User login
Assisting Surgeons with Management: Initial Presentation of Abnormal Bleeding and Diagnosing of Fibroids

As an Advanced Practice Provider, when and why might a patient with uterine fibroids be scheduled to visit with you?
Ms. Haibach: Typically, with the flow of how our practice runs, a patient would schedule with me as an initial visit to explore their abnormal or heavy bleeding. Oftentimes, a patient is unsure with what they have going on medically and will view APPs as a safe place to start. Other times, I will see a patient for a general wellness exam who will mention heavier menses over the years or just a change in their bleeding pattern-- longer flow, things like that.
It may stem from something that seems out of the ordinary for them or a symptom impacting their life. For example, if a patient says, “I have to run home and change my clothes,” or “I'm bleeding through my bed sheets.” Those statements prompt further evaluation. At times, patients who have already been diagnosed with fibroids, will come to see me if they have chosen medical management over surgical management of their fibroids. They continue to follow up with me to reevaluate the success of their treatment plan periodically. So, whether I start them on a plan, or a physician does, they can follow up with me to revisit their medical plan and ensure it remains appropriate.
You touched on this a bit, but can you dive deeper into exactly what you are looking for as part of that visit?
Ms. Haibach: Definitely. With an initial consult to me, the number one question that I would ask my patients first is, what is your most bothersome symptom? With this question, I'm looking to determine: is it pain that brought you to me? Is it heavy bleeding? Do you feel bulk and bloaty? Are you having issues getting pregnant? Do you have bowel or bladder issues?
The information I get from that one initial question, helps guide the remainder of my visit. If bleeding is the main concern, we would focus on getting that under control. So, we need to suppress the menses with medication options. If bulk and bloating is the main concern, for instance the patient feels like they have a pregnant-looking abdomen, typically surgical options are warranted. If the main complaint is infertility, we do have fertility specialists in our practice who remove fibroids to aid patients in achieving pregnancy.
The most important purpose of this visit is to really listen to the patient to find out how these symptoms are impacting their daily lives. From there, I can use that information to guide my treatment plan.
So, once it is determined that the patient is a good surgical candidate, what would be the next steps?
Ms. Haibach: If at the end of my visit, I determine that a patient is potentially a suitable surgical candidate, the first thing I would do is order appropriate imaging. For example, if the patient is interested in uterine preservation for future fertility, she is likely going to opt for a laparoscopic myomectomy, where fibroids would be removed, and her uterus would be left in place. In that case, she would require an MRI for fibroid mapping. If a woman has completed childbearing, then oftentimes a pelvic ultrasound would suffice, at least to start, since she'd likely elect hysterectomy if she has reached her fertility goals.
I would also perform an endometrial biopsy to rule out malignant process before going into surgery. To optimize a patient for our MIGS surgeons, I gather a thorough medical history to ensure their comorbidities are appropriately managed. For example, diabetes is under control, sleep apnea is being treated, no active infections. If there is anything else going on that needs to be addressed, I'd refer them to the appropriate provider first.
Once I have acceptable imaging, a negative endometrial biopsy and an adequate medical history, I would then assist the patient in scheduling with one of the surgeons on my team for a consult and physical exam to determine surgery planning. Once they see our physician, a surgery date is booked. The patient would come back to see me within 30 days of surgery, and we would do a preoperative education appointment. I see them again 2 weeks after surgery for a post-op visit. We’d perform the post-of visit virtually in our practice. We would see the patient sooner if there are any other concerns that arise post-operatively.
What if the patient is not a surgical candidate? How do you as an APP assist in ongoing medical management?
Ms. Haibach: The presence of fibroids alone, without symptoms, often does not require surgical intervention. There are occasions where a patient is, for example, seen in the emergency room for abdominal pain, whereas they’ll get a CT scan of the abdomen pelvis, and a fibroid is incidentally found. At that point, they are instructed to see gynecology for follow-up. If the patient was unaware of the fibroid, has no symptoms and there's no concerning imaging features, then management with ongoing surveillance (repeat imaging and office follow up) and instructions on when to return is usually appropriate.
Depending on the symptoms, medical management typically includes hormonal suppression of menses in the form of a birth control pill or an IUD. If bleeding is the main concern, it is my goal to at least slow her bleeding, if not try to stop it. Not all women are good candidates for hormone therapy, so there is a medication option that is non-hormonal. In my role, I would start a medication plan for a patient and initiate a new medication such as hormonal suppression in the form of birth control, IUD, non-hormonal medications etc.
Typically, when I do that, I'll have the patient follow up with me in about two to three months to reassess the medication’s effectiveness. The goal of the reassessment is to determine if it is working for her life, to be sure there are no major side-effects, and just to make sure she is amenable to the plan. As part of the medical management, sometimes it is necessary to monitor blood counts for anemia to be certain that medical management is still appropriate for her.
From your experience in practicing, are you more likely to be visited by one age bracket or ethnicity over another?
Ms. Haibach: Actually, data tells us that most fibroids occur in women of reproductive age. They are also diagnosed in African American women two to three times more frequently than in white women. Fibroids are infrequently seen in premenstrual women. A relief of symptoms of the fibroids often occurs at the time of menopause, when the menstrual cyclicity seizes and steroid hormone levels decrease. My demographic is consistent with the above statistics. I tend to see women within the ages of 20’s-50’s and more often African Americans.
Was there anything else that you'd like to mention?
Ms. Haibach: Abnormal bleeding can be very stressful for women. APPs are a great place to start an abnormal bleeding or fibroid work-up. Patients should rest assure that although we cannot perform surgery, APPs can help get them in the right direction for the best care possible.
US Department of Health and Human Services, Office on Women’s Health. Uterine fibroids. (https://www.womenshealth.gov/a-z-topics/uterine-fibroids) Accessed 1/26/2022.
The American College of Obstetricians and Gynecologists. Uterine Fibroids. (https://www.acog.org/patient-resources/faqs/gynecologic-problems/uterine-fibroids) Accessed 1/26/2022.
As an Advanced Practice Provider, when and why might a patient with uterine fibroids be scheduled to visit with you?
Ms. Haibach: Typically, with the flow of how our practice runs, a patient would schedule with me as an initial visit to explore their abnormal or heavy bleeding. Oftentimes, a patient is unsure with what they have going on medically and will view APPs as a safe place to start. Other times, I will see a patient for a general wellness exam who will mention heavier menses over the years or just a change in their bleeding pattern-- longer flow, things like that.
It may stem from something that seems out of the ordinary for them or a symptom impacting their life. For example, if a patient says, “I have to run home and change my clothes,” or “I'm bleeding through my bed sheets.” Those statements prompt further evaluation. At times, patients who have already been diagnosed with fibroids, will come to see me if they have chosen medical management over surgical management of their fibroids. They continue to follow up with me to reevaluate the success of their treatment plan periodically. So, whether I start them on a plan, or a physician does, they can follow up with me to revisit their medical plan and ensure it remains appropriate.
You touched on this a bit, but can you dive deeper into exactly what you are looking for as part of that visit?
Ms. Haibach: Definitely. With an initial consult to me, the number one question that I would ask my patients first is, what is your most bothersome symptom? With this question, I'm looking to determine: is it pain that brought you to me? Is it heavy bleeding? Do you feel bulk and bloaty? Are you having issues getting pregnant? Do you have bowel or bladder issues?
The information I get from that one initial question, helps guide the remainder of my visit. If bleeding is the main concern, we would focus on getting that under control. So, we need to suppress the menses with medication options. If bulk and bloating is the main concern, for instance the patient feels like they have a pregnant-looking abdomen, typically surgical options are warranted. If the main complaint is infertility, we do have fertility specialists in our practice who remove fibroids to aid patients in achieving pregnancy.
The most important purpose of this visit is to really listen to the patient to find out how these symptoms are impacting their daily lives. From there, I can use that information to guide my treatment plan.
So, once it is determined that the patient is a good surgical candidate, what would be the next steps?
Ms. Haibach: If at the end of my visit, I determine that a patient is potentially a suitable surgical candidate, the first thing I would do is order appropriate imaging. For example, if the patient is interested in uterine preservation for future fertility, she is likely going to opt for a laparoscopic myomectomy, where fibroids would be removed, and her uterus would be left in place. In that case, she would require an MRI for fibroid mapping. If a woman has completed childbearing, then oftentimes a pelvic ultrasound would suffice, at least to start, since she'd likely elect hysterectomy if she has reached her fertility goals.
I would also perform an endometrial biopsy to rule out malignant process before going into surgery. To optimize a patient for our MIGS surgeons, I gather a thorough medical history to ensure their comorbidities are appropriately managed. For example, diabetes is under control, sleep apnea is being treated, no active infections. If there is anything else going on that needs to be addressed, I'd refer them to the appropriate provider first.
Once I have acceptable imaging, a negative endometrial biopsy and an adequate medical history, I would then assist the patient in scheduling with one of the surgeons on my team for a consult and physical exam to determine surgery planning. Once they see our physician, a surgery date is booked. The patient would come back to see me within 30 days of surgery, and we would do a preoperative education appointment. I see them again 2 weeks after surgery for a post-op visit. We’d perform the post-of visit virtually in our practice. We would see the patient sooner if there are any other concerns that arise post-operatively.
What if the patient is not a surgical candidate? How do you as an APP assist in ongoing medical management?
Ms. Haibach: The presence of fibroids alone, without symptoms, often does not require surgical intervention. There are occasions where a patient is, for example, seen in the emergency room for abdominal pain, whereas they’ll get a CT scan of the abdomen pelvis, and a fibroid is incidentally found. At that point, they are instructed to see gynecology for follow-up. If the patient was unaware of the fibroid, has no symptoms and there's no concerning imaging features, then management with ongoing surveillance (repeat imaging and office follow up) and instructions on when to return is usually appropriate.
Depending on the symptoms, medical management typically includes hormonal suppression of menses in the form of a birth control pill or an IUD. If bleeding is the main concern, it is my goal to at least slow her bleeding, if not try to stop it. Not all women are good candidates for hormone therapy, so there is a medication option that is non-hormonal. In my role, I would start a medication plan for a patient and initiate a new medication such as hormonal suppression in the form of birth control, IUD, non-hormonal medications etc.
Typically, when I do that, I'll have the patient follow up with me in about two to three months to reassess the medication’s effectiveness. The goal of the reassessment is to determine if it is working for her life, to be sure there are no major side-effects, and just to make sure she is amenable to the plan. As part of the medical management, sometimes it is necessary to monitor blood counts for anemia to be certain that medical management is still appropriate for her.
From your experience in practicing, are you more likely to be visited by one age bracket or ethnicity over another?
Ms. Haibach: Actually, data tells us that most fibroids occur in women of reproductive age. They are also diagnosed in African American women two to three times more frequently than in white women. Fibroids are infrequently seen in premenstrual women. A relief of symptoms of the fibroids often occurs at the time of menopause, when the menstrual cyclicity seizes and steroid hormone levels decrease. My demographic is consistent with the above statistics. I tend to see women within the ages of 20’s-50’s and more often African Americans.
Was there anything else that you'd like to mention?
Ms. Haibach: Abnormal bleeding can be very stressful for women. APPs are a great place to start an abnormal bleeding or fibroid work-up. Patients should rest assure that although we cannot perform surgery, APPs can help get them in the right direction for the best care possible.
As an Advanced Practice Provider, when and why might a patient with uterine fibroids be scheduled to visit with you?
Ms. Haibach: Typically, with the flow of how our practice runs, a patient would schedule with me as an initial visit to explore their abnormal or heavy bleeding. Oftentimes, a patient is unsure with what they have going on medically and will view APPs as a safe place to start. Other times, I will see a patient for a general wellness exam who will mention heavier menses over the years or just a change in their bleeding pattern-- longer flow, things like that.
It may stem from something that seems out of the ordinary for them or a symptom impacting their life. For example, if a patient says, “I have to run home and change my clothes,” or “I'm bleeding through my bed sheets.” Those statements prompt further evaluation. At times, patients who have already been diagnosed with fibroids, will come to see me if they have chosen medical management over surgical management of their fibroids. They continue to follow up with me to reevaluate the success of their treatment plan periodically. So, whether I start them on a plan, or a physician does, they can follow up with me to revisit their medical plan and ensure it remains appropriate.
You touched on this a bit, but can you dive deeper into exactly what you are looking for as part of that visit?
Ms. Haibach: Definitely. With an initial consult to me, the number one question that I would ask my patients first is, what is your most bothersome symptom? With this question, I'm looking to determine: is it pain that brought you to me? Is it heavy bleeding? Do you feel bulk and bloaty? Are you having issues getting pregnant? Do you have bowel or bladder issues?
The information I get from that one initial question, helps guide the remainder of my visit. If bleeding is the main concern, we would focus on getting that under control. So, we need to suppress the menses with medication options. If bulk and bloating is the main concern, for instance the patient feels like they have a pregnant-looking abdomen, typically surgical options are warranted. If the main complaint is infertility, we do have fertility specialists in our practice who remove fibroids to aid patients in achieving pregnancy.
The most important purpose of this visit is to really listen to the patient to find out how these symptoms are impacting their daily lives. From there, I can use that information to guide my treatment plan.
So, once it is determined that the patient is a good surgical candidate, what would be the next steps?
Ms. Haibach: If at the end of my visit, I determine that a patient is potentially a suitable surgical candidate, the first thing I would do is order appropriate imaging. For example, if the patient is interested in uterine preservation for future fertility, she is likely going to opt for a laparoscopic myomectomy, where fibroids would be removed, and her uterus would be left in place. In that case, she would require an MRI for fibroid mapping. If a woman has completed childbearing, then oftentimes a pelvic ultrasound would suffice, at least to start, since she'd likely elect hysterectomy if she has reached her fertility goals.
I would also perform an endometrial biopsy to rule out malignant process before going into surgery. To optimize a patient for our MIGS surgeons, I gather a thorough medical history to ensure their comorbidities are appropriately managed. For example, diabetes is under control, sleep apnea is being treated, no active infections. If there is anything else going on that needs to be addressed, I'd refer them to the appropriate provider first.
Once I have acceptable imaging, a negative endometrial biopsy and an adequate medical history, I would then assist the patient in scheduling with one of the surgeons on my team for a consult and physical exam to determine surgery planning. Once they see our physician, a surgery date is booked. The patient would come back to see me within 30 days of surgery, and we would do a preoperative education appointment. I see them again 2 weeks after surgery for a post-op visit. We’d perform the post-of visit virtually in our practice. We would see the patient sooner if there are any other concerns that arise post-operatively.
What if the patient is not a surgical candidate? How do you as an APP assist in ongoing medical management?
Ms. Haibach: The presence of fibroids alone, without symptoms, often does not require surgical intervention. There are occasions where a patient is, for example, seen in the emergency room for abdominal pain, whereas they’ll get a CT scan of the abdomen pelvis, and a fibroid is incidentally found. At that point, they are instructed to see gynecology for follow-up. If the patient was unaware of the fibroid, has no symptoms and there's no concerning imaging features, then management with ongoing surveillance (repeat imaging and office follow up) and instructions on when to return is usually appropriate.
Depending on the symptoms, medical management typically includes hormonal suppression of menses in the form of a birth control pill or an IUD. If bleeding is the main concern, it is my goal to at least slow her bleeding, if not try to stop it. Not all women are good candidates for hormone therapy, so there is a medication option that is non-hormonal. In my role, I would start a medication plan for a patient and initiate a new medication such as hormonal suppression in the form of birth control, IUD, non-hormonal medications etc.
Typically, when I do that, I'll have the patient follow up with me in about two to three months to reassess the medication’s effectiveness. The goal of the reassessment is to determine if it is working for her life, to be sure there are no major side-effects, and just to make sure she is amenable to the plan. As part of the medical management, sometimes it is necessary to monitor blood counts for anemia to be certain that medical management is still appropriate for her.
From your experience in practicing, are you more likely to be visited by one age bracket or ethnicity over another?
Ms. Haibach: Actually, data tells us that most fibroids occur in women of reproductive age. They are also diagnosed in African American women two to three times more frequently than in white women. Fibroids are infrequently seen in premenstrual women. A relief of symptoms of the fibroids often occurs at the time of menopause, when the menstrual cyclicity seizes and steroid hormone levels decrease. My demographic is consistent with the above statistics. I tend to see women within the ages of 20’s-50’s and more often African Americans.
Was there anything else that you'd like to mention?
Ms. Haibach: Abnormal bleeding can be very stressful for women. APPs are a great place to start an abnormal bleeding or fibroid work-up. Patients should rest assure that although we cannot perform surgery, APPs can help get them in the right direction for the best care possible.
US Department of Health and Human Services, Office on Women’s Health. Uterine fibroids. (https://www.womenshealth.gov/a-z-topics/uterine-fibroids) Accessed 1/26/2022.
The American College of Obstetricians and Gynecologists. Uterine Fibroids. (https://www.acog.org/patient-resources/faqs/gynecologic-problems/uterine-fibroids) Accessed 1/26/2022.
US Department of Health and Human Services, Office on Women’s Health. Uterine fibroids. (https://www.womenshealth.gov/a-z-topics/uterine-fibroids) Accessed 1/26/2022.
The American College of Obstetricians and Gynecologists. Uterine Fibroids. (https://www.acog.org/patient-resources/faqs/gynecologic-problems/uterine-fibroids) Accessed 1/26/2022.
Federal Practitioner 2022 Directory
- 4 Explanatory Notes and Abbreviation Key
- 9 Veterans Integrated Service Network (VISN) Guide
- 14 Department of Veterans Affairs Health Care Facilities
- 118 Centers of Excellence
- 135 TRICARE Region Guide
- 146 Department of Defense Health Care Facilities
- 4 Explanatory Notes and Abbreviation Key
- 9 Veterans Integrated Service Network (VISN) Guide
- 14 Department of Veterans Affairs Health Care Facilities
- 118 Centers of Excellence
- 135 TRICARE Region Guide
- 146 Department of Defense Health Care Facilities
- 4 Explanatory Notes and Abbreviation Key
- 9 Veterans Integrated Service Network (VISN) Guide
- 14 Department of Veterans Affairs Health Care Facilities
- 118 Centers of Excellence
- 135 TRICARE Region Guide
- 146 Department of Defense Health Care Facilities
Fewer diabetes complications with NOACs in patients with AFib
The new research, which was published in Annals of Internal Medicine, found that taking non–vitamin K oral anticoagulants was associated with reduced diabetes complications and lower mortality vs. taking warfarin in the group examined.
In their paper, the researchers present the outcomes of a retrospective cohort study involving 30,209 patients with atrial fibrillation and diabetes. Of these, 19,909 were treated with non–vitamin K oral anticoagulants (NOACs) – dabigatran, rivaroxaban, apixaban, or edoxaban – and 10,300 were treated with warfarin.
Dr. Huei-Kai Huang from the Hualien (Taiwan) Tzu Chi Hospital and coauthors wrote that, while diabetes mellitus is an important risk factor for stroke, there’s not yet a good understanding of the effect of different oral anticoagulants on the risk for diabetes-related complications in patients with atrial fibrillation and diabetes.
“Recent evidence has suggested that NOAC and warfarin may have different effects on glycemic control through the vitamin K–related mechanisms,” coauthor Yu-Kang Tu, PhD, from the College of Public Health at the National Taiwan University in Taipei said in an interview. “It was therefore natural to further evaluate whether NOAC could help decrease various diabetes-related complications, compared with warfarin.”
Hazards with NOACS vs. warfarin
The researchers found that patients treated with NOACs had a 16% lower hazard of macrovascular complications – a composite of coronary artery disease, stroke, and peripheral vascular disease (95% confidence interval, 0.78-0.91; P < .001) – and a 21% lower hazard of microvascular complications including dialysis and lower-extremity amputations (95% CI, 0.73-0.85; P < .001).
NOAC therapy was also associated a 22% lower hazard of death (95% CI, 0.75-0.82; P < .001) and a 9% lower hazard for glycemic emergency (95% CI, 0.83-0.99; P = .043), which the authors defined as a composite of diabetic ketoacidosis, hyperosmolar hyperglycemic state, and hypoglycemia.
In particular, patients treated with NOACs showed significantly lower hazards for coronary artery disease, stroke, dialysis, amputation of lower extremities, and death from cardiovascular and noncardiovascular causes, compared with warfarin users.
The study also found that patients on higher volumes of NOAC medication had greater reductions in mortality and diabetes complications.
“Although our main findings can be explained by the potential differences in underlying mechanisms of action between NOAC and warfarin, we were still surprised with the significantly lower risks of retinopathy, neuropathy, and hypoglycemia in patients taking NOAC with high medication possession ratio,” Dr. Tu said.
Study provides more diabetes-specific outcomes data
Commenting on the findings, Dr. Peter Rossing, head of complications research at the Steno Diabetes Center in Copenhagen said there has long been discussion about whether the newer and more expensive NOACs offer greater benefits to patient with diabetes – beyond stroke prevention – compared with the older and cheaper warfarin. As such, this study was important in providing more diabetes-specific outcomes data and in a large population.
“The effect size they find is certainly meaningful and relevant and should support decision-making,” Dr. Rossing noted in an interview. The finding of reduced risk of amputation and mortality “fits in line with theory that maybe if you block vitamin K, you get calcification, you get vascular damage that leads to failure of the kidney and leads to limb amputations, and that is potentially prevented or not developed when you give the NOACs.”
Dr. John Camm, professor of clinical cardiology at St George’s University of London, said the findings of the benefits of NOACs in this patient group ,were confirmation of earlier, smaller studies, and were important not just for patients with atrial fibrillation and diabetes, but also those prone to diabetes.
“We know from previous studies from the same database, and also from Korea, [for example], that patients who are treated with NOACs as opposed to warfarin develop less diabetes,” he explained.
Dr. Camm said many guidelines around the world now suggest NOACs, and, in some cases, even advise against using vitamin K antagonists as a first option, except in certain situations, such as when patients have rheumatic heart disease, mild to moderate mitral stenosis in rheumatic disease, or prosthetic heart valves.
The researchers applied two methods to account for covariates that may have influenced whether patients received one class of treatment or the other. These achieved ‘appropriate balance’ of baseline characteristics such as comorbidities and baseline medication use for diabetes and other conditions, Dr. Tu and colleagues wrote.
The benefits of NOACs were less evident in younger patients, and the reductions in mortality and diabetes complications associated with NOACs did not reach statistical significance in those aged under 65 years. Regarding this, Dr. Camm noted that there was a debate as to whether patients under 65 years with atrial fibrillation and diabetes should be put on an anticoagulant.
The study was funded by Hualien Tzu Chi Hospital. No conflicts of interest were declared.
The new research, which was published in Annals of Internal Medicine, found that taking non–vitamin K oral anticoagulants was associated with reduced diabetes complications and lower mortality vs. taking warfarin in the group examined.
In their paper, the researchers present the outcomes of a retrospective cohort study involving 30,209 patients with atrial fibrillation and diabetes. Of these, 19,909 were treated with non–vitamin K oral anticoagulants (NOACs) – dabigatran, rivaroxaban, apixaban, or edoxaban – and 10,300 were treated with warfarin.
Dr. Huei-Kai Huang from the Hualien (Taiwan) Tzu Chi Hospital and coauthors wrote that, while diabetes mellitus is an important risk factor for stroke, there’s not yet a good understanding of the effect of different oral anticoagulants on the risk for diabetes-related complications in patients with atrial fibrillation and diabetes.
“Recent evidence has suggested that NOAC and warfarin may have different effects on glycemic control through the vitamin K–related mechanisms,” coauthor Yu-Kang Tu, PhD, from the College of Public Health at the National Taiwan University in Taipei said in an interview. “It was therefore natural to further evaluate whether NOAC could help decrease various diabetes-related complications, compared with warfarin.”
Hazards with NOACS vs. warfarin
The researchers found that patients treated with NOACs had a 16% lower hazard of macrovascular complications – a composite of coronary artery disease, stroke, and peripheral vascular disease (95% confidence interval, 0.78-0.91; P < .001) – and a 21% lower hazard of microvascular complications including dialysis and lower-extremity amputations (95% CI, 0.73-0.85; P < .001).
NOAC therapy was also associated a 22% lower hazard of death (95% CI, 0.75-0.82; P < .001) and a 9% lower hazard for glycemic emergency (95% CI, 0.83-0.99; P = .043), which the authors defined as a composite of diabetic ketoacidosis, hyperosmolar hyperglycemic state, and hypoglycemia.
In particular, patients treated with NOACs showed significantly lower hazards for coronary artery disease, stroke, dialysis, amputation of lower extremities, and death from cardiovascular and noncardiovascular causes, compared with warfarin users.
The study also found that patients on higher volumes of NOAC medication had greater reductions in mortality and diabetes complications.
“Although our main findings can be explained by the potential differences in underlying mechanisms of action between NOAC and warfarin, we were still surprised with the significantly lower risks of retinopathy, neuropathy, and hypoglycemia in patients taking NOAC with high medication possession ratio,” Dr. Tu said.
Study provides more diabetes-specific outcomes data
Commenting on the findings, Dr. Peter Rossing, head of complications research at the Steno Diabetes Center in Copenhagen said there has long been discussion about whether the newer and more expensive NOACs offer greater benefits to patient with diabetes – beyond stroke prevention – compared with the older and cheaper warfarin. As such, this study was important in providing more diabetes-specific outcomes data and in a large population.
“The effect size they find is certainly meaningful and relevant and should support decision-making,” Dr. Rossing noted in an interview. The finding of reduced risk of amputation and mortality “fits in line with theory that maybe if you block vitamin K, you get calcification, you get vascular damage that leads to failure of the kidney and leads to limb amputations, and that is potentially prevented or not developed when you give the NOACs.”
Dr. John Camm, professor of clinical cardiology at St George’s University of London, said the findings of the benefits of NOACs in this patient group ,were confirmation of earlier, smaller studies, and were important not just for patients with atrial fibrillation and diabetes, but also those prone to diabetes.
“We know from previous studies from the same database, and also from Korea, [for example], that patients who are treated with NOACs as opposed to warfarin develop less diabetes,” he explained.
Dr. Camm said many guidelines around the world now suggest NOACs, and, in some cases, even advise against using vitamin K antagonists as a first option, except in certain situations, such as when patients have rheumatic heart disease, mild to moderate mitral stenosis in rheumatic disease, or prosthetic heart valves.
The researchers applied two methods to account for covariates that may have influenced whether patients received one class of treatment or the other. These achieved ‘appropriate balance’ of baseline characteristics such as comorbidities and baseline medication use for diabetes and other conditions, Dr. Tu and colleagues wrote.
The benefits of NOACs were less evident in younger patients, and the reductions in mortality and diabetes complications associated with NOACs did not reach statistical significance in those aged under 65 years. Regarding this, Dr. Camm noted that there was a debate as to whether patients under 65 years with atrial fibrillation and diabetes should be put on an anticoagulant.
The study was funded by Hualien Tzu Chi Hospital. No conflicts of interest were declared.
The new research, which was published in Annals of Internal Medicine, found that taking non–vitamin K oral anticoagulants was associated with reduced diabetes complications and lower mortality vs. taking warfarin in the group examined.
In their paper, the researchers present the outcomes of a retrospective cohort study involving 30,209 patients with atrial fibrillation and diabetes. Of these, 19,909 were treated with non–vitamin K oral anticoagulants (NOACs) – dabigatran, rivaroxaban, apixaban, or edoxaban – and 10,300 were treated with warfarin.
Dr. Huei-Kai Huang from the Hualien (Taiwan) Tzu Chi Hospital and coauthors wrote that, while diabetes mellitus is an important risk factor for stroke, there’s not yet a good understanding of the effect of different oral anticoagulants on the risk for diabetes-related complications in patients with atrial fibrillation and diabetes.
“Recent evidence has suggested that NOAC and warfarin may have different effects on glycemic control through the vitamin K–related mechanisms,” coauthor Yu-Kang Tu, PhD, from the College of Public Health at the National Taiwan University in Taipei said in an interview. “It was therefore natural to further evaluate whether NOAC could help decrease various diabetes-related complications, compared with warfarin.”
Hazards with NOACS vs. warfarin
The researchers found that patients treated with NOACs had a 16% lower hazard of macrovascular complications – a composite of coronary artery disease, stroke, and peripheral vascular disease (95% confidence interval, 0.78-0.91; P < .001) – and a 21% lower hazard of microvascular complications including dialysis and lower-extremity amputations (95% CI, 0.73-0.85; P < .001).
NOAC therapy was also associated a 22% lower hazard of death (95% CI, 0.75-0.82; P < .001) and a 9% lower hazard for glycemic emergency (95% CI, 0.83-0.99; P = .043), which the authors defined as a composite of diabetic ketoacidosis, hyperosmolar hyperglycemic state, and hypoglycemia.
In particular, patients treated with NOACs showed significantly lower hazards for coronary artery disease, stroke, dialysis, amputation of lower extremities, and death from cardiovascular and noncardiovascular causes, compared with warfarin users.
The study also found that patients on higher volumes of NOAC medication had greater reductions in mortality and diabetes complications.
“Although our main findings can be explained by the potential differences in underlying mechanisms of action between NOAC and warfarin, we were still surprised with the significantly lower risks of retinopathy, neuropathy, and hypoglycemia in patients taking NOAC with high medication possession ratio,” Dr. Tu said.
Study provides more diabetes-specific outcomes data
Commenting on the findings, Dr. Peter Rossing, head of complications research at the Steno Diabetes Center in Copenhagen said there has long been discussion about whether the newer and more expensive NOACs offer greater benefits to patient with diabetes – beyond stroke prevention – compared with the older and cheaper warfarin. As such, this study was important in providing more diabetes-specific outcomes data and in a large population.
“The effect size they find is certainly meaningful and relevant and should support decision-making,” Dr. Rossing noted in an interview. The finding of reduced risk of amputation and mortality “fits in line with theory that maybe if you block vitamin K, you get calcification, you get vascular damage that leads to failure of the kidney and leads to limb amputations, and that is potentially prevented or not developed when you give the NOACs.”
Dr. John Camm, professor of clinical cardiology at St George’s University of London, said the findings of the benefits of NOACs in this patient group ,were confirmation of earlier, smaller studies, and were important not just for patients with atrial fibrillation and diabetes, but also those prone to diabetes.
“We know from previous studies from the same database, and also from Korea, [for example], that patients who are treated with NOACs as opposed to warfarin develop less diabetes,” he explained.
Dr. Camm said many guidelines around the world now suggest NOACs, and, in some cases, even advise against using vitamin K antagonists as a first option, except in certain situations, such as when patients have rheumatic heart disease, mild to moderate mitral stenosis in rheumatic disease, or prosthetic heart valves.
The researchers applied two methods to account for covariates that may have influenced whether patients received one class of treatment or the other. These achieved ‘appropriate balance’ of baseline characteristics such as comorbidities and baseline medication use for diabetes and other conditions, Dr. Tu and colleagues wrote.
The benefits of NOACs were less evident in younger patients, and the reductions in mortality and diabetes complications associated with NOACs did not reach statistical significance in those aged under 65 years. Regarding this, Dr. Camm noted that there was a debate as to whether patients under 65 years with atrial fibrillation and diabetes should be put on an anticoagulant.
The study was funded by Hualien Tzu Chi Hospital. No conflicts of interest were declared.
FROM ANNALS OF INTERNAL MEDICINE
Early-onset severe COPD: Similar physical symptoms, but higher depression rates
Younger and older patients with severe chronic obstructive pulmonary disease have similar pulmonary and physical health limitations, based on data from 1,058 adults.
Although chronic obstructive pulmonary disease (COPD) generally appears in older patients, the prevalence among adults aged 45-55 years was 6.5% in 2014-2015, wrote Rosanne J.H.C.G. Beijers, PhD, of Maastricht (the Netherlands) University Medical Center, and colleagues. However, data on the early-onset COPD phenotype are limited. In particular, the extent to which younger patients with early-onset severe COPD experienced the same physical and mental health problems as older patients with similar degree of airflow limitation has not been examined, they said.
In a study published in Clinical Nutrition, the researchers analyzed data from adults with COPD who were referred for pulmonary rehabilitation at a single center between July 2013 and August 2018. Severe disease was defined as FEV1< 50%, and early onset was defined as younger than 55 years. The mean age difference between older and younger patient groups was 15.8 years.
The study population included 79 individuals with early-onset severe disease, 54 with early-onset mild to moderate disease, 158 older adults with severe disease, and 103 older adults with mild to moderate disease. The researchers compared disease markers including body composition, physical performance, and mental health between the groups. A significantly greater proportion of the early-onset group were women, compared to the older group (64% vs. 44%).
In comparing early-onset and older patients with severe COPD, the researchers found that clinical characteristics were similar for body composition, skeletal muscle index, fat percentage, and bone mineral content, and for physical performance factors including the percent predicted maximal work capacity (Wmax), 6-minute walk test, and isokinetic strength. However, a higher prevalence of depression appeared in the early-onset severe-disease patients, compared with the older severe-disease patients (51.9% vs. 32.7%; P = .029).
Although the prevalence of depression was not based on a clinical diagnosis, this finding should prompt health care professionals to pay more attention to psychosocial and emotional well-being in early-onset severe COPD patients, the researchers noted.
In comparing early-onset severe-disease patients and early-onset patients with mild to moderate disease, patients with early-onset severe COPD had significantly lower exercise performance, based on a 6-minute walk test and percent predicted Wmax. However, body composition and isokinetic muscle strength were not significantly different between both early-onset groups.
The findings were limited by several factors including the relatively small number of early-onset patients and the lack of data on whether older patients were diagnosed with severe COPD at a younger age, and more research using age and lung function at the time of diagnosis is needed, the researchers noted. However, the results highlight the importance of early identification of patients at risk for early-onset severe COPD, they said. “Within these individuals at risk, special attention should also be paid to the development of extrapulmonary disease manifestations such as exercise limitations, impaired body composition, and psychological and emotional problems,” the researchers said. “Subsequently, intervention strategies need to be applied that not only focus on the regular advice of quitting smoking but also include decreasing the exposure to air pollutants and promoting a healthy lifestyle including physical activity and a healthy diet,” they added.
The study received no outside funding. Lead author Dr. Beijers had no financial conflicts to disclose.
Younger and older patients with severe chronic obstructive pulmonary disease have similar pulmonary and physical health limitations, based on data from 1,058 adults.
Although chronic obstructive pulmonary disease (COPD) generally appears in older patients, the prevalence among adults aged 45-55 years was 6.5% in 2014-2015, wrote Rosanne J.H.C.G. Beijers, PhD, of Maastricht (the Netherlands) University Medical Center, and colleagues. However, data on the early-onset COPD phenotype are limited. In particular, the extent to which younger patients with early-onset severe COPD experienced the same physical and mental health problems as older patients with similar degree of airflow limitation has not been examined, they said.
In a study published in Clinical Nutrition, the researchers analyzed data from adults with COPD who were referred for pulmonary rehabilitation at a single center between July 2013 and August 2018. Severe disease was defined as FEV1< 50%, and early onset was defined as younger than 55 years. The mean age difference between older and younger patient groups was 15.8 years.
The study population included 79 individuals with early-onset severe disease, 54 with early-onset mild to moderate disease, 158 older adults with severe disease, and 103 older adults with mild to moderate disease. The researchers compared disease markers including body composition, physical performance, and mental health between the groups. A significantly greater proportion of the early-onset group were women, compared to the older group (64% vs. 44%).
In comparing early-onset and older patients with severe COPD, the researchers found that clinical characteristics were similar for body composition, skeletal muscle index, fat percentage, and bone mineral content, and for physical performance factors including the percent predicted maximal work capacity (Wmax), 6-minute walk test, and isokinetic strength. However, a higher prevalence of depression appeared in the early-onset severe-disease patients, compared with the older severe-disease patients (51.9% vs. 32.7%; P = .029).
Although the prevalence of depression was not based on a clinical diagnosis, this finding should prompt health care professionals to pay more attention to psychosocial and emotional well-being in early-onset severe COPD patients, the researchers noted.
In comparing early-onset severe-disease patients and early-onset patients with mild to moderate disease, patients with early-onset severe COPD had significantly lower exercise performance, based on a 6-minute walk test and percent predicted Wmax. However, body composition and isokinetic muscle strength were not significantly different between both early-onset groups.
The findings were limited by several factors including the relatively small number of early-onset patients and the lack of data on whether older patients were diagnosed with severe COPD at a younger age, and more research using age and lung function at the time of diagnosis is needed, the researchers noted. However, the results highlight the importance of early identification of patients at risk for early-onset severe COPD, they said. “Within these individuals at risk, special attention should also be paid to the development of extrapulmonary disease manifestations such as exercise limitations, impaired body composition, and psychological and emotional problems,” the researchers said. “Subsequently, intervention strategies need to be applied that not only focus on the regular advice of quitting smoking but also include decreasing the exposure to air pollutants and promoting a healthy lifestyle including physical activity and a healthy diet,” they added.
The study received no outside funding. Lead author Dr. Beijers had no financial conflicts to disclose.
Younger and older patients with severe chronic obstructive pulmonary disease have similar pulmonary and physical health limitations, based on data from 1,058 adults.
Although chronic obstructive pulmonary disease (COPD) generally appears in older patients, the prevalence among adults aged 45-55 years was 6.5% in 2014-2015, wrote Rosanne J.H.C.G. Beijers, PhD, of Maastricht (the Netherlands) University Medical Center, and colleagues. However, data on the early-onset COPD phenotype are limited. In particular, the extent to which younger patients with early-onset severe COPD experienced the same physical and mental health problems as older patients with similar degree of airflow limitation has not been examined, they said.
In a study published in Clinical Nutrition, the researchers analyzed data from adults with COPD who were referred for pulmonary rehabilitation at a single center between July 2013 and August 2018. Severe disease was defined as FEV1< 50%, and early onset was defined as younger than 55 years. The mean age difference between older and younger patient groups was 15.8 years.
The study population included 79 individuals with early-onset severe disease, 54 with early-onset mild to moderate disease, 158 older adults with severe disease, and 103 older adults with mild to moderate disease. The researchers compared disease markers including body composition, physical performance, and mental health between the groups. A significantly greater proportion of the early-onset group were women, compared to the older group (64% vs. 44%).
In comparing early-onset and older patients with severe COPD, the researchers found that clinical characteristics were similar for body composition, skeletal muscle index, fat percentage, and bone mineral content, and for physical performance factors including the percent predicted maximal work capacity (Wmax), 6-minute walk test, and isokinetic strength. However, a higher prevalence of depression appeared in the early-onset severe-disease patients, compared with the older severe-disease patients (51.9% vs. 32.7%; P = .029).
Although the prevalence of depression was not based on a clinical diagnosis, this finding should prompt health care professionals to pay more attention to psychosocial and emotional well-being in early-onset severe COPD patients, the researchers noted.
In comparing early-onset severe-disease patients and early-onset patients with mild to moderate disease, patients with early-onset severe COPD had significantly lower exercise performance, based on a 6-minute walk test and percent predicted Wmax. However, body composition and isokinetic muscle strength were not significantly different between both early-onset groups.
The findings were limited by several factors including the relatively small number of early-onset patients and the lack of data on whether older patients were diagnosed with severe COPD at a younger age, and more research using age and lung function at the time of diagnosis is needed, the researchers noted. However, the results highlight the importance of early identification of patients at risk for early-onset severe COPD, they said. “Within these individuals at risk, special attention should also be paid to the development of extrapulmonary disease manifestations such as exercise limitations, impaired body composition, and psychological and emotional problems,” the researchers said. “Subsequently, intervention strategies need to be applied that not only focus on the regular advice of quitting smoking but also include decreasing the exposure to air pollutants and promoting a healthy lifestyle including physical activity and a healthy diet,” they added.
The study received no outside funding. Lead author Dr. Beijers had no financial conflicts to disclose.
FROM CLINICAL NUTRITION
Medical students help dispel kids’ fears with teddy bear clinics
In December 2021, 26 medical students at Florida State University (FSU) waltzed into the FSU Child Care and Early Learning Center loaded with armfuls of plushy, cute teddy bears. For the first time in several years, the Pediatric Interest Group opened the doors to their teddy bear clinic – an annual event that gives students an opportunity to practice their leadership skills while also helping to demystify trips to the doctor for the young participants.
At the clinic, children aged 2-4 emulate basic medical practices on their fuzzy patients under the guidance of the students.
Teddy bear clinics were started by FSU’s College of Medicine Family Medicine Interest Group in 2018, but it slowed to a halt until second-year medical student Taylor Posey approached the Pediatric Interest Group during her tenure as the group’s president about reinstating a similar program. At FSU, interest groups allow students who are not quite sure which field of medicine they’d like to pursue to gain experience in any they have interest in.
“Pediatrics is the reason I wanted to go to medical school,” Ms. Posey told this news organization. “So it was great that working on this project really solidified the thought that I did the right thing. It’s great to watch the volunteers and children interact together.”
The clinic divides the children into three groups: 2-year-old toddlers, 3-year-old “tweens,” and 4-year-old pre-K children.
The toddlers paint white handprints on black construction paper to “create” x-rays and learn about them. The tweens are given medical equipment such as paper stethoscopes, thermometers, Band Aids, cotton balls, and Q-Tips to put into their very own doctor bags, which are really just folders with the emblematic red plus sign sticker attached to the front. The Pre-K kids are tasked with giving their teddy bears medical exams under the watchful eye of the medical students. Together, they examine the teddy bear’s eyes, heart, and lungs.
“There’s growing research out there that says medical play – which can be defined as children playing as if they were the parents of the teddy bear, learning about a diagnosis, and treating it – decreases the anxiety in children when they go to visit a doctor. Having real medical equipment that the children can manipulate as opposed to plastic toys really makes a big difference,” Ms. Posey said.
One of Ms. Posey’s peers worked with her to create developmentally appropriate activities for the children. Ms. Posey said that some of the ideas for the clinic came from Pinterest boards.
“The planning of it worked really well. I was expecting things to fall through, but they didn’t,” Ms. Posey said. “It can be tough working with young children and trying to do activities with them so that you’re not doing too much but also not having too low of expectations.”
“It was really a massive success on all fronts,” said Mary P. Norton, MD, an assistant professor of pediatrics and faculty Pediatric Interest Group advisor for the clinic. “The ability to be in the community and get hands-on experience has been really cut down by the pandemic, and this allowed for our students to be able to go out in person and apply what they learned in the classroom with the age group they want to work with, which is fantastic.”
Perhaps the most impactful aspect of the clinic is its ability to help ease children’s fears about visits to the doctor. “We want to allow children to have a voice and give them a space to be a part of their treatment plan,” Dr. Norton said. “We want to say, ‘Your voice matters, you’re not a passive being,’ so that they’re a part of that relationship and show them that their experience is important. We hope these clinics aid in forming a partnership between parents, children, and doctors.”
Currently, the Pediatric Interest Group is hoping to have an annual teddy bear clinic. In the future, they hope to increase it to one a semester.
“These registered student organizations are 100% student run – student ideas, student volunteers, connections, and partnerships,” Dr. Norton said. “This clinic was all Taylor and all of the students. I can’t say how proud she is [to be] taking the time out of her busy medical student schedule to organize this for herself, her peers, and for these children.”
A version of this article first appeared on Medscape.com.
In December 2021, 26 medical students at Florida State University (FSU) waltzed into the FSU Child Care and Early Learning Center loaded with armfuls of plushy, cute teddy bears. For the first time in several years, the Pediatric Interest Group opened the doors to their teddy bear clinic – an annual event that gives students an opportunity to practice their leadership skills while also helping to demystify trips to the doctor for the young participants.
At the clinic, children aged 2-4 emulate basic medical practices on their fuzzy patients under the guidance of the students.
Teddy bear clinics were started by FSU’s College of Medicine Family Medicine Interest Group in 2018, but it slowed to a halt until second-year medical student Taylor Posey approached the Pediatric Interest Group during her tenure as the group’s president about reinstating a similar program. At FSU, interest groups allow students who are not quite sure which field of medicine they’d like to pursue to gain experience in any they have interest in.
“Pediatrics is the reason I wanted to go to medical school,” Ms. Posey told this news organization. “So it was great that working on this project really solidified the thought that I did the right thing. It’s great to watch the volunteers and children interact together.”
The clinic divides the children into three groups: 2-year-old toddlers, 3-year-old “tweens,” and 4-year-old pre-K children.
The toddlers paint white handprints on black construction paper to “create” x-rays and learn about them. The tweens are given medical equipment such as paper stethoscopes, thermometers, Band Aids, cotton balls, and Q-Tips to put into their very own doctor bags, which are really just folders with the emblematic red plus sign sticker attached to the front. The Pre-K kids are tasked with giving their teddy bears medical exams under the watchful eye of the medical students. Together, they examine the teddy bear’s eyes, heart, and lungs.
“There’s growing research out there that says medical play – which can be defined as children playing as if they were the parents of the teddy bear, learning about a diagnosis, and treating it – decreases the anxiety in children when they go to visit a doctor. Having real medical equipment that the children can manipulate as opposed to plastic toys really makes a big difference,” Ms. Posey said.
One of Ms. Posey’s peers worked with her to create developmentally appropriate activities for the children. Ms. Posey said that some of the ideas for the clinic came from Pinterest boards.
“The planning of it worked really well. I was expecting things to fall through, but they didn’t,” Ms. Posey said. “It can be tough working with young children and trying to do activities with them so that you’re not doing too much but also not having too low of expectations.”
“It was really a massive success on all fronts,” said Mary P. Norton, MD, an assistant professor of pediatrics and faculty Pediatric Interest Group advisor for the clinic. “The ability to be in the community and get hands-on experience has been really cut down by the pandemic, and this allowed for our students to be able to go out in person and apply what they learned in the classroom with the age group they want to work with, which is fantastic.”
Perhaps the most impactful aspect of the clinic is its ability to help ease children’s fears about visits to the doctor. “We want to allow children to have a voice and give them a space to be a part of their treatment plan,” Dr. Norton said. “We want to say, ‘Your voice matters, you’re not a passive being,’ so that they’re a part of that relationship and show them that their experience is important. We hope these clinics aid in forming a partnership between parents, children, and doctors.”
Currently, the Pediatric Interest Group is hoping to have an annual teddy bear clinic. In the future, they hope to increase it to one a semester.
“These registered student organizations are 100% student run – student ideas, student volunteers, connections, and partnerships,” Dr. Norton said. “This clinic was all Taylor and all of the students. I can’t say how proud she is [to be] taking the time out of her busy medical student schedule to organize this for herself, her peers, and for these children.”
A version of this article first appeared on Medscape.com.
In December 2021, 26 medical students at Florida State University (FSU) waltzed into the FSU Child Care and Early Learning Center loaded with armfuls of plushy, cute teddy bears. For the first time in several years, the Pediatric Interest Group opened the doors to their teddy bear clinic – an annual event that gives students an opportunity to practice their leadership skills while also helping to demystify trips to the doctor for the young participants.
At the clinic, children aged 2-4 emulate basic medical practices on their fuzzy patients under the guidance of the students.
Teddy bear clinics were started by FSU’s College of Medicine Family Medicine Interest Group in 2018, but it slowed to a halt until second-year medical student Taylor Posey approached the Pediatric Interest Group during her tenure as the group’s president about reinstating a similar program. At FSU, interest groups allow students who are not quite sure which field of medicine they’d like to pursue to gain experience in any they have interest in.
“Pediatrics is the reason I wanted to go to medical school,” Ms. Posey told this news organization. “So it was great that working on this project really solidified the thought that I did the right thing. It’s great to watch the volunteers and children interact together.”
The clinic divides the children into three groups: 2-year-old toddlers, 3-year-old “tweens,” and 4-year-old pre-K children.
The toddlers paint white handprints on black construction paper to “create” x-rays and learn about them. The tweens are given medical equipment such as paper stethoscopes, thermometers, Band Aids, cotton balls, and Q-Tips to put into their very own doctor bags, which are really just folders with the emblematic red plus sign sticker attached to the front. The Pre-K kids are tasked with giving their teddy bears medical exams under the watchful eye of the medical students. Together, they examine the teddy bear’s eyes, heart, and lungs.
“There’s growing research out there that says medical play – which can be defined as children playing as if they were the parents of the teddy bear, learning about a diagnosis, and treating it – decreases the anxiety in children when they go to visit a doctor. Having real medical equipment that the children can manipulate as opposed to plastic toys really makes a big difference,” Ms. Posey said.
One of Ms. Posey’s peers worked with her to create developmentally appropriate activities for the children. Ms. Posey said that some of the ideas for the clinic came from Pinterest boards.
“The planning of it worked really well. I was expecting things to fall through, but they didn’t,” Ms. Posey said. “It can be tough working with young children and trying to do activities with them so that you’re not doing too much but also not having too low of expectations.”
“It was really a massive success on all fronts,” said Mary P. Norton, MD, an assistant professor of pediatrics and faculty Pediatric Interest Group advisor for the clinic. “The ability to be in the community and get hands-on experience has been really cut down by the pandemic, and this allowed for our students to be able to go out in person and apply what they learned in the classroom with the age group they want to work with, which is fantastic.”
Perhaps the most impactful aspect of the clinic is its ability to help ease children’s fears about visits to the doctor. “We want to allow children to have a voice and give them a space to be a part of their treatment plan,” Dr. Norton said. “We want to say, ‘Your voice matters, you’re not a passive being,’ so that they’re a part of that relationship and show them that their experience is important. We hope these clinics aid in forming a partnership between parents, children, and doctors.”
Currently, the Pediatric Interest Group is hoping to have an annual teddy bear clinic. In the future, they hope to increase it to one a semester.
“These registered student organizations are 100% student run – student ideas, student volunteers, connections, and partnerships,” Dr. Norton said. “This clinic was all Taylor and all of the students. I can’t say how proud she is [to be] taking the time out of her busy medical student schedule to organize this for herself, her peers, and for these children.”
A version of this article first appeared on Medscape.com.
Treatment duration for acute otitis media – so many choices
Twenty years ago, the dilemma in treating acute otitis media (AOM) was which among 10-plus antibiotics to prescribe. A recent column discussed the evolving pathogen distribution in AOM and its effects on antibiotic choices.1 But here we consider treatment duration. Until the past decade, AOM treatment (except azithromycin) involved 10-day courses. But lately, 10-day antibiotic regimens for uncomplicated infections are disappearing. Shorter-course recommendations are the new norm because of the evolving clinical data showing that an appropriately chosen antibiotic (in partnership with host defenses and source control) resolves infection faster than was previously thought. Shorter courses make sense because of fewer adverse effects, less distortion of normal flora, and less likely induction of pathogen resistance. Table 4.12 in the newest 2021-2024 SOID Redbook lists three antibiotic durations for AOM, and actually there are more than that.
Why so many duration options? Clinical data show that not all AOM is alike and short courses work for subsets of AOM because, besides antibiotics, key elements in AOM resolution are host anatomy and immunity. Bacterial AOM results from a combination of refluxed pathogens in the middle ear being trapped when the eustachian tube malfunctions (infection occurs when middle ear plumbing gets stopped up). If the eustachian tube spontaneously drains and the host immune response slows/stops pathogen growth, no antibiotics are needed. Indeed, a sizable proportion of mild/moderate AOM episodes spontaneously resolve, particularly in children over 2 years old. So a high likelihood of spontaneous remission allows an initial 0-days duration option (watchful waiting) or delayed antibiotics (rescue prescriptions) for older children.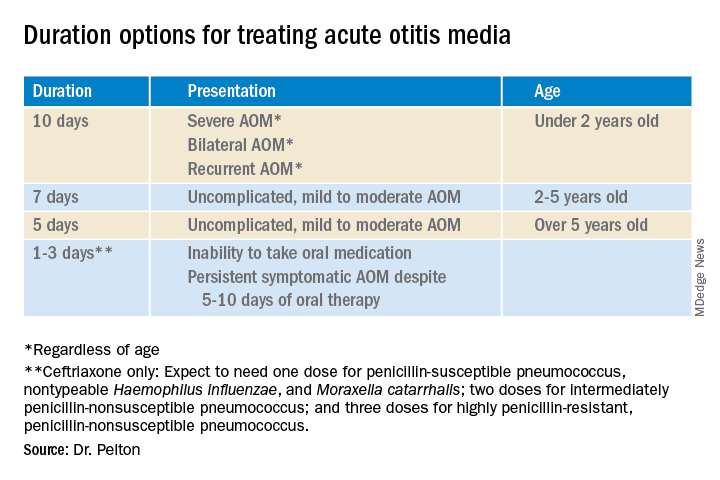
That said, when one chooses to initially prescribe antibiotics for AOM, different durations are recommended. Table 1 has my suggestions.
Data that gave me better microbiological understanding of why oral AOM trials less than 10 days were successful involved purulent AOM drainage from children who had pressure-equalizing (PE) tubes.2 The authors randomized children to either standard-dose amoxicillin-clavulanate or placebo. Of note, 95% of pathogens were susceptible to the antibiotic; 5% were pneumococcus intermediately resistant to penicillin. The authors sampled ear drainage daily for 7 days. Figure 1 shows that cultures remained positive in only around 5% of children by day 3-5 of antibiotics, but viable bacteria persisted through 7 days in over half of placebo recipients. Remember, both groups benefited from a form of source control (drainage of the middle ear via PE tubes). So, if antibiotics can do the job in 3-5 days, why continue antibiotics beyond 5 days?
Anatomy and severity. In children over 5 years old (reasonably mature eustachian tube anatomy) with nonrecurrent (no AOM in past month), nonsevere (no otalgia or high fever) AOM, 5 days is enough. But 2- to 5-year-olds (less mature anatomy) need 7 days and those <2 years old (least mature plumbing) need 10 days. Likewise, severe AOM usually warrants 10 days. Some experts recommend 10 days for bilateral AOM as well.
These age/severity differences make sense because failures are more frequent with:
1. Younger age.3 While not proven, my hypothesis is that “natural” source control (spontaneous internal draining the middle ear into the nasopharynx [NP]) is less frequent in younger children because they have less mature eustachian tube systems. Further, reflux of persisting NP organisms could restart a new AOM episode even if the original pathogen was eliminated by a short 5-day course.
2. Severe AOM. A rationale for longer courses in severe AOM (ear pain, high fever) is that high middle-ear pressures (indicated by degree of tympanic membrane bulging and ear pain) could impede antibiotic penetration, or that high initial bacterial loads (perhaps indicated by systemic fever) require more antibiotic. And finally, return to baseline eustachian tube function may take longer if severe AOM caused enhanced inflammation.
3. Recurrent AOM. (AOM within 1 prior month) – With recurrent AOM, the second “hit” to the eustachian tube may lead to more dysfunction, so a longer antibiotic course may be required to allow more complete source control and more time for more complete functional recovery after a repeated inflammatory injury.
4. Bilateral AOM. Two independent but infected sites mean twice the chance for failure. So, a longer course could allow more time for both sites to undergo “natural” source control.4
More bacteria – more antibiotic? So, is more antibiotic really needed for a higher bacterial load? In vitro this is known as the “inoculum effect,” particularly for beta-lactam drugs, for example, amoxicillin and cephalosporins. Laboratory susceptibility testing is performed with a specifically defined quantity of bacteria (105 bacteria/mL) and the minimum inhibitory concentration (MIC) is the lowest antibiotic concentration that stops bacterial growth. We know that drugs will likely fail if the MIC exceeds the achievable antibiotic concentration at the infection site. But is it as simple as just exceeding the MIC at the infection site? No, pharmacodynamics tell us that overall antibiotic exposure is also important. For example, to be successful, beta-lactam concentrations need to be above the MIC for 40%-50% of the day.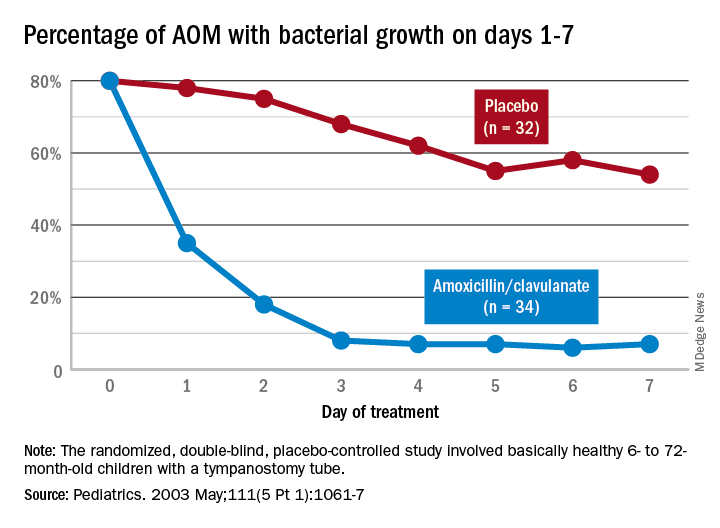
Higher MIC with higher bacterial load. Particularly for beta-lactams, testing with a quantity of bacteria >105/mL produces a higher MIC in vitro. This suggests that clinical failure could occur, even when our in vivo dosing leads to 40%-50% above the “standard” MIC that was obtained from testing the lab standard of 105/mL bacteria, when the infected site’s (middle ear) bacterial load is >105/mL (such higher bacterial loads occur in up to 30% of AOM).5 One way to negate inoculum effect is source control (drain the abscess or debridement), which reduces the bacterial load as well as allowing better antibiotic penetration– both favoring infection resolution. But with suboptimal source control, for example, the middle ear is not drained externally or internally, longer courses (more antibiotic exposure) could aid resolution. Whether the exposure can be administered as higher doses in fewer days or standard doses for more days is debatable but consider that a single parenteral dose of ceftriaxone successfully resolves AOM not attributable to penicillin-nonsusceptible pneumococcus.6Bottom line: Even though the number of potential antibiotics has contracted in the past 20 years, the need to individualize AOM treatment remains important and duration choices are more complex. Indeed, AOM comes in different flavors with patient age, clinical presentation, and episode frequency dictating the choice of duration.
Dr. Christopher J. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics in Kansas City, Mo. Email him at [email protected].
References
1. Pichichero ME. MDedge. 2022 Jan 11.
2. Ruohola A et al. Pediatrics. 2003;111(5):1061-7.
3. Hoberman A et al. N Engl J Med. 2016;375(25):2446-56.
4. Pichichero ME et al. Otolaryngol Head Neck Surg. 2001;124(4):381-7.
5. Harrison CJ et al. Pediatr Infect Dis. 1985;4(6):641-6.
6. Leibovitz E et al. Pediatr Infect Dis. 2000;19(11):1040-5.
Twenty years ago, the dilemma in treating acute otitis media (AOM) was which among 10-plus antibiotics to prescribe. A recent column discussed the evolving pathogen distribution in AOM and its effects on antibiotic choices.1 But here we consider treatment duration. Until the past decade, AOM treatment (except azithromycin) involved 10-day courses. But lately, 10-day antibiotic regimens for uncomplicated infections are disappearing. Shorter-course recommendations are the new norm because of the evolving clinical data showing that an appropriately chosen antibiotic (in partnership with host defenses and source control) resolves infection faster than was previously thought. Shorter courses make sense because of fewer adverse effects, less distortion of normal flora, and less likely induction of pathogen resistance. Table 4.12 in the newest 2021-2024 SOID Redbook lists three antibiotic durations for AOM, and actually there are more than that.
Why so many duration options? Clinical data show that not all AOM is alike and short courses work for subsets of AOM because, besides antibiotics, key elements in AOM resolution are host anatomy and immunity. Bacterial AOM results from a combination of refluxed pathogens in the middle ear being trapped when the eustachian tube malfunctions (infection occurs when middle ear plumbing gets stopped up). If the eustachian tube spontaneously drains and the host immune response slows/stops pathogen growth, no antibiotics are needed. Indeed, a sizable proportion of mild/moderate AOM episodes spontaneously resolve, particularly in children over 2 years old. So a high likelihood of spontaneous remission allows an initial 0-days duration option (watchful waiting) or delayed antibiotics (rescue prescriptions) for older children.
That said, when one chooses to initially prescribe antibiotics for AOM, different durations are recommended. Table 1 has my suggestions.
Data that gave me better microbiological understanding of why oral AOM trials less than 10 days were successful involved purulent AOM drainage from children who had pressure-equalizing (PE) tubes.2 The authors randomized children to either standard-dose amoxicillin-clavulanate or placebo. Of note, 95% of pathogens were susceptible to the antibiotic; 5% were pneumococcus intermediately resistant to penicillin. The authors sampled ear drainage daily for 7 days. Figure 1 shows that cultures remained positive in only around 5% of children by day 3-5 of antibiotics, but viable bacteria persisted through 7 days in over half of placebo recipients. Remember, both groups benefited from a form of source control (drainage of the middle ear via PE tubes). So, if antibiotics can do the job in 3-5 days, why continue antibiotics beyond 5 days?
Anatomy and severity. In children over 5 years old (reasonably mature eustachian tube anatomy) with nonrecurrent (no AOM in past month), nonsevere (no otalgia or high fever) AOM, 5 days is enough. But 2- to 5-year-olds (less mature anatomy) need 7 days and those <2 years old (least mature plumbing) need 10 days. Likewise, severe AOM usually warrants 10 days. Some experts recommend 10 days for bilateral AOM as well.
These age/severity differences make sense because failures are more frequent with:
1. Younger age.3 While not proven, my hypothesis is that “natural” source control (spontaneous internal draining the middle ear into the nasopharynx [NP]) is less frequent in younger children because they have less mature eustachian tube systems. Further, reflux of persisting NP organisms could restart a new AOM episode even if the original pathogen was eliminated by a short 5-day course.
2. Severe AOM. A rationale for longer courses in severe AOM (ear pain, high fever) is that high middle-ear pressures (indicated by degree of tympanic membrane bulging and ear pain) could impede antibiotic penetration, or that high initial bacterial loads (perhaps indicated by systemic fever) require more antibiotic. And finally, return to baseline eustachian tube function may take longer if severe AOM caused enhanced inflammation.
3. Recurrent AOM. (AOM within 1 prior month) – With recurrent AOM, the second “hit” to the eustachian tube may lead to more dysfunction, so a longer antibiotic course may be required to allow more complete source control and more time for more complete functional recovery after a repeated inflammatory injury.
4. Bilateral AOM. Two independent but infected sites mean twice the chance for failure. So, a longer course could allow more time for both sites to undergo “natural” source control.4
More bacteria – more antibiotic? So, is more antibiotic really needed for a higher bacterial load? In vitro this is known as the “inoculum effect,” particularly for beta-lactam drugs, for example, amoxicillin and cephalosporins. Laboratory susceptibility testing is performed with a specifically defined quantity of bacteria (105 bacteria/mL) and the minimum inhibitory concentration (MIC) is the lowest antibiotic concentration that stops bacterial growth. We know that drugs will likely fail if the MIC exceeds the achievable antibiotic concentration at the infection site. But is it as simple as just exceeding the MIC at the infection site? No, pharmacodynamics tell us that overall antibiotic exposure is also important. For example, to be successful, beta-lactam concentrations need to be above the MIC for 40%-50% of the day.
Higher MIC with higher bacterial load. Particularly for beta-lactams, testing with a quantity of bacteria >105/mL produces a higher MIC in vitro. This suggests that clinical failure could occur, even when our in vivo dosing leads to 40%-50% above the “standard” MIC that was obtained from testing the lab standard of 105/mL bacteria, when the infected site’s (middle ear) bacterial load is >105/mL (such higher bacterial loads occur in up to 30% of AOM).5 One way to negate inoculum effect is source control (drain the abscess or debridement), which reduces the bacterial load as well as allowing better antibiotic penetration– both favoring infection resolution. But with suboptimal source control, for example, the middle ear is not drained externally or internally, longer courses (more antibiotic exposure) could aid resolution. Whether the exposure can be administered as higher doses in fewer days or standard doses for more days is debatable but consider that a single parenteral dose of ceftriaxone successfully resolves AOM not attributable to penicillin-nonsusceptible pneumococcus.6Bottom line: Even though the number of potential antibiotics has contracted in the past 20 years, the need to individualize AOM treatment remains important and duration choices are more complex. Indeed, AOM comes in different flavors with patient age, clinical presentation, and episode frequency dictating the choice of duration.
Dr. Christopher J. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics in Kansas City, Mo. Email him at [email protected].
References
1. Pichichero ME. MDedge. 2022 Jan 11.
2. Ruohola A et al. Pediatrics. 2003;111(5):1061-7.
3. Hoberman A et al. N Engl J Med. 2016;375(25):2446-56.
4. Pichichero ME et al. Otolaryngol Head Neck Surg. 2001;124(4):381-7.
5. Harrison CJ et al. Pediatr Infect Dis. 1985;4(6):641-6.
6. Leibovitz E et al. Pediatr Infect Dis. 2000;19(11):1040-5.
Twenty years ago, the dilemma in treating acute otitis media (AOM) was which among 10-plus antibiotics to prescribe. A recent column discussed the evolving pathogen distribution in AOM and its effects on antibiotic choices.1 But here we consider treatment duration. Until the past decade, AOM treatment (except azithromycin) involved 10-day courses. But lately, 10-day antibiotic regimens for uncomplicated infections are disappearing. Shorter-course recommendations are the new norm because of the evolving clinical data showing that an appropriately chosen antibiotic (in partnership with host defenses and source control) resolves infection faster than was previously thought. Shorter courses make sense because of fewer adverse effects, less distortion of normal flora, and less likely induction of pathogen resistance. Table 4.12 in the newest 2021-2024 SOID Redbook lists three antibiotic durations for AOM, and actually there are more than that.
Why so many duration options? Clinical data show that not all AOM is alike and short courses work for subsets of AOM because, besides antibiotics, key elements in AOM resolution are host anatomy and immunity. Bacterial AOM results from a combination of refluxed pathogens in the middle ear being trapped when the eustachian tube malfunctions (infection occurs when middle ear plumbing gets stopped up). If the eustachian tube spontaneously drains and the host immune response slows/stops pathogen growth, no antibiotics are needed. Indeed, a sizable proportion of mild/moderate AOM episodes spontaneously resolve, particularly in children over 2 years old. So a high likelihood of spontaneous remission allows an initial 0-days duration option (watchful waiting) or delayed antibiotics (rescue prescriptions) for older children.
That said, when one chooses to initially prescribe antibiotics for AOM, different durations are recommended. Table 1 has my suggestions.
Data that gave me better microbiological understanding of why oral AOM trials less than 10 days were successful involved purulent AOM drainage from children who had pressure-equalizing (PE) tubes.2 The authors randomized children to either standard-dose amoxicillin-clavulanate or placebo. Of note, 95% of pathogens were susceptible to the antibiotic; 5% were pneumococcus intermediately resistant to penicillin. The authors sampled ear drainage daily for 7 days. Figure 1 shows that cultures remained positive in only around 5% of children by day 3-5 of antibiotics, but viable bacteria persisted through 7 days in over half of placebo recipients. Remember, both groups benefited from a form of source control (drainage of the middle ear via PE tubes). So, if antibiotics can do the job in 3-5 days, why continue antibiotics beyond 5 days?
Anatomy and severity. In children over 5 years old (reasonably mature eustachian tube anatomy) with nonrecurrent (no AOM in past month), nonsevere (no otalgia or high fever) AOM, 5 days is enough. But 2- to 5-year-olds (less mature anatomy) need 7 days and those <2 years old (least mature plumbing) need 10 days. Likewise, severe AOM usually warrants 10 days. Some experts recommend 10 days for bilateral AOM as well.
These age/severity differences make sense because failures are more frequent with:
1. Younger age.3 While not proven, my hypothesis is that “natural” source control (spontaneous internal draining the middle ear into the nasopharynx [NP]) is less frequent in younger children because they have less mature eustachian tube systems. Further, reflux of persisting NP organisms could restart a new AOM episode even if the original pathogen was eliminated by a short 5-day course.
2. Severe AOM. A rationale for longer courses in severe AOM (ear pain, high fever) is that high middle-ear pressures (indicated by degree of tympanic membrane bulging and ear pain) could impede antibiotic penetration, or that high initial bacterial loads (perhaps indicated by systemic fever) require more antibiotic. And finally, return to baseline eustachian tube function may take longer if severe AOM caused enhanced inflammation.
3. Recurrent AOM. (AOM within 1 prior month) – With recurrent AOM, the second “hit” to the eustachian tube may lead to more dysfunction, so a longer antibiotic course may be required to allow more complete source control and more time for more complete functional recovery after a repeated inflammatory injury.
4. Bilateral AOM. Two independent but infected sites mean twice the chance for failure. So, a longer course could allow more time for both sites to undergo “natural” source control.4
More bacteria – more antibiotic? So, is more antibiotic really needed for a higher bacterial load? In vitro this is known as the “inoculum effect,” particularly for beta-lactam drugs, for example, amoxicillin and cephalosporins. Laboratory susceptibility testing is performed with a specifically defined quantity of bacteria (105 bacteria/mL) and the minimum inhibitory concentration (MIC) is the lowest antibiotic concentration that stops bacterial growth. We know that drugs will likely fail if the MIC exceeds the achievable antibiotic concentration at the infection site. But is it as simple as just exceeding the MIC at the infection site? No, pharmacodynamics tell us that overall antibiotic exposure is also important. For example, to be successful, beta-lactam concentrations need to be above the MIC for 40%-50% of the day.
Higher MIC with higher bacterial load. Particularly for beta-lactams, testing with a quantity of bacteria >105/mL produces a higher MIC in vitro. This suggests that clinical failure could occur, even when our in vivo dosing leads to 40%-50% above the “standard” MIC that was obtained from testing the lab standard of 105/mL bacteria, when the infected site’s (middle ear) bacterial load is >105/mL (such higher bacterial loads occur in up to 30% of AOM).5 One way to negate inoculum effect is source control (drain the abscess or debridement), which reduces the bacterial load as well as allowing better antibiotic penetration– both favoring infection resolution. But with suboptimal source control, for example, the middle ear is not drained externally or internally, longer courses (more antibiotic exposure) could aid resolution. Whether the exposure can be administered as higher doses in fewer days or standard doses for more days is debatable but consider that a single parenteral dose of ceftriaxone successfully resolves AOM not attributable to penicillin-nonsusceptible pneumococcus.6Bottom line: Even though the number of potential antibiotics has contracted in the past 20 years, the need to individualize AOM treatment remains important and duration choices are more complex. Indeed, AOM comes in different flavors with patient age, clinical presentation, and episode frequency dictating the choice of duration.
Dr. Christopher J. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics in Kansas City, Mo. Email him at [email protected].
References
1. Pichichero ME. MDedge. 2022 Jan 11.
2. Ruohola A et al. Pediatrics. 2003;111(5):1061-7.
3. Hoberman A et al. N Engl J Med. 2016;375(25):2446-56.
4. Pichichero ME et al. Otolaryngol Head Neck Surg. 2001;124(4):381-7.
5. Harrison CJ et al. Pediatr Infect Dis. 1985;4(6):641-6.
6. Leibovitz E et al. Pediatr Infect Dis. 2000;19(11):1040-5.
Organ transplantation: Unvaccinated need not apply
I agree with most advice given by the affable TV character Ted Lasso. “Every choice is a chance,” he said. Pandemic-era physicians must now consider whether a politically motivated choice to decline COVID-19 vaccination should negatively affect the chance to receive an organ donation.
And in confronting these choices, we have a chance to educate the public on the complexities of the organ allocation process.

A well-informed patient’s personal choice should be honored, even if clinicians disagree, if it does not affect the well-being of others. For example, I once had a patient in acute leukemic crisis who declined blood products because she was a Jehovah’s Witness. She died. Her choice affected her longevity only.
Compare that decision with awarding an organ to an individual who has declined readily available protection of that organ. Weigh that choice against the fact that said protection is against an infectious disease that has killed over 5.5 million worldwide.
Some institutions stand strong, others hedge their bets
Admirably, Loyola University Health System understands that difference. They published a firm stand on transplant candidacy and COVID-19 vaccination status in the Journal of Heart and Lung Transplant. Daniel Dilling, MD, medical director of the lung transplantation program , and Mark Kuczewski, PhD, a professor of medical ethics at Loyola University Chicago, Maywood, Ill., wrote that: “We believe that requiring vaccination against COVID-19 should not be controversial when we focus strictly on established frameworks and practices surrounding eligibility for wait-listing to receive a solid organ transplant.”
The Cleveland Clinic apparently agrees. In October 2021, they denied a liver transplant to Michelle Vitullo of Ohio, whose daughter had been deemed “a perfect match.” Her daughter, also unvaccinated, stated: “Being denied for a nonmedical reason for someone’s beliefs that are different to yours, I mean that’s not how that should be.”
But vaccination status is a medical reason, given well-established data regarding increased mortality among the immunosuppressed. Ms. Vitullo then said: “We are trying to get to UPMC [University of Pittsburgh Medical Center] as they don’t require a vaccination.”
The public information page on transplant candidacy from UPMC reads (my italics): It is recommended that all transplant candidates, transplant recipients, and their household members receive COVID-19 vaccination when the vaccine is available to them. It is preferred that transplant candidates are vaccinated more than 2 weeks before transplantation.
I reached out to UPMC for clarification and was told by email that “we do not have a policy regarding COVID-19 vaccination requirement for current transplant candidates.” Houston Methodist shares the same agnostic stance.
Compare these opinions with Brigham and Women’s Hospital, where the requirements are resolute: “Like most other transplant programs across the country, the COVID-19 vaccine is one of several vaccines and lifestyle behaviors that are required for patients awaiting solid organ transplant.”
They add that “transplant candidates must also receive the seasonal influenza and hepatitis B vaccines, follow other healthy behaviors, and demonstrate they can commit to taking the required medications following transplant.”
In January 2022, Brigham and Women’s Hospital declared 31-year-old D.J. Ferguson ineligible for a heart transplant because he declined to be vaccinated against COVID-19. According to the New York Post and ABC News, his physicians resorted to left ventricular assist device support. His mother, Tracy Ferguson, is quoted as saying: “He’s not an antivaxxer. He has all of his vaccines.” I’ll just leave that right there.
Unfortunately, Michelle Vitullo’s obituary was published in December 2021. Regardless of whether she received her liver transplant, the outcome is tragic, and whatever you think of this family’s battle playing out in the glare of the national spotlight, their loss is no less devastating.
The directed-donation aspect of this case poses an interesting question. A news anchor asked the mother and daughter: “If you both accept the risks, why doesn’t the hospital just let you try?” The answers are obvious to us clinicians. Performing a transplantation in an unvaccinated patient could lead to their early death if they became infected because of their immunocompromised state, would open the door for transplantation of any patient who is unvaccinated for anything, including influenza and hepatitis B, which could result in the preventable waste of organs, and puts other vulnerable hospitalized patients at risk during the initial transplant stay and follow-up.
That’s not to mention the potential legal suit. Never has a consent form dissuaded any party from lodging an accusation of wrongful death or medical malpractice. In the face of strong data on higher mortality in unvaccinated, immunocompromised patients, a good lawyer could charge that the institution and transplant surgeons should have known better, regardless of the donor and recipient’s willingness to accept the risks.
The Vitullo and Ferguson cases are among many similar dilemmas surrounding transplant candidacy across the United States.
University of Virginia Health in Charlottesville denied 42-year-old Shamgar Connors a kidney transplant because he is unvaccinated, despite a previous COVID-19 infection. In October 2021, Leilani Lutali of Colorado was denied a kidney by UCHealth because she declined vaccination.

As Ted Lasso says: “There’s a bunch of crazy stuff on Twitter.”
Predictably, social media is full of public outcry. “Some cold-hearted people on here” tweeted one. “What if it was one of your loved ones who needed a transplant?” Another tweeted the Hippocratic oath with the comment that “They all swore under this noble ‘oat’, but I guess it’s been forgotten.” (This was followed with a photo of a box of Quaker Oats in a failed attempt at humor.) These discussions among the Twitterati highlight the depths of misunderstanding on organ transplantation.
To be fair, unless you have been personally involved in the decision-making process for transplant candidacy, there is little opportunity to be educated. I explain to my anxious patients and their families that a donor organ is like a fumbled football. There may be well over 100 patients at all levels of transplant status in many geographic locations diving for that same organ.
The transplant team is tasked with finding the best match, determining who is the sickest, assessing time for transport of that organ, and, above all, who will be the best steward of that organ.
Take heart transplantation, for instance. Approximately 3,500 patients in the United States are awaiting one each year. Instead of facing an almost certain death within 5 years, a transplant recipient has a chance at a median survival of 12-13 years. The cost of a heart transplant is approximately $1.38 million, according to Milliman, a consulting firm. This is “an incredibly resource intensive procedure,” including expenditures for transportation, antirejection medication, office visits, physician fees, ICU stays, rejection surveillance, and acute rejection therapies.
Transplant denial is nothing new
People get turned down for organ transplants all the time. My patient with end-stage dilated cardiomyopathy was denied a heart transplant when it was discovered that he had scores of outstanding parking tickets. This was seen as a surrogate for an inability to afford his antirejection medication.
Another patient swore that her positive cotinine levels were caused by endless hours at the bingo hall where second-hand smoke swirled. She was also denied. Many potential candidates who are in acute decline hold precariously to newfound sobriety. They are denied. A patient’s boyfriend told the transplant team that he couldn’t be relied upon to drive her to her appointments. She was denied.
Many people who engage in antisocial behaviors have no idea that these actions may result in the denial of an organ transplant should their future selves need one. These are hard lines, but everyone should agree that the odds of survival are heavily in favor of the consistently adherent.
We should take this opportunity to educate the public on how complicated obtaining an organ transplant can be. More than 6,000 people die each year waiting for an organ because of the supply-and-demand disparities in the transplantation arena. I’m willing to bet that many of the loudest protesters in favor of unvaccinated transplant recipients have not signed the organ donor box on the back of their driver’s license. This conversation is an opportunity to change that and remind people that organ donation may be their only opportunity to save a fellow human’s life.
Again, to quote Ted Lasso: “If you care about someone and you got a little love in your heart, there ain’t nothing you can’t get through together.” That philosophy should apply to the tasks of selecting the best organ donors as well as the best organ recipients.
And every organ should go to the one who will honor their donor and their donor’s family by taking the best care of that ultimate gift of life, including being vaccinated against COVID-19.
Dr. Walton-Shirley is a native Kentuckian who retired from full-time invasive cardiology. She enjoys locums work in Montana and is a champion of physician rights and patient safety. She disclosed no relevant conflicts of interest. A version of this article first appeared on Medscape.com.
I agree with most advice given by the affable TV character Ted Lasso. “Every choice is a chance,” he said. Pandemic-era physicians must now consider whether a politically motivated choice to decline COVID-19 vaccination should negatively affect the chance to receive an organ donation.
And in confronting these choices, we have a chance to educate the public on the complexities of the organ allocation process.
A well-informed patient’s personal choice should be honored, even if clinicians disagree, if it does not affect the well-being of others. For example, I once had a patient in acute leukemic crisis who declined blood products because she was a Jehovah’s Witness. She died. Her choice affected her longevity only.
Compare that decision with awarding an organ to an individual who has declined readily available protection of that organ. Weigh that choice against the fact that said protection is against an infectious disease that has killed over 5.5 million worldwide.
Some institutions stand strong, others hedge their bets
Admirably, Loyola University Health System understands that difference. They published a firm stand on transplant candidacy and COVID-19 vaccination status in the Journal of Heart and Lung Transplant. Daniel Dilling, MD, medical director of the lung transplantation program , and Mark Kuczewski, PhD, a professor of medical ethics at Loyola University Chicago, Maywood, Ill., wrote that: “We believe that requiring vaccination against COVID-19 should not be controversial when we focus strictly on established frameworks and practices surrounding eligibility for wait-listing to receive a solid organ transplant.”
The Cleveland Clinic apparently agrees. In October 2021, they denied a liver transplant to Michelle Vitullo of Ohio, whose daughter had been deemed “a perfect match.” Her daughter, also unvaccinated, stated: “Being denied for a nonmedical reason for someone’s beliefs that are different to yours, I mean that’s not how that should be.”
But vaccination status is a medical reason, given well-established data regarding increased mortality among the immunosuppressed. Ms. Vitullo then said: “We are trying to get to UPMC [University of Pittsburgh Medical Center] as they don’t require a vaccination.”
The public information page on transplant candidacy from UPMC reads (my italics): It is recommended that all transplant candidates, transplant recipients, and their household members receive COVID-19 vaccination when the vaccine is available to them. It is preferred that transplant candidates are vaccinated more than 2 weeks before transplantation.
I reached out to UPMC for clarification and was told by email that “we do not have a policy regarding COVID-19 vaccination requirement for current transplant candidates.” Houston Methodist shares the same agnostic stance.
Compare these opinions with Brigham and Women’s Hospital, where the requirements are resolute: “Like most other transplant programs across the country, the COVID-19 vaccine is one of several vaccines and lifestyle behaviors that are required for patients awaiting solid organ transplant.”
They add that “transplant candidates must also receive the seasonal influenza and hepatitis B vaccines, follow other healthy behaviors, and demonstrate they can commit to taking the required medications following transplant.”
In January 2022, Brigham and Women’s Hospital declared 31-year-old D.J. Ferguson ineligible for a heart transplant because he declined to be vaccinated against COVID-19. According to the New York Post and ABC News, his physicians resorted to left ventricular assist device support. His mother, Tracy Ferguson, is quoted as saying: “He’s not an antivaxxer. He has all of his vaccines.” I’ll just leave that right there.
Unfortunately, Michelle Vitullo’s obituary was published in December 2021. Regardless of whether she received her liver transplant, the outcome is tragic, and whatever you think of this family’s battle playing out in the glare of the national spotlight, their loss is no less devastating.
The directed-donation aspect of this case poses an interesting question. A news anchor asked the mother and daughter: “If you both accept the risks, why doesn’t the hospital just let you try?” The answers are obvious to us clinicians. Performing a transplantation in an unvaccinated patient could lead to their early death if they became infected because of their immunocompromised state, would open the door for transplantation of any patient who is unvaccinated for anything, including influenza and hepatitis B, which could result in the preventable waste of organs, and puts other vulnerable hospitalized patients at risk during the initial transplant stay and follow-up.
That’s not to mention the potential legal suit. Never has a consent form dissuaded any party from lodging an accusation of wrongful death or medical malpractice. In the face of strong data on higher mortality in unvaccinated, immunocompromised patients, a good lawyer could charge that the institution and transplant surgeons should have known better, regardless of the donor and recipient’s willingness to accept the risks.
The Vitullo and Ferguson cases are among many similar dilemmas surrounding transplant candidacy across the United States.
University of Virginia Health in Charlottesville denied 42-year-old Shamgar Connors a kidney transplant because he is unvaccinated, despite a previous COVID-19 infection. In October 2021, Leilani Lutali of Colorado was denied a kidney by UCHealth because she declined vaccination.
As Ted Lasso says: “There’s a bunch of crazy stuff on Twitter.”
Predictably, social media is full of public outcry. “Some cold-hearted people on here” tweeted one. “What if it was one of your loved ones who needed a transplant?” Another tweeted the Hippocratic oath with the comment that “They all swore under this noble ‘oat’, but I guess it’s been forgotten.” (This was followed with a photo of a box of Quaker Oats in a failed attempt at humor.) These discussions among the Twitterati highlight the depths of misunderstanding on organ transplantation.
To be fair, unless you have been personally involved in the decision-making process for transplant candidacy, there is little opportunity to be educated. I explain to my anxious patients and their families that a donor organ is like a fumbled football. There may be well over 100 patients at all levels of transplant status in many geographic locations diving for that same organ.
The transplant team is tasked with finding the best match, determining who is the sickest, assessing time for transport of that organ, and, above all, who will be the best steward of that organ.
Take heart transplantation, for instance. Approximately 3,500 patients in the United States are awaiting one each year. Instead of facing an almost certain death within 5 years, a transplant recipient has a chance at a median survival of 12-13 years. The cost of a heart transplant is approximately $1.38 million, according to Milliman, a consulting firm. This is “an incredibly resource intensive procedure,” including expenditures for transportation, antirejection medication, office visits, physician fees, ICU stays, rejection surveillance, and acute rejection therapies.
Transplant denial is nothing new
People get turned down for organ transplants all the time. My patient with end-stage dilated cardiomyopathy was denied a heart transplant when it was discovered that he had scores of outstanding parking tickets. This was seen as a surrogate for an inability to afford his antirejection medication.
Another patient swore that her positive cotinine levels were caused by endless hours at the bingo hall where second-hand smoke swirled. She was also denied. Many potential candidates who are in acute decline hold precariously to newfound sobriety. They are denied. A patient’s boyfriend told the transplant team that he couldn’t be relied upon to drive her to her appointments. She was denied.
Many people who engage in antisocial behaviors have no idea that these actions may result in the denial of an organ transplant should their future selves need one. These are hard lines, but everyone should agree that the odds of survival are heavily in favor of the consistently adherent.
We should take this opportunity to educate the public on how complicated obtaining an organ transplant can be. More than 6,000 people die each year waiting for an organ because of the supply-and-demand disparities in the transplantation arena. I’m willing to bet that many of the loudest protesters in favor of unvaccinated transplant recipients have not signed the organ donor box on the back of their driver’s license. This conversation is an opportunity to change that and remind people that organ donation may be their only opportunity to save a fellow human’s life.
Again, to quote Ted Lasso: “If you care about someone and you got a little love in your heart, there ain’t nothing you can’t get through together.” That philosophy should apply to the tasks of selecting the best organ donors as well as the best organ recipients.
And every organ should go to the one who will honor their donor and their donor’s family by taking the best care of that ultimate gift of life, including being vaccinated against COVID-19.
Dr. Walton-Shirley is a native Kentuckian who retired from full-time invasive cardiology. She enjoys locums work in Montana and is a champion of physician rights and patient safety. She disclosed no relevant conflicts of interest. A version of this article first appeared on Medscape.com.
I agree with most advice given by the affable TV character Ted Lasso. “Every choice is a chance,” he said. Pandemic-era physicians must now consider whether a politically motivated choice to decline COVID-19 vaccination should negatively affect the chance to receive an organ donation.
And in confronting these choices, we have a chance to educate the public on the complexities of the organ allocation process.
A well-informed patient’s personal choice should be honored, even if clinicians disagree, if it does not affect the well-being of others. For example, I once had a patient in acute leukemic crisis who declined blood products because she was a Jehovah’s Witness. She died. Her choice affected her longevity only.
Compare that decision with awarding an organ to an individual who has declined readily available protection of that organ. Weigh that choice against the fact that said protection is against an infectious disease that has killed over 5.5 million worldwide.
Some institutions stand strong, others hedge their bets
Admirably, Loyola University Health System understands that difference. They published a firm stand on transplant candidacy and COVID-19 vaccination status in the Journal of Heart and Lung Transplant. Daniel Dilling, MD, medical director of the lung transplantation program , and Mark Kuczewski, PhD, a professor of medical ethics at Loyola University Chicago, Maywood, Ill., wrote that: “We believe that requiring vaccination against COVID-19 should not be controversial when we focus strictly on established frameworks and practices surrounding eligibility for wait-listing to receive a solid organ transplant.”
The Cleveland Clinic apparently agrees. In October 2021, they denied a liver transplant to Michelle Vitullo of Ohio, whose daughter had been deemed “a perfect match.” Her daughter, also unvaccinated, stated: “Being denied for a nonmedical reason for someone’s beliefs that are different to yours, I mean that’s not how that should be.”
But vaccination status is a medical reason, given well-established data regarding increased mortality among the immunosuppressed. Ms. Vitullo then said: “We are trying to get to UPMC [University of Pittsburgh Medical Center] as they don’t require a vaccination.”
The public information page on transplant candidacy from UPMC reads (my italics): It is recommended that all transplant candidates, transplant recipients, and their household members receive COVID-19 vaccination when the vaccine is available to them. It is preferred that transplant candidates are vaccinated more than 2 weeks before transplantation.
I reached out to UPMC for clarification and was told by email that “we do not have a policy regarding COVID-19 vaccination requirement for current transplant candidates.” Houston Methodist shares the same agnostic stance.
Compare these opinions with Brigham and Women’s Hospital, where the requirements are resolute: “Like most other transplant programs across the country, the COVID-19 vaccine is one of several vaccines and lifestyle behaviors that are required for patients awaiting solid organ transplant.”
They add that “transplant candidates must also receive the seasonal influenza and hepatitis B vaccines, follow other healthy behaviors, and demonstrate they can commit to taking the required medications following transplant.”
In January 2022, Brigham and Women’s Hospital declared 31-year-old D.J. Ferguson ineligible for a heart transplant because he declined to be vaccinated against COVID-19. According to the New York Post and ABC News, his physicians resorted to left ventricular assist device support. His mother, Tracy Ferguson, is quoted as saying: “He’s not an antivaxxer. He has all of his vaccines.” I’ll just leave that right there.
Unfortunately, Michelle Vitullo’s obituary was published in December 2021. Regardless of whether she received her liver transplant, the outcome is tragic, and whatever you think of this family’s battle playing out in the glare of the national spotlight, their loss is no less devastating.
The directed-donation aspect of this case poses an interesting question. A news anchor asked the mother and daughter: “If you both accept the risks, why doesn’t the hospital just let you try?” The answers are obvious to us clinicians. Performing a transplantation in an unvaccinated patient could lead to their early death if they became infected because of their immunocompromised state, would open the door for transplantation of any patient who is unvaccinated for anything, including influenza and hepatitis B, which could result in the preventable waste of organs, and puts other vulnerable hospitalized patients at risk during the initial transplant stay and follow-up.
That’s not to mention the potential legal suit. Never has a consent form dissuaded any party from lodging an accusation of wrongful death or medical malpractice. In the face of strong data on higher mortality in unvaccinated, immunocompromised patients, a good lawyer could charge that the institution and transplant surgeons should have known better, regardless of the donor and recipient’s willingness to accept the risks.
The Vitullo and Ferguson cases are among many similar dilemmas surrounding transplant candidacy across the United States.
University of Virginia Health in Charlottesville denied 42-year-old Shamgar Connors a kidney transplant because he is unvaccinated, despite a previous COVID-19 infection. In October 2021, Leilani Lutali of Colorado was denied a kidney by UCHealth because she declined vaccination.
As Ted Lasso says: “There’s a bunch of crazy stuff on Twitter.”
Predictably, social media is full of public outcry. “Some cold-hearted people on here” tweeted one. “What if it was one of your loved ones who needed a transplant?” Another tweeted the Hippocratic oath with the comment that “They all swore under this noble ‘oat’, but I guess it’s been forgotten.” (This was followed with a photo of a box of Quaker Oats in a failed attempt at humor.) These discussions among the Twitterati highlight the depths of misunderstanding on organ transplantation.
To be fair, unless you have been personally involved in the decision-making process for transplant candidacy, there is little opportunity to be educated. I explain to my anxious patients and their families that a donor organ is like a fumbled football. There may be well over 100 patients at all levels of transplant status in many geographic locations diving for that same organ.
The transplant team is tasked with finding the best match, determining who is the sickest, assessing time for transport of that organ, and, above all, who will be the best steward of that organ.
Take heart transplantation, for instance. Approximately 3,500 patients in the United States are awaiting one each year. Instead of facing an almost certain death within 5 years, a transplant recipient has a chance at a median survival of 12-13 years. The cost of a heart transplant is approximately $1.38 million, according to Milliman, a consulting firm. This is “an incredibly resource intensive procedure,” including expenditures for transportation, antirejection medication, office visits, physician fees, ICU stays, rejection surveillance, and acute rejection therapies.
Transplant denial is nothing new
People get turned down for organ transplants all the time. My patient with end-stage dilated cardiomyopathy was denied a heart transplant when it was discovered that he had scores of outstanding parking tickets. This was seen as a surrogate for an inability to afford his antirejection medication.
Another patient swore that her positive cotinine levels were caused by endless hours at the bingo hall where second-hand smoke swirled. She was also denied. Many potential candidates who are in acute decline hold precariously to newfound sobriety. They are denied. A patient’s boyfriend told the transplant team that he couldn’t be relied upon to drive her to her appointments. She was denied.
Many people who engage in antisocial behaviors have no idea that these actions may result in the denial of an organ transplant should their future selves need one. These are hard lines, but everyone should agree that the odds of survival are heavily in favor of the consistently adherent.
We should take this opportunity to educate the public on how complicated obtaining an organ transplant can be. More than 6,000 people die each year waiting for an organ because of the supply-and-demand disparities in the transplantation arena. I’m willing to bet that many of the loudest protesters in favor of unvaccinated transplant recipients have not signed the organ donor box on the back of their driver’s license. This conversation is an opportunity to change that and remind people that organ donation may be their only opportunity to save a fellow human’s life.
Again, to quote Ted Lasso: “If you care about someone and you got a little love in your heart, there ain’t nothing you can’t get through together.” That philosophy should apply to the tasks of selecting the best organ donors as well as the best organ recipients.
And every organ should go to the one who will honor their donor and their donor’s family by taking the best care of that ultimate gift of life, including being vaccinated against COVID-19.
Dr. Walton-Shirley is a native Kentuckian who retired from full-time invasive cardiology. She enjoys locums work in Montana and is a champion of physician rights and patient safety. She disclosed no relevant conflicts of interest. A version of this article first appeared on Medscape.com.
Fungating Mass on the Abdominal Wall
The Diagnosis: Basal Cell Carcinoma
Histopathology was consistent with fungating basal cell carcinoma (BCC). The nodules were comprised of syncytial basaloid cells with high nuclear to cytoplasmic ratios, numerous mitotic figures, fibromyxoid stroma, and peripheral nuclear palisading (Figure). Fortunately, no perineural or lymphovascular invasion was identified, and the margins of the specimen were negative. Despite the high-risk nature of giant BCC, the mass was solitary without notable local invasion, leaving it amendable to surgery. On follow-up, the patient has remained recurrence free, and her hemoglobin level has since stabilized.

Skin cancer is the most common malignancy worldwide, and BCC accounts for more than 80% of nonmelanoma skin cancers in the United States. The incidence is on the rise due to the aging population and increasing cumulative skin exposure.1 Risk factors include both individual physical characteristics and environmental exposures. Individuals with lighter skin tones, red and blonde hair, and blue and green eyes are at an increased risk.2 UV radiation exposure is the most important cause of BCC.3 Chronic immunosuppression and exposure to arsenic, ionizing radiation, and psoralen plus UVA radiation also have been linked to the development of BCC.4-6 Basal cell carcinomas most commonly arise on sun-exposed areas such as the face, though more than 10% of cases appear on the trunk.7 Lesions characteristically remain localized, and growth rate is variable; however, when left untreated, BCCs have the potential to become locally destructive and difficult to treat.
Advanced BCCs are tumors that penetrate deeply into the skin. They often are not amenable to traditional therapy and/ or metastasize. Those that grow to a diameter greater than 5 cm, as in our patient, are known as giant BCCs. Only 0.5% to 1% of BCCs are giant BCCs8 ; they typically are more aggressive in nature with higher rates of local recurrence and metastasis. Individuals who develop giant BCCs either have had a delay in access to medical care or a history of BCC that was inadequately managed.9,10 During the COVID-19 pandemic, patient access to health care was substantially impacted during lockdowns. As in our patient, skin neoplasms and other medical conditions may present in later stages due to medical neglect.11,12 Metastasis is rare, even in advanced BCCs. A review of the literature from 1984 estimated that the incidence of metastasis of BCCs is 1 in 1000 to 35,000. Metastasis portends a poor prognosis with a median overall survival of 8 to 14 months.13 An updated review in 2013 found similar outcomes.14
The choice of management for BCCs depends on the risk for recurrence as well as individual patient factors. Characteristics such as tumor size, location, histology, whether it is a primary or recurrent lesion, and the presence of chronic skin disease determine the recurrence rate.15 The management of advanced BCCs often requires a multidisciplinary approach, as these neoplasms may not be amenable to local therapy without causing substantial morbidity. Mohs micrographic surgery is the treatment of choice for BCCs at high risk for recurrence.16 Standard surgical excision with postoperative margin assessment is acceptable when Mohs micrographic surgery is not available.17 Radiation therapy is an alternative for patients who are not candidates for surgery.18
Recently, improved understanding of the molecular pathogenesis of BCCs has led to the development of novel systemic therapies. The Hedgehog signaling pathway has been found to play a critical role in the development of most BCCs.19 Vismodegib and sonidegib are small-molecule inhibitors of the Hedgehog signaling pathway approved for the treatment of locally advanced and metastatic BCCs that are not amenable to surgery or radiation. Approximately 50% of advanced BCCs respond to these therapies; however, long-term treatment may be limited by intolerable side effects and the development of resistance.20 Basal cell carcinomas that spread to lymph nodes or distant sites are treated with traditional systemic therapy. Historically, conventional cytotoxic chemotherapies, such as platinum-containing regimens, were employed with limited benefit and notable morbidity.21
The differential diagnosis for our patient included several other cutaneous neoplasms. Squamous cell carcinoma is the second most common type of skin cancer. Similar to BCC, it can reach a substantial size if left untreated. Risk factors include chronic inflammation, exposure to radiation or chemical carcinogens, burns, human papillomavirus, and other chronic infections. Giant squamous cell carcinomas have high malignant potential and require imaging to assess the extent of invasion and for metastasis. Surgery typically is necessary for both staging and treatment. Adjuvant therapy also may be necessary.22,23
Internal malignant neoplasms rarely present as cutaneous metastases. Breast cancer, melanoma, and cancers of the upper respiratory tract most frequently metastasize to the skin. Although colorectal cancer (CRC) rarely metastasizes to the skin, it is an important cause of cutaneous metastasis due to its high incidence in the general population. When it does spread to the skin, CRC preferentially affects the abdominal wall. Lesions typically resemble the primary tumor but may appear anaplastic. The occurrence of cutaneous metastasis suggests latestage disease and carries a poor prognosis.24
Merkel cell carcinoma and melanoma are aggressive skin cancers with high mortality rates. The former is rarer but more lethal. Merkel cell carcinomas typically occur in elderly white men on sun-exposed areas of the skin. Tumors present as asymptomatic, rapidly expanding, blue-red, firm nodules. Immunosuppression and UV light exposure are notable risk factors.25 Of the 4 major subtypes of cutaneous melanoma, superficial spreading is the most common, followed by nodular, lentigo maligna, and acral lentiginous.26 Superficial spreading melanoma characteristically presents as an expanding asymmetric macule or thin plaque with irregular borders and variation in size and color (black, brown, or red). Nodular melanoma usually presents as symmetric in shape and color (amelanotic, black, or brown). Early recognition by both the patient and clinician is essential in preventing tumor growth and progression.27
Our patient’s presentation was highly concerning for cutaneous metastasis given her history of CRC. Furthermore, the finding of severe anemia was atypical for skin cancer and more characteristic of the prior malignancy. Imaging revealed a locally confined mass with no evidence of extension, lymph node involvement, or additional lesions. The diagnosis was clinched with histopathologic examination.
- Rogers HW, Weinstock MA, Harris AR, et al. Incidence estimate of nonmelanoma skin cancer in the United States, 2006. Arch Dermatol. 2010;146:283-287.
- Lear JT, Tan BB, Smith AG, et al. Risk factors for basal cell carcinoma in the UK: case-control study in 806 patients. J R Soc Med. 1997; 90:371-374.
- Gallagher RP, Hill GB, Bajdik CD, et al. Sunlight exposure, pigmentary factors, and risk of nonmelanocytic skin cancer: I. basal cell carcinoma. Arch Dermatol. 1995;131:157-163.
- Guo HR, Yu HS, Hu H, et al. Arsenic in drinking water and skin cancers: cell-type specificity (Taiwan, ROC). Cancer Causes Control. 2001;12:909-916.
- Lichter MD, Karagas MR, Mott LA, et al; The New Hampshire Skin Cancer Study Group. Therapeutic ionizing radiation and the incidence of basal cell carcinoma and squamous cell carcinoma. Arch Dermatol. 2000;136:1007-1011.
- Nijsten TEC, Stern RS. The increased risk of skin cancer is persistent after discontinuation of psoralen plus ultraviolet A: a cohort study. J Invest Dermatol. 2003;121:252-258.
- Scrivener Y, Grosshans E, Cribier B. Variations of basal cell carcinomas according to gender, age, location and histopathological subtype. Br J Dermatol. 2002;147:41-47.
- Gualdi G, Monari P, Calzavara‐Pinton P, et al. When basal cell carcinomas became giant: an Italian multicenter study. Int J Dermatol. 2020;59:377-382.
- Randle HW, Roenigk RK, Brodland DG. Giant basal cell carcinoma (T3). who is at risk? Cancer. 1993;72:1624-1630.
- Archontaki M, Stavrianos SD, Korkolis DP, et al. Giant basal cell carcinoma: clinicopathological analysis of 51 cases and review of the literature. Anticancer Res. 2009;29:2655-2663.
- Shifat Ahmed SAK, Ajisola M, Azeem K, et al. Impact of the societal response to COVID-19 on access to healthcare for non-COVID-19 health issues in slum communities of Bangladesh, Kenya, Nigeria and Pakistan: results of pre-COVID and COVID-19 lockdown ssstakeholder engagements. BMJ Glob Health. 2020;5:E003042.
- Gomolin T, Cline A, Handler MZ. The danger of neglecting melanoma during the COVID-19 pandemic. J Dermatolog Treat. 2020;31:444-445.
- von Domarus H, Stevens PJ. Metastatic basal cell carcinoma. report of five cases and review of 170 cases in the literature. J Am Acad Dermatol. 1984;10:1043-1060.
- Wysong A, Aasi SZ, Tang JY. Update on metastatic basal cell carcinoma: a summary of published cases from 1981 through 2011. JAMA Dermatol. 2013;149:615-616.
- Bøgelund FS, Philipsen PA, Gniadecki R. Factors affecting the recurrence rate of basal cell carcinoma. Acta Derm Venereol. 2007;87:330-334.
- Mosterd K, Krekels GAM, Nieman FH, et al. Surgical excision versus Mohs’ micrographic surgery for primary and recurrent basal-cell carcinoma of the face: a prospective randomised controlled trial with 5-years’ follow-up. Lancet Oncol. 2008;9:1149-1156.
- Wetzig T, Woitek M, Eichhorn K, et al. Surgical excision of basal cell carcinoma with complete margin control: outcome at 5-year follow-up. Dermatology. 2010;220:363-369.
- Silverman MK, Kopf AW, Gladstein AH, et al. Recurrence rates of treated basal cell carcinomas. part 4: X-ray therapy. J Dermatol Surg Oncol. 1992;18:549-554.
- Tanese K, Emoto K, Kubota N, et al. Immunohistochemical visualization of the signature of activated Hedgehog signaling pathway in cutaneous epithelial tumors. J Dermatol. 2018;45:1181-1186.
- Basset-Séguin N, Hauschild A, Kunstfeld R, et al. Vismodegib in patients with advanced basal cell carcinoma: primary analysis of STEVIE, an international, open-label trial. Eur J Cancer. 2017;86:334-348.
- Carneiro BA, Watkin WG, Mehta UK, et al. Metastatic basal cell carcinoma: complete response to chemotherapy and associated pure red cell aplasia. Cancer Invest. 2006;24:396-400.
- Misiakos EP, Damaskou V, Koumarianou A, et al. A giant squamous cell carcinoma of the skin of the thoracic wall: a case report and review of the literature. J Med Case Rep. 2017;11:136.
- Wollina U, Bayyoud Y, Krönert C, et al. Giant epithelial malignancies (basal cell carcinoma, squamous cell carcinoma): a series of 20 tumors from a single center. J Cutan Aesthet Surg. 2012;5:12-19.
- Bittencourt MJS, Imbiriba AA, Oliveira OA, et al. Cutaneous metastasis of colorectal cancer. An Bras Dermatol. 2018;93:884-886.
- Heath M, Jaimes N, Lemos B, et al. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol. 2008;58:375-381.
- Buettner PG, Leiter U, Eigentler TK, et al. Development of prognostic factors and survival in cutaneous melanoma over 25 years: an analysis of the Central Malignant Melanoma Registry of the German Dermatological Society. Cancer. 2005;103:616-624.
- Klebanov N, Gunasekera N, Lin WM, et al. The clinical spectrum of cutaneous melanoma morphology. J Am Acad Dermatol. 2019; 80:178-188.e3.
The Diagnosis: Basal Cell Carcinoma
Histopathology was consistent with fungating basal cell carcinoma (BCC). The nodules were comprised of syncytial basaloid cells with high nuclear to cytoplasmic ratios, numerous mitotic figures, fibromyxoid stroma, and peripheral nuclear palisading (Figure). Fortunately, no perineural or lymphovascular invasion was identified, and the margins of the specimen were negative. Despite the high-risk nature of giant BCC, the mass was solitary without notable local invasion, leaving it amendable to surgery. On follow-up, the patient has remained recurrence free, and her hemoglobin level has since stabilized.
Skin cancer is the most common malignancy worldwide, and BCC accounts for more than 80% of nonmelanoma skin cancers in the United States. The incidence is on the rise due to the aging population and increasing cumulative skin exposure.1 Risk factors include both individual physical characteristics and environmental exposures. Individuals with lighter skin tones, red and blonde hair, and blue and green eyes are at an increased risk.2 UV radiation exposure is the most important cause of BCC.3 Chronic immunosuppression and exposure to arsenic, ionizing radiation, and psoralen plus UVA radiation also have been linked to the development of BCC.4-6 Basal cell carcinomas most commonly arise on sun-exposed areas such as the face, though more than 10% of cases appear on the trunk.7 Lesions characteristically remain localized, and growth rate is variable; however, when left untreated, BCCs have the potential to become locally destructive and difficult to treat.
Advanced BCCs are tumors that penetrate deeply into the skin. They often are not amenable to traditional therapy and/ or metastasize. Those that grow to a diameter greater than 5 cm, as in our patient, are known as giant BCCs. Only 0.5% to 1% of BCCs are giant BCCs8 ; they typically are more aggressive in nature with higher rates of local recurrence and metastasis. Individuals who develop giant BCCs either have had a delay in access to medical care or a history of BCC that was inadequately managed.9,10 During the COVID-19 pandemic, patient access to health care was substantially impacted during lockdowns. As in our patient, skin neoplasms and other medical conditions may present in later stages due to medical neglect.11,12 Metastasis is rare, even in advanced BCCs. A review of the literature from 1984 estimated that the incidence of metastasis of BCCs is 1 in 1000 to 35,000. Metastasis portends a poor prognosis with a median overall survival of 8 to 14 months.13 An updated review in 2013 found similar outcomes.14
The choice of management for BCCs depends on the risk for recurrence as well as individual patient factors. Characteristics such as tumor size, location, histology, whether it is a primary or recurrent lesion, and the presence of chronic skin disease determine the recurrence rate.15 The management of advanced BCCs often requires a multidisciplinary approach, as these neoplasms may not be amenable to local therapy without causing substantial morbidity. Mohs micrographic surgery is the treatment of choice for BCCs at high risk for recurrence.16 Standard surgical excision with postoperative margin assessment is acceptable when Mohs micrographic surgery is not available.17 Radiation therapy is an alternative for patients who are not candidates for surgery.18
Recently, improved understanding of the molecular pathogenesis of BCCs has led to the development of novel systemic therapies. The Hedgehog signaling pathway has been found to play a critical role in the development of most BCCs.19 Vismodegib and sonidegib are small-molecule inhibitors of the Hedgehog signaling pathway approved for the treatment of locally advanced and metastatic BCCs that are not amenable to surgery or radiation. Approximately 50% of advanced BCCs respond to these therapies; however, long-term treatment may be limited by intolerable side effects and the development of resistance.20 Basal cell carcinomas that spread to lymph nodes or distant sites are treated with traditional systemic therapy. Historically, conventional cytotoxic chemotherapies, such as platinum-containing regimens, were employed with limited benefit and notable morbidity.21
The differential diagnosis for our patient included several other cutaneous neoplasms. Squamous cell carcinoma is the second most common type of skin cancer. Similar to BCC, it can reach a substantial size if left untreated. Risk factors include chronic inflammation, exposure to radiation or chemical carcinogens, burns, human papillomavirus, and other chronic infections. Giant squamous cell carcinomas have high malignant potential and require imaging to assess the extent of invasion and for metastasis. Surgery typically is necessary for both staging and treatment. Adjuvant therapy also may be necessary.22,23
Internal malignant neoplasms rarely present as cutaneous metastases. Breast cancer, melanoma, and cancers of the upper respiratory tract most frequently metastasize to the skin. Although colorectal cancer (CRC) rarely metastasizes to the skin, it is an important cause of cutaneous metastasis due to its high incidence in the general population. When it does spread to the skin, CRC preferentially affects the abdominal wall. Lesions typically resemble the primary tumor but may appear anaplastic. The occurrence of cutaneous metastasis suggests latestage disease and carries a poor prognosis.24
Merkel cell carcinoma and melanoma are aggressive skin cancers with high mortality rates. The former is rarer but more lethal. Merkel cell carcinomas typically occur in elderly white men on sun-exposed areas of the skin. Tumors present as asymptomatic, rapidly expanding, blue-red, firm nodules. Immunosuppression and UV light exposure are notable risk factors.25 Of the 4 major subtypes of cutaneous melanoma, superficial spreading is the most common, followed by nodular, lentigo maligna, and acral lentiginous.26 Superficial spreading melanoma characteristically presents as an expanding asymmetric macule or thin plaque with irregular borders and variation in size and color (black, brown, or red). Nodular melanoma usually presents as symmetric in shape and color (amelanotic, black, or brown). Early recognition by both the patient and clinician is essential in preventing tumor growth and progression.27
Our patient’s presentation was highly concerning for cutaneous metastasis given her history of CRC. Furthermore, the finding of severe anemia was atypical for skin cancer and more characteristic of the prior malignancy. Imaging revealed a locally confined mass with no evidence of extension, lymph node involvement, or additional lesions. The diagnosis was clinched with histopathologic examination.
The Diagnosis: Basal Cell Carcinoma
Histopathology was consistent with fungating basal cell carcinoma (BCC). The nodules were comprised of syncytial basaloid cells with high nuclear to cytoplasmic ratios, numerous mitotic figures, fibromyxoid stroma, and peripheral nuclear palisading (Figure). Fortunately, no perineural or lymphovascular invasion was identified, and the margins of the specimen were negative. Despite the high-risk nature of giant BCC, the mass was solitary without notable local invasion, leaving it amendable to surgery. On follow-up, the patient has remained recurrence free, and her hemoglobin level has since stabilized.
Skin cancer is the most common malignancy worldwide, and BCC accounts for more than 80% of nonmelanoma skin cancers in the United States. The incidence is on the rise due to the aging population and increasing cumulative skin exposure.1 Risk factors include both individual physical characteristics and environmental exposures. Individuals with lighter skin tones, red and blonde hair, and blue and green eyes are at an increased risk.2 UV radiation exposure is the most important cause of BCC.3 Chronic immunosuppression and exposure to arsenic, ionizing radiation, and psoralen plus UVA radiation also have been linked to the development of BCC.4-6 Basal cell carcinomas most commonly arise on sun-exposed areas such as the face, though more than 10% of cases appear on the trunk.7 Lesions characteristically remain localized, and growth rate is variable; however, when left untreated, BCCs have the potential to become locally destructive and difficult to treat.
Advanced BCCs are tumors that penetrate deeply into the skin. They often are not amenable to traditional therapy and/ or metastasize. Those that grow to a diameter greater than 5 cm, as in our patient, are known as giant BCCs. Only 0.5% to 1% of BCCs are giant BCCs8 ; they typically are more aggressive in nature with higher rates of local recurrence and metastasis. Individuals who develop giant BCCs either have had a delay in access to medical care or a history of BCC that was inadequately managed.9,10 During the COVID-19 pandemic, patient access to health care was substantially impacted during lockdowns. As in our patient, skin neoplasms and other medical conditions may present in later stages due to medical neglect.11,12 Metastasis is rare, even in advanced BCCs. A review of the literature from 1984 estimated that the incidence of metastasis of BCCs is 1 in 1000 to 35,000. Metastasis portends a poor prognosis with a median overall survival of 8 to 14 months.13 An updated review in 2013 found similar outcomes.14
The choice of management for BCCs depends on the risk for recurrence as well as individual patient factors. Characteristics such as tumor size, location, histology, whether it is a primary or recurrent lesion, and the presence of chronic skin disease determine the recurrence rate.15 The management of advanced BCCs often requires a multidisciplinary approach, as these neoplasms may not be amenable to local therapy without causing substantial morbidity. Mohs micrographic surgery is the treatment of choice for BCCs at high risk for recurrence.16 Standard surgical excision with postoperative margin assessment is acceptable when Mohs micrographic surgery is not available.17 Radiation therapy is an alternative for patients who are not candidates for surgery.18
Recently, improved understanding of the molecular pathogenesis of BCCs has led to the development of novel systemic therapies. The Hedgehog signaling pathway has been found to play a critical role in the development of most BCCs.19 Vismodegib and sonidegib are small-molecule inhibitors of the Hedgehog signaling pathway approved for the treatment of locally advanced and metastatic BCCs that are not amenable to surgery or radiation. Approximately 50% of advanced BCCs respond to these therapies; however, long-term treatment may be limited by intolerable side effects and the development of resistance.20 Basal cell carcinomas that spread to lymph nodes or distant sites are treated with traditional systemic therapy. Historically, conventional cytotoxic chemotherapies, such as platinum-containing regimens, were employed with limited benefit and notable morbidity.21
The differential diagnosis for our patient included several other cutaneous neoplasms. Squamous cell carcinoma is the second most common type of skin cancer. Similar to BCC, it can reach a substantial size if left untreated. Risk factors include chronic inflammation, exposure to radiation or chemical carcinogens, burns, human papillomavirus, and other chronic infections. Giant squamous cell carcinomas have high malignant potential and require imaging to assess the extent of invasion and for metastasis. Surgery typically is necessary for both staging and treatment. Adjuvant therapy also may be necessary.22,23
Internal malignant neoplasms rarely present as cutaneous metastases. Breast cancer, melanoma, and cancers of the upper respiratory tract most frequently metastasize to the skin. Although colorectal cancer (CRC) rarely metastasizes to the skin, it is an important cause of cutaneous metastasis due to its high incidence in the general population. When it does spread to the skin, CRC preferentially affects the abdominal wall. Lesions typically resemble the primary tumor but may appear anaplastic. The occurrence of cutaneous metastasis suggests latestage disease and carries a poor prognosis.24
Merkel cell carcinoma and melanoma are aggressive skin cancers with high mortality rates. The former is rarer but more lethal. Merkel cell carcinomas typically occur in elderly white men on sun-exposed areas of the skin. Tumors present as asymptomatic, rapidly expanding, blue-red, firm nodules. Immunosuppression and UV light exposure are notable risk factors.25 Of the 4 major subtypes of cutaneous melanoma, superficial spreading is the most common, followed by nodular, lentigo maligna, and acral lentiginous.26 Superficial spreading melanoma characteristically presents as an expanding asymmetric macule or thin plaque with irregular borders and variation in size and color (black, brown, or red). Nodular melanoma usually presents as symmetric in shape and color (amelanotic, black, or brown). Early recognition by both the patient and clinician is essential in preventing tumor growth and progression.27
Our patient’s presentation was highly concerning for cutaneous metastasis given her history of CRC. Furthermore, the finding of severe anemia was atypical for skin cancer and more characteristic of the prior malignancy. Imaging revealed a locally confined mass with no evidence of extension, lymph node involvement, or additional lesions. The diagnosis was clinched with histopathologic examination.
- Rogers HW, Weinstock MA, Harris AR, et al. Incidence estimate of nonmelanoma skin cancer in the United States, 2006. Arch Dermatol. 2010;146:283-287.
- Lear JT, Tan BB, Smith AG, et al. Risk factors for basal cell carcinoma in the UK: case-control study in 806 patients. J R Soc Med. 1997; 90:371-374.
- Gallagher RP, Hill GB, Bajdik CD, et al. Sunlight exposure, pigmentary factors, and risk of nonmelanocytic skin cancer: I. basal cell carcinoma. Arch Dermatol. 1995;131:157-163.
- Guo HR, Yu HS, Hu H, et al. Arsenic in drinking water and skin cancers: cell-type specificity (Taiwan, ROC). Cancer Causes Control. 2001;12:909-916.
- Lichter MD, Karagas MR, Mott LA, et al; The New Hampshire Skin Cancer Study Group. Therapeutic ionizing radiation and the incidence of basal cell carcinoma and squamous cell carcinoma. Arch Dermatol. 2000;136:1007-1011.
- Nijsten TEC, Stern RS. The increased risk of skin cancer is persistent after discontinuation of psoralen plus ultraviolet A: a cohort study. J Invest Dermatol. 2003;121:252-258.
- Scrivener Y, Grosshans E, Cribier B. Variations of basal cell carcinomas according to gender, age, location and histopathological subtype. Br J Dermatol. 2002;147:41-47.
- Gualdi G, Monari P, Calzavara‐Pinton P, et al. When basal cell carcinomas became giant: an Italian multicenter study. Int J Dermatol. 2020;59:377-382.
- Randle HW, Roenigk RK, Brodland DG. Giant basal cell carcinoma (T3). who is at risk? Cancer. 1993;72:1624-1630.
- Archontaki M, Stavrianos SD, Korkolis DP, et al. Giant basal cell carcinoma: clinicopathological analysis of 51 cases and review of the literature. Anticancer Res. 2009;29:2655-2663.
- Shifat Ahmed SAK, Ajisola M, Azeem K, et al. Impact of the societal response to COVID-19 on access to healthcare for non-COVID-19 health issues in slum communities of Bangladesh, Kenya, Nigeria and Pakistan: results of pre-COVID and COVID-19 lockdown ssstakeholder engagements. BMJ Glob Health. 2020;5:E003042.
- Gomolin T, Cline A, Handler MZ. The danger of neglecting melanoma during the COVID-19 pandemic. J Dermatolog Treat. 2020;31:444-445.
- von Domarus H, Stevens PJ. Metastatic basal cell carcinoma. report of five cases and review of 170 cases in the literature. J Am Acad Dermatol. 1984;10:1043-1060.
- Wysong A, Aasi SZ, Tang JY. Update on metastatic basal cell carcinoma: a summary of published cases from 1981 through 2011. JAMA Dermatol. 2013;149:615-616.
- Bøgelund FS, Philipsen PA, Gniadecki R. Factors affecting the recurrence rate of basal cell carcinoma. Acta Derm Venereol. 2007;87:330-334.
- Mosterd K, Krekels GAM, Nieman FH, et al. Surgical excision versus Mohs’ micrographic surgery for primary and recurrent basal-cell carcinoma of the face: a prospective randomised controlled trial with 5-years’ follow-up. Lancet Oncol. 2008;9:1149-1156.
- Wetzig T, Woitek M, Eichhorn K, et al. Surgical excision of basal cell carcinoma with complete margin control: outcome at 5-year follow-up. Dermatology. 2010;220:363-369.
- Silverman MK, Kopf AW, Gladstein AH, et al. Recurrence rates of treated basal cell carcinomas. part 4: X-ray therapy. J Dermatol Surg Oncol. 1992;18:549-554.
- Tanese K, Emoto K, Kubota N, et al. Immunohistochemical visualization of the signature of activated Hedgehog signaling pathway in cutaneous epithelial tumors. J Dermatol. 2018;45:1181-1186.
- Basset-Séguin N, Hauschild A, Kunstfeld R, et al. Vismodegib in patients with advanced basal cell carcinoma: primary analysis of STEVIE, an international, open-label trial. Eur J Cancer. 2017;86:334-348.
- Carneiro BA, Watkin WG, Mehta UK, et al. Metastatic basal cell carcinoma: complete response to chemotherapy and associated pure red cell aplasia. Cancer Invest. 2006;24:396-400.
- Misiakos EP, Damaskou V, Koumarianou A, et al. A giant squamous cell carcinoma of the skin of the thoracic wall: a case report and review of the literature. J Med Case Rep. 2017;11:136.
- Wollina U, Bayyoud Y, Krönert C, et al. Giant epithelial malignancies (basal cell carcinoma, squamous cell carcinoma): a series of 20 tumors from a single center. J Cutan Aesthet Surg. 2012;5:12-19.
- Bittencourt MJS, Imbiriba AA, Oliveira OA, et al. Cutaneous metastasis of colorectal cancer. An Bras Dermatol. 2018;93:884-886.
- Heath M, Jaimes N, Lemos B, et al. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol. 2008;58:375-381.
- Buettner PG, Leiter U, Eigentler TK, et al. Development of prognostic factors and survival in cutaneous melanoma over 25 years: an analysis of the Central Malignant Melanoma Registry of the German Dermatological Society. Cancer. 2005;103:616-624.
- Klebanov N, Gunasekera N, Lin WM, et al. The clinical spectrum of cutaneous melanoma morphology. J Am Acad Dermatol. 2019; 80:178-188.e3.
- Rogers HW, Weinstock MA, Harris AR, et al. Incidence estimate of nonmelanoma skin cancer in the United States, 2006. Arch Dermatol. 2010;146:283-287.
- Lear JT, Tan BB, Smith AG, et al. Risk factors for basal cell carcinoma in the UK: case-control study in 806 patients. J R Soc Med. 1997; 90:371-374.
- Gallagher RP, Hill GB, Bajdik CD, et al. Sunlight exposure, pigmentary factors, and risk of nonmelanocytic skin cancer: I. basal cell carcinoma. Arch Dermatol. 1995;131:157-163.
- Guo HR, Yu HS, Hu H, et al. Arsenic in drinking water and skin cancers: cell-type specificity (Taiwan, ROC). Cancer Causes Control. 2001;12:909-916.
- Lichter MD, Karagas MR, Mott LA, et al; The New Hampshire Skin Cancer Study Group. Therapeutic ionizing radiation and the incidence of basal cell carcinoma and squamous cell carcinoma. Arch Dermatol. 2000;136:1007-1011.
- Nijsten TEC, Stern RS. The increased risk of skin cancer is persistent after discontinuation of psoralen plus ultraviolet A: a cohort study. J Invest Dermatol. 2003;121:252-258.
- Scrivener Y, Grosshans E, Cribier B. Variations of basal cell carcinomas according to gender, age, location and histopathological subtype. Br J Dermatol. 2002;147:41-47.
- Gualdi G, Monari P, Calzavara‐Pinton P, et al. When basal cell carcinomas became giant: an Italian multicenter study. Int J Dermatol. 2020;59:377-382.
- Randle HW, Roenigk RK, Brodland DG. Giant basal cell carcinoma (T3). who is at risk? Cancer. 1993;72:1624-1630.
- Archontaki M, Stavrianos SD, Korkolis DP, et al. Giant basal cell carcinoma: clinicopathological analysis of 51 cases and review of the literature. Anticancer Res. 2009;29:2655-2663.
- Shifat Ahmed SAK, Ajisola M, Azeem K, et al. Impact of the societal response to COVID-19 on access to healthcare for non-COVID-19 health issues in slum communities of Bangladesh, Kenya, Nigeria and Pakistan: results of pre-COVID and COVID-19 lockdown ssstakeholder engagements. BMJ Glob Health. 2020;5:E003042.
- Gomolin T, Cline A, Handler MZ. The danger of neglecting melanoma during the COVID-19 pandemic. J Dermatolog Treat. 2020;31:444-445.
- von Domarus H, Stevens PJ. Metastatic basal cell carcinoma. report of five cases and review of 170 cases in the literature. J Am Acad Dermatol. 1984;10:1043-1060.
- Wysong A, Aasi SZ, Tang JY. Update on metastatic basal cell carcinoma: a summary of published cases from 1981 through 2011. JAMA Dermatol. 2013;149:615-616.
- Bøgelund FS, Philipsen PA, Gniadecki R. Factors affecting the recurrence rate of basal cell carcinoma. Acta Derm Venereol. 2007;87:330-334.
- Mosterd K, Krekels GAM, Nieman FH, et al. Surgical excision versus Mohs’ micrographic surgery for primary and recurrent basal-cell carcinoma of the face: a prospective randomised controlled trial with 5-years’ follow-up. Lancet Oncol. 2008;9:1149-1156.
- Wetzig T, Woitek M, Eichhorn K, et al. Surgical excision of basal cell carcinoma with complete margin control: outcome at 5-year follow-up. Dermatology. 2010;220:363-369.
- Silverman MK, Kopf AW, Gladstein AH, et al. Recurrence rates of treated basal cell carcinomas. part 4: X-ray therapy. J Dermatol Surg Oncol. 1992;18:549-554.
- Tanese K, Emoto K, Kubota N, et al. Immunohistochemical visualization of the signature of activated Hedgehog signaling pathway in cutaneous epithelial tumors. J Dermatol. 2018;45:1181-1186.
- Basset-Séguin N, Hauschild A, Kunstfeld R, et al. Vismodegib in patients with advanced basal cell carcinoma: primary analysis of STEVIE, an international, open-label trial. Eur J Cancer. 2017;86:334-348.
- Carneiro BA, Watkin WG, Mehta UK, et al. Metastatic basal cell carcinoma: complete response to chemotherapy and associated pure red cell aplasia. Cancer Invest. 2006;24:396-400.
- Misiakos EP, Damaskou V, Koumarianou A, et al. A giant squamous cell carcinoma of the skin of the thoracic wall: a case report and review of the literature. J Med Case Rep. 2017;11:136.
- Wollina U, Bayyoud Y, Krönert C, et al. Giant epithelial malignancies (basal cell carcinoma, squamous cell carcinoma): a series of 20 tumors from a single center. J Cutan Aesthet Surg. 2012;5:12-19.
- Bittencourt MJS, Imbiriba AA, Oliveira OA, et al. Cutaneous metastasis of colorectal cancer. An Bras Dermatol. 2018;93:884-886.
- Heath M, Jaimes N, Lemos B, et al. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol. 2008;58:375-381.
- Buettner PG, Leiter U, Eigentler TK, et al. Development of prognostic factors and survival in cutaneous melanoma over 25 years: an analysis of the Central Malignant Melanoma Registry of the German Dermatological Society. Cancer. 2005;103:616-624.
- Klebanov N, Gunasekera N, Lin WM, et al. The clinical spectrum of cutaneous melanoma morphology. J Am Acad Dermatol. 2019; 80:178-188.e3.
A 77-year-old woman was admitted to the hospital with anemia (hemoglobin, 5.2 g/dL [reference range, 12.0–15.5 g/dL]) and a rapidly growing abdominal wall mass. She had a history of stage IIA colon cancer (T3N0M0) that was treated 5 years prior with a partial colon resection and adjuvant chemotherapy. She initially noticed a red scaly lesion developing around a scar from a prior surgery that had been stable for years. Over the last 2 months, the lesion rapidly expanded and would intermittently bleed. Physical examination revealed a 13×10×4.5-cm, pink-red, nodular, firm mass over the patient’s right upper quadrant. Computed tomography revealed a mass limited to the skin and superficial tissue. General surgery was consulted for excision of the mass.


ILAE offers first guide to treating depression in epilepsy
The new guidance highlights the high prevalence of depression among patients with epilepsy while offering the first systematic approach to treatment, reported lead author Marco Mula, MD, PhD, of Atkinson Morley Regional Neuroscience Centre at St George’s University Hospital, London, and colleagues.
“Despite evidence that depression represents a frequently encountered comorbidity [among patients with epilepsy], data on the treatment of depression in epilepsy [are] still limited and recommendations rely mostly on individual clinical experience and expertise,” the investigators wrote in Epilepsia.
Recommendations cover first-line treatment of unipolar depression in epilepsy without other psychiatric disorders.
For patients with mild depression, the guidance supports psychological intervention without pharmacologic therapy; however, if the patient wishes to use medication, has had a positive response to medication in the past, or nonpharmacologic treatments have previously failed or are unavailable, then SSRIs should be considered first-choice therapy. For moderate to severe depression, SSRIs are the first choice, according to Dr. Mula and colleagues.
“It has to be acknowledged that there is considerable debate in the psychiatric literature about the treatment of mild depression in adults,” the investigators noted. “A patient-level meta-analysis pointed out that the magnitude of benefit of antidepressant medications compared with placebo increases with severity of depression symptoms and it may be minimal or nonexistent, on average, in patients with mild or moderate symptoms.”
If a patient does not respond to first-line therapy, then venlafaxine should be considered, according to the guidance. When a patient does respond to therapy, treatment should be continued for at least 6 months, and when residual symptoms persist, treatment should be continued until resolution.
“In people with depression it is established that around two-thirds of patients do not achieve full remission with first-line treatment,” Dr. Mula and colleagues wrote. “In people with epilepsy, current data show that up to 50% of patients do not achieve full remission from depression. For this reason, augmentation strategies are often needed. They should be adopted by psychiatrists, neuropsychiatrists, or mental health professionals familiar with such therapeutic strategies.”
Beyond these key recommendations, the guidance covers a range of additional topics, including other pharmacologic options, medication discontinuation strategies, electroconvulsive therapy, light therapy, exercise training, vagus nerve stimulation, and repetitive transcranial magnetic stimulation.
Useful advice that counters common misconceptions
According to Jacqueline A. French, MD, a professor at NYU Langone Medical Center, Dr. Mula and colleagues are “top notch,” and their recommendations “hit every nail on the head.”

Dr. French, chief medical officer of The Epilepsy Foundation, emphasized the importance of the publication, which addresses two common misconceptions within the medical community: First, that standard antidepressants are insufficient to treat depression in patients with epilepsy, and second, that antidepressants may trigger seizures.
“The first purpose [of the publication] is to say, yes, these antidepressants do work,” Dr. French said, “and no, they don’t worsen seizures, and you can use them safely, and they are appropriate to use.”
Dr. French explained that managing depression remains a practice gap among epileptologists and neurologists because it is a diagnosis that doesn’t traditionally fall into their purview, yet many patients with epilepsy forgo visiting their primary care providers, who more frequently diagnose and manage depression. Dr. French agreed with the guidance that epilepsy specialists should fill this gap.
“We need to at least be able to take people through their first antidepressant, even though we were not trained to be psychiatrists,” Dr. French said. “That’s part of the best care of our patients.”
Imad Najm, MD, director of the Charles Shor Epilepsy Center, Cleveland Clinic, said the recommendations are a step forward in the field, as they are supported by clinical data, instead of just clinical experience and expertise.

Still, Dr. Najm noted that more work is needed to stratify risk of depression in epilepsy and evaluate a possible causal relationship between epilepsy therapies and depression.
He went on to emphasizes the scale of issue at hand, and the stakes involved.
“Depression, anxiety, and psychosis affect a large number of patients with epilepsy,” Dr. Najm said. “Clinical screening and recognition of these comorbidities leads to the institution of treatment options and significant improvement in quality of life. Mental health professionals should be an integral part of any comprehensive epilepsy center.”
The investigators disclosed relationships with Esai, UCB, Elsevier, and others. Dr. French is indirectly involved with multiple pharmaceutical companies developing epilepsy drugs through her role as director of The Epilepsy Study Consortium, a nonprofit organization. Dr. Najm reported no conflicts of interest.
The new guidance highlights the high prevalence of depression among patients with epilepsy while offering the first systematic approach to treatment, reported lead author Marco Mula, MD, PhD, of Atkinson Morley Regional Neuroscience Centre at St George’s University Hospital, London, and colleagues.
“Despite evidence that depression represents a frequently encountered comorbidity [among patients with epilepsy], data on the treatment of depression in epilepsy [are] still limited and recommendations rely mostly on individual clinical experience and expertise,” the investigators wrote in Epilepsia.
Recommendations cover first-line treatment of unipolar depression in epilepsy without other psychiatric disorders.
For patients with mild depression, the guidance supports psychological intervention without pharmacologic therapy; however, if the patient wishes to use medication, has had a positive response to medication in the past, or nonpharmacologic treatments have previously failed or are unavailable, then SSRIs should be considered first-choice therapy. For moderate to severe depression, SSRIs are the first choice, according to Dr. Mula and colleagues.
“It has to be acknowledged that there is considerable debate in the psychiatric literature about the treatment of mild depression in adults,” the investigators noted. “A patient-level meta-analysis pointed out that the magnitude of benefit of antidepressant medications compared with placebo increases with severity of depression symptoms and it may be minimal or nonexistent, on average, in patients with mild or moderate symptoms.”
If a patient does not respond to first-line therapy, then venlafaxine should be considered, according to the guidance. When a patient does respond to therapy, treatment should be continued for at least 6 months, and when residual symptoms persist, treatment should be continued until resolution.
“In people with depression it is established that around two-thirds of patients do not achieve full remission with first-line treatment,” Dr. Mula and colleagues wrote. “In people with epilepsy, current data show that up to 50% of patients do not achieve full remission from depression. For this reason, augmentation strategies are often needed. They should be adopted by psychiatrists, neuropsychiatrists, or mental health professionals familiar with such therapeutic strategies.”
Beyond these key recommendations, the guidance covers a range of additional topics, including other pharmacologic options, medication discontinuation strategies, electroconvulsive therapy, light therapy, exercise training, vagus nerve stimulation, and repetitive transcranial magnetic stimulation.
Useful advice that counters common misconceptions
According to Jacqueline A. French, MD, a professor at NYU Langone Medical Center, Dr. Mula and colleagues are “top notch,” and their recommendations “hit every nail on the head.”
Dr. French, chief medical officer of The Epilepsy Foundation, emphasized the importance of the publication, which addresses two common misconceptions within the medical community: First, that standard antidepressants are insufficient to treat depression in patients with epilepsy, and second, that antidepressants may trigger seizures.
“The first purpose [of the publication] is to say, yes, these antidepressants do work,” Dr. French said, “and no, they don’t worsen seizures, and you can use them safely, and they are appropriate to use.”
Dr. French explained that managing depression remains a practice gap among epileptologists and neurologists because it is a diagnosis that doesn’t traditionally fall into their purview, yet many patients with epilepsy forgo visiting their primary care providers, who more frequently diagnose and manage depression. Dr. French agreed with the guidance that epilepsy specialists should fill this gap.
“We need to at least be able to take people through their first antidepressant, even though we were not trained to be psychiatrists,” Dr. French said. “That’s part of the best care of our patients.”
Imad Najm, MD, director of the Charles Shor Epilepsy Center, Cleveland Clinic, said the recommendations are a step forward in the field, as they are supported by clinical data, instead of just clinical experience and expertise.
Still, Dr. Najm noted that more work is needed to stratify risk of depression in epilepsy and evaluate a possible causal relationship between epilepsy therapies and depression.
He went on to emphasizes the scale of issue at hand, and the stakes involved.
“Depression, anxiety, and psychosis affect a large number of patients with epilepsy,” Dr. Najm said. “Clinical screening and recognition of these comorbidities leads to the institution of treatment options and significant improvement in quality of life. Mental health professionals should be an integral part of any comprehensive epilepsy center.”
The investigators disclosed relationships with Esai, UCB, Elsevier, and others. Dr. French is indirectly involved with multiple pharmaceutical companies developing epilepsy drugs through her role as director of The Epilepsy Study Consortium, a nonprofit organization. Dr. Najm reported no conflicts of interest.
The new guidance highlights the high prevalence of depression among patients with epilepsy while offering the first systematic approach to treatment, reported lead author Marco Mula, MD, PhD, of Atkinson Morley Regional Neuroscience Centre at St George’s University Hospital, London, and colleagues.
“Despite evidence that depression represents a frequently encountered comorbidity [among patients with epilepsy], data on the treatment of depression in epilepsy [are] still limited and recommendations rely mostly on individual clinical experience and expertise,” the investigators wrote in Epilepsia.
Recommendations cover first-line treatment of unipolar depression in epilepsy without other psychiatric disorders.
For patients with mild depression, the guidance supports psychological intervention without pharmacologic therapy; however, if the patient wishes to use medication, has had a positive response to medication in the past, or nonpharmacologic treatments have previously failed or are unavailable, then SSRIs should be considered first-choice therapy. For moderate to severe depression, SSRIs are the first choice, according to Dr. Mula and colleagues.
“It has to be acknowledged that there is considerable debate in the psychiatric literature about the treatment of mild depression in adults,” the investigators noted. “A patient-level meta-analysis pointed out that the magnitude of benefit of antidepressant medications compared with placebo increases with severity of depression symptoms and it may be minimal or nonexistent, on average, in patients with mild or moderate symptoms.”
If a patient does not respond to first-line therapy, then venlafaxine should be considered, according to the guidance. When a patient does respond to therapy, treatment should be continued for at least 6 months, and when residual symptoms persist, treatment should be continued until resolution.
“In people with depression it is established that around two-thirds of patients do not achieve full remission with first-line treatment,” Dr. Mula and colleagues wrote. “In people with epilepsy, current data show that up to 50% of patients do not achieve full remission from depression. For this reason, augmentation strategies are often needed. They should be adopted by psychiatrists, neuropsychiatrists, or mental health professionals familiar with such therapeutic strategies.”
Beyond these key recommendations, the guidance covers a range of additional topics, including other pharmacologic options, medication discontinuation strategies, electroconvulsive therapy, light therapy, exercise training, vagus nerve stimulation, and repetitive transcranial magnetic stimulation.
Useful advice that counters common misconceptions
According to Jacqueline A. French, MD, a professor at NYU Langone Medical Center, Dr. Mula and colleagues are “top notch,” and their recommendations “hit every nail on the head.”
Dr. French, chief medical officer of The Epilepsy Foundation, emphasized the importance of the publication, which addresses two common misconceptions within the medical community: First, that standard antidepressants are insufficient to treat depression in patients with epilepsy, and second, that antidepressants may trigger seizures.
“The first purpose [of the publication] is to say, yes, these antidepressants do work,” Dr. French said, “and no, they don’t worsen seizures, and you can use them safely, and they are appropriate to use.”
Dr. French explained that managing depression remains a practice gap among epileptologists and neurologists because it is a diagnosis that doesn’t traditionally fall into their purview, yet many patients with epilepsy forgo visiting their primary care providers, who more frequently diagnose and manage depression. Dr. French agreed with the guidance that epilepsy specialists should fill this gap.
“We need to at least be able to take people through their first antidepressant, even though we were not trained to be psychiatrists,” Dr. French said. “That’s part of the best care of our patients.”
Imad Najm, MD, director of the Charles Shor Epilepsy Center, Cleveland Clinic, said the recommendations are a step forward in the field, as they are supported by clinical data, instead of just clinical experience and expertise.
Still, Dr. Najm noted that more work is needed to stratify risk of depression in epilepsy and evaluate a possible causal relationship between epilepsy therapies and depression.
He went on to emphasizes the scale of issue at hand, and the stakes involved.
“Depression, anxiety, and psychosis affect a large number of patients with epilepsy,” Dr. Najm said. “Clinical screening and recognition of these comorbidities leads to the institution of treatment options and significant improvement in quality of life. Mental health professionals should be an integral part of any comprehensive epilepsy center.”
The investigators disclosed relationships with Esai, UCB, Elsevier, and others. Dr. French is indirectly involved with multiple pharmaceutical companies developing epilepsy drugs through her role as director of The Epilepsy Study Consortium, a nonprofit organization. Dr. Najm reported no conflicts of interest.
FROM EPILEPSIA
Malnutrition common in patients with IBD
Malnutrition is common among patients with inflammatory bowel disease (IBD) and is associated with worse outcomes that can prolong hospitalizations and increase patients’ risk for death.
As many as 85% of inpatients with IBD may be malnourished, with the severity of malnutrition affected by disease activity, extent, and duration, said Kelly Issokson, MS, RD, CNSC, clinical nutrition coordinator in the IBD program in the division of gastroenterology at Cedars-Sinai Medical Center, Los Angeles.
“Malnutrition is a severe complication of IBD, and it should not be overlooked,” she said during an oral presentation at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
In patients with IBD, malabsorption, enteric losses, inadequate intake, and side effects of medical therapy can all lead to malnutrition, which in turn is an independent risk factor for venous thromboembolic events, nonelective surgery, longer hospital stays, and increased mortality.
In addition, malnutrition in IBD increases risk for infection and sepsis, and for perioperative complications, and can more than double the cost of care, compared with adequately nourished IBD patients, she said.
Ms. Issokson cited a definition of malnutrition from the American Society of Parenteral and Enteral Nutrition as “an acute or chronic state of overnutrition or undernutrition with or without inflammatory activity that has led to a change in body composition and diminished function.”
Lab findings of low albumin, low prealbumin, or isolated metrics such as weight loss or change in body mass index do not constitute malnutrition and should not be used to diagnosis it, Ms. Issokson cautioned.
Patients at low risk for malnutrition have no unintentional weight loss, are eating well, have minimal or no dietary restrictions, and no wasting. In contrast, high-risk patients have unintentional weight loss, decreased appetite and/or food intake, restrict multiple foods, or show signs of wasting.
Screening
“Nutrition screening is the first step in diagnosing a patient with malnutrition. This is a process of identifying individuals who may be at nutrition risk and benefit from assessment from a registered dietitian,” Ms. Issokson said.
The Malnutrition Screening Tool is quick, easy to administer, and requires minimal training. It can be used to screen adults for malnutrition regardless of age, medical history, or setting, she said.
The two-item instrument asks, “Have you recently lost weight without trying?” with a “no” scored as 0 and a “yes” scored as 2. The second question is, “Have you been eating poorly because of decreased appetite, with a “no” equal to 0 and a “yes” equal to 1. Patients with a score of 0 or 1 are not at risk, whereas patients with scores of 2 or 3 are deemed to be at risk for malnutrition and require further assessment by a dietitian.
Assessment
Assessment for malnutrition involves a variety of factors, including anthropometric factors such as weight and BMI changes; biochemical markers such as fat-soluble vitamins, water-soluble vitamins, minerals, and urinary sodium; symptoms such as decreased appetite, abdominal pain, cramping or bloating, diarrhea, or urgency or obstructive symptoms; and body composition measures such as handgrip strength, biochemical impedance analysis, skinfold thickness, bone mineral density, and muscle mass.
Other nutritional assessment tools may include 24-hour recall of nutrition intake, diet history, and questions about eating behaviors, food allergies or intolerances, and cultural or religious food preferences.
Assessing food security is also important, especially during the current pandemic, Ms. Issokson emphasized.
“Is your patient running out of food? Do they have money to purchase food? Are they able to go to the grocery store to buy food? This is essential to know when you’re developing a nutrition plan,” she said.
A nutrition-focused physical exam should include assessment of skin manifestation, secondary to malnutrition or malabsorption, such as dry skin, delayed wound healing, stomatitis, scurvy, seborrheic dermatitis, bleeding, and periorificial and acral dermatitis or alopecia.
Diagnosis
Currently available malnutrition criteria have not been validated for use in patients with IBD, and further studies are needed to affirm their applicability to this population, Ms. Issokson said.
The Academy of Nutrition and Dietetics–American Society for Parenteral and Enteral Nutrition (AND-ASPEN) malnutrition criteria require measures of weight loss, energy intake, subcutaneous fat loss, subcutaneous muscle loss, general or local fluid accumulation, and handgrip strength to determine whether a patient is moderately or severely malnourished.
Ms. Issokson said that she finds the European Society for Clinical Nutrition and Metabolism Global Leadership Initiative on Malnutrition (ESPEN GLIM) criteria somewhat easier to use for diagnosis, as they consist of phenotypic and etiologic criteria, with patients who meet at least one of each being considered malnourished.
“When identified, document malnutrition, and of course intervene appropriately by referring to a dietitian providing education and supporting the patient to help them optimize their nutrition and improve their outcomes,” she concluded.
In a discussion following the session, panelist Neha Shah, MPH, RD, CNSC, a dietitian and health education specialist at the University of California, San Francisco, commented on the importance of malnutrition assessment in patients with IBD being considered for surgery.
Patients should be screened for malnutrition, and if they have a positive screen, “should be automatically referred to a registered dietitian specializing in IBD for a nutrition assessment,” she said.
“Certainly, a nutritional assessment, as Kelly has highlighted really well, will encompass an evaluation of various areas of health – patient history, food and nutrition history, changing anthropometrics, alterations in labs – and certainly going into further nutrition history with net food intolerance, intake from each food group, portions, access, support, culture, eating environment, skills in the kitchen, relationship with diet.”
Ms. Issokson is a board member of the Crohn’s & Colitis Foundation and a digital advisory board member of Avant Healthcare. Ms. Shah had no disclosures.
Malnutrition is common among patients with inflammatory bowel disease (IBD) and is associated with worse outcomes that can prolong hospitalizations and increase patients’ risk for death.
As many as 85% of inpatients with IBD may be malnourished, with the severity of malnutrition affected by disease activity, extent, and duration, said Kelly Issokson, MS, RD, CNSC, clinical nutrition coordinator in the IBD program in the division of gastroenterology at Cedars-Sinai Medical Center, Los Angeles.
“Malnutrition is a severe complication of IBD, and it should not be overlooked,” she said during an oral presentation at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
In patients with IBD, malabsorption, enteric losses, inadequate intake, and side effects of medical therapy can all lead to malnutrition, which in turn is an independent risk factor for venous thromboembolic events, nonelective surgery, longer hospital stays, and increased mortality.
In addition, malnutrition in IBD increases risk for infection and sepsis, and for perioperative complications, and can more than double the cost of care, compared with adequately nourished IBD patients, she said.
Ms. Issokson cited a definition of malnutrition from the American Society of Parenteral and Enteral Nutrition as “an acute or chronic state of overnutrition or undernutrition with or without inflammatory activity that has led to a change in body composition and diminished function.”
Lab findings of low albumin, low prealbumin, or isolated metrics such as weight loss or change in body mass index do not constitute malnutrition and should not be used to diagnosis it, Ms. Issokson cautioned.
Patients at low risk for malnutrition have no unintentional weight loss, are eating well, have minimal or no dietary restrictions, and no wasting. In contrast, high-risk patients have unintentional weight loss, decreased appetite and/or food intake, restrict multiple foods, or show signs of wasting.
Screening
“Nutrition screening is the first step in diagnosing a patient with malnutrition. This is a process of identifying individuals who may be at nutrition risk and benefit from assessment from a registered dietitian,” Ms. Issokson said.
The Malnutrition Screening Tool is quick, easy to administer, and requires minimal training. It can be used to screen adults for malnutrition regardless of age, medical history, or setting, she said.
The two-item instrument asks, “Have you recently lost weight without trying?” with a “no” scored as 0 and a “yes” scored as 2. The second question is, “Have you been eating poorly because of decreased appetite, with a “no” equal to 0 and a “yes” equal to 1. Patients with a score of 0 or 1 are not at risk, whereas patients with scores of 2 or 3 are deemed to be at risk for malnutrition and require further assessment by a dietitian.
Assessment
Assessment for malnutrition involves a variety of factors, including anthropometric factors such as weight and BMI changes; biochemical markers such as fat-soluble vitamins, water-soluble vitamins, minerals, and urinary sodium; symptoms such as decreased appetite, abdominal pain, cramping or bloating, diarrhea, or urgency or obstructive symptoms; and body composition measures such as handgrip strength, biochemical impedance analysis, skinfold thickness, bone mineral density, and muscle mass.
Other nutritional assessment tools may include 24-hour recall of nutrition intake, diet history, and questions about eating behaviors, food allergies or intolerances, and cultural or religious food preferences.
Assessing food security is also important, especially during the current pandemic, Ms. Issokson emphasized.
“Is your patient running out of food? Do they have money to purchase food? Are they able to go to the grocery store to buy food? This is essential to know when you’re developing a nutrition plan,” she said.
A nutrition-focused physical exam should include assessment of skin manifestation, secondary to malnutrition or malabsorption, such as dry skin, delayed wound healing, stomatitis, scurvy, seborrheic dermatitis, bleeding, and periorificial and acral dermatitis or alopecia.
Diagnosis
Currently available malnutrition criteria have not been validated for use in patients with IBD, and further studies are needed to affirm their applicability to this population, Ms. Issokson said.
The Academy of Nutrition and Dietetics–American Society for Parenteral and Enteral Nutrition (AND-ASPEN) malnutrition criteria require measures of weight loss, energy intake, subcutaneous fat loss, subcutaneous muscle loss, general or local fluid accumulation, and handgrip strength to determine whether a patient is moderately or severely malnourished.
Ms. Issokson said that she finds the European Society for Clinical Nutrition and Metabolism Global Leadership Initiative on Malnutrition (ESPEN GLIM) criteria somewhat easier to use for diagnosis, as they consist of phenotypic and etiologic criteria, with patients who meet at least one of each being considered malnourished.
“When identified, document malnutrition, and of course intervene appropriately by referring to a dietitian providing education and supporting the patient to help them optimize their nutrition and improve their outcomes,” she concluded.
In a discussion following the session, panelist Neha Shah, MPH, RD, CNSC, a dietitian and health education specialist at the University of California, San Francisco, commented on the importance of malnutrition assessment in patients with IBD being considered for surgery.
Patients should be screened for malnutrition, and if they have a positive screen, “should be automatically referred to a registered dietitian specializing in IBD for a nutrition assessment,” she said.
“Certainly, a nutritional assessment, as Kelly has highlighted really well, will encompass an evaluation of various areas of health – patient history, food and nutrition history, changing anthropometrics, alterations in labs – and certainly going into further nutrition history with net food intolerance, intake from each food group, portions, access, support, culture, eating environment, skills in the kitchen, relationship with diet.”
Ms. Issokson is a board member of the Crohn’s & Colitis Foundation and a digital advisory board member of Avant Healthcare. Ms. Shah had no disclosures.
Malnutrition is common among patients with inflammatory bowel disease (IBD) and is associated with worse outcomes that can prolong hospitalizations and increase patients’ risk for death.
As many as 85% of inpatients with IBD may be malnourished, with the severity of malnutrition affected by disease activity, extent, and duration, said Kelly Issokson, MS, RD, CNSC, clinical nutrition coordinator in the IBD program in the division of gastroenterology at Cedars-Sinai Medical Center, Los Angeles.
“Malnutrition is a severe complication of IBD, and it should not be overlooked,” she said during an oral presentation at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
In patients with IBD, malabsorption, enteric losses, inadequate intake, and side effects of medical therapy can all lead to malnutrition, which in turn is an independent risk factor for venous thromboembolic events, nonelective surgery, longer hospital stays, and increased mortality.
In addition, malnutrition in IBD increases risk for infection and sepsis, and for perioperative complications, and can more than double the cost of care, compared with adequately nourished IBD patients, she said.
Ms. Issokson cited a definition of malnutrition from the American Society of Parenteral and Enteral Nutrition as “an acute or chronic state of overnutrition or undernutrition with or without inflammatory activity that has led to a change in body composition and diminished function.”
Lab findings of low albumin, low prealbumin, or isolated metrics such as weight loss or change in body mass index do not constitute malnutrition and should not be used to diagnosis it, Ms. Issokson cautioned.
Patients at low risk for malnutrition have no unintentional weight loss, are eating well, have minimal or no dietary restrictions, and no wasting. In contrast, high-risk patients have unintentional weight loss, decreased appetite and/or food intake, restrict multiple foods, or show signs of wasting.
Screening
“Nutrition screening is the first step in diagnosing a patient with malnutrition. This is a process of identifying individuals who may be at nutrition risk and benefit from assessment from a registered dietitian,” Ms. Issokson said.
The Malnutrition Screening Tool is quick, easy to administer, and requires minimal training. It can be used to screen adults for malnutrition regardless of age, medical history, or setting, she said.
The two-item instrument asks, “Have you recently lost weight without trying?” with a “no” scored as 0 and a “yes” scored as 2. The second question is, “Have you been eating poorly because of decreased appetite, with a “no” equal to 0 and a “yes” equal to 1. Patients with a score of 0 or 1 are not at risk, whereas patients with scores of 2 or 3 are deemed to be at risk for malnutrition and require further assessment by a dietitian.
Assessment
Assessment for malnutrition involves a variety of factors, including anthropometric factors such as weight and BMI changes; biochemical markers such as fat-soluble vitamins, water-soluble vitamins, minerals, and urinary sodium; symptoms such as decreased appetite, abdominal pain, cramping or bloating, diarrhea, or urgency or obstructive symptoms; and body composition measures such as handgrip strength, biochemical impedance analysis, skinfold thickness, bone mineral density, and muscle mass.
Other nutritional assessment tools may include 24-hour recall of nutrition intake, diet history, and questions about eating behaviors, food allergies or intolerances, and cultural or religious food preferences.
Assessing food security is also important, especially during the current pandemic, Ms. Issokson emphasized.
“Is your patient running out of food? Do they have money to purchase food? Are they able to go to the grocery store to buy food? This is essential to know when you’re developing a nutrition plan,” she said.
A nutrition-focused physical exam should include assessment of skin manifestation, secondary to malnutrition or malabsorption, such as dry skin, delayed wound healing, stomatitis, scurvy, seborrheic dermatitis, bleeding, and periorificial and acral dermatitis or alopecia.
Diagnosis
Currently available malnutrition criteria have not been validated for use in patients with IBD, and further studies are needed to affirm their applicability to this population, Ms. Issokson said.
The Academy of Nutrition and Dietetics–American Society for Parenteral and Enteral Nutrition (AND-ASPEN) malnutrition criteria require measures of weight loss, energy intake, subcutaneous fat loss, subcutaneous muscle loss, general or local fluid accumulation, and handgrip strength to determine whether a patient is moderately or severely malnourished.
Ms. Issokson said that she finds the European Society for Clinical Nutrition and Metabolism Global Leadership Initiative on Malnutrition (ESPEN GLIM) criteria somewhat easier to use for diagnosis, as they consist of phenotypic and etiologic criteria, with patients who meet at least one of each being considered malnourished.
“When identified, document malnutrition, and of course intervene appropriately by referring to a dietitian providing education and supporting the patient to help them optimize their nutrition and improve their outcomes,” she concluded.
In a discussion following the session, panelist Neha Shah, MPH, RD, CNSC, a dietitian and health education specialist at the University of California, San Francisco, commented on the importance of malnutrition assessment in patients with IBD being considered for surgery.
Patients should be screened for malnutrition, and if they have a positive screen, “should be automatically referred to a registered dietitian specializing in IBD for a nutrition assessment,” she said.
“Certainly, a nutritional assessment, as Kelly has highlighted really well, will encompass an evaluation of various areas of health – patient history, food and nutrition history, changing anthropometrics, alterations in labs – and certainly going into further nutrition history with net food intolerance, intake from each food group, portions, access, support, culture, eating environment, skills in the kitchen, relationship with diet.”
Ms. Issokson is a board member of the Crohn’s & Colitis Foundation and a digital advisory board member of Avant Healthcare. Ms. Shah had no disclosures.
FROM THE CROHN’S & COLITIS CONGRESS