User login
Experts Debate How to Best Define Obesity
in three new opinion papers.
The three statements were published on July 22, 2024, in Annals of Internal Medicine. In one, the authors expressed caution about the recent movement away from using BMI alone to define obesity, noting that the measure remains a useful population-level and clinical tool for addressing adiposity, particularly within racial and ethnic groups. But the authors of a second paper pointed out that the use of lower BMI cutoffs to define obesity in Asian populations, in place since 2004, is inadequate in part because it doesn’t account for heterogeneity among different Asian groups.
And in the third paper, an editorial, an Annals editor cautioned that the recent framing of obesity exclusively as a “disease” rather than a “broader, more inclusive construct” may inadvertently reinforce the bias it was meant to combat.
Asked to comment on the issues raised in the papers, Professor Gijs Goossens of Maastricht University Medical Center, Maastricht, the Netherlands, said, “It is important to emphasize that the management and treatment of obesity have wider objectives than weight loss alone and include the prevention, resolution, or improvement of obesity-related complications; achieving better quality of life and mental well-being; and improvement of physical and social functioning.”
Added Dr. Goossens, who was an author of a recent European Association for the Study of Obesity (EASO) framework calling for moving beyond BMI in defining obesity, “Personalized therapeutic goals should be set at the beginning of the treatment, according to the stage of obesity, taking into account available therapeutic options, possible side effects or risks, and patient preferences. The drivers of obesity and possible barriers to treatment should also be discussed with the patient.” Dr. Goossens emphasized that he was providing his personal views and not speaking for the EASO or his coauthors.
BMI: ‘Not a Perfect Measure of Adiposity but Remains Useful’
In their “Ideas and Opinions” paper, Adolfo G. Cuevas, PhD, of New York University School of Global Public Health, New York City, and Walter C. Willett, MD, DrPH, of Harvard T.H. Chan School of Public Health, Boston, argued that “BMI, although not a perfect measure of adiposity, remains a useful population-level and clinical tool for addressing adiposity, including within groups defined by race and ethnicity.”
They added that despite the criticism that BMI doesn’t distinguish between fat and lean body mass, the measure still strongly correlates with fat mass as well as cardiovascular risk and mortality, and it does so similarly across racial and ethnic groups.
Clinically, Dr. Cuevas and Dr. Willett pointed out that BMI correlates fat mass as assessed with the gold standard measure dual x-ray absorptiometry but is far simpler and less expensive. Measuring waist circumference can provide additional information about visceral fat and disease risk but is “more difficult to standardize and suffers from the same limitations as BMI when cut points are used.”
They suggest the addition of change in weight since early adulthood and over time as a “simple and sensitive variable” for assessing adiposity.
Luca Busetto, MD, associate professor of medicine at the University of Padua, Italy, and the first author of the EASO framework, said, “The paper from Cuevas and Willett sounds like a strong defense of BMI, and I can substantially agree with this defense ... We remain anchored on BMI, but we tried to move beyond it adding an estimate of high risk abdominal fat — waist to height ratio — and coupling the anthropometric assessment with a complete clinical evaluation and staging.”
Dr. Goossens said, “I agree with the authors that despite the limitations of BMI as a measure of body fatness, it remains a useful clinical screening tool. Yet the diagnosis of obesity should not be based solely on BMI” due to the stronger association of abdominal fat with cardiometabolic complications.
That link, he noted, “also applies to individuals with a BMI level below the current cutoff values for obesity, who may already have medical, functional, or psychological impairments. We should be aware of the risk of undertreatment in this particular group of patients.”
Does Calling Obesity a ‘Disease’ Have Unintended Consequences?
In her editorial, Christina C. Wee, MD, senior deputy editor, Annals of Internal Medicine, wrote, “Beyond diagnostic challenges, framing obesity exclusively as a disease rather than a broader, more inclusive construct may have unintended consequences — including reinforcing the weight bias this framing was in part intended to combat.”
Focusing solely on biological causes of obesity while ignoring psychosocial, cultural, environmental, and behavioral contexts could undermine public health and policy efforts to address those factors, Dr. Wee argued.
Moreover, she wrote, “Ironically, framing obesity as a disease to justify coverage for treatment reinforces weight bias. It conflates the need to label a condition a disease with healthcare reimbursement and raises the stakes for developing accurate diagnostic criteria ... By exclusively linking obesity as a disease to reimbursement, it sends the message that only those who manifest disease from excess adiposity warrant treatment — and, by inference, those on the continuum who have not yet manifested disease do not warrant treatment.”
Likening obesity to other risk factors such as hypertension or dyslipidemia for which treatment is typically reimbursed, Dr. Wee pointed out that Medicare still prohibits coverage of medications for obesity.
Regarding the high costs of newer obesity medications and the need for payers and clinicians to ration their use, Dr. Wee argued, “Rather than focusing on whether one’s adiposity conforms to an expert panel’s definition of ‘disease,’ we should address how to best stage obesity risk with sufficient accuracy and fairness and reach a consensus on how to prioritize and match treatments to individual patients.”
Dr. Busetto said that EASO stands by its definition of obesity as a disease, adding “we can adhere to the suggestion of a holistic approach deciding treatment modalities according to the risk and the presence of mental, functional, and medical complications of impairments. Of course, we cannot agree on any proposal that is oriented at leaving patients with obesity still in the asymptomatic phase of the disease without treatment. This would be like treating diabetes only after the occurrence of nephropathy or managing hypertension only after a stroke. Prevention of the symptomatic stage is a part of obesity management, even beyond weight loss.”
Dr. Goossens said, “indeed, it is of utmost importance to develop accurate risk stratification tools for adequately clinical staging of obesity, according to the severity of its medical, psychological and functional impairments.”
Do the Current Lower BMI Cutoffs for Defining Obesity in Asian People Make Sense?
Simar S. Bajaj, AB, of Harvard University, Cambridge, Massachusetts, and colleagues, all of Harvard Medical School, Boston, raised several concerns regarding the 2004 World Health Organization’s suggestion to use lower BMI categories for defining overweight and obesity in Asian populations, that is, 23-27.5 kg/m2 and 27.5 kg/m2 or higher for obesity, respectively, as opposed to 25-29.9 and ≥ 30, respectively, for other populations.
Different Asian countries have created their own obesity BMI cutoffs, ranging from 25 kg/m2 in India to 28 kg/m2 in China. But “Asian Americans continue to be treated as a monolith without official disaggregated cutoffs,” Mr. Bajaj and colleagues noted.
The heterogeneity translates to different risk levels across Asian subgroups. For example, in one study, age- and sex-adjusted BMI cutoffs for increased risk of developing type 2 diabetes were 23.9 kg/m2 in South Asian populations, 26.6 kg/m2 in Arab populations, 26.9 kg/m2 in Chinese populations, and 28.1 kg/m2 in Black populations.
These findings raise important questions, the researchers said. “Does it make sense for people of Chinese descent to use the same BMI threshold as the South Asian group when their ‘equivalent risk cutoff’ is closer to that of Arab and Black groups who share the standard BMI threshold?” Most data in this area are cross-sectional rather than the longitudinal data needed to answer those questions, they noted.
They suggest that professional diabetes and obesity organizations consider BMI thresholds to be “placeholders” until more sensitive and specific thresholds can be defined for Asian American populations.
Mr. Bajaj and colleagues also noted the need for disaggregated data is not unique to Asian groups but that they focused on Asian Americans for two main reasons. “First, success would create a precedent for complete disaggregation and help ensure that other groups do not stall at an intermediary level. Second, substantial research into Asian ethnic groups — and the WHO’s precedent 20 years ago — creates a solid foundation to build upon.”
Ultimately, they said, “advancing equity will require funding research that engages diverse Asian communities and developing tailored interventions for all ethnicities.”
Dr. Cuevas, Dr. Willett, Mr. Bajaj, and Dr. Wee had no disclosures. Dr. Goossens received research funding from the European Foundation for the Study of Diabetes, the Dutch Diabetes Research Foundation, and the Dutch Research Council. Dr. Busetto received personal funding from Novo Nordisk, Boehringer Ingelheim, Eli Lilly, Pfizer, and Bruno Farmaceutici as a member of advisory boards and from Rhythm Pharmaceuticals and Pronokal as a speaker.
A version of this article first appeared on Medscape.com.
in three new opinion papers.
The three statements were published on July 22, 2024, in Annals of Internal Medicine. In one, the authors expressed caution about the recent movement away from using BMI alone to define obesity, noting that the measure remains a useful population-level and clinical tool for addressing adiposity, particularly within racial and ethnic groups. But the authors of a second paper pointed out that the use of lower BMI cutoffs to define obesity in Asian populations, in place since 2004, is inadequate in part because it doesn’t account for heterogeneity among different Asian groups.
And in the third paper, an editorial, an Annals editor cautioned that the recent framing of obesity exclusively as a “disease” rather than a “broader, more inclusive construct” may inadvertently reinforce the bias it was meant to combat.
Asked to comment on the issues raised in the papers, Professor Gijs Goossens of Maastricht University Medical Center, Maastricht, the Netherlands, said, “It is important to emphasize that the management and treatment of obesity have wider objectives than weight loss alone and include the prevention, resolution, or improvement of obesity-related complications; achieving better quality of life and mental well-being; and improvement of physical and social functioning.”
Added Dr. Goossens, who was an author of a recent European Association for the Study of Obesity (EASO) framework calling for moving beyond BMI in defining obesity, “Personalized therapeutic goals should be set at the beginning of the treatment, according to the stage of obesity, taking into account available therapeutic options, possible side effects or risks, and patient preferences. The drivers of obesity and possible barriers to treatment should also be discussed with the patient.” Dr. Goossens emphasized that he was providing his personal views and not speaking for the EASO or his coauthors.
BMI: ‘Not a Perfect Measure of Adiposity but Remains Useful’
In their “Ideas and Opinions” paper, Adolfo G. Cuevas, PhD, of New York University School of Global Public Health, New York City, and Walter C. Willett, MD, DrPH, of Harvard T.H. Chan School of Public Health, Boston, argued that “BMI, although not a perfect measure of adiposity, remains a useful population-level and clinical tool for addressing adiposity, including within groups defined by race and ethnicity.”
They added that despite the criticism that BMI doesn’t distinguish between fat and lean body mass, the measure still strongly correlates with fat mass as well as cardiovascular risk and mortality, and it does so similarly across racial and ethnic groups.
Clinically, Dr. Cuevas and Dr. Willett pointed out that BMI correlates fat mass as assessed with the gold standard measure dual x-ray absorptiometry but is far simpler and less expensive. Measuring waist circumference can provide additional information about visceral fat and disease risk but is “more difficult to standardize and suffers from the same limitations as BMI when cut points are used.”
They suggest the addition of change in weight since early adulthood and over time as a “simple and sensitive variable” for assessing adiposity.
Luca Busetto, MD, associate professor of medicine at the University of Padua, Italy, and the first author of the EASO framework, said, “The paper from Cuevas and Willett sounds like a strong defense of BMI, and I can substantially agree with this defense ... We remain anchored on BMI, but we tried to move beyond it adding an estimate of high risk abdominal fat — waist to height ratio — and coupling the anthropometric assessment with a complete clinical evaluation and staging.”
Dr. Goossens said, “I agree with the authors that despite the limitations of BMI as a measure of body fatness, it remains a useful clinical screening tool. Yet the diagnosis of obesity should not be based solely on BMI” due to the stronger association of abdominal fat with cardiometabolic complications.
That link, he noted, “also applies to individuals with a BMI level below the current cutoff values for obesity, who may already have medical, functional, or psychological impairments. We should be aware of the risk of undertreatment in this particular group of patients.”
Does Calling Obesity a ‘Disease’ Have Unintended Consequences?
In her editorial, Christina C. Wee, MD, senior deputy editor, Annals of Internal Medicine, wrote, “Beyond diagnostic challenges, framing obesity exclusively as a disease rather than a broader, more inclusive construct may have unintended consequences — including reinforcing the weight bias this framing was in part intended to combat.”
Focusing solely on biological causes of obesity while ignoring psychosocial, cultural, environmental, and behavioral contexts could undermine public health and policy efforts to address those factors, Dr. Wee argued.
Moreover, she wrote, “Ironically, framing obesity as a disease to justify coverage for treatment reinforces weight bias. It conflates the need to label a condition a disease with healthcare reimbursement and raises the stakes for developing accurate diagnostic criteria ... By exclusively linking obesity as a disease to reimbursement, it sends the message that only those who manifest disease from excess adiposity warrant treatment — and, by inference, those on the continuum who have not yet manifested disease do not warrant treatment.”
Likening obesity to other risk factors such as hypertension or dyslipidemia for which treatment is typically reimbursed, Dr. Wee pointed out that Medicare still prohibits coverage of medications for obesity.
Regarding the high costs of newer obesity medications and the need for payers and clinicians to ration their use, Dr. Wee argued, “Rather than focusing on whether one’s adiposity conforms to an expert panel’s definition of ‘disease,’ we should address how to best stage obesity risk with sufficient accuracy and fairness and reach a consensus on how to prioritize and match treatments to individual patients.”
Dr. Busetto said that EASO stands by its definition of obesity as a disease, adding “we can adhere to the suggestion of a holistic approach deciding treatment modalities according to the risk and the presence of mental, functional, and medical complications of impairments. Of course, we cannot agree on any proposal that is oriented at leaving patients with obesity still in the asymptomatic phase of the disease without treatment. This would be like treating diabetes only after the occurrence of nephropathy or managing hypertension only after a stroke. Prevention of the symptomatic stage is a part of obesity management, even beyond weight loss.”
Dr. Goossens said, “indeed, it is of utmost importance to develop accurate risk stratification tools for adequately clinical staging of obesity, according to the severity of its medical, psychological and functional impairments.”
Do the Current Lower BMI Cutoffs for Defining Obesity in Asian People Make Sense?
Simar S. Bajaj, AB, of Harvard University, Cambridge, Massachusetts, and colleagues, all of Harvard Medical School, Boston, raised several concerns regarding the 2004 World Health Organization’s suggestion to use lower BMI categories for defining overweight and obesity in Asian populations, that is, 23-27.5 kg/m2 and 27.5 kg/m2 or higher for obesity, respectively, as opposed to 25-29.9 and ≥ 30, respectively, for other populations.
Different Asian countries have created their own obesity BMI cutoffs, ranging from 25 kg/m2 in India to 28 kg/m2 in China. But “Asian Americans continue to be treated as a monolith without official disaggregated cutoffs,” Mr. Bajaj and colleagues noted.
The heterogeneity translates to different risk levels across Asian subgroups. For example, in one study, age- and sex-adjusted BMI cutoffs for increased risk of developing type 2 diabetes were 23.9 kg/m2 in South Asian populations, 26.6 kg/m2 in Arab populations, 26.9 kg/m2 in Chinese populations, and 28.1 kg/m2 in Black populations.
These findings raise important questions, the researchers said. “Does it make sense for people of Chinese descent to use the same BMI threshold as the South Asian group when their ‘equivalent risk cutoff’ is closer to that of Arab and Black groups who share the standard BMI threshold?” Most data in this area are cross-sectional rather than the longitudinal data needed to answer those questions, they noted.
They suggest that professional diabetes and obesity organizations consider BMI thresholds to be “placeholders” until more sensitive and specific thresholds can be defined for Asian American populations.
Mr. Bajaj and colleagues also noted the need for disaggregated data is not unique to Asian groups but that they focused on Asian Americans for two main reasons. “First, success would create a precedent for complete disaggregation and help ensure that other groups do not stall at an intermediary level. Second, substantial research into Asian ethnic groups — and the WHO’s precedent 20 years ago — creates a solid foundation to build upon.”
Ultimately, they said, “advancing equity will require funding research that engages diverse Asian communities and developing tailored interventions for all ethnicities.”
Dr. Cuevas, Dr. Willett, Mr. Bajaj, and Dr. Wee had no disclosures. Dr. Goossens received research funding from the European Foundation for the Study of Diabetes, the Dutch Diabetes Research Foundation, and the Dutch Research Council. Dr. Busetto received personal funding from Novo Nordisk, Boehringer Ingelheim, Eli Lilly, Pfizer, and Bruno Farmaceutici as a member of advisory boards and from Rhythm Pharmaceuticals and Pronokal as a speaker.
A version of this article first appeared on Medscape.com.
in three new opinion papers.
The three statements were published on July 22, 2024, in Annals of Internal Medicine. In one, the authors expressed caution about the recent movement away from using BMI alone to define obesity, noting that the measure remains a useful population-level and clinical tool for addressing adiposity, particularly within racial and ethnic groups. But the authors of a second paper pointed out that the use of lower BMI cutoffs to define obesity in Asian populations, in place since 2004, is inadequate in part because it doesn’t account for heterogeneity among different Asian groups.
And in the third paper, an editorial, an Annals editor cautioned that the recent framing of obesity exclusively as a “disease” rather than a “broader, more inclusive construct” may inadvertently reinforce the bias it was meant to combat.
Asked to comment on the issues raised in the papers, Professor Gijs Goossens of Maastricht University Medical Center, Maastricht, the Netherlands, said, “It is important to emphasize that the management and treatment of obesity have wider objectives than weight loss alone and include the prevention, resolution, or improvement of obesity-related complications; achieving better quality of life and mental well-being; and improvement of physical and social functioning.”
Added Dr. Goossens, who was an author of a recent European Association for the Study of Obesity (EASO) framework calling for moving beyond BMI in defining obesity, “Personalized therapeutic goals should be set at the beginning of the treatment, according to the stage of obesity, taking into account available therapeutic options, possible side effects or risks, and patient preferences. The drivers of obesity and possible barriers to treatment should also be discussed with the patient.” Dr. Goossens emphasized that he was providing his personal views and not speaking for the EASO or his coauthors.
BMI: ‘Not a Perfect Measure of Adiposity but Remains Useful’
In their “Ideas and Opinions” paper, Adolfo G. Cuevas, PhD, of New York University School of Global Public Health, New York City, and Walter C. Willett, MD, DrPH, of Harvard T.H. Chan School of Public Health, Boston, argued that “BMI, although not a perfect measure of adiposity, remains a useful population-level and clinical tool for addressing adiposity, including within groups defined by race and ethnicity.”
They added that despite the criticism that BMI doesn’t distinguish between fat and lean body mass, the measure still strongly correlates with fat mass as well as cardiovascular risk and mortality, and it does so similarly across racial and ethnic groups.
Clinically, Dr. Cuevas and Dr. Willett pointed out that BMI correlates fat mass as assessed with the gold standard measure dual x-ray absorptiometry but is far simpler and less expensive. Measuring waist circumference can provide additional information about visceral fat and disease risk but is “more difficult to standardize and suffers from the same limitations as BMI when cut points are used.”
They suggest the addition of change in weight since early adulthood and over time as a “simple and sensitive variable” for assessing adiposity.
Luca Busetto, MD, associate professor of medicine at the University of Padua, Italy, and the first author of the EASO framework, said, “The paper from Cuevas and Willett sounds like a strong defense of BMI, and I can substantially agree with this defense ... We remain anchored on BMI, but we tried to move beyond it adding an estimate of high risk abdominal fat — waist to height ratio — and coupling the anthropometric assessment with a complete clinical evaluation and staging.”
Dr. Goossens said, “I agree with the authors that despite the limitations of BMI as a measure of body fatness, it remains a useful clinical screening tool. Yet the diagnosis of obesity should not be based solely on BMI” due to the stronger association of abdominal fat with cardiometabolic complications.
That link, he noted, “also applies to individuals with a BMI level below the current cutoff values for obesity, who may already have medical, functional, or psychological impairments. We should be aware of the risk of undertreatment in this particular group of patients.”
Does Calling Obesity a ‘Disease’ Have Unintended Consequences?
In her editorial, Christina C. Wee, MD, senior deputy editor, Annals of Internal Medicine, wrote, “Beyond diagnostic challenges, framing obesity exclusively as a disease rather than a broader, more inclusive construct may have unintended consequences — including reinforcing the weight bias this framing was in part intended to combat.”
Focusing solely on biological causes of obesity while ignoring psychosocial, cultural, environmental, and behavioral contexts could undermine public health and policy efforts to address those factors, Dr. Wee argued.
Moreover, she wrote, “Ironically, framing obesity as a disease to justify coverage for treatment reinforces weight bias. It conflates the need to label a condition a disease with healthcare reimbursement and raises the stakes for developing accurate diagnostic criteria ... By exclusively linking obesity as a disease to reimbursement, it sends the message that only those who manifest disease from excess adiposity warrant treatment — and, by inference, those on the continuum who have not yet manifested disease do not warrant treatment.”
Likening obesity to other risk factors such as hypertension or dyslipidemia for which treatment is typically reimbursed, Dr. Wee pointed out that Medicare still prohibits coverage of medications for obesity.
Regarding the high costs of newer obesity medications and the need for payers and clinicians to ration their use, Dr. Wee argued, “Rather than focusing on whether one’s adiposity conforms to an expert panel’s definition of ‘disease,’ we should address how to best stage obesity risk with sufficient accuracy and fairness and reach a consensus on how to prioritize and match treatments to individual patients.”
Dr. Busetto said that EASO stands by its definition of obesity as a disease, adding “we can adhere to the suggestion of a holistic approach deciding treatment modalities according to the risk and the presence of mental, functional, and medical complications of impairments. Of course, we cannot agree on any proposal that is oriented at leaving patients with obesity still in the asymptomatic phase of the disease without treatment. This would be like treating diabetes only after the occurrence of nephropathy or managing hypertension only after a stroke. Prevention of the symptomatic stage is a part of obesity management, even beyond weight loss.”
Dr. Goossens said, “indeed, it is of utmost importance to develop accurate risk stratification tools for adequately clinical staging of obesity, according to the severity of its medical, psychological and functional impairments.”
Do the Current Lower BMI Cutoffs for Defining Obesity in Asian People Make Sense?
Simar S. Bajaj, AB, of Harvard University, Cambridge, Massachusetts, and colleagues, all of Harvard Medical School, Boston, raised several concerns regarding the 2004 World Health Organization’s suggestion to use lower BMI categories for defining overweight and obesity in Asian populations, that is, 23-27.5 kg/m2 and 27.5 kg/m2 or higher for obesity, respectively, as opposed to 25-29.9 and ≥ 30, respectively, for other populations.
Different Asian countries have created their own obesity BMI cutoffs, ranging from 25 kg/m2 in India to 28 kg/m2 in China. But “Asian Americans continue to be treated as a monolith without official disaggregated cutoffs,” Mr. Bajaj and colleagues noted.
The heterogeneity translates to different risk levels across Asian subgroups. For example, in one study, age- and sex-adjusted BMI cutoffs for increased risk of developing type 2 diabetes were 23.9 kg/m2 in South Asian populations, 26.6 kg/m2 in Arab populations, 26.9 kg/m2 in Chinese populations, and 28.1 kg/m2 in Black populations.
These findings raise important questions, the researchers said. “Does it make sense for people of Chinese descent to use the same BMI threshold as the South Asian group when their ‘equivalent risk cutoff’ is closer to that of Arab and Black groups who share the standard BMI threshold?” Most data in this area are cross-sectional rather than the longitudinal data needed to answer those questions, they noted.
They suggest that professional diabetes and obesity organizations consider BMI thresholds to be “placeholders” until more sensitive and specific thresholds can be defined for Asian American populations.
Mr. Bajaj and colleagues also noted the need for disaggregated data is not unique to Asian groups but that they focused on Asian Americans for two main reasons. “First, success would create a precedent for complete disaggregation and help ensure that other groups do not stall at an intermediary level. Second, substantial research into Asian ethnic groups — and the WHO’s precedent 20 years ago — creates a solid foundation to build upon.”
Ultimately, they said, “advancing equity will require funding research that engages diverse Asian communities and developing tailored interventions for all ethnicities.”
Dr. Cuevas, Dr. Willett, Mr. Bajaj, and Dr. Wee had no disclosures. Dr. Goossens received research funding from the European Foundation for the Study of Diabetes, the Dutch Diabetes Research Foundation, and the Dutch Research Council. Dr. Busetto received personal funding from Novo Nordisk, Boehringer Ingelheim, Eli Lilly, Pfizer, and Bruno Farmaceutici as a member of advisory boards and from Rhythm Pharmaceuticals and Pronokal as a speaker.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE
Generalized Fixed Drug Eruptions Require Urgent Care: A Case Series
Recognizing cutaneous drug eruptions is important for treatment and prevention of recurrence. Fixed drug eruptions (FDEs) typically are harmless but can have major negative cosmetic consequences for patients. In its more severe forms, patients are at risk for widespread epithelial necrosis with accompanying complications. We report 1 patient with generalized FDE and 2 with generalized bullous FDE. We also discuss the recognition and treatment of the condition. Two patients previously had been diagnosed with systemic lupus erythematosus (SLE).
Case Series
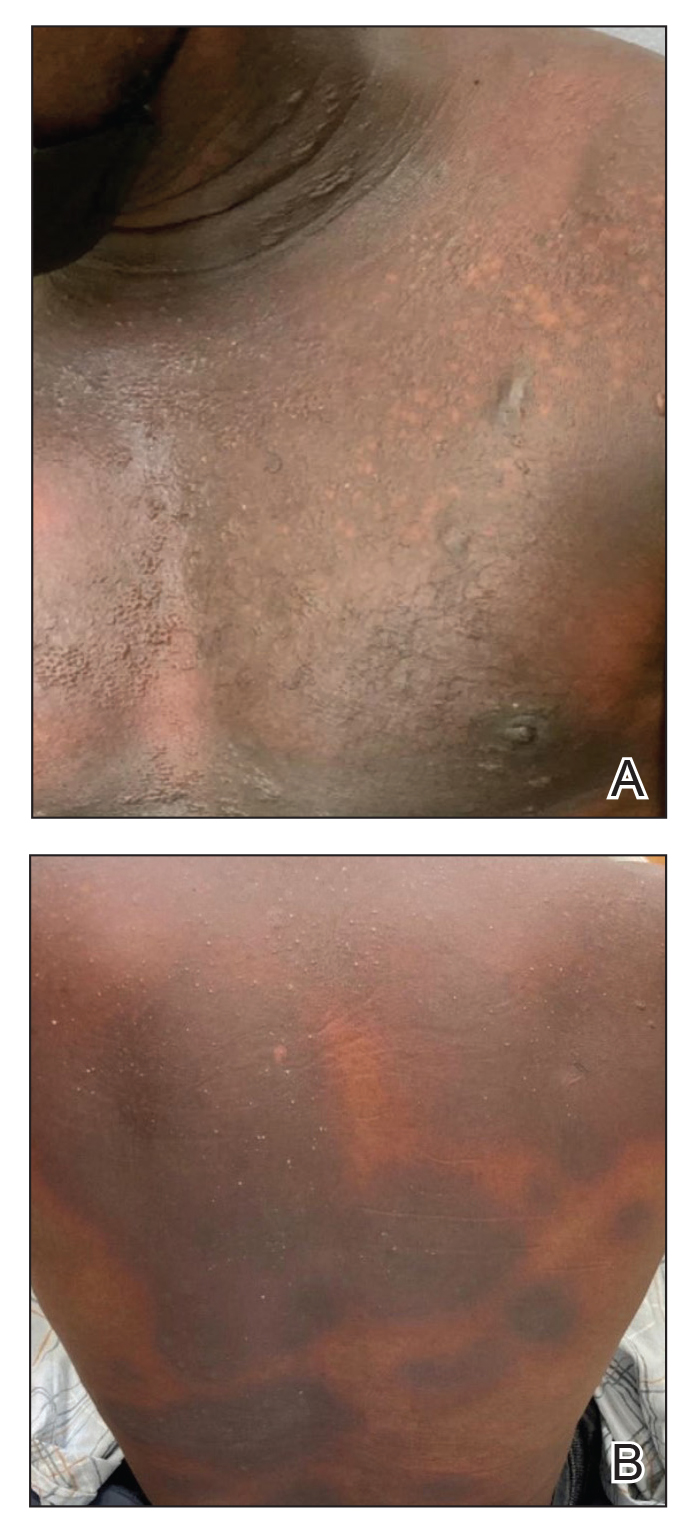
Patient 1—A 60-year-old woman presented to dermatology with a rash on the trunk and groin folds of 4 days’ duration. She had a history of SLE and cutaneous lupus treated with hydroxychloroquine 200 mg twice daily and topical corticosteroids. She had started sulfamethoxazole-trimethoprim for a urinary tract infection with a rash appearing 1 day later. She reported burning skin pain with progression to blisters that “sloughed” off. She denied any known history of allergy to sulfa drugs. Prior to evaluation by dermatology, she visited an urgent care facility and was prescribed hydroxyzine and intramuscular corticosteroids. At presentation to dermatology 3 days after taking sulfamethoxazole-trimethoprim, she had annular flaccid bullae and superficial erosions with dusky borders on the right posterior thigh, right side of the chest, left inframammary fold, and right inguinal fold (Figure 1). She had no ocular, oral, or vaginal erosions. A diagnosis of generalized bullous FDE was favored over erythema multiforme or Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN). Shave biopsies from lesions on the right posterior thigh and right inguinal fold demonstrated interface dermatitis with epidermal necrosis, pigment incontinence, and numerous eosinophils. Direct immunofluorescence of the perilesional skin was negative for immunoprotein deposition. These findings were consistent with the clinical impression of generalized bullous FDE. Prior to receiving the histopathology report, the patient was initiated on a regimen of cyclosporine 5 mg/kg/d in the setting of normal renal function and followed until the eruption resolved completely. Cyclosporine was tapered at 2 weeks and discontinued at 3 weeks.

Patient 2—A 32-year-old woman presented for follow-up management of discoid lupus erythematosus. She had a history of systemic and cutaneous lupus, juvenile rheumatoid arthritis, and mixed connective tissue disease managed with prednisone, hydroxychloroquine, azathioprine, and belimumab. Physical examination revealed scarring alopecia with dyspigmentation and active inflammation consistent with uncontrolled cutaneous lupus. However, she also had oval-shaped hyperpigmented patches over the left breast, clavicle, and anterior chest consistent with a generalized FDE (Figure 2). The patient did not recall a history of similar lesions and could not identify a possible trigger. She was counseled on possible culprits and advised to avoid unnecessary medications. She had an unremarkable clinical course; therefore, no further intervention was necessary.

Patient 3—A 33-year-old man presented to the emergency department with a painful rash on the chest and back of 2 days’ duration that began 1 hour after taking naproxen (dosage unknown) for back pain. He had no notable medical history. The patient stated that the rash had slowly worsened and started to develop blisters. He visited an urgent care facility 1 day prior to the current presentation and was started on a 5-day course of prednisone 40 mg daily; the first 2 doses did not help. He denied any mucosal involvement apart from a tender lesion on the penis. He reported a history of an allergic reaction to penicillin. Physical examination revealed extensive dusky violaceous annular plaques with erythematous borders across the anterior and posterior trunk (Figure 3). Multiple flaccid bullae developed within these plaques, involving 15% of the body surface area. He was diagnosed with generalized bullous FDE based on the clinical history and histopathology. He was admitted to the burn intensive care unit and treated with cyclosporine 3 mg/kg/d with subsequent resolution of the eruption.
Comment
Presentation of FDEs—A fixed drug eruption manifests with 1 or more well-demarcated, red or violaceous, annular patches that resolve with postinflammatory hyperpigmentation; it occasionally may manifest with bullae. Initial eruptions may occur up to 2 weeks following medication exposure, but recurrent eruptions usually happen within minutes to hours later. They often are in the same location as prior lesions. A fixed drug eruption can be solitary, scattered, or generalized; a generalized FDE typically demonstrates multiple bilateral lesions that may itch, burn, or cause no symptoms. Patients can experience an FDE at any age, though the median age is reported as 35 to 60 years of age.1 A fixed drug eruption usually occurs after ingestion of oral medications, though there have been a few reports with iodinated contrast.2 Well-known culprits include antibiotics (eg, sulfamethoxazole-trimethoprim, tetracyclines, penicillins/cephalosporins, quinolones, dapsone), nonsteroidal anti-inflammatory drugs, acetaminophen (eg, paracetamol), barbiturates, antimalarials, and anticonvulsants. It also can occur with vaccines or with certain foods (fixed food eruption).3,4 Clinicians may try an oral drug challenge to identify the cause of an FDE, but in patients with a history of a generalized FDE, the risk for developing an increasingly severe reaction with repeated exposure to the medication is too high.5
Histopathology—Patch testing at the site of prior eruption with suspected drug culprits may be useful.6 Histopathology of FDE typically demonstrates vacuolar changes at the dermoepidermal junction with a lichenoid lymphocytic infiltrate. Early lesions often show a predominance of eosinophils. Subepidermal clefting is a feature of the bullous variant. In an active lesion, there are large numbers of CD8+ T lymphocytes expressing natural killer cell–associated molecules.7 The pathologic mechanism is not well understood, though it has been hypothesized that memory CD8+ cells are maintained in specific regions of the epidermis by IL-15 produced in the microenvironment and are activated upon rechallenge.7Considerations in Generalized Bullous FDE—Generalized FDE is defined in the literature as an FDE with involvement of 3 of 6 body areas: head, neck, trunk, upper limbs, lower limbs, and genital area. It may cover more or less than 10% of the body surface area.8-10 Although an isolated FDE frequently is asymptomatic and may not be cause for alarm, recurring drug eruptions increase the risk for development of generalized bullous FDE. Generalized bullous FDE is a rare subset. It is frequently misdiagnosed, and data on its incidence are uncertain.11 Of note, several pathologies causing bullous lesions may be in the differential diagnosis, including bullous pemphigoid; pemphigus vulgaris; bullous SLE; or bullae from cutaneous lupus, staphylococcal scalded skin syndrome, erythema multiforme, or SJS/TEN.12 When matched for body surface area involvement with SJS/TEN, generalized bullous FDE shares nearly identical mortality rates10; therefore, these patients should be treated with the same level of urgency and admitted to a critical care or burn unit, as they are at serious risk for infection and other complications.13
Clinical history and presentation along with histopathologic findings help to narrow down the differential diagnosis. Clinically, generalized bullous FDE does not affect the surrounding skin and manifests sooner after drug exposure (1–24 hours) with less mucosal involvement than SJS/TEN.9 Additionally, SJS/TEN patients frequently have generalized malaise and/or fever, while generalized bullous FDE patients do not. Finally, patients with generalized bullous FDE may report a history of a cutaneous eruption similar in morphology or in the same location.
Histopathologically, generalized bullous FDE may be similar to FDE with the addition of a subepidermal blister. Generalized bullous FDE patients have greater eosinophil infiltration and dermal melanophages than patients with SJS/TEN.9 Cellular infiltrates in generalized bullous FDE include more dermal CD41 cells, such as Foxp31 regulatory T cells; fewer intraepidermal CD561 cells; and fewer intraepidermal cells with granulysin.9 Occasionally, generalized bullous FDE causes full-thickness necrosis. In those cases, generalized bullous FDE cannot reliably be distinguished from other conditions with epidermal necrolysis on histopathology.13
FDE Diagnostics—A cytotoxin produced by
Management—Avoidance of the inciting drug often is sufficient for patients with an FDE, as demonstrated in patient 2 in our case series. Clinicians also should counsel patients on avoidance of potential cross-reacting drugs. Symptomatic treatment for itch or pain is appropriate and may include antihistamines or topical steroids. Nonsteroidal anti-inflammatory drugs may exacerbate or be causative of FDE. For generalized bullous FDE, cyclosporine is favored in the literature15,16 and was used to successfully treat both patients 1 and 3 in our case series. A short course of systemic corticosteroids or intravenous immunoglobulin also may be considered. Mild cases of generalized bullous FDE may be treated with close outpatient follow-up (patient 1), while severe cases require inpatient or even critical care monitoring with aggressive medical management to prevent the progression of skin desquamation (patient 3). Patients with severe oral lesions may require inpatient support for fluid maintenance.
Lupus History—Two patients in our case series had a history of lupus. Lupus itself can cause primary bullous lesions. Similar to FDE, bullous SLE can involve sun-exposed and nonexposed areas of the skin as well as the mucous membranes with a predilection for the lower vermilion lip.17 In bullous SLE, tense subepidermal blisters with a neutrophil-rich infiltrate form due to circulating antibodies to type VII collagen. These blisters have an erythematous or urticated base, most commonly on the face, upper trunk, and proximal extremities.18 In both SLE with skin manifestations and lupus limited to the skin, bullae may form due to extensive vacuolar degeneration. Similar to TEN, they can form rapidly in a widespread distribution.17 However, there is limited mucosal involvement, no clear drug association, and a better prognosis. Bullae caused by lupus will frequently demonstrate deposition of immunoproteins IgG, IgM, IgA, and complement component 3 at the basement membrane zone in perilesional skin on direct immunofluorescence. However, negative direct immunofluorescence does not rule out lupus.12 At the same time, patients with lupus frequently have comorbidities requiring multiple medications; the need for these medications may predispose patients to higher rates of cutaneous drug eruptions.19 To our knowledge, there is no known association between FDE and lupus.
Conclusion
Patients with acute eruptions following the initiation of a new prescription or over-the-counter medication require urgent evaluation. Generalized bullous FDE requires timely diagnosis and intervention. Patients with lupus have an increased risk for cutaneous drug eruptions due to polypharmacy. Further investigation is necessary to determine if there is a pathophysiologic mechanism responsible for the development of FDE in lupus patients.
- Anderson HJ, Lee JB. A review of fixed drug eruption with a special focus on generalized bullous fixed drug eruption. Medicina (Kaunas). 2021;57:925.
- Gavin M, Sharp L, Walker K, et al. Contrast-induced generalized bullous fixed drug eruption resembling Stevens-Johnson syndrome. Proc (Bayl Univ Med Cent). 2019;32:601-602.
- Kabir S, Feit EJ, Heilman ER. Generalized fixed drug eruption following Pfizer-BioNtech COVID-19 vaccination. Clin Case Rep. 2022;10:E6684.
- Choi S, Kim SH, Hwang JH, et al. Rapidly progressing generalized bullous fixed drug eruption after the first dose of COVID-19 messenger RNA vaccination. J Dermatol. 2023;50:1190-1193.
- Mahboob A, Haroon TS. Drugs causing fixed eruptions: a study of 450 cases. Int J Dermatol. 1998;37:833-838.
- Shiohara T. Fixed drug eruption: pathogenesis and diagnostic tests. Curr Opin Allergy Clin Immunol. 2009;9:316-321.
- Mizukawa Y, Yamazaki Y, Shiohara T. In vivo dynamics of intraepidermal CD8+ T cells and CD4+ T cells during the evolution of fixed drug eruption. Br J Dermatol. 2008;158:1230-1238.
- Lee CH, Chen YC, Cho YT, et al. Fixed-drug eruption: a retrospective study in a single referral center in northern Taiwan. Dermatologica Sinica. 2012;30:11-15.
- Cho YT, Lin JW, Chen YC, et al. Generalized bullous fixed drug eruption is distinct from Stevens-Johnson syndrome/toxic epidermal necrolysis by immunohistopathological features. J Am Acad Dermatol. 2014;70:539-548.
- Lipowicz S, Sekula P, Ingen-Housz-Oro S, et al. Prognosis of generalized bullous fixed drug eruption: comparison with Stevens-Johnson syndrome and toxic epidermal necrolysis. Br J Dermatol. 2013;168:726-732.
- Patel S, John AM, Handler MZ, et al. Fixed drug eruptions: an update, emphasizing the potentially lethal generalized bullous fixed drug eruption. Am J Clin Dermatol. 2020;21:393-399.
- Ranario JS, Smith JL. Bullous lesions in a patient with systemic lupus erythematosus. J Clin Aesthet Dermatol. 2014;7:44-49.
- Perron E, Viarnaud A, Marciano L, et al. Clinical and histological features of fixed drug eruption: a single-centre series of 73 cases with comparison between bullous and non-bullous forms. Eur J Dermatol. 2021;31:372-380.
- Chen CB, Kuo KL, Wang CW, et al. Detecting lesional granulysin levels for rapid diagnosis of cytotoxic T lymphocyte-mediated bullous skin disorders. J Allergy Clin Immunol Pract. 2021;9:1327-1337.e3.
- Beniwal R, Gupta LK, Khare AK, et al. Cyclosporine in generalized bullous-fixed drug eruption. Indian J Dermatol. 2018;63:432-433.
- Vargas Mora P, García S, Valenzuela F, et al. Generalized bullous fixed drug eruption successfully treated with cyclosporine. Dermatol Ther. 2020;33:E13492.
- Montagnon CM, Tolkachjov SN, Murrell DF, et al. Subepithelial autoimmune blistering dermatoses: clinical features and diagnosis. J Am Acad Dermatol. 2021;85:1-14.
- Sebaratnam DF, Murrell DF. Bullous systemic lupus erythematosus. Dermatol Clin. 2011;29:649-653.
- Zonzits E, Aberer W, Tappeiner G. Drug eruptions from mesna. After cyclophosphamide treatment of patients with systemic lupus erythematosus and dermatomyositis. Arch Dermatol. 1992;128:80-82.
Recognizing cutaneous drug eruptions is important for treatment and prevention of recurrence. Fixed drug eruptions (FDEs) typically are harmless but can have major negative cosmetic consequences for patients. In its more severe forms, patients are at risk for widespread epithelial necrosis with accompanying complications. We report 1 patient with generalized FDE and 2 with generalized bullous FDE. We also discuss the recognition and treatment of the condition. Two patients previously had been diagnosed with systemic lupus erythematosus (SLE).
Case Series
Patient 1—A 60-year-old woman presented to dermatology with a rash on the trunk and groin folds of 4 days’ duration. She had a history of SLE and cutaneous lupus treated with hydroxychloroquine 200 mg twice daily and topical corticosteroids. She had started sulfamethoxazole-trimethoprim for a urinary tract infection with a rash appearing 1 day later. She reported burning skin pain with progression to blisters that “sloughed” off. She denied any known history of allergy to sulfa drugs. Prior to evaluation by dermatology, she visited an urgent care facility and was prescribed hydroxyzine and intramuscular corticosteroids. At presentation to dermatology 3 days after taking sulfamethoxazole-trimethoprim, she had annular flaccid bullae and superficial erosions with dusky borders on the right posterior thigh, right side of the chest, left inframammary fold, and right inguinal fold (Figure 1). She had no ocular, oral, or vaginal erosions. A diagnosis of generalized bullous FDE was favored over erythema multiforme or Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN). Shave biopsies from lesions on the right posterior thigh and right inguinal fold demonstrated interface dermatitis with epidermal necrosis, pigment incontinence, and numerous eosinophils. Direct immunofluorescence of the perilesional skin was negative for immunoprotein deposition. These findings were consistent with the clinical impression of generalized bullous FDE. Prior to receiving the histopathology report, the patient was initiated on a regimen of cyclosporine 5 mg/kg/d in the setting of normal renal function and followed until the eruption resolved completely. Cyclosporine was tapered at 2 weeks and discontinued at 3 weeks.
Patient 2—A 32-year-old woman presented for follow-up management of discoid lupus erythematosus. She had a history of systemic and cutaneous lupus, juvenile rheumatoid arthritis, and mixed connective tissue disease managed with prednisone, hydroxychloroquine, azathioprine, and belimumab. Physical examination revealed scarring alopecia with dyspigmentation and active inflammation consistent with uncontrolled cutaneous lupus. However, she also had oval-shaped hyperpigmented patches over the left breast, clavicle, and anterior chest consistent with a generalized FDE (Figure 2). The patient did not recall a history of similar lesions and could not identify a possible trigger. She was counseled on possible culprits and advised to avoid unnecessary medications. She had an unremarkable clinical course; therefore, no further intervention was necessary.
Patient 3—A 33-year-old man presented to the emergency department with a painful rash on the chest and back of 2 days’ duration that began 1 hour after taking naproxen (dosage unknown) for back pain. He had no notable medical history. The patient stated that the rash had slowly worsened and started to develop blisters. He visited an urgent care facility 1 day prior to the current presentation and was started on a 5-day course of prednisone 40 mg daily; the first 2 doses did not help. He denied any mucosal involvement apart from a tender lesion on the penis. He reported a history of an allergic reaction to penicillin. Physical examination revealed extensive dusky violaceous annular plaques with erythematous borders across the anterior and posterior trunk (Figure 3). Multiple flaccid bullae developed within these plaques, involving 15% of the body surface area. He was diagnosed with generalized bullous FDE based on the clinical history and histopathology. He was admitted to the burn intensive care unit and treated with cyclosporine 3 mg/kg/d with subsequent resolution of the eruption.
Comment
Presentation of FDEs—A fixed drug eruption manifests with 1 or more well-demarcated, red or violaceous, annular patches that resolve with postinflammatory hyperpigmentation; it occasionally may manifest with bullae. Initial eruptions may occur up to 2 weeks following medication exposure, but recurrent eruptions usually happen within minutes to hours later. They often are in the same location as prior lesions. A fixed drug eruption can be solitary, scattered, or generalized; a generalized FDE typically demonstrates multiple bilateral lesions that may itch, burn, or cause no symptoms. Patients can experience an FDE at any age, though the median age is reported as 35 to 60 years of age.1 A fixed drug eruption usually occurs after ingestion of oral medications, though there have been a few reports with iodinated contrast.2 Well-known culprits include antibiotics (eg, sulfamethoxazole-trimethoprim, tetracyclines, penicillins/cephalosporins, quinolones, dapsone), nonsteroidal anti-inflammatory drugs, acetaminophen (eg, paracetamol), barbiturates, antimalarials, and anticonvulsants. It also can occur with vaccines or with certain foods (fixed food eruption).3,4 Clinicians may try an oral drug challenge to identify the cause of an FDE, but in patients with a history of a generalized FDE, the risk for developing an increasingly severe reaction with repeated exposure to the medication is too high.5
Histopathology—Patch testing at the site of prior eruption with suspected drug culprits may be useful.6 Histopathology of FDE typically demonstrates vacuolar changes at the dermoepidermal junction with a lichenoid lymphocytic infiltrate. Early lesions often show a predominance of eosinophils. Subepidermal clefting is a feature of the bullous variant. In an active lesion, there are large numbers of CD8+ T lymphocytes expressing natural killer cell–associated molecules.7 The pathologic mechanism is not well understood, though it has been hypothesized that memory CD8+ cells are maintained in specific regions of the epidermis by IL-15 produced in the microenvironment and are activated upon rechallenge.7Considerations in Generalized Bullous FDE—Generalized FDE is defined in the literature as an FDE with involvement of 3 of 6 body areas: head, neck, trunk, upper limbs, lower limbs, and genital area. It may cover more or less than 10% of the body surface area.8-10 Although an isolated FDE frequently is asymptomatic and may not be cause for alarm, recurring drug eruptions increase the risk for development of generalized bullous FDE. Generalized bullous FDE is a rare subset. It is frequently misdiagnosed, and data on its incidence are uncertain.11 Of note, several pathologies causing bullous lesions may be in the differential diagnosis, including bullous pemphigoid; pemphigus vulgaris; bullous SLE; or bullae from cutaneous lupus, staphylococcal scalded skin syndrome, erythema multiforme, or SJS/TEN.12 When matched for body surface area involvement with SJS/TEN, generalized bullous FDE shares nearly identical mortality rates10; therefore, these patients should be treated with the same level of urgency and admitted to a critical care or burn unit, as they are at serious risk for infection and other complications.13
Clinical history and presentation along with histopathologic findings help to narrow down the differential diagnosis. Clinically, generalized bullous FDE does not affect the surrounding skin and manifests sooner after drug exposure (1–24 hours) with less mucosal involvement than SJS/TEN.9 Additionally, SJS/TEN patients frequently have generalized malaise and/or fever, while generalized bullous FDE patients do not. Finally, patients with generalized bullous FDE may report a history of a cutaneous eruption similar in morphology or in the same location.
Histopathologically, generalized bullous FDE may be similar to FDE with the addition of a subepidermal blister. Generalized bullous FDE patients have greater eosinophil infiltration and dermal melanophages than patients with SJS/TEN.9 Cellular infiltrates in generalized bullous FDE include more dermal CD41 cells, such as Foxp31 regulatory T cells; fewer intraepidermal CD561 cells; and fewer intraepidermal cells with granulysin.9 Occasionally, generalized bullous FDE causes full-thickness necrosis. In those cases, generalized bullous FDE cannot reliably be distinguished from other conditions with epidermal necrolysis on histopathology.13
FDE Diagnostics—A cytotoxin produced by
Management—Avoidance of the inciting drug often is sufficient for patients with an FDE, as demonstrated in patient 2 in our case series. Clinicians also should counsel patients on avoidance of potential cross-reacting drugs. Symptomatic treatment for itch or pain is appropriate and may include antihistamines or topical steroids. Nonsteroidal anti-inflammatory drugs may exacerbate or be causative of FDE. For generalized bullous FDE, cyclosporine is favored in the literature15,16 and was used to successfully treat both patients 1 and 3 in our case series. A short course of systemic corticosteroids or intravenous immunoglobulin also may be considered. Mild cases of generalized bullous FDE may be treated with close outpatient follow-up (patient 1), while severe cases require inpatient or even critical care monitoring with aggressive medical management to prevent the progression of skin desquamation (patient 3). Patients with severe oral lesions may require inpatient support for fluid maintenance.
Lupus History—Two patients in our case series had a history of lupus. Lupus itself can cause primary bullous lesions. Similar to FDE, bullous SLE can involve sun-exposed and nonexposed areas of the skin as well as the mucous membranes with a predilection for the lower vermilion lip.17 In bullous SLE, tense subepidermal blisters with a neutrophil-rich infiltrate form due to circulating antibodies to type VII collagen. These blisters have an erythematous or urticated base, most commonly on the face, upper trunk, and proximal extremities.18 In both SLE with skin manifestations and lupus limited to the skin, bullae may form due to extensive vacuolar degeneration. Similar to TEN, they can form rapidly in a widespread distribution.17 However, there is limited mucosal involvement, no clear drug association, and a better prognosis. Bullae caused by lupus will frequently demonstrate deposition of immunoproteins IgG, IgM, IgA, and complement component 3 at the basement membrane zone in perilesional skin on direct immunofluorescence. However, negative direct immunofluorescence does not rule out lupus.12 At the same time, patients with lupus frequently have comorbidities requiring multiple medications; the need for these medications may predispose patients to higher rates of cutaneous drug eruptions.19 To our knowledge, there is no known association between FDE and lupus.
Conclusion
Patients with acute eruptions following the initiation of a new prescription or over-the-counter medication require urgent evaluation. Generalized bullous FDE requires timely diagnosis and intervention. Patients with lupus have an increased risk for cutaneous drug eruptions due to polypharmacy. Further investigation is necessary to determine if there is a pathophysiologic mechanism responsible for the development of FDE in lupus patients.
Recognizing cutaneous drug eruptions is important for treatment and prevention of recurrence. Fixed drug eruptions (FDEs) typically are harmless but can have major negative cosmetic consequences for patients. In its more severe forms, patients are at risk for widespread epithelial necrosis with accompanying complications. We report 1 patient with generalized FDE and 2 with generalized bullous FDE. We also discuss the recognition and treatment of the condition. Two patients previously had been diagnosed with systemic lupus erythematosus (SLE).
Case Series
Patient 1—A 60-year-old woman presented to dermatology with a rash on the trunk and groin folds of 4 days’ duration. She had a history of SLE and cutaneous lupus treated with hydroxychloroquine 200 mg twice daily and topical corticosteroids. She had started sulfamethoxazole-trimethoprim for a urinary tract infection with a rash appearing 1 day later. She reported burning skin pain with progression to blisters that “sloughed” off. She denied any known history of allergy to sulfa drugs. Prior to evaluation by dermatology, she visited an urgent care facility and was prescribed hydroxyzine and intramuscular corticosteroids. At presentation to dermatology 3 days after taking sulfamethoxazole-trimethoprim, she had annular flaccid bullae and superficial erosions with dusky borders on the right posterior thigh, right side of the chest, left inframammary fold, and right inguinal fold (Figure 1). She had no ocular, oral, or vaginal erosions. A diagnosis of generalized bullous FDE was favored over erythema multiforme or Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN). Shave biopsies from lesions on the right posterior thigh and right inguinal fold demonstrated interface dermatitis with epidermal necrosis, pigment incontinence, and numerous eosinophils. Direct immunofluorescence of the perilesional skin was negative for immunoprotein deposition. These findings were consistent with the clinical impression of generalized bullous FDE. Prior to receiving the histopathology report, the patient was initiated on a regimen of cyclosporine 5 mg/kg/d in the setting of normal renal function and followed until the eruption resolved completely. Cyclosporine was tapered at 2 weeks and discontinued at 3 weeks.
Patient 2—A 32-year-old woman presented for follow-up management of discoid lupus erythematosus. She had a history of systemic and cutaneous lupus, juvenile rheumatoid arthritis, and mixed connective tissue disease managed with prednisone, hydroxychloroquine, azathioprine, and belimumab. Physical examination revealed scarring alopecia with dyspigmentation and active inflammation consistent with uncontrolled cutaneous lupus. However, she also had oval-shaped hyperpigmented patches over the left breast, clavicle, and anterior chest consistent with a generalized FDE (Figure 2). The patient did not recall a history of similar lesions and could not identify a possible trigger. She was counseled on possible culprits and advised to avoid unnecessary medications. She had an unremarkable clinical course; therefore, no further intervention was necessary.
Patient 3—A 33-year-old man presented to the emergency department with a painful rash on the chest and back of 2 days’ duration that began 1 hour after taking naproxen (dosage unknown) for back pain. He had no notable medical history. The patient stated that the rash had slowly worsened and started to develop blisters. He visited an urgent care facility 1 day prior to the current presentation and was started on a 5-day course of prednisone 40 mg daily; the first 2 doses did not help. He denied any mucosal involvement apart from a tender lesion on the penis. He reported a history of an allergic reaction to penicillin. Physical examination revealed extensive dusky violaceous annular plaques with erythematous borders across the anterior and posterior trunk (Figure 3). Multiple flaccid bullae developed within these plaques, involving 15% of the body surface area. He was diagnosed with generalized bullous FDE based on the clinical history and histopathology. He was admitted to the burn intensive care unit and treated with cyclosporine 3 mg/kg/d with subsequent resolution of the eruption.
Comment
Presentation of FDEs—A fixed drug eruption manifests with 1 or more well-demarcated, red or violaceous, annular patches that resolve with postinflammatory hyperpigmentation; it occasionally may manifest with bullae. Initial eruptions may occur up to 2 weeks following medication exposure, but recurrent eruptions usually happen within minutes to hours later. They often are in the same location as prior lesions. A fixed drug eruption can be solitary, scattered, or generalized; a generalized FDE typically demonstrates multiple bilateral lesions that may itch, burn, or cause no symptoms. Patients can experience an FDE at any age, though the median age is reported as 35 to 60 years of age.1 A fixed drug eruption usually occurs after ingestion of oral medications, though there have been a few reports with iodinated contrast.2 Well-known culprits include antibiotics (eg, sulfamethoxazole-trimethoprim, tetracyclines, penicillins/cephalosporins, quinolones, dapsone), nonsteroidal anti-inflammatory drugs, acetaminophen (eg, paracetamol), barbiturates, antimalarials, and anticonvulsants. It also can occur with vaccines or with certain foods (fixed food eruption).3,4 Clinicians may try an oral drug challenge to identify the cause of an FDE, but in patients with a history of a generalized FDE, the risk for developing an increasingly severe reaction with repeated exposure to the medication is too high.5
Histopathology—Patch testing at the site of prior eruption with suspected drug culprits may be useful.6 Histopathology of FDE typically demonstrates vacuolar changes at the dermoepidermal junction with a lichenoid lymphocytic infiltrate. Early lesions often show a predominance of eosinophils. Subepidermal clefting is a feature of the bullous variant. In an active lesion, there are large numbers of CD8+ T lymphocytes expressing natural killer cell–associated molecules.7 The pathologic mechanism is not well understood, though it has been hypothesized that memory CD8+ cells are maintained in specific regions of the epidermis by IL-15 produced in the microenvironment and are activated upon rechallenge.7Considerations in Generalized Bullous FDE—Generalized FDE is defined in the literature as an FDE with involvement of 3 of 6 body areas: head, neck, trunk, upper limbs, lower limbs, and genital area. It may cover more or less than 10% of the body surface area.8-10 Although an isolated FDE frequently is asymptomatic and may not be cause for alarm, recurring drug eruptions increase the risk for development of generalized bullous FDE. Generalized bullous FDE is a rare subset. It is frequently misdiagnosed, and data on its incidence are uncertain.11 Of note, several pathologies causing bullous lesions may be in the differential diagnosis, including bullous pemphigoid; pemphigus vulgaris; bullous SLE; or bullae from cutaneous lupus, staphylococcal scalded skin syndrome, erythema multiforme, or SJS/TEN.12 When matched for body surface area involvement with SJS/TEN, generalized bullous FDE shares nearly identical mortality rates10; therefore, these patients should be treated with the same level of urgency and admitted to a critical care or burn unit, as they are at serious risk for infection and other complications.13
Clinical history and presentation along with histopathologic findings help to narrow down the differential diagnosis. Clinically, generalized bullous FDE does not affect the surrounding skin and manifests sooner after drug exposure (1–24 hours) with less mucosal involvement than SJS/TEN.9 Additionally, SJS/TEN patients frequently have generalized malaise and/or fever, while generalized bullous FDE patients do not. Finally, patients with generalized bullous FDE may report a history of a cutaneous eruption similar in morphology or in the same location.
Histopathologically, generalized bullous FDE may be similar to FDE with the addition of a subepidermal blister. Generalized bullous FDE patients have greater eosinophil infiltration and dermal melanophages than patients with SJS/TEN.9 Cellular infiltrates in generalized bullous FDE include more dermal CD41 cells, such as Foxp31 regulatory T cells; fewer intraepidermal CD561 cells; and fewer intraepidermal cells with granulysin.9 Occasionally, generalized bullous FDE causes full-thickness necrosis. In those cases, generalized bullous FDE cannot reliably be distinguished from other conditions with epidermal necrolysis on histopathology.13
FDE Diagnostics—A cytotoxin produced by
Management—Avoidance of the inciting drug often is sufficient for patients with an FDE, as demonstrated in patient 2 in our case series. Clinicians also should counsel patients on avoidance of potential cross-reacting drugs. Symptomatic treatment for itch or pain is appropriate and may include antihistamines or topical steroids. Nonsteroidal anti-inflammatory drugs may exacerbate or be causative of FDE. For generalized bullous FDE, cyclosporine is favored in the literature15,16 and was used to successfully treat both patients 1 and 3 in our case series. A short course of systemic corticosteroids or intravenous immunoglobulin also may be considered. Mild cases of generalized bullous FDE may be treated with close outpatient follow-up (patient 1), while severe cases require inpatient or even critical care monitoring with aggressive medical management to prevent the progression of skin desquamation (patient 3). Patients with severe oral lesions may require inpatient support for fluid maintenance.
Lupus History—Two patients in our case series had a history of lupus. Lupus itself can cause primary bullous lesions. Similar to FDE, bullous SLE can involve sun-exposed and nonexposed areas of the skin as well as the mucous membranes with a predilection for the lower vermilion lip.17 In bullous SLE, tense subepidermal blisters with a neutrophil-rich infiltrate form due to circulating antibodies to type VII collagen. These blisters have an erythematous or urticated base, most commonly on the face, upper trunk, and proximal extremities.18 In both SLE with skin manifestations and lupus limited to the skin, bullae may form due to extensive vacuolar degeneration. Similar to TEN, they can form rapidly in a widespread distribution.17 However, there is limited mucosal involvement, no clear drug association, and a better prognosis. Bullae caused by lupus will frequently demonstrate deposition of immunoproteins IgG, IgM, IgA, and complement component 3 at the basement membrane zone in perilesional skin on direct immunofluorescence. However, negative direct immunofluorescence does not rule out lupus.12 At the same time, patients with lupus frequently have comorbidities requiring multiple medications; the need for these medications may predispose patients to higher rates of cutaneous drug eruptions.19 To our knowledge, there is no known association between FDE and lupus.
Conclusion
Patients with acute eruptions following the initiation of a new prescription or over-the-counter medication require urgent evaluation. Generalized bullous FDE requires timely diagnosis and intervention. Patients with lupus have an increased risk for cutaneous drug eruptions due to polypharmacy. Further investigation is necessary to determine if there is a pathophysiologic mechanism responsible for the development of FDE in lupus patients.
- Anderson HJ, Lee JB. A review of fixed drug eruption with a special focus on generalized bullous fixed drug eruption. Medicina (Kaunas). 2021;57:925.
- Gavin M, Sharp L, Walker K, et al. Contrast-induced generalized bullous fixed drug eruption resembling Stevens-Johnson syndrome. Proc (Bayl Univ Med Cent). 2019;32:601-602.
- Kabir S, Feit EJ, Heilman ER. Generalized fixed drug eruption following Pfizer-BioNtech COVID-19 vaccination. Clin Case Rep. 2022;10:E6684.
- Choi S, Kim SH, Hwang JH, et al. Rapidly progressing generalized bullous fixed drug eruption after the first dose of COVID-19 messenger RNA vaccination. J Dermatol. 2023;50:1190-1193.
- Mahboob A, Haroon TS. Drugs causing fixed eruptions: a study of 450 cases. Int J Dermatol. 1998;37:833-838.
- Shiohara T. Fixed drug eruption: pathogenesis and diagnostic tests. Curr Opin Allergy Clin Immunol. 2009;9:316-321.
- Mizukawa Y, Yamazaki Y, Shiohara T. In vivo dynamics of intraepidermal CD8+ T cells and CD4+ T cells during the evolution of fixed drug eruption. Br J Dermatol. 2008;158:1230-1238.
- Lee CH, Chen YC, Cho YT, et al. Fixed-drug eruption: a retrospective study in a single referral center in northern Taiwan. Dermatologica Sinica. 2012;30:11-15.
- Cho YT, Lin JW, Chen YC, et al. Generalized bullous fixed drug eruption is distinct from Stevens-Johnson syndrome/toxic epidermal necrolysis by immunohistopathological features. J Am Acad Dermatol. 2014;70:539-548.
- Lipowicz S, Sekula P, Ingen-Housz-Oro S, et al. Prognosis of generalized bullous fixed drug eruption: comparison with Stevens-Johnson syndrome and toxic epidermal necrolysis. Br J Dermatol. 2013;168:726-732.
- Patel S, John AM, Handler MZ, et al. Fixed drug eruptions: an update, emphasizing the potentially lethal generalized bullous fixed drug eruption. Am J Clin Dermatol. 2020;21:393-399.
- Ranario JS, Smith JL. Bullous lesions in a patient with systemic lupus erythematosus. J Clin Aesthet Dermatol. 2014;7:44-49.
- Perron E, Viarnaud A, Marciano L, et al. Clinical and histological features of fixed drug eruption: a single-centre series of 73 cases with comparison between bullous and non-bullous forms. Eur J Dermatol. 2021;31:372-380.
- Chen CB, Kuo KL, Wang CW, et al. Detecting lesional granulysin levels for rapid diagnosis of cytotoxic T lymphocyte-mediated bullous skin disorders. J Allergy Clin Immunol Pract. 2021;9:1327-1337.e3.
- Beniwal R, Gupta LK, Khare AK, et al. Cyclosporine in generalized bullous-fixed drug eruption. Indian J Dermatol. 2018;63:432-433.
- Vargas Mora P, García S, Valenzuela F, et al. Generalized bullous fixed drug eruption successfully treated with cyclosporine. Dermatol Ther. 2020;33:E13492.
- Montagnon CM, Tolkachjov SN, Murrell DF, et al. Subepithelial autoimmune blistering dermatoses: clinical features and diagnosis. J Am Acad Dermatol. 2021;85:1-14.
- Sebaratnam DF, Murrell DF. Bullous systemic lupus erythematosus. Dermatol Clin. 2011;29:649-653.
- Zonzits E, Aberer W, Tappeiner G. Drug eruptions from mesna. After cyclophosphamide treatment of patients with systemic lupus erythematosus and dermatomyositis. Arch Dermatol. 1992;128:80-82.
- Anderson HJ, Lee JB. A review of fixed drug eruption with a special focus on generalized bullous fixed drug eruption. Medicina (Kaunas). 2021;57:925.
- Gavin M, Sharp L, Walker K, et al. Contrast-induced generalized bullous fixed drug eruption resembling Stevens-Johnson syndrome. Proc (Bayl Univ Med Cent). 2019;32:601-602.
- Kabir S, Feit EJ, Heilman ER. Generalized fixed drug eruption following Pfizer-BioNtech COVID-19 vaccination. Clin Case Rep. 2022;10:E6684.
- Choi S, Kim SH, Hwang JH, et al. Rapidly progressing generalized bullous fixed drug eruption after the first dose of COVID-19 messenger RNA vaccination. J Dermatol. 2023;50:1190-1193.
- Mahboob A, Haroon TS. Drugs causing fixed eruptions: a study of 450 cases. Int J Dermatol. 1998;37:833-838.
- Shiohara T. Fixed drug eruption: pathogenesis and diagnostic tests. Curr Opin Allergy Clin Immunol. 2009;9:316-321.
- Mizukawa Y, Yamazaki Y, Shiohara T. In vivo dynamics of intraepidermal CD8+ T cells and CD4+ T cells during the evolution of fixed drug eruption. Br J Dermatol. 2008;158:1230-1238.
- Lee CH, Chen YC, Cho YT, et al. Fixed-drug eruption: a retrospective study in a single referral center in northern Taiwan. Dermatologica Sinica. 2012;30:11-15.
- Cho YT, Lin JW, Chen YC, et al. Generalized bullous fixed drug eruption is distinct from Stevens-Johnson syndrome/toxic epidermal necrolysis by immunohistopathological features. J Am Acad Dermatol. 2014;70:539-548.
- Lipowicz S, Sekula P, Ingen-Housz-Oro S, et al. Prognosis of generalized bullous fixed drug eruption: comparison with Stevens-Johnson syndrome and toxic epidermal necrolysis. Br J Dermatol. 2013;168:726-732.
- Patel S, John AM, Handler MZ, et al. Fixed drug eruptions: an update, emphasizing the potentially lethal generalized bullous fixed drug eruption. Am J Clin Dermatol. 2020;21:393-399.
- Ranario JS, Smith JL. Bullous lesions in a patient with systemic lupus erythematosus. J Clin Aesthet Dermatol. 2014;7:44-49.
- Perron E, Viarnaud A, Marciano L, et al. Clinical and histological features of fixed drug eruption: a single-centre series of 73 cases with comparison between bullous and non-bullous forms. Eur J Dermatol. 2021;31:372-380.
- Chen CB, Kuo KL, Wang CW, et al. Detecting lesional granulysin levels for rapid diagnosis of cytotoxic T lymphocyte-mediated bullous skin disorders. J Allergy Clin Immunol Pract. 2021;9:1327-1337.e3.
- Beniwal R, Gupta LK, Khare AK, et al. Cyclosporine in generalized bullous-fixed drug eruption. Indian J Dermatol. 2018;63:432-433.
- Vargas Mora P, García S, Valenzuela F, et al. Generalized bullous fixed drug eruption successfully treated with cyclosporine. Dermatol Ther. 2020;33:E13492.
- Montagnon CM, Tolkachjov SN, Murrell DF, et al. Subepithelial autoimmune blistering dermatoses: clinical features and diagnosis. J Am Acad Dermatol. 2021;85:1-14.
- Sebaratnam DF, Murrell DF. Bullous systemic lupus erythematosus. Dermatol Clin. 2011;29:649-653.
- Zonzits E, Aberer W, Tappeiner G. Drug eruptions from mesna. After cyclophosphamide treatment of patients with systemic lupus erythematosus and dermatomyositis. Arch Dermatol. 1992;128:80-82.
Practice Points
- Although localized fixed drug eruption (FDE) is a relatively benign diagnosis, generalized bullous FDE requires urgent management and may necessitate intensive burn care.
- Patients with lupus are at increased risk for drug eruptions due to polypharmacy, and there is a wide differential for bullous eruptions in these patients.

Mycobacterium interjectum Infection in an Immunocompetent Host Following Contact With Aquarium Fish
To the Editor:
A 48-year-old man presented with nodular lesions in a sporotrichoid pattern on the right hand and forearm of 3 months’ duration (Figure). There were no lymphadeno-pathies, and he had no notable medical history. He denied fever and other systemic symptoms. The patient recently had manipulated a warm water fish aquarium. Although he did not recall a clear injury, inadvertent mild trauma was a possibility. He denied other contact or trauma in relation to animals or vegetables.
Histopathology from a punch biopsy of the forearm revealed a granulomatous infiltrate with necrosis at the deep dermis level at the interface with the subcutaneous cellular tissue that was composed of mainly epithelioid cells with a few multinucleated giant cells. No acid-fast bacilli or fungi were observed with special stains.
A polymerase chain reaction assay for atypical mycobacteria was positive for Mycobacterium interjectum. The culture of the skin biopsy was negative for fungi and mycobacteria after long incubation (6 weeks) on 2 occasions, and an antibiogram was not available. Complementary tests including hemogram, HIV serology, and chest and upper extremity radiographs did not reveal any abnormalities.

The patient was treated with rifampicin 600 mg/d, clarithromycin 500 mg every 12 hours, and co-trimoxazole 160/800 mg every 12 hours for 9 months with some resolution but persistence of some residual scarring lesions. There was no recurrence at 6-month follow-up.
Mycobacterium interjectum is a rare, slow-growing, scotochromogenic mycobacteria. Case reports usually refer to lymphadenitis in healthy children and pulmonary infections in immunocompromised or immunocompetent adults.1,2 A case of M interjectum with cutaneous involvement was reported by Fukuoka et al,3 with ulcerated nodules and abscesses on the leg identified in an immunocompromised patient. Our patient did not present with any cause of immunosuppression or clear injury predisposing him to infection. This microorganism has been detected in water, soil,3 and aquarium fish,4 the latter being the most likely source of infection in our patient. Given its slow growth rate and the need for a specific polymerase chain reaction assay, which is not widely available, M interjectum infection may be underdiagnosed.
No standard antibiotic regimen has been established, but M interjectum has proven to be a multidrug-resistant bacterium with frequent therapy failures. Treatment options have ranged from standard tuberculostatic therapy to combination therapy with medications such as amikacin, levofloxacin, rifampicin, and co-trimoxazole.1 Because an antibiogram was not available for our patient, empiric treatment with rifampicin, clarithromycin, and co-trimoxazole was prescribed for 9 months, with satisfactory response and tolerance. These drugs were selected because of their susceptibility profile in the literature.1,5
- Sotello D, Hata DJ, Reza M, et al. Disseminated Mycobacterium interjectum infection with bacteremia, hepatic and pulmonary involvement associated with a long-term catheter infection. Case Rep Infect Dis. 2017;2017:1-5.
- Dholakia YN. Mycobacterium interjectum isolated from an immunocompetent host with lung infection. Int J Mycobacteriol. 2017;6:401-403.
- Fukuoka M, Matsumura Y, Kore-eda S, et al. Cutaneous infection due to Mycobacterium interjectum in an immunosuppressed patient with microscopic polyangiitis. Br J Dermatol. 2008;159:1382-1384.
- Zanoni RG, Florio D, Fioravanti ML, et al. Occurrence of Mycobacterium spp. in ornamental fish in Italy. J Fish Dis. 2008;31:433-441.
- Emler S, Rochat T, Rohner P, et al. Chronic destructive lung disease associated with a novel mycobacterium. Am J Respir Crit Care Med. 1994;150:261-265.
To the Editor:
A 48-year-old man presented with nodular lesions in a sporotrichoid pattern on the right hand and forearm of 3 months’ duration (Figure). There were no lymphadeno-pathies, and he had no notable medical history. He denied fever and other systemic symptoms. The patient recently had manipulated a warm water fish aquarium. Although he did not recall a clear injury, inadvertent mild trauma was a possibility. He denied other contact or trauma in relation to animals or vegetables.
Histopathology from a punch biopsy of the forearm revealed a granulomatous infiltrate with necrosis at the deep dermis level at the interface with the subcutaneous cellular tissue that was composed of mainly epithelioid cells with a few multinucleated giant cells. No acid-fast bacilli or fungi were observed with special stains.
A polymerase chain reaction assay for atypical mycobacteria was positive for Mycobacterium interjectum. The culture of the skin biopsy was negative for fungi and mycobacteria after long incubation (6 weeks) on 2 occasions, and an antibiogram was not available. Complementary tests including hemogram, HIV serology, and chest and upper extremity radiographs did not reveal any abnormalities.
The patient was treated with rifampicin 600 mg/d, clarithromycin 500 mg every 12 hours, and co-trimoxazole 160/800 mg every 12 hours for 9 months with some resolution but persistence of some residual scarring lesions. There was no recurrence at 6-month follow-up.
Mycobacterium interjectum is a rare, slow-growing, scotochromogenic mycobacteria. Case reports usually refer to lymphadenitis in healthy children and pulmonary infections in immunocompromised or immunocompetent adults.1,2 A case of M interjectum with cutaneous involvement was reported by Fukuoka et al,3 with ulcerated nodules and abscesses on the leg identified in an immunocompromised patient. Our patient did not present with any cause of immunosuppression or clear injury predisposing him to infection. This microorganism has been detected in water, soil,3 and aquarium fish,4 the latter being the most likely source of infection in our patient. Given its slow growth rate and the need for a specific polymerase chain reaction assay, which is not widely available, M interjectum infection may be underdiagnosed.
No standard antibiotic regimen has been established, but M interjectum has proven to be a multidrug-resistant bacterium with frequent therapy failures. Treatment options have ranged from standard tuberculostatic therapy to combination therapy with medications such as amikacin, levofloxacin, rifampicin, and co-trimoxazole.1 Because an antibiogram was not available for our patient, empiric treatment with rifampicin, clarithromycin, and co-trimoxazole was prescribed for 9 months, with satisfactory response and tolerance. These drugs were selected because of their susceptibility profile in the literature.1,5
To the Editor:
A 48-year-old man presented with nodular lesions in a sporotrichoid pattern on the right hand and forearm of 3 months’ duration (Figure). There were no lymphadeno-pathies, and he had no notable medical history. He denied fever and other systemic symptoms. The patient recently had manipulated a warm water fish aquarium. Although he did not recall a clear injury, inadvertent mild trauma was a possibility. He denied other contact or trauma in relation to animals or vegetables.
Histopathology from a punch biopsy of the forearm revealed a granulomatous infiltrate with necrosis at the deep dermis level at the interface with the subcutaneous cellular tissue that was composed of mainly epithelioid cells with a few multinucleated giant cells. No acid-fast bacilli or fungi were observed with special stains.
A polymerase chain reaction assay for atypical mycobacteria was positive for Mycobacterium interjectum. The culture of the skin biopsy was negative for fungi and mycobacteria after long incubation (6 weeks) on 2 occasions, and an antibiogram was not available. Complementary tests including hemogram, HIV serology, and chest and upper extremity radiographs did not reveal any abnormalities.
The patient was treated with rifampicin 600 mg/d, clarithromycin 500 mg every 12 hours, and co-trimoxazole 160/800 mg every 12 hours for 9 months with some resolution but persistence of some residual scarring lesions. There was no recurrence at 6-month follow-up.
Mycobacterium interjectum is a rare, slow-growing, scotochromogenic mycobacteria. Case reports usually refer to lymphadenitis in healthy children and pulmonary infections in immunocompromised or immunocompetent adults.1,2 A case of M interjectum with cutaneous involvement was reported by Fukuoka et al,3 with ulcerated nodules and abscesses on the leg identified in an immunocompromised patient. Our patient did not present with any cause of immunosuppression or clear injury predisposing him to infection. This microorganism has been detected in water, soil,3 and aquarium fish,4 the latter being the most likely source of infection in our patient. Given its slow growth rate and the need for a specific polymerase chain reaction assay, which is not widely available, M interjectum infection may be underdiagnosed.
No standard antibiotic regimen has been established, but M interjectum has proven to be a multidrug-resistant bacterium with frequent therapy failures. Treatment options have ranged from standard tuberculostatic therapy to combination therapy with medications such as amikacin, levofloxacin, rifampicin, and co-trimoxazole.1 Because an antibiogram was not available for our patient, empiric treatment with rifampicin, clarithromycin, and co-trimoxazole was prescribed for 9 months, with satisfactory response and tolerance. These drugs were selected because of their susceptibility profile in the literature.1,5
- Sotello D, Hata DJ, Reza M, et al. Disseminated Mycobacterium interjectum infection with bacteremia, hepatic and pulmonary involvement associated with a long-term catheter infection. Case Rep Infect Dis. 2017;2017:1-5.
- Dholakia YN. Mycobacterium interjectum isolated from an immunocompetent host with lung infection. Int J Mycobacteriol. 2017;6:401-403.
- Fukuoka M, Matsumura Y, Kore-eda S, et al. Cutaneous infection due to Mycobacterium interjectum in an immunosuppressed patient with microscopic polyangiitis. Br J Dermatol. 2008;159:1382-1384.
- Zanoni RG, Florio D, Fioravanti ML, et al. Occurrence of Mycobacterium spp. in ornamental fish in Italy. J Fish Dis. 2008;31:433-441.
- Emler S, Rochat T, Rohner P, et al. Chronic destructive lung disease associated with a novel mycobacterium. Am J Respir Crit Care Med. 1994;150:261-265.
- Sotello D, Hata DJ, Reza M, et al. Disseminated Mycobacterium interjectum infection with bacteremia, hepatic and pulmonary involvement associated with a long-term catheter infection. Case Rep Infect Dis. 2017;2017:1-5.
- Dholakia YN. Mycobacterium interjectum isolated from an immunocompetent host with lung infection. Int J Mycobacteriol. 2017;6:401-403.
- Fukuoka M, Matsumura Y, Kore-eda S, et al. Cutaneous infection due to Mycobacterium interjectum in an immunosuppressed patient with microscopic polyangiitis. Br J Dermatol. 2008;159:1382-1384.
- Zanoni RG, Florio D, Fioravanti ML, et al. Occurrence of Mycobacterium spp. in ornamental fish in Italy. J Fish Dis. 2008;31:433-441.
- Emler S, Rochat T, Rohner P, et al. Chronic destructive lung disease associated with a novel mycobacterium. Am J Respir Crit Care Med. 1994;150:261-265.
Practice Points
- Mycobacterium interjectum can cause cutaneous nodules in a sporotrichoid or lymphocutaneous pattern and may affect immunocompromised and immunocompetent patients.
- This mycobacteria has been detected in water, soil, and aquarium fish. The latter could be a source of infection and should be taken into account in the anamnesis.
- There is no established therapeutic regimen for M interjectum infection. Combination therapy with rifampicin, clarithromycin, and co-trimoxazole could be an option, though it must always be adapted to an antibiogram if results are available.
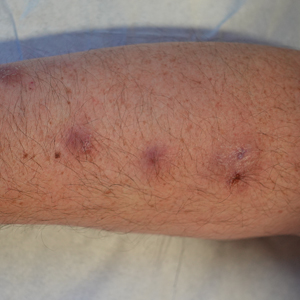
Dermatoporosis in Older Adults: A Condition That Requires Holistic, Creative Management
WASHINGTON — and conveys the skin’s vulnerability to serious medical complications, said Adam Friedman, MD, at the ElderDerm conference on dermatology in the older patient.
Key features of dermatoporosis include atrophic skin, solar purpura, white pseudoscars, easily acquired skin lacerations and tears, bruises, and delayed healing. “We’re going to see more of this, and it will more and more be a chief complaint of patients,” said Dr. Friedman, professor and chair of dermatology at George Washington University (GWU) in Washington, and co-chair of the meeting. GWU hosted the conference, describing it as a first-of-its-kind meeting dedicated to improving dermatologic care for older adults.

Dermatoporosis was described in the literature in 2007 by dermatologists at the University of Geneva in Switzerland. “It is not only a cosmetic problem,” Dr. Friedman said. “This is a medical problem ... which can absolutely lead to comorbidities [such as deep dissecting hematomas] that are a huge strain on the healthcare system.”
Dermatologists can meet the moment with holistic, creative combination treatment and counseling approaches aimed at improving the mechanical strength of skin and preventing potential complications in older patients, Dr. Friedman said at the meeting.
He described the case of a 76-year-old woman who presented with dermatoporosis on her arms involving pronounced skin atrophy, solar purpura, and a small covered laceration. “This was a patient who was both devastated by the appearance” and impacted by the pain and burden of dressing frequent wounds, said Dr. Friedman, who is also the director of the Residency Program, of Translational Research, and of Supportive Oncodermatology, all within the Department of Dermatology at GWU.
With 11 months of topical treatment that included daily application of calcipotriene 0.05% ointment and nightly application of tazarotene 0.045% lotion and oral supplementation with 1000-mg vitamin C twice daily and 1000-mg citrus bioflavonoid complex daily, as well as no changes to the medications she took for various comorbidities, the solar purpura improved significantly and “we made a huge difference in the integrity of her skin,” he said.
Dr. Friedman also described this case in a recently published article in the Journal of Drugs in Dermatology titled “What’s Old Is New: An Emerging Focus on Dermatoporosis”.
Likely Pathophysiology
Advancing age and chronic ultraviolet (UV) radiation exposure are the chief drivers of dermatoporosis. In addition to UVA and UVB light, other secondary drivers include genetic susceptibility, topical and systematic corticosteroid use, and anticoagulant treatment.
Its pathogenesis is not well described in the literature but is easy to envision, Dr. Friedman said. For one, both advancing age and exposure to UV light lead to a reduction in hygroscopic glycosaminoglycans, including hyaluronate (HA), and the impact of this diminishment is believed to go “beyond [the loss of] buoyancy,” he noted. Researchers have “been showing these are not just water-loving molecules, they also have some biologic properties” relating to keratinocyte production and epidermal turnover that appear to be intricately linked to the pathogenesis of dermatoporosis.
HAs have been shown to interact with the cell surface receptor CD44 to stimulate keratinocyte proliferation, and low levels of CD44 have been reported in skin with dermatoporosis compared with a younger control population. (A newly characterized organelle, the hyaluronosome, serves as an HA factory and contains CD44 and heparin-binding epidermal growth factor, Dr. Friedman noted. Inadequate functioning may be involved in skin atrophy.)
Advancing age also brings an increase in matrix metalloproteinases (MMPs)–1, –2, and –3, which are “the demolition workers of the skin,” and downregulation of a tissue inhibitor of MMPs, he said.
Adding insult to injury, dermis-penetrating UVA also activates MMPs, “obliterating collagen and elastin.” UVB generates DNA photoproducts, including oxidative stress and damaging skin cell DNA. “That UV light induces breakdown [of the skin] through different mechanisms and inhibits buildup is a simple concept I think our patients can understand,” Dr. Friedman said.
Multifaceted Treatment
For an older adult, “there is never a wrong time to start sun-protective measures” to prevent or try to halt the progression of dermatoporosis, Dr. Friedman said, noting that “UV radiation is an immunosuppressant, so there are many good reasons to start” if the adult is not already taking measures on a regular basis.
Potential treatments for the syndrome of dermatoporosis are backed by few clinical studies, but dermatologists are skilled at translating the use of products from one disease state to another based on understandings of pathophysiology and mechanistic pathways, Dr. Friedman commented in an interview after the meeting.
For instance, “from decades of research, we know what retinoids will do to the skin,” he said in the interview. “We know they will turn on collagen-1 and -3 genes in the skin, and that they will increase the production of glycosaminoglycans ... By understanding the biology, we can translate this to dermatoporosis.” These changes were demonstrated, for instance, in a small study of topical retinol in older adults.
Studies of topical alpha hydroxy acid (AHA), moreover, have demonstrated epidermal thickening and firmness, and “some studies show they can limit steroid-induced atrophy,” Dr. Friedman said at the meeting. “And things like lactic acid and urea are super accessible.”
Topical dehydroepiandrosterone is backed by even less data than retinoids or AHAs are, “but it’s still something to consider” as part of a multimechanistic approach to dermatoporosis, Dr. Friedman shared, noting that a small study demonstrated beneficial effects on epidermal atrophy in aging skin.
The use of vitamin D analogues such as calcipotriene, which is approved for the treatment of psoriasis, may also be promising. “One concept is that [vitamin D analogues] increase calcium concentrations in the epidermis, and calcium is so central to keratinocyte differentiation” and epidermal function that calcipotriene in combination with topical steroid therapy has been shown to limit skin atrophy, he noted.
Nutritionally, low protein intake is a known problem in the older population and is associated with increased skin fragility and poorer healing. From a prevention and treatment standpoint, therefore, patients can be counseled to be attentive to their diets, Dr. Friedman said. Experts have recommended a higher protein intake for older adults than for younger adults; in 2013, an international group recommended a protein intake of 1-1.5 g/kg/d for healthy older adults and more for those with acute or chronic illness.
“Patients love talking about diet and skin disease ... and they love over-the-counter nutraceuticals as well because they want something natural,” Dr. Friedman said. “I like using bioflavonoids in combination with vitamin C, which can be effective especially for solar purpura.”

A 6-week randomized, placebo-controlled, double-blind trial involving 67 patients with purpura associated with aging found a 50% reduction in purpura lesions among those took a particular citrus bioflavonoid blend twice daily. “I thought this was a pretty well-done study,” he said, noting that patient self-assessment and investigator global assessment were utilized.
Skin Injury and Wound Prevention
In addition to recommending gentle skin cleansers and daily moisturizing, dermatologists should talk to their older patients with dermatoporosis about their home environments. “What is it like? Is there furniture with sharp edges?” Dr. Friedman advised. If so, could they use sleeves or protectors on their arms or legs “to protect against injury?”
In a later meeting session about lower-extremity wounds on geriatric patients, Michael Stempel, DPM, assistant professor of medicine and surgery and chief of podiatry at GWU, said that he was happy to hear the term dermatoporosis being used because like diabetes, it’s a risk factor for developing lower-extremity wounds and poor wound healing.
He shared the case of an older woman with dermatoporosis who “tripped and skinned her knee against a step and then self-treated it for over a month by pouring hydrogen peroxide over it and letting air get to it.” The wound developed into “full-thickness tissue loss,” said Dr. Stempel, also medical director of the Wound Healing and Limb Preservation Center at GWU Hospital.
Misperceptions are common among older patients about how a simple wound should be managed; for instance, the adage “just let it get air” is not uncommon. This makes anticipatory guidance about basic wound care — such as the importance of a moist and occlusive environment and the safe use of hydrogen peroxide — especially important for patients with dermatoporosis, Dr. Friedman commented after the meeting.
Dermatoporosis is quantifiable, Dr. Friedman said during the meeting, with a scoring system having been developed by the researchers in Switzerland who originally coined the term. Its use in practice is unnecessary, but its existence is “nice to share with patients who feel bothered because oftentimes, patients feel it’s been dismissed by other providers,” he said. “Telling your patients there’s an actual name for their problem, and that there are ways to quantify and measure changes over time, is validating.”
Its recognition as a medical condition, Dr. Friedman added, also enables the dermatologist to bring it up and counsel appropriately — without a patient feeling shame — when it is identified in the context of a skin excision, treatment of a primary inflammatory skin disease, or management of another dermatologic problem.
Dr. Friedman disclosed that he is a consultant/advisory board member for L’Oréal, La Roche-Posay, Galderma, and other companies; a speaker for Regeneron/Sanofi, Incyte, BMD, and Janssen; and has grants from Pfizer, Lilly, Incyte, and other companies. Dr. Stempel reported no disclosures.
A version of this article first appeared on Medscape.com.
WASHINGTON — and conveys the skin’s vulnerability to serious medical complications, said Adam Friedman, MD, at the ElderDerm conference on dermatology in the older patient.
Key features of dermatoporosis include atrophic skin, solar purpura, white pseudoscars, easily acquired skin lacerations and tears, bruises, and delayed healing. “We’re going to see more of this, and it will more and more be a chief complaint of patients,” said Dr. Friedman, professor and chair of dermatology at George Washington University (GWU) in Washington, and co-chair of the meeting. GWU hosted the conference, describing it as a first-of-its-kind meeting dedicated to improving dermatologic care for older adults.
Dermatoporosis was described in the literature in 2007 by dermatologists at the University of Geneva in Switzerland. “It is not only a cosmetic problem,” Dr. Friedman said. “This is a medical problem ... which can absolutely lead to comorbidities [such as deep dissecting hematomas] that are a huge strain on the healthcare system.”
Dermatologists can meet the moment with holistic, creative combination treatment and counseling approaches aimed at improving the mechanical strength of skin and preventing potential complications in older patients, Dr. Friedman said at the meeting.
He described the case of a 76-year-old woman who presented with dermatoporosis on her arms involving pronounced skin atrophy, solar purpura, and a small covered laceration. “This was a patient who was both devastated by the appearance” and impacted by the pain and burden of dressing frequent wounds, said Dr. Friedman, who is also the director of the Residency Program, of Translational Research, and of Supportive Oncodermatology, all within the Department of Dermatology at GWU.
With 11 months of topical treatment that included daily application of calcipotriene 0.05% ointment and nightly application of tazarotene 0.045% lotion and oral supplementation with 1000-mg vitamin C twice daily and 1000-mg citrus bioflavonoid complex daily, as well as no changes to the medications she took for various comorbidities, the solar purpura improved significantly and “we made a huge difference in the integrity of her skin,” he said.
Dr. Friedman also described this case in a recently published article in the Journal of Drugs in Dermatology titled “What’s Old Is New: An Emerging Focus on Dermatoporosis”.
Likely Pathophysiology
Advancing age and chronic ultraviolet (UV) radiation exposure are the chief drivers of dermatoporosis. In addition to UVA and UVB light, other secondary drivers include genetic susceptibility, topical and systematic corticosteroid use, and anticoagulant treatment.
Its pathogenesis is not well described in the literature but is easy to envision, Dr. Friedman said. For one, both advancing age and exposure to UV light lead to a reduction in hygroscopic glycosaminoglycans, including hyaluronate (HA), and the impact of this diminishment is believed to go “beyond [the loss of] buoyancy,” he noted. Researchers have “been showing these are not just water-loving molecules, they also have some biologic properties” relating to keratinocyte production and epidermal turnover that appear to be intricately linked to the pathogenesis of dermatoporosis.
HAs have been shown to interact with the cell surface receptor CD44 to stimulate keratinocyte proliferation, and low levels of CD44 have been reported in skin with dermatoporosis compared with a younger control population. (A newly characterized organelle, the hyaluronosome, serves as an HA factory and contains CD44 and heparin-binding epidermal growth factor, Dr. Friedman noted. Inadequate functioning may be involved in skin atrophy.)
Advancing age also brings an increase in matrix metalloproteinases (MMPs)–1, –2, and –3, which are “the demolition workers of the skin,” and downregulation of a tissue inhibitor of MMPs, he said.
Adding insult to injury, dermis-penetrating UVA also activates MMPs, “obliterating collagen and elastin.” UVB generates DNA photoproducts, including oxidative stress and damaging skin cell DNA. “That UV light induces breakdown [of the skin] through different mechanisms and inhibits buildup is a simple concept I think our patients can understand,” Dr. Friedman said.
Multifaceted Treatment
For an older adult, “there is never a wrong time to start sun-protective measures” to prevent or try to halt the progression of dermatoporosis, Dr. Friedman said, noting that “UV radiation is an immunosuppressant, so there are many good reasons to start” if the adult is not already taking measures on a regular basis.
Potential treatments for the syndrome of dermatoporosis are backed by few clinical studies, but dermatologists are skilled at translating the use of products from one disease state to another based on understandings of pathophysiology and mechanistic pathways, Dr. Friedman commented in an interview after the meeting.
For instance, “from decades of research, we know what retinoids will do to the skin,” he said in the interview. “We know they will turn on collagen-1 and -3 genes in the skin, and that they will increase the production of glycosaminoglycans ... By understanding the biology, we can translate this to dermatoporosis.” These changes were demonstrated, for instance, in a small study of topical retinol in older adults.
Studies of topical alpha hydroxy acid (AHA), moreover, have demonstrated epidermal thickening and firmness, and “some studies show they can limit steroid-induced atrophy,” Dr. Friedman said at the meeting. “And things like lactic acid and urea are super accessible.”
Topical dehydroepiandrosterone is backed by even less data than retinoids or AHAs are, “but it’s still something to consider” as part of a multimechanistic approach to dermatoporosis, Dr. Friedman shared, noting that a small study demonstrated beneficial effects on epidermal atrophy in aging skin.
The use of vitamin D analogues such as calcipotriene, which is approved for the treatment of psoriasis, may also be promising. “One concept is that [vitamin D analogues] increase calcium concentrations in the epidermis, and calcium is so central to keratinocyte differentiation” and epidermal function that calcipotriene in combination with topical steroid therapy has been shown to limit skin atrophy, he noted.
Nutritionally, low protein intake is a known problem in the older population and is associated with increased skin fragility and poorer healing. From a prevention and treatment standpoint, therefore, patients can be counseled to be attentive to their diets, Dr. Friedman said. Experts have recommended a higher protein intake for older adults than for younger adults; in 2013, an international group recommended a protein intake of 1-1.5 g/kg/d for healthy older adults and more for those with acute or chronic illness.
“Patients love talking about diet and skin disease ... and they love over-the-counter nutraceuticals as well because they want something natural,” Dr. Friedman said. “I like using bioflavonoids in combination with vitamin C, which can be effective especially for solar purpura.”
A 6-week randomized, placebo-controlled, double-blind trial involving 67 patients with purpura associated with aging found a 50% reduction in purpura lesions among those took a particular citrus bioflavonoid blend twice daily. “I thought this was a pretty well-done study,” he said, noting that patient self-assessment and investigator global assessment were utilized.
Skin Injury and Wound Prevention
In addition to recommending gentle skin cleansers and daily moisturizing, dermatologists should talk to their older patients with dermatoporosis about their home environments. “What is it like? Is there furniture with sharp edges?” Dr. Friedman advised. If so, could they use sleeves or protectors on their arms or legs “to protect against injury?”
In a later meeting session about lower-extremity wounds on geriatric patients, Michael Stempel, DPM, assistant professor of medicine and surgery and chief of podiatry at GWU, said that he was happy to hear the term dermatoporosis being used because like diabetes, it’s a risk factor for developing lower-extremity wounds and poor wound healing.
He shared the case of an older woman with dermatoporosis who “tripped and skinned her knee against a step and then self-treated it for over a month by pouring hydrogen peroxide over it and letting air get to it.” The wound developed into “full-thickness tissue loss,” said Dr. Stempel, also medical director of the Wound Healing and Limb Preservation Center at GWU Hospital.
Misperceptions are common among older patients about how a simple wound should be managed; for instance, the adage “just let it get air” is not uncommon. This makes anticipatory guidance about basic wound care — such as the importance of a moist and occlusive environment and the safe use of hydrogen peroxide — especially important for patients with dermatoporosis, Dr. Friedman commented after the meeting.
Dermatoporosis is quantifiable, Dr. Friedman said during the meeting, with a scoring system having been developed by the researchers in Switzerland who originally coined the term. Its use in practice is unnecessary, but its existence is “nice to share with patients who feel bothered because oftentimes, patients feel it’s been dismissed by other providers,” he said. “Telling your patients there’s an actual name for their problem, and that there are ways to quantify and measure changes over time, is validating.”
Its recognition as a medical condition, Dr. Friedman added, also enables the dermatologist to bring it up and counsel appropriately — without a patient feeling shame — when it is identified in the context of a skin excision, treatment of a primary inflammatory skin disease, or management of another dermatologic problem.
Dr. Friedman disclosed that he is a consultant/advisory board member for L’Oréal, La Roche-Posay, Galderma, and other companies; a speaker for Regeneron/Sanofi, Incyte, BMD, and Janssen; and has grants from Pfizer, Lilly, Incyte, and other companies. Dr. Stempel reported no disclosures.
A version of this article first appeared on Medscape.com.
WASHINGTON — and conveys the skin’s vulnerability to serious medical complications, said Adam Friedman, MD, at the ElderDerm conference on dermatology in the older patient.
Key features of dermatoporosis include atrophic skin, solar purpura, white pseudoscars, easily acquired skin lacerations and tears, bruises, and delayed healing. “We’re going to see more of this, and it will more and more be a chief complaint of patients,” said Dr. Friedman, professor and chair of dermatology at George Washington University (GWU) in Washington, and co-chair of the meeting. GWU hosted the conference, describing it as a first-of-its-kind meeting dedicated to improving dermatologic care for older adults.
Dermatoporosis was described in the literature in 2007 by dermatologists at the University of Geneva in Switzerland. “It is not only a cosmetic problem,” Dr. Friedman said. “This is a medical problem ... which can absolutely lead to comorbidities [such as deep dissecting hematomas] that are a huge strain on the healthcare system.”
Dermatologists can meet the moment with holistic, creative combination treatment and counseling approaches aimed at improving the mechanical strength of skin and preventing potential complications in older patients, Dr. Friedman said at the meeting.
He described the case of a 76-year-old woman who presented with dermatoporosis on her arms involving pronounced skin atrophy, solar purpura, and a small covered laceration. “This was a patient who was both devastated by the appearance” and impacted by the pain and burden of dressing frequent wounds, said Dr. Friedman, who is also the director of the Residency Program, of Translational Research, and of Supportive Oncodermatology, all within the Department of Dermatology at GWU.
With 11 months of topical treatment that included daily application of calcipotriene 0.05% ointment and nightly application of tazarotene 0.045% lotion and oral supplementation with 1000-mg vitamin C twice daily and 1000-mg citrus bioflavonoid complex daily, as well as no changes to the medications she took for various comorbidities, the solar purpura improved significantly and “we made a huge difference in the integrity of her skin,” he said.
Dr. Friedman also described this case in a recently published article in the Journal of Drugs in Dermatology titled “What’s Old Is New: An Emerging Focus on Dermatoporosis”.
Likely Pathophysiology
Advancing age and chronic ultraviolet (UV) radiation exposure are the chief drivers of dermatoporosis. In addition to UVA and UVB light, other secondary drivers include genetic susceptibility, topical and systematic corticosteroid use, and anticoagulant treatment.
Its pathogenesis is not well described in the literature but is easy to envision, Dr. Friedman said. For one, both advancing age and exposure to UV light lead to a reduction in hygroscopic glycosaminoglycans, including hyaluronate (HA), and the impact of this diminishment is believed to go “beyond [the loss of] buoyancy,” he noted. Researchers have “been showing these are not just water-loving molecules, they also have some biologic properties” relating to keratinocyte production and epidermal turnover that appear to be intricately linked to the pathogenesis of dermatoporosis.
HAs have been shown to interact with the cell surface receptor CD44 to stimulate keratinocyte proliferation, and low levels of CD44 have been reported in skin with dermatoporosis compared with a younger control population. (A newly characterized organelle, the hyaluronosome, serves as an HA factory and contains CD44 and heparin-binding epidermal growth factor, Dr. Friedman noted. Inadequate functioning may be involved in skin atrophy.)
Advancing age also brings an increase in matrix metalloproteinases (MMPs)–1, –2, and –3, which are “the demolition workers of the skin,” and downregulation of a tissue inhibitor of MMPs, he said.
Adding insult to injury, dermis-penetrating UVA also activates MMPs, “obliterating collagen and elastin.” UVB generates DNA photoproducts, including oxidative stress and damaging skin cell DNA. “That UV light induces breakdown [of the skin] through different mechanisms and inhibits buildup is a simple concept I think our patients can understand,” Dr. Friedman said.
Multifaceted Treatment
For an older adult, “there is never a wrong time to start sun-protective measures” to prevent or try to halt the progression of dermatoporosis, Dr. Friedman said, noting that “UV radiation is an immunosuppressant, so there are many good reasons to start” if the adult is not already taking measures on a regular basis.
Potential treatments for the syndrome of dermatoporosis are backed by few clinical studies, but dermatologists are skilled at translating the use of products from one disease state to another based on understandings of pathophysiology and mechanistic pathways, Dr. Friedman commented in an interview after the meeting.
For instance, “from decades of research, we know what retinoids will do to the skin,” he said in the interview. “We know they will turn on collagen-1 and -3 genes in the skin, and that they will increase the production of glycosaminoglycans ... By understanding the biology, we can translate this to dermatoporosis.” These changes were demonstrated, for instance, in a small study of topical retinol in older adults.
Studies of topical alpha hydroxy acid (AHA), moreover, have demonstrated epidermal thickening and firmness, and “some studies show they can limit steroid-induced atrophy,” Dr. Friedman said at the meeting. “And things like lactic acid and urea are super accessible.”
Topical dehydroepiandrosterone is backed by even less data than retinoids or AHAs are, “but it’s still something to consider” as part of a multimechanistic approach to dermatoporosis, Dr. Friedman shared, noting that a small study demonstrated beneficial effects on epidermal atrophy in aging skin.
The use of vitamin D analogues such as calcipotriene, which is approved for the treatment of psoriasis, may also be promising. “One concept is that [vitamin D analogues] increase calcium concentrations in the epidermis, and calcium is so central to keratinocyte differentiation” and epidermal function that calcipotriene in combination with topical steroid therapy has been shown to limit skin atrophy, he noted.
Nutritionally, low protein intake is a known problem in the older population and is associated with increased skin fragility and poorer healing. From a prevention and treatment standpoint, therefore, patients can be counseled to be attentive to their diets, Dr. Friedman said. Experts have recommended a higher protein intake for older adults than for younger adults; in 2013, an international group recommended a protein intake of 1-1.5 g/kg/d for healthy older adults and more for those with acute or chronic illness.
“Patients love talking about diet and skin disease ... and they love over-the-counter nutraceuticals as well because they want something natural,” Dr. Friedman said. “I like using bioflavonoids in combination with vitamin C, which can be effective especially for solar purpura.”
A 6-week randomized, placebo-controlled, double-blind trial involving 67 patients with purpura associated with aging found a 50% reduction in purpura lesions among those took a particular citrus bioflavonoid blend twice daily. “I thought this was a pretty well-done study,” he said, noting that patient self-assessment and investigator global assessment were utilized.
Skin Injury and Wound Prevention
In addition to recommending gentle skin cleansers and daily moisturizing, dermatologists should talk to their older patients with dermatoporosis about their home environments. “What is it like? Is there furniture with sharp edges?” Dr. Friedman advised. If so, could they use sleeves or protectors on their arms or legs “to protect against injury?”
In a later meeting session about lower-extremity wounds on geriatric patients, Michael Stempel, DPM, assistant professor of medicine and surgery and chief of podiatry at GWU, said that he was happy to hear the term dermatoporosis being used because like diabetes, it’s a risk factor for developing lower-extremity wounds and poor wound healing.
He shared the case of an older woman with dermatoporosis who “tripped and skinned her knee against a step and then self-treated it for over a month by pouring hydrogen peroxide over it and letting air get to it.” The wound developed into “full-thickness tissue loss,” said Dr. Stempel, also medical director of the Wound Healing and Limb Preservation Center at GWU Hospital.
Misperceptions are common among older patients about how a simple wound should be managed; for instance, the adage “just let it get air” is not uncommon. This makes anticipatory guidance about basic wound care — such as the importance of a moist and occlusive environment and the safe use of hydrogen peroxide — especially important for patients with dermatoporosis, Dr. Friedman commented after the meeting.
Dermatoporosis is quantifiable, Dr. Friedman said during the meeting, with a scoring system having been developed by the researchers in Switzerland who originally coined the term. Its use in practice is unnecessary, but its existence is “nice to share with patients who feel bothered because oftentimes, patients feel it’s been dismissed by other providers,” he said. “Telling your patients there’s an actual name for their problem, and that there are ways to quantify and measure changes over time, is validating.”
Its recognition as a medical condition, Dr. Friedman added, also enables the dermatologist to bring it up and counsel appropriately — without a patient feeling shame — when it is identified in the context of a skin excision, treatment of a primary inflammatory skin disease, or management of another dermatologic problem.
Dr. Friedman disclosed that he is a consultant/advisory board member for L’Oréal, La Roche-Posay, Galderma, and other companies; a speaker for Regeneron/Sanofi, Incyte, BMD, and Janssen; and has grants from Pfizer, Lilly, Incyte, and other companies. Dr. Stempel reported no disclosures.
A version of this article first appeared on Medscape.com.
FROM ELDERDERM 2024
It’s the Television, Stupid
As more and more of us begin to feel (or believe we are feeling) the symptoms of aging, our language has begun to incorporate new words and phrases such as “aging in place” or “healthy aging.” In fact, some scientists have created a diagnostic criteria to define “healthy aging.” If you have reached your 70th birthday without mental health issues, memory issues, physical impairments, or chronic disease, according to some researchers at T.H. Chan School of Public Health and Brigham and Women’s Hospital, you should receive a gold star for healthy aging.
I am now nearly a decade past that milestone and can’t remember where I’ve put my gold star, or even if I had ever received one. But, I get up each morning looking forward to another day of activity and feeling “pretty good.”

Healthy aging is not something you start doing when you turn 65. Aging is something that goes on from the moment you are born. For the first couple decades we call it “maturing.” If you have lived well, the odds are you will age well. And, for that reason we should take note of some recent work by Boston-based researchers.
Looking at recent data from 45,000 participants in the well-known Nurses Health Study, the investigators found that for every 2-hour increase in daily sedentary behavior, the participants cut their chances of healthy aging by 12%. On the other hand, for every 2 hours of light physical activity, they increased their odds of healthy aging by 6 %.
There are two important messages sitting just below the surface of these two observations. First, we continue to overemphasize the importance of “exercise” in our attempt to help our patients achieve wellness. The word “exercise” carries with it whole carousel full of baggage including “fitness programs,” gym memberships, pulse rate monitors, pain, sweat, and spandex, to name just a few. Exercise can conjure up bad memories of suiting up for phys ed class, group showers, and being picked last when teams were being chosen.
It turns out the we should simply be promoting activity, and light activity at that — vacuuming the living room, walking around the block, rearranging the books on your bedroom book shelf, making a pot of soup, doing the laundry. Just getting up off one’s behind and doing something instead of being a passive spectator.
This somewhat counterintuitive notion of the benefit of light activity is beginning to get more attention. Earlier this year, I reported on a study by Andre O. Abaje MD, MPH, in which he showed that light physical activity in children was superior to more vigorous activity in lowering lipids.
The more important message embedded in this paper based on the Nurses Health Study is that the researchers used television watching time as their proxy for sedentary behavior. The investigators chose TV viewing because it is ubiquitous and includes prolonged sitting. Being semi-reclined on the couch or in a lounger requires very little muscle activity, which is in turn linked to disruption of glucose metabolism, increased inflammation, and altered blood flow to the brain, to name just a few of its collateral damages. I would add that TV viewing often prompts viewers to stay up well beyond their healthy bedtime. And, we know sleep deprivation is not compatible with health aging.
A traditional warning issued to new retirees was once “Don’t let the old rocking chair get ya.” In fact, I wonder how many folks watching television even have or use wood rocking chairs anymore, which, if rocked, might qualify as a light exercise if the viewer made the effort to rock. Instead I suspect most television viewing is done cocooned in soft recliners or curled up on a couch.
I will admit that this recent paper merely supports a suspicion I have harbored for decades. Like many of you, I have wondered how our society got to the point where obesity is frequent enough to be labeled a disease, attention deficit diagnoses are becoming increasingly prevalent, and our life expectancy is shrinking. There are dozens of factors, but if I had to pick one, I would paraphrase James Carville’s advice to Bill Clinton: “It’s the television, stupid.”
At least a couple of notches above “Are you wearing your seatbelt?” It can start with a nonjudgmental question such as “What are your favorite television shows?” And then deftly move toward compiling a tally of how many hours the patient watches each day.
How you manage the situation from there is up to you and can be based on the patient’s complaints and problem list. You might suggest he or she start by eliminating 2 hours of viewing a day. Then ask if he or she thinks that new schedule is achievable. If they ask for alternatives, be ready with a list of light activities that they might be surprised are healthier than their current behavior. Follow up with another visit or a call to see how they are doing. It’s that important, and your call will underscore your concern.
Sedentism is a serious health problem in this country and our emphasis on encouraging vigorous exercise isn’t working. Selling a television diet will be a tough sell, but it needs to be done.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
As more and more of us begin to feel (or believe we are feeling) the symptoms of aging, our language has begun to incorporate new words and phrases such as “aging in place” or “healthy aging.” In fact, some scientists have created a diagnostic criteria to define “healthy aging.” If you have reached your 70th birthday without mental health issues, memory issues, physical impairments, or chronic disease, according to some researchers at T.H. Chan School of Public Health and Brigham and Women’s Hospital, you should receive a gold star for healthy aging.
I am now nearly a decade past that milestone and can’t remember where I’ve put my gold star, or even if I had ever received one. But, I get up each morning looking forward to another day of activity and feeling “pretty good.”
Healthy aging is not something you start doing when you turn 65. Aging is something that goes on from the moment you are born. For the first couple decades we call it “maturing.” If you have lived well, the odds are you will age well. And, for that reason we should take note of some recent work by Boston-based researchers.
Looking at recent data from 45,000 participants in the well-known Nurses Health Study, the investigators found that for every 2-hour increase in daily sedentary behavior, the participants cut their chances of healthy aging by 12%. On the other hand, for every 2 hours of light physical activity, they increased their odds of healthy aging by 6 %.
There are two important messages sitting just below the surface of these two observations. First, we continue to overemphasize the importance of “exercise” in our attempt to help our patients achieve wellness. The word “exercise” carries with it whole carousel full of baggage including “fitness programs,” gym memberships, pulse rate monitors, pain, sweat, and spandex, to name just a few. Exercise can conjure up bad memories of suiting up for phys ed class, group showers, and being picked last when teams were being chosen.
It turns out the we should simply be promoting activity, and light activity at that — vacuuming the living room, walking around the block, rearranging the books on your bedroom book shelf, making a pot of soup, doing the laundry. Just getting up off one’s behind and doing something instead of being a passive spectator.
This somewhat counterintuitive notion of the benefit of light activity is beginning to get more attention. Earlier this year, I reported on a study by Andre O. Abaje MD, MPH, in which he showed that light physical activity in children was superior to more vigorous activity in lowering lipids.
The more important message embedded in this paper based on the Nurses Health Study is that the researchers used television watching time as their proxy for sedentary behavior. The investigators chose TV viewing because it is ubiquitous and includes prolonged sitting. Being semi-reclined on the couch or in a lounger requires very little muscle activity, which is in turn linked to disruption of glucose metabolism, increased inflammation, and altered blood flow to the brain, to name just a few of its collateral damages. I would add that TV viewing often prompts viewers to stay up well beyond their healthy bedtime. And, we know sleep deprivation is not compatible with health aging.
A traditional warning issued to new retirees was once “Don’t let the old rocking chair get ya.” In fact, I wonder how many folks watching television even have or use wood rocking chairs anymore, which, if rocked, might qualify as a light exercise if the viewer made the effort to rock. Instead I suspect most television viewing is done cocooned in soft recliners or curled up on a couch.
I will admit that this recent paper merely supports a suspicion I have harbored for decades. Like many of you, I have wondered how our society got to the point where obesity is frequent enough to be labeled a disease, attention deficit diagnoses are becoming increasingly prevalent, and our life expectancy is shrinking. There are dozens of factors, but if I had to pick one, I would paraphrase James Carville’s advice to Bill Clinton: “It’s the television, stupid.”
At least a couple of notches above “Are you wearing your seatbelt?” It can start with a nonjudgmental question such as “What are your favorite television shows?” And then deftly move toward compiling a tally of how many hours the patient watches each day.
How you manage the situation from there is up to you and can be based on the patient’s complaints and problem list. You might suggest he or she start by eliminating 2 hours of viewing a day. Then ask if he or she thinks that new schedule is achievable. If they ask for alternatives, be ready with a list of light activities that they might be surprised are healthier than their current behavior. Follow up with another visit or a call to see how they are doing. It’s that important, and your call will underscore your concern.
Sedentism is a serious health problem in this country and our emphasis on encouraging vigorous exercise isn’t working. Selling a television diet will be a tough sell, but it needs to be done.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
As more and more of us begin to feel (or believe we are feeling) the symptoms of aging, our language has begun to incorporate new words and phrases such as “aging in place” or “healthy aging.” In fact, some scientists have created a diagnostic criteria to define “healthy aging.” If you have reached your 70th birthday without mental health issues, memory issues, physical impairments, or chronic disease, according to some researchers at T.H. Chan School of Public Health and Brigham and Women’s Hospital, you should receive a gold star for healthy aging.
I am now nearly a decade past that milestone and can’t remember where I’ve put my gold star, or even if I had ever received one. But, I get up each morning looking forward to another day of activity and feeling “pretty good.”
Healthy aging is not something you start doing when you turn 65. Aging is something that goes on from the moment you are born. For the first couple decades we call it “maturing.” If you have lived well, the odds are you will age well. And, for that reason we should take note of some recent work by Boston-based researchers.
Looking at recent data from 45,000 participants in the well-known Nurses Health Study, the investigators found that for every 2-hour increase in daily sedentary behavior, the participants cut their chances of healthy aging by 12%. On the other hand, for every 2 hours of light physical activity, they increased their odds of healthy aging by 6 %.
There are two important messages sitting just below the surface of these two observations. First, we continue to overemphasize the importance of “exercise” in our attempt to help our patients achieve wellness. The word “exercise” carries with it whole carousel full of baggage including “fitness programs,” gym memberships, pulse rate monitors, pain, sweat, and spandex, to name just a few. Exercise can conjure up bad memories of suiting up for phys ed class, group showers, and being picked last when teams were being chosen.
It turns out the we should simply be promoting activity, and light activity at that — vacuuming the living room, walking around the block, rearranging the books on your bedroom book shelf, making a pot of soup, doing the laundry. Just getting up off one’s behind and doing something instead of being a passive spectator.
This somewhat counterintuitive notion of the benefit of light activity is beginning to get more attention. Earlier this year, I reported on a study by Andre O. Abaje MD, MPH, in which he showed that light physical activity in children was superior to more vigorous activity in lowering lipids.
The more important message embedded in this paper based on the Nurses Health Study is that the researchers used television watching time as their proxy for sedentary behavior. The investigators chose TV viewing because it is ubiquitous and includes prolonged sitting. Being semi-reclined on the couch or in a lounger requires very little muscle activity, which is in turn linked to disruption of glucose metabolism, increased inflammation, and altered blood flow to the brain, to name just a few of its collateral damages. I would add that TV viewing often prompts viewers to stay up well beyond their healthy bedtime. And, we know sleep deprivation is not compatible with health aging.
A traditional warning issued to new retirees was once “Don’t let the old rocking chair get ya.” In fact, I wonder how many folks watching television even have or use wood rocking chairs anymore, which, if rocked, might qualify as a light exercise if the viewer made the effort to rock. Instead I suspect most television viewing is done cocooned in soft recliners or curled up on a couch.
I will admit that this recent paper merely supports a suspicion I have harbored for decades. Like many of you, I have wondered how our society got to the point where obesity is frequent enough to be labeled a disease, attention deficit diagnoses are becoming increasingly prevalent, and our life expectancy is shrinking. There are dozens of factors, but if I had to pick one, I would paraphrase James Carville’s advice to Bill Clinton: “It’s the television, stupid.”
At least a couple of notches above “Are you wearing your seatbelt?” It can start with a nonjudgmental question such as “What are your favorite television shows?” And then deftly move toward compiling a tally of how many hours the patient watches each day.
How you manage the situation from there is up to you and can be based on the patient’s complaints and problem list. You might suggest he or she start by eliminating 2 hours of viewing a day. Then ask if he or she thinks that new schedule is achievable. If they ask for alternatives, be ready with a list of light activities that they might be surprised are healthier than their current behavior. Follow up with another visit or a call to see how they are doing. It’s that important, and your call will underscore your concern.
Sedentism is a serious health problem in this country and our emphasis on encouraging vigorous exercise isn’t working. Selling a television diet will be a tough sell, but it needs to be done.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Giving Cash to Improve Health
This transcript has been edited for clarity.
It doesn’t really matter what disease you are looking at — cancer, heart disease, dementia, drug abuse, psychiatric disorders. In every case, poverty is associated with worse disease.
But the word “associated” is doing a lot of work there. Many of us feel that poverty itself is causally linked to worse disease outcomes through things like poor access to care and poor access to medicines.
And there is an argument that the arrow goes the other way; perhaps people with worse illness are more likely to be poor because, in this country at least, being sick is incredibly expensive.
Causality is what all medical research is fundamentally about. We want to know if A causes B, because if A causes B, then changing A changes B. If poverty causes bad health outcomes, then alleviating poverty should alleviate bad health outcomes.
But that’s a hard proposition to test. You can’t exactly randomize some people to get extra money and some not to, right? Actually, you can. And in Massachusetts, they did.
What happened in Chelsea, Massachusetts, wasn’t exactly a randomized trial of cash supplementation to avoid bad health outcomes. It was actually a government program instituted during the pandemic. Chelsea has a large immigrant population, many of whom are living in poverty. From April to August 2020, the city ran a food distribution program to aid those in need. But the decision was then made to convert the money spent on that program to cash distributions — free of obligations. Chelsea residents making less than 30% of the median income for the Boston metro area — around $30,000 per family — were invited to enter a lottery. Only one member of any given family could enter. If selected, an individual would receive $200 a month, or $300 for a family of two, or $400 for a family of three or more. These payments went on for about 9 months.
The key thing here is that not everyone won the lottery. The lottery picked winners randomly; 1746 individuals were selected to receive the benefits in the form of a reloadable gift card, and 1134 applied but did not receive any assistance.
This is a perfect natural experiment. As you can see here — and as expected, given that the lottery winners were chosen randomly — winners and losers were similar in terms of age, sex, race, language, income, and more.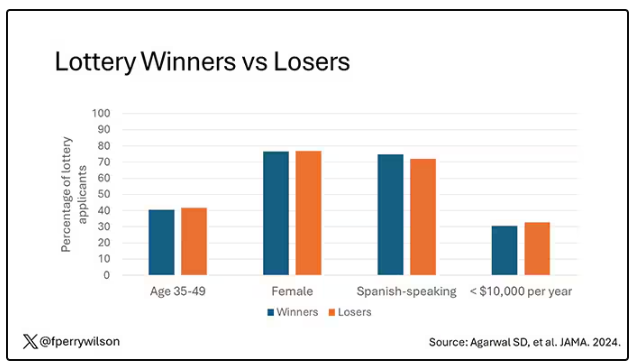
Researchers, led by Sumit Agarwal at the Brigham, leveraged that randomization to ask how these cash benefits would affect healthcare utilization. Their results appeared this week in JAMA.
I know what you’re thinking: Is $400 a month really enough to make a difference? Does $400 a month, less than $5000 a year, really fix poverty? We’ll get to that. But I will point out that the average family income of individuals in this study was about $1400 a month. An extra $400 might not change someone’s life, but it may really make a difference.
The primary outcome of this study was ED visits. There are a few ways this could go. Perhaps the money would lead to improved health and thus fewer ED visits. Or perhaps it would help people get transportation to primary care or other services that would offload the ED. Or maybe it would make things worse. Some folks have suggested that cash payments could increase the use of drugs and alcohol, and lead to more ED visits associated with the complications of using those substances.
Here are the actual data. Per 1000 individuals, there were 217 ED visits in the cash-benefit group, 318 in the no-benefit group. That was a statistically significant finding.
Breaking those ED visits down, you can see that fewer visits resulted in hospital admission, with fewer behavioral health–related visits and — a key finding — fewer visits for substance use disorder. This puts the lie to the idea that cash benefits increase drug use.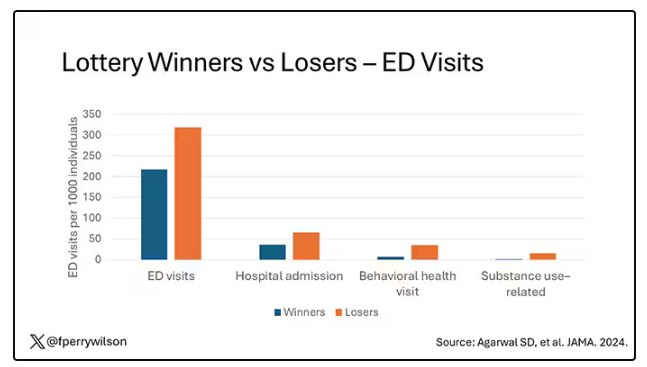
But the authors also looked at other causes of healthcare utilization. Outpatient visits were slightly higher in the cash-benefit group, driven largely by an increase in specialty care visits. The authors note that this is likely due to the fact that reaching a specialist often requires more travel, which can be costly. Indeed, this effect was most pronounced among the people living furthest from a specialty center.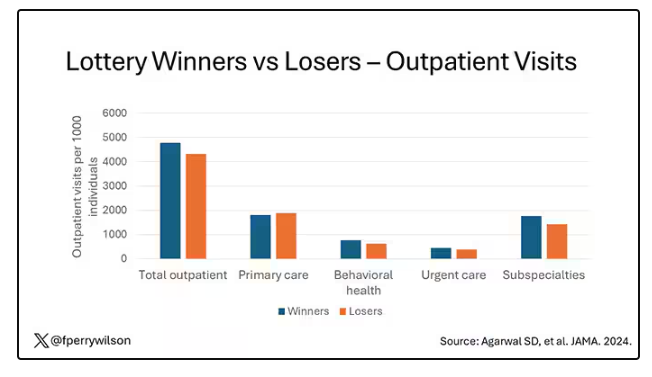
Outside of utilization, the researchers examined a variety of individual health markers — things like blood pressure — to see if the cash benefit had any effect. A bit of caution here because these data were available only among those who interacted with the healthcare system, which may bias the results a bit. Regardless, no major differences were seen in blood pressure, weight, hemoglobin A1c, cholesterol, or COVID vaccination.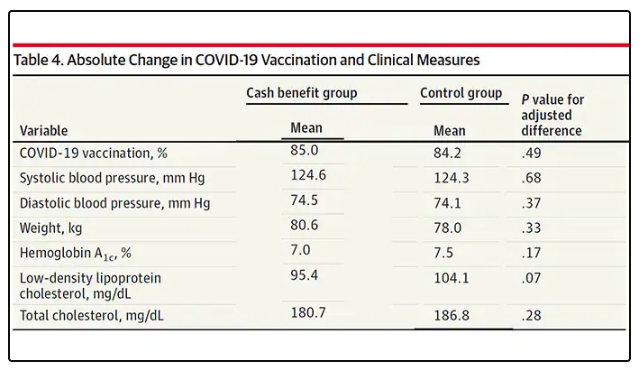
So, it seems that $400 a month doesn’t move the needle too much on risk factors for cardiovascular disease, but the effect on ED visits on their own is fairly impressive.
Is it worth it? The authors did their best to calculate the net effect of this program, accounting for the reduced ED visits and hospitalizations (that’s a big one), but also for the increased number of specialty visits. All told, the program saves about $450 per person in healthcare costs over 9 months. That’s about one seventh of the cost of the overall program.
But remember that they only looked at outcomes for the individual who got the gift cards; it’s likely that there were benefits to their family members as well. And, of course, programs like this can recoup costs indirectly though increases in economic activity, a phenomenon known as the multiplier effect.
I’m not here to tell you whether this program was a good idea; people tend to have quite strong feelings about this sort of thing. But I can tell you what it tells me about healthcare in America. It may not be surprising, but it confirms that access is far from fairly distributed.
I started this story asking about the arrow of causality between poverty and poor health. The truth is, you probably have causality in both directions. 
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It doesn’t really matter what disease you are looking at — cancer, heart disease, dementia, drug abuse, psychiatric disorders. In every case, poverty is associated with worse disease.
But the word “associated” is doing a lot of work there. Many of us feel that poverty itself is causally linked to worse disease outcomes through things like poor access to care and poor access to medicines.
And there is an argument that the arrow goes the other way; perhaps people with worse illness are more likely to be poor because, in this country at least, being sick is incredibly expensive.
Causality is what all medical research is fundamentally about. We want to know if A causes B, because if A causes B, then changing A changes B. If poverty causes bad health outcomes, then alleviating poverty should alleviate bad health outcomes.
But that’s a hard proposition to test. You can’t exactly randomize some people to get extra money and some not to, right? Actually, you can. And in Massachusetts, they did.
What happened in Chelsea, Massachusetts, wasn’t exactly a randomized trial of cash supplementation to avoid bad health outcomes. It was actually a government program instituted during the pandemic. Chelsea has a large immigrant population, many of whom are living in poverty. From April to August 2020, the city ran a food distribution program to aid those in need. But the decision was then made to convert the money spent on that program to cash distributions — free of obligations. Chelsea residents making less than 30% of the median income for the Boston metro area — around $30,000 per family — were invited to enter a lottery. Only one member of any given family could enter. If selected, an individual would receive $200 a month, or $300 for a family of two, or $400 for a family of three or more. These payments went on for about 9 months.
The key thing here is that not everyone won the lottery. The lottery picked winners randomly; 1746 individuals were selected to receive the benefits in the form of a reloadable gift card, and 1134 applied but did not receive any assistance.
This is a perfect natural experiment. As you can see here — and as expected, given that the lottery winners were chosen randomly — winners and losers were similar in terms of age, sex, race, language, income, and more.
Researchers, led by Sumit Agarwal at the Brigham, leveraged that randomization to ask how these cash benefits would affect healthcare utilization. Their results appeared this week in JAMA.
I know what you’re thinking: Is $400 a month really enough to make a difference? Does $400 a month, less than $5000 a year, really fix poverty? We’ll get to that. But I will point out that the average family income of individuals in this study was about $1400 a month. An extra $400 might not change someone’s life, but it may really make a difference.
The primary outcome of this study was ED visits. There are a few ways this could go. Perhaps the money would lead to improved health and thus fewer ED visits. Or perhaps it would help people get transportation to primary care or other services that would offload the ED. Or maybe it would make things worse. Some folks have suggested that cash payments could increase the use of drugs and alcohol, and lead to more ED visits associated with the complications of using those substances.
Here are the actual data. Per 1000 individuals, there were 217 ED visits in the cash-benefit group, 318 in the no-benefit group. That was a statistically significant finding.
Breaking those ED visits down, you can see that fewer visits resulted in hospital admission, with fewer behavioral health–related visits and — a key finding — fewer visits for substance use disorder. This puts the lie to the idea that cash benefits increase drug use.
But the authors also looked at other causes of healthcare utilization. Outpatient visits were slightly higher in the cash-benefit group, driven largely by an increase in specialty care visits. The authors note that this is likely due to the fact that reaching a specialist often requires more travel, which can be costly. Indeed, this effect was most pronounced among the people living furthest from a specialty center.
Outside of utilization, the researchers examined a variety of individual health markers — things like blood pressure — to see if the cash benefit had any effect. A bit of caution here because these data were available only among those who interacted with the healthcare system, which may bias the results a bit. Regardless, no major differences were seen in blood pressure, weight, hemoglobin A1c, cholesterol, or COVID vaccination.
So, it seems that $400 a month doesn’t move the needle too much on risk factors for cardiovascular disease, but the effect on ED visits on their own is fairly impressive.
Is it worth it? The authors did their best to calculate the net effect of this program, accounting for the reduced ED visits and hospitalizations (that’s a big one), but also for the increased number of specialty visits. All told, the program saves about $450 per person in healthcare costs over 9 months. That’s about one seventh of the cost of the overall program.
But remember that they only looked at outcomes for the individual who got the gift cards; it’s likely that there were benefits to their family members as well. And, of course, programs like this can recoup costs indirectly though increases in economic activity, a phenomenon known as the multiplier effect.
I’m not here to tell you whether this program was a good idea; people tend to have quite strong feelings about this sort of thing. But I can tell you what it tells me about healthcare in America. It may not be surprising, but it confirms that access is far from fairly distributed.
I started this story asking about the arrow of causality between poverty and poor health. The truth is, you probably have causality in both directions.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It doesn’t really matter what disease you are looking at — cancer, heart disease, dementia, drug abuse, psychiatric disorders. In every case, poverty is associated with worse disease.
But the word “associated” is doing a lot of work there. Many of us feel that poverty itself is causally linked to worse disease outcomes through things like poor access to care and poor access to medicines.
And there is an argument that the arrow goes the other way; perhaps people with worse illness are more likely to be poor because, in this country at least, being sick is incredibly expensive.
Causality is what all medical research is fundamentally about. We want to know if A causes B, because if A causes B, then changing A changes B. If poverty causes bad health outcomes, then alleviating poverty should alleviate bad health outcomes.
But that’s a hard proposition to test. You can’t exactly randomize some people to get extra money and some not to, right? Actually, you can. And in Massachusetts, they did.
What happened in Chelsea, Massachusetts, wasn’t exactly a randomized trial of cash supplementation to avoid bad health outcomes. It was actually a government program instituted during the pandemic. Chelsea has a large immigrant population, many of whom are living in poverty. From April to August 2020, the city ran a food distribution program to aid those in need. But the decision was then made to convert the money spent on that program to cash distributions — free of obligations. Chelsea residents making less than 30% of the median income for the Boston metro area — around $30,000 per family — were invited to enter a lottery. Only one member of any given family could enter. If selected, an individual would receive $200 a month, or $300 for a family of two, or $400 for a family of three or more. These payments went on for about 9 months.
The key thing here is that not everyone won the lottery. The lottery picked winners randomly; 1746 individuals were selected to receive the benefits in the form of a reloadable gift card, and 1134 applied but did not receive any assistance.
This is a perfect natural experiment. As you can see here — and as expected, given that the lottery winners were chosen randomly — winners and losers were similar in terms of age, sex, race, language, income, and more.
Researchers, led by Sumit Agarwal at the Brigham, leveraged that randomization to ask how these cash benefits would affect healthcare utilization. Their results appeared this week in JAMA.
I know what you’re thinking: Is $400 a month really enough to make a difference? Does $400 a month, less than $5000 a year, really fix poverty? We’ll get to that. But I will point out that the average family income of individuals in this study was about $1400 a month. An extra $400 might not change someone’s life, but it may really make a difference.
The primary outcome of this study was ED visits. There are a few ways this could go. Perhaps the money would lead to improved health and thus fewer ED visits. Or perhaps it would help people get transportation to primary care or other services that would offload the ED. Or maybe it would make things worse. Some folks have suggested that cash payments could increase the use of drugs and alcohol, and lead to more ED visits associated with the complications of using those substances.
Here are the actual data. Per 1000 individuals, there were 217 ED visits in the cash-benefit group, 318 in the no-benefit group. That was a statistically significant finding.
Breaking those ED visits down, you can see that fewer visits resulted in hospital admission, with fewer behavioral health–related visits and — a key finding — fewer visits for substance use disorder. This puts the lie to the idea that cash benefits increase drug use.
But the authors also looked at other causes of healthcare utilization. Outpatient visits were slightly higher in the cash-benefit group, driven largely by an increase in specialty care visits. The authors note that this is likely due to the fact that reaching a specialist often requires more travel, which can be costly. Indeed, this effect was most pronounced among the people living furthest from a specialty center.
Outside of utilization, the researchers examined a variety of individual health markers — things like blood pressure — to see if the cash benefit had any effect. A bit of caution here because these data were available only among those who interacted with the healthcare system, which may bias the results a bit. Regardless, no major differences were seen in blood pressure, weight, hemoglobin A1c, cholesterol, or COVID vaccination.
So, it seems that $400 a month doesn’t move the needle too much on risk factors for cardiovascular disease, but the effect on ED visits on their own is fairly impressive.
Is it worth it? The authors did their best to calculate the net effect of this program, accounting for the reduced ED visits and hospitalizations (that’s a big one), but also for the increased number of specialty visits. All told, the program saves about $450 per person in healthcare costs over 9 months. That’s about one seventh of the cost of the overall program.
But remember that they only looked at outcomes for the individual who got the gift cards; it’s likely that there were benefits to their family members as well. And, of course, programs like this can recoup costs indirectly though increases in economic activity, a phenomenon known as the multiplier effect.
I’m not here to tell you whether this program was a good idea; people tend to have quite strong feelings about this sort of thing. But I can tell you what it tells me about healthcare in America. It may not be surprising, but it confirms that access is far from fairly distributed.
I started this story asking about the arrow of causality between poverty and poor health. The truth is, you probably have causality in both directions.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Doctor on Death Row: Ahmad Reza Djalali Begins Hunger Strike
Ahmad Reza Djalali, an Iranian-Swedish physician specializing in disaster medicine, has begun a hunger strike after being sentenced to death in 2017.
Last year, Iran set a grim record, leading the world in executions. The country carried out at least 853 executions, which accounted for three quarters of the officially recorded executions worldwide. The Iranian government uses the death penalty to intimidate political opponents, especially since the women’s uprising in 2022, and to exert pressure on Western states in diplomatic standoffs.
He emigrated to Sweden in 2009 and joined the Karolinska Institutet in Stockholm, Sweden. Over the years, he became one of Europe’s leading experts in disaster medicine. His work has been cited more than 700 times in medical literature, and he played a key role in establishing the emergency and disaster research center at the University of Piedmont.
In Italy, Denmark, and Sweden, Dr. Djalali helped hospitals and healthcare professionals in preparing for earthquakes, nuclear accidents, and terrorist attacks and designed several disaster medicine training programs.
‘Spreading Corruption’
Despite settling in Sweden with his family, Dr. Djalali never forgot his Iranian roots. His doctoral thesis was dedicated to the victims of the 2003 Bam earthquake in Iran, which killed 23,000 people. He expressed a desire to share his knowledge with his Iranian colleagues to help people. So when he was invited to participate in a 2016 conference at the University of Tehran, he accepted without hesitation.
Unfortunately, this decision had severe consequences. On April 25, 2016, as he was concluding his trip to Iran, the researcher was arrested by intelligence agents. After being held incommunicado for several days, he was officially accused of passing confidential information to Israeli intelligence services. According to his family, this accusation was baseless. They believed he was targeted for refusing to work for Iranian intelligence services in Europe.
On October 21, 2017, Dr. Djalali was sentenced to death for “spreading corruption on Earth,” a vague charge often used by Islamic courts against those who allegedly have challenged the regime. A few days later, a video of his “confessions” was broadcast on Iranian television. These confessions were coerced; Dr. Djalali later revealed that Iranian police had threatened to harm his mother in Iran and his family in Sweden.
Since then, Dr. Djalali and his loved ones have anxiously awaited the moment when the regime might carry out the sentence. Several times over the years, he has seemed on the verge of execution, only to receive a last-minute reprieve each time.
His imprisonment has taken a severe toll on his physical and mental health. He has reportedly lost 24 kg since his incarceration, and his family, who receive sporadic updates, suspect he has leukemia. Despite his deteriorating condition, the authorities have refused him access to a hematologist.
‘Forgotten’ in Exchange
The international medical community has rallied to secure Dr. Djalali’s release, but their efforts have so far been fruitless. The United Nations, the European Union, Amnesty International, several universities, and the World Medical Association have called for his release. In 2018, Sweden granted him citizenship in an attempt to increase pressure on Tehran, but Iranian law does not recognize dual citizenship.
On June 16, after nearly 7 years on death row, Dr. Djalali informed his family that he had begun a hunger strike. “It’s the only way to make my voice heard in the world,” he explained. “As a doctor, Ahmad Reza knows all too well that his fragile physical state makes a hunger strike potentially fatal, but he sees no other option. He suffers from cardiac arrhythmia, bradycardia, hypotension, chronic gastritis, anemia, and extreme weight loss following his two previous hunger strikes,” his wife told the press.
Aside from a potential (and unlikely) act of clemency by the Iranian authorities, Dr. Djalali’s best hope lies in a prisoner exchange. The Iranian government often imprisons foreign nationals to exchange them for Iranians detained in Western countries.
On June 15, Sweden agreed to release an Iranian dignitary serving a life sentence in exchange for the release of Swedish nationals detained in Iran. For a long time, Dr. Djalali’s family had hoped he would be included in this exchange.
However, to avoid jeopardizing the deal, the Swedish prime minister chose to accept the release of only two other Swedish nationals, leaving Dr. Djalali to his grim fate. “Mr Prime Minister, you have decided to abandon me at the enormous risk of being executed,” Dr. Djalali responded bitterly, knowing he could be hanged at any moment.
This story was translated from JIM using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Ahmad Reza Djalali, an Iranian-Swedish physician specializing in disaster medicine, has begun a hunger strike after being sentenced to death in 2017.
Last year, Iran set a grim record, leading the world in executions. The country carried out at least 853 executions, which accounted for three quarters of the officially recorded executions worldwide. The Iranian government uses the death penalty to intimidate political opponents, especially since the women’s uprising in 2022, and to exert pressure on Western states in diplomatic standoffs.
He emigrated to Sweden in 2009 and joined the Karolinska Institutet in Stockholm, Sweden. Over the years, he became one of Europe’s leading experts in disaster medicine. His work has been cited more than 700 times in medical literature, and he played a key role in establishing the emergency and disaster research center at the University of Piedmont.
In Italy, Denmark, and Sweden, Dr. Djalali helped hospitals and healthcare professionals in preparing for earthquakes, nuclear accidents, and terrorist attacks and designed several disaster medicine training programs.
‘Spreading Corruption’
Despite settling in Sweden with his family, Dr. Djalali never forgot his Iranian roots. His doctoral thesis was dedicated to the victims of the 2003 Bam earthquake in Iran, which killed 23,000 people. He expressed a desire to share his knowledge with his Iranian colleagues to help people. So when he was invited to participate in a 2016 conference at the University of Tehran, he accepted without hesitation.
Unfortunately, this decision had severe consequences. On April 25, 2016, as he was concluding his trip to Iran, the researcher was arrested by intelligence agents. After being held incommunicado for several days, he was officially accused of passing confidential information to Israeli intelligence services. According to his family, this accusation was baseless. They believed he was targeted for refusing to work for Iranian intelligence services in Europe.
On October 21, 2017, Dr. Djalali was sentenced to death for “spreading corruption on Earth,” a vague charge often used by Islamic courts against those who allegedly have challenged the regime. A few days later, a video of his “confessions” was broadcast on Iranian television. These confessions were coerced; Dr. Djalali later revealed that Iranian police had threatened to harm his mother in Iran and his family in Sweden.
Since then, Dr. Djalali and his loved ones have anxiously awaited the moment when the regime might carry out the sentence. Several times over the years, he has seemed on the verge of execution, only to receive a last-minute reprieve each time.
His imprisonment has taken a severe toll on his physical and mental health. He has reportedly lost 24 kg since his incarceration, and his family, who receive sporadic updates, suspect he has leukemia. Despite his deteriorating condition, the authorities have refused him access to a hematologist.
‘Forgotten’ in Exchange
The international medical community has rallied to secure Dr. Djalali’s release, but their efforts have so far been fruitless. The United Nations, the European Union, Amnesty International, several universities, and the World Medical Association have called for his release. In 2018, Sweden granted him citizenship in an attempt to increase pressure on Tehran, but Iranian law does not recognize dual citizenship.
On June 16, after nearly 7 years on death row, Dr. Djalali informed his family that he had begun a hunger strike. “It’s the only way to make my voice heard in the world,” he explained. “As a doctor, Ahmad Reza knows all too well that his fragile physical state makes a hunger strike potentially fatal, but he sees no other option. He suffers from cardiac arrhythmia, bradycardia, hypotension, chronic gastritis, anemia, and extreme weight loss following his two previous hunger strikes,” his wife told the press.
Aside from a potential (and unlikely) act of clemency by the Iranian authorities, Dr. Djalali’s best hope lies in a prisoner exchange. The Iranian government often imprisons foreign nationals to exchange them for Iranians detained in Western countries.
On June 15, Sweden agreed to release an Iranian dignitary serving a life sentence in exchange for the release of Swedish nationals detained in Iran. For a long time, Dr. Djalali’s family had hoped he would be included in this exchange.
However, to avoid jeopardizing the deal, the Swedish prime minister chose to accept the release of only two other Swedish nationals, leaving Dr. Djalali to his grim fate. “Mr Prime Minister, you have decided to abandon me at the enormous risk of being executed,” Dr. Djalali responded bitterly, knowing he could be hanged at any moment.
This story was translated from JIM using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Ahmad Reza Djalali, an Iranian-Swedish physician specializing in disaster medicine, has begun a hunger strike after being sentenced to death in 2017.
Last year, Iran set a grim record, leading the world in executions. The country carried out at least 853 executions, which accounted for three quarters of the officially recorded executions worldwide. The Iranian government uses the death penalty to intimidate political opponents, especially since the women’s uprising in 2022, and to exert pressure on Western states in diplomatic standoffs.
He emigrated to Sweden in 2009 and joined the Karolinska Institutet in Stockholm, Sweden. Over the years, he became one of Europe’s leading experts in disaster medicine. His work has been cited more than 700 times in medical literature, and he played a key role in establishing the emergency and disaster research center at the University of Piedmont.
In Italy, Denmark, and Sweden, Dr. Djalali helped hospitals and healthcare professionals in preparing for earthquakes, nuclear accidents, and terrorist attacks and designed several disaster medicine training programs.
‘Spreading Corruption’
Despite settling in Sweden with his family, Dr. Djalali never forgot his Iranian roots. His doctoral thesis was dedicated to the victims of the 2003 Bam earthquake in Iran, which killed 23,000 people. He expressed a desire to share his knowledge with his Iranian colleagues to help people. So when he was invited to participate in a 2016 conference at the University of Tehran, he accepted without hesitation.
Unfortunately, this decision had severe consequences. On April 25, 2016, as he was concluding his trip to Iran, the researcher was arrested by intelligence agents. After being held incommunicado for several days, he was officially accused of passing confidential information to Israeli intelligence services. According to his family, this accusation was baseless. They believed he was targeted for refusing to work for Iranian intelligence services in Europe.
On October 21, 2017, Dr. Djalali was sentenced to death for “spreading corruption on Earth,” a vague charge often used by Islamic courts against those who allegedly have challenged the regime. A few days later, a video of his “confessions” was broadcast on Iranian television. These confessions were coerced; Dr. Djalali later revealed that Iranian police had threatened to harm his mother in Iran and his family in Sweden.
Since then, Dr. Djalali and his loved ones have anxiously awaited the moment when the regime might carry out the sentence. Several times over the years, he has seemed on the verge of execution, only to receive a last-minute reprieve each time.
His imprisonment has taken a severe toll on his physical and mental health. He has reportedly lost 24 kg since his incarceration, and his family, who receive sporadic updates, suspect he has leukemia. Despite his deteriorating condition, the authorities have refused him access to a hematologist.
‘Forgotten’ in Exchange
The international medical community has rallied to secure Dr. Djalali’s release, but their efforts have so far been fruitless. The United Nations, the European Union, Amnesty International, several universities, and the World Medical Association have called for his release. In 2018, Sweden granted him citizenship in an attempt to increase pressure on Tehran, but Iranian law does not recognize dual citizenship.
On June 16, after nearly 7 years on death row, Dr. Djalali informed his family that he had begun a hunger strike. “It’s the only way to make my voice heard in the world,” he explained. “As a doctor, Ahmad Reza knows all too well that his fragile physical state makes a hunger strike potentially fatal, but he sees no other option. He suffers from cardiac arrhythmia, bradycardia, hypotension, chronic gastritis, anemia, and extreme weight loss following his two previous hunger strikes,” his wife told the press.
Aside from a potential (and unlikely) act of clemency by the Iranian authorities, Dr. Djalali’s best hope lies in a prisoner exchange. The Iranian government often imprisons foreign nationals to exchange them for Iranians detained in Western countries.
On June 15, Sweden agreed to release an Iranian dignitary serving a life sentence in exchange for the release of Swedish nationals detained in Iran. For a long time, Dr. Djalali’s family had hoped he would be included in this exchange.
However, to avoid jeopardizing the deal, the Swedish prime minister chose to accept the release of only two other Swedish nationals, leaving Dr. Djalali to his grim fate. “Mr Prime Minister, you have decided to abandon me at the enormous risk of being executed,” Dr. Djalali responded bitterly, knowing he could be hanged at any moment.
This story was translated from JIM using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Disruptive Sleep Linked to Increased Susceptibility to COVID-19
Individuals with preexisting sleep disturbances including obstructive sleep apnea (OSA), insomnia, and abnormal sleep duration showed significantly increased vulnerability to COVID-19, as well as an increased risk for hospitalization, mortality, and long COVID, according to new data from more than 8 million individuals.
, wrote Jiawei Zhou, MD, of The First Hospital of China Medical University, Shenyang, China, and colleagues. Most previous research has focused on the impact of COVID-19 on sleep disturbances, not the impact of sleep disturbances on COVID-19, and most studies on the latter topic have focused only on OSA, the researchers wrote.
In a meta-analysis published in eClinicalMedicine, part of The Lancet Discovery Science, the researchers identified 48 observational studies published between October 27, 2023, and May 8, 2024, that involved COVID-19 and sleep disturbances including OSA, insomnia, abnormal sleep duration, and night shift work, among others. The study population included 8,664,026 adults.
The primary outcomes were COVID-19 susceptibility, hospitalization, mortality, and long COVID. Overall, the presence of preexisting sleep disturbances was associated with a significantly increased risk for each of these outcomes, with odds ratios (ORs) of 1.12, 1.25, 1.45, and 1.36, respectively.
In subgroup analyses, the association between preexisting sleep disturbances and greater susceptibility and hospitalization was higher in younger adults (younger than 60 years) than in older adults (aged 60 years and older), but the risk for death was lower in younger adults with sleep disturbances than in older adults with sleep disturbances (OR, 1.22 vs OR, 2.07, respectively). Men with sleep disturbances had a higher risk for COVID-19 mortality than women with sleep disturbances.
Preexisting sleep disturbances overall were significantly associated with long COVID and more so in a subgroup analysis of patients whose definition of long COVID was symptoms lasting 3 or more months vs those lasting 1 month (P = .029).
When the researchers broke down associations with COVID-19 outcomes and specific sleep disturbances, they found significant associations between OSA and all four primary outcomes. Abnormal sleep duration was associated with an increased risk for COVID-19 susceptibility, hospitalization, and long COVID. Night shift work was associated with an increased risk for COVID-19 susceptibility and hospitalization, and insomnia was associated with an increased risk for long COVID.
Although the exact mechanism behind the associations between preexisting sleep disturbances and COVID-19 outcomes is uncertain, persistent sleep deprivation could set the stage in various ways, including the promotion of elevated C-reactive protein and interleukin-6 levels, the researchers wrote.
“Overall, the compromised innate and adaptive immune functions combined with a persistent inflammatory state may explain the higher risk of susceptibility, severity, and longer recovery time observed in patients with sleep disturbances. Fortunately, early intervention for sleep disturbances could attenuate the adverse effects of COVID-19,” they noted in their discussion.
The findings were limited by several factors including the observational nature of the studies and the heterogeneity of outcomes, the researchers wrote. Looking ahead, randomized, controlled trials are needed to examine the effect of interventions for sleep disturbances in the prevention and course of COVID-19, they said.
However, the study is the first known to examine multiple types of sleep disturbances and their possible influences on the full clinical course of COVID-19 and support the need for early evaluation and intervention for individuals with sleep disturbances to reduce short-term and long-term effects of the disease, the researchers concluded.
Findings Reflect the Need to Address Sleep Issues Early
Although the results of the current study were not surprising, “it is always worth doing meta-analyses to see if there is a potential signal in the published data to suggest a need for a new study,” Arun Chatterjee, MD, professor of pulmonary, critical care, allergy, and immunologic diseases at Wake Forest University, Winston-Salem, North Carolina, said in an interview.
“Lack of sleep, whether acute active deprivation (zero sleep for one night) or subacute/chronic sleep debt, such as only 5 hours per night, has been demonstrated to affect lymphocyte proliferation, reduce immune globulin levels, increase inflammatory markers, shorten telomeres, and affect the immune system in various ways,” said Dr. Chatterjee, who was not involved in the meta-analysis.
The clinical takeaway from the current meta-analysis is that adequate sleep is important for various reasons, Dr. Chatterjee said. “Sleep disruption affects health across a spectrum of systems; adding an annual sleep wellness and screening event to healthcare visits is probably worth the investment,” he noted.
Much more is needed in the way of additional research, Dr. Chatterjee told this news organization. Notably, studies are needed to examine what sleep disruption does to immune status, as well as all other physiologic and mental health systems, he said.
The study was supported by the National Natural Science Foundation of China and the Key Laboratory of Respiratory Diseases of Liaoning Province. The researchers had no financial conflicts to disclose. Chatterjee had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Individuals with preexisting sleep disturbances including obstructive sleep apnea (OSA), insomnia, and abnormal sleep duration showed significantly increased vulnerability to COVID-19, as well as an increased risk for hospitalization, mortality, and long COVID, according to new data from more than 8 million individuals.
, wrote Jiawei Zhou, MD, of The First Hospital of China Medical University, Shenyang, China, and colleagues. Most previous research has focused on the impact of COVID-19 on sleep disturbances, not the impact of sleep disturbances on COVID-19, and most studies on the latter topic have focused only on OSA, the researchers wrote.
In a meta-analysis published in eClinicalMedicine, part of The Lancet Discovery Science, the researchers identified 48 observational studies published between October 27, 2023, and May 8, 2024, that involved COVID-19 and sleep disturbances including OSA, insomnia, abnormal sleep duration, and night shift work, among others. The study population included 8,664,026 adults.
The primary outcomes were COVID-19 susceptibility, hospitalization, mortality, and long COVID. Overall, the presence of preexisting sleep disturbances was associated with a significantly increased risk for each of these outcomes, with odds ratios (ORs) of 1.12, 1.25, 1.45, and 1.36, respectively.
In subgroup analyses, the association between preexisting sleep disturbances and greater susceptibility and hospitalization was higher in younger adults (younger than 60 years) than in older adults (aged 60 years and older), but the risk for death was lower in younger adults with sleep disturbances than in older adults with sleep disturbances (OR, 1.22 vs OR, 2.07, respectively). Men with sleep disturbances had a higher risk for COVID-19 mortality than women with sleep disturbances.
Preexisting sleep disturbances overall were significantly associated with long COVID and more so in a subgroup analysis of patients whose definition of long COVID was symptoms lasting 3 or more months vs those lasting 1 month (P = .029).
When the researchers broke down associations with COVID-19 outcomes and specific sleep disturbances, they found significant associations between OSA and all four primary outcomes. Abnormal sleep duration was associated with an increased risk for COVID-19 susceptibility, hospitalization, and long COVID. Night shift work was associated with an increased risk for COVID-19 susceptibility and hospitalization, and insomnia was associated with an increased risk for long COVID.
Although the exact mechanism behind the associations between preexisting sleep disturbances and COVID-19 outcomes is uncertain, persistent sleep deprivation could set the stage in various ways, including the promotion of elevated C-reactive protein and interleukin-6 levels, the researchers wrote.
“Overall, the compromised innate and adaptive immune functions combined with a persistent inflammatory state may explain the higher risk of susceptibility, severity, and longer recovery time observed in patients with sleep disturbances. Fortunately, early intervention for sleep disturbances could attenuate the adverse effects of COVID-19,” they noted in their discussion.
The findings were limited by several factors including the observational nature of the studies and the heterogeneity of outcomes, the researchers wrote. Looking ahead, randomized, controlled trials are needed to examine the effect of interventions for sleep disturbances in the prevention and course of COVID-19, they said.
However, the study is the first known to examine multiple types of sleep disturbances and their possible influences on the full clinical course of COVID-19 and support the need for early evaluation and intervention for individuals with sleep disturbances to reduce short-term and long-term effects of the disease, the researchers concluded.
Findings Reflect the Need to Address Sleep Issues Early
Although the results of the current study were not surprising, “it is always worth doing meta-analyses to see if there is a potential signal in the published data to suggest a need for a new study,” Arun Chatterjee, MD, professor of pulmonary, critical care, allergy, and immunologic diseases at Wake Forest University, Winston-Salem, North Carolina, said in an interview.
“Lack of sleep, whether acute active deprivation (zero sleep for one night) or subacute/chronic sleep debt, such as only 5 hours per night, has been demonstrated to affect lymphocyte proliferation, reduce immune globulin levels, increase inflammatory markers, shorten telomeres, and affect the immune system in various ways,” said Dr. Chatterjee, who was not involved in the meta-analysis.
The clinical takeaway from the current meta-analysis is that adequate sleep is important for various reasons, Dr. Chatterjee said. “Sleep disruption affects health across a spectrum of systems; adding an annual sleep wellness and screening event to healthcare visits is probably worth the investment,” he noted.
Much more is needed in the way of additional research, Dr. Chatterjee told this news organization. Notably, studies are needed to examine what sleep disruption does to immune status, as well as all other physiologic and mental health systems, he said.
The study was supported by the National Natural Science Foundation of China and the Key Laboratory of Respiratory Diseases of Liaoning Province. The researchers had no financial conflicts to disclose. Chatterjee had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Individuals with preexisting sleep disturbances including obstructive sleep apnea (OSA), insomnia, and abnormal sleep duration showed significantly increased vulnerability to COVID-19, as well as an increased risk for hospitalization, mortality, and long COVID, according to new data from more than 8 million individuals.
, wrote Jiawei Zhou, MD, of The First Hospital of China Medical University, Shenyang, China, and colleagues. Most previous research has focused on the impact of COVID-19 on sleep disturbances, not the impact of sleep disturbances on COVID-19, and most studies on the latter topic have focused only on OSA, the researchers wrote.
In a meta-analysis published in eClinicalMedicine, part of The Lancet Discovery Science, the researchers identified 48 observational studies published between October 27, 2023, and May 8, 2024, that involved COVID-19 and sleep disturbances including OSA, insomnia, abnormal sleep duration, and night shift work, among others. The study population included 8,664,026 adults.
The primary outcomes were COVID-19 susceptibility, hospitalization, mortality, and long COVID. Overall, the presence of preexisting sleep disturbances was associated with a significantly increased risk for each of these outcomes, with odds ratios (ORs) of 1.12, 1.25, 1.45, and 1.36, respectively.
In subgroup analyses, the association between preexisting sleep disturbances and greater susceptibility and hospitalization was higher in younger adults (younger than 60 years) than in older adults (aged 60 years and older), but the risk for death was lower in younger adults with sleep disturbances than in older adults with sleep disturbances (OR, 1.22 vs OR, 2.07, respectively). Men with sleep disturbances had a higher risk for COVID-19 mortality than women with sleep disturbances.
Preexisting sleep disturbances overall were significantly associated with long COVID and more so in a subgroup analysis of patients whose definition of long COVID was symptoms lasting 3 or more months vs those lasting 1 month (P = .029).
When the researchers broke down associations with COVID-19 outcomes and specific sleep disturbances, they found significant associations between OSA and all four primary outcomes. Abnormal sleep duration was associated with an increased risk for COVID-19 susceptibility, hospitalization, and long COVID. Night shift work was associated with an increased risk for COVID-19 susceptibility and hospitalization, and insomnia was associated with an increased risk for long COVID.
Although the exact mechanism behind the associations between preexisting sleep disturbances and COVID-19 outcomes is uncertain, persistent sleep deprivation could set the stage in various ways, including the promotion of elevated C-reactive protein and interleukin-6 levels, the researchers wrote.
“Overall, the compromised innate and adaptive immune functions combined with a persistent inflammatory state may explain the higher risk of susceptibility, severity, and longer recovery time observed in patients with sleep disturbances. Fortunately, early intervention for sleep disturbances could attenuate the adverse effects of COVID-19,” they noted in their discussion.
The findings were limited by several factors including the observational nature of the studies and the heterogeneity of outcomes, the researchers wrote. Looking ahead, randomized, controlled trials are needed to examine the effect of interventions for sleep disturbances in the prevention and course of COVID-19, they said.
However, the study is the first known to examine multiple types of sleep disturbances and their possible influences on the full clinical course of COVID-19 and support the need for early evaluation and intervention for individuals with sleep disturbances to reduce short-term and long-term effects of the disease, the researchers concluded.
Findings Reflect the Need to Address Sleep Issues Early
Although the results of the current study were not surprising, “it is always worth doing meta-analyses to see if there is a potential signal in the published data to suggest a need for a new study,” Arun Chatterjee, MD, professor of pulmonary, critical care, allergy, and immunologic diseases at Wake Forest University, Winston-Salem, North Carolina, said in an interview.
“Lack of sleep, whether acute active deprivation (zero sleep for one night) or subacute/chronic sleep debt, such as only 5 hours per night, has been demonstrated to affect lymphocyte proliferation, reduce immune globulin levels, increase inflammatory markers, shorten telomeres, and affect the immune system in various ways,” said Dr. Chatterjee, who was not involved in the meta-analysis.
The clinical takeaway from the current meta-analysis is that adequate sleep is important for various reasons, Dr. Chatterjee said. “Sleep disruption affects health across a spectrum of systems; adding an annual sleep wellness and screening event to healthcare visits is probably worth the investment,” he noted.
Much more is needed in the way of additional research, Dr. Chatterjee told this news organization. Notably, studies are needed to examine what sleep disruption does to immune status, as well as all other physiologic and mental health systems, he said.
The study was supported by the National Natural Science Foundation of China and the Key Laboratory of Respiratory Diseases of Liaoning Province. The researchers had no financial conflicts to disclose. Chatterjee had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Managing Atopic Dermatitis in Older Adults: A Common, Unique Challenge
WASHINGTON, DC — Jonathan I. Silverberg, MD, PhD, MPH, said at the ElderDerm Conference on dermatology in the older patient hosted by the George Washington University School of Medicine and Health Sciences, Washington, DC.
“I walked out of residency under the impression that if it didn’t start in the first year or two of life, it’s not AD,” said Dr. Silverberg, professor of dermatology and director of clinical research at George Washington University. “The numbers tell us a very different story.”

The prevalence of AD in the United States fluctuates between 6% and 8% through adulthood, including age categories up to 81-85 years, according to 2012 National Health Interview Survey data. And while persistence of childhood-onset AD is common, a systematic review and meta-analysis published in 2018 concluded that one in four adults with AD report adult-onset disease.
The investigators, including Dr. Silverberg, identified 25 observational studies — studies conducted across 16 countries and published during 1956-2017 — that included an analysis of age of onset beyond 10 years of age, and other inclusion criteria. Of the 25 studies, 17 reported age of onset after 16 years of age and had sufficient data for the meta-analysis. Using random-effects weighting, the investigators found a pooled proportion of adult-onset AD of 26.1% (95% CI, 16.5%-37.2%).
The research demonstrates that “the age of onset is distributed well throughout the lifespan,” Dr. Silverberg said, with the data “indicating there are many elderly-onset cases of true AD as well.” (Thirteen of the studies analyzed an age of onset from age ≥ 65, and several looked beyond age 80).
A 2021 study of a primary care database in the United Kingdom of 3.85 million children and adults found a “fascinating” bimodal distribution of incidence across the lifespan, with peaks in both infancy and older adulthood, he said. Incidence in adulthood was relatively stable from ages 18-49 years, after which, “into the 50s, 60s and beyond, you started to see a steady climb again.”
Also intriguing, Dr. Silverberg continued, are findings from a study of outpatient healthcare utilization for AD in which he and his coinvestigator analyzed data from the National Ambulatory Medical Care Survey (NAMCS). In the article, published in 2023 covering data from the 1993-2015 NAMCS, they reported that AD visits were more common among children aged 0-4 years (32.0%) and 5-9 years of age (10.6%), then decreased in adolescents aged 10-19 years (11.6%), remained fairly steady in patients aged 20-89 years (1.0%-4.7%), and increased in patients aged > 90 years (20.7%).
“The peak usage for dermatologists, primary care physicians, etc., is happening in the first few years of life, partially because that’s when the disease is more common and more severe but also partially because that’s when parents and caregivers are first learning [about] the disease and trying to understand how to gain control,” Dr. Silverberg said at the meeting, presenting data from an expanded, unpublished analysis of NAMCS data showing these same outpatient utilization patterns.
“It’s fascinating — there’s a much greater utilization in the elderly population. Why? The short answer is, we don’t know,” he said.
Risk Factors, Immune Differences
People with adult-onset AD were more likely to be women, smokers in adulthood, and have a lower childhood socioeconomic status than those whose AD started in childhood in a longitudinal study of two large birth cohorts from the United Kingdom , Dr. Silverberg pointed out.
Patients with childhood-onset AD, meanwhile, were more likely to have asthma, allergen-specific immunoglobulin E (IgE), and known genetic polymorphisms previously associated with AD. (Each cohort — the 1958 British Cohort Study and the 1970 British Cohort Study — had more than 17,000 participants who were followed from birth through middle age.)
Data is limited, but “mechanistically,” AD in much older adults appears to have a unique serum cytokine pattern, Dr. Silverberg said. He pointed to a cross-sectional study in China of 1312 children and adults with AD in which researchers analyzed clinical features, serum samples, and skin biopsy samples.
Adults aged > 60 years showed more lesions on the trunk and extensor sites of the extremities and lower levels of serum IgE and peripheral eosinophil counts than those in younger age groups. And “interestingly,” compared with healthy controls, older patients with AD had “higher levels of serum expression of a variety of cytokines, including IL [interleukin]-4 but also high TARC levels ... and a variety of cytokines related to the Th17, TH1 axes, etc.,” he said.
“So, we’re seeing a fascinating new profile that may be a little different than younger-onset cases,” he said, noting that TARC (thymus and activation-regulated chemokine) is regarded as a “decent biomarker” for AD.
In addition to higher levels of IL-4 and TARC, the study investigators reported significantly higher levels of IL-17A, IL-6, IL-22, IL-33, and thymic stromal lymphopoietin in older patients, compared with healthy controls.
Research also suggests that air pollution may play a role in the onset of AD in older age, Dr. Silverberg said, referencing a 2023 study that explored the association of air pollution and genetic risk with the onset of AD after age 50. The study analyzed 337,910 participants from the UK Biobank, with a median 12-year follow-up. Genetic risks were assessed as low, intermediate, and high, based on tertiles of polygenic risk scores. Exposure to various air pollutants was assessed using weighted quantile sum and also categorized into tertiles.
The incidence of older adult-onset AD was associated with medium and high air pollution compared with low air pollution, with hazard ratios (HRs) of 1.182 (P = .003) and 1.359 (P < .001), respectively. And “to a lesser extent,” Dr. Silverberg said, incidence was associated with medium and high genetic susceptibility, with HRs of 1.065 (P = .249) and 1.153 (P = .008).
The researchers calculated a greater population-attributable fraction of air pollution (15.5%) than genetic risk (6.4%). “This means that yes, genetics can contribute even to later-onset disease ... but environment may play an even more important role,” Dr. Silverberg said.
In the Clinic
In all patients, and especially in older adults, sleep disturbance associated with AD is a consideration for care. Data collected at the eczema clinic of Northwestern University, Chicago, Illinois, between 2014 and 2019 through previsit, self-administered questionnaires show that patients ≥ 65 years of age have more profound sleep disturbance (especially trouble staying asleep) than patients aged 18-64 years, despite having similar AD severity, said Dr. Silverberg, a coinvestigator of the study.
Older age was associated with having an increased number of nights of sleep disturbance (3-7 nights in the previous week) because of eczema (adjusted odds ratio [aOR], 2.14; 95% CI, 1.16-3.92). It was also associated with itching-attributed delays in falling asleep and nighttime awakenings in the prior 2 weeks (aOR, 1.88; 95% CI, 1.05-3.39).
“The aging population has dysregulated sleep patterns and altered circadian rhythms, so some of this is just natural predisposition,” Dr. Silverberg said. “But it’s amplified [with AD and itching], and it becomes a big clinical problem when we get into treatment because it’s our natural inclination to prescribe antihistamines for their sedative properties.”
Antihistamines can cause more profound sedation, more forgetfulness, and more anticholinergic side effects, he said, noting that “there’s some evidence that high-dose antihistamines may exacerbate dementia.”
Medication side effects and medication interactions, comorbidities, and decreased renal and hepatic clearance all can complicate treatment of AD in older adults. So can mobility, the extent of social/caregiving support, and other aspects of aging. For example, “I’m a big fan of ‘soak and smears’ ... but you have to ask, can you get out of a bathtub safely?” Dr. Silverberg said. “And you have to ask, can you reach the areas you need to [in order] to apply topicals?”
With oral Janus kinase inhibitors and other systemic medications, as with other drugs, “our older population is the most vulnerable from a safety perspective,” he said. A recently published post hoc analysis of four randomized trials of dupilumab in adults ≥ 60 years of age with moderate to severe AD demonstrated efficacy comparable with that in younger patients and “a really clean safety profile,” said Dr. Silverberg, the lead author. “We really need more of these types of post hocs to have some relative contextualization” for older adults.
Dr. Silverberg reported being a speaker for AbbVie, Eli Lilly, Leo Pharma, Pfizer, Regeneron, and Sanofi-Genzyme; a consultant and/or advisory board member for Regeneron, Sanofi-Genzyme, and other companies; and an investigator for several companies.
A version of this article first appeared on Medscape.com.
WASHINGTON, DC — Jonathan I. Silverberg, MD, PhD, MPH, said at the ElderDerm Conference on dermatology in the older patient hosted by the George Washington University School of Medicine and Health Sciences, Washington, DC.
“I walked out of residency under the impression that if it didn’t start in the first year or two of life, it’s not AD,” said Dr. Silverberg, professor of dermatology and director of clinical research at George Washington University. “The numbers tell us a very different story.”
The prevalence of AD in the United States fluctuates between 6% and 8% through adulthood, including age categories up to 81-85 years, according to 2012 National Health Interview Survey data. And while persistence of childhood-onset AD is common, a systematic review and meta-analysis published in 2018 concluded that one in four adults with AD report adult-onset disease.
The investigators, including Dr. Silverberg, identified 25 observational studies — studies conducted across 16 countries and published during 1956-2017 — that included an analysis of age of onset beyond 10 years of age, and other inclusion criteria. Of the 25 studies, 17 reported age of onset after 16 years of age and had sufficient data for the meta-analysis. Using random-effects weighting, the investigators found a pooled proportion of adult-onset AD of 26.1% (95% CI, 16.5%-37.2%).
The research demonstrates that “the age of onset is distributed well throughout the lifespan,” Dr. Silverberg said, with the data “indicating there are many elderly-onset cases of true AD as well.” (Thirteen of the studies analyzed an age of onset from age ≥ 65, and several looked beyond age 80).
A 2021 study of a primary care database in the United Kingdom of 3.85 million children and adults found a “fascinating” bimodal distribution of incidence across the lifespan, with peaks in both infancy and older adulthood, he said. Incidence in adulthood was relatively stable from ages 18-49 years, after which, “into the 50s, 60s and beyond, you started to see a steady climb again.”
Also intriguing, Dr. Silverberg continued, are findings from a study of outpatient healthcare utilization for AD in which he and his coinvestigator analyzed data from the National Ambulatory Medical Care Survey (NAMCS). In the article, published in 2023 covering data from the 1993-2015 NAMCS, they reported that AD visits were more common among children aged 0-4 years (32.0%) and 5-9 years of age (10.6%), then decreased in adolescents aged 10-19 years (11.6%), remained fairly steady in patients aged 20-89 years (1.0%-4.7%), and increased in patients aged > 90 years (20.7%).
“The peak usage for dermatologists, primary care physicians, etc., is happening in the first few years of life, partially because that’s when the disease is more common and more severe but also partially because that’s when parents and caregivers are first learning [about] the disease and trying to understand how to gain control,” Dr. Silverberg said at the meeting, presenting data from an expanded, unpublished analysis of NAMCS data showing these same outpatient utilization patterns.
“It’s fascinating — there’s a much greater utilization in the elderly population. Why? The short answer is, we don’t know,” he said.
Risk Factors, Immune Differences
People with adult-onset AD were more likely to be women, smokers in adulthood, and have a lower childhood socioeconomic status than those whose AD started in childhood in a longitudinal study of two large birth cohorts from the United Kingdom , Dr. Silverberg pointed out.
Patients with childhood-onset AD, meanwhile, were more likely to have asthma, allergen-specific immunoglobulin E (IgE), and known genetic polymorphisms previously associated with AD. (Each cohort — the 1958 British Cohort Study and the 1970 British Cohort Study — had more than 17,000 participants who were followed from birth through middle age.)
Data is limited, but “mechanistically,” AD in much older adults appears to have a unique serum cytokine pattern, Dr. Silverberg said. He pointed to a cross-sectional study in China of 1312 children and adults with AD in which researchers analyzed clinical features, serum samples, and skin biopsy samples.
Adults aged > 60 years showed more lesions on the trunk and extensor sites of the extremities and lower levels of serum IgE and peripheral eosinophil counts than those in younger age groups. And “interestingly,” compared with healthy controls, older patients with AD had “higher levels of serum expression of a variety of cytokines, including IL [interleukin]-4 but also high TARC levels ... and a variety of cytokines related to the Th17, TH1 axes, etc.,” he said.
“So, we’re seeing a fascinating new profile that may be a little different than younger-onset cases,” he said, noting that TARC (thymus and activation-regulated chemokine) is regarded as a “decent biomarker” for AD.
In addition to higher levels of IL-4 and TARC, the study investigators reported significantly higher levels of IL-17A, IL-6, IL-22, IL-33, and thymic stromal lymphopoietin in older patients, compared with healthy controls.
Research also suggests that air pollution may play a role in the onset of AD in older age, Dr. Silverberg said, referencing a 2023 study that explored the association of air pollution and genetic risk with the onset of AD after age 50. The study analyzed 337,910 participants from the UK Biobank, with a median 12-year follow-up. Genetic risks were assessed as low, intermediate, and high, based on tertiles of polygenic risk scores. Exposure to various air pollutants was assessed using weighted quantile sum and also categorized into tertiles.
The incidence of older adult-onset AD was associated with medium and high air pollution compared with low air pollution, with hazard ratios (HRs) of 1.182 (P = .003) and 1.359 (P < .001), respectively. And “to a lesser extent,” Dr. Silverberg said, incidence was associated with medium and high genetic susceptibility, with HRs of 1.065 (P = .249) and 1.153 (P = .008).
The researchers calculated a greater population-attributable fraction of air pollution (15.5%) than genetic risk (6.4%). “This means that yes, genetics can contribute even to later-onset disease ... but environment may play an even more important role,” Dr. Silverberg said.
In the Clinic
In all patients, and especially in older adults, sleep disturbance associated with AD is a consideration for care. Data collected at the eczema clinic of Northwestern University, Chicago, Illinois, between 2014 and 2019 through previsit, self-administered questionnaires show that patients ≥ 65 years of age have more profound sleep disturbance (especially trouble staying asleep) than patients aged 18-64 years, despite having similar AD severity, said Dr. Silverberg, a coinvestigator of the study.
Older age was associated with having an increased number of nights of sleep disturbance (3-7 nights in the previous week) because of eczema (adjusted odds ratio [aOR], 2.14; 95% CI, 1.16-3.92). It was also associated with itching-attributed delays in falling asleep and nighttime awakenings in the prior 2 weeks (aOR, 1.88; 95% CI, 1.05-3.39).
“The aging population has dysregulated sleep patterns and altered circadian rhythms, so some of this is just natural predisposition,” Dr. Silverberg said. “But it’s amplified [with AD and itching], and it becomes a big clinical problem when we get into treatment because it’s our natural inclination to prescribe antihistamines for their sedative properties.”
Antihistamines can cause more profound sedation, more forgetfulness, and more anticholinergic side effects, he said, noting that “there’s some evidence that high-dose antihistamines may exacerbate dementia.”
Medication side effects and medication interactions, comorbidities, and decreased renal and hepatic clearance all can complicate treatment of AD in older adults. So can mobility, the extent of social/caregiving support, and other aspects of aging. For example, “I’m a big fan of ‘soak and smears’ ... but you have to ask, can you get out of a bathtub safely?” Dr. Silverberg said. “And you have to ask, can you reach the areas you need to [in order] to apply topicals?”
With oral Janus kinase inhibitors and other systemic medications, as with other drugs, “our older population is the most vulnerable from a safety perspective,” he said. A recently published post hoc analysis of four randomized trials of dupilumab in adults ≥ 60 years of age with moderate to severe AD demonstrated efficacy comparable with that in younger patients and “a really clean safety profile,” said Dr. Silverberg, the lead author. “We really need more of these types of post hocs to have some relative contextualization” for older adults.
Dr. Silverberg reported being a speaker for AbbVie, Eli Lilly, Leo Pharma, Pfizer, Regeneron, and Sanofi-Genzyme; a consultant and/or advisory board member for Regeneron, Sanofi-Genzyme, and other companies; and an investigator for several companies.
A version of this article first appeared on Medscape.com.
WASHINGTON, DC — Jonathan I. Silverberg, MD, PhD, MPH, said at the ElderDerm Conference on dermatology in the older patient hosted by the George Washington University School of Medicine and Health Sciences, Washington, DC.
“I walked out of residency under the impression that if it didn’t start in the first year or two of life, it’s not AD,” said Dr. Silverberg, professor of dermatology and director of clinical research at George Washington University. “The numbers tell us a very different story.”
The prevalence of AD in the United States fluctuates between 6% and 8% through adulthood, including age categories up to 81-85 years, according to 2012 National Health Interview Survey data. And while persistence of childhood-onset AD is common, a systematic review and meta-analysis published in 2018 concluded that one in four adults with AD report adult-onset disease.
The investigators, including Dr. Silverberg, identified 25 observational studies — studies conducted across 16 countries and published during 1956-2017 — that included an analysis of age of onset beyond 10 years of age, and other inclusion criteria. Of the 25 studies, 17 reported age of onset after 16 years of age and had sufficient data for the meta-analysis. Using random-effects weighting, the investigators found a pooled proportion of adult-onset AD of 26.1% (95% CI, 16.5%-37.2%).
The research demonstrates that “the age of onset is distributed well throughout the lifespan,” Dr. Silverberg said, with the data “indicating there are many elderly-onset cases of true AD as well.” (Thirteen of the studies analyzed an age of onset from age ≥ 65, and several looked beyond age 80).
A 2021 study of a primary care database in the United Kingdom of 3.85 million children and adults found a “fascinating” bimodal distribution of incidence across the lifespan, with peaks in both infancy and older adulthood, he said. Incidence in adulthood was relatively stable from ages 18-49 years, after which, “into the 50s, 60s and beyond, you started to see a steady climb again.”
Also intriguing, Dr. Silverberg continued, are findings from a study of outpatient healthcare utilization for AD in which he and his coinvestigator analyzed data from the National Ambulatory Medical Care Survey (NAMCS). In the article, published in 2023 covering data from the 1993-2015 NAMCS, they reported that AD visits were more common among children aged 0-4 years (32.0%) and 5-9 years of age (10.6%), then decreased in adolescents aged 10-19 years (11.6%), remained fairly steady in patients aged 20-89 years (1.0%-4.7%), and increased in patients aged > 90 years (20.7%).
“The peak usage for dermatologists, primary care physicians, etc., is happening in the first few years of life, partially because that’s when the disease is more common and more severe but also partially because that’s when parents and caregivers are first learning [about] the disease and trying to understand how to gain control,” Dr. Silverberg said at the meeting, presenting data from an expanded, unpublished analysis of NAMCS data showing these same outpatient utilization patterns.
“It’s fascinating — there’s a much greater utilization in the elderly population. Why? The short answer is, we don’t know,” he said.
Risk Factors, Immune Differences
People with adult-onset AD were more likely to be women, smokers in adulthood, and have a lower childhood socioeconomic status than those whose AD started in childhood in a longitudinal study of two large birth cohorts from the United Kingdom , Dr. Silverberg pointed out.
Patients with childhood-onset AD, meanwhile, were more likely to have asthma, allergen-specific immunoglobulin E (IgE), and known genetic polymorphisms previously associated with AD. (Each cohort — the 1958 British Cohort Study and the 1970 British Cohort Study — had more than 17,000 participants who were followed from birth through middle age.)
Data is limited, but “mechanistically,” AD in much older adults appears to have a unique serum cytokine pattern, Dr. Silverberg said. He pointed to a cross-sectional study in China of 1312 children and adults with AD in which researchers analyzed clinical features, serum samples, and skin biopsy samples.
Adults aged > 60 years showed more lesions on the trunk and extensor sites of the extremities and lower levels of serum IgE and peripheral eosinophil counts than those in younger age groups. And “interestingly,” compared with healthy controls, older patients with AD had “higher levels of serum expression of a variety of cytokines, including IL [interleukin]-4 but also high TARC levels ... and a variety of cytokines related to the Th17, TH1 axes, etc.,” he said.
“So, we’re seeing a fascinating new profile that may be a little different than younger-onset cases,” he said, noting that TARC (thymus and activation-regulated chemokine) is regarded as a “decent biomarker” for AD.
In addition to higher levels of IL-4 and TARC, the study investigators reported significantly higher levels of IL-17A, IL-6, IL-22, IL-33, and thymic stromal lymphopoietin in older patients, compared with healthy controls.
Research also suggests that air pollution may play a role in the onset of AD in older age, Dr. Silverberg said, referencing a 2023 study that explored the association of air pollution and genetic risk with the onset of AD after age 50. The study analyzed 337,910 participants from the UK Biobank, with a median 12-year follow-up. Genetic risks were assessed as low, intermediate, and high, based on tertiles of polygenic risk scores. Exposure to various air pollutants was assessed using weighted quantile sum and also categorized into tertiles.
The incidence of older adult-onset AD was associated with medium and high air pollution compared with low air pollution, with hazard ratios (HRs) of 1.182 (P = .003) and 1.359 (P < .001), respectively. And “to a lesser extent,” Dr. Silverberg said, incidence was associated with medium and high genetic susceptibility, with HRs of 1.065 (P = .249) and 1.153 (P = .008).
The researchers calculated a greater population-attributable fraction of air pollution (15.5%) than genetic risk (6.4%). “This means that yes, genetics can contribute even to later-onset disease ... but environment may play an even more important role,” Dr. Silverberg said.
In the Clinic
In all patients, and especially in older adults, sleep disturbance associated with AD is a consideration for care. Data collected at the eczema clinic of Northwestern University, Chicago, Illinois, between 2014 and 2019 through previsit, self-administered questionnaires show that patients ≥ 65 years of age have more profound sleep disturbance (especially trouble staying asleep) than patients aged 18-64 years, despite having similar AD severity, said Dr. Silverberg, a coinvestigator of the study.
Older age was associated with having an increased number of nights of sleep disturbance (3-7 nights in the previous week) because of eczema (adjusted odds ratio [aOR], 2.14; 95% CI, 1.16-3.92). It was also associated with itching-attributed delays in falling asleep and nighttime awakenings in the prior 2 weeks (aOR, 1.88; 95% CI, 1.05-3.39).
“The aging population has dysregulated sleep patterns and altered circadian rhythms, so some of this is just natural predisposition,” Dr. Silverberg said. “But it’s amplified [with AD and itching], and it becomes a big clinical problem when we get into treatment because it’s our natural inclination to prescribe antihistamines for their sedative properties.”
Antihistamines can cause more profound sedation, more forgetfulness, and more anticholinergic side effects, he said, noting that “there’s some evidence that high-dose antihistamines may exacerbate dementia.”
Medication side effects and medication interactions, comorbidities, and decreased renal and hepatic clearance all can complicate treatment of AD in older adults. So can mobility, the extent of social/caregiving support, and other aspects of aging. For example, “I’m a big fan of ‘soak and smears’ ... but you have to ask, can you get out of a bathtub safely?” Dr. Silverberg said. “And you have to ask, can you reach the areas you need to [in order] to apply topicals?”
With oral Janus kinase inhibitors and other systemic medications, as with other drugs, “our older population is the most vulnerable from a safety perspective,” he said. A recently published post hoc analysis of four randomized trials of dupilumab in adults ≥ 60 years of age with moderate to severe AD demonstrated efficacy comparable with that in younger patients and “a really clean safety profile,” said Dr. Silverberg, the lead author. “We really need more of these types of post hocs to have some relative contextualization” for older adults.
Dr. Silverberg reported being a speaker for AbbVie, Eli Lilly, Leo Pharma, Pfizer, Regeneron, and Sanofi-Genzyme; a consultant and/or advisory board member for Regeneron, Sanofi-Genzyme, and other companies; and an investigator for several companies.
A version of this article first appeared on Medscape.com.
FROM ELDERDERM 2024
Treatable Condition Misdiagnosed as Dementia in Almost 13% of Cases
, one of the main causes of the condition, new research suggests.
The study of more than 68,000 individuals in the general population diagnosed with dementia between 2009 and 2019 found that almost 13% had FIB-4 scores indicative of cirrhosis and potential hepatic encephalopathy.
The findings, recently published online in The American Journal of Medicine, corroborate and extend the researchers’ previous work, which showed that about 10% of US veterans with a dementia diagnosis may in fact have hepatic encephalopathy.
“We need to increase awareness that cirrhosis and related brain complications are common, silent, but treatable when found,” said corresponding author Jasmohan Bajaj, MD, of Virginia Commonwealth University and Richmond VA Medical Center, Richmond, Virginia. “Moreover, these are being increasingly diagnosed in older individuals.”
“Cirrhosis can also predispose patients to liver cancer and other complications, so diagnosing it in all patients is important, regardless of the hepatic encephalopathy-dementia connection,” he said.
FIB-4 Is Key
Dr. Bajaj and colleagues analyzed data from 72 healthcare centers on 68,807 nonveteran patients diagnosed with dementia at two or more physician visits between 2009 and 2019. Patients had no prior cirrhosis diagnosis, the mean age was 73 years, 44.7% were men, and 78% were White.
The team measured the prevalence of two high FIB-4 scores (> 2.67 and > 3.25), selected for their strong predictive value for advanced cirrhosis. Researchers also examined associations between high scores and multiple comorbidities and demographic factors.
Alanine aminotransferase (ALT), aspartate aminotransferase (AST), and platelet labs were collected up to 2 years after the index dementia diagnosis because they are used to calculate FIB-4.
The mean FIB-4 score was 1.78, mean ALT was 23.72 U/L, mean AST was 27.42 U/L, and mean platelets were 243.51 × 109/µL.
A total of 8683 participants (12.8%) had a FIB-4 score greater than 2.67 and 5185 (7.6%) had a score greater than 3.25.
In multivariable logistic regression models, FIB-4 greater than 3.25 was associated with viral hepatitis (odds ratio [OR], 2.23), congestive heart failure (OR,1.73), HIV (OR, 1.72), male gender (OR, 1.42), alcohol use disorder (OR, 1.39), and chronic kidney disease (OR, 1.38).
FIB-4 greater than 3.25 was inversely associated with White race (OR, 0.76) and diabetes (OR, 0.82).
The associations were similar when using a threshold score of greater than 2.67.
“With the aging population, including those with cirrhosis, the potential for overlap between hepatic encephalopathy and dementia has risen and should be considered in the differential diagnosis,” the authors wrote. “Undiagnosed cirrhosis and potential hepatic encephalopathy can be a treatable cause of or contributor towards cognitive impairment in patients diagnosed with dementia.”
Providers should use the FIB-4 index as a screening tool to detect cirrhosis in patients with dementia, they concluded.
The team’s next steps will include investigating barriers to the use of FIB-4 among practitioners, Dr. Bajaj said.
Incorporating use of the FIB-4 index into screening guidelines “with input from all stakeholders, including geriatricians, primary care providers, and neurologists … would greatly expand the diagnosis of cirrhosis and potentially hepatic encephalopathy in dementia patients,” Dr. Bajaj said.
The study had a few limitations, including the selected centers in the cohort database, lack of chart review to confirm diagnoses in individual cases, and the use of a modified FIB-4, with age capped at 65 years.
‘Easy to Miss’
Commenting on the research, Nancy Reau, MD, section chief of hepatology at Rush University Medical Center in Chicago, said that it is easy for physicians to miss asymptomatic liver disease that could progress and lead to cognitive decline.
“Most of my patients are already labeled with liver disease; however, it is not uncommon to receive a patient from another specialist who felt their presentation was more consistent with liver disease than the issue they were referred for,” she said.
Still, even in metabolic dysfunction–associated steatotic liver disease, which affects nearly one third of the population, the condition isn’t advanced enough in most patients to cause symptoms similar to those of dementia, said Dr. Reau, who was not associated with the study.
“It is more important for specialists in neurology to exclude liver disease and for hepatologists or gastroenterologists to be equipped with tools to exclude alternative explanations for neurocognitive presentations,” she said. “It is important to not label a patient as having HE and then miss alternative explanations.”
“Every presentation has a differential diagnosis. Using easy tools like FIB-4 can make sure you don’t miss liver disease as a contributing factor in a patient that presents with neurocognitive symptoms,” Dr. Reau said.
This work was partly supported by grants from Department of Veterans Affairs merit review program and the National Institutes of Health’s National Center for Advancing Translational Science. Dr. Bajaj and Dr. Reau reported no conflicts of interest.
A version of this article appeared on Medscape.com.
, one of the main causes of the condition, new research suggests.
The study of more than 68,000 individuals in the general population diagnosed with dementia between 2009 and 2019 found that almost 13% had FIB-4 scores indicative of cirrhosis and potential hepatic encephalopathy.
The findings, recently published online in The American Journal of Medicine, corroborate and extend the researchers’ previous work, which showed that about 10% of US veterans with a dementia diagnosis may in fact have hepatic encephalopathy.
“We need to increase awareness that cirrhosis and related brain complications are common, silent, but treatable when found,” said corresponding author Jasmohan Bajaj, MD, of Virginia Commonwealth University and Richmond VA Medical Center, Richmond, Virginia. “Moreover, these are being increasingly diagnosed in older individuals.”
“Cirrhosis can also predispose patients to liver cancer and other complications, so diagnosing it in all patients is important, regardless of the hepatic encephalopathy-dementia connection,” he said.
FIB-4 Is Key
Dr. Bajaj and colleagues analyzed data from 72 healthcare centers on 68,807 nonveteran patients diagnosed with dementia at two or more physician visits between 2009 and 2019. Patients had no prior cirrhosis diagnosis, the mean age was 73 years, 44.7% were men, and 78% were White.
The team measured the prevalence of two high FIB-4 scores (> 2.67 and > 3.25), selected for their strong predictive value for advanced cirrhosis. Researchers also examined associations between high scores and multiple comorbidities and demographic factors.
Alanine aminotransferase (ALT), aspartate aminotransferase (AST), and platelet labs were collected up to 2 years after the index dementia diagnosis because they are used to calculate FIB-4.
The mean FIB-4 score was 1.78, mean ALT was 23.72 U/L, mean AST was 27.42 U/L, and mean platelets were 243.51 × 109/µL.
A total of 8683 participants (12.8%) had a FIB-4 score greater than 2.67 and 5185 (7.6%) had a score greater than 3.25.
In multivariable logistic regression models, FIB-4 greater than 3.25 was associated with viral hepatitis (odds ratio [OR], 2.23), congestive heart failure (OR,1.73), HIV (OR, 1.72), male gender (OR, 1.42), alcohol use disorder (OR, 1.39), and chronic kidney disease (OR, 1.38).
FIB-4 greater than 3.25 was inversely associated with White race (OR, 0.76) and diabetes (OR, 0.82).
The associations were similar when using a threshold score of greater than 2.67.
“With the aging population, including those with cirrhosis, the potential for overlap between hepatic encephalopathy and dementia has risen and should be considered in the differential diagnosis,” the authors wrote. “Undiagnosed cirrhosis and potential hepatic encephalopathy can be a treatable cause of or contributor towards cognitive impairment in patients diagnosed with dementia.”
Providers should use the FIB-4 index as a screening tool to detect cirrhosis in patients with dementia, they concluded.
The team’s next steps will include investigating barriers to the use of FIB-4 among practitioners, Dr. Bajaj said.
Incorporating use of the FIB-4 index into screening guidelines “with input from all stakeholders, including geriatricians, primary care providers, and neurologists … would greatly expand the diagnosis of cirrhosis and potentially hepatic encephalopathy in dementia patients,” Dr. Bajaj said.
The study had a few limitations, including the selected centers in the cohort database, lack of chart review to confirm diagnoses in individual cases, and the use of a modified FIB-4, with age capped at 65 years.
‘Easy to Miss’
Commenting on the research, Nancy Reau, MD, section chief of hepatology at Rush University Medical Center in Chicago, said that it is easy for physicians to miss asymptomatic liver disease that could progress and lead to cognitive decline.
“Most of my patients are already labeled with liver disease; however, it is not uncommon to receive a patient from another specialist who felt their presentation was more consistent with liver disease than the issue they were referred for,” she said.
Still, even in metabolic dysfunction–associated steatotic liver disease, which affects nearly one third of the population, the condition isn’t advanced enough in most patients to cause symptoms similar to those of dementia, said Dr. Reau, who was not associated with the study.
“It is more important for specialists in neurology to exclude liver disease and for hepatologists or gastroenterologists to be equipped with tools to exclude alternative explanations for neurocognitive presentations,” she said. “It is important to not label a patient as having HE and then miss alternative explanations.”
“Every presentation has a differential diagnosis. Using easy tools like FIB-4 can make sure you don’t miss liver disease as a contributing factor in a patient that presents with neurocognitive symptoms,” Dr. Reau said.
This work was partly supported by grants from Department of Veterans Affairs merit review program and the National Institutes of Health’s National Center for Advancing Translational Science. Dr. Bajaj and Dr. Reau reported no conflicts of interest.
A version of this article appeared on Medscape.com.
, one of the main causes of the condition, new research suggests.
The study of more than 68,000 individuals in the general population diagnosed with dementia between 2009 and 2019 found that almost 13% had FIB-4 scores indicative of cirrhosis and potential hepatic encephalopathy.
The findings, recently published online in The American Journal of Medicine, corroborate and extend the researchers’ previous work, which showed that about 10% of US veterans with a dementia diagnosis may in fact have hepatic encephalopathy.
“We need to increase awareness that cirrhosis and related brain complications are common, silent, but treatable when found,” said corresponding author Jasmohan Bajaj, MD, of Virginia Commonwealth University and Richmond VA Medical Center, Richmond, Virginia. “Moreover, these are being increasingly diagnosed in older individuals.”
“Cirrhosis can also predispose patients to liver cancer and other complications, so diagnosing it in all patients is important, regardless of the hepatic encephalopathy-dementia connection,” he said.
FIB-4 Is Key
Dr. Bajaj and colleagues analyzed data from 72 healthcare centers on 68,807 nonveteran patients diagnosed with dementia at two or more physician visits between 2009 and 2019. Patients had no prior cirrhosis diagnosis, the mean age was 73 years, 44.7% were men, and 78% were White.
The team measured the prevalence of two high FIB-4 scores (> 2.67 and > 3.25), selected for their strong predictive value for advanced cirrhosis. Researchers also examined associations between high scores and multiple comorbidities and demographic factors.
Alanine aminotransferase (ALT), aspartate aminotransferase (AST), and platelet labs were collected up to 2 years after the index dementia diagnosis because they are used to calculate FIB-4.
The mean FIB-4 score was 1.78, mean ALT was 23.72 U/L, mean AST was 27.42 U/L, and mean platelets were 243.51 × 109/µL.
A total of 8683 participants (12.8%) had a FIB-4 score greater than 2.67 and 5185 (7.6%) had a score greater than 3.25.
In multivariable logistic regression models, FIB-4 greater than 3.25 was associated with viral hepatitis (odds ratio [OR], 2.23), congestive heart failure (OR,1.73), HIV (OR, 1.72), male gender (OR, 1.42), alcohol use disorder (OR, 1.39), and chronic kidney disease (OR, 1.38).
FIB-4 greater than 3.25 was inversely associated with White race (OR, 0.76) and diabetes (OR, 0.82).
The associations were similar when using a threshold score of greater than 2.67.
“With the aging population, including those with cirrhosis, the potential for overlap between hepatic encephalopathy and dementia has risen and should be considered in the differential diagnosis,” the authors wrote. “Undiagnosed cirrhosis and potential hepatic encephalopathy can be a treatable cause of or contributor towards cognitive impairment in patients diagnosed with dementia.”
Providers should use the FIB-4 index as a screening tool to detect cirrhosis in patients with dementia, they concluded.
The team’s next steps will include investigating barriers to the use of FIB-4 among practitioners, Dr. Bajaj said.
Incorporating use of the FIB-4 index into screening guidelines “with input from all stakeholders, including geriatricians, primary care providers, and neurologists … would greatly expand the diagnosis of cirrhosis and potentially hepatic encephalopathy in dementia patients,” Dr. Bajaj said.
The study had a few limitations, including the selected centers in the cohort database, lack of chart review to confirm diagnoses in individual cases, and the use of a modified FIB-4, with age capped at 65 years.
‘Easy to Miss’
Commenting on the research, Nancy Reau, MD, section chief of hepatology at Rush University Medical Center in Chicago, said that it is easy for physicians to miss asymptomatic liver disease that could progress and lead to cognitive decline.
“Most of my patients are already labeled with liver disease; however, it is not uncommon to receive a patient from another specialist who felt their presentation was more consistent with liver disease than the issue they were referred for,” she said.
Still, even in metabolic dysfunction–associated steatotic liver disease, which affects nearly one third of the population, the condition isn’t advanced enough in most patients to cause symptoms similar to those of dementia, said Dr. Reau, who was not associated with the study.
“It is more important for specialists in neurology to exclude liver disease and for hepatologists or gastroenterologists to be equipped with tools to exclude alternative explanations for neurocognitive presentations,” she said. “It is important to not label a patient as having HE and then miss alternative explanations.”
“Every presentation has a differential diagnosis. Using easy tools like FIB-4 can make sure you don’t miss liver disease as a contributing factor in a patient that presents with neurocognitive symptoms,” Dr. Reau said.
This work was partly supported by grants from Department of Veterans Affairs merit review program and the National Institutes of Health’s National Center for Advancing Translational Science. Dr. Bajaj and Dr. Reau reported no conflicts of interest.
A version of this article appeared on Medscape.com.
From the American Journal of Medicine