User login
Debate Over Axial Involvement in Psoriatic Arthritis Still Unresolved Despite New Studies
VIENNA — While there is no doubt that some people with psoriatic arthritis (PsA) have axial symptoms, data presented at the annual European Congress of Rheumatology do not appear to add much to what is already known about axial PsA or to further the cause of differentiating it from axial spondyloarthritis (axSpA).
In both the AXIS study and Reuma.pt, around one in three patients with PsA were found to have axial involvement. Notably, the percentage of people with axial PsA was found to vary according to how imaging information was interpreted in the AXIS study. Both studies were discussed during the Axial Involvement in PsA and SpA session at EULAR 2024.
The One-Million-Dollar Question
“So, the one-million-dollar question: What is it, really?” Philippe Carron, MD, PhD, Ghent University Hospital, Ghent, Belgium, said in the presentation that started the session. Despite PsA being described more than 60 years ago, “we still have no internationally accepted definition or a consensus on how we should define these patients and how we should screen them,” he said.
“There are some believers that it is just a form of axial SpA with concomitant psoriasis, but also some people that think that the axial PsA is a typical disease, with typical characteristics which are different from axial disease,” Dr. Carron said.
The lack of consensus makes it difficult to estimate just how many people have axial PsA. Reported prevalences range from 5% to 70%, “all caused by which criteria that you’re using to define axial involvement,” Dr. Carron added.
There are, however, two things that can be agreed upon, according to Dr. Carron. First, the prevalence of axial involvement in people with early PsA is “much, much lower” than that of more established disease. Second, exclusive axial involvement is seen in “just a minority of PsA patients.” Most people with axial disease also have peripheral disease, he added.
Imaging findings in axial PsA “are quite similar to those seen in axial SpA,” although Dr. Carron also said that there were some distinct differences. Radiographic sacroiliitis occurs in around 25%-50% of people with axial PsA, and atypical syndesmophytes are more often found in people with axial PsA than in those with axSpA.
Shared Characteristics
But are axial PsA and axSpA separate diseases or part of the same disease continuum? That’s a question that is still very much open for debate, said Sofia Ramiro, MD, PhD, a senior researcher at Leiden University Medical Center, Leiden, the Netherlands, and rheumatology consultant at Zuyderland Medical Center in Heerlen, the Netherlands.
While many studies have looked to answer this question, there is a big methodological problem — the studies largely cannot be compared as they have used different definitions of axSpA.
Take a patient with inflammatory back pain, psoriasis, and oligoarthritis, Dr. Ramiro said. If the patient goes to one rheumatologist, they may get a diagnosis of axSpA, but if they go to a different rheumatologist, they may get a diagnosis of axial PsA.
“This is influenced by training, expertise, by beliefs, and by belonging to ASAS [Assessment of Spondyloarthritis International Society] or to GRAPPA [Group for Research and Assessment of Psoriasis and Psoriatic Arthritis],” Dr. Ramiro suggested. It’s “a diagnostic bias” that is very difficult to overcome and makes direct comparisons between patient populations recruited into clinical studies “extremely challenging.”
To confuse matters more, axial PsA and axSpA share common characteristics: Inflammatory back pain, HLA-B27 positivity, elevated levels of C-reactive protein (CRP) or a higher erythrocyte sedimentation rate, and structural lesions in the sacroiliac joints and spine.
AXIS Study ‘Gives Answers’
More research into factors associated with axial PsA need to be performed to try to help define the condition and enable classification and ultimately treatment guidelines. This is where the AXIS study comes in.
The AXIS study is a joint project of ASAS and GRAPPA that was started in January 2019 with the aim of defining a homogeneous subgroup of patients who could be studied.
“The objectives of the AXIS study are to determine the frequency of axial involvement in patients with PsA; to identify the frequency of active inflammatory and structural changes on imaging; and to identify factors associated with the presence of axial involvement in PsA,” Murat Torgutalp, MD, of Charité – Universitätsmedizin Berlin, Berlin, Germany, said at EULAR 2024.
The study population consisted of 409 consecutively recruited patients diagnosed with PsA according to CASPAR (Classification for Psoriatic Arthritis) criteria; all have had PsA for up to 10 years and were untreated with biologic or targeted synthetic disease modifying drugs at the time of inclusion.
Dr. Torgutalp, who is the study’s primary research coordinator, reported that a diagnosis of PsA was made in 37% of the population when local investigators considered available clinical, laboratory, and imaging data. However, patients’ imaging data were also centrally assessed, and when the local investigators were party to the expert imaging interpretations, the percentage of people diagnosed with PsA dropped to 27%.
“When we looked at the clinical characteristics, the presence of the back pain, particularly inflammatory back pain, HLA-B27 positivity, elevated CRP, and presence of active, inflammatory and structural changes in the sacroiliac joints and spine were associated with the final conclusion on the presence of axial involvement,” Dr. Torgutalp said.
Despite the title of his presentation being “The Axis Study Gives Answers,” Dr. Torgutalp presented lots of data without giving much insight into how they might be used. He concluded that “overall, there was a trend toward overestimation of the presence of imaging changes indicative of axial involvement across all imaging modalities” by the local investigators.
Dennis McGonagle, MB, MCH, BAO, PhD, of the University of Leeds, Leeds, England,said in an interview that the AXIS study “is a noble, international effort across multiple countries to try and better understand axial PsA.”
Dr. McGonagle, who was not involved in the study, added: “A lot of data are being generated, and a lot of analysis needs to be done to drill down to get a clear message that could influence practice.”
Axial PsA in the Portuguese Population
Separately, Catarina Abreu, a rheumatology intern at Hospital Garcia de Orta, Almada, Portugal, presented some real-world data on axial PsA from Reuma.pt.
Of 2304 patients, 854 (37.1%) reportedly had axial PsA, which had been defined as physician-reported spondylitis or the presence of imaging findings suggestive of axial involvement. This included radiographic- or MRI-detected sacroiliitis or syndesmophytes seen on axial x-rays.
The majority (78.2%) of those with an axial PsA diagnosis had concomitant peripheral involvement, with 8.1% having exclusive axial disease.
About 70% of the axial PsA diagnoses had been made using clinical or laboratory findings alone, and 30% of diagnoses was based on imaging results. Of the latter, Ms. Abreu noted that patients who had imaging data available were more likely to be HLA-B27 positive and less likely to have dactylitis, with respective odds ratios (ORs) of 3.10 and 2.42.
Individuals with axial PsA were more likely to have enthesitis (OR, 1.92), although no data were available on whether this was axial or peripheral enthesitis. Tobacco exposure was also linked to an increased chance of having axial PsA (OR, 1.66).
Ms. Abreu noted that the “scarce number of available imaging exams” and other missing data in Reuma.pt may have led to an underdiagnosis of axial PsA.
“The difference that we found between axial and peripheral [PsA] are similar to the differences found in other studies that compared axial psoriatic arthritis with axial spondyloarthritis,” Ms. Abreu said.
“So, we leave with the question that was already left before here: If these are different diseases or just different phenotypes of the same disease, and what implications will this have in the future?” Ms. Abreu concluded.
Dr. Carron received educational grants, speaker fees, or honoraria for other consultancy work from AbbVie, UCB, Pfizer, Eli Lilly, Novartis, Janssen, and Galapagos/Alfasigma. Dr. Ramiro is an ASAS executive committee member and received research grants or consulting/speaker fees from AbbVie, Eli Lilly, Galapagos, Janssen, Merck Sharp and Dohme, Novartis, Pfizer, Sanofi, and UCB. AXIS is supported by unrestricted research grants from AbbVie, Galapagos, Janssen, Eli Lilly, Novartis, Pfizer, and UCB. Dr. Torgutalp is the primary research coordinator for the study; he reported no financial conflicts of interest. The Reuma.pt registry was developed with the financial support of the pharmaceutical industry and is currently supported by AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp and Dohme, Novartis, Pfizer, and Sobi. Ms. Abreu reported no financial conflicts of interest.
A version of this article appeared on Medscape.com.
VIENNA — While there is no doubt that some people with psoriatic arthritis (PsA) have axial symptoms, data presented at the annual European Congress of Rheumatology do not appear to add much to what is already known about axial PsA or to further the cause of differentiating it from axial spondyloarthritis (axSpA).
In both the AXIS study and Reuma.pt, around one in three patients with PsA were found to have axial involvement. Notably, the percentage of people with axial PsA was found to vary according to how imaging information was interpreted in the AXIS study. Both studies were discussed during the Axial Involvement in PsA and SpA session at EULAR 2024.
The One-Million-Dollar Question
“So, the one-million-dollar question: What is it, really?” Philippe Carron, MD, PhD, Ghent University Hospital, Ghent, Belgium, said in the presentation that started the session. Despite PsA being described more than 60 years ago, “we still have no internationally accepted definition or a consensus on how we should define these patients and how we should screen them,” he said.
“There are some believers that it is just a form of axial SpA with concomitant psoriasis, but also some people that think that the axial PsA is a typical disease, with typical characteristics which are different from axial disease,” Dr. Carron said.
The lack of consensus makes it difficult to estimate just how many people have axial PsA. Reported prevalences range from 5% to 70%, “all caused by which criteria that you’re using to define axial involvement,” Dr. Carron added.
There are, however, two things that can be agreed upon, according to Dr. Carron. First, the prevalence of axial involvement in people with early PsA is “much, much lower” than that of more established disease. Second, exclusive axial involvement is seen in “just a minority of PsA patients.” Most people with axial disease also have peripheral disease, he added.
Imaging findings in axial PsA “are quite similar to those seen in axial SpA,” although Dr. Carron also said that there were some distinct differences. Radiographic sacroiliitis occurs in around 25%-50% of people with axial PsA, and atypical syndesmophytes are more often found in people with axial PsA than in those with axSpA.
Shared Characteristics
But are axial PsA and axSpA separate diseases or part of the same disease continuum? That’s a question that is still very much open for debate, said Sofia Ramiro, MD, PhD, a senior researcher at Leiden University Medical Center, Leiden, the Netherlands, and rheumatology consultant at Zuyderland Medical Center in Heerlen, the Netherlands.
While many studies have looked to answer this question, there is a big methodological problem — the studies largely cannot be compared as they have used different definitions of axSpA.
Take a patient with inflammatory back pain, psoriasis, and oligoarthritis, Dr. Ramiro said. If the patient goes to one rheumatologist, they may get a diagnosis of axSpA, but if they go to a different rheumatologist, they may get a diagnosis of axial PsA.
“This is influenced by training, expertise, by beliefs, and by belonging to ASAS [Assessment of Spondyloarthritis International Society] or to GRAPPA [Group for Research and Assessment of Psoriasis and Psoriatic Arthritis],” Dr. Ramiro suggested. It’s “a diagnostic bias” that is very difficult to overcome and makes direct comparisons between patient populations recruited into clinical studies “extremely challenging.”
To confuse matters more, axial PsA and axSpA share common characteristics: Inflammatory back pain, HLA-B27 positivity, elevated levels of C-reactive protein (CRP) or a higher erythrocyte sedimentation rate, and structural lesions in the sacroiliac joints and spine.
AXIS Study ‘Gives Answers’
More research into factors associated with axial PsA need to be performed to try to help define the condition and enable classification and ultimately treatment guidelines. This is where the AXIS study comes in.
The AXIS study is a joint project of ASAS and GRAPPA that was started in January 2019 with the aim of defining a homogeneous subgroup of patients who could be studied.
“The objectives of the AXIS study are to determine the frequency of axial involvement in patients with PsA; to identify the frequency of active inflammatory and structural changes on imaging; and to identify factors associated with the presence of axial involvement in PsA,” Murat Torgutalp, MD, of Charité – Universitätsmedizin Berlin, Berlin, Germany, said at EULAR 2024.
The study population consisted of 409 consecutively recruited patients diagnosed with PsA according to CASPAR (Classification for Psoriatic Arthritis) criteria; all have had PsA for up to 10 years and were untreated with biologic or targeted synthetic disease modifying drugs at the time of inclusion.
Dr. Torgutalp, who is the study’s primary research coordinator, reported that a diagnosis of PsA was made in 37% of the population when local investigators considered available clinical, laboratory, and imaging data. However, patients’ imaging data were also centrally assessed, and when the local investigators were party to the expert imaging interpretations, the percentage of people diagnosed with PsA dropped to 27%.
“When we looked at the clinical characteristics, the presence of the back pain, particularly inflammatory back pain, HLA-B27 positivity, elevated CRP, and presence of active, inflammatory and structural changes in the sacroiliac joints and spine were associated with the final conclusion on the presence of axial involvement,” Dr. Torgutalp said.
Despite the title of his presentation being “The Axis Study Gives Answers,” Dr. Torgutalp presented lots of data without giving much insight into how they might be used. He concluded that “overall, there was a trend toward overestimation of the presence of imaging changes indicative of axial involvement across all imaging modalities” by the local investigators.
Dennis McGonagle, MB, MCH, BAO, PhD, of the University of Leeds, Leeds, England,said in an interview that the AXIS study “is a noble, international effort across multiple countries to try and better understand axial PsA.”
Dr. McGonagle, who was not involved in the study, added: “A lot of data are being generated, and a lot of analysis needs to be done to drill down to get a clear message that could influence practice.”
Axial PsA in the Portuguese Population
Separately, Catarina Abreu, a rheumatology intern at Hospital Garcia de Orta, Almada, Portugal, presented some real-world data on axial PsA from Reuma.pt.
Of 2304 patients, 854 (37.1%) reportedly had axial PsA, which had been defined as physician-reported spondylitis or the presence of imaging findings suggestive of axial involvement. This included radiographic- or MRI-detected sacroiliitis or syndesmophytes seen on axial x-rays.
The majority (78.2%) of those with an axial PsA diagnosis had concomitant peripheral involvement, with 8.1% having exclusive axial disease.
About 70% of the axial PsA diagnoses had been made using clinical or laboratory findings alone, and 30% of diagnoses was based on imaging results. Of the latter, Ms. Abreu noted that patients who had imaging data available were more likely to be HLA-B27 positive and less likely to have dactylitis, with respective odds ratios (ORs) of 3.10 and 2.42.
Individuals with axial PsA were more likely to have enthesitis (OR, 1.92), although no data were available on whether this was axial or peripheral enthesitis. Tobacco exposure was also linked to an increased chance of having axial PsA (OR, 1.66).
Ms. Abreu noted that the “scarce number of available imaging exams” and other missing data in Reuma.pt may have led to an underdiagnosis of axial PsA.
“The difference that we found between axial and peripheral [PsA] are similar to the differences found in other studies that compared axial psoriatic arthritis with axial spondyloarthritis,” Ms. Abreu said.
“So, we leave with the question that was already left before here: If these are different diseases or just different phenotypes of the same disease, and what implications will this have in the future?” Ms. Abreu concluded.
Dr. Carron received educational grants, speaker fees, or honoraria for other consultancy work from AbbVie, UCB, Pfizer, Eli Lilly, Novartis, Janssen, and Galapagos/Alfasigma. Dr. Ramiro is an ASAS executive committee member and received research grants or consulting/speaker fees from AbbVie, Eli Lilly, Galapagos, Janssen, Merck Sharp and Dohme, Novartis, Pfizer, Sanofi, and UCB. AXIS is supported by unrestricted research grants from AbbVie, Galapagos, Janssen, Eli Lilly, Novartis, Pfizer, and UCB. Dr. Torgutalp is the primary research coordinator for the study; he reported no financial conflicts of interest. The Reuma.pt registry was developed with the financial support of the pharmaceutical industry and is currently supported by AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp and Dohme, Novartis, Pfizer, and Sobi. Ms. Abreu reported no financial conflicts of interest.
A version of this article appeared on Medscape.com.
VIENNA — While there is no doubt that some people with psoriatic arthritis (PsA) have axial symptoms, data presented at the annual European Congress of Rheumatology do not appear to add much to what is already known about axial PsA or to further the cause of differentiating it from axial spondyloarthritis (axSpA).
In both the AXIS study and Reuma.pt, around one in three patients with PsA were found to have axial involvement. Notably, the percentage of people with axial PsA was found to vary according to how imaging information was interpreted in the AXIS study. Both studies were discussed during the Axial Involvement in PsA and SpA session at EULAR 2024.
The One-Million-Dollar Question
“So, the one-million-dollar question: What is it, really?” Philippe Carron, MD, PhD, Ghent University Hospital, Ghent, Belgium, said in the presentation that started the session. Despite PsA being described more than 60 years ago, “we still have no internationally accepted definition or a consensus on how we should define these patients and how we should screen them,” he said.
“There are some believers that it is just a form of axial SpA with concomitant psoriasis, but also some people that think that the axial PsA is a typical disease, with typical characteristics which are different from axial disease,” Dr. Carron said.
The lack of consensus makes it difficult to estimate just how many people have axial PsA. Reported prevalences range from 5% to 70%, “all caused by which criteria that you’re using to define axial involvement,” Dr. Carron added.
There are, however, two things that can be agreed upon, according to Dr. Carron. First, the prevalence of axial involvement in people with early PsA is “much, much lower” than that of more established disease. Second, exclusive axial involvement is seen in “just a minority of PsA patients.” Most people with axial disease also have peripheral disease, he added.
Imaging findings in axial PsA “are quite similar to those seen in axial SpA,” although Dr. Carron also said that there were some distinct differences. Radiographic sacroiliitis occurs in around 25%-50% of people with axial PsA, and atypical syndesmophytes are more often found in people with axial PsA than in those with axSpA.
Shared Characteristics
But are axial PsA and axSpA separate diseases or part of the same disease continuum? That’s a question that is still very much open for debate, said Sofia Ramiro, MD, PhD, a senior researcher at Leiden University Medical Center, Leiden, the Netherlands, and rheumatology consultant at Zuyderland Medical Center in Heerlen, the Netherlands.
While many studies have looked to answer this question, there is a big methodological problem — the studies largely cannot be compared as they have used different definitions of axSpA.
Take a patient with inflammatory back pain, psoriasis, and oligoarthritis, Dr. Ramiro said. If the patient goes to one rheumatologist, they may get a diagnosis of axSpA, but if they go to a different rheumatologist, they may get a diagnosis of axial PsA.
“This is influenced by training, expertise, by beliefs, and by belonging to ASAS [Assessment of Spondyloarthritis International Society] or to GRAPPA [Group for Research and Assessment of Psoriasis and Psoriatic Arthritis],” Dr. Ramiro suggested. It’s “a diagnostic bias” that is very difficult to overcome and makes direct comparisons between patient populations recruited into clinical studies “extremely challenging.”
To confuse matters more, axial PsA and axSpA share common characteristics: Inflammatory back pain, HLA-B27 positivity, elevated levels of C-reactive protein (CRP) or a higher erythrocyte sedimentation rate, and structural lesions in the sacroiliac joints and spine.
AXIS Study ‘Gives Answers’
More research into factors associated with axial PsA need to be performed to try to help define the condition and enable classification and ultimately treatment guidelines. This is where the AXIS study comes in.
The AXIS study is a joint project of ASAS and GRAPPA that was started in January 2019 with the aim of defining a homogeneous subgroup of patients who could be studied.
“The objectives of the AXIS study are to determine the frequency of axial involvement in patients with PsA; to identify the frequency of active inflammatory and structural changes on imaging; and to identify factors associated with the presence of axial involvement in PsA,” Murat Torgutalp, MD, of Charité – Universitätsmedizin Berlin, Berlin, Germany, said at EULAR 2024.
The study population consisted of 409 consecutively recruited patients diagnosed with PsA according to CASPAR (Classification for Psoriatic Arthritis) criteria; all have had PsA for up to 10 years and were untreated with biologic or targeted synthetic disease modifying drugs at the time of inclusion.
Dr. Torgutalp, who is the study’s primary research coordinator, reported that a diagnosis of PsA was made in 37% of the population when local investigators considered available clinical, laboratory, and imaging data. However, patients’ imaging data were also centrally assessed, and when the local investigators were party to the expert imaging interpretations, the percentage of people diagnosed with PsA dropped to 27%.
“When we looked at the clinical characteristics, the presence of the back pain, particularly inflammatory back pain, HLA-B27 positivity, elevated CRP, and presence of active, inflammatory and structural changes in the sacroiliac joints and spine were associated with the final conclusion on the presence of axial involvement,” Dr. Torgutalp said.
Despite the title of his presentation being “The Axis Study Gives Answers,” Dr. Torgutalp presented lots of data without giving much insight into how they might be used. He concluded that “overall, there was a trend toward overestimation of the presence of imaging changes indicative of axial involvement across all imaging modalities” by the local investigators.
Dennis McGonagle, MB, MCH, BAO, PhD, of the University of Leeds, Leeds, England,said in an interview that the AXIS study “is a noble, international effort across multiple countries to try and better understand axial PsA.”
Dr. McGonagle, who was not involved in the study, added: “A lot of data are being generated, and a lot of analysis needs to be done to drill down to get a clear message that could influence practice.”
Axial PsA in the Portuguese Population
Separately, Catarina Abreu, a rheumatology intern at Hospital Garcia de Orta, Almada, Portugal, presented some real-world data on axial PsA from Reuma.pt.
Of 2304 patients, 854 (37.1%) reportedly had axial PsA, which had been defined as physician-reported spondylitis or the presence of imaging findings suggestive of axial involvement. This included radiographic- or MRI-detected sacroiliitis or syndesmophytes seen on axial x-rays.
The majority (78.2%) of those with an axial PsA diagnosis had concomitant peripheral involvement, with 8.1% having exclusive axial disease.
About 70% of the axial PsA diagnoses had been made using clinical or laboratory findings alone, and 30% of diagnoses was based on imaging results. Of the latter, Ms. Abreu noted that patients who had imaging data available were more likely to be HLA-B27 positive and less likely to have dactylitis, with respective odds ratios (ORs) of 3.10 and 2.42.
Individuals with axial PsA were more likely to have enthesitis (OR, 1.92), although no data were available on whether this was axial or peripheral enthesitis. Tobacco exposure was also linked to an increased chance of having axial PsA (OR, 1.66).
Ms. Abreu noted that the “scarce number of available imaging exams” and other missing data in Reuma.pt may have led to an underdiagnosis of axial PsA.
“The difference that we found between axial and peripheral [PsA] are similar to the differences found in other studies that compared axial psoriatic arthritis with axial spondyloarthritis,” Ms. Abreu said.
“So, we leave with the question that was already left before here: If these are different diseases or just different phenotypes of the same disease, and what implications will this have in the future?” Ms. Abreu concluded.
Dr. Carron received educational grants, speaker fees, or honoraria for other consultancy work from AbbVie, UCB, Pfizer, Eli Lilly, Novartis, Janssen, and Galapagos/Alfasigma. Dr. Ramiro is an ASAS executive committee member and received research grants or consulting/speaker fees from AbbVie, Eli Lilly, Galapagos, Janssen, Merck Sharp and Dohme, Novartis, Pfizer, Sanofi, and UCB. AXIS is supported by unrestricted research grants from AbbVie, Galapagos, Janssen, Eli Lilly, Novartis, Pfizer, and UCB. Dr. Torgutalp is the primary research coordinator for the study; he reported no financial conflicts of interest. The Reuma.pt registry was developed with the financial support of the pharmaceutical industry and is currently supported by AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp and Dohme, Novartis, Pfizer, and Sobi. Ms. Abreu reported no financial conflicts of interest.
A version of this article appeared on Medscape.com.
FROM EULAR 2024
Trading TV Time for Physical Activity Boosts Healthy Aging
TOPLINE:
, but substituting it with any physical activity — or even sleeping, in case of women with inadequate sleep — may lead to better overall health.
METHODOLOGY:
- Previous studies have shown that replacing sedentary behavior with physical activity may improve mortality outcomes, but whether this increased lifespan is accompanied by better overall health remains an unanswered question.
- To understand the impact of sedentary behavior and physical activity on healthy aging, researchers analyzed data from the prospective cohort Nurses’ Health Study.
- They included 45,176 women aged > 50 years in 1992 (mean age, 59.2 years) who were free of major chronic diseases and were followed up for 20 years.
- In 1992, validated questionnaires were used to record exposure to sedentary behavior, different levels of physical activity, and sleep. The time spent watching television was the primary exposure in the sedentary behavior category.
- The main outcome was healthy aging, defined as survival to ≥ 70 years of age and maintenance of four domains of health — being free of 11 main chronic diseases and having no impairment of subjective memory, physical function, or mental health.
TAKEAWAY:
- At 20 years of follow-up, 8.6% of the women achieved healthy aging, while 41.4% had none of the 11 chronic diseases, 16.1% had no physical function impairment, 44.1% had no mental health limitation, and 51.9% reported no memory impairment.
- For each increase of 2 hours per day spent sitting and watching television, the odds of healthy aging dropped by 12% (95% confidence interval [CI], 7%-17%).
- Conversely, every additional 2 hours per day of low-level physical activity at work upped the odds of healthy aging by 6% (95% CI, 3%-9%); furthermore, each extra hour per day of standardized moderate to vigorous physical activity (normal pace walking or the equivalent) was associated with 14% higher odds (95% CI, 11%-16%) of healthy aging.
- In a theoretical modeling analysis, individuals could increase their odds of healthy aging by replacing 1 hour of television time per day with low levels of physical activity at home and work or with moderate to vigorous levels of physical activity — or even sleeping, for those who slept for ≤ 7 hours.
IN PRACTICE:
“These findings expand on the literature reporting that replacing sedentary behavior with light or moderate to vigorous physical activity is associated with decreased mortality by suggesting that this increased lifespan might be accompanied by better overall health,” the authors wrote.
SOURCE:
Hongying Shi, PhD, Department of Epidemiology and Health Statistics, School of Public Health, Wenzhou Medical University, Wenzhou, China, led this study, which was published online in JAMA Network Open.
LIMITATIONS:
The measures of different behaviors were self-reported and may, therefore, be less accurate than objective measurement methods. Measurement error may have attenuated the effect of low levels of physical activity. The single exposure assessment at baseline may not reflect the long-term pattern of these activities.
DISCLOSURES:
The lead author was supported by the National Social Science Foundation Project of China and the Zhejiang Provincial Philosophy and Social Sciences Planning Project. A co-author and the Nurses’ Health Study were supported by the US National Institutes of Health. The authors declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
, but substituting it with any physical activity — or even sleeping, in case of women with inadequate sleep — may lead to better overall health.
METHODOLOGY:
- Previous studies have shown that replacing sedentary behavior with physical activity may improve mortality outcomes, but whether this increased lifespan is accompanied by better overall health remains an unanswered question.
- To understand the impact of sedentary behavior and physical activity on healthy aging, researchers analyzed data from the prospective cohort Nurses’ Health Study.
- They included 45,176 women aged > 50 years in 1992 (mean age, 59.2 years) who were free of major chronic diseases and were followed up for 20 years.
- In 1992, validated questionnaires were used to record exposure to sedentary behavior, different levels of physical activity, and sleep. The time spent watching television was the primary exposure in the sedentary behavior category.
- The main outcome was healthy aging, defined as survival to ≥ 70 years of age and maintenance of four domains of health — being free of 11 main chronic diseases and having no impairment of subjective memory, physical function, or mental health.
TAKEAWAY:
- At 20 years of follow-up, 8.6% of the women achieved healthy aging, while 41.4% had none of the 11 chronic diseases, 16.1% had no physical function impairment, 44.1% had no mental health limitation, and 51.9% reported no memory impairment.
- For each increase of 2 hours per day spent sitting and watching television, the odds of healthy aging dropped by 12% (95% confidence interval [CI], 7%-17%).
- Conversely, every additional 2 hours per day of low-level physical activity at work upped the odds of healthy aging by 6% (95% CI, 3%-9%); furthermore, each extra hour per day of standardized moderate to vigorous physical activity (normal pace walking or the equivalent) was associated with 14% higher odds (95% CI, 11%-16%) of healthy aging.
- In a theoretical modeling analysis, individuals could increase their odds of healthy aging by replacing 1 hour of television time per day with low levels of physical activity at home and work or with moderate to vigorous levels of physical activity — or even sleeping, for those who slept for ≤ 7 hours.
IN PRACTICE:
“These findings expand on the literature reporting that replacing sedentary behavior with light or moderate to vigorous physical activity is associated with decreased mortality by suggesting that this increased lifespan might be accompanied by better overall health,” the authors wrote.
SOURCE:
Hongying Shi, PhD, Department of Epidemiology and Health Statistics, School of Public Health, Wenzhou Medical University, Wenzhou, China, led this study, which was published online in JAMA Network Open.
LIMITATIONS:
The measures of different behaviors were self-reported and may, therefore, be less accurate than objective measurement methods. Measurement error may have attenuated the effect of low levels of physical activity. The single exposure assessment at baseline may not reflect the long-term pattern of these activities.
DISCLOSURES:
The lead author was supported by the National Social Science Foundation Project of China and the Zhejiang Provincial Philosophy and Social Sciences Planning Project. A co-author and the Nurses’ Health Study were supported by the US National Institutes of Health. The authors declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
, but substituting it with any physical activity — or even sleeping, in case of women with inadequate sleep — may lead to better overall health.
METHODOLOGY:
- Previous studies have shown that replacing sedentary behavior with physical activity may improve mortality outcomes, but whether this increased lifespan is accompanied by better overall health remains an unanswered question.
- To understand the impact of sedentary behavior and physical activity on healthy aging, researchers analyzed data from the prospective cohort Nurses’ Health Study.
- They included 45,176 women aged > 50 years in 1992 (mean age, 59.2 years) who were free of major chronic diseases and were followed up for 20 years.
- In 1992, validated questionnaires were used to record exposure to sedentary behavior, different levels of physical activity, and sleep. The time spent watching television was the primary exposure in the sedentary behavior category.
- The main outcome was healthy aging, defined as survival to ≥ 70 years of age and maintenance of four domains of health — being free of 11 main chronic diseases and having no impairment of subjective memory, physical function, or mental health.
TAKEAWAY:
- At 20 years of follow-up, 8.6% of the women achieved healthy aging, while 41.4% had none of the 11 chronic diseases, 16.1% had no physical function impairment, 44.1% had no mental health limitation, and 51.9% reported no memory impairment.
- For each increase of 2 hours per day spent sitting and watching television, the odds of healthy aging dropped by 12% (95% confidence interval [CI], 7%-17%).
- Conversely, every additional 2 hours per day of low-level physical activity at work upped the odds of healthy aging by 6% (95% CI, 3%-9%); furthermore, each extra hour per day of standardized moderate to vigorous physical activity (normal pace walking or the equivalent) was associated with 14% higher odds (95% CI, 11%-16%) of healthy aging.
- In a theoretical modeling analysis, individuals could increase their odds of healthy aging by replacing 1 hour of television time per day with low levels of physical activity at home and work or with moderate to vigorous levels of physical activity — or even sleeping, for those who slept for ≤ 7 hours.
IN PRACTICE:
“These findings expand on the literature reporting that replacing sedentary behavior with light or moderate to vigorous physical activity is associated with decreased mortality by suggesting that this increased lifespan might be accompanied by better overall health,” the authors wrote.
SOURCE:
Hongying Shi, PhD, Department of Epidemiology and Health Statistics, School of Public Health, Wenzhou Medical University, Wenzhou, China, led this study, which was published online in JAMA Network Open.
LIMITATIONS:
The measures of different behaviors were self-reported and may, therefore, be less accurate than objective measurement methods. Measurement error may have attenuated the effect of low levels of physical activity. The single exposure assessment at baseline may not reflect the long-term pattern of these activities.
DISCLOSURES:
The lead author was supported by the National Social Science Foundation Project of China and the Zhejiang Provincial Philosophy and Social Sciences Planning Project. A co-author and the Nurses’ Health Study were supported by the US National Institutes of Health. The authors declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
Supreme Court Ruling Overturning Chevron Could ‘Paralyze’ Health Policy Making: Experts
Larry Levitt, executive vice president for health policy at the Kaiser Family Foundation, wrote on X, “my worry is that it will paralyze policymaking in healthcare and other areas,” because “Congress will try to fill in more details, making it harder to pass legislation.” He also wrote that federal agencies “will become very cautious in using their regulatory authority.”
In their 6-3 opinion reversing the “Chevron doctrine” — which has been followed since a 1984 Court opinion — the Justices said that the judiciary should no longer have to defer to federal agency interpretations of laws. Existing federal law “requires courts to exercise their independent judgment in deciding whether an agency has acted within its statutory authority,” said the Court, in stating why Chevron should be overruled.
Writing for the majority in the combined cases — Relentless v. Department of Commerce and Loper Bright Enterprises v. Raimondo — Chief Justice John Roberts Jr. wrote that “agencies have no special competence in resolving statutory ambiguities. Courts do.”
In a dissenting opinion, Justice Elena Kagan said the decision was a judicial power grab and would result in a “jolt to the legal system.” She was joined by Justices Sonia Sotomayor and Ketanji Brown Jackson.
The opinion will have many repercussions, said lawyer and Supreme Court watcher Amy Howe. The Chevron ruling has been “one of the most important rulings on federal administrative law, cited by federal courts more than 18,000 times,” she wrote on her blog.
For example, without the long-standing deference to agencies under Chevron, healthcare providers may have more opportunities to challenge how federal officials set Medicare reimbursement for hospital procedures or prescription drugs, Baker Donelson healthcare attorneys McKenna Cloud and Thomas Barnard wrote in an analysis.
Seventeen health organizations issued a joint statement signaling their disappointment.
“We anticipate that today’s ruling will cause significant disruption to publicly funded health insurance programs, to the stability of this country’s healthcare and food and drug review systems, and to the health and well-being of the patients and consumers we serve,” wrote the organizations, which included American Academy of Pediatrics, American Cancer Society, American Cancer Society Cancer Action Network, ALS Association, American Heart Association, American Lung Association, American Public Health Association, American Thoracic Society, Bazelon Center for Mental Health Law, Campaign for Tobacco-Free Kids, Child Neurology Foundation, Epilepsy Foundation, Muscular Dystrophy Association, National Health Law Program, Physicians for Social Responsibility, The Leukemia & Lymphoma Society, and Truth Initiative.
“It’s much harder for agencies to exercise power without some power to interpret statues. This is big,” wrote Berkeley Law Professor Orin Kerr on X.
A New, Uncertain Landscape for Healthcare
In the original Chevron case, the Court ruled that federal agencies had relevant expertise and should be given deference in resolving ambiguities that Congress had not spelled out in legislation.
In Relentless and Loper Bright, the plaintiffs argued that federal agencies overstepped their authority by issuing a rule that required commercial fishing vessels to pay for professional observers to monitor their catch.
In a statement after Friday’s ruling, the Relentless plaintiffs’ attorneys said that the decision “will recalibrate the balance of power between agencies and courts” and “make it harder for those agencies to adopt regulatory programs that exceed the authority conferred on them by Congress.”
Some predicted chaos in the wake of the ruling.
“Overturning Chevron could invite legal challenges to any and all agency determinations of ambiguous statutes by any stakeholder, leaving individual courts with the impractical task of determining the ‘correct’ meaning of statutes without the benefit of requisite expertise, practical experience, or public engagement,” wrote Sahil Agrawal, MD, PhD, Joseph S. Ross, MD, and Reshma Ramachandran, MD, in JAMA in an opinion piece in March that considered the ramifications of overturning Chevron.
“The spillover effects for medicine and public health, in turn, will be consequential,” they wrote.
In an analysis published in April, the Kaiser Family Foundation noted many potential ramifications on patient and consumer protections in the health insurance market. For instance, courts could vacate current rules governing protections under the Affordable Care Act, including that health plans offer a range of free preventive health services, such as breast, cervical, colon, and lung cancer screening.
Congressional, White House Reaction
Many legal observers said the ruling will have the effect of requiring Congress to write ever-more dense and exacting legislation to prevent agencies from interpreting any gaps.
Some members of Congress welcomed the decision.
Senate Minority Leader Mitch McConnell (R-Kentucky) said in a statement, “The Constitution vests Congress with the sole authority to make law,” adding, “the Supreme Court made it clear today that our system of government leaves no room for an unelected bureaucracy to co-opt this authority for itself.”
In a post on X, Senate Majority Leader Chuck Schumer (D-New York) accused the Court of siding with “special interests and giant corporations.” Added Mr. Schumer, “Their headlong rush to overturn 40 years of precedent and impose their own radical views is appalling.”
White House Press Secretary Karine Jean-Pierre said in a statement that “While this decision undermines the ability of federal agencies to use their expertise as Congress intended to make government work for the people, the Biden-Harris Administration will not relent in our efforts to protect and serve every American.”
A version of this article first appeared on Medscape.com.
Larry Levitt, executive vice president for health policy at the Kaiser Family Foundation, wrote on X, “my worry is that it will paralyze policymaking in healthcare and other areas,” because “Congress will try to fill in more details, making it harder to pass legislation.” He also wrote that federal agencies “will become very cautious in using their regulatory authority.”
In their 6-3 opinion reversing the “Chevron doctrine” — which has been followed since a 1984 Court opinion — the Justices said that the judiciary should no longer have to defer to federal agency interpretations of laws. Existing federal law “requires courts to exercise their independent judgment in deciding whether an agency has acted within its statutory authority,” said the Court, in stating why Chevron should be overruled.
Writing for the majority in the combined cases — Relentless v. Department of Commerce and Loper Bright Enterprises v. Raimondo — Chief Justice John Roberts Jr. wrote that “agencies have no special competence in resolving statutory ambiguities. Courts do.”
In a dissenting opinion, Justice Elena Kagan said the decision was a judicial power grab and would result in a “jolt to the legal system.” She was joined by Justices Sonia Sotomayor and Ketanji Brown Jackson.
The opinion will have many repercussions, said lawyer and Supreme Court watcher Amy Howe. The Chevron ruling has been “one of the most important rulings on federal administrative law, cited by federal courts more than 18,000 times,” she wrote on her blog.
For example, without the long-standing deference to agencies under Chevron, healthcare providers may have more opportunities to challenge how federal officials set Medicare reimbursement for hospital procedures or prescription drugs, Baker Donelson healthcare attorneys McKenna Cloud and Thomas Barnard wrote in an analysis.
Seventeen health organizations issued a joint statement signaling their disappointment.
“We anticipate that today’s ruling will cause significant disruption to publicly funded health insurance programs, to the stability of this country’s healthcare and food and drug review systems, and to the health and well-being of the patients and consumers we serve,” wrote the organizations, which included American Academy of Pediatrics, American Cancer Society, American Cancer Society Cancer Action Network, ALS Association, American Heart Association, American Lung Association, American Public Health Association, American Thoracic Society, Bazelon Center for Mental Health Law, Campaign for Tobacco-Free Kids, Child Neurology Foundation, Epilepsy Foundation, Muscular Dystrophy Association, National Health Law Program, Physicians for Social Responsibility, The Leukemia & Lymphoma Society, and Truth Initiative.
“It’s much harder for agencies to exercise power without some power to interpret statues. This is big,” wrote Berkeley Law Professor Orin Kerr on X.
A New, Uncertain Landscape for Healthcare
In the original Chevron case, the Court ruled that federal agencies had relevant expertise and should be given deference in resolving ambiguities that Congress had not spelled out in legislation.
In Relentless and Loper Bright, the plaintiffs argued that federal agencies overstepped their authority by issuing a rule that required commercial fishing vessels to pay for professional observers to monitor their catch.
In a statement after Friday’s ruling, the Relentless plaintiffs’ attorneys said that the decision “will recalibrate the balance of power between agencies and courts” and “make it harder for those agencies to adopt regulatory programs that exceed the authority conferred on them by Congress.”
Some predicted chaos in the wake of the ruling.
“Overturning Chevron could invite legal challenges to any and all agency determinations of ambiguous statutes by any stakeholder, leaving individual courts with the impractical task of determining the ‘correct’ meaning of statutes without the benefit of requisite expertise, practical experience, or public engagement,” wrote Sahil Agrawal, MD, PhD, Joseph S. Ross, MD, and Reshma Ramachandran, MD, in JAMA in an opinion piece in March that considered the ramifications of overturning Chevron.
“The spillover effects for medicine and public health, in turn, will be consequential,” they wrote.
In an analysis published in April, the Kaiser Family Foundation noted many potential ramifications on patient and consumer protections in the health insurance market. For instance, courts could vacate current rules governing protections under the Affordable Care Act, including that health plans offer a range of free preventive health services, such as breast, cervical, colon, and lung cancer screening.
Congressional, White House Reaction
Many legal observers said the ruling will have the effect of requiring Congress to write ever-more dense and exacting legislation to prevent agencies from interpreting any gaps.
Some members of Congress welcomed the decision.
Senate Minority Leader Mitch McConnell (R-Kentucky) said in a statement, “The Constitution vests Congress with the sole authority to make law,” adding, “the Supreme Court made it clear today that our system of government leaves no room for an unelected bureaucracy to co-opt this authority for itself.”
In a post on X, Senate Majority Leader Chuck Schumer (D-New York) accused the Court of siding with “special interests and giant corporations.” Added Mr. Schumer, “Their headlong rush to overturn 40 years of precedent and impose their own radical views is appalling.”
White House Press Secretary Karine Jean-Pierre said in a statement that “While this decision undermines the ability of federal agencies to use their expertise as Congress intended to make government work for the people, the Biden-Harris Administration will not relent in our efforts to protect and serve every American.”
A version of this article first appeared on Medscape.com.
Larry Levitt, executive vice president for health policy at the Kaiser Family Foundation, wrote on X, “my worry is that it will paralyze policymaking in healthcare and other areas,” because “Congress will try to fill in more details, making it harder to pass legislation.” He also wrote that federal agencies “will become very cautious in using their regulatory authority.”
In their 6-3 opinion reversing the “Chevron doctrine” — which has been followed since a 1984 Court opinion — the Justices said that the judiciary should no longer have to defer to federal agency interpretations of laws. Existing federal law “requires courts to exercise their independent judgment in deciding whether an agency has acted within its statutory authority,” said the Court, in stating why Chevron should be overruled.
Writing for the majority in the combined cases — Relentless v. Department of Commerce and Loper Bright Enterprises v. Raimondo — Chief Justice John Roberts Jr. wrote that “agencies have no special competence in resolving statutory ambiguities. Courts do.”
In a dissenting opinion, Justice Elena Kagan said the decision was a judicial power grab and would result in a “jolt to the legal system.” She was joined by Justices Sonia Sotomayor and Ketanji Brown Jackson.
The opinion will have many repercussions, said lawyer and Supreme Court watcher Amy Howe. The Chevron ruling has been “one of the most important rulings on federal administrative law, cited by federal courts more than 18,000 times,” she wrote on her blog.
For example, without the long-standing deference to agencies under Chevron, healthcare providers may have more opportunities to challenge how federal officials set Medicare reimbursement for hospital procedures or prescription drugs, Baker Donelson healthcare attorneys McKenna Cloud and Thomas Barnard wrote in an analysis.
Seventeen health organizations issued a joint statement signaling their disappointment.
“We anticipate that today’s ruling will cause significant disruption to publicly funded health insurance programs, to the stability of this country’s healthcare and food and drug review systems, and to the health and well-being of the patients and consumers we serve,” wrote the organizations, which included American Academy of Pediatrics, American Cancer Society, American Cancer Society Cancer Action Network, ALS Association, American Heart Association, American Lung Association, American Public Health Association, American Thoracic Society, Bazelon Center for Mental Health Law, Campaign for Tobacco-Free Kids, Child Neurology Foundation, Epilepsy Foundation, Muscular Dystrophy Association, National Health Law Program, Physicians for Social Responsibility, The Leukemia & Lymphoma Society, and Truth Initiative.
“It’s much harder for agencies to exercise power without some power to interpret statues. This is big,” wrote Berkeley Law Professor Orin Kerr on X.
A New, Uncertain Landscape for Healthcare
In the original Chevron case, the Court ruled that federal agencies had relevant expertise and should be given deference in resolving ambiguities that Congress had not spelled out in legislation.
In Relentless and Loper Bright, the plaintiffs argued that federal agencies overstepped their authority by issuing a rule that required commercial fishing vessels to pay for professional observers to monitor their catch.
In a statement after Friday’s ruling, the Relentless plaintiffs’ attorneys said that the decision “will recalibrate the balance of power between agencies and courts” and “make it harder for those agencies to adopt regulatory programs that exceed the authority conferred on them by Congress.”
Some predicted chaos in the wake of the ruling.
“Overturning Chevron could invite legal challenges to any and all agency determinations of ambiguous statutes by any stakeholder, leaving individual courts with the impractical task of determining the ‘correct’ meaning of statutes without the benefit of requisite expertise, practical experience, or public engagement,” wrote Sahil Agrawal, MD, PhD, Joseph S. Ross, MD, and Reshma Ramachandran, MD, in JAMA in an opinion piece in March that considered the ramifications of overturning Chevron.
“The spillover effects for medicine and public health, in turn, will be consequential,” they wrote.
In an analysis published in April, the Kaiser Family Foundation noted many potential ramifications on patient and consumer protections in the health insurance market. For instance, courts could vacate current rules governing protections under the Affordable Care Act, including that health plans offer a range of free preventive health services, such as breast, cervical, colon, and lung cancer screening.
Congressional, White House Reaction
Many legal observers said the ruling will have the effect of requiring Congress to write ever-more dense and exacting legislation to prevent agencies from interpreting any gaps.
Some members of Congress welcomed the decision.
Senate Minority Leader Mitch McConnell (R-Kentucky) said in a statement, “The Constitution vests Congress with the sole authority to make law,” adding, “the Supreme Court made it clear today that our system of government leaves no room for an unelected bureaucracy to co-opt this authority for itself.”
In a post on X, Senate Majority Leader Chuck Schumer (D-New York) accused the Court of siding with “special interests and giant corporations.” Added Mr. Schumer, “Their headlong rush to overturn 40 years of precedent and impose their own radical views is appalling.”
White House Press Secretary Karine Jean-Pierre said in a statement that “While this decision undermines the ability of federal agencies to use their expertise as Congress intended to make government work for the people, the Biden-Harris Administration will not relent in our efforts to protect and serve every American.”
A version of this article first appeared on Medscape.com.
EMA Greenlights Four Drugs for Bladder and Other Cancers
Balversa
The CHMP endorsed the approval of Balversa (erdafitinib, Janssen-Cilag International N.V.), intended for the treatment of urothelial carcinoma, a type of cancer affecting the bladder and urinary system.
As a monotherapy, Balversa is indicated for the treatment of adult patients with unresectable or metastatic urothelial carcinoma harboring susceptible FGFR3 genetic alterations. These patients must have previously received at least one line of therapy containing a programmed death receptor 1 (PD-1) or programmed death-ligand 1 (PD-L1) inhibitor in the unresectable or metastatic treatment setting.
Urothelial carcinoma is the most common form of bladder cancer, the ninth most frequently diagnosed cancer worldwide. In 2022, there were approximately 614,000 new cases of bladder cancer and 220,000 deaths globally.
The highest incidence rates in both men and women are found in Southern Europe. Greece had 5800 new cases and 1537 deaths in 2018. Spain has the highest incidence rate in men globally. Since the 1990s, bladder cancer incidence trends have diverged by sex, with rates decreasing or stabilizing in men but increasing among women in certain European countries.
The CHMP recommendation is based on data from cohort 1 of the phase 3 THOR trial, which compared erdafitinib with standard-of-care chemotherapy (investigator’s choice of docetaxel or vinflunine). Cohort 1 included 266 adults with advanced urothelial cancer harboring selected FGFR3 alterations.
All patients had disease progression after one or two prior treatments, at least one of which included a PD-1 or PD-L1 inhibitor. The major efficacy endpoints were overall survival, progression free survival, and objective response rate (ORR).
Treatment with erdafitinib reduced the risk for death by 36% compared with chemotherapy (hazard ratio [HR], 0.64; P = .005). Median overall survival was 12.1 months in the erdafitinib arm vs 7.8 months in the chemotherapy arm. Median progression-free survival was 5.6 months in the erdafitinib arm vs 2.7 months in the chemotherapy arm (HR, 0.58; P = .0002). ORR was 35.3% with erdafitinib compared with 8.5% with chemotherapy.
Balversa will be available as 3-mg, 4-mg, and 5-mg film-coated tablets. Erdafitinib, the active substance in Balversa, is an antineoplastic protein kinase inhibitor that suppresses fibroblast growth factor receptor (FGFR) tyrosine kinases. Deregulation of FGFR3 signaling is implicated in the pathogenesis of urothelial cancer, and FGFR inhibition has demonstrated antitumor activity in FGFR-expressing cells.
Ordspono
The committee adopted a positive opinion for Ordspono (odronextamab, Regeneron Ireland Designated Activity Company), indicated as a monotherapy for the treatment of adult patients with:
- Relapsed or refractory follicular lymphoma (rrFL), after two or more lines of systemic therapy.
- Relapsed or refractory diffuse large B-cell lymphoma (rrDLBCL), after two or more lines of systemic therapy.
The approval recommendation is based on phase 2 trials (NCT02290951, NCT03888105), which demonstrated high ORRs in patients with rrFL and rrDLBCL.
In the DLBCL cohort, a 49% ORR was achieved in heavily pretreated patients who had not received chimeric antigen receptor T-cell therapy. A total of 31% achieved a complete response.
The FL cohort showed an 82% response rate in patients with grades I-IIIA disease, with 75% of the overall population achieving a complete response.
Ordspono will be available as a 2-mg, 80-mg, and 320-mg concentrate for solution for infusion. The active substance of Ordspono is odronextamab, a bispecific antibody that targets CD20-expressing B cells and CD3-expressing T cells. By binding to both, it induces T-cell activation and generates a polyclonal cytotoxic T-cell response, leading to the lysis of malignant B cells.
Generics
The panel also adopted positive opinions for two generic cancer medicines.
Enzalutamide Viatris (enzalutamide) is indicated for the treatment of adult men with prostate cancer in several scenarios:
- As monotherapy or with androgen-deprivation therapy for high-risk biochemical recurrent nonmetastatic hormone-sensitive prostate cancer in men unsuitable for salvage-radiotherapy.
- In combination with androgen-deprivation therapy for metastatic hormone-sensitive prostate cancer.
- For high-risk nonmetastatic castration-resistant prostate cancer (CRPC).
- For metastatic CRPC in men who are asymptomatic or mildly symptomatic after failure of androgen-deprivation therapy, where chemotherapy is not yet indicated.
- For metastatic CRPC in men whose disease has progressed on or after docetaxel therapy.
Enzalutamide Viatris is a generic version of Xtandi, authorized in the European Union since June 2013. Studies have confirmed the satisfactory quality and bioequivalence of Enzalutamide Viatris to Xtandi.
Enzalutamide Viatris will be available as 40-mg and 80-mg film-coated tablets. The active substance of Enzalutamide Viatris is enzalutamide, a hormone antagonist that blocks multiple steps in the androgen receptor–signaling pathway.
Nilotinib Accord (nilotinib) is indicated for the treatment of Philadelphia chromosome–positive chronic myelogenous leukemia (CML).
It is used in adult and pediatric patients with newly diagnosed CML in the chronic phase, adult patients with chronic phase and accelerated phase CML with resistance or intolerance to prior therapy including imatinib, and pediatric patients with CML with resistance or intolerance to prior therapy including imatinib.
Nilotinib Accord is a generic of Tasigna, authorized in the European Union since November 2007. Studies have demonstrated the satisfactory quality and bioequivalence of Nilotinib Accord to Tasigna.
Nilotinib Accord will be available as 50-mg, 150-mg, and 200-mg hard capsules. The active substance of Nilotinib Accord is nilotinib, an antineoplastic protein kinase inhibitor that targets BCR-ABL kinase and other oncogenic kinases.
A version of this article appeared on Medscape.com.
Balversa
The CHMP endorsed the approval of Balversa (erdafitinib, Janssen-Cilag International N.V.), intended for the treatment of urothelial carcinoma, a type of cancer affecting the bladder and urinary system.
As a monotherapy, Balversa is indicated for the treatment of adult patients with unresectable or metastatic urothelial carcinoma harboring susceptible FGFR3 genetic alterations. These patients must have previously received at least one line of therapy containing a programmed death receptor 1 (PD-1) or programmed death-ligand 1 (PD-L1) inhibitor in the unresectable or metastatic treatment setting.
Urothelial carcinoma is the most common form of bladder cancer, the ninth most frequently diagnosed cancer worldwide. In 2022, there were approximately 614,000 new cases of bladder cancer and 220,000 deaths globally.
The highest incidence rates in both men and women are found in Southern Europe. Greece had 5800 new cases and 1537 deaths in 2018. Spain has the highest incidence rate in men globally. Since the 1990s, bladder cancer incidence trends have diverged by sex, with rates decreasing or stabilizing in men but increasing among women in certain European countries.
The CHMP recommendation is based on data from cohort 1 of the phase 3 THOR trial, which compared erdafitinib with standard-of-care chemotherapy (investigator’s choice of docetaxel or vinflunine). Cohort 1 included 266 adults with advanced urothelial cancer harboring selected FGFR3 alterations.
All patients had disease progression after one or two prior treatments, at least one of which included a PD-1 or PD-L1 inhibitor. The major efficacy endpoints were overall survival, progression free survival, and objective response rate (ORR).
Treatment with erdafitinib reduced the risk for death by 36% compared with chemotherapy (hazard ratio [HR], 0.64; P = .005). Median overall survival was 12.1 months in the erdafitinib arm vs 7.8 months in the chemotherapy arm. Median progression-free survival was 5.6 months in the erdafitinib arm vs 2.7 months in the chemotherapy arm (HR, 0.58; P = .0002). ORR was 35.3% with erdafitinib compared with 8.5% with chemotherapy.
Balversa will be available as 3-mg, 4-mg, and 5-mg film-coated tablets. Erdafitinib, the active substance in Balversa, is an antineoplastic protein kinase inhibitor that suppresses fibroblast growth factor receptor (FGFR) tyrosine kinases. Deregulation of FGFR3 signaling is implicated in the pathogenesis of urothelial cancer, and FGFR inhibition has demonstrated antitumor activity in FGFR-expressing cells.
Ordspono
The committee adopted a positive opinion for Ordspono (odronextamab, Regeneron Ireland Designated Activity Company), indicated as a monotherapy for the treatment of adult patients with:
- Relapsed or refractory follicular lymphoma (rrFL), after two or more lines of systemic therapy.
- Relapsed or refractory diffuse large B-cell lymphoma (rrDLBCL), after two or more lines of systemic therapy.
The approval recommendation is based on phase 2 trials (NCT02290951, NCT03888105), which demonstrated high ORRs in patients with rrFL and rrDLBCL.
In the DLBCL cohort, a 49% ORR was achieved in heavily pretreated patients who had not received chimeric antigen receptor T-cell therapy. A total of 31% achieved a complete response.
The FL cohort showed an 82% response rate in patients with grades I-IIIA disease, with 75% of the overall population achieving a complete response.
Ordspono will be available as a 2-mg, 80-mg, and 320-mg concentrate for solution for infusion. The active substance of Ordspono is odronextamab, a bispecific antibody that targets CD20-expressing B cells and CD3-expressing T cells. By binding to both, it induces T-cell activation and generates a polyclonal cytotoxic T-cell response, leading to the lysis of malignant B cells.
Generics
The panel also adopted positive opinions for two generic cancer medicines.
Enzalutamide Viatris (enzalutamide) is indicated for the treatment of adult men with prostate cancer in several scenarios:
- As monotherapy or with androgen-deprivation therapy for high-risk biochemical recurrent nonmetastatic hormone-sensitive prostate cancer in men unsuitable for salvage-radiotherapy.
- In combination with androgen-deprivation therapy for metastatic hormone-sensitive prostate cancer.
- For high-risk nonmetastatic castration-resistant prostate cancer (CRPC).
- For metastatic CRPC in men who are asymptomatic or mildly symptomatic after failure of androgen-deprivation therapy, where chemotherapy is not yet indicated.
- For metastatic CRPC in men whose disease has progressed on or after docetaxel therapy.
Enzalutamide Viatris is a generic version of Xtandi, authorized in the European Union since June 2013. Studies have confirmed the satisfactory quality and bioequivalence of Enzalutamide Viatris to Xtandi.
Enzalutamide Viatris will be available as 40-mg and 80-mg film-coated tablets. The active substance of Enzalutamide Viatris is enzalutamide, a hormone antagonist that blocks multiple steps in the androgen receptor–signaling pathway.
Nilotinib Accord (nilotinib) is indicated for the treatment of Philadelphia chromosome–positive chronic myelogenous leukemia (CML).
It is used in adult and pediatric patients with newly diagnosed CML in the chronic phase, adult patients with chronic phase and accelerated phase CML with resistance or intolerance to prior therapy including imatinib, and pediatric patients with CML with resistance or intolerance to prior therapy including imatinib.
Nilotinib Accord is a generic of Tasigna, authorized in the European Union since November 2007. Studies have demonstrated the satisfactory quality and bioequivalence of Nilotinib Accord to Tasigna.
Nilotinib Accord will be available as 50-mg, 150-mg, and 200-mg hard capsules. The active substance of Nilotinib Accord is nilotinib, an antineoplastic protein kinase inhibitor that targets BCR-ABL kinase and other oncogenic kinases.
A version of this article appeared on Medscape.com.
Balversa
The CHMP endorsed the approval of Balversa (erdafitinib, Janssen-Cilag International N.V.), intended for the treatment of urothelial carcinoma, a type of cancer affecting the bladder and urinary system.
As a monotherapy, Balversa is indicated for the treatment of adult patients with unresectable or metastatic urothelial carcinoma harboring susceptible FGFR3 genetic alterations. These patients must have previously received at least one line of therapy containing a programmed death receptor 1 (PD-1) or programmed death-ligand 1 (PD-L1) inhibitor in the unresectable or metastatic treatment setting.
Urothelial carcinoma is the most common form of bladder cancer, the ninth most frequently diagnosed cancer worldwide. In 2022, there were approximately 614,000 new cases of bladder cancer and 220,000 deaths globally.
The highest incidence rates in both men and women are found in Southern Europe. Greece had 5800 new cases and 1537 deaths in 2018. Spain has the highest incidence rate in men globally. Since the 1990s, bladder cancer incidence trends have diverged by sex, with rates decreasing or stabilizing in men but increasing among women in certain European countries.
The CHMP recommendation is based on data from cohort 1 of the phase 3 THOR trial, which compared erdafitinib with standard-of-care chemotherapy (investigator’s choice of docetaxel or vinflunine). Cohort 1 included 266 adults with advanced urothelial cancer harboring selected FGFR3 alterations.
All patients had disease progression after one or two prior treatments, at least one of which included a PD-1 or PD-L1 inhibitor. The major efficacy endpoints were overall survival, progression free survival, and objective response rate (ORR).
Treatment with erdafitinib reduced the risk for death by 36% compared with chemotherapy (hazard ratio [HR], 0.64; P = .005). Median overall survival was 12.1 months in the erdafitinib arm vs 7.8 months in the chemotherapy arm. Median progression-free survival was 5.6 months in the erdafitinib arm vs 2.7 months in the chemotherapy arm (HR, 0.58; P = .0002). ORR was 35.3% with erdafitinib compared with 8.5% with chemotherapy.
Balversa will be available as 3-mg, 4-mg, and 5-mg film-coated tablets. Erdafitinib, the active substance in Balversa, is an antineoplastic protein kinase inhibitor that suppresses fibroblast growth factor receptor (FGFR) tyrosine kinases. Deregulation of FGFR3 signaling is implicated in the pathogenesis of urothelial cancer, and FGFR inhibition has demonstrated antitumor activity in FGFR-expressing cells.
Ordspono
The committee adopted a positive opinion for Ordspono (odronextamab, Regeneron Ireland Designated Activity Company), indicated as a monotherapy for the treatment of adult patients with:
- Relapsed or refractory follicular lymphoma (rrFL), after two or more lines of systemic therapy.
- Relapsed or refractory diffuse large B-cell lymphoma (rrDLBCL), after two or more lines of systemic therapy.
The approval recommendation is based on phase 2 trials (NCT02290951, NCT03888105), which demonstrated high ORRs in patients with rrFL and rrDLBCL.
In the DLBCL cohort, a 49% ORR was achieved in heavily pretreated patients who had not received chimeric antigen receptor T-cell therapy. A total of 31% achieved a complete response.
The FL cohort showed an 82% response rate in patients with grades I-IIIA disease, with 75% of the overall population achieving a complete response.
Ordspono will be available as a 2-mg, 80-mg, and 320-mg concentrate for solution for infusion. The active substance of Ordspono is odronextamab, a bispecific antibody that targets CD20-expressing B cells and CD3-expressing T cells. By binding to both, it induces T-cell activation and generates a polyclonal cytotoxic T-cell response, leading to the lysis of malignant B cells.
Generics
The panel also adopted positive opinions for two generic cancer medicines.
Enzalutamide Viatris (enzalutamide) is indicated for the treatment of adult men with prostate cancer in several scenarios:
- As monotherapy or with androgen-deprivation therapy for high-risk biochemical recurrent nonmetastatic hormone-sensitive prostate cancer in men unsuitable for salvage-radiotherapy.
- In combination with androgen-deprivation therapy for metastatic hormone-sensitive prostate cancer.
- For high-risk nonmetastatic castration-resistant prostate cancer (CRPC).
- For metastatic CRPC in men who are asymptomatic or mildly symptomatic after failure of androgen-deprivation therapy, where chemotherapy is not yet indicated.
- For metastatic CRPC in men whose disease has progressed on or after docetaxel therapy.
Enzalutamide Viatris is a generic version of Xtandi, authorized in the European Union since June 2013. Studies have confirmed the satisfactory quality and bioequivalence of Enzalutamide Viatris to Xtandi.
Enzalutamide Viatris will be available as 40-mg and 80-mg film-coated tablets. The active substance of Enzalutamide Viatris is enzalutamide, a hormone antagonist that blocks multiple steps in the androgen receptor–signaling pathway.
Nilotinib Accord (nilotinib) is indicated for the treatment of Philadelphia chromosome–positive chronic myelogenous leukemia (CML).
It is used in adult and pediatric patients with newly diagnosed CML in the chronic phase, adult patients with chronic phase and accelerated phase CML with resistance or intolerance to prior therapy including imatinib, and pediatric patients with CML with resistance or intolerance to prior therapy including imatinib.
Nilotinib Accord is a generic of Tasigna, authorized in the European Union since November 2007. Studies have demonstrated the satisfactory quality and bioequivalence of Nilotinib Accord to Tasigna.
Nilotinib Accord will be available as 50-mg, 150-mg, and 200-mg hard capsules. The active substance of Nilotinib Accord is nilotinib, an antineoplastic protein kinase inhibitor that targets BCR-ABL kinase and other oncogenic kinases.
A version of this article appeared on Medscape.com.
Two Techniques to Avoid Cyst Spray During Excision
Practice Gap
Epidermoid cysts are asymptomatic, well-circumscribed, mobile, subcutaneous masses that elevate the skin. Also known as epidermal, keratin, or infundibular cysts, epidermoid cysts are caused by proliferation of surface epidermoid cells within the dermis and can arise anywhere on the body, most commonly on the face, neck, and trunk.1 Cutaneous cysts often contain fluid or semifluid contents and can be aesthetically displeasing or cause mild pain, prompting patients to seek removal. Definitive treatment of epidermoid cysts is complete surgical removal,2 which can be performed in office in a sterile or clean manner by either dermatologists or primary care providers.
Prior to incision, a local anesthetic—commonly lidocaine with epinephrine—is injected in the region surrounding the cyst sac so as not to rupture the cyst wall. Maintaining the cyst wall throughout the procedure ensures total cyst removal and minimizes the risk for recurrence. However, it often is difficult to approximate the cyst border because it cannot be visualized prior to incision.
Throughout the duration of the procedure, cyst contents may suddenly spray out of the area and pose a risk to providers and their staff (Figure, A). Even with careful application around the periphery, either puncture or pericystic anesthesia between the cyst wall and the dermis can lead to splatter. Larger and wider peripheral anesthesia may not be possible given a shortage of lidocaine and a desire to minimize injection. Even with meticulous use of personal protective equipment in cutaneous surgery, infectious organisms found in ruptured cysts and abscesses may spray the surgical field.3 Therefore, it is in our best interest to minimize the trajectory of cyst spray contents.
The Tools
We have employed 2 simple techniques using equipment normally found on a standard surgical tray for easy safe injection of cysts. Supplies needed include 4×4-inch gauze pads, alcohol and chlorhexidine, a marker, all instruments necessary for cyst excision, and a small clear biohazard bag.
The Technique
Prior to covering the cyst, care is taken to locate the cyst opening. At times, a comedo or punctum can be seen overlying the cyst bulge. We mark the lumen and cyst opening with a surgical marker. If the pore is not easily identified, we draw an 8-mm circle around the mound of the cyst.
One option is to apply a gauze pad over the cyst to allow for stabilization of the surgical field and blanket the area from splatter (Figure, B). Then we cover the cyst using antiseptic-soaked gauze as a protective barrier to avoid potentially contaminated spray. This tool can be constructed from a 4×4-inch gauze pad with the addition of alcohol and chlorhexidine. When the cyst is covered, the surgeon can inject the lesion and surrounding tissue without biohazard splatter.
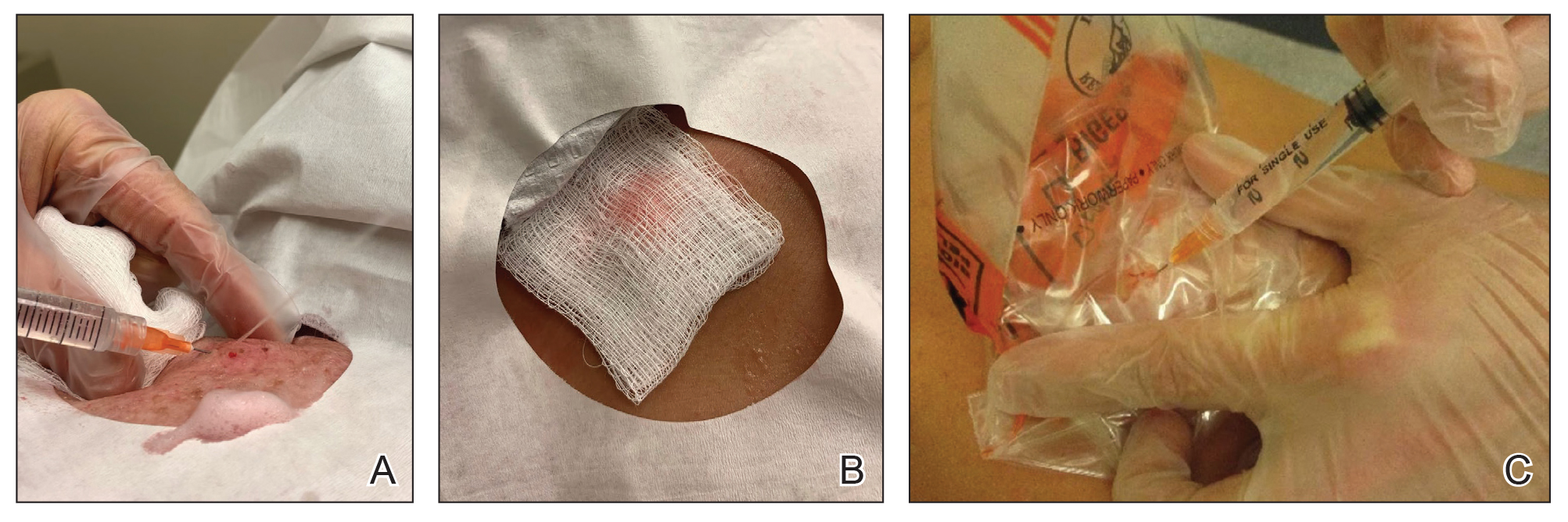
Another method is to cover the cyst with a small clear biohazard bag (Figure, C). When injecting anesthetic through the bag, the spray is captured by the bag and does not reach the surgeon or staff. This method is potentially more effective given that the cyst can still be visualized fully for more accurate injection.
Practice Implications
Outpatient surgical excision is a common effective procedure for epidermoid cysts. However, it is not uncommon for cyst contents to spray during the injection of anesthetic, posing a nuisance to the surgeon, health care staff, and patient. The technique of covering the lesion with antiseptic-soaked gauze or a small clear biohazard bag prevents cyst contents from spraying and reduces risk for contamination. In addition to these protective benefits, the use of readily available items replaces the need to order a splatter control shield.
Limitations—Although we seldom see spray using our technique, covering the cyst with gauze may disguise the region of interest and interfere with accurate incision. Marking the lesion prior to anesthesia administration or using a clear biohazard bag minimizes difficulty visualizing the cyst opening.
- Zito PM, Scharf R. Epidermoid cyst. StatPearls [Internet]. Updated August 8, 2023. Accessed June 13, 2024. https://www.ncbi.nlm.nih.gov/books/NBK499974
- Weir CB, St. Hilaire NJ. Epidermal inclusion cyst. StatPearls [Internet]. Updated August 8, 2023. Accessed June3, 2024. https://www.ncbi.nlm.nih.gov/books/NBK532310/
- Kuniyuki S, Yoshida Y, Maekawa N, et al. Bacteriological study of epidermal cysts. Acta Derm Venereol. 2018;88:23-25. doi:10.2340/00015555-0348
Practice Gap
Epidermoid cysts are asymptomatic, well-circumscribed, mobile, subcutaneous masses that elevate the skin. Also known as epidermal, keratin, or infundibular cysts, epidermoid cysts are caused by proliferation of surface epidermoid cells within the dermis and can arise anywhere on the body, most commonly on the face, neck, and trunk.1 Cutaneous cysts often contain fluid or semifluid contents and can be aesthetically displeasing or cause mild pain, prompting patients to seek removal. Definitive treatment of epidermoid cysts is complete surgical removal,2 which can be performed in office in a sterile or clean manner by either dermatologists or primary care providers.
Prior to incision, a local anesthetic—commonly lidocaine with epinephrine—is injected in the region surrounding the cyst sac so as not to rupture the cyst wall. Maintaining the cyst wall throughout the procedure ensures total cyst removal and minimizes the risk for recurrence. However, it often is difficult to approximate the cyst border because it cannot be visualized prior to incision.
Throughout the duration of the procedure, cyst contents may suddenly spray out of the area and pose a risk to providers and their staff (Figure, A). Even with careful application around the periphery, either puncture or pericystic anesthesia between the cyst wall and the dermis can lead to splatter. Larger and wider peripheral anesthesia may not be possible given a shortage of lidocaine and a desire to minimize injection. Even with meticulous use of personal protective equipment in cutaneous surgery, infectious organisms found in ruptured cysts and abscesses may spray the surgical field.3 Therefore, it is in our best interest to minimize the trajectory of cyst spray contents.
The Tools
We have employed 2 simple techniques using equipment normally found on a standard surgical tray for easy safe injection of cysts. Supplies needed include 4×4-inch gauze pads, alcohol and chlorhexidine, a marker, all instruments necessary for cyst excision, and a small clear biohazard bag.
The Technique
Prior to covering the cyst, care is taken to locate the cyst opening. At times, a comedo or punctum can be seen overlying the cyst bulge. We mark the lumen and cyst opening with a surgical marker. If the pore is not easily identified, we draw an 8-mm circle around the mound of the cyst.
One option is to apply a gauze pad over the cyst to allow for stabilization of the surgical field and blanket the area from splatter (Figure, B). Then we cover the cyst using antiseptic-soaked gauze as a protective barrier to avoid potentially contaminated spray. This tool can be constructed from a 4×4-inch gauze pad with the addition of alcohol and chlorhexidine. When the cyst is covered, the surgeon can inject the lesion and surrounding tissue without biohazard splatter.
Another method is to cover the cyst with a small clear biohazard bag (Figure, C). When injecting anesthetic through the bag, the spray is captured by the bag and does not reach the surgeon or staff. This method is potentially more effective given that the cyst can still be visualized fully for more accurate injection.
Practice Implications
Outpatient surgical excision is a common effective procedure for epidermoid cysts. However, it is not uncommon for cyst contents to spray during the injection of anesthetic, posing a nuisance to the surgeon, health care staff, and patient. The technique of covering the lesion with antiseptic-soaked gauze or a small clear biohazard bag prevents cyst contents from spraying and reduces risk for contamination. In addition to these protective benefits, the use of readily available items replaces the need to order a splatter control shield.
Limitations—Although we seldom see spray using our technique, covering the cyst with gauze may disguise the region of interest and interfere with accurate incision. Marking the lesion prior to anesthesia administration or using a clear biohazard bag minimizes difficulty visualizing the cyst opening.
Practice Gap
Epidermoid cysts are asymptomatic, well-circumscribed, mobile, subcutaneous masses that elevate the skin. Also known as epidermal, keratin, or infundibular cysts, epidermoid cysts are caused by proliferation of surface epidermoid cells within the dermis and can arise anywhere on the body, most commonly on the face, neck, and trunk.1 Cutaneous cysts often contain fluid or semifluid contents and can be aesthetically displeasing or cause mild pain, prompting patients to seek removal. Definitive treatment of epidermoid cysts is complete surgical removal,2 which can be performed in office in a sterile or clean manner by either dermatologists or primary care providers.
Prior to incision, a local anesthetic—commonly lidocaine with epinephrine—is injected in the region surrounding the cyst sac so as not to rupture the cyst wall. Maintaining the cyst wall throughout the procedure ensures total cyst removal and minimizes the risk for recurrence. However, it often is difficult to approximate the cyst border because it cannot be visualized prior to incision.
Throughout the duration of the procedure, cyst contents may suddenly spray out of the area and pose a risk to providers and their staff (Figure, A). Even with careful application around the periphery, either puncture or pericystic anesthesia between the cyst wall and the dermis can lead to splatter. Larger and wider peripheral anesthesia may not be possible given a shortage of lidocaine and a desire to minimize injection. Even with meticulous use of personal protective equipment in cutaneous surgery, infectious organisms found in ruptured cysts and abscesses may spray the surgical field.3 Therefore, it is in our best interest to minimize the trajectory of cyst spray contents.
The Tools
We have employed 2 simple techniques using equipment normally found on a standard surgical tray for easy safe injection of cysts. Supplies needed include 4×4-inch gauze pads, alcohol and chlorhexidine, a marker, all instruments necessary for cyst excision, and a small clear biohazard bag.
The Technique
Prior to covering the cyst, care is taken to locate the cyst opening. At times, a comedo or punctum can be seen overlying the cyst bulge. We mark the lumen and cyst opening with a surgical marker. If the pore is not easily identified, we draw an 8-mm circle around the mound of the cyst.
One option is to apply a gauze pad over the cyst to allow for stabilization of the surgical field and blanket the area from splatter (Figure, B). Then we cover the cyst using antiseptic-soaked gauze as a protective barrier to avoid potentially contaminated spray. This tool can be constructed from a 4×4-inch gauze pad with the addition of alcohol and chlorhexidine. When the cyst is covered, the surgeon can inject the lesion and surrounding tissue without biohazard splatter.
Another method is to cover the cyst with a small clear biohazard bag (Figure, C). When injecting anesthetic through the bag, the spray is captured by the bag and does not reach the surgeon or staff. This method is potentially more effective given that the cyst can still be visualized fully for more accurate injection.
Practice Implications
Outpatient surgical excision is a common effective procedure for epidermoid cysts. However, it is not uncommon for cyst contents to spray during the injection of anesthetic, posing a nuisance to the surgeon, health care staff, and patient. The technique of covering the lesion with antiseptic-soaked gauze or a small clear biohazard bag prevents cyst contents from spraying and reduces risk for contamination. In addition to these protective benefits, the use of readily available items replaces the need to order a splatter control shield.
Limitations—Although we seldom see spray using our technique, covering the cyst with gauze may disguise the region of interest and interfere with accurate incision. Marking the lesion prior to anesthesia administration or using a clear biohazard bag minimizes difficulty visualizing the cyst opening.
- Zito PM, Scharf R. Epidermoid cyst. StatPearls [Internet]. Updated August 8, 2023. Accessed June 13, 2024. https://www.ncbi.nlm.nih.gov/books/NBK499974
- Weir CB, St. Hilaire NJ. Epidermal inclusion cyst. StatPearls [Internet]. Updated August 8, 2023. Accessed June3, 2024. https://www.ncbi.nlm.nih.gov/books/NBK532310/
- Kuniyuki S, Yoshida Y, Maekawa N, et al. Bacteriological study of epidermal cysts. Acta Derm Venereol. 2018;88:23-25. doi:10.2340/00015555-0348
- Zito PM, Scharf R. Epidermoid cyst. StatPearls [Internet]. Updated August 8, 2023. Accessed June 13, 2024. https://www.ncbi.nlm.nih.gov/books/NBK499974
- Weir CB, St. Hilaire NJ. Epidermal inclusion cyst. StatPearls [Internet]. Updated August 8, 2023. Accessed June3, 2024. https://www.ncbi.nlm.nih.gov/books/NBK532310/
- Kuniyuki S, Yoshida Y, Maekawa N, et al. Bacteriological study of epidermal cysts. Acta Derm Venereol. 2018;88:23-25. doi:10.2340/00015555-0348

Children on Medicaid With Asthma Receive Less Specialty Care
Primary care clinicians successfully manage many children with asthma, but data on specialist care according to insurance coverage are lacking, wrote Kimberley H. Geissler, PhD, of the University of Massachusetts Chan Medical School–Baystate, Springfield, Massachusetts, and colleagues.
Despite many interventions over time, “low-income children insured by Medicaid, many of whom are from minoritized racial and ethnic groups, continue to have worse outcomes and higher rates of poorly controlled asthma than children who are privately insured,” Dr. Geissler said in an interview.
“Because differences in whether a child sees an asthma specialist could contribute to these disparities, better understanding specialist use among both groups of kids may help inform potential solutions,” she said.
In a study published in JAMA Network Open, the researchers identified children with asthma aged 2-17 years using data from the Massachusetts All-Payer Claims Database for the years 2015-2020. The study population included 198,101 children and 432,455 child-year observations from children with asthma during a year when they met at least one of three criteria with any asthma diagnosis: One or more hospital visits, two or more outpatient visits, or at least one outpatient visit and at least one asthma medication.
Outpatient Visit Outcome
The primary outcome of asthma specialist care was defined as at least one outpatient visit with any asthma diagnosis to a clinician with a code of allergy and immunology, pulmonology, or otolaryngology.
A total of 66.2% of the child-year observations involved Medicaid and 33.8% involved private insurance. Approximately 15% of the children received asthma specialist care. However, nearly twice as many children with private insurance received asthma specialty care compared with those with Medicaid (20.6% vs 11.9%). In a full logistic regression analysis, children with Medicaid insurance were 55% less likely to receive asthma specialist treatment than children with private insurance.
Allergy and immunology was the most common specialty used, and the child-years for this specialty among children with Medicaid were less than half of those among children with private insurance (7.1% vs 15.9%).
Rates of persistent asthma were 20.0% and 16.9% in children with Medicaid and private insurance, respectively. Overall, children with persistent asthma were nearly four times as likely to receive asthma specialist care (adjusted odds ratio, 3.96). However, the difference in odds of receiving specialty care based on insurance type in favor of private insurance was greater among children with persistent asthma than among those without persistent asthma (−24.0 percentage points vs −20.8 percentage points).
The researchers found a similar pattern of difference in asthma specialty care in a sensitivity analysis limiting the results to child-year observations with at least one outpatient visit with any asthma diagnosis in a calendar year, although they also found a slight narrowing of the difference between the groups over time.
“Contrary to expectations, disparities in specialist care by insurance type were even more striking in children with persistent asthma,” the researchers wrote in their discussion. Notably, the growth of specialty drugs such as biologics for moderate to severe asthma are mainly prescribed by specialists, and ensuring access to specialists for children with Medicaid may reduce disparities in asthma control for those with severe or poorly controlled disease, they added.
The study findings were limited by several factors including the use only of data from Massachusetts, which may not generalize to other states, and the use of completed specialist visits without data on referrals, the researchers noted. Other limitations included a lack of data on asthma symptom frequency or control and on the setting in which an asthma diagnosis was made.
However, the results suggest a need for more attention to disparities in asthma care by insurance type, and more research is needed to determine whether these disparities persist in subsets of children with asthma, such as those with allergies or chronic medical conditions, they concluded.
Takeaways and Next Steps
“Perhaps unsurprisingly, children with private insurance were more likely to receive asthma specialist care than children with Medicaid,” Dr. Geissler told this news organization. The researchers expected a smaller gap between insurance types among children with persistent asthma, a marker for asthma severity, she said. However, “we found that the gap between those with Medicaid and those with private insurance is actually larger” for children with persistent asthma, she added.
As improved treatments for hard-to-control asthma become more available, pediatricians and primary care clinicians should follow the latest clinical guidelines for referring children to specialists for asthma care, said Dr. Geissler.
“Additionally, asthma specialists should ensure that their practices are accessible to children with Medicaid, as these families may face higher barriers to care; for example, transportation needs or scheduling challenges,” she said. Other strategies to overcome barriers to care might include electronic consultations with specialists or primary care–oriented interdisciplinary asthma clinics, which may be useful for all children with asthma but may particularly benefit those insured by Medicaid, she noted.
“Based on data limitations, we could not examine why we observed such big differences in specialist use by insurance type; for example, whether pediatricians were referring to specialists less for Medicaid-insured kids, or whether kids with Medicaid were less likely to see a specialist after a referral was made,” Dr. Geissler said. More research is needed to examine not only these factors but also the appropriateness of specialty care based on clinical guidelines to ensure high-quality evidence-based care for children with asthma who are insured by Medicaid, she said.
Improve Access and Expand Analysis
Asthma is a chronic and prevalent disease and requires a comprehensive approach that sometimes calls for specialist care, Anne Coates, MD, a pediatric pulmonologist in Portland, Maine, said in an interview.
Dr. Coates said she was surprised by the results of the current study but commended the authors for highlighting the limitations of the study, which illustrate areas for additional research. Notably, “the authors couldn’t observe referrals to specialists from primary care physicians; they used completed visits as a proxy,” Dr. Coates said.
More studies are needed to assess the completion of referral visits regardless of children’s insurance in order to better understand and address the barriers to specialty care, she added.
The current study is important because of the extent of asthma coupled with the significant number of children across the United States who are insured by Medicaid, especially underserved populations, she said.
“The burden of asthma differentially affects people of color who are living in lower resourced areas, and it is important in further research to understanding the barriers to helping people get the care they need,” Dr. Coates told this news organization. Some alternatives might include telehealth visits or even a hybrid visit to a primary care provider (PCP) who has high-speed internet, and the specialist could then conduct a telehealth visit from the PCP’s office, with the PCP acting as on-site eyes and ears, said Dr. Coates, who has used this strategy in her practice in Maine, where many patients live far from specialist care.
The study was supported by the National Heart, Lung, and Blood Institute and the University of Massachusetts Center for Clinical and Translational Science-Biostatistics, Epidemiology & Research Design Component. Dr. Geissler and Dr. Coates had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Primary care clinicians successfully manage many children with asthma, but data on specialist care according to insurance coverage are lacking, wrote Kimberley H. Geissler, PhD, of the University of Massachusetts Chan Medical School–Baystate, Springfield, Massachusetts, and colleagues.
Despite many interventions over time, “low-income children insured by Medicaid, many of whom are from minoritized racial and ethnic groups, continue to have worse outcomes and higher rates of poorly controlled asthma than children who are privately insured,” Dr. Geissler said in an interview.
“Because differences in whether a child sees an asthma specialist could contribute to these disparities, better understanding specialist use among both groups of kids may help inform potential solutions,” she said.
In a study published in JAMA Network Open, the researchers identified children with asthma aged 2-17 years using data from the Massachusetts All-Payer Claims Database for the years 2015-2020. The study population included 198,101 children and 432,455 child-year observations from children with asthma during a year when they met at least one of three criteria with any asthma diagnosis: One or more hospital visits, two or more outpatient visits, or at least one outpatient visit and at least one asthma medication.
Outpatient Visit Outcome
The primary outcome of asthma specialist care was defined as at least one outpatient visit with any asthma diagnosis to a clinician with a code of allergy and immunology, pulmonology, or otolaryngology.
A total of 66.2% of the child-year observations involved Medicaid and 33.8% involved private insurance. Approximately 15% of the children received asthma specialist care. However, nearly twice as many children with private insurance received asthma specialty care compared with those with Medicaid (20.6% vs 11.9%). In a full logistic regression analysis, children with Medicaid insurance were 55% less likely to receive asthma specialist treatment than children with private insurance.
Allergy and immunology was the most common specialty used, and the child-years for this specialty among children with Medicaid were less than half of those among children with private insurance (7.1% vs 15.9%).
Rates of persistent asthma were 20.0% and 16.9% in children with Medicaid and private insurance, respectively. Overall, children with persistent asthma were nearly four times as likely to receive asthma specialist care (adjusted odds ratio, 3.96). However, the difference in odds of receiving specialty care based on insurance type in favor of private insurance was greater among children with persistent asthma than among those without persistent asthma (−24.0 percentage points vs −20.8 percentage points).
The researchers found a similar pattern of difference in asthma specialty care in a sensitivity analysis limiting the results to child-year observations with at least one outpatient visit with any asthma diagnosis in a calendar year, although they also found a slight narrowing of the difference between the groups over time.
“Contrary to expectations, disparities in specialist care by insurance type were even more striking in children with persistent asthma,” the researchers wrote in their discussion. Notably, the growth of specialty drugs such as biologics for moderate to severe asthma are mainly prescribed by specialists, and ensuring access to specialists for children with Medicaid may reduce disparities in asthma control for those with severe or poorly controlled disease, they added.
The study findings were limited by several factors including the use only of data from Massachusetts, which may not generalize to other states, and the use of completed specialist visits without data on referrals, the researchers noted. Other limitations included a lack of data on asthma symptom frequency or control and on the setting in which an asthma diagnosis was made.
However, the results suggest a need for more attention to disparities in asthma care by insurance type, and more research is needed to determine whether these disparities persist in subsets of children with asthma, such as those with allergies or chronic medical conditions, they concluded.
Takeaways and Next Steps
“Perhaps unsurprisingly, children with private insurance were more likely to receive asthma specialist care than children with Medicaid,” Dr. Geissler told this news organization. The researchers expected a smaller gap between insurance types among children with persistent asthma, a marker for asthma severity, she said. However, “we found that the gap between those with Medicaid and those with private insurance is actually larger” for children with persistent asthma, she added.
As improved treatments for hard-to-control asthma become more available, pediatricians and primary care clinicians should follow the latest clinical guidelines for referring children to specialists for asthma care, said Dr. Geissler.
“Additionally, asthma specialists should ensure that their practices are accessible to children with Medicaid, as these families may face higher barriers to care; for example, transportation needs or scheduling challenges,” she said. Other strategies to overcome barriers to care might include electronic consultations with specialists or primary care–oriented interdisciplinary asthma clinics, which may be useful for all children with asthma but may particularly benefit those insured by Medicaid, she noted.
“Based on data limitations, we could not examine why we observed such big differences in specialist use by insurance type; for example, whether pediatricians were referring to specialists less for Medicaid-insured kids, or whether kids with Medicaid were less likely to see a specialist after a referral was made,” Dr. Geissler said. More research is needed to examine not only these factors but also the appropriateness of specialty care based on clinical guidelines to ensure high-quality evidence-based care for children with asthma who are insured by Medicaid, she said.
Improve Access and Expand Analysis
Asthma is a chronic and prevalent disease and requires a comprehensive approach that sometimes calls for specialist care, Anne Coates, MD, a pediatric pulmonologist in Portland, Maine, said in an interview.
Dr. Coates said she was surprised by the results of the current study but commended the authors for highlighting the limitations of the study, which illustrate areas for additional research. Notably, “the authors couldn’t observe referrals to specialists from primary care physicians; they used completed visits as a proxy,” Dr. Coates said.
More studies are needed to assess the completion of referral visits regardless of children’s insurance in order to better understand and address the barriers to specialty care, she added.
The current study is important because of the extent of asthma coupled with the significant number of children across the United States who are insured by Medicaid, especially underserved populations, she said.
“The burden of asthma differentially affects people of color who are living in lower resourced areas, and it is important in further research to understanding the barriers to helping people get the care they need,” Dr. Coates told this news organization. Some alternatives might include telehealth visits or even a hybrid visit to a primary care provider (PCP) who has high-speed internet, and the specialist could then conduct a telehealth visit from the PCP’s office, with the PCP acting as on-site eyes and ears, said Dr. Coates, who has used this strategy in her practice in Maine, where many patients live far from specialist care.
The study was supported by the National Heart, Lung, and Blood Institute and the University of Massachusetts Center for Clinical and Translational Science-Biostatistics, Epidemiology & Research Design Component. Dr. Geissler and Dr. Coates had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Primary care clinicians successfully manage many children with asthma, but data on specialist care according to insurance coverage are lacking, wrote Kimberley H. Geissler, PhD, of the University of Massachusetts Chan Medical School–Baystate, Springfield, Massachusetts, and colleagues.
Despite many interventions over time, “low-income children insured by Medicaid, many of whom are from minoritized racial and ethnic groups, continue to have worse outcomes and higher rates of poorly controlled asthma than children who are privately insured,” Dr. Geissler said in an interview.
“Because differences in whether a child sees an asthma specialist could contribute to these disparities, better understanding specialist use among both groups of kids may help inform potential solutions,” she said.
In a study published in JAMA Network Open, the researchers identified children with asthma aged 2-17 years using data from the Massachusetts All-Payer Claims Database for the years 2015-2020. The study population included 198,101 children and 432,455 child-year observations from children with asthma during a year when they met at least one of three criteria with any asthma diagnosis: One or more hospital visits, two or more outpatient visits, or at least one outpatient visit and at least one asthma medication.
Outpatient Visit Outcome
The primary outcome of asthma specialist care was defined as at least one outpatient visit with any asthma diagnosis to a clinician with a code of allergy and immunology, pulmonology, or otolaryngology.
A total of 66.2% of the child-year observations involved Medicaid and 33.8% involved private insurance. Approximately 15% of the children received asthma specialist care. However, nearly twice as many children with private insurance received asthma specialty care compared with those with Medicaid (20.6% vs 11.9%). In a full logistic regression analysis, children with Medicaid insurance were 55% less likely to receive asthma specialist treatment than children with private insurance.
Allergy and immunology was the most common specialty used, and the child-years for this specialty among children with Medicaid were less than half of those among children with private insurance (7.1% vs 15.9%).
Rates of persistent asthma were 20.0% and 16.9% in children with Medicaid and private insurance, respectively. Overall, children with persistent asthma were nearly four times as likely to receive asthma specialist care (adjusted odds ratio, 3.96). However, the difference in odds of receiving specialty care based on insurance type in favor of private insurance was greater among children with persistent asthma than among those without persistent asthma (−24.0 percentage points vs −20.8 percentage points).
The researchers found a similar pattern of difference in asthma specialty care in a sensitivity analysis limiting the results to child-year observations with at least one outpatient visit with any asthma diagnosis in a calendar year, although they also found a slight narrowing of the difference between the groups over time.
“Contrary to expectations, disparities in specialist care by insurance type were even more striking in children with persistent asthma,” the researchers wrote in their discussion. Notably, the growth of specialty drugs such as biologics for moderate to severe asthma are mainly prescribed by specialists, and ensuring access to specialists for children with Medicaid may reduce disparities in asthma control for those with severe or poorly controlled disease, they added.
The study findings were limited by several factors including the use only of data from Massachusetts, which may not generalize to other states, and the use of completed specialist visits without data on referrals, the researchers noted. Other limitations included a lack of data on asthma symptom frequency or control and on the setting in which an asthma diagnosis was made.
However, the results suggest a need for more attention to disparities in asthma care by insurance type, and more research is needed to determine whether these disparities persist in subsets of children with asthma, such as those with allergies or chronic medical conditions, they concluded.
Takeaways and Next Steps
“Perhaps unsurprisingly, children with private insurance were more likely to receive asthma specialist care than children with Medicaid,” Dr. Geissler told this news organization. The researchers expected a smaller gap between insurance types among children with persistent asthma, a marker for asthma severity, she said. However, “we found that the gap between those with Medicaid and those with private insurance is actually larger” for children with persistent asthma, she added.
As improved treatments for hard-to-control asthma become more available, pediatricians and primary care clinicians should follow the latest clinical guidelines for referring children to specialists for asthma care, said Dr. Geissler.
“Additionally, asthma specialists should ensure that their practices are accessible to children with Medicaid, as these families may face higher barriers to care; for example, transportation needs or scheduling challenges,” she said. Other strategies to overcome barriers to care might include electronic consultations with specialists or primary care–oriented interdisciplinary asthma clinics, which may be useful for all children with asthma but may particularly benefit those insured by Medicaid, she noted.
“Based on data limitations, we could not examine why we observed such big differences in specialist use by insurance type; for example, whether pediatricians were referring to specialists less for Medicaid-insured kids, or whether kids with Medicaid were less likely to see a specialist after a referral was made,” Dr. Geissler said. More research is needed to examine not only these factors but also the appropriateness of specialty care based on clinical guidelines to ensure high-quality evidence-based care for children with asthma who are insured by Medicaid, she said.
Improve Access and Expand Analysis
Asthma is a chronic and prevalent disease and requires a comprehensive approach that sometimes calls for specialist care, Anne Coates, MD, a pediatric pulmonologist in Portland, Maine, said in an interview.
Dr. Coates said she was surprised by the results of the current study but commended the authors for highlighting the limitations of the study, which illustrate areas for additional research. Notably, “the authors couldn’t observe referrals to specialists from primary care physicians; they used completed visits as a proxy,” Dr. Coates said.
More studies are needed to assess the completion of referral visits regardless of children’s insurance in order to better understand and address the barriers to specialty care, she added.
The current study is important because of the extent of asthma coupled with the significant number of children across the United States who are insured by Medicaid, especially underserved populations, she said.
“The burden of asthma differentially affects people of color who are living in lower resourced areas, and it is important in further research to understanding the barriers to helping people get the care they need,” Dr. Coates told this news organization. Some alternatives might include telehealth visits or even a hybrid visit to a primary care provider (PCP) who has high-speed internet, and the specialist could then conduct a telehealth visit from the PCP’s office, with the PCP acting as on-site eyes and ears, said Dr. Coates, who has used this strategy in her practice in Maine, where many patients live far from specialist care.
The study was supported by the National Heart, Lung, and Blood Institute and the University of Massachusetts Center for Clinical and Translational Science-Biostatistics, Epidemiology & Research Design Component. Dr. Geissler and Dr. Coates had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Pyzchiva Receives FDA Approval as Third Ustekinumab Biosimilar
The Food and Drug Administration has approved ustekinumab-ttwe (Pyzchiva) as a biosimilar to ustekinumab (Stelara) for the treatment of multiple inflammatory conditions.
In addition, the agency “provisionally determined” that the medication would be interchangeable with the reference product but that designation would not take hold until the interchangeability exclusivity period for the first approved biosimilar ustekinumab-auub (Wezlana) expires, according to a press release. This designation would, depending on state law, allow a pharmacist to substitute the biosimilar for the reference product without involving the prescribing clinician. It’s unclear when ustekinumab-auub’s interchangeability exclusivity ends.
Ustekinumab-ttwe, a human interleukin (IL)-12 and IL-23 antagonist, is indicated for the treatment of:
- Moderate to severe plaque psoriasis in adults and pediatric patients aged 6 years or older who are candidates for phototherapy or systemic therapy
- Active psoriatic arthritis in adults and pediatric patients aged 6 years or older with moderately to severely active Crohn’s disease or ulcerative colitis
It is administered via subcutaneous injection in 45 mg/0.5 mL and 90 mg/mL prefilled syringes or via intravenous infusion in 130 mg/26 mL (5 mg/mL) single-dose vial.
Developed by Samsung Bioepis, ustekinumab-ttwe will be commercialized by Sandoz in the United States. Besides ustekinumab-auub, the other ustekinumab biosimilar is ustekinumab-aekn (Selarsdi).
Ustekinumab-ttwe is expected to launch in February 2025 “in accordance with the settlement and license agreement with Janssen Biotech,” which manufacturers the reference product, Sandoz said. The other approved ustekinumab biosimilars will launch within a similar time frame.
A version of this article appeared on Medscape.com.
The Food and Drug Administration has approved ustekinumab-ttwe (Pyzchiva) as a biosimilar to ustekinumab (Stelara) for the treatment of multiple inflammatory conditions.
In addition, the agency “provisionally determined” that the medication would be interchangeable with the reference product but that designation would not take hold until the interchangeability exclusivity period for the first approved biosimilar ustekinumab-auub (Wezlana) expires, according to a press release. This designation would, depending on state law, allow a pharmacist to substitute the biosimilar for the reference product without involving the prescribing clinician. It’s unclear when ustekinumab-auub’s interchangeability exclusivity ends.
Ustekinumab-ttwe, a human interleukin (IL)-12 and IL-23 antagonist, is indicated for the treatment of:
- Moderate to severe plaque psoriasis in adults and pediatric patients aged 6 years or older who are candidates for phototherapy or systemic therapy
- Active psoriatic arthritis in adults and pediatric patients aged 6 years or older with moderately to severely active Crohn’s disease or ulcerative colitis
It is administered via subcutaneous injection in 45 mg/0.5 mL and 90 mg/mL prefilled syringes or via intravenous infusion in 130 mg/26 mL (5 mg/mL) single-dose vial.
Developed by Samsung Bioepis, ustekinumab-ttwe will be commercialized by Sandoz in the United States. Besides ustekinumab-auub, the other ustekinumab biosimilar is ustekinumab-aekn (Selarsdi).
Ustekinumab-ttwe is expected to launch in February 2025 “in accordance with the settlement and license agreement with Janssen Biotech,” which manufacturers the reference product, Sandoz said. The other approved ustekinumab biosimilars will launch within a similar time frame.
A version of this article appeared on Medscape.com.
The Food and Drug Administration has approved ustekinumab-ttwe (Pyzchiva) as a biosimilar to ustekinumab (Stelara) for the treatment of multiple inflammatory conditions.
In addition, the agency “provisionally determined” that the medication would be interchangeable with the reference product but that designation would not take hold until the interchangeability exclusivity period for the first approved biosimilar ustekinumab-auub (Wezlana) expires, according to a press release. This designation would, depending on state law, allow a pharmacist to substitute the biosimilar for the reference product without involving the prescribing clinician. It’s unclear when ustekinumab-auub’s interchangeability exclusivity ends.
Ustekinumab-ttwe, a human interleukin (IL)-12 and IL-23 antagonist, is indicated for the treatment of:
- Moderate to severe plaque psoriasis in adults and pediatric patients aged 6 years or older who are candidates for phototherapy or systemic therapy
- Active psoriatic arthritis in adults and pediatric patients aged 6 years or older with moderately to severely active Crohn’s disease or ulcerative colitis
It is administered via subcutaneous injection in 45 mg/0.5 mL and 90 mg/mL prefilled syringes or via intravenous infusion in 130 mg/26 mL (5 mg/mL) single-dose vial.
Developed by Samsung Bioepis, ustekinumab-ttwe will be commercialized by Sandoz in the United States. Besides ustekinumab-auub, the other ustekinumab biosimilar is ustekinumab-aekn (Selarsdi).
Ustekinumab-ttwe is expected to launch in February 2025 “in accordance with the settlement and license agreement with Janssen Biotech,” which manufacturers the reference product, Sandoz said. The other approved ustekinumab biosimilars will launch within a similar time frame.
A version of this article appeared on Medscape.com.
Is Anxiety a Prodromal Feature of Parkinson’s Disease?
new research suggested.
Investigators drew on 10-year data from primary care registry to compare almost 110,000 patients who developed anxiety after the age of 50 years with close to 900,000 matched controls without anxiety.
After adjusting for a variety of sociodemographic, lifestyle, psychiatric, and neurological factors, they found that the risk of developing Parkinson’s disease was double in those with anxiety, compared with controls.
“Anxiety is known to be a feature of the early stages of Parkinson’s disease, but prior to our study, the prospective risk of Parkinson’s in those over the age of 50 with new-onset anxiety was unknown,” colead author Juan Bazo Alvarez, a senior research fellow in the Division of Epidemiology and Health at University College London, London, England, said in a news release.
The study was published online in the British Journal of General Practice.
The presence of anxiety is increased in prodromal Parkinson’s disease, but the prospective risk for Parkinson’s disease in those aged 50 years or older with new-onset anxiety was largely unknown.
Investigators analyzed data from a large UK primary care dataset that includes all people aged between 50 and 99 years who were registered with a participating practice from Jan. 1, 2008, to Dec. 31, 2018.
They identified 109,435 people (35% men) with more than one anxiety record in the database but no previous record of anxiety for 1 year or more and 878,256 people (37% men) with no history of anxiety (control group).
Features of Parkinson’s disease such as sleep problems, depression, tremor, and impaired balance were then tracked from the point of the anxiety diagnosis until 1 year before the Parkinson’s disease diagnosis.
Among those with anxiety, 331 developed Parkinson’s disease during the follow-up period, with a median time to diagnosis of 4.9 years after the first recorded episode of anxiety.
The incidence of Parkinson’s disease was 1.2 per 1000 person-years (95% CI, 0.92-1.13) in those with anxiety versus 0.49 (95% CI, 0.47-0.52) in those without anxiety.
After adjustment for age, sex, social deprivation, lifestyle factors, severe mental illness, head trauma, and dementia, the risk for Parkinson’s disease was double in those with anxiety, compared with the non-anxiety group (hazard ratio, 2.1; 95% CI, 1.9-2.4).
Individuals without anxiety also developed Parkinson’s disease later than those with anxiety.
The researchers identified specific symptoms that were associated with later development of Parkinson’s disease in those with anxiety, including depression, sleep disturbance, fatigue, and cognitive impairment, among other symptoms.
“The results suggest that there is a strong association between anxiety and diagnosis of Parkinson’s disease in patients aged over 50 years who present with a new diagnosis of anxiety,” the authors wrote. “This provides evidence for anxiety as a prodromal presentation of Parkinson’s disease.”
Future research “should explore anxiety in relation to other prodromal symptoms and how this symptom complex is associated with the incidence of Parkinson’s disease,” the researchers wrote. Doing so “may lead to earlier diagnosis and better management of Parkinson’s disease.”
This study was funded by the European Union. Specific authors received funding from the National Institute for Health and Care Research and the Alzheimer’s Society Clinical Training Fellowship program. The authors declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggested.
Investigators drew on 10-year data from primary care registry to compare almost 110,000 patients who developed anxiety after the age of 50 years with close to 900,000 matched controls without anxiety.
After adjusting for a variety of sociodemographic, lifestyle, psychiatric, and neurological factors, they found that the risk of developing Parkinson’s disease was double in those with anxiety, compared with controls.
“Anxiety is known to be a feature of the early stages of Parkinson’s disease, but prior to our study, the prospective risk of Parkinson’s in those over the age of 50 with new-onset anxiety was unknown,” colead author Juan Bazo Alvarez, a senior research fellow in the Division of Epidemiology and Health at University College London, London, England, said in a news release.
The study was published online in the British Journal of General Practice.
The presence of anxiety is increased in prodromal Parkinson’s disease, but the prospective risk for Parkinson’s disease in those aged 50 years or older with new-onset anxiety was largely unknown.
Investigators analyzed data from a large UK primary care dataset that includes all people aged between 50 and 99 years who were registered with a participating practice from Jan. 1, 2008, to Dec. 31, 2018.
They identified 109,435 people (35% men) with more than one anxiety record in the database but no previous record of anxiety for 1 year or more and 878,256 people (37% men) with no history of anxiety (control group).
Features of Parkinson’s disease such as sleep problems, depression, tremor, and impaired balance were then tracked from the point of the anxiety diagnosis until 1 year before the Parkinson’s disease diagnosis.
Among those with anxiety, 331 developed Parkinson’s disease during the follow-up period, with a median time to diagnosis of 4.9 years after the first recorded episode of anxiety.
The incidence of Parkinson’s disease was 1.2 per 1000 person-years (95% CI, 0.92-1.13) in those with anxiety versus 0.49 (95% CI, 0.47-0.52) in those without anxiety.
After adjustment for age, sex, social deprivation, lifestyle factors, severe mental illness, head trauma, and dementia, the risk for Parkinson’s disease was double in those with anxiety, compared with the non-anxiety group (hazard ratio, 2.1; 95% CI, 1.9-2.4).
Individuals without anxiety also developed Parkinson’s disease later than those with anxiety.
The researchers identified specific symptoms that were associated with later development of Parkinson’s disease in those with anxiety, including depression, sleep disturbance, fatigue, and cognitive impairment, among other symptoms.
“The results suggest that there is a strong association between anxiety and diagnosis of Parkinson’s disease in patients aged over 50 years who present with a new diagnosis of anxiety,” the authors wrote. “This provides evidence for anxiety as a prodromal presentation of Parkinson’s disease.”
Future research “should explore anxiety in relation to other prodromal symptoms and how this symptom complex is associated with the incidence of Parkinson’s disease,” the researchers wrote. Doing so “may lead to earlier diagnosis and better management of Parkinson’s disease.”
This study was funded by the European Union. Specific authors received funding from the National Institute for Health and Care Research and the Alzheimer’s Society Clinical Training Fellowship program. The authors declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggested.
Investigators drew on 10-year data from primary care registry to compare almost 110,000 patients who developed anxiety after the age of 50 years with close to 900,000 matched controls without anxiety.
After adjusting for a variety of sociodemographic, lifestyle, psychiatric, and neurological factors, they found that the risk of developing Parkinson’s disease was double in those with anxiety, compared with controls.
“Anxiety is known to be a feature of the early stages of Parkinson’s disease, but prior to our study, the prospective risk of Parkinson’s in those over the age of 50 with new-onset anxiety was unknown,” colead author Juan Bazo Alvarez, a senior research fellow in the Division of Epidemiology and Health at University College London, London, England, said in a news release.
The study was published online in the British Journal of General Practice.
The presence of anxiety is increased in prodromal Parkinson’s disease, but the prospective risk for Parkinson’s disease in those aged 50 years or older with new-onset anxiety was largely unknown.
Investigators analyzed data from a large UK primary care dataset that includes all people aged between 50 and 99 years who were registered with a participating practice from Jan. 1, 2008, to Dec. 31, 2018.
They identified 109,435 people (35% men) with more than one anxiety record in the database but no previous record of anxiety for 1 year or more and 878,256 people (37% men) with no history of anxiety (control group).
Features of Parkinson’s disease such as sleep problems, depression, tremor, and impaired balance were then tracked from the point of the anxiety diagnosis until 1 year before the Parkinson’s disease diagnosis.
Among those with anxiety, 331 developed Parkinson’s disease during the follow-up period, with a median time to diagnosis of 4.9 years after the first recorded episode of anxiety.
The incidence of Parkinson’s disease was 1.2 per 1000 person-years (95% CI, 0.92-1.13) in those with anxiety versus 0.49 (95% CI, 0.47-0.52) in those without anxiety.
After adjustment for age, sex, social deprivation, lifestyle factors, severe mental illness, head trauma, and dementia, the risk for Parkinson’s disease was double in those with anxiety, compared with the non-anxiety group (hazard ratio, 2.1; 95% CI, 1.9-2.4).
Individuals without anxiety also developed Parkinson’s disease later than those with anxiety.
The researchers identified specific symptoms that were associated with later development of Parkinson’s disease in those with anxiety, including depression, sleep disturbance, fatigue, and cognitive impairment, among other symptoms.
“The results suggest that there is a strong association between anxiety and diagnosis of Parkinson’s disease in patients aged over 50 years who present with a new diagnosis of anxiety,” the authors wrote. “This provides evidence for anxiety as a prodromal presentation of Parkinson’s disease.”
Future research “should explore anxiety in relation to other prodromal symptoms and how this symptom complex is associated with the incidence of Parkinson’s disease,” the researchers wrote. Doing so “may lead to earlier diagnosis and better management of Parkinson’s disease.”
This study was funded by the European Union. Specific authors received funding from the National Institute for Health and Care Research and the Alzheimer’s Society Clinical Training Fellowship program. The authors declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE BRITISH JOURNAL OF GENERAL PRACTICE
Benzos Are Hard on the Brain, But Do They Raise Dementia Risk?
The study of more than 5000 older adults found that benzodiazepine use was associated with an accelerated reduction in the volume of the hippocampus and amygdala — brain regions involved in memory and mood regulation. However, benzodiazepine use overall was not associated with an increased risk for dementia.
The findings suggest that benzodiazepine use “may have subtle, long-term impact on brain health,” lead investigator Frank Wolters, MD, PhD, with Erasmus University Medical Center, Rotterdam, the Netherlands, and colleagues wrote.
The study was published online in BMC Medicine.
Conflicting Evidence
Benzodiazepines are commonly prescribed in older adults for anxiety and sleep disorders. Though the short-term cognitive side effects are well documented, the long-term impact on neurodegeneration and dementia risk remains unclear. Some studies have linked benzodiazepine use to an increased risk for dementia, whereas others have not.
Dr. Wolters and colleagues assessed the effect of benzodiazepine use on long-term dementia risk and on imaging markers of neurodegeneration in 5443 cognitively healthy adults (mean age, 71 years; 57% women) from the population-based Rotterdam Study.
Benzodiazepine use between 1991 and 2008 was determined using pharmacy dispensing records, and dementia incidence was determined from medical records.
Half of the participants had used benzodiazepines at any time in the 15 years before baseline (2005-2008); 47% used anxiolytics, 20% used sedative-hypnotics, 34% used both, and 13% were still using the drugs at the baseline assessment.
During an average follow-up of 11 years, 13% of participants developed dementia.
Overall, use of benzodiazepines was not associated with dementia risk, compared with never-use (hazard ratio [HR], 1.06), irrespective of cumulative dose.
The risk for dementia was somewhat higher with any use of anxiolytics than with sedative-hypnotics (HR, 1.17 vs HR, 0.92), although neither was statistically significant. The highest risk estimates were observed for high cumulative dose of anxiolytics (HR, 1.33).
Sensitivity analyses of the two most commonly used anxiolytics found no differences in risk between use of short half-life oxazepam and long half-life diazepam (HR, 1.01 and HR, 1.06, respectively, for ever-use, compared with never-use for oxazepam and diazepam).
Brain Atrophy
The researchers investigated potential associations between benzodiazepine use and brain volumes using brain MRI imaging from 4836 participants.
They found that current use of a benzodiazepine at baseline was significantly associated with lower total brain volume — as well as lower hippocampus, amygdala, and thalamus volume cross-sectionally — and with accelerated volume loss of the hippocampus and, to a lesser extent, amygdala longitudinally.
Imaging findings did not differ by type of benzodiazepine used or cumulative dose.
“Given the availability of effective alternative pharmacological and nonpharmacological treatments for anxiety and sleep problems, it is important to carefully consider the necessity of prolonged benzodiazepine use in light of potential detrimental effects on brain health,” the authors wrote.
Risks Go Beyond the Brain
Commenting on the study, Shaheen Lakhan, MD, PhD, a neurologist and researcher based in Miami, Florida, noted that “chronic benzodiazepine use may reduce neuroplasticity, potentially interfering with the brain’s ability to form new connections and adapt.
“Long-term use can lead to down-regulation of GABA receptors, altering the brain’s natural inhibitory mechanisms and potentially contributing to tolerance and withdrawal symptoms. Prolonged use can also disrupt the balance of various neurotransmitter systems beyond just GABA, potentially affecting mood, cognition, and overall brain function,” said Dr. Lakhan, who was not involved in the study.
“While the literature is mixed on chronic benzodiazepine use and dementia risk, prolonged use has consistently been associated with accelerated volume loss in certain brain regions, particularly the hippocampus and amygdala,” which are responsible for memory, learning, and emotional regulation, he noted.
“Beyond cognitive impairments and brain volume loss, chronic benzodiazepine use is associated with tolerance and dependence, potential for abuse, interactions with other drugs, and increased fall risk, especially in older adults,” Dr. Lakhan added.
Current guidelines discourage long-term use of benzodiazepines because of risk for psychological and physical dependence; falls; and cognitive impairment, especially in older adults. Nevertheless, research shows that 30%-40% of older benzodiazepine users stay on the medication beyond the recommended period of several weeks.
Donovan T. Maust, MD, Department of Psychiatry, University of Michigan Medical School, Ann Arbor, said in an interview these new findings are consistent with other recently published observational research that suggest benzodiazepine use is not linked to dementia risk.
“I realize that such meta-analyses that find a positive relationship between benzodiazepines and dementia are out there, but they include older, less rigorous studies,” said Dr. Maust, who was not part of the new study. “In my opinion, the jury is not still out on this topic. However, there are plenty of other reasons to avoid them — and in particular, starting them — in older adults, most notably the increased risk of fall injury as well as increased overdose risk when taken along with opioids.”
A version of this article first appeared on Medscape.com.
The study of more than 5000 older adults found that benzodiazepine use was associated with an accelerated reduction in the volume of the hippocampus and amygdala — brain regions involved in memory and mood regulation. However, benzodiazepine use overall was not associated with an increased risk for dementia.
The findings suggest that benzodiazepine use “may have subtle, long-term impact on brain health,” lead investigator Frank Wolters, MD, PhD, with Erasmus University Medical Center, Rotterdam, the Netherlands, and colleagues wrote.
The study was published online in BMC Medicine.
Conflicting Evidence
Benzodiazepines are commonly prescribed in older adults for anxiety and sleep disorders. Though the short-term cognitive side effects are well documented, the long-term impact on neurodegeneration and dementia risk remains unclear. Some studies have linked benzodiazepine use to an increased risk for dementia, whereas others have not.
Dr. Wolters and colleagues assessed the effect of benzodiazepine use on long-term dementia risk and on imaging markers of neurodegeneration in 5443 cognitively healthy adults (mean age, 71 years; 57% women) from the population-based Rotterdam Study.
Benzodiazepine use between 1991 and 2008 was determined using pharmacy dispensing records, and dementia incidence was determined from medical records.
Half of the participants had used benzodiazepines at any time in the 15 years before baseline (2005-2008); 47% used anxiolytics, 20% used sedative-hypnotics, 34% used both, and 13% were still using the drugs at the baseline assessment.
During an average follow-up of 11 years, 13% of participants developed dementia.
Overall, use of benzodiazepines was not associated with dementia risk, compared with never-use (hazard ratio [HR], 1.06), irrespective of cumulative dose.
The risk for dementia was somewhat higher with any use of anxiolytics than with sedative-hypnotics (HR, 1.17 vs HR, 0.92), although neither was statistically significant. The highest risk estimates were observed for high cumulative dose of anxiolytics (HR, 1.33).
Sensitivity analyses of the two most commonly used anxiolytics found no differences in risk between use of short half-life oxazepam and long half-life diazepam (HR, 1.01 and HR, 1.06, respectively, for ever-use, compared with never-use for oxazepam and diazepam).
Brain Atrophy
The researchers investigated potential associations between benzodiazepine use and brain volumes using brain MRI imaging from 4836 participants.
They found that current use of a benzodiazepine at baseline was significantly associated with lower total brain volume — as well as lower hippocampus, amygdala, and thalamus volume cross-sectionally — and with accelerated volume loss of the hippocampus and, to a lesser extent, amygdala longitudinally.
Imaging findings did not differ by type of benzodiazepine used or cumulative dose.
“Given the availability of effective alternative pharmacological and nonpharmacological treatments for anxiety and sleep problems, it is important to carefully consider the necessity of prolonged benzodiazepine use in light of potential detrimental effects on brain health,” the authors wrote.
Risks Go Beyond the Brain
Commenting on the study, Shaheen Lakhan, MD, PhD, a neurologist and researcher based in Miami, Florida, noted that “chronic benzodiazepine use may reduce neuroplasticity, potentially interfering with the brain’s ability to form new connections and adapt.
“Long-term use can lead to down-regulation of GABA receptors, altering the brain’s natural inhibitory mechanisms and potentially contributing to tolerance and withdrawal symptoms. Prolonged use can also disrupt the balance of various neurotransmitter systems beyond just GABA, potentially affecting mood, cognition, and overall brain function,” said Dr. Lakhan, who was not involved in the study.
“While the literature is mixed on chronic benzodiazepine use and dementia risk, prolonged use has consistently been associated with accelerated volume loss in certain brain regions, particularly the hippocampus and amygdala,” which are responsible for memory, learning, and emotional regulation, he noted.
“Beyond cognitive impairments and brain volume loss, chronic benzodiazepine use is associated with tolerance and dependence, potential for abuse, interactions with other drugs, and increased fall risk, especially in older adults,” Dr. Lakhan added.
Current guidelines discourage long-term use of benzodiazepines because of risk for psychological and physical dependence; falls; and cognitive impairment, especially in older adults. Nevertheless, research shows that 30%-40% of older benzodiazepine users stay on the medication beyond the recommended period of several weeks.
Donovan T. Maust, MD, Department of Psychiatry, University of Michigan Medical School, Ann Arbor, said in an interview these new findings are consistent with other recently published observational research that suggest benzodiazepine use is not linked to dementia risk.
“I realize that such meta-analyses that find a positive relationship between benzodiazepines and dementia are out there, but they include older, less rigorous studies,” said Dr. Maust, who was not part of the new study. “In my opinion, the jury is not still out on this topic. However, there are plenty of other reasons to avoid them — and in particular, starting them — in older adults, most notably the increased risk of fall injury as well as increased overdose risk when taken along with opioids.”
A version of this article first appeared on Medscape.com.
The study of more than 5000 older adults found that benzodiazepine use was associated with an accelerated reduction in the volume of the hippocampus and amygdala — brain regions involved in memory and mood regulation. However, benzodiazepine use overall was not associated with an increased risk for dementia.
The findings suggest that benzodiazepine use “may have subtle, long-term impact on brain health,” lead investigator Frank Wolters, MD, PhD, with Erasmus University Medical Center, Rotterdam, the Netherlands, and colleagues wrote.
The study was published online in BMC Medicine.
Conflicting Evidence
Benzodiazepines are commonly prescribed in older adults for anxiety and sleep disorders. Though the short-term cognitive side effects are well documented, the long-term impact on neurodegeneration and dementia risk remains unclear. Some studies have linked benzodiazepine use to an increased risk for dementia, whereas others have not.
Dr. Wolters and colleagues assessed the effect of benzodiazepine use on long-term dementia risk and on imaging markers of neurodegeneration in 5443 cognitively healthy adults (mean age, 71 years; 57% women) from the population-based Rotterdam Study.
Benzodiazepine use between 1991 and 2008 was determined using pharmacy dispensing records, and dementia incidence was determined from medical records.
Half of the participants had used benzodiazepines at any time in the 15 years before baseline (2005-2008); 47% used anxiolytics, 20% used sedative-hypnotics, 34% used both, and 13% were still using the drugs at the baseline assessment.
During an average follow-up of 11 years, 13% of participants developed dementia.
Overall, use of benzodiazepines was not associated with dementia risk, compared with never-use (hazard ratio [HR], 1.06), irrespective of cumulative dose.
The risk for dementia was somewhat higher with any use of anxiolytics than with sedative-hypnotics (HR, 1.17 vs HR, 0.92), although neither was statistically significant. The highest risk estimates were observed for high cumulative dose of anxiolytics (HR, 1.33).
Sensitivity analyses of the two most commonly used anxiolytics found no differences in risk between use of short half-life oxazepam and long half-life diazepam (HR, 1.01 and HR, 1.06, respectively, for ever-use, compared with never-use for oxazepam and diazepam).
Brain Atrophy
The researchers investigated potential associations between benzodiazepine use and brain volumes using brain MRI imaging from 4836 participants.
They found that current use of a benzodiazepine at baseline was significantly associated with lower total brain volume — as well as lower hippocampus, amygdala, and thalamus volume cross-sectionally — and with accelerated volume loss of the hippocampus and, to a lesser extent, amygdala longitudinally.
Imaging findings did not differ by type of benzodiazepine used or cumulative dose.
“Given the availability of effective alternative pharmacological and nonpharmacological treatments for anxiety and sleep problems, it is important to carefully consider the necessity of prolonged benzodiazepine use in light of potential detrimental effects on brain health,” the authors wrote.
Risks Go Beyond the Brain
Commenting on the study, Shaheen Lakhan, MD, PhD, a neurologist and researcher based in Miami, Florida, noted that “chronic benzodiazepine use may reduce neuroplasticity, potentially interfering with the brain’s ability to form new connections and adapt.
“Long-term use can lead to down-regulation of GABA receptors, altering the brain’s natural inhibitory mechanisms and potentially contributing to tolerance and withdrawal symptoms. Prolonged use can also disrupt the balance of various neurotransmitter systems beyond just GABA, potentially affecting mood, cognition, and overall brain function,” said Dr. Lakhan, who was not involved in the study.
“While the literature is mixed on chronic benzodiazepine use and dementia risk, prolonged use has consistently been associated with accelerated volume loss in certain brain regions, particularly the hippocampus and amygdala,” which are responsible for memory, learning, and emotional regulation, he noted.
“Beyond cognitive impairments and brain volume loss, chronic benzodiazepine use is associated with tolerance and dependence, potential for abuse, interactions with other drugs, and increased fall risk, especially in older adults,” Dr. Lakhan added.
Current guidelines discourage long-term use of benzodiazepines because of risk for psychological and physical dependence; falls; and cognitive impairment, especially in older adults. Nevertheless, research shows that 30%-40% of older benzodiazepine users stay on the medication beyond the recommended period of several weeks.
Donovan T. Maust, MD, Department of Psychiatry, University of Michigan Medical School, Ann Arbor, said in an interview these new findings are consistent with other recently published observational research that suggest benzodiazepine use is not linked to dementia risk.
“I realize that such meta-analyses that find a positive relationship between benzodiazepines and dementia are out there, but they include older, less rigorous studies,” said Dr. Maust, who was not part of the new study. “In my opinion, the jury is not still out on this topic. However, there are plenty of other reasons to avoid them — and in particular, starting them — in older adults, most notably the increased risk of fall injury as well as increased overdose risk when taken along with opioids.”
A version of this article first appeared on Medscape.com.
FROM BMC MEDICINE
Medication Overuse in Mental Health Facilities: Not the Answer, Regardless of Consent, Says Ethicist
This transcript has been edited for clarity.
There’s a growing scandal in mental health care. Recent studies are showing that certain medications that basically are used to, if you will, quiet patients — antipsychotic drugs — are being overused, particularly in facilities that serve poorer people and people who are minorities. This situation is utterly, ethically unacceptable and it’s something that we are starting to get really pressed to solve.
Part of this is due to the fact that numbers of caregivers are in short supply. We need to get more people trained. We need to get more mental health providers at all levels into facilities in order to provide care, and not substitute that inability to have a provider present and minimize risk to patients by having drug-induced sleepiness, soporific behavior, or, if you will, snowing them just because we don’t have enough people to keep an eye on them. Furthermore, we can’t let them engage in some activities, even things like walking around, because we’re worried about falls. The nursing homes or mental health facilities don’t want anybody to get injured, much less killed, because that’s going to really bring government agencies down on them.
What do we do, aside from trying to get more numbers in there? California came up with a law not too long ago that basically put the burden of using these drugs on consent. They passed a law that said the patient, before going under and being administered any type of psychoactive drug, has to consent; or if they’re really unable to do that, their relative or next of kin should have to consent.
California law now puts the burden on getting consent from the patient in order to use these drugs. It’s not a good solution. It still permits the use of the drugs to substitute for the inability to provide adequate numbers of people to provide care in safe environments. It’s almost like saying, “We know you’re going into a dangerous place. We can’t really reduce the danger, so we’re going to make sure that you stay in your seat. You better consent to that because otherwise things could not go well for you in this mental institution.”
That’s not a sound argument for the use of informed consent. Moreover, I’m very skeptical that many of these people in mental institutions do have the capacity to either say, “Fine, give me psychoactive drugs if I have to stay here,” or “No, I don’t want that. I’ll take my chances.”
They’re vulnerable people. Many of them may not be fully incompetent, but they often have compromised competency. Relatives may be thinking, Well, the right thing to do is just to make sure they don’t get hurt or injure themselves. Yes, give them the drugs.
Consent, while I support it, is not the solution to what is fundamentally an infrastructure problem, a personnel problem, and one of the shames of American healthcare, which is lousy long-term mental health care. For too many people, their care is in the street. For too many people, their care is taking place in institutions that have dangerous designs where people either get injured, can’t provide enough spacing, or just don’t have the people to do it.
Let’s move to fix the mental health care system and not be in a situation where we say to people, “The system stinks and you’re at risk. Is it okay with you if we drug you because we can’t think of any other way to keep you safe, given the rotten nature of the institutions that we’ve got?”
Dr. Caplan is director, Division of Medical Ethics, New York University Langone Medical Center, New York. He disclosed ties with Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position) and serves as a contributing author and adviser for Medscape.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
There’s a growing scandal in mental health care. Recent studies are showing that certain medications that basically are used to, if you will, quiet patients — antipsychotic drugs — are being overused, particularly in facilities that serve poorer people and people who are minorities. This situation is utterly, ethically unacceptable and it’s something that we are starting to get really pressed to solve.
Part of this is due to the fact that numbers of caregivers are in short supply. We need to get more people trained. We need to get more mental health providers at all levels into facilities in order to provide care, and not substitute that inability to have a provider present and minimize risk to patients by having drug-induced sleepiness, soporific behavior, or, if you will, snowing them just because we don’t have enough people to keep an eye on them. Furthermore, we can’t let them engage in some activities, even things like walking around, because we’re worried about falls. The nursing homes or mental health facilities don’t want anybody to get injured, much less killed, because that’s going to really bring government agencies down on them.
What do we do, aside from trying to get more numbers in there? California came up with a law not too long ago that basically put the burden of using these drugs on consent. They passed a law that said the patient, before going under and being administered any type of psychoactive drug, has to consent; or if they’re really unable to do that, their relative or next of kin should have to consent.
California law now puts the burden on getting consent from the patient in order to use these drugs. It’s not a good solution. It still permits the use of the drugs to substitute for the inability to provide adequate numbers of people to provide care in safe environments. It’s almost like saying, “We know you’re going into a dangerous place. We can’t really reduce the danger, so we’re going to make sure that you stay in your seat. You better consent to that because otherwise things could not go well for you in this mental institution.”
That’s not a sound argument for the use of informed consent. Moreover, I’m very skeptical that many of these people in mental institutions do have the capacity to either say, “Fine, give me psychoactive drugs if I have to stay here,” or “No, I don’t want that. I’ll take my chances.”
They’re vulnerable people. Many of them may not be fully incompetent, but they often have compromised competency. Relatives may be thinking, Well, the right thing to do is just to make sure they don’t get hurt or injure themselves. Yes, give them the drugs.
Consent, while I support it, is not the solution to what is fundamentally an infrastructure problem, a personnel problem, and one of the shames of American healthcare, which is lousy long-term mental health care. For too many people, their care is in the street. For too many people, their care is taking place in institutions that have dangerous designs where people either get injured, can’t provide enough spacing, or just don’t have the people to do it.
Let’s move to fix the mental health care system and not be in a situation where we say to people, “The system stinks and you’re at risk. Is it okay with you if we drug you because we can’t think of any other way to keep you safe, given the rotten nature of the institutions that we’ve got?”
Dr. Caplan is director, Division of Medical Ethics, New York University Langone Medical Center, New York. He disclosed ties with Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position) and serves as a contributing author and adviser for Medscape.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
There’s a growing scandal in mental health care. Recent studies are showing that certain medications that basically are used to, if you will, quiet patients — antipsychotic drugs — are being overused, particularly in facilities that serve poorer people and people who are minorities. This situation is utterly, ethically unacceptable and it’s something that we are starting to get really pressed to solve.
Part of this is due to the fact that numbers of caregivers are in short supply. We need to get more people trained. We need to get more mental health providers at all levels into facilities in order to provide care, and not substitute that inability to have a provider present and minimize risk to patients by having drug-induced sleepiness, soporific behavior, or, if you will, snowing them just because we don’t have enough people to keep an eye on them. Furthermore, we can’t let them engage in some activities, even things like walking around, because we’re worried about falls. The nursing homes or mental health facilities don’t want anybody to get injured, much less killed, because that’s going to really bring government agencies down on them.
What do we do, aside from trying to get more numbers in there? California came up with a law not too long ago that basically put the burden of using these drugs on consent. They passed a law that said the patient, before going under and being administered any type of psychoactive drug, has to consent; or if they’re really unable to do that, their relative or next of kin should have to consent.
California law now puts the burden on getting consent from the patient in order to use these drugs. It’s not a good solution. It still permits the use of the drugs to substitute for the inability to provide adequate numbers of people to provide care in safe environments. It’s almost like saying, “We know you’re going into a dangerous place. We can’t really reduce the danger, so we’re going to make sure that you stay in your seat. You better consent to that because otherwise things could not go well for you in this mental institution.”
That’s not a sound argument for the use of informed consent. Moreover, I’m very skeptical that many of these people in mental institutions do have the capacity to either say, “Fine, give me psychoactive drugs if I have to stay here,” or “No, I don’t want that. I’ll take my chances.”
They’re vulnerable people. Many of them may not be fully incompetent, but they often have compromised competency. Relatives may be thinking, Well, the right thing to do is just to make sure they don’t get hurt or injure themselves. Yes, give them the drugs.
Consent, while I support it, is not the solution to what is fundamentally an infrastructure problem, a personnel problem, and one of the shames of American healthcare, which is lousy long-term mental health care. For too many people, their care is in the street. For too many people, their care is taking place in institutions that have dangerous designs where people either get injured, can’t provide enough spacing, or just don’t have the people to do it.
Let’s move to fix the mental health care system and not be in a situation where we say to people, “The system stinks and you’re at risk. Is it okay with you if we drug you because we can’t think of any other way to keep you safe, given the rotten nature of the institutions that we’ve got?”
Dr. Caplan is director, Division of Medical Ethics, New York University Langone Medical Center, New York. He disclosed ties with Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position) and serves as a contributing author and adviser for Medscape.
A version of this article first appeared on Medscape.com.