User login
Louisiana HCV program cuts costs – and hassles

Beginning July 15, physicians will no longer have to seek prior authorization or preauthorization to prescribe the authorized generic version of Epclusa (sofosbuvir/velpatasvir) to any Medicaid patient with hepatitis C. There will be no forms to file.
The change comes as part of a supplemental rebate agreement approved June 26 by CMS. That same day, Louisiana announced a deal with Asegua Therapeutics, a wholly owned subsidiary of Epclusa maker Gilead, that essentially caps the annual cost to the state for treating hepatitis C in incarcerated patients and Medicaid recipients.
State officials estimate about 39,000 Louisianans fit those criteria; the goal of the program is to cure at least 31,000 of them by the time the 5-year agreement expires.
“This new model has the potential to save many lives and improve the health of our citizens,” Louisiana Gov. John Bel Edwards (D) said in a statement. “Asegua was willing to come to the table to work with us to help Louisiana residents and we are pleased to initiate this 5-year partnership. Ultimately our goal is to eliminate this disease in Louisiana, and we have taken a big step forward in that effort.”
The agreement was designed to change very little in terms of the mechanics of how Medicaid managed care organizations, which cover most of the state’s Medicaid population and handle coverage and claims. The biggest change is that, when a spending cap is reached, Asegua will rebate 100% excess costs to the state. Louisiana officials did not disclose what the annual financial caps were as part of the agreement.
“We really thought it was important to leave the system – as much as possible – intact because we think that is going to make us most successful,” Alex Billioux, MD, of the Louisiana Department of Health said in an interview. “We think it leverages existing patient relationships and existing [Medicaid managed care organization] care management responsibilities.”
He added that, by keeping current processes unchanged, “it takes what is an otherwise very complicated arrangement with the state and makes it a little simpler.”
Patients will see no change in terms of copayments for the approved generic topping out at $3 depending on income level as they would have prior to the agreement. The biggest difference for them is that “people who couldn’t be treated are now going to have access to those prescriptions,” Dr. Billioux said.
Some cautious optimism surrounds this kind of arrangement and the potential effect it can have on the affected population.
“Innovation geared to improve access to hepatitis C treatment is critical, particularly in areas like Louisiana where treatment rates for Medicaid patients have been very low,” Robert Brown, MD, member of the American Liver Foundation’s National Medical Advisory Committee and hepatologist at Weill Cornell Medical College, New York, said. “If we can enhance patient access to treatment, we know we will improve health outcomes. However, it is too early to tell if this innovation will be a success. At the end of the day, the number of additional patients cured will determine if this was the right approach.”
Visit the AGA GI Patient Center for information to share with your patients about hepatitis C at https://www.gastro.org/practice-guidance/gi-patient-center/topic/hepatitis-c-hcv
Beginning July 15, physicians will no longer have to seek prior authorization or preauthorization to prescribe the authorized generic version of Epclusa (sofosbuvir/velpatasvir) to any Medicaid patient with hepatitis C. There will be no forms to file.
The change comes as part of a supplemental rebate agreement approved June 26 by CMS. That same day, Louisiana announced a deal with Asegua Therapeutics, a wholly owned subsidiary of Epclusa maker Gilead, that essentially caps the annual cost to the state for treating hepatitis C in incarcerated patients and Medicaid recipients.
State officials estimate about 39,000 Louisianans fit those criteria; the goal of the program is to cure at least 31,000 of them by the time the 5-year agreement expires.
“This new model has the potential to save many lives and improve the health of our citizens,” Louisiana Gov. John Bel Edwards (D) said in a statement. “Asegua was willing to come to the table to work with us to help Louisiana residents and we are pleased to initiate this 5-year partnership. Ultimately our goal is to eliminate this disease in Louisiana, and we have taken a big step forward in that effort.”
The agreement was designed to change very little in terms of the mechanics of how Medicaid managed care organizations, which cover most of the state’s Medicaid population and handle coverage and claims. The biggest change is that, when a spending cap is reached, Asegua will rebate 100% excess costs to the state. Louisiana officials did not disclose what the annual financial caps were as part of the agreement.
“We really thought it was important to leave the system – as much as possible – intact because we think that is going to make us most successful,” Alex Billioux, MD, of the Louisiana Department of Health said in an interview. “We think it leverages existing patient relationships and existing [Medicaid managed care organization] care management responsibilities.”
He added that, by keeping current processes unchanged, “it takes what is an otherwise very complicated arrangement with the state and makes it a little simpler.”
Patients will see no change in terms of copayments for the approved generic topping out at $3 depending on income level as they would have prior to the agreement. The biggest difference for them is that “people who couldn’t be treated are now going to have access to those prescriptions,” Dr. Billioux said.
Some cautious optimism surrounds this kind of arrangement and the potential effect it can have on the affected population.
“Innovation geared to improve access to hepatitis C treatment is critical, particularly in areas like Louisiana where treatment rates for Medicaid patients have been very low,” Robert Brown, MD, member of the American Liver Foundation’s National Medical Advisory Committee and hepatologist at Weill Cornell Medical College, New York, said. “If we can enhance patient access to treatment, we know we will improve health outcomes. However, it is too early to tell if this innovation will be a success. At the end of the day, the number of additional patients cured will determine if this was the right approach.”
Visit the AGA GI Patient Center for information to share with your patients about hepatitis C at https://www.gastro.org/practice-guidance/gi-patient-center/topic/hepatitis-c-hcv
Beginning July 15, physicians will no longer have to seek prior authorization or preauthorization to prescribe the authorized generic version of Epclusa (sofosbuvir/velpatasvir) to any Medicaid patient with hepatitis C. There will be no forms to file.
The change comes as part of a supplemental rebate agreement approved June 26 by CMS. That same day, Louisiana announced a deal with Asegua Therapeutics, a wholly owned subsidiary of Epclusa maker Gilead, that essentially caps the annual cost to the state for treating hepatitis C in incarcerated patients and Medicaid recipients.
State officials estimate about 39,000 Louisianans fit those criteria; the goal of the program is to cure at least 31,000 of them by the time the 5-year agreement expires.
“This new model has the potential to save many lives and improve the health of our citizens,” Louisiana Gov. John Bel Edwards (D) said in a statement. “Asegua was willing to come to the table to work with us to help Louisiana residents and we are pleased to initiate this 5-year partnership. Ultimately our goal is to eliminate this disease in Louisiana, and we have taken a big step forward in that effort.”
The agreement was designed to change very little in terms of the mechanics of how Medicaid managed care organizations, which cover most of the state’s Medicaid population and handle coverage and claims. The biggest change is that, when a spending cap is reached, Asegua will rebate 100% excess costs to the state. Louisiana officials did not disclose what the annual financial caps were as part of the agreement.
“We really thought it was important to leave the system – as much as possible – intact because we think that is going to make us most successful,” Alex Billioux, MD, of the Louisiana Department of Health said in an interview. “We think it leverages existing patient relationships and existing [Medicaid managed care organization] care management responsibilities.”
He added that, by keeping current processes unchanged, “it takes what is an otherwise very complicated arrangement with the state and makes it a little simpler.”
Patients will see no change in terms of copayments for the approved generic topping out at $3 depending on income level as they would have prior to the agreement. The biggest difference for them is that “people who couldn’t be treated are now going to have access to those prescriptions,” Dr. Billioux said.
Some cautious optimism surrounds this kind of arrangement and the potential effect it can have on the affected population.
“Innovation geared to improve access to hepatitis C treatment is critical, particularly in areas like Louisiana where treatment rates for Medicaid patients have been very low,” Robert Brown, MD, member of the American Liver Foundation’s National Medical Advisory Committee and hepatologist at Weill Cornell Medical College, New York, said. “If we can enhance patient access to treatment, we know we will improve health outcomes. However, it is too early to tell if this innovation will be a success. At the end of the day, the number of additional patients cured will determine if this was the right approach.”
Visit the AGA GI Patient Center for information to share with your patients about hepatitis C at https://www.gastro.org/practice-guidance/gi-patient-center/topic/hepatitis-c-hcv
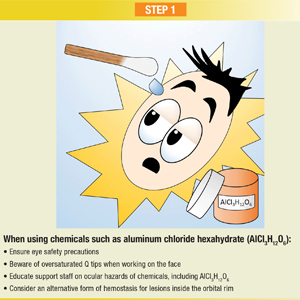
Infographic: Step-by-Step Guide to Managing Ocular Chemical Burns
Memories, flashbacks, and PTSD in NYC
On June 10, 2019, a rainy, foggy day, there was a news flash that a plane had crashed into a building in the middle of New York City. I first saw this notification on my iPhone and my immediate thought was: Could this be a redo of Sept. 11?

I was especially concerned because I knew the area fairly well, in that a clinic I had worked in for more than 10 years was only a few blocks away. However, my memory bank brought me back to that day almost 18 years ago when, from a hospital window, many of us doctors, nurses, social workers, and patients saw the fire in the north tower and then saw the second plane crash into the south tower of the World Trade Center. Once we all knew what happened, we spent that night at the hospital awaiting the arrival of people in need of care. Unfortunately, very few arrived.
On this past June day, before anyone really knew the facts, what we heard and saw on TV was buildings being evacuated in midtown Manhattan, people running and moving in all directions with police officers directing people and diverting traffic, firemen entering the building, and EMT first responders in place. What mayhem!
Gov. Andrew Cuomo got to the scene very quickly and assured us that the incident did not appear to be a terrorist attack. Furthermore, he thoughtfully pointed out, we in New York City all seem to have a version or a form of posttraumatic stress disorder taking us back to Sept. 11, 2001. From my point of view, Gov. Cuomo could not have been more correct in his short, televised talk to a nervous public. The incident, and the governor’s reaction to it, started me thinking about how easily triggered the memories and flashbacks of PTSD can be.
It became clear very soon that a pilot had lost control of the helicopter on that foggy, rainy June day and had tried to make an emergency landing on the roof of a Manhattan high-rise. The roof landing did not go well; the helicopter crashed on the roof; and the lone pilot died.
As it turned out, mental health care workers treated many PTSD sufferers at the Bellevue and Mount Sinai hospital programs set up after Sept. 11, including those who were part of the rescue as well as the clean-up. In addition, it appears that many who witnessed the disaster also were vulnerable to PTSD and were additionally treated in various programs. I have seen and interviewed many of those people over the last 10 years.
PTSD is defined mainly in terms of experiencing a traumatic event during a man-made or natural disaster: torture, assaults, the tragedies of war, or any event that causes physical or psychological injury. According to research, it can occur right after the event or years later. Besides those major traumatic events, I’ve seen PTSD occur from much lesser traumas; much depends on how individuals process what is happening around them. For example, in some people, I’ve seen PTSD occur after job loss, where identity and persona are lost and the brain experiences the psychological shock consistent with more dangerously threatening aspects of PTSD. I’ve seen dog bites, auto accidents, even “fender benders” and emotional break-ups bring out the symptoms of PTSD (J Adv Nurs. 2005 Oct;52[1]:22-30). Luckily, in most of those cases, treatment or time itself can heal the problems.

Going back to that June day, for a few brief moments, my memory was jogged back to Sept. 11. A few people I spoke with about the event last month also reported being taken back to that fateful day (Am Psychol. 2011 Sep;66[6]:429-46).
For some experiencing PTSD, flashbacks to the physically threatening or psychologically shocking event occur as opposed to memory alone. During a flashback, the person actually relives the experience as if it were in the present. Flashbacks are quite different from recall alone. In my experience, the flashback is not unlike age regression, where an individual actually relives an event as opposed to having a memory of an event.
PTSD is a serious emotional problem, and I believe that much of it is undiagnosed in society – partly because we tend to look for the disorder after major traumatic events, such as physical and psychological effects of war or disaster, man-made and natural disasters, as well as assaults and torture. As we know in medicine and mental health care, there are certain vulnerabilities to some disorders. I believe that, whether through education, environment, or genetics, we have vulnerabilities to PTSD (Brain Behav Immun. 2013 May;30:12-21); (Clin Psychol Rev. 2012 Nov;32[7]:630-41), not only from major disastrous physical and psychological shocks but less obvious events in life that might create the same clinical picture we see in more traditional cases of PTSD.
Some PTSD survivors will improve and get better with time. Others do well after getting treatments with interventions such as cognitive-behavioral therapy (CBT) and prolonged exposure therapy, both of which are fairly short term in many instances. An ongoing relationship with a supportive therapist or friends and family is extremely important, in order to keep PTSD survivors from isolating and endlessly “living in their heads” as they relive the experience and face the multiple symptom complexes of PTSD.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including CBT and guided imagery. He recently published a book called “Find Freedom Fast” (New York: Kettlehole Publishing, 2018).
On June 10, 2019, a rainy, foggy day, there was a news flash that a plane had crashed into a building in the middle of New York City. I first saw this notification on my iPhone and my immediate thought was: Could this be a redo of Sept. 11?
I was especially concerned because I knew the area fairly well, in that a clinic I had worked in for more than 10 years was only a few blocks away. However, my memory bank brought me back to that day almost 18 years ago when, from a hospital window, many of us doctors, nurses, social workers, and patients saw the fire in the north tower and then saw the second plane crash into the south tower of the World Trade Center. Once we all knew what happened, we spent that night at the hospital awaiting the arrival of people in need of care. Unfortunately, very few arrived.
On this past June day, before anyone really knew the facts, what we heard and saw on TV was buildings being evacuated in midtown Manhattan, people running and moving in all directions with police officers directing people and diverting traffic, firemen entering the building, and EMT first responders in place. What mayhem!
Gov. Andrew Cuomo got to the scene very quickly and assured us that the incident did not appear to be a terrorist attack. Furthermore, he thoughtfully pointed out, we in New York City all seem to have a version or a form of posttraumatic stress disorder taking us back to Sept. 11, 2001. From my point of view, Gov. Cuomo could not have been more correct in his short, televised talk to a nervous public. The incident, and the governor’s reaction to it, started me thinking about how easily triggered the memories and flashbacks of PTSD can be.
It became clear very soon that a pilot had lost control of the helicopter on that foggy, rainy June day and had tried to make an emergency landing on the roof of a Manhattan high-rise. The roof landing did not go well; the helicopter crashed on the roof; and the lone pilot died.
As it turned out, mental health care workers treated many PTSD sufferers at the Bellevue and Mount Sinai hospital programs set up after Sept. 11, including those who were part of the rescue as well as the clean-up. In addition, it appears that many who witnessed the disaster also were vulnerable to PTSD and were additionally treated in various programs. I have seen and interviewed many of those people over the last 10 years.
PTSD is defined mainly in terms of experiencing a traumatic event during a man-made or natural disaster: torture, assaults, the tragedies of war, or any event that causes physical or psychological injury. According to research, it can occur right after the event or years later. Besides those major traumatic events, I’ve seen PTSD occur from much lesser traumas; much depends on how individuals process what is happening around them. For example, in some people, I’ve seen PTSD occur after job loss, where identity and persona are lost and the brain experiences the psychological shock consistent with more dangerously threatening aspects of PTSD. I’ve seen dog bites, auto accidents, even “fender benders” and emotional break-ups bring out the symptoms of PTSD (J Adv Nurs. 2005 Oct;52[1]:22-30). Luckily, in most of those cases, treatment or time itself can heal the problems.
Going back to that June day, for a few brief moments, my memory was jogged back to Sept. 11. A few people I spoke with about the event last month also reported being taken back to that fateful day (Am Psychol. 2011 Sep;66[6]:429-46).
For some experiencing PTSD, flashbacks to the physically threatening or psychologically shocking event occur as opposed to memory alone. During a flashback, the person actually relives the experience as if it were in the present. Flashbacks are quite different from recall alone. In my experience, the flashback is not unlike age regression, where an individual actually relives an event as opposed to having a memory of an event.
PTSD is a serious emotional problem, and I believe that much of it is undiagnosed in society – partly because we tend to look for the disorder after major traumatic events, such as physical and psychological effects of war or disaster, man-made and natural disasters, as well as assaults and torture. As we know in medicine and mental health care, there are certain vulnerabilities to some disorders. I believe that, whether through education, environment, or genetics, we have vulnerabilities to PTSD (Brain Behav Immun. 2013 May;30:12-21); (Clin Psychol Rev. 2012 Nov;32[7]:630-41), not only from major disastrous physical and psychological shocks but less obvious events in life that might create the same clinical picture we see in more traditional cases of PTSD.
Some PTSD survivors will improve and get better with time. Others do well after getting treatments with interventions such as cognitive-behavioral therapy (CBT) and prolonged exposure therapy, both of which are fairly short term in many instances. An ongoing relationship with a supportive therapist or friends and family is extremely important, in order to keep PTSD survivors from isolating and endlessly “living in their heads” as they relive the experience and face the multiple symptom complexes of PTSD.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including CBT and guided imagery. He recently published a book called “Find Freedom Fast” (New York: Kettlehole Publishing, 2018).
On June 10, 2019, a rainy, foggy day, there was a news flash that a plane had crashed into a building in the middle of New York City. I first saw this notification on my iPhone and my immediate thought was: Could this be a redo of Sept. 11?
I was especially concerned because I knew the area fairly well, in that a clinic I had worked in for more than 10 years was only a few blocks away. However, my memory bank brought me back to that day almost 18 years ago when, from a hospital window, many of us doctors, nurses, social workers, and patients saw the fire in the north tower and then saw the second plane crash into the south tower of the World Trade Center. Once we all knew what happened, we spent that night at the hospital awaiting the arrival of people in need of care. Unfortunately, very few arrived.
On this past June day, before anyone really knew the facts, what we heard and saw on TV was buildings being evacuated in midtown Manhattan, people running and moving in all directions with police officers directing people and diverting traffic, firemen entering the building, and EMT first responders in place. What mayhem!
Gov. Andrew Cuomo got to the scene very quickly and assured us that the incident did not appear to be a terrorist attack. Furthermore, he thoughtfully pointed out, we in New York City all seem to have a version or a form of posttraumatic stress disorder taking us back to Sept. 11, 2001. From my point of view, Gov. Cuomo could not have been more correct in his short, televised talk to a nervous public. The incident, and the governor’s reaction to it, started me thinking about how easily triggered the memories and flashbacks of PTSD can be.
It became clear very soon that a pilot had lost control of the helicopter on that foggy, rainy June day and had tried to make an emergency landing on the roof of a Manhattan high-rise. The roof landing did not go well; the helicopter crashed on the roof; and the lone pilot died.
As it turned out, mental health care workers treated many PTSD sufferers at the Bellevue and Mount Sinai hospital programs set up after Sept. 11, including those who were part of the rescue as well as the clean-up. In addition, it appears that many who witnessed the disaster also were vulnerable to PTSD and were additionally treated in various programs. I have seen and interviewed many of those people over the last 10 years.
PTSD is defined mainly in terms of experiencing a traumatic event during a man-made or natural disaster: torture, assaults, the tragedies of war, or any event that causes physical or psychological injury. According to research, it can occur right after the event or years later. Besides those major traumatic events, I’ve seen PTSD occur from much lesser traumas; much depends on how individuals process what is happening around them. For example, in some people, I’ve seen PTSD occur after job loss, where identity and persona are lost and the brain experiences the psychological shock consistent with more dangerously threatening aspects of PTSD. I’ve seen dog bites, auto accidents, even “fender benders” and emotional break-ups bring out the symptoms of PTSD (J Adv Nurs. 2005 Oct;52[1]:22-30). Luckily, in most of those cases, treatment or time itself can heal the problems.
Going back to that June day, for a few brief moments, my memory was jogged back to Sept. 11. A few people I spoke with about the event last month also reported being taken back to that fateful day (Am Psychol. 2011 Sep;66[6]:429-46).
For some experiencing PTSD, flashbacks to the physically threatening or psychologically shocking event occur as opposed to memory alone. During a flashback, the person actually relives the experience as if it were in the present. Flashbacks are quite different from recall alone. In my experience, the flashback is not unlike age regression, where an individual actually relives an event as opposed to having a memory of an event.
PTSD is a serious emotional problem, and I believe that much of it is undiagnosed in society – partly because we tend to look for the disorder after major traumatic events, such as physical and psychological effects of war or disaster, man-made and natural disasters, as well as assaults and torture. As we know in medicine and mental health care, there are certain vulnerabilities to some disorders. I believe that, whether through education, environment, or genetics, we have vulnerabilities to PTSD (Brain Behav Immun. 2013 May;30:12-21); (Clin Psychol Rev. 2012 Nov;32[7]:630-41), not only from major disastrous physical and psychological shocks but less obvious events in life that might create the same clinical picture we see in more traditional cases of PTSD.
Some PTSD survivors will improve and get better with time. Others do well after getting treatments with interventions such as cognitive-behavioral therapy (CBT) and prolonged exposure therapy, both of which are fairly short term in many instances. An ongoing relationship with a supportive therapist or friends and family is extremely important, in order to keep PTSD survivors from isolating and endlessly “living in their heads” as they relive the experience and face the multiple symptom complexes of PTSD.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including CBT and guided imagery. He recently published a book called “Find Freedom Fast” (New York: Kettlehole Publishing, 2018).
Dealing with staffing shortfalls
Five options for covering unfilled positions
Being in stressful situations is part of being a hospitalist. During a hospitalist’s work shift, one of the key determinants of stress is adequate staffing. With use of survey data from 569 hospital medicine groups (HMGs) across the nation, one of the topics examined in the 2018 State of Hospital Medicine Report is how HMGs cope with unfilled hospitalist physician positions.

The survey presented five options for covering unfilled hospitalist physician positions: use of locum tenens, use of moonlighters, use of voluntary extra shifts by the HMG’s existing hospitalists, use of required extra shifts, and leaving some shifts uncovered. Recipients were instructed to select all options that applied, so totals exceeded 100%. The data is organized according to HMGs that serve adults only, children only, and both adults and children.
For all three types of HMGs, the most common tactic to fill coverage gaps is through voluntary extra shifts by existing clinicians, reportedly used by 70.3% of HMGs that cover adults only, 66.7% by those that cover children only, and 76.9% by those that cover both adults and children. Data for adults-only HMGs was further broken down by geographic region, academic status, teaching status, group size, and employment model. Among adults-only HMGs, there is a direct correlation between group size and having members voluntarily work extra shifts, with 91.1% of groups with 30 or more full-time equivalent positions employing this tactic.
For HMGs that cover adults only and those that cover children only, the second most common tactic is to use moonlighters (57.4% and 53.3% respectively), while use of moonlighters is the third most commonly employed surveyed tactic for HMGs that cover both adults and children (53.8%).
HMGs that serve both adults and children were much more likely to utilize locum tenens to cover unfilled positions (69.2%) than were groups that serve adults only (44.0%) or children only (26.7%). The variability in the use of locum tenens is likely because of the willingness and/or ability of the respective groups to afford this option because it is generally the most expensive option of those surveyed.
Requiring that members of the group work extra shifts is the least popular staffing method among adults-only HMGs (10.0%) and HMGs serving both children and adults (7.7%). This strategy is unpopular, especially when there is little advance warning. Surprisingly, 40.0% of HMGs that see children only require members to work extra shifts to cover unfilled slots. This could be because pediatric HMGs are often smaller, and it would be more difficult to absorb the work if the shift is left uncovered. In fact, many pediatric HMGs staff with only one clinician at a time, so there may be no option besides requiring someone else in the group to come in and work.Of the options surveyed, perhaps the most uncomfortable for those hospitalist physicians on duty is to leave some shifts uncovered. The rapid growth and development of the specialty of hospital medicine has made it difficult for HMGs to continuously hire qualified hospitalists fast enough to meet demand. The survey found 46.2% of HMGs that serve both adults and children and 31.4% of groups that serve adults only have employed the staffing model of going short-staffed for at least some shifts. HMGs serving children-only are much less likely to go short-staffed (20.0%).
I work with a large HMG that has more than 70 members, and when it has been short-staffed, it tries to ensure a full complement of evening and night staff as the top priority because these shifts are typically more stressful. Since we have more hospitalist capacity during the day to absorb the loss of a physician, we pull staff from their daytime rounding schedules to execute this strategy. While going short-staffed is not ideal, this option has worked for many groups out of sheer necessity.
Dr. Stephan is a hospitalist at Allina Health’s Abbott Northwestern Hospital in Minneapolis and is a member of the SHM Practice Analysis Committee.
Five options for covering unfilled positions
Five options for covering unfilled positions
Being in stressful situations is part of being a hospitalist. During a hospitalist’s work shift, one of the key determinants of stress is adequate staffing. With use of survey data from 569 hospital medicine groups (HMGs) across the nation, one of the topics examined in the 2018 State of Hospital Medicine Report is how HMGs cope with unfilled hospitalist physician positions.
The survey presented five options for covering unfilled hospitalist physician positions: use of locum tenens, use of moonlighters, use of voluntary extra shifts by the HMG’s existing hospitalists, use of required extra shifts, and leaving some shifts uncovered. Recipients were instructed to select all options that applied, so totals exceeded 100%. The data is organized according to HMGs that serve adults only, children only, and both adults and children.
For all three types of HMGs, the most common tactic to fill coverage gaps is through voluntary extra shifts by existing clinicians, reportedly used by 70.3% of HMGs that cover adults only, 66.7% by those that cover children only, and 76.9% by those that cover both adults and children. Data for adults-only HMGs was further broken down by geographic region, academic status, teaching status, group size, and employment model. Among adults-only HMGs, there is a direct correlation between group size and having members voluntarily work extra shifts, with 91.1% of groups with 30 or more full-time equivalent positions employing this tactic.
For HMGs that cover adults only and those that cover children only, the second most common tactic is to use moonlighters (57.4% and 53.3% respectively), while use of moonlighters is the third most commonly employed surveyed tactic for HMGs that cover both adults and children (53.8%).
HMGs that serve both adults and children were much more likely to utilize locum tenens to cover unfilled positions (69.2%) than were groups that serve adults only (44.0%) or children only (26.7%). The variability in the use of locum tenens is likely because of the willingness and/or ability of the respective groups to afford this option because it is generally the most expensive option of those surveyed.
Requiring that members of the group work extra shifts is the least popular staffing method among adults-only HMGs (10.0%) and HMGs serving both children and adults (7.7%). This strategy is unpopular, especially when there is little advance warning. Surprisingly, 40.0% of HMGs that see children only require members to work extra shifts to cover unfilled slots. This could be because pediatric HMGs are often smaller, and it would be more difficult to absorb the work if the shift is left uncovered. In fact, many pediatric HMGs staff with only one clinician at a time, so there may be no option besides requiring someone else in the group to come in and work.Of the options surveyed, perhaps the most uncomfortable for those hospitalist physicians on duty is to leave some shifts uncovered. The rapid growth and development of the specialty of hospital medicine has made it difficult for HMGs to continuously hire qualified hospitalists fast enough to meet demand. The survey found 46.2% of HMGs that serve both adults and children and 31.4% of groups that serve adults only have employed the staffing model of going short-staffed for at least some shifts. HMGs serving children-only are much less likely to go short-staffed (20.0%).
I work with a large HMG that has more than 70 members, and when it has been short-staffed, it tries to ensure a full complement of evening and night staff as the top priority because these shifts are typically more stressful. Since we have more hospitalist capacity during the day to absorb the loss of a physician, we pull staff from their daytime rounding schedules to execute this strategy. While going short-staffed is not ideal, this option has worked for many groups out of sheer necessity.
Dr. Stephan is a hospitalist at Allina Health’s Abbott Northwestern Hospital in Minneapolis and is a member of the SHM Practice Analysis Committee.
Being in stressful situations is part of being a hospitalist. During a hospitalist’s work shift, one of the key determinants of stress is adequate staffing. With use of survey data from 569 hospital medicine groups (HMGs) across the nation, one of the topics examined in the 2018 State of Hospital Medicine Report is how HMGs cope with unfilled hospitalist physician positions.
The survey presented five options for covering unfilled hospitalist physician positions: use of locum tenens, use of moonlighters, use of voluntary extra shifts by the HMG’s existing hospitalists, use of required extra shifts, and leaving some shifts uncovered. Recipients were instructed to select all options that applied, so totals exceeded 100%. The data is organized according to HMGs that serve adults only, children only, and both adults and children.
For all three types of HMGs, the most common tactic to fill coverage gaps is through voluntary extra shifts by existing clinicians, reportedly used by 70.3% of HMGs that cover adults only, 66.7% by those that cover children only, and 76.9% by those that cover both adults and children. Data for adults-only HMGs was further broken down by geographic region, academic status, teaching status, group size, and employment model. Among adults-only HMGs, there is a direct correlation between group size and having members voluntarily work extra shifts, with 91.1% of groups with 30 or more full-time equivalent positions employing this tactic.
For HMGs that cover adults only and those that cover children only, the second most common tactic is to use moonlighters (57.4% and 53.3% respectively), while use of moonlighters is the third most commonly employed surveyed tactic for HMGs that cover both adults and children (53.8%).
HMGs that serve both adults and children were much more likely to utilize locum tenens to cover unfilled positions (69.2%) than were groups that serve adults only (44.0%) or children only (26.7%). The variability in the use of locum tenens is likely because of the willingness and/or ability of the respective groups to afford this option because it is generally the most expensive option of those surveyed.
Requiring that members of the group work extra shifts is the least popular staffing method among adults-only HMGs (10.0%) and HMGs serving both children and adults (7.7%). This strategy is unpopular, especially when there is little advance warning. Surprisingly, 40.0% of HMGs that see children only require members to work extra shifts to cover unfilled slots. This could be because pediatric HMGs are often smaller, and it would be more difficult to absorb the work if the shift is left uncovered. In fact, many pediatric HMGs staff with only one clinician at a time, so there may be no option besides requiring someone else in the group to come in and work.Of the options surveyed, perhaps the most uncomfortable for those hospitalist physicians on duty is to leave some shifts uncovered. The rapid growth and development of the specialty of hospital medicine has made it difficult for HMGs to continuously hire qualified hospitalists fast enough to meet demand. The survey found 46.2% of HMGs that serve both adults and children and 31.4% of groups that serve adults only have employed the staffing model of going short-staffed for at least some shifts. HMGs serving children-only are much less likely to go short-staffed (20.0%).
I work with a large HMG that has more than 70 members, and when it has been short-staffed, it tries to ensure a full complement of evening and night staff as the top priority because these shifts are typically more stressful. Since we have more hospitalist capacity during the day to absorb the loss of a physician, we pull staff from their daytime rounding schedules to execute this strategy. While going short-staffed is not ideal, this option has worked for many groups out of sheer necessity.
Dr. Stephan is a hospitalist at Allina Health’s Abbott Northwestern Hospital in Minneapolis and is a member of the SHM Practice Analysis Committee.
CBT intervention tied to Internet addiction remission in men
A manualized cognitive-behavioral therapy (CBT) program that combines group and individual interventions might effectively treat Internet and computer game addiction in men, results of a multicenter randomized trial suggest.
In the study, Klaus Wölfling, PhD, and colleagues randomized 143 men (mean age, 26.2 years) with Internet addiction (IA), which was defined as a score greater than 13 on the Assessment of Internet and Computer Game Addiction Self-Report (AICA-S). The men were recruited at four outpatient clinics in Germany and Austria from Jan. 24, 2012, to June 14, 2017. The primary endpoint of remission, defined as a score of less than 7 on the AICA-S, was achieved by 50 patients (69.4%) in the treatment arm, compared with 17 patients (23.9%) of the wait-list control arm. The greatest declines in AICA-S scores were seen by midtreatment, but mean scores continued at similar levels through follow-up. The study was published in JAMA Psychiatry (2019 Jul 10. doi: 10.1001/jamapsychiatry.2019.1676).
Dr. Wölfling and colleagues chose to limit the scope of the study to male participants because they represent most of those affected by IA; however, the authors admitted this limits the results’ generalizability. They also noted that many of the patients were ambivalent toward treatment, which is a core characteristic of patients affected by IA. Recruitment was slow, so the investigators had to evaluate a smaller number of participants than planned, although they felt their analyses were still statistically powerful enough to detect difference in endpoints. The authors also noted that, although they tried to control for comorbidities, which are often associated with IA, they had to define exclusion criteria for certain conditions such as major depression and some personality disorders.
IA was included in the DSM-5 in 2013 as a condition warranting further research, the authors of this study noted. More recently, it was “introduced as a new diagnosis in the International Classification of Diseases, 11th Revision, in the section Disorders Due to Substance Use or Addictive Behaviors.”
A manualized cognitive-behavioral therapy (CBT) program that combines group and individual interventions might effectively treat Internet and computer game addiction in men, results of a multicenter randomized trial suggest.
In the study, Klaus Wölfling, PhD, and colleagues randomized 143 men (mean age, 26.2 years) with Internet addiction (IA), which was defined as a score greater than 13 on the Assessment of Internet and Computer Game Addiction Self-Report (AICA-S). The men were recruited at four outpatient clinics in Germany and Austria from Jan. 24, 2012, to June 14, 2017. The primary endpoint of remission, defined as a score of less than 7 on the AICA-S, was achieved by 50 patients (69.4%) in the treatment arm, compared with 17 patients (23.9%) of the wait-list control arm. The greatest declines in AICA-S scores were seen by midtreatment, but mean scores continued at similar levels through follow-up. The study was published in JAMA Psychiatry (2019 Jul 10. doi: 10.1001/jamapsychiatry.2019.1676).
Dr. Wölfling and colleagues chose to limit the scope of the study to male participants because they represent most of those affected by IA; however, the authors admitted this limits the results’ generalizability. They also noted that many of the patients were ambivalent toward treatment, which is a core characteristic of patients affected by IA. Recruitment was slow, so the investigators had to evaluate a smaller number of participants than planned, although they felt their analyses were still statistically powerful enough to detect difference in endpoints. The authors also noted that, although they tried to control for comorbidities, which are often associated with IA, they had to define exclusion criteria for certain conditions such as major depression and some personality disorders.
IA was included in the DSM-5 in 2013 as a condition warranting further research, the authors of this study noted. More recently, it was “introduced as a new diagnosis in the International Classification of Diseases, 11th Revision, in the section Disorders Due to Substance Use or Addictive Behaviors.”
A manualized cognitive-behavioral therapy (CBT) program that combines group and individual interventions might effectively treat Internet and computer game addiction in men, results of a multicenter randomized trial suggest.
In the study, Klaus Wölfling, PhD, and colleagues randomized 143 men (mean age, 26.2 years) with Internet addiction (IA), which was defined as a score greater than 13 on the Assessment of Internet and Computer Game Addiction Self-Report (AICA-S). The men were recruited at four outpatient clinics in Germany and Austria from Jan. 24, 2012, to June 14, 2017. The primary endpoint of remission, defined as a score of less than 7 on the AICA-S, was achieved by 50 patients (69.4%) in the treatment arm, compared with 17 patients (23.9%) of the wait-list control arm. The greatest declines in AICA-S scores were seen by midtreatment, but mean scores continued at similar levels through follow-up. The study was published in JAMA Psychiatry (2019 Jul 10. doi: 10.1001/jamapsychiatry.2019.1676).
Dr. Wölfling and colleagues chose to limit the scope of the study to male participants because they represent most of those affected by IA; however, the authors admitted this limits the results’ generalizability. They also noted that many of the patients were ambivalent toward treatment, which is a core characteristic of patients affected by IA. Recruitment was slow, so the investigators had to evaluate a smaller number of participants than planned, although they felt their analyses were still statistically powerful enough to detect difference in endpoints. The authors also noted that, although they tried to control for comorbidities, which are often associated with IA, they had to define exclusion criteria for certain conditions such as major depression and some personality disorders.
IA was included in the DSM-5 in 2013 as a condition warranting further research, the authors of this study noted. More recently, it was “introduced as a new diagnosis in the International Classification of Diseases, 11th Revision, in the section Disorders Due to Substance Use or Addictive Behaviors.”
FROM JAMA PSYCHIATRY
Novel topical psoriasis treatment targets nerve pathways
MILAN – A novel topical nonsteroidal treatment for psoriasis showed sufficient efficacy in phase 2b clinical trials to proceed to phase 3 studies, with improvements in severity, pain, and burning in adults with mild to moderate psoriasis.
At the end of 12 weeks of treatment, 29% of patients receiving the medication – which targets nerve pathways – experienced a decrease of at least 2 grades on the 5-point Investigator’s Global Assessment (IGA) scale, compared with 13% of those receiving the topical vehicle only (P = .036). A similar proportion of patients achieved 75% improvement on the Psoriasis Area and Severity Index (PASI-75)compared with those on vehicle alone (27% versus 13%; P = .045).
, said Paul F. Lizzul, MD, PhD, presenting the findings during a late-breaking abstract session at the World Congress of Dermatology.
Pruritus severity also dropped by about 60%, but the decrease did not differ significantly from the change seen with vehicle alone, said Dr. Lizzul, chief medical officer for Sienna Biopharmaceuticals, Westlake Village, Calif., which funded the study. He and his coinvestigators found this “interesting, surprising, and different from what we had seen previously,” he said. “We think a few things happened here,” including intensive querying on itch by means of daily diaries, a different approach than had been taken in the investigator’s earlier SNA-120 trials. “We think in this way we probably biased patients’ expectations, altering reporting on this subjective measure,” he added.
“There’s been really a lack of innovation in the topical world in developing nonsteroidal therapies for the majority of patients who are treated with topicals, said Dr. Lizzul. Keratinocytes within psoriatic plaques are known to have elevated levels of nerve growth factor (NGF), he explained. Together with tropomyosin receptor kinase A (TrkA), NGF is implicated in the pathogenesis of psoriasis; it stimulates keratinocyte hyperproliferation, is a factor in neurogenic inflammation, and contributes to pruritus. Upregulation of TrkA expression is seen in nerve fibers within pruritic psoriasis plaques as well, said Dr. Lizzul, senior author of the study. (The first author was Kristina Callis Duffin, MD, cochair of the dermatology department at the University of Utah, Salt Lake City.)
In fact, the pruritus that plagues many psoriasis patients, said Dr. Lizzul, may “serve as a clinical biomarker for elevated NGF/TrkA expression.” And certain clinical phenomena observed in psoriasis, such as the Koebner phenomenon and plaque resolution along the path of damaged nerves, provide other clues. “Clearly, astute clinicians going back many, many years have recognized the very important role that nerves and neuropeptides play in psoriasis,” he added.
SNA-120 targets NGF TrKA activity, and “achieves high local drug concentration in the skin, with low systemic availability,” he said.
The randomized, double-blind, vehicle-controlled study enrolled 208 adults with mild to moderate psoriasis (scores of 2 or 3 on the IGA), with pruritus of at least moderate intensity (5 or higher on a 10-point itch numeric rating scale, or I-NRS). The mean age of the patients was 50 years, and about half were male. Most (84%-90% across study arms) were white. At baseline, the mean I-NRS was 7.3-7.4, and the mean PASI score at baseline ranged from 5.9 to 6.5.
Patients were randomized to receive SNA-120 twice daily at either 0.05% (70 patients) or 0.5% (69 patients) in an ointment formulation, or vehicle alone twice daily (69 patients). Efficacy was tracked by measuring decrease in IGA by one or two grades, the number of patients achieving PASI-50 and PASI-75, reduction in itch, and a composite of a decrease of at least 2 grades on the IGA and having clear or almost clear skin.
The investigators also tracked reduction in burning and pain as measured on a 10-point numeric rating scale. Though itch scores didn’t differ significantly from reductions seen with the topical vehicle alone, pain and burning were both reduced significantly compared with vehicle by week 12 of the study (P = .033 for pain; P = .043 for burning).
All improvements were seen only with the lower dose, not the 0.5% dose of SNA-120, noted Dr. Lizzul, adding: “This is not necessarily surprising in the world of kinase inhibitors, where you can see these J-shaped or inverse dose-response curves.”
In addition to recording adverse events, the researchers assessed safety by obtaining laboratory values and electrocardiograms. Plasma SNA-120 levels at study weeks 2, 4, and 8 were obtained for pharmacokinetic analysis. Systemic uptake was virtually nil, and the safety profile overall was good, said Dr. Lizzul.
Next steps are phase 3 clinical trials that will evaluate global improvement as well as pain, burning, and itch in psoriasis, he noted.
Dr. Lizzul is an employee of Sienna Biopharmaceuticals, which is developing SNA-120.
MILAN – A novel topical nonsteroidal treatment for psoriasis showed sufficient efficacy in phase 2b clinical trials to proceed to phase 3 studies, with improvements in severity, pain, and burning in adults with mild to moderate psoriasis.
At the end of 12 weeks of treatment, 29% of patients receiving the medication – which targets nerve pathways – experienced a decrease of at least 2 grades on the 5-point Investigator’s Global Assessment (IGA) scale, compared with 13% of those receiving the topical vehicle only (P = .036). A similar proportion of patients achieved 75% improvement on the Psoriasis Area and Severity Index (PASI-75)compared with those on vehicle alone (27% versus 13%; P = .045).
, said Paul F. Lizzul, MD, PhD, presenting the findings during a late-breaking abstract session at the World Congress of Dermatology.
Pruritus severity also dropped by about 60%, but the decrease did not differ significantly from the change seen with vehicle alone, said Dr. Lizzul, chief medical officer for Sienna Biopharmaceuticals, Westlake Village, Calif., which funded the study. He and his coinvestigators found this “interesting, surprising, and different from what we had seen previously,” he said. “We think a few things happened here,” including intensive querying on itch by means of daily diaries, a different approach than had been taken in the investigator’s earlier SNA-120 trials. “We think in this way we probably biased patients’ expectations, altering reporting on this subjective measure,” he added.
“There’s been really a lack of innovation in the topical world in developing nonsteroidal therapies for the majority of patients who are treated with topicals, said Dr. Lizzul. Keratinocytes within psoriatic plaques are known to have elevated levels of nerve growth factor (NGF), he explained. Together with tropomyosin receptor kinase A (TrkA), NGF is implicated in the pathogenesis of psoriasis; it stimulates keratinocyte hyperproliferation, is a factor in neurogenic inflammation, and contributes to pruritus. Upregulation of TrkA expression is seen in nerve fibers within pruritic psoriasis plaques as well, said Dr. Lizzul, senior author of the study. (The first author was Kristina Callis Duffin, MD, cochair of the dermatology department at the University of Utah, Salt Lake City.)
In fact, the pruritus that plagues many psoriasis patients, said Dr. Lizzul, may “serve as a clinical biomarker for elevated NGF/TrkA expression.” And certain clinical phenomena observed in psoriasis, such as the Koebner phenomenon and plaque resolution along the path of damaged nerves, provide other clues. “Clearly, astute clinicians going back many, many years have recognized the very important role that nerves and neuropeptides play in psoriasis,” he added.
SNA-120 targets NGF TrKA activity, and “achieves high local drug concentration in the skin, with low systemic availability,” he said.
The randomized, double-blind, vehicle-controlled study enrolled 208 adults with mild to moderate psoriasis (scores of 2 or 3 on the IGA), with pruritus of at least moderate intensity (5 or higher on a 10-point itch numeric rating scale, or I-NRS). The mean age of the patients was 50 years, and about half were male. Most (84%-90% across study arms) were white. At baseline, the mean I-NRS was 7.3-7.4, and the mean PASI score at baseline ranged from 5.9 to 6.5.
Patients were randomized to receive SNA-120 twice daily at either 0.05% (70 patients) or 0.5% (69 patients) in an ointment formulation, or vehicle alone twice daily (69 patients). Efficacy was tracked by measuring decrease in IGA by one or two grades, the number of patients achieving PASI-50 and PASI-75, reduction in itch, and a composite of a decrease of at least 2 grades on the IGA and having clear or almost clear skin.
The investigators also tracked reduction in burning and pain as measured on a 10-point numeric rating scale. Though itch scores didn’t differ significantly from reductions seen with the topical vehicle alone, pain and burning were both reduced significantly compared with vehicle by week 12 of the study (P = .033 for pain; P = .043 for burning).
All improvements were seen only with the lower dose, not the 0.5% dose of SNA-120, noted Dr. Lizzul, adding: “This is not necessarily surprising in the world of kinase inhibitors, where you can see these J-shaped or inverse dose-response curves.”
In addition to recording adverse events, the researchers assessed safety by obtaining laboratory values and electrocardiograms. Plasma SNA-120 levels at study weeks 2, 4, and 8 were obtained for pharmacokinetic analysis. Systemic uptake was virtually nil, and the safety profile overall was good, said Dr. Lizzul.
Next steps are phase 3 clinical trials that will evaluate global improvement as well as pain, burning, and itch in psoriasis, he noted.
Dr. Lizzul is an employee of Sienna Biopharmaceuticals, which is developing SNA-120.
MILAN – A novel topical nonsteroidal treatment for psoriasis showed sufficient efficacy in phase 2b clinical trials to proceed to phase 3 studies, with improvements in severity, pain, and burning in adults with mild to moderate psoriasis.
At the end of 12 weeks of treatment, 29% of patients receiving the medication – which targets nerve pathways – experienced a decrease of at least 2 grades on the 5-point Investigator’s Global Assessment (IGA) scale, compared with 13% of those receiving the topical vehicle only (P = .036). A similar proportion of patients achieved 75% improvement on the Psoriasis Area and Severity Index (PASI-75)compared with those on vehicle alone (27% versus 13%; P = .045).
, said Paul F. Lizzul, MD, PhD, presenting the findings during a late-breaking abstract session at the World Congress of Dermatology.
Pruritus severity also dropped by about 60%, but the decrease did not differ significantly from the change seen with vehicle alone, said Dr. Lizzul, chief medical officer for Sienna Biopharmaceuticals, Westlake Village, Calif., which funded the study. He and his coinvestigators found this “interesting, surprising, and different from what we had seen previously,” he said. “We think a few things happened here,” including intensive querying on itch by means of daily diaries, a different approach than had been taken in the investigator’s earlier SNA-120 trials. “We think in this way we probably biased patients’ expectations, altering reporting on this subjective measure,” he added.
“There’s been really a lack of innovation in the topical world in developing nonsteroidal therapies for the majority of patients who are treated with topicals, said Dr. Lizzul. Keratinocytes within psoriatic plaques are known to have elevated levels of nerve growth factor (NGF), he explained. Together with tropomyosin receptor kinase A (TrkA), NGF is implicated in the pathogenesis of psoriasis; it stimulates keratinocyte hyperproliferation, is a factor in neurogenic inflammation, and contributes to pruritus. Upregulation of TrkA expression is seen in nerve fibers within pruritic psoriasis plaques as well, said Dr. Lizzul, senior author of the study. (The first author was Kristina Callis Duffin, MD, cochair of the dermatology department at the University of Utah, Salt Lake City.)
In fact, the pruritus that plagues many psoriasis patients, said Dr. Lizzul, may “serve as a clinical biomarker for elevated NGF/TrkA expression.” And certain clinical phenomena observed in psoriasis, such as the Koebner phenomenon and plaque resolution along the path of damaged nerves, provide other clues. “Clearly, astute clinicians going back many, many years have recognized the very important role that nerves and neuropeptides play in psoriasis,” he added.
SNA-120 targets NGF TrKA activity, and “achieves high local drug concentration in the skin, with low systemic availability,” he said.
The randomized, double-blind, vehicle-controlled study enrolled 208 adults with mild to moderate psoriasis (scores of 2 or 3 on the IGA), with pruritus of at least moderate intensity (5 or higher on a 10-point itch numeric rating scale, or I-NRS). The mean age of the patients was 50 years, and about half were male. Most (84%-90% across study arms) were white. At baseline, the mean I-NRS was 7.3-7.4, and the mean PASI score at baseline ranged from 5.9 to 6.5.
Patients were randomized to receive SNA-120 twice daily at either 0.05% (70 patients) or 0.5% (69 patients) in an ointment formulation, or vehicle alone twice daily (69 patients). Efficacy was tracked by measuring decrease in IGA by one or two grades, the number of patients achieving PASI-50 and PASI-75, reduction in itch, and a composite of a decrease of at least 2 grades on the IGA and having clear or almost clear skin.
The investigators also tracked reduction in burning and pain as measured on a 10-point numeric rating scale. Though itch scores didn’t differ significantly from reductions seen with the topical vehicle alone, pain and burning were both reduced significantly compared with vehicle by week 12 of the study (P = .033 for pain; P = .043 for burning).
All improvements were seen only with the lower dose, not the 0.5% dose of SNA-120, noted Dr. Lizzul, adding: “This is not necessarily surprising in the world of kinase inhibitors, where you can see these J-shaped or inverse dose-response curves.”
In addition to recording adverse events, the researchers assessed safety by obtaining laboratory values and electrocardiograms. Plasma SNA-120 levels at study weeks 2, 4, and 8 were obtained for pharmacokinetic analysis. Systemic uptake was virtually nil, and the safety profile overall was good, said Dr. Lizzul.
Next steps are phase 3 clinical trials that will evaluate global improvement as well as pain, burning, and itch in psoriasis, he noted.
Dr. Lizzul is an employee of Sienna Biopharmaceuticals, which is developing SNA-120.
REPORTING FROM WCD2019
SGLT2 inhibitors, GLP-1 RAs are effective, but costly in T2D
Polyester. Plywood. Pizza. Skin allergens lurk in unusual places
NEWPORT BEACH, CALIF. – , according to dermatologist Jennifer H. Perryman, MD.
Here’s a closer look at the allergens highlighted by Dr. Perryman in a presentation at Skin Disease Education Foundation’s Women’s & Pediatric Dermatology Seminar:
Formaldehyde: It’s everywhere
“In general, formaldehyde is found on everyone in this room in two different places: preservatives in skin care products and in a lot of our clothing,” said Dr. Perryman, who practices in Greeley and Fort Collins, Colo.
The preservative is used in an even wider variety of products, including fluids used in industry (such as metalworking) and topical medications. But people are especially likely to encounter it in clothing – via formaldehyde textile resins – as well as in cosmetics, soaps, and lotions.
On the clothing front, Dr. Perryman said, formaldehyde textile resins have been used since the 1930s. They’re used to treat blends of synthetic and cotton fibers and bed sheets. Beware of “wrinkle resistant” and “permanent press” clothing (although not all have been treated with this resin). “Newer formaldehyde textile resins have less formaldehyde release, but they may be more expensive, and some industries may not use them,” she said.
Avoiding formaldehyde textile resins isn’t a simple matter.” You have to go out of your way to stay away from a polyester-cotton blend,” she said. “And don’t forget bedsheets,” she added, noting that the packaging on some sheets include information about cotton count, “but when you flip over the label it says it’s ‘50% cotton and 50% polyester or other.’ ”
Some patients will bring their own bedsheets to hotels so they don’t experience flares from hotel bedsheets, she added.
Other products can trigger this skin allergy. Beware, Dr. Perryman said, of formaldehyde exposure from paper, cardboard, cigarette smoke, processed wood products like plywood, foam housing and industrial insulation, embalming fluid and tissue fixatives, and some paints and adhesives.
What are the signs that someone may have a case of formaldehyde allergy? It may cause patchy generalized dermatitis, erythroderma, and nummular dermatitis. It may spare the hands, feet, and face because those parts of the body have less exposure to clothing, and it’s likely to especially affect body areas where clothing is tight. And for unknown reasons, this allergy is more common in the elderly, Dr. Perryman said.
Textile dye: Beware polyester
This allergy is mainly triggered by synthetic fabrics like polyester, rayon, and acetate, she noted. Darker colors are more allergenic. Clothes made of natural fibers such as cotton, silk, linen, and wool are alternatives. These are not dyed with these dyes, she said, adding that a reaction to wool will be from irritation, not from the dye.
Paraphenylenediamine: Keep an eye out for this dye ingredient
Paraphenylenediamine, which can trigger allergic reactions, is found in leather dye, fur dye, and some (but not all) hair dyes. Be aware that it can cross-react with other allergens like sulfonamide medications.
If a patch test turns up a reaction to “Black-Rubber Mix,” which includes paraphenylenediamine, consider whether the patient has exposure to the rubber in tires. Car mechanics may be affected by this allergy, Dr. Perryman said.
Neomycin: A drop of trouble
Allergy to the antibiotic neomycin can be triggered by exposure to gentamicin and tobramycin eye drops. Patients may believe they have an infection, Dr. Perryman said, so consider getting a culture. In some cases, an allergic reaction to neomycin may be incorrectly diagnosed as cellulitis.
Nickel: Not just a jewelry hazard
Jewelry and coins can trigger nickel allergies, but be aware that systemic nickel allergy can also trigger skin problems from a patient’s diet. It may be necessary to put patients on a low-nickel diet that avoids foods such as healthy grains, greens (especially spinach), nuts, legumes, and chocolate. “I always feel bad” putting patients on a restrictive diet, Dr. Perryman said, but it can be helpful to take 500 mg of vitamin C three times a day since it binds to nickel.
Cobalt: Watch the chocolate and coffee
Jewelry with cobalt can cause an allergic reaction. Dr. Perryman tells patients to buy an inexpensive “spot test” product online that detects whether jewelry has nickel or cobalt. Cobalt allergy can also trigger symptoms in patients exposed to “hard metal” industrial tools, cement, and masonry. Workers in the plastics and dye industries may be exposed too.
Like nickel, Dr. Perryman said, systemic cobalt allergy related to diet is also possible. The list of foods that contain higher levels of cobalt is long, and includes apricots, beans, beer, chocolate, coffee, nuts, tea, and whole-grain flour.
Dr. Perryman also mentioned several other allergens to keep in mind:
- Chromate can trigger reactions in people who wear leather shoes (the metal can be used in tanning). It can also cause problems in workers exposed to it via cement, bricks, drywall, and metal plating.
- Chromium picolinate, an over-the-counter supplement, can cause systemic dermatitis.
- Gold in jewelry can trigger an allergic reaction. Talk to patients about replating their jewelry, Dr. Perryman said.
- Rubber can trigger reactions due to exposure to rubber bands, makeup sponges, and rubber gloves (even nitrile ones). Be aware that both rubber and latex allergies may coexist and consider a blood test for latex allergy.
- Systemic balsam allergy related to an individual’s diet is possible. Tomato is an especially big villain on this front, along with citrus fruits, spices, cola, chili, and chocolate.
Dr. Perryman disclosed consulting work for IntraDerm. SDEF and this news organization are owned by the same parent company.
NEWPORT BEACH, CALIF. – , according to dermatologist Jennifer H. Perryman, MD.
Here’s a closer look at the allergens highlighted by Dr. Perryman in a presentation at Skin Disease Education Foundation’s Women’s & Pediatric Dermatology Seminar:
Formaldehyde: It’s everywhere
“In general, formaldehyde is found on everyone in this room in two different places: preservatives in skin care products and in a lot of our clothing,” said Dr. Perryman, who practices in Greeley and Fort Collins, Colo.
The preservative is used in an even wider variety of products, including fluids used in industry (such as metalworking) and topical medications. But people are especially likely to encounter it in clothing – via formaldehyde textile resins – as well as in cosmetics, soaps, and lotions.
On the clothing front, Dr. Perryman said, formaldehyde textile resins have been used since the 1930s. They’re used to treat blends of synthetic and cotton fibers and bed sheets. Beware of “wrinkle resistant” and “permanent press” clothing (although not all have been treated with this resin). “Newer formaldehyde textile resins have less formaldehyde release, but they may be more expensive, and some industries may not use them,” she said.
Avoiding formaldehyde textile resins isn’t a simple matter.” You have to go out of your way to stay away from a polyester-cotton blend,” she said. “And don’t forget bedsheets,” she added, noting that the packaging on some sheets include information about cotton count, “but when you flip over the label it says it’s ‘50% cotton and 50% polyester or other.’ ”
Some patients will bring their own bedsheets to hotels so they don’t experience flares from hotel bedsheets, she added.
Other products can trigger this skin allergy. Beware, Dr. Perryman said, of formaldehyde exposure from paper, cardboard, cigarette smoke, processed wood products like plywood, foam housing and industrial insulation, embalming fluid and tissue fixatives, and some paints and adhesives.
What are the signs that someone may have a case of formaldehyde allergy? It may cause patchy generalized dermatitis, erythroderma, and nummular dermatitis. It may spare the hands, feet, and face because those parts of the body have less exposure to clothing, and it’s likely to especially affect body areas where clothing is tight. And for unknown reasons, this allergy is more common in the elderly, Dr. Perryman said.
Textile dye: Beware polyester
This allergy is mainly triggered by synthetic fabrics like polyester, rayon, and acetate, she noted. Darker colors are more allergenic. Clothes made of natural fibers such as cotton, silk, linen, and wool are alternatives. These are not dyed with these dyes, she said, adding that a reaction to wool will be from irritation, not from the dye.
Paraphenylenediamine: Keep an eye out for this dye ingredient
Paraphenylenediamine, which can trigger allergic reactions, is found in leather dye, fur dye, and some (but not all) hair dyes. Be aware that it can cross-react with other allergens like sulfonamide medications.
If a patch test turns up a reaction to “Black-Rubber Mix,” which includes paraphenylenediamine, consider whether the patient has exposure to the rubber in tires. Car mechanics may be affected by this allergy, Dr. Perryman said.
Neomycin: A drop of trouble
Allergy to the antibiotic neomycin can be triggered by exposure to gentamicin and tobramycin eye drops. Patients may believe they have an infection, Dr. Perryman said, so consider getting a culture. In some cases, an allergic reaction to neomycin may be incorrectly diagnosed as cellulitis.
Nickel: Not just a jewelry hazard
Jewelry and coins can trigger nickel allergies, but be aware that systemic nickel allergy can also trigger skin problems from a patient’s diet. It may be necessary to put patients on a low-nickel diet that avoids foods such as healthy grains, greens (especially spinach), nuts, legumes, and chocolate. “I always feel bad” putting patients on a restrictive diet, Dr. Perryman said, but it can be helpful to take 500 mg of vitamin C three times a day since it binds to nickel.
Cobalt: Watch the chocolate and coffee
Jewelry with cobalt can cause an allergic reaction. Dr. Perryman tells patients to buy an inexpensive “spot test” product online that detects whether jewelry has nickel or cobalt. Cobalt allergy can also trigger symptoms in patients exposed to “hard metal” industrial tools, cement, and masonry. Workers in the plastics and dye industries may be exposed too.
Like nickel, Dr. Perryman said, systemic cobalt allergy related to diet is also possible. The list of foods that contain higher levels of cobalt is long, and includes apricots, beans, beer, chocolate, coffee, nuts, tea, and whole-grain flour.
Dr. Perryman also mentioned several other allergens to keep in mind:
- Chromate can trigger reactions in people who wear leather shoes (the metal can be used in tanning). It can also cause problems in workers exposed to it via cement, bricks, drywall, and metal plating.
- Chromium picolinate, an over-the-counter supplement, can cause systemic dermatitis.
- Gold in jewelry can trigger an allergic reaction. Talk to patients about replating their jewelry, Dr. Perryman said.
- Rubber can trigger reactions due to exposure to rubber bands, makeup sponges, and rubber gloves (even nitrile ones). Be aware that both rubber and latex allergies may coexist and consider a blood test for latex allergy.
- Systemic balsam allergy related to an individual’s diet is possible. Tomato is an especially big villain on this front, along with citrus fruits, spices, cola, chili, and chocolate.
Dr. Perryman disclosed consulting work for IntraDerm. SDEF and this news organization are owned by the same parent company.
NEWPORT BEACH, CALIF. – , according to dermatologist Jennifer H. Perryman, MD.
Here’s a closer look at the allergens highlighted by Dr. Perryman in a presentation at Skin Disease Education Foundation’s Women’s & Pediatric Dermatology Seminar:
Formaldehyde: It’s everywhere
“In general, formaldehyde is found on everyone in this room in two different places: preservatives in skin care products and in a lot of our clothing,” said Dr. Perryman, who practices in Greeley and Fort Collins, Colo.
The preservative is used in an even wider variety of products, including fluids used in industry (such as metalworking) and topical medications. But people are especially likely to encounter it in clothing – via formaldehyde textile resins – as well as in cosmetics, soaps, and lotions.
On the clothing front, Dr. Perryman said, formaldehyde textile resins have been used since the 1930s. They’re used to treat blends of synthetic and cotton fibers and bed sheets. Beware of “wrinkle resistant” and “permanent press” clothing (although not all have been treated with this resin). “Newer formaldehyde textile resins have less formaldehyde release, but they may be more expensive, and some industries may not use them,” she said.
Avoiding formaldehyde textile resins isn’t a simple matter.” You have to go out of your way to stay away from a polyester-cotton blend,” she said. “And don’t forget bedsheets,” she added, noting that the packaging on some sheets include information about cotton count, “but when you flip over the label it says it’s ‘50% cotton and 50% polyester or other.’ ”
Some patients will bring their own bedsheets to hotels so they don’t experience flares from hotel bedsheets, she added.
Other products can trigger this skin allergy. Beware, Dr. Perryman said, of formaldehyde exposure from paper, cardboard, cigarette smoke, processed wood products like plywood, foam housing and industrial insulation, embalming fluid and tissue fixatives, and some paints and adhesives.
What are the signs that someone may have a case of formaldehyde allergy? It may cause patchy generalized dermatitis, erythroderma, and nummular dermatitis. It may spare the hands, feet, and face because those parts of the body have less exposure to clothing, and it’s likely to especially affect body areas where clothing is tight. And for unknown reasons, this allergy is more common in the elderly, Dr. Perryman said.
Textile dye: Beware polyester
This allergy is mainly triggered by synthetic fabrics like polyester, rayon, and acetate, she noted. Darker colors are more allergenic. Clothes made of natural fibers such as cotton, silk, linen, and wool are alternatives. These are not dyed with these dyes, she said, adding that a reaction to wool will be from irritation, not from the dye.
Paraphenylenediamine: Keep an eye out for this dye ingredient
Paraphenylenediamine, which can trigger allergic reactions, is found in leather dye, fur dye, and some (but not all) hair dyes. Be aware that it can cross-react with other allergens like sulfonamide medications.
If a patch test turns up a reaction to “Black-Rubber Mix,” which includes paraphenylenediamine, consider whether the patient has exposure to the rubber in tires. Car mechanics may be affected by this allergy, Dr. Perryman said.
Neomycin: A drop of trouble
Allergy to the antibiotic neomycin can be triggered by exposure to gentamicin and tobramycin eye drops. Patients may believe they have an infection, Dr. Perryman said, so consider getting a culture. In some cases, an allergic reaction to neomycin may be incorrectly diagnosed as cellulitis.
Nickel: Not just a jewelry hazard
Jewelry and coins can trigger nickel allergies, but be aware that systemic nickel allergy can also trigger skin problems from a patient’s diet. It may be necessary to put patients on a low-nickel diet that avoids foods such as healthy grains, greens (especially spinach), nuts, legumes, and chocolate. “I always feel bad” putting patients on a restrictive diet, Dr. Perryman said, but it can be helpful to take 500 mg of vitamin C three times a day since it binds to nickel.
Cobalt: Watch the chocolate and coffee
Jewelry with cobalt can cause an allergic reaction. Dr. Perryman tells patients to buy an inexpensive “spot test” product online that detects whether jewelry has nickel or cobalt. Cobalt allergy can also trigger symptoms in patients exposed to “hard metal” industrial tools, cement, and masonry. Workers in the plastics and dye industries may be exposed too.
Like nickel, Dr. Perryman said, systemic cobalt allergy related to diet is also possible. The list of foods that contain higher levels of cobalt is long, and includes apricots, beans, beer, chocolate, coffee, nuts, tea, and whole-grain flour.
Dr. Perryman also mentioned several other allergens to keep in mind:
- Chromate can trigger reactions in people who wear leather shoes (the metal can be used in tanning). It can also cause problems in workers exposed to it via cement, bricks, drywall, and metal plating.
- Chromium picolinate, an over-the-counter supplement, can cause systemic dermatitis.
- Gold in jewelry can trigger an allergic reaction. Talk to patients about replating their jewelry, Dr. Perryman said.
- Rubber can trigger reactions due to exposure to rubber bands, makeup sponges, and rubber gloves (even nitrile ones). Be aware that both rubber and latex allergies may coexist and consider a blood test for latex allergy.
- Systemic balsam allergy related to an individual’s diet is possible. Tomato is an especially big villain on this front, along with citrus fruits, spices, cola, chili, and chocolate.
Dr. Perryman disclosed consulting work for IntraDerm. SDEF and this news organization are owned by the same parent company.
REPORTING FROM SDEF WOMEN’S & PEDIATRIC DERMATOLOGY SEMINAR
Parent education improves pediatric influenza vaccination rates
according to a randomized clinical trial published in Pediatrics.

Vanessa P. Scott, MD, MS, of Columbia University, New York, and colleagues randomized 400 parent-child dyads into any of three arms: receiving a handout based on national data, receiving a handout based on local data, or receiving usual care. This convenience sample was drawn from two pediatric clinics in New York between August 2016 and March 2017.
After adjustment for parents’ education level, the trial found that parents who received either handout were significantly more likely than were those receiving usual care to vaccinate their children by the end of season (75% and 65%, respectively; adjusted odds ratio, 1.68; 95% confidence interval, 1.06-2.67), but the effects of any intervention versus those of usual care on vaccination on day of visit were not statistically significant (59% vs. 53%; aOR, 1.36; 95% CI, 0.89-2.09).The researchers had hoped that using a targeted approach based on local data would increase vaccine receipt, but that was not seen in the results.
They did find that, across all three arms in the trial, baseline parental intent to vaccinate (likely versus unlikely) was associated with vaccination rates: Both vaccination on clinic visit day (70% vs. 22%; aOR, 8.38; 95% CI, 4.85-14.34) and vaccination by end of season (87% vs. 29%; aOR, 18.26; 95% CI, 9.94-33.52) were affected.
Strengths of the study included the randomized, controlled design and assessment of baseline factors, such as intention to vaccinate, to reduce confounding effects. Limitations included use of a convenience sample, which could have introduced selection bias.
One author was an unremunerated coinvestigator of an unrelated trial that received an investigator-initiated grant from the Pfizer Medical Education Group. Two authors were funded by other grants, but no potential conflicts of interests to disclose were indicated by any of the authors in this study.
SOURCE: Scott VP et al. Pediatrics. 2019. doi: 10.1542/peds.2018-2580.
according to a randomized clinical trial published in Pediatrics.
Vanessa P. Scott, MD, MS, of Columbia University, New York, and colleagues randomized 400 parent-child dyads into any of three arms: receiving a handout based on national data, receiving a handout based on local data, or receiving usual care. This convenience sample was drawn from two pediatric clinics in New York between August 2016 and March 2017.
After adjustment for parents’ education level, the trial found that parents who received either handout were significantly more likely than were those receiving usual care to vaccinate their children by the end of season (75% and 65%, respectively; adjusted odds ratio, 1.68; 95% confidence interval, 1.06-2.67), but the effects of any intervention versus those of usual care on vaccination on day of visit were not statistically significant (59% vs. 53%; aOR, 1.36; 95% CI, 0.89-2.09).The researchers had hoped that using a targeted approach based on local data would increase vaccine receipt, but that was not seen in the results.
They did find that, across all three arms in the trial, baseline parental intent to vaccinate (likely versus unlikely) was associated with vaccination rates: Both vaccination on clinic visit day (70% vs. 22%; aOR, 8.38; 95% CI, 4.85-14.34) and vaccination by end of season (87% vs. 29%; aOR, 18.26; 95% CI, 9.94-33.52) were affected.
Strengths of the study included the randomized, controlled design and assessment of baseline factors, such as intention to vaccinate, to reduce confounding effects. Limitations included use of a convenience sample, which could have introduced selection bias.
One author was an unremunerated coinvestigator of an unrelated trial that received an investigator-initiated grant from the Pfizer Medical Education Group. Two authors were funded by other grants, but no potential conflicts of interests to disclose were indicated by any of the authors in this study.
SOURCE: Scott VP et al. Pediatrics. 2019. doi: 10.1542/peds.2018-2580.
according to a randomized clinical trial published in Pediatrics.
Vanessa P. Scott, MD, MS, of Columbia University, New York, and colleagues randomized 400 parent-child dyads into any of three arms: receiving a handout based on national data, receiving a handout based on local data, or receiving usual care. This convenience sample was drawn from two pediatric clinics in New York between August 2016 and March 2017.
After adjustment for parents’ education level, the trial found that parents who received either handout were significantly more likely than were those receiving usual care to vaccinate their children by the end of season (75% and 65%, respectively; adjusted odds ratio, 1.68; 95% confidence interval, 1.06-2.67), but the effects of any intervention versus those of usual care on vaccination on day of visit were not statistically significant (59% vs. 53%; aOR, 1.36; 95% CI, 0.89-2.09).The researchers had hoped that using a targeted approach based on local data would increase vaccine receipt, but that was not seen in the results.
They did find that, across all three arms in the trial, baseline parental intent to vaccinate (likely versus unlikely) was associated with vaccination rates: Both vaccination on clinic visit day (70% vs. 22%; aOR, 8.38; 95% CI, 4.85-14.34) and vaccination by end of season (87% vs. 29%; aOR, 18.26; 95% CI, 9.94-33.52) were affected.
Strengths of the study included the randomized, controlled design and assessment of baseline factors, such as intention to vaccinate, to reduce confounding effects. Limitations included use of a convenience sample, which could have introduced selection bias.
One author was an unremunerated coinvestigator of an unrelated trial that received an investigator-initiated grant from the Pfizer Medical Education Group. Two authors were funded by other grants, but no potential conflicts of interests to disclose were indicated by any of the authors in this study.
SOURCE: Scott VP et al. Pediatrics. 2019. doi: 10.1542/peds.2018-2580.
FROM PEDIATRICS
Hyponatremia is a potential and serious complication of prolonged labor

Sarah C. Lassey, MD, of the Brigham and Women’s Hospital, Boston, and colleagues noted that a rise in the number of women choosing a home labor means health care professionals may be more likely to encounter patients with hyponatremia secondary to prolonged labor and excessive hypotonic fluid consumption.
They presented the cases of two patients who were transferred to their labor and delivery unit with hyponatremia after a prolonged labor, published in Obstetrics & Gynecology. One woman presented with somnolence and confusion. The other woman was alert on arrival, but post partum had slurred speech and blurry vision.
“A likely mechanism for hyponatremia in these cases includes endogenous oxytocin and excessive free water consumption in the setting of hypovolemia,” they suggested.
One of the patients was managed with an intravenous infusion of normal saline and went on to make a full recovery after being monitored in the intensive care unit.
The other patient also was managed with normal saline, but her serum sodium level rose by 6 mmol/L within 3 hours of delivery, raising concern that the serum sodium correction was dangerously rapid. After consultation with a nephrologist, the patient’s saline IV was discontinued, and she was given desmopressin acetate to “reduce rapid diuresis of free water excretion,” they said.
“The goal of treatment should be to raise the serum sodium concentration by 1-2 mmol/L per hour, with a maximum increase ranging from 8 mmol/L in 24 hours to 25 mmol/L in 48 hours,” Dr. Lassey and colleagues noted. “The risk of raising the serum sodium concentration too quickly is osmotic demyelination syndrome, which has been reported with a serum sodium level increase of more than 12 mmol/L in 24 hours.”
Hyponatremia should be considered in women presenting as home birth transfers and in women undergoing prolonged labor at the hospital, they concluded. It also makes sense to perform electrolyte testing on admission for women with a long labor prior to coming to the hospital and for those whose labor becomes prolonged who drink a lot of fluids.
Considering the risks associated with hyponatremia, if suspicion is high, it may be prudent to start isotonic fluids before lab results are back, they said. Symptoms of mild hyponatremia include headache, lethargy, nausea, vomiting, and anorexia. Moderate hyponatremia can present as agitation, disorientation, and psychosis; if severe, hyponatremia may present as seizure, coma, or death.
Also alert your neonatal colleagues in cases of maternal intrapartum hyponatremia, because “neonatal serum sodium level will be reflective of the mother’s serum sodium level,” Dr. Lassey and associates added.
Dr. Daniela Carusi received payment from UptoDate. The other authors did not report any potential conflicts of interest.
SOURCE: Lassey SC et al. Obstet Gynecol. 2019. doi: 10.1097/AOG.0000000000003306.
Sarah C. Lassey, MD, of the Brigham and Women’s Hospital, Boston, and colleagues noted that a rise in the number of women choosing a home labor means health care professionals may be more likely to encounter patients with hyponatremia secondary to prolonged labor and excessive hypotonic fluid consumption.
They presented the cases of two patients who were transferred to their labor and delivery unit with hyponatremia after a prolonged labor, published in Obstetrics & Gynecology. One woman presented with somnolence and confusion. The other woman was alert on arrival, but post partum had slurred speech and blurry vision.
“A likely mechanism for hyponatremia in these cases includes endogenous oxytocin and excessive free water consumption in the setting of hypovolemia,” they suggested.
One of the patients was managed with an intravenous infusion of normal saline and went on to make a full recovery after being monitored in the intensive care unit.
The other patient also was managed with normal saline, but her serum sodium level rose by 6 mmol/L within 3 hours of delivery, raising concern that the serum sodium correction was dangerously rapid. After consultation with a nephrologist, the patient’s saline IV was discontinued, and she was given desmopressin acetate to “reduce rapid diuresis of free water excretion,” they said.
“The goal of treatment should be to raise the serum sodium concentration by 1-2 mmol/L per hour, with a maximum increase ranging from 8 mmol/L in 24 hours to 25 mmol/L in 48 hours,” Dr. Lassey and colleagues noted. “The risk of raising the serum sodium concentration too quickly is osmotic demyelination syndrome, which has been reported with a serum sodium level increase of more than 12 mmol/L in 24 hours.”
Hyponatremia should be considered in women presenting as home birth transfers and in women undergoing prolonged labor at the hospital, they concluded. It also makes sense to perform electrolyte testing on admission for women with a long labor prior to coming to the hospital and for those whose labor becomes prolonged who drink a lot of fluids.
Considering the risks associated with hyponatremia, if suspicion is high, it may be prudent to start isotonic fluids before lab results are back, they said. Symptoms of mild hyponatremia include headache, lethargy, nausea, vomiting, and anorexia. Moderate hyponatremia can present as agitation, disorientation, and psychosis; if severe, hyponatremia may present as seizure, coma, or death.
Also alert your neonatal colleagues in cases of maternal intrapartum hyponatremia, because “neonatal serum sodium level will be reflective of the mother’s serum sodium level,” Dr. Lassey and associates added.
Dr. Daniela Carusi received payment from UptoDate. The other authors did not report any potential conflicts of interest.
SOURCE: Lassey SC et al. Obstet Gynecol. 2019. doi: 10.1097/AOG.0000000000003306.
Sarah C. Lassey, MD, of the Brigham and Women’s Hospital, Boston, and colleagues noted that a rise in the number of women choosing a home labor means health care professionals may be more likely to encounter patients with hyponatremia secondary to prolonged labor and excessive hypotonic fluid consumption.
They presented the cases of two patients who were transferred to their labor and delivery unit with hyponatremia after a prolonged labor, published in Obstetrics & Gynecology. One woman presented with somnolence and confusion. The other woman was alert on arrival, but post partum had slurred speech and blurry vision.
“A likely mechanism for hyponatremia in these cases includes endogenous oxytocin and excessive free water consumption in the setting of hypovolemia,” they suggested.
One of the patients was managed with an intravenous infusion of normal saline and went on to make a full recovery after being monitored in the intensive care unit.
The other patient also was managed with normal saline, but her serum sodium level rose by 6 mmol/L within 3 hours of delivery, raising concern that the serum sodium correction was dangerously rapid. After consultation with a nephrologist, the patient’s saline IV was discontinued, and she was given desmopressin acetate to “reduce rapid diuresis of free water excretion,” they said.
“The goal of treatment should be to raise the serum sodium concentration by 1-2 mmol/L per hour, with a maximum increase ranging from 8 mmol/L in 24 hours to 25 mmol/L in 48 hours,” Dr. Lassey and colleagues noted. “The risk of raising the serum sodium concentration too quickly is osmotic demyelination syndrome, which has been reported with a serum sodium level increase of more than 12 mmol/L in 24 hours.”
Hyponatremia should be considered in women presenting as home birth transfers and in women undergoing prolonged labor at the hospital, they concluded. It also makes sense to perform electrolyte testing on admission for women with a long labor prior to coming to the hospital and for those whose labor becomes prolonged who drink a lot of fluids.
Considering the risks associated with hyponatremia, if suspicion is high, it may be prudent to start isotonic fluids before lab results are back, they said. Symptoms of mild hyponatremia include headache, lethargy, nausea, vomiting, and anorexia. Moderate hyponatremia can present as agitation, disorientation, and psychosis; if severe, hyponatremia may present as seizure, coma, or death.
Also alert your neonatal colleagues in cases of maternal intrapartum hyponatremia, because “neonatal serum sodium level will be reflective of the mother’s serum sodium level,” Dr. Lassey and associates added.
Dr. Daniela Carusi received payment from UptoDate. The other authors did not report any potential conflicts of interest.
SOURCE: Lassey SC et al. Obstet Gynecol. 2019. doi: 10.1097/AOG.0000000000003306.
FROM OBSTETRICS & GYNECOLOGY
