User login
Acute Superior Mesenteric Venous Thrombosis in a Young Patient Without Risk Factors
In this case report, the authors address the diagnostic challenges of a young, healthy patient who presented to the ED with unrelenting abdominal pain.
Acute mesenteric ischemia (AMI) results when oxygen delivery to the mesenteric artery is compromised, and is a serious diagnosis that should be considered in patients of all ages to avoid significant morbidity and mortality. The majority of cases are due to arterial embolism, arterial thrombus, or intestinal hypoperfusion (non-occlusive). Acute mesenteric venous thrombosis (MVT) accounts for only 2% to 10% of AMI cases, and only 0.01% of emergency surgery admissions.1 A large systematic review showed a 44% mortality rate for MVT, in contrast to 66% to 89% for all other forms of AMI.2 The typical age range for MVT is reported between 45 and 60 years, with a slight male predominance.3 Dull, central abdominal pain is the most frequently reported symptom of MVT, although it is generally less impressive than the pain described in other forms of AMI.3Along with the hallmark of abdominal pain out of proportion to the examination, other gastrointestinal symptoms include weight loss and non-specific altered bowel function (constipation, diarrhea, abdominal distention, and bloating), which are present in half of all patients with MVT.1 Peritoneal signs and bloody stools portend poor outcomes, as they often occur with disease progression.4
Case
A 26-year-old man presented to the ED with periumbilical and lower abdominal pain for 1 week. The pain was described as constant and dull, worsened by movement and oral intake, and improved with lying flat. He described bloating and decreased volume of bowel movements. He denied nausea, vomiting, fever, colicky pain, blood in stool, testicular pain, urinary complaints, trauma, or any similar episodes in the past. The patient had no known medical conditions or surgical history, except for a remote history of alcohol dependence (in remission) and tobacco use. There was no personal or family history of coagulopathy. Of note, he was seen by his primary care physician a few days prior to his ED presentation and had been instructed to take acetaminophen, which did not provide relief.
The patient’s vital signs at presentation were: blood pressure, 122/70 mm Hg; heart rate, 93 beats/min; respiratory rate, 18 breaths/min; and temperature, 37.5°C (99.5°F). Oxygen saturation was 99% on room air. The physical examination was remarkable only for mild abdominal tenderness diffusely, greater in the lower and central abdomen than in the upper abdomen. The remainder of the physical examination was unremarkable.
Laboratory studies ordered included a complete blood count, comprehensive metabolic profile, lipase, and urinalysis. The patient did have a mild transaminitis (aspartate aminotransferase, 48 U/L; alanine aminotransferase, 84 U/L); the remainder of the studies were normal. A serum lactate, drawn after the 1 L of normal saline was administered intravenously (IV), was within normal limits (0.7 mmol/L). No prior laboratory studies were available for comparison.
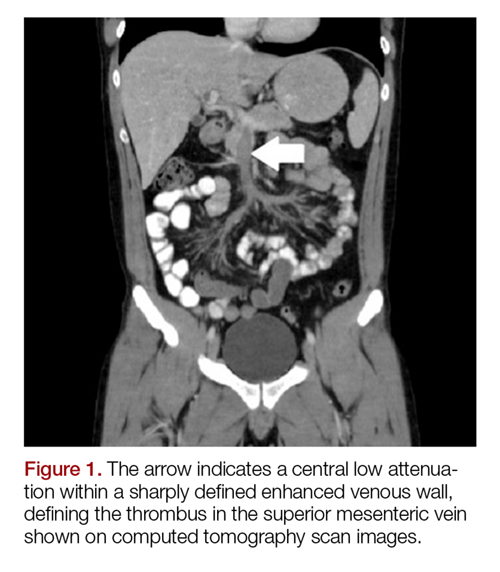
The patient’s continued abdominal pain and transaminitis prompted an ED bedside right upper quadrant ultrasound, which showed a small gallbladder polyp; no signs of gallbladder disease were present. The patient required three doses of morphine 4 mg IV without complete pain relief. Given the concern for pain out of proportion to physical examination, a computed tomography (CT) scan of the abdomen/pelvis with IV and oral contrast was ordered. The radiologist interpreted the scan as showing a superior mesenteric vein (SMV) thrombus extending into the splenic/portal vein confluence and the intrahepatic portal veins (Figures 1 and 2).

Ciprofloxacin and metronidazole were administered IV for antibiotic prophylaxis, and the patient was placed on bowel rest with advancement to regular diet as tolerated. Propranolol was given for variceal prophylaxis. The patient was discharged home the following day in stable condition. Although he still had mild abdominal tenderness, the vital signs and physical examination were within normal limits. The patient was placed on a 6-month course of rivaroxaban therapy. Coagulopathy testing was scheduled at a later date, since ongoing anticoagulation treatment could interfere with test results. Unfortunately, the patient did not attend follow-up appointments to obtain testing.
Discussion
Mesenteric venous thrombosis is seen predominantly in middle-aged patients presenting with vague symptoms, which makes this a challenging diagnosis to make in the acute care setting. Risk factors for MVT include recent injury (causing trauma to the vasculature), recent surgery (causing stagnant blood flow), inflammatory conditions, and hypercoagulable states.1 In this patient’s case, no risk factors were identified; although the majority of cases of MVT will have an identifiable risk factor.2 Still, 21% to 49% of cases of MVT are considered idiopathic.1,3It is possible that our patient had a prior undiagnosed pancreatitis associated with his history of alcoholism that contributed to his thrombosis. Pancreatitis and other inflammatory conditions, including diverticulitis or inflammatory bowel disease, are more commonly associated with thrombus formation in the large veins, as opposed to an undiagnosed hypercoagulable state, which would more likely affect distal venuoles, vasa recta, or venous arcades.1,5 The patient’s mild transaminitis was likely secondary to hepatic congestion from the venous thrombus extending to the splenic-portal vein confluence and intrahepatic portal vein. One study looked at patients with pancreatitis and found that 16.7% of their study population had an SMV thrombus, while 4.1% had a SMV thrombus with a concomitant portal vein thrombus.6
Although there are no pathognomonic laboratory findings of MVT, elevated lactate, leukocytosis, and elevated D-dimer levels may be helpful in supporting the diagnosis.7,8 A recent study found that elevated D-dimer levels may be a specific marker in the early recognition of acute SMV thrombosis, as well as predicting risk, outcomes, and treatment options.8 However, emergency physicians should maintain a high index of suspicion in patients with concerning features of the disease, since normal laboratory values, including lactate, do not reliably exclude the diagnosis.
Computed tomography scanning and CT angiography (CTA) are quite helpful in diagnosing MVT. Ultrasound of the upper abdomen may also play a role, noting dilated or thickened bowel wall with intraluminal air or echogenic material in the superior mesenteric vein or portal vein.9 Although magnetic resonance venography most reliably demonstrates thrombi, its lack of widespread availability makes CT with IV contrast the preferred initial study.3Computed tomography not only has high sensitivity, but also offers alternative diagnoses in the undifferentiated presentation.1One study found CT to be 100% sensitive in detecting any abnormality associated with MVT or bowel ischemia.10 Common CT findings of MVT include dilated and thickened bowel loops, mesenteric fat standing, ascites, a halo or target appearance of bowel, vessel filling defects from a thrombus, and pneumatosis intestinalis.11 The latter usually indicates transmural infarction, and can extend as portomesenteric vein gas.11 Of note, if the initial CT scan is non-diagnostic and a high clinical suspicion for mesenteric ischemia remains with no alternative diagnosis, CTA is the gold standard.3,7Expeditious diagnosis of MVT is imperative, given the potential complications of intestinal infarction, submucosal hemorrhage secondary to edema, and third spacing of the venous outflow into the bowel wall due to collateral vessels being unable to redirect blood flow in conjunction with complete venous occlusion.12Not all MVTs progress to infarction, given the extensive collateral circulation. Early diagnosis, however, is crucial for conservative management to be effective.9Acute MVT without signs of infarction necessitates anticoagulation therapy to decrease clot propagation and recurrence.1 In addition, prophylactic antibiotics to limit bacterial translocation, and bowel rest are advised.13,14 If the patient is unresponsive to anticoagulation, thrombolytic and endovascular therapies may be of benefit in select patients.15 Once intestinal ischemia or infarction develops, the prognosis is poor: mortality approaches 75% with infarction.1 If signs of bowel infarction are present, a laparotomy must be performed promptly, although in most cases, delayed patient presentation makes small bowel resection unavoidable.9 Further testing for hypercoagulability is recommended, particularly in isolated thrombosis, since long-term anticoagulation therapy may be necessary if a coagulopathy is discovered.1
Conclusion
Mesenteric venous thrombosis is atypical in a young, healthy patient. However, due to high mortality rates with disease progression, it is important to consider in any patient with unrelenting abdominal pain and vague gastrointestinal symptoms of uncertain cause, even in those without risk factors. Early detection and management of MVT before progression to mesenteric ischemia and infarction considerably lowers the mortality rate. Emergency physicians must be vigilant when treating a patient with abdominal pain out of proportion to physical examination, unrelenting pain despite analgesic medications, or repeat ED visits for the same abdominal complaints.
1. Harnik IG, Brandt LJ. Mesenteric venous thrombosis. Vasc Med. 2010;15(5):407-418. doi:10.1177/1358863x10379673.
2. Tilsed JV, Casamassima A, Kurihara H, et al. ESTES guidelines: acute mesenteric ischaemia. Eur J Trauma Emerg Surg. 2016;42(2):253-270. doi:10.1007/s00068-016-0634-0.
3. Tendler DA, Lamont JT, Grubel P. Mesenteric venous thrombosis in adults. UpToDate Web site. https://www.uptodate.com/contents/mesenteric-venous-thrombosis-in-adults. Accessed November 16, 2017.
4. Al-Zahrani HA, Lindsay T. Mesenteric ischemia. In: Hall JB, Schmidt GA, Kress JP, eds. Principles of Critical Care. 4th ed. New York, NY: McGraw Hill; 2015:1036-1044.
5. Kumar S, Sarr MG, Kamath PS. Mesenteric venous thrombosis. N Engl J Med. 2001;345(23):1683-1688. doi:10.1056/nejmra010076.
6. Al-Khazraji A, Hasan AQ, Patel I, Alkhawam H, Ghrair F, Lieber J. The role of abdominal computed tomography scan in acute pancreatitis. Pancreas. 2017;46(6):e52-e54. doi:10.1097/mpa.0000000000000837.
7. Bradbury MS, Kavanagh PV, Bechtold RE, et al. Mesenteric venous thrombosis: diagnosis and noninvasive imaging. Radiographics. 2002;22(3):527-541.
8. Yang S, Fan X, Ding W, et al. D-dimer as an early marker of severity in patients with acute superior mesenteric venous thrombosis. Medicine (Baltimore). 2014;93(29):e270. doi:10.1097/md.0000000000000270.
9. Matos C, Van Gansbeke D, Zalcman M, et al. Mesenteric vein thrombosis: early CT and US diagnosis and conservative management. Gastrointest Radiol. 1986;11(4):322-325.
10. Rhee RY, Gloviczki P, Mendonca CT, et al. Mesenteric venous thrombosis: still a lethal disease in the 1990s. J Vasc Surg. 1994;20(5):688-697.
11. Furukawa A, Kanasaki S, Kono N, et al. CT diagnosis of acute mesenteric ischemia from various causes. AJR Am J Roentgenol. 2009;192(2):408-416. doi:10.2214/ajr.08.1138.
12. Johnson CC, Baggenstoss AH. Mesenteric vascular occlusion; study of 99 cases of occlusion of veins. Proc Staff Meet Mayo Clin. 1949;24(25):628-636.13. Hmoud B, Singal AK, Kamath PS. Mesenteric venous thrombosis. J Clin Exp Hepatol. 2014;4(3):257-263. doi:10.1016/j.jceh.2014.03.052.
14. Schoots IG, Koffeman GI, Legemate DA, Levi M, van Gulik TM. Systematic review of survival after acute mesenteric ischaemia according to disease aetiology. Br J Surg. 2004;91(1):17-27.
15. Yang S, Fan X, Ding W, et al. Multidisciplinary stepwise management strategy for acute superior mesenteric venous thrombosis: an intestinal stroke center experience. Thromb Res. 2015;135(1):36-45. doi:10.1016/j.thromres.2014.10.018.
In this case report, the authors address the diagnostic challenges of a young, healthy patient who presented to the ED with unrelenting abdominal pain.
In this case report, the authors address the diagnostic challenges of a young, healthy patient who presented to the ED with unrelenting abdominal pain.
Acute mesenteric ischemia (AMI) results when oxygen delivery to the mesenteric artery is compromised, and is a serious diagnosis that should be considered in patients of all ages to avoid significant morbidity and mortality. The majority of cases are due to arterial embolism, arterial thrombus, or intestinal hypoperfusion (non-occlusive). Acute mesenteric venous thrombosis (MVT) accounts for only 2% to 10% of AMI cases, and only 0.01% of emergency surgery admissions.1 A large systematic review showed a 44% mortality rate for MVT, in contrast to 66% to 89% for all other forms of AMI.2 The typical age range for MVT is reported between 45 and 60 years, with a slight male predominance.3 Dull, central abdominal pain is the most frequently reported symptom of MVT, although it is generally less impressive than the pain described in other forms of AMI.3Along with the hallmark of abdominal pain out of proportion to the examination, other gastrointestinal symptoms include weight loss and non-specific altered bowel function (constipation, diarrhea, abdominal distention, and bloating), which are present in half of all patients with MVT.1 Peritoneal signs and bloody stools portend poor outcomes, as they often occur with disease progression.4
Case
A 26-year-old man presented to the ED with periumbilical and lower abdominal pain for 1 week. The pain was described as constant and dull, worsened by movement and oral intake, and improved with lying flat. He described bloating and decreased volume of bowel movements. He denied nausea, vomiting, fever, colicky pain, blood in stool, testicular pain, urinary complaints, trauma, or any similar episodes in the past. The patient had no known medical conditions or surgical history, except for a remote history of alcohol dependence (in remission) and tobacco use. There was no personal or family history of coagulopathy. Of note, he was seen by his primary care physician a few days prior to his ED presentation and had been instructed to take acetaminophen, which did not provide relief.
The patient’s vital signs at presentation were: blood pressure, 122/70 mm Hg; heart rate, 93 beats/min; respiratory rate, 18 breaths/min; and temperature, 37.5°C (99.5°F). Oxygen saturation was 99% on room air. The physical examination was remarkable only for mild abdominal tenderness diffusely, greater in the lower and central abdomen than in the upper abdomen. The remainder of the physical examination was unremarkable.
Laboratory studies ordered included a complete blood count, comprehensive metabolic profile, lipase, and urinalysis. The patient did have a mild transaminitis (aspartate aminotransferase, 48 U/L; alanine aminotransferase, 84 U/L); the remainder of the studies were normal. A serum lactate, drawn after the 1 L of normal saline was administered intravenously (IV), was within normal limits (0.7 mmol/L). No prior laboratory studies were available for comparison.
The patient’s continued abdominal pain and transaminitis prompted an ED bedside right upper quadrant ultrasound, which showed a small gallbladder polyp; no signs of gallbladder disease were present. The patient required three doses of morphine 4 mg IV without complete pain relief. Given the concern for pain out of proportion to physical examination, a computed tomography (CT) scan of the abdomen/pelvis with IV and oral contrast was ordered. The radiologist interpreted the scan as showing a superior mesenteric vein (SMV) thrombus extending into the splenic/portal vein confluence and the intrahepatic portal veins (Figures 1 and 2).
Ciprofloxacin and metronidazole were administered IV for antibiotic prophylaxis, and the patient was placed on bowel rest with advancement to regular diet as tolerated. Propranolol was given for variceal prophylaxis. The patient was discharged home the following day in stable condition. Although he still had mild abdominal tenderness, the vital signs and physical examination were within normal limits. The patient was placed on a 6-month course of rivaroxaban therapy. Coagulopathy testing was scheduled at a later date, since ongoing anticoagulation treatment could interfere with test results. Unfortunately, the patient did not attend follow-up appointments to obtain testing.
Discussion
Mesenteric venous thrombosis is seen predominantly in middle-aged patients presenting with vague symptoms, which makes this a challenging diagnosis to make in the acute care setting. Risk factors for MVT include recent injury (causing trauma to the vasculature), recent surgery (causing stagnant blood flow), inflammatory conditions, and hypercoagulable states.1 In this patient’s case, no risk factors were identified; although the majority of cases of MVT will have an identifiable risk factor.2 Still, 21% to 49% of cases of MVT are considered idiopathic.1,3It is possible that our patient had a prior undiagnosed pancreatitis associated with his history of alcoholism that contributed to his thrombosis. Pancreatitis and other inflammatory conditions, including diverticulitis or inflammatory bowel disease, are more commonly associated with thrombus formation in the large veins, as opposed to an undiagnosed hypercoagulable state, which would more likely affect distal venuoles, vasa recta, or venous arcades.1,5 The patient’s mild transaminitis was likely secondary to hepatic congestion from the venous thrombus extending to the splenic-portal vein confluence and intrahepatic portal vein. One study looked at patients with pancreatitis and found that 16.7% of their study population had an SMV thrombus, while 4.1% had a SMV thrombus with a concomitant portal vein thrombus.6
Although there are no pathognomonic laboratory findings of MVT, elevated lactate, leukocytosis, and elevated D-dimer levels may be helpful in supporting the diagnosis.7,8 A recent study found that elevated D-dimer levels may be a specific marker in the early recognition of acute SMV thrombosis, as well as predicting risk, outcomes, and treatment options.8 However, emergency physicians should maintain a high index of suspicion in patients with concerning features of the disease, since normal laboratory values, including lactate, do not reliably exclude the diagnosis.
Computed tomography scanning and CT angiography (CTA) are quite helpful in diagnosing MVT. Ultrasound of the upper abdomen may also play a role, noting dilated or thickened bowel wall with intraluminal air or echogenic material in the superior mesenteric vein or portal vein.9 Although magnetic resonance venography most reliably demonstrates thrombi, its lack of widespread availability makes CT with IV contrast the preferred initial study.3Computed tomography not only has high sensitivity, but also offers alternative diagnoses in the undifferentiated presentation.1One study found CT to be 100% sensitive in detecting any abnormality associated with MVT or bowel ischemia.10 Common CT findings of MVT include dilated and thickened bowel loops, mesenteric fat standing, ascites, a halo or target appearance of bowel, vessel filling defects from a thrombus, and pneumatosis intestinalis.11 The latter usually indicates transmural infarction, and can extend as portomesenteric vein gas.11 Of note, if the initial CT scan is non-diagnostic and a high clinical suspicion for mesenteric ischemia remains with no alternative diagnosis, CTA is the gold standard.3,7Expeditious diagnosis of MVT is imperative, given the potential complications of intestinal infarction, submucosal hemorrhage secondary to edema, and third spacing of the venous outflow into the bowel wall due to collateral vessels being unable to redirect blood flow in conjunction with complete venous occlusion.12Not all MVTs progress to infarction, given the extensive collateral circulation. Early diagnosis, however, is crucial for conservative management to be effective.9Acute MVT without signs of infarction necessitates anticoagulation therapy to decrease clot propagation and recurrence.1 In addition, prophylactic antibiotics to limit bacterial translocation, and bowel rest are advised.13,14 If the patient is unresponsive to anticoagulation, thrombolytic and endovascular therapies may be of benefit in select patients.15 Once intestinal ischemia or infarction develops, the prognosis is poor: mortality approaches 75% with infarction.1 If signs of bowel infarction are present, a laparotomy must be performed promptly, although in most cases, delayed patient presentation makes small bowel resection unavoidable.9 Further testing for hypercoagulability is recommended, particularly in isolated thrombosis, since long-term anticoagulation therapy may be necessary if a coagulopathy is discovered.1
Conclusion
Mesenteric venous thrombosis is atypical in a young, healthy patient. However, due to high mortality rates with disease progression, it is important to consider in any patient with unrelenting abdominal pain and vague gastrointestinal symptoms of uncertain cause, even in those without risk factors. Early detection and management of MVT before progression to mesenteric ischemia and infarction considerably lowers the mortality rate. Emergency physicians must be vigilant when treating a patient with abdominal pain out of proportion to physical examination, unrelenting pain despite analgesic medications, or repeat ED visits for the same abdominal complaints.
Acute mesenteric ischemia (AMI) results when oxygen delivery to the mesenteric artery is compromised, and is a serious diagnosis that should be considered in patients of all ages to avoid significant morbidity and mortality. The majority of cases are due to arterial embolism, arterial thrombus, or intestinal hypoperfusion (non-occlusive). Acute mesenteric venous thrombosis (MVT) accounts for only 2% to 10% of AMI cases, and only 0.01% of emergency surgery admissions.1 A large systematic review showed a 44% mortality rate for MVT, in contrast to 66% to 89% for all other forms of AMI.2 The typical age range for MVT is reported between 45 and 60 years, with a slight male predominance.3 Dull, central abdominal pain is the most frequently reported symptom of MVT, although it is generally less impressive than the pain described in other forms of AMI.3Along with the hallmark of abdominal pain out of proportion to the examination, other gastrointestinal symptoms include weight loss and non-specific altered bowel function (constipation, diarrhea, abdominal distention, and bloating), which are present in half of all patients with MVT.1 Peritoneal signs and bloody stools portend poor outcomes, as they often occur with disease progression.4
Case
A 26-year-old man presented to the ED with periumbilical and lower abdominal pain for 1 week. The pain was described as constant and dull, worsened by movement and oral intake, and improved with lying flat. He described bloating and decreased volume of bowel movements. He denied nausea, vomiting, fever, colicky pain, blood in stool, testicular pain, urinary complaints, trauma, or any similar episodes in the past. The patient had no known medical conditions or surgical history, except for a remote history of alcohol dependence (in remission) and tobacco use. There was no personal or family history of coagulopathy. Of note, he was seen by his primary care physician a few days prior to his ED presentation and had been instructed to take acetaminophen, which did not provide relief.
The patient’s vital signs at presentation were: blood pressure, 122/70 mm Hg; heart rate, 93 beats/min; respiratory rate, 18 breaths/min; and temperature, 37.5°C (99.5°F). Oxygen saturation was 99% on room air. The physical examination was remarkable only for mild abdominal tenderness diffusely, greater in the lower and central abdomen than in the upper abdomen. The remainder of the physical examination was unremarkable.
Laboratory studies ordered included a complete blood count, comprehensive metabolic profile, lipase, and urinalysis. The patient did have a mild transaminitis (aspartate aminotransferase, 48 U/L; alanine aminotransferase, 84 U/L); the remainder of the studies were normal. A serum lactate, drawn after the 1 L of normal saline was administered intravenously (IV), was within normal limits (0.7 mmol/L). No prior laboratory studies were available for comparison.
The patient’s continued abdominal pain and transaminitis prompted an ED bedside right upper quadrant ultrasound, which showed a small gallbladder polyp; no signs of gallbladder disease were present. The patient required three doses of morphine 4 mg IV without complete pain relief. Given the concern for pain out of proportion to physical examination, a computed tomography (CT) scan of the abdomen/pelvis with IV and oral contrast was ordered. The radiologist interpreted the scan as showing a superior mesenteric vein (SMV) thrombus extending into the splenic/portal vein confluence and the intrahepatic portal veins (Figures 1 and 2).
Ciprofloxacin and metronidazole were administered IV for antibiotic prophylaxis, and the patient was placed on bowel rest with advancement to regular diet as tolerated. Propranolol was given for variceal prophylaxis. The patient was discharged home the following day in stable condition. Although he still had mild abdominal tenderness, the vital signs and physical examination were within normal limits. The patient was placed on a 6-month course of rivaroxaban therapy. Coagulopathy testing was scheduled at a later date, since ongoing anticoagulation treatment could interfere with test results. Unfortunately, the patient did not attend follow-up appointments to obtain testing.
Discussion
Mesenteric venous thrombosis is seen predominantly in middle-aged patients presenting with vague symptoms, which makes this a challenging diagnosis to make in the acute care setting. Risk factors for MVT include recent injury (causing trauma to the vasculature), recent surgery (causing stagnant blood flow), inflammatory conditions, and hypercoagulable states.1 In this patient’s case, no risk factors were identified; although the majority of cases of MVT will have an identifiable risk factor.2 Still, 21% to 49% of cases of MVT are considered idiopathic.1,3It is possible that our patient had a prior undiagnosed pancreatitis associated with his history of alcoholism that contributed to his thrombosis. Pancreatitis and other inflammatory conditions, including diverticulitis or inflammatory bowel disease, are more commonly associated with thrombus formation in the large veins, as opposed to an undiagnosed hypercoagulable state, which would more likely affect distal venuoles, vasa recta, or venous arcades.1,5 The patient’s mild transaminitis was likely secondary to hepatic congestion from the venous thrombus extending to the splenic-portal vein confluence and intrahepatic portal vein. One study looked at patients with pancreatitis and found that 16.7% of their study population had an SMV thrombus, while 4.1% had a SMV thrombus with a concomitant portal vein thrombus.6
Although there are no pathognomonic laboratory findings of MVT, elevated lactate, leukocytosis, and elevated D-dimer levels may be helpful in supporting the diagnosis.7,8 A recent study found that elevated D-dimer levels may be a specific marker in the early recognition of acute SMV thrombosis, as well as predicting risk, outcomes, and treatment options.8 However, emergency physicians should maintain a high index of suspicion in patients with concerning features of the disease, since normal laboratory values, including lactate, do not reliably exclude the diagnosis.
Computed tomography scanning and CT angiography (CTA) are quite helpful in diagnosing MVT. Ultrasound of the upper abdomen may also play a role, noting dilated or thickened bowel wall with intraluminal air or echogenic material in the superior mesenteric vein or portal vein.9 Although magnetic resonance venography most reliably demonstrates thrombi, its lack of widespread availability makes CT with IV contrast the preferred initial study.3Computed tomography not only has high sensitivity, but also offers alternative diagnoses in the undifferentiated presentation.1One study found CT to be 100% sensitive in detecting any abnormality associated with MVT or bowel ischemia.10 Common CT findings of MVT include dilated and thickened bowel loops, mesenteric fat standing, ascites, a halo or target appearance of bowel, vessel filling defects from a thrombus, and pneumatosis intestinalis.11 The latter usually indicates transmural infarction, and can extend as portomesenteric vein gas.11 Of note, if the initial CT scan is non-diagnostic and a high clinical suspicion for mesenteric ischemia remains with no alternative diagnosis, CTA is the gold standard.3,7Expeditious diagnosis of MVT is imperative, given the potential complications of intestinal infarction, submucosal hemorrhage secondary to edema, and third spacing of the venous outflow into the bowel wall due to collateral vessels being unable to redirect blood flow in conjunction with complete venous occlusion.12Not all MVTs progress to infarction, given the extensive collateral circulation. Early diagnosis, however, is crucial for conservative management to be effective.9Acute MVT without signs of infarction necessitates anticoagulation therapy to decrease clot propagation and recurrence.1 In addition, prophylactic antibiotics to limit bacterial translocation, and bowel rest are advised.13,14 If the patient is unresponsive to anticoagulation, thrombolytic and endovascular therapies may be of benefit in select patients.15 Once intestinal ischemia or infarction develops, the prognosis is poor: mortality approaches 75% with infarction.1 If signs of bowel infarction are present, a laparotomy must be performed promptly, although in most cases, delayed patient presentation makes small bowel resection unavoidable.9 Further testing for hypercoagulability is recommended, particularly in isolated thrombosis, since long-term anticoagulation therapy may be necessary if a coagulopathy is discovered.1
Conclusion
Mesenteric venous thrombosis is atypical in a young, healthy patient. However, due to high mortality rates with disease progression, it is important to consider in any patient with unrelenting abdominal pain and vague gastrointestinal symptoms of uncertain cause, even in those without risk factors. Early detection and management of MVT before progression to mesenteric ischemia and infarction considerably lowers the mortality rate. Emergency physicians must be vigilant when treating a patient with abdominal pain out of proportion to physical examination, unrelenting pain despite analgesic medications, or repeat ED visits for the same abdominal complaints.
1. Harnik IG, Brandt LJ. Mesenteric venous thrombosis. Vasc Med. 2010;15(5):407-418. doi:10.1177/1358863x10379673.
2. Tilsed JV, Casamassima A, Kurihara H, et al. ESTES guidelines: acute mesenteric ischaemia. Eur J Trauma Emerg Surg. 2016;42(2):253-270. doi:10.1007/s00068-016-0634-0.
3. Tendler DA, Lamont JT, Grubel P. Mesenteric venous thrombosis in adults. UpToDate Web site. https://www.uptodate.com/contents/mesenteric-venous-thrombosis-in-adults. Accessed November 16, 2017.
4. Al-Zahrani HA, Lindsay T. Mesenteric ischemia. In: Hall JB, Schmidt GA, Kress JP, eds. Principles of Critical Care. 4th ed. New York, NY: McGraw Hill; 2015:1036-1044.
5. Kumar S, Sarr MG, Kamath PS. Mesenteric venous thrombosis. N Engl J Med. 2001;345(23):1683-1688. doi:10.1056/nejmra010076.
6. Al-Khazraji A, Hasan AQ, Patel I, Alkhawam H, Ghrair F, Lieber J. The role of abdominal computed tomography scan in acute pancreatitis. Pancreas. 2017;46(6):e52-e54. doi:10.1097/mpa.0000000000000837.
7. Bradbury MS, Kavanagh PV, Bechtold RE, et al. Mesenteric venous thrombosis: diagnosis and noninvasive imaging. Radiographics. 2002;22(3):527-541.
8. Yang S, Fan X, Ding W, et al. D-dimer as an early marker of severity in patients with acute superior mesenteric venous thrombosis. Medicine (Baltimore). 2014;93(29):e270. doi:10.1097/md.0000000000000270.
9. Matos C, Van Gansbeke D, Zalcman M, et al. Mesenteric vein thrombosis: early CT and US diagnosis and conservative management. Gastrointest Radiol. 1986;11(4):322-325.
10. Rhee RY, Gloviczki P, Mendonca CT, et al. Mesenteric venous thrombosis: still a lethal disease in the 1990s. J Vasc Surg. 1994;20(5):688-697.
11. Furukawa A, Kanasaki S, Kono N, et al. CT diagnosis of acute mesenteric ischemia from various causes. AJR Am J Roentgenol. 2009;192(2):408-416. doi:10.2214/ajr.08.1138.
12. Johnson CC, Baggenstoss AH. Mesenteric vascular occlusion; study of 99 cases of occlusion of veins. Proc Staff Meet Mayo Clin. 1949;24(25):628-636.13. Hmoud B, Singal AK, Kamath PS. Mesenteric venous thrombosis. J Clin Exp Hepatol. 2014;4(3):257-263. doi:10.1016/j.jceh.2014.03.052.
14. Schoots IG, Koffeman GI, Legemate DA, Levi M, van Gulik TM. Systematic review of survival after acute mesenteric ischaemia according to disease aetiology. Br J Surg. 2004;91(1):17-27.
15. Yang S, Fan X, Ding W, et al. Multidisciplinary stepwise management strategy for acute superior mesenteric venous thrombosis: an intestinal stroke center experience. Thromb Res. 2015;135(1):36-45. doi:10.1016/j.thromres.2014.10.018.
1. Harnik IG, Brandt LJ. Mesenteric venous thrombosis. Vasc Med. 2010;15(5):407-418. doi:10.1177/1358863x10379673.
2. Tilsed JV, Casamassima A, Kurihara H, et al. ESTES guidelines: acute mesenteric ischaemia. Eur J Trauma Emerg Surg. 2016;42(2):253-270. doi:10.1007/s00068-016-0634-0.
3. Tendler DA, Lamont JT, Grubel P. Mesenteric venous thrombosis in adults. UpToDate Web site. https://www.uptodate.com/contents/mesenteric-venous-thrombosis-in-adults. Accessed November 16, 2017.
4. Al-Zahrani HA, Lindsay T. Mesenteric ischemia. In: Hall JB, Schmidt GA, Kress JP, eds. Principles of Critical Care. 4th ed. New York, NY: McGraw Hill; 2015:1036-1044.
5. Kumar S, Sarr MG, Kamath PS. Mesenteric venous thrombosis. N Engl J Med. 2001;345(23):1683-1688. doi:10.1056/nejmra010076.
6. Al-Khazraji A, Hasan AQ, Patel I, Alkhawam H, Ghrair F, Lieber J. The role of abdominal computed tomography scan in acute pancreatitis. Pancreas. 2017;46(6):e52-e54. doi:10.1097/mpa.0000000000000837.
7. Bradbury MS, Kavanagh PV, Bechtold RE, et al. Mesenteric venous thrombosis: diagnosis and noninvasive imaging. Radiographics. 2002;22(3):527-541.
8. Yang S, Fan X, Ding W, et al. D-dimer as an early marker of severity in patients with acute superior mesenteric venous thrombosis. Medicine (Baltimore). 2014;93(29):e270. doi:10.1097/md.0000000000000270.
9. Matos C, Van Gansbeke D, Zalcman M, et al. Mesenteric vein thrombosis: early CT and US diagnosis and conservative management. Gastrointest Radiol. 1986;11(4):322-325.
10. Rhee RY, Gloviczki P, Mendonca CT, et al. Mesenteric venous thrombosis: still a lethal disease in the 1990s. J Vasc Surg. 1994;20(5):688-697.
11. Furukawa A, Kanasaki S, Kono N, et al. CT diagnosis of acute mesenteric ischemia from various causes. AJR Am J Roentgenol. 2009;192(2):408-416. doi:10.2214/ajr.08.1138.
12. Johnson CC, Baggenstoss AH. Mesenteric vascular occlusion; study of 99 cases of occlusion of veins. Proc Staff Meet Mayo Clin. 1949;24(25):628-636.13. Hmoud B, Singal AK, Kamath PS. Mesenteric venous thrombosis. J Clin Exp Hepatol. 2014;4(3):257-263. doi:10.1016/j.jceh.2014.03.052.
14. Schoots IG, Koffeman GI, Legemate DA, Levi M, van Gulik TM. Systematic review of survival after acute mesenteric ischaemia according to disease aetiology. Br J Surg. 2004;91(1):17-27.
15. Yang S, Fan X, Ding W, et al. Multidisciplinary stepwise management strategy for acute superior mesenteric venous thrombosis: an intestinal stroke center experience. Thromb Res. 2015;135(1):36-45. doi:10.1016/j.thromres.2014.10.018.

Crizanlizumab relieves sickle cell crises across subgroups
Crizanlizumab effectively reduced vaso-occlusive crises among patients with sickle cell disease (SCD) who have numerous crises, exhibit the HbSS genotype, and take concomitant hydroxyurea, according to investigators.

Across subgroups, crizanlizumab was safe and more effective than placebo at delaying time to first vaso-occlusive crisis (VOC) and eliminating crises, reported lead author Abdullah Kutlar, MD, of the Sickle Cell Center at the Medical College of Georgia, Augusta, and his colleagues.
The phase 2 SUSTAIN trial recently showed that crizanlizumab – a humanized, anti–P-selectin monoclonal antibody – reduced the frequency of VOCs by 45% and delayed time to first crisis by about 3 months (N Engl J Med. 2017;376:429-39).
Additionally, a subgroup analysis showed that there was a lower frequency of pain crises with crizanlizumab 5 mg/kg, compared with placebo, regardless of the number of prior VOCs, concomitant hydroxyurea use, or the SCD genotype.
The present post hoc analysis took a deeper look at these observations across the same subgroups; specifically, the investigators assessed elimination of VOCs, time to first crisis, and adverse events. They reported the findings in the American Journal of Hematology.
Crizanlizumab eliminated pain crises about seven times more frequently than did placebo in patients who had a high frequency of VOCs before the study (28.0% vs. 4.2%), and about twice as often in patients with the HbSS genotype (31.9% vs. 17.0%), and patients who were using concomitant hydroxyurea (33.3% vs. 17.5%).
Further analysis showed that crizanlizumab delayed time to first pain crisis across all subgroups, most dramatically in patients with the HbSS genotype (4.07 months for crizanlizumab vs. 1.12 months for placebo). Safety was comparable across subgroups.
“These findings provide supportive evidence that crizanlizumab provides a clinically meaningful treatment benefit when used alone or in combination with hydroxyurea for the prevention of VOCs,” the investigators wrote.
An ongoing phase 2 pharmacokinetic/pharmacodynamic study is evaluating a higher dose of crizanlizumab (7.5 mg/kg), and another trial seeks to evaluate pediatric doses of the drug.
The study was sponsored by Novartis. The authors reported financial relationships with Novartis, Bluebird Bio, AstraZeneca, and others.
SOURCE: Kutlar A et al. Am J Hematol. 2018 Oct 8. doi: 10.1002/ajh.25308.
Crizanlizumab effectively reduced vaso-occlusive crises among patients with sickle cell disease (SCD) who have numerous crises, exhibit the HbSS genotype, and take concomitant hydroxyurea, according to investigators.
Across subgroups, crizanlizumab was safe and more effective than placebo at delaying time to first vaso-occlusive crisis (VOC) and eliminating crises, reported lead author Abdullah Kutlar, MD, of the Sickle Cell Center at the Medical College of Georgia, Augusta, and his colleagues.
The phase 2 SUSTAIN trial recently showed that crizanlizumab – a humanized, anti–P-selectin monoclonal antibody – reduced the frequency of VOCs by 45% and delayed time to first crisis by about 3 months (N Engl J Med. 2017;376:429-39).
Additionally, a subgroup analysis showed that there was a lower frequency of pain crises with crizanlizumab 5 mg/kg, compared with placebo, regardless of the number of prior VOCs, concomitant hydroxyurea use, or the SCD genotype.
The present post hoc analysis took a deeper look at these observations across the same subgroups; specifically, the investigators assessed elimination of VOCs, time to first crisis, and adverse events. They reported the findings in the American Journal of Hematology.
Crizanlizumab eliminated pain crises about seven times more frequently than did placebo in patients who had a high frequency of VOCs before the study (28.0% vs. 4.2%), and about twice as often in patients with the HbSS genotype (31.9% vs. 17.0%), and patients who were using concomitant hydroxyurea (33.3% vs. 17.5%).
Further analysis showed that crizanlizumab delayed time to first pain crisis across all subgroups, most dramatically in patients with the HbSS genotype (4.07 months for crizanlizumab vs. 1.12 months for placebo). Safety was comparable across subgroups.
“These findings provide supportive evidence that crizanlizumab provides a clinically meaningful treatment benefit when used alone or in combination with hydroxyurea for the prevention of VOCs,” the investigators wrote.
An ongoing phase 2 pharmacokinetic/pharmacodynamic study is evaluating a higher dose of crizanlizumab (7.5 mg/kg), and another trial seeks to evaluate pediatric doses of the drug.
The study was sponsored by Novartis. The authors reported financial relationships with Novartis, Bluebird Bio, AstraZeneca, and others.
SOURCE: Kutlar A et al. Am J Hematol. 2018 Oct 8. doi: 10.1002/ajh.25308.
Crizanlizumab effectively reduced vaso-occlusive crises among patients with sickle cell disease (SCD) who have numerous crises, exhibit the HbSS genotype, and take concomitant hydroxyurea, according to investigators.
Across subgroups, crizanlizumab was safe and more effective than placebo at delaying time to first vaso-occlusive crisis (VOC) and eliminating crises, reported lead author Abdullah Kutlar, MD, of the Sickle Cell Center at the Medical College of Georgia, Augusta, and his colleagues.
The phase 2 SUSTAIN trial recently showed that crizanlizumab – a humanized, anti–P-selectin monoclonal antibody – reduced the frequency of VOCs by 45% and delayed time to first crisis by about 3 months (N Engl J Med. 2017;376:429-39).
Additionally, a subgroup analysis showed that there was a lower frequency of pain crises with crizanlizumab 5 mg/kg, compared with placebo, regardless of the number of prior VOCs, concomitant hydroxyurea use, or the SCD genotype.
The present post hoc analysis took a deeper look at these observations across the same subgroups; specifically, the investigators assessed elimination of VOCs, time to first crisis, and adverse events. They reported the findings in the American Journal of Hematology.
Crizanlizumab eliminated pain crises about seven times more frequently than did placebo in patients who had a high frequency of VOCs before the study (28.0% vs. 4.2%), and about twice as often in patients with the HbSS genotype (31.9% vs. 17.0%), and patients who were using concomitant hydroxyurea (33.3% vs. 17.5%).
Further analysis showed that crizanlizumab delayed time to first pain crisis across all subgroups, most dramatically in patients with the HbSS genotype (4.07 months for crizanlizumab vs. 1.12 months for placebo). Safety was comparable across subgroups.
“These findings provide supportive evidence that crizanlizumab provides a clinically meaningful treatment benefit when used alone or in combination with hydroxyurea for the prevention of VOCs,” the investigators wrote.
An ongoing phase 2 pharmacokinetic/pharmacodynamic study is evaluating a higher dose of crizanlizumab (7.5 mg/kg), and another trial seeks to evaluate pediatric doses of the drug.
The study was sponsored by Novartis. The authors reported financial relationships with Novartis, Bluebird Bio, AstraZeneca, and others.
SOURCE: Kutlar A et al. Am J Hematol. 2018 Oct 8. doi: 10.1002/ajh.25308.
FROM THE AMERICAN JOURNAL OF HEMATOLOGY
Key clinical point:
Major finding: Crizanlizumab eliminated vaso-occlusive crises about seven times more frequently than did placebo in patients with numerous crises (28.0% vs. 4.2%).
Study details: A post hoc analysis of 132 patients from the phase 2 SUSTAIN trial.
Disclosures: The study was sponsored by Novartis. The authors reported financial relationships with Novartis, Bluebird Bio, AstraZeneca, and others.
Source: Kutlar A et al. Am J Hematol. 2018 Oct 8. doi: 10.1002/ajh.25308.
Updated ThroLy system predicts need for thromboprophylaxis
DUBROVNIK, CROATIA – An updated scoring system can more accurately identify lymphoma patients who may require thromboprophylaxis, according to researchers.
The revised scoring system, ThroLy, proved more effective than other systems for predicting thromboembolic events in lymphoma patients, with a positive predictive value of 22%-25%, a negative predictive value of 96%, sensitivity of 56%-57%, and specificity of 85%-87%.
Darko Antic, MD, PhD, of the University of Belgrade in Serbia, presented these findings at Leukemia and Lymphoma, a meeting jointly sponsored by the University of Texas MD Anderson Cancer Center and the School of Medicine at the University of Zagreb, Croatia.
Dr. Antic said that he and his colleagues developed ThroLy because other systems used to predict venous thromboembolism (VTE) are not quite right for lymphoma. He noted that the Padua score is not designed for cancer patients and the Khorana score is predominantly used for solid tumor malignancies.
The ThroLy scoring system is based on variables used in the Padua and Khorana systems, as well as variables that are specific to lymphoma patients.
In a previous study, the researchers found several variables that were independently associated with risk for VTE in lymphoma, including previous VTE, previous acute MI or stroke, mediastinal involvement, high body mass index, reduced mobility, extranodal localization, neutropenia, and hemoglobin less than 100 g/L (Am J Hematol. 2016 Oct;91[10]:1014-9).
In an initial version of the ThroLy scoring system, previous VTE, previous acute MI/stroke, obesity, and mediastinal involvement were all worth two points, and the other factors were worth a single point in the ThroLy system.
Patients with scores of 0 to 1 were considered low risk, patients with scores of 2 to 3 were considered intermediate risk, and patients with scores of 4 or greater were considered high risk.
To validate and refine ThroLy, Dr. Antic and his colleagues used it to assess 1,723 lymphoma patients treated at eight institutions in Austria, Croatia, France, Jordan, Macedonia, Spain, Switzerland, and the United States.
Patients had indolent non-Hodgkin lymphoma, aggressive non-Hodgkin lymphoma, chronic lymphocytic leukemia/small lymphocytic lymphoma, and Hodgkin lymphoma. Most subjects (84%) were outpatients. A total of 9%of patients had thrombosis, with 7% having VTE.
ThroLy had a positive predictive value of 17%, compared with 11% with Khorana and 13% with Padua. The negative predictive value was 93%, 92%, and 95%, respectively. The sensitivity was 51% with ThroLy, 42% with Khorana, and 70% with Padua; specificity was 72%, 64%, and 52%, respectively.
“The positive predictive value was low [with ThroLy] but definitely higher than the positive predictive value of the other two [scoring systems],” Dr. Antic noted.
Updated models
To further improve ThroLy, the researchers updated the system, creating two new models. Model 1 included the type of lymphoma/clinical stage (1 point), previous VTE (5 points), reduced mobility (2 points), hemoglobin less than 100 g/L (1 point), and the presence of vascular devices (1 point). Model 2 included all of the variables in Model 1 plus the thrombophilic condition, which was worth 1 point.
Patients were considered low risk if they scored 2 points or lower and high risk if they scored more than 2 points.
For Model 1, the positive predictive value was 22%, the negative predictive value was 96%, the sensitivity was 56%, and the specificity was 85%. For Model 2, the positive predictive value was 25%, the negative predictive value was 96%, the sensitivity was 57%, and the specificity was 87%.
There were no major differences in model discrimination and calibration based on the country in which a patient was treated or whether the patient was treated in an inpatient or outpatient setting.
Dr. Antic did not report any conflicts of interest. The Leukemia and Lymphoma meeting is organized by Jonathan Wood & Association, which is owned by the parent company of this news organization.
DUBROVNIK, CROATIA – An updated scoring system can more accurately identify lymphoma patients who may require thromboprophylaxis, according to researchers.
The revised scoring system, ThroLy, proved more effective than other systems for predicting thromboembolic events in lymphoma patients, with a positive predictive value of 22%-25%, a negative predictive value of 96%, sensitivity of 56%-57%, and specificity of 85%-87%.
Darko Antic, MD, PhD, of the University of Belgrade in Serbia, presented these findings at Leukemia and Lymphoma, a meeting jointly sponsored by the University of Texas MD Anderson Cancer Center and the School of Medicine at the University of Zagreb, Croatia.
Dr. Antic said that he and his colleagues developed ThroLy because other systems used to predict venous thromboembolism (VTE) are not quite right for lymphoma. He noted that the Padua score is not designed for cancer patients and the Khorana score is predominantly used for solid tumor malignancies.
The ThroLy scoring system is based on variables used in the Padua and Khorana systems, as well as variables that are specific to lymphoma patients.
In a previous study, the researchers found several variables that were independently associated with risk for VTE in lymphoma, including previous VTE, previous acute MI or stroke, mediastinal involvement, high body mass index, reduced mobility, extranodal localization, neutropenia, and hemoglobin less than 100 g/L (Am J Hematol. 2016 Oct;91[10]:1014-9).
In an initial version of the ThroLy scoring system, previous VTE, previous acute MI/stroke, obesity, and mediastinal involvement were all worth two points, and the other factors were worth a single point in the ThroLy system.
Patients with scores of 0 to 1 were considered low risk, patients with scores of 2 to 3 were considered intermediate risk, and patients with scores of 4 or greater were considered high risk.
To validate and refine ThroLy, Dr. Antic and his colleagues used it to assess 1,723 lymphoma patients treated at eight institutions in Austria, Croatia, France, Jordan, Macedonia, Spain, Switzerland, and the United States.
Patients had indolent non-Hodgkin lymphoma, aggressive non-Hodgkin lymphoma, chronic lymphocytic leukemia/small lymphocytic lymphoma, and Hodgkin lymphoma. Most subjects (84%) were outpatients. A total of 9%of patients had thrombosis, with 7% having VTE.
ThroLy had a positive predictive value of 17%, compared with 11% with Khorana and 13% with Padua. The negative predictive value was 93%, 92%, and 95%, respectively. The sensitivity was 51% with ThroLy, 42% with Khorana, and 70% with Padua; specificity was 72%, 64%, and 52%, respectively.
“The positive predictive value was low [with ThroLy] but definitely higher than the positive predictive value of the other two [scoring systems],” Dr. Antic noted.
Updated models
To further improve ThroLy, the researchers updated the system, creating two new models. Model 1 included the type of lymphoma/clinical stage (1 point), previous VTE (5 points), reduced mobility (2 points), hemoglobin less than 100 g/L (1 point), and the presence of vascular devices (1 point). Model 2 included all of the variables in Model 1 plus the thrombophilic condition, which was worth 1 point.
Patients were considered low risk if they scored 2 points or lower and high risk if they scored more than 2 points.
For Model 1, the positive predictive value was 22%, the negative predictive value was 96%, the sensitivity was 56%, and the specificity was 85%. For Model 2, the positive predictive value was 25%, the negative predictive value was 96%, the sensitivity was 57%, and the specificity was 87%.
There were no major differences in model discrimination and calibration based on the country in which a patient was treated or whether the patient was treated in an inpatient or outpatient setting.
Dr. Antic did not report any conflicts of interest. The Leukemia and Lymphoma meeting is organized by Jonathan Wood & Association, which is owned by the parent company of this news organization.
DUBROVNIK, CROATIA – An updated scoring system can more accurately identify lymphoma patients who may require thromboprophylaxis, according to researchers.
The revised scoring system, ThroLy, proved more effective than other systems for predicting thromboembolic events in lymphoma patients, with a positive predictive value of 22%-25%, a negative predictive value of 96%, sensitivity of 56%-57%, and specificity of 85%-87%.
Darko Antic, MD, PhD, of the University of Belgrade in Serbia, presented these findings at Leukemia and Lymphoma, a meeting jointly sponsored by the University of Texas MD Anderson Cancer Center and the School of Medicine at the University of Zagreb, Croatia.
Dr. Antic said that he and his colleagues developed ThroLy because other systems used to predict venous thromboembolism (VTE) are not quite right for lymphoma. He noted that the Padua score is not designed for cancer patients and the Khorana score is predominantly used for solid tumor malignancies.
The ThroLy scoring system is based on variables used in the Padua and Khorana systems, as well as variables that are specific to lymphoma patients.
In a previous study, the researchers found several variables that were independently associated with risk for VTE in lymphoma, including previous VTE, previous acute MI or stroke, mediastinal involvement, high body mass index, reduced mobility, extranodal localization, neutropenia, and hemoglobin less than 100 g/L (Am J Hematol. 2016 Oct;91[10]:1014-9).
In an initial version of the ThroLy scoring system, previous VTE, previous acute MI/stroke, obesity, and mediastinal involvement were all worth two points, and the other factors were worth a single point in the ThroLy system.
Patients with scores of 0 to 1 were considered low risk, patients with scores of 2 to 3 were considered intermediate risk, and patients with scores of 4 or greater were considered high risk.
To validate and refine ThroLy, Dr. Antic and his colleagues used it to assess 1,723 lymphoma patients treated at eight institutions in Austria, Croatia, France, Jordan, Macedonia, Spain, Switzerland, and the United States.
Patients had indolent non-Hodgkin lymphoma, aggressive non-Hodgkin lymphoma, chronic lymphocytic leukemia/small lymphocytic lymphoma, and Hodgkin lymphoma. Most subjects (84%) were outpatients. A total of 9%of patients had thrombosis, with 7% having VTE.
ThroLy had a positive predictive value of 17%, compared with 11% with Khorana and 13% with Padua. The negative predictive value was 93%, 92%, and 95%, respectively. The sensitivity was 51% with ThroLy, 42% with Khorana, and 70% with Padua; specificity was 72%, 64%, and 52%, respectively.
“The positive predictive value was low [with ThroLy] but definitely higher than the positive predictive value of the other two [scoring systems],” Dr. Antic noted.
Updated models
To further improve ThroLy, the researchers updated the system, creating two new models. Model 1 included the type of lymphoma/clinical stage (1 point), previous VTE (5 points), reduced mobility (2 points), hemoglobin less than 100 g/L (1 point), and the presence of vascular devices (1 point). Model 2 included all of the variables in Model 1 plus the thrombophilic condition, which was worth 1 point.
Patients were considered low risk if they scored 2 points or lower and high risk if they scored more than 2 points.
For Model 1, the positive predictive value was 22%, the negative predictive value was 96%, the sensitivity was 56%, and the specificity was 85%. For Model 2, the positive predictive value was 25%, the negative predictive value was 96%, the sensitivity was 57%, and the specificity was 87%.
There were no major differences in model discrimination and calibration based on the country in which a patient was treated or whether the patient was treated in an inpatient or outpatient setting.
Dr. Antic did not report any conflicts of interest. The Leukemia and Lymphoma meeting is organized by Jonathan Wood & Association, which is owned by the parent company of this news organization.
REPORTING FROM LEUKEMIA AND LYMPHOMA 2018
Key clinical point:
Major finding: The updated ThroLy had a positive predictive value of 22%-25%, a negative predictive value of 96%, sensitivity of 56%-57%, and specificity of 85%-87%.
Study details: The scoring system was validated on 1,723 lymphoma patients treated at eight institutions worldwide.
Disclosures: Dr. Antic reported having no conflicts of interest.
How can we best use diagnostic brain imaging in pregnant women with severe headache?
WHAT DOES THIS MEAN FOR PRACTICE?
- Acute, severe headache in pregnancy needs immediate attention when it includes:
- seizures
- altered sensorium, or
- loss of consciousness
- An appropriate threshold utilizing history and clinical diagnosis must be set for obtaining neurologic consultation and for the consultant to obtain imaging
- Brain scans can identify symptomatic pathologic results (27.6% in this study)
- Theoretical concerns about imaging call for the OB to be very involved in evaluation and management
- OB and neurologist should discuss risks and benefits of imaging throughout care

Black patients present as sicker, more likely to receive liver transplant
PHILADELPHIA – Black patients are more likely to be put on a transplant list because of acute liver failure, be listed as status 1, and receive a liver transplant, compared with white patients, according to a recent presentation at the annual meeting of the American College of Gastroenterology.

Lauren D. Nephew, MD, MSCE, of Indiana University in Indianapolis, and her colleagues performed a retrospective cohort study of black and white patients with a minimum age of 18 years in the United Network of Organ Sharing database who were wait-listed for a liver transplantation during 2002-2016. They examined patient clinical characteristics, acute liver failure (ALF) etiologies, wait-list status, and posttransplant survival outcomes through Kaplan Meier analysis.
“We really wanted to explore this topic in patients with acute liver failure, some of the sickest patients that we see,” Dr. Nephew said in her presentation. “We wanted to really determine whether or not there were differences in clinical characteristics and etiologies of acute liver failure in patients by race who are listed for liver transplantation.”
“Then, we wanted to compare wait-list outcomes,” she added, such as “differences by race in liver transplantation or wait-list removal because of death or becoming too sick for transplant.”
There were 11,289 patients in the white ALF group and 2,112 patients in the black ALF group; 2,876 (25.5%) of patients in the white ALF and 790 (37.4%) in the black ALF group were listed as status 1, which indicated an expected survival of 7 days or less. There were similar clinical characteristics for the white and black ALF status 1 patients regarding age (34.2 years vs. 36.3 years), Model for End-Stage Liver Disease (MELD) score (34 vs. 36; P less than .001), international normalized ratio (INR) test (mean 4.5 vs. mean 5.0; P = .001), creatinine levels (2.1 mg/dL vs. 1.9 mg/dL; P less than .001), and percentage of patients who were hepatic encephalopathy grade 3 or 4 (60.0% vs. 63.2%; P = .10). However, Dr. Nephew noted significantly higher bilirubin levels in the black ALF status 1 cohort (17.9 mg/dL), compared with the white ALF status 1 cohort (11.3 mg/dL; P less than .001).
The causes for ALF in each group included drug-induced liver failure (white status 1 cohort, 34.1%; black status 1 cohort, 20.6%), autoimmune hepatitis (2.7% vs. 9.4%), Wilson’s disease (0.58% vs. 0.13%), unknown etiology (34.5% vs. 42.5%), and other etiology (22.9% vs. 17%). For patients who underwent liver transplant and wait-list removal, there were no significant differences in wait-list removal “despite black patients being sicker at presentation,” Dr. Nephew said. Black patients were more likely to be listed to status 1 and transplanted at 62% (490 patients), compared with white patients at 53% (1,524 patients). There were 713 white patients (24.8%) removed from the transplant list, compared with 114 (13.8%) of black patients.
“If you are transplanted and you don’t die, then you are likely removed from the list for other reasons, and the most common reason is that you improved and became well, and so white patients were significantly more likely to be removed from the wait-list because of improvement, compared with black patients,” Dr. Nephew said.
In a competing risk analysis, the researchers found the hazard ratio for white patients who were status 1 and removed from the wait-list because of death or becoming too sick was 1.04 (95% confidence interval, 0.89-1.21) and those white patients who were listed as status 1 and then transplanted was 1.2 (95% CI, 1.08-1.30). In a multivariate analysis, the hazard ratio for white patients who were listed as status 1 and transplanted, which contained bilirubin at transplant, was 1.08 (95% CI, 0.98-1.19). Kaplan Meier 1-year survival post-transplant was 82.8% in white patients and 79.6% in black patients (P = .09).
“I think the question that we’ve been asking ourselves is, is this because black patients are presenting later with their acute liver disease and are sicker at presentation, or do they just have worse liver disease inherently on presentation that drove these findings?” Dr. Nephew said.
Dr. Nephew reports no relevant conflicts of interest.
SOURCE: Nephew L et al. ACG 2018, Presentation 59.
PHILADELPHIA – Black patients are more likely to be put on a transplant list because of acute liver failure, be listed as status 1, and receive a liver transplant, compared with white patients, according to a recent presentation at the annual meeting of the American College of Gastroenterology.
Lauren D. Nephew, MD, MSCE, of Indiana University in Indianapolis, and her colleagues performed a retrospective cohort study of black and white patients with a minimum age of 18 years in the United Network of Organ Sharing database who were wait-listed for a liver transplantation during 2002-2016. They examined patient clinical characteristics, acute liver failure (ALF) etiologies, wait-list status, and posttransplant survival outcomes through Kaplan Meier analysis.
“We really wanted to explore this topic in patients with acute liver failure, some of the sickest patients that we see,” Dr. Nephew said in her presentation. “We wanted to really determine whether or not there were differences in clinical characteristics and etiologies of acute liver failure in patients by race who are listed for liver transplantation.”
“Then, we wanted to compare wait-list outcomes,” she added, such as “differences by race in liver transplantation or wait-list removal because of death or becoming too sick for transplant.”
There were 11,289 patients in the white ALF group and 2,112 patients in the black ALF group; 2,876 (25.5%) of patients in the white ALF and 790 (37.4%) in the black ALF group were listed as status 1, which indicated an expected survival of 7 days or less. There were similar clinical characteristics for the white and black ALF status 1 patients regarding age (34.2 years vs. 36.3 years), Model for End-Stage Liver Disease (MELD) score (34 vs. 36; P less than .001), international normalized ratio (INR) test (mean 4.5 vs. mean 5.0; P = .001), creatinine levels (2.1 mg/dL vs. 1.9 mg/dL; P less than .001), and percentage of patients who were hepatic encephalopathy grade 3 or 4 (60.0% vs. 63.2%; P = .10). However, Dr. Nephew noted significantly higher bilirubin levels in the black ALF status 1 cohort (17.9 mg/dL), compared with the white ALF status 1 cohort (11.3 mg/dL; P less than .001).
The causes for ALF in each group included drug-induced liver failure (white status 1 cohort, 34.1%; black status 1 cohort, 20.6%), autoimmune hepatitis (2.7% vs. 9.4%), Wilson’s disease (0.58% vs. 0.13%), unknown etiology (34.5% vs. 42.5%), and other etiology (22.9% vs. 17%). For patients who underwent liver transplant and wait-list removal, there were no significant differences in wait-list removal “despite black patients being sicker at presentation,” Dr. Nephew said. Black patients were more likely to be listed to status 1 and transplanted at 62% (490 patients), compared with white patients at 53% (1,524 patients). There were 713 white patients (24.8%) removed from the transplant list, compared with 114 (13.8%) of black patients.
“If you are transplanted and you don’t die, then you are likely removed from the list for other reasons, and the most common reason is that you improved and became well, and so white patients were significantly more likely to be removed from the wait-list because of improvement, compared with black patients,” Dr. Nephew said.
In a competing risk analysis, the researchers found the hazard ratio for white patients who were status 1 and removed from the wait-list because of death or becoming too sick was 1.04 (95% confidence interval, 0.89-1.21) and those white patients who were listed as status 1 and then transplanted was 1.2 (95% CI, 1.08-1.30). In a multivariate analysis, the hazard ratio for white patients who were listed as status 1 and transplanted, which contained bilirubin at transplant, was 1.08 (95% CI, 0.98-1.19). Kaplan Meier 1-year survival post-transplant was 82.8% in white patients and 79.6% in black patients (P = .09).
“I think the question that we’ve been asking ourselves is, is this because black patients are presenting later with their acute liver disease and are sicker at presentation, or do they just have worse liver disease inherently on presentation that drove these findings?” Dr. Nephew said.
Dr. Nephew reports no relevant conflicts of interest.
SOURCE: Nephew L et al. ACG 2018, Presentation 59.
PHILADELPHIA – Black patients are more likely to be put on a transplant list because of acute liver failure, be listed as status 1, and receive a liver transplant, compared with white patients, according to a recent presentation at the annual meeting of the American College of Gastroenterology.
Lauren D. Nephew, MD, MSCE, of Indiana University in Indianapolis, and her colleagues performed a retrospective cohort study of black and white patients with a minimum age of 18 years in the United Network of Organ Sharing database who were wait-listed for a liver transplantation during 2002-2016. They examined patient clinical characteristics, acute liver failure (ALF) etiologies, wait-list status, and posttransplant survival outcomes through Kaplan Meier analysis.
“We really wanted to explore this topic in patients with acute liver failure, some of the sickest patients that we see,” Dr. Nephew said in her presentation. “We wanted to really determine whether or not there were differences in clinical characteristics and etiologies of acute liver failure in patients by race who are listed for liver transplantation.”
“Then, we wanted to compare wait-list outcomes,” she added, such as “differences by race in liver transplantation or wait-list removal because of death or becoming too sick for transplant.”
There were 11,289 patients in the white ALF group and 2,112 patients in the black ALF group; 2,876 (25.5%) of patients in the white ALF and 790 (37.4%) in the black ALF group were listed as status 1, which indicated an expected survival of 7 days or less. There were similar clinical characteristics for the white and black ALF status 1 patients regarding age (34.2 years vs. 36.3 years), Model for End-Stage Liver Disease (MELD) score (34 vs. 36; P less than .001), international normalized ratio (INR) test (mean 4.5 vs. mean 5.0; P = .001), creatinine levels (2.1 mg/dL vs. 1.9 mg/dL; P less than .001), and percentage of patients who were hepatic encephalopathy grade 3 or 4 (60.0% vs. 63.2%; P = .10). However, Dr. Nephew noted significantly higher bilirubin levels in the black ALF status 1 cohort (17.9 mg/dL), compared with the white ALF status 1 cohort (11.3 mg/dL; P less than .001).
The causes for ALF in each group included drug-induced liver failure (white status 1 cohort, 34.1%; black status 1 cohort, 20.6%), autoimmune hepatitis (2.7% vs. 9.4%), Wilson’s disease (0.58% vs. 0.13%), unknown etiology (34.5% vs. 42.5%), and other etiology (22.9% vs. 17%). For patients who underwent liver transplant and wait-list removal, there were no significant differences in wait-list removal “despite black patients being sicker at presentation,” Dr. Nephew said. Black patients were more likely to be listed to status 1 and transplanted at 62% (490 patients), compared with white patients at 53% (1,524 patients). There were 713 white patients (24.8%) removed from the transplant list, compared with 114 (13.8%) of black patients.
“If you are transplanted and you don’t die, then you are likely removed from the list for other reasons, and the most common reason is that you improved and became well, and so white patients were significantly more likely to be removed from the wait-list because of improvement, compared with black patients,” Dr. Nephew said.
In a competing risk analysis, the researchers found the hazard ratio for white patients who were status 1 and removed from the wait-list because of death or becoming too sick was 1.04 (95% confidence interval, 0.89-1.21) and those white patients who were listed as status 1 and then transplanted was 1.2 (95% CI, 1.08-1.30). In a multivariate analysis, the hazard ratio for white patients who were listed as status 1 and transplanted, which contained bilirubin at transplant, was 1.08 (95% CI, 0.98-1.19). Kaplan Meier 1-year survival post-transplant was 82.8% in white patients and 79.6% in black patients (P = .09).
“I think the question that we’ve been asking ourselves is, is this because black patients are presenting later with their acute liver disease and are sicker at presentation, or do they just have worse liver disease inherently on presentation that drove these findings?” Dr. Nephew said.
Dr. Nephew reports no relevant conflicts of interest.
SOURCE: Nephew L et al. ACG 2018, Presentation 59.
REPORTING FROM ACG 2018
Key clinical point: Black patients are sicker than white patients when they present with acute liver failure and are awaiting liver transplantation.
Major finding: Black patients with acute liver failure were more likely to be wait-listed, listed as status 1, and have higher Model for End-Stage Liver Disease (MELD) scores, creatinine levels, and INR tests, compared with white patients.
Study details: A retrospective cohort analysis of patients with acute liver failure awaiting a liver transplant in the United Network of Organ Sharing database.
Disclosures: Dr. Nephew reports no relevant conflicts of interest.
Source: Nephew L et al. ACG 2018, Presentation 59.
Managing asthma in children: Pets don’t always have to go
SAN ANTONIO – It may not always be necessary to tell parents of children with asthma to get rid of the household pet, a recent study suggests.
Children with had significant improvements in a variety of asthma measures, regardless of whether parents reported pets or smoking at home, according to results of the 4-year, 471-patient prospective study.
Those results suggest that clinicians should be working to make sure the guidelines are being closely followed before, for example, telling parents they need to consider getting rid of the family pet, said Shahid Sheikh, MD, FCCP, of Nationwide Children’s Hospital, Columbus, Ohio.
“As the guidelines still work, we need to focus and develop the connections with the family to make sure the patients are on the right treatment, and that they’re getting the medications,” Dr. Sheikh said in an interview at the annual meeting of the American College of Chest Physicians.
The prospective cohort study by Dr. Sheikh and his colleagues, presented in a poster session, included children referred to a pediatric asthma center with the diagnosis of uncontrolled asthma. All patients received asthma care according to National Asthma Education and Prevention Program Expert Panel Report 3 guidelines.
Medications were changed as needed, and the asthma action plan was revised accordingly and reviewed with the family at each visit, Dr. Sheikh reported. After a baseline evaluation, clinic visits for the study occurred at 3 months, 6 months, and then at 1, 2, 3, and 4 years.
Out of 471 patients, 258 had pets, and 125 were in homes where smoking took place, according to parent reports.
Asthma control test scores were 15.1 at baseline for children in no-pet households, and 16.5 for those with pets; by the 3-month visit, scores increased to 20.1 and 20.3 for the no-pet and pet groups, and at 4 years, those scores had edged up to 22.2 and 22.7 (P = .371), Dr. Sheikh reported.
Similarly, after care was started, there was no significant difference between the no-pet and pet groups in mean percent of predicted forced expiratory volume in 1 second (FEV1), wheezing, nighttime cough, albuterol use, and other factors over the 4 years of follow-up, he said.
Likewise, looking at the data by nonsmoking vs. smoking households, asthma control test scores at baseline were 16.1 and 15.1, respectively, and at 4 years they were 22.2 and 22.3 (P = .078), with a similar lack of difference in predicted FEV1, wheezing, and all other factors evaluated.
Getting rid of the family pet may need to be a consideration for some families, but based on these data, that might not be necessary for the majority of families, Dr. Sheikh said in the interview.
“On the other hand, we are not saying that if you are smoking, you should continue to smoke,” he added.
“What we are saying is that smoking is bad, but if your child is not getting better, I don’t want to blame your smoking for it. There may be something else which may be more important than smoking which we are missing – the child may not be getting the medicine, or may not be on the right medicine, or may have other comorbidities.”
Dr. Sheikh and his coinvestigators disclosed that they had no relationships relevant to the study.
SOURCE: Sheikh S et al. CHEST 2018. doi: 10.1016/j.chest.2018.08.666.
SAN ANTONIO – It may not always be necessary to tell parents of children with asthma to get rid of the household pet, a recent study suggests.
Children with had significant improvements in a variety of asthma measures, regardless of whether parents reported pets or smoking at home, according to results of the 4-year, 471-patient prospective study.
Those results suggest that clinicians should be working to make sure the guidelines are being closely followed before, for example, telling parents they need to consider getting rid of the family pet, said Shahid Sheikh, MD, FCCP, of Nationwide Children’s Hospital, Columbus, Ohio.
“As the guidelines still work, we need to focus and develop the connections with the family to make sure the patients are on the right treatment, and that they’re getting the medications,” Dr. Sheikh said in an interview at the annual meeting of the American College of Chest Physicians.
The prospective cohort study by Dr. Sheikh and his colleagues, presented in a poster session, included children referred to a pediatric asthma center with the diagnosis of uncontrolled asthma. All patients received asthma care according to National Asthma Education and Prevention Program Expert Panel Report 3 guidelines.
Medications were changed as needed, and the asthma action plan was revised accordingly and reviewed with the family at each visit, Dr. Sheikh reported. After a baseline evaluation, clinic visits for the study occurred at 3 months, 6 months, and then at 1, 2, 3, and 4 years.
Out of 471 patients, 258 had pets, and 125 were in homes where smoking took place, according to parent reports.
Asthma control test scores were 15.1 at baseline for children in no-pet households, and 16.5 for those with pets; by the 3-month visit, scores increased to 20.1 and 20.3 for the no-pet and pet groups, and at 4 years, those scores had edged up to 22.2 and 22.7 (P = .371), Dr. Sheikh reported.
Similarly, after care was started, there was no significant difference between the no-pet and pet groups in mean percent of predicted forced expiratory volume in 1 second (FEV1), wheezing, nighttime cough, albuterol use, and other factors over the 4 years of follow-up, he said.
Likewise, looking at the data by nonsmoking vs. smoking households, asthma control test scores at baseline were 16.1 and 15.1, respectively, and at 4 years they were 22.2 and 22.3 (P = .078), with a similar lack of difference in predicted FEV1, wheezing, and all other factors evaluated.
Getting rid of the family pet may need to be a consideration for some families, but based on these data, that might not be necessary for the majority of families, Dr. Sheikh said in the interview.
“On the other hand, we are not saying that if you are smoking, you should continue to smoke,” he added.
“What we are saying is that smoking is bad, but if your child is not getting better, I don’t want to blame your smoking for it. There may be something else which may be more important than smoking which we are missing – the child may not be getting the medicine, or may not be on the right medicine, or may have other comorbidities.”
Dr. Sheikh and his coinvestigators disclosed that they had no relationships relevant to the study.
SOURCE: Sheikh S et al. CHEST 2018. doi: 10.1016/j.chest.2018.08.666.
SAN ANTONIO – It may not always be necessary to tell parents of children with asthma to get rid of the household pet, a recent study suggests.
Children with had significant improvements in a variety of asthma measures, regardless of whether parents reported pets or smoking at home, according to results of the 4-year, 471-patient prospective study.
Those results suggest that clinicians should be working to make sure the guidelines are being closely followed before, for example, telling parents they need to consider getting rid of the family pet, said Shahid Sheikh, MD, FCCP, of Nationwide Children’s Hospital, Columbus, Ohio.
“As the guidelines still work, we need to focus and develop the connections with the family to make sure the patients are on the right treatment, and that they’re getting the medications,” Dr. Sheikh said in an interview at the annual meeting of the American College of Chest Physicians.
The prospective cohort study by Dr. Sheikh and his colleagues, presented in a poster session, included children referred to a pediatric asthma center with the diagnosis of uncontrolled asthma. All patients received asthma care according to National Asthma Education and Prevention Program Expert Panel Report 3 guidelines.
Medications were changed as needed, and the asthma action plan was revised accordingly and reviewed with the family at each visit, Dr. Sheikh reported. After a baseline evaluation, clinic visits for the study occurred at 3 months, 6 months, and then at 1, 2, 3, and 4 years.
Out of 471 patients, 258 had pets, and 125 were in homes where smoking took place, according to parent reports.
Asthma control test scores were 15.1 at baseline for children in no-pet households, and 16.5 for those with pets; by the 3-month visit, scores increased to 20.1 and 20.3 for the no-pet and pet groups, and at 4 years, those scores had edged up to 22.2 and 22.7 (P = .371), Dr. Sheikh reported.
Similarly, after care was started, there was no significant difference between the no-pet and pet groups in mean percent of predicted forced expiratory volume in 1 second (FEV1), wheezing, nighttime cough, albuterol use, and other factors over the 4 years of follow-up, he said.
Likewise, looking at the data by nonsmoking vs. smoking households, asthma control test scores at baseline were 16.1 and 15.1, respectively, and at 4 years they were 22.2 and 22.3 (P = .078), with a similar lack of difference in predicted FEV1, wheezing, and all other factors evaluated.
Getting rid of the family pet may need to be a consideration for some families, but based on these data, that might not be necessary for the majority of families, Dr. Sheikh said in the interview.
“On the other hand, we are not saying that if you are smoking, you should continue to smoke,” he added.
“What we are saying is that smoking is bad, but if your child is not getting better, I don’t want to blame your smoking for it. There may be something else which may be more important than smoking which we are missing – the child may not be getting the medicine, or may not be on the right medicine, or may have other comorbidities.”
Dr. Sheikh and his coinvestigators disclosed that they had no relationships relevant to the study.
SOURCE: Sheikh S et al. CHEST 2018. doi: 10.1016/j.chest.2018.08.666.
REPORTING FROM CHEST 2018
Key clinical point: Exposure to pets and tobacco smoke may have very little effect on the improvement of asthma in children who are being managed according to guidelines.
Major finding: ACT scores were 15.1 and 16.5 at baseline for children in no-pet and pet households, respectively, and were 22.2 and 22.7 at the 4-year evaluation.
Study details: A 4-year prospective cohort study of 471 children with uncontrolled asthma seen in a pediatric asthma center.
Disclosures: The study authors had no disclosures.
Source: Sheikh S et al. CHEST 2018. doi: 10.1016/j.chest.2018.08.666.
Mood disorders worsen multiple sclerosis disability
BERLIN – Depression and bipolar disorder are major risk factors for worsening disability in people with multiple sclerosis, according to the results of a large Swedish registry-based study.

The presence of depression increased the risk of having a sustained Expanded Disability Status Scale (EDSS) score of 3.0 by 54% and 4.0 by 87%, and it doubled the risk of an EDSS of 6.0.
Selective serotonin reuptake inhibitor treatment also upped the risk of greater disability, with patients exposed to SSRIs having a 40% increased risk of a sustained EDSS of 3.0, a 97% chance of having a sustained EDSS of 4.0, and 2.2-fold increased risk of a sustained EDSS of 6.0.
“We know that mood disorders are highly prevalent in people with multiple sclerosis,” Stefanie Binzer, MD, said at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis. She gave her presentation at the meeting on Oct. 10, which was World Mental Health Day.
The presence of mood disorders is associated with reduced quality of life, said Dr. Binzer of the department of clinical neuroscience at the Karolinska Institute in Stockholm. Furthermore, depression is the major risk factor for suicidality in patients with MS. However, before this study the effect of having a comorbid mood disorder on MS patients’ disability levels had not been established.
The investigators analyzed data from 5,875 patients in the Swedish MS registry between 2001 and 2014. By matching these patients to records in the Swedish National Patient Registry and the Swedish National Prescribed Drug Registry, they found that 8.5% (n = 502) had an International Classification of Diseases, 10th revision (ICD-10), code for depression. Of these, 261 had received a diagnosis of depression before their diagnosis of MS.
Of 3,817 patients with MS onset between 2005 and 2014, 27.4% (n = 1,048) had collected at least one prescription for an SSRI.
“What we found was that MS patients with either an ICD code for depression or having been exposed to SSRIs had a significantly increased risk of reaching EDSS 3.0,” Dr. Binzer reported. The age at which patients reached these milestones were younger in both groups when compared with MS patients without depression, she observed.
“The difference between the groups [MS with and MS without depression] seemed to increased with EDSS,” Dr. Binzer said.
Although not statistically significant, there was a trend for patients with depression to be more likely to convert to secondary progressive MS, with a hazard ratio of 1.38 (95% confidence interval, 0.91-2.1).
“For a sensitivity analysis, we found that those who had depression prior to their first MS symptom, the median age when they reached EDSS 3.0 and 4.0 was reduced by 3 and 7 years, respectively,” Dr. Binzer said, adding that, unfortunately, there wasn’t enough power to look at the other endpoints.
In regard to bipolar disorder, 1.5% (n = 200) of 13,125 MS patients diagnosed between 1973 and 2014 were identified with this mood disorder. Its presence significantly increased the risk of MS patients reaching an EDSS score of 4.0 by 58% (95% CI, 1.1-2.28), but not EDSS 3.0 (HR = 1.34; 95% CI, 0.94-1.92) or 6.0 (HR = 1.16; 95% CI, 0.79-1.69). The latter could be due to smaller sample size, Dr. Binzer suggested.
The investigators’ analysis of the results stratified by sex, conducted because men tend to fare worse than women with MS and progress faster, showed that for both depression and bipolar disorder, men were at significantly higher risk of reaching sustained disability milestones. Indeed, compared with women, men with depression had a 61% increased risk and those with bipolar disorder a 31% increased risk of reaching an EDSS score of 6.0. They also had 51% and 32% increased risks of conversion to secondary progressive MS.
“We don’t know the mechanisms that underlie these associations,” Dr. Binzer noted. “Irrespective of the underlying mechanisms, [the study] clearly shows that it’s imperative that we recognize, early, mood disorders in MS patients, and manage them effectively in order to provide better care and hopefully reduce MS disability worsening.”
The research was funded by the Swedish Research Council and the Swedish Brain Foundation. Dr. Binzer has received speaker fees and travel grants from Biogen.
SOURCE: Binzer S et al. Mult Scler. 2018;24(Suppl 2):41. Abstract 99.
BERLIN – Depression and bipolar disorder are major risk factors for worsening disability in people with multiple sclerosis, according to the results of a large Swedish registry-based study.
The presence of depression increased the risk of having a sustained Expanded Disability Status Scale (EDSS) score of 3.0 by 54% and 4.0 by 87%, and it doubled the risk of an EDSS of 6.0.
Selective serotonin reuptake inhibitor treatment also upped the risk of greater disability, with patients exposed to SSRIs having a 40% increased risk of a sustained EDSS of 3.0, a 97% chance of having a sustained EDSS of 4.0, and 2.2-fold increased risk of a sustained EDSS of 6.0.
“We know that mood disorders are highly prevalent in people with multiple sclerosis,” Stefanie Binzer, MD, said at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis. She gave her presentation at the meeting on Oct. 10, which was World Mental Health Day.
The presence of mood disorders is associated with reduced quality of life, said Dr. Binzer of the department of clinical neuroscience at the Karolinska Institute in Stockholm. Furthermore, depression is the major risk factor for suicidality in patients with MS. However, before this study the effect of having a comorbid mood disorder on MS patients’ disability levels had not been established.
The investigators analyzed data from 5,875 patients in the Swedish MS registry between 2001 and 2014. By matching these patients to records in the Swedish National Patient Registry and the Swedish National Prescribed Drug Registry, they found that 8.5% (n = 502) had an International Classification of Diseases, 10th revision (ICD-10), code for depression. Of these, 261 had received a diagnosis of depression before their diagnosis of MS.
Of 3,817 patients with MS onset between 2005 and 2014, 27.4% (n = 1,048) had collected at least one prescription for an SSRI.
“What we found was that MS patients with either an ICD code for depression or having been exposed to SSRIs had a significantly increased risk of reaching EDSS 3.0,” Dr. Binzer reported. The age at which patients reached these milestones were younger in both groups when compared with MS patients without depression, she observed.
“The difference between the groups [MS with and MS without depression] seemed to increased with EDSS,” Dr. Binzer said.
Although not statistically significant, there was a trend for patients with depression to be more likely to convert to secondary progressive MS, with a hazard ratio of 1.38 (95% confidence interval, 0.91-2.1).
“For a sensitivity analysis, we found that those who had depression prior to their first MS symptom, the median age when they reached EDSS 3.0 and 4.0 was reduced by 3 and 7 years, respectively,” Dr. Binzer said, adding that, unfortunately, there wasn’t enough power to look at the other endpoints.
In regard to bipolar disorder, 1.5% (n = 200) of 13,125 MS patients diagnosed between 1973 and 2014 were identified with this mood disorder. Its presence significantly increased the risk of MS patients reaching an EDSS score of 4.0 by 58% (95% CI, 1.1-2.28), but not EDSS 3.0 (HR = 1.34; 95% CI, 0.94-1.92) or 6.0 (HR = 1.16; 95% CI, 0.79-1.69). The latter could be due to smaller sample size, Dr. Binzer suggested.
The investigators’ analysis of the results stratified by sex, conducted because men tend to fare worse than women with MS and progress faster, showed that for both depression and bipolar disorder, men were at significantly higher risk of reaching sustained disability milestones. Indeed, compared with women, men with depression had a 61% increased risk and those with bipolar disorder a 31% increased risk of reaching an EDSS score of 6.0. They also had 51% and 32% increased risks of conversion to secondary progressive MS.
“We don’t know the mechanisms that underlie these associations,” Dr. Binzer noted. “Irrespective of the underlying mechanisms, [the study] clearly shows that it’s imperative that we recognize, early, mood disorders in MS patients, and manage them effectively in order to provide better care and hopefully reduce MS disability worsening.”
The research was funded by the Swedish Research Council and the Swedish Brain Foundation. Dr. Binzer has received speaker fees and travel grants from Biogen.
SOURCE: Binzer S et al. Mult Scler. 2018;24(Suppl 2):41. Abstract 99.
BERLIN – Depression and bipolar disorder are major risk factors for worsening disability in people with multiple sclerosis, according to the results of a large Swedish registry-based study.
The presence of depression increased the risk of having a sustained Expanded Disability Status Scale (EDSS) score of 3.0 by 54% and 4.0 by 87%, and it doubled the risk of an EDSS of 6.0.
Selective serotonin reuptake inhibitor treatment also upped the risk of greater disability, with patients exposed to SSRIs having a 40% increased risk of a sustained EDSS of 3.0, a 97% chance of having a sustained EDSS of 4.0, and 2.2-fold increased risk of a sustained EDSS of 6.0.
“We know that mood disorders are highly prevalent in people with multiple sclerosis,” Stefanie Binzer, MD, said at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis. She gave her presentation at the meeting on Oct. 10, which was World Mental Health Day.
The presence of mood disorders is associated with reduced quality of life, said Dr. Binzer of the department of clinical neuroscience at the Karolinska Institute in Stockholm. Furthermore, depression is the major risk factor for suicidality in patients with MS. However, before this study the effect of having a comorbid mood disorder on MS patients’ disability levels had not been established.
The investigators analyzed data from 5,875 patients in the Swedish MS registry between 2001 and 2014. By matching these patients to records in the Swedish National Patient Registry and the Swedish National Prescribed Drug Registry, they found that 8.5% (n = 502) had an International Classification of Diseases, 10th revision (ICD-10), code for depression. Of these, 261 had received a diagnosis of depression before their diagnosis of MS.
Of 3,817 patients with MS onset between 2005 and 2014, 27.4% (n = 1,048) had collected at least one prescription for an SSRI.
“What we found was that MS patients with either an ICD code for depression or having been exposed to SSRIs had a significantly increased risk of reaching EDSS 3.0,” Dr. Binzer reported. The age at which patients reached these milestones were younger in both groups when compared with MS patients without depression, she observed.
“The difference between the groups [MS with and MS without depression] seemed to increased with EDSS,” Dr. Binzer said.
Although not statistically significant, there was a trend for patients with depression to be more likely to convert to secondary progressive MS, with a hazard ratio of 1.38 (95% confidence interval, 0.91-2.1).
“For a sensitivity analysis, we found that those who had depression prior to their first MS symptom, the median age when they reached EDSS 3.0 and 4.0 was reduced by 3 and 7 years, respectively,” Dr. Binzer said, adding that, unfortunately, there wasn’t enough power to look at the other endpoints.
In regard to bipolar disorder, 1.5% (n = 200) of 13,125 MS patients diagnosed between 1973 and 2014 were identified with this mood disorder. Its presence significantly increased the risk of MS patients reaching an EDSS score of 4.0 by 58% (95% CI, 1.1-2.28), but not EDSS 3.0 (HR = 1.34; 95% CI, 0.94-1.92) or 6.0 (HR = 1.16; 95% CI, 0.79-1.69). The latter could be due to smaller sample size, Dr. Binzer suggested.
The investigators’ analysis of the results stratified by sex, conducted because men tend to fare worse than women with MS and progress faster, showed that for both depression and bipolar disorder, men were at significantly higher risk of reaching sustained disability milestones. Indeed, compared with women, men with depression had a 61% increased risk and those with bipolar disorder a 31% increased risk of reaching an EDSS score of 6.0. They also had 51% and 32% increased risks of conversion to secondary progressive MS.
“We don’t know the mechanisms that underlie these associations,” Dr. Binzer noted. “Irrespective of the underlying mechanisms, [the study] clearly shows that it’s imperative that we recognize, early, mood disorders in MS patients, and manage them effectively in order to provide better care and hopefully reduce MS disability worsening.”
The research was funded by the Swedish Research Council and the Swedish Brain Foundation. Dr. Binzer has received speaker fees and travel grants from Biogen.
SOURCE: Binzer S et al. Mult Scler. 2018;24(Suppl 2):41. Abstract 99.
REPORTING FROM ECTRIMS 2018
Key clinical point:
Major finding: Depression and bipolar disorder increased the risk of reaching Expanded Disability Status Scale scores of 3.0, 4.0, and 6.0, particularly in men with MS.
Study details: Swedish registry study of nearly 6,000 individuals with confirmed MS, 8.5% of whom had depression and 1.5% of whom had bipolar disorder.
Disclosures: The research was funded by the Swedish Research Council and the Swedish Brain Foundation. Dr. Binzer has received speaker fees and travel grants from Biogen.
Source: Binzer S et al. Mult Scler. 2018;24(Suppl 2):41. Abstract 99.
The Effect of Playing Position on Injury Risk in Male Soccer Players: Systematic Review of the Literature and Risk Considerations for Each Playing Position
ABSTRACT
Soccer (football) is a complex contact sport with a substantial risk of injury. As injury surveillance is the first step of the injury prevention paradigm, soccer epidemiology is well reported in the existing literature, but less is known about the actual role of player position on the general injury risk.
The goal of this study is to present the existing evidence regarding the influence of player’s position on general injury risk in male soccer.
A systematic review of the Medline database was carried out. Only English written studies on male soccer and citing playing position as a possible determinant of injury risk were included. One hundred and two full texts were evaluated for eligibility, and 11 studies were selected for the qualitative synthesis.
Of the 11 studies included in the systematic review, 5 didn’t find any significant correlation with between player’s position and general injury risk, while the remaining 6 studies found player’s position to be correlated with injury risk, with mixed findings depending on each study. The most consistent finding was a tendency for goalkeepers (GKs) to sustain less injuries compared to outfield players. When considering only the studies reporting just the match injury risk, forwards seemed to be at higher risk, even if there wasn’t a complete agreement.
Few studies have evaluated a possible effect of playing position on general injury risk in male soccer. There is no agreement if weather or not different playing positions are associated to a higher injury risk. GKs seem to be at lower risk of injury when compared to outfield players.
Continue to: Soccer, known worldwide as football, is the most...
Soccer, known worldwide as football, is the most common practiced sport worldwide. Soccer is also a complex contact sport with a substantial injury risk,1 that is well documented in the current literature. According to a recent systematic review, general injury incidence in male soccer ranged from 2.0 injuries to 19.4 injuries per 1000 hours of exposure in youth male soccer and from 2.48 injuries to 9.4 injuries per 1000 hours of exposure in elite male soccer.1 It is also well established that the injury risk is greater in matches than training.1 Soccer’s injuries are well known to be a socioeconomic burden for elite, youth, and recreational players.2 Different authors have underlined the problem that nowadays the game is faster, and players need to have a better physical performance as they are subjected to important efforts both metabolically and biomechanically during match play. In the last decades, thanks to different research groups involved with professional soccer,3 there has been an increasing interest in soccer injuries’ epidemiology and for preventative measures.4 A deep comprehension of injury epidemiology is in fact the first necessary step for successful preventative measures. Regarding a possible correlation between playing position and injury incidence, there is a lack of consensus in the literature. Player position (goalkeeper [GK], defenders, midfielder [MF], or striker) may affect injury risk, as different roles are associated to different intensity during match play5 and experience different combination of anticipated or non-anticipated movement patterns.6 Previous authors underlined that few studies have evaluated a possible influence of playing position on injury incidence and severity.7
The main goal of this systematic review is to present the existing evidence regarding the influence of player position on injury incidence in male soccer and to present practical considerations on each field position in relation to the injury’s risk.
METHODS
DATA SOURCES AND SELECTION CRITERIA
We searched the Medline database for key terms and their variations to identify appropriate studies on injury epidemiology in soccer and specific player position influence. The keywords included: injury epidemiology soccer [OR] injury epidemiology football; position specific injury epidemiology soccer [OR] football. We limited our search to originally published English-language research articles.
Relevant data were extracted for study characteristics to ensure the included studies met certain criteria. The inclusion criteria were prospective design with minimum 6-month observational period, exclusively male soccer players’ cohorts, reported injury incidence, and documented player position in correlation with a measure of injury risk.
As stated above, we only included studies on male soccer. We also did not consider studies limited to a single injury type, considering only studies analyzing and documenting all injuries. We did not exclude studies on youth soccer but we didn’t consider studies on ≥2 more sports or mixed male and female studies.
Data were extracted by an author (FDV) and qualitatively controlled by another one (BM). Controversy were solved through discussion or confrontation with another author (LL).
Results of the included studies are presented only qualitatively because of different methodologies we encountered in documenting the potential effects of player’s role. Some studies reported differences in injury incidence within groups, others reported the proportion of injuries for each subgroup.
Continue to: RESULTS...
RESULTS
STUDY SELECTION
Of the 1609 potential items we found in the existing literature, 102 full-text articles were screened for eligibility. Only 11 papers met the inclusion criteria and were included in the systematic review, including 2 studies on youth soccer and 9 studies on adult soccer (Figure 1). Five of the selected studies tracked only match injuries, while the remaining 6 studies presented data on both match and training injuries. As a matter of fact, the effect of player position was not so commonly evaluated or at least reported in the existing literature. Studies’ characteristics and main findings regarding player’s position are reported in Table.
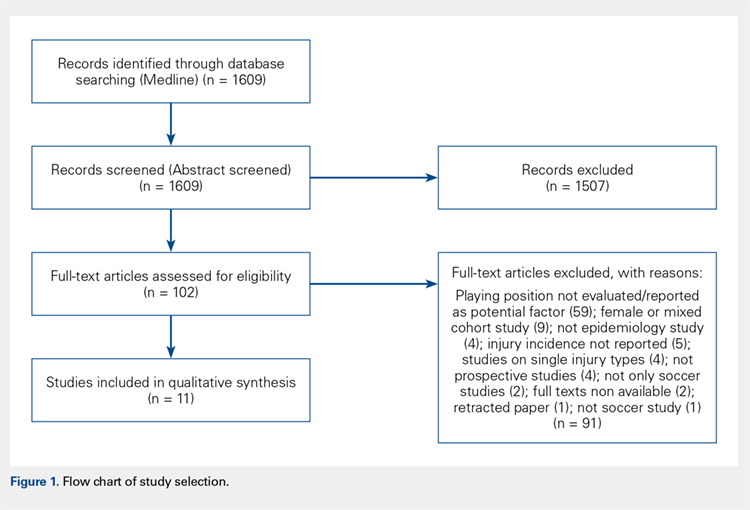
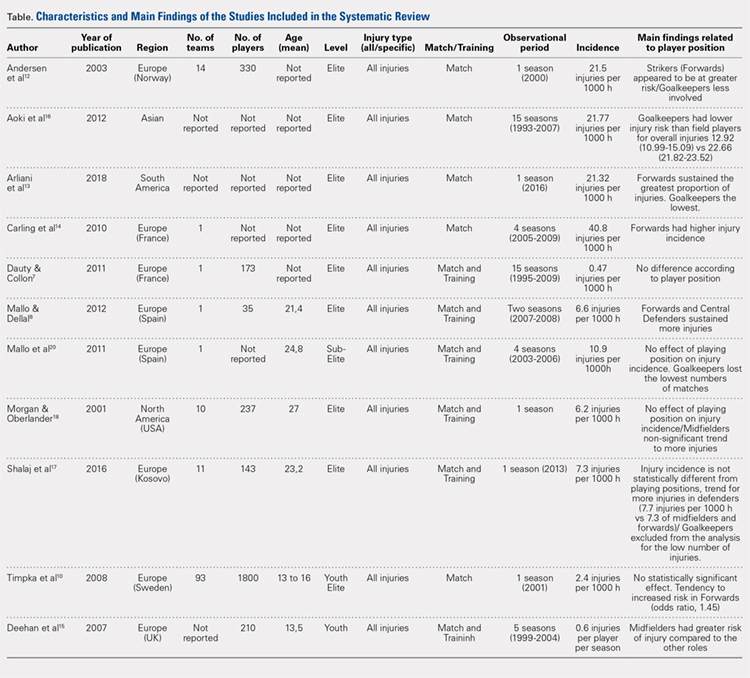
GENERAL INJURY RISK AND PLAYING POSITION
Of the 11 studies included for qualitative synthesis, 5 studies reported no significant effect of player’s position on general risk of injury,7-11 3 studies reported a greater risk in forwards,12-14 1 study reported a greater risk in MFs,15 1 study reported a greater risk in forwards and central defenders,8 and finally 1 study reported a significant lower risk in GKs.16 Additionally, 2 more studies reported GKs to be at the lowest injury risk,12,13 another study reported GKs to have lost the lower number of matches,8 1 study didn’t consider the GK position in the analysis due to the low number of injuries,17 limiting the analysis on the outfield positions.
Out of the 5 studies reporting no significant effect of playing position on injury risk, 1 study found a tendency to more injuries in forward players,10 a second study found a tendency for higher injury risk in midfielders,18 and a third study found a tendency for higher risk in defenders.17 Considering only the 5 studies reporting data on match injuries, 3 reported a higher risk in forwards,12-14 while a fourth one reported a tendency for increased risk in forwards10 even if not statistically significant. On the other hand, evaluating the 6 studies reporting data on match and training injuries, most of the studies, 4 out of 6, reported no effect of playing position.17-20 The main findings of the studies are also expressed graphically in Figures 2A, 2B.
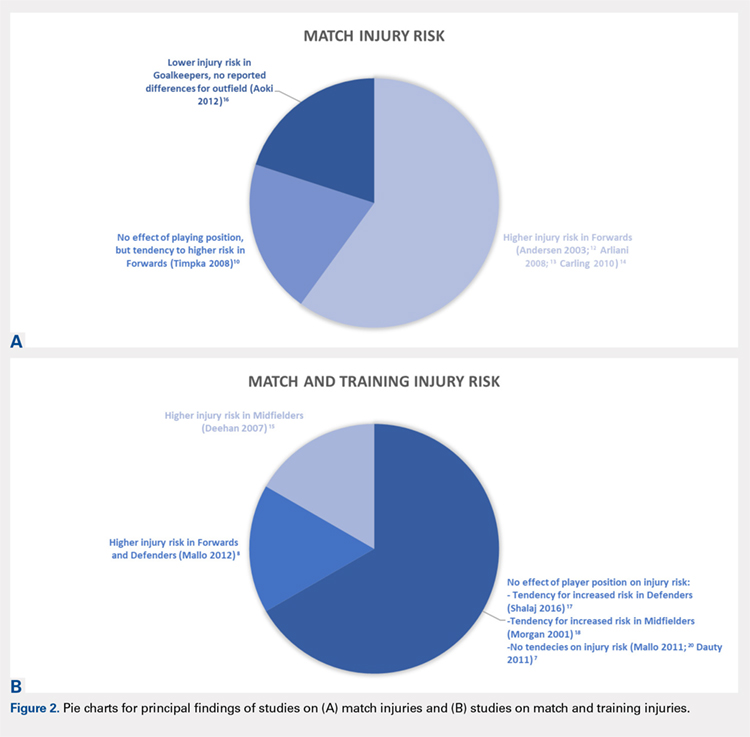
DISCUSSION
The main finding of this study is that there is substantially no agreement regarding the effect of player position on general injury risk in male soccer.
First, we must underline that not many studies have evaluated prospectively the influence of player’s position on injury risk. Of the 11 selected studies, 5 (5/11) reported no significant effect of playing position,7,10,17,18,20 while the remaining studies (6/11)8,12-16 reported a significant effect of player position on the risk of injury, with various results depending on the single study. It should be noted that the 2 studies with the longest observational period (15 consecutive seasons)16,19 did not report any difference in injury risk considering only the outfield playing positions.
Continue to: We will now review the findings...
We will now review the findings of our systematic review based on player position. One of the more consistent trends that we found is the possible occurrence of different injury epidemiology in GKs compared to outfield players. One study reported a significant lower incidence of match injuries for GKs, 12.9 injuries per 1000 game hours vs 22.6 injuries per 1000 game hours of outfield positions.16 This result is remarkable, even considering the very long observational period (15 seasons). Other 2 studies, not reporting position specific injury incidence (but proportion of injuries) also agreed on the topic.12,13 On the other hand, Morgan and Oberlander9 reported no differences between GKs and other positions. Anecdotally, unpublished Major League Soccer data regarding the most recent seasons seems to support these findings with GKs sustaining the lower proportion of injuries. By a physiological point of view, somatotype and body composition have been reported to differ between GKs and the other playing positions in young male soccer players.21 The uniqueness of the GK somatotype and role may reflect on a predisposition to a different pattern of injuries. Ekstrand and colleagues22 reported that GKs have a higher incidence of upper extremity fractures, the same group demonstrated a possible tendency for more head and neck injuries9 and a lower risk of medial collateral ligament injuries.23 On the other hand, GKs seems to be at lower injury risk for the playing pattern differences with outfield players. The reduced distance GKs cover during the match, as well as less direct contacts with opponents, may be factors that potentially explain this finding.
In relation to forwards, 4 studies interestingly stated that forwards were at increased risk of injury,12-14 although 1 report had similar risk of injury with forwards and defenders.8 Most of the studies only on match injuries reported some association between forward position and injury risk (Figures 2A, 2B), so attackers may be at higher risk of match injuries when compared to the other playing positions. There are different possible explanations for this finding. First, it is demonstrated that the clear majority of soccer incidents happen in the mid-defensive zone and in the score-box,24 2 typical attackers’ zones, where most of duels and tackles may happen. So, forwards may be more prone to match injuries because of the intensity of match play in their typical playing zones. Also, fast kicking and acceleration/deceleration activities of the attackers may predispose for thigh muscle injuries, accounting up to 25% of the total lay off time in professional soccer.25 However, these considerations are still yet to be proven.
When considering defenders, 1 report indicated defenders (and forwards) to be at potential greater risk of injury,8which is similar to the report from Shalaj and colleagues,17 although it did not report a statistically significant result. A direct playing style, with defenders and strikers being more involved in the game can potentially explain this finding. However, the specific epidemiology of defenders may be more complicated. Defenders may be predisposed to knee injuries, such as injury to the anterior cruciate ligament (ACL). In fact, Walden and colleagues,11 in a video-analysis study, reported that the 77% of ACL injuries happened in defending situations. In addition, Brophy and colleagues,6 in another video-analysis study, reported a 73% of ACL injuries happened while defending. A likely explanation is the nature of the defender’s role in soccer, reactive to the attacking team actions. Many times, defenders try high risk maneuvers while tackling the opponent, with minimal motor planning time and consciousness. This is well described by Walden and colleagues,11 with the pressing mechanism ACL injury, when the injured player is pressing the opponent in the attempt to get the ball but eventually falls into a high-risk position.
When considering MFs, Deehan and colleagues15 found a significant higher risk in MFs in youth soccer. This result is partially according to Morgan and Oberlander18 who reported a non-statistically significant greater injury incidence in MFs. MFs are generally the players that cover more distance during a soccer match and it is logical to think that they would be predisposed to a large volume of acceleration/deceleration activities,19 potentially relating to injury risk, especially to muscles injuries. A previous study on thigh muscle injuries in youth soccer reporting higher injury risk in MFs, followed by forwards.19 Consistent with these results, another study on a mixed male and female cohort on high school soccer revealed more injuries in MFs, followed by forwards.26
Continue to: The results of this systematic review...
The results of this systematic review reveal mixed reports on injury risk in relation to playing position, the more consistent results through studies was that GKs may be at lower injury risk compared to the outfield players, even if there wasn’t complete agreement. One should note that in modern soccer the specific role of any player at 1 position may not be entirely consistent with another player in the same position. Within the same “position group”, there may also be players with completely different qualitative playing demands (eg, wing defender and central defender). So, even with the strongest study design, it may be difficult to give a simple and clear message about playing position and injury risk due to the variability of the playing styles and players at each position.
This study has several limitations and the results must be considered and interpreted with caution. First, we limited our search to male soccer, so the results may not be applicable to female soccer. Secondly, the interpretation of study findings wasn’t easy because of the different report modalities of the different papers included in the systematic review. Finally, we included reports from a total of a 23-year time span and from different countries and continents. The game may have evolved through years and there may be differences in the style of playing within countries that potentially could interfere with injury risk.
However, this is the first paper systematically evaluating the existing literature on position specific injury risk in male soccer players. Future studies, with prospective design and a consistent method to evaluate the player position as a potential factor related to injury risk, are needed. Match and training injuries should be evaluated separately as playing position may be more related to match injury risk.
CONCLUSION
There is no agreement in the existing literature regarding weather or not player position influence the general injury risk in male soccer. The GKs may have a lower risk of injury if compared to outfield players.
1. Pfirrmann D, Herbst M, Ingelfinger P, Simon P, Tug S. Analysis of injury incidences in male professional adult and elite youth soccer players: a systematic review. J Athl Train. 2016;51(5):410-424. doi:10.4085/1062-6050-51.6.03.
2. Eirale C, Gillogly S, Singh G, Chamari K. Injury and illness epidemiology in soccer - effects of global geographical differences - a call for standardized and consistent research studies. Biol Sport. 2017;34(3):249-254. doi:10.5114/biolsport.2017.66002.
3. Ekstrand J, Hägglund M, Waldén M. Injury incidence and injury patterns in professional football: the UEFA injury study. Br J Sports Med. 2011;45(7):553-558. doi:10.1136/bjsm.2009.060582.
4. Silvers-Granelli HJ, Bizzini M, Arundale A, Mandelbaum BR, Snyder-Mackler L. Does the FIFA 11+ Injury Prevention Program reduce the incidence of ACL injury in male soccer players? Clin Orthop Relat Res. 2017;475(10):2447-2455. doi:10.1007/s11999-017-5342-5.
5. Di Salvo V, Gregson W, Atkinson G, Tordoff P, Drust B. Analysis of high intensity activity in premier league soccer. Int J Sports Med. 2009;30(3):205-212. doi:10.1055/s-0028-1105950.
6. Brophy RH, Stepan JG, Silvers HJ, Mandelbaum BR. Defending puts the anterior cruciate ligament at risk during soccer: a gender-based analysis. Sports Health. 2015;7(3):244-249. doi:10.1177/1941738114535184.
7. Dauty M, Collon S. Incidence of injuries in French professional soccer players. Int J Sports Med. 2011;32(12):965-969. doi:10.1055/s-0031-1283188.
8. Mallo J, Dellal A. Injury risk in professional football players with special reference to the playing position and training periodization. J Sports Med Phys Fitness. 2012;52(6):631-638.
9. Nilsson M, Hägglund M, Ekstrand J, Waldén M. Head and neck injuries in professional soccer. Clin J Sport Med. 2013;23(4):255-260. doi:10.1097/JSM.0b013e31827ee6f8.
10. Timpka T, Risto O, Björmsjö M. Boys soccer league injuries: a community-based study of time-loss from sports participation and long-term sequelae. Eur J Public Health. 2008;18(1):19-24.
11. Waldén M, Krosshaug T, Bjørneboe J, Andersen TE, Faul O, Hägglund M. Three distinct mechanisms predominate in non-contact anterior cruciate ligament injuries in male professional football players: a systematic video analysis of 39 cases. Br J Sports Med. 2015;49(22):1452-1460. doi:10.1136/bjsports-2014-094573.
12. Andersen TE, Larsen Ø, Tenga A, Engebretsen L, Bahr R. Football incident analysis: a new video based method to describe injury mechanisms in professional football. Br J Sports Med. 2003;37(3):226-232.
13. Arliani GG, Lara PHS, Astur DC, Pedrinelli A, Pagura JR, Cohen M. Orthopaedics injuries in male professional football players in Brazil: a prospective comparison between two divisions. Muscles Ligaments Tendons J. 2018;7(3), 524-531. doi:10.11138/mltj/2017.7.3.524.
14. Carling C, Orhant E, LeGall F. Match injuries in professional soccer: inter-seasonal variation and effects of competition type, match congestion and positional role. Int J Sports Med. 2010;31(4):271-276. doi:10.1055/s-0029-1243646.
15. Deehan DJ, Bell K, McCaskie AW. Adolescent musculoskeletal injuries in a football academy. J Bone Joint Surg Br. 2007;89(1):5-8.
16. Aoki H, O'Hata N, Kohno T, Morikawa T, Seki J. A 15-year prospective epidemiological account of acute traumatic injuries during official professional soccer league matches in Japan. Am J Sports Med. 2012;40(5):1006-1014. doi:10.1177/0363546512438695.
17. Shalaj I, Tishukaj F, Bachl N, Tschan H, Wessner B, Csapo R. Injuries in professional male football players in Kosovo: a descriptive epidemiological study. BMC Musculoskelet Disord. 2016;17:338. doi:10.1186/s12891-016-1202-9.
18. Morgan BE, Oberlander MA. An examination of injuries in major league soccer. The inaugural season. Am J Sports Med. 2001;29(4):426-430.
19. Cloke D, Moore O, Shah T, Rushton S, Shirley MD, Deehan DJ. Thigh muscle injuries in youth soccer: predictors of recovery. Am J Sports Med. 2012;40(2):433-439. doi:10.1177/0363546511428800.
20. Mallo J, González P, Veiga S, Navarro E. Injury incidence in a spanish sub-elite professional football team: a prospective study during four consecutive seasons. J Sports Sci Med. 2011;10(4):731-736.
21. Cárdenas-Fernández V, Chinchilla-Minguet JL, Castillo-Rodríguez A. Somatotype and body composition in young soccer players according to the playing position and sport success. J Strength Cond Res. 2017. doi:10.1519/JSC.0000000000002125. [Epub ahead of print]
22. Ekstrand J, Hägglund M, Törnqvist H, et al. Upper extremity injuries in male elite football players. Knee Surg Sports Traumatol Arthrosc. 2013;21(7):1626-1632. doi:10.1007/s00167-012-2164-6.
23. Lundblad M, Waldén M, Magnusson H, Karlsson J, Ekstrand J. The UEFA injury study: 11-year data concerning 346 MCL injuries and time to return to play. Br J Sports Med. 2013;47(12):759-762. doi:10.1136/bjsports-2013-092305.
24. Andersen TE, Tenga A, Engebretsen L, Bahr R. Video analysis of injuries and incidents in Norwegian professional football. Br J Sports Med. 2004;38(5):626-631.
25. Ueblacker P, Müller-Wohlfahrt HW, Ekstrand J. Epidemiological and clinical outcome comparison of indirect (‘strain’) versus direct (‘contusion’) anterior and posterior thigh muscle injuries in male elite football players: UEFA Elite League study of 2287 thigh injuries (2001-2013). Br J Sports Med. 2015;49(22):1461-1465. doi:10.1136/bjsports-2014-094285.
26. Khodaee M, Currie DW, Asif IM, Comstock RD. Nine-year study of US high school soccer injuries: data from a national sports injury surveillance programme. Br J Sports Med. 2017;51(3):185-193. doi:10.1136/bjsports-2015-095946.
ABSTRACT
Soccer (football) is a complex contact sport with a substantial risk of injury. As injury surveillance is the first step of the injury prevention paradigm, soccer epidemiology is well reported in the existing literature, but less is known about the actual role of player position on the general injury risk.
The goal of this study is to present the existing evidence regarding the influence of player’s position on general injury risk in male soccer.
A systematic review of the Medline database was carried out. Only English written studies on male soccer and citing playing position as a possible determinant of injury risk were included. One hundred and two full texts were evaluated for eligibility, and 11 studies were selected for the qualitative synthesis.
Of the 11 studies included in the systematic review, 5 didn’t find any significant correlation with between player’s position and general injury risk, while the remaining 6 studies found player’s position to be correlated with injury risk, with mixed findings depending on each study. The most consistent finding was a tendency for goalkeepers (GKs) to sustain less injuries compared to outfield players. When considering only the studies reporting just the match injury risk, forwards seemed to be at higher risk, even if there wasn’t a complete agreement.
Few studies have evaluated a possible effect of playing position on general injury risk in male soccer. There is no agreement if weather or not different playing positions are associated to a higher injury risk. GKs seem to be at lower risk of injury when compared to outfield players.
Continue to: Soccer, known worldwide as football, is the most...
Soccer, known worldwide as football, is the most common practiced sport worldwide. Soccer is also a complex contact sport with a substantial injury risk,1 that is well documented in the current literature. According to a recent systematic review, general injury incidence in male soccer ranged from 2.0 injuries to 19.4 injuries per 1000 hours of exposure in youth male soccer and from 2.48 injuries to 9.4 injuries per 1000 hours of exposure in elite male soccer.1 It is also well established that the injury risk is greater in matches than training.1 Soccer’s injuries are well known to be a socioeconomic burden for elite, youth, and recreational players.2 Different authors have underlined the problem that nowadays the game is faster, and players need to have a better physical performance as they are subjected to important efforts both metabolically and biomechanically during match play. In the last decades, thanks to different research groups involved with professional soccer,3 there has been an increasing interest in soccer injuries’ epidemiology and for preventative measures.4 A deep comprehension of injury epidemiology is in fact the first necessary step for successful preventative measures. Regarding a possible correlation between playing position and injury incidence, there is a lack of consensus in the literature. Player position (goalkeeper [GK], defenders, midfielder [MF], or striker) may affect injury risk, as different roles are associated to different intensity during match play5 and experience different combination of anticipated or non-anticipated movement patterns.6 Previous authors underlined that few studies have evaluated a possible influence of playing position on injury incidence and severity.7
The main goal of this systematic review is to present the existing evidence regarding the influence of player position on injury incidence in male soccer and to present practical considerations on each field position in relation to the injury’s risk.
METHODS
DATA SOURCES AND SELECTION CRITERIA
We searched the Medline database for key terms and their variations to identify appropriate studies on injury epidemiology in soccer and specific player position influence. The keywords included: injury epidemiology soccer [OR] injury epidemiology football; position specific injury epidemiology soccer [OR] football. We limited our search to originally published English-language research articles.
Relevant data were extracted for study characteristics to ensure the included studies met certain criteria. The inclusion criteria were prospective design with minimum 6-month observational period, exclusively male soccer players’ cohorts, reported injury incidence, and documented player position in correlation with a measure of injury risk.
As stated above, we only included studies on male soccer. We also did not consider studies limited to a single injury type, considering only studies analyzing and documenting all injuries. We did not exclude studies on youth soccer but we didn’t consider studies on ≥2 more sports or mixed male and female studies.
Data were extracted by an author (FDV) and qualitatively controlled by another one (BM). Controversy were solved through discussion or confrontation with another author (LL).
Results of the included studies are presented only qualitatively because of different methodologies we encountered in documenting the potential effects of player’s role. Some studies reported differences in injury incidence within groups, others reported the proportion of injuries for each subgroup.
Continue to: RESULTS...
RESULTS
STUDY SELECTION
Of the 1609 potential items we found in the existing literature, 102 full-text articles were screened for eligibility. Only 11 papers met the inclusion criteria and were included in the systematic review, including 2 studies on youth soccer and 9 studies on adult soccer (Figure 1). Five of the selected studies tracked only match injuries, while the remaining 6 studies presented data on both match and training injuries. As a matter of fact, the effect of player position was not so commonly evaluated or at least reported in the existing literature. Studies’ characteristics and main findings regarding player’s position are reported in Table.
GENERAL INJURY RISK AND PLAYING POSITION
Of the 11 studies included for qualitative synthesis, 5 studies reported no significant effect of player’s position on general risk of injury,7-11 3 studies reported a greater risk in forwards,12-14 1 study reported a greater risk in MFs,15 1 study reported a greater risk in forwards and central defenders,8 and finally 1 study reported a significant lower risk in GKs.16 Additionally, 2 more studies reported GKs to be at the lowest injury risk,12,13 another study reported GKs to have lost the lower number of matches,8 1 study didn’t consider the GK position in the analysis due to the low number of injuries,17 limiting the analysis on the outfield positions.
Out of the 5 studies reporting no significant effect of playing position on injury risk, 1 study found a tendency to more injuries in forward players,10 a second study found a tendency for higher injury risk in midfielders,18 and a third study found a tendency for higher risk in defenders.17 Considering only the 5 studies reporting data on match injuries, 3 reported a higher risk in forwards,12-14 while a fourth one reported a tendency for increased risk in forwards10 even if not statistically significant. On the other hand, evaluating the 6 studies reporting data on match and training injuries, most of the studies, 4 out of 6, reported no effect of playing position.17-20 The main findings of the studies are also expressed graphically in Figures 2A, 2B.
DISCUSSION
The main finding of this study is that there is substantially no agreement regarding the effect of player position on general injury risk in male soccer.
First, we must underline that not many studies have evaluated prospectively the influence of player’s position on injury risk. Of the 11 selected studies, 5 (5/11) reported no significant effect of playing position,7,10,17,18,20 while the remaining studies (6/11)8,12-16 reported a significant effect of player position on the risk of injury, with various results depending on the single study. It should be noted that the 2 studies with the longest observational period (15 consecutive seasons)16,19 did not report any difference in injury risk considering only the outfield playing positions.
Continue to: We will now review the findings...
We will now review the findings of our systematic review based on player position. One of the more consistent trends that we found is the possible occurrence of different injury epidemiology in GKs compared to outfield players. One study reported a significant lower incidence of match injuries for GKs, 12.9 injuries per 1000 game hours vs 22.6 injuries per 1000 game hours of outfield positions.16 This result is remarkable, even considering the very long observational period (15 seasons). Other 2 studies, not reporting position specific injury incidence (but proportion of injuries) also agreed on the topic.12,13 On the other hand, Morgan and Oberlander9 reported no differences between GKs and other positions. Anecdotally, unpublished Major League Soccer data regarding the most recent seasons seems to support these findings with GKs sustaining the lower proportion of injuries. By a physiological point of view, somatotype and body composition have been reported to differ between GKs and the other playing positions in young male soccer players.21 The uniqueness of the GK somatotype and role may reflect on a predisposition to a different pattern of injuries. Ekstrand and colleagues22 reported that GKs have a higher incidence of upper extremity fractures, the same group demonstrated a possible tendency for more head and neck injuries9 and a lower risk of medial collateral ligament injuries.23 On the other hand, GKs seems to be at lower injury risk for the playing pattern differences with outfield players. The reduced distance GKs cover during the match, as well as less direct contacts with opponents, may be factors that potentially explain this finding.
In relation to forwards, 4 studies interestingly stated that forwards were at increased risk of injury,12-14 although 1 report had similar risk of injury with forwards and defenders.8 Most of the studies only on match injuries reported some association between forward position and injury risk (Figures 2A, 2B), so attackers may be at higher risk of match injuries when compared to the other playing positions. There are different possible explanations for this finding. First, it is demonstrated that the clear majority of soccer incidents happen in the mid-defensive zone and in the score-box,24 2 typical attackers’ zones, where most of duels and tackles may happen. So, forwards may be more prone to match injuries because of the intensity of match play in their typical playing zones. Also, fast kicking and acceleration/deceleration activities of the attackers may predispose for thigh muscle injuries, accounting up to 25% of the total lay off time in professional soccer.25 However, these considerations are still yet to be proven.
When considering defenders, 1 report indicated defenders (and forwards) to be at potential greater risk of injury,8which is similar to the report from Shalaj and colleagues,17 although it did not report a statistically significant result. A direct playing style, with defenders and strikers being more involved in the game can potentially explain this finding. However, the specific epidemiology of defenders may be more complicated. Defenders may be predisposed to knee injuries, such as injury to the anterior cruciate ligament (ACL). In fact, Walden and colleagues,11 in a video-analysis study, reported that the 77% of ACL injuries happened in defending situations. In addition, Brophy and colleagues,6 in another video-analysis study, reported a 73% of ACL injuries happened while defending. A likely explanation is the nature of the defender’s role in soccer, reactive to the attacking team actions. Many times, defenders try high risk maneuvers while tackling the opponent, with minimal motor planning time and consciousness. This is well described by Walden and colleagues,11 with the pressing mechanism ACL injury, when the injured player is pressing the opponent in the attempt to get the ball but eventually falls into a high-risk position.
When considering MFs, Deehan and colleagues15 found a significant higher risk in MFs in youth soccer. This result is partially according to Morgan and Oberlander18 who reported a non-statistically significant greater injury incidence in MFs. MFs are generally the players that cover more distance during a soccer match and it is logical to think that they would be predisposed to a large volume of acceleration/deceleration activities,19 potentially relating to injury risk, especially to muscles injuries. A previous study on thigh muscle injuries in youth soccer reporting higher injury risk in MFs, followed by forwards.19 Consistent with these results, another study on a mixed male and female cohort on high school soccer revealed more injuries in MFs, followed by forwards.26
Continue to: The results of this systematic review...
The results of this systematic review reveal mixed reports on injury risk in relation to playing position, the more consistent results through studies was that GKs may be at lower injury risk compared to the outfield players, even if there wasn’t complete agreement. One should note that in modern soccer the specific role of any player at 1 position may not be entirely consistent with another player in the same position. Within the same “position group”, there may also be players with completely different qualitative playing demands (eg, wing defender and central defender). So, even with the strongest study design, it may be difficult to give a simple and clear message about playing position and injury risk due to the variability of the playing styles and players at each position.
This study has several limitations and the results must be considered and interpreted with caution. First, we limited our search to male soccer, so the results may not be applicable to female soccer. Secondly, the interpretation of study findings wasn’t easy because of the different report modalities of the different papers included in the systematic review. Finally, we included reports from a total of a 23-year time span and from different countries and continents. The game may have evolved through years and there may be differences in the style of playing within countries that potentially could interfere with injury risk.
However, this is the first paper systematically evaluating the existing literature on position specific injury risk in male soccer players. Future studies, with prospective design and a consistent method to evaluate the player position as a potential factor related to injury risk, are needed. Match and training injuries should be evaluated separately as playing position may be more related to match injury risk.
CONCLUSION
There is no agreement in the existing literature regarding weather or not player position influence the general injury risk in male soccer. The GKs may have a lower risk of injury if compared to outfield players.
ABSTRACT
Soccer (football) is a complex contact sport with a substantial risk of injury. As injury surveillance is the first step of the injury prevention paradigm, soccer epidemiology is well reported in the existing literature, but less is known about the actual role of player position on the general injury risk.
The goal of this study is to present the existing evidence regarding the influence of player’s position on general injury risk in male soccer.
A systematic review of the Medline database was carried out. Only English written studies on male soccer and citing playing position as a possible determinant of injury risk were included. One hundred and two full texts were evaluated for eligibility, and 11 studies were selected for the qualitative synthesis.
Of the 11 studies included in the systematic review, 5 didn’t find any significant correlation with between player’s position and general injury risk, while the remaining 6 studies found player’s position to be correlated with injury risk, with mixed findings depending on each study. The most consistent finding was a tendency for goalkeepers (GKs) to sustain less injuries compared to outfield players. When considering only the studies reporting just the match injury risk, forwards seemed to be at higher risk, even if there wasn’t a complete agreement.
Few studies have evaluated a possible effect of playing position on general injury risk in male soccer. There is no agreement if weather or not different playing positions are associated to a higher injury risk. GKs seem to be at lower risk of injury when compared to outfield players.
Continue to: Soccer, known worldwide as football, is the most...
Soccer, known worldwide as football, is the most common practiced sport worldwide. Soccer is also a complex contact sport with a substantial injury risk,1 that is well documented in the current literature. According to a recent systematic review, general injury incidence in male soccer ranged from 2.0 injuries to 19.4 injuries per 1000 hours of exposure in youth male soccer and from 2.48 injuries to 9.4 injuries per 1000 hours of exposure in elite male soccer.1 It is also well established that the injury risk is greater in matches than training.1 Soccer’s injuries are well known to be a socioeconomic burden for elite, youth, and recreational players.2 Different authors have underlined the problem that nowadays the game is faster, and players need to have a better physical performance as they are subjected to important efforts both metabolically and biomechanically during match play. In the last decades, thanks to different research groups involved with professional soccer,3 there has been an increasing interest in soccer injuries’ epidemiology and for preventative measures.4 A deep comprehension of injury epidemiology is in fact the first necessary step for successful preventative measures. Regarding a possible correlation between playing position and injury incidence, there is a lack of consensus in the literature. Player position (goalkeeper [GK], defenders, midfielder [MF], or striker) may affect injury risk, as different roles are associated to different intensity during match play5 and experience different combination of anticipated or non-anticipated movement patterns.6 Previous authors underlined that few studies have evaluated a possible influence of playing position on injury incidence and severity.7
The main goal of this systematic review is to present the existing evidence regarding the influence of player position on injury incidence in male soccer and to present practical considerations on each field position in relation to the injury’s risk.
METHODS
DATA SOURCES AND SELECTION CRITERIA
We searched the Medline database for key terms and their variations to identify appropriate studies on injury epidemiology in soccer and specific player position influence. The keywords included: injury epidemiology soccer [OR] injury epidemiology football; position specific injury epidemiology soccer [OR] football. We limited our search to originally published English-language research articles.
Relevant data were extracted for study characteristics to ensure the included studies met certain criteria. The inclusion criteria were prospective design with minimum 6-month observational period, exclusively male soccer players’ cohorts, reported injury incidence, and documented player position in correlation with a measure of injury risk.
As stated above, we only included studies on male soccer. We also did not consider studies limited to a single injury type, considering only studies analyzing and documenting all injuries. We did not exclude studies on youth soccer but we didn’t consider studies on ≥2 more sports or mixed male and female studies.
Data were extracted by an author (FDV) and qualitatively controlled by another one (BM). Controversy were solved through discussion or confrontation with another author (LL).
Results of the included studies are presented only qualitatively because of different methodologies we encountered in documenting the potential effects of player’s role. Some studies reported differences in injury incidence within groups, others reported the proportion of injuries for each subgroup.
Continue to: RESULTS...
RESULTS
STUDY SELECTION
Of the 1609 potential items we found in the existing literature, 102 full-text articles were screened for eligibility. Only 11 papers met the inclusion criteria and were included in the systematic review, including 2 studies on youth soccer and 9 studies on adult soccer (Figure 1). Five of the selected studies tracked only match injuries, while the remaining 6 studies presented data on both match and training injuries. As a matter of fact, the effect of player position was not so commonly evaluated or at least reported in the existing literature. Studies’ characteristics and main findings regarding player’s position are reported in Table.
GENERAL INJURY RISK AND PLAYING POSITION
Of the 11 studies included for qualitative synthesis, 5 studies reported no significant effect of player’s position on general risk of injury,7-11 3 studies reported a greater risk in forwards,12-14 1 study reported a greater risk in MFs,15 1 study reported a greater risk in forwards and central defenders,8 and finally 1 study reported a significant lower risk in GKs.16 Additionally, 2 more studies reported GKs to be at the lowest injury risk,12,13 another study reported GKs to have lost the lower number of matches,8 1 study didn’t consider the GK position in the analysis due to the low number of injuries,17 limiting the analysis on the outfield positions.
Out of the 5 studies reporting no significant effect of playing position on injury risk, 1 study found a tendency to more injuries in forward players,10 a second study found a tendency for higher injury risk in midfielders,18 and a third study found a tendency for higher risk in defenders.17 Considering only the 5 studies reporting data on match injuries, 3 reported a higher risk in forwards,12-14 while a fourth one reported a tendency for increased risk in forwards10 even if not statistically significant. On the other hand, evaluating the 6 studies reporting data on match and training injuries, most of the studies, 4 out of 6, reported no effect of playing position.17-20 The main findings of the studies are also expressed graphically in Figures 2A, 2B.
DISCUSSION
The main finding of this study is that there is substantially no agreement regarding the effect of player position on general injury risk in male soccer.
First, we must underline that not many studies have evaluated prospectively the influence of player’s position on injury risk. Of the 11 selected studies, 5 (5/11) reported no significant effect of playing position,7,10,17,18,20 while the remaining studies (6/11)8,12-16 reported a significant effect of player position on the risk of injury, with various results depending on the single study. It should be noted that the 2 studies with the longest observational period (15 consecutive seasons)16,19 did not report any difference in injury risk considering only the outfield playing positions.
Continue to: We will now review the findings...
We will now review the findings of our systematic review based on player position. One of the more consistent trends that we found is the possible occurrence of different injury epidemiology in GKs compared to outfield players. One study reported a significant lower incidence of match injuries for GKs, 12.9 injuries per 1000 game hours vs 22.6 injuries per 1000 game hours of outfield positions.16 This result is remarkable, even considering the very long observational period (15 seasons). Other 2 studies, not reporting position specific injury incidence (but proportion of injuries) also agreed on the topic.12,13 On the other hand, Morgan and Oberlander9 reported no differences between GKs and other positions. Anecdotally, unpublished Major League Soccer data regarding the most recent seasons seems to support these findings with GKs sustaining the lower proportion of injuries. By a physiological point of view, somatotype and body composition have been reported to differ between GKs and the other playing positions in young male soccer players.21 The uniqueness of the GK somatotype and role may reflect on a predisposition to a different pattern of injuries. Ekstrand and colleagues22 reported that GKs have a higher incidence of upper extremity fractures, the same group demonstrated a possible tendency for more head and neck injuries9 and a lower risk of medial collateral ligament injuries.23 On the other hand, GKs seems to be at lower injury risk for the playing pattern differences with outfield players. The reduced distance GKs cover during the match, as well as less direct contacts with opponents, may be factors that potentially explain this finding.
In relation to forwards, 4 studies interestingly stated that forwards were at increased risk of injury,12-14 although 1 report had similar risk of injury with forwards and defenders.8 Most of the studies only on match injuries reported some association between forward position and injury risk (Figures 2A, 2B), so attackers may be at higher risk of match injuries when compared to the other playing positions. There are different possible explanations for this finding. First, it is demonstrated that the clear majority of soccer incidents happen in the mid-defensive zone and in the score-box,24 2 typical attackers’ zones, where most of duels and tackles may happen. So, forwards may be more prone to match injuries because of the intensity of match play in their typical playing zones. Also, fast kicking and acceleration/deceleration activities of the attackers may predispose for thigh muscle injuries, accounting up to 25% of the total lay off time in professional soccer.25 However, these considerations are still yet to be proven.
When considering defenders, 1 report indicated defenders (and forwards) to be at potential greater risk of injury,8which is similar to the report from Shalaj and colleagues,17 although it did not report a statistically significant result. A direct playing style, with defenders and strikers being more involved in the game can potentially explain this finding. However, the specific epidemiology of defenders may be more complicated. Defenders may be predisposed to knee injuries, such as injury to the anterior cruciate ligament (ACL). In fact, Walden and colleagues,11 in a video-analysis study, reported that the 77% of ACL injuries happened in defending situations. In addition, Brophy and colleagues,6 in another video-analysis study, reported a 73% of ACL injuries happened while defending. A likely explanation is the nature of the defender’s role in soccer, reactive to the attacking team actions. Many times, defenders try high risk maneuvers while tackling the opponent, with minimal motor planning time and consciousness. This is well described by Walden and colleagues,11 with the pressing mechanism ACL injury, when the injured player is pressing the opponent in the attempt to get the ball but eventually falls into a high-risk position.
When considering MFs, Deehan and colleagues15 found a significant higher risk in MFs in youth soccer. This result is partially according to Morgan and Oberlander18 who reported a non-statistically significant greater injury incidence in MFs. MFs are generally the players that cover more distance during a soccer match and it is logical to think that they would be predisposed to a large volume of acceleration/deceleration activities,19 potentially relating to injury risk, especially to muscles injuries. A previous study on thigh muscle injuries in youth soccer reporting higher injury risk in MFs, followed by forwards.19 Consistent with these results, another study on a mixed male and female cohort on high school soccer revealed more injuries in MFs, followed by forwards.26
Continue to: The results of this systematic review...
The results of this systematic review reveal mixed reports on injury risk in relation to playing position, the more consistent results through studies was that GKs may be at lower injury risk compared to the outfield players, even if there wasn’t complete agreement. One should note that in modern soccer the specific role of any player at 1 position may not be entirely consistent with another player in the same position. Within the same “position group”, there may also be players with completely different qualitative playing demands (eg, wing defender and central defender). So, even with the strongest study design, it may be difficult to give a simple and clear message about playing position and injury risk due to the variability of the playing styles and players at each position.
This study has several limitations and the results must be considered and interpreted with caution. First, we limited our search to male soccer, so the results may not be applicable to female soccer. Secondly, the interpretation of study findings wasn’t easy because of the different report modalities of the different papers included in the systematic review. Finally, we included reports from a total of a 23-year time span and from different countries and continents. The game may have evolved through years and there may be differences in the style of playing within countries that potentially could interfere with injury risk.
However, this is the first paper systematically evaluating the existing literature on position specific injury risk in male soccer players. Future studies, with prospective design and a consistent method to evaluate the player position as a potential factor related to injury risk, are needed. Match and training injuries should be evaluated separately as playing position may be more related to match injury risk.
CONCLUSION
There is no agreement in the existing literature regarding weather or not player position influence the general injury risk in male soccer. The GKs may have a lower risk of injury if compared to outfield players.
1. Pfirrmann D, Herbst M, Ingelfinger P, Simon P, Tug S. Analysis of injury incidences in male professional adult and elite youth soccer players: a systematic review. J Athl Train. 2016;51(5):410-424. doi:10.4085/1062-6050-51.6.03.
2. Eirale C, Gillogly S, Singh G, Chamari K. Injury and illness epidemiology in soccer - effects of global geographical differences - a call for standardized and consistent research studies. Biol Sport. 2017;34(3):249-254. doi:10.5114/biolsport.2017.66002.
3. Ekstrand J, Hägglund M, Waldén M. Injury incidence and injury patterns in professional football: the UEFA injury study. Br J Sports Med. 2011;45(7):553-558. doi:10.1136/bjsm.2009.060582.
4. Silvers-Granelli HJ, Bizzini M, Arundale A, Mandelbaum BR, Snyder-Mackler L. Does the FIFA 11+ Injury Prevention Program reduce the incidence of ACL injury in male soccer players? Clin Orthop Relat Res. 2017;475(10):2447-2455. doi:10.1007/s11999-017-5342-5.
5. Di Salvo V, Gregson W, Atkinson G, Tordoff P, Drust B. Analysis of high intensity activity in premier league soccer. Int J Sports Med. 2009;30(3):205-212. doi:10.1055/s-0028-1105950.
6. Brophy RH, Stepan JG, Silvers HJ, Mandelbaum BR. Defending puts the anterior cruciate ligament at risk during soccer: a gender-based analysis. Sports Health. 2015;7(3):244-249. doi:10.1177/1941738114535184.
7. Dauty M, Collon S. Incidence of injuries in French professional soccer players. Int J Sports Med. 2011;32(12):965-969. doi:10.1055/s-0031-1283188.
8. Mallo J, Dellal A. Injury risk in professional football players with special reference to the playing position and training periodization. J Sports Med Phys Fitness. 2012;52(6):631-638.
9. Nilsson M, Hägglund M, Ekstrand J, Waldén M. Head and neck injuries in professional soccer. Clin J Sport Med. 2013;23(4):255-260. doi:10.1097/JSM.0b013e31827ee6f8.
10. Timpka T, Risto O, Björmsjö M. Boys soccer league injuries: a community-based study of time-loss from sports participation and long-term sequelae. Eur J Public Health. 2008;18(1):19-24.
11. Waldén M, Krosshaug T, Bjørneboe J, Andersen TE, Faul O, Hägglund M. Three distinct mechanisms predominate in non-contact anterior cruciate ligament injuries in male professional football players: a systematic video analysis of 39 cases. Br J Sports Med. 2015;49(22):1452-1460. doi:10.1136/bjsports-2014-094573.
12. Andersen TE, Larsen Ø, Tenga A, Engebretsen L, Bahr R. Football incident analysis: a new video based method to describe injury mechanisms in professional football. Br J Sports Med. 2003;37(3):226-232.
13. Arliani GG, Lara PHS, Astur DC, Pedrinelli A, Pagura JR, Cohen M. Orthopaedics injuries in male professional football players in Brazil: a prospective comparison between two divisions. Muscles Ligaments Tendons J. 2018;7(3), 524-531. doi:10.11138/mltj/2017.7.3.524.
14. Carling C, Orhant E, LeGall F. Match injuries in professional soccer: inter-seasonal variation and effects of competition type, match congestion and positional role. Int J Sports Med. 2010;31(4):271-276. doi:10.1055/s-0029-1243646.
15. Deehan DJ, Bell K, McCaskie AW. Adolescent musculoskeletal injuries in a football academy. J Bone Joint Surg Br. 2007;89(1):5-8.
16. Aoki H, O'Hata N, Kohno T, Morikawa T, Seki J. A 15-year prospective epidemiological account of acute traumatic injuries during official professional soccer league matches in Japan. Am J Sports Med. 2012;40(5):1006-1014. doi:10.1177/0363546512438695.
17. Shalaj I, Tishukaj F, Bachl N, Tschan H, Wessner B, Csapo R. Injuries in professional male football players in Kosovo: a descriptive epidemiological study. BMC Musculoskelet Disord. 2016;17:338. doi:10.1186/s12891-016-1202-9.
18. Morgan BE, Oberlander MA. An examination of injuries in major league soccer. The inaugural season. Am J Sports Med. 2001;29(4):426-430.
19. Cloke D, Moore O, Shah T, Rushton S, Shirley MD, Deehan DJ. Thigh muscle injuries in youth soccer: predictors of recovery. Am J Sports Med. 2012;40(2):433-439. doi:10.1177/0363546511428800.
20. Mallo J, González P, Veiga S, Navarro E. Injury incidence in a spanish sub-elite professional football team: a prospective study during four consecutive seasons. J Sports Sci Med. 2011;10(4):731-736.
21. Cárdenas-Fernández V, Chinchilla-Minguet JL, Castillo-Rodríguez A. Somatotype and body composition in young soccer players according to the playing position and sport success. J Strength Cond Res. 2017. doi:10.1519/JSC.0000000000002125. [Epub ahead of print]
22. Ekstrand J, Hägglund M, Törnqvist H, et al. Upper extremity injuries in male elite football players. Knee Surg Sports Traumatol Arthrosc. 2013;21(7):1626-1632. doi:10.1007/s00167-012-2164-6.
23. Lundblad M, Waldén M, Magnusson H, Karlsson J, Ekstrand J. The UEFA injury study: 11-year data concerning 346 MCL injuries and time to return to play. Br J Sports Med. 2013;47(12):759-762. doi:10.1136/bjsports-2013-092305.
24. Andersen TE, Tenga A, Engebretsen L, Bahr R. Video analysis of injuries and incidents in Norwegian professional football. Br J Sports Med. 2004;38(5):626-631.
25. Ueblacker P, Müller-Wohlfahrt HW, Ekstrand J. Epidemiological and clinical outcome comparison of indirect (‘strain’) versus direct (‘contusion’) anterior and posterior thigh muscle injuries in male elite football players: UEFA Elite League study of 2287 thigh injuries (2001-2013). Br J Sports Med. 2015;49(22):1461-1465. doi:10.1136/bjsports-2014-094285.
26. Khodaee M, Currie DW, Asif IM, Comstock RD. Nine-year study of US high school soccer injuries: data from a national sports injury surveillance programme. Br J Sports Med. 2017;51(3):185-193. doi:10.1136/bjsports-2015-095946.
1. Pfirrmann D, Herbst M, Ingelfinger P, Simon P, Tug S. Analysis of injury incidences in male professional adult and elite youth soccer players: a systematic review. J Athl Train. 2016;51(5):410-424. doi:10.4085/1062-6050-51.6.03.
2. Eirale C, Gillogly S, Singh G, Chamari K. Injury and illness epidemiology in soccer - effects of global geographical differences - a call for standardized and consistent research studies. Biol Sport. 2017;34(3):249-254. doi:10.5114/biolsport.2017.66002.
3. Ekstrand J, Hägglund M, Waldén M. Injury incidence and injury patterns in professional football: the UEFA injury study. Br J Sports Med. 2011;45(7):553-558. doi:10.1136/bjsm.2009.060582.
4. Silvers-Granelli HJ, Bizzini M, Arundale A, Mandelbaum BR, Snyder-Mackler L. Does the FIFA 11+ Injury Prevention Program reduce the incidence of ACL injury in male soccer players? Clin Orthop Relat Res. 2017;475(10):2447-2455. doi:10.1007/s11999-017-5342-5.
5. Di Salvo V, Gregson W, Atkinson G, Tordoff P, Drust B. Analysis of high intensity activity in premier league soccer. Int J Sports Med. 2009;30(3):205-212. doi:10.1055/s-0028-1105950.
6. Brophy RH, Stepan JG, Silvers HJ, Mandelbaum BR. Defending puts the anterior cruciate ligament at risk during soccer: a gender-based analysis. Sports Health. 2015;7(3):244-249. doi:10.1177/1941738114535184.
7. Dauty M, Collon S. Incidence of injuries in French professional soccer players. Int J Sports Med. 2011;32(12):965-969. doi:10.1055/s-0031-1283188.
8. Mallo J, Dellal A. Injury risk in professional football players with special reference to the playing position and training periodization. J Sports Med Phys Fitness. 2012;52(6):631-638.
9. Nilsson M, Hägglund M, Ekstrand J, Waldén M. Head and neck injuries in professional soccer. Clin J Sport Med. 2013;23(4):255-260. doi:10.1097/JSM.0b013e31827ee6f8.
10. Timpka T, Risto O, Björmsjö M. Boys soccer league injuries: a community-based study of time-loss from sports participation and long-term sequelae. Eur J Public Health. 2008;18(1):19-24.
11. Waldén M, Krosshaug T, Bjørneboe J, Andersen TE, Faul O, Hägglund M. Three distinct mechanisms predominate in non-contact anterior cruciate ligament injuries in male professional football players: a systematic video analysis of 39 cases. Br J Sports Med. 2015;49(22):1452-1460. doi:10.1136/bjsports-2014-094573.
12. Andersen TE, Larsen Ø, Tenga A, Engebretsen L, Bahr R. Football incident analysis: a new video based method to describe injury mechanisms in professional football. Br J Sports Med. 2003;37(3):226-232.
13. Arliani GG, Lara PHS, Astur DC, Pedrinelli A, Pagura JR, Cohen M. Orthopaedics injuries in male professional football players in Brazil: a prospective comparison between two divisions. Muscles Ligaments Tendons J. 2018;7(3), 524-531. doi:10.11138/mltj/2017.7.3.524.
14. Carling C, Orhant E, LeGall F. Match injuries in professional soccer: inter-seasonal variation and effects of competition type, match congestion and positional role. Int J Sports Med. 2010;31(4):271-276. doi:10.1055/s-0029-1243646.
15. Deehan DJ, Bell K, McCaskie AW. Adolescent musculoskeletal injuries in a football academy. J Bone Joint Surg Br. 2007;89(1):5-8.
16. Aoki H, O'Hata N, Kohno T, Morikawa T, Seki J. A 15-year prospective epidemiological account of acute traumatic injuries during official professional soccer league matches in Japan. Am J Sports Med. 2012;40(5):1006-1014. doi:10.1177/0363546512438695.
17. Shalaj I, Tishukaj F, Bachl N, Tschan H, Wessner B, Csapo R. Injuries in professional male football players in Kosovo: a descriptive epidemiological study. BMC Musculoskelet Disord. 2016;17:338. doi:10.1186/s12891-016-1202-9.
18. Morgan BE, Oberlander MA. An examination of injuries in major league soccer. The inaugural season. Am J Sports Med. 2001;29(4):426-430.
19. Cloke D, Moore O, Shah T, Rushton S, Shirley MD, Deehan DJ. Thigh muscle injuries in youth soccer: predictors of recovery. Am J Sports Med. 2012;40(2):433-439. doi:10.1177/0363546511428800.
20. Mallo J, González P, Veiga S, Navarro E. Injury incidence in a spanish sub-elite professional football team: a prospective study during four consecutive seasons. J Sports Sci Med. 2011;10(4):731-736.
21. Cárdenas-Fernández V, Chinchilla-Minguet JL, Castillo-Rodríguez A. Somatotype and body composition in young soccer players according to the playing position and sport success. J Strength Cond Res. 2017. doi:10.1519/JSC.0000000000002125. [Epub ahead of print]
22. Ekstrand J, Hägglund M, Törnqvist H, et al. Upper extremity injuries in male elite football players. Knee Surg Sports Traumatol Arthrosc. 2013;21(7):1626-1632. doi:10.1007/s00167-012-2164-6.
23. Lundblad M, Waldén M, Magnusson H, Karlsson J, Ekstrand J. The UEFA injury study: 11-year data concerning 346 MCL injuries and time to return to play. Br J Sports Med. 2013;47(12):759-762. doi:10.1136/bjsports-2013-092305.
24. Andersen TE, Tenga A, Engebretsen L, Bahr R. Video analysis of injuries and incidents in Norwegian professional football. Br J Sports Med. 2004;38(5):626-631.
25. Ueblacker P, Müller-Wohlfahrt HW, Ekstrand J. Epidemiological and clinical outcome comparison of indirect (‘strain’) versus direct (‘contusion’) anterior and posterior thigh muscle injuries in male elite football players: UEFA Elite League study of 2287 thigh injuries (2001-2013). Br J Sports Med. 2015;49(22):1461-1465. doi:10.1136/bjsports-2014-094285.
26. Khodaee M, Currie DW, Asif IM, Comstock RD. Nine-year study of US high school soccer injuries: data from a national sports injury surveillance programme. Br J Sports Med. 2017;51(3):185-193. doi:10.1136/bjsports-2015-095946.
TAKE-HOME POINTS
- Playing positions haven’t been extensively evaluated as an injury risk factor in elite, non-elite, and youth soccer (football).
- Different playing positions may have different injury rates and patterns due to different load, different movement patterns, and peculiar combination of anticipated and non-anticipated (reactive movements).
- The existing literature suggests that goalkeepers seem to be at lower general injury risk if compared to outfield players in male soccer (football).
- There is also a tendency towards strikers (forwards) to be at higher risk of match (but not training) injuries. This result is however not consistent between all the studies considered and should be interpreted cautiously.
- When studying injury risk in male soccer match and training injuries should be considered separately and playing position should be evaluated as a potential predictor of injury incidence.
Revamped MS criteria boost pediatric diagnoses
BERLIN –

The increased accuracy largely hinged on a positive finding of oligoclonal bands in cerebrospinal fluid – a diagnostic hallmark that was not included in the earlier criteria, Georgina Arrambide, MD, said at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis.
“Application to children of the new diagnostic criteria is limited,” said Dr. Arrambide, of the University Hospital Vall d’Hebron Multiple Sclerosis Centre of Catalonia, Barcelona. “And there are still some uncertainties with regard to fluid biomarkers and how they predict or confirm a diagnosis of MS in children, and also their relationship to the disease evolution.”
The updated McDonald criteria are intended to boost early, definitive MS diagnosis, leading to earlier initiation of therapy. They are intended primarily for patients aged 11 years and older who present with a typical clinically isolated syndrome and high probability of MS (Lancet Neurol. 2018;17[2]:162-73).
Dr. Arrambide and her colleagues used the revamped criteria to reassess MS diagnoses in a prospective Spanish cohort of children who experienced an acute first demyelinating event and were diagnosed with the 2010 criteria. The Kids-METOMS-MOGBCN Study enrolls children aged younger than 18 years within 1 year of a first acute demyelinating episode. It includes demographic, clinical, and imaging data, as well as data on oligoclonal bands and antibodies against aquaporin-4 and myelin oligodendrocyte glycoprotein (MoG). Of these fluid biomarkers, only oligoclonal bands are included in the new McDonald criteria.
The 55 children in Dr. Arrambide’s analysis were followed for a mean of 16 months. They included 25 (45%) girls with an overall median age of 6 years at the first acute event. Oligoclonal bands were present in 56%, and both anti-MoG and anti–aquaporin-4 antibodies in 82%.
All children had abnormal brain MRI at baseline, with about 33% having gadolinium-enhancing brain lesions. Spinal cord MRI was abnormal in 50%, with 39% having gadolinium-enhancing lesions. According to the 2010 criteria, only three had a definitive MS diagnosis at baseline. The diagnosis was acute disseminated encephalomyelitis in 51%, clinically isolated syndrome in 31%, radiologically isolated syndrome in 2%, and nonencephalopathic disseminated encephalomyelitis in the remainder.
At baseline, three of those had a definitive MS diagnosis, displaying dissemination in both space and time as required by both the 2010 and 2017 criteria. The addition of oligoclonal band positivity added one more patient over the 2010 criteria, and assessing the cohort with the complete 2017 criteria added three more definitive diagnoses. This was a significant increase in definitive MS diagnoses when compared against the earlier criteria (70% vs. 30%).
Diagnoses changed in 10 other patients during follow-up. The single patient with radiologically isolated syndrome was definitively diagnosed with MS. Of the seven with clinically isolated syndrome, six were diagnosed with MS and one with a relapsing optic neuritis. Of the 28 with a nonencephalopathic encephalitis, 2 were diagnosed with optic neuritis.
The study also confirmed the benefit of adding oligoclonal bands as a diagnostic marker in children. Of those with an MS diagnosis at last follow-up, 71% were positive for the cerebrospinal fluid finding, compared with just 4% of those with a non-MS diagnosis. However, none of those children had anti-MoG antibodies, compared with 58% of those with a non-MS diagnosis. None of the patients were positive for anti–aquaporin-4, regardless of diagnosis.
That finding does not necessarily mean that the absence of anti-MoG antibodies can rule out an MS diagnosis in children, Dr. Arrambide cautioned. Nevertheless, the finding is a useful clinical marker during a diagnostic work-up.
“The presence of oligoclonal bands and the absence of MOG-IgG are both useful biomarkers when evaluating the risk of MS in children with a first demyelinating event,” she said.
She disclosed financial relationships with several pharmaceutical companies.
SOURCE: Arrambide G et al. ECTRIMS 2018, Abstract 64
BERLIN –
The increased accuracy largely hinged on a positive finding of oligoclonal bands in cerebrospinal fluid – a diagnostic hallmark that was not included in the earlier criteria, Georgina Arrambide, MD, said at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis.
“Application to children of the new diagnostic criteria is limited,” said Dr. Arrambide, of the University Hospital Vall d’Hebron Multiple Sclerosis Centre of Catalonia, Barcelona. “And there are still some uncertainties with regard to fluid biomarkers and how they predict or confirm a diagnosis of MS in children, and also their relationship to the disease evolution.”
The updated McDonald criteria are intended to boost early, definitive MS diagnosis, leading to earlier initiation of therapy. They are intended primarily for patients aged 11 years and older who present with a typical clinically isolated syndrome and high probability of MS (Lancet Neurol. 2018;17[2]:162-73).
Dr. Arrambide and her colleagues used the revamped criteria to reassess MS diagnoses in a prospective Spanish cohort of children who experienced an acute first demyelinating event and were diagnosed with the 2010 criteria. The Kids-METOMS-MOGBCN Study enrolls children aged younger than 18 years within 1 year of a first acute demyelinating episode. It includes demographic, clinical, and imaging data, as well as data on oligoclonal bands and antibodies against aquaporin-4 and myelin oligodendrocyte glycoprotein (MoG). Of these fluid biomarkers, only oligoclonal bands are included in the new McDonald criteria.
The 55 children in Dr. Arrambide’s analysis were followed for a mean of 16 months. They included 25 (45%) girls with an overall median age of 6 years at the first acute event. Oligoclonal bands were present in 56%, and both anti-MoG and anti–aquaporin-4 antibodies in 82%.
All children had abnormal brain MRI at baseline, with about 33% having gadolinium-enhancing brain lesions. Spinal cord MRI was abnormal in 50%, with 39% having gadolinium-enhancing lesions. According to the 2010 criteria, only three had a definitive MS diagnosis at baseline. The diagnosis was acute disseminated encephalomyelitis in 51%, clinically isolated syndrome in 31%, radiologically isolated syndrome in 2%, and nonencephalopathic disseminated encephalomyelitis in the remainder.
At baseline, three of those had a definitive MS diagnosis, displaying dissemination in both space and time as required by both the 2010 and 2017 criteria. The addition of oligoclonal band positivity added one more patient over the 2010 criteria, and assessing the cohort with the complete 2017 criteria added three more definitive diagnoses. This was a significant increase in definitive MS diagnoses when compared against the earlier criteria (70% vs. 30%).
Diagnoses changed in 10 other patients during follow-up. The single patient with radiologically isolated syndrome was definitively diagnosed with MS. Of the seven with clinically isolated syndrome, six were diagnosed with MS and one with a relapsing optic neuritis. Of the 28 with a nonencephalopathic encephalitis, 2 were diagnosed with optic neuritis.
The study also confirmed the benefit of adding oligoclonal bands as a diagnostic marker in children. Of those with an MS diagnosis at last follow-up, 71% were positive for the cerebrospinal fluid finding, compared with just 4% of those with a non-MS diagnosis. However, none of those children had anti-MoG antibodies, compared with 58% of those with a non-MS diagnosis. None of the patients were positive for anti–aquaporin-4, regardless of diagnosis.
That finding does not necessarily mean that the absence of anti-MoG antibodies can rule out an MS diagnosis in children, Dr. Arrambide cautioned. Nevertheless, the finding is a useful clinical marker during a diagnostic work-up.
“The presence of oligoclonal bands and the absence of MOG-IgG are both useful biomarkers when evaluating the risk of MS in children with a first demyelinating event,” she said.
She disclosed financial relationships with several pharmaceutical companies.
SOURCE: Arrambide G et al. ECTRIMS 2018, Abstract 64
BERLIN –
The increased accuracy largely hinged on a positive finding of oligoclonal bands in cerebrospinal fluid – a diagnostic hallmark that was not included in the earlier criteria, Georgina Arrambide, MD, said at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis.
“Application to children of the new diagnostic criteria is limited,” said Dr. Arrambide, of the University Hospital Vall d’Hebron Multiple Sclerosis Centre of Catalonia, Barcelona. “And there are still some uncertainties with regard to fluid biomarkers and how they predict or confirm a diagnosis of MS in children, and also their relationship to the disease evolution.”
The updated McDonald criteria are intended to boost early, definitive MS diagnosis, leading to earlier initiation of therapy. They are intended primarily for patients aged 11 years and older who present with a typical clinically isolated syndrome and high probability of MS (Lancet Neurol. 2018;17[2]:162-73).
Dr. Arrambide and her colleagues used the revamped criteria to reassess MS diagnoses in a prospective Spanish cohort of children who experienced an acute first demyelinating event and were diagnosed with the 2010 criteria. The Kids-METOMS-MOGBCN Study enrolls children aged younger than 18 years within 1 year of a first acute demyelinating episode. It includes demographic, clinical, and imaging data, as well as data on oligoclonal bands and antibodies against aquaporin-4 and myelin oligodendrocyte glycoprotein (MoG). Of these fluid biomarkers, only oligoclonal bands are included in the new McDonald criteria.
The 55 children in Dr. Arrambide’s analysis were followed for a mean of 16 months. They included 25 (45%) girls with an overall median age of 6 years at the first acute event. Oligoclonal bands were present in 56%, and both anti-MoG and anti–aquaporin-4 antibodies in 82%.
All children had abnormal brain MRI at baseline, with about 33% having gadolinium-enhancing brain lesions. Spinal cord MRI was abnormal in 50%, with 39% having gadolinium-enhancing lesions. According to the 2010 criteria, only three had a definitive MS diagnosis at baseline. The diagnosis was acute disseminated encephalomyelitis in 51%, clinically isolated syndrome in 31%, radiologically isolated syndrome in 2%, and nonencephalopathic disseminated encephalomyelitis in the remainder.
At baseline, three of those had a definitive MS diagnosis, displaying dissemination in both space and time as required by both the 2010 and 2017 criteria. The addition of oligoclonal band positivity added one more patient over the 2010 criteria, and assessing the cohort with the complete 2017 criteria added three more definitive diagnoses. This was a significant increase in definitive MS diagnoses when compared against the earlier criteria (70% vs. 30%).
Diagnoses changed in 10 other patients during follow-up. The single patient with radiologically isolated syndrome was definitively diagnosed with MS. Of the seven with clinically isolated syndrome, six were diagnosed with MS and one with a relapsing optic neuritis. Of the 28 with a nonencephalopathic encephalitis, 2 were diagnosed with optic neuritis.
The study also confirmed the benefit of adding oligoclonal bands as a diagnostic marker in children. Of those with an MS diagnosis at last follow-up, 71% were positive for the cerebrospinal fluid finding, compared with just 4% of those with a non-MS diagnosis. However, none of those children had anti-MoG antibodies, compared with 58% of those with a non-MS diagnosis. None of the patients were positive for anti–aquaporin-4, regardless of diagnosis.
That finding does not necessarily mean that the absence of anti-MoG antibodies can rule out an MS diagnosis in children, Dr. Arrambide cautioned. Nevertheless, the finding is a useful clinical marker during a diagnostic work-up.
“The presence of oligoclonal bands and the absence of MOG-IgG are both useful biomarkers when evaluating the risk of MS in children with a first demyelinating event,” she said.
She disclosed financial relationships with several pharmaceutical companies.
SOURCE: Arrambide G et al. ECTRIMS 2018, Abstract 64
REPORTING FROM ECTRIMS 2018
Key clinical point: The revised McDonald criteria increased definitive multiple sclerosis diagnoses in children.
Major finding: The 2017 criteria boosted pediatric diagnostic accuracy by 40%.
Study details: The prospective cohort study comprised 55 patients.
Disclosures: Dr. Arrambide disclosed relationships with several pharmaceutical companies.
Source: Arrambide G et al. ECTRIMS 2018, Abstract 64.
No elevated cancer risk with MS therapies in COMBAT-MS data
BERLIN – The risk of cancer – and breast cancer in particular – was not elevated above background levels in a large cohort of multiple sclerosis patients taking disease-modifying therapies.
Those findings from the large Nordic cohort study COMBAT-MS stand in contrast to previous work showing an elevated cancer risk for some monoclonal antibodies.
After statistical adjustment and use of rituximab (Rituxan) as the standard, the hazard ratio (HR) for any malignancy with fingolimod (Gilenya) was 1.74 (95% confidence interval, 0.92-3.28). For natalizumab (Tysabri), the malignancy HR was 1.06 (95% CI, 0.53-2.10), said Peter Alping, a PhD student in the department of clinical neuroscience at the Karolinska Institute, Stockholm.
Only limited data exist for real-world multiple sclerosis (MS) cohorts who have been exposed to novel disease-modifying therapies, said Mr. Alping, presenting the findings at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis. Rituximab has been studied in patients with rheumatoid arthritis, but the treatment regimens differ, as do patient characteristics, he noted. However, surveillance for risk of malignancy is important in these therapies, he said, “since modern disease-modifying therapies exert a more profound effect on the immune system, and we know that the immune system is vital in fighting and preventing cancers.”
The anti-CD20 monoclonal antibody ocrelizumab was studied in the ORATORIO trial. “There, they saw an imbalance in the numbers of breast cancers between the ocrelizumab and placebo groups,” said Mr. Alping, with raw data showing four breast cancers in the ocrelizumab population. However, this would translate to 26.1 cancers per 10,000 person-years, as opposed to the zero breast cancers seen in the placebo group (N Engl J Med. 2017;376:209-20).
“To what degree is cancer risk a concern with novel [disease-modifying therapy] use in MS?” Mr. Alping asked.
To answer the question, he and his colleagues from the Karolinska Institute sought to compare the risk of cancer in MS patients who were treated with rituximab, fingolimod, and natalizumab.
To do this, they conducted a nationwide cohort study using the Swedish MS registry, looking at treatment episodes between 2011 and 2016. In Sweden, the MS registry is also linked to the overall patient registry, as well as registries for cancer and prescription drug use. In addition, patient data are linked to national census data.
Mr. Alping and his colleagues looked at data for the first instance of use for an MS patient of rituximab, natalizumab, and/or fingolimod between the years 2011 and 2016. Then, they matched patient records from the general population by age, sex, and geographic location, enrolling the matched controls at the same time point as the MS match entered the study.
Patients treated with mitoxantrone, those who emigrated, and those who died during the study period were excluded from the study.
The statistical analysis, Mr. Alping said, used an ever-treated approach and didn’t attempt to weight exposure duration or dose. However, statistical adjustments were made for patient and control demographics and medical history, for any previous history of cancer, and for MS disease characteristics.
At baseline, 1,558 patients had been treated with fingolimod, 1,761 with natalizumab, and 3,012 with rituximab. A little less than one-third of the patients (26.3%-31.6%) were male, and the mean age was 35-43 years. Most patients (66%-86%) had undergone one or two previous therapies. The mean Expanded Disability Status Scale (EDSS) score was 2.20-2.88. Few patients (0.9%-1.7%) had any history of previous cancer.
Overall, the incidence of cancer in the MS cohort ranged from 23.09 per 10,000 person-years for rituximab ever-takers to 46.28 for those who had ever taken fingolimod. Among the general population, rates of any malignancy were 29.62 per 10,000 person-years.
Looking just at breast cancer, rates in the MS cohort ranged from 2.19 to 2.92/10,000 person-years. For the general population, the rate was 12.07/10,000 person-years.
However, using a Cox regression analysis employing MS-specific covariates and using rituximab as the reference, Mr. Alping and his colleagues calculated an inverse proportion-weighted hazard ratio for any malignancy under the various treatment conditions. Using this analysis, the HR for any cancer with fingolimod was 1.74 (95% CI, 0.92-3.28). For natalizumab, the malignancy HR was 1.06 (95% CI, 0.53-2.10).
Among just women taking rituximab, 2,274 therapy starts occurred, and one breast cancer was seen in 4,050 person-years. This yielded an incidence of 2.32 cancers per 10,000 person-years (95% CI, 0.06-12.9). This contrasts with the adjusted incidence rate in the general female population of 11.06 breast cancers per 10,000 person-years.
Looking at all the therapy episodes captured in the cohort study, there were 6,660 incidences of therapy initiation, and 52 malignancies were seen over 17,283 person-years, Mr. Alping said.
“For malignant cancer of any type, we found no increased risk for rituximab, compared to fingolimod and natalizumab,” Mr. Alping said, pointing to the wide confidence intervals in all the adjusted data. The incidence of breast cancer in women who have taken rituximab, he said, is “comparable to, or possibly lower than, that of the general female population, and lower than the incidence rate reported in the ORATORIO trial for ocrelizumab.
“The overall cancer risk and risk of breast cancer might not be major concerns short term when treating MS patients with rituximab relative to other disease-modifying therapies,” he said.
The study was partially funded by the Patient-Centered Outcomes Research Institute. Mr. Alping reported no conflicts of interest. One study author reported relationships with several pharmaceutical companies.
[email protected]
SOURCE: Alping P et al. Mult Scler. 2018;24(Suppl 2):36. Abstract 89.
BERLIN – The risk of cancer – and breast cancer in particular – was not elevated above background levels in a large cohort of multiple sclerosis patients taking disease-modifying therapies.
Those findings from the large Nordic cohort study COMBAT-MS stand in contrast to previous work showing an elevated cancer risk for some monoclonal antibodies.
After statistical adjustment and use of rituximab (Rituxan) as the standard, the hazard ratio (HR) for any malignancy with fingolimod (Gilenya) was 1.74 (95% confidence interval, 0.92-3.28). For natalizumab (Tysabri), the malignancy HR was 1.06 (95% CI, 0.53-2.10), said Peter Alping, a PhD student in the department of clinical neuroscience at the Karolinska Institute, Stockholm.
Only limited data exist for real-world multiple sclerosis (MS) cohorts who have been exposed to novel disease-modifying therapies, said Mr. Alping, presenting the findings at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis. Rituximab has been studied in patients with rheumatoid arthritis, but the treatment regimens differ, as do patient characteristics, he noted. However, surveillance for risk of malignancy is important in these therapies, he said, “since modern disease-modifying therapies exert a more profound effect on the immune system, and we know that the immune system is vital in fighting and preventing cancers.”
The anti-CD20 monoclonal antibody ocrelizumab was studied in the ORATORIO trial. “There, they saw an imbalance in the numbers of breast cancers between the ocrelizumab and placebo groups,” said Mr. Alping, with raw data showing four breast cancers in the ocrelizumab population. However, this would translate to 26.1 cancers per 10,000 person-years, as opposed to the zero breast cancers seen in the placebo group (N Engl J Med. 2017;376:209-20).
“To what degree is cancer risk a concern with novel [disease-modifying therapy] use in MS?” Mr. Alping asked.
To answer the question, he and his colleagues from the Karolinska Institute sought to compare the risk of cancer in MS patients who were treated with rituximab, fingolimod, and natalizumab.
To do this, they conducted a nationwide cohort study using the Swedish MS registry, looking at treatment episodes between 2011 and 2016. In Sweden, the MS registry is also linked to the overall patient registry, as well as registries for cancer and prescription drug use. In addition, patient data are linked to national census data.
Mr. Alping and his colleagues looked at data for the first instance of use for an MS patient of rituximab, natalizumab, and/or fingolimod between the years 2011 and 2016. Then, they matched patient records from the general population by age, sex, and geographic location, enrolling the matched controls at the same time point as the MS match entered the study.
Patients treated with mitoxantrone, those who emigrated, and those who died during the study period were excluded from the study.
The statistical analysis, Mr. Alping said, used an ever-treated approach and didn’t attempt to weight exposure duration or dose. However, statistical adjustments were made for patient and control demographics and medical history, for any previous history of cancer, and for MS disease characteristics.
At baseline, 1,558 patients had been treated with fingolimod, 1,761 with natalizumab, and 3,012 with rituximab. A little less than one-third of the patients (26.3%-31.6%) were male, and the mean age was 35-43 years. Most patients (66%-86%) had undergone one or two previous therapies. The mean Expanded Disability Status Scale (EDSS) score was 2.20-2.88. Few patients (0.9%-1.7%) had any history of previous cancer.
Overall, the incidence of cancer in the MS cohort ranged from 23.09 per 10,000 person-years for rituximab ever-takers to 46.28 for those who had ever taken fingolimod. Among the general population, rates of any malignancy were 29.62 per 10,000 person-years.
Looking just at breast cancer, rates in the MS cohort ranged from 2.19 to 2.92/10,000 person-years. For the general population, the rate was 12.07/10,000 person-years.
However, using a Cox regression analysis employing MS-specific covariates and using rituximab as the reference, Mr. Alping and his colleagues calculated an inverse proportion-weighted hazard ratio for any malignancy under the various treatment conditions. Using this analysis, the HR for any cancer with fingolimod was 1.74 (95% CI, 0.92-3.28). For natalizumab, the malignancy HR was 1.06 (95% CI, 0.53-2.10).
Among just women taking rituximab, 2,274 therapy starts occurred, and one breast cancer was seen in 4,050 person-years. This yielded an incidence of 2.32 cancers per 10,000 person-years (95% CI, 0.06-12.9). This contrasts with the adjusted incidence rate in the general female population of 11.06 breast cancers per 10,000 person-years.
Looking at all the therapy episodes captured in the cohort study, there were 6,660 incidences of therapy initiation, and 52 malignancies were seen over 17,283 person-years, Mr. Alping said.
“For malignant cancer of any type, we found no increased risk for rituximab, compared to fingolimod and natalizumab,” Mr. Alping said, pointing to the wide confidence intervals in all the adjusted data. The incidence of breast cancer in women who have taken rituximab, he said, is “comparable to, or possibly lower than, that of the general female population, and lower than the incidence rate reported in the ORATORIO trial for ocrelizumab.
“The overall cancer risk and risk of breast cancer might not be major concerns short term when treating MS patients with rituximab relative to other disease-modifying therapies,” he said.
The study was partially funded by the Patient-Centered Outcomes Research Institute. Mr. Alping reported no conflicts of interest. One study author reported relationships with several pharmaceutical companies.
[email protected]
SOURCE: Alping P et al. Mult Scler. 2018;24(Suppl 2):36. Abstract 89.
BERLIN – The risk of cancer – and breast cancer in particular – was not elevated above background levels in a large cohort of multiple sclerosis patients taking disease-modifying therapies.
Those findings from the large Nordic cohort study COMBAT-MS stand in contrast to previous work showing an elevated cancer risk for some monoclonal antibodies.
After statistical adjustment and use of rituximab (Rituxan) as the standard, the hazard ratio (HR) for any malignancy with fingolimod (Gilenya) was 1.74 (95% confidence interval, 0.92-3.28). For natalizumab (Tysabri), the malignancy HR was 1.06 (95% CI, 0.53-2.10), said Peter Alping, a PhD student in the department of clinical neuroscience at the Karolinska Institute, Stockholm.
Only limited data exist for real-world multiple sclerosis (MS) cohorts who have been exposed to novel disease-modifying therapies, said Mr. Alping, presenting the findings at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis. Rituximab has been studied in patients with rheumatoid arthritis, but the treatment regimens differ, as do patient characteristics, he noted. However, surveillance for risk of malignancy is important in these therapies, he said, “since modern disease-modifying therapies exert a more profound effect on the immune system, and we know that the immune system is vital in fighting and preventing cancers.”
The anti-CD20 monoclonal antibody ocrelizumab was studied in the ORATORIO trial. “There, they saw an imbalance in the numbers of breast cancers between the ocrelizumab and placebo groups,” said Mr. Alping, with raw data showing four breast cancers in the ocrelizumab population. However, this would translate to 26.1 cancers per 10,000 person-years, as opposed to the zero breast cancers seen in the placebo group (N Engl J Med. 2017;376:209-20).
“To what degree is cancer risk a concern with novel [disease-modifying therapy] use in MS?” Mr. Alping asked.
To answer the question, he and his colleagues from the Karolinska Institute sought to compare the risk of cancer in MS patients who were treated with rituximab, fingolimod, and natalizumab.
To do this, they conducted a nationwide cohort study using the Swedish MS registry, looking at treatment episodes between 2011 and 2016. In Sweden, the MS registry is also linked to the overall patient registry, as well as registries for cancer and prescription drug use. In addition, patient data are linked to national census data.
Mr. Alping and his colleagues looked at data for the first instance of use for an MS patient of rituximab, natalizumab, and/or fingolimod between the years 2011 and 2016. Then, they matched patient records from the general population by age, sex, and geographic location, enrolling the matched controls at the same time point as the MS match entered the study.
Patients treated with mitoxantrone, those who emigrated, and those who died during the study period were excluded from the study.
The statistical analysis, Mr. Alping said, used an ever-treated approach and didn’t attempt to weight exposure duration or dose. However, statistical adjustments were made for patient and control demographics and medical history, for any previous history of cancer, and for MS disease characteristics.
At baseline, 1,558 patients had been treated with fingolimod, 1,761 with natalizumab, and 3,012 with rituximab. A little less than one-third of the patients (26.3%-31.6%) were male, and the mean age was 35-43 years. Most patients (66%-86%) had undergone one or two previous therapies. The mean Expanded Disability Status Scale (EDSS) score was 2.20-2.88. Few patients (0.9%-1.7%) had any history of previous cancer.
Overall, the incidence of cancer in the MS cohort ranged from 23.09 per 10,000 person-years for rituximab ever-takers to 46.28 for those who had ever taken fingolimod. Among the general population, rates of any malignancy were 29.62 per 10,000 person-years.
Looking just at breast cancer, rates in the MS cohort ranged from 2.19 to 2.92/10,000 person-years. For the general population, the rate was 12.07/10,000 person-years.
However, using a Cox regression analysis employing MS-specific covariates and using rituximab as the reference, Mr. Alping and his colleagues calculated an inverse proportion-weighted hazard ratio for any malignancy under the various treatment conditions. Using this analysis, the HR for any cancer with fingolimod was 1.74 (95% CI, 0.92-3.28). For natalizumab, the malignancy HR was 1.06 (95% CI, 0.53-2.10).
Among just women taking rituximab, 2,274 therapy starts occurred, and one breast cancer was seen in 4,050 person-years. This yielded an incidence of 2.32 cancers per 10,000 person-years (95% CI, 0.06-12.9). This contrasts with the adjusted incidence rate in the general female population of 11.06 breast cancers per 10,000 person-years.
Looking at all the therapy episodes captured in the cohort study, there were 6,660 incidences of therapy initiation, and 52 malignancies were seen over 17,283 person-years, Mr. Alping said.
“For malignant cancer of any type, we found no increased risk for rituximab, compared to fingolimod and natalizumab,” Mr. Alping said, pointing to the wide confidence intervals in all the adjusted data. The incidence of breast cancer in women who have taken rituximab, he said, is “comparable to, or possibly lower than, that of the general female population, and lower than the incidence rate reported in the ORATORIO trial for ocrelizumab.
“The overall cancer risk and risk of breast cancer might not be major concerns short term when treating MS patients with rituximab relative to other disease-modifying therapies,” he said.
The study was partially funded by the Patient-Centered Outcomes Research Institute. Mr. Alping reported no conflicts of interest. One study author reported relationships with several pharmaceutical companies.
[email protected]
SOURCE: Alping P et al. Mult Scler. 2018;24(Suppl 2):36. Abstract 89.
REPORTING FROM ECTRIMS 2018
Key clinical point:
Major finding: The hazard ratios for fingolimod and natalizumab versus rituximab were 1.74 and 1.06, respectively, with confidence intervals crossing 1.
Study details: Case-matched observational cohort study of 6,331 DMT-taking patients with MS.
Disclosures: The study was sponsored in part by the Patient-Centered Outcomes Research Institute. Mr. Alping reported no disclosures; one study author reported financial relationships with multiple pharmaceutical companies.
Source: Alping P et al. Mult Scler. 2018;24(Suppl 2):36. Abstract 89.