User login
More Black mothers deliver by cesarean, not always by choice
When 29-year-old Sakeenah Fowler was pregnant with her first child, doctors kept a close watch. Ms. Fowler has lupus, high blood pressure, a history of blood clotting, and kidney problems that all could have endangered her or the health of her unborn baby.
She saw maternal-fetal specialists who could keep watch of her high-risk pregnancy, and she collected urine samples every 24 hours to make sure her kidneys were functioning properly from her home in Roebuck, S.C.
But the pregnancy ultimately proved uneventful; even her kidneys remained stable. So Ms. Fowler said she was shocked when her doctors ordered an emergency cesarean delivery after she had gone into active labor.
“I was already dilated all the way to 6 cm,” but the baby’s heart rate had decreased by a small amount, she says. “They thought it was best to just go ahead with a C-section.”
Ms. Fowler, who is Black, said she believes the surgical intervention was unnecessary and that she wasn’t given a chance to discuss her options for a vaginal childbirth.
“They already had it in their minds that I wasn’t going to make it through the pregnancy without any issues; then when I did, it was like they wanted to find something that made me have to have a C-section,” Ms. Fowler said. “It was close to the holidays; everybody was ready to go home. It was just like I was pushed to do what they wanted me to do.”
Ms. Fowler’s sense of a lack of choice is important beyond the measure of patient experience. While cesarean deliveries can be a lifeline for mother and baby, they can put up massive roadblocks to maternal and infant health when not necessary.
“The risk of hemorrhage, infection – on average, all of these go up when you have surgery instead of a vaginal delivery,” says Kimberly B. Glazer, PhD, a perinatal epidemiologist at the Icahn School of Medicine at Mount Sinai, New York.
“Birth is one of the most salient experiences you can have. People want to feel like their values and preferences – whatever they may be – were honored and respected. Even if the delivery goes a different way than you wanted, feeling like your values were taken into account is very important.”
More than 1 million women undergo cesarean deliveries in the United States every year, composing over 31% of all births in 2020, according to the Centers for Disease Control and Prevention.
The World Health Organization, meanwhile, recommends a rate of cesarean delivery of no more than 15% per region. Whether or not all the U.S. procedures were medically warranted is unclear, however.
Black women have higher odds of undergoing a cesarean: 36% undergo surgical deliveries annually, compared with about 30% of White women. Black women are also about three times more likely to die of pregnancy-related causes than White women.
Risk becomes reality
Ms. Fowler eventually developed an infection in her cesarean surgical wound, but her doctors initially insisted her alternating chills and fever were merely postpartum hormonal swings, she says.
“I thought something had to be wrong, but they just kept saying nothing was wrong,” she says.
By the time her doctors caught the infection, Ms. Fowler was readmitted to the hospital for several days of IV antibiotic therapy. The infection “almost got into my bloodstream and could have killed me,” she says.
While cesarean deliveries are associated with decreases in maternal, neonatal, and infant mortality, the benefits are only seen up to a certain threshold. The WHO, for instance, has reported that over the 15% threshold, that lower mortality benefit disappears.
“When medically necessary, cesarean delivery can improve outcomes for mother and baby. But the fact that cesarean section rates have increased in recent years without a corresponding improvement in health outcomes indicates overreliance on the procedure,” Dr. Glazer says.
Clinical discretion leads to biased judgment calls
Rates of cesarean deliveries are even higher among low-risk pregnancies in women of color than in White women. Between 2016 and 2019, the overall rate of cesarean deliveries for low-risk births was 23%, according to a recent analysis. But the rate was almost 18% higher among Black women than among White women (27% vs. 22%).
“When you see data about these subjective indications varying by race and ethnicity, I think that’s pointing us toward some answers,” Dr. Glazer says. “Once you adjust for all these measures, prepregnancy characteristics, and risk factors, the research identifies variation in quality and outcomes that is rooted in structural and systemic racism in health care, implicit bias from clinicians.”
Researchers investigating cesarean deliveries have found that Black women are more likely to undergo the surgery for reasons that are highly subjective, such as fetal distress.
“There is a huge range of how concerning a fetal heart rate can be, and some health providers might perform a C-section for only minor changes in the fetal heart rate, while others might wait until it is much worse,” said Rebecca Hamm, MD, an assistant professor of obstetrics and gynecology at the Perelman School of Medicine at the University of Pennsylvania.
At least some of the differences in care can be explained by where women deliver their babies, studies have shown. Women of color disproportionately deliver at hospitals with poorer quality outcomes for moms and babies.
Dealing with the aftermath
There can be costs that reverberate throughout the life of a mother, child, and their family as the result of surgical delivery.
“Cesarean sections cost a lot more,” says Jamila Taylor, PhD, director of health care reform and a senior fellow with The Century Foundation, a progressive policy think tank in Washington, D.C. The cost of a cesarean delivery averages about $17,000, compared with about $12,200 for a vaginal birth; for uninsured patients, surgical deliveries cost about $9,000 more than vaginal deliveries.
Dr. Taylor, who has studied the historical mistreatment of Black women in obstetrics, noted that this cost includes not just the bill for surgery but also a prolonged recovery time that is often spent in a hospital bed.
Beyond the detrimental effect that a large hospital bill for delivery and aftercare can have on families, other costs can crop up later. Infants delivered by cesarean surgery are more likely to develop an infection, breathing problems, and to spend time in the neonatal intensive care unit than babies born vaginally. Although studies suggest these outcomes may result from a medically necessary health concern that spurred the cesarean surgery, they often stem from the delivery itself.
Babies born surgically also miss out on the benefits of passing through the birth canal, such as supporting a newborn’s immune system and preparing their lungs to breathe oxygen after birth.
Most of the efforts to reduce inequities in maternal care are happening at the clinical level, aimed at both patients and providers, Dr. Taylor says.
“As advocates, we’re talking about how we can help Black women be advocates for themselves in the health care system – if the physician suggests a C-section, getting a second opinion, or walking through what a [surgical delivery] will mean and what their recovery will look like,” she says.
Women are also increasingly choosing non-hospital settings to deliver when possible, Dr. Taylor says. Including doulas or midwife practitioners in the maternal care team can reduce unnecessary cesarean deliveries among Black women, according to Camille Clare, MD, chair of the New York chapter of the American College of Obstetricians and Gynecologists.
Also, last year, race was removed from the vaginal birth after C-section (VBAC) calculator, which is used to gauge the safety of vaginal delivery in women with a history of surgical birth. The original calculator included race-based correction factors for Black women and Hispanic women. It predicted a lower likelihood of successful vaginal deliveries for women who already had a C-section and who identify as Black or Hispanic than for White women with otherwise identical characteristics, such as age, weight, and a history of cesarean delivery.
“Those are things that over time should reduce the high rates of cesarean section for Black women in particular,” Dr. Clare says.
In addition to embracing the updated calculator and including nurse-midwives and doulas in their obstetrics services, Penn Medicine, Philadelphia received a federal grant to study the impact of creating a standard plan for deliveries. This includes standardizing the induction of labor and any effect that might have on reducing C-section rates.
“This idea that biases lead to difference in decisionmaking, and that by standardizing practices we could address these differences – people were somewhat resistant at first,” Dr. Hamm says. “They didn’t believe there were differences in their practices.”
People struggle to recognize those differences, she says, and “it takes active participation in reducing disparities to make that happen.”
At the community level, Synergistic Sisters in Science (SIS), a group of maternal health experts and health equity advocates, is working on a project called PM3, to reduce maternal mortality through mobile technology.
The smartphone app will provide information for new moms to empower them to start conversations with health care providers. It also connects users to social support and resources. SIS is especially hoping to engage Black women living in rural areas.
“There is so much mistrust due to things like unnecessary C-sections and the fact that Black women feel they aren’t heard,” said Natalie Hernandez, PhD, executive director of the Center for Maternal Health Equity at Morehouse School of Medicine, Atlanta. “Here is a tool that gives a woman information that’s culturally centered, looks like her, and was informed by her voice.”
A version of this article first appeared on WebMD.com.
When 29-year-old Sakeenah Fowler was pregnant with her first child, doctors kept a close watch. Ms. Fowler has lupus, high blood pressure, a history of blood clotting, and kidney problems that all could have endangered her or the health of her unborn baby.
She saw maternal-fetal specialists who could keep watch of her high-risk pregnancy, and she collected urine samples every 24 hours to make sure her kidneys were functioning properly from her home in Roebuck, S.C.
But the pregnancy ultimately proved uneventful; even her kidneys remained stable. So Ms. Fowler said she was shocked when her doctors ordered an emergency cesarean delivery after she had gone into active labor.
“I was already dilated all the way to 6 cm,” but the baby’s heart rate had decreased by a small amount, she says. “They thought it was best to just go ahead with a C-section.”
Ms. Fowler, who is Black, said she believes the surgical intervention was unnecessary and that she wasn’t given a chance to discuss her options for a vaginal childbirth.
“They already had it in their minds that I wasn’t going to make it through the pregnancy without any issues; then when I did, it was like they wanted to find something that made me have to have a C-section,” Ms. Fowler said. “It was close to the holidays; everybody was ready to go home. It was just like I was pushed to do what they wanted me to do.”
Ms. Fowler’s sense of a lack of choice is important beyond the measure of patient experience. While cesarean deliveries can be a lifeline for mother and baby, they can put up massive roadblocks to maternal and infant health when not necessary.
“The risk of hemorrhage, infection – on average, all of these go up when you have surgery instead of a vaginal delivery,” says Kimberly B. Glazer, PhD, a perinatal epidemiologist at the Icahn School of Medicine at Mount Sinai, New York.
“Birth is one of the most salient experiences you can have. People want to feel like their values and preferences – whatever they may be – were honored and respected. Even if the delivery goes a different way than you wanted, feeling like your values were taken into account is very important.”
More than 1 million women undergo cesarean deliveries in the United States every year, composing over 31% of all births in 2020, according to the Centers for Disease Control and Prevention.
The World Health Organization, meanwhile, recommends a rate of cesarean delivery of no more than 15% per region. Whether or not all the U.S. procedures were medically warranted is unclear, however.
Black women have higher odds of undergoing a cesarean: 36% undergo surgical deliveries annually, compared with about 30% of White women. Black women are also about three times more likely to die of pregnancy-related causes than White women.
Risk becomes reality
Ms. Fowler eventually developed an infection in her cesarean surgical wound, but her doctors initially insisted her alternating chills and fever were merely postpartum hormonal swings, she says.
“I thought something had to be wrong, but they just kept saying nothing was wrong,” she says.
By the time her doctors caught the infection, Ms. Fowler was readmitted to the hospital for several days of IV antibiotic therapy. The infection “almost got into my bloodstream and could have killed me,” she says.
While cesarean deliveries are associated with decreases in maternal, neonatal, and infant mortality, the benefits are only seen up to a certain threshold. The WHO, for instance, has reported that over the 15% threshold, that lower mortality benefit disappears.
“When medically necessary, cesarean delivery can improve outcomes for mother and baby. But the fact that cesarean section rates have increased in recent years without a corresponding improvement in health outcomes indicates overreliance on the procedure,” Dr. Glazer says.
Clinical discretion leads to biased judgment calls
Rates of cesarean deliveries are even higher among low-risk pregnancies in women of color than in White women. Between 2016 and 2019, the overall rate of cesarean deliveries for low-risk births was 23%, according to a recent analysis. But the rate was almost 18% higher among Black women than among White women (27% vs. 22%).
“When you see data about these subjective indications varying by race and ethnicity, I think that’s pointing us toward some answers,” Dr. Glazer says. “Once you adjust for all these measures, prepregnancy characteristics, and risk factors, the research identifies variation in quality and outcomes that is rooted in structural and systemic racism in health care, implicit bias from clinicians.”
Researchers investigating cesarean deliveries have found that Black women are more likely to undergo the surgery for reasons that are highly subjective, such as fetal distress.
“There is a huge range of how concerning a fetal heart rate can be, and some health providers might perform a C-section for only minor changes in the fetal heart rate, while others might wait until it is much worse,” said Rebecca Hamm, MD, an assistant professor of obstetrics and gynecology at the Perelman School of Medicine at the University of Pennsylvania.
At least some of the differences in care can be explained by where women deliver their babies, studies have shown. Women of color disproportionately deliver at hospitals with poorer quality outcomes for moms and babies.
Dealing with the aftermath
There can be costs that reverberate throughout the life of a mother, child, and their family as the result of surgical delivery.
“Cesarean sections cost a lot more,” says Jamila Taylor, PhD, director of health care reform and a senior fellow with The Century Foundation, a progressive policy think tank in Washington, D.C. The cost of a cesarean delivery averages about $17,000, compared with about $12,200 for a vaginal birth; for uninsured patients, surgical deliveries cost about $9,000 more than vaginal deliveries.
Dr. Taylor, who has studied the historical mistreatment of Black women in obstetrics, noted that this cost includes not just the bill for surgery but also a prolonged recovery time that is often spent in a hospital bed.
Beyond the detrimental effect that a large hospital bill for delivery and aftercare can have on families, other costs can crop up later. Infants delivered by cesarean surgery are more likely to develop an infection, breathing problems, and to spend time in the neonatal intensive care unit than babies born vaginally. Although studies suggest these outcomes may result from a medically necessary health concern that spurred the cesarean surgery, they often stem from the delivery itself.
Babies born surgically also miss out on the benefits of passing through the birth canal, such as supporting a newborn’s immune system and preparing their lungs to breathe oxygen after birth.
Most of the efforts to reduce inequities in maternal care are happening at the clinical level, aimed at both patients and providers, Dr. Taylor says.
“As advocates, we’re talking about how we can help Black women be advocates for themselves in the health care system – if the physician suggests a C-section, getting a second opinion, or walking through what a [surgical delivery] will mean and what their recovery will look like,” she says.
Women are also increasingly choosing non-hospital settings to deliver when possible, Dr. Taylor says. Including doulas or midwife practitioners in the maternal care team can reduce unnecessary cesarean deliveries among Black women, according to Camille Clare, MD, chair of the New York chapter of the American College of Obstetricians and Gynecologists.
Also, last year, race was removed from the vaginal birth after C-section (VBAC) calculator, which is used to gauge the safety of vaginal delivery in women with a history of surgical birth. The original calculator included race-based correction factors for Black women and Hispanic women. It predicted a lower likelihood of successful vaginal deliveries for women who already had a C-section and who identify as Black or Hispanic than for White women with otherwise identical characteristics, such as age, weight, and a history of cesarean delivery.
“Those are things that over time should reduce the high rates of cesarean section for Black women in particular,” Dr. Clare says.
In addition to embracing the updated calculator and including nurse-midwives and doulas in their obstetrics services, Penn Medicine, Philadelphia received a federal grant to study the impact of creating a standard plan for deliveries. This includes standardizing the induction of labor and any effect that might have on reducing C-section rates.
“This idea that biases lead to difference in decisionmaking, and that by standardizing practices we could address these differences – people were somewhat resistant at first,” Dr. Hamm says. “They didn’t believe there were differences in their practices.”
People struggle to recognize those differences, she says, and “it takes active participation in reducing disparities to make that happen.”
At the community level, Synergistic Sisters in Science (SIS), a group of maternal health experts and health equity advocates, is working on a project called PM3, to reduce maternal mortality through mobile technology.
The smartphone app will provide information for new moms to empower them to start conversations with health care providers. It also connects users to social support and resources. SIS is especially hoping to engage Black women living in rural areas.
“There is so much mistrust due to things like unnecessary C-sections and the fact that Black women feel they aren’t heard,” said Natalie Hernandez, PhD, executive director of the Center for Maternal Health Equity at Morehouse School of Medicine, Atlanta. “Here is a tool that gives a woman information that’s culturally centered, looks like her, and was informed by her voice.”
A version of this article first appeared on WebMD.com.
When 29-year-old Sakeenah Fowler was pregnant with her first child, doctors kept a close watch. Ms. Fowler has lupus, high blood pressure, a history of blood clotting, and kidney problems that all could have endangered her or the health of her unborn baby.
She saw maternal-fetal specialists who could keep watch of her high-risk pregnancy, and she collected urine samples every 24 hours to make sure her kidneys were functioning properly from her home in Roebuck, S.C.
But the pregnancy ultimately proved uneventful; even her kidneys remained stable. So Ms. Fowler said she was shocked when her doctors ordered an emergency cesarean delivery after she had gone into active labor.
“I was already dilated all the way to 6 cm,” but the baby’s heart rate had decreased by a small amount, she says. “They thought it was best to just go ahead with a C-section.”
Ms. Fowler, who is Black, said she believes the surgical intervention was unnecessary and that she wasn’t given a chance to discuss her options for a vaginal childbirth.
“They already had it in their minds that I wasn’t going to make it through the pregnancy without any issues; then when I did, it was like they wanted to find something that made me have to have a C-section,” Ms. Fowler said. “It was close to the holidays; everybody was ready to go home. It was just like I was pushed to do what they wanted me to do.”
Ms. Fowler’s sense of a lack of choice is important beyond the measure of patient experience. While cesarean deliveries can be a lifeline for mother and baby, they can put up massive roadblocks to maternal and infant health when not necessary.
“The risk of hemorrhage, infection – on average, all of these go up when you have surgery instead of a vaginal delivery,” says Kimberly B. Glazer, PhD, a perinatal epidemiologist at the Icahn School of Medicine at Mount Sinai, New York.
“Birth is one of the most salient experiences you can have. People want to feel like their values and preferences – whatever they may be – were honored and respected. Even if the delivery goes a different way than you wanted, feeling like your values were taken into account is very important.”
More than 1 million women undergo cesarean deliveries in the United States every year, composing over 31% of all births in 2020, according to the Centers for Disease Control and Prevention.
The World Health Organization, meanwhile, recommends a rate of cesarean delivery of no more than 15% per region. Whether or not all the U.S. procedures were medically warranted is unclear, however.
Black women have higher odds of undergoing a cesarean: 36% undergo surgical deliveries annually, compared with about 30% of White women. Black women are also about three times more likely to die of pregnancy-related causes than White women.
Risk becomes reality
Ms. Fowler eventually developed an infection in her cesarean surgical wound, but her doctors initially insisted her alternating chills and fever were merely postpartum hormonal swings, she says.
“I thought something had to be wrong, but they just kept saying nothing was wrong,” she says.
By the time her doctors caught the infection, Ms. Fowler was readmitted to the hospital for several days of IV antibiotic therapy. The infection “almost got into my bloodstream and could have killed me,” she says.
While cesarean deliveries are associated with decreases in maternal, neonatal, and infant mortality, the benefits are only seen up to a certain threshold. The WHO, for instance, has reported that over the 15% threshold, that lower mortality benefit disappears.
“When medically necessary, cesarean delivery can improve outcomes for mother and baby. But the fact that cesarean section rates have increased in recent years without a corresponding improvement in health outcomes indicates overreliance on the procedure,” Dr. Glazer says.
Clinical discretion leads to biased judgment calls
Rates of cesarean deliveries are even higher among low-risk pregnancies in women of color than in White women. Between 2016 and 2019, the overall rate of cesarean deliveries for low-risk births was 23%, according to a recent analysis. But the rate was almost 18% higher among Black women than among White women (27% vs. 22%).
“When you see data about these subjective indications varying by race and ethnicity, I think that’s pointing us toward some answers,” Dr. Glazer says. “Once you adjust for all these measures, prepregnancy characteristics, and risk factors, the research identifies variation in quality and outcomes that is rooted in structural and systemic racism in health care, implicit bias from clinicians.”
Researchers investigating cesarean deliveries have found that Black women are more likely to undergo the surgery for reasons that are highly subjective, such as fetal distress.
“There is a huge range of how concerning a fetal heart rate can be, and some health providers might perform a C-section for only minor changes in the fetal heart rate, while others might wait until it is much worse,” said Rebecca Hamm, MD, an assistant professor of obstetrics and gynecology at the Perelman School of Medicine at the University of Pennsylvania.
At least some of the differences in care can be explained by where women deliver their babies, studies have shown. Women of color disproportionately deliver at hospitals with poorer quality outcomes for moms and babies.
Dealing with the aftermath
There can be costs that reverberate throughout the life of a mother, child, and their family as the result of surgical delivery.
“Cesarean sections cost a lot more,” says Jamila Taylor, PhD, director of health care reform and a senior fellow with The Century Foundation, a progressive policy think tank in Washington, D.C. The cost of a cesarean delivery averages about $17,000, compared with about $12,200 for a vaginal birth; for uninsured patients, surgical deliveries cost about $9,000 more than vaginal deliveries.
Dr. Taylor, who has studied the historical mistreatment of Black women in obstetrics, noted that this cost includes not just the bill for surgery but also a prolonged recovery time that is often spent in a hospital bed.
Beyond the detrimental effect that a large hospital bill for delivery and aftercare can have on families, other costs can crop up later. Infants delivered by cesarean surgery are more likely to develop an infection, breathing problems, and to spend time in the neonatal intensive care unit than babies born vaginally. Although studies suggest these outcomes may result from a medically necessary health concern that spurred the cesarean surgery, they often stem from the delivery itself.
Babies born surgically also miss out on the benefits of passing through the birth canal, such as supporting a newborn’s immune system and preparing their lungs to breathe oxygen after birth.
Most of the efforts to reduce inequities in maternal care are happening at the clinical level, aimed at both patients and providers, Dr. Taylor says.
“As advocates, we’re talking about how we can help Black women be advocates for themselves in the health care system – if the physician suggests a C-section, getting a second opinion, or walking through what a [surgical delivery] will mean and what their recovery will look like,” she says.
Women are also increasingly choosing non-hospital settings to deliver when possible, Dr. Taylor says. Including doulas or midwife practitioners in the maternal care team can reduce unnecessary cesarean deliveries among Black women, according to Camille Clare, MD, chair of the New York chapter of the American College of Obstetricians and Gynecologists.
Also, last year, race was removed from the vaginal birth after C-section (VBAC) calculator, which is used to gauge the safety of vaginal delivery in women with a history of surgical birth. The original calculator included race-based correction factors for Black women and Hispanic women. It predicted a lower likelihood of successful vaginal deliveries for women who already had a C-section and who identify as Black or Hispanic than for White women with otherwise identical characteristics, such as age, weight, and a history of cesarean delivery.
“Those are things that over time should reduce the high rates of cesarean section for Black women in particular,” Dr. Clare says.
In addition to embracing the updated calculator and including nurse-midwives and doulas in their obstetrics services, Penn Medicine, Philadelphia received a federal grant to study the impact of creating a standard plan for deliveries. This includes standardizing the induction of labor and any effect that might have on reducing C-section rates.
“This idea that biases lead to difference in decisionmaking, and that by standardizing practices we could address these differences – people were somewhat resistant at first,” Dr. Hamm says. “They didn’t believe there were differences in their practices.”
People struggle to recognize those differences, she says, and “it takes active participation in reducing disparities to make that happen.”
At the community level, Synergistic Sisters in Science (SIS), a group of maternal health experts and health equity advocates, is working on a project called PM3, to reduce maternal mortality through mobile technology.
The smartphone app will provide information for new moms to empower them to start conversations with health care providers. It also connects users to social support and resources. SIS is especially hoping to engage Black women living in rural areas.
“There is so much mistrust due to things like unnecessary C-sections and the fact that Black women feel they aren’t heard,” said Natalie Hernandez, PhD, executive director of the Center for Maternal Health Equity at Morehouse School of Medicine, Atlanta. “Here is a tool that gives a woman information that’s culturally centered, looks like her, and was informed by her voice.”
A version of this article first appeared on WebMD.com.
Food allergy test breakthrough: Less risk, more useful results
What would you do if you believed you had a serious health issue, but the best way to find out for sure might kill you?
That’s the reality for patients who wish to confirm or rule out a food allergy, says Sindy Tang, PhD, an associate professor of mechanical engineering at Stanford (Calif.) University.
And it’s the reason Dr. Tang and her colleagues are developing a food allergy test that’s not only safer, but also more reliable than today’s tests. In a paper in the journal Lab on a Chip, Dr. Tang and her colleagues outline the basis for this future test, which isolates a food allergy marker from the blood using a magnetic field.
How today’s food allergy tests fall short
The gold standard for food allergy diagnosis is something called the oral food challenge. That’s when the patient eats gradually increasing amounts of a problem food – say, peanuts – every 15 to 30 minutes to see if symptoms occur. This means highly allergic patients may risk anaphylaxis, an allergic reaction that causes inflammation so severe that breathing becomes restricted and blood pressure drops. Because of that, a clinical team must be at the ready with treatments like oxygen, epinephrine, or albuterol.
“The test is very accurate, but it’s also potentially unsafe and even fatal in rare cases,” Dr. Tang says. “That’s led to many sham tests advertised online that claim to use hair samples for food tests, but those are inaccurate and potentially dangerous, since they may give someone a false sense of confidence about a food they should avoid.”
Less risky tests are available, such as skin-prick tests – those involve scratching a small amount of the food into a patient’s arm – as well as blood tests that measure allergen-specific antibodies.
“Unfortunately, both of those are not that accurate and have high false-positive rates,” Dr. Tang says. “The best method is the oral food challenge, which many patients are afraid to do, not surprisingly.”
The future of food allergy testing: faster, safer, more reliable
In their study, the Stanford researchers focused on a type of white blood cell known as basophils, which release histamine when triggered by allergens. By using magnetic nanoparticles that bind to some blood cells but not basophils, they were able to separate basophils from the blood with a magnetic field in just 10 minutes.
Once isolated, the basophils are exposed to potential allergens. If they react, that’s a sign of an allergy.
Basophils have been isolated in labs before but not nearly this quickly and efficiently, Dr. Tang says.
“For true basophil activation, you need the blood to be fresh, which is challenging when you have to send it to a lab,” Dr. Tang says. “Being able to do this kind of test within a clinic or an in-house lab would be a big step forward.”
Next steps
While this represents a breakthrough in basophil activation testing, more research is needed to fully develop the system for clinical use. It must be standardized, automated, and miniaturized, the researchers say.
That said, the results give hope to those with food allergies that tomorrow’s gold-standard test will require only a blood sample without an emergency team standing by.
A version of this article first appeared on WebMD.com.
What would you do if you believed you had a serious health issue, but the best way to find out for sure might kill you?
That’s the reality for patients who wish to confirm or rule out a food allergy, says Sindy Tang, PhD, an associate professor of mechanical engineering at Stanford (Calif.) University.
And it’s the reason Dr. Tang and her colleagues are developing a food allergy test that’s not only safer, but also more reliable than today’s tests. In a paper in the journal Lab on a Chip, Dr. Tang and her colleagues outline the basis for this future test, which isolates a food allergy marker from the blood using a magnetic field.
How today’s food allergy tests fall short
The gold standard for food allergy diagnosis is something called the oral food challenge. That’s when the patient eats gradually increasing amounts of a problem food – say, peanuts – every 15 to 30 minutes to see if symptoms occur. This means highly allergic patients may risk anaphylaxis, an allergic reaction that causes inflammation so severe that breathing becomes restricted and blood pressure drops. Because of that, a clinical team must be at the ready with treatments like oxygen, epinephrine, or albuterol.
“The test is very accurate, but it’s also potentially unsafe and even fatal in rare cases,” Dr. Tang says. “That’s led to many sham tests advertised online that claim to use hair samples for food tests, but those are inaccurate and potentially dangerous, since they may give someone a false sense of confidence about a food they should avoid.”
Less risky tests are available, such as skin-prick tests – those involve scratching a small amount of the food into a patient’s arm – as well as blood tests that measure allergen-specific antibodies.
“Unfortunately, both of those are not that accurate and have high false-positive rates,” Dr. Tang says. “The best method is the oral food challenge, which many patients are afraid to do, not surprisingly.”
The future of food allergy testing: faster, safer, more reliable
In their study, the Stanford researchers focused on a type of white blood cell known as basophils, which release histamine when triggered by allergens. By using magnetic nanoparticles that bind to some blood cells but not basophils, they were able to separate basophils from the blood with a magnetic field in just 10 minutes.
Once isolated, the basophils are exposed to potential allergens. If they react, that’s a sign of an allergy.
Basophils have been isolated in labs before but not nearly this quickly and efficiently, Dr. Tang says.
“For true basophil activation, you need the blood to be fresh, which is challenging when you have to send it to a lab,” Dr. Tang says. “Being able to do this kind of test within a clinic or an in-house lab would be a big step forward.”
Next steps
While this represents a breakthrough in basophil activation testing, more research is needed to fully develop the system for clinical use. It must be standardized, automated, and miniaturized, the researchers say.
That said, the results give hope to those with food allergies that tomorrow’s gold-standard test will require only a blood sample without an emergency team standing by.
A version of this article first appeared on WebMD.com.
What would you do if you believed you had a serious health issue, but the best way to find out for sure might kill you?
That’s the reality for patients who wish to confirm or rule out a food allergy, says Sindy Tang, PhD, an associate professor of mechanical engineering at Stanford (Calif.) University.
And it’s the reason Dr. Tang and her colleagues are developing a food allergy test that’s not only safer, but also more reliable than today’s tests. In a paper in the journal Lab on a Chip, Dr. Tang and her colleagues outline the basis for this future test, which isolates a food allergy marker from the blood using a magnetic field.
How today’s food allergy tests fall short
The gold standard for food allergy diagnosis is something called the oral food challenge. That’s when the patient eats gradually increasing amounts of a problem food – say, peanuts – every 15 to 30 minutes to see if symptoms occur. This means highly allergic patients may risk anaphylaxis, an allergic reaction that causes inflammation so severe that breathing becomes restricted and blood pressure drops. Because of that, a clinical team must be at the ready with treatments like oxygen, epinephrine, or albuterol.
“The test is very accurate, but it’s also potentially unsafe and even fatal in rare cases,” Dr. Tang says. “That’s led to many sham tests advertised online that claim to use hair samples for food tests, but those are inaccurate and potentially dangerous, since they may give someone a false sense of confidence about a food they should avoid.”
Less risky tests are available, such as skin-prick tests – those involve scratching a small amount of the food into a patient’s arm – as well as blood tests that measure allergen-specific antibodies.
“Unfortunately, both of those are not that accurate and have high false-positive rates,” Dr. Tang says. “The best method is the oral food challenge, which many patients are afraid to do, not surprisingly.”
The future of food allergy testing: faster, safer, more reliable
In their study, the Stanford researchers focused on a type of white blood cell known as basophils, which release histamine when triggered by allergens. By using magnetic nanoparticles that bind to some blood cells but not basophils, they were able to separate basophils from the blood with a magnetic field in just 10 minutes.
Once isolated, the basophils are exposed to potential allergens. If they react, that’s a sign of an allergy.
Basophils have been isolated in labs before but not nearly this quickly and efficiently, Dr. Tang says.
“For true basophil activation, you need the blood to be fresh, which is challenging when you have to send it to a lab,” Dr. Tang says. “Being able to do this kind of test within a clinic or an in-house lab would be a big step forward.”
Next steps
While this represents a breakthrough in basophil activation testing, more research is needed to fully develop the system for clinical use. It must be standardized, automated, and miniaturized, the researchers say.
That said, the results give hope to those with food allergies that tomorrow’s gold-standard test will require only a blood sample without an emergency team standing by.
A version of this article first appeared on WebMD.com.
A unique care model for comorbid depression, PTSD
“We know there are strains on the mental health care system, and sometimes something as simple as getting to see a psychiatrist can be incredibly challenging,” coinvestigator Zachary Zuschlag, MD, staff psychiatrist at the James A. Haley Veterans’ Hospital and assistant professor at the University of South Florida, both in Tampa, said in an interview.
“So, a model that encourages primary care doctors, together with consultation from us [psychiatrists] to effectively treat these patients in a more proactive way, is very beneficial,” Dr. Zuschlag said.
The findings were presented at the American Society of Clinical Psychopharmacology annual meeting.
Common bedfellows
Dr. Zuschlag noted that comorbid PTSD and depression is common, but it is often considered too complex to be managed in a primary care setting.
Although treating these patients can be challenging, Dr. Zuschlag, who also heads his Veterans Administration facility’s antidepressant monitoring program (ADM), said that when he started the program for this patient population, he used “a much more inclusive model and welcomed these patients even if they had co-occurring issues.”
“Anecdotally, we had seen that our patients with [depression and] co-occurring PTSD appeared to be doing as well as their peers without PTSD, and we just wanted to look at it more systematically,” he added.
The ADM program is specifically designed for psychopharmacologic management of depression and anxiety in the primary care setting. It involves an interdisciplinary team of RN care managers, consulting psychiatrists, psychologists, and primary care physicians. Patients in primary care clinics deemed likely to benefit from psychiatric medications can be enrolled and followed in the program.
The program consists of structured, protocol-based telephone contacts from the RN care managers at scheduled intervals, usually every 3-4 weeks, said Dr. Zuschlag.
During calls, information is collected via evidence-based mental health symptomatic assessment scales. The consulting psychiatrists use this and other information to help guide treatment and coordinate with patients’ primary care physicians to adjust the treatment plan, including medication changes and additional psychotherapy.
To determine the program’s efficacy the investigators retrospectively reviewed all patients enrolled in the ADM program during its first 10 months. Of the 433 program participants, 112 (26%) were identified with active PTSD symptoms at baseline. Another 43 patients had a prior diagnosis of PTSD.
Program completion rates for the cohort with PTSD did not differ from that of the cohort without PTSD.
Overall, mean improvements in depression and anxiety symptoms were evidenced by changes in Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder Assessment-7 (GAD-7) scores of 44% and 43%, respectively.
No differences in mean reduction in symptoms of depression were observed when comparing those with no history of PTSD with those with any history of PTSD (–6.16 vs. –5.42; P = .3244) or with those with active PTSD symptoms (–6.16 vs. –5.54; P = .4543).
Similarly, for anxiety, a mean reduction of –5.61 on the GAD-7 score was observed for the cohort without PTSD, compared with –4.99 in the cohort with any history of PTSD and –5.35 in the cohort with active PTSD symptoms. Again, these differences were nonsignificant.
Dr. Zuschlag noted that the VA setting is unique, with a lot of resources available to conduct such a program as ADM.
“Care management programs that are multidisciplinary are very effective and, in our experience, those who have completed the program do exceptionally well. The patients love it because there is a lot of contact between them and their various care providers,” he said.
A model for other settings?
Commenting on the study, Nagy A. Youssef, MD, PhD, professor of psychiatry and director of clinical research at Ohio State University, Columbus, called the results “interesting.”
“Treating patients with comorbid mild to moderate depression and current or past PTSD within the primary care setting using a care management program could be a model for other VA hospitals as well as in non-VA settings,” said Dr. Youssef, who was not part of the study.
Dr. Youssef noted that not only was there no difference in symptomatic improvement between the depression-plus-PTSD and depression-only groups, but program completion rates did not differ.
This further emphasizes “the potential utility of this approach in initial patient treatment, especially with limited mental health resources and the need to help more patients,” he said.
Dr. Zuschlag and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“We know there are strains on the mental health care system, and sometimes something as simple as getting to see a psychiatrist can be incredibly challenging,” coinvestigator Zachary Zuschlag, MD, staff psychiatrist at the James A. Haley Veterans’ Hospital and assistant professor at the University of South Florida, both in Tampa, said in an interview.
“So, a model that encourages primary care doctors, together with consultation from us [psychiatrists] to effectively treat these patients in a more proactive way, is very beneficial,” Dr. Zuschlag said.
The findings were presented at the American Society of Clinical Psychopharmacology annual meeting.
Common bedfellows
Dr. Zuschlag noted that comorbid PTSD and depression is common, but it is often considered too complex to be managed in a primary care setting.
Although treating these patients can be challenging, Dr. Zuschlag, who also heads his Veterans Administration facility’s antidepressant monitoring program (ADM), said that when he started the program for this patient population, he used “a much more inclusive model and welcomed these patients even if they had co-occurring issues.”
“Anecdotally, we had seen that our patients with [depression and] co-occurring PTSD appeared to be doing as well as their peers without PTSD, and we just wanted to look at it more systematically,” he added.
The ADM program is specifically designed for psychopharmacologic management of depression and anxiety in the primary care setting. It involves an interdisciplinary team of RN care managers, consulting psychiatrists, psychologists, and primary care physicians. Patients in primary care clinics deemed likely to benefit from psychiatric medications can be enrolled and followed in the program.
The program consists of structured, protocol-based telephone contacts from the RN care managers at scheduled intervals, usually every 3-4 weeks, said Dr. Zuschlag.
During calls, information is collected via evidence-based mental health symptomatic assessment scales. The consulting psychiatrists use this and other information to help guide treatment and coordinate with patients’ primary care physicians to adjust the treatment plan, including medication changes and additional psychotherapy.
To determine the program’s efficacy the investigators retrospectively reviewed all patients enrolled in the ADM program during its first 10 months. Of the 433 program participants, 112 (26%) were identified with active PTSD symptoms at baseline. Another 43 patients had a prior diagnosis of PTSD.
Program completion rates for the cohort with PTSD did not differ from that of the cohort without PTSD.
Overall, mean improvements in depression and anxiety symptoms were evidenced by changes in Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder Assessment-7 (GAD-7) scores of 44% and 43%, respectively.
No differences in mean reduction in symptoms of depression were observed when comparing those with no history of PTSD with those with any history of PTSD (–6.16 vs. –5.42; P = .3244) or with those with active PTSD symptoms (–6.16 vs. –5.54; P = .4543).
Similarly, for anxiety, a mean reduction of –5.61 on the GAD-7 score was observed for the cohort without PTSD, compared with –4.99 in the cohort with any history of PTSD and –5.35 in the cohort with active PTSD symptoms. Again, these differences were nonsignificant.
Dr. Zuschlag noted that the VA setting is unique, with a lot of resources available to conduct such a program as ADM.
“Care management programs that are multidisciplinary are very effective and, in our experience, those who have completed the program do exceptionally well. The patients love it because there is a lot of contact between them and their various care providers,” he said.
A model for other settings?
Commenting on the study, Nagy A. Youssef, MD, PhD, professor of psychiatry and director of clinical research at Ohio State University, Columbus, called the results “interesting.”
“Treating patients with comorbid mild to moderate depression and current or past PTSD within the primary care setting using a care management program could be a model for other VA hospitals as well as in non-VA settings,” said Dr. Youssef, who was not part of the study.
Dr. Youssef noted that not only was there no difference in symptomatic improvement between the depression-plus-PTSD and depression-only groups, but program completion rates did not differ.
This further emphasizes “the potential utility of this approach in initial patient treatment, especially with limited mental health resources and the need to help more patients,” he said.
Dr. Zuschlag and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“We know there are strains on the mental health care system, and sometimes something as simple as getting to see a psychiatrist can be incredibly challenging,” coinvestigator Zachary Zuschlag, MD, staff psychiatrist at the James A. Haley Veterans’ Hospital and assistant professor at the University of South Florida, both in Tampa, said in an interview.
“So, a model that encourages primary care doctors, together with consultation from us [psychiatrists] to effectively treat these patients in a more proactive way, is very beneficial,” Dr. Zuschlag said.
The findings were presented at the American Society of Clinical Psychopharmacology annual meeting.
Common bedfellows
Dr. Zuschlag noted that comorbid PTSD and depression is common, but it is often considered too complex to be managed in a primary care setting.
Although treating these patients can be challenging, Dr. Zuschlag, who also heads his Veterans Administration facility’s antidepressant monitoring program (ADM), said that when he started the program for this patient population, he used “a much more inclusive model and welcomed these patients even if they had co-occurring issues.”
“Anecdotally, we had seen that our patients with [depression and] co-occurring PTSD appeared to be doing as well as their peers without PTSD, and we just wanted to look at it more systematically,” he added.
The ADM program is specifically designed for psychopharmacologic management of depression and anxiety in the primary care setting. It involves an interdisciplinary team of RN care managers, consulting psychiatrists, psychologists, and primary care physicians. Patients in primary care clinics deemed likely to benefit from psychiatric medications can be enrolled and followed in the program.
The program consists of structured, protocol-based telephone contacts from the RN care managers at scheduled intervals, usually every 3-4 weeks, said Dr. Zuschlag.
During calls, information is collected via evidence-based mental health symptomatic assessment scales. The consulting psychiatrists use this and other information to help guide treatment and coordinate with patients’ primary care physicians to adjust the treatment plan, including medication changes and additional psychotherapy.
To determine the program’s efficacy the investigators retrospectively reviewed all patients enrolled in the ADM program during its first 10 months. Of the 433 program participants, 112 (26%) were identified with active PTSD symptoms at baseline. Another 43 patients had a prior diagnosis of PTSD.
Program completion rates for the cohort with PTSD did not differ from that of the cohort without PTSD.
Overall, mean improvements in depression and anxiety symptoms were evidenced by changes in Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder Assessment-7 (GAD-7) scores of 44% and 43%, respectively.
No differences in mean reduction in symptoms of depression were observed when comparing those with no history of PTSD with those with any history of PTSD (–6.16 vs. –5.42; P = .3244) or with those with active PTSD symptoms (–6.16 vs. –5.54; P = .4543).
Similarly, for anxiety, a mean reduction of –5.61 on the GAD-7 score was observed for the cohort without PTSD, compared with –4.99 in the cohort with any history of PTSD and –5.35 in the cohort with active PTSD symptoms. Again, these differences were nonsignificant.
Dr. Zuschlag noted that the VA setting is unique, with a lot of resources available to conduct such a program as ADM.
“Care management programs that are multidisciplinary are very effective and, in our experience, those who have completed the program do exceptionally well. The patients love it because there is a lot of contact between them and their various care providers,” he said.
A model for other settings?
Commenting on the study, Nagy A. Youssef, MD, PhD, professor of psychiatry and director of clinical research at Ohio State University, Columbus, called the results “interesting.”
“Treating patients with comorbid mild to moderate depression and current or past PTSD within the primary care setting using a care management program could be a model for other VA hospitals as well as in non-VA settings,” said Dr. Youssef, who was not part of the study.
Dr. Youssef noted that not only was there no difference in symptomatic improvement between the depression-plus-PTSD and depression-only groups, but program completion rates did not differ.
This further emphasizes “the potential utility of this approach in initial patient treatment, especially with limited mental health resources and the need to help more patients,” he said.
Dr. Zuschlag and Dr. Youssef report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ASCP 2022
It’s hot outside – and that’s bad news for children’s health
Heat waves are getting hotter and becoming more frequent because of rising rates of air pollution, putting children’s health at risk, a wide-ranging new report finds.
An article in the New England Journal of Medicine reviews current research to take a sweeping inventory of how air pollution and climate change interact to adversely affect people’s health, especially that of kids. It examined the link between fossil fuel emissions and a variety of consequences of climate change – including extreme weather events; wildfires; vector-borne illnesses such as malaria, Zika, and Lyme disease; and heat waves, a topic at the forefront of many people’s minds.
This month, for example, record-high temperatures have been reported across the United States, affecting more than 100 million people and touching locations from the Gulf Coast to the Great Lakes, the Southwest, the mid-Atlantic, and the Midwest.
In Texas, Austin has already experienced an 8-day streak of temperatures above the 100° F mark in June, according to the Austin American-Statesman.
These patterns are an important reality to note, said Frederica Perera, DrPH, PhD, the article’s lead author. “My concern is that the threats are rising as temperature is rising,” Dr. Perera, a professor at Columbia University’s Mailman School of Public Health, New York, told KHN. “Temperatures are rising because greenhouse gas emissions are rising, and that’s a great concern for everyone’s health – but especially the most vulnerable.”
Children fit into this category, wrote Dr. Perera and her coauthor, Kari Nadeau, MD, PhD, Naddisy Foundation Endowed Professor of Medicine and Pediatrics at Stanford (Calif.) University, because their ability to regulate temperature, known as thermoregulation, is not fully developed.
They are also more susceptible to heat-related stress because they’re smaller and need to drink and eat more frequently to stay healthy, said Dr. Perera. But because “young children are dependent on parents to provide, sometimes their needs go ignored,” she said.
The authors noted that heat-related illness is “a leading and increasing cause of death and illness among student athletes” in the United States. In addition, they cited studies suggesting that “the heat associated with climate change” takes a toll on the mental health of children and adolescents, as well as their ability to learn.
The review article pointed to previous research. that associated in utero exposure to heat waves with “increased risks of preterm birth or low birth weight; hyperthermia and death among infants; and heat stress, kidney disease, and other illnesses” among kids.
“Being pregnant is very physiologically demanding in itself, and then heat places additional stress on a pregnant woman,” said Dr. Robert Dubrow, a professor of epidemiology at Yale’s School of Public Health, New Haven, Conn., who was not associated with either study. “And the fetus can experience heat stress as well, which could result in adverse birth outcomes.”
And these heat-related risks are across-the-board greater for “low-income communities and communities of color,” wrote the authors of the new article.
Carbon dioxide emissions from burning fossil fuels have risen sharply in the past 70 years, according to the article. “Modeling indicates that some heat waves would be extraordinarily unlikely to occur in the absence of climate change,” it says.
The authors briefly outline solutions that they describe as “climate and environmental strategies” that “should also be seen as essential public health policy.” Beyond big-picture efforts to mitigate fossil fuel and greenhouse gas emissions, they offered various ways to protect children – steps they term “adaptation measures” – which included providing clean water to children and families facing drought or water contamination and creating shaded areas where children play, live, and go to school.
Separately, Austin-based research highlighted why this step could be meaningful.
Researchers tracked the physical activity levels and location of students ages 8 to 10 during recess at three elementary schools in 2019. They compared children’s activity at recess during two weeks in September, the hottest full month during the school year, to a cooler week in November. “We wanted to understand the impact of outdoor temperatures on children’s play in schoolyard environments,” said Dr. Kevin Lanza, the study’s lead investigator, to inform the design of “future school-based interventions for physical activity in the face of climate change.”
During the hotter periods, he said, “children engaged in less physical activity and sought shade.”
As temperatures continue to rise, he said, schools must be flexible in making sure students are getting the daily exercise they need. “Schools should consider adding shade, either by planting trees or installing artificial structures that cover spaces intended for physical activity,” said Dr. Lanza, an assistant professor at UTHealth School of Public Health, Austin, Tex. He also noted that school policies could be updated so that recesses are scheduled during cooler times of the day and moved inside during periods of extreme heat.
But the overall need to protect kids from scorching weather patterns requires action beyond such steps, Dr. Perera said, and more climate and clean air policies must be enacted.
“Governments have the responsibility to protect the population and especially those most vulnerable, which especially includes children,” Dr. Perera said. “Action must be done immediately because we’re absolutely heading in the wrong direction.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Heat waves are getting hotter and becoming more frequent because of rising rates of air pollution, putting children’s health at risk, a wide-ranging new report finds.
An article in the New England Journal of Medicine reviews current research to take a sweeping inventory of how air pollution and climate change interact to adversely affect people’s health, especially that of kids. It examined the link between fossil fuel emissions and a variety of consequences of climate change – including extreme weather events; wildfires; vector-borne illnesses such as malaria, Zika, and Lyme disease; and heat waves, a topic at the forefront of many people’s minds.
This month, for example, record-high temperatures have been reported across the United States, affecting more than 100 million people and touching locations from the Gulf Coast to the Great Lakes, the Southwest, the mid-Atlantic, and the Midwest.
In Texas, Austin has already experienced an 8-day streak of temperatures above the 100° F mark in June, according to the Austin American-Statesman.
These patterns are an important reality to note, said Frederica Perera, DrPH, PhD, the article’s lead author. “My concern is that the threats are rising as temperature is rising,” Dr. Perera, a professor at Columbia University’s Mailman School of Public Health, New York, told KHN. “Temperatures are rising because greenhouse gas emissions are rising, and that’s a great concern for everyone’s health – but especially the most vulnerable.”
Children fit into this category, wrote Dr. Perera and her coauthor, Kari Nadeau, MD, PhD, Naddisy Foundation Endowed Professor of Medicine and Pediatrics at Stanford (Calif.) University, because their ability to regulate temperature, known as thermoregulation, is not fully developed.
They are also more susceptible to heat-related stress because they’re smaller and need to drink and eat more frequently to stay healthy, said Dr. Perera. But because “young children are dependent on parents to provide, sometimes their needs go ignored,” she said.
The authors noted that heat-related illness is “a leading and increasing cause of death and illness among student athletes” in the United States. In addition, they cited studies suggesting that “the heat associated with climate change” takes a toll on the mental health of children and adolescents, as well as their ability to learn.
The review article pointed to previous research. that associated in utero exposure to heat waves with “increased risks of preterm birth or low birth weight; hyperthermia and death among infants; and heat stress, kidney disease, and other illnesses” among kids.
“Being pregnant is very physiologically demanding in itself, and then heat places additional stress on a pregnant woman,” said Dr. Robert Dubrow, a professor of epidemiology at Yale’s School of Public Health, New Haven, Conn., who was not associated with either study. “And the fetus can experience heat stress as well, which could result in adverse birth outcomes.”
And these heat-related risks are across-the-board greater for “low-income communities and communities of color,” wrote the authors of the new article.
Carbon dioxide emissions from burning fossil fuels have risen sharply in the past 70 years, according to the article. “Modeling indicates that some heat waves would be extraordinarily unlikely to occur in the absence of climate change,” it says.
The authors briefly outline solutions that they describe as “climate and environmental strategies” that “should also be seen as essential public health policy.” Beyond big-picture efforts to mitigate fossil fuel and greenhouse gas emissions, they offered various ways to protect children – steps they term “adaptation measures” – which included providing clean water to children and families facing drought or water contamination and creating shaded areas where children play, live, and go to school.
Separately, Austin-based research highlighted why this step could be meaningful.
Researchers tracked the physical activity levels and location of students ages 8 to 10 during recess at three elementary schools in 2019. They compared children’s activity at recess during two weeks in September, the hottest full month during the school year, to a cooler week in November. “We wanted to understand the impact of outdoor temperatures on children’s play in schoolyard environments,” said Dr. Kevin Lanza, the study’s lead investigator, to inform the design of “future school-based interventions for physical activity in the face of climate change.”
During the hotter periods, he said, “children engaged in less physical activity and sought shade.”
As temperatures continue to rise, he said, schools must be flexible in making sure students are getting the daily exercise they need. “Schools should consider adding shade, either by planting trees or installing artificial structures that cover spaces intended for physical activity,” said Dr. Lanza, an assistant professor at UTHealth School of Public Health, Austin, Tex. He also noted that school policies could be updated so that recesses are scheduled during cooler times of the day and moved inside during periods of extreme heat.
But the overall need to protect kids from scorching weather patterns requires action beyond such steps, Dr. Perera said, and more climate and clean air policies must be enacted.
“Governments have the responsibility to protect the population and especially those most vulnerable, which especially includes children,” Dr. Perera said. “Action must be done immediately because we’re absolutely heading in the wrong direction.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Heat waves are getting hotter and becoming more frequent because of rising rates of air pollution, putting children’s health at risk, a wide-ranging new report finds.
An article in the New England Journal of Medicine reviews current research to take a sweeping inventory of how air pollution and climate change interact to adversely affect people’s health, especially that of kids. It examined the link between fossil fuel emissions and a variety of consequences of climate change – including extreme weather events; wildfires; vector-borne illnesses such as malaria, Zika, and Lyme disease; and heat waves, a topic at the forefront of many people’s minds.
This month, for example, record-high temperatures have been reported across the United States, affecting more than 100 million people and touching locations from the Gulf Coast to the Great Lakes, the Southwest, the mid-Atlantic, and the Midwest.
In Texas, Austin has already experienced an 8-day streak of temperatures above the 100° F mark in June, according to the Austin American-Statesman.
These patterns are an important reality to note, said Frederica Perera, DrPH, PhD, the article’s lead author. “My concern is that the threats are rising as temperature is rising,” Dr. Perera, a professor at Columbia University’s Mailman School of Public Health, New York, told KHN. “Temperatures are rising because greenhouse gas emissions are rising, and that’s a great concern for everyone’s health – but especially the most vulnerable.”
Children fit into this category, wrote Dr. Perera and her coauthor, Kari Nadeau, MD, PhD, Naddisy Foundation Endowed Professor of Medicine and Pediatrics at Stanford (Calif.) University, because their ability to regulate temperature, known as thermoregulation, is not fully developed.
They are also more susceptible to heat-related stress because they’re smaller and need to drink and eat more frequently to stay healthy, said Dr. Perera. But because “young children are dependent on parents to provide, sometimes their needs go ignored,” she said.
The authors noted that heat-related illness is “a leading and increasing cause of death and illness among student athletes” in the United States. In addition, they cited studies suggesting that “the heat associated with climate change” takes a toll on the mental health of children and adolescents, as well as their ability to learn.
The review article pointed to previous research. that associated in utero exposure to heat waves with “increased risks of preterm birth or low birth weight; hyperthermia and death among infants; and heat stress, kidney disease, and other illnesses” among kids.
“Being pregnant is very physiologically demanding in itself, and then heat places additional stress on a pregnant woman,” said Dr. Robert Dubrow, a professor of epidemiology at Yale’s School of Public Health, New Haven, Conn., who was not associated with either study. “And the fetus can experience heat stress as well, which could result in adverse birth outcomes.”
And these heat-related risks are across-the-board greater for “low-income communities and communities of color,” wrote the authors of the new article.
Carbon dioxide emissions from burning fossil fuels have risen sharply in the past 70 years, according to the article. “Modeling indicates that some heat waves would be extraordinarily unlikely to occur in the absence of climate change,” it says.
The authors briefly outline solutions that they describe as “climate and environmental strategies” that “should also be seen as essential public health policy.” Beyond big-picture efforts to mitigate fossil fuel and greenhouse gas emissions, they offered various ways to protect children – steps they term “adaptation measures” – which included providing clean water to children and families facing drought or water contamination and creating shaded areas where children play, live, and go to school.
Separately, Austin-based research highlighted why this step could be meaningful.
Researchers tracked the physical activity levels and location of students ages 8 to 10 during recess at three elementary schools in 2019. They compared children’s activity at recess during two weeks in September, the hottest full month during the school year, to a cooler week in November. “We wanted to understand the impact of outdoor temperatures on children’s play in schoolyard environments,” said Dr. Kevin Lanza, the study’s lead investigator, to inform the design of “future school-based interventions for physical activity in the face of climate change.”
During the hotter periods, he said, “children engaged in less physical activity and sought shade.”
As temperatures continue to rise, he said, schools must be flexible in making sure students are getting the daily exercise they need. “Schools should consider adding shade, either by planting trees or installing artificial structures that cover spaces intended for physical activity,” said Dr. Lanza, an assistant professor at UTHealth School of Public Health, Austin, Tex. He also noted that school policies could be updated so that recesses are scheduled during cooler times of the day and moved inside during periods of extreme heat.
But the overall need to protect kids from scorching weather patterns requires action beyond such steps, Dr. Perera said, and more climate and clean air policies must be enacted.
“Governments have the responsibility to protect the population and especially those most vulnerable, which especially includes children,” Dr. Perera said. “Action must be done immediately because we’re absolutely heading in the wrong direction.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Can the ketogenic diet treat polycystic ovary syndrome?
MADRID – During the International Scientific Symposium “New Frontiers in Scientific Research” that recently took place in Barcelona, specialists analyzed the role of the very-low-calorie ketogenic diet. This analysis was in relation to three comorbidities that have a higher incidence among overweight and obese patients: polycystic ovary syndrome, nonalcoholic fatty liver disease, and type 2 diabetes. The experts’ aim? To analyze and update the latest evidence on the benefits of this dietary choice.
Polycystic ovary syndrome
Alessandra Gambineri, MD, PhD, associate professor at the department of medicine and surgery (DIMEC) at the University of Bologna, Italy, addressed the link between obesity and polycystic ovary syndrome, which she described as a chronic disease that affects about 10% of women of childbearing age and that presents diverse phenotypes with different characteristics.
“The pathophysiology of this syndrome is characterized by the interaction of three factors: androgen excess, adipose tissue dysfunction, and insulin resistance. These factors interact with each other and are expressed differently in each phenotype,” said Dr. Gambineri.
She indicated that adipose tissue dysfunction is central to this pathology. This centrality results from its association with secretions, such as free fatty acids, proinflammatory cytokines, certain adipokines that promote insulin resistance, glucocorticosteroids, androgens, and oxidative stress.
“Similarly, the oxidative stress that characterizes this syndrome is increasingly present in obese individuals,” said Dr. Gambineri. “This oxidative stress also produces ovary hypotoxicity that aggravates ovulatory function. In this context, the very-low-calorie ketogenic diet can be useful in several ways: weight reduction; promoting the loss of mainly visceral/abdominal fat; decreasing lipotoxicity; and improving inflammation, hyperinsulinemia, and insulin resistance.”
This was the path followed to carry out a study that aimed to analyze the effects of the very-low-calorie ketogenic diet on manifestations of polycystic ovary syndrome in the obesity phenotype. Dr. Gambineri presented its results.
“The objective was to compare the effects of a very-low-calorie ketogenic diet and the standard low-calorie (hypocaloric) diet as a control group,” she said. “The effects studied include body weight, insulin resistance, menstrual cycle, ovulation, ovarian morphology, and hyperandrogenism in a population of 30 obese women with polycystic ovary syndrome and insulin resistance.”
Study participants had a diagnosis of polycystic ovary syndrome as defined by the National Institutes of Health criteria and were aged 18-45 years. These women were randomly assigned to two groups of equal size: experimental (very-low-calorie ketogenic diet) and control (hypocaloric diet). “The women assigned to the experimental group followed the ketogenic stage for eight weeks and then moved to the second, low-calorie diet phase for an additional eight weeks, while those in the control group (hypocaloric diet) followed the low-calorie diet for all 16 weeks.”
The primary outcomes were changes in weight and body composition, specifically fat mass and lean mass, measured by bioimpedance. “The changes observed in the following aspects were considered secondary outcomes: abdominal fat distribution, metabolic parameters, ovulation, ovarian morphology, hirsutism, hyperandrogenism, psychological well-being, and psychological distress,” said Dr. Gambineri. “Any reduction in the ovarian stroma, the area where androgens are synthesized, was also analyzed.”
The study authors found that although BMI decreased in both groups, this reduction was greater in the group that followed the very-low-calorie ketogenic diet. Significant weight loss was observed in both groups, 12.4 kg versus 4.7 kg. Significant differences were also observed in waist circumference (−8.1% in the experimental group vs. −2.2% in the control group), fat mass (−15.1% vs. −8.5%), and free testosterone (−30.3% vs. +10.6%). Only the experimental group saw a reduction in insulin.
“A key point regarding hyperandrogenism, especially regarding what’s referred to as free testosterone, there was only a significant reduction in the very-low-calorie ketogenic diet group,” said Dr. Gambineri. “This reduction was especially evident in the first part of the study, coinciding with the ketogenic period. The reason for this effect lies in the significant increase in the concentration of sex hormone-binding globulins, SHB6. Said globulins bind to the testosterone present in female blood, producing a reduction in free testosterone, a very important effect considering that this syndrome is an androgenic disorder. Furthermore, current treatments for polycystic ovary syndrome do not reduce free testosterone as much as this dietary approach does.”
For the specialist, among all these positive effects in these patients, perhaps most important is the notable improvement that occurs in ovulation. “At the beginning of the study, only 38.5% of the participants in the experimental group and 14.3% of those in the control group had ovulatory cycles. After the intervention, 84.6% managed to ovulate, compared to 35.7% who achieved this goal in the other group.”
Dr. Gambineri suggested that this method is “valid for reducing fat mass and rapidly improving hyperandrogenism and ovulatory dysfunction in women with obesity and polycystic ovary syndrome.”
Reversing type 2 diabetes?
Daniela Sofrà, MD, an endocrinologist specializing in diabetology at La Source Clinic, Lausanne, Switzerland, reviewed the current evidence on the role of the very-low-calorie ketogenic diet in the management of type 2 diabetes.
“It’s time to rethink diabetes treatment and focus efforts on managing obesity as an associated factor,” she said. “One of the hypotheses being examined in this regard is the twin cycle, which postulates that type 2 diabetes is the result of excess fat in the liver. This in turn is associated with insulin resistance with pancreas dysfunction.”
Dr. Sofrà added that there is a study documenting for the first time the reversibility of the morphology of the diabetic pancreas after caloric restriction with the very-low-calorie ketogenic diet. “The reason for this effect is the use of visceral and intrahepatic fat, which can lead to the remission of the clinical manifestation of type 2 diabetes, understanding as such the definition made by the American Diabetes Association: glycosylated hemoglobin < 6.5% without pharmacological therapy.”
Specifically, the results of this research showed that after following the very-low-calorie ketogenic diet and achieving a 15% weight loss (mean weight loss of the participants), liver glucose levels returned to normal levels within 7 days. Beta cell function returned to near normal within 8 weeks.
“Subsequent studies have shown the durability of remission of type 2 diabetes, thanks to the reactivation of the insulin-secreting function of beta cells that had become dedifferentiated in the face of chronic nutrient excess. Specifically, 6 out of 10 patients maintained glycosylated hemoglobin < 6% after 6 months without the need for pharmacological therapy,” Dr. Sofrà added.
Likewise, she highlighted that the probability of achieving remission is mainly determined by the duration of the disease. “The years with diabetes are one of the main predictors of the response that the patient will have with this dietary intervention. Studies have shown that remission is possible in patients with diabetes for less than 6 years, although there are other projects that indicate that it can be achieved with up to 10 years’ duration.”
Based on these data, Dr. Sofrà emphasized the pleiotropic effects of the very-low-calorie ketogenic diet on glycemic control, favoring the possible remission of diabetes or the reduction of drugs, as well as the reduction of the HOMA-IR index (insulin resistance) and waist circumference in people with type 2 diabetes.
Nonalcoholic fatty liver disease
The third comorbidity of obesity that may benefit from the very-low-calorie ketogenic diet is hepatic steatosis, or nonalcoholic fatty liver disease, said Hardy Walle, MD, an internal medicine specialist and director/founder of the Bodymed center, Kirkel, Germany, and one of the authors of this research.
“Recent research shows that ectopic fat and nonalcoholic fatty liver disease could be considered a cause, or at least one of the causes, of most of the diseases that affect the population as a consequence of overweight and obesity,” said Dr. Walle. “Some authors have stated that without fatty liver, there is no type 2 diabetes.”
Dr. Walle pointed out that between 30% and 40% of the adult population has nonalcoholic fatty liver disease, a percentage that increases considerably in people with obesity, reaching 70% prevalence and increasing, in the case of type 2 diabetes, to almost 90%. “Even normal weight does not rule out fatty liver; in fact, about 15% of people with nonalcoholic fatty liver disease are not overweight.”
In a setting where there are no approved drugs for the treatment of fatty liver (the current standard approach focuses on lifestyle interventions), a short-term hypocaloric diet (or liver fasting) is considered an effective method for management of this pathology. This principle was demonstrated by a study by the Saarland University, Saarbrücken, Germany, that Dr. Walle used to illustrate this statement.
“The participants (60 patients with hepatic steatosis) followed a hypocaloric diet (less than 1,000 kcal/day) for 14 days with a formula rich in protein and fiber specially developed for the treatment of nonalcoholic fatty liver disease. A fibroscan was then performed with controlled attenuation parameter measurement to quantify fatty liver disease. The results showed not only a significant improvement in nonalcoholic fatty liver disease parameters but also a marked improvement in all relevant metabolic parameters (serum lipids, liver enzymes),” explained Dr. Walle.
“This evidence leads us to affirm that the concept of hepatic fasting (by means of a hypocaloric diet) marks a point of reference for a future treatment approach for nonalcoholic fatty liver disease,” he concluded.
The study that Dr. Gambineri presented was carried out with the collaboration of the Pronokal Group (Nestlé Health Science). Dr. Gambineri, Dr. Sofrà, and Dr. Walle disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MADRID – During the International Scientific Symposium “New Frontiers in Scientific Research” that recently took place in Barcelona, specialists analyzed the role of the very-low-calorie ketogenic diet. This analysis was in relation to three comorbidities that have a higher incidence among overweight and obese patients: polycystic ovary syndrome, nonalcoholic fatty liver disease, and type 2 diabetes. The experts’ aim? To analyze and update the latest evidence on the benefits of this dietary choice.
Polycystic ovary syndrome
Alessandra Gambineri, MD, PhD, associate professor at the department of medicine and surgery (DIMEC) at the University of Bologna, Italy, addressed the link between obesity and polycystic ovary syndrome, which she described as a chronic disease that affects about 10% of women of childbearing age and that presents diverse phenotypes with different characteristics.
“The pathophysiology of this syndrome is characterized by the interaction of three factors: androgen excess, adipose tissue dysfunction, and insulin resistance. These factors interact with each other and are expressed differently in each phenotype,” said Dr. Gambineri.
She indicated that adipose tissue dysfunction is central to this pathology. This centrality results from its association with secretions, such as free fatty acids, proinflammatory cytokines, certain adipokines that promote insulin resistance, glucocorticosteroids, androgens, and oxidative stress.
“Similarly, the oxidative stress that characterizes this syndrome is increasingly present in obese individuals,” said Dr. Gambineri. “This oxidative stress also produces ovary hypotoxicity that aggravates ovulatory function. In this context, the very-low-calorie ketogenic diet can be useful in several ways: weight reduction; promoting the loss of mainly visceral/abdominal fat; decreasing lipotoxicity; and improving inflammation, hyperinsulinemia, and insulin resistance.”
This was the path followed to carry out a study that aimed to analyze the effects of the very-low-calorie ketogenic diet on manifestations of polycystic ovary syndrome in the obesity phenotype. Dr. Gambineri presented its results.
“The objective was to compare the effects of a very-low-calorie ketogenic diet and the standard low-calorie (hypocaloric) diet as a control group,” she said. “The effects studied include body weight, insulin resistance, menstrual cycle, ovulation, ovarian morphology, and hyperandrogenism in a population of 30 obese women with polycystic ovary syndrome and insulin resistance.”
Study participants had a diagnosis of polycystic ovary syndrome as defined by the National Institutes of Health criteria and were aged 18-45 years. These women were randomly assigned to two groups of equal size: experimental (very-low-calorie ketogenic diet) and control (hypocaloric diet). “The women assigned to the experimental group followed the ketogenic stage for eight weeks and then moved to the second, low-calorie diet phase for an additional eight weeks, while those in the control group (hypocaloric diet) followed the low-calorie diet for all 16 weeks.”
The primary outcomes were changes in weight and body composition, specifically fat mass and lean mass, measured by bioimpedance. “The changes observed in the following aspects were considered secondary outcomes: abdominal fat distribution, metabolic parameters, ovulation, ovarian morphology, hirsutism, hyperandrogenism, psychological well-being, and psychological distress,” said Dr. Gambineri. “Any reduction in the ovarian stroma, the area where androgens are synthesized, was also analyzed.”
The study authors found that although BMI decreased in both groups, this reduction was greater in the group that followed the very-low-calorie ketogenic diet. Significant weight loss was observed in both groups, 12.4 kg versus 4.7 kg. Significant differences were also observed in waist circumference (−8.1% in the experimental group vs. −2.2% in the control group), fat mass (−15.1% vs. −8.5%), and free testosterone (−30.3% vs. +10.6%). Only the experimental group saw a reduction in insulin.
“A key point regarding hyperandrogenism, especially regarding what’s referred to as free testosterone, there was only a significant reduction in the very-low-calorie ketogenic diet group,” said Dr. Gambineri. “This reduction was especially evident in the first part of the study, coinciding with the ketogenic period. The reason for this effect lies in the significant increase in the concentration of sex hormone-binding globulins, SHB6. Said globulins bind to the testosterone present in female blood, producing a reduction in free testosterone, a very important effect considering that this syndrome is an androgenic disorder. Furthermore, current treatments for polycystic ovary syndrome do not reduce free testosterone as much as this dietary approach does.”
For the specialist, among all these positive effects in these patients, perhaps most important is the notable improvement that occurs in ovulation. “At the beginning of the study, only 38.5% of the participants in the experimental group and 14.3% of those in the control group had ovulatory cycles. After the intervention, 84.6% managed to ovulate, compared to 35.7% who achieved this goal in the other group.”
Dr. Gambineri suggested that this method is “valid for reducing fat mass and rapidly improving hyperandrogenism and ovulatory dysfunction in women with obesity and polycystic ovary syndrome.”
Reversing type 2 diabetes?
Daniela Sofrà, MD, an endocrinologist specializing in diabetology at La Source Clinic, Lausanne, Switzerland, reviewed the current evidence on the role of the very-low-calorie ketogenic diet in the management of type 2 diabetes.
“It’s time to rethink diabetes treatment and focus efforts on managing obesity as an associated factor,” she said. “One of the hypotheses being examined in this regard is the twin cycle, which postulates that type 2 diabetes is the result of excess fat in the liver. This in turn is associated with insulin resistance with pancreas dysfunction.”
Dr. Sofrà added that there is a study documenting for the first time the reversibility of the morphology of the diabetic pancreas after caloric restriction with the very-low-calorie ketogenic diet. “The reason for this effect is the use of visceral and intrahepatic fat, which can lead to the remission of the clinical manifestation of type 2 diabetes, understanding as such the definition made by the American Diabetes Association: glycosylated hemoglobin < 6.5% without pharmacological therapy.”
Specifically, the results of this research showed that after following the very-low-calorie ketogenic diet and achieving a 15% weight loss (mean weight loss of the participants), liver glucose levels returned to normal levels within 7 days. Beta cell function returned to near normal within 8 weeks.
“Subsequent studies have shown the durability of remission of type 2 diabetes, thanks to the reactivation of the insulin-secreting function of beta cells that had become dedifferentiated in the face of chronic nutrient excess. Specifically, 6 out of 10 patients maintained glycosylated hemoglobin < 6% after 6 months without the need for pharmacological therapy,” Dr. Sofrà added.
Likewise, she highlighted that the probability of achieving remission is mainly determined by the duration of the disease. “The years with diabetes are one of the main predictors of the response that the patient will have with this dietary intervention. Studies have shown that remission is possible in patients with diabetes for less than 6 years, although there are other projects that indicate that it can be achieved with up to 10 years’ duration.”
Based on these data, Dr. Sofrà emphasized the pleiotropic effects of the very-low-calorie ketogenic diet on glycemic control, favoring the possible remission of diabetes or the reduction of drugs, as well as the reduction of the HOMA-IR index (insulin resistance) and waist circumference in people with type 2 diabetes.
Nonalcoholic fatty liver disease
The third comorbidity of obesity that may benefit from the very-low-calorie ketogenic diet is hepatic steatosis, or nonalcoholic fatty liver disease, said Hardy Walle, MD, an internal medicine specialist and director/founder of the Bodymed center, Kirkel, Germany, and one of the authors of this research.
“Recent research shows that ectopic fat and nonalcoholic fatty liver disease could be considered a cause, or at least one of the causes, of most of the diseases that affect the population as a consequence of overweight and obesity,” said Dr. Walle. “Some authors have stated that without fatty liver, there is no type 2 diabetes.”
Dr. Walle pointed out that between 30% and 40% of the adult population has nonalcoholic fatty liver disease, a percentage that increases considerably in people with obesity, reaching 70% prevalence and increasing, in the case of type 2 diabetes, to almost 90%. “Even normal weight does not rule out fatty liver; in fact, about 15% of people with nonalcoholic fatty liver disease are not overweight.”
In a setting where there are no approved drugs for the treatment of fatty liver (the current standard approach focuses on lifestyle interventions), a short-term hypocaloric diet (or liver fasting) is considered an effective method for management of this pathology. This principle was demonstrated by a study by the Saarland University, Saarbrücken, Germany, that Dr. Walle used to illustrate this statement.
“The participants (60 patients with hepatic steatosis) followed a hypocaloric diet (less than 1,000 kcal/day) for 14 days with a formula rich in protein and fiber specially developed for the treatment of nonalcoholic fatty liver disease. A fibroscan was then performed with controlled attenuation parameter measurement to quantify fatty liver disease. The results showed not only a significant improvement in nonalcoholic fatty liver disease parameters but also a marked improvement in all relevant metabolic parameters (serum lipids, liver enzymes),” explained Dr. Walle.
“This evidence leads us to affirm that the concept of hepatic fasting (by means of a hypocaloric diet) marks a point of reference for a future treatment approach for nonalcoholic fatty liver disease,” he concluded.
The study that Dr. Gambineri presented was carried out with the collaboration of the Pronokal Group (Nestlé Health Science). Dr. Gambineri, Dr. Sofrà, and Dr. Walle disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MADRID – During the International Scientific Symposium “New Frontiers in Scientific Research” that recently took place in Barcelona, specialists analyzed the role of the very-low-calorie ketogenic diet. This analysis was in relation to three comorbidities that have a higher incidence among overweight and obese patients: polycystic ovary syndrome, nonalcoholic fatty liver disease, and type 2 diabetes. The experts’ aim? To analyze and update the latest evidence on the benefits of this dietary choice.
Polycystic ovary syndrome
Alessandra Gambineri, MD, PhD, associate professor at the department of medicine and surgery (DIMEC) at the University of Bologna, Italy, addressed the link between obesity and polycystic ovary syndrome, which she described as a chronic disease that affects about 10% of women of childbearing age and that presents diverse phenotypes with different characteristics.
“The pathophysiology of this syndrome is characterized by the interaction of three factors: androgen excess, adipose tissue dysfunction, and insulin resistance. These factors interact with each other and are expressed differently in each phenotype,” said Dr. Gambineri.
She indicated that adipose tissue dysfunction is central to this pathology. This centrality results from its association with secretions, such as free fatty acids, proinflammatory cytokines, certain adipokines that promote insulin resistance, glucocorticosteroids, androgens, and oxidative stress.
“Similarly, the oxidative stress that characterizes this syndrome is increasingly present in obese individuals,” said Dr. Gambineri. “This oxidative stress also produces ovary hypotoxicity that aggravates ovulatory function. In this context, the very-low-calorie ketogenic diet can be useful in several ways: weight reduction; promoting the loss of mainly visceral/abdominal fat; decreasing lipotoxicity; and improving inflammation, hyperinsulinemia, and insulin resistance.”
This was the path followed to carry out a study that aimed to analyze the effects of the very-low-calorie ketogenic diet on manifestations of polycystic ovary syndrome in the obesity phenotype. Dr. Gambineri presented its results.
“The objective was to compare the effects of a very-low-calorie ketogenic diet and the standard low-calorie (hypocaloric) diet as a control group,” she said. “The effects studied include body weight, insulin resistance, menstrual cycle, ovulation, ovarian morphology, and hyperandrogenism in a population of 30 obese women with polycystic ovary syndrome and insulin resistance.”
Study participants had a diagnosis of polycystic ovary syndrome as defined by the National Institutes of Health criteria and were aged 18-45 years. These women were randomly assigned to two groups of equal size: experimental (very-low-calorie ketogenic diet) and control (hypocaloric diet). “The women assigned to the experimental group followed the ketogenic stage for eight weeks and then moved to the second, low-calorie diet phase for an additional eight weeks, while those in the control group (hypocaloric diet) followed the low-calorie diet for all 16 weeks.”
The primary outcomes were changes in weight and body composition, specifically fat mass and lean mass, measured by bioimpedance. “The changes observed in the following aspects were considered secondary outcomes: abdominal fat distribution, metabolic parameters, ovulation, ovarian morphology, hirsutism, hyperandrogenism, psychological well-being, and psychological distress,” said Dr. Gambineri. “Any reduction in the ovarian stroma, the area where androgens are synthesized, was also analyzed.”
The study authors found that although BMI decreased in both groups, this reduction was greater in the group that followed the very-low-calorie ketogenic diet. Significant weight loss was observed in both groups, 12.4 kg versus 4.7 kg. Significant differences were also observed in waist circumference (−8.1% in the experimental group vs. −2.2% in the control group), fat mass (−15.1% vs. −8.5%), and free testosterone (−30.3% vs. +10.6%). Only the experimental group saw a reduction in insulin.
“A key point regarding hyperandrogenism, especially regarding what’s referred to as free testosterone, there was only a significant reduction in the very-low-calorie ketogenic diet group,” said Dr. Gambineri. “This reduction was especially evident in the first part of the study, coinciding with the ketogenic period. The reason for this effect lies in the significant increase in the concentration of sex hormone-binding globulins, SHB6. Said globulins bind to the testosterone present in female blood, producing a reduction in free testosterone, a very important effect considering that this syndrome is an androgenic disorder. Furthermore, current treatments for polycystic ovary syndrome do not reduce free testosterone as much as this dietary approach does.”
For the specialist, among all these positive effects in these patients, perhaps most important is the notable improvement that occurs in ovulation. “At the beginning of the study, only 38.5% of the participants in the experimental group and 14.3% of those in the control group had ovulatory cycles. After the intervention, 84.6% managed to ovulate, compared to 35.7% who achieved this goal in the other group.”
Dr. Gambineri suggested that this method is “valid for reducing fat mass and rapidly improving hyperandrogenism and ovulatory dysfunction in women with obesity and polycystic ovary syndrome.”
Reversing type 2 diabetes?
Daniela Sofrà, MD, an endocrinologist specializing in diabetology at La Source Clinic, Lausanne, Switzerland, reviewed the current evidence on the role of the very-low-calorie ketogenic diet in the management of type 2 diabetes.
“It’s time to rethink diabetes treatment and focus efforts on managing obesity as an associated factor,” she said. “One of the hypotheses being examined in this regard is the twin cycle, which postulates that type 2 diabetes is the result of excess fat in the liver. This in turn is associated with insulin resistance with pancreas dysfunction.”
Dr. Sofrà added that there is a study documenting for the first time the reversibility of the morphology of the diabetic pancreas after caloric restriction with the very-low-calorie ketogenic diet. “The reason for this effect is the use of visceral and intrahepatic fat, which can lead to the remission of the clinical manifestation of type 2 diabetes, understanding as such the definition made by the American Diabetes Association: glycosylated hemoglobin < 6.5% without pharmacological therapy.”
Specifically, the results of this research showed that after following the very-low-calorie ketogenic diet and achieving a 15% weight loss (mean weight loss of the participants), liver glucose levels returned to normal levels within 7 days. Beta cell function returned to near normal within 8 weeks.
“Subsequent studies have shown the durability of remission of type 2 diabetes, thanks to the reactivation of the insulin-secreting function of beta cells that had become dedifferentiated in the face of chronic nutrient excess. Specifically, 6 out of 10 patients maintained glycosylated hemoglobin < 6% after 6 months without the need for pharmacological therapy,” Dr. Sofrà added.
Likewise, she highlighted that the probability of achieving remission is mainly determined by the duration of the disease. “The years with diabetes are one of the main predictors of the response that the patient will have with this dietary intervention. Studies have shown that remission is possible in patients with diabetes for less than 6 years, although there are other projects that indicate that it can be achieved with up to 10 years’ duration.”
Based on these data, Dr. Sofrà emphasized the pleiotropic effects of the very-low-calorie ketogenic diet on glycemic control, favoring the possible remission of diabetes or the reduction of drugs, as well as the reduction of the HOMA-IR index (insulin resistance) and waist circumference in people with type 2 diabetes.
Nonalcoholic fatty liver disease
The third comorbidity of obesity that may benefit from the very-low-calorie ketogenic diet is hepatic steatosis, or nonalcoholic fatty liver disease, said Hardy Walle, MD, an internal medicine specialist and director/founder of the Bodymed center, Kirkel, Germany, and one of the authors of this research.
“Recent research shows that ectopic fat and nonalcoholic fatty liver disease could be considered a cause, or at least one of the causes, of most of the diseases that affect the population as a consequence of overweight and obesity,” said Dr. Walle. “Some authors have stated that without fatty liver, there is no type 2 diabetes.”
Dr. Walle pointed out that between 30% and 40% of the adult population has nonalcoholic fatty liver disease, a percentage that increases considerably in people with obesity, reaching 70% prevalence and increasing, in the case of type 2 diabetes, to almost 90%. “Even normal weight does not rule out fatty liver; in fact, about 15% of people with nonalcoholic fatty liver disease are not overweight.”
In a setting where there are no approved drugs for the treatment of fatty liver (the current standard approach focuses on lifestyle interventions), a short-term hypocaloric diet (or liver fasting) is considered an effective method for management of this pathology. This principle was demonstrated by a study by the Saarland University, Saarbrücken, Germany, that Dr. Walle used to illustrate this statement.
“The participants (60 patients with hepatic steatosis) followed a hypocaloric diet (less than 1,000 kcal/day) for 14 days with a formula rich in protein and fiber specially developed for the treatment of nonalcoholic fatty liver disease. A fibroscan was then performed with controlled attenuation parameter measurement to quantify fatty liver disease. The results showed not only a significant improvement in nonalcoholic fatty liver disease parameters but also a marked improvement in all relevant metabolic parameters (serum lipids, liver enzymes),” explained Dr. Walle.
“This evidence leads us to affirm that the concept of hepatic fasting (by means of a hypocaloric diet) marks a point of reference for a future treatment approach for nonalcoholic fatty liver disease,” he concluded.
The study that Dr. Gambineri presented was carried out with the collaboration of the Pronokal Group (Nestlé Health Science). Dr. Gambineri, Dr. Sofrà, and Dr. Walle disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AMA: Insurance should cover treatment for infertility caused by gender-affirming care
CHICAGO – Health insurance should cover treatment for infertility caused by gender-affirming medical interventions, the American Medical Association said June 13 at its House of Delegates meeting.
Speaking on behalf of the Medical Student Section, Justin Magrath, of Louisiana, said, “We as a section feel that these interventions should be considered as additional causes of iatrogenic infertility and be covered by insurance.”
Iatrogenic infertility is infertility caused by surgery, radiotherapy, chemotherapy, or other medically necessary treatment. The AMA voted June 13 to support including the phrase, “impaired fertility as a consequence of gender-affirming hormone therapy and gender-affirming surgery,” in that definition.
The AMA also supports access to fertility preservation services for people who undergo those treatments.
“I’ve had many friends who went through transitions and gender-affirming care and had no idea that these options were available and others who did know they were available but they were so expensive that they couldn’t access them,” said emergency medicine resident Sophia Spadafore, MD, delegate for the Resident and Fellow Section. “So while people might be able to access gender-affirming care, sometimes they have to make the decision between future fertility and having children and accessing this kind of lifesaving care that we support.”
The AMA already had policies that support insurance coverage of treatments for gender dysphoria and the right to seek fertility preservation services for people who undergo gender-affirming hormone therapy or surgery, but until this week, it had not addressed insurance coverage for preserving fertility in those cases.
“The transgender population already faces many barriers to care, such as provider discrimination, legal concerns, financial burden, and emotional cost,” Mr. Magrath said during a reference committee hearing on June 11. “We as a section ask our organization to continue to serve as an ally, providing equitable care for diverse populations and expanding coverage for medically necessary treatments.”
“I am a gender surgeon, so this is pretty important to me,” said Sean Figy, MD, of Nebraska, a delegate for the American Society for Reconstructive Microsurgery.
The original resolution included the words “medically necessary” when referring to gender-affirming treatments, and Dr. Figy expressed hesitancy about those words. An amendment removed them.
“I’ve seen that phrase weaponized against gender-nonconforming patients,” he said.
Ophthalmologist Charles Hickey, MD, of the Ohio delegation, spoke in favor of referral or of waiting to adopt the resolution.
“I think the different amendments being discussed here are evidence that this needs a more thorough and careful treatment than we can do at this point right now,” he said.
A version of this article first appeared on Medscape.com.
CHICAGO – Health insurance should cover treatment for infertility caused by gender-affirming medical interventions, the American Medical Association said June 13 at its House of Delegates meeting.
Speaking on behalf of the Medical Student Section, Justin Magrath, of Louisiana, said, “We as a section feel that these interventions should be considered as additional causes of iatrogenic infertility and be covered by insurance.”
Iatrogenic infertility is infertility caused by surgery, radiotherapy, chemotherapy, or other medically necessary treatment. The AMA voted June 13 to support including the phrase, “impaired fertility as a consequence of gender-affirming hormone therapy and gender-affirming surgery,” in that definition.
The AMA also supports access to fertility preservation services for people who undergo those treatments.
“I’ve had many friends who went through transitions and gender-affirming care and had no idea that these options were available and others who did know they were available but they were so expensive that they couldn’t access them,” said emergency medicine resident Sophia Spadafore, MD, delegate for the Resident and Fellow Section. “So while people might be able to access gender-affirming care, sometimes they have to make the decision between future fertility and having children and accessing this kind of lifesaving care that we support.”
The AMA already had policies that support insurance coverage of treatments for gender dysphoria and the right to seek fertility preservation services for people who undergo gender-affirming hormone therapy or surgery, but until this week, it had not addressed insurance coverage for preserving fertility in those cases.
“The transgender population already faces many barriers to care, such as provider discrimination, legal concerns, financial burden, and emotional cost,” Mr. Magrath said during a reference committee hearing on June 11. “We as a section ask our organization to continue to serve as an ally, providing equitable care for diverse populations and expanding coverage for medically necessary treatments.”
“I am a gender surgeon, so this is pretty important to me,” said Sean Figy, MD, of Nebraska, a delegate for the American Society for Reconstructive Microsurgery.
The original resolution included the words “medically necessary” when referring to gender-affirming treatments, and Dr. Figy expressed hesitancy about those words. An amendment removed them.
“I’ve seen that phrase weaponized against gender-nonconforming patients,” he said.
Ophthalmologist Charles Hickey, MD, of the Ohio delegation, spoke in favor of referral or of waiting to adopt the resolution.
“I think the different amendments being discussed here are evidence that this needs a more thorough and careful treatment than we can do at this point right now,” he said.
A version of this article first appeared on Medscape.com.
CHICAGO – Health insurance should cover treatment for infertility caused by gender-affirming medical interventions, the American Medical Association said June 13 at its House of Delegates meeting.
Speaking on behalf of the Medical Student Section, Justin Magrath, of Louisiana, said, “We as a section feel that these interventions should be considered as additional causes of iatrogenic infertility and be covered by insurance.”
Iatrogenic infertility is infertility caused by surgery, radiotherapy, chemotherapy, or other medically necessary treatment. The AMA voted June 13 to support including the phrase, “impaired fertility as a consequence of gender-affirming hormone therapy and gender-affirming surgery,” in that definition.
The AMA also supports access to fertility preservation services for people who undergo those treatments.
“I’ve had many friends who went through transitions and gender-affirming care and had no idea that these options were available and others who did know they were available but they were so expensive that they couldn’t access them,” said emergency medicine resident Sophia Spadafore, MD, delegate for the Resident and Fellow Section. “So while people might be able to access gender-affirming care, sometimes they have to make the decision between future fertility and having children and accessing this kind of lifesaving care that we support.”
The AMA already had policies that support insurance coverage of treatments for gender dysphoria and the right to seek fertility preservation services for people who undergo gender-affirming hormone therapy or surgery, but until this week, it had not addressed insurance coverage for preserving fertility in those cases.
“The transgender population already faces many barriers to care, such as provider discrimination, legal concerns, financial burden, and emotional cost,” Mr. Magrath said during a reference committee hearing on June 11. “We as a section ask our organization to continue to serve as an ally, providing equitable care for diverse populations and expanding coverage for medically necessary treatments.”
“I am a gender surgeon, so this is pretty important to me,” said Sean Figy, MD, of Nebraska, a delegate for the American Society for Reconstructive Microsurgery.
The original resolution included the words “medically necessary” when referring to gender-affirming treatments, and Dr. Figy expressed hesitancy about those words. An amendment removed them.
“I’ve seen that phrase weaponized against gender-nonconforming patients,” he said.
Ophthalmologist Charles Hickey, MD, of the Ohio delegation, spoke in favor of referral or of waiting to adopt the resolution.
“I think the different amendments being discussed here are evidence that this needs a more thorough and careful treatment than we can do at this point right now,” he said.
A version of this article first appeared on Medscape.com.
Psychedelic drugs ‘truly have potential’ in headache care
DENVER – Psychedelics such as psilocybin “truly have the potential to transform how we treat a number of neuropsychiatric diseases, including headaches,” a neuropharmacologist told colleagues at the annual meeting of the American Headache Society.
However, Bryan Roth, MD, PhD, professor of pharmacology at the University of North Carolina at Chapel Hill, also offered a major cautionary note: There have been no randomized, phase 3 trials of psychedelics, and he bluntly said that “I do not recommend the use of psychedelics for any medical condition.”
The potential disease-altering powers of psychedelics have received a tremendous amount of research and media attention over the past several years. A landmark randomized, double-blind study released in 2016 triggered much of the interest, Dr. Roth said, when it suggested that high-dose psilocybin significantly lowered levels of depressed mood/anxiety in patients with life-threatening cancer. At 6 months, 80% of patients who took the dose reported moderate or greater improvement in well-being/life satisfaction.
“You have the potential – unprecedented in psychiatry – that a single dose of a therapeutic agent may induce a rapid, robust, and sustained antidepressant action,” he said. Also of note: The “vast majority” of subjects say their encounter with a psychedelic was “one of the most meaningful experiences of their lives.”
Dr. Roth said his own research suggests that psychedelics cause a “huge increase” in the asynchronous firing of neurons. “Noise is being injected into the system and is interpreted by the brain or the mind, which always likes to make a story about what’s going on. The story it makes up is idiosyncratic to every person and memorable for reasons that are not understood.”
Now, Dr. Roth said, he and colleagues are working to “create drugs that have this potential remarkable therapeutic efficacy in psychiatric and neurologic disorders without the psychedelic effects.” A $27 million grant from the Defense Advanced Research Projects Agency is providing support for their efforts, he said.
For the moment, he said, there’s no way to know if “the psychedelic experience is essential to the therapeutic action of these drugs. But it’s a testable hypothesis.”
As he noted, a tiny 2010 study of 2-bromo-lysergic acid diethylamide (LSD), which doesn’t cause hallucinations, showed promise as a treatment for cluster headaches.
For now, Dr. Roth said, his lab is synthesizing and testing new compounds that interact with the crucial 5-HT2A receptor.
Additional research
In another presentation at the AHS annual meeting, neurologist Emmanuelle A. D. Schindler, MD, PhD, of Yale School of Medicine, highlighted her 2021 study of an exploratory double-blind, placebo-controlled, cross-over study of psilocybin versus placebo for migraine headache. A single oral dose of the drug, the researchers found, reduced headache frequency and pain over 2 weeks. The study is small, with just 10 subjects, and multiple exclusion criteria.
She also revealed preliminary findings from an ongoing randomized, double-blind, placebo-controlled study of psilocybin versus placebo in cluster headaches. In 14 subjects, a psilocybin pulse was linked to fewer cluster attacks over 3 weeks, although the effect wasn’t statistically significant. However, there was a statistically significant reduction over 8 weeks in patients with chronic headache.
Dr. Schindler noted that “with these early studies, we only looked out to 2 weeks for migraine, and we only looked out to 2 months for cluster.” There are multiple other limitations, she acknowledged. “We have to do a lot more research and consider safety as well.”
However, “there is a really unique capacity for lasting effects after limited dosing,” she added, and the studies do show reductions in headache burden “that do not correlate with acute psychedelic effects.”
Moving forward, Dr. Roth cautioned that while U.S. states are allowing the use of psychedelics for medical purposes, “we don’t know if they ultimately are therapeutic. And we have strong reason to believe that microdosing or chronic dosing of these compounds is ultimately going to be deleterious to the health of our patients.”
Dr. Roth did not provide disclosure information. Dr. Schindler discloses research funding (Ceruvia Lifesciences, Wallace Research Foundation, Clusterbusters, Department of Veterans Affairs), serves on advisory boards (Ceruvia Lifesciences, Clusterbusters), and has a patent.
DENVER – Psychedelics such as psilocybin “truly have the potential to transform how we treat a number of neuropsychiatric diseases, including headaches,” a neuropharmacologist told colleagues at the annual meeting of the American Headache Society.
However, Bryan Roth, MD, PhD, professor of pharmacology at the University of North Carolina at Chapel Hill, also offered a major cautionary note: There have been no randomized, phase 3 trials of psychedelics, and he bluntly said that “I do not recommend the use of psychedelics for any medical condition.”
The potential disease-altering powers of psychedelics have received a tremendous amount of research and media attention over the past several years. A landmark randomized, double-blind study released in 2016 triggered much of the interest, Dr. Roth said, when it suggested that high-dose psilocybin significantly lowered levels of depressed mood/anxiety in patients with life-threatening cancer. At 6 months, 80% of patients who took the dose reported moderate or greater improvement in well-being/life satisfaction.
“You have the potential – unprecedented in psychiatry – that a single dose of a therapeutic agent may induce a rapid, robust, and sustained antidepressant action,” he said. Also of note: The “vast majority” of subjects say their encounter with a psychedelic was “one of the most meaningful experiences of their lives.”
Dr. Roth said his own research suggests that psychedelics cause a “huge increase” in the asynchronous firing of neurons. “Noise is being injected into the system and is interpreted by the brain or the mind, which always likes to make a story about what’s going on. The story it makes up is idiosyncratic to every person and memorable for reasons that are not understood.”
Now, Dr. Roth said, he and colleagues are working to “create drugs that have this potential remarkable therapeutic efficacy in psychiatric and neurologic disorders without the psychedelic effects.” A $27 million grant from the Defense Advanced Research Projects Agency is providing support for their efforts, he said.
For the moment, he said, there’s no way to know if “the psychedelic experience is essential to the therapeutic action of these drugs. But it’s a testable hypothesis.”
As he noted, a tiny 2010 study of 2-bromo-lysergic acid diethylamide (LSD), which doesn’t cause hallucinations, showed promise as a treatment for cluster headaches.
For now, Dr. Roth said, his lab is synthesizing and testing new compounds that interact with the crucial 5-HT2A receptor.
Additional research
In another presentation at the AHS annual meeting, neurologist Emmanuelle A. D. Schindler, MD, PhD, of Yale School of Medicine, highlighted her 2021 study of an exploratory double-blind, placebo-controlled, cross-over study of psilocybin versus placebo for migraine headache. A single oral dose of the drug, the researchers found, reduced headache frequency and pain over 2 weeks. The study is small, with just 10 subjects, and multiple exclusion criteria.
She also revealed preliminary findings from an ongoing randomized, double-blind, placebo-controlled study of psilocybin versus placebo in cluster headaches. In 14 subjects, a psilocybin pulse was linked to fewer cluster attacks over 3 weeks, although the effect wasn’t statistically significant. However, there was a statistically significant reduction over 8 weeks in patients with chronic headache.
Dr. Schindler noted that “with these early studies, we only looked out to 2 weeks for migraine, and we only looked out to 2 months for cluster.” There are multiple other limitations, she acknowledged. “We have to do a lot more research and consider safety as well.”
However, “there is a really unique capacity for lasting effects after limited dosing,” she added, and the studies do show reductions in headache burden “that do not correlate with acute psychedelic effects.”
Moving forward, Dr. Roth cautioned that while U.S. states are allowing the use of psychedelics for medical purposes, “we don’t know if they ultimately are therapeutic. And we have strong reason to believe that microdosing or chronic dosing of these compounds is ultimately going to be deleterious to the health of our patients.”
Dr. Roth did not provide disclosure information. Dr. Schindler discloses research funding (Ceruvia Lifesciences, Wallace Research Foundation, Clusterbusters, Department of Veterans Affairs), serves on advisory boards (Ceruvia Lifesciences, Clusterbusters), and has a patent.
DENVER – Psychedelics such as psilocybin “truly have the potential to transform how we treat a number of neuropsychiatric diseases, including headaches,” a neuropharmacologist told colleagues at the annual meeting of the American Headache Society.
However, Bryan Roth, MD, PhD, professor of pharmacology at the University of North Carolina at Chapel Hill, also offered a major cautionary note: There have been no randomized, phase 3 trials of psychedelics, and he bluntly said that “I do not recommend the use of psychedelics for any medical condition.”
The potential disease-altering powers of psychedelics have received a tremendous amount of research and media attention over the past several years. A landmark randomized, double-blind study released in 2016 triggered much of the interest, Dr. Roth said, when it suggested that high-dose psilocybin significantly lowered levels of depressed mood/anxiety in patients with life-threatening cancer. At 6 months, 80% of patients who took the dose reported moderate or greater improvement in well-being/life satisfaction.
“You have the potential – unprecedented in psychiatry – that a single dose of a therapeutic agent may induce a rapid, robust, and sustained antidepressant action,” he said. Also of note: The “vast majority” of subjects say their encounter with a psychedelic was “one of the most meaningful experiences of their lives.”
Dr. Roth said his own research suggests that psychedelics cause a “huge increase” in the asynchronous firing of neurons. “Noise is being injected into the system and is interpreted by the brain or the mind, which always likes to make a story about what’s going on. The story it makes up is idiosyncratic to every person and memorable for reasons that are not understood.”
Now, Dr. Roth said, he and colleagues are working to “create drugs that have this potential remarkable therapeutic efficacy in psychiatric and neurologic disorders without the psychedelic effects.” A $27 million grant from the Defense Advanced Research Projects Agency is providing support for their efforts, he said.
For the moment, he said, there’s no way to know if “the psychedelic experience is essential to the therapeutic action of these drugs. But it’s a testable hypothesis.”
As he noted, a tiny 2010 study of 2-bromo-lysergic acid diethylamide (LSD), which doesn’t cause hallucinations, showed promise as a treatment for cluster headaches.
For now, Dr. Roth said, his lab is synthesizing and testing new compounds that interact with the crucial 5-HT2A receptor.
Additional research
In another presentation at the AHS annual meeting, neurologist Emmanuelle A. D. Schindler, MD, PhD, of Yale School of Medicine, highlighted her 2021 study of an exploratory double-blind, placebo-controlled, cross-over study of psilocybin versus placebo for migraine headache. A single oral dose of the drug, the researchers found, reduced headache frequency and pain over 2 weeks. The study is small, with just 10 subjects, and multiple exclusion criteria.
She also revealed preliminary findings from an ongoing randomized, double-blind, placebo-controlled study of psilocybin versus placebo in cluster headaches. In 14 subjects, a psilocybin pulse was linked to fewer cluster attacks over 3 weeks, although the effect wasn’t statistically significant. However, there was a statistically significant reduction over 8 weeks in patients with chronic headache.
Dr. Schindler noted that “with these early studies, we only looked out to 2 weeks for migraine, and we only looked out to 2 months for cluster.” There are multiple other limitations, she acknowledged. “We have to do a lot more research and consider safety as well.”
However, “there is a really unique capacity for lasting effects after limited dosing,” she added, and the studies do show reductions in headache burden “that do not correlate with acute psychedelic effects.”
Moving forward, Dr. Roth cautioned that while U.S. states are allowing the use of psychedelics for medical purposes, “we don’t know if they ultimately are therapeutic. And we have strong reason to believe that microdosing or chronic dosing of these compounds is ultimately going to be deleterious to the health of our patients.”
Dr. Roth did not provide disclosure information. Dr. Schindler discloses research funding (Ceruvia Lifesciences, Wallace Research Foundation, Clusterbusters, Department of Veterans Affairs), serves on advisory boards (Ceruvia Lifesciences, Clusterbusters), and has a patent.
FROM AHS 2022
Adolescent female with rash on the arms and posterior legs
Erythema annulare centrifugum
A thorough body examination failed to reveal any other rashes or lesions suggestive of a fungal infection. A blood count and urinalysis were within normal limits. She had no lymphadenopathy or hepatosplenomegaly. A potassium hydroxide analysis of skin scrapings was negative for fungal elements. Punch biopsy of the skin on the left arm revealed focal intermittent parakeratosis, mildly acanthotic and spongiotic epidermis, and a tight superficial perivascular chronic dermatitis consisting of lymphocytes and histiocytes (Figures). Given these findings, a diagnosis of erythema annulare centrifugum (EAC) was rendered.
EAC is a rare, reactive skin rash characterized by redness (erythema) and ring-shaped lesions (annulare) that slowly spread from the center (centrifugum). The lesions present with a characteristic trailing scale on the inner border of the erythematous ring. Lesions may be asymptomatic or mildly pruritic and commonly involve the trunk, buttocks, hips, and upper legs. It is important to note that its duration is highly variable, ranging from weeks to decades, with most cases persisting for 9 months. EAC typically affects young or middle-aged adults but can occur at any age.

Although the etiology of EAC is unknown, it is believed to be a hypersensitivity reaction to a foreign antigen. Cutaneous fungal infections are commonly reported as triggers as well as other viral infections, medications, malignancy, underlying systemic disease, and certain foods. Treatment depends on the underlying condition and removing the implicated agent. However, most cases of EAC are idiopathic and self-limiting. It is possible that our patient’s prior history of tinea capitis could have triggered the skin lesions suggestive of EAC, but interestingly, these lesions did not go away after the fungal infection was cleared and have continued to recur. For patients with refractory lesions or treatment of patients without an identifiable cause, the use of oral antimicrobials has been proposed. Medications such as azithromycin, erythromycin, fluconazole, and metronidazole have been reported to be helpful in some patients with refractory EAC. Our patient wanted to continue topical treatment with betamethasone as needed and may consider antimicrobial therapy if the lesions continue to recur.
Tinea corporis refers to a superficial fungal infection of the skin. It may present as one or more asymmetrical, annular, pruritic plaques with a raised scaly leading edge rather than the trailing scale seen with EAC. Diagnosis is made by KOH examination of skin scrapings. Common risk factors include close contact with an infected person or animal, warm, moist environments, sharing personal items, and prolonged use of systemic corticosteroids. Our patient’s KOH analysis of skin scrapings was negative for fungal elements.

Erythema marginatum is a rare skin rash commonly seen with acute rheumatic fever secondary to streptococcal infection. It presents as annular erythematous lesions on the trunk and proximal extremities that are exacerbated by heat. It is often associated with active carditis related to rheumatic fever. This self-limited rash usually resolves in 2-3 days. Our patient was asymptomatic without involvement of other organs.
Like EAC, granuloma annulare is a benign chronic skin condition that presents with ring-shaped lesions. Its etiology is unknown, and lesions may be asymptomatic or mildly pruritic. Localized granuloma annulare typically presents as reddish-brown papules or plaques on the fingers, hands, elbows, dorsal feet, or ankles. The distinguishing feature of granuloma annulare from other annular lesions is its absence of scale.

Urticaria multiforme is an allergic hypersensitivity reaction commonly linked to viral infections, medications, and immunizations. Clinical features include blanchable annular/polycyclic lesions with a central purplish or dusky hue. Diagnostic pearls include the presence of pruritus, dermatographism, and individual lesions that resolve within 24 hours, all of which were not found in our patient’s case.
Ms. Laborada is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital. Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Ms. Laborada and Dr. Matiz have no relevant financial disclosures.
References
1. Paller A and Mancini AJ. Hurwitz Clinical Pediatric Dermatology: A Textbook of Skin Disorders of Childhood and Adolescence. 4th ed. Philadelphia: Elsevier Saunders, 2011.
2. McDaniel B and Cook C. “Erythema annulare centrifugum” 2021 Aug 27. In: StatPearls [Internet]. Treasure Island, Fla.: StatPearls Publishing, 2022 Jan. PMID: 29494101.
3. Leung AK e al. Drugs Context. 2020 Jul 20;9:5-6.
4. Majmundar VD and Nagalli S. “Erythema marginatum” 2022 May 8. In: StatPearls [Internet]. Treasure Island, Fla.: StatPearls Publishing, 2022 Jan.
5. Piette EW and Rosenbach M. J Am Acad Dermatol. 2016 Sep;75(3):467-79.
6. Barros M et al. BMJ Case Rep. 2021 Jan 28;14(1):e241011.
Erythema annulare centrifugum
A thorough body examination failed to reveal any other rashes or lesions suggestive of a fungal infection. A blood count and urinalysis were within normal limits. She had no lymphadenopathy or hepatosplenomegaly. A potassium hydroxide analysis of skin scrapings was negative for fungal elements. Punch biopsy of the skin on the left arm revealed focal intermittent parakeratosis, mildly acanthotic and spongiotic epidermis, and a tight superficial perivascular chronic dermatitis consisting of lymphocytes and histiocytes (Figures). Given these findings, a diagnosis of erythema annulare centrifugum (EAC) was rendered.
EAC is a rare, reactive skin rash characterized by redness (erythema) and ring-shaped lesions (annulare) that slowly spread from the center (centrifugum). The lesions present with a characteristic trailing scale on the inner border of the erythematous ring. Lesions may be asymptomatic or mildly pruritic and commonly involve the trunk, buttocks, hips, and upper legs. It is important to note that its duration is highly variable, ranging from weeks to decades, with most cases persisting for 9 months. EAC typically affects young or middle-aged adults but can occur at any age.
Although the etiology of EAC is unknown, it is believed to be a hypersensitivity reaction to a foreign antigen. Cutaneous fungal infections are commonly reported as triggers as well as other viral infections, medications, malignancy, underlying systemic disease, and certain foods. Treatment depends on the underlying condition and removing the implicated agent. However, most cases of EAC are idiopathic and self-limiting. It is possible that our patient’s prior history of tinea capitis could have triggered the skin lesions suggestive of EAC, but interestingly, these lesions did not go away after the fungal infection was cleared and have continued to recur. For patients with refractory lesions or treatment of patients without an identifiable cause, the use of oral antimicrobials has been proposed. Medications such as azithromycin, erythromycin, fluconazole, and metronidazole have been reported to be helpful in some patients with refractory EAC. Our patient wanted to continue topical treatment with betamethasone as needed and may consider antimicrobial therapy if the lesions continue to recur.
Tinea corporis refers to a superficial fungal infection of the skin. It may present as one or more asymmetrical, annular, pruritic plaques with a raised scaly leading edge rather than the trailing scale seen with EAC. Diagnosis is made by KOH examination of skin scrapings. Common risk factors include close contact with an infected person or animal, warm, moist environments, sharing personal items, and prolonged use of systemic corticosteroids. Our patient’s KOH analysis of skin scrapings was negative for fungal elements.
Erythema marginatum is a rare skin rash commonly seen with acute rheumatic fever secondary to streptococcal infection. It presents as annular erythematous lesions on the trunk and proximal extremities that are exacerbated by heat. It is often associated with active carditis related to rheumatic fever. This self-limited rash usually resolves in 2-3 days. Our patient was asymptomatic without involvement of other organs.
Like EAC, granuloma annulare is a benign chronic skin condition that presents with ring-shaped lesions. Its etiology is unknown, and lesions may be asymptomatic or mildly pruritic. Localized granuloma annulare typically presents as reddish-brown papules or plaques on the fingers, hands, elbows, dorsal feet, or ankles. The distinguishing feature of granuloma annulare from other annular lesions is its absence of scale.
Urticaria multiforme is an allergic hypersensitivity reaction commonly linked to viral infections, medications, and immunizations. Clinical features include blanchable annular/polycyclic lesions with a central purplish or dusky hue. Diagnostic pearls include the presence of pruritus, dermatographism, and individual lesions that resolve within 24 hours, all of which were not found in our patient’s case.
Ms. Laborada is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital. Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Ms. Laborada and Dr. Matiz have no relevant financial disclosures.
References
1. Paller A and Mancini AJ. Hurwitz Clinical Pediatric Dermatology: A Textbook of Skin Disorders of Childhood and Adolescence. 4th ed. Philadelphia: Elsevier Saunders, 2011.
2. McDaniel B and Cook C. “Erythema annulare centrifugum” 2021 Aug 27. In: StatPearls [Internet]. Treasure Island, Fla.: StatPearls Publishing, 2022 Jan. PMID: 29494101.
3. Leung AK e al. Drugs Context. 2020 Jul 20;9:5-6.
4. Majmundar VD and Nagalli S. “Erythema marginatum” 2022 May 8. In: StatPearls [Internet]. Treasure Island, Fla.: StatPearls Publishing, 2022 Jan.
5. Piette EW and Rosenbach M. J Am Acad Dermatol. 2016 Sep;75(3):467-79.
6. Barros M et al. BMJ Case Rep. 2021 Jan 28;14(1):e241011.
Erythema annulare centrifugum
A thorough body examination failed to reveal any other rashes or lesions suggestive of a fungal infection. A blood count and urinalysis were within normal limits. She had no lymphadenopathy or hepatosplenomegaly. A potassium hydroxide analysis of skin scrapings was negative for fungal elements. Punch biopsy of the skin on the left arm revealed focal intermittent parakeratosis, mildly acanthotic and spongiotic epidermis, and a tight superficial perivascular chronic dermatitis consisting of lymphocytes and histiocytes (Figures). Given these findings, a diagnosis of erythema annulare centrifugum (EAC) was rendered.
EAC is a rare, reactive skin rash characterized by redness (erythema) and ring-shaped lesions (annulare) that slowly spread from the center (centrifugum). The lesions present with a characteristic trailing scale on the inner border of the erythematous ring. Lesions may be asymptomatic or mildly pruritic and commonly involve the trunk, buttocks, hips, and upper legs. It is important to note that its duration is highly variable, ranging from weeks to decades, with most cases persisting for 9 months. EAC typically affects young or middle-aged adults but can occur at any age.
Although the etiology of EAC is unknown, it is believed to be a hypersensitivity reaction to a foreign antigen. Cutaneous fungal infections are commonly reported as triggers as well as other viral infections, medications, malignancy, underlying systemic disease, and certain foods. Treatment depends on the underlying condition and removing the implicated agent. However, most cases of EAC are idiopathic and self-limiting. It is possible that our patient’s prior history of tinea capitis could have triggered the skin lesions suggestive of EAC, but interestingly, these lesions did not go away after the fungal infection was cleared and have continued to recur. For patients with refractory lesions or treatment of patients without an identifiable cause, the use of oral antimicrobials has been proposed. Medications such as azithromycin, erythromycin, fluconazole, and metronidazole have been reported to be helpful in some patients with refractory EAC. Our patient wanted to continue topical treatment with betamethasone as needed and may consider antimicrobial therapy if the lesions continue to recur.
Tinea corporis refers to a superficial fungal infection of the skin. It may present as one or more asymmetrical, annular, pruritic plaques with a raised scaly leading edge rather than the trailing scale seen with EAC. Diagnosis is made by KOH examination of skin scrapings. Common risk factors include close contact with an infected person or animal, warm, moist environments, sharing personal items, and prolonged use of systemic corticosteroids. Our patient’s KOH analysis of skin scrapings was negative for fungal elements.
Erythema marginatum is a rare skin rash commonly seen with acute rheumatic fever secondary to streptococcal infection. It presents as annular erythematous lesions on the trunk and proximal extremities that are exacerbated by heat. It is often associated with active carditis related to rheumatic fever. This self-limited rash usually resolves in 2-3 days. Our patient was asymptomatic without involvement of other organs.
Like EAC, granuloma annulare is a benign chronic skin condition that presents with ring-shaped lesions. Its etiology is unknown, and lesions may be asymptomatic or mildly pruritic. Localized granuloma annulare typically presents as reddish-brown papules or plaques on the fingers, hands, elbows, dorsal feet, or ankles. The distinguishing feature of granuloma annulare from other annular lesions is its absence of scale.
Urticaria multiforme is an allergic hypersensitivity reaction commonly linked to viral infections, medications, and immunizations. Clinical features include blanchable annular/polycyclic lesions with a central purplish or dusky hue. Diagnostic pearls include the presence of pruritus, dermatographism, and individual lesions that resolve within 24 hours, all of which were not found in our patient’s case.
Ms. Laborada is a pediatric dermatology research associate in the division of pediatric and adolescent dermatology at the University of California, San Diego, and Rady Children’s Hospital. Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Ms. Laborada and Dr. Matiz have no relevant financial disclosures.
References
1. Paller A and Mancini AJ. Hurwitz Clinical Pediatric Dermatology: A Textbook of Skin Disorders of Childhood and Adolescence. 4th ed. Philadelphia: Elsevier Saunders, 2011.
2. McDaniel B and Cook C. “Erythema annulare centrifugum” 2021 Aug 27. In: StatPearls [Internet]. Treasure Island, Fla.: StatPearls Publishing, 2022 Jan. PMID: 29494101.
3. Leung AK e al. Drugs Context. 2020 Jul 20;9:5-6.
4. Majmundar VD and Nagalli S. “Erythema marginatum” 2022 May 8. In: StatPearls [Internet]. Treasure Island, Fla.: StatPearls Publishing, 2022 Jan.
5. Piette EW and Rosenbach M. J Am Acad Dermatol. 2016 Sep;75(3):467-79.
6. Barros M et al. BMJ Case Rep. 2021 Jan 28;14(1):e241011.

A review of systems was noncontributory. She was not taking any other medications or vitamin supplements. There were no pets at home and no other affected family members. Physical exam was notable for scattered, pink, annular plaques with central clearing, faint brownish pigmentation, and fine scale.
Employment and buyout agreements
. The most common question was, “Do I really need to go to the trouble and expense of negotiating them?” If you have more than one physician in your group, you absolutely do need written contracts for a variety of reasons, but mostly to avoid conflicts later on. The proverbial “handshake agreement” is worthless in a major business dispute; everyone loses in such situations except the lawyers and accountants.
Mergers and buy-ins were covered at some length in my two previous columns. If the arrangement is to be one of employer and employees rather than a merger of equal partners, you will need an employment agreement to cover duties, requirements, expectations, and benefits. They define how each practitioner/employee will be paid, along with paid time off, health insurance, expense allowances, and malpractice coverage, among other basics. The more that is spelled out in the employment agreement, the fewer disagreements you are likely to have down the road.
Many employment contracts include a “termination without cause” clause, which benefits both the practice and the practitioners. It allows a practice to terminate a new associate if it feels a mistake has been made, even if he or she has done nothing wrong. On the other hand, the newcomer has the option to terminate if a better offer arises, their spouse hates the area, or for any other reason.

Buyouts should be addressed in advance as well. Several recent correspondents told me they didn’t see the necessity of writing a buyout agreement, because they plan to eventually sell their practice, rendering any buyout conditions moot. But what happens if an associate dies, becomes permanently disabled, or abruptly decides to leave the practice? If you haven’t prepared for such eventualities, you could find yourself receiving a demand from your ex-partner (or surviving spouse) for immediate payment of that partner’s portion of the practice’s value. And your valuation of the practice is likely to be severely at odds with the other party’s. Meanwhile, remaining partners must cover all the practice’s expenses and deal with an increased patient load.
A buyout agreement avoids these problems by planning for such eventualities in advance. You must agree on how a buyout amount will be valued. As I’ve said in previous columns, I strongly advise using a formula, not a fixed amount. If a buyout is based on 15- or 20-year-old reimbursements, the buyout will have no relationship to what the partners are currently being paid. Likewise, any buyout calculated at “appraised value” is a problem, because the buyout amount remains a mystery until an appraisal is performed. If the appraised value ends up being too high, the remaining owners may refuse to pay it. Have an actuary create a formula, so that a buyout figure can be calculated at any time. This area, especially, is where you need experienced, competent legal advice.
To avoid surprises, any buyout should require ample notice (6-12 months is common) to allow time to rearrange finances and recruit a new provider. Vesting schedules, similar to those used in retirement plans, are also popular. If a partner leaves before a prescribed time period has elapsed – say, 20 years – the buyout is proportionally reduced.
Buyouts can also be useful when dealing with noncompete agreements, which are notoriously difficult (and expensive) to enforce. One solution is a buyout penalty; a departing partner can compete with his or her former practice, but at the cost of a substantially reduced buyout. This permits competition, but discourages it, and compensates the targeted practice.
Buyouts are also a potential solution to some buy-in issues. A new associate entering an established practice may not be able to contribute assets equal to existing partners’ stakes and may lack the cash necessary to make up the difference. One alternative is to agree that any inequalities will be compensated at the other end in buyout value. Those partners contributing more assets will receive larger buyouts than those contributing less.
As I’ve said many times, these are not negotiations to undertake on your own. Enlist the aid of a consultant or attorney (or both) with ample medical practice experience.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
. The most common question was, “Do I really need to go to the trouble and expense of negotiating them?” If you have more than one physician in your group, you absolutely do need written contracts for a variety of reasons, but mostly to avoid conflicts later on. The proverbial “handshake agreement” is worthless in a major business dispute; everyone loses in such situations except the lawyers and accountants.
Mergers and buy-ins were covered at some length in my two previous columns. If the arrangement is to be one of employer and employees rather than a merger of equal partners, you will need an employment agreement to cover duties, requirements, expectations, and benefits. They define how each practitioner/employee will be paid, along with paid time off, health insurance, expense allowances, and malpractice coverage, among other basics. The more that is spelled out in the employment agreement, the fewer disagreements you are likely to have down the road.
Many employment contracts include a “termination without cause” clause, which benefits both the practice and the practitioners. It allows a practice to terminate a new associate if it feels a mistake has been made, even if he or she has done nothing wrong. On the other hand, the newcomer has the option to terminate if a better offer arises, their spouse hates the area, or for any other reason.
Buyouts should be addressed in advance as well. Several recent correspondents told me they didn’t see the necessity of writing a buyout agreement, because they plan to eventually sell their practice, rendering any buyout conditions moot. But what happens if an associate dies, becomes permanently disabled, or abruptly decides to leave the practice? If you haven’t prepared for such eventualities, you could find yourself receiving a demand from your ex-partner (or surviving spouse) for immediate payment of that partner’s portion of the practice’s value. And your valuation of the practice is likely to be severely at odds with the other party’s. Meanwhile, remaining partners must cover all the practice’s expenses and deal with an increased patient load.
A buyout agreement avoids these problems by planning for such eventualities in advance. You must agree on how a buyout amount will be valued. As I’ve said in previous columns, I strongly advise using a formula, not a fixed amount. If a buyout is based on 15- or 20-year-old reimbursements, the buyout will have no relationship to what the partners are currently being paid. Likewise, any buyout calculated at “appraised value” is a problem, because the buyout amount remains a mystery until an appraisal is performed. If the appraised value ends up being too high, the remaining owners may refuse to pay it. Have an actuary create a formula, so that a buyout figure can be calculated at any time. This area, especially, is where you need experienced, competent legal advice.
To avoid surprises, any buyout should require ample notice (6-12 months is common) to allow time to rearrange finances and recruit a new provider. Vesting schedules, similar to those used in retirement plans, are also popular. If a partner leaves before a prescribed time period has elapsed – say, 20 years – the buyout is proportionally reduced.
Buyouts can also be useful when dealing with noncompete agreements, which are notoriously difficult (and expensive) to enforce. One solution is a buyout penalty; a departing partner can compete with his or her former practice, but at the cost of a substantially reduced buyout. This permits competition, but discourages it, and compensates the targeted practice.
Buyouts are also a potential solution to some buy-in issues. A new associate entering an established practice may not be able to contribute assets equal to existing partners’ stakes and may lack the cash necessary to make up the difference. One alternative is to agree that any inequalities will be compensated at the other end in buyout value. Those partners contributing more assets will receive larger buyouts than those contributing less.
As I’ve said many times, these are not negotiations to undertake on your own. Enlist the aid of a consultant or attorney (or both) with ample medical practice experience.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
. The most common question was, “Do I really need to go to the trouble and expense of negotiating them?” If you have more than one physician in your group, you absolutely do need written contracts for a variety of reasons, but mostly to avoid conflicts later on. The proverbial “handshake agreement” is worthless in a major business dispute; everyone loses in such situations except the lawyers and accountants.
Mergers and buy-ins were covered at some length in my two previous columns. If the arrangement is to be one of employer and employees rather than a merger of equal partners, you will need an employment agreement to cover duties, requirements, expectations, and benefits. They define how each practitioner/employee will be paid, along with paid time off, health insurance, expense allowances, and malpractice coverage, among other basics. The more that is spelled out in the employment agreement, the fewer disagreements you are likely to have down the road.
Many employment contracts include a “termination without cause” clause, which benefits both the practice and the practitioners. It allows a practice to terminate a new associate if it feels a mistake has been made, even if he or she has done nothing wrong. On the other hand, the newcomer has the option to terminate if a better offer arises, their spouse hates the area, or for any other reason.
Buyouts should be addressed in advance as well. Several recent correspondents told me they didn’t see the necessity of writing a buyout agreement, because they plan to eventually sell their practice, rendering any buyout conditions moot. But what happens if an associate dies, becomes permanently disabled, or abruptly decides to leave the practice? If you haven’t prepared for such eventualities, you could find yourself receiving a demand from your ex-partner (or surviving spouse) for immediate payment of that partner’s portion of the practice’s value. And your valuation of the practice is likely to be severely at odds with the other party’s. Meanwhile, remaining partners must cover all the practice’s expenses and deal with an increased patient load.
A buyout agreement avoids these problems by planning for such eventualities in advance. You must agree on how a buyout amount will be valued. As I’ve said in previous columns, I strongly advise using a formula, not a fixed amount. If a buyout is based on 15- or 20-year-old reimbursements, the buyout will have no relationship to what the partners are currently being paid. Likewise, any buyout calculated at “appraised value” is a problem, because the buyout amount remains a mystery until an appraisal is performed. If the appraised value ends up being too high, the remaining owners may refuse to pay it. Have an actuary create a formula, so that a buyout figure can be calculated at any time. This area, especially, is where you need experienced, competent legal advice.
To avoid surprises, any buyout should require ample notice (6-12 months is common) to allow time to rearrange finances and recruit a new provider. Vesting schedules, similar to those used in retirement plans, are also popular. If a partner leaves before a prescribed time period has elapsed – say, 20 years – the buyout is proportionally reduced.
Buyouts can also be useful when dealing with noncompete agreements, which are notoriously difficult (and expensive) to enforce. One solution is a buyout penalty; a departing partner can compete with his or her former practice, but at the cost of a substantially reduced buyout. This permits competition, but discourages it, and compensates the targeted practice.
Buyouts are also a potential solution to some buy-in issues. A new associate entering an established practice may not be able to contribute assets equal to existing partners’ stakes and may lack the cash necessary to make up the difference. One alternative is to agree that any inequalities will be compensated at the other end in buyout value. Those partners contributing more assets will receive larger buyouts than those contributing less.
As I’ve said many times, these are not negotiations to undertake on your own. Enlist the aid of a consultant or attorney (or both) with ample medical practice experience.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

COVID-19 Cycle Threshold/Cycle Number Testing at a Community Living Center
COVID-19, caused by SARS-CoV-2, is more severe in individuals with underlying illnesses. Because complete social distancing might be more difficult in nursing homes and community living centers (CLCs), public health leaders and clinicians have been concerned about the epidemiology and disease course in nursing homes even before the COVID-19 pandemic.1-7 A report of a COVID-19 outbreak in a nursing home facility in King County, Washington, documented a 33.7% overall fatality rate for residents and 52.4% among the most critically ill.4,5 The experience at King County, Washington, shows that proactive steps to identify, monitor, and apply preventive control measures is important for future outbreaks.5
Reverse transcriptase polymerase chain reaction (RT-PCR) testing produces a cycle threshold (CT) or cycle number (CN) that correlates with viral load and infectiousness. 8-14 CT/CN represents the number of RT-PCR cycles required for the fluorescent signal to cross the detection threshold (exceed background level) and is inversely proportional to the viral load. Effectively, the higher the viral load, the lower the CT/ CN value (Figure 1). Tracking CT/CN values was not documented in the Washington nursing home outbreak. Reports of COVID- 19 testing in CLCs during outbreaks are sparse, and CT/CN values and demographic distribution of these veterans has not been reported.15 The CLC veteran population, with known higher vulnerability to infection and chronic diseases, is epidemiologically different from the general nursing home population.15-18 To address these literature gaps, we present the first report of COVID- 19 testing with CT/CN value correlations in the high-risk veteran CLC population.
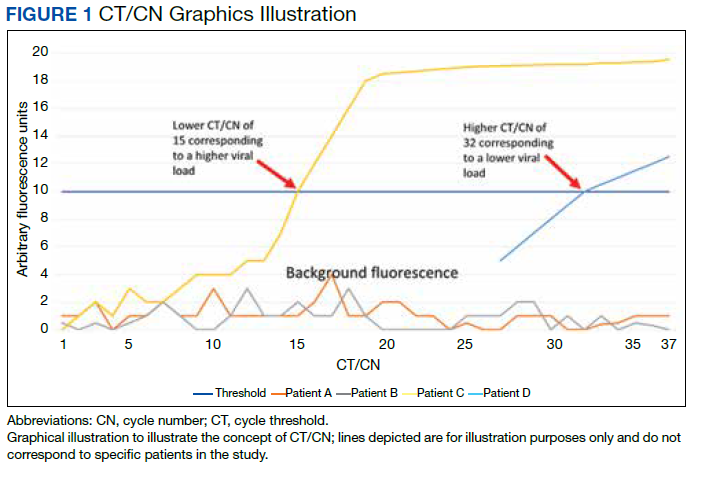
Methods
A retrospective review of all COVID-19 CT/CN testing at the Corporal Michael J. Crescenz Veterans Affairs Medical Center (VAMC) CLC in Philadelphia, Pennsylvania, from March 28, 2020, to April 24, 2020, was performed with a US Department of Veterans Affairs (VA) Veterans Health Information System Architecture VistA/FileMan search. Only veteran residents were included in this review. Data collected included initial and serial test results, CT/CN on positive test results, test dates, testing platform used, demographic information (age, self-reported ethnicity, and sex), and clinical follow-up information. Health records were reviewed retrospectively to identify death, the first day after diagnosis with no documented symptoms, or hospitalization status.
RT-PCR testing was performed with the Abbott RealTime SARS-CoV-2 assay on the Abbott m2000 platform and the Xpert Xpress SARS-CoV-2 assay on the Cepheid Infinity platform. The Xpert Xpress assay gave 2 CT values for the E and N2 targets on positive samples.19 For this assay to indicate a positive specimen, amplification by RT-PCR of the N2 target or both the N2 and E target is required. The Xpert Xpress assay results as presumptive positive if only the E target amplified. This assay counts a maximum of 45 cycles. The Abbott RealTime SARS-CoV-2 assay gave 1 CN derived from the RNA-dependent RNA polymerase and N targets on positive samples.20 The Abbott assay on the m2000 counts a maximum of 37 cycles. The CT/CN value is the number of cycles required by RT-PCR for the fluorescence signal to cross a threshold value exceeding background level.19,20
Samples that are negative for COVID-19 by RT-PCR do not produce a CT/CN value. Although both instruments were used for RT-PCR, the precise CT/CN values are not interchangeable and CT/CN observations over time between the 2 instruments during the disease course would be based on CT/CN value movement (general upward or downward trend) rather than absolute CT/CN differences. Both assays have been approved by emergency use authorization as qualitative tests for the presence/absence of COVID-19. Although the CT/CN value is available to laboratory staff after test completion, the CT/CN value is not reported routinely in the patient health record. All veteran patients identified on the initial review from March 28, 2020, to April 24, 2020, had all serial COVID-19 testing recorded until November 10, 2020. The CN values at the limit of detection (LOD) for the Abbott m2000 platform from the initial validation study were reviewed for reference.21
Results
Of 80 patients, 25 (31%) were COVID-19 positive over the course of testing. The study population had a mean age of 73.5 years; 92% were aged > 60 years. The group was predominantly male (79 male vs 1 female). Among the 77 patients with a stated ethnicity, 39 (51%) were African American. In comparison, 43% of residents in Philadelphia County are African American (Table).22,23 Additionally, a previously published total COVID-19 tested population by ethnicity at the same regional VAMC revealed 46.8% of tested veteran patients were African American. 24 Three patients had no stated ethnicity. Among those who tested positive, 11 were African American patients, 12 were White patients, and 2 had no stated ethnicity. Four patients tested positive on their first test. The other 21 patients were positive on repeat testing. Interestingly, 6 patients had 1 initial negative test before a positive test, 6 patients had 2, 8 patients had 3, and 1 patient had 4 initial negative tests before a positive test result. Among the 25 positive patients, 22 were either positive within 10 days of the initial negative test result or initially positive (Figure 2). Three patients who tested positive after 10 days did so at 16, 20, and 21 days after the initial negative test result. Among the 25 positive patients, 23 had initial and serial testing from both the Abbott and Xpert Xpress assays. The remaining 2 positive patients had initial and serial testing from the Abbott assay exclusively.
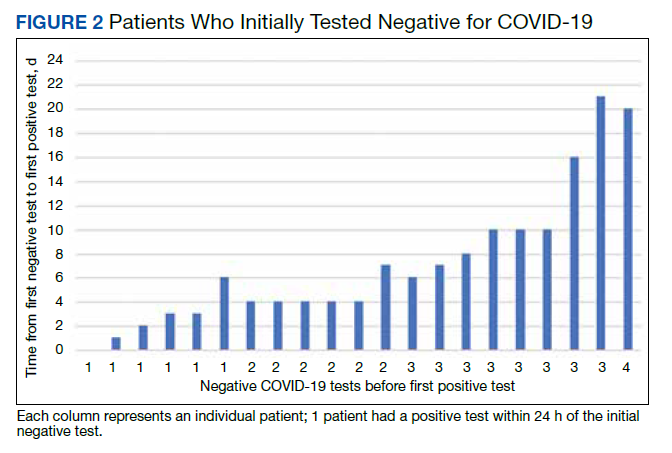
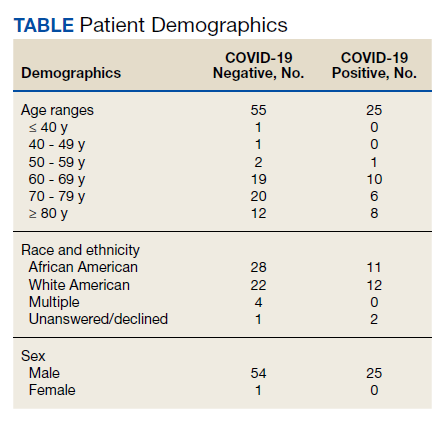
Only positive COVID-19 results by RTPCR produced a CT/CN value. After disease resolution with a negative test, no CT/CN value was produced with the negative test result on either testing platform. Because repeat testing after the initial positive result took place no sooner than 10 days, we observed that the CT/CN value increased after the initial positive result until the disease resolved, and a negative result was obtained (eAppendix 1, available online at doi:10.12788/fp.0276). A t test comparing the initial CT/CN value to the value more than 10 days after the initial positive showed the CT/CN was statistically significantly higher (P < .05).
Prompt repeat testing after the initial test can show a decrease in the CT/CN value because of increasing viral load before the expected increase until disease resolution if the initial test caught the infection early. Twelve patients had a negative test result between 2 serial positive results. These negative test results occurred later, near the end of the disease course. Among the 12 patients with this positive-negativepositive CT/CN pattern, 7 were symptomatic and no longer had documented symptoms or hospitalization around the time of this positive-negative-positive pattern. Four of these individuals were asymptomatic during the entire infection course. One of the 12 patients with this pattern expired with the negative result occurring on day 27 of the disease in the context of rising CT/CN. One of these 12 patients only had a presumptive positive test result on the Cepheid because it detected only the E target with a CT value of 38.7. In 1 of the 12 patients, the negative test result occurred between 2 positive test results with CT/CN values < 20 (12.05 and 19.05 for the positive tests before and after the negative result, respectively). When the initial CT/CN values was separated based on ethnicity, the average CT/CN value for African Americans (23.3) was higher than for other ethnicities (19.9), although it did not reach statistical significance (P = .35).
Ten of the 25 patients testing positive were admitted to the hospital, including 1 admitted 15 days before diagnosis (patient 20) and 1 admitted 80 days after diagnosis (patient 7). Among these 10 patients, 6 were admitted to the intensive care unit, including patient 7. None of the patients were intubated. Three of the 10 admitted patients died (patients 7, 20, and 24). Patient 7 was a 79-year-old male with a history of dementia, cerebrovascular accident, hypertension, hyperlipidemia, and chronic kidney disease with symptoms of lethargy and refusal of oral intake when he was diagnosed with COVID-19. He was admitted 80 days after diagnosis for hyponatremia and acute renal failure, with death on day 87 recorded as complications from the earlier COVID-19 infection. Patient 20, an 89-year-old male with a history of dementia, chronic kidney disease, and hyperlipidemia, had been admitted with fever, cough, and leukocytosis 17 days before COVID-19 diagnosis. He continued to be symptomatic after diagnosis with development of hypotension, dehydration, and refusal of oral intake while on comfort measures/endof- life care and died 15 days after COVID- 19 infection diagnosis. Patient 24 was a 96-year-old male with history of heart failure, hypertension, coronary artery disease, prostate carcinoma, and dementia who developed a cough at the time of diagnosis; because of his underlying condition, he remained in the CLC on comfort care. His symptoms, including hypoxia, worsened until he died 7 days after diagnosis.
Among the 25 patients, 17 were symptomatic at the time of diagnosis; the 14 initially symptomatic patients who survived improved clinically and returned to baseline. Eight of the 25 patients were asymptomatic initially and 3 developed symptoms 2 to 5 days after diagnosis. Only 1 patient who remained asymptomatic was admitted for inability to adhere to quarantine at the CLC. Review of the health records of all surviving symptomatic patients showed symptom resolution with return to baseline that corresponds to an increasing CT/CN value. A 1-tailed t test comparing the initial CT/ CN at the time of diagnosis to the last CT/CN value for symptomatic patients who recovered revealed a statistically significant increase (P < .05). For the symptomatic, symptom resolution and hospital discharge took (if required) a mean 20 days (range, 7-46). Among those who were not hospitalized, symptoms resolved in 7 to 36 days (18 days). Among those requiring hospitalization at any time (excluding patients who died or were asymptomatic), symptom and hospitalization resolution took a mean 22 days (range, 10-46). Asymptomatic patients (patients 8, 10, 15, 16, and 25) also showed increasing CT/CN value during the infection course, although there was no correlation with the continued lack of symptoms.
During the initial validation of the Abbott m2000 instrument, an LOD study included concentrations of 1000, 500, 250, 100, 70, 60, and 50 virus copies/mL (eAppendix 2, available online at doi:10.12788/fp.0276).21 The average CN at 100 virus copies/mL—the manufacturer provided LOD in the instructions for use—was 25.74.20 At a concentration of one-half that (50 virus copies/mL), the average CN was 28.39.
Discussion
This is the first study in the English literature to track CT/CN values as part of serial testing of a veteran CLC. Widescale testing and repeat screening in the absence of symptoms of nursing home residents would identify those who are infected and allow providers to track viral load clearance.9-14 CT/CN values, when serially tracked during the infection course, appear to increase with illness resolution, consistent with earlier reports that CT/CN correlates with viral load.8-14 Serial CT/CN values that are high (> 25) and continue to increase with each test suggest progression toward disease resolution or viral RNA clearance.8-14 After symptom resolution, patients can have a persistent low level of viral shedding (corresponding to a high CT/CN value).10-14,25 Near the end of disease resolution, a negative serial RT-PCR sample test before a subsequent positive might be a promising clinical sign of near disease recovery. Once the viral load is low with a CT/CN significantly higher than 25, some specimens might result as negative but turn up positive on subsequent sampling with a high CT/CN value. This pattern, with attendant high CT/CN values for the positive results, are consistent with the known effect of viral load (ie, a low viral load correlates to a high CT/CN) and adequacy of specimen collection on CT/CN values.25 If the patient’s viral load is low, the sample collected might have a viral load at or near the testing platform’s LOD.
For Abbott m2000, the manufacturer provided LOD is 100 virus copies/mL, although the instrument was able to detect virus concentrations below that level during the initial validation.20 The actual LOD of the instrument at our institution is < 100 virus copies/mL. For the Cepheid Xpert Xpress SARS-CoV-2 assay, the manufacturer-provided LOD is 250 virus copies/mL.19 An LOD study including samples below the manufacturer-provided LOD was not part of the initial validation study for the Xpert Xpress assay. Nonetheless, the virus concentration of samples with very high CT values at or near the maximum CT value of 45 is expected to be at or near the platform’s actual LOD.
If the samples collected near the end of the patient’s disease course have viral loads near these low concentrations, the encouraging positive-negative-positive pattern with high CT/CN values might be a promising sign for viral clearance. On the other hand, a positive-negative-positive pattern in the setting of low CT/CN values before and after the negative test might indicate poor sampling for the negative specimen. The back-and-forth or positive-negative-positive pattern generally appears to indicate near resolution of the infection course, although clinical correlation is necessary to rule out inadequate sampling earlier in the disease course or prolonged viral RNA shedding.9-14 In all of the surviving symptomatic patients who showed the positive-negative-positive pattern, this sign occurred around or after symptom resolution. It also is important to consider that in some patients, SARS-CoV-2 RNA might remain detectable with increasing CT/CN after symptom resolution, and samples from these patients might not result positive. Therefore, CT/CN values cannot be interpreted without considering the clinical picture.25
Studies on infectiousness and virus culture from COVID-19 samples with CT/ CN correlation have shown that patients with high CT/CN at the end of their disease course might not be as infectious.9-14,25 Because 1 patient had a presumptive positive result after the negative result, this study shows that this positive-negative-positive pattern could include presumptive positive results. Also, in the setting of a recent positive result on the same testing platform, a patient with this pattern is presumed to be positive for COVID-19 RNA because of scant viral material.
Taiwan’s public health response to the outbreak illustrates the ability to mitigate an outbreak throughout a society.26 These actions could help blunt an outbreak within a civilian nursing home population.5 Mitigation within a veteran CLC population has been documented, but the study, which focused on mitigation, did not consider CT/CN values, demographic distribution, testing access of the studied population, or laboratory findings related to disease pathophysiology.15 A key ingredient in widescale, serial testing is the availability of a rapid turnaround from testing in-house that allowed identification within 24 hours instead of several days at a reference laboratory. 15 Rapid widescale testing would allow clinical teams to optimize the Triangle of Benefit of Widescale Timely Tests for CLC (Figure 3).15 Timely laboratory testing remains pivotal for CLC veteran residents to aid successful clinical triage and management. Reporting serial CT/CN values can provide additional information to clinicians about the disease course because CT/ CN correlates with viral load, which varies based on where the patient is in the disease course.9-14 CT/CN values carry significant prognostic value, particularly with respect to intubation and mortality.8
Limitations
Important limitations to our study include the use of 2 separate RT-PCR platforms. Using different RT-PCR platforms is common in clinical laboratories trying to take advantage of the unique characteristics of different platforms—for example, turnaround time vs high throughput— to manage COVID-19 testing workflow.25 However, the exact CT/CN values obtained from each platform might not translate to the other, and the general trend (CT/CN values are rising or falling across serial tests) rather than a single value could be useful for clinical correlation. Even when the same platform is used for the serial testing, CT/CN values can be affected by adequacy of specimen collection; therefore, clinical correlation and considering the trend in CT/CN values is necessary for interpretation.10-14,25 Because of the known trend in viral dynamics, a positive specimen collected with a high CT/CN followed by a subsequent (within 2 days) positive specimen collected with a low CT/CN might be compatible with early detection of COVID- 19 infection in the appropriate clinical context. 10-14 However, detection late in the infection course or even after the symptomatic disease resolved with prolonged viral shedding might show serial positive samples with increasing CT/CN values.10-14
Patients with prolonged viral shedding might not be infectious.27 Because of the clinical correlation required for interpretation and the other factors that might affect CT/CN values, recommendations advise against using CT/CN values in clinical practice at this time, although these recommendations could change with future research.25 Serial CT/CN values have the potential, if appropriately correlated with the clinical picture, to provide useful information, such as whether the viral load of the sample is relatively high or low and increasing or decreasing.
Veterans, as a population, are more susceptible to poor health outcomes and morbidity compared with similar civilian counterparts.2,14-16 Veteran CLC patients likely would experience worse outcomes with COVID-19, including more infections, expiration, and morbidity compared with similar general population nursing homes. Similar to what had been reported for the civilian population, a trend (high CT/CN values early in the disease course with repeat testing needed to detect all positives followed by lower CT/CN value to correlate with increased viral load and then increased CT/CN value as the infection resolved) also was observed in this veteran population.
It has been extensively documented that minority groups experience decreased health care access and worse health outcomes. 28-30 Considering the critical medical supply shortages, including personal protective equipment, ventilators, and even testing supplies, there is the potential for a resource access disparity by ethnicity.28-31 Because the VA does not depend on measures of wealth and privilege such as health insurance, there was no disparity noted in access to testing by race or ethnicity at the VAMC CLC. When considering the health outcome of viral load from the measured CT/CN value, the viral loads of African American patients and those of other ethnicities was not significantly different in this study.
Conclusions
This is the first study to bring up critical points including serial CT/CN value correlation in RT-PCR tests, demographic distributions demonstrating easy and equal access in a veteran nursing home to COVID-19 testing, and clinical laboratory signs related to disease pathophysiology. Unlike other populations who have undergone serial CT/CN monitoring, nursing homes represent a particularly vulnerable population who require measures to prevent the spread and mitigate outbreaks of COVID-19.2,4,5 Test measurements obtained such as the CT/CN value during routine clinical care can provide useful information for public health, epidemiologic, or clinical purposes with appropriate correlation to clinical and other laboratory parameters. This study demonstrates early intervention of serial testing of an outbreak in a veterans nursing home with CT/CN value correlation.
1. Chen T, Wu D, Chen H, et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. BMJ. 2020;368:m1091. doi:10.1136/bmj.m1091
2. Tsan L, Davis C, Langberg R, et al. Prevalence of nursing home-associated infections in the Department of Veterans Affairs nursing home care units. Am J Infect Control. 2008;36(3):173-179. doi:10.1016/j.ajic.2007.06.008
3. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054-1062. doi:10.1016/S0140-6736(20)30566-3
4. Arentz M, Yim E, Klaff L, et al. Characteristics and outcomes of 21 critically ill patients with COVID-19 in Washington State. JAMA. 2020;323(16):1612-1614. doi:10.1001/jama.2020.4326
5. McMichael TM, Currie DW, Clark S, et al. Public Health–Seattle and King County, EvergreenHealth, and CDC COVID-19 Investigation Team. Epidemiology of Covid-19 in a long-term care facility in King County, Washington. N Engl J Med. 2020;382(21):2005-2011. doi:10.1056/NEJMoa2005412
6. Childs A, Zullo AR, Joyce NR, et al. The burden of respiratory infections among older adults in long-term care: a systematic review. BMC Geriatr. 2019;19(1):210. doi:10.1186/s12877-019-1236-6
7. Eriksen HM, Iversen BG, Aavitsland PJ. Prevalence of nosocomial infections and use of antibiotics in long-term care facilities in Norway, 2002 and 2003. Hosp Infect. 2004;57(4):316-320. doi:10.1016/j.jhin.2004.03.028
8. Magleby R, Westblade LF, Trzebucki A, et al. Impact Severe acute respiratory syndrome coronavirus 2 viral load on risk of intubation and mortality among hospitalized patients with coronavirus disease 2019. Clin Infect Dis. 2021;73(11):e4197-e4205. doi:10.1093/cid/ciaa851
9. Buchan B, Hoff J, Gmehlin C, et al. Distribution of SARSCoV- 2 PCR cycle threshold values provide practical insight into overall and target-specific sensitivity among symptomatic patients. Am Clin Pathol. 2020;154:479-485. doi:10.1093/ajcp/aqaa133
10. He X, Lau EHY, Wu P, et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med. 2020;26(5):672-675. doi:10.1038/s41591-020-0869-5
11. Zou L, Ruan F, Huang M, et al. SARS-CoV-2 Viral load in upper respiratory specimens of infected patients. N Engl J Med. 2020;382(12):1177-1179. doi:10.1056/NEJMc2001737
12. Singanayagam A, Patel M, Charlett A, et al. Duration of infectiousness and correlation with RT-PCR cycle threshold values in cases of COVID-19, England, January to May 2020. Euro Surveill. 2020;25(32):2001483. doi:10.2807/1560-7917.ES.2020.25.32.2001483
13. Salvatore P, Dawson P, Wadhwa A, et al. Epidemiological correlates of PCR cycles threshold values in the detection of SARS-CoV-2. Clin Infect Dis. 2021;72(11):e761-e767. doi:10.1093/cid/ciaa1469
14. Kissler S, Fauver J, Mack C, et al. Viral dynamics of SARS-CoV-2 infection and the predictive value of repeat testing. medRxiv. 2020;10.21.20217042. doi:10.1101/2020.10.21.20217042 1
5. Escobar DJ, Lanzi M, Saberi P, et al. Mitigation of a COVID-19 outbreak in a nursing home through serial testing of residents and staff. Clin Infect Dis. 2021;72(9):e394- e396. doi:10.1093/cid/ciaa1021
16. Eibner C, Krull H, Brown KM, et al. Current and projected characteristics and unique health care needs of the patient population served by the Department of Veterans Affairs. Rand Health Q. 2016;5(4):13.
17. Agha Z, Lofgren RP, VanRuiswyk JV, Layde PM. Are patients at Veterans Affairs medical centers sicker? A comparative analysis of health status and medical resource use. Arch Intern Med. 2000;160(21):3252-3257. doi:10.1001/archinte.160.21.3252
18. Morgan RO, Teal CR, Reddy SG, Ford ME, Ashton CM. Measurement in Veterans Affairs Health Services Research: veterans as a special population. Health Serv Res. 2005;40(5 Pt 2):1573-1583. doi:10.1111/j.1475-6773.2005.00448.x 1
9. Xpert Xpress SARS-CoV-2. Instructions for use. Cepheid. 302-2562, Rev. C April 2020. Accessed January 7, 2021. https://www.fda.gov/media/136314/download
20. Abbott RealTime SARS-CoV-2. Instructions for use Abbott. 09N77-95. July 2020. Accessed January 7, 2021. https:// www.fda.gov/media/136258/download
21. Petersen JM, Dalal S, Jhala D. Successful implementation of SARS-CoV-2 testing in midst of pandemic with emphasis on all phases of testing. J Clin Pathol. 2021;74:273- 278. doi:10.1136/jclinpath-2020-207175
22. United States Census Bureau. Quick Facts: Philadelphia County, Pennsylvania. Accessed April 16, 2020. https://www .census.gov/quickfacts/philadelphiacountypennsylvania
23. Centers for Disease Control and Prevention. United States COVID-19 cases, deaths, and laboratory testing (NAATS) by state, territory, and jurisdiction. Accessed April 26, 2020. https://www.cdc.gov/coronavirus/2019-ncov/cases -updates/cases-in-us.html 2
4. Petersen J, Jhala D. Ethnicity, comorbid medical conditions, and SARS-CoV-2 test cycle thresholds in the veteran population [published online ahead of print, 2021 Jul 28]. J Racial Ethn Health Disparities. 2021;1-8. doi:10.1007/s40615-021-01114-4
25. Infectious Diseases Society of America, Association for Molecular Pathology. IDSA and AMP joint statement on the use of SARS-CoV-2 PCR cycle threshold (Ct) values for clinical decision-making. Accessed August 28, 2021. https://www.idsociety.org/globalassets/idsa/public-health /covid-19/idsa-amp-statement.pdf
26. Wang J, Ng CY, Brook RH. Response to COVID-19 in Taiwan: big data analysis, new technology, and proactive testing. JAMA. 2020;323(14):1341-1342. doi:10.1001/jama.2020.3151
27. Centers for Disease Control and Prevention. Overview of testing for SARS-CoV-2, the virus that causes COVID- 19. Accessed July 28, 2021. https://www.cdc.gov /coronavirus/2019-ncov/hcp/testing-overview.html
28. Zuvekas SH, Taliaferro GS. Pathways to access: health insurance, the health care delivery system, and racial/ethnic disparities, 1996-1999. Health Aff. 2003;22(2):139-153. doi:10.1377/hlthaff.22.2.139
29. Egede LE. Race, ethnicity, culture, and disparities in health care. J Gen Intern Med. 2006;21(6):667-669. doi:10.1111/j.1525-1497.2006.0512.x
30. Institute of Medicine (US) Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care. Smedley BD, Stith AY, Nelson AR, eds. Unequal treatment: confronting racial and ethnic disparities in health care. National Academies Press; 2003. doi:10.17226/12875
31. Ranney ML, Griffeth V, Jha AK. Critical supply shortages – the need for ventilators and personal protective equipment during the Covid-19 Pandemic. N Engl J Med. 2020;382(18):e41. doi:10.1056/NEJMp2006141
COVID-19, caused by SARS-CoV-2, is more severe in individuals with underlying illnesses. Because complete social distancing might be more difficult in nursing homes and community living centers (CLCs), public health leaders and clinicians have been concerned about the epidemiology and disease course in nursing homes even before the COVID-19 pandemic.1-7 A report of a COVID-19 outbreak in a nursing home facility in King County, Washington, documented a 33.7% overall fatality rate for residents and 52.4% among the most critically ill.4,5 The experience at King County, Washington, shows that proactive steps to identify, monitor, and apply preventive control measures is important for future outbreaks.5
Reverse transcriptase polymerase chain reaction (RT-PCR) testing produces a cycle threshold (CT) or cycle number (CN) that correlates with viral load and infectiousness. 8-14 CT/CN represents the number of RT-PCR cycles required for the fluorescent signal to cross the detection threshold (exceed background level) and is inversely proportional to the viral load. Effectively, the higher the viral load, the lower the CT/ CN value (Figure 1). Tracking CT/CN values was not documented in the Washington nursing home outbreak. Reports of COVID- 19 testing in CLCs during outbreaks are sparse, and CT/CN values and demographic distribution of these veterans has not been reported.15 The CLC veteran population, with known higher vulnerability to infection and chronic diseases, is epidemiologically different from the general nursing home population.15-18 To address these literature gaps, we present the first report of COVID- 19 testing with CT/CN value correlations in the high-risk veteran CLC population.
Methods
A retrospective review of all COVID-19 CT/CN testing at the Corporal Michael J. Crescenz Veterans Affairs Medical Center (VAMC) CLC in Philadelphia, Pennsylvania, from March 28, 2020, to April 24, 2020, was performed with a US Department of Veterans Affairs (VA) Veterans Health Information System Architecture VistA/FileMan search. Only veteran residents were included in this review. Data collected included initial and serial test results, CT/CN on positive test results, test dates, testing platform used, demographic information (age, self-reported ethnicity, and sex), and clinical follow-up information. Health records were reviewed retrospectively to identify death, the first day after diagnosis with no documented symptoms, or hospitalization status.
RT-PCR testing was performed with the Abbott RealTime SARS-CoV-2 assay on the Abbott m2000 platform and the Xpert Xpress SARS-CoV-2 assay on the Cepheid Infinity platform. The Xpert Xpress assay gave 2 CT values for the E and N2 targets on positive samples.19 For this assay to indicate a positive specimen, amplification by RT-PCR of the N2 target or both the N2 and E target is required. The Xpert Xpress assay results as presumptive positive if only the E target amplified. This assay counts a maximum of 45 cycles. The Abbott RealTime SARS-CoV-2 assay gave 1 CN derived from the RNA-dependent RNA polymerase and N targets on positive samples.20 The Abbott assay on the m2000 counts a maximum of 37 cycles. The CT/CN value is the number of cycles required by RT-PCR for the fluorescence signal to cross a threshold value exceeding background level.19,20
Samples that are negative for COVID-19 by RT-PCR do not produce a CT/CN value. Although both instruments were used for RT-PCR, the precise CT/CN values are not interchangeable and CT/CN observations over time between the 2 instruments during the disease course would be based on CT/CN value movement (general upward or downward trend) rather than absolute CT/CN differences. Both assays have been approved by emergency use authorization as qualitative tests for the presence/absence of COVID-19. Although the CT/CN value is available to laboratory staff after test completion, the CT/CN value is not reported routinely in the patient health record. All veteran patients identified on the initial review from March 28, 2020, to April 24, 2020, had all serial COVID-19 testing recorded until November 10, 2020. The CN values at the limit of detection (LOD) for the Abbott m2000 platform from the initial validation study were reviewed for reference.21
Results
Of 80 patients, 25 (31%) were COVID-19 positive over the course of testing. The study population had a mean age of 73.5 years; 92% were aged > 60 years. The group was predominantly male (79 male vs 1 female). Among the 77 patients with a stated ethnicity, 39 (51%) were African American. In comparison, 43% of residents in Philadelphia County are African American (Table).22,23 Additionally, a previously published total COVID-19 tested population by ethnicity at the same regional VAMC revealed 46.8% of tested veteran patients were African American. 24 Three patients had no stated ethnicity. Among those who tested positive, 11 were African American patients, 12 were White patients, and 2 had no stated ethnicity. Four patients tested positive on their first test. The other 21 patients were positive on repeat testing. Interestingly, 6 patients had 1 initial negative test before a positive test, 6 patients had 2, 8 patients had 3, and 1 patient had 4 initial negative tests before a positive test result. Among the 25 positive patients, 22 were either positive within 10 days of the initial negative test result or initially positive (Figure 2). Three patients who tested positive after 10 days did so at 16, 20, and 21 days after the initial negative test result. Among the 25 positive patients, 23 had initial and serial testing from both the Abbott and Xpert Xpress assays. The remaining 2 positive patients had initial and serial testing from the Abbott assay exclusively.
Only positive COVID-19 results by RTPCR produced a CT/CN value. After disease resolution with a negative test, no CT/CN value was produced with the negative test result on either testing platform. Because repeat testing after the initial positive result took place no sooner than 10 days, we observed that the CT/CN value increased after the initial positive result until the disease resolved, and a negative result was obtained (eAppendix 1, available online at doi:10.12788/fp.0276). A t test comparing the initial CT/CN value to the value more than 10 days after the initial positive showed the CT/CN was statistically significantly higher (P < .05).
Prompt repeat testing after the initial test can show a decrease in the CT/CN value because of increasing viral load before the expected increase until disease resolution if the initial test caught the infection early. Twelve patients had a negative test result between 2 serial positive results. These negative test results occurred later, near the end of the disease course. Among the 12 patients with this positive-negativepositive CT/CN pattern, 7 were symptomatic and no longer had documented symptoms or hospitalization around the time of this positive-negative-positive pattern. Four of these individuals were asymptomatic during the entire infection course. One of the 12 patients with this pattern expired with the negative result occurring on day 27 of the disease in the context of rising CT/CN. One of these 12 patients only had a presumptive positive test result on the Cepheid because it detected only the E target with a CT value of 38.7. In 1 of the 12 patients, the negative test result occurred between 2 positive test results with CT/CN values < 20 (12.05 and 19.05 for the positive tests before and after the negative result, respectively). When the initial CT/CN values was separated based on ethnicity, the average CT/CN value for African Americans (23.3) was higher than for other ethnicities (19.9), although it did not reach statistical significance (P = .35).
Ten of the 25 patients testing positive were admitted to the hospital, including 1 admitted 15 days before diagnosis (patient 20) and 1 admitted 80 days after diagnosis (patient 7). Among these 10 patients, 6 were admitted to the intensive care unit, including patient 7. None of the patients were intubated. Three of the 10 admitted patients died (patients 7, 20, and 24). Patient 7 was a 79-year-old male with a history of dementia, cerebrovascular accident, hypertension, hyperlipidemia, and chronic kidney disease with symptoms of lethargy and refusal of oral intake when he was diagnosed with COVID-19. He was admitted 80 days after diagnosis for hyponatremia and acute renal failure, with death on day 87 recorded as complications from the earlier COVID-19 infection. Patient 20, an 89-year-old male with a history of dementia, chronic kidney disease, and hyperlipidemia, had been admitted with fever, cough, and leukocytosis 17 days before COVID-19 diagnosis. He continued to be symptomatic after diagnosis with development of hypotension, dehydration, and refusal of oral intake while on comfort measures/endof- life care and died 15 days after COVID- 19 infection diagnosis. Patient 24 was a 96-year-old male with history of heart failure, hypertension, coronary artery disease, prostate carcinoma, and dementia who developed a cough at the time of diagnosis; because of his underlying condition, he remained in the CLC on comfort care. His symptoms, including hypoxia, worsened until he died 7 days after diagnosis.
Among the 25 patients, 17 were symptomatic at the time of diagnosis; the 14 initially symptomatic patients who survived improved clinically and returned to baseline. Eight of the 25 patients were asymptomatic initially and 3 developed symptoms 2 to 5 days after diagnosis. Only 1 patient who remained asymptomatic was admitted for inability to adhere to quarantine at the CLC. Review of the health records of all surviving symptomatic patients showed symptom resolution with return to baseline that corresponds to an increasing CT/CN value. A 1-tailed t test comparing the initial CT/ CN at the time of diagnosis to the last CT/CN value for symptomatic patients who recovered revealed a statistically significant increase (P < .05). For the symptomatic, symptom resolution and hospital discharge took (if required) a mean 20 days (range, 7-46). Among those who were not hospitalized, symptoms resolved in 7 to 36 days (18 days). Among those requiring hospitalization at any time (excluding patients who died or were asymptomatic), symptom and hospitalization resolution took a mean 22 days (range, 10-46). Asymptomatic patients (patients 8, 10, 15, 16, and 25) also showed increasing CT/CN value during the infection course, although there was no correlation with the continued lack of symptoms.
During the initial validation of the Abbott m2000 instrument, an LOD study included concentrations of 1000, 500, 250, 100, 70, 60, and 50 virus copies/mL (eAppendix 2, available online at doi:10.12788/fp.0276).21 The average CN at 100 virus copies/mL—the manufacturer provided LOD in the instructions for use—was 25.74.20 At a concentration of one-half that (50 virus copies/mL), the average CN was 28.39.
Discussion
This is the first study in the English literature to track CT/CN values as part of serial testing of a veteran CLC. Widescale testing and repeat screening in the absence of symptoms of nursing home residents would identify those who are infected and allow providers to track viral load clearance.9-14 CT/CN values, when serially tracked during the infection course, appear to increase with illness resolution, consistent with earlier reports that CT/CN correlates with viral load.8-14 Serial CT/CN values that are high (> 25) and continue to increase with each test suggest progression toward disease resolution or viral RNA clearance.8-14 After symptom resolution, patients can have a persistent low level of viral shedding (corresponding to a high CT/CN value).10-14,25 Near the end of disease resolution, a negative serial RT-PCR sample test before a subsequent positive might be a promising clinical sign of near disease recovery. Once the viral load is low with a CT/CN significantly higher than 25, some specimens might result as negative but turn up positive on subsequent sampling with a high CT/CN value. This pattern, with attendant high CT/CN values for the positive results, are consistent with the known effect of viral load (ie, a low viral load correlates to a high CT/CN) and adequacy of specimen collection on CT/CN values.25 If the patient’s viral load is low, the sample collected might have a viral load at or near the testing platform’s LOD.
For Abbott m2000, the manufacturer provided LOD is 100 virus copies/mL, although the instrument was able to detect virus concentrations below that level during the initial validation.20 The actual LOD of the instrument at our institution is < 100 virus copies/mL. For the Cepheid Xpert Xpress SARS-CoV-2 assay, the manufacturer-provided LOD is 250 virus copies/mL.19 An LOD study including samples below the manufacturer-provided LOD was not part of the initial validation study for the Xpert Xpress assay. Nonetheless, the virus concentration of samples with very high CT values at or near the maximum CT value of 45 is expected to be at or near the platform’s actual LOD.
If the samples collected near the end of the patient’s disease course have viral loads near these low concentrations, the encouraging positive-negative-positive pattern with high CT/CN values might be a promising sign for viral clearance. On the other hand, a positive-negative-positive pattern in the setting of low CT/CN values before and after the negative test might indicate poor sampling for the negative specimen. The back-and-forth or positive-negative-positive pattern generally appears to indicate near resolution of the infection course, although clinical correlation is necessary to rule out inadequate sampling earlier in the disease course or prolonged viral RNA shedding.9-14 In all of the surviving symptomatic patients who showed the positive-negative-positive pattern, this sign occurred around or after symptom resolution. It also is important to consider that in some patients, SARS-CoV-2 RNA might remain detectable with increasing CT/CN after symptom resolution, and samples from these patients might not result positive. Therefore, CT/CN values cannot be interpreted without considering the clinical picture.25
Studies on infectiousness and virus culture from COVID-19 samples with CT/ CN correlation have shown that patients with high CT/CN at the end of their disease course might not be as infectious.9-14,25 Because 1 patient had a presumptive positive result after the negative result, this study shows that this positive-negative-positive pattern could include presumptive positive results. Also, in the setting of a recent positive result on the same testing platform, a patient with this pattern is presumed to be positive for COVID-19 RNA because of scant viral material.
Taiwan’s public health response to the outbreak illustrates the ability to mitigate an outbreak throughout a society.26 These actions could help blunt an outbreak within a civilian nursing home population.5 Mitigation within a veteran CLC population has been documented, but the study, which focused on mitigation, did not consider CT/CN values, demographic distribution, testing access of the studied population, or laboratory findings related to disease pathophysiology.15 A key ingredient in widescale, serial testing is the availability of a rapid turnaround from testing in-house that allowed identification within 24 hours instead of several days at a reference laboratory. 15 Rapid widescale testing would allow clinical teams to optimize the Triangle of Benefit of Widescale Timely Tests for CLC (Figure 3).15 Timely laboratory testing remains pivotal for CLC veteran residents to aid successful clinical triage and management. Reporting serial CT/CN values can provide additional information to clinicians about the disease course because CT/ CN correlates with viral load, which varies based on where the patient is in the disease course.9-14 CT/CN values carry significant prognostic value, particularly with respect to intubation and mortality.8
Limitations
Important limitations to our study include the use of 2 separate RT-PCR platforms. Using different RT-PCR platforms is common in clinical laboratories trying to take advantage of the unique characteristics of different platforms—for example, turnaround time vs high throughput— to manage COVID-19 testing workflow.25 However, the exact CT/CN values obtained from each platform might not translate to the other, and the general trend (CT/CN values are rising or falling across serial tests) rather than a single value could be useful for clinical correlation. Even when the same platform is used for the serial testing, CT/CN values can be affected by adequacy of specimen collection; therefore, clinical correlation and considering the trend in CT/CN values is necessary for interpretation.10-14,25 Because of the known trend in viral dynamics, a positive specimen collected with a high CT/CN followed by a subsequent (within 2 days) positive specimen collected with a low CT/CN might be compatible with early detection of COVID- 19 infection in the appropriate clinical context. 10-14 However, detection late in the infection course or even after the symptomatic disease resolved with prolonged viral shedding might show serial positive samples with increasing CT/CN values.10-14
Patients with prolonged viral shedding might not be infectious.27 Because of the clinical correlation required for interpretation and the other factors that might affect CT/CN values, recommendations advise against using CT/CN values in clinical practice at this time, although these recommendations could change with future research.25 Serial CT/CN values have the potential, if appropriately correlated with the clinical picture, to provide useful information, such as whether the viral load of the sample is relatively high or low and increasing or decreasing.
Veterans, as a population, are more susceptible to poor health outcomes and morbidity compared with similar civilian counterparts.2,14-16 Veteran CLC patients likely would experience worse outcomes with COVID-19, including more infections, expiration, and morbidity compared with similar general population nursing homes. Similar to what had been reported for the civilian population, a trend (high CT/CN values early in the disease course with repeat testing needed to detect all positives followed by lower CT/CN value to correlate with increased viral load and then increased CT/CN value as the infection resolved) also was observed in this veteran population.
It has been extensively documented that minority groups experience decreased health care access and worse health outcomes. 28-30 Considering the critical medical supply shortages, including personal protective equipment, ventilators, and even testing supplies, there is the potential for a resource access disparity by ethnicity.28-31 Because the VA does not depend on measures of wealth and privilege such as health insurance, there was no disparity noted in access to testing by race or ethnicity at the VAMC CLC. When considering the health outcome of viral load from the measured CT/CN value, the viral loads of African American patients and those of other ethnicities was not significantly different in this study.
Conclusions
This is the first study to bring up critical points including serial CT/CN value correlation in RT-PCR tests, demographic distributions demonstrating easy and equal access in a veteran nursing home to COVID-19 testing, and clinical laboratory signs related to disease pathophysiology. Unlike other populations who have undergone serial CT/CN monitoring, nursing homes represent a particularly vulnerable population who require measures to prevent the spread and mitigate outbreaks of COVID-19.2,4,5 Test measurements obtained such as the CT/CN value during routine clinical care can provide useful information for public health, epidemiologic, or clinical purposes with appropriate correlation to clinical and other laboratory parameters. This study demonstrates early intervention of serial testing of an outbreak in a veterans nursing home with CT/CN value correlation.
COVID-19, caused by SARS-CoV-2, is more severe in individuals with underlying illnesses. Because complete social distancing might be more difficult in nursing homes and community living centers (CLCs), public health leaders and clinicians have been concerned about the epidemiology and disease course in nursing homes even before the COVID-19 pandemic.1-7 A report of a COVID-19 outbreak in a nursing home facility in King County, Washington, documented a 33.7% overall fatality rate for residents and 52.4% among the most critically ill.4,5 The experience at King County, Washington, shows that proactive steps to identify, monitor, and apply preventive control measures is important for future outbreaks.5
Reverse transcriptase polymerase chain reaction (RT-PCR) testing produces a cycle threshold (CT) or cycle number (CN) that correlates with viral load and infectiousness. 8-14 CT/CN represents the number of RT-PCR cycles required for the fluorescent signal to cross the detection threshold (exceed background level) and is inversely proportional to the viral load. Effectively, the higher the viral load, the lower the CT/ CN value (Figure 1). Tracking CT/CN values was not documented in the Washington nursing home outbreak. Reports of COVID- 19 testing in CLCs during outbreaks are sparse, and CT/CN values and demographic distribution of these veterans has not been reported.15 The CLC veteran population, with known higher vulnerability to infection and chronic diseases, is epidemiologically different from the general nursing home population.15-18 To address these literature gaps, we present the first report of COVID- 19 testing with CT/CN value correlations in the high-risk veteran CLC population.
Methods
A retrospective review of all COVID-19 CT/CN testing at the Corporal Michael J. Crescenz Veterans Affairs Medical Center (VAMC) CLC in Philadelphia, Pennsylvania, from March 28, 2020, to April 24, 2020, was performed with a US Department of Veterans Affairs (VA) Veterans Health Information System Architecture VistA/FileMan search. Only veteran residents were included in this review. Data collected included initial and serial test results, CT/CN on positive test results, test dates, testing platform used, demographic information (age, self-reported ethnicity, and sex), and clinical follow-up information. Health records were reviewed retrospectively to identify death, the first day after diagnosis with no documented symptoms, or hospitalization status.
RT-PCR testing was performed with the Abbott RealTime SARS-CoV-2 assay on the Abbott m2000 platform and the Xpert Xpress SARS-CoV-2 assay on the Cepheid Infinity platform. The Xpert Xpress assay gave 2 CT values for the E and N2 targets on positive samples.19 For this assay to indicate a positive specimen, amplification by RT-PCR of the N2 target or both the N2 and E target is required. The Xpert Xpress assay results as presumptive positive if only the E target amplified. This assay counts a maximum of 45 cycles. The Abbott RealTime SARS-CoV-2 assay gave 1 CN derived from the RNA-dependent RNA polymerase and N targets on positive samples.20 The Abbott assay on the m2000 counts a maximum of 37 cycles. The CT/CN value is the number of cycles required by RT-PCR for the fluorescence signal to cross a threshold value exceeding background level.19,20
Samples that are negative for COVID-19 by RT-PCR do not produce a CT/CN value. Although both instruments were used for RT-PCR, the precise CT/CN values are not interchangeable and CT/CN observations over time between the 2 instruments during the disease course would be based on CT/CN value movement (general upward or downward trend) rather than absolute CT/CN differences. Both assays have been approved by emergency use authorization as qualitative tests for the presence/absence of COVID-19. Although the CT/CN value is available to laboratory staff after test completion, the CT/CN value is not reported routinely in the patient health record. All veteran patients identified on the initial review from March 28, 2020, to April 24, 2020, had all serial COVID-19 testing recorded until November 10, 2020. The CN values at the limit of detection (LOD) for the Abbott m2000 platform from the initial validation study were reviewed for reference.21
Results
Of 80 patients, 25 (31%) were COVID-19 positive over the course of testing. The study population had a mean age of 73.5 years; 92% were aged > 60 years. The group was predominantly male (79 male vs 1 female). Among the 77 patients with a stated ethnicity, 39 (51%) were African American. In comparison, 43% of residents in Philadelphia County are African American (Table).22,23 Additionally, a previously published total COVID-19 tested population by ethnicity at the same regional VAMC revealed 46.8% of tested veteran patients were African American. 24 Three patients had no stated ethnicity. Among those who tested positive, 11 were African American patients, 12 were White patients, and 2 had no stated ethnicity. Four patients tested positive on their first test. The other 21 patients were positive on repeat testing. Interestingly, 6 patients had 1 initial negative test before a positive test, 6 patients had 2, 8 patients had 3, and 1 patient had 4 initial negative tests before a positive test result. Among the 25 positive patients, 22 were either positive within 10 days of the initial negative test result or initially positive (Figure 2). Three patients who tested positive after 10 days did so at 16, 20, and 21 days after the initial negative test result. Among the 25 positive patients, 23 had initial and serial testing from both the Abbott and Xpert Xpress assays. The remaining 2 positive patients had initial and serial testing from the Abbott assay exclusively.
Only positive COVID-19 results by RTPCR produced a CT/CN value. After disease resolution with a negative test, no CT/CN value was produced with the negative test result on either testing platform. Because repeat testing after the initial positive result took place no sooner than 10 days, we observed that the CT/CN value increased after the initial positive result until the disease resolved, and a negative result was obtained (eAppendix 1, available online at doi:10.12788/fp.0276). A t test comparing the initial CT/CN value to the value more than 10 days after the initial positive showed the CT/CN was statistically significantly higher (P < .05).
Prompt repeat testing after the initial test can show a decrease in the CT/CN value because of increasing viral load before the expected increase until disease resolution if the initial test caught the infection early. Twelve patients had a negative test result between 2 serial positive results. These negative test results occurred later, near the end of the disease course. Among the 12 patients with this positive-negativepositive CT/CN pattern, 7 were symptomatic and no longer had documented symptoms or hospitalization around the time of this positive-negative-positive pattern. Four of these individuals were asymptomatic during the entire infection course. One of the 12 patients with this pattern expired with the negative result occurring on day 27 of the disease in the context of rising CT/CN. One of these 12 patients only had a presumptive positive test result on the Cepheid because it detected only the E target with a CT value of 38.7. In 1 of the 12 patients, the negative test result occurred between 2 positive test results with CT/CN values < 20 (12.05 and 19.05 for the positive tests before and after the negative result, respectively). When the initial CT/CN values was separated based on ethnicity, the average CT/CN value for African Americans (23.3) was higher than for other ethnicities (19.9), although it did not reach statistical significance (P = .35).
Ten of the 25 patients testing positive were admitted to the hospital, including 1 admitted 15 days before diagnosis (patient 20) and 1 admitted 80 days after diagnosis (patient 7). Among these 10 patients, 6 were admitted to the intensive care unit, including patient 7. None of the patients were intubated. Three of the 10 admitted patients died (patients 7, 20, and 24). Patient 7 was a 79-year-old male with a history of dementia, cerebrovascular accident, hypertension, hyperlipidemia, and chronic kidney disease with symptoms of lethargy and refusal of oral intake when he was diagnosed with COVID-19. He was admitted 80 days after diagnosis for hyponatremia and acute renal failure, with death on day 87 recorded as complications from the earlier COVID-19 infection. Patient 20, an 89-year-old male with a history of dementia, chronic kidney disease, and hyperlipidemia, had been admitted with fever, cough, and leukocytosis 17 days before COVID-19 diagnosis. He continued to be symptomatic after diagnosis with development of hypotension, dehydration, and refusal of oral intake while on comfort measures/endof- life care and died 15 days after COVID- 19 infection diagnosis. Patient 24 was a 96-year-old male with history of heart failure, hypertension, coronary artery disease, prostate carcinoma, and dementia who developed a cough at the time of diagnosis; because of his underlying condition, he remained in the CLC on comfort care. His symptoms, including hypoxia, worsened until he died 7 days after diagnosis.
Among the 25 patients, 17 were symptomatic at the time of diagnosis; the 14 initially symptomatic patients who survived improved clinically and returned to baseline. Eight of the 25 patients were asymptomatic initially and 3 developed symptoms 2 to 5 days after diagnosis. Only 1 patient who remained asymptomatic was admitted for inability to adhere to quarantine at the CLC. Review of the health records of all surviving symptomatic patients showed symptom resolution with return to baseline that corresponds to an increasing CT/CN value. A 1-tailed t test comparing the initial CT/ CN at the time of diagnosis to the last CT/CN value for symptomatic patients who recovered revealed a statistically significant increase (P < .05). For the symptomatic, symptom resolution and hospital discharge took (if required) a mean 20 days (range, 7-46). Among those who were not hospitalized, symptoms resolved in 7 to 36 days (18 days). Among those requiring hospitalization at any time (excluding patients who died or were asymptomatic), symptom and hospitalization resolution took a mean 22 days (range, 10-46). Asymptomatic patients (patients 8, 10, 15, 16, and 25) also showed increasing CT/CN value during the infection course, although there was no correlation with the continued lack of symptoms.
During the initial validation of the Abbott m2000 instrument, an LOD study included concentrations of 1000, 500, 250, 100, 70, 60, and 50 virus copies/mL (eAppendix 2, available online at doi:10.12788/fp.0276).21 The average CN at 100 virus copies/mL—the manufacturer provided LOD in the instructions for use—was 25.74.20 At a concentration of one-half that (50 virus copies/mL), the average CN was 28.39.
Discussion
This is the first study in the English literature to track CT/CN values as part of serial testing of a veteran CLC. Widescale testing and repeat screening in the absence of symptoms of nursing home residents would identify those who are infected and allow providers to track viral load clearance.9-14 CT/CN values, when serially tracked during the infection course, appear to increase with illness resolution, consistent with earlier reports that CT/CN correlates with viral load.8-14 Serial CT/CN values that are high (> 25) and continue to increase with each test suggest progression toward disease resolution or viral RNA clearance.8-14 After symptom resolution, patients can have a persistent low level of viral shedding (corresponding to a high CT/CN value).10-14,25 Near the end of disease resolution, a negative serial RT-PCR sample test before a subsequent positive might be a promising clinical sign of near disease recovery. Once the viral load is low with a CT/CN significantly higher than 25, some specimens might result as negative but turn up positive on subsequent sampling with a high CT/CN value. This pattern, with attendant high CT/CN values for the positive results, are consistent with the known effect of viral load (ie, a low viral load correlates to a high CT/CN) and adequacy of specimen collection on CT/CN values.25 If the patient’s viral load is low, the sample collected might have a viral load at or near the testing platform’s LOD.
For Abbott m2000, the manufacturer provided LOD is 100 virus copies/mL, although the instrument was able to detect virus concentrations below that level during the initial validation.20 The actual LOD of the instrument at our institution is < 100 virus copies/mL. For the Cepheid Xpert Xpress SARS-CoV-2 assay, the manufacturer-provided LOD is 250 virus copies/mL.19 An LOD study including samples below the manufacturer-provided LOD was not part of the initial validation study for the Xpert Xpress assay. Nonetheless, the virus concentration of samples with very high CT values at or near the maximum CT value of 45 is expected to be at or near the platform’s actual LOD.
If the samples collected near the end of the patient’s disease course have viral loads near these low concentrations, the encouraging positive-negative-positive pattern with high CT/CN values might be a promising sign for viral clearance. On the other hand, a positive-negative-positive pattern in the setting of low CT/CN values before and after the negative test might indicate poor sampling for the negative specimen. The back-and-forth or positive-negative-positive pattern generally appears to indicate near resolution of the infection course, although clinical correlation is necessary to rule out inadequate sampling earlier in the disease course or prolonged viral RNA shedding.9-14 In all of the surviving symptomatic patients who showed the positive-negative-positive pattern, this sign occurred around or after symptom resolution. It also is important to consider that in some patients, SARS-CoV-2 RNA might remain detectable with increasing CT/CN after symptom resolution, and samples from these patients might not result positive. Therefore, CT/CN values cannot be interpreted without considering the clinical picture.25
Studies on infectiousness and virus culture from COVID-19 samples with CT/ CN correlation have shown that patients with high CT/CN at the end of their disease course might not be as infectious.9-14,25 Because 1 patient had a presumptive positive result after the negative result, this study shows that this positive-negative-positive pattern could include presumptive positive results. Also, in the setting of a recent positive result on the same testing platform, a patient with this pattern is presumed to be positive for COVID-19 RNA because of scant viral material.
Taiwan’s public health response to the outbreak illustrates the ability to mitigate an outbreak throughout a society.26 These actions could help blunt an outbreak within a civilian nursing home population.5 Mitigation within a veteran CLC population has been documented, but the study, which focused on mitigation, did not consider CT/CN values, demographic distribution, testing access of the studied population, or laboratory findings related to disease pathophysiology.15 A key ingredient in widescale, serial testing is the availability of a rapid turnaround from testing in-house that allowed identification within 24 hours instead of several days at a reference laboratory. 15 Rapid widescale testing would allow clinical teams to optimize the Triangle of Benefit of Widescale Timely Tests for CLC (Figure 3).15 Timely laboratory testing remains pivotal for CLC veteran residents to aid successful clinical triage and management. Reporting serial CT/CN values can provide additional information to clinicians about the disease course because CT/ CN correlates with viral load, which varies based on where the patient is in the disease course.9-14 CT/CN values carry significant prognostic value, particularly with respect to intubation and mortality.8
Limitations
Important limitations to our study include the use of 2 separate RT-PCR platforms. Using different RT-PCR platforms is common in clinical laboratories trying to take advantage of the unique characteristics of different platforms—for example, turnaround time vs high throughput— to manage COVID-19 testing workflow.25 However, the exact CT/CN values obtained from each platform might not translate to the other, and the general trend (CT/CN values are rising or falling across serial tests) rather than a single value could be useful for clinical correlation. Even when the same platform is used for the serial testing, CT/CN values can be affected by adequacy of specimen collection; therefore, clinical correlation and considering the trend in CT/CN values is necessary for interpretation.10-14,25 Because of the known trend in viral dynamics, a positive specimen collected with a high CT/CN followed by a subsequent (within 2 days) positive specimen collected with a low CT/CN might be compatible with early detection of COVID- 19 infection in the appropriate clinical context. 10-14 However, detection late in the infection course or even after the symptomatic disease resolved with prolonged viral shedding might show serial positive samples with increasing CT/CN values.10-14
Patients with prolonged viral shedding might not be infectious.27 Because of the clinical correlation required for interpretation and the other factors that might affect CT/CN values, recommendations advise against using CT/CN values in clinical practice at this time, although these recommendations could change with future research.25 Serial CT/CN values have the potential, if appropriately correlated with the clinical picture, to provide useful information, such as whether the viral load of the sample is relatively high or low and increasing or decreasing.
Veterans, as a population, are more susceptible to poor health outcomes and morbidity compared with similar civilian counterparts.2,14-16 Veteran CLC patients likely would experience worse outcomes with COVID-19, including more infections, expiration, and morbidity compared with similar general population nursing homes. Similar to what had been reported for the civilian population, a trend (high CT/CN values early in the disease course with repeat testing needed to detect all positives followed by lower CT/CN value to correlate with increased viral load and then increased CT/CN value as the infection resolved) also was observed in this veteran population.
It has been extensively documented that minority groups experience decreased health care access and worse health outcomes. 28-30 Considering the critical medical supply shortages, including personal protective equipment, ventilators, and even testing supplies, there is the potential for a resource access disparity by ethnicity.28-31 Because the VA does not depend on measures of wealth and privilege such as health insurance, there was no disparity noted in access to testing by race or ethnicity at the VAMC CLC. When considering the health outcome of viral load from the measured CT/CN value, the viral loads of African American patients and those of other ethnicities was not significantly different in this study.
Conclusions
This is the first study to bring up critical points including serial CT/CN value correlation in RT-PCR tests, demographic distributions demonstrating easy and equal access in a veteran nursing home to COVID-19 testing, and clinical laboratory signs related to disease pathophysiology. Unlike other populations who have undergone serial CT/CN monitoring, nursing homes represent a particularly vulnerable population who require measures to prevent the spread and mitigate outbreaks of COVID-19.2,4,5 Test measurements obtained such as the CT/CN value during routine clinical care can provide useful information for public health, epidemiologic, or clinical purposes with appropriate correlation to clinical and other laboratory parameters. This study demonstrates early intervention of serial testing of an outbreak in a veterans nursing home with CT/CN value correlation.
1. Chen T, Wu D, Chen H, et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. BMJ. 2020;368:m1091. doi:10.1136/bmj.m1091
2. Tsan L, Davis C, Langberg R, et al. Prevalence of nursing home-associated infections in the Department of Veterans Affairs nursing home care units. Am J Infect Control. 2008;36(3):173-179. doi:10.1016/j.ajic.2007.06.008
3. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054-1062. doi:10.1016/S0140-6736(20)30566-3
4. Arentz M, Yim E, Klaff L, et al. Characteristics and outcomes of 21 critically ill patients with COVID-19 in Washington State. JAMA. 2020;323(16):1612-1614. doi:10.1001/jama.2020.4326
5. McMichael TM, Currie DW, Clark S, et al. Public Health–Seattle and King County, EvergreenHealth, and CDC COVID-19 Investigation Team. Epidemiology of Covid-19 in a long-term care facility in King County, Washington. N Engl J Med. 2020;382(21):2005-2011. doi:10.1056/NEJMoa2005412
6. Childs A, Zullo AR, Joyce NR, et al. The burden of respiratory infections among older adults in long-term care: a systematic review. BMC Geriatr. 2019;19(1):210. doi:10.1186/s12877-019-1236-6
7. Eriksen HM, Iversen BG, Aavitsland PJ. Prevalence of nosocomial infections and use of antibiotics in long-term care facilities in Norway, 2002 and 2003. Hosp Infect. 2004;57(4):316-320. doi:10.1016/j.jhin.2004.03.028
8. Magleby R, Westblade LF, Trzebucki A, et al. Impact Severe acute respiratory syndrome coronavirus 2 viral load on risk of intubation and mortality among hospitalized patients with coronavirus disease 2019. Clin Infect Dis. 2021;73(11):e4197-e4205. doi:10.1093/cid/ciaa851
9. Buchan B, Hoff J, Gmehlin C, et al. Distribution of SARSCoV- 2 PCR cycle threshold values provide practical insight into overall and target-specific sensitivity among symptomatic patients. Am Clin Pathol. 2020;154:479-485. doi:10.1093/ajcp/aqaa133
10. He X, Lau EHY, Wu P, et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med. 2020;26(5):672-675. doi:10.1038/s41591-020-0869-5
11. Zou L, Ruan F, Huang M, et al. SARS-CoV-2 Viral load in upper respiratory specimens of infected patients. N Engl J Med. 2020;382(12):1177-1179. doi:10.1056/NEJMc2001737
12. Singanayagam A, Patel M, Charlett A, et al. Duration of infectiousness and correlation with RT-PCR cycle threshold values in cases of COVID-19, England, January to May 2020. Euro Surveill. 2020;25(32):2001483. doi:10.2807/1560-7917.ES.2020.25.32.2001483
13. Salvatore P, Dawson P, Wadhwa A, et al. Epidemiological correlates of PCR cycles threshold values in the detection of SARS-CoV-2. Clin Infect Dis. 2021;72(11):e761-e767. doi:10.1093/cid/ciaa1469
14. Kissler S, Fauver J, Mack C, et al. Viral dynamics of SARS-CoV-2 infection and the predictive value of repeat testing. medRxiv. 2020;10.21.20217042. doi:10.1101/2020.10.21.20217042 1
5. Escobar DJ, Lanzi M, Saberi P, et al. Mitigation of a COVID-19 outbreak in a nursing home through serial testing of residents and staff. Clin Infect Dis. 2021;72(9):e394- e396. doi:10.1093/cid/ciaa1021
16. Eibner C, Krull H, Brown KM, et al. Current and projected characteristics and unique health care needs of the patient population served by the Department of Veterans Affairs. Rand Health Q. 2016;5(4):13.
17. Agha Z, Lofgren RP, VanRuiswyk JV, Layde PM. Are patients at Veterans Affairs medical centers sicker? A comparative analysis of health status and medical resource use. Arch Intern Med. 2000;160(21):3252-3257. doi:10.1001/archinte.160.21.3252
18. Morgan RO, Teal CR, Reddy SG, Ford ME, Ashton CM. Measurement in Veterans Affairs Health Services Research: veterans as a special population. Health Serv Res. 2005;40(5 Pt 2):1573-1583. doi:10.1111/j.1475-6773.2005.00448.x 1
9. Xpert Xpress SARS-CoV-2. Instructions for use. Cepheid. 302-2562, Rev. C April 2020. Accessed January 7, 2021. https://www.fda.gov/media/136314/download
20. Abbott RealTime SARS-CoV-2. Instructions for use Abbott. 09N77-95. July 2020. Accessed January 7, 2021. https:// www.fda.gov/media/136258/download
21. Petersen JM, Dalal S, Jhala D. Successful implementation of SARS-CoV-2 testing in midst of pandemic with emphasis on all phases of testing. J Clin Pathol. 2021;74:273- 278. doi:10.1136/jclinpath-2020-207175
22. United States Census Bureau. Quick Facts: Philadelphia County, Pennsylvania. Accessed April 16, 2020. https://www .census.gov/quickfacts/philadelphiacountypennsylvania
23. Centers for Disease Control and Prevention. United States COVID-19 cases, deaths, and laboratory testing (NAATS) by state, territory, and jurisdiction. Accessed April 26, 2020. https://www.cdc.gov/coronavirus/2019-ncov/cases -updates/cases-in-us.html 2
4. Petersen J, Jhala D. Ethnicity, comorbid medical conditions, and SARS-CoV-2 test cycle thresholds in the veteran population [published online ahead of print, 2021 Jul 28]. J Racial Ethn Health Disparities. 2021;1-8. doi:10.1007/s40615-021-01114-4
25. Infectious Diseases Society of America, Association for Molecular Pathology. IDSA and AMP joint statement on the use of SARS-CoV-2 PCR cycle threshold (Ct) values for clinical decision-making. Accessed August 28, 2021. https://www.idsociety.org/globalassets/idsa/public-health /covid-19/idsa-amp-statement.pdf
26. Wang J, Ng CY, Brook RH. Response to COVID-19 in Taiwan: big data analysis, new technology, and proactive testing. JAMA. 2020;323(14):1341-1342. doi:10.1001/jama.2020.3151
27. Centers for Disease Control and Prevention. Overview of testing for SARS-CoV-2, the virus that causes COVID- 19. Accessed July 28, 2021. https://www.cdc.gov /coronavirus/2019-ncov/hcp/testing-overview.html
28. Zuvekas SH, Taliaferro GS. Pathways to access: health insurance, the health care delivery system, and racial/ethnic disparities, 1996-1999. Health Aff. 2003;22(2):139-153. doi:10.1377/hlthaff.22.2.139
29. Egede LE. Race, ethnicity, culture, and disparities in health care. J Gen Intern Med. 2006;21(6):667-669. doi:10.1111/j.1525-1497.2006.0512.x
30. Institute of Medicine (US) Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care. Smedley BD, Stith AY, Nelson AR, eds. Unequal treatment: confronting racial and ethnic disparities in health care. National Academies Press; 2003. doi:10.17226/12875
31. Ranney ML, Griffeth V, Jha AK. Critical supply shortages – the need for ventilators and personal protective equipment during the Covid-19 Pandemic. N Engl J Med. 2020;382(18):e41. doi:10.1056/NEJMp2006141
1. Chen T, Wu D, Chen H, et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. BMJ. 2020;368:m1091. doi:10.1136/bmj.m1091
2. Tsan L, Davis C, Langberg R, et al. Prevalence of nursing home-associated infections in the Department of Veterans Affairs nursing home care units. Am J Infect Control. 2008;36(3):173-179. doi:10.1016/j.ajic.2007.06.008
3. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054-1062. doi:10.1016/S0140-6736(20)30566-3
4. Arentz M, Yim E, Klaff L, et al. Characteristics and outcomes of 21 critically ill patients with COVID-19 in Washington State. JAMA. 2020;323(16):1612-1614. doi:10.1001/jama.2020.4326
5. McMichael TM, Currie DW, Clark S, et al. Public Health–Seattle and King County, EvergreenHealth, and CDC COVID-19 Investigation Team. Epidemiology of Covid-19 in a long-term care facility in King County, Washington. N Engl J Med. 2020;382(21):2005-2011. doi:10.1056/NEJMoa2005412
6. Childs A, Zullo AR, Joyce NR, et al. The burden of respiratory infections among older adults in long-term care: a systematic review. BMC Geriatr. 2019;19(1):210. doi:10.1186/s12877-019-1236-6
7. Eriksen HM, Iversen BG, Aavitsland PJ. Prevalence of nosocomial infections and use of antibiotics in long-term care facilities in Norway, 2002 and 2003. Hosp Infect. 2004;57(4):316-320. doi:10.1016/j.jhin.2004.03.028
8. Magleby R, Westblade LF, Trzebucki A, et al. Impact Severe acute respiratory syndrome coronavirus 2 viral load on risk of intubation and mortality among hospitalized patients with coronavirus disease 2019. Clin Infect Dis. 2021;73(11):e4197-e4205. doi:10.1093/cid/ciaa851
9. Buchan B, Hoff J, Gmehlin C, et al. Distribution of SARSCoV- 2 PCR cycle threshold values provide practical insight into overall and target-specific sensitivity among symptomatic patients. Am Clin Pathol. 2020;154:479-485. doi:10.1093/ajcp/aqaa133
10. He X, Lau EHY, Wu P, et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med. 2020;26(5):672-675. doi:10.1038/s41591-020-0869-5
11. Zou L, Ruan F, Huang M, et al. SARS-CoV-2 Viral load in upper respiratory specimens of infected patients. N Engl J Med. 2020;382(12):1177-1179. doi:10.1056/NEJMc2001737
12. Singanayagam A, Patel M, Charlett A, et al. Duration of infectiousness and correlation with RT-PCR cycle threshold values in cases of COVID-19, England, January to May 2020. Euro Surveill. 2020;25(32):2001483. doi:10.2807/1560-7917.ES.2020.25.32.2001483
13. Salvatore P, Dawson P, Wadhwa A, et al. Epidemiological correlates of PCR cycles threshold values in the detection of SARS-CoV-2. Clin Infect Dis. 2021;72(11):e761-e767. doi:10.1093/cid/ciaa1469
14. Kissler S, Fauver J, Mack C, et al. Viral dynamics of SARS-CoV-2 infection and the predictive value of repeat testing. medRxiv. 2020;10.21.20217042. doi:10.1101/2020.10.21.20217042 1
5. Escobar DJ, Lanzi M, Saberi P, et al. Mitigation of a COVID-19 outbreak in a nursing home through serial testing of residents and staff. Clin Infect Dis. 2021;72(9):e394- e396. doi:10.1093/cid/ciaa1021
16. Eibner C, Krull H, Brown KM, et al. Current and projected characteristics and unique health care needs of the patient population served by the Department of Veterans Affairs. Rand Health Q. 2016;5(4):13.
17. Agha Z, Lofgren RP, VanRuiswyk JV, Layde PM. Are patients at Veterans Affairs medical centers sicker? A comparative analysis of health status and medical resource use. Arch Intern Med. 2000;160(21):3252-3257. doi:10.1001/archinte.160.21.3252
18. Morgan RO, Teal CR, Reddy SG, Ford ME, Ashton CM. Measurement in Veterans Affairs Health Services Research: veterans as a special population. Health Serv Res. 2005;40(5 Pt 2):1573-1583. doi:10.1111/j.1475-6773.2005.00448.x 1
9. Xpert Xpress SARS-CoV-2. Instructions for use. Cepheid. 302-2562, Rev. C April 2020. Accessed January 7, 2021. https://www.fda.gov/media/136314/download
20. Abbott RealTime SARS-CoV-2. Instructions for use Abbott. 09N77-95. July 2020. Accessed January 7, 2021. https:// www.fda.gov/media/136258/download
21. Petersen JM, Dalal S, Jhala D. Successful implementation of SARS-CoV-2 testing in midst of pandemic with emphasis on all phases of testing. J Clin Pathol. 2021;74:273- 278. doi:10.1136/jclinpath-2020-207175
22. United States Census Bureau. Quick Facts: Philadelphia County, Pennsylvania. Accessed April 16, 2020. https://www .census.gov/quickfacts/philadelphiacountypennsylvania
23. Centers for Disease Control and Prevention. United States COVID-19 cases, deaths, and laboratory testing (NAATS) by state, territory, and jurisdiction. Accessed April 26, 2020. https://www.cdc.gov/coronavirus/2019-ncov/cases -updates/cases-in-us.html 2
4. Petersen J, Jhala D. Ethnicity, comorbid medical conditions, and SARS-CoV-2 test cycle thresholds in the veteran population [published online ahead of print, 2021 Jul 28]. J Racial Ethn Health Disparities. 2021;1-8. doi:10.1007/s40615-021-01114-4
25. Infectious Diseases Society of America, Association for Molecular Pathology. IDSA and AMP joint statement on the use of SARS-CoV-2 PCR cycle threshold (Ct) values for clinical decision-making. Accessed August 28, 2021. https://www.idsociety.org/globalassets/idsa/public-health /covid-19/idsa-amp-statement.pdf
26. Wang J, Ng CY, Brook RH. Response to COVID-19 in Taiwan: big data analysis, new technology, and proactive testing. JAMA. 2020;323(14):1341-1342. doi:10.1001/jama.2020.3151
27. Centers for Disease Control and Prevention. Overview of testing for SARS-CoV-2, the virus that causes COVID- 19. Accessed July 28, 2021. https://www.cdc.gov /coronavirus/2019-ncov/hcp/testing-overview.html
28. Zuvekas SH, Taliaferro GS. Pathways to access: health insurance, the health care delivery system, and racial/ethnic disparities, 1996-1999. Health Aff. 2003;22(2):139-153. doi:10.1377/hlthaff.22.2.139
29. Egede LE. Race, ethnicity, culture, and disparities in health care. J Gen Intern Med. 2006;21(6):667-669. doi:10.1111/j.1525-1497.2006.0512.x
30. Institute of Medicine (US) Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care. Smedley BD, Stith AY, Nelson AR, eds. Unequal treatment: confronting racial and ethnic disparities in health care. National Academies Press; 2003. doi:10.17226/12875
31. Ranney ML, Griffeth V, Jha AK. Critical supply shortages – the need for ventilators and personal protective equipment during the Covid-19 Pandemic. N Engl J Med. 2020;382(18):e41. doi:10.1056/NEJMp2006141