User login
Hair Restoration: The Present and the Future
Don't Miss the Medical Diagnoses: Screen for Causes of Hirsutism
NAPLES, Fla. — Many women with hirsutism have already removed their excess, unwanted hair before they present to dermatology. Look beyond the shaving, bleaching, plucking, and waxing, Dr. Elise A. Olsen said, because dermatologists play an important role in identification of important medical conditions associated with excess hair growth.
"Patients seen for the cosmetic treatment of hirsutism provide an opportunity to screen for [other] common findings." Accurate diagnosis also optimizes dermatology treatment. "Most of your patients with hirsutism will be coming in for laser hair removal. Evaluation for hirsutism will affect your [result]," Dr. Olsen said at the annual meeting of the Florida Society of Dermatology & Dermatologic Surgeons.
Polycystic ovarian syndrome, adrenal abnormalities, and drug reactions are important considerations in a differential diagnosis. Rule out these and other causes of hirsutism, as well as acromegaly and premature ovarian failure, Dr. Olsen said.
Hirsutism is a common problem that affects at least 5% of the female population, said Dr. Olsen, director of the Duke Dermatopharmacology Study Center and professor of dermatology at Duke University Medical Center in Durham, N.C.
Begin your evaluation with patient and family history. Ask about history of menses, acne, and how often the woman removes unwanted hair. Note affected anatomic sites during your physical examination, and use the Ferriman-Gallwey hirsutism index to score results, Dr. Olsen said. Also perform a pelvic examination and order ultrasound if you suspect a tumor or other abnormality.
Measurement of serum dehydroepiandrosterone sulfate (DHEAS), androstenedione, prolactin, and sex-hormone–binding globulin (SHBG) can facilitate diagnosis. Other helpful laboratory assays include luteinizing hormone/follicle stimulating hormone (LH/FSH) levels, a glucose tolerance test with insulin levels, and a fasting lipid panel.
Simple blood work includes a check of testosterone levels, Dr. Olsen said. "You will catch 40% [of hyperandrogenemia in hirsutism] with elevated testosterone alone and 60% with elevated free testosterone." In addition, she added, "I have started to do DHT or dihydrotestosterone because it can catch idiopathic cases."
Polycystic ovarian syndrome (PCOS) affects an estimated 3%-11% of women of reproductive age. Keep in mind that Rotterdam consensus criteria do not apply to adolescent girls, women on oral contraceptive pills, or postmenopausal women, Dr. Olsen said.
"One of the most important things I will talk about is that 50%-60% of these women with PCOS have insulin resistance. They have a three to seven times increased risk of type 2 diabetes, decreased fertility, and increased risk of cardiovascular disease," Dr. Olsen said. Risk of endometrial cancer is also elevated.
Part of ruling in PCOS is ruling out congenital adrenal hyperplasia, which can be challenging because many symptoms overlap, Dr. Olsen said. To diagnose congenital adrenal hyperplasia, look for premature pubarche with early pubic hair, cystic acne, and accelerated growth in girls. These girls also will have advanced bone age but premature closure of epiphyses, "so, ultimately, they have short adult stature." In adult women, include amenorrhea, anovulation, oligomenorrhea, and infertility in your differential diagnosis.
Tumors that cause hirsutism are rare, Dr. Olsen said. "If someone is suddenly developing hirsutism, that should be in the back of your mind."
Not surprisingly, androgen medications can cause excess hair growth in women. Danazol (Danocrine, Sanofi-Synthelabo Inc.; plus generics), valproate sodium (Depacon, Abbott; plus generics), and valproic acid (Depakene, Abbott; plus generics) are other common drug-related causes. Take a thorough medication history that includes these agents as well as progesterone.
There is no drug specifically indicated to treat hirsutism approved for marketing by the Food and Drug Administration. One agent, eflornithine (Vaniqa, SkinMedica Inc.) is approved only for reduction of unwanted facial hair. "It decreases the rate of hair growth and amount of shaving a woman has to do," Dr. Olsen said. "It's a decrease in the rate of hair growth only" and not the amount of hair, so patient education and realistic expectations are important.
Disclosures: Dr. Olsen said she is a consultant for Merck & Co., an investigator for Eisai Pharmaceuticals, and she receives research support from both companies.
NAPLES, Fla. — Many women with hirsutism have already removed their excess, unwanted hair before they present to dermatology. Look beyond the shaving, bleaching, plucking, and waxing, Dr. Elise A. Olsen said, because dermatologists play an important role in identification of important medical conditions associated with excess hair growth.
"Patients seen for the cosmetic treatment of hirsutism provide an opportunity to screen for [other] common findings." Accurate diagnosis also optimizes dermatology treatment. "Most of your patients with hirsutism will be coming in for laser hair removal. Evaluation for hirsutism will affect your [result]," Dr. Olsen said at the annual meeting of the Florida Society of Dermatology & Dermatologic Surgeons.
Polycystic ovarian syndrome, adrenal abnormalities, and drug reactions are important considerations in a differential diagnosis. Rule out these and other causes of hirsutism, as well as acromegaly and premature ovarian failure, Dr. Olsen said.
Hirsutism is a common problem that affects at least 5% of the female population, said Dr. Olsen, director of the Duke Dermatopharmacology Study Center and professor of dermatology at Duke University Medical Center in Durham, N.C.
Begin your evaluation with patient and family history. Ask about history of menses, acne, and how often the woman removes unwanted hair. Note affected anatomic sites during your physical examination, and use the Ferriman-Gallwey hirsutism index to score results, Dr. Olsen said. Also perform a pelvic examination and order ultrasound if you suspect a tumor or other abnormality.
Measurement of serum dehydroepiandrosterone sulfate (DHEAS), androstenedione, prolactin, and sex-hormone–binding globulin (SHBG) can facilitate diagnosis. Other helpful laboratory assays include luteinizing hormone/follicle stimulating hormone (LH/FSH) levels, a glucose tolerance test with insulin levels, and a fasting lipid panel.
Simple blood work includes a check of testosterone levels, Dr. Olsen said. "You will catch 40% [of hyperandrogenemia in hirsutism] with elevated testosterone alone and 60% with elevated free testosterone." In addition, she added, "I have started to do DHT or dihydrotestosterone because it can catch idiopathic cases."
Polycystic ovarian syndrome (PCOS) affects an estimated 3%-11% of women of reproductive age. Keep in mind that Rotterdam consensus criteria do not apply to adolescent girls, women on oral contraceptive pills, or postmenopausal women, Dr. Olsen said.
"One of the most important things I will talk about is that 50%-60% of these women with PCOS have insulin resistance. They have a three to seven times increased risk of type 2 diabetes, decreased fertility, and increased risk of cardiovascular disease," Dr. Olsen said. Risk of endometrial cancer is also elevated.
Part of ruling in PCOS is ruling out congenital adrenal hyperplasia, which can be challenging because many symptoms overlap, Dr. Olsen said. To diagnose congenital adrenal hyperplasia, look for premature pubarche with early pubic hair, cystic acne, and accelerated growth in girls. These girls also will have advanced bone age but premature closure of epiphyses, "so, ultimately, they have short adult stature." In adult women, include amenorrhea, anovulation, oligomenorrhea, and infertility in your differential diagnosis.
Tumors that cause hirsutism are rare, Dr. Olsen said. "If someone is suddenly developing hirsutism, that should be in the back of your mind."
Not surprisingly, androgen medications can cause excess hair growth in women. Danazol (Danocrine, Sanofi-Synthelabo Inc.; plus generics), valproate sodium (Depacon, Abbott; plus generics), and valproic acid (Depakene, Abbott; plus generics) are other common drug-related causes. Take a thorough medication history that includes these agents as well as progesterone.
There is no drug specifically indicated to treat hirsutism approved for marketing by the Food and Drug Administration. One agent, eflornithine (Vaniqa, SkinMedica Inc.) is approved only for reduction of unwanted facial hair. "It decreases the rate of hair growth and amount of shaving a woman has to do," Dr. Olsen said. "It's a decrease in the rate of hair growth only" and not the amount of hair, so patient education and realistic expectations are important.
Disclosures: Dr. Olsen said she is a consultant for Merck & Co., an investigator for Eisai Pharmaceuticals, and she receives research support from both companies.
NAPLES, Fla. — Many women with hirsutism have already removed their excess, unwanted hair before they present to dermatology. Look beyond the shaving, bleaching, plucking, and waxing, Dr. Elise A. Olsen said, because dermatologists play an important role in identification of important medical conditions associated with excess hair growth.
"Patients seen for the cosmetic treatment of hirsutism provide an opportunity to screen for [other] common findings." Accurate diagnosis also optimizes dermatology treatment. "Most of your patients with hirsutism will be coming in for laser hair removal. Evaluation for hirsutism will affect your [result]," Dr. Olsen said at the annual meeting of the Florida Society of Dermatology & Dermatologic Surgeons.
Polycystic ovarian syndrome, adrenal abnormalities, and drug reactions are important considerations in a differential diagnosis. Rule out these and other causes of hirsutism, as well as acromegaly and premature ovarian failure, Dr. Olsen said.
Hirsutism is a common problem that affects at least 5% of the female population, said Dr. Olsen, director of the Duke Dermatopharmacology Study Center and professor of dermatology at Duke University Medical Center in Durham, N.C.
Begin your evaluation with patient and family history. Ask about history of menses, acne, and how often the woman removes unwanted hair. Note affected anatomic sites during your physical examination, and use the Ferriman-Gallwey hirsutism index to score results, Dr. Olsen said. Also perform a pelvic examination and order ultrasound if you suspect a tumor or other abnormality.
Measurement of serum dehydroepiandrosterone sulfate (DHEAS), androstenedione, prolactin, and sex-hormone–binding globulin (SHBG) can facilitate diagnosis. Other helpful laboratory assays include luteinizing hormone/follicle stimulating hormone (LH/FSH) levels, a glucose tolerance test with insulin levels, and a fasting lipid panel.
Simple blood work includes a check of testosterone levels, Dr. Olsen said. "You will catch 40% [of hyperandrogenemia in hirsutism] with elevated testosterone alone and 60% with elevated free testosterone." In addition, she added, "I have started to do DHT or dihydrotestosterone because it can catch idiopathic cases."
Polycystic ovarian syndrome (PCOS) affects an estimated 3%-11% of women of reproductive age. Keep in mind that Rotterdam consensus criteria do not apply to adolescent girls, women on oral contraceptive pills, or postmenopausal women, Dr. Olsen said.
"One of the most important things I will talk about is that 50%-60% of these women with PCOS have insulin resistance. They have a three to seven times increased risk of type 2 diabetes, decreased fertility, and increased risk of cardiovascular disease," Dr. Olsen said. Risk of endometrial cancer is also elevated.
Part of ruling in PCOS is ruling out congenital adrenal hyperplasia, which can be challenging because many symptoms overlap, Dr. Olsen said. To diagnose congenital adrenal hyperplasia, look for premature pubarche with early pubic hair, cystic acne, and accelerated growth in girls. These girls also will have advanced bone age but premature closure of epiphyses, "so, ultimately, they have short adult stature." In adult women, include amenorrhea, anovulation, oligomenorrhea, and infertility in your differential diagnosis.
Tumors that cause hirsutism are rare, Dr. Olsen said. "If someone is suddenly developing hirsutism, that should be in the back of your mind."
Not surprisingly, androgen medications can cause excess hair growth in women. Danazol (Danocrine, Sanofi-Synthelabo Inc.; plus generics), valproate sodium (Depacon, Abbott; plus generics), and valproic acid (Depakene, Abbott; plus generics) are other common drug-related causes. Take a thorough medication history that includes these agents as well as progesterone.
There is no drug specifically indicated to treat hirsutism approved for marketing by the Food and Drug Administration. One agent, eflornithine (Vaniqa, SkinMedica Inc.) is approved only for reduction of unwanted facial hair. "It decreases the rate of hair growth and amount of shaving a woman has to do," Dr. Olsen said. "It's a decrease in the rate of hair growth only" and not the amount of hair, so patient education and realistic expectations are important.
Disclosures: Dr. Olsen said she is a consultant for Merck & Co., an investigator for Eisai Pharmaceuticals, and she receives research support from both companies.
Pilomatrical Carcinoma: Case Report and Review of the Literature
Cutaneous Manifestations of Diabetes Mellitus: A Case Series
Trichotillomania: An Important Psychocutaneous Disorder
Cultural Competence Key to Treating Skin of Color
NAPLES, Fla. — Vitiligo, keloids, acne keloidalis nuchae, and hair and scalp concerns are among the challenges dermatologists face when treating darker skin, Dr. George Cohen said.
Black skin is prone to adverse pigmentary or hyperproliferative responses to cryotherapy, lasers, and chemical skin treatments. Because of these and other concerns in a growing population of patients with skin types IV through VI, Dr. Cohen suggested dermatologists learn more about recognition and treatment of these important differences.

"We are a more diverse society. Become culturally competent and learn as much as you can," Dr. Cohen said at the annual meeting of the Florida Society of Dermatology & Dermatologic Surgeons. Respect, inquire, and do not make assumptions—those are the three pillars of cultural competence, he said.
Cultural competence is not only good for patients; it can be good for your practice as well. "Access and acceptance are good for us—this creates more demand for services," said Dr. Cohen, of the department of dermatology and cutaneous surgery at the University of South Florida in Tampa.
Vitiligo
Vitiligo is the prototypic pigmentary challenge for patients with skin of color, Dr. Cohen said. Although the etiology is not completely understood, it may be related to the immune system. The challenge for dermatologists is that "some people respond to some things some of the time, so we don't always know who is going to respond," Dr. Cohen said.
The myriad of treatments available for vitiligo include:
- Narrow-band UVB therapy.
- Targeted laser treatment with the XeCL Excimer (308 nm).
- Topical steroids.
- Calcineurin inhibitors.
- Surgery.
- Depigmentation (using medications or 694-nm Q-switched Ruby laser).
- Makeup.
Unfortunately, "none of these work perfectly," he said.

He cited the case of a patient with vitiligo who tried steroids, psoralen and UVA (PUVA), and other treatments to no avail. "He was desperate. He came to me with his family and asked: 'Doctor, can you make me one color?' I told him we can only make him one color—white—that is all we are able to do.
"Sometimes you cannot repigment the patient, and you have to know how to judiciously offer depigmentation. Some might say I robbed him of his culture. I say, no, I didn't, I robbed him of a disfiguring condition," said Dr. Cohen.
More research is clearly warranted to improve treatment options for vitiligo, such as studies to assess the biology of melanocytes, he said.
Keloids
Keloids are another challenge in skin of color patients. The therapeutic approach depends in part on the extent of the patient's condition. For example, a single keloid on the earlobe would be treated differently than more widespread presentation.
Again, more research is warranted on optimal treatments, Dr. Cohen said, because studies in the literature are contradictory and provide no consensus.
Acne keloidalis nuchae, "the keloids' cousin," most often occur in black men, he said. These nuchae can advance to plaque and form tumors, "and at the very least will need intralesional therapy." One clinical tip is to make an incision only within the keloid, he said.

If a patient presents with an acne keloidalis tumor, simply excise it. Once you get hemostasis, dress the wound with petroleum jelly only, and let it close by the magic of second intention
"I monitor these people. If I see any evidence of regrowth, I treat with triamcinolone early and often," he said.
Hair and Scalp Challenges
Hair and scalp concerns are common in patients with skin of color, Dr. Cohen said. A scalp biopsy is recommended to determine or confirm a diagnosis and to guide the course of clinical treatment.
These presentations can have a great psychosocial impact. "Do not underestimate the effect on patients," he said. Know your limitations and the limitations of therapy, and make sure you communicate those effectively to the patient. Otherwise, both the patient and provider can become frustrated.
Be honest with genetically-susceptible patients who present with scarring on the scalp from physical insult. In this population, scarring results when fibrous tissue replaces hair follicles. "Let them know up front that creams and other nonsense are not going to work," he said.

Contrary to popular belief, Dr. Cohen said, hair transplants are an option in patients with skin of color. "Hair transplants in black patients are not scary— I've been doing them for years and never had keloids," he said.
Black hair is heterogenous, so not everyone has curved follicles. If a skin of color patient has straight follicles, standard hair transplant procedures—for example, with 4-mm donor grafts—would be an option.
Dr. Cohen said that he did not have any relevant financial disclosures.
NAPLES, Fla. — Vitiligo, keloids, acne keloidalis nuchae, and hair and scalp concerns are among the challenges dermatologists face when treating darker skin, Dr. George Cohen said.
Black skin is prone to adverse pigmentary or hyperproliferative responses to cryotherapy, lasers, and chemical skin treatments. Because of these and other concerns in a growing population of patients with skin types IV through VI, Dr. Cohen suggested dermatologists learn more about recognition and treatment of these important differences.
"We are a more diverse society. Become culturally competent and learn as much as you can," Dr. Cohen said at the annual meeting of the Florida Society of Dermatology & Dermatologic Surgeons. Respect, inquire, and do not make assumptions—those are the three pillars of cultural competence, he said.
Cultural competence is not only good for patients; it can be good for your practice as well. "Access and acceptance are good for us—this creates more demand for services," said Dr. Cohen, of the department of dermatology and cutaneous surgery at the University of South Florida in Tampa.
Vitiligo
Vitiligo is the prototypic pigmentary challenge for patients with skin of color, Dr. Cohen said. Although the etiology is not completely understood, it may be related to the immune system. The challenge for dermatologists is that "some people respond to some things some of the time, so we don't always know who is going to respond," Dr. Cohen said.
The myriad of treatments available for vitiligo include:
- Narrow-band UVB therapy.
- Targeted laser treatment with the XeCL Excimer (308 nm).
- Topical steroids.
- Calcineurin inhibitors.
- Surgery.
- Depigmentation (using medications or 694-nm Q-switched Ruby laser).
- Makeup.
Unfortunately, "none of these work perfectly," he said.
He cited the case of a patient with vitiligo who tried steroids, psoralen and UVA (PUVA), and other treatments to no avail. "He was desperate. He came to me with his family and asked: 'Doctor, can you make me one color?' I told him we can only make him one color—white—that is all we are able to do.
"Sometimes you cannot repigment the patient, and you have to know how to judiciously offer depigmentation. Some might say I robbed him of his culture. I say, no, I didn't, I robbed him of a disfiguring condition," said Dr. Cohen.
More research is clearly warranted to improve treatment options for vitiligo, such as studies to assess the biology of melanocytes, he said.
Keloids
Keloids are another challenge in skin of color patients. The therapeutic approach depends in part on the extent of the patient's condition. For example, a single keloid on the earlobe would be treated differently than more widespread presentation.
Again, more research is warranted on optimal treatments, Dr. Cohen said, because studies in the literature are contradictory and provide no consensus.
Acne keloidalis nuchae, "the keloids' cousin," most often occur in black men, he said. These nuchae can advance to plaque and form tumors, "and at the very least will need intralesional therapy." One clinical tip is to make an incision only within the keloid, he said.
If a patient presents with an acne keloidalis tumor, simply excise it. Once you get hemostasis, dress the wound with petroleum jelly only, and let it close by the magic of second intention
"I monitor these people. If I see any evidence of regrowth, I treat with triamcinolone early and often," he said.
Hair and Scalp Challenges
Hair and scalp concerns are common in patients with skin of color, Dr. Cohen said. A scalp biopsy is recommended to determine or confirm a diagnosis and to guide the course of clinical treatment.
These presentations can have a great psychosocial impact. "Do not underestimate the effect on patients," he said. Know your limitations and the limitations of therapy, and make sure you communicate those effectively to the patient. Otherwise, both the patient and provider can become frustrated.
Be honest with genetically-susceptible patients who present with scarring on the scalp from physical insult. In this population, scarring results when fibrous tissue replaces hair follicles. "Let them know up front that creams and other nonsense are not going to work," he said.
Contrary to popular belief, Dr. Cohen said, hair transplants are an option in patients with skin of color. "Hair transplants in black patients are not scary— I've been doing them for years and never had keloids," he said.
Black hair is heterogenous, so not everyone has curved follicles. If a skin of color patient has straight follicles, standard hair transplant procedures—for example, with 4-mm donor grafts—would be an option.
Dr. Cohen said that he did not have any relevant financial disclosures.
NAPLES, Fla. — Vitiligo, keloids, acne keloidalis nuchae, and hair and scalp concerns are among the challenges dermatologists face when treating darker skin, Dr. George Cohen said.
Black skin is prone to adverse pigmentary or hyperproliferative responses to cryotherapy, lasers, and chemical skin treatments. Because of these and other concerns in a growing population of patients with skin types IV through VI, Dr. Cohen suggested dermatologists learn more about recognition and treatment of these important differences.
"We are a more diverse society. Become culturally competent and learn as much as you can," Dr. Cohen said at the annual meeting of the Florida Society of Dermatology & Dermatologic Surgeons. Respect, inquire, and do not make assumptions—those are the three pillars of cultural competence, he said.
Cultural competence is not only good for patients; it can be good for your practice as well. "Access and acceptance are good for us—this creates more demand for services," said Dr. Cohen, of the department of dermatology and cutaneous surgery at the University of South Florida in Tampa.
Vitiligo
Vitiligo is the prototypic pigmentary challenge for patients with skin of color, Dr. Cohen said. Although the etiology is not completely understood, it may be related to the immune system. The challenge for dermatologists is that "some people respond to some things some of the time, so we don't always know who is going to respond," Dr. Cohen said.
The myriad of treatments available for vitiligo include:
- Narrow-band UVB therapy.
- Targeted laser treatment with the XeCL Excimer (308 nm).
- Topical steroids.
- Calcineurin inhibitors.
- Surgery.
- Depigmentation (using medications or 694-nm Q-switched Ruby laser).
- Makeup.
Unfortunately, "none of these work perfectly," he said.
He cited the case of a patient with vitiligo who tried steroids, psoralen and UVA (PUVA), and other treatments to no avail. "He was desperate. He came to me with his family and asked: 'Doctor, can you make me one color?' I told him we can only make him one color—white—that is all we are able to do.
"Sometimes you cannot repigment the patient, and you have to know how to judiciously offer depigmentation. Some might say I robbed him of his culture. I say, no, I didn't, I robbed him of a disfiguring condition," said Dr. Cohen.
More research is clearly warranted to improve treatment options for vitiligo, such as studies to assess the biology of melanocytes, he said.
Keloids
Keloids are another challenge in skin of color patients. The therapeutic approach depends in part on the extent of the patient's condition. For example, a single keloid on the earlobe would be treated differently than more widespread presentation.
Again, more research is warranted on optimal treatments, Dr. Cohen said, because studies in the literature are contradictory and provide no consensus.
Acne keloidalis nuchae, "the keloids' cousin," most often occur in black men, he said. These nuchae can advance to plaque and form tumors, "and at the very least will need intralesional therapy." One clinical tip is to make an incision only within the keloid, he said.
If a patient presents with an acne keloidalis tumor, simply excise it. Once you get hemostasis, dress the wound with petroleum jelly only, and let it close by the magic of second intention
"I monitor these people. If I see any evidence of regrowth, I treat with triamcinolone early and often," he said.
Hair and Scalp Challenges
Hair and scalp concerns are common in patients with skin of color, Dr. Cohen said. A scalp biopsy is recommended to determine or confirm a diagnosis and to guide the course of clinical treatment.
These presentations can have a great psychosocial impact. "Do not underestimate the effect on patients," he said. Know your limitations and the limitations of therapy, and make sure you communicate those effectively to the patient. Otherwise, both the patient and provider can become frustrated.
Be honest with genetically-susceptible patients who present with scarring on the scalp from physical insult. In this population, scarring results when fibrous tissue replaces hair follicles. "Let them know up front that creams and other nonsense are not going to work," he said.
Contrary to popular belief, Dr. Cohen said, hair transplants are an option in patients with skin of color. "Hair transplants in black patients are not scary— I've been doing them for years and never had keloids," he said.
Black hair is heterogenous, so not everyone has curved follicles. If a skin of color patient has straight follicles, standard hair transplant procedures—for example, with 4-mm donor grafts—would be an option.
Dr. Cohen said that he did not have any relevant financial disclosures.
Are We Giving Nails Away? [editorial]
Two Lasers May Be Better Than One for Hair Removal
Recent advances in laser hair removal include using combination wavelengths, longer pulses, and larger spot sizes for all skin types, and using longer wavelengths for darker skin, according to Dr. E. Victor Ross.
Better pain control and cooling techniques also can make device-based hair removal a more comfortable option for patients, Dr. Ross said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
When using lasers for hair removal, cooling the skin before and after treatment can reduce pain and swelling, and cooling the skin during laser exposure "tends to minimize the dermal epidermal temperature," said Dr. Ross, director of the Scripps Clinic Laser and Cosmetic Dermatology Center in Carmel Valley, Calif.
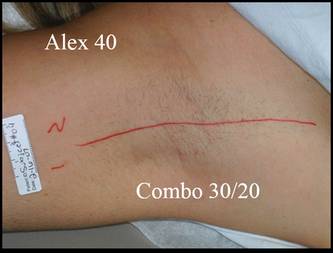
Historically, fair-skinned patients have been treated with a 755-nm alexandrite laser for hair removal. For dark or tanned skin, or coarser hair, a 1064-nm Nd:YAG might be more effective, but it can be more painful for patients, Dr. Ross noted.
In his experience, a blended treatment including both the 755-nm and 1064-nm lasers can be more effective for removing fine hair on the legs than either laser alone, he said, adding that some patients still prefer the 755-nm alexandrite laser because the combination therapy is more painful than the 755 nm, although it is less painful than the 1064 nm alone.
New hair removal technologies include ultrasound and microwave radiation, as well as lower-fluence intense pulsed light and diode options with suction.
Approaches using high repetition with low fluence have been applied in some settings. The advantage is less pain, but more research is needed to determine whether lower fluences at high rates of repetition are effective, and what types of treatments are effective for white hair, said Dr. Ross.
Suction devices are an option to assist with permanent hair reduction over larger areas. A larger spot size allows more photons to remain in the target area, while vacuum-assisted suction concentrates more cumulative energy at any given depth and allows for effective treatment at a lower fluence.
Dr. Ross also addressed laser-diode hair removal devices being marketed for home use. The key issues to consider when evaluating at-home devices are safety for all skin types; safety with open or closed eyes; effectiveness in removing fine, gray, or white hair; and, of course, cost.
The TRIA hair removal device from TRIA Beauty Inc. is approved by the Food and Drug Administration for home use. The device packs an 800-nm wavelength and fluences of 7, 12, or 20 J/cm2, and efficacy data on this product are promising, Dr. Ross said.
Dr. Ross disclosed that he is a researcher for and receives funding from multiple laser companies, including Candela, Cutera, Lumenis, Sciton, and Syneron. SDEF and this news organization are both owned by Elsevier.
Recent advances in laser hair removal include using combination wavelengths, longer pulses, and larger spot sizes for all skin types, and using longer wavelengths for darker skin, according to Dr. E. Victor Ross.
Better pain control and cooling techniques also can make device-based hair removal a more comfortable option for patients, Dr. Ross said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
When using lasers for hair removal, cooling the skin before and after treatment can reduce pain and swelling, and cooling the skin during laser exposure "tends to minimize the dermal epidermal temperature," said Dr. Ross, director of the Scripps Clinic Laser and Cosmetic Dermatology Center in Carmel Valley, Calif.
Historically, fair-skinned patients have been treated with a 755-nm alexandrite laser for hair removal. For dark or tanned skin, or coarser hair, a 1064-nm Nd:YAG might be more effective, but it can be more painful for patients, Dr. Ross noted.
In his experience, a blended treatment including both the 755-nm and 1064-nm lasers can be more effective for removing fine hair on the legs than either laser alone, he said, adding that some patients still prefer the 755-nm alexandrite laser because the combination therapy is more painful than the 755 nm, although it is less painful than the 1064 nm alone.
New hair removal technologies include ultrasound and microwave radiation, as well as lower-fluence intense pulsed light and diode options with suction.
Approaches using high repetition with low fluence have been applied in some settings. The advantage is less pain, but more research is needed to determine whether lower fluences at high rates of repetition are effective, and what types of treatments are effective for white hair, said Dr. Ross.
Suction devices are an option to assist with permanent hair reduction over larger areas. A larger spot size allows more photons to remain in the target area, while vacuum-assisted suction concentrates more cumulative energy at any given depth and allows for effective treatment at a lower fluence.
Dr. Ross also addressed laser-diode hair removal devices being marketed for home use. The key issues to consider when evaluating at-home devices are safety for all skin types; safety with open or closed eyes; effectiveness in removing fine, gray, or white hair; and, of course, cost.
The TRIA hair removal device from TRIA Beauty Inc. is approved by the Food and Drug Administration for home use. The device packs an 800-nm wavelength and fluences of 7, 12, or 20 J/cm2, and efficacy data on this product are promising, Dr. Ross said.
Dr. Ross disclosed that he is a researcher for and receives funding from multiple laser companies, including Candela, Cutera, Lumenis, Sciton, and Syneron. SDEF and this news organization are both owned by Elsevier.
Recent advances in laser hair removal include using combination wavelengths, longer pulses, and larger spot sizes for all skin types, and using longer wavelengths for darker skin, according to Dr. E. Victor Ross.
Better pain control and cooling techniques also can make device-based hair removal a more comfortable option for patients, Dr. Ross said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
When using lasers for hair removal, cooling the skin before and after treatment can reduce pain and swelling, and cooling the skin during laser exposure "tends to minimize the dermal epidermal temperature," said Dr. Ross, director of the Scripps Clinic Laser and Cosmetic Dermatology Center in Carmel Valley, Calif.
Historically, fair-skinned patients have been treated with a 755-nm alexandrite laser for hair removal. For dark or tanned skin, or coarser hair, a 1064-nm Nd:YAG might be more effective, but it can be more painful for patients, Dr. Ross noted.
In his experience, a blended treatment including both the 755-nm and 1064-nm lasers can be more effective for removing fine hair on the legs than either laser alone, he said, adding that some patients still prefer the 755-nm alexandrite laser because the combination therapy is more painful than the 755 nm, although it is less painful than the 1064 nm alone.
New hair removal technologies include ultrasound and microwave radiation, as well as lower-fluence intense pulsed light and diode options with suction.
Approaches using high repetition with low fluence have been applied in some settings. The advantage is less pain, but more research is needed to determine whether lower fluences at high rates of repetition are effective, and what types of treatments are effective for white hair, said Dr. Ross.
Suction devices are an option to assist with permanent hair reduction over larger areas. A larger spot size allows more photons to remain in the target area, while vacuum-assisted suction concentrates more cumulative energy at any given depth and allows for effective treatment at a lower fluence.
Dr. Ross also addressed laser-diode hair removal devices being marketed for home use. The key issues to consider when evaluating at-home devices are safety for all skin types; safety with open or closed eyes; effectiveness in removing fine, gray, or white hair; and, of course, cost.
The TRIA hair removal device from TRIA Beauty Inc. is approved by the Food and Drug Administration for home use. The device packs an 800-nm wavelength and fluences of 7, 12, or 20 J/cm2, and efficacy data on this product are promising, Dr. Ross said.
Dr. Ross disclosed that he is a researcher for and receives funding from multiple laser companies, including Candela, Cutera, Lumenis, Sciton, and Syneron. SDEF and this news organization are both owned by Elsevier.