the very young has been debated in pediatrics for a while, with some centers opting for a few days and others for 2 weeks or more. Shorter courses reduce length of stay, costs, and complications, but there hasn’t been much research to see whether they work as well.
The new investigation has suggested they do. “Young infants with bacteremic UTI who received less than or equal to 7 days of IV antibiotic therapy did not have more recurrent UTIs,” compared “to infants who received longer courses. Short course IV therapy with early conversion to oral antibiotics may be considered in this population,” said lead investigator Sanyukta Desai, MD, at the Pediatric Hospital Medicine meeting.
The team compared outcomes of 58 infants treated for 7 days or less to outcomes of 58 infants treated for more than 7 days at 11 children’s hospitals scattered across the United States.
Urine was collected by catheter, and each child grew the same organism in their blood and urine cultures, confirming the diagnosis of bacteremic UTI. Children with bacterial meningitis, or suspected of having it, were excluded. The subjects had all been admitted through the ED.
There was quite a bit of variation among the 11 hospitals, with the proportion of children treated with short courses ranging from 10% to 81%.
As for the results, two patients in the short-course group (3%) and four in the long-course group (7%) had recurrent UTIs within 30 days. None of them developed meningitis, and none required ICU admission. Propensity-score matching revealed an odds ratio for recurrence that favored shorter treatment, but it wasn’t statistically significant.
The mean length of stay was 5 days in the short-course arm and 11 days in the long-course arm. There were no serious adverse events within 30 days of the index admission in either group.
Among the recurrences, the two children in the short-course arm were initially treated for 3 and 5 days. Both were older than 28 days at their initial presentation, and both had vesicoureteral reflux of at least grade 2, which was not diagnosed in one child until after the recurrence. The other child had been on prophylactic trimethoprim/sulfamethoxazole before the recurrence.
The four recurrent cases in the long arm initially received either 10 or 14 days of IV antibiotics. Two children had grade 4 vesicoureteral reflux and had been on prophylactic amoxicillin.
Infants treated with longer antibiotic courses were more likely to be under 28 days old, appear ill at presentation, have had bacteremia for more than 24 hours, and have and grow out pathogens other than Escherichia coli. The two groups were otherwise balanced for sex, prematurity, complex chronic conditions, and known genitourinary anomalies.
With such low event rates, the study wasn’t powered to detect small but potentially meaningful differences in outcomes, and further work is needed to define which children would benefit from longer treatment courses. Even so, “it was reassuring that patients did well in both arms,” said Dr. Desai, a clinical fellow in the division of hospital medicine at Cincinnati Children’s Hospital.
“At our institution with uncomplicated UTI, we wait to see what the culture grows.” If there’s an oral antibiotic that will work, “we send [infants] home in 3-4 days. We haven’t had any poor outcomes, even when they’re bacteremic,” she said.
The work was funded by the National Institutes of Health. The investigators didn’t have any disclosures.
ATLANTA – A short course of IV antibiotics – 7 days or less – is fine for most infants with uncomplicated bacteremic urinary tract infections, according to a review of 116 children younger than 60 days.
How long to treat bacteremic UTIs in the very young has been debated in pediatrics for a while, with some centers opting for a few days and others for 2 weeks or more. Shorter courses reduce length of stay, costs, and complications, but there hasn’t been much research to see whether they work as well.
The new investigation has suggested they do. “Young infants with bacteremic UTI who received less than or equal to 7 days of IV antibiotic therapy did not have more recurrent UTIs,” compared “to infants who received longer courses. Short course IV therapy with early conversion to oral antibiotics may be considered in this population,” said lead investigator Sanyukta Desai, MD, at the Pediatric Hospital Medicine meeting.
The team compared outcomes of 58 infants treated for 7 days or less to outcomes of 58 infants treated for more than 7 days at 11 children’s hospitals scattered across the United States.
Urine was collected by catheter, and each child grew the same organism in their blood and urine cultures, confirming the diagnosis of bacteremic UTI. Children with bacterial meningitis, or suspected of having it, were excluded. The subjects had all been admitted through the ED.
There was quite a bit of variation among the 11 hospitals, with the proportion of children treated with short courses ranging from 10% to 81%.
As for the results, two patients in the short-course group (3%) and four in the long-course group (7%) had recurrent UTIs within 30 days. None of them developed meningitis, and none required ICU admission. Propensity-score matching revealed an odds ratio for recurrence that favored shorter treatment, but it wasn’t statistically significant.
The mean length of stay was 5 days in the short-course arm and 11 days in the long-course arm. There were no serious adverse events within 30 days of the index admission in either group.
Among the recurrences, the two children in the short-course arm were initially treated for 3 and 5 days. Both were older than 28 days at their initial presentation, and both had vesicoureteral reflux of at least grade 2, which was not diagnosed in one child until after the recurrence. The other child had been on prophylactic trimethoprim/sulfamethoxazole before the recurrence.
The four recurrent cases in the long arm initially received either 10 or 14 days of IV antibiotics. Two children had grade 4 vesicoureteral reflux and had been on prophylactic amoxicillin.
Infants treated with longer antibiotic courses were more likely to be under 28 days old, appear ill at presentation, have had bacteremia for more than 24 hours, and have and grow out pathogens other than Escherichia coli. The two groups were otherwise balanced for sex, prematurity, complex chronic conditions, and known genitourinary anomalies.
With such low event rates, the study wasn’t powered to detect small but potentially meaningful differences in outcomes, and further work is needed to define which children would benefit from longer treatment courses. Even so, “it was reassuring that patients did well in both arms,” said Dr. Desai, a clinical fellow in the division of hospital medicine at Cincinnati Children’s Hospital.
“At our institution with uncomplicated UTI, we wait to see what the culture grows.” If there’s an oral antibiotic that will work, “we send [infants] home in 3-4 days. We haven’t had any poor outcomes, even when they’re bacteremic,” she said.
The work was funded by the National Institutes of Health. The investigators didn’t have any disclosures.
REPORTING FROM PHM 2018
Key clinical point:
Major finding: Two patients in the short-course group (3%) and four in the long-course group (7%) had recurrent UTIs within 30 days.
Study details: Review of 116 infants.
Disclosures: The work was funded by the National Institutes of Health. The investigators didn’t have any disclosures.
Study explores adolescents’ views on their skin tone, pressure to tan
LAKE TAHOE, CALIF. –

During an interview at the annual meeting of the Society for Pediatric Dermatology, lead study author Shivani Patel, MD, said that prior research on skin color had focused mainly on adults and its impact on self-esteem and perceived attractiveness, yet little data are available on perceptions of skin color among adolescents.
“During puberty, adolescents receive pressure from friends, family, and social media to conform to a certain acceptable standard of skin tone,” said Dr. Patel, a chief resident in the department of dermatology at Johns Hopkins University, Baltimore. “They will often engage in risky behaviors such as tanning bed use, suntanning, and use of skin lightening creams.”
In an effort to characterize the attitudes of adolescents about their skin tone, she and her associates recruited 50 patients aged 12-19 years who were seen at the Johns Hopkins dermatology clinics. Slightly more than half (56%) were female. They were asked to complete surveys on their use of sunscreen, tanning beds, and skin-lightening creams, as well as to report any family or friends who have used these interventions.
Next, the researchers used Pantone’s Capsure device to record each subject’s skin tone according to a palate of 110 skin colors available from Pantone’s SkinTone Guide, which is intended to match and reproduce lifelike skin tones in a variety of industries. The adolescents were then given the palette and asked which skin tone they felt best represented their skin and which skin tone they wished they had. These differences were compared with their objective measurement by the study team.
Of all respondents, 20% indicated that they felt pressure to have tan skin and were likely to engage in suntanning (P less than .001), a feeling they said started around the age of 12 years and stemmed from perceived pressure from friends and celebrity figures. Those who suntanned were more likely to wear sunscreen (P less than .01), a finding “that was reassuring and showed that they are aware of sunscreen and sun safety,” Dr. Patel said. However, about half of the respondents reported never wearing sunscreen and only two reported wearing sunscreen daily. No one reported using tanning beds, but 8% reported that a family member used them. One adolescent reported using skin lightening creams, and three reported that their mothers used them.
The researchers also found that black and Asian study participants were significantly more likely to desire a skin tone lighter than what they perceived their skin tone to be, while white participants were significantly more likely to desire a darker skin tone (P less than .011 for both associations).
The findings suggest that sun safety initiatives should target prepubertal patients before they engage in risky behaviors, Dr. Patel said. She acknowledged that the small sample size is a limitation of the study, but said that she and her associates hope to conduct a larger-scale analysis.
She reported having no financial disclosures.
LAKE TAHOE, CALIF. –
During an interview at the annual meeting of the Society for Pediatric Dermatology, lead study author Shivani Patel, MD, said that prior research on skin color had focused mainly on adults and its impact on self-esteem and perceived attractiveness, yet little data are available on perceptions of skin color among adolescents.
“During puberty, adolescents receive pressure from friends, family, and social media to conform to a certain acceptable standard of skin tone,” said Dr. Patel, a chief resident in the department of dermatology at Johns Hopkins University, Baltimore. “They will often engage in risky behaviors such as tanning bed use, suntanning, and use of skin lightening creams.”
In an effort to characterize the attitudes of adolescents about their skin tone, she and her associates recruited 50 patients aged 12-19 years who were seen at the Johns Hopkins dermatology clinics. Slightly more than half (56%) were female. They were asked to complete surveys on their use of sunscreen, tanning beds, and skin-lightening creams, as well as to report any family or friends who have used these interventions.
Next, the researchers used Pantone’s Capsure device to record each subject’s skin tone according to a palate of 110 skin colors available from Pantone’s SkinTone Guide, which is intended to match and reproduce lifelike skin tones in a variety of industries. The adolescents were then given the palette and asked which skin tone they felt best represented their skin and which skin tone they wished they had. These differences were compared with their objective measurement by the study team.
Of all respondents, 20% indicated that they felt pressure to have tan skin and were likely to engage in suntanning (P less than .001), a feeling they said started around the age of 12 years and stemmed from perceived pressure from friends and celebrity figures. Those who suntanned were more likely to wear sunscreen (P less than .01), a finding “that was reassuring and showed that they are aware of sunscreen and sun safety,” Dr. Patel said. However, about half of the respondents reported never wearing sunscreen and only two reported wearing sunscreen daily. No one reported using tanning beds, but 8% reported that a family member used them. One adolescent reported using skin lightening creams, and three reported that their mothers used them.
The researchers also found that black and Asian study participants were significantly more likely to desire a skin tone lighter than what they perceived their skin tone to be, while white participants were significantly more likely to desire a darker skin tone (P less than .011 for both associations).
The findings suggest that sun safety initiatives should target prepubertal patients before they engage in risky behaviors, Dr. Patel said. She acknowledged that the small sample size is a limitation of the study, but said that she and her associates hope to conduct a larger-scale analysis.
She reported having no financial disclosures.
LAKE TAHOE, CALIF. –
During an interview at the annual meeting of the Society for Pediatric Dermatology, lead study author Shivani Patel, MD, said that prior research on skin color had focused mainly on adults and its impact on self-esteem and perceived attractiveness, yet little data are available on perceptions of skin color among adolescents.
“During puberty, adolescents receive pressure from friends, family, and social media to conform to a certain acceptable standard of skin tone,” said Dr. Patel, a chief resident in the department of dermatology at Johns Hopkins University, Baltimore. “They will often engage in risky behaviors such as tanning bed use, suntanning, and use of skin lightening creams.”
In an effort to characterize the attitudes of adolescents about their skin tone, she and her associates recruited 50 patients aged 12-19 years who were seen at the Johns Hopkins dermatology clinics. Slightly more than half (56%) were female. They were asked to complete surveys on their use of sunscreen, tanning beds, and skin-lightening creams, as well as to report any family or friends who have used these interventions.
Next, the researchers used Pantone’s Capsure device to record each subject’s skin tone according to a palate of 110 skin colors available from Pantone’s SkinTone Guide, which is intended to match and reproduce lifelike skin tones in a variety of industries. The adolescents were then given the palette and asked which skin tone they felt best represented their skin and which skin tone they wished they had. These differences were compared with their objective measurement by the study team.
Of all respondents, 20% indicated that they felt pressure to have tan skin and were likely to engage in suntanning (P less than .001), a feeling they said started around the age of 12 years and stemmed from perceived pressure from friends and celebrity figures. Those who suntanned were more likely to wear sunscreen (P less than .01), a finding “that was reassuring and showed that they are aware of sunscreen and sun safety,” Dr. Patel said. However, about half of the respondents reported never wearing sunscreen and only two reported wearing sunscreen daily. No one reported using tanning beds, but 8% reported that a family member used them. One adolescent reported using skin lightening creams, and three reported that their mothers used them.
The researchers also found that black and Asian study participants were significantly more likely to desire a skin tone lighter than what they perceived their skin tone to be, while white participants were significantly more likely to desire a darker skin tone (P less than .011 for both associations).
The findings suggest that sun safety initiatives should target prepubertal patients before they engage in risky behaviors, Dr. Patel said. She acknowledged that the small sample size is a limitation of the study, but said that she and her associates hope to conduct a larger-scale analysis.
She reported having no financial disclosures.
REPORTING FROM SPD 2018
Key clinical point: Sun safety initiatives should target prepubertal patients before they engage in risky behaviors.
Major finding: One in five adolescents indicated that they felt pressure to have tan skin and were likely to engage in suntanning (P less than .001).
Study details: A survey of 50 patients aged 12-19 years.
Disclosures: Dr. Patel reported having no financial disclosures.
Title X and proposed changes: Take action now
The facts
Title X, a bill originally passed in 1970 under President Nixon, is the only federal grant program dedicated to providing family planning services as well as other preventive health care to primarily low-income patients. It is estimated that 70% of patients using Title X services are below the federal poverty level and more than 60% are uninsured or underinsured.1
In 2015 alone, Title X clinics served 3.8 million women, preventing 822,300 unintended pregnancies and 277,800 abortions.2 These clinics provide comprehensive family planning services including information, counseling, and referrals for abortion services. Title X clinics do not use the funding to provide abortion care, and no federal funding from Title X has ever been used to pay for abortions.

Proposed rule changes
The Trump Administration has proposed several new rules for Title X grant recipients.
Here are the main changes3:
- There must be a “financial and physical” separation between a clinic that is a Title X grant recipient and a facility where “abortion is a method of family planning.” This would prevent health centers that receive Title X funding from providing abortions at the same facility. This rule would predominantly affect health centers like Planned Parenthood. Although these clinics already have a financial separation from abortion care, there would not be a physical one in most situations and these clinics would lose Title X funding or be forced to stop providing abortion services.
- Providers who work at a clinic that receives Title X funding but provides abortions at a completely different facility may be ineligible for ongoing Title X grant money. In the new changes, “funds may not be used…to support the separate abortion business of Title X grant subrecipient.” The changes also propose to “protect Title X providers” from choosing between the health of their patients and their consciences. It plans to do this by removing the requirement to provide abortion counseling and referral and allows “non-directive” counseling.
- There would also be a requirement to encourage more parental involvement in minors’ decision making. While clinics already discuss parental involvement, the change would seek to increase the encouragement to young patients to involve parents. Most young patients do involve a parent or guardian in their care; however, many Title X clinics serve young patients who seek care confidentially. Patients seek confidential care due to a multitude of reasons, including history of abuse, lack of trust, and intimate partner violence.
- “A Title X project may not perform, promote, refer for, or support abortion as a method of family planning.” Although the rule does not prevent providers from discussing abortions, clinicians could offer little guidance if a patient opts for an abortion. Providers can give a list of “qualified, comprehensive health service providers” but may not disclose which, if any, of the providers perform abortions.
Take action
Title X provides important health care services to low-income, uninsured, and underinsured patients. These proposals put access to comprehensive health care for vulnerable populations at risk. Medical organizations including the American Medical Association and American College of Obstetricians and Gynecologists have made statements against the proposed changes to Title X. As ObGyns, we need to ensure our patients are fully informed and have access to all family planning and preventive health services.
Call or email your local representative and tell them you oppose the changes to Title X. Find your representatives here.
Follow ACOG’s Action Center on protecting Title X, which includes a flyer for your waiting room.
Send a message to the Health and Human Services Secretary. Submit a formal comment through July 31, 2018, on the Federal Registrar website expressing your thoughts with these proposed changes.
- Title X: Helping ensure access to high-quality care. National family planning website. https://www.nationalfamilyplanning.org/document.doc?id=514. Accessed July 25, 2018.
- Publicly Funded Contraceptive Services at U.S. Clinics, 2015. Guttmacher website. https://www.guttmacher.org/article/2018/06/domestic-gag-rule-and-more-administrations-proposed-changes-title-x. Accessed July 25, 2018.
- Compliance with statutory program integrity requirements. Federal register website. https://www.federalregister.gov/documents/2018/06/01/2018-11673/compliance-with-statutory-program-integrity-requirements. Accessed July 25, 2018.
The facts
Title X, a bill originally passed in 1970 under President Nixon, is the only federal grant program dedicated to providing family planning services as well as other preventive health care to primarily low-income patients. It is estimated that 70% of patients using Title X services are below the federal poverty level and more than 60% are uninsured or underinsured.1
In 2015 alone, Title X clinics served 3.8 million women, preventing 822,300 unintended pregnancies and 277,800 abortions.2 These clinics provide comprehensive family planning services including information, counseling, and referrals for abortion services. Title X clinics do not use the funding to provide abortion care, and no federal funding from Title X has ever been used to pay for abortions.
Proposed rule changes
The Trump Administration has proposed several new rules for Title X grant recipients.
Here are the main changes3:
- There must be a “financial and physical” separation between a clinic that is a Title X grant recipient and a facility where “abortion is a method of family planning.” This would prevent health centers that receive Title X funding from providing abortions at the same facility. This rule would predominantly affect health centers like Planned Parenthood. Although these clinics already have a financial separation from abortion care, there would not be a physical one in most situations and these clinics would lose Title X funding or be forced to stop providing abortion services.
- Providers who work at a clinic that receives Title X funding but provides abortions at a completely different facility may be ineligible for ongoing Title X grant money. In the new changes, “funds may not be used…to support the separate abortion business of Title X grant subrecipient.” The changes also propose to “protect Title X providers” from choosing between the health of their patients and their consciences. It plans to do this by removing the requirement to provide abortion counseling and referral and allows “non-directive” counseling.
- There would also be a requirement to encourage more parental involvement in minors’ decision making. While clinics already discuss parental involvement, the change would seek to increase the encouragement to young patients to involve parents. Most young patients do involve a parent or guardian in their care; however, many Title X clinics serve young patients who seek care confidentially. Patients seek confidential care due to a multitude of reasons, including history of abuse, lack of trust, and intimate partner violence.
- “A Title X project may not perform, promote, refer for, or support abortion as a method of family planning.” Although the rule does not prevent providers from discussing abortions, clinicians could offer little guidance if a patient opts for an abortion. Providers can give a list of “qualified, comprehensive health service providers” but may not disclose which, if any, of the providers perform abortions.
Take action
Title X provides important health care services to low-income, uninsured, and underinsured patients. These proposals put access to comprehensive health care for vulnerable populations at risk. Medical organizations including the American Medical Association and American College of Obstetricians and Gynecologists have made statements against the proposed changes to Title X. As ObGyns, we need to ensure our patients are fully informed and have access to all family planning and preventive health services.
Call or email your local representative and tell them you oppose the changes to Title X. Find your representatives here.
Follow ACOG’s Action Center on protecting Title X, which includes a flyer for your waiting room.
Send a message to the Health and Human Services Secretary. Submit a formal comment through July 31, 2018, on the Federal Registrar website expressing your thoughts with these proposed changes.
The facts
Title X, a bill originally passed in 1970 under President Nixon, is the only federal grant program dedicated to providing family planning services as well as other preventive health care to primarily low-income patients. It is estimated that 70% of patients using Title X services are below the federal poverty level and more than 60% are uninsured or underinsured.1
In 2015 alone, Title X clinics served 3.8 million women, preventing 822,300 unintended pregnancies and 277,800 abortions.2 These clinics provide comprehensive family planning services including information, counseling, and referrals for abortion services. Title X clinics do not use the funding to provide abortion care, and no federal funding from Title X has ever been used to pay for abortions.
Proposed rule changes
The Trump Administration has proposed several new rules for Title X grant recipients.
Here are the main changes3:
- There must be a “financial and physical” separation between a clinic that is a Title X grant recipient and a facility where “abortion is a method of family planning.” This would prevent health centers that receive Title X funding from providing abortions at the same facility. This rule would predominantly affect health centers like Planned Parenthood. Although these clinics already have a financial separation from abortion care, there would not be a physical one in most situations and these clinics would lose Title X funding or be forced to stop providing abortion services.
- Providers who work at a clinic that receives Title X funding but provides abortions at a completely different facility may be ineligible for ongoing Title X grant money. In the new changes, “funds may not be used…to support the separate abortion business of Title X grant subrecipient.” The changes also propose to “protect Title X providers” from choosing between the health of their patients and their consciences. It plans to do this by removing the requirement to provide abortion counseling and referral and allows “non-directive” counseling.
- There would also be a requirement to encourage more parental involvement in minors’ decision making. While clinics already discuss parental involvement, the change would seek to increase the encouragement to young patients to involve parents. Most young patients do involve a parent or guardian in their care; however, many Title X clinics serve young patients who seek care confidentially. Patients seek confidential care due to a multitude of reasons, including history of abuse, lack of trust, and intimate partner violence.
- “A Title X project may not perform, promote, refer for, or support abortion as a method of family planning.” Although the rule does not prevent providers from discussing abortions, clinicians could offer little guidance if a patient opts for an abortion. Providers can give a list of “qualified, comprehensive health service providers” but may not disclose which, if any, of the providers perform abortions.
Take action
Title X provides important health care services to low-income, uninsured, and underinsured patients. These proposals put access to comprehensive health care for vulnerable populations at risk. Medical organizations including the American Medical Association and American College of Obstetricians and Gynecologists have made statements against the proposed changes to Title X. As ObGyns, we need to ensure our patients are fully informed and have access to all family planning and preventive health services.
Call or email your local representative and tell them you oppose the changes to Title X. Find your representatives here.
Follow ACOG’s Action Center on protecting Title X, which includes a flyer for your waiting room.
Send a message to the Health and Human Services Secretary. Submit a formal comment through July 31, 2018, on the Federal Registrar website expressing your thoughts with these proposed changes.
- Title X: Helping ensure access to high-quality care. National family planning website. https://www.nationalfamilyplanning.org/document.doc?id=514. Accessed July 25, 2018.
- Publicly Funded Contraceptive Services at U.S. Clinics, 2015. Guttmacher website. https://www.guttmacher.org/article/2018/06/domestic-gag-rule-and-more-administrations-proposed-changes-title-x. Accessed July 25, 2018.
- Compliance with statutory program integrity requirements. Federal register website. https://www.federalregister.gov/documents/2018/06/01/2018-11673/compliance-with-statutory-program-integrity-requirements. Accessed July 25, 2018.
- Title X: Helping ensure access to high-quality care. National family planning website. https://www.nationalfamilyplanning.org/document.doc?id=514. Accessed July 25, 2018.
- Publicly Funded Contraceptive Services at U.S. Clinics, 2015. Guttmacher website. https://www.guttmacher.org/article/2018/06/domestic-gag-rule-and-more-administrations-proposed-changes-title-x. Accessed July 25, 2018.
- Compliance with statutory program integrity requirements. Federal register website. https://www.federalregister.gov/documents/2018/06/01/2018-11673/compliance-with-statutory-program-integrity-requirements. Accessed July 25, 2018.
Incident heart failure linked to HIV infection
AMSTERDAM –
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“HIV infection is independently associated with a higher risk for developing heart failure, and this excess risk does not appear mediated through atherosclerotic disease pathways or differential use of cardioprotective medications,” Alan S. Go, MD, said at the 22nd International AIDS Conference.
The finding sends two important messages to physicians who care for people living with HIV, Dr. Go said in a video interview. First, have “greater awareness for the risk of heart failure” in people living with HIV, even in those who have excellent [HIV] treatment. Be on the lookout, he recommended, for classic symptoms of heart failure like dyspnea and fatigue, and if found follow-up with an assessment of heart function, usually by echocardiography. The second message is to pay attention to and aggressively treat risk factors for heart failure, such as hypertension, smoking, obesity, diabetes, and hypercholesterolemia, said Dr. Go, director of the Comprehensive Clinical Research Unit of Kaiser Permanente in Oakland, Calif.
Results from a small number of prior studies also suggested an increased heart failure rate in people infected with HIV, but those reports had not been able to untangle this observed increase from a possible relationship to the elevated rate of MIs among people living with HIV. The study led by Dr. Go adjusted for acute coronary syndrome events that occurred during follow-up in the analysis and this showed that the increased incidence of heart failure occurred independently of any preceding MI or unstable angina event.
Dr. Go proposed several potential mechanisms that could tie HIV infection to an elevated heart failure risk that was not linked to a prior ischemic heart disease event. The virus could directly damage cardiac myocytes to produce fibrosis, the virus could trigger cardiac inflammation, and the infected person could have an increased susceptibility to infection by a pathogen know to potentially cause cardiac damage and myocarditis such as coxsackievirus.
For the time being, patients infected by HIV who develop heart failure should receive the same treatments that are recommended for the general population, Dr. Go said, but he also highlighted the need for further study to determine the effectiveness of standard heart failure treatments specifically in people living with HIV. He and his associates are also currently analyzing the relationship of several other variables to the risk for heart failure in HIV-infected people, such as the degree of HIV control, and the types of antiretroviral therapy that patients receive. So far the study has not shown a relationship between HIV infection and any specific type of heart failure. About a quarter of the HIV-infected people who developed heart failure in this study had reduced left ventricular ejection fraction, about a quarter had preserved ejection fraction, and for the remaining patients information on their left ventricular ejection fraction was not available, Dr. Go said.
The Kaiser Permanente HIV Heart Study used data from health records from about 13.5 million people enrolled in the health system during 2000-2016 at locations in northern California, southern California, or the mid-Atlantic region. From these records the researchers identified 38,868 people diagnosed with an HIV infection, free of a heart failure diagnosis, and at least 21 years old, and matched them by age, sex, and race with 386,586 people in the health system who were both uninfected and free of heart failure. At “baseline” in the analysis the two study groups had very similar rates of smoking, but those with HIV had somewhat more alcohol abuse and nearly twice the rate of illicit drug use, although even among those with HIV this rate was low at 4%.
Some clinical characteristics at baseline showed significant differences between the two groups. People living with HIV had substantially less hypertension, 7% compared with 12% in those without HIV; half the rate of dyslipidemia, 8% compared with 16% among the control group; and nearly half the prevalence of diabetes, 3% versus 5% among those without HIV. On the other hand, certain other clinical characteristics were more common among those with HIV. The prevalence at baseline of diagnosed dementia was 15% among people infected with HIV and essentially nonexistent (less than 1%) among controls, and the prevalence of diagnosed depression was 8% among people with HIV and 5% among those without the infection.
Baseline parameters also showed that at the time this review first identified a person with HIV and without heart failure in the system records only 18% of the HIV-infected individuals were on an antiretroviral therapy regimen. Dr. Go said that the study is currently analyzing subsequent HIV treatments that these patients may have received. Also at “baseline” 13% of people with documented HIV infection had a CD4 cell count of fewer than 200 cell/mm3, with 4% having fewer than 50 CD4 cells/mm3, and 29% of those with HIV had a blood level of at least 500 copies of HIV RNA/mL. In addition, information on CD4 cell counts was unavailable for 43% of these people, and information on viral load was unavailable for about half.
During “follow-up” in the system’s medical records for a period of up to 17 years, diagnoses of incident heart failure accumulated significantly faster among people with HIV compared to those without HIV. After adjustment for demographic differences, the time of entry into the health system, cardiovascular and other medical differences, and differences in medication use, people living with HIV had a 75% higher rate of incident heart failure compared with those without HIV. Further adjustment based on incident first episodes of acute coronary syndrome during “follow-up” brought the excess rate of heart failure to 66% higher among people infected by HIV, Dr. Go reported. He cautioned that the findings came from a U.S. population that had access to comprehensive health care.
SOURCE: Go AS et al. AIDS 2018, Abstract 2778, THAB0103.
AMSTERDAM –
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“HIV infection is independently associated with a higher risk for developing heart failure, and this excess risk does not appear mediated through atherosclerotic disease pathways or differential use of cardioprotective medications,” Alan S. Go, MD, said at the 22nd International AIDS Conference.
The finding sends two important messages to physicians who care for people living with HIV, Dr. Go said in a video interview. First, have “greater awareness for the risk of heart failure” in people living with HIV, even in those who have excellent [HIV] treatment. Be on the lookout, he recommended, for classic symptoms of heart failure like dyspnea and fatigue, and if found follow-up with an assessment of heart function, usually by echocardiography. The second message is to pay attention to and aggressively treat risk factors for heart failure, such as hypertension, smoking, obesity, diabetes, and hypercholesterolemia, said Dr. Go, director of the Comprehensive Clinical Research Unit of Kaiser Permanente in Oakland, Calif.
Results from a small number of prior studies also suggested an increased heart failure rate in people infected with HIV, but those reports had not been able to untangle this observed increase from a possible relationship to the elevated rate of MIs among people living with HIV. The study led by Dr. Go adjusted for acute coronary syndrome events that occurred during follow-up in the analysis and this showed that the increased incidence of heart failure occurred independently of any preceding MI or unstable angina event.
Dr. Go proposed several potential mechanisms that could tie HIV infection to an elevated heart failure risk that was not linked to a prior ischemic heart disease event. The virus could directly damage cardiac myocytes to produce fibrosis, the virus could trigger cardiac inflammation, and the infected person could have an increased susceptibility to infection by a pathogen know to potentially cause cardiac damage and myocarditis such as coxsackievirus.
For the time being, patients infected by HIV who develop heart failure should receive the same treatments that are recommended for the general population, Dr. Go said, but he also highlighted the need for further study to determine the effectiveness of standard heart failure treatments specifically in people living with HIV. He and his associates are also currently analyzing the relationship of several other variables to the risk for heart failure in HIV-infected people, such as the degree of HIV control, and the types of antiretroviral therapy that patients receive. So far the study has not shown a relationship between HIV infection and any specific type of heart failure. About a quarter of the HIV-infected people who developed heart failure in this study had reduced left ventricular ejection fraction, about a quarter had preserved ejection fraction, and for the remaining patients information on their left ventricular ejection fraction was not available, Dr. Go said.
The Kaiser Permanente HIV Heart Study used data from health records from about 13.5 million people enrolled in the health system during 2000-2016 at locations in northern California, southern California, or the mid-Atlantic region. From these records the researchers identified 38,868 people diagnosed with an HIV infection, free of a heart failure diagnosis, and at least 21 years old, and matched them by age, sex, and race with 386,586 people in the health system who were both uninfected and free of heart failure. At “baseline” in the analysis the two study groups had very similar rates of smoking, but those with HIV had somewhat more alcohol abuse and nearly twice the rate of illicit drug use, although even among those with HIV this rate was low at 4%.
Some clinical characteristics at baseline showed significant differences between the two groups. People living with HIV had substantially less hypertension, 7% compared with 12% in those without HIV; half the rate of dyslipidemia, 8% compared with 16% among the control group; and nearly half the prevalence of diabetes, 3% versus 5% among those without HIV. On the other hand, certain other clinical characteristics were more common among those with HIV. The prevalence at baseline of diagnosed dementia was 15% among people infected with HIV and essentially nonexistent (less than 1%) among controls, and the prevalence of diagnosed depression was 8% among people with HIV and 5% among those without the infection.
Baseline parameters also showed that at the time this review first identified a person with HIV and without heart failure in the system records only 18% of the HIV-infected individuals were on an antiretroviral therapy regimen. Dr. Go said that the study is currently analyzing subsequent HIV treatments that these patients may have received. Also at “baseline” 13% of people with documented HIV infection had a CD4 cell count of fewer than 200 cell/mm3, with 4% having fewer than 50 CD4 cells/mm3, and 29% of those with HIV had a blood level of at least 500 copies of HIV RNA/mL. In addition, information on CD4 cell counts was unavailable for 43% of these people, and information on viral load was unavailable for about half.
During “follow-up” in the system’s medical records for a period of up to 17 years, diagnoses of incident heart failure accumulated significantly faster among people with HIV compared to those without HIV. After adjustment for demographic differences, the time of entry into the health system, cardiovascular and other medical differences, and differences in medication use, people living with HIV had a 75% higher rate of incident heart failure compared with those without HIV. Further adjustment based on incident first episodes of acute coronary syndrome during “follow-up” brought the excess rate of heart failure to 66% higher among people infected by HIV, Dr. Go reported. He cautioned that the findings came from a U.S. population that had access to comprehensive health care.
SOURCE: Go AS et al. AIDS 2018, Abstract 2778, THAB0103.
AMSTERDAM –
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“HIV infection is independently associated with a higher risk for developing heart failure, and this excess risk does not appear mediated through atherosclerotic disease pathways or differential use of cardioprotective medications,” Alan S. Go, MD, said at the 22nd International AIDS Conference.
The finding sends two important messages to physicians who care for people living with HIV, Dr. Go said in a video interview. First, have “greater awareness for the risk of heart failure” in people living with HIV, even in those who have excellent [HIV] treatment. Be on the lookout, he recommended, for classic symptoms of heart failure like dyspnea and fatigue, and if found follow-up with an assessment of heart function, usually by echocardiography. The second message is to pay attention to and aggressively treat risk factors for heart failure, such as hypertension, smoking, obesity, diabetes, and hypercholesterolemia, said Dr. Go, director of the Comprehensive Clinical Research Unit of Kaiser Permanente in Oakland, Calif.
Results from a small number of prior studies also suggested an increased heart failure rate in people infected with HIV, but those reports had not been able to untangle this observed increase from a possible relationship to the elevated rate of MIs among people living with HIV. The study led by Dr. Go adjusted for acute coronary syndrome events that occurred during follow-up in the analysis and this showed that the increased incidence of heart failure occurred independently of any preceding MI or unstable angina event.
Dr. Go proposed several potential mechanisms that could tie HIV infection to an elevated heart failure risk that was not linked to a prior ischemic heart disease event. The virus could directly damage cardiac myocytes to produce fibrosis, the virus could trigger cardiac inflammation, and the infected person could have an increased susceptibility to infection by a pathogen know to potentially cause cardiac damage and myocarditis such as coxsackievirus.
For the time being, patients infected by HIV who develop heart failure should receive the same treatments that are recommended for the general population, Dr. Go said, but he also highlighted the need for further study to determine the effectiveness of standard heart failure treatments specifically in people living with HIV. He and his associates are also currently analyzing the relationship of several other variables to the risk for heart failure in HIV-infected people, such as the degree of HIV control, and the types of antiretroviral therapy that patients receive. So far the study has not shown a relationship between HIV infection and any specific type of heart failure. About a quarter of the HIV-infected people who developed heart failure in this study had reduced left ventricular ejection fraction, about a quarter had preserved ejection fraction, and for the remaining patients information on their left ventricular ejection fraction was not available, Dr. Go said.
The Kaiser Permanente HIV Heart Study used data from health records from about 13.5 million people enrolled in the health system during 2000-2016 at locations in northern California, southern California, or the mid-Atlantic region. From these records the researchers identified 38,868 people diagnosed with an HIV infection, free of a heart failure diagnosis, and at least 21 years old, and matched them by age, sex, and race with 386,586 people in the health system who were both uninfected and free of heart failure. At “baseline” in the analysis the two study groups had very similar rates of smoking, but those with HIV had somewhat more alcohol abuse and nearly twice the rate of illicit drug use, although even among those with HIV this rate was low at 4%.
Some clinical characteristics at baseline showed significant differences between the two groups. People living with HIV had substantially less hypertension, 7% compared with 12% in those without HIV; half the rate of dyslipidemia, 8% compared with 16% among the control group; and nearly half the prevalence of diabetes, 3% versus 5% among those without HIV. On the other hand, certain other clinical characteristics were more common among those with HIV. The prevalence at baseline of diagnosed dementia was 15% among people infected with HIV and essentially nonexistent (less than 1%) among controls, and the prevalence of diagnosed depression was 8% among people with HIV and 5% among those without the infection.
Baseline parameters also showed that at the time this review first identified a person with HIV and without heart failure in the system records only 18% of the HIV-infected individuals were on an antiretroviral therapy regimen. Dr. Go said that the study is currently analyzing subsequent HIV treatments that these patients may have received. Also at “baseline” 13% of people with documented HIV infection had a CD4 cell count of fewer than 200 cell/mm3, with 4% having fewer than 50 CD4 cells/mm3, and 29% of those with HIV had a blood level of at least 500 copies of HIV RNA/mL. In addition, information on CD4 cell counts was unavailable for 43% of these people, and information on viral load was unavailable for about half.
During “follow-up” in the system’s medical records for a period of up to 17 years, diagnoses of incident heart failure accumulated significantly faster among people with HIV compared to those without HIV. After adjustment for demographic differences, the time of entry into the health system, cardiovascular and other medical differences, and differences in medication use, people living with HIV had a 75% higher rate of incident heart failure compared with those without HIV. Further adjustment based on incident first episodes of acute coronary syndrome during “follow-up” brought the excess rate of heart failure to 66% higher among people infected by HIV, Dr. Go reported. He cautioned that the findings came from a U.S. population that had access to comprehensive health care.
SOURCE: Go AS et al. AIDS 2018, Abstract 2778, THAB0103.
REPORTING FROM AIDS 2018
Key clinical point: HIV infection may be an independent trigger for heart failure.
Major finding: After extensive adjustment for potential confounders, HIV infection linked with a 66% increased rate of incident heart failure.
Study details: The Kaiser Permanente HIV Heart Study, which included medical records for 425,454 people.
Disclosures: Dr. Go had no disclosures.
Source: Go AS et al. AIDS 2018, Abstract 2778, THAB0103.
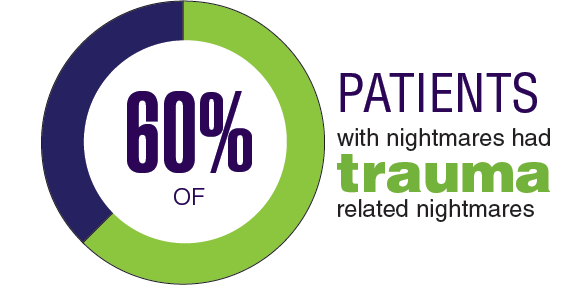
Federal Health Care Data Trends: Sleep Disorders
In 2017, the VA had more than 1 million health care visits related to sleep disorders.1 Although predominantly sleep apnea, other sleep disorders such as insomnia, hypersomnia, narcolepsy, sleep-related bruxism, nightmares, and poor sleep quality present significant health care burdens for both the VA and Military Health Systems.
Click here to continue reading.
In 2017, the VA had more than 1 million health care visits related to sleep disorders.1 Although predominantly sleep apnea, other sleep disorders such as insomnia, hypersomnia, narcolepsy, sleep-related bruxism, nightmares, and poor sleep quality present significant health care burdens for both the VA and Military Health Systems.
Click here to continue reading.
In 2017, the VA had more than 1 million health care visits related to sleep disorders.1 Although predominantly sleep apnea, other sleep disorders such as insomnia, hypersomnia, narcolepsy, sleep-related bruxism, nightmares, and poor sleep quality present significant health care burdens for both the VA and Military Health Systems.
Click here to continue reading.
Study could change treatment of MLSM7

New findings could help improve treatment of an inherited bone marrow disorder known as myelodysplasia and leukemia syndrome with monosomy 7 (MLSM7), according to researchers.
While studying families affected by MLSM7, researchers identified germline mutations in SAMD9L or SAMD9 in patients who had hematologic abnormalities, myelodysplastic syndromes (MDS), or acute myeloid leukemia (AML).
However, these mutations were also present in apparently healthy family members, and the researchers found that bone marrow monosomy 7 sometimes resolved without treatment.
The team recounted these findings in JCI Insight.
The researchers analyzed blood samples from 16 siblings in 5 families affected by MLSM7 and found they all carried germline mutations in SAMD9 or SAMD9L. In 3 of the 5 families, there were apparently healthy parents who also carried the mutations.
“Surprisingly, the health consequences of these mutations varied tremendously for reasons that must still be determined, but the findings are already affecting how we may choose to manage these patients,” said study author Jeffery Klco, MD, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
Three of the 16 siblings developed AML and died of the disease or related complications. Two other siblings were diagnosed with MDS.
The remaining 11 siblings with the mutations were apparently healthy, although several had been treated for anemia and other conditions associated with low blood counts.
Some of these patients had a previous history of bone marrow monosomy 7 that spontaneously corrected over time. These patients, despite no therapy, appeared to have normal bone marrow function.
“This was an even greater surprise,” Dr Klco said. “The spontaneous recovery experienced by some children with the germline mutations suggests some patients with SAMD9 and SAMD9L mutations who were previously considered candidates for bone marrow transplantation may recover hematologic function on their own.”
Dr Klco and his colleagues have a theory that could explain the spontaneous correction. The team noted that SAMD9 and SAMD9L are activated in response to viral infections. While the normal function of both proteins is poorly understood, abnormally activated SAMD9 and SAMD9L are known to inhibit cell growth.
In this study, deep sequencing showed that selective pressure on developing blood cells favors cells without the SAMD9 or SAMD9L mutations. That may increase pressure for cells to selectively jettison chromosome 7 with the gene alteration or take other molecular measures to counteract the mutant protein.
Implications for treatment
This research also showed that, in patients who developed AML, loss of chromosome 7 was associated with the development of mutations in additional genes, including ETV6, KRAS, SETBP1, and RUNX1.
These same mutations are broadly associated with monosomy 7 in AML, which suggests that understanding how SAMD9 and SAMD9L mutations contribute to leukemia has implications beyond familial cases.
The presence of secondary mutations may also help clinicians identify which patients will benefit from immediate treatment, including chemotherapy or transplant to prevent or treat AML or myelodysplasia, Dr Klco said.
For patients without the mutations or significant symptoms due to low blood cell counts, watchful waiting with careful follow-up may sometimes be an option.
“Now that we know this disease can resolve without treatment in some patients, we need to focus on developing screening and treatment guidelines,” Dr Klco said. “We want to reserve hematopoietic bone marrow transplantation for those who truly need the procedure. These findings will help to point the way.”
“So little is known about SAMD9 and SAMD9L that we need to continue working in the lab to better understand how these mutations impact blood cell development and how they are activated in response to infections and other types of stress.”
New findings could help improve treatment of an inherited bone marrow disorder known as myelodysplasia and leukemia syndrome with monosomy 7 (MLSM7), according to researchers.
While studying families affected by MLSM7, researchers identified germline mutations in SAMD9L or SAMD9 in patients who had hematologic abnormalities, myelodysplastic syndromes (MDS), or acute myeloid leukemia (AML).
However, these mutations were also present in apparently healthy family members, and the researchers found that bone marrow monosomy 7 sometimes resolved without treatment.
The team recounted these findings in JCI Insight.
The researchers analyzed blood samples from 16 siblings in 5 families affected by MLSM7 and found they all carried germline mutations in SAMD9 or SAMD9L. In 3 of the 5 families, there were apparently healthy parents who also carried the mutations.
“Surprisingly, the health consequences of these mutations varied tremendously for reasons that must still be determined, but the findings are already affecting how we may choose to manage these patients,” said study author Jeffery Klco, MD, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
Three of the 16 siblings developed AML and died of the disease or related complications. Two other siblings were diagnosed with MDS.
The remaining 11 siblings with the mutations were apparently healthy, although several had been treated for anemia and other conditions associated with low blood counts.
Some of these patients had a previous history of bone marrow monosomy 7 that spontaneously corrected over time. These patients, despite no therapy, appeared to have normal bone marrow function.
“This was an even greater surprise,” Dr Klco said. “The spontaneous recovery experienced by some children with the germline mutations suggests some patients with SAMD9 and SAMD9L mutations who were previously considered candidates for bone marrow transplantation may recover hematologic function on their own.”
Dr Klco and his colleagues have a theory that could explain the spontaneous correction. The team noted that SAMD9 and SAMD9L are activated in response to viral infections. While the normal function of both proteins is poorly understood, abnormally activated SAMD9 and SAMD9L are known to inhibit cell growth.
In this study, deep sequencing showed that selective pressure on developing blood cells favors cells without the SAMD9 or SAMD9L mutations. That may increase pressure for cells to selectively jettison chromosome 7 with the gene alteration or take other molecular measures to counteract the mutant protein.
Implications for treatment
This research also showed that, in patients who developed AML, loss of chromosome 7 was associated with the development of mutations in additional genes, including ETV6, KRAS, SETBP1, and RUNX1.
These same mutations are broadly associated with monosomy 7 in AML, which suggests that understanding how SAMD9 and SAMD9L mutations contribute to leukemia has implications beyond familial cases.
The presence of secondary mutations may also help clinicians identify which patients will benefit from immediate treatment, including chemotherapy or transplant to prevent or treat AML or myelodysplasia, Dr Klco said.
For patients without the mutations or significant symptoms due to low blood cell counts, watchful waiting with careful follow-up may sometimes be an option.
“Now that we know this disease can resolve without treatment in some patients, we need to focus on developing screening and treatment guidelines,” Dr Klco said. “We want to reserve hematopoietic bone marrow transplantation for those who truly need the procedure. These findings will help to point the way.”
“So little is known about SAMD9 and SAMD9L that we need to continue working in the lab to better understand how these mutations impact blood cell development and how they are activated in response to infections and other types of stress.”
New findings could help improve treatment of an inherited bone marrow disorder known as myelodysplasia and leukemia syndrome with monosomy 7 (MLSM7), according to researchers.
While studying families affected by MLSM7, researchers identified germline mutations in SAMD9L or SAMD9 in patients who had hematologic abnormalities, myelodysplastic syndromes (MDS), or acute myeloid leukemia (AML).
However, these mutations were also present in apparently healthy family members, and the researchers found that bone marrow monosomy 7 sometimes resolved without treatment.
The team recounted these findings in JCI Insight.
The researchers analyzed blood samples from 16 siblings in 5 families affected by MLSM7 and found they all carried germline mutations in SAMD9 or SAMD9L. In 3 of the 5 families, there were apparently healthy parents who also carried the mutations.
“Surprisingly, the health consequences of these mutations varied tremendously for reasons that must still be determined, but the findings are already affecting how we may choose to manage these patients,” said study author Jeffery Klco, MD, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
Three of the 16 siblings developed AML and died of the disease or related complications. Two other siblings were diagnosed with MDS.
The remaining 11 siblings with the mutations were apparently healthy, although several had been treated for anemia and other conditions associated with low blood counts.
Some of these patients had a previous history of bone marrow monosomy 7 that spontaneously corrected over time. These patients, despite no therapy, appeared to have normal bone marrow function.
“This was an even greater surprise,” Dr Klco said. “The spontaneous recovery experienced by some children with the germline mutations suggests some patients with SAMD9 and SAMD9L mutations who were previously considered candidates for bone marrow transplantation may recover hematologic function on their own.”
Dr Klco and his colleagues have a theory that could explain the spontaneous correction. The team noted that SAMD9 and SAMD9L are activated in response to viral infections. While the normal function of both proteins is poorly understood, abnormally activated SAMD9 and SAMD9L are known to inhibit cell growth.
In this study, deep sequencing showed that selective pressure on developing blood cells favors cells without the SAMD9 or SAMD9L mutations. That may increase pressure for cells to selectively jettison chromosome 7 with the gene alteration or take other molecular measures to counteract the mutant protein.
Implications for treatment
This research also showed that, in patients who developed AML, loss of chromosome 7 was associated with the development of mutations in additional genes, including ETV6, KRAS, SETBP1, and RUNX1.
These same mutations are broadly associated with monosomy 7 in AML, which suggests that understanding how SAMD9 and SAMD9L mutations contribute to leukemia has implications beyond familial cases.
The presence of secondary mutations may also help clinicians identify which patients will benefit from immediate treatment, including chemotherapy or transplant to prevent or treat AML or myelodysplasia, Dr Klco said.
For patients without the mutations or significant symptoms due to low blood cell counts, watchful waiting with careful follow-up may sometimes be an option.
“Now that we know this disease can resolve without treatment in some patients, we need to focus on developing screening and treatment guidelines,” Dr Klco said. “We want to reserve hematopoietic bone marrow transplantation for those who truly need the procedure. These findings will help to point the way.”
“So little is known about SAMD9 and SAMD9L that we need to continue working in the lab to better understand how these mutations impact blood cell development and how they are activated in response to infections and other types of stress.”
Depression, antidepressants linked to VTE

Depression and the use of antidepressants are each associated with an increased risk of venous thromboembolism (VTE), according to a review and meta-analysis published in Annals of Medicine.
The research also showed that each of the various classes of antidepressant medications is associated with an increased risk of VTE.
The researchers noted that this study does not prove cause and effect, and further studies are needed to determine what is driving the observed increase in VTE risk.
Some previous studies have indicated that depression and antidepressant use might be associated with an increased risk of VTE, but other studies have shown no evidence of associations.
Therefore, Setor Kunutsor, MD, PhD, of the University of Bristol in Bristol, UK, and his colleagues conducted a systematic review and meta-analysis of observational studies evaluating the associations of depression and antidepressant use with VTE risk.
The researchers looked at 8 observational studies with data on 960,113 non-overlapping participants. There were 9027 cases of VTE in this population.
To determine the association between depression and VTE, the researchers conducted a pooled analysis of 3 studies comparing patients with depression and without. These studies included 865,878 participants and 4676 cases of VTE.
The relative risk (RR) for VTE was 1.31 (95% CI, 1.13-1.53) among patients with depression.
The researchers also conducted a pooled analysis of 6 studies comparing antidepressant users to non-users. These studies included 828,327 participants and 8273 cases of VTE.
The RR for VTE was 1.27 (95% CI, 1.06-1.51) among patients taking antidepressants.
In addition, individual antidepressants were associated with an increased risk of VTE. This includes:
- Tricyclic antidepressants—RR=1.16 (95% CI, 1.06-1.27)
- Selective serotonin reuptake inhibitors—RR=1.12 (95% CI, 1.02-1.23)
- “Other” antidepressants*—RR=1.59 (95% CI, 1.21-2.09).
The researchers said these data show that antidepressant use and depression are each associated with an increased risk of VTE, and these results add to accumulating evidence that a relationship exists between depression, antidepressant use, and VTE.
“These findings are very useful to me as both a clinician and a researcher,” Dr Kunutsor said. “It gives me the information I need, especially when prescribing antidepressant medications to my patients.”
Still, Dr Kunutsor and his colleagues conceded that more research is needed to determine if the observed associations are causal and if depression, antidepressant use, or both drive the increased risk of VTE.
To so this, studies would need to isolate depression from antidepressant medications. For example, researchers could assess if non-depressed individuals who use antidepressants for other conditions have an increased risk of VTE.
*The “other” antidepressants include monoamine oxidase inhibitors, triazolopyridine, serotonin norepinephrine reuptake inhibitors, and norepinephrine dopamine reuptake inhibitors.
Depression and the use of antidepressants are each associated with an increased risk of venous thromboembolism (VTE), according to a review and meta-analysis published in Annals of Medicine.
The research also showed that each of the various classes of antidepressant medications is associated with an increased risk of VTE.
The researchers noted that this study does not prove cause and effect, and further studies are needed to determine what is driving the observed increase in VTE risk.
Some previous studies have indicated that depression and antidepressant use might be associated with an increased risk of VTE, but other studies have shown no evidence of associations.
Therefore, Setor Kunutsor, MD, PhD, of the University of Bristol in Bristol, UK, and his colleagues conducted a systematic review and meta-analysis of observational studies evaluating the associations of depression and antidepressant use with VTE risk.
The researchers looked at 8 observational studies with data on 960,113 non-overlapping participants. There were 9027 cases of VTE in this population.
To determine the association between depression and VTE, the researchers conducted a pooled analysis of 3 studies comparing patients with depression and without. These studies included 865,878 participants and 4676 cases of VTE.
The relative risk (RR) for VTE was 1.31 (95% CI, 1.13-1.53) among patients with depression.
The researchers also conducted a pooled analysis of 6 studies comparing antidepressant users to non-users. These studies included 828,327 participants and 8273 cases of VTE.
The RR for VTE was 1.27 (95% CI, 1.06-1.51) among patients taking antidepressants.
In addition, individual antidepressants were associated with an increased risk of VTE. This includes:
- Tricyclic antidepressants—RR=1.16 (95% CI, 1.06-1.27)
- Selective serotonin reuptake inhibitors—RR=1.12 (95% CI, 1.02-1.23)
- “Other” antidepressants*—RR=1.59 (95% CI, 1.21-2.09).
The researchers said these data show that antidepressant use and depression are each associated with an increased risk of VTE, and these results add to accumulating evidence that a relationship exists between depression, antidepressant use, and VTE.
“These findings are very useful to me as both a clinician and a researcher,” Dr Kunutsor said. “It gives me the information I need, especially when prescribing antidepressant medications to my patients.”
Still, Dr Kunutsor and his colleagues conceded that more research is needed to determine if the observed associations are causal and if depression, antidepressant use, or both drive the increased risk of VTE.
To so this, studies would need to isolate depression from antidepressant medications. For example, researchers could assess if non-depressed individuals who use antidepressants for other conditions have an increased risk of VTE.
*The “other” antidepressants include monoamine oxidase inhibitors, triazolopyridine, serotonin norepinephrine reuptake inhibitors, and norepinephrine dopamine reuptake inhibitors.
Depression and the use of antidepressants are each associated with an increased risk of venous thromboembolism (VTE), according to a review and meta-analysis published in Annals of Medicine.
The research also showed that each of the various classes of antidepressant medications is associated with an increased risk of VTE.
The researchers noted that this study does not prove cause and effect, and further studies are needed to determine what is driving the observed increase in VTE risk.
Some previous studies have indicated that depression and antidepressant use might be associated with an increased risk of VTE, but other studies have shown no evidence of associations.
Therefore, Setor Kunutsor, MD, PhD, of the University of Bristol in Bristol, UK, and his colleagues conducted a systematic review and meta-analysis of observational studies evaluating the associations of depression and antidepressant use with VTE risk.
The researchers looked at 8 observational studies with data on 960,113 non-overlapping participants. There were 9027 cases of VTE in this population.
To determine the association between depression and VTE, the researchers conducted a pooled analysis of 3 studies comparing patients with depression and without. These studies included 865,878 participants and 4676 cases of VTE.
The relative risk (RR) for VTE was 1.31 (95% CI, 1.13-1.53) among patients with depression.
The researchers also conducted a pooled analysis of 6 studies comparing antidepressant users to non-users. These studies included 828,327 participants and 8273 cases of VTE.
The RR for VTE was 1.27 (95% CI, 1.06-1.51) among patients taking antidepressants.
In addition, individual antidepressants were associated with an increased risk of VTE. This includes:
- Tricyclic antidepressants—RR=1.16 (95% CI, 1.06-1.27)
- Selective serotonin reuptake inhibitors—RR=1.12 (95% CI, 1.02-1.23)
- “Other” antidepressants*—RR=1.59 (95% CI, 1.21-2.09).
The researchers said these data show that antidepressant use and depression are each associated with an increased risk of VTE, and these results add to accumulating evidence that a relationship exists between depression, antidepressant use, and VTE.
“These findings are very useful to me as both a clinician and a researcher,” Dr Kunutsor said. “It gives me the information I need, especially when prescribing antidepressant medications to my patients.”
Still, Dr Kunutsor and his colleagues conceded that more research is needed to determine if the observed associations are causal and if depression, antidepressant use, or both drive the increased risk of VTE.
To so this, studies would need to isolate depression from antidepressant medications. For example, researchers could assess if non-depressed individuals who use antidepressants for other conditions have an increased risk of VTE.
*The “other” antidepressants include monoamine oxidase inhibitors, triazolopyridine, serotonin norepinephrine reuptake inhibitors, and norepinephrine dopamine reuptake inhibitors.
Gene therapy granted accelerated assessment

The European Medicines Agency’s (EMA) Committee for Medicinal Products for Human Use has granted accelerated assessment for the upcoming marketing authorization application (MAA) for LentiGlobin™.
LentiGlobin is a gene therapy intended for the treatment of adolescents and adults with transfusion-dependent β-thalassemia (TDT) and a non-β0/β0 genotype.
bluebird bio intends to file an MAA for LentiGlobin with the EMA this year.
Accelerated assessment can reduce the active review time of an MAA from 210 days to 150 days once it has been validated by the EMA.
An accelerated assessment is granted to products deemed to be of major interest for public health and represent therapeutic innovation.
The accelerated assessment for LentiGlobin is supported by data from clinical studies, including the phase 1/2 Northstar (HGB-204) study, phase 1/2 HGB-205 study, phase 3 Northstar-2 (HGB-207) study, and the long-term follow-up study LTF-303.
The EMA previously granted PRIME (Priority Medicines) eligibility and orphan designation to LentiGlobin for the treatment of TDT.
LentiGlobin is also part of the EMA’s Adaptive Pathways pilot program, which is part of the EMA’s effort to improve timely access to new medicines.
Phase 1/2 trials
Results from the phase 1/2 trials of LentiGlobin—HGB-204 and HGB-205—were published in NEJM in April.
HGB-204 is a completed study that included 18 patients with TDT. Eight patients had a β0/β0 genotype, 6 had a βE/β0 genotype, and 4 had other genotypes.
HGB-205 is an ongoing study, and results were reported for 4 patients with TDT. Three patients had a βE/β0 genotype. The remaining patient was homozygous for the IVS1-110 mutation and had a severe clinical presentation similar to that seen in β0/β0 genotypes.
For both studies, the researchers harvested hematopoietic stem and progenitor cells (mobilized with filgrastim and plerixafor) from the patients. CD34+ cells were transduced ex vivo with LentiGlobin BB305 vector, which encodes adult hemoglobin (HbA) with a T87Q amino acid substitution (HbAT87Q).
The patients underwent myeloablative conditioning with busulfan, and the final LentiGlobin product was infused into patients after a 72-hour washout period.
In HGB-205 only, patients received enhanced red blood cell (RBC) transfusions for at least 3 months before stem cell mobilization and harvest to maintain a hemoglobin level of more than 11.0 g/dL.
Safety
In HGB-204, there were 5 grade 1 adverse events (AEs) considered possibly or probably related to LentiGlobin—abdominal pain (n=2), dyspnea (n=1), hot flush (n=1), and non-cardiac chest pain (n=1).
There were 9 serious AEs. Grade 3 serious AEs included 2 episodes of veno-occlusive liver disease that were attributed to busulfan, Klebsiella infection, cardiac ventricular thrombosis, cellulitis, hyperglycemia, and gastroenteritis. Grade 2 serious AEs included device-related thrombosis and infectious diarrhea.
In HGB-205, there were no AEs considered possibly or probably related to LentiGlobin. The 3 serious AEs were tooth infection (grade 3), major depression (grade 3), and pneumonia (grade 2).
Efficacy
The median time to neutrophil engraftment was 18.5 days (range, 14.0 to 30.0) in HGB-204 and 16.5 days (range, 14.0 to 29.0) in HGB-205.
The median time to platelet engraftment was 39.5 days (range, 19.0 to 191.0) and 23.0 days (range, 20.0 to 26.0), respectively.
In both studies, the median follow-up was 26 months (range, 15 to 42) after LentiGlobin infusion.
At last follow-up, all but 1 of the 13 patients with a non-β0/β0 genotype had stopped receiving RBC transfusions.
In the 8 patients with a β0/β0 genotype and the 1 patient with 2 copies of the IVS1-110 mutation, the median annualized transfusion volume decreased by 73% after LentiGlobin administration.
Two patients with a β0/β0 genotype were able to stop receiving RBC transfusions, as was the patient with 2 copies of the IVS1-110 mutation.
The European Medicines Agency’s (EMA) Committee for Medicinal Products for Human Use has granted accelerated assessment for the upcoming marketing authorization application (MAA) for LentiGlobin™.
LentiGlobin is a gene therapy intended for the treatment of adolescents and adults with transfusion-dependent β-thalassemia (TDT) and a non-β0/β0 genotype.
bluebird bio intends to file an MAA for LentiGlobin with the EMA this year.
Accelerated assessment can reduce the active review time of an MAA from 210 days to 150 days once it has been validated by the EMA.
An accelerated assessment is granted to products deemed to be of major interest for public health and represent therapeutic innovation.
The accelerated assessment for LentiGlobin is supported by data from clinical studies, including the phase 1/2 Northstar (HGB-204) study, phase 1/2 HGB-205 study, phase 3 Northstar-2 (HGB-207) study, and the long-term follow-up study LTF-303.
The EMA previously granted PRIME (Priority Medicines) eligibility and orphan designation to LentiGlobin for the treatment of TDT.
LentiGlobin is also part of the EMA’s Adaptive Pathways pilot program, which is part of the EMA’s effort to improve timely access to new medicines.
Phase 1/2 trials
Results from the phase 1/2 trials of LentiGlobin—HGB-204 and HGB-205—were published in NEJM in April.
HGB-204 is a completed study that included 18 patients with TDT. Eight patients had a β0/β0 genotype, 6 had a βE/β0 genotype, and 4 had other genotypes.
HGB-205 is an ongoing study, and results were reported for 4 patients with TDT. Three patients had a βE/β0 genotype. The remaining patient was homozygous for the IVS1-110 mutation and had a severe clinical presentation similar to that seen in β0/β0 genotypes.
For both studies, the researchers harvested hematopoietic stem and progenitor cells (mobilized with filgrastim and plerixafor) from the patients. CD34+ cells were transduced ex vivo with LentiGlobin BB305 vector, which encodes adult hemoglobin (HbA) with a T87Q amino acid substitution (HbAT87Q).
The patients underwent myeloablative conditioning with busulfan, and the final LentiGlobin product was infused into patients after a 72-hour washout period.
In HGB-205 only, patients received enhanced red blood cell (RBC) transfusions for at least 3 months before stem cell mobilization and harvest to maintain a hemoglobin level of more than 11.0 g/dL.
Safety
In HGB-204, there were 5 grade 1 adverse events (AEs) considered possibly or probably related to LentiGlobin—abdominal pain (n=2), dyspnea (n=1), hot flush (n=1), and non-cardiac chest pain (n=1).
There were 9 serious AEs. Grade 3 serious AEs included 2 episodes of veno-occlusive liver disease that were attributed to busulfan, Klebsiella infection, cardiac ventricular thrombosis, cellulitis, hyperglycemia, and gastroenteritis. Grade 2 serious AEs included device-related thrombosis and infectious diarrhea.
In HGB-205, there were no AEs considered possibly or probably related to LentiGlobin. The 3 serious AEs were tooth infection (grade 3), major depression (grade 3), and pneumonia (grade 2).
Efficacy
The median time to neutrophil engraftment was 18.5 days (range, 14.0 to 30.0) in HGB-204 and 16.5 days (range, 14.0 to 29.0) in HGB-205.
The median time to platelet engraftment was 39.5 days (range, 19.0 to 191.0) and 23.0 days (range, 20.0 to 26.0), respectively.
In both studies, the median follow-up was 26 months (range, 15 to 42) after LentiGlobin infusion.
At last follow-up, all but 1 of the 13 patients with a non-β0/β0 genotype had stopped receiving RBC transfusions.
In the 8 patients with a β0/β0 genotype and the 1 patient with 2 copies of the IVS1-110 mutation, the median annualized transfusion volume decreased by 73% after LentiGlobin administration.
Two patients with a β0/β0 genotype were able to stop receiving RBC transfusions, as was the patient with 2 copies of the IVS1-110 mutation.
The European Medicines Agency’s (EMA) Committee for Medicinal Products for Human Use has granted accelerated assessment for the upcoming marketing authorization application (MAA) for LentiGlobin™.
LentiGlobin is a gene therapy intended for the treatment of adolescents and adults with transfusion-dependent β-thalassemia (TDT) and a non-β0/β0 genotype.
bluebird bio intends to file an MAA for LentiGlobin with the EMA this year.
Accelerated assessment can reduce the active review time of an MAA from 210 days to 150 days once it has been validated by the EMA.
An accelerated assessment is granted to products deemed to be of major interest for public health and represent therapeutic innovation.
The accelerated assessment for LentiGlobin is supported by data from clinical studies, including the phase 1/2 Northstar (HGB-204) study, phase 1/2 HGB-205 study, phase 3 Northstar-2 (HGB-207) study, and the long-term follow-up study LTF-303.
The EMA previously granted PRIME (Priority Medicines) eligibility and orphan designation to LentiGlobin for the treatment of TDT.
LentiGlobin is also part of the EMA’s Adaptive Pathways pilot program, which is part of the EMA’s effort to improve timely access to new medicines.
Phase 1/2 trials
Results from the phase 1/2 trials of LentiGlobin—HGB-204 and HGB-205—were published in NEJM in April.
HGB-204 is a completed study that included 18 patients with TDT. Eight patients had a β0/β0 genotype, 6 had a βE/β0 genotype, and 4 had other genotypes.
HGB-205 is an ongoing study, and results were reported for 4 patients with TDT. Three patients had a βE/β0 genotype. The remaining patient was homozygous for the IVS1-110 mutation and had a severe clinical presentation similar to that seen in β0/β0 genotypes.
For both studies, the researchers harvested hematopoietic stem and progenitor cells (mobilized with filgrastim and plerixafor) from the patients. CD34+ cells were transduced ex vivo with LentiGlobin BB305 vector, which encodes adult hemoglobin (HbA) with a T87Q amino acid substitution (HbAT87Q).
The patients underwent myeloablative conditioning with busulfan, and the final LentiGlobin product was infused into patients after a 72-hour washout period.
In HGB-205 only, patients received enhanced red blood cell (RBC) transfusions for at least 3 months before stem cell mobilization and harvest to maintain a hemoglobin level of more than 11.0 g/dL.
Safety
In HGB-204, there were 5 grade 1 adverse events (AEs) considered possibly or probably related to LentiGlobin—abdominal pain (n=2), dyspnea (n=1), hot flush (n=1), and non-cardiac chest pain (n=1).
There were 9 serious AEs. Grade 3 serious AEs included 2 episodes of veno-occlusive liver disease that were attributed to busulfan, Klebsiella infection, cardiac ventricular thrombosis, cellulitis, hyperglycemia, and gastroenteritis. Grade 2 serious AEs included device-related thrombosis and infectious diarrhea.
In HGB-205, there were no AEs considered possibly or probably related to LentiGlobin. The 3 serious AEs were tooth infection (grade 3), major depression (grade 3), and pneumonia (grade 2).
Efficacy
The median time to neutrophil engraftment was 18.5 days (range, 14.0 to 30.0) in HGB-204 and 16.5 days (range, 14.0 to 29.0) in HGB-205.
The median time to platelet engraftment was 39.5 days (range, 19.0 to 191.0) and 23.0 days (range, 20.0 to 26.0), respectively.
In both studies, the median follow-up was 26 months (range, 15 to 42) after LentiGlobin infusion.
At last follow-up, all but 1 of the 13 patients with a non-β0/β0 genotype had stopped receiving RBC transfusions.
In the 8 patients with a β0/β0 genotype and the 1 patient with 2 copies of the IVS1-110 mutation, the median annualized transfusion volume decreased by 73% after LentiGlobin administration.
Two patients with a β0/β0 genotype were able to stop receiving RBC transfusions, as was the patient with 2 copies of the IVS1-110 mutation.
Intrathecal methotrexate dosing in acute leukemia falls short
STOCKHOLM – Although intrathecal chemoprophylaxis for prevention of central nervous system involvement is an essential component of modern regimens to treat acute lymphoblastic leukemia (ALL), patients don’t always receive the recommended number of doses, potentially compromising remissions.
But as a large-scale audit of health care delivery in the United Kingdom has suggested, many of the possible causes for suboptimal delivery of intrathecal methotrexate (IT MTX) appear to be modifiable, reported Sven A. Sommerfeld, MD, and his colleagues from the Christie Hospital in Manchester, England.
“In our clinical observations, and confirmed in this audit, patients on intensive chemotherapy, including induction and consolidation protocols for acute lymphoblastic leukemia, can develop a number of issues and toxicities, which can interfere with the administration of IT MTX,” they wrote in a poster presented at the annual congress of the European Hematology Association.
Reasons for canceling or postponing scheduled doses of IT MTX range from “fairly compelling clinical reasons affecting patient safety or tolerance” to more mundane issues, such as scheduling and staffing problems, the investigators found.
“I think there are a number of factors that can improve compliance, including having your cancellation rate as low as possible. You have already prescribed the treatment, the patient is supposed to be attending [clinic], yet for some reason you cannot go ahead,” Dr. Sommerfeld said in an interview. “I think blood product support is important, but there are capacity issues. Organization of complex treatment protocols that involve systemic chemotherapy and concurrent intrathecal administration can be difficult as different people oversee both of these treatments.”
For example, protocols specify delivery of intrathecal chemoprophylaxis on specific days and induction chemotherapy on other days, and it may be difficult to coordinate the care so that the doses don’t overlap, he said.
Dr. Sommerfeld and his colleagues conducted an audit of standard of care for patients aged 16-60 years who were diagnosed with B-cell or T-cell ALL and received IT MTX under one of two clinical protocols: UKALL 2011 or UKALL 14.
The investigators examined data on IT MTX compliance and assigned each patient a compliance score calculated by the number of administered doses divided by protocol-defined number of doses. They also examined pharmacy records of cancellations of protocol-scheduled IT MTX from January 2016 through July 2017.
They found that the total number of IT MTX prescriptions delivered as a proportion of the number prescribed ranged from a low of 61.8% in 2009 to a high of 84.2% in 2007.
When the investigators looked at records for individual patients, including 29 adolescent and young adults receiving IT MTX under the UKALL 2011 protocol and 27 adults receiving it under the UKALL 14 protocol, they found that failure to maintain coagulation levels within parameters accounted for 23% of cancellations. The next most common reasons for cancellation were rescheduling for administrative or clinical reasons in 20% of canceled doses, low platelet levels in 19% of cases, and patient nonattendance or communication failure in 16% of cases. Other factors included problems with lumbar access, vincristine schedule for the same day, recent anticoagulation, and delay of blood results.
“Notable is the variable approach to IT MTX in patients requiring therapeutic dose anticoagulation, reflecting clinical decisions of different physicians on a case-by-case basis. Whilst a full discussion of this topic and management of asparaginase-associated [venous thromboembolism] is beyond the scope of this audit, we generally recognize today that many affected patients can be managed to continue therapy as per protocol,” the investigators wrote.
Integrating relevant prescriptions into a single information system, monitoring clinics for treatment backlogs, and improving clinical resources, such as staffing, could help to improve the efficacy of IT MTX therapy, they suggested.
The study was supported by the National Health Service Foundation Trust. Dr. Sommerfeld reported having no relevant financial disclosures.
SOURCE: Sommerfeld SA et al. EHA Congress, Abstract PS930.
STOCKHOLM – Although intrathecal chemoprophylaxis for prevention of central nervous system involvement is an essential component of modern regimens to treat acute lymphoblastic leukemia (ALL), patients don’t always receive the recommended number of doses, potentially compromising remissions.
But as a large-scale audit of health care delivery in the United Kingdom has suggested, many of the possible causes for suboptimal delivery of intrathecal methotrexate (IT MTX) appear to be modifiable, reported Sven A. Sommerfeld, MD, and his colleagues from the Christie Hospital in Manchester, England.
“In our clinical observations, and confirmed in this audit, patients on intensive chemotherapy, including induction and consolidation protocols for acute lymphoblastic leukemia, can develop a number of issues and toxicities, which can interfere with the administration of IT MTX,” they wrote in a poster presented at the annual congress of the European Hematology Association.
Reasons for canceling or postponing scheduled doses of IT MTX range from “fairly compelling clinical reasons affecting patient safety or tolerance” to more mundane issues, such as scheduling and staffing problems, the investigators found.
“I think there are a number of factors that can improve compliance, including having your cancellation rate as low as possible. You have already prescribed the treatment, the patient is supposed to be attending [clinic], yet for some reason you cannot go ahead,” Dr. Sommerfeld said in an interview. “I think blood product support is important, but there are capacity issues. Organization of complex treatment protocols that involve systemic chemotherapy and concurrent intrathecal administration can be difficult as different people oversee both of these treatments.”
For example, protocols specify delivery of intrathecal chemoprophylaxis on specific days and induction chemotherapy on other days, and it may be difficult to coordinate the care so that the doses don’t overlap, he said.
Dr. Sommerfeld and his colleagues conducted an audit of standard of care for patients aged 16-60 years who were diagnosed with B-cell or T-cell ALL and received IT MTX under one of two clinical protocols: UKALL 2011 or UKALL 14.
The investigators examined data on IT MTX compliance and assigned each patient a compliance score calculated by the number of administered doses divided by protocol-defined number of doses. They also examined pharmacy records of cancellations of protocol-scheduled IT MTX from January 2016 through July 2017.
They found that the total number of IT MTX prescriptions delivered as a proportion of the number prescribed ranged from a low of 61.8% in 2009 to a high of 84.2% in 2007.
When the investigators looked at records for individual patients, including 29 adolescent and young adults receiving IT MTX under the UKALL 2011 protocol and 27 adults receiving it under the UKALL 14 protocol, they found that failure to maintain coagulation levels within parameters accounted for 23% of cancellations. The next most common reasons for cancellation were rescheduling for administrative or clinical reasons in 20% of canceled doses, low platelet levels in 19% of cases, and patient nonattendance or communication failure in 16% of cases. Other factors included problems with lumbar access, vincristine schedule for the same day, recent anticoagulation, and delay of blood results.
“Notable is the variable approach to IT MTX in patients requiring therapeutic dose anticoagulation, reflecting clinical decisions of different physicians on a case-by-case basis. Whilst a full discussion of this topic and management of asparaginase-associated [venous thromboembolism] is beyond the scope of this audit, we generally recognize today that many affected patients can be managed to continue therapy as per protocol,” the investigators wrote.
Integrating relevant prescriptions into a single information system, monitoring clinics for treatment backlogs, and improving clinical resources, such as staffing, could help to improve the efficacy of IT MTX therapy, they suggested.
The study was supported by the National Health Service Foundation Trust. Dr. Sommerfeld reported having no relevant financial disclosures.
SOURCE: Sommerfeld SA et al. EHA Congress, Abstract PS930.
STOCKHOLM – Although intrathecal chemoprophylaxis for prevention of central nervous system involvement is an essential component of modern regimens to treat acute lymphoblastic leukemia (ALL), patients don’t always receive the recommended number of doses, potentially compromising remissions.
But as a large-scale audit of health care delivery in the United Kingdom has suggested, many of the possible causes for suboptimal delivery of intrathecal methotrexate (IT MTX) appear to be modifiable, reported Sven A. Sommerfeld, MD, and his colleagues from the Christie Hospital in Manchester, England.
“In our clinical observations, and confirmed in this audit, patients on intensive chemotherapy, including induction and consolidation protocols for acute lymphoblastic leukemia, can develop a number of issues and toxicities, which can interfere with the administration of IT MTX,” they wrote in a poster presented at the annual congress of the European Hematology Association.
Reasons for canceling or postponing scheduled doses of IT MTX range from “fairly compelling clinical reasons affecting patient safety or tolerance” to more mundane issues, such as scheduling and staffing problems, the investigators found.
“I think there are a number of factors that can improve compliance, including having your cancellation rate as low as possible. You have already prescribed the treatment, the patient is supposed to be attending [clinic], yet for some reason you cannot go ahead,” Dr. Sommerfeld said in an interview. “I think blood product support is important, but there are capacity issues. Organization of complex treatment protocols that involve systemic chemotherapy and concurrent intrathecal administration can be difficult as different people oversee both of these treatments.”
For example, protocols specify delivery of intrathecal chemoprophylaxis on specific days and induction chemotherapy on other days, and it may be difficult to coordinate the care so that the doses don’t overlap, he said.
Dr. Sommerfeld and his colleagues conducted an audit of standard of care for patients aged 16-60 years who were diagnosed with B-cell or T-cell ALL and received IT MTX under one of two clinical protocols: UKALL 2011 or UKALL 14.
The investigators examined data on IT MTX compliance and assigned each patient a compliance score calculated by the number of administered doses divided by protocol-defined number of doses. They also examined pharmacy records of cancellations of protocol-scheduled IT MTX from January 2016 through July 2017.
They found that the total number of IT MTX prescriptions delivered as a proportion of the number prescribed ranged from a low of 61.8% in 2009 to a high of 84.2% in 2007.
When the investigators looked at records for individual patients, including 29 adolescent and young adults receiving IT MTX under the UKALL 2011 protocol and 27 adults receiving it under the UKALL 14 protocol, they found that failure to maintain coagulation levels within parameters accounted for 23% of cancellations. The next most common reasons for cancellation were rescheduling for administrative or clinical reasons in 20% of canceled doses, low platelet levels in 19% of cases, and patient nonattendance or communication failure in 16% of cases. Other factors included problems with lumbar access, vincristine schedule for the same day, recent anticoagulation, and delay of blood results.
“Notable is the variable approach to IT MTX in patients requiring therapeutic dose anticoagulation, reflecting clinical decisions of different physicians on a case-by-case basis. Whilst a full discussion of this topic and management of asparaginase-associated [venous thromboembolism] is beyond the scope of this audit, we generally recognize today that many affected patients can be managed to continue therapy as per protocol,” the investigators wrote.
Integrating relevant prescriptions into a single information system, monitoring clinics for treatment backlogs, and improving clinical resources, such as staffing, could help to improve the efficacy of IT MTX therapy, they suggested.
The study was supported by the National Health Service Foundation Trust. Dr. Sommerfeld reported having no relevant financial disclosures.
SOURCE: Sommerfeld SA et al. EHA Congress, Abstract PS930.
REPORTING FROM THE EHA CONGRESS
Key clinical point:
Major finding: The total number of intrathecal methotrexate prescriptions delivered as a proportion of the number prescribed ranged from a low of 61.8% in 2009 to a high of 84.2% in 2007.
Study details: Audit of standard of care delivery of intrathecal methotrexate in the United Kingdom.
Disclosures: The study was supported by the National Health Service Foundation Trust. Dr. Sommerfeld reported having no relevant financial disclosures.
Source: Sommerfeld SA et al. EHA Congress, Abstract PS930.