User login
New AAD guidelines eye comorbidities in adults with atopic dermatitis
While it’s well established that atopic dermatitis (AD) in adults is associated with asthma, allergic rhinitis, and other atopic conditions, the links between AD and other comorbidities are coming into clearer focus.
, published evidence supports an association between AD and comorbidities that may not be on the radar of clinicians and patients, including substance use, attention-deficit/hyperactivity disorder (ADHD), elements of metabolic syndrome, and various cardiovascular conditions.
“There are more comorbidities with AD than we anticipated, that are supported by data in the literature,” Dawn M.R. Davis, MD, cochair and an author of the guidelines, told this news organization. “We are learning more about the interconnectivity of various medical conditions,” she continued. “Many skin diseases over time have been noted to be impactful to the whole person and not only the skin. A classic example of that is psoriasis. We now understand that psoriasis is a multisystem inflammatory disorder.”
As for AD, “we’ve always appreciated that AD patients tend to be at higher risk for other atopic diseases such as asthma, allergic rhinoconjunctivitis, and food allergies,” said Dr. Davis, of the departments of dermatology and pediatrics at the Mayo Clinic, Rochester, Minn. “With further research, we are now able to delineate those associations more intimately and have data to support our suspicions. Additionally, we’re now understanding that these inflammatory conditions can impact more than the end organ involved, such as the skin and AD. We wanted to look at how AD can affect the whole patient.”
For the guidelines, which are the first of their kind and were published online in the Journal of the American Academy of Dermatology, Dr. Davis and project cochair Robert Sidbury, MD, MPH, chief of dermatology at Seattle Children’s Hospital, led a multidisciplinary group of 12 experts to review the association between AD and selected comorbidities. They applied the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) for prognosis approach for assessing the certainty of the evidence and provided statements of association based on the available evidence.
With respect to highlights for atopic and allergic conditions, the guideline authors found high-quality evidence that AD in adults is associated with food allergies, moderate-quality evidence that AD is associated with asthma, and low-quality evidence that AD in adults may be associated with eosinophilic esophagitis.
In the realm of mental health and substance use, ample evidence exists to support an association between AD and mental health conditions such as depression and anxiety, the guidelines state. “For many patients, low mood may be driven by the symptoms of AD, including chronic itch and poor sleep,” Dr. Davis and her coauthors wrote. “Successfully treating AD may alleviate depressive symptoms for some patients; for others, assessment and treatment specific to their mental health may be needed.”
The guidelines also state that low-quality evidence exists to suggest that AD in adults may be associated with alcohol abuse disorders and cigarette smoking.
The authors noted “limited but consistent evidence” supporting a link between AD and adverse bone health, including osteoporosis and fractures, while associations between AD and cardiovascular risk factors and comorbidities, including hypertension, myocardial infarction, and stroke, are more controversial.
“I have published on bone health and AD so that was not as surprising to me,” Dr. Davis said in the interview. “I found a lot of the evidence in the guidelines to be validating of patterns that we see in our patients. The most significant learning point for me was [the link to] cardiovascular disease and the link to specific mental health and substance use disorders. It validates how impactful AD is to the individual.”
According to the guidelines, moderate-quality evidence exists linking AD in adults to both alopecia areata and urticaria. “Because we are dermatologists and take care of both of those diseases, be mindful of that in your daily practice,” Dr. Davis advised. “I would also encourage our colleagues to remember to educate patients on the comorbidities of AD so that they are empowered, and to screen for those comorbidities in your office based on the patient and their history and physical exam, to the level that you think is appropriate for that person’s individual’s care.”
Christine Ko, MD, who was asked to comment on the guidelines, characterized some of the reported comorbidity associations as predictable, such as asthma, food allergy, allergic rhinitis, and skin infections. “As the authors comment, ‘associations between AD and other atopic and allergic conditions have been recognized for decades and even contribute to diagnostic criteria for AD,’ ” said Dr. Ko, professor of dermatology and pathology at Yale University, New Haven, Conn, who was not involved with the guidelines. “I was a bit surprised to see that atopic dermatitis in adults is associated with osteoporosis and fractures. As the authors suggest, this could be secondary to treatment with oral prednisone, and it is possible that use of dupilumab and JAK inhibitors may lessen this association.”
Shawn G. Kwatra, MD, of the department of dermatology at Johns Hopkins University, Baltimore, who was not involved with the guidelines, and was also asked to comment, said that the guidelines underscore the importance of informing adults with AD “of the risks of unchecked inflammation and the potential for multiple disease comorbidities.” Dr. Kwatra, who has AD, added that “these results make me want to be more proactive in treating my eczema to reduce the potential for development of these comorbidities.”
He pointed out that the guidelines did not address racial and ethnic differences in the observed comorbidities. “Unfortunately, minority populations have a greater comorbidity burden in many inflammatory skin diseases so this will be another area needing further investigation,” he said. “As an example, our group found from multicenter data that black patients with atopic dermatitis have higher levels of C-reactive protein, blood eosinophils, and other inflammatory biomarkers.”
The AAD guidelines are the first in a four-part series on AD expected to be published over the next 1-2 years, Dr. Davis said. The subsequent guidelines will address topicals, phototherapy/systemics, and pediatrics.
The study was funded by internal funds from the AAD. Dr. Davis reported having no financial disclosures. Dr. Sidbury disclosed that he serves as an advisory board member for Pfizer, a principal investigator for Regeneron, and an investigator for Brickell Biotech and Galderma. He is also a consultant for Galderma Global and Microes. Dr. Ko reported having no financial disclosures. Dr. Kwatra is a member of the board of directors of the Skin of Color Society. He is also an advisory board member/consultant for AbbVie, Galderma, Incyte, Pfizer, Regeneron Pharmaceuticals, and Sanofi, and has served as an investigator for Galderma, Pfizer, and Sanofi.
While it’s well established that atopic dermatitis (AD) in adults is associated with asthma, allergic rhinitis, and other atopic conditions, the links between AD and other comorbidities are coming into clearer focus.
, published evidence supports an association between AD and comorbidities that may not be on the radar of clinicians and patients, including substance use, attention-deficit/hyperactivity disorder (ADHD), elements of metabolic syndrome, and various cardiovascular conditions.
“There are more comorbidities with AD than we anticipated, that are supported by data in the literature,” Dawn M.R. Davis, MD, cochair and an author of the guidelines, told this news organization. “We are learning more about the interconnectivity of various medical conditions,” she continued. “Many skin diseases over time have been noted to be impactful to the whole person and not only the skin. A classic example of that is psoriasis. We now understand that psoriasis is a multisystem inflammatory disorder.”
As for AD, “we’ve always appreciated that AD patients tend to be at higher risk for other atopic diseases such as asthma, allergic rhinoconjunctivitis, and food allergies,” said Dr. Davis, of the departments of dermatology and pediatrics at the Mayo Clinic, Rochester, Minn. “With further research, we are now able to delineate those associations more intimately and have data to support our suspicions. Additionally, we’re now understanding that these inflammatory conditions can impact more than the end organ involved, such as the skin and AD. We wanted to look at how AD can affect the whole patient.”
For the guidelines, which are the first of their kind and were published online in the Journal of the American Academy of Dermatology, Dr. Davis and project cochair Robert Sidbury, MD, MPH, chief of dermatology at Seattle Children’s Hospital, led a multidisciplinary group of 12 experts to review the association between AD and selected comorbidities. They applied the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) for prognosis approach for assessing the certainty of the evidence and provided statements of association based on the available evidence.
With respect to highlights for atopic and allergic conditions, the guideline authors found high-quality evidence that AD in adults is associated with food allergies, moderate-quality evidence that AD is associated with asthma, and low-quality evidence that AD in adults may be associated with eosinophilic esophagitis.
In the realm of mental health and substance use, ample evidence exists to support an association between AD and mental health conditions such as depression and anxiety, the guidelines state. “For many patients, low mood may be driven by the symptoms of AD, including chronic itch and poor sleep,” Dr. Davis and her coauthors wrote. “Successfully treating AD may alleviate depressive symptoms for some patients; for others, assessment and treatment specific to their mental health may be needed.”
The guidelines also state that low-quality evidence exists to suggest that AD in adults may be associated with alcohol abuse disorders and cigarette smoking.
The authors noted “limited but consistent evidence” supporting a link between AD and adverse bone health, including osteoporosis and fractures, while associations between AD and cardiovascular risk factors and comorbidities, including hypertension, myocardial infarction, and stroke, are more controversial.
“I have published on bone health and AD so that was not as surprising to me,” Dr. Davis said in the interview. “I found a lot of the evidence in the guidelines to be validating of patterns that we see in our patients. The most significant learning point for me was [the link to] cardiovascular disease and the link to specific mental health and substance use disorders. It validates how impactful AD is to the individual.”
According to the guidelines, moderate-quality evidence exists linking AD in adults to both alopecia areata and urticaria. “Because we are dermatologists and take care of both of those diseases, be mindful of that in your daily practice,” Dr. Davis advised. “I would also encourage our colleagues to remember to educate patients on the comorbidities of AD so that they are empowered, and to screen for those comorbidities in your office based on the patient and their history and physical exam, to the level that you think is appropriate for that person’s individual’s care.”
Christine Ko, MD, who was asked to comment on the guidelines, characterized some of the reported comorbidity associations as predictable, such as asthma, food allergy, allergic rhinitis, and skin infections. “As the authors comment, ‘associations between AD and other atopic and allergic conditions have been recognized for decades and even contribute to diagnostic criteria for AD,’ ” said Dr. Ko, professor of dermatology and pathology at Yale University, New Haven, Conn, who was not involved with the guidelines. “I was a bit surprised to see that atopic dermatitis in adults is associated with osteoporosis and fractures. As the authors suggest, this could be secondary to treatment with oral prednisone, and it is possible that use of dupilumab and JAK inhibitors may lessen this association.”
Shawn G. Kwatra, MD, of the department of dermatology at Johns Hopkins University, Baltimore, who was not involved with the guidelines, and was also asked to comment, said that the guidelines underscore the importance of informing adults with AD “of the risks of unchecked inflammation and the potential for multiple disease comorbidities.” Dr. Kwatra, who has AD, added that “these results make me want to be more proactive in treating my eczema to reduce the potential for development of these comorbidities.”
He pointed out that the guidelines did not address racial and ethnic differences in the observed comorbidities. “Unfortunately, minority populations have a greater comorbidity burden in many inflammatory skin diseases so this will be another area needing further investigation,” he said. “As an example, our group found from multicenter data that black patients with atopic dermatitis have higher levels of C-reactive protein, blood eosinophils, and other inflammatory biomarkers.”
The AAD guidelines are the first in a four-part series on AD expected to be published over the next 1-2 years, Dr. Davis said. The subsequent guidelines will address topicals, phototherapy/systemics, and pediatrics.
The study was funded by internal funds from the AAD. Dr. Davis reported having no financial disclosures. Dr. Sidbury disclosed that he serves as an advisory board member for Pfizer, a principal investigator for Regeneron, and an investigator for Brickell Biotech and Galderma. He is also a consultant for Galderma Global and Microes. Dr. Ko reported having no financial disclosures. Dr. Kwatra is a member of the board of directors of the Skin of Color Society. He is also an advisory board member/consultant for AbbVie, Galderma, Incyte, Pfizer, Regeneron Pharmaceuticals, and Sanofi, and has served as an investigator for Galderma, Pfizer, and Sanofi.
While it’s well established that atopic dermatitis (AD) in adults is associated with asthma, allergic rhinitis, and other atopic conditions, the links between AD and other comorbidities are coming into clearer focus.
, published evidence supports an association between AD and comorbidities that may not be on the radar of clinicians and patients, including substance use, attention-deficit/hyperactivity disorder (ADHD), elements of metabolic syndrome, and various cardiovascular conditions.
“There are more comorbidities with AD than we anticipated, that are supported by data in the literature,” Dawn M.R. Davis, MD, cochair and an author of the guidelines, told this news organization. “We are learning more about the interconnectivity of various medical conditions,” she continued. “Many skin diseases over time have been noted to be impactful to the whole person and not only the skin. A classic example of that is psoriasis. We now understand that psoriasis is a multisystem inflammatory disorder.”
As for AD, “we’ve always appreciated that AD patients tend to be at higher risk for other atopic diseases such as asthma, allergic rhinoconjunctivitis, and food allergies,” said Dr. Davis, of the departments of dermatology and pediatrics at the Mayo Clinic, Rochester, Minn. “With further research, we are now able to delineate those associations more intimately and have data to support our suspicions. Additionally, we’re now understanding that these inflammatory conditions can impact more than the end organ involved, such as the skin and AD. We wanted to look at how AD can affect the whole patient.”
For the guidelines, which are the first of their kind and were published online in the Journal of the American Academy of Dermatology, Dr. Davis and project cochair Robert Sidbury, MD, MPH, chief of dermatology at Seattle Children’s Hospital, led a multidisciplinary group of 12 experts to review the association between AD and selected comorbidities. They applied the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) for prognosis approach for assessing the certainty of the evidence and provided statements of association based on the available evidence.
With respect to highlights for atopic and allergic conditions, the guideline authors found high-quality evidence that AD in adults is associated with food allergies, moderate-quality evidence that AD is associated with asthma, and low-quality evidence that AD in adults may be associated with eosinophilic esophagitis.
In the realm of mental health and substance use, ample evidence exists to support an association between AD and mental health conditions such as depression and anxiety, the guidelines state. “For many patients, low mood may be driven by the symptoms of AD, including chronic itch and poor sleep,” Dr. Davis and her coauthors wrote. “Successfully treating AD may alleviate depressive symptoms for some patients; for others, assessment and treatment specific to their mental health may be needed.”
The guidelines also state that low-quality evidence exists to suggest that AD in adults may be associated with alcohol abuse disorders and cigarette smoking.
The authors noted “limited but consistent evidence” supporting a link between AD and adverse bone health, including osteoporosis and fractures, while associations between AD and cardiovascular risk factors and comorbidities, including hypertension, myocardial infarction, and stroke, are more controversial.
“I have published on bone health and AD so that was not as surprising to me,” Dr. Davis said in the interview. “I found a lot of the evidence in the guidelines to be validating of patterns that we see in our patients. The most significant learning point for me was [the link to] cardiovascular disease and the link to specific mental health and substance use disorders. It validates how impactful AD is to the individual.”
According to the guidelines, moderate-quality evidence exists linking AD in adults to both alopecia areata and urticaria. “Because we are dermatologists and take care of both of those diseases, be mindful of that in your daily practice,” Dr. Davis advised. “I would also encourage our colleagues to remember to educate patients on the comorbidities of AD so that they are empowered, and to screen for those comorbidities in your office based on the patient and their history and physical exam, to the level that you think is appropriate for that person’s individual’s care.”
Christine Ko, MD, who was asked to comment on the guidelines, characterized some of the reported comorbidity associations as predictable, such as asthma, food allergy, allergic rhinitis, and skin infections. “As the authors comment, ‘associations between AD and other atopic and allergic conditions have been recognized for decades and even contribute to diagnostic criteria for AD,’ ” said Dr. Ko, professor of dermatology and pathology at Yale University, New Haven, Conn, who was not involved with the guidelines. “I was a bit surprised to see that atopic dermatitis in adults is associated with osteoporosis and fractures. As the authors suggest, this could be secondary to treatment with oral prednisone, and it is possible that use of dupilumab and JAK inhibitors may lessen this association.”
Shawn G. Kwatra, MD, of the department of dermatology at Johns Hopkins University, Baltimore, who was not involved with the guidelines, and was also asked to comment, said that the guidelines underscore the importance of informing adults with AD “of the risks of unchecked inflammation and the potential for multiple disease comorbidities.” Dr. Kwatra, who has AD, added that “these results make me want to be more proactive in treating my eczema to reduce the potential for development of these comorbidities.”
He pointed out that the guidelines did not address racial and ethnic differences in the observed comorbidities. “Unfortunately, minority populations have a greater comorbidity burden in many inflammatory skin diseases so this will be another area needing further investigation,” he said. “As an example, our group found from multicenter data that black patients with atopic dermatitis have higher levels of C-reactive protein, blood eosinophils, and other inflammatory biomarkers.”
The AAD guidelines are the first in a four-part series on AD expected to be published over the next 1-2 years, Dr. Davis said. The subsequent guidelines will address topicals, phototherapy/systemics, and pediatrics.
The study was funded by internal funds from the AAD. Dr. Davis reported having no financial disclosures. Dr. Sidbury disclosed that he serves as an advisory board member for Pfizer, a principal investigator for Regeneron, and an investigator for Brickell Biotech and Galderma. He is also a consultant for Galderma Global and Microes. Dr. Ko reported having no financial disclosures. Dr. Kwatra is a member of the board of directors of the Skin of Color Society. He is also an advisory board member/consultant for AbbVie, Galderma, Incyte, Pfizer, Regeneron Pharmaceuticals, and Sanofi, and has served as an investigator for Galderma, Pfizer, and Sanofi.
FROM JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Lilly calls it quits on baricitinib’s development for lupus
The company is also in talks with the FDA about how to move forward with the drug’s development for atopic dermatitis.
from two pivotal phase 3 trials, SLE-BRAVE-I and II, the company announced Jan. 28.
Lilly said that the primary endpoint of the SLE-BRAVE-I trial, the proportion of adults with active SLE who met criteria for response on the SLE Responder Index-4 at week 52, was significantly greater among patients treated with 4 mg baricitinib daily than with placebo. However, this endpoint was not met in SLE-BRAVE-II, and no key secondary endpoints were met in either trial. In the announcement, Lilly noted that safety was not a reason for discontinuation because data from these trials were consistent with those previously seen with baricitinib.
The company statement said that it will work with investigators on concluding the combined long-term extension study of the trials.
Baricitinib, a Janus kinase (JAK) inhibitor, had previously shown promising results in a phase 2 trial in patients with SLE. It is approved by the U.S. Food and Drug Administration for treating adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response to one or more tumor necrosis factor blockers at a dose of 2 mg once daily and has an emergency use authorization for the treatment of hospitalized patients with COVID-19.
The decision to stop baricitinib’s development for SLE will not affect other research efforts with the drug, the company said.
Development for atopic dermatitis
Lilly also noted that it is in discussion with the FDA about the status of a supplemental new drug application of baricitinib for the treatment of adults with moderate to severe atopic dermatitis (AD). In its press release, Lilly said, “At this point, the company does not have alignment with the FDA on the indicated population. Given the agency’s position, there is a possibility that this could lead to a Complete Response Letter (CRL). The efficacy and safety profile of Olumiant was evaluated in eight atopic dermatitis clinical trials (six double-blind, randomized, placebo-controlled studies and two long-term extension studies) inclusive of patients whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. The safety profile in these trials was consistent with previously published Olumiant data.”
Baricitinib was the first JAK inhibitor approved to treat patients with moderate to severe AD who have an inadequate response to topical treatments in the European Union and Japan.
The Lilly announcement was made with Incyte, the company that discovered baricitinib.
The company is also in talks with the FDA about how to move forward with the drug’s development for atopic dermatitis.
The company is also in talks with the FDA about how to move forward with the drug’s development for atopic dermatitis.
from two pivotal phase 3 trials, SLE-BRAVE-I and II, the company announced Jan. 28.
Lilly said that the primary endpoint of the SLE-BRAVE-I trial, the proportion of adults with active SLE who met criteria for response on the SLE Responder Index-4 at week 52, was significantly greater among patients treated with 4 mg baricitinib daily than with placebo. However, this endpoint was not met in SLE-BRAVE-II, and no key secondary endpoints were met in either trial. In the announcement, Lilly noted that safety was not a reason for discontinuation because data from these trials were consistent with those previously seen with baricitinib.
The company statement said that it will work with investigators on concluding the combined long-term extension study of the trials.
Baricitinib, a Janus kinase (JAK) inhibitor, had previously shown promising results in a phase 2 trial in patients with SLE. It is approved by the U.S. Food and Drug Administration for treating adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response to one or more tumor necrosis factor blockers at a dose of 2 mg once daily and has an emergency use authorization for the treatment of hospitalized patients with COVID-19.
The decision to stop baricitinib’s development for SLE will not affect other research efforts with the drug, the company said.
Development for atopic dermatitis
Lilly also noted that it is in discussion with the FDA about the status of a supplemental new drug application of baricitinib for the treatment of adults with moderate to severe atopic dermatitis (AD). In its press release, Lilly said, “At this point, the company does not have alignment with the FDA on the indicated population. Given the agency’s position, there is a possibility that this could lead to a Complete Response Letter (CRL). The efficacy and safety profile of Olumiant was evaluated in eight atopic dermatitis clinical trials (six double-blind, randomized, placebo-controlled studies and two long-term extension studies) inclusive of patients whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. The safety profile in these trials was consistent with previously published Olumiant data.”
Baricitinib was the first JAK inhibitor approved to treat patients with moderate to severe AD who have an inadequate response to topical treatments in the European Union and Japan.
The Lilly announcement was made with Incyte, the company that discovered baricitinib.
from two pivotal phase 3 trials, SLE-BRAVE-I and II, the company announced Jan. 28.
Lilly said that the primary endpoint of the SLE-BRAVE-I trial, the proportion of adults with active SLE who met criteria for response on the SLE Responder Index-4 at week 52, was significantly greater among patients treated with 4 mg baricitinib daily than with placebo. However, this endpoint was not met in SLE-BRAVE-II, and no key secondary endpoints were met in either trial. In the announcement, Lilly noted that safety was not a reason for discontinuation because data from these trials were consistent with those previously seen with baricitinib.
The company statement said that it will work with investigators on concluding the combined long-term extension study of the trials.
Baricitinib, a Janus kinase (JAK) inhibitor, had previously shown promising results in a phase 2 trial in patients with SLE. It is approved by the U.S. Food and Drug Administration for treating adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response to one or more tumor necrosis factor blockers at a dose of 2 mg once daily and has an emergency use authorization for the treatment of hospitalized patients with COVID-19.
The decision to stop baricitinib’s development for SLE will not affect other research efforts with the drug, the company said.
Development for atopic dermatitis
Lilly also noted that it is in discussion with the FDA about the status of a supplemental new drug application of baricitinib for the treatment of adults with moderate to severe atopic dermatitis (AD). In its press release, Lilly said, “At this point, the company does not have alignment with the FDA on the indicated population. Given the agency’s position, there is a possibility that this could lead to a Complete Response Letter (CRL). The efficacy and safety profile of Olumiant was evaluated in eight atopic dermatitis clinical trials (six double-blind, randomized, placebo-controlled studies and two long-term extension studies) inclusive of patients whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. The safety profile in these trials was consistent with previously published Olumiant data.”
Baricitinib was the first JAK inhibitor approved to treat patients with moderate to severe AD who have an inadequate response to topical treatments in the European Union and Japan.
The Lilly announcement was made with Incyte, the company that discovered baricitinib.
Perception of atopic dermatitis severity often differs between patients, physicians
It’s no secret that atopic dermatitis (AD) is associated with a high burden of disease, with an impact on sleep disturbance, increased anxiety, depression, reduced function and productivity at work and school, and overall decreased quality of life.
But to complicate matters, , according to Zelma Chiesa Fuxench, MD, a dermatologist at the University of Pennsylvania, Philadelphia. For example, a cross-sectional study of 678 patients with AD, which assessed disease severity based on self-reports and physician-reported disease severity using components of the Eczema Area and Severity Index score, found that the level of agreement matched in about 68% of the cases. However, in about 32% of cases, there was a mismatch between how patients and physicians rated disease severity. In about 11% of the cases, patients reported a higher degree of disease severity, compared with physicians, while in about 20% of cases, patients reported lower disease severity, compared with the physician assessment.
“This has potential implications for overestimating or underestimating disease burden and could impact our treatment of AD patients,” Dr. Chiesa Fuxench said at the Revolutionizing Atopic Dermatitis symposium.
The study also found that, while the pattern of agreement was not affected by the extent of AD in terms of the body surface area, the use of immunomodulatory drugs, or the Eczema Area and Severity Index (EASI) score, increased sleep disturbance did have an influence. Also, quality of life was lower and a higher impact on work productivity was observed when patients rated their disease severity higher than the rating of physicians.
Measures to assess disease severity
“If we understand that there is mismatch between how a patient experiences their disease and how physicians rate it, what can we do to be better at assessing disease severity in AD to truly capture the full disease burden in patients with AD?” Dr. Chiesa Fuxench asked. She noted that different validated measures have been described in the literature, and objective assessment tools often used in clinical trials include the EASI and the SCORing Atopic Dermatitis (SCORAD). “These are measures that are done by the physician that take into account the extent of the body surface area involvement and also the intensity of the lesions such as how red or thick they are,” she said. “In addition, the SCORAD will also take into account the patient-reported intensity level of itch and sleep loss.”
The Patient-Oriented SCORAD (PO-SCORAD) is similar to the SCORAD except that it is completed by the patient or the patient’s caregiver. In all three outcome measures, a higher score indicates a higher level of disease severity. Other measures that have been frequently described in the literature include the Patient-Oriented Eczema Measure (POEM), which takes into account seven symptoms scored over the last week (itch, sleep, weeping/oozing, cracking, flaking, and dryness/roughness), with higher scores indicating increased disease severity, and the Dermatology Life Quality Index (DLQI), which is a generic measure to assess the burden of skin diseases including AD. The DLQI “asks 10 questions as they relate to the impact of health-related quality of life over the last week, with higher scores indicating more severe disease,” Dr. Chiesa Fuxench said.
There are also symptom-specific scales such as the Pruritus Numerical Rating Scale (Pruritus-NRS) that measures the impact of itch on a scale of 0 to 10, and the Three-Item Severity Scale (TIS) and the Validated Investigator Global Assessment (v-IGA) that are used to assess different measures in terms of intensity of the lesions.”
However, the study that looked at the discordance between AD severity reported by physicians and patients also found that awareness and use of clinical and patient-reported measures for assessing AD disease severity among physicians was low. The authors further divided their findings among primary care physicians, dermatologists, and allergists/immunologists. “While dermatologists and allergists/immunologists reported being more aware of these outcome measures, a high proportion of physicians within this group were not using these outcomes measures in daily clinical practice,” Dr. Chiesa Fuxench said.
“Is there a need for us to use more than one outcome measure instrument when trying to assess the impact of AD, understanding that many of us practice in a very busy clinical setting? The answer is probably yes. The use of multiple assessment tools that measure different domains could potentially help better capture the broad manifestations of AD, because of the complex nature of disease burden in this population. In addition, there are studies showing poor correlation between patient-reported and physician-assessed disease severity for various instruments, emphasizing the point that these measures may be capturing very different things.”
With so many measures to choose from and limited time in the office, which ones should clinicians use? Harmonizing Outcome Measures for Eczema (HOME), based at the Center of Evidence-based Dermatology, at the University of Nottingham (England), is a consortium of patients and other key stakeholders in AD aiming to develop a consensus-based core outcome set for clinical trials and clinical practice. At a consensus meeting in 2018, the consortium reported that the PO-SCORAD and the POEM could be used in the clinical setting to better capture the true level of disease severity and burden in patients with AD.
The PO-SCORAD is also available as an App. A PO-SCORAD of less than 25 is associated with mild disease; a PO-SCORAD between 25 and 50 is associated with moderate disease, and a PO-SCORAD of greater than 50 is associated with severe disease.
“It’s recommended that patients capture the PO-SCORAD once or twice a week,” Dr. Chiesa Fuxench said, noting that the newer version of the App includes photos of different skin types to make it more relevant for a larger number of patients.
Another advantage of using the App is that a patient can track their disease severity through time. They can upload photographs, or they can send you a graphical input of their disease severity either through e-mail or print it out and bring it to their office visit to share the results with you.”
A prospective observational European study of 471 adult and pediatric patients with AD found a statistically significant correlation between SCORAD and PO-SCORAD results at day 0 and day 28. A separate large study conducted in 12 countries found that PO-SCORAD was the only self-assessment score to be highly correlated with the SCORAD index and POEM (A Spearman’s correlation coefficient of greater than or equal to 0.70). In that study, PO-SCORAD also correlated most closely with the results of the DLQI (r = 0.67) and the Dermatitis Family Questionnaire Impact DFQI (r = 0.56).
A more recent study of almost 300 adults with AD that examined the correlations between PO-SCORAD, POEM, and DLQI yielded similar findings.
Other researchers are aiming to assess the full burden of AD at the patient level. Drawing from a cross-sectional study called AWARE (Adults With Atopic Dermatitis Reporting on their Experience), an international observational study, investigators sought to identify what terms AD patients were using to describe their disease. The most commonly used terms were itch (37%), embarrassed (37%), annoyed (35%), pain (25%), and frustration (22%). “Although our study did not identify all patient-reported consequences of AD, such as the known impact of AD on sexual health, our qualitative approach has provided an understanding of patient perceptions and the underlying range of physical and emotional consequences of AD, which can inform shared decision-making,” the authors wrote. “These findings suggest the need for broader assessment of the impact of AD on patients’ lives,” they added.
Dr. Chiesa Fuxench reported having no disclosures relevant to her presentation.
The study on AD severity reported by physicians and patients was funded by Sanofi and Regeneron Pharmaceuticals, and several authors were employees of those companies.
It’s no secret that atopic dermatitis (AD) is associated with a high burden of disease, with an impact on sleep disturbance, increased anxiety, depression, reduced function and productivity at work and school, and overall decreased quality of life.
But to complicate matters, , according to Zelma Chiesa Fuxench, MD, a dermatologist at the University of Pennsylvania, Philadelphia. For example, a cross-sectional study of 678 patients with AD, which assessed disease severity based on self-reports and physician-reported disease severity using components of the Eczema Area and Severity Index score, found that the level of agreement matched in about 68% of the cases. However, in about 32% of cases, there was a mismatch between how patients and physicians rated disease severity. In about 11% of the cases, patients reported a higher degree of disease severity, compared with physicians, while in about 20% of cases, patients reported lower disease severity, compared with the physician assessment.
“This has potential implications for overestimating or underestimating disease burden and could impact our treatment of AD patients,” Dr. Chiesa Fuxench said at the Revolutionizing Atopic Dermatitis symposium.
The study also found that, while the pattern of agreement was not affected by the extent of AD in terms of the body surface area, the use of immunomodulatory drugs, or the Eczema Area and Severity Index (EASI) score, increased sleep disturbance did have an influence. Also, quality of life was lower and a higher impact on work productivity was observed when patients rated their disease severity higher than the rating of physicians.
Measures to assess disease severity
“If we understand that there is mismatch between how a patient experiences their disease and how physicians rate it, what can we do to be better at assessing disease severity in AD to truly capture the full disease burden in patients with AD?” Dr. Chiesa Fuxench asked. She noted that different validated measures have been described in the literature, and objective assessment tools often used in clinical trials include the EASI and the SCORing Atopic Dermatitis (SCORAD). “These are measures that are done by the physician that take into account the extent of the body surface area involvement and also the intensity of the lesions such as how red or thick they are,” she said. “In addition, the SCORAD will also take into account the patient-reported intensity level of itch and sleep loss.”
The Patient-Oriented SCORAD (PO-SCORAD) is similar to the SCORAD except that it is completed by the patient or the patient’s caregiver. In all three outcome measures, a higher score indicates a higher level of disease severity. Other measures that have been frequently described in the literature include the Patient-Oriented Eczema Measure (POEM), which takes into account seven symptoms scored over the last week (itch, sleep, weeping/oozing, cracking, flaking, and dryness/roughness), with higher scores indicating increased disease severity, and the Dermatology Life Quality Index (DLQI), which is a generic measure to assess the burden of skin diseases including AD. The DLQI “asks 10 questions as they relate to the impact of health-related quality of life over the last week, with higher scores indicating more severe disease,” Dr. Chiesa Fuxench said.
There are also symptom-specific scales such as the Pruritus Numerical Rating Scale (Pruritus-NRS) that measures the impact of itch on a scale of 0 to 10, and the Three-Item Severity Scale (TIS) and the Validated Investigator Global Assessment (v-IGA) that are used to assess different measures in terms of intensity of the lesions.”
However, the study that looked at the discordance between AD severity reported by physicians and patients also found that awareness and use of clinical and patient-reported measures for assessing AD disease severity among physicians was low. The authors further divided their findings among primary care physicians, dermatologists, and allergists/immunologists. “While dermatologists and allergists/immunologists reported being more aware of these outcome measures, a high proportion of physicians within this group were not using these outcomes measures in daily clinical practice,” Dr. Chiesa Fuxench said.
“Is there a need for us to use more than one outcome measure instrument when trying to assess the impact of AD, understanding that many of us practice in a very busy clinical setting? The answer is probably yes. The use of multiple assessment tools that measure different domains could potentially help better capture the broad manifestations of AD, because of the complex nature of disease burden in this population. In addition, there are studies showing poor correlation between patient-reported and physician-assessed disease severity for various instruments, emphasizing the point that these measures may be capturing very different things.”
With so many measures to choose from and limited time in the office, which ones should clinicians use? Harmonizing Outcome Measures for Eczema (HOME), based at the Center of Evidence-based Dermatology, at the University of Nottingham (England), is a consortium of patients and other key stakeholders in AD aiming to develop a consensus-based core outcome set for clinical trials and clinical practice. At a consensus meeting in 2018, the consortium reported that the PO-SCORAD and the POEM could be used in the clinical setting to better capture the true level of disease severity and burden in patients with AD.
The PO-SCORAD is also available as an App. A PO-SCORAD of less than 25 is associated with mild disease; a PO-SCORAD between 25 and 50 is associated with moderate disease, and a PO-SCORAD of greater than 50 is associated with severe disease.
“It’s recommended that patients capture the PO-SCORAD once or twice a week,” Dr. Chiesa Fuxench said, noting that the newer version of the App includes photos of different skin types to make it more relevant for a larger number of patients.
Another advantage of using the App is that a patient can track their disease severity through time. They can upload photographs, or they can send you a graphical input of their disease severity either through e-mail or print it out and bring it to their office visit to share the results with you.”
A prospective observational European study of 471 adult and pediatric patients with AD found a statistically significant correlation between SCORAD and PO-SCORAD results at day 0 and day 28. A separate large study conducted in 12 countries found that PO-SCORAD was the only self-assessment score to be highly correlated with the SCORAD index and POEM (A Spearman’s correlation coefficient of greater than or equal to 0.70). In that study, PO-SCORAD also correlated most closely with the results of the DLQI (r = 0.67) and the Dermatitis Family Questionnaire Impact DFQI (r = 0.56).
A more recent study of almost 300 adults with AD that examined the correlations between PO-SCORAD, POEM, and DLQI yielded similar findings.
Other researchers are aiming to assess the full burden of AD at the patient level. Drawing from a cross-sectional study called AWARE (Adults With Atopic Dermatitis Reporting on their Experience), an international observational study, investigators sought to identify what terms AD patients were using to describe their disease. The most commonly used terms were itch (37%), embarrassed (37%), annoyed (35%), pain (25%), and frustration (22%). “Although our study did not identify all patient-reported consequences of AD, such as the known impact of AD on sexual health, our qualitative approach has provided an understanding of patient perceptions and the underlying range of physical and emotional consequences of AD, which can inform shared decision-making,” the authors wrote. “These findings suggest the need for broader assessment of the impact of AD on patients’ lives,” they added.
Dr. Chiesa Fuxench reported having no disclosures relevant to her presentation.
The study on AD severity reported by physicians and patients was funded by Sanofi and Regeneron Pharmaceuticals, and several authors were employees of those companies.
It’s no secret that atopic dermatitis (AD) is associated with a high burden of disease, with an impact on sleep disturbance, increased anxiety, depression, reduced function and productivity at work and school, and overall decreased quality of life.
But to complicate matters, , according to Zelma Chiesa Fuxench, MD, a dermatologist at the University of Pennsylvania, Philadelphia. For example, a cross-sectional study of 678 patients with AD, which assessed disease severity based on self-reports and physician-reported disease severity using components of the Eczema Area and Severity Index score, found that the level of agreement matched in about 68% of the cases. However, in about 32% of cases, there was a mismatch between how patients and physicians rated disease severity. In about 11% of the cases, patients reported a higher degree of disease severity, compared with physicians, while in about 20% of cases, patients reported lower disease severity, compared with the physician assessment.
“This has potential implications for overestimating or underestimating disease burden and could impact our treatment of AD patients,” Dr. Chiesa Fuxench said at the Revolutionizing Atopic Dermatitis symposium.
The study also found that, while the pattern of agreement was not affected by the extent of AD in terms of the body surface area, the use of immunomodulatory drugs, or the Eczema Area and Severity Index (EASI) score, increased sleep disturbance did have an influence. Also, quality of life was lower and a higher impact on work productivity was observed when patients rated their disease severity higher than the rating of physicians.
Measures to assess disease severity
“If we understand that there is mismatch between how a patient experiences their disease and how physicians rate it, what can we do to be better at assessing disease severity in AD to truly capture the full disease burden in patients with AD?” Dr. Chiesa Fuxench asked. She noted that different validated measures have been described in the literature, and objective assessment tools often used in clinical trials include the EASI and the SCORing Atopic Dermatitis (SCORAD). “These are measures that are done by the physician that take into account the extent of the body surface area involvement and also the intensity of the lesions such as how red or thick they are,” she said. “In addition, the SCORAD will also take into account the patient-reported intensity level of itch and sleep loss.”
The Patient-Oriented SCORAD (PO-SCORAD) is similar to the SCORAD except that it is completed by the patient or the patient’s caregiver. In all three outcome measures, a higher score indicates a higher level of disease severity. Other measures that have been frequently described in the literature include the Patient-Oriented Eczema Measure (POEM), which takes into account seven symptoms scored over the last week (itch, sleep, weeping/oozing, cracking, flaking, and dryness/roughness), with higher scores indicating increased disease severity, and the Dermatology Life Quality Index (DLQI), which is a generic measure to assess the burden of skin diseases including AD. The DLQI “asks 10 questions as they relate to the impact of health-related quality of life over the last week, with higher scores indicating more severe disease,” Dr. Chiesa Fuxench said.
There are also symptom-specific scales such as the Pruritus Numerical Rating Scale (Pruritus-NRS) that measures the impact of itch on a scale of 0 to 10, and the Three-Item Severity Scale (TIS) and the Validated Investigator Global Assessment (v-IGA) that are used to assess different measures in terms of intensity of the lesions.”
However, the study that looked at the discordance between AD severity reported by physicians and patients also found that awareness and use of clinical and patient-reported measures for assessing AD disease severity among physicians was low. The authors further divided their findings among primary care physicians, dermatologists, and allergists/immunologists. “While dermatologists and allergists/immunologists reported being more aware of these outcome measures, a high proportion of physicians within this group were not using these outcomes measures in daily clinical practice,” Dr. Chiesa Fuxench said.
“Is there a need for us to use more than one outcome measure instrument when trying to assess the impact of AD, understanding that many of us practice in a very busy clinical setting? The answer is probably yes. The use of multiple assessment tools that measure different domains could potentially help better capture the broad manifestations of AD, because of the complex nature of disease burden in this population. In addition, there are studies showing poor correlation between patient-reported and physician-assessed disease severity for various instruments, emphasizing the point that these measures may be capturing very different things.”
With so many measures to choose from and limited time in the office, which ones should clinicians use? Harmonizing Outcome Measures for Eczema (HOME), based at the Center of Evidence-based Dermatology, at the University of Nottingham (England), is a consortium of patients and other key stakeholders in AD aiming to develop a consensus-based core outcome set for clinical trials and clinical practice. At a consensus meeting in 2018, the consortium reported that the PO-SCORAD and the POEM could be used in the clinical setting to better capture the true level of disease severity and burden in patients with AD.
The PO-SCORAD is also available as an App. A PO-SCORAD of less than 25 is associated with mild disease; a PO-SCORAD between 25 and 50 is associated with moderate disease, and a PO-SCORAD of greater than 50 is associated with severe disease.
“It’s recommended that patients capture the PO-SCORAD once or twice a week,” Dr. Chiesa Fuxench said, noting that the newer version of the App includes photos of different skin types to make it more relevant for a larger number of patients.
Another advantage of using the App is that a patient can track their disease severity through time. They can upload photographs, or they can send you a graphical input of their disease severity either through e-mail or print it out and bring it to their office visit to share the results with you.”
A prospective observational European study of 471 adult and pediatric patients with AD found a statistically significant correlation between SCORAD and PO-SCORAD results at day 0 and day 28. A separate large study conducted in 12 countries found that PO-SCORAD was the only self-assessment score to be highly correlated with the SCORAD index and POEM (A Spearman’s correlation coefficient of greater than or equal to 0.70). In that study, PO-SCORAD also correlated most closely with the results of the DLQI (r = 0.67) and the Dermatitis Family Questionnaire Impact DFQI (r = 0.56).
A more recent study of almost 300 adults with AD that examined the correlations between PO-SCORAD, POEM, and DLQI yielded similar findings.
Other researchers are aiming to assess the full burden of AD at the patient level. Drawing from a cross-sectional study called AWARE (Adults With Atopic Dermatitis Reporting on their Experience), an international observational study, investigators sought to identify what terms AD patients were using to describe their disease. The most commonly used terms were itch (37%), embarrassed (37%), annoyed (35%), pain (25%), and frustration (22%). “Although our study did not identify all patient-reported consequences of AD, such as the known impact of AD on sexual health, our qualitative approach has provided an understanding of patient perceptions and the underlying range of physical and emotional consequences of AD, which can inform shared decision-making,” the authors wrote. “These findings suggest the need for broader assessment of the impact of AD on patients’ lives,” they added.
Dr. Chiesa Fuxench reported having no disclosures relevant to her presentation.
The study on AD severity reported by physicians and patients was funded by Sanofi and Regeneron Pharmaceuticals, and several authors were employees of those companies.
FROM REVOLUTIONIZING AD 2021
Brain stimulation for improved memory?
Electrical brain stimulation may have the potential to improve verbal memory, results of a small study of patients with epilepsy suggest.
Investigators observed improvements in patients implanted with a responsive neurostimulation system (RNS) to control seizures, in that the patients had improved word recall when the system was activated.

Beyond epilepsy, “we suspect that our results would be broadly applicable regardless of the underlying condition, for example, memory loss with Alzheimer’s disease or traumatic brain injury,” Zulfi Haneef, MBBS, MD, associate professor of neurology, Baylor College of Medicine, Houston, said in an interview.
“Mental health conditions such as depression or psychosis could also benefit from targeted electrical stimulation. While we focused on enhancing a preferred brain function [such as memory], parallel areas of research may target enhancing function [such as weakness following stroke] or suppressing function [to manage conditions such as chronic pain,]” Dr. Haneef added.
The study was published online Jan. 17, 2022, in Neurosurgery.
As reported by this news organization, Following implantation of the system, patients attend the clinic for adjustments about every 8-12 weeks.
The investigators studied 17 patients with epilepsy and RNS implants who attended the clinic for routine appointments. A clinical neuropsychologist administered the Hopkins Verbal Learning Test–Revised (HVLT-R), a well-validated list-learning measure of memory and verbal learning.
Patients were read a list of 12 semantically related words and asked to recall the list after three different learning trials. Active or sham stimulation was performed for every third word presented for immediate recall.
The investigators found that the HVLT-R delayed recall raw score was higher for the stimulation condition, compared with the nonstimulation condition (paired t-test, P = .04; effect size, d = 0.627).
“The patients were not aware of when the RNS system was being activated. We alternated when patients were undergoing stimulation versus no stimulation, and still found that when patients’ RNS systems were activated, their memory recall score was greater than when there was no stimulation,” Dr. Haneef said in a release.
This suggests the “human memory can be potentially improved by direct electrical brain stimulation at extremely low currents,” Dr. Haneef said in an interview.
Most patients in the study had stimulation of the hippocampus, the brain’s memory center.
“Moving forward we would want to look at how different patterns or standardized stimulation patterns affect memory. Ultimately, the underlying brain rhythms responsible for these changes in brain function need to be understood so that a more targeted and precise application of electrical stimulation can be achieved,” Dr. Haneef said.
The researchers also caution that, for this preliminary study, no follow-up testing was conducted to determine whether the memory improvement was transient and settled back to baseline after a specified period.
However, they note, this study lays the groundwork for larger-scale and extensive studies examining the nuanced effects of brain stimulation on human cognition and memory.
The study was funded by the Mike Hogg Foundation. Dr. Haneef and two coauthors received coverage for travel expenses but no honorarium for a NeuroPace advisory meeting.
A version of this article first appeared on Medscape.com.
Electrical brain stimulation may have the potential to improve verbal memory, results of a small study of patients with epilepsy suggest.
Investigators observed improvements in patients implanted with a responsive neurostimulation system (RNS) to control seizures, in that the patients had improved word recall when the system was activated.
Beyond epilepsy, “we suspect that our results would be broadly applicable regardless of the underlying condition, for example, memory loss with Alzheimer’s disease or traumatic brain injury,” Zulfi Haneef, MBBS, MD, associate professor of neurology, Baylor College of Medicine, Houston, said in an interview.
“Mental health conditions such as depression or psychosis could also benefit from targeted electrical stimulation. While we focused on enhancing a preferred brain function [such as memory], parallel areas of research may target enhancing function [such as weakness following stroke] or suppressing function [to manage conditions such as chronic pain,]” Dr. Haneef added.
The study was published online Jan. 17, 2022, in Neurosurgery.
As reported by this news organization, Following implantation of the system, patients attend the clinic for adjustments about every 8-12 weeks.
The investigators studied 17 patients with epilepsy and RNS implants who attended the clinic for routine appointments. A clinical neuropsychologist administered the Hopkins Verbal Learning Test–Revised (HVLT-R), a well-validated list-learning measure of memory and verbal learning.
Patients were read a list of 12 semantically related words and asked to recall the list after three different learning trials. Active or sham stimulation was performed for every third word presented for immediate recall.
The investigators found that the HVLT-R delayed recall raw score was higher for the stimulation condition, compared with the nonstimulation condition (paired t-test, P = .04; effect size, d = 0.627).
“The patients were not aware of when the RNS system was being activated. We alternated when patients were undergoing stimulation versus no stimulation, and still found that when patients’ RNS systems were activated, their memory recall score was greater than when there was no stimulation,” Dr. Haneef said in a release.
This suggests the “human memory can be potentially improved by direct electrical brain stimulation at extremely low currents,” Dr. Haneef said in an interview.
Most patients in the study had stimulation of the hippocampus, the brain’s memory center.
“Moving forward we would want to look at how different patterns or standardized stimulation patterns affect memory. Ultimately, the underlying brain rhythms responsible for these changes in brain function need to be understood so that a more targeted and precise application of electrical stimulation can be achieved,” Dr. Haneef said.
The researchers also caution that, for this preliminary study, no follow-up testing was conducted to determine whether the memory improvement was transient and settled back to baseline after a specified period.
However, they note, this study lays the groundwork for larger-scale and extensive studies examining the nuanced effects of brain stimulation on human cognition and memory.
The study was funded by the Mike Hogg Foundation. Dr. Haneef and two coauthors received coverage for travel expenses but no honorarium for a NeuroPace advisory meeting.
A version of this article first appeared on Medscape.com.
Electrical brain stimulation may have the potential to improve verbal memory, results of a small study of patients with epilepsy suggest.
Investigators observed improvements in patients implanted with a responsive neurostimulation system (RNS) to control seizures, in that the patients had improved word recall when the system was activated.
Beyond epilepsy, “we suspect that our results would be broadly applicable regardless of the underlying condition, for example, memory loss with Alzheimer’s disease or traumatic brain injury,” Zulfi Haneef, MBBS, MD, associate professor of neurology, Baylor College of Medicine, Houston, said in an interview.
“Mental health conditions such as depression or psychosis could also benefit from targeted electrical stimulation. While we focused on enhancing a preferred brain function [such as memory], parallel areas of research may target enhancing function [such as weakness following stroke] or suppressing function [to manage conditions such as chronic pain,]” Dr. Haneef added.
The study was published online Jan. 17, 2022, in Neurosurgery.
As reported by this news organization, Following implantation of the system, patients attend the clinic for adjustments about every 8-12 weeks.
The investigators studied 17 patients with epilepsy and RNS implants who attended the clinic for routine appointments. A clinical neuropsychologist administered the Hopkins Verbal Learning Test–Revised (HVLT-R), a well-validated list-learning measure of memory and verbal learning.
Patients were read a list of 12 semantically related words and asked to recall the list after three different learning trials. Active or sham stimulation was performed for every third word presented for immediate recall.
The investigators found that the HVLT-R delayed recall raw score was higher for the stimulation condition, compared with the nonstimulation condition (paired t-test, P = .04; effect size, d = 0.627).
“The patients were not aware of when the RNS system was being activated. We alternated when patients were undergoing stimulation versus no stimulation, and still found that when patients’ RNS systems were activated, their memory recall score was greater than when there was no stimulation,” Dr. Haneef said in a release.
This suggests the “human memory can be potentially improved by direct electrical brain stimulation at extremely low currents,” Dr. Haneef said in an interview.
Most patients in the study had stimulation of the hippocampus, the brain’s memory center.
“Moving forward we would want to look at how different patterns or standardized stimulation patterns affect memory. Ultimately, the underlying brain rhythms responsible for these changes in brain function need to be understood so that a more targeted and precise application of electrical stimulation can be achieved,” Dr. Haneef said.
The researchers also caution that, for this preliminary study, no follow-up testing was conducted to determine whether the memory improvement was transient and settled back to baseline after a specified period.
However, they note, this study lays the groundwork for larger-scale and extensive studies examining the nuanced effects of brain stimulation on human cognition and memory.
The study was funded by the Mike Hogg Foundation. Dr. Haneef and two coauthors received coverage for travel expenses but no honorarium for a NeuroPace advisory meeting.
A version of this article first appeared on Medscape.com.
FROM NEUROSURGERY
‘Physiology fights back’ when people are trying to lose weight
Metabolic adaptation – slowing of metabolism in response to weight loss – increases the length of time needed to achieve a target lower weight, a new study of premenopausal women with overweight reports.
All of the 65 sedentary young and middle-aged women with overweight who were on a low-calorie diet (800 calories/day) attained their target lower weight – corresponding to a body mass index (BMI) of 25 kg/m2 or less – after 66-252 days.
But a woman with the largest metabolic adaptation needed to stay on the diet for an extra 70 days, compared with a woman with no metabolic adaptation, to reach the target BMI, after adjusting for dietary adherence.
The study by Catia Martins, PhD, and colleagues was published Jan. 27, 2022, in Obesity.
“Even though adherence to the diet is clearly the most important determinant of time to reach weight loss goals,” wrote Dr. Martins and colleagues, “the present findings are of great clinical relevance as they mean that individuals who are struggling to achieve weight-loss goals, despite assuring compliance with the diet, may indeed be ‘suffering’ from metabolic adaptation during active weight loss.”
Therefore, “clinicians need to consider metabolic adaptation when assessing resistance to weight loss,” they concluded.
Good news: Metabolic adaption ceases when weight stabilizes
“This study shows that a longer than expected duration of intervention to achieve weight loss targets might be due to metabolic adaptation, even after controlling for adherence to the diet,” Dr. Martins said in an interview.
Metabolic adaptation while on a diet makes it harder to lose the last pound than to lose the first pound because as weight loss progresses metabolic adaptation increases, she noted.
However, “the good news is that this mechanism disappears once weight is stabilized (a new energy balance is established), and it is not a predictor of weight regain in the long term,” noted Dr. Martins, associate professor, nutrition sciences research, University of Alabama at Birmingham.
The group published a study in 2020 showing that metabolic adaptation does not predict weight regain at 1 year, and another study, published a few months earlier, showed it is not a barrier to weight-loss maintenance.
The current study findings “provide further evidence of the ways that physiology fights back when people are trying to lose weight,” David B. Sarwer, PhD, who was not involved with this research, said in a press release from the Obesity Society.
“A countless number of environmental variables and other social determinants of health also make weight loss and maintenance challenging for many individuals,” added Dr. Sarwer, director of the Center for Obesity Research and Education at Temple University, Philadelphia.
“Nevertheless, it is import to remember that even a modest weight loss of 5% of initial body weight – much smaller than seen in this study – is associated with clinically significant improvements in weight-related health issues for many individuals,” he stressed.
16% weight loss at 5 weeks with 800-calorie/day diet
It is unclear whether metabolic adaptation contributes to resistance to weight loss by increasing the time necessary to achieve weight-loss goals.
To investigate this, Dr. Martins and associates analyzed data from 36 White women and 29 Black women, aged 20-41 years (mean age, 36), who had a mean BMI of 28.6 and had participated in the diet arms of two studies (ROMEO and JULIET) conducted at Martins’ institution.
Participants received food containing 20% to 22% fat, 20% to 22% protein, and 56% to 58% carbohydrate provided by the center’s research kitchen.
On average, the women were 64% compliant with the diet and lost 12.5 kg (27.6 pounds), a 16% weight loss, over 155 days.
Metabolic adaption was measured 4 weeks after weight stabilization after reaching the weight-loss target.
On average, participants’ resting metabolic rate after weight loss was 46 kcal lower than what would be expected for their lower body weight.
Metabolic adaptation after weight loss was a significant predictor of time to reach the weight-loss goal, after adjusting for target weight loss, energy deficit, and adherence to the diet (R2 adjusted, 0.63; P < .001).
The study findings may not be generalizable to men, older patients, or people with a higher BMI, so further research is needed in a broader population, the researchers concluded.
The research was supported by National Institutes of Health grants. Dr. Martins was supported by a sabbatical grant from the Liaison Committee for Education, Research, and Innovation in Central Norway and the Norwegian University of Science and Technology. The researchers have no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
Metabolic adaptation – slowing of metabolism in response to weight loss – increases the length of time needed to achieve a target lower weight, a new study of premenopausal women with overweight reports.
All of the 65 sedentary young and middle-aged women with overweight who were on a low-calorie diet (800 calories/day) attained their target lower weight – corresponding to a body mass index (BMI) of 25 kg/m2 or less – after 66-252 days.
But a woman with the largest metabolic adaptation needed to stay on the diet for an extra 70 days, compared with a woman with no metabolic adaptation, to reach the target BMI, after adjusting for dietary adherence.
The study by Catia Martins, PhD, and colleagues was published Jan. 27, 2022, in Obesity.
“Even though adherence to the diet is clearly the most important determinant of time to reach weight loss goals,” wrote Dr. Martins and colleagues, “the present findings are of great clinical relevance as they mean that individuals who are struggling to achieve weight-loss goals, despite assuring compliance with the diet, may indeed be ‘suffering’ from metabolic adaptation during active weight loss.”
Therefore, “clinicians need to consider metabolic adaptation when assessing resistance to weight loss,” they concluded.
Good news: Metabolic adaption ceases when weight stabilizes
“This study shows that a longer than expected duration of intervention to achieve weight loss targets might be due to metabolic adaptation, even after controlling for adherence to the diet,” Dr. Martins said in an interview.
Metabolic adaptation while on a diet makes it harder to lose the last pound than to lose the first pound because as weight loss progresses metabolic adaptation increases, she noted.
However, “the good news is that this mechanism disappears once weight is stabilized (a new energy balance is established), and it is not a predictor of weight regain in the long term,” noted Dr. Martins, associate professor, nutrition sciences research, University of Alabama at Birmingham.
The group published a study in 2020 showing that metabolic adaptation does not predict weight regain at 1 year, and another study, published a few months earlier, showed it is not a barrier to weight-loss maintenance.
The current study findings “provide further evidence of the ways that physiology fights back when people are trying to lose weight,” David B. Sarwer, PhD, who was not involved with this research, said in a press release from the Obesity Society.
“A countless number of environmental variables and other social determinants of health also make weight loss and maintenance challenging for many individuals,” added Dr. Sarwer, director of the Center for Obesity Research and Education at Temple University, Philadelphia.
“Nevertheless, it is import to remember that even a modest weight loss of 5% of initial body weight – much smaller than seen in this study – is associated with clinically significant improvements in weight-related health issues for many individuals,” he stressed.
16% weight loss at 5 weeks with 800-calorie/day diet
It is unclear whether metabolic adaptation contributes to resistance to weight loss by increasing the time necessary to achieve weight-loss goals.
To investigate this, Dr. Martins and associates analyzed data from 36 White women and 29 Black women, aged 20-41 years (mean age, 36), who had a mean BMI of 28.6 and had participated in the diet arms of two studies (ROMEO and JULIET) conducted at Martins’ institution.
Participants received food containing 20% to 22% fat, 20% to 22% protein, and 56% to 58% carbohydrate provided by the center’s research kitchen.
On average, the women were 64% compliant with the diet and lost 12.5 kg (27.6 pounds), a 16% weight loss, over 155 days.
Metabolic adaption was measured 4 weeks after weight stabilization after reaching the weight-loss target.
On average, participants’ resting metabolic rate after weight loss was 46 kcal lower than what would be expected for their lower body weight.
Metabolic adaptation after weight loss was a significant predictor of time to reach the weight-loss goal, after adjusting for target weight loss, energy deficit, and adherence to the diet (R2 adjusted, 0.63; P < .001).
The study findings may not be generalizable to men, older patients, or people with a higher BMI, so further research is needed in a broader population, the researchers concluded.
The research was supported by National Institutes of Health grants. Dr. Martins was supported by a sabbatical grant from the Liaison Committee for Education, Research, and Innovation in Central Norway and the Norwegian University of Science and Technology. The researchers have no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
Metabolic adaptation – slowing of metabolism in response to weight loss – increases the length of time needed to achieve a target lower weight, a new study of premenopausal women with overweight reports.
All of the 65 sedentary young and middle-aged women with overweight who were on a low-calorie diet (800 calories/day) attained their target lower weight – corresponding to a body mass index (BMI) of 25 kg/m2 or less – after 66-252 days.
But a woman with the largest metabolic adaptation needed to stay on the diet for an extra 70 days, compared with a woman with no metabolic adaptation, to reach the target BMI, after adjusting for dietary adherence.
The study by Catia Martins, PhD, and colleagues was published Jan. 27, 2022, in Obesity.
“Even though adherence to the diet is clearly the most important determinant of time to reach weight loss goals,” wrote Dr. Martins and colleagues, “the present findings are of great clinical relevance as they mean that individuals who are struggling to achieve weight-loss goals, despite assuring compliance with the diet, may indeed be ‘suffering’ from metabolic adaptation during active weight loss.”
Therefore, “clinicians need to consider metabolic adaptation when assessing resistance to weight loss,” they concluded.
Good news: Metabolic adaption ceases when weight stabilizes
“This study shows that a longer than expected duration of intervention to achieve weight loss targets might be due to metabolic adaptation, even after controlling for adherence to the diet,” Dr. Martins said in an interview.
Metabolic adaptation while on a diet makes it harder to lose the last pound than to lose the first pound because as weight loss progresses metabolic adaptation increases, she noted.
However, “the good news is that this mechanism disappears once weight is stabilized (a new energy balance is established), and it is not a predictor of weight regain in the long term,” noted Dr. Martins, associate professor, nutrition sciences research, University of Alabama at Birmingham.
The group published a study in 2020 showing that metabolic adaptation does not predict weight regain at 1 year, and another study, published a few months earlier, showed it is not a barrier to weight-loss maintenance.
The current study findings “provide further evidence of the ways that physiology fights back when people are trying to lose weight,” David B. Sarwer, PhD, who was not involved with this research, said in a press release from the Obesity Society.
“A countless number of environmental variables and other social determinants of health also make weight loss and maintenance challenging for many individuals,” added Dr. Sarwer, director of the Center for Obesity Research and Education at Temple University, Philadelphia.
“Nevertheless, it is import to remember that even a modest weight loss of 5% of initial body weight – much smaller than seen in this study – is associated with clinically significant improvements in weight-related health issues for many individuals,” he stressed.
16% weight loss at 5 weeks with 800-calorie/day diet
It is unclear whether metabolic adaptation contributes to resistance to weight loss by increasing the time necessary to achieve weight-loss goals.
To investigate this, Dr. Martins and associates analyzed data from 36 White women and 29 Black women, aged 20-41 years (mean age, 36), who had a mean BMI of 28.6 and had participated in the diet arms of two studies (ROMEO and JULIET) conducted at Martins’ institution.
Participants received food containing 20% to 22% fat, 20% to 22% protein, and 56% to 58% carbohydrate provided by the center’s research kitchen.
On average, the women were 64% compliant with the diet and lost 12.5 kg (27.6 pounds), a 16% weight loss, over 155 days.
Metabolic adaption was measured 4 weeks after weight stabilization after reaching the weight-loss target.
On average, participants’ resting metabolic rate after weight loss was 46 kcal lower than what would be expected for their lower body weight.
Metabolic adaptation after weight loss was a significant predictor of time to reach the weight-loss goal, after adjusting for target weight loss, energy deficit, and adherence to the diet (R2 adjusted, 0.63; P < .001).
The study findings may not be generalizable to men, older patients, or people with a higher BMI, so further research is needed in a broader population, the researchers concluded.
The research was supported by National Institutes of Health grants. Dr. Martins was supported by a sabbatical grant from the Liaison Committee for Education, Research, and Innovation in Central Norway and the Norwegian University of Science and Technology. The researchers have no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
FROM OBESITY
Long COVID is real, and many real questions remain
Long story short, we still have a lot to learn about long COVID-19.
But it is a real phenomenon with real long-term health effects for people recovering from coronavirus infections. And diagnosing and managing it can get tricky, as some symptoms of long COVID-19 overlap with those of other conditions – and what many people have as they recover from any challenging stay in the ICU.
Risk factors remain largely unknown as well: What makes one person more likely to have symptoms like fatigue, “brain fog,” or headaches versus someone else? Researchers are just starting to offer some intriguing answers, but the evidence is preliminary at this point, experts said at a media briefing sponsored by the Infectious Diseases Society of America.
Unanswered questions include: Does an autoimmune reaction drive long COVID? Does the coronavirus linger in reservoirs within the body and reactivate later? What protection against long COVID do vaccines and treatments offer, if any?
To get a handle on these and other questions, nailing down a standard definition of long COVID would be a good start.
“Studies so far have used different definitions of long COVID,” Nahid Bhadelia, MD, founding director of the Boston University Center for Emerging Infectious Diseases Policy and Research, said during the briefing.
Fatigue is the most commonly symptom of long COVID in research so far, said Dr. Bhadelia, who is also an associate professor of medicine at Boston University.
“What’s difficult in this situation is it’s been 2 years in a global pandemic. We’re all fatigued. How do you tease this apart?” she asked.
Other common symptoms are a hard time thinking quickly – also known as “brain fog” – and the feeling that, despite normal oxygen levels, breathing is difficult, said Kathleen Bell, MD.
Headache, joint and muscle pain, and persistent loss of smell and taste are also widely reported, said Dr. Bell, a professor and chair of the department of physical medicine and rehabilitation at the University of Texas Southwestern Medical Center in Dallas.
Not all the symptoms are physical either.
“Pretty prominent things that we’re seeing are very high levels of anxiety, depression, and insomnia,” Dr. Bell said. These “actually seem to be associated independently with the virus as opposed to just being a completely reactive component.”
More research will be needed to distinguish the causes of these conditions.
A difficult diagnosis
the experts said.
“We are starting to see some interesting features of inaccurate attributions to COVID, both on the part of perhaps the person with long COVID symptoms and health care providers,” Dr. Bell said.“It’s sometimes a little difficult to sort it out.”
Dr. Bell said she was not suggesting misdiagnoses are common, “but it is difficult for physicians that don’t see a lot of people with long COVID.”
The advice is to consider other conditions. “You can have both a long COVID syndrome and other syndromes as well,” she said. “As one of my teachers used to say: ‘You can have both ticks and fleas.’ ”
Predicting long COVID
In a study getting attention, researchers identified four early things linked to greater chances that someone with COVID-19 will have long-term effects: type 2 diabetes at the time of diagnosis, the presence of specific autoantibodies, unusual levels of SARS-CoV-2 RNA in the blood, and signs of the Epstein-Barr virus in the blood.
The study, published in Cell, followed 309 people 2-3 months after COVID-19.
“That’s important work, but it’s early work,” Dr. Bhadelia said. “I think we still have a while to go in terms of understanding the mechanism of long COVID.”
Unexpected patients getting long COVID care
“We are seeing different populations than we all expected to see when this pandemic first started,” Dr. Bell said.
Instead of seeing primarily patients who had severe COVID-19, “the preponderance of people that we’re seeing in long COVID clinics are people who are enabled, were never hospitalized, and have what people might call mild to moderate cases of coronavirus infection,” she said.
Also, instead of just older patients, people of all ages are seeking long COVID care.
One thing that appears more certain is a lack of diversity in people seeking care at long COVID clinics nationwide.
“Many of us who have long COVID specialty clinics will tell you that we are tending to see fairly educated, socioeconomically stable population in these clinics,” Dr. Bell said. “We know that based on the early statistics of who’s getting COVID and having significant COVID that we may not be seeing those populations for follow-up.”
Is an autoinflammatory process to blame?
It remains unclear if a hyperinflammatory response is driving persistent post–COVID-19 symptoms. Children and some adults have developed multisystem inflammatory conditions associated with COVID-19, for example.
There is a signal, and “I think there is enough data now to show something does happen,” Dr. Bhadelia said. “The question is, how often does it happen?”
Spending time in critical care, even without COVID-19, can result in persistent symptoms after a hospital stay, such as acute respiratory distress syndrome. Recovery can take time because being in an ICU is “basically the physiologically equivalent of a car crash,” Dr. Bhadelia said. “So you’re recovering from that, too.”
Dr. Bell agreed. “You’re not only recovering from the virus itself, you’re recovering from intubation, secondary infections, secondary lung conditions, perhaps other organ failure, and prolonged bed rest. There are so many things that go into that, that it’s a little bit hard to sort that out from what long COVID is and what the direct effects of the virus are.”
Also a research opportunity
“I hate to call it this, but we’ve never had an opportunity [where] we have so many people in such a short amount of time with the same viral disorder,” Dr. Bell said. “We also have the technology to investigate it. This has never happened.
“SARS-CoV-2 is not the only virus. This is just the only one we’ve gotten whacked with in such a huge quantity at one time,” she said.
What researchers learn now about COVID-19 and long COVID “is a model that’s going to be able to be applied in the future to infectious diseases in general,” Dr. Bell predicted.
How long will long COVID last?
The vast majority of people with long COVID will get better over time, given enough support and relief of their symptoms, Dr. Bell said.
Type 2 diabetes, preexisting pulmonary disease, and other things could affect how long it takes to recover from long COVID, she said, although more evidence is needed.
“I don’t think at this point that anyone can say how long this long COVID will last because there are a variety of factors,” Dr. Bell said.
A version of this article first appeared on WebMD.com.
Long story short, we still have a lot to learn about long COVID-19.
But it is a real phenomenon with real long-term health effects for people recovering from coronavirus infections. And diagnosing and managing it can get tricky, as some symptoms of long COVID-19 overlap with those of other conditions – and what many people have as they recover from any challenging stay in the ICU.
Risk factors remain largely unknown as well: What makes one person more likely to have symptoms like fatigue, “brain fog,” or headaches versus someone else? Researchers are just starting to offer some intriguing answers, but the evidence is preliminary at this point, experts said at a media briefing sponsored by the Infectious Diseases Society of America.
Unanswered questions include: Does an autoimmune reaction drive long COVID? Does the coronavirus linger in reservoirs within the body and reactivate later? What protection against long COVID do vaccines and treatments offer, if any?
To get a handle on these and other questions, nailing down a standard definition of long COVID would be a good start.
“Studies so far have used different definitions of long COVID,” Nahid Bhadelia, MD, founding director of the Boston University Center for Emerging Infectious Diseases Policy and Research, said during the briefing.
Fatigue is the most commonly symptom of long COVID in research so far, said Dr. Bhadelia, who is also an associate professor of medicine at Boston University.
“What’s difficult in this situation is it’s been 2 years in a global pandemic. We’re all fatigued. How do you tease this apart?” she asked.
Other common symptoms are a hard time thinking quickly – also known as “brain fog” – and the feeling that, despite normal oxygen levels, breathing is difficult, said Kathleen Bell, MD.
Headache, joint and muscle pain, and persistent loss of smell and taste are also widely reported, said Dr. Bell, a professor and chair of the department of physical medicine and rehabilitation at the University of Texas Southwestern Medical Center in Dallas.
Not all the symptoms are physical either.
“Pretty prominent things that we’re seeing are very high levels of anxiety, depression, and insomnia,” Dr. Bell said. These “actually seem to be associated independently with the virus as opposed to just being a completely reactive component.”
More research will be needed to distinguish the causes of these conditions.
A difficult diagnosis
the experts said.
“We are starting to see some interesting features of inaccurate attributions to COVID, both on the part of perhaps the person with long COVID symptoms and health care providers,” Dr. Bell said.“It’s sometimes a little difficult to sort it out.”
Dr. Bell said she was not suggesting misdiagnoses are common, “but it is difficult for physicians that don’t see a lot of people with long COVID.”
The advice is to consider other conditions. “You can have both a long COVID syndrome and other syndromes as well,” she said. “As one of my teachers used to say: ‘You can have both ticks and fleas.’ ”
Predicting long COVID
In a study getting attention, researchers identified four early things linked to greater chances that someone with COVID-19 will have long-term effects: type 2 diabetes at the time of diagnosis, the presence of specific autoantibodies, unusual levels of SARS-CoV-2 RNA in the blood, and signs of the Epstein-Barr virus in the blood.
The study, published in Cell, followed 309 people 2-3 months after COVID-19.
“That’s important work, but it’s early work,” Dr. Bhadelia said. “I think we still have a while to go in terms of understanding the mechanism of long COVID.”
Unexpected patients getting long COVID care
“We are seeing different populations than we all expected to see when this pandemic first started,” Dr. Bell said.
Instead of seeing primarily patients who had severe COVID-19, “the preponderance of people that we’re seeing in long COVID clinics are people who are enabled, were never hospitalized, and have what people might call mild to moderate cases of coronavirus infection,” she said.
Also, instead of just older patients, people of all ages are seeking long COVID care.
One thing that appears more certain is a lack of diversity in people seeking care at long COVID clinics nationwide.
“Many of us who have long COVID specialty clinics will tell you that we are tending to see fairly educated, socioeconomically stable population in these clinics,” Dr. Bell said. “We know that based on the early statistics of who’s getting COVID and having significant COVID that we may not be seeing those populations for follow-up.”
Is an autoinflammatory process to blame?
It remains unclear if a hyperinflammatory response is driving persistent post–COVID-19 symptoms. Children and some adults have developed multisystem inflammatory conditions associated with COVID-19, for example.
There is a signal, and “I think there is enough data now to show something does happen,” Dr. Bhadelia said. “The question is, how often does it happen?”
Spending time in critical care, even without COVID-19, can result in persistent symptoms after a hospital stay, such as acute respiratory distress syndrome. Recovery can take time because being in an ICU is “basically the physiologically equivalent of a car crash,” Dr. Bhadelia said. “So you’re recovering from that, too.”
Dr. Bell agreed. “You’re not only recovering from the virus itself, you’re recovering from intubation, secondary infections, secondary lung conditions, perhaps other organ failure, and prolonged bed rest. There are so many things that go into that, that it’s a little bit hard to sort that out from what long COVID is and what the direct effects of the virus are.”
Also a research opportunity
“I hate to call it this, but we’ve never had an opportunity [where] we have so many people in such a short amount of time with the same viral disorder,” Dr. Bell said. “We also have the technology to investigate it. This has never happened.
“SARS-CoV-2 is not the only virus. This is just the only one we’ve gotten whacked with in such a huge quantity at one time,” she said.
What researchers learn now about COVID-19 and long COVID “is a model that’s going to be able to be applied in the future to infectious diseases in general,” Dr. Bell predicted.
How long will long COVID last?
The vast majority of people with long COVID will get better over time, given enough support and relief of their symptoms, Dr. Bell said.
Type 2 diabetes, preexisting pulmonary disease, and other things could affect how long it takes to recover from long COVID, she said, although more evidence is needed.
“I don’t think at this point that anyone can say how long this long COVID will last because there are a variety of factors,” Dr. Bell said.
A version of this article first appeared on WebMD.com.
Long story short, we still have a lot to learn about long COVID-19.
But it is a real phenomenon with real long-term health effects for people recovering from coronavirus infections. And diagnosing and managing it can get tricky, as some symptoms of long COVID-19 overlap with those of other conditions – and what many people have as they recover from any challenging stay in the ICU.
Risk factors remain largely unknown as well: What makes one person more likely to have symptoms like fatigue, “brain fog,” or headaches versus someone else? Researchers are just starting to offer some intriguing answers, but the evidence is preliminary at this point, experts said at a media briefing sponsored by the Infectious Diseases Society of America.
Unanswered questions include: Does an autoimmune reaction drive long COVID? Does the coronavirus linger in reservoirs within the body and reactivate later? What protection against long COVID do vaccines and treatments offer, if any?
To get a handle on these and other questions, nailing down a standard definition of long COVID would be a good start.
“Studies so far have used different definitions of long COVID,” Nahid Bhadelia, MD, founding director of the Boston University Center for Emerging Infectious Diseases Policy and Research, said during the briefing.
Fatigue is the most commonly symptom of long COVID in research so far, said Dr. Bhadelia, who is also an associate professor of medicine at Boston University.
“What’s difficult in this situation is it’s been 2 years in a global pandemic. We’re all fatigued. How do you tease this apart?” she asked.
Other common symptoms are a hard time thinking quickly – also known as “brain fog” – and the feeling that, despite normal oxygen levels, breathing is difficult, said Kathleen Bell, MD.
Headache, joint and muscle pain, and persistent loss of smell and taste are also widely reported, said Dr. Bell, a professor and chair of the department of physical medicine and rehabilitation at the University of Texas Southwestern Medical Center in Dallas.
Not all the symptoms are physical either.
“Pretty prominent things that we’re seeing are very high levels of anxiety, depression, and insomnia,” Dr. Bell said. These “actually seem to be associated independently with the virus as opposed to just being a completely reactive component.”
More research will be needed to distinguish the causes of these conditions.
A difficult diagnosis
the experts said.
“We are starting to see some interesting features of inaccurate attributions to COVID, both on the part of perhaps the person with long COVID symptoms and health care providers,” Dr. Bell said.“It’s sometimes a little difficult to sort it out.”
Dr. Bell said she was not suggesting misdiagnoses are common, “but it is difficult for physicians that don’t see a lot of people with long COVID.”
The advice is to consider other conditions. “You can have both a long COVID syndrome and other syndromes as well,” she said. “As one of my teachers used to say: ‘You can have both ticks and fleas.’ ”
Predicting long COVID
In a study getting attention, researchers identified four early things linked to greater chances that someone with COVID-19 will have long-term effects: type 2 diabetes at the time of diagnosis, the presence of specific autoantibodies, unusual levels of SARS-CoV-2 RNA in the blood, and signs of the Epstein-Barr virus in the blood.
The study, published in Cell, followed 309 people 2-3 months after COVID-19.
“That’s important work, but it’s early work,” Dr. Bhadelia said. “I think we still have a while to go in terms of understanding the mechanism of long COVID.”
Unexpected patients getting long COVID care
“We are seeing different populations than we all expected to see when this pandemic first started,” Dr. Bell said.
Instead of seeing primarily patients who had severe COVID-19, “the preponderance of people that we’re seeing in long COVID clinics are people who are enabled, were never hospitalized, and have what people might call mild to moderate cases of coronavirus infection,” she said.
Also, instead of just older patients, people of all ages are seeking long COVID care.
One thing that appears more certain is a lack of diversity in people seeking care at long COVID clinics nationwide.
“Many of us who have long COVID specialty clinics will tell you that we are tending to see fairly educated, socioeconomically stable population in these clinics,” Dr. Bell said. “We know that based on the early statistics of who’s getting COVID and having significant COVID that we may not be seeing those populations for follow-up.”
Is an autoinflammatory process to blame?
It remains unclear if a hyperinflammatory response is driving persistent post–COVID-19 symptoms. Children and some adults have developed multisystem inflammatory conditions associated with COVID-19, for example.
There is a signal, and “I think there is enough data now to show something does happen,” Dr. Bhadelia said. “The question is, how often does it happen?”
Spending time in critical care, even without COVID-19, can result in persistent symptoms after a hospital stay, such as acute respiratory distress syndrome. Recovery can take time because being in an ICU is “basically the physiologically equivalent of a car crash,” Dr. Bhadelia said. “So you’re recovering from that, too.”
Dr. Bell agreed. “You’re not only recovering from the virus itself, you’re recovering from intubation, secondary infections, secondary lung conditions, perhaps other organ failure, and prolonged bed rest. There are so many things that go into that, that it’s a little bit hard to sort that out from what long COVID is and what the direct effects of the virus are.”
Also a research opportunity
“I hate to call it this, but we’ve never had an opportunity [where] we have so many people in such a short amount of time with the same viral disorder,” Dr. Bell said. “We also have the technology to investigate it. This has never happened.
“SARS-CoV-2 is not the only virus. This is just the only one we’ve gotten whacked with in such a huge quantity at one time,” she said.
What researchers learn now about COVID-19 and long COVID “is a model that’s going to be able to be applied in the future to infectious diseases in general,” Dr. Bell predicted.
How long will long COVID last?
The vast majority of people with long COVID will get better over time, given enough support and relief of their symptoms, Dr. Bell said.
Type 2 diabetes, preexisting pulmonary disease, and other things could affect how long it takes to recover from long COVID, she said, although more evidence is needed.
“I don’t think at this point that anyone can say how long this long COVID will last because there are a variety of factors,” Dr. Bell said.
A version of this article first appeared on WebMD.com.
Clinical Edge Journal Scan Commentary: Prostate Cancer February 2022
The STAMPEDE platform included a multiple arm and multiple stage protocol to evaluate abiraterone and enzalutamide in high risk non-metastatic and metastatic disease in separate trials. In the accompanying article by Attard et. al, a meta-analysis of two separate trials conducted as part of the STAMPEDE platform was undertaken. In the first trial, patients with high-risk localized prostate cancer were randomized to androgen deprivation therapy (ADT) with or without abiraterone. In the second trial, similar patients were randomized to ADT versus ADT plus abiraterone plus enzalutamide. The primary outcome of metastasis-free survival and secondary outcome of overall survival [OS] were significantly longer for the treatment arms over ADT; however, the addition of enzalutamide to abiraterone did not result in additional benefit. In appropriately selected patients with high risk localized prostate cancer, abiraterone is a reasonable option to consider in appropriately selected patients.
While bone is the most frequent site of metastasis in men with prostate cancer, visceral metastases (predominantly liver or lung) has been associated with worse outcomes. However, lower incidence of visceral metastases makes conduct of studies focused on visceral disease challenging. Baciarello et al conducted a post-hoc analysis of the LATITUDE study (where men with metastatic castrate-sensitive disease were treated with ADT plus abiraterone or ADT alone) in participants with visceral disease. Overall, patients with visceral metastases derived OS benefit (55.4 versus 33 months). Patients with lung metastases had similar OS to the entire cohort; however, those with liver metastases still derived benefit but had lower OS (36.8 versus 25.6 months). These post-hoc findings suggest that liver metastases present unique challenges compare to other metastatic disease sites, but further study is needed.
In the ENZAMET trial, enzalutamide plus ADT was compared to ADT alone in patients with metastatic castrate-sensitive disease, and enzalutamide treatment was associated with improved OS. In the report by Stockler et al, quality of life metrics as assessed by periodic evaluation utilizing standard questionnaires were reported. Patients who received enzalutamide reported more fatigue and lower cognitive and physical function than those receiving placebo. However, the overall quality of life did not decrease. These important quality of life findings, which are increasingly being reported in similar studies, support the overall net benefit of utilization of enzalutamide in patients with metastatic castrate-sensitive disease.
The STAMPEDE platform included a multiple arm and multiple stage protocol to evaluate abiraterone and enzalutamide in high risk non-metastatic and metastatic disease in separate trials. In the accompanying article by Attard et. al, a meta-analysis of two separate trials conducted as part of the STAMPEDE platform was undertaken. In the first trial, patients with high-risk localized prostate cancer were randomized to androgen deprivation therapy (ADT) with or without abiraterone. In the second trial, similar patients were randomized to ADT versus ADT plus abiraterone plus enzalutamide. The primary outcome of metastasis-free survival and secondary outcome of overall survival [OS] were significantly longer for the treatment arms over ADT; however, the addition of enzalutamide to abiraterone did not result in additional benefit. In appropriately selected patients with high risk localized prostate cancer, abiraterone is a reasonable option to consider in appropriately selected patients.
While bone is the most frequent site of metastasis in men with prostate cancer, visceral metastases (predominantly liver or lung) has been associated with worse outcomes. However, lower incidence of visceral metastases makes conduct of studies focused on visceral disease challenging. Baciarello et al conducted a post-hoc analysis of the LATITUDE study (where men with metastatic castrate-sensitive disease were treated with ADT plus abiraterone or ADT alone) in participants with visceral disease. Overall, patients with visceral metastases derived OS benefit (55.4 versus 33 months). Patients with lung metastases had similar OS to the entire cohort; however, those with liver metastases still derived benefit but had lower OS (36.8 versus 25.6 months). These post-hoc findings suggest that liver metastases present unique challenges compare to other metastatic disease sites, but further study is needed.
In the ENZAMET trial, enzalutamide plus ADT was compared to ADT alone in patients with metastatic castrate-sensitive disease, and enzalutamide treatment was associated with improved OS. In the report by Stockler et al, quality of life metrics as assessed by periodic evaluation utilizing standard questionnaires were reported. Patients who received enzalutamide reported more fatigue and lower cognitive and physical function than those receiving placebo. However, the overall quality of life did not decrease. These important quality of life findings, which are increasingly being reported in similar studies, support the overall net benefit of utilization of enzalutamide in patients with metastatic castrate-sensitive disease.
The STAMPEDE platform included a multiple arm and multiple stage protocol to evaluate abiraterone and enzalutamide in high risk non-metastatic and metastatic disease in separate trials. In the accompanying article by Attard et. al, a meta-analysis of two separate trials conducted as part of the STAMPEDE platform was undertaken. In the first trial, patients with high-risk localized prostate cancer were randomized to androgen deprivation therapy (ADT) with or without abiraterone. In the second trial, similar patients were randomized to ADT versus ADT plus abiraterone plus enzalutamide. The primary outcome of metastasis-free survival and secondary outcome of overall survival [OS] were significantly longer for the treatment arms over ADT; however, the addition of enzalutamide to abiraterone did not result in additional benefit. In appropriately selected patients with high risk localized prostate cancer, abiraterone is a reasonable option to consider in appropriately selected patients.
While bone is the most frequent site of metastasis in men with prostate cancer, visceral metastases (predominantly liver or lung) has been associated with worse outcomes. However, lower incidence of visceral metastases makes conduct of studies focused on visceral disease challenging. Baciarello et al conducted a post-hoc analysis of the LATITUDE study (where men with metastatic castrate-sensitive disease were treated with ADT plus abiraterone or ADT alone) in participants with visceral disease. Overall, patients with visceral metastases derived OS benefit (55.4 versus 33 months). Patients with lung metastases had similar OS to the entire cohort; however, those with liver metastases still derived benefit but had lower OS (36.8 versus 25.6 months). These post-hoc findings suggest that liver metastases present unique challenges compare to other metastatic disease sites, but further study is needed.
In the ENZAMET trial, enzalutamide plus ADT was compared to ADT alone in patients with metastatic castrate-sensitive disease, and enzalutamide treatment was associated with improved OS. In the report by Stockler et al, quality of life metrics as assessed by periodic evaluation utilizing standard questionnaires were reported. Patients who received enzalutamide reported more fatigue and lower cognitive and physical function than those receiving placebo. However, the overall quality of life did not decrease. These important quality of life findings, which are increasingly being reported in similar studies, support the overall net benefit of utilization of enzalutamide in patients with metastatic castrate-sensitive disease.
Early, subtle, cardiac changes tied to midlife cognitive decline
new research suggests.
Cardiovascular disease risk factors such as high blood pressure, high cholesterol, and diabetes have been associated with an increased risk for cognitive impairment, but much less is known about heart structure and function and the risks for cognition.
“We showed for the first time that, even before the occurrence of cardiovascular disease, people with abnormalities in cardiac structure and function as early as in young adulthood have lower midlife cognition,” investigators Laure Rouch, PharmD, PhD, and Kristine Yaffe, MD, both with the department of psychiatry, University of California, San Francisco, said in a joint email.
“This study reminds us that heart health is key to brain health and that the overlap and interplay between the two is not limited to patients with end-stage heart disease,” Dr. Rouch and Dr. Yaffe said.
The findings were published online Jan. 26, 2022, in Neurology.
Heart/brain connection
The analysis included 2,653 participants in the Coronary Artery Risk Development in Young Adults (CARDIA) study.
Echocardiograms were obtained at year 5, 25, and 30 study visits – at mean ages of 30, 50, and 55 years, respectively. At year 30, participants underwent a standard battery of tests measuring global cognition, processing speed, executive function, delayed verbal memory, and verbal fluency.
Over 25 years, there was an average increase in left ventricular mass of 0.27 g/m2 per year – from a mean of 80.5 g/m2 in year 5 to 86.0 g/m2 in year 30.
Left atrial volume increased by an average of 0.42 mL/m2 per year, from 16 mL/m2 in year 5 to 26 mL/m2 in year 30.
Left ventricular ejection fraction (LVEF) decreased by 0.11% per year, from 63.3% in year 5 to 59.7% in year 30.
After adjustment for demographics and education, an increase in left ventricular mass of at least 1 standard deviation over 25 years was associated with lower cognition on most tests (P ≤ .02).
An increase in left atrial volume over the study period was associated with lower global cognition (P = .04), whereas a decrease in LVEF was not associated with cognition. Further adjustment for cardiovascular risk factors yielded similar results.
“A more effective collaboration is needed between cardiologists and neurologists to promote healthy brain aging,” Dr. Rouch and Dr. Yaffe said.
“Echocardiography is a widely available, relatively inexpensive, and noninvasive imaging method that could be integrated into a risk assessment for cognitive impairment,” they added.
Looking ahead, the investigators noted there is a need for further research to determine whether interventions to improve cardiac structure and diastolic function could also benefit brain health.
They should also investigate the role of arterial stiffness and cerebral small vessel disease in the relationship between cardiac structure, function, and cognition, the researchers added.
First structural biomarker
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Newton, Mass., said the study is important because, “thus far, the connections have really been physiological parameters,” such as blood pressure and cognitive health.
“This is really strong evidence of a structural cardiac biomarker that can be measured before and independent of changes in physiology or diseased state,” said Dr. Lakhan, who was not involved with the research.
As more and more interventions are being introduced for addressing disorders of cognition, “this potential structural finding may serve as a solid biomarker to determine” what lifestyle or drug therapy should be taken, he added.
Also weighing in on the findings, Pierre Fayad, MD, professor in the department of neurological sciences and director of the Nebraska Stroke Center, University of Nebraska Medical Center, Omaha, said CARDIA is “an important study” providing “precious data.”
The reported changes in cardiac structure and function “precede the clinical symptomatology, as the follow-up stops before they enter into later adulthood, where the risk of clinical events dramatically rises. Meaning these patients still have not had stroke, congestive heart failure, heart attack or dementia, but some of them could be on that trajectory later in their life,” Dr. Fayad told this news organization.
Documenting such changes over time is “valuable to give an insight into what leads us to such progression,” he noted.
How reliably predictive the findings are for eventual clinical cognitive impairment “will need to be confirmed and verified” in future studies, he added.
“If verified, it could be helpful to provide interventions to those with the left atrial volume enlargement marker and see their effectiveness at preventing eventual clinical cognitive impairment,” said Dr. Fayad.
The CARDIA study is supported by the National Heart, Lung, and Blood Institute in collaboration with the University of Alabama at Birmingham, Northwestern University, the University of Minnesota, and the Kaiser Foundation Research Institute. Rouch, Lakhan, and Dr. Fayad have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
Cardiovascular disease risk factors such as high blood pressure, high cholesterol, and diabetes have been associated with an increased risk for cognitive impairment, but much less is known about heart structure and function and the risks for cognition.
“We showed for the first time that, even before the occurrence of cardiovascular disease, people with abnormalities in cardiac structure and function as early as in young adulthood have lower midlife cognition,” investigators Laure Rouch, PharmD, PhD, and Kristine Yaffe, MD, both with the department of psychiatry, University of California, San Francisco, said in a joint email.
“This study reminds us that heart health is key to brain health and that the overlap and interplay between the two is not limited to patients with end-stage heart disease,” Dr. Rouch and Dr. Yaffe said.
The findings were published online Jan. 26, 2022, in Neurology.
Heart/brain connection
The analysis included 2,653 participants in the Coronary Artery Risk Development in Young Adults (CARDIA) study.
Echocardiograms were obtained at year 5, 25, and 30 study visits – at mean ages of 30, 50, and 55 years, respectively. At year 30, participants underwent a standard battery of tests measuring global cognition, processing speed, executive function, delayed verbal memory, and verbal fluency.
Over 25 years, there was an average increase in left ventricular mass of 0.27 g/m2 per year – from a mean of 80.5 g/m2 in year 5 to 86.0 g/m2 in year 30.
Left atrial volume increased by an average of 0.42 mL/m2 per year, from 16 mL/m2 in year 5 to 26 mL/m2 in year 30.
Left ventricular ejection fraction (LVEF) decreased by 0.11% per year, from 63.3% in year 5 to 59.7% in year 30.
After adjustment for demographics and education, an increase in left ventricular mass of at least 1 standard deviation over 25 years was associated with lower cognition on most tests (P ≤ .02).
An increase in left atrial volume over the study period was associated with lower global cognition (P = .04), whereas a decrease in LVEF was not associated with cognition. Further adjustment for cardiovascular risk factors yielded similar results.
“A more effective collaboration is needed between cardiologists and neurologists to promote healthy brain aging,” Dr. Rouch and Dr. Yaffe said.
“Echocardiography is a widely available, relatively inexpensive, and noninvasive imaging method that could be integrated into a risk assessment for cognitive impairment,” they added.
Looking ahead, the investigators noted there is a need for further research to determine whether interventions to improve cardiac structure and diastolic function could also benefit brain health.
They should also investigate the role of arterial stiffness and cerebral small vessel disease in the relationship between cardiac structure, function, and cognition, the researchers added.
First structural biomarker
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Newton, Mass., said the study is important because, “thus far, the connections have really been physiological parameters,” such as blood pressure and cognitive health.
“This is really strong evidence of a structural cardiac biomarker that can be measured before and independent of changes in physiology or diseased state,” said Dr. Lakhan, who was not involved with the research.
As more and more interventions are being introduced for addressing disorders of cognition, “this potential structural finding may serve as a solid biomarker to determine” what lifestyle or drug therapy should be taken, he added.
Also weighing in on the findings, Pierre Fayad, MD, professor in the department of neurological sciences and director of the Nebraska Stroke Center, University of Nebraska Medical Center, Omaha, said CARDIA is “an important study” providing “precious data.”
The reported changes in cardiac structure and function “precede the clinical symptomatology, as the follow-up stops before they enter into later adulthood, where the risk of clinical events dramatically rises. Meaning these patients still have not had stroke, congestive heart failure, heart attack or dementia, but some of them could be on that trajectory later in their life,” Dr. Fayad told this news organization.
Documenting such changes over time is “valuable to give an insight into what leads us to such progression,” he noted.
How reliably predictive the findings are for eventual clinical cognitive impairment “will need to be confirmed and verified” in future studies, he added.
“If verified, it could be helpful to provide interventions to those with the left atrial volume enlargement marker and see their effectiveness at preventing eventual clinical cognitive impairment,” said Dr. Fayad.
The CARDIA study is supported by the National Heart, Lung, and Blood Institute in collaboration with the University of Alabama at Birmingham, Northwestern University, the University of Minnesota, and the Kaiser Foundation Research Institute. Rouch, Lakhan, and Dr. Fayad have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
Cardiovascular disease risk factors such as high blood pressure, high cholesterol, and diabetes have been associated with an increased risk for cognitive impairment, but much less is known about heart structure and function and the risks for cognition.
“We showed for the first time that, even before the occurrence of cardiovascular disease, people with abnormalities in cardiac structure and function as early as in young adulthood have lower midlife cognition,” investigators Laure Rouch, PharmD, PhD, and Kristine Yaffe, MD, both with the department of psychiatry, University of California, San Francisco, said in a joint email.
“This study reminds us that heart health is key to brain health and that the overlap and interplay between the two is not limited to patients with end-stage heart disease,” Dr. Rouch and Dr. Yaffe said.
The findings were published online Jan. 26, 2022, in Neurology.
Heart/brain connection
The analysis included 2,653 participants in the Coronary Artery Risk Development in Young Adults (CARDIA) study.
Echocardiograms were obtained at year 5, 25, and 30 study visits – at mean ages of 30, 50, and 55 years, respectively. At year 30, participants underwent a standard battery of tests measuring global cognition, processing speed, executive function, delayed verbal memory, and verbal fluency.
Over 25 years, there was an average increase in left ventricular mass of 0.27 g/m2 per year – from a mean of 80.5 g/m2 in year 5 to 86.0 g/m2 in year 30.
Left atrial volume increased by an average of 0.42 mL/m2 per year, from 16 mL/m2 in year 5 to 26 mL/m2 in year 30.
Left ventricular ejection fraction (LVEF) decreased by 0.11% per year, from 63.3% in year 5 to 59.7% in year 30.
After adjustment for demographics and education, an increase in left ventricular mass of at least 1 standard deviation over 25 years was associated with lower cognition on most tests (P ≤ .02).
An increase in left atrial volume over the study period was associated with lower global cognition (P = .04), whereas a decrease in LVEF was not associated with cognition. Further adjustment for cardiovascular risk factors yielded similar results.
“A more effective collaboration is needed between cardiologists and neurologists to promote healthy brain aging,” Dr. Rouch and Dr. Yaffe said.
“Echocardiography is a widely available, relatively inexpensive, and noninvasive imaging method that could be integrated into a risk assessment for cognitive impairment,” they added.
Looking ahead, the investigators noted there is a need for further research to determine whether interventions to improve cardiac structure and diastolic function could also benefit brain health.
They should also investigate the role of arterial stiffness and cerebral small vessel disease in the relationship between cardiac structure, function, and cognition, the researchers added.
First structural biomarker
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Newton, Mass., said the study is important because, “thus far, the connections have really been physiological parameters,” such as blood pressure and cognitive health.
“This is really strong evidence of a structural cardiac biomarker that can be measured before and independent of changes in physiology or diseased state,” said Dr. Lakhan, who was not involved with the research.
As more and more interventions are being introduced for addressing disorders of cognition, “this potential structural finding may serve as a solid biomarker to determine” what lifestyle or drug therapy should be taken, he added.
Also weighing in on the findings, Pierre Fayad, MD, professor in the department of neurological sciences and director of the Nebraska Stroke Center, University of Nebraska Medical Center, Omaha, said CARDIA is “an important study” providing “precious data.”
The reported changes in cardiac structure and function “precede the clinical symptomatology, as the follow-up stops before they enter into later adulthood, where the risk of clinical events dramatically rises. Meaning these patients still have not had stroke, congestive heart failure, heart attack or dementia, but some of them could be on that trajectory later in their life,” Dr. Fayad told this news organization.
Documenting such changes over time is “valuable to give an insight into what leads us to such progression,” he noted.
How reliably predictive the findings are for eventual clinical cognitive impairment “will need to be confirmed and verified” in future studies, he added.
“If verified, it could be helpful to provide interventions to those with the left atrial volume enlargement marker and see their effectiveness at preventing eventual clinical cognitive impairment,” said Dr. Fayad.
The CARDIA study is supported by the National Heart, Lung, and Blood Institute in collaboration with the University of Alabama at Birmingham, Northwestern University, the University of Minnesota, and the Kaiser Foundation Research Institute. Rouch, Lakhan, and Dr. Fayad have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NEUROLOGY
Immunocompromised patients should receive fourth COVID shot: CDC
The Centers for Disease Control and Prevention contacted pharmacies on Jan. 26 to reinforce the message that people with moderate to severe immune suppression should receive a fourth COVID-19 vaccine, according to Kaiser Health News.
The conference call came a day after the news outlet reported that immunocompromised people were being turned away by pharmacies. White House officials also emphasized on Jan. 26 that immunocompromised people should receive an additional shot.
During the call, the CDC “reiterated the recommendations, running through case examples,” Mitchel Rothholz, RPh, MBA, chief of governance and state affiliates for the American Pharmacists Association, told KHN.
While on the call, Mr. Rothholz asked for a “prepared document” with the CDC’s recommendations “so we can clearly and consistently communicate the message.” The CDC officials on the call said they would create a document but “don’t know how long that will take,” Mr. Rothholz told KHN.
The CDC recommends an additional shot -– or a fourth shot – for those who have weak immune systems, which makes them more at risk for severe COVID-19 and death. About 7 million American adults are considered immunocompromised, KHN reported, which includes people who have certain medical conditions that impair their immune response or who take immune-suppressing drugs because of organ transplants, cancer, or autoimmune diseases.
The CDC first recommended fourth shots for immunocompromised people in October. This month, the CDC shortened the time for booster shots from 6 months to 5 months, and some immunocompromised people who are due for another shot have begun to seek them. The agency has been educating pharmacists and other health providers since then, a CDC spokesperson told KHN.
While patients don’t need to provide proof that they are immunocompromised, according to the CDC, some have been turned away, KHN reported.
To improve communication with the public, large pharmacies could issue news releases and update their websites “explicitly stating that they are offering fourth doses” to immunocompromised people, Ameet Kini, MD, a professor of pathology and laboratory medicine at Loyola University Medical Center in Chicago, told KHN.
Pharmacies should also update their patient portals and provide “clear guidance for their pharmacists,” he said.
A version of this article first appeared on WebMD.com.
The Centers for Disease Control and Prevention contacted pharmacies on Jan. 26 to reinforce the message that people with moderate to severe immune suppression should receive a fourth COVID-19 vaccine, according to Kaiser Health News.
The conference call came a day after the news outlet reported that immunocompromised people were being turned away by pharmacies. White House officials also emphasized on Jan. 26 that immunocompromised people should receive an additional shot.
During the call, the CDC “reiterated the recommendations, running through case examples,” Mitchel Rothholz, RPh, MBA, chief of governance and state affiliates for the American Pharmacists Association, told KHN.
While on the call, Mr. Rothholz asked for a “prepared document” with the CDC’s recommendations “so we can clearly and consistently communicate the message.” The CDC officials on the call said they would create a document but “don’t know how long that will take,” Mr. Rothholz told KHN.
The CDC recommends an additional shot -– or a fourth shot – for those who have weak immune systems, which makes them more at risk for severe COVID-19 and death. About 7 million American adults are considered immunocompromised, KHN reported, which includes people who have certain medical conditions that impair their immune response or who take immune-suppressing drugs because of organ transplants, cancer, or autoimmune diseases.
The CDC first recommended fourth shots for immunocompromised people in October. This month, the CDC shortened the time for booster shots from 6 months to 5 months, and some immunocompromised people who are due for another shot have begun to seek them. The agency has been educating pharmacists and other health providers since then, a CDC spokesperson told KHN.
While patients don’t need to provide proof that they are immunocompromised, according to the CDC, some have been turned away, KHN reported.
To improve communication with the public, large pharmacies could issue news releases and update their websites “explicitly stating that they are offering fourth doses” to immunocompromised people, Ameet Kini, MD, a professor of pathology and laboratory medicine at Loyola University Medical Center in Chicago, told KHN.
Pharmacies should also update their patient portals and provide “clear guidance for their pharmacists,” he said.
A version of this article first appeared on WebMD.com.
The Centers for Disease Control and Prevention contacted pharmacies on Jan. 26 to reinforce the message that people with moderate to severe immune suppression should receive a fourth COVID-19 vaccine, according to Kaiser Health News.
The conference call came a day after the news outlet reported that immunocompromised people were being turned away by pharmacies. White House officials also emphasized on Jan. 26 that immunocompromised people should receive an additional shot.
During the call, the CDC “reiterated the recommendations, running through case examples,” Mitchel Rothholz, RPh, MBA, chief of governance and state affiliates for the American Pharmacists Association, told KHN.
While on the call, Mr. Rothholz asked for a “prepared document” with the CDC’s recommendations “so we can clearly and consistently communicate the message.” The CDC officials on the call said they would create a document but “don’t know how long that will take,” Mr. Rothholz told KHN.
The CDC recommends an additional shot -– or a fourth shot – for those who have weak immune systems, which makes them more at risk for severe COVID-19 and death. About 7 million American adults are considered immunocompromised, KHN reported, which includes people who have certain medical conditions that impair their immune response or who take immune-suppressing drugs because of organ transplants, cancer, or autoimmune diseases.
The CDC first recommended fourth shots for immunocompromised people in October. This month, the CDC shortened the time for booster shots from 6 months to 5 months, and some immunocompromised people who are due for another shot have begun to seek them. The agency has been educating pharmacists and other health providers since then, a CDC spokesperson told KHN.
While patients don’t need to provide proof that they are immunocompromised, according to the CDC, some have been turned away, KHN reported.
To improve communication with the public, large pharmacies could issue news releases and update their websites “explicitly stating that they are offering fourth doses” to immunocompromised people, Ameet Kini, MD, a professor of pathology and laboratory medicine at Loyola University Medical Center in Chicago, told KHN.
Pharmacies should also update their patient portals and provide “clear guidance for their pharmacists,” he said.
A version of this article first appeared on WebMD.com.
Hong Kong, U.S., Israeli data illuminate COVID vaccine myocarditis
Why some COVID-19 vaccines seem occasionally to cause a distinctive form of myocarditis, and why adolescent boys and young men appear most vulnerable, remain a mystery. But the entity’s prevalence, nuances of presentation, and likely clinical course have come into sharper view after recent additions to the literature.
Two new publications all but confirm that the rare cases of myocarditis closely following vaccination against SARS-CoV-2, primarily with one of the mRNA-based vaccines from Pfizer-BioNTech and Moderna, is a clinically different creature from myocarditis physicians were likely to see before the pandemic.
A third report unveils rates of hospitalization for myocarditis linked to Pfizer-BioNTech vaccination in the 12- to 15-year age group, based on active surveillance across Israel. Of note, the rates were lower than corresponding numbers among the country’s 16- to 19-year-olds published in late 2021 by the same authors.
No link with CoronaVac
A case-control study covering almost the entire population of Hong Kong from February to August 2021 confirms a slight but significant excess risk for myocarditis and, to a lesser degree, pericarditis, after injections of the Pfizer-BioNTech vaccine. As consistently reported from other studies, the risks were highest in adolescent and young adult males and after a second dose.
The study estimated an overall carditis incidence of 5.7 cases per million doses of Pfizer-BioNTech, for a risk 3.5 times that in the unvaccinated Hong Kong population. Carditis rates after a first dose were about 2.5 per million and 10 per million after a second dose.
Hong Kong launched its public SARS-CoV-2 immunization program in late February 2021 with the Chinese-made CoronaVac (Sinovac) inactivated-virus vaccine, and introduced the mRNA-based alternative several weeks later. By August 2021, the vaccines had reached about 3.3 million people in the region – 49% of the Hong Kong population at least 12 years of age.
In a novel finding, there were no excesses in carditis cases after CoronaVac vaccination. The difference between vaccines likely isn’t caused by chance, because three-fourths of the carditis-associated Pfizer-BioNTech injections arose within a week, whereas “71% of cases following the use of CoronaVac occurred more than 30 days after vaccination,” senior author Ian Chi Kei Wong, PhD, University of Hong Kong, said in an interview.
“This onset distribution for cases having received CoronaVac demonstrates that it is highly unlikely the carditis cases are related to the vaccine,” he said. And that “plausibly implies a specific underlying mechanism between vaccination and carditis that may only be applicable to mRNA vaccines.”
That inference is in line with case reports and other research, including large population-based studies from Israel and Denmark, although a recent study from the United Kingdom hinted at a potential excess myocarditis risk associated with the adenovirus-based AstraZeneca-Oxford vaccine.
The Hong Kong study identified 160 patients age 12 or older with a first diagnosis of carditis during February to August 2021, in electronic health records covering nearly the entire region.
“We used laboratory test results of troponin levels to further eliminate unlikely cases of carditis,” Dr. Wong said. The health records were linked to a “population-based vaccination record” maintained by the government’s department of health.
About 10 control patients from among all hospitalized patients without carditis were matched by age, sex, and admission date to each of the 160 carditis cases. About 83% of cases and 92% of the controls were unvaccinated.
Among those who received the Pfizer-BioNTech vaccine, representing 12.5% of cases and 4.2% of controls, the estimated carditis incidence was 0.57 per 100,000 doses. For those who received CoronaVac, representing 4.4% of cases and 3.9% of controls, it was 0.31 per 100,000 doses.
In adjusted analysis, the odds ratios for carditis among Pfizer-BioNTech vaccine recipients, compared with unvaccinated controls, were 3.57 (95% confidence interval, 1.93-6.60) overall, 4.68 (95% CI, 2.25-9.71) for males, 2.22 (95% CI, 0.57-8.69) for females, 2.41 (95% CI, 1.18-4.90) for ages 18 and older, and 13.8 (95% CI, 2.86-110.4) for ages 12-17
Myocarditis accounted for most of the excess cases, with an overall OR of 9.29 (95% CI, 3.94-21.9). The OR reached only 1.06 (95% CI, 0.35-3.22) for pericarditis alone.
The case-control study is noteworthy for its design, which contrasts with the many recent case series and passive or active surveillance studies, and even the more robust population-based studies of vaccine-related myocarditis, observed Dongngan Truong, MD, University of Utah and Primary Children’s Hospital, both in Salt Lake City, who wasn’t part of the study.
Among its strengths, she said in an interview, are its linkage of comprehensive hospital and vaccination data sets for two different vaccines; and that it corroborates other research suggesting there is “something in particular about mRNA vaccination that seems to be associated with the development of myocarditis.”
Active surveillance in Israel
In an October 2021 report based on an Israeli Ministry of Health database covering up to May 2021, rates of myocarditis arising within 21 days of a second Pfizer-BioNTech dose in 16- to 19-year-olds reached about 1 per 6,637 males and 1 per 99,853 females. Those numbers compared with 1 per 26,000 males and 1 per 218,000 females across all age groups.
Now authors led by Dror Mevorach, MD, Hadassah Medical Center, Jerusalem, have published corresponding numbers from the same data base for myocarditis associated with the same vaccine in males and females aged 12-15.
Their research covers 404,407 people in that age group who received a first dose of the mRNA-based vaccine and 326,463 who received the second dose from June to October, 2021. Only 18 cases of myocarditis were observed within 21 days of either dose.
The estimated rates for males were 0.56 cases per 100,000 after a first dose and 8.09 cases per 100,000 after a second dose.
For females, the estimates were 0 cases per 100,000 after a first dose and 0.69 cases per 100,000 after a second dose.
“The pattern observed, mainly following the second vaccination in males, suggests causality,” the group wrote.
Leveraging passive surveillance reports
Another new report adds a twist to updated numbers from the U.S. Vaccine Adverse Event Reporting System (VAERS).
Prevalences derived from the passive-surveillance data base, known for including case records of inconsistent quality or completeness, are considered especially prone to reporting bias, the authors acknowledged.
The current analysis, however, plunges deep into VAERS-reported cases of presumed SARS-CoV-2 vaccine-associated myocarditis to help clarify “more of the characteristics of the patients and some of the treatments and short-term outcomes,” Matthew E. Oster, MD, MPH, said in an interview.
Dr. Oster, from the Centers for Disease Control and Prevention and Emory University, Atlanta, is lead author on the study’s Jan. 25, 2022, publication in JAMA.
The group reviewed charts and interviewed involved clinicians to adjudicate and document presentations, therapies, and the clinical course of cases reported as SARS-CoV-2 vaccine–associated myocarditis from December 2020 to August 2021. Out of the nearly 2000 reports, which were limited to patients younger than 30, the group identified 1,626 likely cases of such myocarditis arising within 7 days of a second mRNA vaccine dose.
The confirmed cases consistently represented higher prevalences than expected compared with prepandemic myocarditis claims data for both sexes and across age groups spanning 12-29 years.
For example, rates were highest for adolescent males – about 106 and 71 cases per million second doses of the Pfizer-BioNTech vaccine in those aged 16-17 and 12-16, respectively, for example. They were lowest for women aged 25-29, at 2.23 cases per million second Pfizer-BioNTech doses; the highest rate among females was about 11 per million for the 16-17 age group.
The observed rates, Dr. Oster said, represent an update to VAERS numbers published June 2021 in Morbidity and Mortality Weekly Report covering cases through June 2021.
“Overall, the general risk of having myocarditis from the vaccines is still extremely low. Even in the highest risk groups, it is still extremely low, and still lower than the risk of having cardiac complications from COVID,” he noted.
How do patients fare clinically?
From their chart reviews and interviews with case clinicians, Dr. Oster said, “we started to learn quickly that this is really a different type of myocarditis.”
For example, its onset, typically within a few days of the potential immunologic cause, was more rapid than in viral myocarditis, and its symptoms resolved faster, the report notes. Clinical presentations tended to be less severe, treatments not as intensive, and outcomes not as serious, compared with “the kind of typical viral myocarditis that most of the providers were used to taking care of in the past,” he said. “The pattern for these cases was very consistent.”
The study covered VAERS reports of suspected myocarditis arising within a week of first dose of a mRNA-based vaccine from the United States launch of public vaccination in December 2020 to August 2021, the CDC-based group reported. By then, more than 192 million people in the country had received either the Pfizer-BioNTech (age 12 or older) or Moderna (age 18 or older) vaccines.
Of the 1,991 reports of myocarditis, including 391 also involving pericarditis, 1,626 met the study’s definition for myocarditis on adjudication; about 82% of the latter cases were in males.
Based on the investigators’ review of charts and clinician interviews connected with 826 cases that met their definition of myocarditis in patients younger than 30, 89% reported “chest pain, pressure, or discomfort” and 30% reported dyspnea or shortness of breath. Troponin levels were elevated in 98%, 72% of patients who underwent electrocardiography showed abnormalities, and 12% of those with echocardiography had left ventricular ejection fractions less than 50%.
About 96% were hospitalized, and presenting symptoms resolved by discharge in 87% of those with available data, the group noted. Among patients with data on in-hospital therapy, they wrote, NSAIDs were the most common therapy, in 87%.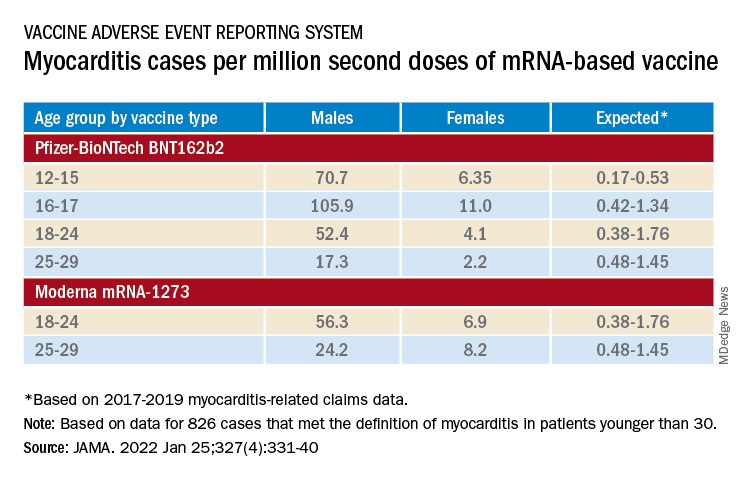
‘Mild and self-limiting’
The case-control study from Hong Kong didn’t specifically examine patients’ treatment and clinical course, but it does portray their vaccine-associated myocarditis as contrasting with more familiar viral myocarditis.
Patients with “typical” myocarditis tend to be “overall much sicker than what we’re seeing with myocarditis following vaccination,” Dr. Truong agreed. None of the 20 patients with myocarditis after Pfizer-BioNTech vaccination in Hong Kong were admitted to the intensive care unit. That, she added, suggests none required extracorporeal membrane oxygenation or vasoactive support, often necessary in viral myocarditis. “And they had shorter hospital stays.”
In contrast, Dr. Wong noted, 14 of the study’s unvaccinated patients required ICU admission; 12 of them died during the follow-up period. None with vaccine-related carditis died during the study’s follow-up. “We also showed that cases following [Pfizer-BioNTech] vaccination were all mild and self-limiting.”
Dr. Truong largely agreed that SARS-CoV-2 vaccine myocarditis and most myocarditis seen before the pandemic can be viewed as distinct clinical entities, “at least in the short term. I think we do need to follow these patients to look at more long-term outcomes, because at this point I don’t think we know the long-term implications. But at least in the short term, it seems like these patients are different, are much less sick, and recover pretty quickly overall.”
Dr. Oster emphasized that the many and varied acute and long-term hazards from contracting COVID-19 far outweigh any risk for myocarditis from vaccination. But for individuals who were hit with myocarditis soon after their first mRNA vaccine dose, who have already established their susceptibility, he and his colleagues would recommend that they “consider alternatives and not get the vaccine again.”
Dr. Oster reported no relevant financial relationships. Dr. Wong and colleagues did not report any relevant disclosures. Dr. Truong has previously disclosed serving as a consultant to Pfizer.
A version of this article first appeared on Medscape.com.
Why some COVID-19 vaccines seem occasionally to cause a distinctive form of myocarditis, and why adolescent boys and young men appear most vulnerable, remain a mystery. But the entity’s prevalence, nuances of presentation, and likely clinical course have come into sharper view after recent additions to the literature.
Two new publications all but confirm that the rare cases of myocarditis closely following vaccination against SARS-CoV-2, primarily with one of the mRNA-based vaccines from Pfizer-BioNTech and Moderna, is a clinically different creature from myocarditis physicians were likely to see before the pandemic.
A third report unveils rates of hospitalization for myocarditis linked to Pfizer-BioNTech vaccination in the 12- to 15-year age group, based on active surveillance across Israel. Of note, the rates were lower than corresponding numbers among the country’s 16- to 19-year-olds published in late 2021 by the same authors.
No link with CoronaVac
A case-control study covering almost the entire population of Hong Kong from February to August 2021 confirms a slight but significant excess risk for myocarditis and, to a lesser degree, pericarditis, after injections of the Pfizer-BioNTech vaccine. As consistently reported from other studies, the risks were highest in adolescent and young adult males and after a second dose.
The study estimated an overall carditis incidence of 5.7 cases per million doses of Pfizer-BioNTech, for a risk 3.5 times that in the unvaccinated Hong Kong population. Carditis rates after a first dose were about 2.5 per million and 10 per million after a second dose.
Hong Kong launched its public SARS-CoV-2 immunization program in late February 2021 with the Chinese-made CoronaVac (Sinovac) inactivated-virus vaccine, and introduced the mRNA-based alternative several weeks later. By August 2021, the vaccines had reached about 3.3 million people in the region – 49% of the Hong Kong population at least 12 years of age.
In a novel finding, there were no excesses in carditis cases after CoronaVac vaccination. The difference between vaccines likely isn’t caused by chance, because three-fourths of the carditis-associated Pfizer-BioNTech injections arose within a week, whereas “71% of cases following the use of CoronaVac occurred more than 30 days after vaccination,” senior author Ian Chi Kei Wong, PhD, University of Hong Kong, said in an interview.
“This onset distribution for cases having received CoronaVac demonstrates that it is highly unlikely the carditis cases are related to the vaccine,” he said. And that “plausibly implies a specific underlying mechanism between vaccination and carditis that may only be applicable to mRNA vaccines.”
That inference is in line with case reports and other research, including large population-based studies from Israel and Denmark, although a recent study from the United Kingdom hinted at a potential excess myocarditis risk associated with the adenovirus-based AstraZeneca-Oxford vaccine.
The Hong Kong study identified 160 patients age 12 or older with a first diagnosis of carditis during February to August 2021, in electronic health records covering nearly the entire region.
“We used laboratory test results of troponin levels to further eliminate unlikely cases of carditis,” Dr. Wong said. The health records were linked to a “population-based vaccination record” maintained by the government’s department of health.
About 10 control patients from among all hospitalized patients without carditis were matched by age, sex, and admission date to each of the 160 carditis cases. About 83% of cases and 92% of the controls were unvaccinated.
Among those who received the Pfizer-BioNTech vaccine, representing 12.5% of cases and 4.2% of controls, the estimated carditis incidence was 0.57 per 100,000 doses. For those who received CoronaVac, representing 4.4% of cases and 3.9% of controls, it was 0.31 per 100,000 doses.
In adjusted analysis, the odds ratios for carditis among Pfizer-BioNTech vaccine recipients, compared with unvaccinated controls, were 3.57 (95% confidence interval, 1.93-6.60) overall, 4.68 (95% CI, 2.25-9.71) for males, 2.22 (95% CI, 0.57-8.69) for females, 2.41 (95% CI, 1.18-4.90) for ages 18 and older, and 13.8 (95% CI, 2.86-110.4) for ages 12-17
Myocarditis accounted for most of the excess cases, with an overall OR of 9.29 (95% CI, 3.94-21.9). The OR reached only 1.06 (95% CI, 0.35-3.22) for pericarditis alone.
The case-control study is noteworthy for its design, which contrasts with the many recent case series and passive or active surveillance studies, and even the more robust population-based studies of vaccine-related myocarditis, observed Dongngan Truong, MD, University of Utah and Primary Children’s Hospital, both in Salt Lake City, who wasn’t part of the study.
Among its strengths, she said in an interview, are its linkage of comprehensive hospital and vaccination data sets for two different vaccines; and that it corroborates other research suggesting there is “something in particular about mRNA vaccination that seems to be associated with the development of myocarditis.”
Active surveillance in Israel
In an October 2021 report based on an Israeli Ministry of Health database covering up to May 2021, rates of myocarditis arising within 21 days of a second Pfizer-BioNTech dose in 16- to 19-year-olds reached about 1 per 6,637 males and 1 per 99,853 females. Those numbers compared with 1 per 26,000 males and 1 per 218,000 females across all age groups.
Now authors led by Dror Mevorach, MD, Hadassah Medical Center, Jerusalem, have published corresponding numbers from the same data base for myocarditis associated with the same vaccine in males and females aged 12-15.
Their research covers 404,407 people in that age group who received a first dose of the mRNA-based vaccine and 326,463 who received the second dose from June to October, 2021. Only 18 cases of myocarditis were observed within 21 days of either dose.
The estimated rates for males were 0.56 cases per 100,000 after a first dose and 8.09 cases per 100,000 after a second dose.
For females, the estimates were 0 cases per 100,000 after a first dose and 0.69 cases per 100,000 after a second dose.
“The pattern observed, mainly following the second vaccination in males, suggests causality,” the group wrote.
Leveraging passive surveillance reports
Another new report adds a twist to updated numbers from the U.S. Vaccine Adverse Event Reporting System (VAERS).
Prevalences derived from the passive-surveillance data base, known for including case records of inconsistent quality or completeness, are considered especially prone to reporting bias, the authors acknowledged.
The current analysis, however, plunges deep into VAERS-reported cases of presumed SARS-CoV-2 vaccine-associated myocarditis to help clarify “more of the characteristics of the patients and some of the treatments and short-term outcomes,” Matthew E. Oster, MD, MPH, said in an interview.
Dr. Oster, from the Centers for Disease Control and Prevention and Emory University, Atlanta, is lead author on the study’s Jan. 25, 2022, publication in JAMA.
The group reviewed charts and interviewed involved clinicians to adjudicate and document presentations, therapies, and the clinical course of cases reported as SARS-CoV-2 vaccine–associated myocarditis from December 2020 to August 2021. Out of the nearly 2000 reports, which were limited to patients younger than 30, the group identified 1,626 likely cases of such myocarditis arising within 7 days of a second mRNA vaccine dose.
The confirmed cases consistently represented higher prevalences than expected compared with prepandemic myocarditis claims data for both sexes and across age groups spanning 12-29 years.
For example, rates were highest for adolescent males – about 106 and 71 cases per million second doses of the Pfizer-BioNTech vaccine in those aged 16-17 and 12-16, respectively, for example. They were lowest for women aged 25-29, at 2.23 cases per million second Pfizer-BioNTech doses; the highest rate among females was about 11 per million for the 16-17 age group.
The observed rates, Dr. Oster said, represent an update to VAERS numbers published June 2021 in Morbidity and Mortality Weekly Report covering cases through June 2021.
“Overall, the general risk of having myocarditis from the vaccines is still extremely low. Even in the highest risk groups, it is still extremely low, and still lower than the risk of having cardiac complications from COVID,” he noted.
How do patients fare clinically?
From their chart reviews and interviews with case clinicians, Dr. Oster said, “we started to learn quickly that this is really a different type of myocarditis.”
For example, its onset, typically within a few days of the potential immunologic cause, was more rapid than in viral myocarditis, and its symptoms resolved faster, the report notes. Clinical presentations tended to be less severe, treatments not as intensive, and outcomes not as serious, compared with “the kind of typical viral myocarditis that most of the providers were used to taking care of in the past,” he said. “The pattern for these cases was very consistent.”
The study covered VAERS reports of suspected myocarditis arising within a week of first dose of a mRNA-based vaccine from the United States launch of public vaccination in December 2020 to August 2021, the CDC-based group reported. By then, more than 192 million people in the country had received either the Pfizer-BioNTech (age 12 or older) or Moderna (age 18 or older) vaccines.
Of the 1,991 reports of myocarditis, including 391 also involving pericarditis, 1,626 met the study’s definition for myocarditis on adjudication; about 82% of the latter cases were in males.
Based on the investigators’ review of charts and clinician interviews connected with 826 cases that met their definition of myocarditis in patients younger than 30, 89% reported “chest pain, pressure, or discomfort” and 30% reported dyspnea or shortness of breath. Troponin levels were elevated in 98%, 72% of patients who underwent electrocardiography showed abnormalities, and 12% of those with echocardiography had left ventricular ejection fractions less than 50%.
About 96% were hospitalized, and presenting symptoms resolved by discharge in 87% of those with available data, the group noted. Among patients with data on in-hospital therapy, they wrote, NSAIDs were the most common therapy, in 87%.
‘Mild and self-limiting’
The case-control study from Hong Kong didn’t specifically examine patients’ treatment and clinical course, but it does portray their vaccine-associated myocarditis as contrasting with more familiar viral myocarditis.
Patients with “typical” myocarditis tend to be “overall much sicker than what we’re seeing with myocarditis following vaccination,” Dr. Truong agreed. None of the 20 patients with myocarditis after Pfizer-BioNTech vaccination in Hong Kong were admitted to the intensive care unit. That, she added, suggests none required extracorporeal membrane oxygenation or vasoactive support, often necessary in viral myocarditis. “And they had shorter hospital stays.”
In contrast, Dr. Wong noted, 14 of the study’s unvaccinated patients required ICU admission; 12 of them died during the follow-up period. None with vaccine-related carditis died during the study’s follow-up. “We also showed that cases following [Pfizer-BioNTech] vaccination were all mild and self-limiting.”
Dr. Truong largely agreed that SARS-CoV-2 vaccine myocarditis and most myocarditis seen before the pandemic can be viewed as distinct clinical entities, “at least in the short term. I think we do need to follow these patients to look at more long-term outcomes, because at this point I don’t think we know the long-term implications. But at least in the short term, it seems like these patients are different, are much less sick, and recover pretty quickly overall.”
Dr. Oster emphasized that the many and varied acute and long-term hazards from contracting COVID-19 far outweigh any risk for myocarditis from vaccination. But for individuals who were hit with myocarditis soon after their first mRNA vaccine dose, who have already established their susceptibility, he and his colleagues would recommend that they “consider alternatives and not get the vaccine again.”
Dr. Oster reported no relevant financial relationships. Dr. Wong and colleagues did not report any relevant disclosures. Dr. Truong has previously disclosed serving as a consultant to Pfizer.
A version of this article first appeared on Medscape.com.
Why some COVID-19 vaccines seem occasionally to cause a distinctive form of myocarditis, and why adolescent boys and young men appear most vulnerable, remain a mystery. But the entity’s prevalence, nuances of presentation, and likely clinical course have come into sharper view after recent additions to the literature.
Two new publications all but confirm that the rare cases of myocarditis closely following vaccination against SARS-CoV-2, primarily with one of the mRNA-based vaccines from Pfizer-BioNTech and Moderna, is a clinically different creature from myocarditis physicians were likely to see before the pandemic.
A third report unveils rates of hospitalization for myocarditis linked to Pfizer-BioNTech vaccination in the 12- to 15-year age group, based on active surveillance across Israel. Of note, the rates were lower than corresponding numbers among the country’s 16- to 19-year-olds published in late 2021 by the same authors.
No link with CoronaVac
A case-control study covering almost the entire population of Hong Kong from February to August 2021 confirms a slight but significant excess risk for myocarditis and, to a lesser degree, pericarditis, after injections of the Pfizer-BioNTech vaccine. As consistently reported from other studies, the risks were highest in adolescent and young adult males and after a second dose.
The study estimated an overall carditis incidence of 5.7 cases per million doses of Pfizer-BioNTech, for a risk 3.5 times that in the unvaccinated Hong Kong population. Carditis rates after a first dose were about 2.5 per million and 10 per million after a second dose.
Hong Kong launched its public SARS-CoV-2 immunization program in late February 2021 with the Chinese-made CoronaVac (Sinovac) inactivated-virus vaccine, and introduced the mRNA-based alternative several weeks later. By August 2021, the vaccines had reached about 3.3 million people in the region – 49% of the Hong Kong population at least 12 years of age.
In a novel finding, there were no excesses in carditis cases after CoronaVac vaccination. The difference between vaccines likely isn’t caused by chance, because three-fourths of the carditis-associated Pfizer-BioNTech injections arose within a week, whereas “71% of cases following the use of CoronaVac occurred more than 30 days after vaccination,” senior author Ian Chi Kei Wong, PhD, University of Hong Kong, said in an interview.
“This onset distribution for cases having received CoronaVac demonstrates that it is highly unlikely the carditis cases are related to the vaccine,” he said. And that “plausibly implies a specific underlying mechanism between vaccination and carditis that may only be applicable to mRNA vaccines.”
That inference is in line with case reports and other research, including large population-based studies from Israel and Denmark, although a recent study from the United Kingdom hinted at a potential excess myocarditis risk associated with the adenovirus-based AstraZeneca-Oxford vaccine.
The Hong Kong study identified 160 patients age 12 or older with a first diagnosis of carditis during February to August 2021, in electronic health records covering nearly the entire region.
“We used laboratory test results of troponin levels to further eliminate unlikely cases of carditis,” Dr. Wong said. The health records were linked to a “population-based vaccination record” maintained by the government’s department of health.
About 10 control patients from among all hospitalized patients without carditis were matched by age, sex, and admission date to each of the 160 carditis cases. About 83% of cases and 92% of the controls were unvaccinated.
Among those who received the Pfizer-BioNTech vaccine, representing 12.5% of cases and 4.2% of controls, the estimated carditis incidence was 0.57 per 100,000 doses. For those who received CoronaVac, representing 4.4% of cases and 3.9% of controls, it was 0.31 per 100,000 doses.
In adjusted analysis, the odds ratios for carditis among Pfizer-BioNTech vaccine recipients, compared with unvaccinated controls, were 3.57 (95% confidence interval, 1.93-6.60) overall, 4.68 (95% CI, 2.25-9.71) for males, 2.22 (95% CI, 0.57-8.69) for females, 2.41 (95% CI, 1.18-4.90) for ages 18 and older, and 13.8 (95% CI, 2.86-110.4) for ages 12-17
Myocarditis accounted for most of the excess cases, with an overall OR of 9.29 (95% CI, 3.94-21.9). The OR reached only 1.06 (95% CI, 0.35-3.22) for pericarditis alone.
The case-control study is noteworthy for its design, which contrasts with the many recent case series and passive or active surveillance studies, and even the more robust population-based studies of vaccine-related myocarditis, observed Dongngan Truong, MD, University of Utah and Primary Children’s Hospital, both in Salt Lake City, who wasn’t part of the study.
Among its strengths, she said in an interview, are its linkage of comprehensive hospital and vaccination data sets for two different vaccines; and that it corroborates other research suggesting there is “something in particular about mRNA vaccination that seems to be associated with the development of myocarditis.”
Active surveillance in Israel
In an October 2021 report based on an Israeli Ministry of Health database covering up to May 2021, rates of myocarditis arising within 21 days of a second Pfizer-BioNTech dose in 16- to 19-year-olds reached about 1 per 6,637 males and 1 per 99,853 females. Those numbers compared with 1 per 26,000 males and 1 per 218,000 females across all age groups.
Now authors led by Dror Mevorach, MD, Hadassah Medical Center, Jerusalem, have published corresponding numbers from the same data base for myocarditis associated with the same vaccine in males and females aged 12-15.
Their research covers 404,407 people in that age group who received a first dose of the mRNA-based vaccine and 326,463 who received the second dose from June to October, 2021. Only 18 cases of myocarditis were observed within 21 days of either dose.
The estimated rates for males were 0.56 cases per 100,000 after a first dose and 8.09 cases per 100,000 after a second dose.
For females, the estimates were 0 cases per 100,000 after a first dose and 0.69 cases per 100,000 after a second dose.
“The pattern observed, mainly following the second vaccination in males, suggests causality,” the group wrote.
Leveraging passive surveillance reports
Another new report adds a twist to updated numbers from the U.S. Vaccine Adverse Event Reporting System (VAERS).
Prevalences derived from the passive-surveillance data base, known for including case records of inconsistent quality or completeness, are considered especially prone to reporting bias, the authors acknowledged.
The current analysis, however, plunges deep into VAERS-reported cases of presumed SARS-CoV-2 vaccine-associated myocarditis to help clarify “more of the characteristics of the patients and some of the treatments and short-term outcomes,” Matthew E. Oster, MD, MPH, said in an interview.
Dr. Oster, from the Centers for Disease Control and Prevention and Emory University, Atlanta, is lead author on the study’s Jan. 25, 2022, publication in JAMA.
The group reviewed charts and interviewed involved clinicians to adjudicate and document presentations, therapies, and the clinical course of cases reported as SARS-CoV-2 vaccine–associated myocarditis from December 2020 to August 2021. Out of the nearly 2000 reports, which were limited to patients younger than 30, the group identified 1,626 likely cases of such myocarditis arising within 7 days of a second mRNA vaccine dose.
The confirmed cases consistently represented higher prevalences than expected compared with prepandemic myocarditis claims data for both sexes and across age groups spanning 12-29 years.
For example, rates were highest for adolescent males – about 106 and 71 cases per million second doses of the Pfizer-BioNTech vaccine in those aged 16-17 and 12-16, respectively, for example. They were lowest for women aged 25-29, at 2.23 cases per million second Pfizer-BioNTech doses; the highest rate among females was about 11 per million for the 16-17 age group.
The observed rates, Dr. Oster said, represent an update to VAERS numbers published June 2021 in Morbidity and Mortality Weekly Report covering cases through June 2021.
“Overall, the general risk of having myocarditis from the vaccines is still extremely low. Even in the highest risk groups, it is still extremely low, and still lower than the risk of having cardiac complications from COVID,” he noted.
How do patients fare clinically?
From their chart reviews and interviews with case clinicians, Dr. Oster said, “we started to learn quickly that this is really a different type of myocarditis.”
For example, its onset, typically within a few days of the potential immunologic cause, was more rapid than in viral myocarditis, and its symptoms resolved faster, the report notes. Clinical presentations tended to be less severe, treatments not as intensive, and outcomes not as serious, compared with “the kind of typical viral myocarditis that most of the providers were used to taking care of in the past,” he said. “The pattern for these cases was very consistent.”
The study covered VAERS reports of suspected myocarditis arising within a week of first dose of a mRNA-based vaccine from the United States launch of public vaccination in December 2020 to August 2021, the CDC-based group reported. By then, more than 192 million people in the country had received either the Pfizer-BioNTech (age 12 or older) or Moderna (age 18 or older) vaccines.
Of the 1,991 reports of myocarditis, including 391 also involving pericarditis, 1,626 met the study’s definition for myocarditis on adjudication; about 82% of the latter cases were in males.
Based on the investigators’ review of charts and clinician interviews connected with 826 cases that met their definition of myocarditis in patients younger than 30, 89% reported “chest pain, pressure, or discomfort” and 30% reported dyspnea or shortness of breath. Troponin levels were elevated in 98%, 72% of patients who underwent electrocardiography showed abnormalities, and 12% of those with echocardiography had left ventricular ejection fractions less than 50%.
About 96% were hospitalized, and presenting symptoms resolved by discharge in 87% of those with available data, the group noted. Among patients with data on in-hospital therapy, they wrote, NSAIDs were the most common therapy, in 87%.
‘Mild and self-limiting’
The case-control study from Hong Kong didn’t specifically examine patients’ treatment and clinical course, but it does portray their vaccine-associated myocarditis as contrasting with more familiar viral myocarditis.
Patients with “typical” myocarditis tend to be “overall much sicker than what we’re seeing with myocarditis following vaccination,” Dr. Truong agreed. None of the 20 patients with myocarditis after Pfizer-BioNTech vaccination in Hong Kong were admitted to the intensive care unit. That, she added, suggests none required extracorporeal membrane oxygenation or vasoactive support, often necessary in viral myocarditis. “And they had shorter hospital stays.”
In contrast, Dr. Wong noted, 14 of the study’s unvaccinated patients required ICU admission; 12 of them died during the follow-up period. None with vaccine-related carditis died during the study’s follow-up. “We also showed that cases following [Pfizer-BioNTech] vaccination were all mild and self-limiting.”
Dr. Truong largely agreed that SARS-CoV-2 vaccine myocarditis and most myocarditis seen before the pandemic can be viewed as distinct clinical entities, “at least in the short term. I think we do need to follow these patients to look at more long-term outcomes, because at this point I don’t think we know the long-term implications. But at least in the short term, it seems like these patients are different, are much less sick, and recover pretty quickly overall.”
Dr. Oster emphasized that the many and varied acute and long-term hazards from contracting COVID-19 far outweigh any risk for myocarditis from vaccination. But for individuals who were hit with myocarditis soon after their first mRNA vaccine dose, who have already established their susceptibility, he and his colleagues would recommend that they “consider alternatives and not get the vaccine again.”
Dr. Oster reported no relevant financial relationships. Dr. Wong and colleagues did not report any relevant disclosures. Dr. Truong has previously disclosed serving as a consultant to Pfizer.
A version of this article first appeared on Medscape.com.