User login
VERTIS CV: Ertugliflozin’s proven benefits fall short of other SGLT2 inhibitors
Further analyses from the cardiovascular outcome trial of the sodium-glucose transporter 2 inhibitor ertugliflozin in patients with type 2 diabetes helped better define positive effects the drug had on preserving renal function, and also gave a tantalizing hint that this drug, and hence possibly the entire SGLT2 inhibitor drug class, may benefit patients with heart failure with reduced ejection fraction.

But the underlying problem for ertugliflozin (Steglatro) – first seen when results from the VERTIS CV trial initially came out in June 2020 at the annual meeting of the American Diabetes Association – was that, while the trial met its primary endpoint of proving noninferiority to placebo for the combined endpoint of cardiovascular death, nonfatal MI, or nonfatal stroke, treatment with ertugliflozin showed no suggestion of benefit, compared with placebo for reducing this endpoint, producing a nonsignificant 3% relative cut in the combined rate of these adverse events, compared with placebo treatment.
‘Somewhat disappointing’ trial performance
Overall, results from VERTIS CV with ertugliflozin were “somewhat disappointing,” commented Melanie J. Davies, MD, who was not involved with the study and chaired a session at the virtual annual meeting of the European Association for the Study of Diabetes that reviewed the main results, put them into perspective, and added a few new exploratory analyses.
Although the results from 8,246-patient VERTIS CV (Evaluation of Ertugliflozin Efficacy and Safety Cardiovascular Outcomes Trial) put ertugliflozin in the same league as other drugs from its class for safety, “we do not see the significant benefits observed in many of the previous cardiovascular outcomes trials” for other drugs in the SGLT2 inhibitor class, specifically canagliflozin (Invokana), dapagliflozin (Farxiga), and empagliflozin (Jardiance), Dr. Davies said in an interview. The upshot, for at least the time being, is that ertugliflozin “is unlikely to receive a label for any new indications,” she predicted. In contrast, the other drugs in the class have, for example, received a U.S. labeled indication to reduce cardiovascular death (empagliflozin) or major cardiovascular disease events (canagliflozin) in adults with type 2 diabetes (T2D) and cardiovascular disease, or to reduce heart failure hospitalizations (dapagliflozin).
The main results from VERTIS CV, posted online in the New England Journal of Medicine after the EASD session, showed a single significant outcome difference between treatment with ertugliflozin and placebo over a median of 3.0 years of follow-up from among 10 reported secondary outcomes: a 30% relative reduction (a 1.1% absolute reduction) in the rate of hospitalization for heart failure, the sole criterion in the report by which ertugliflozin matched the benefits of the other SGLT2 inhibitors.
But the prespecified design of VERTIS CV called for a hierarchical sequence of secondary analyses. The statistically significant noninferiority of the primary endpoint allowed calculation of the initial secondary endpoint, a reduction in the combined rate of cardiovascular death or hospitalization for heart failure. Ertugliflozin treatment cut this outcome by a relative 12%, compared with placebo, a difference that was not significant.
This neutral finding brought to a stop further statistical testing of any of the other secondary endpoints, including impact on hospitalization for heart failure by itself. It also guaranteed that no beneficial effect inferred from the trial’s data would qualify for statistical validity, making it unlikely that ertugliflozin would gain any new label indications from these results. The drug carries a U.S. label that is limited to providing glycemic control.
Choosing among the SGLT2 inhibitors
“What we can say for sure is that there is a glycemic benefit and a heart failure hospitalization benefit” across all four of the SGLT2 inhibitors. “Beyond that, the best we can say today [about using these drugs in practice] is to follow regulatory indications and guidelines recommendations,” commented Javed Butler, MD, a cardiologist and professor and chair of medicine at the University of Mississippi Medical Center, Jackson.

“These results are going to lead to some serious discussions among the research, clinical, and regulatory communities about class effects versus drug effects, and specific trial data versus the totality of evidence,” he said in an interview.
“I think it will influence prescribing ertugliflozin, particularly in patients with established cardiovascular disease, or when the goal is to improve heart failure outcomes of reduce chronic kidney disease,” added Dr. Davies, a professor of diabetes medicine at the University of Leicester (England). “We already have positive benefits [proven for these outcomes] using other agents in the class.”
Perhaps one feature potentially in ertugliflozin’s favor is its price, and whatever impact that might have for payers or patients with inadequate coverage for their drug costs. U.S. websites show a typical retail price for ertugliflozin that is roughly 40% below the three other agents in the class, a difference that can add up to an annual cost savings of about $2,500.
A major consideration for clinicians deciding which SGLT2 inhibitor to prescribe should be “what can the patient afford,” noted Darren K. McGuire, MD, a coinvestigator for VERTIS CV, during discussion of the trial at the EASD virtual meeting.
New analyses show more renal-effect consistency
One surprise in the initial VERTIS CV report was in the study’s key renal outcome, a composite of renal death, need for dialysis, or a doubling of the serum creatinine level, which reflects a cut of at least a 50% in estimated glomerular filtration rate (eGFR). This composite outcome trended toward a significant benefit but fell short, producing a nominal 19% relative reduction. This combined endpoint probably “set the bar too high,” said David Z.I. Cherney, MD, a nephrologist who led the renal assessments run in the trial. He presented several exploratory analyses during the virtual EASD session that provided reassuring evidence that ertugliflozin was not an outlier among the SGLT2 inhibitors when it came to kidney benefits.

Perhaps the most compelling analysis he reported was a slight tweak to the main renal composite endpoint that substituted prevention of a 40% or greater reduction in eGFR for prevention of a 50% or greater reduction. By this somewhat lower bar for efficacy, treatment with ertugliflozin in VERTIS CV linked with a 34% relative risk reduction, compared with placebo (a roughly 1% absolute reduction) that was statistically significant, and importantly came out very close to the effect for this revised endpoint that had been seen for the other three SGLT2 inhibitor drugs.
Focusing on prevention of a 40% or greater drop in eGFR “gives a much more robust measure of renal protection,” Dr. Cherney, a clinician and researcher at the University of Toronto, said in an interview. “The key message is that renal protection is much more uniform” with the rest of the drugs in the class when looked at this way or by some of the other alternative parameters he reported. But the new renal analyses do not address disparities seen among the drugs in the class for several cardiovascular disease effects.
“The overall impression from VERTIS CV is that there was less cardiovascular disease benefit,” except for prevention of heart failure hospitalization, he said.
A teaser for HFpEF
One additional notable new finding discussed during the EASD session stemmed from the investigators ability to mine the medical records of enrolled patients for information about their heart failure history and left ventricular ejection fractions, a data set that was “unique,” compared with the other cardiovascular outcome trials for the drugs in the class, noted Francesco Cosentino, MD, another VERTIS CV coinvestigator and professor of cardiology at the Karolinska Institute in Stockholm.
Roughly a quarter of the enrolled patients had a history of heart failure, and about half of these patients had heart failure with preserved ejection fraction, about 1,000 total patients. In this subgroup treatment with ertugliflozin linked with a 30% relative reduction in hospitalization for heart failure, compared with placebo, a roughly 0.5% absolute reduction. The numbers were small and underpowered for producing convincing evidence, but it provided an intriguing hint of benefit for an unmet need that is currently undergoing further testing in studies designed to specifically explore benefit in this type of heart failure patient, said Dr. Cosentino.
VERTIS CV was sponsored by Merck and Pfizer, the companies that market ertugliflozin. Dr. Davies has been a speaker on behalf of Merck and has had relationships with several other companies. Dr. Butler is a consultant to Merck and several other companies. Dr. McGuire has received honoraria from Merck, nonfinancial support from Pfizer, and has had relationships with several other companies. Dr. Cherney has received honoraria from Merck, nonfinancial research support from Pfizer, and has also had relationships with several other companies. Dr. Cosentino has received fees from Merck and Pfizer, and also from Abbott, AstraZeneca, Bayer, Bristol-Myers Squibb, and Novo Nordisk
Further analyses from the cardiovascular outcome trial of the sodium-glucose transporter 2 inhibitor ertugliflozin in patients with type 2 diabetes helped better define positive effects the drug had on preserving renal function, and also gave a tantalizing hint that this drug, and hence possibly the entire SGLT2 inhibitor drug class, may benefit patients with heart failure with reduced ejection fraction.
But the underlying problem for ertugliflozin (Steglatro) – first seen when results from the VERTIS CV trial initially came out in June 2020 at the annual meeting of the American Diabetes Association – was that, while the trial met its primary endpoint of proving noninferiority to placebo for the combined endpoint of cardiovascular death, nonfatal MI, or nonfatal stroke, treatment with ertugliflozin showed no suggestion of benefit, compared with placebo for reducing this endpoint, producing a nonsignificant 3% relative cut in the combined rate of these adverse events, compared with placebo treatment.
‘Somewhat disappointing’ trial performance
Overall, results from VERTIS CV with ertugliflozin were “somewhat disappointing,” commented Melanie J. Davies, MD, who was not involved with the study and chaired a session at the virtual annual meeting of the European Association for the Study of Diabetes that reviewed the main results, put them into perspective, and added a few new exploratory analyses.
Although the results from 8,246-patient VERTIS CV (Evaluation of Ertugliflozin Efficacy and Safety Cardiovascular Outcomes Trial) put ertugliflozin in the same league as other drugs from its class for safety, “we do not see the significant benefits observed in many of the previous cardiovascular outcomes trials” for other drugs in the SGLT2 inhibitor class, specifically canagliflozin (Invokana), dapagliflozin (Farxiga), and empagliflozin (Jardiance), Dr. Davies said in an interview. The upshot, for at least the time being, is that ertugliflozin “is unlikely to receive a label for any new indications,” she predicted. In contrast, the other drugs in the class have, for example, received a U.S. labeled indication to reduce cardiovascular death (empagliflozin) or major cardiovascular disease events (canagliflozin) in adults with type 2 diabetes (T2D) and cardiovascular disease, or to reduce heart failure hospitalizations (dapagliflozin).
The main results from VERTIS CV, posted online in the New England Journal of Medicine after the EASD session, showed a single significant outcome difference between treatment with ertugliflozin and placebo over a median of 3.0 years of follow-up from among 10 reported secondary outcomes: a 30% relative reduction (a 1.1% absolute reduction) in the rate of hospitalization for heart failure, the sole criterion in the report by which ertugliflozin matched the benefits of the other SGLT2 inhibitors.
But the prespecified design of VERTIS CV called for a hierarchical sequence of secondary analyses. The statistically significant noninferiority of the primary endpoint allowed calculation of the initial secondary endpoint, a reduction in the combined rate of cardiovascular death or hospitalization for heart failure. Ertugliflozin treatment cut this outcome by a relative 12%, compared with placebo, a difference that was not significant.
This neutral finding brought to a stop further statistical testing of any of the other secondary endpoints, including impact on hospitalization for heart failure by itself. It also guaranteed that no beneficial effect inferred from the trial’s data would qualify for statistical validity, making it unlikely that ertugliflozin would gain any new label indications from these results. The drug carries a U.S. label that is limited to providing glycemic control.
Choosing among the SGLT2 inhibitors
“What we can say for sure is that there is a glycemic benefit and a heart failure hospitalization benefit” across all four of the SGLT2 inhibitors. “Beyond that, the best we can say today [about using these drugs in practice] is to follow regulatory indications and guidelines recommendations,” commented Javed Butler, MD, a cardiologist and professor and chair of medicine at the University of Mississippi Medical Center, Jackson.
“These results are going to lead to some serious discussions among the research, clinical, and regulatory communities about class effects versus drug effects, and specific trial data versus the totality of evidence,” he said in an interview.
“I think it will influence prescribing ertugliflozin, particularly in patients with established cardiovascular disease, or when the goal is to improve heart failure outcomes of reduce chronic kidney disease,” added Dr. Davies, a professor of diabetes medicine at the University of Leicester (England). “We already have positive benefits [proven for these outcomes] using other agents in the class.”
Perhaps one feature potentially in ertugliflozin’s favor is its price, and whatever impact that might have for payers or patients with inadequate coverage for their drug costs. U.S. websites show a typical retail price for ertugliflozin that is roughly 40% below the three other agents in the class, a difference that can add up to an annual cost savings of about $2,500.
A major consideration for clinicians deciding which SGLT2 inhibitor to prescribe should be “what can the patient afford,” noted Darren K. McGuire, MD, a coinvestigator for VERTIS CV, during discussion of the trial at the EASD virtual meeting.
New analyses show more renal-effect consistency
One surprise in the initial VERTIS CV report was in the study’s key renal outcome, a composite of renal death, need for dialysis, or a doubling of the serum creatinine level, which reflects a cut of at least a 50% in estimated glomerular filtration rate (eGFR). This composite outcome trended toward a significant benefit but fell short, producing a nominal 19% relative reduction. This combined endpoint probably “set the bar too high,” said David Z.I. Cherney, MD, a nephrologist who led the renal assessments run in the trial. He presented several exploratory analyses during the virtual EASD session that provided reassuring evidence that ertugliflozin was not an outlier among the SGLT2 inhibitors when it came to kidney benefits.
Perhaps the most compelling analysis he reported was a slight tweak to the main renal composite endpoint that substituted prevention of a 40% or greater reduction in eGFR for prevention of a 50% or greater reduction. By this somewhat lower bar for efficacy, treatment with ertugliflozin in VERTIS CV linked with a 34% relative risk reduction, compared with placebo (a roughly 1% absolute reduction) that was statistically significant, and importantly came out very close to the effect for this revised endpoint that had been seen for the other three SGLT2 inhibitor drugs.
Focusing on prevention of a 40% or greater drop in eGFR “gives a much more robust measure of renal protection,” Dr. Cherney, a clinician and researcher at the University of Toronto, said in an interview. “The key message is that renal protection is much more uniform” with the rest of the drugs in the class when looked at this way or by some of the other alternative parameters he reported. But the new renal analyses do not address disparities seen among the drugs in the class for several cardiovascular disease effects.
“The overall impression from VERTIS CV is that there was less cardiovascular disease benefit,” except for prevention of heart failure hospitalization, he said.
A teaser for HFpEF
One additional notable new finding discussed during the EASD session stemmed from the investigators ability to mine the medical records of enrolled patients for information about their heart failure history and left ventricular ejection fractions, a data set that was “unique,” compared with the other cardiovascular outcome trials for the drugs in the class, noted Francesco Cosentino, MD, another VERTIS CV coinvestigator and professor of cardiology at the Karolinska Institute in Stockholm.
Roughly a quarter of the enrolled patients had a history of heart failure, and about half of these patients had heart failure with preserved ejection fraction, about 1,000 total patients. In this subgroup treatment with ertugliflozin linked with a 30% relative reduction in hospitalization for heart failure, compared with placebo, a roughly 0.5% absolute reduction. The numbers were small and underpowered for producing convincing evidence, but it provided an intriguing hint of benefit for an unmet need that is currently undergoing further testing in studies designed to specifically explore benefit in this type of heart failure patient, said Dr. Cosentino.
VERTIS CV was sponsored by Merck and Pfizer, the companies that market ertugliflozin. Dr. Davies has been a speaker on behalf of Merck and has had relationships with several other companies. Dr. Butler is a consultant to Merck and several other companies. Dr. McGuire has received honoraria from Merck, nonfinancial support from Pfizer, and has had relationships with several other companies. Dr. Cherney has received honoraria from Merck, nonfinancial research support from Pfizer, and has also had relationships with several other companies. Dr. Cosentino has received fees from Merck and Pfizer, and also from Abbott, AstraZeneca, Bayer, Bristol-Myers Squibb, and Novo Nordisk
Further analyses from the cardiovascular outcome trial of the sodium-glucose transporter 2 inhibitor ertugliflozin in patients with type 2 diabetes helped better define positive effects the drug had on preserving renal function, and also gave a tantalizing hint that this drug, and hence possibly the entire SGLT2 inhibitor drug class, may benefit patients with heart failure with reduced ejection fraction.
But the underlying problem for ertugliflozin (Steglatro) – first seen when results from the VERTIS CV trial initially came out in June 2020 at the annual meeting of the American Diabetes Association – was that, while the trial met its primary endpoint of proving noninferiority to placebo for the combined endpoint of cardiovascular death, nonfatal MI, or nonfatal stroke, treatment with ertugliflozin showed no suggestion of benefit, compared with placebo for reducing this endpoint, producing a nonsignificant 3% relative cut in the combined rate of these adverse events, compared with placebo treatment.
‘Somewhat disappointing’ trial performance
Overall, results from VERTIS CV with ertugliflozin were “somewhat disappointing,” commented Melanie J. Davies, MD, who was not involved with the study and chaired a session at the virtual annual meeting of the European Association for the Study of Diabetes that reviewed the main results, put them into perspective, and added a few new exploratory analyses.
Although the results from 8,246-patient VERTIS CV (Evaluation of Ertugliflozin Efficacy and Safety Cardiovascular Outcomes Trial) put ertugliflozin in the same league as other drugs from its class for safety, “we do not see the significant benefits observed in many of the previous cardiovascular outcomes trials” for other drugs in the SGLT2 inhibitor class, specifically canagliflozin (Invokana), dapagliflozin (Farxiga), and empagliflozin (Jardiance), Dr. Davies said in an interview. The upshot, for at least the time being, is that ertugliflozin “is unlikely to receive a label for any new indications,” she predicted. In contrast, the other drugs in the class have, for example, received a U.S. labeled indication to reduce cardiovascular death (empagliflozin) or major cardiovascular disease events (canagliflozin) in adults with type 2 diabetes (T2D) and cardiovascular disease, or to reduce heart failure hospitalizations (dapagliflozin).
The main results from VERTIS CV, posted online in the New England Journal of Medicine after the EASD session, showed a single significant outcome difference between treatment with ertugliflozin and placebo over a median of 3.0 years of follow-up from among 10 reported secondary outcomes: a 30% relative reduction (a 1.1% absolute reduction) in the rate of hospitalization for heart failure, the sole criterion in the report by which ertugliflozin matched the benefits of the other SGLT2 inhibitors.
But the prespecified design of VERTIS CV called for a hierarchical sequence of secondary analyses. The statistically significant noninferiority of the primary endpoint allowed calculation of the initial secondary endpoint, a reduction in the combined rate of cardiovascular death or hospitalization for heart failure. Ertugliflozin treatment cut this outcome by a relative 12%, compared with placebo, a difference that was not significant.
This neutral finding brought to a stop further statistical testing of any of the other secondary endpoints, including impact on hospitalization for heart failure by itself. It also guaranteed that no beneficial effect inferred from the trial’s data would qualify for statistical validity, making it unlikely that ertugliflozin would gain any new label indications from these results. The drug carries a U.S. label that is limited to providing glycemic control.
Choosing among the SGLT2 inhibitors
“What we can say for sure is that there is a glycemic benefit and a heart failure hospitalization benefit” across all four of the SGLT2 inhibitors. “Beyond that, the best we can say today [about using these drugs in practice] is to follow regulatory indications and guidelines recommendations,” commented Javed Butler, MD, a cardiologist and professor and chair of medicine at the University of Mississippi Medical Center, Jackson.
“These results are going to lead to some serious discussions among the research, clinical, and regulatory communities about class effects versus drug effects, and specific trial data versus the totality of evidence,” he said in an interview.
“I think it will influence prescribing ertugliflozin, particularly in patients with established cardiovascular disease, or when the goal is to improve heart failure outcomes of reduce chronic kidney disease,” added Dr. Davies, a professor of diabetes medicine at the University of Leicester (England). “We already have positive benefits [proven for these outcomes] using other agents in the class.”
Perhaps one feature potentially in ertugliflozin’s favor is its price, and whatever impact that might have for payers or patients with inadequate coverage for their drug costs. U.S. websites show a typical retail price for ertugliflozin that is roughly 40% below the three other agents in the class, a difference that can add up to an annual cost savings of about $2,500.
A major consideration for clinicians deciding which SGLT2 inhibitor to prescribe should be “what can the patient afford,” noted Darren K. McGuire, MD, a coinvestigator for VERTIS CV, during discussion of the trial at the EASD virtual meeting.
New analyses show more renal-effect consistency
One surprise in the initial VERTIS CV report was in the study’s key renal outcome, a composite of renal death, need for dialysis, or a doubling of the serum creatinine level, which reflects a cut of at least a 50% in estimated glomerular filtration rate (eGFR). This composite outcome trended toward a significant benefit but fell short, producing a nominal 19% relative reduction. This combined endpoint probably “set the bar too high,” said David Z.I. Cherney, MD, a nephrologist who led the renal assessments run in the trial. He presented several exploratory analyses during the virtual EASD session that provided reassuring evidence that ertugliflozin was not an outlier among the SGLT2 inhibitors when it came to kidney benefits.
Perhaps the most compelling analysis he reported was a slight tweak to the main renal composite endpoint that substituted prevention of a 40% or greater reduction in eGFR for prevention of a 50% or greater reduction. By this somewhat lower bar for efficacy, treatment with ertugliflozin in VERTIS CV linked with a 34% relative risk reduction, compared with placebo (a roughly 1% absolute reduction) that was statistically significant, and importantly came out very close to the effect for this revised endpoint that had been seen for the other three SGLT2 inhibitor drugs.
Focusing on prevention of a 40% or greater drop in eGFR “gives a much more robust measure of renal protection,” Dr. Cherney, a clinician and researcher at the University of Toronto, said in an interview. “The key message is that renal protection is much more uniform” with the rest of the drugs in the class when looked at this way or by some of the other alternative parameters he reported. But the new renal analyses do not address disparities seen among the drugs in the class for several cardiovascular disease effects.
“The overall impression from VERTIS CV is that there was less cardiovascular disease benefit,” except for prevention of heart failure hospitalization, he said.
A teaser for HFpEF
One additional notable new finding discussed during the EASD session stemmed from the investigators ability to mine the medical records of enrolled patients for information about their heart failure history and left ventricular ejection fractions, a data set that was “unique,” compared with the other cardiovascular outcome trials for the drugs in the class, noted Francesco Cosentino, MD, another VERTIS CV coinvestigator and professor of cardiology at the Karolinska Institute in Stockholm.
Roughly a quarter of the enrolled patients had a history of heart failure, and about half of these patients had heart failure with preserved ejection fraction, about 1,000 total patients. In this subgroup treatment with ertugliflozin linked with a 30% relative reduction in hospitalization for heart failure, compared with placebo, a roughly 0.5% absolute reduction. The numbers were small and underpowered for producing convincing evidence, but it provided an intriguing hint of benefit for an unmet need that is currently undergoing further testing in studies designed to specifically explore benefit in this type of heart failure patient, said Dr. Cosentino.
VERTIS CV was sponsored by Merck and Pfizer, the companies that market ertugliflozin. Dr. Davies has been a speaker on behalf of Merck and has had relationships with several other companies. Dr. Butler is a consultant to Merck and several other companies. Dr. McGuire has received honoraria from Merck, nonfinancial support from Pfizer, and has had relationships with several other companies. Dr. Cherney has received honoraria from Merck, nonfinancial research support from Pfizer, and has also had relationships with several other companies. Dr. Cosentino has received fees from Merck and Pfizer, and also from Abbott, AstraZeneca, Bayer, Bristol-Myers Squibb, and Novo Nordisk
FROM EASD 2020
What to do when a patient is not ready to stop smoking
Recommendations from the American Thoracic Society
Below is a case involving a patient who is not yet ready to quit smoking. We later provide treatment recommendations for this patient based on a new guideline from the American Thoracic Society.
Case

A 58-year-old female comes into the office for a physical exam. She has been smoking two packs a day since she was 23 years of age. You have tried at previous visits to get her to quit, but she hasn’t been interested. The patient says she has a lot of stress, and that it is still not the right time for her to stop smoking. You tell her she needs to quit and, though the patient understands that quitting would be beneficial for her health, she just isn’t ready to try to kick the habit. How do you proceed?
The Guideline in context
Even though this patient stated that she is not ready to stop smoking, she is still a candidate for pharmacological treatment for her tobacco dependence and can be offered varenicline, according to the ATS guideline.1
In a previously published column, we have discussed the ATS’ recommended approaches for treating patients who are ready to stop smoking cigarettes. The reality is that many patients, if not most, are not ready to quit when we speak to them during any given office visit. The ATS guideline addresses this critical issue by recommending treatment with varenicline in patients who are not ready to stop smoking. It also states that this is a better strategy than waiting to start treatment until patients say they are ready for it.
This recommendation – to prescribe varenicline to smokers even when they are not ready to quit smoking – is based on solid clinical trial evidence. Research has shown that behavior change is dynamic and that the decision to stop smoking is not always a planned one.1 Patients often make quit attempts between office visits, and are often successful in those attempts. Because the decision to try to stop smoking is influenced by the satisfaction and physical addiction that comes from smoking, a medication such as varenicline that is a partial agonist/antagonist at the alpha4-beta2 nicotinic receptor might increase the likelihood that a patient would decide to try to stop smoking. This is because taking this type of a drug would lead the patient to no longer experience the reinforcing effects of nicotine.2 This hypothesis was examined in five randomized trials.1
In these studies, regular smokers who were not ready to make a quit attempt were randomized to varenicline versus placebo. Twice as many individuals who took varenicline stopped smoking 6 months after starting treatment.1
Suggested treatment
This patient should be offered varenicline. This individual meets the criteria for this treatment according to the ATS guideline in that the patient is a regular smoker who doesn’t think she is ready to stop smoking but understands she needs to stop and is open to taking medication to assist her with quitting.
Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Hospital–Jefferson Health. Dr. Sprogell is a third-year resident in the family medicine residency program at Abington Jefferson Health. They have no conflicts related to the content of this piece. For questions or comments, feel free to contact Dr. Skolnik on Twitter @NeilSkolnik.
References
1. Leone F T et al. Initiating pharmacologic treatment in tobacco-dependent adults: An official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020 Jul 15;202(2):e5–e31.
2. Ebbert JO et al. Varenicline for smoking cessation: Efficacy, safety, and treatment recommendations. Patient Prefer Adherence. 2010;4:355-62.
Recommendations from the American Thoracic Society
Recommendations from the American Thoracic Society
Below is a case involving a patient who is not yet ready to quit smoking. We later provide treatment recommendations for this patient based on a new guideline from the American Thoracic Society.
Case
A 58-year-old female comes into the office for a physical exam. She has been smoking two packs a day since she was 23 years of age. You have tried at previous visits to get her to quit, but she hasn’t been interested. The patient says she has a lot of stress, and that it is still not the right time for her to stop smoking. You tell her she needs to quit and, though the patient understands that quitting would be beneficial for her health, she just isn’t ready to try to kick the habit. How do you proceed?
The Guideline in context
Even though this patient stated that she is not ready to stop smoking, she is still a candidate for pharmacological treatment for her tobacco dependence and can be offered varenicline, according to the ATS guideline.1
In a previously published column, we have discussed the ATS’ recommended approaches for treating patients who are ready to stop smoking cigarettes. The reality is that many patients, if not most, are not ready to quit when we speak to them during any given office visit. The ATS guideline addresses this critical issue by recommending treatment with varenicline in patients who are not ready to stop smoking. It also states that this is a better strategy than waiting to start treatment until patients say they are ready for it.
This recommendation – to prescribe varenicline to smokers even when they are not ready to quit smoking – is based on solid clinical trial evidence. Research has shown that behavior change is dynamic and that the decision to stop smoking is not always a planned one.1 Patients often make quit attempts between office visits, and are often successful in those attempts. Because the decision to try to stop smoking is influenced by the satisfaction and physical addiction that comes from smoking, a medication such as varenicline that is a partial agonist/antagonist at the alpha4-beta2 nicotinic receptor might increase the likelihood that a patient would decide to try to stop smoking. This is because taking this type of a drug would lead the patient to no longer experience the reinforcing effects of nicotine.2 This hypothesis was examined in five randomized trials.1
In these studies, regular smokers who were not ready to make a quit attempt were randomized to varenicline versus placebo. Twice as many individuals who took varenicline stopped smoking 6 months after starting treatment.1
Suggested treatment
This patient should be offered varenicline. This individual meets the criteria for this treatment according to the ATS guideline in that the patient is a regular smoker who doesn’t think she is ready to stop smoking but understands she needs to stop and is open to taking medication to assist her with quitting.
Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Hospital–Jefferson Health. Dr. Sprogell is a third-year resident in the family medicine residency program at Abington Jefferson Health. They have no conflicts related to the content of this piece. For questions or comments, feel free to contact Dr. Skolnik on Twitter @NeilSkolnik.
References
1. Leone F T et al. Initiating pharmacologic treatment in tobacco-dependent adults: An official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020 Jul 15;202(2):e5–e31.
2. Ebbert JO et al. Varenicline for smoking cessation: Efficacy, safety, and treatment recommendations. Patient Prefer Adherence. 2010;4:355-62.
Below is a case involving a patient who is not yet ready to quit smoking. We later provide treatment recommendations for this patient based on a new guideline from the American Thoracic Society.
Case
A 58-year-old female comes into the office for a physical exam. She has been smoking two packs a day since she was 23 years of age. You have tried at previous visits to get her to quit, but she hasn’t been interested. The patient says she has a lot of stress, and that it is still not the right time for her to stop smoking. You tell her she needs to quit and, though the patient understands that quitting would be beneficial for her health, she just isn’t ready to try to kick the habit. How do you proceed?
The Guideline in context
Even though this patient stated that she is not ready to stop smoking, she is still a candidate for pharmacological treatment for her tobacco dependence and can be offered varenicline, according to the ATS guideline.1
In a previously published column, we have discussed the ATS’ recommended approaches for treating patients who are ready to stop smoking cigarettes. The reality is that many patients, if not most, are not ready to quit when we speak to them during any given office visit. The ATS guideline addresses this critical issue by recommending treatment with varenicline in patients who are not ready to stop smoking. It also states that this is a better strategy than waiting to start treatment until patients say they are ready for it.
This recommendation – to prescribe varenicline to smokers even when they are not ready to quit smoking – is based on solid clinical trial evidence. Research has shown that behavior change is dynamic and that the decision to stop smoking is not always a planned one.1 Patients often make quit attempts between office visits, and are often successful in those attempts. Because the decision to try to stop smoking is influenced by the satisfaction and physical addiction that comes from smoking, a medication such as varenicline that is a partial agonist/antagonist at the alpha4-beta2 nicotinic receptor might increase the likelihood that a patient would decide to try to stop smoking. This is because taking this type of a drug would lead the patient to no longer experience the reinforcing effects of nicotine.2 This hypothesis was examined in five randomized trials.1
In these studies, regular smokers who were not ready to make a quit attempt were randomized to varenicline versus placebo. Twice as many individuals who took varenicline stopped smoking 6 months after starting treatment.1
Suggested treatment
This patient should be offered varenicline. This individual meets the criteria for this treatment according to the ATS guideline in that the patient is a regular smoker who doesn’t think she is ready to stop smoking but understands she needs to stop and is open to taking medication to assist her with quitting.
Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Hospital–Jefferson Health. Dr. Sprogell is a third-year resident in the family medicine residency program at Abington Jefferson Health. They have no conflicts related to the content of this piece. For questions or comments, feel free to contact Dr. Skolnik on Twitter @NeilSkolnik.
References
1. Leone F T et al. Initiating pharmacologic treatment in tobacco-dependent adults: An official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020 Jul 15;202(2):e5–e31.
2. Ebbert JO et al. Varenicline for smoking cessation: Efficacy, safety, and treatment recommendations. Patient Prefer Adherence. 2010;4:355-62.
Hepatocellular carcinoma shows risk factor shift
Rates of hepatocellular carcinoma (HCC) continue to rise in the United States, but unevenly so given how the incidence has become highest in the Hispanic population, which is reflected in increased rates in the southern and western states, Hashem B. El-Serag, MD, of Baylor College of Medicine, Houston, said in a virtual presentation at the annual Digestive Diseases: New Advances, which is jointly provided by Rutgers and Global Academy for Medical Education.

In addition to this demographic shift, the risk factors for HCC are shifting, he said. Hepatitis C virus (HCV) has been the dominant risk factor for HCC; for patients with active HCV, the factors historically associated with increased HCC risk have included alcohol consumption, obesity, diabetes, coinfection, and genetics, he said.
This pattern is starting to change. In fact, for patients with active HCV, antiviral treatment with a sustained virologic response has surfaced as the most significant risk factor in the development of HCC, said Dr. El-Serag: Among these patients, sustained virologic response from direct-acting antivirals is associated with a significant reduction in HCC risk. However, it is important to recognize that a residual risk of HCC remains that doesn’t go away for several years, he noted.
“Who are those people who got treated, got cured, and still developed HCC? Those with cirrhosis at the time of treatment,” he said. Those with cirrhosis have cumulative incidence of 1.8% per year, but those without cirrhosis had very low risk, he said.
Some good news in HCC is that rates appear to be declining among young men, and this is thought to be one of the groups who are achieving a cure of HCV, he said.
“One would hope, if goals for HCV elimination are met, that will translate into massive reduction of HCC,” he said.
“The issue now for hepatitis is finding infected patients and curing them,” he noted.
Dr. El-Serag touched on hepatitis B (HBV), which continues to be the driving force of hepatitis infections globally. However, in patients who receive and respond to antiviral treatment “there is a significant and considerable reduction in HCC in the context of hepatitis B” similar to that seen with hepatitis C. Vaccination programs for HBV have started to make the desired impact of reducing HCC in HBV-endemic areas, he noted.
However, current risk factors for HCC are related less to HCV and HBV and more to metabolic syndrome because more people are treated for HCV and HBV, Dr. El-Serag said. He went on to address the new dominant global risk factor for HCC: obesity. Based on data from multiple studies, those who are obese, defined as a body mass index greater than 30 kg/m2, carry a twofold increased risk of developing HCC, he said.
To reduce this risk, treatment targets might address intermediate factors such as abdominal obesity, said Dr. El-Serag. He cited a study published in Hepatology in which individuals in the highest tertile for waist-hip ratio had a threefold higher risk of HCC, compared with those in the lowest tertile.
In addition, consideration of obesity must include type 2 diabetes, which is often linked to obesity and occurs in approximately one-third of adults in the United States, Dr. El-Serag said.
Treatment of type 2 diabetes may make a difference in HCC risk reduction, Dr. El-Serag noted. “The impact of treatment of diabetes on HCC risk is an area of intense interest,” he said. Based on the latest research, “the bottom line is that those treated with metformin experience a 50% reduction in the risk of HCC,” he said
Dr. El-Serag also acknowledged the impact of other risk factors for HCC: the use of statins and the presence of nonalcoholic fatty liver disease (NAFLD).
Dr. El-Serag noted that, among NAFLD patients, subgroups at even greater risk for HCC include those with diabetes, those older than 65 years, Hispanic race, and those with cirrhosis. These patients should be candidates for surveillance. Metabolic dysfunction traits such as obesity and diabetes are very common conditions, so it’s important to look at other, more specific factors, he added. “I hope that there will be tools to help clinicians classify or risk-stratify patients into different buckets,” he said.
Areas for further research on HCC continue to include risk stratification, mechanisms of action, and HCC prevention related to treatment of metabolic syndrome, he emphasized.
Dr. El-Serag had no financial conflicts to disclose. Global Academy for Medical Education and this news organization are owned by the same parent company.
*This story was updated on Oct. 28, 2020.
SOURCE: El-Serag HB. Digestive Diseases: New Advances 2020.
Rates of hepatocellular carcinoma (HCC) continue to rise in the United States, but unevenly so given how the incidence has become highest in the Hispanic population, which is reflected in increased rates in the southern and western states, Hashem B. El-Serag, MD, of Baylor College of Medicine, Houston, said in a virtual presentation at the annual Digestive Diseases: New Advances, which is jointly provided by Rutgers and Global Academy for Medical Education.
In addition to this demographic shift, the risk factors for HCC are shifting, he said. Hepatitis C virus (HCV) has been the dominant risk factor for HCC; for patients with active HCV, the factors historically associated with increased HCC risk have included alcohol consumption, obesity, diabetes, coinfection, and genetics, he said.
This pattern is starting to change. In fact, for patients with active HCV, antiviral treatment with a sustained virologic response has surfaced as the most significant risk factor in the development of HCC, said Dr. El-Serag: Among these patients, sustained virologic response from direct-acting antivirals is associated with a significant reduction in HCC risk. However, it is important to recognize that a residual risk of HCC remains that doesn’t go away for several years, he noted.
“Who are those people who got treated, got cured, and still developed HCC? Those with cirrhosis at the time of treatment,” he said. Those with cirrhosis have cumulative incidence of 1.8% per year, but those without cirrhosis had very low risk, he said.
Some good news in HCC is that rates appear to be declining among young men, and this is thought to be one of the groups who are achieving a cure of HCV, he said.
“One would hope, if goals for HCV elimination are met, that will translate into massive reduction of HCC,” he said.
“The issue now for hepatitis is finding infected patients and curing them,” he noted.
Dr. El-Serag touched on hepatitis B (HBV), which continues to be the driving force of hepatitis infections globally. However, in patients who receive and respond to antiviral treatment “there is a significant and considerable reduction in HCC in the context of hepatitis B” similar to that seen with hepatitis C. Vaccination programs for HBV have started to make the desired impact of reducing HCC in HBV-endemic areas, he noted.
However, current risk factors for HCC are related less to HCV and HBV and more to metabolic syndrome because more people are treated for HCV and HBV, Dr. El-Serag said. He went on to address the new dominant global risk factor for HCC: obesity. Based on data from multiple studies, those who are obese, defined as a body mass index greater than 30 kg/m2, carry a twofold increased risk of developing HCC, he said.
To reduce this risk, treatment targets might address intermediate factors such as abdominal obesity, said Dr. El-Serag. He cited a study published in Hepatology in which individuals in the highest tertile for waist-hip ratio had a threefold higher risk of HCC, compared with those in the lowest tertile.
In addition, consideration of obesity must include type 2 diabetes, which is often linked to obesity and occurs in approximately one-third of adults in the United States, Dr. El-Serag said.
Treatment of type 2 diabetes may make a difference in HCC risk reduction, Dr. El-Serag noted. “The impact of treatment of diabetes on HCC risk is an area of intense interest,” he said. Based on the latest research, “the bottom line is that those treated with metformin experience a 50% reduction in the risk of HCC,” he said
Dr. El-Serag also acknowledged the impact of other risk factors for HCC: the use of statins and the presence of nonalcoholic fatty liver disease (NAFLD).
Dr. El-Serag noted that, among NAFLD patients, subgroups at even greater risk for HCC include those with diabetes, those older than 65 years, Hispanic race, and those with cirrhosis. These patients should be candidates for surveillance. Metabolic dysfunction traits such as obesity and diabetes are very common conditions, so it’s important to look at other, more specific factors, he added. “I hope that there will be tools to help clinicians classify or risk-stratify patients into different buckets,” he said.
Areas for further research on HCC continue to include risk stratification, mechanisms of action, and HCC prevention related to treatment of metabolic syndrome, he emphasized.
Dr. El-Serag had no financial conflicts to disclose. Global Academy for Medical Education and this news organization are owned by the same parent company.
*This story was updated on Oct. 28, 2020.
SOURCE: El-Serag HB. Digestive Diseases: New Advances 2020.
Rates of hepatocellular carcinoma (HCC) continue to rise in the United States, but unevenly so given how the incidence has become highest in the Hispanic population, which is reflected in increased rates in the southern and western states, Hashem B. El-Serag, MD, of Baylor College of Medicine, Houston, said in a virtual presentation at the annual Digestive Diseases: New Advances, which is jointly provided by Rutgers and Global Academy for Medical Education.
In addition to this demographic shift, the risk factors for HCC are shifting, he said. Hepatitis C virus (HCV) has been the dominant risk factor for HCC; for patients with active HCV, the factors historically associated with increased HCC risk have included alcohol consumption, obesity, diabetes, coinfection, and genetics, he said.
This pattern is starting to change. In fact, for patients with active HCV, antiviral treatment with a sustained virologic response has surfaced as the most significant risk factor in the development of HCC, said Dr. El-Serag: Among these patients, sustained virologic response from direct-acting antivirals is associated with a significant reduction in HCC risk. However, it is important to recognize that a residual risk of HCC remains that doesn’t go away for several years, he noted.
“Who are those people who got treated, got cured, and still developed HCC? Those with cirrhosis at the time of treatment,” he said. Those with cirrhosis have cumulative incidence of 1.8% per year, but those without cirrhosis had very low risk, he said.
Some good news in HCC is that rates appear to be declining among young men, and this is thought to be one of the groups who are achieving a cure of HCV, he said.
“One would hope, if goals for HCV elimination are met, that will translate into massive reduction of HCC,” he said.
“The issue now for hepatitis is finding infected patients and curing them,” he noted.
Dr. El-Serag touched on hepatitis B (HBV), which continues to be the driving force of hepatitis infections globally. However, in patients who receive and respond to antiviral treatment “there is a significant and considerable reduction in HCC in the context of hepatitis B” similar to that seen with hepatitis C. Vaccination programs for HBV have started to make the desired impact of reducing HCC in HBV-endemic areas, he noted.
However, current risk factors for HCC are related less to HCV and HBV and more to metabolic syndrome because more people are treated for HCV and HBV, Dr. El-Serag said. He went on to address the new dominant global risk factor for HCC: obesity. Based on data from multiple studies, those who are obese, defined as a body mass index greater than 30 kg/m2, carry a twofold increased risk of developing HCC, he said.
To reduce this risk, treatment targets might address intermediate factors such as abdominal obesity, said Dr. El-Serag. He cited a study published in Hepatology in which individuals in the highest tertile for waist-hip ratio had a threefold higher risk of HCC, compared with those in the lowest tertile.
In addition, consideration of obesity must include type 2 diabetes, which is often linked to obesity and occurs in approximately one-third of adults in the United States, Dr. El-Serag said.
Treatment of type 2 diabetes may make a difference in HCC risk reduction, Dr. El-Serag noted. “The impact of treatment of diabetes on HCC risk is an area of intense interest,” he said. Based on the latest research, “the bottom line is that those treated with metformin experience a 50% reduction in the risk of HCC,” he said
Dr. El-Serag also acknowledged the impact of other risk factors for HCC: the use of statins and the presence of nonalcoholic fatty liver disease (NAFLD).
Dr. El-Serag noted that, among NAFLD patients, subgroups at even greater risk for HCC include those with diabetes, those older than 65 years, Hispanic race, and those with cirrhosis. These patients should be candidates for surveillance. Metabolic dysfunction traits such as obesity and diabetes are very common conditions, so it’s important to look at other, more specific factors, he added. “I hope that there will be tools to help clinicians classify or risk-stratify patients into different buckets,” he said.
Areas for further research on HCC continue to include risk stratification, mechanisms of action, and HCC prevention related to treatment of metabolic syndrome, he emphasized.
Dr. El-Serag had no financial conflicts to disclose. Global Academy for Medical Education and this news organization are owned by the same parent company.
*This story was updated on Oct. 28, 2020.
SOURCE: El-Serag HB. Digestive Diseases: New Advances 2020.
FROM DIGESTIVE DISEASES: NEW ADVANCES

NCI may ‘kill’ major mammography trial, says adviser
Reevaluation comes after Medscape report
In September, an advisory board to the National Cancer Institute overwhelmingly voted to form a working group to review the continued funding and running of its largest cancer screening trial. But the lone abstaining board member suggested that the reevaluation was a smoke screen for ending the $100 million Tomosynthesis Mammography Imaging Screening Trial (TMIST).
“We’re going to have a working group to kill the trial,” Peter Adamson, MD, of Sanofi, commented in an interpretation of the NCI’s intent. The randomized trial, which began enrolling women in 2017, is comparing tomosynthesis, or three-dimensional (3-D) mammography, with older, less expensive 2-D technology.
The NCI’s move to reevaluate TMIST comes 6 months after Medscape Medical News reported that the projected 165,000-women study was lagging in enrollment of both patients and participating sites/physicians.
Enlisting sites is difficult, in part because radiologists – informed by their experience and previous research results – already believe that the 3-D technology is superior, commented two TMIST study investigators at that time.
Furthermore, experts who were quoted in the Medscape story said that radiology practice in the United States has substantially transitioned to 3-D and will continue to do so. This point was supported by a review of imaging market data.
At the September virtual meeting of the National Cancer Advisory Board, which was first reported by the Cancer Letter, Philip Castle, PhD, MPH, director of the NCI’s division of cancer prevention, said it was “time to reevaluate TMIST’s feasibility and relevance.”
There is also a need to “examine the utility of TMIST, given the unanticipated challenges due to the pandemic,” he said, referring to low accrual of patients in 2020.
TMIST is “a huge budget item,” and accrual has been a problem “for years – essentially since the trial began,” added Ned Sharpless, MD, director of the NCI.
Fourteen advisory board members voted in favor of creating the working group to review the trial. The lone abstention, as noted above, was from Dr. Adamson, who is global head of oncology development and pediatric innovation at Sanofi and is also professor emeritus, University of Pennsylvania, Philadelphia.
Dr. Adamson said that he was “not denying the impact” of COVID-19 but speculated that other clinical trials have had the same problem.
He also wondered whether COVID-19 was an “excuse” for bringing TMIST to a “public forum” and objected to the fact that TMIST investigators were not present and had not been invited to offer “an action plan” to remedy their trial’s woes.
Dr. Castle explained that COVID-19 had reduced TMIST’s monthly patient accrual by 50% from March to August, compared with recent preceding months. The underaccrual “will likely result in delayed outcomes and escalating costs.”
However, TMIST was staggeringly behind in accrual even before COVID-19. The trial has averaged less than 1,500 women a month over the past 2 years, yet it needed to average 5,500 a month to meet accrual goals, Dr. Castle noted.
Further, Dr. Castle suggested that TMIST’s contribution to mammography practice may be negligible, citing three factors: changes in the imaging market, earlier research results, and other ongoing major trials of 3-D mammography.
“[The] relevance of the [TMIST] data by the completion of the trial is uncertain because of 3-D market ... penetrance by the conclusion of the trial,” Dr. Castle said. Even with optimistic accrual projections, study completion and reporting would occur somewhere between 2029 and 2032 – not in 2025, as originally planned.
Currently, 68% of certified mammography facilities in the United States have one or more 3-D units, and 40% of all units are 3-D, he noted. (However, as previously reported, this latter statistic on total units is likely an undercount because all 3-D units have a built-in 2-D function, but the two components in a single machine are equally counted by the Food and Drug Administration – even when 3-D is exclusively used.)
Dr. Castle also summarized earlier observational and randomized trial data on tomosynthesis mammography: “Evidence is already available suggesting that 3-D is no worse and probably better than 2-D.”
Additionally, he reviewed three other European mammography trials involving 3-D technology (in the United Kingdom, Germany, and Norway) and said that they will contribute “additional informative data.”
Notably, Dr. Adamson did not object to these critical points but said the “approach” taken by the NCI advisory board at this meeting was “incredibly disturbing.”
Dr. Castle defended himself, saying “nowhere” in his presentation was there any mention that the trial would be “shut down.”
Dr. Sharpless then interjected: “There is no easy way to do this. TMIST is the most troubled of our trials [in prevention and screening] from an accrual point of view.”
TMIST investigators respond
A pair of TMIST investigators commented about the NCI’s planned reevaluation – and what it means.
Etta D. Pisano, MD, the study’s principal investigator, accented the positive: “We have heard nothing of suspending TMIST and are ready to work with NCI to reach TMIST endpoints more efficiently,” she said in an interview.
She also offered a positive spin on TMIST enrollment and trial site enlistment. “Enrollment quadrupled and trial sites doubled in the 14 months prior to the COVID-19 pandemic. An unheard of 19% of the 30,000 women enrolled at 99 sites are African American.”
The trial has “momentum,” said Dr. Pisano, who is also chief research officer at the American College of Radiology.
Dr. Castle, however, noted that enrollment is far behind schedule; the 30,000 women who have been enrolled so far represent less than a quarter of the planned enrollment of 165,000 women, due by the end of 2020.
TMIST is designed to learn whether 3-D mammography is better at finding – and reducing the rate of – potentially lethal cancers than older 2-D technology.
Most 3-D systems are used in conjunction with 2-D. First, two static images of the breast are taken (2-D), and then the unit moves in an arc, taking multiple images of the breast (3-D). This allows radiologists to flip through the images like pages in a book and is considered to offer a superior read of the breast.
TMIST uses “advanced” breast cancers as a novel surrogate outcome. The trial period is 4.5 years, during which women are screened annually to determine which imaging technology results in fewer advanced cancers. These include larger HER2-positive and triple-negative malignancies; those associated with positive nodes; and metastatic disease.
These malignancies correlate with breast cancer mortality, Dr. Pisano said.
“We need this trial to help us learn how to improve the process for identifying high-risk patients and how to utilize both of these technologies better,” said Mitchell Schnall, MD, PhD, from the University of Pennsylvania. He is cochair of the ECOG-ACRIN trial group, which is corunning TMIST.
“Look, we all know that 3-D sees more lesions, but consequently, more women are having additional procedures, including biopsies and excisions. The question that TMIST asks is whether that huge expenditure of time, money, and psychological stress is worth it in terms of better outcomes for each person who has the experience,” Dr. Schnall said in an interview.
“One size should not fit all in breast cancer screening, and the TMIST trial can show the way to a precision approach to screening,” he said.
But, earlier this year, Daniel Kopans, MD, professor of radiology, Harvard Medical School, Boston, said in an interview that TMIST is a “huge waste of money.”
He believes that “radiologists who are experienced in using [3-D] for screening will not go back.
“It would be malpractice since they know there are cancers that they will miss on [2-D] that they can find on tomosynthesis,” said Dr. Kopans. He was involved in the development of the first 3-D unit but no longer profits from its sales because his group’s patent has expired.
TMIST was conceived before 3-D mammogram took off clinically, which may explain the trial’s enrollment and site participation woes. In the lag time between the initial trial design (2012) and study start date (2017), clinical practice in the United States and Canada shifted quickly to embrace the newer technology.
This article first appeared on Medscape.com.
Reevaluation comes after Medscape report
Reevaluation comes after Medscape report
In September, an advisory board to the National Cancer Institute overwhelmingly voted to form a working group to review the continued funding and running of its largest cancer screening trial. But the lone abstaining board member suggested that the reevaluation was a smoke screen for ending the $100 million Tomosynthesis Mammography Imaging Screening Trial (TMIST).
“We’re going to have a working group to kill the trial,” Peter Adamson, MD, of Sanofi, commented in an interpretation of the NCI’s intent. The randomized trial, which began enrolling women in 2017, is comparing tomosynthesis, or three-dimensional (3-D) mammography, with older, less expensive 2-D technology.
The NCI’s move to reevaluate TMIST comes 6 months after Medscape Medical News reported that the projected 165,000-women study was lagging in enrollment of both patients and participating sites/physicians.
Enlisting sites is difficult, in part because radiologists – informed by their experience and previous research results – already believe that the 3-D technology is superior, commented two TMIST study investigators at that time.
Furthermore, experts who were quoted in the Medscape story said that radiology practice in the United States has substantially transitioned to 3-D and will continue to do so. This point was supported by a review of imaging market data.
At the September virtual meeting of the National Cancer Advisory Board, which was first reported by the Cancer Letter, Philip Castle, PhD, MPH, director of the NCI’s division of cancer prevention, said it was “time to reevaluate TMIST’s feasibility and relevance.”
There is also a need to “examine the utility of TMIST, given the unanticipated challenges due to the pandemic,” he said, referring to low accrual of patients in 2020.
TMIST is “a huge budget item,” and accrual has been a problem “for years – essentially since the trial began,” added Ned Sharpless, MD, director of the NCI.
Fourteen advisory board members voted in favor of creating the working group to review the trial. The lone abstention, as noted above, was from Dr. Adamson, who is global head of oncology development and pediatric innovation at Sanofi and is also professor emeritus, University of Pennsylvania, Philadelphia.
Dr. Adamson said that he was “not denying the impact” of COVID-19 but speculated that other clinical trials have had the same problem.
He also wondered whether COVID-19 was an “excuse” for bringing TMIST to a “public forum” and objected to the fact that TMIST investigators were not present and had not been invited to offer “an action plan” to remedy their trial’s woes.
Dr. Castle explained that COVID-19 had reduced TMIST’s monthly patient accrual by 50% from March to August, compared with recent preceding months. The underaccrual “will likely result in delayed outcomes and escalating costs.”
However, TMIST was staggeringly behind in accrual even before COVID-19. The trial has averaged less than 1,500 women a month over the past 2 years, yet it needed to average 5,500 a month to meet accrual goals, Dr. Castle noted.
Further, Dr. Castle suggested that TMIST’s contribution to mammography practice may be negligible, citing three factors: changes in the imaging market, earlier research results, and other ongoing major trials of 3-D mammography.
“[The] relevance of the [TMIST] data by the completion of the trial is uncertain because of 3-D market ... penetrance by the conclusion of the trial,” Dr. Castle said. Even with optimistic accrual projections, study completion and reporting would occur somewhere between 2029 and 2032 – not in 2025, as originally planned.
Currently, 68% of certified mammography facilities in the United States have one or more 3-D units, and 40% of all units are 3-D, he noted. (However, as previously reported, this latter statistic on total units is likely an undercount because all 3-D units have a built-in 2-D function, but the two components in a single machine are equally counted by the Food and Drug Administration – even when 3-D is exclusively used.)
Dr. Castle also summarized earlier observational and randomized trial data on tomosynthesis mammography: “Evidence is already available suggesting that 3-D is no worse and probably better than 2-D.”
Additionally, he reviewed three other European mammography trials involving 3-D technology (in the United Kingdom, Germany, and Norway) and said that they will contribute “additional informative data.”
Notably, Dr. Adamson did not object to these critical points but said the “approach” taken by the NCI advisory board at this meeting was “incredibly disturbing.”
Dr. Castle defended himself, saying “nowhere” in his presentation was there any mention that the trial would be “shut down.”
Dr. Sharpless then interjected: “There is no easy way to do this. TMIST is the most troubled of our trials [in prevention and screening] from an accrual point of view.”
TMIST investigators respond
A pair of TMIST investigators commented about the NCI’s planned reevaluation – and what it means.
Etta D. Pisano, MD, the study’s principal investigator, accented the positive: “We have heard nothing of suspending TMIST and are ready to work with NCI to reach TMIST endpoints more efficiently,” she said in an interview.
She also offered a positive spin on TMIST enrollment and trial site enlistment. “Enrollment quadrupled and trial sites doubled in the 14 months prior to the COVID-19 pandemic. An unheard of 19% of the 30,000 women enrolled at 99 sites are African American.”
The trial has “momentum,” said Dr. Pisano, who is also chief research officer at the American College of Radiology.
Dr. Castle, however, noted that enrollment is far behind schedule; the 30,000 women who have been enrolled so far represent less than a quarter of the planned enrollment of 165,000 women, due by the end of 2020.
TMIST is designed to learn whether 3-D mammography is better at finding – and reducing the rate of – potentially lethal cancers than older 2-D technology.
Most 3-D systems are used in conjunction with 2-D. First, two static images of the breast are taken (2-D), and then the unit moves in an arc, taking multiple images of the breast (3-D). This allows radiologists to flip through the images like pages in a book and is considered to offer a superior read of the breast.
TMIST uses “advanced” breast cancers as a novel surrogate outcome. The trial period is 4.5 years, during which women are screened annually to determine which imaging technology results in fewer advanced cancers. These include larger HER2-positive and triple-negative malignancies; those associated with positive nodes; and metastatic disease.
These malignancies correlate with breast cancer mortality, Dr. Pisano said.
“We need this trial to help us learn how to improve the process for identifying high-risk patients and how to utilize both of these technologies better,” said Mitchell Schnall, MD, PhD, from the University of Pennsylvania. He is cochair of the ECOG-ACRIN trial group, which is corunning TMIST.
“Look, we all know that 3-D sees more lesions, but consequently, more women are having additional procedures, including biopsies and excisions. The question that TMIST asks is whether that huge expenditure of time, money, and psychological stress is worth it in terms of better outcomes for each person who has the experience,” Dr. Schnall said in an interview.
“One size should not fit all in breast cancer screening, and the TMIST trial can show the way to a precision approach to screening,” he said.
But, earlier this year, Daniel Kopans, MD, professor of radiology, Harvard Medical School, Boston, said in an interview that TMIST is a “huge waste of money.”
He believes that “radiologists who are experienced in using [3-D] for screening will not go back.
“It would be malpractice since they know there are cancers that they will miss on [2-D] that they can find on tomosynthesis,” said Dr. Kopans. He was involved in the development of the first 3-D unit but no longer profits from its sales because his group’s patent has expired.
TMIST was conceived before 3-D mammogram took off clinically, which may explain the trial’s enrollment and site participation woes. In the lag time between the initial trial design (2012) and study start date (2017), clinical practice in the United States and Canada shifted quickly to embrace the newer technology.
This article first appeared on Medscape.com.
In September, an advisory board to the National Cancer Institute overwhelmingly voted to form a working group to review the continued funding and running of its largest cancer screening trial. But the lone abstaining board member suggested that the reevaluation was a smoke screen for ending the $100 million Tomosynthesis Mammography Imaging Screening Trial (TMIST).
“We’re going to have a working group to kill the trial,” Peter Adamson, MD, of Sanofi, commented in an interpretation of the NCI’s intent. The randomized trial, which began enrolling women in 2017, is comparing tomosynthesis, or three-dimensional (3-D) mammography, with older, less expensive 2-D technology.
The NCI’s move to reevaluate TMIST comes 6 months after Medscape Medical News reported that the projected 165,000-women study was lagging in enrollment of both patients and participating sites/physicians.
Enlisting sites is difficult, in part because radiologists – informed by their experience and previous research results – already believe that the 3-D technology is superior, commented two TMIST study investigators at that time.
Furthermore, experts who were quoted in the Medscape story said that radiology practice in the United States has substantially transitioned to 3-D and will continue to do so. This point was supported by a review of imaging market data.
At the September virtual meeting of the National Cancer Advisory Board, which was first reported by the Cancer Letter, Philip Castle, PhD, MPH, director of the NCI’s division of cancer prevention, said it was “time to reevaluate TMIST’s feasibility and relevance.”
There is also a need to “examine the utility of TMIST, given the unanticipated challenges due to the pandemic,” he said, referring to low accrual of patients in 2020.
TMIST is “a huge budget item,” and accrual has been a problem “for years – essentially since the trial began,” added Ned Sharpless, MD, director of the NCI.
Fourteen advisory board members voted in favor of creating the working group to review the trial. The lone abstention, as noted above, was from Dr. Adamson, who is global head of oncology development and pediatric innovation at Sanofi and is also professor emeritus, University of Pennsylvania, Philadelphia.
Dr. Adamson said that he was “not denying the impact” of COVID-19 but speculated that other clinical trials have had the same problem.
He also wondered whether COVID-19 was an “excuse” for bringing TMIST to a “public forum” and objected to the fact that TMIST investigators were not present and had not been invited to offer “an action plan” to remedy their trial’s woes.
Dr. Castle explained that COVID-19 had reduced TMIST’s monthly patient accrual by 50% from March to August, compared with recent preceding months. The underaccrual “will likely result in delayed outcomes and escalating costs.”
However, TMIST was staggeringly behind in accrual even before COVID-19. The trial has averaged less than 1,500 women a month over the past 2 years, yet it needed to average 5,500 a month to meet accrual goals, Dr. Castle noted.
Further, Dr. Castle suggested that TMIST’s contribution to mammography practice may be negligible, citing three factors: changes in the imaging market, earlier research results, and other ongoing major trials of 3-D mammography.
“[The] relevance of the [TMIST] data by the completion of the trial is uncertain because of 3-D market ... penetrance by the conclusion of the trial,” Dr. Castle said. Even with optimistic accrual projections, study completion and reporting would occur somewhere between 2029 and 2032 – not in 2025, as originally planned.
Currently, 68% of certified mammography facilities in the United States have one or more 3-D units, and 40% of all units are 3-D, he noted. (However, as previously reported, this latter statistic on total units is likely an undercount because all 3-D units have a built-in 2-D function, but the two components in a single machine are equally counted by the Food and Drug Administration – even when 3-D is exclusively used.)
Dr. Castle also summarized earlier observational and randomized trial data on tomosynthesis mammography: “Evidence is already available suggesting that 3-D is no worse and probably better than 2-D.”
Additionally, he reviewed three other European mammography trials involving 3-D technology (in the United Kingdom, Germany, and Norway) and said that they will contribute “additional informative data.”
Notably, Dr. Adamson did not object to these critical points but said the “approach” taken by the NCI advisory board at this meeting was “incredibly disturbing.”
Dr. Castle defended himself, saying “nowhere” in his presentation was there any mention that the trial would be “shut down.”
Dr. Sharpless then interjected: “There is no easy way to do this. TMIST is the most troubled of our trials [in prevention and screening] from an accrual point of view.”
TMIST investigators respond
A pair of TMIST investigators commented about the NCI’s planned reevaluation – and what it means.
Etta D. Pisano, MD, the study’s principal investigator, accented the positive: “We have heard nothing of suspending TMIST and are ready to work with NCI to reach TMIST endpoints more efficiently,” she said in an interview.
She also offered a positive spin on TMIST enrollment and trial site enlistment. “Enrollment quadrupled and trial sites doubled in the 14 months prior to the COVID-19 pandemic. An unheard of 19% of the 30,000 women enrolled at 99 sites are African American.”
The trial has “momentum,” said Dr. Pisano, who is also chief research officer at the American College of Radiology.
Dr. Castle, however, noted that enrollment is far behind schedule; the 30,000 women who have been enrolled so far represent less than a quarter of the planned enrollment of 165,000 women, due by the end of 2020.
TMIST is designed to learn whether 3-D mammography is better at finding – and reducing the rate of – potentially lethal cancers than older 2-D technology.
Most 3-D systems are used in conjunction with 2-D. First, two static images of the breast are taken (2-D), and then the unit moves in an arc, taking multiple images of the breast (3-D). This allows radiologists to flip through the images like pages in a book and is considered to offer a superior read of the breast.
TMIST uses “advanced” breast cancers as a novel surrogate outcome. The trial period is 4.5 years, during which women are screened annually to determine which imaging technology results in fewer advanced cancers. These include larger HER2-positive and triple-negative malignancies; those associated with positive nodes; and metastatic disease.
These malignancies correlate with breast cancer mortality, Dr. Pisano said.
“We need this trial to help us learn how to improve the process for identifying high-risk patients and how to utilize both of these technologies better,” said Mitchell Schnall, MD, PhD, from the University of Pennsylvania. He is cochair of the ECOG-ACRIN trial group, which is corunning TMIST.
“Look, we all know that 3-D sees more lesions, but consequently, more women are having additional procedures, including biopsies and excisions. The question that TMIST asks is whether that huge expenditure of time, money, and psychological stress is worth it in terms of better outcomes for each person who has the experience,” Dr. Schnall said in an interview.
“One size should not fit all in breast cancer screening, and the TMIST trial can show the way to a precision approach to screening,” he said.
But, earlier this year, Daniel Kopans, MD, professor of radiology, Harvard Medical School, Boston, said in an interview that TMIST is a “huge waste of money.”
He believes that “radiologists who are experienced in using [3-D] for screening will not go back.
“It would be malpractice since they know there are cancers that they will miss on [2-D] that they can find on tomosynthesis,” said Dr. Kopans. He was involved in the development of the first 3-D unit but no longer profits from its sales because his group’s patent has expired.
TMIST was conceived before 3-D mammogram took off clinically, which may explain the trial’s enrollment and site participation woes. In the lag time between the initial trial design (2012) and study start date (2017), clinical practice in the United States and Canada shifted quickly to embrace the newer technology.
This article first appeared on Medscape.com.
Initial response to novel agents preps MM patients for favorable transplant outcomes
For patients with multiple myeloma, triplet induction with novel agents beat doublet with regards to early results, according to Lalit Kumar, MD, and colleagues at the All India Institute of Medical sciences Myeloma Group, New Delhi.
The study analyzed 326 multiple myeloma patients who received high-dose, novel agent–based induction therapy prior to autologous stem cell transplant (ASCT) at a single institution, according to a report published in Clinical Lymphoma, Myeloma and Leukemia.
Between January 2005 and December 2018, 326 consecutive patients underwent high-dose chemotherapy and autologous stem cell transplant. The median age of the patients was 52 years; 66% were men, nearly 33% had Revised ISS III disease; almost 16% had high-risk cytogenetics and 23% underwent transplant in second remission after salvage therapy for relapse. A total of 194 patients (59.5%) received induction with two novel agents (thalidomide/dexamethasone, n = 95; lenalidomide/dexamethasone, n = 63; bortezomib/dexamethasone, n = 36) and 132 (40.5%) received three drugs (bortezomib/lenalidomide/dexamethasone, n = 53; bortezomib/liposomal doxorubicin/dexamethasone, n = 42; bortezomib/thalidomide/dexamethasone, n = 31; other n = 3).
Outcomes favorable
After transplant 227 (69.8%) patients achieved a complete response; 48 (14.7%) had a very good partial response, 32 (9.8%) had a partial response, and 9 (2.8%) patients had stable disease. Ten (3.1%) patients died of transplant-related complications (before day 100). Triplet induction beat doublet with regards to early response (95.4% vs. 84.02% [doublets], P < .003), stem cell mobilization (88.6% vs. 76.8%, P < .005) and lower day-100 transplant-related mortality (P < .001), However, at a median follow-up of 62.5 months, the median overall response rate (97.5 months triplet vs. 100.0 months doublet) and the median progression free survival (54.5 months vs. 57 months) were not statistically different between the two induction-treatment groups.
Patients who had undergone transplant in a recent period (2016-18) had a better outcome, compared with initial years, which possibly reflects a combined effect of learning curve, use of triplets, and gradual reduction in day-100 mortality, the authors stated.
“Whether newer regimens incorporating monoclonal antibodies (associated with higher [complete response] rate and [minimal residual disease] negativity) would result in further improvement in survival, needs to be determined in future studies,” the researchers concluded.
The authors reported that they had no conflicts.
SOURCE: Kumar L et al. Clin Lymphoma Myeloma Leuk. 2020 Sep 18. doi: 10.1016/j.clml.2020.08.021.
For patients with multiple myeloma, triplet induction with novel agents beat doublet with regards to early results, according to Lalit Kumar, MD, and colleagues at the All India Institute of Medical sciences Myeloma Group, New Delhi.
The study analyzed 326 multiple myeloma patients who received high-dose, novel agent–based induction therapy prior to autologous stem cell transplant (ASCT) at a single institution, according to a report published in Clinical Lymphoma, Myeloma and Leukemia.
Between January 2005 and December 2018, 326 consecutive patients underwent high-dose chemotherapy and autologous stem cell transplant. The median age of the patients was 52 years; 66% were men, nearly 33% had Revised ISS III disease; almost 16% had high-risk cytogenetics and 23% underwent transplant in second remission after salvage therapy for relapse. A total of 194 patients (59.5%) received induction with two novel agents (thalidomide/dexamethasone, n = 95; lenalidomide/dexamethasone, n = 63; bortezomib/dexamethasone, n = 36) and 132 (40.5%) received three drugs (bortezomib/lenalidomide/dexamethasone, n = 53; bortezomib/liposomal doxorubicin/dexamethasone, n = 42; bortezomib/thalidomide/dexamethasone, n = 31; other n = 3).
Outcomes favorable
After transplant 227 (69.8%) patients achieved a complete response; 48 (14.7%) had a very good partial response, 32 (9.8%) had a partial response, and 9 (2.8%) patients had stable disease. Ten (3.1%) patients died of transplant-related complications (before day 100). Triplet induction beat doublet with regards to early response (95.4% vs. 84.02% [doublets], P < .003), stem cell mobilization (88.6% vs. 76.8%, P < .005) and lower day-100 transplant-related mortality (P < .001), However, at a median follow-up of 62.5 months, the median overall response rate (97.5 months triplet vs. 100.0 months doublet) and the median progression free survival (54.5 months vs. 57 months) were not statistically different between the two induction-treatment groups.
Patients who had undergone transplant in a recent period (2016-18) had a better outcome, compared with initial years, which possibly reflects a combined effect of learning curve, use of triplets, and gradual reduction in day-100 mortality, the authors stated.
“Whether newer regimens incorporating monoclonal antibodies (associated with higher [complete response] rate and [minimal residual disease] negativity) would result in further improvement in survival, needs to be determined in future studies,” the researchers concluded.
The authors reported that they had no conflicts.
SOURCE: Kumar L et al. Clin Lymphoma Myeloma Leuk. 2020 Sep 18. doi: 10.1016/j.clml.2020.08.021.
For patients with multiple myeloma, triplet induction with novel agents beat doublet with regards to early results, according to Lalit Kumar, MD, and colleagues at the All India Institute of Medical sciences Myeloma Group, New Delhi.
The study analyzed 326 multiple myeloma patients who received high-dose, novel agent–based induction therapy prior to autologous stem cell transplant (ASCT) at a single institution, according to a report published in Clinical Lymphoma, Myeloma and Leukemia.
Between January 2005 and December 2018, 326 consecutive patients underwent high-dose chemotherapy and autologous stem cell transplant. The median age of the patients was 52 years; 66% were men, nearly 33% had Revised ISS III disease; almost 16% had high-risk cytogenetics and 23% underwent transplant in second remission after salvage therapy for relapse. A total of 194 patients (59.5%) received induction with two novel agents (thalidomide/dexamethasone, n = 95; lenalidomide/dexamethasone, n = 63; bortezomib/dexamethasone, n = 36) and 132 (40.5%) received three drugs (bortezomib/lenalidomide/dexamethasone, n = 53; bortezomib/liposomal doxorubicin/dexamethasone, n = 42; bortezomib/thalidomide/dexamethasone, n = 31; other n = 3).
Outcomes favorable
After transplant 227 (69.8%) patients achieved a complete response; 48 (14.7%) had a very good partial response, 32 (9.8%) had a partial response, and 9 (2.8%) patients had stable disease. Ten (3.1%) patients died of transplant-related complications (before day 100). Triplet induction beat doublet with regards to early response (95.4% vs. 84.02% [doublets], P < .003), stem cell mobilization (88.6% vs. 76.8%, P < .005) and lower day-100 transplant-related mortality (P < .001), However, at a median follow-up of 62.5 months, the median overall response rate (97.5 months triplet vs. 100.0 months doublet) and the median progression free survival (54.5 months vs. 57 months) were not statistically different between the two induction-treatment groups.
Patients who had undergone transplant in a recent period (2016-18) had a better outcome, compared with initial years, which possibly reflects a combined effect of learning curve, use of triplets, and gradual reduction in day-100 mortality, the authors stated.
“Whether newer regimens incorporating monoclonal antibodies (associated with higher [complete response] rate and [minimal residual disease] negativity) would result in further improvement in survival, needs to be determined in future studies,” the researchers concluded.
The authors reported that they had no conflicts.
SOURCE: Kumar L et al. Clin Lymphoma Myeloma Leuk. 2020 Sep 18. doi: 10.1016/j.clml.2020.08.021.
FROM CLINICAL LYMPHOMA, MYELOMA AND LEUKEMIA
New first-line standard of care for esophageal cancer?
Pembrolizumab (Keytruda) is already approved for use in the treatment of esophageal cancer, but in the second-line setting.
New results show that it also improves outcomes when used in the first-line setting, and the investigators suggest that pembrolizumab in combination with chemotherapy should be the new standard of care.
The results come from an interim analysis of the phase 3 KEYNOTE-590 trial, conducted with 740 patients who had advanced cancers of the esophagus or esophagogastric junction (EGJ). The patients were followed for a median of 10.8 months.
The findings show that the combination offered patients a modest but distinct survival benefit over chemotherapy alone.
Median overall survival (OS), one of two primary endpoints for the trial, was 12.4 months for pembrolizumab plus chemotherapy, compared with 9.8 months for patients who received chemotherapy plus placebo.
This difference translated into a hazard ratio (HR) for death with pembrolizumab of 0.73 (P < .0001), reported Peter Enzinger, MD, from the Dana-Farber Cancer Institute in Boston. Progression-free survival (PFS), the trial’s other primary endpoint, was superior with the combination, at a median of 6.3 months compared with 5.8 months for chemotherapy alone, translating into an HR for progression with pembrolizumab of 0.65 (P < .0001).
“Pembrolizumab plus chemotherapy should be a new standard of care as first-line therapy in patients with locally advanced unresectable or metastastic esophageal cancer, including the EGJ, regardless of the histology and biomarker status,” Enzinger concluded.
He was speaking at a press briefing prior to a presentation of the data in a presidential symposium at the European Society of Medical Oncology (ESMO) Virtual Congress 2020. (The data were presented in oral session by Ken Kato, MD, from the National Cancer Center Hospital in Tokyo, Japan.)
Little change in treatment
“Unfortunately, for esophageal cancer, the standard of care has remained relatively unchanged for a long period of time,” Enzinger said.
Standard first-line therapy for patients with advanced esophageal, EGJ, or gastric adenocarcinoma is primarily a chemotherapy doublet consisting of a fluoropyrimidine plus a platinum agent.
Pembrolizumab was previously shown to have some activity as monotherapy against advanced or metastatic esophageal cancer in the third line in the KEYNOTE-180 trial. It yielded an overall response rate (ORR) of 14%. A median duration of response was not reached among patients with esophageal squamous cell carcinoma (ESCC) and tumors with programmed cell death–ligand-1 (PD-L1) that had combined positive scores (CPSs) of 10 or higher.
Another previous trial, KEYNOTE-181, showed that pembrolizumab monotherapy in the second line was associated with an ORR of 22% vs 7% for chemotherapy and respective median OS of 10.3 vs 6.7 months. This trial led to US Food and Drug Administration approval of pembrolizumab for the treatment of patients with recurrent locally advanced or metastatic ESCC with PD-L1 CPS ≥10 who have experienced disease progression after at least one prior line of therapy.
The trial now being reported, KEYNOTE-590, assessed use of the drug in the first-line setting. It was designed to see whether combining standard-of-care chemotherapy with pembrolizumab would improve outcomes.
Study details
Patients were randomly assigned to receive chemotherapy with 5-fluorauracil (5-FU) 800 mg/m2 intravenously on days 1–5 every 3 weeks for up to 35 cycles and cisplatin 80 mg/m2 IV every 3 weeks for up to 6 cycles, plus either pembrolizumab 200 mg IV every 3 weeks for up to 35 cycles or saline placebo IV.
Rates of treatment-related adverse events of grade 3 or higher were similar between study arms, occurring in 71.9% with the combination and in 67.6% with chemotherapy alone. Adverse events leading to drug discontinuation occurred in 19.5% and 11.6%, respectively. Fatal adverse events occurred in 2.4% of patients who received the combination and in 1.4% of patients who received chemotherapy and placebo.
Immune-mediated adverse events of grade 3 or higher and infusion reactions occurred in 7% and 2.2% of patients, respectively.
Patient-reported quality of life was similar between the groups.
Mixed histologies muddy results
The improvement in OS was observed across all patient populations, including patients with ESCC, esophageal adenocarcinoma (EAC), and EGJ tumors, the researchers noted.
However, invited discussant Andres Cervantes, MD, PhD, from the University of Valencia, Spain, commented that ESCC and EAC have very different histologies and that including patients with both in a single trial can make the results very confusing.
He pointed out that, in the KEYNOTE-590 population, 73% of patients had ESCCs and 27% had EACs.
The OS improvement was seen regardless of PD-L1 expression, although the best results occurred in patients with high expression.
However, Cervantes noted that PD-L1 expression was not used as a stratification factor prior to randomization, even though it was included in the complex, step-wise statistical plan for the study.
Another expert, Salah-Eddin Al-Batran, MD, from the Krankenhaus Nordwest in Frankfurt, Germany, questioned the researchers’ recommendation that all patients with esophageal cancer receive this regimen, regardless of PD-L1 expression.
“We have to be sure that we do not inflate the results for the all-comers by the very responsive group of high [PD-L1] expressers,” he said at the press briefing.
He said the trial report also leaves open the question of efficacy in tumors with microsatellite instability and/or high tumor mutational burden.
“I think these questions have to be addressed to give us a clear picture of how to treat a patient sitting in front of us as doctors,” he said.
Also adding to the concerns about this trial is the fact that the “selected chemotherapy schedule is not much currently used as the standard of care,” said Cervantes, although he added that it “is acceptable for this protocol.”
Despite these caveats, the trial was clearly positive, Cervantes said. The greatest benefit appeared to accrue for patients with ESCC.
“The addition of pembrolizumab to platinum-based chemotherapy significantly increases response rate, PFS, and OS in patients with advanced esophageal carcinomas over chemotherapy alone,” he said, and therefore he agreed with the investigators that “this is a new standard of care.”
The study was funded by Merck Sharp & Dohme. Enzinger disclosed honoraria and advisory or consulting roles for Merck and others. Cervantes disclosed consulting or advising and research funding from Merck Serono and others. He is president-elect of ESMO. Al-Batran has disclosed no relevant financial relationships.
This story first appeared on Medscape.com.
Pembrolizumab (Keytruda) is already approved for use in the treatment of esophageal cancer, but in the second-line setting.
New results show that it also improves outcomes when used in the first-line setting, and the investigators suggest that pembrolizumab in combination with chemotherapy should be the new standard of care.
The results come from an interim analysis of the phase 3 KEYNOTE-590 trial, conducted with 740 patients who had advanced cancers of the esophagus or esophagogastric junction (EGJ). The patients were followed for a median of 10.8 months.
The findings show that the combination offered patients a modest but distinct survival benefit over chemotherapy alone.
Median overall survival (OS), one of two primary endpoints for the trial, was 12.4 months for pembrolizumab plus chemotherapy, compared with 9.8 months for patients who received chemotherapy plus placebo.
This difference translated into a hazard ratio (HR) for death with pembrolizumab of 0.73 (P < .0001), reported Peter Enzinger, MD, from the Dana-Farber Cancer Institute in Boston. Progression-free survival (PFS), the trial’s other primary endpoint, was superior with the combination, at a median of 6.3 months compared with 5.8 months for chemotherapy alone, translating into an HR for progression with pembrolizumab of 0.65 (P < .0001).
“Pembrolizumab plus chemotherapy should be a new standard of care as first-line therapy in patients with locally advanced unresectable or metastastic esophageal cancer, including the EGJ, regardless of the histology and biomarker status,” Enzinger concluded.
He was speaking at a press briefing prior to a presentation of the data in a presidential symposium at the European Society of Medical Oncology (ESMO) Virtual Congress 2020. (The data were presented in oral session by Ken Kato, MD, from the National Cancer Center Hospital in Tokyo, Japan.)
Little change in treatment
“Unfortunately, for esophageal cancer, the standard of care has remained relatively unchanged for a long period of time,” Enzinger said.
Standard first-line therapy for patients with advanced esophageal, EGJ, or gastric adenocarcinoma is primarily a chemotherapy doublet consisting of a fluoropyrimidine plus a platinum agent.
Pembrolizumab was previously shown to have some activity as monotherapy against advanced or metastatic esophageal cancer in the third line in the KEYNOTE-180 trial. It yielded an overall response rate (ORR) of 14%. A median duration of response was not reached among patients with esophageal squamous cell carcinoma (ESCC) and tumors with programmed cell death–ligand-1 (PD-L1) that had combined positive scores (CPSs) of 10 or higher.
Another previous trial, KEYNOTE-181, showed that pembrolizumab monotherapy in the second line was associated with an ORR of 22% vs 7% for chemotherapy and respective median OS of 10.3 vs 6.7 months. This trial led to US Food and Drug Administration approval of pembrolizumab for the treatment of patients with recurrent locally advanced or metastatic ESCC with PD-L1 CPS ≥10 who have experienced disease progression after at least one prior line of therapy.
The trial now being reported, KEYNOTE-590, assessed use of the drug in the first-line setting. It was designed to see whether combining standard-of-care chemotherapy with pembrolizumab would improve outcomes.
Study details
Patients were randomly assigned to receive chemotherapy with 5-fluorauracil (5-FU) 800 mg/m2 intravenously on days 1–5 every 3 weeks for up to 35 cycles and cisplatin 80 mg/m2 IV every 3 weeks for up to 6 cycles, plus either pembrolizumab 200 mg IV every 3 weeks for up to 35 cycles or saline placebo IV.
Rates of treatment-related adverse events of grade 3 or higher were similar between study arms, occurring in 71.9% with the combination and in 67.6% with chemotherapy alone. Adverse events leading to drug discontinuation occurred in 19.5% and 11.6%, respectively. Fatal adverse events occurred in 2.4% of patients who received the combination and in 1.4% of patients who received chemotherapy and placebo.
Immune-mediated adverse events of grade 3 or higher and infusion reactions occurred in 7% and 2.2% of patients, respectively.
Patient-reported quality of life was similar between the groups.
Mixed histologies muddy results
The improvement in OS was observed across all patient populations, including patients with ESCC, esophageal adenocarcinoma (EAC), and EGJ tumors, the researchers noted.
However, invited discussant Andres Cervantes, MD, PhD, from the University of Valencia, Spain, commented that ESCC and EAC have very different histologies and that including patients with both in a single trial can make the results very confusing.
He pointed out that, in the KEYNOTE-590 population, 73% of patients had ESCCs and 27% had EACs.
The OS improvement was seen regardless of PD-L1 expression, although the best results occurred in patients with high expression.
However, Cervantes noted that PD-L1 expression was not used as a stratification factor prior to randomization, even though it was included in the complex, step-wise statistical plan for the study.
Another expert, Salah-Eddin Al-Batran, MD, from the Krankenhaus Nordwest in Frankfurt, Germany, questioned the researchers’ recommendation that all patients with esophageal cancer receive this regimen, regardless of PD-L1 expression.
“We have to be sure that we do not inflate the results for the all-comers by the very responsive group of high [PD-L1] expressers,” he said at the press briefing.
He said the trial report also leaves open the question of efficacy in tumors with microsatellite instability and/or high tumor mutational burden.
“I think these questions have to be addressed to give us a clear picture of how to treat a patient sitting in front of us as doctors,” he said.
Also adding to the concerns about this trial is the fact that the “selected chemotherapy schedule is not much currently used as the standard of care,” said Cervantes, although he added that it “is acceptable for this protocol.”
Despite these caveats, the trial was clearly positive, Cervantes said. The greatest benefit appeared to accrue for patients with ESCC.
“The addition of pembrolizumab to platinum-based chemotherapy significantly increases response rate, PFS, and OS in patients with advanced esophageal carcinomas over chemotherapy alone,” he said, and therefore he agreed with the investigators that “this is a new standard of care.”
The study was funded by Merck Sharp & Dohme. Enzinger disclosed honoraria and advisory or consulting roles for Merck and others. Cervantes disclosed consulting or advising and research funding from Merck Serono and others. He is president-elect of ESMO. Al-Batran has disclosed no relevant financial relationships.
This story first appeared on Medscape.com.
Pembrolizumab (Keytruda) is already approved for use in the treatment of esophageal cancer, but in the second-line setting.
New results show that it also improves outcomes when used in the first-line setting, and the investigators suggest that pembrolizumab in combination with chemotherapy should be the new standard of care.
The results come from an interim analysis of the phase 3 KEYNOTE-590 trial, conducted with 740 patients who had advanced cancers of the esophagus or esophagogastric junction (EGJ). The patients were followed for a median of 10.8 months.
The findings show that the combination offered patients a modest but distinct survival benefit over chemotherapy alone.
Median overall survival (OS), one of two primary endpoints for the trial, was 12.4 months for pembrolizumab plus chemotherapy, compared with 9.8 months for patients who received chemotherapy plus placebo.
This difference translated into a hazard ratio (HR) for death with pembrolizumab of 0.73 (P < .0001), reported Peter Enzinger, MD, from the Dana-Farber Cancer Institute in Boston. Progression-free survival (PFS), the trial’s other primary endpoint, was superior with the combination, at a median of 6.3 months compared with 5.8 months for chemotherapy alone, translating into an HR for progression with pembrolizumab of 0.65 (P < .0001).
“Pembrolizumab plus chemotherapy should be a new standard of care as first-line therapy in patients with locally advanced unresectable or metastastic esophageal cancer, including the EGJ, regardless of the histology and biomarker status,” Enzinger concluded.
He was speaking at a press briefing prior to a presentation of the data in a presidential symposium at the European Society of Medical Oncology (ESMO) Virtual Congress 2020. (The data were presented in oral session by Ken Kato, MD, from the National Cancer Center Hospital in Tokyo, Japan.)
Little change in treatment
“Unfortunately, for esophageal cancer, the standard of care has remained relatively unchanged for a long period of time,” Enzinger said.
Standard first-line therapy for patients with advanced esophageal, EGJ, or gastric adenocarcinoma is primarily a chemotherapy doublet consisting of a fluoropyrimidine plus a platinum agent.
Pembrolizumab was previously shown to have some activity as monotherapy against advanced or metastatic esophageal cancer in the third line in the KEYNOTE-180 trial. It yielded an overall response rate (ORR) of 14%. A median duration of response was not reached among patients with esophageal squamous cell carcinoma (ESCC) and tumors with programmed cell death–ligand-1 (PD-L1) that had combined positive scores (CPSs) of 10 or higher.
Another previous trial, KEYNOTE-181, showed that pembrolizumab monotherapy in the second line was associated with an ORR of 22% vs 7% for chemotherapy and respective median OS of 10.3 vs 6.7 months. This trial led to US Food and Drug Administration approval of pembrolizumab for the treatment of patients with recurrent locally advanced or metastatic ESCC with PD-L1 CPS ≥10 who have experienced disease progression after at least one prior line of therapy.
The trial now being reported, KEYNOTE-590, assessed use of the drug in the first-line setting. It was designed to see whether combining standard-of-care chemotherapy with pembrolizumab would improve outcomes.
Study details
Patients were randomly assigned to receive chemotherapy with 5-fluorauracil (5-FU) 800 mg/m2 intravenously on days 1–5 every 3 weeks for up to 35 cycles and cisplatin 80 mg/m2 IV every 3 weeks for up to 6 cycles, plus either pembrolizumab 200 mg IV every 3 weeks for up to 35 cycles or saline placebo IV.
Rates of treatment-related adverse events of grade 3 or higher were similar between study arms, occurring in 71.9% with the combination and in 67.6% with chemotherapy alone. Adverse events leading to drug discontinuation occurred in 19.5% and 11.6%, respectively. Fatal adverse events occurred in 2.4% of patients who received the combination and in 1.4% of patients who received chemotherapy and placebo.
Immune-mediated adverse events of grade 3 or higher and infusion reactions occurred in 7% and 2.2% of patients, respectively.
Patient-reported quality of life was similar between the groups.
Mixed histologies muddy results
The improvement in OS was observed across all patient populations, including patients with ESCC, esophageal adenocarcinoma (EAC), and EGJ tumors, the researchers noted.
However, invited discussant Andres Cervantes, MD, PhD, from the University of Valencia, Spain, commented that ESCC and EAC have very different histologies and that including patients with both in a single trial can make the results very confusing.
He pointed out that, in the KEYNOTE-590 population, 73% of patients had ESCCs and 27% had EACs.
The OS improvement was seen regardless of PD-L1 expression, although the best results occurred in patients with high expression.
However, Cervantes noted that PD-L1 expression was not used as a stratification factor prior to randomization, even though it was included in the complex, step-wise statistical plan for the study.
Another expert, Salah-Eddin Al-Batran, MD, from the Krankenhaus Nordwest in Frankfurt, Germany, questioned the researchers’ recommendation that all patients with esophageal cancer receive this regimen, regardless of PD-L1 expression.
“We have to be sure that we do not inflate the results for the all-comers by the very responsive group of high [PD-L1] expressers,” he said at the press briefing.
He said the trial report also leaves open the question of efficacy in tumors with microsatellite instability and/or high tumor mutational burden.
“I think these questions have to be addressed to give us a clear picture of how to treat a patient sitting in front of us as doctors,” he said.
Also adding to the concerns about this trial is the fact that the “selected chemotherapy schedule is not much currently used as the standard of care,” said Cervantes, although he added that it “is acceptable for this protocol.”
Despite these caveats, the trial was clearly positive, Cervantes said. The greatest benefit appeared to accrue for patients with ESCC.
“The addition of pembrolizumab to platinum-based chemotherapy significantly increases response rate, PFS, and OS in patients with advanced esophageal carcinomas over chemotherapy alone,” he said, and therefore he agreed with the investigators that “this is a new standard of care.”
The study was funded by Merck Sharp & Dohme. Enzinger disclosed honoraria and advisory or consulting roles for Merck and others. Cervantes disclosed consulting or advising and research funding from Merck Serono and others. He is president-elect of ESMO. Al-Batran has disclosed no relevant financial relationships.
This story first appeared on Medscape.com.
FROM ESMO 2020
Understanding the enduring power of caste
Isabel Wilkerson’s naming of the malady facilitates space for a shift in thinking.
America has been struggling to understand its racial dynamics since the arrival of enslaved Africans more than 400 years ago. Today, with much of the world more polarized than ever, and certainly in our United States, there is a need for something to shift us from our fear and survival paranoid schizoid (us-vs.-them) position to an integrated form if we are to come out of this unusual democratic and societal unrest whole.
Yet, we’ve never had the lexicon to adequately describe the sociopolitical dynamics rooted in race and racism and their power to shape the thinking of all who originate in this country and all who enter its self-made borders whether forcefully or voluntarily. Enter Isabel Wilkerson, a Pulitzer Prize–winning, former New York Times Chicago bureau chief, and author of “The Warmth of Other Suns: The Epic Story of America’s Great Migration” (New York: Random House, 2010) with her second book, “Caste: The Origins of Our Discontents” (New York: Random House, 2020).
Ms. Wilkerson quickly gets to work in an engaging storytelling style of weaving past to present with ideas she supports with letters from the past, historians’ impressions, research studies, and data. Her observations and research are bookended by the lead up to the 2016 presidential election and its aftermath on the one end, and the impending 2020 presidential election on the other. In her view, the reemergence of violence that has accelerated in the 21st century and the renewed commitment to promote white supremacy can be understood if we expand our view of race and racism to consider the enduring power of caste. For, in Ms. Wilkerson’s view, the fear of the 2042 U.S. census (which is predicted to reflect for the first time a non-White majority) is a driving force behind the dominant caste’s determination to maintain the status quo power dynamics in the United States.

In an effort to explain American’s racial hierarchy, Ms. Wilkerson explains the need for a new lexicon “that may sound like a foreign language,” but this is intentional on her part. She writes:
“To recalibrate how we see ourselves, I use language that may be more commonly associated with people in other cultures, to suggest a new way of understanding our hierarchy: Dominant caste, ruling majority, favored caste, or upper caste, instead of, or in addition to, white. Middle castes instead of, or in addition to, Asian or Latino. Subordinate caste, lowest caste, bottom caste, disfavored caste, historically stigmatized instead of African-American. Original, conquered, or indigenous peoples instead of, or in addition to, Native American. Marginalized people in addition to, or instead of, women of any race, or minorities of any kind.”
Early in the book Ms. Wilkerson anchors her argument in Rev. Dr. Martin Luther King Jr.’s sojourn to India. Rather than focus on the known history of Dr. King’s admiration of Mohandas Gandhi, Ms. Wilkerson directs our attention to Dr. King’s discovery of his connection to Dalits, those who had been considered “untouchables” until Bhimrao Ramji Ambedkar, the Indian economist, jurist, social reformer, and Dalit leader, fiercely and successfully advocated for a rebranding of his caste of origin; instead of “untouchables” they would be considered Dalits or “broken people.” Dr. King did not meet Mr. Ambedkar, who died 3 years before this journey, but Ms. Wilkerson writes that Dr. King acknowledged the kinship, “And he said unto himself, Yes, I am an untouchable, and every Negro in the United States is an untouchable.” The Dalits and Dr. King recognized in each other their shared positions as subordinates in a global caste system.

In answering the question about the difference between racism and casteism, Ms. Wilkerson writes:
“Because caste and race are interwoven in America, it can be hard to separate the two. ... Casteism is the investment in keeping the hierarchy as it is in order to maintain your own ranking, advantage, privilege, or to elevate yourself above others or to keep others beneath you.”
Reading “Caste: The Origins of Our Discontents” is akin to the experience of gaining relief after struggling for years with a chronic malady that has a fluctuating course: Under the surface is low-grade pain that is compartmentalized and often met with denial or gaslighting when symptoms and systems are reported to members of the dominant caste. Yet, when there are acute flare-ups and increasingly frequent deadly encounters, the defenses of denial are painfully revealed; structures are broken and sometimes burned down. This has been the clinical course of racism, particularly in the United States. In that vein, an early reaction while reading “Caste” might be comparable to hearing an interpretation that educates, clarifies, resonates, and lands perfectly on the right diagnosis at the right moment.
Approach proves clarifying
In conceptualizing the malady as one of caste, Ms. Wilkerson achieves several things simultaneously – she names the malady, thus providing a lexicon, describes its symptoms, and most importantly, in our opinion, shares some of the compelling data from her field studies. By focusing on India, Nazi Germany, and the United States, she describes how easily one system influences another in the global effort to maintain power among the privileged.
This is not a new way of conceptualizing racial hierarchy; however, what is truly persuasive is Ms. Wilkerson’s ability to weave her rigorous research, sociopolitical analysis, and cogent psychological insights and interpretations to explain the 400-year trajectory of racialized caste in the United States. She achieves this exigent task with beautiful prose that motivates the reader to return time and time again to learn gut-wrenching painful historical details. She summarizes truths that have been unearthed (again) about Germany, India, and, in particular, the United States during her research and travels around the world. In doing so, she provides vivid examples of racism layered on caste. Consider the following:
“The Nazis were impressed by the American custom of lynching its subordinate caste of African-Americans, having become aware of the ritual torture and mutilations that typically accompanied them. Hitler especially marveled at the American ‘knack for maintaining an air of robust innocence in the wake of mass death.’ ” Ms. Wilkerson informs us that Hitler sent emissaries to study America’s Jim Crow system and then imported some features to orchestrate the Holocaust in Nazi Germany.
and a corresponding sense of inadequacy in the presence of someone who is considered to be from a higher caste.
A painful account of interpersonal racism is captured as Ms. Wilkerson recounts her experience after a routine business flight from Chicago to Detroit. She details her difficulty leaving a rental car parking lot because she had become so disoriented after being profiled and accosted by Drug Enforcement Administration agents who had intercepted her in the airport terminal and followed her onto the airport shuttle bus as she attempted to reach her destination. She provides a description of “getting turned around in a parking lot that I had been to dozens of times, going in circles, not able to get out, not registering the signs to the exit, not seeing how to get to Interstate 94, when I knew full well how to get to I-94 after all the times I’d driven it. ... This was the thievery of caste, stealing the time and psychic resources of the marginalized, draining energy in an already uphill competition. They were not, like me, frozen and disoriented, trying to make sense of a public violation that seemed all the more menacing now that I could see it in full. The quiet mundanity of that terror has never left me, the scars outliving the cut.”
This account is consistent with the dissociative, disorienting dynamics of race-based trauma. Her experience is not uncommon and helps to explain the activism of those in the subordinate caste who have attained some measure of wealth, power, and influence, and are motivated to expend their resources (energy, time, fame, and/or wealth) to raise awareness about social and political injustices by calling out structural racism in medicine, protesting police use of force by taking a knee, boycotting sporting events, and even demanding that football stadiums be used as polling sites. At the end of the day, all of us who have “made it” know that when we leave our homes, our relegation to the subordinate caste determines how we are perceived and what landmines we must navigate to make it through the day and that determine whether we will make it home.
This tour de force work of art has the potential to be a game changer in the way that we think about racial polarization in the United States. It is hoped that this new language opens up a space that allows each of us to explore this hegemony while identifying our placement and actions we take to maintain it, for each of us undeniably has a position in this caste system.
Having this new lexicon summons to mind the reactions of patients who gain immediate relief from having their illnesses named. In the case of the U.S. malady that has gripped us all, Ms. Wilkerson reiterates the importance of naming the condition. She writes:
“Because, to truly understand America, we must open our eyes to the hidden work of a caste system that has gone unnamed but prevails among us to our collective detriment, to see that we have more in common with each other and with cultures that we might otherwise dismiss, and to summon the courage to consider that therein may lie the answers.”
The naming allows both doctor and patient to have greater insight, understanding its origins and course, as well as having hope that there is a remedy. Naming facilitates the space for a shift in thinking and implementation of treatment protocols, such as Nazi Germany’s “zero tolerance policy” of swastikas in comparison to the ongoing U.S. controversy about the display of Confederate symbols. At this point in history, we welcome a diagnosis that has the potential to shift us from these poles of dominant and subordinate, black and white, good and bad, toward integration and wholeness of the individual psyche and collective global community. This is similar to what Melanie Klein calls the depressive position. Ms. Wilkerson suggests, in relinquishing these polar splits, we increase our capacity to shift to a space where our psychic integration occurs and our inextricable interdependence and responsibility for one another are honored.
Dr. Dunlap is a psychiatrist and psychoanalyst, and clinical professor of psychiatry and behavioral sciences at George Washington University. She is interested in the management of “difference” – race, gender, ethnicity, and intersectionality – in dyadic relationships and group dynamics; and the impact of racism on interpersonal relationships in institutional structures. Dr. Dunlap practices in Washington and has no disclosures. Dr. Dennis is a clinical psychologist and psychoanalyst. Her interests are in gender and ethnic diversity, health equity, and supervision and training. Dr. Dennis practices in Washington and has no disclosures.
Isabel Wilkerson’s naming of the malady facilitates space for a shift in thinking.
Isabel Wilkerson’s naming of the malady facilitates space for a shift in thinking.
America has been struggling to understand its racial dynamics since the arrival of enslaved Africans more than 400 years ago. Today, with much of the world more polarized than ever, and certainly in our United States, there is a need for something to shift us from our fear and survival paranoid schizoid (us-vs.-them) position to an integrated form if we are to come out of this unusual democratic and societal unrest whole.
Yet, we’ve never had the lexicon to adequately describe the sociopolitical dynamics rooted in race and racism and their power to shape the thinking of all who originate in this country and all who enter its self-made borders whether forcefully or voluntarily. Enter Isabel Wilkerson, a Pulitzer Prize–winning, former New York Times Chicago bureau chief, and author of “The Warmth of Other Suns: The Epic Story of America’s Great Migration” (New York: Random House, 2010) with her second book, “Caste: The Origins of Our Discontents” (New York: Random House, 2020).
Ms. Wilkerson quickly gets to work in an engaging storytelling style of weaving past to present with ideas she supports with letters from the past, historians’ impressions, research studies, and data. Her observations and research are bookended by the lead up to the 2016 presidential election and its aftermath on the one end, and the impending 2020 presidential election on the other. In her view, the reemergence of violence that has accelerated in the 21st century and the renewed commitment to promote white supremacy can be understood if we expand our view of race and racism to consider the enduring power of caste. For, in Ms. Wilkerson’s view, the fear of the 2042 U.S. census (which is predicted to reflect for the first time a non-White majority) is a driving force behind the dominant caste’s determination to maintain the status quo power dynamics in the United States.
In an effort to explain American’s racial hierarchy, Ms. Wilkerson explains the need for a new lexicon “that may sound like a foreign language,” but this is intentional on her part. She writes:
“To recalibrate how we see ourselves, I use language that may be more commonly associated with people in other cultures, to suggest a new way of understanding our hierarchy: Dominant caste, ruling majority, favored caste, or upper caste, instead of, or in addition to, white. Middle castes instead of, or in addition to, Asian or Latino. Subordinate caste, lowest caste, bottom caste, disfavored caste, historically stigmatized instead of African-American. Original, conquered, or indigenous peoples instead of, or in addition to, Native American. Marginalized people in addition to, or instead of, women of any race, or minorities of any kind.”
Early in the book Ms. Wilkerson anchors her argument in Rev. Dr. Martin Luther King Jr.’s sojourn to India. Rather than focus on the known history of Dr. King’s admiration of Mohandas Gandhi, Ms. Wilkerson directs our attention to Dr. King’s discovery of his connection to Dalits, those who had been considered “untouchables” until Bhimrao Ramji Ambedkar, the Indian economist, jurist, social reformer, and Dalit leader, fiercely and successfully advocated for a rebranding of his caste of origin; instead of “untouchables” they would be considered Dalits or “broken people.” Dr. King did not meet Mr. Ambedkar, who died 3 years before this journey, but Ms. Wilkerson writes that Dr. King acknowledged the kinship, “And he said unto himself, Yes, I am an untouchable, and every Negro in the United States is an untouchable.” The Dalits and Dr. King recognized in each other their shared positions as subordinates in a global caste system.
In answering the question about the difference between racism and casteism, Ms. Wilkerson writes:
“Because caste and race are interwoven in America, it can be hard to separate the two. ... Casteism is the investment in keeping the hierarchy as it is in order to maintain your own ranking, advantage, privilege, or to elevate yourself above others or to keep others beneath you.”
Reading “Caste: The Origins of Our Discontents” is akin to the experience of gaining relief after struggling for years with a chronic malady that has a fluctuating course: Under the surface is low-grade pain that is compartmentalized and often met with denial or gaslighting when symptoms and systems are reported to members of the dominant caste. Yet, when there are acute flare-ups and increasingly frequent deadly encounters, the defenses of denial are painfully revealed; structures are broken and sometimes burned down. This has been the clinical course of racism, particularly in the United States. In that vein, an early reaction while reading “Caste” might be comparable to hearing an interpretation that educates, clarifies, resonates, and lands perfectly on the right diagnosis at the right moment.
Approach proves clarifying
In conceptualizing the malady as one of caste, Ms. Wilkerson achieves several things simultaneously – she names the malady, thus providing a lexicon, describes its symptoms, and most importantly, in our opinion, shares some of the compelling data from her field studies. By focusing on India, Nazi Germany, and the United States, she describes how easily one system influences another in the global effort to maintain power among the privileged.
This is not a new way of conceptualizing racial hierarchy; however, what is truly persuasive is Ms. Wilkerson’s ability to weave her rigorous research, sociopolitical analysis, and cogent psychological insights and interpretations to explain the 400-year trajectory of racialized caste in the United States. She achieves this exigent task with beautiful prose that motivates the reader to return time and time again to learn gut-wrenching painful historical details. She summarizes truths that have been unearthed (again) about Germany, India, and, in particular, the United States during her research and travels around the world. In doing so, she provides vivid examples of racism layered on caste. Consider the following:
“The Nazis were impressed by the American custom of lynching its subordinate caste of African-Americans, having become aware of the ritual torture and mutilations that typically accompanied them. Hitler especially marveled at the American ‘knack for maintaining an air of robust innocence in the wake of mass death.’ ” Ms. Wilkerson informs us that Hitler sent emissaries to study America’s Jim Crow system and then imported some features to orchestrate the Holocaust in Nazi Germany.
and a corresponding sense of inadequacy in the presence of someone who is considered to be from a higher caste.
A painful account of interpersonal racism is captured as Ms. Wilkerson recounts her experience after a routine business flight from Chicago to Detroit. She details her difficulty leaving a rental car parking lot because she had become so disoriented after being profiled and accosted by Drug Enforcement Administration agents who had intercepted her in the airport terminal and followed her onto the airport shuttle bus as she attempted to reach her destination. She provides a description of “getting turned around in a parking lot that I had been to dozens of times, going in circles, not able to get out, not registering the signs to the exit, not seeing how to get to Interstate 94, when I knew full well how to get to I-94 after all the times I’d driven it. ... This was the thievery of caste, stealing the time and psychic resources of the marginalized, draining energy in an already uphill competition. They were not, like me, frozen and disoriented, trying to make sense of a public violation that seemed all the more menacing now that I could see it in full. The quiet mundanity of that terror has never left me, the scars outliving the cut.”
This account is consistent with the dissociative, disorienting dynamics of race-based trauma. Her experience is not uncommon and helps to explain the activism of those in the subordinate caste who have attained some measure of wealth, power, and influence, and are motivated to expend their resources (energy, time, fame, and/or wealth) to raise awareness about social and political injustices by calling out structural racism in medicine, protesting police use of force by taking a knee, boycotting sporting events, and even demanding that football stadiums be used as polling sites. At the end of the day, all of us who have “made it” know that when we leave our homes, our relegation to the subordinate caste determines how we are perceived and what landmines we must navigate to make it through the day and that determine whether we will make it home.
This tour de force work of art has the potential to be a game changer in the way that we think about racial polarization in the United States. It is hoped that this new language opens up a space that allows each of us to explore this hegemony while identifying our placement and actions we take to maintain it, for each of us undeniably has a position in this caste system.
Having this new lexicon summons to mind the reactions of patients who gain immediate relief from having their illnesses named. In the case of the U.S. malady that has gripped us all, Ms. Wilkerson reiterates the importance of naming the condition. She writes:
“Because, to truly understand America, we must open our eyes to the hidden work of a caste system that has gone unnamed but prevails among us to our collective detriment, to see that we have more in common with each other and with cultures that we might otherwise dismiss, and to summon the courage to consider that therein may lie the answers.”
The naming allows both doctor and patient to have greater insight, understanding its origins and course, as well as having hope that there is a remedy. Naming facilitates the space for a shift in thinking and implementation of treatment protocols, such as Nazi Germany’s “zero tolerance policy” of swastikas in comparison to the ongoing U.S. controversy about the display of Confederate symbols. At this point in history, we welcome a diagnosis that has the potential to shift us from these poles of dominant and subordinate, black and white, good and bad, toward integration and wholeness of the individual psyche and collective global community. This is similar to what Melanie Klein calls the depressive position. Ms. Wilkerson suggests, in relinquishing these polar splits, we increase our capacity to shift to a space where our psychic integration occurs and our inextricable interdependence and responsibility for one another are honored.
Dr. Dunlap is a psychiatrist and psychoanalyst, and clinical professor of psychiatry and behavioral sciences at George Washington University. She is interested in the management of “difference” – race, gender, ethnicity, and intersectionality – in dyadic relationships and group dynamics; and the impact of racism on interpersonal relationships in institutional structures. Dr. Dunlap practices in Washington and has no disclosures. Dr. Dennis is a clinical psychologist and psychoanalyst. Her interests are in gender and ethnic diversity, health equity, and supervision and training. Dr. Dennis practices in Washington and has no disclosures.
America has been struggling to understand its racial dynamics since the arrival of enslaved Africans more than 400 years ago. Today, with much of the world more polarized than ever, and certainly in our United States, there is a need for something to shift us from our fear and survival paranoid schizoid (us-vs.-them) position to an integrated form if we are to come out of this unusual democratic and societal unrest whole.
Yet, we’ve never had the lexicon to adequately describe the sociopolitical dynamics rooted in race and racism and their power to shape the thinking of all who originate in this country and all who enter its self-made borders whether forcefully or voluntarily. Enter Isabel Wilkerson, a Pulitzer Prize–winning, former New York Times Chicago bureau chief, and author of “The Warmth of Other Suns: The Epic Story of America’s Great Migration” (New York: Random House, 2010) with her second book, “Caste: The Origins of Our Discontents” (New York: Random House, 2020).
Ms. Wilkerson quickly gets to work in an engaging storytelling style of weaving past to present with ideas she supports with letters from the past, historians’ impressions, research studies, and data. Her observations and research are bookended by the lead up to the 2016 presidential election and its aftermath on the one end, and the impending 2020 presidential election on the other. In her view, the reemergence of violence that has accelerated in the 21st century and the renewed commitment to promote white supremacy can be understood if we expand our view of race and racism to consider the enduring power of caste. For, in Ms. Wilkerson’s view, the fear of the 2042 U.S. census (which is predicted to reflect for the first time a non-White majority) is a driving force behind the dominant caste’s determination to maintain the status quo power dynamics in the United States.
In an effort to explain American’s racial hierarchy, Ms. Wilkerson explains the need for a new lexicon “that may sound like a foreign language,” but this is intentional on her part. She writes:
“To recalibrate how we see ourselves, I use language that may be more commonly associated with people in other cultures, to suggest a new way of understanding our hierarchy: Dominant caste, ruling majority, favored caste, or upper caste, instead of, or in addition to, white. Middle castes instead of, or in addition to, Asian or Latino. Subordinate caste, lowest caste, bottom caste, disfavored caste, historically stigmatized instead of African-American. Original, conquered, or indigenous peoples instead of, or in addition to, Native American. Marginalized people in addition to, or instead of, women of any race, or minorities of any kind.”
Early in the book Ms. Wilkerson anchors her argument in Rev. Dr. Martin Luther King Jr.’s sojourn to India. Rather than focus on the known history of Dr. King’s admiration of Mohandas Gandhi, Ms. Wilkerson directs our attention to Dr. King’s discovery of his connection to Dalits, those who had been considered “untouchables” until Bhimrao Ramji Ambedkar, the Indian economist, jurist, social reformer, and Dalit leader, fiercely and successfully advocated for a rebranding of his caste of origin; instead of “untouchables” they would be considered Dalits or “broken people.” Dr. King did not meet Mr. Ambedkar, who died 3 years before this journey, but Ms. Wilkerson writes that Dr. King acknowledged the kinship, “And he said unto himself, Yes, I am an untouchable, and every Negro in the United States is an untouchable.” The Dalits and Dr. King recognized in each other their shared positions as subordinates in a global caste system.
In answering the question about the difference between racism and casteism, Ms. Wilkerson writes:
“Because caste and race are interwoven in America, it can be hard to separate the two. ... Casteism is the investment in keeping the hierarchy as it is in order to maintain your own ranking, advantage, privilege, or to elevate yourself above others or to keep others beneath you.”
Reading “Caste: The Origins of Our Discontents” is akin to the experience of gaining relief after struggling for years with a chronic malady that has a fluctuating course: Under the surface is low-grade pain that is compartmentalized and often met with denial or gaslighting when symptoms and systems are reported to members of the dominant caste. Yet, when there are acute flare-ups and increasingly frequent deadly encounters, the defenses of denial are painfully revealed; structures are broken and sometimes burned down. This has been the clinical course of racism, particularly in the United States. In that vein, an early reaction while reading “Caste” might be comparable to hearing an interpretation that educates, clarifies, resonates, and lands perfectly on the right diagnosis at the right moment.
Approach proves clarifying
In conceptualizing the malady as one of caste, Ms. Wilkerson achieves several things simultaneously – she names the malady, thus providing a lexicon, describes its symptoms, and most importantly, in our opinion, shares some of the compelling data from her field studies. By focusing on India, Nazi Germany, and the United States, she describes how easily one system influences another in the global effort to maintain power among the privileged.
This is not a new way of conceptualizing racial hierarchy; however, what is truly persuasive is Ms. Wilkerson’s ability to weave her rigorous research, sociopolitical analysis, and cogent psychological insights and interpretations to explain the 400-year trajectory of racialized caste in the United States. She achieves this exigent task with beautiful prose that motivates the reader to return time and time again to learn gut-wrenching painful historical details. She summarizes truths that have been unearthed (again) about Germany, India, and, in particular, the United States during her research and travels around the world. In doing so, she provides vivid examples of racism layered on caste. Consider the following:
“The Nazis were impressed by the American custom of lynching its subordinate caste of African-Americans, having become aware of the ritual torture and mutilations that typically accompanied them. Hitler especially marveled at the American ‘knack for maintaining an air of robust innocence in the wake of mass death.’ ” Ms. Wilkerson informs us that Hitler sent emissaries to study America’s Jim Crow system and then imported some features to orchestrate the Holocaust in Nazi Germany.
and a corresponding sense of inadequacy in the presence of someone who is considered to be from a higher caste.
A painful account of interpersonal racism is captured as Ms. Wilkerson recounts her experience after a routine business flight from Chicago to Detroit. She details her difficulty leaving a rental car parking lot because she had become so disoriented after being profiled and accosted by Drug Enforcement Administration agents who had intercepted her in the airport terminal and followed her onto the airport shuttle bus as she attempted to reach her destination. She provides a description of “getting turned around in a parking lot that I had been to dozens of times, going in circles, not able to get out, not registering the signs to the exit, not seeing how to get to Interstate 94, when I knew full well how to get to I-94 after all the times I’d driven it. ... This was the thievery of caste, stealing the time and psychic resources of the marginalized, draining energy in an already uphill competition. They were not, like me, frozen and disoriented, trying to make sense of a public violation that seemed all the more menacing now that I could see it in full. The quiet mundanity of that terror has never left me, the scars outliving the cut.”
This account is consistent with the dissociative, disorienting dynamics of race-based trauma. Her experience is not uncommon and helps to explain the activism of those in the subordinate caste who have attained some measure of wealth, power, and influence, and are motivated to expend their resources (energy, time, fame, and/or wealth) to raise awareness about social and political injustices by calling out structural racism in medicine, protesting police use of force by taking a knee, boycotting sporting events, and even demanding that football stadiums be used as polling sites. At the end of the day, all of us who have “made it” know that when we leave our homes, our relegation to the subordinate caste determines how we are perceived and what landmines we must navigate to make it through the day and that determine whether we will make it home.
This tour de force work of art has the potential to be a game changer in the way that we think about racial polarization in the United States. It is hoped that this new language opens up a space that allows each of us to explore this hegemony while identifying our placement and actions we take to maintain it, for each of us undeniably has a position in this caste system.
Having this new lexicon summons to mind the reactions of patients who gain immediate relief from having their illnesses named. In the case of the U.S. malady that has gripped us all, Ms. Wilkerson reiterates the importance of naming the condition. She writes:
“Because, to truly understand America, we must open our eyes to the hidden work of a caste system that has gone unnamed but prevails among us to our collective detriment, to see that we have more in common with each other and with cultures that we might otherwise dismiss, and to summon the courage to consider that therein may lie the answers.”
The naming allows both doctor and patient to have greater insight, understanding its origins and course, as well as having hope that there is a remedy. Naming facilitates the space for a shift in thinking and implementation of treatment protocols, such as Nazi Germany’s “zero tolerance policy” of swastikas in comparison to the ongoing U.S. controversy about the display of Confederate symbols. At this point in history, we welcome a diagnosis that has the potential to shift us from these poles of dominant and subordinate, black and white, good and bad, toward integration and wholeness of the individual psyche and collective global community. This is similar to what Melanie Klein calls the depressive position. Ms. Wilkerson suggests, in relinquishing these polar splits, we increase our capacity to shift to a space where our psychic integration occurs and our inextricable interdependence and responsibility for one another are honored.
Dr. Dunlap is a psychiatrist and psychoanalyst, and clinical professor of psychiatry and behavioral sciences at George Washington University. She is interested in the management of “difference” – race, gender, ethnicity, and intersectionality – in dyadic relationships and group dynamics; and the impact of racism on interpersonal relationships in institutional structures. Dr. Dunlap practices in Washington and has no disclosures. Dr. Dennis is a clinical psychologist and psychoanalyst. Her interests are in gender and ethnic diversity, health equity, and supervision and training. Dr. Dennis practices in Washington and has no disclosures.
Suicide rates up significantly among adolescents, young adults
Suicide rates in young people aged 10-24 years increased significantly in 42 states from 2007-2009 to 2016-2018, according to a recent analysis from the National Center for Health Statistics.
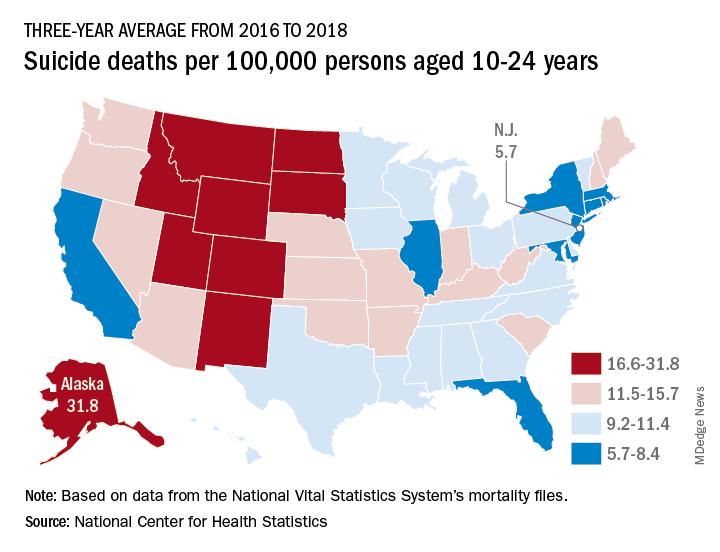
Nationally, the suicide rate jumped 47%, based on the averages for the two 3-year periods, rising from 7.0 per 100,000 persons aged 10-24 years to 10.3 per 100,000. For all ages, the corresponding increase was 47%, Sally C. Curtin, MA, of the NCHS, said in a National Vital Statistics Report.
There was no state with a decrease in suicide rates for adolescents and young adults, as the other eight all had nonsignificant increases, the smallest being 14% in South Dakota. Three-year averages were used to increase statistical power for states with relatively small numbers of deaths but were still not enough to show significance for some large increases, such as the 48% rise in Delaware, Ms. Curtin noted.
In 2016-2018, Alaska’s suicide rate of 31.8 per 100,000 persons aged 10-24 years was the highest in the country, followed by South Dakota (23.6), Montana (23.2), and Wyoming (20.5). New Jersey had the lowest rate at 5.7 per 100,000, with New York and Rhode Island both slightly higher at 5.9 and Connecticut at 6.3, based on data from the National Vital Statistics System.
Even the low numbers, however, hide some large changes, as New Jersey (up by 39%) and New York (up by 44%) were among the 42 states with statistically significant increases, which ranged from 21.7% in Maryland to 110% in New Hampshire, Ms. Curtin said in the report. The increases seen in this analysis contrast with data from the preceding time period, as “the suicide rate among persons aged 10-24 was statistically stable from 2000 to 2007.”
SOURCE: Curtin SC. National Vital Statistics Reports. 2020;69(11)1-9.
Suicide rates in young people aged 10-24 years increased significantly in 42 states from 2007-2009 to 2016-2018, according to a recent analysis from the National Center for Health Statistics.
Nationally, the suicide rate jumped 47%, based on the averages for the two 3-year periods, rising from 7.0 per 100,000 persons aged 10-24 years to 10.3 per 100,000. For all ages, the corresponding increase was 47%, Sally C. Curtin, MA, of the NCHS, said in a National Vital Statistics Report.
There was no state with a decrease in suicide rates for adolescents and young adults, as the other eight all had nonsignificant increases, the smallest being 14% in South Dakota. Three-year averages were used to increase statistical power for states with relatively small numbers of deaths but were still not enough to show significance for some large increases, such as the 48% rise in Delaware, Ms. Curtin noted.
In 2016-2018, Alaska’s suicide rate of 31.8 per 100,000 persons aged 10-24 years was the highest in the country, followed by South Dakota (23.6), Montana (23.2), and Wyoming (20.5). New Jersey had the lowest rate at 5.7 per 100,000, with New York and Rhode Island both slightly higher at 5.9 and Connecticut at 6.3, based on data from the National Vital Statistics System.
Even the low numbers, however, hide some large changes, as New Jersey (up by 39%) and New York (up by 44%) were among the 42 states with statistically significant increases, which ranged from 21.7% in Maryland to 110% in New Hampshire, Ms. Curtin said in the report. The increases seen in this analysis contrast with data from the preceding time period, as “the suicide rate among persons aged 10-24 was statistically stable from 2000 to 2007.”
SOURCE: Curtin SC. National Vital Statistics Reports. 2020;69(11)1-9.
Suicide rates in young people aged 10-24 years increased significantly in 42 states from 2007-2009 to 2016-2018, according to a recent analysis from the National Center for Health Statistics.
Nationally, the suicide rate jumped 47%, based on the averages for the two 3-year periods, rising from 7.0 per 100,000 persons aged 10-24 years to 10.3 per 100,000. For all ages, the corresponding increase was 47%, Sally C. Curtin, MA, of the NCHS, said in a National Vital Statistics Report.
There was no state with a decrease in suicide rates for adolescents and young adults, as the other eight all had nonsignificant increases, the smallest being 14% in South Dakota. Three-year averages were used to increase statistical power for states with relatively small numbers of deaths but were still not enough to show significance for some large increases, such as the 48% rise in Delaware, Ms. Curtin noted.
In 2016-2018, Alaska’s suicide rate of 31.8 per 100,000 persons aged 10-24 years was the highest in the country, followed by South Dakota (23.6), Montana (23.2), and Wyoming (20.5). New Jersey had the lowest rate at 5.7 per 100,000, with New York and Rhode Island both slightly higher at 5.9 and Connecticut at 6.3, based on data from the National Vital Statistics System.
Even the low numbers, however, hide some large changes, as New Jersey (up by 39%) and New York (up by 44%) were among the 42 states with statistically significant increases, which ranged from 21.7% in Maryland to 110% in New Hampshire, Ms. Curtin said in the report. The increases seen in this analysis contrast with data from the preceding time period, as “the suicide rate among persons aged 10-24 was statistically stable from 2000 to 2007.”
SOURCE: Curtin SC. National Vital Statistics Reports. 2020;69(11)1-9.
Is psychiatry coddling the American mind?
A trainee recently observed that psychiatrists frequently seem motivated to protect patients from emotional and internal disruption. He suggested that we often did so by validating their maladaptive perspectives regarding their impaired relationships to society and close attachments. These maneuvers were justified by referring to the need to establish a therapeutic alliance and reduce patients’ suffering.

As an example, he mentioned a patient with alcohol use disorder. The patient came in with complaints that he could not stay sober with his current level of depression. The patient also complained of a family member who was setting limits. To the trainee’s surprise, the patient was not challenged on his perceived victimhood and his fantasy that a sober life should mean a life without negative effect. Instead, the patient was validated in his anger toward the family member. In addition, his medications were adjusted, seemingly confirming to the patient that one could only ask for sobriety once life is empty of pain.
The observation of the trainee reminded us of the three great “untruths” mentioned by Greg Lukianoff and Jonathan Haidt, PhD, in their famous book, “The Coddling of the American Mind.”1 In the book they warn against the idea of fragility – what doesn’t kill you makes you weaker; emotional reasoning – always trust your feelings; and us-versus-them thinking – life is a battle between good people and evil people. The authors compare these three great untruths with the cognitive distortions of cognitive-behavioral therapy.
We ponder the trainee’s observation that psychiatrists appear to encourage the untruths rather than challenge them. Part of psychiatric and all medical training involves learning nonjudgmental approaches to human suffering and an identification with individual needs over societal demands. Our suspicion is that a nonjudgmental approach to the understanding of the human condition generates a desire to protect patients from a moralistic shaming position. However, we wonder if, at times, psychiatry takes this approach too far.
Reconceptualizing shame
Shame can be a toxic presence in the overwhelmed superego of a patient, but it can serve an important role in psychic development and should not be avoided out of hand. We suggest that it can be appropriate for a patient with an alcohol use disorder to feel some shame for the harm caused by their drinking, and we question the limit of psychiatry’s current pursuit of incessant validation. As an extreme example, would modern psychiatry discourage a patient who killed someone while driving in an intoxicated state from feeling remorse and shame?
Modern psychiatry appears to have other examples of the three great untruths on display. In our work, we are often faced with patients who are prematurely placed on disability, an example of fragility. Instead of encouraging patients to return to the workforce, they are “protected” from the emotional difficulty of work. In many patients this results in a decline in functioning and worsening of psychiatric symptoms. We are also confronted with patients who define themselves by how they feel, an example of emotional reasoning. Instead of using our clinical judgments to define and assess symptoms, patients are left to decide for themselves through self-rated scales with questionable validity.2 This can result in patients having their emotional experiences not only validated when inappropriate but can also give emotional reasoning a false sense of medical legitimacy.
Finally, we commonly see patients who endlessly blame family members and others for any life difficulties, a form of us-versus-them thinking. Instead of acknowledging and then integrating life challenges to achieve recovery, patients are affirmed despite clinicians having little evidence on the veracity of the patients’ perspective. As a consequence, patients can be further isolated from their greatest source of support.

In some ways, a mindlessly validating approach in psychiatry is unexpected since the practice of psychiatry would seem to promote the development of strong attachments and resilience. After all, connections to family, employment, social institutions, and even religious worship are associated with vastly better outcomes. Those who have become alienated to these pillars of social cohesion fare much worse. One may deplore the static and at times oppressive nature of these institutions but the empirical experience of practicing psychiatry leads one to a healthy respect for the stabilizing influence they accord for individuals struggling with life’s vicissitudes, unpredictability, and loneliness. Overcoming the fear of responsibility, living up to the demands and expectations of society, and having the strength to overcome difficult emotions should be the standard goals of psychiatric treatment.
From the knowledge gained from working with patients struggling from psychic pain, we wonder how to encourage patients to pursue those adaptive approaches to life. We argue that a stoic emphasis on learning to manage one’s affective and mental response to the inevitable changes of life is key to achieving wisdom and stability in our humble lives. This perspective is a common denominator of multiple different psychotherapies. The goal is to provide patients with the ability to be in a place where they are engaged with the world in a meaningful way that is not overwhelmed by distorted, self-absorbed psychic anguish. This perspective discourages externalization as a relatively low-yield way to understand and overcome one’s problems. One identifies childhood experiences with one’s mother as a source of adult distress not for the purpose of blaming her, but for the purpose of recognizing one’s own childish motivations for making maladaptive decisions as an adult.
For many patients, the goal should be to emphasize an internal locus of control and responsibility. We should also avoid constantly relying on society and government’s role in helping the individual achieve a satisfactory life. We wonder if this endless pursuit of nonjudgment and validation corrupts the doctor-patient interaction. In other words, and individual responsibility for their own psychic development. Psychotherapy that ends with the patient being able to identify all the traumas that led to their sorrow has simply left the patient in the role of helpless and sorrowful victim. Instead, we should allow patients to proceed to the next step, which is empowerment and transformation. From this angle, the field of psychiatry should be cautious of encouraging movements that promote victimhood and grievance as a meaningful psychic position to take in society.
Mr. Lukianoff and Dr. Haidt use cognitive therapy as an analogy throughout their books for how to confront the great untruths. They perceive those modern forms of thinking as cognitive distortions, which can be remedied using the techniques of cognitive restructuring found in cognitive-behavioral therapy. They encourage us to recognize those maladaptive thoughts, and create more accurate and adaptive ways of viewing the world – a view that would be able to grow from challenges not just survive them; a view referred to as antifragile.3 We believe that those techniques and others would certainly be of assistance in our current times. However, the first step is to recognize our problem – a problem that is not rooted in the DSM, research, or biology but in an exaggerated intention to be patient centered. We should, however, remember that, when a patient has negative schemas, being too patient centered can be encouraging to maladaptive behaviors.
In conclusion, we wonder what modern psychiatry could look like if it made a concerted effort at also treating mental illness by reinforcing the importance of individual agency and responsibility. Modern psychiatry has been so focused on describing biological symptoms needing biological treatments that we sometimes forget that having no symptom (being asymptomatic) is not the only goal. Having a fulfilling and meaningful life, which is resilient to future symptoms is just as important to patients. We seem to have entrenched ourselves so deeply in an overly basic approach of problem-solution and diagnosis-treatment paradigm. However, we don’t need to renege on modern advances to promote the patient’s strength, adaptability, and antifragility. An emphasis on patient growth can complement the medical model. We wonder what effect such an approach would have if the trainee’s patient with alcohol use disorder was instead told: “Given the suffering you have and have caused because of your alcohol use disorder, how do you plan to make changes in your life to help the treatment plan we create together?”
Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He also is the course director for the UCSD third-year medical student psychiatry clerkship. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at UCSD and the University of San Diego. Dr. Badre can be reached at his website, BadreMD.com.
References
1. Lukianoff G, Haidt J. The Coddling of the American Mind: How Good Intentions and Bad Ideas are Setting Up a Generation for Failure. New York: Penguin Books, 2019.
2. Levis B et al. J Clin Epidemiol. 2020 Jun;122:115-128.e1.,
3. Taleb NN. Antifragile: Things That Gain from Disorder. Vol. 3. New York: Random House, 2012.
A trainee recently observed that psychiatrists frequently seem motivated to protect patients from emotional and internal disruption. He suggested that we often did so by validating their maladaptive perspectives regarding their impaired relationships to society and close attachments. These maneuvers were justified by referring to the need to establish a therapeutic alliance and reduce patients’ suffering.
As an example, he mentioned a patient with alcohol use disorder. The patient came in with complaints that he could not stay sober with his current level of depression. The patient also complained of a family member who was setting limits. To the trainee’s surprise, the patient was not challenged on his perceived victimhood and his fantasy that a sober life should mean a life without negative effect. Instead, the patient was validated in his anger toward the family member. In addition, his medications were adjusted, seemingly confirming to the patient that one could only ask for sobriety once life is empty of pain.
The observation of the trainee reminded us of the three great “untruths” mentioned by Greg Lukianoff and Jonathan Haidt, PhD, in their famous book, “The Coddling of the American Mind.”1 In the book they warn against the idea of fragility – what doesn’t kill you makes you weaker; emotional reasoning – always trust your feelings; and us-versus-them thinking – life is a battle between good people and evil people. The authors compare these three great untruths with the cognitive distortions of cognitive-behavioral therapy.
We ponder the trainee’s observation that psychiatrists appear to encourage the untruths rather than challenge them. Part of psychiatric and all medical training involves learning nonjudgmental approaches to human suffering and an identification with individual needs over societal demands. Our suspicion is that a nonjudgmental approach to the understanding of the human condition generates a desire to protect patients from a moralistic shaming position. However, we wonder if, at times, psychiatry takes this approach too far.
Reconceptualizing shame
Shame can be a toxic presence in the overwhelmed superego of a patient, but it can serve an important role in psychic development and should not be avoided out of hand. We suggest that it can be appropriate for a patient with an alcohol use disorder to feel some shame for the harm caused by their drinking, and we question the limit of psychiatry’s current pursuit of incessant validation. As an extreme example, would modern psychiatry discourage a patient who killed someone while driving in an intoxicated state from feeling remorse and shame?
Modern psychiatry appears to have other examples of the three great untruths on display. In our work, we are often faced with patients who are prematurely placed on disability, an example of fragility. Instead of encouraging patients to return to the workforce, they are “protected” from the emotional difficulty of work. In many patients this results in a decline in functioning and worsening of psychiatric symptoms. We are also confronted with patients who define themselves by how they feel, an example of emotional reasoning. Instead of using our clinical judgments to define and assess symptoms, patients are left to decide for themselves through self-rated scales with questionable validity.2 This can result in patients having their emotional experiences not only validated when inappropriate but can also give emotional reasoning a false sense of medical legitimacy.
Finally, we commonly see patients who endlessly blame family members and others for any life difficulties, a form of us-versus-them thinking. Instead of acknowledging and then integrating life challenges to achieve recovery, patients are affirmed despite clinicians having little evidence on the veracity of the patients’ perspective. As a consequence, patients can be further isolated from their greatest source of support.
In some ways, a mindlessly validating approach in psychiatry is unexpected since the practice of psychiatry would seem to promote the development of strong attachments and resilience. After all, connections to family, employment, social institutions, and even religious worship are associated with vastly better outcomes. Those who have become alienated to these pillars of social cohesion fare much worse. One may deplore the static and at times oppressive nature of these institutions but the empirical experience of practicing psychiatry leads one to a healthy respect for the stabilizing influence they accord for individuals struggling with life’s vicissitudes, unpredictability, and loneliness. Overcoming the fear of responsibility, living up to the demands and expectations of society, and having the strength to overcome difficult emotions should be the standard goals of psychiatric treatment.
From the knowledge gained from working with patients struggling from psychic pain, we wonder how to encourage patients to pursue those adaptive approaches to life. We argue that a stoic emphasis on learning to manage one’s affective and mental response to the inevitable changes of life is key to achieving wisdom and stability in our humble lives. This perspective is a common denominator of multiple different psychotherapies. The goal is to provide patients with the ability to be in a place where they are engaged with the world in a meaningful way that is not overwhelmed by distorted, self-absorbed psychic anguish. This perspective discourages externalization as a relatively low-yield way to understand and overcome one’s problems. One identifies childhood experiences with one’s mother as a source of adult distress not for the purpose of blaming her, but for the purpose of recognizing one’s own childish motivations for making maladaptive decisions as an adult.
For many patients, the goal should be to emphasize an internal locus of control and responsibility. We should also avoid constantly relying on society and government’s role in helping the individual achieve a satisfactory life. We wonder if this endless pursuit of nonjudgment and validation corrupts the doctor-patient interaction. In other words, and individual responsibility for their own psychic development. Psychotherapy that ends with the patient being able to identify all the traumas that led to their sorrow has simply left the patient in the role of helpless and sorrowful victim. Instead, we should allow patients to proceed to the next step, which is empowerment and transformation. From this angle, the field of psychiatry should be cautious of encouraging movements that promote victimhood and grievance as a meaningful psychic position to take in society.
Mr. Lukianoff and Dr. Haidt use cognitive therapy as an analogy throughout their books for how to confront the great untruths. They perceive those modern forms of thinking as cognitive distortions, which can be remedied using the techniques of cognitive restructuring found in cognitive-behavioral therapy. They encourage us to recognize those maladaptive thoughts, and create more accurate and adaptive ways of viewing the world – a view that would be able to grow from challenges not just survive them; a view referred to as antifragile.3 We believe that those techniques and others would certainly be of assistance in our current times. However, the first step is to recognize our problem – a problem that is not rooted in the DSM, research, or biology but in an exaggerated intention to be patient centered. We should, however, remember that, when a patient has negative schemas, being too patient centered can be encouraging to maladaptive behaviors.
In conclusion, we wonder what modern psychiatry could look like if it made a concerted effort at also treating mental illness by reinforcing the importance of individual agency and responsibility. Modern psychiatry has been so focused on describing biological symptoms needing biological treatments that we sometimes forget that having no symptom (being asymptomatic) is not the only goal. Having a fulfilling and meaningful life, which is resilient to future symptoms is just as important to patients. We seem to have entrenched ourselves so deeply in an overly basic approach of problem-solution and diagnosis-treatment paradigm. However, we don’t need to renege on modern advances to promote the patient’s strength, adaptability, and antifragility. An emphasis on patient growth can complement the medical model. We wonder what effect such an approach would have if the trainee’s patient with alcohol use disorder was instead told: “Given the suffering you have and have caused because of your alcohol use disorder, how do you plan to make changes in your life to help the treatment plan we create together?”
Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He also is the course director for the UCSD third-year medical student psychiatry clerkship. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at UCSD and the University of San Diego. Dr. Badre can be reached at his website, BadreMD.com.
References
1. Lukianoff G, Haidt J. The Coddling of the American Mind: How Good Intentions and Bad Ideas are Setting Up a Generation for Failure. New York: Penguin Books, 2019.
2. Levis B et al. J Clin Epidemiol. 2020 Jun;122:115-128.e1.,
3. Taleb NN. Antifragile: Things That Gain from Disorder. Vol. 3. New York: Random House, 2012.
A trainee recently observed that psychiatrists frequently seem motivated to protect patients from emotional and internal disruption. He suggested that we often did so by validating their maladaptive perspectives regarding their impaired relationships to society and close attachments. These maneuvers were justified by referring to the need to establish a therapeutic alliance and reduce patients’ suffering.
As an example, he mentioned a patient with alcohol use disorder. The patient came in with complaints that he could not stay sober with his current level of depression. The patient also complained of a family member who was setting limits. To the trainee’s surprise, the patient was not challenged on his perceived victimhood and his fantasy that a sober life should mean a life without negative effect. Instead, the patient was validated in his anger toward the family member. In addition, his medications were adjusted, seemingly confirming to the patient that one could only ask for sobriety once life is empty of pain.
The observation of the trainee reminded us of the three great “untruths” mentioned by Greg Lukianoff and Jonathan Haidt, PhD, in their famous book, “The Coddling of the American Mind.”1 In the book they warn against the idea of fragility – what doesn’t kill you makes you weaker; emotional reasoning – always trust your feelings; and us-versus-them thinking – life is a battle between good people and evil people. The authors compare these three great untruths with the cognitive distortions of cognitive-behavioral therapy.
We ponder the trainee’s observation that psychiatrists appear to encourage the untruths rather than challenge them. Part of psychiatric and all medical training involves learning nonjudgmental approaches to human suffering and an identification with individual needs over societal demands. Our suspicion is that a nonjudgmental approach to the understanding of the human condition generates a desire to protect patients from a moralistic shaming position. However, we wonder if, at times, psychiatry takes this approach too far.
Reconceptualizing shame
Shame can be a toxic presence in the overwhelmed superego of a patient, but it can serve an important role in psychic development and should not be avoided out of hand. We suggest that it can be appropriate for a patient with an alcohol use disorder to feel some shame for the harm caused by their drinking, and we question the limit of psychiatry’s current pursuit of incessant validation. As an extreme example, would modern psychiatry discourage a patient who killed someone while driving in an intoxicated state from feeling remorse and shame?
Modern psychiatry appears to have other examples of the three great untruths on display. In our work, we are often faced with patients who are prematurely placed on disability, an example of fragility. Instead of encouraging patients to return to the workforce, they are “protected” from the emotional difficulty of work. In many patients this results in a decline in functioning and worsening of psychiatric symptoms. We are also confronted with patients who define themselves by how they feel, an example of emotional reasoning. Instead of using our clinical judgments to define and assess symptoms, patients are left to decide for themselves through self-rated scales with questionable validity.2 This can result in patients having their emotional experiences not only validated when inappropriate but can also give emotional reasoning a false sense of medical legitimacy.
Finally, we commonly see patients who endlessly blame family members and others for any life difficulties, a form of us-versus-them thinking. Instead of acknowledging and then integrating life challenges to achieve recovery, patients are affirmed despite clinicians having little evidence on the veracity of the patients’ perspective. As a consequence, patients can be further isolated from their greatest source of support.
In some ways, a mindlessly validating approach in psychiatry is unexpected since the practice of psychiatry would seem to promote the development of strong attachments and resilience. After all, connections to family, employment, social institutions, and even religious worship are associated with vastly better outcomes. Those who have become alienated to these pillars of social cohesion fare much worse. One may deplore the static and at times oppressive nature of these institutions but the empirical experience of practicing psychiatry leads one to a healthy respect for the stabilizing influence they accord for individuals struggling with life’s vicissitudes, unpredictability, and loneliness. Overcoming the fear of responsibility, living up to the demands and expectations of society, and having the strength to overcome difficult emotions should be the standard goals of psychiatric treatment.
From the knowledge gained from working with patients struggling from psychic pain, we wonder how to encourage patients to pursue those adaptive approaches to life. We argue that a stoic emphasis on learning to manage one’s affective and mental response to the inevitable changes of life is key to achieving wisdom and stability in our humble lives. This perspective is a common denominator of multiple different psychotherapies. The goal is to provide patients with the ability to be in a place where they are engaged with the world in a meaningful way that is not overwhelmed by distorted, self-absorbed psychic anguish. This perspective discourages externalization as a relatively low-yield way to understand and overcome one’s problems. One identifies childhood experiences with one’s mother as a source of adult distress not for the purpose of blaming her, but for the purpose of recognizing one’s own childish motivations for making maladaptive decisions as an adult.
For many patients, the goal should be to emphasize an internal locus of control and responsibility. We should also avoid constantly relying on society and government’s role in helping the individual achieve a satisfactory life. We wonder if this endless pursuit of nonjudgment and validation corrupts the doctor-patient interaction. In other words, and individual responsibility for their own psychic development. Psychotherapy that ends with the patient being able to identify all the traumas that led to their sorrow has simply left the patient in the role of helpless and sorrowful victim. Instead, we should allow patients to proceed to the next step, which is empowerment and transformation. From this angle, the field of psychiatry should be cautious of encouraging movements that promote victimhood and grievance as a meaningful psychic position to take in society.
Mr. Lukianoff and Dr. Haidt use cognitive therapy as an analogy throughout their books for how to confront the great untruths. They perceive those modern forms of thinking as cognitive distortions, which can be remedied using the techniques of cognitive restructuring found in cognitive-behavioral therapy. They encourage us to recognize those maladaptive thoughts, and create more accurate and adaptive ways of viewing the world – a view that would be able to grow from challenges not just survive them; a view referred to as antifragile.3 We believe that those techniques and others would certainly be of assistance in our current times. However, the first step is to recognize our problem – a problem that is not rooted in the DSM, research, or biology but in an exaggerated intention to be patient centered. We should, however, remember that, when a patient has negative schemas, being too patient centered can be encouraging to maladaptive behaviors.
In conclusion, we wonder what modern psychiatry could look like if it made a concerted effort at also treating mental illness by reinforcing the importance of individual agency and responsibility. Modern psychiatry has been so focused on describing biological symptoms needing biological treatments that we sometimes forget that having no symptom (being asymptomatic) is not the only goal. Having a fulfilling and meaningful life, which is resilient to future symptoms is just as important to patients. We seem to have entrenched ourselves so deeply in an overly basic approach of problem-solution and diagnosis-treatment paradigm. However, we don’t need to renege on modern advances to promote the patient’s strength, adaptability, and antifragility. An emphasis on patient growth can complement the medical model. We wonder what effect such an approach would have if the trainee’s patient with alcohol use disorder was instead told: “Given the suffering you have and have caused because of your alcohol use disorder, how do you plan to make changes in your life to help the treatment plan we create together?”
Dr. Lehman is a professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He also is the course director for the UCSD third-year medical student psychiatry clerkship. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at UCSD and the University of San Diego. Dr. Badre can be reached at his website, BadreMD.com.
References
1. Lukianoff G, Haidt J. The Coddling of the American Mind: How Good Intentions and Bad Ideas are Setting Up a Generation for Failure. New York: Penguin Books, 2019.
2. Levis B et al. J Clin Epidemiol. 2020 Jun;122:115-128.e1.,
3. Taleb NN. Antifragile: Things That Gain from Disorder. Vol. 3. New York: Random House, 2012.
No prior use of insulin predicts postsurgical diabetes remission
Type 2 diabetes patients who had never used insulin showed sustained remission 10 years after bariatric surgery in a prospective study of 85 patients.
Having diabetes for less than 5 years was also predictive of achieving long-term diabetes remission, Diego Moriconi, MD, of the University of Pisa (Italy) and presenting study investigator, reported at the virtual annual meeting of the European Association for the Study of Diabetes.
“Weight loss was associated with type 2 diabetes remission 1 year after surgery, but it had no impact on the long-term relapse of diabetes,” Dr. Moriconi said.
The findings are important, commented Tina Vilsbøll, MD, DMSc, chief consultant at the Steno Diabetes Centre Copenhagen, who chaired the session. They’re important because they would help “to set the expectations for patients before they have surgery, what to expect in respect to resolution or remission of diabetes.”
If patients were taking insulin, for instance, the take home would seem to be not to expect too much in terms of remission of their diabetes, Dr. Vilsbøll said. She added: “Usually I am not a big fan of [relying on] diabetes duration, because often we know that patients with type 2 diabetes have had diabetes for a long time before they’re actually diagnosed.” However, “it seems to be very important here.”
Dr. Moriconi reported the findings of an observational study that had started in 2006 and recruited individuals about to undergo bariatric surgery for type 2 diabetes. Participants were evaluated before surgery and every 6-12 months after, undergoing various clinical and laboratory investigations, for a period of 10 years.
The majority of the recruited patients (76%) were women. Most (also 76%) had undergone gastric bypass (Roux-en-Y) surgery, and the remainder had undergone sleeve gastrectomy. Both types of surgery were equally as good at getting people into remission, as defined by the American Diabetes Association Standards of Medical Care in Diabetes, Dr. Moriconi said. As such, remission was achieved if the fasting blood glucose fell below 100 mg/dL and the hemoglobin A1c below 5.7%.
In the first year following surgery, 75% of patients had met diabetes remission criteria. This fell to 61% of patients after 5 years, and to 55% at 10 years. At each of these time points, 25% of patients had type 2 diabetes, with 14% relapsing back at 5 years and 20% at 10 years.
Dr. Moriconi pointed out some of the different characteristics of the 47 patients who had achieved diabetes remission at 10 years, compared with the 17 who had “relapsed” back to having type 2 diabetes and the 21 who had remained with type 2 diabetes.
The decrease in body mass index achieved at 10 years was no different between the three groups. However, 1 year after surgery, there had been a significantly greater drop in body in those who achieved remission, compared with those who did not (P = .04).
“Glycemic control improved with time in all the three groups after bariatric surgery, although more markedly so in the remission group,” Dr. Moriconi said.
He highlighted how none of the patients who had achieved remission had used insulin, whereas 12% of those who had relapsed and half (52%) of those who remained with type 2 diabetes had used insulin (P < .0001).
Patients who achieved remission at 1, 5, and 10 years were more likely to have had diabetes for less than 5 years than those who remained with type 2 diabetes. The average duration of diabetes was 2 years in those achieving remission versus 8 years in those who had relapsed and 13 years in those who had remained diabetic (P < .0001).
Logistic regression analysis, which adjusted for all major confounding factors such as age, sex, and type of surgery, showed that only the duration of diabetes and insulin therapy before surgery were the only predictors of long-term diabetes remission.
The study had no commercial funding. Dr. Moriconi and Dr. Vilsbøll had no conflicts of interest to disclose.
SOURCE: Moriconi D. EASD 2020, Oral presentation 120.
Type 2 diabetes patients who had never used insulin showed sustained remission 10 years after bariatric surgery in a prospective study of 85 patients.
Having diabetes for less than 5 years was also predictive of achieving long-term diabetes remission, Diego Moriconi, MD, of the University of Pisa (Italy) and presenting study investigator, reported at the virtual annual meeting of the European Association for the Study of Diabetes.
“Weight loss was associated with type 2 diabetes remission 1 year after surgery, but it had no impact on the long-term relapse of diabetes,” Dr. Moriconi said.
The findings are important, commented Tina Vilsbøll, MD, DMSc, chief consultant at the Steno Diabetes Centre Copenhagen, who chaired the session. They’re important because they would help “to set the expectations for patients before they have surgery, what to expect in respect to resolution or remission of diabetes.”
If patients were taking insulin, for instance, the take home would seem to be not to expect too much in terms of remission of their diabetes, Dr. Vilsbøll said. She added: “Usually I am not a big fan of [relying on] diabetes duration, because often we know that patients with type 2 diabetes have had diabetes for a long time before they’re actually diagnosed.” However, “it seems to be very important here.”
Dr. Moriconi reported the findings of an observational study that had started in 2006 and recruited individuals about to undergo bariatric surgery for type 2 diabetes. Participants were evaluated before surgery and every 6-12 months after, undergoing various clinical and laboratory investigations, for a period of 10 years.
The majority of the recruited patients (76%) were women. Most (also 76%) had undergone gastric bypass (Roux-en-Y) surgery, and the remainder had undergone sleeve gastrectomy. Both types of surgery were equally as good at getting people into remission, as defined by the American Diabetes Association Standards of Medical Care in Diabetes, Dr. Moriconi said. As such, remission was achieved if the fasting blood glucose fell below 100 mg/dL and the hemoglobin A1c below 5.7%.
In the first year following surgery, 75% of patients had met diabetes remission criteria. This fell to 61% of patients after 5 years, and to 55% at 10 years. At each of these time points, 25% of patients had type 2 diabetes, with 14% relapsing back at 5 years and 20% at 10 years.
Dr. Moriconi pointed out some of the different characteristics of the 47 patients who had achieved diabetes remission at 10 years, compared with the 17 who had “relapsed” back to having type 2 diabetes and the 21 who had remained with type 2 diabetes.
The decrease in body mass index achieved at 10 years was no different between the three groups. However, 1 year after surgery, there had been a significantly greater drop in body in those who achieved remission, compared with those who did not (P = .04).
“Glycemic control improved with time in all the three groups after bariatric surgery, although more markedly so in the remission group,” Dr. Moriconi said.
He highlighted how none of the patients who had achieved remission had used insulin, whereas 12% of those who had relapsed and half (52%) of those who remained with type 2 diabetes had used insulin (P < .0001).
Patients who achieved remission at 1, 5, and 10 years were more likely to have had diabetes for less than 5 years than those who remained with type 2 diabetes. The average duration of diabetes was 2 years in those achieving remission versus 8 years in those who had relapsed and 13 years in those who had remained diabetic (P < .0001).
Logistic regression analysis, which adjusted for all major confounding factors such as age, sex, and type of surgery, showed that only the duration of diabetes and insulin therapy before surgery were the only predictors of long-term diabetes remission.
The study had no commercial funding. Dr. Moriconi and Dr. Vilsbøll had no conflicts of interest to disclose.
SOURCE: Moriconi D. EASD 2020, Oral presentation 120.
Type 2 diabetes patients who had never used insulin showed sustained remission 10 years after bariatric surgery in a prospective study of 85 patients.
Having diabetes for less than 5 years was also predictive of achieving long-term diabetes remission, Diego Moriconi, MD, of the University of Pisa (Italy) and presenting study investigator, reported at the virtual annual meeting of the European Association for the Study of Diabetes.
“Weight loss was associated with type 2 diabetes remission 1 year after surgery, but it had no impact on the long-term relapse of diabetes,” Dr. Moriconi said.
The findings are important, commented Tina Vilsbøll, MD, DMSc, chief consultant at the Steno Diabetes Centre Copenhagen, who chaired the session. They’re important because they would help “to set the expectations for patients before they have surgery, what to expect in respect to resolution or remission of diabetes.”
If patients were taking insulin, for instance, the take home would seem to be not to expect too much in terms of remission of their diabetes, Dr. Vilsbøll said. She added: “Usually I am not a big fan of [relying on] diabetes duration, because often we know that patients with type 2 diabetes have had diabetes for a long time before they’re actually diagnosed.” However, “it seems to be very important here.”
Dr. Moriconi reported the findings of an observational study that had started in 2006 and recruited individuals about to undergo bariatric surgery for type 2 diabetes. Participants were evaluated before surgery and every 6-12 months after, undergoing various clinical and laboratory investigations, for a period of 10 years.
The majority of the recruited patients (76%) were women. Most (also 76%) had undergone gastric bypass (Roux-en-Y) surgery, and the remainder had undergone sleeve gastrectomy. Both types of surgery were equally as good at getting people into remission, as defined by the American Diabetes Association Standards of Medical Care in Diabetes, Dr. Moriconi said. As such, remission was achieved if the fasting blood glucose fell below 100 mg/dL and the hemoglobin A1c below 5.7%.
In the first year following surgery, 75% of patients had met diabetes remission criteria. This fell to 61% of patients after 5 years, and to 55% at 10 years. At each of these time points, 25% of patients had type 2 diabetes, with 14% relapsing back at 5 years and 20% at 10 years.
Dr. Moriconi pointed out some of the different characteristics of the 47 patients who had achieved diabetes remission at 10 years, compared with the 17 who had “relapsed” back to having type 2 diabetes and the 21 who had remained with type 2 diabetes.
The decrease in body mass index achieved at 10 years was no different between the three groups. However, 1 year after surgery, there had been a significantly greater drop in body in those who achieved remission, compared with those who did not (P = .04).
“Glycemic control improved with time in all the three groups after bariatric surgery, although more markedly so in the remission group,” Dr. Moriconi said.
He highlighted how none of the patients who had achieved remission had used insulin, whereas 12% of those who had relapsed and half (52%) of those who remained with type 2 diabetes had used insulin (P < .0001).
Patients who achieved remission at 1, 5, and 10 years were more likely to have had diabetes for less than 5 years than those who remained with type 2 diabetes. The average duration of diabetes was 2 years in those achieving remission versus 8 years in those who had relapsed and 13 years in those who had remained diabetic (P < .0001).
Logistic regression analysis, which adjusted for all major confounding factors such as age, sex, and type of surgery, showed that only the duration of diabetes and insulin therapy before surgery were the only predictors of long-term diabetes remission.
The study had no commercial funding. Dr. Moriconi and Dr. Vilsbøll had no conflicts of interest to disclose.
SOURCE: Moriconi D. EASD 2020, Oral presentation 120.
FROM EASD 2020