User login
Primary, metastatic ccRCC share mutational features
A comparison of the genomic landscapes of both primary and metastatic clear cell renal cell carcinoma (ccRCC) found no significant differences in gene expression or mutational burden between the disease states, suggesting that there is no single genetic driver of metastases, investigators reported.
An analysis of targeted next-generation sequencing of both primary tumors and metastases in two independent patient cohorts showed that only the gene encoding for the tumor suppressor TP53 was significantly more frequently mutated in metastases, compared with primary tumors, but this finding did not pass a false positive test (false discovery rate), noted Toni K. Choueiri, MD, from the Dana-Farber Cancer Institute in Boston, and his colleagues, in the British Journal of Cancer.
“No other gene had significant difference in the cohort frequency of mutations between the metastases and primary tumors. Mutation burden was not significantly different between the metastases and primary tumors or between metastatic sites,” they wrote.
Frequently mutated genes in ccRCC include VHL, the gene encoding for von Hippel–Lindau syndrome, as well as tumor suppressor genes such as PBRM1, SEDT2, BAP1 and KDM5C, but few mutations are clinically actionable, the investigators noted. “However, the value of genomic alterations will be determined by understanding the interactions between acquired genetic alterations, treatments received, heterogeneity, and the dynamics of mutations during evolution of disease.”
To see whether they could improve understanding of the genomic differences between primary and metastatic ccRCC and potentially develop personalized therapies, the investigators studied targeted next-generation sequencing data from two separate cohorts.
The first cohort included data on 349 ccRCC primary tumors and 229 unmatched cases of metastatic ccRCC from the Foundation Medicine database. The second, a validation cohort, included data on 177 ccRCC primary tumors and 80 metastases from patients treated at Dana-Farber. In each cohort, sequencing was performed on 275 genes and intronic regions in 30 genes for a total of 282 unique genes.
In cohort 1, which included tumor samples from 417 men and 169 women with a median age of 58 years, the frequency of mutations was similar in primary tumors and metastases. As noted before, mutations in TP53 were significantly more frequent in metastases than in primary tumors, detected in 14.85% versus 8.90% of samples, respectively (P = .031). This difference did not, however, pass the false discovery rate test (q = 0.21). Two other tumor suppressor genes, PBRM1 and KDM5C, were numerically but not significantly more frequent in metastases.
There were no differences in median tumor mutational burden between primary and metastatic samples and no difference in either mutations or mutational burden across different metastatic sites.
In cohort 2 there were no significantly different mutational frequencies between primary and metastatic samples for any gene and no differences in median tumor mutational burden.
An analysis comparing the frequency of gene mutations in primary tumors of patients in this cohort who went on to develop metastatic disease versus those of patients with only localized disease showed that, after a median follow-up of 21.9 months, there were no significant differences in either mutational frequency or tumor mutational burden.
“It is currently unknown if cohortwide genomic alterations in RCC metastases have a different genomic profile, including potential actionable mutations, compared to samples derived from the primary site. To our knowledge, our analysis is the largest genomic ccRCC study that compares cohortwide mutational differences between metastases and primary tumors,” the investigators wrote.
They acknowledged that because they did not match primary tumors with metastatic tumors in the same patients they were unable to evaluate how individual tumors evolve over time or how systemic therapies may alter the tumor genomic landscape.
Dr. Choueri is supported in part by the Dana-Farber/Harvard Cancer Center Kidney SPORE, the Kohlberg Chair at Harvard Medical School and the Trust Family, Michael Brigham, and Loker Pinard Funds for Kidney Cancer Research at the Dana-Farber Cancer Institute. Six of the study’s coauthors are employed by Foundation Medicine. The remaining authors declared no competing interests.
SOURCE: Choueiri TK et al. Br J Cancer. 2018 May;118(9):1238-42.
A comparison of the genomic landscapes of both primary and metastatic clear cell renal cell carcinoma (ccRCC) found no significant differences in gene expression or mutational burden between the disease states, suggesting that there is no single genetic driver of metastases, investigators reported.
An analysis of targeted next-generation sequencing of both primary tumors and metastases in two independent patient cohorts showed that only the gene encoding for the tumor suppressor TP53 was significantly more frequently mutated in metastases, compared with primary tumors, but this finding did not pass a false positive test (false discovery rate), noted Toni K. Choueiri, MD, from the Dana-Farber Cancer Institute in Boston, and his colleagues, in the British Journal of Cancer.
“No other gene had significant difference in the cohort frequency of mutations between the metastases and primary tumors. Mutation burden was not significantly different between the metastases and primary tumors or between metastatic sites,” they wrote.
Frequently mutated genes in ccRCC include VHL, the gene encoding for von Hippel–Lindau syndrome, as well as tumor suppressor genes such as PBRM1, SEDT2, BAP1 and KDM5C, but few mutations are clinically actionable, the investigators noted. “However, the value of genomic alterations will be determined by understanding the interactions between acquired genetic alterations, treatments received, heterogeneity, and the dynamics of mutations during evolution of disease.”
To see whether they could improve understanding of the genomic differences between primary and metastatic ccRCC and potentially develop personalized therapies, the investigators studied targeted next-generation sequencing data from two separate cohorts.
The first cohort included data on 349 ccRCC primary tumors and 229 unmatched cases of metastatic ccRCC from the Foundation Medicine database. The second, a validation cohort, included data on 177 ccRCC primary tumors and 80 metastases from patients treated at Dana-Farber. In each cohort, sequencing was performed on 275 genes and intronic regions in 30 genes for a total of 282 unique genes.
In cohort 1, which included tumor samples from 417 men and 169 women with a median age of 58 years, the frequency of mutations was similar in primary tumors and metastases. As noted before, mutations in TP53 were significantly more frequent in metastases than in primary tumors, detected in 14.85% versus 8.90% of samples, respectively (P = .031). This difference did not, however, pass the false discovery rate test (q = 0.21). Two other tumor suppressor genes, PBRM1 and KDM5C, were numerically but not significantly more frequent in metastases.
There were no differences in median tumor mutational burden between primary and metastatic samples and no difference in either mutations or mutational burden across different metastatic sites.
In cohort 2 there were no significantly different mutational frequencies between primary and metastatic samples for any gene and no differences in median tumor mutational burden.
An analysis comparing the frequency of gene mutations in primary tumors of patients in this cohort who went on to develop metastatic disease versus those of patients with only localized disease showed that, after a median follow-up of 21.9 months, there were no significant differences in either mutational frequency or tumor mutational burden.
“It is currently unknown if cohortwide genomic alterations in RCC metastases have a different genomic profile, including potential actionable mutations, compared to samples derived from the primary site. To our knowledge, our analysis is the largest genomic ccRCC study that compares cohortwide mutational differences between metastases and primary tumors,” the investigators wrote.
They acknowledged that because they did not match primary tumors with metastatic tumors in the same patients they were unable to evaluate how individual tumors evolve over time or how systemic therapies may alter the tumor genomic landscape.
Dr. Choueri is supported in part by the Dana-Farber/Harvard Cancer Center Kidney SPORE, the Kohlberg Chair at Harvard Medical School and the Trust Family, Michael Brigham, and Loker Pinard Funds for Kidney Cancer Research at the Dana-Farber Cancer Institute. Six of the study’s coauthors are employed by Foundation Medicine. The remaining authors declared no competing interests.
SOURCE: Choueiri TK et al. Br J Cancer. 2018 May;118(9):1238-42.
A comparison of the genomic landscapes of both primary and metastatic clear cell renal cell carcinoma (ccRCC) found no significant differences in gene expression or mutational burden between the disease states, suggesting that there is no single genetic driver of metastases, investigators reported.
An analysis of targeted next-generation sequencing of both primary tumors and metastases in two independent patient cohorts showed that only the gene encoding for the tumor suppressor TP53 was significantly more frequently mutated in metastases, compared with primary tumors, but this finding did not pass a false positive test (false discovery rate), noted Toni K. Choueiri, MD, from the Dana-Farber Cancer Institute in Boston, and his colleagues, in the British Journal of Cancer.
“No other gene had significant difference in the cohort frequency of mutations between the metastases and primary tumors. Mutation burden was not significantly different between the metastases and primary tumors or between metastatic sites,” they wrote.
Frequently mutated genes in ccRCC include VHL, the gene encoding for von Hippel–Lindau syndrome, as well as tumor suppressor genes such as PBRM1, SEDT2, BAP1 and KDM5C, but few mutations are clinically actionable, the investigators noted. “However, the value of genomic alterations will be determined by understanding the interactions between acquired genetic alterations, treatments received, heterogeneity, and the dynamics of mutations during evolution of disease.”
To see whether they could improve understanding of the genomic differences between primary and metastatic ccRCC and potentially develop personalized therapies, the investigators studied targeted next-generation sequencing data from two separate cohorts.
The first cohort included data on 349 ccRCC primary tumors and 229 unmatched cases of metastatic ccRCC from the Foundation Medicine database. The second, a validation cohort, included data on 177 ccRCC primary tumors and 80 metastases from patients treated at Dana-Farber. In each cohort, sequencing was performed on 275 genes and intronic regions in 30 genes for a total of 282 unique genes.
In cohort 1, which included tumor samples from 417 men and 169 women with a median age of 58 years, the frequency of mutations was similar in primary tumors and metastases. As noted before, mutations in TP53 were significantly more frequent in metastases than in primary tumors, detected in 14.85% versus 8.90% of samples, respectively (P = .031). This difference did not, however, pass the false discovery rate test (q = 0.21). Two other tumor suppressor genes, PBRM1 and KDM5C, were numerically but not significantly more frequent in metastases.
There were no differences in median tumor mutational burden between primary and metastatic samples and no difference in either mutations or mutational burden across different metastatic sites.
In cohort 2 there were no significantly different mutational frequencies between primary and metastatic samples for any gene and no differences in median tumor mutational burden.
An analysis comparing the frequency of gene mutations in primary tumors of patients in this cohort who went on to develop metastatic disease versus those of patients with only localized disease showed that, after a median follow-up of 21.9 months, there were no significant differences in either mutational frequency or tumor mutational burden.
“It is currently unknown if cohortwide genomic alterations in RCC metastases have a different genomic profile, including potential actionable mutations, compared to samples derived from the primary site. To our knowledge, our analysis is the largest genomic ccRCC study that compares cohortwide mutational differences between metastases and primary tumors,” the investigators wrote.
They acknowledged that because they did not match primary tumors with metastatic tumors in the same patients they were unable to evaluate how individual tumors evolve over time or how systemic therapies may alter the tumor genomic landscape.
Dr. Choueri is supported in part by the Dana-Farber/Harvard Cancer Center Kidney SPORE, the Kohlberg Chair at Harvard Medical School and the Trust Family, Michael Brigham, and Loker Pinard Funds for Kidney Cancer Research at the Dana-Farber Cancer Institute. Six of the study’s coauthors are employed by Foundation Medicine. The remaining authors declared no competing interests.
SOURCE: Choueiri TK et al. Br J Cancer. 2018 May;118(9):1238-42.
FROM THE BRITISH JOURNAL OF CANCER
Key clinical point: There does not appear to be a single-gene driver of metastases in patients with clear cell renal cell carcinoma.
Major finding: There were no significant differences in mutational frequency or tumor mutational burden between primary and metastatic clear cell renal cell carcinoma.
Study details: A targeted next-generation sequencing analysis of data from two independent patient cohorts.
Disclosures: Dr. Choueri is supported in part by the Dana-Farber/Harvard Cancer Center Kidney SPORE, the Kohlberg Chair at Harvard Medical School and the Trust Family, Michael Brigham, and Loker Pinard Funds for Kidney Cancer Research at the Dana-Farber Cancer Institute. Six of the study’s coauthors are employed by Foundation Medicine. The remaining authors reported no competing interests.
Source: Choueiri TK et al. Br J Cancer. 2018 May;118(9):1238-42.
Do Dimethyl Fumarate and Teriflunomide Have Equivalent Efficacy?
New T2 lesions are more likely on teriflunomide, which may contribute to its higher rate of discontinuation.
BERLIN—Dimethyl fumarate and teriflunomide have similar efficacy in terms of risk of relapse and worsening of Expanded Disability Status Scale (EDSS) score after one and two years of treatment, according to data presented at ECTRIMS 2018. Significantly more patients have new T2 lesions after two years of teriflunomide, however, compared with dimethyl fumarate, and this outcome may explain an increased treatment withdrawal for lack of efficacy among patients receiving teriflunomide.
Teriflunomide and dimethyl fumarate have been approved as first-line treatments for patients with relapsing-remitting multiple sclerosis (MS). To date, no randomized controlled nor observational studies have compared their relative efficacies. David A. Laplaud, MD, PhD, a team leader at the Center of Research in Transplantation and Immunology in Nantes, France, and colleagues conducted a study to compare the effects of teriflunomide and dimethyl fumarate on clinical and MRI outcomes in patients with relapsing-remitting MS from 34 MS centers participating in the French prospective national cohort of MS patients.
The investigators included 1,770 patients with relapsing-remitting MS in the study. In all, 713 participants received teriflunomide, and 1,057 received dimethyl fumarate. Participants were aged 18 to 65 and had an EDSS score of 0 to 5.5 and an available brain MRI performed within six months before treatment initiation. The outcomes under investigation were the proportion of patients with at least one relapse in the year and the two years following teriflunomide or dimethyl fumarate initiation, the proportion of patients with at least one new T2 lesion at one and two years, the number of patients with an increased EDSS score at one and two years, and reasons for treatment cessation at one and two years. For statistical analyses, the outcomes were modeled with propensity scores and logistic regressions by using weighted likelihood maximization and a robust variance estimator.
The confounder-adjusted proportion of patients with at least one relapse at one and two years of treatment was similar in the teriflunomide group and the dimethyl fumarate group (21.6% vs 20.2% for the first year, 30.4% vs 29.5% at two years). Likewise, a similar percentage of patients had an increase of EDSS score at one and two years in the teriflunomide group (27.4% and 41.6%, respectively) and the dimethyl fumarate group (27.1% and 40.6%, respectively). MRI comparisons, however, revealed that the confounder-adjusted proportion of patients with at least one new T2 lesion at two years was significantly lower in patients treated with dimethyl fumarate, compared with teriflunomide (60.8% vs 72.2%; odds ratio [OR], 0.6). The reason for treatment withdrawal at two years was lack of efficacy in 8.5% of patients who received dimethyl fumarate versus 14.5% of patients who received teriflunomide (OR, 0.54).
New T2 lesions are more likely on teriflunomide, which may contribute to its higher rate of discontinuation.
New T2 lesions are more likely on teriflunomide, which may contribute to its higher rate of discontinuation.
BERLIN—Dimethyl fumarate and teriflunomide have similar efficacy in terms of risk of relapse and worsening of Expanded Disability Status Scale (EDSS) score after one and two years of treatment, according to data presented at ECTRIMS 2018. Significantly more patients have new T2 lesions after two years of teriflunomide, however, compared with dimethyl fumarate, and this outcome may explain an increased treatment withdrawal for lack of efficacy among patients receiving teriflunomide.
Teriflunomide and dimethyl fumarate have been approved as first-line treatments for patients with relapsing-remitting multiple sclerosis (MS). To date, no randomized controlled nor observational studies have compared their relative efficacies. David A. Laplaud, MD, PhD, a team leader at the Center of Research in Transplantation and Immunology in Nantes, France, and colleagues conducted a study to compare the effects of teriflunomide and dimethyl fumarate on clinical and MRI outcomes in patients with relapsing-remitting MS from 34 MS centers participating in the French prospective national cohort of MS patients.
The investigators included 1,770 patients with relapsing-remitting MS in the study. In all, 713 participants received teriflunomide, and 1,057 received dimethyl fumarate. Participants were aged 18 to 65 and had an EDSS score of 0 to 5.5 and an available brain MRI performed within six months before treatment initiation. The outcomes under investigation were the proportion of patients with at least one relapse in the year and the two years following teriflunomide or dimethyl fumarate initiation, the proportion of patients with at least one new T2 lesion at one and two years, the number of patients with an increased EDSS score at one and two years, and reasons for treatment cessation at one and two years. For statistical analyses, the outcomes were modeled with propensity scores and logistic regressions by using weighted likelihood maximization and a robust variance estimator.
The confounder-adjusted proportion of patients with at least one relapse at one and two years of treatment was similar in the teriflunomide group and the dimethyl fumarate group (21.6% vs 20.2% for the first year, 30.4% vs 29.5% at two years). Likewise, a similar percentage of patients had an increase of EDSS score at one and two years in the teriflunomide group (27.4% and 41.6%, respectively) and the dimethyl fumarate group (27.1% and 40.6%, respectively). MRI comparisons, however, revealed that the confounder-adjusted proportion of patients with at least one new T2 lesion at two years was significantly lower in patients treated with dimethyl fumarate, compared with teriflunomide (60.8% vs 72.2%; odds ratio [OR], 0.6). The reason for treatment withdrawal at two years was lack of efficacy in 8.5% of patients who received dimethyl fumarate versus 14.5% of patients who received teriflunomide (OR, 0.54).
BERLIN—Dimethyl fumarate and teriflunomide have similar efficacy in terms of risk of relapse and worsening of Expanded Disability Status Scale (EDSS) score after one and two years of treatment, according to data presented at ECTRIMS 2018. Significantly more patients have new T2 lesions after two years of teriflunomide, however, compared with dimethyl fumarate, and this outcome may explain an increased treatment withdrawal for lack of efficacy among patients receiving teriflunomide.
Teriflunomide and dimethyl fumarate have been approved as first-line treatments for patients with relapsing-remitting multiple sclerosis (MS). To date, no randomized controlled nor observational studies have compared their relative efficacies. David A. Laplaud, MD, PhD, a team leader at the Center of Research in Transplantation and Immunology in Nantes, France, and colleagues conducted a study to compare the effects of teriflunomide and dimethyl fumarate on clinical and MRI outcomes in patients with relapsing-remitting MS from 34 MS centers participating in the French prospective national cohort of MS patients.
The investigators included 1,770 patients with relapsing-remitting MS in the study. In all, 713 participants received teriflunomide, and 1,057 received dimethyl fumarate. Participants were aged 18 to 65 and had an EDSS score of 0 to 5.5 and an available brain MRI performed within six months before treatment initiation. The outcomes under investigation were the proportion of patients with at least one relapse in the year and the two years following teriflunomide or dimethyl fumarate initiation, the proportion of patients with at least one new T2 lesion at one and two years, the number of patients with an increased EDSS score at one and two years, and reasons for treatment cessation at one and two years. For statistical analyses, the outcomes were modeled with propensity scores and logistic regressions by using weighted likelihood maximization and a robust variance estimator.
The confounder-adjusted proportion of patients with at least one relapse at one and two years of treatment was similar in the teriflunomide group and the dimethyl fumarate group (21.6% vs 20.2% for the first year, 30.4% vs 29.5% at two years). Likewise, a similar percentage of patients had an increase of EDSS score at one and two years in the teriflunomide group (27.4% and 41.6%, respectively) and the dimethyl fumarate group (27.1% and 40.6%, respectively). MRI comparisons, however, revealed that the confounder-adjusted proportion of patients with at least one new T2 lesion at two years was significantly lower in patients treated with dimethyl fumarate, compared with teriflunomide (60.8% vs 72.2%; odds ratio [OR], 0.6). The reason for treatment withdrawal at two years was lack of efficacy in 8.5% of patients who received dimethyl fumarate versus 14.5% of patients who received teriflunomide (OR, 0.54).
Task force advises behavioral intervention for obese adults
The U.S. Preventive Services Task Force advises clinicians to refer or offer intensive behavioral weight-loss interventions to obese adults, according to an updated recommendation statement published in JAMA.

Obesity affects more than one-third of U.S. adults, according to federal statistics. It carries increased risk for comorbidities including heart disease, diabetes, and various cancers, as well as increased risk of death among adults younger than 65 years, noted lead author Susan J. Curry, PhD, of the University of Iowa, Iowa City, and members of the Task Force.
The B recommendation applies to obese adults; obesity was defined as a body mass index of 30 kg/m2 or higher. The evidence review focused on interventions for weight loss and weight maintenance that could be provided in primary care or referred from primary care, such as nutrition counseling, exercise strategies, and goal setting.
The Task Force found adequate evidence that behavior-based weight-loss interventions improved weight, reduced incidence of type 2 diabetes, and helped maintain weight loss after interventions ended.
The Task Force found small to no evidence of harm associated with any of the behavioral weight-loss interventions, which included group sessions, personal sessions, print-based interventions, and technology-based interventions (such as text messages). Although interventions that combined drug therapy with behavioral intervention resulted in greater weight loss over 12-18 months, compared with behavioral interventions alone, the attrition rates were high and data on weight-loss maintenance after discontinuation of the drugs were limited, the Task Force noted.
“As a result, the USPSTF encourages clinicians to promote behavioral interventions as the primary focus of effective interventions for weight loss in adults,” they wrote.
The Task Force acknowledged the need for future research in subgroups and to explore whether factors such as genetics and untreated conditions are barriers to behavior-based weight loss interventions.
In the evidence review published in JAMA, Erin S. LeBlanc, MD, of Kaiser Permanente in Portland, Ore., and her colleagues reviewed data from 122 randomized, controlled trials including more than 62,000 persons and 2 observational studies including more than 209,000 persons.
The researchers found behavioral interventions were associated with greater weight loss and less risk of developing diabetes, compared with control interventions.
Intensive behavioral interventions included counseling patients about healthy eating, encouraging physical activity, setting weight and health goals, and assisting with weight monitoring. The interventions ranged from text messaging to in-person sessions for individuals or groups. The average absolute weight loss in the trials included in the review ranged from –0.5 kg to –9.3 kg (–1.1 lb to –20.5 lb) for intervention patients and from +1.4 kg to –5.6 kg (+3.1 lb to –12.3 lb) in controls.
Limitations of the review included a lack of data on population subgroups and a lack of long-term data on weight and health outcomes, the researchers noted. However, the results support the value of behavior-based therapy for obesity treatment.
The final recommendation is consistent with the 2018 draft recommendation and updates the 2012 final recommendation on obesity management.
The researchers and Task Force members had no relevant financial conflicts to disclose.
SOURCE: U.S. Preventive Services Task Force. JAMA. 2018;320(11):1163-71. doi: 10.1001/jama.2018.13022.
In the USPSTF Recommendation Statement on Behavioral Weight Loss Interventions to Prevent Obesity-Related Morbidity and Mortality in Adults the Task Force updates their 2012 statement and recommends that patients with obesity be referred for intensive, multicomponent behavioral weight loss interventions and weight loss maintenance. Reiterating the importance of intensive behavioral and lifestyle support is to be commended and should be the cornerstone of treatment for people with overweight disorders. As thoughtfully discussed in accompanying editorials by Haire-Joshu, Hill-Briggs, and Yanovski, moving from recommendation to reality will require access to high-quality programs for patients of all socioeconomic and ethnic backgrounds, less restrictive reimbursement for services, and broader involvement of the public health and food industry sectors.
However, the task force recommendations were limited in scope: they pertained to people with obesity defined as a BMI greater than 30 kg/m2, to those without diagnosed obesity-associated disorders, and to patients seen in a primary care setting. This lessens the impact of the report for a disease which continues to be epidemic in the United States. Leaving out the overweight pre-obese in whom efforts toward prevention are essential, as well as people with obesity who have coexisting comorbidities restricts the recommendations to one slice of the large obesity pie. As more high-quality data pertaining to a broader range of people impacted by overweight disorders become available, more expansive guidelines for treatment will be important.
Furthermore, while behavioral weight loss interventions are meaningful, they fall short for many in bringing about sustained efficacy. The primary care setting should include referral for appropriate patients to be evaluated for combined multidisciplinary behavioral and surgical, endoscopic, or pharmacologic therapies that can improve clinical outcomes for those refractory to behavioral weight loss interventions alone. Finally, tackling the obesity epidemic requires that health care providers across a broad range of specialties become involved in a coordinated effort to help our patients. As digestive disease specialists treating a myriad of obesity-related diseases from fatty liver to colorectal cancer, we too need to help address the underlying disease by providing obesity therapy within our practices or making referrals for its multidisciplinary treatment.
Sarah Streett, MD, AGAF, clinical associate professor of medicine, division of gastroenterology and hepatology, Stanford University School of Medicine, Stanford, Calif. She has no relevant disclosures.
In the USPSTF Recommendation Statement on Behavioral Weight Loss Interventions to Prevent Obesity-Related Morbidity and Mortality in Adults the Task Force updates their 2012 statement and recommends that patients with obesity be referred for intensive, multicomponent behavioral weight loss interventions and weight loss maintenance. Reiterating the importance of intensive behavioral and lifestyle support is to be commended and should be the cornerstone of treatment for people with overweight disorders. As thoughtfully discussed in accompanying editorials by Haire-Joshu, Hill-Briggs, and Yanovski, moving from recommendation to reality will require access to high-quality programs for patients of all socioeconomic and ethnic backgrounds, less restrictive reimbursement for services, and broader involvement of the public health and food industry sectors.
However, the task force recommendations were limited in scope: they pertained to people with obesity defined as a BMI greater than 30 kg/m2, to those without diagnosed obesity-associated disorders, and to patients seen in a primary care setting. This lessens the impact of the report for a disease which continues to be epidemic in the United States. Leaving out the overweight pre-obese in whom efforts toward prevention are essential, as well as people with obesity who have coexisting comorbidities restricts the recommendations to one slice of the large obesity pie. As more high-quality data pertaining to a broader range of people impacted by overweight disorders become available, more expansive guidelines for treatment will be important.
Furthermore, while behavioral weight loss interventions are meaningful, they fall short for many in bringing about sustained efficacy. The primary care setting should include referral for appropriate patients to be evaluated for combined multidisciplinary behavioral and surgical, endoscopic, or pharmacologic therapies that can improve clinical outcomes for those refractory to behavioral weight loss interventions alone. Finally, tackling the obesity epidemic requires that health care providers across a broad range of specialties become involved in a coordinated effort to help our patients. As digestive disease specialists treating a myriad of obesity-related diseases from fatty liver to colorectal cancer, we too need to help address the underlying disease by providing obesity therapy within our practices or making referrals for its multidisciplinary treatment.
Sarah Streett, MD, AGAF, clinical associate professor of medicine, division of gastroenterology and hepatology, Stanford University School of Medicine, Stanford, Calif. She has no relevant disclosures.
In the USPSTF Recommendation Statement on Behavioral Weight Loss Interventions to Prevent Obesity-Related Morbidity and Mortality in Adults the Task Force updates their 2012 statement and recommends that patients with obesity be referred for intensive, multicomponent behavioral weight loss interventions and weight loss maintenance. Reiterating the importance of intensive behavioral and lifestyle support is to be commended and should be the cornerstone of treatment for people with overweight disorders. As thoughtfully discussed in accompanying editorials by Haire-Joshu, Hill-Briggs, and Yanovski, moving from recommendation to reality will require access to high-quality programs for patients of all socioeconomic and ethnic backgrounds, less restrictive reimbursement for services, and broader involvement of the public health and food industry sectors.
However, the task force recommendations were limited in scope: they pertained to people with obesity defined as a BMI greater than 30 kg/m2, to those without diagnosed obesity-associated disorders, and to patients seen in a primary care setting. This lessens the impact of the report for a disease which continues to be epidemic in the United States. Leaving out the overweight pre-obese in whom efforts toward prevention are essential, as well as people with obesity who have coexisting comorbidities restricts the recommendations to one slice of the large obesity pie. As more high-quality data pertaining to a broader range of people impacted by overweight disorders become available, more expansive guidelines for treatment will be important.
Furthermore, while behavioral weight loss interventions are meaningful, they fall short for many in bringing about sustained efficacy. The primary care setting should include referral for appropriate patients to be evaluated for combined multidisciplinary behavioral and surgical, endoscopic, or pharmacologic therapies that can improve clinical outcomes for those refractory to behavioral weight loss interventions alone. Finally, tackling the obesity epidemic requires that health care providers across a broad range of specialties become involved in a coordinated effort to help our patients. As digestive disease specialists treating a myriad of obesity-related diseases from fatty liver to colorectal cancer, we too need to help address the underlying disease by providing obesity therapy within our practices or making referrals for its multidisciplinary treatment.
Sarah Streett, MD, AGAF, clinical associate professor of medicine, division of gastroenterology and hepatology, Stanford University School of Medicine, Stanford, Calif. She has no relevant disclosures.
The U.S. Preventive Services Task Force advises clinicians to refer or offer intensive behavioral weight-loss interventions to obese adults, according to an updated recommendation statement published in JAMA.
Obesity affects more than one-third of U.S. adults, according to federal statistics. It carries increased risk for comorbidities including heart disease, diabetes, and various cancers, as well as increased risk of death among adults younger than 65 years, noted lead author Susan J. Curry, PhD, of the University of Iowa, Iowa City, and members of the Task Force.
The B recommendation applies to obese adults; obesity was defined as a body mass index of 30 kg/m2 or higher. The evidence review focused on interventions for weight loss and weight maintenance that could be provided in primary care or referred from primary care, such as nutrition counseling, exercise strategies, and goal setting.
The Task Force found adequate evidence that behavior-based weight-loss interventions improved weight, reduced incidence of type 2 diabetes, and helped maintain weight loss after interventions ended.
The Task Force found small to no evidence of harm associated with any of the behavioral weight-loss interventions, which included group sessions, personal sessions, print-based interventions, and technology-based interventions (such as text messages). Although interventions that combined drug therapy with behavioral intervention resulted in greater weight loss over 12-18 months, compared with behavioral interventions alone, the attrition rates were high and data on weight-loss maintenance after discontinuation of the drugs were limited, the Task Force noted.
“As a result, the USPSTF encourages clinicians to promote behavioral interventions as the primary focus of effective interventions for weight loss in adults,” they wrote.
The Task Force acknowledged the need for future research in subgroups and to explore whether factors such as genetics and untreated conditions are barriers to behavior-based weight loss interventions.
In the evidence review published in JAMA, Erin S. LeBlanc, MD, of Kaiser Permanente in Portland, Ore., and her colleagues reviewed data from 122 randomized, controlled trials including more than 62,000 persons and 2 observational studies including more than 209,000 persons.
The researchers found behavioral interventions were associated with greater weight loss and less risk of developing diabetes, compared with control interventions.
Intensive behavioral interventions included counseling patients about healthy eating, encouraging physical activity, setting weight and health goals, and assisting with weight monitoring. The interventions ranged from text messaging to in-person sessions for individuals or groups. The average absolute weight loss in the trials included in the review ranged from –0.5 kg to –9.3 kg (–1.1 lb to –20.5 lb) for intervention patients and from +1.4 kg to –5.6 kg (+3.1 lb to –12.3 lb) in controls.
Limitations of the review included a lack of data on population subgroups and a lack of long-term data on weight and health outcomes, the researchers noted. However, the results support the value of behavior-based therapy for obesity treatment.
The final recommendation is consistent with the 2018 draft recommendation and updates the 2012 final recommendation on obesity management.
The researchers and Task Force members had no relevant financial conflicts to disclose.
SOURCE: U.S. Preventive Services Task Force. JAMA. 2018;320(11):1163-71. doi: 10.1001/jama.2018.13022.
The U.S. Preventive Services Task Force advises clinicians to refer or offer intensive behavioral weight-loss interventions to obese adults, according to an updated recommendation statement published in JAMA.
Obesity affects more than one-third of U.S. adults, according to federal statistics. It carries increased risk for comorbidities including heart disease, diabetes, and various cancers, as well as increased risk of death among adults younger than 65 years, noted lead author Susan J. Curry, PhD, of the University of Iowa, Iowa City, and members of the Task Force.
The B recommendation applies to obese adults; obesity was defined as a body mass index of 30 kg/m2 or higher. The evidence review focused on interventions for weight loss and weight maintenance that could be provided in primary care or referred from primary care, such as nutrition counseling, exercise strategies, and goal setting.
The Task Force found adequate evidence that behavior-based weight-loss interventions improved weight, reduced incidence of type 2 diabetes, and helped maintain weight loss after interventions ended.
The Task Force found small to no evidence of harm associated with any of the behavioral weight-loss interventions, which included group sessions, personal sessions, print-based interventions, and technology-based interventions (such as text messages). Although interventions that combined drug therapy with behavioral intervention resulted in greater weight loss over 12-18 months, compared with behavioral interventions alone, the attrition rates were high and data on weight-loss maintenance after discontinuation of the drugs were limited, the Task Force noted.
“As a result, the USPSTF encourages clinicians to promote behavioral interventions as the primary focus of effective interventions for weight loss in adults,” they wrote.
The Task Force acknowledged the need for future research in subgroups and to explore whether factors such as genetics and untreated conditions are barriers to behavior-based weight loss interventions.
In the evidence review published in JAMA, Erin S. LeBlanc, MD, of Kaiser Permanente in Portland, Ore., and her colleagues reviewed data from 122 randomized, controlled trials including more than 62,000 persons and 2 observational studies including more than 209,000 persons.
The researchers found behavioral interventions were associated with greater weight loss and less risk of developing diabetes, compared with control interventions.
Intensive behavioral interventions included counseling patients about healthy eating, encouraging physical activity, setting weight and health goals, and assisting with weight monitoring. The interventions ranged from text messaging to in-person sessions for individuals or groups. The average absolute weight loss in the trials included in the review ranged from –0.5 kg to –9.3 kg (–1.1 lb to –20.5 lb) for intervention patients and from +1.4 kg to –5.6 kg (+3.1 lb to –12.3 lb) in controls.
Limitations of the review included a lack of data on population subgroups and a lack of long-term data on weight and health outcomes, the researchers noted. However, the results support the value of behavior-based therapy for obesity treatment.
The final recommendation is consistent with the 2018 draft recommendation and updates the 2012 final recommendation on obesity management.
The researchers and Task Force members had no relevant financial conflicts to disclose.
SOURCE: U.S. Preventive Services Task Force. JAMA. 2018;320(11):1163-71. doi: 10.1001/jama.2018.13022.
FROM JAMA
Cortical Damage at Onset May Indicate Risk of Secondary Progressive MS
This observation may aid patient stratification and guide the choice of appropriate therapy.
BERLIN—Widespread focal cortical damage at multiple sclerosis (MS) onset identifies patients likely to have frequent early relapses and a rapid development of progressive disease, which results from worsening global cortical pathology over time, according to a study presented at ECTRIMS 2018. The results provide a basis for patient stratification with the goal of therapeutic optimization. In addition, the data “highlight the importance of elucidating mechanisms involved in early cortical pathology,” according to the investigators.
Following Patients With Relapsing-Remitting MS
Among patients with relapsing-remitting MS, a high frequency of early relapses is associated with increased risk of developing severe disability, which suggests that early biologic mechanisms influence long-term disease evolution. Antonio Scalfari, MD, PhD, a consultant neurologist at Imperial College Healthcare in London, and colleagues sought to investigate the relationship between early cortical pathology, early relapses, and the risk of converting to secondary progressive MS.

Dr. Scalfari and colleagues examined 219 patients with relapsing-remitting MS. Participants had one (n = 116), two (n = 53), or three or more (n = 50) relapses during the first two years. Follow-up lasted for a mean of 7.9 years. The researchers assessed the number of cortical lesions and white matter lesions and the rate of cortical thinning using 3D double inversion recovery, 3D T1-weighted imaging, and Freesurfer analysis.
Cortical Lesions Predicted Cortical Thinning
During the observation period, 59 (27%) patients converted to secondary progressive MS in a mean of 6.1 years. At disease onset, the investigators detected 674 cortical lesions in 166 (76%) patients. A larger number of cortical lesions was associated with a significantly higher risk of secondary progressive MS. The hazard ratios (HR) for secondary progressive MS were 2.16 for patients with two lesions, 4.79 for patients with five lesions, and 12.3 for patients with seven lesions. A large number of cortical lesions also was associated with shorter latency to secondary progressive MS and a faster rate of global cortical thinning. The mean loss per year was 0.93% for patients with no lesions, 0.99% for patients with one to three lesions, 1.13% for patients with four to six lesions, and 1.33% for patients with seven or more lesions. In the group with no cortical lesions (n = 53), no patients entered the secondary progressive phase, and four reached an Expanded Disability Status Scale score of 4.
Patients with a high number of early relapses, compared with those with low and moderate numbers, had a larger volume of white matter lesions and cortical lesions at onset. The mean volumes of cortical lesions were 181.6 mm3, 386.8 mm3, and 544.0 mm3 for patients with one, two, and three or more early relapses, respectively. Patients with a high number of early relapses also accrued more cortical lesions (mean cortical lesion volumes were 118.8 mm3, 138.8 mm3, and 790.5 mm3 for patients with one, two, and three or more early relapses, respectively), had a faster rate of cortical atrophy (mean loss/year was 0.47%, 0.79%, and 0.94% for patients with one, two, and three or more early relapses, respectively), and entered the secondary progressive phase more rapidly.
In the multivariate model, older age at onset (HR, 1.97), a larger baseline cortical lesion (HR, 2.21) and white matter lesion (HR, 1.32) volume, early changes of global cortical thickness (HR, 1.36), and three or more early relapses (HR, 6.08) independently predicted a higher probability of secondary progressive MS.
This observation may aid patient stratification and guide the choice of appropriate therapy.
This observation may aid patient stratification and guide the choice of appropriate therapy.
BERLIN—Widespread focal cortical damage at multiple sclerosis (MS) onset identifies patients likely to have frequent early relapses and a rapid development of progressive disease, which results from worsening global cortical pathology over time, according to a study presented at ECTRIMS 2018. The results provide a basis for patient stratification with the goal of therapeutic optimization. In addition, the data “highlight the importance of elucidating mechanisms involved in early cortical pathology,” according to the investigators.
Following Patients With Relapsing-Remitting MS
Among patients with relapsing-remitting MS, a high frequency of early relapses is associated with increased risk of developing severe disability, which suggests that early biologic mechanisms influence long-term disease evolution. Antonio Scalfari, MD, PhD, a consultant neurologist at Imperial College Healthcare in London, and colleagues sought to investigate the relationship between early cortical pathology, early relapses, and the risk of converting to secondary progressive MS.
Dr. Scalfari and colleagues examined 219 patients with relapsing-remitting MS. Participants had one (n = 116), two (n = 53), or three or more (n = 50) relapses during the first two years. Follow-up lasted for a mean of 7.9 years. The researchers assessed the number of cortical lesions and white matter lesions and the rate of cortical thinning using 3D double inversion recovery, 3D T1-weighted imaging, and Freesurfer analysis.
Cortical Lesions Predicted Cortical Thinning
During the observation period, 59 (27%) patients converted to secondary progressive MS in a mean of 6.1 years. At disease onset, the investigators detected 674 cortical lesions in 166 (76%) patients. A larger number of cortical lesions was associated with a significantly higher risk of secondary progressive MS. The hazard ratios (HR) for secondary progressive MS were 2.16 for patients with two lesions, 4.79 for patients with five lesions, and 12.3 for patients with seven lesions. A large number of cortical lesions also was associated with shorter latency to secondary progressive MS and a faster rate of global cortical thinning. The mean loss per year was 0.93% for patients with no lesions, 0.99% for patients with one to three lesions, 1.13% for patients with four to six lesions, and 1.33% for patients with seven or more lesions. In the group with no cortical lesions (n = 53), no patients entered the secondary progressive phase, and four reached an Expanded Disability Status Scale score of 4.
Patients with a high number of early relapses, compared with those with low and moderate numbers, had a larger volume of white matter lesions and cortical lesions at onset. The mean volumes of cortical lesions were 181.6 mm3, 386.8 mm3, and 544.0 mm3 for patients with one, two, and three or more early relapses, respectively. Patients with a high number of early relapses also accrued more cortical lesions (mean cortical lesion volumes were 118.8 mm3, 138.8 mm3, and 790.5 mm3 for patients with one, two, and three or more early relapses, respectively), had a faster rate of cortical atrophy (mean loss/year was 0.47%, 0.79%, and 0.94% for patients with one, two, and three or more early relapses, respectively), and entered the secondary progressive phase more rapidly.
In the multivariate model, older age at onset (HR, 1.97), a larger baseline cortical lesion (HR, 2.21) and white matter lesion (HR, 1.32) volume, early changes of global cortical thickness (HR, 1.36), and three or more early relapses (HR, 6.08) independently predicted a higher probability of secondary progressive MS.
BERLIN—Widespread focal cortical damage at multiple sclerosis (MS) onset identifies patients likely to have frequent early relapses and a rapid development of progressive disease, which results from worsening global cortical pathology over time, according to a study presented at ECTRIMS 2018. The results provide a basis for patient stratification with the goal of therapeutic optimization. In addition, the data “highlight the importance of elucidating mechanisms involved in early cortical pathology,” according to the investigators.
Following Patients With Relapsing-Remitting MS
Among patients with relapsing-remitting MS, a high frequency of early relapses is associated with increased risk of developing severe disability, which suggests that early biologic mechanisms influence long-term disease evolution. Antonio Scalfari, MD, PhD, a consultant neurologist at Imperial College Healthcare in London, and colleagues sought to investigate the relationship between early cortical pathology, early relapses, and the risk of converting to secondary progressive MS.
Dr. Scalfari and colleagues examined 219 patients with relapsing-remitting MS. Participants had one (n = 116), two (n = 53), or three or more (n = 50) relapses during the first two years. Follow-up lasted for a mean of 7.9 years. The researchers assessed the number of cortical lesions and white matter lesions and the rate of cortical thinning using 3D double inversion recovery, 3D T1-weighted imaging, and Freesurfer analysis.
Cortical Lesions Predicted Cortical Thinning
During the observation period, 59 (27%) patients converted to secondary progressive MS in a mean of 6.1 years. At disease onset, the investigators detected 674 cortical lesions in 166 (76%) patients. A larger number of cortical lesions was associated with a significantly higher risk of secondary progressive MS. The hazard ratios (HR) for secondary progressive MS were 2.16 for patients with two lesions, 4.79 for patients with five lesions, and 12.3 for patients with seven lesions. A large number of cortical lesions also was associated with shorter latency to secondary progressive MS and a faster rate of global cortical thinning. The mean loss per year was 0.93% for patients with no lesions, 0.99% for patients with one to three lesions, 1.13% for patients with four to six lesions, and 1.33% for patients with seven or more lesions. In the group with no cortical lesions (n = 53), no patients entered the secondary progressive phase, and four reached an Expanded Disability Status Scale score of 4.
Patients with a high number of early relapses, compared with those with low and moderate numbers, had a larger volume of white matter lesions and cortical lesions at onset. The mean volumes of cortical lesions were 181.6 mm3, 386.8 mm3, and 544.0 mm3 for patients with one, two, and three or more early relapses, respectively. Patients with a high number of early relapses also accrued more cortical lesions (mean cortical lesion volumes were 118.8 mm3, 138.8 mm3, and 790.5 mm3 for patients with one, two, and three or more early relapses, respectively), had a faster rate of cortical atrophy (mean loss/year was 0.47%, 0.79%, and 0.94% for patients with one, two, and three or more early relapses, respectively), and entered the secondary progressive phase more rapidly.
In the multivariate model, older age at onset (HR, 1.97), a larger baseline cortical lesion (HR, 2.21) and white matter lesion (HR, 1.32) volume, early changes of global cortical thickness (HR, 1.36), and three or more early relapses (HR, 6.08) independently predicted a higher probability of secondary progressive MS.
When Is the Optimal Time to Start Treatment in Patients With Relapsing-Remitting MS?
Real-world data identify when therapy initiation has the best chance of reducing long-term disability.
BERLIN—Data from the Big Multiple Sclerosis Data (BMSD) Network indicate that the optimal time to start disease-modifying therapy in patients with multiple sclerosis (MS) to prevent the long-term accumulation of disability is within six months of disease onset. This finding was presented by Pietro Iaffaldano, MD, and colleagues at ECTRIMS 2018. Dr. Iaffaldano is Assistant Professor of Neurology at the University of Bari, Italy.

Many randomized clinical trials support the early start of disease-modifying therapies in MS. However, there is still an ongoing discussion on the optimal timing of treatment. For insight into this and other questions, the Danish, Italian, and Swedish national MS registries, MSBase, and the OFSEP of France pooled data for specific research projects in the BMSD Network. One question they sought to answer with this large, real-world data set was the optimal time to start disease-modifying therapy to prevent long-term disability accumulation in MS.
A cohort of patients with relapsing-remitting MS who had 10 or more years of follow-up, three or more years of cumulative disease-modifying therapy exposure, and three or more Expanded Disability Status Scale (EDSS) score evaluations was selected from the pooled cohort of the BMSD Network. The researchers conducted a set of pairwise (1:1) propensity score matching analyses with 10 different cut-offs for early versus delayed treatment (> 0.5 year up to > 5.0 years, using 0.5-year intervals) to allow an unbiased comparison between groups. The logistic model to predict propensity score included the following covariates: age at onset of the disease, sex, baseline EDSS, number of relapses in the two years before disease-modifying therapy start, number of EDSS evaluations, decade of birth, and registry source. To estimate the risk of reaching 12 months-confirmed EDSS progression (EDSSpr), a set of Cox models, adjusted for disease duration and relapses after disease-modifying therapy start as time-dependent covariates, was calculated.
A cohort of 11,871 patients with relapsing-remitting MS (71.0% female) was retrieved from the pooled BMSD Network database. The median (interquartile range) age at onset was 27.7 (22.3–34.6), median follow-up was 13.2 (11.4–15.4) years, and median time to the first disease-modifying therapy start was 3.8 (1.5–8.5) years. During the follow-up, an EDSSpr was reached by 4,138 (34.9%) patients. The lowest hazard ratio (HR) with relative 95% confidence interval (CI) for the propensity score matched models was obtained by a cutoff of treatment start within six months from disease onset (n = 873 per group). Early treatment significantly reduced the risk of reaching an EDSSpr (HR, 0.72 ). All subsequent comparisons between early and delayed treatment were not statistically significant.
This project was supported by Biogen International (Zug, Switzerland) on the basis of a sponsored research agreement with the BMSD Network.
Real-world data identify when therapy initiation has the best chance of reducing long-term disability.
Real-world data identify when therapy initiation has the best chance of reducing long-term disability.
BERLIN—Data from the Big Multiple Sclerosis Data (BMSD) Network indicate that the optimal time to start disease-modifying therapy in patients with multiple sclerosis (MS) to prevent the long-term accumulation of disability is within six months of disease onset. This finding was presented by Pietro Iaffaldano, MD, and colleagues at ECTRIMS 2018. Dr. Iaffaldano is Assistant Professor of Neurology at the University of Bari, Italy.
Many randomized clinical trials support the early start of disease-modifying therapies in MS. However, there is still an ongoing discussion on the optimal timing of treatment. For insight into this and other questions, the Danish, Italian, and Swedish national MS registries, MSBase, and the OFSEP of France pooled data for specific research projects in the BMSD Network. One question they sought to answer with this large, real-world data set was the optimal time to start disease-modifying therapy to prevent long-term disability accumulation in MS.
A cohort of patients with relapsing-remitting MS who had 10 or more years of follow-up, three or more years of cumulative disease-modifying therapy exposure, and three or more Expanded Disability Status Scale (EDSS) score evaluations was selected from the pooled cohort of the BMSD Network. The researchers conducted a set of pairwise (1:1) propensity score matching analyses with 10 different cut-offs for early versus delayed treatment (> 0.5 year up to > 5.0 years, using 0.5-year intervals) to allow an unbiased comparison between groups. The logistic model to predict propensity score included the following covariates: age at onset of the disease, sex, baseline EDSS, number of relapses in the two years before disease-modifying therapy start, number of EDSS evaluations, decade of birth, and registry source. To estimate the risk of reaching 12 months-confirmed EDSS progression (EDSSpr), a set of Cox models, adjusted for disease duration and relapses after disease-modifying therapy start as time-dependent covariates, was calculated.
A cohort of 11,871 patients with relapsing-remitting MS (71.0% female) was retrieved from the pooled BMSD Network database. The median (interquartile range) age at onset was 27.7 (22.3–34.6), median follow-up was 13.2 (11.4–15.4) years, and median time to the first disease-modifying therapy start was 3.8 (1.5–8.5) years. During the follow-up, an EDSSpr was reached by 4,138 (34.9%) patients. The lowest hazard ratio (HR) with relative 95% confidence interval (CI) for the propensity score matched models was obtained by a cutoff of treatment start within six months from disease onset (n = 873 per group). Early treatment significantly reduced the risk of reaching an EDSSpr (HR, 0.72 ). All subsequent comparisons between early and delayed treatment were not statistically significant.
This project was supported by Biogen International (Zug, Switzerland) on the basis of a sponsored research agreement with the BMSD Network.
BERLIN—Data from the Big Multiple Sclerosis Data (BMSD) Network indicate that the optimal time to start disease-modifying therapy in patients with multiple sclerosis (MS) to prevent the long-term accumulation of disability is within six months of disease onset. This finding was presented by Pietro Iaffaldano, MD, and colleagues at ECTRIMS 2018. Dr. Iaffaldano is Assistant Professor of Neurology at the University of Bari, Italy.
Many randomized clinical trials support the early start of disease-modifying therapies in MS. However, there is still an ongoing discussion on the optimal timing of treatment. For insight into this and other questions, the Danish, Italian, and Swedish national MS registries, MSBase, and the OFSEP of France pooled data for specific research projects in the BMSD Network. One question they sought to answer with this large, real-world data set was the optimal time to start disease-modifying therapy to prevent long-term disability accumulation in MS.
A cohort of patients with relapsing-remitting MS who had 10 or more years of follow-up, three or more years of cumulative disease-modifying therapy exposure, and three or more Expanded Disability Status Scale (EDSS) score evaluations was selected from the pooled cohort of the BMSD Network. The researchers conducted a set of pairwise (1:1) propensity score matching analyses with 10 different cut-offs for early versus delayed treatment (> 0.5 year up to > 5.0 years, using 0.5-year intervals) to allow an unbiased comparison between groups. The logistic model to predict propensity score included the following covariates: age at onset of the disease, sex, baseline EDSS, number of relapses in the two years before disease-modifying therapy start, number of EDSS evaluations, decade of birth, and registry source. To estimate the risk of reaching 12 months-confirmed EDSS progression (EDSSpr), a set of Cox models, adjusted for disease duration and relapses after disease-modifying therapy start as time-dependent covariates, was calculated.
A cohort of 11,871 patients with relapsing-remitting MS (71.0% female) was retrieved from the pooled BMSD Network database. The median (interquartile range) age at onset was 27.7 (22.3–34.6), median follow-up was 13.2 (11.4–15.4) years, and median time to the first disease-modifying therapy start was 3.8 (1.5–8.5) years. During the follow-up, an EDSSpr was reached by 4,138 (34.9%) patients. The lowest hazard ratio (HR) with relative 95% confidence interval (CI) for the propensity score matched models was obtained by a cutoff of treatment start within six months from disease onset (n = 873 per group). Early treatment significantly reduced the risk of reaching an EDSSpr (HR, 0.72 ). All subsequent comparisons between early and delayed treatment were not statistically significant.
This project was supported by Biogen International (Zug, Switzerland) on the basis of a sponsored research agreement with the BMSD Network.
Rivaroxaban gains indication for prevention of major cardiovascular events in CAD/PAD
when taken with aspirin, Janssen Pharmaceuticals announced on October 11.

The Food and Drug Administration’s approval was based on a review of the 27,000-patient COMPASS trial, which showed last year that a low dosage of rivaroxaban (Xarelto) plus aspirin reduced the combined rate of cardiovascular disease events by 24% in patients with coronary artery disease and by 28% in participants with peripheral artery disease, compared with aspirin alone. (N Engl J Med. 2017 Oct 5;377[14]:1319-30)
The flip side to the reduction in COMPASS’s combined primary endpoint was a 51% increase in major bleeding. However, that bump did not translate to increases in fatal bleeds, intracerebral bleeds, or bleeding in other critical organs.
COMPASS (Cardiovascular Outcomes for People Using Anticoagulation Strategies) studied two dosages of rivaroxaban, 2.5 mg and 5 mg twice daily, and it was the lower dosage that did the trick. Until this approval, that formulation wasn’t available; Janssen announced the coming of the 2.5-mg pill in its release.
The new prescribing information states specifically that Xarelto 2.5 mg is indicated, in combination with aspirin, to reduce the risk of major cardiovascular events, cardiovascular death, MI, and stroke in patients with chronic coronary artery disease or peripheral artery disease.
This is the sixth indication for rivaroxaban, a factor Xa inhibitor that was first approved in 2011. It is also the first indication for cardiovascular prevention for any factor Xa inhibitor. Others on the U.S. market are apixaban (Eliquis), edoxaban (Savaysa), and betrixaban (Bevyxxa).
COMPASS was presented at the 2017 annual congress of the European Society of Cardiology. At that time, Eugene Braunwald, MD, of Harvard Medical School and Brigham and Women’s Hospital in Boston, commented that the trial produced “unambiguous results that should change guidelines and the management of stable coronary artery disease.” He added that the results are “an important step for thrombocardiology.”
when taken with aspirin, Janssen Pharmaceuticals announced on October 11.
The Food and Drug Administration’s approval was based on a review of the 27,000-patient COMPASS trial, which showed last year that a low dosage of rivaroxaban (Xarelto) plus aspirin reduced the combined rate of cardiovascular disease events by 24% in patients with coronary artery disease and by 28% in participants with peripheral artery disease, compared with aspirin alone. (N Engl J Med. 2017 Oct 5;377[14]:1319-30)
The flip side to the reduction in COMPASS’s combined primary endpoint was a 51% increase in major bleeding. However, that bump did not translate to increases in fatal bleeds, intracerebral bleeds, or bleeding in other critical organs.
COMPASS (Cardiovascular Outcomes for People Using Anticoagulation Strategies) studied two dosages of rivaroxaban, 2.5 mg and 5 mg twice daily, and it was the lower dosage that did the trick. Until this approval, that formulation wasn’t available; Janssen announced the coming of the 2.5-mg pill in its release.
The new prescribing information states specifically that Xarelto 2.5 mg is indicated, in combination with aspirin, to reduce the risk of major cardiovascular events, cardiovascular death, MI, and stroke in patients with chronic coronary artery disease or peripheral artery disease.
This is the sixth indication for rivaroxaban, a factor Xa inhibitor that was first approved in 2011. It is also the first indication for cardiovascular prevention for any factor Xa inhibitor. Others on the U.S. market are apixaban (Eliquis), edoxaban (Savaysa), and betrixaban (Bevyxxa).
COMPASS was presented at the 2017 annual congress of the European Society of Cardiology. At that time, Eugene Braunwald, MD, of Harvard Medical School and Brigham and Women’s Hospital in Boston, commented that the trial produced “unambiguous results that should change guidelines and the management of stable coronary artery disease.” He added that the results are “an important step for thrombocardiology.”
when taken with aspirin, Janssen Pharmaceuticals announced on October 11.
The Food and Drug Administration’s approval was based on a review of the 27,000-patient COMPASS trial, which showed last year that a low dosage of rivaroxaban (Xarelto) plus aspirin reduced the combined rate of cardiovascular disease events by 24% in patients with coronary artery disease and by 28% in participants with peripheral artery disease, compared with aspirin alone. (N Engl J Med. 2017 Oct 5;377[14]:1319-30)
The flip side to the reduction in COMPASS’s combined primary endpoint was a 51% increase in major bleeding. However, that bump did not translate to increases in fatal bleeds, intracerebral bleeds, or bleeding in other critical organs.
COMPASS (Cardiovascular Outcomes for People Using Anticoagulation Strategies) studied two dosages of rivaroxaban, 2.5 mg and 5 mg twice daily, and it was the lower dosage that did the trick. Until this approval, that formulation wasn’t available; Janssen announced the coming of the 2.5-mg pill in its release.
The new prescribing information states specifically that Xarelto 2.5 mg is indicated, in combination with aspirin, to reduce the risk of major cardiovascular events, cardiovascular death, MI, and stroke in patients with chronic coronary artery disease or peripheral artery disease.
This is the sixth indication for rivaroxaban, a factor Xa inhibitor that was first approved in 2011. It is also the first indication for cardiovascular prevention for any factor Xa inhibitor. Others on the U.S. market are apixaban (Eliquis), edoxaban (Savaysa), and betrixaban (Bevyxxa).
COMPASS was presented at the 2017 annual congress of the European Society of Cardiology. At that time, Eugene Braunwald, MD, of Harvard Medical School and Brigham and Women’s Hospital in Boston, commented that the trial produced “unambiguous results that should change guidelines and the management of stable coronary artery disease.” He added that the results are “an important step for thrombocardiology.”
Bias in the clinical setting can impact patient care
SAN ANTONIO – Physicians and other health care providers may harbor implicit, or unconscious, biases that contribute to health care disparities, patient communication researcher Stacey Passalacqua, PhD, said here at the annual meeting of the American College of Chest Physicians.
Implicit biases are beliefs or attitudes, for example, about certain social groups, that exist outside of a health care provider’s conscious awareness, said Dr. Passalacqua of the department of communication at the University of Texas, San Antonio. If bias is implicit, it can be difficult self-assess.
among other social, ethnic, and racial groups, Dr. Passalacqua told attendees in workshops at the meeting.
“If a health care provider has negative biases toward a particular patient – maybe they think that these patients doesn’t care that much about their health or that they really have no interest in participating – then obviously that health care provider is far less likely to engage that patient in shared decision making,” she said in a video interview.
Diagnosis and treatment are subject to influence by the bias that physicians have toward certain patient groups, according to Dr. Passalacqua. For example, she said women with heart disease are less likely to be accurately diagnosed.
The bias in the medical setting might be mitigated by the presence of more individuals from the at-risk groups in the health care workforce, she added. In one recent retrospective study, investigators found that after an MI, a woman treated by a male physician was associated with higher mortality, while women and men had similar outcomes when treated by female physicians.
“That is one of the reasons why it is so important to have a diverse workforce, to have health care providers of different ethnicities, of different genders, or different backgrounds, because they are less subject to some of these implicit biases that we know are highly problematic in health care,” she said in the interview.
Dr. Passalacqua had no disclosures related to her presentation.
SAN ANTONIO – Physicians and other health care providers may harbor implicit, or unconscious, biases that contribute to health care disparities, patient communication researcher Stacey Passalacqua, PhD, said here at the annual meeting of the American College of Chest Physicians.
Implicit biases are beliefs or attitudes, for example, about certain social groups, that exist outside of a health care provider’s conscious awareness, said Dr. Passalacqua of the department of communication at the University of Texas, San Antonio. If bias is implicit, it can be difficult self-assess.
among other social, ethnic, and racial groups, Dr. Passalacqua told attendees in workshops at the meeting.
“If a health care provider has negative biases toward a particular patient – maybe they think that these patients doesn’t care that much about their health or that they really have no interest in participating – then obviously that health care provider is far less likely to engage that patient in shared decision making,” she said in a video interview.
Diagnosis and treatment are subject to influence by the bias that physicians have toward certain patient groups, according to Dr. Passalacqua. For example, she said women with heart disease are less likely to be accurately diagnosed.
The bias in the medical setting might be mitigated by the presence of more individuals from the at-risk groups in the health care workforce, she added. In one recent retrospective study, investigators found that after an MI, a woman treated by a male physician was associated with higher mortality, while women and men had similar outcomes when treated by female physicians.
“That is one of the reasons why it is so important to have a diverse workforce, to have health care providers of different ethnicities, of different genders, or different backgrounds, because they are less subject to some of these implicit biases that we know are highly problematic in health care,” she said in the interview.
Dr. Passalacqua had no disclosures related to her presentation.
SAN ANTONIO – Physicians and other health care providers may harbor implicit, or unconscious, biases that contribute to health care disparities, patient communication researcher Stacey Passalacqua, PhD, said here at the annual meeting of the American College of Chest Physicians.
Implicit biases are beliefs or attitudes, for example, about certain social groups, that exist outside of a health care provider’s conscious awareness, said Dr. Passalacqua of the department of communication at the University of Texas, San Antonio. If bias is implicit, it can be difficult self-assess.
among other social, ethnic, and racial groups, Dr. Passalacqua told attendees in workshops at the meeting.
“If a health care provider has negative biases toward a particular patient – maybe they think that these patients doesn’t care that much about their health or that they really have no interest in participating – then obviously that health care provider is far less likely to engage that patient in shared decision making,” she said in a video interview.
Diagnosis and treatment are subject to influence by the bias that physicians have toward certain patient groups, according to Dr. Passalacqua. For example, she said women with heart disease are less likely to be accurately diagnosed.
The bias in the medical setting might be mitigated by the presence of more individuals from the at-risk groups in the health care workforce, she added. In one recent retrospective study, investigators found that after an MI, a woman treated by a male physician was associated with higher mortality, while women and men had similar outcomes when treated by female physicians.
“That is one of the reasons why it is so important to have a diverse workforce, to have health care providers of different ethnicities, of different genders, or different backgrounds, because they are less subject to some of these implicit biases that we know are highly problematic in health care,” she said in the interview.
Dr. Passalacqua had no disclosures related to her presentation.
REPORTING FROM CHEST 2018

Diffuse Nonscarring Alopecia
The Diagnosis: Trichotillomania
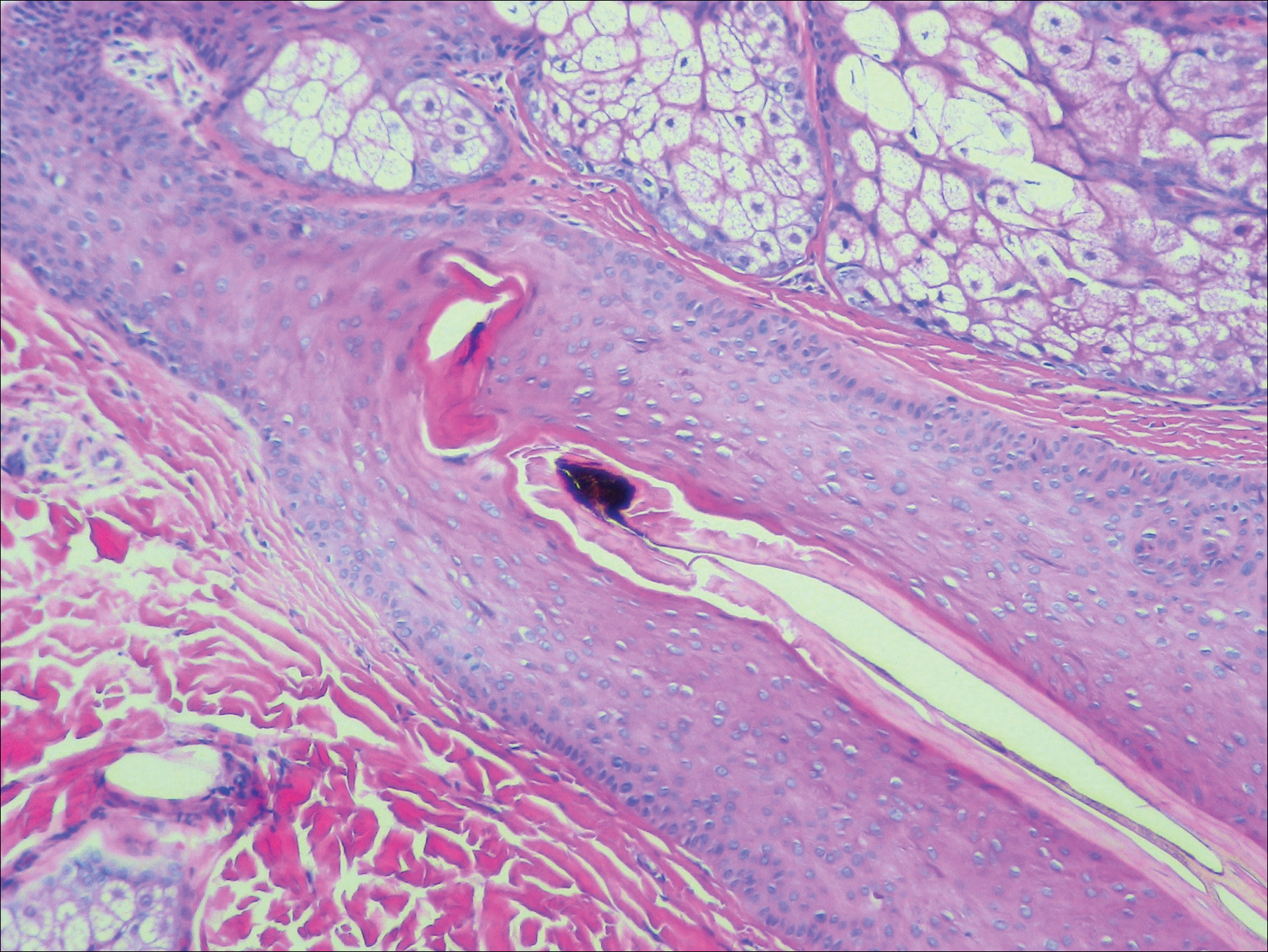
A scalp punch biopsy revealed pigmented hair casts, an increase in catagen and telogen follicles, and a lack of perifollicular inflammation (Figure). Based on the clinical and histopathological findings, a diagnosis of trichotillomania (TTM) was established.
Trichotillomania is a hairpulling disorder with notable dermatologic and psychiatric overlap. Although previously considered an impulse control disorder, the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) reclassified it within obsessive-compulsive and related disorders, which also include body dysmorphic disorder and excoriation (skin-picking) disorder. Diagnostic criteria for TTM include the following: the patient must have recurrent pulling out of his/her hair resulting in hair loss despite repeated attempts to stop; underlying medical conditions and other psychiatric diagnoses must be excluded; and the patient must experience distress or impairment in social, occupational, or other areas of functioning from the hairpulling.1 Trichotillomania mainly occurs in children and young adults, with a lifetime prevalence of approximately 1% to 2%.2 The coexistence of a mood or anxiety disorder is common, as seen in our patient.
The diagnosis of TTM requires strong clinical suspicion because patients and their parents/guardians usually deny hairpulling. The main clinical differential diagnosis often is alopecia areata (AA) because both conditions can present as well-defined patches of nonscarring hair loss. Trichoscopy provides an invaluable noninvasive diagnostic tool that can be particularly useful in pediatric patients who may be reluctant to have a scalp biopsy. There are many overlapping trichoscopic findings of TTM and AA, including yellow dots, black dots, broken hairs, coiled hairs, and exclamation mark hairs.3 More specific trichoscopy findings for TTM include flame hairs (wavy proximal hair residue), V-sign (2 shafts within 1 follicle broken at the same length), and tulip hairs (dark, tulip-shaped ends of broken hairs).4 Hair breakage of varying lengths and trichoptilosis (split ends) can be better visualized using trichoscopy and support a diagnosis of TTM over AA.
Androgenetic alopecia (female pattern hair loss) presents with gradual thinning around the part line of the frontal and parietal scalp with trichoscopy showing miniaturization of hairs and decreased follicle density. The moth-eaten-like appearance of alopecia due to secondary syphilis may mimic alopecia areata clinically, but serologic testing can confirm the diagnosis of syphilis. Telogen effluvium does not have the trichoscopic features that are seen in TTM and is clinically distinguished by hair shedding and a positive hair pull test.
Biopsy can provide objective yet nonspecific support for the diagnosis, demonstrating trichomalacia, pigmented hair casts, empty follicles, and an increase in catagen hairs with a lack of inflammation. Normal and damaged hair follicles may be seen in close proximity, and hemorrhage may be seen secondary to trauma. Pigmented hair casts are not specific to TTM and are present in other traumatic hair disorders, such as traction alopecia; therefore, clinical correlation is essential for diagnosis.
Habit reversal training is the most effective treatment of TTM and involves 3 major components: awareness training with self-monitoring, stimulus control, and competing response procedures.5 Although numerous pharmacotherapies have been reported as effective treatments for TTM, a 2013 Cochrane review of 8 randomized controlled trials concluded that no medication has demonstrated reliable efficacy. Reported therapies included selective serotonin reuptake inhibitors, naltrexone, olanzapine, N-acetylcysteine, and clomipramine.6
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013.
- Schumer MC, Panza KE, Mulqueen JM, et al. Long-term outcome in pediatric trichotillomania. Depress Anxiety. 2015;32:737-743.
- Lencastre A, Tosti A. Role of trichoscopy on children's scalp and hair disorders. Pediatr Dermatol. 2013;30:674-682.
- Rakowska A, Slowinska M, Olszewska M, et al. New trichoscopy findings in trichotillomania: flame hairs, V-sign, hook hairs, hair powder, tulip hairs. Acta Derm Venereol. 2014;94:303-306.
- Morris S, Zickgraf H, Dingfelder H, et al. Habit reversal training in trichotillomania: guide for the clinician. Expert Rev Neurother. 2013;13:1069-1177.
- Rothbart R, Amos T, Siegfried N, et al. Pharmacotherapy for trichotillomania. Cochrane Database Syst Rev. 2013;11:CD007662.
The Diagnosis: Trichotillomania
A scalp punch biopsy revealed pigmented hair casts, an increase in catagen and telogen follicles, and a lack of perifollicular inflammation (Figure). Based on the clinical and histopathological findings, a diagnosis of trichotillomania (TTM) was established.
Trichotillomania is a hairpulling disorder with notable dermatologic and psychiatric overlap. Although previously considered an impulse control disorder, the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) reclassified it within obsessive-compulsive and related disorders, which also include body dysmorphic disorder and excoriation (skin-picking) disorder. Diagnostic criteria for TTM include the following: the patient must have recurrent pulling out of his/her hair resulting in hair loss despite repeated attempts to stop; underlying medical conditions and other psychiatric diagnoses must be excluded; and the patient must experience distress or impairment in social, occupational, or other areas of functioning from the hairpulling.1 Trichotillomania mainly occurs in children and young adults, with a lifetime prevalence of approximately 1% to 2%.2 The coexistence of a mood or anxiety disorder is common, as seen in our patient.
The diagnosis of TTM requires strong clinical suspicion because patients and their parents/guardians usually deny hairpulling. The main clinical differential diagnosis often is alopecia areata (AA) because both conditions can present as well-defined patches of nonscarring hair loss. Trichoscopy provides an invaluable noninvasive diagnostic tool that can be particularly useful in pediatric patients who may be reluctant to have a scalp biopsy. There are many overlapping trichoscopic findings of TTM and AA, including yellow dots, black dots, broken hairs, coiled hairs, and exclamation mark hairs.3 More specific trichoscopy findings for TTM include flame hairs (wavy proximal hair residue), V-sign (2 shafts within 1 follicle broken at the same length), and tulip hairs (dark, tulip-shaped ends of broken hairs).4 Hair breakage of varying lengths and trichoptilosis (split ends) can be better visualized using trichoscopy and support a diagnosis of TTM over AA.
Androgenetic alopecia (female pattern hair loss) presents with gradual thinning around the part line of the frontal and parietal scalp with trichoscopy showing miniaturization of hairs and decreased follicle density. The moth-eaten-like appearance of alopecia due to secondary syphilis may mimic alopecia areata clinically, but serologic testing can confirm the diagnosis of syphilis. Telogen effluvium does not have the trichoscopic features that are seen in TTM and is clinically distinguished by hair shedding and a positive hair pull test.
Biopsy can provide objective yet nonspecific support for the diagnosis, demonstrating trichomalacia, pigmented hair casts, empty follicles, and an increase in catagen hairs with a lack of inflammation. Normal and damaged hair follicles may be seen in close proximity, and hemorrhage may be seen secondary to trauma. Pigmented hair casts are not specific to TTM and are present in other traumatic hair disorders, such as traction alopecia; therefore, clinical correlation is essential for diagnosis.
Habit reversal training is the most effective treatment of TTM and involves 3 major components: awareness training with self-monitoring, stimulus control, and competing response procedures.5 Although numerous pharmacotherapies have been reported as effective treatments for TTM, a 2013 Cochrane review of 8 randomized controlled trials concluded that no medication has demonstrated reliable efficacy. Reported therapies included selective serotonin reuptake inhibitors, naltrexone, olanzapine, N-acetylcysteine, and clomipramine.6
The Diagnosis: Trichotillomania
A scalp punch biopsy revealed pigmented hair casts, an increase in catagen and telogen follicles, and a lack of perifollicular inflammation (Figure). Based on the clinical and histopathological findings, a diagnosis of trichotillomania (TTM) was established.
Trichotillomania is a hairpulling disorder with notable dermatologic and psychiatric overlap. Although previously considered an impulse control disorder, the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) reclassified it within obsessive-compulsive and related disorders, which also include body dysmorphic disorder and excoriation (skin-picking) disorder. Diagnostic criteria for TTM include the following: the patient must have recurrent pulling out of his/her hair resulting in hair loss despite repeated attempts to stop; underlying medical conditions and other psychiatric diagnoses must be excluded; and the patient must experience distress or impairment in social, occupational, or other areas of functioning from the hairpulling.1 Trichotillomania mainly occurs in children and young adults, with a lifetime prevalence of approximately 1% to 2%.2 The coexistence of a mood or anxiety disorder is common, as seen in our patient.
The diagnosis of TTM requires strong clinical suspicion because patients and their parents/guardians usually deny hairpulling. The main clinical differential diagnosis often is alopecia areata (AA) because both conditions can present as well-defined patches of nonscarring hair loss. Trichoscopy provides an invaluable noninvasive diagnostic tool that can be particularly useful in pediatric patients who may be reluctant to have a scalp biopsy. There are many overlapping trichoscopic findings of TTM and AA, including yellow dots, black dots, broken hairs, coiled hairs, and exclamation mark hairs.3 More specific trichoscopy findings for TTM include flame hairs (wavy proximal hair residue), V-sign (2 shafts within 1 follicle broken at the same length), and tulip hairs (dark, tulip-shaped ends of broken hairs).4 Hair breakage of varying lengths and trichoptilosis (split ends) can be better visualized using trichoscopy and support a diagnosis of TTM over AA.
Androgenetic alopecia (female pattern hair loss) presents with gradual thinning around the part line of the frontal and parietal scalp with trichoscopy showing miniaturization of hairs and decreased follicle density. The moth-eaten-like appearance of alopecia due to secondary syphilis may mimic alopecia areata clinically, but serologic testing can confirm the diagnosis of syphilis. Telogen effluvium does not have the trichoscopic features that are seen in TTM and is clinically distinguished by hair shedding and a positive hair pull test.
Biopsy can provide objective yet nonspecific support for the diagnosis, demonstrating trichomalacia, pigmented hair casts, empty follicles, and an increase in catagen hairs with a lack of inflammation. Normal and damaged hair follicles may be seen in close proximity, and hemorrhage may be seen secondary to trauma. Pigmented hair casts are not specific to TTM and are present in other traumatic hair disorders, such as traction alopecia; therefore, clinical correlation is essential for diagnosis.
Habit reversal training is the most effective treatment of TTM and involves 3 major components: awareness training with self-monitoring, stimulus control, and competing response procedures.5 Although numerous pharmacotherapies have been reported as effective treatments for TTM, a 2013 Cochrane review of 8 randomized controlled trials concluded that no medication has demonstrated reliable efficacy. Reported therapies included selective serotonin reuptake inhibitors, naltrexone, olanzapine, N-acetylcysteine, and clomipramine.6
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013.
- Schumer MC, Panza KE, Mulqueen JM, et al. Long-term outcome in pediatric trichotillomania. Depress Anxiety. 2015;32:737-743.
- Lencastre A, Tosti A. Role of trichoscopy on children's scalp and hair disorders. Pediatr Dermatol. 2013;30:674-682.
- Rakowska A, Slowinska M, Olszewska M, et al. New trichoscopy findings in trichotillomania: flame hairs, V-sign, hook hairs, hair powder, tulip hairs. Acta Derm Venereol. 2014;94:303-306.
- Morris S, Zickgraf H, Dingfelder H, et al. Habit reversal training in trichotillomania: guide for the clinician. Expert Rev Neurother. 2013;13:1069-1177.
- Rothbart R, Amos T, Siegfried N, et al. Pharmacotherapy for trichotillomania. Cochrane Database Syst Rev. 2013;11:CD007662.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013.
- Schumer MC, Panza KE, Mulqueen JM, et al. Long-term outcome in pediatric trichotillomania. Depress Anxiety. 2015;32:737-743.
- Lencastre A, Tosti A. Role of trichoscopy on children's scalp and hair disorders. Pediatr Dermatol. 2013;30:674-682.
- Rakowska A, Slowinska M, Olszewska M, et al. New trichoscopy findings in trichotillomania: flame hairs, V-sign, hook hairs, hair powder, tulip hairs. Acta Derm Venereol. 2014;94:303-306.
- Morris S, Zickgraf H, Dingfelder H, et al. Habit reversal training in trichotillomania: guide for the clinician. Expert Rev Neurother. 2013;13:1069-1177.
- Rothbart R, Amos T, Siegfried N, et al. Pharmacotherapy for trichotillomania. Cochrane Database Syst Rev. 2013;11:CD007662.

A 19-year-old woman with attention deficit hyperactivity disorder and an anxiety disorder presented with hair loss of 2 years' duration. She initially had small circular bald areas throughout the scalp that had progressed to diffuse hair loss of the entire scalp. She denied recent hairpulling but admitted to a remote prior history of eyelash and eyebrow pulling. She denied any voice changes, acne, or menstrual irregularities. Physical examination revealed short hairs of varying lengths throughout the scalp with no loss of follicles, erythema, scale, or exclamation point hairs. Eyebrows and eyelashes were normal. A hair-pull test was negative. Trichoscopy illuminated variation in hair shaft diameters, as well as short, irregularly broken hairs of different lengths (inset).

Introducing the Postcall Podcast
At MDedge, we know that medicine can be a bit of an awakening at every step of your career. So, we launched the Postcall Podcast as a way to share your stories: what you love about medicine and what you love outside of your career. This podcast is meant to be a place for you to find your truth.
In the first episode, Nick Andrews welcomes the Editor-In-Chief of MDedge Psychiatry and the host of the MDedge Psychcast, Dr. Lorenzo Norris.
Apple Podcasts
Google Podcasts
At MDedge, we know that medicine can be a bit of an awakening at every step of your career. So, we launched the Postcall Podcast as a way to share your stories: what you love about medicine and what you love outside of your career. This podcast is meant to be a place for you to find your truth.
In the first episode, Nick Andrews welcomes the Editor-In-Chief of MDedge Psychiatry and the host of the MDedge Psychcast, Dr. Lorenzo Norris.
Apple Podcasts
Google Podcasts
At MDedge, we know that medicine can be a bit of an awakening at every step of your career. So, we launched the Postcall Podcast as a way to share your stories: what you love about medicine and what you love outside of your career. This podcast is meant to be a place for you to find your truth.
In the first episode, Nick Andrews welcomes the Editor-In-Chief of MDedge Psychiatry and the host of the MDedge Psychcast, Dr. Lorenzo Norris.
Apple Podcasts
Google Podcasts

Dupilumab offers extra benefits to asthmatic teens
SAN ANTONIO – For adolescents with asthma, treatment with the biologic agent dupilumab provided benefits that were at least comparable with what was seen in adults, results from a retrospective analysis of a randomized, phase 3 study suggest.

Adolescents had reduced asthma exacerbations in line with what was seen in adults and had improvements in lung function that were at a greater magnitude than adults, according to study coauthor Neil M.H. Graham, MD, of Regeneron Pharmaceuticals, Tarrytown, N.Y.
“We think, overall, it’s a very good treatment response from this drug in this high-risk population, and it is generally well tolerated, as we’ve seen in other studies,” Dr. Graham said in a podium presentation at the annual meeting of the American College of Chest Physicians.
Dr. Graham presented results of an analysis of the 1,902-patient, phase 3 Liberty Asthma QUEST trial, published in May 2018 in the New England Journal of Medicine.
Top-line results of QUEST showed that treatment with dupilumab, a fully human anti–IL-4Ra monoclonal antibody, resulted in significantly lower rates of severe asthma exacerbation, along with improved lung function, in patients aged 12 years and older with moderate to severe asthma.
Now, this retrospective analysis shows that, in adolescents, improvements from baseline to week 12 in forced expiratory volume in 1 second (FEV1) were significant and at a greater magnitude than in adults, according to Dr. Graham and his coinvestigators.
The improvement over 12 weeks in FEV1 for adolescents was 0.36 L and 0.27 L, respectively, for the 200- and 300-mg doses of dupilumab (P less than .05 vs. placebo for both), Dr. Graham and his coinvestigators reported. In adults, the improvement was 0.12 L.
The annualized exacerbation rate dropped by 46.4% for those adolescents who received 200 mg dupilumab, though there was no treatment effect versus placebo for dupilumab 300 mg; the investigators said the lack of effect in this retrospective analysis could have been caused by imbalances in prior event rates or the small sample size.
A total of 107 out of 1,902 patients in QUEST were adolescents, and of those, 68 were randomly assigned to dupilumab, according to the report. Injection site reaction was the most common adverse event in adolescents in both dosing groups.
Dr. Graham reported disclosures related to his employment with Regeneron. Study coauthors reported disclosures related to Regeneron, AstraZeneca, Sanofi, Teva Pharmaceutical, GlaxoSmithKline, Boehringer Ingelheim, Merck, Genentech, and others.
SOURCE: Graham NMH et al. CHEST. 2018 Oct. doi: 10.1016/j.chest.2018.08.022.
SAN ANTONIO – For adolescents with asthma, treatment with the biologic agent dupilumab provided benefits that were at least comparable with what was seen in adults, results from a retrospective analysis of a randomized, phase 3 study suggest.
Adolescents had reduced asthma exacerbations in line with what was seen in adults and had improvements in lung function that were at a greater magnitude than adults, according to study coauthor Neil M.H. Graham, MD, of Regeneron Pharmaceuticals, Tarrytown, N.Y.
“We think, overall, it’s a very good treatment response from this drug in this high-risk population, and it is generally well tolerated, as we’ve seen in other studies,” Dr. Graham said in a podium presentation at the annual meeting of the American College of Chest Physicians.
Dr. Graham presented results of an analysis of the 1,902-patient, phase 3 Liberty Asthma QUEST trial, published in May 2018 in the New England Journal of Medicine.
Top-line results of QUEST showed that treatment with dupilumab, a fully human anti–IL-4Ra monoclonal antibody, resulted in significantly lower rates of severe asthma exacerbation, along with improved lung function, in patients aged 12 years and older with moderate to severe asthma.
Now, this retrospective analysis shows that, in adolescents, improvements from baseline to week 12 in forced expiratory volume in 1 second (FEV1) were significant and at a greater magnitude than in adults, according to Dr. Graham and his coinvestigators.
The improvement over 12 weeks in FEV1 for adolescents was 0.36 L and 0.27 L, respectively, for the 200- and 300-mg doses of dupilumab (P less than .05 vs. placebo for both), Dr. Graham and his coinvestigators reported. In adults, the improvement was 0.12 L.
The annualized exacerbation rate dropped by 46.4% for those adolescents who received 200 mg dupilumab, though there was no treatment effect versus placebo for dupilumab 300 mg; the investigators said the lack of effect in this retrospective analysis could have been caused by imbalances in prior event rates or the small sample size.
A total of 107 out of 1,902 patients in QUEST were adolescents, and of those, 68 were randomly assigned to dupilumab, according to the report. Injection site reaction was the most common adverse event in adolescents in both dosing groups.
Dr. Graham reported disclosures related to his employment with Regeneron. Study coauthors reported disclosures related to Regeneron, AstraZeneca, Sanofi, Teva Pharmaceutical, GlaxoSmithKline, Boehringer Ingelheim, Merck, Genentech, and others.
SOURCE: Graham NMH et al. CHEST. 2018 Oct. doi: 10.1016/j.chest.2018.08.022.
SAN ANTONIO – For adolescents with asthma, treatment with the biologic agent dupilumab provided benefits that were at least comparable with what was seen in adults, results from a retrospective analysis of a randomized, phase 3 study suggest.
Adolescents had reduced asthma exacerbations in line with what was seen in adults and had improvements in lung function that were at a greater magnitude than adults, according to study coauthor Neil M.H. Graham, MD, of Regeneron Pharmaceuticals, Tarrytown, N.Y.
“We think, overall, it’s a very good treatment response from this drug in this high-risk population, and it is generally well tolerated, as we’ve seen in other studies,” Dr. Graham said in a podium presentation at the annual meeting of the American College of Chest Physicians.
Dr. Graham presented results of an analysis of the 1,902-patient, phase 3 Liberty Asthma QUEST trial, published in May 2018 in the New England Journal of Medicine.
Top-line results of QUEST showed that treatment with dupilumab, a fully human anti–IL-4Ra monoclonal antibody, resulted in significantly lower rates of severe asthma exacerbation, along with improved lung function, in patients aged 12 years and older with moderate to severe asthma.
Now, this retrospective analysis shows that, in adolescents, improvements from baseline to week 12 in forced expiratory volume in 1 second (FEV1) were significant and at a greater magnitude than in adults, according to Dr. Graham and his coinvestigators.
The improvement over 12 weeks in FEV1 for adolescents was 0.36 L and 0.27 L, respectively, for the 200- and 300-mg doses of dupilumab (P less than .05 vs. placebo for both), Dr. Graham and his coinvestigators reported. In adults, the improvement was 0.12 L.
The annualized exacerbation rate dropped by 46.4% for those adolescents who received 200 mg dupilumab, though there was no treatment effect versus placebo for dupilumab 300 mg; the investigators said the lack of effect in this retrospective analysis could have been caused by imbalances in prior event rates or the small sample size.
A total of 107 out of 1,902 patients in QUEST were adolescents, and of those, 68 were randomly assigned to dupilumab, according to the report. Injection site reaction was the most common adverse event in adolescents in both dosing groups.
Dr. Graham reported disclosures related to his employment with Regeneron. Study coauthors reported disclosures related to Regeneron, AstraZeneca, Sanofi, Teva Pharmaceutical, GlaxoSmithKline, Boehringer Ingelheim, Merck, Genentech, and others.
SOURCE: Graham NMH et al. CHEST. 2018 Oct. doi: 10.1016/j.chest.2018.08.022.
REPORTING FROM CHEST 2018
Key clinical point: Dupilumab’s benefits in adolescents with moderate to severe asthma are at least comparable with what has been reported in adults.
Major finding: The improvement over 12 weeks in forced expiratory volume in 1 second for adolescents was 0.36 L and 0.27 L, respectively, for the 200- and 300-mg doses of dupilumab versus 0.12 L for adults.
Study details: A retrospective analysis of 1,902 patients (including 107 adolescents) in Liberty Asthma QUEST, a recently reported randomized, phase 3 trial.
Disclosures: Several study coauthors reported employment with Regeneron. Dr. Graham reported disclosures related to his employment with Regeneron. Other reported disclosures were related to AstraZeneca, Sanofi, Teva Pharmaceutical, GlaxoSmithKline, Boehringer Ingelheim, Merck, and Genentech, among other entities.
Source: Graham NMH et al. CHEST. 2018 Oct. doi: 10.1016/j/chest.2018.08.002.