User login
Magnesium Sulfate for Fetal Neuroprotection in Preterm Birth
Introduction: The Many Lanes of Research on Magnesium Sulfate
The research that improves human health in the most expedient and most impactful ways is multitiered, with basic or fundamental research, translational research, interventional studies, and retrospective research often occurring simultaneously. There should be no “single lane” of research and one type of research does not preclude the other.
Too often, we fall short in one of these lanes. While we have achieved many moonshots in obstetrics and maternal-fetal medicine, we have tended not to place a high priority on basic research, which can provide a strong understanding of the biology of major diseases and conditions affecting women and their offspring. When conducted with proper commitment and funding, such research can lead to biologically directed therapy.
Within our specialty, research on how we can effectively prevent preterm birth, prematurity, and preeclampsia has taken a long road, with various types of therapies being tried, but none being overwhelmingly effective — with an ongoing need for more basic or fundamental research. Nevertheless, we can benefit and gain great insights from retrospective and interventional studies associated with clinical therapies used to treat premature labor and preeclampsia when these therapies have an unanticipated and important secondary benefit.
This month our Master Class is focused on the neuroprotection of prematurity. Magnesium sulfate is a valuable tool for the treatment of both premature labor and preeclampsia, and more recently, also for neuroprotection of the fetus. Interestingly, this use stemmed from researchers looking retrospectively at outcomes in women who received the compound for other reasons. It took many years for researchers to prove its neuroprotective value through interventional trials, while researchers simultaneously strove to understand on a basic biologic level how magnesium sulfate works to prevent outcomes such as cerebral palsy.
Basic research underway today continues to improve our understanding of its precise mechanisms of action. Combined with other tiers of research — including more interventional studies and more translational research — we can improve its utility for the neuroprotection of prematurity. Alternatively, ongoing research may lead to different, even more effective treatments.
Our guest author is Irina Burd, MD, PhD, Sylvan Freiman, MD Endowed Professor and Chair of the department of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine.* Dr. Burd is also a physician-scientist. She recounts the important story of magnesium sulfate and what is currently known about its biologic plausibility in neuroprotection — including through her own studies – as well as what may be coming in the future.

E. Albert Reece, MD, PhD, MBA, a maternal-fetal medicine specialist, is dean emeritus of the University of Maryland School of Medicine, former university executive vice president; currently the endowed professor and director of the Center for Advanced Research Training and Innovation (CARTI), and senior scientist in the Center for Birth Defects Research. Dr. Reece reported no relevant disclosures. He is the medical editor of this column. Contact him at [email protected].
Magnesium Sulfate for Fetal Neuroprotection in Preterm Birth
Without a doubt, magnesium sulfate (MgSO4) given before anticipated preterm birth reduces the risk of cerebral palsy. It is a valuable tool for fetal neuroprotection at a time when there are no proven alternatives. Yet without the persistent research that occurred over more than 20 years, it may not have won the endorsement of the American College of Obstetrics and Gynecologists in 2010 and worked its way into routine practice.
Its history is worthy of reflection. It took years of observational trials (not all of which showed neuroprotective effects), six randomized controlled trials (none of which met their primary endpoint), three meta-analyses, and a Cochrane Database Systematic Review to arrive at the conclusion that antenatal magnesium sulfate therapy given to women at risk of preterm birth has definitive neuroprotective benefit.

This history also holds lessons for our specialty given the dearth of drugs approved for use in pregnancy and the recent withdrawal from the market of Makena — one of only nine drugs to ever be approved by the Food and Drug Administration for use in pregnancy — after a second trial showed lack of benefit in preventing recurrent preterm birth. The story of MgSO4 tells us it’s acceptable to have major stumbling blocks: At one point, MgSO4 was considered to be not only not helpful, but harmful, causing neonatal death. Further research disproved this initial finding.
Moreover, the MgSO4 story is one that remains unfinished, as my laboratory and other researchers work to better understand its biologic plausibility and to discover additional neuroprotective agents for anticipated preterm birth that may further reduce the risk of cerebral palsy. This leading cause of chronic childhood disability is estimated by the United Cerebral Palsy Foundation to affect approximately 800,000 people in the United States.
Origins and Biologic Plausibility
The MgSO4 story is rooted in the late seventeenth century discovery by physician Nehemiah Grew that the compound was the key component of the then-famous medicinal spring waters in Epsom, England.1 MgSO4 was first used for eclampsia in 1906,2 and was first reported in the American literature for eclampsia in 1925.3 In 1959, its effect as a tocolytic agent was reported.4
More than 30 years later, in 1995, an observational study coauthored by Karin B. Nelson, MD, and Judith K. Grether, PhD of the National Institutes of Health, showed a reduced risk of cerebral palsy in very-low-birth-weight infants (VLBW).5 The report marked a turning point in research interest on neuroprotection for anticipated preterm birth.
The precise molecular mechanisms of action of MgSO4 for neuroprotection are still not well understood. However, research findings from the University of Maryland and other institutions have provided biologic plausibility for its use to prevent cerebral palsy. Our current thinking is that it involves the prevention of periventricular white matter injury and/or the prevention of oxidative stress and a neuronal injury mechanism called excitotoxicity.
Periventricular white matter injury involving injury to preoligodendrocytes before 32 weeks’ gestation is the most prevalent injury seen in cerebral palsy; preoligodendrocytes are precursors of myelinating oligodendrocytes, which constitute a major glial population in the white matter. Our research in a mouse model demonstrated that the intrauterine inflammation frequently associated with preterm birth can lead to neuronal injury as well as white matter damage, and that MgSO4 may ameliorate both.6,7
Excitotoxicity results from excessive stimulation of N-methyl-D-aspartate (NMDA) glutamatergic receptors on preoligodendrocytes and a rush of calcium through the voltage-gated channels. This calcium influx leads to the production of nitric oxide, oxidative stress, and subsequent mitochondrial damage and cell death. As a bivalent ion, MgSO4 sits in the voltage-gated channels of the NMDA receptors and reduces glutamatergic signaling, thus serving as a calcium antagonist and modulating calcium influx (See Figure).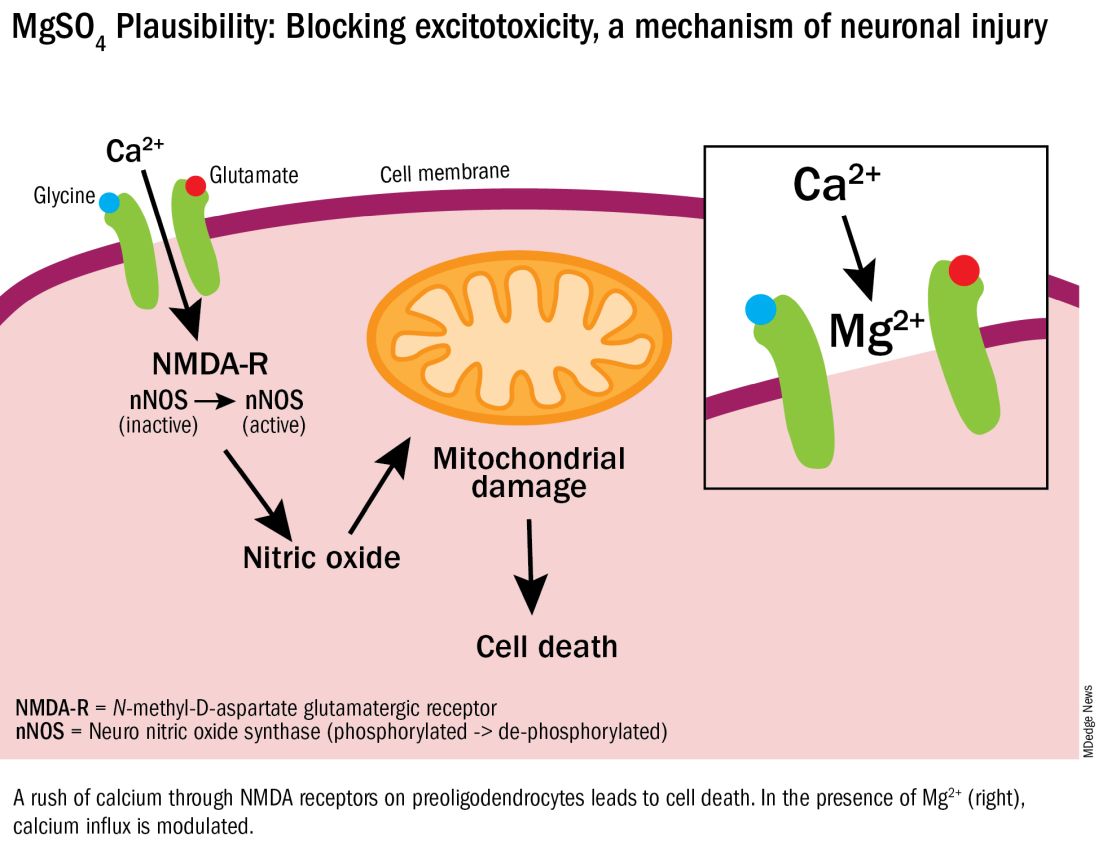
In vitro research in our laboratory has also shown that MgSO4 may dampen inflammatory reactions driven by intrauterine infections, which, like preterm birth, increase the risk of cerebral palsy and adverse neurodevelopmental outcomes.8 MgSO4 appears to do so by blocking the voltage-gated P2X7 receptor in umbilical vein endothelial cells, thus blocking endothelial secretion of the proinflammatory cytokine interleukin (IL)–1beta. Much more research is needed to determine whether MgSO4 could help prevent cerebral palsy through this mechanism.
The Long Route of Research
The 1995 Nelson-Grether study compared VLBW (< 1500 g) infants who survived and developed moderate/severe cerebral palsy within 3 years to randomly selected VLBW controls with respect to whether their mothers had received MgSO4 to prevent seizures in preeclampsia or as a tocolytic agent.5 In a population of more than 155,000 children born between 1983 and 1985, in utero exposure to MgSO4 was reported in 7.1% of 42 VLBW infants with cerebral palsy and 36% of 75 VLBW controls (odds ratio [OR], 0.14; 95% CI, 0.05-0.51). In women without preeclampsia the OR increased to 0.25.
This motivating study had been preceded by several observational studies showing that infants born to women with preeclampsia who received MgSO4 had significantly lower risks of developing intraventricular hemorrhage (IVH) and germinal matrix hemorrhage (GMH). In one of these studies, published in 1992, Karl C. Kuban, MD, and coauthors reported that “maternal receipt of magnesium sulfate was associated with diminished risk of GMH-IVH even in those babies born to mothers who apparently did not have preeclampsia.”9
In the several years following the 1995 Nelson-Grether study, several other case-control/observational studies were reported, with conflicting conclusions, and investigators around the world began designing and conducting needed randomized controlled trials.
The six published randomized controlled trials looking at MgSO4 and neuroprotection varied in their inclusion and exclusion criteria, their recruitment and enrollment style, the gestational ages for MgSO4 administration, loading and maintenance doses, how cerebral palsy or neuroprotection was assessed, and other factors (See Table for RCT characteristics and main outcomes).10-14 One of the trials aimed primarily at evaluating the efficacy of MgSO4 for preventing preeclampsia.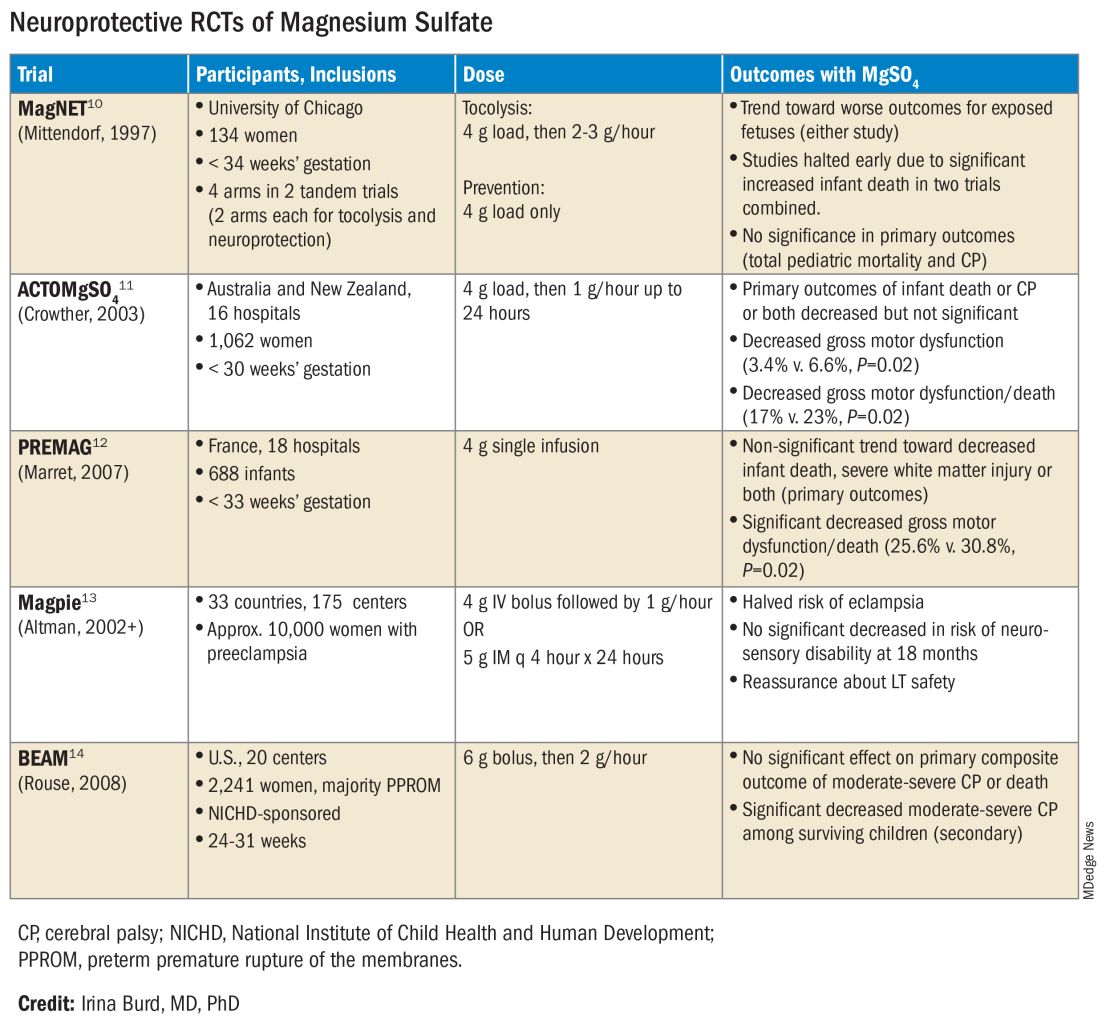
Again, none of the randomized controlled trials demonstrated statistical significance for their primary outcomes or concluded that there was a significant neuroprotective effect for cerebral palsy. Rather, most suggested benefit through secondary analyses. Moreover, as mentioned earlier, research that proceeded after the first published randomized controlled trial — the Magnesium and Neurologic Endpoints (MAGnet) trial — was suspended early when an interim analysis showed a significantly increased risk of mortality in MgSO4-exposed fetuses. All told, it wasn’t until researchers obtained unpublished data and conducted meta-analyses and systematic reviews that a significant effect of MgSO4 on cerebral palsy could be seen.
The three systematic reviews and the Cochrane review, each of which used slightly different methodologies, were published in rapid succession in 2009. One review calculated a relative risk of cerebral palsy of 0.71 (95% CI, 0.55-0.91) — and a relative risk for the combined outcome of death and cerebral palsy at 0.85 (95% CI, 0.74-0.98) — when women at risk of preterm birth were given MgSO4.15 The number needed to treat (NNT) to prevent one case of cerebral palsy was 63, investigators determined, and the NNT to prevent one case of cerebral palsy or infant death was 44.
Another review estimated the NNT for prevention of one case of cerebral palsy at 52 when MgSO4 is given at less than 34 weeks’ gestation, and similarly concluded that MgSO4 is associated with a significantly “reduced risk of moderate/severe CP and substantial gross motor dysfunction without any statistically significant effect on the risk of total pediatric mortality.”16
A third review, from the National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units Network (MFMU), estimated an NNT of 46 to prevent one case of cerebral palsy in infants exposed to MgSO4 before 30 weeks, and an NNT of 56 when exposure occurs before 32-34 weeks.17
The Cochrane Review, meanwhile, reported a relative reduction in the risk of cerebral palsy of 0.68 (95% CI, 0.54-0.87) when antenatal MgSO4 is given at less than 37 weeks’ gestation, as well as a significant reduction in the rate of substantial gross motor dysfunction (RR, 0.61; 95% CI, 0.44-0.85).18 The NNT to avoid one case of cerebral palsy, researchers reported, was 63.
Moving Forward
The NNTs calculated in these reviews — ranging from 44 to 63 — are convincing, and are comparable with evidence-based medicine data for prevention of other common diseases.19 For instance, the NNT for a life saved when aspirin is given immediately after a heart attack is 42. Statins given for 5 years in people with known heart disease have an NNT of 83 to save one life, an NNT of 39 to prevent one nonfatal heart attack, and an NNT of 125 to prevent one stroke. For oral anticoagulants used in nonvalvular atrial fibrillation for primary stroke prevention, the NNTs to prevent one stroke, and one death, are 22 and 42, respectively.19
In its 2010 Committee Opinion on Magnesium Sulfate Before Anticipated Preterm Birth for Neuroprotection (reaffirmed in 2020), the American College of Obstetricians and Gynecologists left it to institutions to develop their own guidelines “regarding inclusion criteria, treatment regimens, concurrent tocolysis, and monitoring in accordance with one of the larger trials.”20
Not surprisingly, most if not all hospitals have chosen a higher dose of MgSO4 administered up to 31 weeks’ gestation in keeping with the protocols employed in the NICHD-sponsored BEAM trial (See Table).
The hope moving forward is to expand treatment options for neuroprotection in cases of imminent preterm birth. Researchers have been assessing the ability of melatonin to provide neuroprotection in cases of growth restriction and neonatal asphyxia. Melatonin has anti-inflammatory and antioxidant properties and is known to mediate neuronal generation and synaptic plasticity.21
N-acetyl-L-cysteine is another potential neuroprotective agent. It acts as an antioxidant, a precursor to glutathione, and a modulator of the glutamate system and has been studied as a neuroprotective agent in cases of maternal chorioamnionitis.21 Both melatonin and N-acetyl-L-cysteine are regarded as safe in pregnancy, but much more clinical study is needed to prove their neuroprotective potential when given shortly before birth or earlier.
Dr. Burd is the Sylvan Freiman, MD Endowed Professor and Chair of the department of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, Baltimore. She has no conflicts of interest.
References
1. Clio Med. 1984;19(1-2):1-21.
2. Medicinsk Rev. (Bergen) 1906;32:264-272.
3. Am J Obstet Gynecol. 1996;174(4):1390-1391.
4. Am J Obstet Gynecol. 1959;78(1):27-32.
5. Pediatrics. 1995;95(2):263-269.
6. Am J Obstet Gynecol. 2009;201(3):279.e1-279.e8.
7. Am J Obstet Gynecol. 2010;202(3):292.e1-292.e9.
8. Pediatr Res. 2020;87(3):463-471.
9. J Child Neurol. 1992;7(1):70-76.
10. Lancet. 1997;350:1517-1518.
11. JAMA. 2003;290:2669-2676.
12. BJOG. 2007;114(3):310-318.
13. Lancet. 2002;359(9321):1877-1890.
14. N Engl J Med. 2008;359:895-905.
15. Obstet Gynecol. 2009;113(6):1327-1333.
16. Am J Obstet Gynecol. 2009;200(6):595-609.
17. Obstet Gynecol 2009;114:354-364.
18. Cochrane Database Syst Rev. 2009 Jan 21:(1):CD004661.
19. www.thennt.com.
20. Obstet Gynecol. 2010;115:669-671.
21. Front Synaptic Neurosci. 2012;13:680899.
*This story was corrected on June 10, 2024.
Introduction: The Many Lanes of Research on Magnesium Sulfate
The research that improves human health in the most expedient and most impactful ways is multitiered, with basic or fundamental research, translational research, interventional studies, and retrospective research often occurring simultaneously. There should be no “single lane” of research and one type of research does not preclude the other.
Too often, we fall short in one of these lanes. While we have achieved many moonshots in obstetrics and maternal-fetal medicine, we have tended not to place a high priority on basic research, which can provide a strong understanding of the biology of major diseases and conditions affecting women and their offspring. When conducted with proper commitment and funding, such research can lead to biologically directed therapy.
Within our specialty, research on how we can effectively prevent preterm birth, prematurity, and preeclampsia has taken a long road, with various types of therapies being tried, but none being overwhelmingly effective — with an ongoing need for more basic or fundamental research. Nevertheless, we can benefit and gain great insights from retrospective and interventional studies associated with clinical therapies used to treat premature labor and preeclampsia when these therapies have an unanticipated and important secondary benefit.
This month our Master Class is focused on the neuroprotection of prematurity. Magnesium sulfate is a valuable tool for the treatment of both premature labor and preeclampsia, and more recently, also for neuroprotection of the fetus. Interestingly, this use stemmed from researchers looking retrospectively at outcomes in women who received the compound for other reasons. It took many years for researchers to prove its neuroprotective value through interventional trials, while researchers simultaneously strove to understand on a basic biologic level how magnesium sulfate works to prevent outcomes such as cerebral palsy.
Basic research underway today continues to improve our understanding of its precise mechanisms of action. Combined with other tiers of research — including more interventional studies and more translational research — we can improve its utility for the neuroprotection of prematurity. Alternatively, ongoing research may lead to different, even more effective treatments.
Our guest author is Irina Burd, MD, PhD, Sylvan Freiman, MD Endowed Professor and Chair of the department of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine.* Dr. Burd is also a physician-scientist. She recounts the important story of magnesium sulfate and what is currently known about its biologic plausibility in neuroprotection — including through her own studies – as well as what may be coming in the future.
E. Albert Reece, MD, PhD, MBA, a maternal-fetal medicine specialist, is dean emeritus of the University of Maryland School of Medicine, former university executive vice president; currently the endowed professor and director of the Center for Advanced Research Training and Innovation (CARTI), and senior scientist in the Center for Birth Defects Research. Dr. Reece reported no relevant disclosures. He is the medical editor of this column. Contact him at [email protected].
Magnesium Sulfate for Fetal Neuroprotection in Preterm Birth
Without a doubt, magnesium sulfate (MgSO4) given before anticipated preterm birth reduces the risk of cerebral palsy. It is a valuable tool for fetal neuroprotection at a time when there are no proven alternatives. Yet without the persistent research that occurred over more than 20 years, it may not have won the endorsement of the American College of Obstetrics and Gynecologists in 2010 and worked its way into routine practice.
Its history is worthy of reflection. It took years of observational trials (not all of which showed neuroprotective effects), six randomized controlled trials (none of which met their primary endpoint), three meta-analyses, and a Cochrane Database Systematic Review to arrive at the conclusion that antenatal magnesium sulfate therapy given to women at risk of preterm birth has definitive neuroprotective benefit.
This history also holds lessons for our specialty given the dearth of drugs approved for use in pregnancy and the recent withdrawal from the market of Makena — one of only nine drugs to ever be approved by the Food and Drug Administration for use in pregnancy — after a second trial showed lack of benefit in preventing recurrent preterm birth. The story of MgSO4 tells us it’s acceptable to have major stumbling blocks: At one point, MgSO4 was considered to be not only not helpful, but harmful, causing neonatal death. Further research disproved this initial finding.
Moreover, the MgSO4 story is one that remains unfinished, as my laboratory and other researchers work to better understand its biologic plausibility and to discover additional neuroprotective agents for anticipated preterm birth that may further reduce the risk of cerebral palsy. This leading cause of chronic childhood disability is estimated by the United Cerebral Palsy Foundation to affect approximately 800,000 people in the United States.
Origins and Biologic Plausibility
The MgSO4 story is rooted in the late seventeenth century discovery by physician Nehemiah Grew that the compound was the key component of the then-famous medicinal spring waters in Epsom, England.1 MgSO4 was first used for eclampsia in 1906,2 and was first reported in the American literature for eclampsia in 1925.3 In 1959, its effect as a tocolytic agent was reported.4
More than 30 years later, in 1995, an observational study coauthored by Karin B. Nelson, MD, and Judith K. Grether, PhD of the National Institutes of Health, showed a reduced risk of cerebral palsy in very-low-birth-weight infants (VLBW).5 The report marked a turning point in research interest on neuroprotection for anticipated preterm birth.
The precise molecular mechanisms of action of MgSO4 for neuroprotection are still not well understood. However, research findings from the University of Maryland and other institutions have provided biologic plausibility for its use to prevent cerebral palsy. Our current thinking is that it involves the prevention of periventricular white matter injury and/or the prevention of oxidative stress and a neuronal injury mechanism called excitotoxicity.
Periventricular white matter injury involving injury to preoligodendrocytes before 32 weeks’ gestation is the most prevalent injury seen in cerebral palsy; preoligodendrocytes are precursors of myelinating oligodendrocytes, which constitute a major glial population in the white matter. Our research in a mouse model demonstrated that the intrauterine inflammation frequently associated with preterm birth can lead to neuronal injury as well as white matter damage, and that MgSO4 may ameliorate both.6,7
Excitotoxicity results from excessive stimulation of N-methyl-D-aspartate (NMDA) glutamatergic receptors on preoligodendrocytes and a rush of calcium through the voltage-gated channels. This calcium influx leads to the production of nitric oxide, oxidative stress, and subsequent mitochondrial damage and cell death. As a bivalent ion, MgSO4 sits in the voltage-gated channels of the NMDA receptors and reduces glutamatergic signaling, thus serving as a calcium antagonist and modulating calcium influx (See Figure).
In vitro research in our laboratory has also shown that MgSO4 may dampen inflammatory reactions driven by intrauterine infections, which, like preterm birth, increase the risk of cerebral palsy and adverse neurodevelopmental outcomes.8 MgSO4 appears to do so by blocking the voltage-gated P2X7 receptor in umbilical vein endothelial cells, thus blocking endothelial secretion of the proinflammatory cytokine interleukin (IL)–1beta. Much more research is needed to determine whether MgSO4 could help prevent cerebral palsy through this mechanism.
The Long Route of Research
The 1995 Nelson-Grether study compared VLBW (< 1500 g) infants who survived and developed moderate/severe cerebral palsy within 3 years to randomly selected VLBW controls with respect to whether their mothers had received MgSO4 to prevent seizures in preeclampsia or as a tocolytic agent.5 In a population of more than 155,000 children born between 1983 and 1985, in utero exposure to MgSO4 was reported in 7.1% of 42 VLBW infants with cerebral palsy and 36% of 75 VLBW controls (odds ratio [OR], 0.14; 95% CI, 0.05-0.51). In women without preeclampsia the OR increased to 0.25.
This motivating study had been preceded by several observational studies showing that infants born to women with preeclampsia who received MgSO4 had significantly lower risks of developing intraventricular hemorrhage (IVH) and germinal matrix hemorrhage (GMH). In one of these studies, published in 1992, Karl C. Kuban, MD, and coauthors reported that “maternal receipt of magnesium sulfate was associated with diminished risk of GMH-IVH even in those babies born to mothers who apparently did not have preeclampsia.”9
In the several years following the 1995 Nelson-Grether study, several other case-control/observational studies were reported, with conflicting conclusions, and investigators around the world began designing and conducting needed randomized controlled trials.
The six published randomized controlled trials looking at MgSO4 and neuroprotection varied in their inclusion and exclusion criteria, their recruitment and enrollment style, the gestational ages for MgSO4 administration, loading and maintenance doses, how cerebral palsy or neuroprotection was assessed, and other factors (See Table for RCT characteristics and main outcomes).10-14 One of the trials aimed primarily at evaluating the efficacy of MgSO4 for preventing preeclampsia.
Again, none of the randomized controlled trials demonstrated statistical significance for their primary outcomes or concluded that there was a significant neuroprotective effect for cerebral palsy. Rather, most suggested benefit through secondary analyses. Moreover, as mentioned earlier, research that proceeded after the first published randomized controlled trial — the Magnesium and Neurologic Endpoints (MAGnet) trial — was suspended early when an interim analysis showed a significantly increased risk of mortality in MgSO4-exposed fetuses. All told, it wasn’t until researchers obtained unpublished data and conducted meta-analyses and systematic reviews that a significant effect of MgSO4 on cerebral palsy could be seen.
The three systematic reviews and the Cochrane review, each of which used slightly different methodologies, were published in rapid succession in 2009. One review calculated a relative risk of cerebral palsy of 0.71 (95% CI, 0.55-0.91) — and a relative risk for the combined outcome of death and cerebral palsy at 0.85 (95% CI, 0.74-0.98) — when women at risk of preterm birth were given MgSO4.15 The number needed to treat (NNT) to prevent one case of cerebral palsy was 63, investigators determined, and the NNT to prevent one case of cerebral palsy or infant death was 44.
Another review estimated the NNT for prevention of one case of cerebral palsy at 52 when MgSO4 is given at less than 34 weeks’ gestation, and similarly concluded that MgSO4 is associated with a significantly “reduced risk of moderate/severe CP and substantial gross motor dysfunction without any statistically significant effect on the risk of total pediatric mortality.”16
A third review, from the National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units Network (MFMU), estimated an NNT of 46 to prevent one case of cerebral palsy in infants exposed to MgSO4 before 30 weeks, and an NNT of 56 when exposure occurs before 32-34 weeks.17
The Cochrane Review, meanwhile, reported a relative reduction in the risk of cerebral palsy of 0.68 (95% CI, 0.54-0.87) when antenatal MgSO4 is given at less than 37 weeks’ gestation, as well as a significant reduction in the rate of substantial gross motor dysfunction (RR, 0.61; 95% CI, 0.44-0.85).18 The NNT to avoid one case of cerebral palsy, researchers reported, was 63.
Moving Forward
The NNTs calculated in these reviews — ranging from 44 to 63 — are convincing, and are comparable with evidence-based medicine data for prevention of other common diseases.19 For instance, the NNT for a life saved when aspirin is given immediately after a heart attack is 42. Statins given for 5 years in people with known heart disease have an NNT of 83 to save one life, an NNT of 39 to prevent one nonfatal heart attack, and an NNT of 125 to prevent one stroke. For oral anticoagulants used in nonvalvular atrial fibrillation for primary stroke prevention, the NNTs to prevent one stroke, and one death, are 22 and 42, respectively.19
In its 2010 Committee Opinion on Magnesium Sulfate Before Anticipated Preterm Birth for Neuroprotection (reaffirmed in 2020), the American College of Obstetricians and Gynecologists left it to institutions to develop their own guidelines “regarding inclusion criteria, treatment regimens, concurrent tocolysis, and monitoring in accordance with one of the larger trials.”20
Not surprisingly, most if not all hospitals have chosen a higher dose of MgSO4 administered up to 31 weeks’ gestation in keeping with the protocols employed in the NICHD-sponsored BEAM trial (See Table).
The hope moving forward is to expand treatment options for neuroprotection in cases of imminent preterm birth. Researchers have been assessing the ability of melatonin to provide neuroprotection in cases of growth restriction and neonatal asphyxia. Melatonin has anti-inflammatory and antioxidant properties and is known to mediate neuronal generation and synaptic plasticity.21
N-acetyl-L-cysteine is another potential neuroprotective agent. It acts as an antioxidant, a precursor to glutathione, and a modulator of the glutamate system and has been studied as a neuroprotective agent in cases of maternal chorioamnionitis.21 Both melatonin and N-acetyl-L-cysteine are regarded as safe in pregnancy, but much more clinical study is needed to prove their neuroprotective potential when given shortly before birth or earlier.
Dr. Burd is the Sylvan Freiman, MD Endowed Professor and Chair of the department of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, Baltimore. She has no conflicts of interest.
References
1. Clio Med. 1984;19(1-2):1-21.
2. Medicinsk Rev. (Bergen) 1906;32:264-272.
3. Am J Obstet Gynecol. 1996;174(4):1390-1391.
4. Am J Obstet Gynecol. 1959;78(1):27-32.
5. Pediatrics. 1995;95(2):263-269.
6. Am J Obstet Gynecol. 2009;201(3):279.e1-279.e8.
7. Am J Obstet Gynecol. 2010;202(3):292.e1-292.e9.
8. Pediatr Res. 2020;87(3):463-471.
9. J Child Neurol. 1992;7(1):70-76.
10. Lancet. 1997;350:1517-1518.
11. JAMA. 2003;290:2669-2676.
12. BJOG. 2007;114(3):310-318.
13. Lancet. 2002;359(9321):1877-1890.
14. N Engl J Med. 2008;359:895-905.
15. Obstet Gynecol. 2009;113(6):1327-1333.
16. Am J Obstet Gynecol. 2009;200(6):595-609.
17. Obstet Gynecol 2009;114:354-364.
18. Cochrane Database Syst Rev. 2009 Jan 21:(1):CD004661.
19. www.thennt.com.
20. Obstet Gynecol. 2010;115:669-671.
21. Front Synaptic Neurosci. 2012;13:680899.
*This story was corrected on June 10, 2024.
Introduction: The Many Lanes of Research on Magnesium Sulfate
The research that improves human health in the most expedient and most impactful ways is multitiered, with basic or fundamental research, translational research, interventional studies, and retrospective research often occurring simultaneously. There should be no “single lane” of research and one type of research does not preclude the other.
Too often, we fall short in one of these lanes. While we have achieved many moonshots in obstetrics and maternal-fetal medicine, we have tended not to place a high priority on basic research, which can provide a strong understanding of the biology of major diseases and conditions affecting women and their offspring. When conducted with proper commitment and funding, such research can lead to biologically directed therapy.
Within our specialty, research on how we can effectively prevent preterm birth, prematurity, and preeclampsia has taken a long road, with various types of therapies being tried, but none being overwhelmingly effective — with an ongoing need for more basic or fundamental research. Nevertheless, we can benefit and gain great insights from retrospective and interventional studies associated with clinical therapies used to treat premature labor and preeclampsia when these therapies have an unanticipated and important secondary benefit.
This month our Master Class is focused on the neuroprotection of prematurity. Magnesium sulfate is a valuable tool for the treatment of both premature labor and preeclampsia, and more recently, also for neuroprotection of the fetus. Interestingly, this use stemmed from researchers looking retrospectively at outcomes in women who received the compound for other reasons. It took many years for researchers to prove its neuroprotective value through interventional trials, while researchers simultaneously strove to understand on a basic biologic level how magnesium sulfate works to prevent outcomes such as cerebral palsy.
Basic research underway today continues to improve our understanding of its precise mechanisms of action. Combined with other tiers of research — including more interventional studies and more translational research — we can improve its utility for the neuroprotection of prematurity. Alternatively, ongoing research may lead to different, even more effective treatments.
Our guest author is Irina Burd, MD, PhD, Sylvan Freiman, MD Endowed Professor and Chair of the department of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine.* Dr. Burd is also a physician-scientist. She recounts the important story of magnesium sulfate and what is currently known about its biologic plausibility in neuroprotection — including through her own studies – as well as what may be coming in the future.
E. Albert Reece, MD, PhD, MBA, a maternal-fetal medicine specialist, is dean emeritus of the University of Maryland School of Medicine, former university executive vice president; currently the endowed professor and director of the Center for Advanced Research Training and Innovation (CARTI), and senior scientist in the Center for Birth Defects Research. Dr. Reece reported no relevant disclosures. He is the medical editor of this column. Contact him at [email protected].
Magnesium Sulfate for Fetal Neuroprotection in Preterm Birth
Without a doubt, magnesium sulfate (MgSO4) given before anticipated preterm birth reduces the risk of cerebral palsy. It is a valuable tool for fetal neuroprotection at a time when there are no proven alternatives. Yet without the persistent research that occurred over more than 20 years, it may not have won the endorsement of the American College of Obstetrics and Gynecologists in 2010 and worked its way into routine practice.
Its history is worthy of reflection. It took years of observational trials (not all of which showed neuroprotective effects), six randomized controlled trials (none of which met their primary endpoint), three meta-analyses, and a Cochrane Database Systematic Review to arrive at the conclusion that antenatal magnesium sulfate therapy given to women at risk of preterm birth has definitive neuroprotective benefit.
This history also holds lessons for our specialty given the dearth of drugs approved for use in pregnancy and the recent withdrawal from the market of Makena — one of only nine drugs to ever be approved by the Food and Drug Administration for use in pregnancy — after a second trial showed lack of benefit in preventing recurrent preterm birth. The story of MgSO4 tells us it’s acceptable to have major stumbling blocks: At one point, MgSO4 was considered to be not only not helpful, but harmful, causing neonatal death. Further research disproved this initial finding.
Moreover, the MgSO4 story is one that remains unfinished, as my laboratory and other researchers work to better understand its biologic plausibility and to discover additional neuroprotective agents for anticipated preterm birth that may further reduce the risk of cerebral palsy. This leading cause of chronic childhood disability is estimated by the United Cerebral Palsy Foundation to affect approximately 800,000 people in the United States.
Origins and Biologic Plausibility
The MgSO4 story is rooted in the late seventeenth century discovery by physician Nehemiah Grew that the compound was the key component of the then-famous medicinal spring waters in Epsom, England.1 MgSO4 was first used for eclampsia in 1906,2 and was first reported in the American literature for eclampsia in 1925.3 In 1959, its effect as a tocolytic agent was reported.4
More than 30 years later, in 1995, an observational study coauthored by Karin B. Nelson, MD, and Judith K. Grether, PhD of the National Institutes of Health, showed a reduced risk of cerebral palsy in very-low-birth-weight infants (VLBW).5 The report marked a turning point in research interest on neuroprotection for anticipated preterm birth.
The precise molecular mechanisms of action of MgSO4 for neuroprotection are still not well understood. However, research findings from the University of Maryland and other institutions have provided biologic plausibility for its use to prevent cerebral palsy. Our current thinking is that it involves the prevention of periventricular white matter injury and/or the prevention of oxidative stress and a neuronal injury mechanism called excitotoxicity.
Periventricular white matter injury involving injury to preoligodendrocytes before 32 weeks’ gestation is the most prevalent injury seen in cerebral palsy; preoligodendrocytes are precursors of myelinating oligodendrocytes, which constitute a major glial population in the white matter. Our research in a mouse model demonstrated that the intrauterine inflammation frequently associated with preterm birth can lead to neuronal injury as well as white matter damage, and that MgSO4 may ameliorate both.6,7
Excitotoxicity results from excessive stimulation of N-methyl-D-aspartate (NMDA) glutamatergic receptors on preoligodendrocytes and a rush of calcium through the voltage-gated channels. This calcium influx leads to the production of nitric oxide, oxidative stress, and subsequent mitochondrial damage and cell death. As a bivalent ion, MgSO4 sits in the voltage-gated channels of the NMDA receptors and reduces glutamatergic signaling, thus serving as a calcium antagonist and modulating calcium influx (See Figure).
In vitro research in our laboratory has also shown that MgSO4 may dampen inflammatory reactions driven by intrauterine infections, which, like preterm birth, increase the risk of cerebral palsy and adverse neurodevelopmental outcomes.8 MgSO4 appears to do so by blocking the voltage-gated P2X7 receptor in umbilical vein endothelial cells, thus blocking endothelial secretion of the proinflammatory cytokine interleukin (IL)–1beta. Much more research is needed to determine whether MgSO4 could help prevent cerebral palsy through this mechanism.
The Long Route of Research
The 1995 Nelson-Grether study compared VLBW (< 1500 g) infants who survived and developed moderate/severe cerebral palsy within 3 years to randomly selected VLBW controls with respect to whether their mothers had received MgSO4 to prevent seizures in preeclampsia or as a tocolytic agent.5 In a population of more than 155,000 children born between 1983 and 1985, in utero exposure to MgSO4 was reported in 7.1% of 42 VLBW infants with cerebral palsy and 36% of 75 VLBW controls (odds ratio [OR], 0.14; 95% CI, 0.05-0.51). In women without preeclampsia the OR increased to 0.25.
This motivating study had been preceded by several observational studies showing that infants born to women with preeclampsia who received MgSO4 had significantly lower risks of developing intraventricular hemorrhage (IVH) and germinal matrix hemorrhage (GMH). In one of these studies, published in 1992, Karl C. Kuban, MD, and coauthors reported that “maternal receipt of magnesium sulfate was associated with diminished risk of GMH-IVH even in those babies born to mothers who apparently did not have preeclampsia.”9
In the several years following the 1995 Nelson-Grether study, several other case-control/observational studies were reported, with conflicting conclusions, and investigators around the world began designing and conducting needed randomized controlled trials.
The six published randomized controlled trials looking at MgSO4 and neuroprotection varied in their inclusion and exclusion criteria, their recruitment and enrollment style, the gestational ages for MgSO4 administration, loading and maintenance doses, how cerebral palsy or neuroprotection was assessed, and other factors (See Table for RCT characteristics and main outcomes).10-14 One of the trials aimed primarily at evaluating the efficacy of MgSO4 for preventing preeclampsia.
Again, none of the randomized controlled trials demonstrated statistical significance for their primary outcomes or concluded that there was a significant neuroprotective effect for cerebral palsy. Rather, most suggested benefit through secondary analyses. Moreover, as mentioned earlier, research that proceeded after the first published randomized controlled trial — the Magnesium and Neurologic Endpoints (MAGnet) trial — was suspended early when an interim analysis showed a significantly increased risk of mortality in MgSO4-exposed fetuses. All told, it wasn’t until researchers obtained unpublished data and conducted meta-analyses and systematic reviews that a significant effect of MgSO4 on cerebral palsy could be seen.
The three systematic reviews and the Cochrane review, each of which used slightly different methodologies, were published in rapid succession in 2009. One review calculated a relative risk of cerebral palsy of 0.71 (95% CI, 0.55-0.91) — and a relative risk for the combined outcome of death and cerebral palsy at 0.85 (95% CI, 0.74-0.98) — when women at risk of preterm birth were given MgSO4.15 The number needed to treat (NNT) to prevent one case of cerebral palsy was 63, investigators determined, and the NNT to prevent one case of cerebral palsy or infant death was 44.
Another review estimated the NNT for prevention of one case of cerebral palsy at 52 when MgSO4 is given at less than 34 weeks’ gestation, and similarly concluded that MgSO4 is associated with a significantly “reduced risk of moderate/severe CP and substantial gross motor dysfunction without any statistically significant effect on the risk of total pediatric mortality.”16
A third review, from the National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units Network (MFMU), estimated an NNT of 46 to prevent one case of cerebral palsy in infants exposed to MgSO4 before 30 weeks, and an NNT of 56 when exposure occurs before 32-34 weeks.17
The Cochrane Review, meanwhile, reported a relative reduction in the risk of cerebral palsy of 0.68 (95% CI, 0.54-0.87) when antenatal MgSO4 is given at less than 37 weeks’ gestation, as well as a significant reduction in the rate of substantial gross motor dysfunction (RR, 0.61; 95% CI, 0.44-0.85).18 The NNT to avoid one case of cerebral palsy, researchers reported, was 63.
Moving Forward
The NNTs calculated in these reviews — ranging from 44 to 63 — are convincing, and are comparable with evidence-based medicine data for prevention of other common diseases.19 For instance, the NNT for a life saved when aspirin is given immediately after a heart attack is 42. Statins given for 5 years in people with known heart disease have an NNT of 83 to save one life, an NNT of 39 to prevent one nonfatal heart attack, and an NNT of 125 to prevent one stroke. For oral anticoagulants used in nonvalvular atrial fibrillation for primary stroke prevention, the NNTs to prevent one stroke, and one death, are 22 and 42, respectively.19
In its 2010 Committee Opinion on Magnesium Sulfate Before Anticipated Preterm Birth for Neuroprotection (reaffirmed in 2020), the American College of Obstetricians and Gynecologists left it to institutions to develop their own guidelines “regarding inclusion criteria, treatment regimens, concurrent tocolysis, and monitoring in accordance with one of the larger trials.”20
Not surprisingly, most if not all hospitals have chosen a higher dose of MgSO4 administered up to 31 weeks’ gestation in keeping with the protocols employed in the NICHD-sponsored BEAM trial (See Table).
The hope moving forward is to expand treatment options for neuroprotection in cases of imminent preterm birth. Researchers have been assessing the ability of melatonin to provide neuroprotection in cases of growth restriction and neonatal asphyxia. Melatonin has anti-inflammatory and antioxidant properties and is known to mediate neuronal generation and synaptic plasticity.21
N-acetyl-L-cysteine is another potential neuroprotective agent. It acts as an antioxidant, a precursor to glutathione, and a modulator of the glutamate system and has been studied as a neuroprotective agent in cases of maternal chorioamnionitis.21 Both melatonin and N-acetyl-L-cysteine are regarded as safe in pregnancy, but much more clinical study is needed to prove their neuroprotective potential when given shortly before birth or earlier.
Dr. Burd is the Sylvan Freiman, MD Endowed Professor and Chair of the department of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, Baltimore. She has no conflicts of interest.
References
1. Clio Med. 1984;19(1-2):1-21.
2. Medicinsk Rev. (Bergen) 1906;32:264-272.
3. Am J Obstet Gynecol. 1996;174(4):1390-1391.
4. Am J Obstet Gynecol. 1959;78(1):27-32.
5. Pediatrics. 1995;95(2):263-269.
6. Am J Obstet Gynecol. 2009;201(3):279.e1-279.e8.
7. Am J Obstet Gynecol. 2010;202(3):292.e1-292.e9.
8. Pediatr Res. 2020;87(3):463-471.
9. J Child Neurol. 1992;7(1):70-76.
10. Lancet. 1997;350:1517-1518.
11. JAMA. 2003;290:2669-2676.
12. BJOG. 2007;114(3):310-318.
13. Lancet. 2002;359(9321):1877-1890.
14. N Engl J Med. 2008;359:895-905.
15. Obstet Gynecol. 2009;113(6):1327-1333.
16. Am J Obstet Gynecol. 2009;200(6):595-609.
17. Obstet Gynecol 2009;114:354-364.
18. Cochrane Database Syst Rev. 2009 Jan 21:(1):CD004661.
19. www.thennt.com.
20. Obstet Gynecol. 2010;115:669-671.
21. Front Synaptic Neurosci. 2012;13:680899.
*This story was corrected on June 10, 2024.
Direct Measurement of T3 Is Likely Vital, Say Researchers
To assess thyroid function, clinicians typically determine blood levels of thyroid-stimulating hormone (TSH) and thyroxine (T4) and do not directly measure triiodothyronine (T3).
However, linking socioeconomic forces, human biology, and aging,” researchers reported.
The study, with lead author Ralph I. Lawton, an MD-PhD student at Harvard Medical School, Boston, was published online on January 4, 2024, in Proceedings of the National Academy of Sciences. In this national sample of healthy adults older than 20, free T3 was negatively related to household income. At age 40 and older, free T3 was significantly linked to being employed. Among adults from age 51 to 80, free T3 levels were inversely related to mortality.
“It is important to note that the more typically measured biomarkers for thyroid function (T4 and TSH) are poorly linked to free T3 levels,” Dr. Lawton and colleagues wrote.
The ratio of TSH:T4 explained only 1.7% of variation in T3 levels, they noted, which suggested that TSH and T4 may not be accurate surrogates of free T3. Thus, “direct measurement of free T3 is likely vital to properly stratify the effects of HPT-axis variation,” they maintained. “Improved methods for measurement [of T3] and further investigation of the role of free T3 in clinical conditions may be high yield,” according to the researchers.
Further studies of the relationship between the action of deiodinase in converting T4 to T3 and social forces and aging could elucidate critical biology. “New therapeutics targeting T3/T4 ratios,” they suggested, “may be more beneficial for a significant cohort of older individuals [with hypothyroidism] currently treated with levothyroxine [(LT4)].”
‘Cherry on Top’
“I think this is a really important paper,” thyroidology expert Antonio Bianco, MD, PhD, professor of medicine, The University of Chicago, who was not involved with this research, told this news organization.
His research group and others “have slowly been providing evidence of the relevance of measuring T3 levels,” he said. “This paper is sort of a cherry on top. It is really the most recent strong evidence that looking at T3 levels in plasma is really important. We need to do a better job at developing a much more precise assay for T3,” he said, “because now we know T3 is a very important parameter that endocrinologists should be looking for. We know that about 20 million Americans have hypothyroidism, and are being treated with T4 (levothyroxine),” Dr. Bianco continued.
“As endocrinologists, we believe that if you treat someone with levothyroxine, you normalize T3 levels. However, many times, with standard of care with levothyroxine, T3 levels are not normalized.”
Larger Variations in T3
Thyroid hormones (TSH, free T4, and free T3) influence many aspects of human physiology and behavior, but it is not known how variations in these levels in a population free of thyroid disease are associated with mortality and socioeconomic factors.
The researchers analyzed data from 7626 adults over age 20 up to age 80 who participated in the National Health and Nutrition Examination Survey during 2007-2012 and had blood tests to determine TSH, free T4, and free T3 and were not being actively treated for thyroid conditions. Among the 3603 older adults (over age 50), there were 981 deaths up until the end of 2019. TSH levels were not linked to mortality, but increasing levels of free T3 and decreasing levels of free T4 were protective for mortality (hazard ratios, 0.88 and 1.26, respectively; P < .01).
There was a robust negative relationship between household income and employment and free T3 but no relationship between these factors and T4. There was a much larger variation across age in levels of free T3 than in levels of TSH or free T4. Free T4 and free T3 diverged at older ages, when free T4 increased and free T3 continually decreased.
Older adults with symptoms of hypothyroidism may have high free T4 levels despite low free T3, the researchers noted.
“In a nonclinical sample representative of the US population,” they summarized, “we find that free T3 is much more strongly related to all domains studied — age, sex, seasonality, household income, employment, and longevity — than the other molecules of the HPT axis.”
This work was supported by the Burroughs Wellcome Fund Career at Scientific Interface award, a Brain and Behavior Research Foundation young investigator award, the Howard Hughes Medical Institute, the National Institute of Aging, and the National Institute of General Medical Sciences. Dr. Bianco served as a consultant for AbbVie, Avion Pharmaceuticals, Synthonics, Synthion, and Thyron and recently published the book Rethinking Hypothyroidism: Why Treatment Must Change and What Patients Can Do.
A version of this article appeared on Medscape.com.
To assess thyroid function, clinicians typically determine blood levels of thyroid-stimulating hormone (TSH) and thyroxine (T4) and do not directly measure triiodothyronine (T3).
However, linking socioeconomic forces, human biology, and aging,” researchers reported.
The study, with lead author Ralph I. Lawton, an MD-PhD student at Harvard Medical School, Boston, was published online on January 4, 2024, in Proceedings of the National Academy of Sciences. In this national sample of healthy adults older than 20, free T3 was negatively related to household income. At age 40 and older, free T3 was significantly linked to being employed. Among adults from age 51 to 80, free T3 levels were inversely related to mortality.
“It is important to note that the more typically measured biomarkers for thyroid function (T4 and TSH) are poorly linked to free T3 levels,” Dr. Lawton and colleagues wrote.
The ratio of TSH:T4 explained only 1.7% of variation in T3 levels, they noted, which suggested that TSH and T4 may not be accurate surrogates of free T3. Thus, “direct measurement of free T3 is likely vital to properly stratify the effects of HPT-axis variation,” they maintained. “Improved methods for measurement [of T3] and further investigation of the role of free T3 in clinical conditions may be high yield,” according to the researchers.
Further studies of the relationship between the action of deiodinase in converting T4 to T3 and social forces and aging could elucidate critical biology. “New therapeutics targeting T3/T4 ratios,” they suggested, “may be more beneficial for a significant cohort of older individuals [with hypothyroidism] currently treated with levothyroxine [(LT4)].”
‘Cherry on Top’
“I think this is a really important paper,” thyroidology expert Antonio Bianco, MD, PhD, professor of medicine, The University of Chicago, who was not involved with this research, told this news organization.
His research group and others “have slowly been providing evidence of the relevance of measuring T3 levels,” he said. “This paper is sort of a cherry on top. It is really the most recent strong evidence that looking at T3 levels in plasma is really important. We need to do a better job at developing a much more precise assay for T3,” he said, “because now we know T3 is a very important parameter that endocrinologists should be looking for. We know that about 20 million Americans have hypothyroidism, and are being treated with T4 (levothyroxine),” Dr. Bianco continued.
“As endocrinologists, we believe that if you treat someone with levothyroxine, you normalize T3 levels. However, many times, with standard of care with levothyroxine, T3 levels are not normalized.”
Larger Variations in T3
Thyroid hormones (TSH, free T4, and free T3) influence many aspects of human physiology and behavior, but it is not known how variations in these levels in a population free of thyroid disease are associated with mortality and socioeconomic factors.
The researchers analyzed data from 7626 adults over age 20 up to age 80 who participated in the National Health and Nutrition Examination Survey during 2007-2012 and had blood tests to determine TSH, free T4, and free T3 and were not being actively treated for thyroid conditions. Among the 3603 older adults (over age 50), there were 981 deaths up until the end of 2019. TSH levels were not linked to mortality, but increasing levels of free T3 and decreasing levels of free T4 were protective for mortality (hazard ratios, 0.88 and 1.26, respectively; P < .01).
There was a robust negative relationship between household income and employment and free T3 but no relationship between these factors and T4. There was a much larger variation across age in levels of free T3 than in levels of TSH or free T4. Free T4 and free T3 diverged at older ages, when free T4 increased and free T3 continually decreased.
Older adults with symptoms of hypothyroidism may have high free T4 levels despite low free T3, the researchers noted.
“In a nonclinical sample representative of the US population,” they summarized, “we find that free T3 is much more strongly related to all domains studied — age, sex, seasonality, household income, employment, and longevity — than the other molecules of the HPT axis.”
This work was supported by the Burroughs Wellcome Fund Career at Scientific Interface award, a Brain and Behavior Research Foundation young investigator award, the Howard Hughes Medical Institute, the National Institute of Aging, and the National Institute of General Medical Sciences. Dr. Bianco served as a consultant for AbbVie, Avion Pharmaceuticals, Synthonics, Synthion, and Thyron and recently published the book Rethinking Hypothyroidism: Why Treatment Must Change and What Patients Can Do.
A version of this article appeared on Medscape.com.
To assess thyroid function, clinicians typically determine blood levels of thyroid-stimulating hormone (TSH) and thyroxine (T4) and do not directly measure triiodothyronine (T3).
However, linking socioeconomic forces, human biology, and aging,” researchers reported.
The study, with lead author Ralph I. Lawton, an MD-PhD student at Harvard Medical School, Boston, was published online on January 4, 2024, in Proceedings of the National Academy of Sciences. In this national sample of healthy adults older than 20, free T3 was negatively related to household income. At age 40 and older, free T3 was significantly linked to being employed. Among adults from age 51 to 80, free T3 levels were inversely related to mortality.
“It is important to note that the more typically measured biomarkers for thyroid function (T4 and TSH) are poorly linked to free T3 levels,” Dr. Lawton and colleagues wrote.
The ratio of TSH:T4 explained only 1.7% of variation in T3 levels, they noted, which suggested that TSH and T4 may not be accurate surrogates of free T3. Thus, “direct measurement of free T3 is likely vital to properly stratify the effects of HPT-axis variation,” they maintained. “Improved methods for measurement [of T3] and further investigation of the role of free T3 in clinical conditions may be high yield,” according to the researchers.
Further studies of the relationship between the action of deiodinase in converting T4 to T3 and social forces and aging could elucidate critical biology. “New therapeutics targeting T3/T4 ratios,” they suggested, “may be more beneficial for a significant cohort of older individuals [with hypothyroidism] currently treated with levothyroxine [(LT4)].”
‘Cherry on Top’
“I think this is a really important paper,” thyroidology expert Antonio Bianco, MD, PhD, professor of medicine, The University of Chicago, who was not involved with this research, told this news organization.
His research group and others “have slowly been providing evidence of the relevance of measuring T3 levels,” he said. “This paper is sort of a cherry on top. It is really the most recent strong evidence that looking at T3 levels in plasma is really important. We need to do a better job at developing a much more precise assay for T3,” he said, “because now we know T3 is a very important parameter that endocrinologists should be looking for. We know that about 20 million Americans have hypothyroidism, and are being treated with T4 (levothyroxine),” Dr. Bianco continued.
“As endocrinologists, we believe that if you treat someone with levothyroxine, you normalize T3 levels. However, many times, with standard of care with levothyroxine, T3 levels are not normalized.”
Larger Variations in T3
Thyroid hormones (TSH, free T4, and free T3) influence many aspects of human physiology and behavior, but it is not known how variations in these levels in a population free of thyroid disease are associated with mortality and socioeconomic factors.
The researchers analyzed data from 7626 adults over age 20 up to age 80 who participated in the National Health and Nutrition Examination Survey during 2007-2012 and had blood tests to determine TSH, free T4, and free T3 and were not being actively treated for thyroid conditions. Among the 3603 older adults (over age 50), there were 981 deaths up until the end of 2019. TSH levels were not linked to mortality, but increasing levels of free T3 and decreasing levels of free T4 were protective for mortality (hazard ratios, 0.88 and 1.26, respectively; P < .01).
There was a robust negative relationship between household income and employment and free T3 but no relationship between these factors and T4. There was a much larger variation across age in levels of free T3 than in levels of TSH or free T4. Free T4 and free T3 diverged at older ages, when free T4 increased and free T3 continually decreased.
Older adults with symptoms of hypothyroidism may have high free T4 levels despite low free T3, the researchers noted.
“In a nonclinical sample representative of the US population,” they summarized, “we find that free T3 is much more strongly related to all domains studied — age, sex, seasonality, household income, employment, and longevity — than the other molecules of the HPT axis.”
This work was supported by the Burroughs Wellcome Fund Career at Scientific Interface award, a Brain and Behavior Research Foundation young investigator award, the Howard Hughes Medical Institute, the National Institute of Aging, and the National Institute of General Medical Sciences. Dr. Bianco served as a consultant for AbbVie, Avion Pharmaceuticals, Synthonics, Synthion, and Thyron and recently published the book Rethinking Hypothyroidism: Why Treatment Must Change and What Patients Can Do.
A version of this article appeared on Medscape.com.
Are You Unwittingly Aiding the Rise of Superfungi?
Unnecessary or incorrect use of topical antifungal medications is driving the spread of fungal infections like ringworm, which are becoming more difficult to treat, according to a January 11 study published in Morbidity and Mortality Weekly Report.
If a patient’s condition is not caused by a fungus but is treated as such, treatment will be ineffective.
such as clotrimazole or combinations of antifungals and corticosteroids. And because many topical treatments are also available over-the-counter, doctors should advise patients about how to use them correctly.
“In the last few years, there have been many antifungal resistant cases of tinea corporisand onychomycosisreported,” or ringworm and finger or toenail infections, respectively, said Shari Lipner, MD, PhD, a dermatologist at Weill Cornell Medicine in New York, and an author of the study.
Many of these cases originated in South Asia and have also been reported in Europe and Canada. In 2023, the first cases of a new strain of antifungal-resistant ringworm were reported in the United States. This species, Trichophyton indotineae, does not respond to topical medications, requiring oral treatment instead.
“It’s really a serious problem and a huge public health concern,” Dr. Lipner said.
For the new study, Dr. Lipner and colleagues examined prescription patterns from 2021 Medicare Part D claims of topical antifungals. They report that 6.5 million topical antifungal prescriptions were filled that year, some of which included steroids in the formulation. Primary care clinicians wrote 40% of these prescriptions, the most for any clinician group. The estimate is almost certainly an undercount of topical antifungal use because the database did not include over-the-counter purchases or data from other insurance payers.
The number of prescriptions equate to 1 in every 8 Medicare Part D beneficiary receiving an antifungal, the researchers reported.
“If I think about the patients that come into my office, I’m certainly not giving an antifungal to 1 in 8 of them, and I see a lot of fungal infections,” Dr. Lipner said. The findings suggest to Dr. Lipner that some clinicians are diagnosing ringworm by eyesight alone rather than confirming the diagnosis with techniques such as microscopy, fungal culture testing, or polymerase chain reaction testing.
Sometimes what looks like ringworm may actually be eczema, in which case, the topical antifungal would not be appropriate, according to Avrom Caplan, MD, a dermatologist at NYU Langone Health in New York.
“If you’re prescribing something to somebody that they don’t need, you’re basically exposing them to the side effects without the benefit,” Dr. Caplan, who was not part of the study, said.
Dr. Caplan, who reported the first cases of ringworm that only responded to oral medications in the United States, stressed that topical treatments work fine for many ringworm cases today. But if indiscriminate prescribing spurs the development of more resilient fungi, more situations may arise in which only oral medications work in the future, Dr. Caplan said. In addition, oral medications are inherently more demanding on a patient than something they can rub on their skin, Dr. Caplan added.
“We hope that physicians will really think hard about this study and change their practices if they’re not confirming the diagnosis,” Dr. Lipner said.
Dr. Lipner and Dr. Caplan report no relevant financial relationships.
A version of this article appeared on Medscape.com.
Unnecessary or incorrect use of topical antifungal medications is driving the spread of fungal infections like ringworm, which are becoming more difficult to treat, according to a January 11 study published in Morbidity and Mortality Weekly Report.
If a patient’s condition is not caused by a fungus but is treated as such, treatment will be ineffective.
such as clotrimazole or combinations of antifungals and corticosteroids. And because many topical treatments are also available over-the-counter, doctors should advise patients about how to use them correctly.
“In the last few years, there have been many antifungal resistant cases of tinea corporisand onychomycosisreported,” or ringworm and finger or toenail infections, respectively, said Shari Lipner, MD, PhD, a dermatologist at Weill Cornell Medicine in New York, and an author of the study.
Many of these cases originated in South Asia and have also been reported in Europe and Canada. In 2023, the first cases of a new strain of antifungal-resistant ringworm were reported in the United States. This species, Trichophyton indotineae, does not respond to topical medications, requiring oral treatment instead.
“It’s really a serious problem and a huge public health concern,” Dr. Lipner said.
For the new study, Dr. Lipner and colleagues examined prescription patterns from 2021 Medicare Part D claims of topical antifungals. They report that 6.5 million topical antifungal prescriptions were filled that year, some of which included steroids in the formulation. Primary care clinicians wrote 40% of these prescriptions, the most for any clinician group. The estimate is almost certainly an undercount of topical antifungal use because the database did not include over-the-counter purchases or data from other insurance payers.
The number of prescriptions equate to 1 in every 8 Medicare Part D beneficiary receiving an antifungal, the researchers reported.
“If I think about the patients that come into my office, I’m certainly not giving an antifungal to 1 in 8 of them, and I see a lot of fungal infections,” Dr. Lipner said. The findings suggest to Dr. Lipner that some clinicians are diagnosing ringworm by eyesight alone rather than confirming the diagnosis with techniques such as microscopy, fungal culture testing, or polymerase chain reaction testing.
Sometimes what looks like ringworm may actually be eczema, in which case, the topical antifungal would not be appropriate, according to Avrom Caplan, MD, a dermatologist at NYU Langone Health in New York.
“If you’re prescribing something to somebody that they don’t need, you’re basically exposing them to the side effects without the benefit,” Dr. Caplan, who was not part of the study, said.
Dr. Caplan, who reported the first cases of ringworm that only responded to oral medications in the United States, stressed that topical treatments work fine for many ringworm cases today. But if indiscriminate prescribing spurs the development of more resilient fungi, more situations may arise in which only oral medications work in the future, Dr. Caplan said. In addition, oral medications are inherently more demanding on a patient than something they can rub on their skin, Dr. Caplan added.
“We hope that physicians will really think hard about this study and change their practices if they’re not confirming the diagnosis,” Dr. Lipner said.
Dr. Lipner and Dr. Caplan report no relevant financial relationships.
A version of this article appeared on Medscape.com.
Unnecessary or incorrect use of topical antifungal medications is driving the spread of fungal infections like ringworm, which are becoming more difficult to treat, according to a January 11 study published in Morbidity and Mortality Weekly Report.
If a patient’s condition is not caused by a fungus but is treated as such, treatment will be ineffective.
such as clotrimazole or combinations of antifungals and corticosteroids. And because many topical treatments are also available over-the-counter, doctors should advise patients about how to use them correctly.
“In the last few years, there have been many antifungal resistant cases of tinea corporisand onychomycosisreported,” or ringworm and finger or toenail infections, respectively, said Shari Lipner, MD, PhD, a dermatologist at Weill Cornell Medicine in New York, and an author of the study.
Many of these cases originated in South Asia and have also been reported in Europe and Canada. In 2023, the first cases of a new strain of antifungal-resistant ringworm were reported in the United States. This species, Trichophyton indotineae, does not respond to topical medications, requiring oral treatment instead.
“It’s really a serious problem and a huge public health concern,” Dr. Lipner said.
For the new study, Dr. Lipner and colleagues examined prescription patterns from 2021 Medicare Part D claims of topical antifungals. They report that 6.5 million topical antifungal prescriptions were filled that year, some of which included steroids in the formulation. Primary care clinicians wrote 40% of these prescriptions, the most for any clinician group. The estimate is almost certainly an undercount of topical antifungal use because the database did not include over-the-counter purchases or data from other insurance payers.
The number of prescriptions equate to 1 in every 8 Medicare Part D beneficiary receiving an antifungal, the researchers reported.
“If I think about the patients that come into my office, I’m certainly not giving an antifungal to 1 in 8 of them, and I see a lot of fungal infections,” Dr. Lipner said. The findings suggest to Dr. Lipner that some clinicians are diagnosing ringworm by eyesight alone rather than confirming the diagnosis with techniques such as microscopy, fungal culture testing, or polymerase chain reaction testing.
Sometimes what looks like ringworm may actually be eczema, in which case, the topical antifungal would not be appropriate, according to Avrom Caplan, MD, a dermatologist at NYU Langone Health in New York.
“If you’re prescribing something to somebody that they don’t need, you’re basically exposing them to the side effects without the benefit,” Dr. Caplan, who was not part of the study, said.
Dr. Caplan, who reported the first cases of ringworm that only responded to oral medications in the United States, stressed that topical treatments work fine for many ringworm cases today. But if indiscriminate prescribing spurs the development of more resilient fungi, more situations may arise in which only oral medications work in the future, Dr. Caplan said. In addition, oral medications are inherently more demanding on a patient than something they can rub on their skin, Dr. Caplan added.
“We hope that physicians will really think hard about this study and change their practices if they’re not confirming the diagnosis,” Dr. Lipner said.
Dr. Lipner and Dr. Caplan report no relevant financial relationships.
A version of this article appeared on Medscape.com.
Chronic Fatigue Syndrome and Fibromyalgia: A Single Disease Entity?
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and fibromyalgia (FM) have overlapping neurologic symptoms — particularly profound fatigue. The similarity between these two conditions has led to the question of whether they are indeed distinct central nervous system (CNS) entities, or whether they exist along a spectrum and are actually two different manifestations of the same disease process.
A new study utilized a novel methodology — unbiased quantitative mass spectrometry-based proteomics — to investigate this question by analyzing cerebrospinal fluid (CSF) in a group of patients with ME/CFS and another group of patients diagnosed with both ME/CFS and FM.
Close to 2,100 proteins were identified, of which nearly 1,800 were common to both conditions.
“ME/CFS and fibromyalgia do not appear to be distinct entities, with respect to their cerebrospinal fluid proteins,” lead author Steven Schutzer, MD, professor of medicine, Rutgers New Jersey School of Medicine, told this news organization.
“Work is underway to solve the multiple mysteries of ME/CFS, fibromyalgia, and other neurologic-associated diseases,” he continued. “We have further affirmed that we have a precise objective discovery tool in our hands. Collectively studying multiple diseases brings clarity to each individual disease.”
The study was published in the December 2023 issue of Annals of Medicine.
Cutting-Edge Technology
“ME/CFS is characterized by disabling fatigue, and FM is an illness characterized by body-wide pain,” Dr. Schutzer said. These “medically unexplained” illnesses often coexist by current definitions, and the overlap between them has suggested that they may be part of the “same illness spectrum.”
But co-investigator Benjamin Natelson, MD, professor of neurology and director of the Pain and Fatigue Study Center, Mount Sinai, New York, and others found in previous research that there are distinct differences between the conditions, raising the possibility that there may be different pathophysiological processes.
“The physicians and scientists on our team have had longstanding interest in studying neurologic diseases with cutting-edge tools such as mass spectrometry applied to CSF,” Dr. Schutzer said. “We have had success using this message to distinguish diseases such as ME/CFS from post-treatment Lyme disease, multiple sclerosis, and healthy normal people.”
Dr. Schutzer explained that Dr. Natelson had acquired CSF samples from “well-characterized [ME/CFS] patients and controls.”
Since the cause of ME/CFS is “unknown,” it seemed “ripe to investigate it further with the discovery tool of mass spectrometry” by harnessing the “most advanced equipment in the country at the pacific Northwest National Laboratory, which is part of the US Department of Energy.”
Dr. Schutzer noted that it was the “merger of different clinical and laboratory expertise” that enabled them to address whether ME/CFS and FM are two distinct disease processes.
The choice of analyzing CSF is that it’s the fluid closest to the brain, he added. “A lot of people have studied ME/CFS peripherally because they don’t have access to spinal fluid or it’s easier to look peripherally in the blood, but that doesn’t mean that the blood is where the real ‘action’ is occurring.”
The researchers compared the CSF of 15 patients with ME/CFS only to 15 patients with ME/CFS+FM using mass spectrometry-based proteomics, which they had employed in previous research to see whether ME/CFS was distinct from persistent neurologic Lyme disease syndrome.
This technology has become the “method of choice and discovery tool to rapidly uncover protein biomarkers that can distinguish one disease from another,” the authors stated.
In particular, in unbiased quantitative mass spectrometry-based proteomics, the researchers do not have to know in advance what’s in a sample before studying it, Dr. Schutzer explained.
Shared Pathophysiology?
Both groups of patients were of similar age (41.3 ± 9.4 years and 40.1 ± 11.0 years, respectively), with no differences in gender or rates of current comorbid psychiatric diagnoses between the groups.
The researchers quantified a total of 2,083 proteins, including 1,789 that were specifically quantified in all of the CSF samples, regardless of the presence or absence of FM.
Several analyses (including an ANOVA analysis with adjusted P values, a Random Forest machine learning approach that looked at relative protein abundance changes between those with ME/CFS and ME/CFS+FM, and unsupervised hierarchical clustering analyses) did not find distinguishing differences between the groups.
the authors stated.
They noted that both conditions are “medically unexplained,” with core symptoms of pain, fatigue, sleep problems, and cognitive difficulty. The fact that these two syndromes coexist so often has led to the assumption that the “similarities between them outweigh the differences,” they wrote.
They pointed to some differences between the conditions, including an increase in substance P in the CSF of FM patients, but not in ME/CFS patients reported by others. There are also some immunological, physiological and genetic differences.
But if the conclusion that the two illnesses may share a similar pathophysiological basis is supported by other research that includes FM-only patients as comparators to those with ME/CFS, “this would support the notion that the two illnesses fall along a common illness spectrum and may be approached as a single entity — with implications for both diagnosis and the development of new treatment approaches,” they concluded.
‘Noncontributory’ Findings
Commenting on the research, Robert G. Lahita, MD, PhD, director of the Institute for Autoimmune and Rheumatic Diseases, St. Joseph Health, Wayne, New Jersey, stated that he does not regard these diseases as neurologic but rather as rheumatologic.
“Most neurologists don’t see these diseases, but as a rheumatologist, I see them every day,” said Dr. Lahita, professor of medicine at Hackensack (New Jersey) Meridian School of Medicine and a clinical professor of medicine at Rutgers New Jersey Medical School, New Brunswick. “ME/CFS isn’t as common in my practice, but we do deal with many post-COVID patients who are afflicted mostly with ME/CFS.”
He noted that an important reason for fatigue in FM is that patients generally don’t sleep, or their sleep is disrupted. This is different from the cause of fatigue in ME/CFS.
In addition, the small sample size and the lack of difference between males and females were both limitations of the current study, said Dr. Lahita, who was not involved in this research. “We know that FM disproportionately affects women — in my practice, for example, over 95% of the patients with FM are female — while ME/CFS affects both genders similarly.”
Using proteomics as a biomarker was also problematic, according to Dr. Lahita. “It would have been more valuable to investigate differences in cytokines, for example,” he suggested.
Ultimately, Dr. Lahita thinks that the study is “non-contributory to the field and, as complex as the analysis was, it does nothing to shed differentiate the two conditions or explain the syndromes themselves.”
He added that it would have been more valuable to compare ME/CFS not only to ME/CFS plus FM but also with FM without ME/CFS and to healthy controls, and perhaps to a group with an autoimmune condition, such as lupus or Hashimoto’s thyroiditis.
Dr. Schutzer acknowledged that a limitation of the current study is that his team was unable analyze the CSF of patients with only FM. He and his colleagues “combed the world’s labs” for existing CSF samples of patients with FM alone but were unable to obtain any. “We see this study as a ‘stepping stone’ and hope that future studies will include patients with FM who are willing to donate CSF samples that we can use for comparison,” he said.
The authors received support from the National Institutes of Health, National Institute of Allergy and Infectious Diseases, and National Institute of Neurological Disorders and Stroke. Dr. Schutzer, coauthors, and Dr. Lahita reported no relevant financial relationships.
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and fibromyalgia (FM) have overlapping neurologic symptoms — particularly profound fatigue. The similarity between these two conditions has led to the question of whether they are indeed distinct central nervous system (CNS) entities, or whether they exist along a spectrum and are actually two different manifestations of the same disease process.
A new study utilized a novel methodology — unbiased quantitative mass spectrometry-based proteomics — to investigate this question by analyzing cerebrospinal fluid (CSF) in a group of patients with ME/CFS and another group of patients diagnosed with both ME/CFS and FM.
Close to 2,100 proteins were identified, of which nearly 1,800 were common to both conditions.
“ME/CFS and fibromyalgia do not appear to be distinct entities, with respect to their cerebrospinal fluid proteins,” lead author Steven Schutzer, MD, professor of medicine, Rutgers New Jersey School of Medicine, told this news organization.
“Work is underway to solve the multiple mysteries of ME/CFS, fibromyalgia, and other neurologic-associated diseases,” he continued. “We have further affirmed that we have a precise objective discovery tool in our hands. Collectively studying multiple diseases brings clarity to each individual disease.”
The study was published in the December 2023 issue of Annals of Medicine.
Cutting-Edge Technology
“ME/CFS is characterized by disabling fatigue, and FM is an illness characterized by body-wide pain,” Dr. Schutzer said. These “medically unexplained” illnesses often coexist by current definitions, and the overlap between them has suggested that they may be part of the “same illness spectrum.”
But co-investigator Benjamin Natelson, MD, professor of neurology and director of the Pain and Fatigue Study Center, Mount Sinai, New York, and others found in previous research that there are distinct differences between the conditions, raising the possibility that there may be different pathophysiological processes.
“The physicians and scientists on our team have had longstanding interest in studying neurologic diseases with cutting-edge tools such as mass spectrometry applied to CSF,” Dr. Schutzer said. “We have had success using this message to distinguish diseases such as ME/CFS from post-treatment Lyme disease, multiple sclerosis, and healthy normal people.”
Dr. Schutzer explained that Dr. Natelson had acquired CSF samples from “well-characterized [ME/CFS] patients and controls.”
Since the cause of ME/CFS is “unknown,” it seemed “ripe to investigate it further with the discovery tool of mass spectrometry” by harnessing the “most advanced equipment in the country at the pacific Northwest National Laboratory, which is part of the US Department of Energy.”
Dr. Schutzer noted that it was the “merger of different clinical and laboratory expertise” that enabled them to address whether ME/CFS and FM are two distinct disease processes.
The choice of analyzing CSF is that it’s the fluid closest to the brain, he added. “A lot of people have studied ME/CFS peripherally because they don’t have access to spinal fluid or it’s easier to look peripherally in the blood, but that doesn’t mean that the blood is where the real ‘action’ is occurring.”
The researchers compared the CSF of 15 patients with ME/CFS only to 15 patients with ME/CFS+FM using mass spectrometry-based proteomics, which they had employed in previous research to see whether ME/CFS was distinct from persistent neurologic Lyme disease syndrome.
This technology has become the “method of choice and discovery tool to rapidly uncover protein biomarkers that can distinguish one disease from another,” the authors stated.
In particular, in unbiased quantitative mass spectrometry-based proteomics, the researchers do not have to know in advance what’s in a sample before studying it, Dr. Schutzer explained.
Shared Pathophysiology?
Both groups of patients were of similar age (41.3 ± 9.4 years and 40.1 ± 11.0 years, respectively), with no differences in gender or rates of current comorbid psychiatric diagnoses between the groups.
The researchers quantified a total of 2,083 proteins, including 1,789 that were specifically quantified in all of the CSF samples, regardless of the presence or absence of FM.
Several analyses (including an ANOVA analysis with adjusted P values, a Random Forest machine learning approach that looked at relative protein abundance changes between those with ME/CFS and ME/CFS+FM, and unsupervised hierarchical clustering analyses) did not find distinguishing differences between the groups.
the authors stated.
They noted that both conditions are “medically unexplained,” with core symptoms of pain, fatigue, sleep problems, and cognitive difficulty. The fact that these two syndromes coexist so often has led to the assumption that the “similarities between them outweigh the differences,” they wrote.
They pointed to some differences between the conditions, including an increase in substance P in the CSF of FM patients, but not in ME/CFS patients reported by others. There are also some immunological, physiological and genetic differences.
But if the conclusion that the two illnesses may share a similar pathophysiological basis is supported by other research that includes FM-only patients as comparators to those with ME/CFS, “this would support the notion that the two illnesses fall along a common illness spectrum and may be approached as a single entity — with implications for both diagnosis and the development of new treatment approaches,” they concluded.
‘Noncontributory’ Findings
Commenting on the research, Robert G. Lahita, MD, PhD, director of the Institute for Autoimmune and Rheumatic Diseases, St. Joseph Health, Wayne, New Jersey, stated that he does not regard these diseases as neurologic but rather as rheumatologic.
“Most neurologists don’t see these diseases, but as a rheumatologist, I see them every day,” said Dr. Lahita, professor of medicine at Hackensack (New Jersey) Meridian School of Medicine and a clinical professor of medicine at Rutgers New Jersey Medical School, New Brunswick. “ME/CFS isn’t as common in my practice, but we do deal with many post-COVID patients who are afflicted mostly with ME/CFS.”
He noted that an important reason for fatigue in FM is that patients generally don’t sleep, or their sleep is disrupted. This is different from the cause of fatigue in ME/CFS.
In addition, the small sample size and the lack of difference between males and females were both limitations of the current study, said Dr. Lahita, who was not involved in this research. “We know that FM disproportionately affects women — in my practice, for example, over 95% of the patients with FM are female — while ME/CFS affects both genders similarly.”
Using proteomics as a biomarker was also problematic, according to Dr. Lahita. “It would have been more valuable to investigate differences in cytokines, for example,” he suggested.
Ultimately, Dr. Lahita thinks that the study is “non-contributory to the field and, as complex as the analysis was, it does nothing to shed differentiate the two conditions or explain the syndromes themselves.”
He added that it would have been more valuable to compare ME/CFS not only to ME/CFS plus FM but also with FM without ME/CFS and to healthy controls, and perhaps to a group with an autoimmune condition, such as lupus or Hashimoto’s thyroiditis.
Dr. Schutzer acknowledged that a limitation of the current study is that his team was unable analyze the CSF of patients with only FM. He and his colleagues “combed the world’s labs” for existing CSF samples of patients with FM alone but were unable to obtain any. “We see this study as a ‘stepping stone’ and hope that future studies will include patients with FM who are willing to donate CSF samples that we can use for comparison,” he said.
The authors received support from the National Institutes of Health, National Institute of Allergy and Infectious Diseases, and National Institute of Neurological Disorders and Stroke. Dr. Schutzer, coauthors, and Dr. Lahita reported no relevant financial relationships.
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and fibromyalgia (FM) have overlapping neurologic symptoms — particularly profound fatigue. The similarity between these two conditions has led to the question of whether they are indeed distinct central nervous system (CNS) entities, or whether they exist along a spectrum and are actually two different manifestations of the same disease process.
A new study utilized a novel methodology — unbiased quantitative mass spectrometry-based proteomics — to investigate this question by analyzing cerebrospinal fluid (CSF) in a group of patients with ME/CFS and another group of patients diagnosed with both ME/CFS and FM.
Close to 2,100 proteins were identified, of which nearly 1,800 were common to both conditions.
“ME/CFS and fibromyalgia do not appear to be distinct entities, with respect to their cerebrospinal fluid proteins,” lead author Steven Schutzer, MD, professor of medicine, Rutgers New Jersey School of Medicine, told this news organization.
“Work is underway to solve the multiple mysteries of ME/CFS, fibromyalgia, and other neurologic-associated diseases,” he continued. “We have further affirmed that we have a precise objective discovery tool in our hands. Collectively studying multiple diseases brings clarity to each individual disease.”
The study was published in the December 2023 issue of Annals of Medicine.
Cutting-Edge Technology
“ME/CFS is characterized by disabling fatigue, and FM is an illness characterized by body-wide pain,” Dr. Schutzer said. These “medically unexplained” illnesses often coexist by current definitions, and the overlap between them has suggested that they may be part of the “same illness spectrum.”
But co-investigator Benjamin Natelson, MD, professor of neurology and director of the Pain and Fatigue Study Center, Mount Sinai, New York, and others found in previous research that there are distinct differences between the conditions, raising the possibility that there may be different pathophysiological processes.
“The physicians and scientists on our team have had longstanding interest in studying neurologic diseases with cutting-edge tools such as mass spectrometry applied to CSF,” Dr. Schutzer said. “We have had success using this message to distinguish diseases such as ME/CFS from post-treatment Lyme disease, multiple sclerosis, and healthy normal people.”
Dr. Schutzer explained that Dr. Natelson had acquired CSF samples from “well-characterized [ME/CFS] patients and controls.”
Since the cause of ME/CFS is “unknown,” it seemed “ripe to investigate it further with the discovery tool of mass spectrometry” by harnessing the “most advanced equipment in the country at the pacific Northwest National Laboratory, which is part of the US Department of Energy.”
Dr. Schutzer noted that it was the “merger of different clinical and laboratory expertise” that enabled them to address whether ME/CFS and FM are two distinct disease processes.
The choice of analyzing CSF is that it’s the fluid closest to the brain, he added. “A lot of people have studied ME/CFS peripherally because they don’t have access to spinal fluid or it’s easier to look peripherally in the blood, but that doesn’t mean that the blood is where the real ‘action’ is occurring.”
The researchers compared the CSF of 15 patients with ME/CFS only to 15 patients with ME/CFS+FM using mass spectrometry-based proteomics, which they had employed in previous research to see whether ME/CFS was distinct from persistent neurologic Lyme disease syndrome.
This technology has become the “method of choice and discovery tool to rapidly uncover protein biomarkers that can distinguish one disease from another,” the authors stated.
In particular, in unbiased quantitative mass spectrometry-based proteomics, the researchers do not have to know in advance what’s in a sample before studying it, Dr. Schutzer explained.
Shared Pathophysiology?
Both groups of patients were of similar age (41.3 ± 9.4 years and 40.1 ± 11.0 years, respectively), with no differences in gender or rates of current comorbid psychiatric diagnoses between the groups.
The researchers quantified a total of 2,083 proteins, including 1,789 that were specifically quantified in all of the CSF samples, regardless of the presence or absence of FM.
Several analyses (including an ANOVA analysis with adjusted P values, a Random Forest machine learning approach that looked at relative protein abundance changes between those with ME/CFS and ME/CFS+FM, and unsupervised hierarchical clustering analyses) did not find distinguishing differences between the groups.
the authors stated.
They noted that both conditions are “medically unexplained,” with core symptoms of pain, fatigue, sleep problems, and cognitive difficulty. The fact that these two syndromes coexist so often has led to the assumption that the “similarities between them outweigh the differences,” they wrote.
They pointed to some differences between the conditions, including an increase in substance P in the CSF of FM patients, but not in ME/CFS patients reported by others. There are also some immunological, physiological and genetic differences.
But if the conclusion that the two illnesses may share a similar pathophysiological basis is supported by other research that includes FM-only patients as comparators to those with ME/CFS, “this would support the notion that the two illnesses fall along a common illness spectrum and may be approached as a single entity — with implications for both diagnosis and the development of new treatment approaches,” they concluded.
‘Noncontributory’ Findings
Commenting on the research, Robert G. Lahita, MD, PhD, director of the Institute for Autoimmune and Rheumatic Diseases, St. Joseph Health, Wayne, New Jersey, stated that he does not regard these diseases as neurologic but rather as rheumatologic.
“Most neurologists don’t see these diseases, but as a rheumatologist, I see them every day,” said Dr. Lahita, professor of medicine at Hackensack (New Jersey) Meridian School of Medicine and a clinical professor of medicine at Rutgers New Jersey Medical School, New Brunswick. “ME/CFS isn’t as common in my practice, but we do deal with many post-COVID patients who are afflicted mostly with ME/CFS.”
He noted that an important reason for fatigue in FM is that patients generally don’t sleep, or their sleep is disrupted. This is different from the cause of fatigue in ME/CFS.
In addition, the small sample size and the lack of difference between males and females were both limitations of the current study, said Dr. Lahita, who was not involved in this research. “We know that FM disproportionately affects women — in my practice, for example, over 95% of the patients with FM are female — while ME/CFS affects both genders similarly.”
Using proteomics as a biomarker was also problematic, according to Dr. Lahita. “It would have been more valuable to investigate differences in cytokines, for example,” he suggested.
Ultimately, Dr. Lahita thinks that the study is “non-contributory to the field and, as complex as the analysis was, it does nothing to shed differentiate the two conditions or explain the syndromes themselves.”
He added that it would have been more valuable to compare ME/CFS not only to ME/CFS plus FM but also with FM without ME/CFS and to healthy controls, and perhaps to a group with an autoimmune condition, such as lupus or Hashimoto’s thyroiditis.
Dr. Schutzer acknowledged that a limitation of the current study is that his team was unable analyze the CSF of patients with only FM. He and his colleagues “combed the world’s labs” for existing CSF samples of patients with FM alone but were unable to obtain any. “We see this study as a ‘stepping stone’ and hope that future studies will include patients with FM who are willing to donate CSF samples that we can use for comparison,” he said.
The authors received support from the National Institutes of Health, National Institute of Allergy and Infectious Diseases, and National Institute of Neurological Disorders and Stroke. Dr. Schutzer, coauthors, and Dr. Lahita reported no relevant financial relationships.
Coming Soon: The First mRNA Vaccine for Melanoma?
Moderna and Merck have presented promising results from their phase 2b clinical trial that investigated a combination of a messenger RNA (mRNA) vaccine and a cancer drug for the treatment of melanoma.
Is mRNA set to shake up the world of cancer treatment? This is certainly what Moderna seems to think; the pharmaceutical company has published the results of a phase 2b trial combining its mRNA vaccine (mRNA-4157 [V940]) with Merck’s cancer drug KEYTRUDA. While these are not the final results but rather mid-term data from the 3-year follow-up, they are somewhat promising. The randomized KEYNOTE-942/mRNA-4157-P201 clinical trial involves patients with high-risk (stage III/IV) melanoma following complete resection.
Relapse Risk Halved
Treatment with mRNA-4157 (V940) in combination with pembrolizumab led to a clinically meaningful improvement in recurrence-free survival, reducing the risk for recurrence or death by 49%, compared with pembrolizumab alone. T, reducing the risk of developing distant metastasis or death by 62%. “The KEYNOTE-942/mRNA-4157-P201 study was the first demonstration of efficacy for an investigational mRNA cancer treatment in a randomized clinical trial and the first combination therapy to show a significant benefit over pembrolizumab alone in adjuvant melanoma,” said Kyle Holen, MD, Moderna’s senior vice president, after presenting these results.
Side Effects
The combined treatment also did not demonstrate more significant side effects than pembrolizumab alone. The number of patients reporting treatment-related adverse events of grade 3 or greater was similar between the arms (25% for mRNA-4157 [V940] with pembrolizumab vs 20% for KEYTRUDA alone). The most common adverse events of any grade attributed to mRNA-4157 (V940) were fatigue (60.6%), injection site pain (56.7%), and chills (49%). Based on data from the phase 2b KEYNOTE-942/mRNA-4157-P201 study, the US Food and Drug Administration and European Medicines Agency granted breakthrough therapy designation and recognition under the the Priority Medicines scheme, respectively, for mRNA-4157 (V940) in combination with KEYTRUDA for the adjuvant treatment of patients with high-risk melanoma.
Phase 3 Trial
In July, Moderna and Merck announced the launch of a phase 3 trial, assessing “mRNA-4157 [V940] in combination with pembrolizumab as adjuvant treatment in patients with high-risk resected melanoma [stages IIB-IV].” Stéphane Bancel, Moderna’s director general, believes that an mRNA vaccine for melanoma could be available in 2025.
Other Cancer Vaccines
Moderna is not the only laboratory to set its sights on developing a vaccine for cancer. In May, BioNTech, in partnership with Roche, proposed a phase 1 clinical trial of a vaccine targeting pancreatic cancer in Nature. In June, at the American Society of Clinical Oncology›s conference, Transgene presented its conclusions concerning its viral vector vaccines against ENT and papillomavirus-linked cancers. And in September, Ose Immunotherapeutics made headlines with its vaccine for advanced lung cancer.
This article was translated from Univadis France, which is part of the Medscape Professional Network.
Moderna and Merck have presented promising results from their phase 2b clinical trial that investigated a combination of a messenger RNA (mRNA) vaccine and a cancer drug for the treatment of melanoma.
Is mRNA set to shake up the world of cancer treatment? This is certainly what Moderna seems to think; the pharmaceutical company has published the results of a phase 2b trial combining its mRNA vaccine (mRNA-4157 [V940]) with Merck’s cancer drug KEYTRUDA. While these are not the final results but rather mid-term data from the 3-year follow-up, they are somewhat promising. The randomized KEYNOTE-942/mRNA-4157-P201 clinical trial involves patients with high-risk (stage III/IV) melanoma following complete resection.
Relapse Risk Halved
Treatment with mRNA-4157 (V940) in combination with pembrolizumab led to a clinically meaningful improvement in recurrence-free survival, reducing the risk for recurrence or death by 49%, compared with pembrolizumab alone. T, reducing the risk of developing distant metastasis or death by 62%. “The KEYNOTE-942/mRNA-4157-P201 study was the first demonstration of efficacy for an investigational mRNA cancer treatment in a randomized clinical trial and the first combination therapy to show a significant benefit over pembrolizumab alone in adjuvant melanoma,” said Kyle Holen, MD, Moderna’s senior vice president, after presenting these results.
Side Effects
The combined treatment also did not demonstrate more significant side effects than pembrolizumab alone. The number of patients reporting treatment-related adverse events of grade 3 or greater was similar between the arms (25% for mRNA-4157 [V940] with pembrolizumab vs 20% for KEYTRUDA alone). The most common adverse events of any grade attributed to mRNA-4157 (V940) were fatigue (60.6%), injection site pain (56.7%), and chills (49%). Based on data from the phase 2b KEYNOTE-942/mRNA-4157-P201 study, the US Food and Drug Administration and European Medicines Agency granted breakthrough therapy designation and recognition under the the Priority Medicines scheme, respectively, for mRNA-4157 (V940) in combination with KEYTRUDA for the adjuvant treatment of patients with high-risk melanoma.
Phase 3 Trial
In July, Moderna and Merck announced the launch of a phase 3 trial, assessing “mRNA-4157 [V940] in combination with pembrolizumab as adjuvant treatment in patients with high-risk resected melanoma [stages IIB-IV].” Stéphane Bancel, Moderna’s director general, believes that an mRNA vaccine for melanoma could be available in 2025.
Other Cancer Vaccines
Moderna is not the only laboratory to set its sights on developing a vaccine for cancer. In May, BioNTech, in partnership with Roche, proposed a phase 1 clinical trial of a vaccine targeting pancreatic cancer in Nature. In June, at the American Society of Clinical Oncology›s conference, Transgene presented its conclusions concerning its viral vector vaccines against ENT and papillomavirus-linked cancers. And in September, Ose Immunotherapeutics made headlines with its vaccine for advanced lung cancer.
This article was translated from Univadis France, which is part of the Medscape Professional Network.
Moderna and Merck have presented promising results from their phase 2b clinical trial that investigated a combination of a messenger RNA (mRNA) vaccine and a cancer drug for the treatment of melanoma.
Is mRNA set to shake up the world of cancer treatment? This is certainly what Moderna seems to think; the pharmaceutical company has published the results of a phase 2b trial combining its mRNA vaccine (mRNA-4157 [V940]) with Merck’s cancer drug KEYTRUDA. While these are not the final results but rather mid-term data from the 3-year follow-up, they are somewhat promising. The randomized KEYNOTE-942/mRNA-4157-P201 clinical trial involves patients with high-risk (stage III/IV) melanoma following complete resection.
Relapse Risk Halved
Treatment with mRNA-4157 (V940) in combination with pembrolizumab led to a clinically meaningful improvement in recurrence-free survival, reducing the risk for recurrence or death by 49%, compared with pembrolizumab alone. T, reducing the risk of developing distant metastasis or death by 62%. “The KEYNOTE-942/mRNA-4157-P201 study was the first demonstration of efficacy for an investigational mRNA cancer treatment in a randomized clinical trial and the first combination therapy to show a significant benefit over pembrolizumab alone in adjuvant melanoma,” said Kyle Holen, MD, Moderna’s senior vice president, after presenting these results.
Side Effects
The combined treatment also did not demonstrate more significant side effects than pembrolizumab alone. The number of patients reporting treatment-related adverse events of grade 3 or greater was similar between the arms (25% for mRNA-4157 [V940] with pembrolizumab vs 20% for KEYTRUDA alone). The most common adverse events of any grade attributed to mRNA-4157 (V940) were fatigue (60.6%), injection site pain (56.7%), and chills (49%). Based on data from the phase 2b KEYNOTE-942/mRNA-4157-P201 study, the US Food and Drug Administration and European Medicines Agency granted breakthrough therapy designation and recognition under the the Priority Medicines scheme, respectively, for mRNA-4157 (V940) in combination with KEYTRUDA for the adjuvant treatment of patients with high-risk melanoma.
Phase 3 Trial
In July, Moderna and Merck announced the launch of a phase 3 trial, assessing “mRNA-4157 [V940] in combination with pembrolizumab as adjuvant treatment in patients with high-risk resected melanoma [stages IIB-IV].” Stéphane Bancel, Moderna’s director general, believes that an mRNA vaccine for melanoma could be available in 2025.
Other Cancer Vaccines
Moderna is not the only laboratory to set its sights on developing a vaccine for cancer. In May, BioNTech, in partnership with Roche, proposed a phase 1 clinical trial of a vaccine targeting pancreatic cancer in Nature. In June, at the American Society of Clinical Oncology›s conference, Transgene presented its conclusions concerning its viral vector vaccines against ENT and papillomavirus-linked cancers. And in September, Ose Immunotherapeutics made headlines with its vaccine for advanced lung cancer.
This article was translated from Univadis France, which is part of the Medscape Professional Network.
Efficacy of Topical Clascoterone for Acne Increased Over Time, Analysis Shows
TOPLINE:
METHODOLOGY:
- A 1% cream formulation of clascoterone, a topical androgen receptor inhibitor, is approved for the treatment of acne vulgaris in patients aged 12 years and older based on results from two identical phase 3 12-week trials, NCT02608450 and NCT02608476, and a long-term extension (LTE) study.
- The purpose of the current study was to evaluate the integrated efficacy of clascoterone cream 1% (Winlevi) in the intention-to-treat population of patients from all three trials.
- In the pivotal trials, investigators randomized patients with acne 1:1 to receive clascoterone cream 1% or vehicle twice daily for 12 weeks. Participants were eligible to enter the LTE study, in which patients applied clascoterone to the face, and if they wanted to, the trunk for up to 9 more months.
- To assess combined efficacy, researchers evaluated the proportion of patients who achieved an Investigator’s Global Assessment (IGA) of 0 or 1.
TAKEAWAY:
- Of the 1143 patients from the pivotal trials who completed 12 weeks of treatment, 576 were in the clascoterone group and 567 were in the vehicle group. Of the 600 patients who entered the LTE study, 311 were in the clascoterone group and 289 were in the vehicle group. Of these, 343 completed the LTE study.
- At week 12, the proportion of patients who achieved treatment success was higher in the clascoterone group than in the vehicle group (19.9% vs 7.7%, respectively; P < .0001).
- In the LTE study, the proportion of patients previously treated with clascoterone who achieved a facial IGA of 0/1 increased from 13.5% at extension day 0 to 29.9% at extension day 274, while the proportion of patients previously treated with vehicle and switched to clascoterone who achieved a facial IGA of 0/1 increased from 6.2% at extension day 0 to 30.4% at extension day 274.
- Similarly, the proportion of patients in the LTE study with a truncal IGA of 0/1 increased from 4.9% at extension day 0 to 31.7% on extension day 274.
IN PRACTICE:
“Clinicians may consider counseling patients that treatment persistence is required to maximize the efficacy of clascoterone treatment,” the authors concluded.
SOURCE:
Lawrence F. Eichenfield, MD, of the departments of dermatology and pediatrics at the University of California and Rady Children’s Hospital, San Diego, California, led the research. The study was published in the January 2024 issue of the Journal of Drugs in Dermatology.
LIMITATIONS:
There was a high patient discontinuation rate before and during the LET study. Also, no assessment was made as to how clascoterone affected patients’ quality of life.
DISCLOSURES:
Clascoterone manufacturer Cassiopea funded the studies. Dr. Eichenfield and fellow investigators Adelaide A. Hebert, MD, and Linda Stein Gold, MD, received compensation from Cassiopea as advisers and disclosed ties to many other pharmaceutical companies.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- A 1% cream formulation of clascoterone, a topical androgen receptor inhibitor, is approved for the treatment of acne vulgaris in patients aged 12 years and older based on results from two identical phase 3 12-week trials, NCT02608450 and NCT02608476, and a long-term extension (LTE) study.
- The purpose of the current study was to evaluate the integrated efficacy of clascoterone cream 1% (Winlevi) in the intention-to-treat population of patients from all three trials.
- In the pivotal trials, investigators randomized patients with acne 1:1 to receive clascoterone cream 1% or vehicle twice daily for 12 weeks. Participants were eligible to enter the LTE study, in which patients applied clascoterone to the face, and if they wanted to, the trunk for up to 9 more months.
- To assess combined efficacy, researchers evaluated the proportion of patients who achieved an Investigator’s Global Assessment (IGA) of 0 or 1.
TAKEAWAY:
- Of the 1143 patients from the pivotal trials who completed 12 weeks of treatment, 576 were in the clascoterone group and 567 were in the vehicle group. Of the 600 patients who entered the LTE study, 311 were in the clascoterone group and 289 were in the vehicle group. Of these, 343 completed the LTE study.
- At week 12, the proportion of patients who achieved treatment success was higher in the clascoterone group than in the vehicle group (19.9% vs 7.7%, respectively; P < .0001).
- In the LTE study, the proportion of patients previously treated with clascoterone who achieved a facial IGA of 0/1 increased from 13.5% at extension day 0 to 29.9% at extension day 274, while the proportion of patients previously treated with vehicle and switched to clascoterone who achieved a facial IGA of 0/1 increased from 6.2% at extension day 0 to 30.4% at extension day 274.
- Similarly, the proportion of patients in the LTE study with a truncal IGA of 0/1 increased from 4.9% at extension day 0 to 31.7% on extension day 274.
IN PRACTICE:
“Clinicians may consider counseling patients that treatment persistence is required to maximize the efficacy of clascoterone treatment,” the authors concluded.
SOURCE:
Lawrence F. Eichenfield, MD, of the departments of dermatology and pediatrics at the University of California and Rady Children’s Hospital, San Diego, California, led the research. The study was published in the January 2024 issue of the Journal of Drugs in Dermatology.
LIMITATIONS:
There was a high patient discontinuation rate before and during the LET study. Also, no assessment was made as to how clascoterone affected patients’ quality of life.
DISCLOSURES:
Clascoterone manufacturer Cassiopea funded the studies. Dr. Eichenfield and fellow investigators Adelaide A. Hebert, MD, and Linda Stein Gold, MD, received compensation from Cassiopea as advisers and disclosed ties to many other pharmaceutical companies.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- A 1% cream formulation of clascoterone, a topical androgen receptor inhibitor, is approved for the treatment of acne vulgaris in patients aged 12 years and older based on results from two identical phase 3 12-week trials, NCT02608450 and NCT02608476, and a long-term extension (LTE) study.
- The purpose of the current study was to evaluate the integrated efficacy of clascoterone cream 1% (Winlevi) in the intention-to-treat population of patients from all three trials.
- In the pivotal trials, investigators randomized patients with acne 1:1 to receive clascoterone cream 1% or vehicle twice daily for 12 weeks. Participants were eligible to enter the LTE study, in which patients applied clascoterone to the face, and if they wanted to, the trunk for up to 9 more months.
- To assess combined efficacy, researchers evaluated the proportion of patients who achieved an Investigator’s Global Assessment (IGA) of 0 or 1.
TAKEAWAY:
- Of the 1143 patients from the pivotal trials who completed 12 weeks of treatment, 576 were in the clascoterone group and 567 were in the vehicle group. Of the 600 patients who entered the LTE study, 311 were in the clascoterone group and 289 were in the vehicle group. Of these, 343 completed the LTE study.
- At week 12, the proportion of patients who achieved treatment success was higher in the clascoterone group than in the vehicle group (19.9% vs 7.7%, respectively; P < .0001).
- In the LTE study, the proportion of patients previously treated with clascoterone who achieved a facial IGA of 0/1 increased from 13.5% at extension day 0 to 29.9% at extension day 274, while the proportion of patients previously treated with vehicle and switched to clascoterone who achieved a facial IGA of 0/1 increased from 6.2% at extension day 0 to 30.4% at extension day 274.
- Similarly, the proportion of patients in the LTE study with a truncal IGA of 0/1 increased from 4.9% at extension day 0 to 31.7% on extension day 274.
IN PRACTICE:
“Clinicians may consider counseling patients that treatment persistence is required to maximize the efficacy of clascoterone treatment,” the authors concluded.
SOURCE:
Lawrence F. Eichenfield, MD, of the departments of dermatology and pediatrics at the University of California and Rady Children’s Hospital, San Diego, California, led the research. The study was published in the January 2024 issue of the Journal of Drugs in Dermatology.
LIMITATIONS:
There was a high patient discontinuation rate before and during the LET study. Also, no assessment was made as to how clascoterone affected patients’ quality of life.
DISCLOSURES:
Clascoterone manufacturer Cassiopea funded the studies. Dr. Eichenfield and fellow investigators Adelaide A. Hebert, MD, and Linda Stein Gold, MD, received compensation from Cassiopea as advisers and disclosed ties to many other pharmaceutical companies.
A version of this article appeared on Medscape.com.
Gestational Diabetes May Double Chronic Kidney Disease Risk
TOPLINE:
Previous gestational diabetes mellitus (GDM) nearly doubles future chronic kidney disease (CKD) risk, irrespective of subsequent diabetes and hypertension, a study showed.
METHODOLOGY:
- A nationwide, cohort study was based on data from the Danish Medical Birth Register and included 697,622 women who gave birth between 1997 and 2018.
- Of all study participants, 3.4% reported GDM in at least one pregnancy, and 12.8% of women with GDM received insulin, a proxy for a more severe metabolic dysfunction.
- The women were followed up for a median of 11.9 years.
- Researchers studied CKD and acute kidney disease as the outcomes of interest, the mediating effects of subsequent diabetes and hypertension on future CKD, and how GDM severity affected later risk for kidney disease.
TAKEAWAY:
- Women with GDM showed significantly higher CKD risk than those without GDM (adjusted hazard ratio [aHR], 1.92; 95% CI, 1.67-2.21).
- Women who received insulin during pregnancy due to severe metabolic dysfunction but did not develop subsequent diabetes had a proportionally higher risk for CKD (aHR, 2.35; 95% CI, 1.39-3.97).
- Women with GDM who went on to develop diabetes or hypertension faced even higher risks for CKD, suggesting that preventing diabetes and hypertension after GDM may reduce the development of CKD.
- GDM did not affect the risk for acute kidney disease (aHR, 1.08; 95% CI, 0.90-1.29).
IN PRACTICE:
“Women with severe metabolic dysfunction during pregnancy constitute a high-risk group regarding future CKD,” the authors wrote. “The significantly elevated CKD risk was observed from 2 years after pregnancy and beyond.”
SOURCE:
The study, with first author Maria Hornstrup Christensen, of Odense University Hospital, Odense, Denmark, was published online on December 15 in Diabetes Care.
LIMITATIONS:
GDM may be underdiagnosed, and undiagnosed diabetes may be misclassified as GDM. The proxies of GDM and insulin treatment may not have captured the increasing severity of metabolic dysfunction. The prevalence of insulin treatment was lower than expected, perhaps due to the practice of providing a patient’s first insulin pen without a prescription and perhaps not recording it in a patient’s health record.
DISCLOSURES:
This work received financial support from the University of Southern Denmark, the Region of Southern Denmark, and the Danish Diabetes Academy, which is funded by the Novo Nordisk Foundation. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Previous gestational diabetes mellitus (GDM) nearly doubles future chronic kidney disease (CKD) risk, irrespective of subsequent diabetes and hypertension, a study showed.
METHODOLOGY:
- A nationwide, cohort study was based on data from the Danish Medical Birth Register and included 697,622 women who gave birth between 1997 and 2018.
- Of all study participants, 3.4% reported GDM in at least one pregnancy, and 12.8% of women with GDM received insulin, a proxy for a more severe metabolic dysfunction.
- The women were followed up for a median of 11.9 years.
- Researchers studied CKD and acute kidney disease as the outcomes of interest, the mediating effects of subsequent diabetes and hypertension on future CKD, and how GDM severity affected later risk for kidney disease.
TAKEAWAY:
- Women with GDM showed significantly higher CKD risk than those without GDM (adjusted hazard ratio [aHR], 1.92; 95% CI, 1.67-2.21).
- Women who received insulin during pregnancy due to severe metabolic dysfunction but did not develop subsequent diabetes had a proportionally higher risk for CKD (aHR, 2.35; 95% CI, 1.39-3.97).
- Women with GDM who went on to develop diabetes or hypertension faced even higher risks for CKD, suggesting that preventing diabetes and hypertension after GDM may reduce the development of CKD.
- GDM did not affect the risk for acute kidney disease (aHR, 1.08; 95% CI, 0.90-1.29).
IN PRACTICE:
“Women with severe metabolic dysfunction during pregnancy constitute a high-risk group regarding future CKD,” the authors wrote. “The significantly elevated CKD risk was observed from 2 years after pregnancy and beyond.”
SOURCE:
The study, with first author Maria Hornstrup Christensen, of Odense University Hospital, Odense, Denmark, was published online on December 15 in Diabetes Care.
LIMITATIONS:
GDM may be underdiagnosed, and undiagnosed diabetes may be misclassified as GDM. The proxies of GDM and insulin treatment may not have captured the increasing severity of metabolic dysfunction. The prevalence of insulin treatment was lower than expected, perhaps due to the practice of providing a patient’s first insulin pen without a prescription and perhaps not recording it in a patient’s health record.
DISCLOSURES:
This work received financial support from the University of Southern Denmark, the Region of Southern Denmark, and the Danish Diabetes Academy, which is funded by the Novo Nordisk Foundation. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Previous gestational diabetes mellitus (GDM) nearly doubles future chronic kidney disease (CKD) risk, irrespective of subsequent diabetes and hypertension, a study showed.
METHODOLOGY:
- A nationwide, cohort study was based on data from the Danish Medical Birth Register and included 697,622 women who gave birth between 1997 and 2018.
- Of all study participants, 3.4% reported GDM in at least one pregnancy, and 12.8% of women with GDM received insulin, a proxy for a more severe metabolic dysfunction.
- The women were followed up for a median of 11.9 years.
- Researchers studied CKD and acute kidney disease as the outcomes of interest, the mediating effects of subsequent diabetes and hypertension on future CKD, and how GDM severity affected later risk for kidney disease.
TAKEAWAY:
- Women with GDM showed significantly higher CKD risk than those without GDM (adjusted hazard ratio [aHR], 1.92; 95% CI, 1.67-2.21).
- Women who received insulin during pregnancy due to severe metabolic dysfunction but did not develop subsequent diabetes had a proportionally higher risk for CKD (aHR, 2.35; 95% CI, 1.39-3.97).
- Women with GDM who went on to develop diabetes or hypertension faced even higher risks for CKD, suggesting that preventing diabetes and hypertension after GDM may reduce the development of CKD.
- GDM did not affect the risk for acute kidney disease (aHR, 1.08; 95% CI, 0.90-1.29).
IN PRACTICE:
“Women with severe metabolic dysfunction during pregnancy constitute a high-risk group regarding future CKD,” the authors wrote. “The significantly elevated CKD risk was observed from 2 years after pregnancy and beyond.”
SOURCE:
The study, with first author Maria Hornstrup Christensen, of Odense University Hospital, Odense, Denmark, was published online on December 15 in Diabetes Care.
LIMITATIONS:
GDM may be underdiagnosed, and undiagnosed diabetes may be misclassified as GDM. The proxies of GDM and insulin treatment may not have captured the increasing severity of metabolic dysfunction. The prevalence of insulin treatment was lower than expected, perhaps due to the practice of providing a patient’s first insulin pen without a prescription and perhaps not recording it in a patient’s health record.
DISCLOSURES:
This work received financial support from the University of Southern Denmark, the Region of Southern Denmark, and the Danish Diabetes Academy, which is funded by the Novo Nordisk Foundation. The authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
Dispelling Common Headache Myths

Patients may be familiar with several myths and have misconceptions about headaches and migraine, which often arise due to a combination of factors, including limited understanding of the conditions, cultural beliefs, misinformation, and the complex nature of headaches. Being aware of these myths and seeking accurate information help patients to better understand and manage their headaches.
Myth: Migraine Is the Most Common Type of Headache
This is not true. The most common type of headache is tension-type headache, and it's the kind of headache that almost everyone has from time to time. Between 40% and 80% of the US population have had some form of tension-type headache, but only about 13% of the adult population have migraine. Stress can make muscles in the head and neck tense and knotted, and these muscles can be the source of a tension-type headache. Sometimes these headaches are not at all related to muscles or stress. Neck position may also be a factor. Pain from this type of headache is usually felt on both sides of the head and presents more often as steady, dull pressure or pain that’s usually mild to moderate in intensity. The pain can be in the forehead and eyes or further back in the head. Tension-type headaches are not usually associated with nausea, vomiting, or light and sound sensitivity.
When a tension-type headache is really severe, patients could consider this headache a migraine. Clinicians can easily distinguish tension-type headache from migraine, which often presents on one side of the head, with moderate or severe intensity, is throbbing, and is associated with nausea, vomiting, and light and sound sensitivity.
Myth: Only Adults Get Headaches
False. Headaches aren’t experienced just by adults. However, unlike adults, children find it harder to explain their headaches. It is true that adults have more migraines than children; children’s migraines are often hard for doctors to recognize. A 6- to 9-year-old child is 50% less likely than an adult to have migraine, and their attacks are more often bilateral, are shorter, and respond to sleep quickly.
Myth: Migraines Are Just Really Bad Headaches
False. They are bad, but that is only a small part of the story. A migraine attack is different from other headaches; they actually are 1 of the 3 primary headache disorders, along with tension-type headache and cluster headache. A moderate or severe headache is one of the many characteristics of migraine, and some patients do not even have a headache during a migraine attack. Migraine is an inherited disease of the brain and other parts of the nervous system and can feel much worse than a normal headache. During a migraine attack, the brain does not process sensory data, such as lights, sound, or touch, properly. Patients might even experience visual, sensory, or speech problems (ie, auras) and sometime see flashing lights or zigzag lines that blink on and off or blind spots in their vision. Patients with migraine are often nauseated and severely bothered by light, sound, and even smells. Migraine headaches can last between 4 and 72 hours on average, causing disability, tiredness, and inability to think clearly or work productively, which adds to the burden of the disease. So, migraine is not just a headache.
Myth: More Women Than Men Experience Migraine
This is true. Epidemiologic data show a 3-fold higher incidence of migraine in women than men, starting from puberty and throughout life. From about 6 to 12 years, boys have a slightly higher incidence than girls, but then migraine occurrence levels off and becomes a disease primarily of women. The modulation of neuronal and vascular reactivity by hormones (namely estrogens and progesterone) is a crucial aspect of migraine in some women only. These hormones exert influence on a spectrum of neuromediators and neurotransmitters, potentially leading to functional and structural variations in specific brain regions associated with migraine pathogenesis. Beyond their central effects, sex hormones also modulate vascular tone. Therefore, migraine follows a pattern throughout a woman’s life corresponding to the fluctuation of estrogen. Within a year of their first menstrual period, many girls with migraine have their first attack. They are more likely to have a migraine attack just before and at the start of menses, and at other times of the month as well. They feel better when pregnant and worse after they stop breastfeeding, and they start to feel worse prior to menopause. Then they improve a few years after menopause.
While men are less at risk of having migraine, they’re more likely to have cluster headache than women (although this type of headache is rare compared with other headaches like migraine). Only about 0.1% or less of the population of adults in the US experience this type of headache. Cluster headache gets its name from the clustering of attacks occurring 2 to 6 times per day for 4 to 10 weeks and disappearing as quickly as they came. This headache pain is felt exclusively in or behind 1 eye and rarely elsewhere, on the same side of the head. There is also a clustering of other symptoms called autonomic findings, such as tearing and redness of 1 eye, stuffiness and running in 1 nostril, sweating over 1 eyebrow, drooping of 1 eyelid, and a small pupil—all on the same side of the head the pain is radiating from. Most patients have only some of these findings. Cluster headaches tend to occur every year around the same time (circannual). When a patient is in a cycle of cluster headaches, they often occur at the same time each day (circadian). These set times of the year and of the day are caused by the biological clock deep down under the brain in the hypothalamus.
Myth: All Headaches Are Psychological
This is not true. Usually the underlying cause of migraine is genetically-inherited, but each attack may be triggered by an underlying cause (eg, drop in barometric pressure, menses, certain food/drinks, lack of sleep, stress, etc). Even tension-type headaches can be triggered by muscles in the head and neck becoming tense, stressful events, or jaw issues, which in turn send out pain signals that are felt on both sides of the head.
Many years ago (ie, 1950s-1960s), it was thought that the underlying cause of migraine in women was psychological issues; that has been disproven many times. Both men and women have migraine, and they both can have coexisting psychological issues (ie, depression, anxiety, and other psychiatric problems).
Myth: Migraines Aren’t Serious
Most types of migraine in and of themselves are not serious; however, chronic migraine can continue for years and is debilitating and disabling—becoming a serious issue for patients. These patients usually take many medications, are obese, can have big changes in weight and severe insomnia, don’t exercise enough, and develop other illnesses. Migraine can severely impact quality of life; many people living with migraine have reported reduced productivity while at work, lack of promotion, loss of jobs, and a disruption in their family, social, and leisure activities.
Migraine attacks vary from one person to another and can be quite different from one attack to another in the same person. Hemiplegic migraine, a rare and distinct subtype that is sometimes inherited, is characterized by neurologic symptoms (multiple auras, including a significant weakness or paralysis on 1 side of the body). Although these patients seem much sicker and have multiple types of auras and 1-sided weakness with a prolonged headache, most recover without serious consequences.
Myth: Lack of Sleep Causes Migraine
Yes, lack of sleep is a known trigger for migraine in many people, but lack of sleep is not the cause of migraine. Sleep deprivation and irregular sleep patterns can disrupt the delicate balance of neurotransmitters and hormones in the brain, potentially triggering migraine in susceptible individuals. Additionally, inadequate sleep may contribute to increased stress and tension, which are also common triggers for migraine. In fact, many people with migraine do have sleep issues, which can range from trouble falling asleep to early morning awakening without being able to get back to sleep or frequently interrupted sleep each night. Correcting the sleep problem is part of the migraine therapy. Patients should be checked for sleep apnea if they wake with headache in the morning. Medication overuse headache should also be considered.
Establishing a regular sleep routine and ensuring an adequate amount of sleep can be important components of managing migraine symptoms, particularly for those who find a connection between their sleep patterns and the onset of a migraine attack. However, the relationship between sleep and migraine can vary widely among individuals, and other factors may also contribute to migraine triggers.
Myth: Caffeine Causes Migraine
This is a myth; caffeine does not cause migraine but definitely can be a trigger for some people. Coffee and caffeine and migraine have a complex relationship: excessive caffeine consumption or withdrawal can trigger migraine attacks, but caffeine can also help alleviate headaches (including migraine) due to its analgesic properties. Caffeine is a major component of many over-the-counter medicines for migraine. Some people find drinking coffee or a soda or taking a caffeine tablet at the onset of a migraine attack lowers the intensity of a migraine headache. Regular use of caffeine, either as “treatment” or for pleasure, is not advised in patients with migraine. Most doctors limit caffeine to a regular cup of coffee or tea per day, with no caffeine-containing sodas or chocolate in their patients with migraine; caffeine withdrawal is also a frequent migraine trigger. Patients can notice withdrawal headaches when they stop coffee, even if they are only consuming 1 cup per day. Most people drink a lot more.
Myth: Headache Medicine Will Cure Migraine
False. There currently is no “cure” for migraine. There are several medicines available that certainly can help prevent, abort, or control symptoms of migraine. Some of these medications include over-the-counter analgesics; triptans (like sumatriptan or rizatriptan); gepants, which are small molecule CGRP (calcitonin gene-related peptide) antagonists; CGRP antibodies given by injection; antidepressants; antiseizure medicines; and beta-blockers.
Myth: You Cannot Take Any Migraine Medications During Pregnancy
Migraine medications, such as triptans, are relatively safe during pregnancy, particularly after the first trimester. Acetaminophen in low doses is safe as well, but some of the preventive antiseizure medications should be avoided due to the risk of halting the pregnancy or producing a congenital malformation. Noninvasive wearable devices (such as Nerivio), biofeedback training, mindfulness, and relaxation techniques are particularly appealing to pregnant women as they have high efficacy with virtually no lasting side effects.
Although patients who are pregnant might have an increased flurry of migraine headaches in the first trimester of their pregnancy, they will most likely have a decreased number of attacks in the next 2 trimesters of their pregnancy, making them feel really well. The first trimester is a dangerous time for fetuses to be exposed to certain medicines that are foreign to them, as their organs are still being formed. There are medicines that doctors feel are less problematic both for acute care and prevention of migraine during pregnancy; therefore, patients with a history of migraine should always consult with their obstetrician-gynecologist and a neurologist (or other doctor they usually see for their migraine care) before taking any medication if they are planning a pregnancy or are pregnant.
Effective nonpharmaceutical options are available for all patients with migraine, whether pregnant or not. Maintaining a healthy lifestyle, which includes getting 7 to 10 hours of sleep each night, drinking plenty of water each day, getting ample nutrition from healthy foods, and eliminating as many sources of extra stress as possible can help reduce the risk of a migraine, even when exposed to a known trigger.
Medications may also lead to headaches by a phenomenon called medication overuse headache, if the rescue medication is taken too often. Clinicians recommend no more than 2 days per week of any acute care medication and taking a good preventive medication if needed.
Myth: “Migraine Diets” Cure Migraine
This is false. Avoiding known food triggers can reduce the risk of a migraine attack, but a diet regimen is not a cure. Although eating healthy foods and avoiding certain kinds of food that trigger migraine can eliminate triggering the episodes, there are other factors to take into account. For instance, the migraine diet cannot address a lack of sleep, stress, or hormonal changes a person experiences. Only very few patients with migraine can say their medication has cured their migraine, but it could happen.
Myth: Dietary Supplements Can Cure Migraine
This myth is not true. Supplements can help migraine headache or prevent triggering it, but they won’t cure it. Supplements, such as magnesium, vitamin D3, coenzyme Q10, vitamin B2 (riboflavin), feverfew, melatonin, and vitamin B2 are important additions to the migraine treatment armamentarium, but no one specific vitamin/mineral or supplement has been proven to help prevent or relieve migraine for everyone. They help some people immensely and do little for others, just as with any pharmacologic agent.
Myth: It’s Not a Migraine Unless You Experience Aura
This is not true, as most migraines present without aura. Migraine with typical aura affects 30% of patients with migraine.
Myth: Researchers No Longer Investigate Migraine
False; there are several ongoing studies working to address the pathophysiology of migraine and find new treatment options. Recently, neuromodulation devices have entered the market. One such device from Theranica (called Nerivio) now has clearance from the US Food and Drug Administration for acute and preventive migraine treatment from age 12 and up. One phase 4 study by Theranica shows that Nerivio appears to be safe during pregnancy.
Several migraine studies of note include the following:
OnabotulinumtoxinA as a treatment for hemiplegic migraine: This project aims to evaluate the response to onabotulinumtoxinA treatments in patients with hemiplegic migraine evaluated at Mayo Clinic.
Occipital nerve stimulation for migraine: OPTIMISE. This study is evaluating the safety and efficacy of occipital nerve stimulation (ONS) using the Boston Scientific Corporation (BSC) Precision™ System in the management of intractable chronic migraine, when used in conjunction with antimigraine medications.
The Medication Overuse Treatment Strategy trial: This study is comparing the outcomes among patients randomized to 1 of the 2 treatment strategies for treating patients who have chronic migraine with medication overuse.
Metformin is being investigated as a treatment for the prevention of episodic migraine.
Myth: Migraine Cannot Be Diagnosed Without an Imaging Exam
This is false. Migraine is a clinical diagnosis and does not need any imaging to confirm. Imaging is indicated only if the symptoms are not clear or if there are neurologic symptoms or warning signs accompanying the migraine. In such cases, imaging would be warranted to rule out other pathologies. A magnetic resonance imaging scan is performed to rule out other pathology, not to diagnose migraine. A clinician must identify a pattern in the patient’s history according to the diagnostic criteria of the International Headache Society to diagnose migraine, which include that the patient had 5 previous attacks without aura or 2 attacks with aura.
Summary
Headaches, especially migraine, can be unpleasant and disabling and can significantly affect a patient’s quality of life. However, pharmaceutical and nonpharmaceutical interventions that can help are available. Lifestyle changes, including diet, sleep, and stress reduction can ease symptoms and reduce the frequency of migraine attacks. As researchers continue to investigate the pathophysiology of migraine, they are sure to identify better treatments and, perhaps one day—a cure.
Patients may be familiar with several myths and have misconceptions about headaches and migraine, which often arise due to a combination of factors, including limited understanding of the conditions, cultural beliefs, misinformation, and the complex nature of headaches. Being aware of these myths and seeking accurate information help patients to better understand and manage their headaches.
Myth: Migraine Is the Most Common Type of Headache
This is not true. The most common type of headache is tension-type headache, and it's the kind of headache that almost everyone has from time to time. Between 40% and 80% of the US population have had some form of tension-type headache, but only about 13% of the adult population have migraine. Stress can make muscles in the head and neck tense and knotted, and these muscles can be the source of a tension-type headache. Sometimes these headaches are not at all related to muscles or stress. Neck position may also be a factor. Pain from this type of headache is usually felt on both sides of the head and presents more often as steady, dull pressure or pain that’s usually mild to moderate in intensity. The pain can be in the forehead and eyes or further back in the head. Tension-type headaches are not usually associated with nausea, vomiting, or light and sound sensitivity.
When a tension-type headache is really severe, patients could consider this headache a migraine. Clinicians can easily distinguish tension-type headache from migraine, which often presents on one side of the head, with moderate or severe intensity, is throbbing, and is associated with nausea, vomiting, and light and sound sensitivity.
Myth: Only Adults Get Headaches
False. Headaches aren’t experienced just by adults. However, unlike adults, children find it harder to explain their headaches. It is true that adults have more migraines than children; children’s migraines are often hard for doctors to recognize. A 6- to 9-year-old child is 50% less likely than an adult to have migraine, and their attacks are more often bilateral, are shorter, and respond to sleep quickly.
Myth: Migraines Are Just Really Bad Headaches
False. They are bad, but that is only a small part of the story. A migraine attack is different from other headaches; they actually are 1 of the 3 primary headache disorders, along with tension-type headache and cluster headache. A moderate or severe headache is one of the many characteristics of migraine, and some patients do not even have a headache during a migraine attack. Migraine is an inherited disease of the brain and other parts of the nervous system and can feel much worse than a normal headache. During a migraine attack, the brain does not process sensory data, such as lights, sound, or touch, properly. Patients might even experience visual, sensory, or speech problems (ie, auras) and sometime see flashing lights or zigzag lines that blink on and off or blind spots in their vision. Patients with migraine are often nauseated and severely bothered by light, sound, and even smells. Migraine headaches can last between 4 and 72 hours on average, causing disability, tiredness, and inability to think clearly or work productively, which adds to the burden of the disease. So, migraine is not just a headache.
Myth: More Women Than Men Experience Migraine
This is true. Epidemiologic data show a 3-fold higher incidence of migraine in women than men, starting from puberty and throughout life. From about 6 to 12 years, boys have a slightly higher incidence than girls, but then migraine occurrence levels off and becomes a disease primarily of women. The modulation of neuronal and vascular reactivity by hormones (namely estrogens and progesterone) is a crucial aspect of migraine in some women only. These hormones exert influence on a spectrum of neuromediators and neurotransmitters, potentially leading to functional and structural variations in specific brain regions associated with migraine pathogenesis. Beyond their central effects, sex hormones also modulate vascular tone. Therefore, migraine follows a pattern throughout a woman’s life corresponding to the fluctuation of estrogen. Within a year of their first menstrual period, many girls with migraine have their first attack. They are more likely to have a migraine attack just before and at the start of menses, and at other times of the month as well. They feel better when pregnant and worse after they stop breastfeeding, and they start to feel worse prior to menopause. Then they improve a few years after menopause.
While men are less at risk of having migraine, they’re more likely to have cluster headache than women (although this type of headache is rare compared with other headaches like migraine). Only about 0.1% or less of the population of adults in the US experience this type of headache. Cluster headache gets its name from the clustering of attacks occurring 2 to 6 times per day for 4 to 10 weeks and disappearing as quickly as they came. This headache pain is felt exclusively in or behind 1 eye and rarely elsewhere, on the same side of the head. There is also a clustering of other symptoms called autonomic findings, such as tearing and redness of 1 eye, stuffiness and running in 1 nostril, sweating over 1 eyebrow, drooping of 1 eyelid, and a small pupil—all on the same side of the head the pain is radiating from. Most patients have only some of these findings. Cluster headaches tend to occur every year around the same time (circannual). When a patient is in a cycle of cluster headaches, they often occur at the same time each day (circadian). These set times of the year and of the day are caused by the biological clock deep down under the brain in the hypothalamus.
Myth: All Headaches Are Psychological
This is not true. Usually the underlying cause of migraine is genetically-inherited, but each attack may be triggered by an underlying cause (eg, drop in barometric pressure, menses, certain food/drinks, lack of sleep, stress, etc). Even tension-type headaches can be triggered by muscles in the head and neck becoming tense, stressful events, or jaw issues, which in turn send out pain signals that are felt on both sides of the head.
Many years ago (ie, 1950s-1960s), it was thought that the underlying cause of migraine in women was psychological issues; that has been disproven many times. Both men and women have migraine, and they both can have coexisting psychological issues (ie, depression, anxiety, and other psychiatric problems).
Myth: Migraines Aren’t Serious
Most types of migraine in and of themselves are not serious; however, chronic migraine can continue for years and is debilitating and disabling—becoming a serious issue for patients. These patients usually take many medications, are obese, can have big changes in weight and severe insomnia, don’t exercise enough, and develop other illnesses. Migraine can severely impact quality of life; many people living with migraine have reported reduced productivity while at work, lack of promotion, loss of jobs, and a disruption in their family, social, and leisure activities.
Migraine attacks vary from one person to another and can be quite different from one attack to another in the same person. Hemiplegic migraine, a rare and distinct subtype that is sometimes inherited, is characterized by neurologic symptoms (multiple auras, including a significant weakness or paralysis on 1 side of the body). Although these patients seem much sicker and have multiple types of auras and 1-sided weakness with a prolonged headache, most recover without serious consequences.
Myth: Lack of Sleep Causes Migraine
Yes, lack of sleep is a known trigger for migraine in many people, but lack of sleep is not the cause of migraine. Sleep deprivation and irregular sleep patterns can disrupt the delicate balance of neurotransmitters and hormones in the brain, potentially triggering migraine in susceptible individuals. Additionally, inadequate sleep may contribute to increased stress and tension, which are also common triggers for migraine. In fact, many people with migraine do have sleep issues, which can range from trouble falling asleep to early morning awakening without being able to get back to sleep or frequently interrupted sleep each night. Correcting the sleep problem is part of the migraine therapy. Patients should be checked for sleep apnea if they wake with headache in the morning. Medication overuse headache should also be considered.
Establishing a regular sleep routine and ensuring an adequate amount of sleep can be important components of managing migraine symptoms, particularly for those who find a connection between their sleep patterns and the onset of a migraine attack. However, the relationship between sleep and migraine can vary widely among individuals, and other factors may also contribute to migraine triggers.
Myth: Caffeine Causes Migraine
This is a myth; caffeine does not cause migraine but definitely can be a trigger for some people. Coffee and caffeine and migraine have a complex relationship: excessive caffeine consumption or withdrawal can trigger migraine attacks, but caffeine can also help alleviate headaches (including migraine) due to its analgesic properties. Caffeine is a major component of many over-the-counter medicines for migraine. Some people find drinking coffee or a soda or taking a caffeine tablet at the onset of a migraine attack lowers the intensity of a migraine headache. Regular use of caffeine, either as “treatment” or for pleasure, is not advised in patients with migraine. Most doctors limit caffeine to a regular cup of coffee or tea per day, with no caffeine-containing sodas or chocolate in their patients with migraine; caffeine withdrawal is also a frequent migraine trigger. Patients can notice withdrawal headaches when they stop coffee, even if they are only consuming 1 cup per day. Most people drink a lot more.
Myth: Headache Medicine Will Cure Migraine
False. There currently is no “cure” for migraine. There are several medicines available that certainly can help prevent, abort, or control symptoms of migraine. Some of these medications include over-the-counter analgesics; triptans (like sumatriptan or rizatriptan); gepants, which are small molecule CGRP (calcitonin gene-related peptide) antagonists; CGRP antibodies given by injection; antidepressants; antiseizure medicines; and beta-blockers.
Myth: You Cannot Take Any Migraine Medications During Pregnancy
Migraine medications, such as triptans, are relatively safe during pregnancy, particularly after the first trimester. Acetaminophen in low doses is safe as well, but some of the preventive antiseizure medications should be avoided due to the risk of halting the pregnancy or producing a congenital malformation. Noninvasive wearable devices (such as Nerivio), biofeedback training, mindfulness, and relaxation techniques are particularly appealing to pregnant women as they have high efficacy with virtually no lasting side effects.
Although patients who are pregnant might have an increased flurry of migraine headaches in the first trimester of their pregnancy, they will most likely have a decreased number of attacks in the next 2 trimesters of their pregnancy, making them feel really well. The first trimester is a dangerous time for fetuses to be exposed to certain medicines that are foreign to them, as their organs are still being formed. There are medicines that doctors feel are less problematic both for acute care and prevention of migraine during pregnancy; therefore, patients with a history of migraine should always consult with their obstetrician-gynecologist and a neurologist (or other doctor they usually see for their migraine care) before taking any medication if they are planning a pregnancy or are pregnant.
Effective nonpharmaceutical options are available for all patients with migraine, whether pregnant or not. Maintaining a healthy lifestyle, which includes getting 7 to 10 hours of sleep each night, drinking plenty of water each day, getting ample nutrition from healthy foods, and eliminating as many sources of extra stress as possible can help reduce the risk of a migraine, even when exposed to a known trigger.
Medications may also lead to headaches by a phenomenon called medication overuse headache, if the rescue medication is taken too often. Clinicians recommend no more than 2 days per week of any acute care medication and taking a good preventive medication if needed.
Myth: “Migraine Diets” Cure Migraine
This is false. Avoiding known food triggers can reduce the risk of a migraine attack, but a diet regimen is not a cure. Although eating healthy foods and avoiding certain kinds of food that trigger migraine can eliminate triggering the episodes, there are other factors to take into account. For instance, the migraine diet cannot address a lack of sleep, stress, or hormonal changes a person experiences. Only very few patients with migraine can say their medication has cured their migraine, but it could happen.
Myth: Dietary Supplements Can Cure Migraine
This myth is not true. Supplements can help migraine headache or prevent triggering it, but they won’t cure it. Supplements, such as magnesium, vitamin D3, coenzyme Q10, vitamin B2 (riboflavin), feverfew, melatonin, and vitamin B2 are important additions to the migraine treatment armamentarium, but no one specific vitamin/mineral or supplement has been proven to help prevent or relieve migraine for everyone. They help some people immensely and do little for others, just as with any pharmacologic agent.
Myth: It’s Not a Migraine Unless You Experience Aura
This is not true, as most migraines present without aura. Migraine with typical aura affects 30% of patients with migraine.
Myth: Researchers No Longer Investigate Migraine
False; there are several ongoing studies working to address the pathophysiology of migraine and find new treatment options. Recently, neuromodulation devices have entered the market. One such device from Theranica (called Nerivio) now has clearance from the US Food and Drug Administration for acute and preventive migraine treatment from age 12 and up. One phase 4 study by Theranica shows that Nerivio appears to be safe during pregnancy.
Several migraine studies of note include the following:
OnabotulinumtoxinA as a treatment for hemiplegic migraine: This project aims to evaluate the response to onabotulinumtoxinA treatments in patients with hemiplegic migraine evaluated at Mayo Clinic.
Occipital nerve stimulation for migraine: OPTIMISE. This study is evaluating the safety and efficacy of occipital nerve stimulation (ONS) using the Boston Scientific Corporation (BSC) Precision™ System in the management of intractable chronic migraine, when used in conjunction with antimigraine medications.
The Medication Overuse Treatment Strategy trial: This study is comparing the outcomes among patients randomized to 1 of the 2 treatment strategies for treating patients who have chronic migraine with medication overuse.
Metformin is being investigated as a treatment for the prevention of episodic migraine.
Myth: Migraine Cannot Be Diagnosed Without an Imaging Exam
This is false. Migraine is a clinical diagnosis and does not need any imaging to confirm. Imaging is indicated only if the symptoms are not clear or if there are neurologic symptoms or warning signs accompanying the migraine. In such cases, imaging would be warranted to rule out other pathologies. A magnetic resonance imaging scan is performed to rule out other pathology, not to diagnose migraine. A clinician must identify a pattern in the patient’s history according to the diagnostic criteria of the International Headache Society to diagnose migraine, which include that the patient had 5 previous attacks without aura or 2 attacks with aura.
Summary
Headaches, especially migraine, can be unpleasant and disabling and can significantly affect a patient’s quality of life. However, pharmaceutical and nonpharmaceutical interventions that can help are available. Lifestyle changes, including diet, sleep, and stress reduction can ease symptoms and reduce the frequency of migraine attacks. As researchers continue to investigate the pathophysiology of migraine, they are sure to identify better treatments and, perhaps one day—a cure.
Patients may be familiar with several myths and have misconceptions about headaches and migraine, which often arise due to a combination of factors, including limited understanding of the conditions, cultural beliefs, misinformation, and the complex nature of headaches. Being aware of these myths and seeking accurate information help patients to better understand and manage their headaches.
Myth: Migraine Is the Most Common Type of Headache
This is not true. The most common type of headache is tension-type headache, and it's the kind of headache that almost everyone has from time to time. Between 40% and 80% of the US population have had some form of tension-type headache, but only about 13% of the adult population have migraine. Stress can make muscles in the head and neck tense and knotted, and these muscles can be the source of a tension-type headache. Sometimes these headaches are not at all related to muscles or stress. Neck position may also be a factor. Pain from this type of headache is usually felt on both sides of the head and presents more often as steady, dull pressure or pain that’s usually mild to moderate in intensity. The pain can be in the forehead and eyes or further back in the head. Tension-type headaches are not usually associated with nausea, vomiting, or light and sound sensitivity.
When a tension-type headache is really severe, patients could consider this headache a migraine. Clinicians can easily distinguish tension-type headache from migraine, which often presents on one side of the head, with moderate or severe intensity, is throbbing, and is associated with nausea, vomiting, and light and sound sensitivity.
Myth: Only Adults Get Headaches
False. Headaches aren’t experienced just by adults. However, unlike adults, children find it harder to explain their headaches. It is true that adults have more migraines than children; children’s migraines are often hard for doctors to recognize. A 6- to 9-year-old child is 50% less likely than an adult to have migraine, and their attacks are more often bilateral, are shorter, and respond to sleep quickly.
Myth: Migraines Are Just Really Bad Headaches
False. They are bad, but that is only a small part of the story. A migraine attack is different from other headaches; they actually are 1 of the 3 primary headache disorders, along with tension-type headache and cluster headache. A moderate or severe headache is one of the many characteristics of migraine, and some patients do not even have a headache during a migraine attack. Migraine is an inherited disease of the brain and other parts of the nervous system and can feel much worse than a normal headache. During a migraine attack, the brain does not process sensory data, such as lights, sound, or touch, properly. Patients might even experience visual, sensory, or speech problems (ie, auras) and sometime see flashing lights or zigzag lines that blink on and off or blind spots in their vision. Patients with migraine are often nauseated and severely bothered by light, sound, and even smells. Migraine headaches can last between 4 and 72 hours on average, causing disability, tiredness, and inability to think clearly or work productively, which adds to the burden of the disease. So, migraine is not just a headache.
Myth: More Women Than Men Experience Migraine
This is true. Epidemiologic data show a 3-fold higher incidence of migraine in women than men, starting from puberty and throughout life. From about 6 to 12 years, boys have a slightly higher incidence than girls, but then migraine occurrence levels off and becomes a disease primarily of women. The modulation of neuronal and vascular reactivity by hormones (namely estrogens and progesterone) is a crucial aspect of migraine in some women only. These hormones exert influence on a spectrum of neuromediators and neurotransmitters, potentially leading to functional and structural variations in specific brain regions associated with migraine pathogenesis. Beyond their central effects, sex hormones also modulate vascular tone. Therefore, migraine follows a pattern throughout a woman’s life corresponding to the fluctuation of estrogen. Within a year of their first menstrual period, many girls with migraine have their first attack. They are more likely to have a migraine attack just before and at the start of menses, and at other times of the month as well. They feel better when pregnant and worse after they stop breastfeeding, and they start to feel worse prior to menopause. Then they improve a few years after menopause.
While men are less at risk of having migraine, they’re more likely to have cluster headache than women (although this type of headache is rare compared with other headaches like migraine). Only about 0.1% or less of the population of adults in the US experience this type of headache. Cluster headache gets its name from the clustering of attacks occurring 2 to 6 times per day for 4 to 10 weeks and disappearing as quickly as they came. This headache pain is felt exclusively in or behind 1 eye and rarely elsewhere, on the same side of the head. There is also a clustering of other symptoms called autonomic findings, such as tearing and redness of 1 eye, stuffiness and running in 1 nostril, sweating over 1 eyebrow, drooping of 1 eyelid, and a small pupil—all on the same side of the head the pain is radiating from. Most patients have only some of these findings. Cluster headaches tend to occur every year around the same time (circannual). When a patient is in a cycle of cluster headaches, they often occur at the same time each day (circadian). These set times of the year and of the day are caused by the biological clock deep down under the brain in the hypothalamus.
Myth: All Headaches Are Psychological
This is not true. Usually the underlying cause of migraine is genetically-inherited, but each attack may be triggered by an underlying cause (eg, drop in barometric pressure, menses, certain food/drinks, lack of sleep, stress, etc). Even tension-type headaches can be triggered by muscles in the head and neck becoming tense, stressful events, or jaw issues, which in turn send out pain signals that are felt on both sides of the head.
Many years ago (ie, 1950s-1960s), it was thought that the underlying cause of migraine in women was psychological issues; that has been disproven many times. Both men and women have migraine, and they both can have coexisting psychological issues (ie, depression, anxiety, and other psychiatric problems).
Myth: Migraines Aren’t Serious
Most types of migraine in and of themselves are not serious; however, chronic migraine can continue for years and is debilitating and disabling—becoming a serious issue for patients. These patients usually take many medications, are obese, can have big changes in weight and severe insomnia, don’t exercise enough, and develop other illnesses. Migraine can severely impact quality of life; many people living with migraine have reported reduced productivity while at work, lack of promotion, loss of jobs, and a disruption in their family, social, and leisure activities.
Migraine attacks vary from one person to another and can be quite different from one attack to another in the same person. Hemiplegic migraine, a rare and distinct subtype that is sometimes inherited, is characterized by neurologic symptoms (multiple auras, including a significant weakness or paralysis on 1 side of the body). Although these patients seem much sicker and have multiple types of auras and 1-sided weakness with a prolonged headache, most recover without serious consequences.
Myth: Lack of Sleep Causes Migraine
Yes, lack of sleep is a known trigger for migraine in many people, but lack of sleep is not the cause of migraine. Sleep deprivation and irregular sleep patterns can disrupt the delicate balance of neurotransmitters and hormones in the brain, potentially triggering migraine in susceptible individuals. Additionally, inadequate sleep may contribute to increased stress and tension, which are also common triggers for migraine. In fact, many people with migraine do have sleep issues, which can range from trouble falling asleep to early morning awakening without being able to get back to sleep or frequently interrupted sleep each night. Correcting the sleep problem is part of the migraine therapy. Patients should be checked for sleep apnea if they wake with headache in the morning. Medication overuse headache should also be considered.
Establishing a regular sleep routine and ensuring an adequate amount of sleep can be important components of managing migraine symptoms, particularly for those who find a connection between their sleep patterns and the onset of a migraine attack. However, the relationship between sleep and migraine can vary widely among individuals, and other factors may also contribute to migraine triggers.
Myth: Caffeine Causes Migraine
This is a myth; caffeine does not cause migraine but definitely can be a trigger for some people. Coffee and caffeine and migraine have a complex relationship: excessive caffeine consumption or withdrawal can trigger migraine attacks, but caffeine can also help alleviate headaches (including migraine) due to its analgesic properties. Caffeine is a major component of many over-the-counter medicines for migraine. Some people find drinking coffee or a soda or taking a caffeine tablet at the onset of a migraine attack lowers the intensity of a migraine headache. Regular use of caffeine, either as “treatment” or for pleasure, is not advised in patients with migraine. Most doctors limit caffeine to a regular cup of coffee or tea per day, with no caffeine-containing sodas or chocolate in their patients with migraine; caffeine withdrawal is also a frequent migraine trigger. Patients can notice withdrawal headaches when they stop coffee, even if they are only consuming 1 cup per day. Most people drink a lot more.
Myth: Headache Medicine Will Cure Migraine
False. There currently is no “cure” for migraine. There are several medicines available that certainly can help prevent, abort, or control symptoms of migraine. Some of these medications include over-the-counter analgesics; triptans (like sumatriptan or rizatriptan); gepants, which are small molecule CGRP (calcitonin gene-related peptide) antagonists; CGRP antibodies given by injection; antidepressants; antiseizure medicines; and beta-blockers.
Myth: You Cannot Take Any Migraine Medications During Pregnancy
Migraine medications, such as triptans, are relatively safe during pregnancy, particularly after the first trimester. Acetaminophen in low doses is safe as well, but some of the preventive antiseizure medications should be avoided due to the risk of halting the pregnancy or producing a congenital malformation. Noninvasive wearable devices (such as Nerivio), biofeedback training, mindfulness, and relaxation techniques are particularly appealing to pregnant women as they have high efficacy with virtually no lasting side effects.
Although patients who are pregnant might have an increased flurry of migraine headaches in the first trimester of their pregnancy, they will most likely have a decreased number of attacks in the next 2 trimesters of their pregnancy, making them feel really well. The first trimester is a dangerous time for fetuses to be exposed to certain medicines that are foreign to them, as their organs are still being formed. There are medicines that doctors feel are less problematic both for acute care and prevention of migraine during pregnancy; therefore, patients with a history of migraine should always consult with their obstetrician-gynecologist and a neurologist (or other doctor they usually see for their migraine care) before taking any medication if they are planning a pregnancy or are pregnant.
Effective nonpharmaceutical options are available for all patients with migraine, whether pregnant or not. Maintaining a healthy lifestyle, which includes getting 7 to 10 hours of sleep each night, drinking plenty of water each day, getting ample nutrition from healthy foods, and eliminating as many sources of extra stress as possible can help reduce the risk of a migraine, even when exposed to a known trigger.
Medications may also lead to headaches by a phenomenon called medication overuse headache, if the rescue medication is taken too often. Clinicians recommend no more than 2 days per week of any acute care medication and taking a good preventive medication if needed.
Myth: “Migraine Diets” Cure Migraine
This is false. Avoiding known food triggers can reduce the risk of a migraine attack, but a diet regimen is not a cure. Although eating healthy foods and avoiding certain kinds of food that trigger migraine can eliminate triggering the episodes, there are other factors to take into account. For instance, the migraine diet cannot address a lack of sleep, stress, or hormonal changes a person experiences. Only very few patients with migraine can say their medication has cured their migraine, but it could happen.
Myth: Dietary Supplements Can Cure Migraine
This myth is not true. Supplements can help migraine headache or prevent triggering it, but they won’t cure it. Supplements, such as magnesium, vitamin D3, coenzyme Q10, vitamin B2 (riboflavin), feverfew, melatonin, and vitamin B2 are important additions to the migraine treatment armamentarium, but no one specific vitamin/mineral or supplement has been proven to help prevent or relieve migraine for everyone. They help some people immensely and do little for others, just as with any pharmacologic agent.
Myth: It’s Not a Migraine Unless You Experience Aura
This is not true, as most migraines present without aura. Migraine with typical aura affects 30% of patients with migraine.
Myth: Researchers No Longer Investigate Migraine
False; there are several ongoing studies working to address the pathophysiology of migraine and find new treatment options. Recently, neuromodulation devices have entered the market. One such device from Theranica (called Nerivio) now has clearance from the US Food and Drug Administration for acute and preventive migraine treatment from age 12 and up. One phase 4 study by Theranica shows that Nerivio appears to be safe during pregnancy.
Several migraine studies of note include the following:
OnabotulinumtoxinA as a treatment for hemiplegic migraine: This project aims to evaluate the response to onabotulinumtoxinA treatments in patients with hemiplegic migraine evaluated at Mayo Clinic.
Occipital nerve stimulation for migraine: OPTIMISE. This study is evaluating the safety and efficacy of occipital nerve stimulation (ONS) using the Boston Scientific Corporation (BSC) Precision™ System in the management of intractable chronic migraine, when used in conjunction with antimigraine medications.
The Medication Overuse Treatment Strategy trial: This study is comparing the outcomes among patients randomized to 1 of the 2 treatment strategies for treating patients who have chronic migraine with medication overuse.
Metformin is being investigated as a treatment for the prevention of episodic migraine.
Myth: Migraine Cannot Be Diagnosed Without an Imaging Exam
This is false. Migraine is a clinical diagnosis and does not need any imaging to confirm. Imaging is indicated only if the symptoms are not clear or if there are neurologic symptoms or warning signs accompanying the migraine. In such cases, imaging would be warranted to rule out other pathologies. A magnetic resonance imaging scan is performed to rule out other pathology, not to diagnose migraine. A clinician must identify a pattern in the patient’s history according to the diagnostic criteria of the International Headache Society to diagnose migraine, which include that the patient had 5 previous attacks without aura or 2 attacks with aura.
Summary
Headaches, especially migraine, can be unpleasant and disabling and can significantly affect a patient’s quality of life. However, pharmaceutical and nonpharmaceutical interventions that can help are available. Lifestyle changes, including diet, sleep, and stress reduction can ease symptoms and reduce the frequency of migraine attacks. As researchers continue to investigate the pathophysiology of migraine, they are sure to identify better treatments and, perhaps one day—a cure.
AGA members save on registration for DDW® 2024
, the world’s largest and most comprehensive gathering of gastroenterology clinicians, researchers and industry. Registration and housing are now open, and AGA members can save up to $380 on registration fees. Discounted registration rates are also available through the March 13 early bird deadline. AGA member trainees, students, residents and postdoctoral fellows can register for free through this date. Visit ddw.org/register to join us.
This year, DDW takes place May 18-21, in Washington, D.C., and online. Whether you work in patient care, research, training or academia, you’ll find content tailored to your essential role at every step.
Add on to your DDW experience with AGA’s one-day Postgraduate Course. Join us on May 18, from D.C. or online, to explore challenging patient cases, high-impact papers, and important practice updates that you can use immediately upon your return to the clinic. Learn more at pgcourse.gastro.org.
, the world’s largest and most comprehensive gathering of gastroenterology clinicians, researchers and industry. Registration and housing are now open, and AGA members can save up to $380 on registration fees. Discounted registration rates are also available through the March 13 early bird deadline. AGA member trainees, students, residents and postdoctoral fellows can register for free through this date. Visit ddw.org/register to join us.
This year, DDW takes place May 18-21, in Washington, D.C., and online. Whether you work in patient care, research, training or academia, you’ll find content tailored to your essential role at every step.
Add on to your DDW experience with AGA’s one-day Postgraduate Course. Join us on May 18, from D.C. or online, to explore challenging patient cases, high-impact papers, and important practice updates that you can use immediately upon your return to the clinic. Learn more at pgcourse.gastro.org.
, the world’s largest and most comprehensive gathering of gastroenterology clinicians, researchers and industry. Registration and housing are now open, and AGA members can save up to $380 on registration fees. Discounted registration rates are also available through the March 13 early bird deadline. AGA member trainees, students, residents and postdoctoral fellows can register for free through this date. Visit ddw.org/register to join us.
This year, DDW takes place May 18-21, in Washington, D.C., and online. Whether you work in patient care, research, training or academia, you’ll find content tailored to your essential role at every step.
Add on to your DDW experience with AGA’s one-day Postgraduate Course. Join us on May 18, from D.C. or online, to explore challenging patient cases, high-impact papers, and important practice updates that you can use immediately upon your return to the clinic. Learn more at pgcourse.gastro.org.
Resistance Training Formats Compared in Patients With PsA
TOPLINE:
Exercise with weight machines or elastic resistance bands yielded similar improvements in strength and function in adults with psoriatic arthritis (PsA) after 12 weeks.
METHODOLOGY:
- Researchers recruited 41 adults aged 18-65 years with PsA who were then randomized to a functional training group (FT) or a resistance exercise group (RE) for 12 weeks of twice-weekly, 55-minute sessions under the supervision of a physical trainer.
- Functional training involved the use of elastic bands to work upper body, lower body, and trunk muscles including the biceps, triceps, back quadriceps, glutes, and hips; the RE used weight machines instead of bands.
- Participants were evaluated at baseline and after 6 and 12 weeks of training sessions; the primary outcome was functional status based on the Health Assessment Questionnaire for the Spondyloarthropathies (HAQ-S).
- Secondary outcomes included the Bath Ankylosing Spondylitis Functional Index (BASFI) to assess functional capacity, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and Disease Activity Score in 28 joints (DAS28) to assess disease activity, and the Short Form 36 (SF-36) to measure quality of life.
TAKEAWAY:
- Participants in both groups showed significant improvement from baseline on the primary outcome measure, with no significant differences between the groups on the primary outcome of function or secondary measures of function and disease activity after 12 weeks.
- Significant intragroup changes occurred between times for both groups on the HAQ-S, BASFI, BASDAI, and DAS28 (P = .001, .007, .001, and .001, respectively).
- Improvement in quality of life was significant from baseline and similar between the FT and RE, with the exception of the “social aspects” domain, for which only the FT showed significant improvement.
- No intervention-related adverse events were reported in either group.
IN PRACTICE:
Despite the absence of consensus guidelines on the use and effectiveness of FT and RE, “we can conclude that both FT and RE have similar effectiveness in improving functional capacity, functional status, disease activity, general quality of life, and muscle strength in patients with psoriatic arthritis,” the researchers wrote.
SOURCE:
The study was led by Diego Roger Silva, MD, of the Universidade Federal de São Paulo, Brazil, and published online in Advances in Rheumatology.
LIMITATIONS:
The study population was recruited from outpatient clinics, and the mean age of 52 years was higher than in previous studies; the study also lacked long-term follow-up data.
DISCLOSURES:
The study received no outside funding. The researchers had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
Exercise with weight machines or elastic resistance bands yielded similar improvements in strength and function in adults with psoriatic arthritis (PsA) after 12 weeks.
METHODOLOGY:
- Researchers recruited 41 adults aged 18-65 years with PsA who were then randomized to a functional training group (FT) or a resistance exercise group (RE) for 12 weeks of twice-weekly, 55-minute sessions under the supervision of a physical trainer.
- Functional training involved the use of elastic bands to work upper body, lower body, and trunk muscles including the biceps, triceps, back quadriceps, glutes, and hips; the RE used weight machines instead of bands.
- Participants were evaluated at baseline and after 6 and 12 weeks of training sessions; the primary outcome was functional status based on the Health Assessment Questionnaire for the Spondyloarthropathies (HAQ-S).
- Secondary outcomes included the Bath Ankylosing Spondylitis Functional Index (BASFI) to assess functional capacity, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and Disease Activity Score in 28 joints (DAS28) to assess disease activity, and the Short Form 36 (SF-36) to measure quality of life.
TAKEAWAY:
- Participants in both groups showed significant improvement from baseline on the primary outcome measure, with no significant differences between the groups on the primary outcome of function or secondary measures of function and disease activity after 12 weeks.
- Significant intragroup changes occurred between times for both groups on the HAQ-S, BASFI, BASDAI, and DAS28 (P = .001, .007, .001, and .001, respectively).
- Improvement in quality of life was significant from baseline and similar between the FT and RE, with the exception of the “social aspects” domain, for which only the FT showed significant improvement.
- No intervention-related adverse events were reported in either group.
IN PRACTICE:
Despite the absence of consensus guidelines on the use and effectiveness of FT and RE, “we can conclude that both FT and RE have similar effectiveness in improving functional capacity, functional status, disease activity, general quality of life, and muscle strength in patients with psoriatic arthritis,” the researchers wrote.
SOURCE:
The study was led by Diego Roger Silva, MD, of the Universidade Federal de São Paulo, Brazil, and published online in Advances in Rheumatology.
LIMITATIONS:
The study population was recruited from outpatient clinics, and the mean age of 52 years was higher than in previous studies; the study also lacked long-term follow-up data.
DISCLOSURES:
The study received no outside funding. The researchers had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
Exercise with weight machines or elastic resistance bands yielded similar improvements in strength and function in adults with psoriatic arthritis (PsA) after 12 weeks.
METHODOLOGY:
- Researchers recruited 41 adults aged 18-65 years with PsA who were then randomized to a functional training group (FT) or a resistance exercise group (RE) for 12 weeks of twice-weekly, 55-minute sessions under the supervision of a physical trainer.
- Functional training involved the use of elastic bands to work upper body, lower body, and trunk muscles including the biceps, triceps, back quadriceps, glutes, and hips; the RE used weight machines instead of bands.
- Participants were evaluated at baseline and after 6 and 12 weeks of training sessions; the primary outcome was functional status based on the Health Assessment Questionnaire for the Spondyloarthropathies (HAQ-S).
- Secondary outcomes included the Bath Ankylosing Spondylitis Functional Index (BASFI) to assess functional capacity, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and Disease Activity Score in 28 joints (DAS28) to assess disease activity, and the Short Form 36 (SF-36) to measure quality of life.
TAKEAWAY:
- Participants in both groups showed significant improvement from baseline on the primary outcome measure, with no significant differences between the groups on the primary outcome of function or secondary measures of function and disease activity after 12 weeks.
- Significant intragroup changes occurred between times for both groups on the HAQ-S, BASFI, BASDAI, and DAS28 (P = .001, .007, .001, and .001, respectively).
- Improvement in quality of life was significant from baseline and similar between the FT and RE, with the exception of the “social aspects” domain, for which only the FT showed significant improvement.
- No intervention-related adverse events were reported in either group.
IN PRACTICE:
Despite the absence of consensus guidelines on the use and effectiveness of FT and RE, “we can conclude that both FT and RE have similar effectiveness in improving functional capacity, functional status, disease activity, general quality of life, and muscle strength in patients with psoriatic arthritis,” the researchers wrote.
SOURCE:
The study was led by Diego Roger Silva, MD, of the Universidade Federal de São Paulo, Brazil, and published online in Advances in Rheumatology.
LIMITATIONS:
The study population was recruited from outpatient clinics, and the mean age of 52 years was higher than in previous studies; the study also lacked long-term follow-up data.
DISCLOSURES:
The study received no outside funding. The researchers had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.