User login
Diagnosis and Monitoring Highlights From ECTRIMS 2020
Promising imaging developments may soon improve clinicians' ability to diagnose and monitor the progression of multiple sclerosis (MS). Dr Patricia Coyle, director of the Multiple Sclerosis Comprehensive Care Center at Stony Brook University Medical Center, reports on findings presented at the 8th Joint ACTRIMS-ECTRIMS Conference, this year known as MSVirtual 2020.
Dr Coyle emphasizes the importance of appropriate diagnosis as well as the need to improve the misdiagnosis rate. Advanced monitoring techniques that can detect MS with more accuracy are key.
She highlights exciting research in novel MRI markers, including central vein sign and paramagnetic rim sign (PRS). One study shows reliable methods for quantification of PRS, which is especially critical if this prognostic marker is to be adopted for clinical practice.
INFORMATION FROM INDUSTRY
Resources
Have You Seen the Head-to-Head Efficacy Data for ZEPOSIA® (ozanimod)?
Clinical Trial Safety Findings for an S1P Therapy
Discover How to Start Appropriate Patients on an S1P
US-ZEP-20-0997 10/20
Dr Coyle highlights other studies focused on techniques that help monitor the damage from progressing MS, including further analysis of optical coherence tomography.
Patricia K. Coyle, MD, Professor, Interim Chair, Director, Multiple Sclerosis Comprehensive Care Center, Department of Neurology, Stony Brook University Medical Center, Stony Brook, New York
Promising imaging developments may soon improve clinicians' ability to diagnose and monitor the progression of multiple sclerosis (MS). Dr Patricia Coyle, director of the Multiple Sclerosis Comprehensive Care Center at Stony Brook University Medical Center, reports on findings presented at the 8th Joint ACTRIMS-ECTRIMS Conference, this year known as MSVirtual 2020.
Dr Coyle emphasizes the importance of appropriate diagnosis as well as the need to improve the misdiagnosis rate. Advanced monitoring techniques that can detect MS with more accuracy are key.
She highlights exciting research in novel MRI markers, including central vein sign and paramagnetic rim sign (PRS). One study shows reliable methods for quantification of PRS, which is especially critical if this prognostic marker is to be adopted for clinical practice.
INFORMATION FROM INDUSTRY
Resources
Have You Seen the Head-to-Head Efficacy Data for ZEPOSIA® (ozanimod)?
Clinical Trial Safety Findings for an S1P Therapy
Discover How to Start Appropriate Patients on an S1P
US-ZEP-20-0997 10/20
Dr Coyle highlights other studies focused on techniques that help monitor the damage from progressing MS, including further analysis of optical coherence tomography.
Patricia K. Coyle, MD, Professor, Interim Chair, Director, Multiple Sclerosis Comprehensive Care Center, Department of Neurology, Stony Brook University Medical Center, Stony Brook, New York
Promising imaging developments may soon improve clinicians' ability to diagnose and monitor the progression of multiple sclerosis (MS). Dr Patricia Coyle, director of the Multiple Sclerosis Comprehensive Care Center at Stony Brook University Medical Center, reports on findings presented at the 8th Joint ACTRIMS-ECTRIMS Conference, this year known as MSVirtual 2020.
Dr Coyle emphasizes the importance of appropriate diagnosis as well as the need to improve the misdiagnosis rate. Advanced monitoring techniques that can detect MS with more accuracy are key.
She highlights exciting research in novel MRI markers, including central vein sign and paramagnetic rim sign (PRS). One study shows reliable methods for quantification of PRS, which is especially critical if this prognostic marker is to be adopted for clinical practice.
INFORMATION FROM INDUSTRY
Resources
Have You Seen the Head-to-Head Efficacy Data for ZEPOSIA® (ozanimod)?
Clinical Trial Safety Findings for an S1P Therapy
Discover How to Start Appropriate Patients on an S1P
US-ZEP-20-0997 10/20
Dr Coyle highlights other studies focused on techniques that help monitor the damage from progressing MS, including further analysis of optical coherence tomography.
Patricia K. Coyle, MD, Professor, Interim Chair, Director, Multiple Sclerosis Comprehensive Care Center, Department of Neurology, Stony Brook University Medical Center, Stony Brook, New York

CRC risk: Raised by meat/alcohol, lowered by aspirin/NSAIDs
A new meta-analysis has largely confirmed what is already known about the lifestyle factors that increase and those that decrease the risk of developing colorectal cancer.
The use of aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs) is associated with a decreased risk for colorectal cancer, the new article concludes. But it also adds a number of other factors that are associated with a decreased risk for the disease, including taking magnesium and folate supplements and eating dairy products, fiber, soy, and fruits and vegetables.
On the other hand, consumption of meat and alcohol was associated with an increased risk for colorectal cancer in almost all of the analyses included in this article.
The study was published online September 28 in Gut.
However, the authors pointed out that it is important to keep in mind that in most cases, the level of evidence is low or very low, primarily because of the heterogeneity of the various published studies, as well as the type of study.
“Furthermore, in most cases, we were unable to identify an optimal dose and duration of exposure/intake for any of the products, even in the case of low-dose aspirin and other compounds that have been extensively assessed,” they wrote.
The findings of this new meta-analysis echo previous findings on this issue.
A number of studies, for example, have found varying associations between the consumption of red meat and cancer. The American Institute for Cancer Research and the World Cancer Research Fund have published several reports during the past 10 years on the effect of diet, nutrition, and/or physical activity on risk for several cancer types. Their most recent study, published in 2017, concluded that eating red meat and processed meat may increase the risk for colorectal cancer, as may drinking two or more alcoholic beverages per day.
Another large meta-analysis published earlier this year found that regular use of aspirin reduced the risk for cancers of the digestive tract by 22%-38%, compared with nonuse.
Umbrella review
In the latest article in Gut, researchers led by Marc Bardou, MD, PhD, Centre Hospitalier Universitaire de Dijon (France), conducted an umbrella review of systematic reviews and meta-analyses of interventions that assessed chemopreventive products for colorectal cancer in an average-risk population.
A total of 80 meta-analyses of interventional and observational studies were included. The studies investigated a wide range of chemopreventive agents in an average-risk population and the risk for colorectal cancer. Agents included medications (aspirin, NSAIDs, statins), vitamins or supplements (magnesium; calcium; folic acid; vitamin A, B, C, E, and D; beta-carotene; and selenium), and dietary items (coffee, tea, fish, dairy products, fiber, fruits, vegetables, meat, and alcohol).
The studies included randomized controlled trials and observational studies. Most of the meta-analyses found a protective effect for aspirin, which lowered the risk by between 14% and 29% even at doses as low as 75 mg/day, with a dose-response effect of up to 325 mg/day. The certainty of evidence was moderate.
NSAID use was also associated with a protective effect, with a significant 26%-43% decrease in the incidence in colorectal cancer. The optimal duration for the observed protective effect remains unclear. Two meta-analyses suggested that NSAIDs may need to be taken for at least 5 years, although one article suggested a protective effect after the first year. The certainty of evidence was low.
Use of magnesium was found to be protective, with a relative risk (RR) of 0.78-0.87. High intake of folic acid was associated with a significant decrease in risk (RR, 0.85-0.88). The certainty of evidence was low and very low, respectively.
Consumption of dairy products was associated with 13%-19% lower risk for the disease. However, the authors note that, because of the small number of available meta-analyses, the multiplicity of outcomes, and the variety of dairy products, it was not possible to reach any firm conclusions about the amount needed or the duration necessary for a protective effect.
Another dietary item, fiber, was associated with a 22%-43% lower risk. Consumption of fruits and vegetables was associated with up to a 52% lower risk, with an added benefit for every additional 100 g/day increase in intake. Soy intake was also associated with a small but significant decrease in risk (8%-15%).
For many of the other items reviewed, evidence was either weak or no beneficial effect was seen.
Increased risk
Consumption of both meat and alcohol was found to increase the risk for colorectal cancer.
Most of the meta-analyses of observational studies have reported a significant increase in risk (RR, 1.12-1.21) with meat consumption (particularly red and processed) and the incidence of colorectal cancer. Studies of the dose effect reported a 10%-30% increased risk for each increment of 100 g/day of total or red meat.
Alcohol consumption was also associated with a significantly increased risk. The higher the intake, the greater the risk. The risk was evident even at the lowest consumption doses that were investigated (1-2 drinks per day).
Balanced for the individual patient
Commenting on the article, Thomas J. George Jr, MD, professor of medicine and director, GI Oncology Program, the University of Florida Health Cancer Center, Gainesville, feels that the take-home message for clinicians and patients alike is that these data help to reinforce behaviors that have already been recommended.
“We know that excessive alcohol and red meat consumption is not healthy, so seeing that there may be a negative effect on colorectal cancer is just more evidence that we should be avoiding that and recommend avoiding that,” said Dr. George. “So yes, I recommend minimizing those, and likewise, a diet that is inclusive of fruits, vegetables, fiber, soy – perhaps as an alternative to meat consumption – is healthier than a diet devoid of these, so again, more reassuring data to support doing what we should already be doing.”
However, he pointed out that there are risks associated with medications such as NSAIDs and aspirin, including bleeding, gastric ulcer formation, and kidney damage. “The risks are low but very real,” Dr. George said. “So I think those recommendations need to be considered on a very individual level, balancing any other risk factors that the patient may have for both colorectal cancer, as well as risks from the medications.”
The study had no outside funding. The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Share AGA GI Patient Center education on colorectal cancer to help your patients better understand their risks and treatment options at http://ow.ly/mZ9q30rcz1U.
A new meta-analysis has largely confirmed what is already known about the lifestyle factors that increase and those that decrease the risk of developing colorectal cancer.
The use of aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs) is associated with a decreased risk for colorectal cancer, the new article concludes. But it also adds a number of other factors that are associated with a decreased risk for the disease, including taking magnesium and folate supplements and eating dairy products, fiber, soy, and fruits and vegetables.
On the other hand, consumption of meat and alcohol was associated with an increased risk for colorectal cancer in almost all of the analyses included in this article.
The study was published online September 28 in Gut.
However, the authors pointed out that it is important to keep in mind that in most cases, the level of evidence is low or very low, primarily because of the heterogeneity of the various published studies, as well as the type of study.
“Furthermore, in most cases, we were unable to identify an optimal dose and duration of exposure/intake for any of the products, even in the case of low-dose aspirin and other compounds that have been extensively assessed,” they wrote.
The findings of this new meta-analysis echo previous findings on this issue.
A number of studies, for example, have found varying associations between the consumption of red meat and cancer. The American Institute for Cancer Research and the World Cancer Research Fund have published several reports during the past 10 years on the effect of diet, nutrition, and/or physical activity on risk for several cancer types. Their most recent study, published in 2017, concluded that eating red meat and processed meat may increase the risk for colorectal cancer, as may drinking two or more alcoholic beverages per day.
Another large meta-analysis published earlier this year found that regular use of aspirin reduced the risk for cancers of the digestive tract by 22%-38%, compared with nonuse.
Umbrella review
In the latest article in Gut, researchers led by Marc Bardou, MD, PhD, Centre Hospitalier Universitaire de Dijon (France), conducted an umbrella review of systematic reviews and meta-analyses of interventions that assessed chemopreventive products for colorectal cancer in an average-risk population.
A total of 80 meta-analyses of interventional and observational studies were included. The studies investigated a wide range of chemopreventive agents in an average-risk population and the risk for colorectal cancer. Agents included medications (aspirin, NSAIDs, statins), vitamins or supplements (magnesium; calcium; folic acid; vitamin A, B, C, E, and D; beta-carotene; and selenium), and dietary items (coffee, tea, fish, dairy products, fiber, fruits, vegetables, meat, and alcohol).
The studies included randomized controlled trials and observational studies. Most of the meta-analyses found a protective effect for aspirin, which lowered the risk by between 14% and 29% even at doses as low as 75 mg/day, with a dose-response effect of up to 325 mg/day. The certainty of evidence was moderate.
NSAID use was also associated with a protective effect, with a significant 26%-43% decrease in the incidence in colorectal cancer. The optimal duration for the observed protective effect remains unclear. Two meta-analyses suggested that NSAIDs may need to be taken for at least 5 years, although one article suggested a protective effect after the first year. The certainty of evidence was low.
Use of magnesium was found to be protective, with a relative risk (RR) of 0.78-0.87. High intake of folic acid was associated with a significant decrease in risk (RR, 0.85-0.88). The certainty of evidence was low and very low, respectively.
Consumption of dairy products was associated with 13%-19% lower risk for the disease. However, the authors note that, because of the small number of available meta-analyses, the multiplicity of outcomes, and the variety of dairy products, it was not possible to reach any firm conclusions about the amount needed or the duration necessary for a protective effect.
Another dietary item, fiber, was associated with a 22%-43% lower risk. Consumption of fruits and vegetables was associated with up to a 52% lower risk, with an added benefit for every additional 100 g/day increase in intake. Soy intake was also associated with a small but significant decrease in risk (8%-15%).
For many of the other items reviewed, evidence was either weak or no beneficial effect was seen.
Increased risk
Consumption of both meat and alcohol was found to increase the risk for colorectal cancer.
Most of the meta-analyses of observational studies have reported a significant increase in risk (RR, 1.12-1.21) with meat consumption (particularly red and processed) and the incidence of colorectal cancer. Studies of the dose effect reported a 10%-30% increased risk for each increment of 100 g/day of total or red meat.
Alcohol consumption was also associated with a significantly increased risk. The higher the intake, the greater the risk. The risk was evident even at the lowest consumption doses that were investigated (1-2 drinks per day).
Balanced for the individual patient
Commenting on the article, Thomas J. George Jr, MD, professor of medicine and director, GI Oncology Program, the University of Florida Health Cancer Center, Gainesville, feels that the take-home message for clinicians and patients alike is that these data help to reinforce behaviors that have already been recommended.
“We know that excessive alcohol and red meat consumption is not healthy, so seeing that there may be a negative effect on colorectal cancer is just more evidence that we should be avoiding that and recommend avoiding that,” said Dr. George. “So yes, I recommend minimizing those, and likewise, a diet that is inclusive of fruits, vegetables, fiber, soy – perhaps as an alternative to meat consumption – is healthier than a diet devoid of these, so again, more reassuring data to support doing what we should already be doing.”
However, he pointed out that there are risks associated with medications such as NSAIDs and aspirin, including bleeding, gastric ulcer formation, and kidney damage. “The risks are low but very real,” Dr. George said. “So I think those recommendations need to be considered on a very individual level, balancing any other risk factors that the patient may have for both colorectal cancer, as well as risks from the medications.”
The study had no outside funding. The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Share AGA GI Patient Center education on colorectal cancer to help your patients better understand their risks and treatment options at http://ow.ly/mZ9q30rcz1U.
A new meta-analysis has largely confirmed what is already known about the lifestyle factors that increase and those that decrease the risk of developing colorectal cancer.
The use of aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs) is associated with a decreased risk for colorectal cancer, the new article concludes. But it also adds a number of other factors that are associated with a decreased risk for the disease, including taking magnesium and folate supplements and eating dairy products, fiber, soy, and fruits and vegetables.
On the other hand, consumption of meat and alcohol was associated with an increased risk for colorectal cancer in almost all of the analyses included in this article.
The study was published online September 28 in Gut.
However, the authors pointed out that it is important to keep in mind that in most cases, the level of evidence is low or very low, primarily because of the heterogeneity of the various published studies, as well as the type of study.
“Furthermore, in most cases, we were unable to identify an optimal dose and duration of exposure/intake for any of the products, even in the case of low-dose aspirin and other compounds that have been extensively assessed,” they wrote.
The findings of this new meta-analysis echo previous findings on this issue.
A number of studies, for example, have found varying associations between the consumption of red meat and cancer. The American Institute for Cancer Research and the World Cancer Research Fund have published several reports during the past 10 years on the effect of diet, nutrition, and/or physical activity on risk for several cancer types. Their most recent study, published in 2017, concluded that eating red meat and processed meat may increase the risk for colorectal cancer, as may drinking two or more alcoholic beverages per day.
Another large meta-analysis published earlier this year found that regular use of aspirin reduced the risk for cancers of the digestive tract by 22%-38%, compared with nonuse.
Umbrella review
In the latest article in Gut, researchers led by Marc Bardou, MD, PhD, Centre Hospitalier Universitaire de Dijon (France), conducted an umbrella review of systematic reviews and meta-analyses of interventions that assessed chemopreventive products for colorectal cancer in an average-risk population.
A total of 80 meta-analyses of interventional and observational studies were included. The studies investigated a wide range of chemopreventive agents in an average-risk population and the risk for colorectal cancer. Agents included medications (aspirin, NSAIDs, statins), vitamins or supplements (magnesium; calcium; folic acid; vitamin A, B, C, E, and D; beta-carotene; and selenium), and dietary items (coffee, tea, fish, dairy products, fiber, fruits, vegetables, meat, and alcohol).
The studies included randomized controlled trials and observational studies. Most of the meta-analyses found a protective effect for aspirin, which lowered the risk by between 14% and 29% even at doses as low as 75 mg/day, with a dose-response effect of up to 325 mg/day. The certainty of evidence was moderate.
NSAID use was also associated with a protective effect, with a significant 26%-43% decrease in the incidence in colorectal cancer. The optimal duration for the observed protective effect remains unclear. Two meta-analyses suggested that NSAIDs may need to be taken for at least 5 years, although one article suggested a protective effect after the first year. The certainty of evidence was low.
Use of magnesium was found to be protective, with a relative risk (RR) of 0.78-0.87. High intake of folic acid was associated with a significant decrease in risk (RR, 0.85-0.88). The certainty of evidence was low and very low, respectively.
Consumption of dairy products was associated with 13%-19% lower risk for the disease. However, the authors note that, because of the small number of available meta-analyses, the multiplicity of outcomes, and the variety of dairy products, it was not possible to reach any firm conclusions about the amount needed or the duration necessary for a protective effect.
Another dietary item, fiber, was associated with a 22%-43% lower risk. Consumption of fruits and vegetables was associated with up to a 52% lower risk, with an added benefit for every additional 100 g/day increase in intake. Soy intake was also associated with a small but significant decrease in risk (8%-15%).
For many of the other items reviewed, evidence was either weak or no beneficial effect was seen.
Increased risk
Consumption of both meat and alcohol was found to increase the risk for colorectal cancer.
Most of the meta-analyses of observational studies have reported a significant increase in risk (RR, 1.12-1.21) with meat consumption (particularly red and processed) and the incidence of colorectal cancer. Studies of the dose effect reported a 10%-30% increased risk for each increment of 100 g/day of total or red meat.
Alcohol consumption was also associated with a significantly increased risk. The higher the intake, the greater the risk. The risk was evident even at the lowest consumption doses that were investigated (1-2 drinks per day).
Balanced for the individual patient
Commenting on the article, Thomas J. George Jr, MD, professor of medicine and director, GI Oncology Program, the University of Florida Health Cancer Center, Gainesville, feels that the take-home message for clinicians and patients alike is that these data help to reinforce behaviors that have already been recommended.
“We know that excessive alcohol and red meat consumption is not healthy, so seeing that there may be a negative effect on colorectal cancer is just more evidence that we should be avoiding that and recommend avoiding that,” said Dr. George. “So yes, I recommend minimizing those, and likewise, a diet that is inclusive of fruits, vegetables, fiber, soy – perhaps as an alternative to meat consumption – is healthier than a diet devoid of these, so again, more reassuring data to support doing what we should already be doing.”
However, he pointed out that there are risks associated with medications such as NSAIDs and aspirin, including bleeding, gastric ulcer formation, and kidney damage. “The risks are low but very real,” Dr. George said. “So I think those recommendations need to be considered on a very individual level, balancing any other risk factors that the patient may have for both colorectal cancer, as well as risks from the medications.”
The study had no outside funding. The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Share AGA GI Patient Center education on colorectal cancer to help your patients better understand their risks and treatment options at http://ow.ly/mZ9q30rcz1U.
Breast cancer screening complexities
Breast cancer in women remains one of the most common types of cancer in the United States, affecting about one in eight women1 over the course of their lifetime. Despite its pervasiveness, the 5-year survival rate for women with breast cancer remains high, estimated at around 90%2 based on data from 2010-2016, in large part because of early detection and treatment through screening. However, many organizations disagree on when to start and how often to screen women at average risk.

Important to discussions about breast cancer screening is the trend that many women delay childbirth until their 30s and 40s. In 2018 the birth rate increased for women ages 35-44, and the mean age of first birth increased from the prior year across all racial and ethnic groups.3 Therefore, ob.gyns. may need to consider that their patients not only may have increased risk of developing breast cancer based on age alone – women aged 35-44 have four times greater risk of disease than women aged 20-342 – but that the pregnancy itself may further exacerbate risk in older women. A 2019 pooled analysis found that women who were older at first birth had a greater chance of developing breast cancer compared with women with no children.4
In addition, ob.gyns. should consider that their patients may have received a breast cancer diagnosis prior to initiation or completion of their family plans or that their patients are cancer survivors – in 2013-2017, breast cancer was the most common form of cancer in adolescents and young adults.5 Thus, practitioners should be prepared to discuss not only options for fertility preservation but the evidence regarding cancer recurrence after pregnancy.
We have invited Dr. Katherine Tkaczuk, professor of medicine at the University of Maryland School of Medicine* and director of the breast evaluation and treatment program at the Marlene and Stewart Greenebaum Comprehensive Cancer Center, to discuss the vital role of screening in the shared decision-making process of breast cancer prevention.
Dr. Reece, who specializes in maternal-fetal medicine, is executive vice president for medical affairs at the University of Maryland, Baltimore,* as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. He is the medical editor of this column. He said he had no relevant financial disclosures. Contact him at [email protected].
Correction, 1/8/21: *An earlier version of this article misstated the university affiliations for Dr. Tkaczuk and Dr. Reece.
References
1. U.S. Breast Cancer Statistics. breastcancer.org.
2. “Cancer Stat Facts: Female Breast Cancer,” Surveillance, Epidemiology, and End Results Program. National Cancer Institute.
3. Martin JA et al. “Births: Final Data for 2018.” National Vital Statistics Reports. 2019 Nov 27;68(13):1-46.
4. Nichols HB et al. Ann Intern Med. 2019 Jan;170(1):22-30.
5. “Cancer Stat Facts: Cancer Among Adolescents and Young Adults (AYAs) (Ages 15-39),” Surveillance, Epidemiology, and End Results Program. National Cancer Institute.
Breast cancer in women remains one of the most common types of cancer in the United States, affecting about one in eight women1 over the course of their lifetime. Despite its pervasiveness, the 5-year survival rate for women with breast cancer remains high, estimated at around 90%2 based on data from 2010-2016, in large part because of early detection and treatment through screening. However, many organizations disagree on when to start and how often to screen women at average risk.
Important to discussions about breast cancer screening is the trend that many women delay childbirth until their 30s and 40s. In 2018 the birth rate increased for women ages 35-44, and the mean age of first birth increased from the prior year across all racial and ethnic groups.3 Therefore, ob.gyns. may need to consider that their patients not only may have increased risk of developing breast cancer based on age alone – women aged 35-44 have four times greater risk of disease than women aged 20-342 – but that the pregnancy itself may further exacerbate risk in older women. A 2019 pooled analysis found that women who were older at first birth had a greater chance of developing breast cancer compared with women with no children.4
In addition, ob.gyns. should consider that their patients may have received a breast cancer diagnosis prior to initiation or completion of their family plans or that their patients are cancer survivors – in 2013-2017, breast cancer was the most common form of cancer in adolescents and young adults.5 Thus, practitioners should be prepared to discuss not only options for fertility preservation but the evidence regarding cancer recurrence after pregnancy.
We have invited Dr. Katherine Tkaczuk, professor of medicine at the University of Maryland School of Medicine* and director of the breast evaluation and treatment program at the Marlene and Stewart Greenebaum Comprehensive Cancer Center, to discuss the vital role of screening in the shared decision-making process of breast cancer prevention.
Dr. Reece, who specializes in maternal-fetal medicine, is executive vice president for medical affairs at the University of Maryland, Baltimore,* as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. He is the medical editor of this column. He said he had no relevant financial disclosures. Contact him at [email protected].
Correction, 1/8/21: *An earlier version of this article misstated the university affiliations for Dr. Tkaczuk and Dr. Reece.
References
1. U.S. Breast Cancer Statistics. breastcancer.org.
2. “Cancer Stat Facts: Female Breast Cancer,” Surveillance, Epidemiology, and End Results Program. National Cancer Institute.
3. Martin JA et al. “Births: Final Data for 2018.” National Vital Statistics Reports. 2019 Nov 27;68(13):1-46.
4. Nichols HB et al. Ann Intern Med. 2019 Jan;170(1):22-30.
5. “Cancer Stat Facts: Cancer Among Adolescents and Young Adults (AYAs) (Ages 15-39),” Surveillance, Epidemiology, and End Results Program. National Cancer Institute.
Breast cancer in women remains one of the most common types of cancer in the United States, affecting about one in eight women1 over the course of their lifetime. Despite its pervasiveness, the 5-year survival rate for women with breast cancer remains high, estimated at around 90%2 based on data from 2010-2016, in large part because of early detection and treatment through screening. However, many organizations disagree on when to start and how often to screen women at average risk.
Important to discussions about breast cancer screening is the trend that many women delay childbirth until their 30s and 40s. In 2018 the birth rate increased for women ages 35-44, and the mean age of first birth increased from the prior year across all racial and ethnic groups.3 Therefore, ob.gyns. may need to consider that their patients not only may have increased risk of developing breast cancer based on age alone – women aged 35-44 have four times greater risk of disease than women aged 20-342 – but that the pregnancy itself may further exacerbate risk in older women. A 2019 pooled analysis found that women who were older at first birth had a greater chance of developing breast cancer compared with women with no children.4
In addition, ob.gyns. should consider that their patients may have received a breast cancer diagnosis prior to initiation or completion of their family plans or that their patients are cancer survivors – in 2013-2017, breast cancer was the most common form of cancer in adolescents and young adults.5 Thus, practitioners should be prepared to discuss not only options for fertility preservation but the evidence regarding cancer recurrence after pregnancy.
We have invited Dr. Katherine Tkaczuk, professor of medicine at the University of Maryland School of Medicine* and director of the breast evaluation and treatment program at the Marlene and Stewart Greenebaum Comprehensive Cancer Center, to discuss the vital role of screening in the shared decision-making process of breast cancer prevention.
Dr. Reece, who specializes in maternal-fetal medicine, is executive vice president for medical affairs at the University of Maryland, Baltimore,* as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. He is the medical editor of this column. He said he had no relevant financial disclosures. Contact him at [email protected].
Correction, 1/8/21: *An earlier version of this article misstated the university affiliations for Dr. Tkaczuk and Dr. Reece.
References
1. U.S. Breast Cancer Statistics. breastcancer.org.
2. “Cancer Stat Facts: Female Breast Cancer,” Surveillance, Epidemiology, and End Results Program. National Cancer Institute.
3. Martin JA et al. “Births: Final Data for 2018.” National Vital Statistics Reports. 2019 Nov 27;68(13):1-46.
4. Nichols HB et al. Ann Intern Med. 2019 Jan;170(1):22-30.
5. “Cancer Stat Facts: Cancer Among Adolescents and Young Adults (AYAs) (Ages 15-39),” Surveillance, Epidemiology, and End Results Program. National Cancer Institute.
An oncologist’s view on screening mammography
Screening mammography has contributed to the lowering of mortality from breast cancer by facilitating earlier diagnosis and a lower stage at diagnosis. With more effective treatment options for women who are diagnosed with lower-stage breast cancer, the current 5-year survival rate has risen to 90% – significantly higher than the 5-year survival rate of 75% in 1975.1

Women who are at much higher risk for developing breast cancer – mainly because of family history, certain genetic mutations, or a history of radiation therapy to the chest – will benefit the most from earlier and more frequent screening mammography as well as enhanced screening with non-x-ray methods of breast imaging. It is important that ob.gyns. help to identify these women.
However, the majority of women who are screened with mammography are at “average risk,” with a lifetime risk for developing breast cancer of 12.9%, based on 2015-2017 data from the National Cancer Institute’s (NCI) Surveillance, Epidemiology, and End Results Program (SEER).1 The median age at diagnosis of breast cancer in the U.S. is 62 years,1 and advancing age is the most important risk factor for these women.
A 20% relative risk reduction in breast cancer mortality with screening mammography has been demonstrated both in systematic reviews of randomized and observational studies2 and in a meta-analysis of 11 randomized trials comparing screening and no screening.3 Even though the majority of randomized trials were done in the age of film mammography, experts believe that we still see at least a 20% reduction today.
Among average-risk women, those aged 50-74 with a life expectancy of at least 10 years will benefit the most from regular screening. According to the 2016 screening guideline of the United States Preventive Services Task Force (USPSTF), relative risk reductions in breast cancer mortality from mammography screening, by age group, are 0.88 (confidence interval, 0.73-1.003) for ages 39-49; 0.86 (CI, 0.68-0.97) for ages 50-59; 0.67 (CI, 0.55-0.91) for ages 60-69; and 0.80 (CI, 0.51 to 1.28) for ages 70-74.2
For women aged 40-49 years, most of the guidelines in the United States recommend individualized screening every 1 or 2 years – screening that is guided by shared decision-making that takes into account each woman’s values regarding relative harms and benefits. This is because their risk of developing breast cancer is relatively low while the risk of false-positive results can be higher.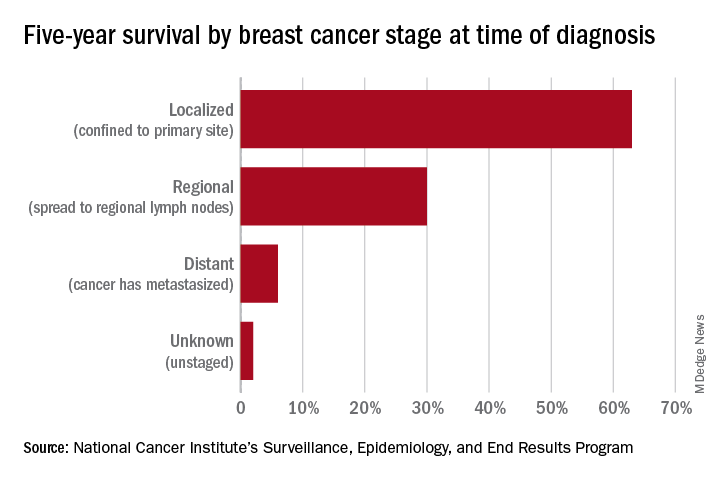
A few exceptions include guidelines by the National Comprehensive Cancer Network (NCCN) and the American College of Radiology, which recommend annual screening mammography starting at age 40 years for all average-risk women. In our program, we adhere to these latter recommendations and advise annual digital 3-D mammograms starting at age 40 and continuing until age 74, or longer if the woman is otherwise healthy with a life expectancy greater than 10 years.
Screening and overdiagnosis
Overdiagnosis – the diagnosis of cancers that may not actually cause mortality or may not even have become apparent without screening – is a concern for all women undergoing routine screening for breast cancer. There is significant uncertainty about its frequency, however.
Research cited by the USPSTF suggests that as many as one in five women diagnosed with breast cancer over approximately 10 years will be overdiagnosed. Other modeling studies have estimated one in eight overdiagnoses, for women aged 50-75 years specifically. By the more conservative estimate, according to the USPSTF, one breast cancer death will be prevented for every 2-3 cases of unnecessary treatment.2
Ductal carcinoma in situ is confined to the mammary ductal-lobular system and lacks the classic characteristics of cancer. Technically, it should not metastasize. But we do not know with certainty which cases of DCIS will or will not progress to invasive cancer. Therefore these women often are offered surgical approaches mirroring invasive cancer treatments (lumpectomy with radiation or even mastectomy in some cases), while for some, such treatments may be unnecessary.
Screening younger women (40-49)
Shared decision-making is always important for breast cancer screening, but in our program we routinely recommend annual screening in average-risk women starting at age 40 for several reasons. For one, younger women may present with more aggressive types of breast cancer such as triple-negative breast cancer. These are much less common than hormone-receptor positive breast cancers – they represent 15%-20% of all breast cancers – but they are faster growing and may develop in the interim if women are screened less often (at 2-year intervals).
In addition, finding an invasive breast cancer early is almost always beneficial. Earlier diagnosis (lower stage at diagnosis) is associated with increased breast cancer-specific and overall survival, as well as less-aggressive treatment approaches.
As a medical oncologist who treats women with breast cancer, I see these benefits firsthand. With earlier diagnosis, we are more likely to offer less aggressive surgical approaches such as partial mastectomy (lumpectomy) and sentinel lymph node biopsy as opposed to total mastectomy with axillary lymph node dissection, the latter of which is more likely to be associated with lymphedema and which can lead to postmastectomy chest wall pain syndromes.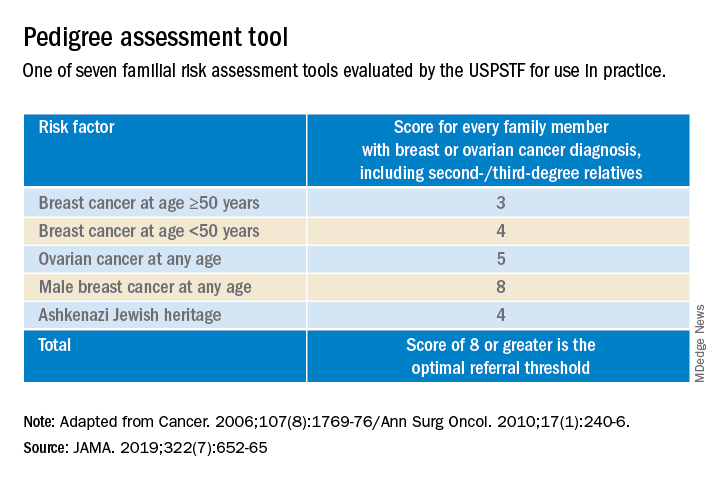
We also are able to use less aggressive radiation therapy approaches such as partial breast radiation, and less aggressive breast cancer–specific systemic treatments for women with a lower stage of breast cancer at diagnosis. In some cases, adjuvant or neoadjuvant chemotherapy may not be needed – and when it is necessary, shorter courses of chemotherapy or targeted chemotherapeutic regimens may be offered. This means lower systemic toxicities, both early and late, such as less cytopenias, risk of infections, mucositis, hair loss, cardiotoxicity, secondary malignancies/leukemia, and peripheral sensory neuropathy.
It is important to note that Black women in the United States have the highest death rate from breast cancer – 27.3 per 100,000 per year, versus 19.6 per 100,000 per year for White women1 – and that younger Black women appear to have a higher risk of developing triple-negative breast cancer, a more aggressive type of breast cancer. The higher breast cancer mortality in Black women is likely multifactorial and may be attributed partly to disparities in health care and partly to tumor biology. The case for annual screening in this population thus seems especially strong.
Screening modalities
Digital 3-D mammography, or digital breast tomosynthesis (DBT), is widely considered to be a more sensitive screening tool than conventional digital mammography alone. The NCCN recommends DBT for women with an average risk of developing breast cancer starting at age 40,4,5 and the USPSTF, while offering no recommendation on DBT as a primary screening method (“insufficient evidence”), says that DBT appears to increase cancer detection rates.2 So, I do routinely recommend it.
DBT may be especially beneficial for women with dense breast tissue (determined mammographically), who are most often premenopausal women – particularly non-Hispanic White women. Dense breast tissue itself can contribute to an increased risk of breast cancer – an approximately 20% higher relative risk in an average-risk woman with heterogeneously dense breast tissue, and an approximately 100% higher relative risk in a woman with extremely dense breasts6 – but unfortunately it affects the sensitivity and specificity of screening mammography.
I do not recommend routine supplemental screening with other methods (breast ultrasonography or MRI) for women at average risk of breast cancer who have dense breasts. MRI with gadolinium contrast is recommended as an adjunct to mammography for women who have a lifetime risk of developing breast cancer of more than 20%-25% (e.g., women with known BRCA1/2 mutations or radiation to breast tissue), and can be done annually at the same time as the screening mammogram is done. Some clinicians and patients prefer to alternate these two tests – one every 6 months.
Screening breast MRI is more sensitive but less specific than mammography; combining the two screening modalities leads to overall increased sensitivity and specificity in high-risk populations.
Risk assessment
Identifying higher-risk women who need to be sent to a genetic counselor is critically important. The USPSTF recommends that women who have family members with breast, ovarian, tubal or peritoneal cancer, or who have an ancestry associated with BRCA1/2 gene mutations, be assessed with a brief familial risk assessment tool such as the Pedigree Assessment Tool. This and other validated tools have been evaluated by the USPSTF and can be used to guide referrals to genetic counseling for more definitive risk assessment.7
These tools are different from general breast cancer risk assessment models, such as the NCI’s Breast Cancer Risk Assessment Tool,8 which are designed to calculate the 5-year and lifetime risk of developing invasive breast cancer for an average-risk woman but not to identify BRCA-related cancer risk. (The NCI’s tool is based on the Gail model, which has been widely used over the years.)
The general risk assessment models use a women’s personal medical and reproductive history as well as the history of breast cancer among her first-degree relatives to estimate her risk.
Dr. Tkaczuk reported that she has no disclosures.
References
1. “Cancer Stat Facts: Female Breast Cancer.” Surveillance, Epidemiology, and End Results Program. National Cancer Institute.
2. Siu AL et al. Ann Intern Med. 2016 Feb 16. doi: 10.7326/M15-2886.
3. Independent UK Panel on Breast Cancer Screening. Lancet. 2012 Nov 17;380(9855):1778-86.
4. NCCN guidelines for Detection, Prevention, & Risk Reduction: Breast Cancer Screening and Diagnosis. National Comprehensive Cancer Network.
5. NCCN guidelines for Detection, Prevention, & Risk Reduction: Breast Cancer Risk Reduction. National Comprehensive Cancer Network.
6. Ziv E et al. Cancer Epidemiol Biomarkers Prev. 2004;13(12):2090-5.
7. USPSTF. JAMA. 2019;322(7):652-65.
8. The Breast Cancer Risk Assessment Tool. National Cancer Institute.
Screening mammography has contributed to the lowering of mortality from breast cancer by facilitating earlier diagnosis and a lower stage at diagnosis. With more effective treatment options for women who are diagnosed with lower-stage breast cancer, the current 5-year survival rate has risen to 90% – significantly higher than the 5-year survival rate of 75% in 1975.1
Women who are at much higher risk for developing breast cancer – mainly because of family history, certain genetic mutations, or a history of radiation therapy to the chest – will benefit the most from earlier and more frequent screening mammography as well as enhanced screening with non-x-ray methods of breast imaging. It is important that ob.gyns. help to identify these women.
However, the majority of women who are screened with mammography are at “average risk,” with a lifetime risk for developing breast cancer of 12.9%, based on 2015-2017 data from the National Cancer Institute’s (NCI) Surveillance, Epidemiology, and End Results Program (SEER).1 The median age at diagnosis of breast cancer in the U.S. is 62 years,1 and advancing age is the most important risk factor for these women.
A 20% relative risk reduction in breast cancer mortality with screening mammography has been demonstrated both in systematic reviews of randomized and observational studies2 and in a meta-analysis of 11 randomized trials comparing screening and no screening.3 Even though the majority of randomized trials were done in the age of film mammography, experts believe that we still see at least a 20% reduction today.
Among average-risk women, those aged 50-74 with a life expectancy of at least 10 years will benefit the most from regular screening. According to the 2016 screening guideline of the United States Preventive Services Task Force (USPSTF), relative risk reductions in breast cancer mortality from mammography screening, by age group, are 0.88 (confidence interval, 0.73-1.003) for ages 39-49; 0.86 (CI, 0.68-0.97) for ages 50-59; 0.67 (CI, 0.55-0.91) for ages 60-69; and 0.80 (CI, 0.51 to 1.28) for ages 70-74.2
For women aged 40-49 years, most of the guidelines in the United States recommend individualized screening every 1 or 2 years – screening that is guided by shared decision-making that takes into account each woman’s values regarding relative harms and benefits. This is because their risk of developing breast cancer is relatively low while the risk of false-positive results can be higher.
A few exceptions include guidelines by the National Comprehensive Cancer Network (NCCN) and the American College of Radiology, which recommend annual screening mammography starting at age 40 years for all average-risk women. In our program, we adhere to these latter recommendations and advise annual digital 3-D mammograms starting at age 40 and continuing until age 74, or longer if the woman is otherwise healthy with a life expectancy greater than 10 years.
Screening and overdiagnosis
Overdiagnosis – the diagnosis of cancers that may not actually cause mortality or may not even have become apparent without screening – is a concern for all women undergoing routine screening for breast cancer. There is significant uncertainty about its frequency, however.
Research cited by the USPSTF suggests that as many as one in five women diagnosed with breast cancer over approximately 10 years will be overdiagnosed. Other modeling studies have estimated one in eight overdiagnoses, for women aged 50-75 years specifically. By the more conservative estimate, according to the USPSTF, one breast cancer death will be prevented for every 2-3 cases of unnecessary treatment.2
Ductal carcinoma in situ is confined to the mammary ductal-lobular system and lacks the classic characteristics of cancer. Technically, it should not metastasize. But we do not know with certainty which cases of DCIS will or will not progress to invasive cancer. Therefore these women often are offered surgical approaches mirroring invasive cancer treatments (lumpectomy with radiation or even mastectomy in some cases), while for some, such treatments may be unnecessary.
Screening younger women (40-49)
Shared decision-making is always important for breast cancer screening, but in our program we routinely recommend annual screening in average-risk women starting at age 40 for several reasons. For one, younger women may present with more aggressive types of breast cancer such as triple-negative breast cancer. These are much less common than hormone-receptor positive breast cancers – they represent 15%-20% of all breast cancers – but they are faster growing and may develop in the interim if women are screened less often (at 2-year intervals).
In addition, finding an invasive breast cancer early is almost always beneficial. Earlier diagnosis (lower stage at diagnosis) is associated with increased breast cancer-specific and overall survival, as well as less-aggressive treatment approaches.
As a medical oncologist who treats women with breast cancer, I see these benefits firsthand. With earlier diagnosis, we are more likely to offer less aggressive surgical approaches such as partial mastectomy (lumpectomy) and sentinel lymph node biopsy as opposed to total mastectomy with axillary lymph node dissection, the latter of which is more likely to be associated with lymphedema and which can lead to postmastectomy chest wall pain syndromes.
We also are able to use less aggressive radiation therapy approaches such as partial breast radiation, and less aggressive breast cancer–specific systemic treatments for women with a lower stage of breast cancer at diagnosis. In some cases, adjuvant or neoadjuvant chemotherapy may not be needed – and when it is necessary, shorter courses of chemotherapy or targeted chemotherapeutic regimens may be offered. This means lower systemic toxicities, both early and late, such as less cytopenias, risk of infections, mucositis, hair loss, cardiotoxicity, secondary malignancies/leukemia, and peripheral sensory neuropathy.
It is important to note that Black women in the United States have the highest death rate from breast cancer – 27.3 per 100,000 per year, versus 19.6 per 100,000 per year for White women1 – and that younger Black women appear to have a higher risk of developing triple-negative breast cancer, a more aggressive type of breast cancer. The higher breast cancer mortality in Black women is likely multifactorial and may be attributed partly to disparities in health care and partly to tumor biology. The case for annual screening in this population thus seems especially strong.
Screening modalities
Digital 3-D mammography, or digital breast tomosynthesis (DBT), is widely considered to be a more sensitive screening tool than conventional digital mammography alone. The NCCN recommends DBT for women with an average risk of developing breast cancer starting at age 40,4,5 and the USPSTF, while offering no recommendation on DBT as a primary screening method (“insufficient evidence”), says that DBT appears to increase cancer detection rates.2 So, I do routinely recommend it.
DBT may be especially beneficial for women with dense breast tissue (determined mammographically), who are most often premenopausal women – particularly non-Hispanic White women. Dense breast tissue itself can contribute to an increased risk of breast cancer – an approximately 20% higher relative risk in an average-risk woman with heterogeneously dense breast tissue, and an approximately 100% higher relative risk in a woman with extremely dense breasts6 – but unfortunately it affects the sensitivity and specificity of screening mammography.
I do not recommend routine supplemental screening with other methods (breast ultrasonography or MRI) for women at average risk of breast cancer who have dense breasts. MRI with gadolinium contrast is recommended as an adjunct to mammography for women who have a lifetime risk of developing breast cancer of more than 20%-25% (e.g., women with known BRCA1/2 mutations or radiation to breast tissue), and can be done annually at the same time as the screening mammogram is done. Some clinicians and patients prefer to alternate these two tests – one every 6 months.
Screening breast MRI is more sensitive but less specific than mammography; combining the two screening modalities leads to overall increased sensitivity and specificity in high-risk populations.
Risk assessment
Identifying higher-risk women who need to be sent to a genetic counselor is critically important. The USPSTF recommends that women who have family members with breast, ovarian, tubal or peritoneal cancer, or who have an ancestry associated with BRCA1/2 gene mutations, be assessed with a brief familial risk assessment tool such as the Pedigree Assessment Tool. This and other validated tools have been evaluated by the USPSTF and can be used to guide referrals to genetic counseling for more definitive risk assessment.7
These tools are different from general breast cancer risk assessment models, such as the NCI’s Breast Cancer Risk Assessment Tool,8 which are designed to calculate the 5-year and lifetime risk of developing invasive breast cancer for an average-risk woman but not to identify BRCA-related cancer risk. (The NCI’s tool is based on the Gail model, which has been widely used over the years.)
The general risk assessment models use a women’s personal medical and reproductive history as well as the history of breast cancer among her first-degree relatives to estimate her risk.
Dr. Tkaczuk reported that she has no disclosures.
References
1. “Cancer Stat Facts: Female Breast Cancer.” Surveillance, Epidemiology, and End Results Program. National Cancer Institute.
2. Siu AL et al. Ann Intern Med. 2016 Feb 16. doi: 10.7326/M15-2886.
3. Independent UK Panel on Breast Cancer Screening. Lancet. 2012 Nov 17;380(9855):1778-86.
4. NCCN guidelines for Detection, Prevention, & Risk Reduction: Breast Cancer Screening and Diagnosis. National Comprehensive Cancer Network.
5. NCCN guidelines for Detection, Prevention, & Risk Reduction: Breast Cancer Risk Reduction. National Comprehensive Cancer Network.
6. Ziv E et al. Cancer Epidemiol Biomarkers Prev. 2004;13(12):2090-5.
7. USPSTF. JAMA. 2019;322(7):652-65.
8. The Breast Cancer Risk Assessment Tool. National Cancer Institute.
Screening mammography has contributed to the lowering of mortality from breast cancer by facilitating earlier diagnosis and a lower stage at diagnosis. With more effective treatment options for women who are diagnosed with lower-stage breast cancer, the current 5-year survival rate has risen to 90% – significantly higher than the 5-year survival rate of 75% in 1975.1
Women who are at much higher risk for developing breast cancer – mainly because of family history, certain genetic mutations, or a history of radiation therapy to the chest – will benefit the most from earlier and more frequent screening mammography as well as enhanced screening with non-x-ray methods of breast imaging. It is important that ob.gyns. help to identify these women.
However, the majority of women who are screened with mammography are at “average risk,” with a lifetime risk for developing breast cancer of 12.9%, based on 2015-2017 data from the National Cancer Institute’s (NCI) Surveillance, Epidemiology, and End Results Program (SEER).1 The median age at diagnosis of breast cancer in the U.S. is 62 years,1 and advancing age is the most important risk factor for these women.
A 20% relative risk reduction in breast cancer mortality with screening mammography has been demonstrated both in systematic reviews of randomized and observational studies2 and in a meta-analysis of 11 randomized trials comparing screening and no screening.3 Even though the majority of randomized trials were done in the age of film mammography, experts believe that we still see at least a 20% reduction today.
Among average-risk women, those aged 50-74 with a life expectancy of at least 10 years will benefit the most from regular screening. According to the 2016 screening guideline of the United States Preventive Services Task Force (USPSTF), relative risk reductions in breast cancer mortality from mammography screening, by age group, are 0.88 (confidence interval, 0.73-1.003) for ages 39-49; 0.86 (CI, 0.68-0.97) for ages 50-59; 0.67 (CI, 0.55-0.91) for ages 60-69; and 0.80 (CI, 0.51 to 1.28) for ages 70-74.2
For women aged 40-49 years, most of the guidelines in the United States recommend individualized screening every 1 or 2 years – screening that is guided by shared decision-making that takes into account each woman’s values regarding relative harms and benefits. This is because their risk of developing breast cancer is relatively low while the risk of false-positive results can be higher.
A few exceptions include guidelines by the National Comprehensive Cancer Network (NCCN) and the American College of Radiology, which recommend annual screening mammography starting at age 40 years for all average-risk women. In our program, we adhere to these latter recommendations and advise annual digital 3-D mammograms starting at age 40 and continuing until age 74, or longer if the woman is otherwise healthy with a life expectancy greater than 10 years.
Screening and overdiagnosis
Overdiagnosis – the diagnosis of cancers that may not actually cause mortality or may not even have become apparent without screening – is a concern for all women undergoing routine screening for breast cancer. There is significant uncertainty about its frequency, however.
Research cited by the USPSTF suggests that as many as one in five women diagnosed with breast cancer over approximately 10 years will be overdiagnosed. Other modeling studies have estimated one in eight overdiagnoses, for women aged 50-75 years specifically. By the more conservative estimate, according to the USPSTF, one breast cancer death will be prevented for every 2-3 cases of unnecessary treatment.2
Ductal carcinoma in situ is confined to the mammary ductal-lobular system and lacks the classic characteristics of cancer. Technically, it should not metastasize. But we do not know with certainty which cases of DCIS will or will not progress to invasive cancer. Therefore these women often are offered surgical approaches mirroring invasive cancer treatments (lumpectomy with radiation or even mastectomy in some cases), while for some, such treatments may be unnecessary.
Screening younger women (40-49)
Shared decision-making is always important for breast cancer screening, but in our program we routinely recommend annual screening in average-risk women starting at age 40 for several reasons. For one, younger women may present with more aggressive types of breast cancer such as triple-negative breast cancer. These are much less common than hormone-receptor positive breast cancers – they represent 15%-20% of all breast cancers – but they are faster growing and may develop in the interim if women are screened less often (at 2-year intervals).
In addition, finding an invasive breast cancer early is almost always beneficial. Earlier diagnosis (lower stage at diagnosis) is associated with increased breast cancer-specific and overall survival, as well as less-aggressive treatment approaches.
As a medical oncologist who treats women with breast cancer, I see these benefits firsthand. With earlier diagnosis, we are more likely to offer less aggressive surgical approaches such as partial mastectomy (lumpectomy) and sentinel lymph node biopsy as opposed to total mastectomy with axillary lymph node dissection, the latter of which is more likely to be associated with lymphedema and which can lead to postmastectomy chest wall pain syndromes.
We also are able to use less aggressive radiation therapy approaches such as partial breast radiation, and less aggressive breast cancer–specific systemic treatments for women with a lower stage of breast cancer at diagnosis. In some cases, adjuvant or neoadjuvant chemotherapy may not be needed – and when it is necessary, shorter courses of chemotherapy or targeted chemotherapeutic regimens may be offered. This means lower systemic toxicities, both early and late, such as less cytopenias, risk of infections, mucositis, hair loss, cardiotoxicity, secondary malignancies/leukemia, and peripheral sensory neuropathy.
It is important to note that Black women in the United States have the highest death rate from breast cancer – 27.3 per 100,000 per year, versus 19.6 per 100,000 per year for White women1 – and that younger Black women appear to have a higher risk of developing triple-negative breast cancer, a more aggressive type of breast cancer. The higher breast cancer mortality in Black women is likely multifactorial and may be attributed partly to disparities in health care and partly to tumor biology. The case for annual screening in this population thus seems especially strong.
Screening modalities
Digital 3-D mammography, or digital breast tomosynthesis (DBT), is widely considered to be a more sensitive screening tool than conventional digital mammography alone. The NCCN recommends DBT for women with an average risk of developing breast cancer starting at age 40,4,5 and the USPSTF, while offering no recommendation on DBT as a primary screening method (“insufficient evidence”), says that DBT appears to increase cancer detection rates.2 So, I do routinely recommend it.
DBT may be especially beneficial for women with dense breast tissue (determined mammographically), who are most often premenopausal women – particularly non-Hispanic White women. Dense breast tissue itself can contribute to an increased risk of breast cancer – an approximately 20% higher relative risk in an average-risk woman with heterogeneously dense breast tissue, and an approximately 100% higher relative risk in a woman with extremely dense breasts6 – but unfortunately it affects the sensitivity and specificity of screening mammography.
I do not recommend routine supplemental screening with other methods (breast ultrasonography or MRI) for women at average risk of breast cancer who have dense breasts. MRI with gadolinium contrast is recommended as an adjunct to mammography for women who have a lifetime risk of developing breast cancer of more than 20%-25% (e.g., women with known BRCA1/2 mutations or radiation to breast tissue), and can be done annually at the same time as the screening mammogram is done. Some clinicians and patients prefer to alternate these two tests – one every 6 months.
Screening breast MRI is more sensitive but less specific than mammography; combining the two screening modalities leads to overall increased sensitivity and specificity in high-risk populations.
Risk assessment
Identifying higher-risk women who need to be sent to a genetic counselor is critically important. The USPSTF recommends that women who have family members with breast, ovarian, tubal or peritoneal cancer, or who have an ancestry associated with BRCA1/2 gene mutations, be assessed with a brief familial risk assessment tool such as the Pedigree Assessment Tool. This and other validated tools have been evaluated by the USPSTF and can be used to guide referrals to genetic counseling for more definitive risk assessment.7
These tools are different from general breast cancer risk assessment models, such as the NCI’s Breast Cancer Risk Assessment Tool,8 which are designed to calculate the 5-year and lifetime risk of developing invasive breast cancer for an average-risk woman but not to identify BRCA-related cancer risk. (The NCI’s tool is based on the Gail model, which has been widely used over the years.)
The general risk assessment models use a women’s personal medical and reproductive history as well as the history of breast cancer among her first-degree relatives to estimate her risk.
Dr. Tkaczuk reported that she has no disclosures.
References
1. “Cancer Stat Facts: Female Breast Cancer.” Surveillance, Epidemiology, and End Results Program. National Cancer Institute.
2. Siu AL et al. Ann Intern Med. 2016 Feb 16. doi: 10.7326/M15-2886.
3. Independent UK Panel on Breast Cancer Screening. Lancet. 2012 Nov 17;380(9855):1778-86.
4. NCCN guidelines for Detection, Prevention, & Risk Reduction: Breast Cancer Screening and Diagnosis. National Comprehensive Cancer Network.
5. NCCN guidelines for Detection, Prevention, & Risk Reduction: Breast Cancer Risk Reduction. National Comprehensive Cancer Network.
6. Ziv E et al. Cancer Epidemiol Biomarkers Prev. 2004;13(12):2090-5.
7. USPSTF. JAMA. 2019;322(7):652-65.
8. The Breast Cancer Risk Assessment Tool. National Cancer Institute.
CRC risk: Raised by meat/alcohol, lowered by aspirin/NSAIDs
A new meta-analysis has largely confirmed what is already known about the lifestyle factors that increase and those that decrease the risk of developing colorectal cancer.
The use of aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs) is associated with a decreased risk for colorectal cancer, the new article concludes. But it also adds a number of other factors that are associated with a decreased risk for the disease, including taking magnesium and folate supplements and eating dairy products, fiber, soy, and fruits and vegetables.
On the other hand, consumption of meat and alcohol was associated with an increased risk for colorectal cancer in almost all of the analyses included in this article.
The study was published online September 28 in Gut.
However, the authors pointed out that it is important to keep in mind that in most cases, the level of evidence is low or very low, primarily because of the heterogeneity of the various published studies, as well as the type of study.
“Furthermore, in most cases, we were unable to identify an optimal dose and duration of exposure/intake for any of the products, even in the case of low-dose aspirin and other compounds that have been extensively assessed,” they wrote.
The findings of this new meta-analysis echo previous findings on this issue.
A number of studies, for example, have found varying associations between the consumption of red meat and cancer. The American Institute for Cancer Research and the World Cancer Research Fund have published several reports during the past 10 years on the effect of diet, nutrition, and/or physical activity on risk for several cancer types. Their most recent study, published in 2017, concluded that eating red meat and processed meat may increase the risk for colorectal cancer, as may drinking two or more alcoholic beverages per day.
Another large meta-analysis published earlier this year found that regular use of aspirin reduced the risk for cancers of the digestive tract by 22%-38%, compared with nonuse.
Umbrella review
In the latest article in Gut, researchers led by Marc Bardou, MD, PhD, Centre Hospitalier Universitaire de Dijon (France), conducted an umbrella review of systematic reviews and meta-analyses of interventions that assessed chemopreventive products for colorectal cancer in an average-risk population.
A total of 80 meta-analyses of interventional and observational studies were included. The studies investigated a wide range of chemopreventive agents in an average-risk population and the risk for colorectal cancer. Agents included medications (aspirin, NSAIDs, statins), vitamins or supplements (magnesium; calcium; folic acid; vitamin A, B, C, E, and D; beta-carotene; and selenium), and dietary items (coffee, tea, fish, dairy products, fiber, fruits, vegetables, meat, and alcohol).
The studies included randomized controlled trials and observational studies. Most of the meta-analyses found a protective effect for aspirin, which lowered the risk by between 14% and 29% even at doses as low as 75 mg/day, with a dose-response effect of up to 325 mg/day. The certainty of evidence was moderate.
NSAID use was also associated with a protective effect, with a significant 26%-43% decrease in the incidence in colorectal cancer. The optimal duration for the observed protective effect remains unclear. Two meta-analyses suggested that NSAIDs may need to be taken for at least 5 years, although one article suggested a protective effect after the first year. The certainty of evidence was low.
Use of magnesium was found to be protective, with a relative risk (RR) of 0.78-0.87. High intake of folic acid was associated with a significant decrease in risk (RR, 0.85-0.88). The certainty of evidence was low and very low, respectively.
Consumption of dairy products was associated with 13%-19% lower risk for the disease. However, the authors note that, because of the small number of available meta-analyses, the multiplicity of outcomes, and the variety of dairy products, it was not possible to reach any firm conclusions about the amount needed or the duration necessary for a protective effect.
Another dietary item, fiber, was associated with a 22%-43% lower risk. Consumption of fruits and vegetables was associated with up to a 52% lower risk, with an added benefit for every additional 100 g/day increase in intake. Soy intake was also associated with a small but significant decrease in risk (8%-15%).
For many of the other items reviewed, evidence was either weak or no beneficial effect was seen.
Increased risk
Consumption of both meat and alcohol was found to increase the risk for colorectal cancer.
Most of the meta-analyses of observational studies have reported a significant increase in risk (RR, 1.12-1.21) with meat consumption (particularly red and processed) and the incidence of colorectal cancer. Studies of the dose effect reported a 10%-30% increased risk for each increment of 100 g/day of total or red meat.
Alcohol consumption was also associated with a significantly increased risk. The higher the intake, the greater the risk. The risk was evident even at the lowest consumption doses that were investigated (1-2 drinks per day).
Balanced for the individual patient
Commenting on the article, Thomas J. George Jr, MD, professor of medicine and director, GI Oncology Program, the University of Florida Health Cancer Center, Gainesville, feels that the take-home message for clinicians and patients alike is that these data help to reinforce behaviors that have already been recommended.
“We know that excessive alcohol and red meat consumption is not healthy, so seeing that there may be a negative effect on colorectal cancer is just more evidence that we should be avoiding that and recommend avoiding that,” said Dr. George. “So yes, I recommend minimizing those, and likewise, a diet that is inclusive of fruits, vegetables, fiber, soy – perhaps as an alternative to meat consumption – is healthier than a diet devoid of these, so again, more reassuring data to support doing what we should already be doing.”
However, he pointed out that there are risks associated with medications such as NSAIDs and aspirin, including bleeding, gastric ulcer formation, and kidney damage. “The risks are low but very real,” Dr. George said. “So I think those recommendations need to be considered on a very individual level, balancing any other risk factors that the patient may have for both colorectal cancer, as well as risks from the medications.”
The study had no outside funding. The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
A new meta-analysis has largely confirmed what is already known about the lifestyle factors that increase and those that decrease the risk of developing colorectal cancer.
The use of aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs) is associated with a decreased risk for colorectal cancer, the new article concludes. But it also adds a number of other factors that are associated with a decreased risk for the disease, including taking magnesium and folate supplements and eating dairy products, fiber, soy, and fruits and vegetables.
On the other hand, consumption of meat and alcohol was associated with an increased risk for colorectal cancer in almost all of the analyses included in this article.
The study was published online September 28 in Gut.
However, the authors pointed out that it is important to keep in mind that in most cases, the level of evidence is low or very low, primarily because of the heterogeneity of the various published studies, as well as the type of study.
“Furthermore, in most cases, we were unable to identify an optimal dose and duration of exposure/intake for any of the products, even in the case of low-dose aspirin and other compounds that have been extensively assessed,” they wrote.
The findings of this new meta-analysis echo previous findings on this issue.
A number of studies, for example, have found varying associations between the consumption of red meat and cancer. The American Institute for Cancer Research and the World Cancer Research Fund have published several reports during the past 10 years on the effect of diet, nutrition, and/or physical activity on risk for several cancer types. Their most recent study, published in 2017, concluded that eating red meat and processed meat may increase the risk for colorectal cancer, as may drinking two or more alcoholic beverages per day.
Another large meta-analysis published earlier this year found that regular use of aspirin reduced the risk for cancers of the digestive tract by 22%-38%, compared with nonuse.
Umbrella review
In the latest article in Gut, researchers led by Marc Bardou, MD, PhD, Centre Hospitalier Universitaire de Dijon (France), conducted an umbrella review of systematic reviews and meta-analyses of interventions that assessed chemopreventive products for colorectal cancer in an average-risk population.
A total of 80 meta-analyses of interventional and observational studies were included. The studies investigated a wide range of chemopreventive agents in an average-risk population and the risk for colorectal cancer. Agents included medications (aspirin, NSAIDs, statins), vitamins or supplements (magnesium; calcium; folic acid; vitamin A, B, C, E, and D; beta-carotene; and selenium), and dietary items (coffee, tea, fish, dairy products, fiber, fruits, vegetables, meat, and alcohol).
The studies included randomized controlled trials and observational studies. Most of the meta-analyses found a protective effect for aspirin, which lowered the risk by between 14% and 29% even at doses as low as 75 mg/day, with a dose-response effect of up to 325 mg/day. The certainty of evidence was moderate.
NSAID use was also associated with a protective effect, with a significant 26%-43% decrease in the incidence in colorectal cancer. The optimal duration for the observed protective effect remains unclear. Two meta-analyses suggested that NSAIDs may need to be taken for at least 5 years, although one article suggested a protective effect after the first year. The certainty of evidence was low.
Use of magnesium was found to be protective, with a relative risk (RR) of 0.78-0.87. High intake of folic acid was associated with a significant decrease in risk (RR, 0.85-0.88). The certainty of evidence was low and very low, respectively.
Consumption of dairy products was associated with 13%-19% lower risk for the disease. However, the authors note that, because of the small number of available meta-analyses, the multiplicity of outcomes, and the variety of dairy products, it was not possible to reach any firm conclusions about the amount needed or the duration necessary for a protective effect.
Another dietary item, fiber, was associated with a 22%-43% lower risk. Consumption of fruits and vegetables was associated with up to a 52% lower risk, with an added benefit for every additional 100 g/day increase in intake. Soy intake was also associated with a small but significant decrease in risk (8%-15%).
For many of the other items reviewed, evidence was either weak or no beneficial effect was seen.
Increased risk
Consumption of both meat and alcohol was found to increase the risk for colorectal cancer.
Most of the meta-analyses of observational studies have reported a significant increase in risk (RR, 1.12-1.21) with meat consumption (particularly red and processed) and the incidence of colorectal cancer. Studies of the dose effect reported a 10%-30% increased risk for each increment of 100 g/day of total or red meat.
Alcohol consumption was also associated with a significantly increased risk. The higher the intake, the greater the risk. The risk was evident even at the lowest consumption doses that were investigated (1-2 drinks per day).
Balanced for the individual patient
Commenting on the article, Thomas J. George Jr, MD, professor of medicine and director, GI Oncology Program, the University of Florida Health Cancer Center, Gainesville, feels that the take-home message for clinicians and patients alike is that these data help to reinforce behaviors that have already been recommended.
“We know that excessive alcohol and red meat consumption is not healthy, so seeing that there may be a negative effect on colorectal cancer is just more evidence that we should be avoiding that and recommend avoiding that,” said Dr. George. “So yes, I recommend minimizing those, and likewise, a diet that is inclusive of fruits, vegetables, fiber, soy – perhaps as an alternative to meat consumption – is healthier than a diet devoid of these, so again, more reassuring data to support doing what we should already be doing.”
However, he pointed out that there are risks associated with medications such as NSAIDs and aspirin, including bleeding, gastric ulcer formation, and kidney damage. “The risks are low but very real,” Dr. George said. “So I think those recommendations need to be considered on a very individual level, balancing any other risk factors that the patient may have for both colorectal cancer, as well as risks from the medications.”
The study had no outside funding. The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
A new meta-analysis has largely confirmed what is already known about the lifestyle factors that increase and those that decrease the risk of developing colorectal cancer.
The use of aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs) is associated with a decreased risk for colorectal cancer, the new article concludes. But it also adds a number of other factors that are associated with a decreased risk for the disease, including taking magnesium and folate supplements and eating dairy products, fiber, soy, and fruits and vegetables.
On the other hand, consumption of meat and alcohol was associated with an increased risk for colorectal cancer in almost all of the analyses included in this article.
The study was published online September 28 in Gut.
However, the authors pointed out that it is important to keep in mind that in most cases, the level of evidence is low or very low, primarily because of the heterogeneity of the various published studies, as well as the type of study.
“Furthermore, in most cases, we were unable to identify an optimal dose and duration of exposure/intake for any of the products, even in the case of low-dose aspirin and other compounds that have been extensively assessed,” they wrote.
The findings of this new meta-analysis echo previous findings on this issue.
A number of studies, for example, have found varying associations between the consumption of red meat and cancer. The American Institute for Cancer Research and the World Cancer Research Fund have published several reports during the past 10 years on the effect of diet, nutrition, and/or physical activity on risk for several cancer types. Their most recent study, published in 2017, concluded that eating red meat and processed meat may increase the risk for colorectal cancer, as may drinking two or more alcoholic beverages per day.
Another large meta-analysis published earlier this year found that regular use of aspirin reduced the risk for cancers of the digestive tract by 22%-38%, compared with nonuse.
Umbrella review
In the latest article in Gut, researchers led by Marc Bardou, MD, PhD, Centre Hospitalier Universitaire de Dijon (France), conducted an umbrella review of systematic reviews and meta-analyses of interventions that assessed chemopreventive products for colorectal cancer in an average-risk population.
A total of 80 meta-analyses of interventional and observational studies were included. The studies investigated a wide range of chemopreventive agents in an average-risk population and the risk for colorectal cancer. Agents included medications (aspirin, NSAIDs, statins), vitamins or supplements (magnesium; calcium; folic acid; vitamin A, B, C, E, and D; beta-carotene; and selenium), and dietary items (coffee, tea, fish, dairy products, fiber, fruits, vegetables, meat, and alcohol).
The studies included randomized controlled trials and observational studies. Most of the meta-analyses found a protective effect for aspirin, which lowered the risk by between 14% and 29% even at doses as low as 75 mg/day, with a dose-response effect of up to 325 mg/day. The certainty of evidence was moderate.
NSAID use was also associated with a protective effect, with a significant 26%-43% decrease in the incidence in colorectal cancer. The optimal duration for the observed protective effect remains unclear. Two meta-analyses suggested that NSAIDs may need to be taken for at least 5 years, although one article suggested a protective effect after the first year. The certainty of evidence was low.
Use of magnesium was found to be protective, with a relative risk (RR) of 0.78-0.87. High intake of folic acid was associated with a significant decrease in risk (RR, 0.85-0.88). The certainty of evidence was low and very low, respectively.
Consumption of dairy products was associated with 13%-19% lower risk for the disease. However, the authors note that, because of the small number of available meta-analyses, the multiplicity of outcomes, and the variety of dairy products, it was not possible to reach any firm conclusions about the amount needed or the duration necessary for a protective effect.
Another dietary item, fiber, was associated with a 22%-43% lower risk. Consumption of fruits and vegetables was associated with up to a 52% lower risk, with an added benefit for every additional 100 g/day increase in intake. Soy intake was also associated with a small but significant decrease in risk (8%-15%).
For many of the other items reviewed, evidence was either weak or no beneficial effect was seen.
Increased risk
Consumption of both meat and alcohol was found to increase the risk for colorectal cancer.
Most of the meta-analyses of observational studies have reported a significant increase in risk (RR, 1.12-1.21) with meat consumption (particularly red and processed) and the incidence of colorectal cancer. Studies of the dose effect reported a 10%-30% increased risk for each increment of 100 g/day of total or red meat.
Alcohol consumption was also associated with a significantly increased risk. The higher the intake, the greater the risk. The risk was evident even at the lowest consumption doses that were investigated (1-2 drinks per day).
Balanced for the individual patient
Commenting on the article, Thomas J. George Jr, MD, professor of medicine and director, GI Oncology Program, the University of Florida Health Cancer Center, Gainesville, feels that the take-home message for clinicians and patients alike is that these data help to reinforce behaviors that have already been recommended.
“We know that excessive alcohol and red meat consumption is not healthy, so seeing that there may be a negative effect on colorectal cancer is just more evidence that we should be avoiding that and recommend avoiding that,” said Dr. George. “So yes, I recommend minimizing those, and likewise, a diet that is inclusive of fruits, vegetables, fiber, soy – perhaps as an alternative to meat consumption – is healthier than a diet devoid of these, so again, more reassuring data to support doing what we should already be doing.”
However, he pointed out that there are risks associated with medications such as NSAIDs and aspirin, including bleeding, gastric ulcer formation, and kidney damage. “The risks are low but very real,” Dr. George said. “So I think those recommendations need to be considered on a very individual level, balancing any other risk factors that the patient may have for both colorectal cancer, as well as risks from the medications.”
The study had no outside funding. The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
AHA scientific statement highlights cardiorenal benefit of new diabetes drugs
To protect the heart and kidneys, sodium-glucose transporter 2 (SGLT2) inhibitors and glucagonlike peptide–1 (GLP-1) receptor agonists should be considered for people with type 2 diabetes and chronic kidney disease (CKD), the American Heart Association advised in a new scientific statement.
Taken together, the results of relevant clinical trials indicate that SGLT2 inhibitors and GLP-1 receptor agonists safely and significantly reduce the risk for cardiovascular (CV) events, death, and the slow progression of CKD to end-stage kidney disease, including the risks for dialysis, transplantation, and death, the writing group says.
The scientific statement was published online Sept. 28 in Circulation.
“There has been rapid reporting of high-quality data in the cardio-renal-metabolic space with significant heart and kidney benefits, particularly with these two newer classes of antihyperglycemic agents,” Janani Rangaswami, MD, who chaired the writing group, said in an interview.
“More recent data show benefits in chronic kidney disease and heart failure even in patients without diabetes,” said Dr. Rangaswami, Einstein Medical Center and Sidney Kimmel Medical College, both in Philadelphia.
“These data are practice-changing in both cardiology and nephrology, and usher in a new era of disease-modifying therapies in heart and kidney disease,” Dr. Rangaswami added.
Recommendations at a glance
- Provide early and ongoing assessment of risks for CVD and CKD to patients who may benefit from SGLT2 inhibitors of GLP-1 receptor agonists.
- Tailor medication choices that meet the needs of individual patients. Realize that, given “consistent class-wide effects,” the choice of a specific SGLT2 inhibitor or GLP-1 receptor agonist may be dictated by affordability, coverage, and formulary considerations.
- Adjust all medications in tandem with these medicines and consider the burden of polypharmacy, which is common among people with type 2 diabetes. Adjust concomitant therapies and deprescribe where possible.
- Identify risks for hypoglycemia and educate patients on the signs so they can seek treatment quickly.
- Monitor and control high blood pressure.
- Counsel patients about the risks for and symptoms of euglycemic diabetic ketoacidosis when taking SGLT2 inhibitors, as well as classic DKA, which can be fatal.
- Regularly screen and counsel patients about foot care to prevent foot ulcers or blisters that can quickly become infected and lead to amputation.
The writing group identified two additional patient subgroups that may benefit from SGLT2 inhibitors and GLP-1 receptor agonists: those with heart failure with reduced ejection fraction with or without diabetes; and those with CKD who do not have diabetes. They say more data are anticipated to validate the use of SGLT2 inhibitors and GLP-1 receptor agonists in these “at-risk” patients.
Collaborative care model
The writing group proposed a collaborative care model, bridging cardiologists, nephrologists, endocrinologists, and primary care physicians, to help facilitate the “prompt and appropriate” integration of these new classes of medications in the management of patients with type 2 diabetes and CKD.
There is “an unmet need for a cardio-renal-metabolic care model that incorporates best practices in the real world to help align these therapies, especially with vulnerable high-risk patients with cardiorenal disease, and to overcome barriers toward uptake of these agents. Hopefully this statement provides some guidance to the cardiology and nephrology communities in that area,” Dr. Rangaswami said in an interview.
But old habits die hard, as research continues to show the slow adoption of these newer medications in the real world.
For example, a large observational study published last year showed a “striking” discordance between evidence-based, guideline-recommended use of SGLT2 inhibitors for the treatment of type 2 diabetes and their actual uptake in clinical practice.
Paradoxically, patients with CVD, heart failure, hypertension, CKD, and those at risk for hypoglycemia were less apt to receive an SGLT2 inhibitor than other patients.
“The relatively slow uptake of these agents is multifactorial,” Dr. Rangaswami said. “Cardiologists and nephrologists may suffer from some level of ‘therapeutic inertia’ when using new agents they are unfamiliar with and originally branded as ‘antidiabetic’ agents, with the perception of these agents being outside the scope of their practice.”
Two other factors are also at play. “The current health care system is based on ‘specialty silos,’ where specialists tend to stick to the traditional scope of their specialty and are reluctant to view these agents as part of their therapeutic armamentarium. Finally, insurance coverage barriers and affordability also limit the use on a widespread basis,” Dr. Rangaswami said.
A version of this article originally appeared on Medscape.com .
To protect the heart and kidneys, sodium-glucose transporter 2 (SGLT2) inhibitors and glucagonlike peptide–1 (GLP-1) receptor agonists should be considered for people with type 2 diabetes and chronic kidney disease (CKD), the American Heart Association advised in a new scientific statement.
Taken together, the results of relevant clinical trials indicate that SGLT2 inhibitors and GLP-1 receptor agonists safely and significantly reduce the risk for cardiovascular (CV) events, death, and the slow progression of CKD to end-stage kidney disease, including the risks for dialysis, transplantation, and death, the writing group says.
The scientific statement was published online Sept. 28 in Circulation.
“There has been rapid reporting of high-quality data in the cardio-renal-metabolic space with significant heart and kidney benefits, particularly with these two newer classes of antihyperglycemic agents,” Janani Rangaswami, MD, who chaired the writing group, said in an interview.
“More recent data show benefits in chronic kidney disease and heart failure even in patients without diabetes,” said Dr. Rangaswami, Einstein Medical Center and Sidney Kimmel Medical College, both in Philadelphia.
“These data are practice-changing in both cardiology and nephrology, and usher in a new era of disease-modifying therapies in heart and kidney disease,” Dr. Rangaswami added.
Recommendations at a glance
- Provide early and ongoing assessment of risks for CVD and CKD to patients who may benefit from SGLT2 inhibitors of GLP-1 receptor agonists.
- Tailor medication choices that meet the needs of individual patients. Realize that, given “consistent class-wide effects,” the choice of a specific SGLT2 inhibitor or GLP-1 receptor agonist may be dictated by affordability, coverage, and formulary considerations.
- Adjust all medications in tandem with these medicines and consider the burden of polypharmacy, which is common among people with type 2 diabetes. Adjust concomitant therapies and deprescribe where possible.
- Identify risks for hypoglycemia and educate patients on the signs so they can seek treatment quickly.
- Monitor and control high blood pressure.
- Counsel patients about the risks for and symptoms of euglycemic diabetic ketoacidosis when taking SGLT2 inhibitors, as well as classic DKA, which can be fatal.
- Regularly screen and counsel patients about foot care to prevent foot ulcers or blisters that can quickly become infected and lead to amputation.
The writing group identified two additional patient subgroups that may benefit from SGLT2 inhibitors and GLP-1 receptor agonists: those with heart failure with reduced ejection fraction with or without diabetes; and those with CKD who do not have diabetes. They say more data are anticipated to validate the use of SGLT2 inhibitors and GLP-1 receptor agonists in these “at-risk” patients.
Collaborative care model
The writing group proposed a collaborative care model, bridging cardiologists, nephrologists, endocrinologists, and primary care physicians, to help facilitate the “prompt and appropriate” integration of these new classes of medications in the management of patients with type 2 diabetes and CKD.
There is “an unmet need for a cardio-renal-metabolic care model that incorporates best practices in the real world to help align these therapies, especially with vulnerable high-risk patients with cardiorenal disease, and to overcome barriers toward uptake of these agents. Hopefully this statement provides some guidance to the cardiology and nephrology communities in that area,” Dr. Rangaswami said in an interview.
But old habits die hard, as research continues to show the slow adoption of these newer medications in the real world.
For example, a large observational study published last year showed a “striking” discordance between evidence-based, guideline-recommended use of SGLT2 inhibitors for the treatment of type 2 diabetes and their actual uptake in clinical practice.
Paradoxically, patients with CVD, heart failure, hypertension, CKD, and those at risk for hypoglycemia were less apt to receive an SGLT2 inhibitor than other patients.
“The relatively slow uptake of these agents is multifactorial,” Dr. Rangaswami said. “Cardiologists and nephrologists may suffer from some level of ‘therapeutic inertia’ when using new agents they are unfamiliar with and originally branded as ‘antidiabetic’ agents, with the perception of these agents being outside the scope of their practice.”
Two other factors are also at play. “The current health care system is based on ‘specialty silos,’ where specialists tend to stick to the traditional scope of their specialty and are reluctant to view these agents as part of their therapeutic armamentarium. Finally, insurance coverage barriers and affordability also limit the use on a widespread basis,” Dr. Rangaswami said.
A version of this article originally appeared on Medscape.com .
To protect the heart and kidneys, sodium-glucose transporter 2 (SGLT2) inhibitors and glucagonlike peptide–1 (GLP-1) receptor agonists should be considered for people with type 2 diabetes and chronic kidney disease (CKD), the American Heart Association advised in a new scientific statement.
Taken together, the results of relevant clinical trials indicate that SGLT2 inhibitors and GLP-1 receptor agonists safely and significantly reduce the risk for cardiovascular (CV) events, death, and the slow progression of CKD to end-stage kidney disease, including the risks for dialysis, transplantation, and death, the writing group says.
The scientific statement was published online Sept. 28 in Circulation.
“There has been rapid reporting of high-quality data in the cardio-renal-metabolic space with significant heart and kidney benefits, particularly with these two newer classes of antihyperglycemic agents,” Janani Rangaswami, MD, who chaired the writing group, said in an interview.
“More recent data show benefits in chronic kidney disease and heart failure even in patients without diabetes,” said Dr. Rangaswami, Einstein Medical Center and Sidney Kimmel Medical College, both in Philadelphia.
“These data are practice-changing in both cardiology and nephrology, and usher in a new era of disease-modifying therapies in heart and kidney disease,” Dr. Rangaswami added.
Recommendations at a glance
- Provide early and ongoing assessment of risks for CVD and CKD to patients who may benefit from SGLT2 inhibitors of GLP-1 receptor agonists.
- Tailor medication choices that meet the needs of individual patients. Realize that, given “consistent class-wide effects,” the choice of a specific SGLT2 inhibitor or GLP-1 receptor agonist may be dictated by affordability, coverage, and formulary considerations.
- Adjust all medications in tandem with these medicines and consider the burden of polypharmacy, which is common among people with type 2 diabetes. Adjust concomitant therapies and deprescribe where possible.
- Identify risks for hypoglycemia and educate patients on the signs so they can seek treatment quickly.
- Monitor and control high blood pressure.
- Counsel patients about the risks for and symptoms of euglycemic diabetic ketoacidosis when taking SGLT2 inhibitors, as well as classic DKA, which can be fatal.
- Regularly screen and counsel patients about foot care to prevent foot ulcers or blisters that can quickly become infected and lead to amputation.
The writing group identified two additional patient subgroups that may benefit from SGLT2 inhibitors and GLP-1 receptor agonists: those with heart failure with reduced ejection fraction with or without diabetes; and those with CKD who do not have diabetes. They say more data are anticipated to validate the use of SGLT2 inhibitors and GLP-1 receptor agonists in these “at-risk” patients.
Collaborative care model
The writing group proposed a collaborative care model, bridging cardiologists, nephrologists, endocrinologists, and primary care physicians, to help facilitate the “prompt and appropriate” integration of these new classes of medications in the management of patients with type 2 diabetes and CKD.
There is “an unmet need for a cardio-renal-metabolic care model that incorporates best practices in the real world to help align these therapies, especially with vulnerable high-risk patients with cardiorenal disease, and to overcome barriers toward uptake of these agents. Hopefully this statement provides some guidance to the cardiology and nephrology communities in that area,” Dr. Rangaswami said in an interview.
But old habits die hard, as research continues to show the slow adoption of these newer medications in the real world.
For example, a large observational study published last year showed a “striking” discordance between evidence-based, guideline-recommended use of SGLT2 inhibitors for the treatment of type 2 diabetes and their actual uptake in clinical practice.
Paradoxically, patients with CVD, heart failure, hypertension, CKD, and those at risk for hypoglycemia were less apt to receive an SGLT2 inhibitor than other patients.
“The relatively slow uptake of these agents is multifactorial,” Dr. Rangaswami said. “Cardiologists and nephrologists may suffer from some level of ‘therapeutic inertia’ when using new agents they are unfamiliar with and originally branded as ‘antidiabetic’ agents, with the perception of these agents being outside the scope of their practice.”
Two other factors are also at play. “The current health care system is based on ‘specialty silos,’ where specialists tend to stick to the traditional scope of their specialty and are reluctant to view these agents as part of their therapeutic armamentarium. Finally, insurance coverage barriers and affordability also limit the use on a widespread basis,” Dr. Rangaswami said.
A version of this article originally appeared on Medscape.com .
Geriatric patients: My three rules for them
I have been in practice for 31 years, so many of my patients are now in their 80s and 90s. Practices age with us, and I have been seeing many of these patients for 25-30 years.
Absolutely, positively make sure you move!

Our older patients often have many reasons not to move, including pain from arthritis, deconditioning, muscle weakness, fatigue, and depression. “Keeping moving” is probably the most important thing a patient can do for their health.
Holme and Anderssen studied a large cohort of men for cardiovascular risk in 1972 and again in 2000. The surviving men were followed over an additional 12 years.1 They found that 30 minutes of physical activity 6 days a week was associated with a 40% reduction in mortality. Sedentary men had a reduced life expectancy of about 5 years, compared with men who were moderately to vigorously physically active.
Stewart etal. studied the benefit of physical activity in people with stable coronary disease.2 They concluded that, in patients with stable coronary heart disease, more physical activity was associated with lower mortality, and the largest benefit occurred in the sedentary patient groups and the highest cardiac risk groups.
Saint-Maurice et al. studied the effects of total daily step count and step intensity on mortality risk.3 They found that the risk of all-cause mortality decreases as the total number of daily steps increases, but that the speed of those steps did not make a difference. This is very encouraging data for our elderly patients. Moving is the secret, even if it may not be moving at a fast pace!
Never, ever get on a ladder!
This one should be part of every geriatric’s assessment and every Medicare wellness exam. I first experienced the horror of what can happen when elderly people climb when a 96-year-old healthy patient of mine fell off his roof and died. I never thought to tell him climbing on the roof was an awful idea.
Akland et al. looked at the epidemiology and outcomes of ladder-related falls that required ICU admission.4 Hospital mortality was 26%, and almost all of the mortalities occurred in older males in domestic falls, who died as a result of traumatic brain injury. Fewer than half of the survivors were living independently 1 year after the fall.
Valmuur et al. studied ladder related falls in Australia.5 They found that rates of ladder related falls requiring hospitalization rose from about 20/100,000 for men ages 15-29 years to 78/100,000 for men aged over 60 years. Of those who died from fall-related injury, 82% were over the age of 60, with more than 70% dying from head injuries.
Schaffarczyk et al. looked at the impact of nonoccupational falls from ladders in men aged over 50 years.6 The mean age of the patients in the study was 64 years (range, 50-85), with 27% suffering severe trauma. There was a striking impact on long-term function occurring in over half the study patients. The authors did interviews with patients in follow-up long after the falls and found that most never thought of themselves at risk for a fall, and after the experience of a bad fall, would never consider going on a ladder again. I think it is important for health care professionals to discuss the dangers of ladder use with our older patients, pointing out the higher risk of falling and the potential for the fall to be a life-changing or life-ending event.
Let them eat!
Many patients have a reduced appetite as they age. We work hard with our patients to choose a healthy diet throughout their lives, to help ward off obesity, treat hypertension, prevent or control diabetes, or provide heart health. Many patients just stop being interested in food, reduce intake, and may lose weight and muscle mass. When my patients pass the age of 85, I change my focus to encouraging them to eat for calories, socialization, and joy. I think the marginal benefits of more restrictive diets are small, compared with the benefits of helping your patients enjoy eating again. I ask patients what their very favorite foods are and encourage them to have them.
Pearl
Keep your patients eating and moving, except not onto a ladder!
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. Holme I, Anderssen SA. Increases in physical activity is as important as smoking cessation for reduction in total mortality in elderly men: 12 years of follow-up of the Oslo II study. Br J Sports Med. 2015; 49:743-8.
2. Stewart RAH et al. Physical activity and mortality in patients with stable coronary heart disease. J Am Coll Cardiol. 2017 Oct 3;70(14):1689-1700..
3. Saint-Maurice PF et al. Association of daily step count and step intensity with mortality among U.S. adults. JAMA 2020;323:1151-60.
4. Ackland HM et al. Danger at every rung: Epidemiology and outcomes of ICU-admitted ladder-related trauma. Injury. 2016;47:1109-117.
5. Vallmuur K et al. Falls from ladders in Australia: comparing occupational and nonoccupational injuries across age groups. Aust N Z J Public Health. 2016 Dec;40(6):559-63.
6. Schaffarczyk K et al. Nonoccupational falls from ladders in men 50 years and over: Contributing factors and impact. Injury. 2020 Aug;51(8):1798-1804.
I have been in practice for 31 years, so many of my patients are now in their 80s and 90s. Practices age with us, and I have been seeing many of these patients for 25-30 years.
Absolutely, positively make sure you move!
Our older patients often have many reasons not to move, including pain from arthritis, deconditioning, muscle weakness, fatigue, and depression. “Keeping moving” is probably the most important thing a patient can do for their health.
Holme and Anderssen studied a large cohort of men for cardiovascular risk in 1972 and again in 2000. The surviving men were followed over an additional 12 years.1 They found that 30 minutes of physical activity 6 days a week was associated with a 40% reduction in mortality. Sedentary men had a reduced life expectancy of about 5 years, compared with men who were moderately to vigorously physically active.
Stewart etal. studied the benefit of physical activity in people with stable coronary disease.2 They concluded that, in patients with stable coronary heart disease, more physical activity was associated with lower mortality, and the largest benefit occurred in the sedentary patient groups and the highest cardiac risk groups.
Saint-Maurice et al. studied the effects of total daily step count and step intensity on mortality risk.3 They found that the risk of all-cause mortality decreases as the total number of daily steps increases, but that the speed of those steps did not make a difference. This is very encouraging data for our elderly patients. Moving is the secret, even if it may not be moving at a fast pace!
Never, ever get on a ladder!
This one should be part of every geriatric’s assessment and every Medicare wellness exam. I first experienced the horror of what can happen when elderly people climb when a 96-year-old healthy patient of mine fell off his roof and died. I never thought to tell him climbing on the roof was an awful idea.
Akland et al. looked at the epidemiology and outcomes of ladder-related falls that required ICU admission.4 Hospital mortality was 26%, and almost all of the mortalities occurred in older males in domestic falls, who died as a result of traumatic brain injury. Fewer than half of the survivors were living independently 1 year after the fall.
Valmuur et al. studied ladder related falls in Australia.5 They found that rates of ladder related falls requiring hospitalization rose from about 20/100,000 for men ages 15-29 years to 78/100,000 for men aged over 60 years. Of those who died from fall-related injury, 82% were over the age of 60, with more than 70% dying from head injuries.
Schaffarczyk et al. looked at the impact of nonoccupational falls from ladders in men aged over 50 years.6 The mean age of the patients in the study was 64 years (range, 50-85), with 27% suffering severe trauma. There was a striking impact on long-term function occurring in over half the study patients. The authors did interviews with patients in follow-up long after the falls and found that most never thought of themselves at risk for a fall, and after the experience of a bad fall, would never consider going on a ladder again. I think it is important for health care professionals to discuss the dangers of ladder use with our older patients, pointing out the higher risk of falling and the potential for the fall to be a life-changing or life-ending event.
Let them eat!
Many patients have a reduced appetite as they age. We work hard with our patients to choose a healthy diet throughout their lives, to help ward off obesity, treat hypertension, prevent or control diabetes, or provide heart health. Many patients just stop being interested in food, reduce intake, and may lose weight and muscle mass. When my patients pass the age of 85, I change my focus to encouraging them to eat for calories, socialization, and joy. I think the marginal benefits of more restrictive diets are small, compared with the benefits of helping your patients enjoy eating again. I ask patients what their very favorite foods are and encourage them to have them.
Pearl
Keep your patients eating and moving, except not onto a ladder!
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. Holme I, Anderssen SA. Increases in physical activity is as important as smoking cessation for reduction in total mortality in elderly men: 12 years of follow-up of the Oslo II study. Br J Sports Med. 2015; 49:743-8.
2. Stewart RAH et al. Physical activity and mortality in patients with stable coronary heart disease. J Am Coll Cardiol. 2017 Oct 3;70(14):1689-1700..
3. Saint-Maurice PF et al. Association of daily step count and step intensity with mortality among U.S. adults. JAMA 2020;323:1151-60.
4. Ackland HM et al. Danger at every rung: Epidemiology and outcomes of ICU-admitted ladder-related trauma. Injury. 2016;47:1109-117.
5. Vallmuur K et al. Falls from ladders in Australia: comparing occupational and nonoccupational injuries across age groups. Aust N Z J Public Health. 2016 Dec;40(6):559-63.
6. Schaffarczyk K et al. Nonoccupational falls from ladders in men 50 years and over: Contributing factors and impact. Injury. 2020 Aug;51(8):1798-1804.
I have been in practice for 31 years, so many of my patients are now in their 80s and 90s. Practices age with us, and I have been seeing many of these patients for 25-30 years.
Absolutely, positively make sure you move!
Our older patients often have many reasons not to move, including pain from arthritis, deconditioning, muscle weakness, fatigue, and depression. “Keeping moving” is probably the most important thing a patient can do for their health.
Holme and Anderssen studied a large cohort of men for cardiovascular risk in 1972 and again in 2000. The surviving men were followed over an additional 12 years.1 They found that 30 minutes of physical activity 6 days a week was associated with a 40% reduction in mortality. Sedentary men had a reduced life expectancy of about 5 years, compared with men who were moderately to vigorously physically active.
Stewart etal. studied the benefit of physical activity in people with stable coronary disease.2 They concluded that, in patients with stable coronary heart disease, more physical activity was associated with lower mortality, and the largest benefit occurred in the sedentary patient groups and the highest cardiac risk groups.
Saint-Maurice et al. studied the effects of total daily step count and step intensity on mortality risk.3 They found that the risk of all-cause mortality decreases as the total number of daily steps increases, but that the speed of those steps did not make a difference. This is very encouraging data for our elderly patients. Moving is the secret, even if it may not be moving at a fast pace!
Never, ever get on a ladder!
This one should be part of every geriatric’s assessment and every Medicare wellness exam. I first experienced the horror of what can happen when elderly people climb when a 96-year-old healthy patient of mine fell off his roof and died. I never thought to tell him climbing on the roof was an awful idea.
Akland et al. looked at the epidemiology and outcomes of ladder-related falls that required ICU admission.4 Hospital mortality was 26%, and almost all of the mortalities occurred in older males in domestic falls, who died as a result of traumatic brain injury. Fewer than half of the survivors were living independently 1 year after the fall.
Valmuur et al. studied ladder related falls in Australia.5 They found that rates of ladder related falls requiring hospitalization rose from about 20/100,000 for men ages 15-29 years to 78/100,000 for men aged over 60 years. Of those who died from fall-related injury, 82% were over the age of 60, with more than 70% dying from head injuries.
Schaffarczyk et al. looked at the impact of nonoccupational falls from ladders in men aged over 50 years.6 The mean age of the patients in the study was 64 years (range, 50-85), with 27% suffering severe trauma. There was a striking impact on long-term function occurring in over half the study patients. The authors did interviews with patients in follow-up long after the falls and found that most never thought of themselves at risk for a fall, and after the experience of a bad fall, would never consider going on a ladder again. I think it is important for health care professionals to discuss the dangers of ladder use with our older patients, pointing out the higher risk of falling and the potential for the fall to be a life-changing or life-ending event.
Let them eat!
Many patients have a reduced appetite as they age. We work hard with our patients to choose a healthy diet throughout their lives, to help ward off obesity, treat hypertension, prevent or control diabetes, or provide heart health. Many patients just stop being interested in food, reduce intake, and may lose weight and muscle mass. When my patients pass the age of 85, I change my focus to encouraging them to eat for calories, socialization, and joy. I think the marginal benefits of more restrictive diets are small, compared with the benefits of helping your patients enjoy eating again. I ask patients what their very favorite foods are and encourage them to have them.
Pearl
Keep your patients eating and moving, except not onto a ladder!
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. Holme I, Anderssen SA. Increases in physical activity is as important as smoking cessation for reduction in total mortality in elderly men: 12 years of follow-up of the Oslo II study. Br J Sports Med. 2015; 49:743-8.
2. Stewart RAH et al. Physical activity and mortality in patients with stable coronary heart disease. J Am Coll Cardiol. 2017 Oct 3;70(14):1689-1700..
3. Saint-Maurice PF et al. Association of daily step count and step intensity with mortality among U.S. adults. JAMA 2020;323:1151-60.
4. Ackland HM et al. Danger at every rung: Epidemiology and outcomes of ICU-admitted ladder-related trauma. Injury. 2016;47:1109-117.
5. Vallmuur K et al. Falls from ladders in Australia: comparing occupational and nonoccupational injuries across age groups. Aust N Z J Public Health. 2016 Dec;40(6):559-63.
6. Schaffarczyk K et al. Nonoccupational falls from ladders in men 50 years and over: Contributing factors and impact. Injury. 2020 Aug;51(8):1798-1804.
Pregnancy studies on psoriasis, PsA medications pick up
Christina Chambers, PhD, MPH, who runs the MotherToBaby Pregnancy Studies research center at the University of California, San Diego, has found most pregnant women to be “entirely altruistic” about sharing their experiences with drug treatment during pregnancy.

– but dermatologists, rheumatologists, and their female patients with psoriasis and psoriatic arthritis (PsA) want much more.
And women’s participation in the MotherToBaby studies conducted by the nonprofit Organization of Teratology Information Specialists (OTIS) is key, say physicians who are treating women of reproductive age. OTIS is now listed in drug labeling as the “pregnancy registry” contact for many of the medications they may be discussing with patients.
Dr. Chambers said that most women appreciate “that participating in a study may not help her with her pregnancy, but it can help her sister or her friend or someone else who has these same questions in planning a pregnancy of ‘Can I stay on my treatment?’ or, in the case of an unplanned pregnancy, ‘Should I be concerned?’ ”
OTIS has enrolled women with psoriasis and/or PsA in studies of nine medications, most of them biologics (both TNF-alpha blockers and newer anti-interleukin agents).
Four of the studies – those evaluating etanercept (Enbrel), adalimumab (Humira), abatacept (Orencia), and ustekinumab (Stelara) – are now closed to enrollment with analyses either underway or completed. The other five are currently enrolling patients and involve treatment with certolizumab pegol (Cimzia), tildrakizumab (Ilumya), apremilast (Otezla), guselkumab (Tremfya), and tofacitinib (Xeljanz).

Lisa R. Sammaritano, MD, a rheumatologist at the Hospital for Special Surgery, New York, who led the development of the American College of Rheumatology’s first guideline for the management of reproductive health in rheumatic and musculoskeletal diseases, recommends to some of her patients that they contact OTIS. “Their pregnancy registry studies have added important information to the field over the years,” she said.
Most recently, a study of the anti–TNF-alpha medication adalimumab that began in 2004 in pregnant patients with RA and Crohn’s disease culminated in a 2019 PLOS ONE paper reporting no associations between exposure to the medication and an increased risk of adverse outcomes. The outcomes studied were major structural birth defects, minor defects, spontaneous abortion, preterm delivery, prenatal and postnatal growth deficiency, serious or opportunistic infections, and malignancies.
An analysis is underway of adalimumab exposure in women with PsA – a patient subset that was added after the study started. But in the meantime, Dr. Chambers said, the 2019 research article is relevant to questions of drug safety across indications.
OTIS’s MothertoBaby studies are structured as prospective cohort studies. Dr. Chambers, a perinatal epidemiologist, is president of OTIS, which recruits women who have an exposure to the medication under study – at least one dose, for any length of time. And in most cases, it also recruits women with the underlying condition but no exposure and healthy women without the condition to represent the general population.
It’s the disease-matched comparison group that makes OTIS’s studies different from traditional pregnancy registries involving “a simple exposure series and outcomes that are described in the context of what you’d expect in the general population,” said Dr. Chambers, professor in the department of pediatrics, as well as family and preventative medicine, at UCSD and codirector of the Center for Better Beginnings at that university. “Many maternal conditions themselves [or their comorbidities] carry some risk of adverse outcomes in pregnancy.”
The OTIS studies typically involve at least 100 exposed pregnancies and a similar number of unexposed pregnancies; some have cohorts of 200-300.
The recently published study of adalimumab, for instance, included 257 women with exposure to the drug and 120 women in a disease comparison group with no exposure. In addition to finding no associations between drug exposure and adverse outcomes, the study found that women with RA or Crohn’s were at increased risk of preterm delivery, irrespective of adalimumab exposure.
“There’s insufficient [power with any of these numbers] to come to the conclusion that a drug is safe,” she said. “But what we have been able to say [through our studies] is that we’ve looked carefully at the whole array of outcomes ... and we don’t see anything unusual. That early view can be reassuring” until large population-based studies or claims analyses become possible.
Dr. Sammaritano, also with Weill Cornell Medicine, New York, said that she does not recommend registry participation for patients who stop biologics at the diagnosis of pregnancy. Since “the start of IgG antibody transfer during pregnancy is about 16 weeks,” she worries that including these patients might lead to falsely reassuring findings. “We are most interested in [knowing the outcomes of] patients who must continue the drugs through pregnancy,” she said.
Dr. Chambers, however, said that in her view, placental transfer is not a requirement for a medication to have some effect on the outcome of pregnancy. “The outcome could be influenced by an effect of the medication that doesn’t require placental transfer or require placental transfer in large amounts,” she said. “So it’s relevant to examine exposures that have occurred only in the first trimester, and this is especially true for the outcome of major birth defects, most of which are initiated in the first trimester.”
The MotherToBaby studies typically include both early, short exposures and longer exposures, she said. “And certainly, duration of use is a factor that we do consider in looking at specific outcomes such as growth, preterm delivery, and risk of serious or opportunistic infections.”
(In the published study of adalimumab, 65.3% of women in the medication-exposed cohort used the medication in all three trimesters, 10.5% in the first and second trimesters, and 22.4% in the first trimester only.)
Women participating in the MotherToBaby studies complete two to four interviews during pregnancy and may be interviewed again after delivery. They are asked for their permission to share a copy of their medical records – and their baby’s medical records – and their babies receive a follow-up pediatric exam by a pediatrician with expertise in dysmorphology/genetics (who is blinded to exposure status), most commonly in the participant’s home. Providers are not asked to enter any data.

Eliza Chakravarty, MD, a rheumatologist with the Oklahoma Medical Research Foundation in Oklahoma City who treats patients with PsA who are pregnant or considering pregnancy, said that her referrals for research participation “have been mostly to MothertoBaby.”
“Most drug companies [in the autoimmune space] are now contracting with them [for their pregnancy exposure research],” she said. “I really like that it’s become so centralized.”
She tells patients that many questions can be answered through research, that their experience matters, and that “there are benefits” to the extra pediatric examination. “I give them the information and let them decide whether or not they want to call [MotherToBaby],” she said. “I don’t want to impose. I want to make them aware.”
Dr. Chambers emphasizes to patients and physicians that the studies are strictly observational and do not require any changes in personal or medical regimens. “When people hear the word ‘research’ they think of clinical trials. We’re saying, you and your provider do everything you normally would do, just let us observe what happens during your pregnancy.”
Physicians should assure patients, moreover, that “just because the drug is being studied doesn’t mean there’s a known risk or even a suspected risk,” she said.
The MotherToBaby studies receive funding from the pharmaceutical companies, which are required by the Food and Drug Administration to conduct pregnancy exposure registries for medications used during pregnancy or in women of reproductive age. OTIS has an independent advisory board, however, and independently analyzes and publishes its findings. Progress reports are shared with the pharmaceutical companies, and in turn, the FDA, Dr. Chambers said.
To refer patients for MotherToBaby studies, physicians can use an online referral form found on the MothertoBaby web site, a service of OTIS, or call the pregnancy studies team at 877-311-8972 to provide them with the patient’s name or number. Patients may also be given the number and advised to consider calling. MotherToBaby offers medication fact sheets that answer questions about exposures during pregnancy and breastfeeding, and runs a free and confidential teratogen counseling service: 866-626-6847.
Christina Chambers, PhD, MPH, who runs the MotherToBaby Pregnancy Studies research center at the University of California, San Diego, has found most pregnant women to be “entirely altruistic” about sharing their experiences with drug treatment during pregnancy.
– but dermatologists, rheumatologists, and their female patients with psoriasis and psoriatic arthritis (PsA) want much more.
And women’s participation in the MotherToBaby studies conducted by the nonprofit Organization of Teratology Information Specialists (OTIS) is key, say physicians who are treating women of reproductive age. OTIS is now listed in drug labeling as the “pregnancy registry” contact for many of the medications they may be discussing with patients.
Dr. Chambers said that most women appreciate “that participating in a study may not help her with her pregnancy, but it can help her sister or her friend or someone else who has these same questions in planning a pregnancy of ‘Can I stay on my treatment?’ or, in the case of an unplanned pregnancy, ‘Should I be concerned?’ ”
OTIS has enrolled women with psoriasis and/or PsA in studies of nine medications, most of them biologics (both TNF-alpha blockers and newer anti-interleukin agents).
Four of the studies – those evaluating etanercept (Enbrel), adalimumab (Humira), abatacept (Orencia), and ustekinumab (Stelara) – are now closed to enrollment with analyses either underway or completed. The other five are currently enrolling patients and involve treatment with certolizumab pegol (Cimzia), tildrakizumab (Ilumya), apremilast (Otezla), guselkumab (Tremfya), and tofacitinib (Xeljanz).
Lisa R. Sammaritano, MD, a rheumatologist at the Hospital for Special Surgery, New York, who led the development of the American College of Rheumatology’s first guideline for the management of reproductive health in rheumatic and musculoskeletal diseases, recommends to some of her patients that they contact OTIS. “Their pregnancy registry studies have added important information to the field over the years,” she said.
Most recently, a study of the anti–TNF-alpha medication adalimumab that began in 2004 in pregnant patients with RA and Crohn’s disease culminated in a 2019 PLOS ONE paper reporting no associations between exposure to the medication and an increased risk of adverse outcomes. The outcomes studied were major structural birth defects, minor defects, spontaneous abortion, preterm delivery, prenatal and postnatal growth deficiency, serious or opportunistic infections, and malignancies.
An analysis is underway of adalimumab exposure in women with PsA – a patient subset that was added after the study started. But in the meantime, Dr. Chambers said, the 2019 research article is relevant to questions of drug safety across indications.
OTIS’s MothertoBaby studies are structured as prospective cohort studies. Dr. Chambers, a perinatal epidemiologist, is president of OTIS, which recruits women who have an exposure to the medication under study – at least one dose, for any length of time. And in most cases, it also recruits women with the underlying condition but no exposure and healthy women without the condition to represent the general population.
It’s the disease-matched comparison group that makes OTIS’s studies different from traditional pregnancy registries involving “a simple exposure series and outcomes that are described in the context of what you’d expect in the general population,” said Dr. Chambers, professor in the department of pediatrics, as well as family and preventative medicine, at UCSD and codirector of the Center for Better Beginnings at that university. “Many maternal conditions themselves [or their comorbidities] carry some risk of adverse outcomes in pregnancy.”
The OTIS studies typically involve at least 100 exposed pregnancies and a similar number of unexposed pregnancies; some have cohorts of 200-300.
The recently published study of adalimumab, for instance, included 257 women with exposure to the drug and 120 women in a disease comparison group with no exposure. In addition to finding no associations between drug exposure and adverse outcomes, the study found that women with RA or Crohn’s were at increased risk of preterm delivery, irrespective of adalimumab exposure.
“There’s insufficient [power with any of these numbers] to come to the conclusion that a drug is safe,” she said. “But what we have been able to say [through our studies] is that we’ve looked carefully at the whole array of outcomes ... and we don’t see anything unusual. That early view can be reassuring” until large population-based studies or claims analyses become possible.
Dr. Sammaritano, also with Weill Cornell Medicine, New York, said that she does not recommend registry participation for patients who stop biologics at the diagnosis of pregnancy. Since “the start of IgG antibody transfer during pregnancy is about 16 weeks,” she worries that including these patients might lead to falsely reassuring findings. “We are most interested in [knowing the outcomes of] patients who must continue the drugs through pregnancy,” she said.
Dr. Chambers, however, said that in her view, placental transfer is not a requirement for a medication to have some effect on the outcome of pregnancy. “The outcome could be influenced by an effect of the medication that doesn’t require placental transfer or require placental transfer in large amounts,” she said. “So it’s relevant to examine exposures that have occurred only in the first trimester, and this is especially true for the outcome of major birth defects, most of which are initiated in the first trimester.”
The MotherToBaby studies typically include both early, short exposures and longer exposures, she said. “And certainly, duration of use is a factor that we do consider in looking at specific outcomes such as growth, preterm delivery, and risk of serious or opportunistic infections.”
(In the published study of adalimumab, 65.3% of women in the medication-exposed cohort used the medication in all three trimesters, 10.5% in the first and second trimesters, and 22.4% in the first trimester only.)
Women participating in the MotherToBaby studies complete two to four interviews during pregnancy and may be interviewed again after delivery. They are asked for their permission to share a copy of their medical records – and their baby’s medical records – and their babies receive a follow-up pediatric exam by a pediatrician with expertise in dysmorphology/genetics (who is blinded to exposure status), most commonly in the participant’s home. Providers are not asked to enter any data.
Eliza Chakravarty, MD, a rheumatologist with the Oklahoma Medical Research Foundation in Oklahoma City who treats patients with PsA who are pregnant or considering pregnancy, said that her referrals for research participation “have been mostly to MothertoBaby.”
“Most drug companies [in the autoimmune space] are now contracting with them [for their pregnancy exposure research],” she said. “I really like that it’s become so centralized.”
She tells patients that many questions can be answered through research, that their experience matters, and that “there are benefits” to the extra pediatric examination. “I give them the information and let them decide whether or not they want to call [MotherToBaby],” she said. “I don’t want to impose. I want to make them aware.”
Dr. Chambers emphasizes to patients and physicians that the studies are strictly observational and do not require any changes in personal or medical regimens. “When people hear the word ‘research’ they think of clinical trials. We’re saying, you and your provider do everything you normally would do, just let us observe what happens during your pregnancy.”
Physicians should assure patients, moreover, that “just because the drug is being studied doesn’t mean there’s a known risk or even a suspected risk,” she said.
The MotherToBaby studies receive funding from the pharmaceutical companies, which are required by the Food and Drug Administration to conduct pregnancy exposure registries for medications used during pregnancy or in women of reproductive age. OTIS has an independent advisory board, however, and independently analyzes and publishes its findings. Progress reports are shared with the pharmaceutical companies, and in turn, the FDA, Dr. Chambers said.
To refer patients for MotherToBaby studies, physicians can use an online referral form found on the MothertoBaby web site, a service of OTIS, or call the pregnancy studies team at 877-311-8972 to provide them with the patient’s name or number. Patients may also be given the number and advised to consider calling. MotherToBaby offers medication fact sheets that answer questions about exposures during pregnancy and breastfeeding, and runs a free and confidential teratogen counseling service: 866-626-6847.
Christina Chambers, PhD, MPH, who runs the MotherToBaby Pregnancy Studies research center at the University of California, San Diego, has found most pregnant women to be “entirely altruistic” about sharing their experiences with drug treatment during pregnancy.
– but dermatologists, rheumatologists, and their female patients with psoriasis and psoriatic arthritis (PsA) want much more.
And women’s participation in the MotherToBaby studies conducted by the nonprofit Organization of Teratology Information Specialists (OTIS) is key, say physicians who are treating women of reproductive age. OTIS is now listed in drug labeling as the “pregnancy registry” contact for many of the medications they may be discussing with patients.
Dr. Chambers said that most women appreciate “that participating in a study may not help her with her pregnancy, but it can help her sister or her friend or someone else who has these same questions in planning a pregnancy of ‘Can I stay on my treatment?’ or, in the case of an unplanned pregnancy, ‘Should I be concerned?’ ”
OTIS has enrolled women with psoriasis and/or PsA in studies of nine medications, most of them biologics (both TNF-alpha blockers and newer anti-interleukin agents).
Four of the studies – those evaluating etanercept (Enbrel), adalimumab (Humira), abatacept (Orencia), and ustekinumab (Stelara) – are now closed to enrollment with analyses either underway or completed. The other five are currently enrolling patients and involve treatment with certolizumab pegol (Cimzia), tildrakizumab (Ilumya), apremilast (Otezla), guselkumab (Tremfya), and tofacitinib (Xeljanz).
Lisa R. Sammaritano, MD, a rheumatologist at the Hospital for Special Surgery, New York, who led the development of the American College of Rheumatology’s first guideline for the management of reproductive health in rheumatic and musculoskeletal diseases, recommends to some of her patients that they contact OTIS. “Their pregnancy registry studies have added important information to the field over the years,” she said.
Most recently, a study of the anti–TNF-alpha medication adalimumab that began in 2004 in pregnant patients with RA and Crohn’s disease culminated in a 2019 PLOS ONE paper reporting no associations between exposure to the medication and an increased risk of adverse outcomes. The outcomes studied were major structural birth defects, minor defects, spontaneous abortion, preterm delivery, prenatal and postnatal growth deficiency, serious or opportunistic infections, and malignancies.
An analysis is underway of adalimumab exposure in women with PsA – a patient subset that was added after the study started. But in the meantime, Dr. Chambers said, the 2019 research article is relevant to questions of drug safety across indications.
OTIS’s MothertoBaby studies are structured as prospective cohort studies. Dr. Chambers, a perinatal epidemiologist, is president of OTIS, which recruits women who have an exposure to the medication under study – at least one dose, for any length of time. And in most cases, it also recruits women with the underlying condition but no exposure and healthy women without the condition to represent the general population.
It’s the disease-matched comparison group that makes OTIS’s studies different from traditional pregnancy registries involving “a simple exposure series and outcomes that are described in the context of what you’d expect in the general population,” said Dr. Chambers, professor in the department of pediatrics, as well as family and preventative medicine, at UCSD and codirector of the Center for Better Beginnings at that university. “Many maternal conditions themselves [or their comorbidities] carry some risk of adverse outcomes in pregnancy.”
The OTIS studies typically involve at least 100 exposed pregnancies and a similar number of unexposed pregnancies; some have cohorts of 200-300.
The recently published study of adalimumab, for instance, included 257 women with exposure to the drug and 120 women in a disease comparison group with no exposure. In addition to finding no associations between drug exposure and adverse outcomes, the study found that women with RA or Crohn’s were at increased risk of preterm delivery, irrespective of adalimumab exposure.
“There’s insufficient [power with any of these numbers] to come to the conclusion that a drug is safe,” she said. “But what we have been able to say [through our studies] is that we’ve looked carefully at the whole array of outcomes ... and we don’t see anything unusual. That early view can be reassuring” until large population-based studies or claims analyses become possible.
Dr. Sammaritano, also with Weill Cornell Medicine, New York, said that she does not recommend registry participation for patients who stop biologics at the diagnosis of pregnancy. Since “the start of IgG antibody transfer during pregnancy is about 16 weeks,” she worries that including these patients might lead to falsely reassuring findings. “We are most interested in [knowing the outcomes of] patients who must continue the drugs through pregnancy,” she said.
Dr. Chambers, however, said that in her view, placental transfer is not a requirement for a medication to have some effect on the outcome of pregnancy. “The outcome could be influenced by an effect of the medication that doesn’t require placental transfer or require placental transfer in large amounts,” she said. “So it’s relevant to examine exposures that have occurred only in the first trimester, and this is especially true for the outcome of major birth defects, most of which are initiated in the first trimester.”
The MotherToBaby studies typically include both early, short exposures and longer exposures, she said. “And certainly, duration of use is a factor that we do consider in looking at specific outcomes such as growth, preterm delivery, and risk of serious or opportunistic infections.”
(In the published study of adalimumab, 65.3% of women in the medication-exposed cohort used the medication in all three trimesters, 10.5% in the first and second trimesters, and 22.4% in the first trimester only.)
Women participating in the MotherToBaby studies complete two to four interviews during pregnancy and may be interviewed again after delivery. They are asked for their permission to share a copy of their medical records – and their baby’s medical records – and their babies receive a follow-up pediatric exam by a pediatrician with expertise in dysmorphology/genetics (who is blinded to exposure status), most commonly in the participant’s home. Providers are not asked to enter any data.
Eliza Chakravarty, MD, a rheumatologist with the Oklahoma Medical Research Foundation in Oklahoma City who treats patients with PsA who are pregnant or considering pregnancy, said that her referrals for research participation “have been mostly to MothertoBaby.”
“Most drug companies [in the autoimmune space] are now contracting with them [for their pregnancy exposure research],” she said. “I really like that it’s become so centralized.”
She tells patients that many questions can be answered through research, that their experience matters, and that “there are benefits” to the extra pediatric examination. “I give them the information and let them decide whether or not they want to call [MotherToBaby],” she said. “I don’t want to impose. I want to make them aware.”
Dr. Chambers emphasizes to patients and physicians that the studies are strictly observational and do not require any changes in personal or medical regimens. “When people hear the word ‘research’ they think of clinical trials. We’re saying, you and your provider do everything you normally would do, just let us observe what happens during your pregnancy.”
Physicians should assure patients, moreover, that “just because the drug is being studied doesn’t mean there’s a known risk or even a suspected risk,” she said.
The MotherToBaby studies receive funding from the pharmaceutical companies, which are required by the Food and Drug Administration to conduct pregnancy exposure registries for medications used during pregnancy or in women of reproductive age. OTIS has an independent advisory board, however, and independently analyzes and publishes its findings. Progress reports are shared with the pharmaceutical companies, and in turn, the FDA, Dr. Chambers said.
To refer patients for MotherToBaby studies, physicians can use an online referral form found on the MothertoBaby web site, a service of OTIS, or call the pregnancy studies team at 877-311-8972 to provide them with the patient’s name or number. Patients may also be given the number and advised to consider calling. MotherToBaby offers medication fact sheets that answer questions about exposures during pregnancy and breastfeeding, and runs a free and confidential teratogen counseling service: 866-626-6847.
New data challenge primary care’s inattention to aldosterone in hypertension
Jun Yang, MBBS, had watched as her father, who had battled hypertension for decades, ended up on four medications that still couldn’t bring his blood pressure to a healthy level. The cardiovascular endocrinologist then ran some tests, and soon thereafter her father had his blood pressure optimized on just one targeted medication.

Dr. Yang’s father was found to have a hormonal condition known as primary aldosteronism (PA) as the cause of his hypertension.
It turns out that PA is not as rare as once thought.
An eye-catching report in Annals of Internal Medicine this spring of an unexpectedly high prevalence of primary aldosteronism among a diverse cross section of U.S. patients with hypertension has raised issues that could dramatically change the way doctors in America, and elsewhere, assess and manage high blood pressure.
Foremost is the question of whether primary care physicians – the clinicians at the front line for diagnosing and initially treating most patients with hypertension – will absorb and act on this new evidence. For them, aldosteronism doesn’t automatically come to mind when they see high numbers on a BP monitor, and yet this latest research found that up to a third of all 726 patients in the study who were diagnosed with hypertension and with high urinary salt levels had PA.
That translates to a roughly three- to fivefold increase over standard prevalence estimates, and is a ”game changer” for how clinicians should approach hypertension management and PA diagnosis going forward, said John W. Funder, MD, in an editorial accompanying the Annals study.
Long considered relatively uncommon, hypertension driven by an excess of the hormone aldosterone, often because of an adenoma on the adrenal gland, is not the same as conventional “essential” hypertension. The former benefits from early diagnosis because its treatment is completely different – close to half of all PA patients can be treated definitively and quickly with surgical removal of an adenoma from one side of the adrenal gland.
For other PA patients, who have bilateral adrenal hyperplasia that is impossible to resolve surgically, treatment with drugs called mineralocorticoid receptor antagonists (MRAs), such as spironolactone, is needed because they target the hormonal cause of the high BP.
But what usually happens is that a patient with PA is mistakenly diagnosed with essential hypertension, in which the classic approach to treatment is to start with one regular antihypertensive drug, and add on further ones from different drug classes if blood pressure is not adequately controlled. When patients are taking three drugs, without adequate control, they are labeled as having “resistant hypertension.”
But in the case of PA, none of these conventional antihypertensives work, and the process of continuing to monitor and add different drugs wastes time, during which patients deteriorate.
“We need to change the culture of waiting for hypertension to be resistant and have patients riddled with end-organ damage,” due to years of persistently high BP and excess aldosterone “before we look for a secondary cause” like PA, declared Dr. Yang, of Hudson Institute of Medical Research and Monash University in Melbourne, during an interview.
So early diagnosis and prompt treatment of PA is key.
In addition to boosting the public health importance of early PA detection in hypertensive patients, the new up-sized PA prevalence numbers throw a spotlight on primary care physicians (PCPs) as key players who will need to apply the findings to practice on a public health scale.
These novel results create a need for “new guidelines, and a radically revised game plan with the key role of PCPs” emphasized in future management of patients with hypertension, said Dr. Funder, a professor of medicine at Monash University, in a second recent editorial in Hypertension.

“Buy-in by PCPs is essential,” agrees Robert M. Carey, MD, a cardiovascular endocrinologist and professor of medicine at the University of Virginia in Charlottesville, and a coauthor of the new study.
But he too acknowledges that this presents a major challenge. PCPs and internists, who diagnose a lot of hypertension, are “not used to thinking about aldosterone,” he said in an interview, encapsulating the key problem faced by proponents of earlier and more widespread PA assessment.
This dilemma looms as a “huge public health issue,” Dr. Carey warned.
‘We’re a long way from getting’ PCPs to buy in to PA screening
Will PCPs grow more comfortable with screening patients for PA themselves, or might they become more willing to refer hypertensive individuals for assessment at an expert center?
One skeptic is Ross D. Feldman, MD, a hypertension-management researcher and professor of medicine at the University of Manitoba in Winnipeg. The finding about high PA prevalence in patients with hypertension “is brand new, [and] the message needs to get to PCPs,” he said. But, “We’re a long way from getting it” to them. “I don’t know how to do that. It will be a tough sell.”
In addition, repositioning MRAs as an earlier option for many hypertensive patients won’t be easy either, because “we’ll never have outcome-trial data for MRAs,” given that they are now generic drugs, he noted.
“No clinical trial data show [MRAs] are first-line drugs,” said Dr. Feldman, who explained that, instead, MRAs are considered “go-to drugs” for patients with treatment-resistant hypertension, a niche therapeutic area. Results from the PATHWAY-2 trial published 5 years ago in Lancet showed “spironolactone was clearly the most effective treatment for the condition,” according to the report authors.
But even among patients with resistant hypertension, screening for PA dramatically lags despite being enshrined in guidelines.

“PCPs should start checking aldosterone-to-renin ratios [a widely used PA screen] in all patients with resistant hypertension or hypertension with hypokalemia, and then refer patients to specialists for testing and management,” said Jordana B. Cohen, MD, a nephrologist and hypertension researcher at the University of Pennsylvania in Philadelphia.
But recent studies of U.S. patient populations with clinical characteristics that meet existing criteria for PA screening showed that just 1%-2% of these individuals underwent an initial PA assessment, she noted, citing reports in the journals Surgery and Hypertension.
“We need to prioritize improving screening in these high-risk patients,” she stressed in an interview.
This illustrates that, in some respects, the new prevalence numbers are beside the point, because PA has been going unscreened and overlooked far too often even in the context of historical, lower prevalence rates, said Dr. Yang.
“The key point is that approximately 1 in 10 people with hypertension, and even more with resistant hypertension, have a form of the disease that is worse than essential hypertension but is routinely missed at present” and is also highly treatable.
“Evidence for the need for increased awareness of PA has been building for 2 decades,” stressed Dr. Yang, who has coauthored several commentaries and reviews that have bemoaned PA’s underappreciated status.
Interest in partnering with PCPs on guidance grows
One potential solution is to have endocrinologists and hypertension specialists’ partner with PCPs to come up with diagnostic and management recommendations. Both Dr. Funder and Dr. Carey are opinion leaders regarding the role of aldosterone in hypertension, and both were coauthors of the 2016 Endocrine Society guideline for PA assessment and management published in the Journal of Clinical Endocrinology & Metabolism , with Dr. Funder chairing the writing panel.
Now approaching its fifth year in effect, this guideline is “due for revision,” and “my hope is that we’ll be able to partner with one or more PCP organizations to come up with a version of the guideline targeted to PCPs,” Dr. Carey said.
He voiced interest in working on this with the American College of Physicians, which represents U.S. internal medicine physicians, and the American Academy of Family Physicians.
“We definitely need a partnership and educational efforts to get the word out from these organizations and not from a specialty society,” said Dr. Carey.
Dr. Funder said he has submitted a proposal to the Endocrine Society for a guidelines update he would chair with Dr. Carey’s assistance and with a diverse writing group that includes PCPs. Dr. Carey said that ideally this panel would write and release a revised guideline in 2021.
“Several of us are chomping at the bit to get this done,” he noted.
But participation by the ACP and AAFP remain uncertain as of September 2020. When approached about this, an ACP spokesperson said the organization had no comment. A spokesperson for the AAFP said, “It’s too early to tell if we will partner with any other organizations to develop guidelines specific to excess aldosterone, and how such guidelines might be received by our members.”
Recent history shows little cooperation between ACP, AAFP, and what might be termed the U.S. hypertension “establishment.” For example, when the American College of Cardiology and the American Heart Association released their most recent essential hypertension management guidelines in Hypertension in 2018, it was never adopted by ACP or AAFP.
The latter two organizations continue to endorse a higher BP threshold for diagnosing hypertension, and higher treatment targets set by alternative expert panels to those of the AHA/ACC.
Collaboration feasible, although PCPs overworked
Dr. Carey hopes that this episode will not preclude agreement over PA screening.
“I think it is still possible to partner with [the ACP and AAFP],” he observed, adding that he believes high PA prevalence among hypertensive patients and its consequences when unrecognized is “noncontentious.”
But he acknowledges that other, substantial hurdles also exist, notably the “overwhelming workload” that American PCPs already face.
David O’Gurek, MD, a family and community medicine physician at the Lewis Katz School of Medicine of Temple University in Philadelphia, agrees that a revamped approach to PA screening developed cooperatively between PCPs and specialists is an important goal and potentially feasible despite prior disagreements. “There has to be room for collaboration,” he said, but also emphasized the need for developing policies based on a systematic evidence review and a focus on patient-centered outcomes.
“We’re certainly missing patients with PA, but there needs to be greater clarity and standardization about the most appropriate screening approach and cutoff level” for flagging patients who need specialized assessment, Dr. O’Gurek said in an interview.
The current endocrinology literature also shows that experts remain divided on how best to accomplish this.
And some hypertension specialists question whether existing evidence is conclusive enough to warrant revised guidelines.
Dr. Cohen, the nephrologist and hypertension researcher, said that, while the recent prevalence report in Annals of Internal Medicine is “intriguing, hypothesis-generating information that suggests we are missing many cases of hyperaldosteronism in routine care,” she nevertheless believes that “we need additional data to be able to truly understand the breadth and implications of the findings.”
William C. Cushman, MD, a hypertension management specialist at the University of Tennessee Health Science Center in Memphis, agrees.
Changing existing practice guidelines “really needs randomized, controlled trials demonstrating a difference in long-term outcomes, ideally major cardiovascular outcomes,” that result from broader PA screening, he said.
Dr. Carey concurs that more evidence is needed to confirm the Annals report, but is confident this evidence will be in hand by the time a guideline-revision panel meets in 2021.
Australian model of PCPs screening for PA could be implemented in United States
An example of what might be possible when PCPs, endocrinologists, and hypertension specialists work together to make PA screening more accessible can be found in Melbourne, at the Endocrine Hypertension Service of Monash Health, in association with the Hudson Institute of Medical Research.
This began operating in July 2016, cofounded by Dr. Yang, whose experiences with her own father made her sensitive to the issue.
The service’s aim is to “address the underdiagnosis of PA, and to offer a streamlined diagnostic service for patients with hypertension,” with an “extensive outreach program” targeted to regional PCPs that, among other messages, encourages them to screen patients for PA when blood pressures exceed 140/90 mm Hg.
During its first 3 years of operation, the service saw 267 patients, with PA diagnosed in 135 and ruled out in 73 patients.
Notably, the proportion of these patients referred from PCPs jumped from 21% of 70 patients during the first year of operation to 47% of 70 patients during year 2, and 52% of 127 patients during the third year, ending in July 2019, said Dr. Yang, who continues to help run the service.
During the first year, a scant 3% of referred patients had recently diagnosed hypertension, but this rose to 14% during the second year, and to 19% during the most recent year with data available.
The median duration of diagnosed hypertension among referred patients fell from 11 years during year 1, to 7 years during year 3.
Service clinicians diagnosed 37 patients with unilateral adenomas, and removed them from 23 patients with four more awaiting surgery and the remaining 10 opting instead for medical management. Another 95 patients went on therapy with a MRA, and during the most recent year studied all patients who began a MRA regimen had a partial or complete clinical response.
Dr. Carey said the “creative program represents a model for implementation in U.S. practice.
Dr. Funder, Dr. Carey, Dr. Feldman, Dr. Yang, Dr. Cohen, and Dr. O’Gurek had no relevant disclosures. Dr. Cushman has been a consultant to Novartis, received personal fees from Sanofi, and research funding from Eli Lilly.
Jun Yang, MBBS, had watched as her father, who had battled hypertension for decades, ended up on four medications that still couldn’t bring his blood pressure to a healthy level. The cardiovascular endocrinologist then ran some tests, and soon thereafter her father had his blood pressure optimized on just one targeted medication.
Dr. Yang’s father was found to have a hormonal condition known as primary aldosteronism (PA) as the cause of his hypertension.
It turns out that PA is not as rare as once thought.
An eye-catching report in Annals of Internal Medicine this spring of an unexpectedly high prevalence of primary aldosteronism among a diverse cross section of U.S. patients with hypertension has raised issues that could dramatically change the way doctors in America, and elsewhere, assess and manage high blood pressure.
Foremost is the question of whether primary care physicians – the clinicians at the front line for diagnosing and initially treating most patients with hypertension – will absorb and act on this new evidence. For them, aldosteronism doesn’t automatically come to mind when they see high numbers on a BP monitor, and yet this latest research found that up to a third of all 726 patients in the study who were diagnosed with hypertension and with high urinary salt levels had PA.
That translates to a roughly three- to fivefold increase over standard prevalence estimates, and is a ”game changer” for how clinicians should approach hypertension management and PA diagnosis going forward, said John W. Funder, MD, in an editorial accompanying the Annals study.
Long considered relatively uncommon, hypertension driven by an excess of the hormone aldosterone, often because of an adenoma on the adrenal gland, is not the same as conventional “essential” hypertension. The former benefits from early diagnosis because its treatment is completely different – close to half of all PA patients can be treated definitively and quickly with surgical removal of an adenoma from one side of the adrenal gland.
For other PA patients, who have bilateral adrenal hyperplasia that is impossible to resolve surgically, treatment with drugs called mineralocorticoid receptor antagonists (MRAs), such as spironolactone, is needed because they target the hormonal cause of the high BP.
But what usually happens is that a patient with PA is mistakenly diagnosed with essential hypertension, in which the classic approach to treatment is to start with one regular antihypertensive drug, and add on further ones from different drug classes if blood pressure is not adequately controlled. When patients are taking three drugs, without adequate control, they are labeled as having “resistant hypertension.”
But in the case of PA, none of these conventional antihypertensives work, and the process of continuing to monitor and add different drugs wastes time, during which patients deteriorate.
“We need to change the culture of waiting for hypertension to be resistant and have patients riddled with end-organ damage,” due to years of persistently high BP and excess aldosterone “before we look for a secondary cause” like PA, declared Dr. Yang, of Hudson Institute of Medical Research and Monash University in Melbourne, during an interview.
So early diagnosis and prompt treatment of PA is key.
In addition to boosting the public health importance of early PA detection in hypertensive patients, the new up-sized PA prevalence numbers throw a spotlight on primary care physicians (PCPs) as key players who will need to apply the findings to practice on a public health scale.
These novel results create a need for “new guidelines, and a radically revised game plan with the key role of PCPs” emphasized in future management of patients with hypertension, said Dr. Funder, a professor of medicine at Monash University, in a second recent editorial in Hypertension.
“Buy-in by PCPs is essential,” agrees Robert M. Carey, MD, a cardiovascular endocrinologist and professor of medicine at the University of Virginia in Charlottesville, and a coauthor of the new study.
But he too acknowledges that this presents a major challenge. PCPs and internists, who diagnose a lot of hypertension, are “not used to thinking about aldosterone,” he said in an interview, encapsulating the key problem faced by proponents of earlier and more widespread PA assessment.
This dilemma looms as a “huge public health issue,” Dr. Carey warned.
‘We’re a long way from getting’ PCPs to buy in to PA screening
Will PCPs grow more comfortable with screening patients for PA themselves, or might they become more willing to refer hypertensive individuals for assessment at an expert center?
One skeptic is Ross D. Feldman, MD, a hypertension-management researcher and professor of medicine at the University of Manitoba in Winnipeg. The finding about high PA prevalence in patients with hypertension “is brand new, [and] the message needs to get to PCPs,” he said. But, “We’re a long way from getting it” to them. “I don’t know how to do that. It will be a tough sell.”
In addition, repositioning MRAs as an earlier option for many hypertensive patients won’t be easy either, because “we’ll never have outcome-trial data for MRAs,” given that they are now generic drugs, he noted.
“No clinical trial data show [MRAs] are first-line drugs,” said Dr. Feldman, who explained that, instead, MRAs are considered “go-to drugs” for patients with treatment-resistant hypertension, a niche therapeutic area. Results from the PATHWAY-2 trial published 5 years ago in Lancet showed “spironolactone was clearly the most effective treatment for the condition,” according to the report authors.
But even among patients with resistant hypertension, screening for PA dramatically lags despite being enshrined in guidelines.
“PCPs should start checking aldosterone-to-renin ratios [a widely used PA screen] in all patients with resistant hypertension or hypertension with hypokalemia, and then refer patients to specialists for testing and management,” said Jordana B. Cohen, MD, a nephrologist and hypertension researcher at the University of Pennsylvania in Philadelphia.
But recent studies of U.S. patient populations with clinical characteristics that meet existing criteria for PA screening showed that just 1%-2% of these individuals underwent an initial PA assessment, she noted, citing reports in the journals Surgery and Hypertension.
“We need to prioritize improving screening in these high-risk patients,” she stressed in an interview.
This illustrates that, in some respects, the new prevalence numbers are beside the point, because PA has been going unscreened and overlooked far too often even in the context of historical, lower prevalence rates, said Dr. Yang.
“The key point is that approximately 1 in 10 people with hypertension, and even more with resistant hypertension, have a form of the disease that is worse than essential hypertension but is routinely missed at present” and is also highly treatable.
“Evidence for the need for increased awareness of PA has been building for 2 decades,” stressed Dr. Yang, who has coauthored several commentaries and reviews that have bemoaned PA’s underappreciated status.
Interest in partnering with PCPs on guidance grows
One potential solution is to have endocrinologists and hypertension specialists’ partner with PCPs to come up with diagnostic and management recommendations. Both Dr. Funder and Dr. Carey are opinion leaders regarding the role of aldosterone in hypertension, and both were coauthors of the 2016 Endocrine Society guideline for PA assessment and management published in the Journal of Clinical Endocrinology & Metabolism , with Dr. Funder chairing the writing panel.
Now approaching its fifth year in effect, this guideline is “due for revision,” and “my hope is that we’ll be able to partner with one or more PCP organizations to come up with a version of the guideline targeted to PCPs,” Dr. Carey said.
He voiced interest in working on this with the American College of Physicians, which represents U.S. internal medicine physicians, and the American Academy of Family Physicians.
“We definitely need a partnership and educational efforts to get the word out from these organizations and not from a specialty society,” said Dr. Carey.
Dr. Funder said he has submitted a proposal to the Endocrine Society for a guidelines update he would chair with Dr. Carey’s assistance and with a diverse writing group that includes PCPs. Dr. Carey said that ideally this panel would write and release a revised guideline in 2021.
“Several of us are chomping at the bit to get this done,” he noted.
But participation by the ACP and AAFP remain uncertain as of September 2020. When approached about this, an ACP spokesperson said the organization had no comment. A spokesperson for the AAFP said, “It’s too early to tell if we will partner with any other organizations to develop guidelines specific to excess aldosterone, and how such guidelines might be received by our members.”
Recent history shows little cooperation between ACP, AAFP, and what might be termed the U.S. hypertension “establishment.” For example, when the American College of Cardiology and the American Heart Association released their most recent essential hypertension management guidelines in Hypertension in 2018, it was never adopted by ACP or AAFP.
The latter two organizations continue to endorse a higher BP threshold for diagnosing hypertension, and higher treatment targets set by alternative expert panels to those of the AHA/ACC.
Collaboration feasible, although PCPs overworked
Dr. Carey hopes that this episode will not preclude agreement over PA screening.
“I think it is still possible to partner with [the ACP and AAFP],” he observed, adding that he believes high PA prevalence among hypertensive patients and its consequences when unrecognized is “noncontentious.”
But he acknowledges that other, substantial hurdles also exist, notably the “overwhelming workload” that American PCPs already face.
David O’Gurek, MD, a family and community medicine physician at the Lewis Katz School of Medicine of Temple University in Philadelphia, agrees that a revamped approach to PA screening developed cooperatively between PCPs and specialists is an important goal and potentially feasible despite prior disagreements. “There has to be room for collaboration,” he said, but also emphasized the need for developing policies based on a systematic evidence review and a focus on patient-centered outcomes.
“We’re certainly missing patients with PA, but there needs to be greater clarity and standardization about the most appropriate screening approach and cutoff level” for flagging patients who need specialized assessment, Dr. O’Gurek said in an interview.
The current endocrinology literature also shows that experts remain divided on how best to accomplish this.
And some hypertension specialists question whether existing evidence is conclusive enough to warrant revised guidelines.
Dr. Cohen, the nephrologist and hypertension researcher, said that, while the recent prevalence report in Annals of Internal Medicine is “intriguing, hypothesis-generating information that suggests we are missing many cases of hyperaldosteronism in routine care,” she nevertheless believes that “we need additional data to be able to truly understand the breadth and implications of the findings.”
William C. Cushman, MD, a hypertension management specialist at the University of Tennessee Health Science Center in Memphis, agrees.
Changing existing practice guidelines “really needs randomized, controlled trials demonstrating a difference in long-term outcomes, ideally major cardiovascular outcomes,” that result from broader PA screening, he said.
Dr. Carey concurs that more evidence is needed to confirm the Annals report, but is confident this evidence will be in hand by the time a guideline-revision panel meets in 2021.
Australian model of PCPs screening for PA could be implemented in United States
An example of what might be possible when PCPs, endocrinologists, and hypertension specialists work together to make PA screening more accessible can be found in Melbourne, at the Endocrine Hypertension Service of Monash Health, in association with the Hudson Institute of Medical Research.
This began operating in July 2016, cofounded by Dr. Yang, whose experiences with her own father made her sensitive to the issue.
The service’s aim is to “address the underdiagnosis of PA, and to offer a streamlined diagnostic service for patients with hypertension,” with an “extensive outreach program” targeted to regional PCPs that, among other messages, encourages them to screen patients for PA when blood pressures exceed 140/90 mm Hg.
During its first 3 years of operation, the service saw 267 patients, with PA diagnosed in 135 and ruled out in 73 patients.
Notably, the proportion of these patients referred from PCPs jumped from 21% of 70 patients during the first year of operation to 47% of 70 patients during year 2, and 52% of 127 patients during the third year, ending in July 2019, said Dr. Yang, who continues to help run the service.
During the first year, a scant 3% of referred patients had recently diagnosed hypertension, but this rose to 14% during the second year, and to 19% during the most recent year with data available.
The median duration of diagnosed hypertension among referred patients fell from 11 years during year 1, to 7 years during year 3.
Service clinicians diagnosed 37 patients with unilateral adenomas, and removed them from 23 patients with four more awaiting surgery and the remaining 10 opting instead for medical management. Another 95 patients went on therapy with a MRA, and during the most recent year studied all patients who began a MRA regimen had a partial or complete clinical response.
Dr. Carey said the “creative program represents a model for implementation in U.S. practice.
Dr. Funder, Dr. Carey, Dr. Feldman, Dr. Yang, Dr. Cohen, and Dr. O’Gurek had no relevant disclosures. Dr. Cushman has been a consultant to Novartis, received personal fees from Sanofi, and research funding from Eli Lilly.
Jun Yang, MBBS, had watched as her father, who had battled hypertension for decades, ended up on four medications that still couldn’t bring his blood pressure to a healthy level. The cardiovascular endocrinologist then ran some tests, and soon thereafter her father had his blood pressure optimized on just one targeted medication.
Dr. Yang’s father was found to have a hormonal condition known as primary aldosteronism (PA) as the cause of his hypertension.
It turns out that PA is not as rare as once thought.
An eye-catching report in Annals of Internal Medicine this spring of an unexpectedly high prevalence of primary aldosteronism among a diverse cross section of U.S. patients with hypertension has raised issues that could dramatically change the way doctors in America, and elsewhere, assess and manage high blood pressure.
Foremost is the question of whether primary care physicians – the clinicians at the front line for diagnosing and initially treating most patients with hypertension – will absorb and act on this new evidence. For them, aldosteronism doesn’t automatically come to mind when they see high numbers on a BP monitor, and yet this latest research found that up to a third of all 726 patients in the study who were diagnosed with hypertension and with high urinary salt levels had PA.
That translates to a roughly three- to fivefold increase over standard prevalence estimates, and is a ”game changer” for how clinicians should approach hypertension management and PA diagnosis going forward, said John W. Funder, MD, in an editorial accompanying the Annals study.
Long considered relatively uncommon, hypertension driven by an excess of the hormone aldosterone, often because of an adenoma on the adrenal gland, is not the same as conventional “essential” hypertension. The former benefits from early diagnosis because its treatment is completely different – close to half of all PA patients can be treated definitively and quickly with surgical removal of an adenoma from one side of the adrenal gland.
For other PA patients, who have bilateral adrenal hyperplasia that is impossible to resolve surgically, treatment with drugs called mineralocorticoid receptor antagonists (MRAs), such as spironolactone, is needed because they target the hormonal cause of the high BP.
But what usually happens is that a patient with PA is mistakenly diagnosed with essential hypertension, in which the classic approach to treatment is to start with one regular antihypertensive drug, and add on further ones from different drug classes if blood pressure is not adequately controlled. When patients are taking three drugs, without adequate control, they are labeled as having “resistant hypertension.”
But in the case of PA, none of these conventional antihypertensives work, and the process of continuing to monitor and add different drugs wastes time, during which patients deteriorate.
“We need to change the culture of waiting for hypertension to be resistant and have patients riddled with end-organ damage,” due to years of persistently high BP and excess aldosterone “before we look for a secondary cause” like PA, declared Dr. Yang, of Hudson Institute of Medical Research and Monash University in Melbourne, during an interview.
So early diagnosis and prompt treatment of PA is key.
In addition to boosting the public health importance of early PA detection in hypertensive patients, the new up-sized PA prevalence numbers throw a spotlight on primary care physicians (PCPs) as key players who will need to apply the findings to practice on a public health scale.
These novel results create a need for “new guidelines, and a radically revised game plan with the key role of PCPs” emphasized in future management of patients with hypertension, said Dr. Funder, a professor of medicine at Monash University, in a second recent editorial in Hypertension.
“Buy-in by PCPs is essential,” agrees Robert M. Carey, MD, a cardiovascular endocrinologist and professor of medicine at the University of Virginia in Charlottesville, and a coauthor of the new study.
But he too acknowledges that this presents a major challenge. PCPs and internists, who diagnose a lot of hypertension, are “not used to thinking about aldosterone,” he said in an interview, encapsulating the key problem faced by proponents of earlier and more widespread PA assessment.
This dilemma looms as a “huge public health issue,” Dr. Carey warned.
‘We’re a long way from getting’ PCPs to buy in to PA screening
Will PCPs grow more comfortable with screening patients for PA themselves, or might they become more willing to refer hypertensive individuals for assessment at an expert center?
One skeptic is Ross D. Feldman, MD, a hypertension-management researcher and professor of medicine at the University of Manitoba in Winnipeg. The finding about high PA prevalence in patients with hypertension “is brand new, [and] the message needs to get to PCPs,” he said. But, “We’re a long way from getting it” to them. “I don’t know how to do that. It will be a tough sell.”
In addition, repositioning MRAs as an earlier option for many hypertensive patients won’t be easy either, because “we’ll never have outcome-trial data for MRAs,” given that they are now generic drugs, he noted.
“No clinical trial data show [MRAs] are first-line drugs,” said Dr. Feldman, who explained that, instead, MRAs are considered “go-to drugs” for patients with treatment-resistant hypertension, a niche therapeutic area. Results from the PATHWAY-2 trial published 5 years ago in Lancet showed “spironolactone was clearly the most effective treatment for the condition,” according to the report authors.
But even among patients with resistant hypertension, screening for PA dramatically lags despite being enshrined in guidelines.
“PCPs should start checking aldosterone-to-renin ratios [a widely used PA screen] in all patients with resistant hypertension or hypertension with hypokalemia, and then refer patients to specialists for testing and management,” said Jordana B. Cohen, MD, a nephrologist and hypertension researcher at the University of Pennsylvania in Philadelphia.
But recent studies of U.S. patient populations with clinical characteristics that meet existing criteria for PA screening showed that just 1%-2% of these individuals underwent an initial PA assessment, she noted, citing reports in the journals Surgery and Hypertension.
“We need to prioritize improving screening in these high-risk patients,” she stressed in an interview.
This illustrates that, in some respects, the new prevalence numbers are beside the point, because PA has been going unscreened and overlooked far too often even in the context of historical, lower prevalence rates, said Dr. Yang.
“The key point is that approximately 1 in 10 people with hypertension, and even more with resistant hypertension, have a form of the disease that is worse than essential hypertension but is routinely missed at present” and is also highly treatable.
“Evidence for the need for increased awareness of PA has been building for 2 decades,” stressed Dr. Yang, who has coauthored several commentaries and reviews that have bemoaned PA’s underappreciated status.
Interest in partnering with PCPs on guidance grows
One potential solution is to have endocrinologists and hypertension specialists’ partner with PCPs to come up with diagnostic and management recommendations. Both Dr. Funder and Dr. Carey are opinion leaders regarding the role of aldosterone in hypertension, and both were coauthors of the 2016 Endocrine Society guideline for PA assessment and management published in the Journal of Clinical Endocrinology & Metabolism , with Dr. Funder chairing the writing panel.
Now approaching its fifth year in effect, this guideline is “due for revision,” and “my hope is that we’ll be able to partner with one or more PCP organizations to come up with a version of the guideline targeted to PCPs,” Dr. Carey said.
He voiced interest in working on this with the American College of Physicians, which represents U.S. internal medicine physicians, and the American Academy of Family Physicians.
“We definitely need a partnership and educational efforts to get the word out from these organizations and not from a specialty society,” said Dr. Carey.
Dr. Funder said he has submitted a proposal to the Endocrine Society for a guidelines update he would chair with Dr. Carey’s assistance and with a diverse writing group that includes PCPs. Dr. Carey said that ideally this panel would write and release a revised guideline in 2021.
“Several of us are chomping at the bit to get this done,” he noted.
But participation by the ACP and AAFP remain uncertain as of September 2020. When approached about this, an ACP spokesperson said the organization had no comment. A spokesperson for the AAFP said, “It’s too early to tell if we will partner with any other organizations to develop guidelines specific to excess aldosterone, and how such guidelines might be received by our members.”
Recent history shows little cooperation between ACP, AAFP, and what might be termed the U.S. hypertension “establishment.” For example, when the American College of Cardiology and the American Heart Association released their most recent essential hypertension management guidelines in Hypertension in 2018, it was never adopted by ACP or AAFP.
The latter two organizations continue to endorse a higher BP threshold for diagnosing hypertension, and higher treatment targets set by alternative expert panels to those of the AHA/ACC.
Collaboration feasible, although PCPs overworked
Dr. Carey hopes that this episode will not preclude agreement over PA screening.
“I think it is still possible to partner with [the ACP and AAFP],” he observed, adding that he believes high PA prevalence among hypertensive patients and its consequences when unrecognized is “noncontentious.”
But he acknowledges that other, substantial hurdles also exist, notably the “overwhelming workload” that American PCPs already face.
David O’Gurek, MD, a family and community medicine physician at the Lewis Katz School of Medicine of Temple University in Philadelphia, agrees that a revamped approach to PA screening developed cooperatively between PCPs and specialists is an important goal and potentially feasible despite prior disagreements. “There has to be room for collaboration,” he said, but also emphasized the need for developing policies based on a systematic evidence review and a focus on patient-centered outcomes.
“We’re certainly missing patients with PA, but there needs to be greater clarity and standardization about the most appropriate screening approach and cutoff level” for flagging patients who need specialized assessment, Dr. O’Gurek said in an interview.
The current endocrinology literature also shows that experts remain divided on how best to accomplish this.
And some hypertension specialists question whether existing evidence is conclusive enough to warrant revised guidelines.
Dr. Cohen, the nephrologist and hypertension researcher, said that, while the recent prevalence report in Annals of Internal Medicine is “intriguing, hypothesis-generating information that suggests we are missing many cases of hyperaldosteronism in routine care,” she nevertheless believes that “we need additional data to be able to truly understand the breadth and implications of the findings.”
William C. Cushman, MD, a hypertension management specialist at the University of Tennessee Health Science Center in Memphis, agrees.
Changing existing practice guidelines “really needs randomized, controlled trials demonstrating a difference in long-term outcomes, ideally major cardiovascular outcomes,” that result from broader PA screening, he said.
Dr. Carey concurs that more evidence is needed to confirm the Annals report, but is confident this evidence will be in hand by the time a guideline-revision panel meets in 2021.
Australian model of PCPs screening for PA could be implemented in United States
An example of what might be possible when PCPs, endocrinologists, and hypertension specialists work together to make PA screening more accessible can be found in Melbourne, at the Endocrine Hypertension Service of Monash Health, in association with the Hudson Institute of Medical Research.
This began operating in July 2016, cofounded by Dr. Yang, whose experiences with her own father made her sensitive to the issue.
The service’s aim is to “address the underdiagnosis of PA, and to offer a streamlined diagnostic service for patients with hypertension,” with an “extensive outreach program” targeted to regional PCPs that, among other messages, encourages them to screen patients for PA when blood pressures exceed 140/90 mm Hg.
During its first 3 years of operation, the service saw 267 patients, with PA diagnosed in 135 and ruled out in 73 patients.
Notably, the proportion of these patients referred from PCPs jumped from 21% of 70 patients during the first year of operation to 47% of 70 patients during year 2, and 52% of 127 patients during the third year, ending in July 2019, said Dr. Yang, who continues to help run the service.
During the first year, a scant 3% of referred patients had recently diagnosed hypertension, but this rose to 14% during the second year, and to 19% during the most recent year with data available.
The median duration of diagnosed hypertension among referred patients fell from 11 years during year 1, to 7 years during year 3.
Service clinicians diagnosed 37 patients with unilateral adenomas, and removed them from 23 patients with four more awaiting surgery and the remaining 10 opting instead for medical management. Another 95 patients went on therapy with a MRA, and during the most recent year studied all patients who began a MRA regimen had a partial or complete clinical response.
Dr. Carey said the “creative program represents a model for implementation in U.S. practice.
Dr. Funder, Dr. Carey, Dr. Feldman, Dr. Yang, Dr. Cohen, and Dr. O’Gurek had no relevant disclosures. Dr. Cushman has been a consultant to Novartis, received personal fees from Sanofi, and research funding from Eli Lilly.
‘Overwhelming evidence’ FDA’s opioid approval process is shoddy
Despite the ongoing epidemic of misuse, overuse, and diversion of opioids, the Food and Drug Administration has set a low bar for approval of these medications over the past 20 years, new research suggests.
The study results also show that the FDA did not require manufacturers to collect safety data on tolerance, withdrawal, overdose, misuse, and diversion in any rigorous fashion.
In addition, during the study period, 17 of the 39 new drug applications (NDAs) (only one was an innovator product, known as a new molecular entity) for chronic pain were approved with an “enriched enrollment randomized withdrawal” (EERW) trial design. Such a design, in this case, allowed manufacturers to exclude 32%-43% of the initially enrolled patients from the double-blind treatment phase.
“The question for regulators, policy makers, and others is: How did we get to a point where these approvals took place based on trials that were by design unlikely to yield some of the most important information about safety and efficacy that patients and clinicians would care about?” study investigator G. Caleb Alexander, MD, Johns Hopkins University, Baltimore, said in an interview.
The study was published online Sept. 29 in the Annals of Internal Medicine.
‘Cooking the books’
Little is known about the evidence required by the FDA for new approvals of opioid analgesics.
To characterize the quality of safety and efficacy data in NDAs for opioid analgesics approved by the FDA between 1997 and 2018, the investigators conducted the cross-sectional analysis using data from ClinicalTrials.gov, FDA reviews, and peer-reviewed publications regarding phase 3 pivotal trials.
The investigators examined the key characteristics of each NDA, including the number, size, and duration of pivotal trials, trial control groups, use of EERW, and systematically measured safety outcomes.
Results showed that most of the 48 NDAs evaluated were for new dosage forms (52.1%) or new formulations (18.8%). Only one (2.1%) was for a new molecular entity.
Of 39 NDAs approved for the treatment of chronic pain, only 21 products were supported by at least one pivotal trial. The mean duration of these 28 trials was 84 days, and they enrolled a median of 299 patients.
Results showed that, for 17 of the 39 opioids approved for chronic pain, pivotal trials had an EERW design. For the latest period – 2012-2018 – trials of all eight of the approved opioids used the EERW method.
This EERW design allows the manufacturer to assess efficacy “among a subset of patients most likely to respond and least likely to have adverse effects, reducing generalizability to real-world settings,” the investigators noted.
They called on the FDA to stop relying on this type of trial to assess opioid efficacy.
In an August 2020 article, Andrew Kolodny, MD, pointed out the pitfalls of the EERW approach. In such a study, all participants are made physiologically dependent on the opioid in a 4- to 6-week open-label phase. Only those who tolerate the drug and find it helpful are included in the randomized study. Dr. Kolodny is codirector of opioid policy research at Brandeis University, Waltham, Mass.
“Critics of EERW have correctly described this methodology as ‘cooking the books,’ ” Dr. Kolodny writes.
He noted that the agency’s decision to rely on EERW trials for opioids was “based on discussions at private meetings between FDA officials and pharmaceutical company executives hosted by an organization called Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials.” The 2013 meetings were reported in an article published in the Washington Post.
Little sign of change
Among NDAs for chronic pain, the investigators found that eight (20.5%) included pooled safety reviews that reported systematic assessment of diversion. Seven (17.9%) reported systematic measurement of nonmedical use, and 15 (38.5%) assessed incident tolerance.
The study revealed that eight of nine products that were approved for acute pain were supported by at least one pivotal trial. The median duration of these 19 trials was 1 day, and they enrolled a median of 329 patients.
The investigators noted that the findings “underscore the evidence gaps that have limited clinicians’ and patients’ understanding and appreciation of the inherent risks of prescription opioid analgesics.”
Dr. Alexander, who has been an FDA advisory committee chairman and currently serves as a consultant to plaintiffs who are suing opioid manufacturers in federal multidistrict litigation, said the study “is a story about missed opportunities to improve the safety and to improve the regulatory review of these products.”
Coinvestigator Peter Lurie, MD, who was an official at the FDA from 2009 to 2017, said that “there’s not a lot of signs that things are changing” at the agency.
The study shows that the FDA has “accepted what the companies have been presenting,” said Dr. Lurie, who is president of the Center for Science in the Public Interest.
The FDA “absolutely has the authority” to require manufacturers to undertake more rigorous trials, but agency culture keeps it from making such demands, especially if doing so means a new applicant might have to conduct trials that weren’t previously required, Dr. Lurie said in an interview.
“FDA is pretty rigorous about trying to establish a level playing field. That’s a virtuous thing, but it becomes problematic when that prevents change,” said Dr. Lurie.
The most recent FDA guidance to manufacturers, issued in 2019, does not provide advice on criteria for endpoints, study duration, or which populations are most likely to benefit from opioid treatment. The agency also does not require drug manufacturers to formally collect data on safety, tolerance, overdose symptoms, or constipation.
The guidance does suggest that the agency would likely take into account public health considerations when evaluating opioids, such as the risk to the overall population for overdose and diversion.
‘Overwhelming evidence’
Dr. Kolodny said that, as far as he is aware, “this is the first scientific publication in a peer-reviewed journal demonstrating clearly the problems with FDA’s opioid approval process.”
The article offers “overwhelming evidence that they are improperly approving the most dangerous medications – medications that killed more people than any other medication on the market,” added Dr. Kolodny, who is also president of Physicians for Responsible Opioid Prescribing.
Asked to respond to the study findings, FDA spokesperson Charles Kohler said the agency “does not comment on specific studies but evaluates them as part of the body of evidence to further our understanding about a particular issue and assist in our mission to protect public health.”
A version of this article originally appeared on Medscape.com.
Despite the ongoing epidemic of misuse, overuse, and diversion of opioids, the Food and Drug Administration has set a low bar for approval of these medications over the past 20 years, new research suggests.
The study results also show that the FDA did not require manufacturers to collect safety data on tolerance, withdrawal, overdose, misuse, and diversion in any rigorous fashion.
In addition, during the study period, 17 of the 39 new drug applications (NDAs) (only one was an innovator product, known as a new molecular entity) for chronic pain were approved with an “enriched enrollment randomized withdrawal” (EERW) trial design. Such a design, in this case, allowed manufacturers to exclude 32%-43% of the initially enrolled patients from the double-blind treatment phase.
“The question for regulators, policy makers, and others is: How did we get to a point where these approvals took place based on trials that were by design unlikely to yield some of the most important information about safety and efficacy that patients and clinicians would care about?” study investigator G. Caleb Alexander, MD, Johns Hopkins University, Baltimore, said in an interview.
The study was published online Sept. 29 in the Annals of Internal Medicine.
‘Cooking the books’
Little is known about the evidence required by the FDA for new approvals of opioid analgesics.
To characterize the quality of safety and efficacy data in NDAs for opioid analgesics approved by the FDA between 1997 and 2018, the investigators conducted the cross-sectional analysis using data from ClinicalTrials.gov, FDA reviews, and peer-reviewed publications regarding phase 3 pivotal trials.
The investigators examined the key characteristics of each NDA, including the number, size, and duration of pivotal trials, trial control groups, use of EERW, and systematically measured safety outcomes.
Results showed that most of the 48 NDAs evaluated were for new dosage forms (52.1%) or new formulations (18.8%). Only one (2.1%) was for a new molecular entity.
Of 39 NDAs approved for the treatment of chronic pain, only 21 products were supported by at least one pivotal trial. The mean duration of these 28 trials was 84 days, and they enrolled a median of 299 patients.
Results showed that, for 17 of the 39 opioids approved for chronic pain, pivotal trials had an EERW design. For the latest period – 2012-2018 – trials of all eight of the approved opioids used the EERW method.
This EERW design allows the manufacturer to assess efficacy “among a subset of patients most likely to respond and least likely to have adverse effects, reducing generalizability to real-world settings,” the investigators noted.
They called on the FDA to stop relying on this type of trial to assess opioid efficacy.
In an August 2020 article, Andrew Kolodny, MD, pointed out the pitfalls of the EERW approach. In such a study, all participants are made physiologically dependent on the opioid in a 4- to 6-week open-label phase. Only those who tolerate the drug and find it helpful are included in the randomized study. Dr. Kolodny is codirector of opioid policy research at Brandeis University, Waltham, Mass.
“Critics of EERW have correctly described this methodology as ‘cooking the books,’ ” Dr. Kolodny writes.
He noted that the agency’s decision to rely on EERW trials for opioids was “based on discussions at private meetings between FDA officials and pharmaceutical company executives hosted by an organization called Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials.” The 2013 meetings were reported in an article published in the Washington Post.
Little sign of change
Among NDAs for chronic pain, the investigators found that eight (20.5%) included pooled safety reviews that reported systematic assessment of diversion. Seven (17.9%) reported systematic measurement of nonmedical use, and 15 (38.5%) assessed incident tolerance.
The study revealed that eight of nine products that were approved for acute pain were supported by at least one pivotal trial. The median duration of these 19 trials was 1 day, and they enrolled a median of 329 patients.
The investigators noted that the findings “underscore the evidence gaps that have limited clinicians’ and patients’ understanding and appreciation of the inherent risks of prescription opioid analgesics.”
Dr. Alexander, who has been an FDA advisory committee chairman and currently serves as a consultant to plaintiffs who are suing opioid manufacturers in federal multidistrict litigation, said the study “is a story about missed opportunities to improve the safety and to improve the regulatory review of these products.”
Coinvestigator Peter Lurie, MD, who was an official at the FDA from 2009 to 2017, said that “there’s not a lot of signs that things are changing” at the agency.
The study shows that the FDA has “accepted what the companies have been presenting,” said Dr. Lurie, who is president of the Center for Science in the Public Interest.
The FDA “absolutely has the authority” to require manufacturers to undertake more rigorous trials, but agency culture keeps it from making such demands, especially if doing so means a new applicant might have to conduct trials that weren’t previously required, Dr. Lurie said in an interview.
“FDA is pretty rigorous about trying to establish a level playing field. That’s a virtuous thing, but it becomes problematic when that prevents change,” said Dr. Lurie.
The most recent FDA guidance to manufacturers, issued in 2019, does not provide advice on criteria for endpoints, study duration, or which populations are most likely to benefit from opioid treatment. The agency also does not require drug manufacturers to formally collect data on safety, tolerance, overdose symptoms, or constipation.
The guidance does suggest that the agency would likely take into account public health considerations when evaluating opioids, such as the risk to the overall population for overdose and diversion.
‘Overwhelming evidence’
Dr. Kolodny said that, as far as he is aware, “this is the first scientific publication in a peer-reviewed journal demonstrating clearly the problems with FDA’s opioid approval process.”
The article offers “overwhelming evidence that they are improperly approving the most dangerous medications – medications that killed more people than any other medication on the market,” added Dr. Kolodny, who is also president of Physicians for Responsible Opioid Prescribing.
Asked to respond to the study findings, FDA spokesperson Charles Kohler said the agency “does not comment on specific studies but evaluates them as part of the body of evidence to further our understanding about a particular issue and assist in our mission to protect public health.”
A version of this article originally appeared on Medscape.com.
Despite the ongoing epidemic of misuse, overuse, and diversion of opioids, the Food and Drug Administration has set a low bar for approval of these medications over the past 20 years, new research suggests.
The study results also show that the FDA did not require manufacturers to collect safety data on tolerance, withdrawal, overdose, misuse, and diversion in any rigorous fashion.
In addition, during the study period, 17 of the 39 new drug applications (NDAs) (only one was an innovator product, known as a new molecular entity) for chronic pain were approved with an “enriched enrollment randomized withdrawal” (EERW) trial design. Such a design, in this case, allowed manufacturers to exclude 32%-43% of the initially enrolled patients from the double-blind treatment phase.
“The question for regulators, policy makers, and others is: How did we get to a point where these approvals took place based on trials that were by design unlikely to yield some of the most important information about safety and efficacy that patients and clinicians would care about?” study investigator G. Caleb Alexander, MD, Johns Hopkins University, Baltimore, said in an interview.
The study was published online Sept. 29 in the Annals of Internal Medicine.
‘Cooking the books’
Little is known about the evidence required by the FDA for new approvals of opioid analgesics.
To characterize the quality of safety and efficacy data in NDAs for opioid analgesics approved by the FDA between 1997 and 2018, the investigators conducted the cross-sectional analysis using data from ClinicalTrials.gov, FDA reviews, and peer-reviewed publications regarding phase 3 pivotal trials.
The investigators examined the key characteristics of each NDA, including the number, size, and duration of pivotal trials, trial control groups, use of EERW, and systematically measured safety outcomes.
Results showed that most of the 48 NDAs evaluated were for new dosage forms (52.1%) or new formulations (18.8%). Only one (2.1%) was for a new molecular entity.
Of 39 NDAs approved for the treatment of chronic pain, only 21 products were supported by at least one pivotal trial. The mean duration of these 28 trials was 84 days, and they enrolled a median of 299 patients.
Results showed that, for 17 of the 39 opioids approved for chronic pain, pivotal trials had an EERW design. For the latest period – 2012-2018 – trials of all eight of the approved opioids used the EERW method.
This EERW design allows the manufacturer to assess efficacy “among a subset of patients most likely to respond and least likely to have adverse effects, reducing generalizability to real-world settings,” the investigators noted.
They called on the FDA to stop relying on this type of trial to assess opioid efficacy.
In an August 2020 article, Andrew Kolodny, MD, pointed out the pitfalls of the EERW approach. In such a study, all participants are made physiologically dependent on the opioid in a 4- to 6-week open-label phase. Only those who tolerate the drug and find it helpful are included in the randomized study. Dr. Kolodny is codirector of opioid policy research at Brandeis University, Waltham, Mass.
“Critics of EERW have correctly described this methodology as ‘cooking the books,’ ” Dr. Kolodny writes.
He noted that the agency’s decision to rely on EERW trials for opioids was “based on discussions at private meetings between FDA officials and pharmaceutical company executives hosted by an organization called Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials.” The 2013 meetings were reported in an article published in the Washington Post.
Little sign of change
Among NDAs for chronic pain, the investigators found that eight (20.5%) included pooled safety reviews that reported systematic assessment of diversion. Seven (17.9%) reported systematic measurement of nonmedical use, and 15 (38.5%) assessed incident tolerance.
The study revealed that eight of nine products that were approved for acute pain were supported by at least one pivotal trial. The median duration of these 19 trials was 1 day, and they enrolled a median of 329 patients.
The investigators noted that the findings “underscore the evidence gaps that have limited clinicians’ and patients’ understanding and appreciation of the inherent risks of prescription opioid analgesics.”
Dr. Alexander, who has been an FDA advisory committee chairman and currently serves as a consultant to plaintiffs who are suing opioid manufacturers in federal multidistrict litigation, said the study “is a story about missed opportunities to improve the safety and to improve the regulatory review of these products.”
Coinvestigator Peter Lurie, MD, who was an official at the FDA from 2009 to 2017, said that “there’s not a lot of signs that things are changing” at the agency.
The study shows that the FDA has “accepted what the companies have been presenting,” said Dr. Lurie, who is president of the Center for Science in the Public Interest.
The FDA “absolutely has the authority” to require manufacturers to undertake more rigorous trials, but agency culture keeps it from making such demands, especially if doing so means a new applicant might have to conduct trials that weren’t previously required, Dr. Lurie said in an interview.
“FDA is pretty rigorous about trying to establish a level playing field. That’s a virtuous thing, but it becomes problematic when that prevents change,” said Dr. Lurie.
The most recent FDA guidance to manufacturers, issued in 2019, does not provide advice on criteria for endpoints, study duration, or which populations are most likely to benefit from opioid treatment. The agency also does not require drug manufacturers to formally collect data on safety, tolerance, overdose symptoms, or constipation.
The guidance does suggest that the agency would likely take into account public health considerations when evaluating opioids, such as the risk to the overall population for overdose and diversion.
‘Overwhelming evidence’
Dr. Kolodny said that, as far as he is aware, “this is the first scientific publication in a peer-reviewed journal demonstrating clearly the problems with FDA’s opioid approval process.”
The article offers “overwhelming evidence that they are improperly approving the most dangerous medications – medications that killed more people than any other medication on the market,” added Dr. Kolodny, who is also president of Physicians for Responsible Opioid Prescribing.
Asked to respond to the study findings, FDA spokesperson Charles Kohler said the agency “does not comment on specific studies but evaluates them as part of the body of evidence to further our understanding about a particular issue and assist in our mission to protect public health.”
A version of this article originally appeared on Medscape.com.