User login
Bringing trainee wellness to the forefront
Researching the impact of reflection in medical training
Before the spread of COVID-19, and increasingly during the pandemic, Ilana Krumm, MD, noticed a burgeoning focus on wellness for trainees and how to combat burnout in the medical space.
But Dr. Krumm also noticed that most of the existing programs focused on the individual level, rather than the system level. The onus was on the trainees to manage their wellness and burnout.
“I wanted to look at something that could be instituted at a systems level as opposed to putting all the burden of this wellness on the resident, as someone who already has a huge burden of work, stress, and time constraints as they try to learn their discipline,” Dr. Krumm said. “Asking them to meditate on their own time seemed very impractical.”

Eager to research this idea, Dr. Krumm applied for the CHEST Research Grant in Medical Education.
“The fact that CHEST is willing to support medical education research is really important for all those trying to better the educational environment. Although there’s a movement toward more support for medical education research and more recognition of its value, I think the fact that CHEST has already done so has helped advance the field and the support for the field as a whole,” Dr. Krumm said.
“Having the support from a reputable institution like CHEST inherently gave the work that I was doing value,” Dr. Krumm said. “It gave folks an understanding that this research in medical education has importance.”
Dr. Krumm’s project focused on the monthly Reflection Rounds between the ICU, palliative care, and chaplaincy staff that were held at the Seattle VA Medical Center, where residents could discuss the challenges of caring for critically ill patients during a protected time. While similar interventions around death and dying have been shown to help residents reduce burnout in medical intensive care rotations, it was unknown which aspects of these sessions would be most effective.
Participant interviews were conducted before and after the residents’ monthly sessions to understand the impact these sessions had on wellness and burnout levels.
“With the grant funding from CHEST, our team was able to purchase the recording equipment, transcription, and software necessary to complete a thorough qualitative research project, which greatly accelerated the project timeline,” she said.
Through these interviews, Dr. Krumm’s team identified three key themes that shed light on the impact of Reflection Rounds.
1. Cultural precedent
Participants were encouraged to participate as little or as much as they wanted during the session. Despite some residents being less vocal during these discussions, every resident agreed that this type of session set an important cultural precedent in their program and acknowledged the value of a program that encouraged space for decompression and reflection.
2. Shared experiences
During this project, many residents experienced an increased sense of isolation, as COVID-19 precautions were stricter in the ICU. Having this protected time together allowed residents to discover their shared experiences and find comfort in them while feeling supported.
“A lot of residents commented that it was nice to know that others were going through this as well or that they were also finding this particular instance difficult,” Dr. Krumm said.
3. Ritual
At the opening of each hour-long session, participants were invited to light a candle and say aloud or think to themselves the name of a patient they had lost, had a hard time with, or cared for during their time in the ICU.
“Every single person pointed to that moment as meaningful and impactful,” Dr. Krumm said.
This ritual gave the residents time to center and have a common focus with their peers to think about patient stories that they were carrying with them.
“Maybe just incorporating a small moment like that, a point of reflection, could potentially have a big impact on the weight we carry as providers who care for [patients who are] critically ill,” Dr. Krumm said. “What I’ve learned from this project will make me a better leader in the ICU, not only in taking care of critically ill individuals but also in taking care of the team doing that work.”
Dr. Krumm credits the CHEST grant funding and subsequent research project with helping her join a highly competitive fellowship program at the University of California San Francisco, where she can continue to conduct research in the field of medical education.
“I am working closely with medical education faculty and peers to design new research studies and further establish myself in the field of medical education, leading to my ultimate goal of becoming a program director at a strong med-ed-focused program.”
This article was adapted from the Spring 2024 online issue of CHEST Advocates. For the full article—and to engage with the other content from this issue—visit chestnet.org/chest-advocates.
Support CHEST grants like this
Through clinical research grants, CHEST assists in acquiring vital data and clinically important results that can advance medical care. You can help support projects like this by making a gift to CHEST.
MAKE A GIFT » | LEARN ABOUT CHEST PHILANTHROPY »
Researching the impact of reflection in medical training
Researching the impact of reflection in medical training
Before the spread of COVID-19, and increasingly during the pandemic, Ilana Krumm, MD, noticed a burgeoning focus on wellness for trainees and how to combat burnout in the medical space.
But Dr. Krumm also noticed that most of the existing programs focused on the individual level, rather than the system level. The onus was on the trainees to manage their wellness and burnout.
“I wanted to look at something that could be instituted at a systems level as opposed to putting all the burden of this wellness on the resident, as someone who already has a huge burden of work, stress, and time constraints as they try to learn their discipline,” Dr. Krumm said. “Asking them to meditate on their own time seemed very impractical.”
Eager to research this idea, Dr. Krumm applied for the CHEST Research Grant in Medical Education.
“The fact that CHEST is willing to support medical education research is really important for all those trying to better the educational environment. Although there’s a movement toward more support for medical education research and more recognition of its value, I think the fact that CHEST has already done so has helped advance the field and the support for the field as a whole,” Dr. Krumm said.
“Having the support from a reputable institution like CHEST inherently gave the work that I was doing value,” Dr. Krumm said. “It gave folks an understanding that this research in medical education has importance.”
Dr. Krumm’s project focused on the monthly Reflection Rounds between the ICU, palliative care, and chaplaincy staff that were held at the Seattle VA Medical Center, where residents could discuss the challenges of caring for critically ill patients during a protected time. While similar interventions around death and dying have been shown to help residents reduce burnout in medical intensive care rotations, it was unknown which aspects of these sessions would be most effective.
Participant interviews were conducted before and after the residents’ monthly sessions to understand the impact these sessions had on wellness and burnout levels.
“With the grant funding from CHEST, our team was able to purchase the recording equipment, transcription, and software necessary to complete a thorough qualitative research project, which greatly accelerated the project timeline,” she said.
Through these interviews, Dr. Krumm’s team identified three key themes that shed light on the impact of Reflection Rounds.
1. Cultural precedent
Participants were encouraged to participate as little or as much as they wanted during the session. Despite some residents being less vocal during these discussions, every resident agreed that this type of session set an important cultural precedent in their program and acknowledged the value of a program that encouraged space for decompression and reflection.
2. Shared experiences
During this project, many residents experienced an increased sense of isolation, as COVID-19 precautions were stricter in the ICU. Having this protected time together allowed residents to discover their shared experiences and find comfort in them while feeling supported.
“A lot of residents commented that it was nice to know that others were going through this as well or that they were also finding this particular instance difficult,” Dr. Krumm said.
3. Ritual
At the opening of each hour-long session, participants were invited to light a candle and say aloud or think to themselves the name of a patient they had lost, had a hard time with, or cared for during their time in the ICU.
“Every single person pointed to that moment as meaningful and impactful,” Dr. Krumm said.
This ritual gave the residents time to center and have a common focus with their peers to think about patient stories that they were carrying with them.
“Maybe just incorporating a small moment like that, a point of reflection, could potentially have a big impact on the weight we carry as providers who care for [patients who are] critically ill,” Dr. Krumm said. “What I’ve learned from this project will make me a better leader in the ICU, not only in taking care of critically ill individuals but also in taking care of the team doing that work.”
Dr. Krumm credits the CHEST grant funding and subsequent research project with helping her join a highly competitive fellowship program at the University of California San Francisco, where she can continue to conduct research in the field of medical education.
“I am working closely with medical education faculty and peers to design new research studies and further establish myself in the field of medical education, leading to my ultimate goal of becoming a program director at a strong med-ed-focused program.”
This article was adapted from the Spring 2024 online issue of CHEST Advocates. For the full article—and to engage with the other content from this issue—visit chestnet.org/chest-advocates.
Support CHEST grants like this
Through clinical research grants, CHEST assists in acquiring vital data and clinically important results that can advance medical care. You can help support projects like this by making a gift to CHEST.
MAKE A GIFT » | LEARN ABOUT CHEST PHILANTHROPY »
Before the spread of COVID-19, and increasingly during the pandemic, Ilana Krumm, MD, noticed a burgeoning focus on wellness for trainees and how to combat burnout in the medical space.
But Dr. Krumm also noticed that most of the existing programs focused on the individual level, rather than the system level. The onus was on the trainees to manage their wellness and burnout.
“I wanted to look at something that could be instituted at a systems level as opposed to putting all the burden of this wellness on the resident, as someone who already has a huge burden of work, stress, and time constraints as they try to learn their discipline,” Dr. Krumm said. “Asking them to meditate on their own time seemed very impractical.”
Eager to research this idea, Dr. Krumm applied for the CHEST Research Grant in Medical Education.
“The fact that CHEST is willing to support medical education research is really important for all those trying to better the educational environment. Although there’s a movement toward more support for medical education research and more recognition of its value, I think the fact that CHEST has already done so has helped advance the field and the support for the field as a whole,” Dr. Krumm said.
“Having the support from a reputable institution like CHEST inherently gave the work that I was doing value,” Dr. Krumm said. “It gave folks an understanding that this research in medical education has importance.”
Dr. Krumm’s project focused on the monthly Reflection Rounds between the ICU, palliative care, and chaplaincy staff that were held at the Seattle VA Medical Center, where residents could discuss the challenges of caring for critically ill patients during a protected time. While similar interventions around death and dying have been shown to help residents reduce burnout in medical intensive care rotations, it was unknown which aspects of these sessions would be most effective.
Participant interviews were conducted before and after the residents’ monthly sessions to understand the impact these sessions had on wellness and burnout levels.
“With the grant funding from CHEST, our team was able to purchase the recording equipment, transcription, and software necessary to complete a thorough qualitative research project, which greatly accelerated the project timeline,” she said.
Through these interviews, Dr. Krumm’s team identified three key themes that shed light on the impact of Reflection Rounds.
1. Cultural precedent
Participants were encouraged to participate as little or as much as they wanted during the session. Despite some residents being less vocal during these discussions, every resident agreed that this type of session set an important cultural precedent in their program and acknowledged the value of a program that encouraged space for decompression and reflection.
2. Shared experiences
During this project, many residents experienced an increased sense of isolation, as COVID-19 precautions were stricter in the ICU. Having this protected time together allowed residents to discover their shared experiences and find comfort in them while feeling supported.
“A lot of residents commented that it was nice to know that others were going through this as well or that they were also finding this particular instance difficult,” Dr. Krumm said.
3. Ritual
At the opening of each hour-long session, participants were invited to light a candle and say aloud or think to themselves the name of a patient they had lost, had a hard time with, or cared for during their time in the ICU.
“Every single person pointed to that moment as meaningful and impactful,” Dr. Krumm said.
This ritual gave the residents time to center and have a common focus with their peers to think about patient stories that they were carrying with them.
“Maybe just incorporating a small moment like that, a point of reflection, could potentially have a big impact on the weight we carry as providers who care for [patients who are] critically ill,” Dr. Krumm said. “What I’ve learned from this project will make me a better leader in the ICU, not only in taking care of critically ill individuals but also in taking care of the team doing that work.”
Dr. Krumm credits the CHEST grant funding and subsequent research project with helping her join a highly competitive fellowship program at the University of California San Francisco, where she can continue to conduct research in the field of medical education.
“I am working closely with medical education faculty and peers to design new research studies and further establish myself in the field of medical education, leading to my ultimate goal of becoming a program director at a strong med-ed-focused program.”
This article was adapted from the Spring 2024 online issue of CHEST Advocates. For the full article—and to engage with the other content from this issue—visit chestnet.org/chest-advocates.
Support CHEST grants like this
Through clinical research grants, CHEST assists in acquiring vital data and clinically important results that can advance medical care. You can help support projects like this by making a gift to CHEST.
MAKE A GIFT » | LEARN ABOUT CHEST PHILANTHROPY »
Coding & billing: A look into G2211 for visit complexities
This add-on code is for new (99202-99205) and established (99212-99215) office visits. CMS created this add-on code to address the additional costs and resources associated with providing longitudinal care.
G2211 – Visit complexity inherent to evaluation and management (E/M) associated with medical care services that serve as the continuing focal point for all needed health care services and/or with medical care services that are part of ongoing care related to a patient’s single, serious condition, or a complex condition (Add-on code; list separately in addition to office/outpatient (O/O) E/M visit, new or established)
The documentation should demonstrate the intent and need for ongoing care. Otherwise, no additional documentation is required. CMS pays $16.04 for each service (wRVU = 0.33). It may be reported each time the patient is seen, and there is currently no limit to how often it may be used. Also, there is no additional copay requirement for patients.
Do’s and don’ts
Do report in the following situations when longitudinal care is provided:
- The provider has or intends to have a long-term, ongoing relationship with the patient (ie, G2211 can be used for a new patient visit)
- Audio/video virtual visits
- May be reported with Prolonged Care Services G2212
- When advanced practice providers or physician colleagues in the same specialty practice see the patient (ie, if you see the patient for an urgent visit, but the patient is usually followed by your partner, you can still use G2211)
- When working with graduate medical education trainees (along with the -GC modifier), and as long as the conditions described in the description of G2211 are met
Do NOT report in the following situations:
- If modifier -25 is appended to the E/M service when another service is provided on the same day (eg, pulmonary function tests, 6-minute walk tests, immunization)
- Audio-only virtual visits, hospital, skilled nursing facility, or long-term acute care hospital
- If the patient is not expected to return for ongoing care
- If the reason for longitudinal care does not include a “single, serious condition or a complex condition” (eg, annual visits for a stable 6 mm lung nodule)
CMS expects that this will be billed with 38% of all E/M services initially and potentially up to 54% over time. We feel this is reimbursement for the work being done to care for our patients with single, serious, or complex conditions. Both Medicare and Medicare Advantage plans are expected to reimburse for this service. Whether other payers will do the same is unclear, but it will become clear with time and further negotiation at the local level. In the meantime, members are encouraged to report this code for all appropriate patient encounters.
Questions and answers — G2211
Question: What private insurances cover G2211?
Answer: As of March 1, 2024, four national payers have confirmed coverage of G2211:
- Cigna (Medicare Advantage only),
- Humana (commercial and Medicare Advantage),
- United Healthcare (commercial and Medicare Advantage), and
- Aetna (Medicare Advantage).
Question: What needs to be documented for G2211?
Answer: CMS states, “You must document the reason for billing the office and outpatient (O/O) and evaluation and management (E/M). The visits themselves would need to be medically reasonable and necessary for the practitioner to report G2211. In addition, the documentation would need to illustrate medical necessity of the O/O E/M visit. We [CMS] haven’t required additional documentation.”
American Thoracic Society (ATS) and CHEST also recommend including a detailed assessment and plan for the visit, as well as any follow-up. The complexity of the visit should be clear in your documentation to support the medical necessity for reporting the G2211.
Question: How can a provider show that a new patient visit (99202-99205) is part of continuing care?
Answer: The treating practitioner should make sure their documentation supports their intent to provide ongoing care to the patient. Establishing such intent goes beyond a statement that the provider plans to provide ongoing care or schedule a follow-up visit. The circumstances of the visit should support the extra work involved in becoming the focal point of the patient’s care or providing ongoing care for a serious or complex condition.
Question: Dr. Red works at a primary care practice, is the focal point for a patient’s care, and has reported G2211. If Dr. Yellow, who is in the same specialty, or Mr. Green, a nurse practitioner, is covering for Dr. Red, and the patient comes in for a visit, can they report G2211 for that visit?
Answer: Yes. The same specialty/same provider rules would apply in this situation. But remember that Dr. Yellow’s or Mr. Green’s documentation for that encounter must support the code.
Question: Can a resident report G2211 under the primary care exemption?
Answer: Yes, according to CMS staff, so long as the service and the documentation meet all the requirements for the exemption and the visit complexity code. For example, the resident can only report low-level E/M codes, and the resident must be “the focal point for that person’s care.”
Question: Are there frequency limits for how often we can report G2211, either for a single patient in a given time period or by a provider or a practice?
Answer: Not at this time, but make sure your providers are following the rules for reporting the code. “There’s got to be documentation that suggests why the practitioner believes they are treating the patient on this long-standing, longitudinal trajectory, and we’ll be able to see how that interaction is happening,” senior CMS staff said. CMS staff further issued a subtle warning to providers by reminding them that CMS has a very strong integrity program. Your practice can avoid problems with thorough training, frequent chart review, and encouraging the team to ask questions until you feel that everyone is comfortable with the code.
Question: Are there any limits on the specialties that can report the code? Is it just for primary care providers?
Answer: No. Remember that a provider who is managing a single serious or complex condition can also report the code. But CMS expects the documentation to support the ongoing nature of the treatment. If a patient sees a provider as a one-off encounter, perhaps to manage an acute problem, that visit wouldn’t qualify. But if the provider clearly documents that they are actively managing the patient’s condition, the encounters could qualify.
Question: Will CMS issue a list of conditions that meet the code’s serious or complex condition requirement?
Answer: CMS has included the examples of HIV and sickle cell anemia in existing guidance, and it plans to issue a few more examples “that help folks understand what is expected.” However, it won’t be a complete list of every condition that might qualify.
Originally published in the May 2023 issue of the American Thoracic Society’s ATS Coding & Billing Quarterly. Republished with permission from the American Thoracic Society.
This add-on code is for new (99202-99205) and established (99212-99215) office visits. CMS created this add-on code to address the additional costs and resources associated with providing longitudinal care.
G2211 – Visit complexity inherent to evaluation and management (E/M) associated with medical care services that serve as the continuing focal point for all needed health care services and/or with medical care services that are part of ongoing care related to a patient’s single, serious condition, or a complex condition (Add-on code; list separately in addition to office/outpatient (O/O) E/M visit, new or established)
The documentation should demonstrate the intent and need for ongoing care. Otherwise, no additional documentation is required. CMS pays $16.04 for each service (wRVU = 0.33). It may be reported each time the patient is seen, and there is currently no limit to how often it may be used. Also, there is no additional copay requirement for patients.
Do’s and don’ts
Do report in the following situations when longitudinal care is provided:
- The provider has or intends to have a long-term, ongoing relationship with the patient (ie, G2211 can be used for a new patient visit)
- Audio/video virtual visits
- May be reported with Prolonged Care Services G2212
- When advanced practice providers or physician colleagues in the same specialty practice see the patient (ie, if you see the patient for an urgent visit, but the patient is usually followed by your partner, you can still use G2211)
- When working with graduate medical education trainees (along with the -GC modifier), and as long as the conditions described in the description of G2211 are met
Do NOT report in the following situations:
- If modifier -25 is appended to the E/M service when another service is provided on the same day (eg, pulmonary function tests, 6-minute walk tests, immunization)
- Audio-only virtual visits, hospital, skilled nursing facility, or long-term acute care hospital
- If the patient is not expected to return for ongoing care
- If the reason for longitudinal care does not include a “single, serious condition or a complex condition” (eg, annual visits for a stable 6 mm lung nodule)
CMS expects that this will be billed with 38% of all E/M services initially and potentially up to 54% over time. We feel this is reimbursement for the work being done to care for our patients with single, serious, or complex conditions. Both Medicare and Medicare Advantage plans are expected to reimburse for this service. Whether other payers will do the same is unclear, but it will become clear with time and further negotiation at the local level. In the meantime, members are encouraged to report this code for all appropriate patient encounters.
Questions and answers — G2211
Question: What private insurances cover G2211?
Answer: As of March 1, 2024, four national payers have confirmed coverage of G2211:
- Cigna (Medicare Advantage only),
- Humana (commercial and Medicare Advantage),
- United Healthcare (commercial and Medicare Advantage), and
- Aetna (Medicare Advantage).
Question: What needs to be documented for G2211?
Answer: CMS states, “You must document the reason for billing the office and outpatient (O/O) and evaluation and management (E/M). The visits themselves would need to be medically reasonable and necessary for the practitioner to report G2211. In addition, the documentation would need to illustrate medical necessity of the O/O E/M visit. We [CMS] haven’t required additional documentation.”
American Thoracic Society (ATS) and CHEST also recommend including a detailed assessment and plan for the visit, as well as any follow-up. The complexity of the visit should be clear in your documentation to support the medical necessity for reporting the G2211.
Question: How can a provider show that a new patient visit (99202-99205) is part of continuing care?
Answer: The treating practitioner should make sure their documentation supports their intent to provide ongoing care to the patient. Establishing such intent goes beyond a statement that the provider plans to provide ongoing care or schedule a follow-up visit. The circumstances of the visit should support the extra work involved in becoming the focal point of the patient’s care or providing ongoing care for a serious or complex condition.
Question: Dr. Red works at a primary care practice, is the focal point for a patient’s care, and has reported G2211. If Dr. Yellow, who is in the same specialty, or Mr. Green, a nurse practitioner, is covering for Dr. Red, and the patient comes in for a visit, can they report G2211 for that visit?
Answer: Yes. The same specialty/same provider rules would apply in this situation. But remember that Dr. Yellow’s or Mr. Green’s documentation for that encounter must support the code.
Question: Can a resident report G2211 under the primary care exemption?
Answer: Yes, according to CMS staff, so long as the service and the documentation meet all the requirements for the exemption and the visit complexity code. For example, the resident can only report low-level E/M codes, and the resident must be “the focal point for that person’s care.”
Question: Are there frequency limits for how often we can report G2211, either for a single patient in a given time period or by a provider or a practice?
Answer: Not at this time, but make sure your providers are following the rules for reporting the code. “There’s got to be documentation that suggests why the practitioner believes they are treating the patient on this long-standing, longitudinal trajectory, and we’ll be able to see how that interaction is happening,” senior CMS staff said. CMS staff further issued a subtle warning to providers by reminding them that CMS has a very strong integrity program. Your practice can avoid problems with thorough training, frequent chart review, and encouraging the team to ask questions until you feel that everyone is comfortable with the code.
Question: Are there any limits on the specialties that can report the code? Is it just for primary care providers?
Answer: No. Remember that a provider who is managing a single serious or complex condition can also report the code. But CMS expects the documentation to support the ongoing nature of the treatment. If a patient sees a provider as a one-off encounter, perhaps to manage an acute problem, that visit wouldn’t qualify. But if the provider clearly documents that they are actively managing the patient’s condition, the encounters could qualify.
Question: Will CMS issue a list of conditions that meet the code’s serious or complex condition requirement?
Answer: CMS has included the examples of HIV and sickle cell anemia in existing guidance, and it plans to issue a few more examples “that help folks understand what is expected.” However, it won’t be a complete list of every condition that might qualify.
Originally published in the May 2023 issue of the American Thoracic Society’s ATS Coding & Billing Quarterly. Republished with permission from the American Thoracic Society.
This add-on code is for new (99202-99205) and established (99212-99215) office visits. CMS created this add-on code to address the additional costs and resources associated with providing longitudinal care.
G2211 – Visit complexity inherent to evaluation and management (E/M) associated with medical care services that serve as the continuing focal point for all needed health care services and/or with medical care services that are part of ongoing care related to a patient’s single, serious condition, or a complex condition (Add-on code; list separately in addition to office/outpatient (O/O) E/M visit, new or established)
The documentation should demonstrate the intent and need for ongoing care. Otherwise, no additional documentation is required. CMS pays $16.04 for each service (wRVU = 0.33). It may be reported each time the patient is seen, and there is currently no limit to how often it may be used. Also, there is no additional copay requirement for patients.
Do’s and don’ts
Do report in the following situations when longitudinal care is provided:
- The provider has or intends to have a long-term, ongoing relationship with the patient (ie, G2211 can be used for a new patient visit)
- Audio/video virtual visits
- May be reported with Prolonged Care Services G2212
- When advanced practice providers or physician colleagues in the same specialty practice see the patient (ie, if you see the patient for an urgent visit, but the patient is usually followed by your partner, you can still use G2211)
- When working with graduate medical education trainees (along with the -GC modifier), and as long as the conditions described in the description of G2211 are met
Do NOT report in the following situations:
- If modifier -25 is appended to the E/M service when another service is provided on the same day (eg, pulmonary function tests, 6-minute walk tests, immunization)
- Audio-only virtual visits, hospital, skilled nursing facility, or long-term acute care hospital
- If the patient is not expected to return for ongoing care
- If the reason for longitudinal care does not include a “single, serious condition or a complex condition” (eg, annual visits for a stable 6 mm lung nodule)
CMS expects that this will be billed with 38% of all E/M services initially and potentially up to 54% over time. We feel this is reimbursement for the work being done to care for our patients with single, serious, or complex conditions. Both Medicare and Medicare Advantage plans are expected to reimburse for this service. Whether other payers will do the same is unclear, but it will become clear with time and further negotiation at the local level. In the meantime, members are encouraged to report this code for all appropriate patient encounters.
Questions and answers — G2211
Question: What private insurances cover G2211?
Answer: As of March 1, 2024, four national payers have confirmed coverage of G2211:
- Cigna (Medicare Advantage only),
- Humana (commercial and Medicare Advantage),
- United Healthcare (commercial and Medicare Advantage), and
- Aetna (Medicare Advantage).
Question: What needs to be documented for G2211?
Answer: CMS states, “You must document the reason for billing the office and outpatient (O/O) and evaluation and management (E/M). The visits themselves would need to be medically reasonable and necessary for the practitioner to report G2211. In addition, the documentation would need to illustrate medical necessity of the O/O E/M visit. We [CMS] haven’t required additional documentation.”
American Thoracic Society (ATS) and CHEST also recommend including a detailed assessment and plan for the visit, as well as any follow-up. The complexity of the visit should be clear in your documentation to support the medical necessity for reporting the G2211.
Question: How can a provider show that a new patient visit (99202-99205) is part of continuing care?
Answer: The treating practitioner should make sure their documentation supports their intent to provide ongoing care to the patient. Establishing such intent goes beyond a statement that the provider plans to provide ongoing care or schedule a follow-up visit. The circumstances of the visit should support the extra work involved in becoming the focal point of the patient’s care or providing ongoing care for a serious or complex condition.
Question: Dr. Red works at a primary care practice, is the focal point for a patient’s care, and has reported G2211. If Dr. Yellow, who is in the same specialty, or Mr. Green, a nurse practitioner, is covering for Dr. Red, and the patient comes in for a visit, can they report G2211 for that visit?
Answer: Yes. The same specialty/same provider rules would apply in this situation. But remember that Dr. Yellow’s or Mr. Green’s documentation for that encounter must support the code.
Question: Can a resident report G2211 under the primary care exemption?
Answer: Yes, according to CMS staff, so long as the service and the documentation meet all the requirements for the exemption and the visit complexity code. For example, the resident can only report low-level E/M codes, and the resident must be “the focal point for that person’s care.”
Question: Are there frequency limits for how often we can report G2211, either for a single patient in a given time period or by a provider or a practice?
Answer: Not at this time, but make sure your providers are following the rules for reporting the code. “There’s got to be documentation that suggests why the practitioner believes they are treating the patient on this long-standing, longitudinal trajectory, and we’ll be able to see how that interaction is happening,” senior CMS staff said. CMS staff further issued a subtle warning to providers by reminding them that CMS has a very strong integrity program. Your practice can avoid problems with thorough training, frequent chart review, and encouraging the team to ask questions until you feel that everyone is comfortable with the code.
Question: Are there any limits on the specialties that can report the code? Is it just for primary care providers?
Answer: No. Remember that a provider who is managing a single serious or complex condition can also report the code. But CMS expects the documentation to support the ongoing nature of the treatment. If a patient sees a provider as a one-off encounter, perhaps to manage an acute problem, that visit wouldn’t qualify. But if the provider clearly documents that they are actively managing the patient’s condition, the encounters could qualify.
Question: Will CMS issue a list of conditions that meet the code’s serious or complex condition requirement?
Answer: CMS has included the examples of HIV and sickle cell anemia in existing guidance, and it plans to issue a few more examples “that help folks understand what is expected.” However, it won’t be a complete list of every condition that might qualify.
Originally published in the May 2023 issue of the American Thoracic Society’s ATS Coding & Billing Quarterly. Republished with permission from the American Thoracic Society.
Top reads from the CHEST journal portfolio
Understanding RA with COPD, lung cancer prediction models, and chronic cardiac dysfunction
Journal CHEST®
Does Rheumatoid Arthritis Increase the Risk of COPD?
By: Chiwook Chung, MD, and colleagues
Notably, individuals with seropositive RA exhibit a greater risk of COPD onset than those with seronegative RA. Although smoking history didn’t affect the relationship between RA and COPD, monitoring respiratory symptoms and pulmonary function in patients with RA, especially patients who are seropositive, is crucial. These findings underscore the importance of interdisciplinary collaboration between rheumatologists and pulmonologists to enhance early detection and management strategies for pulmonary complications in patients with RA.

– Commentary by Corinne Young, MSN, FNP-C, FCCP, Member of the CHEST Physician® Editorial Board
CHEST Pulmonary®
The Lung Cancer Prediction Model “Stress Test”
By: Brent E. Heideman, MD, and colleagues
Current lung cancer prediction models have limited utility in high-risk patients referred for diagnostic biopsy. In a study of 322 indeterminate pulmonary nodules, the Brock, Mayo Clinic, Herder, and Veterans Affairs models showed modest discrimination between benign and malignant nodules (AUCs 0.67-0.77). The models performed poorly for low-risk patients (negative predictive values 63%-71%) and suboptimally for high-risk patients (positive predictive values 73%-87%), suggesting referring physicians use additional clinical information not captured in these models to identify high-risk patients needing biopsy. New prediction models and biomarkers specifically developed and calibrated for high-risk populations are needed to better inform clinical decision-making. Incorporating interval imaging to assess changes in nodule characteristics could potentially improve model performance. Tailored risk assessment tools are crucial for optimizing management and reducing unnecessary invasive procedures in this challenging patient population.

– Commentary by Russell Miller, MD, Member of the CHEST Physician Editorial Board
CHEST Critical Care ®
Characterizing Cardiac Function in ICU Survivors of Sepsis
By: Kevin Garrity, MBChB, and colleagues
While chronic cardiac dysfunction is one of the proposed mechanisms of long-term impairment post critical illness, its prevalence, mechanisms, and associations with disability following admission for sepsis are not well understood. Garrity and colleagues describe the Characterization of Cardiovascular Function in ICU Survivors of Sepsis (CONDUCT-ICU) protocol, a prospective study including two ICUs in Scotland aimed to better define cardiovascular dysfunction in survivors of sepsis. Designed to enroll 69 patients, demographics, cardiac and inflammatory biomarkers, and echocardiograms will be obtained on ICU discharge with additional laboratory data, cardiac magnetic resonance imaging, and patient-reported outcome measures to be obtained at 6 to 10 weeks. This novel multimodal approach will provide understanding into the role of cardiovascular dysfunction following critical illness as well as offer mechanistic insights. The investigators hope to obtain operational and pilot data for larger future studies.

– Commentary by Eugene Yuriditsky, MD, FCCP, Member of the CHEST Physician Editorial Board
Understanding RA with COPD, lung cancer prediction models, and chronic cardiac dysfunction
Understanding RA with COPD, lung cancer prediction models, and chronic cardiac dysfunction
Journal CHEST®
Does Rheumatoid Arthritis Increase the Risk of COPD?
By: Chiwook Chung, MD, and colleagues
Notably, individuals with seropositive RA exhibit a greater risk of COPD onset than those with seronegative RA. Although smoking history didn’t affect the relationship between RA and COPD, monitoring respiratory symptoms and pulmonary function in patients with RA, especially patients who are seropositive, is crucial. These findings underscore the importance of interdisciplinary collaboration between rheumatologists and pulmonologists to enhance early detection and management strategies for pulmonary complications in patients with RA.
– Commentary by Corinne Young, MSN, FNP-C, FCCP, Member of the CHEST Physician® Editorial Board
CHEST Pulmonary®
The Lung Cancer Prediction Model “Stress Test”
By: Brent E. Heideman, MD, and colleagues
Current lung cancer prediction models have limited utility in high-risk patients referred for diagnostic biopsy. In a study of 322 indeterminate pulmonary nodules, the Brock, Mayo Clinic, Herder, and Veterans Affairs models showed modest discrimination between benign and malignant nodules (AUCs 0.67-0.77). The models performed poorly for low-risk patients (negative predictive values 63%-71%) and suboptimally for high-risk patients (positive predictive values 73%-87%), suggesting referring physicians use additional clinical information not captured in these models to identify high-risk patients needing biopsy. New prediction models and biomarkers specifically developed and calibrated for high-risk populations are needed to better inform clinical decision-making. Incorporating interval imaging to assess changes in nodule characteristics could potentially improve model performance. Tailored risk assessment tools are crucial for optimizing management and reducing unnecessary invasive procedures in this challenging patient population.
– Commentary by Russell Miller, MD, Member of the CHEST Physician Editorial Board
CHEST Critical Care ®
Characterizing Cardiac Function in ICU Survivors of Sepsis
By: Kevin Garrity, MBChB, and colleagues
While chronic cardiac dysfunction is one of the proposed mechanisms of long-term impairment post critical illness, its prevalence, mechanisms, and associations with disability following admission for sepsis are not well understood. Garrity and colleagues describe the Characterization of Cardiovascular Function in ICU Survivors of Sepsis (CONDUCT-ICU) protocol, a prospective study including two ICUs in Scotland aimed to better define cardiovascular dysfunction in survivors of sepsis. Designed to enroll 69 patients, demographics, cardiac and inflammatory biomarkers, and echocardiograms will be obtained on ICU discharge with additional laboratory data, cardiac magnetic resonance imaging, and patient-reported outcome measures to be obtained at 6 to 10 weeks. This novel multimodal approach will provide understanding into the role of cardiovascular dysfunction following critical illness as well as offer mechanistic insights. The investigators hope to obtain operational and pilot data for larger future studies.
– Commentary by Eugene Yuriditsky, MD, FCCP, Member of the CHEST Physician Editorial Board
Journal CHEST®
Does Rheumatoid Arthritis Increase the Risk of COPD?
By: Chiwook Chung, MD, and colleagues
Notably, individuals with seropositive RA exhibit a greater risk of COPD onset than those with seronegative RA. Although smoking history didn’t affect the relationship between RA and COPD, monitoring respiratory symptoms and pulmonary function in patients with RA, especially patients who are seropositive, is crucial. These findings underscore the importance of interdisciplinary collaboration between rheumatologists and pulmonologists to enhance early detection and management strategies for pulmonary complications in patients with RA.
– Commentary by Corinne Young, MSN, FNP-C, FCCP, Member of the CHEST Physician® Editorial Board
CHEST Pulmonary®
The Lung Cancer Prediction Model “Stress Test”
By: Brent E. Heideman, MD, and colleagues
Current lung cancer prediction models have limited utility in high-risk patients referred for diagnostic biopsy. In a study of 322 indeterminate pulmonary nodules, the Brock, Mayo Clinic, Herder, and Veterans Affairs models showed modest discrimination between benign and malignant nodules (AUCs 0.67-0.77). The models performed poorly for low-risk patients (negative predictive values 63%-71%) and suboptimally for high-risk patients (positive predictive values 73%-87%), suggesting referring physicians use additional clinical information not captured in these models to identify high-risk patients needing biopsy. New prediction models and biomarkers specifically developed and calibrated for high-risk populations are needed to better inform clinical decision-making. Incorporating interval imaging to assess changes in nodule characteristics could potentially improve model performance. Tailored risk assessment tools are crucial for optimizing management and reducing unnecessary invasive procedures in this challenging patient population.
– Commentary by Russell Miller, MD, Member of the CHEST Physician Editorial Board
CHEST Critical Care ®
Characterizing Cardiac Function in ICU Survivors of Sepsis
By: Kevin Garrity, MBChB, and colleagues
While chronic cardiac dysfunction is one of the proposed mechanisms of long-term impairment post critical illness, its prevalence, mechanisms, and associations with disability following admission for sepsis are not well understood. Garrity and colleagues describe the Characterization of Cardiovascular Function in ICU Survivors of Sepsis (CONDUCT-ICU) protocol, a prospective study including two ICUs in Scotland aimed to better define cardiovascular dysfunction in survivors of sepsis. Designed to enroll 69 patients, demographics, cardiac and inflammatory biomarkers, and echocardiograms will be obtained on ICU discharge with additional laboratory data, cardiac magnetic resonance imaging, and patient-reported outcome measures to be obtained at 6 to 10 weeks. This novel multimodal approach will provide understanding into the role of cardiovascular dysfunction following critical illness as well as offer mechanistic insights. The investigators hope to obtain operational and pilot data for larger future studies.
– Commentary by Eugene Yuriditsky, MD, FCCP, Member of the CHEST Physician Editorial Board
Use of albumin in critically ill patients
Intravenous albumin is a human-derived blood product studied widely in a variety of patient populations. Despite its frequent use in critical care, few high-quality studies have demonstrated improvements in patient-important outcomes. Compared with crystalloids, albumin increases the risk of fluid overload and bleeding and infections in patients undergoing cardiac surgery.1,2 In addition, albumin is costly, and its production is fraught with donor supply chain ethical concerns (the majority of albumin is derived from paid plasma donors).

Albumin use is highly variable between countries, hospitals, and even clinicians within the same specialty due to several factors, including the perception of minimal risk with albumin, concerns regarding insufficient short-term hemodynamic response to crystalloid, and lack of high-quality evidence to inform clinical practice. We will discuss when intensivists should consider albumin use (with prescription personalized to patient context) and when it should be avoided due to the concerns for patient harm.
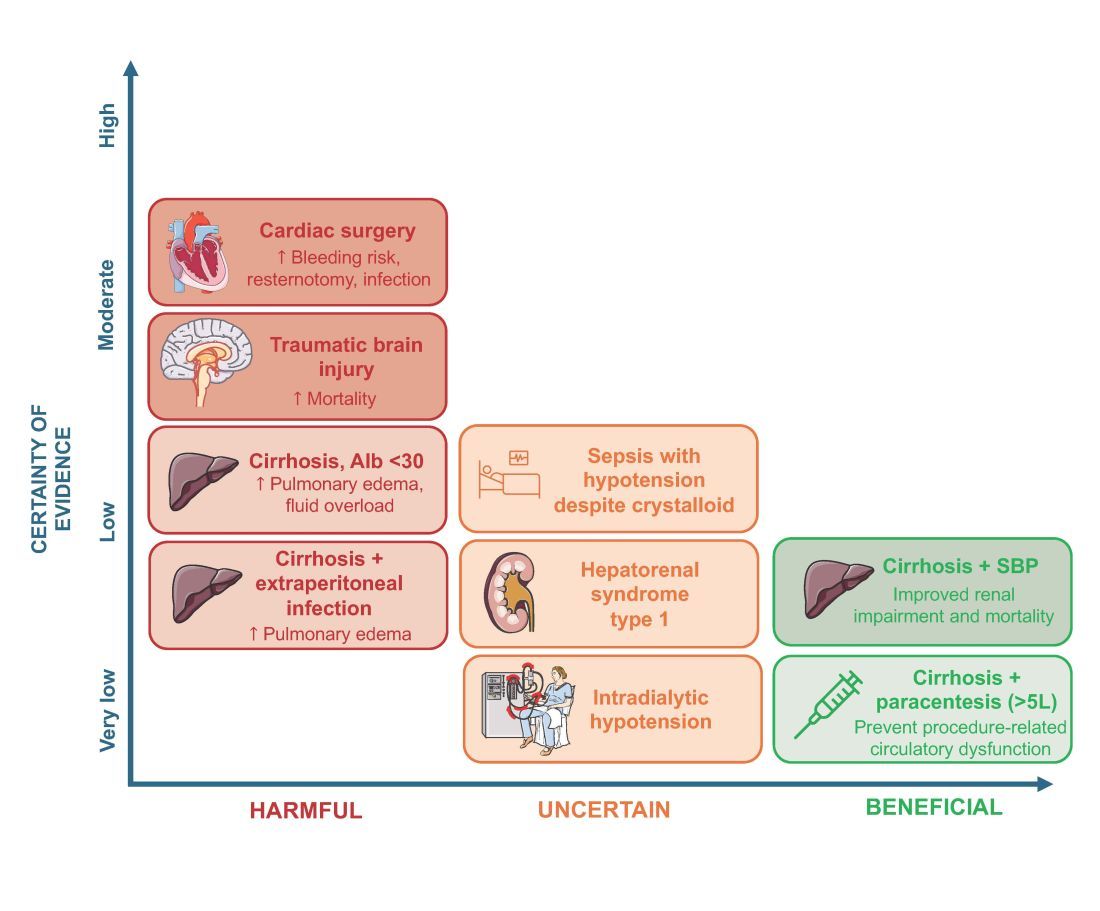
An intensivist might consider albumin as a reasonable treatment option in patients with cirrhosis undergoing large volume paracentesis to prevent paracentesis-induced circulatory dysfunction, and in patients with cirrhosis and spontaneous bacterial peritonitis (SBP), as data suggests use in this setting leads to a reduction in mortality.3 Clinicians should be aware that even for these widely accepted albumin indications, which are supported by published guidelines, the certainty of evidence is low, recommendations are weak (conditional), and, therefore, albumin should always be personalized to the patient based on volume of paracentesis fluid removed, prior history of hypotension after procedures, and degree of renal dysfunction.4

There are also several conditions for which an intensivist might consider albumin and for which albumin is commonly administered but lacks high-quality studies to support its use either as a frontline or rescue fluid therapy. One such condition is type 1 hepatorenal syndrome (HRS), for which albumin is widely used; however, there are no randomized controlled trials that have compared albumin with placebo.
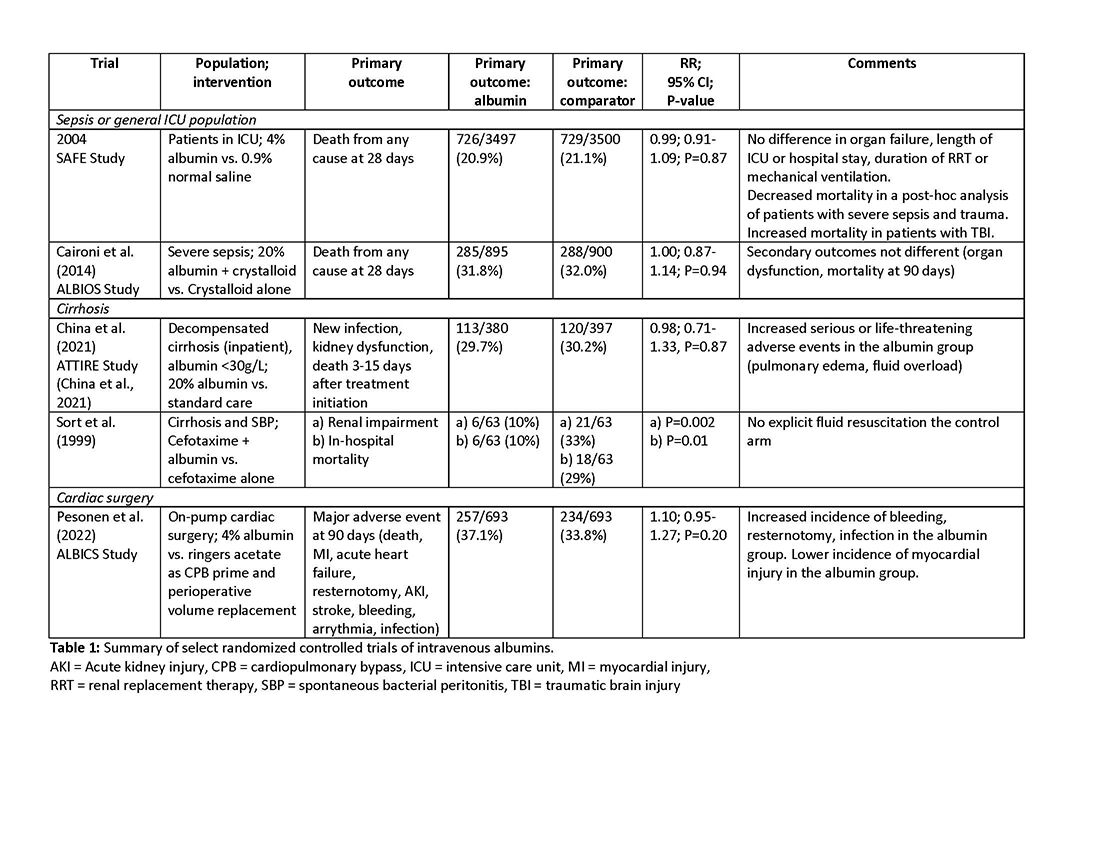
As with any intervention, the use of albumin is associated with risks. In patients undergoing on-pump cardiac surgery, the ALBICS study showed that albumin did not reduce the risk of major adverse events and, instead, increased risk of bleeding, resternotomy, and infection.2 The ATTIRE trial showed that in patients hospitalized with decompensated cirrhosis and serum albumin <30 g/L, albumin failed to reduce infection, renal impairment, or mortality while increasing life-threatening adverse events, including pulmonary edema and fluid overload.1 Similarly, in patients with cirrhosis and extraperitoneal infections, albumin showed no benefit in reducing renal impairment or mortality, and its use was associated with higher rates of pulmonary edema.6 Lastly, critically ill patients with traumatic brain injury (TBI) who received fluid resuscitation with albumin have been shown to experience higher mortality compared with saline.7 Thus, based on current evidence, intravenous albumin is not recommended for patients undergoing cardiac surgery (priming of the bypass circuit or volume replacement), patients hospitalized with decompensated cirrhosis and hypoalbuminemia, patients hospitalized with cirrhosis and extraperitoneal infections, and critically ill patients with TBI.4

Overall, intravenous albumin prescription in critical care patients requires a personalized approach informed by current best evidence and is not without potential harm.
High-quality evidence is currently lacking in many clinical settings, and large randomized controlled trials are underway to provide further insights into the utility of albumin. These trials will address albumin use in the following: acute kidney injury requiring renal replacement therapy (ALTER-AKI, NCT04705896), inpatients with community-acquired pneumonia (NCT04071041), high-risk cardiac surgery (ACTRN1261900135516703), and septic shock (NCT03869385).

Financial/nonfinancial disclosures
Nicole Relke: None. Mark Hewitt: None. Bram Rochwerg: None. Jeannie Callum: Research support from Canadian Blood Services and Octapharma.
References
1. China L, Freemantle N, Forrest E, et al. A randomized trial of albumin infusions in hospitalized patients with cirrhosis. N Engl J Med. 2021;384(9):808-817. doi:10.1056/NEJMoa2022166
2. Pesonen E, Vlasov H, Suojaranta R, et al. Effect of 4% albumin solution vs ringer acetate on major adverse events in patients undergoing cardiac surgery with cardiopulmonary bypass: a randomized clinical trial. JAMA. 2022;328(3):251-258. doi:10.1001/jama.2022.10461
3. Sort P, Navasa M, Arroyo V, et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. NEJM. 1999;341:403-409.
4. Callum J, Skubas NJ, Bathla A, et al. Use of intravenous albumin: a guideline from the international collaboration for transfusion medicine guidelines. Chest. 2024:S0012-3692(24)00285-X. doi:10.1016/j.chest.2024.02.049
5. Torp N. High doses of albumin increases mortality and complications in terlipressin treated patients with cirrhosis: insights from the ATTIRE trial. Paper presented at the AASLD; 2023; San Diego, CA. https://www.aasld.org/the-liver-meeting/high-doses-albumin-increases-mortality-and-complications-terlipressin-treated
6. Wong YJ, Qiu TY, Tam YC, Mohan BP, Gallegos-Orozco JF, Adler DG. Efficacy and safety of IV albumin for non-spontaneous bacterial peritonitis infection among patients with cirrhosis: a systematic review and meta-analysis. Dig Liver Dis. 2020;52(10):1137-1142. doi:10.1016/j.dld.2020.05.047
7. Myburgh J, Cooper JD, Finfer S, et al. Saline or albumin for fluid resuscitation in patients with traumatic brain injury. N Engl J Med. 2007;357(9):874-884.
Intravenous albumin is a human-derived blood product studied widely in a variety of patient populations. Despite its frequent use in critical care, few high-quality studies have demonstrated improvements in patient-important outcomes. Compared with crystalloids, albumin increases the risk of fluid overload and bleeding and infections in patients undergoing cardiac surgery.1,2 In addition, albumin is costly, and its production is fraught with donor supply chain ethical concerns (the majority of albumin is derived from paid plasma donors).
Albumin use is highly variable between countries, hospitals, and even clinicians within the same specialty due to several factors, including the perception of minimal risk with albumin, concerns regarding insufficient short-term hemodynamic response to crystalloid, and lack of high-quality evidence to inform clinical practice. We will discuss when intensivists should consider albumin use (with prescription personalized to patient context) and when it should be avoided due to the concerns for patient harm.
An intensivist might consider albumin as a reasonable treatment option in patients with cirrhosis undergoing large volume paracentesis to prevent paracentesis-induced circulatory dysfunction, and in patients with cirrhosis and spontaneous bacterial peritonitis (SBP), as data suggests use in this setting leads to a reduction in mortality.3 Clinicians should be aware that even for these widely accepted albumin indications, which are supported by published guidelines, the certainty of evidence is low, recommendations are weak (conditional), and, therefore, albumin should always be personalized to the patient based on volume of paracentesis fluid removed, prior history of hypotension after procedures, and degree of renal dysfunction.4
There are also several conditions for which an intensivist might consider albumin and for which albumin is commonly administered but lacks high-quality studies to support its use either as a frontline or rescue fluid therapy. One such condition is type 1 hepatorenal syndrome (HRS), for which albumin is widely used; however, there are no randomized controlled trials that have compared albumin with placebo.
As with any intervention, the use of albumin is associated with risks. In patients undergoing on-pump cardiac surgery, the ALBICS study showed that albumin did not reduce the risk of major adverse events and, instead, increased risk of bleeding, resternotomy, and infection.2 The ATTIRE trial showed that in patients hospitalized with decompensated cirrhosis and serum albumin <30 g/L, albumin failed to reduce infection, renal impairment, or mortality while increasing life-threatening adverse events, including pulmonary edema and fluid overload.1 Similarly, in patients with cirrhosis and extraperitoneal infections, albumin showed no benefit in reducing renal impairment or mortality, and its use was associated with higher rates of pulmonary edema.6 Lastly, critically ill patients with traumatic brain injury (TBI) who received fluid resuscitation with albumin have been shown to experience higher mortality compared with saline.7 Thus, based on current evidence, intravenous albumin is not recommended for patients undergoing cardiac surgery (priming of the bypass circuit or volume replacement), patients hospitalized with decompensated cirrhosis and hypoalbuminemia, patients hospitalized with cirrhosis and extraperitoneal infections, and critically ill patients with TBI.4
Overall, intravenous albumin prescription in critical care patients requires a personalized approach informed by current best evidence and is not without potential harm.
High-quality evidence is currently lacking in many clinical settings, and large randomized controlled trials are underway to provide further insights into the utility of albumin. These trials will address albumin use in the following: acute kidney injury requiring renal replacement therapy (ALTER-AKI, NCT04705896), inpatients with community-acquired pneumonia (NCT04071041), high-risk cardiac surgery (ACTRN1261900135516703), and septic shock (NCT03869385).
Financial/nonfinancial disclosures
Nicole Relke: None. Mark Hewitt: None. Bram Rochwerg: None. Jeannie Callum: Research support from Canadian Blood Services and Octapharma.
References
1. China L, Freemantle N, Forrest E, et al. A randomized trial of albumin infusions in hospitalized patients with cirrhosis. N Engl J Med. 2021;384(9):808-817. doi:10.1056/NEJMoa2022166
2. Pesonen E, Vlasov H, Suojaranta R, et al. Effect of 4% albumin solution vs ringer acetate on major adverse events in patients undergoing cardiac surgery with cardiopulmonary bypass: a randomized clinical trial. JAMA. 2022;328(3):251-258. doi:10.1001/jama.2022.10461
3. Sort P, Navasa M, Arroyo V, et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. NEJM. 1999;341:403-409.
4. Callum J, Skubas NJ, Bathla A, et al. Use of intravenous albumin: a guideline from the international collaboration for transfusion medicine guidelines. Chest. 2024:S0012-3692(24)00285-X. doi:10.1016/j.chest.2024.02.049
5. Torp N. High doses of albumin increases mortality and complications in terlipressin treated patients with cirrhosis: insights from the ATTIRE trial. Paper presented at the AASLD; 2023; San Diego, CA. https://www.aasld.org/the-liver-meeting/high-doses-albumin-increases-mortality-and-complications-terlipressin-treated
6. Wong YJ, Qiu TY, Tam YC, Mohan BP, Gallegos-Orozco JF, Adler DG. Efficacy and safety of IV albumin for non-spontaneous bacterial peritonitis infection among patients with cirrhosis: a systematic review and meta-analysis. Dig Liver Dis. 2020;52(10):1137-1142. doi:10.1016/j.dld.2020.05.047
7. Myburgh J, Cooper JD, Finfer S, et al. Saline or albumin for fluid resuscitation in patients with traumatic brain injury. N Engl J Med. 2007;357(9):874-884.
Intravenous albumin is a human-derived blood product studied widely in a variety of patient populations. Despite its frequent use in critical care, few high-quality studies have demonstrated improvements in patient-important outcomes. Compared with crystalloids, albumin increases the risk of fluid overload and bleeding and infections in patients undergoing cardiac surgery.1,2 In addition, albumin is costly, and its production is fraught with donor supply chain ethical concerns (the majority of albumin is derived from paid plasma donors).
Albumin use is highly variable between countries, hospitals, and even clinicians within the same specialty due to several factors, including the perception of minimal risk with albumin, concerns regarding insufficient short-term hemodynamic response to crystalloid, and lack of high-quality evidence to inform clinical practice. We will discuss when intensivists should consider albumin use (with prescription personalized to patient context) and when it should be avoided due to the concerns for patient harm.
An intensivist might consider albumin as a reasonable treatment option in patients with cirrhosis undergoing large volume paracentesis to prevent paracentesis-induced circulatory dysfunction, and in patients with cirrhosis and spontaneous bacterial peritonitis (SBP), as data suggests use in this setting leads to a reduction in mortality.3 Clinicians should be aware that even for these widely accepted albumin indications, which are supported by published guidelines, the certainty of evidence is low, recommendations are weak (conditional), and, therefore, albumin should always be personalized to the patient based on volume of paracentesis fluid removed, prior history of hypotension after procedures, and degree of renal dysfunction.4
There are also several conditions for which an intensivist might consider albumin and for which albumin is commonly administered but lacks high-quality studies to support its use either as a frontline or rescue fluid therapy. One such condition is type 1 hepatorenal syndrome (HRS), for which albumin is widely used; however, there are no randomized controlled trials that have compared albumin with placebo.
As with any intervention, the use of albumin is associated with risks. In patients undergoing on-pump cardiac surgery, the ALBICS study showed that albumin did not reduce the risk of major adverse events and, instead, increased risk of bleeding, resternotomy, and infection.2 The ATTIRE trial showed that in patients hospitalized with decompensated cirrhosis and serum albumin <30 g/L, albumin failed to reduce infection, renal impairment, or mortality while increasing life-threatening adverse events, including pulmonary edema and fluid overload.1 Similarly, in patients with cirrhosis and extraperitoneal infections, albumin showed no benefit in reducing renal impairment or mortality, and its use was associated with higher rates of pulmonary edema.6 Lastly, critically ill patients with traumatic brain injury (TBI) who received fluid resuscitation with albumin have been shown to experience higher mortality compared with saline.7 Thus, based on current evidence, intravenous albumin is not recommended for patients undergoing cardiac surgery (priming of the bypass circuit or volume replacement), patients hospitalized with decompensated cirrhosis and hypoalbuminemia, patients hospitalized with cirrhosis and extraperitoneal infections, and critically ill patients with TBI.4
Overall, intravenous albumin prescription in critical care patients requires a personalized approach informed by current best evidence and is not without potential harm.
High-quality evidence is currently lacking in many clinical settings, and large randomized controlled trials are underway to provide further insights into the utility of albumin. These trials will address albumin use in the following: acute kidney injury requiring renal replacement therapy (ALTER-AKI, NCT04705896), inpatients with community-acquired pneumonia (NCT04071041), high-risk cardiac surgery (ACTRN1261900135516703), and septic shock (NCT03869385).
Financial/nonfinancial disclosures
Nicole Relke: None. Mark Hewitt: None. Bram Rochwerg: None. Jeannie Callum: Research support from Canadian Blood Services and Octapharma.
References
1. China L, Freemantle N, Forrest E, et al. A randomized trial of albumin infusions in hospitalized patients with cirrhosis. N Engl J Med. 2021;384(9):808-817. doi:10.1056/NEJMoa2022166
2. Pesonen E, Vlasov H, Suojaranta R, et al. Effect of 4% albumin solution vs ringer acetate on major adverse events in patients undergoing cardiac surgery with cardiopulmonary bypass: a randomized clinical trial. JAMA. 2022;328(3):251-258. doi:10.1001/jama.2022.10461
3. Sort P, Navasa M, Arroyo V, et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. NEJM. 1999;341:403-409.
4. Callum J, Skubas NJ, Bathla A, et al. Use of intravenous albumin: a guideline from the international collaboration for transfusion medicine guidelines. Chest. 2024:S0012-3692(24)00285-X. doi:10.1016/j.chest.2024.02.049
5. Torp N. High doses of albumin increases mortality and complications in terlipressin treated patients with cirrhosis: insights from the ATTIRE trial. Paper presented at the AASLD; 2023; San Diego, CA. https://www.aasld.org/the-liver-meeting/high-doses-albumin-increases-mortality-and-complications-terlipressin-treated
6. Wong YJ, Qiu TY, Tam YC, Mohan BP, Gallegos-Orozco JF, Adler DG. Efficacy and safety of IV albumin for non-spontaneous bacterial peritonitis infection among patients with cirrhosis: a systematic review and meta-analysis. Dig Liver Dis. 2020;52(10):1137-1142. doi:10.1016/j.dld.2020.05.047
7. Myburgh J, Cooper JD, Finfer S, et al. Saline or albumin for fluid resuscitation in patients with traumatic brain injury. N Engl J Med. 2007;357(9):874-884.
ASCO 2024: Treating Myeloma Just Got More Complicated
For brevity’s sake, I’ll focus on trials about newly diagnosed MM and myeloma at first relapse. Here’s my take on how to interpret those studies in light of broader evidence, what I view as their key limitations, and how what came out of ASCO 2024 changes my approach.
The Return of Belantamab
Belantamab, a BCMA targeting antibody-drug conjugate, previously had shown a response rate of 34% in a single-arm, heavily pretreated population, albeit with modest progression free survival (PFS), only to fail its confirmatory randomized study against pomalidomide/dexamethasone. Given the ocular toxicity associated with belantamab, many — including myself — had written off this drug (save in exceptional/unique circumstances), especially with the rise of novel immunotherapies targeting BCMA, such as chimeric antigen receptor (CAR T-cell) therapy and bispecific antibodies.

However, this year at ASCO, two key randomized trials were presented with concurrent publications, a trial of belantamab/bortezomib/dexamethasone versus daratumumab/bortezomib/dexamethasone (DVd) (DREAMM-7), and a trial of belantamab/pomalidomide/dexamethasone versus bortezomib/pomalidomide/dexamethasone (DREAMM-8). Both trials evaluated patients with myeloma who had relapsed disease and had received at least one prior line of therapy.
In both trials, the belantamab triplet beat the other triplets for the endpoint of PFS (median PFS 36.6 vs 13 months for DREAMM-7, and 12 months PFS 71% vs 51% for DREAMM-8). We must commend the bold three-versus-three design and a convincing result.
What are the caveats? Some censoring of information happened in DREAMM-7, which helped make the intervention arm look better than reality and the control arm look even worse than reality. To illustrate this point: the control arm of DVd (PFS 13 months) underperformed, compared to the CASTOR trial, where DVd led to a PFS of 16.7 months. The drug remains toxic, with high rates of keratopathy and vision problems in its current dosing schema. (Perhaps the future lies in less frequent dosing.) This toxicity is almost always reversible, but it is a huge problem to deal with, and our current quality-of-life instruments fail miserably at capturing this.
Furthermore, DVd is now emerging as perhaps the weakest daratumumab triplet that exists. Almost all patients in this trial had disease sensitivity to lenalidomide, and daratumumab/lenalidomide/dexamethasone (PFS of 45 months in the POLLUX trial) is unequivocally easier to use and handle (in my opinion) than this belantamab triplet--which is quite literally “an eyesore.” Would belantamab-based triplets beat dara/len/dex for patients with lenalidomide sensitive disease? Or, for that matter, would belantamab combos beat anti-CD38+carfilzomib+dex combinations, or cilta-cel (which is also now approved for first relapse)?
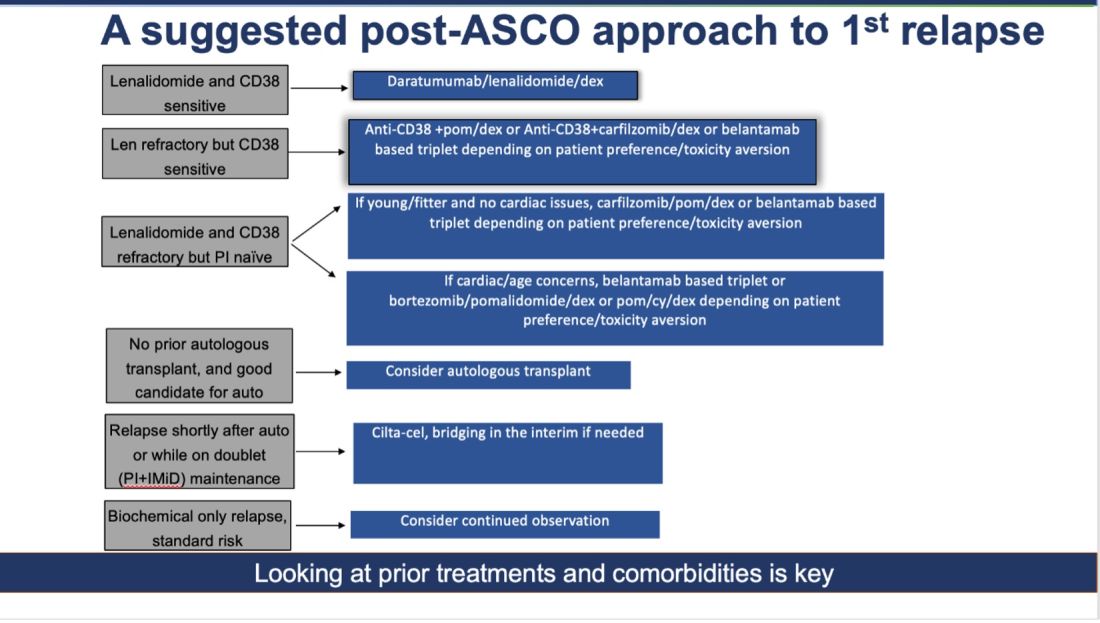
How do I foresee the future of belantamab? Despite these unequivocally positive results, I am not enthused about using it for most patients at first relapse. When trials for bispecifics at first relapse read out, my enthusiasm will likely wane even more. Still, it is useful to have belantamab in the armamentarium. For some patients perceived to be at very high risk of infection, belantamab-based triplets may indeed prove to be a better option than bispecifics. However, I suspect that with better dosing strategies for bispecifics, perhaps even that trend may be mitigated. Since we do not yet have bispecifics available in this line, my suggested algorithm for first relapse is as follows:
Newly Diagnosed MM: The Era of Quads Solidifies
At ASCO 2024, two key trials with concurrent publications assessed the role of quadruplets (without the use of transplant): the IMROZ trial of a quadruplet of isatuximab/bortezomib/lenalidomide/dexamethasone versus bortezomib/lenalidomide/dexamethasone (VRd), and the BENEFIT trial (isatuximab/lenalidomide/bortezomib/dexamethasone versus isatuximab/lenalidomide/dexamethasone).
The IMROZ trial tested the addition of an anti-CD38 antibody to a triplet backbone, and the results are compelling. The PFS was not reached for the quad vs 54 months for VRd. Unlike in the belantamab trial (where the control arm underperformed), here the control arm really overperformed. In this case, we have never seen such a compelling PFS of 54 months for VRd before. (Based on other trials, VRd PFS has been more in the ballpark of 35-43 months.) This speaks to the fitness and biology of the patients enrolled in this trial, and perhaps to how we will not see such stellar results with this quad recreated in real life.
The addition of isatuximab did not seem to impair quality of life, and although there were more treatment-related deaths with isatuximab, those higher numbers seem to have been driven by longer treatment durations. For this study, the upper age limit was 80 years, and most patients enrolled had an excellent functional status--making it clear that frail patients were greatly underrepresented.
What can we conclude from this study? For fit, older patients (who would have been transplant-eligible in the United States), this study provides excellent proof of concept that very good outcomes can be obtained without the use of transplantation. In treating frail patients, we do not know if quads are safe (or even necessary, compared to gentler sequencing), so these data are not applicable.
High-risk cytogenetics were underrepresented, and although the subgroup analysis for such patients did not show a benefit, it is hard to draw conclusions either way. For me, this trial is further evidence that for many older patients with MM, even if you “can” do a transplant, you probably “shouldn’t, they will experience increasingly better outcomes.
The standard for newly diagnosed MM in older patients for whom transplant is not intended is currently dara/len/dex. Is isa/bort/len/dex better? I do not know. It may give a better PFS, but the addition of bortezomib will lead to more neuropathy: 60% of patients developed neuropathy here, with 7% developing Grade III/IV peripheral neuropathy.
To resolve this issue, highly individualized discussions with patients will be needed. The BENEFIT trial evaluated this question more directly, with a randomized comparison of Isa-VRd versus Isa-Rd (the role of bortezomib being the main variable assessed here) with a primary endpoint of MRD negativity at 10-5 at 18 months. Although MRD negativity allows for a quick read-out, having MRD as an endpoint is a foregone conclusion. Adding another drug will almost certainly lead to deeper responses. But is it worth it?
In the BENEFIT trial, the MRD negativity at 10-5 was 26% versus 53% with the quad. However, peripheral neuropathy rates were much higher with the quad (28% vs 52%). Without longer-term data such as PFS and OS, I do not know whether it is worth the extra risks of neuropathy for older patients. Their priority may not be eradication of cancer cells at all costs. Instead, it may be better quality of life and functioning while preserving survival.
To sum up: Post-ASCO 2024, the approach to newly diagnosed MM just got a lot more complicated. For fit, older patients willing to endure extra toxicities of neuropathy (and acknowledging that we do not know whether survival will be any better with this approach), a quad is a very reasonable option to offer while forgoing transplant, in resource-rich areas of the world, such as the United States. Omitting a transplant now seems very reasonable for most older adults. However, a nuanced and individualized approach remains paramount. And given the speed of new developments, even this suggested approach will be outdated soon!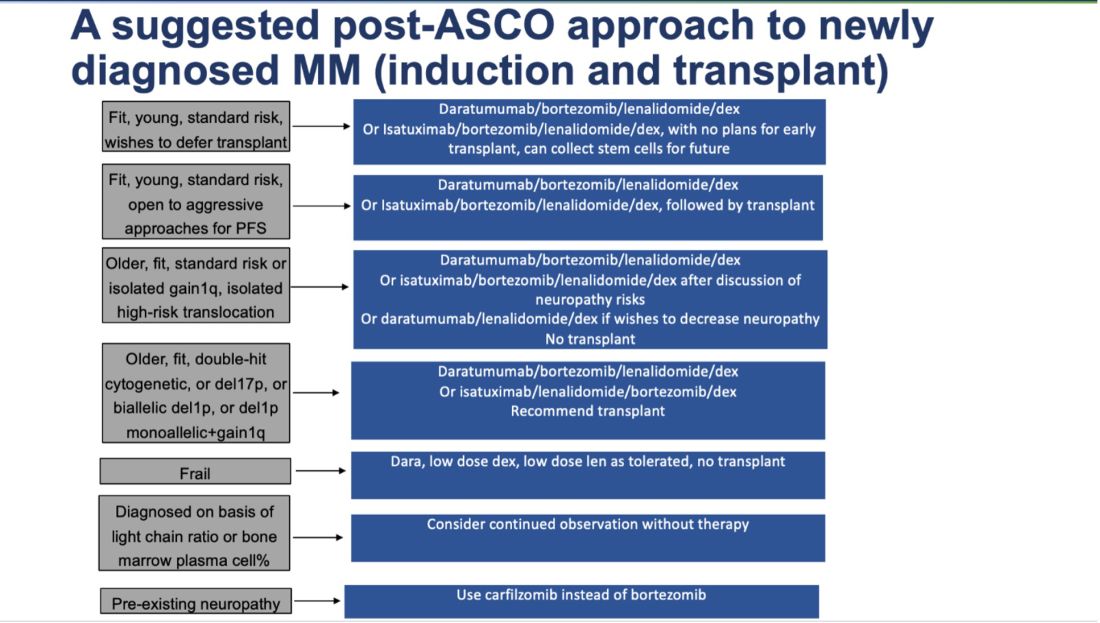
Dr. Mohyuddin is assistant professor in the multiple myeloma program at the Huntsman Cancer Institute at the University of Utah in Salt Lake City.
For brevity’s sake, I’ll focus on trials about newly diagnosed MM and myeloma at first relapse. Here’s my take on how to interpret those studies in light of broader evidence, what I view as their key limitations, and how what came out of ASCO 2024 changes my approach.
The Return of Belantamab
Belantamab, a BCMA targeting antibody-drug conjugate, previously had shown a response rate of 34% in a single-arm, heavily pretreated population, albeit with modest progression free survival (PFS), only to fail its confirmatory randomized study against pomalidomide/dexamethasone. Given the ocular toxicity associated with belantamab, many — including myself — had written off this drug (save in exceptional/unique circumstances), especially with the rise of novel immunotherapies targeting BCMA, such as chimeric antigen receptor (CAR T-cell) therapy and bispecific antibodies.
However, this year at ASCO, two key randomized trials were presented with concurrent publications, a trial of belantamab/bortezomib/dexamethasone versus daratumumab/bortezomib/dexamethasone (DVd) (DREAMM-7), and a trial of belantamab/pomalidomide/dexamethasone versus bortezomib/pomalidomide/dexamethasone (DREAMM-8). Both trials evaluated patients with myeloma who had relapsed disease and had received at least one prior line of therapy.
In both trials, the belantamab triplet beat the other triplets for the endpoint of PFS (median PFS 36.6 vs 13 months for DREAMM-7, and 12 months PFS 71% vs 51% for DREAMM-8). We must commend the bold three-versus-three design and a convincing result.
What are the caveats? Some censoring of information happened in DREAMM-7, which helped make the intervention arm look better than reality and the control arm look even worse than reality. To illustrate this point: the control arm of DVd (PFS 13 months) underperformed, compared to the CASTOR trial, where DVd led to a PFS of 16.7 months. The drug remains toxic, with high rates of keratopathy and vision problems in its current dosing schema. (Perhaps the future lies in less frequent dosing.) This toxicity is almost always reversible, but it is a huge problem to deal with, and our current quality-of-life instruments fail miserably at capturing this.
Furthermore, DVd is now emerging as perhaps the weakest daratumumab triplet that exists. Almost all patients in this trial had disease sensitivity to lenalidomide, and daratumumab/lenalidomide/dexamethasone (PFS of 45 months in the POLLUX trial) is unequivocally easier to use and handle (in my opinion) than this belantamab triplet--which is quite literally “an eyesore.” Would belantamab-based triplets beat dara/len/dex for patients with lenalidomide sensitive disease? Or, for that matter, would belantamab combos beat anti-CD38+carfilzomib+dex combinations, or cilta-cel (which is also now approved for first relapse)?
How do I foresee the future of belantamab? Despite these unequivocally positive results, I am not enthused about using it for most patients at first relapse. When trials for bispecifics at first relapse read out, my enthusiasm will likely wane even more. Still, it is useful to have belantamab in the armamentarium. For some patients perceived to be at very high risk of infection, belantamab-based triplets may indeed prove to be a better option than bispecifics. However, I suspect that with better dosing strategies for bispecifics, perhaps even that trend may be mitigated. Since we do not yet have bispecifics available in this line, my suggested algorithm for first relapse is as follows:
Newly Diagnosed MM: The Era of Quads Solidifies
At ASCO 2024, two key trials with concurrent publications assessed the role of quadruplets (without the use of transplant): the IMROZ trial of a quadruplet of isatuximab/bortezomib/lenalidomide/dexamethasone versus bortezomib/lenalidomide/dexamethasone (VRd), and the BENEFIT trial (isatuximab/lenalidomide/bortezomib/dexamethasone versus isatuximab/lenalidomide/dexamethasone).
The IMROZ trial tested the addition of an anti-CD38 antibody to a triplet backbone, and the results are compelling. The PFS was not reached for the quad vs 54 months for VRd. Unlike in the belantamab trial (where the control arm underperformed), here the control arm really overperformed. In this case, we have never seen such a compelling PFS of 54 months for VRd before. (Based on other trials, VRd PFS has been more in the ballpark of 35-43 months.) This speaks to the fitness and biology of the patients enrolled in this trial, and perhaps to how we will not see such stellar results with this quad recreated in real life.
The addition of isatuximab did not seem to impair quality of life, and although there were more treatment-related deaths with isatuximab, those higher numbers seem to have been driven by longer treatment durations. For this study, the upper age limit was 80 years, and most patients enrolled had an excellent functional status--making it clear that frail patients were greatly underrepresented.
What can we conclude from this study? For fit, older patients (who would have been transplant-eligible in the United States), this study provides excellent proof of concept that very good outcomes can be obtained without the use of transplantation. In treating frail patients, we do not know if quads are safe (or even necessary, compared to gentler sequencing), so these data are not applicable.
High-risk cytogenetics were underrepresented, and although the subgroup analysis for such patients did not show a benefit, it is hard to draw conclusions either way. For me, this trial is further evidence that for many older patients with MM, even if you “can” do a transplant, you probably “shouldn’t, they will experience increasingly better outcomes.
The standard for newly diagnosed MM in older patients for whom transplant is not intended is currently dara/len/dex. Is isa/bort/len/dex better? I do not know. It may give a better PFS, but the addition of bortezomib will lead to more neuropathy: 60% of patients developed neuropathy here, with 7% developing Grade III/IV peripheral neuropathy.
To resolve this issue, highly individualized discussions with patients will be needed. The BENEFIT trial evaluated this question more directly, with a randomized comparison of Isa-VRd versus Isa-Rd (the role of bortezomib being the main variable assessed here) with a primary endpoint of MRD negativity at 10-5 at 18 months. Although MRD negativity allows for a quick read-out, having MRD as an endpoint is a foregone conclusion. Adding another drug will almost certainly lead to deeper responses. But is it worth it?
In the BENEFIT trial, the MRD negativity at 10-5 was 26% versus 53% with the quad. However, peripheral neuropathy rates were much higher with the quad (28% vs 52%). Without longer-term data such as PFS and OS, I do not know whether it is worth the extra risks of neuropathy for older patients. Their priority may not be eradication of cancer cells at all costs. Instead, it may be better quality of life and functioning while preserving survival.
To sum up: Post-ASCO 2024, the approach to newly diagnosed MM just got a lot more complicated. For fit, older patients willing to endure extra toxicities of neuropathy (and acknowledging that we do not know whether survival will be any better with this approach), a quad is a very reasonable option to offer while forgoing transplant, in resource-rich areas of the world, such as the United States. Omitting a transplant now seems very reasonable for most older adults. However, a nuanced and individualized approach remains paramount. And given the speed of new developments, even this suggested approach will be outdated soon!
Dr. Mohyuddin is assistant professor in the multiple myeloma program at the Huntsman Cancer Institute at the University of Utah in Salt Lake City.
For brevity’s sake, I’ll focus on trials about newly diagnosed MM and myeloma at first relapse. Here’s my take on how to interpret those studies in light of broader evidence, what I view as their key limitations, and how what came out of ASCO 2024 changes my approach.
The Return of Belantamab
Belantamab, a BCMA targeting antibody-drug conjugate, previously had shown a response rate of 34% in a single-arm, heavily pretreated population, albeit with modest progression free survival (PFS), only to fail its confirmatory randomized study against pomalidomide/dexamethasone. Given the ocular toxicity associated with belantamab, many — including myself — had written off this drug (save in exceptional/unique circumstances), especially with the rise of novel immunotherapies targeting BCMA, such as chimeric antigen receptor (CAR T-cell) therapy and bispecific antibodies.
However, this year at ASCO, two key randomized trials were presented with concurrent publications, a trial of belantamab/bortezomib/dexamethasone versus daratumumab/bortezomib/dexamethasone (DVd) (DREAMM-7), and a trial of belantamab/pomalidomide/dexamethasone versus bortezomib/pomalidomide/dexamethasone (DREAMM-8). Both trials evaluated patients with myeloma who had relapsed disease and had received at least one prior line of therapy.
In both trials, the belantamab triplet beat the other triplets for the endpoint of PFS (median PFS 36.6 vs 13 months for DREAMM-7, and 12 months PFS 71% vs 51% for DREAMM-8). We must commend the bold three-versus-three design and a convincing result.
What are the caveats? Some censoring of information happened in DREAMM-7, which helped make the intervention arm look better than reality and the control arm look even worse than reality. To illustrate this point: the control arm of DVd (PFS 13 months) underperformed, compared to the CASTOR trial, where DVd led to a PFS of 16.7 months. The drug remains toxic, with high rates of keratopathy and vision problems in its current dosing schema. (Perhaps the future lies in less frequent dosing.) This toxicity is almost always reversible, but it is a huge problem to deal with, and our current quality-of-life instruments fail miserably at capturing this.
Furthermore, DVd is now emerging as perhaps the weakest daratumumab triplet that exists. Almost all patients in this trial had disease sensitivity to lenalidomide, and daratumumab/lenalidomide/dexamethasone (PFS of 45 months in the POLLUX trial) is unequivocally easier to use and handle (in my opinion) than this belantamab triplet--which is quite literally “an eyesore.” Would belantamab-based triplets beat dara/len/dex for patients with lenalidomide sensitive disease? Or, for that matter, would belantamab combos beat anti-CD38+carfilzomib+dex combinations, or cilta-cel (which is also now approved for first relapse)?
How do I foresee the future of belantamab? Despite these unequivocally positive results, I am not enthused about using it for most patients at first relapse. When trials for bispecifics at first relapse read out, my enthusiasm will likely wane even more. Still, it is useful to have belantamab in the armamentarium. For some patients perceived to be at very high risk of infection, belantamab-based triplets may indeed prove to be a better option than bispecifics. However, I suspect that with better dosing strategies for bispecifics, perhaps even that trend may be mitigated. Since we do not yet have bispecifics available in this line, my suggested algorithm for first relapse is as follows:
Newly Diagnosed MM: The Era of Quads Solidifies
At ASCO 2024, two key trials with concurrent publications assessed the role of quadruplets (without the use of transplant): the IMROZ trial of a quadruplet of isatuximab/bortezomib/lenalidomide/dexamethasone versus bortezomib/lenalidomide/dexamethasone (VRd), and the BENEFIT trial (isatuximab/lenalidomide/bortezomib/dexamethasone versus isatuximab/lenalidomide/dexamethasone).
The IMROZ trial tested the addition of an anti-CD38 antibody to a triplet backbone, and the results are compelling. The PFS was not reached for the quad vs 54 months for VRd. Unlike in the belantamab trial (where the control arm underperformed), here the control arm really overperformed. In this case, we have never seen such a compelling PFS of 54 months for VRd before. (Based on other trials, VRd PFS has been more in the ballpark of 35-43 months.) This speaks to the fitness and biology of the patients enrolled in this trial, and perhaps to how we will not see such stellar results with this quad recreated in real life.
The addition of isatuximab did not seem to impair quality of life, and although there were more treatment-related deaths with isatuximab, those higher numbers seem to have been driven by longer treatment durations. For this study, the upper age limit was 80 years, and most patients enrolled had an excellent functional status--making it clear that frail patients were greatly underrepresented.
What can we conclude from this study? For fit, older patients (who would have been transplant-eligible in the United States), this study provides excellent proof of concept that very good outcomes can be obtained without the use of transplantation. In treating frail patients, we do not know if quads are safe (or even necessary, compared to gentler sequencing), so these data are not applicable.
High-risk cytogenetics were underrepresented, and although the subgroup analysis for such patients did not show a benefit, it is hard to draw conclusions either way. For me, this trial is further evidence that for many older patients with MM, even if you “can” do a transplant, you probably “shouldn’t, they will experience increasingly better outcomes.
The standard for newly diagnosed MM in older patients for whom transplant is not intended is currently dara/len/dex. Is isa/bort/len/dex better? I do not know. It may give a better PFS, but the addition of bortezomib will lead to more neuropathy: 60% of patients developed neuropathy here, with 7% developing Grade III/IV peripheral neuropathy.
To resolve this issue, highly individualized discussions with patients will be needed. The BENEFIT trial evaluated this question more directly, with a randomized comparison of Isa-VRd versus Isa-Rd (the role of bortezomib being the main variable assessed here) with a primary endpoint of MRD negativity at 10-5 at 18 months. Although MRD negativity allows for a quick read-out, having MRD as an endpoint is a foregone conclusion. Adding another drug will almost certainly lead to deeper responses. But is it worth it?
In the BENEFIT trial, the MRD negativity at 10-5 was 26% versus 53% with the quad. However, peripheral neuropathy rates were much higher with the quad (28% vs 52%). Without longer-term data such as PFS and OS, I do not know whether it is worth the extra risks of neuropathy for older patients. Their priority may not be eradication of cancer cells at all costs. Instead, it may be better quality of life and functioning while preserving survival.
To sum up: Post-ASCO 2024, the approach to newly diagnosed MM just got a lot more complicated. For fit, older patients willing to endure extra toxicities of neuropathy (and acknowledging that we do not know whether survival will be any better with this approach), a quad is a very reasonable option to offer while forgoing transplant, in resource-rich areas of the world, such as the United States. Omitting a transplant now seems very reasonable for most older adults. However, a nuanced and individualized approach remains paramount. And given the speed of new developments, even this suggested approach will be outdated soon!
Dr. Mohyuddin is assistant professor in the multiple myeloma program at the Huntsman Cancer Institute at the University of Utah in Salt Lake City.
Cardiovascular Health Becoming a Major Risk Factor for Dementia
That’s according to researchers from University College London (UCL) in the United Kingdom who analyzed 27 papers about dementia that had data collected over more than 70 years. They calculated what share of dementia cases were due to different risk factors. Their findings were recently published in the Lancet Public Health.
Top risk factors for dementia over the years have been hypertension, obesity, diabetes, education, and smoking, according to a news release on the findings. But the prevalence of risk factors has changed over the decades.
Researchers said smoking and education have become less important risk factors because of “population-level interventions,” such as stop-smoking campaigns and compulsory public education. On the other hand, obesity and diabetes rates have increased and become bigger risk factors.
Hypertension remains the greatest risk factor, even though doctors and public health groups are putting more emphasis on managing the condition, the study said.
“Cardiovascular risk factors may have contributed more to dementia risk over time, so these deserve more targeted action for future dementia prevention efforts,” said Naaheed Mukadam, PhD, an associate professor at UCL and the lead author of the study.
Eliminating modifiable risk factors could theoretically prevent 40% of dementia cases, the release said.
The CDC says that an estimated 5.8 million people in the United States have Alzheimer’s disease and related dementias, including 5.6 million people ages 65 and older and about 200,000 under age 65. The UCL release said an estimated 944,000 in the U.K. have dementia.
A version of this article first appeared on WebMD.com.
That’s according to researchers from University College London (UCL) in the United Kingdom who analyzed 27 papers about dementia that had data collected over more than 70 years. They calculated what share of dementia cases were due to different risk factors. Their findings were recently published in the Lancet Public Health.
Top risk factors for dementia over the years have been hypertension, obesity, diabetes, education, and smoking, according to a news release on the findings. But the prevalence of risk factors has changed over the decades.
Researchers said smoking and education have become less important risk factors because of “population-level interventions,” such as stop-smoking campaigns and compulsory public education. On the other hand, obesity and diabetes rates have increased and become bigger risk factors.
Hypertension remains the greatest risk factor, even though doctors and public health groups are putting more emphasis on managing the condition, the study said.
“Cardiovascular risk factors may have contributed more to dementia risk over time, so these deserve more targeted action for future dementia prevention efforts,” said Naaheed Mukadam, PhD, an associate professor at UCL and the lead author of the study.
Eliminating modifiable risk factors could theoretically prevent 40% of dementia cases, the release said.
The CDC says that an estimated 5.8 million people in the United States have Alzheimer’s disease and related dementias, including 5.6 million people ages 65 and older and about 200,000 under age 65. The UCL release said an estimated 944,000 in the U.K. have dementia.
A version of this article first appeared on WebMD.com.
That’s according to researchers from University College London (UCL) in the United Kingdom who analyzed 27 papers about dementia that had data collected over more than 70 years. They calculated what share of dementia cases were due to different risk factors. Their findings were recently published in the Lancet Public Health.
Top risk factors for dementia over the years have been hypertension, obesity, diabetes, education, and smoking, according to a news release on the findings. But the prevalence of risk factors has changed over the decades.
Researchers said smoking and education have become less important risk factors because of “population-level interventions,” such as stop-smoking campaigns and compulsory public education. On the other hand, obesity and diabetes rates have increased and become bigger risk factors.
Hypertension remains the greatest risk factor, even though doctors and public health groups are putting more emphasis on managing the condition, the study said.
“Cardiovascular risk factors may have contributed more to dementia risk over time, so these deserve more targeted action for future dementia prevention efforts,” said Naaheed Mukadam, PhD, an associate professor at UCL and the lead author of the study.
Eliminating modifiable risk factors could theoretically prevent 40% of dementia cases, the release said.
The CDC says that an estimated 5.8 million people in the United States have Alzheimer’s disease and related dementias, including 5.6 million people ages 65 and older and about 200,000 under age 65. The UCL release said an estimated 944,000 in the U.K. have dementia.
A version of this article first appeared on WebMD.com.
FROM THE LANCET PUBLIC HEALTH
Revised Criteria for Alzheimer’s Diagnosis, Staging Released
, including a new biomarker classification system that incorporates fluid and imaging biomarkers as well as an updated disease staging system.
“Plasma markers are here now, and it’s very important to incorporate them into the criteria for diagnosis,” said senior author Maria C. Carrillo, PhD, Alzheimer’s Association chief science officer and medical affairs lead.
The revised criteria are the first updates since 2018.
“Defining diseases biologically, rather than based on syndromic presentation, has long been standard in many areas of medicine — including cancer, heart disease, and diabetes — and is becoming a unifying concept common to all neurodegenerative diseases,” lead author Clifford Jack Jr, MD, with Mayo Clinic, Rochester, Minnesota, said in a news release from the Alzheimer’s Association.
“These updates to the diagnostic criteria are needed now because we know more about the underlying biology of Alzheimer’s and we are able to measure those changes,” Dr. Jack added.
The 2024 revised criteria for diagnosis and staging of Alzheimer’s disease were published online in Alzheimer’s & Dementia.
Core Biomarkers Defined
The revised criteria define Alzheimer’s disease as a biologic process that begins with the appearance of Alzheimer’s disease neuropathologic change (ADNPC) in the absence of symptoms. Progression of the neuropathologic burden leads to the later appearance and progression of clinical symptoms.
The work group organized Alzheimer’s disease biomarkers into three broad categories: (1) core biomarkers of ADNPC, (2) nonspecific biomarkers that are important in Alzheimer’s disease but are also involved in other brain diseases, and (3) biomarkers of diseases or conditions that commonly coexist with Alzheimer’s disease.
Core Alzheimer’s biomarkers are subdivided into Core 1 and Core 2.
Core 1 biomarkers become abnormal early in the disease course and directly measure either amyloid plaques or phosphorylated tau (p-tau). They include amyloid PET; cerebrospinal fluid (CSF) amyloid beta 42/40 ratio, CSF p-tau181/amyloid beta 42 ratio, and CSF total (t)-tau/amyloid beta 42 ratio; and “accurate” plasma biomarkers, such as p-tau217.
“An abnormal Core 1 biomarker result is sufficient to establish a diagnosis of Alzheimer’s disease and to inform clinical decision making [sic] throughout the disease continuum,” the work group wrote.
Core 2 biomarkers become abnormal later in the disease process and are more closely linked with the onset of symptoms. Core 2 biomarkers include tau PET and certain soluble tau fragments associated with tau proteinopathy (eg, MTBR-tau243) but also pT205 and nonphosphorylated mid-region tau fragments.
Core 2 biomarkers, when combined with Core 1, may be used to stage biologic disease severity; abnormal Core 2 biomarkers “increase confidence that Alzheimer’s disease is contributing to symptoms,” the work group noted.
The revised criteria give clinicians “the flexibility to use plasma or PET scans or CSF,” Dr. Carrillo said. “They will have several tools that they can choose from and offer this variety of tools to their patients. We need different tools for different individuals. There will be differences in coverage and access to these diagnostics.”
The revised criteria also include an integrated biologic and clinical staging scheme that acknowledges the fact that common co-pathologies, cognitive reserve, and resistance may modify relationships between clinical and biologic Alzheimer’s disease stages.
Formal Guidelines to Come
The work group noted that currently, the clinical use of Alzheimer’s disease biomarkers is intended for the evaluation of symptomatic patients, not cognitively unimpaired individuals.
Disease-targeted therapies have not yet been approved for cognitively unimpaired individuals. For this reason, the work group currently recommends against diagnostic testing in cognitively unimpaired individuals outside the context of observational or therapeutic research studies.
This recommendation would change in the future if disease-targeted therapies that are currently being evaluated in trials demonstrate a benefit in preventing cognitive decline and are approved for use in preclinical Alzheimer’s disease, they wrote.
They emphasize that the revised criteria are not intended to provide step-by-step clinical practice guidelines for clinicians. Rather, they provide general principles to inform diagnosis and staging of Alzheimer’s disease that reflect current science.
“This is just the beginning,” said Dr. Carrillo. “This is a gathering of the evidence to date and putting it in one place so we can have a consensus and actually a way to test it and make it better as we add new science.”
This also serves as a “springboard” for the Alzheimer’s Association to create formal clinical guidelines. “That will come, hopefully, over the next 12 months. We’ll be working on it, and we hope to have that in 2025,” Dr. Carrillo said.
The revised criteria also emphasize the role of the clinician.
“The biologically based diagnosis of Alzheimer’s disease is meant to assist, rather than supplant, the clinical evaluation of individuals with cognitive impairment,” the work group wrote in a related commentary published online in Nature Medicine.
Recent diagnostics and therapeutic developments “herald a virtuous cycle in which improvements in diagnostic methods enable more sophisticated treatment approaches, which in turn steer advances in diagnostic methods,” they continued. “An unchanging principle, however, is that effective treatment will always rely on the ability to diagnose and stage the biology driving the disease process.”
Funding for this research was provided by the National Institutes of Health, Alexander family professorship, GHR Foundation, Alzheimer’s Association, Veterans Administration, Life Molecular Imaging, Michael J. Fox Foundation for Parkinson’s Research, Avid Radiopharmaceuticals, Eli Lilly, Gates Foundation, Biogen, C2N Diagnostics, Eisai, Fujirebio, GE Healthcare, Roche, National Institute on Aging, Roche/Genentech, BrightFocus Foundation, Hoffmann-La Roche, Novo Nordisk, Toyama, National MS Society, Alzheimer Drug Discovery Foundation, and others. A complete list of donors and disclosures is included in the original article.
A version of this article appeared on Medscape.com.
, including a new biomarker classification system that incorporates fluid and imaging biomarkers as well as an updated disease staging system.
“Plasma markers are here now, and it’s very important to incorporate them into the criteria for diagnosis,” said senior author Maria C. Carrillo, PhD, Alzheimer’s Association chief science officer and medical affairs lead.
The revised criteria are the first updates since 2018.
“Defining diseases biologically, rather than based on syndromic presentation, has long been standard in many areas of medicine — including cancer, heart disease, and diabetes — and is becoming a unifying concept common to all neurodegenerative diseases,” lead author Clifford Jack Jr, MD, with Mayo Clinic, Rochester, Minnesota, said in a news release from the Alzheimer’s Association.
“These updates to the diagnostic criteria are needed now because we know more about the underlying biology of Alzheimer’s and we are able to measure those changes,” Dr. Jack added.
The 2024 revised criteria for diagnosis and staging of Alzheimer’s disease were published online in Alzheimer’s & Dementia.
Core Biomarkers Defined
The revised criteria define Alzheimer’s disease as a biologic process that begins with the appearance of Alzheimer’s disease neuropathologic change (ADNPC) in the absence of symptoms. Progression of the neuropathologic burden leads to the later appearance and progression of clinical symptoms.
The work group organized Alzheimer’s disease biomarkers into three broad categories: (1) core biomarkers of ADNPC, (2) nonspecific biomarkers that are important in Alzheimer’s disease but are also involved in other brain diseases, and (3) biomarkers of diseases or conditions that commonly coexist with Alzheimer’s disease.
Core Alzheimer’s biomarkers are subdivided into Core 1 and Core 2.
Core 1 biomarkers become abnormal early in the disease course and directly measure either amyloid plaques or phosphorylated tau (p-tau). They include amyloid PET; cerebrospinal fluid (CSF) amyloid beta 42/40 ratio, CSF p-tau181/amyloid beta 42 ratio, and CSF total (t)-tau/amyloid beta 42 ratio; and “accurate” plasma biomarkers, such as p-tau217.
“An abnormal Core 1 biomarker result is sufficient to establish a diagnosis of Alzheimer’s disease and to inform clinical decision making [sic] throughout the disease continuum,” the work group wrote.
Core 2 biomarkers become abnormal later in the disease process and are more closely linked with the onset of symptoms. Core 2 biomarkers include tau PET and certain soluble tau fragments associated with tau proteinopathy (eg, MTBR-tau243) but also pT205 and nonphosphorylated mid-region tau fragments.
Core 2 biomarkers, when combined with Core 1, may be used to stage biologic disease severity; abnormal Core 2 biomarkers “increase confidence that Alzheimer’s disease is contributing to symptoms,” the work group noted.
The revised criteria give clinicians “the flexibility to use plasma or PET scans or CSF,” Dr. Carrillo said. “They will have several tools that they can choose from and offer this variety of tools to their patients. We need different tools for different individuals. There will be differences in coverage and access to these diagnostics.”
The revised criteria also include an integrated biologic and clinical staging scheme that acknowledges the fact that common co-pathologies, cognitive reserve, and resistance may modify relationships between clinical and biologic Alzheimer’s disease stages.
Formal Guidelines to Come
The work group noted that currently, the clinical use of Alzheimer’s disease biomarkers is intended for the evaluation of symptomatic patients, not cognitively unimpaired individuals.
Disease-targeted therapies have not yet been approved for cognitively unimpaired individuals. For this reason, the work group currently recommends against diagnostic testing in cognitively unimpaired individuals outside the context of observational or therapeutic research studies.
This recommendation would change in the future if disease-targeted therapies that are currently being evaluated in trials demonstrate a benefit in preventing cognitive decline and are approved for use in preclinical Alzheimer’s disease, they wrote.
They emphasize that the revised criteria are not intended to provide step-by-step clinical practice guidelines for clinicians. Rather, they provide general principles to inform diagnosis and staging of Alzheimer’s disease that reflect current science.
“This is just the beginning,” said Dr. Carrillo. “This is a gathering of the evidence to date and putting it in one place so we can have a consensus and actually a way to test it and make it better as we add new science.”
This also serves as a “springboard” for the Alzheimer’s Association to create formal clinical guidelines. “That will come, hopefully, over the next 12 months. We’ll be working on it, and we hope to have that in 2025,” Dr. Carrillo said.
The revised criteria also emphasize the role of the clinician.
“The biologically based diagnosis of Alzheimer’s disease is meant to assist, rather than supplant, the clinical evaluation of individuals with cognitive impairment,” the work group wrote in a related commentary published online in Nature Medicine.
Recent diagnostics and therapeutic developments “herald a virtuous cycle in which improvements in diagnostic methods enable more sophisticated treatment approaches, which in turn steer advances in diagnostic methods,” they continued. “An unchanging principle, however, is that effective treatment will always rely on the ability to diagnose and stage the biology driving the disease process.”
Funding for this research was provided by the National Institutes of Health, Alexander family professorship, GHR Foundation, Alzheimer’s Association, Veterans Administration, Life Molecular Imaging, Michael J. Fox Foundation for Parkinson’s Research, Avid Radiopharmaceuticals, Eli Lilly, Gates Foundation, Biogen, C2N Diagnostics, Eisai, Fujirebio, GE Healthcare, Roche, National Institute on Aging, Roche/Genentech, BrightFocus Foundation, Hoffmann-La Roche, Novo Nordisk, Toyama, National MS Society, Alzheimer Drug Discovery Foundation, and others. A complete list of donors and disclosures is included in the original article.
A version of this article appeared on Medscape.com.
, including a new biomarker classification system that incorporates fluid and imaging biomarkers as well as an updated disease staging system.
“Plasma markers are here now, and it’s very important to incorporate them into the criteria for diagnosis,” said senior author Maria C. Carrillo, PhD, Alzheimer’s Association chief science officer and medical affairs lead.
The revised criteria are the first updates since 2018.
“Defining diseases biologically, rather than based on syndromic presentation, has long been standard in many areas of medicine — including cancer, heart disease, and diabetes — and is becoming a unifying concept common to all neurodegenerative diseases,” lead author Clifford Jack Jr, MD, with Mayo Clinic, Rochester, Minnesota, said in a news release from the Alzheimer’s Association.
“These updates to the diagnostic criteria are needed now because we know more about the underlying biology of Alzheimer’s and we are able to measure those changes,” Dr. Jack added.
The 2024 revised criteria for diagnosis and staging of Alzheimer’s disease were published online in Alzheimer’s & Dementia.
Core Biomarkers Defined
The revised criteria define Alzheimer’s disease as a biologic process that begins with the appearance of Alzheimer’s disease neuropathologic change (ADNPC) in the absence of symptoms. Progression of the neuropathologic burden leads to the later appearance and progression of clinical symptoms.
The work group organized Alzheimer’s disease biomarkers into three broad categories: (1) core biomarkers of ADNPC, (2) nonspecific biomarkers that are important in Alzheimer’s disease but are also involved in other brain diseases, and (3) biomarkers of diseases or conditions that commonly coexist with Alzheimer’s disease.
Core Alzheimer’s biomarkers are subdivided into Core 1 and Core 2.
Core 1 biomarkers become abnormal early in the disease course and directly measure either amyloid plaques or phosphorylated tau (p-tau). They include amyloid PET; cerebrospinal fluid (CSF) amyloid beta 42/40 ratio, CSF p-tau181/amyloid beta 42 ratio, and CSF total (t)-tau/amyloid beta 42 ratio; and “accurate” plasma biomarkers, such as p-tau217.
“An abnormal Core 1 biomarker result is sufficient to establish a diagnosis of Alzheimer’s disease and to inform clinical decision making [sic] throughout the disease continuum,” the work group wrote.
Core 2 biomarkers become abnormal later in the disease process and are more closely linked with the onset of symptoms. Core 2 biomarkers include tau PET and certain soluble tau fragments associated with tau proteinopathy (eg, MTBR-tau243) but also pT205 and nonphosphorylated mid-region tau fragments.
Core 2 biomarkers, when combined with Core 1, may be used to stage biologic disease severity; abnormal Core 2 biomarkers “increase confidence that Alzheimer’s disease is contributing to symptoms,” the work group noted.
The revised criteria give clinicians “the flexibility to use plasma or PET scans or CSF,” Dr. Carrillo said. “They will have several tools that they can choose from and offer this variety of tools to their patients. We need different tools for different individuals. There will be differences in coverage and access to these diagnostics.”
The revised criteria also include an integrated biologic and clinical staging scheme that acknowledges the fact that common co-pathologies, cognitive reserve, and resistance may modify relationships between clinical and biologic Alzheimer’s disease stages.
Formal Guidelines to Come
The work group noted that currently, the clinical use of Alzheimer’s disease biomarkers is intended for the evaluation of symptomatic patients, not cognitively unimpaired individuals.
Disease-targeted therapies have not yet been approved for cognitively unimpaired individuals. For this reason, the work group currently recommends against diagnostic testing in cognitively unimpaired individuals outside the context of observational or therapeutic research studies.
This recommendation would change in the future if disease-targeted therapies that are currently being evaluated in trials demonstrate a benefit in preventing cognitive decline and are approved for use in preclinical Alzheimer’s disease, they wrote.
They emphasize that the revised criteria are not intended to provide step-by-step clinical practice guidelines for clinicians. Rather, they provide general principles to inform diagnosis and staging of Alzheimer’s disease that reflect current science.
“This is just the beginning,” said Dr. Carrillo. “This is a gathering of the evidence to date and putting it in one place so we can have a consensus and actually a way to test it and make it better as we add new science.”
This also serves as a “springboard” for the Alzheimer’s Association to create formal clinical guidelines. “That will come, hopefully, over the next 12 months. We’ll be working on it, and we hope to have that in 2025,” Dr. Carrillo said.
The revised criteria also emphasize the role of the clinician.
“The biologically based diagnosis of Alzheimer’s disease is meant to assist, rather than supplant, the clinical evaluation of individuals with cognitive impairment,” the work group wrote in a related commentary published online in Nature Medicine.
Recent diagnostics and therapeutic developments “herald a virtuous cycle in which improvements in diagnostic methods enable more sophisticated treatment approaches, which in turn steer advances in diagnostic methods,” they continued. “An unchanging principle, however, is that effective treatment will always rely on the ability to diagnose and stage the biology driving the disease process.”
Funding for this research was provided by the National Institutes of Health, Alexander family professorship, GHR Foundation, Alzheimer’s Association, Veterans Administration, Life Molecular Imaging, Michael J. Fox Foundation for Parkinson’s Research, Avid Radiopharmaceuticals, Eli Lilly, Gates Foundation, Biogen, C2N Diagnostics, Eisai, Fujirebio, GE Healthcare, Roche, National Institute on Aging, Roche/Genentech, BrightFocus Foundation, Hoffmann-La Roche, Novo Nordisk, Toyama, National MS Society, Alzheimer Drug Discovery Foundation, and others. A complete list of donors and disclosures is included in the original article.
A version of this article appeared on Medscape.com.
FROM ALZHEIMER’S & DEMENTIA
Common Cognitive Test Falls Short for Concussion Diagnosis
, a new study showed.
Investigators found that almost half of athletes diagnosed with a concussion tested normally on the Sports Concussion Assessment Tool 5 (SCAT5), the recommended tool for measuring cognitive skills in concussion evaluations. The most accurate measure of concussion was symptoms reported by the athletes.
“If you don’t do well on the cognitive exam, it suggests you have a concussion. But many people who are concussed do fine on the exam,” lead author Kimberly Harmon, MD, professor of family medicine and section head of sports medicine at the University of Washington School of Medicine, Seattle, said in a news release.
The study was published online in JAMA Network Open.
Introduced in 2004, the SCAT was created to standardize the collection of information clinicians use to diagnose concussion, including evaluation of symptoms, orientation, and balance. It also uses a 10-word list to assess immediate memory and delayed recall.
Dr. Harmon’s own experiences as a team physician led her to wonder about the accuracy of the cognitive screening portion of the SCAT. She saw that “some people were concussed, and they did well on the recall test. Some people weren’t concussed, and they didn’t do well. So I thought we should study it,” she said.
Investigators compared 92 National Collegiate Athletic Association (NCAA) Division 1 athletes who had sustained a concussion between 2020 and 2022 and had a concussion evaluation within 48 hours to 92 matched nonconcussed teammates (overall cohort, 52% men). Most concussions occurred in those who played football, followed by volleyball.
All athletes had previously completed NCAA-required baseline concussion screenings. Participants completed the SCAT5 screening test within 2 weeks of the incident concussion.
No significant differences were found between the baseline scores of athletes with and without concussion. Moreover, responses on the word recall section of the SCAT5 held little predictive value for concussion.
Nearly half (45%) of athletes with concussion performed at or even above their baseline cognitive report, which the authors said highlights the limitations of the cognitive components of SCAT5.
The most accurate predictor of concussion was participants’ responses to questions about their symptoms.
“If you get hit in the head and go to the sideline and say, ‘I have a headache, I’m dizzy, I don’t feel right,’ I can say with pretty good assurance that you have a concussion,” Dr. Harmon continued. “I don’t need to do any testing.”
Unfortunately, the problem is “that some athletes don’t want to come out. They don’t report their symptoms or may not recognize their symptoms. So then you need an objective, accurate test to tell you whether you can safely put the athlete back on the field. We don’t have that right now.”
The study did not control for concussion history, and the all–Division 1 cohort means the findings may not be generalizable to other athletes.
Nevertheless, investigators said the study “affirms that reported symptoms are the most sensitive indicator of concussion, and there are limitations to the objective cognitive testing included in the SCAT.” They concluded that concussion “remains a clinical diagnosis that should be based on a thorough review of signs, symptoms, and clinical findings.”
This study was funded in part by donations from University of Washington alumni Jack and Luellen Cherneski and the Chisholm Foundation. Dr. Harmon reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new study showed.
Investigators found that almost half of athletes diagnosed with a concussion tested normally on the Sports Concussion Assessment Tool 5 (SCAT5), the recommended tool for measuring cognitive skills in concussion evaluations. The most accurate measure of concussion was symptoms reported by the athletes.
“If you don’t do well on the cognitive exam, it suggests you have a concussion. But many people who are concussed do fine on the exam,” lead author Kimberly Harmon, MD, professor of family medicine and section head of sports medicine at the University of Washington School of Medicine, Seattle, said in a news release.
The study was published online in JAMA Network Open.
Introduced in 2004, the SCAT was created to standardize the collection of information clinicians use to diagnose concussion, including evaluation of symptoms, orientation, and balance. It also uses a 10-word list to assess immediate memory and delayed recall.
Dr. Harmon’s own experiences as a team physician led her to wonder about the accuracy of the cognitive screening portion of the SCAT. She saw that “some people were concussed, and they did well on the recall test. Some people weren’t concussed, and they didn’t do well. So I thought we should study it,” she said.
Investigators compared 92 National Collegiate Athletic Association (NCAA) Division 1 athletes who had sustained a concussion between 2020 and 2022 and had a concussion evaluation within 48 hours to 92 matched nonconcussed teammates (overall cohort, 52% men). Most concussions occurred in those who played football, followed by volleyball.
All athletes had previously completed NCAA-required baseline concussion screenings. Participants completed the SCAT5 screening test within 2 weeks of the incident concussion.
No significant differences were found between the baseline scores of athletes with and without concussion. Moreover, responses on the word recall section of the SCAT5 held little predictive value for concussion.
Nearly half (45%) of athletes with concussion performed at or even above their baseline cognitive report, which the authors said highlights the limitations of the cognitive components of SCAT5.
The most accurate predictor of concussion was participants’ responses to questions about their symptoms.
“If you get hit in the head and go to the sideline and say, ‘I have a headache, I’m dizzy, I don’t feel right,’ I can say with pretty good assurance that you have a concussion,” Dr. Harmon continued. “I don’t need to do any testing.”
Unfortunately, the problem is “that some athletes don’t want to come out. They don’t report their symptoms or may not recognize their symptoms. So then you need an objective, accurate test to tell you whether you can safely put the athlete back on the field. We don’t have that right now.”
The study did not control for concussion history, and the all–Division 1 cohort means the findings may not be generalizable to other athletes.
Nevertheless, investigators said the study “affirms that reported symptoms are the most sensitive indicator of concussion, and there are limitations to the objective cognitive testing included in the SCAT.” They concluded that concussion “remains a clinical diagnosis that should be based on a thorough review of signs, symptoms, and clinical findings.”
This study was funded in part by donations from University of Washington alumni Jack and Luellen Cherneski and the Chisholm Foundation. Dr. Harmon reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new study showed.
Investigators found that almost half of athletes diagnosed with a concussion tested normally on the Sports Concussion Assessment Tool 5 (SCAT5), the recommended tool for measuring cognitive skills in concussion evaluations. The most accurate measure of concussion was symptoms reported by the athletes.
“If you don’t do well on the cognitive exam, it suggests you have a concussion. But many people who are concussed do fine on the exam,” lead author Kimberly Harmon, MD, professor of family medicine and section head of sports medicine at the University of Washington School of Medicine, Seattle, said in a news release.
The study was published online in JAMA Network Open.
Introduced in 2004, the SCAT was created to standardize the collection of information clinicians use to diagnose concussion, including evaluation of symptoms, orientation, and balance. It also uses a 10-word list to assess immediate memory and delayed recall.
Dr. Harmon’s own experiences as a team physician led her to wonder about the accuracy of the cognitive screening portion of the SCAT. She saw that “some people were concussed, and they did well on the recall test. Some people weren’t concussed, and they didn’t do well. So I thought we should study it,” she said.
Investigators compared 92 National Collegiate Athletic Association (NCAA) Division 1 athletes who had sustained a concussion between 2020 and 2022 and had a concussion evaluation within 48 hours to 92 matched nonconcussed teammates (overall cohort, 52% men). Most concussions occurred in those who played football, followed by volleyball.
All athletes had previously completed NCAA-required baseline concussion screenings. Participants completed the SCAT5 screening test within 2 weeks of the incident concussion.
No significant differences were found between the baseline scores of athletes with and without concussion. Moreover, responses on the word recall section of the SCAT5 held little predictive value for concussion.
Nearly half (45%) of athletes with concussion performed at or even above their baseline cognitive report, which the authors said highlights the limitations of the cognitive components of SCAT5.
The most accurate predictor of concussion was participants’ responses to questions about their symptoms.
“If you get hit in the head and go to the sideline and say, ‘I have a headache, I’m dizzy, I don’t feel right,’ I can say with pretty good assurance that you have a concussion,” Dr. Harmon continued. “I don’t need to do any testing.”
Unfortunately, the problem is “that some athletes don’t want to come out. They don’t report their symptoms or may not recognize their symptoms. So then you need an objective, accurate test to tell you whether you can safely put the athlete back on the field. We don’t have that right now.”
The study did not control for concussion history, and the all–Division 1 cohort means the findings may not be generalizable to other athletes.
Nevertheless, investigators said the study “affirms that reported symptoms are the most sensitive indicator of concussion, and there are limitations to the objective cognitive testing included in the SCAT.” They concluded that concussion “remains a clinical diagnosis that should be based on a thorough review of signs, symptoms, and clinical findings.”
This study was funded in part by donations from University of Washington alumni Jack and Luellen Cherneski and the Chisholm Foundation. Dr. Harmon reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Form of B12 Deficiency Affecting the Central Nervous System May Be New Autoimmune Disease
Discovered while studying a puzzling case of one patient with inexplicable neurological systems, the same autoantibody was detected in a small percentage of healthy individuals and was nearly four times as prevalent in patients with neuropsychiatric systemic lupus erythematosus (SLE).
“I didn’t think this single investigation was going to yield a broader phenomenon with other patients,” lead author John V. Pluvinage, MD, PhD, a neurology resident at the University of California San Francisco, said in an interview. “It started as an N-of-one study just based on scientific curiosity.”
“It’s a beautifully done study,” added Betty Diamond, MD, director of the Institute of Molecular Medicine at the Feinstein Institutes for Medical Research in Manhasset, New York, commenting on the research. It uncovers “yet another example of a disease where antibodies getting into the brain are the problem.”
The research was published in Science Translational Medicine.
The Patient
The investigation began in 2014 with a 67-year-old woman presenting with difficulty speaking, ataxia, and tremor. Her blood tests showed no signs of B12 deficiency, and testing for known autoantibodies came back negative.
Solving this mystery required a more exhaustive approach. The patient enrolled in a research study focused on identifying novel autoantibodies in suspected neuroinflammatory disease, using a screening technology called phage immunoprecipitation sequencing.
“We adapted this technology to screen for autoantibodies in an unbiased manner by displaying every peptide across the human proteome and then mixing those peptides with patient antibodies in order to figure out what the antibodies are binding to,” explained Dr. Pluvinage.
Using this method, he and colleagues discovered that this woman had autoantibodies that target CD320 — a receptor important in the cellular uptake of B12. While her blood tests were normal, B12 in the patient’s cerebral spinal fluid (CSF) was “nearly undetectable,” Dr. Pluvinage said. Using an in vitro model of the blood-brain barrier (BBB), the researchers determined that anti-CD320 impaired the transport of B12 across the BBB by targeting receptors on the cell surface.
Treating the patient with a combination of immunosuppressant medication and high-dose B12 supplementation increased B12 levels in the patient’s CSF and improved clinical symptoms.
Identifying More Cases
Dr. Pluvinage and colleagues tested the 254 other individuals enrolled in the neuroinflammatory disease study and identified seven participants with CSF anti-CD320 autoantibodies — four of whom had low B12 in the CSF.
In a group of healthy controls, anti-CD320 seropositivity was 6%, similar to the positivity rate in 132 paired serum and CSF samples from a cohort of patients with multiple sclerosis (5.7%). In this group of patients with multiple sclerosis, anti-CD320 presence in the blood was highly predictive of high levels of CSF methylmalonic acid, a metabolic marker of B12 deficiency.
Researchers also screened for anti-CD320 seropositivity in 408 patients with non-neurologic SLE and 28 patients with neuropsychiatric SLE and found that the autoantibody was nearly four times as prevalent in patients with neurologic symptoms (21.4%) compared with in those with non-neurologic SLE (5.6%).
“The clinical relevance of anti-CD320 in healthy controls remains uncertain,” the authors wrote. However, it is not uncommon to have healthy patients with known autoantibodies.
“There are always people who have autoantibodies who don’t get disease, and why that is we don’t know,” said Dr. Diamond. Some individuals may develop clinical symptoms later, or there may be other reasons why they are protected against disease.
Pluvinage is eager to follow some seropositive healthy individuals to track their neurologic health overtime, to see if the presence of anti-CD320 “alters their neurologic trajectories.”
Alternative Pathways
Lastly, Dr. Pluvinage and colleagues set out to explain why patients with anti-CD320 in their blood did not show any signs of B12 deficiency. They hypothesized that another receptor may be compensating and still allowing blood cells to take up B12. Using CRISPR screening, the team identified the low-density lipoprotein receptor as an alternative pathway to B12 uptake.
“These findings suggest a model in which anti-CD320 impairs transport of B12 across the BBB, leading to autoimmune B12 central deficiency (ABCD) with varied neurologic manifestations but sparing peripheral manifestations of B12 deficiency,” the authors wrote.
The work was supported by the National Institute of Mental Health, National Center for Chronic Disease Prevention and Health Promotion, Department of Defense, UCSF Helen Diller Family Comprehensive Cancer Center Laboratory for Cell Analysis Shared Resource Facility, National Multiple Sclerosis Society, Valhalla Foundation, and the Westridge Foundation. Dr. Pluvinage is a co-inventor on a patent application related to this work. Dr. Diamond had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Discovered while studying a puzzling case of one patient with inexplicable neurological systems, the same autoantibody was detected in a small percentage of healthy individuals and was nearly four times as prevalent in patients with neuropsychiatric systemic lupus erythematosus (SLE).
“I didn’t think this single investigation was going to yield a broader phenomenon with other patients,” lead author John V. Pluvinage, MD, PhD, a neurology resident at the University of California San Francisco, said in an interview. “It started as an N-of-one study just based on scientific curiosity.”
“It’s a beautifully done study,” added Betty Diamond, MD, director of the Institute of Molecular Medicine at the Feinstein Institutes for Medical Research in Manhasset, New York, commenting on the research. It uncovers “yet another example of a disease where antibodies getting into the brain are the problem.”
The research was published in Science Translational Medicine.
The Patient
The investigation began in 2014 with a 67-year-old woman presenting with difficulty speaking, ataxia, and tremor. Her blood tests showed no signs of B12 deficiency, and testing for known autoantibodies came back negative.
Solving this mystery required a more exhaustive approach. The patient enrolled in a research study focused on identifying novel autoantibodies in suspected neuroinflammatory disease, using a screening technology called phage immunoprecipitation sequencing.
“We adapted this technology to screen for autoantibodies in an unbiased manner by displaying every peptide across the human proteome and then mixing those peptides with patient antibodies in order to figure out what the antibodies are binding to,” explained Dr. Pluvinage.
Using this method, he and colleagues discovered that this woman had autoantibodies that target CD320 — a receptor important in the cellular uptake of B12. While her blood tests were normal, B12 in the patient’s cerebral spinal fluid (CSF) was “nearly undetectable,” Dr. Pluvinage said. Using an in vitro model of the blood-brain barrier (BBB), the researchers determined that anti-CD320 impaired the transport of B12 across the BBB by targeting receptors on the cell surface.
Treating the patient with a combination of immunosuppressant medication and high-dose B12 supplementation increased B12 levels in the patient’s CSF and improved clinical symptoms.
Identifying More Cases
Dr. Pluvinage and colleagues tested the 254 other individuals enrolled in the neuroinflammatory disease study and identified seven participants with CSF anti-CD320 autoantibodies — four of whom had low B12 in the CSF.
In a group of healthy controls, anti-CD320 seropositivity was 6%, similar to the positivity rate in 132 paired serum and CSF samples from a cohort of patients with multiple sclerosis (5.7%). In this group of patients with multiple sclerosis, anti-CD320 presence in the blood was highly predictive of high levels of CSF methylmalonic acid, a metabolic marker of B12 deficiency.
Researchers also screened for anti-CD320 seropositivity in 408 patients with non-neurologic SLE and 28 patients with neuropsychiatric SLE and found that the autoantibody was nearly four times as prevalent in patients with neurologic symptoms (21.4%) compared with in those with non-neurologic SLE (5.6%).
“The clinical relevance of anti-CD320 in healthy controls remains uncertain,” the authors wrote. However, it is not uncommon to have healthy patients with known autoantibodies.
“There are always people who have autoantibodies who don’t get disease, and why that is we don’t know,” said Dr. Diamond. Some individuals may develop clinical symptoms later, or there may be other reasons why they are protected against disease.
Pluvinage is eager to follow some seropositive healthy individuals to track their neurologic health overtime, to see if the presence of anti-CD320 “alters their neurologic trajectories.”
Alternative Pathways
Lastly, Dr. Pluvinage and colleagues set out to explain why patients with anti-CD320 in their blood did not show any signs of B12 deficiency. They hypothesized that another receptor may be compensating and still allowing blood cells to take up B12. Using CRISPR screening, the team identified the low-density lipoprotein receptor as an alternative pathway to B12 uptake.
“These findings suggest a model in which anti-CD320 impairs transport of B12 across the BBB, leading to autoimmune B12 central deficiency (ABCD) with varied neurologic manifestations but sparing peripheral manifestations of B12 deficiency,” the authors wrote.
The work was supported by the National Institute of Mental Health, National Center for Chronic Disease Prevention and Health Promotion, Department of Defense, UCSF Helen Diller Family Comprehensive Cancer Center Laboratory for Cell Analysis Shared Resource Facility, National Multiple Sclerosis Society, Valhalla Foundation, and the Westridge Foundation. Dr. Pluvinage is a co-inventor on a patent application related to this work. Dr. Diamond had no relevant disclosures.
A version of this article first appeared on Medscape.com.
Discovered while studying a puzzling case of one patient with inexplicable neurological systems, the same autoantibody was detected in a small percentage of healthy individuals and was nearly four times as prevalent in patients with neuropsychiatric systemic lupus erythematosus (SLE).
“I didn’t think this single investigation was going to yield a broader phenomenon with other patients,” lead author John V. Pluvinage, MD, PhD, a neurology resident at the University of California San Francisco, said in an interview. “It started as an N-of-one study just based on scientific curiosity.”
“It’s a beautifully done study,” added Betty Diamond, MD, director of the Institute of Molecular Medicine at the Feinstein Institutes for Medical Research in Manhasset, New York, commenting on the research. It uncovers “yet another example of a disease where antibodies getting into the brain are the problem.”
The research was published in Science Translational Medicine.
The Patient
The investigation began in 2014 with a 67-year-old woman presenting with difficulty speaking, ataxia, and tremor. Her blood tests showed no signs of B12 deficiency, and testing for known autoantibodies came back negative.
Solving this mystery required a more exhaustive approach. The patient enrolled in a research study focused on identifying novel autoantibodies in suspected neuroinflammatory disease, using a screening technology called phage immunoprecipitation sequencing.
“We adapted this technology to screen for autoantibodies in an unbiased manner by displaying every peptide across the human proteome and then mixing those peptides with patient antibodies in order to figure out what the antibodies are binding to,” explained Dr. Pluvinage.
Using this method, he and colleagues discovered that this woman had autoantibodies that target CD320 — a receptor important in the cellular uptake of B12. While her blood tests were normal, B12 in the patient’s cerebral spinal fluid (CSF) was “nearly undetectable,” Dr. Pluvinage said. Using an in vitro model of the blood-brain barrier (BBB), the researchers determined that anti-CD320 impaired the transport of B12 across the BBB by targeting receptors on the cell surface.
Treating the patient with a combination of immunosuppressant medication and high-dose B12 supplementation increased B12 levels in the patient’s CSF and improved clinical symptoms.
Identifying More Cases
Dr. Pluvinage and colleagues tested the 254 other individuals enrolled in the neuroinflammatory disease study and identified seven participants with CSF anti-CD320 autoantibodies — four of whom had low B12 in the CSF.
In a group of healthy controls, anti-CD320 seropositivity was 6%, similar to the positivity rate in 132 paired serum and CSF samples from a cohort of patients with multiple sclerosis (5.7%). In this group of patients with multiple sclerosis, anti-CD320 presence in the blood was highly predictive of high levels of CSF methylmalonic acid, a metabolic marker of B12 deficiency.
Researchers also screened for anti-CD320 seropositivity in 408 patients with non-neurologic SLE and 28 patients with neuropsychiatric SLE and found that the autoantibody was nearly four times as prevalent in patients with neurologic symptoms (21.4%) compared with in those with non-neurologic SLE (5.6%).
“The clinical relevance of anti-CD320 in healthy controls remains uncertain,” the authors wrote. However, it is not uncommon to have healthy patients with known autoantibodies.
“There are always people who have autoantibodies who don’t get disease, and why that is we don’t know,” said Dr. Diamond. Some individuals may develop clinical symptoms later, or there may be other reasons why they are protected against disease.
Pluvinage is eager to follow some seropositive healthy individuals to track their neurologic health overtime, to see if the presence of anti-CD320 “alters their neurologic trajectories.”
Alternative Pathways
Lastly, Dr. Pluvinage and colleagues set out to explain why patients with anti-CD320 in their blood did not show any signs of B12 deficiency. They hypothesized that another receptor may be compensating and still allowing blood cells to take up B12. Using CRISPR screening, the team identified the low-density lipoprotein receptor as an alternative pathway to B12 uptake.
“These findings suggest a model in which anti-CD320 impairs transport of B12 across the BBB, leading to autoimmune B12 central deficiency (ABCD) with varied neurologic manifestations but sparing peripheral manifestations of B12 deficiency,” the authors wrote.
The work was supported by the National Institute of Mental Health, National Center for Chronic Disease Prevention and Health Promotion, Department of Defense, UCSF Helen Diller Family Comprehensive Cancer Center Laboratory for Cell Analysis Shared Resource Facility, National Multiple Sclerosis Society, Valhalla Foundation, and the Westridge Foundation. Dr. Pluvinage is a co-inventor on a patent application related to this work. Dr. Diamond had no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM SCIENCE TRANSLATIONAL MEDICINE
Is Screen Time to Blame for Rising Rates of Myopia in Children?
TOPLINE:
More time spent exposed to screens is associated with a higher risk for myopia in children and adolescents; the use of computers and televisions appears to have the most significant effects on eye health.
METHODOLOGY:
- Researchers conducted a meta-analysis of 19 studies involving 102,360 children and adolescents to assess the association between screen time and myopia.
- Data were collected from studies published before June 1, 2023, in three databases: PubMed, Embase, and Web of Science.
- Screen time was categorized by device type, including computers, televisions, and smartphones, and analyzed using random or fixed-effect models.
- The analysis included both cohort and cross-sectional studies.
TAKEAWAY:
- High exposure to screen time was significantly associated with myopia in both cross-sectional (odds ratio [OR], 2.24; 95% confidence interval (CI), 1.47-3.42) and cohort studies (OR, 2.39; 95% CI, 2.07-2.76).
- In cohort studies, each extra hour per day spent using screens increased the risk for myopia by 7% (95% CI, 1.01-1.13).
- Subgroup analyses revealed significant associations between myopia and screen time on computers (OR, 8.19; 95% CI, 4.78-14.04) and televisions (OR, 1.46; 95% CI, 1.02-2.10), whereas time spent using smartphones was not significantly associated with myopia.
IN PRACTICE:
“With the development of technology and GDP [gross domestic product], educational pressure may lead students to use screen devices such as smartphones and computers for long periods of time to learn online courses, receive additional tutoring or practice, and increase the incidence of myopia,” wrote the authors.
SOURCE:
The study was led by Zhiqiang Zong of Anhui Medical University in Hefei, China. It was published online in BMC Public Health.
LIMITATIONS:
The majority of the studies included were cross-sectional, which cannot establish causality. High heterogeneity was found among the included studies, possibly due to differences in research design, population characteristics, and exposure levels. Some studies did not adjust for important confounding factors such as outdoor activities.
DISCLOSURES:
The study was supported by grants from the Educational Commission of Anhui Province of China, Research Fund of Anhui Institute of Translational Medicine, and National Natural Science Foundation of China. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
More time spent exposed to screens is associated with a higher risk for myopia in children and adolescents; the use of computers and televisions appears to have the most significant effects on eye health.
METHODOLOGY:
- Researchers conducted a meta-analysis of 19 studies involving 102,360 children and adolescents to assess the association between screen time and myopia.
- Data were collected from studies published before June 1, 2023, in three databases: PubMed, Embase, and Web of Science.
- Screen time was categorized by device type, including computers, televisions, and smartphones, and analyzed using random or fixed-effect models.
- The analysis included both cohort and cross-sectional studies.
TAKEAWAY:
- High exposure to screen time was significantly associated with myopia in both cross-sectional (odds ratio [OR], 2.24; 95% confidence interval (CI), 1.47-3.42) and cohort studies (OR, 2.39; 95% CI, 2.07-2.76).
- In cohort studies, each extra hour per day spent using screens increased the risk for myopia by 7% (95% CI, 1.01-1.13).
- Subgroup analyses revealed significant associations between myopia and screen time on computers (OR, 8.19; 95% CI, 4.78-14.04) and televisions (OR, 1.46; 95% CI, 1.02-2.10), whereas time spent using smartphones was not significantly associated with myopia.
IN PRACTICE:
“With the development of technology and GDP [gross domestic product], educational pressure may lead students to use screen devices such as smartphones and computers for long periods of time to learn online courses, receive additional tutoring or practice, and increase the incidence of myopia,” wrote the authors.
SOURCE:
The study was led by Zhiqiang Zong of Anhui Medical University in Hefei, China. It was published online in BMC Public Health.
LIMITATIONS:
The majority of the studies included were cross-sectional, which cannot establish causality. High heterogeneity was found among the included studies, possibly due to differences in research design, population characteristics, and exposure levels. Some studies did not adjust for important confounding factors such as outdoor activities.
DISCLOSURES:
The study was supported by grants from the Educational Commission of Anhui Province of China, Research Fund of Anhui Institute of Translational Medicine, and National Natural Science Foundation of China. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
More time spent exposed to screens is associated with a higher risk for myopia in children and adolescents; the use of computers and televisions appears to have the most significant effects on eye health.
METHODOLOGY:
- Researchers conducted a meta-analysis of 19 studies involving 102,360 children and adolescents to assess the association between screen time and myopia.
- Data were collected from studies published before June 1, 2023, in three databases: PubMed, Embase, and Web of Science.
- Screen time was categorized by device type, including computers, televisions, and smartphones, and analyzed using random or fixed-effect models.
- The analysis included both cohort and cross-sectional studies.
TAKEAWAY:
- High exposure to screen time was significantly associated with myopia in both cross-sectional (odds ratio [OR], 2.24; 95% confidence interval (CI), 1.47-3.42) and cohort studies (OR, 2.39; 95% CI, 2.07-2.76).
- In cohort studies, each extra hour per day spent using screens increased the risk for myopia by 7% (95% CI, 1.01-1.13).
- Subgroup analyses revealed significant associations between myopia and screen time on computers (OR, 8.19; 95% CI, 4.78-14.04) and televisions (OR, 1.46; 95% CI, 1.02-2.10), whereas time spent using smartphones was not significantly associated with myopia.
IN PRACTICE:
“With the development of technology and GDP [gross domestic product], educational pressure may lead students to use screen devices such as smartphones and computers for long periods of time to learn online courses, receive additional tutoring or practice, and increase the incidence of myopia,” wrote the authors.
SOURCE:
The study was led by Zhiqiang Zong of Anhui Medical University in Hefei, China. It was published online in BMC Public Health.
LIMITATIONS:
The majority of the studies included were cross-sectional, which cannot establish causality. High heterogeneity was found among the included studies, possibly due to differences in research design, population characteristics, and exposure levels. Some studies did not adjust for important confounding factors such as outdoor activities.
DISCLOSURES:
The study was supported by grants from the Educational Commission of Anhui Province of China, Research Fund of Anhui Institute of Translational Medicine, and National Natural Science Foundation of China. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.