User login
Respiratory particles generated by speech can remain airborne for up to 14 minutes
Stadnytskyi and colleagues explored the size of droplets created by speech using a highly sensitive laser system. They reported in PNAS that speaking resulted in the generation of a high number of medium-sized droplets (10- to 100-µm in diameter). Under the conditions of their experiment (27% humidity and 23° C) they reported that speech probably generates droplets that originate at a size of 12 to 21 µm in diameter and quickly dehydrate to an estimated diameter of 4 µm. The 4 µm-sized particles had a falling rate of only 0.06 cm·s−1 and remained airborne for 8 to 14 minutes.1
As reported by Hamner and colleagues, on March 10, 2020, 61 persons attended a 2.5-hour choir practice. One choir member had symptoms of an upper respiratory infection that began on March 7. Eventually that choir member tested positive for SARS-CoV-2. Of the 60 remaining persons, 52 (86.7%) eventually developed an upper respiratory illness. In total, 33 cases of SARS-CoV-2 were confirmed by nucleic acid testing and 20 probable cases were diagnosed (these individuals declined testing). The choir attendees developed symptoms at a median of 3 days following the practice, with a range of 1 to 12 days. Three of the 53 ill people were hospitalized, and two died.2
The Stadnytskyi study suggests that speech generates large respiratory droplets that dehydrate into very small droplets that may remain in the air for an extended period of time. If the SARS-CoV-2 virus were in the original large droplet, the rapid dehydration of the droplet would result in prolonged airborne presence of the virus and enhance its infectivity.
The Hamner study highlights the importance of vocalization and respiratory particles in transmitting the SARS-CoV-2 virus. For clinicians and patients, both studies support many recommendations to reduce viral transmission, including:
- all clinicians and patients need to wear face masks
- all clinicians and patients should avoid face-to-face contact if alternative approaches to communication are possible
- all clinicians and patients should avoid gathering in large groups or crowded public spaces and need to maintain physical distancing.
The COVID pandemic has dramatically changed how we practice medicine and socialize.
- Stadnytskyi V, Bax CE, Bax A, et al. The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. PNAS. May 13, 2020. https://doi.org/10.1073/pnas.2006874117.
- Hamner L, Dubbel P, Capron I, et al. High SARS-CoV-2 attack rate following exposure at choir practice—Skagit County, Washington, March 2020. MMWR Morb Mortal Wkly Rep. 2020;69:606-610. Early release, May 12, 2020.

Robert L. Barbieri, MD
Editor in Chief, OBG MANAGEMENT
Chair, Obstetrics and Gynecology
Brigham and Women’s Hospital
Boston, Massachusetts
Kate Macy Ladd Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG MANAGEMENT
Chair, Obstetrics and Gynecology
Brigham and Women’s Hospital
Boston, Massachusetts
Kate Macy Ladd Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief, OBG MANAGEMENT
Chair, Obstetrics and Gynecology
Brigham and Women’s Hospital
Boston, Massachusetts
Kate Macy Ladd Professor of Obstetrics,
Gynecology and Reproductive Biology
Harvard Medical School
Dr. Barbieri reports no financial relationships relevant to this article.
Stadnytskyi and colleagues explored the size of droplets created by speech using a highly sensitive laser system. They reported in PNAS that speaking resulted in the generation of a high number of medium-sized droplets (10- to 100-µm in diameter). Under the conditions of their experiment (27% humidity and 23° C) they reported that speech probably generates droplets that originate at a size of 12 to 21 µm in diameter and quickly dehydrate to an estimated diameter of 4 µm. The 4 µm-sized particles had a falling rate of only 0.06 cm·s−1 and remained airborne for 8 to 14 minutes.1
As reported by Hamner and colleagues, on March 10, 2020, 61 persons attended a 2.5-hour choir practice. One choir member had symptoms of an upper respiratory infection that began on March 7. Eventually that choir member tested positive for SARS-CoV-2. Of the 60 remaining persons, 52 (86.7%) eventually developed an upper respiratory illness. In total, 33 cases of SARS-CoV-2 were confirmed by nucleic acid testing and 20 probable cases were diagnosed (these individuals declined testing). The choir attendees developed symptoms at a median of 3 days following the practice, with a range of 1 to 12 days. Three of the 53 ill people were hospitalized, and two died.2
The Stadnytskyi study suggests that speech generates large respiratory droplets that dehydrate into very small droplets that may remain in the air for an extended period of time. If the SARS-CoV-2 virus were in the original large droplet, the rapid dehydration of the droplet would result in prolonged airborne presence of the virus and enhance its infectivity.
The Hamner study highlights the importance of vocalization and respiratory particles in transmitting the SARS-CoV-2 virus. For clinicians and patients, both studies support many recommendations to reduce viral transmission, including:
- all clinicians and patients need to wear face masks
- all clinicians and patients should avoid face-to-face contact if alternative approaches to communication are possible
- all clinicians and patients should avoid gathering in large groups or crowded public spaces and need to maintain physical distancing.
The COVID pandemic has dramatically changed how we practice medicine and socialize.
Stadnytskyi and colleagues explored the size of droplets created by speech using a highly sensitive laser system. They reported in PNAS that speaking resulted in the generation of a high number of medium-sized droplets (10- to 100-µm in diameter). Under the conditions of their experiment (27% humidity and 23° C) they reported that speech probably generates droplets that originate at a size of 12 to 21 µm in diameter and quickly dehydrate to an estimated diameter of 4 µm. The 4 µm-sized particles had a falling rate of only 0.06 cm·s−1 and remained airborne for 8 to 14 minutes.1
As reported by Hamner and colleagues, on March 10, 2020, 61 persons attended a 2.5-hour choir practice. One choir member had symptoms of an upper respiratory infection that began on March 7. Eventually that choir member tested positive for SARS-CoV-2. Of the 60 remaining persons, 52 (86.7%) eventually developed an upper respiratory illness. In total, 33 cases of SARS-CoV-2 were confirmed by nucleic acid testing and 20 probable cases were diagnosed (these individuals declined testing). The choir attendees developed symptoms at a median of 3 days following the practice, with a range of 1 to 12 days. Three of the 53 ill people were hospitalized, and two died.2
The Stadnytskyi study suggests that speech generates large respiratory droplets that dehydrate into very small droplets that may remain in the air for an extended period of time. If the SARS-CoV-2 virus were in the original large droplet, the rapid dehydration of the droplet would result in prolonged airborne presence of the virus and enhance its infectivity.
The Hamner study highlights the importance of vocalization and respiratory particles in transmitting the SARS-CoV-2 virus. For clinicians and patients, both studies support many recommendations to reduce viral transmission, including:
- all clinicians and patients need to wear face masks
- all clinicians and patients should avoid face-to-face contact if alternative approaches to communication are possible
- all clinicians and patients should avoid gathering in large groups or crowded public spaces and need to maintain physical distancing.
The COVID pandemic has dramatically changed how we practice medicine and socialize.
- Stadnytskyi V, Bax CE, Bax A, et al. The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. PNAS. May 13, 2020. https://doi.org/10.1073/pnas.2006874117.
- Hamner L, Dubbel P, Capron I, et al. High SARS-CoV-2 attack rate following exposure at choir practice—Skagit County, Washington, March 2020. MMWR Morb Mortal Wkly Rep. 2020;69:606-610. Early release, May 12, 2020.
- Stadnytskyi V, Bax CE, Bax A, et al. The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. PNAS. May 13, 2020. https://doi.org/10.1073/pnas.2006874117.
- Hamner L, Dubbel P, Capron I, et al. High SARS-CoV-2 attack rate following exposure at choir practice—Skagit County, Washington, March 2020. MMWR Morb Mortal Wkly Rep. 2020;69:606-610. Early release, May 12, 2020.
Hazard pay included in new COVID-19 relief bill
Hazard pay for frontline health care workers – an idea that has been championed by President Donald J. Trump and Senate Minority Leader Chuck Schumer, among others – is included in a just-released COVID-19 relief package assembled by Democrats in the House of Representatives.
according to a report in the Washington Post.
But it is far from a done deal. “The Democrats’ spending bill is a Pelosi-led pipe dream written in private,” said House Republican Leader Kevin McCarthy (Calif.) in a Fox News interview posted May 12 on Facebook.
Senate Majority Leader Mitch McConnell condemned the package. “This is exactly the wrong approach,” he said in a prepared statement that instead laid out a variety of liability protections, which he said should be the first priority.
“We are not going to let health care heroes emerge from this crisis facing a tidal wave of medical malpractice lawsuits so that trial lawyers can line their pockets,” said Sen. McConnell, adding that his plan would “raise the liability threshold for COVID-related malpractice lawsuits.”
Ingrida Lusis, vice president of government affairs and health policy at the American Nurses Association, said in an interview that the ANA had lobbied for hazard pay and was told it would be in the next relief package.
“Though there is an inherent risk in the nursing profession, we think that this is really critical to ensuring that we have a workforce to meet the intense demands of this pandemic,” said Ms. Lusis.
“If health care workers are not treated and compensated appropriately for what they’re going through right now, then we may not have a next generation that will want to enter the field,” she said.
Various nursing organizations, nurses’ unions, and health care unions, such as the American Federation of State, County and Municipal Employees (AFSCME) and the Service Employees International Union, have advocated for hazard pay.
Physicians’ organizations have not been vocal on the issue, however. The American Medical Association, for instance, pushed for hazard pay for residents but has not made any further public statements. An AMA spokesman said that the group was monitoring the situation but declined further comment.
Multiple online petitions seeking hazard pay for health care workers have been circulated, including one seeking the same $600 bump for essential workers that was given out as part of unemployment benefits in the first COVID-19 relief package. More than 1.2 million had signed the petition as of May 12.
‘Heroes fund’
The president first suggested hazard pay for health care workers on March 30 Fox News broadcast. “These are really brave people,” he said, adding that the administration was considering different ways of boosting pay, primarily through hospitals.
“We are asking the hospitals to do it and to consider something, including bonuses,” said Trump. “If anybody’s entitled to it, they are.”
On April 7, Sen. Schumer proposed a “Heroes Fund.” It would give public, private, and tribal frontline employees – including doctors, nurses, first responders, and transit, grocery, and postal workers – a $13 per hour raise up to $25,000 in additional pay through Dec. 31 for workers earning up to $200,000 and $5,000 in additional pay for those earning more than $200,000. It would also provide a $15,000 signing bonus to those who agree to take on such a position.
Rep. Matt Cartwright (D-Pa.) introduced a bill in mid-April, the Coronavirus Frontline Workers Fair Pay Act (HR 6709), that would provide similar pay increases. Health care workers would receive an additional $13 per hour. It would be retroactive to Jan. 31, 2020, and would be available through the end of 2020.
Molly Kinder of the Brookings Institution, a self-described nonpartisan Washington policy institute, estimates that Sen. Schumer’s proposal would represent the equivalent of double-time pay for the average low-wage worker, a 50% pay increase for a mail carrier, a 20% boost for a pharmacist, and less than a 15% increase for a surgeon, as determined from median 2018 wages.
Before the House Democrats unveiled their bill, Isabel Soto of the center-right group American Action Forum estimated that a $13 per hour wage increase could cost $398.9 billion just from the end of March to the end of September. A great proportion of that amount – $264 billion – would go to some 10 million health care workers, Ms. Soto calculated.
Some already offering pay boost
A few states and hospital systems are already offering hazard pay.
On April 12, Massachusetts agreed to give about 6,500 AFSCME union members who work at state human services facilities and group homes a $5 or a $10 per hour pay increase, depending on duties. It was to stay in effect until at least May 30.
Maine Governor Janet Mills (D) also agreed to increase pay by $3-$5 an hour for AFSCME workers in state correctional and mental health facilities beginning March 29.
In New York City, the biggest hospital network, Northwell Health, in late April gave 45,000 workers – including nurses, physicians, respiratory therapists, environmental services workers, housekeepers, and people in outpatient and corporate roles – a lump sum bonus payment of up to $2,500 and 1 week of paid time off. The money came out of the system’s general fund.
“As an organization, we want to continue to support, motivate and inspire our team members,” said Northwell President and CEO Michael Dowling in a statement at the time.
On April 2, New York–Presbyterian Hospital’s chair of the department of surgery, Craig Smith, MD, announced that the facility was “providing a $1,250 bonus for everyone who has worked in or supported the COVID-19 front lines, for at least 1 week.”
Advocate Aurora, with 15 hospitals and 32,000 employees in Wisconsin, said in early April that it was giving increases of $6.25-$15.00 an hour at least through the end of May.
A version of this article originally appeared on Medscape.com.
Hazard pay for frontline health care workers – an idea that has been championed by President Donald J. Trump and Senate Minority Leader Chuck Schumer, among others – is included in a just-released COVID-19 relief package assembled by Democrats in the House of Representatives.
according to a report in the Washington Post.
But it is far from a done deal. “The Democrats’ spending bill is a Pelosi-led pipe dream written in private,” said House Republican Leader Kevin McCarthy (Calif.) in a Fox News interview posted May 12 on Facebook.
Senate Majority Leader Mitch McConnell condemned the package. “This is exactly the wrong approach,” he said in a prepared statement that instead laid out a variety of liability protections, which he said should be the first priority.
“We are not going to let health care heroes emerge from this crisis facing a tidal wave of medical malpractice lawsuits so that trial lawyers can line their pockets,” said Sen. McConnell, adding that his plan would “raise the liability threshold for COVID-related malpractice lawsuits.”
Ingrida Lusis, vice president of government affairs and health policy at the American Nurses Association, said in an interview that the ANA had lobbied for hazard pay and was told it would be in the next relief package.
“Though there is an inherent risk in the nursing profession, we think that this is really critical to ensuring that we have a workforce to meet the intense demands of this pandemic,” said Ms. Lusis.
“If health care workers are not treated and compensated appropriately for what they’re going through right now, then we may not have a next generation that will want to enter the field,” she said.
Various nursing organizations, nurses’ unions, and health care unions, such as the American Federation of State, County and Municipal Employees (AFSCME) and the Service Employees International Union, have advocated for hazard pay.
Physicians’ organizations have not been vocal on the issue, however. The American Medical Association, for instance, pushed for hazard pay for residents but has not made any further public statements. An AMA spokesman said that the group was monitoring the situation but declined further comment.
Multiple online petitions seeking hazard pay for health care workers have been circulated, including one seeking the same $600 bump for essential workers that was given out as part of unemployment benefits in the first COVID-19 relief package. More than 1.2 million had signed the petition as of May 12.
‘Heroes fund’
The president first suggested hazard pay for health care workers on March 30 Fox News broadcast. “These are really brave people,” he said, adding that the administration was considering different ways of boosting pay, primarily through hospitals.
“We are asking the hospitals to do it and to consider something, including bonuses,” said Trump. “If anybody’s entitled to it, they are.”
On April 7, Sen. Schumer proposed a “Heroes Fund.” It would give public, private, and tribal frontline employees – including doctors, nurses, first responders, and transit, grocery, and postal workers – a $13 per hour raise up to $25,000 in additional pay through Dec. 31 for workers earning up to $200,000 and $5,000 in additional pay for those earning more than $200,000. It would also provide a $15,000 signing bonus to those who agree to take on such a position.
Rep. Matt Cartwright (D-Pa.) introduced a bill in mid-April, the Coronavirus Frontline Workers Fair Pay Act (HR 6709), that would provide similar pay increases. Health care workers would receive an additional $13 per hour. It would be retroactive to Jan. 31, 2020, and would be available through the end of 2020.
Molly Kinder of the Brookings Institution, a self-described nonpartisan Washington policy institute, estimates that Sen. Schumer’s proposal would represent the equivalent of double-time pay for the average low-wage worker, a 50% pay increase for a mail carrier, a 20% boost for a pharmacist, and less than a 15% increase for a surgeon, as determined from median 2018 wages.
Before the House Democrats unveiled their bill, Isabel Soto of the center-right group American Action Forum estimated that a $13 per hour wage increase could cost $398.9 billion just from the end of March to the end of September. A great proportion of that amount – $264 billion – would go to some 10 million health care workers, Ms. Soto calculated.
Some already offering pay boost
A few states and hospital systems are already offering hazard pay.
On April 12, Massachusetts agreed to give about 6,500 AFSCME union members who work at state human services facilities and group homes a $5 or a $10 per hour pay increase, depending on duties. It was to stay in effect until at least May 30.
Maine Governor Janet Mills (D) also agreed to increase pay by $3-$5 an hour for AFSCME workers in state correctional and mental health facilities beginning March 29.
In New York City, the biggest hospital network, Northwell Health, in late April gave 45,000 workers – including nurses, physicians, respiratory therapists, environmental services workers, housekeepers, and people in outpatient and corporate roles – a lump sum bonus payment of up to $2,500 and 1 week of paid time off. The money came out of the system’s general fund.
“As an organization, we want to continue to support, motivate and inspire our team members,” said Northwell President and CEO Michael Dowling in a statement at the time.
On April 2, New York–Presbyterian Hospital’s chair of the department of surgery, Craig Smith, MD, announced that the facility was “providing a $1,250 bonus for everyone who has worked in or supported the COVID-19 front lines, for at least 1 week.”
Advocate Aurora, with 15 hospitals and 32,000 employees in Wisconsin, said in early April that it was giving increases of $6.25-$15.00 an hour at least through the end of May.
A version of this article originally appeared on Medscape.com.
Hazard pay for frontline health care workers – an idea that has been championed by President Donald J. Trump and Senate Minority Leader Chuck Schumer, among others – is included in a just-released COVID-19 relief package assembled by Democrats in the House of Representatives.
according to a report in the Washington Post.
But it is far from a done deal. “The Democrats’ spending bill is a Pelosi-led pipe dream written in private,” said House Republican Leader Kevin McCarthy (Calif.) in a Fox News interview posted May 12 on Facebook.
Senate Majority Leader Mitch McConnell condemned the package. “This is exactly the wrong approach,” he said in a prepared statement that instead laid out a variety of liability protections, which he said should be the first priority.
“We are not going to let health care heroes emerge from this crisis facing a tidal wave of medical malpractice lawsuits so that trial lawyers can line their pockets,” said Sen. McConnell, adding that his plan would “raise the liability threshold for COVID-related malpractice lawsuits.”
Ingrida Lusis, vice president of government affairs and health policy at the American Nurses Association, said in an interview that the ANA had lobbied for hazard pay and was told it would be in the next relief package.
“Though there is an inherent risk in the nursing profession, we think that this is really critical to ensuring that we have a workforce to meet the intense demands of this pandemic,” said Ms. Lusis.
“If health care workers are not treated and compensated appropriately for what they’re going through right now, then we may not have a next generation that will want to enter the field,” she said.
Various nursing organizations, nurses’ unions, and health care unions, such as the American Federation of State, County and Municipal Employees (AFSCME) and the Service Employees International Union, have advocated for hazard pay.
Physicians’ organizations have not been vocal on the issue, however. The American Medical Association, for instance, pushed for hazard pay for residents but has not made any further public statements. An AMA spokesman said that the group was monitoring the situation but declined further comment.
Multiple online petitions seeking hazard pay for health care workers have been circulated, including one seeking the same $600 bump for essential workers that was given out as part of unemployment benefits in the first COVID-19 relief package. More than 1.2 million had signed the petition as of May 12.
‘Heroes fund’
The president first suggested hazard pay for health care workers on March 30 Fox News broadcast. “These are really brave people,” he said, adding that the administration was considering different ways of boosting pay, primarily through hospitals.
“We are asking the hospitals to do it and to consider something, including bonuses,” said Trump. “If anybody’s entitled to it, they are.”
On April 7, Sen. Schumer proposed a “Heroes Fund.” It would give public, private, and tribal frontline employees – including doctors, nurses, first responders, and transit, grocery, and postal workers – a $13 per hour raise up to $25,000 in additional pay through Dec. 31 for workers earning up to $200,000 and $5,000 in additional pay for those earning more than $200,000. It would also provide a $15,000 signing bonus to those who agree to take on such a position.
Rep. Matt Cartwright (D-Pa.) introduced a bill in mid-April, the Coronavirus Frontline Workers Fair Pay Act (HR 6709), that would provide similar pay increases. Health care workers would receive an additional $13 per hour. It would be retroactive to Jan. 31, 2020, and would be available through the end of 2020.
Molly Kinder of the Brookings Institution, a self-described nonpartisan Washington policy institute, estimates that Sen. Schumer’s proposal would represent the equivalent of double-time pay for the average low-wage worker, a 50% pay increase for a mail carrier, a 20% boost for a pharmacist, and less than a 15% increase for a surgeon, as determined from median 2018 wages.
Before the House Democrats unveiled their bill, Isabel Soto of the center-right group American Action Forum estimated that a $13 per hour wage increase could cost $398.9 billion just from the end of March to the end of September. A great proportion of that amount – $264 billion – would go to some 10 million health care workers, Ms. Soto calculated.
Some already offering pay boost
A few states and hospital systems are already offering hazard pay.
On April 12, Massachusetts agreed to give about 6,500 AFSCME union members who work at state human services facilities and group homes a $5 or a $10 per hour pay increase, depending on duties. It was to stay in effect until at least May 30.
Maine Governor Janet Mills (D) also agreed to increase pay by $3-$5 an hour for AFSCME workers in state correctional and mental health facilities beginning March 29.
In New York City, the biggest hospital network, Northwell Health, in late April gave 45,000 workers – including nurses, physicians, respiratory therapists, environmental services workers, housekeepers, and people in outpatient and corporate roles – a lump sum bonus payment of up to $2,500 and 1 week of paid time off. The money came out of the system’s general fund.
“As an organization, we want to continue to support, motivate and inspire our team members,” said Northwell President and CEO Michael Dowling in a statement at the time.
On April 2, New York–Presbyterian Hospital’s chair of the department of surgery, Craig Smith, MD, announced that the facility was “providing a $1,250 bonus for everyone who has worked in or supported the COVID-19 front lines, for at least 1 week.”
Advocate Aurora, with 15 hospitals and 32,000 employees in Wisconsin, said in early April that it was giving increases of $6.25-$15.00 an hour at least through the end of May.
A version of this article originally appeared on Medscape.com.
COVID-19 will likely change docs’ incentive targets, bonuses: Survey
“Employed physicians are often getting a guaranteed salary for a month or two, but no bonuses or extra distributions,” Joel Greenwald, MD, a financial adviser for physicians in St. Louis Park, Minn., told Medscape Medical News.
“This amounts to salary reductions of 10% to 30%,” he said.
The COVID-19 crisis dramatically reversed the consistent upward trajectory of physician compensation, according to a Medical Group Management Association (MGMA) survey, as reported by Medscape Medical News.
The survey, conducted April 7-8, found that practices have reported an average 55% drop in income. The report also found an average decrease in patient volume of 60%.
Before pandemic, salaries were rising
The pandemic interrupted a steady gain in compensation for this year compared to last, according to the Medscape Physician Compensation Report 2020.
The report reflects data gathered from October 4, 2019, to February 10, 2020, and includes online survey responses from 17,000 physicians in more than 30 specialties.
Before the pandemic, primary care physician (PCP) pay was up 2.5%, to $243,000, from the previous year’s average of $237,000. Specialists saw a 1.5% increase, from $341,000 in 2019 to $346,000 this year.
Reported compensation for employed physicians included salary, bonus, and profit-sharing contributions. For those self-employed, compensation includes earnings after taxes and deductible business expenses before income tax.
This report reflects only full-time salaries. But most physicians work more than full time. The report notes that physicians overall spent 37.8 hours a week seeing patients. Add to that the 15.6 average hours spent on paperwork, and doctors are averaging 53.4 hours a week.
Administrative demands varied widely by specialty. Physicians in critical care, for example, spent the most hours on paperwork (19.1 per week), and ophthalmologists spent the least on those tasks, at 9.8.
Orthopedists top earners again
The top four specialties were the same this year as they were last year and were ranked in the same order: orthopedists made the most, at $511,000, followed by plastic surgeons, at $479,000, otolaryngologists, at $455,000, and cardiologists, at $438,000.
Pediatricians and public health/preventive medicine physicians made the least, at $232,000, followed by family physicians ($234,000) and diabetes/endocrinology specialists ($236,000).
Despite the low ranking, public health/preventive medicine providers had the biggest compensation increase of all physicians, up 11% from last year. Two specialties saw a decrease: otolaryngology salaries dropped 1%, and dermatology pay dropped 2%. Pay in gastroenterology and diabetes/endocrinology was virtually unchanged from last year.
Kentucky has highest pay
Ranked by state, physicians in Kentucky made the most on average ($346,000). Utah, Ohio, and North Carolina were new to the top 10 in physician pay this year, pushing out Connecticut, Arkansas, and Nevada.
More than half of all physicians receive incentive bonuses (58% of PCPs and 55% of specialists).
The average incentive bonus is 13% of salary, but that varies by specialty. Orthopedists got an average $96,000 bonus, whereas family physicians got $24,000.
According to the report, “Among physicians who have an incentive bonus, about a third of both PCPs and specialists say the prospect of an incentive bonus has encouraged them to work longer hours.”
Gender gap similar to previous year
Consistent with Medscape compensation reports over the past decade, this year’s report shows a large gender gap in pay. Among PCPs, men made 25% more than women ($264,000 vs. $212,000); among specialists, they made 31% more than their female colleagues ($375,000 vs. $286,000).
Some specialties report positive changes from growing awareness of the gap.
“Many organizations have been carefully analyzing their culture, transparency, and pay practices to make sure they aren’t unintentionally discriminating against any group of employees,” Halee Fischer-Wright, MD, pediatrician and CEO of MGMA, told Medscape Medical News.
She added that the growing physician shortage has given all physicians more leverage in salary demands and that increased recognition of the gender gap is giving women more confidence and more evidence to use in negotiations.
Three specialties have seen large increases in the past 5 years in the percentage of women physicians. Obstetrics/gynecology and pediatrics both saw increases from 50% in 2015 to 58% in 2020. Additionally, women now account for 54% of rheumatologists, up from 29% in 2015.
Would you choose your specialty again?
Of responding physicians who were asked if they would choose their specialty again, internists were least likely to say yes (66%), followed by nephrologists (69%) and family physicians (70%).
Orthopedists were most likely to say they would choose the same specialty (97%), followed by oncologists (96%) and ophthalmologists and dermatologists (both at 95%).
Most physicians overall (77%) said they would choose medicine again.
Despite aggravations and pressures, in this survey and in previous years, physicians have indicated that the top rewards are “gratitude/relationships with patients,” “being very good at what I do/finding answers, diagnoses,” and “knowing that I make the world a better place.” From 24% to 27% ranked those rewards most important.
“Making good money at a job I like” came in fourth, at 12%.
This article first appeared on Medscape.com.
“Employed physicians are often getting a guaranteed salary for a month or two, but no bonuses or extra distributions,” Joel Greenwald, MD, a financial adviser for physicians in St. Louis Park, Minn., told Medscape Medical News.
“This amounts to salary reductions of 10% to 30%,” he said.
The COVID-19 crisis dramatically reversed the consistent upward trajectory of physician compensation, according to a Medical Group Management Association (MGMA) survey, as reported by Medscape Medical News.
The survey, conducted April 7-8, found that practices have reported an average 55% drop in income. The report also found an average decrease in patient volume of 60%.
Before pandemic, salaries were rising
The pandemic interrupted a steady gain in compensation for this year compared to last, according to the Medscape Physician Compensation Report 2020.
The report reflects data gathered from October 4, 2019, to February 10, 2020, and includes online survey responses from 17,000 physicians in more than 30 specialties.
Before the pandemic, primary care physician (PCP) pay was up 2.5%, to $243,000, from the previous year’s average of $237,000. Specialists saw a 1.5% increase, from $341,000 in 2019 to $346,000 this year.
Reported compensation for employed physicians included salary, bonus, and profit-sharing contributions. For those self-employed, compensation includes earnings after taxes and deductible business expenses before income tax.
This report reflects only full-time salaries. But most physicians work more than full time. The report notes that physicians overall spent 37.8 hours a week seeing patients. Add to that the 15.6 average hours spent on paperwork, and doctors are averaging 53.4 hours a week.
Administrative demands varied widely by specialty. Physicians in critical care, for example, spent the most hours on paperwork (19.1 per week), and ophthalmologists spent the least on those tasks, at 9.8.
Orthopedists top earners again
The top four specialties were the same this year as they were last year and were ranked in the same order: orthopedists made the most, at $511,000, followed by plastic surgeons, at $479,000, otolaryngologists, at $455,000, and cardiologists, at $438,000.
Pediatricians and public health/preventive medicine physicians made the least, at $232,000, followed by family physicians ($234,000) and diabetes/endocrinology specialists ($236,000).
Despite the low ranking, public health/preventive medicine providers had the biggest compensation increase of all physicians, up 11% from last year. Two specialties saw a decrease: otolaryngology salaries dropped 1%, and dermatology pay dropped 2%. Pay in gastroenterology and diabetes/endocrinology was virtually unchanged from last year.
Kentucky has highest pay
Ranked by state, physicians in Kentucky made the most on average ($346,000). Utah, Ohio, and North Carolina were new to the top 10 in physician pay this year, pushing out Connecticut, Arkansas, and Nevada.
More than half of all physicians receive incentive bonuses (58% of PCPs and 55% of specialists).
The average incentive bonus is 13% of salary, but that varies by specialty. Orthopedists got an average $96,000 bonus, whereas family physicians got $24,000.
According to the report, “Among physicians who have an incentive bonus, about a third of both PCPs and specialists say the prospect of an incentive bonus has encouraged them to work longer hours.”
Gender gap similar to previous year
Consistent with Medscape compensation reports over the past decade, this year’s report shows a large gender gap in pay. Among PCPs, men made 25% more than women ($264,000 vs. $212,000); among specialists, they made 31% more than their female colleagues ($375,000 vs. $286,000).
Some specialties report positive changes from growing awareness of the gap.
“Many organizations have been carefully analyzing their culture, transparency, and pay practices to make sure they aren’t unintentionally discriminating against any group of employees,” Halee Fischer-Wright, MD, pediatrician and CEO of MGMA, told Medscape Medical News.
She added that the growing physician shortage has given all physicians more leverage in salary demands and that increased recognition of the gender gap is giving women more confidence and more evidence to use in negotiations.
Three specialties have seen large increases in the past 5 years in the percentage of women physicians. Obstetrics/gynecology and pediatrics both saw increases from 50% in 2015 to 58% in 2020. Additionally, women now account for 54% of rheumatologists, up from 29% in 2015.
Would you choose your specialty again?
Of responding physicians who were asked if they would choose their specialty again, internists were least likely to say yes (66%), followed by nephrologists (69%) and family physicians (70%).
Orthopedists were most likely to say they would choose the same specialty (97%), followed by oncologists (96%) and ophthalmologists and dermatologists (both at 95%).
Most physicians overall (77%) said they would choose medicine again.
Despite aggravations and pressures, in this survey and in previous years, physicians have indicated that the top rewards are “gratitude/relationships with patients,” “being very good at what I do/finding answers, diagnoses,” and “knowing that I make the world a better place.” From 24% to 27% ranked those rewards most important.
“Making good money at a job I like” came in fourth, at 12%.
This article first appeared on Medscape.com.
“Employed physicians are often getting a guaranteed salary for a month or two, but no bonuses or extra distributions,” Joel Greenwald, MD, a financial adviser for physicians in St. Louis Park, Minn., told Medscape Medical News.
“This amounts to salary reductions of 10% to 30%,” he said.
The COVID-19 crisis dramatically reversed the consistent upward trajectory of physician compensation, according to a Medical Group Management Association (MGMA) survey, as reported by Medscape Medical News.
The survey, conducted April 7-8, found that practices have reported an average 55% drop in income. The report also found an average decrease in patient volume of 60%.
Before pandemic, salaries were rising
The pandemic interrupted a steady gain in compensation for this year compared to last, according to the Medscape Physician Compensation Report 2020.
The report reflects data gathered from October 4, 2019, to February 10, 2020, and includes online survey responses from 17,000 physicians in more than 30 specialties.
Before the pandemic, primary care physician (PCP) pay was up 2.5%, to $243,000, from the previous year’s average of $237,000. Specialists saw a 1.5% increase, from $341,000 in 2019 to $346,000 this year.
Reported compensation for employed physicians included salary, bonus, and profit-sharing contributions. For those self-employed, compensation includes earnings after taxes and deductible business expenses before income tax.
This report reflects only full-time salaries. But most physicians work more than full time. The report notes that physicians overall spent 37.8 hours a week seeing patients. Add to that the 15.6 average hours spent on paperwork, and doctors are averaging 53.4 hours a week.
Administrative demands varied widely by specialty. Physicians in critical care, for example, spent the most hours on paperwork (19.1 per week), and ophthalmologists spent the least on those tasks, at 9.8.
Orthopedists top earners again
The top four specialties were the same this year as they were last year and were ranked in the same order: orthopedists made the most, at $511,000, followed by plastic surgeons, at $479,000, otolaryngologists, at $455,000, and cardiologists, at $438,000.
Pediatricians and public health/preventive medicine physicians made the least, at $232,000, followed by family physicians ($234,000) and diabetes/endocrinology specialists ($236,000).
Despite the low ranking, public health/preventive medicine providers had the biggest compensation increase of all physicians, up 11% from last year. Two specialties saw a decrease: otolaryngology salaries dropped 1%, and dermatology pay dropped 2%. Pay in gastroenterology and diabetes/endocrinology was virtually unchanged from last year.
Kentucky has highest pay
Ranked by state, physicians in Kentucky made the most on average ($346,000). Utah, Ohio, and North Carolina were new to the top 10 in physician pay this year, pushing out Connecticut, Arkansas, and Nevada.
More than half of all physicians receive incentive bonuses (58% of PCPs and 55% of specialists).
The average incentive bonus is 13% of salary, but that varies by specialty. Orthopedists got an average $96,000 bonus, whereas family physicians got $24,000.
According to the report, “Among physicians who have an incentive bonus, about a third of both PCPs and specialists say the prospect of an incentive bonus has encouraged them to work longer hours.”
Gender gap similar to previous year
Consistent with Medscape compensation reports over the past decade, this year’s report shows a large gender gap in pay. Among PCPs, men made 25% more than women ($264,000 vs. $212,000); among specialists, they made 31% more than their female colleagues ($375,000 vs. $286,000).
Some specialties report positive changes from growing awareness of the gap.
“Many organizations have been carefully analyzing their culture, transparency, and pay practices to make sure they aren’t unintentionally discriminating against any group of employees,” Halee Fischer-Wright, MD, pediatrician and CEO of MGMA, told Medscape Medical News.
She added that the growing physician shortage has given all physicians more leverage in salary demands and that increased recognition of the gender gap is giving women more confidence and more evidence to use in negotiations.
Three specialties have seen large increases in the past 5 years in the percentage of women physicians. Obstetrics/gynecology and pediatrics both saw increases from 50% in 2015 to 58% in 2020. Additionally, women now account for 54% of rheumatologists, up from 29% in 2015.
Would you choose your specialty again?
Of responding physicians who were asked if they would choose their specialty again, internists were least likely to say yes (66%), followed by nephrologists (69%) and family physicians (70%).
Orthopedists were most likely to say they would choose the same specialty (97%), followed by oncologists (96%) and ophthalmologists and dermatologists (both at 95%).
Most physicians overall (77%) said they would choose medicine again.
Despite aggravations and pressures, in this survey and in previous years, physicians have indicated that the top rewards are “gratitude/relationships with patients,” “being very good at what I do/finding answers, diagnoses,” and “knowing that I make the world a better place.” From 24% to 27% ranked those rewards most important.
“Making good money at a job I like” came in fourth, at 12%.
This article first appeared on Medscape.com.
Video coaching may relieve anxiety and distress for long-distance cancer caregivers
Anxiety and distress related to caring for a cancer patient who lives far away may be alleviated through an intervention that includes video-based coaching sessions with a nurse practitioner or social worker, a randomized study suggests.

About 20% of long-distance caregivers had a significant reduction in anxiety and 25% had a significant reduction in distress when they received video coaching sessions, attended oncologist visits via video, and had access to a website specifically designed for their needs.
Adding the caregiver to oncologist office visits made the patients feel better supported and didn’t add a significant amount of time to the encounter, said Sara L. Douglas, PhD, RN, of Case Western Reserve University, Cleveland.
Taken together, these results suggest that fairly simple technologies can be leveraged to help caregivers cope with psychological strains related to supporting a patient who doesn’t live nearby, Dr. Douglas said.
Distance caregivers, defined as those who live an hour or more away from the patient, can experience high rates of distress and anxiety because they lack first-hand information or may have uncertainty about the patient’s current condition, according to Dr. Douglas and colleagues.
“Caregivers’ high rates of anxiety and distress have been found to have a negative impact not only upon their own health but upon their ability to provide high quality care to the patient,” Dr. Douglas said.
With this in mind, she and her colleagues conducted a 4-month study of distance caregivers. Dr. Douglas presented results from the study at the American Society of Clinical Oncology virtual scientific program during a press briefing in advance of the meeting. This year, ASCO’s annual meeting is split into two parts. The virtual scientific program will be presented online on May 29-31, and the virtual education program will be available Aug. 8-10.
Study details
The study enrolled 441 distance caregivers of cancer patients, and Dr. Douglas presented results in 311 of those caregivers. (Data in the presentation differ from the abstract.) The caregivers were, on average, 47 years of age. Most were female (72%), white (67%), the child of the patient (63%), currently employed (81%), and new to the distance caregiver role (89%).
The caregivers were randomized to one of three study arms.
One arm received the full intervention, which consisted of four video-coaching sessions with an advanced practice nurse or social worker, videoconference office visits with the physician and patient, and access to a website with information for cancer distance caregivers. A second arm received no video coaching but had access to the website and participated in video visits with the physician and patient. The third arm, which only received access to the website, served as the study’s control group.
Results
Dr. Douglas said that the full intervention had the biggest impact on caregivers’ distress and anxiety.
Among distance caregivers who received the full intervention, 19.2% had a significant reduction in anxiety (P = .03), as measured in online surveys before and after the intervention using the PROMIS Anxiety instrument. Furthermore, 24.8% of these caregivers had a significant reduction in distress (P = .02) from preintervention to post intervention, as measured by the National Comprehensive Cancer Network Distress Thermometer. Overall, distress and anxiety scores decreased in this arm.
Distance caregivers who only had physician-patient video visits and website access had a “moderate” reduction in distress and anxiety, Dr. Douglas said. Among these caregivers, 17.3% had an improvement in anxiety from baseline, and 19.8% had an improvement in distress. Overall, distress scores decreased, but anxiety scores increased slightly in this arm.
In the control arm, 13.1% of caregivers had an improvement in anxiety from baseline, and 18% had an improvement in distress. Overall, both anxiety and distress scores increased in this arm.
“While the full intervention yielded the best results for distance caregivers, we recognize that not all health care systems have the resources to provide individualized coaching sessions to distance caregivers,” Dr. Douglas said. “Therefore, it is worth noting that videoconference office visits alone are found to be of some benefit in improving distress and anxiety in this group of cancer caregivers.”
The study results suggest videoconferencing interventions can improve the emotional well-being of remote caregivers who provide “critical support” for cancer patients, said ASCO President Howard A. “Skip” Burris III, MD.
“As COVID-19 forces separation from loved ones and increases anxiety for people with cancer and their caregivers, providing emotional support virtually is more important than ever,” Dr. Burris said in a news release highlighting the study.
This study was funded by the National Institutes of Health and Case Comprehensive Cancer Center. Dr. Douglas reported having no disclosures. Other researchers involved in the study disclosed relationships with BridgeBio Pharma, Cardinal Health, Apexigen, Roche/Genentech, Seattle Genetics, Tesaro, Array BioPharma, Abbvie, Bristol-Myers Squibb, and Celgene. A full list of Dr. Burris’s financial disclosures is available on the ASCO website.
SOURCE: Douglas SL et al. ASCO 2020, Abstract 12123.
Anxiety and distress related to caring for a cancer patient who lives far away may be alleviated through an intervention that includes video-based coaching sessions with a nurse practitioner or social worker, a randomized study suggests.
About 20% of long-distance caregivers had a significant reduction in anxiety and 25% had a significant reduction in distress when they received video coaching sessions, attended oncologist visits via video, and had access to a website specifically designed for their needs.
Adding the caregiver to oncologist office visits made the patients feel better supported and didn’t add a significant amount of time to the encounter, said Sara L. Douglas, PhD, RN, of Case Western Reserve University, Cleveland.
Taken together, these results suggest that fairly simple technologies can be leveraged to help caregivers cope with psychological strains related to supporting a patient who doesn’t live nearby, Dr. Douglas said.
Distance caregivers, defined as those who live an hour or more away from the patient, can experience high rates of distress and anxiety because they lack first-hand information or may have uncertainty about the patient’s current condition, according to Dr. Douglas and colleagues.
“Caregivers’ high rates of anxiety and distress have been found to have a negative impact not only upon their own health but upon their ability to provide high quality care to the patient,” Dr. Douglas said.
With this in mind, she and her colleagues conducted a 4-month study of distance caregivers. Dr. Douglas presented results from the study at the American Society of Clinical Oncology virtual scientific program during a press briefing in advance of the meeting. This year, ASCO’s annual meeting is split into two parts. The virtual scientific program will be presented online on May 29-31, and the virtual education program will be available Aug. 8-10.
Study details
The study enrolled 441 distance caregivers of cancer patients, and Dr. Douglas presented results in 311 of those caregivers. (Data in the presentation differ from the abstract.) The caregivers were, on average, 47 years of age. Most were female (72%), white (67%), the child of the patient (63%), currently employed (81%), and new to the distance caregiver role (89%).
The caregivers were randomized to one of three study arms.
One arm received the full intervention, which consisted of four video-coaching sessions with an advanced practice nurse or social worker, videoconference office visits with the physician and patient, and access to a website with information for cancer distance caregivers. A second arm received no video coaching but had access to the website and participated in video visits with the physician and patient. The third arm, which only received access to the website, served as the study’s control group.
Results
Dr. Douglas said that the full intervention had the biggest impact on caregivers’ distress and anxiety.
Among distance caregivers who received the full intervention, 19.2% had a significant reduction in anxiety (P = .03), as measured in online surveys before and after the intervention using the PROMIS Anxiety instrument. Furthermore, 24.8% of these caregivers had a significant reduction in distress (P = .02) from preintervention to post intervention, as measured by the National Comprehensive Cancer Network Distress Thermometer. Overall, distress and anxiety scores decreased in this arm.
Distance caregivers who only had physician-patient video visits and website access had a “moderate” reduction in distress and anxiety, Dr. Douglas said. Among these caregivers, 17.3% had an improvement in anxiety from baseline, and 19.8% had an improvement in distress. Overall, distress scores decreased, but anxiety scores increased slightly in this arm.
In the control arm, 13.1% of caregivers had an improvement in anxiety from baseline, and 18% had an improvement in distress. Overall, both anxiety and distress scores increased in this arm.
“While the full intervention yielded the best results for distance caregivers, we recognize that not all health care systems have the resources to provide individualized coaching sessions to distance caregivers,” Dr. Douglas said. “Therefore, it is worth noting that videoconference office visits alone are found to be of some benefit in improving distress and anxiety in this group of cancer caregivers.”
The study results suggest videoconferencing interventions can improve the emotional well-being of remote caregivers who provide “critical support” for cancer patients, said ASCO President Howard A. “Skip” Burris III, MD.
“As COVID-19 forces separation from loved ones and increases anxiety for people with cancer and their caregivers, providing emotional support virtually is more important than ever,” Dr. Burris said in a news release highlighting the study.
This study was funded by the National Institutes of Health and Case Comprehensive Cancer Center. Dr. Douglas reported having no disclosures. Other researchers involved in the study disclosed relationships with BridgeBio Pharma, Cardinal Health, Apexigen, Roche/Genentech, Seattle Genetics, Tesaro, Array BioPharma, Abbvie, Bristol-Myers Squibb, and Celgene. A full list of Dr. Burris’s financial disclosures is available on the ASCO website.
SOURCE: Douglas SL et al. ASCO 2020, Abstract 12123.
Anxiety and distress related to caring for a cancer patient who lives far away may be alleviated through an intervention that includes video-based coaching sessions with a nurse practitioner or social worker, a randomized study suggests.
About 20% of long-distance caregivers had a significant reduction in anxiety and 25% had a significant reduction in distress when they received video coaching sessions, attended oncologist visits via video, and had access to a website specifically designed for their needs.
Adding the caregiver to oncologist office visits made the patients feel better supported and didn’t add a significant amount of time to the encounter, said Sara L. Douglas, PhD, RN, of Case Western Reserve University, Cleveland.
Taken together, these results suggest that fairly simple technologies can be leveraged to help caregivers cope with psychological strains related to supporting a patient who doesn’t live nearby, Dr. Douglas said.
Distance caregivers, defined as those who live an hour or more away from the patient, can experience high rates of distress and anxiety because they lack first-hand information or may have uncertainty about the patient’s current condition, according to Dr. Douglas and colleagues.
“Caregivers’ high rates of anxiety and distress have been found to have a negative impact not only upon their own health but upon their ability to provide high quality care to the patient,” Dr. Douglas said.
With this in mind, she and her colleagues conducted a 4-month study of distance caregivers. Dr. Douglas presented results from the study at the American Society of Clinical Oncology virtual scientific program during a press briefing in advance of the meeting. This year, ASCO’s annual meeting is split into two parts. The virtual scientific program will be presented online on May 29-31, and the virtual education program will be available Aug. 8-10.
Study details
The study enrolled 441 distance caregivers of cancer patients, and Dr. Douglas presented results in 311 of those caregivers. (Data in the presentation differ from the abstract.) The caregivers were, on average, 47 years of age. Most were female (72%), white (67%), the child of the patient (63%), currently employed (81%), and new to the distance caregiver role (89%).
The caregivers were randomized to one of three study arms.
One arm received the full intervention, which consisted of four video-coaching sessions with an advanced practice nurse or social worker, videoconference office visits with the physician and patient, and access to a website with information for cancer distance caregivers. A second arm received no video coaching but had access to the website and participated in video visits with the physician and patient. The third arm, which only received access to the website, served as the study’s control group.
Results
Dr. Douglas said that the full intervention had the biggest impact on caregivers’ distress and anxiety.
Among distance caregivers who received the full intervention, 19.2% had a significant reduction in anxiety (P = .03), as measured in online surveys before and after the intervention using the PROMIS Anxiety instrument. Furthermore, 24.8% of these caregivers had a significant reduction in distress (P = .02) from preintervention to post intervention, as measured by the National Comprehensive Cancer Network Distress Thermometer. Overall, distress and anxiety scores decreased in this arm.
Distance caregivers who only had physician-patient video visits and website access had a “moderate” reduction in distress and anxiety, Dr. Douglas said. Among these caregivers, 17.3% had an improvement in anxiety from baseline, and 19.8% had an improvement in distress. Overall, distress scores decreased, but anxiety scores increased slightly in this arm.
In the control arm, 13.1% of caregivers had an improvement in anxiety from baseline, and 18% had an improvement in distress. Overall, both anxiety and distress scores increased in this arm.
“While the full intervention yielded the best results for distance caregivers, we recognize that not all health care systems have the resources to provide individualized coaching sessions to distance caregivers,” Dr. Douglas said. “Therefore, it is worth noting that videoconference office visits alone are found to be of some benefit in improving distress and anxiety in this group of cancer caregivers.”
The study results suggest videoconferencing interventions can improve the emotional well-being of remote caregivers who provide “critical support” for cancer patients, said ASCO President Howard A. “Skip” Burris III, MD.
“As COVID-19 forces separation from loved ones and increases anxiety for people with cancer and their caregivers, providing emotional support virtually is more important than ever,” Dr. Burris said in a news release highlighting the study.
This study was funded by the National Institutes of Health and Case Comprehensive Cancer Center. Dr. Douglas reported having no disclosures. Other researchers involved in the study disclosed relationships with BridgeBio Pharma, Cardinal Health, Apexigen, Roche/Genentech, Seattle Genetics, Tesaro, Array BioPharma, Abbvie, Bristol-Myers Squibb, and Celgene. A full list of Dr. Burris’s financial disclosures is available on the ASCO website.
SOURCE: Douglas SL et al. ASCO 2020, Abstract 12123.
FROM ASCO 2020
COVID-19: What will happen to physician income this year?
“At a combined system and hospital board meeting yesterday, there was a financial presentation,” said a cardiologist in Minnesota, who declined to be named. “We have ‘salary support’ through May 16, which means we will be receiving base pay at our 2019 level. After May 16, I think it’s fairly certain salaries will be decreased.”
A general internist in the same area added: “The system has decided to pay physicians and other employees for 8 weeks, until May 15, and they are borrowing about $150 million to do this. We don’t know what will happen after May 15, but we are supposed to have an update in early May.”
Physician income is of huge interest, and many aspects of it are discussed in Medscape’s Physician Compensation Report 2020, just released.
The worst may be yet to come
Of all the categories of physicians, “I am worried about private practices the most,” said Travis Singleton, senior vice president at Merritt Hawkins, a physician search firm. “They don’t have a financial cushion, and will start seeing big drops in revenue at the end of May.”
“A lot of the A/R [accounts receivables] for practices come within 30 days, and very little comes in after 90 days,” said Terrence R. McWilliams, MD, chief clinical consultant at HSG Advisors, a consultancy for not-for-profit hospitals and their employed physician networks around the country. “So private practices are reaching the point where prior A/R will start to dwindle and they will start feeling the decline in new claims submissions.”
Large practices may have a bigger financial cushion, but in many cases, they also have more liabilities. “We don’t know the financial loss yet, but I think it’s been devastating,” said Paul M. Yonover, MD, a urologist at UroPartners, a large single-specialty practice in Chicago with 62 urologists. “In fact, the financial loss may well be larger than our loss in volume, because we have to support our own surgery center, pathology lab, radiation center, and other in-house services.”
Employed physicians in limbo
In contrast to physicians in private practices, many employed physicians at hospitals and health systems have been shielded from the impact of COVID-19 – at least for now.
“The experiences of employed physicians are very mixed,” said Mr. Singleton at Merritt Hawkins. “Some health systems have reduced physicians’ pay by 20%, but other systems have been putting off any reductions.”
Hospitals and health systems are struggling. “Stopping elective surgeries deeply affected hospitals,” said Ryan Inman, founder of Physician Wealth Services in San Diego. “With fewer elective surgeries, they have much less income coming in. Some big hospitals that are pillars of their community are under great financial stress.”
“Hospitals’ patient volumes have fallen by 50%-90%,” Mr. McWilliams reported. “Lower volume means lower pay for employed physicians, who are paid by straight productivity or other models that require high volumes. However, some health systems have intervened to make sure these physicians get some money.”
Base pay is often safe for now, but quarterly bonuses are on the chopping block. “Employed physicians are often getting a guaranteed salary for a month or two, but no bonuses or extra distributions,” said Joel Greenwald, MD, a financial adviser for physicians in St. Louis Park, Minn., a state mecca for physician employment. “They’ve been told that they will continue to get their base salary but forget about the quarterly bonuses. This amounts to salary reductions of 10%-30%.”
Ensuring payment for these doctors means lowering their productivity benchmarks, but the benchmarks might still be too high for these times. An internist at a large health system in Minneapolis–St. Paul reports that, at a lunch meeting, employed doctors learned that payment benchmarks will be reduced to 70% of their 2019 monthly average.
“I am seeing nowhere near 70% of what I was seeing last year,” he said in an interview, asking that his name not be used. “Given how slow things have been, I am probably closer to 30%, but have not been given any data on this, so I am guessing at this point.”
Adapting to a brave new world
Even as they face a dark financial future, physicians have had to completely revamp the way they practice medicine – a cumbersome process that, in itself, incurred some financial losses. They had to obtain masks and other PPE, reposition or even close down their waiting rooms, cut back on unneeded staff, and adapt to telemedicine.
“It’s been an incredibly challenging time,” said Dr. Yonover, the Chicago urologist. “As a doctor. I cannot avoid contact, and it’s not totally clear yet how the virus spreads. But I don’t have the option of closing the door. As a practice owner, you’re responsible for the health and well-being of employees, patients, and the business.”
“A practice’s daily routine is somewhat slower and costlier,” said David N. Gans, MSHA, senior fellow at the Medical Group Management Association (MGMA), which represents group practices. “Between each patient, you have to clean a lot more than previously, and you have to stock up on PPE such as masks and gowns. PPE used to be limited to infectious patients, but now it’s universal.”
At PA Clinical Network, a clinically integrated network in Pennsylvania, volume fell 40%-50% and income fell 30%-50% from late March to late April, according to Jaan Sidorov, MD, an internist who is CEO of the network, which has 158 physicians in a variety of specialties working in 54 practices around the state.
“Revenue went down but it didn’t crash,” he said. “And our physicians pivoted very quickly. They adapted to telehealth and applied for the federal loan programs. They didn’t use waiting rooms. In some cases, staff was out in the parking lot, putting stethoscopes through patients’ windows.”
“None of the practices closed, not even temporarily,” Dr. Sidorov said. “But clearly this cannot go forever without having serious consequences.”
How much can telemedicine help?
Telemedicine has been a lifeline for many struggling practices. “As much as 20%-40% of a practice’s losses can be recouped through telemedicine, depending on variables like patients’ attitudes,” said Mr. Singleton at Merritt Hawkins.
The rise in telemedicine was made possible by a temporary relaxation of the limits on telemedicine payments by Medicare and many private payers. Medicare is currently paying the same rates for telemedicine as it does for in-office visits.
In a recent MGMA Stat survey, 97% of practices reported that they had taken up telemedicine, according to Mr. Gans. He estimates that 80% of primary care could be converted to telemedicine, including medication refills, ongoing care of chronic patients, and recording patients’ vital signs from home.
Some primary care physicians are now using telemedicine for 100% of their visits. “I voluntarily closed my practice weeks ago except for virtual visits due to the risk of exposure for my patients,” a doctor in South Carolina told the Primary Care Collaborative in mid-April. “I continue to pay my staff out of pocket but have reduced hours and am not receiving any income myself.”
However, Mr. Inman of Physician Wealth Services said family medicine clients using telemedicine for all of their patients are earning less per visit, even though the Medicare reimbursement is the same as for an office visit. “They earn less because they cannot charge for any ancillaries, such as labs or imaging,” he said.
“Telemedicine has its limits,” Mr. Singleton said. It cannot replace elective surgeries, and even in primary care practices, “there is a lot of work for which patients have to come in, such as physicals or providing vaccines,” he said. “I know of one doctor who has refrigerator full of vaccines to give out. That pays his bills.”
In many cases, “telemedicine” simply means using the phone, with no video. Many patients can only use the phone, and Medicare now reimburses for some kinds of phone visits. In a mid-April survey of primary care providers, 44% were using the telephone for the majority of their visits, and 14% were not using video at all. Medicare recently decided to pay physicians the same amount for telephone visits as in-person visits.
Financial boosts will run out soon
Many private practices are surviving only because they have managed to tap into new federal programs that can finance them for the short-term. Here are the main examples:
Receiving advance Medicare payments. Through the Medicare Accelerated and Advance Payment Program, physicians can be paid up to 3 months of their average Medicare reimbursement in advance. However, repayment starts 120 days after receiving the money and must be completed within 210 days.
Obtaining a federal loan. Under the Paycheck Protection Program (PPP), which is available to all kinds of small businesses, practices can apply for up to 2.5 times their average monthly payroll costs.
PPP money can be used for payroll, rent, mortgage interest, or utility payments for up to 8 weeks. The loan will be entirely forgiven as long as the rules are followed. For example, three quarters of the money must go to payroll, and laid-off employees must be rehired by June 30.
There was such a rush for the first round of PPP loans that many physicians failed to get the loan. “Many of my physician clients applied for the loan as soon as they could, but none of them got it,” said Mr. Inman, the San Diego financial adviser. “We are hoping that the next round of funding will provide them some relief.” The second round started on April 27.
Physicians who have already obtained the PPP loan are very relieved. “This loan made it possible for us to pay our employees,” said George W. Monks, MD, a dermatologist in Tulsa, Okla., and president of the Oklahoma Medical Association.
Staff benefiting from higher unemployment payments. Many practices and hospitals are laying off their staff so that they can collect unemployment benefits. This is a good time to do that because the federal government has boosted unemployment payments by $600 a week, creating a total benefit that is greater than many people earned at their regular jobs.
This extra boost ends in July, but practices with PPP loans will have to rehire their laid-off workers a month before that. Getting laid-off staffers to come back in is going to be critical, and some practices are already having a hard time convincing them to come back, said Michael La Penna, a physician practice manager in Grand Rapids, Mich.
“They are finding that those people don’t want to come back in yet,” he said. “In many cases they have to care for children at home or have been getting generous unemployment checks.”
The problem with all these temporary financial boosts is that they will disappear within weeks or months from now. Mr. La Penna is concerned that the sudden loss of this support could send some practices spinning into bankruptcy. “Unless volume gets better very soon, time is running out for a lot of practices,” he said.
Hospitals, which also have been depending on federal assistance, may run out of money, too. Daniel Wrenne, a financial planner for physicians in Lexington, Ky., said smaller hospitals are particularly vulnerable because they lack the capital. He said a friend who is an attorney for hospitals predicted that 25% of small regional hospitals “won’t make it through this.”
Such financial turmoil might prompt many physicians to retire or find a new job, said Gary Price, MD, a plastic surgeon in New Haven, Conn., and president of the Physicians Foundation, an advocacy group for the profession. In a survey of doctors by the Physicians Foundation and Merritt Hawkins, released on April 21, 18% planned to retire, temporarily close their practices, or opt out of patient care, and another 14%, presumably employed physicians, planned to change jobs.
Is recovery around the corner?
In early May, practices in many parts of the country were seeing the possibility of a return to normal business – or at least what could pass for normal in these unusual times.
“From mid-March to mid-April, hospitals and practices were in panic mode,” said MGMA’s Mr. Gans. “They were focusing on the here and now. But from mid-April to mid-May, they could begin looking at the big picture and decide how they will get back into business.”
Surgeons devastated by bans on elective surgeries might see a bounce in cases, as the backlog of patients comes back in. By late April, 10 states reinstituted elective surgeries, including California, Arizona, Georgia, Indiana, Colorado, and Oklahoma, and New York has reinstituted elective surgeries for some counties.
Dr. Price said he hopes to reopen his plastic surgery practice by the end of June. “If it takes longer than that, I’m not sure that the practice will survive.” His PPP loan would have run out and he would have to lay off his staff. “At that point, ongoing viability of practice would become a real question.”
Dr. Monks said he hopes a lot more patients will come to his dermatology practice. As of the end of April, “we’re starting to see an uptick in the number of patients wanting to come in,” he said. “They seem to be more comfortable with the new world we’re living in.
“Viewing the backlog of cases that haven’t been attended to,” Dr. Monks added, “I think we’ll be really busy for a while.”
But Mr. La Penna said he thinks the expected backlog of elective patients will be more like a trickle than a flood. “Many patients aren’t going to want to return that fast,” he said. “They may have a condition that makes exposure to COVID-19 more risky, like diabetes or high blood pressure, or they’re elderly, or they live in a household with one of these risk groups.”
Andrew Musbach, cofounder of MD Wealth Management in Chelsea, Mich., said he expects a slow recovery for primary care physicians as well. “Even when the lockdowns are over, not everyone is going to feel comfortable coming to a hospital or visiting a doctor’s office unless it’s absolutely necessary,” he said.
Getting back to normal patient volumes will involve finding better ways to protect patients and staff from COVID-19, Dr. Yonover said. At his urology practice, “we take all the usual precautions, but nothing yet has made it dramatically easier to protect patients and staff,” he said. “Rapid, accurate testing for COVID-19 would change the landscape, but I have no idea when that will come.”
Mr. Wrenne advises his physician clients that a financial recovery will take months. “I tell them to plan for 6 months, until October, before income returns to pre–COVID-19 levels. Reimbursement lags appointments by as much as 3 months, plus it will probably take the economy 2-3 months more to get back to normal.”
“We are facing a recession, and how long it will last is anyone’s guess,” said Alex Kilian, a physician wealth manager at Aldrich Wealth in San Diego. “The federal government’s efforts to stimulate the economy is keeping it from crashing, but there are no real signs that it will actually pick up. It may take years for the travel and entertainment industries to come back.”
A recession means patients will have less spending power, and health care sectors like laser eye surgery may be damaged for years to come, said John B. Pinto, an ophthalmology practice management consultant in San Diego. “[That kind of surgery] is purely elective and relatively costly,” he said. “When people get back to work, they are going to be building up their savings and avoiding new debt. They won’t be having [laser eye surgery].”
“There won’t be any quick return to normal for me,” said Dr. Price, the Connecticut plastic surgeon. “The damage this time will probably be worse than in the Great Recession. Back then, plastic surgery was off by 20%, but this time you have the extra problem of patients reluctant to come into medical offices.”
“To get patients to come in, facilities are going to have to convince patients that they are safe,” Mr. Singleton said. “That may mean undertaking some marketing and promotion, and hospitals tend to be much better at that than practices.”
What a new wave of COVID-19 would mean
Some states have begun reopening public places, which could signal patients to return to doctors’ offices even though doctors’ offices were never officially closed. Oklahoma, for example, reopened restaurants, movie theaters, and sports venues on May 1.
Dr. Monks, president of the Oklahoma Medical Association, said his group opposes states reopening. “The governor’s order is too hasty and overly ambitious,” he said. “Oklahoma has seen an ongoing growth in the number of cases, hospitalizations, and deaths in the past week alone [in late April].”
The concern is that opening up public places too soon would create a new wave of COVID-19, which would not only be a public health disaster, but also a financial disaster for physicians. Doctors would be back where they were in March, but unlike in March, they would not benefit from revenues from previously busy times.
Mr. Pinto said the number of COVID-19 cases will rise and fall in the next 2 years, forcing states to reenact new bans on public gatherings and on elective surgeries until the numbers subside again.
Mr. Pinto said authorities in Singapore have successfully handled such waves of the disease through short bans that are tantamount to tapping the brakes of a car. “As the car gathers speed down the hill, you tap the brake,” he said. “I suspect we’ll be seeing a lot of brake-tapping until a vaccine can be developed and distributed.”
Gary LeRoy, MD, president of the American Academy of Family Physicians, recalled the worldwide Spanish Flu pandemic a century ago. “People were allowed out of their houses after 2 months, and the flu spiked up again,” he said. “I hope we don’t make that mistake this time.”
Dr. LeRoy said it’s not possible to predict how the COVID-19 crisis will play out. “What will the future be like? I don’t know the answer,” he said. “The information we learn in next hours, days, or months will probably change everything.”
A version of this article originally appeared on Medscape.com.
“At a combined system and hospital board meeting yesterday, there was a financial presentation,” said a cardiologist in Minnesota, who declined to be named. “We have ‘salary support’ through May 16, which means we will be receiving base pay at our 2019 level. After May 16, I think it’s fairly certain salaries will be decreased.”
A general internist in the same area added: “The system has decided to pay physicians and other employees for 8 weeks, until May 15, and they are borrowing about $150 million to do this. We don’t know what will happen after May 15, but we are supposed to have an update in early May.”
Physician income is of huge interest, and many aspects of it are discussed in Medscape’s Physician Compensation Report 2020, just released.
The worst may be yet to come
Of all the categories of physicians, “I am worried about private practices the most,” said Travis Singleton, senior vice president at Merritt Hawkins, a physician search firm. “They don’t have a financial cushion, and will start seeing big drops in revenue at the end of May.”
“A lot of the A/R [accounts receivables] for practices come within 30 days, and very little comes in after 90 days,” said Terrence R. McWilliams, MD, chief clinical consultant at HSG Advisors, a consultancy for not-for-profit hospitals and their employed physician networks around the country. “So private practices are reaching the point where prior A/R will start to dwindle and they will start feeling the decline in new claims submissions.”
Large practices may have a bigger financial cushion, but in many cases, they also have more liabilities. “We don’t know the financial loss yet, but I think it’s been devastating,” said Paul M. Yonover, MD, a urologist at UroPartners, a large single-specialty practice in Chicago with 62 urologists. “In fact, the financial loss may well be larger than our loss in volume, because we have to support our own surgery center, pathology lab, radiation center, and other in-house services.”
Employed physicians in limbo
In contrast to physicians in private practices, many employed physicians at hospitals and health systems have been shielded from the impact of COVID-19 – at least for now.
“The experiences of employed physicians are very mixed,” said Mr. Singleton at Merritt Hawkins. “Some health systems have reduced physicians’ pay by 20%, but other systems have been putting off any reductions.”
Hospitals and health systems are struggling. “Stopping elective surgeries deeply affected hospitals,” said Ryan Inman, founder of Physician Wealth Services in San Diego. “With fewer elective surgeries, they have much less income coming in. Some big hospitals that are pillars of their community are under great financial stress.”
“Hospitals’ patient volumes have fallen by 50%-90%,” Mr. McWilliams reported. “Lower volume means lower pay for employed physicians, who are paid by straight productivity or other models that require high volumes. However, some health systems have intervened to make sure these physicians get some money.”
Base pay is often safe for now, but quarterly bonuses are on the chopping block. “Employed physicians are often getting a guaranteed salary for a month or two, but no bonuses or extra distributions,” said Joel Greenwald, MD, a financial adviser for physicians in St. Louis Park, Minn., a state mecca for physician employment. “They’ve been told that they will continue to get their base salary but forget about the quarterly bonuses. This amounts to salary reductions of 10%-30%.”
Ensuring payment for these doctors means lowering their productivity benchmarks, but the benchmarks might still be too high for these times. An internist at a large health system in Minneapolis–St. Paul reports that, at a lunch meeting, employed doctors learned that payment benchmarks will be reduced to 70% of their 2019 monthly average.
“I am seeing nowhere near 70% of what I was seeing last year,” he said in an interview, asking that his name not be used. “Given how slow things have been, I am probably closer to 30%, but have not been given any data on this, so I am guessing at this point.”
Adapting to a brave new world
Even as they face a dark financial future, physicians have had to completely revamp the way they practice medicine – a cumbersome process that, in itself, incurred some financial losses. They had to obtain masks and other PPE, reposition or even close down their waiting rooms, cut back on unneeded staff, and adapt to telemedicine.
“It’s been an incredibly challenging time,” said Dr. Yonover, the Chicago urologist. “As a doctor. I cannot avoid contact, and it’s not totally clear yet how the virus spreads. But I don’t have the option of closing the door. As a practice owner, you’re responsible for the health and well-being of employees, patients, and the business.”
“A practice’s daily routine is somewhat slower and costlier,” said David N. Gans, MSHA, senior fellow at the Medical Group Management Association (MGMA), which represents group practices. “Between each patient, you have to clean a lot more than previously, and you have to stock up on PPE such as masks and gowns. PPE used to be limited to infectious patients, but now it’s universal.”
At PA Clinical Network, a clinically integrated network in Pennsylvania, volume fell 40%-50% and income fell 30%-50% from late March to late April, according to Jaan Sidorov, MD, an internist who is CEO of the network, which has 158 physicians in a variety of specialties working in 54 practices around the state.
“Revenue went down but it didn’t crash,” he said. “And our physicians pivoted very quickly. They adapted to telehealth and applied for the federal loan programs. They didn’t use waiting rooms. In some cases, staff was out in the parking lot, putting stethoscopes through patients’ windows.”
“None of the practices closed, not even temporarily,” Dr. Sidorov said. “But clearly this cannot go forever without having serious consequences.”
How much can telemedicine help?
Telemedicine has been a lifeline for many struggling practices. “As much as 20%-40% of a practice’s losses can be recouped through telemedicine, depending on variables like patients’ attitudes,” said Mr. Singleton at Merritt Hawkins.
The rise in telemedicine was made possible by a temporary relaxation of the limits on telemedicine payments by Medicare and many private payers. Medicare is currently paying the same rates for telemedicine as it does for in-office visits.
In a recent MGMA Stat survey, 97% of practices reported that they had taken up telemedicine, according to Mr. Gans. He estimates that 80% of primary care could be converted to telemedicine, including medication refills, ongoing care of chronic patients, and recording patients’ vital signs from home.
Some primary care physicians are now using telemedicine for 100% of their visits. “I voluntarily closed my practice weeks ago except for virtual visits due to the risk of exposure for my patients,” a doctor in South Carolina told the Primary Care Collaborative in mid-April. “I continue to pay my staff out of pocket but have reduced hours and am not receiving any income myself.”
However, Mr. Inman of Physician Wealth Services said family medicine clients using telemedicine for all of their patients are earning less per visit, even though the Medicare reimbursement is the same as for an office visit. “They earn less because they cannot charge for any ancillaries, such as labs or imaging,” he said.
“Telemedicine has its limits,” Mr. Singleton said. It cannot replace elective surgeries, and even in primary care practices, “there is a lot of work for which patients have to come in, such as physicals or providing vaccines,” he said. “I know of one doctor who has refrigerator full of vaccines to give out. That pays his bills.”
In many cases, “telemedicine” simply means using the phone, with no video. Many patients can only use the phone, and Medicare now reimburses for some kinds of phone visits. In a mid-April survey of primary care providers, 44% were using the telephone for the majority of their visits, and 14% were not using video at all. Medicare recently decided to pay physicians the same amount for telephone visits as in-person visits.
Financial boosts will run out soon
Many private practices are surviving only because they have managed to tap into new federal programs that can finance them for the short-term. Here are the main examples:
Receiving advance Medicare payments. Through the Medicare Accelerated and Advance Payment Program, physicians can be paid up to 3 months of their average Medicare reimbursement in advance. However, repayment starts 120 days after receiving the money and must be completed within 210 days.
Obtaining a federal loan. Under the Paycheck Protection Program (PPP), which is available to all kinds of small businesses, practices can apply for up to 2.5 times their average monthly payroll costs.
PPP money can be used for payroll, rent, mortgage interest, or utility payments for up to 8 weeks. The loan will be entirely forgiven as long as the rules are followed. For example, three quarters of the money must go to payroll, and laid-off employees must be rehired by June 30.
There was such a rush for the first round of PPP loans that many physicians failed to get the loan. “Many of my physician clients applied for the loan as soon as they could, but none of them got it,” said Mr. Inman, the San Diego financial adviser. “We are hoping that the next round of funding will provide them some relief.” The second round started on April 27.
Physicians who have already obtained the PPP loan are very relieved. “This loan made it possible for us to pay our employees,” said George W. Monks, MD, a dermatologist in Tulsa, Okla., and president of the Oklahoma Medical Association.
Staff benefiting from higher unemployment payments. Many practices and hospitals are laying off their staff so that they can collect unemployment benefits. This is a good time to do that because the federal government has boosted unemployment payments by $600 a week, creating a total benefit that is greater than many people earned at their regular jobs.
This extra boost ends in July, but practices with PPP loans will have to rehire their laid-off workers a month before that. Getting laid-off staffers to come back in is going to be critical, and some practices are already having a hard time convincing them to come back, said Michael La Penna, a physician practice manager in Grand Rapids, Mich.
“They are finding that those people don’t want to come back in yet,” he said. “In many cases they have to care for children at home or have been getting generous unemployment checks.”
The problem with all these temporary financial boosts is that they will disappear within weeks or months from now. Mr. La Penna is concerned that the sudden loss of this support could send some practices spinning into bankruptcy. “Unless volume gets better very soon, time is running out for a lot of practices,” he said.
Hospitals, which also have been depending on federal assistance, may run out of money, too. Daniel Wrenne, a financial planner for physicians in Lexington, Ky., said smaller hospitals are particularly vulnerable because they lack the capital. He said a friend who is an attorney for hospitals predicted that 25% of small regional hospitals “won’t make it through this.”
Such financial turmoil might prompt many physicians to retire or find a new job, said Gary Price, MD, a plastic surgeon in New Haven, Conn., and president of the Physicians Foundation, an advocacy group for the profession. In a survey of doctors by the Physicians Foundation and Merritt Hawkins, released on April 21, 18% planned to retire, temporarily close their practices, or opt out of patient care, and another 14%, presumably employed physicians, planned to change jobs.
Is recovery around the corner?
In early May, practices in many parts of the country were seeing the possibility of a return to normal business – or at least what could pass for normal in these unusual times.
“From mid-March to mid-April, hospitals and practices were in panic mode,” said MGMA’s Mr. Gans. “They were focusing on the here and now. But from mid-April to mid-May, they could begin looking at the big picture and decide how they will get back into business.”
Surgeons devastated by bans on elective surgeries might see a bounce in cases, as the backlog of patients comes back in. By late April, 10 states reinstituted elective surgeries, including California, Arizona, Georgia, Indiana, Colorado, and Oklahoma, and New York has reinstituted elective surgeries for some counties.
Dr. Price said he hopes to reopen his plastic surgery practice by the end of June. “If it takes longer than that, I’m not sure that the practice will survive.” His PPP loan would have run out and he would have to lay off his staff. “At that point, ongoing viability of practice would become a real question.”
Dr. Monks said he hopes a lot more patients will come to his dermatology practice. As of the end of April, “we’re starting to see an uptick in the number of patients wanting to come in,” he said. “They seem to be more comfortable with the new world we’re living in.
“Viewing the backlog of cases that haven’t been attended to,” Dr. Monks added, “I think we’ll be really busy for a while.”
But Mr. La Penna said he thinks the expected backlog of elective patients will be more like a trickle than a flood. “Many patients aren’t going to want to return that fast,” he said. “They may have a condition that makes exposure to COVID-19 more risky, like diabetes or high blood pressure, or they’re elderly, or they live in a household with one of these risk groups.”
Andrew Musbach, cofounder of MD Wealth Management in Chelsea, Mich., said he expects a slow recovery for primary care physicians as well. “Even when the lockdowns are over, not everyone is going to feel comfortable coming to a hospital or visiting a doctor’s office unless it’s absolutely necessary,” he said.
Getting back to normal patient volumes will involve finding better ways to protect patients and staff from COVID-19, Dr. Yonover said. At his urology practice, “we take all the usual precautions, but nothing yet has made it dramatically easier to protect patients and staff,” he said. “Rapid, accurate testing for COVID-19 would change the landscape, but I have no idea when that will come.”
Mr. Wrenne advises his physician clients that a financial recovery will take months. “I tell them to plan for 6 months, until October, before income returns to pre–COVID-19 levels. Reimbursement lags appointments by as much as 3 months, plus it will probably take the economy 2-3 months more to get back to normal.”
“We are facing a recession, and how long it will last is anyone’s guess,” said Alex Kilian, a physician wealth manager at Aldrich Wealth in San Diego. “The federal government’s efforts to stimulate the economy is keeping it from crashing, but there are no real signs that it will actually pick up. It may take years for the travel and entertainment industries to come back.”
A recession means patients will have less spending power, and health care sectors like laser eye surgery may be damaged for years to come, said John B. Pinto, an ophthalmology practice management consultant in San Diego. “[That kind of surgery] is purely elective and relatively costly,” he said. “When people get back to work, they are going to be building up their savings and avoiding new debt. They won’t be having [laser eye surgery].”
“There won’t be any quick return to normal for me,” said Dr. Price, the Connecticut plastic surgeon. “The damage this time will probably be worse than in the Great Recession. Back then, plastic surgery was off by 20%, but this time you have the extra problem of patients reluctant to come into medical offices.”
“To get patients to come in, facilities are going to have to convince patients that they are safe,” Mr. Singleton said. “That may mean undertaking some marketing and promotion, and hospitals tend to be much better at that than practices.”
What a new wave of COVID-19 would mean
Some states have begun reopening public places, which could signal patients to return to doctors’ offices even though doctors’ offices were never officially closed. Oklahoma, for example, reopened restaurants, movie theaters, and sports venues on May 1.
Dr. Monks, president of the Oklahoma Medical Association, said his group opposes states reopening. “The governor’s order is too hasty and overly ambitious,” he said. “Oklahoma has seen an ongoing growth in the number of cases, hospitalizations, and deaths in the past week alone [in late April].”
The concern is that opening up public places too soon would create a new wave of COVID-19, which would not only be a public health disaster, but also a financial disaster for physicians. Doctors would be back where they were in March, but unlike in March, they would not benefit from revenues from previously busy times.
Mr. Pinto said the number of COVID-19 cases will rise and fall in the next 2 years, forcing states to reenact new bans on public gatherings and on elective surgeries until the numbers subside again.
Mr. Pinto said authorities in Singapore have successfully handled such waves of the disease through short bans that are tantamount to tapping the brakes of a car. “As the car gathers speed down the hill, you tap the brake,” he said. “I suspect we’ll be seeing a lot of brake-tapping until a vaccine can be developed and distributed.”
Gary LeRoy, MD, president of the American Academy of Family Physicians, recalled the worldwide Spanish Flu pandemic a century ago. “People were allowed out of their houses after 2 months, and the flu spiked up again,” he said. “I hope we don’t make that mistake this time.”
Dr. LeRoy said it’s not possible to predict how the COVID-19 crisis will play out. “What will the future be like? I don’t know the answer,” he said. “The information we learn in next hours, days, or months will probably change everything.”
A version of this article originally appeared on Medscape.com.
“At a combined system and hospital board meeting yesterday, there was a financial presentation,” said a cardiologist in Minnesota, who declined to be named. “We have ‘salary support’ through May 16, which means we will be receiving base pay at our 2019 level. After May 16, I think it’s fairly certain salaries will be decreased.”
A general internist in the same area added: “The system has decided to pay physicians and other employees for 8 weeks, until May 15, and they are borrowing about $150 million to do this. We don’t know what will happen after May 15, but we are supposed to have an update in early May.”
Physician income is of huge interest, and many aspects of it are discussed in Medscape’s Physician Compensation Report 2020, just released.
The worst may be yet to come
Of all the categories of physicians, “I am worried about private practices the most,” said Travis Singleton, senior vice president at Merritt Hawkins, a physician search firm. “They don’t have a financial cushion, and will start seeing big drops in revenue at the end of May.”
“A lot of the A/R [accounts receivables] for practices come within 30 days, and very little comes in after 90 days,” said Terrence R. McWilliams, MD, chief clinical consultant at HSG Advisors, a consultancy for not-for-profit hospitals and their employed physician networks around the country. “So private practices are reaching the point where prior A/R will start to dwindle and they will start feeling the decline in new claims submissions.”
Large practices may have a bigger financial cushion, but in many cases, they also have more liabilities. “We don’t know the financial loss yet, but I think it’s been devastating,” said Paul M. Yonover, MD, a urologist at UroPartners, a large single-specialty practice in Chicago with 62 urologists. “In fact, the financial loss may well be larger than our loss in volume, because we have to support our own surgery center, pathology lab, radiation center, and other in-house services.”
Employed physicians in limbo
In contrast to physicians in private practices, many employed physicians at hospitals and health systems have been shielded from the impact of COVID-19 – at least for now.
“The experiences of employed physicians are very mixed,” said Mr. Singleton at Merritt Hawkins. “Some health systems have reduced physicians’ pay by 20%, but other systems have been putting off any reductions.”
Hospitals and health systems are struggling. “Stopping elective surgeries deeply affected hospitals,” said Ryan Inman, founder of Physician Wealth Services in San Diego. “With fewer elective surgeries, they have much less income coming in. Some big hospitals that are pillars of their community are under great financial stress.”
“Hospitals’ patient volumes have fallen by 50%-90%,” Mr. McWilliams reported. “Lower volume means lower pay for employed physicians, who are paid by straight productivity or other models that require high volumes. However, some health systems have intervened to make sure these physicians get some money.”
Base pay is often safe for now, but quarterly bonuses are on the chopping block. “Employed physicians are often getting a guaranteed salary for a month or two, but no bonuses or extra distributions,” said Joel Greenwald, MD, a financial adviser for physicians in St. Louis Park, Minn., a state mecca for physician employment. “They’ve been told that they will continue to get their base salary but forget about the quarterly bonuses. This amounts to salary reductions of 10%-30%.”
Ensuring payment for these doctors means lowering their productivity benchmarks, but the benchmarks might still be too high for these times. An internist at a large health system in Minneapolis–St. Paul reports that, at a lunch meeting, employed doctors learned that payment benchmarks will be reduced to 70% of their 2019 monthly average.
“I am seeing nowhere near 70% of what I was seeing last year,” he said in an interview, asking that his name not be used. “Given how slow things have been, I am probably closer to 30%, but have not been given any data on this, so I am guessing at this point.”
Adapting to a brave new world
Even as they face a dark financial future, physicians have had to completely revamp the way they practice medicine – a cumbersome process that, in itself, incurred some financial losses. They had to obtain masks and other PPE, reposition or even close down their waiting rooms, cut back on unneeded staff, and adapt to telemedicine.
“It’s been an incredibly challenging time,” said Dr. Yonover, the Chicago urologist. “As a doctor. I cannot avoid contact, and it’s not totally clear yet how the virus spreads. But I don’t have the option of closing the door. As a practice owner, you’re responsible for the health and well-being of employees, patients, and the business.”
“A practice’s daily routine is somewhat slower and costlier,” said David N. Gans, MSHA, senior fellow at the Medical Group Management Association (MGMA), which represents group practices. “Between each patient, you have to clean a lot more than previously, and you have to stock up on PPE such as masks and gowns. PPE used to be limited to infectious patients, but now it’s universal.”
At PA Clinical Network, a clinically integrated network in Pennsylvania, volume fell 40%-50% and income fell 30%-50% from late March to late April, according to Jaan Sidorov, MD, an internist who is CEO of the network, which has 158 physicians in a variety of specialties working in 54 practices around the state.
“Revenue went down but it didn’t crash,” he said. “And our physicians pivoted very quickly. They adapted to telehealth and applied for the federal loan programs. They didn’t use waiting rooms. In some cases, staff was out in the parking lot, putting stethoscopes through patients’ windows.”
“None of the practices closed, not even temporarily,” Dr. Sidorov said. “But clearly this cannot go forever without having serious consequences.”
How much can telemedicine help?
Telemedicine has been a lifeline for many struggling practices. “As much as 20%-40% of a practice’s losses can be recouped through telemedicine, depending on variables like patients’ attitudes,” said Mr. Singleton at Merritt Hawkins.
The rise in telemedicine was made possible by a temporary relaxation of the limits on telemedicine payments by Medicare and many private payers. Medicare is currently paying the same rates for telemedicine as it does for in-office visits.
In a recent MGMA Stat survey, 97% of practices reported that they had taken up telemedicine, according to Mr. Gans. He estimates that 80% of primary care could be converted to telemedicine, including medication refills, ongoing care of chronic patients, and recording patients’ vital signs from home.
Some primary care physicians are now using telemedicine for 100% of their visits. “I voluntarily closed my practice weeks ago except for virtual visits due to the risk of exposure for my patients,” a doctor in South Carolina told the Primary Care Collaborative in mid-April. “I continue to pay my staff out of pocket but have reduced hours and am not receiving any income myself.”
However, Mr. Inman of Physician Wealth Services said family medicine clients using telemedicine for all of their patients are earning less per visit, even though the Medicare reimbursement is the same as for an office visit. “They earn less because they cannot charge for any ancillaries, such as labs or imaging,” he said.
“Telemedicine has its limits,” Mr. Singleton said. It cannot replace elective surgeries, and even in primary care practices, “there is a lot of work for which patients have to come in, such as physicals or providing vaccines,” he said. “I know of one doctor who has refrigerator full of vaccines to give out. That pays his bills.”
In many cases, “telemedicine” simply means using the phone, with no video. Many patients can only use the phone, and Medicare now reimburses for some kinds of phone visits. In a mid-April survey of primary care providers, 44% were using the telephone for the majority of their visits, and 14% were not using video at all. Medicare recently decided to pay physicians the same amount for telephone visits as in-person visits.
Financial boosts will run out soon
Many private practices are surviving only because they have managed to tap into new federal programs that can finance them for the short-term. Here are the main examples:
Receiving advance Medicare payments. Through the Medicare Accelerated and Advance Payment Program, physicians can be paid up to 3 months of their average Medicare reimbursement in advance. However, repayment starts 120 days after receiving the money and must be completed within 210 days.
Obtaining a federal loan. Under the Paycheck Protection Program (PPP), which is available to all kinds of small businesses, practices can apply for up to 2.5 times their average monthly payroll costs.
PPP money can be used for payroll, rent, mortgage interest, or utility payments for up to 8 weeks. The loan will be entirely forgiven as long as the rules are followed. For example, three quarters of the money must go to payroll, and laid-off employees must be rehired by June 30.
There was such a rush for the first round of PPP loans that many physicians failed to get the loan. “Many of my physician clients applied for the loan as soon as they could, but none of them got it,” said Mr. Inman, the San Diego financial adviser. “We are hoping that the next round of funding will provide them some relief.” The second round started on April 27.
Physicians who have already obtained the PPP loan are very relieved. “This loan made it possible for us to pay our employees,” said George W. Monks, MD, a dermatologist in Tulsa, Okla., and president of the Oklahoma Medical Association.
Staff benefiting from higher unemployment payments. Many practices and hospitals are laying off their staff so that they can collect unemployment benefits. This is a good time to do that because the federal government has boosted unemployment payments by $600 a week, creating a total benefit that is greater than many people earned at their regular jobs.
This extra boost ends in July, but practices with PPP loans will have to rehire their laid-off workers a month before that. Getting laid-off staffers to come back in is going to be critical, and some practices are already having a hard time convincing them to come back, said Michael La Penna, a physician practice manager in Grand Rapids, Mich.
“They are finding that those people don’t want to come back in yet,” he said. “In many cases they have to care for children at home or have been getting generous unemployment checks.”
The problem with all these temporary financial boosts is that they will disappear within weeks or months from now. Mr. La Penna is concerned that the sudden loss of this support could send some practices spinning into bankruptcy. “Unless volume gets better very soon, time is running out for a lot of practices,” he said.
Hospitals, which also have been depending on federal assistance, may run out of money, too. Daniel Wrenne, a financial planner for physicians in Lexington, Ky., said smaller hospitals are particularly vulnerable because they lack the capital. He said a friend who is an attorney for hospitals predicted that 25% of small regional hospitals “won’t make it through this.”
Such financial turmoil might prompt many physicians to retire or find a new job, said Gary Price, MD, a plastic surgeon in New Haven, Conn., and president of the Physicians Foundation, an advocacy group for the profession. In a survey of doctors by the Physicians Foundation and Merritt Hawkins, released on April 21, 18% planned to retire, temporarily close their practices, or opt out of patient care, and another 14%, presumably employed physicians, planned to change jobs.
Is recovery around the corner?
In early May, practices in many parts of the country were seeing the possibility of a return to normal business – or at least what could pass for normal in these unusual times.
“From mid-March to mid-April, hospitals and practices were in panic mode,” said MGMA’s Mr. Gans. “They were focusing on the here and now. But from mid-April to mid-May, they could begin looking at the big picture and decide how they will get back into business.”
Surgeons devastated by bans on elective surgeries might see a bounce in cases, as the backlog of patients comes back in. By late April, 10 states reinstituted elective surgeries, including California, Arizona, Georgia, Indiana, Colorado, and Oklahoma, and New York has reinstituted elective surgeries for some counties.
Dr. Price said he hopes to reopen his plastic surgery practice by the end of June. “If it takes longer than that, I’m not sure that the practice will survive.” His PPP loan would have run out and he would have to lay off his staff. “At that point, ongoing viability of practice would become a real question.”
Dr. Monks said he hopes a lot more patients will come to his dermatology practice. As of the end of April, “we’re starting to see an uptick in the number of patients wanting to come in,” he said. “They seem to be more comfortable with the new world we’re living in.
“Viewing the backlog of cases that haven’t been attended to,” Dr. Monks added, “I think we’ll be really busy for a while.”
But Mr. La Penna said he thinks the expected backlog of elective patients will be more like a trickle than a flood. “Many patients aren’t going to want to return that fast,” he said. “They may have a condition that makes exposure to COVID-19 more risky, like diabetes or high blood pressure, or they’re elderly, or they live in a household with one of these risk groups.”
Andrew Musbach, cofounder of MD Wealth Management in Chelsea, Mich., said he expects a slow recovery for primary care physicians as well. “Even when the lockdowns are over, not everyone is going to feel comfortable coming to a hospital or visiting a doctor’s office unless it’s absolutely necessary,” he said.
Getting back to normal patient volumes will involve finding better ways to protect patients and staff from COVID-19, Dr. Yonover said. At his urology practice, “we take all the usual precautions, but nothing yet has made it dramatically easier to protect patients and staff,” he said. “Rapid, accurate testing for COVID-19 would change the landscape, but I have no idea when that will come.”
Mr. Wrenne advises his physician clients that a financial recovery will take months. “I tell them to plan for 6 months, until October, before income returns to pre–COVID-19 levels. Reimbursement lags appointments by as much as 3 months, plus it will probably take the economy 2-3 months more to get back to normal.”
“We are facing a recession, and how long it will last is anyone’s guess,” said Alex Kilian, a physician wealth manager at Aldrich Wealth in San Diego. “The federal government’s efforts to stimulate the economy is keeping it from crashing, but there are no real signs that it will actually pick up. It may take years for the travel and entertainment industries to come back.”
A recession means patients will have less spending power, and health care sectors like laser eye surgery may be damaged for years to come, said John B. Pinto, an ophthalmology practice management consultant in San Diego. “[That kind of surgery] is purely elective and relatively costly,” he said. “When people get back to work, they are going to be building up their savings and avoiding new debt. They won’t be having [laser eye surgery].”
“There won’t be any quick return to normal for me,” said Dr. Price, the Connecticut plastic surgeon. “The damage this time will probably be worse than in the Great Recession. Back then, plastic surgery was off by 20%, but this time you have the extra problem of patients reluctant to come into medical offices.”
“To get patients to come in, facilities are going to have to convince patients that they are safe,” Mr. Singleton said. “That may mean undertaking some marketing and promotion, and hospitals tend to be much better at that than practices.”
What a new wave of COVID-19 would mean
Some states have begun reopening public places, which could signal patients to return to doctors’ offices even though doctors’ offices were never officially closed. Oklahoma, for example, reopened restaurants, movie theaters, and sports venues on May 1.
Dr. Monks, president of the Oklahoma Medical Association, said his group opposes states reopening. “The governor’s order is too hasty and overly ambitious,” he said. “Oklahoma has seen an ongoing growth in the number of cases, hospitalizations, and deaths in the past week alone [in late April].”
The concern is that opening up public places too soon would create a new wave of COVID-19, which would not only be a public health disaster, but also a financial disaster for physicians. Doctors would be back where they were in March, but unlike in March, they would not benefit from revenues from previously busy times.
Mr. Pinto said the number of COVID-19 cases will rise and fall in the next 2 years, forcing states to reenact new bans on public gatherings and on elective surgeries until the numbers subside again.
Mr. Pinto said authorities in Singapore have successfully handled such waves of the disease through short bans that are tantamount to tapping the brakes of a car. “As the car gathers speed down the hill, you tap the brake,” he said. “I suspect we’ll be seeing a lot of brake-tapping until a vaccine can be developed and distributed.”
Gary LeRoy, MD, president of the American Academy of Family Physicians, recalled the worldwide Spanish Flu pandemic a century ago. “People were allowed out of their houses after 2 months, and the flu spiked up again,” he said. “I hope we don’t make that mistake this time.”
Dr. LeRoy said it’s not possible to predict how the COVID-19 crisis will play out. “What will the future be like? I don’t know the answer,” he said. “The information we learn in next hours, days, or months will probably change everything.”
A version of this article originally appeared on Medscape.com.
Practice During the Pandemic
The first installment of my new column was obsolete on arrival. It referred to walking abroad at midday, with no mention of masks and social distancing. The whole thing was so February 2020.

My last day in the office was in mid-March. Friday the 13th.
, using stored and forwarded images.
What I had in mind was visits by patients in nursing homes or too sick at home to come in. It always bothered me to see very aged and infirm patients brought to the office at great inconvenience and expense for what often turned out to be problems like xerosis or eczema that could have been managed quite well remotely.
The HMO never got back to me, though. There were too many hurdles, mostly bureaucratic rather than medical. Would insurance pay? What about consent? Malpractice? It has been interesting to watch the current crisis sweep away the inertia of such obstacles, including licensure considerations (seeing patients across state lines for cutaneous purposes). People get around to fixing the roof when it pours. Perhaps next time there will be tests, masks, respirators. Perhaps.
Seeing patients remotely has acquainted me with all the technical headaches everyone stuck at home talks and jokes about: Balky transmission (What did you say after, “and then the blood ...”?); patients who can’t figure out how to log on, or start the video, or unmute themselves, and on and on. Picture resolution is not great, as anyone knows from watching TV newscasters interview talking heads stuck in their homes.
I was never all that image-conscious, but my beard has grown fuller and my hair unkempter. Even though I sit at my desk, I do take care to keep my trousers on. Not taking any chances.
Everyone agonizes over what the “new normal” may be. Will people come back to doctors’ offices? Will practices survive economically if many patients don’t return to the office? Stay tuned. For a long time.
Mostly, though, remote visits seem to work. Helped if needed by additional, better-resolution emailed photos, it’s possible to make useful decisions, including which lesions can wait for in-person evaluation, until ...
... Until what? In an effort to keep this column up-to-the-nanosecond, I am writing it as many countries tentatively “open up.” Careful analysis of the knowledge behind this world-wide project shows ... not much. It seems to come down to some educated guesswork about what might work and what the risks might be, which leads to advice that differs widely from state to state and country to country. It’s as if people everywhere just decided that locking everyone down is a real drag, is financially ruinous, has a duration both uncertain and longer than most people and governments think they can handle, so let’s get out there and “be careful,” whatever that is said to mean.
And the risks? Well, more people will get sick and some will die. How many “extra” deaths are ethically acceptable? Thoughtful people are working on that. They’ll get back sometime to those who are still around.
I don’t blame anyone for our staggering ignorance about this terrifying new reality. But absorbing the ignorance in real time is not reassuring.
I have nothing but sympathy for those who are not emeritus, who have practices to sustain and families to feed. I didn’t ask to be born 73 years ago, and take no credit for having done so. So much of what happens to us depends on when and where we were born – two factors for which we deserve absolutely no credit – that it’s a wonder we take such pride in praising ourselves for what we think we accomplish. Having no better choice, we do the best we can.
Meantime, I am in a “high-risk” category. If I were obese, I could try to lose weight. But my risk factor is age, which tends not to decline. Risk-wise, there is just one way to exit my group.
So I don’t expect to get back to the office anytime soon. To paraphrase a comedian who shall remain nameless: I don’t want to live on in the hearts of men. I want to live on in my house.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semiretired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available online. Write to him at [email protected].
The first installment of my new column was obsolete on arrival. It referred to walking abroad at midday, with no mention of masks and social distancing. The whole thing was so February 2020.
My last day in the office was in mid-March. Friday the 13th.
, using stored and forwarded images.
What I had in mind was visits by patients in nursing homes or too sick at home to come in. It always bothered me to see very aged and infirm patients brought to the office at great inconvenience and expense for what often turned out to be problems like xerosis or eczema that could have been managed quite well remotely.
The HMO never got back to me, though. There were too many hurdles, mostly bureaucratic rather than medical. Would insurance pay? What about consent? Malpractice? It has been interesting to watch the current crisis sweep away the inertia of such obstacles, including licensure considerations (seeing patients across state lines for cutaneous purposes). People get around to fixing the roof when it pours. Perhaps next time there will be tests, masks, respirators. Perhaps.
Seeing patients remotely has acquainted me with all the technical headaches everyone stuck at home talks and jokes about: Balky transmission (What did you say after, “and then the blood ...”?); patients who can’t figure out how to log on, or start the video, or unmute themselves, and on and on. Picture resolution is not great, as anyone knows from watching TV newscasters interview talking heads stuck in their homes.
I was never all that image-conscious, but my beard has grown fuller and my hair unkempter. Even though I sit at my desk, I do take care to keep my trousers on. Not taking any chances.
Everyone agonizes over what the “new normal” may be. Will people come back to doctors’ offices? Will practices survive economically if many patients don’t return to the office? Stay tuned. For a long time.
Mostly, though, remote visits seem to work. Helped if needed by additional, better-resolution emailed photos, it’s possible to make useful decisions, including which lesions can wait for in-person evaluation, until ...
... Until what? In an effort to keep this column up-to-the-nanosecond, I am writing it as many countries tentatively “open up.” Careful analysis of the knowledge behind this world-wide project shows ... not much. It seems to come down to some educated guesswork about what might work and what the risks might be, which leads to advice that differs widely from state to state and country to country. It’s as if people everywhere just decided that locking everyone down is a real drag, is financially ruinous, has a duration both uncertain and longer than most people and governments think they can handle, so let’s get out there and “be careful,” whatever that is said to mean.
And the risks? Well, more people will get sick and some will die. How many “extra” deaths are ethically acceptable? Thoughtful people are working on that. They’ll get back sometime to those who are still around.
I don’t blame anyone for our staggering ignorance about this terrifying new reality. But absorbing the ignorance in real time is not reassuring.
I have nothing but sympathy for those who are not emeritus, who have practices to sustain and families to feed. I didn’t ask to be born 73 years ago, and take no credit for having done so. So much of what happens to us depends on when and where we were born – two factors for which we deserve absolutely no credit – that it’s a wonder we take such pride in praising ourselves for what we think we accomplish. Having no better choice, we do the best we can.
Meantime, I am in a “high-risk” category. If I were obese, I could try to lose weight. But my risk factor is age, which tends not to decline. Risk-wise, there is just one way to exit my group.
So I don’t expect to get back to the office anytime soon. To paraphrase a comedian who shall remain nameless: I don’t want to live on in the hearts of men. I want to live on in my house.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semiretired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available online. Write to him at [email protected].
The first installment of my new column was obsolete on arrival. It referred to walking abroad at midday, with no mention of masks and social distancing. The whole thing was so February 2020.
My last day in the office was in mid-March. Friday the 13th.
, using stored and forwarded images.
What I had in mind was visits by patients in nursing homes or too sick at home to come in. It always bothered me to see very aged and infirm patients brought to the office at great inconvenience and expense for what often turned out to be problems like xerosis or eczema that could have been managed quite well remotely.
The HMO never got back to me, though. There were too many hurdles, mostly bureaucratic rather than medical. Would insurance pay? What about consent? Malpractice? It has been interesting to watch the current crisis sweep away the inertia of such obstacles, including licensure considerations (seeing patients across state lines for cutaneous purposes). People get around to fixing the roof when it pours. Perhaps next time there will be tests, masks, respirators. Perhaps.
Seeing patients remotely has acquainted me with all the technical headaches everyone stuck at home talks and jokes about: Balky transmission (What did you say after, “and then the blood ...”?); patients who can’t figure out how to log on, or start the video, or unmute themselves, and on and on. Picture resolution is not great, as anyone knows from watching TV newscasters interview talking heads stuck in their homes.
I was never all that image-conscious, but my beard has grown fuller and my hair unkempter. Even though I sit at my desk, I do take care to keep my trousers on. Not taking any chances.
Everyone agonizes over what the “new normal” may be. Will people come back to doctors’ offices? Will practices survive economically if many patients don’t return to the office? Stay tuned. For a long time.
Mostly, though, remote visits seem to work. Helped if needed by additional, better-resolution emailed photos, it’s possible to make useful decisions, including which lesions can wait for in-person evaluation, until ...
... Until what? In an effort to keep this column up-to-the-nanosecond, I am writing it as many countries tentatively “open up.” Careful analysis of the knowledge behind this world-wide project shows ... not much. It seems to come down to some educated guesswork about what might work and what the risks might be, which leads to advice that differs widely from state to state and country to country. It’s as if people everywhere just decided that locking everyone down is a real drag, is financially ruinous, has a duration both uncertain and longer than most people and governments think they can handle, so let’s get out there and “be careful,” whatever that is said to mean.
And the risks? Well, more people will get sick and some will die. How many “extra” deaths are ethically acceptable? Thoughtful people are working on that. They’ll get back sometime to those who are still around.
I don’t blame anyone for our staggering ignorance about this terrifying new reality. But absorbing the ignorance in real time is not reassuring.
I have nothing but sympathy for those who are not emeritus, who have practices to sustain and families to feed. I didn’t ask to be born 73 years ago, and take no credit for having done so. So much of what happens to us depends on when and where we were born – two factors for which we deserve absolutely no credit – that it’s a wonder we take such pride in praising ourselves for what we think we accomplish. Having no better choice, we do the best we can.
Meantime, I am in a “high-risk” category. If I were obese, I could try to lose weight. But my risk factor is age, which tends not to decline. Risk-wise, there is just one way to exit my group.
So I don’t expect to get back to the office anytime soon. To paraphrase a comedian who shall remain nameless: I don’t want to live on in the hearts of men. I want to live on in my house.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semiretired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available online. Write to him at [email protected].
Operation Quack Hack: FDA moves to stop fraudulent COVID-19 products
No form of human misery can be allowed to go unexploited, and the pandemic, it seems, is no exception.
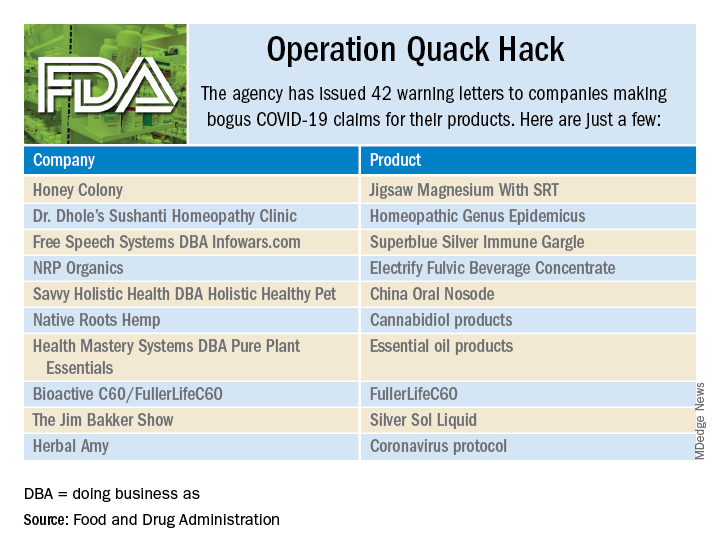
As part of Operation Quack Hack, the Food and Drug Administration has stepped up its investigation and enforcement efforts against companies and individuals that are “taking advantage of widespread fear among consumers during the COVID-19 pandemic” by selling fake products and treatments for coronavirus.
As of May 7, 2020, the agency had issued 42 warning letters to companies that were “selling unapproved products that fraudulently claim to mitigate, prevent, treat, diagnose or cure COVID-19,” the FDA announced in a written statement. Of those 42 products, 29 are no longer being sold with any sort of COVID-19 claim.
Since the beginning of the pandemic, Operation Quack Hack has uncovered hundreds of such products – drugs, testing kits, and personal protective equipment – being sold online, and complaints were sent to domain-name registrars and Internet marketplaces that have, in most cases, removed the postings, the FDA said.
“We will continue to monitor the online ecosystem for fraudulent products peddled by bad actors seeking to profit from this global pandemic. We encourage anyone aware of suspected fraudulent medical products for COVID-19 to report them to the FDA,” the statement said.
No form of human misery can be allowed to go unexploited, and the pandemic, it seems, is no exception.
As part of Operation Quack Hack, the Food and Drug Administration has stepped up its investigation and enforcement efforts against companies and individuals that are “taking advantage of widespread fear among consumers during the COVID-19 pandemic” by selling fake products and treatments for coronavirus.
As of May 7, 2020, the agency had issued 42 warning letters to companies that were “selling unapproved products that fraudulently claim to mitigate, prevent, treat, diagnose or cure COVID-19,” the FDA announced in a written statement. Of those 42 products, 29 are no longer being sold with any sort of COVID-19 claim.
Since the beginning of the pandemic, Operation Quack Hack has uncovered hundreds of such products – drugs, testing kits, and personal protective equipment – being sold online, and complaints were sent to domain-name registrars and Internet marketplaces that have, in most cases, removed the postings, the FDA said.
“We will continue to monitor the online ecosystem for fraudulent products peddled by bad actors seeking to profit from this global pandemic. We encourage anyone aware of suspected fraudulent medical products for COVID-19 to report them to the FDA,” the statement said.
No form of human misery can be allowed to go unexploited, and the pandemic, it seems, is no exception.
As part of Operation Quack Hack, the Food and Drug Administration has stepped up its investigation and enforcement efforts against companies and individuals that are “taking advantage of widespread fear among consumers during the COVID-19 pandemic” by selling fake products and treatments for coronavirus.
As of May 7, 2020, the agency had issued 42 warning letters to companies that were “selling unapproved products that fraudulently claim to mitigate, prevent, treat, diagnose or cure COVID-19,” the FDA announced in a written statement. Of those 42 products, 29 are no longer being sold with any sort of COVID-19 claim.
Since the beginning of the pandemic, Operation Quack Hack has uncovered hundreds of such products – drugs, testing kits, and personal protective equipment – being sold online, and complaints were sent to domain-name registrars and Internet marketplaces that have, in most cases, removed the postings, the FDA said.
“We will continue to monitor the online ecosystem for fraudulent products peddled by bad actors seeking to profit from this global pandemic. We encourage anyone aware of suspected fraudulent medical products for COVID-19 to report them to the FDA,” the statement said.
Volunteering during the pandemic: What doctors need to know
A couple of weeks ago, I posted a silly picture of myself with one N95 mask and asked the folks on Twitter what else I might need. In a matter of a few days, I had filled out a form online for volunteering through the Society of Critical Care Medicine, been assigned to work at a hospital in New York City, and booked a hotel and flight.

I was going to volunteer, although I wasn’t sure of exactly what I would be doing. I’m trained as a bariatric surgeon – not obviously suited for critical care, but arguably even less suited for medicine wards.
I undoubtedly would have been less prepared if I hadn’t sought guidance on what to bring with me and generally what to expect. Less than a day after seeking advice, two local women physicians donated N95s, face shields, gowns, bouffants, and coveralls to me. I also received a laminated photo of myself to attach to my gown in the mail from a stranger I met online.
Others suggested I bring goggles, chocolate, protein bars, hand sanitizer, powdered laundry detergent, and alcohol wipes. After running around all over town, I was able find everything but the wipes.
Just as others helped me achieve my goal of volunteering, I hope I can guide those who would like to do similar work by sharing details about my experience and other information I have collected about volunteering.
Below I answer some questions that those considering volunteering might have, including why I went, who I contacted to set this up, who paid for my flight, and what I observed in the hospital.
Motivation and logistics
I am currently serving in a nonclinical role at my institution. So when the pandemic hit the United States, I felt an immense amount of guilt for not being on the front lines caring for patients. I offered my services to local hospitals and registered for the California Health Corps. I live in northern California, which was the first part of the country to shelter in place. Since my home was actually relatively spared, my services weren’t needed.
As the weeks passed, I was slowly getting more and more fit, exercising in my house since there was little else I could do, and the guilt became a cloud gathering over my head.
I decided to volunteer in a place where demands for help were higher – New York. I tried very hard to sign up to volunteer through the state’s registry for health care volunteers, but was unable to do so. Coincidentally, around that same time, I saw on Twitter that Josh Mugele, MD, emergency medicine physician and program director of the emergency medicine residency at Northeast Georgia Medical Center in Gainesville, was on his way to New York. He shared the Society of Critical Care Medicine’s form for volunteering with me, and in less than 48 hours, I was assigned to a hospital in New York City. Five days later I was on a plane from San Francisco to my destination on the opposite side of the country. The airline paid for my flight.
This is not the only path to volunteering. Another volunteer, Sara Pauk, MD, ob.gyn. at the University of Washington, Seattle, found her volunteer role through contacting the New York City Health and Hospitals system directly. Other who have volunteered told me they had contacted specific hospitals or worked with agencies that were placing physicians.
PPE

The Brooklyn hospital where I volunteered provided me with two sets of scrubs and two N95s. Gowns were variably available on our unit, and there was no eye protection. As a colleague of mine, Ben Daxon, MD, anesthesia and critical care physician at the Mayo Clinic in Rochester, Minn., had suggested, anyone volunteering in this context should bring personal protective equipment (PPE) – That includes gowns, bouffants/scrub caps, eye protection, masks, and scrubs.
The “COVID corner”
Once I arrived in New York, I did not feel particularly safe in my hotel, so I moved to another the next day. Then I had to sort out how to keep the whole room from being contaminated. I created a “COVID corner” right by the door where I kept almost everything that had been outside the door.
Every time I walked in the door, I immediately took off my shoes and left them in that corner. I could not find alcohol wipes, even after looking around in the city, so I relied on time to kill the virus, which I presumed was on everything that came from outside.
Groceries stayed by the door for 48-72 hours if possible. After that, I would move them to the “clean” parts of the room. I wore the same outfit to and from the hospital everyday, putting it on right before I left and taking it off immediately after walking into the room (and then proceeding directly to the shower). Those clothes – “my COVID outfit” – lived in the COVID corner. Anything else I wore, including exercise clothes and underwear, got washed right after I wore it.
At the hospital, I would change into scrubs and leave my COVID outfit in a plastic bag inside my handbag. Note: I fully accepted that my handbag was now a COVID handbag. I kept a pair of clogs in the hospital for daily wear. Without alcohol wipes, my room did not feel clean. But I did start to become at peace with my system, even though it was inferior to the system I use in my own home.
Meal time
In addition to bringing snacks from home, I gathered some meal items at a grocery store during my first day in New York. These included water, yogurt, a few protein drinks, fruit, and some mini chocolate croissants. It’s a pandemic – chocolate is encouraged, right?
Neither any of the volunteers I knew nor I had access to a kitchen, so this was about the best I could do.
My first week I worked nights and ate sporadically. A couple of days I bought bagel sandwiches on the way back to the hotel in the morning. Other times, I would eat yogurt or a protein bar.
I had trouble sleeping, so I would wake up early and either do yoga in my room or go for a run in a nearby park. Usually I didn’t plan well enough to eat before I went into the hospital, so I would take yogurt, some fruit, and a croissant with me as I headed out. It was hard eating on the run with a mask on my face.
When I switched to working days, I actually ordered proper dinners from local Thai, Mexican, and Indian restaurants. I paid around $20 a meal.
One night I even had dinner with a coworker who was staying at a hotel close to mine – what a luxury! Prior to all this I had been sheltering in place alone for weeks, so in that sense, this experience was a delight. I interacted with other people, in person, every day!
My commute
My hotel was about 20 minutes from the hospital. Well-meaning folks informed me that Hertz had free car rentals and Uber had discounts for health care workers. When I investigated these options, I found that only employees of certain hospitals were eligible. As a volunteer, I was not eligible.

I ultimately took Uber back and forth, and I was lucky that a few friends had sent me Uber gift cards to defray the costs. Most days, I paid about $20 each way, although 1 day there actually was “surge pricing.” The grand total for the trip was close to $800.
Many of the Uber drivers had put up plastic partitions – reminiscent of the plastic Dexter would use to contain his crime scenes – to increase their separation from their passengers. It was a bit eerie, but also somewhat welcome.
New normal
The actual work at the hospital in Brooklyn where I volunteered was different from usual practice in numerous ways. One of the things I immediately noticed was how difficult it was to get chest x-rays. After placing an emergent chest tube for a tension pneumothorax, it took about 6 hours to get a chest x-ray to assess placement.
Because code medications were needed much more frequently than normal times, these medications were kept in an open supply closet for ease of access. Many of the ventilators looked like they were from the 1970s. (They had been borrowed from the Federal Emergency Management Agency.)
What was most distinct about this work was the sheer volume of deaths and dying patients -- at least one death on our unit occurred every day I was there -- and the way families communicated with their loved ones. Countless times I held my phone over the faces of my unconscious patients to let their family profess their love and beg them to fight. While I have had to deliver bad news over the phone many times in my career, I have never had to intrude on families’ last conversations with their dying loved ones or witness that conversation occurring via a tiny screen.
Reentry
In many ways, I am lucky that I do not do clinical work in my hometown. So while other volunteers were figuring out how many more vacation days they would have to use, or whether they would have to take unpaid leave, and when and how they would get tested, all I had to do was prepare to go back home and quarantine myself for a couple of weeks.
I used up 2 weeks of vacation to volunteer in New York, but luckily, I could resume my normal work the day after I returned home.
Obviously, living in the pandemic is unique to anything we have ever experienced. Recognizing that, I recorded video diaries the whole time I was in New York. I laughed (like when I tried to fit all of my PPE on my tiny head), and I cried – several times. I suppose 1 day I may actually watch them and be reminded of what it was like to have been able to serve in this historic moment. Until then, they will remain locked up on the same phone that served as the only communication vehicle between my patients and their loved ones.
Dr. Salles is a bariatric surgeon and is currently a Scholar in Residence at Stanford (Calif.) University.
A couple of weeks ago, I posted a silly picture of myself with one N95 mask and asked the folks on Twitter what else I might need. In a matter of a few days, I had filled out a form online for volunteering through the Society of Critical Care Medicine, been assigned to work at a hospital in New York City, and booked a hotel and flight.
I was going to volunteer, although I wasn’t sure of exactly what I would be doing. I’m trained as a bariatric surgeon – not obviously suited for critical care, but arguably even less suited for medicine wards.
I undoubtedly would have been less prepared if I hadn’t sought guidance on what to bring with me and generally what to expect. Less than a day after seeking advice, two local women physicians donated N95s, face shields, gowns, bouffants, and coveralls to me. I also received a laminated photo of myself to attach to my gown in the mail from a stranger I met online.
Others suggested I bring goggles, chocolate, protein bars, hand sanitizer, powdered laundry detergent, and alcohol wipes. After running around all over town, I was able find everything but the wipes.
Just as others helped me achieve my goal of volunteering, I hope I can guide those who would like to do similar work by sharing details about my experience and other information I have collected about volunteering.
Below I answer some questions that those considering volunteering might have, including why I went, who I contacted to set this up, who paid for my flight, and what I observed in the hospital.
Motivation and logistics
I am currently serving in a nonclinical role at my institution. So when the pandemic hit the United States, I felt an immense amount of guilt for not being on the front lines caring for patients. I offered my services to local hospitals and registered for the California Health Corps. I live in northern California, which was the first part of the country to shelter in place. Since my home was actually relatively spared, my services weren’t needed.
As the weeks passed, I was slowly getting more and more fit, exercising in my house since there was little else I could do, and the guilt became a cloud gathering over my head.
I decided to volunteer in a place where demands for help were higher – New York. I tried very hard to sign up to volunteer through the state’s registry for health care volunteers, but was unable to do so. Coincidentally, around that same time, I saw on Twitter that Josh Mugele, MD, emergency medicine physician and program director of the emergency medicine residency at Northeast Georgia Medical Center in Gainesville, was on his way to New York. He shared the Society of Critical Care Medicine’s form for volunteering with me, and in less than 48 hours, I was assigned to a hospital in New York City. Five days later I was on a plane from San Francisco to my destination on the opposite side of the country. The airline paid for my flight.
This is not the only path to volunteering. Another volunteer, Sara Pauk, MD, ob.gyn. at the University of Washington, Seattle, found her volunteer role through contacting the New York City Health and Hospitals system directly. Other who have volunteered told me they had contacted specific hospitals or worked with agencies that were placing physicians.
PPE
The Brooklyn hospital where I volunteered provided me with two sets of scrubs and two N95s. Gowns were variably available on our unit, and there was no eye protection. As a colleague of mine, Ben Daxon, MD, anesthesia and critical care physician at the Mayo Clinic in Rochester, Minn., had suggested, anyone volunteering in this context should bring personal protective equipment (PPE) – That includes gowns, bouffants/scrub caps, eye protection, masks, and scrubs.
The “COVID corner”
Once I arrived in New York, I did not feel particularly safe in my hotel, so I moved to another the next day. Then I had to sort out how to keep the whole room from being contaminated. I created a “COVID corner” right by the door where I kept almost everything that had been outside the door.
Every time I walked in the door, I immediately took off my shoes and left them in that corner. I could not find alcohol wipes, even after looking around in the city, so I relied on time to kill the virus, which I presumed was on everything that came from outside.
Groceries stayed by the door for 48-72 hours if possible. After that, I would move them to the “clean” parts of the room. I wore the same outfit to and from the hospital everyday, putting it on right before I left and taking it off immediately after walking into the room (and then proceeding directly to the shower). Those clothes – “my COVID outfit” – lived in the COVID corner. Anything else I wore, including exercise clothes and underwear, got washed right after I wore it.
At the hospital, I would change into scrubs and leave my COVID outfit in a plastic bag inside my handbag. Note: I fully accepted that my handbag was now a COVID handbag. I kept a pair of clogs in the hospital for daily wear. Without alcohol wipes, my room did not feel clean. But I did start to become at peace with my system, even though it was inferior to the system I use in my own home.
Meal time
In addition to bringing snacks from home, I gathered some meal items at a grocery store during my first day in New York. These included water, yogurt, a few protein drinks, fruit, and some mini chocolate croissants. It’s a pandemic – chocolate is encouraged, right?
Neither any of the volunteers I knew nor I had access to a kitchen, so this was about the best I could do.
My first week I worked nights and ate sporadically. A couple of days I bought bagel sandwiches on the way back to the hotel in the morning. Other times, I would eat yogurt or a protein bar.
I had trouble sleeping, so I would wake up early and either do yoga in my room or go for a run in a nearby park. Usually I didn’t plan well enough to eat before I went into the hospital, so I would take yogurt, some fruit, and a croissant with me as I headed out. It was hard eating on the run with a mask on my face.
When I switched to working days, I actually ordered proper dinners from local Thai, Mexican, and Indian restaurants. I paid around $20 a meal.
One night I even had dinner with a coworker who was staying at a hotel close to mine – what a luxury! Prior to all this I had been sheltering in place alone for weeks, so in that sense, this experience was a delight. I interacted with other people, in person, every day!
My commute
My hotel was about 20 minutes from the hospital. Well-meaning folks informed me that Hertz had free car rentals and Uber had discounts for health care workers. When I investigated these options, I found that only employees of certain hospitals were eligible. As a volunteer, I was not eligible.
I ultimately took Uber back and forth, and I was lucky that a few friends had sent me Uber gift cards to defray the costs. Most days, I paid about $20 each way, although 1 day there actually was “surge pricing.” The grand total for the trip was close to $800.
Many of the Uber drivers had put up plastic partitions – reminiscent of the plastic Dexter would use to contain his crime scenes – to increase their separation from their passengers. It was a bit eerie, but also somewhat welcome.
New normal
The actual work at the hospital in Brooklyn where I volunteered was different from usual practice in numerous ways. One of the things I immediately noticed was how difficult it was to get chest x-rays. After placing an emergent chest tube for a tension pneumothorax, it took about 6 hours to get a chest x-ray to assess placement.
Because code medications were needed much more frequently than normal times, these medications were kept in an open supply closet for ease of access. Many of the ventilators looked like they were from the 1970s. (They had been borrowed from the Federal Emergency Management Agency.)
What was most distinct about this work was the sheer volume of deaths and dying patients -- at least one death on our unit occurred every day I was there -- and the way families communicated with their loved ones. Countless times I held my phone over the faces of my unconscious patients to let their family profess their love and beg them to fight. While I have had to deliver bad news over the phone many times in my career, I have never had to intrude on families’ last conversations with their dying loved ones or witness that conversation occurring via a tiny screen.
Reentry
In many ways, I am lucky that I do not do clinical work in my hometown. So while other volunteers were figuring out how many more vacation days they would have to use, or whether they would have to take unpaid leave, and when and how they would get tested, all I had to do was prepare to go back home and quarantine myself for a couple of weeks.
I used up 2 weeks of vacation to volunteer in New York, but luckily, I could resume my normal work the day after I returned home.
Obviously, living in the pandemic is unique to anything we have ever experienced. Recognizing that, I recorded video diaries the whole time I was in New York. I laughed (like when I tried to fit all of my PPE on my tiny head), and I cried – several times. I suppose 1 day I may actually watch them and be reminded of what it was like to have been able to serve in this historic moment. Until then, they will remain locked up on the same phone that served as the only communication vehicle between my patients and their loved ones.
Dr. Salles is a bariatric surgeon and is currently a Scholar in Residence at Stanford (Calif.) University.
A couple of weeks ago, I posted a silly picture of myself with one N95 mask and asked the folks on Twitter what else I might need. In a matter of a few days, I had filled out a form online for volunteering through the Society of Critical Care Medicine, been assigned to work at a hospital in New York City, and booked a hotel and flight.
I was going to volunteer, although I wasn’t sure of exactly what I would be doing. I’m trained as a bariatric surgeon – not obviously suited for critical care, but arguably even less suited for medicine wards.
I undoubtedly would have been less prepared if I hadn’t sought guidance on what to bring with me and generally what to expect. Less than a day after seeking advice, two local women physicians donated N95s, face shields, gowns, bouffants, and coveralls to me. I also received a laminated photo of myself to attach to my gown in the mail from a stranger I met online.
Others suggested I bring goggles, chocolate, protein bars, hand sanitizer, powdered laundry detergent, and alcohol wipes. After running around all over town, I was able find everything but the wipes.
Just as others helped me achieve my goal of volunteering, I hope I can guide those who would like to do similar work by sharing details about my experience and other information I have collected about volunteering.
Below I answer some questions that those considering volunteering might have, including why I went, who I contacted to set this up, who paid for my flight, and what I observed in the hospital.
Motivation and logistics
I am currently serving in a nonclinical role at my institution. So when the pandemic hit the United States, I felt an immense amount of guilt for not being on the front lines caring for patients. I offered my services to local hospitals and registered for the California Health Corps. I live in northern California, which was the first part of the country to shelter in place. Since my home was actually relatively spared, my services weren’t needed.
As the weeks passed, I was slowly getting more and more fit, exercising in my house since there was little else I could do, and the guilt became a cloud gathering over my head.
I decided to volunteer in a place where demands for help were higher – New York. I tried very hard to sign up to volunteer through the state’s registry for health care volunteers, but was unable to do so. Coincidentally, around that same time, I saw on Twitter that Josh Mugele, MD, emergency medicine physician and program director of the emergency medicine residency at Northeast Georgia Medical Center in Gainesville, was on his way to New York. He shared the Society of Critical Care Medicine’s form for volunteering with me, and in less than 48 hours, I was assigned to a hospital in New York City. Five days later I was on a plane from San Francisco to my destination on the opposite side of the country. The airline paid for my flight.
This is not the only path to volunteering. Another volunteer, Sara Pauk, MD, ob.gyn. at the University of Washington, Seattle, found her volunteer role through contacting the New York City Health and Hospitals system directly. Other who have volunteered told me they had contacted specific hospitals or worked with agencies that were placing physicians.
PPE
The Brooklyn hospital where I volunteered provided me with two sets of scrubs and two N95s. Gowns were variably available on our unit, and there was no eye protection. As a colleague of mine, Ben Daxon, MD, anesthesia and critical care physician at the Mayo Clinic in Rochester, Minn., had suggested, anyone volunteering in this context should bring personal protective equipment (PPE) – That includes gowns, bouffants/scrub caps, eye protection, masks, and scrubs.
The “COVID corner”
Once I arrived in New York, I did not feel particularly safe in my hotel, so I moved to another the next day. Then I had to sort out how to keep the whole room from being contaminated. I created a “COVID corner” right by the door where I kept almost everything that had been outside the door.
Every time I walked in the door, I immediately took off my shoes and left them in that corner. I could not find alcohol wipes, even after looking around in the city, so I relied on time to kill the virus, which I presumed was on everything that came from outside.
Groceries stayed by the door for 48-72 hours if possible. After that, I would move them to the “clean” parts of the room. I wore the same outfit to and from the hospital everyday, putting it on right before I left and taking it off immediately after walking into the room (and then proceeding directly to the shower). Those clothes – “my COVID outfit” – lived in the COVID corner. Anything else I wore, including exercise clothes and underwear, got washed right after I wore it.
At the hospital, I would change into scrubs and leave my COVID outfit in a plastic bag inside my handbag. Note: I fully accepted that my handbag was now a COVID handbag. I kept a pair of clogs in the hospital for daily wear. Without alcohol wipes, my room did not feel clean. But I did start to become at peace with my system, even though it was inferior to the system I use in my own home.
Meal time
In addition to bringing snacks from home, I gathered some meal items at a grocery store during my first day in New York. These included water, yogurt, a few protein drinks, fruit, and some mini chocolate croissants. It’s a pandemic – chocolate is encouraged, right?
Neither any of the volunteers I knew nor I had access to a kitchen, so this was about the best I could do.
My first week I worked nights and ate sporadically. A couple of days I bought bagel sandwiches on the way back to the hotel in the morning. Other times, I would eat yogurt or a protein bar.
I had trouble sleeping, so I would wake up early and either do yoga in my room or go for a run in a nearby park. Usually I didn’t plan well enough to eat before I went into the hospital, so I would take yogurt, some fruit, and a croissant with me as I headed out. It was hard eating on the run with a mask on my face.
When I switched to working days, I actually ordered proper dinners from local Thai, Mexican, and Indian restaurants. I paid around $20 a meal.
One night I even had dinner with a coworker who was staying at a hotel close to mine – what a luxury! Prior to all this I had been sheltering in place alone for weeks, so in that sense, this experience was a delight. I interacted with other people, in person, every day!
My commute
My hotel was about 20 minutes from the hospital. Well-meaning folks informed me that Hertz had free car rentals and Uber had discounts for health care workers. When I investigated these options, I found that only employees of certain hospitals were eligible. As a volunteer, I was not eligible.
I ultimately took Uber back and forth, and I was lucky that a few friends had sent me Uber gift cards to defray the costs. Most days, I paid about $20 each way, although 1 day there actually was “surge pricing.” The grand total for the trip was close to $800.
Many of the Uber drivers had put up plastic partitions – reminiscent of the plastic Dexter would use to contain his crime scenes – to increase their separation from their passengers. It was a bit eerie, but also somewhat welcome.
New normal
The actual work at the hospital in Brooklyn where I volunteered was different from usual practice in numerous ways. One of the things I immediately noticed was how difficult it was to get chest x-rays. After placing an emergent chest tube for a tension pneumothorax, it took about 6 hours to get a chest x-ray to assess placement.
Because code medications were needed much more frequently than normal times, these medications were kept in an open supply closet for ease of access. Many of the ventilators looked like they were from the 1970s. (They had been borrowed from the Federal Emergency Management Agency.)
What was most distinct about this work was the sheer volume of deaths and dying patients -- at least one death on our unit occurred every day I was there -- and the way families communicated with their loved ones. Countless times I held my phone over the faces of my unconscious patients to let their family profess their love and beg them to fight. While I have had to deliver bad news over the phone many times in my career, I have never had to intrude on families’ last conversations with their dying loved ones or witness that conversation occurring via a tiny screen.
Reentry
In many ways, I am lucky that I do not do clinical work in my hometown. So while other volunteers were figuring out how many more vacation days they would have to use, or whether they would have to take unpaid leave, and when and how they would get tested, all I had to do was prepare to go back home and quarantine myself for a couple of weeks.
I used up 2 weeks of vacation to volunteer in New York, but luckily, I could resume my normal work the day after I returned home.
Obviously, living in the pandemic is unique to anything we have ever experienced. Recognizing that, I recorded video diaries the whole time I was in New York. I laughed (like when I tried to fit all of my PPE on my tiny head), and I cried – several times. I suppose 1 day I may actually watch them and be reminded of what it was like to have been able to serve in this historic moment. Until then, they will remain locked up on the same phone that served as the only communication vehicle between my patients and their loved ones.
Dr. Salles is a bariatric surgeon and is currently a Scholar in Residence at Stanford (Calif.) University.
COVID-19: Eight steps for getting ready to see patients again
After COVID-19 hit the Denver area, internist Jean Kutner, MD, and her clinical colleagues drastically reduced the number of patients they saw and kept a minimum number of people in the office. A small team sees patients who still require in-person visits on one side of the clinic; on the other side, another team conducts clinic-based telehealth visits. A rotating schedule allows for social distancing.
The rest of the practice’s physicians are home, conducting more virtual visits.
Dr. Kutner said she is looking forward to reopening her practice completely at some point. She said she realizes that the practice probably won’t be exactly the same as before.
“We have to embrace the fact that the way we practice medicine has fundamentally changed,” said Dr. Kutner, professor of medicine at the University of Colorado at Denver, Aurora, and incoming president of the Society of General Internal Medicine. She anticipates keeping many of these changes in place for the foreseeable future.
Nearly half of 2,600 primary care physicians who responded to a recent national survey said they were struggling to remain open during the crisis. Most have had to limit wellness/chronic-disease management visits, and nearly half reported that physicians or staff were out sick. Layoffs, furloughs, and reduced hours are commonplace; some practices were forced to shut down entirely.
Social distancing helps reduce the rates of hospitalizations and deaths.
For example, remote monitoring capabilities have reduced the need for in-person checks of vital signs, such as respiratory rate oxygenation, blood glucose levels, and heart rate. “We can’t go back,” she said.
Dr. Kutner sees the pandemic as an opportunity to innovate, to think about how primary practices can best utilize their resources, face-to-face time with patients, and when and how to best leverage virtual visits in a way that improves patient health. The goal, of course, is to meet the needs of the patients while keeping everyone safe.
Like many physicians in private practice, Dr. Kutner is concerned about revenue. She hopes the Centers for Medicare & Medicaid Services makes its temporary waivers permanent.
What you need to consider when planning to reopen your office
Physicians say their post-COVID-19 practices will look very different from their prepandemic practices. Many plan to maintain guidelines, such as those from the AAFP, long after the pandemic has peaked.
If you are starting to think about reopening, here are some major considerations.
1. Develop procedures and practices that will keep your patients and staff safe.
“When we return, the first thing we need to do is limit the number of patients in the waiting room,” said Clinton Coleman, MD, who practices internal medicine and nephrology in Teaneck, N.J. “No one is comfortable in a waiting room any longer,” said Dr. Coleman, chief of internal medicine at Holy Name Medical Center in Teaneck.
Careful planning is required to resume in-person care of patients requiring non-COVID-19 care, as well as all aspects of care, according to the CMS. Adequate staff, testing, supplies, and support services, such as pathology services, are just a few considerations. The CMS recommends that physicians “evaluate the necessity of the care based on clinical needs. Providers should prioritize surgical/procedural care and high-complexity chronic disease management; however, select preventive services may also be highly necessary.”
The American Medical Association recently unveiled a checklist for reopening. One key recommendation was for practices to select a date for reopening the office, ideally preceded by a “soft” or incremental reopening to ensure that new procedures are working. The AMA also recommends opening incrementally, continuing telehealth while also inviting patients back into the office.
2. Figure out how to safely see patients, particularly in your waiting areas and common spaces.
Logistic factors, such as managing patient flow, will change. Waiting rooms will be emptier; in some locations, patients may be asked to wait in their cars until an exam room is available.
The AMA also suggests limiting nonpatient visitors by posting the practice’s policy at the entrance and on the practice’s website. If service calls for repairs are needed, have those visitors come outside of normal operating hours.
Commonly shared objects such magazines or toys in pediatric offices will likely disappear. Wipes, hand sanitizers, and the wearing of masks will become even more commonplace. Those who suspect they’re ill or who have respiratory symptoms may be relegated to specific “sick visit” appointment times or taken to designated exam rooms, which will be thoroughly sanitized between patients.
3. Prepare for routine screening of staff and other facility workers.
According to recent CMS guidelines, you and your staff will need to undergo routine screening, as will others who work in the facility (housekeeping, delivery personnel, and anyone else who enters the area). This may mean regularly stocking screening tests and setting guidelines for what to do if one of your staff tests positive.
You may need to hire temporary workers if your staff tests positive. The CDC recommends at the very least understanding the minimum staffing requirements to ensure good patient care and a safe work environment. Consider adjusting staff schedules and rotating clinical personnel to positions that support patient care activities. You may also want to look into cross-training your office staff so that they can fill in or help out with each other’s responsibilities if one or more persons are ill.
Dr. Kutner is on board with these changes. “We don’t want to get rid of social distancing right away, because it will give us a new spike in cases – how do we figure out patient flow while honoring that?”
4. Develop a strategy for triaging and caring for a potential backlog of patients.
“Many of my partners are scared right now because they have no income except for emergencies,” said Andrew Gonzalez, MD, JD, MPH, a vascular surgeon and assistant professor of surgery at Indiana University, Indianapolis. Almost all nonemergency surgery has been put on hold.
“If we don’t operate, the practice makes no money,” he said. He thinks revenue will continue to be a problem as long as patients fear in-person consultations or undergoing surgery for nonacute problems such as hernias.
As restrictions ease, most physicians will face an enormous backlog of patients and will need to find new ways of triaging the most serious cases, he says. Telehealth will help, but Dr. Gonzalez predicts many of his colleagues will be working longer hours and on weekends to catch up. “Physicians are going to have to really think about ways of optimizing their time and workflow to be very efficient, because the backlog is going to prodigious.”
5. Anticipate changes in patient expectations.
This may entail your reconsidering tests and procedures you previously performed and considering developing new sources for some services, phasing some others out, and revising your current approach. It will most likely also mean that you make telemedicine and televisits a greater part of your practice.
Carolyn Kaloostian, MD, a family medicine and geriatric practitioner in Los Angeles, points to increased reliance on community agencies for conducting common office-based procedures, such as performing blood tests and taking ECGs and x-rays. “A lot of patients are using telemedicine or telephone visits and get the lab work or x-rays somewhere that’s less congested,” she said. To become sustainable, many of these changes will hinge on economics – whether and how they are reimbursed.
The pandemic will leave lasting effects in our health care delivery, according to Dr. Kaloostian. She is sure many of her colleagues’ and patients’ current experiences will be infused into future care. “I can’t say we’ll ever be back to normal, necessarily.”
Even if the CMS rolls back its telehealth waivers, some physicians, like Dr. Coleman, plan to continue using the technology extensively. He’s confident about the level of care he’s currently providing patients in his practice. It allows him to better manage many low-income patients who can’t access his office regularly. Not only does splitting his time between the clinic and telehealth allow him to be more available for more patients, he says it also empowers patients to take better care of themselves.
6. Consider a new way to conduct “check-in visits.”
One thing that will likely go by the wayside are “check-in” visits, or so-called “social visits,” those interval appointments that can just as easily be completed virtually. “Patients are going to ask why they need to drive 3 hours so you can tell them their incision looks fine from an operation you did 5 years ago,” Dr. Gonzalez said.
He’s concerned that some people will remain so fearful of the health care system that a formerly busy practice may see the pendulum swing in the opposite direction. If an aneurysm patient skips a visit, that person may also decide not to undergo a CT scan – and something preventable will be missed. “Not everybody has the option to stay away until they feel comfortable. They’re basically playing hot potato. And at some point, the music’s going to stop,” Dr. Gonzalez said.
The pandemic has prompted some very honest conversations with his patients about what truly needs to get done and what may be optional. “Everyone has now become a hyper-rational user of health care,” he said.
7. If you haven’t yet, consider becoming more involved with technology.
In addition to greater use of telehealth, Dr. Kaloostian, assistant professor of clinical family medicine at the University of Southern California, Los Angeles, foresees continued reliance upon technology such as smartphone apps that connect with a user’s smartwatch. This allows for more proactive, remote monitoring.
“For example, any time a patient is having recurrent nighttime trips to the bathroom, I’ll get pinged and know that,” she explained. It means she can reach out and ask about any changes before a fall occurs or a condition worsens. “It provides reassurance to the provider and to the patient that you’re doing all you can to keep an eye on them from afar.”
8. Update or reformulate your business plans.
Some physicians in smaller practices may have to temporarily or permanently rethink their situation. Those who have struggled or who have closed down and are considering reopening need to update their business plans. It may be safer economically to become part of a bigger group that is affiliated with an academic center or join a larger health care system that has more funds or resources.
In addition, Dr. Kaloostian suggests that primary care physicians become more flexible in the short term, perhaps working part time in an urgent care clinic or larger organization to gain additional sources of revenue until their own practice finances pick back up.
For offices that reopen, the AMA recommends contacting medical malpractice insurance carriers to check on possible liability concerns. Congress has provided certain protections for clinicians during this time, but malpractice carriers may have more information and may offer more coverage.
Dr. Coleman said a hybrid model of fewer in-person and more telehealth visits “will allow me to practice in a different way.” If the CMS reimposes prior restrictions, reimbursement may be affected initially, but that will likely change once insurers see the increased cost-effectiveness of this approach. Patients with minor complaints, those who need to have medications refilled, and patients with chronic diseases that need managing won’t have to deal with crowded waiting rooms, and it will help mitigate problems with infection control.
If there’s any upside to the pandemic, it’s an increase in attention given to advanced care planning, said Dr. Kutner. It’s something she hopes continues after everyone stops being in crisis mode. “We’re realizing how important it is to have these conversations and document people’s goals and values and code status,” she said.
Are offices likely to open soon?
An assumption that may or may not be valid is that a practice will remain viable and can return to former capacity. Prior to passage of the CARES Act on March 27, a survey from Kareo, a company in Irvine, California, that makes a technology platform for independent physician practices, found that 9% of respondents reported practice closures. Many more reported concern about potential closures as patient office visits plummet because of stay-at-home orders and other concerns.
By mid-April, a survey from the Primary Care Collaborative and the Larry A. Green Center found that 42% of practices had experienced layoffs and had furloughed staff. Most (85%) have seen dramatic decreases in patient volume.
“Reopening the economy or loosening physical distancing restrictions will be difficult when 20% of primary care practices predict closure within 4 weeks,” the survey concluded.
For the practices and the doctors who make it through this, we’re going to probably be better, stronger, and more efficient, Dr. Gonzalez predicts. This shock has uncovered a lot of weaknesses in the American health care system that doctors have known about and have been complaining about for a long time. It will take an open mind and lots of continued flexibility on the part of physicians, hospitals, health care systems, and the government for these changes to stick.
A version of this article originally appeared on Medscape.com.
After COVID-19 hit the Denver area, internist Jean Kutner, MD, and her clinical colleagues drastically reduced the number of patients they saw and kept a minimum number of people in the office. A small team sees patients who still require in-person visits on one side of the clinic; on the other side, another team conducts clinic-based telehealth visits. A rotating schedule allows for social distancing.
The rest of the practice’s physicians are home, conducting more virtual visits.
Dr. Kutner said she is looking forward to reopening her practice completely at some point. She said she realizes that the practice probably won’t be exactly the same as before.
“We have to embrace the fact that the way we practice medicine has fundamentally changed,” said Dr. Kutner, professor of medicine at the University of Colorado at Denver, Aurora, and incoming president of the Society of General Internal Medicine. She anticipates keeping many of these changes in place for the foreseeable future.
Nearly half of 2,600 primary care physicians who responded to a recent national survey said they were struggling to remain open during the crisis. Most have had to limit wellness/chronic-disease management visits, and nearly half reported that physicians or staff were out sick. Layoffs, furloughs, and reduced hours are commonplace; some practices were forced to shut down entirely.
Social distancing helps reduce the rates of hospitalizations and deaths.
For example, remote monitoring capabilities have reduced the need for in-person checks of vital signs, such as respiratory rate oxygenation, blood glucose levels, and heart rate. “We can’t go back,” she said.
Dr. Kutner sees the pandemic as an opportunity to innovate, to think about how primary practices can best utilize their resources, face-to-face time with patients, and when and how to best leverage virtual visits in a way that improves patient health. The goal, of course, is to meet the needs of the patients while keeping everyone safe.
Like many physicians in private practice, Dr. Kutner is concerned about revenue. She hopes the Centers for Medicare & Medicaid Services makes its temporary waivers permanent.
What you need to consider when planning to reopen your office
Physicians say their post-COVID-19 practices will look very different from their prepandemic practices. Many plan to maintain guidelines, such as those from the AAFP, long after the pandemic has peaked.
If you are starting to think about reopening, here are some major considerations.
1. Develop procedures and practices that will keep your patients and staff safe.
“When we return, the first thing we need to do is limit the number of patients in the waiting room,” said Clinton Coleman, MD, who practices internal medicine and nephrology in Teaneck, N.J. “No one is comfortable in a waiting room any longer,” said Dr. Coleman, chief of internal medicine at Holy Name Medical Center in Teaneck.
Careful planning is required to resume in-person care of patients requiring non-COVID-19 care, as well as all aspects of care, according to the CMS. Adequate staff, testing, supplies, and support services, such as pathology services, are just a few considerations. The CMS recommends that physicians “evaluate the necessity of the care based on clinical needs. Providers should prioritize surgical/procedural care and high-complexity chronic disease management; however, select preventive services may also be highly necessary.”
The American Medical Association recently unveiled a checklist for reopening. One key recommendation was for practices to select a date for reopening the office, ideally preceded by a “soft” or incremental reopening to ensure that new procedures are working. The AMA also recommends opening incrementally, continuing telehealth while also inviting patients back into the office.
2. Figure out how to safely see patients, particularly in your waiting areas and common spaces.
Logistic factors, such as managing patient flow, will change. Waiting rooms will be emptier; in some locations, patients may be asked to wait in their cars until an exam room is available.
The AMA also suggests limiting nonpatient visitors by posting the practice’s policy at the entrance and on the practice’s website. If service calls for repairs are needed, have those visitors come outside of normal operating hours.
Commonly shared objects such magazines or toys in pediatric offices will likely disappear. Wipes, hand sanitizers, and the wearing of masks will become even more commonplace. Those who suspect they’re ill or who have respiratory symptoms may be relegated to specific “sick visit” appointment times or taken to designated exam rooms, which will be thoroughly sanitized between patients.
3. Prepare for routine screening of staff and other facility workers.
According to recent CMS guidelines, you and your staff will need to undergo routine screening, as will others who work in the facility (housekeeping, delivery personnel, and anyone else who enters the area). This may mean regularly stocking screening tests and setting guidelines for what to do if one of your staff tests positive.
You may need to hire temporary workers if your staff tests positive. The CDC recommends at the very least understanding the minimum staffing requirements to ensure good patient care and a safe work environment. Consider adjusting staff schedules and rotating clinical personnel to positions that support patient care activities. You may also want to look into cross-training your office staff so that they can fill in or help out with each other’s responsibilities if one or more persons are ill.
Dr. Kutner is on board with these changes. “We don’t want to get rid of social distancing right away, because it will give us a new spike in cases – how do we figure out patient flow while honoring that?”
4. Develop a strategy for triaging and caring for a potential backlog of patients.
“Many of my partners are scared right now because they have no income except for emergencies,” said Andrew Gonzalez, MD, JD, MPH, a vascular surgeon and assistant professor of surgery at Indiana University, Indianapolis. Almost all nonemergency surgery has been put on hold.
“If we don’t operate, the practice makes no money,” he said. He thinks revenue will continue to be a problem as long as patients fear in-person consultations or undergoing surgery for nonacute problems such as hernias.
As restrictions ease, most physicians will face an enormous backlog of patients and will need to find new ways of triaging the most serious cases, he says. Telehealth will help, but Dr. Gonzalez predicts many of his colleagues will be working longer hours and on weekends to catch up. “Physicians are going to have to really think about ways of optimizing their time and workflow to be very efficient, because the backlog is going to prodigious.”
5. Anticipate changes in patient expectations.
This may entail your reconsidering tests and procedures you previously performed and considering developing new sources for some services, phasing some others out, and revising your current approach. It will most likely also mean that you make telemedicine and televisits a greater part of your practice.
Carolyn Kaloostian, MD, a family medicine and geriatric practitioner in Los Angeles, points to increased reliance on community agencies for conducting common office-based procedures, such as performing blood tests and taking ECGs and x-rays. “A lot of patients are using telemedicine or telephone visits and get the lab work or x-rays somewhere that’s less congested,” she said. To become sustainable, many of these changes will hinge on economics – whether and how they are reimbursed.
The pandemic will leave lasting effects in our health care delivery, according to Dr. Kaloostian. She is sure many of her colleagues’ and patients’ current experiences will be infused into future care. “I can’t say we’ll ever be back to normal, necessarily.”
Even if the CMS rolls back its telehealth waivers, some physicians, like Dr. Coleman, plan to continue using the technology extensively. He’s confident about the level of care he’s currently providing patients in his practice. It allows him to better manage many low-income patients who can’t access his office regularly. Not only does splitting his time between the clinic and telehealth allow him to be more available for more patients, he says it also empowers patients to take better care of themselves.
6. Consider a new way to conduct “check-in visits.”
One thing that will likely go by the wayside are “check-in” visits, or so-called “social visits,” those interval appointments that can just as easily be completed virtually. “Patients are going to ask why they need to drive 3 hours so you can tell them their incision looks fine from an operation you did 5 years ago,” Dr. Gonzalez said.
He’s concerned that some people will remain so fearful of the health care system that a formerly busy practice may see the pendulum swing in the opposite direction. If an aneurysm patient skips a visit, that person may also decide not to undergo a CT scan – and something preventable will be missed. “Not everybody has the option to stay away until they feel comfortable. They’re basically playing hot potato. And at some point, the music’s going to stop,” Dr. Gonzalez said.
The pandemic has prompted some very honest conversations with his patients about what truly needs to get done and what may be optional. “Everyone has now become a hyper-rational user of health care,” he said.
7. If you haven’t yet, consider becoming more involved with technology.
In addition to greater use of telehealth, Dr. Kaloostian, assistant professor of clinical family medicine at the University of Southern California, Los Angeles, foresees continued reliance upon technology such as smartphone apps that connect with a user’s smartwatch. This allows for more proactive, remote monitoring.
“For example, any time a patient is having recurrent nighttime trips to the bathroom, I’ll get pinged and know that,” she explained. It means she can reach out and ask about any changes before a fall occurs or a condition worsens. “It provides reassurance to the provider and to the patient that you’re doing all you can to keep an eye on them from afar.”
8. Update or reformulate your business plans.
Some physicians in smaller practices may have to temporarily or permanently rethink their situation. Those who have struggled or who have closed down and are considering reopening need to update their business plans. It may be safer economically to become part of a bigger group that is affiliated with an academic center or join a larger health care system that has more funds or resources.
In addition, Dr. Kaloostian suggests that primary care physicians become more flexible in the short term, perhaps working part time in an urgent care clinic or larger organization to gain additional sources of revenue until their own practice finances pick back up.
For offices that reopen, the AMA recommends contacting medical malpractice insurance carriers to check on possible liability concerns. Congress has provided certain protections for clinicians during this time, but malpractice carriers may have more information and may offer more coverage.
Dr. Coleman said a hybrid model of fewer in-person and more telehealth visits “will allow me to practice in a different way.” If the CMS reimposes prior restrictions, reimbursement may be affected initially, but that will likely change once insurers see the increased cost-effectiveness of this approach. Patients with minor complaints, those who need to have medications refilled, and patients with chronic diseases that need managing won’t have to deal with crowded waiting rooms, and it will help mitigate problems with infection control.
If there’s any upside to the pandemic, it’s an increase in attention given to advanced care planning, said Dr. Kutner. It’s something she hopes continues after everyone stops being in crisis mode. “We’re realizing how important it is to have these conversations and document people’s goals and values and code status,” she said.
Are offices likely to open soon?
An assumption that may or may not be valid is that a practice will remain viable and can return to former capacity. Prior to passage of the CARES Act on March 27, a survey from Kareo, a company in Irvine, California, that makes a technology platform for independent physician practices, found that 9% of respondents reported practice closures. Many more reported concern about potential closures as patient office visits plummet because of stay-at-home orders and other concerns.
By mid-April, a survey from the Primary Care Collaborative and the Larry A. Green Center found that 42% of practices had experienced layoffs and had furloughed staff. Most (85%) have seen dramatic decreases in patient volume.
“Reopening the economy or loosening physical distancing restrictions will be difficult when 20% of primary care practices predict closure within 4 weeks,” the survey concluded.
For the practices and the doctors who make it through this, we’re going to probably be better, stronger, and more efficient, Dr. Gonzalez predicts. This shock has uncovered a lot of weaknesses in the American health care system that doctors have known about and have been complaining about for a long time. It will take an open mind and lots of continued flexibility on the part of physicians, hospitals, health care systems, and the government for these changes to stick.
A version of this article originally appeared on Medscape.com.
After COVID-19 hit the Denver area, internist Jean Kutner, MD, and her clinical colleagues drastically reduced the number of patients they saw and kept a minimum number of people in the office. A small team sees patients who still require in-person visits on one side of the clinic; on the other side, another team conducts clinic-based telehealth visits. A rotating schedule allows for social distancing.
The rest of the practice’s physicians are home, conducting more virtual visits.
Dr. Kutner said she is looking forward to reopening her practice completely at some point. She said she realizes that the practice probably won’t be exactly the same as before.
“We have to embrace the fact that the way we practice medicine has fundamentally changed,” said Dr. Kutner, professor of medicine at the University of Colorado at Denver, Aurora, and incoming president of the Society of General Internal Medicine. She anticipates keeping many of these changes in place for the foreseeable future.
Nearly half of 2,600 primary care physicians who responded to a recent national survey said they were struggling to remain open during the crisis. Most have had to limit wellness/chronic-disease management visits, and nearly half reported that physicians or staff were out sick. Layoffs, furloughs, and reduced hours are commonplace; some practices were forced to shut down entirely.
Social distancing helps reduce the rates of hospitalizations and deaths.
For example, remote monitoring capabilities have reduced the need for in-person checks of vital signs, such as respiratory rate oxygenation, blood glucose levels, and heart rate. “We can’t go back,” she said.
Dr. Kutner sees the pandemic as an opportunity to innovate, to think about how primary practices can best utilize their resources, face-to-face time with patients, and when and how to best leverage virtual visits in a way that improves patient health. The goal, of course, is to meet the needs of the patients while keeping everyone safe.
Like many physicians in private practice, Dr. Kutner is concerned about revenue. She hopes the Centers for Medicare & Medicaid Services makes its temporary waivers permanent.
What you need to consider when planning to reopen your office
Physicians say their post-COVID-19 practices will look very different from their prepandemic practices. Many plan to maintain guidelines, such as those from the AAFP, long after the pandemic has peaked.
If you are starting to think about reopening, here are some major considerations.
1. Develop procedures and practices that will keep your patients and staff safe.
“When we return, the first thing we need to do is limit the number of patients in the waiting room,” said Clinton Coleman, MD, who practices internal medicine and nephrology in Teaneck, N.J. “No one is comfortable in a waiting room any longer,” said Dr. Coleman, chief of internal medicine at Holy Name Medical Center in Teaneck.
Careful planning is required to resume in-person care of patients requiring non-COVID-19 care, as well as all aspects of care, according to the CMS. Adequate staff, testing, supplies, and support services, such as pathology services, are just a few considerations. The CMS recommends that physicians “evaluate the necessity of the care based on clinical needs. Providers should prioritize surgical/procedural care and high-complexity chronic disease management; however, select preventive services may also be highly necessary.”
The American Medical Association recently unveiled a checklist for reopening. One key recommendation was for practices to select a date for reopening the office, ideally preceded by a “soft” or incremental reopening to ensure that new procedures are working. The AMA also recommends opening incrementally, continuing telehealth while also inviting patients back into the office.
2. Figure out how to safely see patients, particularly in your waiting areas and common spaces.
Logistic factors, such as managing patient flow, will change. Waiting rooms will be emptier; in some locations, patients may be asked to wait in their cars until an exam room is available.
The AMA also suggests limiting nonpatient visitors by posting the practice’s policy at the entrance and on the practice’s website. If service calls for repairs are needed, have those visitors come outside of normal operating hours.
Commonly shared objects such magazines or toys in pediatric offices will likely disappear. Wipes, hand sanitizers, and the wearing of masks will become even more commonplace. Those who suspect they’re ill or who have respiratory symptoms may be relegated to specific “sick visit” appointment times or taken to designated exam rooms, which will be thoroughly sanitized between patients.
3. Prepare for routine screening of staff and other facility workers.
According to recent CMS guidelines, you and your staff will need to undergo routine screening, as will others who work in the facility (housekeeping, delivery personnel, and anyone else who enters the area). This may mean regularly stocking screening tests and setting guidelines for what to do if one of your staff tests positive.
You may need to hire temporary workers if your staff tests positive. The CDC recommends at the very least understanding the minimum staffing requirements to ensure good patient care and a safe work environment. Consider adjusting staff schedules and rotating clinical personnel to positions that support patient care activities. You may also want to look into cross-training your office staff so that they can fill in or help out with each other’s responsibilities if one or more persons are ill.
Dr. Kutner is on board with these changes. “We don’t want to get rid of social distancing right away, because it will give us a new spike in cases – how do we figure out patient flow while honoring that?”
4. Develop a strategy for triaging and caring for a potential backlog of patients.
“Many of my partners are scared right now because they have no income except for emergencies,” said Andrew Gonzalez, MD, JD, MPH, a vascular surgeon and assistant professor of surgery at Indiana University, Indianapolis. Almost all nonemergency surgery has been put on hold.
“If we don’t operate, the practice makes no money,” he said. He thinks revenue will continue to be a problem as long as patients fear in-person consultations or undergoing surgery for nonacute problems such as hernias.
As restrictions ease, most physicians will face an enormous backlog of patients and will need to find new ways of triaging the most serious cases, he says. Telehealth will help, but Dr. Gonzalez predicts many of his colleagues will be working longer hours and on weekends to catch up. “Physicians are going to have to really think about ways of optimizing their time and workflow to be very efficient, because the backlog is going to prodigious.”
5. Anticipate changes in patient expectations.
This may entail your reconsidering tests and procedures you previously performed and considering developing new sources for some services, phasing some others out, and revising your current approach. It will most likely also mean that you make telemedicine and televisits a greater part of your practice.
Carolyn Kaloostian, MD, a family medicine and geriatric practitioner in Los Angeles, points to increased reliance on community agencies for conducting common office-based procedures, such as performing blood tests and taking ECGs and x-rays. “A lot of patients are using telemedicine or telephone visits and get the lab work or x-rays somewhere that’s less congested,” she said. To become sustainable, many of these changes will hinge on economics – whether and how they are reimbursed.
The pandemic will leave lasting effects in our health care delivery, according to Dr. Kaloostian. She is sure many of her colleagues’ and patients’ current experiences will be infused into future care. “I can’t say we’ll ever be back to normal, necessarily.”
Even if the CMS rolls back its telehealth waivers, some physicians, like Dr. Coleman, plan to continue using the technology extensively. He’s confident about the level of care he’s currently providing patients in his practice. It allows him to better manage many low-income patients who can’t access his office regularly. Not only does splitting his time between the clinic and telehealth allow him to be more available for more patients, he says it also empowers patients to take better care of themselves.
6. Consider a new way to conduct “check-in visits.”
One thing that will likely go by the wayside are “check-in” visits, or so-called “social visits,” those interval appointments that can just as easily be completed virtually. “Patients are going to ask why they need to drive 3 hours so you can tell them their incision looks fine from an operation you did 5 years ago,” Dr. Gonzalez said.
He’s concerned that some people will remain so fearful of the health care system that a formerly busy practice may see the pendulum swing in the opposite direction. If an aneurysm patient skips a visit, that person may also decide not to undergo a CT scan – and something preventable will be missed. “Not everybody has the option to stay away until they feel comfortable. They’re basically playing hot potato. And at some point, the music’s going to stop,” Dr. Gonzalez said.
The pandemic has prompted some very honest conversations with his patients about what truly needs to get done and what may be optional. “Everyone has now become a hyper-rational user of health care,” he said.
7. If you haven’t yet, consider becoming more involved with technology.
In addition to greater use of telehealth, Dr. Kaloostian, assistant professor of clinical family medicine at the University of Southern California, Los Angeles, foresees continued reliance upon technology such as smartphone apps that connect with a user’s smartwatch. This allows for more proactive, remote monitoring.
“For example, any time a patient is having recurrent nighttime trips to the bathroom, I’ll get pinged and know that,” she explained. It means she can reach out and ask about any changes before a fall occurs or a condition worsens. “It provides reassurance to the provider and to the patient that you’re doing all you can to keep an eye on them from afar.”
8. Update or reformulate your business plans.
Some physicians in smaller practices may have to temporarily or permanently rethink their situation. Those who have struggled or who have closed down and are considering reopening need to update their business plans. It may be safer economically to become part of a bigger group that is affiliated with an academic center or join a larger health care system that has more funds or resources.
In addition, Dr. Kaloostian suggests that primary care physicians become more flexible in the short term, perhaps working part time in an urgent care clinic or larger organization to gain additional sources of revenue until their own practice finances pick back up.
For offices that reopen, the AMA recommends contacting medical malpractice insurance carriers to check on possible liability concerns. Congress has provided certain protections for clinicians during this time, but malpractice carriers may have more information and may offer more coverage.
Dr. Coleman said a hybrid model of fewer in-person and more telehealth visits “will allow me to practice in a different way.” If the CMS reimposes prior restrictions, reimbursement may be affected initially, but that will likely change once insurers see the increased cost-effectiveness of this approach. Patients with minor complaints, those who need to have medications refilled, and patients with chronic diseases that need managing won’t have to deal with crowded waiting rooms, and it will help mitigate problems with infection control.
If there’s any upside to the pandemic, it’s an increase in attention given to advanced care planning, said Dr. Kutner. It’s something she hopes continues after everyone stops being in crisis mode. “We’re realizing how important it is to have these conversations and document people’s goals and values and code status,” she said.
Are offices likely to open soon?
An assumption that may or may not be valid is that a practice will remain viable and can return to former capacity. Prior to passage of the CARES Act on March 27, a survey from Kareo, a company in Irvine, California, that makes a technology platform for independent physician practices, found that 9% of respondents reported practice closures. Many more reported concern about potential closures as patient office visits plummet because of stay-at-home orders and other concerns.
By mid-April, a survey from the Primary Care Collaborative and the Larry A. Green Center found that 42% of practices had experienced layoffs and had furloughed staff. Most (85%) have seen dramatic decreases in patient volume.
“Reopening the economy or loosening physical distancing restrictions will be difficult when 20% of primary care practices predict closure within 4 weeks,” the survey concluded.
For the practices and the doctors who make it through this, we’re going to probably be better, stronger, and more efficient, Dr. Gonzalez predicts. This shock has uncovered a lot of weaknesses in the American health care system that doctors have known about and have been complaining about for a long time. It will take an open mind and lots of continued flexibility on the part of physicians, hospitals, health care systems, and the government for these changes to stick.
A version of this article originally appeared on Medscape.com.
Telemedicine: A primer for today’s ObGyn
If telemedicine had not yet begun to play a significant role in your ObGyn practice, it is almost certain to now as the COVID-19 pandemic demands new ways of caring for our patients while keeping others safe from disease. According to the American College of Obstetricians and Gynecologists (ACOG), the term “telemedicine” refers to delivering traditional clinical diagnosis and monitoring via technology (see “ACOG weighs in on telehealth”).1
Whether they realize it or not, most ObGyns have practiced a simple form of telemedicine when they take phone calls from patients who are seeking medication refills. In these cases, physicians either can call the pharmacy to refill the medication or suggest patients make an office appointment to receive a new prescription (much to the chagrin of many patients—especially millennials). Physicians who acquiesce to patients’ phone requests to have prescriptions filled or to others seeking free medical advice are not compensated for these services, yet are legally responsible for their actions and advice—a situation that does not make for good medicine.
This is where telemedicine can be an important addition to an ObGyn practice. Telemedicine saves the patient the time and effort of coming to the office, while providing compensation to the physician for his/her time and advice and providing a record of the interaction, all of which makes for far better medicine. This article—the first of 3 on the subject—discusses the process of integrating telemedicine into a practice with minimal time, energy, and expense.
Telemedicine and the ObGyn practice
Many ObGyn patients do not require an in-person visit in order to receive effective care. There is even the potential to provide prenatal care via telemedicine by replacing some of the many prenatal well-care office visits with at-home care for pregnant women with low-risk pregnancies. A typical virtual visit for a low-risk pregnancy includes utilizing home monitoring equipment to track fetal heart rate, maternal blood pressure, and fundal height.2
Practices typically use telemedicine platforms to manage one or both of the following types of encounters: 1) walk-in visits through the practice’s web site; for most of these, patients tend not to care which physicians they see; their priority is usually the first available provider; and 2) appointment-based consultations, where patients schedule video chats in advance, usually with a specific provider.
Although incorporating telemedicine into a practice may seem overwhelming, it requires minimal additional equipment, interfaces easily with a practice’s web site and electronic medical record (EMR) system, increases productivity, and improves workflow. And patients generally appreciate the option of not having to travel to the office for an appointment.
Most patients and physicians are already comfortable with their mobile phones, tablets, social media, and wearable technology, such as Fitbits. Telemedicine is a logical next step. And given the current situation with COVID-19, it is really not a matter of “if,” but rather “when” to incorporate telemedicine as a communication and practice tool, and the sooner the better.
Continue to: Getting started...
Getting started
Physicians and their colleagues and staff first need to become comfortable with telemedicine technology. Physicians can begin by using video communication for other purposes, such as for conducting staff meetings. They should practice starting and ending calls and adjusting audio volume and video quality to ensure good reception.
Selecting a video platform
TABLE 1 provides a list of the most popular video providers and the advantages and disadvantages of each, and TABLE 2 shows a list of free video chat apps. Apps are available that can:
- share and mark up lab tests, magnetic resonance images, and other medical documents without exposing the entire desktop
- securely send documents over a Health Insurance Portability and Accountability Act (HIPAA)-compliant video
- stream digital device images live while still seeing patients’ faces.
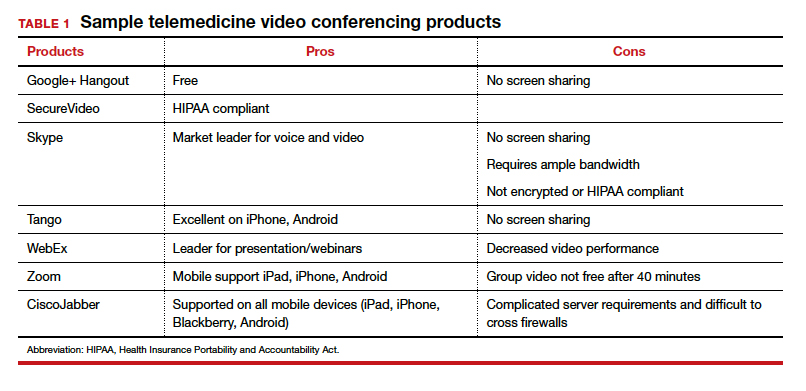
Physicians should make sure their implementation team has the necessary equipment, including webcams, microphones, and speakers, and they should take the time to do research and test out a few programs before selecting one for their practice. Consider appointing a telemedicine point person who is knowledgeable about the technology and can patiently explain it to others. And keep in mind that video chatting is dependent upon a fast, strong Internet connection that has sufficient bandwidth to transport a large amount of data. If your practice has connectivity problems, consider consulting with an information technology (IT) expert.
Testing it out and obtaining feedback
Once a team is comfortable using video within the practice, it is time to test it out with a few patients and perhaps a few payers. Most patients are eager to start using video for their medical encounters. Even senior patients are often willing to try consults via video. According to a recent survey, 64% of patients are willing to see a physician over video.3 And among those who were comfortable accepting an invitation to participate in a video encounter, increasing age was actually associated with a higher likelihood to accept an invite.
Physician colleagues, medical assistants, and nurse practitioners will need some basic telemedicine skills, and physicians and staff should be prepared to make video connections seamless for patients. Usually, patients need some guidance and encouragement, such as telling them to check their spam folder for their invites if the invites fail to arrive in their email inbox, adjusting audio settings, or setting up a webcam. In the beginning, ObGyns should make sure they build in plenty of buffer time for the unexpected, as there will certainly be some “bugs” that need to be worked out.
ObGyns should encourage and collect patient feedback to such questions as:
- What kinds of devices (laptop, mobile) do they prefer using?
- What kind of networks are they using (3G, corporate, home)?
- What features do they like? What features do they have a hard time finding?
- What do they like or not like about the video experience?
- Keep track of the types of questions patients ask, and be patient as patients become acclimated to the video consultation experience.
Continue to: Streamlining online workflow...
Streamlining online workflow
Armed with feedback from patients, it is time to start streamlining online workflow. Most ObGyns want to be able to manage video visits in a way that is similar to the way they manage face-to-face visits with patients. This may mean experimenting with a virtual waiting room. A virtual waiting room is a simple web page or link that can be sent to patients. On that page, patients sign in with minimal demographic information and select one of the time slots when the physician is available. Typically, these programs are designed to alert the physicians and/or staff when a patient enters the virtual waiting room. Patients have access to the online patient queue and can start a chat or video call when both parties are ready. Such a waiting room model serves as a stepping stone for new practices to familiarize themselves with video conferencing. This approach is also perfect for practices that already have a practice management system and just want to add a video component.
Influences on practice workflow
With good time management, telemedicine can improve the efficiency and productivity of your practice. Your daily schedule and management of patients will need some minor changes, but significant alterations to your existing schedule and workflow are generally unnecessary. One of the advantages of telemedicine is the convenience of prompt care and the easy access patients have to your practice. This decreases visits to the emergency department and to urgent care centers.
Consider scheduling telemedicine appointments at the end of the day when your staff has left the office, as no staff members are required for a telemedicine visit. Ideally, you should offer a set time to communicate with patients, as this avoids having to make multiple calls to reach a patient. Another advantage of telemedicine is that you can provide care in the evenings and on weekends if you want. Whereas before you might have been fielding calls from patients during these times and not being compensated, with telemedicine you can conduct a virtual visit from any location and any computer or mobile phone and receive remuneration for your care.
And while access to care has been a problem in many ObGyn practices, many additional patients can be accommodated into a busy ObGyn practice by using telemedicine.
Telemedicine and the coronavirus
The current health care crisis makes implementing telemedicine essential. Patients who think they may have COVID-19 or who have been diagnosed need to be quarantined. Such patients can be helped safely in the comfort of their own homes without endangering others. Patients can be triaged virtually. All those who are febrile or have respiratory symptoms can continue to avail themselves of virtual visits.
According to reports in the media, COVID-19 is stretching the health care workforce to its limits and creating a shortage, both because of the sheer number of cases and because health care workers are getting sick themselves. Physicians who test positive do not have to be completely removed from the workforce if they have the ability to care for patients remotely from their homes. And not incidentally the new environment has prompted the Centers for Medicaid and Medicare Services (CMS) and private payers to initiate national payment policies that create parity between office and telemedicine visits.4
Continue to: Bottom line...
Bottom line
Patient-driven care is the future, and telemedicine is part of that. Patients want to have ready access to their health care providers without having to devote hours to a medical encounter that could be completed in a matter of minutes via telemedicine.
In the next article in this series, we will review the proper coding for a telemedicine visit so that appropriate compensation is gleaned. We will also review the barriers to implementing telemedicine visits. The third article is written with the assistance of 2 health care attorneys, Anjali Dooley and Nadia de la Houssaye, who are experts in telemedicine and who have helped dozens of practices and hospitals implement the technology. They provide legal guidelines for ObGyns who are considering adding telemedicine to their practice. ●
The American College of Obstetricians and Gynecologists (ACOG) encourages all practices and facilities without telemedicine capabilities “to strategize about how telehealth could be integrated into their services as appropriate.”1 In doing so, they also encourage consideration of ways to care for those who may not have access to such technology or who do not know how to use it. They also explain that a number of federal telehealth policy changes have been made in response to the COVID-19 pandemic, and that most private health insurers are following suit.2 Such changes include:
- covering all telehealth visits for all traditional Medicare beneficiaries regardless of geographic location or originating site
- not requiring physicians to have a pre-existing relationship with a patient to provide a telehealth visit
- permitting the use of FaceTime, Skype, and other everyday communication technologies to provide telehealth visits.
A summary of the major telehealth policy changes, as well as information on how to code and bill for telehealth visits can be found at https://www.acog.org/clinical-information/physician-faqs/~/link .aspx?_id=3803296EAAD940C69525D4DD2679A00E&_z=z.
References
- American College of Obstetricians and Gynecologists. COVID-19 FAQs for obstetriciangynecologists, gynecology. https://www.acog.org/clinical-information/physician-faqs/covid19faqs-for-ob-gyns-gynecology. Accessed April 8, 2020.
- American College of Obstetricians and Gynecologists. Managing patients remotely: billing for digital and telehealth services. Updated April 2, 2020. https://www.acog.org/clinicalinformation/physician-faqs/~/link.aspx?_id=3803296EAAD940C69525D4DD2679A00E&_z=z. Accessed April 8, 2020.
- Implementing telehealth in practice. ACOG Committee Opinion. February 2020. https://www.acog.org/clinical /clinical-guidance/committee-opinion/articles/2020/02 /implementing-telehealth-in-practice. Accessed April 6, 2020.
- de Mooij MJM, Hodny RL, O’Neil DA, et al. OB nest: reimagining low-risk prenatal care. Mayo Clin Proc. 2018;93:458-466.
- Gardner MR, Jenkins SM, O’Neil DA, et al. Perceptions of video-based appointments from the patient’s home: a patient survey. Telemed J E Health. 2015;21:281-285.
- American College of Obstetricians and Gynecologists. Managing patients remotely: billing for digital and telehealth services. Updated April 2, 2020. https://www.acog.org /clinical-information/physician-faqs/~/link.aspx?_id=380 3296EAAD940C69525D4DD2679A00E&_z=z. Accessed April 8, 2020.

Dr. Karram is Clinical Professor of Obstetrics and Gynecology, University of Cincinnati, and Director of Urogynecology, The Christ Hospital, Cincinnati, Ohio.

Dr. Baum is Professor of Clinical Urology, Tulane Medical School, New Orleans, Louisiana.
The authors report no financial relationships relevant to this article.
Dr. Karram is Clinical Professor of Obstetrics and Gynecology, University of Cincinnati, and Director of Urogynecology, The Christ Hospital, Cincinnati, Ohio.
Dr. Baum is Professor of Clinical Urology, Tulane Medical School, New Orleans, Louisiana.
The authors report no financial relationships relevant to this article.
Dr. Karram is Clinical Professor of Obstetrics and Gynecology, University of Cincinnati, and Director of Urogynecology, The Christ Hospital, Cincinnati, Ohio.
Dr. Baum is Professor of Clinical Urology, Tulane Medical School, New Orleans, Louisiana.
The authors report no financial relationships relevant to this article.
If telemedicine had not yet begun to play a significant role in your ObGyn practice, it is almost certain to now as the COVID-19 pandemic demands new ways of caring for our patients while keeping others safe from disease. According to the American College of Obstetricians and Gynecologists (ACOG), the term “telemedicine” refers to delivering traditional clinical diagnosis and monitoring via technology (see “ACOG weighs in on telehealth”).1
Whether they realize it or not, most ObGyns have practiced a simple form of telemedicine when they take phone calls from patients who are seeking medication refills. In these cases, physicians either can call the pharmacy to refill the medication or suggest patients make an office appointment to receive a new prescription (much to the chagrin of many patients—especially millennials). Physicians who acquiesce to patients’ phone requests to have prescriptions filled or to others seeking free medical advice are not compensated for these services, yet are legally responsible for their actions and advice—a situation that does not make for good medicine.
This is where telemedicine can be an important addition to an ObGyn practice. Telemedicine saves the patient the time and effort of coming to the office, while providing compensation to the physician for his/her time and advice and providing a record of the interaction, all of which makes for far better medicine. This article—the first of 3 on the subject—discusses the process of integrating telemedicine into a practice with minimal time, energy, and expense.
Telemedicine and the ObGyn practice
Many ObGyn patients do not require an in-person visit in order to receive effective care. There is even the potential to provide prenatal care via telemedicine by replacing some of the many prenatal well-care office visits with at-home care for pregnant women with low-risk pregnancies. A typical virtual visit for a low-risk pregnancy includes utilizing home monitoring equipment to track fetal heart rate, maternal blood pressure, and fundal height.2
Practices typically use telemedicine platforms to manage one or both of the following types of encounters: 1) walk-in visits through the practice’s web site; for most of these, patients tend not to care which physicians they see; their priority is usually the first available provider; and 2) appointment-based consultations, where patients schedule video chats in advance, usually with a specific provider.
Although incorporating telemedicine into a practice may seem overwhelming, it requires minimal additional equipment, interfaces easily with a practice’s web site and electronic medical record (EMR) system, increases productivity, and improves workflow. And patients generally appreciate the option of not having to travel to the office for an appointment.
Most patients and physicians are already comfortable with their mobile phones, tablets, social media, and wearable technology, such as Fitbits. Telemedicine is a logical next step. And given the current situation with COVID-19, it is really not a matter of “if,” but rather “when” to incorporate telemedicine as a communication and practice tool, and the sooner the better.
Continue to: Getting started...
Getting started
Physicians and their colleagues and staff first need to become comfortable with telemedicine technology. Physicians can begin by using video communication for other purposes, such as for conducting staff meetings. They should practice starting and ending calls and adjusting audio volume and video quality to ensure good reception.
Selecting a video platform
TABLE 1 provides a list of the most popular video providers and the advantages and disadvantages of each, and TABLE 2 shows a list of free video chat apps. Apps are available that can:
- share and mark up lab tests, magnetic resonance images, and other medical documents without exposing the entire desktop
- securely send documents over a Health Insurance Portability and Accountability Act (HIPAA)-compliant video
- stream digital device images live while still seeing patients’ faces.
Physicians should make sure their implementation team has the necessary equipment, including webcams, microphones, and speakers, and they should take the time to do research and test out a few programs before selecting one for their practice. Consider appointing a telemedicine point person who is knowledgeable about the technology and can patiently explain it to others. And keep in mind that video chatting is dependent upon a fast, strong Internet connection that has sufficient bandwidth to transport a large amount of data. If your practice has connectivity problems, consider consulting with an information technology (IT) expert.
Testing it out and obtaining feedback
Once a team is comfortable using video within the practice, it is time to test it out with a few patients and perhaps a few payers. Most patients are eager to start using video for their medical encounters. Even senior patients are often willing to try consults via video. According to a recent survey, 64% of patients are willing to see a physician over video.3 And among those who were comfortable accepting an invitation to participate in a video encounter, increasing age was actually associated with a higher likelihood to accept an invite.
Physician colleagues, medical assistants, and nurse practitioners will need some basic telemedicine skills, and physicians and staff should be prepared to make video connections seamless for patients. Usually, patients need some guidance and encouragement, such as telling them to check their spam folder for their invites if the invites fail to arrive in their email inbox, adjusting audio settings, or setting up a webcam. In the beginning, ObGyns should make sure they build in plenty of buffer time for the unexpected, as there will certainly be some “bugs” that need to be worked out.
ObGyns should encourage and collect patient feedback to such questions as:
- What kinds of devices (laptop, mobile) do they prefer using?
- What kind of networks are they using (3G, corporate, home)?
- What features do they like? What features do they have a hard time finding?
- What do they like or not like about the video experience?
- Keep track of the types of questions patients ask, and be patient as patients become acclimated to the video consultation experience.
Continue to: Streamlining online workflow...
Streamlining online workflow
Armed with feedback from patients, it is time to start streamlining online workflow. Most ObGyns want to be able to manage video visits in a way that is similar to the way they manage face-to-face visits with patients. This may mean experimenting with a virtual waiting room. A virtual waiting room is a simple web page or link that can be sent to patients. On that page, patients sign in with minimal demographic information and select one of the time slots when the physician is available. Typically, these programs are designed to alert the physicians and/or staff when a patient enters the virtual waiting room. Patients have access to the online patient queue and can start a chat or video call when both parties are ready. Such a waiting room model serves as a stepping stone for new practices to familiarize themselves with video conferencing. This approach is also perfect for practices that already have a practice management system and just want to add a video component.
Influences on practice workflow
With good time management, telemedicine can improve the efficiency and productivity of your practice. Your daily schedule and management of patients will need some minor changes, but significant alterations to your existing schedule and workflow are generally unnecessary. One of the advantages of telemedicine is the convenience of prompt care and the easy access patients have to your practice. This decreases visits to the emergency department and to urgent care centers.
Consider scheduling telemedicine appointments at the end of the day when your staff has left the office, as no staff members are required for a telemedicine visit. Ideally, you should offer a set time to communicate with patients, as this avoids having to make multiple calls to reach a patient. Another advantage of telemedicine is that you can provide care in the evenings and on weekends if you want. Whereas before you might have been fielding calls from patients during these times and not being compensated, with telemedicine you can conduct a virtual visit from any location and any computer or mobile phone and receive remuneration for your care.
And while access to care has been a problem in many ObGyn practices, many additional patients can be accommodated into a busy ObGyn practice by using telemedicine.
Telemedicine and the coronavirus
The current health care crisis makes implementing telemedicine essential. Patients who think they may have COVID-19 or who have been diagnosed need to be quarantined. Such patients can be helped safely in the comfort of their own homes without endangering others. Patients can be triaged virtually. All those who are febrile or have respiratory symptoms can continue to avail themselves of virtual visits.
According to reports in the media, COVID-19 is stretching the health care workforce to its limits and creating a shortage, both because of the sheer number of cases and because health care workers are getting sick themselves. Physicians who test positive do not have to be completely removed from the workforce if they have the ability to care for patients remotely from their homes. And not incidentally the new environment has prompted the Centers for Medicaid and Medicare Services (CMS) and private payers to initiate national payment policies that create parity between office and telemedicine visits.4
Continue to: Bottom line...
Bottom line
Patient-driven care is the future, and telemedicine is part of that. Patients want to have ready access to their health care providers without having to devote hours to a medical encounter that could be completed in a matter of minutes via telemedicine.
In the next article in this series, we will review the proper coding for a telemedicine visit so that appropriate compensation is gleaned. We will also review the barriers to implementing telemedicine visits. The third article is written with the assistance of 2 health care attorneys, Anjali Dooley and Nadia de la Houssaye, who are experts in telemedicine and who have helped dozens of practices and hospitals implement the technology. They provide legal guidelines for ObGyns who are considering adding telemedicine to their practice. ●
The American College of Obstetricians and Gynecologists (ACOG) encourages all practices and facilities without telemedicine capabilities “to strategize about how telehealth could be integrated into their services as appropriate.”1 In doing so, they also encourage consideration of ways to care for those who may not have access to such technology or who do not know how to use it. They also explain that a number of federal telehealth policy changes have been made in response to the COVID-19 pandemic, and that most private health insurers are following suit.2 Such changes include:
- covering all telehealth visits for all traditional Medicare beneficiaries regardless of geographic location or originating site
- not requiring physicians to have a pre-existing relationship with a patient to provide a telehealth visit
- permitting the use of FaceTime, Skype, and other everyday communication technologies to provide telehealth visits.
A summary of the major telehealth policy changes, as well as information on how to code and bill for telehealth visits can be found at https://www.acog.org/clinical-information/physician-faqs/~/link .aspx?_id=3803296EAAD940C69525D4DD2679A00E&_z=z.
References
- American College of Obstetricians and Gynecologists. COVID-19 FAQs for obstetriciangynecologists, gynecology. https://www.acog.org/clinical-information/physician-faqs/covid19faqs-for-ob-gyns-gynecology. Accessed April 8, 2020.
- American College of Obstetricians and Gynecologists. Managing patients remotely: billing for digital and telehealth services. Updated April 2, 2020. https://www.acog.org/clinicalinformation/physician-faqs/~/link.aspx?_id=3803296EAAD940C69525D4DD2679A00E&_z=z. Accessed April 8, 2020.
If telemedicine had not yet begun to play a significant role in your ObGyn practice, it is almost certain to now as the COVID-19 pandemic demands new ways of caring for our patients while keeping others safe from disease. According to the American College of Obstetricians and Gynecologists (ACOG), the term “telemedicine” refers to delivering traditional clinical diagnosis and monitoring via technology (see “ACOG weighs in on telehealth”).1
Whether they realize it or not, most ObGyns have practiced a simple form of telemedicine when they take phone calls from patients who are seeking medication refills. In these cases, physicians either can call the pharmacy to refill the medication or suggest patients make an office appointment to receive a new prescription (much to the chagrin of many patients—especially millennials). Physicians who acquiesce to patients’ phone requests to have prescriptions filled or to others seeking free medical advice are not compensated for these services, yet are legally responsible for their actions and advice—a situation that does not make for good medicine.
This is where telemedicine can be an important addition to an ObGyn practice. Telemedicine saves the patient the time and effort of coming to the office, while providing compensation to the physician for his/her time and advice and providing a record of the interaction, all of which makes for far better medicine. This article—the first of 3 on the subject—discusses the process of integrating telemedicine into a practice with minimal time, energy, and expense.
Telemedicine and the ObGyn practice
Many ObGyn patients do not require an in-person visit in order to receive effective care. There is even the potential to provide prenatal care via telemedicine by replacing some of the many prenatal well-care office visits with at-home care for pregnant women with low-risk pregnancies. A typical virtual visit for a low-risk pregnancy includes utilizing home monitoring equipment to track fetal heart rate, maternal blood pressure, and fundal height.2
Practices typically use telemedicine platforms to manage one or both of the following types of encounters: 1) walk-in visits through the practice’s web site; for most of these, patients tend not to care which physicians they see; their priority is usually the first available provider; and 2) appointment-based consultations, where patients schedule video chats in advance, usually with a specific provider.
Although incorporating telemedicine into a practice may seem overwhelming, it requires minimal additional equipment, interfaces easily with a practice’s web site and electronic medical record (EMR) system, increases productivity, and improves workflow. And patients generally appreciate the option of not having to travel to the office for an appointment.
Most patients and physicians are already comfortable with their mobile phones, tablets, social media, and wearable technology, such as Fitbits. Telemedicine is a logical next step. And given the current situation with COVID-19, it is really not a matter of “if,” but rather “when” to incorporate telemedicine as a communication and practice tool, and the sooner the better.
Continue to: Getting started...
Getting started
Physicians and their colleagues and staff first need to become comfortable with telemedicine technology. Physicians can begin by using video communication for other purposes, such as for conducting staff meetings. They should practice starting and ending calls and adjusting audio volume and video quality to ensure good reception.
Selecting a video platform
TABLE 1 provides a list of the most popular video providers and the advantages and disadvantages of each, and TABLE 2 shows a list of free video chat apps. Apps are available that can:
- share and mark up lab tests, magnetic resonance images, and other medical documents without exposing the entire desktop
- securely send documents over a Health Insurance Portability and Accountability Act (HIPAA)-compliant video
- stream digital device images live while still seeing patients’ faces.
Physicians should make sure their implementation team has the necessary equipment, including webcams, microphones, and speakers, and they should take the time to do research and test out a few programs before selecting one for their practice. Consider appointing a telemedicine point person who is knowledgeable about the technology and can patiently explain it to others. And keep in mind that video chatting is dependent upon a fast, strong Internet connection that has sufficient bandwidth to transport a large amount of data. If your practice has connectivity problems, consider consulting with an information technology (IT) expert.
Testing it out and obtaining feedback
Once a team is comfortable using video within the practice, it is time to test it out with a few patients and perhaps a few payers. Most patients are eager to start using video for their medical encounters. Even senior patients are often willing to try consults via video. According to a recent survey, 64% of patients are willing to see a physician over video.3 And among those who were comfortable accepting an invitation to participate in a video encounter, increasing age was actually associated with a higher likelihood to accept an invite.
Physician colleagues, medical assistants, and nurse practitioners will need some basic telemedicine skills, and physicians and staff should be prepared to make video connections seamless for patients. Usually, patients need some guidance and encouragement, such as telling them to check their spam folder for their invites if the invites fail to arrive in their email inbox, adjusting audio settings, or setting up a webcam. In the beginning, ObGyns should make sure they build in plenty of buffer time for the unexpected, as there will certainly be some “bugs” that need to be worked out.
ObGyns should encourage and collect patient feedback to such questions as:
- What kinds of devices (laptop, mobile) do they prefer using?
- What kind of networks are they using (3G, corporate, home)?
- What features do they like? What features do they have a hard time finding?
- What do they like or not like about the video experience?
- Keep track of the types of questions patients ask, and be patient as patients become acclimated to the video consultation experience.
Continue to: Streamlining online workflow...
Streamlining online workflow
Armed with feedback from patients, it is time to start streamlining online workflow. Most ObGyns want to be able to manage video visits in a way that is similar to the way they manage face-to-face visits with patients. This may mean experimenting with a virtual waiting room. A virtual waiting room is a simple web page or link that can be sent to patients. On that page, patients sign in with minimal demographic information and select one of the time slots when the physician is available. Typically, these programs are designed to alert the physicians and/or staff when a patient enters the virtual waiting room. Patients have access to the online patient queue and can start a chat or video call when both parties are ready. Such a waiting room model serves as a stepping stone for new practices to familiarize themselves with video conferencing. This approach is also perfect for practices that already have a practice management system and just want to add a video component.
Influences on practice workflow
With good time management, telemedicine can improve the efficiency and productivity of your practice. Your daily schedule and management of patients will need some minor changes, but significant alterations to your existing schedule and workflow are generally unnecessary. One of the advantages of telemedicine is the convenience of prompt care and the easy access patients have to your practice. This decreases visits to the emergency department and to urgent care centers.
Consider scheduling telemedicine appointments at the end of the day when your staff has left the office, as no staff members are required for a telemedicine visit. Ideally, you should offer a set time to communicate with patients, as this avoids having to make multiple calls to reach a patient. Another advantage of telemedicine is that you can provide care in the evenings and on weekends if you want. Whereas before you might have been fielding calls from patients during these times and not being compensated, with telemedicine you can conduct a virtual visit from any location and any computer or mobile phone and receive remuneration for your care.
And while access to care has been a problem in many ObGyn practices, many additional patients can be accommodated into a busy ObGyn practice by using telemedicine.
Telemedicine and the coronavirus
The current health care crisis makes implementing telemedicine essential. Patients who think they may have COVID-19 or who have been diagnosed need to be quarantined. Such patients can be helped safely in the comfort of their own homes without endangering others. Patients can be triaged virtually. All those who are febrile or have respiratory symptoms can continue to avail themselves of virtual visits.
According to reports in the media, COVID-19 is stretching the health care workforce to its limits and creating a shortage, both because of the sheer number of cases and because health care workers are getting sick themselves. Physicians who test positive do not have to be completely removed from the workforce if they have the ability to care for patients remotely from their homes. And not incidentally the new environment has prompted the Centers for Medicaid and Medicare Services (CMS) and private payers to initiate national payment policies that create parity between office and telemedicine visits.4
Continue to: Bottom line...
Bottom line
Patient-driven care is the future, and telemedicine is part of that. Patients want to have ready access to their health care providers without having to devote hours to a medical encounter that could be completed in a matter of minutes via telemedicine.
In the next article in this series, we will review the proper coding for a telemedicine visit so that appropriate compensation is gleaned. We will also review the barriers to implementing telemedicine visits. The third article is written with the assistance of 2 health care attorneys, Anjali Dooley and Nadia de la Houssaye, who are experts in telemedicine and who have helped dozens of practices and hospitals implement the technology. They provide legal guidelines for ObGyns who are considering adding telemedicine to their practice. ●
The American College of Obstetricians and Gynecologists (ACOG) encourages all practices and facilities without telemedicine capabilities “to strategize about how telehealth could be integrated into their services as appropriate.”1 In doing so, they also encourage consideration of ways to care for those who may not have access to such technology or who do not know how to use it. They also explain that a number of federal telehealth policy changes have been made in response to the COVID-19 pandemic, and that most private health insurers are following suit.2 Such changes include:
- covering all telehealth visits for all traditional Medicare beneficiaries regardless of geographic location or originating site
- not requiring physicians to have a pre-existing relationship with a patient to provide a telehealth visit
- permitting the use of FaceTime, Skype, and other everyday communication technologies to provide telehealth visits.
A summary of the major telehealth policy changes, as well as information on how to code and bill for telehealth visits can be found at https://www.acog.org/clinical-information/physician-faqs/~/link .aspx?_id=3803296EAAD940C69525D4DD2679A00E&_z=z.
References
- American College of Obstetricians and Gynecologists. COVID-19 FAQs for obstetriciangynecologists, gynecology. https://www.acog.org/clinical-information/physician-faqs/covid19faqs-for-ob-gyns-gynecology. Accessed April 8, 2020.
- American College of Obstetricians and Gynecologists. Managing patients remotely: billing for digital and telehealth services. Updated April 2, 2020. https://www.acog.org/clinicalinformation/physician-faqs/~/link.aspx?_id=3803296EAAD940C69525D4DD2679A00E&_z=z. Accessed April 8, 2020.
- Implementing telehealth in practice. ACOG Committee Opinion. February 2020. https://www.acog.org/clinical /clinical-guidance/committee-opinion/articles/2020/02 /implementing-telehealth-in-practice. Accessed April 6, 2020.
- de Mooij MJM, Hodny RL, O’Neil DA, et al. OB nest: reimagining low-risk prenatal care. Mayo Clin Proc. 2018;93:458-466.
- Gardner MR, Jenkins SM, O’Neil DA, et al. Perceptions of video-based appointments from the patient’s home: a patient survey. Telemed J E Health. 2015;21:281-285.
- American College of Obstetricians and Gynecologists. Managing patients remotely: billing for digital and telehealth services. Updated April 2, 2020. https://www.acog.org /clinical-information/physician-faqs/~/link.aspx?_id=380 3296EAAD940C69525D4DD2679A00E&_z=z. Accessed April 8, 2020.
- Implementing telehealth in practice. ACOG Committee Opinion. February 2020. https://www.acog.org/clinical /clinical-guidance/committee-opinion/articles/2020/02 /implementing-telehealth-in-practice. Accessed April 6, 2020.
- de Mooij MJM, Hodny RL, O’Neil DA, et al. OB nest: reimagining low-risk prenatal care. Mayo Clin Proc. 2018;93:458-466.
- Gardner MR, Jenkins SM, O’Neil DA, et al. Perceptions of video-based appointments from the patient’s home: a patient survey. Telemed J E Health. 2015;21:281-285.
- American College of Obstetricians and Gynecologists. Managing patients remotely: billing for digital and telehealth services. Updated April 2, 2020. https://www.acog.org /clinical-information/physician-faqs/~/link.aspx?_id=380 3296EAAD940C69525D4DD2679A00E&_z=z. Accessed April 8, 2020.