User login
Consider COVID-19–associated multisystem hyperinflammatory syndrome
A 21-year-old young adult presented to the ED with a 1-week history of high fever, vomiting, diarrhea, and abdominal pain. His mother was SARS-CoV-2 positive by polymerase chain reaction approximately 3 weeks prior; his PCR was negative for SARS-CoV-2.

Following admission, he became hypotensive and tachycardic with evidence of myocarditis. His chest x-ray was normal and his O2 saturation was 100% on room air. His clinical presentation was initially suggestive of toxic shock syndrome without a rash, but despite aggressive fluid resuscitation and broad-spectrum antibiotics, he continued to clinically deteriorate with persistent high fever and increasing cardiac stress. Echocardiography revealed biventricular dysfunction. His laboratory abnormalities included rising inflammatory markers and troponin I and B-type natriuretic peptide (BNP). A repeat PCR for SARS-CoV-2 was negative on day 2 of illness. He was diagnosed as likely having macrophage-activation syndrome (MAS) despite the atypical features (myocarditis), and he received Anakinra with no apparent response. He also was given intravenous immunoglobulin (IVIg) for his myocarditis and subsequently high-dose steroids. He became afebrile, his blood pressure stabilized, his inflammatory markers declined, and over several days he returned to normal. His COVID-19 antibody test IgG was positive on day 4 of illness.
This case challenged us for several reasons. First, the PCR from his nasopharynx was negative on two occasions, which raises the issue of how sensitive and accurate these PCR tests are for SARS-CoV-2 or are patients with COVID-19–associated hyperinflammatory syndrome still PCR positive? Second, although we have seen many adult cases with a cytokine storm picture similar to this patient, nearly all of the prior cases had chest x-ray abnormalities and hypoxia. Third, the severity of the myocardial dysfunction and rising troponin and BNP also was unusual in our experience with COVID-19 infection. Lastly, the use of antibody detection to SARS-CoV-2 enabled us to confirm recent COIVD-19 disease and see his illness as part of the likely spectrum of clinical syndromes seen with this virus.

The Lancet reported eight children, aged 4-14 years, with a hyperinflammatory shock-like syndrome in early May.1 The cases had features similar to atypical Kawasaki disease, KD shock syndrome, and toxic shock syndrome. Each case had high fever for multiple days; diarrhea and abdominal pain was present in even children; elevated ferritin, C-reactive protein, d-dimer, increased troponins, and ventricular dysfunction also was present in seven. Most patients had no pulmonary involvement, and most tested negative for SARS-CoV-2 despite four of the eight having direct contact with a COVID-positive family member. All received IVIg and antibiotics; six received aspirin. Seven of the eight made a full recovery; one child died from a large cerebrovascular infarct.
Also in early May, the New York Times described a “mysterious” hyperinflammatory syndrome in children thought to be linked to COVID-19. A total of 76 suspected cases in children had been reported in New York state, three of whom died. The syndrome has been given the name pediatric multisystem inflammatory syndrome. The syndrome can resemble KD shock syndrome with rash; fever; conjunctivitis; hypotension; and redness in the lips, tongue and mucous membranes . It also can resemble toxic shock syndrome with abdominal pain, vomiting, and diarrhea. However, the degree of cardiac inflammation and dysfunction is substantial in many cases and usually beyond that seen in KD or toxic shock.
The syndrome is not limited to the United States. The Royal College of Pediatrics and Child Health has created a case definition:2
- A child presenting with persistent fever, inflammation (elevated C-reactive protein, neutrophilia, and lymphopenia) and evidence of single or multiorgan dysfunction (shock, cardiac, respiratory, renal, gastrointestinal, or neurologic) with additional features.
- Exclusion of any other microbial causes such as bacterial sepsis or staphylococcal or streptococcal shock syndromes, infections known to be associated with myocarditis (such as enterovirus).
- SARS-CoV-2 testing may or may not be positive.

As with our young adult, treatment is supportive, nonspecific, and aimed at quieting the inflammatory response. The current thinking is the syndrome is seen as antibody to SARS-CoV-2 appears and frequently the nasopharyngeal PCR is negative. It is hypothesized that the syndrome occurs in genetically predisposed hosts and potentially is a late-onset inflammatory process or potentially an antibody-triggered inflammatory process. The negative PCR from nasopharyngeal specimens reflects that the onset is later in the course of disease; whether fecal samples would be COVID positive is unknown. As with our case, antibody testing for IgG against SARS-CoV-2 is appropriate to confirm COVID-19 disease and may be positive as early as day 7.
The approach needs to be team oriented and include cardiology, rheumatology, infectious diseases, and intensive care specialists working collaboratively. Such cases should be considered COVID positive despite negative PCR tests, and full personal protective equipment should be used as we do not as yet know if live virus could be found in stool. We initiated treatment with Anakinra (an interleukin-1 type-1 receptor inhibitor) as part of our treatment protocol for MAS; we did not appreciate a response. He then received IVIg and high-dose steroids, and he recovered over several days with improved cardiac function and stable blood pressure.
What is the pathogenesis? Is SARS-CoV-2 causative or just an associated finding? Who are the at-risk children, adolescents, and adults? Is there a genetic predisposition? What therapies work best? The eight cases described in London all received IVIg, as did our case, and all but one improved and survived. In adults we have seen substantial inflammation with elevated C-reactive protein (often as high as 300), ferritin, lactate dehydrogenase, triglycerides, fibrinogen, and d-dimers, but nearly all have extensive pulmonary disease, hypoxia, and are SARS-CoV-2 positive by PCR. Influenza is also associated with a cytokine storm syndrome in adolescents and young adults.3 The mechanisms influenza virus uses to initiate a cytokine storm and strategies for immunomodulatory treatment may provide insights into COVID-19–associated multisystem hyperinflammatory syndrome.
Dr. Pelton is professor of pediatrics and epidemiology at Boston University and public health and senior attending physician in pediatric infectious diseases at Boston Medical Center. Dr. Camelo is a senior fellow in pediatric infectious diseases at Boston Medical Center. They have no relevant financial disclosures. Email them at [email protected].
References
1. Riphagen S et al. Lancet. 2020 May 6. doi: 10.1016/S0140-6736(20)31094-1.
2. Royal College of Paediatrics and Child Health Guidance: Paediatric multisystem inflammatory syndrome temporally associated with COVID-19.
3. Liu Q et al.Cell Mol Immunol. 2016 Jan;13(1):3-10.
A 21-year-old young adult presented to the ED with a 1-week history of high fever, vomiting, diarrhea, and abdominal pain. His mother was SARS-CoV-2 positive by polymerase chain reaction approximately 3 weeks prior; his PCR was negative for SARS-CoV-2.
Following admission, he became hypotensive and tachycardic with evidence of myocarditis. His chest x-ray was normal and his O2 saturation was 100% on room air. His clinical presentation was initially suggestive of toxic shock syndrome without a rash, but despite aggressive fluid resuscitation and broad-spectrum antibiotics, he continued to clinically deteriorate with persistent high fever and increasing cardiac stress. Echocardiography revealed biventricular dysfunction. His laboratory abnormalities included rising inflammatory markers and troponin I and B-type natriuretic peptide (BNP). A repeat PCR for SARS-CoV-2 was negative on day 2 of illness. He was diagnosed as likely having macrophage-activation syndrome (MAS) despite the atypical features (myocarditis), and he received Anakinra with no apparent response. He also was given intravenous immunoglobulin (IVIg) for his myocarditis and subsequently high-dose steroids. He became afebrile, his blood pressure stabilized, his inflammatory markers declined, and over several days he returned to normal. His COVID-19 antibody test IgG was positive on day 4 of illness.
This case challenged us for several reasons. First, the PCR from his nasopharynx was negative on two occasions, which raises the issue of how sensitive and accurate these PCR tests are for SARS-CoV-2 or are patients with COVID-19–associated hyperinflammatory syndrome still PCR positive? Second, although we have seen many adult cases with a cytokine storm picture similar to this patient, nearly all of the prior cases had chest x-ray abnormalities and hypoxia. Third, the severity of the myocardial dysfunction and rising troponin and BNP also was unusual in our experience with COVID-19 infection. Lastly, the use of antibody detection to SARS-CoV-2 enabled us to confirm recent COIVD-19 disease and see his illness as part of the likely spectrum of clinical syndromes seen with this virus.
The Lancet reported eight children, aged 4-14 years, with a hyperinflammatory shock-like syndrome in early May.1 The cases had features similar to atypical Kawasaki disease, KD shock syndrome, and toxic shock syndrome. Each case had high fever for multiple days; diarrhea and abdominal pain was present in even children; elevated ferritin, C-reactive protein, d-dimer, increased troponins, and ventricular dysfunction also was present in seven. Most patients had no pulmonary involvement, and most tested negative for SARS-CoV-2 despite four of the eight having direct contact with a COVID-positive family member. All received IVIg and antibiotics; six received aspirin. Seven of the eight made a full recovery; one child died from a large cerebrovascular infarct.
Also in early May, the New York Times described a “mysterious” hyperinflammatory syndrome in children thought to be linked to COVID-19. A total of 76 suspected cases in children had been reported in New York state, three of whom died. The syndrome has been given the name pediatric multisystem inflammatory syndrome. The syndrome can resemble KD shock syndrome with rash; fever; conjunctivitis; hypotension; and redness in the lips, tongue and mucous membranes . It also can resemble toxic shock syndrome with abdominal pain, vomiting, and diarrhea. However, the degree of cardiac inflammation and dysfunction is substantial in many cases and usually beyond that seen in KD or toxic shock.
The syndrome is not limited to the United States. The Royal College of Pediatrics and Child Health has created a case definition:2
- A child presenting with persistent fever, inflammation (elevated C-reactive protein, neutrophilia, and lymphopenia) and evidence of single or multiorgan dysfunction (shock, cardiac, respiratory, renal, gastrointestinal, or neurologic) with additional features.
- Exclusion of any other microbial causes such as bacterial sepsis or staphylococcal or streptococcal shock syndromes, infections known to be associated with myocarditis (such as enterovirus).
- SARS-CoV-2 testing may or may not be positive.
As with our young adult, treatment is supportive, nonspecific, and aimed at quieting the inflammatory response. The current thinking is the syndrome is seen as antibody to SARS-CoV-2 appears and frequently the nasopharyngeal PCR is negative. It is hypothesized that the syndrome occurs in genetically predisposed hosts and potentially is a late-onset inflammatory process or potentially an antibody-triggered inflammatory process. The negative PCR from nasopharyngeal specimens reflects that the onset is later in the course of disease; whether fecal samples would be COVID positive is unknown. As with our case, antibody testing for IgG against SARS-CoV-2 is appropriate to confirm COVID-19 disease and may be positive as early as day 7.
The approach needs to be team oriented and include cardiology, rheumatology, infectious diseases, and intensive care specialists working collaboratively. Such cases should be considered COVID positive despite negative PCR tests, and full personal protective equipment should be used as we do not as yet know if live virus could be found in stool. We initiated treatment with Anakinra (an interleukin-1 type-1 receptor inhibitor) as part of our treatment protocol for MAS; we did not appreciate a response. He then received IVIg and high-dose steroids, and he recovered over several days with improved cardiac function and stable blood pressure.
What is the pathogenesis? Is SARS-CoV-2 causative or just an associated finding? Who are the at-risk children, adolescents, and adults? Is there a genetic predisposition? What therapies work best? The eight cases described in London all received IVIg, as did our case, and all but one improved and survived. In adults we have seen substantial inflammation with elevated C-reactive protein (often as high as 300), ferritin, lactate dehydrogenase, triglycerides, fibrinogen, and d-dimers, but nearly all have extensive pulmonary disease, hypoxia, and are SARS-CoV-2 positive by PCR. Influenza is also associated with a cytokine storm syndrome in adolescents and young adults.3 The mechanisms influenza virus uses to initiate a cytokine storm and strategies for immunomodulatory treatment may provide insights into COVID-19–associated multisystem hyperinflammatory syndrome.
Dr. Pelton is professor of pediatrics and epidemiology at Boston University and public health and senior attending physician in pediatric infectious diseases at Boston Medical Center. Dr. Camelo is a senior fellow in pediatric infectious diseases at Boston Medical Center. They have no relevant financial disclosures. Email them at [email protected].
References
1. Riphagen S et al. Lancet. 2020 May 6. doi: 10.1016/S0140-6736(20)31094-1.
2. Royal College of Paediatrics and Child Health Guidance: Paediatric multisystem inflammatory syndrome temporally associated with COVID-19.
3. Liu Q et al.Cell Mol Immunol. 2016 Jan;13(1):3-10.
A 21-year-old young adult presented to the ED with a 1-week history of high fever, vomiting, diarrhea, and abdominal pain. His mother was SARS-CoV-2 positive by polymerase chain reaction approximately 3 weeks prior; his PCR was negative for SARS-CoV-2.
Following admission, he became hypotensive and tachycardic with evidence of myocarditis. His chest x-ray was normal and his O2 saturation was 100% on room air. His clinical presentation was initially suggestive of toxic shock syndrome without a rash, but despite aggressive fluid resuscitation and broad-spectrum antibiotics, he continued to clinically deteriorate with persistent high fever and increasing cardiac stress. Echocardiography revealed biventricular dysfunction. His laboratory abnormalities included rising inflammatory markers and troponin I and B-type natriuretic peptide (BNP). A repeat PCR for SARS-CoV-2 was negative on day 2 of illness. He was diagnosed as likely having macrophage-activation syndrome (MAS) despite the atypical features (myocarditis), and he received Anakinra with no apparent response. He also was given intravenous immunoglobulin (IVIg) for his myocarditis and subsequently high-dose steroids. He became afebrile, his blood pressure stabilized, his inflammatory markers declined, and over several days he returned to normal. His COVID-19 antibody test IgG was positive on day 4 of illness.
This case challenged us for several reasons. First, the PCR from his nasopharynx was negative on two occasions, which raises the issue of how sensitive and accurate these PCR tests are for SARS-CoV-2 or are patients with COVID-19–associated hyperinflammatory syndrome still PCR positive? Second, although we have seen many adult cases with a cytokine storm picture similar to this patient, nearly all of the prior cases had chest x-ray abnormalities and hypoxia. Third, the severity of the myocardial dysfunction and rising troponin and BNP also was unusual in our experience with COVID-19 infection. Lastly, the use of antibody detection to SARS-CoV-2 enabled us to confirm recent COIVD-19 disease and see his illness as part of the likely spectrum of clinical syndromes seen with this virus.
The Lancet reported eight children, aged 4-14 years, with a hyperinflammatory shock-like syndrome in early May.1 The cases had features similar to atypical Kawasaki disease, KD shock syndrome, and toxic shock syndrome. Each case had high fever for multiple days; diarrhea and abdominal pain was present in even children; elevated ferritin, C-reactive protein, d-dimer, increased troponins, and ventricular dysfunction also was present in seven. Most patients had no pulmonary involvement, and most tested negative for SARS-CoV-2 despite four of the eight having direct contact with a COVID-positive family member. All received IVIg and antibiotics; six received aspirin. Seven of the eight made a full recovery; one child died from a large cerebrovascular infarct.
Also in early May, the New York Times described a “mysterious” hyperinflammatory syndrome in children thought to be linked to COVID-19. A total of 76 suspected cases in children had been reported in New York state, three of whom died. The syndrome has been given the name pediatric multisystem inflammatory syndrome. The syndrome can resemble KD shock syndrome with rash; fever; conjunctivitis; hypotension; and redness in the lips, tongue and mucous membranes . It also can resemble toxic shock syndrome with abdominal pain, vomiting, and diarrhea. However, the degree of cardiac inflammation and dysfunction is substantial in many cases and usually beyond that seen in KD or toxic shock.
The syndrome is not limited to the United States. The Royal College of Pediatrics and Child Health has created a case definition:2
- A child presenting with persistent fever, inflammation (elevated C-reactive protein, neutrophilia, and lymphopenia) and evidence of single or multiorgan dysfunction (shock, cardiac, respiratory, renal, gastrointestinal, or neurologic) with additional features.
- Exclusion of any other microbial causes such as bacterial sepsis or staphylococcal or streptococcal shock syndromes, infections known to be associated with myocarditis (such as enterovirus).
- SARS-CoV-2 testing may or may not be positive.
As with our young adult, treatment is supportive, nonspecific, and aimed at quieting the inflammatory response. The current thinking is the syndrome is seen as antibody to SARS-CoV-2 appears and frequently the nasopharyngeal PCR is negative. It is hypothesized that the syndrome occurs in genetically predisposed hosts and potentially is a late-onset inflammatory process or potentially an antibody-triggered inflammatory process. The negative PCR from nasopharyngeal specimens reflects that the onset is later in the course of disease; whether fecal samples would be COVID positive is unknown. As with our case, antibody testing for IgG against SARS-CoV-2 is appropriate to confirm COVID-19 disease and may be positive as early as day 7.
The approach needs to be team oriented and include cardiology, rheumatology, infectious diseases, and intensive care specialists working collaboratively. Such cases should be considered COVID positive despite negative PCR tests, and full personal protective equipment should be used as we do not as yet know if live virus could be found in stool. We initiated treatment with Anakinra (an interleukin-1 type-1 receptor inhibitor) as part of our treatment protocol for MAS; we did not appreciate a response. He then received IVIg and high-dose steroids, and he recovered over several days with improved cardiac function and stable blood pressure.
What is the pathogenesis? Is SARS-CoV-2 causative or just an associated finding? Who are the at-risk children, adolescents, and adults? Is there a genetic predisposition? What therapies work best? The eight cases described in London all received IVIg, as did our case, and all but one improved and survived. In adults we have seen substantial inflammation with elevated C-reactive protein (often as high as 300), ferritin, lactate dehydrogenase, triglycerides, fibrinogen, and d-dimers, but nearly all have extensive pulmonary disease, hypoxia, and are SARS-CoV-2 positive by PCR. Influenza is also associated with a cytokine storm syndrome in adolescents and young adults.3 The mechanisms influenza virus uses to initiate a cytokine storm and strategies for immunomodulatory treatment may provide insights into COVID-19–associated multisystem hyperinflammatory syndrome.
Dr. Pelton is professor of pediatrics and epidemiology at Boston University and public health and senior attending physician in pediatric infectious diseases at Boston Medical Center. Dr. Camelo is a senior fellow in pediatric infectious diseases at Boston Medical Center. They have no relevant financial disclosures. Email them at [email protected].
References
1. Riphagen S et al. Lancet. 2020 May 6. doi: 10.1016/S0140-6736(20)31094-1.
2. Royal College of Paediatrics and Child Health Guidance: Paediatric multisystem inflammatory syndrome temporally associated with COVID-19.
3. Liu Q et al.Cell Mol Immunol. 2016 Jan;13(1):3-10.
COVID-19 fears tied to dangerous drop in child vaccinations
The social distancing and sheltering in place mandated because of the COVID-19 pandemic are keeping parents and kids out of their doctors’ offices, and that has prompted a steep decline in recommended routine vaccinations for U.S. children, according to Centers for Disease Control and Prevention researchers.
Pediatric vaccinations dropped sharply after the national emergency was declared on March 13, suggesting that some children may be at increased risk for other serious infectious diseases, such as measles.
The researchers compared weekly orders for federally funded vaccines from Jan. 6 to April 19, 2020, with those during the same period in 2019.
They noted that, by the end of the study period, there was a cumulative COVID-19–related decline of 2.5 million doses in orders for routine noninfluenza pediatric childhood vaccines recommended by the Advisory Committee on Immunization Practices, as well as a cumulative decline in orders of 250,000 doses of measles vaccines.
Although the overall decrease in vaccinations during the study period was larger, according to CDC spokesperson Richard Quartarone, the above figures represent declines clearly associated with the pandemic.
The weekly number of measles vaccines ordered for children aged 24 months or older fell dramatically to about 500 during the week beginning March 16, 2020, and fell further to approximately 250 during the week beginning March 23. It stayed at that level until the week beginning April 13. By comparison, more than 2,500 were ordered during the week starting March 2, before the emergency was declared.
The decline was notably less for children younger than 2 years. For those children, orders dropped to about 750 during the week starting March 23 and climbed slightly for 3 weeks. By comparison, during the week of March 2, about 2,000 vaccines were ordered.
The findings, which were published in the CDC’s Morbidity and Mortality Weekly Report, stem from an analysis of ordering data from the federal Vaccines for Children (VFC) Program, as well as from vaccine administration data from the CDC’s Vaccine Tracking System and the collaborative Vaccine Safety Datalink (VSD).
The VFC provides federally purchased vaccines at no cost to about half of persons aged 18 years or younger. The VSD collaborates on vaccine coverage with the CDC’s Immunization Safety Office and eight large health care organizations across the country. Vaccination coverage is the usual metric for assessing vaccine usage; providers’ orders and the number of doses administered are two proxy measures, the authors explained.
“The substantial reduction in VFC-funded pediatric vaccine ordering after the COVID-19 emergency declaration is consistent with changes in vaccine administration among children in the VSD population receiving care through eight large U.S. health care organizations,” wrote Jeanne M. Santoli, MD, and colleagues, of the immunization services division at the National Center for Immunization and Respiratory Diseases. “The smaller decline in measles-containing vaccine administration among children aged ≤24 months suggests that system-level strategies to prioritize well child care and immunization for this age group are being implemented.”
Dr. Santoli, who is an Atlanta-based pediatrician, and associates stressed the importance of maintaining regular vaccinations during the pandemic. “The identified declines in routine pediatric vaccine ordering and doses administered might indicate that U.S. children and their communities face increased risks for outbreaks of vaccine-preventable diseases,” they wrote. “Parental concerns about potentially exposing their children to COVID-19 during well child visits might contribute to the declines observed.” Parents should therefore be reminded of the necessity of protecting their children against vaccine-preventable diseases.
In 2019, a Gallup survey reported that overall support for vaccination continued to decline in the United States.
The researchers predicted that, as social distancing relaxes, unvaccinated children will be more susceptible to other serious diseases. “In response, continued coordinated efforts between health care providers and public health officials at the local, state, and federal levels will be necessary to achieve rapid catch-up vaccination,” they concluded.
The authors disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
The social distancing and sheltering in place mandated because of the COVID-19 pandemic are keeping parents and kids out of their doctors’ offices, and that has prompted a steep decline in recommended routine vaccinations for U.S. children, according to Centers for Disease Control and Prevention researchers.
Pediatric vaccinations dropped sharply after the national emergency was declared on March 13, suggesting that some children may be at increased risk for other serious infectious diseases, such as measles.
The researchers compared weekly orders for federally funded vaccines from Jan. 6 to April 19, 2020, with those during the same period in 2019.
They noted that, by the end of the study period, there was a cumulative COVID-19–related decline of 2.5 million doses in orders for routine noninfluenza pediatric childhood vaccines recommended by the Advisory Committee on Immunization Practices, as well as a cumulative decline in orders of 250,000 doses of measles vaccines.
Although the overall decrease in vaccinations during the study period was larger, according to CDC spokesperson Richard Quartarone, the above figures represent declines clearly associated with the pandemic.
The weekly number of measles vaccines ordered for children aged 24 months or older fell dramatically to about 500 during the week beginning March 16, 2020, and fell further to approximately 250 during the week beginning March 23. It stayed at that level until the week beginning April 13. By comparison, more than 2,500 were ordered during the week starting March 2, before the emergency was declared.
The decline was notably less for children younger than 2 years. For those children, orders dropped to about 750 during the week starting March 23 and climbed slightly for 3 weeks. By comparison, during the week of March 2, about 2,000 vaccines were ordered.
The findings, which were published in the CDC’s Morbidity and Mortality Weekly Report, stem from an analysis of ordering data from the federal Vaccines for Children (VFC) Program, as well as from vaccine administration data from the CDC’s Vaccine Tracking System and the collaborative Vaccine Safety Datalink (VSD).
The VFC provides federally purchased vaccines at no cost to about half of persons aged 18 years or younger. The VSD collaborates on vaccine coverage with the CDC’s Immunization Safety Office and eight large health care organizations across the country. Vaccination coverage is the usual metric for assessing vaccine usage; providers’ orders and the number of doses administered are two proxy measures, the authors explained.
“The substantial reduction in VFC-funded pediatric vaccine ordering after the COVID-19 emergency declaration is consistent with changes in vaccine administration among children in the VSD population receiving care through eight large U.S. health care organizations,” wrote Jeanne M. Santoli, MD, and colleagues, of the immunization services division at the National Center for Immunization and Respiratory Diseases. “The smaller decline in measles-containing vaccine administration among children aged ≤24 months suggests that system-level strategies to prioritize well child care and immunization for this age group are being implemented.”
Dr. Santoli, who is an Atlanta-based pediatrician, and associates stressed the importance of maintaining regular vaccinations during the pandemic. “The identified declines in routine pediatric vaccine ordering and doses administered might indicate that U.S. children and their communities face increased risks for outbreaks of vaccine-preventable diseases,” they wrote. “Parental concerns about potentially exposing their children to COVID-19 during well child visits might contribute to the declines observed.” Parents should therefore be reminded of the necessity of protecting their children against vaccine-preventable diseases.
In 2019, a Gallup survey reported that overall support for vaccination continued to decline in the United States.
The researchers predicted that, as social distancing relaxes, unvaccinated children will be more susceptible to other serious diseases. “In response, continued coordinated efforts between health care providers and public health officials at the local, state, and federal levels will be necessary to achieve rapid catch-up vaccination,” they concluded.
The authors disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
The social distancing and sheltering in place mandated because of the COVID-19 pandemic are keeping parents and kids out of their doctors’ offices, and that has prompted a steep decline in recommended routine vaccinations for U.S. children, according to Centers for Disease Control and Prevention researchers.
Pediatric vaccinations dropped sharply after the national emergency was declared on March 13, suggesting that some children may be at increased risk for other serious infectious diseases, such as measles.
The researchers compared weekly orders for federally funded vaccines from Jan. 6 to April 19, 2020, with those during the same period in 2019.
They noted that, by the end of the study period, there was a cumulative COVID-19–related decline of 2.5 million doses in orders for routine noninfluenza pediatric childhood vaccines recommended by the Advisory Committee on Immunization Practices, as well as a cumulative decline in orders of 250,000 doses of measles vaccines.
Although the overall decrease in vaccinations during the study period was larger, according to CDC spokesperson Richard Quartarone, the above figures represent declines clearly associated with the pandemic.
The weekly number of measles vaccines ordered for children aged 24 months or older fell dramatically to about 500 during the week beginning March 16, 2020, and fell further to approximately 250 during the week beginning March 23. It stayed at that level until the week beginning April 13. By comparison, more than 2,500 were ordered during the week starting March 2, before the emergency was declared.
The decline was notably less for children younger than 2 years. For those children, orders dropped to about 750 during the week starting March 23 and climbed slightly for 3 weeks. By comparison, during the week of March 2, about 2,000 vaccines were ordered.
The findings, which were published in the CDC’s Morbidity and Mortality Weekly Report, stem from an analysis of ordering data from the federal Vaccines for Children (VFC) Program, as well as from vaccine administration data from the CDC’s Vaccine Tracking System and the collaborative Vaccine Safety Datalink (VSD).
The VFC provides federally purchased vaccines at no cost to about half of persons aged 18 years or younger. The VSD collaborates on vaccine coverage with the CDC’s Immunization Safety Office and eight large health care organizations across the country. Vaccination coverage is the usual metric for assessing vaccine usage; providers’ orders and the number of doses administered are two proxy measures, the authors explained.
“The substantial reduction in VFC-funded pediatric vaccine ordering after the COVID-19 emergency declaration is consistent with changes in vaccine administration among children in the VSD population receiving care through eight large U.S. health care organizations,” wrote Jeanne M. Santoli, MD, and colleagues, of the immunization services division at the National Center for Immunization and Respiratory Diseases. “The smaller decline in measles-containing vaccine administration among children aged ≤24 months suggests that system-level strategies to prioritize well child care and immunization for this age group are being implemented.”
Dr. Santoli, who is an Atlanta-based pediatrician, and associates stressed the importance of maintaining regular vaccinations during the pandemic. “The identified declines in routine pediatric vaccine ordering and doses administered might indicate that U.S. children and their communities face increased risks for outbreaks of vaccine-preventable diseases,” they wrote. “Parental concerns about potentially exposing their children to COVID-19 during well child visits might contribute to the declines observed.” Parents should therefore be reminded of the necessity of protecting their children against vaccine-preventable diseases.
In 2019, a Gallup survey reported that overall support for vaccination continued to decline in the United States.
The researchers predicted that, as social distancing relaxes, unvaccinated children will be more susceptible to other serious diseases. “In response, continued coordinated efforts between health care providers and public health officials at the local, state, and federal levels will be necessary to achieve rapid catch-up vaccination,” they concluded.
The authors disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Nucleoside polymers show early promise in HBV
For patients with chronic hepatitis B virus (HBV) infection, triple-combination therapy with tenofovir disoproxil fumarate, pegylated interferon alfa-2a (TDF-pegIFN), and either of two investigational nucleic acid polymers was tolerable and led to long-term functional cures in an open-label phase 2 trial.
The addition of either REP 2139 or REP 2165 to backbone TDF-pegIFN therapy produced functional cures in 39% of patients without lessening HBV DNA control or exacerbating treatment-induced neutropenia or thrombocytopenia, said Michel Bazinet, MD, of Replicor in Montreal and his associates. “Increases in levels of transaminases were significantly more frequent (P < .001 vs. controls) and greater (P = .002 vs. controls) in the nucleic acid polymer groups but did not produce symptoms, correlated with [an] initial decrease in hepatitis B surface antigen [HBsAg], and normalized during therapy and follow-up,” the investigators wrote in Gastroenterology.
Nucleic acid polymers (NAPs) suppress the assembly and secretion of HBV subviral particles. NAP monotherapy is active against HBV but usually does not provide long-term virologic control. In a small study, adding pegIFN or thymosin alpha-1 to an investigational NAP achieved functional control (HBsAg positive, HBV DNA ≤ 2000 IU/mL, and normal alanine aminotransferase levels) in eight of nine patients.
Building on these findings, two triple-combination NAP regimens were evaluated in 40 noncirrhotic HB envelope antigen–negative adults with chronic HBV infection. After 24 weeks of TDF monotherapy, participants were randomly assigned to either 48 weeks of REP 2139 or REP 2165 plus backbone therapy with TDF and pegIFN, or 24 weeks of backbone therapy followed by 48 weeks of triple-combination treatment. Patients were then followed without treatment for 24-48 weeks.
Backbone TDF-pegIFN therapy produced no HBsAg seroconversions, and HBsAg levels dropped by more than 1 log10 IU/mL in only three patients. In contrast, triple-combination NAP therapy produced undetectable HBsAg and HBsAg seroconversions (up to 233,055 mIU/mL) for 60% of patients. Among 36 patients followed for 24-48 weeks after completing treatment, 78% maintained virologic control and 39% showed functional cures (HBsAg < 0.05 IU/mL, undetectable HBV DNA, and normal ALT). “Additional follow-up is planned to confirm the long-term stability of [these] outcomes,” the researchers said.
Both NAPs were formulated with chelated magnesium to improve their tolerability. Although 95% of patients experienced transaminase flares, these “self-resolved or declined during continuing NAP therapy and normalized in 32 of 34 (94%) of participants completing 48 weeks of follow-up,” the researchers said. In keeping with prior studies, transaminase flares were associated with early declines in HBsAg but not with altered liver function or liver disease symptoms.
The study was conducted at three sites in Maldova. Most participants were men with HBV genotype D infection. “During follow-up, viral rebound occurred in participants [in whom] HBsAg was still detectable at the end of 48 weeks of combination therapy (≥ 57.9 IU/mL), who did not complete therapy, or [for whom] HBsAg clearance occurred very late in therapy,” the researchers wrote. Thus, “persistent exposure to pegIFN while HBsAg is cleared may be important for the establishment of virologic control and functional cure.” They recommended evaluating NAP plus nucleos(t)ide analogue (NUC) therapy to assess response in the absence of pegIFN. Such studies should enroll “NUC-experienced participants with well-controlled HBV DNA.”
Replicor provided funding. Dr. Bazinet and the senior investigator reported that they are employees and shareholders of Replicor and have invented patents that Replicor holds. One coinvestigator reported compensation from Replicor to his institution. The remaining 11 coinvestigators reported having no relevant disclosures.
SOURCE: Bazinet M et al. Gastroenterology. 2020 Mar 5. doi: 0.1053/j.gastro.2020.02.058.

Manhal Izzy, MD, is assistant professor of medicine, Vanderbilt University Medical Center, division of gastroenterology, hepatology, and nutrition, and transplant hepatology at the Vanderbilt Clinic, Nashville, Tenn. He has no conflicts.
Manhal Izzy, MD, is assistant professor of medicine, Vanderbilt University Medical Center, division of gastroenterology, hepatology, and nutrition, and transplant hepatology at the Vanderbilt Clinic, Nashville, Tenn. He has no conflicts.
Manhal Izzy, MD, is assistant professor of medicine, Vanderbilt University Medical Center, division of gastroenterology, hepatology, and nutrition, and transplant hepatology at the Vanderbilt Clinic, Nashville, Tenn. He has no conflicts.
For patients with chronic hepatitis B virus (HBV) infection, triple-combination therapy with tenofovir disoproxil fumarate, pegylated interferon alfa-2a (TDF-pegIFN), and either of two investigational nucleic acid polymers was tolerable and led to long-term functional cures in an open-label phase 2 trial.
The addition of either REP 2139 or REP 2165 to backbone TDF-pegIFN therapy produced functional cures in 39% of patients without lessening HBV DNA control or exacerbating treatment-induced neutropenia or thrombocytopenia, said Michel Bazinet, MD, of Replicor in Montreal and his associates. “Increases in levels of transaminases were significantly more frequent (P < .001 vs. controls) and greater (P = .002 vs. controls) in the nucleic acid polymer groups but did not produce symptoms, correlated with [an] initial decrease in hepatitis B surface antigen [HBsAg], and normalized during therapy and follow-up,” the investigators wrote in Gastroenterology.
Nucleic acid polymers (NAPs) suppress the assembly and secretion of HBV subviral particles. NAP monotherapy is active against HBV but usually does not provide long-term virologic control. In a small study, adding pegIFN or thymosin alpha-1 to an investigational NAP achieved functional control (HBsAg positive, HBV DNA ≤ 2000 IU/mL, and normal alanine aminotransferase levels) in eight of nine patients.
Building on these findings, two triple-combination NAP regimens were evaluated in 40 noncirrhotic HB envelope antigen–negative adults with chronic HBV infection. After 24 weeks of TDF monotherapy, participants were randomly assigned to either 48 weeks of REP 2139 or REP 2165 plus backbone therapy with TDF and pegIFN, or 24 weeks of backbone therapy followed by 48 weeks of triple-combination treatment. Patients were then followed without treatment for 24-48 weeks.
Backbone TDF-pegIFN therapy produced no HBsAg seroconversions, and HBsAg levels dropped by more than 1 log10 IU/mL in only three patients. In contrast, triple-combination NAP therapy produced undetectable HBsAg and HBsAg seroconversions (up to 233,055 mIU/mL) for 60% of patients. Among 36 patients followed for 24-48 weeks after completing treatment, 78% maintained virologic control and 39% showed functional cures (HBsAg < 0.05 IU/mL, undetectable HBV DNA, and normal ALT). “Additional follow-up is planned to confirm the long-term stability of [these] outcomes,” the researchers said.
Both NAPs were formulated with chelated magnesium to improve their tolerability. Although 95% of patients experienced transaminase flares, these “self-resolved or declined during continuing NAP therapy and normalized in 32 of 34 (94%) of participants completing 48 weeks of follow-up,” the researchers said. In keeping with prior studies, transaminase flares were associated with early declines in HBsAg but not with altered liver function or liver disease symptoms.
The study was conducted at three sites in Maldova. Most participants were men with HBV genotype D infection. “During follow-up, viral rebound occurred in participants [in whom] HBsAg was still detectable at the end of 48 weeks of combination therapy (≥ 57.9 IU/mL), who did not complete therapy, or [for whom] HBsAg clearance occurred very late in therapy,” the researchers wrote. Thus, “persistent exposure to pegIFN while HBsAg is cleared may be important for the establishment of virologic control and functional cure.” They recommended evaluating NAP plus nucleos(t)ide analogue (NUC) therapy to assess response in the absence of pegIFN. Such studies should enroll “NUC-experienced participants with well-controlled HBV DNA.”
Replicor provided funding. Dr. Bazinet and the senior investigator reported that they are employees and shareholders of Replicor and have invented patents that Replicor holds. One coinvestigator reported compensation from Replicor to his institution. The remaining 11 coinvestigators reported having no relevant disclosures.
SOURCE: Bazinet M et al. Gastroenterology. 2020 Mar 5. doi: 0.1053/j.gastro.2020.02.058.
For patients with chronic hepatitis B virus (HBV) infection, triple-combination therapy with tenofovir disoproxil fumarate, pegylated interferon alfa-2a (TDF-pegIFN), and either of two investigational nucleic acid polymers was tolerable and led to long-term functional cures in an open-label phase 2 trial.
The addition of either REP 2139 or REP 2165 to backbone TDF-pegIFN therapy produced functional cures in 39% of patients without lessening HBV DNA control or exacerbating treatment-induced neutropenia or thrombocytopenia, said Michel Bazinet, MD, of Replicor in Montreal and his associates. “Increases in levels of transaminases were significantly more frequent (P < .001 vs. controls) and greater (P = .002 vs. controls) in the nucleic acid polymer groups but did not produce symptoms, correlated with [an] initial decrease in hepatitis B surface antigen [HBsAg], and normalized during therapy and follow-up,” the investigators wrote in Gastroenterology.
Nucleic acid polymers (NAPs) suppress the assembly and secretion of HBV subviral particles. NAP monotherapy is active against HBV but usually does not provide long-term virologic control. In a small study, adding pegIFN or thymosin alpha-1 to an investigational NAP achieved functional control (HBsAg positive, HBV DNA ≤ 2000 IU/mL, and normal alanine aminotransferase levels) in eight of nine patients.
Building on these findings, two triple-combination NAP regimens were evaluated in 40 noncirrhotic HB envelope antigen–negative adults with chronic HBV infection. After 24 weeks of TDF monotherapy, participants were randomly assigned to either 48 weeks of REP 2139 or REP 2165 plus backbone therapy with TDF and pegIFN, or 24 weeks of backbone therapy followed by 48 weeks of triple-combination treatment. Patients were then followed without treatment for 24-48 weeks.
Backbone TDF-pegIFN therapy produced no HBsAg seroconversions, and HBsAg levels dropped by more than 1 log10 IU/mL in only three patients. In contrast, triple-combination NAP therapy produced undetectable HBsAg and HBsAg seroconversions (up to 233,055 mIU/mL) for 60% of patients. Among 36 patients followed for 24-48 weeks after completing treatment, 78% maintained virologic control and 39% showed functional cures (HBsAg < 0.05 IU/mL, undetectable HBV DNA, and normal ALT). “Additional follow-up is planned to confirm the long-term stability of [these] outcomes,” the researchers said.
Both NAPs were formulated with chelated magnesium to improve their tolerability. Although 95% of patients experienced transaminase flares, these “self-resolved or declined during continuing NAP therapy and normalized in 32 of 34 (94%) of participants completing 48 weeks of follow-up,” the researchers said. In keeping with prior studies, transaminase flares were associated with early declines in HBsAg but not with altered liver function or liver disease symptoms.
The study was conducted at three sites in Maldova. Most participants were men with HBV genotype D infection. “During follow-up, viral rebound occurred in participants [in whom] HBsAg was still detectable at the end of 48 weeks of combination therapy (≥ 57.9 IU/mL), who did not complete therapy, or [for whom] HBsAg clearance occurred very late in therapy,” the researchers wrote. Thus, “persistent exposure to pegIFN while HBsAg is cleared may be important for the establishment of virologic control and functional cure.” They recommended evaluating NAP plus nucleos(t)ide analogue (NUC) therapy to assess response in the absence of pegIFN. Such studies should enroll “NUC-experienced participants with well-controlled HBV DNA.”
Replicor provided funding. Dr. Bazinet and the senior investigator reported that they are employees and shareholders of Replicor and have invented patents that Replicor holds. One coinvestigator reported compensation from Replicor to his institution. The remaining 11 coinvestigators reported having no relevant disclosures.
SOURCE: Bazinet M et al. Gastroenterology. 2020 Mar 5. doi: 0.1053/j.gastro.2020.02.058.
FROM GASTROENTEROLOGY
Modify risk factors to manage ICU delirium in patients with COVID-19
, and a bedside risk management strategy based on modifiable risk factors can help prevent lingering effects on cognition, according to an article published in Critical Care.

Several factors can contribute to an increased risk of ICU delirium in COVID-19 patients, wrote Katarzyna Kotfis, MD, of Pomeranian Medical University, Szczecin, Poland, and colleagues.
“In patients with COVID-19, delirium may be a manifestation of direct central nervous system invasion, induction of CNS inflammatory mediators, a secondary effect of other organ system failure, an effect of sedative strategies, prolonged mechanical ventilation time, or environmental factors, including social isolation,” they said.
Delirium in the context of COVID-19 can mean an early sign of infection, so patients should be screened using dedicated psychometric tools, the researchers wrote. Also, COVID-19 has been shown to cause pneumonia in elderly patients, who are at high risk for severe pulmonary disease related to COVID-19 and for ICU delirium generally, they said.
In addition, don’t underestimate the impact of social isolation created by quarantines, the researchers said.
“What is needed now, is not only high-quality ICU care, concentrated on providing adequate respiratory support to critically ill patients, but an identification of the source and degree of mental and spiritual suffering of patients as well as their families to provide the most ethical and person-centered care during this humanitarian crisis,” they emphasized. However, they acknowledged that nonpharmacologic interventions such as mobility outside the ICU room and interactions with family members are limited by the COVID-19 situation.
The researchers noted several mechanisms by which the COVID-19 virus may cause brain damage, including through the dysfunction of the renin-angiotensin system.
“Inflammatory response of the CNS to viral infection seems to be another important reason for poor neurological outcome and occurrence of delirium,” in COVID-19 patients, they said.
As for risk-reduction strategies, the researchers noted that “delirium in mechanically ventilated patients can be reduced dramatically to 50% using a culture of lighter sedation and mobilization via the implementation of the safety bundle called the ABCDEFs promoted by the Society of Critical Care Medicine in their ICU Liberation Collaborative,” although COVID-19 isolation is a barrier, they said.
The ABCDEF bundle consists of Assessment of pain, Both spontaneous awakening trials and spontaneous breathing trials, Choice of sedation, Delirium (hyperactive or hypoactive), Early mobility, and Family presence; all of which are challenging in the COVID-19 environment, the researchers said.
They advised implementing easy screening methods for delirium to reduce the burden on medical staff, and emphasized the importance of regular patient orientation, despite social separation from family and caregivers.
“No drugs can be recommended for the prevention or treatment of ICU delirium other than avoidance of overuse of potent psychoactive agents like sedatives and neuromuscular blockers (NMB) unless patients absolutely require such management,” they added.

“Delirium is so common and so hard to manage in the COVID-19 population,” Mangala Narasimhan, DO, of Northwell Health in New Hyde Park, N.Y., said in an interview. Delirium is impacted by many sources including a viral encephalopathy, the amount and duration of sedation medications, and prolonged intubation and hypoxemia, she said. “Managing the delirium allows you to wake the patient up successfully and without a lot of discoordination. This will help with weaning,” she noted. Barriers to delirium management for COVID-19 patients include the length of time on a ventilator, as well as amount of sedatives and paralytics, and the added issues of renal insufficiency, she noted. “How they can be addressed is thoughtful plans on the addition of long-term sedation for withdrawal symptoms, and anxiolytics for the profound anxiety associated with arousal from this type of sedation on ventilators, she said. The take-home message for clinicians is the need to perform weaning trials to manage delirium in the ICU. “We have to combat this delirium in order to be successful in taking these patients off of ventilators,” she said. Dr. Narasimhan added that more research is needed on areas including drug-to-drug interactions, duration of efficacy of various drugs, and how the virus affects the brain.

“Adherence to the ABCDEF bundle can reduce the incidence of delirium, from approximately 75% of mechanically ventilated patients to 50% or less,” David L. Bowton, MD, of Wake Forest Baptist Health in Winston-Salem, N.C., said in an interview.
“Importantly, in most studies, bundle adherence reduces mortality and ICU length of stay and lowers the total cost of care. However, isolation of patients and protection of staff, visitor restrictions, and potentially stressed staffing will likely alter how most institutions approach bundle compliance,” he said. “Gathering input from infection control clinicians and bedside providers from multiple disciplines that consider these factors to critically examine current bundle procedures and workflow will be essential to the creation and/or revision of bundle processes of care that maintain the integrity of the ABCDEF bundle yet preserve staff, patient, and family safety,” he said.
“We did not have strong evidence to suggest an optimal approach to treating delirium before the advent of the COVID-19 pandemic, so I do not believe we know what the best approach is in the current environment,” Dr. Bowton added. “Further, vigilance will be necessary to ensure that altered consciousness or cognition is ICU delirium and not attributable to another cause such as drug withdrawal, drug adverse effect, or primary central nervous system infection or immune response that mandates specific therapy,” he emphasized.
For clinicians, “this study reminds us of the importance of the ABCDEF bundle to improve outcomes of critical illness,” said Dr. Bowton. “It highlights the difficulties of providing frequent reassessment of pain, comfort, reassurance, and reorientation to critically ill patients. To me, it underscores the importance of each institution critically examining staffing needs and staffing roles to mitigate these difficulties and to explore novel methods of maintaining staff-patient and family-patient interactions to enhance compliance with all elements of the ABCDEF bundle while maintaining the safety of staff and families.”
Dr. Bowton added, “When necessary, explicit modifications to existing ABCDEF bundles should be developed and disseminated to provide realistic, readily understood guidance to achieve the best possible compliance with each bundle element. One potentially underrecognized issue will be the large, hopefully temporary, number of people requiring post–critical illness rehabilitation and mental health services,” he said. “In many regions these services are already underfunded and ill-equipped to handle an increased demand for these services,” he noted.
Additional research is needed in many areas, said Dr. Bowton. “While compliance with the ABCDEF bundle decreases the incidence and duration of delirium, decreases ICU length of stay, decreases duration of mechanical ventilation, and improves mortality, many questions remain. Individual elements of the bundle have been inconsistently associated with improved outcomes,” he said. “What is the relative importance of specific elements and what are the mechanisms by which they improve outcomes?” he asked. “We still do not know how to best achieve physical/functional recovery following critical illness, which, in light of these authors’ studies relating persisting physical debility to depression (Lancet Respir Med. 2014; 2[5]:369-79), may be a key component to improving long-term outcomes,” he said.
The study received no specific funding, although several coauthors disclosed grants from agencies including the National Center for Advancing Translational Sciences, National Institute of General Medical Sciences, National Heart, Lung, and Blood Institute, and National Institute on Aging. Dr. Narasimhan and Dr. Bowton had no financial conflicts to disclose.
SOURCE: Kotfis K et al. Critical Care. 2020 Apr 28. doi: 10.1186/s13054-020-02882-x.
, and a bedside risk management strategy based on modifiable risk factors can help prevent lingering effects on cognition, according to an article published in Critical Care.
Several factors can contribute to an increased risk of ICU delirium in COVID-19 patients, wrote Katarzyna Kotfis, MD, of Pomeranian Medical University, Szczecin, Poland, and colleagues.
“In patients with COVID-19, delirium may be a manifestation of direct central nervous system invasion, induction of CNS inflammatory mediators, a secondary effect of other organ system failure, an effect of sedative strategies, prolonged mechanical ventilation time, or environmental factors, including social isolation,” they said.
Delirium in the context of COVID-19 can mean an early sign of infection, so patients should be screened using dedicated psychometric tools, the researchers wrote. Also, COVID-19 has been shown to cause pneumonia in elderly patients, who are at high risk for severe pulmonary disease related to COVID-19 and for ICU delirium generally, they said.
In addition, don’t underestimate the impact of social isolation created by quarantines, the researchers said.
“What is needed now, is not only high-quality ICU care, concentrated on providing adequate respiratory support to critically ill patients, but an identification of the source and degree of mental and spiritual suffering of patients as well as their families to provide the most ethical and person-centered care during this humanitarian crisis,” they emphasized. However, they acknowledged that nonpharmacologic interventions such as mobility outside the ICU room and interactions with family members are limited by the COVID-19 situation.
The researchers noted several mechanisms by which the COVID-19 virus may cause brain damage, including through the dysfunction of the renin-angiotensin system.
“Inflammatory response of the CNS to viral infection seems to be another important reason for poor neurological outcome and occurrence of delirium,” in COVID-19 patients, they said.
As for risk-reduction strategies, the researchers noted that “delirium in mechanically ventilated patients can be reduced dramatically to 50% using a culture of lighter sedation and mobilization via the implementation of the safety bundle called the ABCDEFs promoted by the Society of Critical Care Medicine in their ICU Liberation Collaborative,” although COVID-19 isolation is a barrier, they said.
The ABCDEF bundle consists of Assessment of pain, Both spontaneous awakening trials and spontaneous breathing trials, Choice of sedation, Delirium (hyperactive or hypoactive), Early mobility, and Family presence; all of which are challenging in the COVID-19 environment, the researchers said.
They advised implementing easy screening methods for delirium to reduce the burden on medical staff, and emphasized the importance of regular patient orientation, despite social separation from family and caregivers.
“No drugs can be recommended for the prevention or treatment of ICU delirium other than avoidance of overuse of potent psychoactive agents like sedatives and neuromuscular blockers (NMB) unless patients absolutely require such management,” they added.
“Delirium is so common and so hard to manage in the COVID-19 population,” Mangala Narasimhan, DO, of Northwell Health in New Hyde Park, N.Y., said in an interview. Delirium is impacted by many sources including a viral encephalopathy, the amount and duration of sedation medications, and prolonged intubation and hypoxemia, she said. “Managing the delirium allows you to wake the patient up successfully and without a lot of discoordination. This will help with weaning,” she noted. Barriers to delirium management for COVID-19 patients include the length of time on a ventilator, as well as amount of sedatives and paralytics, and the added issues of renal insufficiency, she noted. “How they can be addressed is thoughtful plans on the addition of long-term sedation for withdrawal symptoms, and anxiolytics for the profound anxiety associated with arousal from this type of sedation on ventilators, she said. The take-home message for clinicians is the need to perform weaning trials to manage delirium in the ICU. “We have to combat this delirium in order to be successful in taking these patients off of ventilators,” she said. Dr. Narasimhan added that more research is needed on areas including drug-to-drug interactions, duration of efficacy of various drugs, and how the virus affects the brain.
“Adherence to the ABCDEF bundle can reduce the incidence of delirium, from approximately 75% of mechanically ventilated patients to 50% or less,” David L. Bowton, MD, of Wake Forest Baptist Health in Winston-Salem, N.C., said in an interview.
“Importantly, in most studies, bundle adherence reduces mortality and ICU length of stay and lowers the total cost of care. However, isolation of patients and protection of staff, visitor restrictions, and potentially stressed staffing will likely alter how most institutions approach bundle compliance,” he said. “Gathering input from infection control clinicians and bedside providers from multiple disciplines that consider these factors to critically examine current bundle procedures and workflow will be essential to the creation and/or revision of bundle processes of care that maintain the integrity of the ABCDEF bundle yet preserve staff, patient, and family safety,” he said.
“We did not have strong evidence to suggest an optimal approach to treating delirium before the advent of the COVID-19 pandemic, so I do not believe we know what the best approach is in the current environment,” Dr. Bowton added. “Further, vigilance will be necessary to ensure that altered consciousness or cognition is ICU delirium and not attributable to another cause such as drug withdrawal, drug adverse effect, or primary central nervous system infection or immune response that mandates specific therapy,” he emphasized.
For clinicians, “this study reminds us of the importance of the ABCDEF bundle to improve outcomes of critical illness,” said Dr. Bowton. “It highlights the difficulties of providing frequent reassessment of pain, comfort, reassurance, and reorientation to critically ill patients. To me, it underscores the importance of each institution critically examining staffing needs and staffing roles to mitigate these difficulties and to explore novel methods of maintaining staff-patient and family-patient interactions to enhance compliance with all elements of the ABCDEF bundle while maintaining the safety of staff and families.”
Dr. Bowton added, “When necessary, explicit modifications to existing ABCDEF bundles should be developed and disseminated to provide realistic, readily understood guidance to achieve the best possible compliance with each bundle element. One potentially underrecognized issue will be the large, hopefully temporary, number of people requiring post–critical illness rehabilitation and mental health services,” he said. “In many regions these services are already underfunded and ill-equipped to handle an increased demand for these services,” he noted.
Additional research is needed in many areas, said Dr. Bowton. “While compliance with the ABCDEF bundle decreases the incidence and duration of delirium, decreases ICU length of stay, decreases duration of mechanical ventilation, and improves mortality, many questions remain. Individual elements of the bundle have been inconsistently associated with improved outcomes,” he said. “What is the relative importance of specific elements and what are the mechanisms by which they improve outcomes?” he asked. “We still do not know how to best achieve physical/functional recovery following critical illness, which, in light of these authors’ studies relating persisting physical debility to depression (Lancet Respir Med. 2014; 2[5]:369-79), may be a key component to improving long-term outcomes,” he said.
The study received no specific funding, although several coauthors disclosed grants from agencies including the National Center for Advancing Translational Sciences, National Institute of General Medical Sciences, National Heart, Lung, and Blood Institute, and National Institute on Aging. Dr. Narasimhan and Dr. Bowton had no financial conflicts to disclose.
SOURCE: Kotfis K et al. Critical Care. 2020 Apr 28. doi: 10.1186/s13054-020-02882-x.
, and a bedside risk management strategy based on modifiable risk factors can help prevent lingering effects on cognition, according to an article published in Critical Care.
Several factors can contribute to an increased risk of ICU delirium in COVID-19 patients, wrote Katarzyna Kotfis, MD, of Pomeranian Medical University, Szczecin, Poland, and colleagues.
“In patients with COVID-19, delirium may be a manifestation of direct central nervous system invasion, induction of CNS inflammatory mediators, a secondary effect of other organ system failure, an effect of sedative strategies, prolonged mechanical ventilation time, or environmental factors, including social isolation,” they said.
Delirium in the context of COVID-19 can mean an early sign of infection, so patients should be screened using dedicated psychometric tools, the researchers wrote. Also, COVID-19 has been shown to cause pneumonia in elderly patients, who are at high risk for severe pulmonary disease related to COVID-19 and for ICU delirium generally, they said.
In addition, don’t underestimate the impact of social isolation created by quarantines, the researchers said.
“What is needed now, is not only high-quality ICU care, concentrated on providing adequate respiratory support to critically ill patients, but an identification of the source and degree of mental and spiritual suffering of patients as well as their families to provide the most ethical and person-centered care during this humanitarian crisis,” they emphasized. However, they acknowledged that nonpharmacologic interventions such as mobility outside the ICU room and interactions with family members are limited by the COVID-19 situation.
The researchers noted several mechanisms by which the COVID-19 virus may cause brain damage, including through the dysfunction of the renin-angiotensin system.
“Inflammatory response of the CNS to viral infection seems to be another important reason for poor neurological outcome and occurrence of delirium,” in COVID-19 patients, they said.
As for risk-reduction strategies, the researchers noted that “delirium in mechanically ventilated patients can be reduced dramatically to 50% using a culture of lighter sedation and mobilization via the implementation of the safety bundle called the ABCDEFs promoted by the Society of Critical Care Medicine in their ICU Liberation Collaborative,” although COVID-19 isolation is a barrier, they said.
The ABCDEF bundle consists of Assessment of pain, Both spontaneous awakening trials and spontaneous breathing trials, Choice of sedation, Delirium (hyperactive or hypoactive), Early mobility, and Family presence; all of which are challenging in the COVID-19 environment, the researchers said.
They advised implementing easy screening methods for delirium to reduce the burden on medical staff, and emphasized the importance of regular patient orientation, despite social separation from family and caregivers.
“No drugs can be recommended for the prevention or treatment of ICU delirium other than avoidance of overuse of potent psychoactive agents like sedatives and neuromuscular blockers (NMB) unless patients absolutely require such management,” they added.
“Delirium is so common and so hard to manage in the COVID-19 population,” Mangala Narasimhan, DO, of Northwell Health in New Hyde Park, N.Y., said in an interview. Delirium is impacted by many sources including a viral encephalopathy, the amount and duration of sedation medications, and prolonged intubation and hypoxemia, she said. “Managing the delirium allows you to wake the patient up successfully and without a lot of discoordination. This will help with weaning,” she noted. Barriers to delirium management for COVID-19 patients include the length of time on a ventilator, as well as amount of sedatives and paralytics, and the added issues of renal insufficiency, she noted. “How they can be addressed is thoughtful plans on the addition of long-term sedation for withdrawal symptoms, and anxiolytics for the profound anxiety associated with arousal from this type of sedation on ventilators, she said. The take-home message for clinicians is the need to perform weaning trials to manage delirium in the ICU. “We have to combat this delirium in order to be successful in taking these patients off of ventilators,” she said. Dr. Narasimhan added that more research is needed on areas including drug-to-drug interactions, duration of efficacy of various drugs, and how the virus affects the brain.
“Adherence to the ABCDEF bundle can reduce the incidence of delirium, from approximately 75% of mechanically ventilated patients to 50% or less,” David L. Bowton, MD, of Wake Forest Baptist Health in Winston-Salem, N.C., said in an interview.
“Importantly, in most studies, bundle adherence reduces mortality and ICU length of stay and lowers the total cost of care. However, isolation of patients and protection of staff, visitor restrictions, and potentially stressed staffing will likely alter how most institutions approach bundle compliance,” he said. “Gathering input from infection control clinicians and bedside providers from multiple disciplines that consider these factors to critically examine current bundle procedures and workflow will be essential to the creation and/or revision of bundle processes of care that maintain the integrity of the ABCDEF bundle yet preserve staff, patient, and family safety,” he said.
“We did not have strong evidence to suggest an optimal approach to treating delirium before the advent of the COVID-19 pandemic, so I do not believe we know what the best approach is in the current environment,” Dr. Bowton added. “Further, vigilance will be necessary to ensure that altered consciousness or cognition is ICU delirium and not attributable to another cause such as drug withdrawal, drug adverse effect, or primary central nervous system infection or immune response that mandates specific therapy,” he emphasized.
For clinicians, “this study reminds us of the importance of the ABCDEF bundle to improve outcomes of critical illness,” said Dr. Bowton. “It highlights the difficulties of providing frequent reassessment of pain, comfort, reassurance, and reorientation to critically ill patients. To me, it underscores the importance of each institution critically examining staffing needs and staffing roles to mitigate these difficulties and to explore novel methods of maintaining staff-patient and family-patient interactions to enhance compliance with all elements of the ABCDEF bundle while maintaining the safety of staff and families.”
Dr. Bowton added, “When necessary, explicit modifications to existing ABCDEF bundles should be developed and disseminated to provide realistic, readily understood guidance to achieve the best possible compliance with each bundle element. One potentially underrecognized issue will be the large, hopefully temporary, number of people requiring post–critical illness rehabilitation and mental health services,” he said. “In many regions these services are already underfunded and ill-equipped to handle an increased demand for these services,” he noted.
Additional research is needed in many areas, said Dr. Bowton. “While compliance with the ABCDEF bundle decreases the incidence and duration of delirium, decreases ICU length of stay, decreases duration of mechanical ventilation, and improves mortality, many questions remain. Individual elements of the bundle have been inconsistently associated with improved outcomes,” he said. “What is the relative importance of specific elements and what are the mechanisms by which they improve outcomes?” he asked. “We still do not know how to best achieve physical/functional recovery following critical illness, which, in light of these authors’ studies relating persisting physical debility to depression (Lancet Respir Med. 2014; 2[5]:369-79), may be a key component to improving long-term outcomes,” he said.
The study received no specific funding, although several coauthors disclosed grants from agencies including the National Center for Advancing Translational Sciences, National Institute of General Medical Sciences, National Heart, Lung, and Blood Institute, and National Institute on Aging. Dr. Narasimhan and Dr. Bowton had no financial conflicts to disclose.
SOURCE: Kotfis K et al. Critical Care. 2020 Apr 28. doi: 10.1186/s13054-020-02882-x.
FROM CRITICAL CARE
U.S. is poised to produce a COVID-19 vaccine, but don’t expect it soon
Manufacturers will begin producing COVID-19 vaccine doses in anticipation of approval so that if a product gets the okay for usage, distribution can begin quickly, according to Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases.

“We will be producing vaccine at risk, which means we’ll be [investing] considerable resources in developing doses even before we know any given candidate or candidates work,” he testified during a May 12, 2020, hearing of the Senate Health, Education, Labor, and Pensions Committee.
During the hearing, Dr. Fauci did not elaborate on how the production at risk would be undertaken, what criteria would be in place for selecting which candidates would be in the pipeline, or how much would be spent on the advanced production of these vaccines.
And while Dr. Fauci, a member of the White House coronavirus task force, remained optimistic that one or more vaccine candidates would ultimately be viable, he cautioned that there remain many unknowns that could slow the development of a vaccine for COVID-19.
“I must warn that there’s also the possibility of negative consequences that certain vaccines can actually enhance the negative effect of the infection,” he said. “The big unknown is efficacy. Will it be present or absent and how durable will it be?”
It’s unlikely that either a vaccine or an effective treatment will be available in the next 3 months, Dr. Fauci told the committee.
Sen. Lamar Alexander (R-Tenn.), the committee chairman, asked Dr. Fauci what he would say to college, primary, and secondary school administrators about how the availability of treatments and vaccines could influence the ability to reopen campuses to students. Dr. Fauci replied that the idea of having treatments or a vaccine available to facilitate the reentry of students in the fall term would be “a bit of a bridge too far.”
The emphasis in the coming months should be on testing, contact tracing, and isolation of those infected with the virus, Dr. Fauci said.
Manufacturers will begin producing COVID-19 vaccine doses in anticipation of approval so that if a product gets the okay for usage, distribution can begin quickly, according to Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases.
“We will be producing vaccine at risk, which means we’ll be [investing] considerable resources in developing doses even before we know any given candidate or candidates work,” he testified during a May 12, 2020, hearing of the Senate Health, Education, Labor, and Pensions Committee.
During the hearing, Dr. Fauci did not elaborate on how the production at risk would be undertaken, what criteria would be in place for selecting which candidates would be in the pipeline, or how much would be spent on the advanced production of these vaccines.
And while Dr. Fauci, a member of the White House coronavirus task force, remained optimistic that one or more vaccine candidates would ultimately be viable, he cautioned that there remain many unknowns that could slow the development of a vaccine for COVID-19.
“I must warn that there’s also the possibility of negative consequences that certain vaccines can actually enhance the negative effect of the infection,” he said. “The big unknown is efficacy. Will it be present or absent and how durable will it be?”
It’s unlikely that either a vaccine or an effective treatment will be available in the next 3 months, Dr. Fauci told the committee.
Sen. Lamar Alexander (R-Tenn.), the committee chairman, asked Dr. Fauci what he would say to college, primary, and secondary school administrators about how the availability of treatments and vaccines could influence the ability to reopen campuses to students. Dr. Fauci replied that the idea of having treatments or a vaccine available to facilitate the reentry of students in the fall term would be “a bit of a bridge too far.”
The emphasis in the coming months should be on testing, contact tracing, and isolation of those infected with the virus, Dr. Fauci said.
Manufacturers will begin producing COVID-19 vaccine doses in anticipation of approval so that if a product gets the okay for usage, distribution can begin quickly, according to Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases.
“We will be producing vaccine at risk, which means we’ll be [investing] considerable resources in developing doses even before we know any given candidate or candidates work,” he testified during a May 12, 2020, hearing of the Senate Health, Education, Labor, and Pensions Committee.
During the hearing, Dr. Fauci did not elaborate on how the production at risk would be undertaken, what criteria would be in place for selecting which candidates would be in the pipeline, or how much would be spent on the advanced production of these vaccines.
And while Dr. Fauci, a member of the White House coronavirus task force, remained optimistic that one or more vaccine candidates would ultimately be viable, he cautioned that there remain many unknowns that could slow the development of a vaccine for COVID-19.
“I must warn that there’s also the possibility of negative consequences that certain vaccines can actually enhance the negative effect of the infection,” he said. “The big unknown is efficacy. Will it be present or absent and how durable will it be?”
It’s unlikely that either a vaccine or an effective treatment will be available in the next 3 months, Dr. Fauci told the committee.
Sen. Lamar Alexander (R-Tenn.), the committee chairman, asked Dr. Fauci what he would say to college, primary, and secondary school administrators about how the availability of treatments and vaccines could influence the ability to reopen campuses to students. Dr. Fauci replied that the idea of having treatments or a vaccine available to facilitate the reentry of students in the fall term would be “a bit of a bridge too far.”
The emphasis in the coming months should be on testing, contact tracing, and isolation of those infected with the virus, Dr. Fauci said.
States vary in vulnerability to COVID-19 impact
West Virginia’s large elderly population and high rates of chronic kidney disease, cardiovascular disease, diabetes, and COPD make it the most vulnerable state to the coronavirus, according to a new analysis.

Vulnerability to the virus “isn’t just health related, though, as many people are harmed by the economic effects of the pandemic,” personal finance website WalletHub said May 12.
“It’s important for the U.S. to dedicate a large portion of its resources to providing medical support during the coronavirus pandemic, but we should also support people who don’t have adequate housing or enough money to survive the pandemic,” said WalletHub analyst Jill Gonzalez.
WalletHub graded each state on 28 measures – including share of obese adults, share of homes lacking access to basic hygienic facilities, and biggest increases in unemployment because of COVID-19 – grouped into three dimensions of vulnerability: medical (60% of the total score), housing (15%), and financial (25%).
Using those measures, Louisiana is the most vulnerable state after West Virginia, followed by Mississippi, Arkansas, and Alabama. All 5 states finished in the top 6 for medical vulnerability, and 4 were in the top 10 for financial vulnerability, but only 1 (Arkansas) was in the top 10 for housing vulnerability, WalletHub said.
Among the three vulnerability dimensions, West Virginia was first in medical, Hawaii (33rd overall) was first in housing, and Louisiana was first in financial. Utah is the least vulnerable state, overall, and the least vulnerable states in each dimension are, respectively, Colorado (50th overall), the District of Columbia (29th overall), and Iowa (45th overall), the report showed.
A look at the individual metrics WalletHub used shows some serious disparities:
- New Jersey’s unemployment recipiency rate of 57.2%, the highest in the country, is 6.1 times higher than North Carolina’s 9.3%.
- The highest uninsured rate, 17.4% in Texas, is 6.2 times higher than in Massachusetts, which is the lowest at 2.8%.
- In California, the share of the homeless population that is unsheltered (71.7%) is more than 33 times higher than in North Dakota (2.2%).
“The financial damage caused by COVID-19 is leaving many Americans without the means to pay their bills and purchase necessities. … The U.S. must continue to support its financially vulnerable populations even after the virus has subsided,” Ms. Gonzalez said.
West Virginia’s large elderly population and high rates of chronic kidney disease, cardiovascular disease, diabetes, and COPD make it the most vulnerable state to the coronavirus, according to a new analysis.
Vulnerability to the virus “isn’t just health related, though, as many people are harmed by the economic effects of the pandemic,” personal finance website WalletHub said May 12.
“It’s important for the U.S. to dedicate a large portion of its resources to providing medical support during the coronavirus pandemic, but we should also support people who don’t have adequate housing or enough money to survive the pandemic,” said WalletHub analyst Jill Gonzalez.
WalletHub graded each state on 28 measures – including share of obese adults, share of homes lacking access to basic hygienic facilities, and biggest increases in unemployment because of COVID-19 – grouped into three dimensions of vulnerability: medical (60% of the total score), housing (15%), and financial (25%).
Using those measures, Louisiana is the most vulnerable state after West Virginia, followed by Mississippi, Arkansas, and Alabama. All 5 states finished in the top 6 for medical vulnerability, and 4 were in the top 10 for financial vulnerability, but only 1 (Arkansas) was in the top 10 for housing vulnerability, WalletHub said.
Among the three vulnerability dimensions, West Virginia was first in medical, Hawaii (33rd overall) was first in housing, and Louisiana was first in financial. Utah is the least vulnerable state, overall, and the least vulnerable states in each dimension are, respectively, Colorado (50th overall), the District of Columbia (29th overall), and Iowa (45th overall), the report showed.
A look at the individual metrics WalletHub used shows some serious disparities:
- New Jersey’s unemployment recipiency rate of 57.2%, the highest in the country, is 6.1 times higher than North Carolina’s 9.3%.
- The highest uninsured rate, 17.4% in Texas, is 6.2 times higher than in Massachusetts, which is the lowest at 2.8%.
- In California, the share of the homeless population that is unsheltered (71.7%) is more than 33 times higher than in North Dakota (2.2%).
“The financial damage caused by COVID-19 is leaving many Americans without the means to pay their bills and purchase necessities. … The U.S. must continue to support its financially vulnerable populations even after the virus has subsided,” Ms. Gonzalez said.
West Virginia’s large elderly population and high rates of chronic kidney disease, cardiovascular disease, diabetes, and COPD make it the most vulnerable state to the coronavirus, according to a new analysis.
Vulnerability to the virus “isn’t just health related, though, as many people are harmed by the economic effects of the pandemic,” personal finance website WalletHub said May 12.
“It’s important for the U.S. to dedicate a large portion of its resources to providing medical support during the coronavirus pandemic, but we should also support people who don’t have adequate housing or enough money to survive the pandemic,” said WalletHub analyst Jill Gonzalez.
WalletHub graded each state on 28 measures – including share of obese adults, share of homes lacking access to basic hygienic facilities, and biggest increases in unemployment because of COVID-19 – grouped into three dimensions of vulnerability: medical (60% of the total score), housing (15%), and financial (25%).
Using those measures, Louisiana is the most vulnerable state after West Virginia, followed by Mississippi, Arkansas, and Alabama. All 5 states finished in the top 6 for medical vulnerability, and 4 were in the top 10 for financial vulnerability, but only 1 (Arkansas) was in the top 10 for housing vulnerability, WalletHub said.
Among the three vulnerability dimensions, West Virginia was first in medical, Hawaii (33rd overall) was first in housing, and Louisiana was first in financial. Utah is the least vulnerable state, overall, and the least vulnerable states in each dimension are, respectively, Colorado (50th overall), the District of Columbia (29th overall), and Iowa (45th overall), the report showed.
A look at the individual metrics WalletHub used shows some serious disparities:
- New Jersey’s unemployment recipiency rate of 57.2%, the highest in the country, is 6.1 times higher than North Carolina’s 9.3%.
- The highest uninsured rate, 17.4% in Texas, is 6.2 times higher than in Massachusetts, which is the lowest at 2.8%.
- In California, the share of the homeless population that is unsheltered (71.7%) is more than 33 times higher than in North Dakota (2.2%).
“The financial damage caused by COVID-19 is leaving many Americans without the means to pay their bills and purchase necessities. … The U.S. must continue to support its financially vulnerable populations even after the virus has subsided,” Ms. Gonzalez said.
Many hydroxychloroquine COVID-19 prophylaxis trials lack ECG screening
Many planned randomized trials to test the efficacy of hydroxychloroquine or related drugs for preventing COVID-19 infection have, as of the end of April 2020, failed to include ECG assessment to either exclude people at the highest risk for possibly developing a life-threatening cardiac arrhythmia or to flag people who achieve a dangerous QTc interval on treatment, according to an analysis of the posted designs of several dozen studies.

Hydroxychloroquine, the related agent chloroquine, and azithromycin have all recently received attention as potentially effective but unproven agents for both reducing the severity and duration of established COVID-19 infection as well as possibly preventing or mitigating an incident infection. As of April 30, 155 randomized, control trials listed on a major index for pending and in-progress trials, clinicaltrials.gov, had designs that intended to randomized an overall total of more than 85,000 healthy people to receive hydroxychloroquine or chloroquine, in some cases in combination with azithromycin, to test their efficacy and safety for COVID-19 prophylaxis, Michael H. Gollob, MD, said in an article posted by the Journal of the American College of Cardiology (2020 May 11. doi: 10.1016/j.jacc.2020.05.008).
The problem is that all three agents are documented to potentially produce lengthening of the corrected QT interval (QTc), and if this happens in a person who starts treatment with a QTc on the high end, the incremental prolongation from drug treatment could push their heart rhythm into a range where their risk for a life-threatening arrhythmia becomes substantial, said Dr. Gollob, a cardiac arrhythmia researcher at Toronto General Hospital and the University of Toronto. As a consequence, he recommended excluding from these prophylaxis trials anyone with a resting QTc at baseline assessment of greater than 450 msec, as well as discontinuing treatment from anyone who develops a resting QTc of more than 480 ms while on treatment.
“Though this may seem like a conservative value for subject withdrawal from a study, this is a prudent QTc cut-off, particularly when the severity of the adverse event, sudden death, may be worse than the study endpoint” of reduced incidence of COVID-19 infection, he wrote in his opinion piece.
“We cannot provide an accurate number for elevated risk” faced by people whose QTc climbs above these thresholds, “but we know that events will occur, which is why most trials that involve QT-prolonging drugs typically have an ECG exclusion criterion of QTc greater than 450 msec,” Dr. Gollob said in an interview.
His analysis of the 155 planned randomized prophylaxis trials on clinicaltrials.gov that he examined in detail had enrollment goals that would translate into more than 85,000 uninfected people who would receive hydroxychloroquine or chloroquine plus, in come cases, azithromycin. Only six relatively small studies from among these 155 included a plan for ECG screening and monitoring in its design, he noted. “It is reasonable to estimate that among the 80,000 patients randomized to a QT-prolonging drug [without ECG screening or monitoring] there will certainly be arrhythmic events.” If some of these people were to then die from a drug-induced arrhythmic event that could have been prevented by ECG screening or monitoring, it would be a “tragedy,” Dr. Gollob said.
“It is not only inexplicable, but also inexcusable that clinical investigators would dare to include healthy individuals in a clinical trial involving QT-prolonging medications without bothering to screen their electrocardiogram,” commented Sami Viskin, MD, an electrophysiologist at Tel Aviv Sourasky Medical Center. “The fact that we needed Dr. Gollob to ring this alarm is, itself, shocking,” he said in an interview.
“ECG screening is a good option to minimize the risk. You don’t eliminate the risk, but you can minimize it,” commented Arthur Wilde, MD, a cardiac electrophysiologist and professor of medicine at the Academic Medical Center in Amsterdam. Both Dr. Viskin and Dr. Wilde agreed with the QTc interval thresholds Dr. Gollob recommended using for excluding or discontinuing study participants.
In his commentary, Dr. Gollob estimated that if 85,000 otherwise healthy adults were randomized to received a drug that can increase the QTc interval, as many as about 3,400 people (4%) in the group could statistically be expected to have an especially high vulnerability to QT prolongation because of genetic variants they might carry that collectively have roughly this prevalence. In some people of African heritage, the prevalence of genetic risk for excessive QTc lengthening can be even higher, approaching about 10%, noted Dr. Wilde.
Dr. Gollob hoped the concerns he raised will prompt the organizers of many of these studies to revise their design, and he said he already knew of one study based in Toronto that recently added an ECG-monitoring strategy in response to the concerns he raised. He expressed optimism that more studies will follow.
“It’s a real issue to have these trials designed without ECG exclusions or monitoring. I’m glad that Dr. Gollob sent this warning, because he is right. ECG monitoring during treatment is important so you can stop the treatment in time,” Dr. Wilde said. Dr. Wilde also noted that many, if not most, of the studies listed on clinicaltrials.gov may not actually launch.
In April, representatives from several cardiology societies coauthored a document of considerations when using hydroxychloroquine, chloroquine, or azithromycin to treat patients with a diagnosed COVID-19 infection, and highlighted a QTc interval of 500 msec or greater as flagging patients who should no longer receive these drugs (J Am Coll Cardiol. 2020 Apr 10. doi: 10.1016/j.jacc.2020.04.016). For patients who do not yet have COVID-19 disease and the goal from treatment is prevention the potential efficacy of these drugs is reasonable to explore, but “does not exclude the need to minimize risk to research participants, especially when enrolling healthy subjects,” Dr. Gollob said.
Dr. Gollob, Dr. Viskin, and Dr. Wilde had no relevant financial disclosures.
Many planned randomized trials to test the efficacy of hydroxychloroquine or related drugs for preventing COVID-19 infection have, as of the end of April 2020, failed to include ECG assessment to either exclude people at the highest risk for possibly developing a life-threatening cardiac arrhythmia or to flag people who achieve a dangerous QTc interval on treatment, according to an analysis of the posted designs of several dozen studies.
Hydroxychloroquine, the related agent chloroquine, and azithromycin have all recently received attention as potentially effective but unproven agents for both reducing the severity and duration of established COVID-19 infection as well as possibly preventing or mitigating an incident infection. As of April 30, 155 randomized, control trials listed on a major index for pending and in-progress trials, clinicaltrials.gov, had designs that intended to randomized an overall total of more than 85,000 healthy people to receive hydroxychloroquine or chloroquine, in some cases in combination with azithromycin, to test their efficacy and safety for COVID-19 prophylaxis, Michael H. Gollob, MD, said in an article posted by the Journal of the American College of Cardiology (2020 May 11. doi: 10.1016/j.jacc.2020.05.008).
The problem is that all three agents are documented to potentially produce lengthening of the corrected QT interval (QTc), and if this happens in a person who starts treatment with a QTc on the high end, the incremental prolongation from drug treatment could push their heart rhythm into a range where their risk for a life-threatening arrhythmia becomes substantial, said Dr. Gollob, a cardiac arrhythmia researcher at Toronto General Hospital and the University of Toronto. As a consequence, he recommended excluding from these prophylaxis trials anyone with a resting QTc at baseline assessment of greater than 450 msec, as well as discontinuing treatment from anyone who develops a resting QTc of more than 480 ms while on treatment.
“Though this may seem like a conservative value for subject withdrawal from a study, this is a prudent QTc cut-off, particularly when the severity of the adverse event, sudden death, may be worse than the study endpoint” of reduced incidence of COVID-19 infection, he wrote in his opinion piece.
“We cannot provide an accurate number for elevated risk” faced by people whose QTc climbs above these thresholds, “but we know that events will occur, which is why most trials that involve QT-prolonging drugs typically have an ECG exclusion criterion of QTc greater than 450 msec,” Dr. Gollob said in an interview.
His analysis of the 155 planned randomized prophylaxis trials on clinicaltrials.gov that he examined in detail had enrollment goals that would translate into more than 85,000 uninfected people who would receive hydroxychloroquine or chloroquine plus, in come cases, azithromycin. Only six relatively small studies from among these 155 included a plan for ECG screening and monitoring in its design, he noted. “It is reasonable to estimate that among the 80,000 patients randomized to a QT-prolonging drug [without ECG screening or monitoring] there will certainly be arrhythmic events.” If some of these people were to then die from a drug-induced arrhythmic event that could have been prevented by ECG screening or monitoring, it would be a “tragedy,” Dr. Gollob said.
“It is not only inexplicable, but also inexcusable that clinical investigators would dare to include healthy individuals in a clinical trial involving QT-prolonging medications without bothering to screen their electrocardiogram,” commented Sami Viskin, MD, an electrophysiologist at Tel Aviv Sourasky Medical Center. “The fact that we needed Dr. Gollob to ring this alarm is, itself, shocking,” he said in an interview.
“ECG screening is a good option to minimize the risk. You don’t eliminate the risk, but you can minimize it,” commented Arthur Wilde, MD, a cardiac electrophysiologist and professor of medicine at the Academic Medical Center in Amsterdam. Both Dr. Viskin and Dr. Wilde agreed with the QTc interval thresholds Dr. Gollob recommended using for excluding or discontinuing study participants.
In his commentary, Dr. Gollob estimated that if 85,000 otherwise healthy adults were randomized to received a drug that can increase the QTc interval, as many as about 3,400 people (4%) in the group could statistically be expected to have an especially high vulnerability to QT prolongation because of genetic variants they might carry that collectively have roughly this prevalence. In some people of African heritage, the prevalence of genetic risk for excessive QTc lengthening can be even higher, approaching about 10%, noted Dr. Wilde.
Dr. Gollob hoped the concerns he raised will prompt the organizers of many of these studies to revise their design, and he said he already knew of one study based in Toronto that recently added an ECG-monitoring strategy in response to the concerns he raised. He expressed optimism that more studies will follow.
“It’s a real issue to have these trials designed without ECG exclusions or monitoring. I’m glad that Dr. Gollob sent this warning, because he is right. ECG monitoring during treatment is important so you can stop the treatment in time,” Dr. Wilde said. Dr. Wilde also noted that many, if not most, of the studies listed on clinicaltrials.gov may not actually launch.
In April, representatives from several cardiology societies coauthored a document of considerations when using hydroxychloroquine, chloroquine, or azithromycin to treat patients with a diagnosed COVID-19 infection, and highlighted a QTc interval of 500 msec or greater as flagging patients who should no longer receive these drugs (J Am Coll Cardiol. 2020 Apr 10. doi: 10.1016/j.jacc.2020.04.016). For patients who do not yet have COVID-19 disease and the goal from treatment is prevention the potential efficacy of these drugs is reasonable to explore, but “does not exclude the need to minimize risk to research participants, especially when enrolling healthy subjects,” Dr. Gollob said.
Dr. Gollob, Dr. Viskin, and Dr. Wilde had no relevant financial disclosures.
Many planned randomized trials to test the efficacy of hydroxychloroquine or related drugs for preventing COVID-19 infection have, as of the end of April 2020, failed to include ECG assessment to either exclude people at the highest risk for possibly developing a life-threatening cardiac arrhythmia or to flag people who achieve a dangerous QTc interval on treatment, according to an analysis of the posted designs of several dozen studies.
Hydroxychloroquine, the related agent chloroquine, and azithromycin have all recently received attention as potentially effective but unproven agents for both reducing the severity and duration of established COVID-19 infection as well as possibly preventing or mitigating an incident infection. As of April 30, 155 randomized, control trials listed on a major index for pending and in-progress trials, clinicaltrials.gov, had designs that intended to randomized an overall total of more than 85,000 healthy people to receive hydroxychloroquine or chloroquine, in some cases in combination with azithromycin, to test their efficacy and safety for COVID-19 prophylaxis, Michael H. Gollob, MD, said in an article posted by the Journal of the American College of Cardiology (2020 May 11. doi: 10.1016/j.jacc.2020.05.008).
The problem is that all three agents are documented to potentially produce lengthening of the corrected QT interval (QTc), and if this happens in a person who starts treatment with a QTc on the high end, the incremental prolongation from drug treatment could push their heart rhythm into a range where their risk for a life-threatening arrhythmia becomes substantial, said Dr. Gollob, a cardiac arrhythmia researcher at Toronto General Hospital and the University of Toronto. As a consequence, he recommended excluding from these prophylaxis trials anyone with a resting QTc at baseline assessment of greater than 450 msec, as well as discontinuing treatment from anyone who develops a resting QTc of more than 480 ms while on treatment.
“Though this may seem like a conservative value for subject withdrawal from a study, this is a prudent QTc cut-off, particularly when the severity of the adverse event, sudden death, may be worse than the study endpoint” of reduced incidence of COVID-19 infection, he wrote in his opinion piece.
“We cannot provide an accurate number for elevated risk” faced by people whose QTc climbs above these thresholds, “but we know that events will occur, which is why most trials that involve QT-prolonging drugs typically have an ECG exclusion criterion of QTc greater than 450 msec,” Dr. Gollob said in an interview.
His analysis of the 155 planned randomized prophylaxis trials on clinicaltrials.gov that he examined in detail had enrollment goals that would translate into more than 85,000 uninfected people who would receive hydroxychloroquine or chloroquine plus, in come cases, azithromycin. Only six relatively small studies from among these 155 included a plan for ECG screening and monitoring in its design, he noted. “It is reasonable to estimate that among the 80,000 patients randomized to a QT-prolonging drug [without ECG screening or monitoring] there will certainly be arrhythmic events.” If some of these people were to then die from a drug-induced arrhythmic event that could have been prevented by ECG screening or monitoring, it would be a “tragedy,” Dr. Gollob said.
“It is not only inexplicable, but also inexcusable that clinical investigators would dare to include healthy individuals in a clinical trial involving QT-prolonging medications without bothering to screen their electrocardiogram,” commented Sami Viskin, MD, an electrophysiologist at Tel Aviv Sourasky Medical Center. “The fact that we needed Dr. Gollob to ring this alarm is, itself, shocking,” he said in an interview.
“ECG screening is a good option to minimize the risk. You don’t eliminate the risk, but you can minimize it,” commented Arthur Wilde, MD, a cardiac electrophysiologist and professor of medicine at the Academic Medical Center in Amsterdam. Both Dr. Viskin and Dr. Wilde agreed with the QTc interval thresholds Dr. Gollob recommended using for excluding or discontinuing study participants.
In his commentary, Dr. Gollob estimated that if 85,000 otherwise healthy adults were randomized to received a drug that can increase the QTc interval, as many as about 3,400 people (4%) in the group could statistically be expected to have an especially high vulnerability to QT prolongation because of genetic variants they might carry that collectively have roughly this prevalence. In some people of African heritage, the prevalence of genetic risk for excessive QTc lengthening can be even higher, approaching about 10%, noted Dr. Wilde.
Dr. Gollob hoped the concerns he raised will prompt the organizers of many of these studies to revise their design, and he said he already knew of one study based in Toronto that recently added an ECG-monitoring strategy in response to the concerns he raised. He expressed optimism that more studies will follow.
“It’s a real issue to have these trials designed without ECG exclusions or monitoring. I’m glad that Dr. Gollob sent this warning, because he is right. ECG monitoring during treatment is important so you can stop the treatment in time,” Dr. Wilde said. Dr. Wilde also noted that many, if not most, of the studies listed on clinicaltrials.gov may not actually launch.
In April, representatives from several cardiology societies coauthored a document of considerations when using hydroxychloroquine, chloroquine, or azithromycin to treat patients with a diagnosed COVID-19 infection, and highlighted a QTc interval of 500 msec or greater as flagging patients who should no longer receive these drugs (J Am Coll Cardiol. 2020 Apr 10. doi: 10.1016/j.jacc.2020.04.016). For patients who do not yet have COVID-19 disease and the goal from treatment is prevention the potential efficacy of these drugs is reasonable to explore, but “does not exclude the need to minimize risk to research participants, especially when enrolling healthy subjects,” Dr. Gollob said.
Dr. Gollob, Dr. Viskin, and Dr. Wilde had no relevant financial disclosures.
REPORTING FROM JACC
COVID-19: Telehealth at the forefront of the pandemic
On Jan. 20, 2020, the first confirmed case of the 2019 novel coronavirus in the United States was admitted to Providence Regional Medical Center in Everett, Wash. Less than 3 months later, the COVID-19 pandemic has put enormous stress on the U.S. health care system, which is confronting acute resource shortage because of the surge of acute and critically ill patients, health care provider safety and burnout, and an ongoing need for managing vulnerable populations while minimizing the infection spread.

With the onset of these unprecedented challenges, telehealth has emerged as a powerful new resource for health care providers, hospitals, and health care systems across the country. This article offers a summary of government regulations that enabled telehealth expansion, and provides an overview of how two health care organizations, Providence St. Joseph Health and Sound Physicians, are employing telehealth services to combat the COVID-19 health care crisis.
The government response: Telehealth expansion
In response to the pandemic, the Centers for Medicare and Medicaid Services (CMS) have significantly increased access to telehealth services for Medicare and Medicaid beneficiaries. CMS swiftly put measures in place such as:
- Expanding telehealth beyond rural areas.
- Adding 80 services that can be provided in all settings, including patient homes
- Allowing providers to bill for telehealth visits at the same rate as in-person visits.
The U.S. Department of Health and Human Services also aided this effort by:
- Waiving requirements that physicians or other health care professionals must have licenses in the state in which they provide services, if they have an equivalent license from another state.
- Waving penalties for HIPAA violations against health care providers that serve patients in good faith through everyday communications technologies, such as FaceTime or Skype
Without prior regulatory and reimbursement restrictions, telehealth rapidly became a powerful tool in helping to solve some of the problems brought about by the COVID-19 pandemic.
Providence Telehealth for COVID-19

Providence St. Joseph Health is a not-for-profit health care system operating 51 hospitals and 1,085 clinics across Alaska, California, Montana, New Mexico, Oregon, Texas, and Washington. Providence has developed an enterprise telemedicine network with more than 100 virtual programs. Several of these services – including Telestroke, Telepsychiatry, TeleICU, and Telehospitalist – have been scaled across several states as a clinical cloud. More than 400 telemedicine endpoints are deployed, such as robotic carts and fixed InTouch TVs. In fact, the first U.S. COVID-19 patient was treated at Providence Regional Medical Center in Everett, Wash., using the telemedical robot Vici from InTouch Health.
According to Todd Czartoski, MD, chief medical technology officer at Providence, “while telehealth has been around for many years, COVID-19 opened a lot of people’s eyes to the value of virtual care delivery.”
Providence’s telehealth response to COVID-19 has encompassed five main areas: COVID-19 home care, COVID-19 acute care, ambulatory virtual visits, behavioral health concierge (BHC) expansion, and additional support for outside partnerships.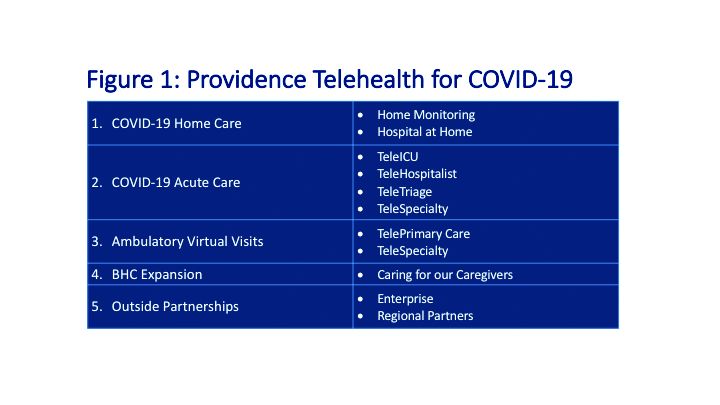
COVID-19 Home Care
Providence rapidly deployed home monitoring for nearly 2,000 positive or presumptive COVID-19 patients. Those symptomatic, clinically stable patients are given a thermometer and a pulse oximeter, and are monitored from home by a central team of nurses and physicians using the Xealth and Twistle programs.
Providence is evaluating expansion of home monitoring to other diagnoses, including higher acuity conditions.
COVID-19 Acute Care
TeleTriage expedites the triage of suspected COVID-19 patients and reduces the use of personal protective equipment (PPE) by 50% per patient per day. To date, TeleTriage has resulted in the conservation of more than 90,000 PPE units.
TeleHospitalist services expanded from traditional night coverage to caring for patients in COVID-19 units around the clock. Currently, there are 25 telehospitalists who practice both in-person and virtual medicine.
TeleICU offers remote management of more than 180 ICU beds across 17 hospitals from two central command centers in Washington state and Alaska. The services include night-time intensivist and ICU nurse coverage, including medication and ventilator management, and family conferences. COVID-19 increased the demand for TeleICU, with anticipated expansion to more than 300 beds.
Core TeleSpecialty services include TeleStroke and TelePsychiatry across 135 remote sites.
Ambulatory Virtual Visits
Providence launched the COVID-19 hub microsite to help educate patients by providing accurate and timely information. A chatbot named Grace helps screen patients who are worried about COVID-19. Grace also suggests next steps, such as a video visit with a patient’s primary care provider or a visit using Express Care/Virtual team, a direct-to-consumer service available to patients within and outside of the health care system.
In less than 2 weeks, Providence enabled virtual visits for more than 7,000 outpatient providers, with more than 14,000 alternative visits now occurring daily. This has allowed primary and specialty providers to continue to manage their patient panels remotely. The number of Express Care/Virtual visits increased from 60 to more than 1,000 per day.
BHC Expansion
In the effort to improve care for its caregivers, Providence launched a behavioral health concierge (BHC) service that offers employees and their dependents virtual access to licensed mental health professionals. Over the last half of 2019, BHC provided more than 1,000 phone and virtual visits, depending on the individual preference of patients. Notably, 21% percent of users were physicians; 65% of users were seen the same day and 100% of users were seen within 48 hours.
COVID-19 increased demand for services that initially started in Seattle and rapidly expanded to Montana, Oregon, and California.
Outside Partnerships
Providence has established partnerships with outside facilities by providing services to 135 sites across eight states. COVID-19 accelerated the employment of new services, including TeleICU.
Telemedicine at Sound Physicians
Sound Physicians is a national physician-founded and -led organization that provides emergency medicine, critical care, hospital medicine, population health, and physician advisory services. Five years ago, Sound launched a telemedicine service line. I spoke with Brian Carpenter, MD, national medical director for TeleHospitalist Services at Sound, to learn about his experience implementing Telehospitalist programs across 22 hospitals and 22 skilled nursing facilities.

Prior to COVID-19, Sound offered a spectrum of telemedicine services including night-time telephonic cross coverage, as well as video-assisted admissions, transfers, and rapid responses. In 2019, Sound Telehospitalists received 88,000 connect requests, including 6,400 video-assisted new admissions and 82 rapid responses. Typically, one physician covers four to eight hospitals with back-up available for surges. The team uses a predictive model for staffing and developed an acuity-based algorithm to ensure that patients in distress are evaluated immediately, new stable admissions on average are seen within 12 minutes, and order clarifications are provided within 30 minutes.
The COVID-19 pandemic created an urgent demand for providers to support an overwhelmed health care system. Without the traditional barriers to implementation – such as lack of acceptance by medical staff, nurses and patients, strict state licensing and technology requirements, lack of reimbursement, and delays in hospital credentialing – Sound was able to develop a rapid implementation model for telemedicine services. Currently, four new hospitals are in the active implementation phase, with 40 more hospitals in the pipeline.
Implementing a telemedicine program at your hospital
In order to successfully launch a telemedicine program, Dr. Carpenter outlined the following critical implementation steps:
- In collaboration with local leadership, define the problem you are trying to solve, which helps inform the scope of the telemedicine practice and technology requirements (for example, night-time cross-coverage vs. full telemedicine service).
- Complete a discovery process (for example, existing workflow for patient admission and transfer) with the end-goal of developing a workflow and rules of engagement.
- Obtain hospital credentialing/privileges and EMR access.
- Train end-users, including physicians and nurse telepresenters.
Dr. Carpenter offered this advice to those considering a telemedicine program: “Telemedicine is not just about technology; a true telemedicine program encompasses change management, workflow development, end-user training, compliance, and mechanisms for continuous process improvement. We want to make things better for the physicians, nurses, and patients.”
Telehealth is offering support to health care providers on the front lines, patients in need of care, and health care systems managing the unprecedented surges in volume.
Dr. Farah is a hospitalist, physician adviser, and Lean Six Sigma Black Belt. She is a performance improvement consultant based in Corvallis, Ore., and a member of The Hospitalist’s editorial advisory board.
On Jan. 20, 2020, the first confirmed case of the 2019 novel coronavirus in the United States was admitted to Providence Regional Medical Center in Everett, Wash. Less than 3 months later, the COVID-19 pandemic has put enormous stress on the U.S. health care system, which is confronting acute resource shortage because of the surge of acute and critically ill patients, health care provider safety and burnout, and an ongoing need for managing vulnerable populations while minimizing the infection spread.
With the onset of these unprecedented challenges, telehealth has emerged as a powerful new resource for health care providers, hospitals, and health care systems across the country. This article offers a summary of government regulations that enabled telehealth expansion, and provides an overview of how two health care organizations, Providence St. Joseph Health and Sound Physicians, are employing telehealth services to combat the COVID-19 health care crisis.
The government response: Telehealth expansion
In response to the pandemic, the Centers for Medicare and Medicaid Services (CMS) have significantly increased access to telehealth services for Medicare and Medicaid beneficiaries. CMS swiftly put measures in place such as:
- Expanding telehealth beyond rural areas.
- Adding 80 services that can be provided in all settings, including patient homes
- Allowing providers to bill for telehealth visits at the same rate as in-person visits.
The U.S. Department of Health and Human Services also aided this effort by:
- Waiving requirements that physicians or other health care professionals must have licenses in the state in which they provide services, if they have an equivalent license from another state.
- Waving penalties for HIPAA violations against health care providers that serve patients in good faith through everyday communications technologies, such as FaceTime or Skype
Without prior regulatory and reimbursement restrictions, telehealth rapidly became a powerful tool in helping to solve some of the problems brought about by the COVID-19 pandemic.
Providence Telehealth for COVID-19
Providence St. Joseph Health is a not-for-profit health care system operating 51 hospitals and 1,085 clinics across Alaska, California, Montana, New Mexico, Oregon, Texas, and Washington. Providence has developed an enterprise telemedicine network with more than 100 virtual programs. Several of these services – including Telestroke, Telepsychiatry, TeleICU, and Telehospitalist – have been scaled across several states as a clinical cloud. More than 400 telemedicine endpoints are deployed, such as robotic carts and fixed InTouch TVs. In fact, the first U.S. COVID-19 patient was treated at Providence Regional Medical Center in Everett, Wash., using the telemedical robot Vici from InTouch Health.
According to Todd Czartoski, MD, chief medical technology officer at Providence, “while telehealth has been around for many years, COVID-19 opened a lot of people’s eyes to the value of virtual care delivery.”
Providence’s telehealth response to COVID-19 has encompassed five main areas: COVID-19 home care, COVID-19 acute care, ambulatory virtual visits, behavioral health concierge (BHC) expansion, and additional support for outside partnerships.
COVID-19 Home Care
Providence rapidly deployed home monitoring for nearly 2,000 positive or presumptive COVID-19 patients. Those symptomatic, clinically stable patients are given a thermometer and a pulse oximeter, and are monitored from home by a central team of nurses and physicians using the Xealth and Twistle programs.
Providence is evaluating expansion of home monitoring to other diagnoses, including higher acuity conditions.
COVID-19 Acute Care
TeleTriage expedites the triage of suspected COVID-19 patients and reduces the use of personal protective equipment (PPE) by 50% per patient per day. To date, TeleTriage has resulted in the conservation of more than 90,000 PPE units.
TeleHospitalist services expanded from traditional night coverage to caring for patients in COVID-19 units around the clock. Currently, there are 25 telehospitalists who practice both in-person and virtual medicine.
TeleICU offers remote management of more than 180 ICU beds across 17 hospitals from two central command centers in Washington state and Alaska. The services include night-time intensivist and ICU nurse coverage, including medication and ventilator management, and family conferences. COVID-19 increased the demand for TeleICU, with anticipated expansion to more than 300 beds.
Core TeleSpecialty services include TeleStroke and TelePsychiatry across 135 remote sites.
Ambulatory Virtual Visits
Providence launched the COVID-19 hub microsite to help educate patients by providing accurate and timely information. A chatbot named Grace helps screen patients who are worried about COVID-19. Grace also suggests next steps, such as a video visit with a patient’s primary care provider or a visit using Express Care/Virtual team, a direct-to-consumer service available to patients within and outside of the health care system.
In less than 2 weeks, Providence enabled virtual visits for more than 7,000 outpatient providers, with more than 14,000 alternative visits now occurring daily. This has allowed primary and specialty providers to continue to manage their patient panels remotely. The number of Express Care/Virtual visits increased from 60 to more than 1,000 per day.
BHC Expansion
In the effort to improve care for its caregivers, Providence launched a behavioral health concierge (BHC) service that offers employees and their dependents virtual access to licensed mental health professionals. Over the last half of 2019, BHC provided more than 1,000 phone and virtual visits, depending on the individual preference of patients. Notably, 21% percent of users were physicians; 65% of users were seen the same day and 100% of users were seen within 48 hours.
COVID-19 increased demand for services that initially started in Seattle and rapidly expanded to Montana, Oregon, and California.
Outside Partnerships
Providence has established partnerships with outside facilities by providing services to 135 sites across eight states. COVID-19 accelerated the employment of new services, including TeleICU.
Telemedicine at Sound Physicians
Sound Physicians is a national physician-founded and -led organization that provides emergency medicine, critical care, hospital medicine, population health, and physician advisory services. Five years ago, Sound launched a telemedicine service line. I spoke with Brian Carpenter, MD, national medical director for TeleHospitalist Services at Sound, to learn about his experience implementing Telehospitalist programs across 22 hospitals and 22 skilled nursing facilities.
Prior to COVID-19, Sound offered a spectrum of telemedicine services including night-time telephonic cross coverage, as well as video-assisted admissions, transfers, and rapid responses. In 2019, Sound Telehospitalists received 88,000 connect requests, including 6,400 video-assisted new admissions and 82 rapid responses. Typically, one physician covers four to eight hospitals with back-up available for surges. The team uses a predictive model for staffing and developed an acuity-based algorithm to ensure that patients in distress are evaluated immediately, new stable admissions on average are seen within 12 minutes, and order clarifications are provided within 30 minutes.
The COVID-19 pandemic created an urgent demand for providers to support an overwhelmed health care system. Without the traditional barriers to implementation – such as lack of acceptance by medical staff, nurses and patients, strict state licensing and technology requirements, lack of reimbursement, and delays in hospital credentialing – Sound was able to develop a rapid implementation model for telemedicine services. Currently, four new hospitals are in the active implementation phase, with 40 more hospitals in the pipeline.
Implementing a telemedicine program at your hospital
In order to successfully launch a telemedicine program, Dr. Carpenter outlined the following critical implementation steps:
- In collaboration with local leadership, define the problem you are trying to solve, which helps inform the scope of the telemedicine practice and technology requirements (for example, night-time cross-coverage vs. full telemedicine service).
- Complete a discovery process (for example, existing workflow for patient admission and transfer) with the end-goal of developing a workflow and rules of engagement.
- Obtain hospital credentialing/privileges and EMR access.
- Train end-users, including physicians and nurse telepresenters.
Dr. Carpenter offered this advice to those considering a telemedicine program: “Telemedicine is not just about technology; a true telemedicine program encompasses change management, workflow development, end-user training, compliance, and mechanisms for continuous process improvement. We want to make things better for the physicians, nurses, and patients.”
Telehealth is offering support to health care providers on the front lines, patients in need of care, and health care systems managing the unprecedented surges in volume.
Dr. Farah is a hospitalist, physician adviser, and Lean Six Sigma Black Belt. She is a performance improvement consultant based in Corvallis, Ore., and a member of The Hospitalist’s editorial advisory board.
On Jan. 20, 2020, the first confirmed case of the 2019 novel coronavirus in the United States was admitted to Providence Regional Medical Center in Everett, Wash. Less than 3 months later, the COVID-19 pandemic has put enormous stress on the U.S. health care system, which is confronting acute resource shortage because of the surge of acute and critically ill patients, health care provider safety and burnout, and an ongoing need for managing vulnerable populations while minimizing the infection spread.
With the onset of these unprecedented challenges, telehealth has emerged as a powerful new resource for health care providers, hospitals, and health care systems across the country. This article offers a summary of government regulations that enabled telehealth expansion, and provides an overview of how two health care organizations, Providence St. Joseph Health and Sound Physicians, are employing telehealth services to combat the COVID-19 health care crisis.
The government response: Telehealth expansion
In response to the pandemic, the Centers for Medicare and Medicaid Services (CMS) have significantly increased access to telehealth services for Medicare and Medicaid beneficiaries. CMS swiftly put measures in place such as:
- Expanding telehealth beyond rural areas.
- Adding 80 services that can be provided in all settings, including patient homes
- Allowing providers to bill for telehealth visits at the same rate as in-person visits.
The U.S. Department of Health and Human Services also aided this effort by:
- Waiving requirements that physicians or other health care professionals must have licenses in the state in which they provide services, if they have an equivalent license from another state.
- Waving penalties for HIPAA violations against health care providers that serve patients in good faith through everyday communications technologies, such as FaceTime or Skype
Without prior regulatory and reimbursement restrictions, telehealth rapidly became a powerful tool in helping to solve some of the problems brought about by the COVID-19 pandemic.
Providence Telehealth for COVID-19
Providence St. Joseph Health is a not-for-profit health care system operating 51 hospitals and 1,085 clinics across Alaska, California, Montana, New Mexico, Oregon, Texas, and Washington. Providence has developed an enterprise telemedicine network with more than 100 virtual programs. Several of these services – including Telestroke, Telepsychiatry, TeleICU, and Telehospitalist – have been scaled across several states as a clinical cloud. More than 400 telemedicine endpoints are deployed, such as robotic carts and fixed InTouch TVs. In fact, the first U.S. COVID-19 patient was treated at Providence Regional Medical Center in Everett, Wash., using the telemedical robot Vici from InTouch Health.
According to Todd Czartoski, MD, chief medical technology officer at Providence, “while telehealth has been around for many years, COVID-19 opened a lot of people’s eyes to the value of virtual care delivery.”
Providence’s telehealth response to COVID-19 has encompassed five main areas: COVID-19 home care, COVID-19 acute care, ambulatory virtual visits, behavioral health concierge (BHC) expansion, and additional support for outside partnerships.
COVID-19 Home Care
Providence rapidly deployed home monitoring for nearly 2,000 positive or presumptive COVID-19 patients. Those symptomatic, clinically stable patients are given a thermometer and a pulse oximeter, and are monitored from home by a central team of nurses and physicians using the Xealth and Twistle programs.
Providence is evaluating expansion of home monitoring to other diagnoses, including higher acuity conditions.
COVID-19 Acute Care
TeleTriage expedites the triage of suspected COVID-19 patients and reduces the use of personal protective equipment (PPE) by 50% per patient per day. To date, TeleTriage has resulted in the conservation of more than 90,000 PPE units.
TeleHospitalist services expanded from traditional night coverage to caring for patients in COVID-19 units around the clock. Currently, there are 25 telehospitalists who practice both in-person and virtual medicine.
TeleICU offers remote management of more than 180 ICU beds across 17 hospitals from two central command centers in Washington state and Alaska. The services include night-time intensivist and ICU nurse coverage, including medication and ventilator management, and family conferences. COVID-19 increased the demand for TeleICU, with anticipated expansion to more than 300 beds.
Core TeleSpecialty services include TeleStroke and TelePsychiatry across 135 remote sites.
Ambulatory Virtual Visits
Providence launched the COVID-19 hub microsite to help educate patients by providing accurate and timely information. A chatbot named Grace helps screen patients who are worried about COVID-19. Grace also suggests next steps, such as a video visit with a patient’s primary care provider or a visit using Express Care/Virtual team, a direct-to-consumer service available to patients within and outside of the health care system.
In less than 2 weeks, Providence enabled virtual visits for more than 7,000 outpatient providers, with more than 14,000 alternative visits now occurring daily. This has allowed primary and specialty providers to continue to manage their patient panels remotely. The number of Express Care/Virtual visits increased from 60 to more than 1,000 per day.
BHC Expansion
In the effort to improve care for its caregivers, Providence launched a behavioral health concierge (BHC) service that offers employees and their dependents virtual access to licensed mental health professionals. Over the last half of 2019, BHC provided more than 1,000 phone and virtual visits, depending on the individual preference of patients. Notably, 21% percent of users were physicians; 65% of users were seen the same day and 100% of users were seen within 48 hours.
COVID-19 increased demand for services that initially started in Seattle and rapidly expanded to Montana, Oregon, and California.
Outside Partnerships
Providence has established partnerships with outside facilities by providing services to 135 sites across eight states. COVID-19 accelerated the employment of new services, including TeleICU.
Telemedicine at Sound Physicians
Sound Physicians is a national physician-founded and -led organization that provides emergency medicine, critical care, hospital medicine, population health, and physician advisory services. Five years ago, Sound launched a telemedicine service line. I spoke with Brian Carpenter, MD, national medical director for TeleHospitalist Services at Sound, to learn about his experience implementing Telehospitalist programs across 22 hospitals and 22 skilled nursing facilities.
Prior to COVID-19, Sound offered a spectrum of telemedicine services including night-time telephonic cross coverage, as well as video-assisted admissions, transfers, and rapid responses. In 2019, Sound Telehospitalists received 88,000 connect requests, including 6,400 video-assisted new admissions and 82 rapid responses. Typically, one physician covers four to eight hospitals with back-up available for surges. The team uses a predictive model for staffing and developed an acuity-based algorithm to ensure that patients in distress are evaluated immediately, new stable admissions on average are seen within 12 minutes, and order clarifications are provided within 30 minutes.
The COVID-19 pandemic created an urgent demand for providers to support an overwhelmed health care system. Without the traditional barriers to implementation – such as lack of acceptance by medical staff, nurses and patients, strict state licensing and technology requirements, lack of reimbursement, and delays in hospital credentialing – Sound was able to develop a rapid implementation model for telemedicine services. Currently, four new hospitals are in the active implementation phase, with 40 more hospitals in the pipeline.
Implementing a telemedicine program at your hospital
In order to successfully launch a telemedicine program, Dr. Carpenter outlined the following critical implementation steps:
- In collaboration with local leadership, define the problem you are trying to solve, which helps inform the scope of the telemedicine practice and technology requirements (for example, night-time cross-coverage vs. full telemedicine service).
- Complete a discovery process (for example, existing workflow for patient admission and transfer) with the end-goal of developing a workflow and rules of engagement.
- Obtain hospital credentialing/privileges and EMR access.
- Train end-users, including physicians and nurse telepresenters.
Dr. Carpenter offered this advice to those considering a telemedicine program: “Telemedicine is not just about technology; a true telemedicine program encompasses change management, workflow development, end-user training, compliance, and mechanisms for continuous process improvement. We want to make things better for the physicians, nurses, and patients.”
Telehealth is offering support to health care providers on the front lines, patients in need of care, and health care systems managing the unprecedented surges in volume.
Dr. Farah is a hospitalist, physician adviser, and Lean Six Sigma Black Belt. She is a performance improvement consultant based in Corvallis, Ore., and a member of The Hospitalist’s editorial advisory board.
COVID-19: “You’re gonna need a bigger boat”
Every family physician has experienced the onset of a bad flu season, when suddenly the phone starts ringing off the hook. As the family medicine lead physician for Cleveland Clinic Express Care Online (ECO)—specifically its on-demand virtual visit platform—I have been performing virtual visits as part of a small team of physicians and nurse practitioners for 5 years, and was capably seeing 5 to 15 patients in an afternoon across the 18 states in which I am licensed. Until recently, our Distance Health team collectively would perform between 3000 and 4000 virtual visits per month.
On Saturday, March 14, 2020, we had the virtual visit equivalent of the phone ringing off the hook—to the point of breaking the phone. The ECO Medical Director, Matthew Faiman, MD, texted me to ask if I would be willing to sign on to the platform for a bit to help out with high volume—and whoosh, just by signing on, I had 20 patients waiting in the queue, with hundreds more trying to get a visit, all related to COVID-19. And patients who would normally leave a line if the wait time was more than 5 minutes were willing to stay online for more than 3 hours, if necessary, to consult with a provider.
After handling in excess of 38 patients that afternoon (some of whom were unfortunately dropped by the platform, which was overwhelmed by sheer volume), I did my best impression of Roy Scheider in Jaws: I emailed Matt, “You’re gonna need a bigger boat.”
How we got a bigger boat
As an early pioneer in telemedicine, Cleveland Clinic was well suited to quickly ramp up its use of virtual visits (both synchronous ECO visits, which occur in real time, and asynchronous e-Visits, in which the patient provides information via images, video, audio, or text file, to be evaluated and responded to by the provider within a specified timeframe). Even with a robust existing infrastructure, however, we faced challenges that necessitated a dynamic response.
The first step was to increase available personnel. Cleveland Clinic leadership immediately put out a call for volunteers to sign on to the on-demand platform, and more than 200 primary care physicians and advanced practice providers responded. We also dedicated an additional 30 full-time nurse practitioners to our ECO team of physicians, nurse practitioners, and physician assistants.
Daily live online training sessions were launched to walk staff through how to set up and conduct a virtual visit. As we navigated the day-to-day reality of increased virtual visits, our accumulated experience informed the development of what we refer to as a “distance health playbook.” This single repository of information is accessible to all caregivers, and we also created a digital pocket card containing the most pertinent information from the playbook and automatically pushed it to all Cleveland Clinic–issued iPhones. Providers literally have what they need at their fingertips, no matter where they are when they “see” a patient.
The full playbook outlines how to adopt and ramp up telemedicine services. This includes details on clinician training, scheduling visits, coding for services provided during a telemedicine visit, and demonstrating empathy from a distance. There are also patient-facing resources on how to access various digital platforms, which may be handy for less tech-savvy patients. For example, if your patient does not already have FaceTime or Skype installed on his phone, or is not familiar with the use of such programs, the playbook includes specific instructions (with screencaps) that you can share.
Continue to: While initially available...
While initially available only to Cleveland Clinic staff, the Cleveland Clinic Response to COVID-19 Digital Health Playbook is now accessible to the medical community at large via the Cleveland Clinic Web site (learn more at https://consultqd.clevelandclinic.org/cleveland-clinics-digital-health-playbook/) and a link from the US Department of Health and Human Services Web site.
What we accomplished
Within 1 week, providers who previously had little experience conducting virtual visits were helping out like seasoned professionals, and we were able to reduce wait times back to pre-COVID-19 levels while performing 8000 virtual visits in a single week. Those who were less fluent with virtual visits contributed by assessing the queue to identify patients who would be well handled with a telephone encounter; this helped to successfully meet patients’ needs and alleviate the burden on the system.
The capacity to accommodate (more) remote visits became increasingly important when, as happened in many states, Ohio Governor Mike DeWine announced social-distancing measures and restriction of business in response to the growing surge of COVID-19 cases. This culminated in a stay-at-home order issued on March 22.
With care needs increasing, the early experience gained by our primary care teams was an invaluable asset as we transitioned patients who had upcoming in-person evaluation and management visits to virtual, phone, and e-Visits. Daily huddles were instituted to help with this process, and additional training materials and support tools were created and uploaded to an easily accessible online “toolkit.”
When the volume of video visits overwhelmed the ECO platform, upgrades were made to accommodate increased bandwidth and traffic. Permission was also granted to utilize FaceTime and Google Duo for visits, provided patients gave consent (and in accordance with HIPAA COVID-19 guidelines), when and if a disconnection occurred due to volume overloads.
Continue to: During the period from...
During the period from March 12 to March 24, more than 200 Cleveland Clinic primary care providers and APPs performed more than 54,000 digital and nontraditional encounters, serving more than 26,000 unique patients. By April 11, total outpatient visits at Cleveland Clinic had shifted from 2% remote (virtual or phone) to 75% remote.
What we learned
For medical practices currently grappling with telemedicine during the COVID-19 pandemic—many of whom may be starting from scratch as opposed to ramping up existing services—I offer the following “take-aways” from our recent experience:
Recognize that you are not alone in feeling overwhelmed in ramping up telemedicine. Our experience at Cleveland Clinic has shown that it only takes 5 to 10 virtual visits for most providers to gain comfort with the platforms.
Be innovative. There will be technical issues along the way; work with whatever platform is available: FaceTime, Google Duo, Doximity, Zoom, etc. The patient should be asked to consent to the use of these platforms.
Start with phone visits for patients who are technologically challenged.
Continue to: Utilize existing techniques when you can
Utilize existing techniques when you can. We are all developing our own innovative physical diagnosis techniques with video, but there are some evidence-based recommended techniques for use in special circumstances (eg, Ottawa ankle rules). Gaining familiarity with these and developing standard disease-specific documentation templates can be helpful.
Keep in mind that many systems were not designed to handle high volume, whether that means the platform itself or the workflow for providers. Problems require troubleshooting to determine whether the issue is related to the platform, user error, or design flaws, in order to provide the right solution in the right environment.
Even with our robust existing system, Cleveland Clinic required upgrades to accommodate the increased volume in virtual visits. By contrast, a physician in private practice may have purchased access to an entry-level system that was designed to work for occasional use but when asked to perform outside its design, simply cannot meet the needs of its client. Furthermore, small practices do not have an IT department on hand to address technical issues. This is why I would advise my family medicine colleagues to deal with the present need with a present solution: FaceTime, Google Duo, Zoom, and Doximity are low-cost options to get your feet wet if you have no prior experience with virtual visits.
As you get a better handle on your needs and capabilities, you will be better able to prepare for your future practice needs, including a more robust and HIPAA-compliant virtual visit platform. You will have built yourself that “bigger boat.”

Cleveland Clinic, Chagrin Falls, Ohio; Department of Family Medicine, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University
The author reported no potential conflict of interest relevant to this article.
Cleveland Clinic, Chagrin Falls, Ohio; Department of Family Medicine, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University
The author reported no potential conflict of interest relevant to this article.
Cleveland Clinic, Chagrin Falls, Ohio; Department of Family Medicine, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University
The author reported no potential conflict of interest relevant to this article.
Every family physician has experienced the onset of a bad flu season, when suddenly the phone starts ringing off the hook. As the family medicine lead physician for Cleveland Clinic Express Care Online (ECO)—specifically its on-demand virtual visit platform—I have been performing virtual visits as part of a small team of physicians and nurse practitioners for 5 years, and was capably seeing 5 to 15 patients in an afternoon across the 18 states in which I am licensed. Until recently, our Distance Health team collectively would perform between 3000 and 4000 virtual visits per month.
On Saturday, March 14, 2020, we had the virtual visit equivalent of the phone ringing off the hook—to the point of breaking the phone. The ECO Medical Director, Matthew Faiman, MD, texted me to ask if I would be willing to sign on to the platform for a bit to help out with high volume—and whoosh, just by signing on, I had 20 patients waiting in the queue, with hundreds more trying to get a visit, all related to COVID-19. And patients who would normally leave a line if the wait time was more than 5 minutes were willing to stay online for more than 3 hours, if necessary, to consult with a provider.
After handling in excess of 38 patients that afternoon (some of whom were unfortunately dropped by the platform, which was overwhelmed by sheer volume), I did my best impression of Roy Scheider in Jaws: I emailed Matt, “You’re gonna need a bigger boat.”
How we got a bigger boat
As an early pioneer in telemedicine, Cleveland Clinic was well suited to quickly ramp up its use of virtual visits (both synchronous ECO visits, which occur in real time, and asynchronous e-Visits, in which the patient provides information via images, video, audio, or text file, to be evaluated and responded to by the provider within a specified timeframe). Even with a robust existing infrastructure, however, we faced challenges that necessitated a dynamic response.
The first step was to increase available personnel. Cleveland Clinic leadership immediately put out a call for volunteers to sign on to the on-demand platform, and more than 200 primary care physicians and advanced practice providers responded. We also dedicated an additional 30 full-time nurse practitioners to our ECO team of physicians, nurse practitioners, and physician assistants.
Daily live online training sessions were launched to walk staff through how to set up and conduct a virtual visit. As we navigated the day-to-day reality of increased virtual visits, our accumulated experience informed the development of what we refer to as a “distance health playbook.” This single repository of information is accessible to all caregivers, and we also created a digital pocket card containing the most pertinent information from the playbook and automatically pushed it to all Cleveland Clinic–issued iPhones. Providers literally have what they need at their fingertips, no matter where they are when they “see” a patient.
The full playbook outlines how to adopt and ramp up telemedicine services. This includes details on clinician training, scheduling visits, coding for services provided during a telemedicine visit, and demonstrating empathy from a distance. There are also patient-facing resources on how to access various digital platforms, which may be handy for less tech-savvy patients. For example, if your patient does not already have FaceTime or Skype installed on his phone, or is not familiar with the use of such programs, the playbook includes specific instructions (with screencaps) that you can share.
Continue to: While initially available...
While initially available only to Cleveland Clinic staff, the Cleveland Clinic Response to COVID-19 Digital Health Playbook is now accessible to the medical community at large via the Cleveland Clinic Web site (learn more at https://consultqd.clevelandclinic.org/cleveland-clinics-digital-health-playbook/) and a link from the US Department of Health and Human Services Web site.
What we accomplished
Within 1 week, providers who previously had little experience conducting virtual visits were helping out like seasoned professionals, and we were able to reduce wait times back to pre-COVID-19 levels while performing 8000 virtual visits in a single week. Those who were less fluent with virtual visits contributed by assessing the queue to identify patients who would be well handled with a telephone encounter; this helped to successfully meet patients’ needs and alleviate the burden on the system.
The capacity to accommodate (more) remote visits became increasingly important when, as happened in many states, Ohio Governor Mike DeWine announced social-distancing measures and restriction of business in response to the growing surge of COVID-19 cases. This culminated in a stay-at-home order issued on March 22.
With care needs increasing, the early experience gained by our primary care teams was an invaluable asset as we transitioned patients who had upcoming in-person evaluation and management visits to virtual, phone, and e-Visits. Daily huddles were instituted to help with this process, and additional training materials and support tools were created and uploaded to an easily accessible online “toolkit.”
When the volume of video visits overwhelmed the ECO platform, upgrades were made to accommodate increased bandwidth and traffic. Permission was also granted to utilize FaceTime and Google Duo for visits, provided patients gave consent (and in accordance with HIPAA COVID-19 guidelines), when and if a disconnection occurred due to volume overloads.
Continue to: During the period from...
During the period from March 12 to March 24, more than 200 Cleveland Clinic primary care providers and APPs performed more than 54,000 digital and nontraditional encounters, serving more than 26,000 unique patients. By April 11, total outpatient visits at Cleveland Clinic had shifted from 2% remote (virtual or phone) to 75% remote.
What we learned
For medical practices currently grappling with telemedicine during the COVID-19 pandemic—many of whom may be starting from scratch as opposed to ramping up existing services—I offer the following “take-aways” from our recent experience:
Recognize that you are not alone in feeling overwhelmed in ramping up telemedicine. Our experience at Cleveland Clinic has shown that it only takes 5 to 10 virtual visits for most providers to gain comfort with the platforms.
Be innovative. There will be technical issues along the way; work with whatever platform is available: FaceTime, Google Duo, Doximity, Zoom, etc. The patient should be asked to consent to the use of these platforms.
Start with phone visits for patients who are technologically challenged.
Continue to: Utilize existing techniques when you can
Utilize existing techniques when you can. We are all developing our own innovative physical diagnosis techniques with video, but there are some evidence-based recommended techniques for use in special circumstances (eg, Ottawa ankle rules). Gaining familiarity with these and developing standard disease-specific documentation templates can be helpful.
Keep in mind that many systems were not designed to handle high volume, whether that means the platform itself or the workflow for providers. Problems require troubleshooting to determine whether the issue is related to the platform, user error, or design flaws, in order to provide the right solution in the right environment.
Even with our robust existing system, Cleveland Clinic required upgrades to accommodate the increased volume in virtual visits. By contrast, a physician in private practice may have purchased access to an entry-level system that was designed to work for occasional use but when asked to perform outside its design, simply cannot meet the needs of its client. Furthermore, small practices do not have an IT department on hand to address technical issues. This is why I would advise my family medicine colleagues to deal with the present need with a present solution: FaceTime, Google Duo, Zoom, and Doximity are low-cost options to get your feet wet if you have no prior experience with virtual visits.
As you get a better handle on your needs and capabilities, you will be better able to prepare for your future practice needs, including a more robust and HIPAA-compliant virtual visit platform. You will have built yourself that “bigger boat.”
Every family physician has experienced the onset of a bad flu season, when suddenly the phone starts ringing off the hook. As the family medicine lead physician for Cleveland Clinic Express Care Online (ECO)—specifically its on-demand virtual visit platform—I have been performing virtual visits as part of a small team of physicians and nurse practitioners for 5 years, and was capably seeing 5 to 15 patients in an afternoon across the 18 states in which I am licensed. Until recently, our Distance Health team collectively would perform between 3000 and 4000 virtual visits per month.
On Saturday, March 14, 2020, we had the virtual visit equivalent of the phone ringing off the hook—to the point of breaking the phone. The ECO Medical Director, Matthew Faiman, MD, texted me to ask if I would be willing to sign on to the platform for a bit to help out with high volume—and whoosh, just by signing on, I had 20 patients waiting in the queue, with hundreds more trying to get a visit, all related to COVID-19. And patients who would normally leave a line if the wait time was more than 5 minutes were willing to stay online for more than 3 hours, if necessary, to consult with a provider.
After handling in excess of 38 patients that afternoon (some of whom were unfortunately dropped by the platform, which was overwhelmed by sheer volume), I did my best impression of Roy Scheider in Jaws: I emailed Matt, “You’re gonna need a bigger boat.”
How we got a bigger boat
As an early pioneer in telemedicine, Cleveland Clinic was well suited to quickly ramp up its use of virtual visits (both synchronous ECO visits, which occur in real time, and asynchronous e-Visits, in which the patient provides information via images, video, audio, or text file, to be evaluated and responded to by the provider within a specified timeframe). Even with a robust existing infrastructure, however, we faced challenges that necessitated a dynamic response.
The first step was to increase available personnel. Cleveland Clinic leadership immediately put out a call for volunteers to sign on to the on-demand platform, and more than 200 primary care physicians and advanced practice providers responded. We also dedicated an additional 30 full-time nurse practitioners to our ECO team of physicians, nurse practitioners, and physician assistants.
Daily live online training sessions were launched to walk staff through how to set up and conduct a virtual visit. As we navigated the day-to-day reality of increased virtual visits, our accumulated experience informed the development of what we refer to as a “distance health playbook.” This single repository of information is accessible to all caregivers, and we also created a digital pocket card containing the most pertinent information from the playbook and automatically pushed it to all Cleveland Clinic–issued iPhones. Providers literally have what they need at their fingertips, no matter where they are when they “see” a patient.
The full playbook outlines how to adopt and ramp up telemedicine services. This includes details on clinician training, scheduling visits, coding for services provided during a telemedicine visit, and demonstrating empathy from a distance. There are also patient-facing resources on how to access various digital platforms, which may be handy for less tech-savvy patients. For example, if your patient does not already have FaceTime or Skype installed on his phone, or is not familiar with the use of such programs, the playbook includes specific instructions (with screencaps) that you can share.
Continue to: While initially available...
While initially available only to Cleveland Clinic staff, the Cleveland Clinic Response to COVID-19 Digital Health Playbook is now accessible to the medical community at large via the Cleveland Clinic Web site (learn more at https://consultqd.clevelandclinic.org/cleveland-clinics-digital-health-playbook/) and a link from the US Department of Health and Human Services Web site.
What we accomplished
Within 1 week, providers who previously had little experience conducting virtual visits were helping out like seasoned professionals, and we were able to reduce wait times back to pre-COVID-19 levels while performing 8000 virtual visits in a single week. Those who were less fluent with virtual visits contributed by assessing the queue to identify patients who would be well handled with a telephone encounter; this helped to successfully meet patients’ needs and alleviate the burden on the system.
The capacity to accommodate (more) remote visits became increasingly important when, as happened in many states, Ohio Governor Mike DeWine announced social-distancing measures and restriction of business in response to the growing surge of COVID-19 cases. This culminated in a stay-at-home order issued on March 22.
With care needs increasing, the early experience gained by our primary care teams was an invaluable asset as we transitioned patients who had upcoming in-person evaluation and management visits to virtual, phone, and e-Visits. Daily huddles were instituted to help with this process, and additional training materials and support tools were created and uploaded to an easily accessible online “toolkit.”
When the volume of video visits overwhelmed the ECO platform, upgrades were made to accommodate increased bandwidth and traffic. Permission was also granted to utilize FaceTime and Google Duo for visits, provided patients gave consent (and in accordance with HIPAA COVID-19 guidelines), when and if a disconnection occurred due to volume overloads.
Continue to: During the period from...
During the period from March 12 to March 24, more than 200 Cleveland Clinic primary care providers and APPs performed more than 54,000 digital and nontraditional encounters, serving more than 26,000 unique patients. By April 11, total outpatient visits at Cleveland Clinic had shifted from 2% remote (virtual or phone) to 75% remote.
What we learned
For medical practices currently grappling with telemedicine during the COVID-19 pandemic—many of whom may be starting from scratch as opposed to ramping up existing services—I offer the following “take-aways” from our recent experience:
Recognize that you are not alone in feeling overwhelmed in ramping up telemedicine. Our experience at Cleveland Clinic has shown that it only takes 5 to 10 virtual visits for most providers to gain comfort with the platforms.
Be innovative. There will be technical issues along the way; work with whatever platform is available: FaceTime, Google Duo, Doximity, Zoom, etc. The patient should be asked to consent to the use of these platforms.
Start with phone visits for patients who are technologically challenged.
Continue to: Utilize existing techniques when you can
Utilize existing techniques when you can. We are all developing our own innovative physical diagnosis techniques with video, but there are some evidence-based recommended techniques for use in special circumstances (eg, Ottawa ankle rules). Gaining familiarity with these and developing standard disease-specific documentation templates can be helpful.
Keep in mind that many systems were not designed to handle high volume, whether that means the platform itself or the workflow for providers. Problems require troubleshooting to determine whether the issue is related to the platform, user error, or design flaws, in order to provide the right solution in the right environment.
Even with our robust existing system, Cleveland Clinic required upgrades to accommodate the increased volume in virtual visits. By contrast, a physician in private practice may have purchased access to an entry-level system that was designed to work for occasional use but when asked to perform outside its design, simply cannot meet the needs of its client. Furthermore, small practices do not have an IT department on hand to address technical issues. This is why I would advise my family medicine colleagues to deal with the present need with a present solution: FaceTime, Google Duo, Zoom, and Doximity are low-cost options to get your feet wet if you have no prior experience with virtual visits.
As you get a better handle on your needs and capabilities, you will be better able to prepare for your future practice needs, including a more robust and HIPAA-compliant virtual visit platform. You will have built yourself that “bigger boat.”
Obesity can shift severe COVID-19 to younger age groups
published in The Lancet.
“By itself, obesity seems to be a sufficient risk factor to start seeing younger people landing in the ICU,” said the study’s lead author, David Kass, MD, a professor of cardiology and medicine at Johns Hopkins University School of Medicine in Baltimore, Maryland.
“In that sense, there’s a simple message: If you’re very, very overweight, don’t think that if you’re 35 you’re that much safer [from severe COVID-19] than your mother or grandparents or others in their 60s or 70s,” Kass told Medscape Medical News.
The findings, which Kass describes as a “2-week snapshot” of 265 patients (58% male) in late March and early April at a handful of university hospitals in the United States reinforces other recent research indicating that obesity is one of the biggest risk factors for severe COVID-19 disease, particularly among younger patients. In addition, a large British study showed that, after adjusting for comorbidities, obesity was a significant factor associated with in-hospital death in COVID-19.
But this new analysis stands out as the only dataset to date that specifically “asks the question relative to age” of whether severe COVID-19 disease correlates to ICU treatment, he said.
The mean age of his study population of ICU patients was 55, Kass said, “and that was young, not what we were expecting.”
“Even with the first 20 patients, we were already seeing younger people and they definitely were heavier, with plenty of patients with a BMI over 35 kg/m2,” he added. “The relationship was pretty tight, pretty quick.”
“Just don’t make the assumption that any of us are too young to be vulnerable if, in fact, this is an aspect of our bodies,” he said.
Steven Heymsfield, MD, past president and a spokesperson for the Obesity Society, agrees with Kass’ conclusions.
“One thing we’ve had on our minds is that the prototype of a person with this disease is older...but now if we get [a patient] who’s symptomatic and 40 and obese, we shouldn’t assume they have some other disease,” Heymsfield told Medscape Medical News.
“We should think of them as a susceptible population.”
Kass and colleagues agree. “Public messaging to younger adults, reducing the threshold for virus testing in obese individuals, and maintaining greater vigilance for this at-risk population should reduce the prevalence of severe COVID-19 disease [among those with obesity],” they state.
“I think it’s a mental adjustment from a health care standpoint, which might hopefully help target the folks who are at higher risk before they get into trouble,” Kass told Medscape Medical News.
Trio of mechanisms explain obesity’s extra COVID-19 risks
Kass and coauthors write that, in analyzing their data, they anticipated similar results to the largest study of 1591 ICU patients from Italy in which only 203 were younger than 51 years. Common comorbidities among those patients included hypertension, cardiovascular disease, and type 2 diabetes, with similar data reported from China.
When the COVID-19 epidemic accelerated in the United States, older age was also identified as a risk factor. Obesity had not yet been added to this list, Kass noted. But following informal discussions with colleagues in other ICUs around the country, he decided to investigate further as to whether it was an underappreciated risk factor.
Kass and colleagues did a quick evaluation of the link between BMI and age of patients with COVID-19 admitted to ICUs at Johns Hopkins, University of Cincinnati, New York University, University of Washington, Florida Health, and University of Pennsylvania.
The “significant inverse correlation between age and BMI” showed younger ICU patients were more likely to be obese, with no difference by gender.
Median BMI among study participants was 29.3 kg/m2, with only a quarter having a BMI lower than 26 kg/m2 and another 25% having a BMI higher than 34.7 kg/m2.
Kass acknowledged that it wasn’t possible with this simple dataset to account for any other potential confounders, but he told Medscape Medical News that, “while diabetes, cardiovascular disease, and hypertension, for example, can occur with obesity, this is generally less so in younger populations as it takes time for the other comorbidities to develop.”
He said several mechanisms could explain why obesity predisposes patients with COVID-19 to severe disease.
For one, obesity places extra pressure on the diaphragm while lying on the back, restricting breathing.
“Morbid obesity itself is sort of proinflammatory,” he continued.
“Here we’ve got a viral infection where the early reports suggest that cytokine storms and immune mishandling of the virus are why it’s so much more severe than other forms of coronavirus we’ve seen before. So if you have someone with an already underlying proinflammatory state, this could be a reason there’s higher risk.”
Additionally, the angiotensin-converting enzyme-2 (ACE-2) receptor to which the SARS-CoV-2 virus that causes COVID-19 attaches is expressed in higher amounts in adipose tissue than the lungs, Kass noted.
“This could turn into kind of a viral replication depot,” he explained. “You may well be brewing more virus as a component of obesity.”
Sensitivity needed in public messaging about risks, but test sooner
With an obesity rate of about 40% in the United States, the results are particularly relevant for Americans, Kass and Heymsfield say, noting that the country’s “obesity belt” runs through the South.
Heymsfield, who wasn’t part of the new analysis, notes that public messaging around severe COVID-19 risks to younger adults with obesity is “tricky,” especially because the virus is “still pretty common in nonobese people.”
Kass agrees, noting, “it’s difficult to turn to 40% of the population and say: ‘You guys have to watch it.’ ”
But the mounting research findings necessitate linking obesity with severe COVID-19 disease and perhaps testing patients in this category for the virus sooner before symptoms become severe.
And of note, since shortness of breath is common among people with obesity regardless of illness, similar COVID-19 symptoms might catch these individuals unaware, pointed out Heymsfield, who is also a professor in the Metabolism and Body Composition Lab at Pennington Biomedical Research Center at Louisiana State University, Baton Rouge.
“They may find themselves literally unable to breathe, and the concern would be that they wait much too long to come in” for treatment, he said. Typically, people can deteriorate between day 7 and 10 of the COVID-19 infection.
Individuals with obesity “need to be educated to recognize the serious complications of COVID-19 often appear suddenly, although the virus has sometimes been working its way through the body for a long time,” he concluded.
Kass and Heymsfield have declared no relevant financial relationships.
This article first appeared on Medscape.com.
published in The Lancet.
“By itself, obesity seems to be a sufficient risk factor to start seeing younger people landing in the ICU,” said the study’s lead author, David Kass, MD, a professor of cardiology and medicine at Johns Hopkins University School of Medicine in Baltimore, Maryland.
“In that sense, there’s a simple message: If you’re very, very overweight, don’t think that if you’re 35 you’re that much safer [from severe COVID-19] than your mother or grandparents or others in their 60s or 70s,” Kass told Medscape Medical News.
The findings, which Kass describes as a “2-week snapshot” of 265 patients (58% male) in late March and early April at a handful of university hospitals in the United States reinforces other recent research indicating that obesity is one of the biggest risk factors for severe COVID-19 disease, particularly among younger patients. In addition, a large British study showed that, after adjusting for comorbidities, obesity was a significant factor associated with in-hospital death in COVID-19.
But this new analysis stands out as the only dataset to date that specifically “asks the question relative to age” of whether severe COVID-19 disease correlates to ICU treatment, he said.
The mean age of his study population of ICU patients was 55, Kass said, “and that was young, not what we were expecting.”
“Even with the first 20 patients, we were already seeing younger people and they definitely were heavier, with plenty of patients with a BMI over 35 kg/m2,” he added. “The relationship was pretty tight, pretty quick.”
“Just don’t make the assumption that any of us are too young to be vulnerable if, in fact, this is an aspect of our bodies,” he said.
Steven Heymsfield, MD, past president and a spokesperson for the Obesity Society, agrees with Kass’ conclusions.
“One thing we’ve had on our minds is that the prototype of a person with this disease is older...but now if we get [a patient] who’s symptomatic and 40 and obese, we shouldn’t assume they have some other disease,” Heymsfield told Medscape Medical News.
“We should think of them as a susceptible population.”
Kass and colleagues agree. “Public messaging to younger adults, reducing the threshold for virus testing in obese individuals, and maintaining greater vigilance for this at-risk population should reduce the prevalence of severe COVID-19 disease [among those with obesity],” they state.
“I think it’s a mental adjustment from a health care standpoint, which might hopefully help target the folks who are at higher risk before they get into trouble,” Kass told Medscape Medical News.
Trio of mechanisms explain obesity’s extra COVID-19 risks
Kass and coauthors write that, in analyzing their data, they anticipated similar results to the largest study of 1591 ICU patients from Italy in which only 203 were younger than 51 years. Common comorbidities among those patients included hypertension, cardiovascular disease, and type 2 diabetes, with similar data reported from China.
When the COVID-19 epidemic accelerated in the United States, older age was also identified as a risk factor. Obesity had not yet been added to this list, Kass noted. But following informal discussions with colleagues in other ICUs around the country, he decided to investigate further as to whether it was an underappreciated risk factor.
Kass and colleagues did a quick evaluation of the link between BMI and age of patients with COVID-19 admitted to ICUs at Johns Hopkins, University of Cincinnati, New York University, University of Washington, Florida Health, and University of Pennsylvania.
The “significant inverse correlation between age and BMI” showed younger ICU patients were more likely to be obese, with no difference by gender.
Median BMI among study participants was 29.3 kg/m2, with only a quarter having a BMI lower than 26 kg/m2 and another 25% having a BMI higher than 34.7 kg/m2.
Kass acknowledged that it wasn’t possible with this simple dataset to account for any other potential confounders, but he told Medscape Medical News that, “while diabetes, cardiovascular disease, and hypertension, for example, can occur with obesity, this is generally less so in younger populations as it takes time for the other comorbidities to develop.”
He said several mechanisms could explain why obesity predisposes patients with COVID-19 to severe disease.
For one, obesity places extra pressure on the diaphragm while lying on the back, restricting breathing.
“Morbid obesity itself is sort of proinflammatory,” he continued.
“Here we’ve got a viral infection where the early reports suggest that cytokine storms and immune mishandling of the virus are why it’s so much more severe than other forms of coronavirus we’ve seen before. So if you have someone with an already underlying proinflammatory state, this could be a reason there’s higher risk.”
Additionally, the angiotensin-converting enzyme-2 (ACE-2) receptor to which the SARS-CoV-2 virus that causes COVID-19 attaches is expressed in higher amounts in adipose tissue than the lungs, Kass noted.
“This could turn into kind of a viral replication depot,” he explained. “You may well be brewing more virus as a component of obesity.”
Sensitivity needed in public messaging about risks, but test sooner
With an obesity rate of about 40% in the United States, the results are particularly relevant for Americans, Kass and Heymsfield say, noting that the country’s “obesity belt” runs through the South.
Heymsfield, who wasn’t part of the new analysis, notes that public messaging around severe COVID-19 risks to younger adults with obesity is “tricky,” especially because the virus is “still pretty common in nonobese people.”
Kass agrees, noting, “it’s difficult to turn to 40% of the population and say: ‘You guys have to watch it.’ ”
But the mounting research findings necessitate linking obesity with severe COVID-19 disease and perhaps testing patients in this category for the virus sooner before symptoms become severe.
And of note, since shortness of breath is common among people with obesity regardless of illness, similar COVID-19 symptoms might catch these individuals unaware, pointed out Heymsfield, who is also a professor in the Metabolism and Body Composition Lab at Pennington Biomedical Research Center at Louisiana State University, Baton Rouge.
“They may find themselves literally unable to breathe, and the concern would be that they wait much too long to come in” for treatment, he said. Typically, people can deteriorate between day 7 and 10 of the COVID-19 infection.
Individuals with obesity “need to be educated to recognize the serious complications of COVID-19 often appear suddenly, although the virus has sometimes been working its way through the body for a long time,” he concluded.
Kass and Heymsfield have declared no relevant financial relationships.
This article first appeared on Medscape.com.
published in The Lancet.
“By itself, obesity seems to be a sufficient risk factor to start seeing younger people landing in the ICU,” said the study’s lead author, David Kass, MD, a professor of cardiology and medicine at Johns Hopkins University School of Medicine in Baltimore, Maryland.
“In that sense, there’s a simple message: If you’re very, very overweight, don’t think that if you’re 35 you’re that much safer [from severe COVID-19] than your mother or grandparents or others in their 60s or 70s,” Kass told Medscape Medical News.
The findings, which Kass describes as a “2-week snapshot” of 265 patients (58% male) in late March and early April at a handful of university hospitals in the United States reinforces other recent research indicating that obesity is one of the biggest risk factors for severe COVID-19 disease, particularly among younger patients. In addition, a large British study showed that, after adjusting for comorbidities, obesity was a significant factor associated with in-hospital death in COVID-19.
But this new analysis stands out as the only dataset to date that specifically “asks the question relative to age” of whether severe COVID-19 disease correlates to ICU treatment, he said.
The mean age of his study population of ICU patients was 55, Kass said, “and that was young, not what we were expecting.”
“Even with the first 20 patients, we were already seeing younger people and they definitely were heavier, with plenty of patients with a BMI over 35 kg/m2,” he added. “The relationship was pretty tight, pretty quick.”
“Just don’t make the assumption that any of us are too young to be vulnerable if, in fact, this is an aspect of our bodies,” he said.
Steven Heymsfield, MD, past president and a spokesperson for the Obesity Society, agrees with Kass’ conclusions.
“One thing we’ve had on our minds is that the prototype of a person with this disease is older...but now if we get [a patient] who’s symptomatic and 40 and obese, we shouldn’t assume they have some other disease,” Heymsfield told Medscape Medical News.
“We should think of them as a susceptible population.”
Kass and colleagues agree. “Public messaging to younger adults, reducing the threshold for virus testing in obese individuals, and maintaining greater vigilance for this at-risk population should reduce the prevalence of severe COVID-19 disease [among those with obesity],” they state.
“I think it’s a mental adjustment from a health care standpoint, which might hopefully help target the folks who are at higher risk before they get into trouble,” Kass told Medscape Medical News.
Trio of mechanisms explain obesity’s extra COVID-19 risks
Kass and coauthors write that, in analyzing their data, they anticipated similar results to the largest study of 1591 ICU patients from Italy in which only 203 were younger than 51 years. Common comorbidities among those patients included hypertension, cardiovascular disease, and type 2 diabetes, with similar data reported from China.
When the COVID-19 epidemic accelerated in the United States, older age was also identified as a risk factor. Obesity had not yet been added to this list, Kass noted. But following informal discussions with colleagues in other ICUs around the country, he decided to investigate further as to whether it was an underappreciated risk factor.
Kass and colleagues did a quick evaluation of the link between BMI and age of patients with COVID-19 admitted to ICUs at Johns Hopkins, University of Cincinnati, New York University, University of Washington, Florida Health, and University of Pennsylvania.
The “significant inverse correlation between age and BMI” showed younger ICU patients were more likely to be obese, with no difference by gender.
Median BMI among study participants was 29.3 kg/m2, with only a quarter having a BMI lower than 26 kg/m2 and another 25% having a BMI higher than 34.7 kg/m2.
Kass acknowledged that it wasn’t possible with this simple dataset to account for any other potential confounders, but he told Medscape Medical News that, “while diabetes, cardiovascular disease, and hypertension, for example, can occur with obesity, this is generally less so in younger populations as it takes time for the other comorbidities to develop.”
He said several mechanisms could explain why obesity predisposes patients with COVID-19 to severe disease.
For one, obesity places extra pressure on the diaphragm while lying on the back, restricting breathing.
“Morbid obesity itself is sort of proinflammatory,” he continued.
“Here we’ve got a viral infection where the early reports suggest that cytokine storms and immune mishandling of the virus are why it’s so much more severe than other forms of coronavirus we’ve seen before. So if you have someone with an already underlying proinflammatory state, this could be a reason there’s higher risk.”
Additionally, the angiotensin-converting enzyme-2 (ACE-2) receptor to which the SARS-CoV-2 virus that causes COVID-19 attaches is expressed in higher amounts in adipose tissue than the lungs, Kass noted.
“This could turn into kind of a viral replication depot,” he explained. “You may well be brewing more virus as a component of obesity.”
Sensitivity needed in public messaging about risks, but test sooner
With an obesity rate of about 40% in the United States, the results are particularly relevant for Americans, Kass and Heymsfield say, noting that the country’s “obesity belt” runs through the South.
Heymsfield, who wasn’t part of the new analysis, notes that public messaging around severe COVID-19 risks to younger adults with obesity is “tricky,” especially because the virus is “still pretty common in nonobese people.”
Kass agrees, noting, “it’s difficult to turn to 40% of the population and say: ‘You guys have to watch it.’ ”
But the mounting research findings necessitate linking obesity with severe COVID-19 disease and perhaps testing patients in this category for the virus sooner before symptoms become severe.
And of note, since shortness of breath is common among people with obesity regardless of illness, similar COVID-19 symptoms might catch these individuals unaware, pointed out Heymsfield, who is also a professor in the Metabolism and Body Composition Lab at Pennington Biomedical Research Center at Louisiana State University, Baton Rouge.
“They may find themselves literally unable to breathe, and the concern would be that they wait much too long to come in” for treatment, he said. Typically, people can deteriorate between day 7 and 10 of the COVID-19 infection.
Individuals with obesity “need to be educated to recognize the serious complications of COVID-19 often appear suddenly, although the virus has sometimes been working its way through the body for a long time,” he concluded.
Kass and Heymsfield have declared no relevant financial relationships.
This article first appeared on Medscape.com.