User login
PD-L1 test debated in gastroesophageal cancer immunotherapy
on whether measuring programmed death–ligand 1 (PD-L1) is essential before prescribing checkpoint inhibitors for gastroesophageal cancer.
“In the last couple of years, the incorporation of PD-1 antibodies is really changing our standard of care and international guidelines in this disease,” said Ian Chau, MD, a consultant medical oncologist at the Royal Marsden Hospital, London.
He moderated a debate at the 2022 Gastrointestinal Cancers Symposium on the importance of measuring PD-L1 expression levels before administering immune checkpoint inhibitor therapy.
Tumor cells can use PD-1 signaling to deactivate the response of T cells that would otherwise destroy them, and several new drugs are designed to block that signaling.
Multiple randomized controlled trials have shown the benefit of adding such checkpoint inhibitors to chemotherapy for gastroesophageal cancer and currently, chemotherapy plus a checkpoint inhibitor is standard care, Dr. Chau said.
PD-1–blocking antibodies include pembrolizumab (Keytruda, Merck) for colorectal cancer, gastric cancer, esophageal cancer, hepatocellular carcinoma, and renal cell carcinoma, among other cancers. And, nivolumab (Opdivo, Bristol-Myers Squibb) approved for renal cell carcinoma, colorectal cancer, hepatocellular carcinoma, and esophageal squamous cell carcinoma, among other cancers.
Regulators differ on whether these treatments should be limited to patients whose expression level of PD-L1 reaches a defined threshold. The FDA has not required the measurement of any biomarker before starting therapy with either of these drugs. However, the EMA requires a PD-L1 combined positive score (CPS) of at least 10 for pembrolizumab and at least 5 for nivolumab.
In a poll conducted before the start of the debate, 83% of physician attendees said they favor of the EMA position, while 17% disagreed.
Florian Lordick, MD, PhD, director of the University of Leipzig (Germany) Cancer Center, argued that tests for PD-L1 expression are accurate. About half of patients have CPS of at least 1. And, pathologists are in agreement in interpreting the tests about 97% of the time.
Pivotal decision-making clinical trials
The EMA requires a PD-L1 assay primarily based on its interpretation of the data from KEYNOTE-590 and CheckMate-648.
KEYNOTE-590 included 749 patients with esophageal carcinoma who were randomized to receive either pembrolizumab with standard of care chemotherapy, or placebo and standard of care chemotherapy. Patients receiving pembrolizumab who had PD-L1 CPS scores of 10 or more survived a few months longer on average. But in a post hoc analysis, the investigators found that, in patients with PD-L1 CPS scores less than 10, the difference between the treatment and placebo groups was not statistically significant.
In CheckMate-648, 970 patients with esophageal carcinoma were randomized to receive nivolumab with ipilimumab, nivolumab with chemotherapy, or chemotherapy alone. Investigators used a slightly different measurement of PD-L1 tumor proportion score (TPS), in comparing chemotherapy plus nivolumab to chemotherapy alone for advanced esophageal squamous cell carcinoma.
The median survival time of patients with TPS of at least 1% was 15.4 months in the nivolumab group and 9.2 months in the control group. But among patients with a TPS of less than 1%, the median overall survival was 12.0 months in the nivolumab group and 12.2 in the control group. CPS thresholds of 5 or 1 resulted in similar effects.
Dr. Lordick cited a systematic review of four studies in press at ESMO Open. Hazard ratios for three of the studies favored immunotherapy only in patients with CPS of at least 10.
Deciding which patients to treat matters because these drugs are expensive, he said. A single dose of 240 mg nivolumab costs $7,228.70, and treatment for 1 year can cost $173,488.80 in addition to costs for hospitalization because of immune-related adverse events, labs, imaging, colonoscopy, and other related costs.
“This is a lot of money, isn’t it? It’s the same price the hospital pay for two registered nurses in the U.S., at least when we are talking about the average price. I’m not sure I want to spend this money for a drug that does not work,” Dr. Lordick said.
Aaron Scott, MD, an oncologist with the University of Arizona Cancer Center, Tucson, said that “patients and clinicians want and need options” because there may be other factors that should be considered.
“PD-L1 has shown inconsistent results. And while I agree it is the best that we have for predictive biomarker in the space, it is far from perfect. PD-L1 has not been predictive for response in a variety of settings and trials. In first-line, second-line, third-line trials we have examples where it does not predict response,” he said.
JUPITER06 compared toripalimab or placebo with paclitaxel and cisplatin for patients with esophageal squamous cell carcinoma. Patients who received toripalimab lived longer than patients who received the placebo, but within the toripalimab group, there was no difference in median overall survival between those patients above and those below the threshold of CPS 1.
ORIENT-15 compared sintilimab or placebo with chemotherapy as first-line therapy for patients with esophageal squamous cell carcinoma. Although the treatment group fared better, survival rates were the same whether patients were above or below the CPS 10 threshold.
Dr. Scott cited three other trials in which PD-L1 was not predictive of response to checkpoint inhibitors.
The differences among studies could be attributed to different assays, he said. “Where you biopsy and when you biopsy seems to matter.”
In a second opinion poll conducted after the presentations, the proportion of physician attendees saying PD-L1 was essential before initiating checkpoint inhibitors, dropped to about two-thirds.
Dr. Chau reported financial relationships with Bristol-Myers Squibb, Merck Serono, and other pharmaceutical companies. Dr. Lordick reported financial relationships Bristol-Myers Squibb, Merck Sharp & Dohme, Merck, and other pharmaceutical companies.
on whether measuring programmed death–ligand 1 (PD-L1) is essential before prescribing checkpoint inhibitors for gastroesophageal cancer.
“In the last couple of years, the incorporation of PD-1 antibodies is really changing our standard of care and international guidelines in this disease,” said Ian Chau, MD, a consultant medical oncologist at the Royal Marsden Hospital, London.
He moderated a debate at the 2022 Gastrointestinal Cancers Symposium on the importance of measuring PD-L1 expression levels before administering immune checkpoint inhibitor therapy.
Tumor cells can use PD-1 signaling to deactivate the response of T cells that would otherwise destroy them, and several new drugs are designed to block that signaling.
Multiple randomized controlled trials have shown the benefit of adding such checkpoint inhibitors to chemotherapy for gastroesophageal cancer and currently, chemotherapy plus a checkpoint inhibitor is standard care, Dr. Chau said.
PD-1–blocking antibodies include pembrolizumab (Keytruda, Merck) for colorectal cancer, gastric cancer, esophageal cancer, hepatocellular carcinoma, and renal cell carcinoma, among other cancers. And, nivolumab (Opdivo, Bristol-Myers Squibb) approved for renal cell carcinoma, colorectal cancer, hepatocellular carcinoma, and esophageal squamous cell carcinoma, among other cancers.
Regulators differ on whether these treatments should be limited to patients whose expression level of PD-L1 reaches a defined threshold. The FDA has not required the measurement of any biomarker before starting therapy with either of these drugs. However, the EMA requires a PD-L1 combined positive score (CPS) of at least 10 for pembrolizumab and at least 5 for nivolumab.
In a poll conducted before the start of the debate, 83% of physician attendees said they favor of the EMA position, while 17% disagreed.
Florian Lordick, MD, PhD, director of the University of Leipzig (Germany) Cancer Center, argued that tests for PD-L1 expression are accurate. About half of patients have CPS of at least 1. And, pathologists are in agreement in interpreting the tests about 97% of the time.
Pivotal decision-making clinical trials
The EMA requires a PD-L1 assay primarily based on its interpretation of the data from KEYNOTE-590 and CheckMate-648.
KEYNOTE-590 included 749 patients with esophageal carcinoma who were randomized to receive either pembrolizumab with standard of care chemotherapy, or placebo and standard of care chemotherapy. Patients receiving pembrolizumab who had PD-L1 CPS scores of 10 or more survived a few months longer on average. But in a post hoc analysis, the investigators found that, in patients with PD-L1 CPS scores less than 10, the difference between the treatment and placebo groups was not statistically significant.
In CheckMate-648, 970 patients with esophageal carcinoma were randomized to receive nivolumab with ipilimumab, nivolumab with chemotherapy, or chemotherapy alone. Investigators used a slightly different measurement of PD-L1 tumor proportion score (TPS), in comparing chemotherapy plus nivolumab to chemotherapy alone for advanced esophageal squamous cell carcinoma.
The median survival time of patients with TPS of at least 1% was 15.4 months in the nivolumab group and 9.2 months in the control group. But among patients with a TPS of less than 1%, the median overall survival was 12.0 months in the nivolumab group and 12.2 in the control group. CPS thresholds of 5 or 1 resulted in similar effects.
Dr. Lordick cited a systematic review of four studies in press at ESMO Open. Hazard ratios for three of the studies favored immunotherapy only in patients with CPS of at least 10.
Deciding which patients to treat matters because these drugs are expensive, he said. A single dose of 240 mg nivolumab costs $7,228.70, and treatment for 1 year can cost $173,488.80 in addition to costs for hospitalization because of immune-related adverse events, labs, imaging, colonoscopy, and other related costs.
“This is a lot of money, isn’t it? It’s the same price the hospital pay for two registered nurses in the U.S., at least when we are talking about the average price. I’m not sure I want to spend this money for a drug that does not work,” Dr. Lordick said.
Aaron Scott, MD, an oncologist with the University of Arizona Cancer Center, Tucson, said that “patients and clinicians want and need options” because there may be other factors that should be considered.
“PD-L1 has shown inconsistent results. And while I agree it is the best that we have for predictive biomarker in the space, it is far from perfect. PD-L1 has not been predictive for response in a variety of settings and trials. In first-line, second-line, third-line trials we have examples where it does not predict response,” he said.
JUPITER06 compared toripalimab or placebo with paclitaxel and cisplatin for patients with esophageal squamous cell carcinoma. Patients who received toripalimab lived longer than patients who received the placebo, but within the toripalimab group, there was no difference in median overall survival between those patients above and those below the threshold of CPS 1.
ORIENT-15 compared sintilimab or placebo with chemotherapy as first-line therapy for patients with esophageal squamous cell carcinoma. Although the treatment group fared better, survival rates were the same whether patients were above or below the CPS 10 threshold.
Dr. Scott cited three other trials in which PD-L1 was not predictive of response to checkpoint inhibitors.
The differences among studies could be attributed to different assays, he said. “Where you biopsy and when you biopsy seems to matter.”
In a second opinion poll conducted after the presentations, the proportion of physician attendees saying PD-L1 was essential before initiating checkpoint inhibitors, dropped to about two-thirds.
Dr. Chau reported financial relationships with Bristol-Myers Squibb, Merck Serono, and other pharmaceutical companies. Dr. Lordick reported financial relationships Bristol-Myers Squibb, Merck Sharp & Dohme, Merck, and other pharmaceutical companies.
on whether measuring programmed death–ligand 1 (PD-L1) is essential before prescribing checkpoint inhibitors for gastroesophageal cancer.
“In the last couple of years, the incorporation of PD-1 antibodies is really changing our standard of care and international guidelines in this disease,” said Ian Chau, MD, a consultant medical oncologist at the Royal Marsden Hospital, London.
He moderated a debate at the 2022 Gastrointestinal Cancers Symposium on the importance of measuring PD-L1 expression levels before administering immune checkpoint inhibitor therapy.
Tumor cells can use PD-1 signaling to deactivate the response of T cells that would otherwise destroy them, and several new drugs are designed to block that signaling.
Multiple randomized controlled trials have shown the benefit of adding such checkpoint inhibitors to chemotherapy for gastroesophageal cancer and currently, chemotherapy plus a checkpoint inhibitor is standard care, Dr. Chau said.
PD-1–blocking antibodies include pembrolizumab (Keytruda, Merck) for colorectal cancer, gastric cancer, esophageal cancer, hepatocellular carcinoma, and renal cell carcinoma, among other cancers. And, nivolumab (Opdivo, Bristol-Myers Squibb) approved for renal cell carcinoma, colorectal cancer, hepatocellular carcinoma, and esophageal squamous cell carcinoma, among other cancers.
Regulators differ on whether these treatments should be limited to patients whose expression level of PD-L1 reaches a defined threshold. The FDA has not required the measurement of any biomarker before starting therapy with either of these drugs. However, the EMA requires a PD-L1 combined positive score (CPS) of at least 10 for pembrolizumab and at least 5 for nivolumab.
In a poll conducted before the start of the debate, 83% of physician attendees said they favor of the EMA position, while 17% disagreed.
Florian Lordick, MD, PhD, director of the University of Leipzig (Germany) Cancer Center, argued that tests for PD-L1 expression are accurate. About half of patients have CPS of at least 1. And, pathologists are in agreement in interpreting the tests about 97% of the time.
Pivotal decision-making clinical trials
The EMA requires a PD-L1 assay primarily based on its interpretation of the data from KEYNOTE-590 and CheckMate-648.
KEYNOTE-590 included 749 patients with esophageal carcinoma who were randomized to receive either pembrolizumab with standard of care chemotherapy, or placebo and standard of care chemotherapy. Patients receiving pembrolizumab who had PD-L1 CPS scores of 10 or more survived a few months longer on average. But in a post hoc analysis, the investigators found that, in patients with PD-L1 CPS scores less than 10, the difference between the treatment and placebo groups was not statistically significant.
In CheckMate-648, 970 patients with esophageal carcinoma were randomized to receive nivolumab with ipilimumab, nivolumab with chemotherapy, or chemotherapy alone. Investigators used a slightly different measurement of PD-L1 tumor proportion score (TPS), in comparing chemotherapy plus nivolumab to chemotherapy alone for advanced esophageal squamous cell carcinoma.
The median survival time of patients with TPS of at least 1% was 15.4 months in the nivolumab group and 9.2 months in the control group. But among patients with a TPS of less than 1%, the median overall survival was 12.0 months in the nivolumab group and 12.2 in the control group. CPS thresholds of 5 or 1 resulted in similar effects.
Dr. Lordick cited a systematic review of four studies in press at ESMO Open. Hazard ratios for three of the studies favored immunotherapy only in patients with CPS of at least 10.
Deciding which patients to treat matters because these drugs are expensive, he said. A single dose of 240 mg nivolumab costs $7,228.70, and treatment for 1 year can cost $173,488.80 in addition to costs for hospitalization because of immune-related adverse events, labs, imaging, colonoscopy, and other related costs.
“This is a lot of money, isn’t it? It’s the same price the hospital pay for two registered nurses in the U.S., at least when we are talking about the average price. I’m not sure I want to spend this money for a drug that does not work,” Dr. Lordick said.
Aaron Scott, MD, an oncologist with the University of Arizona Cancer Center, Tucson, said that “patients and clinicians want and need options” because there may be other factors that should be considered.
“PD-L1 has shown inconsistent results. And while I agree it is the best that we have for predictive biomarker in the space, it is far from perfect. PD-L1 has not been predictive for response in a variety of settings and trials. In first-line, second-line, third-line trials we have examples where it does not predict response,” he said.
JUPITER06 compared toripalimab or placebo with paclitaxel and cisplatin for patients with esophageal squamous cell carcinoma. Patients who received toripalimab lived longer than patients who received the placebo, but within the toripalimab group, there was no difference in median overall survival between those patients above and those below the threshold of CPS 1.
ORIENT-15 compared sintilimab or placebo with chemotherapy as first-line therapy for patients with esophageal squamous cell carcinoma. Although the treatment group fared better, survival rates were the same whether patients were above or below the CPS 10 threshold.
Dr. Scott cited three other trials in which PD-L1 was not predictive of response to checkpoint inhibitors.
The differences among studies could be attributed to different assays, he said. “Where you biopsy and when you biopsy seems to matter.”
In a second opinion poll conducted after the presentations, the proportion of physician attendees saying PD-L1 was essential before initiating checkpoint inhibitors, dropped to about two-thirds.
Dr. Chau reported financial relationships with Bristol-Myers Squibb, Merck Serono, and other pharmaceutical companies. Dr. Lordick reported financial relationships Bristol-Myers Squibb, Merck Sharp & Dohme, Merck, and other pharmaceutical companies.
FROM ASCO GI 2022
Zanubrutinib shows worth against standard CLL drugs
MANCHESTER, ENGLAND – A new treatment option may soon be available for patients with chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL).
Zanubrutinib (Brukinsa), an irreversible, next-generation Bruton tyrosine kinase (BTK) inhibitor, is designed to minimize the off-target cardiovascular toxicities, such as atrial fibrillation and hypertension, seen with the first-generation ibrutinib (Imbruvica).
Zanubrutinib is already approved for use in mantle cell and marginal zone lymphomas and Waldenström’s macroglobulinemia.
Now it has also shown efficacy in CLL.
However, experts question whether the drug will find its place in an increasingly crowded space for the management of CLL.
Data from two phase 3 trials
The new data from two phase 3 clinical trials were presented recently at the British Society for Haematology 62nd annual scientific meeting, held in Manchester, England.
The ALPINE trial compared zanubrutinib with ibrutinib in 415 patients with CLL/SLL and showed that the novel drug was associated with a significant improvement in overall response rate, at 78% versus 63%.
This first interim analysis also showed that there was an increase in progression-free survival (PFS) with zanubrutinib, and crucially, it was associated with a lower atrial fibrillation/flutter rate than ibrutinib.
“These data support that more selective BTK inhibition, with more complete and sustained BTK occupancy, results in improved efficacy and safety outcomes,” said lead author Peter Hillmen, MBChB, FRCP, PhD, St. James’s University Hospital, Leeds, England.
The SEQUOIA study looked at zanubrutinib versus bendamustine plus rituximab in patients with untreated CLL/SLL with a 17p deletion and showed that PFS was improved with zanubrutinib by 58%.
Zanubrutinib was also associated with improved overall response rates and was well tolerated.
The results therefore “support the potential utility of zanubrutinib in the frontline management of patients with previously untreated CLL/SLL,” said lead author Talha Munir, MBBS, also of St. James’s University Hospital.
Improvement over ibrutinib
Ibrutinib, the first BTK inhibitor, “truly revolutionized the way we treat CLL,” commented Renata Walewska, MRCP, PhD, consultant hematologist at the Royal Bournemouth (England) Hospital and chair of the UKCLL Forum.
“But it has got quite a lot of, especially cardiac, problems, with atrial fibrillation and hypertension,” she said in an interview. The problem is that it acts not only as an inhibitor of Bruton kinase, but also affects other kinases, she explained.
Zanubrutinib is “much cleaner,” continued Dr. Walewska, who was lead author of the recently published British Society of Haematology guideline for the treatment of CLL.
However, the drug “is not that groundbreaking,” she commented, as acalabrutinib (Calquence), another next-generation BTK inhibitor, is already available for use in the clinic.
“We’re really lucky in CLL,” Dr. Walewska said, “we’ve got so many new drugs available, and it’s getting quite crowded. Trying to find a place for zanubrutinib is going be tricky.”
Lee Greenberger, PhD, chief scientific officer at the Leukemia & Lymphoma Society, commented that he “gives a lot of credit” to BeiGene, the company behind zanubrutinib, for “taking on these big studies.”
He said that, with the improvements in PFS and reduced atrial fibrillation with the drug, “there will be many clinicians paying attention to this and zanubrutinib could be preferred over conventional options.”
However, he agreed that it will have to compete with acalabrutinib, adding that, beyond BTK inhibitors, there are “a lot of options” for patients with CLL.
“That makes it very difficult for physicians to figure out what is the best type of therapy” to use in these patients, he added.
Dr. Greenberger told this news organization that further studies will need to demonstrate that zanubrutinib is associated with extended survival, which is “just not possible to show” at the moment with the current follow-up period.
He also noted that, in 10 years, ibrutinib will be off-patent, but zanubrutinib will not, at which point the “substantial” cost of the medication, which is a source of “hardship to patients,” will be increasingly relevant.
Study details
The phase 3 ALPINE study involved 415 adults with CLL/SLL refractory to one or more prior systemic therapies and measurable lymphadenopathy on imaging.
They were randomized 1:1 to zanubrutinib or ibrutinib until disease progression or withdrawal from the study.
Most patients had Binet stage A/B or Ann Arbor stage I/II disease, and 7.3% of patients treated with zanubrutinib and 10.1% of those assigned to ibrutinib had received more than three prior lines of therapy.
Over 60% of patients were aged 65 years or older and around 70% were men, with no significant differences between treatment groups.
Patients were randomized 1:1 to zanubrutinib or ibrutinib until disease progression or study withdrawal.
After a median follow-up of 15 months, the overall response rate was significantly higher with zanubrutinib than ibrutinib, at 78.3% versus 62.5% (P = .0006).
Subgroup analysis confirmed that the effect was seen regardless of age, sex, disease stage, number of prior lines of therapy, mutation status, or bulky disease.
Over a median follow-up of 14 months, the investigator-assessed 12-month PFS was 94.9% for zanubrutinib and 84.0% for ibrutinib (P = .0007). Overall survival at 12 months was 97% versus 92.7%, but the difference was not significant (P = .1081).
Patients treated with zanubrutinib experienced more grade 3 or higher adverse events than those given ibrutinib, at 55.9% versus 51.2%, although they had fewer adverse events leading to treatment discontinuation, at 7.8% versus 13.0%.
More importantly, there were fewer cardiac disorders of any grade with zanubrutinib versus ibrutinib, and any-grade atrial fibrillation was significantly less common, at 2.5% versus 10.1% (P = .0014).
Rates of hypertension and hemorrhage were similar between the two treatments, while rates of neutropenia were higher with zanubrutinib versus ibrutinib, at 28.4% versus 21.7%.
The phase 3 SEQUOIA study looked at an earlier stage of disease and included patients with previously untreated CLL/SLL (without 17p depletion) who were unsuitable for treatment with fludarabine, cyclophosphamide, and rituximab.
This trial involved 479 patients randomized to zanubrutinib or bendamustine (days 1 and 2) plus rituximab for six cycles of 28 days each (B+R).
The median age of patients was 70 years, and approximately 80% were at least 65 years old. Just over 60% were men and most (over 70%) were from Europe.
After a median of 26.2 months, independent review committee–assessed PFS was significantly longer with zanubrutinib versus B+R (hazard ratio, 0.42; P < .0001), with an estimated 24-month PFS of 85.5% versus 69.5%.
These results held whether patients were stratified by age, Binet stage, bulky disease, or 11q deletion status, and for patients with an unmutated, but not mutated, immunoglobulin heavy chain gene.
The overall response rate with zanubrutinib was 94.6% versus 85.3% with B+R, and estimated 24-month overall survival was 94.3% versus 94.6%.
Rates of adverse events of any grade were similar between the two treatment groups, although B+R was associated with a higher (grade ≥ 3) adverse event rate, at 79.7%, versus 52.5% for zanubrutinib, and a higher rate of treatment discontinuation because of adverse events, at 13.7% versus 8.3%.
Interestingly, any-grade hypertension was more common with zanubrutinib versus B+R, at 14.2% versus 10.6%, but much lower rates of neutropenia were more common with zanubrutinib, at 15.8% versus 56.8%.
The studies were sponsored by BeiGene. Dr. Hillmen has reported relationships with Janssen, AbbVie, Pharmacyclics, Roche, Gilead, AstraZeneca, SOBI, and BeiGene. Dr. Munir has reported relationships with AbbVie, AstraZeneca, Roche, Alexion, Janssen, MorphoSys, and SOBI. Other authors have also declared numerous relationships.
A version of this article first appeared on Medscape.com.
MANCHESTER, ENGLAND – A new treatment option may soon be available for patients with chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL).
Zanubrutinib (Brukinsa), an irreversible, next-generation Bruton tyrosine kinase (BTK) inhibitor, is designed to minimize the off-target cardiovascular toxicities, such as atrial fibrillation and hypertension, seen with the first-generation ibrutinib (Imbruvica).
Zanubrutinib is already approved for use in mantle cell and marginal zone lymphomas and Waldenström’s macroglobulinemia.
Now it has also shown efficacy in CLL.
However, experts question whether the drug will find its place in an increasingly crowded space for the management of CLL.
Data from two phase 3 trials
The new data from two phase 3 clinical trials were presented recently at the British Society for Haematology 62nd annual scientific meeting, held in Manchester, England.
The ALPINE trial compared zanubrutinib with ibrutinib in 415 patients with CLL/SLL and showed that the novel drug was associated with a significant improvement in overall response rate, at 78% versus 63%.
This first interim analysis also showed that there was an increase in progression-free survival (PFS) with zanubrutinib, and crucially, it was associated with a lower atrial fibrillation/flutter rate than ibrutinib.
“These data support that more selective BTK inhibition, with more complete and sustained BTK occupancy, results in improved efficacy and safety outcomes,” said lead author Peter Hillmen, MBChB, FRCP, PhD, St. James’s University Hospital, Leeds, England.
The SEQUOIA study looked at zanubrutinib versus bendamustine plus rituximab in patients with untreated CLL/SLL with a 17p deletion and showed that PFS was improved with zanubrutinib by 58%.
Zanubrutinib was also associated with improved overall response rates and was well tolerated.
The results therefore “support the potential utility of zanubrutinib in the frontline management of patients with previously untreated CLL/SLL,” said lead author Talha Munir, MBBS, also of St. James’s University Hospital.
Improvement over ibrutinib
Ibrutinib, the first BTK inhibitor, “truly revolutionized the way we treat CLL,” commented Renata Walewska, MRCP, PhD, consultant hematologist at the Royal Bournemouth (England) Hospital and chair of the UKCLL Forum.
“But it has got quite a lot of, especially cardiac, problems, with atrial fibrillation and hypertension,” she said in an interview. The problem is that it acts not only as an inhibitor of Bruton kinase, but also affects other kinases, she explained.
Zanubrutinib is “much cleaner,” continued Dr. Walewska, who was lead author of the recently published British Society of Haematology guideline for the treatment of CLL.
However, the drug “is not that groundbreaking,” she commented, as acalabrutinib (Calquence), another next-generation BTK inhibitor, is already available for use in the clinic.
“We’re really lucky in CLL,” Dr. Walewska said, “we’ve got so many new drugs available, and it’s getting quite crowded. Trying to find a place for zanubrutinib is going be tricky.”
Lee Greenberger, PhD, chief scientific officer at the Leukemia & Lymphoma Society, commented that he “gives a lot of credit” to BeiGene, the company behind zanubrutinib, for “taking on these big studies.”
He said that, with the improvements in PFS and reduced atrial fibrillation with the drug, “there will be many clinicians paying attention to this and zanubrutinib could be preferred over conventional options.”
However, he agreed that it will have to compete with acalabrutinib, adding that, beyond BTK inhibitors, there are “a lot of options” for patients with CLL.
“That makes it very difficult for physicians to figure out what is the best type of therapy” to use in these patients, he added.
Dr. Greenberger told this news organization that further studies will need to demonstrate that zanubrutinib is associated with extended survival, which is “just not possible to show” at the moment with the current follow-up period.
He also noted that, in 10 years, ibrutinib will be off-patent, but zanubrutinib will not, at which point the “substantial” cost of the medication, which is a source of “hardship to patients,” will be increasingly relevant.
Study details
The phase 3 ALPINE study involved 415 adults with CLL/SLL refractory to one or more prior systemic therapies and measurable lymphadenopathy on imaging.
They were randomized 1:1 to zanubrutinib or ibrutinib until disease progression or withdrawal from the study.
Most patients had Binet stage A/B or Ann Arbor stage I/II disease, and 7.3% of patients treated with zanubrutinib and 10.1% of those assigned to ibrutinib had received more than three prior lines of therapy.
Over 60% of patients were aged 65 years or older and around 70% were men, with no significant differences between treatment groups.
Patients were randomized 1:1 to zanubrutinib or ibrutinib until disease progression or study withdrawal.
After a median follow-up of 15 months, the overall response rate was significantly higher with zanubrutinib than ibrutinib, at 78.3% versus 62.5% (P = .0006).
Subgroup analysis confirmed that the effect was seen regardless of age, sex, disease stage, number of prior lines of therapy, mutation status, or bulky disease.
Over a median follow-up of 14 months, the investigator-assessed 12-month PFS was 94.9% for zanubrutinib and 84.0% for ibrutinib (P = .0007). Overall survival at 12 months was 97% versus 92.7%, but the difference was not significant (P = .1081).
Patients treated with zanubrutinib experienced more grade 3 or higher adverse events than those given ibrutinib, at 55.9% versus 51.2%, although they had fewer adverse events leading to treatment discontinuation, at 7.8% versus 13.0%.
More importantly, there were fewer cardiac disorders of any grade with zanubrutinib versus ibrutinib, and any-grade atrial fibrillation was significantly less common, at 2.5% versus 10.1% (P = .0014).
Rates of hypertension and hemorrhage were similar between the two treatments, while rates of neutropenia were higher with zanubrutinib versus ibrutinib, at 28.4% versus 21.7%.
The phase 3 SEQUOIA study looked at an earlier stage of disease and included patients with previously untreated CLL/SLL (without 17p depletion) who were unsuitable for treatment with fludarabine, cyclophosphamide, and rituximab.
This trial involved 479 patients randomized to zanubrutinib or bendamustine (days 1 and 2) plus rituximab for six cycles of 28 days each (B+R).
The median age of patients was 70 years, and approximately 80% were at least 65 years old. Just over 60% were men and most (over 70%) were from Europe.
After a median of 26.2 months, independent review committee–assessed PFS was significantly longer with zanubrutinib versus B+R (hazard ratio, 0.42; P < .0001), with an estimated 24-month PFS of 85.5% versus 69.5%.
These results held whether patients were stratified by age, Binet stage, bulky disease, or 11q deletion status, and for patients with an unmutated, but not mutated, immunoglobulin heavy chain gene.
The overall response rate with zanubrutinib was 94.6% versus 85.3% with B+R, and estimated 24-month overall survival was 94.3% versus 94.6%.
Rates of adverse events of any grade were similar between the two treatment groups, although B+R was associated with a higher (grade ≥ 3) adverse event rate, at 79.7%, versus 52.5% for zanubrutinib, and a higher rate of treatment discontinuation because of adverse events, at 13.7% versus 8.3%.
Interestingly, any-grade hypertension was more common with zanubrutinib versus B+R, at 14.2% versus 10.6%, but much lower rates of neutropenia were more common with zanubrutinib, at 15.8% versus 56.8%.
The studies were sponsored by BeiGene. Dr. Hillmen has reported relationships with Janssen, AbbVie, Pharmacyclics, Roche, Gilead, AstraZeneca, SOBI, and BeiGene. Dr. Munir has reported relationships with AbbVie, AstraZeneca, Roche, Alexion, Janssen, MorphoSys, and SOBI. Other authors have also declared numerous relationships.
A version of this article first appeared on Medscape.com.
MANCHESTER, ENGLAND – A new treatment option may soon be available for patients with chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL).
Zanubrutinib (Brukinsa), an irreversible, next-generation Bruton tyrosine kinase (BTK) inhibitor, is designed to minimize the off-target cardiovascular toxicities, such as atrial fibrillation and hypertension, seen with the first-generation ibrutinib (Imbruvica).
Zanubrutinib is already approved for use in mantle cell and marginal zone lymphomas and Waldenström’s macroglobulinemia.
Now it has also shown efficacy in CLL.
However, experts question whether the drug will find its place in an increasingly crowded space for the management of CLL.
Data from two phase 3 trials
The new data from two phase 3 clinical trials were presented recently at the British Society for Haematology 62nd annual scientific meeting, held in Manchester, England.
The ALPINE trial compared zanubrutinib with ibrutinib in 415 patients with CLL/SLL and showed that the novel drug was associated with a significant improvement in overall response rate, at 78% versus 63%.
This first interim analysis also showed that there was an increase in progression-free survival (PFS) with zanubrutinib, and crucially, it was associated with a lower atrial fibrillation/flutter rate than ibrutinib.
“These data support that more selective BTK inhibition, with more complete and sustained BTK occupancy, results in improved efficacy and safety outcomes,” said lead author Peter Hillmen, MBChB, FRCP, PhD, St. James’s University Hospital, Leeds, England.
The SEQUOIA study looked at zanubrutinib versus bendamustine plus rituximab in patients with untreated CLL/SLL with a 17p deletion and showed that PFS was improved with zanubrutinib by 58%.
Zanubrutinib was also associated with improved overall response rates and was well tolerated.
The results therefore “support the potential utility of zanubrutinib in the frontline management of patients with previously untreated CLL/SLL,” said lead author Talha Munir, MBBS, also of St. James’s University Hospital.
Improvement over ibrutinib
Ibrutinib, the first BTK inhibitor, “truly revolutionized the way we treat CLL,” commented Renata Walewska, MRCP, PhD, consultant hematologist at the Royal Bournemouth (England) Hospital and chair of the UKCLL Forum.
“But it has got quite a lot of, especially cardiac, problems, with atrial fibrillation and hypertension,” she said in an interview. The problem is that it acts not only as an inhibitor of Bruton kinase, but also affects other kinases, she explained.
Zanubrutinib is “much cleaner,” continued Dr. Walewska, who was lead author of the recently published British Society of Haematology guideline for the treatment of CLL.
However, the drug “is not that groundbreaking,” she commented, as acalabrutinib (Calquence), another next-generation BTK inhibitor, is already available for use in the clinic.
“We’re really lucky in CLL,” Dr. Walewska said, “we’ve got so many new drugs available, and it’s getting quite crowded. Trying to find a place for zanubrutinib is going be tricky.”
Lee Greenberger, PhD, chief scientific officer at the Leukemia & Lymphoma Society, commented that he “gives a lot of credit” to BeiGene, the company behind zanubrutinib, for “taking on these big studies.”
He said that, with the improvements in PFS and reduced atrial fibrillation with the drug, “there will be many clinicians paying attention to this and zanubrutinib could be preferred over conventional options.”
However, he agreed that it will have to compete with acalabrutinib, adding that, beyond BTK inhibitors, there are “a lot of options” for patients with CLL.
“That makes it very difficult for physicians to figure out what is the best type of therapy” to use in these patients, he added.
Dr. Greenberger told this news organization that further studies will need to demonstrate that zanubrutinib is associated with extended survival, which is “just not possible to show” at the moment with the current follow-up period.
He also noted that, in 10 years, ibrutinib will be off-patent, but zanubrutinib will not, at which point the “substantial” cost of the medication, which is a source of “hardship to patients,” will be increasingly relevant.
Study details
The phase 3 ALPINE study involved 415 adults with CLL/SLL refractory to one or more prior systemic therapies and measurable lymphadenopathy on imaging.
They were randomized 1:1 to zanubrutinib or ibrutinib until disease progression or withdrawal from the study.
Most patients had Binet stage A/B or Ann Arbor stage I/II disease, and 7.3% of patients treated with zanubrutinib and 10.1% of those assigned to ibrutinib had received more than three prior lines of therapy.
Over 60% of patients were aged 65 years or older and around 70% were men, with no significant differences between treatment groups.
Patients were randomized 1:1 to zanubrutinib or ibrutinib until disease progression or study withdrawal.
After a median follow-up of 15 months, the overall response rate was significantly higher with zanubrutinib than ibrutinib, at 78.3% versus 62.5% (P = .0006).
Subgroup analysis confirmed that the effect was seen regardless of age, sex, disease stage, number of prior lines of therapy, mutation status, or bulky disease.
Over a median follow-up of 14 months, the investigator-assessed 12-month PFS was 94.9% for zanubrutinib and 84.0% for ibrutinib (P = .0007). Overall survival at 12 months was 97% versus 92.7%, but the difference was not significant (P = .1081).
Patients treated with zanubrutinib experienced more grade 3 or higher adverse events than those given ibrutinib, at 55.9% versus 51.2%, although they had fewer adverse events leading to treatment discontinuation, at 7.8% versus 13.0%.
More importantly, there were fewer cardiac disorders of any grade with zanubrutinib versus ibrutinib, and any-grade atrial fibrillation was significantly less common, at 2.5% versus 10.1% (P = .0014).
Rates of hypertension and hemorrhage were similar between the two treatments, while rates of neutropenia were higher with zanubrutinib versus ibrutinib, at 28.4% versus 21.7%.
The phase 3 SEQUOIA study looked at an earlier stage of disease and included patients with previously untreated CLL/SLL (without 17p depletion) who were unsuitable for treatment with fludarabine, cyclophosphamide, and rituximab.
This trial involved 479 patients randomized to zanubrutinib or bendamustine (days 1 and 2) plus rituximab for six cycles of 28 days each (B+R).
The median age of patients was 70 years, and approximately 80% were at least 65 years old. Just over 60% were men and most (over 70%) were from Europe.
After a median of 26.2 months, independent review committee–assessed PFS was significantly longer with zanubrutinib versus B+R (hazard ratio, 0.42; P < .0001), with an estimated 24-month PFS of 85.5% versus 69.5%.
These results held whether patients were stratified by age, Binet stage, bulky disease, or 11q deletion status, and for patients with an unmutated, but not mutated, immunoglobulin heavy chain gene.
The overall response rate with zanubrutinib was 94.6% versus 85.3% with B+R, and estimated 24-month overall survival was 94.3% versus 94.6%.
Rates of adverse events of any grade were similar between the two treatment groups, although B+R was associated with a higher (grade ≥ 3) adverse event rate, at 79.7%, versus 52.5% for zanubrutinib, and a higher rate of treatment discontinuation because of adverse events, at 13.7% versus 8.3%.
Interestingly, any-grade hypertension was more common with zanubrutinib versus B+R, at 14.2% versus 10.6%, but much lower rates of neutropenia were more common with zanubrutinib, at 15.8% versus 56.8%.
The studies were sponsored by BeiGene. Dr. Hillmen has reported relationships with Janssen, AbbVie, Pharmacyclics, Roche, Gilead, AstraZeneca, SOBI, and BeiGene. Dr. Munir has reported relationships with AbbVie, AstraZeneca, Roche, Alexion, Janssen, MorphoSys, and SOBI. Other authors have also declared numerous relationships.
A version of this article first appeared on Medscape.com.
Cancer diet studies: Veggies get another rave, while red meat’s busted again
Researchers report that high consumption of vegetables – especially lettuce, legumes, and cruciferous varieties – appears to lower the risk of liver cancer/liver disease. A separate team suggests that high consumption of red meat, organ meats, and processed meats boosts the risk of gastric cancer.
The findings of the latter study “reinforce the idea that avoidance of red meat and processed meat is probably good beyond [the prevention of] colorectal cancer,” said corresponding author and epidemiologist Paolo Boffetta, MD, MPH, of Stony Brook University Cancer Center, New York, in an interview. “The possible carcinogenic effect may extend beyond the colon.”
Both studies were released at the annual meeting of the American Association for Cancer Research.
For the red meat study, researchers examined statistics from the Golestan cohort study, which is prospectively tracking 50,045 people aged 40-75 from northeastern Iran. The study focuses on esophageal cancer due to the region’s high rate of the disease.
Red meat consumption is fairly rare in the region, where residents typically prefer chicken, said study lead author Giulia Collatuzzo, MD, a resident physician in occupational medicine at the University of Bologna, Italy, in an interview. On average, participants reported eating 18.4 grams daily of red meat and 72.1 grams daily of white meat.
The researchers tracked study participants for a median 12-year follow-up, during which 369 developed esophageal cancer and 368 developed gastric cancer. Red meat was only linked to more esophageal cancer in women (hazard ratio, 1.13, 95% confidence interval, 1.00-1.18, for each quintile increase in consumption).
Overall red meat consumption (including red meat, organ meat, and processed meat) was linked to higher rates of gastric cancer (HR, 1.08, 95% CI, 1.00-1.17) for each quartile increase in consumption, as was consumption of the red meat subtype alone (HR, 1.09, 95% CI, 1.00-1.18).
According to Dr. Collatuzzo, the findings suggest that those in the highest quartile of overall red meat consumption may have around a 25% increase in risk, compared with the lowest quartile.
Overall, she said, the study findings aren’t surprising. The lack of a connection between red meat consumption and esophageal cancer may be due to the fact that meat only temporarily transits through the esophagus, she said.
For the liver cancer/liver disease study, researchers examined the medical records of 470,653 subjects in the NIH-AARP Diet and Health Study. They were recruited in 1995-1996 when they were 50-71 years old. Over a median follow-up of 15.5 years, 899 developed liver cancer, and 934 died of chronic liver disease.
The median intakes of vegetables in quintile 5 (highest) and quintile 1 (lowest) were 3.7 cups daily and 1.0 cups daily, respectively, said study lead author Long-Gang Zhao, MS, a graduate student at Harvard University.
After adjusting for possible cofounders, those in the highest quintile of vegetable consumption were a third less likely to develop liver cancer, compared with the lowest quintile (HR, 0.66, 95% CI, 0.53-0.82, P < 0.01). Several types of vegetables appeared to be the strongest cancer fighters: cruciferous (broccoli, cauliflower), lettuce, legumes, and carrots. These kinds of vegetables were also linked to lower rates of chronic liver disease mortality (all P < 0.01), as was total vegetable intake for the top quintile versus the lowest quintile (HR, 0.60, 95% CI, 0.49-0.74, P = < 0.01).
“A one-cup increase (8 oz or 225 g) in vegetable intake was associated with about 20% decreased risk of liver cancer incidence and chronic liver mortality,” Zhao said.
There was no statistically significant link between fruit consumption and liver cancer or chronic liver disease mortality.
The findings provide more insight into diet and liver disease, Zhao said. “Chronic liver disease, which predisposes to liver cancer, is the tenth cause of death worldwide, causing two million deaths each year. It shares some etiological processes with liver cancer. Therefore, examining both chronic liver disease mortality and liver cancer incidence in our study may provide a more general picture for the prevention of liver diseases.”
As for limitations, both studies are based on self-reports about food consumption, which can be unreliable, and the subjects in the fruit/vegetable analysis were mainly of European origin.
The authors of both studies report no relevant disclosures. No funding is reported for either study.
Researchers report that high consumption of vegetables – especially lettuce, legumes, and cruciferous varieties – appears to lower the risk of liver cancer/liver disease. A separate team suggests that high consumption of red meat, organ meats, and processed meats boosts the risk of gastric cancer.
The findings of the latter study “reinforce the idea that avoidance of red meat and processed meat is probably good beyond [the prevention of] colorectal cancer,” said corresponding author and epidemiologist Paolo Boffetta, MD, MPH, of Stony Brook University Cancer Center, New York, in an interview. “The possible carcinogenic effect may extend beyond the colon.”
Both studies were released at the annual meeting of the American Association for Cancer Research.
For the red meat study, researchers examined statistics from the Golestan cohort study, which is prospectively tracking 50,045 people aged 40-75 from northeastern Iran. The study focuses on esophageal cancer due to the region’s high rate of the disease.
Red meat consumption is fairly rare in the region, where residents typically prefer chicken, said study lead author Giulia Collatuzzo, MD, a resident physician in occupational medicine at the University of Bologna, Italy, in an interview. On average, participants reported eating 18.4 grams daily of red meat and 72.1 grams daily of white meat.
The researchers tracked study participants for a median 12-year follow-up, during which 369 developed esophageal cancer and 368 developed gastric cancer. Red meat was only linked to more esophageal cancer in women (hazard ratio, 1.13, 95% confidence interval, 1.00-1.18, for each quintile increase in consumption).
Overall red meat consumption (including red meat, organ meat, and processed meat) was linked to higher rates of gastric cancer (HR, 1.08, 95% CI, 1.00-1.17) for each quartile increase in consumption, as was consumption of the red meat subtype alone (HR, 1.09, 95% CI, 1.00-1.18).
According to Dr. Collatuzzo, the findings suggest that those in the highest quartile of overall red meat consumption may have around a 25% increase in risk, compared with the lowest quartile.
Overall, she said, the study findings aren’t surprising. The lack of a connection between red meat consumption and esophageal cancer may be due to the fact that meat only temporarily transits through the esophagus, she said.
For the liver cancer/liver disease study, researchers examined the medical records of 470,653 subjects in the NIH-AARP Diet and Health Study. They were recruited in 1995-1996 when they were 50-71 years old. Over a median follow-up of 15.5 years, 899 developed liver cancer, and 934 died of chronic liver disease.
The median intakes of vegetables in quintile 5 (highest) and quintile 1 (lowest) were 3.7 cups daily and 1.0 cups daily, respectively, said study lead author Long-Gang Zhao, MS, a graduate student at Harvard University.
After adjusting for possible cofounders, those in the highest quintile of vegetable consumption were a third less likely to develop liver cancer, compared with the lowest quintile (HR, 0.66, 95% CI, 0.53-0.82, P < 0.01). Several types of vegetables appeared to be the strongest cancer fighters: cruciferous (broccoli, cauliflower), lettuce, legumes, and carrots. These kinds of vegetables were also linked to lower rates of chronic liver disease mortality (all P < 0.01), as was total vegetable intake for the top quintile versus the lowest quintile (HR, 0.60, 95% CI, 0.49-0.74, P = < 0.01).
“A one-cup increase (8 oz or 225 g) in vegetable intake was associated with about 20% decreased risk of liver cancer incidence and chronic liver mortality,” Zhao said.
There was no statistically significant link between fruit consumption and liver cancer or chronic liver disease mortality.
The findings provide more insight into diet and liver disease, Zhao said. “Chronic liver disease, which predisposes to liver cancer, is the tenth cause of death worldwide, causing two million deaths each year. It shares some etiological processes with liver cancer. Therefore, examining both chronic liver disease mortality and liver cancer incidence in our study may provide a more general picture for the prevention of liver diseases.”
As for limitations, both studies are based on self-reports about food consumption, which can be unreliable, and the subjects in the fruit/vegetable analysis were mainly of European origin.
The authors of both studies report no relevant disclosures. No funding is reported for either study.
Researchers report that high consumption of vegetables – especially lettuce, legumes, and cruciferous varieties – appears to lower the risk of liver cancer/liver disease. A separate team suggests that high consumption of red meat, organ meats, and processed meats boosts the risk of gastric cancer.
The findings of the latter study “reinforce the idea that avoidance of red meat and processed meat is probably good beyond [the prevention of] colorectal cancer,” said corresponding author and epidemiologist Paolo Boffetta, MD, MPH, of Stony Brook University Cancer Center, New York, in an interview. “The possible carcinogenic effect may extend beyond the colon.”
Both studies were released at the annual meeting of the American Association for Cancer Research.
For the red meat study, researchers examined statistics from the Golestan cohort study, which is prospectively tracking 50,045 people aged 40-75 from northeastern Iran. The study focuses on esophageal cancer due to the region’s high rate of the disease.
Red meat consumption is fairly rare in the region, where residents typically prefer chicken, said study lead author Giulia Collatuzzo, MD, a resident physician in occupational medicine at the University of Bologna, Italy, in an interview. On average, participants reported eating 18.4 grams daily of red meat and 72.1 grams daily of white meat.
The researchers tracked study participants for a median 12-year follow-up, during which 369 developed esophageal cancer and 368 developed gastric cancer. Red meat was only linked to more esophageal cancer in women (hazard ratio, 1.13, 95% confidence interval, 1.00-1.18, for each quintile increase in consumption).
Overall red meat consumption (including red meat, organ meat, and processed meat) was linked to higher rates of gastric cancer (HR, 1.08, 95% CI, 1.00-1.17) for each quartile increase in consumption, as was consumption of the red meat subtype alone (HR, 1.09, 95% CI, 1.00-1.18).
According to Dr. Collatuzzo, the findings suggest that those in the highest quartile of overall red meat consumption may have around a 25% increase in risk, compared with the lowest quartile.
Overall, she said, the study findings aren’t surprising. The lack of a connection between red meat consumption and esophageal cancer may be due to the fact that meat only temporarily transits through the esophagus, she said.
For the liver cancer/liver disease study, researchers examined the medical records of 470,653 subjects in the NIH-AARP Diet and Health Study. They were recruited in 1995-1996 when they were 50-71 years old. Over a median follow-up of 15.5 years, 899 developed liver cancer, and 934 died of chronic liver disease.
The median intakes of vegetables in quintile 5 (highest) and quintile 1 (lowest) were 3.7 cups daily and 1.0 cups daily, respectively, said study lead author Long-Gang Zhao, MS, a graduate student at Harvard University.
After adjusting for possible cofounders, those in the highest quintile of vegetable consumption were a third less likely to develop liver cancer, compared with the lowest quintile (HR, 0.66, 95% CI, 0.53-0.82, P < 0.01). Several types of vegetables appeared to be the strongest cancer fighters: cruciferous (broccoli, cauliflower), lettuce, legumes, and carrots. These kinds of vegetables were also linked to lower rates of chronic liver disease mortality (all P < 0.01), as was total vegetable intake for the top quintile versus the lowest quintile (HR, 0.60, 95% CI, 0.49-0.74, P = < 0.01).
“A one-cup increase (8 oz or 225 g) in vegetable intake was associated with about 20% decreased risk of liver cancer incidence and chronic liver mortality,” Zhao said.
There was no statistically significant link between fruit consumption and liver cancer or chronic liver disease mortality.
The findings provide more insight into diet and liver disease, Zhao said. “Chronic liver disease, which predisposes to liver cancer, is the tenth cause of death worldwide, causing two million deaths each year. It shares some etiological processes with liver cancer. Therefore, examining both chronic liver disease mortality and liver cancer incidence in our study may provide a more general picture for the prevention of liver diseases.”
As for limitations, both studies are based on self-reports about food consumption, which can be unreliable, and the subjects in the fruit/vegetable analysis were mainly of European origin.
The authors of both studies report no relevant disclosures. No funding is reported for either study.
FROM AACR 2022
‘Time is blood’: Researchers devise shortcut to AHA diagnosis
“A simple algorithm for unexplained bleeding might be helpful to emergency department physicians and other frontline workers to improve recognition of the disease,” said Amar Kelkar, MD, a fellow at the Dana-Farber Cancer Institute, Boston, and corresponding author of “Time is blood: The impact of diagnostic delays on acquired hemophilia A,” a report that appeared in the journal Cureus.
According to Dr. Kelkar, AHA is an autoimmune disease caused by the formation of autoantibodies against factor VIII (FVIII). “Classically, patients present with various forms of bleeding symptoms, including extensive bruising, spontaneous prolonged or persistent bleeding, and blood in the urine. These symptoms are usually accompanied by a prolonged activated partial thromboplastin time (aPTT) test,” he said in an interview. “While this is a rare diagnosis to be seen in primary, critical, or emergency care, it’s a disease that most hematologists should have seen and managed before.”
For the new study, researchers retrospectively tracked patients with AHA at the OSF Healthcare System in Illinois from 2010 to 2017. They focused on six patients (mean age, 79.5; male = 5). Cancer was considered a cause in four cases, and autoimmune disease in one. The sixth case was idiopathic. Five of the six patients died, with all but one death related to bleeding.
The researchers note that they saw more cases than expected (6 per 2.1 million vs. an estimated incidence of 1.48 per 1 million per year), although they attributed this high incidence to the population being made up of older hospitalized patients. In fact, Dr. Kelkar said, researchers believe this is an undercount reflecting diagnostic misses.
The median time to diagnosis was 14 days, the authors report, reflecting other studies that have also shown delays. Pseudo-thrombosis and preexisting anticoagulant therapy likely contribute to the diagnostic delays, they write.
In their new report, the authors developed an algorithm to speed diagnosis.
“The initial step is the identification of a patient with new, unexplained bleeding,” they write. “In the setting of unexplained bleeding, a detailed clinical history, including medication use, along with a thorough physical examination is critical. Prompt primary laboratory testing should include a complete blood count, a metabolic panel including creatinine and bilirubin, and coagulation testing including aPTT and prothrombin time with international normalized ratio (PT/INR). A resulting isolated aPTT elevation will initiate subsequent steps. Early inpatient hematology consultation is recommended.”
The authors add: “An important point to highlight is that we recommend concurrently ordering an aPTT mixing study and a factor VIII activity (FVIII:C) once a prolonged aPTT is confirmed. This may decrease the time to initiate treatment and improve patient outcomes. If the mixing study result is abnormal with low FVIII:C, hemostatic treatment could be initiated with concurrent confirmatory Bethesda assay or anti-FVIII ELISA, preventing further delay in patient recovery and hopefully reducing potential complications. If there is limited availability of specialty testing or prolonged delays in getting test results, such as for FVIII:C, or an inability to confirm a diagnosis at any stage of the algorithm, transferring the patient to a higher level of care with these laboratory and hematology services should be strongly considered.”
The authors also note that “when the diagnostic delay is greater than 1 month, there will be a significant increase in the days that the patient is required to be on hemostatic therapy, compared to diagnosis before 1 month (23.8 ± 13 vs. 7.6 ± 5.7 days, respectively; P = .003).”
The algorithm is meant to be widely available, Dr. Kelkar said. “That is why we targeted an open-source, general medicine journal like Cureus.”
Jerome Teitel, MD, a hematologist with St. Michael’s Hospital in Toronto, said in an interview that the algorithm “might be a useful guide for initial investigation at community hospitals.”
However, he recommended against emphasizing the use of mixing studies. They are “often ambiguous and just delay ordering the definitive tests (FVIII activity and inhibitor assay), which will need to be done regardless,” he said. “The most important message should be that patients with AHA should be referred to, or at least comanaged with, a hematologist who has specific experience and expertise in the field, and who will likely have access to specialized coagulation tests with short turnaround times.”
Another hematologist, George M. Rodgers III, MD, of the University of Utah, Salt Lake City, said in an interview that the algorithm is appropriate for the evaluation of possible AHA. “Patients with the disorder who present with minor bleeding are not evaluated with high priority by physicians,” he said. “Patients with bleeding and a prolonged PTT should be taken very seriously because AHA patients can develop spontaneous fatal bleeding.”
No study funding is reported. The authors, Dr. Teitel, and Dr. Rodgers report no relevant disclosures.
“A simple algorithm for unexplained bleeding might be helpful to emergency department physicians and other frontline workers to improve recognition of the disease,” said Amar Kelkar, MD, a fellow at the Dana-Farber Cancer Institute, Boston, and corresponding author of “Time is blood: The impact of diagnostic delays on acquired hemophilia A,” a report that appeared in the journal Cureus.
According to Dr. Kelkar, AHA is an autoimmune disease caused by the formation of autoantibodies against factor VIII (FVIII). “Classically, patients present with various forms of bleeding symptoms, including extensive bruising, spontaneous prolonged or persistent bleeding, and blood in the urine. These symptoms are usually accompanied by a prolonged activated partial thromboplastin time (aPTT) test,” he said in an interview. “While this is a rare diagnosis to be seen in primary, critical, or emergency care, it’s a disease that most hematologists should have seen and managed before.”
For the new study, researchers retrospectively tracked patients with AHA at the OSF Healthcare System in Illinois from 2010 to 2017. They focused on six patients (mean age, 79.5; male = 5). Cancer was considered a cause in four cases, and autoimmune disease in one. The sixth case was idiopathic. Five of the six patients died, with all but one death related to bleeding.
The researchers note that they saw more cases than expected (6 per 2.1 million vs. an estimated incidence of 1.48 per 1 million per year), although they attributed this high incidence to the population being made up of older hospitalized patients. In fact, Dr. Kelkar said, researchers believe this is an undercount reflecting diagnostic misses.
The median time to diagnosis was 14 days, the authors report, reflecting other studies that have also shown delays. Pseudo-thrombosis and preexisting anticoagulant therapy likely contribute to the diagnostic delays, they write.
In their new report, the authors developed an algorithm to speed diagnosis.
“The initial step is the identification of a patient with new, unexplained bleeding,” they write. “In the setting of unexplained bleeding, a detailed clinical history, including medication use, along with a thorough physical examination is critical. Prompt primary laboratory testing should include a complete blood count, a metabolic panel including creatinine and bilirubin, and coagulation testing including aPTT and prothrombin time with international normalized ratio (PT/INR). A resulting isolated aPTT elevation will initiate subsequent steps. Early inpatient hematology consultation is recommended.”
The authors add: “An important point to highlight is that we recommend concurrently ordering an aPTT mixing study and a factor VIII activity (FVIII:C) once a prolonged aPTT is confirmed. This may decrease the time to initiate treatment and improve patient outcomes. If the mixing study result is abnormal with low FVIII:C, hemostatic treatment could be initiated with concurrent confirmatory Bethesda assay or anti-FVIII ELISA, preventing further delay in patient recovery and hopefully reducing potential complications. If there is limited availability of specialty testing or prolonged delays in getting test results, such as for FVIII:C, or an inability to confirm a diagnosis at any stage of the algorithm, transferring the patient to a higher level of care with these laboratory and hematology services should be strongly considered.”
The authors also note that “when the diagnostic delay is greater than 1 month, there will be a significant increase in the days that the patient is required to be on hemostatic therapy, compared to diagnosis before 1 month (23.8 ± 13 vs. 7.6 ± 5.7 days, respectively; P = .003).”
The algorithm is meant to be widely available, Dr. Kelkar said. “That is why we targeted an open-source, general medicine journal like Cureus.”
Jerome Teitel, MD, a hematologist with St. Michael’s Hospital in Toronto, said in an interview that the algorithm “might be a useful guide for initial investigation at community hospitals.”
However, he recommended against emphasizing the use of mixing studies. They are “often ambiguous and just delay ordering the definitive tests (FVIII activity and inhibitor assay), which will need to be done regardless,” he said. “The most important message should be that patients with AHA should be referred to, or at least comanaged with, a hematologist who has specific experience and expertise in the field, and who will likely have access to specialized coagulation tests with short turnaround times.”
Another hematologist, George M. Rodgers III, MD, of the University of Utah, Salt Lake City, said in an interview that the algorithm is appropriate for the evaluation of possible AHA. “Patients with the disorder who present with minor bleeding are not evaluated with high priority by physicians,” he said. “Patients with bleeding and a prolonged PTT should be taken very seriously because AHA patients can develop spontaneous fatal bleeding.”
No study funding is reported. The authors, Dr. Teitel, and Dr. Rodgers report no relevant disclosures.
“A simple algorithm for unexplained bleeding might be helpful to emergency department physicians and other frontline workers to improve recognition of the disease,” said Amar Kelkar, MD, a fellow at the Dana-Farber Cancer Institute, Boston, and corresponding author of “Time is blood: The impact of diagnostic delays on acquired hemophilia A,” a report that appeared in the journal Cureus.
According to Dr. Kelkar, AHA is an autoimmune disease caused by the formation of autoantibodies against factor VIII (FVIII). “Classically, patients present with various forms of bleeding symptoms, including extensive bruising, spontaneous prolonged or persistent bleeding, and blood in the urine. These symptoms are usually accompanied by a prolonged activated partial thromboplastin time (aPTT) test,” he said in an interview. “While this is a rare diagnosis to be seen in primary, critical, or emergency care, it’s a disease that most hematologists should have seen and managed before.”
For the new study, researchers retrospectively tracked patients with AHA at the OSF Healthcare System in Illinois from 2010 to 2017. They focused on six patients (mean age, 79.5; male = 5). Cancer was considered a cause in four cases, and autoimmune disease in one. The sixth case was idiopathic. Five of the six patients died, with all but one death related to bleeding.
The researchers note that they saw more cases than expected (6 per 2.1 million vs. an estimated incidence of 1.48 per 1 million per year), although they attributed this high incidence to the population being made up of older hospitalized patients. In fact, Dr. Kelkar said, researchers believe this is an undercount reflecting diagnostic misses.
The median time to diagnosis was 14 days, the authors report, reflecting other studies that have also shown delays. Pseudo-thrombosis and preexisting anticoagulant therapy likely contribute to the diagnostic delays, they write.
In their new report, the authors developed an algorithm to speed diagnosis.
“The initial step is the identification of a patient with new, unexplained bleeding,” they write. “In the setting of unexplained bleeding, a detailed clinical history, including medication use, along with a thorough physical examination is critical. Prompt primary laboratory testing should include a complete blood count, a metabolic panel including creatinine and bilirubin, and coagulation testing including aPTT and prothrombin time with international normalized ratio (PT/INR). A resulting isolated aPTT elevation will initiate subsequent steps. Early inpatient hematology consultation is recommended.”
The authors add: “An important point to highlight is that we recommend concurrently ordering an aPTT mixing study and a factor VIII activity (FVIII:C) once a prolonged aPTT is confirmed. This may decrease the time to initiate treatment and improve patient outcomes. If the mixing study result is abnormal with low FVIII:C, hemostatic treatment could be initiated with concurrent confirmatory Bethesda assay or anti-FVIII ELISA, preventing further delay in patient recovery and hopefully reducing potential complications. If there is limited availability of specialty testing or prolonged delays in getting test results, such as for FVIII:C, or an inability to confirm a diagnosis at any stage of the algorithm, transferring the patient to a higher level of care with these laboratory and hematology services should be strongly considered.”
The authors also note that “when the diagnostic delay is greater than 1 month, there will be a significant increase in the days that the patient is required to be on hemostatic therapy, compared to diagnosis before 1 month (23.8 ± 13 vs. 7.6 ± 5.7 days, respectively; P = .003).”
The algorithm is meant to be widely available, Dr. Kelkar said. “That is why we targeted an open-source, general medicine journal like Cureus.”
Jerome Teitel, MD, a hematologist with St. Michael’s Hospital in Toronto, said in an interview that the algorithm “might be a useful guide for initial investigation at community hospitals.”
However, he recommended against emphasizing the use of mixing studies. They are “often ambiguous and just delay ordering the definitive tests (FVIII activity and inhibitor assay), which will need to be done regardless,” he said. “The most important message should be that patients with AHA should be referred to, or at least comanaged with, a hematologist who has specific experience and expertise in the field, and who will likely have access to specialized coagulation tests with short turnaround times.”
Another hematologist, George M. Rodgers III, MD, of the University of Utah, Salt Lake City, said in an interview that the algorithm is appropriate for the evaluation of possible AHA. “Patients with the disorder who present with minor bleeding are not evaluated with high priority by physicians,” he said. “Patients with bleeding and a prolonged PTT should be taken very seriously because AHA patients can develop spontaneous fatal bleeding.”
No study funding is reported. The authors, Dr. Teitel, and Dr. Rodgers report no relevant disclosures.
FROM CUREUS
Judge strikes down Biden mask mandate for planes, transit
The mandate, enacted in February 2021, is unconstitutional because Congress never granted the Centers for Disease Control and Prevention the power to create such a requirement, U.S. District Judge Kathryn Kimball Mizelle said in her order issued April 18.
“Congress addressed whether the CDC may enact preventative measures that condition the interstate travel of an entire population to CDC dictates. It may not,” the order says.
While the government argued that the definition of “sanitation” in federal law allows it to create travel restrictions like the use of masks, Judge Mizelle disagreed.
“A power to improve ‘sanitation’ would easily extend to requiring vaccinations against COVID-19, the seasonal flu, or other diseases. Or to mandatory social distancing, coughing-into-elbows, and daily multivitamins,” she wrote.
The Biden administration has extended the mask mandate several times since it was first announced. Most recently, the mandate was extended last week and was set to end May 3.
The rule has been alternately praised and criticized by airlines, pilots, and flight attendants. Lawsuits have been filed over the mandate, but Judge Mizelle ruled in favor of two people and the Health Freedom Defense Fund, who filed suit in July 2021.
It is not yet clear if the Biden administration will appeal the decision.
A version of this article first appeared on WebMD.com.
The mandate, enacted in February 2021, is unconstitutional because Congress never granted the Centers for Disease Control and Prevention the power to create such a requirement, U.S. District Judge Kathryn Kimball Mizelle said in her order issued April 18.
“Congress addressed whether the CDC may enact preventative measures that condition the interstate travel of an entire population to CDC dictates. It may not,” the order says.
While the government argued that the definition of “sanitation” in federal law allows it to create travel restrictions like the use of masks, Judge Mizelle disagreed.
“A power to improve ‘sanitation’ would easily extend to requiring vaccinations against COVID-19, the seasonal flu, or other diseases. Or to mandatory social distancing, coughing-into-elbows, and daily multivitamins,” she wrote.
The Biden administration has extended the mask mandate several times since it was first announced. Most recently, the mandate was extended last week and was set to end May 3.
The rule has been alternately praised and criticized by airlines, pilots, and flight attendants. Lawsuits have been filed over the mandate, but Judge Mizelle ruled in favor of two people and the Health Freedom Defense Fund, who filed suit in July 2021.
It is not yet clear if the Biden administration will appeal the decision.
A version of this article first appeared on WebMD.com.
The mandate, enacted in February 2021, is unconstitutional because Congress never granted the Centers for Disease Control and Prevention the power to create such a requirement, U.S. District Judge Kathryn Kimball Mizelle said in her order issued April 18.
“Congress addressed whether the CDC may enact preventative measures that condition the interstate travel of an entire population to CDC dictates. It may not,” the order says.
While the government argued that the definition of “sanitation” in federal law allows it to create travel restrictions like the use of masks, Judge Mizelle disagreed.
“A power to improve ‘sanitation’ would easily extend to requiring vaccinations against COVID-19, the seasonal flu, or other diseases. Or to mandatory social distancing, coughing-into-elbows, and daily multivitamins,” she wrote.
The Biden administration has extended the mask mandate several times since it was first announced. Most recently, the mandate was extended last week and was set to end May 3.
The rule has been alternately praised and criticized by airlines, pilots, and flight attendants. Lawsuits have been filed over the mandate, but Judge Mizelle ruled in favor of two people and the Health Freedom Defense Fund, who filed suit in July 2021.
It is not yet clear if the Biden administration will appeal the decision.
A version of this article first appeared on WebMD.com.
Fresh data confirm healthy plant foods link to lower diabetes risk
A scientific analysis of metabolites from plant-based-diets – especially those rich in whole grains, fruits, and vegetables – may in the future yield clues as to how such eating patterns lower the risk of type 2 diabetes, finds a new study of more than 8,000 people.
The research looked at healthy, unhealthy, and overall plant-based diets, but only metabolic profiles for the healthy and overall plant-based diets showed an inverse relationship with type 2 diabetes.
A primarily “unhealthy” plant-based diet was one including mainly refined grains (e.g., white bread and pasta), fruit juices, potatoes, sugar-sweetened beverages, and sweets/desserts.
“Individual metabolites from consumption of polyphenol-rich plant foods like fruits, vegetables, coffee, and legumes are all closely linked to healthy plant-based diet and lower risk of diabetes,” lead author Frank Hu, MD, said in a press release.
Dr. Hu, of the department of nutrition at Harvard T.H. Chan School of Public Health, Boston, and colleagues reported their findings in Diabetologia.
High-throughput profiling of the metabolome
Given that an individual’s metabolic profile reflects their diet, there is a growing trend in nutritional research to use a technique called high-throughput metabolomics to profile biological samples.
The team conducted an analysis of blood plasma samples and dietary intake using food frequency questionnaires of 10,684 participants from three prospective cohorts (Nurses’ Health Study, Nurses’ Health Study II, and Health Professionals Follow-Up Study). Participants were predominantly White and middle-aged (mean age 54 years), with a mean body mass index of 25.6 kg/m2.
Metabolite profile scores were generated from the blood samples, taken in the 1980s and 1990s, and matched to any cases of incident type 2 diabetes reported during follow-up, which ended in 2016-2017.
The team looked at three different plant-based diets – by definition, higher in plant foods and lower in animal foods – and further categorized them according to the actual foods consumed, to generate an overall plant diet index (PDI), a healthy PDI, or an unhealthy PDI.
In all, 8,827 participants completed the study, and 270 cases of diabetes were reported.
Multi-metabolite profiles were composed of 55 metabolites for the overall PDI, 93 metabolites for healthy PDI, and 75 metabolites for unhealthy PDI.
The findings are that metabolomics can be harnessed and “the identified metabolic profiles could be used to assess adherence to ... plant-based diets as part of type 2 diabetes prevention ... and provide new insights for future investigation,” the researchers concluded.
One coauthor received research support from the California Walnut Commission and Swiss ReManagement; another reported being a scientific consultant to LayerIV. The other authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A scientific analysis of metabolites from plant-based-diets – especially those rich in whole grains, fruits, and vegetables – may in the future yield clues as to how such eating patterns lower the risk of type 2 diabetes, finds a new study of more than 8,000 people.
The research looked at healthy, unhealthy, and overall plant-based diets, but only metabolic profiles for the healthy and overall plant-based diets showed an inverse relationship with type 2 diabetes.
A primarily “unhealthy” plant-based diet was one including mainly refined grains (e.g., white bread and pasta), fruit juices, potatoes, sugar-sweetened beverages, and sweets/desserts.
“Individual metabolites from consumption of polyphenol-rich plant foods like fruits, vegetables, coffee, and legumes are all closely linked to healthy plant-based diet and lower risk of diabetes,” lead author Frank Hu, MD, said in a press release.
Dr. Hu, of the department of nutrition at Harvard T.H. Chan School of Public Health, Boston, and colleagues reported their findings in Diabetologia.
High-throughput profiling of the metabolome
Given that an individual’s metabolic profile reflects their diet, there is a growing trend in nutritional research to use a technique called high-throughput metabolomics to profile biological samples.
The team conducted an analysis of blood plasma samples and dietary intake using food frequency questionnaires of 10,684 participants from three prospective cohorts (Nurses’ Health Study, Nurses’ Health Study II, and Health Professionals Follow-Up Study). Participants were predominantly White and middle-aged (mean age 54 years), with a mean body mass index of 25.6 kg/m2.
Metabolite profile scores were generated from the blood samples, taken in the 1980s and 1990s, and matched to any cases of incident type 2 diabetes reported during follow-up, which ended in 2016-2017.
The team looked at three different plant-based diets – by definition, higher in plant foods and lower in animal foods – and further categorized them according to the actual foods consumed, to generate an overall plant diet index (PDI), a healthy PDI, or an unhealthy PDI.
In all, 8,827 participants completed the study, and 270 cases of diabetes were reported.
Multi-metabolite profiles were composed of 55 metabolites for the overall PDI, 93 metabolites for healthy PDI, and 75 metabolites for unhealthy PDI.
The findings are that metabolomics can be harnessed and “the identified metabolic profiles could be used to assess adherence to ... plant-based diets as part of type 2 diabetes prevention ... and provide new insights for future investigation,” the researchers concluded.
One coauthor received research support from the California Walnut Commission and Swiss ReManagement; another reported being a scientific consultant to LayerIV. The other authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A scientific analysis of metabolites from plant-based-diets – especially those rich in whole grains, fruits, and vegetables – may in the future yield clues as to how such eating patterns lower the risk of type 2 diabetes, finds a new study of more than 8,000 people.
The research looked at healthy, unhealthy, and overall plant-based diets, but only metabolic profiles for the healthy and overall plant-based diets showed an inverse relationship with type 2 diabetes.
A primarily “unhealthy” plant-based diet was one including mainly refined grains (e.g., white bread and pasta), fruit juices, potatoes, sugar-sweetened beverages, and sweets/desserts.
“Individual metabolites from consumption of polyphenol-rich plant foods like fruits, vegetables, coffee, and legumes are all closely linked to healthy plant-based diet and lower risk of diabetes,” lead author Frank Hu, MD, said in a press release.
Dr. Hu, of the department of nutrition at Harvard T.H. Chan School of Public Health, Boston, and colleagues reported their findings in Diabetologia.
High-throughput profiling of the metabolome
Given that an individual’s metabolic profile reflects their diet, there is a growing trend in nutritional research to use a technique called high-throughput metabolomics to profile biological samples.
The team conducted an analysis of blood plasma samples and dietary intake using food frequency questionnaires of 10,684 participants from three prospective cohorts (Nurses’ Health Study, Nurses’ Health Study II, and Health Professionals Follow-Up Study). Participants were predominantly White and middle-aged (mean age 54 years), with a mean body mass index of 25.6 kg/m2.
Metabolite profile scores were generated from the blood samples, taken in the 1980s and 1990s, and matched to any cases of incident type 2 diabetes reported during follow-up, which ended in 2016-2017.
The team looked at three different plant-based diets – by definition, higher in plant foods and lower in animal foods – and further categorized them according to the actual foods consumed, to generate an overall plant diet index (PDI), a healthy PDI, or an unhealthy PDI.
In all, 8,827 participants completed the study, and 270 cases of diabetes were reported.
Multi-metabolite profiles were composed of 55 metabolites for the overall PDI, 93 metabolites for healthy PDI, and 75 metabolites for unhealthy PDI.
The findings are that metabolomics can be harnessed and “the identified metabolic profiles could be used to assess adherence to ... plant-based diets as part of type 2 diabetes prevention ... and provide new insights for future investigation,” the researchers concluded.
One coauthor received research support from the California Walnut Commission and Swiss ReManagement; another reported being a scientific consultant to LayerIV. The other authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM DIABETOLOGIA
Novel COVID-19 vaccine could fill the void for patients with blood cancers
according to study results presented at the annual meeting of the American Association for Cancer Research.
The phase 1/2 trial included 54 patients with a B-cell deficiency (mean age, 63 years; 28% female): 4 had congenital B-cell deficiency and 50 had a blood cancer (lymphocytic leukemia or lymphoma). T-cell immune responses were observed in 86% of patients 28 days after vaccination with a single CoVac-1 dose. The potency of CoVac-1–induced T-cell responses exceeded those seen typically with B cell–deficient patient responses after mRNA vaccine treatment and were comparable with those seen among nonimmunocompromised COVID-19 patients.
In the majority of individuals, currently approved SARS-CoV-2 vaccines induce a robust immune response, however, their efficacy, has been shown to be decreased among individuals who are immunocompromised. Patients treated for hematologic cancers, in particular, receive treatment regimens that damage healthy immune cells, particularly B cells, said Juliane Walz, MD, the study’s senior author and professor of medicine at University Hospital Tübingen (Germany).
“In the clinic, we see many cancer patients who do not mount sufficient humoral immune responses after vaccination with available SARS-CoV-2 vaccines,” Dr. Walz said. “These patients are at a high risk for a severe course of COVID-19.”
B-cell deficiency, she stated, can be compensated for by enhancing T-cell responses against SARS-CoV-2, which can then combat infections in the absence of neutralizing antibodies.
In a prior study of CoVac-1 among 36 adults without immune deficiency, the vaccine elicited T-cell responses that were still robust 3 months post vaccination, and that included responses against omicron and other key SARS-CoV-2 variants.
While mRNA-based or adenoviral vector-based vaccines are limited to the spike protein and are thus prone to loss of activity because of viral mutations, CoVac-1–induced T-cell immunity is far more intense and broader, Dr. Walz said.
CoVac-1 is a peptide vaccine that is injected directly rather than being encoded via mRNA and targets different viral components. It would not be given, however, to healthy, immunocompetent adults because it is important for them to have both B-cell antibody and T-cell response.
The patients with B-cell deficiency recruited for the study were given a single dose of CoVac-1 and assessed for safety and immunogenicity until day 56. Prior vaccinations with an approved SARS-CoV-2 vaccine had failed to elicit a humoral response in 87% of the subjects.
“Our vaccine does not induce antibody responses,” Dr. Walz said. “However, it could be used to induce broad T-cell responses as a complementary or additive vaccine for elderly adults. In the elderly, antibody responses decline very, very fast after vaccination.”
Dr. Walz said that CoVac-1 could find application in various syndromes associated with congenital B-cell deficiencies, in autoimmune diseases such as rheumatoid arthritis and multiple sclerosis, or diseases treated with rituximab or other B cell–depleting therapies (for example, ofatumumab, blinatumomab, or chimeric antigen receptor T cells), and in transplant patients.
A phase 3 study of CoVac-1 versus placebo is under discussion and would require about 300-500 subjects, Dr. Walz said.
“CoVac-1 is designed to induce broad and long-lasting SARS-CoV-2 T-cell immunity, even in individuals who have impaired ability to mount sufficient immunity from a currently approved vaccine, and thus protect these high-risk patients from a severe course of COVID-19,” Dr. Walz said.
“Having an option for these patients is just critical – so this is significant work,” said Ana Maria Lopez, MD, MPH, of the Sidney Kimmel Cancer Center–Jefferson Health, Philadelphia.
Limitations of this study included the small sample size with low racial and ethnic diversity, Dr. Walz stated.
Funding was provided by the Ministry of Science, Research and the Arts of the state of Baden-Württemberg; the Federal Ministry of Research and Education in Germany; the German Research Foundation under Germany’s Excellence Strategy; and the Clinical Cooperation Unit Translational Immunology at University Hospital Tübingen. Dr. Walz holds the CoVac-1 patent.
according to study results presented at the annual meeting of the American Association for Cancer Research.
The phase 1/2 trial included 54 patients with a B-cell deficiency (mean age, 63 years; 28% female): 4 had congenital B-cell deficiency and 50 had a blood cancer (lymphocytic leukemia or lymphoma). T-cell immune responses were observed in 86% of patients 28 days after vaccination with a single CoVac-1 dose. The potency of CoVac-1–induced T-cell responses exceeded those seen typically with B cell–deficient patient responses after mRNA vaccine treatment and were comparable with those seen among nonimmunocompromised COVID-19 patients.
In the majority of individuals, currently approved SARS-CoV-2 vaccines induce a robust immune response, however, their efficacy, has been shown to be decreased among individuals who are immunocompromised. Patients treated for hematologic cancers, in particular, receive treatment regimens that damage healthy immune cells, particularly B cells, said Juliane Walz, MD, the study’s senior author and professor of medicine at University Hospital Tübingen (Germany).
“In the clinic, we see many cancer patients who do not mount sufficient humoral immune responses after vaccination with available SARS-CoV-2 vaccines,” Dr. Walz said. “These patients are at a high risk for a severe course of COVID-19.”
B-cell deficiency, she stated, can be compensated for by enhancing T-cell responses against SARS-CoV-2, which can then combat infections in the absence of neutralizing antibodies.
In a prior study of CoVac-1 among 36 adults without immune deficiency, the vaccine elicited T-cell responses that were still robust 3 months post vaccination, and that included responses against omicron and other key SARS-CoV-2 variants.
While mRNA-based or adenoviral vector-based vaccines are limited to the spike protein and are thus prone to loss of activity because of viral mutations, CoVac-1–induced T-cell immunity is far more intense and broader, Dr. Walz said.
CoVac-1 is a peptide vaccine that is injected directly rather than being encoded via mRNA and targets different viral components. It would not be given, however, to healthy, immunocompetent adults because it is important for them to have both B-cell antibody and T-cell response.
The patients with B-cell deficiency recruited for the study were given a single dose of CoVac-1 and assessed for safety and immunogenicity until day 56. Prior vaccinations with an approved SARS-CoV-2 vaccine had failed to elicit a humoral response in 87% of the subjects.
“Our vaccine does not induce antibody responses,” Dr. Walz said. “However, it could be used to induce broad T-cell responses as a complementary or additive vaccine for elderly adults. In the elderly, antibody responses decline very, very fast after vaccination.”
Dr. Walz said that CoVac-1 could find application in various syndromes associated with congenital B-cell deficiencies, in autoimmune diseases such as rheumatoid arthritis and multiple sclerosis, or diseases treated with rituximab or other B cell–depleting therapies (for example, ofatumumab, blinatumomab, or chimeric antigen receptor T cells), and in transplant patients.
A phase 3 study of CoVac-1 versus placebo is under discussion and would require about 300-500 subjects, Dr. Walz said.
“CoVac-1 is designed to induce broad and long-lasting SARS-CoV-2 T-cell immunity, even in individuals who have impaired ability to mount sufficient immunity from a currently approved vaccine, and thus protect these high-risk patients from a severe course of COVID-19,” Dr. Walz said.
“Having an option for these patients is just critical – so this is significant work,” said Ana Maria Lopez, MD, MPH, of the Sidney Kimmel Cancer Center–Jefferson Health, Philadelphia.
Limitations of this study included the small sample size with low racial and ethnic diversity, Dr. Walz stated.
Funding was provided by the Ministry of Science, Research and the Arts of the state of Baden-Württemberg; the Federal Ministry of Research and Education in Germany; the German Research Foundation under Germany’s Excellence Strategy; and the Clinical Cooperation Unit Translational Immunology at University Hospital Tübingen. Dr. Walz holds the CoVac-1 patent.
according to study results presented at the annual meeting of the American Association for Cancer Research.
The phase 1/2 trial included 54 patients with a B-cell deficiency (mean age, 63 years; 28% female): 4 had congenital B-cell deficiency and 50 had a blood cancer (lymphocytic leukemia or lymphoma). T-cell immune responses were observed in 86% of patients 28 days after vaccination with a single CoVac-1 dose. The potency of CoVac-1–induced T-cell responses exceeded those seen typically with B cell–deficient patient responses after mRNA vaccine treatment and were comparable with those seen among nonimmunocompromised COVID-19 patients.
In the majority of individuals, currently approved SARS-CoV-2 vaccines induce a robust immune response, however, their efficacy, has been shown to be decreased among individuals who are immunocompromised. Patients treated for hematologic cancers, in particular, receive treatment regimens that damage healthy immune cells, particularly B cells, said Juliane Walz, MD, the study’s senior author and professor of medicine at University Hospital Tübingen (Germany).
“In the clinic, we see many cancer patients who do not mount sufficient humoral immune responses after vaccination with available SARS-CoV-2 vaccines,” Dr. Walz said. “These patients are at a high risk for a severe course of COVID-19.”
B-cell deficiency, she stated, can be compensated for by enhancing T-cell responses against SARS-CoV-2, which can then combat infections in the absence of neutralizing antibodies.
In a prior study of CoVac-1 among 36 adults without immune deficiency, the vaccine elicited T-cell responses that were still robust 3 months post vaccination, and that included responses against omicron and other key SARS-CoV-2 variants.
While mRNA-based or adenoviral vector-based vaccines are limited to the spike protein and are thus prone to loss of activity because of viral mutations, CoVac-1–induced T-cell immunity is far more intense and broader, Dr. Walz said.
CoVac-1 is a peptide vaccine that is injected directly rather than being encoded via mRNA and targets different viral components. It would not be given, however, to healthy, immunocompetent adults because it is important for them to have both B-cell antibody and T-cell response.
The patients with B-cell deficiency recruited for the study were given a single dose of CoVac-1 and assessed for safety and immunogenicity until day 56. Prior vaccinations with an approved SARS-CoV-2 vaccine had failed to elicit a humoral response in 87% of the subjects.
“Our vaccine does not induce antibody responses,” Dr. Walz said. “However, it could be used to induce broad T-cell responses as a complementary or additive vaccine for elderly adults. In the elderly, antibody responses decline very, very fast after vaccination.”
Dr. Walz said that CoVac-1 could find application in various syndromes associated with congenital B-cell deficiencies, in autoimmune diseases such as rheumatoid arthritis and multiple sclerosis, or diseases treated with rituximab or other B cell–depleting therapies (for example, ofatumumab, blinatumomab, or chimeric antigen receptor T cells), and in transplant patients.
A phase 3 study of CoVac-1 versus placebo is under discussion and would require about 300-500 subjects, Dr. Walz said.
“CoVac-1 is designed to induce broad and long-lasting SARS-CoV-2 T-cell immunity, even in individuals who have impaired ability to mount sufficient immunity from a currently approved vaccine, and thus protect these high-risk patients from a severe course of COVID-19,” Dr. Walz said.
“Having an option for these patients is just critical – so this is significant work,” said Ana Maria Lopez, MD, MPH, of the Sidney Kimmel Cancer Center–Jefferson Health, Philadelphia.
Limitations of this study included the small sample size with low racial and ethnic diversity, Dr. Walz stated.
Funding was provided by the Ministry of Science, Research and the Arts of the state of Baden-Württemberg; the Federal Ministry of Research and Education in Germany; the German Research Foundation under Germany’s Excellence Strategy; and the Clinical Cooperation Unit Translational Immunology at University Hospital Tübingen. Dr. Walz holds the CoVac-1 patent.
FROM AACR 2022
1 in 7 breast cancer patients report worsening personal finances
a new study found. Factors like disease severity and treatment type didn’t seem to have an impact on financial status.
The findings, presented at the annual meeting of the American Association for Cancer Research, were unexpected. “We were surprised that we did not find that patients who received more aggressive therapies were more likely to experience worsening financial concerns,” said corresponding author and medical oncologist Kathryn J. Ruddy, MD, of the Mayo Clinici in Rochester, Minn.
The study was undertaken to understand the financial stress facing patients with breast cancer. The question was whether individual or disease factors, or both, were at play.
The study is based on results from the Mayo Clinic Breast Disease Registry, a prospective cohort of patient who were at Mayo Clinic Rochester. Participants answered questions about their finances at baseline and then again at annual follow-ups.
Researchers examined survey findings from 1,957 patients (mean age 58.5, 99.1% female, 95.4% White, 54.9% bachelor degree or higher) who answered questions at least twice from 2015-2020. The average time between diagnosis and the most recent follow-up was 25.6 months.
Of the 1,957 patients, 357 (18.2%) said their finances deteriorated as measured by a 1 point or higher decline on a 10-point scale.
There was no statistically significant link between deteriorating finances and age, race, employment status, stage of cancer at diagnosis, type of cancer, or treatment type. There was a slight link between deteriorating finances and reporting that they were in the category of “pay bills, no money for special things” near diagnosis.
Other research has suggested that breast cancer may not disrupt finances to a large extent, at least early on. Earlier in 2022, Stanford (Calif.) University researchers reported the results of a survey of 273 breast and gynecologic cancer patients who were surveyed about their finances at a mean of 3.4 years after diagnosis. While one-third said their cancer caused career changes, the study described overall financial toxicity as mild.
In regard to limitations, the subject population of the new study is overwhelmingly White, and the finances were self-reported by those who participated in the survey. Also, “because our participants were recruited at a tertiary medical center, there were relatively financially secure at baseline,” Dr. Ruddy said. “More financial hardship would be expected in a more financially diverse population.”
In an interview, Cathy Bradley, PhD, associate dean for research at the University of Colorado at Denver and deputy director of the University of Colorado Cancer Center, both in Aurora, praised the study as “an important start toward assessing financial burden in the clinic. Having more universal assessments in the clinic would remove stigma.”
She cautioned about interpreting a seemingly low number of patients whose financial situation worsened. “This was for a single site where there is a high rate of health insurance either through Medicare or Medicaid. There may be some selection bias as well given that Mayo may attract a wealthier patient population. Most women completed treatment and may not have been on long-term therapies.”
Moving forward, Dr. Ruddy said, “we hope to study cost of oncologic care in more geographically and financially diverse populations with breast cancer and other cancers.”
The study was funded by the Breast Cancer Research Foundation and National Cancer Institute. The study authors and Dr. Ruddy report no relevant disclosures.
a new study found. Factors like disease severity and treatment type didn’t seem to have an impact on financial status.
The findings, presented at the annual meeting of the American Association for Cancer Research, were unexpected. “We were surprised that we did not find that patients who received more aggressive therapies were more likely to experience worsening financial concerns,” said corresponding author and medical oncologist Kathryn J. Ruddy, MD, of the Mayo Clinici in Rochester, Minn.
The study was undertaken to understand the financial stress facing patients with breast cancer. The question was whether individual or disease factors, or both, were at play.
The study is based on results from the Mayo Clinic Breast Disease Registry, a prospective cohort of patient who were at Mayo Clinic Rochester. Participants answered questions about their finances at baseline and then again at annual follow-ups.
Researchers examined survey findings from 1,957 patients (mean age 58.5, 99.1% female, 95.4% White, 54.9% bachelor degree or higher) who answered questions at least twice from 2015-2020. The average time between diagnosis and the most recent follow-up was 25.6 months.
Of the 1,957 patients, 357 (18.2%) said their finances deteriorated as measured by a 1 point or higher decline on a 10-point scale.
There was no statistically significant link between deteriorating finances and age, race, employment status, stage of cancer at diagnosis, type of cancer, or treatment type. There was a slight link between deteriorating finances and reporting that they were in the category of “pay bills, no money for special things” near diagnosis.
Other research has suggested that breast cancer may not disrupt finances to a large extent, at least early on. Earlier in 2022, Stanford (Calif.) University researchers reported the results of a survey of 273 breast and gynecologic cancer patients who were surveyed about their finances at a mean of 3.4 years after diagnosis. While one-third said their cancer caused career changes, the study described overall financial toxicity as mild.
In regard to limitations, the subject population of the new study is overwhelmingly White, and the finances were self-reported by those who participated in the survey. Also, “because our participants were recruited at a tertiary medical center, there were relatively financially secure at baseline,” Dr. Ruddy said. “More financial hardship would be expected in a more financially diverse population.”
In an interview, Cathy Bradley, PhD, associate dean for research at the University of Colorado at Denver and deputy director of the University of Colorado Cancer Center, both in Aurora, praised the study as “an important start toward assessing financial burden in the clinic. Having more universal assessments in the clinic would remove stigma.”
She cautioned about interpreting a seemingly low number of patients whose financial situation worsened. “This was for a single site where there is a high rate of health insurance either through Medicare or Medicaid. There may be some selection bias as well given that Mayo may attract a wealthier patient population. Most women completed treatment and may not have been on long-term therapies.”
Moving forward, Dr. Ruddy said, “we hope to study cost of oncologic care in more geographically and financially diverse populations with breast cancer and other cancers.”
The study was funded by the Breast Cancer Research Foundation and National Cancer Institute. The study authors and Dr. Ruddy report no relevant disclosures.
a new study found. Factors like disease severity and treatment type didn’t seem to have an impact on financial status.
The findings, presented at the annual meeting of the American Association for Cancer Research, were unexpected. “We were surprised that we did not find that patients who received more aggressive therapies were more likely to experience worsening financial concerns,” said corresponding author and medical oncologist Kathryn J. Ruddy, MD, of the Mayo Clinici in Rochester, Minn.
The study was undertaken to understand the financial stress facing patients with breast cancer. The question was whether individual or disease factors, or both, were at play.
The study is based on results from the Mayo Clinic Breast Disease Registry, a prospective cohort of patient who were at Mayo Clinic Rochester. Participants answered questions about their finances at baseline and then again at annual follow-ups.
Researchers examined survey findings from 1,957 patients (mean age 58.5, 99.1% female, 95.4% White, 54.9% bachelor degree or higher) who answered questions at least twice from 2015-2020. The average time between diagnosis and the most recent follow-up was 25.6 months.
Of the 1,957 patients, 357 (18.2%) said their finances deteriorated as measured by a 1 point or higher decline on a 10-point scale.
There was no statistically significant link between deteriorating finances and age, race, employment status, stage of cancer at diagnosis, type of cancer, or treatment type. There was a slight link between deteriorating finances and reporting that they were in the category of “pay bills, no money for special things” near diagnosis.
Other research has suggested that breast cancer may not disrupt finances to a large extent, at least early on. Earlier in 2022, Stanford (Calif.) University researchers reported the results of a survey of 273 breast and gynecologic cancer patients who were surveyed about their finances at a mean of 3.4 years after diagnosis. While one-third said their cancer caused career changes, the study described overall financial toxicity as mild.
In regard to limitations, the subject population of the new study is overwhelmingly White, and the finances were self-reported by those who participated in the survey. Also, “because our participants were recruited at a tertiary medical center, there were relatively financially secure at baseline,” Dr. Ruddy said. “More financial hardship would be expected in a more financially diverse population.”
In an interview, Cathy Bradley, PhD, associate dean for research at the University of Colorado at Denver and deputy director of the University of Colorado Cancer Center, both in Aurora, praised the study as “an important start toward assessing financial burden in the clinic. Having more universal assessments in the clinic would remove stigma.”
She cautioned about interpreting a seemingly low number of patients whose financial situation worsened. “This was for a single site where there is a high rate of health insurance either through Medicare or Medicaid. There may be some selection bias as well given that Mayo may attract a wealthier patient population. Most women completed treatment and may not have been on long-term therapies.”
Moving forward, Dr. Ruddy said, “we hope to study cost of oncologic care in more geographically and financially diverse populations with breast cancer and other cancers.”
The study was funded by the Breast Cancer Research Foundation and National Cancer Institute. The study authors and Dr. Ruddy report no relevant disclosures.
FROM AACR 2022
Aged black garlic supplement may help lower BP
After 6 weeks, consumption of ABG with a high concentration of s-allyl-L-cystine (SAC) was associated with a nearly 6-mm Hg reduction in DBP in men. Other cardiovascular disease (CVD) risk factors were not significantly affected.
“The observed reduction in DBP by ABG extract was similar to the effects of dietary approaches, including the effects of the Dietary Approaches to Stop Hypertension(DASH) diet on BP,” say Rosa M. Valls, PhD, Universitat Rovira i Virgili, Reus, Spain, and colleagues.
“The potential beneficial effects of ABG may contribute to obtaining an optimal DBP” but were “better observed in men and in nonoptimal DBP populations,” they write in the study, published in Nutrients.
Pure SAC and aged garlics have shown healthy effects on multiple targets in in vitro and in vivo tests. However, previous studies in humans have not focused on ABG but rather on other types of aged garlic in patients with some type of CVD risk factor and suffered from methodologic or design weaknesses, the authors note.
To address this gap, Dr. Valls and colleagues randomly assigned 67 individuals with moderate hypercholesterolemia (defined as LDL levels of at least 115 mg/dL) to receive one ABG tablet (250 mg ABG extract/1.25 mg SAC) or placebo daily for 6 weeks. Following a 3-week washout, the groups were reversed and the new intervention continued for another 6 weeks.
Participants received dietary recommendations regarding CVD risk factors and had their dietary habits assessed through a 3-day food record at baseline and after 6 weeks during both treatments.
Individuals receiving lipid-lowering treatment or antihypertensives were excluded, as were those with a body mass index of 35 kg/m2 or higher, those with a fasting blood glucose of at least 126 mg/dL, or active smokers.
There were no differences in baseline characteristics between the two groups. The mean systolic and diastolic pressures at baseline were 124/75 mm Hg in the ABG group and 121/74 mm Hg in the placebo group. Their mean age was 53 years.
Adherence with the protocol was “high” at 96.5% in both groups, and no adverse effects were reported.
Reduced risk of death from stroke, ischemic heart disease
Although no significant differences between ABG and placebo were observed at 3 weeks, the decline in DBP after consumption of the ABG extract became significant at 6 weeks (mean change, –3.7 mm Hg vs. –0.10 mm Hg; P = .007).
When stratified by sex and categories of DBP, the mean change in DBP after 6 weeks of ABG consumption was particularly prominent in men and in those with a baseline DBP of at least 75 mm Hg.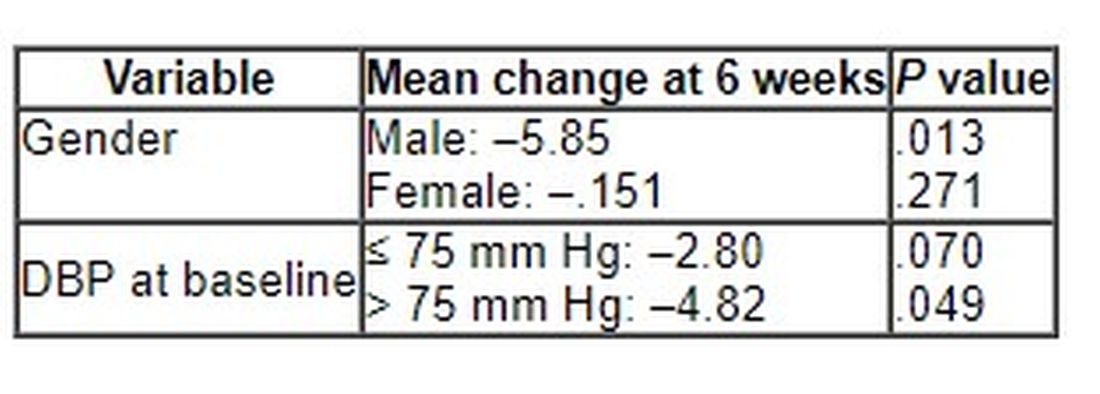
The 6-week change in systolic blood pressure with ABG and placebo was 1.32 mm Hg and 2.84 mm Hg, respectively (P = .694).
At week 6, total cholesterol levels showed a “quadratic decreasing trend” after ABG treatment (P = .047), but no other significant differences between groups were observed for lipid profile, apolipoproteins, or other outcomes of interest, including serum insulin, waist circumference, and body mass index.
The authors note that although systolic BP elevation “has a greater effect on outcomes, both systolic and diastolic hypertension independently influence the risk of adverse cardiovascular events, regardless of the definition of hypertension” and that the risk of death from ischemic heart disease and stroke doubles with every 10 mm Hg increase in DBP in people between the ages of 40 and 89 years.
“Thus, reducing DBP by 5 mm Hg results in a 40% lower risk of death from stroke and a 30% lower risk of death from ischemic heart disease or other vascular death,” they state.
Small study
Commenting for this news organization, Linda Van Horn, PhD, RDN, professor and chief of the department of preventive medicine’s nutrition division, Northwestern University, Chicago, said that for many years, garlic has been “reported to be an adjunct to the benefits of a healthy eating pattern, with inconclusive results.”
She noted that ABG is “literally aged for many months to years, and the resulting concentrate is found higher in many organosulfur compounds and phytochemicals that suggest enhanced response.”
Dr. Van Horn, a member of the American Heart Association’s Nutrition Committee, who was not involved with the study, continued: “The data suggest that ABG that is much more highly concentrated than fresh or processed garlic might be helpful in lowering BP in certain subgroups, in this case men with higher BP.”
However, she cautioned, “these results are limited in a small study, and ... potential other issues, such as sodium, potassium, or other nutrients known to be associated with blood pressure, were not reported, thereby raising questions about the exclusivity of the ABG over other accompanying dietary factors.”
The study was funded by the Center for the Development of Industrial Technology of the Spanish Ministry of Science and Innovation. Two authors are employees of Pharmactive Biotech Products, SL (Madrid), which manufactured the ABG product, but neither played a role in any result or conclusion. The other authors and Dr. Van Horn report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
After 6 weeks, consumption of ABG with a high concentration of s-allyl-L-cystine (SAC) was associated with a nearly 6-mm Hg reduction in DBP in men. Other cardiovascular disease (CVD) risk factors were not significantly affected.
“The observed reduction in DBP by ABG extract was similar to the effects of dietary approaches, including the effects of the Dietary Approaches to Stop Hypertension(DASH) diet on BP,” say Rosa M. Valls, PhD, Universitat Rovira i Virgili, Reus, Spain, and colleagues.
“The potential beneficial effects of ABG may contribute to obtaining an optimal DBP” but were “better observed in men and in nonoptimal DBP populations,” they write in the study, published in Nutrients.
Pure SAC and aged garlics have shown healthy effects on multiple targets in in vitro and in vivo tests. However, previous studies in humans have not focused on ABG but rather on other types of aged garlic in patients with some type of CVD risk factor and suffered from methodologic or design weaknesses, the authors note.
To address this gap, Dr. Valls and colleagues randomly assigned 67 individuals with moderate hypercholesterolemia (defined as LDL levels of at least 115 mg/dL) to receive one ABG tablet (250 mg ABG extract/1.25 mg SAC) or placebo daily for 6 weeks. Following a 3-week washout, the groups were reversed and the new intervention continued for another 6 weeks.
Participants received dietary recommendations regarding CVD risk factors and had their dietary habits assessed through a 3-day food record at baseline and after 6 weeks during both treatments.
Individuals receiving lipid-lowering treatment or antihypertensives were excluded, as were those with a body mass index of 35 kg/m2 or higher, those with a fasting blood glucose of at least 126 mg/dL, or active smokers.
There were no differences in baseline characteristics between the two groups. The mean systolic and diastolic pressures at baseline were 124/75 mm Hg in the ABG group and 121/74 mm Hg in the placebo group. Their mean age was 53 years.
Adherence with the protocol was “high” at 96.5% in both groups, and no adverse effects were reported.
Reduced risk of death from stroke, ischemic heart disease
Although no significant differences between ABG and placebo were observed at 3 weeks, the decline in DBP after consumption of the ABG extract became significant at 6 weeks (mean change, –3.7 mm Hg vs. –0.10 mm Hg; P = .007).
When stratified by sex and categories of DBP, the mean change in DBP after 6 weeks of ABG consumption was particularly prominent in men and in those with a baseline DBP of at least 75 mm Hg.
The 6-week change in systolic blood pressure with ABG and placebo was 1.32 mm Hg and 2.84 mm Hg, respectively (P = .694).
At week 6, total cholesterol levels showed a “quadratic decreasing trend” after ABG treatment (P = .047), but no other significant differences between groups were observed for lipid profile, apolipoproteins, or other outcomes of interest, including serum insulin, waist circumference, and body mass index.
The authors note that although systolic BP elevation “has a greater effect on outcomes, both systolic and diastolic hypertension independently influence the risk of adverse cardiovascular events, regardless of the definition of hypertension” and that the risk of death from ischemic heart disease and stroke doubles with every 10 mm Hg increase in DBP in people between the ages of 40 and 89 years.
“Thus, reducing DBP by 5 mm Hg results in a 40% lower risk of death from stroke and a 30% lower risk of death from ischemic heart disease or other vascular death,” they state.
Small study
Commenting for this news organization, Linda Van Horn, PhD, RDN, professor and chief of the department of preventive medicine’s nutrition division, Northwestern University, Chicago, said that for many years, garlic has been “reported to be an adjunct to the benefits of a healthy eating pattern, with inconclusive results.”
She noted that ABG is “literally aged for many months to years, and the resulting concentrate is found higher in many organosulfur compounds and phytochemicals that suggest enhanced response.”
Dr. Van Horn, a member of the American Heart Association’s Nutrition Committee, who was not involved with the study, continued: “The data suggest that ABG that is much more highly concentrated than fresh or processed garlic might be helpful in lowering BP in certain subgroups, in this case men with higher BP.”
However, she cautioned, “these results are limited in a small study, and ... potential other issues, such as sodium, potassium, or other nutrients known to be associated with blood pressure, were not reported, thereby raising questions about the exclusivity of the ABG over other accompanying dietary factors.”
The study was funded by the Center for the Development of Industrial Technology of the Spanish Ministry of Science and Innovation. Two authors are employees of Pharmactive Biotech Products, SL (Madrid), which manufactured the ABG product, but neither played a role in any result or conclusion. The other authors and Dr. Van Horn report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
After 6 weeks, consumption of ABG with a high concentration of s-allyl-L-cystine (SAC) was associated with a nearly 6-mm Hg reduction in DBP in men. Other cardiovascular disease (CVD) risk factors were not significantly affected.
“The observed reduction in DBP by ABG extract was similar to the effects of dietary approaches, including the effects of the Dietary Approaches to Stop Hypertension(DASH) diet on BP,” say Rosa M. Valls, PhD, Universitat Rovira i Virgili, Reus, Spain, and colleagues.
“The potential beneficial effects of ABG may contribute to obtaining an optimal DBP” but were “better observed in men and in nonoptimal DBP populations,” they write in the study, published in Nutrients.
Pure SAC and aged garlics have shown healthy effects on multiple targets in in vitro and in vivo tests. However, previous studies in humans have not focused on ABG but rather on other types of aged garlic in patients with some type of CVD risk factor and suffered from methodologic or design weaknesses, the authors note.
To address this gap, Dr. Valls and colleagues randomly assigned 67 individuals with moderate hypercholesterolemia (defined as LDL levels of at least 115 mg/dL) to receive one ABG tablet (250 mg ABG extract/1.25 mg SAC) or placebo daily for 6 weeks. Following a 3-week washout, the groups were reversed and the new intervention continued for another 6 weeks.
Participants received dietary recommendations regarding CVD risk factors and had their dietary habits assessed through a 3-day food record at baseline and after 6 weeks during both treatments.
Individuals receiving lipid-lowering treatment or antihypertensives were excluded, as were those with a body mass index of 35 kg/m2 or higher, those with a fasting blood glucose of at least 126 mg/dL, or active smokers.
There were no differences in baseline characteristics between the two groups. The mean systolic and diastolic pressures at baseline were 124/75 mm Hg in the ABG group and 121/74 mm Hg in the placebo group. Their mean age was 53 years.
Adherence with the protocol was “high” at 96.5% in both groups, and no adverse effects were reported.
Reduced risk of death from stroke, ischemic heart disease
Although no significant differences between ABG and placebo were observed at 3 weeks, the decline in DBP after consumption of the ABG extract became significant at 6 weeks (mean change, –3.7 mm Hg vs. –0.10 mm Hg; P = .007).
When stratified by sex and categories of DBP, the mean change in DBP after 6 weeks of ABG consumption was particularly prominent in men and in those with a baseline DBP of at least 75 mm Hg.
The 6-week change in systolic blood pressure with ABG and placebo was 1.32 mm Hg and 2.84 mm Hg, respectively (P = .694).
At week 6, total cholesterol levels showed a “quadratic decreasing trend” after ABG treatment (P = .047), but no other significant differences between groups were observed for lipid profile, apolipoproteins, or other outcomes of interest, including serum insulin, waist circumference, and body mass index.
The authors note that although systolic BP elevation “has a greater effect on outcomes, both systolic and diastolic hypertension independently influence the risk of adverse cardiovascular events, regardless of the definition of hypertension” and that the risk of death from ischemic heart disease and stroke doubles with every 10 mm Hg increase in DBP in people between the ages of 40 and 89 years.
“Thus, reducing DBP by 5 mm Hg results in a 40% lower risk of death from stroke and a 30% lower risk of death from ischemic heart disease or other vascular death,” they state.
Small study
Commenting for this news organization, Linda Van Horn, PhD, RDN, professor and chief of the department of preventive medicine’s nutrition division, Northwestern University, Chicago, said that for many years, garlic has been “reported to be an adjunct to the benefits of a healthy eating pattern, with inconclusive results.”
She noted that ABG is “literally aged for many months to years, and the resulting concentrate is found higher in many organosulfur compounds and phytochemicals that suggest enhanced response.”
Dr. Van Horn, a member of the American Heart Association’s Nutrition Committee, who was not involved with the study, continued: “The data suggest that ABG that is much more highly concentrated than fresh or processed garlic might be helpful in lowering BP in certain subgroups, in this case men with higher BP.”
However, she cautioned, “these results are limited in a small study, and ... potential other issues, such as sodium, potassium, or other nutrients known to be associated with blood pressure, were not reported, thereby raising questions about the exclusivity of the ABG over other accompanying dietary factors.”
The study was funded by the Center for the Development of Industrial Technology of the Spanish Ministry of Science and Innovation. Two authors are employees of Pharmactive Biotech Products, SL (Madrid), which manufactured the ABG product, but neither played a role in any result or conclusion. The other authors and Dr. Van Horn report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NUTRIENTS
Pediatric hepatitis cases may be linked to adenovirus, CDC says
Internationally, 108 cases have been reported in the United Kingdom, with 79 cases occurring in England. There are three documented cases in Spain, and similar cases are being reported in Denmark and the Netherlands, according to an article in Science. In the United Kingdom, cases have been reported in children up to 16 years old, but most affected children are between 2 and 5 years old. Eight children in the United Kingdom have required liver transplants.
On April 14, the CDC said that nine cases have been recorded in Alabama since the fall of 2021. All of these cases have been in children between 1 and 6 years old, and two children have needed liver transplants. Two additional cases have been reported in North Carolina, according to Stat News, and both children have since recovered.
Hepatitis A, B, C, D, and E viruses—common causes of hepatitis—have been ruled out in the U.K. and Spanish cases. More than three-fourths (77%) of the children sickened in the United Kingdom and all nine cases in Alabama have tested positive for a form of the adenovirus. While adenovirus can cause hepatitis in children, it is usually in those who are immunocompromised.
The CDC health alert advises clinicians who have cases of unexplained hepatitis in children to test for adenovirus and report these cases to the CDC as well as state public health authorities. The agency recommends nucleic acid amplification testing to detect adenovirus using respiratory swabs, stool samples or rectal swabs, or blood.
Officials are exploring whether these cases are linked to a version of the virus called adenovirus 41, which is associated with gut inflammation. The most recent case in Alabama was reported in February, and five of the nine children in the state with these puzzling cases of hepatitis have tested positive for adenovirus 41.
There have yet to be any links among the cases in Alabama or North Carolina, and investigators in the United Kingdom have also not found any connections in their cases, STAT News reports.
“CDC is working with state health departments to see if there are additional U.S. cases and what may be causing these cases,” said Kristen Nordlund, a CDC spokesperson, in a statement to STAT News. “At this time, adenovirus may be the cause for these, but investigators are still learning more – including ruling out the more common causes of hepatitis.”
Looking for other explanations
None of the children in the United States with hepatitis had COVID-19, but a few children in the United Kingdom have tested positive for the virus; none of these children have received the COVID-19 vaccine.
While the U.K. Health Security Agency says their investigation “continues to point toward a link to adenovirus infection,” they are also considering other contributing factors such as an environmental cause or COVID-19.
“COVID has been consistently shown to increase liver test numbers,” Nancy Reau, MD, the section chief of hepatology at Rush University in Chicago, said in an interview with this news organization. “It has been shown to cause other organ involvement besides just pulmonary symptoms and respiratory failure. As this virus evolves, it might be that in children, it is more able to present as hepatitis.”
A version of this article first appeared on Medscape.com.
This article was updated 4/22/22.
Internationally, 108 cases have been reported in the United Kingdom, with 79 cases occurring in England. There are three documented cases in Spain, and similar cases are being reported in Denmark and the Netherlands, according to an article in Science. In the United Kingdom, cases have been reported in children up to 16 years old, but most affected children are between 2 and 5 years old. Eight children in the United Kingdom have required liver transplants.
On April 14, the CDC said that nine cases have been recorded in Alabama since the fall of 2021. All of these cases have been in children between 1 and 6 years old, and two children have needed liver transplants. Two additional cases have been reported in North Carolina, according to Stat News, and both children have since recovered.
Hepatitis A, B, C, D, and E viruses—common causes of hepatitis—have been ruled out in the U.K. and Spanish cases. More than three-fourths (77%) of the children sickened in the United Kingdom and all nine cases in Alabama have tested positive for a form of the adenovirus. While adenovirus can cause hepatitis in children, it is usually in those who are immunocompromised.
The CDC health alert advises clinicians who have cases of unexplained hepatitis in children to test for adenovirus and report these cases to the CDC as well as state public health authorities. The agency recommends nucleic acid amplification testing to detect adenovirus using respiratory swabs, stool samples or rectal swabs, or blood.
Officials are exploring whether these cases are linked to a version of the virus called adenovirus 41, which is associated with gut inflammation. The most recent case in Alabama was reported in February, and five of the nine children in the state with these puzzling cases of hepatitis have tested positive for adenovirus 41.
There have yet to be any links among the cases in Alabama or North Carolina, and investigators in the United Kingdom have also not found any connections in their cases, STAT News reports.
“CDC is working with state health departments to see if there are additional U.S. cases and what may be causing these cases,” said Kristen Nordlund, a CDC spokesperson, in a statement to STAT News. “At this time, adenovirus may be the cause for these, but investigators are still learning more – including ruling out the more common causes of hepatitis.”
Looking for other explanations
None of the children in the United States with hepatitis had COVID-19, but a few children in the United Kingdom have tested positive for the virus; none of these children have received the COVID-19 vaccine.
While the U.K. Health Security Agency says their investigation “continues to point toward a link to adenovirus infection,” they are also considering other contributing factors such as an environmental cause or COVID-19.
“COVID has been consistently shown to increase liver test numbers,” Nancy Reau, MD, the section chief of hepatology at Rush University in Chicago, said in an interview with this news organization. “It has been shown to cause other organ involvement besides just pulmonary symptoms and respiratory failure. As this virus evolves, it might be that in children, it is more able to present as hepatitis.”
A version of this article first appeared on Medscape.com.
This article was updated 4/22/22.
Internationally, 108 cases have been reported in the United Kingdom, with 79 cases occurring in England. There are three documented cases in Spain, and similar cases are being reported in Denmark and the Netherlands, according to an article in Science. In the United Kingdom, cases have been reported in children up to 16 years old, but most affected children are between 2 and 5 years old. Eight children in the United Kingdom have required liver transplants.
On April 14, the CDC said that nine cases have been recorded in Alabama since the fall of 2021. All of these cases have been in children between 1 and 6 years old, and two children have needed liver transplants. Two additional cases have been reported in North Carolina, according to Stat News, and both children have since recovered.
Hepatitis A, B, C, D, and E viruses—common causes of hepatitis—have been ruled out in the U.K. and Spanish cases. More than three-fourths (77%) of the children sickened in the United Kingdom and all nine cases in Alabama have tested positive for a form of the adenovirus. While adenovirus can cause hepatitis in children, it is usually in those who are immunocompromised.
The CDC health alert advises clinicians who have cases of unexplained hepatitis in children to test for adenovirus and report these cases to the CDC as well as state public health authorities. The agency recommends nucleic acid amplification testing to detect adenovirus using respiratory swabs, stool samples or rectal swabs, or blood.
Officials are exploring whether these cases are linked to a version of the virus called adenovirus 41, which is associated with gut inflammation. The most recent case in Alabama was reported in February, and five of the nine children in the state with these puzzling cases of hepatitis have tested positive for adenovirus 41.
There have yet to be any links among the cases in Alabama or North Carolina, and investigators in the United Kingdom have also not found any connections in their cases, STAT News reports.
“CDC is working with state health departments to see if there are additional U.S. cases and what may be causing these cases,” said Kristen Nordlund, a CDC spokesperson, in a statement to STAT News. “At this time, adenovirus may be the cause for these, but investigators are still learning more – including ruling out the more common causes of hepatitis.”
Looking for other explanations
None of the children in the United States with hepatitis had COVID-19, but a few children in the United Kingdom have tested positive for the virus; none of these children have received the COVID-19 vaccine.
While the U.K. Health Security Agency says their investigation “continues to point toward a link to adenovirus infection,” they are also considering other contributing factors such as an environmental cause or COVID-19.
“COVID has been consistently shown to increase liver test numbers,” Nancy Reau, MD, the section chief of hepatology at Rush University in Chicago, said in an interview with this news organization. “It has been shown to cause other organ involvement besides just pulmonary symptoms and respiratory failure. As this virus evolves, it might be that in children, it is more able to present as hepatitis.”
A version of this article first appeared on Medscape.com.
This article was updated 4/22/22.