User login
Racial and ethnic disparities persist in pregnant women with gestational diabetes
Between 2014 and 2020, the frequency of adverse pregnancy outcomes in the United States increased among women with gestational diabetes, with persisting differences in adverse outcomes by race and ethnicity, according to a report in JAMA
“[Previous] population-based studies on racial and ethnic disparities in gestational diabetes have focused on differences in the rate of diagnosis, rather than adverse pregnancy outcomes,” lead author Kartik K. Venkatesh, MD, PhD, of Ohio State University, Columbus, and colleagues explained.

The researchers conducted a cross-sectional, descriptive study to evaluate whether the frequency of adverse pregnancy outcomes with gestational diabetes changed over time and whether the risk of these outcomes differed by maternal race and ethnicity.
The data were obtained from the Centers for Disease Control and Prevention’s National Center for Health Statistics Natality Files. Exposures of interest were year of delivery, as well as race and ethnicity.
Results
The study cohort included 1,560,822 pregnant women with gestational diabetes aged 15-44 years. Among the study participants the mean age was 31 years (standard deviation, 5.5 years) and the majority were White (48%), followed by Hispanic/Latina (27%), Asian/Pacific Islander (13%), and Black (12%).
There was a significant increase in the overall frequency of transfusion (8.0%; 95% confidence interval, 3.8%-12.4%), preeclampsia or gestational hypertension (4.2%; 95% CI, 3.3%-5.2%), NICU admission (1.0%; 95% CI, 0.3%-1.7%), and preterm birth at less than 37 weeks (0.9%; 95% CI, 0.3%-1.5%) from 2014 to 2020 for these women and their infants.
In addition, there was a significant decrease in the following outcomes: macrosomia (–4.7%; 95% CI, –5.3% to –4.0%), cesarean delivery (–1.4%; 95% CI, –1.7% to –1.1%), primary cesarean delivery (–1.2%; 95% CI, –1.5% to –0.9%), and large for gestational age (–2.3%; 95% CI, –2.8% to –1.8%), but there was no significant differences in maternal ICU admission and small-for-gestational-age infants.
From 2014 through 2020, differences in adverse outcomes by race and ethnicity persisted; in comparison with Whites, Black participants were at significantly higher risk of all evaluated outcomes, except for macrosomia and large for gestational age.
Hispanic/Latina and Asian/Pacific Islander individuals were also at significantly higher risk of preterm birth, NICU admission, maternal ICU admission, and small for gestational age. Furthermore, American Indian participants were at significantly higher risk of all evaluated outcomes, except for cesarean delivery and small for gestational age.
Results in context
Health policy researcher Felicia Hill-Briggs, PhD, at the Feinstein Institutes for Medical Research in Manhasset, N.Y. commented: “Two alarming trends highlighted by this study: 1) Racial and ethnic inequities in adverse gestational diabetes outcomes; and 2) the rising rates of gestational diabetes overall – both must and can be halted.”

“Optimizing medical management of gestational diabetes, whether through improved access to diabetes care in pregnancy, behavioral interventions, and pharmacotherapy can decrease the risk of adverse pregnancy outcomes,” Dr. Venkatesh commented. “It is possible that the equitable delivery of these interventions to address glycemic control could decrease racial and ethnic disparities in adverse pregnancy outcomes among individuals with gestational diabetes.”
Dr. Venkatesh and his colleagues acknowledged that a key limitation of the study was the use of administrative data; thus, inferences on maternal care improvements could not be determined.
“Further research could focus on greater understanding of racial and ethnic differences in the management of gestational diabetes,” the researchers concluded.
This study was supported by the Care Innovation and Community Improvement Program at Ohio State University. One author reported receiving grants from the National Institutes of Health outside of this study. The other authors reported no relevant disclosures. Dr. Hill-Briggs had no relevant disclosures.
Between 2014 and 2020, the frequency of adverse pregnancy outcomes in the United States increased among women with gestational diabetes, with persisting differences in adverse outcomes by race and ethnicity, according to a report in JAMA
“[Previous] population-based studies on racial and ethnic disparities in gestational diabetes have focused on differences in the rate of diagnosis, rather than adverse pregnancy outcomes,” lead author Kartik K. Venkatesh, MD, PhD, of Ohio State University, Columbus, and colleagues explained.
The researchers conducted a cross-sectional, descriptive study to evaluate whether the frequency of adverse pregnancy outcomes with gestational diabetes changed over time and whether the risk of these outcomes differed by maternal race and ethnicity.
The data were obtained from the Centers for Disease Control and Prevention’s National Center for Health Statistics Natality Files. Exposures of interest were year of delivery, as well as race and ethnicity.
Results
The study cohort included 1,560,822 pregnant women with gestational diabetes aged 15-44 years. Among the study participants the mean age was 31 years (standard deviation, 5.5 years) and the majority were White (48%), followed by Hispanic/Latina (27%), Asian/Pacific Islander (13%), and Black (12%).
There was a significant increase in the overall frequency of transfusion (8.0%; 95% confidence interval, 3.8%-12.4%), preeclampsia or gestational hypertension (4.2%; 95% CI, 3.3%-5.2%), NICU admission (1.0%; 95% CI, 0.3%-1.7%), and preterm birth at less than 37 weeks (0.9%; 95% CI, 0.3%-1.5%) from 2014 to 2020 for these women and their infants.
In addition, there was a significant decrease in the following outcomes: macrosomia (–4.7%; 95% CI, –5.3% to –4.0%), cesarean delivery (–1.4%; 95% CI, –1.7% to –1.1%), primary cesarean delivery (–1.2%; 95% CI, –1.5% to –0.9%), and large for gestational age (–2.3%; 95% CI, –2.8% to –1.8%), but there was no significant differences in maternal ICU admission and small-for-gestational-age infants.
From 2014 through 2020, differences in adverse outcomes by race and ethnicity persisted; in comparison with Whites, Black participants were at significantly higher risk of all evaluated outcomes, except for macrosomia and large for gestational age.
Hispanic/Latina and Asian/Pacific Islander individuals were also at significantly higher risk of preterm birth, NICU admission, maternal ICU admission, and small for gestational age. Furthermore, American Indian participants were at significantly higher risk of all evaluated outcomes, except for cesarean delivery and small for gestational age.
Results in context
Health policy researcher Felicia Hill-Briggs, PhD, at the Feinstein Institutes for Medical Research in Manhasset, N.Y. commented: “Two alarming trends highlighted by this study: 1) Racial and ethnic inequities in adverse gestational diabetes outcomes; and 2) the rising rates of gestational diabetes overall – both must and can be halted.”
“Optimizing medical management of gestational diabetes, whether through improved access to diabetes care in pregnancy, behavioral interventions, and pharmacotherapy can decrease the risk of adverse pregnancy outcomes,” Dr. Venkatesh commented. “It is possible that the equitable delivery of these interventions to address glycemic control could decrease racial and ethnic disparities in adverse pregnancy outcomes among individuals with gestational diabetes.”
Dr. Venkatesh and his colleagues acknowledged that a key limitation of the study was the use of administrative data; thus, inferences on maternal care improvements could not be determined.
“Further research could focus on greater understanding of racial and ethnic differences in the management of gestational diabetes,” the researchers concluded.
This study was supported by the Care Innovation and Community Improvement Program at Ohio State University. One author reported receiving grants from the National Institutes of Health outside of this study. The other authors reported no relevant disclosures. Dr. Hill-Briggs had no relevant disclosures.
Between 2014 and 2020, the frequency of adverse pregnancy outcomes in the United States increased among women with gestational diabetes, with persisting differences in adverse outcomes by race and ethnicity, according to a report in JAMA
“[Previous] population-based studies on racial and ethnic disparities in gestational diabetes have focused on differences in the rate of diagnosis, rather than adverse pregnancy outcomes,” lead author Kartik K. Venkatesh, MD, PhD, of Ohio State University, Columbus, and colleagues explained.
The researchers conducted a cross-sectional, descriptive study to evaluate whether the frequency of adverse pregnancy outcomes with gestational diabetes changed over time and whether the risk of these outcomes differed by maternal race and ethnicity.
The data were obtained from the Centers for Disease Control and Prevention’s National Center for Health Statistics Natality Files. Exposures of interest were year of delivery, as well as race and ethnicity.
Results
The study cohort included 1,560,822 pregnant women with gestational diabetes aged 15-44 years. Among the study participants the mean age was 31 years (standard deviation, 5.5 years) and the majority were White (48%), followed by Hispanic/Latina (27%), Asian/Pacific Islander (13%), and Black (12%).
There was a significant increase in the overall frequency of transfusion (8.0%; 95% confidence interval, 3.8%-12.4%), preeclampsia or gestational hypertension (4.2%; 95% CI, 3.3%-5.2%), NICU admission (1.0%; 95% CI, 0.3%-1.7%), and preterm birth at less than 37 weeks (0.9%; 95% CI, 0.3%-1.5%) from 2014 to 2020 for these women and their infants.
In addition, there was a significant decrease in the following outcomes: macrosomia (–4.7%; 95% CI, –5.3% to –4.0%), cesarean delivery (–1.4%; 95% CI, –1.7% to –1.1%), primary cesarean delivery (–1.2%; 95% CI, –1.5% to –0.9%), and large for gestational age (–2.3%; 95% CI, –2.8% to –1.8%), but there was no significant differences in maternal ICU admission and small-for-gestational-age infants.
From 2014 through 2020, differences in adverse outcomes by race and ethnicity persisted; in comparison with Whites, Black participants were at significantly higher risk of all evaluated outcomes, except for macrosomia and large for gestational age.
Hispanic/Latina and Asian/Pacific Islander individuals were also at significantly higher risk of preterm birth, NICU admission, maternal ICU admission, and small for gestational age. Furthermore, American Indian participants were at significantly higher risk of all evaluated outcomes, except for cesarean delivery and small for gestational age.
Results in context
Health policy researcher Felicia Hill-Briggs, PhD, at the Feinstein Institutes for Medical Research in Manhasset, N.Y. commented: “Two alarming trends highlighted by this study: 1) Racial and ethnic inequities in adverse gestational diabetes outcomes; and 2) the rising rates of gestational diabetes overall – both must and can be halted.”
“Optimizing medical management of gestational diabetes, whether through improved access to diabetes care in pregnancy, behavioral interventions, and pharmacotherapy can decrease the risk of adverse pregnancy outcomes,” Dr. Venkatesh commented. “It is possible that the equitable delivery of these interventions to address glycemic control could decrease racial and ethnic disparities in adverse pregnancy outcomes among individuals with gestational diabetes.”
Dr. Venkatesh and his colleagues acknowledged that a key limitation of the study was the use of administrative data; thus, inferences on maternal care improvements could not be determined.
“Further research could focus on greater understanding of racial and ethnic differences in the management of gestational diabetes,” the researchers concluded.
This study was supported by the Care Innovation and Community Improvement Program at Ohio State University. One author reported receiving grants from the National Institutes of Health outside of this study. The other authors reported no relevant disclosures. Dr. Hill-Briggs had no relevant disclosures.
FROM JAMA
Less cirrhosis but worse outcomes for Black patients with NASH
Compared with White people, Black people are less likely to develop cirrhosis from nonalcoholic steatohepatitis (NASH) but are more likely to die when hospitalized with this condition, researchers say.
The finding highlights the importance of addressing hepatic complications and nonhepatic comorbidities with a comprehensive and interdisciplinary approach that includes social determinants of health, said Emad Qayed, MD, MPH, an associate professor of medicine at Emory University School of Medicine, Atlanta.
“Clinicians should realize that in Black patients with NASH and NASH cirrhosis, mortality can be high despite a low rate of hepatic complications,” he told this news organization.
The study by Dr. Qayed and colleagues was published in the Journal of Clinical Gastroenterology.
A nationwide analysis
Previous studies have indicated that Black people are less likely than White people to develop nonalcoholic fatty liver disease (NAFLD), despite the fact that prevalence is increasing. Furthermore, when Black people do develop NAFLD, the disease is less likely to progress to NASH. In cases in which NASH does develop, the evidence has been mixed as to the effect of race on hospital outcomes.
To shed new light on that question, Dr. Qayed and colleagues analyzed data from 2016 to 2018 from the National Inpatient Sample, which is produced by the Healthcare Cost and Utilization Project and is sponsored by the Agency of Healthcare Research and Quality.
They identified 43,409 hospitalizations for NASH, with 41,143 White patients and 2,266 Black patients. The mean age of the Black patients was less than that of the White patients (56.4 years vs. 63.0 years), and Black patients were more likely to be women (69.9% vs. 61.6%).
More of the Black patients had hypertension, obesity, chronic kidney disease, and congestive heart failure, while more of the White patients had diabetes, dyslipidemia, and ischemic heart disease.
Among the Black patients, 33.6% had cirrhosis, compared with 56.4% of the White patients. Likewise, among the Black patients, there were fewer manifestations of decompensated cirrhosis, compared with the White patients. Black patients were also less likely to have had to undergo upper endoscopy and paracentesis.
The Black patients died in the hospital at a rate of 3.9%, which was not significantly higher than the 3.7% rate for the White patients (unadjusted odds ratio = 1.06; 95% confidence interval: 0.84-1.32; P = .6). But, when the researchers adjusted for age, sex, cirrhosis, risk of mortality (based on the overall number and severity of diseases), and insurance status, there were significantly higher odds of mortality among the Black patients (adjusted OR, 1.34; 95% CI: 1.05-1.71; P = .018).
They did not find any association between hospital size, location, or region with mortality.
They also found no difference in mortality between Black patients and White patients among those those with and those without cirrhosis. However, they found that Black patients were more likely to have acute kidney injury, chronic kidney disease, and congestive heart failure.
Regarding the reasons for hospitalization, the researchers found liver-related illnesses, such as hepatic failure and noninfectious hepatitis, to be most common among the White patients. Circulatory disorders, such as heart failure, and endocrine disorders, such as diabetes mellitus with complications, were found to be most common among the Black patients.
The length of time in the hospital was longer for the Black patients than the White patients (6.3 days vs. 5.6 days; P < .0001). The cost of hospitalization was higher for Black patients as well ($18,603 vs. $17,467). This suggests that Black patients were sicker overall, despite their lower rates of liver complications.
“Some of these differences are likely related to socioeconomic factors and clinical comorbidities, such as cardiac and renal disease,” Dr. Qayed said. “However, the underlying etiologies for such disparities in NASH and cirrhosis remain unclear. Further research is warranted to clarify these etiologies.”
NASH as part of the metabolic syndrome
“Clinicians should consider NASH as part of the metabolic syndrome,” Paul Martin, MD, chief of digestive health and liver diseases at the University of Miami, told this news organization. He was not involved in the study.
“Typically, these patients have a number of risk factors for fatty liver, including obesity and often hyperlipidemia, hypertension, and sleep apnea,” he said. “Clinicians should screen their patients for such comorbidities and then treat them.”
Genetic factors could also play a role in the difference in susceptibility to fatty liver disease found between Black and White patients, he added.
Dr. Martin noted a prevalence of fatty liver in many Hispanic populations and that it is found in Asia but sometimes in the absence of the risk factors associated with it in the United States.
Dr. Qayed and Dr. Martin reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Compared with White people, Black people are less likely to develop cirrhosis from nonalcoholic steatohepatitis (NASH) but are more likely to die when hospitalized with this condition, researchers say.
The finding highlights the importance of addressing hepatic complications and nonhepatic comorbidities with a comprehensive and interdisciplinary approach that includes social determinants of health, said Emad Qayed, MD, MPH, an associate professor of medicine at Emory University School of Medicine, Atlanta.
“Clinicians should realize that in Black patients with NASH and NASH cirrhosis, mortality can be high despite a low rate of hepatic complications,” he told this news organization.
The study by Dr. Qayed and colleagues was published in the Journal of Clinical Gastroenterology.
A nationwide analysis
Previous studies have indicated that Black people are less likely than White people to develop nonalcoholic fatty liver disease (NAFLD), despite the fact that prevalence is increasing. Furthermore, when Black people do develop NAFLD, the disease is less likely to progress to NASH. In cases in which NASH does develop, the evidence has been mixed as to the effect of race on hospital outcomes.
To shed new light on that question, Dr. Qayed and colleagues analyzed data from 2016 to 2018 from the National Inpatient Sample, which is produced by the Healthcare Cost and Utilization Project and is sponsored by the Agency of Healthcare Research and Quality.
They identified 43,409 hospitalizations for NASH, with 41,143 White patients and 2,266 Black patients. The mean age of the Black patients was less than that of the White patients (56.4 years vs. 63.0 years), and Black patients were more likely to be women (69.9% vs. 61.6%).
More of the Black patients had hypertension, obesity, chronic kidney disease, and congestive heart failure, while more of the White patients had diabetes, dyslipidemia, and ischemic heart disease.
Among the Black patients, 33.6% had cirrhosis, compared with 56.4% of the White patients. Likewise, among the Black patients, there were fewer manifestations of decompensated cirrhosis, compared with the White patients. Black patients were also less likely to have had to undergo upper endoscopy and paracentesis.
The Black patients died in the hospital at a rate of 3.9%, which was not significantly higher than the 3.7% rate for the White patients (unadjusted odds ratio = 1.06; 95% confidence interval: 0.84-1.32; P = .6). But, when the researchers adjusted for age, sex, cirrhosis, risk of mortality (based on the overall number and severity of diseases), and insurance status, there were significantly higher odds of mortality among the Black patients (adjusted OR, 1.34; 95% CI: 1.05-1.71; P = .018).
They did not find any association between hospital size, location, or region with mortality.
They also found no difference in mortality between Black patients and White patients among those those with and those without cirrhosis. However, they found that Black patients were more likely to have acute kidney injury, chronic kidney disease, and congestive heart failure.
Regarding the reasons for hospitalization, the researchers found liver-related illnesses, such as hepatic failure and noninfectious hepatitis, to be most common among the White patients. Circulatory disorders, such as heart failure, and endocrine disorders, such as diabetes mellitus with complications, were found to be most common among the Black patients.
The length of time in the hospital was longer for the Black patients than the White patients (6.3 days vs. 5.6 days; P < .0001). The cost of hospitalization was higher for Black patients as well ($18,603 vs. $17,467). This suggests that Black patients were sicker overall, despite their lower rates of liver complications.
“Some of these differences are likely related to socioeconomic factors and clinical comorbidities, such as cardiac and renal disease,” Dr. Qayed said. “However, the underlying etiologies for such disparities in NASH and cirrhosis remain unclear. Further research is warranted to clarify these etiologies.”
NASH as part of the metabolic syndrome
“Clinicians should consider NASH as part of the metabolic syndrome,” Paul Martin, MD, chief of digestive health and liver diseases at the University of Miami, told this news organization. He was not involved in the study.
“Typically, these patients have a number of risk factors for fatty liver, including obesity and often hyperlipidemia, hypertension, and sleep apnea,” he said. “Clinicians should screen their patients for such comorbidities and then treat them.”
Genetic factors could also play a role in the difference in susceptibility to fatty liver disease found between Black and White patients, he added.
Dr. Martin noted a prevalence of fatty liver in many Hispanic populations and that it is found in Asia but sometimes in the absence of the risk factors associated with it in the United States.
Dr. Qayed and Dr. Martin reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Compared with White people, Black people are less likely to develop cirrhosis from nonalcoholic steatohepatitis (NASH) but are more likely to die when hospitalized with this condition, researchers say.
The finding highlights the importance of addressing hepatic complications and nonhepatic comorbidities with a comprehensive and interdisciplinary approach that includes social determinants of health, said Emad Qayed, MD, MPH, an associate professor of medicine at Emory University School of Medicine, Atlanta.
“Clinicians should realize that in Black patients with NASH and NASH cirrhosis, mortality can be high despite a low rate of hepatic complications,” he told this news organization.
The study by Dr. Qayed and colleagues was published in the Journal of Clinical Gastroenterology.
A nationwide analysis
Previous studies have indicated that Black people are less likely than White people to develop nonalcoholic fatty liver disease (NAFLD), despite the fact that prevalence is increasing. Furthermore, when Black people do develop NAFLD, the disease is less likely to progress to NASH. In cases in which NASH does develop, the evidence has been mixed as to the effect of race on hospital outcomes.
To shed new light on that question, Dr. Qayed and colleagues analyzed data from 2016 to 2018 from the National Inpatient Sample, which is produced by the Healthcare Cost and Utilization Project and is sponsored by the Agency of Healthcare Research and Quality.
They identified 43,409 hospitalizations for NASH, with 41,143 White patients and 2,266 Black patients. The mean age of the Black patients was less than that of the White patients (56.4 years vs. 63.0 years), and Black patients were more likely to be women (69.9% vs. 61.6%).
More of the Black patients had hypertension, obesity, chronic kidney disease, and congestive heart failure, while more of the White patients had diabetes, dyslipidemia, and ischemic heart disease.
Among the Black patients, 33.6% had cirrhosis, compared with 56.4% of the White patients. Likewise, among the Black patients, there were fewer manifestations of decompensated cirrhosis, compared with the White patients. Black patients were also less likely to have had to undergo upper endoscopy and paracentesis.
The Black patients died in the hospital at a rate of 3.9%, which was not significantly higher than the 3.7% rate for the White patients (unadjusted odds ratio = 1.06; 95% confidence interval: 0.84-1.32; P = .6). But, when the researchers adjusted for age, sex, cirrhosis, risk of mortality (based on the overall number and severity of diseases), and insurance status, there were significantly higher odds of mortality among the Black patients (adjusted OR, 1.34; 95% CI: 1.05-1.71; P = .018).
They did not find any association between hospital size, location, or region with mortality.
They also found no difference in mortality between Black patients and White patients among those those with and those without cirrhosis. However, they found that Black patients were more likely to have acute kidney injury, chronic kidney disease, and congestive heart failure.
Regarding the reasons for hospitalization, the researchers found liver-related illnesses, such as hepatic failure and noninfectious hepatitis, to be most common among the White patients. Circulatory disorders, such as heart failure, and endocrine disorders, such as diabetes mellitus with complications, were found to be most common among the Black patients.
The length of time in the hospital was longer for the Black patients than the White patients (6.3 days vs. 5.6 days; P < .0001). The cost of hospitalization was higher for Black patients as well ($18,603 vs. $17,467). This suggests that Black patients were sicker overall, despite their lower rates of liver complications.
“Some of these differences are likely related to socioeconomic factors and clinical comorbidities, such as cardiac and renal disease,” Dr. Qayed said. “However, the underlying etiologies for such disparities in NASH and cirrhosis remain unclear. Further research is warranted to clarify these etiologies.”
NASH as part of the metabolic syndrome
“Clinicians should consider NASH as part of the metabolic syndrome,” Paul Martin, MD, chief of digestive health and liver diseases at the University of Miami, told this news organization. He was not involved in the study.
“Typically, these patients have a number of risk factors for fatty liver, including obesity and often hyperlipidemia, hypertension, and sleep apnea,” he said. “Clinicians should screen their patients for such comorbidities and then treat them.”
Genetic factors could also play a role in the difference in susceptibility to fatty liver disease found between Black and White patients, he added.
Dr. Martin noted a prevalence of fatty liver in many Hispanic populations and that it is found in Asia but sometimes in the absence of the risk factors associated with it in the United States.
Dr. Qayed and Dr. Martin reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Two rounds of FIT vs. single colonoscopy as a one-time CRC screening
A fecal immunochemical test (FIT) conducted 2 years apart could form the basis for population-based colorectal cancer screening if this approach goes on to show a mortality benefit, according to a preliminary analysis.
Researchers are investigating the effect of this time frame of FIT screening as well as a single colonoscopy on colorectal cancer incidence and mortality as the primary endpoints of a randomized controlled trial called SCREESCO. Both were compared to a control of no intervention.
“The rationale is to have the FIT test for a 2-year interval and then no more [colorectal cancer screening] after that,” Anna Forsberg, MD, PhD, lead author and a researcher at the Karolinska Institute in Stockholm, told this news organization.
In addition to the spacing of the FIT screening, the cutoff value in the stool sample of 10 micrograms of hemoglobin per gram is also unique to SCREESCO.
“In most other studies, the cutoff is either 20 micrograms or 40 micrograms,” Dr. Forsberg said. “With this very low cutoff, we hope that we find cancer, including advanced adenomas that are precancerous and can be removed.”
The preliminary analysis reporting the trial’s baseline findings was published online in The Lancet Gastroenterology & Hepatology.
Comparing two interventions
Between 2014 and 2020, the study included 278,280 individuals, with 31,140 assigned to the colonoscopy group, 60,300 to the FIT group, and 186,840 to the control group. Both colonoscopy and FIT screening occurred at age 60 years.
Of the individuals in the colonoscopy group, 35.1% had a colonoscopy, compared with 55.5% in the FIT group who participated in at least one round of testing; 41.4% completed both rounds of FIT screening.
In the FIT group, 6.3% of the test results were positive, and 90.8% of individuals with a positive FIT test underwent a follow-up colonoscopy.
Polyps were found in 45.2% of colonoscopies in the colonoscopy group and in 58.2% in the FIT group. The median adenoma detection rate was 20% in the colonoscopy group and 34% in the FIT group.
The intention-to-treat analysis found a colorectal cancer detection rate of 0.16% in the colonoscopy group and 0.20% in the FIT group, but it was not statistically significant. Advanced adenomas were detected more often in the colonoscopy group than in the FIT group (2.05% vs. 1.61%; relative risk, 1.27; 95% confidence interval, 1.15-1.41).
The number of colonoscopies needed to detect one cancer was 218 in the colonoscopy group and 49 in the FIT group; to detect a single advanced adenoma, 17 and 6 colonoscopies had to be done, respectively.
Too early to change screening strategies
When asked to comment on the study, David Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School in Norfolk, said that the results should be understood as preliminary.
“This is only a description of what they have to date and not of what they proposed for their endpoints,” said Dr. Johnson, who wasn’t associated with the research. “A recommendation for changing screening strategies based on these findings would be very inappropriate at this point.”
Dr. Johnson raised concerns about the quality of the colonoscopies, noting that the procedures were carried out by a mix of gastroenterologists and surgeons. He said that several measures, including the surprisingly low yields for the colonoscopy group and even more so for the FIT-positive group, were concerning.
“They are much lower than even the minimum standard that we would use as benchmark quality indicators in the United States,” he said. “That raises a considerable flag to me that the quality of the colonoscopy confirmation [after a positive FIT test] and screening were both low.”
Dr. Johnson said the ultimate goal of colorectal cancer screening is to detect and remove polyps, a strategy that has been shown to reduce mortality. But FIT tests are not well suited to detecting adenomatous polyps and are of little value in detecting sessile serrated lesions.
“FIT is a detection for cancer, not a detection for polyps. The true value of screening is not just detection but prevention by identification and removal of precancerous polyps,” he said.
Still, Dr. Forsberg emphasized the importance of maximizing uptake of colorectal cancer screening.
“When we pooled the results from the two interventions, the participation in the FIT arm was 56%, which is good. If you look at international figures, that is also high for participation in colonoscopy screening,” Dr. Forsberg said.
“Participation is the main thing. You can have the most fantastic test, but if people don’t participate, then it’s not worth much.”
SCREESCO is one of several ongoing studies comparing screening strategies that employ colonoscopy or FIT. Other studies of colon cancer surveillance methods include the COLONPREV and CONFIRM trials comparing colonoscopy to FIT, and the NordICC trial comparing colonoscopy to no intervention. None of these trials have yet published their final results on colorectal cancer mortality.
Dr. Forsberg and Dr. Johnson have disclosed no relevant financial disclosures. The study was funded by Swedish regions, County Council, Regional Cancer Center Mellansverige, Swedish Cancer Society, Aleris Research and Development Fund, and Eiken Chemical.
A version of this article first appeared on Medscape.com.
A fecal immunochemical test (FIT) conducted 2 years apart could form the basis for population-based colorectal cancer screening if this approach goes on to show a mortality benefit, according to a preliminary analysis.
Researchers are investigating the effect of this time frame of FIT screening as well as a single colonoscopy on colorectal cancer incidence and mortality as the primary endpoints of a randomized controlled trial called SCREESCO. Both were compared to a control of no intervention.
“The rationale is to have the FIT test for a 2-year interval and then no more [colorectal cancer screening] after that,” Anna Forsberg, MD, PhD, lead author and a researcher at the Karolinska Institute in Stockholm, told this news organization.
In addition to the spacing of the FIT screening, the cutoff value in the stool sample of 10 micrograms of hemoglobin per gram is also unique to SCREESCO.
“In most other studies, the cutoff is either 20 micrograms or 40 micrograms,” Dr. Forsberg said. “With this very low cutoff, we hope that we find cancer, including advanced adenomas that are precancerous and can be removed.”
The preliminary analysis reporting the trial’s baseline findings was published online in The Lancet Gastroenterology & Hepatology.
Comparing two interventions
Between 2014 and 2020, the study included 278,280 individuals, with 31,140 assigned to the colonoscopy group, 60,300 to the FIT group, and 186,840 to the control group. Both colonoscopy and FIT screening occurred at age 60 years.
Of the individuals in the colonoscopy group, 35.1% had a colonoscopy, compared with 55.5% in the FIT group who participated in at least one round of testing; 41.4% completed both rounds of FIT screening.
In the FIT group, 6.3% of the test results were positive, and 90.8% of individuals with a positive FIT test underwent a follow-up colonoscopy.
Polyps were found in 45.2% of colonoscopies in the colonoscopy group and in 58.2% in the FIT group. The median adenoma detection rate was 20% in the colonoscopy group and 34% in the FIT group.
The intention-to-treat analysis found a colorectal cancer detection rate of 0.16% in the colonoscopy group and 0.20% in the FIT group, but it was not statistically significant. Advanced adenomas were detected more often in the colonoscopy group than in the FIT group (2.05% vs. 1.61%; relative risk, 1.27; 95% confidence interval, 1.15-1.41).
The number of colonoscopies needed to detect one cancer was 218 in the colonoscopy group and 49 in the FIT group; to detect a single advanced adenoma, 17 and 6 colonoscopies had to be done, respectively.
Too early to change screening strategies
When asked to comment on the study, David Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School in Norfolk, said that the results should be understood as preliminary.
“This is only a description of what they have to date and not of what they proposed for their endpoints,” said Dr. Johnson, who wasn’t associated with the research. “A recommendation for changing screening strategies based on these findings would be very inappropriate at this point.”
Dr. Johnson raised concerns about the quality of the colonoscopies, noting that the procedures were carried out by a mix of gastroenterologists and surgeons. He said that several measures, including the surprisingly low yields for the colonoscopy group and even more so for the FIT-positive group, were concerning.
“They are much lower than even the minimum standard that we would use as benchmark quality indicators in the United States,” he said. “That raises a considerable flag to me that the quality of the colonoscopy confirmation [after a positive FIT test] and screening were both low.”
Dr. Johnson said the ultimate goal of colorectal cancer screening is to detect and remove polyps, a strategy that has been shown to reduce mortality. But FIT tests are not well suited to detecting adenomatous polyps and are of little value in detecting sessile serrated lesions.
“FIT is a detection for cancer, not a detection for polyps. The true value of screening is not just detection but prevention by identification and removal of precancerous polyps,” he said.
Still, Dr. Forsberg emphasized the importance of maximizing uptake of colorectal cancer screening.
“When we pooled the results from the two interventions, the participation in the FIT arm was 56%, which is good. If you look at international figures, that is also high for participation in colonoscopy screening,” Dr. Forsberg said.
“Participation is the main thing. You can have the most fantastic test, but if people don’t participate, then it’s not worth much.”
SCREESCO is one of several ongoing studies comparing screening strategies that employ colonoscopy or FIT. Other studies of colon cancer surveillance methods include the COLONPREV and CONFIRM trials comparing colonoscopy to FIT, and the NordICC trial comparing colonoscopy to no intervention. None of these trials have yet published their final results on colorectal cancer mortality.
Dr. Forsberg and Dr. Johnson have disclosed no relevant financial disclosures. The study was funded by Swedish regions, County Council, Regional Cancer Center Mellansverige, Swedish Cancer Society, Aleris Research and Development Fund, and Eiken Chemical.
A version of this article first appeared on Medscape.com.
A fecal immunochemical test (FIT) conducted 2 years apart could form the basis for population-based colorectal cancer screening if this approach goes on to show a mortality benefit, according to a preliminary analysis.
Researchers are investigating the effect of this time frame of FIT screening as well as a single colonoscopy on colorectal cancer incidence and mortality as the primary endpoints of a randomized controlled trial called SCREESCO. Both were compared to a control of no intervention.
“The rationale is to have the FIT test for a 2-year interval and then no more [colorectal cancer screening] after that,” Anna Forsberg, MD, PhD, lead author and a researcher at the Karolinska Institute in Stockholm, told this news organization.
In addition to the spacing of the FIT screening, the cutoff value in the stool sample of 10 micrograms of hemoglobin per gram is also unique to SCREESCO.
“In most other studies, the cutoff is either 20 micrograms or 40 micrograms,” Dr. Forsberg said. “With this very low cutoff, we hope that we find cancer, including advanced adenomas that are precancerous and can be removed.”
The preliminary analysis reporting the trial’s baseline findings was published online in The Lancet Gastroenterology & Hepatology.
Comparing two interventions
Between 2014 and 2020, the study included 278,280 individuals, with 31,140 assigned to the colonoscopy group, 60,300 to the FIT group, and 186,840 to the control group. Both colonoscopy and FIT screening occurred at age 60 years.
Of the individuals in the colonoscopy group, 35.1% had a colonoscopy, compared with 55.5% in the FIT group who participated in at least one round of testing; 41.4% completed both rounds of FIT screening.
In the FIT group, 6.3% of the test results were positive, and 90.8% of individuals with a positive FIT test underwent a follow-up colonoscopy.
Polyps were found in 45.2% of colonoscopies in the colonoscopy group and in 58.2% in the FIT group. The median adenoma detection rate was 20% in the colonoscopy group and 34% in the FIT group.
The intention-to-treat analysis found a colorectal cancer detection rate of 0.16% in the colonoscopy group and 0.20% in the FIT group, but it was not statistically significant. Advanced adenomas were detected more often in the colonoscopy group than in the FIT group (2.05% vs. 1.61%; relative risk, 1.27; 95% confidence interval, 1.15-1.41).
The number of colonoscopies needed to detect one cancer was 218 in the colonoscopy group and 49 in the FIT group; to detect a single advanced adenoma, 17 and 6 colonoscopies had to be done, respectively.
Too early to change screening strategies
When asked to comment on the study, David Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School in Norfolk, said that the results should be understood as preliminary.
“This is only a description of what they have to date and not of what they proposed for their endpoints,” said Dr. Johnson, who wasn’t associated with the research. “A recommendation for changing screening strategies based on these findings would be very inappropriate at this point.”
Dr. Johnson raised concerns about the quality of the colonoscopies, noting that the procedures were carried out by a mix of gastroenterologists and surgeons. He said that several measures, including the surprisingly low yields for the colonoscopy group and even more so for the FIT-positive group, were concerning.
“They are much lower than even the minimum standard that we would use as benchmark quality indicators in the United States,” he said. “That raises a considerable flag to me that the quality of the colonoscopy confirmation [after a positive FIT test] and screening were both low.”
Dr. Johnson said the ultimate goal of colorectal cancer screening is to detect and remove polyps, a strategy that has been shown to reduce mortality. But FIT tests are not well suited to detecting adenomatous polyps and are of little value in detecting sessile serrated lesions.
“FIT is a detection for cancer, not a detection for polyps. The true value of screening is not just detection but prevention by identification and removal of precancerous polyps,” he said.
Still, Dr. Forsberg emphasized the importance of maximizing uptake of colorectal cancer screening.
“When we pooled the results from the two interventions, the participation in the FIT arm was 56%, which is good. If you look at international figures, that is also high for participation in colonoscopy screening,” Dr. Forsberg said.
“Participation is the main thing. You can have the most fantastic test, but if people don’t participate, then it’s not worth much.”
SCREESCO is one of several ongoing studies comparing screening strategies that employ colonoscopy or FIT. Other studies of colon cancer surveillance methods include the COLONPREV and CONFIRM trials comparing colonoscopy to FIT, and the NordICC trial comparing colonoscopy to no intervention. None of these trials have yet published their final results on colorectal cancer mortality.
Dr. Forsberg and Dr. Johnson have disclosed no relevant financial disclosures. The study was funded by Swedish regions, County Council, Regional Cancer Center Mellansverige, Swedish Cancer Society, Aleris Research and Development Fund, and Eiken Chemical.
A version of this article first appeared on Medscape.com.
Vibrating wearable device may help night time GERD
A vibrating wearable device helped people with gastroesophageal reflux disease (GERD) stay positioned on their left side while sleeping, alleviating night time reflux symptoms, compared with sham treatment, a small, randomized study suggests.
People often report having more reflux symptoms when sleeping on their right side, and experimental studies suggest that sleeping on the right side is associated with higher esophageal acid exposure time and slower esophageal acid clearance, compared with sleeping on the left side, the authors wrote.
They cite a possible cause as the stomach being above the esophagus when a person is sleeping on their right side, resulting in more reflux.
“There are two very exciting new things that can be learned,” Arjan Bredenoord, MD, PhD, a principal investigator of the study and professor of neurogastroenterology and motility at the Academic Medical Center in Amsterdam, told this news organization. “First, we show that a device that trains people to sleep on the left side really helps to relieve nocturnal reflux symptoms. Second, the study was performed completely remotely, with the patients being at home.”
“The devices were shipped to the patients. All contact was via video calling, and questionnaires were done via links in emails that were linked to secure databases to store the patients’ symptom responses,” he added.
The findings were published online in Clinical Gastroenterology and Hepatology.
A study in sleep positional therapy
Researchers performed a double-blind, randomized, sham-controlled trial in 100 patients with night time GERD symptoms who wore a programmed device (about 1.5 inches square) on their chest, midsternum.
Patients were advised to sleep on their left side and randomly assigned (1:1) either to a group whose device produced a gentle vibration when they flipped onto their right side throughout sleep or to the group whose device vibrated when they flipped to the right side but only for the first 20 minutes of use (the sham intervention).
The primary outcome for success was at least a 50% reduction in the Nocturnal Gastroesophageal Reflux Disease Symptom Severity and Impact Questionnaire (N-GSSIQ) score. Secondary outcomes included change in sleep position and reflux symptoms.
In the intention-to-treat analysis, the rate of treatment success was 44% in the intervention group versus 24% in the sham group. The risk difference was 20% (95% confidence interval, 1.8% to 38.2%; P = .03).
Treatment led to a significant avoidance of sleeping on the right side (intervention 2.2% vs. sham 23.5%; P ≤ .0001) and an increased time of sleeping on the left side (intervention 60.9% vs. sham 38.5%; P ≤ .0001).
Patients in the intervention group also had more reflux-free nights (9 nights vs. 6 nights for the sham group).
After 2 weeks of treatment, the average total N-GSSIQ scores were lower in the active device group (18.8 vs. 23.7 in the sham group; P = .04).
Most with GERD have night time symptoms
The authors pointed out that up to 80% of patients with GERD experience symptoms during the night, such as heartburn and regurgitation, which can significantly impair sleep quality and daytime functioning.
Solutions are of high interest because current measures have shortcomings.
Raising the head-end of the bed and lengthening the time between dinner and bedtime have limited effect, the authors explained. And while proton pump inhibitors are very effective for daytime symptoms, they have limited efficacy for night time reflux symptoms.
Antireflux pillows, which are designed to keep patients on their left side through the night, have been found to result in less recumbent acid exposure and less self-reported night time reflux symptoms, but they do not allow for spontaneous body movements and can be uncomfortable, they explained.
The lightweight vibration device, made by Side Sleep Technologies BV, registers the sleep position of a subject at 30-second intervals. It categorizes sleep position as supine, right, left, prone, or upright.
Michiel Allessie, CEO of Side Sleep Technologies, told this news organization that the wearable V1.0 is sold as a consumer electronic device rather than a medical device in the United Kingdom for £99. He said the company expects to sell the V1.0 in the United States starting in June, with a target price of $99.
Promising but device still needs real-world testing
When asked to comment, Philip Katz, MD, a gastroenterologist at Weill Cornell Medicine, New York, said it was a fantastic study scientifically and academically incredibly interesting, but the device is not a panacea.
Dr. Katz said he will remain skeptical until the device is tested in real life and added that it’s important to remember this is one study with 100 people.
He also wondered whether there might be an even better solution in a well-designed wedge, for example, and whether the buzzing of this product might affect sleep quality. If so, would that be worth the tradeoff?
Dr. Katz noted that busy physicians may not have the time to determine whether patients truly have nocturnal GERD or just similar symptoms. This study included people who were carefully screened by the researchers for nocturnal reflux symptoms, he pointed out.
Based on this study, Dr. Katz said he would tell patients, “You have a 50% chance to be helped because their primary outcome was met by 44%.”
He said the decision is up to the patients and comes down to this: “It’s better than nothing for sure. Is it worth $100? You tell me.”
Dr. Bredenoord said the next step is a study using pH-impedance monitoring of the esophagus to show that there is also an effect on reflux episodes.
The investigational medical devices were provided free of charge and without restrictions by Side Sleep Technologies BV. Dr. Bredenoord disclosed research funding from Nutricia, Norgine, SST, Thelial, and Bayer; speaker and/or consulting fees from Laborie, EsoCap, Medtronic, Dr. Falk Pharma, Calypso Biotech, Alimentiv, Reckett Benkiser, Regeneron, and AstraZeneca; and previously owned shares in Side Sleep Technologies BV. Another coauthor received research funding from Boston Scientific and speaker and/or consulting fees from Cook and Olympus. The remaining authors have disclosed no relevant financial relationships. Dr. Katz reported being a consultant for Phathom Pharmaceuticals and Sebela.
A version of this article first appeared on Medscape.com.
A vibrating wearable device helped people with gastroesophageal reflux disease (GERD) stay positioned on their left side while sleeping, alleviating night time reflux symptoms, compared with sham treatment, a small, randomized study suggests.
People often report having more reflux symptoms when sleeping on their right side, and experimental studies suggest that sleeping on the right side is associated with higher esophageal acid exposure time and slower esophageal acid clearance, compared with sleeping on the left side, the authors wrote.
They cite a possible cause as the stomach being above the esophagus when a person is sleeping on their right side, resulting in more reflux.
“There are two very exciting new things that can be learned,” Arjan Bredenoord, MD, PhD, a principal investigator of the study and professor of neurogastroenterology and motility at the Academic Medical Center in Amsterdam, told this news organization. “First, we show that a device that trains people to sleep on the left side really helps to relieve nocturnal reflux symptoms. Second, the study was performed completely remotely, with the patients being at home.”
“The devices were shipped to the patients. All contact was via video calling, and questionnaires were done via links in emails that were linked to secure databases to store the patients’ symptom responses,” he added.
The findings were published online in Clinical Gastroenterology and Hepatology.
A study in sleep positional therapy
Researchers performed a double-blind, randomized, sham-controlled trial in 100 patients with night time GERD symptoms who wore a programmed device (about 1.5 inches square) on their chest, midsternum.
Patients were advised to sleep on their left side and randomly assigned (1:1) either to a group whose device produced a gentle vibration when they flipped onto their right side throughout sleep or to the group whose device vibrated when they flipped to the right side but only for the first 20 minutes of use (the sham intervention).
The primary outcome for success was at least a 50% reduction in the Nocturnal Gastroesophageal Reflux Disease Symptom Severity and Impact Questionnaire (N-GSSIQ) score. Secondary outcomes included change in sleep position and reflux symptoms.
In the intention-to-treat analysis, the rate of treatment success was 44% in the intervention group versus 24% in the sham group. The risk difference was 20% (95% confidence interval, 1.8% to 38.2%; P = .03).
Treatment led to a significant avoidance of sleeping on the right side (intervention 2.2% vs. sham 23.5%; P ≤ .0001) and an increased time of sleeping on the left side (intervention 60.9% vs. sham 38.5%; P ≤ .0001).
Patients in the intervention group also had more reflux-free nights (9 nights vs. 6 nights for the sham group).
After 2 weeks of treatment, the average total N-GSSIQ scores were lower in the active device group (18.8 vs. 23.7 in the sham group; P = .04).
Most with GERD have night time symptoms
The authors pointed out that up to 80% of patients with GERD experience symptoms during the night, such as heartburn and regurgitation, which can significantly impair sleep quality and daytime functioning.
Solutions are of high interest because current measures have shortcomings.
Raising the head-end of the bed and lengthening the time between dinner and bedtime have limited effect, the authors explained. And while proton pump inhibitors are very effective for daytime symptoms, they have limited efficacy for night time reflux symptoms.
Antireflux pillows, which are designed to keep patients on their left side through the night, have been found to result in less recumbent acid exposure and less self-reported night time reflux symptoms, but they do not allow for spontaneous body movements and can be uncomfortable, they explained.
The lightweight vibration device, made by Side Sleep Technologies BV, registers the sleep position of a subject at 30-second intervals. It categorizes sleep position as supine, right, left, prone, or upright.
Michiel Allessie, CEO of Side Sleep Technologies, told this news organization that the wearable V1.0 is sold as a consumer electronic device rather than a medical device in the United Kingdom for £99. He said the company expects to sell the V1.0 in the United States starting in June, with a target price of $99.
Promising but device still needs real-world testing
When asked to comment, Philip Katz, MD, a gastroenterologist at Weill Cornell Medicine, New York, said it was a fantastic study scientifically and academically incredibly interesting, but the device is not a panacea.
Dr. Katz said he will remain skeptical until the device is tested in real life and added that it’s important to remember this is one study with 100 people.
He also wondered whether there might be an even better solution in a well-designed wedge, for example, and whether the buzzing of this product might affect sleep quality. If so, would that be worth the tradeoff?
Dr. Katz noted that busy physicians may not have the time to determine whether patients truly have nocturnal GERD or just similar symptoms. This study included people who were carefully screened by the researchers for nocturnal reflux symptoms, he pointed out.
Based on this study, Dr. Katz said he would tell patients, “You have a 50% chance to be helped because their primary outcome was met by 44%.”
He said the decision is up to the patients and comes down to this: “It’s better than nothing for sure. Is it worth $100? You tell me.”
Dr. Bredenoord said the next step is a study using pH-impedance monitoring of the esophagus to show that there is also an effect on reflux episodes.
The investigational medical devices were provided free of charge and without restrictions by Side Sleep Technologies BV. Dr. Bredenoord disclosed research funding from Nutricia, Norgine, SST, Thelial, and Bayer; speaker and/or consulting fees from Laborie, EsoCap, Medtronic, Dr. Falk Pharma, Calypso Biotech, Alimentiv, Reckett Benkiser, Regeneron, and AstraZeneca; and previously owned shares in Side Sleep Technologies BV. Another coauthor received research funding from Boston Scientific and speaker and/or consulting fees from Cook and Olympus. The remaining authors have disclosed no relevant financial relationships. Dr. Katz reported being a consultant for Phathom Pharmaceuticals and Sebela.
A version of this article first appeared on Medscape.com.
A vibrating wearable device helped people with gastroesophageal reflux disease (GERD) stay positioned on their left side while sleeping, alleviating night time reflux symptoms, compared with sham treatment, a small, randomized study suggests.
People often report having more reflux symptoms when sleeping on their right side, and experimental studies suggest that sleeping on the right side is associated with higher esophageal acid exposure time and slower esophageal acid clearance, compared with sleeping on the left side, the authors wrote.
They cite a possible cause as the stomach being above the esophagus when a person is sleeping on their right side, resulting in more reflux.
“There are two very exciting new things that can be learned,” Arjan Bredenoord, MD, PhD, a principal investigator of the study and professor of neurogastroenterology and motility at the Academic Medical Center in Amsterdam, told this news organization. “First, we show that a device that trains people to sleep on the left side really helps to relieve nocturnal reflux symptoms. Second, the study was performed completely remotely, with the patients being at home.”
“The devices were shipped to the patients. All contact was via video calling, and questionnaires were done via links in emails that were linked to secure databases to store the patients’ symptom responses,” he added.
The findings were published online in Clinical Gastroenterology and Hepatology.
A study in sleep positional therapy
Researchers performed a double-blind, randomized, sham-controlled trial in 100 patients with night time GERD symptoms who wore a programmed device (about 1.5 inches square) on their chest, midsternum.
Patients were advised to sleep on their left side and randomly assigned (1:1) either to a group whose device produced a gentle vibration when they flipped onto their right side throughout sleep or to the group whose device vibrated when they flipped to the right side but only for the first 20 minutes of use (the sham intervention).
The primary outcome for success was at least a 50% reduction in the Nocturnal Gastroesophageal Reflux Disease Symptom Severity and Impact Questionnaire (N-GSSIQ) score. Secondary outcomes included change in sleep position and reflux symptoms.
In the intention-to-treat analysis, the rate of treatment success was 44% in the intervention group versus 24% in the sham group. The risk difference was 20% (95% confidence interval, 1.8% to 38.2%; P = .03).
Treatment led to a significant avoidance of sleeping on the right side (intervention 2.2% vs. sham 23.5%; P ≤ .0001) and an increased time of sleeping on the left side (intervention 60.9% vs. sham 38.5%; P ≤ .0001).
Patients in the intervention group also had more reflux-free nights (9 nights vs. 6 nights for the sham group).
After 2 weeks of treatment, the average total N-GSSIQ scores were lower in the active device group (18.8 vs. 23.7 in the sham group; P = .04).
Most with GERD have night time symptoms
The authors pointed out that up to 80% of patients with GERD experience symptoms during the night, such as heartburn and regurgitation, which can significantly impair sleep quality and daytime functioning.
Solutions are of high interest because current measures have shortcomings.
Raising the head-end of the bed and lengthening the time between dinner and bedtime have limited effect, the authors explained. And while proton pump inhibitors are very effective for daytime symptoms, they have limited efficacy for night time reflux symptoms.
Antireflux pillows, which are designed to keep patients on their left side through the night, have been found to result in less recumbent acid exposure and less self-reported night time reflux symptoms, but they do not allow for spontaneous body movements and can be uncomfortable, they explained.
The lightweight vibration device, made by Side Sleep Technologies BV, registers the sleep position of a subject at 30-second intervals. It categorizes sleep position as supine, right, left, prone, or upright.
Michiel Allessie, CEO of Side Sleep Technologies, told this news organization that the wearable V1.0 is sold as a consumer electronic device rather than a medical device in the United Kingdom for £99. He said the company expects to sell the V1.0 in the United States starting in June, with a target price of $99.
Promising but device still needs real-world testing
When asked to comment, Philip Katz, MD, a gastroenterologist at Weill Cornell Medicine, New York, said it was a fantastic study scientifically and academically incredibly interesting, but the device is not a panacea.
Dr. Katz said he will remain skeptical until the device is tested in real life and added that it’s important to remember this is one study with 100 people.
He also wondered whether there might be an even better solution in a well-designed wedge, for example, and whether the buzzing of this product might affect sleep quality. If so, would that be worth the tradeoff?
Dr. Katz noted that busy physicians may not have the time to determine whether patients truly have nocturnal GERD or just similar symptoms. This study included people who were carefully screened by the researchers for nocturnal reflux symptoms, he pointed out.
Based on this study, Dr. Katz said he would tell patients, “You have a 50% chance to be helped because their primary outcome was met by 44%.”
He said the decision is up to the patients and comes down to this: “It’s better than nothing for sure. Is it worth $100? You tell me.”
Dr. Bredenoord said the next step is a study using pH-impedance monitoring of the esophagus to show that there is also an effect on reflux episodes.
The investigational medical devices were provided free of charge and without restrictions by Side Sleep Technologies BV. Dr. Bredenoord disclosed research funding from Nutricia, Norgine, SST, Thelial, and Bayer; speaker and/or consulting fees from Laborie, EsoCap, Medtronic, Dr. Falk Pharma, Calypso Biotech, Alimentiv, Reckett Benkiser, Regeneron, and AstraZeneca; and previously owned shares in Side Sleep Technologies BV. Another coauthor received research funding from Boston Scientific and speaker and/or consulting fees from Cook and Olympus. The remaining authors have disclosed no relevant financial relationships. Dr. Katz reported being a consultant for Phathom Pharmaceuticals and Sebela.
A version of this article first appeared on Medscape.com.
Gaps in follow-up care put kids with asthma at risk of severe recurrence
Jo Ward’s twin boys have been to the emergency department for respiratory problems about as many times as the dozen years they’ve been alive. Both have asthma and bronchopulmonary dysplasia, a form of chronic airway damage that can occur in children born premature, as the twins were. But each time Ms. Ward took them in for treatment during an acute bout of breathing distress, the staff told her to schedule a follow-up visit for the children with their physician only if they didn’t get better, not regardless of the outcome – as medical guidelines recommend.
“They asked questions, they did the exams, but they really didn’t give you a lot of information to help you at home,” Ms. Ward told this news organization. If they had, she doesn’t think she’d have needed to take them in for emergency care so often.
A new study, published in Academic Pediatrics, suggests she’s right.
Current clinical guidelines for asthma recommend that patients who visit the ED for an asthma-related problem should have a follow-up appointment within a month after the visit, independent of how well they have recovered once home, according to Naomi S. Bardach, MD, a professor of pediatrics and health policy at the University of California, San Francisco, who led the new study.
Her research found that children who have a follow-up appointment within 2 weeks of such a visit are less likely to come back again the next year. Yet the study also found that only about one in five youth had a follow-up visit within that 2-week window.
“The emergency department visit is probably a sign that they need some additional attention for their asthma,” Dr. Bardach said. “We know we can prevent emergency department visits if they get the right kind of medication or if they figure out how to avoid the things that are going to cause an asthma exacerbation or flare.”
For the study, Dr. Bardach and colleagues analyzed data from California, Vermont, and Massachusetts for all asthma-related emergency visits for patients aged 3-21 years between 2013 and 2016.
Out of the 90,267 such visits they identified, 22.6% of patients had a follow-up within 2 weeks, more often by patients who were younger, had commercial insurance, had evidence of prior asthma, or had complex chronic conditions.
Whereas 5.7% of patients who had follow-up visits returned to the ED within 60 days, 6.4% of those who didn’t came back – a 12% difference (P < .001). The gap was larger a year out, with 25% of those with follow-ups returning to the ED, compared with 28.3% of those without follow-ups returning (P < .001), according to the researchers.
Overall, Dr. Bardach’s group estimates that for every 30 children who have follow-up visits with a physician, one would avoid a return trip to the emergency department for asthma within a year.
But given the sheer number of asthma-related trips to the ED each year – 164,145 for kids age 1-17 years in the United States in 2016 alone – that translates into big numbers of kids not going back to the hospital: approximately 72,000 such trips avoided at a savings to the health care system of at least $8.6 million annually.
Missed opportunities
Had Ms. Ward’s boys been among the one in five to receive follow-up care earlier in their lives, she might have saved a significant amount of time, money, anxiety, and heartache. When the twins were 9 years old, she took them to a new pediatric pulmonologist. That changed everything. In that first visit, “they gave me way more information than I ever had in the first 9 years,” she said.
The doctor told Ms. Ward to keep steroids on hand, gave her a prescription for extra doses of the powerful medication, and explained that they needed to be used within 24 hours of the first sign of a breathing problem.
“She said if you give them the steroids right away, it keeps them out of the emergency room, and that’s actually worked,” Ms. Ward said. “She made sure we had care plans every visit and asked me each time if I still had it or we needed to rewrite it. They gave me signs to look for, for when to go to hospital visits. I think that when you go to the doctor, they should be telling you stuff like that.”
Dr. Bardach said visits with a primary care doctor or asthma specialist offer families a chance to receive information to keep the condition from becoming critical.
“Going to that follow-up visit, they can get access to education from the provider about how to avoid things that trigger asthma, and there’s medication that kids can take that keeps the lungs calm and less likely to have a big asthma reaction, so getting access to that medication can be really helpful,” she said.
That was the case for Amy Davenport, of Chapel Hill, N.C., whose 6-year-old son has been to the ED twice for his asthma.
The first time, when he was 3, he was having trouble breathing with a respiratory tract infection and received nebulizer treatment – although he received it in the ED since no beds were available in the ICU. The staff did tell Ms. Davenport to follow up with her primary care provider, but her son’s pediatrician was reluctant to diagnose him with asthma at such a young age and didn’t prescribe any maintenance medications.
A few months later, Ms. Davenport and her son found themselves back in the hospital, and an ICU bed was open this time. The critical care staff referred Davenport to a pediatric pulmonary specialist, and they haven’t been back to the hospital since. Ms. Davenport said she believes if they’d received a maintenance medication after the first visit, it likely would have prevented the second one.
“I’ve definitely seen now that, after the second admission, we got an asthma action plan and it said exactly what to do,” she said. “I felt like we had really good follow-up. We had that action plan on our refrigerator for a long time, and it helped us as parents with three small children to manage.”
Of course, follow-up care takes time – time away from work and school that not all families can spare, the researchers acknowledged. Telehealth may be an option, especially after its use expanded during the COVID-19 pandemic.
“We know that health systems have a hard time being flexible enough to actually have a kid be able to make an appointment within a short period of time, and we also know it’s hard for families sometimes to go back into a clinical setting within a certain period of time,” Dr. Bardach said. The urgency for the appointment may wane for those whose children seem to be doing better.
When the researchers adjusted their calculations for socioeconomic status, the results didn’t change much. But the study did find that patients with private insurance were about twice as likely to have follow-up visits as those on Medicaid (43.7% vs. 21.7%). And “the content and conduct” of the follow-up visit makes a difference as well.
Ms. Ward, whose boys are insured through Medicaid, recalled several visits to the ED where she had to push the staff to get the care her children needed. In one case, when one of her boys was a year old and struggling to breathe, the emergency doctor handed her a prescription and recommended she fill it at a neighborhood drugstore that would be cheaper than the hospital’s pharmacy. Then a nurse came in to begin the discharge process.
“I said no, ‘we’re not ready yet. Look at him,’” Ms. Ward said. The nurse took a pulse oximeter reading that showed the boy’s oxygen levels were at 84%, dangerously low. “If I wasn’t so knowledgeable and paid attention when they were born, since they were preemies, if it would have been somebody else, they probably would’ve went home and he’d have died.”
With the pediatric pulmonologist the boys have now, Ms. Ward said she feels more capable of managing their asthma and knowing how to reduce the likelihood that they’ll need to visit the ED.
“Part of what we’re seeing here is that having an existing and trusting relationship with a clinician can be helpful to kids with asthma,” Dr. Bardach said. “If we help establish and maintain those connections, and explain how important that connection can be, that can also help somebody with asthma overall.”
The research was funded by the Agency for Healthcare Research and Quality. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Jo Ward’s twin boys have been to the emergency department for respiratory problems about as many times as the dozen years they’ve been alive. Both have asthma and bronchopulmonary dysplasia, a form of chronic airway damage that can occur in children born premature, as the twins were. But each time Ms. Ward took them in for treatment during an acute bout of breathing distress, the staff told her to schedule a follow-up visit for the children with their physician only if they didn’t get better, not regardless of the outcome – as medical guidelines recommend.
“They asked questions, they did the exams, but they really didn’t give you a lot of information to help you at home,” Ms. Ward told this news organization. If they had, she doesn’t think she’d have needed to take them in for emergency care so often.
A new study, published in Academic Pediatrics, suggests she’s right.
Current clinical guidelines for asthma recommend that patients who visit the ED for an asthma-related problem should have a follow-up appointment within a month after the visit, independent of how well they have recovered once home, according to Naomi S. Bardach, MD, a professor of pediatrics and health policy at the University of California, San Francisco, who led the new study.
Her research found that children who have a follow-up appointment within 2 weeks of such a visit are less likely to come back again the next year. Yet the study also found that only about one in five youth had a follow-up visit within that 2-week window.
“The emergency department visit is probably a sign that they need some additional attention for their asthma,” Dr. Bardach said. “We know we can prevent emergency department visits if they get the right kind of medication or if they figure out how to avoid the things that are going to cause an asthma exacerbation or flare.”
For the study, Dr. Bardach and colleagues analyzed data from California, Vermont, and Massachusetts for all asthma-related emergency visits for patients aged 3-21 years between 2013 and 2016.
Out of the 90,267 such visits they identified, 22.6% of patients had a follow-up within 2 weeks, more often by patients who were younger, had commercial insurance, had evidence of prior asthma, or had complex chronic conditions.
Whereas 5.7% of patients who had follow-up visits returned to the ED within 60 days, 6.4% of those who didn’t came back – a 12% difference (P < .001). The gap was larger a year out, with 25% of those with follow-ups returning to the ED, compared with 28.3% of those without follow-ups returning (P < .001), according to the researchers.
Overall, Dr. Bardach’s group estimates that for every 30 children who have follow-up visits with a physician, one would avoid a return trip to the emergency department for asthma within a year.
But given the sheer number of asthma-related trips to the ED each year – 164,145 for kids age 1-17 years in the United States in 2016 alone – that translates into big numbers of kids not going back to the hospital: approximately 72,000 such trips avoided at a savings to the health care system of at least $8.6 million annually.
Missed opportunities
Had Ms. Ward’s boys been among the one in five to receive follow-up care earlier in their lives, she might have saved a significant amount of time, money, anxiety, and heartache. When the twins were 9 years old, she took them to a new pediatric pulmonologist. That changed everything. In that first visit, “they gave me way more information than I ever had in the first 9 years,” she said.
The doctor told Ms. Ward to keep steroids on hand, gave her a prescription for extra doses of the powerful medication, and explained that they needed to be used within 24 hours of the first sign of a breathing problem.
“She said if you give them the steroids right away, it keeps them out of the emergency room, and that’s actually worked,” Ms. Ward said. “She made sure we had care plans every visit and asked me each time if I still had it or we needed to rewrite it. They gave me signs to look for, for when to go to hospital visits. I think that when you go to the doctor, they should be telling you stuff like that.”
Dr. Bardach said visits with a primary care doctor or asthma specialist offer families a chance to receive information to keep the condition from becoming critical.
“Going to that follow-up visit, they can get access to education from the provider about how to avoid things that trigger asthma, and there’s medication that kids can take that keeps the lungs calm and less likely to have a big asthma reaction, so getting access to that medication can be really helpful,” she said.
That was the case for Amy Davenport, of Chapel Hill, N.C., whose 6-year-old son has been to the ED twice for his asthma.
The first time, when he was 3, he was having trouble breathing with a respiratory tract infection and received nebulizer treatment – although he received it in the ED since no beds were available in the ICU. The staff did tell Ms. Davenport to follow up with her primary care provider, but her son’s pediatrician was reluctant to diagnose him with asthma at such a young age and didn’t prescribe any maintenance medications.
A few months later, Ms. Davenport and her son found themselves back in the hospital, and an ICU bed was open this time. The critical care staff referred Davenport to a pediatric pulmonary specialist, and they haven’t been back to the hospital since. Ms. Davenport said she believes if they’d received a maintenance medication after the first visit, it likely would have prevented the second one.
“I’ve definitely seen now that, after the second admission, we got an asthma action plan and it said exactly what to do,” she said. “I felt like we had really good follow-up. We had that action plan on our refrigerator for a long time, and it helped us as parents with three small children to manage.”
Of course, follow-up care takes time – time away from work and school that not all families can spare, the researchers acknowledged. Telehealth may be an option, especially after its use expanded during the COVID-19 pandemic.
“We know that health systems have a hard time being flexible enough to actually have a kid be able to make an appointment within a short period of time, and we also know it’s hard for families sometimes to go back into a clinical setting within a certain period of time,” Dr. Bardach said. The urgency for the appointment may wane for those whose children seem to be doing better.
When the researchers adjusted their calculations for socioeconomic status, the results didn’t change much. But the study did find that patients with private insurance were about twice as likely to have follow-up visits as those on Medicaid (43.7% vs. 21.7%). And “the content and conduct” of the follow-up visit makes a difference as well.
Ms. Ward, whose boys are insured through Medicaid, recalled several visits to the ED where she had to push the staff to get the care her children needed. In one case, when one of her boys was a year old and struggling to breathe, the emergency doctor handed her a prescription and recommended she fill it at a neighborhood drugstore that would be cheaper than the hospital’s pharmacy. Then a nurse came in to begin the discharge process.
“I said no, ‘we’re not ready yet. Look at him,’” Ms. Ward said. The nurse took a pulse oximeter reading that showed the boy’s oxygen levels were at 84%, dangerously low. “If I wasn’t so knowledgeable and paid attention when they were born, since they were preemies, if it would have been somebody else, they probably would’ve went home and he’d have died.”
With the pediatric pulmonologist the boys have now, Ms. Ward said she feels more capable of managing their asthma and knowing how to reduce the likelihood that they’ll need to visit the ED.
“Part of what we’re seeing here is that having an existing and trusting relationship with a clinician can be helpful to kids with asthma,” Dr. Bardach said. “If we help establish and maintain those connections, and explain how important that connection can be, that can also help somebody with asthma overall.”
The research was funded by the Agency for Healthcare Research and Quality. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Jo Ward’s twin boys have been to the emergency department for respiratory problems about as many times as the dozen years they’ve been alive. Both have asthma and bronchopulmonary dysplasia, a form of chronic airway damage that can occur in children born premature, as the twins were. But each time Ms. Ward took them in for treatment during an acute bout of breathing distress, the staff told her to schedule a follow-up visit for the children with their physician only if they didn’t get better, not regardless of the outcome – as medical guidelines recommend.
“They asked questions, they did the exams, but they really didn’t give you a lot of information to help you at home,” Ms. Ward told this news organization. If they had, she doesn’t think she’d have needed to take them in for emergency care so often.
A new study, published in Academic Pediatrics, suggests she’s right.
Current clinical guidelines for asthma recommend that patients who visit the ED for an asthma-related problem should have a follow-up appointment within a month after the visit, independent of how well they have recovered once home, according to Naomi S. Bardach, MD, a professor of pediatrics and health policy at the University of California, San Francisco, who led the new study.
Her research found that children who have a follow-up appointment within 2 weeks of such a visit are less likely to come back again the next year. Yet the study also found that only about one in five youth had a follow-up visit within that 2-week window.
“The emergency department visit is probably a sign that they need some additional attention for their asthma,” Dr. Bardach said. “We know we can prevent emergency department visits if they get the right kind of medication or if they figure out how to avoid the things that are going to cause an asthma exacerbation or flare.”
For the study, Dr. Bardach and colleagues analyzed data from California, Vermont, and Massachusetts for all asthma-related emergency visits for patients aged 3-21 years between 2013 and 2016.
Out of the 90,267 such visits they identified, 22.6% of patients had a follow-up within 2 weeks, more often by patients who were younger, had commercial insurance, had evidence of prior asthma, or had complex chronic conditions.
Whereas 5.7% of patients who had follow-up visits returned to the ED within 60 days, 6.4% of those who didn’t came back – a 12% difference (P < .001). The gap was larger a year out, with 25% of those with follow-ups returning to the ED, compared with 28.3% of those without follow-ups returning (P < .001), according to the researchers.
Overall, Dr. Bardach’s group estimates that for every 30 children who have follow-up visits with a physician, one would avoid a return trip to the emergency department for asthma within a year.
But given the sheer number of asthma-related trips to the ED each year – 164,145 for kids age 1-17 years in the United States in 2016 alone – that translates into big numbers of kids not going back to the hospital: approximately 72,000 such trips avoided at a savings to the health care system of at least $8.6 million annually.
Missed opportunities
Had Ms. Ward’s boys been among the one in five to receive follow-up care earlier in their lives, she might have saved a significant amount of time, money, anxiety, and heartache. When the twins were 9 years old, she took them to a new pediatric pulmonologist. That changed everything. In that first visit, “they gave me way more information than I ever had in the first 9 years,” she said.
The doctor told Ms. Ward to keep steroids on hand, gave her a prescription for extra doses of the powerful medication, and explained that they needed to be used within 24 hours of the first sign of a breathing problem.
“She said if you give them the steroids right away, it keeps them out of the emergency room, and that’s actually worked,” Ms. Ward said. “She made sure we had care plans every visit and asked me each time if I still had it or we needed to rewrite it. They gave me signs to look for, for when to go to hospital visits. I think that when you go to the doctor, they should be telling you stuff like that.”
Dr. Bardach said visits with a primary care doctor or asthma specialist offer families a chance to receive information to keep the condition from becoming critical.
“Going to that follow-up visit, they can get access to education from the provider about how to avoid things that trigger asthma, and there’s medication that kids can take that keeps the lungs calm and less likely to have a big asthma reaction, so getting access to that medication can be really helpful,” she said.
That was the case for Amy Davenport, of Chapel Hill, N.C., whose 6-year-old son has been to the ED twice for his asthma.
The first time, when he was 3, he was having trouble breathing with a respiratory tract infection and received nebulizer treatment – although he received it in the ED since no beds were available in the ICU. The staff did tell Ms. Davenport to follow up with her primary care provider, but her son’s pediatrician was reluctant to diagnose him with asthma at such a young age and didn’t prescribe any maintenance medications.
A few months later, Ms. Davenport and her son found themselves back in the hospital, and an ICU bed was open this time. The critical care staff referred Davenport to a pediatric pulmonary specialist, and they haven’t been back to the hospital since. Ms. Davenport said she believes if they’d received a maintenance medication after the first visit, it likely would have prevented the second one.
“I’ve definitely seen now that, after the second admission, we got an asthma action plan and it said exactly what to do,” she said. “I felt like we had really good follow-up. We had that action plan on our refrigerator for a long time, and it helped us as parents with three small children to manage.”
Of course, follow-up care takes time – time away from work and school that not all families can spare, the researchers acknowledged. Telehealth may be an option, especially after its use expanded during the COVID-19 pandemic.
“We know that health systems have a hard time being flexible enough to actually have a kid be able to make an appointment within a short period of time, and we also know it’s hard for families sometimes to go back into a clinical setting within a certain period of time,” Dr. Bardach said. The urgency for the appointment may wane for those whose children seem to be doing better.
When the researchers adjusted their calculations for socioeconomic status, the results didn’t change much. But the study did find that patients with private insurance were about twice as likely to have follow-up visits as those on Medicaid (43.7% vs. 21.7%). And “the content and conduct” of the follow-up visit makes a difference as well.
Ms. Ward, whose boys are insured through Medicaid, recalled several visits to the ED where she had to push the staff to get the care her children needed. In one case, when one of her boys was a year old and struggling to breathe, the emergency doctor handed her a prescription and recommended she fill it at a neighborhood drugstore that would be cheaper than the hospital’s pharmacy. Then a nurse came in to begin the discharge process.
“I said no, ‘we’re not ready yet. Look at him,’” Ms. Ward said. The nurse took a pulse oximeter reading that showed the boy’s oxygen levels were at 84%, dangerously low. “If I wasn’t so knowledgeable and paid attention when they were born, since they were preemies, if it would have been somebody else, they probably would’ve went home and he’d have died.”
With the pediatric pulmonologist the boys have now, Ms. Ward said she feels more capable of managing their asthma and knowing how to reduce the likelihood that they’ll need to visit the ED.
“Part of what we’re seeing here is that having an existing and trusting relationship with a clinician can be helpful to kids with asthma,” Dr. Bardach said. “If we help establish and maintain those connections, and explain how important that connection can be, that can also help somebody with asthma overall.”
The research was funded by the Agency for Healthcare Research and Quality. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACADEMIC PEDIATRICS
New Barrett’s esophagus guideline reduces reliance on endoscopy
A swallowable, capsule-sponge device used to sample biomarkers offers a reliable, noninvasive alternative to endoscopy for diagnosing Barrett’s esophagus, according to a new guideline from the American College of Gastroenterology.
In addition, the guideline recommends that patients with Barrett’s esophagus with segments of less than 3 cm be screened every 5 years, but if their Barrett’s esophagus segments are 5 cm or greater, they should be screened every 3 years.
“We don’t want to scope everyone for the lowest risk of cancer,” lead author Nicholas J. Shaheen, MD, MPH, chief of gastroenterology and hepatology at the University of North Carolina School of Medicine, Chapel Hill, told this news organization.
“The traditional way to diagnose Barrett’s esophagus is by upper endoscopy, but it’s expensive and not available everywhere,” he said. “One big change since the last iteration of this guideline is that there’s been a development of nonendoscopic screening modalities.”
The guideline was published in The American Journal of Gastroenterology.
Progress with swallowable devices
Solid evidence supports the Cytosponge, a capsule containing a compressed spherical polyurethane sponge attached to a string. The sponge expands to a sphere when the capsule dissolves after being swallowed, Dr. Shaheen said.
When withdrawn, the sponge contains esophageal cytology samples that can be used to identify biomarkers for Barrett’s esophagus, either the protein trefoil factor 3 expressed in intestinal metaplasia or methylated DNA markers associated with Barrett’s esophagus mucosa.
More than 90% of participants in trials have been able to swallow the device. Some mild gagging or throat discomfort has been reported.
In one trial, patients with chronic reflux were randomly assigned to either swallow the Cytosponge or be screened by endoscopy based on the practitioner’s usual care. Any diagnosis with the Cytosponge was confirmed with endoscopy. Barrett’s esophagus was found in 2% of patients who had undergone the Cytosponge procedure, versus less than 1% of those screened in the usual way. Of the 6,834 patients in the Cytosponge group, nine were diagnosed with dysplastic Barrett’s esophagus or stage I esophagogastric cancer, versus none of the 6,388 participants in the usual-care group.
“At least for now, we’re using the same guidance that we used for endoscopy to decide who might be best served by these devices,” Dr. Shaheen said. “There are not good data to make a recommendation yet, but you could easily imagine how you could broaden screening guidelines by having a cheaper, more available test.”
Screening for esophageal cancer may one day be as common as screening for colon cancer, said Herbert C. Wolfsen, MD, a consultant in gastroenterology at the Mayo Clinic in Jacksonville, Florida, and professor of medicine at the Mayo Clinic College of Medicine, Rochester, Minn. He was not involved in writing the new guideline.
“We’ve known for years that at least half of patients with esophageal cancer have little, if any, reflux symptoms,” he told this news organization. “This is an area where the guidelines have been consistent, but I think we’re going to see them start to change.”
Additional recommendations
The expert panel of the new guideline held off on recommending the use of biomarkers more generally, deeming the evidence insufficient.
The new guideline also endorses endoscopic treatment for dysplastic Barrett’s esophagus but not for Barrett’s esophagus with no dysplasia.
For the first time, it recommends that patients undergo surveillance after successful ablation.
Dr. Wolfsen took note of the guideline’s recommendation that clinicians benchmark their practices against published standards.
The guideline mentions “documentation of landmarks and extent of [Barrett’s esophagus], not obtaining biopsies in the setting of a normal-appearing squamocolumnar junction, sampling using the Seattle biopsy protocol, and performing surveillance endoscopy in patients with [nondysplastic Barrett’s esophagus] no sooner than 3-5 years.”
“The acceptance and implementation of these quality metrics is important,” Dr. Wolfsen said.
However, the guideline underscores the need for considerably more research, he added.
“This group did a fabulous job,” Dr. Wolfsen said. “But when it comes to getting a consensus and people on board, all headed in the same direction, it’s hard when you’re not working with very good data.”
Dr. Shaheen reports financial relationships with Medtronic, Steris, Pentax, CDx Diagnostics, Interpace Diagnostics, Lucid Medical, Cernostics, Phathom Pharmaceuticals, Exact Sciences, Aqua Medical, and Cook Medical. Dr. Wolfsen reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A swallowable, capsule-sponge device used to sample biomarkers offers a reliable, noninvasive alternative to endoscopy for diagnosing Barrett’s esophagus, according to a new guideline from the American College of Gastroenterology.
In addition, the guideline recommends that patients with Barrett’s esophagus with segments of less than 3 cm be screened every 5 years, but if their Barrett’s esophagus segments are 5 cm or greater, they should be screened every 3 years.
“We don’t want to scope everyone for the lowest risk of cancer,” lead author Nicholas J. Shaheen, MD, MPH, chief of gastroenterology and hepatology at the University of North Carolina School of Medicine, Chapel Hill, told this news organization.
“The traditional way to diagnose Barrett’s esophagus is by upper endoscopy, but it’s expensive and not available everywhere,” he said. “One big change since the last iteration of this guideline is that there’s been a development of nonendoscopic screening modalities.”
The guideline was published in The American Journal of Gastroenterology.
Progress with swallowable devices
Solid evidence supports the Cytosponge, a capsule containing a compressed spherical polyurethane sponge attached to a string. The sponge expands to a sphere when the capsule dissolves after being swallowed, Dr. Shaheen said.
When withdrawn, the sponge contains esophageal cytology samples that can be used to identify biomarkers for Barrett’s esophagus, either the protein trefoil factor 3 expressed in intestinal metaplasia or methylated DNA markers associated with Barrett’s esophagus mucosa.
More than 90% of participants in trials have been able to swallow the device. Some mild gagging or throat discomfort has been reported.
In one trial, patients with chronic reflux were randomly assigned to either swallow the Cytosponge or be screened by endoscopy based on the practitioner’s usual care. Any diagnosis with the Cytosponge was confirmed with endoscopy. Barrett’s esophagus was found in 2% of patients who had undergone the Cytosponge procedure, versus less than 1% of those screened in the usual way. Of the 6,834 patients in the Cytosponge group, nine were diagnosed with dysplastic Barrett’s esophagus or stage I esophagogastric cancer, versus none of the 6,388 participants in the usual-care group.
“At least for now, we’re using the same guidance that we used for endoscopy to decide who might be best served by these devices,” Dr. Shaheen said. “There are not good data to make a recommendation yet, but you could easily imagine how you could broaden screening guidelines by having a cheaper, more available test.”
Screening for esophageal cancer may one day be as common as screening for colon cancer, said Herbert C. Wolfsen, MD, a consultant in gastroenterology at the Mayo Clinic in Jacksonville, Florida, and professor of medicine at the Mayo Clinic College of Medicine, Rochester, Minn. He was not involved in writing the new guideline.
“We’ve known for years that at least half of patients with esophageal cancer have little, if any, reflux symptoms,” he told this news organization. “This is an area where the guidelines have been consistent, but I think we’re going to see them start to change.”
Additional recommendations
The expert panel of the new guideline held off on recommending the use of biomarkers more generally, deeming the evidence insufficient.
The new guideline also endorses endoscopic treatment for dysplastic Barrett’s esophagus but not for Barrett’s esophagus with no dysplasia.
For the first time, it recommends that patients undergo surveillance after successful ablation.
Dr. Wolfsen took note of the guideline’s recommendation that clinicians benchmark their practices against published standards.
The guideline mentions “documentation of landmarks and extent of [Barrett’s esophagus], not obtaining biopsies in the setting of a normal-appearing squamocolumnar junction, sampling using the Seattle biopsy protocol, and performing surveillance endoscopy in patients with [nondysplastic Barrett’s esophagus] no sooner than 3-5 years.”
“The acceptance and implementation of these quality metrics is important,” Dr. Wolfsen said.
However, the guideline underscores the need for considerably more research, he added.
“This group did a fabulous job,” Dr. Wolfsen said. “But when it comes to getting a consensus and people on board, all headed in the same direction, it’s hard when you’re not working with very good data.”
Dr. Shaheen reports financial relationships with Medtronic, Steris, Pentax, CDx Diagnostics, Interpace Diagnostics, Lucid Medical, Cernostics, Phathom Pharmaceuticals, Exact Sciences, Aqua Medical, and Cook Medical. Dr. Wolfsen reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A swallowable, capsule-sponge device used to sample biomarkers offers a reliable, noninvasive alternative to endoscopy for diagnosing Barrett’s esophagus, according to a new guideline from the American College of Gastroenterology.
In addition, the guideline recommends that patients with Barrett’s esophagus with segments of less than 3 cm be screened every 5 years, but if their Barrett’s esophagus segments are 5 cm or greater, they should be screened every 3 years.
“We don’t want to scope everyone for the lowest risk of cancer,” lead author Nicholas J. Shaheen, MD, MPH, chief of gastroenterology and hepatology at the University of North Carolina School of Medicine, Chapel Hill, told this news organization.
“The traditional way to diagnose Barrett’s esophagus is by upper endoscopy, but it’s expensive and not available everywhere,” he said. “One big change since the last iteration of this guideline is that there’s been a development of nonendoscopic screening modalities.”
The guideline was published in The American Journal of Gastroenterology.
Progress with swallowable devices
Solid evidence supports the Cytosponge, a capsule containing a compressed spherical polyurethane sponge attached to a string. The sponge expands to a sphere when the capsule dissolves after being swallowed, Dr. Shaheen said.
When withdrawn, the sponge contains esophageal cytology samples that can be used to identify biomarkers for Barrett’s esophagus, either the protein trefoil factor 3 expressed in intestinal metaplasia or methylated DNA markers associated with Barrett’s esophagus mucosa.
More than 90% of participants in trials have been able to swallow the device. Some mild gagging or throat discomfort has been reported.
In one trial, patients with chronic reflux were randomly assigned to either swallow the Cytosponge or be screened by endoscopy based on the practitioner’s usual care. Any diagnosis with the Cytosponge was confirmed with endoscopy. Barrett’s esophagus was found in 2% of patients who had undergone the Cytosponge procedure, versus less than 1% of those screened in the usual way. Of the 6,834 patients in the Cytosponge group, nine were diagnosed with dysplastic Barrett’s esophagus or stage I esophagogastric cancer, versus none of the 6,388 participants in the usual-care group.
“At least for now, we’re using the same guidance that we used for endoscopy to decide who might be best served by these devices,” Dr. Shaheen said. “There are not good data to make a recommendation yet, but you could easily imagine how you could broaden screening guidelines by having a cheaper, more available test.”
Screening for esophageal cancer may one day be as common as screening for colon cancer, said Herbert C. Wolfsen, MD, a consultant in gastroenterology at the Mayo Clinic in Jacksonville, Florida, and professor of medicine at the Mayo Clinic College of Medicine, Rochester, Minn. He was not involved in writing the new guideline.
“We’ve known for years that at least half of patients with esophageal cancer have little, if any, reflux symptoms,” he told this news organization. “This is an area where the guidelines have been consistent, but I think we’re going to see them start to change.”
Additional recommendations
The expert panel of the new guideline held off on recommending the use of biomarkers more generally, deeming the evidence insufficient.
The new guideline also endorses endoscopic treatment for dysplastic Barrett’s esophagus but not for Barrett’s esophagus with no dysplasia.
For the first time, it recommends that patients undergo surveillance after successful ablation.
Dr. Wolfsen took note of the guideline’s recommendation that clinicians benchmark their practices against published standards.
The guideline mentions “documentation of landmarks and extent of [Barrett’s esophagus], not obtaining biopsies in the setting of a normal-appearing squamocolumnar junction, sampling using the Seattle biopsy protocol, and performing surveillance endoscopy in patients with [nondysplastic Barrett’s esophagus] no sooner than 3-5 years.”
“The acceptance and implementation of these quality metrics is important,” Dr. Wolfsen said.
However, the guideline underscores the need for considerably more research, he added.
“This group did a fabulous job,” Dr. Wolfsen said. “But when it comes to getting a consensus and people on board, all headed in the same direction, it’s hard when you’re not working with very good data.”
Dr. Shaheen reports financial relationships with Medtronic, Steris, Pentax, CDx Diagnostics, Interpace Diagnostics, Lucid Medical, Cernostics, Phathom Pharmaceuticals, Exact Sciences, Aqua Medical, and Cook Medical. Dr. Wolfsen reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Statins tied to lower risk for parkinsonism
, new research suggests. An observational study showed older adults taking statins had a lower risk for parkinsonism than their counterparts not taking statins – an effect that may be partially mediated by less severe intracranial atherosclerosis in statin users.
“These findings further support the idea that cerebrovascular disease pathologies accumulating in older brains may be an unrecognized contributor to the common occurrence of parkinsonism in old age,” the investigators wrote. “More importantly, these findings suggest that statins may have a potential therapeutic role in decreasing the magnitude of parkinsonism in older adults,” they added.
The study was published online in Neurology.
No clinical recommendations ... yet
The findings are based on 2,841 older adults enrolled in one of three ongoing clinical pathological studies at Rush Alzheimer’s Disease Center, Chicago.
Participants’ average age at baseline was 76 years, and 75% were women. None had parkinsonism at the start of the study. One-third of participants (n = 936) were taking statins. During an average follow-up of 6 years, 1,432 (50%) participants developed parkinsonism.
After controlling for demographics, vascular risk factors, and diseases, use of a statin at baseline was associated with a 16% lower risk for parkinsonism (hazard ratio, 0.84; 95% confidence interval, 0.74-0.96; P = .008). Compared with low-intensity statin therapy, moderate- or high-intensity statin therapy was associated with a 7% lower risk for parkinsonism (HR, 0.93; 95% CI, 0.87-1.00; P = .043).
The researchers also examined the brains of 1,044 people who died during the study at a mean age of 89 years. They found statin use prior to death was associated with a 37% lower odds of cerebral atherosclerosis, compared with no statin use prior to death (odds ratio, 0.63; 95% CI, 0.50-0.79; P < .001).
In a mediation analysis, both a direct (OR, 0.73; 95% CI, 0.54-0.93; P = .008) and an indirect (OR, 0.92; 95% CI, 0.88-0.97; P = .002) pathway via less severe cerebrovascular disease linked statins to parkinsonism, indicating that cerebral atherosclerosis mediated 17% of the association between statins and parkinsonism.
In line with other studies, there was no association between statins and other neurodegenerative pathologies, including Parkinson’s disease pathology. However, even older adults with a clinical diagnosis of Parkinson’s disease often show mixed brain pathologies, including cerebrovascular disease pathologies.
“Therefore, we think that statins may be beneficial against parkinsonism in patients with Parkinson’s disease, dependent on how much cerebrovascular disease pathologies they have, including atherosclerosis,” said study investigator Shahram Oveisgharan, MD, with Rush Alzheimer’s Disease Center, Rush University Medical Center, Chicago.
However, since the results stem from an observational study, “we do not yet recommend using statins in large scale for older adults at risk for parkinsonism,” Dr. Oveisgharan said.
A mixed picture
Reached for comment, Shaheen Lakhan, MD, neurologist in Newton, Massachusetts, noted that since statins were first discovered in the fermented broth of a common soil fungus in the late 1970s, they have proven to reduce cholesterol, heart disease, and stroke.
“The jury is out, however, on [their] effects on diseases such as dementia, autoimmune/inflammatory conditions, bacterial/viral infections, cancer, and parkinsonism,” he said.
“Also, the question often remains whether any benefit gained from statins is from cholesterol-lowering or through another mechanism. When there is such a mixed picture, it generally means that the drug has an effect, but not for everyone,” Dr. Lakhan said. “Much work must now be done to stratify for which patients are statins effective, ineffective, or even harmful in these conditions,” he added.
The study was supported by the National Institutes of Health. Dr. Oveisgharan and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. An observational study showed older adults taking statins had a lower risk for parkinsonism than their counterparts not taking statins – an effect that may be partially mediated by less severe intracranial atherosclerosis in statin users.
“These findings further support the idea that cerebrovascular disease pathologies accumulating in older brains may be an unrecognized contributor to the common occurrence of parkinsonism in old age,” the investigators wrote. “More importantly, these findings suggest that statins may have a potential therapeutic role in decreasing the magnitude of parkinsonism in older adults,” they added.
The study was published online in Neurology.
No clinical recommendations ... yet
The findings are based on 2,841 older adults enrolled in one of three ongoing clinical pathological studies at Rush Alzheimer’s Disease Center, Chicago.
Participants’ average age at baseline was 76 years, and 75% were women. None had parkinsonism at the start of the study. One-third of participants (n = 936) were taking statins. During an average follow-up of 6 years, 1,432 (50%) participants developed parkinsonism.
After controlling for demographics, vascular risk factors, and diseases, use of a statin at baseline was associated with a 16% lower risk for parkinsonism (hazard ratio, 0.84; 95% confidence interval, 0.74-0.96; P = .008). Compared with low-intensity statin therapy, moderate- or high-intensity statin therapy was associated with a 7% lower risk for parkinsonism (HR, 0.93; 95% CI, 0.87-1.00; P = .043).
The researchers also examined the brains of 1,044 people who died during the study at a mean age of 89 years. They found statin use prior to death was associated with a 37% lower odds of cerebral atherosclerosis, compared with no statin use prior to death (odds ratio, 0.63; 95% CI, 0.50-0.79; P < .001).
In a mediation analysis, both a direct (OR, 0.73; 95% CI, 0.54-0.93; P = .008) and an indirect (OR, 0.92; 95% CI, 0.88-0.97; P = .002) pathway via less severe cerebrovascular disease linked statins to parkinsonism, indicating that cerebral atherosclerosis mediated 17% of the association between statins and parkinsonism.
In line with other studies, there was no association between statins and other neurodegenerative pathologies, including Parkinson’s disease pathology. However, even older adults with a clinical diagnosis of Parkinson’s disease often show mixed brain pathologies, including cerebrovascular disease pathologies.
“Therefore, we think that statins may be beneficial against parkinsonism in patients with Parkinson’s disease, dependent on how much cerebrovascular disease pathologies they have, including atherosclerosis,” said study investigator Shahram Oveisgharan, MD, with Rush Alzheimer’s Disease Center, Rush University Medical Center, Chicago.
However, since the results stem from an observational study, “we do not yet recommend using statins in large scale for older adults at risk for parkinsonism,” Dr. Oveisgharan said.
A mixed picture
Reached for comment, Shaheen Lakhan, MD, neurologist in Newton, Massachusetts, noted that since statins were first discovered in the fermented broth of a common soil fungus in the late 1970s, they have proven to reduce cholesterol, heart disease, and stroke.
“The jury is out, however, on [their] effects on diseases such as dementia, autoimmune/inflammatory conditions, bacterial/viral infections, cancer, and parkinsonism,” he said.
“Also, the question often remains whether any benefit gained from statins is from cholesterol-lowering or through another mechanism. When there is such a mixed picture, it generally means that the drug has an effect, but not for everyone,” Dr. Lakhan said. “Much work must now be done to stratify for which patients are statins effective, ineffective, or even harmful in these conditions,” he added.
The study was supported by the National Institutes of Health. Dr. Oveisgharan and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. An observational study showed older adults taking statins had a lower risk for parkinsonism than their counterparts not taking statins – an effect that may be partially mediated by less severe intracranial atherosclerosis in statin users.
“These findings further support the idea that cerebrovascular disease pathologies accumulating in older brains may be an unrecognized contributor to the common occurrence of parkinsonism in old age,” the investigators wrote. “More importantly, these findings suggest that statins may have a potential therapeutic role in decreasing the magnitude of parkinsonism in older adults,” they added.
The study was published online in Neurology.
No clinical recommendations ... yet
The findings are based on 2,841 older adults enrolled in one of three ongoing clinical pathological studies at Rush Alzheimer’s Disease Center, Chicago.
Participants’ average age at baseline was 76 years, and 75% were women. None had parkinsonism at the start of the study. One-third of participants (n = 936) were taking statins. During an average follow-up of 6 years, 1,432 (50%) participants developed parkinsonism.
After controlling for demographics, vascular risk factors, and diseases, use of a statin at baseline was associated with a 16% lower risk for parkinsonism (hazard ratio, 0.84; 95% confidence interval, 0.74-0.96; P = .008). Compared with low-intensity statin therapy, moderate- or high-intensity statin therapy was associated with a 7% lower risk for parkinsonism (HR, 0.93; 95% CI, 0.87-1.00; P = .043).
The researchers also examined the brains of 1,044 people who died during the study at a mean age of 89 years. They found statin use prior to death was associated with a 37% lower odds of cerebral atherosclerosis, compared with no statin use prior to death (odds ratio, 0.63; 95% CI, 0.50-0.79; P < .001).
In a mediation analysis, both a direct (OR, 0.73; 95% CI, 0.54-0.93; P = .008) and an indirect (OR, 0.92; 95% CI, 0.88-0.97; P = .002) pathway via less severe cerebrovascular disease linked statins to parkinsonism, indicating that cerebral atherosclerosis mediated 17% of the association between statins and parkinsonism.
In line with other studies, there was no association between statins and other neurodegenerative pathologies, including Parkinson’s disease pathology. However, even older adults with a clinical diagnosis of Parkinson’s disease often show mixed brain pathologies, including cerebrovascular disease pathologies.
“Therefore, we think that statins may be beneficial against parkinsonism in patients with Parkinson’s disease, dependent on how much cerebrovascular disease pathologies they have, including atherosclerosis,” said study investigator Shahram Oveisgharan, MD, with Rush Alzheimer’s Disease Center, Rush University Medical Center, Chicago.
However, since the results stem from an observational study, “we do not yet recommend using statins in large scale for older adults at risk for parkinsonism,” Dr. Oveisgharan said.
A mixed picture
Reached for comment, Shaheen Lakhan, MD, neurologist in Newton, Massachusetts, noted that since statins were first discovered in the fermented broth of a common soil fungus in the late 1970s, they have proven to reduce cholesterol, heart disease, and stroke.
“The jury is out, however, on [their] effects on diseases such as dementia, autoimmune/inflammatory conditions, bacterial/viral infections, cancer, and parkinsonism,” he said.
“Also, the question often remains whether any benefit gained from statins is from cholesterol-lowering or through another mechanism. When there is such a mixed picture, it generally means that the drug has an effect, but not for everyone,” Dr. Lakhan said. “Much work must now be done to stratify for which patients are statins effective, ineffective, or even harmful in these conditions,” he added.
The study was supported by the National Institutes of Health. Dr. Oveisgharan and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Anticipation key to tackling perioperative anemia
MANCHESTER, ENGLAND –
Anemia management may include dietary changes, iron supplementation, blood transfusion, perioperative physiological optimization, delay or review of the surgical plan, medication reviews, and greater intraoperative care.
It is quite clear that patients have a better experience if management covers the whole pathway, said lead author of the guidelines, Scarlett McNally, MD, PhD, East Sussex Healthcare NHS Trust, Eastbourne, England.
It’s much better for the patient “if every individual member of staff knows what’s supposed to happen, not just for their bit, but the whole way along,” she said. “Otherwise things go wrong, and people don’t anticipate things early enough.”
The new guidelines, to be published in full later this year by the Centre for Perioperative Care, cover emergency and elective surgery for all ages.
It follows the 2021 publication of a guideline for perioperative diabetes management, and a previous document that covered frailty.
Dr. McNally was presenting the new guidelines on perioperative anemia at the British Society for Haematology 62nd Annual Scientific Meeting.
Although perioperative anemia is a “big issue” in clinical management, “some health care professionals know a lot about one area,” but tend to work in “silos,” Dr. McNally said.
The result is clinicians believe that all other areas are “complex” and opaque, and they “don’t make the simple decisions” that could have a big impact on patient care.
As an example, she said there are already some excellent guidelines out there, but they are not widely read.
One example of a comprehensive guideline, Dr. McNally said, is that issued by the British Society of Gastroenterology. This guideline notes that in cases where a man or a postmenopausal woman has anemia of unknown cause, about 30% of those cases end up having a gastrointestinal cause, and so gastroenterologists are happy to have those patients referred to them.
But Dr. McNally said that she personally, as an orthopedic surgeon, wouldn’t have known what to do with such a patient, and may have referred that person back to primary care to be investigated.
The new guidelines contain algorithms to help staff plan care. Without those, she said, “a lot is resting on the preassessment nurses, but they are having to think about everything else.”
The guidance suggests proactive measures to identify and manage anemia. These include testing for anemia while assessing renal function ahead of a CT scan, or asking patients about their nutrition.
For low-risk patients, it may be enough to give general advice about a good diet and exercise to try to get them through the operation.
However, patients who are high risk (defined as likely to lose > 500 mL or > 10% of blood volume during surgery) need to be identified as such early on, so that early measures can be put in place, as well as a senior review of their care plan.
The guidelines also recommend that operating room staff consider tranexamic acid and other bloodless minimization strategies, and that senior staff give clinical input in cases of functional iron deficiency, a marker of ill health.
To maximize postoperative outcomes, it is suggested that staff work with prehabilitation services and mobilize patients, as symptoms allow.
More importantly, they emphasize the need for shared decision-making about potential surgery, ensuring that the patients understand “Benefits, Risks, Alternatives, and what if we do Nothing (BRAN).”
No funding was declared. One study author declared relationships with the National Institute for Health Research and Pfizer.
A version of this article first appeared on Medscape.com.
MANCHESTER, ENGLAND –
Anemia management may include dietary changes, iron supplementation, blood transfusion, perioperative physiological optimization, delay or review of the surgical plan, medication reviews, and greater intraoperative care.
It is quite clear that patients have a better experience if management covers the whole pathway, said lead author of the guidelines, Scarlett McNally, MD, PhD, East Sussex Healthcare NHS Trust, Eastbourne, England.
It’s much better for the patient “if every individual member of staff knows what’s supposed to happen, not just for their bit, but the whole way along,” she said. “Otherwise things go wrong, and people don’t anticipate things early enough.”
The new guidelines, to be published in full later this year by the Centre for Perioperative Care, cover emergency and elective surgery for all ages.
It follows the 2021 publication of a guideline for perioperative diabetes management, and a previous document that covered frailty.
Dr. McNally was presenting the new guidelines on perioperative anemia at the British Society for Haematology 62nd Annual Scientific Meeting.
Although perioperative anemia is a “big issue” in clinical management, “some health care professionals know a lot about one area,” but tend to work in “silos,” Dr. McNally said.
The result is clinicians believe that all other areas are “complex” and opaque, and they “don’t make the simple decisions” that could have a big impact on patient care.
As an example, she said there are already some excellent guidelines out there, but they are not widely read.
One example of a comprehensive guideline, Dr. McNally said, is that issued by the British Society of Gastroenterology. This guideline notes that in cases where a man or a postmenopausal woman has anemia of unknown cause, about 30% of those cases end up having a gastrointestinal cause, and so gastroenterologists are happy to have those patients referred to them.
But Dr. McNally said that she personally, as an orthopedic surgeon, wouldn’t have known what to do with such a patient, and may have referred that person back to primary care to be investigated.
The new guidelines contain algorithms to help staff plan care. Without those, she said, “a lot is resting on the preassessment nurses, but they are having to think about everything else.”
The guidance suggests proactive measures to identify and manage anemia. These include testing for anemia while assessing renal function ahead of a CT scan, or asking patients about their nutrition.
For low-risk patients, it may be enough to give general advice about a good diet and exercise to try to get them through the operation.
However, patients who are high risk (defined as likely to lose > 500 mL or > 10% of blood volume during surgery) need to be identified as such early on, so that early measures can be put in place, as well as a senior review of their care plan.
The guidelines also recommend that operating room staff consider tranexamic acid and other bloodless minimization strategies, and that senior staff give clinical input in cases of functional iron deficiency, a marker of ill health.
To maximize postoperative outcomes, it is suggested that staff work with prehabilitation services and mobilize patients, as symptoms allow.
More importantly, they emphasize the need for shared decision-making about potential surgery, ensuring that the patients understand “Benefits, Risks, Alternatives, and what if we do Nothing (BRAN).”
No funding was declared. One study author declared relationships with the National Institute for Health Research and Pfizer.
A version of this article first appeared on Medscape.com.
MANCHESTER, ENGLAND –
Anemia management may include dietary changes, iron supplementation, blood transfusion, perioperative physiological optimization, delay or review of the surgical plan, medication reviews, and greater intraoperative care.
It is quite clear that patients have a better experience if management covers the whole pathway, said lead author of the guidelines, Scarlett McNally, MD, PhD, East Sussex Healthcare NHS Trust, Eastbourne, England.
It’s much better for the patient “if every individual member of staff knows what’s supposed to happen, not just for their bit, but the whole way along,” she said. “Otherwise things go wrong, and people don’t anticipate things early enough.”
The new guidelines, to be published in full later this year by the Centre for Perioperative Care, cover emergency and elective surgery for all ages.
It follows the 2021 publication of a guideline for perioperative diabetes management, and a previous document that covered frailty.
Dr. McNally was presenting the new guidelines on perioperative anemia at the British Society for Haematology 62nd Annual Scientific Meeting.
Although perioperative anemia is a “big issue” in clinical management, “some health care professionals know a lot about one area,” but tend to work in “silos,” Dr. McNally said.
The result is clinicians believe that all other areas are “complex” and opaque, and they “don’t make the simple decisions” that could have a big impact on patient care.
As an example, she said there are already some excellent guidelines out there, but they are not widely read.
One example of a comprehensive guideline, Dr. McNally said, is that issued by the British Society of Gastroenterology. This guideline notes that in cases where a man or a postmenopausal woman has anemia of unknown cause, about 30% of those cases end up having a gastrointestinal cause, and so gastroenterologists are happy to have those patients referred to them.
But Dr. McNally said that she personally, as an orthopedic surgeon, wouldn’t have known what to do with such a patient, and may have referred that person back to primary care to be investigated.
The new guidelines contain algorithms to help staff plan care. Without those, she said, “a lot is resting on the preassessment nurses, but they are having to think about everything else.”
The guidance suggests proactive measures to identify and manage anemia. These include testing for anemia while assessing renal function ahead of a CT scan, or asking patients about their nutrition.
For low-risk patients, it may be enough to give general advice about a good diet and exercise to try to get them through the operation.
However, patients who are high risk (defined as likely to lose > 500 mL or > 10% of blood volume during surgery) need to be identified as such early on, so that early measures can be put in place, as well as a senior review of their care plan.
The guidelines also recommend that operating room staff consider tranexamic acid and other bloodless minimization strategies, and that senior staff give clinical input in cases of functional iron deficiency, a marker of ill health.
To maximize postoperative outcomes, it is suggested that staff work with prehabilitation services and mobilize patients, as symptoms allow.
More importantly, they emphasize the need for shared decision-making about potential surgery, ensuring that the patients understand “Benefits, Risks, Alternatives, and what if we do Nothing (BRAN).”
No funding was declared. One study author declared relationships with the National Institute for Health Research and Pfizer.
A version of this article first appeared on Medscape.com.
Psilocybin ‘rewires’ the brain to alleviate depression
Led by investigators from the University of California, San Francisco, and Imperial College London’s Centre for Psychedelic Research, the findings come from a new analysis of brain scans of almost 60 patients with resistant depression treated with psilocybin.

“Not much is known about the changes in brain function after psychedelic experience. There has been much more research done on the acute brain action of psychedelics, but there is very little on the postacute or subacute changes in brain function,” study investigator Robin Carhart-Harris, PhD, former head of the Imperial Centre for Psychedelic Research and now director of the Neuroscape psychedelics division at UCSF, and senior author of the study, told this news organization.
“This research is a major advance because it is showing replication across two datasets with different designs. One in which the scanning is done 1 day after intervention and the other one when the posttreatment scanning is done 3 weeks after the second of two psilocybin therapy sessions,” Dr. Carhart-Harris added.
The study was published online in Nature Medicine.
A disruptor?
Psilocybin is one of a number of psychedelics under investigation as a potential therapy for psychiatric disorders. In the last 15 years, at least six separate clinical trials have reported impressive improvements in depressive symptoms with psilocybin therapy. Several studies have tested a synthesized a form of the drug to treat patients with depression and anxiety – with promising results.
However, the therapeutic action of psilocybin and other serotonergic psychedelics is still not completely understood, although it is known that they affect 5-HT2A receptors and are hypothesized to briefly disrupt these connections, allowing them to reform in new ways in the days and weeks following treatment.
This research assessed the subacute impact of psilocybin on brain function in two clinical trials of depression:
The first trial was an open-label trial of oral psilocybin in patients with treatment-resistant depression.
Patients had baseline clinical assessment and resting-state functional MRI, followed by fixed-order “low” (10 mg) and “high” (25 mg) psilocybin therapy dosing days separated by 1 week. Of the 19 patients recruited, 3 were excluded as a result of excessive fMRI head motion. The team confirmed an antidepressant effect of psilocybin in 16 patients via reduced questionnaire scores from baseline.
Brain network modularity was significantly reduced 1 day after psilocybin therapy in 10 of 16 participants (mean difference, –0.29; t15, 2.87; 95% confidence interval, 0.07-0.50; P = .012; d = 0.72). This result implies an increase in functional connectivity between the brain’s main intrinsic networks.
Pre- vs posttreatment change in modularity significantly correlated with change in Beck Depression Inventory (BDI) score at 6 months, relative to baseline (r14 = 0.54, 95% CI, 0.14-0.78, P = .033). Results imply that decreased brain modularity 1 day after psilocybin therapy relates to long-term improvements in symptom severity.
Effective antidepressant alternative?
The second trial was a double-blind, phase 2, randomized, controlled trial comparing psilocybin with escitalopram (Lexapro). Twenty-one patients were included in the escitalopram imaging sample and 22 patients were included in the psilocybin imaging sample.
Patients received either 2 x 25 mg oral psilocybin, 3 weeks apart, plus 6 weeks of daily placebo (psilocybin arm) or 2 x 1 mg oral psilocybin, 3 weeks apart, plus 6 weeks of daily escitalopram (10-20 mg) (escitalopram arm). Functional MRI was recorded at baseline and 3 weeks after the second psilocybin dose.
On average, BDI-measured reductions in depressive symptom severity were significantly greater under psilocybin than escitalopram, indicating superior efficacy of psilocybin therapy versus escitalopram.
Evidence indicated that the reduction in network modularity and its relationship to depression severity was specific to the psilocybin group. In the escitalopram group, network modularity did not change from baseline and there was no significant correlation between changes in modularity and changes in BDI scores.
Post–psilocybin therapy changes in network flexibility were correlated with changes in BDI score. After false discovery rate correction, increased executive network dynamic flexibility strongly correlated with greater symptom improvement at the 6-week primary endpoint for the psilocybin arm (r20, –0.76, 95% CI, −0.90 to –0.50, P = .001).
There were no significant correlations between changes in BDI scores and changes in dynamic flexibility in the escitalopram arm.

“These findings are important because for the first time we find that psilocybin works differently from conventional antidepressants, making the brain more flexible and fluid and less entrenched in the negative thinking patterns associated with depression. This supports our initial predictions and confirms psilocybin could be a real alternative approach to depression treatments,” study investigator David Nutt, DM, head of the Imperial Centre for Psychedelic Research, London, said in a release.
“In previous studies we had seen a similar effect in the brain when people were scanned whilst on a psychedelic, but here we’re seeing it weeks after treatment for depression, which suggests a carryover of the acute drug action,” said Dr. Carhart-Harris.
Durable effect?
“We don’t yet know how long the changes in brain activity seen with psilocybin therapy last, and we need to do more research to understand this,” said Dr. Carhart-Harris, who is a member of the UCSF Weill Institute for Neurosciences. “If the changes don’t last, then is it related to relapse into a depressive episode? We need to do follow-up scans to see where people’s brains are at 3 months or even 6 months after treatment.
“We do know that some people relapse, and it may be that after a while their brains revert to the rigid patterns of activity we see in depression.
“One exciting implication of our findings is that we have discovered a fundamental mechanism via which psychedelic therapy works not just for depression but other mental illnesses, such as anorexia or addiction. We now need to test if this is the case, and if it is, then we have found something important,” added Dr. Carhart-Harris.
Successful phase 3, double-blind randomized, controlled trials will be required to achieve licensing for psilocybin therapy, but pragmatic trials may better address questions regarding treatment practicability, specificity, and optimization. Given the emerging research into psychedelic therapy, it is important for large-scale trials to establish the generalizability, reliability, and specificity of the drug’s antidepressant response.
So how close are we to full federal approval for psilocybin in the treatment of depression? Dr. Carhart-Harris estimated that within 4-5 years is realistic at the federal level. At the state level, in Oregon psilocybin therapy is on track for approval in 2023, including for patients currently undergoing treatment for depressive disorders. In addition, things are opening up in Canada, with some special-access opportunities.
The researchers cautioned that, while these findings are encouraging, trials assessing psilocybin for depression have taken place under controlled, clinical conditions, using a regulated dose formulated in a laboratory, and involved extensive psychological support by a mental health professional – before, during, and after dosing. Taking psychedelics in the absence of these combined safeguards may not have a positive outcome.
The research was supported by funding from the Alex Mosley Charitable Trust and founding donors of the Imperial Centre for Psychedelic Research. One coauthor was supported by the Imperial College London EPSRC Centre London for doctoral training in neurotechnology.
A version of this article first appeared on Medscape.com.
Led by investigators from the University of California, San Francisco, and Imperial College London’s Centre for Psychedelic Research, the findings come from a new analysis of brain scans of almost 60 patients with resistant depression treated with psilocybin.
“Not much is known about the changes in brain function after psychedelic experience. There has been much more research done on the acute brain action of psychedelics, but there is very little on the postacute or subacute changes in brain function,” study investigator Robin Carhart-Harris, PhD, former head of the Imperial Centre for Psychedelic Research and now director of the Neuroscape psychedelics division at UCSF, and senior author of the study, told this news organization.
“This research is a major advance because it is showing replication across two datasets with different designs. One in which the scanning is done 1 day after intervention and the other one when the posttreatment scanning is done 3 weeks after the second of two psilocybin therapy sessions,” Dr. Carhart-Harris added.
The study was published online in Nature Medicine.
A disruptor?
Psilocybin is one of a number of psychedelics under investigation as a potential therapy for psychiatric disorders. In the last 15 years, at least six separate clinical trials have reported impressive improvements in depressive symptoms with psilocybin therapy. Several studies have tested a synthesized a form of the drug to treat patients with depression and anxiety – with promising results.
However, the therapeutic action of psilocybin and other serotonergic psychedelics is still not completely understood, although it is known that they affect 5-HT2A receptors and are hypothesized to briefly disrupt these connections, allowing them to reform in new ways in the days and weeks following treatment.
This research assessed the subacute impact of psilocybin on brain function in two clinical trials of depression:
The first trial was an open-label trial of oral psilocybin in patients with treatment-resistant depression.
Patients had baseline clinical assessment and resting-state functional MRI, followed by fixed-order “low” (10 mg) and “high” (25 mg) psilocybin therapy dosing days separated by 1 week. Of the 19 patients recruited, 3 were excluded as a result of excessive fMRI head motion. The team confirmed an antidepressant effect of psilocybin in 16 patients via reduced questionnaire scores from baseline.
Brain network modularity was significantly reduced 1 day after psilocybin therapy in 10 of 16 participants (mean difference, –0.29; t15, 2.87; 95% confidence interval, 0.07-0.50; P = .012; d = 0.72). This result implies an increase in functional connectivity between the brain’s main intrinsic networks.
Pre- vs posttreatment change in modularity significantly correlated with change in Beck Depression Inventory (BDI) score at 6 months, relative to baseline (r14 = 0.54, 95% CI, 0.14-0.78, P = .033). Results imply that decreased brain modularity 1 day after psilocybin therapy relates to long-term improvements in symptom severity.
Effective antidepressant alternative?
The second trial was a double-blind, phase 2, randomized, controlled trial comparing psilocybin with escitalopram (Lexapro). Twenty-one patients were included in the escitalopram imaging sample and 22 patients were included in the psilocybin imaging sample.
Patients received either 2 x 25 mg oral psilocybin, 3 weeks apart, plus 6 weeks of daily placebo (psilocybin arm) or 2 x 1 mg oral psilocybin, 3 weeks apart, plus 6 weeks of daily escitalopram (10-20 mg) (escitalopram arm). Functional MRI was recorded at baseline and 3 weeks after the second psilocybin dose.
On average, BDI-measured reductions in depressive symptom severity were significantly greater under psilocybin than escitalopram, indicating superior efficacy of psilocybin therapy versus escitalopram.
Evidence indicated that the reduction in network modularity and its relationship to depression severity was specific to the psilocybin group. In the escitalopram group, network modularity did not change from baseline and there was no significant correlation between changes in modularity and changes in BDI scores.
Post–psilocybin therapy changes in network flexibility were correlated with changes in BDI score. After false discovery rate correction, increased executive network dynamic flexibility strongly correlated with greater symptom improvement at the 6-week primary endpoint for the psilocybin arm (r20, –0.76, 95% CI, −0.90 to –0.50, P = .001).
There were no significant correlations between changes in BDI scores and changes in dynamic flexibility in the escitalopram arm.
“These findings are important because for the first time we find that psilocybin works differently from conventional antidepressants, making the brain more flexible and fluid and less entrenched in the negative thinking patterns associated with depression. This supports our initial predictions and confirms psilocybin could be a real alternative approach to depression treatments,” study investigator David Nutt, DM, head of the Imperial Centre for Psychedelic Research, London, said in a release.
“In previous studies we had seen a similar effect in the brain when people were scanned whilst on a psychedelic, but here we’re seeing it weeks after treatment for depression, which suggests a carryover of the acute drug action,” said Dr. Carhart-Harris.
Durable effect?
“We don’t yet know how long the changes in brain activity seen with psilocybin therapy last, and we need to do more research to understand this,” said Dr. Carhart-Harris, who is a member of the UCSF Weill Institute for Neurosciences. “If the changes don’t last, then is it related to relapse into a depressive episode? We need to do follow-up scans to see where people’s brains are at 3 months or even 6 months after treatment.
“We do know that some people relapse, and it may be that after a while their brains revert to the rigid patterns of activity we see in depression.
“One exciting implication of our findings is that we have discovered a fundamental mechanism via which psychedelic therapy works not just for depression but other mental illnesses, such as anorexia or addiction. We now need to test if this is the case, and if it is, then we have found something important,” added Dr. Carhart-Harris.
Successful phase 3, double-blind randomized, controlled trials will be required to achieve licensing for psilocybin therapy, but pragmatic trials may better address questions regarding treatment practicability, specificity, and optimization. Given the emerging research into psychedelic therapy, it is important for large-scale trials to establish the generalizability, reliability, and specificity of the drug’s antidepressant response.
So how close are we to full federal approval for psilocybin in the treatment of depression? Dr. Carhart-Harris estimated that within 4-5 years is realistic at the federal level. At the state level, in Oregon psilocybin therapy is on track for approval in 2023, including for patients currently undergoing treatment for depressive disorders. In addition, things are opening up in Canada, with some special-access opportunities.
The researchers cautioned that, while these findings are encouraging, trials assessing psilocybin for depression have taken place under controlled, clinical conditions, using a regulated dose formulated in a laboratory, and involved extensive psychological support by a mental health professional – before, during, and after dosing. Taking psychedelics in the absence of these combined safeguards may not have a positive outcome.
The research was supported by funding from the Alex Mosley Charitable Trust and founding donors of the Imperial Centre for Psychedelic Research. One coauthor was supported by the Imperial College London EPSRC Centre London for doctoral training in neurotechnology.
A version of this article first appeared on Medscape.com.
Led by investigators from the University of California, San Francisco, and Imperial College London’s Centre for Psychedelic Research, the findings come from a new analysis of brain scans of almost 60 patients with resistant depression treated with psilocybin.
“Not much is known about the changes in brain function after psychedelic experience. There has been much more research done on the acute brain action of psychedelics, but there is very little on the postacute or subacute changes in brain function,” study investigator Robin Carhart-Harris, PhD, former head of the Imperial Centre for Psychedelic Research and now director of the Neuroscape psychedelics division at UCSF, and senior author of the study, told this news organization.
“This research is a major advance because it is showing replication across two datasets with different designs. One in which the scanning is done 1 day after intervention and the other one when the posttreatment scanning is done 3 weeks after the second of two psilocybin therapy sessions,” Dr. Carhart-Harris added.
The study was published online in Nature Medicine.
A disruptor?
Psilocybin is one of a number of psychedelics under investigation as a potential therapy for psychiatric disorders. In the last 15 years, at least six separate clinical trials have reported impressive improvements in depressive symptoms with psilocybin therapy. Several studies have tested a synthesized a form of the drug to treat patients with depression and anxiety – with promising results.
However, the therapeutic action of psilocybin and other serotonergic psychedelics is still not completely understood, although it is known that they affect 5-HT2A receptors and are hypothesized to briefly disrupt these connections, allowing them to reform in new ways in the days and weeks following treatment.
This research assessed the subacute impact of psilocybin on brain function in two clinical trials of depression:
The first trial was an open-label trial of oral psilocybin in patients with treatment-resistant depression.
Patients had baseline clinical assessment and resting-state functional MRI, followed by fixed-order “low” (10 mg) and “high” (25 mg) psilocybin therapy dosing days separated by 1 week. Of the 19 patients recruited, 3 were excluded as a result of excessive fMRI head motion. The team confirmed an antidepressant effect of psilocybin in 16 patients via reduced questionnaire scores from baseline.
Brain network modularity was significantly reduced 1 day after psilocybin therapy in 10 of 16 participants (mean difference, –0.29; t15, 2.87; 95% confidence interval, 0.07-0.50; P = .012; d = 0.72). This result implies an increase in functional connectivity between the brain’s main intrinsic networks.
Pre- vs posttreatment change in modularity significantly correlated with change in Beck Depression Inventory (BDI) score at 6 months, relative to baseline (r14 = 0.54, 95% CI, 0.14-0.78, P = .033). Results imply that decreased brain modularity 1 day after psilocybin therapy relates to long-term improvements in symptom severity.
Effective antidepressant alternative?
The second trial was a double-blind, phase 2, randomized, controlled trial comparing psilocybin with escitalopram (Lexapro). Twenty-one patients were included in the escitalopram imaging sample and 22 patients were included in the psilocybin imaging sample.
Patients received either 2 x 25 mg oral psilocybin, 3 weeks apart, plus 6 weeks of daily placebo (psilocybin arm) or 2 x 1 mg oral psilocybin, 3 weeks apart, plus 6 weeks of daily escitalopram (10-20 mg) (escitalopram arm). Functional MRI was recorded at baseline and 3 weeks after the second psilocybin dose.
On average, BDI-measured reductions in depressive symptom severity were significantly greater under psilocybin than escitalopram, indicating superior efficacy of psilocybin therapy versus escitalopram.
Evidence indicated that the reduction in network modularity and its relationship to depression severity was specific to the psilocybin group. In the escitalopram group, network modularity did not change from baseline and there was no significant correlation between changes in modularity and changes in BDI scores.
Post–psilocybin therapy changes in network flexibility were correlated with changes in BDI score. After false discovery rate correction, increased executive network dynamic flexibility strongly correlated with greater symptom improvement at the 6-week primary endpoint for the psilocybin arm (r20, –0.76, 95% CI, −0.90 to –0.50, P = .001).
There were no significant correlations between changes in BDI scores and changes in dynamic flexibility in the escitalopram arm.
“These findings are important because for the first time we find that psilocybin works differently from conventional antidepressants, making the brain more flexible and fluid and less entrenched in the negative thinking patterns associated with depression. This supports our initial predictions and confirms psilocybin could be a real alternative approach to depression treatments,” study investigator David Nutt, DM, head of the Imperial Centre for Psychedelic Research, London, said in a release.
“In previous studies we had seen a similar effect in the brain when people were scanned whilst on a psychedelic, but here we’re seeing it weeks after treatment for depression, which suggests a carryover of the acute drug action,” said Dr. Carhart-Harris.
Durable effect?
“We don’t yet know how long the changes in brain activity seen with psilocybin therapy last, and we need to do more research to understand this,” said Dr. Carhart-Harris, who is a member of the UCSF Weill Institute for Neurosciences. “If the changes don’t last, then is it related to relapse into a depressive episode? We need to do follow-up scans to see where people’s brains are at 3 months or even 6 months after treatment.
“We do know that some people relapse, and it may be that after a while their brains revert to the rigid patterns of activity we see in depression.
“One exciting implication of our findings is that we have discovered a fundamental mechanism via which psychedelic therapy works not just for depression but other mental illnesses, such as anorexia or addiction. We now need to test if this is the case, and if it is, then we have found something important,” added Dr. Carhart-Harris.
Successful phase 3, double-blind randomized, controlled trials will be required to achieve licensing for psilocybin therapy, but pragmatic trials may better address questions regarding treatment practicability, specificity, and optimization. Given the emerging research into psychedelic therapy, it is important for large-scale trials to establish the generalizability, reliability, and specificity of the drug’s antidepressant response.
So how close are we to full federal approval for psilocybin in the treatment of depression? Dr. Carhart-Harris estimated that within 4-5 years is realistic at the federal level. At the state level, in Oregon psilocybin therapy is on track for approval in 2023, including for patients currently undergoing treatment for depressive disorders. In addition, things are opening up in Canada, with some special-access opportunities.
The researchers cautioned that, while these findings are encouraging, trials assessing psilocybin for depression have taken place under controlled, clinical conditions, using a regulated dose formulated in a laboratory, and involved extensive psychological support by a mental health professional – before, during, and after dosing. Taking psychedelics in the absence of these combined safeguards may not have a positive outcome.
The research was supported by funding from the Alex Mosley Charitable Trust and founding donors of the Imperial Centre for Psychedelic Research. One coauthor was supported by the Imperial College London EPSRC Centre London for doctoral training in neurotechnology.
A version of this article first appeared on Medscape.com.
FROM NATURE MEDICINE
Erectile dysfunction drugs linked to ocular conditions
, researchers say.
Patients in an insurance database who were prescribed sildenafil (Viagra), tadalafil (Cialis), vardenafil (Levitra), or avanafil (Stendra) were almost twice as likely as were patients not prescribed the drugs to have ischemic optic neuropathy, retinal vascular occlusion, or serous retinal detachment.
In 2020, physicians wrote about 20 million monthly prescriptions for PDE5Is in the United States alone, said Mahyar Etminan, PharmD, associate professor of ophthalmology at the University of British Columbia, Vancouver.
“We don’t want to alarm people taking them, but generally speaking, if they experience visual problems or changes in vision, then these drugs may be the culprits, and they should check it out,” he said in an interview.
The study was published in JAMA Ophthalmology.
Previous reports, including postmarketing studies by the drug makers, have documented ocular events. The monographs for sildenafil, tadalafil, vardenafil, and avanafil warn users about ischemic optic neuropathy, the researchers found.
The monographs for sildenafil, tadalafil, and vardenafil list retinal vascular occlusion as a potential adverse event but do not quantify the risk. None of the drug monographs mention serous retinal detachment.
Previous research has associated PDE5Is with compromised perfusion of the optic nerve. Some researchers have speculated that the choroid blood vessels can undergo smooth muscle relaxation through a cyclic guanosine monophosphate pathway that can lead to choroidal congestion.
To get a better handle on the ocular risks of PDE51s, Dr. Etminan and his colleagues analyzed health insurance claim records from the PharMetrics Plus database of 213,033 men who had not experienced any of the three ocular conditions in the year before they became regular users of the medications.
They identified 1,146 patients who had been diagnosed with at least one of the three conditions.
The overall number of conditions diagnosed was small relative to the size of the population, 15.5 cases per 10,000 person-years. “So that’s still relatively rare, but the problem is that these are very heavily used medications,” Dr. Etminan said.
For each man diagnosed with one of the ocular conditions, the researchers matched four control persons who were the same age and could be followed for the same length of time. There was a total of 4,584 control persons.
The researchers compared regular users of PDE5Is (those who had received at least one prescription for a PDE5I every 3 months in the year before the ocular diagnosis) with nonusers (those who had not received a PDE5I prescription during that time).
Patients with the ocular conditions were more likely than were those in the control group to have hypertension, diabetes, cardiovascular disease, or sleep apnea. After controlling for these covariates, the researchers found that the users were overall 85% more likely to be diagnosed with one or more of them (incidence rate ratio [IRR], 1.85).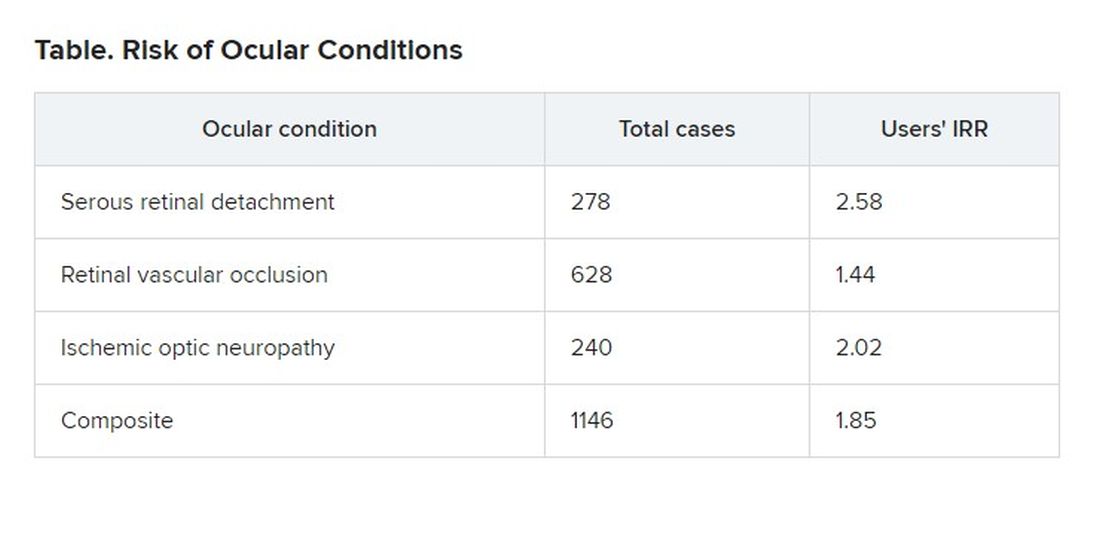
The researchers also found that the risk was even greater for those patients who were given five or more prescriptions of PDE5Is, compared to those given fewer than five prescriptions, suggesting a dose response.
On the basis of these findings, Dr. Etminan thinks drug companies should add warnings about serous retinal detachment and retinal vascular occlusion to the drug monographs.
Asked to comment, Pfizer, which developed Viagra, referred questions to its spinoff company, Viatris, which did not respond. Eli Lilly, which makes Cialis, also did not respond to a request for comment. Vivus, which makes Stendra, could not be reached by press time.
Bayer, which makes Levitra, declined to provide anyone who could answer questions, but it provided a statement noting that the occurrence of ocular adverse events is already known among PDE5I users and that retinal vascular occlusion and ischemic optic neuropathy are mentioned in the product information.
“For example, non-arteritic anterior ischemic optic neuropathy (NAION) is a very rare condition which occurs with an overall higher risk in the population usually suffering from erectile dysfunction (ED) – that is, elderly men with concomitant diseases such as diabetes, dyslipidemia, and hypertension – compared to the general population,” the statement said.
Because of the retrospective nature of the analysis, Dr. Etminan acknowledged that researchers could not prove that the increased risk of ocular disease was associated with use of the drugs rather than some underlying condition. But in addition to adjusting for known risk factors, they also separately analyzed men without hypertension, diabetes, or coronary artery disease and still found that the risk of the ocular conditions was roughly double for men with PDE5I prescriptions.
Howard Pomeranz, MD, PhD, professor of ophthalmology at Northwell Health in Great Neck, N.Y., who was not involved in this study, said its findings confirmed similar research that he conducted on ischemic optic neuropathy.
He told this news organization that people taking PDE5Is should weigh the risk against the benefit, but added that the calculation might be different for people who use them to treat pulmonary hypertension rather than erectile dysfunction.
Although people taking the drugs should discuss any changes in their vision with their practitioners, he said they should not be concerned about a “bluish type of tint to the vision that may occur transiently for anywhere from a few minutes up to 40 or 45 minutes.”
Drug companies and regulators should consider changing the monographs in light of this new evidence, Dr. Pomeranz said. “Perhaps this data might drive the warning to be perhaps a little bit stronger, now that there’s more data to suggest maybe a bit of a stronger association and not just some chance association between using these drugs and these visual events.”
The study was funded by the University of British Columbia. Dr. Etminan and Dr. Pomeranz have disclosed no relevant financial interests.
A version of this article first appeared on Medscape.com
, researchers say.
Patients in an insurance database who were prescribed sildenafil (Viagra), tadalafil (Cialis), vardenafil (Levitra), or avanafil (Stendra) were almost twice as likely as were patients not prescribed the drugs to have ischemic optic neuropathy, retinal vascular occlusion, or serous retinal detachment.
In 2020, physicians wrote about 20 million monthly prescriptions for PDE5Is in the United States alone, said Mahyar Etminan, PharmD, associate professor of ophthalmology at the University of British Columbia, Vancouver.
“We don’t want to alarm people taking them, but generally speaking, if they experience visual problems or changes in vision, then these drugs may be the culprits, and they should check it out,” he said in an interview.
The study was published in JAMA Ophthalmology.
Previous reports, including postmarketing studies by the drug makers, have documented ocular events. The monographs for sildenafil, tadalafil, vardenafil, and avanafil warn users about ischemic optic neuropathy, the researchers found.
The monographs for sildenafil, tadalafil, and vardenafil list retinal vascular occlusion as a potential adverse event but do not quantify the risk. None of the drug monographs mention serous retinal detachment.
Previous research has associated PDE5Is with compromised perfusion of the optic nerve. Some researchers have speculated that the choroid blood vessels can undergo smooth muscle relaxation through a cyclic guanosine monophosphate pathway that can lead to choroidal congestion.
To get a better handle on the ocular risks of PDE51s, Dr. Etminan and his colleagues analyzed health insurance claim records from the PharMetrics Plus database of 213,033 men who had not experienced any of the three ocular conditions in the year before they became regular users of the medications.
They identified 1,146 patients who had been diagnosed with at least one of the three conditions.
The overall number of conditions diagnosed was small relative to the size of the population, 15.5 cases per 10,000 person-years. “So that’s still relatively rare, but the problem is that these are very heavily used medications,” Dr. Etminan said.
For each man diagnosed with one of the ocular conditions, the researchers matched four control persons who were the same age and could be followed for the same length of time. There was a total of 4,584 control persons.
The researchers compared regular users of PDE5Is (those who had received at least one prescription for a PDE5I every 3 months in the year before the ocular diagnosis) with nonusers (those who had not received a PDE5I prescription during that time).
Patients with the ocular conditions were more likely than were those in the control group to have hypertension, diabetes, cardiovascular disease, or sleep apnea. After controlling for these covariates, the researchers found that the users were overall 85% more likely to be diagnosed with one or more of them (incidence rate ratio [IRR], 1.85).
The researchers also found that the risk was even greater for those patients who were given five or more prescriptions of PDE5Is, compared to those given fewer than five prescriptions, suggesting a dose response.
On the basis of these findings, Dr. Etminan thinks drug companies should add warnings about serous retinal detachment and retinal vascular occlusion to the drug monographs.
Asked to comment, Pfizer, which developed Viagra, referred questions to its spinoff company, Viatris, which did not respond. Eli Lilly, which makes Cialis, also did not respond to a request for comment. Vivus, which makes Stendra, could not be reached by press time.
Bayer, which makes Levitra, declined to provide anyone who could answer questions, but it provided a statement noting that the occurrence of ocular adverse events is already known among PDE5I users and that retinal vascular occlusion and ischemic optic neuropathy are mentioned in the product information.
“For example, non-arteritic anterior ischemic optic neuropathy (NAION) is a very rare condition which occurs with an overall higher risk in the population usually suffering from erectile dysfunction (ED) – that is, elderly men with concomitant diseases such as diabetes, dyslipidemia, and hypertension – compared to the general population,” the statement said.
Because of the retrospective nature of the analysis, Dr. Etminan acknowledged that researchers could not prove that the increased risk of ocular disease was associated with use of the drugs rather than some underlying condition. But in addition to adjusting for known risk factors, they also separately analyzed men without hypertension, diabetes, or coronary artery disease and still found that the risk of the ocular conditions was roughly double for men with PDE5I prescriptions.
Howard Pomeranz, MD, PhD, professor of ophthalmology at Northwell Health in Great Neck, N.Y., who was not involved in this study, said its findings confirmed similar research that he conducted on ischemic optic neuropathy.
He told this news organization that people taking PDE5Is should weigh the risk against the benefit, but added that the calculation might be different for people who use them to treat pulmonary hypertension rather than erectile dysfunction.
Although people taking the drugs should discuss any changes in their vision with their practitioners, he said they should not be concerned about a “bluish type of tint to the vision that may occur transiently for anywhere from a few minutes up to 40 or 45 minutes.”
Drug companies and regulators should consider changing the monographs in light of this new evidence, Dr. Pomeranz said. “Perhaps this data might drive the warning to be perhaps a little bit stronger, now that there’s more data to suggest maybe a bit of a stronger association and not just some chance association between using these drugs and these visual events.”
The study was funded by the University of British Columbia. Dr. Etminan and Dr. Pomeranz have disclosed no relevant financial interests.
A version of this article first appeared on Medscape.com
, researchers say.
Patients in an insurance database who were prescribed sildenafil (Viagra), tadalafil (Cialis), vardenafil (Levitra), or avanafil (Stendra) were almost twice as likely as were patients not prescribed the drugs to have ischemic optic neuropathy, retinal vascular occlusion, or serous retinal detachment.
In 2020, physicians wrote about 20 million monthly prescriptions for PDE5Is in the United States alone, said Mahyar Etminan, PharmD, associate professor of ophthalmology at the University of British Columbia, Vancouver.
“We don’t want to alarm people taking them, but generally speaking, if they experience visual problems or changes in vision, then these drugs may be the culprits, and they should check it out,” he said in an interview.
The study was published in JAMA Ophthalmology.
Previous reports, including postmarketing studies by the drug makers, have documented ocular events. The monographs for sildenafil, tadalafil, vardenafil, and avanafil warn users about ischemic optic neuropathy, the researchers found.
The monographs for sildenafil, tadalafil, and vardenafil list retinal vascular occlusion as a potential adverse event but do not quantify the risk. None of the drug monographs mention serous retinal detachment.
Previous research has associated PDE5Is with compromised perfusion of the optic nerve. Some researchers have speculated that the choroid blood vessels can undergo smooth muscle relaxation through a cyclic guanosine monophosphate pathway that can lead to choroidal congestion.
To get a better handle on the ocular risks of PDE51s, Dr. Etminan and his colleagues analyzed health insurance claim records from the PharMetrics Plus database of 213,033 men who had not experienced any of the three ocular conditions in the year before they became regular users of the medications.
They identified 1,146 patients who had been diagnosed with at least one of the three conditions.
The overall number of conditions diagnosed was small relative to the size of the population, 15.5 cases per 10,000 person-years. “So that’s still relatively rare, but the problem is that these are very heavily used medications,” Dr. Etminan said.
For each man diagnosed with one of the ocular conditions, the researchers matched four control persons who were the same age and could be followed for the same length of time. There was a total of 4,584 control persons.
The researchers compared regular users of PDE5Is (those who had received at least one prescription for a PDE5I every 3 months in the year before the ocular diagnosis) with nonusers (those who had not received a PDE5I prescription during that time).
Patients with the ocular conditions were more likely than were those in the control group to have hypertension, diabetes, cardiovascular disease, or sleep apnea. After controlling for these covariates, the researchers found that the users were overall 85% more likely to be diagnosed with one or more of them (incidence rate ratio [IRR], 1.85).
The researchers also found that the risk was even greater for those patients who were given five or more prescriptions of PDE5Is, compared to those given fewer than five prescriptions, suggesting a dose response.
On the basis of these findings, Dr. Etminan thinks drug companies should add warnings about serous retinal detachment and retinal vascular occlusion to the drug monographs.
Asked to comment, Pfizer, which developed Viagra, referred questions to its spinoff company, Viatris, which did not respond. Eli Lilly, which makes Cialis, also did not respond to a request for comment. Vivus, which makes Stendra, could not be reached by press time.
Bayer, which makes Levitra, declined to provide anyone who could answer questions, but it provided a statement noting that the occurrence of ocular adverse events is already known among PDE5I users and that retinal vascular occlusion and ischemic optic neuropathy are mentioned in the product information.
“For example, non-arteritic anterior ischemic optic neuropathy (NAION) is a very rare condition which occurs with an overall higher risk in the population usually suffering from erectile dysfunction (ED) – that is, elderly men with concomitant diseases such as diabetes, dyslipidemia, and hypertension – compared to the general population,” the statement said.
Because of the retrospective nature of the analysis, Dr. Etminan acknowledged that researchers could not prove that the increased risk of ocular disease was associated with use of the drugs rather than some underlying condition. But in addition to adjusting for known risk factors, they also separately analyzed men without hypertension, diabetes, or coronary artery disease and still found that the risk of the ocular conditions was roughly double for men with PDE5I prescriptions.
Howard Pomeranz, MD, PhD, professor of ophthalmology at Northwell Health in Great Neck, N.Y., who was not involved in this study, said its findings confirmed similar research that he conducted on ischemic optic neuropathy.
He told this news organization that people taking PDE5Is should weigh the risk against the benefit, but added that the calculation might be different for people who use them to treat pulmonary hypertension rather than erectile dysfunction.
Although people taking the drugs should discuss any changes in their vision with their practitioners, he said they should not be concerned about a “bluish type of tint to the vision that may occur transiently for anywhere from a few minutes up to 40 or 45 minutes.”
Drug companies and regulators should consider changing the monographs in light of this new evidence, Dr. Pomeranz said. “Perhaps this data might drive the warning to be perhaps a little bit stronger, now that there’s more data to suggest maybe a bit of a stronger association and not just some chance association between using these drugs and these visual events.”
The study was funded by the University of British Columbia. Dr. Etminan and Dr. Pomeranz have disclosed no relevant financial interests.
A version of this article first appeared on Medscape.com