User login
Docs push back on step therapy in Medicare Advantage
A new policy that allows Medicare Advantage plans to use step therapy to control spending on prescription drug administered in the office is not going over well with doctors.

The Centers for Medicare & Medicaid Services announced the policy change Aug. 7, which will give Medicare Advantage plan sponsors the “choice of implementing step therapy to manage Part B drugs, beginning Jan. 1, 2019,” the agency said in a statement.
The action is part of the broader Trump administration initiative to lower the prices and out-of-pocket costs of prescription drugs as outlined in the American Patients First blueprint.
By “implementing step therapy along with care coordination and drug adherence programs in [Medicare Advantage], it will lower costs and improve the quality of care for Medicare beneficiaries,” CMS officials said in a statement. The move to allow step therapy will give Medicare Advantage plan sponsors the ability to negotiate the designation of a preferred drug, something the agency believes could result in lower prices for these drugs, which in turn will lower the copays for Medicare beneficiaries.
Plan sponsors will be required to pass savings onto beneficiaries through some sort of rewards program, according to a memo detailing the policy change, which also notes that plan rewards “cannot be offered in the form of cash or monetary rebate, but may be offered as gift cards or other items value to all eligible enrollees.”
The value of the rewards must be more than half of the savings generated from implementing the step therapy program, according to the memo.
CMS officials noted that there will be a process that beneficiaries can follow if they believe they need direct access to a drug that would otherwise be available only after failing on another drug.
The American Gastroenterological Association “is concerned that the proposal could limit access for current and future beneficiaries and could add to the growing regulatory burden that physicians already face,” according to a statement. AGA stated that “any change in policy must ensure that patients have access to the appropriate therapies to manage their diseases and not contribute to additional administrative burdens for physician practices.” In addition to responding to CMS, AGA continues to advocate to Congress for patient protections for those subject to step therapy protocols in employer-sponsored health plans; learn more at http:/ow.ly/kp8l30lnDmp.

The new policy applies to only new prescriptions or administrations of Part B drugs. Patients will not have current treatments disrupted if that drug is not the first drug on the step therapy ladder. Additionally, patients will have the opportunity to make a one-time change in plans during the first quarter annually if they are finding the plan is not working for them. Plan sponsors must disclose that Part B drugs may be subject to step therapy.
A new policy that allows Medicare Advantage plans to use step therapy to control spending on prescription drug administered in the office is not going over well with doctors.
The Centers for Medicare & Medicaid Services announced the policy change Aug. 7, which will give Medicare Advantage plan sponsors the “choice of implementing step therapy to manage Part B drugs, beginning Jan. 1, 2019,” the agency said in a statement.
The action is part of the broader Trump administration initiative to lower the prices and out-of-pocket costs of prescription drugs as outlined in the American Patients First blueprint.
By “implementing step therapy along with care coordination and drug adherence programs in [Medicare Advantage], it will lower costs and improve the quality of care for Medicare beneficiaries,” CMS officials said in a statement. The move to allow step therapy will give Medicare Advantage plan sponsors the ability to negotiate the designation of a preferred drug, something the agency believes could result in lower prices for these drugs, which in turn will lower the copays for Medicare beneficiaries.
Plan sponsors will be required to pass savings onto beneficiaries through some sort of rewards program, according to a memo detailing the policy change, which also notes that plan rewards “cannot be offered in the form of cash or monetary rebate, but may be offered as gift cards or other items value to all eligible enrollees.”
The value of the rewards must be more than half of the savings generated from implementing the step therapy program, according to the memo.
CMS officials noted that there will be a process that beneficiaries can follow if they believe they need direct access to a drug that would otherwise be available only after failing on another drug.
The American Gastroenterological Association “is concerned that the proposal could limit access for current and future beneficiaries and could add to the growing regulatory burden that physicians already face,” according to a statement. AGA stated that “any change in policy must ensure that patients have access to the appropriate therapies to manage their diseases and not contribute to additional administrative burdens for physician practices.” In addition to responding to CMS, AGA continues to advocate to Congress for patient protections for those subject to step therapy protocols in employer-sponsored health plans; learn more at http:/ow.ly/kp8l30lnDmp.
The new policy applies to only new prescriptions or administrations of Part B drugs. Patients will not have current treatments disrupted if that drug is not the first drug on the step therapy ladder. Additionally, patients will have the opportunity to make a one-time change in plans during the first quarter annually if they are finding the plan is not working for them. Plan sponsors must disclose that Part B drugs may be subject to step therapy.
A new policy that allows Medicare Advantage plans to use step therapy to control spending on prescription drug administered in the office is not going over well with doctors.
The Centers for Medicare & Medicaid Services announced the policy change Aug. 7, which will give Medicare Advantage plan sponsors the “choice of implementing step therapy to manage Part B drugs, beginning Jan. 1, 2019,” the agency said in a statement.
The action is part of the broader Trump administration initiative to lower the prices and out-of-pocket costs of prescription drugs as outlined in the American Patients First blueprint.
By “implementing step therapy along with care coordination and drug adherence programs in [Medicare Advantage], it will lower costs and improve the quality of care for Medicare beneficiaries,” CMS officials said in a statement. The move to allow step therapy will give Medicare Advantage plan sponsors the ability to negotiate the designation of a preferred drug, something the agency believes could result in lower prices for these drugs, which in turn will lower the copays for Medicare beneficiaries.
Plan sponsors will be required to pass savings onto beneficiaries through some sort of rewards program, according to a memo detailing the policy change, which also notes that plan rewards “cannot be offered in the form of cash or monetary rebate, but may be offered as gift cards or other items value to all eligible enrollees.”
The value of the rewards must be more than half of the savings generated from implementing the step therapy program, according to the memo.
CMS officials noted that there will be a process that beneficiaries can follow if they believe they need direct access to a drug that would otherwise be available only after failing on another drug.
The American Gastroenterological Association “is concerned that the proposal could limit access for current and future beneficiaries and could add to the growing regulatory burden that physicians already face,” according to a statement. AGA stated that “any change in policy must ensure that patients have access to the appropriate therapies to manage their diseases and not contribute to additional administrative burdens for physician practices.” In addition to responding to CMS, AGA continues to advocate to Congress for patient protections for those subject to step therapy protocols in employer-sponsored health plans; learn more at http:/ow.ly/kp8l30lnDmp.
The new policy applies to only new prescriptions or administrations of Part B drugs. Patients will not have current treatments disrupted if that drug is not the first drug on the step therapy ladder. Additionally, patients will have the opportunity to make a one-time change in plans during the first quarter annually if they are finding the plan is not working for them. Plan sponsors must disclose that Part B drugs may be subject to step therapy.
CMS proposes site-neutral payments for hospital outpatient settings

In the proposed update to the Outpatient Prospective Payment System (OPPS) and Ambulatory Surgical Center (ASC) Payment System for 2019, CMS is proposing to apply a physician fee schedule–equivalent for the clinic visit service when provided at an off-campus, provider-based department that is paid under OPPS.
According to CMS, the average current clinical visit paid by CMS is $116 with $23 being the average copay by the patient. If the proposal is finalized, the payment would drop to about $46 with an average patient copay of $9.
“This is intended to address concerns about recent consolidations in the market that reduce competition,” CMS Administrator Seema Verma said during a July 25 press conference.
The American Hospital Association already is pushing back on this proposal.
“With today’s proposed rule, CMS has once again showed a lack of understanding about the reality in which hospitals and health systems operate daily to serve the needs of their communities,” AHA Executive Vice President Tom Nickels said in a statement. “In 2015, Congress clearly intended to provide current off-campus hospital clinics with the existing outpatient payment rate in recognition of the critical role they play in their communities. But CMS’s proposal runs counter to this and will instead impede access to care for the most vulnerable patients.”
The OPPS/ASC update also includes proposals to expand the list of covered surgical procedures that can be performed in an ASC, a move that Ms. Verma said would “provide patients with more choices and options for lower-priced care.”
“For CY 2019, CMS is proposing to allow certain CPT codes outside of the surgical code range that directly crosswalk or are clinically similar to procedures within the CPT surgical code range to be included on the [covered procedure list] and is proposing to add certain cardiovascular codes to the ASC [covered procedure list] as a result,” the CMS fact sheet notes.
Another change proposed by CMS relates to how ASC reimbursement rates are updated. They have been based on the consumer price index-urban, which has resulted in a decline in ASC payments relative to hospitals for the same service. For 2019-2023, CMS proposes to use the hospital market basket instead, which will help promote site neutrality between hospitals and ASCs. The AGA applauds this proposal, and has been working for it with the ACG and ASGE for nearly a decade.
In addition, the OPPS is seeking feedback on a number of topics.
One is related to price transparency. The agency is asking “whether providers and suppliers can and should be required to inform patients about charges and payment information for healthcare services and out-of-pocket costs, what data elements the public would find most useful, and what other charges are needed to empower patients,” according to the fact sheet.
Finally, the agency is seeking more information on solutions to better promote interoperability.
In the proposed update to the Outpatient Prospective Payment System (OPPS) and Ambulatory Surgical Center (ASC) Payment System for 2019, CMS is proposing to apply a physician fee schedule–equivalent for the clinic visit service when provided at an off-campus, provider-based department that is paid under OPPS.
According to CMS, the average current clinical visit paid by CMS is $116 with $23 being the average copay by the patient. If the proposal is finalized, the payment would drop to about $46 with an average patient copay of $9.
“This is intended to address concerns about recent consolidations in the market that reduce competition,” CMS Administrator Seema Verma said during a July 25 press conference.
The American Hospital Association already is pushing back on this proposal.
“With today’s proposed rule, CMS has once again showed a lack of understanding about the reality in which hospitals and health systems operate daily to serve the needs of their communities,” AHA Executive Vice President Tom Nickels said in a statement. “In 2015, Congress clearly intended to provide current off-campus hospital clinics with the existing outpatient payment rate in recognition of the critical role they play in their communities. But CMS’s proposal runs counter to this and will instead impede access to care for the most vulnerable patients.”
The OPPS/ASC update also includes proposals to expand the list of covered surgical procedures that can be performed in an ASC, a move that Ms. Verma said would “provide patients with more choices and options for lower-priced care.”
“For CY 2019, CMS is proposing to allow certain CPT codes outside of the surgical code range that directly crosswalk or are clinically similar to procedures within the CPT surgical code range to be included on the [covered procedure list] and is proposing to add certain cardiovascular codes to the ASC [covered procedure list] as a result,” the CMS fact sheet notes.
Another change proposed by CMS relates to how ASC reimbursement rates are updated. They have been based on the consumer price index-urban, which has resulted in a decline in ASC payments relative to hospitals for the same service. For 2019-2023, CMS proposes to use the hospital market basket instead, which will help promote site neutrality between hospitals and ASCs. The AGA applauds this proposal, and has been working for it with the ACG and ASGE for nearly a decade.
In addition, the OPPS is seeking feedback on a number of topics.
One is related to price transparency. The agency is asking “whether providers and suppliers can and should be required to inform patients about charges and payment information for healthcare services and out-of-pocket costs, what data elements the public would find most useful, and what other charges are needed to empower patients,” according to the fact sheet.
Finally, the agency is seeking more information on solutions to better promote interoperability.
In the proposed update to the Outpatient Prospective Payment System (OPPS) and Ambulatory Surgical Center (ASC) Payment System for 2019, CMS is proposing to apply a physician fee schedule–equivalent for the clinic visit service when provided at an off-campus, provider-based department that is paid under OPPS.
According to CMS, the average current clinical visit paid by CMS is $116 with $23 being the average copay by the patient. If the proposal is finalized, the payment would drop to about $46 with an average patient copay of $9.
“This is intended to address concerns about recent consolidations in the market that reduce competition,” CMS Administrator Seema Verma said during a July 25 press conference.
The American Hospital Association already is pushing back on this proposal.
“With today’s proposed rule, CMS has once again showed a lack of understanding about the reality in which hospitals and health systems operate daily to serve the needs of their communities,” AHA Executive Vice President Tom Nickels said in a statement. “In 2015, Congress clearly intended to provide current off-campus hospital clinics with the existing outpatient payment rate in recognition of the critical role they play in their communities. But CMS’s proposal runs counter to this and will instead impede access to care for the most vulnerable patients.”
The OPPS/ASC update also includes proposals to expand the list of covered surgical procedures that can be performed in an ASC, a move that Ms. Verma said would “provide patients with more choices and options for lower-priced care.”
“For CY 2019, CMS is proposing to allow certain CPT codes outside of the surgical code range that directly crosswalk or are clinically similar to procedures within the CPT surgical code range to be included on the [covered procedure list] and is proposing to add certain cardiovascular codes to the ASC [covered procedure list] as a result,” the CMS fact sheet notes.
Another change proposed by CMS relates to how ASC reimbursement rates are updated. They have been based on the consumer price index-urban, which has resulted in a decline in ASC payments relative to hospitals for the same service. For 2019-2023, CMS proposes to use the hospital market basket instead, which will help promote site neutrality between hospitals and ASCs. The AGA applauds this proposal, and has been working for it with the ACG and ASGE for nearly a decade.
In addition, the OPPS is seeking feedback on a number of topics.
One is related to price transparency. The agency is asking “whether providers and suppliers can and should be required to inform patients about charges and payment information for healthcare services and out-of-pocket costs, what data elements the public would find most useful, and what other charges are needed to empower patients,” according to the fact sheet.
Finally, the agency is seeking more information on solutions to better promote interoperability.
CMS proposal to level E/M payments raises concerns
Citing the need to reduce paperwork hassles, officials at the Centers for Medicare & Medicaid Services are proposing to flatten the payment for evaluation and management (E/M) visits coded at levels 2-5.
The CMS outlined how the proposal would affect payment using 2018 rates to model the change. The proposal would set the payment rate for level 1 E/M office visits for new patients at $44, down from the $45 using the current methodology. Levels 2-5 would receive $135. Currently, payments for level 2 visits are set at $76, level 3 at $110, level 4 at $167, and level 5 at $211.
For office visits with established patients, the proposed rate would be $24, up from the current payment of $22 for a level 1 visit. Levels 2-5 would receive $93. Under the current methodology, payments for level 2 visits are set at $45, level 3 at $74, level 4 at $109, and level 5 at $148.
The change also comes with a reduced documentation burden, so the same documentation is needed regardless of which level between 2 and 5 the office visit is, a move that is expected to save time.
The CMS outlined its vision for changes to the E/M payment in the proposed update to the 2019 Medicare physician fee schedule. Comments on the proposal are due Sept. 10, 2018.
The agency estimated that for most specialties, there would be minimal effect on this proposed change. However, for 10 specialties, payment reductions could result from this change. The proposal is raising concerns, particularly from those who stand to see their pay reduced.
CMS officials estimate the proposal would save time. CMS Administrator Seema Verma said that the documentation change would result in an additional 51 hours for patient care per clinician per year.
“The agency has clearly heard from physicians about the need to reduce administrative burdens for physicians,” stated Lisa Gangarosa, MD, AGAF, chair, AGA Government Affairs Committee. “In that regard, CMS should be commended. Unfortunately, in their efforts to reduce burden, CMS has proposed changes that drastically undervalue the care gastroenterologists and hepatologists provide to patients with inflammatory bowel disease, motility disorders, chronic liver disease and other complex gastrointestinal diseases.”
Angus B. Worthing, MD, chair of the American College of Rheumatology’s Committee on Government Affairs, said he was doubtful that any increase in volume would offset the losses from the proposed flat payment across levels 2-5 E/M visits, especially if the pay decrease results in access issues.
SOURCE: CMS proposed rule, CMS-1693-P.
On July 12, 2018, CMS published a set of “proposed rules” that will have substantial impact on your practice. CMS released a 665-page document with 26 proposed changes in Medicare. A public comment period is open until Sept. 10, 2018. Final rules will be published in the fall with implementation expected in January 2019.

Medicare proposes to reduce the number of E/M coding levels to two (from five: these relate to current CPT codes 99201-99205 and 99211-99215), with documentation requirements reduced to those required for current level 2. If you tend to bill levels 4-5, your bottom line will be affected.
CMS wants to eliminate site-of-service differences in both clinic and ASC payments. This will modify the financial advantages gained by practices who sold their centers to hospital systems and for health systems that have HOPD endoscopy centers and clinics.
Endoscopy with biopsy and colonoscopy with polypectomy were again identified as being potentially overvalued and thus may trigger a re-analysis.
A policy change announced recently by CMS would allow Medicare Advantage plans to establish sequence requirements (step therapy) for medical therapies, including biologics.
While community practices clearly will be affected by these changes, the financial pressures on academic medical centers will be immense. AMC’s have high fixed costs and deteriorating clinical margins. Clinical revenue supports not only clinical enterprises (including faculty salaries) but also a large portion of research and education costs. Loss of 340b pharmacy income, the more government payers, CMS regulations and potential penalties, and narrowing clinical networks all have reduced revenue for many AMCs. Adding these proposed rule changes will send many AMCs further into negative margins: This will affect the training of our next-generation leaders and discoveries of new science.
John I. Allen, MD, MBA, AGAF, professor of medicine, division of gastroenterology, University of Michigan School of Medicine, Ann Arbor. He reported no conflicts.
On July 12, 2018, CMS published a set of “proposed rules” that will have substantial impact on your practice. CMS released a 665-page document with 26 proposed changes in Medicare. A public comment period is open until Sept. 10, 2018. Final rules will be published in the fall with implementation expected in January 2019.
Medicare proposes to reduce the number of E/M coding levels to two (from five: these relate to current CPT codes 99201-99205 and 99211-99215), with documentation requirements reduced to those required for current level 2. If you tend to bill levels 4-5, your bottom line will be affected.
CMS wants to eliminate site-of-service differences in both clinic and ASC payments. This will modify the financial advantages gained by practices who sold their centers to hospital systems and for health systems that have HOPD endoscopy centers and clinics.
Endoscopy with biopsy and colonoscopy with polypectomy were again identified as being potentially overvalued and thus may trigger a re-analysis.
A policy change announced recently by CMS would allow Medicare Advantage plans to establish sequence requirements (step therapy) for medical therapies, including biologics.
While community practices clearly will be affected by these changes, the financial pressures on academic medical centers will be immense. AMC’s have high fixed costs and deteriorating clinical margins. Clinical revenue supports not only clinical enterprises (including faculty salaries) but also a large portion of research and education costs. Loss of 340b pharmacy income, the more government payers, CMS regulations and potential penalties, and narrowing clinical networks all have reduced revenue for many AMCs. Adding these proposed rule changes will send many AMCs further into negative margins: This will affect the training of our next-generation leaders and discoveries of new science.
John I. Allen, MD, MBA, AGAF, professor of medicine, division of gastroenterology, University of Michigan School of Medicine, Ann Arbor. He reported no conflicts.
On July 12, 2018, CMS published a set of “proposed rules” that will have substantial impact on your practice. CMS released a 665-page document with 26 proposed changes in Medicare. A public comment period is open until Sept. 10, 2018. Final rules will be published in the fall with implementation expected in January 2019.
Medicare proposes to reduce the number of E/M coding levels to two (from five: these relate to current CPT codes 99201-99205 and 99211-99215), with documentation requirements reduced to those required for current level 2. If you tend to bill levels 4-5, your bottom line will be affected.
CMS wants to eliminate site-of-service differences in both clinic and ASC payments. This will modify the financial advantages gained by practices who sold their centers to hospital systems and for health systems that have HOPD endoscopy centers and clinics.
Endoscopy with biopsy and colonoscopy with polypectomy were again identified as being potentially overvalued and thus may trigger a re-analysis.
A policy change announced recently by CMS would allow Medicare Advantage plans to establish sequence requirements (step therapy) for medical therapies, including biologics.
While community practices clearly will be affected by these changes, the financial pressures on academic medical centers will be immense. AMC’s have high fixed costs and deteriorating clinical margins. Clinical revenue supports not only clinical enterprises (including faculty salaries) but also a large portion of research and education costs. Loss of 340b pharmacy income, the more government payers, CMS regulations and potential penalties, and narrowing clinical networks all have reduced revenue for many AMCs. Adding these proposed rule changes will send many AMCs further into negative margins: This will affect the training of our next-generation leaders and discoveries of new science.
John I. Allen, MD, MBA, AGAF, professor of medicine, division of gastroenterology, University of Michigan School of Medicine, Ann Arbor. He reported no conflicts.
Citing the need to reduce paperwork hassles, officials at the Centers for Medicare & Medicaid Services are proposing to flatten the payment for evaluation and management (E/M) visits coded at levels 2-5.
The CMS outlined how the proposal would affect payment using 2018 rates to model the change. The proposal would set the payment rate for level 1 E/M office visits for new patients at $44, down from the $45 using the current methodology. Levels 2-5 would receive $135. Currently, payments for level 2 visits are set at $76, level 3 at $110, level 4 at $167, and level 5 at $211.
For office visits with established patients, the proposed rate would be $24, up from the current payment of $22 for a level 1 visit. Levels 2-5 would receive $93. Under the current methodology, payments for level 2 visits are set at $45, level 3 at $74, level 4 at $109, and level 5 at $148.
The change also comes with a reduced documentation burden, so the same documentation is needed regardless of which level between 2 and 5 the office visit is, a move that is expected to save time.
The CMS outlined its vision for changes to the E/M payment in the proposed update to the 2019 Medicare physician fee schedule. Comments on the proposal are due Sept. 10, 2018.
The agency estimated that for most specialties, there would be minimal effect on this proposed change. However, for 10 specialties, payment reductions could result from this change. The proposal is raising concerns, particularly from those who stand to see their pay reduced.
CMS officials estimate the proposal would save time. CMS Administrator Seema Verma said that the documentation change would result in an additional 51 hours for patient care per clinician per year.
“The agency has clearly heard from physicians about the need to reduce administrative burdens for physicians,” stated Lisa Gangarosa, MD, AGAF, chair, AGA Government Affairs Committee. “In that regard, CMS should be commended. Unfortunately, in their efforts to reduce burden, CMS has proposed changes that drastically undervalue the care gastroenterologists and hepatologists provide to patients with inflammatory bowel disease, motility disorders, chronic liver disease and other complex gastrointestinal diseases.”
Angus B. Worthing, MD, chair of the American College of Rheumatology’s Committee on Government Affairs, said he was doubtful that any increase in volume would offset the losses from the proposed flat payment across levels 2-5 E/M visits, especially if the pay decrease results in access issues.
SOURCE: CMS proposed rule, CMS-1693-P.
Citing the need to reduce paperwork hassles, officials at the Centers for Medicare & Medicaid Services are proposing to flatten the payment for evaluation and management (E/M) visits coded at levels 2-5.
The CMS outlined how the proposal would affect payment using 2018 rates to model the change. The proposal would set the payment rate for level 1 E/M office visits for new patients at $44, down from the $45 using the current methodology. Levels 2-5 would receive $135. Currently, payments for level 2 visits are set at $76, level 3 at $110, level 4 at $167, and level 5 at $211.
For office visits with established patients, the proposed rate would be $24, up from the current payment of $22 for a level 1 visit. Levels 2-5 would receive $93. Under the current methodology, payments for level 2 visits are set at $45, level 3 at $74, level 4 at $109, and level 5 at $148.
The change also comes with a reduced documentation burden, so the same documentation is needed regardless of which level between 2 and 5 the office visit is, a move that is expected to save time.
The CMS outlined its vision for changes to the E/M payment in the proposed update to the 2019 Medicare physician fee schedule. Comments on the proposal are due Sept. 10, 2018.
The agency estimated that for most specialties, there would be minimal effect on this proposed change. However, for 10 specialties, payment reductions could result from this change. The proposal is raising concerns, particularly from those who stand to see their pay reduced.
CMS officials estimate the proposal would save time. CMS Administrator Seema Verma said that the documentation change would result in an additional 51 hours for patient care per clinician per year.
“The agency has clearly heard from physicians about the need to reduce administrative burdens for physicians,” stated Lisa Gangarosa, MD, AGAF, chair, AGA Government Affairs Committee. “In that regard, CMS should be commended. Unfortunately, in their efforts to reduce burden, CMS has proposed changes that drastically undervalue the care gastroenterologists and hepatologists provide to patients with inflammatory bowel disease, motility disorders, chronic liver disease and other complex gastrointestinal diseases.”
Angus B. Worthing, MD, chair of the American College of Rheumatology’s Committee on Government Affairs, said he was doubtful that any increase in volume would offset the losses from the proposed flat payment across levels 2-5 E/M visits, especially if the pay decrease results in access issues.
SOURCE: CMS proposed rule, CMS-1693-P.
Rapid-onset rash in child
A 7-year-old boy was brought to his family physician for evaluation of a mildly pruritic spreading rash. Ten days earlier, the skin eruption had appeared, and he was given a diagnosis of streptococcal pharyngitis, which was confirmed by a throat swab and a positive antistreptolysin O titer. The child had no personal or family history of skin disorders, including eczema or psoriasis. He hadn’t used any topical agents or new medications recently, nor had he been exposed to triggering plants, animals, or chemicals. There was no history of trauma, friction, or rubbing in the area.
Physical examination revealed multiple erythematous, scaly papules and plaques of varying size on the patient’s trunk, arms, and legs (FIGURE). His palms and soles were spared.

WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Guttate psoriasis
A diagnosis of guttate psoriasis was made based on the physical exam findings and the preceding group A beta-hemolytic streptococcal infection.
This condition affects approximately 2% of all patients with psoriasis; it is characterized by the acute onset of multiple erythematosquamous papules and small plaques that look like droplets (“gutta”).1 It tends to affect children and young adults and typically occurs following an acute infection (eg, streptococcal pharyngitis).2,3 In this case, a rapid strep test and throat culture positive for group A Streptococcus supported the diagnosis.
Although this particular phenotype of psoriasis is usually associated with streptococcal infection and mainly occurs in patients with the HLA-Cw6+ allele, the specific immunologic response that causes these skin lesions is poorly understood.4 Antigenic similarities between streptococcal proteins and keratinocyte antigens might explain why the condition is triggered by streptococcal infections.5
Pityriasis rosea and tinea corporis are part of the differential
The differential includes skin conditions such as pityriasis rosea, tinea corporis, varicella, and insect bites.
Pityriasis rosea can manifest as a papulosquamous eruption, but it has an inward-facing scale, called a collarette. The “Christmas tree” pattern on the back that is preceded by a solitary 2- to 10-cm oval, pink, scaly herald patch (in 17%-50% of cases) is key to the diagnosis.6 (For more information, see “Rash on trunk and upper arms.”)
Continue to: Tinea corporis...
Tinea corporis is a dermatophyte infection that causes flat, red, scaly lesions that progress into annular lesions with central clearing or brown discoloration. The plaques can range from a few centimeters to several inches in size, but are always characterized by the slowly advancing border.6
Varicella also affects the trunk and extremities, but a key clinical finding is crops of characteristic lesions, including papules, vesicles, pustules, and crusted lesions in different stages that manifest simultaneously.6
Insect bites usually appear as urticarial papules and plaques associated with outdoor exposure. The lesions are distributed where insects are likely to bite.6
Treat the infection, control the psoriasis
The first-line treatment for streptococcal infection is amoxicillin (50 mg/kg/d [maximum: 1000 mg/d] orally for 10 d) or penicillin G benzathine (for children < 60 lb, 6 × 105 units intramuscularly; children ≥ 60 lb, 1.2 × 106 units intramuscularly).7 For the psoriasis lesions, treatment options include topical glucocorticosteroids, vitamin D derivatives, or combinations of both.5 In most cases, guttate psoriasis completely resolves. However, one-third of children with guttate psoriasis go on to develop plaque psoriasis later in life.8
Our patient was treated with penicillin G benzathine (1.2 × 106 units intramuscularly) and a calcipotriol/betamethasone combination gel. The streptococcal infection and skin lesions completely resolved. No adverse events were reported, and no relapse was observed after 3 months.
CORRESPONDENCE
Rita Matos, MD, Rua Actor Mário Viegas SN Rio Tinto, Portugal; [email protected]
1. Maciejewska-Radomska A, Szczerkowska-Dobosz A, Rebała K, et al. Frequency of streptococcal upper respiratory tract infections and HLA-Cw*06 allele in 70 patients with guttate psoriasis from northern Poland. Postepy Dermatol Alergol. 2015;32:455-458.
2. Garritsen FM, Kraag DE, de Graaf M. Guttate psoriasis triggered by perianal streptococcal infection. Clin Exp Dermatol. 2017;42:536-538.
3. Pfingstler LF, Maroon M, Mowad C. Guttate psoriasis outcomes. Cutis. 2016;97:140-144.
4. Ruiz-Romeu E, Ferran M, Sagristà M, et al. Streptococcus pyogenes-induced cutaneous lymphocyte antigen-positive T cell-dependent epidermal cell activation triggers TH17 responses in patients with guttate psoriasis. J Allergy Clin Immunol. 2016;138:491-499.
5. Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386:983-994.
6. Ely JW, Seabury Stone M. The generalized rash: part I. Differential diagnosis. Am Fam Physician. 2010;81:726-734.
7. Kalra MG, Higgins KE, Perez ED. Common questions about streptococcal pharyngitis. Am Fam Physician. 2016;94:24-31.
8. Martin BA, Chalmers RJ, Telfer NR. How great is the risk of further psoriasis following a single episode of acute guttate psoriasis? Arch Dermatol. 1996;132: 717-718.
A 7-year-old boy was brought to his family physician for evaluation of a mildly pruritic spreading rash. Ten days earlier, the skin eruption had appeared, and he was given a diagnosis of streptococcal pharyngitis, which was confirmed by a throat swab and a positive antistreptolysin O titer. The child had no personal or family history of skin disorders, including eczema or psoriasis. He hadn’t used any topical agents or new medications recently, nor had he been exposed to triggering plants, animals, or chemicals. There was no history of trauma, friction, or rubbing in the area.
Physical examination revealed multiple erythematous, scaly papules and plaques of varying size on the patient’s trunk, arms, and legs (FIGURE). His palms and soles were spared.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Guttate psoriasis
A diagnosis of guttate psoriasis was made based on the physical exam findings and the preceding group A beta-hemolytic streptococcal infection.
This condition affects approximately 2% of all patients with psoriasis; it is characterized by the acute onset of multiple erythematosquamous papules and small plaques that look like droplets (“gutta”).1 It tends to affect children and young adults and typically occurs following an acute infection (eg, streptococcal pharyngitis).2,3 In this case, a rapid strep test and throat culture positive for group A Streptococcus supported the diagnosis.
Although this particular phenotype of psoriasis is usually associated with streptococcal infection and mainly occurs in patients with the HLA-Cw6+ allele, the specific immunologic response that causes these skin lesions is poorly understood.4 Antigenic similarities between streptococcal proteins and keratinocyte antigens might explain why the condition is triggered by streptococcal infections.5
Pityriasis rosea and tinea corporis are part of the differential
The differential includes skin conditions such as pityriasis rosea, tinea corporis, varicella, and insect bites.
Pityriasis rosea can manifest as a papulosquamous eruption, but it has an inward-facing scale, called a collarette. The “Christmas tree” pattern on the back that is preceded by a solitary 2- to 10-cm oval, pink, scaly herald patch (in 17%-50% of cases) is key to the diagnosis.6 (For more information, see “Rash on trunk and upper arms.”)
Continue to: Tinea corporis...
Tinea corporis is a dermatophyte infection that causes flat, red, scaly lesions that progress into annular lesions with central clearing or brown discoloration. The plaques can range from a few centimeters to several inches in size, but are always characterized by the slowly advancing border.6
Varicella also affects the trunk and extremities, but a key clinical finding is crops of characteristic lesions, including papules, vesicles, pustules, and crusted lesions in different stages that manifest simultaneously.6
Insect bites usually appear as urticarial papules and plaques associated with outdoor exposure. The lesions are distributed where insects are likely to bite.6
Treat the infection, control the psoriasis
The first-line treatment for streptococcal infection is amoxicillin (50 mg/kg/d [maximum: 1000 mg/d] orally for 10 d) or penicillin G benzathine (for children < 60 lb, 6 × 105 units intramuscularly; children ≥ 60 lb, 1.2 × 106 units intramuscularly).7 For the psoriasis lesions, treatment options include topical glucocorticosteroids, vitamin D derivatives, or combinations of both.5 In most cases, guttate psoriasis completely resolves. However, one-third of children with guttate psoriasis go on to develop plaque psoriasis later in life.8
Our patient was treated with penicillin G benzathine (1.2 × 106 units intramuscularly) and a calcipotriol/betamethasone combination gel. The streptococcal infection and skin lesions completely resolved. No adverse events were reported, and no relapse was observed after 3 months.
CORRESPONDENCE
Rita Matos, MD, Rua Actor Mário Viegas SN Rio Tinto, Portugal; [email protected]
A 7-year-old boy was brought to his family physician for evaluation of a mildly pruritic spreading rash. Ten days earlier, the skin eruption had appeared, and he was given a diagnosis of streptococcal pharyngitis, which was confirmed by a throat swab and a positive antistreptolysin O titer. The child had no personal or family history of skin disorders, including eczema or psoriasis. He hadn’t used any topical agents or new medications recently, nor had he been exposed to triggering plants, animals, or chemicals. There was no history of trauma, friction, or rubbing in the area.
Physical examination revealed multiple erythematous, scaly papules and plaques of varying size on the patient’s trunk, arms, and legs (FIGURE). His palms and soles were spared.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Guttate psoriasis
A diagnosis of guttate psoriasis was made based on the physical exam findings and the preceding group A beta-hemolytic streptococcal infection.
This condition affects approximately 2% of all patients with psoriasis; it is characterized by the acute onset of multiple erythematosquamous papules and small plaques that look like droplets (“gutta”).1 It tends to affect children and young adults and typically occurs following an acute infection (eg, streptococcal pharyngitis).2,3 In this case, a rapid strep test and throat culture positive for group A Streptococcus supported the diagnosis.
Although this particular phenotype of psoriasis is usually associated with streptococcal infection and mainly occurs in patients with the HLA-Cw6+ allele, the specific immunologic response that causes these skin lesions is poorly understood.4 Antigenic similarities between streptococcal proteins and keratinocyte antigens might explain why the condition is triggered by streptococcal infections.5
Pityriasis rosea and tinea corporis are part of the differential
The differential includes skin conditions such as pityriasis rosea, tinea corporis, varicella, and insect bites.
Pityriasis rosea can manifest as a papulosquamous eruption, but it has an inward-facing scale, called a collarette. The “Christmas tree” pattern on the back that is preceded by a solitary 2- to 10-cm oval, pink, scaly herald patch (in 17%-50% of cases) is key to the diagnosis.6 (For more information, see “Rash on trunk and upper arms.”)
Continue to: Tinea corporis...
Tinea corporis is a dermatophyte infection that causes flat, red, scaly lesions that progress into annular lesions with central clearing or brown discoloration. The plaques can range from a few centimeters to several inches in size, but are always characterized by the slowly advancing border.6
Varicella also affects the trunk and extremities, but a key clinical finding is crops of characteristic lesions, including papules, vesicles, pustules, and crusted lesions in different stages that manifest simultaneously.6
Insect bites usually appear as urticarial papules and plaques associated with outdoor exposure. The lesions are distributed where insects are likely to bite.6
Treat the infection, control the psoriasis
The first-line treatment for streptococcal infection is amoxicillin (50 mg/kg/d [maximum: 1000 mg/d] orally for 10 d) or penicillin G benzathine (for children < 60 lb, 6 × 105 units intramuscularly; children ≥ 60 lb, 1.2 × 106 units intramuscularly).7 For the psoriasis lesions, treatment options include topical glucocorticosteroids, vitamin D derivatives, or combinations of both.5 In most cases, guttate psoriasis completely resolves. However, one-third of children with guttate psoriasis go on to develop plaque psoriasis later in life.8
Our patient was treated with penicillin G benzathine (1.2 × 106 units intramuscularly) and a calcipotriol/betamethasone combination gel. The streptococcal infection and skin lesions completely resolved. No adverse events were reported, and no relapse was observed after 3 months.
CORRESPONDENCE
Rita Matos, MD, Rua Actor Mário Viegas SN Rio Tinto, Portugal; [email protected]
1. Maciejewska-Radomska A, Szczerkowska-Dobosz A, Rebała K, et al. Frequency of streptococcal upper respiratory tract infections and HLA-Cw*06 allele in 70 patients with guttate psoriasis from northern Poland. Postepy Dermatol Alergol. 2015;32:455-458.
2. Garritsen FM, Kraag DE, de Graaf M. Guttate psoriasis triggered by perianal streptococcal infection. Clin Exp Dermatol. 2017;42:536-538.
3. Pfingstler LF, Maroon M, Mowad C. Guttate psoriasis outcomes. Cutis. 2016;97:140-144.
4. Ruiz-Romeu E, Ferran M, Sagristà M, et al. Streptococcus pyogenes-induced cutaneous lymphocyte antigen-positive T cell-dependent epidermal cell activation triggers TH17 responses in patients with guttate psoriasis. J Allergy Clin Immunol. 2016;138:491-499.
5. Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386:983-994.
6. Ely JW, Seabury Stone M. The generalized rash: part I. Differential diagnosis. Am Fam Physician. 2010;81:726-734.
7. Kalra MG, Higgins KE, Perez ED. Common questions about streptococcal pharyngitis. Am Fam Physician. 2016;94:24-31.
8. Martin BA, Chalmers RJ, Telfer NR. How great is the risk of further psoriasis following a single episode of acute guttate psoriasis? Arch Dermatol. 1996;132: 717-718.
1. Maciejewska-Radomska A, Szczerkowska-Dobosz A, Rebała K, et al. Frequency of streptococcal upper respiratory tract infections and HLA-Cw*06 allele in 70 patients with guttate psoriasis from northern Poland. Postepy Dermatol Alergol. 2015;32:455-458.
2. Garritsen FM, Kraag DE, de Graaf M. Guttate psoriasis triggered by perianal streptococcal infection. Clin Exp Dermatol. 2017;42:536-538.
3. Pfingstler LF, Maroon M, Mowad C. Guttate psoriasis outcomes. Cutis. 2016;97:140-144.
4. Ruiz-Romeu E, Ferran M, Sagristà M, et al. Streptococcus pyogenes-induced cutaneous lymphocyte antigen-positive T cell-dependent epidermal cell activation triggers TH17 responses in patients with guttate psoriasis. J Allergy Clin Immunol. 2016;138:491-499.
5. Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386:983-994.
6. Ely JW, Seabury Stone M. The generalized rash: part I. Differential diagnosis. Am Fam Physician. 2010;81:726-734.
7. Kalra MG, Higgins KE, Perez ED. Common questions about streptococcal pharyngitis. Am Fam Physician. 2016;94:24-31.
8. Martin BA, Chalmers RJ, Telfer NR. How great is the risk of further psoriasis following a single episode of acute guttate psoriasis? Arch Dermatol. 1996;132: 717-718.

Strides in digestive cancer research: Two research projects to note
The AGA Research Foundation Research Awards Program includes two grants dedicated to digestive cancer research: the AGA–Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer and the AGA–R. Robert & Sally Funderburg Research Award in Gastric Cancer.
Continue reading to learn about the novel research projects being conducted by our 2018 digestive cancer grant recipients.
AGA–Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer
Ravikanth Maddipati, MD
University of Pennsylvania Hospital System, Philadelphia
Dr. Maddipati’s research focuses on understanding and treating metastatic disease in pancreatic cancer. With this grant, Dr. Maddipati will use advanced lineage-traced mouse models and innovative bioengineering approaches to identify the molecular pathways involved in tumor cell cooperation and define the role of circulating tumor cell-clusters in pancreatic cancer progression. This work will lead to a noninvasive method for monitoring disease progression and response to treatment in pancreatic cancer patients.
AGA’s take: Pancreatic cancer, namely pancreatic ductal adenocarcinoma, is one of the deadliest cancers in the U.S. The AGA Research Foundation is pleased to fund Dr. Maddipati’s research. As a physician-scientist, he is in a unique position to translate findings from basic research, using preclinical models, to develop improved approaches to treating patients with pancreatic cancer.
AGA–R. Robert & Sally Funderburg Research Award in Gastric Cancer
Jingwu Xie, PhD
Indiana University, Indianapolis
Dr. Xie’s research focuses on drug resistance in gastric cancer. His team recently had a monumental discovery — activated hedgehog signaling, via GLI1 and GLI2 gene up-regulation, is responsible for drug resistance in gastric cancer. Dr. Xie’s AGA-funded research will work to identify novel ways to sensitize gastric cancer cells to drug treatment by suppressing GLI1 and GLI2 activity.
AGA’s take: Gastric cancer is a very underfunded area of research in the U.S., and with limited treatment options for patients, there is a great need for novel research projects. The AGA Research Foundation is proud to fund Dr. Xie’s research, which we believe has the potential to translate into a new treatment that will improve outcomes for gastric cancer patients.
To see the full class of 2018 AGA Research Foundation awardees, visit the Meet Our Awardees section of our website, www.gastro.org/foundation-awardees.
The AGA Research Foundation Research Awards Program includes two grants dedicated to digestive cancer research: the AGA–Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer and the AGA–R. Robert & Sally Funderburg Research Award in Gastric Cancer.
Continue reading to learn about the novel research projects being conducted by our 2018 digestive cancer grant recipients.
AGA–Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer
Ravikanth Maddipati, MD
University of Pennsylvania Hospital System, Philadelphia
Dr. Maddipati’s research focuses on understanding and treating metastatic disease in pancreatic cancer. With this grant, Dr. Maddipati will use advanced lineage-traced mouse models and innovative bioengineering approaches to identify the molecular pathways involved in tumor cell cooperation and define the role of circulating tumor cell-clusters in pancreatic cancer progression. This work will lead to a noninvasive method for monitoring disease progression and response to treatment in pancreatic cancer patients.
AGA’s take: Pancreatic cancer, namely pancreatic ductal adenocarcinoma, is one of the deadliest cancers in the U.S. The AGA Research Foundation is pleased to fund Dr. Maddipati’s research. As a physician-scientist, he is in a unique position to translate findings from basic research, using preclinical models, to develop improved approaches to treating patients with pancreatic cancer.
AGA–R. Robert & Sally Funderburg Research Award in Gastric Cancer
Jingwu Xie, PhD
Indiana University, Indianapolis
Dr. Xie’s research focuses on drug resistance in gastric cancer. His team recently had a monumental discovery — activated hedgehog signaling, via GLI1 and GLI2 gene up-regulation, is responsible for drug resistance in gastric cancer. Dr. Xie’s AGA-funded research will work to identify novel ways to sensitize gastric cancer cells to drug treatment by suppressing GLI1 and GLI2 activity.
AGA’s take: Gastric cancer is a very underfunded area of research in the U.S., and with limited treatment options for patients, there is a great need for novel research projects. The AGA Research Foundation is proud to fund Dr. Xie’s research, which we believe has the potential to translate into a new treatment that will improve outcomes for gastric cancer patients.
To see the full class of 2018 AGA Research Foundation awardees, visit the Meet Our Awardees section of our website, www.gastro.org/foundation-awardees.
The AGA Research Foundation Research Awards Program includes two grants dedicated to digestive cancer research: the AGA–Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer and the AGA–R. Robert & Sally Funderburg Research Award in Gastric Cancer.
Continue reading to learn about the novel research projects being conducted by our 2018 digestive cancer grant recipients.
AGA–Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer
Ravikanth Maddipati, MD
University of Pennsylvania Hospital System, Philadelphia
Dr. Maddipati’s research focuses on understanding and treating metastatic disease in pancreatic cancer. With this grant, Dr. Maddipati will use advanced lineage-traced mouse models and innovative bioengineering approaches to identify the molecular pathways involved in tumor cell cooperation and define the role of circulating tumor cell-clusters in pancreatic cancer progression. This work will lead to a noninvasive method for monitoring disease progression and response to treatment in pancreatic cancer patients.
AGA’s take: Pancreatic cancer, namely pancreatic ductal adenocarcinoma, is one of the deadliest cancers in the U.S. The AGA Research Foundation is pleased to fund Dr. Maddipati’s research. As a physician-scientist, he is in a unique position to translate findings from basic research, using preclinical models, to develop improved approaches to treating patients with pancreatic cancer.
AGA–R. Robert & Sally Funderburg Research Award in Gastric Cancer
Jingwu Xie, PhD
Indiana University, Indianapolis
Dr. Xie’s research focuses on drug resistance in gastric cancer. His team recently had a monumental discovery — activated hedgehog signaling, via GLI1 and GLI2 gene up-regulation, is responsible for drug resistance in gastric cancer. Dr. Xie’s AGA-funded research will work to identify novel ways to sensitize gastric cancer cells to drug treatment by suppressing GLI1 and GLI2 activity.
AGA’s take: Gastric cancer is a very underfunded area of research in the U.S., and with limited treatment options for patients, there is a great need for novel research projects. The AGA Research Foundation is proud to fund Dr. Xie’s research, which we believe has the potential to translate into a new treatment that will improve outcomes for gastric cancer patients.
To see the full class of 2018 AGA Research Foundation awardees, visit the Meet Our Awardees section of our website, www.gastro.org/foundation-awardees.
Rivaroxaban superior to aspirin for extended VTE treatment
Both low-dose and full-dose rivaroxaban had superior benefit-risk profiles for extended venous thromboembolism (VTE) treatment compared with aspirin, according to results published in Thrombosis Research.

Incidences of the combined outcome of recurrent VTE and major bleeding were 2.8% and 3.4% lower for patients treated with rivaroxaban at 20 mg and 10 mg, respectively, than for those treated with aspirin, reported Paolo Prandoni, MD, of the department of cardiothoracic and vascular sciences at the University of Padua, Italy, and his coauthors.
Investigators analyzed data from the EINSTEIN-CHOICE trial, a double-blind, randomized study of 3,365 patients aged 18 years or older with deep vein thrombosis or pulmonary embolism who had previously received anticoagulant treatment for 6-12 months. Patients were given either once-daily rivaroxaban at a low dose (10 mg), once-daily rivaroxaban at full dose (20 mg), or once- daily aspirin at a dose of 100 mg.
Benefit and risk were calculated using “excess numbers of events,” or the difference in cumulative incidences in a hypothetical population of 10,000 VTE patients treated for 1 year. Excess numbers of events were defined as the number of patients in this hypothetical population who would experience a particular event when treated with rivaroxaban (at either dose), minus that in the same population treated with aspirin.
The cumulative incidences of recurrent VTE in the full-dose rivaroxaban, low-dose rivaroxaban, and aspirin groups were 1.9%, 1.6%, and 5.0%, respectively. The cumulative incidences of major bleeding in these groups were 0.7%, 0.4% and 0.5%, respectively.
In patients treated with 20 mg of rivaroxaban instead of aspirin, there would be 123 fewer episodes of pulmonary embolism (95% confidence interval, 21-226) and 198 fewer episodes of deep vein thrombosis (95% CI, 62-333).
In patients given 10 mg of rivaroxaban instead of aspirin, there would be 121 fewer episodes of pulmonary embolism (95% CI, 4-238) and 217 fewer episodes of deep vein thrombosis (95% CI, 92-342), Dr. Prandoni and his colleagues wrote.
Net clinical benefit was defined as the composite of symptomatic recurrent VTE and major bleeding events, and occurred in 23 patients in the full-dose rivaroxaban group, 17 patients in the low-dose rivaroxaban group, and 53 patients in the aspirin group.
For 10,000 patients treated for 1 year with rivaroxaban instead of aspirin, there would be 284 fewer net clinical benefit outcomes for the 20-mg dose (95% CI, 106-462) and 339 fewer (95% CI, 165-512) for the 10-mg dose. “Thus, compared with aspirin, one additional symptomatic recurrent VTE or major bleed would be avoided for every 36 or 30 patients treated with rivaroxaban 20 mg or 10 mg, respectively,” the investigators wrote.
The findings indicate that there is “no longer a place” for extended VTE treatment with aspirin, the investigators said.
“Extended anticoagulation with once daily rivaroxaban ... provides a clinically important benefit in terms of reduction in recurrent VTE,” they wrote. “Regardless of which dose is chosen ... rivaroxaban has a favourable benefit-risk profile relative to aspirin.”
Bayer AG funded the study. Dr. Prandoni reported financial relationships with Bayer, Sanofi, Daiichi Sankyo, and Pfizer.
SOURCE: Prandoni P et al. Thromb Res. 2018 Aug;168:121-9.
Both low-dose and full-dose rivaroxaban had superior benefit-risk profiles for extended venous thromboembolism (VTE) treatment compared with aspirin, according to results published in Thrombosis Research.
Incidences of the combined outcome of recurrent VTE and major bleeding were 2.8% and 3.4% lower for patients treated with rivaroxaban at 20 mg and 10 mg, respectively, than for those treated with aspirin, reported Paolo Prandoni, MD, of the department of cardiothoracic and vascular sciences at the University of Padua, Italy, and his coauthors.
Investigators analyzed data from the EINSTEIN-CHOICE trial, a double-blind, randomized study of 3,365 patients aged 18 years or older with deep vein thrombosis or pulmonary embolism who had previously received anticoagulant treatment for 6-12 months. Patients were given either once-daily rivaroxaban at a low dose (10 mg), once-daily rivaroxaban at full dose (20 mg), or once- daily aspirin at a dose of 100 mg.
Benefit and risk were calculated using “excess numbers of events,” or the difference in cumulative incidences in a hypothetical population of 10,000 VTE patients treated for 1 year. Excess numbers of events were defined as the number of patients in this hypothetical population who would experience a particular event when treated with rivaroxaban (at either dose), minus that in the same population treated with aspirin.
The cumulative incidences of recurrent VTE in the full-dose rivaroxaban, low-dose rivaroxaban, and aspirin groups were 1.9%, 1.6%, and 5.0%, respectively. The cumulative incidences of major bleeding in these groups were 0.7%, 0.4% and 0.5%, respectively.
In patients treated with 20 mg of rivaroxaban instead of aspirin, there would be 123 fewer episodes of pulmonary embolism (95% confidence interval, 21-226) and 198 fewer episodes of deep vein thrombosis (95% CI, 62-333).
In patients given 10 mg of rivaroxaban instead of aspirin, there would be 121 fewer episodes of pulmonary embolism (95% CI, 4-238) and 217 fewer episodes of deep vein thrombosis (95% CI, 92-342), Dr. Prandoni and his colleagues wrote.
Net clinical benefit was defined as the composite of symptomatic recurrent VTE and major bleeding events, and occurred in 23 patients in the full-dose rivaroxaban group, 17 patients in the low-dose rivaroxaban group, and 53 patients in the aspirin group.
For 10,000 patients treated for 1 year with rivaroxaban instead of aspirin, there would be 284 fewer net clinical benefit outcomes for the 20-mg dose (95% CI, 106-462) and 339 fewer (95% CI, 165-512) for the 10-mg dose. “Thus, compared with aspirin, one additional symptomatic recurrent VTE or major bleed would be avoided for every 36 or 30 patients treated with rivaroxaban 20 mg or 10 mg, respectively,” the investigators wrote.
The findings indicate that there is “no longer a place” for extended VTE treatment with aspirin, the investigators said.
“Extended anticoagulation with once daily rivaroxaban ... provides a clinically important benefit in terms of reduction in recurrent VTE,” they wrote. “Regardless of which dose is chosen ... rivaroxaban has a favourable benefit-risk profile relative to aspirin.”
Bayer AG funded the study. Dr. Prandoni reported financial relationships with Bayer, Sanofi, Daiichi Sankyo, and Pfizer.
SOURCE: Prandoni P et al. Thromb Res. 2018 Aug;168:121-9.
Both low-dose and full-dose rivaroxaban had superior benefit-risk profiles for extended venous thromboembolism (VTE) treatment compared with aspirin, according to results published in Thrombosis Research.
Incidences of the combined outcome of recurrent VTE and major bleeding were 2.8% and 3.4% lower for patients treated with rivaroxaban at 20 mg and 10 mg, respectively, than for those treated with aspirin, reported Paolo Prandoni, MD, of the department of cardiothoracic and vascular sciences at the University of Padua, Italy, and his coauthors.
Investigators analyzed data from the EINSTEIN-CHOICE trial, a double-blind, randomized study of 3,365 patients aged 18 years or older with deep vein thrombosis or pulmonary embolism who had previously received anticoagulant treatment for 6-12 months. Patients were given either once-daily rivaroxaban at a low dose (10 mg), once-daily rivaroxaban at full dose (20 mg), or once- daily aspirin at a dose of 100 mg.
Benefit and risk were calculated using “excess numbers of events,” or the difference in cumulative incidences in a hypothetical population of 10,000 VTE patients treated for 1 year. Excess numbers of events were defined as the number of patients in this hypothetical population who would experience a particular event when treated with rivaroxaban (at either dose), minus that in the same population treated with aspirin.
The cumulative incidences of recurrent VTE in the full-dose rivaroxaban, low-dose rivaroxaban, and aspirin groups were 1.9%, 1.6%, and 5.0%, respectively. The cumulative incidences of major bleeding in these groups were 0.7%, 0.4% and 0.5%, respectively.
In patients treated with 20 mg of rivaroxaban instead of aspirin, there would be 123 fewer episodes of pulmonary embolism (95% confidence interval, 21-226) and 198 fewer episodes of deep vein thrombosis (95% CI, 62-333).
In patients given 10 mg of rivaroxaban instead of aspirin, there would be 121 fewer episodes of pulmonary embolism (95% CI, 4-238) and 217 fewer episodes of deep vein thrombosis (95% CI, 92-342), Dr. Prandoni and his colleagues wrote.
Net clinical benefit was defined as the composite of symptomatic recurrent VTE and major bleeding events, and occurred in 23 patients in the full-dose rivaroxaban group, 17 patients in the low-dose rivaroxaban group, and 53 patients in the aspirin group.
For 10,000 patients treated for 1 year with rivaroxaban instead of aspirin, there would be 284 fewer net clinical benefit outcomes for the 20-mg dose (95% CI, 106-462) and 339 fewer (95% CI, 165-512) for the 10-mg dose. “Thus, compared with aspirin, one additional symptomatic recurrent VTE or major bleed would be avoided for every 36 or 30 patients treated with rivaroxaban 20 mg or 10 mg, respectively,” the investigators wrote.
The findings indicate that there is “no longer a place” for extended VTE treatment with aspirin, the investigators said.
“Extended anticoagulation with once daily rivaroxaban ... provides a clinically important benefit in terms of reduction in recurrent VTE,” they wrote. “Regardless of which dose is chosen ... rivaroxaban has a favourable benefit-risk profile relative to aspirin.”
Bayer AG funded the study. Dr. Prandoni reported financial relationships with Bayer, Sanofi, Daiichi Sankyo, and Pfizer.
SOURCE: Prandoni P et al. Thromb Res. 2018 Aug;168:121-9.
FROM THROMBOSIS RESEARCH
Key clinical point:
Major finding: Incidences of the combined outcome of recurrent VTE and major bleeding were 2.8% and 3.4% lower in the rivaroxaban 20-mg and 10-mg groups, respectively, than in the aspirin group.
Study details: Analysis of data from 3,365 patients in the EINSTEIN-CHOICE trial, a double-blind, randomized study comparing rivaroxaban with aspirin for extended treatment of VTE.
Disclosures: Bayer AG funded the study. Dr. Prandoni disclosed financial relationships with Bayer, Sanofi, Daiichi Sankyo, and Pfizer.
Source: Prandoni P et al. Thromb Res. 2018 Aug;168:121-9.
Headless Compression Screw Fixation of Vertical Medial Malleolus Fractures is Superior to Unicortical Screw Fixation
ABSTRACT
This study is the first biomechanical research of headless compression screws for fixation of vertical shear fractures of the medial malleolus, a promising alternative that potentially offers several advantages for fixation.
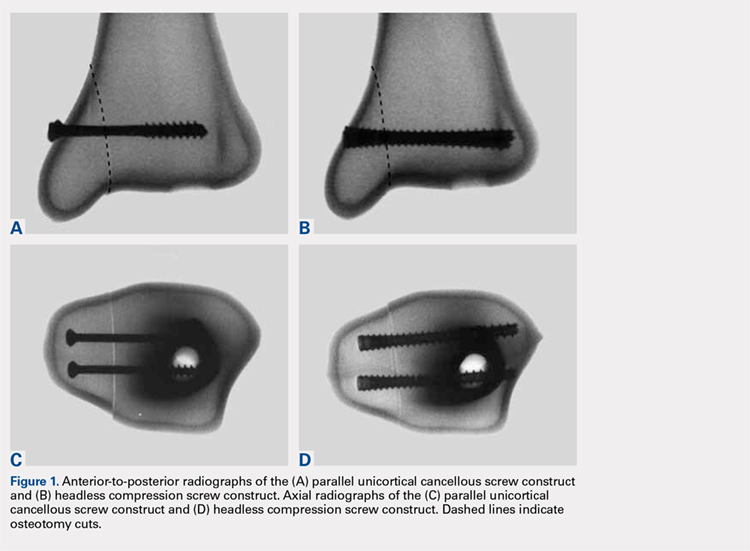
Vertical shear fractures were simulated by osteotomies in 20 synthetic distal tibiae. Models were randomly assigned to fixation with either 2 parallel cancellous screws or 2 parallel Acutrak 2 headless compression screws (Acumed). Specimens were subjected to offset axial loading to simulate supination-adduction loading and tracked using high-resolution video.
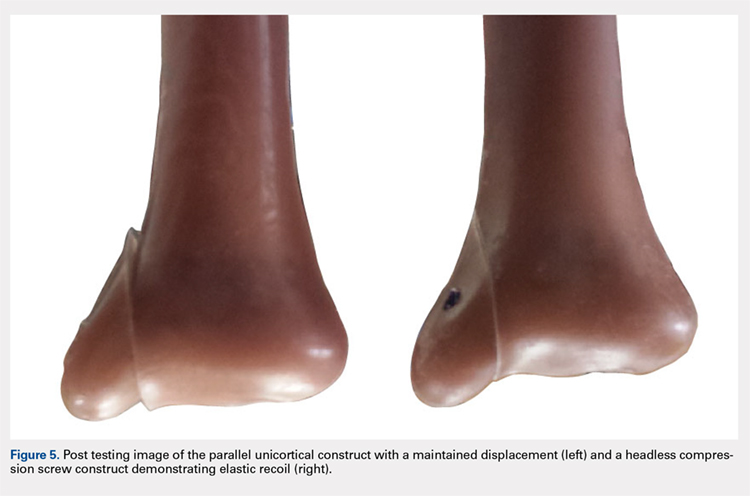
The headless compression screw construct was significantly stiffer (P < .0001) (360 ± 131 N/mm) than the partially threaded cancellous screws (180 ± 48 N/mm) and demonstrated a significantly increased (P < .0001) mean load to clinical failure (719 ± 91 N vs 343 ± 83 N). When specimens were displaced to 6 mm and allowed to relax, the headless compression screw constructs demonstrated an elastic recoil and were reduced to the pretesting fragment alignment, whereas the parallel cancellous screw constructs remained displaced.
Along with the headless design that may decrease soft tissue irritation, the increased stiffness and elastic recoil of the headless compression screw construct offers improved fixation of medial malleolus vertical shear fractures over the traditional methods.
Continue to: Headless compressions screws...
Headless compressions screws are cannulated tapered titanium screws with variable thread pitch angle, allowing a fully threaded screw to apply compression along its entire length. These screws have been most commonly used for scaphoid fractures1 but have also been studied in fractures of small bones, such as capitellum, midfoot, and talar neck,2-4 and arthrodesis in the foot, ankle, and hand.5-7 Headless compression screws have been found to produce equivalent fragment compression to partially threaded cancellous screws while allowing less fragment displacement.8,9 The lack of a head may decrease soft tissue irritation compared with the partially threaded cancellous screws. Finally, headless compression screws are independent of cortical integrity, as the entire length of the screw features a wide thread diameter to capture cancellous bone in the proximal fragment, unlike partially threaded cancellous screws, which only possess a thread purchase in the distal fragment and depend on an intact cortex.
Vertical shear fractures of the medial malleolus occur through the supination-adduction of the talus exerted onto the articular surface of the medial malleolus.10 Optimal fixation of these fractures must be sufficient to maintain stable anatomic reduction of the ankle joint articular surface, allowing early range of motion, maintaining congruency of the ankle joint, and decreasing the risk of future post-traumatic arthritis to maximize functional outcome.11
A wide variety of techniques are available for fixation of these fractures, including various configurations of cortical screws, cancellous screws, tension bands, and antiglide plates. Clinically, 2 parallel 4.0-mm partially threaded cancellous screws are most often used. Limited evidence indicates that headless compression screws may be a viable option for fixation of medial malleolus fractures. One case reports the use of a headless compression screw for a horizontal medial malleolar fracture,12 and a small retrospective case series that used headless compression screws for all medial malleolar fractures showed satisfactory outcomes, a high union rate, and low patient-reported pain.13
We evaluate the stiffness, force to 2-mm displacement of the joint surface, and elastic properties of these 2 different constructs in vertical medial malleolar fractures in synthetic distal tibiae. We hypothesize that the parallel headless compression screw fixation will be stiffer and require more force to 2-mm displacement than parallel unicortical cancellous screw fixation.
MATERIALS AND METHODS
Identical vertical osteotomies (17.5 mm) were made from the medial border of the medial malleolus using a custom jig in 20 left 4th-generation composite synthetic distal tibiae (Sawbones, Pacific Research Labs; Model No. 3401) to simulate an Orthopaedic Trauma Association type 44-A2.3 fracture. The tibiae were then cut 18 cm from the tibial plafond and randomized to 2 fixation groups (n = 10 specimens for each group): parallel unicortical screw fixation or parallel unicortical headless compression screw fixation (Figures 1A-1D). Custom polymethylmethacrylate jigs were used to reproducibly drill identical holes with a 3.2-mm drill for the parallel unicortical screw construct and the drill bits provided by the Acutrak 2 Headless Compression Screw System (Acumed). The parallel unicortical screw construct consisted of 2 parallel 4.0-mm-diameter, 40-mm partially threaded cancellous screws (Depuy Synthes), and the headless compression fixation construct consisted of 2 parallel 4.7-mm-diameter, 45-mm titanium Acutrak 2 screws parallel to each other in the transverse plane. The Acutrak screws were placed per manufacturer instructions by first drilling with the Acutrak 2-4.7 Long Drill bit (Acumed), followed by the Acutrak 2-4.7 Profile Drill bit for the near cortex.
Continue to: Specimens...
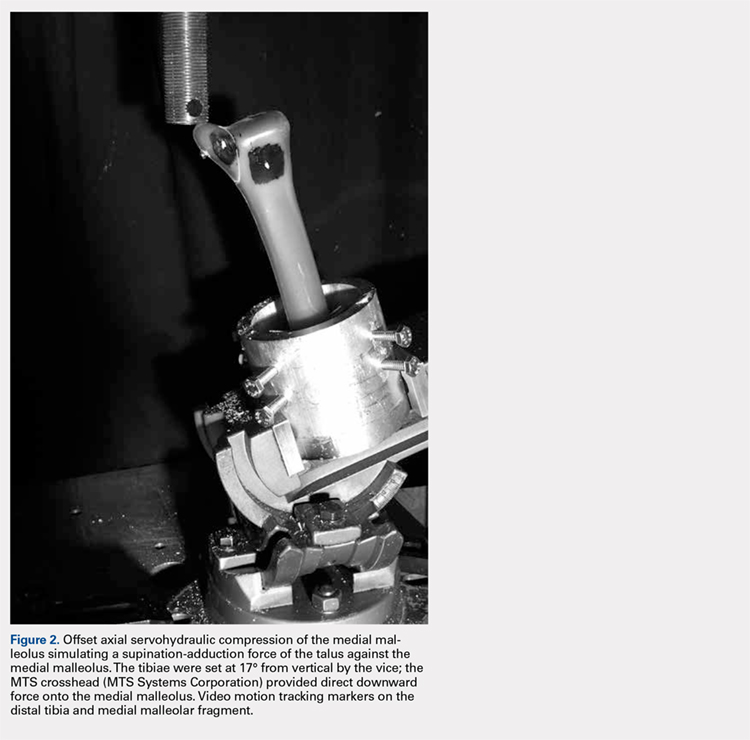
Specimens were fixed to the base of a servohydraulic testing machine (Model 809, MTS Systems Corporation) with an axial-torsional load transducer (Model No. 662.20-01; Axial capacity of 250 kg, torsional capacity 2.88 kg-m; MTS Systems Corporation). The specimens were set in a vice tilted at 17° in the coronal plane to allow the MTS crosshead to apply an offset axial load simulating supination-adduction loading, which has been described previously (Figure 2).14,15 Load was applied to the inferolateral articular surface of the medial malleolus at 1 mm/s to a crosshead displacement of 6 mm and then cycled back to 0 mm. Load and axial displacement were measured at 60 Hz. The markers on the distal tibia and medial malleolus fracture fragment were tracked using high-resolution video (Fastcam PCI, Photron USA Inc). The motion of the video markers was determined using digitization and motion analysis software (Motus 9, Vicon).
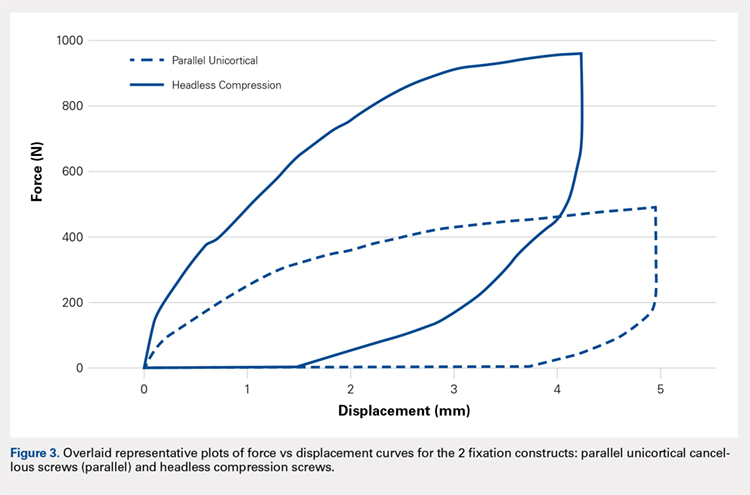
Stiffness was calculated as the slope of the linear portion of the load-displacement curve over a range of 0.5 to 2.0 mm (Figure 3) and reported as mean (standard deviation). The force at 2 mm of fragment displacement was defined as a clinical failure.16,17 Student’s t test was used to determine the difference in construct stiffness and force for 2 mm displacement of the 2 groups. Significance was defined as P < .05. Institutional Review Board approval was not required for this study.
RESULTS
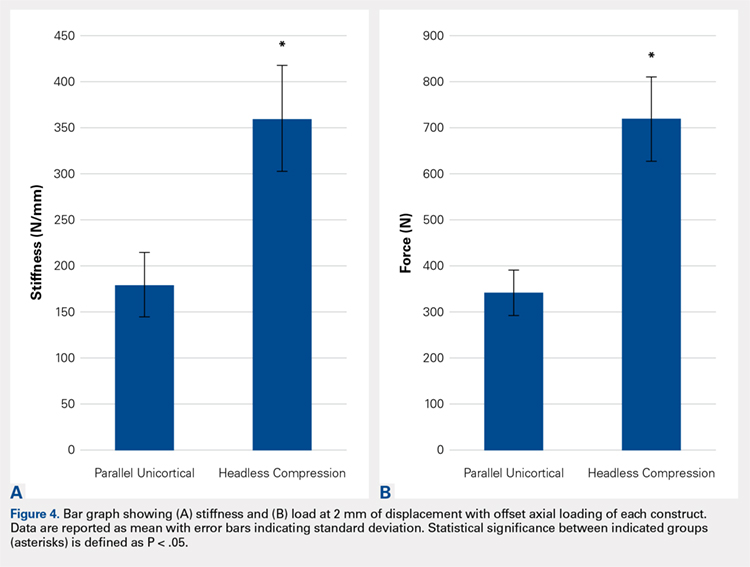
With offset axial testing to simulate supination-adduction force along with video motion analysis, the mean stiffness (± standard deviation) measured 180 ± 48 N/mm for the parallel unicortical screw fixation construct and 360 ± 131 N/mm for the headless compression screw fixation construct (Figure 4A). The headless compression screw fixation construct was over 2 times stiffer than the parallel unicortical construct during initial displacement of the fracture, indicating a statistically significant difference (P < .0001).
The mean force for 2 mm of fracture displacement, defined as clinical failure, reached 342 ± 83 N for the parallel unicortical screw fixation construct and 719 ± 91 N for the headless compression screw fixation construct (Figure 4B). The headless compression screw fixation construct resisted displacement significantly more (P = .0001) than the parallel unicortical screw construct, presenting a 100% increase.
Upon cycling of the servohydraulic testing machine back to 0-mm displacement, the parallel unicortical construct demonstrated no elastic recoil, remaining displaced at 4 mm, whereas the headless compression screw construct rebounded to almost 0-mm displacement, which is well below the clinical definition of fixation failure of 2 mm (Figure 5).
Continue to: Discussion...
DISCUSSION
When subjected to offset axial load, we observed that the headless compression screw construct exhibited significantly increased stiffness and load to 2 mm of displacement compared with a parallel unicortical screw construct. The headless compression screw also demonstrated elastic recoil to almost 0 mm of displacement, which is well below the 2-mm displacement.
We made reproducible fractures and fixation methods in synthetic distal tibiae, which feature less variability in size and quality than the cadaveric bone. Offset axial loading, rather than direct axial loading previously described by Amanatullah and colleagues,18 is the most physiologically relevant mode of force application to simulate the loading of the tauls onto the medial malleolus in the supination-adduction mechanism of injury.
The limitations of this study include the use of synthetic rather than cadaveric bone. Fourth-generation sawbones have been validated as possessing similar biomechanical properties as real bone.7,19 These results may also be inapplicable to osteoporotic bone, which would be significantly less dense than sawbones. This study is also an artificial situation designed to only test construct stiffness and load to clinical failure in a single mode of stress, offset axial loading and neglects other possible modes of force. This testing setup also disregards the structures surrounding the medial malleolus and tibia, including the talus, fibula, or soft tissue attachments, including the deltoid ligament and flexor retinaculum. These results are only relevant immediately after fixation and before bone healing occurs. We also tested the load to clinical failure rather than cyclic loading. Our testing more closely modeled a single traumatic force rather than the considerably smaller stresses that would be repeatedly exerted on the construct over several weeks after fixation in a clinical situation. This research is also not a clinical outcome study, rather, it suggests that headless compression screws are a viable, stronger, and possibly superior method for the initial fixation of vertical medial malleolar fractures.
As the load is offset axial, the larger thread purchase of the headless compression screws may lead to increased pullout strength, possibly increasing headless compression screw construct stiffness. Also, the variable diameter of headless compression screw, which reaches up to 4.7 mm, would increase the stiffness of the construct compared with the diameter of the cancellous screws. The elasticity of the headless compression construct may be because screws are made of titanium rather than stainless steel. Such property and given that the screws are cannulated rather than solid may also play a role, although several studies have shown variable results for cannulated vs solid screws of the same diameter.20,21 The elastic section modulus of both screws would have to be calculated to determine their exact effect on fixation.
CONCLUSION
The headless compression screw construct was found to be stiffer and features a higher load to clinical failure than a parallel unicortical cancellous screw construct for fixation of vertical medial malleolus fractures. Although significantly increased cost occurs with this construct, the headless design may decrease soft tissue irritation, and the elastic recoil of the construct after displacement may decrease clinical failure rates of this fixation method. This condition would eliminate the need for revision surgeries and thus be a cost effective alternative overall.
This paper will be judged for the Resident Writer’s Award.
- Fowler JR, Ilyas AM. Headless compression screw fixation of scaphoid fractures. Hand Clin. 2010;26(3):351-361, vi. doi:10.1016/j.hcl.2010.04.005.
- Karakasli A, Hapa O, Erduran M, Dincer C, Cecen B, Havitcioglu H. Mechanical comparison of headless screw fixation and locking plate fixation for talar neck fractures. J Foot Ankle Surg. 2015;54(5):905-909. doi:10.1053/j.jfas.2015.04.002.
- Elkowitz SJ, Polatsch DB, Egol KA, Kummer FJ, Koval KJ. Capitellum fractures: a biomechanical evaluation of three fixation methods. J Orthop Trauma. 2002;16(7):503-506. doi:10.1097/00005131-200208000-00009.
- Zhang H, Min L, Wang GL, et al. Primary open reduction and internal fixation with headless compression screws in the treatment of Chinese patients with acute Lisfranc joint injuries. J Trauma Acute Care Surg. 2012;72(5):1380-1385. doi:10.1097/TA.0b013e318246eabc.
- Lucas KJ, Morris RP, Buford WL Jr, Panchbhavi VK. Biomechanical comparison of first metatarsophalangeal joint arthrodeses using triple-threaded headless screws versus partially threaded lag screws. Foot Ankle Surg. 2014;20(2):144-148. doi:10.1016/j.fas.2014.02.009.
- Iwamoto T, Matsumura N, Sato K, Momohara S, Toyama Y, Nakamura T. An obliquely placed headless compression screw for distal interphalangeal joint arthrodesis. J Hand Surg. 2013;38(12):2360-2364. doi:10.1016/j.jhsa.2013.09.026.
- Odutola AA, Sheridan BD, Kelly AJ. Headless compression screw fixation prevents symptomatic metalwork in arthroscopic ankle arthrodesis. Foot Ankle Surg. 2012;18(2):111-113. doi:10.1016/j.fas.2011.03.013.
- Capelle JH, Couch CG, Wells KM, et al. Fixation strength of anteriorly inserted headless screws for talar neck fractures. Foot Ankle Int. 2013;34(7):1012-1016. doi:10.1177/1071100713479586.
- Wheeler DL, McLoughlin SW. Biomechanical assessment of compression screws. Clin Orthop Relat Res. 1998;350(350):237-245. doi:10.1097/00003086-199805000-00032.
- Rockwood CA, Green DP, Bucholz RW. Rockwood and Green's Fractures in Adults. 7th ed. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2010.
- Simanski CJ, Maegele MG, Lefering R, et al. Functional treatment and early weightbearing after an ankle fracture: a prospective study. J Orthop Trauma. 2006;20(2):108-114. doi:10.1097/01.bot.0000197701.96954.8c.
- Reimer H, Kreibich M, Oettinger W. Extended uses for the Herbert/Whipple screw: six case reports out of 35 illustrating technique. J Orthop Trauma. 1996;10(1):7-14. doi:10.1097/00005131-199601000-00002.
- Barnes H, Cannada LK, Watson JT. A clinical evaluation of alternative fixation techniques for medial malleolus fractures. Injury. 2014;45(9):1365-1367. doi:10.1016/j.injury.2014.05.031.
- Dumigan RM, Bronson DG, Early JS. Analysis of fixation methods for vertical shear fractures of the medial malleolus. J Orthop Trauma. 2006;20(10):687-691. doi:10.1097/01.bot.0000247075.17548.3a.
- Toolan BC, Koval KJ, Kummer FJ, Sanders R, Zuckerman JD. Vertical shear fractures of the medial malleolus: a biomechanical study of five internal fixation techniques. Foot Ankle Int. 1994;15(9):483-489. doi:10.1177/107110079401500905.
- Ramsey PL, Hamilton W. Changes in tibiotalar area of contact caused by lateral talar shift. J Bone Joint Surg Am. 1976;58(3):356-357. doi:10.2106/00004623-197658030-00010.
- Thordarson DB, Motamed S, Hedman T, Ebramzadeh E, Bakshian S. The effect of fibular malreduction on contact pressures in an ankle fracture malunion model. J Bone Joint Surg Am. 1997;79(12):1809-1815. doi:10.2106/00004623-199712000-00006.
- Amanatullah DF, Khan SN, Curtiss S, Wolinsky PR. Effect of divergent screw fixation in vertical medial malleolus fractures. J Trauma Acute Care Surg. 2012;72(3):751-754. doi:10.1097/TA.0b013e31823b8b9f.
- Heiner AD. Structural properties of fourth-generation composite femurs and tibias. J Biomech. 2008;41(15):3282-3284. doi:10.1016/j.jbiomech.2008.08.013.
- Brown GA, McCarthy T, Bourgeault CA, Callahan DJ. Mechanical performance of standard and cannulated 4.0-mm cancellous bone screws. J Orthop Res. 2000;18(2):307-312. doi:10.1002/jor.1100180220.
- Merk BR, Stern SH, Cordes S, Lautenschlager EP. A fatigue life analysis of small fragment screws. J Orthop Trauma. 2001;15(7):494-499. doi:10.1097/00005131-200109000-00006.
ABSTRACT
This study is the first biomechanical research of headless compression screws for fixation of vertical shear fractures of the medial malleolus, a promising alternative that potentially offers several advantages for fixation.
Vertical shear fractures were simulated by osteotomies in 20 synthetic distal tibiae. Models were randomly assigned to fixation with either 2 parallel cancellous screws or 2 parallel Acutrak 2 headless compression screws (Acumed). Specimens were subjected to offset axial loading to simulate supination-adduction loading and tracked using high-resolution video.
The headless compression screw construct was significantly stiffer (P < .0001) (360 ± 131 N/mm) than the partially threaded cancellous screws (180 ± 48 N/mm) and demonstrated a significantly increased (P < .0001) mean load to clinical failure (719 ± 91 N vs 343 ± 83 N). When specimens were displaced to 6 mm and allowed to relax, the headless compression screw constructs demonstrated an elastic recoil and were reduced to the pretesting fragment alignment, whereas the parallel cancellous screw constructs remained displaced.
Along with the headless design that may decrease soft tissue irritation, the increased stiffness and elastic recoil of the headless compression screw construct offers improved fixation of medial malleolus vertical shear fractures over the traditional methods.
Continue to: Headless compressions screws...
Headless compressions screws are cannulated tapered titanium screws with variable thread pitch angle, allowing a fully threaded screw to apply compression along its entire length. These screws have been most commonly used for scaphoid fractures1 but have also been studied in fractures of small bones, such as capitellum, midfoot, and talar neck,2-4 and arthrodesis in the foot, ankle, and hand.5-7 Headless compression screws have been found to produce equivalent fragment compression to partially threaded cancellous screws while allowing less fragment displacement.8,9 The lack of a head may decrease soft tissue irritation compared with the partially threaded cancellous screws. Finally, headless compression screws are independent of cortical integrity, as the entire length of the screw features a wide thread diameter to capture cancellous bone in the proximal fragment, unlike partially threaded cancellous screws, which only possess a thread purchase in the distal fragment and depend on an intact cortex.
Vertical shear fractures of the medial malleolus occur through the supination-adduction of the talus exerted onto the articular surface of the medial malleolus.10 Optimal fixation of these fractures must be sufficient to maintain stable anatomic reduction of the ankle joint articular surface, allowing early range of motion, maintaining congruency of the ankle joint, and decreasing the risk of future post-traumatic arthritis to maximize functional outcome.11
A wide variety of techniques are available for fixation of these fractures, including various configurations of cortical screws, cancellous screws, tension bands, and antiglide plates. Clinically, 2 parallel 4.0-mm partially threaded cancellous screws are most often used. Limited evidence indicates that headless compression screws may be a viable option for fixation of medial malleolus fractures. One case reports the use of a headless compression screw for a horizontal medial malleolar fracture,12 and a small retrospective case series that used headless compression screws for all medial malleolar fractures showed satisfactory outcomes, a high union rate, and low patient-reported pain.13
We evaluate the stiffness, force to 2-mm displacement of the joint surface, and elastic properties of these 2 different constructs in vertical medial malleolar fractures in synthetic distal tibiae. We hypothesize that the parallel headless compression screw fixation will be stiffer and require more force to 2-mm displacement than parallel unicortical cancellous screw fixation.
MATERIALS AND METHODS
Identical vertical osteotomies (17.5 mm) were made from the medial border of the medial malleolus using a custom jig in 20 left 4th-generation composite synthetic distal tibiae (Sawbones, Pacific Research Labs; Model No. 3401) to simulate an Orthopaedic Trauma Association type 44-A2.3 fracture. The tibiae were then cut 18 cm from the tibial plafond and randomized to 2 fixation groups (n = 10 specimens for each group): parallel unicortical screw fixation or parallel unicortical headless compression screw fixation (Figures 1A-1D). Custom polymethylmethacrylate jigs were used to reproducibly drill identical holes with a 3.2-mm drill for the parallel unicortical screw construct and the drill bits provided by the Acutrak 2 Headless Compression Screw System (Acumed). The parallel unicortical screw construct consisted of 2 parallel 4.0-mm-diameter, 40-mm partially threaded cancellous screws (Depuy Synthes), and the headless compression fixation construct consisted of 2 parallel 4.7-mm-diameter, 45-mm titanium Acutrak 2 screws parallel to each other in the transverse plane. The Acutrak screws were placed per manufacturer instructions by first drilling with the Acutrak 2-4.7 Long Drill bit (Acumed), followed by the Acutrak 2-4.7 Profile Drill bit for the near cortex.
Continue to: Specimens...
Specimens were fixed to the base of a servohydraulic testing machine (Model 809, MTS Systems Corporation) with an axial-torsional load transducer (Model No. 662.20-01; Axial capacity of 250 kg, torsional capacity 2.88 kg-m; MTS Systems Corporation). The specimens were set in a vice tilted at 17° in the coronal plane to allow the MTS crosshead to apply an offset axial load simulating supination-adduction loading, which has been described previously (Figure 2).14,15 Load was applied to the inferolateral articular surface of the medial malleolus at 1 mm/s to a crosshead displacement of 6 mm and then cycled back to 0 mm. Load and axial displacement were measured at 60 Hz. The markers on the distal tibia and medial malleolus fracture fragment were tracked using high-resolution video (Fastcam PCI, Photron USA Inc). The motion of the video markers was determined using digitization and motion analysis software (Motus 9, Vicon).
Stiffness was calculated as the slope of the linear portion of the load-displacement curve over a range of 0.5 to 2.0 mm (Figure 3) and reported as mean (standard deviation). The force at 2 mm of fragment displacement was defined as a clinical failure.16,17 Student’s t test was used to determine the difference in construct stiffness and force for 2 mm displacement of the 2 groups. Significance was defined as P < .05. Institutional Review Board approval was not required for this study.
RESULTS
With offset axial testing to simulate supination-adduction force along with video motion analysis, the mean stiffness (± standard deviation) measured 180 ± 48 N/mm for the parallel unicortical screw fixation construct and 360 ± 131 N/mm for the headless compression screw fixation construct (Figure 4A). The headless compression screw fixation construct was over 2 times stiffer than the parallel unicortical construct during initial displacement of the fracture, indicating a statistically significant difference (P < .0001).
The mean force for 2 mm of fracture displacement, defined as clinical failure, reached 342 ± 83 N for the parallel unicortical screw fixation construct and 719 ± 91 N for the headless compression screw fixation construct (Figure 4B). The headless compression screw fixation construct resisted displacement significantly more (P = .0001) than the parallel unicortical screw construct, presenting a 100% increase.
Upon cycling of the servohydraulic testing machine back to 0-mm displacement, the parallel unicortical construct demonstrated no elastic recoil, remaining displaced at 4 mm, whereas the headless compression screw construct rebounded to almost 0-mm displacement, which is well below the clinical definition of fixation failure of 2 mm (Figure 5).
Continue to: Discussion...
DISCUSSION
When subjected to offset axial load, we observed that the headless compression screw construct exhibited significantly increased stiffness and load to 2 mm of displacement compared with a parallel unicortical screw construct. The headless compression screw also demonstrated elastic recoil to almost 0 mm of displacement, which is well below the 2-mm displacement.
We made reproducible fractures and fixation methods in synthetic distal tibiae, which feature less variability in size and quality than the cadaveric bone. Offset axial loading, rather than direct axial loading previously described by Amanatullah and colleagues,18 is the most physiologically relevant mode of force application to simulate the loading of the tauls onto the medial malleolus in the supination-adduction mechanism of injury.
The limitations of this study include the use of synthetic rather than cadaveric bone. Fourth-generation sawbones have been validated as possessing similar biomechanical properties as real bone.7,19 These results may also be inapplicable to osteoporotic bone, which would be significantly less dense than sawbones. This study is also an artificial situation designed to only test construct stiffness and load to clinical failure in a single mode of stress, offset axial loading and neglects other possible modes of force. This testing setup also disregards the structures surrounding the medial malleolus and tibia, including the talus, fibula, or soft tissue attachments, including the deltoid ligament and flexor retinaculum. These results are only relevant immediately after fixation and before bone healing occurs. We also tested the load to clinical failure rather than cyclic loading. Our testing more closely modeled a single traumatic force rather than the considerably smaller stresses that would be repeatedly exerted on the construct over several weeks after fixation in a clinical situation. This research is also not a clinical outcome study, rather, it suggests that headless compression screws are a viable, stronger, and possibly superior method for the initial fixation of vertical medial malleolar fractures.
As the load is offset axial, the larger thread purchase of the headless compression screws may lead to increased pullout strength, possibly increasing headless compression screw construct stiffness. Also, the variable diameter of headless compression screw, which reaches up to 4.7 mm, would increase the stiffness of the construct compared with the diameter of the cancellous screws. The elasticity of the headless compression construct may be because screws are made of titanium rather than stainless steel. Such property and given that the screws are cannulated rather than solid may also play a role, although several studies have shown variable results for cannulated vs solid screws of the same diameter.20,21 The elastic section modulus of both screws would have to be calculated to determine their exact effect on fixation.
CONCLUSION
The headless compression screw construct was found to be stiffer and features a higher load to clinical failure than a parallel unicortical cancellous screw construct for fixation of vertical medial malleolus fractures. Although significantly increased cost occurs with this construct, the headless design may decrease soft tissue irritation, and the elastic recoil of the construct after displacement may decrease clinical failure rates of this fixation method. This condition would eliminate the need for revision surgeries and thus be a cost effective alternative overall.
This paper will be judged for the Resident Writer’s Award.
ABSTRACT
This study is the first biomechanical research of headless compression screws for fixation of vertical shear fractures of the medial malleolus, a promising alternative that potentially offers several advantages for fixation.
Vertical shear fractures were simulated by osteotomies in 20 synthetic distal tibiae. Models were randomly assigned to fixation with either 2 parallel cancellous screws or 2 parallel Acutrak 2 headless compression screws (Acumed). Specimens were subjected to offset axial loading to simulate supination-adduction loading and tracked using high-resolution video.
The headless compression screw construct was significantly stiffer (P < .0001) (360 ± 131 N/mm) than the partially threaded cancellous screws (180 ± 48 N/mm) and demonstrated a significantly increased (P < .0001) mean load to clinical failure (719 ± 91 N vs 343 ± 83 N). When specimens were displaced to 6 mm and allowed to relax, the headless compression screw constructs demonstrated an elastic recoil and were reduced to the pretesting fragment alignment, whereas the parallel cancellous screw constructs remained displaced.
Along with the headless design that may decrease soft tissue irritation, the increased stiffness and elastic recoil of the headless compression screw construct offers improved fixation of medial malleolus vertical shear fractures over the traditional methods.
Continue to: Headless compressions screws...
Headless compressions screws are cannulated tapered titanium screws with variable thread pitch angle, allowing a fully threaded screw to apply compression along its entire length. These screws have been most commonly used for scaphoid fractures1 but have also been studied in fractures of small bones, such as capitellum, midfoot, and talar neck,2-4 and arthrodesis in the foot, ankle, and hand.5-7 Headless compression screws have been found to produce equivalent fragment compression to partially threaded cancellous screws while allowing less fragment displacement.8,9 The lack of a head may decrease soft tissue irritation compared with the partially threaded cancellous screws. Finally, headless compression screws are independent of cortical integrity, as the entire length of the screw features a wide thread diameter to capture cancellous bone in the proximal fragment, unlike partially threaded cancellous screws, which only possess a thread purchase in the distal fragment and depend on an intact cortex.
Vertical shear fractures of the medial malleolus occur through the supination-adduction of the talus exerted onto the articular surface of the medial malleolus.10 Optimal fixation of these fractures must be sufficient to maintain stable anatomic reduction of the ankle joint articular surface, allowing early range of motion, maintaining congruency of the ankle joint, and decreasing the risk of future post-traumatic arthritis to maximize functional outcome.11
A wide variety of techniques are available for fixation of these fractures, including various configurations of cortical screws, cancellous screws, tension bands, and antiglide plates. Clinically, 2 parallel 4.0-mm partially threaded cancellous screws are most often used. Limited evidence indicates that headless compression screws may be a viable option for fixation of medial malleolus fractures. One case reports the use of a headless compression screw for a horizontal medial malleolar fracture,12 and a small retrospective case series that used headless compression screws for all medial malleolar fractures showed satisfactory outcomes, a high union rate, and low patient-reported pain.13
We evaluate the stiffness, force to 2-mm displacement of the joint surface, and elastic properties of these 2 different constructs in vertical medial malleolar fractures in synthetic distal tibiae. We hypothesize that the parallel headless compression screw fixation will be stiffer and require more force to 2-mm displacement than parallel unicortical cancellous screw fixation.
MATERIALS AND METHODS
Identical vertical osteotomies (17.5 mm) were made from the medial border of the medial malleolus using a custom jig in 20 left 4th-generation composite synthetic distal tibiae (Sawbones, Pacific Research Labs; Model No. 3401) to simulate an Orthopaedic Trauma Association type 44-A2.3 fracture. The tibiae were then cut 18 cm from the tibial plafond and randomized to 2 fixation groups (n = 10 specimens for each group): parallel unicortical screw fixation or parallel unicortical headless compression screw fixation (Figures 1A-1D). Custom polymethylmethacrylate jigs were used to reproducibly drill identical holes with a 3.2-mm drill for the parallel unicortical screw construct and the drill bits provided by the Acutrak 2 Headless Compression Screw System (Acumed). The parallel unicortical screw construct consisted of 2 parallel 4.0-mm-diameter, 40-mm partially threaded cancellous screws (Depuy Synthes), and the headless compression fixation construct consisted of 2 parallel 4.7-mm-diameter, 45-mm titanium Acutrak 2 screws parallel to each other in the transverse plane. The Acutrak screws were placed per manufacturer instructions by first drilling with the Acutrak 2-4.7 Long Drill bit (Acumed), followed by the Acutrak 2-4.7 Profile Drill bit for the near cortex.
Continue to: Specimens...
Specimens were fixed to the base of a servohydraulic testing machine (Model 809, MTS Systems Corporation) with an axial-torsional load transducer (Model No. 662.20-01; Axial capacity of 250 kg, torsional capacity 2.88 kg-m; MTS Systems Corporation). The specimens were set in a vice tilted at 17° in the coronal plane to allow the MTS crosshead to apply an offset axial load simulating supination-adduction loading, which has been described previously (Figure 2).14,15 Load was applied to the inferolateral articular surface of the medial malleolus at 1 mm/s to a crosshead displacement of 6 mm and then cycled back to 0 mm. Load and axial displacement were measured at 60 Hz. The markers on the distal tibia and medial malleolus fracture fragment were tracked using high-resolution video (Fastcam PCI, Photron USA Inc). The motion of the video markers was determined using digitization and motion analysis software (Motus 9, Vicon).
Stiffness was calculated as the slope of the linear portion of the load-displacement curve over a range of 0.5 to 2.0 mm (Figure 3) and reported as mean (standard deviation). The force at 2 mm of fragment displacement was defined as a clinical failure.16,17 Student’s t test was used to determine the difference in construct stiffness and force for 2 mm displacement of the 2 groups. Significance was defined as P < .05. Institutional Review Board approval was not required for this study.
RESULTS
With offset axial testing to simulate supination-adduction force along with video motion analysis, the mean stiffness (± standard deviation) measured 180 ± 48 N/mm for the parallel unicortical screw fixation construct and 360 ± 131 N/mm for the headless compression screw fixation construct (Figure 4A). The headless compression screw fixation construct was over 2 times stiffer than the parallel unicortical construct during initial displacement of the fracture, indicating a statistically significant difference (P < .0001).
The mean force for 2 mm of fracture displacement, defined as clinical failure, reached 342 ± 83 N for the parallel unicortical screw fixation construct and 719 ± 91 N for the headless compression screw fixation construct (Figure 4B). The headless compression screw fixation construct resisted displacement significantly more (P = .0001) than the parallel unicortical screw construct, presenting a 100% increase.
Upon cycling of the servohydraulic testing machine back to 0-mm displacement, the parallel unicortical construct demonstrated no elastic recoil, remaining displaced at 4 mm, whereas the headless compression screw construct rebounded to almost 0-mm displacement, which is well below the clinical definition of fixation failure of 2 mm (Figure 5).
Continue to: Discussion...
DISCUSSION
When subjected to offset axial load, we observed that the headless compression screw construct exhibited significantly increased stiffness and load to 2 mm of displacement compared with a parallel unicortical screw construct. The headless compression screw also demonstrated elastic recoil to almost 0 mm of displacement, which is well below the 2-mm displacement.
We made reproducible fractures and fixation methods in synthetic distal tibiae, which feature less variability in size and quality than the cadaveric bone. Offset axial loading, rather than direct axial loading previously described by Amanatullah and colleagues,18 is the most physiologically relevant mode of force application to simulate the loading of the tauls onto the medial malleolus in the supination-adduction mechanism of injury.
The limitations of this study include the use of synthetic rather than cadaveric bone. Fourth-generation sawbones have been validated as possessing similar biomechanical properties as real bone.7,19 These results may also be inapplicable to osteoporotic bone, which would be significantly less dense than sawbones. This study is also an artificial situation designed to only test construct stiffness and load to clinical failure in a single mode of stress, offset axial loading and neglects other possible modes of force. This testing setup also disregards the structures surrounding the medial malleolus and tibia, including the talus, fibula, or soft tissue attachments, including the deltoid ligament and flexor retinaculum. These results are only relevant immediately after fixation and before bone healing occurs. We also tested the load to clinical failure rather than cyclic loading. Our testing more closely modeled a single traumatic force rather than the considerably smaller stresses that would be repeatedly exerted on the construct over several weeks after fixation in a clinical situation. This research is also not a clinical outcome study, rather, it suggests that headless compression screws are a viable, stronger, and possibly superior method for the initial fixation of vertical medial malleolar fractures.
As the load is offset axial, the larger thread purchase of the headless compression screws may lead to increased pullout strength, possibly increasing headless compression screw construct stiffness. Also, the variable diameter of headless compression screw, which reaches up to 4.7 mm, would increase the stiffness of the construct compared with the diameter of the cancellous screws. The elasticity of the headless compression construct may be because screws are made of titanium rather than stainless steel. Such property and given that the screws are cannulated rather than solid may also play a role, although several studies have shown variable results for cannulated vs solid screws of the same diameter.20,21 The elastic section modulus of both screws would have to be calculated to determine their exact effect on fixation.
CONCLUSION
The headless compression screw construct was found to be stiffer and features a higher load to clinical failure than a parallel unicortical cancellous screw construct for fixation of vertical medial malleolus fractures. Although significantly increased cost occurs with this construct, the headless design may decrease soft tissue irritation, and the elastic recoil of the construct after displacement may decrease clinical failure rates of this fixation method. This condition would eliminate the need for revision surgeries and thus be a cost effective alternative overall.
This paper will be judged for the Resident Writer’s Award.
- Fowler JR, Ilyas AM. Headless compression screw fixation of scaphoid fractures. Hand Clin. 2010;26(3):351-361, vi. doi:10.1016/j.hcl.2010.04.005.
- Karakasli A, Hapa O, Erduran M, Dincer C, Cecen B, Havitcioglu H. Mechanical comparison of headless screw fixation and locking plate fixation for talar neck fractures. J Foot Ankle Surg. 2015;54(5):905-909. doi:10.1053/j.jfas.2015.04.002.
- Elkowitz SJ, Polatsch DB, Egol KA, Kummer FJ, Koval KJ. Capitellum fractures: a biomechanical evaluation of three fixation methods. J Orthop Trauma. 2002;16(7):503-506. doi:10.1097/00005131-200208000-00009.
- Zhang H, Min L, Wang GL, et al. Primary open reduction and internal fixation with headless compression screws in the treatment of Chinese patients with acute Lisfranc joint injuries. J Trauma Acute Care Surg. 2012;72(5):1380-1385. doi:10.1097/TA.0b013e318246eabc.
- Lucas KJ, Morris RP, Buford WL Jr, Panchbhavi VK. Biomechanical comparison of first metatarsophalangeal joint arthrodeses using triple-threaded headless screws versus partially threaded lag screws. Foot Ankle Surg. 2014;20(2):144-148. doi:10.1016/j.fas.2014.02.009.
- Iwamoto T, Matsumura N, Sato K, Momohara S, Toyama Y, Nakamura T. An obliquely placed headless compression screw for distal interphalangeal joint arthrodesis. J Hand Surg. 2013;38(12):2360-2364. doi:10.1016/j.jhsa.2013.09.026.
- Odutola AA, Sheridan BD, Kelly AJ. Headless compression screw fixation prevents symptomatic metalwork in arthroscopic ankle arthrodesis. Foot Ankle Surg. 2012;18(2):111-113. doi:10.1016/j.fas.2011.03.013.
- Capelle JH, Couch CG, Wells KM, et al. Fixation strength of anteriorly inserted headless screws for talar neck fractures. Foot Ankle Int. 2013;34(7):1012-1016. doi:10.1177/1071100713479586.
- Wheeler DL, McLoughlin SW. Biomechanical assessment of compression screws. Clin Orthop Relat Res. 1998;350(350):237-245. doi:10.1097/00003086-199805000-00032.
- Rockwood CA, Green DP, Bucholz RW. Rockwood and Green's Fractures in Adults. 7th ed. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2010.
- Simanski CJ, Maegele MG, Lefering R, et al. Functional treatment and early weightbearing after an ankle fracture: a prospective study. J Orthop Trauma. 2006;20(2):108-114. doi:10.1097/01.bot.0000197701.96954.8c.
- Reimer H, Kreibich M, Oettinger W. Extended uses for the Herbert/Whipple screw: six case reports out of 35 illustrating technique. J Orthop Trauma. 1996;10(1):7-14. doi:10.1097/00005131-199601000-00002.
- Barnes H, Cannada LK, Watson JT. A clinical evaluation of alternative fixation techniques for medial malleolus fractures. Injury. 2014;45(9):1365-1367. doi:10.1016/j.injury.2014.05.031.
- Dumigan RM, Bronson DG, Early JS. Analysis of fixation methods for vertical shear fractures of the medial malleolus. J Orthop Trauma. 2006;20(10):687-691. doi:10.1097/01.bot.0000247075.17548.3a.
- Toolan BC, Koval KJ, Kummer FJ, Sanders R, Zuckerman JD. Vertical shear fractures of the medial malleolus: a biomechanical study of five internal fixation techniques. Foot Ankle Int. 1994;15(9):483-489. doi:10.1177/107110079401500905.
- Ramsey PL, Hamilton W. Changes in tibiotalar area of contact caused by lateral talar shift. J Bone Joint Surg Am. 1976;58(3):356-357. doi:10.2106/00004623-197658030-00010.
- Thordarson DB, Motamed S, Hedman T, Ebramzadeh E, Bakshian S. The effect of fibular malreduction on contact pressures in an ankle fracture malunion model. J Bone Joint Surg Am. 1997;79(12):1809-1815. doi:10.2106/00004623-199712000-00006.
- Amanatullah DF, Khan SN, Curtiss S, Wolinsky PR. Effect of divergent screw fixation in vertical medial malleolus fractures. J Trauma Acute Care Surg. 2012;72(3):751-754. doi:10.1097/TA.0b013e31823b8b9f.
- Heiner AD. Structural properties of fourth-generation composite femurs and tibias. J Biomech. 2008;41(15):3282-3284. doi:10.1016/j.jbiomech.2008.08.013.
- Brown GA, McCarthy T, Bourgeault CA, Callahan DJ. Mechanical performance of standard and cannulated 4.0-mm cancellous bone screws. J Orthop Res. 2000;18(2):307-312. doi:10.1002/jor.1100180220.
- Merk BR, Stern SH, Cordes S, Lautenschlager EP. A fatigue life analysis of small fragment screws. J Orthop Trauma. 2001;15(7):494-499. doi:10.1097/00005131-200109000-00006.
- Fowler JR, Ilyas AM. Headless compression screw fixation of scaphoid fractures. Hand Clin. 2010;26(3):351-361, vi. doi:10.1016/j.hcl.2010.04.005.
- Karakasli A, Hapa O, Erduran M, Dincer C, Cecen B, Havitcioglu H. Mechanical comparison of headless screw fixation and locking plate fixation for talar neck fractures. J Foot Ankle Surg. 2015;54(5):905-909. doi:10.1053/j.jfas.2015.04.002.
- Elkowitz SJ, Polatsch DB, Egol KA, Kummer FJ, Koval KJ. Capitellum fractures: a biomechanical evaluation of three fixation methods. J Orthop Trauma. 2002;16(7):503-506. doi:10.1097/00005131-200208000-00009.
- Zhang H, Min L, Wang GL, et al. Primary open reduction and internal fixation with headless compression screws in the treatment of Chinese patients with acute Lisfranc joint injuries. J Trauma Acute Care Surg. 2012;72(5):1380-1385. doi:10.1097/TA.0b013e318246eabc.
- Lucas KJ, Morris RP, Buford WL Jr, Panchbhavi VK. Biomechanical comparison of first metatarsophalangeal joint arthrodeses using triple-threaded headless screws versus partially threaded lag screws. Foot Ankle Surg. 2014;20(2):144-148. doi:10.1016/j.fas.2014.02.009.
- Iwamoto T, Matsumura N, Sato K, Momohara S, Toyama Y, Nakamura T. An obliquely placed headless compression screw for distal interphalangeal joint arthrodesis. J Hand Surg. 2013;38(12):2360-2364. doi:10.1016/j.jhsa.2013.09.026.
- Odutola AA, Sheridan BD, Kelly AJ. Headless compression screw fixation prevents symptomatic metalwork in arthroscopic ankle arthrodesis. Foot Ankle Surg. 2012;18(2):111-113. doi:10.1016/j.fas.2011.03.013.
- Capelle JH, Couch CG, Wells KM, et al. Fixation strength of anteriorly inserted headless screws for talar neck fractures. Foot Ankle Int. 2013;34(7):1012-1016. doi:10.1177/1071100713479586.
- Wheeler DL, McLoughlin SW. Biomechanical assessment of compression screws. Clin Orthop Relat Res. 1998;350(350):237-245. doi:10.1097/00003086-199805000-00032.
- Rockwood CA, Green DP, Bucholz RW. Rockwood and Green's Fractures in Adults. 7th ed. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2010.
- Simanski CJ, Maegele MG, Lefering R, et al. Functional treatment and early weightbearing after an ankle fracture: a prospective study. J Orthop Trauma. 2006;20(2):108-114. doi:10.1097/01.bot.0000197701.96954.8c.
- Reimer H, Kreibich M, Oettinger W. Extended uses for the Herbert/Whipple screw: six case reports out of 35 illustrating technique. J Orthop Trauma. 1996;10(1):7-14. doi:10.1097/00005131-199601000-00002.
- Barnes H, Cannada LK, Watson JT. A clinical evaluation of alternative fixation techniques for medial malleolus fractures. Injury. 2014;45(9):1365-1367. doi:10.1016/j.injury.2014.05.031.
- Dumigan RM, Bronson DG, Early JS. Analysis of fixation methods for vertical shear fractures of the medial malleolus. J Orthop Trauma. 2006;20(10):687-691. doi:10.1097/01.bot.0000247075.17548.3a.
- Toolan BC, Koval KJ, Kummer FJ, Sanders R, Zuckerman JD. Vertical shear fractures of the medial malleolus: a biomechanical study of five internal fixation techniques. Foot Ankle Int. 1994;15(9):483-489. doi:10.1177/107110079401500905.
- Ramsey PL, Hamilton W. Changes in tibiotalar area of contact caused by lateral talar shift. J Bone Joint Surg Am. 1976;58(3):356-357. doi:10.2106/00004623-197658030-00010.
- Thordarson DB, Motamed S, Hedman T, Ebramzadeh E, Bakshian S. The effect of fibular malreduction on contact pressures in an ankle fracture malunion model. J Bone Joint Surg Am. 1997;79(12):1809-1815. doi:10.2106/00004623-199712000-00006.
- Amanatullah DF, Khan SN, Curtiss S, Wolinsky PR. Effect of divergent screw fixation in vertical medial malleolus fractures. J Trauma Acute Care Surg. 2012;72(3):751-754. doi:10.1097/TA.0b013e31823b8b9f.
- Heiner AD. Structural properties of fourth-generation composite femurs and tibias. J Biomech. 2008;41(15):3282-3284. doi:10.1016/j.jbiomech.2008.08.013.
- Brown GA, McCarthy T, Bourgeault CA, Callahan DJ. Mechanical performance of standard and cannulated 4.0-mm cancellous bone screws. J Orthop Res. 2000;18(2):307-312. doi:10.1002/jor.1100180220.
- Merk BR, Stern SH, Cordes S, Lautenschlager EP. A fatigue life analysis of small fragment screws. J Orthop Trauma. 2001;15(7):494-499. doi:10.1097/00005131-200109000-00006.
TAKE-HOME POINTS
- Optimal fixation of vertical sheer ankle fractures is unknown.
- Headless compression screws are stiffer than cancellous screws in offset axial load.
- Headless compression screws have a higher load to failure than cancellous screws.
- Headless compression screws may offer a soft tissue friendly fixation of method for vertical sheer ankle fractures.
- These findings may not apply when subject to cyclic loads or in osteoporotic bone.
Patient transfers between hospitals contribute substantially to CDI burden
ATLANTA – Patient sharing among hospital facilities contributed substantially to the overall Clostridium difficile infection rate, an analysis of interhospital contamination effects showed.
In fact, 7.6% of all Clostridium difficile infection (CDI) cases at the nearly 400 California hospitals included in the study were directly attributable to the patient-sharing network, Daniel Sewell, PhD, reported at the International Conference on Emerging Infectious Diseases.
“The methods that we employed allowed us to estimate the expected increase in CDI cases due to transfers as a function of the CDI rate at the hospital from which those patients were brought. These transfer patients were responsible for about 3.06 times the number of CDI cases as a normal patient,” said Dr. Sewell, a biostatistician at the University of Iowa, Iowa City.
The findings, which underscored the importance of regional (rather than local) efforts to minimize the spread of health care–associated infections, are based on an analysis of 27,200,873 hospital admissions and 532,320 same-day patient transfers identified from the Healthcare Cost and Utilization Project California State Inpatient Database for 2005-2011.
Transfer networks based on the monthly average number of patients discharged from one hospital and admitted to another on the same day were constructed, and the monthly average number of CDI cases per hospital were considered, along with hospital-level characteristics such as patient length of stay, age, and number of diagnoses. Network autocorrelation models that help eliminate bias were then used to assess the contamination effects between hospitals, he explained.
This led to development of an equation that can be used to determine the expected number of CDI cases in a hospital as a function of the number of transfers coming in and the contamination level of the source hospitals. The ability to calculate the expected number of CDI cases in this fashion is an important factor for the success of regional versus local intervention efforts, which are increasingly thought to be important for reducing health care–associated infections.
“If we want to design a coordinated or regional approach, we’ve got to have a much better understanding of the role that patient transfers have in these diseases,” Dr. Sewell said.
As most hospitals included in the study had a low CDI rate and a low transfer rate, the CDIs attributable to transfers represent a minority of cases, but they are a substantial minority, he said, noting that the main concern is with the “perfect storm” of high CDI rate plus high transfer rate.
The methodological approach used in this study to estimate CDI rates can be used for any health care–associated infection of interest, he added.
Dr. Sewell reported that he had no disclosures.
The AGA Fecal Microbiota Transplantation (FMT) National Registry will assess short- and long-term patient outcomes associated with FMT. Learn more at http://ow.ly/WdQE30lBuSu
ATLANTA – Patient sharing among hospital facilities contributed substantially to the overall Clostridium difficile infection rate, an analysis of interhospital contamination effects showed.
In fact, 7.6% of all Clostridium difficile infection (CDI) cases at the nearly 400 California hospitals included in the study were directly attributable to the patient-sharing network, Daniel Sewell, PhD, reported at the International Conference on Emerging Infectious Diseases.
“The methods that we employed allowed us to estimate the expected increase in CDI cases due to transfers as a function of the CDI rate at the hospital from which those patients were brought. These transfer patients were responsible for about 3.06 times the number of CDI cases as a normal patient,” said Dr. Sewell, a biostatistician at the University of Iowa, Iowa City.
The findings, which underscored the importance of regional (rather than local) efforts to minimize the spread of health care–associated infections, are based on an analysis of 27,200,873 hospital admissions and 532,320 same-day patient transfers identified from the Healthcare Cost and Utilization Project California State Inpatient Database for 2005-2011.
Transfer networks based on the monthly average number of patients discharged from one hospital and admitted to another on the same day were constructed, and the monthly average number of CDI cases per hospital were considered, along with hospital-level characteristics such as patient length of stay, age, and number of diagnoses. Network autocorrelation models that help eliminate bias were then used to assess the contamination effects between hospitals, he explained.
This led to development of an equation that can be used to determine the expected number of CDI cases in a hospital as a function of the number of transfers coming in and the contamination level of the source hospitals. The ability to calculate the expected number of CDI cases in this fashion is an important factor for the success of regional versus local intervention efforts, which are increasingly thought to be important for reducing health care–associated infections.
“If we want to design a coordinated or regional approach, we’ve got to have a much better understanding of the role that patient transfers have in these diseases,” Dr. Sewell said.
As most hospitals included in the study had a low CDI rate and a low transfer rate, the CDIs attributable to transfers represent a minority of cases, but they are a substantial minority, he said, noting that the main concern is with the “perfect storm” of high CDI rate plus high transfer rate.
The methodological approach used in this study to estimate CDI rates can be used for any health care–associated infection of interest, he added.
Dr. Sewell reported that he had no disclosures.
The AGA Fecal Microbiota Transplantation (FMT) National Registry will assess short- and long-term patient outcomes associated with FMT. Learn more at http://ow.ly/WdQE30lBuSu
ATLANTA – Patient sharing among hospital facilities contributed substantially to the overall Clostridium difficile infection rate, an analysis of interhospital contamination effects showed.
In fact, 7.6% of all Clostridium difficile infection (CDI) cases at the nearly 400 California hospitals included in the study were directly attributable to the patient-sharing network, Daniel Sewell, PhD, reported at the International Conference on Emerging Infectious Diseases.
“The methods that we employed allowed us to estimate the expected increase in CDI cases due to transfers as a function of the CDI rate at the hospital from which those patients were brought. These transfer patients were responsible for about 3.06 times the number of CDI cases as a normal patient,” said Dr. Sewell, a biostatistician at the University of Iowa, Iowa City.
The findings, which underscored the importance of regional (rather than local) efforts to minimize the spread of health care–associated infections, are based on an analysis of 27,200,873 hospital admissions and 532,320 same-day patient transfers identified from the Healthcare Cost and Utilization Project California State Inpatient Database for 2005-2011.
Transfer networks based on the monthly average number of patients discharged from one hospital and admitted to another on the same day were constructed, and the monthly average number of CDI cases per hospital were considered, along with hospital-level characteristics such as patient length of stay, age, and number of diagnoses. Network autocorrelation models that help eliminate bias were then used to assess the contamination effects between hospitals, he explained.
This led to development of an equation that can be used to determine the expected number of CDI cases in a hospital as a function of the number of transfers coming in and the contamination level of the source hospitals. The ability to calculate the expected number of CDI cases in this fashion is an important factor for the success of regional versus local intervention efforts, which are increasingly thought to be important for reducing health care–associated infections.
“If we want to design a coordinated or regional approach, we’ve got to have a much better understanding of the role that patient transfers have in these diseases,” Dr. Sewell said.
As most hospitals included in the study had a low CDI rate and a low transfer rate, the CDIs attributable to transfers represent a minority of cases, but they are a substantial minority, he said, noting that the main concern is with the “perfect storm” of high CDI rate plus high transfer rate.
The methodological approach used in this study to estimate CDI rates can be used for any health care–associated infection of interest, he added.
Dr. Sewell reported that he had no disclosures.
The AGA Fecal Microbiota Transplantation (FMT) National Registry will assess short- and long-term patient outcomes associated with FMT. Learn more at http://ow.ly/WdQE30lBuSu
REPORTING FROM ICEID 2018
Key clinical point: Patient sharing among hospitals contributes substantially to Clostridium difficile infection (CDI) rates.
Major finding: Patient transfers account for 7.6% of the overall CDI burden.
Study details: A statistical analysis to estimate interhospital CDI transmissions.
Disclosures: Dr. Sewell reported that he had no disclosures.
Bone biopsy in suspected osteomyelitis: Culture and histology matter
Diabetic foot ulcers and infections can lead to osteomyelitis, a potentially devastating infection in the bone.

How much of a difference can osteomyelitis make to a patient’s prognosis? A 2014 commentary by Benjamin A. Lipsky, MD, a prominent expert in problems associated with diabetic patients’ feet who’s with the University of Washington, Seattle, hints at the potential toll: “Overall, about 20% of patients with a diabetic foot infection (and over 60% of those with severe infections) have underlying osteomyelitis, which dramatically increases the risk of lower-extremity amputation” (Diabetes Care. 2014 Mar;37[3]:593-5).
Diagnosis of osteomyelitis, which relies on a bone biopsy, is clearly important. But there’s a big gap in diagnostic findings depending on whether doctors request culture or histology results, according to a new study released at the 2018 scientific meeting of the American Diabetes Association (Diabetes. 2018 Jul. doi: 10.2337/db18-110-OR).

In an interview, lead author and podiatrist Peter A. Crisologo, DPM, of University of Texas Southwestern Medical Center, Dallas, explained the study findings and offered guidance for requesting bone biopsies in possible cases of osteomyelitis.
Q: What makes diagnosis and treatment of osteomyelitis unique?
A: In the foot, there’s not a lot of soft tissue between the outside world and your bone. If the wounds on the feet go deep enough, they can spread a bacterial infection to the bone. This changes how foot infections are treated.
If you have a skin infection, it requires 11-12 days of antibiotics. Things start ramping up once you start getting into the bone. You’re talking potential surgery and 6 weeks of antibiotics through IV treatments. This is why it’s really important that you get your diagnosis right.
A lot of people say “I’m going to do the safe thing” and treat a bone infection with an extended course of antibiotics.
That’s not necessarily safe. If you’re overdiagnosing – for example, you identify bacteria that’s just a contaminant – you could put a patient through 6 weeks of IV treatment along with the risks of a PICC (peripherally inserted central catheter ) line infection, complications from IV placement, and complications from the antibiotic.
Also, acute kidney injury develops in at least a third of the patients who undergo 6 weeks of antibiotics. That’s not to mention the cost of the visits and the labs you have to draw. But we don’t want to underdiagnose either. If osteomyelitis is underdiagnosed and then not treated, the infection can smolder and continue to progress and worsen.
Q: Your study looks at the bone biopsy. How does it fit into care of osteomyelitis in the diabetic foot?
A: A bone biopsy is the standard for diagnosis under the guidelines of the Infectious Diseases Society of America/International Working Group on the Diabetic Foot (Clin Infect Dis. 2012;54[12]:e132-73 ).
But beyond that, nobody says anything. Everyone has an operational definition of how a bone biopsy is interpreted, and there’s a need for a consensus on how a bone biopsy can be used to diagnose osteomyelitis.
You’ll get different percentages of your patients diagnosed with osteomyelitis. For example, someone may say the biopsy is only positive if the histology is positive, while another says the histology doesn’t matter if the culture is positive.
Q: Your study looks at histology and culture analyses. What do these reveal?
A: A traditional culture helps you identify the bacteria, as well as guide your treatment when it’s tested against antibiotics.
A traditional histology allows the pathologist to look under a microscope for signs of osteomyelitis: Do they see the right inflammatory cells, white cells, lymphocytes, combinations of cells? Does this look like an acute or chronic osteomyelitis?
Q: Why might it be wise to combine culture and histology analyses?
A: If you have bacteria that’s difficult to culture via traditional methods, it may be a bacteria that doesn’t grow well or easily. If you combine culture with histology, pathologists can look and say, “Your culture was negative but we see these other signs, so we feel this is osteomyelitis.”
Q: Your study examined 35 consecutive patients aged at least 21 years who had moderate or severe infections bone infections in the foot linked with type 1 diabetes (n = 4) or type 2 diabetes (n = 31).
The samples were analyzed via culture, histology, and culture/histology examinations. You also performed genetic sequencing (quantitative polymerase chain reaction targeting 16S rRNA). How does this test fit in to bone biopsies in the clinic?
A: That’s a newer method and not a standard of care treatment for the diabetic foot. This analysis looks at DNA that’s present, bypassing the analysis of difficult-to-grow bacteria.
Q: What did you discover?
A: In this study, histology had the lowest incidence of positively detecting osteomyelitis. (45.7%). The level increases when a culture is taken (68.6% vs. histology; P = .02).
Then it goes up when DNA is used because it’s catching everything (82.9%, P = .001 vs. histology and P = .31 vs. culture).
[The study also found that adding histology to culture or to genetic sequencing did not change positive findings.]
Q: Does the study suggest one approach is better than the others?
A: This paper doesn’t provide enough evidence to use one method over another. The main purpose was to raise the concern that diagnosis can change dramatically depending on how the gold standard of bone biopsy is interpreted.
Q: What were the pros and cons of the genetic sequencing approach?
A: When we use this approach, our positive diagnostic rate significantly increases. But there are also downsides. We don’t know whether the bacteria we see is alive or dead. We just know it was there. So are the patients truly positive? That’s a question we can’t answer.
Genetic sequencing also doesn’t tell us about susceptibilities to antibiotics.
Q: What is the take-home message here for physicians who may order bone biopsies?
A: The thing to do is request both traditional culture and traditional histology.
As far as DNA sequencing, that not something I’d recommend as a standard of care.
Q: Can you comment on cost and insurance coverage for these approaches?
A: As far as I know, genetic sequencing is not covered as it is not standard of care in the diabetic foot and is used mainly for research at this time.
Pathology and culture are standard of care when evaluating for osteomyelitis and should be a covered service. However, a patient should call their insurance company first prior to having the procedure done to see whether it is covered.
Q: What’s next for research in this area?
A: From here, the next step is bigger numbers: Increase the study size and look at this again. Also, we may be able to identify susceptibilities by identifying resistance within the DNA.
Dr. Crisologo and two other study authors report no relevant disclosures. One study author reported various disclosures including research support, consulting, and service on speakers' bureaus.
Diabetic foot ulcers and infections can lead to osteomyelitis, a potentially devastating infection in the bone.
How much of a difference can osteomyelitis make to a patient’s prognosis? A 2014 commentary by Benjamin A. Lipsky, MD, a prominent expert in problems associated with diabetic patients’ feet who’s with the University of Washington, Seattle, hints at the potential toll: “Overall, about 20% of patients with a diabetic foot infection (and over 60% of those with severe infections) have underlying osteomyelitis, which dramatically increases the risk of lower-extremity amputation” (Diabetes Care. 2014 Mar;37[3]:593-5).
Diagnosis of osteomyelitis, which relies on a bone biopsy, is clearly important. But there’s a big gap in diagnostic findings depending on whether doctors request culture or histology results, according to a new study released at the 2018 scientific meeting of the American Diabetes Association (Diabetes. 2018 Jul. doi: 10.2337/db18-110-OR).
In an interview, lead author and podiatrist Peter A. Crisologo, DPM, of University of Texas Southwestern Medical Center, Dallas, explained the study findings and offered guidance for requesting bone biopsies in possible cases of osteomyelitis.
Q: What makes diagnosis and treatment of osteomyelitis unique?
A: In the foot, there’s not a lot of soft tissue between the outside world and your bone. If the wounds on the feet go deep enough, they can spread a bacterial infection to the bone. This changes how foot infections are treated.
If you have a skin infection, it requires 11-12 days of antibiotics. Things start ramping up once you start getting into the bone. You’re talking potential surgery and 6 weeks of antibiotics through IV treatments. This is why it’s really important that you get your diagnosis right.
A lot of people say “I’m going to do the safe thing” and treat a bone infection with an extended course of antibiotics.
That’s not necessarily safe. If you’re overdiagnosing – for example, you identify bacteria that’s just a contaminant – you could put a patient through 6 weeks of IV treatment along with the risks of a PICC (peripherally inserted central catheter ) line infection, complications from IV placement, and complications from the antibiotic.
Also, acute kidney injury develops in at least a third of the patients who undergo 6 weeks of antibiotics. That’s not to mention the cost of the visits and the labs you have to draw. But we don’t want to underdiagnose either. If osteomyelitis is underdiagnosed and then not treated, the infection can smolder and continue to progress and worsen.
Q: Your study looks at the bone biopsy. How does it fit into care of osteomyelitis in the diabetic foot?
A: A bone biopsy is the standard for diagnosis under the guidelines of the Infectious Diseases Society of America/International Working Group on the Diabetic Foot (Clin Infect Dis. 2012;54[12]:e132-73 ).
But beyond that, nobody says anything. Everyone has an operational definition of how a bone biopsy is interpreted, and there’s a need for a consensus on how a bone biopsy can be used to diagnose osteomyelitis.
You’ll get different percentages of your patients diagnosed with osteomyelitis. For example, someone may say the biopsy is only positive if the histology is positive, while another says the histology doesn’t matter if the culture is positive.
Q: Your study looks at histology and culture analyses. What do these reveal?
A: A traditional culture helps you identify the bacteria, as well as guide your treatment when it’s tested against antibiotics.
A traditional histology allows the pathologist to look under a microscope for signs of osteomyelitis: Do they see the right inflammatory cells, white cells, lymphocytes, combinations of cells? Does this look like an acute or chronic osteomyelitis?
Q: Why might it be wise to combine culture and histology analyses?
A: If you have bacteria that’s difficult to culture via traditional methods, it may be a bacteria that doesn’t grow well or easily. If you combine culture with histology, pathologists can look and say, “Your culture was negative but we see these other signs, so we feel this is osteomyelitis.”
Q: Your study examined 35 consecutive patients aged at least 21 years who had moderate or severe infections bone infections in the foot linked with type 1 diabetes (n = 4) or type 2 diabetes (n = 31).
The samples were analyzed via culture, histology, and culture/histology examinations. You also performed genetic sequencing (quantitative polymerase chain reaction targeting 16S rRNA). How does this test fit in to bone biopsies in the clinic?
A: That’s a newer method and not a standard of care treatment for the diabetic foot. This analysis looks at DNA that’s present, bypassing the analysis of difficult-to-grow bacteria.
Q: What did you discover?
A: In this study, histology had the lowest incidence of positively detecting osteomyelitis. (45.7%). The level increases when a culture is taken (68.6% vs. histology; P = .02).
Then it goes up when DNA is used because it’s catching everything (82.9%, P = .001 vs. histology and P = .31 vs. culture).
[The study also found that adding histology to culture or to genetic sequencing did not change positive findings.]
Q: Does the study suggest one approach is better than the others?
A: This paper doesn’t provide enough evidence to use one method over another. The main purpose was to raise the concern that diagnosis can change dramatically depending on how the gold standard of bone biopsy is interpreted.
Q: What were the pros and cons of the genetic sequencing approach?
A: When we use this approach, our positive diagnostic rate significantly increases. But there are also downsides. We don’t know whether the bacteria we see is alive or dead. We just know it was there. So are the patients truly positive? That’s a question we can’t answer.
Genetic sequencing also doesn’t tell us about susceptibilities to antibiotics.
Q: What is the take-home message here for physicians who may order bone biopsies?
A: The thing to do is request both traditional culture and traditional histology.
As far as DNA sequencing, that not something I’d recommend as a standard of care.
Q: Can you comment on cost and insurance coverage for these approaches?
A: As far as I know, genetic sequencing is not covered as it is not standard of care in the diabetic foot and is used mainly for research at this time.
Pathology and culture are standard of care when evaluating for osteomyelitis and should be a covered service. However, a patient should call their insurance company first prior to having the procedure done to see whether it is covered.
Q: What’s next for research in this area?
A: From here, the next step is bigger numbers: Increase the study size and look at this again. Also, we may be able to identify susceptibilities by identifying resistance within the DNA.
Dr. Crisologo and two other study authors report no relevant disclosures. One study author reported various disclosures including research support, consulting, and service on speakers' bureaus.
Diabetic foot ulcers and infections can lead to osteomyelitis, a potentially devastating infection in the bone.
How much of a difference can osteomyelitis make to a patient’s prognosis? A 2014 commentary by Benjamin A. Lipsky, MD, a prominent expert in problems associated with diabetic patients’ feet who’s with the University of Washington, Seattle, hints at the potential toll: “Overall, about 20% of patients with a diabetic foot infection (and over 60% of those with severe infections) have underlying osteomyelitis, which dramatically increases the risk of lower-extremity amputation” (Diabetes Care. 2014 Mar;37[3]:593-5).
Diagnosis of osteomyelitis, which relies on a bone biopsy, is clearly important. But there’s a big gap in diagnostic findings depending on whether doctors request culture or histology results, according to a new study released at the 2018 scientific meeting of the American Diabetes Association (Diabetes. 2018 Jul. doi: 10.2337/db18-110-OR).
In an interview, lead author and podiatrist Peter A. Crisologo, DPM, of University of Texas Southwestern Medical Center, Dallas, explained the study findings and offered guidance for requesting bone biopsies in possible cases of osteomyelitis.
Q: What makes diagnosis and treatment of osteomyelitis unique?
A: In the foot, there’s not a lot of soft tissue between the outside world and your bone. If the wounds on the feet go deep enough, they can spread a bacterial infection to the bone. This changes how foot infections are treated.
If you have a skin infection, it requires 11-12 days of antibiotics. Things start ramping up once you start getting into the bone. You’re talking potential surgery and 6 weeks of antibiotics through IV treatments. This is why it’s really important that you get your diagnosis right.
A lot of people say “I’m going to do the safe thing” and treat a bone infection with an extended course of antibiotics.
That’s not necessarily safe. If you’re overdiagnosing – for example, you identify bacteria that’s just a contaminant – you could put a patient through 6 weeks of IV treatment along with the risks of a PICC (peripherally inserted central catheter ) line infection, complications from IV placement, and complications from the antibiotic.
Also, acute kidney injury develops in at least a third of the patients who undergo 6 weeks of antibiotics. That’s not to mention the cost of the visits and the labs you have to draw. But we don’t want to underdiagnose either. If osteomyelitis is underdiagnosed and then not treated, the infection can smolder and continue to progress and worsen.
Q: Your study looks at the bone biopsy. How does it fit into care of osteomyelitis in the diabetic foot?
A: A bone biopsy is the standard for diagnosis under the guidelines of the Infectious Diseases Society of America/International Working Group on the Diabetic Foot (Clin Infect Dis. 2012;54[12]:e132-73 ).
But beyond that, nobody says anything. Everyone has an operational definition of how a bone biopsy is interpreted, and there’s a need for a consensus on how a bone biopsy can be used to diagnose osteomyelitis.
You’ll get different percentages of your patients diagnosed with osteomyelitis. For example, someone may say the biopsy is only positive if the histology is positive, while another says the histology doesn’t matter if the culture is positive.
Q: Your study looks at histology and culture analyses. What do these reveal?
A: A traditional culture helps you identify the bacteria, as well as guide your treatment when it’s tested against antibiotics.
A traditional histology allows the pathologist to look under a microscope for signs of osteomyelitis: Do they see the right inflammatory cells, white cells, lymphocytes, combinations of cells? Does this look like an acute or chronic osteomyelitis?
Q: Why might it be wise to combine culture and histology analyses?
A: If you have bacteria that’s difficult to culture via traditional methods, it may be a bacteria that doesn’t grow well or easily. If you combine culture with histology, pathologists can look and say, “Your culture was negative but we see these other signs, so we feel this is osteomyelitis.”
Q: Your study examined 35 consecutive patients aged at least 21 years who had moderate or severe infections bone infections in the foot linked with type 1 diabetes (n = 4) or type 2 diabetes (n = 31).
The samples were analyzed via culture, histology, and culture/histology examinations. You also performed genetic sequencing (quantitative polymerase chain reaction targeting 16S rRNA). How does this test fit in to bone biopsies in the clinic?
A: That’s a newer method and not a standard of care treatment for the diabetic foot. This analysis looks at DNA that’s present, bypassing the analysis of difficult-to-grow bacteria.
Q: What did you discover?
A: In this study, histology had the lowest incidence of positively detecting osteomyelitis. (45.7%). The level increases when a culture is taken (68.6% vs. histology; P = .02).
Then it goes up when DNA is used because it’s catching everything (82.9%, P = .001 vs. histology and P = .31 vs. culture).
[The study also found that adding histology to culture or to genetic sequencing did not change positive findings.]
Q: Does the study suggest one approach is better than the others?
A: This paper doesn’t provide enough evidence to use one method over another. The main purpose was to raise the concern that diagnosis can change dramatically depending on how the gold standard of bone biopsy is interpreted.
Q: What were the pros and cons of the genetic sequencing approach?
A: When we use this approach, our positive diagnostic rate significantly increases. But there are also downsides. We don’t know whether the bacteria we see is alive or dead. We just know it was there. So are the patients truly positive? That’s a question we can’t answer.
Genetic sequencing also doesn’t tell us about susceptibilities to antibiotics.
Q: What is the take-home message here for physicians who may order bone biopsies?
A: The thing to do is request both traditional culture and traditional histology.
As far as DNA sequencing, that not something I’d recommend as a standard of care.
Q: Can you comment on cost and insurance coverage for these approaches?
A: As far as I know, genetic sequencing is not covered as it is not standard of care in the diabetic foot and is used mainly for research at this time.
Pathology and culture are standard of care when evaluating for osteomyelitis and should be a covered service. However, a patient should call their insurance company first prior to having the procedure done to see whether it is covered.
Q: What’s next for research in this area?
A: From here, the next step is bigger numbers: Increase the study size and look at this again. Also, we may be able to identify susceptibilities by identifying resistance within the DNA.
Dr. Crisologo and two other study authors report no relevant disclosures. One study author reported various disclosures including research support, consulting, and service on speakers' bureaus.
EXPERT ANALYSIS FROM ADA 2018
Does Screen Time Reduce Sleep Time?
BALTIMORE—Sleeping with a bed partner’s smartphone notifications within earshot relates to daytime sleepiness. Insomnia symptoms and sleep duration may explain associations between technology use and depressive symptoms in teens. Among students, nighttime cell phone use reduces the likelihood of getting at least eight hours of sleep per night and increases the likelihood of receiving hurtful messages.
Those were among the findings from three studies about technology use and sleep that researchers presented at the 32nd Annual Meeting of the Associated Professional Sleep Societies. The results suggest possible interventions such as education and regulating screen time to improve patients’ sleep and overall health, investigators said.
Screen Time, Depressive Symptoms, and Sleep
“Although screen-based activities, insomnia symptoms, and insufficient sleep are known risk factors for adolescent depressive symptoms, limited research has investigated whether sleep mediates the association between screen time and depressive symptoms,” said Xian Stella Li, PhD, a postdoctoral researcher at Stony Brook University in New York, and colleagues.
To examine how screen activities are associated with depressive symptoms and how sleep mediates these associations, Dr. Li and colleagues analyzed data from 2,865 participants (51% male) in the Fragile Families and Child Wellbeing Study’s teen survey. Participants completed the survey at age 15 and reported problems falling asleep, problems staying asleep, and habitual weeknight sleep duration, as well as depressive symptoms. They also reported the typical daily time spent on four screen-based activities—social messaging, web surfing, watching TV or movies, and gaming. The investigators constructed a multiple mediation model to examine associations between screen time, insomnia symptoms and sleep duration, and depressive symptoms. Covariates included gender, age, race, family structure and income, and primary caregiver’s education.
For social messaging, web surfing, and watching TV or movies, “insomnia symptoms and sleep duration fully mediated the association between screen activities and depressive symptoms,” the researchers said. Furthermore, all four types of screen-based activities “have significant associations with teens’ depressive symptoms mediated by insomnia symptoms and sleep duration.”

“These results suggest that parents, educators, and health care professionals could consider educating adolescents and regulating their screen time as possible interventions for improving sleep health and reducing depression,” said Lauren Hale, PhD, Professor of Family, Population, and Preventive Medicine at Stony Brook University and the study’s principal investigator.
Can a Bed Partner’s Phone Affect Daytime Sleepiness?
Studies have found that the use of interactive social technology around bedtime is related to difficulty falling asleep, unrefreshing sleep, and nighttime awakenings. At the same time, “evidence suggests that bed partners can play a role in the onset and maintenance of insomnia” and that “sleep problems might better be treated as a couple-level phenomenon,” said David F. Mastin, PhD, Professor of Psychology at the University of Arkansas at Little Rock, and colleagues.
To examine whether a bed partner’s passive social technology use is a useful addition to the Sleep Hygiene Index, Dr. Mastin and colleagues analyzed data from 220 introductory psychology students (mean age, 20.1). Participants completed the Epworth Sleepiness Scale, the Pittsburgh Sleep Quality Index, and the Sleep Hygiene Index. “For this study, three additional questions were added [to the Sleep Hygiene Index], two assessing self-bedtime social technology use (active and passive) and one assessing partner (passive) use (ie, I sleep with my bed partner’s phone sounds or vibrations turned on where I could hear them if I were awake).”
In addition, participants indicated how frequently they experienced daytime sleepiness, preoccupation with sleep, mood disturbance, avolition (ie, decreased motivation), and impaired cognition.
Many students frequently or always used social technology at bedtime themselves (60% actively and 64% passively) or were able to hear a partner’s social technology at bedtime (35%).
“Both self and partner social technology use during sleep time were associated with greater daytime sleepiness,” the researchers said. In addition, six of the of the 13 original sleep hygiene items, as well as passive, active, and partner technology use, significantly correlated with greater daytime sleepiness. “The addition of self-use sleep-time technology items strengthened the correlation between the Sleep Hygiene Index and daytime sleepiness, and the addition of partner sleep-time technology use strengthened it even further,” Dr. Mastin and colleagues said. “We suggest social technology use in a dyadic context is an important new aspect of understanding sleep hygiene. Future research should investigate whether bed partner active social technology use similarly disrupts sleep.”
Nighttime Cell Phone Use by Students as Young as 7
Cell phone use at night may be common among children as young as 7, according to an Australian study. This practice “may not only impact negatively on sleep, but may also increase angry or hurtful communication and mental health issues,” researchers said. “On the other hand, it may also facilitate friendship building. Interventions must consider the benefits and potential losses associated with change.”
To study nighttime smartphone use by students and its associations with sleep, indicators of impaired communication, mental health, and relationship building, Jillian Dorrian, PhD, Associate Professor of Psychology at the University of South Australia in Adelaide, and colleagues analyzed data from more than 160,000 Australian students.
Primary and high school students completed an in-class survey about phone use, sleep, and friendships, as well as the General Health Questionnaire. The researchers included data from 169,352 students between ages 7 and 18 (49.9% male) in their analyses.
Fifty-five percent of respondents reported phone use between 10 PM and 6 AM at least once in the past week, including 25% of 7- and 8-year-olds and 83% of 17- and 18-year-olds.
After controlling for age and gender, nighttime phone use was associated with significantly increased odds of having responded to a text in anger (odds ratio, 4.9), having received hurtful messages (odds ratio, 4), or having been cyberbullied in the past month (odds ratio, 2.8). It also increased the likelihood of building friendships, however (odd ratio, 1.2).
In addition, nighttime phone use was associated with reduced odds of getting eight or more hours of sleep per night (odds ratio, 0.5) and less favorable General Health Questionnaire scores.
“Smartphones in the bedroom rob sleep time and facilitate communication during the circadian low,” Dr. Dorrian and colleagues said. “These factors may lead to impaired communication and disturbed mental health. However, nighttime messaging may also foster social connection…. These data highlight the ubiquity of smartphones in the bedroom, and the potential for health-related costs for developing teens, as well as a potential social cost if smartphones are removed without attention to the complete biopsychosocial context.”
—Jake Remaly
BALTIMORE—Sleeping with a bed partner’s smartphone notifications within earshot relates to daytime sleepiness. Insomnia symptoms and sleep duration may explain associations between technology use and depressive symptoms in teens. Among students, nighttime cell phone use reduces the likelihood of getting at least eight hours of sleep per night and increases the likelihood of receiving hurtful messages.
Those were among the findings from three studies about technology use and sleep that researchers presented at the 32nd Annual Meeting of the Associated Professional Sleep Societies. The results suggest possible interventions such as education and regulating screen time to improve patients’ sleep and overall health, investigators said.
Screen Time, Depressive Symptoms, and Sleep
“Although screen-based activities, insomnia symptoms, and insufficient sleep are known risk factors for adolescent depressive symptoms, limited research has investigated whether sleep mediates the association between screen time and depressive symptoms,” said Xian Stella Li, PhD, a postdoctoral researcher at Stony Brook University in New York, and colleagues.
To examine how screen activities are associated with depressive symptoms and how sleep mediates these associations, Dr. Li and colleagues analyzed data from 2,865 participants (51% male) in the Fragile Families and Child Wellbeing Study’s teen survey. Participants completed the survey at age 15 and reported problems falling asleep, problems staying asleep, and habitual weeknight sleep duration, as well as depressive symptoms. They also reported the typical daily time spent on four screen-based activities—social messaging, web surfing, watching TV or movies, and gaming. The investigators constructed a multiple mediation model to examine associations between screen time, insomnia symptoms and sleep duration, and depressive symptoms. Covariates included gender, age, race, family structure and income, and primary caregiver’s education.
For social messaging, web surfing, and watching TV or movies, “insomnia symptoms and sleep duration fully mediated the association between screen activities and depressive symptoms,” the researchers said. Furthermore, all four types of screen-based activities “have significant associations with teens’ depressive symptoms mediated by insomnia symptoms and sleep duration.”
“These results suggest that parents, educators, and health care professionals could consider educating adolescents and regulating their screen time as possible interventions for improving sleep health and reducing depression,” said Lauren Hale, PhD, Professor of Family, Population, and Preventive Medicine at Stony Brook University and the study’s principal investigator.
Can a Bed Partner’s Phone Affect Daytime Sleepiness?
Studies have found that the use of interactive social technology around bedtime is related to difficulty falling asleep, unrefreshing sleep, and nighttime awakenings. At the same time, “evidence suggests that bed partners can play a role in the onset and maintenance of insomnia” and that “sleep problems might better be treated as a couple-level phenomenon,” said David F. Mastin, PhD, Professor of Psychology at the University of Arkansas at Little Rock, and colleagues.
To examine whether a bed partner’s passive social technology use is a useful addition to the Sleep Hygiene Index, Dr. Mastin and colleagues analyzed data from 220 introductory psychology students (mean age, 20.1). Participants completed the Epworth Sleepiness Scale, the Pittsburgh Sleep Quality Index, and the Sleep Hygiene Index. “For this study, three additional questions were added [to the Sleep Hygiene Index], two assessing self-bedtime social technology use (active and passive) and one assessing partner (passive) use (ie, I sleep with my bed partner’s phone sounds or vibrations turned on where I could hear them if I were awake).”
In addition, participants indicated how frequently they experienced daytime sleepiness, preoccupation with sleep, mood disturbance, avolition (ie, decreased motivation), and impaired cognition.
Many students frequently or always used social technology at bedtime themselves (60% actively and 64% passively) or were able to hear a partner’s social technology at bedtime (35%).
“Both self and partner social technology use during sleep time were associated with greater daytime sleepiness,” the researchers said. In addition, six of the of the 13 original sleep hygiene items, as well as passive, active, and partner technology use, significantly correlated with greater daytime sleepiness. “The addition of self-use sleep-time technology items strengthened the correlation between the Sleep Hygiene Index and daytime sleepiness, and the addition of partner sleep-time technology use strengthened it even further,” Dr. Mastin and colleagues said. “We suggest social technology use in a dyadic context is an important new aspect of understanding sleep hygiene. Future research should investigate whether bed partner active social technology use similarly disrupts sleep.”
Nighttime Cell Phone Use by Students as Young as 7
Cell phone use at night may be common among children as young as 7, according to an Australian study. This practice “may not only impact negatively on sleep, but may also increase angry or hurtful communication and mental health issues,” researchers said. “On the other hand, it may also facilitate friendship building. Interventions must consider the benefits and potential losses associated with change.”
To study nighttime smartphone use by students and its associations with sleep, indicators of impaired communication, mental health, and relationship building, Jillian Dorrian, PhD, Associate Professor of Psychology at the University of South Australia in Adelaide, and colleagues analyzed data from more than 160,000 Australian students.
Primary and high school students completed an in-class survey about phone use, sleep, and friendships, as well as the General Health Questionnaire. The researchers included data from 169,352 students between ages 7 and 18 (49.9% male) in their analyses.
Fifty-five percent of respondents reported phone use between 10 PM and 6 AM at least once in the past week, including 25% of 7- and 8-year-olds and 83% of 17- and 18-year-olds.
After controlling for age and gender, nighttime phone use was associated with significantly increased odds of having responded to a text in anger (odds ratio, 4.9), having received hurtful messages (odds ratio, 4), or having been cyberbullied in the past month (odds ratio, 2.8). It also increased the likelihood of building friendships, however (odd ratio, 1.2).
In addition, nighttime phone use was associated with reduced odds of getting eight or more hours of sleep per night (odds ratio, 0.5) and less favorable General Health Questionnaire scores.
“Smartphones in the bedroom rob sleep time and facilitate communication during the circadian low,” Dr. Dorrian and colleagues said. “These factors may lead to impaired communication and disturbed mental health. However, nighttime messaging may also foster social connection…. These data highlight the ubiquity of smartphones in the bedroom, and the potential for health-related costs for developing teens, as well as a potential social cost if smartphones are removed without attention to the complete biopsychosocial context.”
—Jake Remaly
BALTIMORE—Sleeping with a bed partner’s smartphone notifications within earshot relates to daytime sleepiness. Insomnia symptoms and sleep duration may explain associations between technology use and depressive symptoms in teens. Among students, nighttime cell phone use reduces the likelihood of getting at least eight hours of sleep per night and increases the likelihood of receiving hurtful messages.
Those were among the findings from three studies about technology use and sleep that researchers presented at the 32nd Annual Meeting of the Associated Professional Sleep Societies. The results suggest possible interventions such as education and regulating screen time to improve patients’ sleep and overall health, investigators said.
Screen Time, Depressive Symptoms, and Sleep
“Although screen-based activities, insomnia symptoms, and insufficient sleep are known risk factors for adolescent depressive symptoms, limited research has investigated whether sleep mediates the association between screen time and depressive symptoms,” said Xian Stella Li, PhD, a postdoctoral researcher at Stony Brook University in New York, and colleagues.
To examine how screen activities are associated with depressive symptoms and how sleep mediates these associations, Dr. Li and colleagues analyzed data from 2,865 participants (51% male) in the Fragile Families and Child Wellbeing Study’s teen survey. Participants completed the survey at age 15 and reported problems falling asleep, problems staying asleep, and habitual weeknight sleep duration, as well as depressive symptoms. They also reported the typical daily time spent on four screen-based activities—social messaging, web surfing, watching TV or movies, and gaming. The investigators constructed a multiple mediation model to examine associations between screen time, insomnia symptoms and sleep duration, and depressive symptoms. Covariates included gender, age, race, family structure and income, and primary caregiver’s education.
For social messaging, web surfing, and watching TV or movies, “insomnia symptoms and sleep duration fully mediated the association between screen activities and depressive symptoms,” the researchers said. Furthermore, all four types of screen-based activities “have significant associations with teens’ depressive symptoms mediated by insomnia symptoms and sleep duration.”
“These results suggest that parents, educators, and health care professionals could consider educating adolescents and regulating their screen time as possible interventions for improving sleep health and reducing depression,” said Lauren Hale, PhD, Professor of Family, Population, and Preventive Medicine at Stony Brook University and the study’s principal investigator.
Can a Bed Partner’s Phone Affect Daytime Sleepiness?
Studies have found that the use of interactive social technology around bedtime is related to difficulty falling asleep, unrefreshing sleep, and nighttime awakenings. At the same time, “evidence suggests that bed partners can play a role in the onset and maintenance of insomnia” and that “sleep problems might better be treated as a couple-level phenomenon,” said David F. Mastin, PhD, Professor of Psychology at the University of Arkansas at Little Rock, and colleagues.
To examine whether a bed partner’s passive social technology use is a useful addition to the Sleep Hygiene Index, Dr. Mastin and colleagues analyzed data from 220 introductory psychology students (mean age, 20.1). Participants completed the Epworth Sleepiness Scale, the Pittsburgh Sleep Quality Index, and the Sleep Hygiene Index. “For this study, three additional questions were added [to the Sleep Hygiene Index], two assessing self-bedtime social technology use (active and passive) and one assessing partner (passive) use (ie, I sleep with my bed partner’s phone sounds or vibrations turned on where I could hear them if I were awake).”
In addition, participants indicated how frequently they experienced daytime sleepiness, preoccupation with sleep, mood disturbance, avolition (ie, decreased motivation), and impaired cognition.
Many students frequently or always used social technology at bedtime themselves (60% actively and 64% passively) or were able to hear a partner’s social technology at bedtime (35%).
“Both self and partner social technology use during sleep time were associated with greater daytime sleepiness,” the researchers said. In addition, six of the of the 13 original sleep hygiene items, as well as passive, active, and partner technology use, significantly correlated with greater daytime sleepiness. “The addition of self-use sleep-time technology items strengthened the correlation between the Sleep Hygiene Index and daytime sleepiness, and the addition of partner sleep-time technology use strengthened it even further,” Dr. Mastin and colleagues said. “We suggest social technology use in a dyadic context is an important new aspect of understanding sleep hygiene. Future research should investigate whether bed partner active social technology use similarly disrupts sleep.”
Nighttime Cell Phone Use by Students as Young as 7
Cell phone use at night may be common among children as young as 7, according to an Australian study. This practice “may not only impact negatively on sleep, but may also increase angry or hurtful communication and mental health issues,” researchers said. “On the other hand, it may also facilitate friendship building. Interventions must consider the benefits and potential losses associated with change.”
To study nighttime smartphone use by students and its associations with sleep, indicators of impaired communication, mental health, and relationship building, Jillian Dorrian, PhD, Associate Professor of Psychology at the University of South Australia in Adelaide, and colleagues analyzed data from more than 160,000 Australian students.
Primary and high school students completed an in-class survey about phone use, sleep, and friendships, as well as the General Health Questionnaire. The researchers included data from 169,352 students between ages 7 and 18 (49.9% male) in their analyses.
Fifty-five percent of respondents reported phone use between 10 PM and 6 AM at least once in the past week, including 25% of 7- and 8-year-olds and 83% of 17- and 18-year-olds.
After controlling for age and gender, nighttime phone use was associated with significantly increased odds of having responded to a text in anger (odds ratio, 4.9), having received hurtful messages (odds ratio, 4), or having been cyberbullied in the past month (odds ratio, 2.8). It also increased the likelihood of building friendships, however (odd ratio, 1.2).
In addition, nighttime phone use was associated with reduced odds of getting eight or more hours of sleep per night (odds ratio, 0.5) and less favorable General Health Questionnaire scores.
“Smartphones in the bedroom rob sleep time and facilitate communication during the circadian low,” Dr. Dorrian and colleagues said. “These factors may lead to impaired communication and disturbed mental health. However, nighttime messaging may also foster social connection…. These data highlight the ubiquity of smartphones in the bedroom, and the potential for health-related costs for developing teens, as well as a potential social cost if smartphones are removed without attention to the complete biopsychosocial context.”
—Jake Remaly