User login
Adenoma detection rate removed from 2020 MIPS, or was it?
Every year, the Centers for Medicare & Medicaid Services (CMS) releases their proposed recommendations for the next performance year and in 2019, the gastroenterology community was surprised that CMS recommended removal of QPP 0343 – Screening Colonoscopy Adenoma Detection Rate from a reportable measure in the Quality Payment Program. So what happened? Why was the measure removed from the QPP? Is there anything that we can do?

Over the next several months we will be publishing a series of articles related to the Adenoma Detection Rate Measure to give every gastroenterologist an inside look at the work that is done on your behalf and steps that you can take in the future to help your fellow gastroenterologists.
This current article explains the joint effort made by all GI societies to try to save the Adenoma Detection Rate measure from removal from the 2020 Quality Payment Program. All societies uniformly submitted a letter to CMS in disapproval of the recommendation and outlined the importance of this measure as follows:
Measure 343: Screening Colonoscopy Adenoma Detection Rate
Our societies are disappointed and disagree with CMS’s decision to remove Measure 343: Screening Colonoscopy Adenoma Detection Rate (ADR) from the Quality Payment Program (QPP) beginning with the 2020 performance year.
The ADR plays a central role in quality improvement and colorectal cancer screening. We urge CMS to reconsider this decision and issue a technical correction to reinstate the measure back into the QPP, as it is the only outcome measure specific to endoscopic skills of gastroenterologists currently available for public reporting.
Studies show that high adenoma detection rates are associated with a significant reduction in colorectal cancer risk.1 Virtually all studies on this subject have demonstrated that there is, in fact, marked variation in adenoma detection rates among physicians. Further, ADR is essential to recommended intervals2 between screening and surveillance examinations.2,3
1. Variables influencing ADR. CMS explained that the measure does not account for variables that may influence the ADR such as geographic location, socioeconomic status of patient population, community compliance of screening, etc. The agency further states that according to the risk factors outlined by the American Cancer Society, African Americans have the highest colorectal cancer incidence and mortality rates of all racial groups in the United States. “In addition, dietary factors, such as consumption of highly processed meats will contribute to an increased risk of colorectal cancer. This diet is more prevalent in lower socioeconomic areas, which could influence the outcome of the measure. There are other patient factors like education, health literacy, etc. that might also affect things like the adequacy of bowel preparation, which in turn could affect performance.”
The societies advised CMS that this rationale reflects a misunderstanding of the definition of ADR, which includes all average-risk patients in whom the physician finds at least one adenoma. Further, ADR only includes colonoscopies with adequate bowel preparation and complete examinations. Studies demonstrate that ADR is not influenced by socioeconomic status and sex mix of the provider’s patient population, or by the rate of screening in the community.
Socioeconomics, ethnicity, and diet are not relevant factors of ADR. That said, our societies welcome the opportunity to work with CMS on creating age and sex standardized ADRs for the U.S. population, if feasible, in order to capture information that CMS deems important.
2. Failure to detect all adenomas. CMS stated that the measure does not account for MIPS eligible clinicians that fail to detect adenomas but may score higher based on the patient population.
The societies pushed back with CMS explaining that this rationale again reflects a misunderstanding of the definition of ADR, which includes average-risk patients for whom the physician finds at least one adenoma. Colonoscopy is heavily operator dependent. In an average-risk, mixed population, the variability in ADR reflects quality of the provider’s endoscopic skills and pathology recognition, rather than the risk of the underlying population.
3. Incidence measure. CMS concluded that Measure 343: Screening Colonoscopy Adenoma Detection Rate is considered an “incidence measure” that does not assess the quality of the care provided. In essence, according to CMS, the measure is based on happenstance rather than the eligible clinician providing a thorough examination.
The societies strongly disagreed with this characterization of ADR. Measure 343: Screening Colonoscopy Adenoma Detection Rate is the only measure that assess the quality of the exam performed by the physician in an average-risk patient with an adequate bowel preparation. Physicians can improve their adenoma detection rate by paying attention to detail, spending more time looking for adenomas, and learning better techniques.
4. Benchmarking. CMS stated that because of the measure construct, benchmarks calculated from this measure are misrepresented and do not align with the MIPS scoring methodology where 100% indicates better clinical care or control. Guidelines and supplemental literature support a performance target for adenoma detection rate of 25% for a mixed sex population (20% in women and 30% in men). CMS determined that Measure 343: Screening Colonoscopy Adenoma Detection Rate may be appropriate for other programs but does not align with the scoring logic within MIPS. When this measure was introduced, according to the agency, it was under the legacy program, Physician Quality Reporting System (PQRS), a pay-for-reporting program that does not have the same scoring implications as MIPS.
The societies reminded CMS that the 25% is the minimum requirement for performance and is not a benchmark. This minimum requirement continues to increase as well. With 25% being the threshold, for every 1% increase in ADR the risk of fatal interval colon cancer decreases by 3%. In one important study by Corley et al, the lowest quintile of ADR was 19% or lower, and was associated with the highest risk of interval colon cancer.4
CMS must begin to move beyond traditional approaches toward benchmarking performance where 100% compliance is expected. It was encouraging to see CMS acknowledge that nuances to evaluating scores are needed based on the ability of a measure to accurately identify and capture performance based on the patient population and measure specifications. For example, these adjustments were finalized for the blood pressure and diabetes HbA1c measures, where the highest number of points will be achieved for anyone scoring 90% or higher. This modification was based on the knowledge that it is not realistic nor in the interest of patients to assume that clinicians will be able to achieve the desired targeted outcome for every patient. The potential for unintended consequences was factored into an assessment of what performance could be considered achievable.
In our view, ADR is a similar example where 100% performance across a clinician’s population of patients is biologically impossible since not every individual who receives a screening colonoscopy will have an adenoma detected. ADR is the best-established colorectal neoplasia-related quality indicator and research demonstrates that high rates are associated with significant reductions in colorectal cancer risk.
CMS must continue to explore alternative strategies toward benchmarking in MIPS to ensure that achievement is fairly assessed, and top performance scores are determined not solely based on peer performance but also based on clinical evidence balanced with minimizing unintended consequences. The MIPS program and its benchmarking and scoring methodologies must continue to innovate to ensure that physicians provide the best possible care to their patients while also accurately and fairly representing and rewarding clinicians’ performance. Continuing to promote a siloed view toward quality will only reduce the relevance of the MIPS program and lead our members to question the integrity and validity of the program.
5. Lack of alignment between cost and quality measures. CMS noted that the agency will consider the relationship between cost and quality, viewing it as an essential component of episode-based measures. Our societies agree that a value-based payment system must balance cost and quality, and as such, members of our societies have been highly engaged in the development of episode-based cost measures as part of episode group prioritization for development, CMS’ measure development contractor asked clinical subcommittee members to consider a measure’s potential for alignment with established quality measures. This includes consideration of whether there is potential for overlap in covering the same patient cohort and the dimensions of care that the quality measure would be capturing in relation to a procedure or condition on which the episode-based cost measure would be focused.
The societies believe that given the well-established role of ADR in gastroenterology practices’ quality improvement programs nationwide, and internationally, the introduction of the Screening/Surveillance Colonoscopy episode-based cost measure beginning in the 2019 performance year, and the proposal from CMS to introduce “MIPS Value Pathways” beginning with the 2021 performance year, the removal of Measure 343: Screening Colonoscopy Adenoma Detection Rate undermines the collective desire of CMS and our organizations to move toward aligned reporting of quality and cost measures relevant to a gastroenterologist’s scope of practice and meaningful to patient care.
6. Development of a new measure. CMS suggested that there is the need for an alternate measure, however, the agency does not agree that Measure 343: Screening Colonoscopy Adenoma Detection Rate should be maintained in the interim.
Our societies welcomed the opportunity to work with CMS on developing a revised version for quality reporting purposes. We also welcomed the opportunity to suggest specific changes with CMS staff to further our shared goal on improving quality reporting and patient care. However, as of now, ADR remains the only validated, relevant, outcome-based measure to evaluate gastroenterologists’ endoscopic quality. It is important that the measure be maintained in the QPP in the interim.
The importance of ADR lies in its association with long-term outcomes. Corley et al. published in the New England Journal of Medicine an examination of the association between adenoma detection rate and risks of subsequent colorectal cancer and death among 264,792 colonoscopies by 136 gastroenterologists. Patients were followed from their baseline examinations for either 10 years or until another colonoscopy with negative results, left the health care system, or were diagnosed with colorectal cancer. There was a 3% reduction in colorectal cancer incidence and a 5% reduction in cancer mortality for each 1% increase in adenoma detection rate. This observation remained for both proximal and distal cancer in both men and women.4 Kaminski et al published a study on the association between adenoma detection rate and interval cancer in Gastroenterology of 294 endoscopists and data on 146,860 colonoscopies that reviewed 895,916 person-years of follow-up evaluation through the National Cancer Registry. The study concluded that there is an association between increased adenoma detection rate and reduced risk of interval cancer and death.5
The focus of any quality improvement program relative to colorectal cancer screening is to reduce colorectal cancer incidence and deaths. As discussed, the literature clearly supports driving improvement in each gastroenterologist’s ADR as the mechanism to achieve these outcomes. Indeed, the first step in any gastroenterology practice’s quality improvement program relative to CRC screening is to measure the endoscopist’s ADR and report to it to the physician, ideally benchmarked against a group or national study. Best practice is to measure and report ADR quarterly. There are a variety of well-established and emerging techniques6-11 technologies,12 and education,13,14 with varying associated cost and effort that can be deployed as systemic interventions aimed at improving adenoma detection rate. The effect of multiple interventions over time aimed at improving ADR has demonstrated increased ADRs with notable increases in the identification of difficult to identify colorectal cancer precursors (i.e., sessile serrated adenomas) and advanced adenomas.15 While the landscape of gastroenterology is changing, the constant is the importance of measuring an endoscopist’s ADR. ADR is fundamental to training and definitions of competency for gastroenterologists.
CMS appears to have listened to the concerns brought to their attention and has been willing to have external discussions with the GI societies in an effort to placate some of these concerns. Over the next several months we will explain the current progress with CMS including reinstating a modified ADR measure as a non-MIPS measure available for reporting in a QCDR. We will also discuss what you can do as a gastroenterologist to help propel some of these efforts forward.
References
1. Kaminski MF, Regula J, et al. Quality indicators for colonoscopy and the risk of interval cancer. N Engl J Med. 2010;362(19):1795-803.
2. Lieberman DA, Rex DK, Winawer SJ, et al. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012;143:844-57.
3. Rubin CE, Haggitt RC, Burmer GC, et al. DNA aneuploidy in colonic biopsies predicts future development of dysplasia in ulcerative colitis. Gastroenterology. 1992;103:1611-20.
4. Corley D, Jensen CD, Marks AR, et al. Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med. 2014;370:1298-306.
5. Kaminski MF, et al. Increased rate of adenoma detection associates with reduced risk of colorectal cancer and death. Gastroenterology. 2017 Jul;153[1]:98-105. doi: 10.1053/j.gastro.2017.04.006. Epub 2017 Apr 17.
6. ASGE practice guideline: Measuring the quality of endoscopy. Gastrointest Endosc. 2006;58:S1-S38.
7. Rex DK. Colonoscopic withdrawal technique is associated with adenoma miss rate. Gastrointest Endosc. 2000;51:33-6.
8. Barclay RL, et al. Effect of a time-dependent colonoscopic withdrawal protocol on adenoma detection during screening colonoscopy. Clin Gastroenterol Hepatol. 2008;6:1091-8.
9. Shaukat A, et al. Longer withdrawal time is associated with a reduced incidence of interval cancer after screening colonoscopy. Gastroenterology. 2015 Oct;149[4]:952-7
10. Lee S, et al. Am J Gastroenterol. 2016 Jan;111(1):63-9.
11. Jia H, et al. Water exchange method significantly improves adenoma detection rate: A multicenter, randomized controlled trial. Am J Gastroenterol. 2017;112(4):568-76.
12. ASGE. Endoscopes and devices to improve colon polyp detection. GIE 2015;81:1122-9.
13. Ussui V, et al. Am J Gastroenterol. 2015;110:489-96.
14. Kaminski MF, et al. Leadership training to improve adenoma detection rate in screening colonoscopy: a randomized trial. Gut 2016;65:616-24.
15. Shaukat A, et al. Rates of detection of adenoma, sessile serrated adenoma, and advanced adenoma are stable over time and modifiable. Gastroenterology 2018(Feb);156:816-7.
Dr. Adams is a gastroenterologist and assistant professor at the University of Michigan, Ann Arbor; Dr. Leiman is a gastroenterologist and assistant professor of medicine at Duke Health, Durham, N.C.; Dr. Mathews is a gastroenterologist and leader of Clinical Innovation at the Johns Hopkins Armstrong Institute for Patient Safety and Quality, Baltimore.
Every year, the Centers for Medicare & Medicaid Services (CMS) releases their proposed recommendations for the next performance year and in 2019, the gastroenterology community was surprised that CMS recommended removal of QPP 0343 – Screening Colonoscopy Adenoma Detection Rate from a reportable measure in the Quality Payment Program. So what happened? Why was the measure removed from the QPP? Is there anything that we can do?
Over the next several months we will be publishing a series of articles related to the Adenoma Detection Rate Measure to give every gastroenterologist an inside look at the work that is done on your behalf and steps that you can take in the future to help your fellow gastroenterologists.
This current article explains the joint effort made by all GI societies to try to save the Adenoma Detection Rate measure from removal from the 2020 Quality Payment Program. All societies uniformly submitted a letter to CMS in disapproval of the recommendation and outlined the importance of this measure as follows:
Measure 343: Screening Colonoscopy Adenoma Detection Rate
Our societies are disappointed and disagree with CMS’s decision to remove Measure 343: Screening Colonoscopy Adenoma Detection Rate (ADR) from the Quality Payment Program (QPP) beginning with the 2020 performance year.
The ADR plays a central role in quality improvement and colorectal cancer screening. We urge CMS to reconsider this decision and issue a technical correction to reinstate the measure back into the QPP, as it is the only outcome measure specific to endoscopic skills of gastroenterologists currently available for public reporting.
Studies show that high adenoma detection rates are associated with a significant reduction in colorectal cancer risk.1 Virtually all studies on this subject have demonstrated that there is, in fact, marked variation in adenoma detection rates among physicians. Further, ADR is essential to recommended intervals2 between screening and surveillance examinations.2,3
1. Variables influencing ADR. CMS explained that the measure does not account for variables that may influence the ADR such as geographic location, socioeconomic status of patient population, community compliance of screening, etc. The agency further states that according to the risk factors outlined by the American Cancer Society, African Americans have the highest colorectal cancer incidence and mortality rates of all racial groups in the United States. “In addition, dietary factors, such as consumption of highly processed meats will contribute to an increased risk of colorectal cancer. This diet is more prevalent in lower socioeconomic areas, which could influence the outcome of the measure. There are other patient factors like education, health literacy, etc. that might also affect things like the adequacy of bowel preparation, which in turn could affect performance.”
The societies advised CMS that this rationale reflects a misunderstanding of the definition of ADR, which includes all average-risk patients in whom the physician finds at least one adenoma. Further, ADR only includes colonoscopies with adequate bowel preparation and complete examinations. Studies demonstrate that ADR is not influenced by socioeconomic status and sex mix of the provider’s patient population, or by the rate of screening in the community.
Socioeconomics, ethnicity, and diet are not relevant factors of ADR. That said, our societies welcome the opportunity to work with CMS on creating age and sex standardized ADRs for the U.S. population, if feasible, in order to capture information that CMS deems important.
2. Failure to detect all adenomas. CMS stated that the measure does not account for MIPS eligible clinicians that fail to detect adenomas but may score higher based on the patient population.
The societies pushed back with CMS explaining that this rationale again reflects a misunderstanding of the definition of ADR, which includes average-risk patients for whom the physician finds at least one adenoma. Colonoscopy is heavily operator dependent. In an average-risk, mixed population, the variability in ADR reflects quality of the provider’s endoscopic skills and pathology recognition, rather than the risk of the underlying population.
3. Incidence measure. CMS concluded that Measure 343: Screening Colonoscopy Adenoma Detection Rate is considered an “incidence measure” that does not assess the quality of the care provided. In essence, according to CMS, the measure is based on happenstance rather than the eligible clinician providing a thorough examination.
The societies strongly disagreed with this characterization of ADR. Measure 343: Screening Colonoscopy Adenoma Detection Rate is the only measure that assess the quality of the exam performed by the physician in an average-risk patient with an adequate bowel preparation. Physicians can improve their adenoma detection rate by paying attention to detail, spending more time looking for adenomas, and learning better techniques.
4. Benchmarking. CMS stated that because of the measure construct, benchmarks calculated from this measure are misrepresented and do not align with the MIPS scoring methodology where 100% indicates better clinical care or control. Guidelines and supplemental literature support a performance target for adenoma detection rate of 25% for a mixed sex population (20% in women and 30% in men). CMS determined that Measure 343: Screening Colonoscopy Adenoma Detection Rate may be appropriate for other programs but does not align with the scoring logic within MIPS. When this measure was introduced, according to the agency, it was under the legacy program, Physician Quality Reporting System (PQRS), a pay-for-reporting program that does not have the same scoring implications as MIPS.
The societies reminded CMS that the 25% is the minimum requirement for performance and is not a benchmark. This minimum requirement continues to increase as well. With 25% being the threshold, for every 1% increase in ADR the risk of fatal interval colon cancer decreases by 3%. In one important study by Corley et al, the lowest quintile of ADR was 19% or lower, and was associated with the highest risk of interval colon cancer.4
CMS must begin to move beyond traditional approaches toward benchmarking performance where 100% compliance is expected. It was encouraging to see CMS acknowledge that nuances to evaluating scores are needed based on the ability of a measure to accurately identify and capture performance based on the patient population and measure specifications. For example, these adjustments were finalized for the blood pressure and diabetes HbA1c measures, where the highest number of points will be achieved for anyone scoring 90% or higher. This modification was based on the knowledge that it is not realistic nor in the interest of patients to assume that clinicians will be able to achieve the desired targeted outcome for every patient. The potential for unintended consequences was factored into an assessment of what performance could be considered achievable.
In our view, ADR is a similar example where 100% performance across a clinician’s population of patients is biologically impossible since not every individual who receives a screening colonoscopy will have an adenoma detected. ADR is the best-established colorectal neoplasia-related quality indicator and research demonstrates that high rates are associated with significant reductions in colorectal cancer risk.
CMS must continue to explore alternative strategies toward benchmarking in MIPS to ensure that achievement is fairly assessed, and top performance scores are determined not solely based on peer performance but also based on clinical evidence balanced with minimizing unintended consequences. The MIPS program and its benchmarking and scoring methodologies must continue to innovate to ensure that physicians provide the best possible care to their patients while also accurately and fairly representing and rewarding clinicians’ performance. Continuing to promote a siloed view toward quality will only reduce the relevance of the MIPS program and lead our members to question the integrity and validity of the program.
5. Lack of alignment between cost and quality measures. CMS noted that the agency will consider the relationship between cost and quality, viewing it as an essential component of episode-based measures. Our societies agree that a value-based payment system must balance cost and quality, and as such, members of our societies have been highly engaged in the development of episode-based cost measures as part of episode group prioritization for development, CMS’ measure development contractor asked clinical subcommittee members to consider a measure’s potential for alignment with established quality measures. This includes consideration of whether there is potential for overlap in covering the same patient cohort and the dimensions of care that the quality measure would be capturing in relation to a procedure or condition on which the episode-based cost measure would be focused.
The societies believe that given the well-established role of ADR in gastroenterology practices’ quality improvement programs nationwide, and internationally, the introduction of the Screening/Surveillance Colonoscopy episode-based cost measure beginning in the 2019 performance year, and the proposal from CMS to introduce “MIPS Value Pathways” beginning with the 2021 performance year, the removal of Measure 343: Screening Colonoscopy Adenoma Detection Rate undermines the collective desire of CMS and our organizations to move toward aligned reporting of quality and cost measures relevant to a gastroenterologist’s scope of practice and meaningful to patient care.
6. Development of a new measure. CMS suggested that there is the need for an alternate measure, however, the agency does not agree that Measure 343: Screening Colonoscopy Adenoma Detection Rate should be maintained in the interim.
Our societies welcomed the opportunity to work with CMS on developing a revised version for quality reporting purposes. We also welcomed the opportunity to suggest specific changes with CMS staff to further our shared goal on improving quality reporting and patient care. However, as of now, ADR remains the only validated, relevant, outcome-based measure to evaluate gastroenterologists’ endoscopic quality. It is important that the measure be maintained in the QPP in the interim.
The importance of ADR lies in its association with long-term outcomes. Corley et al. published in the New England Journal of Medicine an examination of the association between adenoma detection rate and risks of subsequent colorectal cancer and death among 264,792 colonoscopies by 136 gastroenterologists. Patients were followed from their baseline examinations for either 10 years or until another colonoscopy with negative results, left the health care system, or were diagnosed with colorectal cancer. There was a 3% reduction in colorectal cancer incidence and a 5% reduction in cancer mortality for each 1% increase in adenoma detection rate. This observation remained for both proximal and distal cancer in both men and women.4 Kaminski et al published a study on the association between adenoma detection rate and interval cancer in Gastroenterology of 294 endoscopists and data on 146,860 colonoscopies that reviewed 895,916 person-years of follow-up evaluation through the National Cancer Registry. The study concluded that there is an association between increased adenoma detection rate and reduced risk of interval cancer and death.5
The focus of any quality improvement program relative to colorectal cancer screening is to reduce colorectal cancer incidence and deaths. As discussed, the literature clearly supports driving improvement in each gastroenterologist’s ADR as the mechanism to achieve these outcomes. Indeed, the first step in any gastroenterology practice’s quality improvement program relative to CRC screening is to measure the endoscopist’s ADR and report to it to the physician, ideally benchmarked against a group or national study. Best practice is to measure and report ADR quarterly. There are a variety of well-established and emerging techniques6-11 technologies,12 and education,13,14 with varying associated cost and effort that can be deployed as systemic interventions aimed at improving adenoma detection rate. The effect of multiple interventions over time aimed at improving ADR has demonstrated increased ADRs with notable increases in the identification of difficult to identify colorectal cancer precursors (i.e., sessile serrated adenomas) and advanced adenomas.15 While the landscape of gastroenterology is changing, the constant is the importance of measuring an endoscopist’s ADR. ADR is fundamental to training and definitions of competency for gastroenterologists.
CMS appears to have listened to the concerns brought to their attention and has been willing to have external discussions with the GI societies in an effort to placate some of these concerns. Over the next several months we will explain the current progress with CMS including reinstating a modified ADR measure as a non-MIPS measure available for reporting in a QCDR. We will also discuss what you can do as a gastroenterologist to help propel some of these efforts forward.
References
1. Kaminski MF, Regula J, et al. Quality indicators for colonoscopy and the risk of interval cancer. N Engl J Med. 2010;362(19):1795-803.
2. Lieberman DA, Rex DK, Winawer SJ, et al. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012;143:844-57.
3. Rubin CE, Haggitt RC, Burmer GC, et al. DNA aneuploidy in colonic biopsies predicts future development of dysplasia in ulcerative colitis. Gastroenterology. 1992;103:1611-20.
4. Corley D, Jensen CD, Marks AR, et al. Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med. 2014;370:1298-306.
5. Kaminski MF, et al. Increased rate of adenoma detection associates with reduced risk of colorectal cancer and death. Gastroenterology. 2017 Jul;153[1]:98-105. doi: 10.1053/j.gastro.2017.04.006. Epub 2017 Apr 17.
6. ASGE practice guideline: Measuring the quality of endoscopy. Gastrointest Endosc. 2006;58:S1-S38.
7. Rex DK. Colonoscopic withdrawal technique is associated with adenoma miss rate. Gastrointest Endosc. 2000;51:33-6.
8. Barclay RL, et al. Effect of a time-dependent colonoscopic withdrawal protocol on adenoma detection during screening colonoscopy. Clin Gastroenterol Hepatol. 2008;6:1091-8.
9. Shaukat A, et al. Longer withdrawal time is associated with a reduced incidence of interval cancer after screening colonoscopy. Gastroenterology. 2015 Oct;149[4]:952-7
10. Lee S, et al. Am J Gastroenterol. 2016 Jan;111(1):63-9.
11. Jia H, et al. Water exchange method significantly improves adenoma detection rate: A multicenter, randomized controlled trial. Am J Gastroenterol. 2017;112(4):568-76.
12. ASGE. Endoscopes and devices to improve colon polyp detection. GIE 2015;81:1122-9.
13. Ussui V, et al. Am J Gastroenterol. 2015;110:489-96.
14. Kaminski MF, et al. Leadership training to improve adenoma detection rate in screening colonoscopy: a randomized trial. Gut 2016;65:616-24.
15. Shaukat A, et al. Rates of detection of adenoma, sessile serrated adenoma, and advanced adenoma are stable over time and modifiable. Gastroenterology 2018(Feb);156:816-7.
Dr. Adams is a gastroenterologist and assistant professor at the University of Michigan, Ann Arbor; Dr. Leiman is a gastroenterologist and assistant professor of medicine at Duke Health, Durham, N.C.; Dr. Mathews is a gastroenterologist and leader of Clinical Innovation at the Johns Hopkins Armstrong Institute for Patient Safety and Quality, Baltimore.
Every year, the Centers for Medicare & Medicaid Services (CMS) releases their proposed recommendations for the next performance year and in 2019, the gastroenterology community was surprised that CMS recommended removal of QPP 0343 – Screening Colonoscopy Adenoma Detection Rate from a reportable measure in the Quality Payment Program. So what happened? Why was the measure removed from the QPP? Is there anything that we can do?
Over the next several months we will be publishing a series of articles related to the Adenoma Detection Rate Measure to give every gastroenterologist an inside look at the work that is done on your behalf and steps that you can take in the future to help your fellow gastroenterologists.
This current article explains the joint effort made by all GI societies to try to save the Adenoma Detection Rate measure from removal from the 2020 Quality Payment Program. All societies uniformly submitted a letter to CMS in disapproval of the recommendation and outlined the importance of this measure as follows:
Measure 343: Screening Colonoscopy Adenoma Detection Rate
Our societies are disappointed and disagree with CMS’s decision to remove Measure 343: Screening Colonoscopy Adenoma Detection Rate (ADR) from the Quality Payment Program (QPP) beginning with the 2020 performance year.
The ADR plays a central role in quality improvement and colorectal cancer screening. We urge CMS to reconsider this decision and issue a technical correction to reinstate the measure back into the QPP, as it is the only outcome measure specific to endoscopic skills of gastroenterologists currently available for public reporting.
Studies show that high adenoma detection rates are associated with a significant reduction in colorectal cancer risk.1 Virtually all studies on this subject have demonstrated that there is, in fact, marked variation in adenoma detection rates among physicians. Further, ADR is essential to recommended intervals2 between screening and surveillance examinations.2,3
1. Variables influencing ADR. CMS explained that the measure does not account for variables that may influence the ADR such as geographic location, socioeconomic status of patient population, community compliance of screening, etc. The agency further states that according to the risk factors outlined by the American Cancer Society, African Americans have the highest colorectal cancer incidence and mortality rates of all racial groups in the United States. “In addition, dietary factors, such as consumption of highly processed meats will contribute to an increased risk of colorectal cancer. This diet is more prevalent in lower socioeconomic areas, which could influence the outcome of the measure. There are other patient factors like education, health literacy, etc. that might also affect things like the adequacy of bowel preparation, which in turn could affect performance.”
The societies advised CMS that this rationale reflects a misunderstanding of the definition of ADR, which includes all average-risk patients in whom the physician finds at least one adenoma. Further, ADR only includes colonoscopies with adequate bowel preparation and complete examinations. Studies demonstrate that ADR is not influenced by socioeconomic status and sex mix of the provider’s patient population, or by the rate of screening in the community.
Socioeconomics, ethnicity, and diet are not relevant factors of ADR. That said, our societies welcome the opportunity to work with CMS on creating age and sex standardized ADRs for the U.S. population, if feasible, in order to capture information that CMS deems important.
2. Failure to detect all adenomas. CMS stated that the measure does not account for MIPS eligible clinicians that fail to detect adenomas but may score higher based on the patient population.
The societies pushed back with CMS explaining that this rationale again reflects a misunderstanding of the definition of ADR, which includes average-risk patients for whom the physician finds at least one adenoma. Colonoscopy is heavily operator dependent. In an average-risk, mixed population, the variability in ADR reflects quality of the provider’s endoscopic skills and pathology recognition, rather than the risk of the underlying population.
3. Incidence measure. CMS concluded that Measure 343: Screening Colonoscopy Adenoma Detection Rate is considered an “incidence measure” that does not assess the quality of the care provided. In essence, according to CMS, the measure is based on happenstance rather than the eligible clinician providing a thorough examination.
The societies strongly disagreed with this characterization of ADR. Measure 343: Screening Colonoscopy Adenoma Detection Rate is the only measure that assess the quality of the exam performed by the physician in an average-risk patient with an adequate bowel preparation. Physicians can improve their adenoma detection rate by paying attention to detail, spending more time looking for adenomas, and learning better techniques.
4. Benchmarking. CMS stated that because of the measure construct, benchmarks calculated from this measure are misrepresented and do not align with the MIPS scoring methodology where 100% indicates better clinical care or control. Guidelines and supplemental literature support a performance target for adenoma detection rate of 25% for a mixed sex population (20% in women and 30% in men). CMS determined that Measure 343: Screening Colonoscopy Adenoma Detection Rate may be appropriate for other programs but does not align with the scoring logic within MIPS. When this measure was introduced, according to the agency, it was under the legacy program, Physician Quality Reporting System (PQRS), a pay-for-reporting program that does not have the same scoring implications as MIPS.
The societies reminded CMS that the 25% is the minimum requirement for performance and is not a benchmark. This minimum requirement continues to increase as well. With 25% being the threshold, for every 1% increase in ADR the risk of fatal interval colon cancer decreases by 3%. In one important study by Corley et al, the lowest quintile of ADR was 19% or lower, and was associated with the highest risk of interval colon cancer.4
CMS must begin to move beyond traditional approaches toward benchmarking performance where 100% compliance is expected. It was encouraging to see CMS acknowledge that nuances to evaluating scores are needed based on the ability of a measure to accurately identify and capture performance based on the patient population and measure specifications. For example, these adjustments were finalized for the blood pressure and diabetes HbA1c measures, where the highest number of points will be achieved for anyone scoring 90% or higher. This modification was based on the knowledge that it is not realistic nor in the interest of patients to assume that clinicians will be able to achieve the desired targeted outcome for every patient. The potential for unintended consequences was factored into an assessment of what performance could be considered achievable.
In our view, ADR is a similar example where 100% performance across a clinician’s population of patients is biologically impossible since not every individual who receives a screening colonoscopy will have an adenoma detected. ADR is the best-established colorectal neoplasia-related quality indicator and research demonstrates that high rates are associated with significant reductions in colorectal cancer risk.
CMS must continue to explore alternative strategies toward benchmarking in MIPS to ensure that achievement is fairly assessed, and top performance scores are determined not solely based on peer performance but also based on clinical evidence balanced with minimizing unintended consequences. The MIPS program and its benchmarking and scoring methodologies must continue to innovate to ensure that physicians provide the best possible care to their patients while also accurately and fairly representing and rewarding clinicians’ performance. Continuing to promote a siloed view toward quality will only reduce the relevance of the MIPS program and lead our members to question the integrity and validity of the program.
5. Lack of alignment between cost and quality measures. CMS noted that the agency will consider the relationship between cost and quality, viewing it as an essential component of episode-based measures. Our societies agree that a value-based payment system must balance cost and quality, and as such, members of our societies have been highly engaged in the development of episode-based cost measures as part of episode group prioritization for development, CMS’ measure development contractor asked clinical subcommittee members to consider a measure’s potential for alignment with established quality measures. This includes consideration of whether there is potential for overlap in covering the same patient cohort and the dimensions of care that the quality measure would be capturing in relation to a procedure or condition on which the episode-based cost measure would be focused.
The societies believe that given the well-established role of ADR in gastroenterology practices’ quality improvement programs nationwide, and internationally, the introduction of the Screening/Surveillance Colonoscopy episode-based cost measure beginning in the 2019 performance year, and the proposal from CMS to introduce “MIPS Value Pathways” beginning with the 2021 performance year, the removal of Measure 343: Screening Colonoscopy Adenoma Detection Rate undermines the collective desire of CMS and our organizations to move toward aligned reporting of quality and cost measures relevant to a gastroenterologist’s scope of practice and meaningful to patient care.
6. Development of a new measure. CMS suggested that there is the need for an alternate measure, however, the agency does not agree that Measure 343: Screening Colonoscopy Adenoma Detection Rate should be maintained in the interim.
Our societies welcomed the opportunity to work with CMS on developing a revised version for quality reporting purposes. We also welcomed the opportunity to suggest specific changes with CMS staff to further our shared goal on improving quality reporting and patient care. However, as of now, ADR remains the only validated, relevant, outcome-based measure to evaluate gastroenterologists’ endoscopic quality. It is important that the measure be maintained in the QPP in the interim.
The importance of ADR lies in its association with long-term outcomes. Corley et al. published in the New England Journal of Medicine an examination of the association between adenoma detection rate and risks of subsequent colorectal cancer and death among 264,792 colonoscopies by 136 gastroenterologists. Patients were followed from their baseline examinations for either 10 years or until another colonoscopy with negative results, left the health care system, or were diagnosed with colorectal cancer. There was a 3% reduction in colorectal cancer incidence and a 5% reduction in cancer mortality for each 1% increase in adenoma detection rate. This observation remained for both proximal and distal cancer in both men and women.4 Kaminski et al published a study on the association between adenoma detection rate and interval cancer in Gastroenterology of 294 endoscopists and data on 146,860 colonoscopies that reviewed 895,916 person-years of follow-up evaluation through the National Cancer Registry. The study concluded that there is an association between increased adenoma detection rate and reduced risk of interval cancer and death.5
The focus of any quality improvement program relative to colorectal cancer screening is to reduce colorectal cancer incidence and deaths. As discussed, the literature clearly supports driving improvement in each gastroenterologist’s ADR as the mechanism to achieve these outcomes. Indeed, the first step in any gastroenterology practice’s quality improvement program relative to CRC screening is to measure the endoscopist’s ADR and report to it to the physician, ideally benchmarked against a group or national study. Best practice is to measure and report ADR quarterly. There are a variety of well-established and emerging techniques6-11 technologies,12 and education,13,14 with varying associated cost and effort that can be deployed as systemic interventions aimed at improving adenoma detection rate. The effect of multiple interventions over time aimed at improving ADR has demonstrated increased ADRs with notable increases in the identification of difficult to identify colorectal cancer precursors (i.e., sessile serrated adenomas) and advanced adenomas.15 While the landscape of gastroenterology is changing, the constant is the importance of measuring an endoscopist’s ADR. ADR is fundamental to training and definitions of competency for gastroenterologists.
CMS appears to have listened to the concerns brought to their attention and has been willing to have external discussions with the GI societies in an effort to placate some of these concerns. Over the next several months we will explain the current progress with CMS including reinstating a modified ADR measure as a non-MIPS measure available for reporting in a QCDR. We will also discuss what you can do as a gastroenterologist to help propel some of these efforts forward.
References
1. Kaminski MF, Regula J, et al. Quality indicators for colonoscopy and the risk of interval cancer. N Engl J Med. 2010;362(19):1795-803.
2. Lieberman DA, Rex DK, Winawer SJ, et al. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012;143:844-57.
3. Rubin CE, Haggitt RC, Burmer GC, et al. DNA aneuploidy in colonic biopsies predicts future development of dysplasia in ulcerative colitis. Gastroenterology. 1992;103:1611-20.
4. Corley D, Jensen CD, Marks AR, et al. Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med. 2014;370:1298-306.
5. Kaminski MF, et al. Increased rate of adenoma detection associates with reduced risk of colorectal cancer and death. Gastroenterology. 2017 Jul;153[1]:98-105. doi: 10.1053/j.gastro.2017.04.006. Epub 2017 Apr 17.
6. ASGE practice guideline: Measuring the quality of endoscopy. Gastrointest Endosc. 2006;58:S1-S38.
7. Rex DK. Colonoscopic withdrawal technique is associated with adenoma miss rate. Gastrointest Endosc. 2000;51:33-6.
8. Barclay RL, et al. Effect of a time-dependent colonoscopic withdrawal protocol on adenoma detection during screening colonoscopy. Clin Gastroenterol Hepatol. 2008;6:1091-8.
9. Shaukat A, et al. Longer withdrawal time is associated with a reduced incidence of interval cancer after screening colonoscopy. Gastroenterology. 2015 Oct;149[4]:952-7
10. Lee S, et al. Am J Gastroenterol. 2016 Jan;111(1):63-9.
11. Jia H, et al. Water exchange method significantly improves adenoma detection rate: A multicenter, randomized controlled trial. Am J Gastroenterol. 2017;112(4):568-76.
12. ASGE. Endoscopes and devices to improve colon polyp detection. GIE 2015;81:1122-9.
13. Ussui V, et al. Am J Gastroenterol. 2015;110:489-96.
14. Kaminski MF, et al. Leadership training to improve adenoma detection rate in screening colonoscopy: a randomized trial. Gut 2016;65:616-24.
15. Shaukat A, et al. Rates of detection of adenoma, sessile serrated adenoma, and advanced adenoma are stable over time and modifiable. Gastroenterology 2018(Feb);156:816-7.
Dr. Adams is a gastroenterologist and assistant professor at the University of Michigan, Ann Arbor; Dr. Leiman is a gastroenterologist and assistant professor of medicine at Duke Health, Durham, N.C.; Dr. Mathews is a gastroenterologist and leader of Clinical Innovation at the Johns Hopkins Armstrong Institute for Patient Safety and Quality, Baltimore.
The power and promise of person-generated health data (Part II)
In Part I of our discussion we introduced the concept of person-generated health data (PGHD), defined as wellness and/or health-related data created, recorded, or gathered by individuals.

Such rich, longitudinal information is now being used in combination with traditional clinical information to predict, diagnose, and formulate treatment plans for diseases, as well as understand the safety and effectiveness of medical interventions.
Identifying a disease early
One novel example of digital technologies being used for early identification of disease was a promising 2019 study by Eli Lilly (in collaboration with Apple and Evidation Health) called the Lilly Exploratory Digital Assessment Study.
In this study, the feasibility of using PGHD for identifying physiological and behavioral signatures of cognitive impairment was examined for the purpose of seeking new methods to detect mild cognitive impairment (MCI) in a timely and cost-effective manner. The study enrolled 31 study participants with cognitive impairment and 82 without cognitive impairment. It used consumer-grade sensor technologies (the iPhone, Apple Watch, iPad, and Beddit sleep monitor) to continuously and unobtrusively collect data. Among the information the researchers collected were interaction with the phone keyboard, accelerometer data from the Apple Watch, volume of messages sent/received, and sleep cycles.1
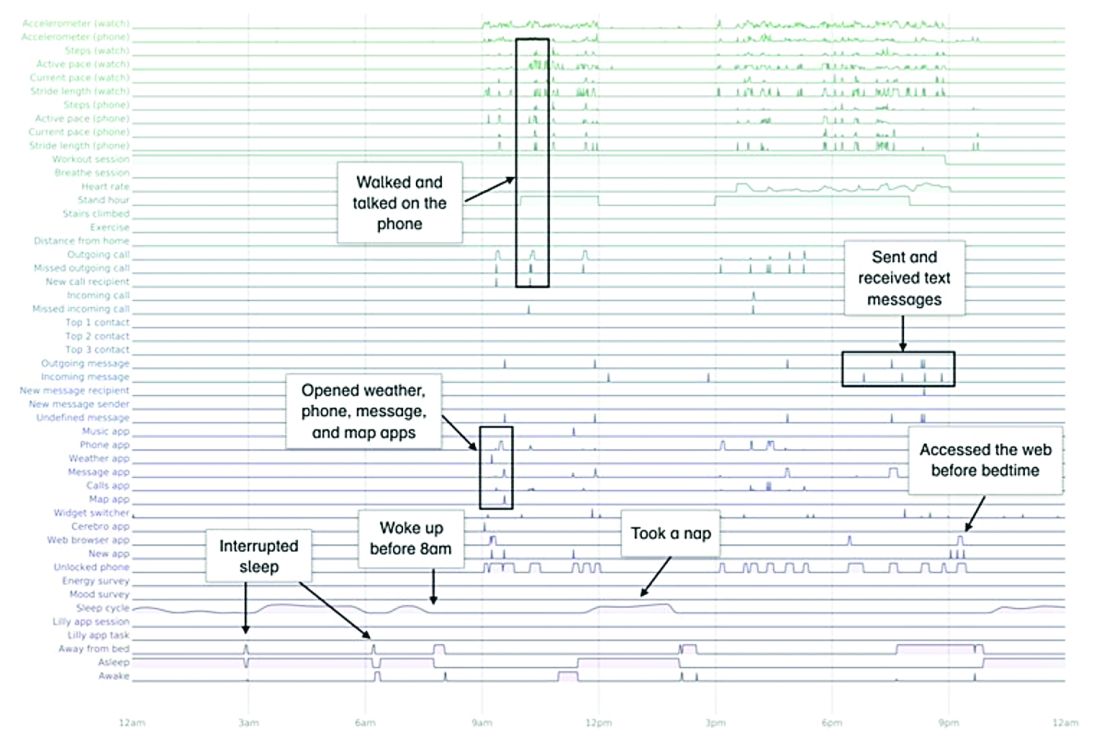
A total of 16 terabytes of data were collected over the course of 12 weeks. Data were organized into a behaviorgram (See Figure 1) that gives a holistic picture of a day in a patient’s life. A machine learning model was used to distinguish between behaviorgrams of symptomatic versus healthy controls, identifying typing speed, circadian rhythm shifts, and reliance on helper apps, among other things, as differentiating cognitively impaired from healthy controls. These behaviorgrams may someday serve as “fingerprints” of different diseases, with specific diseases displaying predictable patterns. In the near future, digital measures like the ones investigated in this study are likely to be used to help clinicians predict and diagnose disease, as well as to better understand disease progression and treatment response.
Leading to better health outcomes

The potential of PGHD to detect diseases early and lead to better health outcomes is being investigated in the Heartline study, a collaboration between Johnson & Johnson and Apple, which is supported by Evidation.2
This study aims to enroll 150,000 adults age 65 years and over to analyze the impact of Apple Watch–based early detection of irregular heart rhythms consistent with atrial fibrillation (AFib). The researchers’ hypothesis is that jointly detecting atrial fibrillation early and providing cardiovascular health programs to new AFib patients, will lead to patients being treated by a medical provider for AFib that otherwise would not have been detected. This, in turn, would lead to these AFib patients decreasing their risks of stroke and other serious cardiovascular events, including death, the study authors speculated.
Presenting new challenges
While PGHD has the potential to help people, it also presents new challenges. It is highly sensitive and personal – it can be as identifying as DNA.3
The vast amount of data that PGHD can collect from interaction with consumer wearable devices poses serious privacy risks if done improperly. To address those risks, companies like Evidation have built in protections. Evidation has an app, Achievement, that has enlisted a connected population of more than 3.5 million members who earn rewards for performing health-related actions, as tracked by wearables devices and apps. Through the Achievement app (See Figure 2.), members are provided opportunities to join research studies. As part of these studies, data collected from sensors and apps is used by permission of the member so that it is clear how their data are contributing to specific research questions or use cases.
This is a collaborative model of data collection built upon trust and permission and is substantially different than the collection of data from electronic health records (EHRs) – which is typically aggregated, deidentified, and commercialized, often without the patients’ knowledge or consent. Stringent protections, explicit permission, and transparency are absolutely imperative until privacy frameworks for data outside of HIPAA regulation catches up and protects patients from discrimination and unintended uses of their data.

Large connected cohorts can help advance our understanding of public health. In one study run on Achievement during the 2017-2018 flu season, a survey was sent to the Achievement population every week asking about symptoms of influenza-like illness and requesting permission to access historical data from their wearable around the influenza-like illness event.4 With the data, it was possible to analyze patterns of activity, sleep, and resting heart rate change around flu events. Resting heart rate, in particular, is shown to increase during fever and at the population level. In fact, through the use of PGHD, it is possible to use the fraction of people with resting heart rate above their usual baseline as a proxy to quantify the number of infected people in a region.5 This resting heart rate–informed flu surveillance method, if refined to increased accuracy, can work in near real time. This means it may be able detect influenza outbreaks days earlier than current epidemiological methods.
Health data generated by connected populations are in the early stages of development. It is clear that it will yield novel insights into health and disease. Only time will tell if it will be able to help clinicians and patients better predict, diagnose, and formulate treatment plans for disease.
Neil Skolnik, M.D. is a professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, and associate director of the Family Medicine Residency Program at Abington Jefferson Health. Luca Foschini PhD, is co-founder & chief data scientist at Evidation Health. Bray Patrick-Lake, MFS, is a patient thought leader and director of strategic partnerships at Evidation Health.
References
1. Chen R et al. Developing measures of cognitive impairment in the real world from consumer-grade multimodal sensor streams. KDD ’19. August 4–8, 2019 Aug 4-8.
2. The Heartline Study. https://www.heartline.com.
3. Foschini L. Privacy of Wearable and Sensors Data (or, the Lack Thereof?). Data Driven Investor, Medium. 2019.
4. Bradshaw B et al. Influenza surveillance using wearable mobile health devices. Online J Public Health Inform. 2019;11(1):e249.
5. Radin JM et al. Harnessing wearable device data to improve state-level real-time surveillance of influenza-like illness in the USA: a population-based study. Lancet Digital Health. 2020. doi: 10.1016/S2589-7500(19)30222-5.
In Part I of our discussion we introduced the concept of person-generated health data (PGHD), defined as wellness and/or health-related data created, recorded, or gathered by individuals.
Such rich, longitudinal information is now being used in combination with traditional clinical information to predict, diagnose, and formulate treatment plans for diseases, as well as understand the safety and effectiveness of medical interventions.
Identifying a disease early
One novel example of digital technologies being used for early identification of disease was a promising 2019 study by Eli Lilly (in collaboration with Apple and Evidation Health) called the Lilly Exploratory Digital Assessment Study.
In this study, the feasibility of using PGHD for identifying physiological and behavioral signatures of cognitive impairment was examined for the purpose of seeking new methods to detect mild cognitive impairment (MCI) in a timely and cost-effective manner. The study enrolled 31 study participants with cognitive impairment and 82 without cognitive impairment. It used consumer-grade sensor technologies (the iPhone, Apple Watch, iPad, and Beddit sleep monitor) to continuously and unobtrusively collect data. Among the information the researchers collected were interaction with the phone keyboard, accelerometer data from the Apple Watch, volume of messages sent/received, and sleep cycles.1
A total of 16 terabytes of data were collected over the course of 12 weeks. Data were organized into a behaviorgram (See Figure 1) that gives a holistic picture of a day in a patient’s life. A machine learning model was used to distinguish between behaviorgrams of symptomatic versus healthy controls, identifying typing speed, circadian rhythm shifts, and reliance on helper apps, among other things, as differentiating cognitively impaired from healthy controls. These behaviorgrams may someday serve as “fingerprints” of different diseases, with specific diseases displaying predictable patterns. In the near future, digital measures like the ones investigated in this study are likely to be used to help clinicians predict and diagnose disease, as well as to better understand disease progression and treatment response.
Leading to better health outcomes
The potential of PGHD to detect diseases early and lead to better health outcomes is being investigated in the Heartline study, a collaboration between Johnson & Johnson and Apple, which is supported by Evidation.2
This study aims to enroll 150,000 adults age 65 years and over to analyze the impact of Apple Watch–based early detection of irregular heart rhythms consistent with atrial fibrillation (AFib). The researchers’ hypothesis is that jointly detecting atrial fibrillation early and providing cardiovascular health programs to new AFib patients, will lead to patients being treated by a medical provider for AFib that otherwise would not have been detected. This, in turn, would lead to these AFib patients decreasing their risks of stroke and other serious cardiovascular events, including death, the study authors speculated.
Presenting new challenges
While PGHD has the potential to help people, it also presents new challenges. It is highly sensitive and personal – it can be as identifying as DNA.3
The vast amount of data that PGHD can collect from interaction with consumer wearable devices poses serious privacy risks if done improperly. To address those risks, companies like Evidation have built in protections. Evidation has an app, Achievement, that has enlisted a connected population of more than 3.5 million members who earn rewards for performing health-related actions, as tracked by wearables devices and apps. Through the Achievement app (See Figure 2.), members are provided opportunities to join research studies. As part of these studies, data collected from sensors and apps is used by permission of the member so that it is clear how their data are contributing to specific research questions or use cases.
This is a collaborative model of data collection built upon trust and permission and is substantially different than the collection of data from electronic health records (EHRs) – which is typically aggregated, deidentified, and commercialized, often without the patients’ knowledge or consent. Stringent protections, explicit permission, and transparency are absolutely imperative until privacy frameworks for data outside of HIPAA regulation catches up and protects patients from discrimination and unintended uses of their data.
Large connected cohorts can help advance our understanding of public health. In one study run on Achievement during the 2017-2018 flu season, a survey was sent to the Achievement population every week asking about symptoms of influenza-like illness and requesting permission to access historical data from their wearable around the influenza-like illness event.4 With the data, it was possible to analyze patterns of activity, sleep, and resting heart rate change around flu events. Resting heart rate, in particular, is shown to increase during fever and at the population level. In fact, through the use of PGHD, it is possible to use the fraction of people with resting heart rate above their usual baseline as a proxy to quantify the number of infected people in a region.5 This resting heart rate–informed flu surveillance method, if refined to increased accuracy, can work in near real time. This means it may be able detect influenza outbreaks days earlier than current epidemiological methods.
Health data generated by connected populations are in the early stages of development. It is clear that it will yield novel insights into health and disease. Only time will tell if it will be able to help clinicians and patients better predict, diagnose, and formulate treatment plans for disease.
Neil Skolnik, M.D. is a professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, and associate director of the Family Medicine Residency Program at Abington Jefferson Health. Luca Foschini PhD, is co-founder & chief data scientist at Evidation Health. Bray Patrick-Lake, MFS, is a patient thought leader and director of strategic partnerships at Evidation Health.
References
1. Chen R et al. Developing measures of cognitive impairment in the real world from consumer-grade multimodal sensor streams. KDD ’19. August 4–8, 2019 Aug 4-8.
2. The Heartline Study. https://www.heartline.com.
3. Foschini L. Privacy of Wearable and Sensors Data (or, the Lack Thereof?). Data Driven Investor, Medium. 2019.
4. Bradshaw B et al. Influenza surveillance using wearable mobile health devices. Online J Public Health Inform. 2019;11(1):e249.
5. Radin JM et al. Harnessing wearable device data to improve state-level real-time surveillance of influenza-like illness in the USA: a population-based study. Lancet Digital Health. 2020. doi: 10.1016/S2589-7500(19)30222-5.
In Part I of our discussion we introduced the concept of person-generated health data (PGHD), defined as wellness and/or health-related data created, recorded, or gathered by individuals.
Such rich, longitudinal information is now being used in combination with traditional clinical information to predict, diagnose, and formulate treatment plans for diseases, as well as understand the safety and effectiveness of medical interventions.
Identifying a disease early
One novel example of digital technologies being used for early identification of disease was a promising 2019 study by Eli Lilly (in collaboration with Apple and Evidation Health) called the Lilly Exploratory Digital Assessment Study.
In this study, the feasibility of using PGHD for identifying physiological and behavioral signatures of cognitive impairment was examined for the purpose of seeking new methods to detect mild cognitive impairment (MCI) in a timely and cost-effective manner. The study enrolled 31 study participants with cognitive impairment and 82 without cognitive impairment. It used consumer-grade sensor technologies (the iPhone, Apple Watch, iPad, and Beddit sleep monitor) to continuously and unobtrusively collect data. Among the information the researchers collected were interaction with the phone keyboard, accelerometer data from the Apple Watch, volume of messages sent/received, and sleep cycles.1
A total of 16 terabytes of data were collected over the course of 12 weeks. Data were organized into a behaviorgram (See Figure 1) that gives a holistic picture of a day in a patient’s life. A machine learning model was used to distinguish between behaviorgrams of symptomatic versus healthy controls, identifying typing speed, circadian rhythm shifts, and reliance on helper apps, among other things, as differentiating cognitively impaired from healthy controls. These behaviorgrams may someday serve as “fingerprints” of different diseases, with specific diseases displaying predictable patterns. In the near future, digital measures like the ones investigated in this study are likely to be used to help clinicians predict and diagnose disease, as well as to better understand disease progression and treatment response.
Leading to better health outcomes
The potential of PGHD to detect diseases early and lead to better health outcomes is being investigated in the Heartline study, a collaboration between Johnson & Johnson and Apple, which is supported by Evidation.2
This study aims to enroll 150,000 adults age 65 years and over to analyze the impact of Apple Watch–based early detection of irregular heart rhythms consistent with atrial fibrillation (AFib). The researchers’ hypothesis is that jointly detecting atrial fibrillation early and providing cardiovascular health programs to new AFib patients, will lead to patients being treated by a medical provider for AFib that otherwise would not have been detected. This, in turn, would lead to these AFib patients decreasing their risks of stroke and other serious cardiovascular events, including death, the study authors speculated.
Presenting new challenges
While PGHD has the potential to help people, it also presents new challenges. It is highly sensitive and personal – it can be as identifying as DNA.3
The vast amount of data that PGHD can collect from interaction with consumer wearable devices poses serious privacy risks if done improperly. To address those risks, companies like Evidation have built in protections. Evidation has an app, Achievement, that has enlisted a connected population of more than 3.5 million members who earn rewards for performing health-related actions, as tracked by wearables devices and apps. Through the Achievement app (See Figure 2.), members are provided opportunities to join research studies. As part of these studies, data collected from sensors and apps is used by permission of the member so that it is clear how their data are contributing to specific research questions or use cases.
This is a collaborative model of data collection built upon trust and permission and is substantially different than the collection of data from electronic health records (EHRs) – which is typically aggregated, deidentified, and commercialized, often without the patients’ knowledge or consent. Stringent protections, explicit permission, and transparency are absolutely imperative until privacy frameworks for data outside of HIPAA regulation catches up and protects patients from discrimination and unintended uses of their data.
Large connected cohorts can help advance our understanding of public health. In one study run on Achievement during the 2017-2018 flu season, a survey was sent to the Achievement population every week asking about symptoms of influenza-like illness and requesting permission to access historical data from their wearable around the influenza-like illness event.4 With the data, it was possible to analyze patterns of activity, sleep, and resting heart rate change around flu events. Resting heart rate, in particular, is shown to increase during fever and at the population level. In fact, through the use of PGHD, it is possible to use the fraction of people with resting heart rate above their usual baseline as a proxy to quantify the number of infected people in a region.5 This resting heart rate–informed flu surveillance method, if refined to increased accuracy, can work in near real time. This means it may be able detect influenza outbreaks days earlier than current epidemiological methods.
Health data generated by connected populations are in the early stages of development. It is clear that it will yield novel insights into health and disease. Only time will tell if it will be able to help clinicians and patients better predict, diagnose, and formulate treatment plans for disease.
Neil Skolnik, M.D. is a professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, and associate director of the Family Medicine Residency Program at Abington Jefferson Health. Luca Foschini PhD, is co-founder & chief data scientist at Evidation Health. Bray Patrick-Lake, MFS, is a patient thought leader and director of strategic partnerships at Evidation Health.
References
1. Chen R et al. Developing measures of cognitive impairment in the real world from consumer-grade multimodal sensor streams. KDD ’19. August 4–8, 2019 Aug 4-8.
2. The Heartline Study. https://www.heartline.com.
3. Foschini L. Privacy of Wearable and Sensors Data (or, the Lack Thereof?). Data Driven Investor, Medium. 2019.
4. Bradshaw B et al. Influenza surveillance using wearable mobile health devices. Online J Public Health Inform. 2019;11(1):e249.
5. Radin JM et al. Harnessing wearable device data to improve state-level real-time surveillance of influenza-like illness in the USA: a population-based study. Lancet Digital Health. 2020. doi: 10.1016/S2589-7500(19)30222-5.
Should the practice of counseling patients to present to the office for a string check after IUD insertion be halted?
[polldaddy:10527068]
[polldaddy:10527068]
[polldaddy:10527068]
White House expands seniors’ telehealth for COVID-19

“Medicare can pay for office, hospital, and other visits furnished via telehealth across the country and including in patients’ places of residence, starting March 6, 2020,” the Centers for Medicare & Medicaid Services said in a fact sheet issued March 17.
Some of the existing benefits were previously limited to rural communities.
“These services can also be provided in a variety of settings, including nursing homes, hospital outpatient departments, and more,” said CMS Administrator Seema Verma during a March 17 White House press briefing on administration actions to contain the spread of COVID-19.
That means that seniors can continue to receive their routine care without having to leave the home and risk infection, or they can get medical guidance if they have mild symptoms, which would help mitigate the spread to others.
“This shift is very important for clinicians and providers who, over the coming weeks, will face considerable strain on their time and resources,” Dr. Verma said. “[It] allows the health care system to prioritize care for those who have more needs or who are in dire need, and it also preserves protective equipment.”
A range of providers will be able to deliver telehealth services, including doctors, nurse practitioners, clinical psychologists, and licensed clinical social workers. Visits using telehealth services will be considered the same as in-person visits and will be paid as if the patient were seen in the office.
This expansion of Medicare telehealth services will continue for the duration of the COVID-19 public health emergency.
“In addition, the [Health & Human Services’] office of inspector general is providing flexibility for health care providers to reduce or waive cost-sharing for telehealth visits paid by federal health care programs,” the fact sheet states.Key to the expansion is that it will cover the entire United States and will not be limited to rural areas.
Dr. Verma also noted that the administration “will be temporarily suspending certain HIPAA requirements so that doctors can provide telehealth with their own phones.”
She added that state Medicaid agencies can expand their telehealth services without the approval of CMS during this emergency.
AGA has released a guide to commercial telehealth COVID-19 coding policies (http://ow.ly/8CIH30qsU0B) that supplements their guide to public payors.
“Medicare can pay for office, hospital, and other visits furnished via telehealth across the country and including in patients’ places of residence, starting March 6, 2020,” the Centers for Medicare & Medicaid Services said in a fact sheet issued March 17.
Some of the existing benefits were previously limited to rural communities.
“These services can also be provided in a variety of settings, including nursing homes, hospital outpatient departments, and more,” said CMS Administrator Seema Verma during a March 17 White House press briefing on administration actions to contain the spread of COVID-19.
That means that seniors can continue to receive their routine care without having to leave the home and risk infection, or they can get medical guidance if they have mild symptoms, which would help mitigate the spread to others.
“This shift is very important for clinicians and providers who, over the coming weeks, will face considerable strain on their time and resources,” Dr. Verma said. “[It] allows the health care system to prioritize care for those who have more needs or who are in dire need, and it also preserves protective equipment.”
A range of providers will be able to deliver telehealth services, including doctors, nurse practitioners, clinical psychologists, and licensed clinical social workers. Visits using telehealth services will be considered the same as in-person visits and will be paid as if the patient were seen in the office.
This expansion of Medicare telehealth services will continue for the duration of the COVID-19 public health emergency.
“In addition, the [Health & Human Services’] office of inspector general is providing flexibility for health care providers to reduce or waive cost-sharing for telehealth visits paid by federal health care programs,” the fact sheet states.Key to the expansion is that it will cover the entire United States and will not be limited to rural areas.
Dr. Verma also noted that the administration “will be temporarily suspending certain HIPAA requirements so that doctors can provide telehealth with their own phones.”
She added that state Medicaid agencies can expand their telehealth services without the approval of CMS during this emergency.
AGA has released a guide to commercial telehealth COVID-19 coding policies (http://ow.ly/8CIH30qsU0B) that supplements their guide to public payors.
“Medicare can pay for office, hospital, and other visits furnished via telehealth across the country and including in patients’ places of residence, starting March 6, 2020,” the Centers for Medicare & Medicaid Services said in a fact sheet issued March 17.
Some of the existing benefits were previously limited to rural communities.
“These services can also be provided in a variety of settings, including nursing homes, hospital outpatient departments, and more,” said CMS Administrator Seema Verma during a March 17 White House press briefing on administration actions to contain the spread of COVID-19.
That means that seniors can continue to receive their routine care without having to leave the home and risk infection, or they can get medical guidance if they have mild symptoms, which would help mitigate the spread to others.
“This shift is very important for clinicians and providers who, over the coming weeks, will face considerable strain on their time and resources,” Dr. Verma said. “[It] allows the health care system to prioritize care for those who have more needs or who are in dire need, and it also preserves protective equipment.”
A range of providers will be able to deliver telehealth services, including doctors, nurse practitioners, clinical psychologists, and licensed clinical social workers. Visits using telehealth services will be considered the same as in-person visits and will be paid as if the patient were seen in the office.
This expansion of Medicare telehealth services will continue for the duration of the COVID-19 public health emergency.
“In addition, the [Health & Human Services’] office of inspector general is providing flexibility for health care providers to reduce or waive cost-sharing for telehealth visits paid by federal health care programs,” the fact sheet states.Key to the expansion is that it will cover the entire United States and will not be limited to rural areas.
Dr. Verma also noted that the administration “will be temporarily suspending certain HIPAA requirements so that doctors can provide telehealth with their own phones.”
She added that state Medicaid agencies can expand their telehealth services without the approval of CMS during this emergency.
AGA has released a guide to commercial telehealth COVID-19 coding policies (http://ow.ly/8CIH30qsU0B) that supplements their guide to public payors.
Perspective from the heartland: Cancer care and research during a public health crisis
I have no knowledge of, or experience with, managing a cancer patient during a pandemic. However, from the published and otherwise shared experience of others, we should not allow ourselves to underestimate the voracity of the coronavirus pandemic on our patients, communities, and health care systems.

Data from China suggest cancer patients infected with SARS-CoV-2 face a 3.5 times higher risk of mechanical ventilation, intensive care unit admission, or death, compared with infected patients without cancer (Lancet Oncol 2020;21:335-7).
Health care workers in Seattle have also shared their experiences battling coronavirus infections in cancer patients (J Natl Compr Canc Netw. 2020 Mar 20. doi: 10.6004/jnccn.2020.7560). Masumi Ueda, MD, of Seattle Cancer Care Alliance, and colleagues reviewed their decisions in multiple domains over a 7-week period, during which the state of Washington went from a single case of SARS-CoV-2 infection to nearly 650 cases and 40 deaths.
Making tough treatment decisions
Dr. Ueda and colleagues contrasted their customary resource-rich, innovation-oriented, cancer-combatting environment with their current circumstance, in which they must prioritize treatment for patients for whom the risk-reward balance has tilted substantially toward “risk.”
The authors noted that their most difficult decisions were those regarding delay of cancer treatment. They suggested that plans for potentially curative adjuvant therapy should likely proceed, but, for patients with metastatic disease, the equation is more nuanced.
In some cases, treatment should be delayed or interrupted with recognition of how that could result in worsening performance status and admission for symptom palliation, further stressing inpatient resources.
The authors suggested scenarios for prioritizing cancer surgery. For example, several months of systemic therapy (ideally, low-risk systemic therapy such as hormone therapy for breast or prostate cancer) and surgical delay may be worthwhile, without compromising patient care.
Patients with aggressive hematologic malignancy requiring urgent systemic treatment (potentially stem cell transplantation and cellular immunotherapies) should be treated promptly. However, even in those cases, opportunities should be sought to lessen immunosuppression and transition care as quickly as possible to the outpatient clinic, according to guidelines from the American Society of Transplantation and Cellular Therapy.
See one, do one, teach one
Rendering patient care during a pandemic would be unique for me. However, I, like all physicians, am familiar with feelings of inadequacy at times of professional challenge. On countless occasions, I have started my day or walked into a patient’s room wondering whether I will have the fortitude, knowledge, creativity, or help I need to get through that day or make that patient “better” by any definition of that word.
We all know the formula: “Work hard. Make evidence-based, personalized decisions for those who have entrusted their care to us. Learn from those encounters. Teach from our knowledge and experience – that is, ‘See one, do one, teach one.’ ”
The Seattle oncologists are living the lives of first responders and deserve our admiration for putting pen to paper so we can learn from their considerable, relevant experience.
Similar admiration is due to Giuseppe Curigliano, MD, of the European Institute of Oncology in Milan. In the ASCO Daily News, Dr. Curigliano described an epidemic that, within 3 weeks, overloaded the health care system across northern Italy.
Hospitalization was needed for over 60% of infected patients, and nearly 15% of those patients needed intensive care unit services for respiratory distress. The Italians centralized oncology care in specialized hubs, with spokes of institutions working in parallel to provide cancer-specific care in a COVID-free environment.
To build upon cancer-specific information from Italy and other areas hard-hit by COVID-19, more than 30 cancer centers have joined together to form the COVID-19 and Cancer Consortium. The consortium’s website hosts a survey designed to “capture details related to cancer patients presumed to have COVID-19.”
Calculating deaths and long-term consequences for cancer care delivery
It is proper that the authors from China, Italy, and Seattle did not focus attention on the case fatality rate from the COVID-19 pandemic among cancer patients. To say the least, it would be complicated to tally the direct mortality – either overall or in clinically important subsets of patients, including country-specific cohorts.
What we know from published reports is that, in Italy, cancer patients account for about 20% of deaths from coronavirus. In China, the case-fatality rate for patients with cancer was 5.6% (JAMA. 2020 Feb 24. doi: 10.1001/jama.2020.2648).
However, we know nothing about the indirect death toll from malignancy (without coronavirus infection) that was untreated or managed less than optimally because of personnel and physical resources that were diverted to COVID-19–associated cases.
Similarly, we cannot begin to estimate indirect consequences of the pandemic to oncology practices, such as accelerated burnout and posttraumatic stress disorder, as well as the long-range effects of economic turmoil on patients, health care workers, and provider organizations.
What happens to cancer trials?
From China, Italy, and Seattle, thus far, there is little information about how the pandemic will affect the vital clinical research endeavor. The Seattle physicians did say they plan to enroll patients on clinical trials only when the trial offers a high chance of benefiting the patient over standard therapy alone.
Fortunately, the National Institutes of Health and Food and Drug Administration have released guidance documents related to clinical trials.
The National Cancer Institute (NCI) has also released guidance documents (March 13 guidance; March 23 guidance) for patients on clinical trials supported by the NCI Cancer Therapy Evaluation Program (CTEP) and the NCI Community Oncology Research Program (NCORP).
CTEP and NCORP are making reasonable accommodations to suspend monitoring visits and audits, allow tele–follow-up visits for patients, and permit local physicians to provide care for patients on study. In addition, with appropriate procedural adherence and documentation, CTEP and NCORP will allow oral investigational medicines to be mailed directly to patients’ homes.
Planned NCI National Clinical Trials Network meetings will be conducted via remote access webinars, conference calls, and similar technology. These adjustments – and probably many more to come – are geared toward facilitating ongoing care to proceed safely and with minimal risk for patients currently receiving investigational therapies and for the sites and investigators engaged in those studies.
Each of us has probably faced a personal “defining professional moment,” when we had to utilize every skill in our arsenal and examine the motivations that led us to a career in oncology. However, it is clear from the forgoing clinical and research processes and guidelines that the COVID-19 pandemic is such a defining professional moment for each of us, in every community we serve.
Critical junctures like this cause more rapid behavior change and innovation than the slow-moving pace that characterizes our idealized preferences. As oncologists who embrace new data and behavioral change, we stand to learn processes that will facilitate more perfected systems of care than the one that preceded this unprecedented crisis, promote more efficient sharing of high-quality information, and improve the outcome for our future patients.
Dr. Lyss was an oncologist and researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
I have no knowledge of, or experience with, managing a cancer patient during a pandemic. However, from the published and otherwise shared experience of others, we should not allow ourselves to underestimate the voracity of the coronavirus pandemic on our patients, communities, and health care systems.
Data from China suggest cancer patients infected with SARS-CoV-2 face a 3.5 times higher risk of mechanical ventilation, intensive care unit admission, or death, compared with infected patients without cancer (Lancet Oncol 2020;21:335-7).
Health care workers in Seattle have also shared their experiences battling coronavirus infections in cancer patients (J Natl Compr Canc Netw. 2020 Mar 20. doi: 10.6004/jnccn.2020.7560). Masumi Ueda, MD, of Seattle Cancer Care Alliance, and colleagues reviewed their decisions in multiple domains over a 7-week period, during which the state of Washington went from a single case of SARS-CoV-2 infection to nearly 650 cases and 40 deaths.
Making tough treatment decisions
Dr. Ueda and colleagues contrasted their customary resource-rich, innovation-oriented, cancer-combatting environment with their current circumstance, in which they must prioritize treatment for patients for whom the risk-reward balance has tilted substantially toward “risk.”
The authors noted that their most difficult decisions were those regarding delay of cancer treatment. They suggested that plans for potentially curative adjuvant therapy should likely proceed, but, for patients with metastatic disease, the equation is more nuanced.
In some cases, treatment should be delayed or interrupted with recognition of how that could result in worsening performance status and admission for symptom palliation, further stressing inpatient resources.
The authors suggested scenarios for prioritizing cancer surgery. For example, several months of systemic therapy (ideally, low-risk systemic therapy such as hormone therapy for breast or prostate cancer) and surgical delay may be worthwhile, without compromising patient care.
Patients with aggressive hematologic malignancy requiring urgent systemic treatment (potentially stem cell transplantation and cellular immunotherapies) should be treated promptly. However, even in those cases, opportunities should be sought to lessen immunosuppression and transition care as quickly as possible to the outpatient clinic, according to guidelines from the American Society of Transplantation and Cellular Therapy.
See one, do one, teach one
Rendering patient care during a pandemic would be unique for me. However, I, like all physicians, am familiar with feelings of inadequacy at times of professional challenge. On countless occasions, I have started my day or walked into a patient’s room wondering whether I will have the fortitude, knowledge, creativity, or help I need to get through that day or make that patient “better” by any definition of that word.
We all know the formula: “Work hard. Make evidence-based, personalized decisions for those who have entrusted their care to us. Learn from those encounters. Teach from our knowledge and experience – that is, ‘See one, do one, teach one.’ ”
The Seattle oncologists are living the lives of first responders and deserve our admiration for putting pen to paper so we can learn from their considerable, relevant experience.
Similar admiration is due to Giuseppe Curigliano, MD, of the European Institute of Oncology in Milan. In the ASCO Daily News, Dr. Curigliano described an epidemic that, within 3 weeks, overloaded the health care system across northern Italy.
Hospitalization was needed for over 60% of infected patients, and nearly 15% of those patients needed intensive care unit services for respiratory distress. The Italians centralized oncology care in specialized hubs, with spokes of institutions working in parallel to provide cancer-specific care in a COVID-free environment.
To build upon cancer-specific information from Italy and other areas hard-hit by COVID-19, more than 30 cancer centers have joined together to form the COVID-19 and Cancer Consortium. The consortium’s website hosts a survey designed to “capture details related to cancer patients presumed to have COVID-19.”
Calculating deaths and long-term consequences for cancer care delivery
It is proper that the authors from China, Italy, and Seattle did not focus attention on the case fatality rate from the COVID-19 pandemic among cancer patients. To say the least, it would be complicated to tally the direct mortality – either overall or in clinically important subsets of patients, including country-specific cohorts.
What we know from published reports is that, in Italy, cancer patients account for about 20% of deaths from coronavirus. In China, the case-fatality rate for patients with cancer was 5.6% (JAMA. 2020 Feb 24. doi: 10.1001/jama.2020.2648).
However, we know nothing about the indirect death toll from malignancy (without coronavirus infection) that was untreated or managed less than optimally because of personnel and physical resources that were diverted to COVID-19–associated cases.
Similarly, we cannot begin to estimate indirect consequences of the pandemic to oncology practices, such as accelerated burnout and posttraumatic stress disorder, as well as the long-range effects of economic turmoil on patients, health care workers, and provider organizations.
What happens to cancer trials?
From China, Italy, and Seattle, thus far, there is little information about how the pandemic will affect the vital clinical research endeavor. The Seattle physicians did say they plan to enroll patients on clinical trials only when the trial offers a high chance of benefiting the patient over standard therapy alone.
Fortunately, the National Institutes of Health and Food and Drug Administration have released guidance documents related to clinical trials.
The National Cancer Institute (NCI) has also released guidance documents (March 13 guidance; March 23 guidance) for patients on clinical trials supported by the NCI Cancer Therapy Evaluation Program (CTEP) and the NCI Community Oncology Research Program (NCORP).
CTEP and NCORP are making reasonable accommodations to suspend monitoring visits and audits, allow tele–follow-up visits for patients, and permit local physicians to provide care for patients on study. In addition, with appropriate procedural adherence and documentation, CTEP and NCORP will allow oral investigational medicines to be mailed directly to patients’ homes.
Planned NCI National Clinical Trials Network meetings will be conducted via remote access webinars, conference calls, and similar technology. These adjustments – and probably many more to come – are geared toward facilitating ongoing care to proceed safely and with minimal risk for patients currently receiving investigational therapies and for the sites and investigators engaged in those studies.
Each of us has probably faced a personal “defining professional moment,” when we had to utilize every skill in our arsenal and examine the motivations that led us to a career in oncology. However, it is clear from the forgoing clinical and research processes and guidelines that the COVID-19 pandemic is such a defining professional moment for each of us, in every community we serve.
Critical junctures like this cause more rapid behavior change and innovation than the slow-moving pace that characterizes our idealized preferences. As oncologists who embrace new data and behavioral change, we stand to learn processes that will facilitate more perfected systems of care than the one that preceded this unprecedented crisis, promote more efficient sharing of high-quality information, and improve the outcome for our future patients.
Dr. Lyss was an oncologist and researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
I have no knowledge of, or experience with, managing a cancer patient during a pandemic. However, from the published and otherwise shared experience of others, we should not allow ourselves to underestimate the voracity of the coronavirus pandemic on our patients, communities, and health care systems.
Data from China suggest cancer patients infected with SARS-CoV-2 face a 3.5 times higher risk of mechanical ventilation, intensive care unit admission, or death, compared with infected patients without cancer (Lancet Oncol 2020;21:335-7).
Health care workers in Seattle have also shared their experiences battling coronavirus infections in cancer patients (J Natl Compr Canc Netw. 2020 Mar 20. doi: 10.6004/jnccn.2020.7560). Masumi Ueda, MD, of Seattle Cancer Care Alliance, and colleagues reviewed their decisions in multiple domains over a 7-week period, during which the state of Washington went from a single case of SARS-CoV-2 infection to nearly 650 cases and 40 deaths.
Making tough treatment decisions
Dr. Ueda and colleagues contrasted their customary resource-rich, innovation-oriented, cancer-combatting environment with their current circumstance, in which they must prioritize treatment for patients for whom the risk-reward balance has tilted substantially toward “risk.”
The authors noted that their most difficult decisions were those regarding delay of cancer treatment. They suggested that plans for potentially curative adjuvant therapy should likely proceed, but, for patients with metastatic disease, the equation is more nuanced.
In some cases, treatment should be delayed or interrupted with recognition of how that could result in worsening performance status and admission for symptom palliation, further stressing inpatient resources.
The authors suggested scenarios for prioritizing cancer surgery. For example, several months of systemic therapy (ideally, low-risk systemic therapy such as hormone therapy for breast or prostate cancer) and surgical delay may be worthwhile, without compromising patient care.
Patients with aggressive hematologic malignancy requiring urgent systemic treatment (potentially stem cell transplantation and cellular immunotherapies) should be treated promptly. However, even in those cases, opportunities should be sought to lessen immunosuppression and transition care as quickly as possible to the outpatient clinic, according to guidelines from the American Society of Transplantation and Cellular Therapy.
See one, do one, teach one
Rendering patient care during a pandemic would be unique for me. However, I, like all physicians, am familiar with feelings of inadequacy at times of professional challenge. On countless occasions, I have started my day or walked into a patient’s room wondering whether I will have the fortitude, knowledge, creativity, or help I need to get through that day or make that patient “better” by any definition of that word.
We all know the formula: “Work hard. Make evidence-based, personalized decisions for those who have entrusted their care to us. Learn from those encounters. Teach from our knowledge and experience – that is, ‘See one, do one, teach one.’ ”
The Seattle oncologists are living the lives of first responders and deserve our admiration for putting pen to paper so we can learn from their considerable, relevant experience.
Similar admiration is due to Giuseppe Curigliano, MD, of the European Institute of Oncology in Milan. In the ASCO Daily News, Dr. Curigliano described an epidemic that, within 3 weeks, overloaded the health care system across northern Italy.
Hospitalization was needed for over 60% of infected patients, and nearly 15% of those patients needed intensive care unit services for respiratory distress. The Italians centralized oncology care in specialized hubs, with spokes of institutions working in parallel to provide cancer-specific care in a COVID-free environment.
To build upon cancer-specific information from Italy and other areas hard-hit by COVID-19, more than 30 cancer centers have joined together to form the COVID-19 and Cancer Consortium. The consortium’s website hosts a survey designed to “capture details related to cancer patients presumed to have COVID-19.”
Calculating deaths and long-term consequences for cancer care delivery
It is proper that the authors from China, Italy, and Seattle did not focus attention on the case fatality rate from the COVID-19 pandemic among cancer patients. To say the least, it would be complicated to tally the direct mortality – either overall or in clinically important subsets of patients, including country-specific cohorts.
What we know from published reports is that, in Italy, cancer patients account for about 20% of deaths from coronavirus. In China, the case-fatality rate for patients with cancer was 5.6% (JAMA. 2020 Feb 24. doi: 10.1001/jama.2020.2648).
However, we know nothing about the indirect death toll from malignancy (without coronavirus infection) that was untreated or managed less than optimally because of personnel and physical resources that were diverted to COVID-19–associated cases.
Similarly, we cannot begin to estimate indirect consequences of the pandemic to oncology practices, such as accelerated burnout and posttraumatic stress disorder, as well as the long-range effects of economic turmoil on patients, health care workers, and provider organizations.
What happens to cancer trials?
From China, Italy, and Seattle, thus far, there is little information about how the pandemic will affect the vital clinical research endeavor. The Seattle physicians did say they plan to enroll patients on clinical trials only when the trial offers a high chance of benefiting the patient over standard therapy alone.
Fortunately, the National Institutes of Health and Food and Drug Administration have released guidance documents related to clinical trials.
The National Cancer Institute (NCI) has also released guidance documents (March 13 guidance; March 23 guidance) for patients on clinical trials supported by the NCI Cancer Therapy Evaluation Program (CTEP) and the NCI Community Oncology Research Program (NCORP).
CTEP and NCORP are making reasonable accommodations to suspend monitoring visits and audits, allow tele–follow-up visits for patients, and permit local physicians to provide care for patients on study. In addition, with appropriate procedural adherence and documentation, CTEP and NCORP will allow oral investigational medicines to be mailed directly to patients’ homes.
Planned NCI National Clinical Trials Network meetings will be conducted via remote access webinars, conference calls, and similar technology. These adjustments – and probably many more to come – are geared toward facilitating ongoing care to proceed safely and with minimal risk for patients currently receiving investigational therapies and for the sites and investigators engaged in those studies.
Each of us has probably faced a personal “defining professional moment,” when we had to utilize every skill in our arsenal and examine the motivations that led us to a career in oncology. However, it is clear from the forgoing clinical and research processes and guidelines that the COVID-19 pandemic is such a defining professional moment for each of us, in every community we serve.
Critical junctures like this cause more rapid behavior change and innovation than the slow-moving pace that characterizes our idealized preferences. As oncologists who embrace new data and behavioral change, we stand to learn processes that will facilitate more perfected systems of care than the one that preceded this unprecedented crisis, promote more efficient sharing of high-quality information, and improve the outcome for our future patients.
Dr. Lyss was an oncologist and researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
Hospitals muzzle doctors and nurses on PPE, COVID-19 cases
Over the past month, an orthopedic surgeon has watched as the crowd of sick patients at his hospital has grown, while the supply of personal protective equipment (PPE) for staff has diminished. As he prepares for another day of staffing testing tents and places his one and only mask across his face, he also receives a daily reminder from hospital management: Don’t talk about it.

“It’s very clear; no one is allowed to speak for the institution or of the institution,” he said in an interview. “We get a daily warning about being very prudent about posts on personal accounts. They’ve talked about this with respect to various issues: case numbers, case severity, testing availability, [and] PPEs.”
The warnings mean staff at the hospital suffer in silence, unable to share the troubling situation with the public or request assistance with supplies.
“I have one mask. We’re expected to reuse them, unless you were exposed or worked with a known COVID victim,” the surgeon said. “However, with the numbers in our region rapidly increasing, you can’t assume that people don’t have it or that you don’t have particles on your mask, even if you’re not in a known quarantine zone within the institution.”
As the COVID-19 health crisis rages on, online platforms have become a common place for health professionals to lament short supplies, share concerns, tell stories, and plead for help. But at the same time, other physicians, nurses, and health care workers are being muzzled by hospital administrators and threatened with discipline for speaking out about coronavirus caseloads and dwindling supplies. Some worry the gag orders are muddying the picture of how hospitals are faring in the pandemic, while placing the safety of frontline workers at risk.
The silencing of physicians by hospitals about PPE shortages and other COVID-19 issues has become widespread, said Nisha Mehta, MD, a physician advocate and community leader who writes about PPE on social media. Physicians are being warned not to speak or post publicly about their COVID-19 experiences, including PPE shortages, case specifics, and the percentage of full hospital beds, Dr. Mehta said in an interview. In some cases, physicians who have posted have been forced to take down the posts or have faced retribution for speaking out, she said.
“There’s definitely a big fear among physicians, particularly employed physicians, in terms of what the consequences may be for telling their stories,” Dr. Mehta said. “I find that counterproductive. I understand not inducing panic, but these are real stories that are important for people to understand so they do stay home and increase the systemic pressure to get sufficient PPE, so that we can preserve our health care workforce for a problem that is going to get worse before it gets better.”
Meanwhile, an Indiana hospitalist who took to social media to ask for masks for hospitals in his area says he was immediately reprimanded by his management after the posts came to light. The hospitalist posted on a social media platform to request donations of N95 masks after hearing members of the public had purchased such masks. He hoped his plea would aid preparation for the pandemic at local hospitals, explained the physician, who spoke on the condition of anonymity.
Shortly afterward, administrators from his hospital contacted the online forum’s moderator and the posts were removed, he said. During a subsequent conversation, administrators warned the doctor not to make such posts about PPE because it made the hospital appear incompetent.
“I was told, ‘we can handle this, we don’t need the public’s help,’” the physician said. “I was hurt and upset. I was trying to help protect my peers.”
After landing on the management’s radar, the hospitalist said he was reprimanded a second time about posts on a separate personal social media account. The second time, the private posts to friends and family were related to COVID-19 and PPE, but did not include any protected health information, he said. However, administrators did not like the content of the posts, and he was told management was monitoring his activity on social media, he said.
“The larger message is that patients are money,” the hospitalist said. “The corporate side of medicine rules out over the medicine side. Image and making sure there is a consistent cash flow trumps all else.”
Another frontline physician who works at a large New York hospital, said staff have been cautioned not to talk with the media and to be careful what they post on social media regarding COVID-19. The general rule is that only information approved by administrators can be shared, said the physician, who spoke on the condition of anonymity.
“[The health system] is very protective of their public image,” he said. “In the past, people that have posted things that they don’t like get spoken to quickly and/or fired depending on what was written. I could only imagine that would be the situation regarding COVID-19. They are very strict.”
The frontline physician, who has close contact with COVID-19 patients, said he has access to N95 masks at the moment, but when he requested higher-level protective gear, hospital management refused the request and denied that such supplies were needed.
“Safety of frontline workers appears to not be taken seriously,” he said of his hospital. “Everyone is stressed, but at the end of the day, the administration is sitting there, while the rest of us are putting ourselves at risk.”
We reached out to one hospital for comment, but messages were not returned. Other hospitals were not contacted because physicians feared they would face retribution. We also contacted the American Hospital Association but they did not immediately respond.
In Chicago, an email by a nurse to her coworkers about the safety of masks has resulted in a lawsuit after the nurse says she was fired for sharing her concerns with staff. The nurse, Lauri Mazurkiewicz, sent an email to staffers at Northwestern Memorial Hospital stating the surgical masks provided by the hospital were less effective against airborne particles than were N95 masks, according to a lawsuit filed March 23 in Cook County Circuit Court. Ms. Mazurkiewicz was terminated the next day in retaliation for her email, the lawsuit alleges.
Ms. Mazurkiewicz could not be reached for comment by press time.
Christopher King, a spokesman for Northwestern Medicine, said the hospital is reviewing the lawsuit.
“As Northwestern Medicine continues to respond to this unprecedented health care pandemic, the health and well-being of our patients, our staff and our employees is our highest priority,” he said in a statement. “We take these matters seriously and we are currently reviewing the complaint. At this time, we will not be commenting further.”
John Mandrola, MD, a Louisville, Ky.–based cardiologist who has written about the recent muzzling of frontline physicians with respect to the coronavirus, said he is not surprised that some hospitals are preventing physicians from sharing their experiences.
“Before C19, in many hospital systems, there was a culture of fear amongst employed clinicians,” he said. “Employed clinicians see other employed physicians being terminated for speaking frankly about problems. It takes scant few of these cases to create a culture of silence.”
Dr. Mandrola, who is a regular Medscape contributor, said that a number of doctors have reached out to him privately about PPE scarcity and shared that they were explicitly warned by administrators not to talk about the shortfalls. Leadership at Dr. Mandrola’s hospital has not issued the same warnings, he said.
“From the hat of total transparency, I think the public is not getting a full view of the impending potential problems that are going to come by doctors not speaking publicly,” he said. “On the other hand, hospital leadership is doing the best they can. It’s not the hospitals’ fault. Hospital administrators can’t manufacture masks.”
From a public health standpoint, Dr. Mehta said that not allowing health professionals to speak publicly about the situations at their hospitals is “irresponsible.” The public deserves to know what is happening, she said, and the health care workforce needs to prepare for what is to come.
“It’s so important that we hear from our colleagues,” she said. “It’s important to hear those accounts so we can prepare for what we’re about to face. Data is crucial. The more you learn from each other, the better shot we have at successfully treating cases and ultimately beating this.”
With the critical shortage of PPE at his hospital and the inability to speak out about the problem, the orthopedic surgeon foresees the dilemma continuing to worsen.
“It’s not only the lives of front-line health care workers that are at risk, but it’s those that they’re going to spread it to and those that are going to be coming to the hospital requiring our care,” he said. “If we don’t have a fully functioning health care force, our capacity is going to be diminished that much further.”
The American Gastroenterological Association, along with 44 other medical specialty societies representing more than 800,000 physicians, signed onto the Council of Medical Specialty Societies letter stating that all frontline health care professionals must have access to PPEs and be able to speak publicly about the lack of PPEs without retribution while pushing for adequate supply and distribution. Review the statement at https://cmss.org/cmss-statement-ppe.
[email protected]
Over the past month, an orthopedic surgeon has watched as the crowd of sick patients at his hospital has grown, while the supply of personal protective equipment (PPE) for staff has diminished. As he prepares for another day of staffing testing tents and places his one and only mask across his face, he also receives a daily reminder from hospital management: Don’t talk about it.
“It’s very clear; no one is allowed to speak for the institution or of the institution,” he said in an interview. “We get a daily warning about being very prudent about posts on personal accounts. They’ve talked about this with respect to various issues: case numbers, case severity, testing availability, [and] PPEs.”
The warnings mean staff at the hospital suffer in silence, unable to share the troubling situation with the public or request assistance with supplies.
“I have one mask. We’re expected to reuse them, unless you were exposed or worked with a known COVID victim,” the surgeon said. “However, with the numbers in our region rapidly increasing, you can’t assume that people don’t have it or that you don’t have particles on your mask, even if you’re not in a known quarantine zone within the institution.”
As the COVID-19 health crisis rages on, online platforms have become a common place for health professionals to lament short supplies, share concerns, tell stories, and plead for help. But at the same time, other physicians, nurses, and health care workers are being muzzled by hospital administrators and threatened with discipline for speaking out about coronavirus caseloads and dwindling supplies. Some worry the gag orders are muddying the picture of how hospitals are faring in the pandemic, while placing the safety of frontline workers at risk.
The silencing of physicians by hospitals about PPE shortages and other COVID-19 issues has become widespread, said Nisha Mehta, MD, a physician advocate and community leader who writes about PPE on social media. Physicians are being warned not to speak or post publicly about their COVID-19 experiences, including PPE shortages, case specifics, and the percentage of full hospital beds, Dr. Mehta said in an interview. In some cases, physicians who have posted have been forced to take down the posts or have faced retribution for speaking out, she said.
“There’s definitely a big fear among physicians, particularly employed physicians, in terms of what the consequences may be for telling their stories,” Dr. Mehta said. “I find that counterproductive. I understand not inducing panic, but these are real stories that are important for people to understand so they do stay home and increase the systemic pressure to get sufficient PPE, so that we can preserve our health care workforce for a problem that is going to get worse before it gets better.”
Meanwhile, an Indiana hospitalist who took to social media to ask for masks for hospitals in his area says he was immediately reprimanded by his management after the posts came to light. The hospitalist posted on a social media platform to request donations of N95 masks after hearing members of the public had purchased such masks. He hoped his plea would aid preparation for the pandemic at local hospitals, explained the physician, who spoke on the condition of anonymity.
Shortly afterward, administrators from his hospital contacted the online forum’s moderator and the posts were removed, he said. During a subsequent conversation, administrators warned the doctor not to make such posts about PPE because it made the hospital appear incompetent.
“I was told, ‘we can handle this, we don’t need the public’s help,’” the physician said. “I was hurt and upset. I was trying to help protect my peers.”
After landing on the management’s radar, the hospitalist said he was reprimanded a second time about posts on a separate personal social media account. The second time, the private posts to friends and family were related to COVID-19 and PPE, but did not include any protected health information, he said. However, administrators did not like the content of the posts, and he was told management was monitoring his activity on social media, he said.
“The larger message is that patients are money,” the hospitalist said. “The corporate side of medicine rules out over the medicine side. Image and making sure there is a consistent cash flow trumps all else.”
Another frontline physician who works at a large New York hospital, said staff have been cautioned not to talk with the media and to be careful what they post on social media regarding COVID-19. The general rule is that only information approved by administrators can be shared, said the physician, who spoke on the condition of anonymity.
“[The health system] is very protective of their public image,” he said. “In the past, people that have posted things that they don’t like get spoken to quickly and/or fired depending on what was written. I could only imagine that would be the situation regarding COVID-19. They are very strict.”
The frontline physician, who has close contact with COVID-19 patients, said he has access to N95 masks at the moment, but when he requested higher-level protective gear, hospital management refused the request and denied that such supplies were needed.
“Safety of frontline workers appears to not be taken seriously,” he said of his hospital. “Everyone is stressed, but at the end of the day, the administration is sitting there, while the rest of us are putting ourselves at risk.”
We reached out to one hospital for comment, but messages were not returned. Other hospitals were not contacted because physicians feared they would face retribution. We also contacted the American Hospital Association but they did not immediately respond.
In Chicago, an email by a nurse to her coworkers about the safety of masks has resulted in a lawsuit after the nurse says she was fired for sharing her concerns with staff. The nurse, Lauri Mazurkiewicz, sent an email to staffers at Northwestern Memorial Hospital stating the surgical masks provided by the hospital were less effective against airborne particles than were N95 masks, according to a lawsuit filed March 23 in Cook County Circuit Court. Ms. Mazurkiewicz was terminated the next day in retaliation for her email, the lawsuit alleges.
Ms. Mazurkiewicz could not be reached for comment by press time.
Christopher King, a spokesman for Northwestern Medicine, said the hospital is reviewing the lawsuit.
“As Northwestern Medicine continues to respond to this unprecedented health care pandemic, the health and well-being of our patients, our staff and our employees is our highest priority,” he said in a statement. “We take these matters seriously and we are currently reviewing the complaint. At this time, we will not be commenting further.”
John Mandrola, MD, a Louisville, Ky.–based cardiologist who has written about the recent muzzling of frontline physicians with respect to the coronavirus, said he is not surprised that some hospitals are preventing physicians from sharing their experiences.
“Before C19, in many hospital systems, there was a culture of fear amongst employed clinicians,” he said. “Employed clinicians see other employed physicians being terminated for speaking frankly about problems. It takes scant few of these cases to create a culture of silence.”
Dr. Mandrola, who is a regular Medscape contributor, said that a number of doctors have reached out to him privately about PPE scarcity and shared that they were explicitly warned by administrators not to talk about the shortfalls. Leadership at Dr. Mandrola’s hospital has not issued the same warnings, he said.
“From the hat of total transparency, I think the public is not getting a full view of the impending potential problems that are going to come by doctors not speaking publicly,” he said. “On the other hand, hospital leadership is doing the best they can. It’s not the hospitals’ fault. Hospital administrators can’t manufacture masks.”
From a public health standpoint, Dr. Mehta said that not allowing health professionals to speak publicly about the situations at their hospitals is “irresponsible.” The public deserves to know what is happening, she said, and the health care workforce needs to prepare for what is to come.
“It’s so important that we hear from our colleagues,” she said. “It’s important to hear those accounts so we can prepare for what we’re about to face. Data is crucial. The more you learn from each other, the better shot we have at successfully treating cases and ultimately beating this.”
With the critical shortage of PPE at his hospital and the inability to speak out about the problem, the orthopedic surgeon foresees the dilemma continuing to worsen.
“It’s not only the lives of front-line health care workers that are at risk, but it’s those that they’re going to spread it to and those that are going to be coming to the hospital requiring our care,” he said. “If we don’t have a fully functioning health care force, our capacity is going to be diminished that much further.”
The American Gastroenterological Association, along with 44 other medical specialty societies representing more than 800,000 physicians, signed onto the Council of Medical Specialty Societies letter stating that all frontline health care professionals must have access to PPEs and be able to speak publicly about the lack of PPEs without retribution while pushing for adequate supply and distribution. Review the statement at https://cmss.org/cmss-statement-ppe.
[email protected]
Over the past month, an orthopedic surgeon has watched as the crowd of sick patients at his hospital has grown, while the supply of personal protective equipment (PPE) for staff has diminished. As he prepares for another day of staffing testing tents and places his one and only mask across his face, he also receives a daily reminder from hospital management: Don’t talk about it.
“It’s very clear; no one is allowed to speak for the institution or of the institution,” he said in an interview. “We get a daily warning about being very prudent about posts on personal accounts. They’ve talked about this with respect to various issues: case numbers, case severity, testing availability, [and] PPEs.”
The warnings mean staff at the hospital suffer in silence, unable to share the troubling situation with the public or request assistance with supplies.
“I have one mask. We’re expected to reuse them, unless you were exposed or worked with a known COVID victim,” the surgeon said. “However, with the numbers in our region rapidly increasing, you can’t assume that people don’t have it or that you don’t have particles on your mask, even if you’re not in a known quarantine zone within the institution.”
As the COVID-19 health crisis rages on, online platforms have become a common place for health professionals to lament short supplies, share concerns, tell stories, and plead for help. But at the same time, other physicians, nurses, and health care workers are being muzzled by hospital administrators and threatened with discipline for speaking out about coronavirus caseloads and dwindling supplies. Some worry the gag orders are muddying the picture of how hospitals are faring in the pandemic, while placing the safety of frontline workers at risk.
The silencing of physicians by hospitals about PPE shortages and other COVID-19 issues has become widespread, said Nisha Mehta, MD, a physician advocate and community leader who writes about PPE on social media. Physicians are being warned not to speak or post publicly about their COVID-19 experiences, including PPE shortages, case specifics, and the percentage of full hospital beds, Dr. Mehta said in an interview. In some cases, physicians who have posted have been forced to take down the posts or have faced retribution for speaking out, she said.
“There’s definitely a big fear among physicians, particularly employed physicians, in terms of what the consequences may be for telling their stories,” Dr. Mehta said. “I find that counterproductive. I understand not inducing panic, but these are real stories that are important for people to understand so they do stay home and increase the systemic pressure to get sufficient PPE, so that we can preserve our health care workforce for a problem that is going to get worse before it gets better.”
Meanwhile, an Indiana hospitalist who took to social media to ask for masks for hospitals in his area says he was immediately reprimanded by his management after the posts came to light. The hospitalist posted on a social media platform to request donations of N95 masks after hearing members of the public had purchased such masks. He hoped his plea would aid preparation for the pandemic at local hospitals, explained the physician, who spoke on the condition of anonymity.
Shortly afterward, administrators from his hospital contacted the online forum’s moderator and the posts were removed, he said. During a subsequent conversation, administrators warned the doctor not to make such posts about PPE because it made the hospital appear incompetent.
“I was told, ‘we can handle this, we don’t need the public’s help,’” the physician said. “I was hurt and upset. I was trying to help protect my peers.”
After landing on the management’s radar, the hospitalist said he was reprimanded a second time about posts on a separate personal social media account. The second time, the private posts to friends and family were related to COVID-19 and PPE, but did not include any protected health information, he said. However, administrators did not like the content of the posts, and he was told management was monitoring his activity on social media, he said.
“The larger message is that patients are money,” the hospitalist said. “The corporate side of medicine rules out over the medicine side. Image and making sure there is a consistent cash flow trumps all else.”
Another frontline physician who works at a large New York hospital, said staff have been cautioned not to talk with the media and to be careful what they post on social media regarding COVID-19. The general rule is that only information approved by administrators can be shared, said the physician, who spoke on the condition of anonymity.
“[The health system] is very protective of their public image,” he said. “In the past, people that have posted things that they don’t like get spoken to quickly and/or fired depending on what was written. I could only imagine that would be the situation regarding COVID-19. They are very strict.”
The frontline physician, who has close contact with COVID-19 patients, said he has access to N95 masks at the moment, but when he requested higher-level protective gear, hospital management refused the request and denied that such supplies were needed.
“Safety of frontline workers appears to not be taken seriously,” he said of his hospital. “Everyone is stressed, but at the end of the day, the administration is sitting there, while the rest of us are putting ourselves at risk.”
We reached out to one hospital for comment, but messages were not returned. Other hospitals were not contacted because physicians feared they would face retribution. We also contacted the American Hospital Association but they did not immediately respond.
In Chicago, an email by a nurse to her coworkers about the safety of masks has resulted in a lawsuit after the nurse says she was fired for sharing her concerns with staff. The nurse, Lauri Mazurkiewicz, sent an email to staffers at Northwestern Memorial Hospital stating the surgical masks provided by the hospital were less effective against airborne particles than were N95 masks, according to a lawsuit filed March 23 in Cook County Circuit Court. Ms. Mazurkiewicz was terminated the next day in retaliation for her email, the lawsuit alleges.
Ms. Mazurkiewicz could not be reached for comment by press time.
Christopher King, a spokesman for Northwestern Medicine, said the hospital is reviewing the lawsuit.
“As Northwestern Medicine continues to respond to this unprecedented health care pandemic, the health and well-being of our patients, our staff and our employees is our highest priority,” he said in a statement. “We take these matters seriously and we are currently reviewing the complaint. At this time, we will not be commenting further.”
John Mandrola, MD, a Louisville, Ky.–based cardiologist who has written about the recent muzzling of frontline physicians with respect to the coronavirus, said he is not surprised that some hospitals are preventing physicians from sharing their experiences.
“Before C19, in many hospital systems, there was a culture of fear amongst employed clinicians,” he said. “Employed clinicians see other employed physicians being terminated for speaking frankly about problems. It takes scant few of these cases to create a culture of silence.”
Dr. Mandrola, who is a regular Medscape contributor, said that a number of doctors have reached out to him privately about PPE scarcity and shared that they were explicitly warned by administrators not to talk about the shortfalls. Leadership at Dr. Mandrola’s hospital has not issued the same warnings, he said.
“From the hat of total transparency, I think the public is not getting a full view of the impending potential problems that are going to come by doctors not speaking publicly,” he said. “On the other hand, hospital leadership is doing the best they can. It’s not the hospitals’ fault. Hospital administrators can’t manufacture masks.”
From a public health standpoint, Dr. Mehta said that not allowing health professionals to speak publicly about the situations at their hospitals is “irresponsible.” The public deserves to know what is happening, she said, and the health care workforce needs to prepare for what is to come.
“It’s so important that we hear from our colleagues,” she said. “It’s important to hear those accounts so we can prepare for what we’re about to face. Data is crucial. The more you learn from each other, the better shot we have at successfully treating cases and ultimately beating this.”
With the critical shortage of PPE at his hospital and the inability to speak out about the problem, the orthopedic surgeon foresees the dilemma continuing to worsen.
“It’s not only the lives of front-line health care workers that are at risk, but it’s those that they’re going to spread it to and those that are going to be coming to the hospital requiring our care,” he said. “If we don’t have a fully functioning health care force, our capacity is going to be diminished that much further.”
The American Gastroenterological Association, along with 44 other medical specialty societies representing more than 800,000 physicians, signed onto the Council of Medical Specialty Societies letter stating that all frontline health care professionals must have access to PPEs and be able to speak publicly about the lack of PPEs without retribution while pushing for adequate supply and distribution. Review the statement at https://cmss.org/cmss-statement-ppe.
[email protected]
AMA offers resources for front-line physicians
.
The literature include news, advocacy, and other information to help front-line physicians provide care to patients and keep themselves safe “in a rapidly changing environment,” the organization said in a statement.
“The AMA continues to forcefully advocate for [personal protective equipment] and critical policy and regulatory changes needed to address our public health and health system needs. Because so many of the challenges of the pandemic are felt at a practice level, we are also providing new tools and information to help physicians respond,” AMA President Patrice A. Harris, MD, said in the statement.
The COVID-19 physician and practice resources released by the AMA include:
- A Physicians Guide to COVID-19 .
- An AMA COVID-19 online resource center and a COVID-19 FAQ.
- A Quick Guide to Telemedicine in Practice.
- Ethical guidance for physicians .
- Evidence-based resources from the The JAMA Network COVID-19 Resource Center.
- CME for physicians through the JAMA Network’s JN Learning website.
.
The literature include news, advocacy, and other information to help front-line physicians provide care to patients and keep themselves safe “in a rapidly changing environment,” the organization said in a statement.
“The AMA continues to forcefully advocate for [personal protective equipment] and critical policy and regulatory changes needed to address our public health and health system needs. Because so many of the challenges of the pandemic are felt at a practice level, we are also providing new tools and information to help physicians respond,” AMA President Patrice A. Harris, MD, said in the statement.
The COVID-19 physician and practice resources released by the AMA include:
- A Physicians Guide to COVID-19 .
- An AMA COVID-19 online resource center and a COVID-19 FAQ.
- A Quick Guide to Telemedicine in Practice.
- Ethical guidance for physicians .
- Evidence-based resources from the The JAMA Network COVID-19 Resource Center.
- CME for physicians through the JAMA Network’s JN Learning website.
.
The literature include news, advocacy, and other information to help front-line physicians provide care to patients and keep themselves safe “in a rapidly changing environment,” the organization said in a statement.
“The AMA continues to forcefully advocate for [personal protective equipment] and critical policy and regulatory changes needed to address our public health and health system needs. Because so many of the challenges of the pandemic are felt at a practice level, we are also providing new tools and information to help physicians respond,” AMA President Patrice A. Harris, MD, said in the statement.
The COVID-19 physician and practice resources released by the AMA include:
- A Physicians Guide to COVID-19 .
- An AMA COVID-19 online resource center and a COVID-19 FAQ.
- A Quick Guide to Telemedicine in Practice.
- Ethical guidance for physicians .
- Evidence-based resources from the The JAMA Network COVID-19 Resource Center.
- CME for physicians through the JAMA Network’s JN Learning website.
Cancer care and COVID-19 in Seattle, the first U.S. epicenter
Two months after the first patient with COVID-19 was identified in China, the first case was reported in the United States in the Seattle, Washington, metropolitan area.
Seattle rapidly became the first US epicenter for COVID-19, and local experts are now offering their expertise and advice on how to provide optimal cancer care during the pandemic in a special feature published online March 20 in the Journal of the National Comprehensive Cancer Network.
“We began implementing measures in early March, including infection control and screening of visitors, staff, and patients at the door,” said lead author Masumi Ueda, MD, who holds positions at the Seattle Cancer Care Alliance, the University of Washington, and the Fred Hutchinson Research Center.
“A lot of changes have been implemented, and it changes on a daily basis. We are responding to the growing rate of COVID-19 infection in the community,” she told Medscape Medical News.
Ueda notes that as a result of the quick implementation of new procedures, so far, very few cancer patients at their facilities have been infected by the virus. “It has not hit our cancer population hard, which is a good thing,” she said.
Create “Incident Command Structure”
In sharing their experience, the authors emphasize the importance of keeping channels of communication open between all stakeholders ― administrators and staff, patients, caregivers, and the general public. They also recommend that each facility create an “incident command structure” that can provide early coordination of institution-wide efforts and that can rapidly respond to changing information.
Ueda noted that their command structure was set up very early on, “so we could get communication set up and start building an infrastructure for response.”
Several areas of care that required new strategies were addressed, both to protect patients and to work around staff shortages caused by possible exposure and/or school closings, as well as projected shortages of supplies and hospital resources.
First and foremost was to identify patients and visitors who had respiratory symptoms and to provide them with masks. Although this is always routine practice during the respiratory virus season, screening has now been initiated at entry points throughout the system.
“We were lucky in Seattle and Washington state in that the University of Washington virology lab developed PCR [polymerase chain reaction] testing early on for COVID-19, which subsequently got FDA approval,” said Ueda. “So we were able to have local testing and didn’t have to rely on the state lab. Testing has also been rapidly scaled up.”
Initiating a comprehensive policy for testing staff, tracking results and exposures for persons under investigation, and defining when it is possible to return to work are essential elements for maintaining a stable workforce. In addition, reinforcing a strict “stay at home when ill” policy and providing access to testing for symptomatic staff have been key to limiting exposures.
“What is unique to our region is that we had testing early on, and we are turning it around in 24 hours,” she pointed out. “This is important for staff to be able to return to work.” Currently, staff, patients, and visitors are being tested only if they show the cardinal symptoms associated with COVID-19: fever, shortness of breath, and cough, although muscle aches have recently been added to their testing protocol.
“I think if we had unlimited capacity, we might consider testing people who are asymptomatic,” Ueda noted, “although if you don’t have symptoms, you may not have the viral load needed for an accurate test.”
Educational materials explaining infection control were also needed for patients and families, along with signs and a website to provide COVID-19 education. These were quickly developed.
In addition, a telephone triage line was established for patients with mild symptoms in order to minimize exposures in clinics and to lessen the number of patients presenting at emergency departments.
Outpatient Care
Because theirs is a referral center, many cancer patients come from out of town, and so there is concern about exposing nonlocal patients to COVID-19 as the virus spreads in the Seattle area. In addition, staffing shortages due to factors such as illness, exposure, and school closures are anticipated.
To address these problems, an initial priority was to establish a “multilayer” coverage system for the clinics in the event that practitioners had to be quarantined on short notice, the authors explain.
One decision was to reschedule all wellness visits for current patients or to use telemedicine. Capacity for that option expanded quickly, which was greatly helped by the recent decision by the Centers for Medicare & Medicaid Services to lift Medicare restrictions on the use of certain telemedicine services.
Another approach is to defer all consultations for second opinions for patients who were already undergoing treatment and to increase clinic hours of operations and capabilities for acute evaluations. This helps reserve emergency departments and hospital resources for patients who require higher-level care, the authors comment.
Treatment Decisions
Treatment decisions were more challenging to make, the authors note. One decision was that, despite the risk for COVID-19 for patients with solid tumors, adjuvant therapy with curative intent should proceed, they note. Similarly, patients with metastatic disease might lose the window of opportunity for treatment if it is delayed.
Treatment for aggressive hematologic malignancies is usually urgent, and stem cell transplant and cellular immunotherapies that provide curative treatments cannot be delayed in many cases.
Enrollment in clinical trials will most likely be limited to those trials that are most likely to benefit the patient.
Ueda noted that, because their patients come from all over the country, they are now conducting consultations for stem cell transplant by telephone so that nonlocal patients do not have to travel to Seattle. “If there is some way we can delay the treatment, we have taken that approach,” Ueda told Medscape Medical News. “If we can divert a patient to an area that is not as heavily affected, that’s another option we are taking.”
Although cancer surgery is not considered elective, surgical intervention needs to be prioritized, the authors comment. In the Seattle system, there is currently a 2-week ban on elective surgery in the healthcare system, owing to limited availability of personal protective equipment (PPE), staffing, and beds.
The oncology teams are currently reviewing treatment regimens to determine which treatments might lessen immunosuppression and which treatment options can be moved from the inpatient to the outpatient setting or can be delayed.
Inpatient Care
For hospitalized patients, several issues are being addressed. The priority is to prepare for an upcoming shortage of beds and resources because of the surge of patients with COVID-19 that is predicted. For both clinic and hospitalized patients, shortages of blood products have necessitated stricter adherence to thresholds for transfusion, and consideration is being given to lowering those thresholds.
Another important problem is the need to conserve PPE, which includes masks, gowns, gloves, and other products. The Seattle teams have implemented solutions such as favoring handwashing with soap and water over the use of hand gel for standard-precaution rooms, limiting the number of personnel entering patient rooms (so as to use less PPE), and reducing nursing procedures that require PPE, such as measuring urine output, unless they are necessary.
In addition, a no-visitor policy has been adopted in inpatient units to conserve PPE, with the exception of end-of-life situations.
The Future
The future trajectory of the COVID-19 pandemic is uncertain, Ueda commented. She emphasized that “we must continue to prepare for its widespread impact. The unknown is what we are looking at. We are expecting it to evolve, and the number of infections cannot go down.”
Ueda and coauthors end their article on a positive note. “To many of us, this has become the health care challenge of our generation, one that modern cancer therapy has never had to face. We will prevail, and when the pandemic ends, we will all be proud of what we did for our patients and each other in this critical moment for humanity.”
Two months after the first patient with COVID-19 was identified in China, the first case was reported in the United States in the Seattle, Washington, metropolitan area.
Seattle rapidly became the first US epicenter for COVID-19, and local experts are now offering their expertise and advice on how to provide optimal cancer care during the pandemic in a special feature published online March 20 in the Journal of the National Comprehensive Cancer Network.
“We began implementing measures in early March, including infection control and screening of visitors, staff, and patients at the door,” said lead author Masumi Ueda, MD, who holds positions at the Seattle Cancer Care Alliance, the University of Washington, and the Fred Hutchinson Research Center.
“A lot of changes have been implemented, and it changes on a daily basis. We are responding to the growing rate of COVID-19 infection in the community,” she told Medscape Medical News.
Ueda notes that as a result of the quick implementation of new procedures, so far, very few cancer patients at their facilities have been infected by the virus. “It has not hit our cancer population hard, which is a good thing,” she said.
Create “Incident Command Structure”
In sharing their experience, the authors emphasize the importance of keeping channels of communication open between all stakeholders ― administrators and staff, patients, caregivers, and the general public. They also recommend that each facility create an “incident command structure” that can provide early coordination of institution-wide efforts and that can rapidly respond to changing information.
Ueda noted that their command structure was set up very early on, “so we could get communication set up and start building an infrastructure for response.”
Several areas of care that required new strategies were addressed, both to protect patients and to work around staff shortages caused by possible exposure and/or school closings, as well as projected shortages of supplies and hospital resources.
First and foremost was to identify patients and visitors who had respiratory symptoms and to provide them with masks. Although this is always routine practice during the respiratory virus season, screening has now been initiated at entry points throughout the system.
“We were lucky in Seattle and Washington state in that the University of Washington virology lab developed PCR [polymerase chain reaction] testing early on for COVID-19, which subsequently got FDA approval,” said Ueda. “So we were able to have local testing and didn’t have to rely on the state lab. Testing has also been rapidly scaled up.”
Initiating a comprehensive policy for testing staff, tracking results and exposures for persons under investigation, and defining when it is possible to return to work are essential elements for maintaining a stable workforce. In addition, reinforcing a strict “stay at home when ill” policy and providing access to testing for symptomatic staff have been key to limiting exposures.
“What is unique to our region is that we had testing early on, and we are turning it around in 24 hours,” she pointed out. “This is important for staff to be able to return to work.” Currently, staff, patients, and visitors are being tested only if they show the cardinal symptoms associated with COVID-19: fever, shortness of breath, and cough, although muscle aches have recently been added to their testing protocol.
“I think if we had unlimited capacity, we might consider testing people who are asymptomatic,” Ueda noted, “although if you don’t have symptoms, you may not have the viral load needed for an accurate test.”
Educational materials explaining infection control were also needed for patients and families, along with signs and a website to provide COVID-19 education. These were quickly developed.
In addition, a telephone triage line was established for patients with mild symptoms in order to minimize exposures in clinics and to lessen the number of patients presenting at emergency departments.
Outpatient Care
Because theirs is a referral center, many cancer patients come from out of town, and so there is concern about exposing nonlocal patients to COVID-19 as the virus spreads in the Seattle area. In addition, staffing shortages due to factors such as illness, exposure, and school closures are anticipated.
To address these problems, an initial priority was to establish a “multilayer” coverage system for the clinics in the event that practitioners had to be quarantined on short notice, the authors explain.
One decision was to reschedule all wellness visits for current patients or to use telemedicine. Capacity for that option expanded quickly, which was greatly helped by the recent decision by the Centers for Medicare & Medicaid Services to lift Medicare restrictions on the use of certain telemedicine services.
Another approach is to defer all consultations for second opinions for patients who were already undergoing treatment and to increase clinic hours of operations and capabilities for acute evaluations. This helps reserve emergency departments and hospital resources for patients who require higher-level care, the authors comment.
Treatment Decisions
Treatment decisions were more challenging to make, the authors note. One decision was that, despite the risk for COVID-19 for patients with solid tumors, adjuvant therapy with curative intent should proceed, they note. Similarly, patients with metastatic disease might lose the window of opportunity for treatment if it is delayed.
Treatment for aggressive hematologic malignancies is usually urgent, and stem cell transplant and cellular immunotherapies that provide curative treatments cannot be delayed in many cases.
Enrollment in clinical trials will most likely be limited to those trials that are most likely to benefit the patient.
Ueda noted that, because their patients come from all over the country, they are now conducting consultations for stem cell transplant by telephone so that nonlocal patients do not have to travel to Seattle. “If there is some way we can delay the treatment, we have taken that approach,” Ueda told Medscape Medical News. “If we can divert a patient to an area that is not as heavily affected, that’s another option we are taking.”
Although cancer surgery is not considered elective, surgical intervention needs to be prioritized, the authors comment. In the Seattle system, there is currently a 2-week ban on elective surgery in the healthcare system, owing to limited availability of personal protective equipment (PPE), staffing, and beds.
The oncology teams are currently reviewing treatment regimens to determine which treatments might lessen immunosuppression and which treatment options can be moved from the inpatient to the outpatient setting or can be delayed.
Inpatient Care
For hospitalized patients, several issues are being addressed. The priority is to prepare for an upcoming shortage of beds and resources because of the surge of patients with COVID-19 that is predicted. For both clinic and hospitalized patients, shortages of blood products have necessitated stricter adherence to thresholds for transfusion, and consideration is being given to lowering those thresholds.
Another important problem is the need to conserve PPE, which includes masks, gowns, gloves, and other products. The Seattle teams have implemented solutions such as favoring handwashing with soap and water over the use of hand gel for standard-precaution rooms, limiting the number of personnel entering patient rooms (so as to use less PPE), and reducing nursing procedures that require PPE, such as measuring urine output, unless they are necessary.
In addition, a no-visitor policy has been adopted in inpatient units to conserve PPE, with the exception of end-of-life situations.
The Future
The future trajectory of the COVID-19 pandemic is uncertain, Ueda commented. She emphasized that “we must continue to prepare for its widespread impact. The unknown is what we are looking at. We are expecting it to evolve, and the number of infections cannot go down.”
Ueda and coauthors end their article on a positive note. “To many of us, this has become the health care challenge of our generation, one that modern cancer therapy has never had to face. We will prevail, and when the pandemic ends, we will all be proud of what we did for our patients and each other in this critical moment for humanity.”
Two months after the first patient with COVID-19 was identified in China, the first case was reported in the United States in the Seattle, Washington, metropolitan area.
Seattle rapidly became the first US epicenter for COVID-19, and local experts are now offering their expertise and advice on how to provide optimal cancer care during the pandemic in a special feature published online March 20 in the Journal of the National Comprehensive Cancer Network.
“We began implementing measures in early March, including infection control and screening of visitors, staff, and patients at the door,” said lead author Masumi Ueda, MD, who holds positions at the Seattle Cancer Care Alliance, the University of Washington, and the Fred Hutchinson Research Center.
“A lot of changes have been implemented, and it changes on a daily basis. We are responding to the growing rate of COVID-19 infection in the community,” she told Medscape Medical News.
Ueda notes that as a result of the quick implementation of new procedures, so far, very few cancer patients at their facilities have been infected by the virus. “It has not hit our cancer population hard, which is a good thing,” she said.
Create “Incident Command Structure”
In sharing their experience, the authors emphasize the importance of keeping channels of communication open between all stakeholders ― administrators and staff, patients, caregivers, and the general public. They also recommend that each facility create an “incident command structure” that can provide early coordination of institution-wide efforts and that can rapidly respond to changing information.
Ueda noted that their command structure was set up very early on, “so we could get communication set up and start building an infrastructure for response.”
Several areas of care that required new strategies were addressed, both to protect patients and to work around staff shortages caused by possible exposure and/or school closings, as well as projected shortages of supplies and hospital resources.
First and foremost was to identify patients and visitors who had respiratory symptoms and to provide them with masks. Although this is always routine practice during the respiratory virus season, screening has now been initiated at entry points throughout the system.
“We were lucky in Seattle and Washington state in that the University of Washington virology lab developed PCR [polymerase chain reaction] testing early on for COVID-19, which subsequently got FDA approval,” said Ueda. “So we were able to have local testing and didn’t have to rely on the state lab. Testing has also been rapidly scaled up.”
Initiating a comprehensive policy for testing staff, tracking results and exposures for persons under investigation, and defining when it is possible to return to work are essential elements for maintaining a stable workforce. In addition, reinforcing a strict “stay at home when ill” policy and providing access to testing for symptomatic staff have been key to limiting exposures.
“What is unique to our region is that we had testing early on, and we are turning it around in 24 hours,” she pointed out. “This is important for staff to be able to return to work.” Currently, staff, patients, and visitors are being tested only if they show the cardinal symptoms associated with COVID-19: fever, shortness of breath, and cough, although muscle aches have recently been added to their testing protocol.
“I think if we had unlimited capacity, we might consider testing people who are asymptomatic,” Ueda noted, “although if you don’t have symptoms, you may not have the viral load needed for an accurate test.”
Educational materials explaining infection control were also needed for patients and families, along with signs and a website to provide COVID-19 education. These were quickly developed.
In addition, a telephone triage line was established for patients with mild symptoms in order to minimize exposures in clinics and to lessen the number of patients presenting at emergency departments.
Outpatient Care
Because theirs is a referral center, many cancer patients come from out of town, and so there is concern about exposing nonlocal patients to COVID-19 as the virus spreads in the Seattle area. In addition, staffing shortages due to factors such as illness, exposure, and school closures are anticipated.
To address these problems, an initial priority was to establish a “multilayer” coverage system for the clinics in the event that practitioners had to be quarantined on short notice, the authors explain.
One decision was to reschedule all wellness visits for current patients or to use telemedicine. Capacity for that option expanded quickly, which was greatly helped by the recent decision by the Centers for Medicare & Medicaid Services to lift Medicare restrictions on the use of certain telemedicine services.
Another approach is to defer all consultations for second opinions for patients who were already undergoing treatment and to increase clinic hours of operations and capabilities for acute evaluations. This helps reserve emergency departments and hospital resources for patients who require higher-level care, the authors comment.
Treatment Decisions
Treatment decisions were more challenging to make, the authors note. One decision was that, despite the risk for COVID-19 for patients with solid tumors, adjuvant therapy with curative intent should proceed, they note. Similarly, patients with metastatic disease might lose the window of opportunity for treatment if it is delayed.
Treatment for aggressive hematologic malignancies is usually urgent, and stem cell transplant and cellular immunotherapies that provide curative treatments cannot be delayed in many cases.
Enrollment in clinical trials will most likely be limited to those trials that are most likely to benefit the patient.
Ueda noted that, because their patients come from all over the country, they are now conducting consultations for stem cell transplant by telephone so that nonlocal patients do not have to travel to Seattle. “If there is some way we can delay the treatment, we have taken that approach,” Ueda told Medscape Medical News. “If we can divert a patient to an area that is not as heavily affected, that’s another option we are taking.”
Although cancer surgery is not considered elective, surgical intervention needs to be prioritized, the authors comment. In the Seattle system, there is currently a 2-week ban on elective surgery in the healthcare system, owing to limited availability of personal protective equipment (PPE), staffing, and beds.
The oncology teams are currently reviewing treatment regimens to determine which treatments might lessen immunosuppression and which treatment options can be moved from the inpatient to the outpatient setting or can be delayed.
Inpatient Care
For hospitalized patients, several issues are being addressed. The priority is to prepare for an upcoming shortage of beds and resources because of the surge of patients with COVID-19 that is predicted. For both clinic and hospitalized patients, shortages of blood products have necessitated stricter adherence to thresholds for transfusion, and consideration is being given to lowering those thresholds.
Another important problem is the need to conserve PPE, which includes masks, gowns, gloves, and other products. The Seattle teams have implemented solutions such as favoring handwashing with soap and water over the use of hand gel for standard-precaution rooms, limiting the number of personnel entering patient rooms (so as to use less PPE), and reducing nursing procedures that require PPE, such as measuring urine output, unless they are necessary.
In addition, a no-visitor policy has been adopted in inpatient units to conserve PPE, with the exception of end-of-life situations.
The Future
The future trajectory of the COVID-19 pandemic is uncertain, Ueda commented. She emphasized that “we must continue to prepare for its widespread impact. The unknown is what we are looking at. We are expecting it to evolve, and the number of infections cannot go down.”
Ueda and coauthors end their article on a positive note. “To many of us, this has become the health care challenge of our generation, one that modern cancer therapy has never had to face. We will prevail, and when the pandemic ends, we will all be proud of what we did for our patients and each other in this critical moment for humanity.”
7 tips for running your practice in the coronavirus crisis
At one large practice in Bergen County, New Jersey, the waiting room is empty — but its patients are still receiving care. As of mid-March, the practice is still operating, thanks to the group’s willingness to adapt its work flow, sometimes radically, to mitigate the threat of the COVID-19 pandemic.
For example, patients now call the receptionist from their vehicles when they arrive, and wait there until receiving a call back telling them the clinician is ready. The practice has also started using telemedicine for the first time, to the extent it can be adopted in a hurry, and some clinicians are working from home on tasks such as medication refills.
Still, the rapidly increasing numbers of COVID-19 cases in the United States raises the possibility that some physician offices will decide or be forced to close temporarily, as occurred in London last month.
Many practices across the country are having to adjust the way they operate, amid daily changes in the pandemic. What should you do to adapt to this new way of operating your practice?
1. Create a task force to manage change
The readiness of medical practices to address the myriad challenges posed by this crisis has so far been a mixed bag, said Owen Dahl, MBA, a Texas-based medical practice management consultant. “Leadership is going to have to assess what’s happening in the community, what’s happening with staff members who may or may not have the disease and may or may not have to self-quarantine,” Dahl said.
The physicians, the administrator, CEO, or managing partner should be involved in decision making as the global crisis unfolds, added Laurie Morgan, MBA, a California-based practice management consultant. And depending on the size of the practice, it may be useful to delegate specific components of this work to various department managers or other individuals in the group.
The team should assess:
- Recommendations and/or mandates from local, state, and federal governments
- Guidance from specialty and state medical societies
- How to triage patients over the phone, virtual visits, or referral to an alternate site of care
- Where to send patients for testing
- The practice’s inventory of personal protective equipment (PPE)
- Review of and possible revision of current infection control policies
- Possible collaborations within the community
- Reimbursement policies for suspected COVID-19 triage, testing, and follow-up treatment — in office or virtually
- Whether some employees’ work (eg, billing, coding) can be done remotely
- Options for paying personnel in the case of a temporary shutdown
- What’s covered and excluded by the group’s business interruption insurance
2. Consider postponing nonessential appointments
What’s more, it’s crucial for practices to form a strategy that does not involve bringing patients into the office, said Javeed Siddiqui, MD, MPH, an infectious disease physician, epidemiologist, and chief medical officer of TeleMed2U. “One thing we really have to recognize in this pandemic is that we don’t want people going and sitting in our waiting room. We don’t want people coming, and not only exposing other patients, but also further exposing staff. Forward triaging is going to be essential in this type of pandemic.”
Reliant Medical Group, with multiple locations in Massachusetts, for example, announced to patients recently that it will postpone appointments for some routine and elective procedures, as determined by the group’s physicians and clinical staff.
“Taking this step will help limit the number of people passing through our facilities, which will help slow the spread of illness [as recommended by the CDC],” noted an email blast to patients.
3. Overcommunicate to patients
With a situation as dynamic and unprecedented as this, constant and clear communication with patients is crucial. “In general, in my experience, practices don’t realize how much communication is necessary,” said Morgan. “In order to be effective and get the word out, you have to be overcommunicating.”
Today’s practices have multiple ways to communicate to keep people informed, including email, text messaging, social media, patient portals, and even local television and radio.
One email or text message to the patient population can help direct them to the appropriate streams of information. Helping direct patients to updated information is critical.
In contrast, having the front desk field multitudes of calls from concerned patients ties up precious resources, according Siddiqui. “Right now, practices are absolutely inundated, patients are waiting on hold, and that creates a great deal of frustration,” he said.
“We really need to take a page from every other industry in the United States, and that is using secure SMS, email communication, and telehealth,” Siddiqui said. “Healthcare generally tends to be a laggard in this because so many people think, ‘Well, you can’t do that in healthcare,’ as opposed to thinking, ‘How can we do that in healthcare?’”
4. Take advantage of telemedicine
Fortunately, technology to interact with patients remotely is almost ubiquitous. Even for practices with little experience in this arena, various vendors exist that can get secure, HIPAA-compliant technologies up and running quickly.
Various payers have issued guidance regarding reimbursement for telemedicine specific to COVID-19, and on March 6, Congress passed a law regarding Medicare coverage and payment for virtual services during a government-declared state of emergency. Some of the rules about HIPAA compliance in telemedicine have been eased for this emergency.
But even with well-established telemedicine modalities in place, it’s crunch time for applying it to COVID-19. “You need to find a way to have telemedicine available and use it, because depending on how this goes, that’s going to be clearly the safest, best way to care for a huge number of people,” said Darryl Elmouchi, MD, MBA, chief medical officer of Spectrum Health System and president of Spectrum Health Medical Group in Michigan.
“What we recognize now, both with our past experience with telehealth for many years and specifically with this coronavirus testing we’ve done, is that it’s incredibly useful both for the clinicians and the patients,” Elmouchi said.
One possibility to consider is the tactic used by Spectrum, a large integrated healthcare system. The company mobilized its existing telemedicine program to offer free virtual screenings for anyone in Michigan showing possible symptoms of COVID-19. “We wanted to keep people out of our clinics, emergency rooms, and urgent care centers if they didn’t need to be there, and help allay fears,” he said.
Elmouchi said his company faced the problems that other physicians would also have to deal with. “It was a ton of work with a dedicated team that was focused on this. The hardest part was probably trying to determine how we can staff it,” he said.
With their dedicated virtual team still seeing regularly scheduled virtual patients, the system had to reassign its traditional teams, such as urgent care and primary care clinicians, to the virtual screening effort. “Then we had to figure out how we could operationalize it. It was a lot of work,” Elmouchi said.
Telemedicine capabilities are not limited to screening patients, but can also be used to stay in touch with patients who may be quarantined and provide follow-up care, he noted.
5. Identify COVID-19 testing sites
Access to tests remains a problem in the US, but is improving by the week. For practices that can attain the tests themselves, it will still require some creativity to administer them with as little risk as possible. In South Korea, for example, and increasingly in the United States, healthcare organizations are instructing patients waiting to be tested to stay in their cars and have a practitioner wearing the proper PPE go out to patients to test them there.
Alternatively, some practices may opt to have PPE-wearing staff members bring PPE to patients in their cars and then escort them to a designated testing area in the building —through the back door if noninfected patients are still being seen.
“Once in the office, you still need to isolate virus patients in any way you can,” Dahl said. “In fact, you want a negative-pressure environment if possible, with the air being sucked out rather than circulating,” he said, adding that a large restroom with a ventilation system could be repurposed as a makeshift exam room.
Community testing sites are another possibility, given proper coordination with other healthcare organizations and community officials. Siddiqui has been working with several communities in which individual clinics and hospitals are unable to handle testing on their own, and have instead collaborated to create community testing sites in tents on local athletic fields.
“One of our communities is looking at using the local college parking lot to do drive-through testing there,” he said. “We really need to embrace collaboration much more than we’ve ever done.”
Collaboration also requires sharing supplies and PPE, noted Dahl. “Don’t hoard them because of the shortage. Look at your inventory and make sure you can help out whomever you may be sending patients to.” And if your office is falling short, Dahl advises checking with offices in your community that may be closing — such as dentists or plastic surgeons — for supplies you can purchase or simply have.
The US Food and Drug Administration has issued some guidance to healthcare providers about shortages of surgical masks and gowns, including advice about reusable cloth alternatives to gowns.
In addition, some hospitals have asked clinicians to keep their masks and provided guidance on how to conserve supplies.
6. Preparing to potentially shut down
A temporary closure may be inevitable for some practices. “Maybe the physician owners will not feel like they have a choice,” said Morgan. “They might feel like they want to stay open for as long as they can; but if it’s not safe for patients or not safe for employees, maybe they’ll feel it’s better if they check out for a bit.”
Should practices make the decision to close or reduce hours, multimodal communication with patients and the public is paramount. Patients will want to know whom to call if they are feeling ill for any reason, where to seek care, and when the practice expects to reopen. Again, proactive outreach will be more efficient and comforting to patients.
Handling financial ramifications of closure is a top priority as well, and will require a full understanding of what is and isn’t covered by the practice’s business interruption insurance. Practices that don’t have a line of credit should reach out to banks and the Small Business Administration immediately, according to Dahl. Practices that have lines of credit already may want to ask for an increase, added Morgan.
Protecting employees’ income is challenging as well. For employees who are furloughed, consider allowing them to use their sick and vacation time during the shutdown — and possibly let staff ‘borrow’ not-yet accrued paid time off.
“However, there’s a risk with certain jobs in a medical practice that tend to have extremely high turnover, so physicians and administrators may be reluctant to pay people too much because they don’t know for sure those employees will come back to those jobs,” Morgan said. “On the other hand, if you have had a stable team for a very long time and feel confident that those employees are going to stay, then you may make a different decision.”
7. Seize work-from-home opportunities
Even if the practice isn’t seeing patients, there may be opportunities for some employees, such as billers and schedulers, to continue to work from home,” Morgan noted. Particularly if a practice is behind on its billing, a closure or slowdown is an ideal time to catch up. This measure will keep at least some people working — perhaps including some individuals who can be cross-trained to do other tasks — and maintain some cashflow when the practice needs it most.
Other remote-friendly jobs that often fall by the wayside when practices are busy include marketing tasks such as setting up or updating Google business pages, Healthgrades profiles, and so on, noted Morgan.
“Another thing that can be even more important, and is often overlooked, is making sure health plan directories have correct information about your practice,” she added. “These are pesky, often tedious tasks that may require repeated contact with health plans to fix things — perfect things to do when the office is not busy or closed.”
For administrators and billers, if the practice is able to keep paying these employees while partially or fully closed, it can also be an excellent time to do the sort of analysis that takes a lot of focused attention and is hard to do when busy. Some examples: a detailed comparison of payer performance, analysis of referral patterns, or a review of coding accuracy, Morgan suggested.
Although practices have varying levels of comfort in letting employees work from home, it’s not much different from working with external billing or scheduling services that have grown more popular in recent years, Morgan said.
As with many technologies, HIPAA is a leading concern, though it needn’t be, according to Morgan. “If you are on a cloud-based electronic medical record and practice management system, there’s a good chance that it’s very straightforward to set someone up to work from elsewhere and have that data be secure,” she said.
Finally, as the crisis begins to abate, practices must keep working in teams to evaluate and structure an orderly return to business as usual, gleaning best practices from colleagues whenever possible.
“I would tell practices this is not a time when anyone is competing with anyone,” said Elmouchi. “The more collaboration between practices and health systems that have larger resources, the better.”
This article was originally published on Medscape.com.
At one large practice in Bergen County, New Jersey, the waiting room is empty — but its patients are still receiving care. As of mid-March, the practice is still operating, thanks to the group’s willingness to adapt its work flow, sometimes radically, to mitigate the threat of the COVID-19 pandemic.
For example, patients now call the receptionist from their vehicles when they arrive, and wait there until receiving a call back telling them the clinician is ready. The practice has also started using telemedicine for the first time, to the extent it can be adopted in a hurry, and some clinicians are working from home on tasks such as medication refills.
Still, the rapidly increasing numbers of COVID-19 cases in the United States raises the possibility that some physician offices will decide or be forced to close temporarily, as occurred in London last month.
Many practices across the country are having to adjust the way they operate, amid daily changes in the pandemic. What should you do to adapt to this new way of operating your practice?
1. Create a task force to manage change
The readiness of medical practices to address the myriad challenges posed by this crisis has so far been a mixed bag, said Owen Dahl, MBA, a Texas-based medical practice management consultant. “Leadership is going to have to assess what’s happening in the community, what’s happening with staff members who may or may not have the disease and may or may not have to self-quarantine,” Dahl said.
The physicians, the administrator, CEO, or managing partner should be involved in decision making as the global crisis unfolds, added Laurie Morgan, MBA, a California-based practice management consultant. And depending on the size of the practice, it may be useful to delegate specific components of this work to various department managers or other individuals in the group.
The team should assess:
- Recommendations and/or mandates from local, state, and federal governments
- Guidance from specialty and state medical societies
- How to triage patients over the phone, virtual visits, or referral to an alternate site of care
- Where to send patients for testing
- The practice’s inventory of personal protective equipment (PPE)
- Review of and possible revision of current infection control policies
- Possible collaborations within the community
- Reimbursement policies for suspected COVID-19 triage, testing, and follow-up treatment — in office or virtually
- Whether some employees’ work (eg, billing, coding) can be done remotely
- Options for paying personnel in the case of a temporary shutdown
- What’s covered and excluded by the group’s business interruption insurance
2. Consider postponing nonessential appointments
What’s more, it’s crucial for practices to form a strategy that does not involve bringing patients into the office, said Javeed Siddiqui, MD, MPH, an infectious disease physician, epidemiologist, and chief medical officer of TeleMed2U. “One thing we really have to recognize in this pandemic is that we don’t want people going and sitting in our waiting room. We don’t want people coming, and not only exposing other patients, but also further exposing staff. Forward triaging is going to be essential in this type of pandemic.”
Reliant Medical Group, with multiple locations in Massachusetts, for example, announced to patients recently that it will postpone appointments for some routine and elective procedures, as determined by the group’s physicians and clinical staff.
“Taking this step will help limit the number of people passing through our facilities, which will help slow the spread of illness [as recommended by the CDC],” noted an email blast to patients.
3. Overcommunicate to patients
With a situation as dynamic and unprecedented as this, constant and clear communication with patients is crucial. “In general, in my experience, practices don’t realize how much communication is necessary,” said Morgan. “In order to be effective and get the word out, you have to be overcommunicating.”
Today’s practices have multiple ways to communicate to keep people informed, including email, text messaging, social media, patient portals, and even local television and radio.
One email or text message to the patient population can help direct them to the appropriate streams of information. Helping direct patients to updated information is critical.
In contrast, having the front desk field multitudes of calls from concerned patients ties up precious resources, according Siddiqui. “Right now, practices are absolutely inundated, patients are waiting on hold, and that creates a great deal of frustration,” he said.
“We really need to take a page from every other industry in the United States, and that is using secure SMS, email communication, and telehealth,” Siddiqui said. “Healthcare generally tends to be a laggard in this because so many people think, ‘Well, you can’t do that in healthcare,’ as opposed to thinking, ‘How can we do that in healthcare?’”
4. Take advantage of telemedicine
Fortunately, technology to interact with patients remotely is almost ubiquitous. Even for practices with little experience in this arena, various vendors exist that can get secure, HIPAA-compliant technologies up and running quickly.
Various payers have issued guidance regarding reimbursement for telemedicine specific to COVID-19, and on March 6, Congress passed a law regarding Medicare coverage and payment for virtual services during a government-declared state of emergency. Some of the rules about HIPAA compliance in telemedicine have been eased for this emergency.
But even with well-established telemedicine modalities in place, it’s crunch time for applying it to COVID-19. “You need to find a way to have telemedicine available and use it, because depending on how this goes, that’s going to be clearly the safest, best way to care for a huge number of people,” said Darryl Elmouchi, MD, MBA, chief medical officer of Spectrum Health System and president of Spectrum Health Medical Group in Michigan.
“What we recognize now, both with our past experience with telehealth for many years and specifically with this coronavirus testing we’ve done, is that it’s incredibly useful both for the clinicians and the patients,” Elmouchi said.
One possibility to consider is the tactic used by Spectrum, a large integrated healthcare system. The company mobilized its existing telemedicine program to offer free virtual screenings for anyone in Michigan showing possible symptoms of COVID-19. “We wanted to keep people out of our clinics, emergency rooms, and urgent care centers if they didn’t need to be there, and help allay fears,” he said.
Elmouchi said his company faced the problems that other physicians would also have to deal with. “It was a ton of work with a dedicated team that was focused on this. The hardest part was probably trying to determine how we can staff it,” he said.
With their dedicated virtual team still seeing regularly scheduled virtual patients, the system had to reassign its traditional teams, such as urgent care and primary care clinicians, to the virtual screening effort. “Then we had to figure out how we could operationalize it. It was a lot of work,” Elmouchi said.
Telemedicine capabilities are not limited to screening patients, but can also be used to stay in touch with patients who may be quarantined and provide follow-up care, he noted.
5. Identify COVID-19 testing sites
Access to tests remains a problem in the US, but is improving by the week. For practices that can attain the tests themselves, it will still require some creativity to administer them with as little risk as possible. In South Korea, for example, and increasingly in the United States, healthcare organizations are instructing patients waiting to be tested to stay in their cars and have a practitioner wearing the proper PPE go out to patients to test them there.
Alternatively, some practices may opt to have PPE-wearing staff members bring PPE to patients in their cars and then escort them to a designated testing area in the building —through the back door if noninfected patients are still being seen.
“Once in the office, you still need to isolate virus patients in any way you can,” Dahl said. “In fact, you want a negative-pressure environment if possible, with the air being sucked out rather than circulating,” he said, adding that a large restroom with a ventilation system could be repurposed as a makeshift exam room.
Community testing sites are another possibility, given proper coordination with other healthcare organizations and community officials. Siddiqui has been working with several communities in which individual clinics and hospitals are unable to handle testing on their own, and have instead collaborated to create community testing sites in tents on local athletic fields.
“One of our communities is looking at using the local college parking lot to do drive-through testing there,” he said. “We really need to embrace collaboration much more than we’ve ever done.”
Collaboration also requires sharing supplies and PPE, noted Dahl. “Don’t hoard them because of the shortage. Look at your inventory and make sure you can help out whomever you may be sending patients to.” And if your office is falling short, Dahl advises checking with offices in your community that may be closing — such as dentists or plastic surgeons — for supplies you can purchase or simply have.
The US Food and Drug Administration has issued some guidance to healthcare providers about shortages of surgical masks and gowns, including advice about reusable cloth alternatives to gowns.
In addition, some hospitals have asked clinicians to keep their masks and provided guidance on how to conserve supplies.
6. Preparing to potentially shut down
A temporary closure may be inevitable for some practices. “Maybe the physician owners will not feel like they have a choice,” said Morgan. “They might feel like they want to stay open for as long as they can; but if it’s not safe for patients or not safe for employees, maybe they’ll feel it’s better if they check out for a bit.”
Should practices make the decision to close or reduce hours, multimodal communication with patients and the public is paramount. Patients will want to know whom to call if they are feeling ill for any reason, where to seek care, and when the practice expects to reopen. Again, proactive outreach will be more efficient and comforting to patients.
Handling financial ramifications of closure is a top priority as well, and will require a full understanding of what is and isn’t covered by the practice’s business interruption insurance. Practices that don’t have a line of credit should reach out to banks and the Small Business Administration immediately, according to Dahl. Practices that have lines of credit already may want to ask for an increase, added Morgan.
Protecting employees’ income is challenging as well. For employees who are furloughed, consider allowing them to use their sick and vacation time during the shutdown — and possibly let staff ‘borrow’ not-yet accrued paid time off.
“However, there’s a risk with certain jobs in a medical practice that tend to have extremely high turnover, so physicians and administrators may be reluctant to pay people too much because they don’t know for sure those employees will come back to those jobs,” Morgan said. “On the other hand, if you have had a stable team for a very long time and feel confident that those employees are going to stay, then you may make a different decision.”
7. Seize work-from-home opportunities
Even if the practice isn’t seeing patients, there may be opportunities for some employees, such as billers and schedulers, to continue to work from home,” Morgan noted. Particularly if a practice is behind on its billing, a closure or slowdown is an ideal time to catch up. This measure will keep at least some people working — perhaps including some individuals who can be cross-trained to do other tasks — and maintain some cashflow when the practice needs it most.
Other remote-friendly jobs that often fall by the wayside when practices are busy include marketing tasks such as setting up or updating Google business pages, Healthgrades profiles, and so on, noted Morgan.
“Another thing that can be even more important, and is often overlooked, is making sure health plan directories have correct information about your practice,” she added. “These are pesky, often tedious tasks that may require repeated contact with health plans to fix things — perfect things to do when the office is not busy or closed.”
For administrators and billers, if the practice is able to keep paying these employees while partially or fully closed, it can also be an excellent time to do the sort of analysis that takes a lot of focused attention and is hard to do when busy. Some examples: a detailed comparison of payer performance, analysis of referral patterns, or a review of coding accuracy, Morgan suggested.
Although practices have varying levels of comfort in letting employees work from home, it’s not much different from working with external billing or scheduling services that have grown more popular in recent years, Morgan said.
As with many technologies, HIPAA is a leading concern, though it needn’t be, according to Morgan. “If you are on a cloud-based electronic medical record and practice management system, there’s a good chance that it’s very straightforward to set someone up to work from elsewhere and have that data be secure,” she said.
Finally, as the crisis begins to abate, practices must keep working in teams to evaluate and structure an orderly return to business as usual, gleaning best practices from colleagues whenever possible.
“I would tell practices this is not a time when anyone is competing with anyone,” said Elmouchi. “The more collaboration between practices and health systems that have larger resources, the better.”
This article was originally published on Medscape.com.
At one large practice in Bergen County, New Jersey, the waiting room is empty — but its patients are still receiving care. As of mid-March, the practice is still operating, thanks to the group’s willingness to adapt its work flow, sometimes radically, to mitigate the threat of the COVID-19 pandemic.
For example, patients now call the receptionist from their vehicles when they arrive, and wait there until receiving a call back telling them the clinician is ready. The practice has also started using telemedicine for the first time, to the extent it can be adopted in a hurry, and some clinicians are working from home on tasks such as medication refills.
Still, the rapidly increasing numbers of COVID-19 cases in the United States raises the possibility that some physician offices will decide or be forced to close temporarily, as occurred in London last month.
Many practices across the country are having to adjust the way they operate, amid daily changes in the pandemic. What should you do to adapt to this new way of operating your practice?
1. Create a task force to manage change
The readiness of medical practices to address the myriad challenges posed by this crisis has so far been a mixed bag, said Owen Dahl, MBA, a Texas-based medical practice management consultant. “Leadership is going to have to assess what’s happening in the community, what’s happening with staff members who may or may not have the disease and may or may not have to self-quarantine,” Dahl said.
The physicians, the administrator, CEO, or managing partner should be involved in decision making as the global crisis unfolds, added Laurie Morgan, MBA, a California-based practice management consultant. And depending on the size of the practice, it may be useful to delegate specific components of this work to various department managers or other individuals in the group.
The team should assess:
- Recommendations and/or mandates from local, state, and federal governments
- Guidance from specialty and state medical societies
- How to triage patients over the phone, virtual visits, or referral to an alternate site of care
- Where to send patients for testing
- The practice’s inventory of personal protective equipment (PPE)
- Review of and possible revision of current infection control policies
- Possible collaborations within the community
- Reimbursement policies for suspected COVID-19 triage, testing, and follow-up treatment — in office or virtually
- Whether some employees’ work (eg, billing, coding) can be done remotely
- Options for paying personnel in the case of a temporary shutdown
- What’s covered and excluded by the group’s business interruption insurance
2. Consider postponing nonessential appointments
What’s more, it’s crucial for practices to form a strategy that does not involve bringing patients into the office, said Javeed Siddiqui, MD, MPH, an infectious disease physician, epidemiologist, and chief medical officer of TeleMed2U. “One thing we really have to recognize in this pandemic is that we don’t want people going and sitting in our waiting room. We don’t want people coming, and not only exposing other patients, but also further exposing staff. Forward triaging is going to be essential in this type of pandemic.”
Reliant Medical Group, with multiple locations in Massachusetts, for example, announced to patients recently that it will postpone appointments for some routine and elective procedures, as determined by the group’s physicians and clinical staff.
“Taking this step will help limit the number of people passing through our facilities, which will help slow the spread of illness [as recommended by the CDC],” noted an email blast to patients.
3. Overcommunicate to patients
With a situation as dynamic and unprecedented as this, constant and clear communication with patients is crucial. “In general, in my experience, practices don’t realize how much communication is necessary,” said Morgan. “In order to be effective and get the word out, you have to be overcommunicating.”
Today’s practices have multiple ways to communicate to keep people informed, including email, text messaging, social media, patient portals, and even local television and radio.
One email or text message to the patient population can help direct them to the appropriate streams of information. Helping direct patients to updated information is critical.
In contrast, having the front desk field multitudes of calls from concerned patients ties up precious resources, according Siddiqui. “Right now, practices are absolutely inundated, patients are waiting on hold, and that creates a great deal of frustration,” he said.
“We really need to take a page from every other industry in the United States, and that is using secure SMS, email communication, and telehealth,” Siddiqui said. “Healthcare generally tends to be a laggard in this because so many people think, ‘Well, you can’t do that in healthcare,’ as opposed to thinking, ‘How can we do that in healthcare?’”
4. Take advantage of telemedicine
Fortunately, technology to interact with patients remotely is almost ubiquitous. Even for practices with little experience in this arena, various vendors exist that can get secure, HIPAA-compliant technologies up and running quickly.
Various payers have issued guidance regarding reimbursement for telemedicine specific to COVID-19, and on March 6, Congress passed a law regarding Medicare coverage and payment for virtual services during a government-declared state of emergency. Some of the rules about HIPAA compliance in telemedicine have been eased for this emergency.
But even with well-established telemedicine modalities in place, it’s crunch time for applying it to COVID-19. “You need to find a way to have telemedicine available and use it, because depending on how this goes, that’s going to be clearly the safest, best way to care for a huge number of people,” said Darryl Elmouchi, MD, MBA, chief medical officer of Spectrum Health System and president of Spectrum Health Medical Group in Michigan.
“What we recognize now, both with our past experience with telehealth for many years and specifically with this coronavirus testing we’ve done, is that it’s incredibly useful both for the clinicians and the patients,” Elmouchi said.
One possibility to consider is the tactic used by Spectrum, a large integrated healthcare system. The company mobilized its existing telemedicine program to offer free virtual screenings for anyone in Michigan showing possible symptoms of COVID-19. “We wanted to keep people out of our clinics, emergency rooms, and urgent care centers if they didn’t need to be there, and help allay fears,” he said.
Elmouchi said his company faced the problems that other physicians would also have to deal with. “It was a ton of work with a dedicated team that was focused on this. The hardest part was probably trying to determine how we can staff it,” he said.
With their dedicated virtual team still seeing regularly scheduled virtual patients, the system had to reassign its traditional teams, such as urgent care and primary care clinicians, to the virtual screening effort. “Then we had to figure out how we could operationalize it. It was a lot of work,” Elmouchi said.
Telemedicine capabilities are not limited to screening patients, but can also be used to stay in touch with patients who may be quarantined and provide follow-up care, he noted.
5. Identify COVID-19 testing sites
Access to tests remains a problem in the US, but is improving by the week. For practices that can attain the tests themselves, it will still require some creativity to administer them with as little risk as possible. In South Korea, for example, and increasingly in the United States, healthcare organizations are instructing patients waiting to be tested to stay in their cars and have a practitioner wearing the proper PPE go out to patients to test them there.
Alternatively, some practices may opt to have PPE-wearing staff members bring PPE to patients in their cars and then escort them to a designated testing area in the building —through the back door if noninfected patients are still being seen.
“Once in the office, you still need to isolate virus patients in any way you can,” Dahl said. “In fact, you want a negative-pressure environment if possible, with the air being sucked out rather than circulating,” he said, adding that a large restroom with a ventilation system could be repurposed as a makeshift exam room.
Community testing sites are another possibility, given proper coordination with other healthcare organizations and community officials. Siddiqui has been working with several communities in which individual clinics and hospitals are unable to handle testing on their own, and have instead collaborated to create community testing sites in tents on local athletic fields.
“One of our communities is looking at using the local college parking lot to do drive-through testing there,” he said. “We really need to embrace collaboration much more than we’ve ever done.”
Collaboration also requires sharing supplies and PPE, noted Dahl. “Don’t hoard them because of the shortage. Look at your inventory and make sure you can help out whomever you may be sending patients to.” And if your office is falling short, Dahl advises checking with offices in your community that may be closing — such as dentists or plastic surgeons — for supplies you can purchase or simply have.
The US Food and Drug Administration has issued some guidance to healthcare providers about shortages of surgical masks and gowns, including advice about reusable cloth alternatives to gowns.
In addition, some hospitals have asked clinicians to keep their masks and provided guidance on how to conserve supplies.
6. Preparing to potentially shut down
A temporary closure may be inevitable for some practices. “Maybe the physician owners will not feel like they have a choice,” said Morgan. “They might feel like they want to stay open for as long as they can; but if it’s not safe for patients or not safe for employees, maybe they’ll feel it’s better if they check out for a bit.”
Should practices make the decision to close or reduce hours, multimodal communication with patients and the public is paramount. Patients will want to know whom to call if they are feeling ill for any reason, where to seek care, and when the practice expects to reopen. Again, proactive outreach will be more efficient and comforting to patients.
Handling financial ramifications of closure is a top priority as well, and will require a full understanding of what is and isn’t covered by the practice’s business interruption insurance. Practices that don’t have a line of credit should reach out to banks and the Small Business Administration immediately, according to Dahl. Practices that have lines of credit already may want to ask for an increase, added Morgan.
Protecting employees’ income is challenging as well. For employees who are furloughed, consider allowing them to use their sick and vacation time during the shutdown — and possibly let staff ‘borrow’ not-yet accrued paid time off.
“However, there’s a risk with certain jobs in a medical practice that tend to have extremely high turnover, so physicians and administrators may be reluctant to pay people too much because they don’t know for sure those employees will come back to those jobs,” Morgan said. “On the other hand, if you have had a stable team for a very long time and feel confident that those employees are going to stay, then you may make a different decision.”
7. Seize work-from-home opportunities
Even if the practice isn’t seeing patients, there may be opportunities for some employees, such as billers and schedulers, to continue to work from home,” Morgan noted. Particularly if a practice is behind on its billing, a closure or slowdown is an ideal time to catch up. This measure will keep at least some people working — perhaps including some individuals who can be cross-trained to do other tasks — and maintain some cashflow when the practice needs it most.
Other remote-friendly jobs that often fall by the wayside when practices are busy include marketing tasks such as setting up or updating Google business pages, Healthgrades profiles, and so on, noted Morgan.
“Another thing that can be even more important, and is often overlooked, is making sure health plan directories have correct information about your practice,” she added. “These are pesky, often tedious tasks that may require repeated contact with health plans to fix things — perfect things to do when the office is not busy or closed.”
For administrators and billers, if the practice is able to keep paying these employees while partially or fully closed, it can also be an excellent time to do the sort of analysis that takes a lot of focused attention and is hard to do when busy. Some examples: a detailed comparison of payer performance, analysis of referral patterns, or a review of coding accuracy, Morgan suggested.
Although practices have varying levels of comfort in letting employees work from home, it’s not much different from working with external billing or scheduling services that have grown more popular in recent years, Morgan said.
As with many technologies, HIPAA is a leading concern, though it needn’t be, according to Morgan. “If you are on a cloud-based electronic medical record and practice management system, there’s a good chance that it’s very straightforward to set someone up to work from elsewhere and have that data be secure,” she said.
Finally, as the crisis begins to abate, practices must keep working in teams to evaluate and structure an orderly return to business as usual, gleaning best practices from colleagues whenever possible.
“I would tell practices this is not a time when anyone is competing with anyone,” said Elmouchi. “The more collaboration between practices and health systems that have larger resources, the better.”
This article was originally published on Medscape.com.
How is oncology adapting to COVID-19?
As the coronavirus pandemic escalates in the United States, Medscape Oncology reached out to a group of our contributors and asked them to provide their perspective on how their oncology departments and centers are preparing. Here are their responses to a number of issues facing oncologists in the US and around the world.
Have you shifted nonurgent follow-up visits to telemedicine, either via video or phone?
Kathy Miller, MD, Associate Director of Indiana University Simon Cancer Center: We are reviewing our clinic schedules and identifying “routine” follow-up patients who can be rescheduled. When patients are contacted to reschedule, they are asked if they have any urgent, immediate concerns that need to be addressed before the new appointment. If yes, they are offered a virtual visit.
Don Dizon, MD, Director of Women’s Cancers, Lifespan Cancer Institute; Director of Medical Oncology, Rhode Island Hospital: We have started to do this in preparation for a surge of people with COVID-19. Patients who are in long-term follow-up (no evidence of disease at 3 years or longer, being seen annually) or those in routine surveillance after curative treatment (that is, seen every 3 months) as well as those being seen for supportive care–type visits, like sexual health or survivorship, are all being contacted and visits are being moved to telehealth.
Jeffrey S. Weber, MD, PhD, Deputy Director of the Laura and Isaac Perlmutter Cancer Center at NYU Langone Medical Center: Yes. Any follow-up, nontreatment visits are done by phone or video if the patient agrees. (They all have).
Have you delayed or canceled cancer surgeries?
Ravi B. Parikh, MD, MPP, Medical oncologist at the University of Pennsylvania and the Philadelphia VA Medical Center: The University of Pennsylvania has taken this seriously. We’ve canceled all elective surgeries, have ramped up our telemedicine (video and phone) capabilities significantly, are limiting our appointments mostly to on-treatment visits, and have been asked to reconsider regular scans and reviews.
Dizon: We have not done this. There are apparently differences in interpretation in what institutions might mean as “elective surgeries.” At our institution, surgery for invasive malignancies is not elective. However, this may (or will) change if resources become an issue.
Lidia Schapira, MD, Associate Professor of Medicine and Director of Cancer Survivorship at the Stanford Comprehensive Cancer Institute: Delaying elective surgery is something that hospitals here have already implemented, and I imagine that this trend will spread. But it may be difficult to decide in situations that are not exactly “life-saving” but where an earlier intervention could preserve function or improve quality of life.
Mark A. Lewis, MD, Director of Gastrointestinal Oncology at Intermountain Healthcare in Utah: Cancer surgeries have not been deemed elective or delayed.
Have you delayed or altered the delivery of potentially immune-comprising treatments?
David Kerr, MD, Professor of Cancer Medicine at the University of Oxford in England: We are considering delaying initiation of our adjuvant colorectal cancer treatments, as we have data from our own QUASAR trials suggesting that patients who commence chemotherapy between 2 and 6 weeks do equally as well as those who begin 6-12 weeks after surgery.
Parikh: I personally haven’t delayed giving chemotherapy to avoid immune compromise, but I believe some others may have. It’s a delicate balance between wanting to ensure cancer control and making sure we are flattening the curve. As an example, though, I delayed three on-treatment visits for my clinic last Monday, and I converted 70% of my visits to telemedicine. However, I’m a genitourinary cancer specialist and the treatments I give are very different from others.
Lewis: The most difficult calculus is around adjuvant therapy. For metastatic patients, I am trying to use the least immunosuppressive regimen possible that will still control their disease. As you can imagine, it’s an assessment of competing risks.
Schapira: Patients who need essential anticancer therapy should still get it, but attempts to deintensify therapy should continue—for example, holding or postponing treatment without harm (based on evidence, not opinion). This may be possible for patients considering hormonal therapies for breast or prostate cancer.
Patients who need radiation should discuss the timing with their radiation oncologist. In some cases, it may be possible to delay treatment without affecting outcomes, but these decisions should be made carefully. Alternatively, shorter courses of radiation may be appropriate.
Have you advised your own patients differently given the high risk to cancer patients?
Kerr: We have factored potential infection with the virus into discussions where the benefits of chemotherapy are very marginal. This could tip the balance toward the patient deciding not to pursue chemotherapy.
Dizon: The data from China are not entirely crystal-clear. While they noted that people with active cancer and those who had a history of cancer are at increased risk for more severe infections and worse outcomes, the Chinese cohort was small, and compared with people without cancer, it tended to be much older and to be smokers (former or current). Having said this, we are counseling everyone about the importance of social distancing, washing hands, and not touching your face.
Lewis: If I have a complete blood count with a differential that includes lymphocytes, I can advise my lymphopenic patients (who are particularly vulnerable to viral infection) to take special precautions regarding social distancing in their own families.
Have any of your hospitalized patients been affected by policy changes to prepare beds/departments for the expected increase in COVID-19–positive patients?
Weber: Not yet.
Dizon: No, not at the moment.
Have you been asked to assist with other services or COVID-19 task forces?
Dizon: I am keenly involved in the preparations and modifications to procedures, including staffing decisions in outpatient, movement to telehealth, and work-from-home policies.
Lewis: I am engaged in system-wide COVID-19 efforts around oncology.
Kerr: Perhaps oddest of all, I am learning with some of our junior doctors to care for ventilated patients. I still consider myself enough of a general physician that I would hope to be able to contribute to the truly sick, but I accept that I do need an appropriate refresher course.
Bishal Gyawali, MD, PhD, medical oncologist at Queen’s University Cancer Research Institute: Queen’s Hospital medical students are now volunteering to help with daycare, groceries, and other tasks for staff who are working in the hospital.
Are you experiencing any shortages in personal protective equipment (PPE) at your center?
Miller: Some supplies are running short, though none are frankly out at this point. However, rationing and controls are in place to stretch the supplies as far as possible, including reusing some PPE.
Dizon: We are rationing face masks and N95 respirators, eye shields, and even surgical scrubs. We are talking about postponing elective surgery to save PPE but are not yet to that point. We’re asking that face masks be reused for at least 2 days, maybe longer. PPEs are one per day. Scrubs are kept secure.
Lewis: We are being very careful not to overuse PPE but currently have an adequate inventory. We have had to move gloves and masks to areas where they are not accessible to the general public, as otherwise they were being stolen (this started weeks ago).
Kerr: Our National Health System has an adequate supply of PPE equipment centrally, but there seems to be a problem with distribution, as some hospitals are reporting shortages.
Weber: Masks are in short supply, so they are being used for several days if not wet. We are short of plastic gowns and are using paper chemo gowns. Similar story at many places.
This article first appeared on Medscape.com.
As the coronavirus pandemic escalates in the United States, Medscape Oncology reached out to a group of our contributors and asked them to provide their perspective on how their oncology departments and centers are preparing. Here are their responses to a number of issues facing oncologists in the US and around the world.
Have you shifted nonurgent follow-up visits to telemedicine, either via video or phone?
Kathy Miller, MD, Associate Director of Indiana University Simon Cancer Center: We are reviewing our clinic schedules and identifying “routine” follow-up patients who can be rescheduled. When patients are contacted to reschedule, they are asked if they have any urgent, immediate concerns that need to be addressed before the new appointment. If yes, they are offered a virtual visit.
Don Dizon, MD, Director of Women’s Cancers, Lifespan Cancer Institute; Director of Medical Oncology, Rhode Island Hospital: We have started to do this in preparation for a surge of people with COVID-19. Patients who are in long-term follow-up (no evidence of disease at 3 years or longer, being seen annually) or those in routine surveillance after curative treatment (that is, seen every 3 months) as well as those being seen for supportive care–type visits, like sexual health or survivorship, are all being contacted and visits are being moved to telehealth.
Jeffrey S. Weber, MD, PhD, Deputy Director of the Laura and Isaac Perlmutter Cancer Center at NYU Langone Medical Center: Yes. Any follow-up, nontreatment visits are done by phone or video if the patient agrees. (They all have).
Have you delayed or canceled cancer surgeries?
Ravi B. Parikh, MD, MPP, Medical oncologist at the University of Pennsylvania and the Philadelphia VA Medical Center: The University of Pennsylvania has taken this seriously. We’ve canceled all elective surgeries, have ramped up our telemedicine (video and phone) capabilities significantly, are limiting our appointments mostly to on-treatment visits, and have been asked to reconsider regular scans and reviews.
Dizon: We have not done this. There are apparently differences in interpretation in what institutions might mean as “elective surgeries.” At our institution, surgery for invasive malignancies is not elective. However, this may (or will) change if resources become an issue.
Lidia Schapira, MD, Associate Professor of Medicine and Director of Cancer Survivorship at the Stanford Comprehensive Cancer Institute: Delaying elective surgery is something that hospitals here have already implemented, and I imagine that this trend will spread. But it may be difficult to decide in situations that are not exactly “life-saving” but where an earlier intervention could preserve function or improve quality of life.
Mark A. Lewis, MD, Director of Gastrointestinal Oncology at Intermountain Healthcare in Utah: Cancer surgeries have not been deemed elective or delayed.
Have you delayed or altered the delivery of potentially immune-comprising treatments?
David Kerr, MD, Professor of Cancer Medicine at the University of Oxford in England: We are considering delaying initiation of our adjuvant colorectal cancer treatments, as we have data from our own QUASAR trials suggesting that patients who commence chemotherapy between 2 and 6 weeks do equally as well as those who begin 6-12 weeks after surgery.
Parikh: I personally haven’t delayed giving chemotherapy to avoid immune compromise, but I believe some others may have. It’s a delicate balance between wanting to ensure cancer control and making sure we are flattening the curve. As an example, though, I delayed three on-treatment visits for my clinic last Monday, and I converted 70% of my visits to telemedicine. However, I’m a genitourinary cancer specialist and the treatments I give are very different from others.
Lewis: The most difficult calculus is around adjuvant therapy. For metastatic patients, I am trying to use the least immunosuppressive regimen possible that will still control their disease. As you can imagine, it’s an assessment of competing risks.
Schapira: Patients who need essential anticancer therapy should still get it, but attempts to deintensify therapy should continue—for example, holding or postponing treatment without harm (based on evidence, not opinion). This may be possible for patients considering hormonal therapies for breast or prostate cancer.
Patients who need radiation should discuss the timing with their radiation oncologist. In some cases, it may be possible to delay treatment without affecting outcomes, but these decisions should be made carefully. Alternatively, shorter courses of radiation may be appropriate.
Have you advised your own patients differently given the high risk to cancer patients?
Kerr: We have factored potential infection with the virus into discussions where the benefits of chemotherapy are very marginal. This could tip the balance toward the patient deciding not to pursue chemotherapy.
Dizon: The data from China are not entirely crystal-clear. While they noted that people with active cancer and those who had a history of cancer are at increased risk for more severe infections and worse outcomes, the Chinese cohort was small, and compared with people without cancer, it tended to be much older and to be smokers (former or current). Having said this, we are counseling everyone about the importance of social distancing, washing hands, and not touching your face.
Lewis: If I have a complete blood count with a differential that includes lymphocytes, I can advise my lymphopenic patients (who are particularly vulnerable to viral infection) to take special precautions regarding social distancing in their own families.
Have any of your hospitalized patients been affected by policy changes to prepare beds/departments for the expected increase in COVID-19–positive patients?
Weber: Not yet.
Dizon: No, not at the moment.
Have you been asked to assist with other services or COVID-19 task forces?
Dizon: I am keenly involved in the preparations and modifications to procedures, including staffing decisions in outpatient, movement to telehealth, and work-from-home policies.
Lewis: I am engaged in system-wide COVID-19 efforts around oncology.
Kerr: Perhaps oddest of all, I am learning with some of our junior doctors to care for ventilated patients. I still consider myself enough of a general physician that I would hope to be able to contribute to the truly sick, but I accept that I do need an appropriate refresher course.
Bishal Gyawali, MD, PhD, medical oncologist at Queen’s University Cancer Research Institute: Queen’s Hospital medical students are now volunteering to help with daycare, groceries, and other tasks for staff who are working in the hospital.
Are you experiencing any shortages in personal protective equipment (PPE) at your center?
Miller: Some supplies are running short, though none are frankly out at this point. However, rationing and controls are in place to stretch the supplies as far as possible, including reusing some PPE.
Dizon: We are rationing face masks and N95 respirators, eye shields, and even surgical scrubs. We are talking about postponing elective surgery to save PPE but are not yet to that point. We’re asking that face masks be reused for at least 2 days, maybe longer. PPEs are one per day. Scrubs are kept secure.
Lewis: We are being very careful not to overuse PPE but currently have an adequate inventory. We have had to move gloves and masks to areas where they are not accessible to the general public, as otherwise they were being stolen (this started weeks ago).
Kerr: Our National Health System has an adequate supply of PPE equipment centrally, but there seems to be a problem with distribution, as some hospitals are reporting shortages.
Weber: Masks are in short supply, so they are being used for several days if not wet. We are short of plastic gowns and are using paper chemo gowns. Similar story at many places.
This article first appeared on Medscape.com.
As the coronavirus pandemic escalates in the United States, Medscape Oncology reached out to a group of our contributors and asked them to provide their perspective on how their oncology departments and centers are preparing. Here are their responses to a number of issues facing oncologists in the US and around the world.
Have you shifted nonurgent follow-up visits to telemedicine, either via video or phone?
Kathy Miller, MD, Associate Director of Indiana University Simon Cancer Center: We are reviewing our clinic schedules and identifying “routine” follow-up patients who can be rescheduled. When patients are contacted to reschedule, they are asked if they have any urgent, immediate concerns that need to be addressed before the new appointment. If yes, they are offered a virtual visit.
Don Dizon, MD, Director of Women’s Cancers, Lifespan Cancer Institute; Director of Medical Oncology, Rhode Island Hospital: We have started to do this in preparation for a surge of people with COVID-19. Patients who are in long-term follow-up (no evidence of disease at 3 years or longer, being seen annually) or those in routine surveillance after curative treatment (that is, seen every 3 months) as well as those being seen for supportive care–type visits, like sexual health or survivorship, are all being contacted and visits are being moved to telehealth.
Jeffrey S. Weber, MD, PhD, Deputy Director of the Laura and Isaac Perlmutter Cancer Center at NYU Langone Medical Center: Yes. Any follow-up, nontreatment visits are done by phone or video if the patient agrees. (They all have).
Have you delayed or canceled cancer surgeries?
Ravi B. Parikh, MD, MPP, Medical oncologist at the University of Pennsylvania and the Philadelphia VA Medical Center: The University of Pennsylvania has taken this seriously. We’ve canceled all elective surgeries, have ramped up our telemedicine (video and phone) capabilities significantly, are limiting our appointments mostly to on-treatment visits, and have been asked to reconsider regular scans and reviews.
Dizon: We have not done this. There are apparently differences in interpretation in what institutions might mean as “elective surgeries.” At our institution, surgery for invasive malignancies is not elective. However, this may (or will) change if resources become an issue.
Lidia Schapira, MD, Associate Professor of Medicine and Director of Cancer Survivorship at the Stanford Comprehensive Cancer Institute: Delaying elective surgery is something that hospitals here have already implemented, and I imagine that this trend will spread. But it may be difficult to decide in situations that are not exactly “life-saving” but where an earlier intervention could preserve function or improve quality of life.
Mark A. Lewis, MD, Director of Gastrointestinal Oncology at Intermountain Healthcare in Utah: Cancer surgeries have not been deemed elective or delayed.
Have you delayed or altered the delivery of potentially immune-comprising treatments?
David Kerr, MD, Professor of Cancer Medicine at the University of Oxford in England: We are considering delaying initiation of our adjuvant colorectal cancer treatments, as we have data from our own QUASAR trials suggesting that patients who commence chemotherapy between 2 and 6 weeks do equally as well as those who begin 6-12 weeks after surgery.
Parikh: I personally haven’t delayed giving chemotherapy to avoid immune compromise, but I believe some others may have. It’s a delicate balance between wanting to ensure cancer control and making sure we are flattening the curve. As an example, though, I delayed three on-treatment visits for my clinic last Monday, and I converted 70% of my visits to telemedicine. However, I’m a genitourinary cancer specialist and the treatments I give are very different from others.
Lewis: The most difficult calculus is around adjuvant therapy. For metastatic patients, I am trying to use the least immunosuppressive regimen possible that will still control their disease. As you can imagine, it’s an assessment of competing risks.
Schapira: Patients who need essential anticancer therapy should still get it, but attempts to deintensify therapy should continue—for example, holding or postponing treatment without harm (based on evidence, not opinion). This may be possible for patients considering hormonal therapies for breast or prostate cancer.
Patients who need radiation should discuss the timing with their radiation oncologist. In some cases, it may be possible to delay treatment without affecting outcomes, but these decisions should be made carefully. Alternatively, shorter courses of radiation may be appropriate.
Have you advised your own patients differently given the high risk to cancer patients?
Kerr: We have factored potential infection with the virus into discussions where the benefits of chemotherapy are very marginal. This could tip the balance toward the patient deciding not to pursue chemotherapy.
Dizon: The data from China are not entirely crystal-clear. While they noted that people with active cancer and those who had a history of cancer are at increased risk for more severe infections and worse outcomes, the Chinese cohort was small, and compared with people without cancer, it tended to be much older and to be smokers (former or current). Having said this, we are counseling everyone about the importance of social distancing, washing hands, and not touching your face.
Lewis: If I have a complete blood count with a differential that includes lymphocytes, I can advise my lymphopenic patients (who are particularly vulnerable to viral infection) to take special precautions regarding social distancing in their own families.
Have any of your hospitalized patients been affected by policy changes to prepare beds/departments for the expected increase in COVID-19–positive patients?
Weber: Not yet.
Dizon: No, not at the moment.
Have you been asked to assist with other services or COVID-19 task forces?
Dizon: I am keenly involved in the preparations and modifications to procedures, including staffing decisions in outpatient, movement to telehealth, and work-from-home policies.
Lewis: I am engaged in system-wide COVID-19 efforts around oncology.
Kerr: Perhaps oddest of all, I am learning with some of our junior doctors to care for ventilated patients. I still consider myself enough of a general physician that I would hope to be able to contribute to the truly sick, but I accept that I do need an appropriate refresher course.
Bishal Gyawali, MD, PhD, medical oncologist at Queen’s University Cancer Research Institute: Queen’s Hospital medical students are now volunteering to help with daycare, groceries, and other tasks for staff who are working in the hospital.
Are you experiencing any shortages in personal protective equipment (PPE) at your center?
Miller: Some supplies are running short, though none are frankly out at this point. However, rationing and controls are in place to stretch the supplies as far as possible, including reusing some PPE.
Dizon: We are rationing face masks and N95 respirators, eye shields, and even surgical scrubs. We are talking about postponing elective surgery to save PPE but are not yet to that point. We’re asking that face masks be reused for at least 2 days, maybe longer. PPEs are one per day. Scrubs are kept secure.
Lewis: We are being very careful not to overuse PPE but currently have an adequate inventory. We have had to move gloves and masks to areas where they are not accessible to the general public, as otherwise they were being stolen (this started weeks ago).
Kerr: Our National Health System has an adequate supply of PPE equipment centrally, but there seems to be a problem with distribution, as some hospitals are reporting shortages.
Weber: Masks are in short supply, so they are being used for several days if not wet. We are short of plastic gowns and are using paper chemo gowns. Similar story at many places.
This article first appeared on Medscape.com.