User login
As Populations Age, Occam’s Razor Loses Its Diagnostic Edge
The principle of parsimony, often referred to as “Occam’s razor,” favors a unifying explanation over multiple ones, as long as both explain the data equally well. This heuristic, widely used in medical practice, advocates for simpler explanations rather than complex theories. However, its application in modern medicine has sparked debate.
“Hickam’s dictum,” a counterargument to Occam’s razor, asserts that patients — especially as populations grow older and more fragile — can simultaneously have multiple, unrelated diagnoses. These contrasting perspectives on clinical reasoning, balancing diagnostic simplicity and complexity, are both used in daily medical practice.
But are these two axioms truly in conflict, or is this a false dichotomy?
Occam’s Razor and Simple Diagnoses
Interpersonal variability in diagnostic approaches, shaped by the subjective nature of many judgments, complicates the formal evaluation of diagnostic parsimony (Occam’s razor). Indirect evidence suggests that prioritizing simplicity in diagnosis can result in under-detection of secondary conditions, particularly in patients with chronic illnesses.
For example, older patients with a known chronic illness were found to have a 30%-60% lower likelihood of being treated for an unrelated secondary diagnosis than matched peers without the chronic condition. Other studies indicate that a readily available, simple diagnosis can lead clinicians to prematurely close their diagnostic reasoning, overlooking other significant illnesses.
Beyond Hickam’s Dictum and Occam’s Razor
A recent study explored the phenomenon of multiple diagnoses by examining the supposed conflict between Hickam’s dictum and Occam’s razor, as well as the ambiguities in how they are interpreted and used by physicians in clinical reasoning.
Part 1: Researchers identified articles on PubMed related to Hickam’s dictum or conflicting with Occam’s razor, categorizing instances into four models of Hickam’s dictum:
1. Incidentaloma: An asymptomatic condition discovered accidentally.
2. Preexisting diagnosis: A known condition in the patient’s medical history.
3. Causally related disease: A complication, association, epiphenomenon, or underlying cause connected to the primary diagnosis.
4. Coincidental and independent disease: A symptomatic condition unrelated to the primary diagnosis.
Part 2: Researchers analyzed 220 case records from Massachusetts General Hospital, Boston, and clinical problem-solving reports published in The New England Journal of Medicine between 2017 and 2023. They found no cases where the final diagnosis was not a unifying one.
Part 3: In an online survey of 265 physicians, 79% identified coincidental symptomatic conditions (category 4) as the least likely type of multiple diagnoses. Preexisting conditions (category 2) emerged as the most common, reflecting the tendency to add new diagnoses to a patient’s existing health profile. Almost one third of instances referencing Hickam’s dictum or violations of Occam’s razor fell into category 2.
Causally related diseases (category 3) were probabilistically dependent, meaning that the presence of one condition increased the likelihood of the other, based on the strength (often unknown) of the causal relationship.
Practical Insights
The significant finding of this work was that multiple diagnoses occur in predictable patterns, informed by causal connections between conditions, symptom onset timing, and likelihood. The principle of common causation supports the search for a unifying diagnosis for coincidental symptoms. It is not surprising that causally related phenomena often co-occur, as reflected by the fact that 40% of multiple diagnoses in the study’s first part were causally linked.
Thus, understanding multiple diagnoses goes beyond Hickam’s dictum and Occam’s razor. It requires not only identifying diseases but also examining their causal relationships and the timing of symptom onset. A unifying diagnosis is not equivalent to a single diagnosis; rather, it represents a causal pathway linking underlying pathologic changes to acute presentations.
This story was translated from Univadis Italy using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
The principle of parsimony, often referred to as “Occam’s razor,” favors a unifying explanation over multiple ones, as long as both explain the data equally well. This heuristic, widely used in medical practice, advocates for simpler explanations rather than complex theories. However, its application in modern medicine has sparked debate.
“Hickam’s dictum,” a counterargument to Occam’s razor, asserts that patients — especially as populations grow older and more fragile — can simultaneously have multiple, unrelated diagnoses. These contrasting perspectives on clinical reasoning, balancing diagnostic simplicity and complexity, are both used in daily medical practice.
But are these two axioms truly in conflict, or is this a false dichotomy?
Occam’s Razor and Simple Diagnoses
Interpersonal variability in diagnostic approaches, shaped by the subjective nature of many judgments, complicates the formal evaluation of diagnostic parsimony (Occam’s razor). Indirect evidence suggests that prioritizing simplicity in diagnosis can result in under-detection of secondary conditions, particularly in patients with chronic illnesses.
For example, older patients with a known chronic illness were found to have a 30%-60% lower likelihood of being treated for an unrelated secondary diagnosis than matched peers without the chronic condition. Other studies indicate that a readily available, simple diagnosis can lead clinicians to prematurely close their diagnostic reasoning, overlooking other significant illnesses.
Beyond Hickam’s Dictum and Occam’s Razor
A recent study explored the phenomenon of multiple diagnoses by examining the supposed conflict between Hickam’s dictum and Occam’s razor, as well as the ambiguities in how they are interpreted and used by physicians in clinical reasoning.
Part 1: Researchers identified articles on PubMed related to Hickam’s dictum or conflicting with Occam’s razor, categorizing instances into four models of Hickam’s dictum:
1. Incidentaloma: An asymptomatic condition discovered accidentally.
2. Preexisting diagnosis: A known condition in the patient’s medical history.
3. Causally related disease: A complication, association, epiphenomenon, or underlying cause connected to the primary diagnosis.
4. Coincidental and independent disease: A symptomatic condition unrelated to the primary diagnosis.
Part 2: Researchers analyzed 220 case records from Massachusetts General Hospital, Boston, and clinical problem-solving reports published in The New England Journal of Medicine between 2017 and 2023. They found no cases where the final diagnosis was not a unifying one.
Part 3: In an online survey of 265 physicians, 79% identified coincidental symptomatic conditions (category 4) as the least likely type of multiple diagnoses. Preexisting conditions (category 2) emerged as the most common, reflecting the tendency to add new diagnoses to a patient’s existing health profile. Almost one third of instances referencing Hickam’s dictum or violations of Occam’s razor fell into category 2.
Causally related diseases (category 3) were probabilistically dependent, meaning that the presence of one condition increased the likelihood of the other, based on the strength (often unknown) of the causal relationship.
Practical Insights
The significant finding of this work was that multiple diagnoses occur in predictable patterns, informed by causal connections between conditions, symptom onset timing, and likelihood. The principle of common causation supports the search for a unifying diagnosis for coincidental symptoms. It is not surprising that causally related phenomena often co-occur, as reflected by the fact that 40% of multiple diagnoses in the study’s first part were causally linked.
Thus, understanding multiple diagnoses goes beyond Hickam’s dictum and Occam’s razor. It requires not only identifying diseases but also examining their causal relationships and the timing of symptom onset. A unifying diagnosis is not equivalent to a single diagnosis; rather, it represents a causal pathway linking underlying pathologic changes to acute presentations.
This story was translated from Univadis Italy using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
The principle of parsimony, often referred to as “Occam’s razor,” favors a unifying explanation over multiple ones, as long as both explain the data equally well. This heuristic, widely used in medical practice, advocates for simpler explanations rather than complex theories. However, its application in modern medicine has sparked debate.
“Hickam’s dictum,” a counterargument to Occam’s razor, asserts that patients — especially as populations grow older and more fragile — can simultaneously have multiple, unrelated diagnoses. These contrasting perspectives on clinical reasoning, balancing diagnostic simplicity and complexity, are both used in daily medical practice.
But are these two axioms truly in conflict, or is this a false dichotomy?
Occam’s Razor and Simple Diagnoses
Interpersonal variability in diagnostic approaches, shaped by the subjective nature of many judgments, complicates the formal evaluation of diagnostic parsimony (Occam’s razor). Indirect evidence suggests that prioritizing simplicity in diagnosis can result in under-detection of secondary conditions, particularly in patients with chronic illnesses.
For example, older patients with a known chronic illness were found to have a 30%-60% lower likelihood of being treated for an unrelated secondary diagnosis than matched peers without the chronic condition. Other studies indicate that a readily available, simple diagnosis can lead clinicians to prematurely close their diagnostic reasoning, overlooking other significant illnesses.
Beyond Hickam’s Dictum and Occam’s Razor
A recent study explored the phenomenon of multiple diagnoses by examining the supposed conflict between Hickam’s dictum and Occam’s razor, as well as the ambiguities in how they are interpreted and used by physicians in clinical reasoning.
Part 1: Researchers identified articles on PubMed related to Hickam’s dictum or conflicting with Occam’s razor, categorizing instances into four models of Hickam’s dictum:
1. Incidentaloma: An asymptomatic condition discovered accidentally.
2. Preexisting diagnosis: A known condition in the patient’s medical history.
3. Causally related disease: A complication, association, epiphenomenon, or underlying cause connected to the primary diagnosis.
4. Coincidental and independent disease: A symptomatic condition unrelated to the primary diagnosis.
Part 2: Researchers analyzed 220 case records from Massachusetts General Hospital, Boston, and clinical problem-solving reports published in The New England Journal of Medicine between 2017 and 2023. They found no cases where the final diagnosis was not a unifying one.
Part 3: In an online survey of 265 physicians, 79% identified coincidental symptomatic conditions (category 4) as the least likely type of multiple diagnoses. Preexisting conditions (category 2) emerged as the most common, reflecting the tendency to add new diagnoses to a patient’s existing health profile. Almost one third of instances referencing Hickam’s dictum or violations of Occam’s razor fell into category 2.
Causally related diseases (category 3) were probabilistically dependent, meaning that the presence of one condition increased the likelihood of the other, based on the strength (often unknown) of the causal relationship.
Practical Insights
The significant finding of this work was that multiple diagnoses occur in predictable patterns, informed by causal connections between conditions, symptom onset timing, and likelihood. The principle of common causation supports the search for a unifying diagnosis for coincidental symptoms. It is not surprising that causally related phenomena often co-occur, as reflected by the fact that 40% of multiple diagnoses in the study’s first part were causally linked.
Thus, understanding multiple diagnoses goes beyond Hickam’s dictum and Occam’s razor. It requires not only identifying diseases but also examining their causal relationships and the timing of symptom onset. A unifying diagnosis is not equivalent to a single diagnosis; rather, it represents a causal pathway linking underlying pathologic changes to acute presentations.
This story was translated from Univadis Italy using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Does Semaglutide Increase Risk for Optic Neuropathy?
TOPLINE:
METHODOLOGY:
- Researchers conducted a retrospective cohort study using data from the TriNetX Analytics Network to investigate the potential risk for NAION associated with semaglutide use in a broader population worldwide.
- They included Caucasians aged ≥ 18 years with only type 2 diabetes (n = 37,245) , only obesity (n = 138,391), or both (n = 64,989) who visited healthcare facilities three or more times.
- The participants were further grouped into those prescribed semaglutide and those using non–GLP-1 RA medications.
- Propensity score matching was performed to balance age, sex, body mass index, A1C levels, medications, and underlying comorbidities between the participants using semaglutide or non–GLP-1 RAs.
- The main outcome measure was the occurrence of NAION, evaluated at 1, 2, and 3 years of follow-up.
TAKEAWAY:
- The use of semaglutide vs non–GLP-1 RAs was not associated with an increased risk for NAION in people with only type 2 diabetes during the 1-year (hazard ratio [HR], 2.32; 95% CI, 0.60-8.97), 2-year (HR, 2.31; 95% CI, 0.86-6.17), and 3-year (HR, 1.51; 0.71-3.25) follow-up periods.
- Similarly, in the obesity-only cohort, use of semaglutide was not linked to the development of NAION across 1-year (HR, 0.41; 95% CI, 0.08-2.09), 2-year (HR, 0.67; 95% CI, 0.20-2.24), and 3-year (HR, 0.72; 95% CI, 0.24-2.17) follow-up periods.
- The patients with both diabetes and obesity also showed no significant association between use of semaglutide and the risk for NAION across each follow-up period.
- Sensitivity analysis confirmed the prescription of semaglutide was not associated with an increased risk for NAION compared with non–GLP-1 RA medications.
IN PRACTICE:
“Our large, multinational, population-based, real-world study found that semaglutide is not associated with an increased risk of NAION in the general population,” the authors of the study wrote.
SOURCE:
The study was led by Chien-Chih Chou, MD, PhD, of National Yang Ming Chiao Tung University, in Taipei City, Taiwan, and was published online on November 02, 2024, in Ophthalmology.
LIMITATIONS:
The retrospective nature of the study may have limited the ability to establish causality between the use of semaglutide and the risk for NAION. The reliance on diagnosis coding for NAION may have introduced a potential misclassification of cases. Moreover, approximately half of the healthcare organizations in the TriNetX network are based in the United States, potentially limiting the diversity of the data.
DISCLOSURES:
This study was supported by a grant from Taichung Veterans General Hospital. The authors declared no potential conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Researchers conducted a retrospective cohort study using data from the TriNetX Analytics Network to investigate the potential risk for NAION associated with semaglutide use in a broader population worldwide.
- They included Caucasians aged ≥ 18 years with only type 2 diabetes (n = 37,245) , only obesity (n = 138,391), or both (n = 64,989) who visited healthcare facilities three or more times.
- The participants were further grouped into those prescribed semaglutide and those using non–GLP-1 RA medications.
- Propensity score matching was performed to balance age, sex, body mass index, A1C levels, medications, and underlying comorbidities between the participants using semaglutide or non–GLP-1 RAs.
- The main outcome measure was the occurrence of NAION, evaluated at 1, 2, and 3 years of follow-up.
TAKEAWAY:
- The use of semaglutide vs non–GLP-1 RAs was not associated with an increased risk for NAION in people with only type 2 diabetes during the 1-year (hazard ratio [HR], 2.32; 95% CI, 0.60-8.97), 2-year (HR, 2.31; 95% CI, 0.86-6.17), and 3-year (HR, 1.51; 0.71-3.25) follow-up periods.
- Similarly, in the obesity-only cohort, use of semaglutide was not linked to the development of NAION across 1-year (HR, 0.41; 95% CI, 0.08-2.09), 2-year (HR, 0.67; 95% CI, 0.20-2.24), and 3-year (HR, 0.72; 95% CI, 0.24-2.17) follow-up periods.
- The patients with both diabetes and obesity also showed no significant association between use of semaglutide and the risk for NAION across each follow-up period.
- Sensitivity analysis confirmed the prescription of semaglutide was not associated with an increased risk for NAION compared with non–GLP-1 RA medications.
IN PRACTICE:
“Our large, multinational, population-based, real-world study found that semaglutide is not associated with an increased risk of NAION in the general population,” the authors of the study wrote.
SOURCE:
The study was led by Chien-Chih Chou, MD, PhD, of National Yang Ming Chiao Tung University, in Taipei City, Taiwan, and was published online on November 02, 2024, in Ophthalmology.
LIMITATIONS:
The retrospective nature of the study may have limited the ability to establish causality between the use of semaglutide and the risk for NAION. The reliance on diagnosis coding for NAION may have introduced a potential misclassification of cases. Moreover, approximately half of the healthcare organizations in the TriNetX network are based in the United States, potentially limiting the diversity of the data.
DISCLOSURES:
This study was supported by a grant from Taichung Veterans General Hospital. The authors declared no potential conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Researchers conducted a retrospective cohort study using data from the TriNetX Analytics Network to investigate the potential risk for NAION associated with semaglutide use in a broader population worldwide.
- They included Caucasians aged ≥ 18 years with only type 2 diabetes (n = 37,245) , only obesity (n = 138,391), or both (n = 64,989) who visited healthcare facilities three or more times.
- The participants were further grouped into those prescribed semaglutide and those using non–GLP-1 RA medications.
- Propensity score matching was performed to balance age, sex, body mass index, A1C levels, medications, and underlying comorbidities between the participants using semaglutide or non–GLP-1 RAs.
- The main outcome measure was the occurrence of NAION, evaluated at 1, 2, and 3 years of follow-up.
TAKEAWAY:
- The use of semaglutide vs non–GLP-1 RAs was not associated with an increased risk for NAION in people with only type 2 diabetes during the 1-year (hazard ratio [HR], 2.32; 95% CI, 0.60-8.97), 2-year (HR, 2.31; 95% CI, 0.86-6.17), and 3-year (HR, 1.51; 0.71-3.25) follow-up periods.
- Similarly, in the obesity-only cohort, use of semaglutide was not linked to the development of NAION across 1-year (HR, 0.41; 95% CI, 0.08-2.09), 2-year (HR, 0.67; 95% CI, 0.20-2.24), and 3-year (HR, 0.72; 95% CI, 0.24-2.17) follow-up periods.
- The patients with both diabetes and obesity also showed no significant association between use of semaglutide and the risk for NAION across each follow-up period.
- Sensitivity analysis confirmed the prescription of semaglutide was not associated with an increased risk for NAION compared with non–GLP-1 RA medications.
IN PRACTICE:
“Our large, multinational, population-based, real-world study found that semaglutide is not associated with an increased risk of NAION in the general population,” the authors of the study wrote.
SOURCE:
The study was led by Chien-Chih Chou, MD, PhD, of National Yang Ming Chiao Tung University, in Taipei City, Taiwan, and was published online on November 02, 2024, in Ophthalmology.
LIMITATIONS:
The retrospective nature of the study may have limited the ability to establish causality between the use of semaglutide and the risk for NAION. The reliance on diagnosis coding for NAION may have introduced a potential misclassification of cases. Moreover, approximately half of the healthcare organizations in the TriNetX network are based in the United States, potentially limiting the diversity of the data.
DISCLOSURES:
This study was supported by a grant from Taichung Veterans General Hospital. The authors declared no potential conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Satisfaction With Department of Veterans Affairs Prosthetics and Support Services as Reported by Women and Men Veterans
Satisfaction With Department of Veterans Affairs Prosthetics and Support Services as Reported by Women and Men Veterans
Limb loss is a significant and growing concern in the United States. Nearly 2 million Americans are living with limb loss, and up to 185,000 people undergo amputations annually.1-4 Of these patients, about 35% are women.5 The Veterans Health Administration (VHA) provides about 10% of US amputations.6-8 Between 2015 and 2019, the number of prosthetic devices provided to female veterans increased from 3.3 million to 4.6 million.5,9,10
Previous research identified disparities in prosthetic care between men and women, both within and outside the VHA. These disparities include slower prosthesis prescription and receipt among women, in addition to differences in self-reported mobility, satisfaction, rates of prosthesis rejection, and challenges related to prosthesis appearance and fit.5,10,11 Recent studies suggest women tend to have worse outcomes following amputation, and are underrepresented in amputation research.12,13 However, these disparities are poorly described in a large, national sample. Because women represent a growing portion of patients with limb loss in the VHA, understanding their needs is critical.14
The Johnny Isakson and David P. Roe, MD Veterans Health Care and Benefits Improvement Act of 2020 was enacted, in part, to improve the care provided to women veterans.15 The law required the VHA to conduct a survey of ≥ 50,000 veterans to assess the satisfaction of women veterans with prostheses provided by the VHA. To comply with this legislation and understand how women veterans rate their prostheses and related care in the VHA, the US Department of Veterans Affairs (VA) Center for Collaborative Evaluation (VACE) conducted a large national survey of veterans with limb loss that oversampled women veterans. This article describes the survey results, including characteristics of female veterans with limb loss receiving care from the VHA, assesses their satisfaction with prostheses and prosthetic care, and highlights where their responses differ from those of male veterans.
Methods
We conducted a cross-sectional, mixedmode survey of eligible amputees in the VHA Support Service Capital Assets Amputee Data Cube. We identified a cohort of veterans with any major amputation (above the ankle or wrist) or partial hand or foot amputation who received VHA care between October 1, 2019, and September 30, 2020. The final cohort yielded 46,646 potentially eligible veterans. Thirty-three had invalid contact information, leaving 46,613 veterans who were asked to participate, including 1356 women.
Survey
We created a survey instrument de novo that included questions from validated instruments, including the Trinity Amputation Prosthesis and Experience Scales to assess prosthetic device satisfaction, the Prosthesis Evaluation Questionnaire to assess quality of life (QOL) satisfaction, and the Orthotics Prosthetics Users Survey to assess prosthesis-related care satisfaction. 16-18 Additional questions were incorporated from a survey of veterans with upper limb amputation to assess the importance of cosmetic considerations related to the prosthesis and comfort with prosthesis use in intimate relationships.19 Questions were also included to assess amputation type, year of amputation, if a prosthesis was currently used, reasons for ceasing use of a prosthesis, reasons for never using a prosthesis, the types of prostheses used, intensity of prosthesis use, satisfaction with time required to receive a prosthetic limb, and if the prosthesis reflected the veteran’s selfidentified gender. Veterans were asked to answer questions based on their most recent amputation.
We tested the survey using cognitive interviews with 6 veterans to refine the survey and better understand how veterans interpreted the questions. Pilot testers completed the survey and participated in individual interviews with experienced interviewers (CL and RRK) to describe how they selected their responses.20 This feedback was used to refine the survey. The online survey was programmed using Qualtrics Software and manually translated into Spanish.
Given the multimodal design, surveys were distributed by email, text message, and US Postal Service (USPS). Surveys were emailed to all veterans for whom a valid email address was available. If emails were undeliverable, veterans were contacted via text message or the USPS. Surveys were distributed by text message to all veterans without an email address but with a cellphone number. We were unable to consistently identify invalid numbers among all text message recipients. Invitations with a survey URL and QR code were sent via USPS to veterans who had no valid email address or cellphone number. Targeted efforts were made to increase the response rate for women. A random sample of 200 women who had not completed the survey 2 weeks prior to the closing date (15% of women in sample) was selected to receive personal phone calls. Another random sample of 400 women was selected to receive personalized outreach emails. The survey data were confidential, and responses could not be traced to identifying information.
Data Analyses
We conducted a descriptive analysis, including percentages and means for responses to variables focused on describing amputation characteristics, prosthesis characteristics, and QOL. All data, including missing values, were used to document the percentage of respondents for each question. Removing missing data from the denominator when calculating percentages could introduce bias to the analysis because we cannot be certain data are missing at random. Missing variables were removed to avoid underinflation of mean scores.
We compared responses across 2 groups: individuals who self-identified as men and individuals who self-identified as women. For each question, we assessed whether each of these groups differed significantly from the remaining sample. For example, we examined whether the percentage of men who answered affirmatively to a question was significantly higher or lower than that of individuals not identifying as male, and whether the percentage of women who answered affirmatively was significantly higher or lower than that of individuals not identifying as female. We utilized x2 tests to determine significant differences for percentage calculations and t tests to determine significant differences in means across gender.
Since conducting multiple comparisons within a dataset may result in inflating statistical significance (type 1 errors), we used a more conservative estimate of statistical significance (α = 0.01) and high significance (α = 0.001). This study was deemed quality improvement by the VHA Rehabilitation and Prosthetic Services (12RPS) and acknowledged by the VA Research Office at Eastern Colorado Health Care System and was not subject to institutional review board review.
Results
Surveys were distributed to 46,613 veterans and were completed by 4981 respondents for a 10.7% overall response rate. Survey respondents were generally similar to the eligible population invited to participate, but the proportion of women who completed the survey was higher than the proportion of women eligible to participate (2.0% of eligible population vs 16.7% of respondents), likely due to specific efforts to target women. Survey respondents were slightly younger than the general population (67.3 years vs 68.7 years), less likely to be male (97.1% vs 83.3%), showed similar representation of Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) veterans (4.4% vs 4.1%), and were less likely to have diabetes (58.0% vs 52.7% had diabetes) (Table 1).
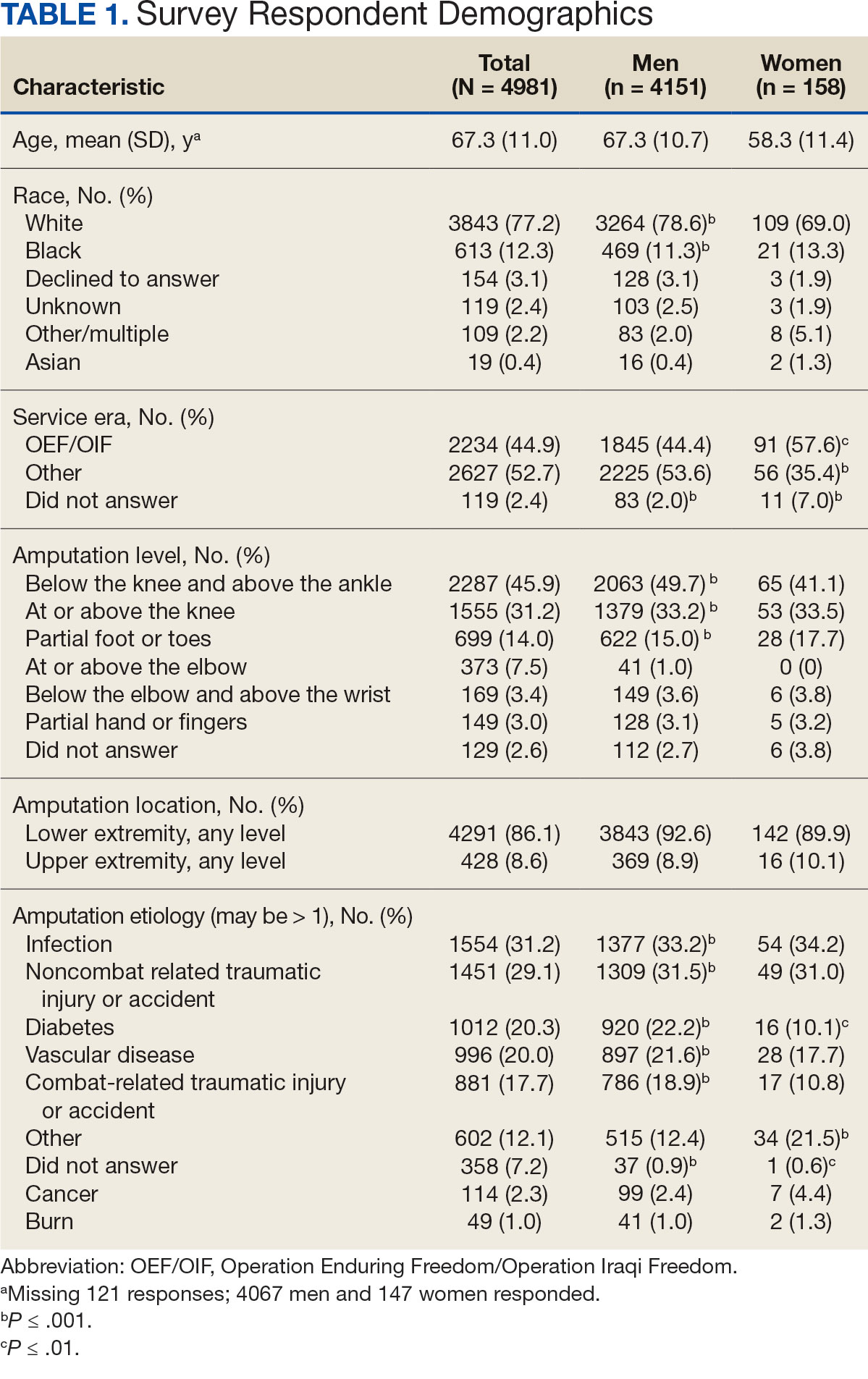
The mean age of male respondents was 67.3 years, while the mean age of female respondents was 58.3 years. The majority of respondents were male (83.3%) and White (77.2%). Female respondents were less likely to have diabetes (35.4% of women vs 53.5% of men) and less likely to report that their most recent amputation resulted from diabetes (10.1% of women vs 22.2% of men). Women respondents were more likely to report an amputation due to other causes, such as adverse results of surgery, neurologic disease, suicide attempt, blood clots, tumors, rheumatoid arthritis, and revisions of previous amputations. Most women respondents did not serve during the OEF or OIF eras. The most common amputation site for women respondents was lower limb, either below the knee and above the ankle or above the knee.
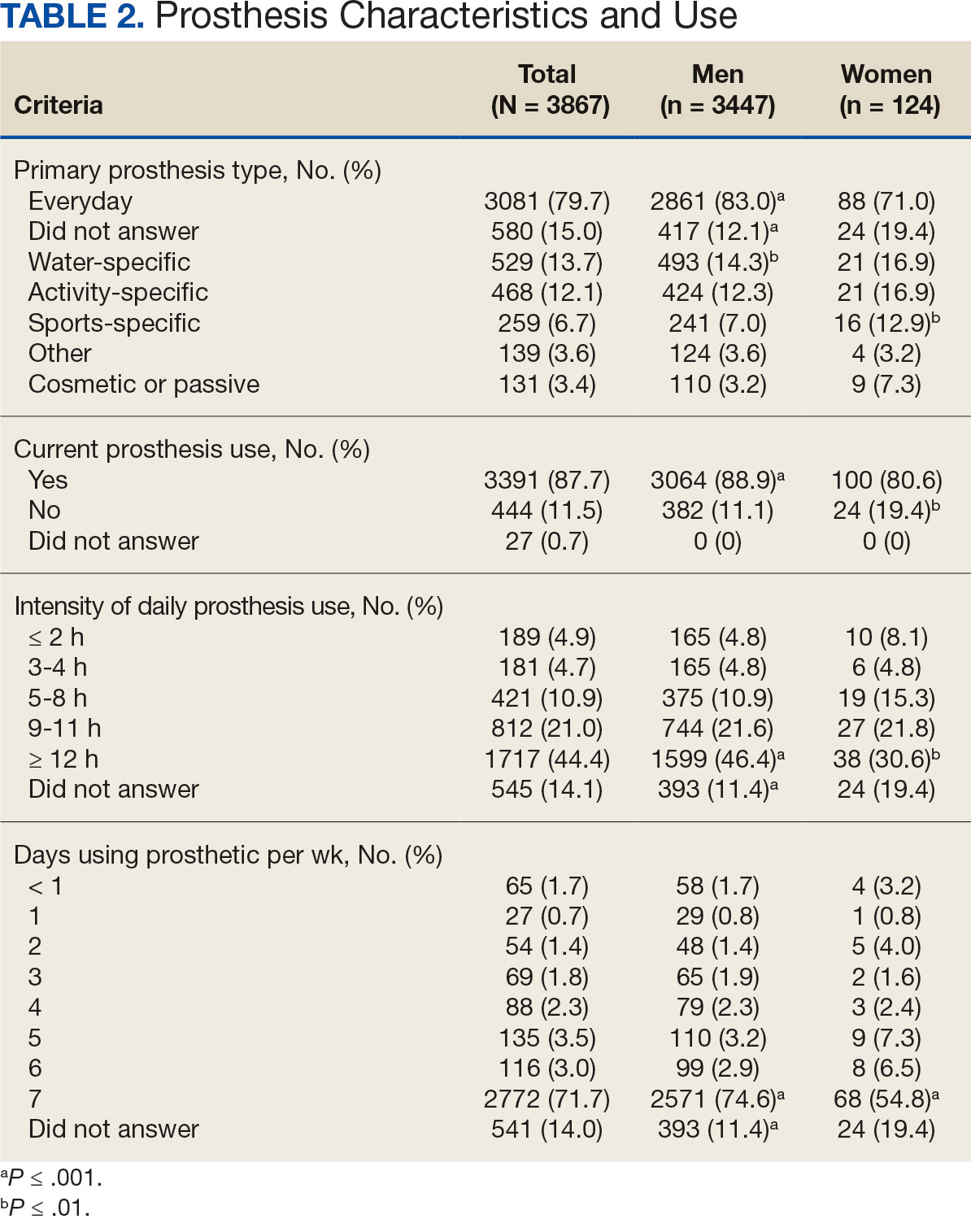
Most participants use an everyday prosthesis, but women were more likely to report using a sports-specific prosthesis (Table 2). Overall, most respondents report using a prosthesis (87.7%); however, women were more likely to report not using a prosthesis (19.4% of women vs 11.1% of men; P ≤ .01). Additionally, a lower proportion of women report using a prosthesis for < 12 hours per day (30.6% of women vs 46.4% of men; P ≤ .01) or using a prosthesis every day (54.8% of women vs 74.6% of men; P ≤ .001).
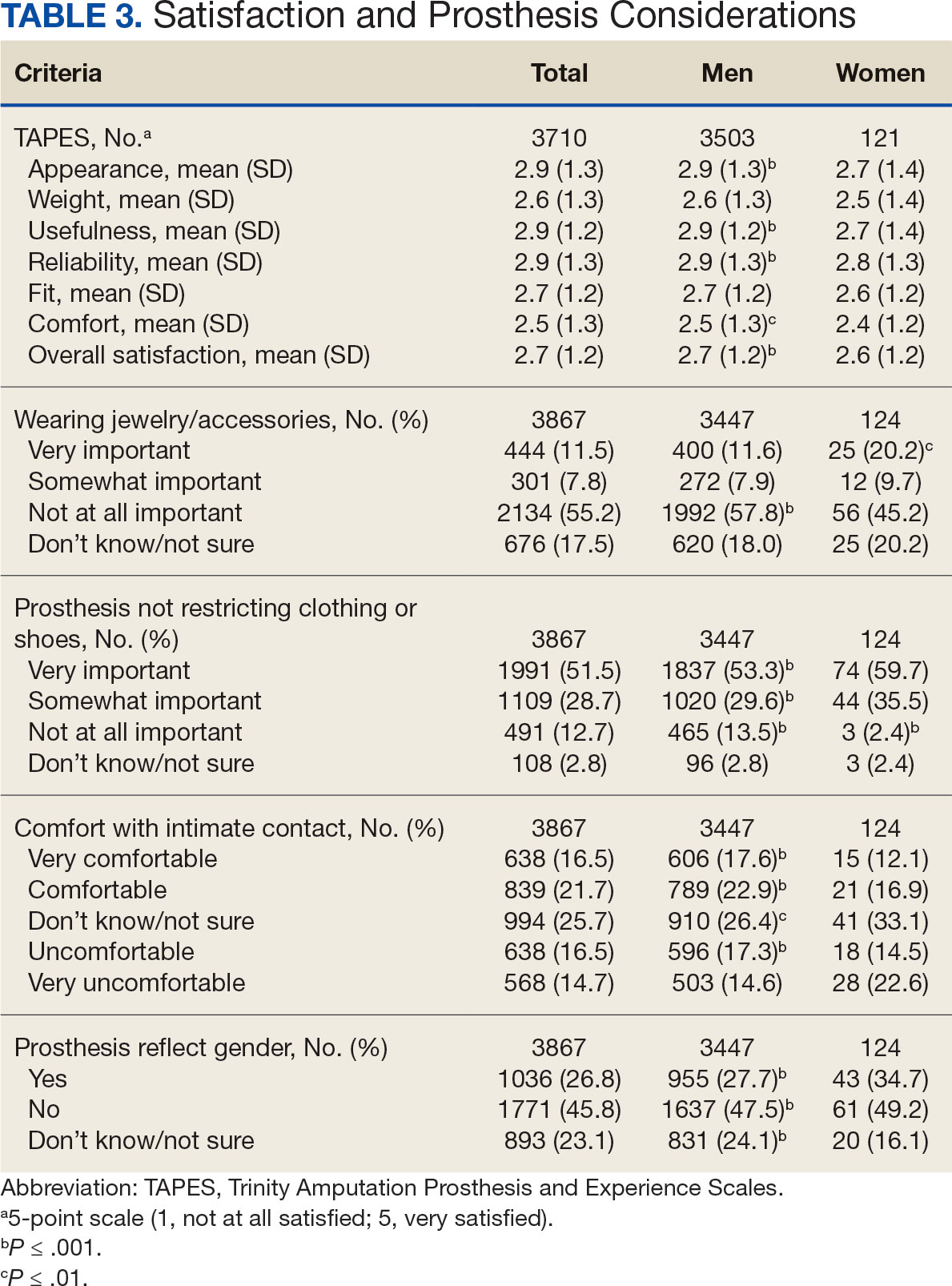
In the overall sample, the mean satisfaction score with a prosthesis was 2.7 on a 5-point scale, and women had slightly lower overall satisfaction scores (2.6 for women vs 2.7 for men; P ≤ .001) (Table 3). Women also had lower satisfaction scores related to appearance, usefulness, reliability, and comfort. Women were more likely to indicate that it was very important to be able to wear jewelry and accessories (20.2% of women vs 11.6% of men; P ≤ .01), while men were less likely to indicate that it was somewhat or very important that the prosthesis not restrict clothing or shoes (95.2% of women vs 82.9% of men; P ≤ .001). Men were more likely than women to report being comfortable or very comfortable using their prosthesis in intimate contact: 40.5% vs 29.0%, respectively (P ≤ .001).
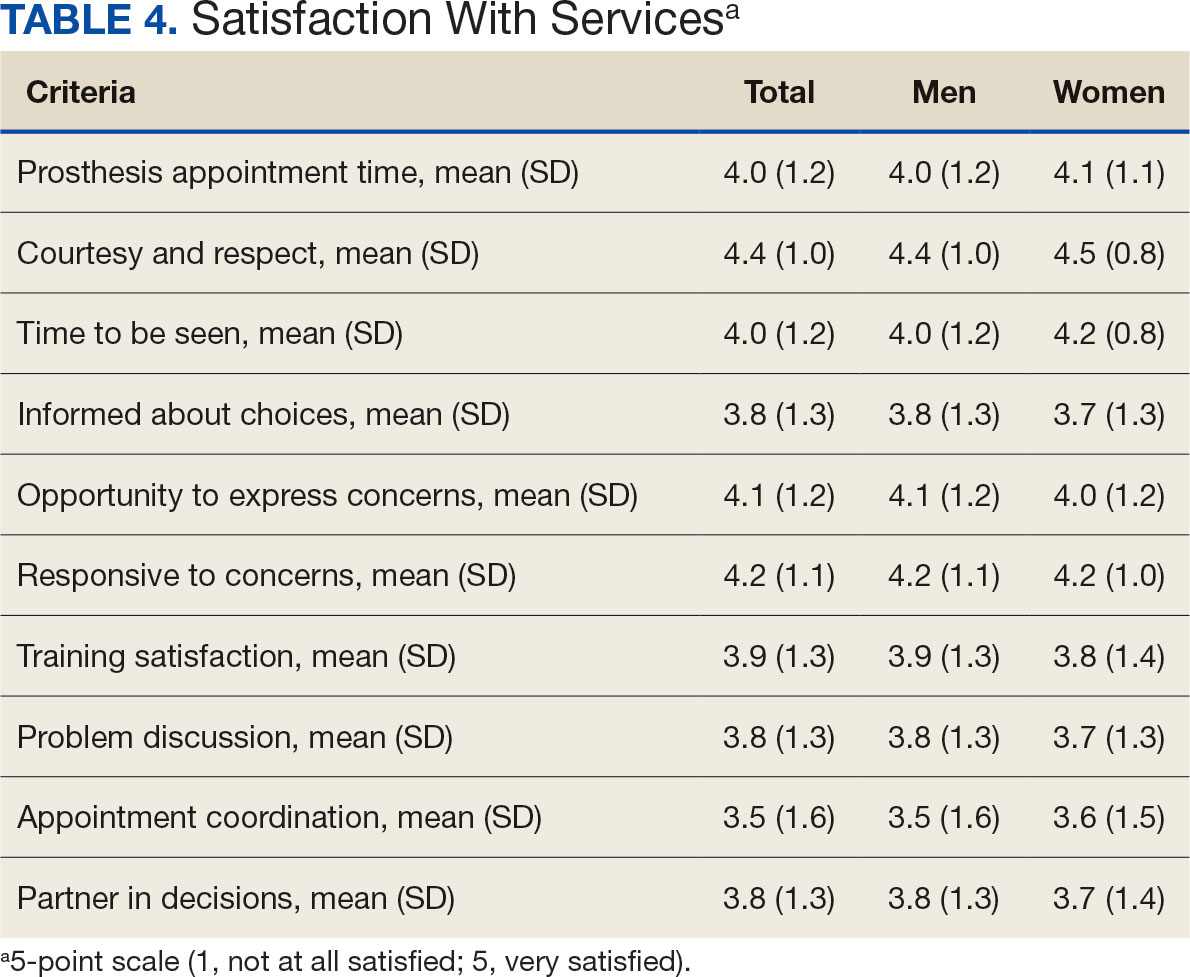
Overall, participants reported high satisfaction with appointment times, wait times, courteous treatment, opportunities to express concerns, and staff responsiveness. Men were slightly more likely than women to be satisfied with training (P ≤ 0.001) and problem discussion (P ≤ 0.01) (Table 4). There were no statistically significant differences in satisfaction or QOL ratings between women and men. The overall sample rated both QOL and satisfaction with QOL 6.7 on a 10-point scale.
Discussion
The goal of this study was to characterize the experience of veterans with limb loss receiving care in the VHA and assess their satisfaction with prostheses and prosthetic care. We received responses from nearly 5000 veterans, 158 of whom were women. Women veteran respondents were slightly younger and less likely to have an amputation due to diabetes. We did not observe significant differences in amputation level between men and women but women were less likely to use a prosthesis, reported lower intensity of prosthesis use, and were less satisfied with certain aspects of their prostheses. Women may also be less satisfied with prosthesis training and problem discussion. However, we found no differences in QOL ratings between men and women.
Findings indicating women were more likely to report not using a prosthesis and that a lower proportion of women report using a prosthesis for > 12 hours a day or every day are consistent with previous research. 21,22 Interestingly, women were more likely to report using a sports-specific prosthesis. This is notable because prior research suggests that individuals with amputations may avoid participating in sports and exercise, and a lack of access to sports-specific prostheses may inhibit physical activity.23,24 Women in this sample were slightly less satisfied with their prostheses overall and reported lower satisfaction scores regarding appearance, usefulness, reliability, and comfort, consistent with previous findings.25
A lower percentage of women in this sample reported being comfortable or very comfortable using their prosthesis during intimate contact. Previous research on prosthesis satisfaction suggests individuals who rate prosthesis satisfaction lower also report lower body image across genders. 26 While women in this sample did not rate their prosthesis satisfaction lower than men, they did report lower intensity of prosthesis use, suggesting potential issues with their prostheses this survey did not evaluate. Women indicated the importance of prostheses not restricting jewelry, accessories, clothing, or shoes. These results have significant clinical and social implications. A recent qualitative study emphasizes that women veterans feel prostheses are primarily designed for men and may not work well with their physiological needs.9 Research focused on limbs better suited to women’s bodies could result in better fitting sockets, lightweight limbs, or less bulky designs. Additional research has also explored the difficulties in accommodating a range of footwear for patients with lower limb amputation. One study found that varying footwear heights affect the function of adjustable prosthetic feet in ways that may not be optimal.27
Ratings of satisfaction with prosthesisrelated services between men and women in this sample are consistent with a recent study showing that women veterans do not have significant differences in satisfaction with prosthesis-related services.28 However, this study focused specifically on lower limb amputations, while the respondents of this study include those with both upper and lower limb amputations. Importantly, our findings that women are less likely to be satisfied with prosthesis training and problem discussions support recent qualitative findings in which women expressed a desire to work with prosthetists who listen to them, take their concerns seriously, and seek solutions that fit their needs. We did not observe a difference in QOL ratings between men and women in the sample despite lower satisfaction among women with some elements of prosthesis-related services. Previous research suggests many factors impact QOL after amputation, most notably time since amputation.16,29
Limitations
This survey was deployed in a short timeline that did not allow for careful sample selection or implementing strategies to increase response rate. Additionally, the study was conducted among veterans receiving care in the VHA, and findings may not be generalizable to limb loss in other settings. Finally, the discrepancy in number of respondents who identified as men vs women made it difficult to compare differences between the 2 groups.
Conclusions
This is the largest sample of survey respondents of veterans with limb loss to date. While the findings suggest veterans are generally satisfied with prosthetic-related services overall, they also highlight several areas for improvement with services or prostheses. Given that most veterans with limb loss are men, there is a significant discrepancy between the number of women and men respondents. Additional studies with more comparable numbers of men and women have found similar ratings of satisfaction with prostheses and services.28 Further research specifically focused on improving the experiences of women should focus on better characterizing their experiences and identifying how they differ from those of male veterans. For example, understanding how to engage female veterans with limb loss in prosthesis training and problem discussions may improve their experience with their care teams and improve their use of prostheses. Understanding experiences and needs that are specific to women could lead to the development of processes, resources, or devices that are tailored to the unique requirements of women with limb loss.
- Ziegler-Graham K, MacKenzie EJ, Ephraim PL, Travison TG, Brookmeyer R. Estimating the prevalence of limb loss in the United States: 2005 to 2050. Arch Phys Med Rehabil. 2008;89(3):422-429. doi:10.1016/j.apmr.2007.11.005
- Dillingham TR, Pezzin LE, MacKenzie EJ. Limb amputation and limb deficiency: epidemiology and recent trends in the united states. South Med J. 2002;95(8):875-883. doi:10.1097/00007611-200208000-00018
- Dillingham TR, Pezzin LE, Shore AD. Reamputation, mortality, and health care costs among persons with dysvascular lower-limb amputations. Arch Phys Med Rehabil. 2005;86(3):480-486. doi:10.1016/j.apmr.2004.06.072
- Centers for Disease Control and Prevention. Ambulatory and inpatient procedures in the United States. Accessed September 30, 2024. https://www.cdc.gov/nchs/pressroom/98facts/ambulat.htm
- Ljung J, Iacangelo A. Identifying and acknowledging a sex gap in lower-limb prosthetics. JPO. 2024;36(1):e18-e24. doi:10.1097/JPO.0000000000000470
- Feinglass J, Brown JL, LoSasso A, et al. Rates of lower-extremity amputation and arterial reconstruction in the united states, 1979 to 1996. Am J Public Health. 1999;89(8):1222- 1227. doi:10.2105/ajph.89.8.1222
- Mayfield JA, Reiber GE, Maynard C, Czerniecki JM, Caps MT, Sangeorzan BJ. Trends in lower limb amputation in the Veterans Health Administration, 1989-1998. J Rehabil Res Dev. 2000;37(1):23-30.
- Feinglass J, Pearce WH, Martin GJ, et al. Postoperative and late survival outcomes after major amputation: findings from the department of veterans affairs national surgical quality improvement program. Surgery. 2001;130(1):21-29. doi:10.1067/msy.2001.115359
- Lehavot K, Young JP, Thomas RM, et al. Voices of women veterans with lower limb prostheses: a qualitative study. J Gen Intern Med. 2022;37(3):799-805. doi:10.1007/s11606-022-07572-8
- US Government Accountability Office. COVID-19: Opportunities to improve federal response. GAO-21-60. Published November 12, 2020. Accessed September 30, 2024. https://www.gao.gov/products/gao-21-60
- Littman AJ, Peterson AC, Korpak A, et al. Differences in prosthetic prescription between men and women veterans after transtibial or transfemoral lowerextremity amputation: a longitudinal cohort study. Arch Phys Med Rehabil. 2023;104(8)1274-1281. doi:10.1016/j.amjsurg.2023.02.011
- Cimino SR, Vijayakumar A, MacKay C, Mayo AL, Hitzig SL, Guilcher SJT. Sex and gender differences in quality of life and related domains for individuals with adult acquired lower-limb amputation: a scoping review. Disabil Rehabil. 2022 Oct 23;44(22):6899-6925. doi:10.1080/09638288.2021.1974106
- DadeMatthews OO, Roper JA, Vazquez A, Shannon DM, Sefton JM. Prosthetic device and service satisfaction, quality of life, and functional performance in lower limb prosthesis clients. Prosthet Orthot Int. 2024;48(4):422-430. doi:10.1097/PXR.0000000000000285
- Hamilton AB, Schwarz EB, Thomas HN, Goldstein KM. Moving women veterans’ health research forward: a special supplement. J Gen Intern Med. 2022;37(Suppl3):665– 667. doi:10.1007/s11606-022-07606-1
- US Congress. Public Law 116-315: An Act to Improve the Lives of Veterans, S 5108 (2) (F). 116th Congress; 2021. Accessed September 30, 2024. https://www.congress.gov/116/plaws/publ315/PLAW-116publ315.pdf
- Gallagher P, MacLachlan M. The Trinity amputation and prosthesis experience scales and quality of life in people with lower-limb amputation. Arch Phys Med Rehabil. 2004;85(5):730-736. doi:10.1016/j.apmr.2003.07.009
- Legro MW, Reiber GD, Smith DG, del Aguila M, Larsen J, Boone D. Prosthesis evaluation questionnaire for persons with lower limb amputations: assessing prosthesis-related quality of life. Arch Phys Med Rehabil. 1998;79(8):931-938. doi:10.1016/s0003-9993(98)90090-9
- Legro MW, Reiber GD, Smith DG, del Aguila M, Larsen J, Boone D. Prosthesis evaluation questionnaire for persons with lower limb amputations: assessing prosthesis-related quality of life. Arch Phys Med Rehabil. 1998;79(8):931-938. doi:10.1016/s0003-9993(98)90090-9
- Heinemann AW, Bode RK, O’Reilly C. Development and measurement properties of the orthotics and prosthetics users’ survey (OPUS): a comprehensive set of clinical outcome instruments. Prosthet Orthot Int. 2003;27(3):191-206. doi:10.1080/03093640308726682
- Resnik LJ, Borgia ML, Clark MA. A national survey of prosthesis use in veterans with major upper limb amputation: comparisons by gender. PM R. 2020;12(11):1086-1098. doi:10.1002/pmrj.12351
- Collins D. Pretesting survey instruments: an overview of cognitive methods. Qual Life Res. 2003;12(3):229-238. doi:10.1023/a:1023254226592
- Østlie K, Lesjø IM, Franklin RJ, Garfelt B, Skjeldal OH, Magnus P. Prosthesis rejection in acquired major upper-limb amputees: a population-based survey. Disabil Rehabil Assist Technol. 2012;7(4):294-303. doi:10.3109/17483107.2011.635405
- Pezzin LE, Dillingham TR, MacKenzie EJ, Ephraim P, Rossbach P. Use and satisfaction with prosthetic limb devices and related services. Arch Phys Med Rehabil. 2004;85(5):723-729. doi:10.1016/j.apmr.2003.06.002
- Deans S, Burns D, McGarry A, Murray K, Mutrie N. Motivations and barriers to prosthesis users participation in physical activity, exercise and sport: a review of the literature. Prosthet Orthot Int. 2012;36(3):260-269. doi:10.1177/0309364612437905
- McDonald CL, Kahn A, Hafner BJ, Morgan SJ. Prevalence of secondary prosthesis use in lower limb prosthesis users. Disabil Rehabil. 2023;46(5):1016-1022. doi:10.1080/09638288.2023.2182919
- Baars EC, Schrier E, Dijkstra PU, Geertzen JHB. Prosthesis satisfaction in lower limb amputees: a systematic review of associated factors and questionnaires. Medicine (Baltimore). 2018;97(39):e12296. doi:10.1097/MD.0000000000012296
- Murray CD, Fox J. Body image and prosthesis satisfaction in the lower limb amputee. Disabil Rehabil. 2002;24(17):925–931. doi:10.1080/09638280210150014
- Major MJ, Quinlan J, Hansen AH, Esposito ER. Effects of women’s footwear on the mechanical function of heel-height accommodating prosthetic feet. PLoS One. 2022;17(1). doi:10.1371/journal.pone.0262910.
- Kuo PB, Lehavot K, Thomas RM, et al. Gender differences in prosthesis-related outcomes among veterans: results of a national survey of U.S. veterans. PM R. 2024;16(3):239- 249. doi:10.1002/pmrj.13028
- Asano M, Rushton P, Miller WC, Deathe BA. Predictors of quality of life among individuals who have a lower limb amputation. Prosthet Orthot Int. 2008;32(2):231-243. doi:10.1080/03093640802024955
Limb loss is a significant and growing concern in the United States. Nearly 2 million Americans are living with limb loss, and up to 185,000 people undergo amputations annually.1-4 Of these patients, about 35% are women.5 The Veterans Health Administration (VHA) provides about 10% of US amputations.6-8 Between 2015 and 2019, the number of prosthetic devices provided to female veterans increased from 3.3 million to 4.6 million.5,9,10
Previous research identified disparities in prosthetic care between men and women, both within and outside the VHA. These disparities include slower prosthesis prescription and receipt among women, in addition to differences in self-reported mobility, satisfaction, rates of prosthesis rejection, and challenges related to prosthesis appearance and fit.5,10,11 Recent studies suggest women tend to have worse outcomes following amputation, and are underrepresented in amputation research.12,13 However, these disparities are poorly described in a large, national sample. Because women represent a growing portion of patients with limb loss in the VHA, understanding their needs is critical.14
The Johnny Isakson and David P. Roe, MD Veterans Health Care and Benefits Improvement Act of 2020 was enacted, in part, to improve the care provided to women veterans.15 The law required the VHA to conduct a survey of ≥ 50,000 veterans to assess the satisfaction of women veterans with prostheses provided by the VHA. To comply with this legislation and understand how women veterans rate their prostheses and related care in the VHA, the US Department of Veterans Affairs (VA) Center for Collaborative Evaluation (VACE) conducted a large national survey of veterans with limb loss that oversampled women veterans. This article describes the survey results, including characteristics of female veterans with limb loss receiving care from the VHA, assesses their satisfaction with prostheses and prosthetic care, and highlights where their responses differ from those of male veterans.
Methods
We conducted a cross-sectional, mixedmode survey of eligible amputees in the VHA Support Service Capital Assets Amputee Data Cube. We identified a cohort of veterans with any major amputation (above the ankle or wrist) or partial hand or foot amputation who received VHA care between October 1, 2019, and September 30, 2020. The final cohort yielded 46,646 potentially eligible veterans. Thirty-three had invalid contact information, leaving 46,613 veterans who were asked to participate, including 1356 women.
Survey
We created a survey instrument de novo that included questions from validated instruments, including the Trinity Amputation Prosthesis and Experience Scales to assess prosthetic device satisfaction, the Prosthesis Evaluation Questionnaire to assess quality of life (QOL) satisfaction, and the Orthotics Prosthetics Users Survey to assess prosthesis-related care satisfaction. 16-18 Additional questions were incorporated from a survey of veterans with upper limb amputation to assess the importance of cosmetic considerations related to the prosthesis and comfort with prosthesis use in intimate relationships.19 Questions were also included to assess amputation type, year of amputation, if a prosthesis was currently used, reasons for ceasing use of a prosthesis, reasons for never using a prosthesis, the types of prostheses used, intensity of prosthesis use, satisfaction with time required to receive a prosthetic limb, and if the prosthesis reflected the veteran’s selfidentified gender. Veterans were asked to answer questions based on their most recent amputation.
We tested the survey using cognitive interviews with 6 veterans to refine the survey and better understand how veterans interpreted the questions. Pilot testers completed the survey and participated in individual interviews with experienced interviewers (CL and RRK) to describe how they selected their responses.20 This feedback was used to refine the survey. The online survey was programmed using Qualtrics Software and manually translated into Spanish.
Given the multimodal design, surveys were distributed by email, text message, and US Postal Service (USPS). Surveys were emailed to all veterans for whom a valid email address was available. If emails were undeliverable, veterans were contacted via text message or the USPS. Surveys were distributed by text message to all veterans without an email address but with a cellphone number. We were unable to consistently identify invalid numbers among all text message recipients. Invitations with a survey URL and QR code were sent via USPS to veterans who had no valid email address or cellphone number. Targeted efforts were made to increase the response rate for women. A random sample of 200 women who had not completed the survey 2 weeks prior to the closing date (15% of women in sample) was selected to receive personal phone calls. Another random sample of 400 women was selected to receive personalized outreach emails. The survey data were confidential, and responses could not be traced to identifying information.
Data Analyses
We conducted a descriptive analysis, including percentages and means for responses to variables focused on describing amputation characteristics, prosthesis characteristics, and QOL. All data, including missing values, were used to document the percentage of respondents for each question. Removing missing data from the denominator when calculating percentages could introduce bias to the analysis because we cannot be certain data are missing at random. Missing variables were removed to avoid underinflation of mean scores.
We compared responses across 2 groups: individuals who self-identified as men and individuals who self-identified as women. For each question, we assessed whether each of these groups differed significantly from the remaining sample. For example, we examined whether the percentage of men who answered affirmatively to a question was significantly higher or lower than that of individuals not identifying as male, and whether the percentage of women who answered affirmatively was significantly higher or lower than that of individuals not identifying as female. We utilized x2 tests to determine significant differences for percentage calculations and t tests to determine significant differences in means across gender.
Since conducting multiple comparisons within a dataset may result in inflating statistical significance (type 1 errors), we used a more conservative estimate of statistical significance (α = 0.01) and high significance (α = 0.001). This study was deemed quality improvement by the VHA Rehabilitation and Prosthetic Services (12RPS) and acknowledged by the VA Research Office at Eastern Colorado Health Care System and was not subject to institutional review board review.
Results
Surveys were distributed to 46,613 veterans and were completed by 4981 respondents for a 10.7% overall response rate. Survey respondents were generally similar to the eligible population invited to participate, but the proportion of women who completed the survey was higher than the proportion of women eligible to participate (2.0% of eligible population vs 16.7% of respondents), likely due to specific efforts to target women. Survey respondents were slightly younger than the general population (67.3 years vs 68.7 years), less likely to be male (97.1% vs 83.3%), showed similar representation of Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) veterans (4.4% vs 4.1%), and were less likely to have diabetes (58.0% vs 52.7% had diabetes) (Table 1).
The mean age of male respondents was 67.3 years, while the mean age of female respondents was 58.3 years. The majority of respondents were male (83.3%) and White (77.2%). Female respondents were less likely to have diabetes (35.4% of women vs 53.5% of men) and less likely to report that their most recent amputation resulted from diabetes (10.1% of women vs 22.2% of men). Women respondents were more likely to report an amputation due to other causes, such as adverse results of surgery, neurologic disease, suicide attempt, blood clots, tumors, rheumatoid arthritis, and revisions of previous amputations. Most women respondents did not serve during the OEF or OIF eras. The most common amputation site for women respondents was lower limb, either below the knee and above the ankle or above the knee.
Most participants use an everyday prosthesis, but women were more likely to report using a sports-specific prosthesis (Table 2). Overall, most respondents report using a prosthesis (87.7%); however, women were more likely to report not using a prosthesis (19.4% of women vs 11.1% of men; P ≤ .01). Additionally, a lower proportion of women report using a prosthesis for < 12 hours per day (30.6% of women vs 46.4% of men; P ≤ .01) or using a prosthesis every day (54.8% of women vs 74.6% of men; P ≤ .001).
In the overall sample, the mean satisfaction score with a prosthesis was 2.7 on a 5-point scale, and women had slightly lower overall satisfaction scores (2.6 for women vs 2.7 for men; P ≤ .001) (Table 3). Women also had lower satisfaction scores related to appearance, usefulness, reliability, and comfort. Women were more likely to indicate that it was very important to be able to wear jewelry and accessories (20.2% of women vs 11.6% of men; P ≤ .01), while men were less likely to indicate that it was somewhat or very important that the prosthesis not restrict clothing or shoes (95.2% of women vs 82.9% of men; P ≤ .001). Men were more likely than women to report being comfortable or very comfortable using their prosthesis in intimate contact: 40.5% vs 29.0%, respectively (P ≤ .001).
Overall, participants reported high satisfaction with appointment times, wait times, courteous treatment, opportunities to express concerns, and staff responsiveness. Men were slightly more likely than women to be satisfied with training (P ≤ 0.001) and problem discussion (P ≤ 0.01) (Table 4). There were no statistically significant differences in satisfaction or QOL ratings between women and men. The overall sample rated both QOL and satisfaction with QOL 6.7 on a 10-point scale.
Discussion
The goal of this study was to characterize the experience of veterans with limb loss receiving care in the VHA and assess their satisfaction with prostheses and prosthetic care. We received responses from nearly 5000 veterans, 158 of whom were women. Women veteran respondents were slightly younger and less likely to have an amputation due to diabetes. We did not observe significant differences in amputation level between men and women but women were less likely to use a prosthesis, reported lower intensity of prosthesis use, and were less satisfied with certain aspects of their prostheses. Women may also be less satisfied with prosthesis training and problem discussion. However, we found no differences in QOL ratings between men and women.
Findings indicating women were more likely to report not using a prosthesis and that a lower proportion of women report using a prosthesis for > 12 hours a day or every day are consistent with previous research. 21,22 Interestingly, women were more likely to report using a sports-specific prosthesis. This is notable because prior research suggests that individuals with amputations may avoid participating in sports and exercise, and a lack of access to sports-specific prostheses may inhibit physical activity.23,24 Women in this sample were slightly less satisfied with their prostheses overall and reported lower satisfaction scores regarding appearance, usefulness, reliability, and comfort, consistent with previous findings.25
A lower percentage of women in this sample reported being comfortable or very comfortable using their prosthesis during intimate contact. Previous research on prosthesis satisfaction suggests individuals who rate prosthesis satisfaction lower also report lower body image across genders. 26 While women in this sample did not rate their prosthesis satisfaction lower than men, they did report lower intensity of prosthesis use, suggesting potential issues with their prostheses this survey did not evaluate. Women indicated the importance of prostheses not restricting jewelry, accessories, clothing, or shoes. These results have significant clinical and social implications. A recent qualitative study emphasizes that women veterans feel prostheses are primarily designed for men and may not work well with their physiological needs.9 Research focused on limbs better suited to women’s bodies could result in better fitting sockets, lightweight limbs, or less bulky designs. Additional research has also explored the difficulties in accommodating a range of footwear for patients with lower limb amputation. One study found that varying footwear heights affect the function of adjustable prosthetic feet in ways that may not be optimal.27
Ratings of satisfaction with prosthesisrelated services between men and women in this sample are consistent with a recent study showing that women veterans do not have significant differences in satisfaction with prosthesis-related services.28 However, this study focused specifically on lower limb amputations, while the respondents of this study include those with both upper and lower limb amputations. Importantly, our findings that women are less likely to be satisfied with prosthesis training and problem discussions support recent qualitative findings in which women expressed a desire to work with prosthetists who listen to them, take their concerns seriously, and seek solutions that fit their needs. We did not observe a difference in QOL ratings between men and women in the sample despite lower satisfaction among women with some elements of prosthesis-related services. Previous research suggests many factors impact QOL after amputation, most notably time since amputation.16,29
Limitations
This survey was deployed in a short timeline that did not allow for careful sample selection or implementing strategies to increase response rate. Additionally, the study was conducted among veterans receiving care in the VHA, and findings may not be generalizable to limb loss in other settings. Finally, the discrepancy in number of respondents who identified as men vs women made it difficult to compare differences between the 2 groups.
Conclusions
This is the largest sample of survey respondents of veterans with limb loss to date. While the findings suggest veterans are generally satisfied with prosthetic-related services overall, they also highlight several areas for improvement with services or prostheses. Given that most veterans with limb loss are men, there is a significant discrepancy between the number of women and men respondents. Additional studies with more comparable numbers of men and women have found similar ratings of satisfaction with prostheses and services.28 Further research specifically focused on improving the experiences of women should focus on better characterizing their experiences and identifying how they differ from those of male veterans. For example, understanding how to engage female veterans with limb loss in prosthesis training and problem discussions may improve their experience with their care teams and improve their use of prostheses. Understanding experiences and needs that are specific to women could lead to the development of processes, resources, or devices that are tailored to the unique requirements of women with limb loss.
Limb loss is a significant and growing concern in the United States. Nearly 2 million Americans are living with limb loss, and up to 185,000 people undergo amputations annually.1-4 Of these patients, about 35% are women.5 The Veterans Health Administration (VHA) provides about 10% of US amputations.6-8 Between 2015 and 2019, the number of prosthetic devices provided to female veterans increased from 3.3 million to 4.6 million.5,9,10
Previous research identified disparities in prosthetic care between men and women, both within and outside the VHA. These disparities include slower prosthesis prescription and receipt among women, in addition to differences in self-reported mobility, satisfaction, rates of prosthesis rejection, and challenges related to prosthesis appearance and fit.5,10,11 Recent studies suggest women tend to have worse outcomes following amputation, and are underrepresented in amputation research.12,13 However, these disparities are poorly described in a large, national sample. Because women represent a growing portion of patients with limb loss in the VHA, understanding their needs is critical.14
The Johnny Isakson and David P. Roe, MD Veterans Health Care and Benefits Improvement Act of 2020 was enacted, in part, to improve the care provided to women veterans.15 The law required the VHA to conduct a survey of ≥ 50,000 veterans to assess the satisfaction of women veterans with prostheses provided by the VHA. To comply with this legislation and understand how women veterans rate their prostheses and related care in the VHA, the US Department of Veterans Affairs (VA) Center for Collaborative Evaluation (VACE) conducted a large national survey of veterans with limb loss that oversampled women veterans. This article describes the survey results, including characteristics of female veterans with limb loss receiving care from the VHA, assesses their satisfaction with prostheses and prosthetic care, and highlights where their responses differ from those of male veterans.
Methods
We conducted a cross-sectional, mixedmode survey of eligible amputees in the VHA Support Service Capital Assets Amputee Data Cube. We identified a cohort of veterans with any major amputation (above the ankle or wrist) or partial hand or foot amputation who received VHA care between October 1, 2019, and September 30, 2020. The final cohort yielded 46,646 potentially eligible veterans. Thirty-three had invalid contact information, leaving 46,613 veterans who were asked to participate, including 1356 women.
Survey
We created a survey instrument de novo that included questions from validated instruments, including the Trinity Amputation Prosthesis and Experience Scales to assess prosthetic device satisfaction, the Prosthesis Evaluation Questionnaire to assess quality of life (QOL) satisfaction, and the Orthotics Prosthetics Users Survey to assess prosthesis-related care satisfaction. 16-18 Additional questions were incorporated from a survey of veterans with upper limb amputation to assess the importance of cosmetic considerations related to the prosthesis and comfort with prosthesis use in intimate relationships.19 Questions were also included to assess amputation type, year of amputation, if a prosthesis was currently used, reasons for ceasing use of a prosthesis, reasons for never using a prosthesis, the types of prostheses used, intensity of prosthesis use, satisfaction with time required to receive a prosthetic limb, and if the prosthesis reflected the veteran’s selfidentified gender. Veterans were asked to answer questions based on their most recent amputation.
We tested the survey using cognitive interviews with 6 veterans to refine the survey and better understand how veterans interpreted the questions. Pilot testers completed the survey and participated in individual interviews with experienced interviewers (CL and RRK) to describe how they selected their responses.20 This feedback was used to refine the survey. The online survey was programmed using Qualtrics Software and manually translated into Spanish.
Given the multimodal design, surveys were distributed by email, text message, and US Postal Service (USPS). Surveys were emailed to all veterans for whom a valid email address was available. If emails were undeliverable, veterans were contacted via text message or the USPS. Surveys were distributed by text message to all veterans without an email address but with a cellphone number. We were unable to consistently identify invalid numbers among all text message recipients. Invitations with a survey URL and QR code were sent via USPS to veterans who had no valid email address or cellphone number. Targeted efforts were made to increase the response rate for women. A random sample of 200 women who had not completed the survey 2 weeks prior to the closing date (15% of women in sample) was selected to receive personal phone calls. Another random sample of 400 women was selected to receive personalized outreach emails. The survey data were confidential, and responses could not be traced to identifying information.
Data Analyses
We conducted a descriptive analysis, including percentages and means for responses to variables focused on describing amputation characteristics, prosthesis characteristics, and QOL. All data, including missing values, were used to document the percentage of respondents for each question. Removing missing data from the denominator when calculating percentages could introduce bias to the analysis because we cannot be certain data are missing at random. Missing variables were removed to avoid underinflation of mean scores.
We compared responses across 2 groups: individuals who self-identified as men and individuals who self-identified as women. For each question, we assessed whether each of these groups differed significantly from the remaining sample. For example, we examined whether the percentage of men who answered affirmatively to a question was significantly higher or lower than that of individuals not identifying as male, and whether the percentage of women who answered affirmatively was significantly higher or lower than that of individuals not identifying as female. We utilized x2 tests to determine significant differences for percentage calculations and t tests to determine significant differences in means across gender.
Since conducting multiple comparisons within a dataset may result in inflating statistical significance (type 1 errors), we used a more conservative estimate of statistical significance (α = 0.01) and high significance (α = 0.001). This study was deemed quality improvement by the VHA Rehabilitation and Prosthetic Services (12RPS) and acknowledged by the VA Research Office at Eastern Colorado Health Care System and was not subject to institutional review board review.
Results
Surveys were distributed to 46,613 veterans and were completed by 4981 respondents for a 10.7% overall response rate. Survey respondents were generally similar to the eligible population invited to participate, but the proportion of women who completed the survey was higher than the proportion of women eligible to participate (2.0% of eligible population vs 16.7% of respondents), likely due to specific efforts to target women. Survey respondents were slightly younger than the general population (67.3 years vs 68.7 years), less likely to be male (97.1% vs 83.3%), showed similar representation of Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) veterans (4.4% vs 4.1%), and were less likely to have diabetes (58.0% vs 52.7% had diabetes) (Table 1).
The mean age of male respondents was 67.3 years, while the mean age of female respondents was 58.3 years. The majority of respondents were male (83.3%) and White (77.2%). Female respondents were less likely to have diabetes (35.4% of women vs 53.5% of men) and less likely to report that their most recent amputation resulted from diabetes (10.1% of women vs 22.2% of men). Women respondents were more likely to report an amputation due to other causes, such as adverse results of surgery, neurologic disease, suicide attempt, blood clots, tumors, rheumatoid arthritis, and revisions of previous amputations. Most women respondents did not serve during the OEF or OIF eras. The most common amputation site for women respondents was lower limb, either below the knee and above the ankle or above the knee.
Most participants use an everyday prosthesis, but women were more likely to report using a sports-specific prosthesis (Table 2). Overall, most respondents report using a prosthesis (87.7%); however, women were more likely to report not using a prosthesis (19.4% of women vs 11.1% of men; P ≤ .01). Additionally, a lower proportion of women report using a prosthesis for < 12 hours per day (30.6% of women vs 46.4% of men; P ≤ .01) or using a prosthesis every day (54.8% of women vs 74.6% of men; P ≤ .001).
In the overall sample, the mean satisfaction score with a prosthesis was 2.7 on a 5-point scale, and women had slightly lower overall satisfaction scores (2.6 for women vs 2.7 for men; P ≤ .001) (Table 3). Women also had lower satisfaction scores related to appearance, usefulness, reliability, and comfort. Women were more likely to indicate that it was very important to be able to wear jewelry and accessories (20.2% of women vs 11.6% of men; P ≤ .01), while men were less likely to indicate that it was somewhat or very important that the prosthesis not restrict clothing or shoes (95.2% of women vs 82.9% of men; P ≤ .001). Men were more likely than women to report being comfortable or very comfortable using their prosthesis in intimate contact: 40.5% vs 29.0%, respectively (P ≤ .001).
Overall, participants reported high satisfaction with appointment times, wait times, courteous treatment, opportunities to express concerns, and staff responsiveness. Men were slightly more likely than women to be satisfied with training (P ≤ 0.001) and problem discussion (P ≤ 0.01) (Table 4). There were no statistically significant differences in satisfaction or QOL ratings between women and men. The overall sample rated both QOL and satisfaction with QOL 6.7 on a 10-point scale.
Discussion
The goal of this study was to characterize the experience of veterans with limb loss receiving care in the VHA and assess their satisfaction with prostheses and prosthetic care. We received responses from nearly 5000 veterans, 158 of whom were women. Women veteran respondents were slightly younger and less likely to have an amputation due to diabetes. We did not observe significant differences in amputation level between men and women but women were less likely to use a prosthesis, reported lower intensity of prosthesis use, and were less satisfied with certain aspects of their prostheses. Women may also be less satisfied with prosthesis training and problem discussion. However, we found no differences in QOL ratings between men and women.
Findings indicating women were more likely to report not using a prosthesis and that a lower proportion of women report using a prosthesis for > 12 hours a day or every day are consistent with previous research. 21,22 Interestingly, women were more likely to report using a sports-specific prosthesis. This is notable because prior research suggests that individuals with amputations may avoid participating in sports and exercise, and a lack of access to sports-specific prostheses may inhibit physical activity.23,24 Women in this sample were slightly less satisfied with their prostheses overall and reported lower satisfaction scores regarding appearance, usefulness, reliability, and comfort, consistent with previous findings.25
A lower percentage of women in this sample reported being comfortable or very comfortable using their prosthesis during intimate contact. Previous research on prosthesis satisfaction suggests individuals who rate prosthesis satisfaction lower also report lower body image across genders. 26 While women in this sample did not rate their prosthesis satisfaction lower than men, they did report lower intensity of prosthesis use, suggesting potential issues with their prostheses this survey did not evaluate. Women indicated the importance of prostheses not restricting jewelry, accessories, clothing, or shoes. These results have significant clinical and social implications. A recent qualitative study emphasizes that women veterans feel prostheses are primarily designed for men and may not work well with their physiological needs.9 Research focused on limbs better suited to women’s bodies could result in better fitting sockets, lightweight limbs, or less bulky designs. Additional research has also explored the difficulties in accommodating a range of footwear for patients with lower limb amputation. One study found that varying footwear heights affect the function of adjustable prosthetic feet in ways that may not be optimal.27
Ratings of satisfaction with prosthesisrelated services between men and women in this sample are consistent with a recent study showing that women veterans do not have significant differences in satisfaction with prosthesis-related services.28 However, this study focused specifically on lower limb amputations, while the respondents of this study include those with both upper and lower limb amputations. Importantly, our findings that women are less likely to be satisfied with prosthesis training and problem discussions support recent qualitative findings in which women expressed a desire to work with prosthetists who listen to them, take their concerns seriously, and seek solutions that fit their needs. We did not observe a difference in QOL ratings between men and women in the sample despite lower satisfaction among women with some elements of prosthesis-related services. Previous research suggests many factors impact QOL after amputation, most notably time since amputation.16,29
Limitations
This survey was deployed in a short timeline that did not allow for careful sample selection or implementing strategies to increase response rate. Additionally, the study was conducted among veterans receiving care in the VHA, and findings may not be generalizable to limb loss in other settings. Finally, the discrepancy in number of respondents who identified as men vs women made it difficult to compare differences between the 2 groups.
Conclusions
This is the largest sample of survey respondents of veterans with limb loss to date. While the findings suggest veterans are generally satisfied with prosthetic-related services overall, they also highlight several areas for improvement with services or prostheses. Given that most veterans with limb loss are men, there is a significant discrepancy between the number of women and men respondents. Additional studies with more comparable numbers of men and women have found similar ratings of satisfaction with prostheses and services.28 Further research specifically focused on improving the experiences of women should focus on better characterizing their experiences and identifying how they differ from those of male veterans. For example, understanding how to engage female veterans with limb loss in prosthesis training and problem discussions may improve their experience with their care teams and improve their use of prostheses. Understanding experiences and needs that are specific to women could lead to the development of processes, resources, or devices that are tailored to the unique requirements of women with limb loss.
- Ziegler-Graham K, MacKenzie EJ, Ephraim PL, Travison TG, Brookmeyer R. Estimating the prevalence of limb loss in the United States: 2005 to 2050. Arch Phys Med Rehabil. 2008;89(3):422-429. doi:10.1016/j.apmr.2007.11.005
- Dillingham TR, Pezzin LE, MacKenzie EJ. Limb amputation and limb deficiency: epidemiology and recent trends in the united states. South Med J. 2002;95(8):875-883. doi:10.1097/00007611-200208000-00018
- Dillingham TR, Pezzin LE, Shore AD. Reamputation, mortality, and health care costs among persons with dysvascular lower-limb amputations. Arch Phys Med Rehabil. 2005;86(3):480-486. doi:10.1016/j.apmr.2004.06.072
- Centers for Disease Control and Prevention. Ambulatory and inpatient procedures in the United States. Accessed September 30, 2024. https://www.cdc.gov/nchs/pressroom/98facts/ambulat.htm
- Ljung J, Iacangelo A. Identifying and acknowledging a sex gap in lower-limb prosthetics. JPO. 2024;36(1):e18-e24. doi:10.1097/JPO.0000000000000470
- Feinglass J, Brown JL, LoSasso A, et al. Rates of lower-extremity amputation and arterial reconstruction in the united states, 1979 to 1996. Am J Public Health. 1999;89(8):1222- 1227. doi:10.2105/ajph.89.8.1222
- Mayfield JA, Reiber GE, Maynard C, Czerniecki JM, Caps MT, Sangeorzan BJ. Trends in lower limb amputation in the Veterans Health Administration, 1989-1998. J Rehabil Res Dev. 2000;37(1):23-30.
- Feinglass J, Pearce WH, Martin GJ, et al. Postoperative and late survival outcomes after major amputation: findings from the department of veterans affairs national surgical quality improvement program. Surgery. 2001;130(1):21-29. doi:10.1067/msy.2001.115359
- Lehavot K, Young JP, Thomas RM, et al. Voices of women veterans with lower limb prostheses: a qualitative study. J Gen Intern Med. 2022;37(3):799-805. doi:10.1007/s11606-022-07572-8
- US Government Accountability Office. COVID-19: Opportunities to improve federal response. GAO-21-60. Published November 12, 2020. Accessed September 30, 2024. https://www.gao.gov/products/gao-21-60
- Littman AJ, Peterson AC, Korpak A, et al. Differences in prosthetic prescription between men and women veterans after transtibial or transfemoral lowerextremity amputation: a longitudinal cohort study. Arch Phys Med Rehabil. 2023;104(8)1274-1281. doi:10.1016/j.amjsurg.2023.02.011
- Cimino SR, Vijayakumar A, MacKay C, Mayo AL, Hitzig SL, Guilcher SJT. Sex and gender differences in quality of life and related domains for individuals with adult acquired lower-limb amputation: a scoping review. Disabil Rehabil. 2022 Oct 23;44(22):6899-6925. doi:10.1080/09638288.2021.1974106
- DadeMatthews OO, Roper JA, Vazquez A, Shannon DM, Sefton JM. Prosthetic device and service satisfaction, quality of life, and functional performance in lower limb prosthesis clients. Prosthet Orthot Int. 2024;48(4):422-430. doi:10.1097/PXR.0000000000000285
- Hamilton AB, Schwarz EB, Thomas HN, Goldstein KM. Moving women veterans’ health research forward: a special supplement. J Gen Intern Med. 2022;37(Suppl3):665– 667. doi:10.1007/s11606-022-07606-1
- US Congress. Public Law 116-315: An Act to Improve the Lives of Veterans, S 5108 (2) (F). 116th Congress; 2021. Accessed September 30, 2024. https://www.congress.gov/116/plaws/publ315/PLAW-116publ315.pdf
- Gallagher P, MacLachlan M. The Trinity amputation and prosthesis experience scales and quality of life in people with lower-limb amputation. Arch Phys Med Rehabil. 2004;85(5):730-736. doi:10.1016/j.apmr.2003.07.009
- Legro MW, Reiber GD, Smith DG, del Aguila M, Larsen J, Boone D. Prosthesis evaluation questionnaire for persons with lower limb amputations: assessing prosthesis-related quality of life. Arch Phys Med Rehabil. 1998;79(8):931-938. doi:10.1016/s0003-9993(98)90090-9
- Legro MW, Reiber GD, Smith DG, del Aguila M, Larsen J, Boone D. Prosthesis evaluation questionnaire for persons with lower limb amputations: assessing prosthesis-related quality of life. Arch Phys Med Rehabil. 1998;79(8):931-938. doi:10.1016/s0003-9993(98)90090-9
- Heinemann AW, Bode RK, O’Reilly C. Development and measurement properties of the orthotics and prosthetics users’ survey (OPUS): a comprehensive set of clinical outcome instruments. Prosthet Orthot Int. 2003;27(3):191-206. doi:10.1080/03093640308726682
- Resnik LJ, Borgia ML, Clark MA. A national survey of prosthesis use in veterans with major upper limb amputation: comparisons by gender. PM R. 2020;12(11):1086-1098. doi:10.1002/pmrj.12351
- Collins D. Pretesting survey instruments: an overview of cognitive methods. Qual Life Res. 2003;12(3):229-238. doi:10.1023/a:1023254226592
- Østlie K, Lesjø IM, Franklin RJ, Garfelt B, Skjeldal OH, Magnus P. Prosthesis rejection in acquired major upper-limb amputees: a population-based survey. Disabil Rehabil Assist Technol. 2012;7(4):294-303. doi:10.3109/17483107.2011.635405
- Pezzin LE, Dillingham TR, MacKenzie EJ, Ephraim P, Rossbach P. Use and satisfaction with prosthetic limb devices and related services. Arch Phys Med Rehabil. 2004;85(5):723-729. doi:10.1016/j.apmr.2003.06.002
- Deans S, Burns D, McGarry A, Murray K, Mutrie N. Motivations and barriers to prosthesis users participation in physical activity, exercise and sport: a review of the literature. Prosthet Orthot Int. 2012;36(3):260-269. doi:10.1177/0309364612437905
- McDonald CL, Kahn A, Hafner BJ, Morgan SJ. Prevalence of secondary prosthesis use in lower limb prosthesis users. Disabil Rehabil. 2023;46(5):1016-1022. doi:10.1080/09638288.2023.2182919
- Baars EC, Schrier E, Dijkstra PU, Geertzen JHB. Prosthesis satisfaction in lower limb amputees: a systematic review of associated factors and questionnaires. Medicine (Baltimore). 2018;97(39):e12296. doi:10.1097/MD.0000000000012296
- Murray CD, Fox J. Body image and prosthesis satisfaction in the lower limb amputee. Disabil Rehabil. 2002;24(17):925–931. doi:10.1080/09638280210150014
- Major MJ, Quinlan J, Hansen AH, Esposito ER. Effects of women’s footwear on the mechanical function of heel-height accommodating prosthetic feet. PLoS One. 2022;17(1). doi:10.1371/journal.pone.0262910.
- Kuo PB, Lehavot K, Thomas RM, et al. Gender differences in prosthesis-related outcomes among veterans: results of a national survey of U.S. veterans. PM R. 2024;16(3):239- 249. doi:10.1002/pmrj.13028
- Asano M, Rushton P, Miller WC, Deathe BA. Predictors of quality of life among individuals who have a lower limb amputation. Prosthet Orthot Int. 2008;32(2):231-243. doi:10.1080/03093640802024955
- Ziegler-Graham K, MacKenzie EJ, Ephraim PL, Travison TG, Brookmeyer R. Estimating the prevalence of limb loss in the United States: 2005 to 2050. Arch Phys Med Rehabil. 2008;89(3):422-429. doi:10.1016/j.apmr.2007.11.005
- Dillingham TR, Pezzin LE, MacKenzie EJ. Limb amputation and limb deficiency: epidemiology and recent trends in the united states. South Med J. 2002;95(8):875-883. doi:10.1097/00007611-200208000-00018
- Dillingham TR, Pezzin LE, Shore AD. Reamputation, mortality, and health care costs among persons with dysvascular lower-limb amputations. Arch Phys Med Rehabil. 2005;86(3):480-486. doi:10.1016/j.apmr.2004.06.072
- Centers for Disease Control and Prevention. Ambulatory and inpatient procedures in the United States. Accessed September 30, 2024. https://www.cdc.gov/nchs/pressroom/98facts/ambulat.htm
- Ljung J, Iacangelo A. Identifying and acknowledging a sex gap in lower-limb prosthetics. JPO. 2024;36(1):e18-e24. doi:10.1097/JPO.0000000000000470
- Feinglass J, Brown JL, LoSasso A, et al. Rates of lower-extremity amputation and arterial reconstruction in the united states, 1979 to 1996. Am J Public Health. 1999;89(8):1222- 1227. doi:10.2105/ajph.89.8.1222
- Mayfield JA, Reiber GE, Maynard C, Czerniecki JM, Caps MT, Sangeorzan BJ. Trends in lower limb amputation in the Veterans Health Administration, 1989-1998. J Rehabil Res Dev. 2000;37(1):23-30.
- Feinglass J, Pearce WH, Martin GJ, et al. Postoperative and late survival outcomes after major amputation: findings from the department of veterans affairs national surgical quality improvement program. Surgery. 2001;130(1):21-29. doi:10.1067/msy.2001.115359
- Lehavot K, Young JP, Thomas RM, et al. Voices of women veterans with lower limb prostheses: a qualitative study. J Gen Intern Med. 2022;37(3):799-805. doi:10.1007/s11606-022-07572-8
- US Government Accountability Office. COVID-19: Opportunities to improve federal response. GAO-21-60. Published November 12, 2020. Accessed September 30, 2024. https://www.gao.gov/products/gao-21-60
- Littman AJ, Peterson AC, Korpak A, et al. Differences in prosthetic prescription between men and women veterans after transtibial or transfemoral lowerextremity amputation: a longitudinal cohort study. Arch Phys Med Rehabil. 2023;104(8)1274-1281. doi:10.1016/j.amjsurg.2023.02.011
- Cimino SR, Vijayakumar A, MacKay C, Mayo AL, Hitzig SL, Guilcher SJT. Sex and gender differences in quality of life and related domains for individuals with adult acquired lower-limb amputation: a scoping review. Disabil Rehabil. 2022 Oct 23;44(22):6899-6925. doi:10.1080/09638288.2021.1974106
- DadeMatthews OO, Roper JA, Vazquez A, Shannon DM, Sefton JM. Prosthetic device and service satisfaction, quality of life, and functional performance in lower limb prosthesis clients. Prosthet Orthot Int. 2024;48(4):422-430. doi:10.1097/PXR.0000000000000285
- Hamilton AB, Schwarz EB, Thomas HN, Goldstein KM. Moving women veterans’ health research forward: a special supplement. J Gen Intern Med. 2022;37(Suppl3):665– 667. doi:10.1007/s11606-022-07606-1
- US Congress. Public Law 116-315: An Act to Improve the Lives of Veterans, S 5108 (2) (F). 116th Congress; 2021. Accessed September 30, 2024. https://www.congress.gov/116/plaws/publ315/PLAW-116publ315.pdf
- Gallagher P, MacLachlan M. The Trinity amputation and prosthesis experience scales and quality of life in people with lower-limb amputation. Arch Phys Med Rehabil. 2004;85(5):730-736. doi:10.1016/j.apmr.2003.07.009
- Legro MW, Reiber GD, Smith DG, del Aguila M, Larsen J, Boone D. Prosthesis evaluation questionnaire for persons with lower limb amputations: assessing prosthesis-related quality of life. Arch Phys Med Rehabil. 1998;79(8):931-938. doi:10.1016/s0003-9993(98)90090-9
- Legro MW, Reiber GD, Smith DG, del Aguila M, Larsen J, Boone D. Prosthesis evaluation questionnaire for persons with lower limb amputations: assessing prosthesis-related quality of life. Arch Phys Med Rehabil. 1998;79(8):931-938. doi:10.1016/s0003-9993(98)90090-9
- Heinemann AW, Bode RK, O’Reilly C. Development and measurement properties of the orthotics and prosthetics users’ survey (OPUS): a comprehensive set of clinical outcome instruments. Prosthet Orthot Int. 2003;27(3):191-206. doi:10.1080/03093640308726682
- Resnik LJ, Borgia ML, Clark MA. A national survey of prosthesis use in veterans with major upper limb amputation: comparisons by gender. PM R. 2020;12(11):1086-1098. doi:10.1002/pmrj.12351
- Collins D. Pretesting survey instruments: an overview of cognitive methods. Qual Life Res. 2003;12(3):229-238. doi:10.1023/a:1023254226592
- Østlie K, Lesjø IM, Franklin RJ, Garfelt B, Skjeldal OH, Magnus P. Prosthesis rejection in acquired major upper-limb amputees: a population-based survey. Disabil Rehabil Assist Technol. 2012;7(4):294-303. doi:10.3109/17483107.2011.635405
- Pezzin LE, Dillingham TR, MacKenzie EJ, Ephraim P, Rossbach P. Use and satisfaction with prosthetic limb devices and related services. Arch Phys Med Rehabil. 2004;85(5):723-729. doi:10.1016/j.apmr.2003.06.002
- Deans S, Burns D, McGarry A, Murray K, Mutrie N. Motivations and barriers to prosthesis users participation in physical activity, exercise and sport: a review of the literature. Prosthet Orthot Int. 2012;36(3):260-269. doi:10.1177/0309364612437905
- McDonald CL, Kahn A, Hafner BJ, Morgan SJ. Prevalence of secondary prosthesis use in lower limb prosthesis users. Disabil Rehabil. 2023;46(5):1016-1022. doi:10.1080/09638288.2023.2182919
- Baars EC, Schrier E, Dijkstra PU, Geertzen JHB. Prosthesis satisfaction in lower limb amputees: a systematic review of associated factors and questionnaires. Medicine (Baltimore). 2018;97(39):e12296. doi:10.1097/MD.0000000000012296
- Murray CD, Fox J. Body image and prosthesis satisfaction in the lower limb amputee. Disabil Rehabil. 2002;24(17):925–931. doi:10.1080/09638280210150014
- Major MJ, Quinlan J, Hansen AH, Esposito ER. Effects of women’s footwear on the mechanical function of heel-height accommodating prosthetic feet. PLoS One. 2022;17(1). doi:10.1371/journal.pone.0262910.
- Kuo PB, Lehavot K, Thomas RM, et al. Gender differences in prosthesis-related outcomes among veterans: results of a national survey of U.S. veterans. PM R. 2024;16(3):239- 249. doi:10.1002/pmrj.13028
- Asano M, Rushton P, Miller WC, Deathe BA. Predictors of quality of life among individuals who have a lower limb amputation. Prosthet Orthot Int. 2008;32(2):231-243. doi:10.1080/03093640802024955
Satisfaction With Department of Veterans Affairs Prosthetics and Support Services as Reported by Women and Men Veterans
Satisfaction With Department of Veterans Affairs Prosthetics and Support Services as Reported by Women and Men Veterans
 visual information does not imply or constitute DoD endorsement.")
Telehealth Vs In-Person Diabetes Care: Is One Better?
Adults with diabetes who participated in telehealth visits reported similar levels of care, trust in the healthcare system, and patient-centered communication compared to those who had in-person visits, a cross-sectional study suggested.
The authors urged continued integration of telehealth into diabetes care beyond December 31, 2024, when the pandemic public health emergency ends, potentially limiting such services.
The study “provides population-level evidence that telehealth can deliver care quality comparable to in-person visits in diabetes management,” lead author Young-Rock Hong, PhD, MPH, an assistant professor in the University of Florida, Gainesville, told this news organization.
“Perhaps the most meaningful finding was the high utilization of telephone-only visits among older adults,” he said. “This has important policy implications, particularly as some insurers and healthcare systems have pushed to restrict telehealth coverage to video-only visits.”
“Maintaining telephone visit coverage is crucial for equitable access, especially for older adults who may be less comfortable with video technology; those with limited internet access; or patients facing other barriers to video visits,” he explained.
The study was published online in BMJ Open.
Video-only, Voice-only, Both
The researchers did a secondary analysis of data from the 2022 Health Information National Trends Survey, a nationally representative survey that includes information on health communication and knowledge and perceptions about all health conditions among US adults aged ≥ 18 years.
Participants had a self-reported diagnosis of type 1 or type 2 diabetes. The mean age was 59.4 years; 50% were women; and 53% were non-Hispanic White individuals.
Primary and secondary outcomes were use of telehealth in the last 12-months; telehealth modality; overall perception of quality of care; perceived trust in the healthcare system; and patient-centered communication score.
In the analysis of 1116 participants representing 33.6 million individuals, 48.1% reported telehealth use in the past 12 months.
Telehealth users were more likely to be younger and women with higher household incomes and health insurance coverage; live in metropolitan areas; and have multiple chronic conditions, poorer perceived health status, and more frequent physician visits than nonusers.
After adjustment, adults aged ≥ 65 years had a significantly lower likelihood of telehealth use than those ages 18-49 years (odds ratio [OR], 0.43).
Higher income and more frequent healthcare visits were predictors of telehealth usage, with no significant differences across race, education, or location.
Those with a household income between $35,000 and $74,999 had more than double the likelihood of telehealth use (OR, 2.14) than those with incomes below $35,000.
Among telehealth users, 39.3% reported having video-only; 35%, phone (voice)-only; and 25.7%, both modalities. Among those aged ≥ 65 years, 55.5% used phone calls only and 25.5% used video only. In contrast, those aged 18-49 years had higher rates of video-only use (36.1%) and combined video/phone use (31.2%).
Healthcare provider recommendation (68.1%) was the most common reason for telehealth use, followed by convenience (57.7%), avoiding potential COVID-19 exposure (48.1%), and obtaining advice about the need for in-person care (23.6%).
Nonusers said they preferred in-person visits and also cited privacy concerns and technology challenges.
Patient-reported quality-of-care outcomes were comparable between telehealth users and nonusers, with no significant differences by telehealth modality or area of residence (urban or rural).
Around 70% of individuals with diabetes in both groups rated their quality of care as “excellent” and “very good;” fewer than 10% rated their care as “fair” and “poor.”
Similarly, trust in the healthcare system was comparable between users and nonusers: 41.3% of telehealth users 41% of nonusers reported trusting the healthcare system “very much.” Patient-centered communication scores were also similar between users and nonusers.
Telehealth appears to be a good option from the providers’ perspective as well, according to the authors. A previous study by the team found more than 80% of US physicians intended to continue telehealth beyond the pandemic.
“The recent unanimous bipartisan passage of the Telehealth Modernization Act by the House Energy & Commerce Committee signals strong political support for extending telehealth flexibilities through 2026,” Hong said. “The bill addresses key access issues by permanently removing geographic restrictions, expanding eligible providers, and maintaining audio-only coverage — provisions that align with our study’s findings about the importance of telephone visits, particularly for older adults and underserved populations.”
There is concern that extending telehealth services might increase Medicare spending by over $2 billion, he added. “While this may be a valid concern, there is a need for more robust evidence regarding the overall value of telehealth services — ie, the ‘benefits’ they provide relative to their costs and outcomes.”
Reassuring, but More Research Needed
COVID prompted “dramatic shifts” in care delivery from in-person to telehealth, Kevin Peterson, MD, MPH, American Diabetes Association vice president of primary care told this news organization. “The authors’ findings provide reassurance that these changes provided for additional convenience in care delivery without being associated with compromises in patient-reported care quality.”
However, he said, “the study does not necessarily capture representative samples of rural and underserved populations, making the impact of telehealth on health equity difficult to determine.” In addition, although patient-perceived care quality did not change with telehealth delivery, the study “does not address impacts on safety, clinical outcomes, equity, costs, or other important measures.”
Furthermore, he noted, “this is an association study that occurred during the dramatic changes brought about by COVID. It may not represent provider or patient preferences that characterize the role of telehealth under more normal circumstances.”
For now, clinicians should be aware that “initial evidence suggests that telehealth can be integrated into care without significantly compromising the patient’s perception of the quality of care,” he concluded.
No funding was declared. Hong and Peterson reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Adults with diabetes who participated in telehealth visits reported similar levels of care, trust in the healthcare system, and patient-centered communication compared to those who had in-person visits, a cross-sectional study suggested.
The authors urged continued integration of telehealth into diabetes care beyond December 31, 2024, when the pandemic public health emergency ends, potentially limiting such services.
The study “provides population-level evidence that telehealth can deliver care quality comparable to in-person visits in diabetes management,” lead author Young-Rock Hong, PhD, MPH, an assistant professor in the University of Florida, Gainesville, told this news organization.
“Perhaps the most meaningful finding was the high utilization of telephone-only visits among older adults,” he said. “This has important policy implications, particularly as some insurers and healthcare systems have pushed to restrict telehealth coverage to video-only visits.”
“Maintaining telephone visit coverage is crucial for equitable access, especially for older adults who may be less comfortable with video technology; those with limited internet access; or patients facing other barriers to video visits,” he explained.
The study was published online in BMJ Open.
Video-only, Voice-only, Both
The researchers did a secondary analysis of data from the 2022 Health Information National Trends Survey, a nationally representative survey that includes information on health communication and knowledge and perceptions about all health conditions among US adults aged ≥ 18 years.
Participants had a self-reported diagnosis of type 1 or type 2 diabetes. The mean age was 59.4 years; 50% were women; and 53% were non-Hispanic White individuals.
Primary and secondary outcomes were use of telehealth in the last 12-months; telehealth modality; overall perception of quality of care; perceived trust in the healthcare system; and patient-centered communication score.
In the analysis of 1116 participants representing 33.6 million individuals, 48.1% reported telehealth use in the past 12 months.
Telehealth users were more likely to be younger and women with higher household incomes and health insurance coverage; live in metropolitan areas; and have multiple chronic conditions, poorer perceived health status, and more frequent physician visits than nonusers.
After adjustment, adults aged ≥ 65 years had a significantly lower likelihood of telehealth use than those ages 18-49 years (odds ratio [OR], 0.43).
Higher income and more frequent healthcare visits were predictors of telehealth usage, with no significant differences across race, education, or location.
Those with a household income between $35,000 and $74,999 had more than double the likelihood of telehealth use (OR, 2.14) than those with incomes below $35,000.
Among telehealth users, 39.3% reported having video-only; 35%, phone (voice)-only; and 25.7%, both modalities. Among those aged ≥ 65 years, 55.5% used phone calls only and 25.5% used video only. In contrast, those aged 18-49 years had higher rates of video-only use (36.1%) and combined video/phone use (31.2%).
Healthcare provider recommendation (68.1%) was the most common reason for telehealth use, followed by convenience (57.7%), avoiding potential COVID-19 exposure (48.1%), and obtaining advice about the need for in-person care (23.6%).
Nonusers said they preferred in-person visits and also cited privacy concerns and technology challenges.
Patient-reported quality-of-care outcomes were comparable between telehealth users and nonusers, with no significant differences by telehealth modality or area of residence (urban or rural).
Around 70% of individuals with diabetes in both groups rated their quality of care as “excellent” and “very good;” fewer than 10% rated their care as “fair” and “poor.”
Similarly, trust in the healthcare system was comparable between users and nonusers: 41.3% of telehealth users 41% of nonusers reported trusting the healthcare system “very much.” Patient-centered communication scores were also similar between users and nonusers.
Telehealth appears to be a good option from the providers’ perspective as well, according to the authors. A previous study by the team found more than 80% of US physicians intended to continue telehealth beyond the pandemic.
“The recent unanimous bipartisan passage of the Telehealth Modernization Act by the House Energy & Commerce Committee signals strong political support for extending telehealth flexibilities through 2026,” Hong said. “The bill addresses key access issues by permanently removing geographic restrictions, expanding eligible providers, and maintaining audio-only coverage — provisions that align with our study’s findings about the importance of telephone visits, particularly for older adults and underserved populations.”
There is concern that extending telehealth services might increase Medicare spending by over $2 billion, he added. “While this may be a valid concern, there is a need for more robust evidence regarding the overall value of telehealth services — ie, the ‘benefits’ they provide relative to their costs and outcomes.”
Reassuring, but More Research Needed
COVID prompted “dramatic shifts” in care delivery from in-person to telehealth, Kevin Peterson, MD, MPH, American Diabetes Association vice president of primary care told this news organization. “The authors’ findings provide reassurance that these changes provided for additional convenience in care delivery without being associated with compromises in patient-reported care quality.”
However, he said, “the study does not necessarily capture representative samples of rural and underserved populations, making the impact of telehealth on health equity difficult to determine.” In addition, although patient-perceived care quality did not change with telehealth delivery, the study “does not address impacts on safety, clinical outcomes, equity, costs, or other important measures.”
Furthermore, he noted, “this is an association study that occurred during the dramatic changes brought about by COVID. It may not represent provider or patient preferences that characterize the role of telehealth under more normal circumstances.”
For now, clinicians should be aware that “initial evidence suggests that telehealth can be integrated into care without significantly compromising the patient’s perception of the quality of care,” he concluded.
No funding was declared. Hong and Peterson reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Adults with diabetes who participated in telehealth visits reported similar levels of care, trust in the healthcare system, and patient-centered communication compared to those who had in-person visits, a cross-sectional study suggested.
The authors urged continued integration of telehealth into diabetes care beyond December 31, 2024, when the pandemic public health emergency ends, potentially limiting such services.
The study “provides population-level evidence that telehealth can deliver care quality comparable to in-person visits in diabetes management,” lead author Young-Rock Hong, PhD, MPH, an assistant professor in the University of Florida, Gainesville, told this news organization.
“Perhaps the most meaningful finding was the high utilization of telephone-only visits among older adults,” he said. “This has important policy implications, particularly as some insurers and healthcare systems have pushed to restrict telehealth coverage to video-only visits.”
“Maintaining telephone visit coverage is crucial for equitable access, especially for older adults who may be less comfortable with video technology; those with limited internet access; or patients facing other barriers to video visits,” he explained.
The study was published online in BMJ Open.
Video-only, Voice-only, Both
The researchers did a secondary analysis of data from the 2022 Health Information National Trends Survey, a nationally representative survey that includes information on health communication and knowledge and perceptions about all health conditions among US adults aged ≥ 18 years.
Participants had a self-reported diagnosis of type 1 or type 2 diabetes. The mean age was 59.4 years; 50% were women; and 53% were non-Hispanic White individuals.
Primary and secondary outcomes were use of telehealth in the last 12-months; telehealth modality; overall perception of quality of care; perceived trust in the healthcare system; and patient-centered communication score.
In the analysis of 1116 participants representing 33.6 million individuals, 48.1% reported telehealth use in the past 12 months.
Telehealth users were more likely to be younger and women with higher household incomes and health insurance coverage; live in metropolitan areas; and have multiple chronic conditions, poorer perceived health status, and more frequent physician visits than nonusers.
After adjustment, adults aged ≥ 65 years had a significantly lower likelihood of telehealth use than those ages 18-49 years (odds ratio [OR], 0.43).
Higher income and more frequent healthcare visits were predictors of telehealth usage, with no significant differences across race, education, or location.
Those with a household income between $35,000 and $74,999 had more than double the likelihood of telehealth use (OR, 2.14) than those with incomes below $35,000.
Among telehealth users, 39.3% reported having video-only; 35%, phone (voice)-only; and 25.7%, both modalities. Among those aged ≥ 65 years, 55.5% used phone calls only and 25.5% used video only. In contrast, those aged 18-49 years had higher rates of video-only use (36.1%) and combined video/phone use (31.2%).
Healthcare provider recommendation (68.1%) was the most common reason for telehealth use, followed by convenience (57.7%), avoiding potential COVID-19 exposure (48.1%), and obtaining advice about the need for in-person care (23.6%).
Nonusers said they preferred in-person visits and also cited privacy concerns and technology challenges.
Patient-reported quality-of-care outcomes were comparable between telehealth users and nonusers, with no significant differences by telehealth modality or area of residence (urban or rural).
Around 70% of individuals with diabetes in both groups rated their quality of care as “excellent” and “very good;” fewer than 10% rated their care as “fair” and “poor.”
Similarly, trust in the healthcare system was comparable between users and nonusers: 41.3% of telehealth users 41% of nonusers reported trusting the healthcare system “very much.” Patient-centered communication scores were also similar between users and nonusers.
Telehealth appears to be a good option from the providers’ perspective as well, according to the authors. A previous study by the team found more than 80% of US physicians intended to continue telehealth beyond the pandemic.
“The recent unanimous bipartisan passage of the Telehealth Modernization Act by the House Energy & Commerce Committee signals strong political support for extending telehealth flexibilities through 2026,” Hong said. “The bill addresses key access issues by permanently removing geographic restrictions, expanding eligible providers, and maintaining audio-only coverage — provisions that align with our study’s findings about the importance of telephone visits, particularly for older adults and underserved populations.”
There is concern that extending telehealth services might increase Medicare spending by over $2 billion, he added. “While this may be a valid concern, there is a need for more robust evidence regarding the overall value of telehealth services — ie, the ‘benefits’ they provide relative to their costs and outcomes.”
Reassuring, but More Research Needed
COVID prompted “dramatic shifts” in care delivery from in-person to telehealth, Kevin Peterson, MD, MPH, American Diabetes Association vice president of primary care told this news organization. “The authors’ findings provide reassurance that these changes provided for additional convenience in care delivery without being associated with compromises in patient-reported care quality.”
However, he said, “the study does not necessarily capture representative samples of rural and underserved populations, making the impact of telehealth on health equity difficult to determine.” In addition, although patient-perceived care quality did not change with telehealth delivery, the study “does not address impacts on safety, clinical outcomes, equity, costs, or other important measures.”
Furthermore, he noted, “this is an association study that occurred during the dramatic changes brought about by COVID. It may not represent provider or patient preferences that characterize the role of telehealth under more normal circumstances.”
For now, clinicians should be aware that “initial evidence suggests that telehealth can be integrated into care without significantly compromising the patient’s perception of the quality of care,” he concluded.
No funding was declared. Hong and Peterson reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM BMJ OPEN
Oral Semaglutide 25-mg Dose May Provide Most Benefit
SAN ANTONIO — Oral semaglutide 25 mg appears to be just as effective in promoting weight loss and other beneficial outcomes as are the investigational 50-mg oral dose and the injectable 2.4-mg dose (Wegovy), in new research.
Data from Novo Nordisk’s OASIS 4 trial suggest that “oral semaglutide 25 mg may represent an efficacious option for the treatment of overweight and obesity, particularly in patients who prefer oral administration,” W. Timothy Garvey, MD, professor in the Department of Nutrition Sciences at the University of Alabama at Birmingham (UAB), said at the Obesity Society’s Obesity Week 2024 meeting.
In an interview, Garvey, who is also senior scientist at the UAB Nutrition Obesity Research Center, added: “There’s a principle in medicine that you always use the lowest dose that has highest efficacy, and for oral semaglutide for obesity, that appears to be the 25-mg dose. We need oral medicines to offer as an option for patients that could lead to a longer persistence in adherence to obesity medications, which is a big problem. Less than half the people maintain their adherence after a year.”
Asked to comment, session moderator and obesity researcher Joseph A. Skelton, MD, professor of pediatrics at Wake Forest University School of Medicine, Winston-Salem, North Carolina, said that OASIS 4 was “extremely well done, especially given that we’re all concerned about the high prevalence of people stopping these medications at a year. ... I love the idea of trying to find these lower doses and increasing options for people.”
(The oral semaglutide approved for treating type 2 diabetes [Rybelsus] is sold in 7-mg and 14-mg doses.)
With Oral Semaglutide, Lower May Be Better
OASIS 4 was a double-blind, randomized, placebo-controlled 64-week multicenter trial involving a total of 307 participants with overweight/obesity randomized 2:1 to oral semaglutide 25 mg or placebo. Of those, 167 in the semaglutide 25 mg and 76 in the placebo groups completed the trial.
For the co–primary endpoint change in body weight at week 64 (including 52-week maintenance and 7-week follow-up periods), there was a drop of 13.6% with oral semaglutide vs just 2.2% with placebo (P < .0001), based on in-trial observation regardless of adherence. For the analysis including just the on-treatment period, those reductions were 16.6% and 2.7%, respectively (P < .0001).
For the other co–primary endpoint, 79.2% semaglutide vs 31.1% placebo lost at least 5% of their body weight, 63.0% vs 14.4% lost ≥ 10%, 50.0% vs 5.6% lost ≥ 15%, and 29.7% vs 3.3% lost ≥ 20%. All were statistically significant differences, at P < .0001.
On the Impact of Weight on Quality of Life-Lite Clinical Trials Version, change from baseline scores were 16.2 with oral semaglutide vs 8.4 for placebo (P = .0006) and the proportion of participants achieving clinically meaningful increases in those scores (≥ 14.6 points) were 55.3% vs 34.8% (P = .0022).
Waist circumference was also significantly reduced from baseline with oral semaglutide, by 12.2 cm vs 2.8 cm (P < .0001). Both systolic and diastolic blood pressure dropped more with semaglutide than placebo, but not significantly. However, the inflammatory marker C-reactive protein dropped from baseline by 46.4% vs just 4.2% with placebo, a significant difference (P < .0001).
Hemoglobin A1c dropped by 0.29 percentage points vs just 0.06 with placebo (P = .0012) and fasting plasma glucose by 6.6 mg/dL, while rising by 0.4 mg/dL in the placebo group (P = .0012). Lipid levels also improved more with oral semaglutide.
Overall adverse events occurred in 93.1% on oral semaglutide and 85.3% with placebo, and gastrointestinal adverse events in 74% and 42.2%, respectively. Other types of adverse events didn’t differ between the groups. The proportions experiencing severe adverse events were less in the semaglutide group (3.9% vs 8.8%), although adverse events leading to permanent treatment discontinuation were slightly higher with oral semaglutide (6.9% vs 5.9%). There were no deaths.
The estimated treatment difference from placebo in body weight change of −11.4% in OASIS 4 (P < .0001) was similar to the –12.7% (P < .0001) seen with the 50-mg oral semaglutide dose studied in OASIS 1 and the –12.4% (P < .0001) difference with subcutaneous semaglutide 2.4 mg in the STEP 1 trial. “All had pretty comparable efficacy,” Garvey noted.
The side-effect profiles, including frequency of gastrointestinal side effects, were also similar across the three trials. However, Garvey added, “the mean duration of nausea in those patients that experienced nausea was shorter in patients on a 25-mg dose, 13 days, whereas the mean duration of nausea was greater, 19 days, in those in OASIS 1 taking 50 mg a day.”
Garvey has consulted for Boehringer Ingelheim, Carmot Therapeutics/Roche, Eli Lilly, Fractyl Laboratories, Inogen, Lilly, Merck, Novo Nordisk, and Zealand Pharma; has ownership interest (stock, stock options in a publicly owned company) for Bristol-Myers Squibb, Isis, Lilly, and Novartis; serves as site principal investigator for Carmot Therapeutics/Roche, Eli Lilly, Epitomee Medical, Lilly, Neurovalens, Novo Nordisk, and Zealand Pharmaceuticals; and as a data monitoring committee member for Boehringer Ingelheim and Eli Lilly. Skelton is editor in chief of the journal Childhood Obesity.
A version of this article first appeared on Medscape.com.
SAN ANTONIO — Oral semaglutide 25 mg appears to be just as effective in promoting weight loss and other beneficial outcomes as are the investigational 50-mg oral dose and the injectable 2.4-mg dose (Wegovy), in new research.
Data from Novo Nordisk’s OASIS 4 trial suggest that “oral semaglutide 25 mg may represent an efficacious option for the treatment of overweight and obesity, particularly in patients who prefer oral administration,” W. Timothy Garvey, MD, professor in the Department of Nutrition Sciences at the University of Alabama at Birmingham (UAB), said at the Obesity Society’s Obesity Week 2024 meeting.
In an interview, Garvey, who is also senior scientist at the UAB Nutrition Obesity Research Center, added: “There’s a principle in medicine that you always use the lowest dose that has highest efficacy, and for oral semaglutide for obesity, that appears to be the 25-mg dose. We need oral medicines to offer as an option for patients that could lead to a longer persistence in adherence to obesity medications, which is a big problem. Less than half the people maintain their adherence after a year.”
Asked to comment, session moderator and obesity researcher Joseph A. Skelton, MD, professor of pediatrics at Wake Forest University School of Medicine, Winston-Salem, North Carolina, said that OASIS 4 was “extremely well done, especially given that we’re all concerned about the high prevalence of people stopping these medications at a year. ... I love the idea of trying to find these lower doses and increasing options for people.”
(The oral semaglutide approved for treating type 2 diabetes [Rybelsus] is sold in 7-mg and 14-mg doses.)
With Oral Semaglutide, Lower May Be Better
OASIS 4 was a double-blind, randomized, placebo-controlled 64-week multicenter trial involving a total of 307 participants with overweight/obesity randomized 2:1 to oral semaglutide 25 mg or placebo. Of those, 167 in the semaglutide 25 mg and 76 in the placebo groups completed the trial.
For the co–primary endpoint change in body weight at week 64 (including 52-week maintenance and 7-week follow-up periods), there was a drop of 13.6% with oral semaglutide vs just 2.2% with placebo (P < .0001), based on in-trial observation regardless of adherence. For the analysis including just the on-treatment period, those reductions were 16.6% and 2.7%, respectively (P < .0001).
For the other co–primary endpoint, 79.2% semaglutide vs 31.1% placebo lost at least 5% of their body weight, 63.0% vs 14.4% lost ≥ 10%, 50.0% vs 5.6% lost ≥ 15%, and 29.7% vs 3.3% lost ≥ 20%. All were statistically significant differences, at P < .0001.
On the Impact of Weight on Quality of Life-Lite Clinical Trials Version, change from baseline scores were 16.2 with oral semaglutide vs 8.4 for placebo (P = .0006) and the proportion of participants achieving clinically meaningful increases in those scores (≥ 14.6 points) were 55.3% vs 34.8% (P = .0022).
Waist circumference was also significantly reduced from baseline with oral semaglutide, by 12.2 cm vs 2.8 cm (P < .0001). Both systolic and diastolic blood pressure dropped more with semaglutide than placebo, but not significantly. However, the inflammatory marker C-reactive protein dropped from baseline by 46.4% vs just 4.2% with placebo, a significant difference (P < .0001).
Hemoglobin A1c dropped by 0.29 percentage points vs just 0.06 with placebo (P = .0012) and fasting plasma glucose by 6.6 mg/dL, while rising by 0.4 mg/dL in the placebo group (P = .0012). Lipid levels also improved more with oral semaglutide.
Overall adverse events occurred in 93.1% on oral semaglutide and 85.3% with placebo, and gastrointestinal adverse events in 74% and 42.2%, respectively. Other types of adverse events didn’t differ between the groups. The proportions experiencing severe adverse events were less in the semaglutide group (3.9% vs 8.8%), although adverse events leading to permanent treatment discontinuation were slightly higher with oral semaglutide (6.9% vs 5.9%). There were no deaths.
The estimated treatment difference from placebo in body weight change of −11.4% in OASIS 4 (P < .0001) was similar to the –12.7% (P < .0001) seen with the 50-mg oral semaglutide dose studied in OASIS 1 and the –12.4% (P < .0001) difference with subcutaneous semaglutide 2.4 mg in the STEP 1 trial. “All had pretty comparable efficacy,” Garvey noted.
The side-effect profiles, including frequency of gastrointestinal side effects, were also similar across the three trials. However, Garvey added, “the mean duration of nausea in those patients that experienced nausea was shorter in patients on a 25-mg dose, 13 days, whereas the mean duration of nausea was greater, 19 days, in those in OASIS 1 taking 50 mg a day.”
Garvey has consulted for Boehringer Ingelheim, Carmot Therapeutics/Roche, Eli Lilly, Fractyl Laboratories, Inogen, Lilly, Merck, Novo Nordisk, and Zealand Pharma; has ownership interest (stock, stock options in a publicly owned company) for Bristol-Myers Squibb, Isis, Lilly, and Novartis; serves as site principal investigator for Carmot Therapeutics/Roche, Eli Lilly, Epitomee Medical, Lilly, Neurovalens, Novo Nordisk, and Zealand Pharmaceuticals; and as a data monitoring committee member for Boehringer Ingelheim and Eli Lilly. Skelton is editor in chief of the journal Childhood Obesity.
A version of this article first appeared on Medscape.com.
SAN ANTONIO — Oral semaglutide 25 mg appears to be just as effective in promoting weight loss and other beneficial outcomes as are the investigational 50-mg oral dose and the injectable 2.4-mg dose (Wegovy), in new research.
Data from Novo Nordisk’s OASIS 4 trial suggest that “oral semaglutide 25 mg may represent an efficacious option for the treatment of overweight and obesity, particularly in patients who prefer oral administration,” W. Timothy Garvey, MD, professor in the Department of Nutrition Sciences at the University of Alabama at Birmingham (UAB), said at the Obesity Society’s Obesity Week 2024 meeting.
In an interview, Garvey, who is also senior scientist at the UAB Nutrition Obesity Research Center, added: “There’s a principle in medicine that you always use the lowest dose that has highest efficacy, and for oral semaglutide for obesity, that appears to be the 25-mg dose. We need oral medicines to offer as an option for patients that could lead to a longer persistence in adherence to obesity medications, which is a big problem. Less than half the people maintain their adherence after a year.”
Asked to comment, session moderator and obesity researcher Joseph A. Skelton, MD, professor of pediatrics at Wake Forest University School of Medicine, Winston-Salem, North Carolina, said that OASIS 4 was “extremely well done, especially given that we’re all concerned about the high prevalence of people stopping these medications at a year. ... I love the idea of trying to find these lower doses and increasing options for people.”
(The oral semaglutide approved for treating type 2 diabetes [Rybelsus] is sold in 7-mg and 14-mg doses.)
With Oral Semaglutide, Lower May Be Better
OASIS 4 was a double-blind, randomized, placebo-controlled 64-week multicenter trial involving a total of 307 participants with overweight/obesity randomized 2:1 to oral semaglutide 25 mg or placebo. Of those, 167 in the semaglutide 25 mg and 76 in the placebo groups completed the trial.
For the co–primary endpoint change in body weight at week 64 (including 52-week maintenance and 7-week follow-up periods), there was a drop of 13.6% with oral semaglutide vs just 2.2% with placebo (P < .0001), based on in-trial observation regardless of adherence. For the analysis including just the on-treatment period, those reductions were 16.6% and 2.7%, respectively (P < .0001).
For the other co–primary endpoint, 79.2% semaglutide vs 31.1% placebo lost at least 5% of their body weight, 63.0% vs 14.4% lost ≥ 10%, 50.0% vs 5.6% lost ≥ 15%, and 29.7% vs 3.3% lost ≥ 20%. All were statistically significant differences, at P < .0001.
On the Impact of Weight on Quality of Life-Lite Clinical Trials Version, change from baseline scores were 16.2 with oral semaglutide vs 8.4 for placebo (P = .0006) and the proportion of participants achieving clinically meaningful increases in those scores (≥ 14.6 points) were 55.3% vs 34.8% (P = .0022).
Waist circumference was also significantly reduced from baseline with oral semaglutide, by 12.2 cm vs 2.8 cm (P < .0001). Both systolic and diastolic blood pressure dropped more with semaglutide than placebo, but not significantly. However, the inflammatory marker C-reactive protein dropped from baseline by 46.4% vs just 4.2% with placebo, a significant difference (P < .0001).
Hemoglobin A1c dropped by 0.29 percentage points vs just 0.06 with placebo (P = .0012) and fasting plasma glucose by 6.6 mg/dL, while rising by 0.4 mg/dL in the placebo group (P = .0012). Lipid levels also improved more with oral semaglutide.
Overall adverse events occurred in 93.1% on oral semaglutide and 85.3% with placebo, and gastrointestinal adverse events in 74% and 42.2%, respectively. Other types of adverse events didn’t differ between the groups. The proportions experiencing severe adverse events were less in the semaglutide group (3.9% vs 8.8%), although adverse events leading to permanent treatment discontinuation were slightly higher with oral semaglutide (6.9% vs 5.9%). There were no deaths.
The estimated treatment difference from placebo in body weight change of −11.4% in OASIS 4 (P < .0001) was similar to the –12.7% (P < .0001) seen with the 50-mg oral semaglutide dose studied in OASIS 1 and the –12.4% (P < .0001) difference with subcutaneous semaglutide 2.4 mg in the STEP 1 trial. “All had pretty comparable efficacy,” Garvey noted.
The side-effect profiles, including frequency of gastrointestinal side effects, were also similar across the three trials. However, Garvey added, “the mean duration of nausea in those patients that experienced nausea was shorter in patients on a 25-mg dose, 13 days, whereas the mean duration of nausea was greater, 19 days, in those in OASIS 1 taking 50 mg a day.”
Garvey has consulted for Boehringer Ingelheim, Carmot Therapeutics/Roche, Eli Lilly, Fractyl Laboratories, Inogen, Lilly, Merck, Novo Nordisk, and Zealand Pharma; has ownership interest (stock, stock options in a publicly owned company) for Bristol-Myers Squibb, Isis, Lilly, and Novartis; serves as site principal investigator for Carmot Therapeutics/Roche, Eli Lilly, Epitomee Medical, Lilly, Neurovalens, Novo Nordisk, and Zealand Pharmaceuticals; and as a data monitoring committee member for Boehringer Ingelheim and Eli Lilly. Skelton is editor in chief of the journal Childhood Obesity.
A version of this article first appeared on Medscape.com.
FROM OBESITY WEEK 2024
Does Light-Intensity Walking Benefit Blood Glucose?
TOPLINE:
METHODOLOGY:
- Researchers conducted a randomized crossover trial with 16 young adults aged 18-34 years with body mass index (BMI) ≥ 25 in Bangkok, Thailand, to examine the effects of different light-intensity walking patterns on postprandial cardiometabolic responses.
- Participants (mean age, 25; mean BMI, 29.8) engaged in four 7-hour experimental conditions, each involving a different activity: Uninterrupted sitting, 30-minutes of light-intensity walking, 3-minute light-intensity walking every 30 minutes, or a combination of both walking regimens. There was a 7- to 20-day washout period between each experiment period.
- Baseline and 6-hour postprandial concentrations of glucose, insulin, triglycerides, and blood pressure were measured.
- Incremental areas under the curve (iAUC) for each outcome and average blood pressure were compared between sitting and walking conditions.
TAKEAWAY:
- All the walking interventions reduced postprandial glucose concentrations and diastolic blood pressure compared with uninterrupted sitting.
- Continuous 30-minute light-intensity walking alone or combined with brief 3-minute bouts also attenuated postprandial insulin concentrations.
- No significant differences were found for triglycerides iAUC and systolic blood pressure between the four experiment conditions.
IN PRACTICE:
“These findings support the notion that engaging in light-intensity walking, regardless of the pattern, provides benefits to glycemic control. Moreover, the timing and patterns of light-intensity physical activity may be an important factor in reducing postprandial insulin concentrations,” the authors wrote.
SOURCE:
The study, led by Waris Wongpipit, PhD, Division of Health and Physical Education, Chulalongkorn University in Bangkok, Thailand, was published online in The Journal of Clinical Endocrinology & Metabolism.
LIMITATIONS:
The study’s small sample size of 16 participants may limit the generalizability of the findings. The short duration of the study (7-hour experimental conditions) may not reflect long-term effects. The prescribed activities and dietary profiles, along with the controlled laboratory setting, may not accurately represent real-world conditions. The lack of objective physical activity/sedentary behavior measurement to confirm compliance between conditions is a limitation.
DISCLOSURES:
This study was supported by grants from the Office of the Permanent Secretary, Ministry of Higher Education, Science, Research and Innovation, Thailand Science Research and Innovation, and Chulalongkorn University. Wongpipit received grant support from these organizations. Paddy C. Dempsey is supported by a National Health and Medical Research Council of Australia research fellowship. The other authors had no disclosures.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Researchers conducted a randomized crossover trial with 16 young adults aged 18-34 years with body mass index (BMI) ≥ 25 in Bangkok, Thailand, to examine the effects of different light-intensity walking patterns on postprandial cardiometabolic responses.
- Participants (mean age, 25; mean BMI, 29.8) engaged in four 7-hour experimental conditions, each involving a different activity: Uninterrupted sitting, 30-minutes of light-intensity walking, 3-minute light-intensity walking every 30 minutes, or a combination of both walking regimens. There was a 7- to 20-day washout period between each experiment period.
- Baseline and 6-hour postprandial concentrations of glucose, insulin, triglycerides, and blood pressure were measured.
- Incremental areas under the curve (iAUC) for each outcome and average blood pressure were compared between sitting and walking conditions.
TAKEAWAY:
- All the walking interventions reduced postprandial glucose concentrations and diastolic blood pressure compared with uninterrupted sitting.
- Continuous 30-minute light-intensity walking alone or combined with brief 3-minute bouts also attenuated postprandial insulin concentrations.
- No significant differences were found for triglycerides iAUC and systolic blood pressure between the four experiment conditions.
IN PRACTICE:
“These findings support the notion that engaging in light-intensity walking, regardless of the pattern, provides benefits to glycemic control. Moreover, the timing and patterns of light-intensity physical activity may be an important factor in reducing postprandial insulin concentrations,” the authors wrote.
SOURCE:
The study, led by Waris Wongpipit, PhD, Division of Health and Physical Education, Chulalongkorn University in Bangkok, Thailand, was published online in The Journal of Clinical Endocrinology & Metabolism.
LIMITATIONS:
The study’s small sample size of 16 participants may limit the generalizability of the findings. The short duration of the study (7-hour experimental conditions) may not reflect long-term effects. The prescribed activities and dietary profiles, along with the controlled laboratory setting, may not accurately represent real-world conditions. The lack of objective physical activity/sedentary behavior measurement to confirm compliance between conditions is a limitation.
DISCLOSURES:
This study was supported by grants from the Office of the Permanent Secretary, Ministry of Higher Education, Science, Research and Innovation, Thailand Science Research and Innovation, and Chulalongkorn University. Wongpipit received grant support from these organizations. Paddy C. Dempsey is supported by a National Health and Medical Research Council of Australia research fellowship. The other authors had no disclosures.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Researchers conducted a randomized crossover trial with 16 young adults aged 18-34 years with body mass index (BMI) ≥ 25 in Bangkok, Thailand, to examine the effects of different light-intensity walking patterns on postprandial cardiometabolic responses.
- Participants (mean age, 25; mean BMI, 29.8) engaged in four 7-hour experimental conditions, each involving a different activity: Uninterrupted sitting, 30-minutes of light-intensity walking, 3-minute light-intensity walking every 30 minutes, or a combination of both walking regimens. There was a 7- to 20-day washout period between each experiment period.
- Baseline and 6-hour postprandial concentrations of glucose, insulin, triglycerides, and blood pressure were measured.
- Incremental areas under the curve (iAUC) for each outcome and average blood pressure were compared between sitting and walking conditions.
TAKEAWAY:
- All the walking interventions reduced postprandial glucose concentrations and diastolic blood pressure compared with uninterrupted sitting.
- Continuous 30-minute light-intensity walking alone or combined with brief 3-minute bouts also attenuated postprandial insulin concentrations.
- No significant differences were found for triglycerides iAUC and systolic blood pressure between the four experiment conditions.
IN PRACTICE:
“These findings support the notion that engaging in light-intensity walking, regardless of the pattern, provides benefits to glycemic control. Moreover, the timing and patterns of light-intensity physical activity may be an important factor in reducing postprandial insulin concentrations,” the authors wrote.
SOURCE:
The study, led by Waris Wongpipit, PhD, Division of Health and Physical Education, Chulalongkorn University in Bangkok, Thailand, was published online in The Journal of Clinical Endocrinology & Metabolism.
LIMITATIONS:
The study’s small sample size of 16 participants may limit the generalizability of the findings. The short duration of the study (7-hour experimental conditions) may not reflect long-term effects. The prescribed activities and dietary profiles, along with the controlled laboratory setting, may not accurately represent real-world conditions. The lack of objective physical activity/sedentary behavior measurement to confirm compliance between conditions is a limitation.
DISCLOSURES:
This study was supported by grants from the Office of the Permanent Secretary, Ministry of Higher Education, Science, Research and Innovation, Thailand Science Research and Innovation, and Chulalongkorn University. Wongpipit received grant support from these organizations. Paddy C. Dempsey is supported by a National Health and Medical Research Council of Australia research fellowship. The other authors had no disclosures.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Gout and SGLT2 Inhibitors: Evidence Points to Reduced Need for ULT, Flare Drugs
WASHINGTON — Use of sodium-glucose cotransporter 2 inhibitors (SGLT2i) reduced the need for urate-lowering therapy (ULT) and gout flare therapies in people who had both type 2 diabetes (T2D) and gout, new research has found.
Data from a large US claims database showed that SGLT2i use was associated with a 31% lower rate of initiation of ULT. “This provides further support for the use of SLGT2i therapy in patients with gout, particularly those with high-risk multimorbidity and polypharmacy,” Greg Challener, MD, a postdoctoral fellow at the Rheumatology and Allergy Clinical Epidemiology Research Center, Massachusetts General Hospital, Boston, said in his presentation of the data at the annual meeting of the American College of Rheumatology.
The first agent of the SGLT2i class, dapagliflozin, was initially approved in the United States a decade ago for treating T2D. Since then, several other “flozins” have become available, and some have also received additional indications for heart failure and albuminuric chronic kidney disease. Several prior studies have linked SGLT2i use with lower rates of gout flares as well as lower likelihood of developing gout in the first place, although not all studies have found this benefit.
Asked about the clinical implications of the new data, Challener said in an interview that “I don’t think we’re quite at the point where this is changing gout management per se, but this just helps us understand that [SGT2is] may have a role at some point, maybe as a combination on top of another agent. Or, in some patients, it really may be enough if they’re already on an SGLT2i where we don’t need to jump to adding allopurinol. Maybe they have tophi, but they were just started on an SGLT2i and they’re not flaring. Typically, you would start those patients on allopurinol, but you could potentially just monitor them if they were just started on one of those [SGLT2i] agents.”
Asked to comment, session moderator J. Antonio Aviña-Zubieta, MD, PhD, head of the Division of Rheumatology at the University of British Columbia, Vancouver, Canada, and senior scientist at Arthritis Research Canada, said in an interview: “What I can see possibly happening when there’s more evidence is that SGLT2is may be used or even become standard of care as an adjuvant therapy to decrease flares, and by that, decrease the risk of complications.”
Reductions in ULT, Flares, and Healthcare Visits
The new study used administrative health data from the multicenter TriNetX Diamond network of electronic medical record and claims data from 92 healthcare sites with 212 million patients. Among those with both T2D and gout who were not taking ULT at baseline, a total of 16,104 initiated SGLT2is and 16,046 initiated glucagon-like peptide 1 receptor agonists (GLP-1 RA).
Propensity score matching was conducted for demographics including age, race, and sex; comorbidities; use of emergency, inpatient, and critical care services; medications; labs; and body mass index. That yielded 11,800 individuals each in the SGLT2i and GLP-1 RA groups.
Over 5 years, 9.9% of the SGLT2i group vs 13.4% of those using GLP-1 RA had initiated ULT, a significant difference with a hazard ratio (HR) of 0.69 (95% CI, 0.64-0.75). The risk for initiation of colchicine for gout flares was 4.7% with SGLT2i vs 6.0% for GLP-1 RA — also a significant difference with an HR of 0.74 (0.65-0.83).
Medical visits for gout occurred in 28.0% vs 28.4% of patients, which also reached statistical significance (HR, 0.94; 95% CI, 0.89-0.99).
Aviña-Zubieta, an author of one of the previous studies finding a reduction in gout flares with SGLT2i, said, “many patients do not want to start gout therapy until they start having more acute attacks. ... So, for a lot of people, it’s a burden taking another pill to prevent one attack. But, if you don’t treat it over time, the attacks come more often. So, can we still delay the initiation of therapy? If you’re not having that many flares, you’re decreasing the burden of the disease and polypharmacy, which I think is the potential benefit in the long run if you already have an indication for the therapy for diabetes. ... These data are supporting that.”
Indeed, Challener said these data can help in counseling patients. “Taking your SGLT2i for your heart failure and your diabetes is also providing some benefit for your gout, and we know that there is also cardiac benefit when gout is controlled.”
Challener and Aviña-Zubieta had no disclosures.
A version of this article first appeared on Medscape.com.
WASHINGTON — Use of sodium-glucose cotransporter 2 inhibitors (SGLT2i) reduced the need for urate-lowering therapy (ULT) and gout flare therapies in people who had both type 2 diabetes (T2D) and gout, new research has found.
Data from a large US claims database showed that SGLT2i use was associated with a 31% lower rate of initiation of ULT. “This provides further support for the use of SLGT2i therapy in patients with gout, particularly those with high-risk multimorbidity and polypharmacy,” Greg Challener, MD, a postdoctoral fellow at the Rheumatology and Allergy Clinical Epidemiology Research Center, Massachusetts General Hospital, Boston, said in his presentation of the data at the annual meeting of the American College of Rheumatology.
The first agent of the SGLT2i class, dapagliflozin, was initially approved in the United States a decade ago for treating T2D. Since then, several other “flozins” have become available, and some have also received additional indications for heart failure and albuminuric chronic kidney disease. Several prior studies have linked SGLT2i use with lower rates of gout flares as well as lower likelihood of developing gout in the first place, although not all studies have found this benefit.
Asked about the clinical implications of the new data, Challener said in an interview that “I don’t think we’re quite at the point where this is changing gout management per se, but this just helps us understand that [SGT2is] may have a role at some point, maybe as a combination on top of another agent. Or, in some patients, it really may be enough if they’re already on an SGLT2i where we don’t need to jump to adding allopurinol. Maybe they have tophi, but they were just started on an SGLT2i and they’re not flaring. Typically, you would start those patients on allopurinol, but you could potentially just monitor them if they were just started on one of those [SGLT2i] agents.”
Asked to comment, session moderator J. Antonio Aviña-Zubieta, MD, PhD, head of the Division of Rheumatology at the University of British Columbia, Vancouver, Canada, and senior scientist at Arthritis Research Canada, said in an interview: “What I can see possibly happening when there’s more evidence is that SGLT2is may be used or even become standard of care as an adjuvant therapy to decrease flares, and by that, decrease the risk of complications.”
Reductions in ULT, Flares, and Healthcare Visits
The new study used administrative health data from the multicenter TriNetX Diamond network of electronic medical record and claims data from 92 healthcare sites with 212 million patients. Among those with both T2D and gout who were not taking ULT at baseline, a total of 16,104 initiated SGLT2is and 16,046 initiated glucagon-like peptide 1 receptor agonists (GLP-1 RA).
Propensity score matching was conducted for demographics including age, race, and sex; comorbidities; use of emergency, inpatient, and critical care services; medications; labs; and body mass index. That yielded 11,800 individuals each in the SGLT2i and GLP-1 RA groups.
Over 5 years, 9.9% of the SGLT2i group vs 13.4% of those using GLP-1 RA had initiated ULT, a significant difference with a hazard ratio (HR) of 0.69 (95% CI, 0.64-0.75). The risk for initiation of colchicine for gout flares was 4.7% with SGLT2i vs 6.0% for GLP-1 RA — also a significant difference with an HR of 0.74 (0.65-0.83).
Medical visits for gout occurred in 28.0% vs 28.4% of patients, which also reached statistical significance (HR, 0.94; 95% CI, 0.89-0.99).
Aviña-Zubieta, an author of one of the previous studies finding a reduction in gout flares with SGLT2i, said, “many patients do not want to start gout therapy until they start having more acute attacks. ... So, for a lot of people, it’s a burden taking another pill to prevent one attack. But, if you don’t treat it over time, the attacks come more often. So, can we still delay the initiation of therapy? If you’re not having that many flares, you’re decreasing the burden of the disease and polypharmacy, which I think is the potential benefit in the long run if you already have an indication for the therapy for diabetes. ... These data are supporting that.”
Indeed, Challener said these data can help in counseling patients. “Taking your SGLT2i for your heart failure and your diabetes is also providing some benefit for your gout, and we know that there is also cardiac benefit when gout is controlled.”
Challener and Aviña-Zubieta had no disclosures.
A version of this article first appeared on Medscape.com.
WASHINGTON — Use of sodium-glucose cotransporter 2 inhibitors (SGLT2i) reduced the need for urate-lowering therapy (ULT) and gout flare therapies in people who had both type 2 diabetes (T2D) and gout, new research has found.
Data from a large US claims database showed that SGLT2i use was associated with a 31% lower rate of initiation of ULT. “This provides further support for the use of SLGT2i therapy in patients with gout, particularly those with high-risk multimorbidity and polypharmacy,” Greg Challener, MD, a postdoctoral fellow at the Rheumatology and Allergy Clinical Epidemiology Research Center, Massachusetts General Hospital, Boston, said in his presentation of the data at the annual meeting of the American College of Rheumatology.
The first agent of the SGLT2i class, dapagliflozin, was initially approved in the United States a decade ago for treating T2D. Since then, several other “flozins” have become available, and some have also received additional indications for heart failure and albuminuric chronic kidney disease. Several prior studies have linked SGLT2i use with lower rates of gout flares as well as lower likelihood of developing gout in the first place, although not all studies have found this benefit.
Asked about the clinical implications of the new data, Challener said in an interview that “I don’t think we’re quite at the point where this is changing gout management per se, but this just helps us understand that [SGT2is] may have a role at some point, maybe as a combination on top of another agent. Or, in some patients, it really may be enough if they’re already on an SGLT2i where we don’t need to jump to adding allopurinol. Maybe they have tophi, but they were just started on an SGLT2i and they’re not flaring. Typically, you would start those patients on allopurinol, but you could potentially just monitor them if they were just started on one of those [SGLT2i] agents.”
Asked to comment, session moderator J. Antonio Aviña-Zubieta, MD, PhD, head of the Division of Rheumatology at the University of British Columbia, Vancouver, Canada, and senior scientist at Arthritis Research Canada, said in an interview: “What I can see possibly happening when there’s more evidence is that SGLT2is may be used or even become standard of care as an adjuvant therapy to decrease flares, and by that, decrease the risk of complications.”
Reductions in ULT, Flares, and Healthcare Visits
The new study used administrative health data from the multicenter TriNetX Diamond network of electronic medical record and claims data from 92 healthcare sites with 212 million patients. Among those with both T2D and gout who were not taking ULT at baseline, a total of 16,104 initiated SGLT2is and 16,046 initiated glucagon-like peptide 1 receptor agonists (GLP-1 RA).
Propensity score matching was conducted for demographics including age, race, and sex; comorbidities; use of emergency, inpatient, and critical care services; medications; labs; and body mass index. That yielded 11,800 individuals each in the SGLT2i and GLP-1 RA groups.
Over 5 years, 9.9% of the SGLT2i group vs 13.4% of those using GLP-1 RA had initiated ULT, a significant difference with a hazard ratio (HR) of 0.69 (95% CI, 0.64-0.75). The risk for initiation of colchicine for gout flares was 4.7% with SGLT2i vs 6.0% for GLP-1 RA — also a significant difference with an HR of 0.74 (0.65-0.83).
Medical visits for gout occurred in 28.0% vs 28.4% of patients, which also reached statistical significance (HR, 0.94; 95% CI, 0.89-0.99).
Aviña-Zubieta, an author of one of the previous studies finding a reduction in gout flares with SGLT2i, said, “many patients do not want to start gout therapy until they start having more acute attacks. ... So, for a lot of people, it’s a burden taking another pill to prevent one attack. But, if you don’t treat it over time, the attacks come more often. So, can we still delay the initiation of therapy? If you’re not having that many flares, you’re decreasing the burden of the disease and polypharmacy, which I think is the potential benefit in the long run if you already have an indication for the therapy for diabetes. ... These data are supporting that.”
Indeed, Challener said these data can help in counseling patients. “Taking your SGLT2i for your heart failure and your diabetes is also providing some benefit for your gout, and we know that there is also cardiac benefit when gout is controlled.”
Challener and Aviña-Zubieta had no disclosures.
A version of this article first appeared on Medscape.com.
FROM ACR 2024
Managing Diabetes and Dementia in Long-Term Care
VANCOUVER, BRITISH COLUMBIA — Conditions like diabetes and dementia are common in patients who are admitted to long-term care facilities, but aggressive management of these conditions in long-term care residents is not recommended, according to a presentation given at the Family Medicine Forum (FMF) 2024.
Hospitalizations for hypoglycemia are risky for patients with diabetes who are residents of long-term care facilities, particularly those aged 75 years or older, said Adam Gurau, MD, a family physician in Toronto. Gurau completed a fellowship in care of the elderly at the University of Toronto, in Ontario, Canada.
“A lot of studies have shown diabetes-related hospitalizations,” said Gurau. He cited a 2014 study that found that hypoglycemia hospitalization rates were twice as high in older patients (age, 75 years or older) as in younger patients (age, 65-74 years).
“It is important to keep in mind that our residents in long-term care are at increasing risk for hypoglycemia, and we really should try to reduce [this risk] and not use dangerous medications or potentially dangerous [means of] diabetes management,” said Gurau.
A Canadian study that examined the composite risk for emergency department visits, hospitalizations, or death within 30 days of reaching intensive glycemic control with high-risk agents (such as insulin or sulfonylureas) suggested little benefit and possible harm in using these agents in adults aged 75 years or older.
In addition, current guidelines on diabetes management encourage a different approach. “Looking at some of the more recent North American guidelines, many of them actually now recommend relaxing glycemic targets to reduce overtreatment and prevent hypoglycemia,” said Gurau.
Deprescribing Medications
Medication reviews present opportunities for taking a global view of a patient’s treatments and determining whether any drug can be removed from the list. “What we want to do is optimize medications,” said Gurau. “We’re not talking about adding medications. We’re talking about removing medications, which is, I think, what we should be doing.”
Some research suggests that patients are open to deprescribing. One survey examined older adults (mean age, 79.1 years) with three or more chronic conditions who had been prescribed at least five medications. The researchers found that most participants (77%) were willing to deprescribe one or more medicines if a doctor advised that it was possible. “General practitioners may be able to increase deprescribing by building trust with their patients and communicating evidence about the risks of medication use,” the researchers wrote.
About 62% of seniors living in a residential care home have a diagnosis of Alzheimer’s disease or another dementia, according to the Alzheimer Society of Canada. Evidence suggests that nonpharmacologic approaches, such as massage and touch therapy and music, can manage neuropsychiatric symptoms, such as aggression and agitation, that are associated with dementia in older adults, noted Gurau.
“We want to focus on nonpharmacologic approaches for many of these [long-term care] residents,” said Gurau. “We have to do as much as we can to exhaust all the nonpharmacologic approaches.”
Preventing Hospitalizations
Another challenge to tackle in long-term care is the unnecessary transfer of residents to hospital emergency departments, according to Gurau. “In many situations, it’s worth trying as hard as we can to treat them in the nursing home, as opposed to having them go to hospital.”
Researchers estimated that 25% of the transfers from long-term care facilities in Canada to hospital emergency departments in 2014 were potentially preventable.
Urinary tract infections accounted for 30% of hospital emergency department visits for potentially preventable conditions by older patients who are residents in long-term care, according to 2013-2014 data from the Canadian Institute for Health Information.
“There are lots of downsides to going to the hospital [from long-term care],” Gurau told this news organization. “There are risks for infections, risks for increasing delirium and agitation [in patients with dementia], and risks for other behavior that can really impact somebody’s life.”
Gurau reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VANCOUVER, BRITISH COLUMBIA — Conditions like diabetes and dementia are common in patients who are admitted to long-term care facilities, but aggressive management of these conditions in long-term care residents is not recommended, according to a presentation given at the Family Medicine Forum (FMF) 2024.
Hospitalizations for hypoglycemia are risky for patients with diabetes who are residents of long-term care facilities, particularly those aged 75 years or older, said Adam Gurau, MD, a family physician in Toronto. Gurau completed a fellowship in care of the elderly at the University of Toronto, in Ontario, Canada.
“A lot of studies have shown diabetes-related hospitalizations,” said Gurau. He cited a 2014 study that found that hypoglycemia hospitalization rates were twice as high in older patients (age, 75 years or older) as in younger patients (age, 65-74 years).
“It is important to keep in mind that our residents in long-term care are at increasing risk for hypoglycemia, and we really should try to reduce [this risk] and not use dangerous medications or potentially dangerous [means of] diabetes management,” said Gurau.
A Canadian study that examined the composite risk for emergency department visits, hospitalizations, or death within 30 days of reaching intensive glycemic control with high-risk agents (such as insulin or sulfonylureas) suggested little benefit and possible harm in using these agents in adults aged 75 years or older.
In addition, current guidelines on diabetes management encourage a different approach. “Looking at some of the more recent North American guidelines, many of them actually now recommend relaxing glycemic targets to reduce overtreatment and prevent hypoglycemia,” said Gurau.
Deprescribing Medications
Medication reviews present opportunities for taking a global view of a patient’s treatments and determining whether any drug can be removed from the list. “What we want to do is optimize medications,” said Gurau. “We’re not talking about adding medications. We’re talking about removing medications, which is, I think, what we should be doing.”
Some research suggests that patients are open to deprescribing. One survey examined older adults (mean age, 79.1 years) with three or more chronic conditions who had been prescribed at least five medications. The researchers found that most participants (77%) were willing to deprescribe one or more medicines if a doctor advised that it was possible. “General practitioners may be able to increase deprescribing by building trust with their patients and communicating evidence about the risks of medication use,” the researchers wrote.
About 62% of seniors living in a residential care home have a diagnosis of Alzheimer’s disease or another dementia, according to the Alzheimer Society of Canada. Evidence suggests that nonpharmacologic approaches, such as massage and touch therapy and music, can manage neuropsychiatric symptoms, such as aggression and agitation, that are associated with dementia in older adults, noted Gurau.
“We want to focus on nonpharmacologic approaches for many of these [long-term care] residents,” said Gurau. “We have to do as much as we can to exhaust all the nonpharmacologic approaches.”
Preventing Hospitalizations
Another challenge to tackle in long-term care is the unnecessary transfer of residents to hospital emergency departments, according to Gurau. “In many situations, it’s worth trying as hard as we can to treat them in the nursing home, as opposed to having them go to hospital.”
Researchers estimated that 25% of the transfers from long-term care facilities in Canada to hospital emergency departments in 2014 were potentially preventable.
Urinary tract infections accounted for 30% of hospital emergency department visits for potentially preventable conditions by older patients who are residents in long-term care, according to 2013-2014 data from the Canadian Institute for Health Information.
“There are lots of downsides to going to the hospital [from long-term care],” Gurau told this news organization. “There are risks for infections, risks for increasing delirium and agitation [in patients with dementia], and risks for other behavior that can really impact somebody’s life.”
Gurau reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VANCOUVER, BRITISH COLUMBIA — Conditions like diabetes and dementia are common in patients who are admitted to long-term care facilities, but aggressive management of these conditions in long-term care residents is not recommended, according to a presentation given at the Family Medicine Forum (FMF) 2024.
Hospitalizations for hypoglycemia are risky for patients with diabetes who are residents of long-term care facilities, particularly those aged 75 years or older, said Adam Gurau, MD, a family physician in Toronto. Gurau completed a fellowship in care of the elderly at the University of Toronto, in Ontario, Canada.
“A lot of studies have shown diabetes-related hospitalizations,” said Gurau. He cited a 2014 study that found that hypoglycemia hospitalization rates were twice as high in older patients (age, 75 years or older) as in younger patients (age, 65-74 years).
“It is important to keep in mind that our residents in long-term care are at increasing risk for hypoglycemia, and we really should try to reduce [this risk] and not use dangerous medications or potentially dangerous [means of] diabetes management,” said Gurau.
A Canadian study that examined the composite risk for emergency department visits, hospitalizations, or death within 30 days of reaching intensive glycemic control with high-risk agents (such as insulin or sulfonylureas) suggested little benefit and possible harm in using these agents in adults aged 75 years or older.
In addition, current guidelines on diabetes management encourage a different approach. “Looking at some of the more recent North American guidelines, many of them actually now recommend relaxing glycemic targets to reduce overtreatment and prevent hypoglycemia,” said Gurau.
Deprescribing Medications
Medication reviews present opportunities for taking a global view of a patient’s treatments and determining whether any drug can be removed from the list. “What we want to do is optimize medications,” said Gurau. “We’re not talking about adding medications. We’re talking about removing medications, which is, I think, what we should be doing.”
Some research suggests that patients are open to deprescribing. One survey examined older adults (mean age, 79.1 years) with three or more chronic conditions who had been prescribed at least five medications. The researchers found that most participants (77%) were willing to deprescribe one or more medicines if a doctor advised that it was possible. “General practitioners may be able to increase deprescribing by building trust with their patients and communicating evidence about the risks of medication use,” the researchers wrote.
About 62% of seniors living in a residential care home have a diagnosis of Alzheimer’s disease or another dementia, according to the Alzheimer Society of Canada. Evidence suggests that nonpharmacologic approaches, such as massage and touch therapy and music, can manage neuropsychiatric symptoms, such as aggression and agitation, that are associated with dementia in older adults, noted Gurau.
“We want to focus on nonpharmacologic approaches for many of these [long-term care] residents,” said Gurau. “We have to do as much as we can to exhaust all the nonpharmacologic approaches.”
Preventing Hospitalizations
Another challenge to tackle in long-term care is the unnecessary transfer of residents to hospital emergency departments, according to Gurau. “In many situations, it’s worth trying as hard as we can to treat them in the nursing home, as opposed to having them go to hospital.”
Researchers estimated that 25% of the transfers from long-term care facilities in Canada to hospital emergency departments in 2014 were potentially preventable.
Urinary tract infections accounted for 30% of hospital emergency department visits for potentially preventable conditions by older patients who are residents in long-term care, according to 2013-2014 data from the Canadian Institute for Health Information.
“There are lots of downsides to going to the hospital [from long-term care],” Gurau told this news organization. “There are risks for infections, risks for increasing delirium and agitation [in patients with dementia], and risks for other behavior that can really impact somebody’s life.”
Gurau reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM FMF 2024
Reassuring Data on GLP-1 RAs and Pancreatic Cancer Risk
PHILADELPHIA —
Instead, the large electronic health record (EHR) analysis of patients with type 2 diabetes (T2D) found those taking GLP-1 RAs had a significantly lower risk for pancreatic cancer than peers on other antidiabetic medications.
“Although there were previous reports suggesting possible association between pancreatic cancer and GLP-1 receptor agonist medications, this study provides reassurance that there is no observed increased incidence of pancreatic cancer in patients prescribed these medications,” said Khaled Alsabbagh Alchirazi, MD, a gastroenterology fellow with Aurora Healthcare in Brookfield, Wisconsin.
He presented the study findings at the American College of Gastroenterology (ACG) 2024 Annual Scientific Meeting.
Important Topic
Patients with T2D are at increased risk for several malignancies, including pancreatic cancer. Given the unique mechanism of action of GLP-1 RAs in the pancreas, it was important to investigate the relationship between use of these drugs and incidence of pancreatic cancer, he explained.
Using the TriNetX database, the study team identified 4.95 million antidiabetic drug naive T2D patients who were prescribed antidiabetic medications for the first time between 2005 and 2020. None had a history of pancreatic cancer.
A total of 245,532 were prescribed a GLP-1 RA. The researchers compared GLP-1 RAs users to users of other antidiabetic medications — namely, insulin, metformin, alpha-glucosidase inhibitors, dipeptidyl-peptidase 4 inhibitors (DPP-4i), sodium-glucose cotransporter-2 inhibitors (SGLT2i), sulfonylureas, and thiazolidinediones.
Patients were propensity score-matched based on demographics, health determinants, lifestyle factors, medical history, family history of cancers, and acute/chronic pancreatitis.
The risk for pancreatic cancer was significantly lower among patients on GLP-1 RAs vs insulin (hazard ratio [HR], 0.47; 95% CI, 0.40-0.55), DPP-4i (HR, 0.80; 95% CI, 0.73-0.89), SGLT2i (HR, 0.78; 95% CI, 0.69-0.89), and sulfonylureas (HR, 0.84; 95% CI, 0.74-0.95), Alchirazi reported.
The results were consistent across different groups, including patients with obesity/ overweight on GLP-1 RAs vs insulin (HR, 0.53; 95% CI, 0.43-0.65) and SGLT2i (HR, 0.81; 95% CI, 0.69-0.96).
Strengths of the analysis included the large and diverse cohort of propensity score-matched patients. Limitations included the retrospective design and use of claims data that did not provide granular data on pathology reports.
The study by Alchirazi and colleagues aligns with a large population-based cohort study from Israel that found no evidence that GLP-1 RAs increase risk for pancreatic cancer over 7 years following initiation.
Separately, a study of more than 1.6 million patients with T2D found that treatment with a GLP-1 RA (vs insulin or metformin) was associated with lower risks for specific types of obesity-related cancers, including pancreatic cancer.
The study had no specific funding. Alchirazi had no relevant disclosures.
A version of this article appeared on Medscape.com.
PHILADELPHIA —
Instead, the large electronic health record (EHR) analysis of patients with type 2 diabetes (T2D) found those taking GLP-1 RAs had a significantly lower risk for pancreatic cancer than peers on other antidiabetic medications.
“Although there were previous reports suggesting possible association between pancreatic cancer and GLP-1 receptor agonist medications, this study provides reassurance that there is no observed increased incidence of pancreatic cancer in patients prescribed these medications,” said Khaled Alsabbagh Alchirazi, MD, a gastroenterology fellow with Aurora Healthcare in Brookfield, Wisconsin.
He presented the study findings at the American College of Gastroenterology (ACG) 2024 Annual Scientific Meeting.
Important Topic
Patients with T2D are at increased risk for several malignancies, including pancreatic cancer. Given the unique mechanism of action of GLP-1 RAs in the pancreas, it was important to investigate the relationship between use of these drugs and incidence of pancreatic cancer, he explained.
Using the TriNetX database, the study team identified 4.95 million antidiabetic drug naive T2D patients who were prescribed antidiabetic medications for the first time between 2005 and 2020. None had a history of pancreatic cancer.
A total of 245,532 were prescribed a GLP-1 RA. The researchers compared GLP-1 RAs users to users of other antidiabetic medications — namely, insulin, metformin, alpha-glucosidase inhibitors, dipeptidyl-peptidase 4 inhibitors (DPP-4i), sodium-glucose cotransporter-2 inhibitors (SGLT2i), sulfonylureas, and thiazolidinediones.
Patients were propensity score-matched based on demographics, health determinants, lifestyle factors, medical history, family history of cancers, and acute/chronic pancreatitis.
The risk for pancreatic cancer was significantly lower among patients on GLP-1 RAs vs insulin (hazard ratio [HR], 0.47; 95% CI, 0.40-0.55), DPP-4i (HR, 0.80; 95% CI, 0.73-0.89), SGLT2i (HR, 0.78; 95% CI, 0.69-0.89), and sulfonylureas (HR, 0.84; 95% CI, 0.74-0.95), Alchirazi reported.
The results were consistent across different groups, including patients with obesity/ overweight on GLP-1 RAs vs insulin (HR, 0.53; 95% CI, 0.43-0.65) and SGLT2i (HR, 0.81; 95% CI, 0.69-0.96).
Strengths of the analysis included the large and diverse cohort of propensity score-matched patients. Limitations included the retrospective design and use of claims data that did not provide granular data on pathology reports.
The study by Alchirazi and colleagues aligns with a large population-based cohort study from Israel that found no evidence that GLP-1 RAs increase risk for pancreatic cancer over 7 years following initiation.
Separately, a study of more than 1.6 million patients with T2D found that treatment with a GLP-1 RA (vs insulin or metformin) was associated with lower risks for specific types of obesity-related cancers, including pancreatic cancer.
The study had no specific funding. Alchirazi had no relevant disclosures.
A version of this article appeared on Medscape.com.
PHILADELPHIA —
Instead, the large electronic health record (EHR) analysis of patients with type 2 diabetes (T2D) found those taking GLP-1 RAs had a significantly lower risk for pancreatic cancer than peers on other antidiabetic medications.
“Although there were previous reports suggesting possible association between pancreatic cancer and GLP-1 receptor agonist medications, this study provides reassurance that there is no observed increased incidence of pancreatic cancer in patients prescribed these medications,” said Khaled Alsabbagh Alchirazi, MD, a gastroenterology fellow with Aurora Healthcare in Brookfield, Wisconsin.
He presented the study findings at the American College of Gastroenterology (ACG) 2024 Annual Scientific Meeting.
Important Topic
Patients with T2D are at increased risk for several malignancies, including pancreatic cancer. Given the unique mechanism of action of GLP-1 RAs in the pancreas, it was important to investigate the relationship between use of these drugs and incidence of pancreatic cancer, he explained.
Using the TriNetX database, the study team identified 4.95 million antidiabetic drug naive T2D patients who were prescribed antidiabetic medications for the first time between 2005 and 2020. None had a history of pancreatic cancer.
A total of 245,532 were prescribed a GLP-1 RA. The researchers compared GLP-1 RAs users to users of other antidiabetic medications — namely, insulin, metformin, alpha-glucosidase inhibitors, dipeptidyl-peptidase 4 inhibitors (DPP-4i), sodium-glucose cotransporter-2 inhibitors (SGLT2i), sulfonylureas, and thiazolidinediones.
Patients were propensity score-matched based on demographics, health determinants, lifestyle factors, medical history, family history of cancers, and acute/chronic pancreatitis.
The risk for pancreatic cancer was significantly lower among patients on GLP-1 RAs vs insulin (hazard ratio [HR], 0.47; 95% CI, 0.40-0.55), DPP-4i (HR, 0.80; 95% CI, 0.73-0.89), SGLT2i (HR, 0.78; 95% CI, 0.69-0.89), and sulfonylureas (HR, 0.84; 95% CI, 0.74-0.95), Alchirazi reported.
The results were consistent across different groups, including patients with obesity/ overweight on GLP-1 RAs vs insulin (HR, 0.53; 95% CI, 0.43-0.65) and SGLT2i (HR, 0.81; 95% CI, 0.69-0.96).
Strengths of the analysis included the large and diverse cohort of propensity score-matched patients. Limitations included the retrospective design and use of claims data that did not provide granular data on pathology reports.
The study by Alchirazi and colleagues aligns with a large population-based cohort study from Israel that found no evidence that GLP-1 RAs increase risk for pancreatic cancer over 7 years following initiation.
Separately, a study of more than 1.6 million patients with T2D found that treatment with a GLP-1 RA (vs insulin or metformin) was associated with lower risks for specific types of obesity-related cancers, including pancreatic cancer.
The study had no specific funding. Alchirazi had no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM ACG 2024
Periodontitis Management: GPs Should Play a Role
Periodontitis is a chronic inflammatory disease that triggers a local immuno-inflammatory response, potentially leading to periodontal tissue destruction and tooth loss. Affecting 1.1 billion people worldwide, periodontitis is recognized as a significant public health issue. It is also linked to a number of other conditions, such as diabetes, cardiovascular disease, and respiratory disorders. The European Federation of Periodontology recently published a consensus report recommending that the optimal management of periodontitis should involve a collaboration between general practitioners (GPs) and oral health professionals.
Diabetes and Periodontitis
A bidirectional association exists between diabetes and periodontitis. Hyperglycemia accelerates periodontitis progression by promoting inflammation and hindering the healing process, while periodontitis is associated with higher hemoglobin A1c levels in patients with diabetes and an increased risk for diabetes development in others. Intervention studies have demonstrated the positive effect of glycemic control on periodontitis and vice versa, with periodontal treatment improving A1c levels.
GPs can raise awareness of the links between these conditions as well as emphasize the benefits of addressing both metabolic and periodontal abnormalities. They should refer patients with diabetes to oral health specialists and look for signs of periodontitis, such as bleeding gums and loose teeth, in patients with diabetes and those with prediabetes.
Cardiovascular Diseases and Periodontitis
Cardiovascular diseases and periodontitis are linked by their epidemiological associations and common biologic mechanisms. This connection can be explained by some of their shared risk factors, such as smoking and systemic inflammatory pathways. Although no intervention studies have shown a direct reduction in cardiovascular risk from periodontal care, two studies have demonstrated improvements in surrogate markers such as blood pressure and arterial stiffness. GPs should inquire about symptoms of periodontitis in cardiovascular patients and, if necessary, refer them to oral health specialists. Periodontal treatments, whether surgical or nonsurgical, pose no risk for patients receiving well-managed secondary preventive treatments.
Respiratory Diseases and Periodontitis
The primary evidence linking periodontitis with chronic respiratory diseases concerns chronic obstructive pulmonary disease (COPD). Individuals with periodontitis have a 33% higher risk of developing COPD, and patients with COPD and periodontitis may experience a greater decline in lung function. An established association also exists between periodontitis and obstructive sleep apnea, although the data remain inconclusive regarding a link with asthma. GPs should encourage patients with COPD to quit smoking, as it benefits both respiratory and oral health.
Finally, based on meta-analyses of COVID-19, experts note significant associations between periodontitis and the need for assisted ventilation or the risk for death during a COVID-19 infection.
This story was translated from Univadis France using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Periodontitis is a chronic inflammatory disease that triggers a local immuno-inflammatory response, potentially leading to periodontal tissue destruction and tooth loss. Affecting 1.1 billion people worldwide, periodontitis is recognized as a significant public health issue. It is also linked to a number of other conditions, such as diabetes, cardiovascular disease, and respiratory disorders. The European Federation of Periodontology recently published a consensus report recommending that the optimal management of periodontitis should involve a collaboration between general practitioners (GPs) and oral health professionals.
Diabetes and Periodontitis
A bidirectional association exists between diabetes and periodontitis. Hyperglycemia accelerates periodontitis progression by promoting inflammation and hindering the healing process, while periodontitis is associated with higher hemoglobin A1c levels in patients with diabetes and an increased risk for diabetes development in others. Intervention studies have demonstrated the positive effect of glycemic control on periodontitis and vice versa, with periodontal treatment improving A1c levels.
GPs can raise awareness of the links between these conditions as well as emphasize the benefits of addressing both metabolic and periodontal abnormalities. They should refer patients with diabetes to oral health specialists and look for signs of periodontitis, such as bleeding gums and loose teeth, in patients with diabetes and those with prediabetes.
Cardiovascular Diseases and Periodontitis
Cardiovascular diseases and periodontitis are linked by their epidemiological associations and common biologic mechanisms. This connection can be explained by some of their shared risk factors, such as smoking and systemic inflammatory pathways. Although no intervention studies have shown a direct reduction in cardiovascular risk from periodontal care, two studies have demonstrated improvements in surrogate markers such as blood pressure and arterial stiffness. GPs should inquire about symptoms of periodontitis in cardiovascular patients and, if necessary, refer them to oral health specialists. Periodontal treatments, whether surgical or nonsurgical, pose no risk for patients receiving well-managed secondary preventive treatments.
Respiratory Diseases and Periodontitis
The primary evidence linking periodontitis with chronic respiratory diseases concerns chronic obstructive pulmonary disease (COPD). Individuals with periodontitis have a 33% higher risk of developing COPD, and patients with COPD and periodontitis may experience a greater decline in lung function. An established association also exists between periodontitis and obstructive sleep apnea, although the data remain inconclusive regarding a link with asthma. GPs should encourage patients with COPD to quit smoking, as it benefits both respiratory and oral health.
Finally, based on meta-analyses of COVID-19, experts note significant associations between periodontitis and the need for assisted ventilation or the risk for death during a COVID-19 infection.
This story was translated from Univadis France using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Periodontitis is a chronic inflammatory disease that triggers a local immuno-inflammatory response, potentially leading to periodontal tissue destruction and tooth loss. Affecting 1.1 billion people worldwide, periodontitis is recognized as a significant public health issue. It is also linked to a number of other conditions, such as diabetes, cardiovascular disease, and respiratory disorders. The European Federation of Periodontology recently published a consensus report recommending that the optimal management of periodontitis should involve a collaboration between general practitioners (GPs) and oral health professionals.
Diabetes and Periodontitis
A bidirectional association exists between diabetes and periodontitis. Hyperglycemia accelerates periodontitis progression by promoting inflammation and hindering the healing process, while periodontitis is associated with higher hemoglobin A1c levels in patients with diabetes and an increased risk for diabetes development in others. Intervention studies have demonstrated the positive effect of glycemic control on periodontitis and vice versa, with periodontal treatment improving A1c levels.
GPs can raise awareness of the links between these conditions as well as emphasize the benefits of addressing both metabolic and periodontal abnormalities. They should refer patients with diabetes to oral health specialists and look for signs of periodontitis, such as bleeding gums and loose teeth, in patients with diabetes and those with prediabetes.
Cardiovascular Diseases and Periodontitis
Cardiovascular diseases and periodontitis are linked by their epidemiological associations and common biologic mechanisms. This connection can be explained by some of their shared risk factors, such as smoking and systemic inflammatory pathways. Although no intervention studies have shown a direct reduction in cardiovascular risk from periodontal care, two studies have demonstrated improvements in surrogate markers such as blood pressure and arterial stiffness. GPs should inquire about symptoms of periodontitis in cardiovascular patients and, if necessary, refer them to oral health specialists. Periodontal treatments, whether surgical or nonsurgical, pose no risk for patients receiving well-managed secondary preventive treatments.
Respiratory Diseases and Periodontitis
The primary evidence linking periodontitis with chronic respiratory diseases concerns chronic obstructive pulmonary disease (COPD). Individuals with periodontitis have a 33% higher risk of developing COPD, and patients with COPD and periodontitis may experience a greater decline in lung function. An established association also exists between periodontitis and obstructive sleep apnea, although the data remain inconclusive regarding a link with asthma. GPs should encourage patients with COPD to quit smoking, as it benefits both respiratory and oral health.
Finally, based on meta-analyses of COVID-19, experts note significant associations between periodontitis and the need for assisted ventilation or the risk for death during a COVID-19 infection.
This story was translated from Univadis France using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.