User login
A 19-month-old vaccinated female with 2 days of rash
Acute hemorrhagic edema of infancy (AHEI) is a leukocytoclastic vasculitis that typically affects children between 4 months and 2 years of age.1 Etiology is unknown but the majority of cases are preceded by infections, vaccinations, or certain medications.2
AHEI is a self-limited disease that runs a benign course with spontaneous resolution within days to 3 weeks.3 Classic presentation involves acute onset of fever, purpura, ecchymosis, and inflammatory edema. Edema is often the first sign, and may involve the face, ears, scrotum, or extremities. Hemorrhagic lesions may vary in size but often coalesce and present in a distinctive “cockade” or rosette pattern with scalloped borders. Systemic manifestations are rare, but renal and joint involvement may occur.4 Despite the dramatic and sometimes extensive appearance of the dermatologic manifestations, patients with AHEI are usually not in significant distress.

Diagnosis is clinical, but skin biopsy may show leukocytoclastic vasculitis of the superficial small vessels with infiltrations of neutrophils, extravasation of red blood cells, and fibrinoid necrosis.5 In most cases, immunofluorescence is negative for perivascular IgA deposition. Treatment is symptomatic as the disease resolves spontaneously. Recurrence is uncommon but may occur, and usually occurs early.

What is on the differential?
Kawasaki disease. Similar to AHEI, patients with Kawasaki disease also may present with facial and extremity edema. However, patients with Kawasaki disease appear sicker, have associated lymphadenopathy, conjunctivitis, and fever longer than 5 days. The lack of elevated inflammatory markers, acute-onset, classic dermatologic lesions, and nontoxic appearance in our patient rule out Kawasaki disease and make AHEI more likely.

IgA vasculitis/Henoch-Schönlein purpura. The distinction between AHEI and Henoch-Schönlein purpura is among the most challenging. AHEI commonly afflicts younger children ranging from 4 months to 2 years, whereas Henoch-Schönlein purpura occurs in older children from 3 to 6 years of age. Visceral involvement is rare in AHEI, but frequently presents in Henoch-Schönlein purpura with gastrointestinal and renal complications. Although our patient had both mild renal involvement and a distribution primarily on the buttocks and lower limbs, similar to the classic distribution of Henoch-Schönlein purpura, the younger age and lack of gastrointestinal and arthritic manifestations make AHEI more likely.
Gianotti-Crosti syndrome. Gianotti-Crosti syndrome, also known as papulovesicular acrodermatitis of childhood, mainly affects children between the ages of 6 months and 12 years. Like AHEI, Gianotti-Crosti is a self-limiting condition likely triggered by viral infection or immunization. However, Gianotti-Crosti is characterized by a papular rash that may last for several weeks. Neither AHEI nor Gianotti-Crosti are pruritic, but patients with Gianotti-Crosti tend to have either inguinal or axillary lymphadenopathy. Our patient’s large, coalescing dusky red patches and edematous plaques without lymphadenopathy are more consistent with AHEI.

Erythema multiforme. Erythema multiforme is an acute, immune-mediated condition characterized by distinctive target-like lesions on the skin often accompanied by erosions or bullae. Unlike AHEI, erythema multiforme can involve the oral, genital, and/or ocular mucosae. Erythema multiforme is rare before the age of 4 years. Although the targetoid or annular purpuric configuration of erythema multiforme may present similarly to AHEI in some cases, the young age of our patient and the lack of mucosal involvement make AHEI more likely.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Ms. Kleinman is a pediatric dermatology research associate at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Neither Dr. Matiz nor Ms. Kleinman has any relevant financial disclosures.
References
1. Savino F et al. Pediatr Dermatol. 2013;30(6):e149-e152.
2. Carboni E et al. F1000Res. 2019;8:1771. 2019 Oct 17.
3. Fiore E et al. J Am Acad Dermatol. 2008;59(4):684-95.
4. Watanabe T and Sato Y. Pediatr Nephrol. 2007;22(11):1979-81.
5. Cunha DF et al. Autops Case Rep. 2015;5(3):37-41.
Acute hemorrhagic edema of infancy (AHEI) is a leukocytoclastic vasculitis that typically affects children between 4 months and 2 years of age.1 Etiology is unknown but the majority of cases are preceded by infections, vaccinations, or certain medications.2
AHEI is a self-limited disease that runs a benign course with spontaneous resolution within days to 3 weeks.3 Classic presentation involves acute onset of fever, purpura, ecchymosis, and inflammatory edema. Edema is often the first sign, and may involve the face, ears, scrotum, or extremities. Hemorrhagic lesions may vary in size but often coalesce and present in a distinctive “cockade” or rosette pattern with scalloped borders. Systemic manifestations are rare, but renal and joint involvement may occur.4 Despite the dramatic and sometimes extensive appearance of the dermatologic manifestations, patients with AHEI are usually not in significant distress.
Diagnosis is clinical, but skin biopsy may show leukocytoclastic vasculitis of the superficial small vessels with infiltrations of neutrophils, extravasation of red blood cells, and fibrinoid necrosis.5 In most cases, immunofluorescence is negative for perivascular IgA deposition. Treatment is symptomatic as the disease resolves spontaneously. Recurrence is uncommon but may occur, and usually occurs early.
What is on the differential?
Kawasaki disease. Similar to AHEI, patients with Kawasaki disease also may present with facial and extremity edema. However, patients with Kawasaki disease appear sicker, have associated lymphadenopathy, conjunctivitis, and fever longer than 5 days. The lack of elevated inflammatory markers, acute-onset, classic dermatologic lesions, and nontoxic appearance in our patient rule out Kawasaki disease and make AHEI more likely.
IgA vasculitis/Henoch-Schönlein purpura. The distinction between AHEI and Henoch-Schönlein purpura is among the most challenging. AHEI commonly afflicts younger children ranging from 4 months to 2 years, whereas Henoch-Schönlein purpura occurs in older children from 3 to 6 years of age. Visceral involvement is rare in AHEI, but frequently presents in Henoch-Schönlein purpura with gastrointestinal and renal complications. Although our patient had both mild renal involvement and a distribution primarily on the buttocks and lower limbs, similar to the classic distribution of Henoch-Schönlein purpura, the younger age and lack of gastrointestinal and arthritic manifestations make AHEI more likely.
Gianotti-Crosti syndrome. Gianotti-Crosti syndrome, also known as papulovesicular acrodermatitis of childhood, mainly affects children between the ages of 6 months and 12 years. Like AHEI, Gianotti-Crosti is a self-limiting condition likely triggered by viral infection or immunization. However, Gianotti-Crosti is characterized by a papular rash that may last for several weeks. Neither AHEI nor Gianotti-Crosti are pruritic, but patients with Gianotti-Crosti tend to have either inguinal or axillary lymphadenopathy. Our patient’s large, coalescing dusky red patches and edematous plaques without lymphadenopathy are more consistent with AHEI.
Erythema multiforme. Erythema multiforme is an acute, immune-mediated condition characterized by distinctive target-like lesions on the skin often accompanied by erosions or bullae. Unlike AHEI, erythema multiforme can involve the oral, genital, and/or ocular mucosae. Erythema multiforme is rare before the age of 4 years. Although the targetoid or annular purpuric configuration of erythema multiforme may present similarly to AHEI in some cases, the young age of our patient and the lack of mucosal involvement make AHEI more likely.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Ms. Kleinman is a pediatric dermatology research associate at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Neither Dr. Matiz nor Ms. Kleinman has any relevant financial disclosures.
References
1. Savino F et al. Pediatr Dermatol. 2013;30(6):e149-e152.
2. Carboni E et al. F1000Res. 2019;8:1771. 2019 Oct 17.
3. Fiore E et al. J Am Acad Dermatol. 2008;59(4):684-95.
4. Watanabe T and Sato Y. Pediatr Nephrol. 2007;22(11):1979-81.
5. Cunha DF et al. Autops Case Rep. 2015;5(3):37-41.
Acute hemorrhagic edema of infancy (AHEI) is a leukocytoclastic vasculitis that typically affects children between 4 months and 2 years of age.1 Etiology is unknown but the majority of cases are preceded by infections, vaccinations, or certain medications.2
AHEI is a self-limited disease that runs a benign course with spontaneous resolution within days to 3 weeks.3 Classic presentation involves acute onset of fever, purpura, ecchymosis, and inflammatory edema. Edema is often the first sign, and may involve the face, ears, scrotum, or extremities. Hemorrhagic lesions may vary in size but often coalesce and present in a distinctive “cockade” or rosette pattern with scalloped borders. Systemic manifestations are rare, but renal and joint involvement may occur.4 Despite the dramatic and sometimes extensive appearance of the dermatologic manifestations, patients with AHEI are usually not in significant distress.
Diagnosis is clinical, but skin biopsy may show leukocytoclastic vasculitis of the superficial small vessels with infiltrations of neutrophils, extravasation of red blood cells, and fibrinoid necrosis.5 In most cases, immunofluorescence is negative for perivascular IgA deposition. Treatment is symptomatic as the disease resolves spontaneously. Recurrence is uncommon but may occur, and usually occurs early.
What is on the differential?
Kawasaki disease. Similar to AHEI, patients with Kawasaki disease also may present with facial and extremity edema. However, patients with Kawasaki disease appear sicker, have associated lymphadenopathy, conjunctivitis, and fever longer than 5 days. The lack of elevated inflammatory markers, acute-onset, classic dermatologic lesions, and nontoxic appearance in our patient rule out Kawasaki disease and make AHEI more likely.
IgA vasculitis/Henoch-Schönlein purpura. The distinction between AHEI and Henoch-Schönlein purpura is among the most challenging. AHEI commonly afflicts younger children ranging from 4 months to 2 years, whereas Henoch-Schönlein purpura occurs in older children from 3 to 6 years of age. Visceral involvement is rare in AHEI, but frequently presents in Henoch-Schönlein purpura with gastrointestinal and renal complications. Although our patient had both mild renal involvement and a distribution primarily on the buttocks and lower limbs, similar to the classic distribution of Henoch-Schönlein purpura, the younger age and lack of gastrointestinal and arthritic manifestations make AHEI more likely.
Gianotti-Crosti syndrome. Gianotti-Crosti syndrome, also known as papulovesicular acrodermatitis of childhood, mainly affects children between the ages of 6 months and 12 years. Like AHEI, Gianotti-Crosti is a self-limiting condition likely triggered by viral infection or immunization. However, Gianotti-Crosti is characterized by a papular rash that may last for several weeks. Neither AHEI nor Gianotti-Crosti are pruritic, but patients with Gianotti-Crosti tend to have either inguinal or axillary lymphadenopathy. Our patient’s large, coalescing dusky red patches and edematous plaques without lymphadenopathy are more consistent with AHEI.
Erythema multiforme. Erythema multiforme is an acute, immune-mediated condition characterized by distinctive target-like lesions on the skin often accompanied by erosions or bullae. Unlike AHEI, erythema multiforme can involve the oral, genital, and/or ocular mucosae. Erythema multiforme is rare before the age of 4 years. Although the targetoid or annular purpuric configuration of erythema multiforme may present similarly to AHEI in some cases, the young age of our patient and the lack of mucosal involvement make AHEI more likely.
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Ms. Kleinman is a pediatric dermatology research associate at the University of California, San Diego, and Rady Children’s Hospital, San Diego. Neither Dr. Matiz nor Ms. Kleinman has any relevant financial disclosures.
References
1. Savino F et al. Pediatr Dermatol. 2013;30(6):e149-e152.
2. Carboni E et al. F1000Res. 2019;8:1771. 2019 Oct 17.
3. Fiore E et al. J Am Acad Dermatol. 2008;59(4):684-95.
4. Watanabe T and Sato Y. Pediatr Nephrol. 2007;22(11):1979-81.
5. Cunha DF et al. Autops Case Rep. 2015;5(3):37-41.

A 34-year-old male presented with 10 days of a pruritic rash
Less frequently observable infectious agents associated with EM are Mycoplasma pneumoniae, Histoplasma capsulatum, and parapoxvirus (orf). Rarely, EM is triggered by drug eruption or systemic disease. Individuals of all age groups and races can be affected by EM. However, it is predominantly observed in young adult patients (20-40 years of age), and there is a male predominance.
Patients typically present with the abrupt onset of symmetrical red papules that evolve into typical and atypical targetoid lesions. Lesions evolve in 48-72 hours, favoring acrofacial sites that then spread down towards the trunk. Systemic symptoms such as fever and arthralgia may accompany the skin lesions.1-3
Erythema multiforme is recognized in two forms: EM minor and EM major. Both forms share the same characteristic of target lesions. However, the presence of mucosal involvement distinguishes the two. Mucosal involvement is absent or mild in EM minor, while mucosal involvement in EM major is often severe.2,3 Painful bullous lesions are commonly present in the mouth, genital, and ocular mucous membranes. Severe symptoms can often result in difficulty eating and drinking.
Diagnosis is largely clinical. Further histologic study may accompany diagnoses to exclude differential diagnosis. In EM, direct immunofluorescence (DIF) is negative. Histopathology reveals apoptosis of individual keratinocytes.1,2
Therapeutic treatment for painful bullous lesions in the mouth involve antiseptic rinses and anesthetic solutions. Preventive treatment for patients with HSV-associated EM recurrence includes oral acyclovir or valacyclovir.2
In this patient, a punch biopsy was performed, confirming the diagnosis. A DIF was negative, and a chest x-ray was negative. Treatment was initiated with oral acyclovir, doxycycline, and a prednisone taper. In addition, topical clobetasol propionate and magic mouthwash (Maalox/lidocaine/nystatin) was prescribed. The patient was placed on daily suppressive valacyclovir to prevent frequent recurrence of EM.

This case and photo were submitted by Ms. Pham, the University of California, Los Angeles, and Dr. Sateesh, San Diego Family Dermatology. Dr. Bilu-Martin edited the column.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
1. Hafsi W and Badri T. Erythema Multiforme, in “StatPearls [Internet].” Treasure Island, Fla.: StatPearls Publishing, 2022 Jan.
2. Bolognia J et al. Dermatology. St. Louis: Mosby/Elsevier, 2008.
3. Oakley A. Erythema Multiforme. DermNet NZ. 2015 Oct.
Less frequently observable infectious agents associated with EM are Mycoplasma pneumoniae, Histoplasma capsulatum, and parapoxvirus (orf). Rarely, EM is triggered by drug eruption or systemic disease. Individuals of all age groups and races can be affected by EM. However, it is predominantly observed in young adult patients (20-40 years of age), and there is a male predominance.
Patients typically present with the abrupt onset of symmetrical red papules that evolve into typical and atypical targetoid lesions. Lesions evolve in 48-72 hours, favoring acrofacial sites that then spread down towards the trunk. Systemic symptoms such as fever and arthralgia may accompany the skin lesions.1-3
Erythema multiforme is recognized in two forms: EM minor and EM major. Both forms share the same characteristic of target lesions. However, the presence of mucosal involvement distinguishes the two. Mucosal involvement is absent or mild in EM minor, while mucosal involvement in EM major is often severe.2,3 Painful bullous lesions are commonly present in the mouth, genital, and ocular mucous membranes. Severe symptoms can often result in difficulty eating and drinking.
Diagnosis is largely clinical. Further histologic study may accompany diagnoses to exclude differential diagnosis. In EM, direct immunofluorescence (DIF) is negative. Histopathology reveals apoptosis of individual keratinocytes.1,2
Therapeutic treatment for painful bullous lesions in the mouth involve antiseptic rinses and anesthetic solutions. Preventive treatment for patients with HSV-associated EM recurrence includes oral acyclovir or valacyclovir.2
In this patient, a punch biopsy was performed, confirming the diagnosis. A DIF was negative, and a chest x-ray was negative. Treatment was initiated with oral acyclovir, doxycycline, and a prednisone taper. In addition, topical clobetasol propionate and magic mouthwash (Maalox/lidocaine/nystatin) was prescribed. The patient was placed on daily suppressive valacyclovir to prevent frequent recurrence of EM.
This case and photo were submitted by Ms. Pham, the University of California, Los Angeles, and Dr. Sateesh, San Diego Family Dermatology. Dr. Bilu-Martin edited the column.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
1. Hafsi W and Badri T. Erythema Multiforme, in “StatPearls [Internet].” Treasure Island, Fla.: StatPearls Publishing, 2022 Jan.
2. Bolognia J et al. Dermatology. St. Louis: Mosby/Elsevier, 2008.
3. Oakley A. Erythema Multiforme. DermNet NZ. 2015 Oct.
Less frequently observable infectious agents associated with EM are Mycoplasma pneumoniae, Histoplasma capsulatum, and parapoxvirus (orf). Rarely, EM is triggered by drug eruption or systemic disease. Individuals of all age groups and races can be affected by EM. However, it is predominantly observed in young adult patients (20-40 years of age), and there is a male predominance.
Patients typically present with the abrupt onset of symmetrical red papules that evolve into typical and atypical targetoid lesions. Lesions evolve in 48-72 hours, favoring acrofacial sites that then spread down towards the trunk. Systemic symptoms such as fever and arthralgia may accompany the skin lesions.1-3
Erythema multiforme is recognized in two forms: EM minor and EM major. Both forms share the same characteristic of target lesions. However, the presence of mucosal involvement distinguishes the two. Mucosal involvement is absent or mild in EM minor, while mucosal involvement in EM major is often severe.2,3 Painful bullous lesions are commonly present in the mouth, genital, and ocular mucous membranes. Severe symptoms can often result in difficulty eating and drinking.
Diagnosis is largely clinical. Further histologic study may accompany diagnoses to exclude differential diagnosis. In EM, direct immunofluorescence (DIF) is negative. Histopathology reveals apoptosis of individual keratinocytes.1,2
Therapeutic treatment for painful bullous lesions in the mouth involve antiseptic rinses and anesthetic solutions. Preventive treatment for patients with HSV-associated EM recurrence includes oral acyclovir or valacyclovir.2
In this patient, a punch biopsy was performed, confirming the diagnosis. A DIF was negative, and a chest x-ray was negative. Treatment was initiated with oral acyclovir, doxycycline, and a prednisone taper. In addition, topical clobetasol propionate and magic mouthwash (Maalox/lidocaine/nystatin) was prescribed. The patient was placed on daily suppressive valacyclovir to prevent frequent recurrence of EM.
This case and photo were submitted by Ms. Pham, the University of California, Los Angeles, and Dr. Sateesh, San Diego Family Dermatology. Dr. Bilu-Martin edited the column.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
1. Hafsi W and Badri T. Erythema Multiforme, in “StatPearls [Internet].” Treasure Island, Fla.: StatPearls Publishing, 2022 Jan.
2. Bolognia J et al. Dermatology. St. Louis: Mosby/Elsevier, 2008.
3. Oakley A. Erythema Multiforme. DermNet NZ. 2015 Oct.

New hemophilia treatments: ‘Our cup runneth over’
It’s a problem many clinicians would love to have: A whole variety of new or emerging therapeutic options to use in the care of their patients.
In a session titled “Hemophilia Update: Our Cup Runneth Over,” presented at the 2021 annual meeting of the American Society of Hematology, .
Factor concentrates
Prophylaxis – as opposed to episodic treatment – is the standard of care in the use of factor concentrates in patients with hemophilia, said Ming Y. Lim, MB BChir, from the University of Utah in Salt Lake City.
“Effective prophylaxis is an ongoing collaborative effort that relies on shared decision-making between the patient and the clinician,” she told the audience.
As the complexity of therapeutic options, including gene therapy, continues to increase “it is critical that both patients and clinicians are actively involved in this collaborative process to optimize treatment and overall patient outcomes,” she added.
Historically, clinicians who treat patients with hemophilia aimed for trough levels of factor concentrates of at least 1% to prevent spontaneous joint bleeding. But as updated World Federation of Hemophilia (WFH) guidelines now recommend, trough levels should be sufficient to prevent spontaneous bleeding based on the individual patient’s bleeding phenotype and activity levels, starting in the range between 3% and 5%, and going higher as necessary.
“The appropriate target trough level is that at which a person with hemophilia experiences zero bleeds while pursuing an active or sedentary lifestyle,” she said.
The choice of factor concentrates between standard and extended half-life products will depend on multiple factors, including availability, patient and provider preferences, cost, and access to assays for monitoring extended half-life products.
The prolonged action of extended half-life products translates into dosing twice per week or every 3 days for factor VIII concentrates, and every 7-14 days for factor IX concentrates.
“All available extended half-life products have been shown to be efficacious in the prevention and treatment of bleeds, with no evidence for any clinical safety issues,” Dr. Lim said.
There are theoretical concerns, however, regarding the lifelong use of PEGylated clotting factor concentrates, leading to some variations in the regulatory approval for some PEGylated product intended for bleeding prophylaxis in children with hemophilia, she noted.
The pharmacokinetics of prophylaxis with factor concentrates can vary according to age, body mass, blood type, and von Willebrand factor levels, so WFH guidelines recommend pharmacokinetic assessment of people with hemophilia for optimization of prophylaxis, she said.
Factor mimetic and rebalancing therapies
With the commercial availability of one factor mimetic for treatment of hemophilia A and with other factor mimetics and rebalancing therapies such as fitusiran in the works, it raises the question, “Is this the beginning of the end of the use of factor?” said Alice Ma, MD, FACP, of the University of North Carolina in Chapel Hill.
Factors that may determine the answer to that question include the convenience of subcutaneous administration of factor VIII mimetics compared with intravenous delivery of factor concentrates, relative cost of factors versus nonfactor products, and safety.
She reviewed the current state of alternatives to factor concentrates, including the factor mimetic emicizumab (Hemlibra), which was approved by the Food and Drug Administration in 2018 for bleeding prophylaxis in patients with hemophilia A with inhibitors, and is currently the only FDA-approved and licensed agent in its class.
Although emicizumab is widely regarded as a major advance, there are still unanswered clinical questions about its long-term use, Dr. Ma said. It is unknown, for example, whether it can prevent inhibitor development in previously untreated patients, and whether it can prevent intracranial hemorrhage in early years of life prior to the start of traditional prophylaxis.
It’s also unknown whether the factor VIII mimetic activity of emicizumab provides the same physiological benefits of coagulation factors, and the mechanism of thrombotic adverse events seen with this agent is still unclear, she added.
Other factor VIII mimetics in the pipeline include Mim8, which is being developed in Denmark by Novo Nordisk; this is a next-generation bispecific antibody with enhanced activity over emicizumab in both mouse models and in vitro hemophilia A assays. There are also two others bispecific antibodies designed to generate thrombin in preclinical development: BS-027125 (Bioverativ, U.S.) and NIBX-2101 (Takeda, Japan).
One of the most promising rebalancing factors in development is fitusiran, a small interfering RNA molecule that targets mRNA encoding antithrombin. As reported during ASH 2021, fitusiran was associated with an approximately 90% reduction in annualized bleeding rates in patients with hemophilia A and hemophilia B, both with inhibitors, in two clinical trials. It was described at the meeting “as a great leap forward” in the treatment of hemophilia.
However, during its clinical development fitusiran has been consistently associated with thrombotic complications, Dr. Ma noted.
Also in development are several drugs targeted against tissue factor pathway inhibitor (TFPI), an anticoagulant protein that inhibits early phases of the procoagulant response. These agents included marstacimab (Pfizer, U.S.) which has been reported to normalize coagulation in plasma from hemophilia patients ex vivo and is currently being evaluated in patients with hemophilia A and B. There is also MG1113 (Green Cross Corporation, South Korea), a monoclonal antibody currently being tested in healthy volunteers, and BAX499 (Takeda), an aptamer derived from recombinant human TFPI that has been shown to inhibit TFPI in vitro and in vivo. However, development of this agent is on hold due to bleeding in study subjects, Dr. Ma noted.
“It is really notable that none of the replacements of factor have been free of thrombotic side effects,” Dr. Ma said. “And so I think it shows that you mess with Mother Nature at your peril. If you poke at the hemostasis-thrombosis arm and reduce antithrombotic proteins, and something triggers bleeding and you start to treat with a therapy for hemorrhage, it’s not a surprise that the first patient treated with fitusiran had a thrombosis, and I think we were just not potentially savvy enough to predict that.”
Considerable optimism over gene therapy
“There is now repeated proof of concept success for hemophilia A and B gene therapy. I think this supports the considerable optimism that’s really driving this field,” said Lindsey A. George, MD, of the University of Pennsylvania and Children’s Hospital of Philadelphia.
She reviewed adeno-associated virus (AAV) vector and AAV-mediated gene transfer approaches for hemophilia A and B.
There are currently four clinical trials of gene therapy for patients with hemophilia B, and five for patients with hemophilia A.
Because AAV efficiently targets the liver, most safety considerations about systemic AAV-mediated gene therapy are focused around potential hepatotoxicity, Dr. George said.
“Thankfully, short-term safety in the context of hemophilia has really been quite good,” she said.
Patients who undergo gene therapy for hemophilia are typically monitored twice weekly for 3 months for evidence of a capsid-specific CD8 T cell response, also called a capsid immune response. This presents with transient transaminase elevations (primarily ALT) and a decline in factor VIII and factor IX activity.
In clinical trials for patients with hemophilia, the capsid immune response has limited the efficacy of the therapy in the short term, but has not been a major cause for safety concerns. It is typically managed with glucocorticoids or other immunomodulating agents such as mycophenolate mofetil or tacrolimus.
There have also been reported cases of transaminase elevations without evidence of a capsid immune response, which warrants further investigation, she added.
Regarding efficacy, she noted that across clinical trials, the observed annualized bleeding rate has been less than 1%, despite heterogeneity of vectors and dosing used.
“That’s obviously quite optimistic for the field, but it also sort of raises the point that the heterogeneity at which we’re achieving the same phenotypic observations deserves a bit of a deeper dive,” she said.
Although hemophilia B gene transfer appears to be durable, the same cannot be said as yet for hemophilia A.
In canine models for hemophilia A and B, factor VIII and factor IX expression have been demonstrated for 8-10 years post vector, and in humans factor IX expression in patients with hemophilia B has been reported for up to 8 years.
In contrast, in the three hemophilia A trials in which patients have been followed for a minimum of 2 years, there was an approximately 40% loss of transgene vector from year 1 to year 2 with two vectors, but not a third.
Potential explanations for the loss of expression seen include an unfolded protein response, promoter silence, and an ongoing undetected or unmitigated immune response to AAV or to the transgene.
Regarding the future of gene therapy, Dr. George said that “we anticipate that there will be licensed vectors in the very near future, and predicted that gene therapy “will fulfill its promise to alter the paradigm of hemophilia care.”
Dr. Lim disclosed honoraria from several companies and travel support from Novo Nordisk. Dr. Ma disclosed honoraria and research funding from Takeda. Dr. George disclosed FVIII-QQ patents and royalties, research funding from AskBio, and consulting activities/advisory board participation with others.
A version of this article first appeared on Medscape.com.
It’s a problem many clinicians would love to have: A whole variety of new or emerging therapeutic options to use in the care of their patients.
In a session titled “Hemophilia Update: Our Cup Runneth Over,” presented at the 2021 annual meeting of the American Society of Hematology, .
Factor concentrates
Prophylaxis – as opposed to episodic treatment – is the standard of care in the use of factor concentrates in patients with hemophilia, said Ming Y. Lim, MB BChir, from the University of Utah in Salt Lake City.
“Effective prophylaxis is an ongoing collaborative effort that relies on shared decision-making between the patient and the clinician,” she told the audience.
As the complexity of therapeutic options, including gene therapy, continues to increase “it is critical that both patients and clinicians are actively involved in this collaborative process to optimize treatment and overall patient outcomes,” she added.
Historically, clinicians who treat patients with hemophilia aimed for trough levels of factor concentrates of at least 1% to prevent spontaneous joint bleeding. But as updated World Federation of Hemophilia (WFH) guidelines now recommend, trough levels should be sufficient to prevent spontaneous bleeding based on the individual patient’s bleeding phenotype and activity levels, starting in the range between 3% and 5%, and going higher as necessary.
“The appropriate target trough level is that at which a person with hemophilia experiences zero bleeds while pursuing an active or sedentary lifestyle,” she said.
The choice of factor concentrates between standard and extended half-life products will depend on multiple factors, including availability, patient and provider preferences, cost, and access to assays for monitoring extended half-life products.
The prolonged action of extended half-life products translates into dosing twice per week or every 3 days for factor VIII concentrates, and every 7-14 days for factor IX concentrates.
“All available extended half-life products have been shown to be efficacious in the prevention and treatment of bleeds, with no evidence for any clinical safety issues,” Dr. Lim said.
There are theoretical concerns, however, regarding the lifelong use of PEGylated clotting factor concentrates, leading to some variations in the regulatory approval for some PEGylated product intended for bleeding prophylaxis in children with hemophilia, she noted.
The pharmacokinetics of prophylaxis with factor concentrates can vary according to age, body mass, blood type, and von Willebrand factor levels, so WFH guidelines recommend pharmacokinetic assessment of people with hemophilia for optimization of prophylaxis, she said.
Factor mimetic and rebalancing therapies
With the commercial availability of one factor mimetic for treatment of hemophilia A and with other factor mimetics and rebalancing therapies such as fitusiran in the works, it raises the question, “Is this the beginning of the end of the use of factor?” said Alice Ma, MD, FACP, of the University of North Carolina in Chapel Hill.
Factors that may determine the answer to that question include the convenience of subcutaneous administration of factor VIII mimetics compared with intravenous delivery of factor concentrates, relative cost of factors versus nonfactor products, and safety.
She reviewed the current state of alternatives to factor concentrates, including the factor mimetic emicizumab (Hemlibra), which was approved by the Food and Drug Administration in 2018 for bleeding prophylaxis in patients with hemophilia A with inhibitors, and is currently the only FDA-approved and licensed agent in its class.
Although emicizumab is widely regarded as a major advance, there are still unanswered clinical questions about its long-term use, Dr. Ma said. It is unknown, for example, whether it can prevent inhibitor development in previously untreated patients, and whether it can prevent intracranial hemorrhage in early years of life prior to the start of traditional prophylaxis.
It’s also unknown whether the factor VIII mimetic activity of emicizumab provides the same physiological benefits of coagulation factors, and the mechanism of thrombotic adverse events seen with this agent is still unclear, she added.
Other factor VIII mimetics in the pipeline include Mim8, which is being developed in Denmark by Novo Nordisk; this is a next-generation bispecific antibody with enhanced activity over emicizumab in both mouse models and in vitro hemophilia A assays. There are also two others bispecific antibodies designed to generate thrombin in preclinical development: BS-027125 (Bioverativ, U.S.) and NIBX-2101 (Takeda, Japan).
One of the most promising rebalancing factors in development is fitusiran, a small interfering RNA molecule that targets mRNA encoding antithrombin. As reported during ASH 2021, fitusiran was associated with an approximately 90% reduction in annualized bleeding rates in patients with hemophilia A and hemophilia B, both with inhibitors, in two clinical trials. It was described at the meeting “as a great leap forward” in the treatment of hemophilia.
However, during its clinical development fitusiran has been consistently associated with thrombotic complications, Dr. Ma noted.
Also in development are several drugs targeted against tissue factor pathway inhibitor (TFPI), an anticoagulant protein that inhibits early phases of the procoagulant response. These agents included marstacimab (Pfizer, U.S.) which has been reported to normalize coagulation in plasma from hemophilia patients ex vivo and is currently being evaluated in patients with hemophilia A and B. There is also MG1113 (Green Cross Corporation, South Korea), a monoclonal antibody currently being tested in healthy volunteers, and BAX499 (Takeda), an aptamer derived from recombinant human TFPI that has been shown to inhibit TFPI in vitro and in vivo. However, development of this agent is on hold due to bleeding in study subjects, Dr. Ma noted.
“It is really notable that none of the replacements of factor have been free of thrombotic side effects,” Dr. Ma said. “And so I think it shows that you mess with Mother Nature at your peril. If you poke at the hemostasis-thrombosis arm and reduce antithrombotic proteins, and something triggers bleeding and you start to treat with a therapy for hemorrhage, it’s not a surprise that the first patient treated with fitusiran had a thrombosis, and I think we were just not potentially savvy enough to predict that.”
Considerable optimism over gene therapy
“There is now repeated proof of concept success for hemophilia A and B gene therapy. I think this supports the considerable optimism that’s really driving this field,” said Lindsey A. George, MD, of the University of Pennsylvania and Children’s Hospital of Philadelphia.
She reviewed adeno-associated virus (AAV) vector and AAV-mediated gene transfer approaches for hemophilia A and B.
There are currently four clinical trials of gene therapy for patients with hemophilia B, and five for patients with hemophilia A.
Because AAV efficiently targets the liver, most safety considerations about systemic AAV-mediated gene therapy are focused around potential hepatotoxicity, Dr. George said.
“Thankfully, short-term safety in the context of hemophilia has really been quite good,” she said.
Patients who undergo gene therapy for hemophilia are typically monitored twice weekly for 3 months for evidence of a capsid-specific CD8 T cell response, also called a capsid immune response. This presents with transient transaminase elevations (primarily ALT) and a decline in factor VIII and factor IX activity.
In clinical trials for patients with hemophilia, the capsid immune response has limited the efficacy of the therapy in the short term, but has not been a major cause for safety concerns. It is typically managed with glucocorticoids or other immunomodulating agents such as mycophenolate mofetil or tacrolimus.
There have also been reported cases of transaminase elevations without evidence of a capsid immune response, which warrants further investigation, she added.
Regarding efficacy, she noted that across clinical trials, the observed annualized bleeding rate has been less than 1%, despite heterogeneity of vectors and dosing used.
“That’s obviously quite optimistic for the field, but it also sort of raises the point that the heterogeneity at which we’re achieving the same phenotypic observations deserves a bit of a deeper dive,” she said.
Although hemophilia B gene transfer appears to be durable, the same cannot be said as yet for hemophilia A.
In canine models for hemophilia A and B, factor VIII and factor IX expression have been demonstrated for 8-10 years post vector, and in humans factor IX expression in patients with hemophilia B has been reported for up to 8 years.
In contrast, in the three hemophilia A trials in which patients have been followed for a minimum of 2 years, there was an approximately 40% loss of transgene vector from year 1 to year 2 with two vectors, but not a third.
Potential explanations for the loss of expression seen include an unfolded protein response, promoter silence, and an ongoing undetected or unmitigated immune response to AAV or to the transgene.
Regarding the future of gene therapy, Dr. George said that “we anticipate that there will be licensed vectors in the very near future, and predicted that gene therapy “will fulfill its promise to alter the paradigm of hemophilia care.”
Dr. Lim disclosed honoraria from several companies and travel support from Novo Nordisk. Dr. Ma disclosed honoraria and research funding from Takeda. Dr. George disclosed FVIII-QQ patents and royalties, research funding from AskBio, and consulting activities/advisory board participation with others.
A version of this article first appeared on Medscape.com.
It’s a problem many clinicians would love to have: A whole variety of new or emerging therapeutic options to use in the care of their patients.
In a session titled “Hemophilia Update: Our Cup Runneth Over,” presented at the 2021 annual meeting of the American Society of Hematology, .
Factor concentrates
Prophylaxis – as opposed to episodic treatment – is the standard of care in the use of factor concentrates in patients with hemophilia, said Ming Y. Lim, MB BChir, from the University of Utah in Salt Lake City.
“Effective prophylaxis is an ongoing collaborative effort that relies on shared decision-making between the patient and the clinician,” she told the audience.
As the complexity of therapeutic options, including gene therapy, continues to increase “it is critical that both patients and clinicians are actively involved in this collaborative process to optimize treatment and overall patient outcomes,” she added.
Historically, clinicians who treat patients with hemophilia aimed for trough levels of factor concentrates of at least 1% to prevent spontaneous joint bleeding. But as updated World Federation of Hemophilia (WFH) guidelines now recommend, trough levels should be sufficient to prevent spontaneous bleeding based on the individual patient’s bleeding phenotype and activity levels, starting in the range between 3% and 5%, and going higher as necessary.
“The appropriate target trough level is that at which a person with hemophilia experiences zero bleeds while pursuing an active or sedentary lifestyle,” she said.
The choice of factor concentrates between standard and extended half-life products will depend on multiple factors, including availability, patient and provider preferences, cost, and access to assays for monitoring extended half-life products.
The prolonged action of extended half-life products translates into dosing twice per week or every 3 days for factor VIII concentrates, and every 7-14 days for factor IX concentrates.
“All available extended half-life products have been shown to be efficacious in the prevention and treatment of bleeds, with no evidence for any clinical safety issues,” Dr. Lim said.
There are theoretical concerns, however, regarding the lifelong use of PEGylated clotting factor concentrates, leading to some variations in the regulatory approval for some PEGylated product intended for bleeding prophylaxis in children with hemophilia, she noted.
The pharmacokinetics of prophylaxis with factor concentrates can vary according to age, body mass, blood type, and von Willebrand factor levels, so WFH guidelines recommend pharmacokinetic assessment of people with hemophilia for optimization of prophylaxis, she said.
Factor mimetic and rebalancing therapies
With the commercial availability of one factor mimetic for treatment of hemophilia A and with other factor mimetics and rebalancing therapies such as fitusiran in the works, it raises the question, “Is this the beginning of the end of the use of factor?” said Alice Ma, MD, FACP, of the University of North Carolina in Chapel Hill.
Factors that may determine the answer to that question include the convenience of subcutaneous administration of factor VIII mimetics compared with intravenous delivery of factor concentrates, relative cost of factors versus nonfactor products, and safety.
She reviewed the current state of alternatives to factor concentrates, including the factor mimetic emicizumab (Hemlibra), which was approved by the Food and Drug Administration in 2018 for bleeding prophylaxis in patients with hemophilia A with inhibitors, and is currently the only FDA-approved and licensed agent in its class.
Although emicizumab is widely regarded as a major advance, there are still unanswered clinical questions about its long-term use, Dr. Ma said. It is unknown, for example, whether it can prevent inhibitor development in previously untreated patients, and whether it can prevent intracranial hemorrhage in early years of life prior to the start of traditional prophylaxis.
It’s also unknown whether the factor VIII mimetic activity of emicizumab provides the same physiological benefits of coagulation factors, and the mechanism of thrombotic adverse events seen with this agent is still unclear, she added.
Other factor VIII mimetics in the pipeline include Mim8, which is being developed in Denmark by Novo Nordisk; this is a next-generation bispecific antibody with enhanced activity over emicizumab in both mouse models and in vitro hemophilia A assays. There are also two others bispecific antibodies designed to generate thrombin in preclinical development: BS-027125 (Bioverativ, U.S.) and NIBX-2101 (Takeda, Japan).
One of the most promising rebalancing factors in development is fitusiran, a small interfering RNA molecule that targets mRNA encoding antithrombin. As reported during ASH 2021, fitusiran was associated with an approximately 90% reduction in annualized bleeding rates in patients with hemophilia A and hemophilia B, both with inhibitors, in two clinical trials. It was described at the meeting “as a great leap forward” in the treatment of hemophilia.
However, during its clinical development fitusiran has been consistently associated with thrombotic complications, Dr. Ma noted.
Also in development are several drugs targeted against tissue factor pathway inhibitor (TFPI), an anticoagulant protein that inhibits early phases of the procoagulant response. These agents included marstacimab (Pfizer, U.S.) which has been reported to normalize coagulation in plasma from hemophilia patients ex vivo and is currently being evaluated in patients with hemophilia A and B. There is also MG1113 (Green Cross Corporation, South Korea), a monoclonal antibody currently being tested in healthy volunteers, and BAX499 (Takeda), an aptamer derived from recombinant human TFPI that has been shown to inhibit TFPI in vitro and in vivo. However, development of this agent is on hold due to bleeding in study subjects, Dr. Ma noted.
“It is really notable that none of the replacements of factor have been free of thrombotic side effects,” Dr. Ma said. “And so I think it shows that you mess with Mother Nature at your peril. If you poke at the hemostasis-thrombosis arm and reduce antithrombotic proteins, and something triggers bleeding and you start to treat with a therapy for hemorrhage, it’s not a surprise that the first patient treated with fitusiran had a thrombosis, and I think we were just not potentially savvy enough to predict that.”
Considerable optimism over gene therapy
“There is now repeated proof of concept success for hemophilia A and B gene therapy. I think this supports the considerable optimism that’s really driving this field,” said Lindsey A. George, MD, of the University of Pennsylvania and Children’s Hospital of Philadelphia.
She reviewed adeno-associated virus (AAV) vector and AAV-mediated gene transfer approaches for hemophilia A and B.
There are currently four clinical trials of gene therapy for patients with hemophilia B, and five for patients with hemophilia A.
Because AAV efficiently targets the liver, most safety considerations about systemic AAV-mediated gene therapy are focused around potential hepatotoxicity, Dr. George said.
“Thankfully, short-term safety in the context of hemophilia has really been quite good,” she said.
Patients who undergo gene therapy for hemophilia are typically monitored twice weekly for 3 months for evidence of a capsid-specific CD8 T cell response, also called a capsid immune response. This presents with transient transaminase elevations (primarily ALT) and a decline in factor VIII and factor IX activity.
In clinical trials for patients with hemophilia, the capsid immune response has limited the efficacy of the therapy in the short term, but has not been a major cause for safety concerns. It is typically managed with glucocorticoids or other immunomodulating agents such as mycophenolate mofetil or tacrolimus.
There have also been reported cases of transaminase elevations without evidence of a capsid immune response, which warrants further investigation, she added.
Regarding efficacy, she noted that across clinical trials, the observed annualized bleeding rate has been less than 1%, despite heterogeneity of vectors and dosing used.
“That’s obviously quite optimistic for the field, but it also sort of raises the point that the heterogeneity at which we’re achieving the same phenotypic observations deserves a bit of a deeper dive,” she said.
Although hemophilia B gene transfer appears to be durable, the same cannot be said as yet for hemophilia A.
In canine models for hemophilia A and B, factor VIII and factor IX expression have been demonstrated for 8-10 years post vector, and in humans factor IX expression in patients with hemophilia B has been reported for up to 8 years.
In contrast, in the three hemophilia A trials in which patients have been followed for a minimum of 2 years, there was an approximately 40% loss of transgene vector from year 1 to year 2 with two vectors, but not a third.
Potential explanations for the loss of expression seen include an unfolded protein response, promoter silence, and an ongoing undetected or unmitigated immune response to AAV or to the transgene.
Regarding the future of gene therapy, Dr. George said that “we anticipate that there will be licensed vectors in the very near future, and predicted that gene therapy “will fulfill its promise to alter the paradigm of hemophilia care.”
Dr. Lim disclosed honoraria from several companies and travel support from Novo Nordisk. Dr. Ma disclosed honoraria and research funding from Takeda. Dr. George disclosed FVIII-QQ patents and royalties, research funding from AskBio, and consulting activities/advisory board participation with others.
A version of this article first appeared on Medscape.com.
REPORTING FROM ASH 2021
Late-onset recurrence in breast cancer: Implications for women’s health clinicians in survivorship care
Improved treatments for breast cancer (BC) and effective screening programs have resulted in a BC mortality rate reduction of 41% since 1989.1 Because BC is the leading cause of cancer in women, these mortality improvements have resulted in more than 3 million BC survivors in the United States.2,3 With longer-term survival, there is increasing interest in late-onset recurrences.4,5 A recent study has provided an improved understanding of the risk of lateonset recurrence in women with 10 years of disease-free survival, an important finding for women’s health providers because oncologists do not typically follow survivors after 10 years of disease-free survival.4
Recent study looks at incidence of late-onset recurrence
Pederson and colleagues evaluated all patients diagnosed with BC in Denmark from 1987 through 2004.4 Those patients without evidence of recurrence at 10 years were then followed utilizing population-based linked registries to identify patients who subsequently developed a local, regional, or distant late-onset recurrence. The authors evaluated the frequency of late recurrence and identified associations with demographic and tumor characteristics.
What they found
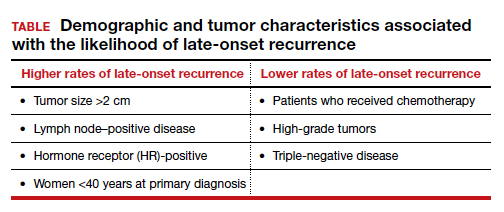
A total of 36,920 patients were diagnosed with BC in Denmark between 1987-2004, of whom 20,315 (55%) were identified as disease free for at least 10 years. Late-onset recurrence occurred in 2,595 (12.8%) with the strongest associations of recurrence seen in patients who had a tumor size >2 cm and lymph node‒positive (involving 4 or more nodes) disease (24.6%), compared with 12.7% in patients with tumors <2 cm and node-negative disease. Several other factors were associated with a higher risk of late-onset recurrence and are included in the TABLE. Half of the recurrences occurred between 10 and 15 years after the primary diagnosis.
Prior research
These findings are consistent with another recent study showing that BC patients have a 1% to 2%/year risk of recurrence after 10 disease-free years.5 Strengths of this study include:
- population-based, including all women with BC
- long-term follow-up for up to 32 years
- universal health care in Denmark, which results in robust and linked databases and very few missing data points.
There were two notable weaknesses to consider:
- Treatment regimens changed considerably during the time frame of the study (1997-2018), particularly the duration of tamoxifen use in patients with HR-positive disease. In this study nearly all patients received 5 years or less of tamoxifen. Since the mid-2010s, 10 years of hormonal adjuvant therapy has become routine in HR-positive BC, which reduces recurrences, including late-onset recurrence.6 The effect of 10 years of tamoxifen would very likely have resulted in less late-onset recurrence in the HR-positive population in this study.
- There is a lack of racial diversity in the Danish population, and the study findings may not translate to Black patients who have a higher frequency of triple-negative BC with a different risk of late-onset recurrence.7
Practice takeaways
Cancer surveillance. There are 3+ million BC survivors in the United States, and a 55%+ likelihood that they will be disease free for 10 years. This is clearly an important population to the women’s health care provider. This study, and previous research, suggests that among 10-year-disease-free survivors, 1% to 2% will recur annually, with higher rates amongst HR-positive, lymph-node positive women under age 40, and in the first 5 years following the 10-year post–initial diagnosis mark, so ongoing surveillance is imperative. Annual clinical breast examinations along with annual (not biennial) mammography should be performed.8 Digital breast tomosynthesis has improved specificity and sensitivity for BC detection and is the preferred modality when it is available.
Management of menopausal symptoms. These findings also have implications for menopausal hormone therapy for patients with symptoms. Because HR-positive patients have an increased risk of late-onset recurrence, nonhormonal therapies should be considered as first-line therapy for patients with menopausal symptoms. If hormone therapy is being considered, providers and patients should use shared decision making to balance the potential benefits (reduction in symptoms, possible cardiovascular benefits, and reduction in bone loss) with the risks (increased risk of recurrence and venous thromboembolism), even if patients are remote from the original diagnosis (ie, 10-year disease-free survival).
Topical estrogen therapies would be preferred for patients with significant urogenital atrophic symptoms who fail nonhormonal therapies due to substantially less systemic absorption and the lack of need to add a progestin.9,10 If oral therapy is being considered, I carefully counsel these women about the likely increased risk of recurrence and, if possible, include their breast oncologist in the discussion. ●
- Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021. CA Cancer J Clin. 2021;71:7-33. doi: 10.3322/caac.21654.
- de Moor JS, Mariotto AB, Parry C, et al. Cancer survivors in the United States: prevalence across the survivorship trajectory and implications for care. Cancer Epidemiol Biomarkers Prev. 2013;22:561- 570. doi: 10.1158/1055-9965.EPI-12-1356.
- Carreira H, Williams R, Funston G, et al. Associations between breast cancer survivorship and adverse mental health outcomes: a matched population-based cohort study in the United Kingdom. PLOS Med. 2021;18:e1003504. doi: 10.1371/journal.pmed.1003504.
- Pedersen RN, Esen BÖ, Mellemkjær L, et al. The incidence of breast cancer recurrence 10-32 years after primary diagnosis. J Natl Cancer Inst. November 8, 2021. doi: 10.1093/jnci/djab202.
- Pan H, Gray R, Braybrooke J, et al. 20-year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years. N Engl J Med. 2017;377:1836- 1846. doi: 10.1056/NEJMoa1701830.
- Davies C, Pan H, Godwin J, et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet. 2013;381:805-816. doi: 10.1016/S0140-6736(12)61963-1.
- Scott LC, Mobley LR, Kuo TM, et al. Update on triple‐negative breast cancer disparities for the United States: a population‐based study from the United States Cancer Statistics database, 2010 through 2014. Cancer. 2019;125:3412-3417. doi: 10.1002/cncr.32207.
- NCCN Clinical Practice Guidelines in Oncology: Breast Cancer. 2021; Version 2.2022.
- Crandall CJ, Diamant A, Santoro N. Safety of vaginal estrogens: a systematic review. Menopause. 2020;27:339-360. doi: 10.1097 /GME.0000000000001468.
- Treatment of urogenital symptoms in individuals with a history of estrogen-dependent breast cancer: clinical consensus. Obstet Gynecol. 2021;138:950-960. doi: 10.1097/AOG .0000000000004601.
Mark D. Pearlman, MD
Dr. Pearlman is Professor Active Emeritus, Departments of Obstetrics & Gynecology and Surgery University of Michigan Health System, Ann Arbor. He serves as an OBG Management Contributing Editor
The author reports no financial relationships relevant to this article.
Mark D. Pearlman, MD
Dr. Pearlman is Professor Active Emeritus, Departments of Obstetrics & Gynecology and Surgery University of Michigan Health System, Ann Arbor. He serves as an OBG Management Contributing Editor
The author reports no financial relationships relevant to this article.
Mark D. Pearlman, MD
Dr. Pearlman is Professor Active Emeritus, Departments of Obstetrics & Gynecology and Surgery University of Michigan Health System, Ann Arbor. He serves as an OBG Management Contributing Editor
The author reports no financial relationships relevant to this article.
Improved treatments for breast cancer (BC) and effective screening programs have resulted in a BC mortality rate reduction of 41% since 1989.1 Because BC is the leading cause of cancer in women, these mortality improvements have resulted in more than 3 million BC survivors in the United States.2,3 With longer-term survival, there is increasing interest in late-onset recurrences.4,5 A recent study has provided an improved understanding of the risk of lateonset recurrence in women with 10 years of disease-free survival, an important finding for women’s health providers because oncologists do not typically follow survivors after 10 years of disease-free survival.4
Recent study looks at incidence of late-onset recurrence
Pederson and colleagues evaluated all patients diagnosed with BC in Denmark from 1987 through 2004.4 Those patients without evidence of recurrence at 10 years were then followed utilizing population-based linked registries to identify patients who subsequently developed a local, regional, or distant late-onset recurrence. The authors evaluated the frequency of late recurrence and identified associations with demographic and tumor characteristics.
What they found
A total of 36,920 patients were diagnosed with BC in Denmark between 1987-2004, of whom 20,315 (55%) were identified as disease free for at least 10 years. Late-onset recurrence occurred in 2,595 (12.8%) with the strongest associations of recurrence seen in patients who had a tumor size >2 cm and lymph node‒positive (involving 4 or more nodes) disease (24.6%), compared with 12.7% in patients with tumors <2 cm and node-negative disease. Several other factors were associated with a higher risk of late-onset recurrence and are included in the TABLE. Half of the recurrences occurred between 10 and 15 years after the primary diagnosis.
Prior research
These findings are consistent with another recent study showing that BC patients have a 1% to 2%/year risk of recurrence after 10 disease-free years.5 Strengths of this study include:
- population-based, including all women with BC
- long-term follow-up for up to 32 years
- universal health care in Denmark, which results in robust and linked databases and very few missing data points.
There were two notable weaknesses to consider:
- Treatment regimens changed considerably during the time frame of the study (1997-2018), particularly the duration of tamoxifen use in patients with HR-positive disease. In this study nearly all patients received 5 years or less of tamoxifen. Since the mid-2010s, 10 years of hormonal adjuvant therapy has become routine in HR-positive BC, which reduces recurrences, including late-onset recurrence.6 The effect of 10 years of tamoxifen would very likely have resulted in less late-onset recurrence in the HR-positive population in this study.
- There is a lack of racial diversity in the Danish population, and the study findings may not translate to Black patients who have a higher frequency of triple-negative BC with a different risk of late-onset recurrence.7
Practice takeaways
Cancer surveillance. There are 3+ million BC survivors in the United States, and a 55%+ likelihood that they will be disease free for 10 years. This is clearly an important population to the women’s health care provider. This study, and previous research, suggests that among 10-year-disease-free survivors, 1% to 2% will recur annually, with higher rates amongst HR-positive, lymph-node positive women under age 40, and in the first 5 years following the 10-year post–initial diagnosis mark, so ongoing surveillance is imperative. Annual clinical breast examinations along with annual (not biennial) mammography should be performed.8 Digital breast tomosynthesis has improved specificity and sensitivity for BC detection and is the preferred modality when it is available.
Management of menopausal symptoms. These findings also have implications for menopausal hormone therapy for patients with symptoms. Because HR-positive patients have an increased risk of late-onset recurrence, nonhormonal therapies should be considered as first-line therapy for patients with menopausal symptoms. If hormone therapy is being considered, providers and patients should use shared decision making to balance the potential benefits (reduction in symptoms, possible cardiovascular benefits, and reduction in bone loss) with the risks (increased risk of recurrence and venous thromboembolism), even if patients are remote from the original diagnosis (ie, 10-year disease-free survival).
Topical estrogen therapies would be preferred for patients with significant urogenital atrophic symptoms who fail nonhormonal therapies due to substantially less systemic absorption and the lack of need to add a progestin.9,10 If oral therapy is being considered, I carefully counsel these women about the likely increased risk of recurrence and, if possible, include their breast oncologist in the discussion. ●
Improved treatments for breast cancer (BC) and effective screening programs have resulted in a BC mortality rate reduction of 41% since 1989.1 Because BC is the leading cause of cancer in women, these mortality improvements have resulted in more than 3 million BC survivors in the United States.2,3 With longer-term survival, there is increasing interest in late-onset recurrences.4,5 A recent study has provided an improved understanding of the risk of lateonset recurrence in women with 10 years of disease-free survival, an important finding for women’s health providers because oncologists do not typically follow survivors after 10 years of disease-free survival.4
Recent study looks at incidence of late-onset recurrence
Pederson and colleagues evaluated all patients diagnosed with BC in Denmark from 1987 through 2004.4 Those patients without evidence of recurrence at 10 years were then followed utilizing population-based linked registries to identify patients who subsequently developed a local, regional, or distant late-onset recurrence. The authors evaluated the frequency of late recurrence and identified associations with demographic and tumor characteristics.
What they found
A total of 36,920 patients were diagnosed with BC in Denmark between 1987-2004, of whom 20,315 (55%) were identified as disease free for at least 10 years. Late-onset recurrence occurred in 2,595 (12.8%) with the strongest associations of recurrence seen in patients who had a tumor size >2 cm and lymph node‒positive (involving 4 or more nodes) disease (24.6%), compared with 12.7% in patients with tumors <2 cm and node-negative disease. Several other factors were associated with a higher risk of late-onset recurrence and are included in the TABLE. Half of the recurrences occurred between 10 and 15 years after the primary diagnosis.
Prior research
These findings are consistent with another recent study showing that BC patients have a 1% to 2%/year risk of recurrence after 10 disease-free years.5 Strengths of this study include:
- population-based, including all women with BC
- long-term follow-up for up to 32 years
- universal health care in Denmark, which results in robust and linked databases and very few missing data points.
There were two notable weaknesses to consider:
- Treatment regimens changed considerably during the time frame of the study (1997-2018), particularly the duration of tamoxifen use in patients with HR-positive disease. In this study nearly all patients received 5 years or less of tamoxifen. Since the mid-2010s, 10 years of hormonal adjuvant therapy has become routine in HR-positive BC, which reduces recurrences, including late-onset recurrence.6 The effect of 10 years of tamoxifen would very likely have resulted in less late-onset recurrence in the HR-positive population in this study.
- There is a lack of racial diversity in the Danish population, and the study findings may not translate to Black patients who have a higher frequency of triple-negative BC with a different risk of late-onset recurrence.7
Practice takeaways
Cancer surveillance. There are 3+ million BC survivors in the United States, and a 55%+ likelihood that they will be disease free for 10 years. This is clearly an important population to the women’s health care provider. This study, and previous research, suggests that among 10-year-disease-free survivors, 1% to 2% will recur annually, with higher rates amongst HR-positive, lymph-node positive women under age 40, and in the first 5 years following the 10-year post–initial diagnosis mark, so ongoing surveillance is imperative. Annual clinical breast examinations along with annual (not biennial) mammography should be performed.8 Digital breast tomosynthesis has improved specificity and sensitivity for BC detection and is the preferred modality when it is available.
Management of menopausal symptoms. These findings also have implications for menopausal hormone therapy for patients with symptoms. Because HR-positive patients have an increased risk of late-onset recurrence, nonhormonal therapies should be considered as first-line therapy for patients with menopausal symptoms. If hormone therapy is being considered, providers and patients should use shared decision making to balance the potential benefits (reduction in symptoms, possible cardiovascular benefits, and reduction in bone loss) with the risks (increased risk of recurrence and venous thromboembolism), even if patients are remote from the original diagnosis (ie, 10-year disease-free survival).
Topical estrogen therapies would be preferred for patients with significant urogenital atrophic symptoms who fail nonhormonal therapies due to substantially less systemic absorption and the lack of need to add a progestin.9,10 If oral therapy is being considered, I carefully counsel these women about the likely increased risk of recurrence and, if possible, include their breast oncologist in the discussion. ●
- Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021. CA Cancer J Clin. 2021;71:7-33. doi: 10.3322/caac.21654.
- de Moor JS, Mariotto AB, Parry C, et al. Cancer survivors in the United States: prevalence across the survivorship trajectory and implications for care. Cancer Epidemiol Biomarkers Prev. 2013;22:561- 570. doi: 10.1158/1055-9965.EPI-12-1356.
- Carreira H, Williams R, Funston G, et al. Associations between breast cancer survivorship and adverse mental health outcomes: a matched population-based cohort study in the United Kingdom. PLOS Med. 2021;18:e1003504. doi: 10.1371/journal.pmed.1003504.
- Pedersen RN, Esen BÖ, Mellemkjær L, et al. The incidence of breast cancer recurrence 10-32 years after primary diagnosis. J Natl Cancer Inst. November 8, 2021. doi: 10.1093/jnci/djab202.
- Pan H, Gray R, Braybrooke J, et al. 20-year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years. N Engl J Med. 2017;377:1836- 1846. doi: 10.1056/NEJMoa1701830.
- Davies C, Pan H, Godwin J, et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet. 2013;381:805-816. doi: 10.1016/S0140-6736(12)61963-1.
- Scott LC, Mobley LR, Kuo TM, et al. Update on triple‐negative breast cancer disparities for the United States: a population‐based study from the United States Cancer Statistics database, 2010 through 2014. Cancer. 2019;125:3412-3417. doi: 10.1002/cncr.32207.
- NCCN Clinical Practice Guidelines in Oncology: Breast Cancer. 2021; Version 2.2022.
- Crandall CJ, Diamant A, Santoro N. Safety of vaginal estrogens: a systematic review. Menopause. 2020;27:339-360. doi: 10.1097 /GME.0000000000001468.
- Treatment of urogenital symptoms in individuals with a history of estrogen-dependent breast cancer: clinical consensus. Obstet Gynecol. 2021;138:950-960. doi: 10.1097/AOG .0000000000004601.
- Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021. CA Cancer J Clin. 2021;71:7-33. doi: 10.3322/caac.21654.
- de Moor JS, Mariotto AB, Parry C, et al. Cancer survivors in the United States: prevalence across the survivorship trajectory and implications for care. Cancer Epidemiol Biomarkers Prev. 2013;22:561- 570. doi: 10.1158/1055-9965.EPI-12-1356.
- Carreira H, Williams R, Funston G, et al. Associations between breast cancer survivorship and adverse mental health outcomes: a matched population-based cohort study in the United Kingdom. PLOS Med. 2021;18:e1003504. doi: 10.1371/journal.pmed.1003504.
- Pedersen RN, Esen BÖ, Mellemkjær L, et al. The incidence of breast cancer recurrence 10-32 years after primary diagnosis. J Natl Cancer Inst. November 8, 2021. doi: 10.1093/jnci/djab202.
- Pan H, Gray R, Braybrooke J, et al. 20-year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years. N Engl J Med. 2017;377:1836- 1846. doi: 10.1056/NEJMoa1701830.
- Davies C, Pan H, Godwin J, et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet. 2013;381:805-816. doi: 10.1016/S0140-6736(12)61963-1.
- Scott LC, Mobley LR, Kuo TM, et al. Update on triple‐negative breast cancer disparities for the United States: a population‐based study from the United States Cancer Statistics database, 2010 through 2014. Cancer. 2019;125:3412-3417. doi: 10.1002/cncr.32207.
- NCCN Clinical Practice Guidelines in Oncology: Breast Cancer. 2021; Version 2.2022.
- Crandall CJ, Diamant A, Santoro N. Safety of vaginal estrogens: a systematic review. Menopause. 2020;27:339-360. doi: 10.1097 /GME.0000000000001468.
- Treatment of urogenital symptoms in individuals with a history of estrogen-dependent breast cancer: clinical consensus. Obstet Gynecol. 2021;138:950-960. doi: 10.1097/AOG .0000000000004601.
Children and COVID: Weekly cases down by more than half
A third consecutive week of declines in new COVID-19 cases among children has brought the weekly count down by 74% since the Omicron surge peaked in mid-January, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
and by 74% from the peak of 1.15 million cases recorded for the week of Jan. 14-20, the AAP and CHA said in their weekly COVID report. They also noted that the weekly tally was still higher than anything seen during the Delta surge.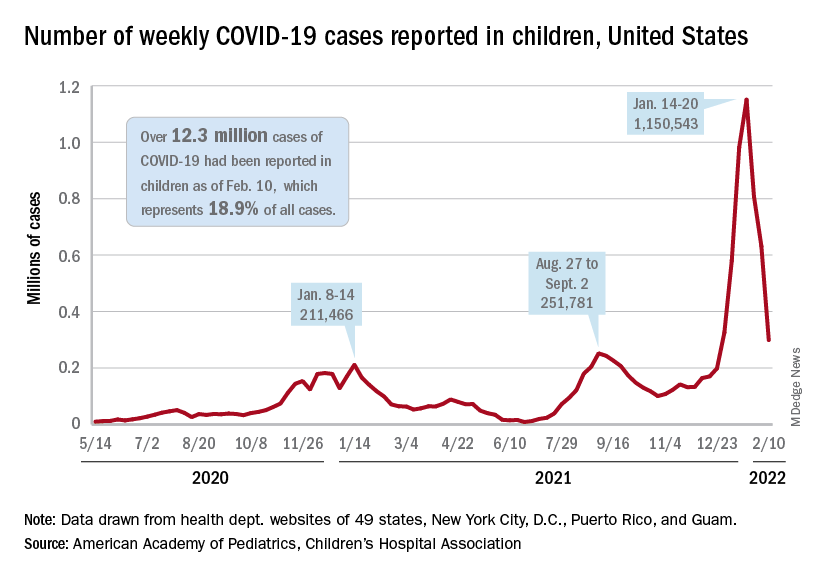
The total number of pediatric cases was over 12.3 million as of Feb. 10, with children representing 18.9% of cases in all ages, according to the AAP/CHA report. The Centers for Disease Control and Prevention puts the two measures at 10.4 million and 17.3% on its COVID Data Tracker, based on availability of age data for 59.6 million total cases as of Feb. 14. The CDC also reported that 1,282 children have died from COVID-19 so far, which is about 0.17% of all deaths with age data available.
The AAP and CHA have been collecting data from state and territorial health departments, which have not always been consistently available over the course of the pandemic. Also, the CDC defines children as those under age 18 years, but that upper boundary varies from 14 to 20 among the states.
The decline of the Omicron variant also can be seen in new admissions of children with confirmed COVID-19, which continued to drop. The 7-day average of 435 admissions per day for the week of Feb. 6-12 was less than half of the peak seen in mid-January, when it reached 914 per day. The daily admission rate on Feb. 12 was 0.60 per 100,000 children aged 0-17 years – again, less than half the peak rate of 1.25 reported on Jan. 16, CDC data show.
The fading threat of Omicron also seems to be reflected in recent vaccination trends. Both initial doses and completions declined for the fourth consecutive week (Feb. 3-9) among children aged 5-11 years, while initiations held steady for 12- to 17-year-olds but completions declined for the third straight week, the AAP said in its separate vaccination report, which is based on data from the CDC.
As of Feb. 14, almost 32% of children aged 5-11 – that’s almost 9.2 million individuals – had received at least one dose of the COVID-19 vaccine and just over 24% (6.9 million) were fully vaccinated, the CDC reported. For children aged 12-17, the corresponding figures are 67% (16.9 million) and 57% (14.4 million). Newly available data from the CDC also indicate that 19.5% (2.8 million) of children aged 12-17 have received a booster dose.
A third consecutive week of declines in new COVID-19 cases among children has brought the weekly count down by 74% since the Omicron surge peaked in mid-January, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
and by 74% from the peak of 1.15 million cases recorded for the week of Jan. 14-20, the AAP and CHA said in their weekly COVID report. They also noted that the weekly tally was still higher than anything seen during the Delta surge.
The total number of pediatric cases was over 12.3 million as of Feb. 10, with children representing 18.9% of cases in all ages, according to the AAP/CHA report. The Centers for Disease Control and Prevention puts the two measures at 10.4 million and 17.3% on its COVID Data Tracker, based on availability of age data for 59.6 million total cases as of Feb. 14. The CDC also reported that 1,282 children have died from COVID-19 so far, which is about 0.17% of all deaths with age data available.
The AAP and CHA have been collecting data from state and territorial health departments, which have not always been consistently available over the course of the pandemic. Also, the CDC defines children as those under age 18 years, but that upper boundary varies from 14 to 20 among the states.
The decline of the Omicron variant also can be seen in new admissions of children with confirmed COVID-19, which continued to drop. The 7-day average of 435 admissions per day for the week of Feb. 6-12 was less than half of the peak seen in mid-January, when it reached 914 per day. The daily admission rate on Feb. 12 was 0.60 per 100,000 children aged 0-17 years – again, less than half the peak rate of 1.25 reported on Jan. 16, CDC data show.
The fading threat of Omicron also seems to be reflected in recent vaccination trends. Both initial doses and completions declined for the fourth consecutive week (Feb. 3-9) among children aged 5-11 years, while initiations held steady for 12- to 17-year-olds but completions declined for the third straight week, the AAP said in its separate vaccination report, which is based on data from the CDC.
As of Feb. 14, almost 32% of children aged 5-11 – that’s almost 9.2 million individuals – had received at least one dose of the COVID-19 vaccine and just over 24% (6.9 million) were fully vaccinated, the CDC reported. For children aged 12-17, the corresponding figures are 67% (16.9 million) and 57% (14.4 million). Newly available data from the CDC also indicate that 19.5% (2.8 million) of children aged 12-17 have received a booster dose.
A third consecutive week of declines in new COVID-19 cases among children has brought the weekly count down by 74% since the Omicron surge peaked in mid-January, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
and by 74% from the peak of 1.15 million cases recorded for the week of Jan. 14-20, the AAP and CHA said in their weekly COVID report. They also noted that the weekly tally was still higher than anything seen during the Delta surge.
The total number of pediatric cases was over 12.3 million as of Feb. 10, with children representing 18.9% of cases in all ages, according to the AAP/CHA report. The Centers for Disease Control and Prevention puts the two measures at 10.4 million and 17.3% on its COVID Data Tracker, based on availability of age data for 59.6 million total cases as of Feb. 14. The CDC also reported that 1,282 children have died from COVID-19 so far, which is about 0.17% of all deaths with age data available.
The AAP and CHA have been collecting data from state and territorial health departments, which have not always been consistently available over the course of the pandemic. Also, the CDC defines children as those under age 18 years, but that upper boundary varies from 14 to 20 among the states.
The decline of the Omicron variant also can be seen in new admissions of children with confirmed COVID-19, which continued to drop. The 7-day average of 435 admissions per day for the week of Feb. 6-12 was less than half of the peak seen in mid-January, when it reached 914 per day. The daily admission rate on Feb. 12 was 0.60 per 100,000 children aged 0-17 years – again, less than half the peak rate of 1.25 reported on Jan. 16, CDC data show.
The fading threat of Omicron also seems to be reflected in recent vaccination trends. Both initial doses and completions declined for the fourth consecutive week (Feb. 3-9) among children aged 5-11 years, while initiations held steady for 12- to 17-year-olds but completions declined for the third straight week, the AAP said in its separate vaccination report, which is based on data from the CDC.
As of Feb. 14, almost 32% of children aged 5-11 – that’s almost 9.2 million individuals – had received at least one dose of the COVID-19 vaccine and just over 24% (6.9 million) were fully vaccinated, the CDC reported. For children aged 12-17, the corresponding figures are 67% (16.9 million) and 57% (14.4 million). Newly available data from the CDC also indicate that 19.5% (2.8 million) of children aged 12-17 have received a booster dose.
Handle with care: Managing IBD in older patients
As the saying goes: "Age is a case of mind over matter: If you don't mind, it don't matter."
But for older patients with inflammatory bowel disease (IBD) and the clinicians who treat them, it’s hard to ignore the complications that aging can bring, such as comorbidities, functional limitations, and polypharmacy, said Nana Bernasko, CRNP, DNP, WHNP-BC, a nurse practitioner in the department of gastroenterology at Penn State Milton S. Hershey Medical Center in Hershey, Pa.
“We are seeing a large number of patients in our clinics that are being diagnosed later on in life,” she said in an oral presentation at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
Between 10% and 30% of all patients with IBD are older than 60, and roughly 10%-15% of patients with IBD are diagnosed after age 60, she said.
The diagnosis of IBD is often delayed in older patients as well, with an estimated 60% of patients initially given an incorrect or incomplete diagnosis that may lead to significant delays in the initiation of appropriate therapy, she said.
Differential diagnoses for IBD in older patients include diverticulitis, ischemic colitis, infectious colitis, and radiation colitis.
Bharati Kochar, MD, MS, from the Crohn’s and Colitis Center at Massachusetts General Hospital in Boston, who was not involved in the presentation, agreed that older adults need special handling.
“The management of IBD in older adults is challenging for a number of reasons, but primarily because until very recently, we have not invested in understanding how IBD should be optimally managed at older ages,” she said in an interview.
“Additionally, like in all fields, older adults with IBD are disproportionately under-represented in clinical trials, meaning that we have less rigorous data guiding the management of older adults,” she added.
Clinical presentations
Older adults tend to differ in clinical presentation, compared with younger adults, Dr. Bernasko said.
For example, among patients with Crohn’s disease, rectal bleeding is a more common symptom among older adults, whereas diarrhea and weight loss are more common among younger adults.
Disease location may also differ, with more senior adults having predominantly colonic disease (L2 according to the Montreal Classification of IBD), compared with more prevalent ileocolonic disease (L3) among their more junior counterparts. And although both generations of patients have inflammatory behavior (B1) at diagnosis, younger patients have more prevalent structuring (B2) and penetrating disease (B3), Dr. Bernasko noted.
Among patients with ulcerative colitis, rectal bleeding, abdominal pain, and extraintestinal manifestations are more common among the younger set, whereas left-sided colitis is more common among older patients. In addition, extensive ulcerative colitis (E3) is more common in younger patients, compared with older patients.
Management considerations
Dr. Kochar noted that “older adults have higher baseline risks for all adverse events – like infections, malignancies, polypharmacy, procedural complications – than younger adults, so any additional risk conferred by treatments seem amplified, but that should not mean that we should avoid effectively treating older adults. It should mean we need to invest in understanding how to best mitigate those risks.”
While younger patients are sometimes on multiple medications prior to starting on IBD therapy, polypharmacy is common among the older set, who may be taking drugs for diabetes, hypertension, prostate disease, and so on.
“There’s just so much going on in terms of their medical background to start off with, so many medications, and then we’re adding more things to it,” Dr. Bernasko said.
She echoed Dr. Kochar in noting that older patients as a subgroup are under-represented in clinical trials, making it difficult to know what treatment approaches may work best for them.
In addition, older patients are at higher risk for malignancies, and for complications from surgery.
Medication adherence in older patients is frequently compromised by memory issues, she added, noting that “I can’t tell you enough how sometimes our older patients forget to take their medications.”
Other challenges for the management of older patients with IBD included psychosocial issues, cognitive decline, and malnutrition.
Medications and adverse events
Dr. Bernasko also discussed specific medications and potential adverse events and drug interactions in older patients.
For example, aminosalicylic acids (5-ASA) are associated with higher risk for nephrotoxicity and pancreatitis in older patients and can interact with thiopurines to cause leukopenia.
Steroids are associated with elevated risk for osteopenia, myopathy, cataracts, glaucoma, diabetes, and hypertension, and can interact with thiazide and loop diuretics to cause hypokalemia.
Methotrexate use in this population is linked to pancytopenia and hepatotoxicity, and it can interact with NSAIDs and multiple antibiotics to cause decreased renal secretion.
Thiopurines in older patients are associated with increased risk for leukopenia, myelosuppression, non-Hodgkin lymphoma, skin cancer, pancreatitis, and hepatotoxicity, and drugs in this class interact with allopurinol and angiotensin-converting enzyme inhibitors to increase risk for myelosuppression. Additionally, warfarin can inhibit the efficacy of thiopurines, and when these drugs are used in combination with tumor necrosis factor (TNF)–alpha inhibitors they can further increase risk of malignancy through immunosuppression.
Cyclosporine is associated with worsening hypertension and renal insufficiency among older patients.
TNF-alpha inhibitors are associated with increased risk for tuberculosis; hepatitis B; and fungal infections, malignant lymphoma, and New York Heart Association class 3 or 4 heart failure.
Ciprofloxacin in older patients with IBD has been linked to tendinopathy and increased risk for Clostridioides difficile infections. Metronidazole increases the likelihood of peripheral neuropathy in these patients.
Colon cancer screening
“When it comes to colon cancer screening, definitely assess the risk prior to doing this,” Dr. Bernasko recommended. “Weigh all the risks and benefits. Why are we doing this for these elderly patients, because there are definitely risks associated with this.”
Older patients with IBD may have difficulty with bowel prep and are at elevated risk, compared with younger patients, for cardiopulmonary complications, perforation, adverse events from sedation, and procedural complications, she cautioned.
“When it comes to our elderly patients, you want to focus on a more personalized approach – not all older people present the same way in terms of comorbidities or medications,” Dr. Bernasko advised in her summary.
Dr. Bernasko and Dr. Kochar reported having no relevant conflicts of interest to disclose. Dr. Kochar is a member of the board of editors for GI & Hepatology News.
This article was updated 2/18/22.
As the saying goes: "Age is a case of mind over matter: If you don't mind, it don't matter."
But for older patients with inflammatory bowel disease (IBD) and the clinicians who treat them, it’s hard to ignore the complications that aging can bring, such as comorbidities, functional limitations, and polypharmacy, said Nana Bernasko, CRNP, DNP, WHNP-BC, a nurse practitioner in the department of gastroenterology at Penn State Milton S. Hershey Medical Center in Hershey, Pa.
“We are seeing a large number of patients in our clinics that are being diagnosed later on in life,” she said in an oral presentation at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
Between 10% and 30% of all patients with IBD are older than 60, and roughly 10%-15% of patients with IBD are diagnosed after age 60, she said.
The diagnosis of IBD is often delayed in older patients as well, with an estimated 60% of patients initially given an incorrect or incomplete diagnosis that may lead to significant delays in the initiation of appropriate therapy, she said.
Differential diagnoses for IBD in older patients include diverticulitis, ischemic colitis, infectious colitis, and radiation colitis.
Bharati Kochar, MD, MS, from the Crohn’s and Colitis Center at Massachusetts General Hospital in Boston, who was not involved in the presentation, agreed that older adults need special handling.
“The management of IBD in older adults is challenging for a number of reasons, but primarily because until very recently, we have not invested in understanding how IBD should be optimally managed at older ages,” she said in an interview.
“Additionally, like in all fields, older adults with IBD are disproportionately under-represented in clinical trials, meaning that we have less rigorous data guiding the management of older adults,” she added.
Clinical presentations
Older adults tend to differ in clinical presentation, compared with younger adults, Dr. Bernasko said.
For example, among patients with Crohn’s disease, rectal bleeding is a more common symptom among older adults, whereas diarrhea and weight loss are more common among younger adults.
Disease location may also differ, with more senior adults having predominantly colonic disease (L2 according to the Montreal Classification of IBD), compared with more prevalent ileocolonic disease (L3) among their more junior counterparts. And although both generations of patients have inflammatory behavior (B1) at diagnosis, younger patients have more prevalent structuring (B2) and penetrating disease (B3), Dr. Bernasko noted.
Among patients with ulcerative colitis, rectal bleeding, abdominal pain, and extraintestinal manifestations are more common among the younger set, whereas left-sided colitis is more common among older patients. In addition, extensive ulcerative colitis (E3) is more common in younger patients, compared with older patients.
Management considerations
Dr. Kochar noted that “older adults have higher baseline risks for all adverse events – like infections, malignancies, polypharmacy, procedural complications – than younger adults, so any additional risk conferred by treatments seem amplified, but that should not mean that we should avoid effectively treating older adults. It should mean we need to invest in understanding how to best mitigate those risks.”
While younger patients are sometimes on multiple medications prior to starting on IBD therapy, polypharmacy is common among the older set, who may be taking drugs for diabetes, hypertension, prostate disease, and so on.
“There’s just so much going on in terms of their medical background to start off with, so many medications, and then we’re adding more things to it,” Dr. Bernasko said.
She echoed Dr. Kochar in noting that older patients as a subgroup are under-represented in clinical trials, making it difficult to know what treatment approaches may work best for them.
In addition, older patients are at higher risk for malignancies, and for complications from surgery.
Medication adherence in older patients is frequently compromised by memory issues, she added, noting that “I can’t tell you enough how sometimes our older patients forget to take their medications.”
Other challenges for the management of older patients with IBD included psychosocial issues, cognitive decline, and malnutrition.
Medications and adverse events
Dr. Bernasko also discussed specific medications and potential adverse events and drug interactions in older patients.
For example, aminosalicylic acids (5-ASA) are associated with higher risk for nephrotoxicity and pancreatitis in older patients and can interact with thiopurines to cause leukopenia.
Steroids are associated with elevated risk for osteopenia, myopathy, cataracts, glaucoma, diabetes, and hypertension, and can interact with thiazide and loop diuretics to cause hypokalemia.
Methotrexate use in this population is linked to pancytopenia and hepatotoxicity, and it can interact with NSAIDs and multiple antibiotics to cause decreased renal secretion.
Thiopurines in older patients are associated with increased risk for leukopenia, myelosuppression, non-Hodgkin lymphoma, skin cancer, pancreatitis, and hepatotoxicity, and drugs in this class interact with allopurinol and angiotensin-converting enzyme inhibitors to increase risk for myelosuppression. Additionally, warfarin can inhibit the efficacy of thiopurines, and when these drugs are used in combination with tumor necrosis factor (TNF)–alpha inhibitors they can further increase risk of malignancy through immunosuppression.
Cyclosporine is associated with worsening hypertension and renal insufficiency among older patients.
TNF-alpha inhibitors are associated with increased risk for tuberculosis; hepatitis B; and fungal infections, malignant lymphoma, and New York Heart Association class 3 or 4 heart failure.
Ciprofloxacin in older patients with IBD has been linked to tendinopathy and increased risk for Clostridioides difficile infections. Metronidazole increases the likelihood of peripheral neuropathy in these patients.
Colon cancer screening
“When it comes to colon cancer screening, definitely assess the risk prior to doing this,” Dr. Bernasko recommended. “Weigh all the risks and benefits. Why are we doing this for these elderly patients, because there are definitely risks associated with this.”
Older patients with IBD may have difficulty with bowel prep and are at elevated risk, compared with younger patients, for cardiopulmonary complications, perforation, adverse events from sedation, and procedural complications, she cautioned.
“When it comes to our elderly patients, you want to focus on a more personalized approach – not all older people present the same way in terms of comorbidities or medications,” Dr. Bernasko advised in her summary.
Dr. Bernasko and Dr. Kochar reported having no relevant conflicts of interest to disclose. Dr. Kochar is a member of the board of editors for GI & Hepatology News.
This article was updated 2/18/22.
As the saying goes: "Age is a case of mind over matter: If you don't mind, it don't matter."
But for older patients with inflammatory bowel disease (IBD) and the clinicians who treat them, it’s hard to ignore the complications that aging can bring, such as comorbidities, functional limitations, and polypharmacy, said Nana Bernasko, CRNP, DNP, WHNP-BC, a nurse practitioner in the department of gastroenterology at Penn State Milton S. Hershey Medical Center in Hershey, Pa.
“We are seeing a large number of patients in our clinics that are being diagnosed later on in life,” she said in an oral presentation at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
Between 10% and 30% of all patients with IBD are older than 60, and roughly 10%-15% of patients with IBD are diagnosed after age 60, she said.
The diagnosis of IBD is often delayed in older patients as well, with an estimated 60% of patients initially given an incorrect or incomplete diagnosis that may lead to significant delays in the initiation of appropriate therapy, she said.
Differential diagnoses for IBD in older patients include diverticulitis, ischemic colitis, infectious colitis, and radiation colitis.
Bharati Kochar, MD, MS, from the Crohn’s and Colitis Center at Massachusetts General Hospital in Boston, who was not involved in the presentation, agreed that older adults need special handling.
“The management of IBD in older adults is challenging for a number of reasons, but primarily because until very recently, we have not invested in understanding how IBD should be optimally managed at older ages,” she said in an interview.
“Additionally, like in all fields, older adults with IBD are disproportionately under-represented in clinical trials, meaning that we have less rigorous data guiding the management of older adults,” she added.
Clinical presentations
Older adults tend to differ in clinical presentation, compared with younger adults, Dr. Bernasko said.
For example, among patients with Crohn’s disease, rectal bleeding is a more common symptom among older adults, whereas diarrhea and weight loss are more common among younger adults.
Disease location may also differ, with more senior adults having predominantly colonic disease (L2 according to the Montreal Classification of IBD), compared with more prevalent ileocolonic disease (L3) among their more junior counterparts. And although both generations of patients have inflammatory behavior (B1) at diagnosis, younger patients have more prevalent structuring (B2) and penetrating disease (B3), Dr. Bernasko noted.
Among patients with ulcerative colitis, rectal bleeding, abdominal pain, and extraintestinal manifestations are more common among the younger set, whereas left-sided colitis is more common among older patients. In addition, extensive ulcerative colitis (E3) is more common in younger patients, compared with older patients.
Management considerations
Dr. Kochar noted that “older adults have higher baseline risks for all adverse events – like infections, malignancies, polypharmacy, procedural complications – than younger adults, so any additional risk conferred by treatments seem amplified, but that should not mean that we should avoid effectively treating older adults. It should mean we need to invest in understanding how to best mitigate those risks.”
While younger patients are sometimes on multiple medications prior to starting on IBD therapy, polypharmacy is common among the older set, who may be taking drugs for diabetes, hypertension, prostate disease, and so on.
“There’s just so much going on in terms of their medical background to start off with, so many medications, and then we’re adding more things to it,” Dr. Bernasko said.
She echoed Dr. Kochar in noting that older patients as a subgroup are under-represented in clinical trials, making it difficult to know what treatment approaches may work best for them.
In addition, older patients are at higher risk for malignancies, and for complications from surgery.
Medication adherence in older patients is frequently compromised by memory issues, she added, noting that “I can’t tell you enough how sometimes our older patients forget to take their medications.”
Other challenges for the management of older patients with IBD included psychosocial issues, cognitive decline, and malnutrition.
Medications and adverse events
Dr. Bernasko also discussed specific medications and potential adverse events and drug interactions in older patients.
For example, aminosalicylic acids (5-ASA) are associated with higher risk for nephrotoxicity and pancreatitis in older patients and can interact with thiopurines to cause leukopenia.
Steroids are associated with elevated risk for osteopenia, myopathy, cataracts, glaucoma, diabetes, and hypertension, and can interact with thiazide and loop diuretics to cause hypokalemia.
Methotrexate use in this population is linked to pancytopenia and hepatotoxicity, and it can interact with NSAIDs and multiple antibiotics to cause decreased renal secretion.
Thiopurines in older patients are associated with increased risk for leukopenia, myelosuppression, non-Hodgkin lymphoma, skin cancer, pancreatitis, and hepatotoxicity, and drugs in this class interact with allopurinol and angiotensin-converting enzyme inhibitors to increase risk for myelosuppression. Additionally, warfarin can inhibit the efficacy of thiopurines, and when these drugs are used in combination with tumor necrosis factor (TNF)–alpha inhibitors they can further increase risk of malignancy through immunosuppression.
Cyclosporine is associated with worsening hypertension and renal insufficiency among older patients.
TNF-alpha inhibitors are associated with increased risk for tuberculosis; hepatitis B; and fungal infections, malignant lymphoma, and New York Heart Association class 3 or 4 heart failure.
Ciprofloxacin in older patients with IBD has been linked to tendinopathy and increased risk for Clostridioides difficile infections. Metronidazole increases the likelihood of peripheral neuropathy in these patients.
Colon cancer screening
“When it comes to colon cancer screening, definitely assess the risk prior to doing this,” Dr. Bernasko recommended. “Weigh all the risks and benefits. Why are we doing this for these elderly patients, because there are definitely risks associated with this.”
Older patients with IBD may have difficulty with bowel prep and are at elevated risk, compared with younger patients, for cardiopulmonary complications, perforation, adverse events from sedation, and procedural complications, she cautioned.
“When it comes to our elderly patients, you want to focus on a more personalized approach – not all older people present the same way in terms of comorbidities or medications,” Dr. Bernasko advised in her summary.
Dr. Bernasko and Dr. Kochar reported having no relevant conflicts of interest to disclose. Dr. Kochar is a member of the board of editors for GI & Hepatology News.
This article was updated 2/18/22.
FROM CROHN’S & COLITIS CONGRESS
Growth hormone therapy for certain children may help them reach their potential
“Dr. Lilley, you’ll always be my favorite doctor; you helped me grow.”
These were the parting words from the last patient that I treated during my endocrinology fellowship. I had watched this young man grow from a prepubertal 17-year-old to a young man who had reached his predicted family height as I treated his delayed puberty caused by Kallmann syndrome, a problem that had been missed for years. It was the appropriate bookend for my chosen specialty.

Watching children grow and develop into who they were meant to be is one of my favorite things about endocrinology, as well as forming meaningful relationships with families. Treating detectable deficiencies in logical and measurable ways is also extremely satisfying.
Too little testosterone? That’s a problem I can solve. Too much thyroid hormone? There’s a blocker for that! Endocrinology can be a straightforward field, and when all goes well, everyone leaves happy.
Except when they don’t.
Gatekeepers for treatment for children’s growth
“Nice to meet you. We’re here to get growth hormone.”
“We’re here because his pediatrician made us come. We’ve already decided we’re not going to put hormones into his body.”
These are common statements I hear when I first meet new patients whose parents are concerned about their children’s growth. Pediatric endocrinologists, after all, are the usual gatekeepers for this treatment.
Growth hormone (GH) often makes the news for controversial reasons – most commonly for its abuse by elite athletes hoping to exploit its anabolic effects – causing parents to have varied opinions about its possible use in their children.
Some refuse endocrinology referrals at all owing to concerns that we will push daily injections on their children. Others demand referrals for their children of average height, hoping for every perceived advantage.
GH deficiency (GHD) – a condition where the pituitary gland fails to produce enough GH – can occur because of congenital pituitary malformations; anatomic, surgical, or traumatic interruptions to the gland; or enzyme deficiencies leading to faulty production.
GHD is just one reason for poor growth, however.
Growth is one of the most important indicators of health in children. A waning growth rate may be an early symptom of serious problems. In my clinic, I’ve diagnosed severe hypothyroidism in a marathon runner, a brain tumor, celiac disease in a teenager with no gastrointestinal complaints, autoimmune hepatitis, and several other diseases needing treatment in children who show no symptoms other than poor growth.
Barriers to normal growth
Sometimes, the die is cast for children to have barriers to normal growth. Several genetic conditions can lead to poor GH production or response, and GH treatment is often necessary to approximate normal height.
These may include:
- Turner syndrome (in females who are missing an X chromosome in whole or part) should be considered in every girl with abnormally short stature; mosaic forms of the condition may be subtle and lack classic features.
- Noonan syndrome is important to detect owing to the possibility of cardiac or renal malformations that may also occur in this condition, caused by a mutation in one of the genes in the RAS-MAPK pathway.
- Russell-Silver syndrome can cause intrauterine GH restriction and has been traced to uniparental disomy of chromosome 7 or duplications, mutations, or methylation defects in chromosome 11.
- Individuals with Prader-Willi syndrome, which is characterized by low muscle tone, hyperphagia, and hypogonadism, have demonstrated dramatic benefits from GH therapy, primarily in maintaining a normal body mass index.
Children who are small for their gestational age may be GH resistant, and those who do not catch up to their growth curve by the age of 2 years may require GH treatment to reach their height potential.
GH therapy isn’t entirely benign. Rare adverse effects of overtreatment can include slipped capital femoral epiphysis (a fracture to the growth plate) and pseudotumor cerebri (idiopathic intracranial hypertension).
Overtreatment can cause acromegaly, which results in coarsened features and large hands and feet.
When is GH therapy warranted?
“Growth hormone therapy has been denied by her insurer. They want you to fill out an appeal.”
Insurance approval in the United States can be a herculean effort because GH is expensive: Out-of-pocket costs are prohibitive for most people without insurance assistance, ranging from $7,000 to $30,000 annually.
Pediatric endocrinologists aren’t in the business of cosmetic endocrinology. Treatment of idiopathic short stature has been controversial since this became an indication for GH treatment.
GH isn’t always necessary. Diagnosing the underlying cause for poor growth is the most important step.
Often, we find constitutional delay of growth and puberty, or “late bloomers.” This condition is characterized by a delayed bone age (growth plates more open than expected for age) and delayed pubertal onset. These children will often reach a normal height despite starting as some of the smallest of their peers.
However, GH plays other roles in the body than simply propelling height. Children with congenital GHD will require GH treatment to prevent hypoglycemia, especially in infancy.
GH is needed even in adults with fused growth plates for normal lipid metabolism, bone accrual, and maintaining normal muscle mass.
I have noticed marked improvements in muscle tone in many children with developmental delays who are treated with GH, and research supports cognitive benefits for certain populations.
The most common regimens for GH focus on treatment via subcutaneous injection nightly, when GH is naturally produced; sometimes, injections are given six nights out of seven to provide a break or for splitting time between households.
Newer once-weekly formulations have recently received approval, as reported by this news organization, and are coming into use.
Pediatric endocrinologists measure height and follow growth factors closely with visits every 3-6 months. GH levels are not useful outside of provocative diagnostic (stimulation) testing.
Insulinlike growth factor 1 or insulinlike growth factor binding protein levels are analyzed per Tanner stage of puberty to assess appropriate response and to make dose adjustments.
Annual standardized films of the left hand help predict progress and anticipated adult height. Treatment usually persists through puberty until growth plates are closed; if true GHD is noticed, much smaller doses are continued through adulthood.
Regardless, conversations about GH happen with your friendly local pediatric endocrinologist.
We are thrilled to help shepherd patients through their growing age to meet their potential. For more information about GH treatment for children, the MAGIC Foundation is the perfect place to start.
Dr. Lilley is director of the pediatric diabetes and lipid program, Mississippi Center for Advanced Medicine, Madison. She disclosed no relevant conflicts of interest. A version of this article first appeared on Medscape.com.
“Dr. Lilley, you’ll always be my favorite doctor; you helped me grow.”
These were the parting words from the last patient that I treated during my endocrinology fellowship. I had watched this young man grow from a prepubertal 17-year-old to a young man who had reached his predicted family height as I treated his delayed puberty caused by Kallmann syndrome, a problem that had been missed for years. It was the appropriate bookend for my chosen specialty.
Watching children grow and develop into who they were meant to be is one of my favorite things about endocrinology, as well as forming meaningful relationships with families. Treating detectable deficiencies in logical and measurable ways is also extremely satisfying.
Too little testosterone? That’s a problem I can solve. Too much thyroid hormone? There’s a blocker for that! Endocrinology can be a straightforward field, and when all goes well, everyone leaves happy.
Except when they don’t.
Gatekeepers for treatment for children’s growth
“Nice to meet you. We’re here to get growth hormone.”
“We’re here because his pediatrician made us come. We’ve already decided we’re not going to put hormones into his body.”
These are common statements I hear when I first meet new patients whose parents are concerned about their children’s growth. Pediatric endocrinologists, after all, are the usual gatekeepers for this treatment.
Growth hormone (GH) often makes the news for controversial reasons – most commonly for its abuse by elite athletes hoping to exploit its anabolic effects – causing parents to have varied opinions about its possible use in their children.
Some refuse endocrinology referrals at all owing to concerns that we will push daily injections on their children. Others demand referrals for their children of average height, hoping for every perceived advantage.
GH deficiency (GHD) – a condition where the pituitary gland fails to produce enough GH – can occur because of congenital pituitary malformations; anatomic, surgical, or traumatic interruptions to the gland; or enzyme deficiencies leading to faulty production.
GHD is just one reason for poor growth, however.
Growth is one of the most important indicators of health in children. A waning growth rate may be an early symptom of serious problems. In my clinic, I’ve diagnosed severe hypothyroidism in a marathon runner, a brain tumor, celiac disease in a teenager with no gastrointestinal complaints, autoimmune hepatitis, and several other diseases needing treatment in children who show no symptoms other than poor growth.
Barriers to normal growth
Sometimes, the die is cast for children to have barriers to normal growth. Several genetic conditions can lead to poor GH production or response, and GH treatment is often necessary to approximate normal height.
These may include:
- Turner syndrome (in females who are missing an X chromosome in whole or part) should be considered in every girl with abnormally short stature; mosaic forms of the condition may be subtle and lack classic features.
- Noonan syndrome is important to detect owing to the possibility of cardiac or renal malformations that may also occur in this condition, caused by a mutation in one of the genes in the RAS-MAPK pathway.
- Russell-Silver syndrome can cause intrauterine GH restriction and has been traced to uniparental disomy of chromosome 7 or duplications, mutations, or methylation defects in chromosome 11.
- Individuals with Prader-Willi syndrome, which is characterized by low muscle tone, hyperphagia, and hypogonadism, have demonstrated dramatic benefits from GH therapy, primarily in maintaining a normal body mass index.
Children who are small for their gestational age may be GH resistant, and those who do not catch up to their growth curve by the age of 2 years may require GH treatment to reach their height potential.
GH therapy isn’t entirely benign. Rare adverse effects of overtreatment can include slipped capital femoral epiphysis (a fracture to the growth plate) and pseudotumor cerebri (idiopathic intracranial hypertension).
Overtreatment can cause acromegaly, which results in coarsened features and large hands and feet.
When is GH therapy warranted?
“Growth hormone therapy has been denied by her insurer. They want you to fill out an appeal.”
Insurance approval in the United States can be a herculean effort because GH is expensive: Out-of-pocket costs are prohibitive for most people without insurance assistance, ranging from $7,000 to $30,000 annually.
Pediatric endocrinologists aren’t in the business of cosmetic endocrinology. Treatment of idiopathic short stature has been controversial since this became an indication for GH treatment.
GH isn’t always necessary. Diagnosing the underlying cause for poor growth is the most important step.
Often, we find constitutional delay of growth and puberty, or “late bloomers.” This condition is characterized by a delayed bone age (growth plates more open than expected for age) and delayed pubertal onset. These children will often reach a normal height despite starting as some of the smallest of their peers.
However, GH plays other roles in the body than simply propelling height. Children with congenital GHD will require GH treatment to prevent hypoglycemia, especially in infancy.
GH is needed even in adults with fused growth plates for normal lipid metabolism, bone accrual, and maintaining normal muscle mass.
I have noticed marked improvements in muscle tone in many children with developmental delays who are treated with GH, and research supports cognitive benefits for certain populations.
The most common regimens for GH focus on treatment via subcutaneous injection nightly, when GH is naturally produced; sometimes, injections are given six nights out of seven to provide a break or for splitting time between households.
Newer once-weekly formulations have recently received approval, as reported by this news organization, and are coming into use.
Pediatric endocrinologists measure height and follow growth factors closely with visits every 3-6 months. GH levels are not useful outside of provocative diagnostic (stimulation) testing.
Insulinlike growth factor 1 or insulinlike growth factor binding protein levels are analyzed per Tanner stage of puberty to assess appropriate response and to make dose adjustments.
Annual standardized films of the left hand help predict progress and anticipated adult height. Treatment usually persists through puberty until growth plates are closed; if true GHD is noticed, much smaller doses are continued through adulthood.
Regardless, conversations about GH happen with your friendly local pediatric endocrinologist.
We are thrilled to help shepherd patients through their growing age to meet their potential. For more information about GH treatment for children, the MAGIC Foundation is the perfect place to start.
Dr. Lilley is director of the pediatric diabetes and lipid program, Mississippi Center for Advanced Medicine, Madison. She disclosed no relevant conflicts of interest. A version of this article first appeared on Medscape.com.
“Dr. Lilley, you’ll always be my favorite doctor; you helped me grow.”
These were the parting words from the last patient that I treated during my endocrinology fellowship. I had watched this young man grow from a prepubertal 17-year-old to a young man who had reached his predicted family height as I treated his delayed puberty caused by Kallmann syndrome, a problem that had been missed for years. It was the appropriate bookend for my chosen specialty.
Watching children grow and develop into who they were meant to be is one of my favorite things about endocrinology, as well as forming meaningful relationships with families. Treating detectable deficiencies in logical and measurable ways is also extremely satisfying.
Too little testosterone? That’s a problem I can solve. Too much thyroid hormone? There’s a blocker for that! Endocrinology can be a straightforward field, and when all goes well, everyone leaves happy.
Except when they don’t.
Gatekeepers for treatment for children’s growth
“Nice to meet you. We’re here to get growth hormone.”
“We’re here because his pediatrician made us come. We’ve already decided we’re not going to put hormones into his body.”
These are common statements I hear when I first meet new patients whose parents are concerned about their children’s growth. Pediatric endocrinologists, after all, are the usual gatekeepers for this treatment.
Growth hormone (GH) often makes the news for controversial reasons – most commonly for its abuse by elite athletes hoping to exploit its anabolic effects – causing parents to have varied opinions about its possible use in their children.
Some refuse endocrinology referrals at all owing to concerns that we will push daily injections on their children. Others demand referrals for their children of average height, hoping for every perceived advantage.
GH deficiency (GHD) – a condition where the pituitary gland fails to produce enough GH – can occur because of congenital pituitary malformations; anatomic, surgical, or traumatic interruptions to the gland; or enzyme deficiencies leading to faulty production.
GHD is just one reason for poor growth, however.
Growth is one of the most important indicators of health in children. A waning growth rate may be an early symptom of serious problems. In my clinic, I’ve diagnosed severe hypothyroidism in a marathon runner, a brain tumor, celiac disease in a teenager with no gastrointestinal complaints, autoimmune hepatitis, and several other diseases needing treatment in children who show no symptoms other than poor growth.
Barriers to normal growth
Sometimes, the die is cast for children to have barriers to normal growth. Several genetic conditions can lead to poor GH production or response, and GH treatment is often necessary to approximate normal height.
These may include:
- Turner syndrome (in females who are missing an X chromosome in whole or part) should be considered in every girl with abnormally short stature; mosaic forms of the condition may be subtle and lack classic features.
- Noonan syndrome is important to detect owing to the possibility of cardiac or renal malformations that may also occur in this condition, caused by a mutation in one of the genes in the RAS-MAPK pathway.
- Russell-Silver syndrome can cause intrauterine GH restriction and has been traced to uniparental disomy of chromosome 7 or duplications, mutations, or methylation defects in chromosome 11.
- Individuals with Prader-Willi syndrome, which is characterized by low muscle tone, hyperphagia, and hypogonadism, have demonstrated dramatic benefits from GH therapy, primarily in maintaining a normal body mass index.
Children who are small for their gestational age may be GH resistant, and those who do not catch up to their growth curve by the age of 2 years may require GH treatment to reach their height potential.
GH therapy isn’t entirely benign. Rare adverse effects of overtreatment can include slipped capital femoral epiphysis (a fracture to the growth plate) and pseudotumor cerebri (idiopathic intracranial hypertension).
Overtreatment can cause acromegaly, which results in coarsened features and large hands and feet.
When is GH therapy warranted?
“Growth hormone therapy has been denied by her insurer. They want you to fill out an appeal.”
Insurance approval in the United States can be a herculean effort because GH is expensive: Out-of-pocket costs are prohibitive for most people without insurance assistance, ranging from $7,000 to $30,000 annually.
Pediatric endocrinologists aren’t in the business of cosmetic endocrinology. Treatment of idiopathic short stature has been controversial since this became an indication for GH treatment.
GH isn’t always necessary. Diagnosing the underlying cause for poor growth is the most important step.
Often, we find constitutional delay of growth and puberty, or “late bloomers.” This condition is characterized by a delayed bone age (growth plates more open than expected for age) and delayed pubertal onset. These children will often reach a normal height despite starting as some of the smallest of their peers.
However, GH plays other roles in the body than simply propelling height. Children with congenital GHD will require GH treatment to prevent hypoglycemia, especially in infancy.
GH is needed even in adults with fused growth plates for normal lipid metabolism, bone accrual, and maintaining normal muscle mass.
I have noticed marked improvements in muscle tone in many children with developmental delays who are treated with GH, and research supports cognitive benefits for certain populations.
The most common regimens for GH focus on treatment via subcutaneous injection nightly, when GH is naturally produced; sometimes, injections are given six nights out of seven to provide a break or for splitting time between households.
Newer once-weekly formulations have recently received approval, as reported by this news organization, and are coming into use.
Pediatric endocrinologists measure height and follow growth factors closely with visits every 3-6 months. GH levels are not useful outside of provocative diagnostic (stimulation) testing.
Insulinlike growth factor 1 or insulinlike growth factor binding protein levels are analyzed per Tanner stage of puberty to assess appropriate response and to make dose adjustments.
Annual standardized films of the left hand help predict progress and anticipated adult height. Treatment usually persists through puberty until growth plates are closed; if true GHD is noticed, much smaller doses are continued through adulthood.
Regardless, conversations about GH happen with your friendly local pediatric endocrinologist.
We are thrilled to help shepherd patients through their growing age to meet their potential. For more information about GH treatment for children, the MAGIC Foundation is the perfect place to start.
Dr. Lilley is director of the pediatric diabetes and lipid program, Mississippi Center for Advanced Medicine, Madison. She disclosed no relevant conflicts of interest. A version of this article first appeared on Medscape.com.
Long COVID symptoms linked to effects on vagus nerve
Several long COVID symptoms could be linked to the effects of the coronavirus on a vital central nerve, according to new research being released in the spring.
The vagus nerve, which runs from the brain into the body, connects to the heart, lungs, intestines, and several muscles involved with swallowing. It plays a role in several body functions that control heart rate, speech, the gag reflex, sweating, and digestion.
Those with long COVID and vagus nerve problems could face long-term issues with their voice, a hard time swallowing, dizziness, a high heart rate, low blood pressure, and diarrhea, the study authors found.
Their findings will be presented at the 2022 European Congress of Clinical Microbiology and Infectious Diseases in late April.
“Most long COVID subjects with vagus nerve dysfunction symptoms had a range of significant, clinically relevant, structural and/or functional alterations in their vagus nerve, including nerve thickening, trouble swallowing, and symptoms of impaired breathing,” the study authors wrote. “Our findings so far thus point at vagus nerve dysfunction as a central pathophysiological feature of long COVID.”
Researchers from the University Hospital Germans Trias i Pujol in Barcelona performed a study to look at vagus nerve functioning in long COVID patients. Among 348 patients, about 66% had at least one symptom that suggested vagus nerve dysfunction. The researchers did a broad evaluation with imaging and functional tests for 22 patients in the university’s Long COVID Clinic from March to June 2021.
Of the 22 patients, 20 were women, and the median age was 44. The most frequent symptoms related to vagus nerve dysfunction were diarrhea (73%), high heart rates (59%), dizziness (45%), swallowing problems (45%), voice problems (45%), and low blood pressure (14%).
Almost all (19 of 22 patients) had three or more symptoms related to vagus nerve dysfunction. The average length of symptoms was 14 months.
Of 22 patients, 6 had a change in the vagus nerve in the neck, which the researchers observed by ultrasound. They had a thickening of the vagus nerve and increased “echogenicity,” which suggests inflammation.
What’s more, 10 of 22 patients had flattened “diaphragmatic curves” during a thoracic ultrasound, which means the diaphragm doesn’t move as well as it should during breathing, and abnormal breathing. In another assessment, 10 of 16 patients had lower maximum inspiration pressures, suggesting a weakness in breathing muscles.
Eating and digestion were also impaired in some patients, with 13 reporting trouble with swallowing. During a gastric and bowel function assessment, eight patients couldn’t move food from the esophagus to the stomach as well as they should, while nine patients had acid reflux. Three patients had a hiatal hernia, which happens when the upper part of the stomach bulges through the diaphragm into the chest cavity.
The voices of some patients changed as well. Eight patients had an abnormal voice handicap index 30 test, which is a standard way to measure voice function. Among those, seven patients had dysphonia, or persistent voice problems.
The study is ongoing, and the research team is continuing to recruit patients to study the links between long COVID and the vagus nerve. The full paper isn’t yet available, and the research hasn’t yet been peer reviewed.
“The study appears to add to a growing collection of data suggesting at least some of the symptoms of long COVID is mediated through a direct impact on the nervous system,” David Strain, MD, a clinical senior lecturer at the University of Exeter (England), told the Science Media Centre.
“Establishing vagal nerve damage is useful information, as there are recognized, albeit not perfect, treatments for other causes of vagal nerve dysfunction that may be extrapolated to be beneficial for people with this type of long COVID,” he said.
A version of this article first appeared on WebMD.com.
Several long COVID symptoms could be linked to the effects of the coronavirus on a vital central nerve, according to new research being released in the spring.
The vagus nerve, which runs from the brain into the body, connects to the heart, lungs, intestines, and several muscles involved with swallowing. It plays a role in several body functions that control heart rate, speech, the gag reflex, sweating, and digestion.
Those with long COVID and vagus nerve problems could face long-term issues with their voice, a hard time swallowing, dizziness, a high heart rate, low blood pressure, and diarrhea, the study authors found.
Their findings will be presented at the 2022 European Congress of Clinical Microbiology and Infectious Diseases in late April.
“Most long COVID subjects with vagus nerve dysfunction symptoms had a range of significant, clinically relevant, structural and/or functional alterations in their vagus nerve, including nerve thickening, trouble swallowing, and symptoms of impaired breathing,” the study authors wrote. “Our findings so far thus point at vagus nerve dysfunction as a central pathophysiological feature of long COVID.”
Researchers from the University Hospital Germans Trias i Pujol in Barcelona performed a study to look at vagus nerve functioning in long COVID patients. Among 348 patients, about 66% had at least one symptom that suggested vagus nerve dysfunction. The researchers did a broad evaluation with imaging and functional tests for 22 patients in the university’s Long COVID Clinic from March to June 2021.
Of the 22 patients, 20 were women, and the median age was 44. The most frequent symptoms related to vagus nerve dysfunction were diarrhea (73%), high heart rates (59%), dizziness (45%), swallowing problems (45%), voice problems (45%), and low blood pressure (14%).
Almost all (19 of 22 patients) had three or more symptoms related to vagus nerve dysfunction. The average length of symptoms was 14 months.
Of 22 patients, 6 had a change in the vagus nerve in the neck, which the researchers observed by ultrasound. They had a thickening of the vagus nerve and increased “echogenicity,” which suggests inflammation.
What’s more, 10 of 22 patients had flattened “diaphragmatic curves” during a thoracic ultrasound, which means the diaphragm doesn’t move as well as it should during breathing, and abnormal breathing. In another assessment, 10 of 16 patients had lower maximum inspiration pressures, suggesting a weakness in breathing muscles.
Eating and digestion were also impaired in some patients, with 13 reporting trouble with swallowing. During a gastric and bowel function assessment, eight patients couldn’t move food from the esophagus to the stomach as well as they should, while nine patients had acid reflux. Three patients had a hiatal hernia, which happens when the upper part of the stomach bulges through the diaphragm into the chest cavity.
The voices of some patients changed as well. Eight patients had an abnormal voice handicap index 30 test, which is a standard way to measure voice function. Among those, seven patients had dysphonia, or persistent voice problems.
The study is ongoing, and the research team is continuing to recruit patients to study the links between long COVID and the vagus nerve. The full paper isn’t yet available, and the research hasn’t yet been peer reviewed.
“The study appears to add to a growing collection of data suggesting at least some of the symptoms of long COVID is mediated through a direct impact on the nervous system,” David Strain, MD, a clinical senior lecturer at the University of Exeter (England), told the Science Media Centre.
“Establishing vagal nerve damage is useful information, as there are recognized, albeit not perfect, treatments for other causes of vagal nerve dysfunction that may be extrapolated to be beneficial for people with this type of long COVID,” he said.
A version of this article first appeared on WebMD.com.
Several long COVID symptoms could be linked to the effects of the coronavirus on a vital central nerve, according to new research being released in the spring.
The vagus nerve, which runs from the brain into the body, connects to the heart, lungs, intestines, and several muscles involved with swallowing. It plays a role in several body functions that control heart rate, speech, the gag reflex, sweating, and digestion.
Those with long COVID and vagus nerve problems could face long-term issues with their voice, a hard time swallowing, dizziness, a high heart rate, low blood pressure, and diarrhea, the study authors found.
Their findings will be presented at the 2022 European Congress of Clinical Microbiology and Infectious Diseases in late April.
“Most long COVID subjects with vagus nerve dysfunction symptoms had a range of significant, clinically relevant, structural and/or functional alterations in their vagus nerve, including nerve thickening, trouble swallowing, and symptoms of impaired breathing,” the study authors wrote. “Our findings so far thus point at vagus nerve dysfunction as a central pathophysiological feature of long COVID.”
Researchers from the University Hospital Germans Trias i Pujol in Barcelona performed a study to look at vagus nerve functioning in long COVID patients. Among 348 patients, about 66% had at least one symptom that suggested vagus nerve dysfunction. The researchers did a broad evaluation with imaging and functional tests for 22 patients in the university’s Long COVID Clinic from March to June 2021.
Of the 22 patients, 20 were women, and the median age was 44. The most frequent symptoms related to vagus nerve dysfunction were diarrhea (73%), high heart rates (59%), dizziness (45%), swallowing problems (45%), voice problems (45%), and low blood pressure (14%).
Almost all (19 of 22 patients) had three or more symptoms related to vagus nerve dysfunction. The average length of symptoms was 14 months.
Of 22 patients, 6 had a change in the vagus nerve in the neck, which the researchers observed by ultrasound. They had a thickening of the vagus nerve and increased “echogenicity,” which suggests inflammation.
What’s more, 10 of 22 patients had flattened “diaphragmatic curves” during a thoracic ultrasound, which means the diaphragm doesn’t move as well as it should during breathing, and abnormal breathing. In another assessment, 10 of 16 patients had lower maximum inspiration pressures, suggesting a weakness in breathing muscles.
Eating and digestion were also impaired in some patients, with 13 reporting trouble with swallowing. During a gastric and bowel function assessment, eight patients couldn’t move food from the esophagus to the stomach as well as they should, while nine patients had acid reflux. Three patients had a hiatal hernia, which happens when the upper part of the stomach bulges through the diaphragm into the chest cavity.
The voices of some patients changed as well. Eight patients had an abnormal voice handicap index 30 test, which is a standard way to measure voice function. Among those, seven patients had dysphonia, or persistent voice problems.
The study is ongoing, and the research team is continuing to recruit patients to study the links between long COVID and the vagus nerve. The full paper isn’t yet available, and the research hasn’t yet been peer reviewed.
“The study appears to add to a growing collection of data suggesting at least some of the symptoms of long COVID is mediated through a direct impact on the nervous system,” David Strain, MD, a clinical senior lecturer at the University of Exeter (England), told the Science Media Centre.
“Establishing vagal nerve damage is useful information, as there are recognized, albeit not perfect, treatments for other causes of vagal nerve dysfunction that may be extrapolated to be beneficial for people with this type of long COVID,” he said.
A version of this article first appeared on WebMD.com.
Can periodontal treatment reduce cardiovascular events in stroke patients?
The first randomized trial to investigate whether periodontal treatment can reduce future risk of cardiovascular events or stroke suggests some promise with this strategy.
The PREMIERS study, which was conducted in patients with a recent stroke or transient ischemic attack (TIA) who also had gum disease, did not show a statistically significant difference between intensive periodontal treatment and standard treatment in the rate of recurrent stroke, myocardial infarction (MI), or death in the 1-year follow-up, although there was a strong trend toward benefit in the intensive group.
Both groups had a much lower event rate compared with a historical control group made up of similar patients.
In addition, the number of dental visits significantly correlated with a reduction in the composite event rate in the study.
“My take-home message from this study is that periodontal treatment does appear to impact cardiovascular outcomes in stroke/TIA patients,” said lead author Souvik Sen, MD, MPH, professor of neurology at the University of South Carolina School of Medicine.
“Even standard periodontal care – a dental cleaning every 3 months – was beneficial.”
Dr. Sen presented the study at the hybrid International Stroke Conference (ISC), taking place in New Orleans and virtually.
“This was a very ambitious study, and it turned out to be very underpowered for the comparisons involved, but I was impressed that we saw such a strong trend toward benefit in the intensive group,” he said at the meeting, presented by the American Stroke Association, a division of the American Heart Association.
Dr. Sen explained that they initially set out to compare periodontal treatment with no treatment, but they were unable to have a control group who received no treatment for ethical reasons, so they ended up comparing standard treatment with intensive treatment.
“We probably needed a study of twice the size for that comparison. But our results are encouraging, and we now plan to do a larger study,” he said.
Dr. Sen reported that gum disease (periodontitis) is extremely prevalent, occurring in around half the U.S. population. It is particularly prevalent in the southeastern part of the United States, known as the “Stroke Belt” because of a much higher incidence of stroke compared with the rest of the country. Gum disease is known to be associated with an increased risk of cardiovascular events and stroke.
For the study, 280 patients from the Stroke Belt area with a recent stroke or TIA and periodontal disease were randomly assigned to standard periodontal treatment or intensive periodontal treatment and followed for 1 year.
Standard treatment was composed of regular (every 3 months) supragingival removal of plaque and calculus; patients were also given a regular toothbrush and advice about dental care.
The intensive group received supragingival and subgingival removal of plaque and calculus (also every 3 months), extraction of hopeless teeth, locally delivered antibiotics. In addition, patients were given an electric toothbrush, mouthwash, and an air flosser for dental care.
All patients received comprehensive conventional stroke risk factor treatment.
The study had an adaptive randomization design to ensure both groups were balanced in terms of age, stroke causes, race, socioeconomic status, and stroke risk factors.
Results showed that after 1 year of follow-up, the primary outcome (stroke/myocardial infarction/death) had occurred in 7.7% of the intensive treatment group versus 12.3% of the standard care group, giving a hazard ratio of 0.65 (95% confidence interval, 0.30-1.38; P = .26).
But both groups had a much lower rate of recurrent events, compared with a historical control group which showed a 1-year rate of stroke/MI/death of 24%. The historical controls were part of an observational study that the same group of researchers conducted previously in a similar population.
In both standard treatment and intensive treatment groups, the combined number of dental visits strongly correlated with a reduction in cardiovascular events. Of the study participants, 65% attended all five visits, 25% attended two to four, and 10% did not attend any after the baseline assessment.
Those who attended all visits in the year had a rate of stroke/MI/death at 1 year of 8%. And those who did not attend any further visits after the baseline visit had an event rate of 25% at 1-year follow-up, which Dr. Sen noted was very similar to that of the historical controls. The P value for this trend was “very significant” (P = .0017), he said.
Secondary outcomes showed a reduction in blood pressure, A1c levels, carotid intima-media thickness, and better lipid profiles in all patients who underwent treatment – in both standard treatment and intensive treatment.
A new part of routine post-stroke care?
“Previous data on how gum disease and periodontal treatment relates to cardiovascular outcomes have all come from observational studies. They have shown that regular dental care is associated with reduced incidence of future cardiovascular events. But until now, we haven’t had any randomized data,” Dr. Sen noted.
He believes advice on oral and dental care should be part of routine clinical practice for patients who have suffered stroke. “This is not something we currently think about, but it could make a big difference in future event rates.”
Dr. Sen said the current study had raised interest in the topic, and his presentation was received with enthusiasm from the audience.
“We are in South Carolina in the Stroke Belt. Previous studies have shown that gum disease is very prevalent in this area. People in this area have a high risk of stroke, but we don’t know all the attributable risk factors. The traditional stroke risk factors do not seem to account for all the excess risk,” Dr. Sen said. “Periodontal disease could be one of the additional risk factors that accounts for the increased stroke risk in this population.”
“I believe doctors treating stroke patients should advise that they pay particular attention to oral care and visit the dentist frequently for periodontal treatment if they have gum disease. It is very unusual for people to get regular dental cleaning. They don’t understand that they need to do this,” he said.
But he acknowledges that larger studies are needed to show statistically significant results to be able to achieve a strong recommendation in the secondary prevention clinical guidelines.
“Even in individuals who haven’t had a stroke or cardiovascular event, population-based observational studies clearly show that gum infection is linked to future risk of myocardial infarction and stroke and that regular dental care (one or more visits per year) can reduce this risk. I don’t think we can do a randomized trial in the general population – that would need enormous numbers. We will have to rely on the observational studies here,” he added.
‘Promising’ results
Commenting on the current study, Louise McCullough, MD, ISC 2022 program chair, said she thought the results were promising.
“There was no difference in the intensive cleaning group versus standard cleaning, but the number of events was small, so it was underpowered to see differences. I think the main take home point is that both groups that came for dental visits had a much lower risk of another event than the group that did not show up for follow-up,” said Dr. McCullough, chair of the department of neurology, McGovern Medical School, University of Texas Health Science Center, Houston. “Clearly, seeing a provider made a difference. It is likely that contact with a dentist, getting blood pressure checked, etc., made a dramatic difference.”
The study was funded by the National Institute of Minority Health Disparity, Phillips Oral Healthcare, and Orapharma (which provided the study antibiotic medication).
A version of this article first appeared on Medscape.com.
The first randomized trial to investigate whether periodontal treatment can reduce future risk of cardiovascular events or stroke suggests some promise with this strategy.
The PREMIERS study, which was conducted in patients with a recent stroke or transient ischemic attack (TIA) who also had gum disease, did not show a statistically significant difference between intensive periodontal treatment and standard treatment in the rate of recurrent stroke, myocardial infarction (MI), or death in the 1-year follow-up, although there was a strong trend toward benefit in the intensive group.
Both groups had a much lower event rate compared with a historical control group made up of similar patients.
In addition, the number of dental visits significantly correlated with a reduction in the composite event rate in the study.
“My take-home message from this study is that periodontal treatment does appear to impact cardiovascular outcomes in stroke/TIA patients,” said lead author Souvik Sen, MD, MPH, professor of neurology at the University of South Carolina School of Medicine.
“Even standard periodontal care – a dental cleaning every 3 months – was beneficial.”
Dr. Sen presented the study at the hybrid International Stroke Conference (ISC), taking place in New Orleans and virtually.
“This was a very ambitious study, and it turned out to be very underpowered for the comparisons involved, but I was impressed that we saw such a strong trend toward benefit in the intensive group,” he said at the meeting, presented by the American Stroke Association, a division of the American Heart Association.
Dr. Sen explained that they initially set out to compare periodontal treatment with no treatment, but they were unable to have a control group who received no treatment for ethical reasons, so they ended up comparing standard treatment with intensive treatment.
“We probably needed a study of twice the size for that comparison. But our results are encouraging, and we now plan to do a larger study,” he said.
Dr. Sen reported that gum disease (periodontitis) is extremely prevalent, occurring in around half the U.S. population. It is particularly prevalent in the southeastern part of the United States, known as the “Stroke Belt” because of a much higher incidence of stroke compared with the rest of the country. Gum disease is known to be associated with an increased risk of cardiovascular events and stroke.
For the study, 280 patients from the Stroke Belt area with a recent stroke or TIA and periodontal disease were randomly assigned to standard periodontal treatment or intensive periodontal treatment and followed for 1 year.
Standard treatment was composed of regular (every 3 months) supragingival removal of plaque and calculus; patients were also given a regular toothbrush and advice about dental care.
The intensive group received supragingival and subgingival removal of plaque and calculus (also every 3 months), extraction of hopeless teeth, locally delivered antibiotics. In addition, patients were given an electric toothbrush, mouthwash, and an air flosser for dental care.
All patients received comprehensive conventional stroke risk factor treatment.
The study had an adaptive randomization design to ensure both groups were balanced in terms of age, stroke causes, race, socioeconomic status, and stroke risk factors.
Results showed that after 1 year of follow-up, the primary outcome (stroke/myocardial infarction/death) had occurred in 7.7% of the intensive treatment group versus 12.3% of the standard care group, giving a hazard ratio of 0.65 (95% confidence interval, 0.30-1.38; P = .26).
But both groups had a much lower rate of recurrent events, compared with a historical control group which showed a 1-year rate of stroke/MI/death of 24%. The historical controls were part of an observational study that the same group of researchers conducted previously in a similar population.
In both standard treatment and intensive treatment groups, the combined number of dental visits strongly correlated with a reduction in cardiovascular events. Of the study participants, 65% attended all five visits, 25% attended two to four, and 10% did not attend any after the baseline assessment.
Those who attended all visits in the year had a rate of stroke/MI/death at 1 year of 8%. And those who did not attend any further visits after the baseline visit had an event rate of 25% at 1-year follow-up, which Dr. Sen noted was very similar to that of the historical controls. The P value for this trend was “very significant” (P = .0017), he said.
Secondary outcomes showed a reduction in blood pressure, A1c levels, carotid intima-media thickness, and better lipid profiles in all patients who underwent treatment – in both standard treatment and intensive treatment.
A new part of routine post-stroke care?
“Previous data on how gum disease and periodontal treatment relates to cardiovascular outcomes have all come from observational studies. They have shown that regular dental care is associated with reduced incidence of future cardiovascular events. But until now, we haven’t had any randomized data,” Dr. Sen noted.
He believes advice on oral and dental care should be part of routine clinical practice for patients who have suffered stroke. “This is not something we currently think about, but it could make a big difference in future event rates.”
Dr. Sen said the current study had raised interest in the topic, and his presentation was received with enthusiasm from the audience.
“We are in South Carolina in the Stroke Belt. Previous studies have shown that gum disease is very prevalent in this area. People in this area have a high risk of stroke, but we don’t know all the attributable risk factors. The traditional stroke risk factors do not seem to account for all the excess risk,” Dr. Sen said. “Periodontal disease could be one of the additional risk factors that accounts for the increased stroke risk in this population.”
“I believe doctors treating stroke patients should advise that they pay particular attention to oral care and visit the dentist frequently for periodontal treatment if they have gum disease. It is very unusual for people to get regular dental cleaning. They don’t understand that they need to do this,” he said.
But he acknowledges that larger studies are needed to show statistically significant results to be able to achieve a strong recommendation in the secondary prevention clinical guidelines.
“Even in individuals who haven’t had a stroke or cardiovascular event, population-based observational studies clearly show that gum infection is linked to future risk of myocardial infarction and stroke and that regular dental care (one or more visits per year) can reduce this risk. I don’t think we can do a randomized trial in the general population – that would need enormous numbers. We will have to rely on the observational studies here,” he added.
‘Promising’ results
Commenting on the current study, Louise McCullough, MD, ISC 2022 program chair, said she thought the results were promising.
“There was no difference in the intensive cleaning group versus standard cleaning, but the number of events was small, so it was underpowered to see differences. I think the main take home point is that both groups that came for dental visits had a much lower risk of another event than the group that did not show up for follow-up,” said Dr. McCullough, chair of the department of neurology, McGovern Medical School, University of Texas Health Science Center, Houston. “Clearly, seeing a provider made a difference. It is likely that contact with a dentist, getting blood pressure checked, etc., made a dramatic difference.”
The study was funded by the National Institute of Minority Health Disparity, Phillips Oral Healthcare, and Orapharma (which provided the study antibiotic medication).
A version of this article first appeared on Medscape.com.
The first randomized trial to investigate whether periodontal treatment can reduce future risk of cardiovascular events or stroke suggests some promise with this strategy.
The PREMIERS study, which was conducted in patients with a recent stroke or transient ischemic attack (TIA) who also had gum disease, did not show a statistically significant difference between intensive periodontal treatment and standard treatment in the rate of recurrent stroke, myocardial infarction (MI), or death in the 1-year follow-up, although there was a strong trend toward benefit in the intensive group.
Both groups had a much lower event rate compared with a historical control group made up of similar patients.
In addition, the number of dental visits significantly correlated with a reduction in the composite event rate in the study.
“My take-home message from this study is that periodontal treatment does appear to impact cardiovascular outcomes in stroke/TIA patients,” said lead author Souvik Sen, MD, MPH, professor of neurology at the University of South Carolina School of Medicine.
“Even standard periodontal care – a dental cleaning every 3 months – was beneficial.”
Dr. Sen presented the study at the hybrid International Stroke Conference (ISC), taking place in New Orleans and virtually.
“This was a very ambitious study, and it turned out to be very underpowered for the comparisons involved, but I was impressed that we saw such a strong trend toward benefit in the intensive group,” he said at the meeting, presented by the American Stroke Association, a division of the American Heart Association.
Dr. Sen explained that they initially set out to compare periodontal treatment with no treatment, but they were unable to have a control group who received no treatment for ethical reasons, so they ended up comparing standard treatment with intensive treatment.
“We probably needed a study of twice the size for that comparison. But our results are encouraging, and we now plan to do a larger study,” he said.
Dr. Sen reported that gum disease (periodontitis) is extremely prevalent, occurring in around half the U.S. population. It is particularly prevalent in the southeastern part of the United States, known as the “Stroke Belt” because of a much higher incidence of stroke compared with the rest of the country. Gum disease is known to be associated with an increased risk of cardiovascular events and stroke.
For the study, 280 patients from the Stroke Belt area with a recent stroke or TIA and periodontal disease were randomly assigned to standard periodontal treatment or intensive periodontal treatment and followed for 1 year.
Standard treatment was composed of regular (every 3 months) supragingival removal of plaque and calculus; patients were also given a regular toothbrush and advice about dental care.
The intensive group received supragingival and subgingival removal of plaque and calculus (also every 3 months), extraction of hopeless teeth, locally delivered antibiotics. In addition, patients were given an electric toothbrush, mouthwash, and an air flosser for dental care.
All patients received comprehensive conventional stroke risk factor treatment.
The study had an adaptive randomization design to ensure both groups were balanced in terms of age, stroke causes, race, socioeconomic status, and stroke risk factors.
Results showed that after 1 year of follow-up, the primary outcome (stroke/myocardial infarction/death) had occurred in 7.7% of the intensive treatment group versus 12.3% of the standard care group, giving a hazard ratio of 0.65 (95% confidence interval, 0.30-1.38; P = .26).
But both groups had a much lower rate of recurrent events, compared with a historical control group which showed a 1-year rate of stroke/MI/death of 24%. The historical controls were part of an observational study that the same group of researchers conducted previously in a similar population.
In both standard treatment and intensive treatment groups, the combined number of dental visits strongly correlated with a reduction in cardiovascular events. Of the study participants, 65% attended all five visits, 25% attended two to four, and 10% did not attend any after the baseline assessment.
Those who attended all visits in the year had a rate of stroke/MI/death at 1 year of 8%. And those who did not attend any further visits after the baseline visit had an event rate of 25% at 1-year follow-up, which Dr. Sen noted was very similar to that of the historical controls. The P value for this trend was “very significant” (P = .0017), he said.
Secondary outcomes showed a reduction in blood pressure, A1c levels, carotid intima-media thickness, and better lipid profiles in all patients who underwent treatment – in both standard treatment and intensive treatment.
A new part of routine post-stroke care?
“Previous data on how gum disease and periodontal treatment relates to cardiovascular outcomes have all come from observational studies. They have shown that regular dental care is associated with reduced incidence of future cardiovascular events. But until now, we haven’t had any randomized data,” Dr. Sen noted.
He believes advice on oral and dental care should be part of routine clinical practice for patients who have suffered stroke. “This is not something we currently think about, but it could make a big difference in future event rates.”
Dr. Sen said the current study had raised interest in the topic, and his presentation was received with enthusiasm from the audience.
“We are in South Carolina in the Stroke Belt. Previous studies have shown that gum disease is very prevalent in this area. People in this area have a high risk of stroke, but we don’t know all the attributable risk factors. The traditional stroke risk factors do not seem to account for all the excess risk,” Dr. Sen said. “Periodontal disease could be one of the additional risk factors that accounts for the increased stroke risk in this population.”
“I believe doctors treating stroke patients should advise that they pay particular attention to oral care and visit the dentist frequently for periodontal treatment if they have gum disease. It is very unusual for people to get regular dental cleaning. They don’t understand that they need to do this,” he said.
But he acknowledges that larger studies are needed to show statistically significant results to be able to achieve a strong recommendation in the secondary prevention clinical guidelines.
“Even in individuals who haven’t had a stroke or cardiovascular event, population-based observational studies clearly show that gum infection is linked to future risk of myocardial infarction and stroke and that regular dental care (one or more visits per year) can reduce this risk. I don’t think we can do a randomized trial in the general population – that would need enormous numbers. We will have to rely on the observational studies here,” he added.
‘Promising’ results
Commenting on the current study, Louise McCullough, MD, ISC 2022 program chair, said she thought the results were promising.
“There was no difference in the intensive cleaning group versus standard cleaning, but the number of events was small, so it was underpowered to see differences. I think the main take home point is that both groups that came for dental visits had a much lower risk of another event than the group that did not show up for follow-up,” said Dr. McCullough, chair of the department of neurology, McGovern Medical School, University of Texas Health Science Center, Houston. “Clearly, seeing a provider made a difference. It is likely that contact with a dentist, getting blood pressure checked, etc., made a dramatic difference.”
The study was funded by the National Institute of Minority Health Disparity, Phillips Oral Healthcare, and Orapharma (which provided the study antibiotic medication).
A version of this article first appeared on Medscape.com.
FROM ISC 2022
Tenecteplase for stroke linked to reduced ICH risk
preliminary results from a large, multicenter registry study suggest.
“In clinical practice where centers are using tenecteplase, we’re seeing that the rate of symptomatic hemorrhage after getting a thrombolytic is half that with tenecteplase than with alteplase,” said lead author Steven J. Warach, MD, PhD, professor of neurology at Dell Medical School, University of Texas, Austin.
“For clinicians who have switched or are considering switching to tenecteplase, I think these results are very reassuring,” he said at the International Stroke Conference, presented by the American Stroke Association, a division of the American Heart Association.
Tenecteplase is a relatively new agent that is approved by the U.S. Food and Drug Administration to treat myocardial infarction but not ischemic stroke, although clinicians sometimes use it off-label for this purpose. American Heart Association guidelines recommend tenecteplase might be reasonable to consider for ischemic stroke in select patients.
The current standard of care for stroke is alteplase, which has been approved for this indication since 1996.
Five randomized clinical trials comparing the two thrombolytics weren’t large enough to make definitive conclusions about differences, said Dr. Warach. “The event rate for serious bleeding into the brain was thankfully low in both groups.”
Results from a meta-analysis that combined data from those five trials were also not definitive. “Numerically, it looked like the rate was lower for tenecteplase, but the sample size was just too low to make any statistically confident statement.”
However, tenecteplase has practical advantages over alteplase. Tenecteplase is a single bolus injection lasting 5 seconds while alteplase is administered by injection followed by an hour-long infusion.
Given these potential advantages, some centers have changed their practice and started using the newer drug beginning in July 2018.
The current study used an ongoing large registry to compare rates of symptomatic intracranial hemorrhage in patients treated with either of these drugs. The registry includes data collected July 2018 to June 2021 from various hospitals and programs in New Zealand, Australia, and the U.S.
Symptomatic intracranial hemorrhage was defined as a severe bleed causing pressure on the brain, extensive swelling, and worsening by at least four points on the National Institutes of Health Stroke Scale (NIHSS).
Researchers abstracted data from the various registries. As not all centers record data in the same format, statisticians then “cleaned” or harmonized the data to make it more standardized, said Dr. Warach.
They controlled for factors known to put a patient at higher risk for symptomatic hemorrhage, including age, sex, baseline NIHSS, and time to treatment.
Dr. Warach noted that at baseline, the tenecteplase group had higher values on most of these factors “that would predict intracranial hemorrhage.”
In an earlier analysis of 7,891 patients, the tenecteplase group was older (73 vs. 70 years; P < .001), less likely to be female (44.1% vs. 48.7%; P = .001), and had higher NIHSS scores (9 vs. 7; P < .001).
Also, a greater percentage of those in the tenecteplase group underwent mechanical thrombectomy (36.7% vs. 18.0%; P < .001). Dr. Warach explained that some centers would opt for tenecteplase if they knew the patient was a candidate for thrombectomy “because that was where the data was clearly strong and positive.”
An updated analysis included 9,238 patients – 7,313 who received alteplase and 1,925 tenecteplase. In the updated unadjusted analysis, the symptomatic intracranial hemorrhage rate was 3.6% for alteplase and 1.8% for tenecteplase (odds ratio, 0.49; P < .001). The adjusted OR was 0.42 (P < .001.)
The difference was even greater in those who underwent thrombectomy. For patients undergoing this procedure after a thrombolytic, the symptomatic intracranial hemorrhage rate was 5.9% for alteplase and 2.4% for tenecteplase.
“That even in those higher-risk patients we’re seeing an even greater difference is promising,” said Dr. Warach.
He and his colleagues plan to assess other potential benefits of tenecteplase, for example, the time it takes for patients to recover, “once we have all the data standardized and cleaned.”
Results of three large phase 3 trials comparing the two thrombolytics are expected within the next year or two, said Dr. Warach.
Joseph Broderick, MD, professor and director of the UC Gardner Neuroscience Institute, director of the National Coordinating Center for NIH’s StrokeNet, and professor of medicine at the University of Cincinnati College of Medicine, Cincinnati, stressed that for both drugs, speed is of the utmost importance to protect the brain.
“No matter which of these drugs is going to be used, the key thing is that they have to be used as quickly as possible,” he said.
Also important is imaging the brain before administering either of these medications to ensure the issue is an ischemic stroke and not an intracerebral hemorrhage, said Dr. Broderick. “If you have a broken blood vessel, you want to seal the leak, not break up the clot and make the bleeding worse.”
Dr. Warach receives payment as chair of the safety committee of another Genentech study comparing tenecteplase versus placebo in patients with large vessel occlusion whose stroke began more than 4.5 hours before treatment.
A version of this article first appeared on Medscape.com.
preliminary results from a large, multicenter registry study suggest.
“In clinical practice where centers are using tenecteplase, we’re seeing that the rate of symptomatic hemorrhage after getting a thrombolytic is half that with tenecteplase than with alteplase,” said lead author Steven J. Warach, MD, PhD, professor of neurology at Dell Medical School, University of Texas, Austin.
“For clinicians who have switched or are considering switching to tenecteplase, I think these results are very reassuring,” he said at the International Stroke Conference, presented by the American Stroke Association, a division of the American Heart Association.
Tenecteplase is a relatively new agent that is approved by the U.S. Food and Drug Administration to treat myocardial infarction but not ischemic stroke, although clinicians sometimes use it off-label for this purpose. American Heart Association guidelines recommend tenecteplase might be reasonable to consider for ischemic stroke in select patients.
The current standard of care for stroke is alteplase, which has been approved for this indication since 1996.
Five randomized clinical trials comparing the two thrombolytics weren’t large enough to make definitive conclusions about differences, said Dr. Warach. “The event rate for serious bleeding into the brain was thankfully low in both groups.”
Results from a meta-analysis that combined data from those five trials were also not definitive. “Numerically, it looked like the rate was lower for tenecteplase, but the sample size was just too low to make any statistically confident statement.”
However, tenecteplase has practical advantages over alteplase. Tenecteplase is a single bolus injection lasting 5 seconds while alteplase is administered by injection followed by an hour-long infusion.
Given these potential advantages, some centers have changed their practice and started using the newer drug beginning in July 2018.
The current study used an ongoing large registry to compare rates of symptomatic intracranial hemorrhage in patients treated with either of these drugs. The registry includes data collected July 2018 to June 2021 from various hospitals and programs in New Zealand, Australia, and the U.S.
Symptomatic intracranial hemorrhage was defined as a severe bleed causing pressure on the brain, extensive swelling, and worsening by at least four points on the National Institutes of Health Stroke Scale (NIHSS).
Researchers abstracted data from the various registries. As not all centers record data in the same format, statisticians then “cleaned” or harmonized the data to make it more standardized, said Dr. Warach.
They controlled for factors known to put a patient at higher risk for symptomatic hemorrhage, including age, sex, baseline NIHSS, and time to treatment.
Dr. Warach noted that at baseline, the tenecteplase group had higher values on most of these factors “that would predict intracranial hemorrhage.”
In an earlier analysis of 7,891 patients, the tenecteplase group was older (73 vs. 70 years; P < .001), less likely to be female (44.1% vs. 48.7%; P = .001), and had higher NIHSS scores (9 vs. 7; P < .001).
Also, a greater percentage of those in the tenecteplase group underwent mechanical thrombectomy (36.7% vs. 18.0%; P < .001). Dr. Warach explained that some centers would opt for tenecteplase if they knew the patient was a candidate for thrombectomy “because that was where the data was clearly strong and positive.”
An updated analysis included 9,238 patients – 7,313 who received alteplase and 1,925 tenecteplase. In the updated unadjusted analysis, the symptomatic intracranial hemorrhage rate was 3.6% for alteplase and 1.8% for tenecteplase (odds ratio, 0.49; P < .001). The adjusted OR was 0.42 (P < .001.)
The difference was even greater in those who underwent thrombectomy. For patients undergoing this procedure after a thrombolytic, the symptomatic intracranial hemorrhage rate was 5.9% for alteplase and 2.4% for tenecteplase.
“That even in those higher-risk patients we’re seeing an even greater difference is promising,” said Dr. Warach.
He and his colleagues plan to assess other potential benefits of tenecteplase, for example, the time it takes for patients to recover, “once we have all the data standardized and cleaned.”
Results of three large phase 3 trials comparing the two thrombolytics are expected within the next year or two, said Dr. Warach.
Joseph Broderick, MD, professor and director of the UC Gardner Neuroscience Institute, director of the National Coordinating Center for NIH’s StrokeNet, and professor of medicine at the University of Cincinnati College of Medicine, Cincinnati, stressed that for both drugs, speed is of the utmost importance to protect the brain.
“No matter which of these drugs is going to be used, the key thing is that they have to be used as quickly as possible,” he said.
Also important is imaging the brain before administering either of these medications to ensure the issue is an ischemic stroke and not an intracerebral hemorrhage, said Dr. Broderick. “If you have a broken blood vessel, you want to seal the leak, not break up the clot and make the bleeding worse.”
Dr. Warach receives payment as chair of the safety committee of another Genentech study comparing tenecteplase versus placebo in patients with large vessel occlusion whose stroke began more than 4.5 hours before treatment.
A version of this article first appeared on Medscape.com.
preliminary results from a large, multicenter registry study suggest.
“In clinical practice where centers are using tenecteplase, we’re seeing that the rate of symptomatic hemorrhage after getting a thrombolytic is half that with tenecteplase than with alteplase,” said lead author Steven J. Warach, MD, PhD, professor of neurology at Dell Medical School, University of Texas, Austin.
“For clinicians who have switched or are considering switching to tenecteplase, I think these results are very reassuring,” he said at the International Stroke Conference, presented by the American Stroke Association, a division of the American Heart Association.
Tenecteplase is a relatively new agent that is approved by the U.S. Food and Drug Administration to treat myocardial infarction but not ischemic stroke, although clinicians sometimes use it off-label for this purpose. American Heart Association guidelines recommend tenecteplase might be reasonable to consider for ischemic stroke in select patients.
The current standard of care for stroke is alteplase, which has been approved for this indication since 1996.
Five randomized clinical trials comparing the two thrombolytics weren’t large enough to make definitive conclusions about differences, said Dr. Warach. “The event rate for serious bleeding into the brain was thankfully low in both groups.”
Results from a meta-analysis that combined data from those five trials were also not definitive. “Numerically, it looked like the rate was lower for tenecteplase, but the sample size was just too low to make any statistically confident statement.”
However, tenecteplase has practical advantages over alteplase. Tenecteplase is a single bolus injection lasting 5 seconds while alteplase is administered by injection followed by an hour-long infusion.
Given these potential advantages, some centers have changed their practice and started using the newer drug beginning in July 2018.
The current study used an ongoing large registry to compare rates of symptomatic intracranial hemorrhage in patients treated with either of these drugs. The registry includes data collected July 2018 to June 2021 from various hospitals and programs in New Zealand, Australia, and the U.S.
Symptomatic intracranial hemorrhage was defined as a severe bleed causing pressure on the brain, extensive swelling, and worsening by at least four points on the National Institutes of Health Stroke Scale (NIHSS).
Researchers abstracted data from the various registries. As not all centers record data in the same format, statisticians then “cleaned” or harmonized the data to make it more standardized, said Dr. Warach.
They controlled for factors known to put a patient at higher risk for symptomatic hemorrhage, including age, sex, baseline NIHSS, and time to treatment.
Dr. Warach noted that at baseline, the tenecteplase group had higher values on most of these factors “that would predict intracranial hemorrhage.”
In an earlier analysis of 7,891 patients, the tenecteplase group was older (73 vs. 70 years; P < .001), less likely to be female (44.1% vs. 48.7%; P = .001), and had higher NIHSS scores (9 vs. 7; P < .001).
Also, a greater percentage of those in the tenecteplase group underwent mechanical thrombectomy (36.7% vs. 18.0%; P < .001). Dr. Warach explained that some centers would opt for tenecteplase if they knew the patient was a candidate for thrombectomy “because that was where the data was clearly strong and positive.”
An updated analysis included 9,238 patients – 7,313 who received alteplase and 1,925 tenecteplase. In the updated unadjusted analysis, the symptomatic intracranial hemorrhage rate was 3.6% for alteplase and 1.8% for tenecteplase (odds ratio, 0.49; P < .001). The adjusted OR was 0.42 (P < .001.)
The difference was even greater in those who underwent thrombectomy. For patients undergoing this procedure after a thrombolytic, the symptomatic intracranial hemorrhage rate was 5.9% for alteplase and 2.4% for tenecteplase.
“That even in those higher-risk patients we’re seeing an even greater difference is promising,” said Dr. Warach.
He and his colleagues plan to assess other potential benefits of tenecteplase, for example, the time it takes for patients to recover, “once we have all the data standardized and cleaned.”
Results of three large phase 3 trials comparing the two thrombolytics are expected within the next year or two, said Dr. Warach.
Joseph Broderick, MD, professor and director of the UC Gardner Neuroscience Institute, director of the National Coordinating Center for NIH’s StrokeNet, and professor of medicine at the University of Cincinnati College of Medicine, Cincinnati, stressed that for both drugs, speed is of the utmost importance to protect the brain.
“No matter which of these drugs is going to be used, the key thing is that they have to be used as quickly as possible,” he said.
Also important is imaging the brain before administering either of these medications to ensure the issue is an ischemic stroke and not an intracerebral hemorrhage, said Dr. Broderick. “If you have a broken blood vessel, you want to seal the leak, not break up the clot and make the bleeding worse.”
Dr. Warach receives payment as chair of the safety committee of another Genentech study comparing tenecteplase versus placebo in patients with large vessel occlusion whose stroke began more than 4.5 hours before treatment.
A version of this article first appeared on Medscape.com.
FROM ISC 2022