User login
Hospital medicine, it’s time to vote
Whether physicians or advanced practice practitioners, we are the backbone of our nation’s network of acute care facilities, and on a daily basis, we see just about everything. We have valuable insight into how to improve our nation’s health care system, especially now, as our nation continues to battle COVID-19.

Our role, squarely on the front lines during this pandemic, has given us an important perspective that needs to be heard. We spend our days managing patients with complexity, coordinating with specialists and subspecialists, and advocating – at local, state, and national levels – so that our patients can more easily transition to their lives out of the hospital.
Our current polarized political climate makes it seem that individual voices will not make a difference. It is easy to feel frustrated and powerless. However, those in our specialty are actually in a perfect position to have an educated and influential say in how we move forward, not only about the immediate health crises, but also regarding future health care issues. That voice begins with voting.
Historically, physicians have had surprisingly low rates of voting. For example, a 2007 study found significantly lower rates of voting among physicians, compared with the general public.1 While physician voter turnout may have improved in the past decade, given the substantial changes in health care and the increasing amount of physician engagement in the public sphere, our participation should be greater still. Elected officials listen to, and follow up with, constituents who make their voices heard. Each of us can ensure that the health care policy priorities of our fast-growing specialty are addressed by mobilizing to the voting booth.
Candidates we elect shape our health care system for the future, directly impacting us and our patients. Cost, coverage, access to health care, the Centers for Medicare & Medicaid Services inpatient fee schedules, the ongoing pandemic response, surprise billing, use of telehealth, observation status, and the three-midnight rule are just a few of the issues most important to hospital medicine.
Therefore, we, the SHM Public Policy Committee, urge all of our colleagues, regardless of political sway, to make your voice heard this and every election henceforth. The first step is to register to vote, if you have not done so already.2 Next, exercise that privilege. Given the pandemic, this is not as simple a process as it has been in the past. Take the time to plan your approach to early voting, mail-in voting, or election day voting. Check your County Supervisor of Elections’ website for further information, including how to register, view candidate profiles, check your precinct, and request a mail-in ballot.
In addition to casting your vote, we encourage you to share your opinions and engage in dialogue about health care issues. Clinical fact can dispel rumor and misinformation, and daily experiences can personalize our patients’ health care stories and the impact laws and rules have on our ability to practice. We are part of a trusted profession and have a unique perspective; others need and want to hear it. They can only do that if we are part of the process. Arming yourself with information and voting are the first steps on the path of advocacy. Interpersonal advocacy can also be done on social media. For example, SHM has an active grassroots advocacy network on Twitter. Tag @SHMadvocacy in your tweets to share your thoughts with their network.
Finally, as advocates for our patients in health care, we can also help ensure their safety during this election, in particular regarding COVID-19. Some patients may not wish to engage us in politics, and we must respect their decision. Others may seek our counsel and we should provide it in an unbiased fashion. We can ask our patients if they have considered a safe voting plan, help patients review the alternatives to voting in person if desired, and inform those who wish to physically cast a vote on Election Day of how to mitigate the risk of in-person voting.
Every election is important and health care is front and center for a multitude of reasons. We who practice hospital medicine are integral to our communities and need to be more politically involved. This is our chance to share our voice through our vote, not just this year, but in future elections as well.
Ann Sheehy, MD, SFHM, is division chief of the Division of Hospital Medicine at the University of Wisconsin, Madison, and chair of the SHM Public Policy Committee. Other members of the SHM PPC include Marta Almli, MD; John Biebelhausen, MD; Robert Burke, MD, MS, FHM; George Cheely, MD; Hyung (Harry) Cho, MD, SFHM; Jennifer Cowart, MD, FHM; Suparna Dutta, MD, MS, MPH; Bradley Flansbaum, DO, MPH, MHM; Alain Folefack, MD; Rick Hilger MD SFHM; Melinda Johnson, MD; Sevan Karadolian, MD; Joshua D. Lenchus, DO, FACP, SFHM; Steve Phillipson, MD; Dahlia Rizk, DO; Kendall Rogers, MD, SFHM; Brett Stauffer, MD, MHS; Amit Vashist, MD, SFHM; Robert Zipper, MD, SFHM.
References
1. Grande D et al. Do doctors vote? J Gen Int Med. 2007 May;22(5):585-9.
2. How to register to vote, confirm or change your registration and get a voter registration card. https://www.usa.gov/voter-registration/.
Whether physicians or advanced practice practitioners, we are the backbone of our nation’s network of acute care facilities, and on a daily basis, we see just about everything. We have valuable insight into how to improve our nation’s health care system, especially now, as our nation continues to battle COVID-19.
Our role, squarely on the front lines during this pandemic, has given us an important perspective that needs to be heard. We spend our days managing patients with complexity, coordinating with specialists and subspecialists, and advocating – at local, state, and national levels – so that our patients can more easily transition to their lives out of the hospital.
Our current polarized political climate makes it seem that individual voices will not make a difference. It is easy to feel frustrated and powerless. However, those in our specialty are actually in a perfect position to have an educated and influential say in how we move forward, not only about the immediate health crises, but also regarding future health care issues. That voice begins with voting.
Historically, physicians have had surprisingly low rates of voting. For example, a 2007 study found significantly lower rates of voting among physicians, compared with the general public.1 While physician voter turnout may have improved in the past decade, given the substantial changes in health care and the increasing amount of physician engagement in the public sphere, our participation should be greater still. Elected officials listen to, and follow up with, constituents who make their voices heard. Each of us can ensure that the health care policy priorities of our fast-growing specialty are addressed by mobilizing to the voting booth.
Candidates we elect shape our health care system for the future, directly impacting us and our patients. Cost, coverage, access to health care, the Centers for Medicare & Medicaid Services inpatient fee schedules, the ongoing pandemic response, surprise billing, use of telehealth, observation status, and the three-midnight rule are just a few of the issues most important to hospital medicine.
Therefore, we, the SHM Public Policy Committee, urge all of our colleagues, regardless of political sway, to make your voice heard this and every election henceforth. The first step is to register to vote, if you have not done so already.2 Next, exercise that privilege. Given the pandemic, this is not as simple a process as it has been in the past. Take the time to plan your approach to early voting, mail-in voting, or election day voting. Check your County Supervisor of Elections’ website for further information, including how to register, view candidate profiles, check your precinct, and request a mail-in ballot.
In addition to casting your vote, we encourage you to share your opinions and engage in dialogue about health care issues. Clinical fact can dispel rumor and misinformation, and daily experiences can personalize our patients’ health care stories and the impact laws and rules have on our ability to practice. We are part of a trusted profession and have a unique perspective; others need and want to hear it. They can only do that if we are part of the process. Arming yourself with information and voting are the first steps on the path of advocacy. Interpersonal advocacy can also be done on social media. For example, SHM has an active grassroots advocacy network on Twitter. Tag @SHMadvocacy in your tweets to share your thoughts with their network.
Finally, as advocates for our patients in health care, we can also help ensure their safety during this election, in particular regarding COVID-19. Some patients may not wish to engage us in politics, and we must respect their decision. Others may seek our counsel and we should provide it in an unbiased fashion. We can ask our patients if they have considered a safe voting plan, help patients review the alternatives to voting in person if desired, and inform those who wish to physically cast a vote on Election Day of how to mitigate the risk of in-person voting.
Every election is important and health care is front and center for a multitude of reasons. We who practice hospital medicine are integral to our communities and need to be more politically involved. This is our chance to share our voice through our vote, not just this year, but in future elections as well.
Ann Sheehy, MD, SFHM, is division chief of the Division of Hospital Medicine at the University of Wisconsin, Madison, and chair of the SHM Public Policy Committee. Other members of the SHM PPC include Marta Almli, MD; John Biebelhausen, MD; Robert Burke, MD, MS, FHM; George Cheely, MD; Hyung (Harry) Cho, MD, SFHM; Jennifer Cowart, MD, FHM; Suparna Dutta, MD, MS, MPH; Bradley Flansbaum, DO, MPH, MHM; Alain Folefack, MD; Rick Hilger MD SFHM; Melinda Johnson, MD; Sevan Karadolian, MD; Joshua D. Lenchus, DO, FACP, SFHM; Steve Phillipson, MD; Dahlia Rizk, DO; Kendall Rogers, MD, SFHM; Brett Stauffer, MD, MHS; Amit Vashist, MD, SFHM; Robert Zipper, MD, SFHM.
References
1. Grande D et al. Do doctors vote? J Gen Int Med. 2007 May;22(5):585-9.
2. How to register to vote, confirm or change your registration and get a voter registration card. https://www.usa.gov/voter-registration/.
Whether physicians or advanced practice practitioners, we are the backbone of our nation’s network of acute care facilities, and on a daily basis, we see just about everything. We have valuable insight into how to improve our nation’s health care system, especially now, as our nation continues to battle COVID-19.
Our role, squarely on the front lines during this pandemic, has given us an important perspective that needs to be heard. We spend our days managing patients with complexity, coordinating with specialists and subspecialists, and advocating – at local, state, and national levels – so that our patients can more easily transition to their lives out of the hospital.
Our current polarized political climate makes it seem that individual voices will not make a difference. It is easy to feel frustrated and powerless. However, those in our specialty are actually in a perfect position to have an educated and influential say in how we move forward, not only about the immediate health crises, but also regarding future health care issues. That voice begins with voting.
Historically, physicians have had surprisingly low rates of voting. For example, a 2007 study found significantly lower rates of voting among physicians, compared with the general public.1 While physician voter turnout may have improved in the past decade, given the substantial changes in health care and the increasing amount of physician engagement in the public sphere, our participation should be greater still. Elected officials listen to, and follow up with, constituents who make their voices heard. Each of us can ensure that the health care policy priorities of our fast-growing specialty are addressed by mobilizing to the voting booth.
Candidates we elect shape our health care system for the future, directly impacting us and our patients. Cost, coverage, access to health care, the Centers for Medicare & Medicaid Services inpatient fee schedules, the ongoing pandemic response, surprise billing, use of telehealth, observation status, and the three-midnight rule are just a few of the issues most important to hospital medicine.
Therefore, we, the SHM Public Policy Committee, urge all of our colleagues, regardless of political sway, to make your voice heard this and every election henceforth. The first step is to register to vote, if you have not done so already.2 Next, exercise that privilege. Given the pandemic, this is not as simple a process as it has been in the past. Take the time to plan your approach to early voting, mail-in voting, or election day voting. Check your County Supervisor of Elections’ website for further information, including how to register, view candidate profiles, check your precinct, and request a mail-in ballot.
In addition to casting your vote, we encourage you to share your opinions and engage in dialogue about health care issues. Clinical fact can dispel rumor and misinformation, and daily experiences can personalize our patients’ health care stories and the impact laws and rules have on our ability to practice. We are part of a trusted profession and have a unique perspective; others need and want to hear it. They can only do that if we are part of the process. Arming yourself with information and voting are the first steps on the path of advocacy. Interpersonal advocacy can also be done on social media. For example, SHM has an active grassroots advocacy network on Twitter. Tag @SHMadvocacy in your tweets to share your thoughts with their network.
Finally, as advocates for our patients in health care, we can also help ensure their safety during this election, in particular regarding COVID-19. Some patients may not wish to engage us in politics, and we must respect their decision. Others may seek our counsel and we should provide it in an unbiased fashion. We can ask our patients if they have considered a safe voting plan, help patients review the alternatives to voting in person if desired, and inform those who wish to physically cast a vote on Election Day of how to mitigate the risk of in-person voting.
Every election is important and health care is front and center for a multitude of reasons. We who practice hospital medicine are integral to our communities and need to be more politically involved. This is our chance to share our voice through our vote, not just this year, but in future elections as well.
Ann Sheehy, MD, SFHM, is division chief of the Division of Hospital Medicine at the University of Wisconsin, Madison, and chair of the SHM Public Policy Committee. Other members of the SHM PPC include Marta Almli, MD; John Biebelhausen, MD; Robert Burke, MD, MS, FHM; George Cheely, MD; Hyung (Harry) Cho, MD, SFHM; Jennifer Cowart, MD, FHM; Suparna Dutta, MD, MS, MPH; Bradley Flansbaum, DO, MPH, MHM; Alain Folefack, MD; Rick Hilger MD SFHM; Melinda Johnson, MD; Sevan Karadolian, MD; Joshua D. Lenchus, DO, FACP, SFHM; Steve Phillipson, MD; Dahlia Rizk, DO; Kendall Rogers, MD, SFHM; Brett Stauffer, MD, MHS; Amit Vashist, MD, SFHM; Robert Zipper, MD, SFHM.
References
1. Grande D et al. Do doctors vote? J Gen Int Med. 2007 May;22(5):585-9.
2. How to register to vote, confirm or change your registration and get a voter registration card. https://www.usa.gov/voter-registration/.
LSD microdosing to boost attention: Too soon to tell?
Microdosing with lysergic acid diethylamide (LSD) is associated with improved mood and increased attention, early research suggests. However, at least one expert believes it’s far too soon to tell and warns against endorsing patient microdosing.
In a dose-finding exploratory study, three low doses of LSD were compared with placebo in healthy volunteers who were all recreational drug users. Adjusted results showed that the highest dose boosted attention and mood, although participants were aware of psychedelic effects, prompting researchers to conclude the results demonstrated “selective, beneficial effects.”
“The majority of participants have improved attention,” study investigator Nadia Hutten, PhD, Department of Neuropsychology and Psychopharmacology, Maastricht University, the Netherlands, told Medscape Medical News.
“So we think that patients with attention deficits might have more beneficial effects,” she added, noting her team plans to study LSD microdosing in patients with attention deficit hyperactivity disorder.
The study was presented at the 33rd European College of Neuropsychopharmacology (ECNP) Congress, which was held online this year because of the COVID-19 pandemic.
Growing interest
Over the past 10 years there has been growing interest in psychedelic microdosing, which is defined as a dose that aims to enhance mood and/or performance but does not affect perception.
However, there has been considerable debate over what constitutes a “microdose.” One tenth of a “full” psychedelic dose is typically suggested, but users report a much wider dose range in practice, suggesting potential “individual variation in response to low doses,” the researchers note.
In the current dose-finding study, the researchers explored whether the effects of LSD on cognition and subjective measures differed between individuals.
The study included 24 healthy recreational drug users and compared the acute effects of 5 mcg, 20 mcg, and 20 mcg LSD with placebo on a computer-based psychomotor vigilance task (PVT) that measured attention and on a Digit Symbol Substitution Test (DSST).
Participants also completed the 72-item Profile of Mood States (POMS) questionnaire, a visual analog scale (VAS) on mood, and the 94-item 5-Dimensional Altered States of Consciousness Rating scales (5D-ASC).
Unadjusted results showed that the 20-mcg LSD dose significantly reduced correct substitutions on the DSST vs placebo (P < .05), but had no effect on attentional lapses on the PCT or on positive mood on the POMS.
Correcting the DSST score for the number of total responses revealed no dose effect of LSD. This suggested that participants were no less accurate when under the influence of LSD, even though they encoded fewer digits, the researchers note.
Participants also reported that both the 10-mcg and 20-mcg dose of LSD increased subjective experiences on the VAS and alternated states of consciousness on the 5D-ASC compared with placebo.
After stratifying the results by dose and participant, the effect of LSD differed between individuals. For example, both the 5-mcg and 20-mcg doses were associated with improvement in attention on the PVT (P < .05), but not the 10-mcg dose.
These results also indicated that the 20-mcg dose was associated with a significant increase in the correct number of substitutions on the DSST and with a significant increase in positive mood on the POMS (P < .05 for both outcomes).
The findings suggest that future studies in patient populations with impaired attention are needed, “including biological parameters involved in LSD receptor-binding and metabolism, in order to understand the inter-individual variation in response to LSD,” the investigators note.
In an educational session at the meeting, the study’s lead researcher, Kim Kuypers, PhD, associate professor at Maastricht University, said research shows individuals are already self-medicating with psychedelic microdosing to treat a wide range of mental health problems, and rated it as significantly more effective than conventional therapy at alleviating symptoms and improving quality of life.
Nevertheless, Kuypers noted there have been fewer than 20 published placebo-controlled studies examining psychedelic microdosing in humans – and much of the current evidence is anecdotal.
However, there is some clinical research suggesting that low-dose LSD is associated with improved mood and cognitive performance and that it also has an effect on resting-state amygdala functional connectivity and acutely increases brain-derived neurotrophic factor plasma levels.
Furthermore, said Kuypers, the evidence in healthy volunteers thus far suggests microdosing is “safe.”
Jumping ahead of the science?
Commenting on the study for Medscape Medical News, Jeffrey A. Lieberman, MD, professor and chair of psychiatry at Columbia University, New York City, said he “gives the investigators credit for doing such a study” but does not believe anything can be gleaned from the findings.
He said he is also concerned that the resurgence of psychedelic research is not congruent with “the methodologic rigor and scientific thinking that accompanies treatment development in other disease areas.”
Lieberman, who is also psychiatrist-in-chief at the NewYork–Presbyterian Hospital Columbia Medical Center and was not involved with the study, added that some of the research is also being conducted in individuals who are “true believers and not sufficiently dispassionate and objective.”
“ But because these are such notorious and interesting compounds, they have attracted a lot of peripheral interest to promote and to disseminate; and the risk is that it will be done in the wrong way and there may be consequences,” he said.
Moreover, Lieberman noted that the psychedelic drugs may be used in practice ahead of strong evidence of safety and efficacy. As an example, he pointed to ketamine, a drug that was identified as a treatment for people with depression who had not responded to standard treatments, he noted.
“But before you knew it, there were clinics being opened up all over the place by anesthesiologists or other people that were trying to make a quick buck,” he said.
“That was alarming because they were stretching the criteria for whom the treatment was appropriate; there were no protocols for dosing, for frequency of administration, and there was inadequate psychiatric follow-up,” Lieberman added.
Preliminary but promising
He agreed with Kuypers that cases of microdosing with psychedelics are largely anecdotal.
“So in that context, when these investigators tried to put it to a test, which is commendable, the results in no way tell you whether it’s good, bad, or indifferent,” Lieberman said. In fact, the results are “disappointing in terms of suggesting any beneficial effect.”
Lieberman said more and larger studies are needed in order to determine whether LSD microdosing is beneficial.
In response to Lieberman’s comments, Kuypers told Medscape Medical News that the investigators tried to base their placebo-controlled research on previous anecdotal research.
She emphasized that the “whole field is still in its infancy,” including research on the use of “full” doses of psychedelics.
“I sometimes think that the message is too positive. We should never forget to communicate that not a lot of research has been done.” In addition, she agreed that researchers should “keep a balanced message.”
“All the data to date is preliminary, in my view, but promising,” she stressed, “and the evidence is growing.”
The study received financial support from the Beckley Foundation. The study authors and Lieberman have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Microdosing with lysergic acid diethylamide (LSD) is associated with improved mood and increased attention, early research suggests. However, at least one expert believes it’s far too soon to tell and warns against endorsing patient microdosing.
In a dose-finding exploratory study, three low doses of LSD were compared with placebo in healthy volunteers who were all recreational drug users. Adjusted results showed that the highest dose boosted attention and mood, although participants were aware of psychedelic effects, prompting researchers to conclude the results demonstrated “selective, beneficial effects.”
“The majority of participants have improved attention,” study investigator Nadia Hutten, PhD, Department of Neuropsychology and Psychopharmacology, Maastricht University, the Netherlands, told Medscape Medical News.
“So we think that patients with attention deficits might have more beneficial effects,” she added, noting her team plans to study LSD microdosing in patients with attention deficit hyperactivity disorder.
The study was presented at the 33rd European College of Neuropsychopharmacology (ECNP) Congress, which was held online this year because of the COVID-19 pandemic.
Growing interest
Over the past 10 years there has been growing interest in psychedelic microdosing, which is defined as a dose that aims to enhance mood and/or performance but does not affect perception.
However, there has been considerable debate over what constitutes a “microdose.” One tenth of a “full” psychedelic dose is typically suggested, but users report a much wider dose range in practice, suggesting potential “individual variation in response to low doses,” the researchers note.
In the current dose-finding study, the researchers explored whether the effects of LSD on cognition and subjective measures differed between individuals.
The study included 24 healthy recreational drug users and compared the acute effects of 5 mcg, 20 mcg, and 20 mcg LSD with placebo on a computer-based psychomotor vigilance task (PVT) that measured attention and on a Digit Symbol Substitution Test (DSST).
Participants also completed the 72-item Profile of Mood States (POMS) questionnaire, a visual analog scale (VAS) on mood, and the 94-item 5-Dimensional Altered States of Consciousness Rating scales (5D-ASC).
Unadjusted results showed that the 20-mcg LSD dose significantly reduced correct substitutions on the DSST vs placebo (P < .05), but had no effect on attentional lapses on the PCT or on positive mood on the POMS.
Correcting the DSST score for the number of total responses revealed no dose effect of LSD. This suggested that participants were no less accurate when under the influence of LSD, even though they encoded fewer digits, the researchers note.
Participants also reported that both the 10-mcg and 20-mcg dose of LSD increased subjective experiences on the VAS and alternated states of consciousness on the 5D-ASC compared with placebo.
After stratifying the results by dose and participant, the effect of LSD differed between individuals. For example, both the 5-mcg and 20-mcg doses were associated with improvement in attention on the PVT (P < .05), but not the 10-mcg dose.
These results also indicated that the 20-mcg dose was associated with a significant increase in the correct number of substitutions on the DSST and with a significant increase in positive mood on the POMS (P < .05 for both outcomes).
The findings suggest that future studies in patient populations with impaired attention are needed, “including biological parameters involved in LSD receptor-binding and metabolism, in order to understand the inter-individual variation in response to LSD,” the investigators note.
In an educational session at the meeting, the study’s lead researcher, Kim Kuypers, PhD, associate professor at Maastricht University, said research shows individuals are already self-medicating with psychedelic microdosing to treat a wide range of mental health problems, and rated it as significantly more effective than conventional therapy at alleviating symptoms and improving quality of life.
Nevertheless, Kuypers noted there have been fewer than 20 published placebo-controlled studies examining psychedelic microdosing in humans – and much of the current evidence is anecdotal.
However, there is some clinical research suggesting that low-dose LSD is associated with improved mood and cognitive performance and that it also has an effect on resting-state amygdala functional connectivity and acutely increases brain-derived neurotrophic factor plasma levels.
Furthermore, said Kuypers, the evidence in healthy volunteers thus far suggests microdosing is “safe.”
Jumping ahead of the science?
Commenting on the study for Medscape Medical News, Jeffrey A. Lieberman, MD, professor and chair of psychiatry at Columbia University, New York City, said he “gives the investigators credit for doing such a study” but does not believe anything can be gleaned from the findings.
He said he is also concerned that the resurgence of psychedelic research is not congruent with “the methodologic rigor and scientific thinking that accompanies treatment development in other disease areas.”
Lieberman, who is also psychiatrist-in-chief at the NewYork–Presbyterian Hospital Columbia Medical Center and was not involved with the study, added that some of the research is also being conducted in individuals who are “true believers and not sufficiently dispassionate and objective.”
“ But because these are such notorious and interesting compounds, they have attracted a lot of peripheral interest to promote and to disseminate; and the risk is that it will be done in the wrong way and there may be consequences,” he said.
Moreover, Lieberman noted that the psychedelic drugs may be used in practice ahead of strong evidence of safety and efficacy. As an example, he pointed to ketamine, a drug that was identified as a treatment for people with depression who had not responded to standard treatments, he noted.
“But before you knew it, there were clinics being opened up all over the place by anesthesiologists or other people that were trying to make a quick buck,” he said.
“That was alarming because they were stretching the criteria for whom the treatment was appropriate; there were no protocols for dosing, for frequency of administration, and there was inadequate psychiatric follow-up,” Lieberman added.
Preliminary but promising
He agreed with Kuypers that cases of microdosing with psychedelics are largely anecdotal.
“So in that context, when these investigators tried to put it to a test, which is commendable, the results in no way tell you whether it’s good, bad, or indifferent,” Lieberman said. In fact, the results are “disappointing in terms of suggesting any beneficial effect.”
Lieberman said more and larger studies are needed in order to determine whether LSD microdosing is beneficial.
In response to Lieberman’s comments, Kuypers told Medscape Medical News that the investigators tried to base their placebo-controlled research on previous anecdotal research.
She emphasized that the “whole field is still in its infancy,” including research on the use of “full” doses of psychedelics.
“I sometimes think that the message is too positive. We should never forget to communicate that not a lot of research has been done.” In addition, she agreed that researchers should “keep a balanced message.”
“All the data to date is preliminary, in my view, but promising,” she stressed, “and the evidence is growing.”
The study received financial support from the Beckley Foundation. The study authors and Lieberman have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Microdosing with lysergic acid diethylamide (LSD) is associated with improved mood and increased attention, early research suggests. However, at least one expert believes it’s far too soon to tell and warns against endorsing patient microdosing.
In a dose-finding exploratory study, three low doses of LSD were compared with placebo in healthy volunteers who were all recreational drug users. Adjusted results showed that the highest dose boosted attention and mood, although participants were aware of psychedelic effects, prompting researchers to conclude the results demonstrated “selective, beneficial effects.”
“The majority of participants have improved attention,” study investigator Nadia Hutten, PhD, Department of Neuropsychology and Psychopharmacology, Maastricht University, the Netherlands, told Medscape Medical News.
“So we think that patients with attention deficits might have more beneficial effects,” she added, noting her team plans to study LSD microdosing in patients with attention deficit hyperactivity disorder.
The study was presented at the 33rd European College of Neuropsychopharmacology (ECNP) Congress, which was held online this year because of the COVID-19 pandemic.
Growing interest
Over the past 10 years there has been growing interest in psychedelic microdosing, which is defined as a dose that aims to enhance mood and/or performance but does not affect perception.
However, there has been considerable debate over what constitutes a “microdose.” One tenth of a “full” psychedelic dose is typically suggested, but users report a much wider dose range in practice, suggesting potential “individual variation in response to low doses,” the researchers note.
In the current dose-finding study, the researchers explored whether the effects of LSD on cognition and subjective measures differed between individuals.
The study included 24 healthy recreational drug users and compared the acute effects of 5 mcg, 20 mcg, and 20 mcg LSD with placebo on a computer-based psychomotor vigilance task (PVT) that measured attention and on a Digit Symbol Substitution Test (DSST).
Participants also completed the 72-item Profile of Mood States (POMS) questionnaire, a visual analog scale (VAS) on mood, and the 94-item 5-Dimensional Altered States of Consciousness Rating scales (5D-ASC).
Unadjusted results showed that the 20-mcg LSD dose significantly reduced correct substitutions on the DSST vs placebo (P < .05), but had no effect on attentional lapses on the PCT or on positive mood on the POMS.
Correcting the DSST score for the number of total responses revealed no dose effect of LSD. This suggested that participants were no less accurate when under the influence of LSD, even though they encoded fewer digits, the researchers note.
Participants also reported that both the 10-mcg and 20-mcg dose of LSD increased subjective experiences on the VAS and alternated states of consciousness on the 5D-ASC compared with placebo.
After stratifying the results by dose and participant, the effect of LSD differed between individuals. For example, both the 5-mcg and 20-mcg doses were associated with improvement in attention on the PVT (P < .05), but not the 10-mcg dose.
These results also indicated that the 20-mcg dose was associated with a significant increase in the correct number of substitutions on the DSST and with a significant increase in positive mood on the POMS (P < .05 for both outcomes).
The findings suggest that future studies in patient populations with impaired attention are needed, “including biological parameters involved in LSD receptor-binding and metabolism, in order to understand the inter-individual variation in response to LSD,” the investigators note.
In an educational session at the meeting, the study’s lead researcher, Kim Kuypers, PhD, associate professor at Maastricht University, said research shows individuals are already self-medicating with psychedelic microdosing to treat a wide range of mental health problems, and rated it as significantly more effective than conventional therapy at alleviating symptoms and improving quality of life.
Nevertheless, Kuypers noted there have been fewer than 20 published placebo-controlled studies examining psychedelic microdosing in humans – and much of the current evidence is anecdotal.
However, there is some clinical research suggesting that low-dose LSD is associated with improved mood and cognitive performance and that it also has an effect on resting-state amygdala functional connectivity and acutely increases brain-derived neurotrophic factor plasma levels.
Furthermore, said Kuypers, the evidence in healthy volunteers thus far suggests microdosing is “safe.”
Jumping ahead of the science?
Commenting on the study for Medscape Medical News, Jeffrey A. Lieberman, MD, professor and chair of psychiatry at Columbia University, New York City, said he “gives the investigators credit for doing such a study” but does not believe anything can be gleaned from the findings.
He said he is also concerned that the resurgence of psychedelic research is not congruent with “the methodologic rigor and scientific thinking that accompanies treatment development in other disease areas.”
Lieberman, who is also psychiatrist-in-chief at the NewYork–Presbyterian Hospital Columbia Medical Center and was not involved with the study, added that some of the research is also being conducted in individuals who are “true believers and not sufficiently dispassionate and objective.”
“ But because these are such notorious and interesting compounds, they have attracted a lot of peripheral interest to promote and to disseminate; and the risk is that it will be done in the wrong way and there may be consequences,” he said.
Moreover, Lieberman noted that the psychedelic drugs may be used in practice ahead of strong evidence of safety and efficacy. As an example, he pointed to ketamine, a drug that was identified as a treatment for people with depression who had not responded to standard treatments, he noted.
“But before you knew it, there were clinics being opened up all over the place by anesthesiologists or other people that were trying to make a quick buck,” he said.
“That was alarming because they were stretching the criteria for whom the treatment was appropriate; there were no protocols for dosing, for frequency of administration, and there was inadequate psychiatric follow-up,” Lieberman added.
Preliminary but promising
He agreed with Kuypers that cases of microdosing with psychedelics are largely anecdotal.
“So in that context, when these investigators tried to put it to a test, which is commendable, the results in no way tell you whether it’s good, bad, or indifferent,” Lieberman said. In fact, the results are “disappointing in terms of suggesting any beneficial effect.”
Lieberman said more and larger studies are needed in order to determine whether LSD microdosing is beneficial.
In response to Lieberman’s comments, Kuypers told Medscape Medical News that the investigators tried to base their placebo-controlled research on previous anecdotal research.
She emphasized that the “whole field is still in its infancy,” including research on the use of “full” doses of psychedelics.
“I sometimes think that the message is too positive. We should never forget to communicate that not a lot of research has been done.” In addition, she agreed that researchers should “keep a balanced message.”
“All the data to date is preliminary, in my view, but promising,” she stressed, “and the evidence is growing.”
The study received financial support from the Beckley Foundation. The study authors and Lieberman have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
PEDIATRIC BEHAVIORAL AND MENTAL HEALTH
- Reduce mental illness stigma
- Ready for school? Not many preschoolers with ADHD are
- Suicide screening is key
- Alcohol, opioid misuse tied to risky behaviors
- Identify runaway risk
- Reduce mental illness stigma
- Ready for school? Not many preschoolers with ADHD are
- Suicide screening is key
- Alcohol, opioid misuse tied to risky behaviors
- Identify runaway risk
- Reduce mental illness stigma
- Ready for school? Not many preschoolers with ADHD are
- Suicide screening is key
- Alcohol, opioid misuse tied to risky behaviors
- Identify runaway risk
Telemedicine feasible and reliable in Parkinson’s trial
, a 1-year, phase 3 clinical trial has shown. The trial was an add-on study involving a subset of subjects from the STEADY-PD III trial of isradipine in early Parkinson’s disease.
Although the trial was conducted before SARS-CoV-2 arrived on the scene, the findings have particular relevance for being able to conduct a variety of clinical trials in the face of COVID-19 and the need to limit in-person interactions.
The 40 participants used tablets to complete three remote, video-based assessments during 1 year, with each remote visit planned to be completed within 4 weeks of an in-person visit. It was easy to enroll patients, and they completed about 95% of planned visits, said neurologist Christopher Tarolli, MD, of the University of Rochester (N.Y.).
He presented the study findings at the Movement Disorder Society’s 23rd International Congress of Parkinson’s Disease and Movement Disorders (Virtual) 2020.
“The visits were clearly feasible, and we were able to do them [84%] within that 4-week time frame around the in-person visit,” he said. “The visits were also reasonably reliable, particularly so for what we call the nonmotor outcomes and the patient-reported outcomes.”
In-person versus remote assessment
For the remote visits, participants completed primarily the same battery of tests as the in-person visits. Responses on the Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) subscales demonstrated “that there was excellent correlation between patient-reported and nonmotor outcome measures and moderate correlation between in-person and remote-performed motor assessments,” Dr. Tarolli said.
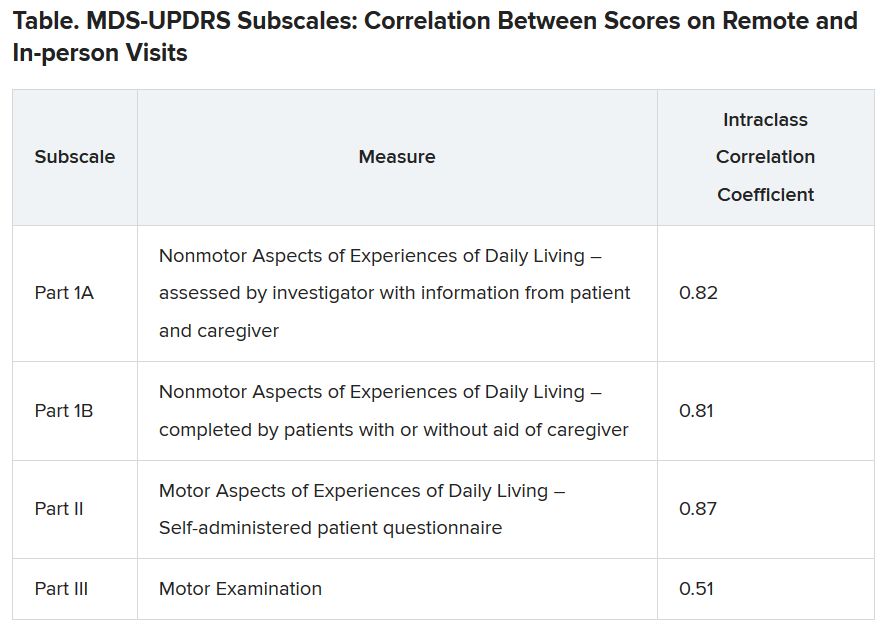
He explained that the study used modified motor assessments (MDS-UPDRS Part III) that excluded testing of rigidity and postural instability, which require hands-on testing by a trained examiner and thus are impossible to do remotely.
Additionally, the somewhat lower correlation on this subscale was probably the result of different investigators conducting in-person versus remote assessments, with a subset of in-person investigators who tended to rate participants more severely driving down the correlation. “I think if these methods were applied in future trials, the in-person and remote investigators would optimally be the same person,” Dr. Tarolli suggested.
Room for error?
Indu Subramanian, MD, of the department of neurology at the University of California, Los Angeles, and director of the Parkinson’s Disease Research, Education, and Clinical Center at the West Los Angeles Veterans Affairs Hospital, commented that “the reliability of UPDRS [part] III is where I would want to have, for sure, a little bit more of a deep dive. … possibly the same patient be rated by the same person.”
She also noted that doing remote and in-person assessments within 4 weeks of each other leaves a lot of room for variability. “You could see the same patient in the morning and then do UPDRS in the afternoon, and it can be totally different depending on when you meet the person,” she said.
Only so much testing can be done remotely. Nonetheless, she questioned whether it is really a valid UPDRS if rigidity and postural stability measures are eliminated. “[Is] this now a new modified UPDRS that we’re going to use that is as good as the old UPDRS moving forward, a home version of UPDRS or whatever we’re going to call it?”
Dr. Subramanian mentioned that patients have told her that UPDRS part III does not really measure what is most important to them, such as making pastries for their grandchildren rather than rapidly tapping their fingers.
“That speaks a little bit to the fact that we should have more patient-centered outcomes and things that patients can report. … things that are not going to require necessarily an in-person exam as maybe measures that really can be used moving forward in studies,” she suggested.
Patient satisfaction with remote visits
Greater than 90% of the patients were satisfied or very satisfied overall with the remote visits, including the convenience, comfort, and connection (using the devices and Internet connection), with “patients describing enjoying being able to do these visits from the comfort of their own home, not having to travel,” Dr. Tarolli said. Not having to drive in an ‘off’ state “was actually something that some participants identified as a safety benefit from this as well.”
There was also a time benefit to the patients and investigators. The average length of the remote visits was 54.3 minutes each versus 74 minutes of interaction for in-person visits, mainly a result of more efficient hand-offs between the neurologist and the study coordinator during the remote visits, plus being able to pause the remote visit to give a medication dose time to take effect.
For the patient, there was a large amount of time saved when travel time was considered – a total of 190.2 minutes on average for travel and testing for the in-person visits.
About three-quarters (76%) of the study patients said that remote visits would increase their likelihood of participating in future trials. However, that result may be skewed by the fact that these were already people willing to participate in a remote trial, so the generalizability of the result may be affected. Nonetheless, Dr. Tarolli said he thinks that, as technology gets better and older people become more comfortable with it, remote visits within Parkinson’s research studies may become more common.
One caveat he mentioned is that, with remote visits, the neurologist misses a chance to observe a patient’s whole body and construct a global impression of how he or she is moving. On the other hand, remote video gives the investigator the chance to see the living environment of the patient and suggest changes for safety, such as to reduce the risk of falling for a person with unsteadiness of gait living in a crowded house.
“It really allows us to make a more holistic assessment of how our patient is functioning outside the clinic, which I think we’ve traditionally had really no way of doing,” Dr. Tarolli said.
His final suggestion for anyone contemplating conducting studies with remote visits is to develop a team that is comfortable troubleshooting the technological aspects of those visits.
UCLA’s Dr. Subramanian lauded the University of Rochester team for their efforts in moving remote visits forward. “They’re at the cutting edge of these sorts of things,” she said. “So I’m assuming that they’ll come out with more things [for visits] to become better that are going to move this forward, which is exciting.”
Dr. Tarolli has disclosed no relevant financial relationships. Dr. Subramanian has given talks for Acorda Pharmaceuticals and Acadia Pharmaceuticals in the past. The study had only university, government, foundation, and other nonprofit support.
A version of this article originally appeared on Medscape.com.
, a 1-year, phase 3 clinical trial has shown. The trial was an add-on study involving a subset of subjects from the STEADY-PD III trial of isradipine in early Parkinson’s disease.
Although the trial was conducted before SARS-CoV-2 arrived on the scene, the findings have particular relevance for being able to conduct a variety of clinical trials in the face of COVID-19 and the need to limit in-person interactions.
The 40 participants used tablets to complete three remote, video-based assessments during 1 year, with each remote visit planned to be completed within 4 weeks of an in-person visit. It was easy to enroll patients, and they completed about 95% of planned visits, said neurologist Christopher Tarolli, MD, of the University of Rochester (N.Y.).
He presented the study findings at the Movement Disorder Society’s 23rd International Congress of Parkinson’s Disease and Movement Disorders (Virtual) 2020.
“The visits were clearly feasible, and we were able to do them [84%] within that 4-week time frame around the in-person visit,” he said. “The visits were also reasonably reliable, particularly so for what we call the nonmotor outcomes and the patient-reported outcomes.”
In-person versus remote assessment
For the remote visits, participants completed primarily the same battery of tests as the in-person visits. Responses on the Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) subscales demonstrated “that there was excellent correlation between patient-reported and nonmotor outcome measures and moderate correlation between in-person and remote-performed motor assessments,” Dr. Tarolli said.
He explained that the study used modified motor assessments (MDS-UPDRS Part III) that excluded testing of rigidity and postural instability, which require hands-on testing by a trained examiner and thus are impossible to do remotely.
Additionally, the somewhat lower correlation on this subscale was probably the result of different investigators conducting in-person versus remote assessments, with a subset of in-person investigators who tended to rate participants more severely driving down the correlation. “I think if these methods were applied in future trials, the in-person and remote investigators would optimally be the same person,” Dr. Tarolli suggested.
Room for error?
Indu Subramanian, MD, of the department of neurology at the University of California, Los Angeles, and director of the Parkinson’s Disease Research, Education, and Clinical Center at the West Los Angeles Veterans Affairs Hospital, commented that “the reliability of UPDRS [part] III is where I would want to have, for sure, a little bit more of a deep dive. … possibly the same patient be rated by the same person.”
She also noted that doing remote and in-person assessments within 4 weeks of each other leaves a lot of room for variability. “You could see the same patient in the morning and then do UPDRS in the afternoon, and it can be totally different depending on when you meet the person,” she said.
Only so much testing can be done remotely. Nonetheless, she questioned whether it is really a valid UPDRS if rigidity and postural stability measures are eliminated. “[Is] this now a new modified UPDRS that we’re going to use that is as good as the old UPDRS moving forward, a home version of UPDRS or whatever we’re going to call it?”
Dr. Subramanian mentioned that patients have told her that UPDRS part III does not really measure what is most important to them, such as making pastries for their grandchildren rather than rapidly tapping their fingers.
“That speaks a little bit to the fact that we should have more patient-centered outcomes and things that patients can report. … things that are not going to require necessarily an in-person exam as maybe measures that really can be used moving forward in studies,” she suggested.
Patient satisfaction with remote visits
Greater than 90% of the patients were satisfied or very satisfied overall with the remote visits, including the convenience, comfort, and connection (using the devices and Internet connection), with “patients describing enjoying being able to do these visits from the comfort of their own home, not having to travel,” Dr. Tarolli said. Not having to drive in an ‘off’ state “was actually something that some participants identified as a safety benefit from this as well.”
There was also a time benefit to the patients and investigators. The average length of the remote visits was 54.3 minutes each versus 74 minutes of interaction for in-person visits, mainly a result of more efficient hand-offs between the neurologist and the study coordinator during the remote visits, plus being able to pause the remote visit to give a medication dose time to take effect.
For the patient, there was a large amount of time saved when travel time was considered – a total of 190.2 minutes on average for travel and testing for the in-person visits.
About three-quarters (76%) of the study patients said that remote visits would increase their likelihood of participating in future trials. However, that result may be skewed by the fact that these were already people willing to participate in a remote trial, so the generalizability of the result may be affected. Nonetheless, Dr. Tarolli said he thinks that, as technology gets better and older people become more comfortable with it, remote visits within Parkinson’s research studies may become more common.
One caveat he mentioned is that, with remote visits, the neurologist misses a chance to observe a patient’s whole body and construct a global impression of how he or she is moving. On the other hand, remote video gives the investigator the chance to see the living environment of the patient and suggest changes for safety, such as to reduce the risk of falling for a person with unsteadiness of gait living in a crowded house.
“It really allows us to make a more holistic assessment of how our patient is functioning outside the clinic, which I think we’ve traditionally had really no way of doing,” Dr. Tarolli said.
His final suggestion for anyone contemplating conducting studies with remote visits is to develop a team that is comfortable troubleshooting the technological aspects of those visits.
UCLA’s Dr. Subramanian lauded the University of Rochester team for their efforts in moving remote visits forward. “They’re at the cutting edge of these sorts of things,” she said. “So I’m assuming that they’ll come out with more things [for visits] to become better that are going to move this forward, which is exciting.”
Dr. Tarolli has disclosed no relevant financial relationships. Dr. Subramanian has given talks for Acorda Pharmaceuticals and Acadia Pharmaceuticals in the past. The study had only university, government, foundation, and other nonprofit support.
A version of this article originally appeared on Medscape.com.
, a 1-year, phase 3 clinical trial has shown. The trial was an add-on study involving a subset of subjects from the STEADY-PD III trial of isradipine in early Parkinson’s disease.
Although the trial was conducted before SARS-CoV-2 arrived on the scene, the findings have particular relevance for being able to conduct a variety of clinical trials in the face of COVID-19 and the need to limit in-person interactions.
The 40 participants used tablets to complete three remote, video-based assessments during 1 year, with each remote visit planned to be completed within 4 weeks of an in-person visit. It was easy to enroll patients, and they completed about 95% of planned visits, said neurologist Christopher Tarolli, MD, of the University of Rochester (N.Y.).
He presented the study findings at the Movement Disorder Society’s 23rd International Congress of Parkinson’s Disease and Movement Disorders (Virtual) 2020.
“The visits were clearly feasible, and we were able to do them [84%] within that 4-week time frame around the in-person visit,” he said. “The visits were also reasonably reliable, particularly so for what we call the nonmotor outcomes and the patient-reported outcomes.”
In-person versus remote assessment
For the remote visits, participants completed primarily the same battery of tests as the in-person visits. Responses on the Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) subscales demonstrated “that there was excellent correlation between patient-reported and nonmotor outcome measures and moderate correlation between in-person and remote-performed motor assessments,” Dr. Tarolli said.
He explained that the study used modified motor assessments (MDS-UPDRS Part III) that excluded testing of rigidity and postural instability, which require hands-on testing by a trained examiner and thus are impossible to do remotely.
Additionally, the somewhat lower correlation on this subscale was probably the result of different investigators conducting in-person versus remote assessments, with a subset of in-person investigators who tended to rate participants more severely driving down the correlation. “I think if these methods were applied in future trials, the in-person and remote investigators would optimally be the same person,” Dr. Tarolli suggested.
Room for error?
Indu Subramanian, MD, of the department of neurology at the University of California, Los Angeles, and director of the Parkinson’s Disease Research, Education, and Clinical Center at the West Los Angeles Veterans Affairs Hospital, commented that “the reliability of UPDRS [part] III is where I would want to have, for sure, a little bit more of a deep dive. … possibly the same patient be rated by the same person.”
She also noted that doing remote and in-person assessments within 4 weeks of each other leaves a lot of room for variability. “You could see the same patient in the morning and then do UPDRS in the afternoon, and it can be totally different depending on when you meet the person,” she said.
Only so much testing can be done remotely. Nonetheless, she questioned whether it is really a valid UPDRS if rigidity and postural stability measures are eliminated. “[Is] this now a new modified UPDRS that we’re going to use that is as good as the old UPDRS moving forward, a home version of UPDRS or whatever we’re going to call it?”
Dr. Subramanian mentioned that patients have told her that UPDRS part III does not really measure what is most important to them, such as making pastries for their grandchildren rather than rapidly tapping their fingers.
“That speaks a little bit to the fact that we should have more patient-centered outcomes and things that patients can report. … things that are not going to require necessarily an in-person exam as maybe measures that really can be used moving forward in studies,” she suggested.
Patient satisfaction with remote visits
Greater than 90% of the patients were satisfied or very satisfied overall with the remote visits, including the convenience, comfort, and connection (using the devices and Internet connection), with “patients describing enjoying being able to do these visits from the comfort of their own home, not having to travel,” Dr. Tarolli said. Not having to drive in an ‘off’ state “was actually something that some participants identified as a safety benefit from this as well.”
There was also a time benefit to the patients and investigators. The average length of the remote visits was 54.3 minutes each versus 74 minutes of interaction for in-person visits, mainly a result of more efficient hand-offs between the neurologist and the study coordinator during the remote visits, plus being able to pause the remote visit to give a medication dose time to take effect.
For the patient, there was a large amount of time saved when travel time was considered – a total of 190.2 minutes on average for travel and testing for the in-person visits.
About three-quarters (76%) of the study patients said that remote visits would increase their likelihood of participating in future trials. However, that result may be skewed by the fact that these were already people willing to participate in a remote trial, so the generalizability of the result may be affected. Nonetheless, Dr. Tarolli said he thinks that, as technology gets better and older people become more comfortable with it, remote visits within Parkinson’s research studies may become more common.
One caveat he mentioned is that, with remote visits, the neurologist misses a chance to observe a patient’s whole body and construct a global impression of how he or she is moving. On the other hand, remote video gives the investigator the chance to see the living environment of the patient and suggest changes for safety, such as to reduce the risk of falling for a person with unsteadiness of gait living in a crowded house.
“It really allows us to make a more holistic assessment of how our patient is functioning outside the clinic, which I think we’ve traditionally had really no way of doing,” Dr. Tarolli said.
His final suggestion for anyone contemplating conducting studies with remote visits is to develop a team that is comfortable troubleshooting the technological aspects of those visits.
UCLA’s Dr. Subramanian lauded the University of Rochester team for their efforts in moving remote visits forward. “They’re at the cutting edge of these sorts of things,” she said. “So I’m assuming that they’ll come out with more things [for visits] to become better that are going to move this forward, which is exciting.”
Dr. Tarolli has disclosed no relevant financial relationships. Dr. Subramanian has given talks for Acorda Pharmaceuticals and Acadia Pharmaceuticals in the past. The study had only university, government, foundation, and other nonprofit support.
A version of this article originally appeared on Medscape.com.
COVID-19 vaccine hesitancy ‘somewhat understandable,’ expert says
“I worry that vaccines are going to be sold like magic powder that we sprinkle across the land and make the virus go away,” Paul Offit, MD, said at the virtual American Academy of Pediatrics (AAP) 2020 National Conference. “That’s not true.”
according to Dr. Offit, director of the Vaccine Education Center and an attending physician in the Division of Infectious Diseases at Children’s Hospital of Philadelphia.
“I think we can get a vaccine that’s 75%-80% effective at preventing mild to moderate disease, but that means one of every four people can still get moderate to severe disease,” Dr. Offit continued.
And that’s if there is high uptake of the vaccine, which may not be the case. Recent polls have suggested there is considerable concern about the pending vaccines.
“It’s somewhat understandable,” Dr. Offitt acknowledged, especially given the “frightening” language used to describe vaccine development. Terms such as “warp speed” may suggest that haste might trump safety considerations. Before COVID-19, the fastest vaccine ever developed was for mumps, he said, with the virus isolated in 1963 and a commercial product available in 1967.
Addressing hesitancy in clinics
In a wide-ranging livestream plenary presentation, Dr. Offit, coinventor of a rotavirus vaccine, shed light on SARS-CoV-2 vaccine development and his impressions of vaccine hesitancy among patients and families. He also offered advice for how to reassure those skeptical of the safety and efficacy of any SARS-COV-2 vaccine, given the accelerated development process.
With more than 180 different vaccines in various stages of investigation, Dr. Offit called the effort to develop COVID-19 vaccines “unprecedented.” Part of that is a result of governments relieving pharmaceutical companies of much of the typical financial risk – which often climbs to hundreds of millions of dollars – by underwriting the costs of vaccine development to battle the pandemic-inducing virus, he said.
But this very swiftness is also stoking antivaccine sentiment. Dr. Offit, part of vaccine advisory groups for the National Institutes of Health and U.S. Food and Drug Administration, cited recent research reporting nearly half of American adults definitely or probably would not get a COVID-19 vaccine if it were available today.
“One way you convince skeptics is with data presented in a clear, compassionate, and compelling way,” he said.
“The other group is vaccine cynics, who are basically conspiracy theorists who believe pharmaceutical companies control the world, the government, the medical establishment. I think there’s no talking them down from this.”
Numerous strategies are being used in COVID-19 vaccine development, he noted, including messenger RNA, DNA, viral vectors, purified protein, and whole killed virus. Dr. Offit believes any candidates approved for distribution will likely be in the range of 75% effective at preventing mild to moderate symptoms.
But clinicians should be ready to face immediate questions of safety. “Even if this vaccination is given to 20,000 [trial participants] safely, that’s not 20 million,” Dr. Offit said. “Anyone could reasonably ask questions about if it causes rare, serious side effects.
“The good news is, there are systems in place,” such as adverse event reporting systems, to identify rare events, even those that occur in one in a million vaccine recipients. Reminding patients of that continued surveillance can be reassuring.
Another reassuring point is that COVID-19 vaccine trial participants have included people from many diverse populations, he said. But children, notably absent so far, should be added to trials immediately, Dr. Offit contends.
“This is going to be important when you consider strategies to get children universally back into school,” he said, which is a “critical issue” from both learning and wellness standpoints. “It breaks my heart that we’ve been unable to do this when other countries have.”
Transparency will be paramount
While presenting data transparently to patients is key in helping them accept COVID-19 vaccination, Dr. Offit said, he also believes “telling stories” can be just as effective, if not more so. When the varicella vaccine was approved in 1995, he said, the “uptake the first few years was pretty miserable” until public service messaging emphasized that some children die from chickenpox.
“Fear works,” he said. “You always worry about pushback of something being oversold, but hopefully we’re scared enough about this virus” to convince people that vaccination is wise. “I do think personal stories carry weight on both sides,” Dr. Offit said.
Mark Sawyer, MD, of University of California San Diego School of Medicine and Rady Children’s Hospital in San Diego, California, said Offit’s presentation offered important takeaways for clinicians about how to broach the topic of COVID-19 vaccination with patients and families.
“We need to communicate clearly and transparently to patients about what we do and don’t know” about the vaccines, Dr. Sawyer said in an interview. “We will know if they have common side effects, but we will not know about very rare side effects until we have used the vaccines for a while.
“We will know how well the vaccine works over the short-term, but we won’t know over the long term,” added Dr. Sawyer, a member of the AAP Committee on Infectious Diseases.
“We can reassure the community that SARS-CoV-2 vaccines are being evaluated in trials in the same way and with the same thoroughness as other vaccines have been,” he said. “That should give people confidence that shortcuts are not being taken with regard to safety and effectiveness evaluations.”
Dr. Offit and Dr. Sawyer have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
“I worry that vaccines are going to be sold like magic powder that we sprinkle across the land and make the virus go away,” Paul Offit, MD, said at the virtual American Academy of Pediatrics (AAP) 2020 National Conference. “That’s not true.”
according to Dr. Offit, director of the Vaccine Education Center and an attending physician in the Division of Infectious Diseases at Children’s Hospital of Philadelphia.
“I think we can get a vaccine that’s 75%-80% effective at preventing mild to moderate disease, but that means one of every four people can still get moderate to severe disease,” Dr. Offit continued.
And that’s if there is high uptake of the vaccine, which may not be the case. Recent polls have suggested there is considerable concern about the pending vaccines.
“It’s somewhat understandable,” Dr. Offitt acknowledged, especially given the “frightening” language used to describe vaccine development. Terms such as “warp speed” may suggest that haste might trump safety considerations. Before COVID-19, the fastest vaccine ever developed was for mumps, he said, with the virus isolated in 1963 and a commercial product available in 1967.
Addressing hesitancy in clinics
In a wide-ranging livestream plenary presentation, Dr. Offit, coinventor of a rotavirus vaccine, shed light on SARS-CoV-2 vaccine development and his impressions of vaccine hesitancy among patients and families. He also offered advice for how to reassure those skeptical of the safety and efficacy of any SARS-COV-2 vaccine, given the accelerated development process.
With more than 180 different vaccines in various stages of investigation, Dr. Offit called the effort to develop COVID-19 vaccines “unprecedented.” Part of that is a result of governments relieving pharmaceutical companies of much of the typical financial risk – which often climbs to hundreds of millions of dollars – by underwriting the costs of vaccine development to battle the pandemic-inducing virus, he said.
But this very swiftness is also stoking antivaccine sentiment. Dr. Offit, part of vaccine advisory groups for the National Institutes of Health and U.S. Food and Drug Administration, cited recent research reporting nearly half of American adults definitely or probably would not get a COVID-19 vaccine if it were available today.
“One way you convince skeptics is with data presented in a clear, compassionate, and compelling way,” he said.
“The other group is vaccine cynics, who are basically conspiracy theorists who believe pharmaceutical companies control the world, the government, the medical establishment. I think there’s no talking them down from this.”
Numerous strategies are being used in COVID-19 vaccine development, he noted, including messenger RNA, DNA, viral vectors, purified protein, and whole killed virus. Dr. Offit believes any candidates approved for distribution will likely be in the range of 75% effective at preventing mild to moderate symptoms.
But clinicians should be ready to face immediate questions of safety. “Even if this vaccination is given to 20,000 [trial participants] safely, that’s not 20 million,” Dr. Offit said. “Anyone could reasonably ask questions about if it causes rare, serious side effects.
“The good news is, there are systems in place,” such as adverse event reporting systems, to identify rare events, even those that occur in one in a million vaccine recipients. Reminding patients of that continued surveillance can be reassuring.
Another reassuring point is that COVID-19 vaccine trial participants have included people from many diverse populations, he said. But children, notably absent so far, should be added to trials immediately, Dr. Offit contends.
“This is going to be important when you consider strategies to get children universally back into school,” he said, which is a “critical issue” from both learning and wellness standpoints. “It breaks my heart that we’ve been unable to do this when other countries have.”
Transparency will be paramount
While presenting data transparently to patients is key in helping them accept COVID-19 vaccination, Dr. Offit said, he also believes “telling stories” can be just as effective, if not more so. When the varicella vaccine was approved in 1995, he said, the “uptake the first few years was pretty miserable” until public service messaging emphasized that some children die from chickenpox.
“Fear works,” he said. “You always worry about pushback of something being oversold, but hopefully we’re scared enough about this virus” to convince people that vaccination is wise. “I do think personal stories carry weight on both sides,” Dr. Offit said.
Mark Sawyer, MD, of University of California San Diego School of Medicine and Rady Children’s Hospital in San Diego, California, said Offit’s presentation offered important takeaways for clinicians about how to broach the topic of COVID-19 vaccination with patients and families.
“We need to communicate clearly and transparently to patients about what we do and don’t know” about the vaccines, Dr. Sawyer said in an interview. “We will know if they have common side effects, but we will not know about very rare side effects until we have used the vaccines for a while.
“We will know how well the vaccine works over the short-term, but we won’t know over the long term,” added Dr. Sawyer, a member of the AAP Committee on Infectious Diseases.
“We can reassure the community that SARS-CoV-2 vaccines are being evaluated in trials in the same way and with the same thoroughness as other vaccines have been,” he said. “That should give people confidence that shortcuts are not being taken with regard to safety and effectiveness evaluations.”
Dr. Offit and Dr. Sawyer have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
“I worry that vaccines are going to be sold like magic powder that we sprinkle across the land and make the virus go away,” Paul Offit, MD, said at the virtual American Academy of Pediatrics (AAP) 2020 National Conference. “That’s not true.”
according to Dr. Offit, director of the Vaccine Education Center and an attending physician in the Division of Infectious Diseases at Children’s Hospital of Philadelphia.
“I think we can get a vaccine that’s 75%-80% effective at preventing mild to moderate disease, but that means one of every four people can still get moderate to severe disease,” Dr. Offit continued.
And that’s if there is high uptake of the vaccine, which may not be the case. Recent polls have suggested there is considerable concern about the pending vaccines.
“It’s somewhat understandable,” Dr. Offitt acknowledged, especially given the “frightening” language used to describe vaccine development. Terms such as “warp speed” may suggest that haste might trump safety considerations. Before COVID-19, the fastest vaccine ever developed was for mumps, he said, with the virus isolated in 1963 and a commercial product available in 1967.
Addressing hesitancy in clinics
In a wide-ranging livestream plenary presentation, Dr. Offit, coinventor of a rotavirus vaccine, shed light on SARS-CoV-2 vaccine development and his impressions of vaccine hesitancy among patients and families. He also offered advice for how to reassure those skeptical of the safety and efficacy of any SARS-COV-2 vaccine, given the accelerated development process.
With more than 180 different vaccines in various stages of investigation, Dr. Offit called the effort to develop COVID-19 vaccines “unprecedented.” Part of that is a result of governments relieving pharmaceutical companies of much of the typical financial risk – which often climbs to hundreds of millions of dollars – by underwriting the costs of vaccine development to battle the pandemic-inducing virus, he said.
But this very swiftness is also stoking antivaccine sentiment. Dr. Offit, part of vaccine advisory groups for the National Institutes of Health and U.S. Food and Drug Administration, cited recent research reporting nearly half of American adults definitely or probably would not get a COVID-19 vaccine if it were available today.
“One way you convince skeptics is with data presented in a clear, compassionate, and compelling way,” he said.
“The other group is vaccine cynics, who are basically conspiracy theorists who believe pharmaceutical companies control the world, the government, the medical establishment. I think there’s no talking them down from this.”
Numerous strategies are being used in COVID-19 vaccine development, he noted, including messenger RNA, DNA, viral vectors, purified protein, and whole killed virus. Dr. Offit believes any candidates approved for distribution will likely be in the range of 75% effective at preventing mild to moderate symptoms.
But clinicians should be ready to face immediate questions of safety. “Even if this vaccination is given to 20,000 [trial participants] safely, that’s not 20 million,” Dr. Offit said. “Anyone could reasonably ask questions about if it causes rare, serious side effects.
“The good news is, there are systems in place,” such as adverse event reporting systems, to identify rare events, even those that occur in one in a million vaccine recipients. Reminding patients of that continued surveillance can be reassuring.
Another reassuring point is that COVID-19 vaccine trial participants have included people from many diverse populations, he said. But children, notably absent so far, should be added to trials immediately, Dr. Offit contends.
“This is going to be important when you consider strategies to get children universally back into school,” he said, which is a “critical issue” from both learning and wellness standpoints. “It breaks my heart that we’ve been unable to do this when other countries have.”
Transparency will be paramount
While presenting data transparently to patients is key in helping them accept COVID-19 vaccination, Dr. Offit said, he also believes “telling stories” can be just as effective, if not more so. When the varicella vaccine was approved in 1995, he said, the “uptake the first few years was pretty miserable” until public service messaging emphasized that some children die from chickenpox.
“Fear works,” he said. “You always worry about pushback of something being oversold, but hopefully we’re scared enough about this virus” to convince people that vaccination is wise. “I do think personal stories carry weight on both sides,” Dr. Offit said.
Mark Sawyer, MD, of University of California San Diego School of Medicine and Rady Children’s Hospital in San Diego, California, said Offit’s presentation offered important takeaways for clinicians about how to broach the topic of COVID-19 vaccination with patients and families.
“We need to communicate clearly and transparently to patients about what we do and don’t know” about the vaccines, Dr. Sawyer said in an interview. “We will know if they have common side effects, but we will not know about very rare side effects until we have used the vaccines for a while.
“We will know how well the vaccine works over the short-term, but we won’t know over the long term,” added Dr. Sawyer, a member of the AAP Committee on Infectious Diseases.
“We can reassure the community that SARS-CoV-2 vaccines are being evaluated in trials in the same way and with the same thoroughness as other vaccines have been,” he said. “That should give people confidence that shortcuts are not being taken with regard to safety and effectiveness evaluations.”
Dr. Offit and Dr. Sawyer have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Flexibility, innovation key to practice management during pandemic
Practice management is the responsibility of every pediatrician, and leadership is more important than ever in a crisis like the COVID-19 pandemic.

“Ultimately you have a critical role in ensuring that your practice remains sustainable so that you can continue to deliver great care,” Sue Kressly, MD, a retired pediatrician from Warrington, Pa., said at the virtual annual meeting of the American Academy of Pediatrics. “None of us escaped some impact of the COVID crisis, and many of us are going to experience lasting change.”
Dr. Kressly and Suzanne Berman, MD, a pediatrician in central Tennessee, presented a live online session on how the pandemic is affecting practices and how pediatricians can effectively address those challenges.
Three ways a crisis impacts practices
“When a practice experiences a crisis, it really exposes what your practice is made of, for better or for worse,” Dr. Berman said. “The COVID crisis has been profound and broad and long enough to really stress the core tensile strength of practices along at least three axes.” Those are staffing, financial health, and partnerships.
It’s a normal human response to enter survival mode during a crisis, so staff management becomes more important than ever. Some things to consider are whether you have a truly collaborative team culture in your practice and whether you’re really listening to the staff’s struggles and suggestions.
“Staffing challenges can be very difficult,” Dr. Berman said. “Permitting staff to work from home is the single biggest thing you can do when staff needs to self-isolate.”
Financially, most medical practices have adequate cash on hand not to have to pay close attention to the numbers, Dr. Kressly said, but if physicians are looking at their books for the first time during a crisis, they have no way of knowing what their baseline expectations should be or how much to worry about their finances. It’s important to understand your practice’s or department’s budget.
Jesse Hackell, MD, a private practice pediatrician in a suburb of New York City and vice president of the New York AAP Chapter 3, attended the session and appreciated this point on finances.
“In order to provide good quality care to kids, you need to be financially successful because otherwise you’ll close your doors,” Dr. Hackell said in an interview. “It’s making yourself available to be able to provide care.”
Stressors among partners during a crisis arise from responding to the challenges of the crisis, such as who should be impacted by pay cuts or furloughs, how to account for overhead, how to distribute revenue and how to divide the work equitably. Other issues include how to protect higher risk providers fairly and how to shift schedules or case load based on unforeseen events, including quarantining.
“There is no ‘fair’ in a crisis,” Dr. Berman said. “We must use the equity paradigm to be sure everyone has what they need to survive and have the best outcome possible.”
The speakers also discussed the importance of a practice’s situation before the pandemic began, a point that resonated with attendee Jason Terk, MD, a pediatrician who practices in a large pediatric health care system near Fort Worth, Texas.
“Just like the pandemic impacts the health of people in different ways based upon their baseline health, the pandemic impacts practices in different ways based on the practice’s baseline health,” he said in an interview. “If you had good operations, a good culture, good communication and all those other good indicators of practice health before, then you stood a much better chance of surviving the pandemic as a practice than practices that had weaknesses before.”
The size of a practice did not necessarily predict the impact of the crisis, Dr. Berman said. Rather, practices with good patient engagement, active recall programs, and good fiscal planning did better.
Dr. Hackell said. “We had never seen anything like this before,” he said in an interview. “From the start we had no idea what was going to work. Try something and see if it works. If it fails, try something else. We were all operating blind here.”
The focus of most practices in the spring was on well visits, chronic care follow-up, and telehealth. Going into fall and winter, innovation will be necessary to provide appropriate care for all children while keeping in mind that the choices pediatricians make will have long-lasting implications for their staff and patients. The speakers stressed the importance of communication and transparency within the office team and to patients and the community.
Dr. Hackell appreciated the speakers’ point that kids need care, and pediatricians need to meet that need.
“Kids need well care and immunizations, and kids get sick and need sick care,” he said. “Parents need a lot more reassurance during times like this. We need to be able to provide that care and be sure that we do it safely. To give the right care at the right time in the right location is key.”
Making practice adaptations
In balancing risk and access to care, Dr. Kressly described the importance of multiple interventions, including managing some patients out of the office and making physical changes, such as putting in physical barriers and eliminating waiting rooms.
“Many practices are highly focused on PPE [personal protective equipment],” Dr. Kressly said, but even Centers for Disease Control and Prevention guidance emphasizes that PPE is the last line of defense. “There are many things we can do to protect our teams and our patients, and we know that not one single adaption is going to be 100% effective. But like the Swiss cheese model indicates, when you layer all of these efforts on top of one another, many defenses allow for the protection of the majority of people.”
Other changes include restricting office visitors to one per patient, implementing social distancing, requiring visitors to wear masks, and considering alternate locations for visits, including car and parking lot visits.
“No idea is too crazy, and some of the best ideas come from your staff,” Dr. Kressly said. She also recommended asking families where they feel most comfortable meeting.
“Don’t make any assumptions about where they want to be seen, but ask and together decide where the patient can most safely and effectively be given appropriate care,” she said.
Dr. Kressly also noted the new CPT code, 99072, that can be used to bill for “additional supplies, materials, and clinical staff time over and above those usually included in an office visit or other nonfacility service(s), when performed during a public health emergency as defined by law, due to respiratory-transmitted infectious disease.”
Pediatricians should think of ways they can remove barriers to access, such as adjusting no-show cancellation penalties and adjusting practice policies as needed when things change. “Avoid creating a culture where families do not disclose all information for fear of not being seen,” Dr. Kressly said.
A slower pace because of delays and hiccups is also normal at this time, Dr. Berman said. “If you feel like you’re just not as efficient as you were prior to COVID, it’s not just you,” she said. “It’s true. Everyone has to grapple with new things now. It takes longer.”
Things that add time include remote check-in and paperwork, more time to don and doff PPE and disinfect, dealing with technology failures, adjusting to new procedures or policies, and the general mental fatigue of adhering to PPE best practices. Patience is vital during this time, Dr. Berman said.
Several ways to improve efficiency include cutting out unnecessary steps, using standing orders and Advance Beneficiary Notice of Noncoverage (ABNs) for flu vaccinations, keeping credit card numbers on file for contactless payment, and considering the clinical and financial value of lab testing before ordering it.
“Effective triage helps patient satisfaction, access to care, and efficiency of your office workload,” Dr. Kressly said. “Use technology where it’s appropriate, but then add people where it’s needed. Connections to caring people matter even more in a time of crisis.”
The speakers also highlighted the importance of early flu vaccinations.
“One of the single biggest things you can do for value in COVID is to get your flu vaccine numbers up,” Dr. Berman said. “Severely reducing the burden of influenza will help flatten the curve, it will reduce febrile respiratory illness, and it will protect your most fragile patients.”
Two ways to do that include flu clinics and making a strong push for immunizations during the first 8 weeks after getting the vaccines. Dr Berman shared numbers from two practices showing how many more total immunizations were done in the practice that began vaccinating in early August versus early September.
A crisis is an opportunity
The speakers closed on an optimistic note that emphasized the opportunities that can grow out of the challenges presented by the pandemic, a point Dr Terk elaborated on.
“One of the most important things is realizing how we can potentially use a crisis to transform our practices,” Dr. Terk said in the interview. “As had been said before, a crisis is a terrible thing to waste. Those practices that have the gumption to innovate and find different ways to improve the way they provide care are probably going to be in better shape as we go forward.”
Critical to that success is taking risks, he added.
“When you’re innovating, failure has to be something you are permissive of because if you’re risk-averse and failure-averse, you’re not going to have the opportunity to grow and innovate, and this is another opportunity to innovate,” Dr. Terk said.
He also stressed the value of learning from one another. “We need to help each other by sharing our good practices, and on the flip side, be open to learning from each other,” he said. “Those pediatricians who are struggling need to be open-minded and open-hearted to understanding how we can operate our practices better and know that the things we think are barriers we can’t change are probably things we probably haven’t allowed ourselves to think about changing.”
Dr. Kressly and Dr. Berman recommended several specific actions for pediatricians to take:
- Creating a SWOT (Strengths, Weaknesses, Opportunities, and Threats) analysis regarding your practice management response to the pandemic.
- Articulating three goals for improving your understanding or the implementation of management in your practice.
- Creating a working group to identify and implement ways to improve clinical work flow and communication strategies.
“Now is the time to meaningfully address disparities of access to appropriate health care and the impact of social determinants of health,” Dr. Kressly said. It’s also an opportunity to build meaningful relationships with patient families based on trust, science, and “true shared decision-making with health literacy in mind.”
Dr Kressly is the medical director of and owns shares in Office Practicum. Dr. Berman is the assistant medical director of and owns shares in Office Practicum, and is the owner of Script Doctor LLC. Dr. Terk and Dr. Hackell had no relevant financial disclosures.
Practice management is the responsibility of every pediatrician, and leadership is more important than ever in a crisis like the COVID-19 pandemic.
“Ultimately you have a critical role in ensuring that your practice remains sustainable so that you can continue to deliver great care,” Sue Kressly, MD, a retired pediatrician from Warrington, Pa., said at the virtual annual meeting of the American Academy of Pediatrics. “None of us escaped some impact of the COVID crisis, and many of us are going to experience lasting change.”
Dr. Kressly and Suzanne Berman, MD, a pediatrician in central Tennessee, presented a live online session on how the pandemic is affecting practices and how pediatricians can effectively address those challenges.
Three ways a crisis impacts practices
“When a practice experiences a crisis, it really exposes what your practice is made of, for better or for worse,” Dr. Berman said. “The COVID crisis has been profound and broad and long enough to really stress the core tensile strength of practices along at least three axes.” Those are staffing, financial health, and partnerships.
It’s a normal human response to enter survival mode during a crisis, so staff management becomes more important than ever. Some things to consider are whether you have a truly collaborative team culture in your practice and whether you’re really listening to the staff’s struggles and suggestions.
“Staffing challenges can be very difficult,” Dr. Berman said. “Permitting staff to work from home is the single biggest thing you can do when staff needs to self-isolate.”
Financially, most medical practices have adequate cash on hand not to have to pay close attention to the numbers, Dr. Kressly said, but if physicians are looking at their books for the first time during a crisis, they have no way of knowing what their baseline expectations should be or how much to worry about their finances. It’s important to understand your practice’s or department’s budget.
Jesse Hackell, MD, a private practice pediatrician in a suburb of New York City and vice president of the New York AAP Chapter 3, attended the session and appreciated this point on finances.
“In order to provide good quality care to kids, you need to be financially successful because otherwise you’ll close your doors,” Dr. Hackell said in an interview. “It’s making yourself available to be able to provide care.”
Stressors among partners during a crisis arise from responding to the challenges of the crisis, such as who should be impacted by pay cuts or furloughs, how to account for overhead, how to distribute revenue and how to divide the work equitably. Other issues include how to protect higher risk providers fairly and how to shift schedules or case load based on unforeseen events, including quarantining.
“There is no ‘fair’ in a crisis,” Dr. Berman said. “We must use the equity paradigm to be sure everyone has what they need to survive and have the best outcome possible.”
The speakers also discussed the importance of a practice’s situation before the pandemic began, a point that resonated with attendee Jason Terk, MD, a pediatrician who practices in a large pediatric health care system near Fort Worth, Texas.
“Just like the pandemic impacts the health of people in different ways based upon their baseline health, the pandemic impacts practices in different ways based on the practice’s baseline health,” he said in an interview. “If you had good operations, a good culture, good communication and all those other good indicators of practice health before, then you stood a much better chance of surviving the pandemic as a practice than practices that had weaknesses before.”
The size of a practice did not necessarily predict the impact of the crisis, Dr. Berman said. Rather, practices with good patient engagement, active recall programs, and good fiscal planning did better.
Dr. Hackell said. “We had never seen anything like this before,” he said in an interview. “From the start we had no idea what was going to work. Try something and see if it works. If it fails, try something else. We were all operating blind here.”
The focus of most practices in the spring was on well visits, chronic care follow-up, and telehealth. Going into fall and winter, innovation will be necessary to provide appropriate care for all children while keeping in mind that the choices pediatricians make will have long-lasting implications for their staff and patients. The speakers stressed the importance of communication and transparency within the office team and to patients and the community.
Dr. Hackell appreciated the speakers’ point that kids need care, and pediatricians need to meet that need.
“Kids need well care and immunizations, and kids get sick and need sick care,” he said. “Parents need a lot more reassurance during times like this. We need to be able to provide that care and be sure that we do it safely. To give the right care at the right time in the right location is key.”
Making practice adaptations
In balancing risk and access to care, Dr. Kressly described the importance of multiple interventions, including managing some patients out of the office and making physical changes, such as putting in physical barriers and eliminating waiting rooms.
“Many practices are highly focused on PPE [personal protective equipment],” Dr. Kressly said, but even Centers for Disease Control and Prevention guidance emphasizes that PPE is the last line of defense. “There are many things we can do to protect our teams and our patients, and we know that not one single adaption is going to be 100% effective. But like the Swiss cheese model indicates, when you layer all of these efforts on top of one another, many defenses allow for the protection of the majority of people.”
Other changes include restricting office visitors to one per patient, implementing social distancing, requiring visitors to wear masks, and considering alternate locations for visits, including car and parking lot visits.
“No idea is too crazy, and some of the best ideas come from your staff,” Dr. Kressly said. She also recommended asking families where they feel most comfortable meeting.
“Don’t make any assumptions about where they want to be seen, but ask and together decide where the patient can most safely and effectively be given appropriate care,” she said.
Dr. Kressly also noted the new CPT code, 99072, that can be used to bill for “additional supplies, materials, and clinical staff time over and above those usually included in an office visit or other nonfacility service(s), when performed during a public health emergency as defined by law, due to respiratory-transmitted infectious disease.”
Pediatricians should think of ways they can remove barriers to access, such as adjusting no-show cancellation penalties and adjusting practice policies as needed when things change. “Avoid creating a culture where families do not disclose all information for fear of not being seen,” Dr. Kressly said.
A slower pace because of delays and hiccups is also normal at this time, Dr. Berman said. “If you feel like you’re just not as efficient as you were prior to COVID, it’s not just you,” she said. “It’s true. Everyone has to grapple with new things now. It takes longer.”
Things that add time include remote check-in and paperwork, more time to don and doff PPE and disinfect, dealing with technology failures, adjusting to new procedures or policies, and the general mental fatigue of adhering to PPE best practices. Patience is vital during this time, Dr. Berman said.
Several ways to improve efficiency include cutting out unnecessary steps, using standing orders and Advance Beneficiary Notice of Noncoverage (ABNs) for flu vaccinations, keeping credit card numbers on file for contactless payment, and considering the clinical and financial value of lab testing before ordering it.
“Effective triage helps patient satisfaction, access to care, and efficiency of your office workload,” Dr. Kressly said. “Use technology where it’s appropriate, but then add people where it’s needed. Connections to caring people matter even more in a time of crisis.”
The speakers also highlighted the importance of early flu vaccinations.
“One of the single biggest things you can do for value in COVID is to get your flu vaccine numbers up,” Dr. Berman said. “Severely reducing the burden of influenza will help flatten the curve, it will reduce febrile respiratory illness, and it will protect your most fragile patients.”
Two ways to do that include flu clinics and making a strong push for immunizations during the first 8 weeks after getting the vaccines. Dr Berman shared numbers from two practices showing how many more total immunizations were done in the practice that began vaccinating in early August versus early September.
A crisis is an opportunity
The speakers closed on an optimistic note that emphasized the opportunities that can grow out of the challenges presented by the pandemic, a point Dr Terk elaborated on.
“One of the most important things is realizing how we can potentially use a crisis to transform our practices,” Dr. Terk said in the interview. “As had been said before, a crisis is a terrible thing to waste. Those practices that have the gumption to innovate and find different ways to improve the way they provide care are probably going to be in better shape as we go forward.”
Critical to that success is taking risks, he added.
“When you’re innovating, failure has to be something you are permissive of because if you’re risk-averse and failure-averse, you’re not going to have the opportunity to grow and innovate, and this is another opportunity to innovate,” Dr. Terk said.
He also stressed the value of learning from one another. “We need to help each other by sharing our good practices, and on the flip side, be open to learning from each other,” he said. “Those pediatricians who are struggling need to be open-minded and open-hearted to understanding how we can operate our practices better and know that the things we think are barriers we can’t change are probably things we probably haven’t allowed ourselves to think about changing.”
Dr. Kressly and Dr. Berman recommended several specific actions for pediatricians to take:
- Creating a SWOT (Strengths, Weaknesses, Opportunities, and Threats) analysis regarding your practice management response to the pandemic.
- Articulating three goals for improving your understanding or the implementation of management in your practice.
- Creating a working group to identify and implement ways to improve clinical work flow and communication strategies.
“Now is the time to meaningfully address disparities of access to appropriate health care and the impact of social determinants of health,” Dr. Kressly said. It’s also an opportunity to build meaningful relationships with patient families based on trust, science, and “true shared decision-making with health literacy in mind.”
Dr Kressly is the medical director of and owns shares in Office Practicum. Dr. Berman is the assistant medical director of and owns shares in Office Practicum, and is the owner of Script Doctor LLC. Dr. Terk and Dr. Hackell had no relevant financial disclosures.
Practice management is the responsibility of every pediatrician, and leadership is more important than ever in a crisis like the COVID-19 pandemic.
“Ultimately you have a critical role in ensuring that your practice remains sustainable so that you can continue to deliver great care,” Sue Kressly, MD, a retired pediatrician from Warrington, Pa., said at the virtual annual meeting of the American Academy of Pediatrics. “None of us escaped some impact of the COVID crisis, and many of us are going to experience lasting change.”
Dr. Kressly and Suzanne Berman, MD, a pediatrician in central Tennessee, presented a live online session on how the pandemic is affecting practices and how pediatricians can effectively address those challenges.
Three ways a crisis impacts practices
“When a practice experiences a crisis, it really exposes what your practice is made of, for better or for worse,” Dr. Berman said. “The COVID crisis has been profound and broad and long enough to really stress the core tensile strength of practices along at least three axes.” Those are staffing, financial health, and partnerships.
It’s a normal human response to enter survival mode during a crisis, so staff management becomes more important than ever. Some things to consider are whether you have a truly collaborative team culture in your practice and whether you’re really listening to the staff’s struggles and suggestions.
“Staffing challenges can be very difficult,” Dr. Berman said. “Permitting staff to work from home is the single biggest thing you can do when staff needs to self-isolate.”
Financially, most medical practices have adequate cash on hand not to have to pay close attention to the numbers, Dr. Kressly said, but if physicians are looking at their books for the first time during a crisis, they have no way of knowing what their baseline expectations should be or how much to worry about their finances. It’s important to understand your practice’s or department’s budget.
Jesse Hackell, MD, a private practice pediatrician in a suburb of New York City and vice president of the New York AAP Chapter 3, attended the session and appreciated this point on finances.
“In order to provide good quality care to kids, you need to be financially successful because otherwise you’ll close your doors,” Dr. Hackell said in an interview. “It’s making yourself available to be able to provide care.”
Stressors among partners during a crisis arise from responding to the challenges of the crisis, such as who should be impacted by pay cuts or furloughs, how to account for overhead, how to distribute revenue and how to divide the work equitably. Other issues include how to protect higher risk providers fairly and how to shift schedules or case load based on unforeseen events, including quarantining.
“There is no ‘fair’ in a crisis,” Dr. Berman said. “We must use the equity paradigm to be sure everyone has what they need to survive and have the best outcome possible.”
The speakers also discussed the importance of a practice’s situation before the pandemic began, a point that resonated with attendee Jason Terk, MD, a pediatrician who practices in a large pediatric health care system near Fort Worth, Texas.
“Just like the pandemic impacts the health of people in different ways based upon their baseline health, the pandemic impacts practices in different ways based on the practice’s baseline health,” he said in an interview. “If you had good operations, a good culture, good communication and all those other good indicators of practice health before, then you stood a much better chance of surviving the pandemic as a practice than practices that had weaknesses before.”
The size of a practice did not necessarily predict the impact of the crisis, Dr. Berman said. Rather, practices with good patient engagement, active recall programs, and good fiscal planning did better.
Dr. Hackell said. “We had never seen anything like this before,” he said in an interview. “From the start we had no idea what was going to work. Try something and see if it works. If it fails, try something else. We were all operating blind here.”
The focus of most practices in the spring was on well visits, chronic care follow-up, and telehealth. Going into fall and winter, innovation will be necessary to provide appropriate care for all children while keeping in mind that the choices pediatricians make will have long-lasting implications for their staff and patients. The speakers stressed the importance of communication and transparency within the office team and to patients and the community.
Dr. Hackell appreciated the speakers’ point that kids need care, and pediatricians need to meet that need.
“Kids need well care and immunizations, and kids get sick and need sick care,” he said. “Parents need a lot more reassurance during times like this. We need to be able to provide that care and be sure that we do it safely. To give the right care at the right time in the right location is key.”
Making practice adaptations
In balancing risk and access to care, Dr. Kressly described the importance of multiple interventions, including managing some patients out of the office and making physical changes, such as putting in physical barriers and eliminating waiting rooms.
“Many practices are highly focused on PPE [personal protective equipment],” Dr. Kressly said, but even Centers for Disease Control and Prevention guidance emphasizes that PPE is the last line of defense. “There are many things we can do to protect our teams and our patients, and we know that not one single adaption is going to be 100% effective. But like the Swiss cheese model indicates, when you layer all of these efforts on top of one another, many defenses allow for the protection of the majority of people.”
Other changes include restricting office visitors to one per patient, implementing social distancing, requiring visitors to wear masks, and considering alternate locations for visits, including car and parking lot visits.
“No idea is too crazy, and some of the best ideas come from your staff,” Dr. Kressly said. She also recommended asking families where they feel most comfortable meeting.
“Don’t make any assumptions about where they want to be seen, but ask and together decide where the patient can most safely and effectively be given appropriate care,” she said.
Dr. Kressly also noted the new CPT code, 99072, that can be used to bill for “additional supplies, materials, and clinical staff time over and above those usually included in an office visit or other nonfacility service(s), when performed during a public health emergency as defined by law, due to respiratory-transmitted infectious disease.”
Pediatricians should think of ways they can remove barriers to access, such as adjusting no-show cancellation penalties and adjusting practice policies as needed when things change. “Avoid creating a culture where families do not disclose all information for fear of not being seen,” Dr. Kressly said.
A slower pace because of delays and hiccups is also normal at this time, Dr. Berman said. “If you feel like you’re just not as efficient as you were prior to COVID, it’s not just you,” she said. “It’s true. Everyone has to grapple with new things now. It takes longer.”
Things that add time include remote check-in and paperwork, more time to don and doff PPE and disinfect, dealing with technology failures, adjusting to new procedures or policies, and the general mental fatigue of adhering to PPE best practices. Patience is vital during this time, Dr. Berman said.
Several ways to improve efficiency include cutting out unnecessary steps, using standing orders and Advance Beneficiary Notice of Noncoverage (ABNs) for flu vaccinations, keeping credit card numbers on file for contactless payment, and considering the clinical and financial value of lab testing before ordering it.
“Effective triage helps patient satisfaction, access to care, and efficiency of your office workload,” Dr. Kressly said. “Use technology where it’s appropriate, but then add people where it’s needed. Connections to caring people matter even more in a time of crisis.”
The speakers also highlighted the importance of early flu vaccinations.
“One of the single biggest things you can do for value in COVID is to get your flu vaccine numbers up,” Dr. Berman said. “Severely reducing the burden of influenza will help flatten the curve, it will reduce febrile respiratory illness, and it will protect your most fragile patients.”
Two ways to do that include flu clinics and making a strong push for immunizations during the first 8 weeks after getting the vaccines. Dr Berman shared numbers from two practices showing how many more total immunizations were done in the practice that began vaccinating in early August versus early September.
A crisis is an opportunity
The speakers closed on an optimistic note that emphasized the opportunities that can grow out of the challenges presented by the pandemic, a point Dr Terk elaborated on.
“One of the most important things is realizing how we can potentially use a crisis to transform our practices,” Dr. Terk said in the interview. “As had been said before, a crisis is a terrible thing to waste. Those practices that have the gumption to innovate and find different ways to improve the way they provide care are probably going to be in better shape as we go forward.”
Critical to that success is taking risks, he added.
“When you’re innovating, failure has to be something you are permissive of because if you’re risk-averse and failure-averse, you’re not going to have the opportunity to grow and innovate, and this is another opportunity to innovate,” Dr. Terk said.
He also stressed the value of learning from one another. “We need to help each other by sharing our good practices, and on the flip side, be open to learning from each other,” he said. “Those pediatricians who are struggling need to be open-minded and open-hearted to understanding how we can operate our practices better and know that the things we think are barriers we can’t change are probably things we probably haven’t allowed ourselves to think about changing.”
Dr. Kressly and Dr. Berman recommended several specific actions for pediatricians to take:
- Creating a SWOT (Strengths, Weaknesses, Opportunities, and Threats) analysis regarding your practice management response to the pandemic.
- Articulating three goals for improving your understanding or the implementation of management in your practice.
- Creating a working group to identify and implement ways to improve clinical work flow and communication strategies.
“Now is the time to meaningfully address disparities of access to appropriate health care and the impact of social determinants of health,” Dr. Kressly said. It’s also an opportunity to build meaningful relationships with patient families based on trust, science, and “true shared decision-making with health literacy in mind.”
Dr Kressly is the medical director of and owns shares in Office Practicum. Dr. Berman is the assistant medical director of and owns shares in Office Practicum, and is the owner of Script Doctor LLC. Dr. Terk and Dr. Hackell had no relevant financial disclosures.
FROM AAP 2020
COVID-19 and the superspreaders: Teens
Although cases of COVID-19 in children is reported to be low, we are seeing a surge in Wisconsin with a 27.6% positivity rate reported on Sept. 27. Numerous other states across the country are reporting similar jumps of 10% or more.

According to the Wisconsin Department of Health Services as of Sept. 20, 2020, there were 10,644 cumulative cases in persons aged less than 18 years. This rise in cases is consistent with a return to school and sports. This cumulative case load amounts to 836.7/100, 000 cases. This population may not experience the level of illness seen in the older populations with hospitalization rates of only 3% under the age of 9 years and 13% of those age 10- 19-years, yet exposing older family and members of the community is driving the death rates. The combined influenza and COVID-19 season may greatly impact hospitalization rates of young and old. Additionally, we may see a surge in pediatric cancer rates and autoimmune diseases secondary to these trends.
I believe the overall number of adolescents with COVID-19 is underreported. Teens admit to a lack of understanding of symptoms. Many do not realize they have COVID-19 until someone points out the symptoms they describe such as a loss of taste or smell are COVID-19 symptoms. Others report they do not report symptoms to prevent quarantine. Additionally, others endorse ridicule from peers if they have tested positive and contract tracing identifies others potentially exposed and forced to sit out of sports because of quarantine. They have been bullied into amnesia when contract tracers call to prevent identifying others at school or in the community. All these behaviors proliferate the spread of disease within the community and will continue to drive both exposures and death rates.
Teens in high schools require increased education of the symptoms of COVID-19, promotion of the flu vaccine, and knowledge of the impact they can have on preventing the spread of viruses.
Ms. Thew is the medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She said she had no relevant financial disclosures. Email her at [email protected].
Reference
COVID-19: Wisconsin Cases, Wisconsin Department of Health Services. Accessed 2020 Sep 27.
Although cases of COVID-19 in children is reported to be low, we are seeing a surge in Wisconsin with a 27.6% positivity rate reported on Sept. 27. Numerous other states across the country are reporting similar jumps of 10% or more.
According to the Wisconsin Department of Health Services as of Sept. 20, 2020, there were 10,644 cumulative cases in persons aged less than 18 years. This rise in cases is consistent with a return to school and sports. This cumulative case load amounts to 836.7/100, 000 cases. This population may not experience the level of illness seen in the older populations with hospitalization rates of only 3% under the age of 9 years and 13% of those age 10- 19-years, yet exposing older family and members of the community is driving the death rates. The combined influenza and COVID-19 season may greatly impact hospitalization rates of young and old. Additionally, we may see a surge in pediatric cancer rates and autoimmune diseases secondary to these trends.
I believe the overall number of adolescents with COVID-19 is underreported. Teens admit to a lack of understanding of symptoms. Many do not realize they have COVID-19 until someone points out the symptoms they describe such as a loss of taste or smell are COVID-19 symptoms. Others report they do not report symptoms to prevent quarantine. Additionally, others endorse ridicule from peers if they have tested positive and contract tracing identifies others potentially exposed and forced to sit out of sports because of quarantine. They have been bullied into amnesia when contract tracers call to prevent identifying others at school or in the community. All these behaviors proliferate the spread of disease within the community and will continue to drive both exposures and death rates.
Teens in high schools require increased education of the symptoms of COVID-19, promotion of the flu vaccine, and knowledge of the impact they can have on preventing the spread of viruses.
Ms. Thew is the medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She said she had no relevant financial disclosures. Email her at [email protected].
Reference
COVID-19: Wisconsin Cases, Wisconsin Department of Health Services. Accessed 2020 Sep 27.
Although cases of COVID-19 in children is reported to be low, we are seeing a surge in Wisconsin with a 27.6% positivity rate reported on Sept. 27. Numerous other states across the country are reporting similar jumps of 10% or more.
According to the Wisconsin Department of Health Services as of Sept. 20, 2020, there were 10,644 cumulative cases in persons aged less than 18 years. This rise in cases is consistent with a return to school and sports. This cumulative case load amounts to 836.7/100, 000 cases. This population may not experience the level of illness seen in the older populations with hospitalization rates of only 3% under the age of 9 years and 13% of those age 10- 19-years, yet exposing older family and members of the community is driving the death rates. The combined influenza and COVID-19 season may greatly impact hospitalization rates of young and old. Additionally, we may see a surge in pediatric cancer rates and autoimmune diseases secondary to these trends.
I believe the overall number of adolescents with COVID-19 is underreported. Teens admit to a lack of understanding of symptoms. Many do not realize they have COVID-19 until someone points out the symptoms they describe such as a loss of taste or smell are COVID-19 symptoms. Others report they do not report symptoms to prevent quarantine. Additionally, others endorse ridicule from peers if they have tested positive and contract tracing identifies others potentially exposed and forced to sit out of sports because of quarantine. They have been bullied into amnesia when contract tracers call to prevent identifying others at school or in the community. All these behaviors proliferate the spread of disease within the community and will continue to drive both exposures and death rates.
Teens in high schools require increased education of the symptoms of COVID-19, promotion of the flu vaccine, and knowledge of the impact they can have on preventing the spread of viruses.
Ms. Thew is the medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She said she had no relevant financial disclosures. Email her at [email protected].
Reference
COVID-19: Wisconsin Cases, Wisconsin Department of Health Services. Accessed 2020 Sep 27.
Pediatric fractures shift during pandemic
Pediatric fractures dropped by 2.5-fold during the early months of the COVID-19 pandemic, but more breaks happened at home and on bicycles, and younger kids were more affected, new research indicates.
The study of 1,745 patients also found that those with distal radius torus fractures were more likely to receive a Velcro splint during the pandemic. Experts said this key trend points toward widespread shifts to streamline treatment, which should persist after the pandemic.
“We expected to see a drop in fracture volume, but what was a bit unexpected was the proportional rise in at-home injuries, which we weren’t immediately aware of,” said senior author Apurva Shah, MD, MBA, of Children’s Hospital of Philadelphia (CHOP) and the University of Pennsylvania in Philadelphia.
“As time went on, it became more apparent that trampoline and bicycle injuries were on the rise, but at the beginning of the pandemic, we didn’t intuitively expect that,” he added.
“Whenever there’s a major shift in how the world is working, we want to understand how that impacts child safety,” Dr. Shah said in an interview. “The message to get out to parents is that it’s obviously difficult to supervise kids while working from home” during the pandemic “and that supervision obviously is not always working as well as intended.”
Joshua T. Bram, a medical student, presented the study at the virtual American Academy of Pediatrics (AAP) 2020 National Conference.
Dr. Bram, Dr. Shah, and colleagues compared patients with acute fractures who presented at CHOP between March and April 2020 with those who presented during the same months in 2018 and 2019.
Overall, the number of patients with pediatric fractures who presented to CHOP fell to an average of just under 10 per day, compared with more than 22 per day in prior years (P < .001). In addition, the age of the patients fell from an average of 9.4 years to 7.5 years (P < .001), with fewer adolescents affected in 2020.
“I think when you cancel a 14-year-old’s baseball season” because of the pandemic, “unfortunately, that lost outdoor time might be substituted with time on a screen,” he explained. “But canceling a 6-year-old’s soccer season might mean substituting that with more time outside on bikes or on a trampoline.”
As noted, because of the pandemic, a higher proportion of pediatric fractures occurred at home (57.8% vs. 32.5%; P < .001) or on bicycles (18.3% vs. 8.2%; P < .001), but there were fewer organized sports–related (7.2% vs. 26.0%; P < .001) or playground-related injuries (5.2% vs. 9.0%; P < .001).
In the study period this year, the researchers saw no increase in the amount of time between injury and presentation. However, data suggest that, in more recent months, “kids are presenting with fractures late, with sometimes great consequences,” Dr. Shah said.
“What has changed is that a lot of adults have lost their jobs, and as a consequence, a lot of children have lost their access to private insurance,” he said. “But fracture is really a major injury, and this is a reminder for pediatricians and primary care physicians to recognize that families are going through these changes and that delays in care can really be detrimental to children.”
Velcro splints more common
A potential upside to shifts seen during the pandemic, Dr. Shah said, is the finding that distal radius torus fractures were more likely to be treated with a Velcro splint than in previous years (44.2% vs. 25.9%; P = .010).
“This is hitting on something important – that sometimes it’s crisis that forces us as physicians to evolve,” he said. “This is something I think is here to stay.
“Although research had already been there suggesting a close equivalent between splints and casting, culturally, a lot of surgeons hadn’t made that shift when historically the gold standard had been casting,” Dr. Shah added. “But with the pandemic, the shift to minimize contact with the health care system to keep families safe in their COVID bubble helped [usage of] splints take off.
“I suspect – and we’ll only know when we’re on the other side of this – when physicians see good results in splints in their own patients, they’re going to adopt those strategies more permanently,” he said.
Benjamin Shore, MD, MPH, of Boston Children’s Hospital, agreed with Dr. Shah’s prediction that fracture care will be more streamlined after the pandemic. Dr. Shore, who wasn’t involved in the study, said not only are more orthopedic providers treating patients with Velcro splints and bivalve casts, but they are also monitoring patients via telehealth.
“All of these are great examples of innovation, and one of the unique parts of the pandemic is it created a lot of rapid change across healthcare because it caused us to scrutinize the ways we practice and make a change,” Dr. Shore said in an interview.
“It wasn’t a very fancy study, but it’s very important in terms of demonstrating a change in practice,” Dr. Shore said. “The research here basically validated what many of us are seeing and hopefully will help us in future pandemics – which hopefully won’t happen – to tell families what to be proactive about.”
Dr. Shah and Dr. Shore agreed that, because fewer fractures are occurring in kids during the pandemic, there is an opportunity to redeploy orthopedic providers to other clinical areas on the basis of volume and need.
Dr. Shah and Dr. Shore have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Pediatric fractures dropped by 2.5-fold during the early months of the COVID-19 pandemic, but more breaks happened at home and on bicycles, and younger kids were more affected, new research indicates.
The study of 1,745 patients also found that those with distal radius torus fractures were more likely to receive a Velcro splint during the pandemic. Experts said this key trend points toward widespread shifts to streamline treatment, which should persist after the pandemic.
“We expected to see a drop in fracture volume, but what was a bit unexpected was the proportional rise in at-home injuries, which we weren’t immediately aware of,” said senior author Apurva Shah, MD, MBA, of Children’s Hospital of Philadelphia (CHOP) and the University of Pennsylvania in Philadelphia.
“As time went on, it became more apparent that trampoline and bicycle injuries were on the rise, but at the beginning of the pandemic, we didn’t intuitively expect that,” he added.
“Whenever there’s a major shift in how the world is working, we want to understand how that impacts child safety,” Dr. Shah said in an interview. “The message to get out to parents is that it’s obviously difficult to supervise kids while working from home” during the pandemic “and that supervision obviously is not always working as well as intended.”
Joshua T. Bram, a medical student, presented the study at the virtual American Academy of Pediatrics (AAP) 2020 National Conference.
Dr. Bram, Dr. Shah, and colleagues compared patients with acute fractures who presented at CHOP between March and April 2020 with those who presented during the same months in 2018 and 2019.
Overall, the number of patients with pediatric fractures who presented to CHOP fell to an average of just under 10 per day, compared with more than 22 per day in prior years (P < .001). In addition, the age of the patients fell from an average of 9.4 years to 7.5 years (P < .001), with fewer adolescents affected in 2020.
“I think when you cancel a 14-year-old’s baseball season” because of the pandemic, “unfortunately, that lost outdoor time might be substituted with time on a screen,” he explained. “But canceling a 6-year-old’s soccer season might mean substituting that with more time outside on bikes or on a trampoline.”
As noted, because of the pandemic, a higher proportion of pediatric fractures occurred at home (57.8% vs. 32.5%; P < .001) or on bicycles (18.3% vs. 8.2%; P < .001), but there were fewer organized sports–related (7.2% vs. 26.0%; P < .001) or playground-related injuries (5.2% vs. 9.0%; P < .001).
In the study period this year, the researchers saw no increase in the amount of time between injury and presentation. However, data suggest that, in more recent months, “kids are presenting with fractures late, with sometimes great consequences,” Dr. Shah said.
“What has changed is that a lot of adults have lost their jobs, and as a consequence, a lot of children have lost their access to private insurance,” he said. “But fracture is really a major injury, and this is a reminder for pediatricians and primary care physicians to recognize that families are going through these changes and that delays in care can really be detrimental to children.”
Velcro splints more common
A potential upside to shifts seen during the pandemic, Dr. Shah said, is the finding that distal radius torus fractures were more likely to be treated with a Velcro splint than in previous years (44.2% vs. 25.9%; P = .010).
“This is hitting on something important – that sometimes it’s crisis that forces us as physicians to evolve,” he said. “This is something I think is here to stay.
“Although research had already been there suggesting a close equivalent between splints and casting, culturally, a lot of surgeons hadn’t made that shift when historically the gold standard had been casting,” Dr. Shah added. “But with the pandemic, the shift to minimize contact with the health care system to keep families safe in their COVID bubble helped [usage of] splints take off.
“I suspect – and we’ll only know when we’re on the other side of this – when physicians see good results in splints in their own patients, they’re going to adopt those strategies more permanently,” he said.
Benjamin Shore, MD, MPH, of Boston Children’s Hospital, agreed with Dr. Shah’s prediction that fracture care will be more streamlined after the pandemic. Dr. Shore, who wasn’t involved in the study, said not only are more orthopedic providers treating patients with Velcro splints and bivalve casts, but they are also monitoring patients via telehealth.
“All of these are great examples of innovation, and one of the unique parts of the pandemic is it created a lot of rapid change across healthcare because it caused us to scrutinize the ways we practice and make a change,” Dr. Shore said in an interview.
“It wasn’t a very fancy study, but it’s very important in terms of demonstrating a change in practice,” Dr. Shore said. “The research here basically validated what many of us are seeing and hopefully will help us in future pandemics – which hopefully won’t happen – to tell families what to be proactive about.”
Dr. Shah and Dr. Shore agreed that, because fewer fractures are occurring in kids during the pandemic, there is an opportunity to redeploy orthopedic providers to other clinical areas on the basis of volume and need.
Dr. Shah and Dr. Shore have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Pediatric fractures dropped by 2.5-fold during the early months of the COVID-19 pandemic, but more breaks happened at home and on bicycles, and younger kids were more affected, new research indicates.
The study of 1,745 patients also found that those with distal radius torus fractures were more likely to receive a Velcro splint during the pandemic. Experts said this key trend points toward widespread shifts to streamline treatment, which should persist after the pandemic.
“We expected to see a drop in fracture volume, but what was a bit unexpected was the proportional rise in at-home injuries, which we weren’t immediately aware of,” said senior author Apurva Shah, MD, MBA, of Children’s Hospital of Philadelphia (CHOP) and the University of Pennsylvania in Philadelphia.
“As time went on, it became more apparent that trampoline and bicycle injuries were on the rise, but at the beginning of the pandemic, we didn’t intuitively expect that,” he added.
“Whenever there’s a major shift in how the world is working, we want to understand how that impacts child safety,” Dr. Shah said in an interview. “The message to get out to parents is that it’s obviously difficult to supervise kids while working from home” during the pandemic “and that supervision obviously is not always working as well as intended.”
Joshua T. Bram, a medical student, presented the study at the virtual American Academy of Pediatrics (AAP) 2020 National Conference.
Dr. Bram, Dr. Shah, and colleagues compared patients with acute fractures who presented at CHOP between March and April 2020 with those who presented during the same months in 2018 and 2019.
Overall, the number of patients with pediatric fractures who presented to CHOP fell to an average of just under 10 per day, compared with more than 22 per day in prior years (P < .001). In addition, the age of the patients fell from an average of 9.4 years to 7.5 years (P < .001), with fewer adolescents affected in 2020.
“I think when you cancel a 14-year-old’s baseball season” because of the pandemic, “unfortunately, that lost outdoor time might be substituted with time on a screen,” he explained. “But canceling a 6-year-old’s soccer season might mean substituting that with more time outside on bikes or on a trampoline.”
As noted, because of the pandemic, a higher proportion of pediatric fractures occurred at home (57.8% vs. 32.5%; P < .001) or on bicycles (18.3% vs. 8.2%; P < .001), but there were fewer organized sports–related (7.2% vs. 26.0%; P < .001) or playground-related injuries (5.2% vs. 9.0%; P < .001).
In the study period this year, the researchers saw no increase in the amount of time between injury and presentation. However, data suggest that, in more recent months, “kids are presenting with fractures late, with sometimes great consequences,” Dr. Shah said.
“What has changed is that a lot of adults have lost their jobs, and as a consequence, a lot of children have lost their access to private insurance,” he said. “But fracture is really a major injury, and this is a reminder for pediatricians and primary care physicians to recognize that families are going through these changes and that delays in care can really be detrimental to children.”
Velcro splints more common
A potential upside to shifts seen during the pandemic, Dr. Shah said, is the finding that distal radius torus fractures were more likely to be treated with a Velcro splint than in previous years (44.2% vs. 25.9%; P = .010).
“This is hitting on something important – that sometimes it’s crisis that forces us as physicians to evolve,” he said. “This is something I think is here to stay.
“Although research had already been there suggesting a close equivalent between splints and casting, culturally, a lot of surgeons hadn’t made that shift when historically the gold standard had been casting,” Dr. Shah added. “But with the pandemic, the shift to minimize contact with the health care system to keep families safe in their COVID bubble helped [usage of] splints take off.
“I suspect – and we’ll only know when we’re on the other side of this – when physicians see good results in splints in their own patients, they’re going to adopt those strategies more permanently,” he said.
Benjamin Shore, MD, MPH, of Boston Children’s Hospital, agreed with Dr. Shah’s prediction that fracture care will be more streamlined after the pandemic. Dr. Shore, who wasn’t involved in the study, said not only are more orthopedic providers treating patients with Velcro splints and bivalve casts, but they are also monitoring patients via telehealth.
“All of these are great examples of innovation, and one of the unique parts of the pandemic is it created a lot of rapid change across healthcare because it caused us to scrutinize the ways we practice and make a change,” Dr. Shore said in an interview.
“It wasn’t a very fancy study, but it’s very important in terms of demonstrating a change in practice,” Dr. Shore said. “The research here basically validated what many of us are seeing and hopefully will help us in future pandemics – which hopefully won’t happen – to tell families what to be proactive about.”
Dr. Shah and Dr. Shore agreed that, because fewer fractures are occurring in kids during the pandemic, there is an opportunity to redeploy orthopedic providers to other clinical areas on the basis of volume and need.
Dr. Shah and Dr. Shore have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Burnout/depression: Half of pulmonology trainees report symptoms
results from a national survey demonstrated.

“Given the high prevalence of burnout and depressive symptoms among fellows training in pulmonary and critical care medicine, it is crucial for fellowship training programs and academic hospitals to consider policies and programs that can improve this public health crisis,” first author Michelle Sharp, MD, MHS, and colleagues wrote in a study published in CHEST.
Dr. Sharp, of the division of pulmonary and critical care medicine at Johns Hopkins University, Baltimore, and colleagues developed a cross-sectional electronic survey to assess burnout and depression symptoms in fellows enrolled in pulmonary and critical care medicine training programs in the United States. Between January and February 2019, a total of 976 fellows received the survey, which used the Maslach Burnout Index two-item measure to assess burnout and the two-item Primary Care Evaluation of Mental Disorders Procedure to screen for depressive symptoms. For both burnout and depression, the researchers constructed three multivariate logistic regression models to assess individual fellow characteristics, program structure, and institutional policies associated with the symptoms.
Of the 976 surveys sent, 502 completed both outcome measures, for a response rate of 51%. More than half (59%) were male, 57% described themselves as White/non-Hispanic, and 39% reported at least $200,000 in student loan debt. The researchers found that 50% of respondents screened positive for either burnout of depressive symptoms. Specifically, 41% met criteria for depressive symptoms, 32% were positive for burnout, and 23% were positive for both.
Factors significantly associated with a higher odds of burnout included working more than 70 hours in an average clinical week (adjusted odds ratio, 2.80) and reporting a somewhat negative or very negative impact of the EHR on joy in medicine (aOR, 1.91).
Factors significantly associated with a higher odds of depressive symptoms were financial concern (aOR, 1.13), being located in the Association of American Medical Colleges West region (aOR 3.96), working more than 70 hours in an average clinical week (aOR, 2.24), and spending a moderately high or excessive amount of time at home on the EHR (aOR, 1.71).
Of respondents who reported working in an institution with a coverage system for personal illness or emergency, 29% were uncomfortable accessing the system or felt comfortable only if unable to find their own coverage. In addition, among respondents who indicated that they had access to mental health resources through their place of employment, 15% said they were reluctant to access those resources if needed. Formal use of these programs was not measured by the survey.
“Our results suggest that further study of systemic solutions at the programmatic and institutional levels rather than at the individual level are needed,” Dr. Sharp and colleagues wrote. “Strategies such as providing an easily accessible coverage system, providing access to mental health resources, addressing work hour burden, reducing the EHR burden, and addressing financial concerns among trainees may help reduce burnout and/or depressive symptoms and should be further studied.”

In an interview, David Schulman, MD, FCCP, characterized the survey findings as “disheartening” but not surprising. “Burnout and depressive symptoms are a problem because almost everything we do to mitigate them works a little, but nothing works a lot,” said Dr. Schulman, professor of medicine in the division of pulmonary, allergy, critical care, and sleep medicine at Emory University, Atlanta, who was not affiliated with the study. “The limited availability of resources to fight this is a challenge. The thing that seems to correlate best with mitigating burnout and depression rates is just giving people time. In my experience, most people just want the space and time they need to mitigate burnout in their own way by having schedule flexibility or arranging time to spend with family or involved in other wellness activities.”
Dr. Schulman, who served as training program director of pulmonary and critical care medicine fellows at Emory for 14 years until stepping down from that role in September 2020, said that nurturing a culture where trainees and seasoned colleagues are comfortable talking about burnout and depressive symptoms is one way to foster change. “It’s weird to say that we should try to normalize burnout, but I don’t think the health care system is changing anytime soon. The health care system is a harsh mistress. It will continue to take and take from everyone involved in it until they have nothing left to give. It’s unfortunate, because people are sick, and hospitals can be relatively understaffed, particularly in the context of a major public health emergency. What we really need to do is try to normalize this by saying to trainees: ‘Hey. Everybody is under the gun. We’re going to share in this workload together because we can’t abandon our patients. We will do our best to make sure that the workload is shared amongst everybody.’ ”
He emphasized that most trainees recognize the importance of the work they do, “and they don’t shirk from it. But I think that drive sometimes gets in the way of self-care. I do think there needs to be a happy medium, where we definitely want you to work, because that’s how you learn and the system needs you, but we also recognize that there’s a need for you to take care of yourself.”
Dr. Schulman recommended that such discussions take place not remotely on Zoom calls and the like but rather in person with small groups of trainees and seasoned clinicians, “where people are more comfortable candidly discussing how they’re feeling. I don’t think grand rounds on burnout or depression are particularly effective. It needs to be interactive, and we need to listen as much as we’re talking.”
Although the survey by Dr. Sharp and colleagues was completed prior to the COVID-19 pandemic, Dr. Schulman has a hunch that the current driver of burnout and depression has more to do with trainees feeling a sense of physical isolation than with being overwhelmed by their workload. “I don’t think that’s unique to medicine,” he said. “When people get home from work, they can’t go out with friends or out to dinner, or travel, whatever they do to decompress. I think that’s a major driver for the current phenomenon, and I don’t think that’s unique to medicine. The psychological ramifications of isolation due to the coronavirus may eventually outpace the physical ramifications of all the illness that we have seen. Depression and burnout may not be as obviously damaging to people, but I think they’re affecting many more people than the virus itself.”
The survey was supported by the Association of Pulmonary and Critical Care Medicine Program Directors.
results from a national survey demonstrated.
“Given the high prevalence of burnout and depressive symptoms among fellows training in pulmonary and critical care medicine, it is crucial for fellowship training programs and academic hospitals to consider policies and programs that can improve this public health crisis,” first author Michelle Sharp, MD, MHS, and colleagues wrote in a study published in CHEST.
Dr. Sharp, of the division of pulmonary and critical care medicine at Johns Hopkins University, Baltimore, and colleagues developed a cross-sectional electronic survey to assess burnout and depression symptoms in fellows enrolled in pulmonary and critical care medicine training programs in the United States. Between January and February 2019, a total of 976 fellows received the survey, which used the Maslach Burnout Index two-item measure to assess burnout and the two-item Primary Care Evaluation of Mental Disorders Procedure to screen for depressive symptoms. For both burnout and depression, the researchers constructed three multivariate logistic regression models to assess individual fellow characteristics, program structure, and institutional policies associated with the symptoms.
Of the 976 surveys sent, 502 completed both outcome measures, for a response rate of 51%. More than half (59%) were male, 57% described themselves as White/non-Hispanic, and 39% reported at least $200,000 in student loan debt. The researchers found that 50% of respondents screened positive for either burnout of depressive symptoms. Specifically, 41% met criteria for depressive symptoms, 32% were positive for burnout, and 23% were positive for both.
Factors significantly associated with a higher odds of burnout included working more than 70 hours in an average clinical week (adjusted odds ratio, 2.80) and reporting a somewhat negative or very negative impact of the EHR on joy in medicine (aOR, 1.91).
Factors significantly associated with a higher odds of depressive symptoms were financial concern (aOR, 1.13), being located in the Association of American Medical Colleges West region (aOR 3.96), working more than 70 hours in an average clinical week (aOR, 2.24), and spending a moderately high or excessive amount of time at home on the EHR (aOR, 1.71).
Of respondents who reported working in an institution with a coverage system for personal illness or emergency, 29% were uncomfortable accessing the system or felt comfortable only if unable to find their own coverage. In addition, among respondents who indicated that they had access to mental health resources through their place of employment, 15% said they were reluctant to access those resources if needed. Formal use of these programs was not measured by the survey.
“Our results suggest that further study of systemic solutions at the programmatic and institutional levels rather than at the individual level are needed,” Dr. Sharp and colleagues wrote. “Strategies such as providing an easily accessible coverage system, providing access to mental health resources, addressing work hour burden, reducing the EHR burden, and addressing financial concerns among trainees may help reduce burnout and/or depressive symptoms and should be further studied.”
In an interview, David Schulman, MD, FCCP, characterized the survey findings as “disheartening” but not surprising. “Burnout and depressive symptoms are a problem because almost everything we do to mitigate them works a little, but nothing works a lot,” said Dr. Schulman, professor of medicine in the division of pulmonary, allergy, critical care, and sleep medicine at Emory University, Atlanta, who was not affiliated with the study. “The limited availability of resources to fight this is a challenge. The thing that seems to correlate best with mitigating burnout and depression rates is just giving people time. In my experience, most people just want the space and time they need to mitigate burnout in their own way by having schedule flexibility or arranging time to spend with family or involved in other wellness activities.”
Dr. Schulman, who served as training program director of pulmonary and critical care medicine fellows at Emory for 14 years until stepping down from that role in September 2020, said that nurturing a culture where trainees and seasoned colleagues are comfortable talking about burnout and depressive symptoms is one way to foster change. “It’s weird to say that we should try to normalize burnout, but I don’t think the health care system is changing anytime soon. The health care system is a harsh mistress. It will continue to take and take from everyone involved in it until they have nothing left to give. It’s unfortunate, because people are sick, and hospitals can be relatively understaffed, particularly in the context of a major public health emergency. What we really need to do is try to normalize this by saying to trainees: ‘Hey. Everybody is under the gun. We’re going to share in this workload together because we can’t abandon our patients. We will do our best to make sure that the workload is shared amongst everybody.’ ”
He emphasized that most trainees recognize the importance of the work they do, “and they don’t shirk from it. But I think that drive sometimes gets in the way of self-care. I do think there needs to be a happy medium, where we definitely want you to work, because that’s how you learn and the system needs you, but we also recognize that there’s a need for you to take care of yourself.”
Dr. Schulman recommended that such discussions take place not remotely on Zoom calls and the like but rather in person with small groups of trainees and seasoned clinicians, “where people are more comfortable candidly discussing how they’re feeling. I don’t think grand rounds on burnout or depression are particularly effective. It needs to be interactive, and we need to listen as much as we’re talking.”
Although the survey by Dr. Sharp and colleagues was completed prior to the COVID-19 pandemic, Dr. Schulman has a hunch that the current driver of burnout and depression has more to do with trainees feeling a sense of physical isolation than with being overwhelmed by their workload. “I don’t think that’s unique to medicine,” he said. “When people get home from work, they can’t go out with friends or out to dinner, or travel, whatever they do to decompress. I think that’s a major driver for the current phenomenon, and I don’t think that’s unique to medicine. The psychological ramifications of isolation due to the coronavirus may eventually outpace the physical ramifications of all the illness that we have seen. Depression and burnout may not be as obviously damaging to people, but I think they’re affecting many more people than the virus itself.”
The survey was supported by the Association of Pulmonary and Critical Care Medicine Program Directors.
results from a national survey demonstrated.
“Given the high prevalence of burnout and depressive symptoms among fellows training in pulmonary and critical care medicine, it is crucial for fellowship training programs and academic hospitals to consider policies and programs that can improve this public health crisis,” first author Michelle Sharp, MD, MHS, and colleagues wrote in a study published in CHEST.
Dr. Sharp, of the division of pulmonary and critical care medicine at Johns Hopkins University, Baltimore, and colleagues developed a cross-sectional electronic survey to assess burnout and depression symptoms in fellows enrolled in pulmonary and critical care medicine training programs in the United States. Between January and February 2019, a total of 976 fellows received the survey, which used the Maslach Burnout Index two-item measure to assess burnout and the two-item Primary Care Evaluation of Mental Disorders Procedure to screen for depressive symptoms. For both burnout and depression, the researchers constructed three multivariate logistic regression models to assess individual fellow characteristics, program structure, and institutional policies associated with the symptoms.
Of the 976 surveys sent, 502 completed both outcome measures, for a response rate of 51%. More than half (59%) were male, 57% described themselves as White/non-Hispanic, and 39% reported at least $200,000 in student loan debt. The researchers found that 50% of respondents screened positive for either burnout of depressive symptoms. Specifically, 41% met criteria for depressive symptoms, 32% were positive for burnout, and 23% were positive for both.
Factors significantly associated with a higher odds of burnout included working more than 70 hours in an average clinical week (adjusted odds ratio, 2.80) and reporting a somewhat negative or very negative impact of the EHR on joy in medicine (aOR, 1.91).
Factors significantly associated with a higher odds of depressive symptoms were financial concern (aOR, 1.13), being located in the Association of American Medical Colleges West region (aOR 3.96), working more than 70 hours in an average clinical week (aOR, 2.24), and spending a moderately high or excessive amount of time at home on the EHR (aOR, 1.71).
Of respondents who reported working in an institution with a coverage system for personal illness or emergency, 29% were uncomfortable accessing the system or felt comfortable only if unable to find their own coverage. In addition, among respondents who indicated that they had access to mental health resources through their place of employment, 15% said they were reluctant to access those resources if needed. Formal use of these programs was not measured by the survey.
“Our results suggest that further study of systemic solutions at the programmatic and institutional levels rather than at the individual level are needed,” Dr. Sharp and colleagues wrote. “Strategies such as providing an easily accessible coverage system, providing access to mental health resources, addressing work hour burden, reducing the EHR burden, and addressing financial concerns among trainees may help reduce burnout and/or depressive symptoms and should be further studied.”
In an interview, David Schulman, MD, FCCP, characterized the survey findings as “disheartening” but not surprising. “Burnout and depressive symptoms are a problem because almost everything we do to mitigate them works a little, but nothing works a lot,” said Dr. Schulman, professor of medicine in the division of pulmonary, allergy, critical care, and sleep medicine at Emory University, Atlanta, who was not affiliated with the study. “The limited availability of resources to fight this is a challenge. The thing that seems to correlate best with mitigating burnout and depression rates is just giving people time. In my experience, most people just want the space and time they need to mitigate burnout in their own way by having schedule flexibility or arranging time to spend with family or involved in other wellness activities.”
Dr. Schulman, who served as training program director of pulmonary and critical care medicine fellows at Emory for 14 years until stepping down from that role in September 2020, said that nurturing a culture where trainees and seasoned colleagues are comfortable talking about burnout and depressive symptoms is one way to foster change. “It’s weird to say that we should try to normalize burnout, but I don’t think the health care system is changing anytime soon. The health care system is a harsh mistress. It will continue to take and take from everyone involved in it until they have nothing left to give. It’s unfortunate, because people are sick, and hospitals can be relatively understaffed, particularly in the context of a major public health emergency. What we really need to do is try to normalize this by saying to trainees: ‘Hey. Everybody is under the gun. We’re going to share in this workload together because we can’t abandon our patients. We will do our best to make sure that the workload is shared amongst everybody.’ ”
He emphasized that most trainees recognize the importance of the work they do, “and they don’t shirk from it. But I think that drive sometimes gets in the way of self-care. I do think there needs to be a happy medium, where we definitely want you to work, because that’s how you learn and the system needs you, but we also recognize that there’s a need for you to take care of yourself.”
Dr. Schulman recommended that such discussions take place not remotely on Zoom calls and the like but rather in person with small groups of trainees and seasoned clinicians, “where people are more comfortable candidly discussing how they’re feeling. I don’t think grand rounds on burnout or depression are particularly effective. It needs to be interactive, and we need to listen as much as we’re talking.”
Although the survey by Dr. Sharp and colleagues was completed prior to the COVID-19 pandemic, Dr. Schulman has a hunch that the current driver of burnout and depression has more to do with trainees feeling a sense of physical isolation than with being overwhelmed by their workload. “I don’t think that’s unique to medicine,” he said. “When people get home from work, they can’t go out with friends or out to dinner, or travel, whatever they do to decompress. I think that’s a major driver for the current phenomenon, and I don’t think that’s unique to medicine. The psychological ramifications of isolation due to the coronavirus may eventually outpace the physical ramifications of all the illness that we have seen. Depression and burnout may not be as obviously damaging to people, but I think they’re affecting many more people than the virus itself.”
The survey was supported by the Association of Pulmonary and Critical Care Medicine Program Directors.
FROM CHEST
New lupus classification criteria perform well in children, young adults
, according to results from a single-center, retrospective study.
However, the 2019 criteria, which were developed using cohorts of adult patients with SLE, were statistically no better than the 1997 ACR criteria at identifying those without the disease, first author Najla Aljaberi, MBBS, of the Cincinnati Children’s Hospital Medical Center, and colleagues reported in Arthritis Care & Research.
The 2019 criteria were especially good at correctly classifying SLE in non-White youths, but the two sets of criteria performed equally well among male and female youths with SLE and across age groups.
“Our study confirms superior sensitivity of the new criteria over the 1997-ACR criteria in youths with SLE. The difference in sensitivity estimates between the two criteria sets (2019-EULAR/ACR vs. 1997-ACR) may be explained by a higher weight being assigned to immunologic criteria, less strict hematologic criteria (not requiring >2 occurrences), and the inclusion of subjective features of arthritis. Notably, our estimates of the sensitivity of the 2019-EULAR/ACR criteria were similar to those reported from a Brazilian pediatric study by Fonseca et al. (87.7%) that also used physician diagnosis as reference standard,” the researchers wrote.
Dr. Aljaberi and colleagues reviewed electronic medical records of 112 patients with SLE aged 2-21 years and 105 controls aged 1-19 years at Cincinnati Children’s Hospital Medical Center during 2008-2019. Patients identified in the records at the center were considered to have SLE based on ICD-10 codes assigned by experienced pediatric rheumatologists. The control patients included 69 (66%) with juvenile dermatomyositis and 36 with juvenile scleroderma/systemic sclerosis, based on corresponding ICD-10 codes.
Among the SLE cases, 57% were White and 81% were female, while Whites represented 83% and females 71% of control patients. Young adults aged 18-21 years represented a minority of SLE cases (18%) and controls (7%).
The 2019 criteria had significantly higher sensitivity than did the 1997 criteria (85% vs. 72%, respectively; P = .023) but similar specificity (83% vs. 87%; P = .456). A total of 17 out of the 112 SLE cases failed to meet the 2019 criteria, 13 (76%) of whom were White. Overall, 31 SLE cases did not meet the 1997 criteria, but 15 of those fulfilled the 2019 criteria. While there was no statistically significant difference in the sensitivity of the 2019 criteria between non-White and White cases (92% vs. 80%, respectively; P = .08), the difference in sensitivity was significant with the 1997 criteria (83% vs. 64%; P < .02).
The 2019 criteria had similar sensitivity in males and females (86% vs. 81%, respectively), as well as specificity (81% vs. 87%). The 1997 criteria also provided similar sensitivity between males and females (71% vs. 76%) as well as specificity (85% vs. 90%).
In only four instances did SLE cases meet 2019 criteria before ICD-10 diagnosis of SLE, whereas in the other 108 cases the ICD-10 diagnosis coincided with reaching the threshold for meeting 2019 criteria.
There was no funding secured for the study, and the authors had no conflicts of interest to disclose.
SOURCE: Aljaberi N et al. Arthritis Care Res. 2020 Aug 25. doi: 10.1002/acr.24430.
, according to results from a single-center, retrospective study.
However, the 2019 criteria, which were developed using cohorts of adult patients with SLE, were statistically no better than the 1997 ACR criteria at identifying those without the disease, first author Najla Aljaberi, MBBS, of the Cincinnati Children’s Hospital Medical Center, and colleagues reported in Arthritis Care & Research.
The 2019 criteria were especially good at correctly classifying SLE in non-White youths, but the two sets of criteria performed equally well among male and female youths with SLE and across age groups.
“Our study confirms superior sensitivity of the new criteria over the 1997-ACR criteria in youths with SLE. The difference in sensitivity estimates between the two criteria sets (2019-EULAR/ACR vs. 1997-ACR) may be explained by a higher weight being assigned to immunologic criteria, less strict hematologic criteria (not requiring >2 occurrences), and the inclusion of subjective features of arthritis. Notably, our estimates of the sensitivity of the 2019-EULAR/ACR criteria were similar to those reported from a Brazilian pediatric study by Fonseca et al. (87.7%) that also used physician diagnosis as reference standard,” the researchers wrote.
Dr. Aljaberi and colleagues reviewed electronic medical records of 112 patients with SLE aged 2-21 years and 105 controls aged 1-19 years at Cincinnati Children’s Hospital Medical Center during 2008-2019. Patients identified in the records at the center were considered to have SLE based on ICD-10 codes assigned by experienced pediatric rheumatologists. The control patients included 69 (66%) with juvenile dermatomyositis and 36 with juvenile scleroderma/systemic sclerosis, based on corresponding ICD-10 codes.
Among the SLE cases, 57% were White and 81% were female, while Whites represented 83% and females 71% of control patients. Young adults aged 18-21 years represented a minority of SLE cases (18%) and controls (7%).
The 2019 criteria had significantly higher sensitivity than did the 1997 criteria (85% vs. 72%, respectively; P = .023) but similar specificity (83% vs. 87%; P = .456). A total of 17 out of the 112 SLE cases failed to meet the 2019 criteria, 13 (76%) of whom were White. Overall, 31 SLE cases did not meet the 1997 criteria, but 15 of those fulfilled the 2019 criteria. While there was no statistically significant difference in the sensitivity of the 2019 criteria between non-White and White cases (92% vs. 80%, respectively; P = .08), the difference in sensitivity was significant with the 1997 criteria (83% vs. 64%; P < .02).
The 2019 criteria had similar sensitivity in males and females (86% vs. 81%, respectively), as well as specificity (81% vs. 87%). The 1997 criteria also provided similar sensitivity between males and females (71% vs. 76%) as well as specificity (85% vs. 90%).
In only four instances did SLE cases meet 2019 criteria before ICD-10 diagnosis of SLE, whereas in the other 108 cases the ICD-10 diagnosis coincided with reaching the threshold for meeting 2019 criteria.
There was no funding secured for the study, and the authors had no conflicts of interest to disclose.
SOURCE: Aljaberi N et al. Arthritis Care Res. 2020 Aug 25. doi: 10.1002/acr.24430.
, according to results from a single-center, retrospective study.
However, the 2019 criteria, which were developed using cohorts of adult patients with SLE, were statistically no better than the 1997 ACR criteria at identifying those without the disease, first author Najla Aljaberi, MBBS, of the Cincinnati Children’s Hospital Medical Center, and colleagues reported in Arthritis Care & Research.
The 2019 criteria were especially good at correctly classifying SLE in non-White youths, but the two sets of criteria performed equally well among male and female youths with SLE and across age groups.
“Our study confirms superior sensitivity of the new criteria over the 1997-ACR criteria in youths with SLE. The difference in sensitivity estimates between the two criteria sets (2019-EULAR/ACR vs. 1997-ACR) may be explained by a higher weight being assigned to immunologic criteria, less strict hematologic criteria (not requiring >2 occurrences), and the inclusion of subjective features of arthritis. Notably, our estimates of the sensitivity of the 2019-EULAR/ACR criteria were similar to those reported from a Brazilian pediatric study by Fonseca et al. (87.7%) that also used physician diagnosis as reference standard,” the researchers wrote.
Dr. Aljaberi and colleagues reviewed electronic medical records of 112 patients with SLE aged 2-21 years and 105 controls aged 1-19 years at Cincinnati Children’s Hospital Medical Center during 2008-2019. Patients identified in the records at the center were considered to have SLE based on ICD-10 codes assigned by experienced pediatric rheumatologists. The control patients included 69 (66%) with juvenile dermatomyositis and 36 with juvenile scleroderma/systemic sclerosis, based on corresponding ICD-10 codes.
Among the SLE cases, 57% were White and 81% were female, while Whites represented 83% and females 71% of control patients. Young adults aged 18-21 years represented a minority of SLE cases (18%) and controls (7%).
The 2019 criteria had significantly higher sensitivity than did the 1997 criteria (85% vs. 72%, respectively; P = .023) but similar specificity (83% vs. 87%; P = .456). A total of 17 out of the 112 SLE cases failed to meet the 2019 criteria, 13 (76%) of whom were White. Overall, 31 SLE cases did not meet the 1997 criteria, but 15 of those fulfilled the 2019 criteria. While there was no statistically significant difference in the sensitivity of the 2019 criteria between non-White and White cases (92% vs. 80%, respectively; P = .08), the difference in sensitivity was significant with the 1997 criteria (83% vs. 64%; P < .02).
The 2019 criteria had similar sensitivity in males and females (86% vs. 81%, respectively), as well as specificity (81% vs. 87%). The 1997 criteria also provided similar sensitivity between males and females (71% vs. 76%) as well as specificity (85% vs. 90%).
In only four instances did SLE cases meet 2019 criteria before ICD-10 diagnosis of SLE, whereas in the other 108 cases the ICD-10 diagnosis coincided with reaching the threshold for meeting 2019 criteria.
There was no funding secured for the study, and the authors had no conflicts of interest to disclose.
SOURCE: Aljaberi N et al. Arthritis Care Res. 2020 Aug 25. doi: 10.1002/acr.24430.
FROM ARTHRITIS CARE & RESEARCH