User login
Algorithm helps assess surgical trade-offs of hernia repair
BOSTON – Choosing an operative approach for ventral hernia can be a matter of weighing the trade-offs between infection risk, postop quality of life, and patient and defect characteristics. A predictive algorithm has been developed to help with this decision, according to a study presented at the annual clinical congress of the American College of Surgeons.

Predictive modeling indicates that open repair might be considered, for example, in low BMI patients with large defects because of potentially fewer anticipated complications and improved quality of life, according to authors of the study. Conversely, laparoscopic repair might be considered in high BMI patients with recurrent hernias to decrease the associated risk of infection, the authors noted in a published abstract of the study.
The retrospective study was based on data on ventral hernia repairs in the International Hernia Mesh Registry that were performed between 2007 and 2017. Investigators used that data to build a predictive algorithm that took into account the impact on outcomes of BMI, hernia size, and operative approach, as well as age, sex, and diabetes status.
They identified 1,906 repairs, of which about 60% were open procedures. The mean patient age was 54.9 years, while mean BMI was 31.2 kg/m2 and the mean defect area was 44.8 cm2. Patients undergoing open procedures were significantly more likely to have infections, at 3.1% versus 0.3% for the laparoscopic approach (P less than .0001), investigators found.
A multivariate regression analysis controlling for confounding variables found that patients undergoing laparoscopic repair had an increased risk of seroma (odds ratio 1.78, confidence interval 1.05-3.03) but a decreased risk of infection (OR 0.05, CI 0.01-0.42). In addition, those undergoing laparoscopic procedures were more likely to have non-ideal quality of life at 1, 6, 12, and 24 months postoperatively, said the study’s lead author, Kathryn A. Schlosser, MD, a resident in the division of gastrointestinal and minimally invasive surgery, department of surgery, Carolinas Medical Center, Charlotte, N.C.
“These are both important factors — infection and non-ideal quality of life — and need to be part of our preoperative discussion with our patients when we start managing their expectations around the time of surgery,” Dr. Schlosser said in a podium presentation.
She and her colleagues calculated probability of infection based on the ratio of BMI to defect area. They found that, for example, the probability of postoperative infection was 21% for a diabetic 69-year-old female with a recurrent hernia who had a BMI of 39 and a defect area of 20 cm2. By contrast, infection probability was 3% in a 66-year-old female with a BMI of 37, a defect area of 1 cm2, and no diabetes, Dr. Schlosser said at the meeting.
Laparoscopic versus open procedures represented a trade-off between infection risk and quality of life in this algorithm. For patients at medium risk for infection based on BMI, defect size, and other variables, switching to a laparoscopic approach dropped the infection probability from 3%-8% down to 0.1%-0.5%, Dr. Schlosser told attendees. On the other hand, switching to a laparoscopic approach increased the risk of non-ideal quality of life, she said.
One sample patient Dr. Schlosser described had an infection risk of 7.2% with the open procedure that dropped to just 0.4% for the laparoscopic procedure; however, that switch would mean that her likelihood of non-ideal quality of life 12 months after surgery increased from 24% with the open repair to 44% with the laparoscopic repair.
Dr. Schlosser had no disclosures related to the study. Co-authors provided disclosures related to Acelity, Allergan, Intuitive, Stryker, and W.L. Gore.
SOURCE: Schlosser KA, et al. abstract SF215 presented at the American College of Surgeons Clinical Congress 2018.
BOSTON – Choosing an operative approach for ventral hernia can be a matter of weighing the trade-offs between infection risk, postop quality of life, and patient and defect characteristics. A predictive algorithm has been developed to help with this decision, according to a study presented at the annual clinical congress of the American College of Surgeons.
Predictive modeling indicates that open repair might be considered, for example, in low BMI patients with large defects because of potentially fewer anticipated complications and improved quality of life, according to authors of the study. Conversely, laparoscopic repair might be considered in high BMI patients with recurrent hernias to decrease the associated risk of infection, the authors noted in a published abstract of the study.
The retrospective study was based on data on ventral hernia repairs in the International Hernia Mesh Registry that were performed between 2007 and 2017. Investigators used that data to build a predictive algorithm that took into account the impact on outcomes of BMI, hernia size, and operative approach, as well as age, sex, and diabetes status.
They identified 1,906 repairs, of which about 60% were open procedures. The mean patient age was 54.9 years, while mean BMI was 31.2 kg/m2 and the mean defect area was 44.8 cm2. Patients undergoing open procedures were significantly more likely to have infections, at 3.1% versus 0.3% for the laparoscopic approach (P less than .0001), investigators found.
A multivariate regression analysis controlling for confounding variables found that patients undergoing laparoscopic repair had an increased risk of seroma (odds ratio 1.78, confidence interval 1.05-3.03) but a decreased risk of infection (OR 0.05, CI 0.01-0.42). In addition, those undergoing laparoscopic procedures were more likely to have non-ideal quality of life at 1, 6, 12, and 24 months postoperatively, said the study’s lead author, Kathryn A. Schlosser, MD, a resident in the division of gastrointestinal and minimally invasive surgery, department of surgery, Carolinas Medical Center, Charlotte, N.C.
“These are both important factors — infection and non-ideal quality of life — and need to be part of our preoperative discussion with our patients when we start managing their expectations around the time of surgery,” Dr. Schlosser said in a podium presentation.
She and her colleagues calculated probability of infection based on the ratio of BMI to defect area. They found that, for example, the probability of postoperative infection was 21% for a diabetic 69-year-old female with a recurrent hernia who had a BMI of 39 and a defect area of 20 cm2. By contrast, infection probability was 3% in a 66-year-old female with a BMI of 37, a defect area of 1 cm2, and no diabetes, Dr. Schlosser said at the meeting.
Laparoscopic versus open procedures represented a trade-off between infection risk and quality of life in this algorithm. For patients at medium risk for infection based on BMI, defect size, and other variables, switching to a laparoscopic approach dropped the infection probability from 3%-8% down to 0.1%-0.5%, Dr. Schlosser told attendees. On the other hand, switching to a laparoscopic approach increased the risk of non-ideal quality of life, she said.
One sample patient Dr. Schlosser described had an infection risk of 7.2% with the open procedure that dropped to just 0.4% for the laparoscopic procedure; however, that switch would mean that her likelihood of non-ideal quality of life 12 months after surgery increased from 24% with the open repair to 44% with the laparoscopic repair.
Dr. Schlosser had no disclosures related to the study. Co-authors provided disclosures related to Acelity, Allergan, Intuitive, Stryker, and W.L. Gore.
SOURCE: Schlosser KA, et al. abstract SF215 presented at the American College of Surgeons Clinical Congress 2018.
BOSTON – Choosing an operative approach for ventral hernia can be a matter of weighing the trade-offs between infection risk, postop quality of life, and patient and defect characteristics. A predictive algorithm has been developed to help with this decision, according to a study presented at the annual clinical congress of the American College of Surgeons.
Predictive modeling indicates that open repair might be considered, for example, in low BMI patients with large defects because of potentially fewer anticipated complications and improved quality of life, according to authors of the study. Conversely, laparoscopic repair might be considered in high BMI patients with recurrent hernias to decrease the associated risk of infection, the authors noted in a published abstract of the study.
The retrospective study was based on data on ventral hernia repairs in the International Hernia Mesh Registry that were performed between 2007 and 2017. Investigators used that data to build a predictive algorithm that took into account the impact on outcomes of BMI, hernia size, and operative approach, as well as age, sex, and diabetes status.
They identified 1,906 repairs, of which about 60% were open procedures. The mean patient age was 54.9 years, while mean BMI was 31.2 kg/m2 and the mean defect area was 44.8 cm2. Patients undergoing open procedures were significantly more likely to have infections, at 3.1% versus 0.3% for the laparoscopic approach (P less than .0001), investigators found.
A multivariate regression analysis controlling for confounding variables found that patients undergoing laparoscopic repair had an increased risk of seroma (odds ratio 1.78, confidence interval 1.05-3.03) but a decreased risk of infection (OR 0.05, CI 0.01-0.42). In addition, those undergoing laparoscopic procedures were more likely to have non-ideal quality of life at 1, 6, 12, and 24 months postoperatively, said the study’s lead author, Kathryn A. Schlosser, MD, a resident in the division of gastrointestinal and minimally invasive surgery, department of surgery, Carolinas Medical Center, Charlotte, N.C.
“These are both important factors — infection and non-ideal quality of life — and need to be part of our preoperative discussion with our patients when we start managing their expectations around the time of surgery,” Dr. Schlosser said in a podium presentation.
She and her colleagues calculated probability of infection based on the ratio of BMI to defect area. They found that, for example, the probability of postoperative infection was 21% for a diabetic 69-year-old female with a recurrent hernia who had a BMI of 39 and a defect area of 20 cm2. By contrast, infection probability was 3% in a 66-year-old female with a BMI of 37, a defect area of 1 cm2, and no diabetes, Dr. Schlosser said at the meeting.
Laparoscopic versus open procedures represented a trade-off between infection risk and quality of life in this algorithm. For patients at medium risk for infection based on BMI, defect size, and other variables, switching to a laparoscopic approach dropped the infection probability from 3%-8% down to 0.1%-0.5%, Dr. Schlosser told attendees. On the other hand, switching to a laparoscopic approach increased the risk of non-ideal quality of life, she said.
One sample patient Dr. Schlosser described had an infection risk of 7.2% with the open procedure that dropped to just 0.4% for the laparoscopic procedure; however, that switch would mean that her likelihood of non-ideal quality of life 12 months after surgery increased from 24% with the open repair to 44% with the laparoscopic repair.
Dr. Schlosser had no disclosures related to the study. Co-authors provided disclosures related to Acelity, Allergan, Intuitive, Stryker, and W.L. Gore.
SOURCE: Schlosser KA, et al. abstract SF215 presented at the American College of Surgeons Clinical Congress 2018.
REPORTING FROM THE ACS CLINICAL CONGRESS
Key clinical point: BMI and defect size are key factors for choosing laparoscopic or open surgery for ventral hernia repair.
Major finding: Patients undergoing open procedures were significantly more likely to have infections, at 3.1% versus 0.3% for the laparoscopic approach.
Study details: Retrospective study including 1,906 ventral hernia repairs in the International Hernia Mesh Registry conducted between 2007 and 2017.
Disclosures: Study authors provided disclosures related to Acelity, Allergan, Intuitive, Stryker, and W.L. Gore.
Source: Schlosser KA, et al. abstract SF215 presented at the American College of Surgeons Clinical Congress 2018.
Primary care holds key to curbing early-onset colorectal cancer
ESTES PARK, CO – , said gastroenterologist Swati G. Patel, MD, at a conference on internal medicine sponsored by the University of Colorado.

The startling rise in the incidence of colorectal cancer (CRC) in younger individuals in recent decades has generated much media coverage and considerable public concern. Reliable national data document a steady decline in CRC incidence over the past several decades in every age group 50 years and older – but a steady rise in incidence in those under age 50.
“The overall decline in CRC incidence and mortality beginning in the mid-1980s is an extremely amazing success story in cancer prevention. But there is still substantial work to be done,” observed Dr. Patel, who directs the Gastrointestinal Cancer Risk and Prevention Center at the university and is a staff physician at the Denver Veterans Affairs Medical Center.
Toward that end, in May 2018 the American Cancer Society issued updated guidelines recommending that people at average risk for CRC should now start undergoing regular screening for the disease at age 45. Models show that starting at age 45 rather than 50 would result in a 6.2% boost in life-years gained and a 17% increase in colonoscopies (CA Cancer J Clin. 2018 Jul;68(4):250-281).
“A different clinical and pathological entity”
Compared to CRC with onset at age 50 or later, early-onset disease is more often symptomatic at presentation. It is also significantly more likely to be located in the left colon or rectum, have a mucinous or signet ring histology, and be Stage III or IV.
“The disease seems to be a different clinical and pathological entity in younger patients,” Dr. Patel said.
The incidence of CRC before age 50 increased by 51% from 1994 to 2014. Mortality due to early-onset CRC rose by 11% during 2005-2015. Up to 90% of cases of early-onset CRC are diagnosed in individuals in their 40s. At the current rate of increase, early-onset CRC is projected to account for 20% of all cases of CRC by the year 2030.
The steadily rising incidence of early-onset CRC can’t be explained away as being due to earlier detection through greater availability of colonoscopy, in Dr. Patel’s view.
Numerous hypotheses have been put forth regarding the etiology of the rise in early-onset CRC. Correlations have variously been noted with the obesity epidemic, red meat consumption, diabetes, metabolic syndrome, increased early childhood exposure to antibiotics with resultant changes in gut microbiota in recent decades, and atopy.
“These are all fascinating hypotheses that will take decades to answer,” she said. “But in the meantime, what can we do about it now?”
Vital role for primary care
It’s going to take time to unravel the etiologies of early-onset CRC, both genetic and non-genetic. In the interim, opportunities abound for prevention and earlier detection. These opportunities are most available to primary care clinicians, since they provide continuity of care and are best positioned to detect red flags for patients at high risk for hereditary cancers.
“This is a time when we should concentrate our efforts on picking the low-hanging fruit,” Dr. Patel advised. She explained that this will entail a three-pronged approach: doing a better job of promptly evaluating potential symptoms of CRC, casting a wider net in search of patients with a hereditary cancer syndrome, and initiating earlier screening, especially in high-risk patients – a category that she said should include all African-Americans.
Prompt evaluation of symptoms
In one major study, the average time from symptom onset – bleeding, unexplained abdominal pain, changes in bowel habits, and/or iron deficiency – to diagnosis of CRC was 217 days in those with early-onset CRC, compared with 29.5 days in patients age 50 or older.
This huge disparity in time to diagnosis occurs largely because physicians typically assume that scant blood present in the stool of younger patients is due to hemorrhoids. Also frequently overlooked is the fact that the presence of hemorrhoids on physical examination can obscure an upstream malignant lesion.
“The initial plan is often to treat assumed benign pathology and only if symptoms persist to consider other causes,” Dr. Patel noted. That practice, she said, has to change: “The tools that we rely on in the clinic for this particular complaint – history and physical examination – are just not as reliable as we need them to be.”
Assessing for increased genetic/familial risk
The best estimate is that 16%-25% of early-onset CRC may be due to a high- or moderate-penetrance genetic mutation. Another 35% or so of cases are associated with a positive family history for CRC without a defined genetic condition.
In a 2011 study a mere 1.2% of Americans carrying a Lynch mutation were aware of it. “I suspect today it’s still less than 10%. We’re still not doing a very good job of identifying high-risk patients,” Dr. Patel said.
The National Comprehensive Cancer Network has published a guideline for assessment of genetic/familial high risk for CRC, but it’s far too complex and detailed for practical use in a busy primary care practice, in her view.
“You don’t have to remember all the detailed branching algorithms and criteria in the NCCN guideline. I propose a gut check. Increased risk boils down to three key points: any patient with onset of advanced neoplasia before age 50, or a personal history of multiple cancers, whether synchronous or metachronous, or with a strong family history of cancer on one side of the family should be sent on for a detailed risk assessment,” she said.
Similarly, don’t sweat trying to remember all the types of cancer associated with Lynch syndrome.
“We’re learning that the true answer is that it could be any kind of cancer,” Dr. Patel said.
It’s worth bearing in mind, however, that just because a patient doesn’t have a positive family history doesn’t mean that a hereditary cancer syndrome can be ruled out. Incomplete penetrance is characteristic of all of these hereditary syndromes. Indeed, 2 out of 10 patients with Lynch syndrome will never develop CRC.
Multiple gastroenterology societies now recommend routine PCR screening of all colon cancers for microsatellite instability markers – the hallmark of Lynch syndrome tumors – even if the cancer occurs in an 88-year-old. And if the screen is positive, genetic testing is appropriate. The University of Colorado is among a growing number of medical centers that have implemented this policy.
Dr. Patel noted that the American Cancer Society characterized its start-screening-at-45 guideline for average-risk patients as “conditional” rather than a “strong” recommendation. She advised applying it without reservation – and in some instances even starting at age 40 – for three groups clearly at high risk for early-onset CRC: African Americans, patients with a family history of CRC, and those with a family history of advanced adenoma, such as a tubular adenoma, which if not removed has an 80% chance of progressing to cancer.
She reported having no financial conflicts regarding her presentation.
ESTES PARK, CO – , said gastroenterologist Swati G. Patel, MD, at a conference on internal medicine sponsored by the University of Colorado.
The startling rise in the incidence of colorectal cancer (CRC) in younger individuals in recent decades has generated much media coverage and considerable public concern. Reliable national data document a steady decline in CRC incidence over the past several decades in every age group 50 years and older – but a steady rise in incidence in those under age 50.
“The overall decline in CRC incidence and mortality beginning in the mid-1980s is an extremely amazing success story in cancer prevention. But there is still substantial work to be done,” observed Dr. Patel, who directs the Gastrointestinal Cancer Risk and Prevention Center at the university and is a staff physician at the Denver Veterans Affairs Medical Center.
Toward that end, in May 2018 the American Cancer Society issued updated guidelines recommending that people at average risk for CRC should now start undergoing regular screening for the disease at age 45. Models show that starting at age 45 rather than 50 would result in a 6.2% boost in life-years gained and a 17% increase in colonoscopies (CA Cancer J Clin. 2018 Jul;68(4):250-281).
“A different clinical and pathological entity”
Compared to CRC with onset at age 50 or later, early-onset disease is more often symptomatic at presentation. It is also significantly more likely to be located in the left colon or rectum, have a mucinous or signet ring histology, and be Stage III or IV.
“The disease seems to be a different clinical and pathological entity in younger patients,” Dr. Patel said.
The incidence of CRC before age 50 increased by 51% from 1994 to 2014. Mortality due to early-onset CRC rose by 11% during 2005-2015. Up to 90% of cases of early-onset CRC are diagnosed in individuals in their 40s. At the current rate of increase, early-onset CRC is projected to account for 20% of all cases of CRC by the year 2030.
The steadily rising incidence of early-onset CRC can’t be explained away as being due to earlier detection through greater availability of colonoscopy, in Dr. Patel’s view.
Numerous hypotheses have been put forth regarding the etiology of the rise in early-onset CRC. Correlations have variously been noted with the obesity epidemic, red meat consumption, diabetes, metabolic syndrome, increased early childhood exposure to antibiotics with resultant changes in gut microbiota in recent decades, and atopy.
“These are all fascinating hypotheses that will take decades to answer,” she said. “But in the meantime, what can we do about it now?”
Vital role for primary care
It’s going to take time to unravel the etiologies of early-onset CRC, both genetic and non-genetic. In the interim, opportunities abound for prevention and earlier detection. These opportunities are most available to primary care clinicians, since they provide continuity of care and are best positioned to detect red flags for patients at high risk for hereditary cancers.
“This is a time when we should concentrate our efforts on picking the low-hanging fruit,” Dr. Patel advised. She explained that this will entail a three-pronged approach: doing a better job of promptly evaluating potential symptoms of CRC, casting a wider net in search of patients with a hereditary cancer syndrome, and initiating earlier screening, especially in high-risk patients – a category that she said should include all African-Americans.
Prompt evaluation of symptoms
In one major study, the average time from symptom onset – bleeding, unexplained abdominal pain, changes in bowel habits, and/or iron deficiency – to diagnosis of CRC was 217 days in those with early-onset CRC, compared with 29.5 days in patients age 50 or older.
This huge disparity in time to diagnosis occurs largely because physicians typically assume that scant blood present in the stool of younger patients is due to hemorrhoids. Also frequently overlooked is the fact that the presence of hemorrhoids on physical examination can obscure an upstream malignant lesion.
“The initial plan is often to treat assumed benign pathology and only if symptoms persist to consider other causes,” Dr. Patel noted. That practice, she said, has to change: “The tools that we rely on in the clinic for this particular complaint – history and physical examination – are just not as reliable as we need them to be.”
Assessing for increased genetic/familial risk
The best estimate is that 16%-25% of early-onset CRC may be due to a high- or moderate-penetrance genetic mutation. Another 35% or so of cases are associated with a positive family history for CRC without a defined genetic condition.
In a 2011 study a mere 1.2% of Americans carrying a Lynch mutation were aware of it. “I suspect today it’s still less than 10%. We’re still not doing a very good job of identifying high-risk patients,” Dr. Patel said.
The National Comprehensive Cancer Network has published a guideline for assessment of genetic/familial high risk for CRC, but it’s far too complex and detailed for practical use in a busy primary care practice, in her view.
“You don’t have to remember all the detailed branching algorithms and criteria in the NCCN guideline. I propose a gut check. Increased risk boils down to three key points: any patient with onset of advanced neoplasia before age 50, or a personal history of multiple cancers, whether synchronous or metachronous, or with a strong family history of cancer on one side of the family should be sent on for a detailed risk assessment,” she said.
Similarly, don’t sweat trying to remember all the types of cancer associated with Lynch syndrome.
“We’re learning that the true answer is that it could be any kind of cancer,” Dr. Patel said.
It’s worth bearing in mind, however, that just because a patient doesn’t have a positive family history doesn’t mean that a hereditary cancer syndrome can be ruled out. Incomplete penetrance is characteristic of all of these hereditary syndromes. Indeed, 2 out of 10 patients with Lynch syndrome will never develop CRC.
Multiple gastroenterology societies now recommend routine PCR screening of all colon cancers for microsatellite instability markers – the hallmark of Lynch syndrome tumors – even if the cancer occurs in an 88-year-old. And if the screen is positive, genetic testing is appropriate. The University of Colorado is among a growing number of medical centers that have implemented this policy.
Dr. Patel noted that the American Cancer Society characterized its start-screening-at-45 guideline for average-risk patients as “conditional” rather than a “strong” recommendation. She advised applying it without reservation – and in some instances even starting at age 40 – for three groups clearly at high risk for early-onset CRC: African Americans, patients with a family history of CRC, and those with a family history of advanced adenoma, such as a tubular adenoma, which if not removed has an 80% chance of progressing to cancer.
She reported having no financial conflicts regarding her presentation.
ESTES PARK, CO – , said gastroenterologist Swati G. Patel, MD, at a conference on internal medicine sponsored by the University of Colorado.
The startling rise in the incidence of colorectal cancer (CRC) in younger individuals in recent decades has generated much media coverage and considerable public concern. Reliable national data document a steady decline in CRC incidence over the past several decades in every age group 50 years and older – but a steady rise in incidence in those under age 50.
“The overall decline in CRC incidence and mortality beginning in the mid-1980s is an extremely amazing success story in cancer prevention. But there is still substantial work to be done,” observed Dr. Patel, who directs the Gastrointestinal Cancer Risk and Prevention Center at the university and is a staff physician at the Denver Veterans Affairs Medical Center.
Toward that end, in May 2018 the American Cancer Society issued updated guidelines recommending that people at average risk for CRC should now start undergoing regular screening for the disease at age 45. Models show that starting at age 45 rather than 50 would result in a 6.2% boost in life-years gained and a 17% increase in colonoscopies (CA Cancer J Clin. 2018 Jul;68(4):250-281).
“A different clinical and pathological entity”
Compared to CRC with onset at age 50 or later, early-onset disease is more often symptomatic at presentation. It is also significantly more likely to be located in the left colon or rectum, have a mucinous or signet ring histology, and be Stage III or IV.
“The disease seems to be a different clinical and pathological entity in younger patients,” Dr. Patel said.
The incidence of CRC before age 50 increased by 51% from 1994 to 2014. Mortality due to early-onset CRC rose by 11% during 2005-2015. Up to 90% of cases of early-onset CRC are diagnosed in individuals in their 40s. At the current rate of increase, early-onset CRC is projected to account for 20% of all cases of CRC by the year 2030.
The steadily rising incidence of early-onset CRC can’t be explained away as being due to earlier detection through greater availability of colonoscopy, in Dr. Patel’s view.
Numerous hypotheses have been put forth regarding the etiology of the rise in early-onset CRC. Correlations have variously been noted with the obesity epidemic, red meat consumption, diabetes, metabolic syndrome, increased early childhood exposure to antibiotics with resultant changes in gut microbiota in recent decades, and atopy.
“These are all fascinating hypotheses that will take decades to answer,” she said. “But in the meantime, what can we do about it now?”
Vital role for primary care
It’s going to take time to unravel the etiologies of early-onset CRC, both genetic and non-genetic. In the interim, opportunities abound for prevention and earlier detection. These opportunities are most available to primary care clinicians, since they provide continuity of care and are best positioned to detect red flags for patients at high risk for hereditary cancers.
“This is a time when we should concentrate our efforts on picking the low-hanging fruit,” Dr. Patel advised. She explained that this will entail a three-pronged approach: doing a better job of promptly evaluating potential symptoms of CRC, casting a wider net in search of patients with a hereditary cancer syndrome, and initiating earlier screening, especially in high-risk patients – a category that she said should include all African-Americans.
Prompt evaluation of symptoms
In one major study, the average time from symptom onset – bleeding, unexplained abdominal pain, changes in bowel habits, and/or iron deficiency – to diagnosis of CRC was 217 days in those with early-onset CRC, compared with 29.5 days in patients age 50 or older.
This huge disparity in time to diagnosis occurs largely because physicians typically assume that scant blood present in the stool of younger patients is due to hemorrhoids. Also frequently overlooked is the fact that the presence of hemorrhoids on physical examination can obscure an upstream malignant lesion.
“The initial plan is often to treat assumed benign pathology and only if symptoms persist to consider other causes,” Dr. Patel noted. That practice, she said, has to change: “The tools that we rely on in the clinic for this particular complaint – history and physical examination – are just not as reliable as we need them to be.”
Assessing for increased genetic/familial risk
The best estimate is that 16%-25% of early-onset CRC may be due to a high- or moderate-penetrance genetic mutation. Another 35% or so of cases are associated with a positive family history for CRC without a defined genetic condition.
In a 2011 study a mere 1.2% of Americans carrying a Lynch mutation were aware of it. “I suspect today it’s still less than 10%. We’re still not doing a very good job of identifying high-risk patients,” Dr. Patel said.
The National Comprehensive Cancer Network has published a guideline for assessment of genetic/familial high risk for CRC, but it’s far too complex and detailed for practical use in a busy primary care practice, in her view.
“You don’t have to remember all the detailed branching algorithms and criteria in the NCCN guideline. I propose a gut check. Increased risk boils down to three key points: any patient with onset of advanced neoplasia before age 50, or a personal history of multiple cancers, whether synchronous or metachronous, or with a strong family history of cancer on one side of the family should be sent on for a detailed risk assessment,” she said.
Similarly, don’t sweat trying to remember all the types of cancer associated with Lynch syndrome.
“We’re learning that the true answer is that it could be any kind of cancer,” Dr. Patel said.
It’s worth bearing in mind, however, that just because a patient doesn’t have a positive family history doesn’t mean that a hereditary cancer syndrome can be ruled out. Incomplete penetrance is characteristic of all of these hereditary syndromes. Indeed, 2 out of 10 patients with Lynch syndrome will never develop CRC.
Multiple gastroenterology societies now recommend routine PCR screening of all colon cancers for microsatellite instability markers – the hallmark of Lynch syndrome tumors – even if the cancer occurs in an 88-year-old. And if the screen is positive, genetic testing is appropriate. The University of Colorado is among a growing number of medical centers that have implemented this policy.
Dr. Patel noted that the American Cancer Society characterized its start-screening-at-45 guideline for average-risk patients as “conditional” rather than a “strong” recommendation. She advised applying it without reservation – and in some instances even starting at age 40 – for three groups clearly at high risk for early-onset CRC: African Americans, patients with a family history of CRC, and those with a family history of advanced adenoma, such as a tubular adenoma, which if not removed has an 80% chance of progressing to cancer.
She reported having no financial conflicts regarding her presentation.
REPORTING FROM COLORADO IM
EHR-guided strategy reduces postop VTE events
BOSTON – Avoiding could result in a reduction in VTE rates, a speaker said at the annual clinical congress of the American College of Surgeons.

The VTE rate dropped by about one-quarter in the trauma care pathway at the University of Pittsburgh Medical Center (UPMC) after implementation of algorithms to risk-stratify patients and guide nursing staff, said Matthew D. Neal, MD, FACS, the Roberta G. Simmons Assistant Professor of Surgery at the University of Pittsburgh.
By incorporating algorithms into the electronic health record (EHR), UPMC was able to realize a “dramatic” 72% reduction in missed doses, from 4,331 missed doses in 2014 to 1,193 in 2015, Dr. Neal told attendees in a session focused on hot topics in surgical patient safety.
That decrease in missed doses has translated into a decreased rate of VTE, from an already relatively low rate of 1.5% in 2015, to 1.1% in 2017, representing a 26.7% reduction, according to data Dr. Neal shared in his podium presentation.
“This has been a sustainable event for us, largely linked to the implementation of an EHR-guided risk assessment pathway to guide the implementation of VTE prophylaxis,” he said.
The change was safe, he added, noting that, since utilization of this pathway, there have been no significant increases in the rate of bleeding events among patients who have mandatory orders.
These results corroborate those of some previous investigations, including one key study from the Johns Hopkins Hospital that described the adoption of a mandatory computerized clinical decision support tool to improve adherence to best practices for VTE prophylaxis.
After incorporation of the tool in the computerized order entry system, there was a significant increase in VTE prophylaxis, translating into a significant drop in preventable harm from VTE, from 1.0% to 0.17% (P = .04), investigators reported in JAMA Surgery.
Reducing missed doses is one of the major contributing factors to decreased VTE rates, according to Dr. Neal.
Missed doses of enoxaparin correlate with increased incidence of deep vein thrombosis (DVT) in trauma and general surgery patients, according to results of one prospective study Dr. Neal described. In that study of 202 patients, reported in JAMA Surgery, DVTs were seen in 23.5% of patients with missed doses, compared with 4.8 for patients with no missed doses (P < .01).
“We need to understand how to risk assess and how to utilize our EHR as a tool,” Dr. Neal told attendees.
Dr. Neal reported disclosures related to Janssen Pharmaceuticals, CSL Behring, Accriva Diagnostics, and Haemonetics, as well as a U.S. patent for a treatment of infectious and inflammatory disorders, and laboratory funding from the National Institutes of Health, Department of Defense, and the Biomedical Advanced Research and Development Authority.
SOURCE: Neal MD. Presentation at the American College of Surgeons Clinical Congress. 2018 Oct 25.
BOSTON – Avoiding could result in a reduction in VTE rates, a speaker said at the annual clinical congress of the American College of Surgeons.
The VTE rate dropped by about one-quarter in the trauma care pathway at the University of Pittsburgh Medical Center (UPMC) after implementation of algorithms to risk-stratify patients and guide nursing staff, said Matthew D. Neal, MD, FACS, the Roberta G. Simmons Assistant Professor of Surgery at the University of Pittsburgh.
By incorporating algorithms into the electronic health record (EHR), UPMC was able to realize a “dramatic” 72% reduction in missed doses, from 4,331 missed doses in 2014 to 1,193 in 2015, Dr. Neal told attendees in a session focused on hot topics in surgical patient safety.
That decrease in missed doses has translated into a decreased rate of VTE, from an already relatively low rate of 1.5% in 2015, to 1.1% in 2017, representing a 26.7% reduction, according to data Dr. Neal shared in his podium presentation.
“This has been a sustainable event for us, largely linked to the implementation of an EHR-guided risk assessment pathway to guide the implementation of VTE prophylaxis,” he said.
The change was safe, he added, noting that, since utilization of this pathway, there have been no significant increases in the rate of bleeding events among patients who have mandatory orders.
These results corroborate those of some previous investigations, including one key study from the Johns Hopkins Hospital that described the adoption of a mandatory computerized clinical decision support tool to improve adherence to best practices for VTE prophylaxis.
After incorporation of the tool in the computerized order entry system, there was a significant increase in VTE prophylaxis, translating into a significant drop in preventable harm from VTE, from 1.0% to 0.17% (P = .04), investigators reported in JAMA Surgery.
Reducing missed doses is one of the major contributing factors to decreased VTE rates, according to Dr. Neal.
Missed doses of enoxaparin correlate with increased incidence of deep vein thrombosis (DVT) in trauma and general surgery patients, according to results of one prospective study Dr. Neal described. In that study of 202 patients, reported in JAMA Surgery, DVTs were seen in 23.5% of patients with missed doses, compared with 4.8 for patients with no missed doses (P < .01).
“We need to understand how to risk assess and how to utilize our EHR as a tool,” Dr. Neal told attendees.
Dr. Neal reported disclosures related to Janssen Pharmaceuticals, CSL Behring, Accriva Diagnostics, and Haemonetics, as well as a U.S. patent for a treatment of infectious and inflammatory disorders, and laboratory funding from the National Institutes of Health, Department of Defense, and the Biomedical Advanced Research and Development Authority.
SOURCE: Neal MD. Presentation at the American College of Surgeons Clinical Congress. 2018 Oct 25.
BOSTON – Avoiding could result in a reduction in VTE rates, a speaker said at the annual clinical congress of the American College of Surgeons.
The VTE rate dropped by about one-quarter in the trauma care pathway at the University of Pittsburgh Medical Center (UPMC) after implementation of algorithms to risk-stratify patients and guide nursing staff, said Matthew D. Neal, MD, FACS, the Roberta G. Simmons Assistant Professor of Surgery at the University of Pittsburgh.
By incorporating algorithms into the electronic health record (EHR), UPMC was able to realize a “dramatic” 72% reduction in missed doses, from 4,331 missed doses in 2014 to 1,193 in 2015, Dr. Neal told attendees in a session focused on hot topics in surgical patient safety.
That decrease in missed doses has translated into a decreased rate of VTE, from an already relatively low rate of 1.5% in 2015, to 1.1% in 2017, representing a 26.7% reduction, according to data Dr. Neal shared in his podium presentation.
“This has been a sustainable event for us, largely linked to the implementation of an EHR-guided risk assessment pathway to guide the implementation of VTE prophylaxis,” he said.
The change was safe, he added, noting that, since utilization of this pathway, there have been no significant increases in the rate of bleeding events among patients who have mandatory orders.
These results corroborate those of some previous investigations, including one key study from the Johns Hopkins Hospital that described the adoption of a mandatory computerized clinical decision support tool to improve adherence to best practices for VTE prophylaxis.
After incorporation of the tool in the computerized order entry system, there was a significant increase in VTE prophylaxis, translating into a significant drop in preventable harm from VTE, from 1.0% to 0.17% (P = .04), investigators reported in JAMA Surgery.
Reducing missed doses is one of the major contributing factors to decreased VTE rates, according to Dr. Neal.
Missed doses of enoxaparin correlate with increased incidence of deep vein thrombosis (DVT) in trauma and general surgery patients, according to results of one prospective study Dr. Neal described. In that study of 202 patients, reported in JAMA Surgery, DVTs were seen in 23.5% of patients with missed doses, compared with 4.8 for patients with no missed doses (P < .01).
“We need to understand how to risk assess and how to utilize our EHR as a tool,” Dr. Neal told attendees.
Dr. Neal reported disclosures related to Janssen Pharmaceuticals, CSL Behring, Accriva Diagnostics, and Haemonetics, as well as a U.S. patent for a treatment of infectious and inflammatory disorders, and laboratory funding from the National Institutes of Health, Department of Defense, and the Biomedical Advanced Research and Development Authority.
SOURCE: Neal MD. Presentation at the American College of Surgeons Clinical Congress. 2018 Oct 25.
AT THE ACS CLINICAL CONGRESS
Frailty tied to higher mortality after major vascular surgery
Frailty defined as functional dependence is a predictor of mortality risk in elderly patients having major vascular surgery, a meta-analysis of studies has found
“Functional dependency may be recommended for use in rapid screening for frailty in major vascular surgery because of the high quality of associated evidence. Additionally, information on central muscle mass also adds incremental predictive value to long-term survival of elderly patients after major vascular surgery,” the study investigaters stated. However, they pointed out that “other newly developed frailty tools require further validation in more studies” before they should be adopted.
The report, published in the European Journal of Vascular and Endovascular Surgery, evaluated the effect of frailty in major vascular surgery from a search of MEDLINE, Embase, Cochrane Database, and Scopus through May 2018. Data were extracted from the articles related to surgery for abdominal aortic aneurysms (AAA) and lower extremity artery disease (LEAD), and a modified Newcastle-Ottawa scale was used to assess the quality of the included studies, according to Jiarong Wang, MD, of the department of vascular surgery, Sichuan University, Sichuan Province, China, and colleagues. A total of 22 cohort studies and one randomized controlled trial was used in the final analysis. The reviewers expressed the impact of frailty on outcomes as odds ratios (OR) or hazard ratios (HR) using a random effects model.
The researchers found that frailty, in terms of functional dependence, was associated with a significantly increased 30-day mortality risk in patients with AAA without heterogeneity (OR 5.15) and also in LEAD patients (OR 3.29). Functionally dependent patients also had a significantly increased 30-day mortality risk, compared with independent patients (OR 4.49), and similar results were observed after stratifying those who underwent AAA repair (OR 5.14) or lower extremity revascularization (OR 4.18). Even for patients who underwent endovascular procedures rather than open surgery, functional dependency was also associated with a significantly increased 30-day mortality risk (OR 4.90). In addition, with regard to 30-day morbidity, frailty was associated with a significantly increased risk in both AAA (OR 2.79) and LEAD (OR 1.40) patients.
As far as long-term outcomes were concerned, frailty was associated with a significantly increased risk of long-term all-cause mortality in the overall studied population (HR 2.22), as well as in patients with AAA repair (HR 2.10) and LEAD revascularization (HR 2.46). Dr. Wang and colleagues found that central muscle mass was the only tool with moderate quality of evidence predicting long-term survival after major vascular surgery (HR .48), with other single-domain tools such as nutrition or cognition scoring being of low quality. The modified Frailty Index was the only multi-domain tool with moderate quality in predicting mortality for AAA, while others were scored as low or very low, the authors added.
“Future research is warranted to establish consensus on how to select the optimal frailty tool for certain clinical settings,” they concluded.
The authors reported that they had no conflicts of interest and no funding sources for the study.
SOURCE: Wang, J et al. Eur J Vasc Endovasc Surg. 2018;56:591-602.
Frailty defined as functional dependence is a predictor of mortality risk in elderly patients having major vascular surgery, a meta-analysis of studies has found
“Functional dependency may be recommended for use in rapid screening for frailty in major vascular surgery because of the high quality of associated evidence. Additionally, information on central muscle mass also adds incremental predictive value to long-term survival of elderly patients after major vascular surgery,” the study investigaters stated. However, they pointed out that “other newly developed frailty tools require further validation in more studies” before they should be adopted.
The report, published in the European Journal of Vascular and Endovascular Surgery, evaluated the effect of frailty in major vascular surgery from a search of MEDLINE, Embase, Cochrane Database, and Scopus through May 2018. Data were extracted from the articles related to surgery for abdominal aortic aneurysms (AAA) and lower extremity artery disease (LEAD), and a modified Newcastle-Ottawa scale was used to assess the quality of the included studies, according to Jiarong Wang, MD, of the department of vascular surgery, Sichuan University, Sichuan Province, China, and colleagues. A total of 22 cohort studies and one randomized controlled trial was used in the final analysis. The reviewers expressed the impact of frailty on outcomes as odds ratios (OR) or hazard ratios (HR) using a random effects model.
The researchers found that frailty, in terms of functional dependence, was associated with a significantly increased 30-day mortality risk in patients with AAA without heterogeneity (OR 5.15) and also in LEAD patients (OR 3.29). Functionally dependent patients also had a significantly increased 30-day mortality risk, compared with independent patients (OR 4.49), and similar results were observed after stratifying those who underwent AAA repair (OR 5.14) or lower extremity revascularization (OR 4.18). Even for patients who underwent endovascular procedures rather than open surgery, functional dependency was also associated with a significantly increased 30-day mortality risk (OR 4.90). In addition, with regard to 30-day morbidity, frailty was associated with a significantly increased risk in both AAA (OR 2.79) and LEAD (OR 1.40) patients.
As far as long-term outcomes were concerned, frailty was associated with a significantly increased risk of long-term all-cause mortality in the overall studied population (HR 2.22), as well as in patients with AAA repair (HR 2.10) and LEAD revascularization (HR 2.46). Dr. Wang and colleagues found that central muscle mass was the only tool with moderate quality of evidence predicting long-term survival after major vascular surgery (HR .48), with other single-domain tools such as nutrition or cognition scoring being of low quality. The modified Frailty Index was the only multi-domain tool with moderate quality in predicting mortality for AAA, while others were scored as low or very low, the authors added.
“Future research is warranted to establish consensus on how to select the optimal frailty tool for certain clinical settings,” they concluded.
The authors reported that they had no conflicts of interest and no funding sources for the study.
SOURCE: Wang, J et al. Eur J Vasc Endovasc Surg. 2018;56:591-602.
Frailty defined as functional dependence is a predictor of mortality risk in elderly patients having major vascular surgery, a meta-analysis of studies has found
“Functional dependency may be recommended for use in rapid screening for frailty in major vascular surgery because of the high quality of associated evidence. Additionally, information on central muscle mass also adds incremental predictive value to long-term survival of elderly patients after major vascular surgery,” the study investigaters stated. However, they pointed out that “other newly developed frailty tools require further validation in more studies” before they should be adopted.
The report, published in the European Journal of Vascular and Endovascular Surgery, evaluated the effect of frailty in major vascular surgery from a search of MEDLINE, Embase, Cochrane Database, and Scopus through May 2018. Data were extracted from the articles related to surgery for abdominal aortic aneurysms (AAA) and lower extremity artery disease (LEAD), and a modified Newcastle-Ottawa scale was used to assess the quality of the included studies, according to Jiarong Wang, MD, of the department of vascular surgery, Sichuan University, Sichuan Province, China, and colleagues. A total of 22 cohort studies and one randomized controlled trial was used in the final analysis. The reviewers expressed the impact of frailty on outcomes as odds ratios (OR) or hazard ratios (HR) using a random effects model.
The researchers found that frailty, in terms of functional dependence, was associated with a significantly increased 30-day mortality risk in patients with AAA without heterogeneity (OR 5.15) and also in LEAD patients (OR 3.29). Functionally dependent patients also had a significantly increased 30-day mortality risk, compared with independent patients (OR 4.49), and similar results were observed after stratifying those who underwent AAA repair (OR 5.14) or lower extremity revascularization (OR 4.18). Even for patients who underwent endovascular procedures rather than open surgery, functional dependency was also associated with a significantly increased 30-day mortality risk (OR 4.90). In addition, with regard to 30-day morbidity, frailty was associated with a significantly increased risk in both AAA (OR 2.79) and LEAD (OR 1.40) patients.
As far as long-term outcomes were concerned, frailty was associated with a significantly increased risk of long-term all-cause mortality in the overall studied population (HR 2.22), as well as in patients with AAA repair (HR 2.10) and LEAD revascularization (HR 2.46). Dr. Wang and colleagues found that central muscle mass was the only tool with moderate quality of evidence predicting long-term survival after major vascular surgery (HR .48), with other single-domain tools such as nutrition or cognition scoring being of low quality. The modified Frailty Index was the only multi-domain tool with moderate quality in predicting mortality for AAA, while others were scored as low or very low, the authors added.
“Future research is warranted to establish consensus on how to select the optimal frailty tool for certain clinical settings,” they concluded.
The authors reported that they had no conflicts of interest and no funding sources for the study.
SOURCE: Wang, J et al. Eur J Vasc Endovasc Surg. 2018;56:591-602.
FROM EUROPEAN JOURNAL OF VASCULAR AND ENDOVASCULAR SURGERY
Key clinical point: Frailty was associated with increased short- and long-term mortality in major vascular surgery.
Major finding: Frailty was associated with a fourfold increased risk of 30-day mortality and a doubled increased risk of long-term mortality after major vascular surgery.
Study details: A meta-analysis of 22 cohort studies and one randomized controlled trial.
Disclosures: The authors reported that they had no conflicts of interest and no funding sources for the study.
Source: Wang, J et al., 2018. Eur J Vasc Endovasc Surg. 56:591-602.
Post-mastectomy pain strategy allows for safe, same-day discharge
BOSTON – A multimodal pain regimen allowed for safe and effective same-day discharge of women undergoing mastectomy procedures, a recent study showed.
Women had little need for stronger oral narcotic use in the single center, retrospective study presented at the annual clinical congress of the American College of Surgeons.
The analysis included 72 consecutive mastectomies performed at a single center from November 2015 to July 2017. Most mastectomies were bilateral (61, or 84.7%) while 11 (15.3%) were unilateral.
Patients received a standardized pain regimen including 1 gram of IV acetaminophen interoperatively, combined with 30 mg of IV ketorolac and a 4-level intercostal nerve block with liposomal bupivacaine.
Liposomal bupivacaine has a longer half-life than other anesthetics, according to lead study author Radbeh Torabi, MD, a fifth-year plastic surgery resident at Louisiana State University (LSU) Health Science Center in New Orleans.
“That allows for prolonged pain control, especially during the time when the patient’s going to have the most amount of pain, which is the first day to two days postoperatively,” Dr. Torabi said in an interview.
All 72 patients were discharged home on the same day with just a 1-week prescription for acetaminophen with codeine.
Only 5 patients presented to the emergency room in the 30-day postoperative period, and of those, only 2 (2.8%) required readmission for reasons other than mastectomy-related pain, investigators said. The remaining 3 patients did present with pain, but did not require hospital admission.
Taken together, these findings suggest that this multimodal strategy offers excellent pain control and has the potential to minimize inpatient admissions while decreasing oral narcotic use, investigators said in an interview following their presentation.
“The main takeaway is reducing the amount of prescriptions we give,” Dr. Torabi said.
Study co-author Cameron T. Ward Coker, MD, a fourth-year general surgery resident at LSU, said the multimodal pain strategy used in this study could represent a step toward eliminating the risks associated with opioid prescribing.
“From the feedback we got from our lecture and the other surgeons in the room, it seems like that’s already becoming a widespread phenomenon,” Dr. Coker said.
Patients in the study had an average age of about 57 years and an average BMI of 30, according to the investigators.
Dr. Coker and Dr. Torabi had no disclosures related to the presentation.
SOURCE: Torabi R, et al. Scientific forum abstract at American College of Surgeons Clinical Congress. 2018 Oct 23.
BOSTON – A multimodal pain regimen allowed for safe and effective same-day discharge of women undergoing mastectomy procedures, a recent study showed.
Women had little need for stronger oral narcotic use in the single center, retrospective study presented at the annual clinical congress of the American College of Surgeons.
The analysis included 72 consecutive mastectomies performed at a single center from November 2015 to July 2017. Most mastectomies were bilateral (61, or 84.7%) while 11 (15.3%) were unilateral.
Patients received a standardized pain regimen including 1 gram of IV acetaminophen interoperatively, combined with 30 mg of IV ketorolac and a 4-level intercostal nerve block with liposomal bupivacaine.
Liposomal bupivacaine has a longer half-life than other anesthetics, according to lead study author Radbeh Torabi, MD, a fifth-year plastic surgery resident at Louisiana State University (LSU) Health Science Center in New Orleans.
“That allows for prolonged pain control, especially during the time when the patient’s going to have the most amount of pain, which is the first day to two days postoperatively,” Dr. Torabi said in an interview.
All 72 patients were discharged home on the same day with just a 1-week prescription for acetaminophen with codeine.
Only 5 patients presented to the emergency room in the 30-day postoperative period, and of those, only 2 (2.8%) required readmission for reasons other than mastectomy-related pain, investigators said. The remaining 3 patients did present with pain, but did not require hospital admission.
Taken together, these findings suggest that this multimodal strategy offers excellent pain control and has the potential to minimize inpatient admissions while decreasing oral narcotic use, investigators said in an interview following their presentation.
“The main takeaway is reducing the amount of prescriptions we give,” Dr. Torabi said.
Study co-author Cameron T. Ward Coker, MD, a fourth-year general surgery resident at LSU, said the multimodal pain strategy used in this study could represent a step toward eliminating the risks associated with opioid prescribing.
“From the feedback we got from our lecture and the other surgeons in the room, it seems like that’s already becoming a widespread phenomenon,” Dr. Coker said.
Patients in the study had an average age of about 57 years and an average BMI of 30, according to the investigators.
Dr. Coker and Dr. Torabi had no disclosures related to the presentation.
SOURCE: Torabi R, et al. Scientific forum abstract at American College of Surgeons Clinical Congress. 2018 Oct 23.
BOSTON – A multimodal pain regimen allowed for safe and effective same-day discharge of women undergoing mastectomy procedures, a recent study showed.
Women had little need for stronger oral narcotic use in the single center, retrospective study presented at the annual clinical congress of the American College of Surgeons.
The analysis included 72 consecutive mastectomies performed at a single center from November 2015 to July 2017. Most mastectomies were bilateral (61, or 84.7%) while 11 (15.3%) were unilateral.
Patients received a standardized pain regimen including 1 gram of IV acetaminophen interoperatively, combined with 30 mg of IV ketorolac and a 4-level intercostal nerve block with liposomal bupivacaine.
Liposomal bupivacaine has a longer half-life than other anesthetics, according to lead study author Radbeh Torabi, MD, a fifth-year plastic surgery resident at Louisiana State University (LSU) Health Science Center in New Orleans.
“That allows for prolonged pain control, especially during the time when the patient’s going to have the most amount of pain, which is the first day to two days postoperatively,” Dr. Torabi said in an interview.
All 72 patients were discharged home on the same day with just a 1-week prescription for acetaminophen with codeine.
Only 5 patients presented to the emergency room in the 30-day postoperative period, and of those, only 2 (2.8%) required readmission for reasons other than mastectomy-related pain, investigators said. The remaining 3 patients did present with pain, but did not require hospital admission.
Taken together, these findings suggest that this multimodal strategy offers excellent pain control and has the potential to minimize inpatient admissions while decreasing oral narcotic use, investigators said in an interview following their presentation.
“The main takeaway is reducing the amount of prescriptions we give,” Dr. Torabi said.
Study co-author Cameron T. Ward Coker, MD, a fourth-year general surgery resident at LSU, said the multimodal pain strategy used in this study could represent a step toward eliminating the risks associated with opioid prescribing.
“From the feedback we got from our lecture and the other surgeons in the room, it seems like that’s already becoming a widespread phenomenon,” Dr. Coker said.
Patients in the study had an average age of about 57 years and an average BMI of 30, according to the investigators.
Dr. Coker and Dr. Torabi had no disclosures related to the presentation.
SOURCE: Torabi R, et al. Scientific forum abstract at American College of Surgeons Clinical Congress. 2018 Oct 23.
REPORTING FROM THE ACS CLINICAL CONGRESS
Key clinical point:
Major finding: Of 72 women who had same-day discharge after mastectomy, only 3 presented for pain in the 30-day postoperative period.
Study details: A retrospective review of 72 consecutive mastectomies performed at a single surgical center.
Disclosures: The lead author had no disclosures related to the presentation.
Source: Torabi R, et al. Scientific forum abstract at American College of Surgeons Clinical Congress. 2018 Oct 23.
Ruxolitinib under priority review for acute GVHD

The U.S. Food and Drug Administration (FDA) has accepted for priority review a supplemental new drug application (sNDA) for the JAK1/JAK2 inhibitor ruxolitinib (Jakafi®).
With this sNDA, Incyte Corporation is seeking approval for ruxolitinib as a treatment for patients with acute graft-versus-host-disease (GVHD) who have had an inadequate response to corticosteroids.
“If approved, ruxolitinib will be the first and only treatment available in the U.S. for patients with acute GVHD who have not responded adequately to corticosteroid therapy,” said Steven Stein, MD, chief medical officer at Incyte.
The FDA grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions. The agency intends to take action on a priority review application within 6 months of receiving it rather than the standard 10 months.
In addition to priority review, ruxolitinib has received breakthrough therapy and orphan drug designations from the FDA as a treatment for acute GVHD.
The sNDA submission for ruxolitinib in acute GVHD is based on data from the phase 2 REACH1 trial (NCT02953678).
In this ongoing trial, researchers are evaluating ruxolitinib in combination with corticosteroids in patients who have steroid-refractory acute GVHD.
Incyte announced topline results from REACH1 in June, reporting on outcomes in 71 patients.
The study’s primary endpoint—overall response rate at day 28—was met. Ruxolitinib produced an overall response rate of 55% (39/71) at that time.
However, 73% of patients (52/71) responded to ruxolitinib at some point during the trial.
Incyte said the most common treatment-emergent adverse events were anemia (61%), thrombocytopenia (61%), and neutropenia (56%).
The U.S. Food and Drug Administration (FDA) has accepted for priority review a supplemental new drug application (sNDA) for the JAK1/JAK2 inhibitor ruxolitinib (Jakafi®).
With this sNDA, Incyte Corporation is seeking approval for ruxolitinib as a treatment for patients with acute graft-versus-host-disease (GVHD) who have had an inadequate response to corticosteroids.
“If approved, ruxolitinib will be the first and only treatment available in the U.S. for patients with acute GVHD who have not responded adequately to corticosteroid therapy,” said Steven Stein, MD, chief medical officer at Incyte.
The FDA grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions. The agency intends to take action on a priority review application within 6 months of receiving it rather than the standard 10 months.
In addition to priority review, ruxolitinib has received breakthrough therapy and orphan drug designations from the FDA as a treatment for acute GVHD.
The sNDA submission for ruxolitinib in acute GVHD is based on data from the phase 2 REACH1 trial (NCT02953678).
In this ongoing trial, researchers are evaluating ruxolitinib in combination with corticosteroids in patients who have steroid-refractory acute GVHD.
Incyte announced topline results from REACH1 in June, reporting on outcomes in 71 patients.
The study’s primary endpoint—overall response rate at day 28—was met. Ruxolitinib produced an overall response rate of 55% (39/71) at that time.
However, 73% of patients (52/71) responded to ruxolitinib at some point during the trial.
Incyte said the most common treatment-emergent adverse events were anemia (61%), thrombocytopenia (61%), and neutropenia (56%).
The U.S. Food and Drug Administration (FDA) has accepted for priority review a supplemental new drug application (sNDA) for the JAK1/JAK2 inhibitor ruxolitinib (Jakafi®).
With this sNDA, Incyte Corporation is seeking approval for ruxolitinib as a treatment for patients with acute graft-versus-host-disease (GVHD) who have had an inadequate response to corticosteroids.
“If approved, ruxolitinib will be the first and only treatment available in the U.S. for patients with acute GVHD who have not responded adequately to corticosteroid therapy,” said Steven Stein, MD, chief medical officer at Incyte.
The FDA grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions. The agency intends to take action on a priority review application within 6 months of receiving it rather than the standard 10 months.
In addition to priority review, ruxolitinib has received breakthrough therapy and orphan drug designations from the FDA as a treatment for acute GVHD.
The sNDA submission for ruxolitinib in acute GVHD is based on data from the phase 2 REACH1 trial (NCT02953678).
In this ongoing trial, researchers are evaluating ruxolitinib in combination with corticosteroids in patients who have steroid-refractory acute GVHD.
Incyte announced topline results from REACH1 in June, reporting on outcomes in 71 patients.
The study’s primary endpoint—overall response rate at day 28—was met. Ruxolitinib produced an overall response rate of 55% (39/71) at that time.
However, 73% of patients (52/71) responded to ruxolitinib at some point during the trial.
Incyte said the most common treatment-emergent adverse events were anemia (61%), thrombocytopenia (61%), and neutropenia (56%).
Ruxolitinib receives priority review for acute GVHD
The Food and Drug Administration has accepted the JAK1/JAK2 inhibitor ruxolitinib (Jakafi) for priority review.
Incyte is seeking approval for ruxolitinib as a treatment for patients with acute graft-versus-host disease (GVHD) who have had an inadequate response to corticosteroids.
“If approved, ruxolitinib will be the first and only treatment available in the U.S. for patients with acute GVHD who have not responded adequately to corticosteroid therapy,” Steven Stein, MD, chief medical officer at Incyte, said in a statement.
The FDA grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions. The designation generally means that the agency will act on the application within 6 months, rather than 10 months.
In addition to priority review, the FDA previously granted ruxolitinib breakthrough therapy and orphan drug designations.
The application is based on data from the ongoing, phase 2 REACH1 trial (NCT02953678), which is evaluating ruxolitinib in combination with corticosteroids in patients who have steroid-refractory acute GVHD.
Incyte announced top-line results from REACH1 in June, reporting on outcomes in 71 patients.
The study’s primary endpoint – overall response rate at day 28 – was met. Ruxolitinib produced an overall response rate of 55% at that time. However, 73% of patients responded to ruxolitinib at some point during the trial. Incyte said the most common treatment-emergent adverse events were anemia, thrombocytopenia, and neutropenia.
The Food and Drug Administration has accepted the JAK1/JAK2 inhibitor ruxolitinib (Jakafi) for priority review.
Incyte is seeking approval for ruxolitinib as a treatment for patients with acute graft-versus-host disease (GVHD) who have had an inadequate response to corticosteroids.
“If approved, ruxolitinib will be the first and only treatment available in the U.S. for patients with acute GVHD who have not responded adequately to corticosteroid therapy,” Steven Stein, MD, chief medical officer at Incyte, said in a statement.
The FDA grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions. The designation generally means that the agency will act on the application within 6 months, rather than 10 months.
In addition to priority review, the FDA previously granted ruxolitinib breakthrough therapy and orphan drug designations.
The application is based on data from the ongoing, phase 2 REACH1 trial (NCT02953678), which is evaluating ruxolitinib in combination with corticosteroids in patients who have steroid-refractory acute GVHD.
Incyte announced top-line results from REACH1 in June, reporting on outcomes in 71 patients.
The study’s primary endpoint – overall response rate at day 28 – was met. Ruxolitinib produced an overall response rate of 55% at that time. However, 73% of patients responded to ruxolitinib at some point during the trial. Incyte said the most common treatment-emergent adverse events were anemia, thrombocytopenia, and neutropenia.
The Food and Drug Administration has accepted the JAK1/JAK2 inhibitor ruxolitinib (Jakafi) for priority review.
Incyte is seeking approval for ruxolitinib as a treatment for patients with acute graft-versus-host disease (GVHD) who have had an inadequate response to corticosteroids.
“If approved, ruxolitinib will be the first and only treatment available in the U.S. for patients with acute GVHD who have not responded adequately to corticosteroid therapy,” Steven Stein, MD, chief medical officer at Incyte, said in a statement.
The FDA grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions. The designation generally means that the agency will act on the application within 6 months, rather than 10 months.
In addition to priority review, the FDA previously granted ruxolitinib breakthrough therapy and orphan drug designations.
The application is based on data from the ongoing, phase 2 REACH1 trial (NCT02953678), which is evaluating ruxolitinib in combination with corticosteroids in patients who have steroid-refractory acute GVHD.
Incyte announced top-line results from REACH1 in June, reporting on outcomes in 71 patients.
The study’s primary endpoint – overall response rate at day 28 – was met. Ruxolitinib produced an overall response rate of 55% at that time. However, 73% of patients responded to ruxolitinib at some point during the trial. Incyte said the most common treatment-emergent adverse events were anemia, thrombocytopenia, and neutropenia.
OMS721 gains orphan designation for HSCT-associated thrombotic microangiopathy
The Food and Drug Administration has granted OMS721 orphan designation for the treatment of hematopoietic stem cell transplant–associated thrombotic microangiopathy (HSCT-TMA).

OMS721 is a monoclonal antibody targeting MASP-2, the effector enzyme of the lectin pathway of the complement system.
The FDA previously granted OMS721 breakthrough therapy designation for HSCT-TMA and orphan designation for the prevention of complement-mediated TMA, including HSCT-TMA.
Omeros, the company developing OMS721, has established a compassionate use program for OMS721, which is active in the United States and Europe.
Phase 3 clinical programs are in progress for OMS721 in atypical hemolytic uremic syndrome, immunoglobulin A nephropathy, and HSCT-TMA. Two phase 2 trials of OMS721 – one in TMA and one in immunoglobulin A nephropathy – are ongoing.
Omeros announced results from the phase 2 TMA trial (NCT02222545) in February. The study includes adults with HSCT-TMA persisting for at least 2 weeks following immunosuppressive regimen modification or more than 30 days post transplant. Patients receive weekly OMS721 treatments for 4-8 weeks at the discretion of the investigator.
At the time of Omeros’s announcement, 18 HSCT-TMA patients had been treated.
These patients had a significantly longer median overall survival at 347 days, compared with historical controls at 21 days (P less than .0001).
Omeros also reported that markers of TMA activity significantly improved following OMS721 treatment.
The mean platelet count increased from 18,100 x 106/mL at baseline to 52,300 x 106/mL (P = .017). The mean lactate dehydrogenase decreased from 591 U/L to 250 U/L (P less than .001). And the mean haptoglobin increased from 8 mg/dL to 141 mg/dL (P = .003).
The most commonly reported adverse events were diarrhea and neutropenia. Four deaths occurred during the study. One of these – attributable to acute renal and respiratory failure – was considered possibly related to OMS721.
The Food and Drug Administration has granted OMS721 orphan designation for the treatment of hematopoietic stem cell transplant–associated thrombotic microangiopathy (HSCT-TMA).
OMS721 is a monoclonal antibody targeting MASP-2, the effector enzyme of the lectin pathway of the complement system.
The FDA previously granted OMS721 breakthrough therapy designation for HSCT-TMA and orphan designation for the prevention of complement-mediated TMA, including HSCT-TMA.
Omeros, the company developing OMS721, has established a compassionate use program for OMS721, which is active in the United States and Europe.
Phase 3 clinical programs are in progress for OMS721 in atypical hemolytic uremic syndrome, immunoglobulin A nephropathy, and HSCT-TMA. Two phase 2 trials of OMS721 – one in TMA and one in immunoglobulin A nephropathy – are ongoing.
Omeros announced results from the phase 2 TMA trial (NCT02222545) in February. The study includes adults with HSCT-TMA persisting for at least 2 weeks following immunosuppressive regimen modification or more than 30 days post transplant. Patients receive weekly OMS721 treatments for 4-8 weeks at the discretion of the investigator.
At the time of Omeros’s announcement, 18 HSCT-TMA patients had been treated.
These patients had a significantly longer median overall survival at 347 days, compared with historical controls at 21 days (P less than .0001).
Omeros also reported that markers of TMA activity significantly improved following OMS721 treatment.
The mean platelet count increased from 18,100 x 106/mL at baseline to 52,300 x 106/mL (P = .017). The mean lactate dehydrogenase decreased from 591 U/L to 250 U/L (P less than .001). And the mean haptoglobin increased from 8 mg/dL to 141 mg/dL (P = .003).
The most commonly reported adverse events were diarrhea and neutropenia. Four deaths occurred during the study. One of these – attributable to acute renal and respiratory failure – was considered possibly related to OMS721.
The Food and Drug Administration has granted OMS721 orphan designation for the treatment of hematopoietic stem cell transplant–associated thrombotic microangiopathy (HSCT-TMA).
OMS721 is a monoclonal antibody targeting MASP-2, the effector enzyme of the lectin pathway of the complement system.
The FDA previously granted OMS721 breakthrough therapy designation for HSCT-TMA and orphan designation for the prevention of complement-mediated TMA, including HSCT-TMA.
Omeros, the company developing OMS721, has established a compassionate use program for OMS721, which is active in the United States and Europe.
Phase 3 clinical programs are in progress for OMS721 in atypical hemolytic uremic syndrome, immunoglobulin A nephropathy, and HSCT-TMA. Two phase 2 trials of OMS721 – one in TMA and one in immunoglobulin A nephropathy – are ongoing.
Omeros announced results from the phase 2 TMA trial (NCT02222545) in February. The study includes adults with HSCT-TMA persisting for at least 2 weeks following immunosuppressive regimen modification or more than 30 days post transplant. Patients receive weekly OMS721 treatments for 4-8 weeks at the discretion of the investigator.
At the time of Omeros’s announcement, 18 HSCT-TMA patients had been treated.
These patients had a significantly longer median overall survival at 347 days, compared with historical controls at 21 days (P less than .0001).
Omeros also reported that markers of TMA activity significantly improved following OMS721 treatment.
The mean platelet count increased from 18,100 x 106/mL at baseline to 52,300 x 106/mL (P = .017). The mean lactate dehydrogenase decreased from 591 U/L to 250 U/L (P less than .001). And the mean haptoglobin increased from 8 mg/dL to 141 mg/dL (P = .003).
The most commonly reported adverse events were diarrhea and neutropenia. Four deaths occurred during the study. One of these – attributable to acute renal and respiratory failure – was considered possibly related to OMS721.
Pigmented Pruritic Macules in the Genital Area
The Diagnosis: Pediculosis Pubis
Dermoscopy of the pubic hair demonstrated a louse clutching multiple shafts of hairs (Figure) as well as scattered nits, confirming the presence of Phthirus pubis and diagnosis of pediculosis pubis. The key clinical diagnostic feature in this case was severe itching of the pubic area, with visible nits present on pubic hairs. Itching and infestation also can involve other hair-bearing areas such as the chest, legs, and axillae. The patient was treated with permethrin cream 5% applied to the pubic area and chest. Symptoms and infestation were resolved at 1-week follow-up.
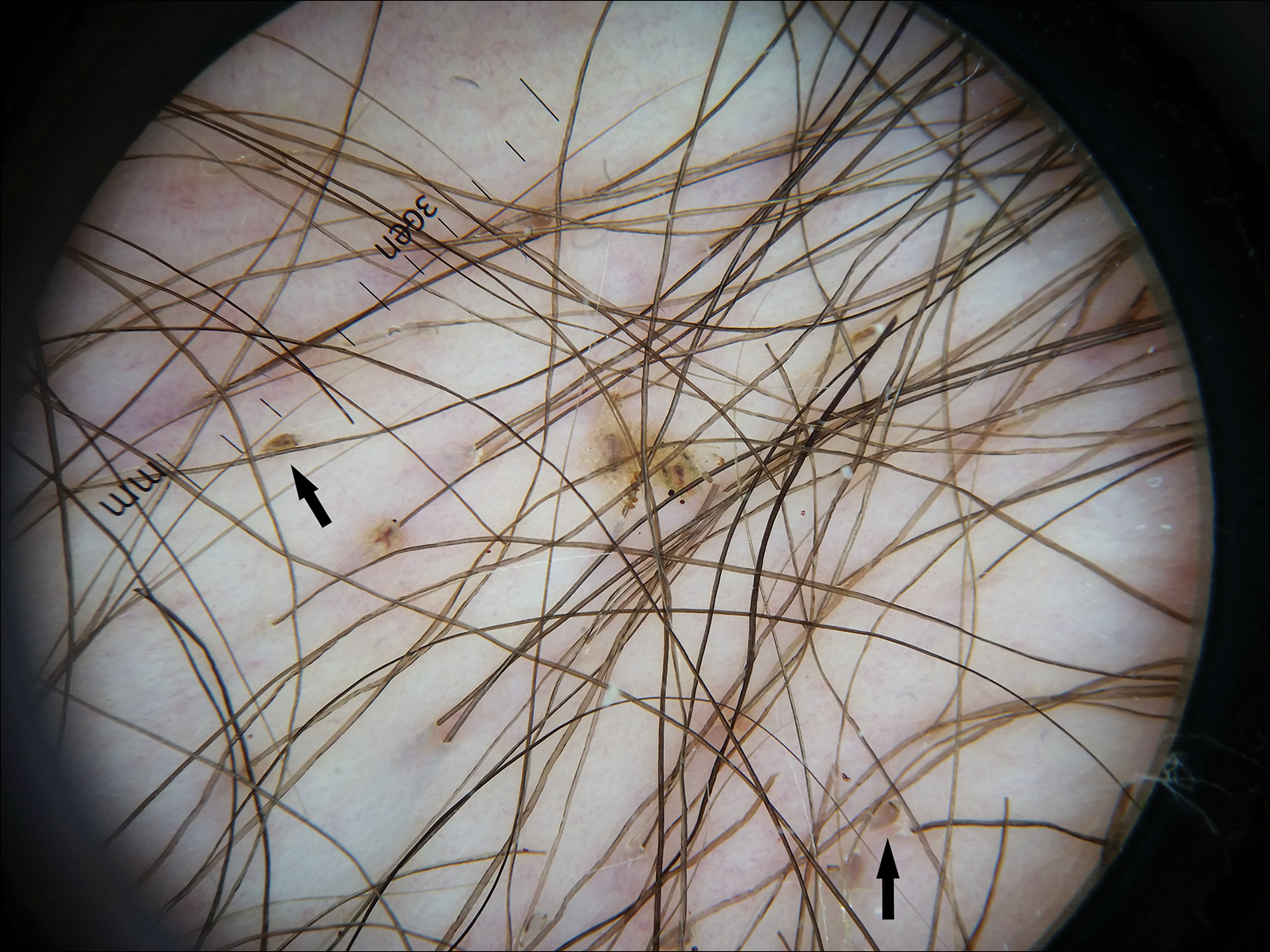
Pediculosis pubis is an infestation of pubic hairs by the pubic (crab) louse P pubis, which feeds on host blood. Other body areas covered with dense hair also may be involved; 60% of patients are infested in at least 2 different sites.1 Pediculosis pubis is most commonly sexually transmitted through direct contact.2 Worldwide prevalence has been estimated at approximately 2% of the adult population, and a survey of 817 US college students in 2009 indicated a lifetime prevalence of 1.3%.3 The prevalence is slightly higher in men, highest in men who have sex with men, and rare in individuals with shaved pubic hair.1 The most common symptom is pruritus of the genital area. Infested patients also may develop asymptomatic bluish gray macules (maculae ceruleae) secondary to hemosiderin deposition from louse bites.4
The diagnosis of pediculosis pubis is made by identification of P pubis, either by examination with the naked eye or confirmation with dermoscopy or microscopy. Although the 0.8- to 1.2-mm lice are visible to the naked eye, they can be difficult to see if not filled with blood, and nits on the hairs can be mistaken for white piedra (fungal infection of the hair shafts) or trichomycosis pubis (bacterial infection of the hair shafts).4 Scabies and tinea cruris do not present with attachments to the hairs. Scabies may present with papules and burrows and tinea cruris with scaly erythematous plaques. Small numbers of lice and nits may be missed by the naked eye or a traditional magnifying glass.5 The use of dermoscopy allows for fast and accurate identification of the characteristic lice and nits, even in these more challenging cases.5 Accurate diagnosis is important, as approximately 31% of infested patients have other concurrent sexually transmitted infections that warrant screening.6
The Centers for Disease Control and Prevention recommends first-line treatment with permethrin cream (1% or 5%) or pyrethrin with piperonyl butoxide applied to all affected areas and washed off after 10 minutes.7 Patients should be reevaluated after 1 week if symptoms persist and re-treated if lice are found on examination.7,8 Malathion lotion 0.5% (applied and washed off after 8-12 hours) or oral ivermectin (250 µg/kg, repeated after 2 weeks) may be used for alternative therapies or cases of permethrin or pyrethrin resistance.7 Ivermectin also is effective for involvement of eyelashes where topical insecticides should not be used.9 Sexual partners should be treated to prevent repeat transmission.7,8 Bedding and clothing can be decontaminated by machine wash on hot cycle or isolating from body contact for 72 hours.7 Patients also should be screened for other sexually transmitted infections, including human immunodeficiency virus.6
- Burkhart CN, Burkhart CG, Morrell DS. Infestations. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. Vol 2. 3rd ed. China: Elsevier/Saunders; 2012:1429-1430.
- Chosidow O. Scabies and pediculosis. Lancet. 2000;355:819-826.
- Anderson AL, Chaney E. Pubic lice (Pthirus pubis): history, biology and treatment vs. knowledge and beliefs of US college students. Int J Environ Res Public Health. 2009;6:592-600.
- Ko CJ, Elston DM. Pediculosis. J Am Acad Dermatol. 2004;50:1-12; quiz 13-14.
- Chuh A, Lee A, Wong W, et al. Diagnosis of pediculosis pubis: a novel application of digital epiluminescence dermatoscopy. J Eur Acad Dermatol Venereol. 2007;21:837-838.
- Chapel TA, Katta T, Kuszmar T, et al. Pediculosis pubis in a clinic for treatment of sexually transmitted diseases. Sex Transm Dis. 1979;6:257-260.
- Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64:1-137.
- Leone PA. Scabies and pediculosis pubis: an update of treatment regimens and general review. Clin Infect Dis. 2007;44(suppl 3):S153-S159.
- Burkhart CN, Burkhart CG. Oral ivermectin therapy for phthiriasis palpebrum. Arch Ophthalmol. 2000;118:134-135.
The Diagnosis: Pediculosis Pubis
Dermoscopy of the pubic hair demonstrated a louse clutching multiple shafts of hairs (Figure) as well as scattered nits, confirming the presence of Phthirus pubis and diagnosis of pediculosis pubis. The key clinical diagnostic feature in this case was severe itching of the pubic area, with visible nits present on pubic hairs. Itching and infestation also can involve other hair-bearing areas such as the chest, legs, and axillae. The patient was treated with permethrin cream 5% applied to the pubic area and chest. Symptoms and infestation were resolved at 1-week follow-up.
Pediculosis pubis is an infestation of pubic hairs by the pubic (crab) louse P pubis, which feeds on host blood. Other body areas covered with dense hair also may be involved; 60% of patients are infested in at least 2 different sites.1 Pediculosis pubis is most commonly sexually transmitted through direct contact.2 Worldwide prevalence has been estimated at approximately 2% of the adult population, and a survey of 817 US college students in 2009 indicated a lifetime prevalence of 1.3%.3 The prevalence is slightly higher in men, highest in men who have sex with men, and rare in individuals with shaved pubic hair.1 The most common symptom is pruritus of the genital area. Infested patients also may develop asymptomatic bluish gray macules (maculae ceruleae) secondary to hemosiderin deposition from louse bites.4
The diagnosis of pediculosis pubis is made by identification of P pubis, either by examination with the naked eye or confirmation with dermoscopy or microscopy. Although the 0.8- to 1.2-mm lice are visible to the naked eye, they can be difficult to see if not filled with blood, and nits on the hairs can be mistaken for white piedra (fungal infection of the hair shafts) or trichomycosis pubis (bacterial infection of the hair shafts).4 Scabies and tinea cruris do not present with attachments to the hairs. Scabies may present with papules and burrows and tinea cruris with scaly erythematous plaques. Small numbers of lice and nits may be missed by the naked eye or a traditional magnifying glass.5 The use of dermoscopy allows for fast and accurate identification of the characteristic lice and nits, even in these more challenging cases.5 Accurate diagnosis is important, as approximately 31% of infested patients have other concurrent sexually transmitted infections that warrant screening.6
The Centers for Disease Control and Prevention recommends first-line treatment with permethrin cream (1% or 5%) or pyrethrin with piperonyl butoxide applied to all affected areas and washed off after 10 minutes.7 Patients should be reevaluated after 1 week if symptoms persist and re-treated if lice are found on examination.7,8 Malathion lotion 0.5% (applied and washed off after 8-12 hours) or oral ivermectin (250 µg/kg, repeated after 2 weeks) may be used for alternative therapies or cases of permethrin or pyrethrin resistance.7 Ivermectin also is effective for involvement of eyelashes where topical insecticides should not be used.9 Sexual partners should be treated to prevent repeat transmission.7,8 Bedding and clothing can be decontaminated by machine wash on hot cycle or isolating from body contact for 72 hours.7 Patients also should be screened for other sexually transmitted infections, including human immunodeficiency virus.6
The Diagnosis: Pediculosis Pubis
Dermoscopy of the pubic hair demonstrated a louse clutching multiple shafts of hairs (Figure) as well as scattered nits, confirming the presence of Phthirus pubis and diagnosis of pediculosis pubis. The key clinical diagnostic feature in this case was severe itching of the pubic area, with visible nits present on pubic hairs. Itching and infestation also can involve other hair-bearing areas such as the chest, legs, and axillae. The patient was treated with permethrin cream 5% applied to the pubic area and chest. Symptoms and infestation were resolved at 1-week follow-up.
Pediculosis pubis is an infestation of pubic hairs by the pubic (crab) louse P pubis, which feeds on host blood. Other body areas covered with dense hair also may be involved; 60% of patients are infested in at least 2 different sites.1 Pediculosis pubis is most commonly sexually transmitted through direct contact.2 Worldwide prevalence has been estimated at approximately 2% of the adult population, and a survey of 817 US college students in 2009 indicated a lifetime prevalence of 1.3%.3 The prevalence is slightly higher in men, highest in men who have sex with men, and rare in individuals with shaved pubic hair.1 The most common symptom is pruritus of the genital area. Infested patients also may develop asymptomatic bluish gray macules (maculae ceruleae) secondary to hemosiderin deposition from louse bites.4
The diagnosis of pediculosis pubis is made by identification of P pubis, either by examination with the naked eye or confirmation with dermoscopy or microscopy. Although the 0.8- to 1.2-mm lice are visible to the naked eye, they can be difficult to see if not filled with blood, and nits on the hairs can be mistaken for white piedra (fungal infection of the hair shafts) or trichomycosis pubis (bacterial infection of the hair shafts).4 Scabies and tinea cruris do not present with attachments to the hairs. Scabies may present with papules and burrows and tinea cruris with scaly erythematous plaques. Small numbers of lice and nits may be missed by the naked eye or a traditional magnifying glass.5 The use of dermoscopy allows for fast and accurate identification of the characteristic lice and nits, even in these more challenging cases.5 Accurate diagnosis is important, as approximately 31% of infested patients have other concurrent sexually transmitted infections that warrant screening.6
The Centers for Disease Control and Prevention recommends first-line treatment with permethrin cream (1% or 5%) or pyrethrin with piperonyl butoxide applied to all affected areas and washed off after 10 minutes.7 Patients should be reevaluated after 1 week if symptoms persist and re-treated if lice are found on examination.7,8 Malathion lotion 0.5% (applied and washed off after 8-12 hours) or oral ivermectin (250 µg/kg, repeated after 2 weeks) may be used for alternative therapies or cases of permethrin or pyrethrin resistance.7 Ivermectin also is effective for involvement of eyelashes where topical insecticides should not be used.9 Sexual partners should be treated to prevent repeat transmission.7,8 Bedding and clothing can be decontaminated by machine wash on hot cycle or isolating from body contact for 72 hours.7 Patients also should be screened for other sexually transmitted infections, including human immunodeficiency virus.6
- Burkhart CN, Burkhart CG, Morrell DS. Infestations. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. Vol 2. 3rd ed. China: Elsevier/Saunders; 2012:1429-1430.
- Chosidow O. Scabies and pediculosis. Lancet. 2000;355:819-826.
- Anderson AL, Chaney E. Pubic lice (Pthirus pubis): history, biology and treatment vs. knowledge and beliefs of US college students. Int J Environ Res Public Health. 2009;6:592-600.
- Ko CJ, Elston DM. Pediculosis. J Am Acad Dermatol. 2004;50:1-12; quiz 13-14.
- Chuh A, Lee A, Wong W, et al. Diagnosis of pediculosis pubis: a novel application of digital epiluminescence dermatoscopy. J Eur Acad Dermatol Venereol. 2007;21:837-838.
- Chapel TA, Katta T, Kuszmar T, et al. Pediculosis pubis in a clinic for treatment of sexually transmitted diseases. Sex Transm Dis. 1979;6:257-260.
- Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64:1-137.
- Leone PA. Scabies and pediculosis pubis: an update of treatment regimens and general review. Clin Infect Dis. 2007;44(suppl 3):S153-S159.
- Burkhart CN, Burkhart CG. Oral ivermectin therapy for phthiriasis palpebrum. Arch Ophthalmol. 2000;118:134-135.
- Burkhart CN, Burkhart CG, Morrell DS. Infestations. In: Bolognia J, Jorizzo JL, Schaffer JV, eds. Dermatology. Vol 2. 3rd ed. China: Elsevier/Saunders; 2012:1429-1430.
- Chosidow O. Scabies and pediculosis. Lancet. 2000;355:819-826.
- Anderson AL, Chaney E. Pubic lice (Pthirus pubis): history, biology and treatment vs. knowledge and beliefs of US college students. Int J Environ Res Public Health. 2009;6:592-600.
- Ko CJ, Elston DM. Pediculosis. J Am Acad Dermatol. 2004;50:1-12; quiz 13-14.
- Chuh A, Lee A, Wong W, et al. Diagnosis of pediculosis pubis: a novel application of digital epiluminescence dermatoscopy. J Eur Acad Dermatol Venereol. 2007;21:837-838.
- Chapel TA, Katta T, Kuszmar T, et al. Pediculosis pubis in a clinic for treatment of sexually transmitted diseases. Sex Transm Dis. 1979;6:257-260.
- Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64:1-137.
- Leone PA. Scabies and pediculosis pubis: an update of treatment regimens and general review. Clin Infect Dis. 2007;44(suppl 3):S153-S159.
- Burkhart CN, Burkhart CG. Oral ivermectin therapy for phthiriasis palpebrum. Arch Ophthalmol. 2000;118:134-135.

A 50-year-old man with a history of cerebrovascular accident presented with severe itching along the inguinal folds and over the chest of 2 months' duration. His last sexual encounter was 5 months prior. He had previously seen a primary care physician who told him he needed to clean the hair better. Examination of the genital area revealed pigmented macules and overlying particles among the pubic hair.

‘Woeful lack of awareness’ leads to delayed diagnoses for women with ovarian cancer
Lack of knowledge about ovarian cancer prevents many women from seeking medical attention, which delays diagnosis and treatment and may prove increasingly dangerous as incidence rises by an expected 55% over the next 2 decades, according to the World Ovarian Cancer Coalition.
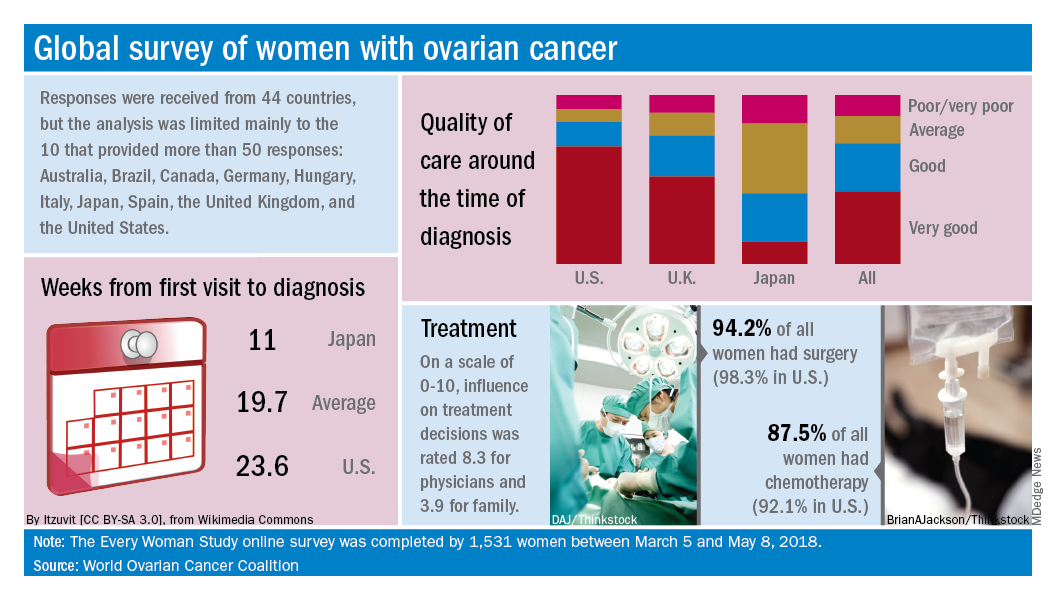
Data from the coalition’s 2018 survey of women with ovarian cancer show that 18% had never heard of the disease before their diagnosis and 51% had heard of it but did not know anything about it. The Every Women Study survey, completed by 1,531 women in 44 countries, also reveals that nine out of ten had experienced symptoms prior to diagnosis but fewer than half saw a physician within a month of noticing those symptoms, the coalition said.
“This study, for the first time, provides powerful evidence of the challenges faced by women diagnosed with ovarian cancer across the world and sets an agenda for global change. We were especially shocked by the widespread, woeful lack of awareness of ovarian cancer,” Annwen Jones, coalition vice-chair and cochair of the study, said in a separate written statement.
Results varied considerably by country, and only 10 countries provided enough responses to allow comparisons: Australia (120), Brazil (52), Canada (167), Germany (141), Hungary (58), Italy (92), Japan (250), Spain (70), the United Kingdom (176), and the United States (248).
Among those comparisons, women in Germany (5.5 weeks) and Spain (7.9 weeks) were the first to visit a physician after first experiencing symptoms, while those in Italy (15.2 weeks) and the United States (12.9 weeks) were last. The United States was also longest in time from first visit to diagnosis (23.6 weeks), and Japan was the shortest (11 weeks). Despite that world-longest time to diagnosis, however, over 69% of U.S. women said that their care around the time of diagnosis was very good, which was higher than any other country, the coalition reported.
Surgery statistics were closer among countries, with an average of 94% of all women undergoing surgery to treat their ovarian cancer. The United States, at 98.3%, was second to Spain’s 98.5%, and Hungary was the largest outlier on the low side at 59%. Over 87% of all women reported having chemotherapy to treat or control their cancer, and 9.8% of women said that they had received intraperitoneal chemotherapy. In the United States, 22.5% of women received intraperitoneal therapy, compared with 0.7% for the United Kingdom.
“No one country has all the answers, and whilst there is still an urgent need for a step-change in the level of investment in research for better treatments and tools for early diagnosis, there are significant opportunities to improve survival and quality of life for women in the immediate and short term to make a series of marginal gains if these variations are addressed by individual countries,” the coalition said in the report.
Lack of knowledge about ovarian cancer prevents many women from seeking medical attention, which delays diagnosis and treatment and may prove increasingly dangerous as incidence rises by an expected 55% over the next 2 decades, according to the World Ovarian Cancer Coalition.
Data from the coalition’s 2018 survey of women with ovarian cancer show that 18% had never heard of the disease before their diagnosis and 51% had heard of it but did not know anything about it. The Every Women Study survey, completed by 1,531 women in 44 countries, also reveals that nine out of ten had experienced symptoms prior to diagnosis but fewer than half saw a physician within a month of noticing those symptoms, the coalition said.
“This study, for the first time, provides powerful evidence of the challenges faced by women diagnosed with ovarian cancer across the world and sets an agenda for global change. We were especially shocked by the widespread, woeful lack of awareness of ovarian cancer,” Annwen Jones, coalition vice-chair and cochair of the study, said in a separate written statement.
Results varied considerably by country, and only 10 countries provided enough responses to allow comparisons: Australia (120), Brazil (52), Canada (167), Germany (141), Hungary (58), Italy (92), Japan (250), Spain (70), the United Kingdom (176), and the United States (248).
Among those comparisons, women in Germany (5.5 weeks) and Spain (7.9 weeks) were the first to visit a physician after first experiencing symptoms, while those in Italy (15.2 weeks) and the United States (12.9 weeks) were last. The United States was also longest in time from first visit to diagnosis (23.6 weeks), and Japan was the shortest (11 weeks). Despite that world-longest time to diagnosis, however, over 69% of U.S. women said that their care around the time of diagnosis was very good, which was higher than any other country, the coalition reported.
Surgery statistics were closer among countries, with an average of 94% of all women undergoing surgery to treat their ovarian cancer. The United States, at 98.3%, was second to Spain’s 98.5%, and Hungary was the largest outlier on the low side at 59%. Over 87% of all women reported having chemotherapy to treat or control their cancer, and 9.8% of women said that they had received intraperitoneal chemotherapy. In the United States, 22.5% of women received intraperitoneal therapy, compared with 0.7% for the United Kingdom.
“No one country has all the answers, and whilst there is still an urgent need for a step-change in the level of investment in research for better treatments and tools for early diagnosis, there are significant opportunities to improve survival and quality of life for women in the immediate and short term to make a series of marginal gains if these variations are addressed by individual countries,” the coalition said in the report.
Lack of knowledge about ovarian cancer prevents many women from seeking medical attention, which delays diagnosis and treatment and may prove increasingly dangerous as incidence rises by an expected 55% over the next 2 decades, according to the World Ovarian Cancer Coalition.
Data from the coalition’s 2018 survey of women with ovarian cancer show that 18% had never heard of the disease before their diagnosis and 51% had heard of it but did not know anything about it. The Every Women Study survey, completed by 1,531 women in 44 countries, also reveals that nine out of ten had experienced symptoms prior to diagnosis but fewer than half saw a physician within a month of noticing those symptoms, the coalition said.
“This study, for the first time, provides powerful evidence of the challenges faced by women diagnosed with ovarian cancer across the world and sets an agenda for global change. We were especially shocked by the widespread, woeful lack of awareness of ovarian cancer,” Annwen Jones, coalition vice-chair and cochair of the study, said in a separate written statement.
Results varied considerably by country, and only 10 countries provided enough responses to allow comparisons: Australia (120), Brazil (52), Canada (167), Germany (141), Hungary (58), Italy (92), Japan (250), Spain (70), the United Kingdom (176), and the United States (248).
Among those comparisons, women in Germany (5.5 weeks) and Spain (7.9 weeks) were the first to visit a physician after first experiencing symptoms, while those in Italy (15.2 weeks) and the United States (12.9 weeks) were last. The United States was also longest in time from first visit to diagnosis (23.6 weeks), and Japan was the shortest (11 weeks). Despite that world-longest time to diagnosis, however, over 69% of U.S. women said that their care around the time of diagnosis was very good, which was higher than any other country, the coalition reported.
Surgery statistics were closer among countries, with an average of 94% of all women undergoing surgery to treat their ovarian cancer. The United States, at 98.3%, was second to Spain’s 98.5%, and Hungary was the largest outlier on the low side at 59%. Over 87% of all women reported having chemotherapy to treat or control their cancer, and 9.8% of women said that they had received intraperitoneal chemotherapy. In the United States, 22.5% of women received intraperitoneal therapy, compared with 0.7% for the United Kingdom.
“No one country has all the answers, and whilst there is still an urgent need for a step-change in the level of investment in research for better treatments and tools for early diagnosis, there are significant opportunities to improve survival and quality of life for women in the immediate and short term to make a series of marginal gains if these variations are addressed by individual countries,” the coalition said in the report.