User login
Liquid albuterol shortage effects reduced by alternative drugs, similar shortages may be increasingly common
The shortage of 0.5% albuterol sulfate inhalation solution, first reported by the FDA last October, gained increasing attention earlier this month when Akorn Pharmaceuticals – one of just two companies making the product – shut down after years of financial and regulatory troubles.
The other manufacturer, Nephron Pharmaceuticals, is producing 0.5% albuterol “as fast as possible” to overcome the shortage, CEO Lou Kennedy said in a written comment.
Meanwhile, the more commonly used version of liquid albuterol, with a concentration of 0.083%, remains in “good supply from several manufacturers,” according to an FDA spokesperson.

Still, headlines concerning the shortage have caused “a bit of a panic” for patients with asthma and parents with asthmatic children, according to David R. Stukus, MD, professor of clinical pediatrics in the division of allergy and immunology at Nationwide Children’s, Columbus, Ohio.
Much of the media coverage has lacked context, causing unnecessary worry, he said, as the shortage only affects one type of albuterol generally reserved for inpatient and emergency use.
“The shortage has not impacted our albuterol inhalers thus far,” Dr. Stukus said in an interview. “So I certainly don’t want people with asthma to panic that they’re going to run out of their inhaler anytime soon.”
Even infants and toddlers can use inhalers
Although Dr. Stukus noted that certain patients do require nebulizers, such as those with conditions that physically limit their breathing, like muscular dystrophy, most patients can use inhalers just fine. He said it’s a “pretty common misconception, even among medical professionals,” that infants and toddlers need nebulizers instead.
“In our institution, for example, we rarely ever start babies on a nebulizer when we diagnose them with asthma,” Dr. Stukus said. “We often just start right away with an inhaler with a spacer and a face mask.”
The shortage of liquid albuterol may therefore have a silver lining, he suggested, as it prompts clinicians to reconsider their routine practice.
“When situations like this arise, it’s a great opportunity for all of us to just take a step back and reevaluate the way we do things,” Dr. Stukus said. “Sometimes we just get caught up with inertia and we continue to do things the same way even though new options are available, or evidence has changed to the contrary.”

Nathan Rabinovitch, MD, professor of pediatrics in the division of pediatric allergy and clinical immunology at National Jewish Health, Denver, said that his center had trouble obtaining liquid albuterol about 2 weeks ago, so they pivoted to the more expensive levalbuterol for about a week and a half, until their albuterol supply was restored.
While Dr. Rabinovitch agreed that most children don’t need a nebulizer, he said about 5%-10% of kids with severe asthma should have one on hand in case their inhaler fails to control an exacerbation.
Personal preferences may also considered, he added.
“If [a parent] says, ‘I like to use the nebulizer. The kid likes it,’ I’m fine if they just use a nebulizer.”

One possible downside of relying on a nebulizer, however, is portability, according to Kelly O’Shea, MD, assistant professor in the division of allergy and clinical immunology at the University of Michigan, Ann Arbor.
“If you’re out at the park or out at a soccer game with your kids, and they are having trouble breathing ... and they need their albuterol, you don’t have that ability if you are tied to a nebulizer,” Dr. O’Shea said in an interview. “As long as a parent feels comfortable – they feel like [their child] can get deep breaths in, I agree that you can use [an inhaler] in the infant and toddler population.”
She also agreed that a nebulizer may serve as a kind of second step if an inhaler isn’t controlling an exacerbation; however, she emphasized that a nebulizer should not be considered a replacement for professional care, and should not give a false sense of security.
“I caution parents to make sure that when they need it, they also take the next step and head over to the emergency room,” Dr. O’Shea said.
Generic drug shortages becoming more common
While the present scarcity of liquid albuterol appears relatively mild in terms of clinical impact, it brings up broader concerns about generic drug supply, and why shortages like this are becoming more common, according to Katie J. Suda, PharmD, MS, professor of medicine and pharmacy, and associate director, center for pharmaceutical policy and prescribing at the University of Pittsburgh.

“Drug shortages continue to increase in frequency, and the duration and severity of the shortages are also getting worse,” Dr. Suda said in an interview.
The reasons for these shortages can be elusive, according to 2022 report by the American Society of Health-System Pharmacists, which found that more than half of shortages came with no explanation from manufacturers.
The same report showed that only 5% of shortages were due to a “business decision,” but this factor is likely more central than publicly stated.
A recent FDA analysis on drug shortages, for instance, lists “lack of incentives to produce less profitable drugs,” as the first “root cause,” and Dr. Suda agrees.
“It’s important that we have generic medicines to decrease costs to our health systems, as well as for our patients,” Dr. Suda said. “But frequently, with those generic products, the price is driven so low that it increases the risk of a shortage.”
The drive to maintain profit margins may motivate companies to cut corners in production, Dr. Suda explained. She emphasized that this connection is speculative, because motivations are effectively unknowable, but the rationale is supported by past and present shortages.
Akorn Pharmaceuticals, for example, received a warning letter from the FDA in 2019 because of a variety of manufacturing issues, including defective bottles, questionable data, and metal shavings on aseptic filling equipment.
When a manufacturer like Akorn fails, the effects can be far-reaching, Dr. Suda said, noting their broad catalog of agents. Beyond liquid albuterol, Akorn was producing cardiac drugs, antibiotics, vitamins, local anesthetics, eye products, and others.
Drug shortages cause “a significant strain on our health care system,” Dr. Suda said, and substituting other medications increases risk of medical errors.
Fortunately, the increasing number of drug shortages is not going unnoticed, according to Dr. Suda. The FDA and multiple other organizations, including the ASHP, American Medical Association, and National Academies of Sciences, Engineering, and Medicine, are all taking steps to ensure that essential medicines are in steady supply, including moves to gather more data from manufacturers.
“I hope that a lot of the efforts that are moving forward ... will help us decrease the impact of shortages on our patients,” Dr. Suda said.
Lou Kennedy is the CEO of Nephron Pharmaceuticals, which commercially produces liquid albuterol. The other interviewees disclosed no relevant conflicts of interest.
The shortage of 0.5% albuterol sulfate inhalation solution, first reported by the FDA last October, gained increasing attention earlier this month when Akorn Pharmaceuticals – one of just two companies making the product – shut down after years of financial and regulatory troubles.
The other manufacturer, Nephron Pharmaceuticals, is producing 0.5% albuterol “as fast as possible” to overcome the shortage, CEO Lou Kennedy said in a written comment.
Meanwhile, the more commonly used version of liquid albuterol, with a concentration of 0.083%, remains in “good supply from several manufacturers,” according to an FDA spokesperson.
Still, headlines concerning the shortage have caused “a bit of a panic” for patients with asthma and parents with asthmatic children, according to David R. Stukus, MD, professor of clinical pediatrics in the division of allergy and immunology at Nationwide Children’s, Columbus, Ohio.
Much of the media coverage has lacked context, causing unnecessary worry, he said, as the shortage only affects one type of albuterol generally reserved for inpatient and emergency use.
“The shortage has not impacted our albuterol inhalers thus far,” Dr. Stukus said in an interview. “So I certainly don’t want people with asthma to panic that they’re going to run out of their inhaler anytime soon.”
Even infants and toddlers can use inhalers
Although Dr. Stukus noted that certain patients do require nebulizers, such as those with conditions that physically limit their breathing, like muscular dystrophy, most patients can use inhalers just fine. He said it’s a “pretty common misconception, even among medical professionals,” that infants and toddlers need nebulizers instead.
“In our institution, for example, we rarely ever start babies on a nebulizer when we diagnose them with asthma,” Dr. Stukus said. “We often just start right away with an inhaler with a spacer and a face mask.”
The shortage of liquid albuterol may therefore have a silver lining, he suggested, as it prompts clinicians to reconsider their routine practice.
“When situations like this arise, it’s a great opportunity for all of us to just take a step back and reevaluate the way we do things,” Dr. Stukus said. “Sometimes we just get caught up with inertia and we continue to do things the same way even though new options are available, or evidence has changed to the contrary.”
Nathan Rabinovitch, MD, professor of pediatrics in the division of pediatric allergy and clinical immunology at National Jewish Health, Denver, said that his center had trouble obtaining liquid albuterol about 2 weeks ago, so they pivoted to the more expensive levalbuterol for about a week and a half, until their albuterol supply was restored.
While Dr. Rabinovitch agreed that most children don’t need a nebulizer, he said about 5%-10% of kids with severe asthma should have one on hand in case their inhaler fails to control an exacerbation.
Personal preferences may also considered, he added.
“If [a parent] says, ‘I like to use the nebulizer. The kid likes it,’ I’m fine if they just use a nebulizer.”
One possible downside of relying on a nebulizer, however, is portability, according to Kelly O’Shea, MD, assistant professor in the division of allergy and clinical immunology at the University of Michigan, Ann Arbor.
“If you’re out at the park or out at a soccer game with your kids, and they are having trouble breathing ... and they need their albuterol, you don’t have that ability if you are tied to a nebulizer,” Dr. O’Shea said in an interview. “As long as a parent feels comfortable – they feel like [their child] can get deep breaths in, I agree that you can use [an inhaler] in the infant and toddler population.”
She also agreed that a nebulizer may serve as a kind of second step if an inhaler isn’t controlling an exacerbation; however, she emphasized that a nebulizer should not be considered a replacement for professional care, and should not give a false sense of security.
“I caution parents to make sure that when they need it, they also take the next step and head over to the emergency room,” Dr. O’Shea said.
Generic drug shortages becoming more common
While the present scarcity of liquid albuterol appears relatively mild in terms of clinical impact, it brings up broader concerns about generic drug supply, and why shortages like this are becoming more common, according to Katie J. Suda, PharmD, MS, professor of medicine and pharmacy, and associate director, center for pharmaceutical policy and prescribing at the University of Pittsburgh.
“Drug shortages continue to increase in frequency, and the duration and severity of the shortages are also getting worse,” Dr. Suda said in an interview.
The reasons for these shortages can be elusive, according to 2022 report by the American Society of Health-System Pharmacists, which found that more than half of shortages came with no explanation from manufacturers.
The same report showed that only 5% of shortages were due to a “business decision,” but this factor is likely more central than publicly stated.
A recent FDA analysis on drug shortages, for instance, lists “lack of incentives to produce less profitable drugs,” as the first “root cause,” and Dr. Suda agrees.
“It’s important that we have generic medicines to decrease costs to our health systems, as well as for our patients,” Dr. Suda said. “But frequently, with those generic products, the price is driven so low that it increases the risk of a shortage.”
The drive to maintain profit margins may motivate companies to cut corners in production, Dr. Suda explained. She emphasized that this connection is speculative, because motivations are effectively unknowable, but the rationale is supported by past and present shortages.
Akorn Pharmaceuticals, for example, received a warning letter from the FDA in 2019 because of a variety of manufacturing issues, including defective bottles, questionable data, and metal shavings on aseptic filling equipment.
When a manufacturer like Akorn fails, the effects can be far-reaching, Dr. Suda said, noting their broad catalog of agents. Beyond liquid albuterol, Akorn was producing cardiac drugs, antibiotics, vitamins, local anesthetics, eye products, and others.
Drug shortages cause “a significant strain on our health care system,” Dr. Suda said, and substituting other medications increases risk of medical errors.
Fortunately, the increasing number of drug shortages is not going unnoticed, according to Dr. Suda. The FDA and multiple other organizations, including the ASHP, American Medical Association, and National Academies of Sciences, Engineering, and Medicine, are all taking steps to ensure that essential medicines are in steady supply, including moves to gather more data from manufacturers.
“I hope that a lot of the efforts that are moving forward ... will help us decrease the impact of shortages on our patients,” Dr. Suda said.
Lou Kennedy is the CEO of Nephron Pharmaceuticals, which commercially produces liquid albuterol. The other interviewees disclosed no relevant conflicts of interest.
The shortage of 0.5% albuterol sulfate inhalation solution, first reported by the FDA last October, gained increasing attention earlier this month when Akorn Pharmaceuticals – one of just two companies making the product – shut down after years of financial and regulatory troubles.
The other manufacturer, Nephron Pharmaceuticals, is producing 0.5% albuterol “as fast as possible” to overcome the shortage, CEO Lou Kennedy said in a written comment.
Meanwhile, the more commonly used version of liquid albuterol, with a concentration of 0.083%, remains in “good supply from several manufacturers,” according to an FDA spokesperson.
Still, headlines concerning the shortage have caused “a bit of a panic” for patients with asthma and parents with asthmatic children, according to David R. Stukus, MD, professor of clinical pediatrics in the division of allergy and immunology at Nationwide Children’s, Columbus, Ohio.
Much of the media coverage has lacked context, causing unnecessary worry, he said, as the shortage only affects one type of albuterol generally reserved for inpatient and emergency use.
“The shortage has not impacted our albuterol inhalers thus far,” Dr. Stukus said in an interview. “So I certainly don’t want people with asthma to panic that they’re going to run out of their inhaler anytime soon.”
Even infants and toddlers can use inhalers
Although Dr. Stukus noted that certain patients do require nebulizers, such as those with conditions that physically limit their breathing, like muscular dystrophy, most patients can use inhalers just fine. He said it’s a “pretty common misconception, even among medical professionals,” that infants and toddlers need nebulizers instead.
“In our institution, for example, we rarely ever start babies on a nebulizer when we diagnose them with asthma,” Dr. Stukus said. “We often just start right away with an inhaler with a spacer and a face mask.”
The shortage of liquid albuterol may therefore have a silver lining, he suggested, as it prompts clinicians to reconsider their routine practice.
“When situations like this arise, it’s a great opportunity for all of us to just take a step back and reevaluate the way we do things,” Dr. Stukus said. “Sometimes we just get caught up with inertia and we continue to do things the same way even though new options are available, or evidence has changed to the contrary.”
Nathan Rabinovitch, MD, professor of pediatrics in the division of pediatric allergy and clinical immunology at National Jewish Health, Denver, said that his center had trouble obtaining liquid albuterol about 2 weeks ago, so they pivoted to the more expensive levalbuterol for about a week and a half, until their albuterol supply was restored.
While Dr. Rabinovitch agreed that most children don’t need a nebulizer, he said about 5%-10% of kids with severe asthma should have one on hand in case their inhaler fails to control an exacerbation.
Personal preferences may also considered, he added.
“If [a parent] says, ‘I like to use the nebulizer. The kid likes it,’ I’m fine if they just use a nebulizer.”
One possible downside of relying on a nebulizer, however, is portability, according to Kelly O’Shea, MD, assistant professor in the division of allergy and clinical immunology at the University of Michigan, Ann Arbor.
“If you’re out at the park or out at a soccer game with your kids, and they are having trouble breathing ... and they need their albuterol, you don’t have that ability if you are tied to a nebulizer,” Dr. O’Shea said in an interview. “As long as a parent feels comfortable – they feel like [their child] can get deep breaths in, I agree that you can use [an inhaler] in the infant and toddler population.”
She also agreed that a nebulizer may serve as a kind of second step if an inhaler isn’t controlling an exacerbation; however, she emphasized that a nebulizer should not be considered a replacement for professional care, and should not give a false sense of security.
“I caution parents to make sure that when they need it, they also take the next step and head over to the emergency room,” Dr. O’Shea said.
Generic drug shortages becoming more common
While the present scarcity of liquid albuterol appears relatively mild in terms of clinical impact, it brings up broader concerns about generic drug supply, and why shortages like this are becoming more common, according to Katie J. Suda, PharmD, MS, professor of medicine and pharmacy, and associate director, center for pharmaceutical policy and prescribing at the University of Pittsburgh.
“Drug shortages continue to increase in frequency, and the duration and severity of the shortages are also getting worse,” Dr. Suda said in an interview.
The reasons for these shortages can be elusive, according to 2022 report by the American Society of Health-System Pharmacists, which found that more than half of shortages came with no explanation from manufacturers.
The same report showed that only 5% of shortages were due to a “business decision,” but this factor is likely more central than publicly stated.
A recent FDA analysis on drug shortages, for instance, lists “lack of incentives to produce less profitable drugs,” as the first “root cause,” and Dr. Suda agrees.
“It’s important that we have generic medicines to decrease costs to our health systems, as well as for our patients,” Dr. Suda said. “But frequently, with those generic products, the price is driven so low that it increases the risk of a shortage.”
The drive to maintain profit margins may motivate companies to cut corners in production, Dr. Suda explained. She emphasized that this connection is speculative, because motivations are effectively unknowable, but the rationale is supported by past and present shortages.
Akorn Pharmaceuticals, for example, received a warning letter from the FDA in 2019 because of a variety of manufacturing issues, including defective bottles, questionable data, and metal shavings on aseptic filling equipment.
When a manufacturer like Akorn fails, the effects can be far-reaching, Dr. Suda said, noting their broad catalog of agents. Beyond liquid albuterol, Akorn was producing cardiac drugs, antibiotics, vitamins, local anesthetics, eye products, and others.
Drug shortages cause “a significant strain on our health care system,” Dr. Suda said, and substituting other medications increases risk of medical errors.
Fortunately, the increasing number of drug shortages is not going unnoticed, according to Dr. Suda. The FDA and multiple other organizations, including the ASHP, American Medical Association, and National Academies of Sciences, Engineering, and Medicine, are all taking steps to ensure that essential medicines are in steady supply, including moves to gather more data from manufacturers.
“I hope that a lot of the efforts that are moving forward ... will help us decrease the impact of shortages on our patients,” Dr. Suda said.
Lou Kennedy is the CEO of Nephron Pharmaceuticals, which commercially produces liquid albuterol. The other interviewees disclosed no relevant conflicts of interest.

New hope for MDS, with AML treatments
Until just over a year ago, Pat Trueman, an 82-year-old in New Hampshire, had always been a “go-go-go” kind of person. Then she started feeling tired easily, even while doing basic housework.
“I had no stamina,” Ms. Trueman said. “I didn’t feel that bad, but I just couldn’t do anything.” She had also begun noticing black and blue bruises appearing on her body, so she met with her cardiologist. But when switching medications and getting a pacemaker didn’t rid Ms. Trueman of the symptoms, her doctor referred her to a hematologist oncologist.
A bone marrow biopsy eventually revealed that Ms. Trueman had myelodysplastic neoplasms, or MDS, a blood cancer affecting an estimated 60,000-170,000 people in the United States, mostly over age 60. MDS includes several bone marrow disorders in which the bone marrow does not produce enough healthy, normal blood cells. Cytopenias are therefore a key feature of MDS, whether it’s anemia (in Ms. Trueman’s case), neutropenia, or thrombocytopenia.
Jamie Koprivnikar, MD, a hematologist oncologist at Hackensack (N.J) University Medical Center, describes the condition to her patients using a factory metaphor: “Our bone marrow is the factory where the red blood cells, white blood cells, and platelets are made, and MDS is where the machinery of the factory is broken, so the factory is making defective parts and not enough parts.”
The paradox of MDS is that too many cells are in the bone marrow while too few are in the blood, since most in the marrow die before reaching the blood, explained Azra Raza, MD, a professor of medicine and director of the MDS Center at Columbia University Medical Center, New York, and author of The First Cell (New York: Basic Books, 2019).
“We’re looking at taking a lot of the therapies that we’ve used to treat AML and then trying to apply them to MDS,” Dr. Koprivnikar said. “With all the improvement that we’re seeing there with leukemia, we’re definitely expecting this trickle-down effect to also help our high-risk MDS patients.”
Workup begins with risk stratification
While different types of MDS exist, based on morphology of the blood cells, after diagnosis the most important determination to make is of the patient’s risk level, based on the International Prognostic Scoring System–Revised (IPSS-R), updated in 2022.
While there are six MDS risk levels, patients generally fall into the high-risk and low-risk categories. The risk-level workup includes “a bone marrow biopsy with morphology, looking at how many blasts they have, looking for dysplasia, cytogenetics, and a full spectrum myeloid mutation testing, or molecular testing,” according to Anna Halpern, MD, an assistant professor of hematology in the clinical research division at Fred Hutchinson Cancer Center, Seattle. ”I use that information and along with their age, in some cases to calculate an IPSS-M or IPPS-R score, and what goes into that risk stratification includes how low their blood counts are as well as any adverse risks features we might see in their marrow, like adverse risk genetics, adverse risk mutations or increased blasts.”
Treatment decisions then turn on whether a patient is high risk – about a third of MDS patients – or low risk, because those treatment goals differ.
“With low-risk, the goal is to improve quality of life,” Dr. Raza said. “For higher-risk MDS, the goal is to prolong survival and delay progression to acute leukemia” since nearly a third of MDS patients will eventually develop AML.
More specifically, the aim with low-risk MDS is “to foster transfusion independence, either to prevent transfusions or to decrease the need for transfusions in people already receiving them,” explained Ellen Ritchie, MD, an assistant professor of medicine and hematologist-oncologist at Weill Cornell Medicine, New York. “We’re not hoping so much to cure the myelofibrosis at that point, but rather to improve blood counts.”
Sometimes, Dr. Halpern said, such treatment means active surveillance monitoring of blood counts, and at other times, it means treating cytopenia – most often anemia. The erythropoiesis-stimulating agents used to treat anemia are epoetin alfa (Epogen/Procrit) or darbepoetin alfa (Aranesp).
Ms. Trueman, whose MDS is low risk, started taking Aranesp, but she didn’t feel well on the drug and didn’t think it was helping much. She was taken off that drug and now relies only on transfusions for treatment, when her blood counts fall too low.
A newer anemia medication, luspatercept (Reblozyl), was approved in 2020 but is reserved primarily for those who fail one of the other erythropoiesis-stimulating agents and have a subtype of MDS with ring sideroblasts. Although white blood cell and platelet growth factors exist for other cytopenias, they’re rarely used because they offer little survival benefit and carry risks, Dr. Halpern said. The only other medication typically used for low-risk MDS is lenalidomide (Revlimid), which is reserved only for those with 5q-deletion syndrome.
The goal of treating high-risk MDS, on the other hand, is to cure it – when possible.
“The only curative approach for MDS is an allogeneic stem cell transplant or bone marrow transplant,” Dr. Halpern said, but transplants carry high rates of morbidity and mortality and therefore require a base level of physical fitness for a patient to consider it.
Dr. Koprivnikar observed that “MDS is certainly a disease of the elderly, and with each increasing decade of life, incidence increases. So there are a lot of patients who do not qualify for transplant.”
Age is not the sole determining factor, however. Dr. Ritchie noted that transplants can be offered to patients up to age 75 and sometimes older, depending on their physical condition. “It all depends upon the patient, their fitness, how much caretaker support they have, and what their comorbid illnesses are.”
If a transplant isn’t an option, Dr. Halpern and Dr. Raza said, they steer patients toward clinical trial participation. Otherwise, the first-line treatment is chemotherapy with hypomethylating agents to hopefully put patients in remission, Dr. Ritchie said.
The main chemo agents for high-risk patients ineligible for transplant are azacitidine (Vidaza) or decitabine (Dacogen), offered indefinitely until patients stop responding or experience progression or intolerance, Dr. Koprivnikar said. The only recently approved drug in this space is Inqovi, which is not a new agent, but it provides decitabine and cedazuridine in an oral pill form, so that patients can avoid infusions.
Treatment gaps
Few treatments options currently exist for patients with MDS, beyond erythropoiesis-stimulating agents for low-risk MDS and chemotherapy or transplant for high-risk MDS, as well as lenalidomide and luspatercept for specific subpopulations. With few breakthroughs occurring, Dr. Halpern expects that progress will only happen gradually, with new treatments coming primarily in the form of AML therapies.
“The biggest gap in our MDS regimen is treatment that can successfully treat or alter the natural history of TP53-mutated disease,” said Dr. Halpern, referring to an adverse risk mutation that can occur spontaneously or as a result of exposure to chemotherapy or radiation. “TP53-mutated MDS is very challenging to treat, and we have not had any successful therapy, so that is the biggest area of need.”
The most promising possibility in that area is an anti-CD47 drug called magrolimab, a drug being tested in a trial of which Dr. Halpern is a principal investigator. Not yet approved, magrolimab has been showing promise for AML when given with azacitidine (Vidaza) and venetoclax (Venclexta).
Venetoclax, currently used for AML, is another drug that Dr. Halpern expects to be approved for MDS soon. A phase 1b trial presented at the 2021 annual meeting of the American Hematology Society found that more than three-quarters of patients with high-risk MDS responded to the combination of venetoclax and azacitidine.
Unlike so many other cancers, MDS has seen little success with immunotherapy, which tends to have too much toxicity for patients with MDS. While Dr. Halpern sees potential for more exploration in this realm, she doesn’t anticipate immunotherapy or chimeric antigen receptor T-cell therapy becoming treatments for MDS in the near future.
“What I do think is, hopefully, we will have better treatment for TP53-mutated disease,” she said, while adding that there are currently no standard options for patients who stopped responding or don’t respond to hypomethylating agents.
Similarly, few new treatments have emerged for low-risk MDS, but there a couple of possibilities on the horizon.
“For a while, low-risk, transfusion-dependent MDS was an area that was being overlooked, and we are starting to see more activity in that area as well, with more drugs being developed,” Dr. Koprivnikar said. Drugs showing promise include imetelstat – an investigative telomerase inhibitor – and IRAK inhibitors. A phase 3 trial of imetelstat recently met its primary endpoint of 8 weeks of transfusion independence in low-risk MDS patients who aren’t responding to or cannot take erythropoiesis-stimulating agents, like Ms. Trueman. If effective and approved, a drug like imetelstat may allow patients like Ms. Trueman to resume some activities that she misses now.
“I have so much energy in my head, and I want to do so much, but I can’t,” Ms. Trueman said. “Now I think I’m getting lazy and I don’t like it because I’m not that kind of person. It’s pretty hard.”
Dr. Raza disclosed relationships with Epizyme, Grail, Vor, Taiho, RareCells, and TFC Therapeutics. Dr Ritchie reported ties with Jazz Pharmaceuticals, Novartis, Takeda, Incyte, AbbVie, Astellas, and Imago Biosciences. Dr. Halpern disclosed relationships with AbbVie, Notable Labs, Imago, Bayer, Gilead, Jazz, Incyte, Karyopharm, and Disc Medicine.
Until just over a year ago, Pat Trueman, an 82-year-old in New Hampshire, had always been a “go-go-go” kind of person. Then she started feeling tired easily, even while doing basic housework.
“I had no stamina,” Ms. Trueman said. “I didn’t feel that bad, but I just couldn’t do anything.” She had also begun noticing black and blue bruises appearing on her body, so she met with her cardiologist. But when switching medications and getting a pacemaker didn’t rid Ms. Trueman of the symptoms, her doctor referred her to a hematologist oncologist.
A bone marrow biopsy eventually revealed that Ms. Trueman had myelodysplastic neoplasms, or MDS, a blood cancer affecting an estimated 60,000-170,000 people in the United States, mostly over age 60. MDS includes several bone marrow disorders in which the bone marrow does not produce enough healthy, normal blood cells. Cytopenias are therefore a key feature of MDS, whether it’s anemia (in Ms. Trueman’s case), neutropenia, or thrombocytopenia.
Jamie Koprivnikar, MD, a hematologist oncologist at Hackensack (N.J) University Medical Center, describes the condition to her patients using a factory metaphor: “Our bone marrow is the factory where the red blood cells, white blood cells, and platelets are made, and MDS is where the machinery of the factory is broken, so the factory is making defective parts and not enough parts.”
The paradox of MDS is that too many cells are in the bone marrow while too few are in the blood, since most in the marrow die before reaching the blood, explained Azra Raza, MD, a professor of medicine and director of the MDS Center at Columbia University Medical Center, New York, and author of The First Cell (New York: Basic Books, 2019).
“We’re looking at taking a lot of the therapies that we’ve used to treat AML and then trying to apply them to MDS,” Dr. Koprivnikar said. “With all the improvement that we’re seeing there with leukemia, we’re definitely expecting this trickle-down effect to also help our high-risk MDS patients.”
Workup begins with risk stratification
While different types of MDS exist, based on morphology of the blood cells, after diagnosis the most important determination to make is of the patient’s risk level, based on the International Prognostic Scoring System–Revised (IPSS-R), updated in 2022.
While there are six MDS risk levels, patients generally fall into the high-risk and low-risk categories. The risk-level workup includes “a bone marrow biopsy with morphology, looking at how many blasts they have, looking for dysplasia, cytogenetics, and a full spectrum myeloid mutation testing, or molecular testing,” according to Anna Halpern, MD, an assistant professor of hematology in the clinical research division at Fred Hutchinson Cancer Center, Seattle. ”I use that information and along with their age, in some cases to calculate an IPSS-M or IPPS-R score, and what goes into that risk stratification includes how low their blood counts are as well as any adverse risks features we might see in their marrow, like adverse risk genetics, adverse risk mutations or increased blasts.”
Treatment decisions then turn on whether a patient is high risk – about a third of MDS patients – or low risk, because those treatment goals differ.
“With low-risk, the goal is to improve quality of life,” Dr. Raza said. “For higher-risk MDS, the goal is to prolong survival and delay progression to acute leukemia” since nearly a third of MDS patients will eventually develop AML.
More specifically, the aim with low-risk MDS is “to foster transfusion independence, either to prevent transfusions or to decrease the need for transfusions in people already receiving them,” explained Ellen Ritchie, MD, an assistant professor of medicine and hematologist-oncologist at Weill Cornell Medicine, New York. “We’re not hoping so much to cure the myelofibrosis at that point, but rather to improve blood counts.”
Sometimes, Dr. Halpern said, such treatment means active surveillance monitoring of blood counts, and at other times, it means treating cytopenia – most often anemia. The erythropoiesis-stimulating agents used to treat anemia are epoetin alfa (Epogen/Procrit) or darbepoetin alfa (Aranesp).
Ms. Trueman, whose MDS is low risk, started taking Aranesp, but she didn’t feel well on the drug and didn’t think it was helping much. She was taken off that drug and now relies only on transfusions for treatment, when her blood counts fall too low.
A newer anemia medication, luspatercept (Reblozyl), was approved in 2020 but is reserved primarily for those who fail one of the other erythropoiesis-stimulating agents and have a subtype of MDS with ring sideroblasts. Although white blood cell and platelet growth factors exist for other cytopenias, they’re rarely used because they offer little survival benefit and carry risks, Dr. Halpern said. The only other medication typically used for low-risk MDS is lenalidomide (Revlimid), which is reserved only for those with 5q-deletion syndrome.
The goal of treating high-risk MDS, on the other hand, is to cure it – when possible.
“The only curative approach for MDS is an allogeneic stem cell transplant or bone marrow transplant,” Dr. Halpern said, but transplants carry high rates of morbidity and mortality and therefore require a base level of physical fitness for a patient to consider it.
Dr. Koprivnikar observed that “MDS is certainly a disease of the elderly, and with each increasing decade of life, incidence increases. So there are a lot of patients who do not qualify for transplant.”
Age is not the sole determining factor, however. Dr. Ritchie noted that transplants can be offered to patients up to age 75 and sometimes older, depending on their physical condition. “It all depends upon the patient, their fitness, how much caretaker support they have, and what their comorbid illnesses are.”
If a transplant isn’t an option, Dr. Halpern and Dr. Raza said, they steer patients toward clinical trial participation. Otherwise, the first-line treatment is chemotherapy with hypomethylating agents to hopefully put patients in remission, Dr. Ritchie said.
The main chemo agents for high-risk patients ineligible for transplant are azacitidine (Vidaza) or decitabine (Dacogen), offered indefinitely until patients stop responding or experience progression or intolerance, Dr. Koprivnikar said. The only recently approved drug in this space is Inqovi, which is not a new agent, but it provides decitabine and cedazuridine in an oral pill form, so that patients can avoid infusions.
Treatment gaps
Few treatments options currently exist for patients with MDS, beyond erythropoiesis-stimulating agents for low-risk MDS and chemotherapy or transplant for high-risk MDS, as well as lenalidomide and luspatercept for specific subpopulations. With few breakthroughs occurring, Dr. Halpern expects that progress will only happen gradually, with new treatments coming primarily in the form of AML therapies.
“The biggest gap in our MDS regimen is treatment that can successfully treat or alter the natural history of TP53-mutated disease,” said Dr. Halpern, referring to an adverse risk mutation that can occur spontaneously or as a result of exposure to chemotherapy or radiation. “TP53-mutated MDS is very challenging to treat, and we have not had any successful therapy, so that is the biggest area of need.”
The most promising possibility in that area is an anti-CD47 drug called magrolimab, a drug being tested in a trial of which Dr. Halpern is a principal investigator. Not yet approved, magrolimab has been showing promise for AML when given with azacitidine (Vidaza) and venetoclax (Venclexta).
Venetoclax, currently used for AML, is another drug that Dr. Halpern expects to be approved for MDS soon. A phase 1b trial presented at the 2021 annual meeting of the American Hematology Society found that more than three-quarters of patients with high-risk MDS responded to the combination of venetoclax and azacitidine.
Unlike so many other cancers, MDS has seen little success with immunotherapy, which tends to have too much toxicity for patients with MDS. While Dr. Halpern sees potential for more exploration in this realm, she doesn’t anticipate immunotherapy or chimeric antigen receptor T-cell therapy becoming treatments for MDS in the near future.
“What I do think is, hopefully, we will have better treatment for TP53-mutated disease,” she said, while adding that there are currently no standard options for patients who stopped responding or don’t respond to hypomethylating agents.
Similarly, few new treatments have emerged for low-risk MDS, but there a couple of possibilities on the horizon.
“For a while, low-risk, transfusion-dependent MDS was an area that was being overlooked, and we are starting to see more activity in that area as well, with more drugs being developed,” Dr. Koprivnikar said. Drugs showing promise include imetelstat – an investigative telomerase inhibitor – and IRAK inhibitors. A phase 3 trial of imetelstat recently met its primary endpoint of 8 weeks of transfusion independence in low-risk MDS patients who aren’t responding to or cannot take erythropoiesis-stimulating agents, like Ms. Trueman. If effective and approved, a drug like imetelstat may allow patients like Ms. Trueman to resume some activities that she misses now.
“I have so much energy in my head, and I want to do so much, but I can’t,” Ms. Trueman said. “Now I think I’m getting lazy and I don’t like it because I’m not that kind of person. It’s pretty hard.”
Dr. Raza disclosed relationships with Epizyme, Grail, Vor, Taiho, RareCells, and TFC Therapeutics. Dr Ritchie reported ties with Jazz Pharmaceuticals, Novartis, Takeda, Incyte, AbbVie, Astellas, and Imago Biosciences. Dr. Halpern disclosed relationships with AbbVie, Notable Labs, Imago, Bayer, Gilead, Jazz, Incyte, Karyopharm, and Disc Medicine.
Until just over a year ago, Pat Trueman, an 82-year-old in New Hampshire, had always been a “go-go-go” kind of person. Then she started feeling tired easily, even while doing basic housework.
“I had no stamina,” Ms. Trueman said. “I didn’t feel that bad, but I just couldn’t do anything.” She had also begun noticing black and blue bruises appearing on her body, so she met with her cardiologist. But when switching medications and getting a pacemaker didn’t rid Ms. Trueman of the symptoms, her doctor referred her to a hematologist oncologist.
A bone marrow biopsy eventually revealed that Ms. Trueman had myelodysplastic neoplasms, or MDS, a blood cancer affecting an estimated 60,000-170,000 people in the United States, mostly over age 60. MDS includes several bone marrow disorders in which the bone marrow does not produce enough healthy, normal blood cells. Cytopenias are therefore a key feature of MDS, whether it’s anemia (in Ms. Trueman’s case), neutropenia, or thrombocytopenia.
Jamie Koprivnikar, MD, a hematologist oncologist at Hackensack (N.J) University Medical Center, describes the condition to her patients using a factory metaphor: “Our bone marrow is the factory where the red blood cells, white blood cells, and platelets are made, and MDS is where the machinery of the factory is broken, so the factory is making defective parts and not enough parts.”
The paradox of MDS is that too many cells are in the bone marrow while too few are in the blood, since most in the marrow die before reaching the blood, explained Azra Raza, MD, a professor of medicine and director of the MDS Center at Columbia University Medical Center, New York, and author of The First Cell (New York: Basic Books, 2019).
“We’re looking at taking a lot of the therapies that we’ve used to treat AML and then trying to apply them to MDS,” Dr. Koprivnikar said. “With all the improvement that we’re seeing there with leukemia, we’re definitely expecting this trickle-down effect to also help our high-risk MDS patients.”
Workup begins with risk stratification
While different types of MDS exist, based on morphology of the blood cells, after diagnosis the most important determination to make is of the patient’s risk level, based on the International Prognostic Scoring System–Revised (IPSS-R), updated in 2022.
While there are six MDS risk levels, patients generally fall into the high-risk and low-risk categories. The risk-level workup includes “a bone marrow biopsy with morphology, looking at how many blasts they have, looking for dysplasia, cytogenetics, and a full spectrum myeloid mutation testing, or molecular testing,” according to Anna Halpern, MD, an assistant professor of hematology in the clinical research division at Fred Hutchinson Cancer Center, Seattle. ”I use that information and along with their age, in some cases to calculate an IPSS-M or IPPS-R score, and what goes into that risk stratification includes how low their blood counts are as well as any adverse risks features we might see in their marrow, like adverse risk genetics, adverse risk mutations or increased blasts.”
Treatment decisions then turn on whether a patient is high risk – about a third of MDS patients – or low risk, because those treatment goals differ.
“With low-risk, the goal is to improve quality of life,” Dr. Raza said. “For higher-risk MDS, the goal is to prolong survival and delay progression to acute leukemia” since nearly a third of MDS patients will eventually develop AML.
More specifically, the aim with low-risk MDS is “to foster transfusion independence, either to prevent transfusions or to decrease the need for transfusions in people already receiving them,” explained Ellen Ritchie, MD, an assistant professor of medicine and hematologist-oncologist at Weill Cornell Medicine, New York. “We’re not hoping so much to cure the myelofibrosis at that point, but rather to improve blood counts.”
Sometimes, Dr. Halpern said, such treatment means active surveillance monitoring of blood counts, and at other times, it means treating cytopenia – most often anemia. The erythropoiesis-stimulating agents used to treat anemia are epoetin alfa (Epogen/Procrit) or darbepoetin alfa (Aranesp).
Ms. Trueman, whose MDS is low risk, started taking Aranesp, but she didn’t feel well on the drug and didn’t think it was helping much. She was taken off that drug and now relies only on transfusions for treatment, when her blood counts fall too low.
A newer anemia medication, luspatercept (Reblozyl), was approved in 2020 but is reserved primarily for those who fail one of the other erythropoiesis-stimulating agents and have a subtype of MDS with ring sideroblasts. Although white blood cell and platelet growth factors exist for other cytopenias, they’re rarely used because they offer little survival benefit and carry risks, Dr. Halpern said. The only other medication typically used for low-risk MDS is lenalidomide (Revlimid), which is reserved only for those with 5q-deletion syndrome.
The goal of treating high-risk MDS, on the other hand, is to cure it – when possible.
“The only curative approach for MDS is an allogeneic stem cell transplant or bone marrow transplant,” Dr. Halpern said, but transplants carry high rates of morbidity and mortality and therefore require a base level of physical fitness for a patient to consider it.
Dr. Koprivnikar observed that “MDS is certainly a disease of the elderly, and with each increasing decade of life, incidence increases. So there are a lot of patients who do not qualify for transplant.”
Age is not the sole determining factor, however. Dr. Ritchie noted that transplants can be offered to patients up to age 75 and sometimes older, depending on their physical condition. “It all depends upon the patient, their fitness, how much caretaker support they have, and what their comorbid illnesses are.”
If a transplant isn’t an option, Dr. Halpern and Dr. Raza said, they steer patients toward clinical trial participation. Otherwise, the first-line treatment is chemotherapy with hypomethylating agents to hopefully put patients in remission, Dr. Ritchie said.
The main chemo agents for high-risk patients ineligible for transplant are azacitidine (Vidaza) or decitabine (Dacogen), offered indefinitely until patients stop responding or experience progression or intolerance, Dr. Koprivnikar said. The only recently approved drug in this space is Inqovi, which is not a new agent, but it provides decitabine and cedazuridine in an oral pill form, so that patients can avoid infusions.
Treatment gaps
Few treatments options currently exist for patients with MDS, beyond erythropoiesis-stimulating agents for low-risk MDS and chemotherapy or transplant for high-risk MDS, as well as lenalidomide and luspatercept for specific subpopulations. With few breakthroughs occurring, Dr. Halpern expects that progress will only happen gradually, with new treatments coming primarily in the form of AML therapies.
“The biggest gap in our MDS regimen is treatment that can successfully treat or alter the natural history of TP53-mutated disease,” said Dr. Halpern, referring to an adverse risk mutation that can occur spontaneously or as a result of exposure to chemotherapy or radiation. “TP53-mutated MDS is very challenging to treat, and we have not had any successful therapy, so that is the biggest area of need.”
The most promising possibility in that area is an anti-CD47 drug called magrolimab, a drug being tested in a trial of which Dr. Halpern is a principal investigator. Not yet approved, magrolimab has been showing promise for AML when given with azacitidine (Vidaza) and venetoclax (Venclexta).
Venetoclax, currently used for AML, is another drug that Dr. Halpern expects to be approved for MDS soon. A phase 1b trial presented at the 2021 annual meeting of the American Hematology Society found that more than three-quarters of patients with high-risk MDS responded to the combination of venetoclax and azacitidine.
Unlike so many other cancers, MDS has seen little success with immunotherapy, which tends to have too much toxicity for patients with MDS. While Dr. Halpern sees potential for more exploration in this realm, she doesn’t anticipate immunotherapy or chimeric antigen receptor T-cell therapy becoming treatments for MDS in the near future.
“What I do think is, hopefully, we will have better treatment for TP53-mutated disease,” she said, while adding that there are currently no standard options for patients who stopped responding or don’t respond to hypomethylating agents.
Similarly, few new treatments have emerged for low-risk MDS, but there a couple of possibilities on the horizon.
“For a while, low-risk, transfusion-dependent MDS was an area that was being overlooked, and we are starting to see more activity in that area as well, with more drugs being developed,” Dr. Koprivnikar said. Drugs showing promise include imetelstat – an investigative telomerase inhibitor – and IRAK inhibitors. A phase 3 trial of imetelstat recently met its primary endpoint of 8 weeks of transfusion independence in low-risk MDS patients who aren’t responding to or cannot take erythropoiesis-stimulating agents, like Ms. Trueman. If effective and approved, a drug like imetelstat may allow patients like Ms. Trueman to resume some activities that she misses now.
“I have so much energy in my head, and I want to do so much, but I can’t,” Ms. Trueman said. “Now I think I’m getting lazy and I don’t like it because I’m not that kind of person. It’s pretty hard.”
Dr. Raza disclosed relationships with Epizyme, Grail, Vor, Taiho, RareCells, and TFC Therapeutics. Dr Ritchie reported ties with Jazz Pharmaceuticals, Novartis, Takeda, Incyte, AbbVie, Astellas, and Imago Biosciences. Dr. Halpern disclosed relationships with AbbVie, Notable Labs, Imago, Bayer, Gilead, Jazz, Incyte, Karyopharm, and Disc Medicine.
California picks generic drug company Civica to produce low-cost insulin
Gov. Gavin Newsom on March 18 announced the selection of Utah-based generic drug manufacturer Civica to produce low-cost insulin for California, an unprecedented move that makes good on his promise to put state government in direct competition with the brand-name drug companies that dominate the market.
“People should not be forced to go into debt to get lifesaving prescriptions,” Gov. Newsom said. “Californians will have access to some of the most inexpensive insulin available, helping them save thousands of dollars each year.”
The contract, with an initial cost of $50 million that Gov. Newsom and his fellow Democratic lawmakers approved last year, calls for Civica to manufacture state-branded insulin and make the lifesaving drug available to any Californian who needs it, regardless of insurance coverage, by mail order and at local pharmacies. But insulin is just the beginning. Gov. Newsom said the state will also look to produce the opioid overdose reversal drug naloxone.
Allan Coukell, Civica’s senior vice president of public policy, said in an interview that the nonprofit drugmaker is also in talks with the Newsom administration to potentially produce other generic medications, but he declined to elaborate, saying the company is focused on making cheap insulin widely available first.
“We are very excited about this partnership with the state of California,” Mr. Coukell said. “We’re not looking to have 100% of the market, but we do want 100% of people to have access to fair insulin prices.”
As insulin costs for consumers have soared, Democratic lawmakers and activists have called on the industry to rein in prices. Just weeks after President Joe Biden attacked Big Pharma for jacking up insulin prices, the three drugmakers that control the insulin market – Eli Lilly, Novo Nordisk, and Sanofi – announced they would slash the list prices of some products.
Gov. Newsom, who has previously accused the pharmaceutical industry of gouging Californians with “sky-high prices,” argued that the launch of the state’s generic drug label, CalRx, will add competition and apply pressure on the industry. Administration officials declined to say when California’s insulin products would be available, but experts say it could be as soon as 2025. Mr. Coukell said the state-branded medication will still require approval from the Food and Drug Administration, which can take roughly 10 months.
The Pharmaceutical Research and Manufacturers of America, which lobbies on behalf of brand-name companies, blasted California’s move. Reid Porter, senior director of state public affairs for PhRMA, said Gov. Newsom just “wants to score political points.”
“If the governor wants to impact what patients pay for insulins and other medicines meaningfully, he should expand his focus to others in the system that often make patients pay more than they do for medicines,” Mr. Porter said, blaming pharmaceutical go-between companies, known as pharmacy benefit managers, that negotiate with manufacturers on behalf of insurers for rebates and discounts on drugs.
The Pharmaceutical Care Management Association, which represents pharmacy benefit managers argued in turn that it’s pharmaceutical companies that are to blame for high prices.
Drug pricing experts, however, say pharmacy benefit managers and drugmakers share the blame.
Gov. Newsom administration officials say that inflated insulin costs force some to pay as much as $300 per vial or $500 for a box of injectable pens, and that too many Californians with diabetes skip or ration their medication. Doing so can lead to blindness, amputations, and life-threatening conditions such as heart disease and kidney failure. Nearly 10% of California adults have diabetes.
Civica is developing three types of generic insulin, known as a biosimilar, which will be available both in vials and in injectable pens. They are expected to be interchangeable with brand-name products including Lantus, Humalog, and NovoLog. Mr. Coukell said the company would make the drug available for no more than $30 a vial, or $55 for five injectable pens.
Gov. Newsom said the state’s insulin will save many patients $2,000-$4,000 a year, though critical questions about how California would get the products into the hands of consumers remain unanswered, including how it would persuade pharmacies, insurers, and retailers to distribute the drugs.
In 2022, Gov. Newsom also secured $50 million in seed money to build a facility to manufacture insulin; Mr. Coukell said Civica is exploring building a plant in California.
California’s move, though never previously tried by a state government, could be blunted by recent industry decisions to lower insulin prices. In March, Lilly, Novo Nordisk, and Sanofi vowed to cut prices, with Lilly offering a vial at $25 per month, Novo Nordisk promising major reductions that would bring the price of a particular generic vial to $48, and Sanofi pegging one vial at $64.
The governor’s office said it will cost the state $30 per vial to manufacture and distribute insulin and it will be sold at that price. Doing so, the administration argued, “will prevent the egregious cost-shifting that happens in traditional pharmaceutical price games.”
Drug pricing experts said generic production in California could further lower costs for insulin, and benefit people with high-deductible health insurance plans or no insurance.
“This is an extraordinary move in the pharmaceutical industry, not just for insulin but potentially for all kinds of drugs,” said Robin Feldman, a professor at the University of California, San Francisco. “It’s a very difficult industry to disrupt, but California is poised to do just that.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Gov. Gavin Newsom on March 18 announced the selection of Utah-based generic drug manufacturer Civica to produce low-cost insulin for California, an unprecedented move that makes good on his promise to put state government in direct competition with the brand-name drug companies that dominate the market.
“People should not be forced to go into debt to get lifesaving prescriptions,” Gov. Newsom said. “Californians will have access to some of the most inexpensive insulin available, helping them save thousands of dollars each year.”
The contract, with an initial cost of $50 million that Gov. Newsom and his fellow Democratic lawmakers approved last year, calls for Civica to manufacture state-branded insulin and make the lifesaving drug available to any Californian who needs it, regardless of insurance coverage, by mail order and at local pharmacies. But insulin is just the beginning. Gov. Newsom said the state will also look to produce the opioid overdose reversal drug naloxone.
Allan Coukell, Civica’s senior vice president of public policy, said in an interview that the nonprofit drugmaker is also in talks with the Newsom administration to potentially produce other generic medications, but he declined to elaborate, saying the company is focused on making cheap insulin widely available first.
“We are very excited about this partnership with the state of California,” Mr. Coukell said. “We’re not looking to have 100% of the market, but we do want 100% of people to have access to fair insulin prices.”
As insulin costs for consumers have soared, Democratic lawmakers and activists have called on the industry to rein in prices. Just weeks after President Joe Biden attacked Big Pharma for jacking up insulin prices, the three drugmakers that control the insulin market – Eli Lilly, Novo Nordisk, and Sanofi – announced they would slash the list prices of some products.
Gov. Newsom, who has previously accused the pharmaceutical industry of gouging Californians with “sky-high prices,” argued that the launch of the state’s generic drug label, CalRx, will add competition and apply pressure on the industry. Administration officials declined to say when California’s insulin products would be available, but experts say it could be as soon as 2025. Mr. Coukell said the state-branded medication will still require approval from the Food and Drug Administration, which can take roughly 10 months.
The Pharmaceutical Research and Manufacturers of America, which lobbies on behalf of brand-name companies, blasted California’s move. Reid Porter, senior director of state public affairs for PhRMA, said Gov. Newsom just “wants to score political points.”
“If the governor wants to impact what patients pay for insulins and other medicines meaningfully, he should expand his focus to others in the system that often make patients pay more than they do for medicines,” Mr. Porter said, blaming pharmaceutical go-between companies, known as pharmacy benefit managers, that negotiate with manufacturers on behalf of insurers for rebates and discounts on drugs.
The Pharmaceutical Care Management Association, which represents pharmacy benefit managers argued in turn that it’s pharmaceutical companies that are to blame for high prices.
Drug pricing experts, however, say pharmacy benefit managers and drugmakers share the blame.
Gov. Newsom administration officials say that inflated insulin costs force some to pay as much as $300 per vial or $500 for a box of injectable pens, and that too many Californians with diabetes skip or ration their medication. Doing so can lead to blindness, amputations, and life-threatening conditions such as heart disease and kidney failure. Nearly 10% of California adults have diabetes.
Civica is developing three types of generic insulin, known as a biosimilar, which will be available both in vials and in injectable pens. They are expected to be interchangeable with brand-name products including Lantus, Humalog, and NovoLog. Mr. Coukell said the company would make the drug available for no more than $30 a vial, or $55 for five injectable pens.
Gov. Newsom said the state’s insulin will save many patients $2,000-$4,000 a year, though critical questions about how California would get the products into the hands of consumers remain unanswered, including how it would persuade pharmacies, insurers, and retailers to distribute the drugs.
In 2022, Gov. Newsom also secured $50 million in seed money to build a facility to manufacture insulin; Mr. Coukell said Civica is exploring building a plant in California.
California’s move, though never previously tried by a state government, could be blunted by recent industry decisions to lower insulin prices. In March, Lilly, Novo Nordisk, and Sanofi vowed to cut prices, with Lilly offering a vial at $25 per month, Novo Nordisk promising major reductions that would bring the price of a particular generic vial to $48, and Sanofi pegging one vial at $64.
The governor’s office said it will cost the state $30 per vial to manufacture and distribute insulin and it will be sold at that price. Doing so, the administration argued, “will prevent the egregious cost-shifting that happens in traditional pharmaceutical price games.”
Drug pricing experts said generic production in California could further lower costs for insulin, and benefit people with high-deductible health insurance plans or no insurance.
“This is an extraordinary move in the pharmaceutical industry, not just for insulin but potentially for all kinds of drugs,” said Robin Feldman, a professor at the University of California, San Francisco. “It’s a very difficult industry to disrupt, but California is poised to do just that.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Gov. Gavin Newsom on March 18 announced the selection of Utah-based generic drug manufacturer Civica to produce low-cost insulin for California, an unprecedented move that makes good on his promise to put state government in direct competition with the brand-name drug companies that dominate the market.
“People should not be forced to go into debt to get lifesaving prescriptions,” Gov. Newsom said. “Californians will have access to some of the most inexpensive insulin available, helping them save thousands of dollars each year.”
The contract, with an initial cost of $50 million that Gov. Newsom and his fellow Democratic lawmakers approved last year, calls for Civica to manufacture state-branded insulin and make the lifesaving drug available to any Californian who needs it, regardless of insurance coverage, by mail order and at local pharmacies. But insulin is just the beginning. Gov. Newsom said the state will also look to produce the opioid overdose reversal drug naloxone.
Allan Coukell, Civica’s senior vice president of public policy, said in an interview that the nonprofit drugmaker is also in talks with the Newsom administration to potentially produce other generic medications, but he declined to elaborate, saying the company is focused on making cheap insulin widely available first.
“We are very excited about this partnership with the state of California,” Mr. Coukell said. “We’re not looking to have 100% of the market, but we do want 100% of people to have access to fair insulin prices.”
As insulin costs for consumers have soared, Democratic lawmakers and activists have called on the industry to rein in prices. Just weeks after President Joe Biden attacked Big Pharma for jacking up insulin prices, the three drugmakers that control the insulin market – Eli Lilly, Novo Nordisk, and Sanofi – announced they would slash the list prices of some products.
Gov. Newsom, who has previously accused the pharmaceutical industry of gouging Californians with “sky-high prices,” argued that the launch of the state’s generic drug label, CalRx, will add competition and apply pressure on the industry. Administration officials declined to say when California’s insulin products would be available, but experts say it could be as soon as 2025. Mr. Coukell said the state-branded medication will still require approval from the Food and Drug Administration, which can take roughly 10 months.
The Pharmaceutical Research and Manufacturers of America, which lobbies on behalf of brand-name companies, blasted California’s move. Reid Porter, senior director of state public affairs for PhRMA, said Gov. Newsom just “wants to score political points.”
“If the governor wants to impact what patients pay for insulins and other medicines meaningfully, he should expand his focus to others in the system that often make patients pay more than they do for medicines,” Mr. Porter said, blaming pharmaceutical go-between companies, known as pharmacy benefit managers, that negotiate with manufacturers on behalf of insurers for rebates and discounts on drugs.
The Pharmaceutical Care Management Association, which represents pharmacy benefit managers argued in turn that it’s pharmaceutical companies that are to blame for high prices.
Drug pricing experts, however, say pharmacy benefit managers and drugmakers share the blame.
Gov. Newsom administration officials say that inflated insulin costs force some to pay as much as $300 per vial or $500 for a box of injectable pens, and that too many Californians with diabetes skip or ration their medication. Doing so can lead to blindness, amputations, and life-threatening conditions such as heart disease and kidney failure. Nearly 10% of California adults have diabetes.
Civica is developing three types of generic insulin, known as a biosimilar, which will be available both in vials and in injectable pens. They are expected to be interchangeable with brand-name products including Lantus, Humalog, and NovoLog. Mr. Coukell said the company would make the drug available for no more than $30 a vial, or $55 for five injectable pens.
Gov. Newsom said the state’s insulin will save many patients $2,000-$4,000 a year, though critical questions about how California would get the products into the hands of consumers remain unanswered, including how it would persuade pharmacies, insurers, and retailers to distribute the drugs.
In 2022, Gov. Newsom also secured $50 million in seed money to build a facility to manufacture insulin; Mr. Coukell said Civica is exploring building a plant in California.
California’s move, though never previously tried by a state government, could be blunted by recent industry decisions to lower insulin prices. In March, Lilly, Novo Nordisk, and Sanofi vowed to cut prices, with Lilly offering a vial at $25 per month, Novo Nordisk promising major reductions that would bring the price of a particular generic vial to $48, and Sanofi pegging one vial at $64.
The governor’s office said it will cost the state $30 per vial to manufacture and distribute insulin and it will be sold at that price. Doing so, the administration argued, “will prevent the egregious cost-shifting that happens in traditional pharmaceutical price games.”
Drug pricing experts said generic production in California could further lower costs for insulin, and benefit people with high-deductible health insurance plans or no insurance.
“This is an extraordinary move in the pharmaceutical industry, not just for insulin but potentially for all kinds of drugs,” said Robin Feldman, a professor at the University of California, San Francisco. “It’s a very difficult industry to disrupt, but California is poised to do just that.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
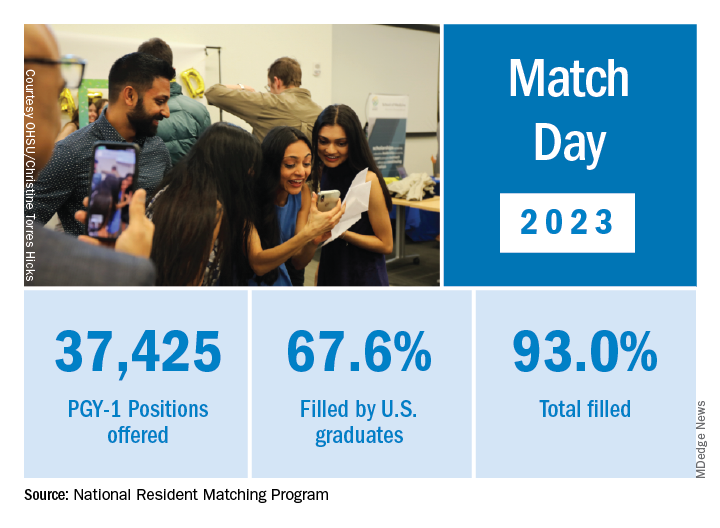
Match Day: Record number of residencies offered
Baily Nagle, vice president of her graduating class at Harvard Medical School, Boston, celebrated “the luck of the Irish” on St. Patrick’s Day that allowed her to match into her chosen specialty and top choice of residency programs: anesthesia at Brigham and Women’s Hospital.
“I am feeling very excited and relieved – I matched,” she said in an interview upon hearing her good fortune on Match Monday, March 13. She had a similar reaction on Match Day, March 17. “After a lot of long nights and hard work, happy to have it pay off.”
Ms. Nagle was so determined to match into her specialty that she didn’t have any other specialties in mind as a backup.
The annual process of matching medical school graduates with compatible residency programs is an emotional roller coaster for all applicants, their personal March Madness, so to speak. But Ms. Nagle was one of the more fortunate applicants. She didn’t have to confront the heartbreak other applicants felt when the National Resident Matching Program (NRMP) announced results of the main residency match and the Supplemental Offer and Acceptance Program (SOAP), which offers alternate programs for unfilled positions or unmatched applicants.
During the 2023 Match process, this news organization has been following a handful of students, checking in with them periodically for updates on their progress. Most of them matched successfully, but at least one international medical graduate (IMG) did not. What the others have in common is that their hearts were set on a chosen specialty. Like Ms. Nagle, another student banked on landing his chosen specialty without a backup plan, whereas another said that she’d continue through the SOAP if she didn’t match successfully.
Overall, Match Day resulted in a record number of residency positions offered, most notably in primary care, which “hit an all-time high,” according to NRMP President and CEO Donna L. Lamb, DHSc, MBA, BSN. The number of positions has “consistently increased over the past 5 years, and most importantly the fill rate for primary care has remained steady,” Dr.. Lamb noted in the NRMP release of Match Day results. The release coincided with students learning through emails at noon Eastern Time to which residency or supplemental programs they were matched.
Though more applicants registered for the Match in 2023 than in 2022 – driven primarily by non-U.S. IMGs – the NRMP stated that it was surprised by the decrease in U.S. MD senior applicants.
U.S. MD seniors had a nearly 94% Match rate, a small increase over 2022. U.S. citizen IMGs saw a nearly 68% Match rate, which NRMP reported as an “all-time high” and about six percentage points over in 2022, whereas non-U.S. IMGs had a nearly 60% Match rate, a 1.3 percentage point increase over 2022.
Among the specialties that filled all available positions in 2023 were orthopedic surgery, plastic surgery (integrated), and radiology – diagnostic and thoracic surgery.
Not everyone matches
On March 13, the American College of Emergency Physicians issued a joint statement with other emergency medicine (EM) organizations about a high rate of unfilled EM positions expected in 2023.
NRMP acknowledged March 17 that 554 positions remained unfilled, an increase of 335 more unfilled positions than 2022. NRMP attributed the increase in unfilled positions in part to a decrease in the number of U.S. MD and U.S. DO seniors who submitted ranks for the specialty, which “could reflect changing applicant interests or projections about workforce opportunities post residency.”
Applicants who didn’t match usually try to obtain an unfilled position through SOAP. In 2023, 2,685 positions were unfilled after the matching algorithm was processed, an increase of nearly 19% over 2022. The vast majority of those positions were placed in SOAP, an increase of 17.5% over 2022.
Asim Ansari was one of the unlucky ones. Mr. Ansari was trying to match for the fifth time. He was unsuccessful in doing so again in 2023 in the Match and SOAP. Still, he was offered and accepted a child and adolescent psychiatry fellowship at Kansas University Medical Center in Kansas City. Psychiatry was his chosen specialty, so he was “feeling good. It’s a nice place to go to do the next 2 years.”
Mr. Ansari, who started the #MatchMadness support group for unmatched doctors on Twitter Spaces, was quick to cheer on his fellow matching peers on March 13 while revealing his own fate: “Congratulations to everyone who matched!!! Y’all are amazing. So proud of each one of you!!! I didn’t.”
Soon after the results, #MatchMadness held a #Soap2023 support session, and Mr. Ansari sought advice for those willing to review SOAP applications. Elsewhere on Twitter Match Day threads, a few doctors offered their support to those who planned to SOAP, students announced their matches, and others either congratulated or encouraged those still trying to match.
Couples match
Not everyone who matched considered the alternative. Before March 13, William Boyer said that he hadn’t given much thought to what would happen if he didn’t match because he was “optimistically confident” he would match into his chosen EM specialty. But he did and got his top choice of programs: Yale New Haven (Conn.) Hospital.
“I feel great,” he said in an interview. “I was definitely nervous opening the envelope” that revealed his residency program, “but there was a rush of relief” when he saw he landed Yale.
Earlier in the match cycle, he said in an interview that he “interviewed at a few ‘reach’ programs, so I hope I don’t match lower than expected on my rank list.”
Mr. Boyer considers himself “a mature applicant,” entering the University of South Carolina, Columbia, after 4 years as an insurance broker.
“I am celebrating today by playing pickleball with a few close medical friends who also matched this morning,” Mr. Boyer said on March 13. “I definitely had periods of nervousness leading up to this morning though that quickly turned into joy and relief” after learning he matched.
Mr. Boyer believes that his professional experience in the insurance industry and health care lobbying efforts with the National Association of Health Underwriters set him apart from other applicants.
“I changed careers to pursue this aspiration, which demonstrates my full dedication to the medical profession.”
He applied to 48 programs and was offered interviews to nearly half. Mr. Boyer visited the majority of those virtually. He said he targeted programs close to where his and his partner’s families are located: Massachusetts, North Carolina, and Texas. “My partner, who I met in medical school, matched into ortho as well so the whole household is very happy,” Mr. Boyer said.
She matched into her top choice as well on March 17, though a distance away at UT Health in San Antonio, he said. “We are both ecstatic. We both got our no. 1 choice. That was the plan going into it. We will make it work. I have 4 weeks of vacation.”
In his program choices, Mr. Boyer prioritized access to nature, minimal leadership turnover, a mix of clinical training sites, and adequate elective rotations and fellowship opportunities, such as in wilderness medicine and health policy.
NRMP reported that there were 1,239 couples participating in the Match; 1,095 had both partners match, and 114 had one partner match to residency training programs for a match rate of 93%.
Like Mr. Boyer, Hannah Hedriana matched into EM, one of the more popular despite the reported unfilled positions. In the past few years, it has consistently been one of the fastest-growing specialties, according to the NRMP.
Still Ms. Hedriana had a fall-back plan. “If I don’t match, then I do plan on going through SOAP. With the number of EM spots that were unfilled in 2022, there’s a chance I could still be an EM physician, but if not, then that’s okay with me.”
Her reaction on March 13, after learning she matched? “Super excited, celebrating with my friends right now.” On Match Day, she said she was “ecstatic” to be matched into Lakeland (Fla.) Regional Health. “This was my first choice so now I can stay close to family and friends,” she said in an interview soon after the results were released.
A first-generation, Filipino American student from the University of South Florida, Tampa, Ms. Hedriana comes from a family of health care professionals. Her father is a respiratory therapist turned physical therapist; her mother a registered nurse. Her sister is a patient care technician applying to nursing school.
Ms. Hedriana applied to 70 programs and interviewed mostly online with 24. Her goal was to stay on the East Coast.
“My partner is a licensed dentist in the state of Florida, and so for his career it would be more practical to stay in state, rather than get relicensed in another state, which could take months,” she said earlier in the matching cycle. “However, when we discussed choosing a residency program, he ultimately left it up to me and wanted me to pick where I thought I’d flourish best,” Ms. Hedriana said, adding that her family lives in Florida, too.
She said she sought a residency program that values family and teamwork.
“A program gets more points in my book if they have sites at nonprofit hospitals or has residents that regularly volunteer throughout their communities or participate in DEI [diversity, equity, and inclusion] initiatives.”
Ms. Hedriana noted that some specialties exclusively offered virtual interviews in 2023, whereas other specialties favored in-person interviews. “This year, many of my classmates were able to do multiple away rotations, which they saw as a positive regarding their chances of matching.” During COVID, in-person visits were limited.
“However, I’ve noticed that many of my classmates are not fond of the signaling aspect that was present for this year’s cycle,” she said. Signaling is a relatively new process that allows applicants to indicate interest in a limited number of residency programs. Not all residencies participate, but it’s growing in popularity among specialties, according to the American Medical Association.
‘Extremely competitive’
Ms. Nagle, a second lieutenant in the U.S. Air Force, applied to 12 programs and interviewed with half of them online. She said that she wasn’t targeting any specific type of program through the match.
“I believe you can get phenomenal training anywhere where you mesh with the residents and leadership. My ultimate priority is to (1) be near good people, (2) be near good food (Indian and Thai are a must), and (3) be near an international airport so I can flee the country during breaks.”
Meanwhile, she said that she found the application process, in which students have to articulate their entire medical school experience, extremely competitive. “I think this process is so easy to get wound up in and the anxiety can be palpable,” Ms. Nagle said. “People around you match your energy. So if you are a ball of anxiety then so are your attendings and residents – and that doesn’t bode well for passing the ‘do I want to be on call with them’ test.”
Looking back at medical school, Ms. Nagle recalled having a baby named after her during her first anesthesia rotation and being featured on The Kelly Clarkson Show. Ms. Nagle said that she had walked into the delivery room where new parents had been debating names of babies beginning with the letter B. “And when I introduced myself, they looked at each other and said, ‘Yep, that’s the one.’”
Mr. Boyer recounted how the majority of his medical school experience involved online education. “Roughly two-thirds of my first year was in-person prior to the pandemic. However, from spring break first year to in-person clinical rotations at the beginning of third year, we were all virtual. While I missed interacting with my classmates, I benefited from the virtual learning environment as I learn more efficiently from reading and visual aids than auditory lectures.”
Ms. Hedriana cited the friends and memories she made while learning to be a doctor. “Medical school was hard, but I wouldn’t have changed a thing.”
A version of this article first appeared on Medscape.com.
Baily Nagle, vice president of her graduating class at Harvard Medical School, Boston, celebrated “the luck of the Irish” on St. Patrick’s Day that allowed her to match into her chosen specialty and top choice of residency programs: anesthesia at Brigham and Women’s Hospital.
“I am feeling very excited and relieved – I matched,” she said in an interview upon hearing her good fortune on Match Monday, March 13. She had a similar reaction on Match Day, March 17. “After a lot of long nights and hard work, happy to have it pay off.”
Ms. Nagle was so determined to match into her specialty that she didn’t have any other specialties in mind as a backup.
The annual process of matching medical school graduates with compatible residency programs is an emotional roller coaster for all applicants, their personal March Madness, so to speak. But Ms. Nagle was one of the more fortunate applicants. She didn’t have to confront the heartbreak other applicants felt when the National Resident Matching Program (NRMP) announced results of the main residency match and the Supplemental Offer and Acceptance Program (SOAP), which offers alternate programs for unfilled positions or unmatched applicants.
During the 2023 Match process, this news organization has been following a handful of students, checking in with them periodically for updates on their progress. Most of them matched successfully, but at least one international medical graduate (IMG) did not. What the others have in common is that their hearts were set on a chosen specialty. Like Ms. Nagle, another student banked on landing his chosen specialty without a backup plan, whereas another said that she’d continue through the SOAP if she didn’t match successfully.
Overall, Match Day resulted in a record number of residency positions offered, most notably in primary care, which “hit an all-time high,” according to NRMP President and CEO Donna L. Lamb, DHSc, MBA, BSN. The number of positions has “consistently increased over the past 5 years, and most importantly the fill rate for primary care has remained steady,” Dr.. Lamb noted in the NRMP release of Match Day results. The release coincided with students learning through emails at noon Eastern Time to which residency or supplemental programs they were matched.
Though more applicants registered for the Match in 2023 than in 2022 – driven primarily by non-U.S. IMGs – the NRMP stated that it was surprised by the decrease in U.S. MD senior applicants.
U.S. MD seniors had a nearly 94% Match rate, a small increase over 2022. U.S. citizen IMGs saw a nearly 68% Match rate, which NRMP reported as an “all-time high” and about six percentage points over in 2022, whereas non-U.S. IMGs had a nearly 60% Match rate, a 1.3 percentage point increase over 2022.
Among the specialties that filled all available positions in 2023 were orthopedic surgery, plastic surgery (integrated), and radiology – diagnostic and thoracic surgery.
Not everyone matches
On March 13, the American College of Emergency Physicians issued a joint statement with other emergency medicine (EM) organizations about a high rate of unfilled EM positions expected in 2023.
NRMP acknowledged March 17 that 554 positions remained unfilled, an increase of 335 more unfilled positions than 2022. NRMP attributed the increase in unfilled positions in part to a decrease in the number of U.S. MD and U.S. DO seniors who submitted ranks for the specialty, which “could reflect changing applicant interests or projections about workforce opportunities post residency.”
Applicants who didn’t match usually try to obtain an unfilled position through SOAP. In 2023, 2,685 positions were unfilled after the matching algorithm was processed, an increase of nearly 19% over 2022. The vast majority of those positions were placed in SOAP, an increase of 17.5% over 2022.
Asim Ansari was one of the unlucky ones. Mr. Ansari was trying to match for the fifth time. He was unsuccessful in doing so again in 2023 in the Match and SOAP. Still, he was offered and accepted a child and adolescent psychiatry fellowship at Kansas University Medical Center in Kansas City. Psychiatry was his chosen specialty, so he was “feeling good. It’s a nice place to go to do the next 2 years.”
Mr. Ansari, who started the #MatchMadness support group for unmatched doctors on Twitter Spaces, was quick to cheer on his fellow matching peers on March 13 while revealing his own fate: “Congratulations to everyone who matched!!! Y’all are amazing. So proud of each one of you!!! I didn’t.”
Soon after the results, #MatchMadness held a #Soap2023 support session, and Mr. Ansari sought advice for those willing to review SOAP applications. Elsewhere on Twitter Match Day threads, a few doctors offered their support to those who planned to SOAP, students announced their matches, and others either congratulated or encouraged those still trying to match.
Couples match
Not everyone who matched considered the alternative. Before March 13, William Boyer said that he hadn’t given much thought to what would happen if he didn’t match because he was “optimistically confident” he would match into his chosen EM specialty. But he did and got his top choice of programs: Yale New Haven (Conn.) Hospital.
“I feel great,” he said in an interview. “I was definitely nervous opening the envelope” that revealed his residency program, “but there was a rush of relief” when he saw he landed Yale.
Earlier in the match cycle, he said in an interview that he “interviewed at a few ‘reach’ programs, so I hope I don’t match lower than expected on my rank list.”
Mr. Boyer considers himself “a mature applicant,” entering the University of South Carolina, Columbia, after 4 years as an insurance broker.
“I am celebrating today by playing pickleball with a few close medical friends who also matched this morning,” Mr. Boyer said on March 13. “I definitely had periods of nervousness leading up to this morning though that quickly turned into joy and relief” after learning he matched.
Mr. Boyer believes that his professional experience in the insurance industry and health care lobbying efforts with the National Association of Health Underwriters set him apart from other applicants.
“I changed careers to pursue this aspiration, which demonstrates my full dedication to the medical profession.”
He applied to 48 programs and was offered interviews to nearly half. Mr. Boyer visited the majority of those virtually. He said he targeted programs close to where his and his partner’s families are located: Massachusetts, North Carolina, and Texas. “My partner, who I met in medical school, matched into ortho as well so the whole household is very happy,” Mr. Boyer said.
She matched into her top choice as well on March 17, though a distance away at UT Health in San Antonio, he said. “We are both ecstatic. We both got our no. 1 choice. That was the plan going into it. We will make it work. I have 4 weeks of vacation.”
In his program choices, Mr. Boyer prioritized access to nature, minimal leadership turnover, a mix of clinical training sites, and adequate elective rotations and fellowship opportunities, such as in wilderness medicine and health policy.
NRMP reported that there were 1,239 couples participating in the Match; 1,095 had both partners match, and 114 had one partner match to residency training programs for a match rate of 93%.
Like Mr. Boyer, Hannah Hedriana matched into EM, one of the more popular despite the reported unfilled positions. In the past few years, it has consistently been one of the fastest-growing specialties, according to the NRMP.
Still Ms. Hedriana had a fall-back plan. “If I don’t match, then I do plan on going through SOAP. With the number of EM spots that were unfilled in 2022, there’s a chance I could still be an EM physician, but if not, then that’s okay with me.”
Her reaction on March 13, after learning she matched? “Super excited, celebrating with my friends right now.” On Match Day, she said she was “ecstatic” to be matched into Lakeland (Fla.) Regional Health. “This was my first choice so now I can stay close to family and friends,” she said in an interview soon after the results were released.
A first-generation, Filipino American student from the University of South Florida, Tampa, Ms. Hedriana comes from a family of health care professionals. Her father is a respiratory therapist turned physical therapist; her mother a registered nurse. Her sister is a patient care technician applying to nursing school.
Ms. Hedriana applied to 70 programs and interviewed mostly online with 24. Her goal was to stay on the East Coast.
“My partner is a licensed dentist in the state of Florida, and so for his career it would be more practical to stay in state, rather than get relicensed in another state, which could take months,” she said earlier in the matching cycle. “However, when we discussed choosing a residency program, he ultimately left it up to me and wanted me to pick where I thought I’d flourish best,” Ms. Hedriana said, adding that her family lives in Florida, too.
She said she sought a residency program that values family and teamwork.
“A program gets more points in my book if they have sites at nonprofit hospitals or has residents that regularly volunteer throughout their communities or participate in DEI [diversity, equity, and inclusion] initiatives.”
Ms. Hedriana noted that some specialties exclusively offered virtual interviews in 2023, whereas other specialties favored in-person interviews. “This year, many of my classmates were able to do multiple away rotations, which they saw as a positive regarding their chances of matching.” During COVID, in-person visits were limited.
“However, I’ve noticed that many of my classmates are not fond of the signaling aspect that was present for this year’s cycle,” she said. Signaling is a relatively new process that allows applicants to indicate interest in a limited number of residency programs. Not all residencies participate, but it’s growing in popularity among specialties, according to the American Medical Association.
‘Extremely competitive’
Ms. Nagle, a second lieutenant in the U.S. Air Force, applied to 12 programs and interviewed with half of them online. She said that she wasn’t targeting any specific type of program through the match.
“I believe you can get phenomenal training anywhere where you mesh with the residents and leadership. My ultimate priority is to (1) be near good people, (2) be near good food (Indian and Thai are a must), and (3) be near an international airport so I can flee the country during breaks.”
Meanwhile, she said that she found the application process, in which students have to articulate their entire medical school experience, extremely competitive. “I think this process is so easy to get wound up in and the anxiety can be palpable,” Ms. Nagle said. “People around you match your energy. So if you are a ball of anxiety then so are your attendings and residents – and that doesn’t bode well for passing the ‘do I want to be on call with them’ test.”
Looking back at medical school, Ms. Nagle recalled having a baby named after her during her first anesthesia rotation and being featured on The Kelly Clarkson Show. Ms. Nagle said that she had walked into the delivery room where new parents had been debating names of babies beginning with the letter B. “And when I introduced myself, they looked at each other and said, ‘Yep, that’s the one.’”
Mr. Boyer recounted how the majority of his medical school experience involved online education. “Roughly two-thirds of my first year was in-person prior to the pandemic. However, from spring break first year to in-person clinical rotations at the beginning of third year, we were all virtual. While I missed interacting with my classmates, I benefited from the virtual learning environment as I learn more efficiently from reading and visual aids than auditory lectures.”
Ms. Hedriana cited the friends and memories she made while learning to be a doctor. “Medical school was hard, but I wouldn’t have changed a thing.”
A version of this article first appeared on Medscape.com.
Baily Nagle, vice president of her graduating class at Harvard Medical School, Boston, celebrated “the luck of the Irish” on St. Patrick’s Day that allowed her to match into her chosen specialty and top choice of residency programs: anesthesia at Brigham and Women’s Hospital.
“I am feeling very excited and relieved – I matched,” she said in an interview upon hearing her good fortune on Match Monday, March 13. She had a similar reaction on Match Day, March 17. “After a lot of long nights and hard work, happy to have it pay off.”
Ms. Nagle was so determined to match into her specialty that she didn’t have any other specialties in mind as a backup.
The annual process of matching medical school graduates with compatible residency programs is an emotional roller coaster for all applicants, their personal March Madness, so to speak. But Ms. Nagle was one of the more fortunate applicants. She didn’t have to confront the heartbreak other applicants felt when the National Resident Matching Program (NRMP) announced results of the main residency match and the Supplemental Offer and Acceptance Program (SOAP), which offers alternate programs for unfilled positions or unmatched applicants.
During the 2023 Match process, this news organization has been following a handful of students, checking in with them periodically for updates on their progress. Most of them matched successfully, but at least one international medical graduate (IMG) did not. What the others have in common is that their hearts were set on a chosen specialty. Like Ms. Nagle, another student banked on landing his chosen specialty without a backup plan, whereas another said that she’d continue through the SOAP if she didn’t match successfully.
Overall, Match Day resulted in a record number of residency positions offered, most notably in primary care, which “hit an all-time high,” according to NRMP President and CEO Donna L. Lamb, DHSc, MBA, BSN. The number of positions has “consistently increased over the past 5 years, and most importantly the fill rate for primary care has remained steady,” Dr.. Lamb noted in the NRMP release of Match Day results. The release coincided with students learning through emails at noon Eastern Time to which residency or supplemental programs they were matched.
Though more applicants registered for the Match in 2023 than in 2022 – driven primarily by non-U.S. IMGs – the NRMP stated that it was surprised by the decrease in U.S. MD senior applicants.
U.S. MD seniors had a nearly 94% Match rate, a small increase over 2022. U.S. citizen IMGs saw a nearly 68% Match rate, which NRMP reported as an “all-time high” and about six percentage points over in 2022, whereas non-U.S. IMGs had a nearly 60% Match rate, a 1.3 percentage point increase over 2022.
Among the specialties that filled all available positions in 2023 were orthopedic surgery, plastic surgery (integrated), and radiology – diagnostic and thoracic surgery.
Not everyone matches
On March 13, the American College of Emergency Physicians issued a joint statement with other emergency medicine (EM) organizations about a high rate of unfilled EM positions expected in 2023.
NRMP acknowledged March 17 that 554 positions remained unfilled, an increase of 335 more unfilled positions than 2022. NRMP attributed the increase in unfilled positions in part to a decrease in the number of U.S. MD and U.S. DO seniors who submitted ranks for the specialty, which “could reflect changing applicant interests or projections about workforce opportunities post residency.”
Applicants who didn’t match usually try to obtain an unfilled position through SOAP. In 2023, 2,685 positions were unfilled after the matching algorithm was processed, an increase of nearly 19% over 2022. The vast majority of those positions were placed in SOAP, an increase of 17.5% over 2022.
Asim Ansari was one of the unlucky ones. Mr. Ansari was trying to match for the fifth time. He was unsuccessful in doing so again in 2023 in the Match and SOAP. Still, he was offered and accepted a child and adolescent psychiatry fellowship at Kansas University Medical Center in Kansas City. Psychiatry was his chosen specialty, so he was “feeling good. It’s a nice place to go to do the next 2 years.”
Mr. Ansari, who started the #MatchMadness support group for unmatched doctors on Twitter Spaces, was quick to cheer on his fellow matching peers on March 13 while revealing his own fate: “Congratulations to everyone who matched!!! Y’all are amazing. So proud of each one of you!!! I didn’t.”
Soon after the results, #MatchMadness held a #Soap2023 support session, and Mr. Ansari sought advice for those willing to review SOAP applications. Elsewhere on Twitter Match Day threads, a few doctors offered their support to those who planned to SOAP, students announced their matches, and others either congratulated or encouraged those still trying to match.
Couples match
Not everyone who matched considered the alternative. Before March 13, William Boyer said that he hadn’t given much thought to what would happen if he didn’t match because he was “optimistically confident” he would match into his chosen EM specialty. But he did and got his top choice of programs: Yale New Haven (Conn.) Hospital.
“I feel great,” he said in an interview. “I was definitely nervous opening the envelope” that revealed his residency program, “but there was a rush of relief” when he saw he landed Yale.
Earlier in the match cycle, he said in an interview that he “interviewed at a few ‘reach’ programs, so I hope I don’t match lower than expected on my rank list.”
Mr. Boyer considers himself “a mature applicant,” entering the University of South Carolina, Columbia, after 4 years as an insurance broker.
“I am celebrating today by playing pickleball with a few close medical friends who also matched this morning,” Mr. Boyer said on March 13. “I definitely had periods of nervousness leading up to this morning though that quickly turned into joy and relief” after learning he matched.
Mr. Boyer believes that his professional experience in the insurance industry and health care lobbying efforts with the National Association of Health Underwriters set him apart from other applicants.
“I changed careers to pursue this aspiration, which demonstrates my full dedication to the medical profession.”
He applied to 48 programs and was offered interviews to nearly half. Mr. Boyer visited the majority of those virtually. He said he targeted programs close to where his and his partner’s families are located: Massachusetts, North Carolina, and Texas. “My partner, who I met in medical school, matched into ortho as well so the whole household is very happy,” Mr. Boyer said.
She matched into her top choice as well on March 17, though a distance away at UT Health in San Antonio, he said. “We are both ecstatic. We both got our no. 1 choice. That was the plan going into it. We will make it work. I have 4 weeks of vacation.”
In his program choices, Mr. Boyer prioritized access to nature, minimal leadership turnover, a mix of clinical training sites, and adequate elective rotations and fellowship opportunities, such as in wilderness medicine and health policy.
NRMP reported that there were 1,239 couples participating in the Match; 1,095 had both partners match, and 114 had one partner match to residency training programs for a match rate of 93%.
Like Mr. Boyer, Hannah Hedriana matched into EM, one of the more popular despite the reported unfilled positions. In the past few years, it has consistently been one of the fastest-growing specialties, according to the NRMP.
Still Ms. Hedriana had a fall-back plan. “If I don’t match, then I do plan on going through SOAP. With the number of EM spots that were unfilled in 2022, there’s a chance I could still be an EM physician, but if not, then that’s okay with me.”
Her reaction on March 13, after learning she matched? “Super excited, celebrating with my friends right now.” On Match Day, she said she was “ecstatic” to be matched into Lakeland (Fla.) Regional Health. “This was my first choice so now I can stay close to family and friends,” she said in an interview soon after the results were released.
A first-generation, Filipino American student from the University of South Florida, Tampa, Ms. Hedriana comes from a family of health care professionals. Her father is a respiratory therapist turned physical therapist; her mother a registered nurse. Her sister is a patient care technician applying to nursing school.
Ms. Hedriana applied to 70 programs and interviewed mostly online with 24. Her goal was to stay on the East Coast.
“My partner is a licensed dentist in the state of Florida, and so for his career it would be more practical to stay in state, rather than get relicensed in another state, which could take months,” she said earlier in the matching cycle. “However, when we discussed choosing a residency program, he ultimately left it up to me and wanted me to pick where I thought I’d flourish best,” Ms. Hedriana said, adding that her family lives in Florida, too.
She said she sought a residency program that values family and teamwork.
“A program gets more points in my book if they have sites at nonprofit hospitals or has residents that regularly volunteer throughout their communities or participate in DEI [diversity, equity, and inclusion] initiatives.”
Ms. Hedriana noted that some specialties exclusively offered virtual interviews in 2023, whereas other specialties favored in-person interviews. “This year, many of my classmates were able to do multiple away rotations, which they saw as a positive regarding their chances of matching.” During COVID, in-person visits were limited.
“However, I’ve noticed that many of my classmates are not fond of the signaling aspect that was present for this year’s cycle,” she said. Signaling is a relatively new process that allows applicants to indicate interest in a limited number of residency programs. Not all residencies participate, but it’s growing in popularity among specialties, according to the American Medical Association.
‘Extremely competitive’
Ms. Nagle, a second lieutenant in the U.S. Air Force, applied to 12 programs and interviewed with half of them online. She said that she wasn’t targeting any specific type of program through the match.
“I believe you can get phenomenal training anywhere where you mesh with the residents and leadership. My ultimate priority is to (1) be near good people, (2) be near good food (Indian and Thai are a must), and (3) be near an international airport so I can flee the country during breaks.”
Meanwhile, she said that she found the application process, in which students have to articulate their entire medical school experience, extremely competitive. “I think this process is so easy to get wound up in and the anxiety can be palpable,” Ms. Nagle said. “People around you match your energy. So if you are a ball of anxiety then so are your attendings and residents – and that doesn’t bode well for passing the ‘do I want to be on call with them’ test.”
Looking back at medical school, Ms. Nagle recalled having a baby named after her during her first anesthesia rotation and being featured on The Kelly Clarkson Show. Ms. Nagle said that she had walked into the delivery room where new parents had been debating names of babies beginning with the letter B. “And when I introduced myself, they looked at each other and said, ‘Yep, that’s the one.’”
Mr. Boyer recounted how the majority of his medical school experience involved online education. “Roughly two-thirds of my first year was in-person prior to the pandemic. However, from spring break first year to in-person clinical rotations at the beginning of third year, we were all virtual. While I missed interacting with my classmates, I benefited from the virtual learning environment as I learn more efficiently from reading and visual aids than auditory lectures.”
Ms. Hedriana cited the friends and memories she made while learning to be a doctor. “Medical school was hard, but I wouldn’t have changed a thing.”
A version of this article first appeared on Medscape.com.
Increased cancer in military pilots and ground crew: Pentagon
“Military aircrew and ground crew were overall more likely to be diagnosed with cancer, but less likely to die from cancer compared to the U.S. population,” the report concludes.
The study involved 156,050 aircrew and 737,891 ground crew. Participants were followed between 1992 and 2017. Both groups were predominantly male and non-Hispanic.
Data on cancer incidence and mortality for these two groups were compared with data from groups of similar age in the general population through use of the Surveillance, Epidemiology, and End Results (SEER) Database of the National Cancer Institute.
For aircrew, the study found an 87% higher rate of melanoma, a 39% higher rate of thyroid cancer, a 16% higher rate of prostate cancer, and a 24% higher rate of cancer for all sites combined.
A higher rate of melanoma and prostate cancer among aircrew has been reported previously, but the increased rate of thyroid cancer is a new finding, the authors note.
The uptick in melanoma has also been reported in studies of civilian pilots and cabin crew. It has been attributed to exposure to hazardous ultraviolet and cosmic radiation.
For ground crew members, the analysis found a 19% higher rate of cancers of the brain and nervous system, a 15% higher rate of thyroid cancer, a 9% higher rate of melanoma and of kidney and renal pelvis cancers, and a 3% higher rate of cancer for all sites combined.
There is little to compare these findings with: This is the first time that cancer risk has been evaluated in such a large population of military ground crew.
Lower rates of cancer mortality
In contrast to the increase in cancer incidence, the report found a decrease in cancer mortality.
When compared with a demographically similar U.S. population, the mortality rate among aircrew was 56% lower for all cancer sites; for ground crew, the mortality rate was 35% lower.
However, the report authors emphasize that “it is important to note that the military study population was relatively young.”
The median age at the end of follow-up for the cancer incidence analysis was 41 years for aircrew and 26 years for ground crew. The median age at the end of follow-up for the cancer mortality analysis was 48 years for aircrew and 41 years for ground crew.
“Results may have differed if additional older former Service members had been included in the study, since cancer risk and mortality rates increase with age,” the authors comment.
Other studies have found an increase in deaths from melanoma as well as an increase in the incidence of melanoma. A meta-analysis published in 2019 in the British Journal of Dermatology found that airline pilots and cabin crew have about twice the risk of melanoma and other skin cancers than the general population. Pilots are also more likely to die from melanoma.
Further study underway
The findings on military air and ground crew come from phase 1 of a study that was required by Congress in the 2021 defense bill. Because the investigators found an increase in the incidence of cancer, phase 2 of the study is now necessary.
The report authors explain that phase 2 will consist of identifying the carcinogenic toxicants or hazardous materials associated with military flight operations; identifying operating environments that could be associated with increased amounts of ionizing and nonionizing radiation; identifying specific duties, dates of service, and types of aircraft flown that could have increased the risk for cancer; identifying duty locations associated with a higher incidence of cancers; identifying potential exposures through military service that are not related to aviation; and determining the appropriate age to begin screening military aircrew and ground crew for cancers.
A version of this article first appeared on Medscape.com.
“Military aircrew and ground crew were overall more likely to be diagnosed with cancer, but less likely to die from cancer compared to the U.S. population,” the report concludes.
The study involved 156,050 aircrew and 737,891 ground crew. Participants were followed between 1992 and 2017. Both groups were predominantly male and non-Hispanic.
Data on cancer incidence and mortality for these two groups were compared with data from groups of similar age in the general population through use of the Surveillance, Epidemiology, and End Results (SEER) Database of the National Cancer Institute.
For aircrew, the study found an 87% higher rate of melanoma, a 39% higher rate of thyroid cancer, a 16% higher rate of prostate cancer, and a 24% higher rate of cancer for all sites combined.
A higher rate of melanoma and prostate cancer among aircrew has been reported previously, but the increased rate of thyroid cancer is a new finding, the authors note.
The uptick in melanoma has also been reported in studies of civilian pilots and cabin crew. It has been attributed to exposure to hazardous ultraviolet and cosmic radiation.
For ground crew members, the analysis found a 19% higher rate of cancers of the brain and nervous system, a 15% higher rate of thyroid cancer, a 9% higher rate of melanoma and of kidney and renal pelvis cancers, and a 3% higher rate of cancer for all sites combined.
There is little to compare these findings with: This is the first time that cancer risk has been evaluated in such a large population of military ground crew.
Lower rates of cancer mortality
In contrast to the increase in cancer incidence, the report found a decrease in cancer mortality.
When compared with a demographically similar U.S. population, the mortality rate among aircrew was 56% lower for all cancer sites; for ground crew, the mortality rate was 35% lower.
However, the report authors emphasize that “it is important to note that the military study population was relatively young.”
The median age at the end of follow-up for the cancer incidence analysis was 41 years for aircrew and 26 years for ground crew. The median age at the end of follow-up for the cancer mortality analysis was 48 years for aircrew and 41 years for ground crew.
“Results may have differed if additional older former Service members had been included in the study, since cancer risk and mortality rates increase with age,” the authors comment.
Other studies have found an increase in deaths from melanoma as well as an increase in the incidence of melanoma. A meta-analysis published in 2019 in the British Journal of Dermatology found that airline pilots and cabin crew have about twice the risk of melanoma and other skin cancers than the general population. Pilots are also more likely to die from melanoma.
Further study underway
The findings on military air and ground crew come from phase 1 of a study that was required by Congress in the 2021 defense bill. Because the investigators found an increase in the incidence of cancer, phase 2 of the study is now necessary.
The report authors explain that phase 2 will consist of identifying the carcinogenic toxicants or hazardous materials associated with military flight operations; identifying operating environments that could be associated with increased amounts of ionizing and nonionizing radiation; identifying specific duties, dates of service, and types of aircraft flown that could have increased the risk for cancer; identifying duty locations associated with a higher incidence of cancers; identifying potential exposures through military service that are not related to aviation; and determining the appropriate age to begin screening military aircrew and ground crew for cancers.
A version of this article first appeared on Medscape.com.
“Military aircrew and ground crew were overall more likely to be diagnosed with cancer, but less likely to die from cancer compared to the U.S. population,” the report concludes.
The study involved 156,050 aircrew and 737,891 ground crew. Participants were followed between 1992 and 2017. Both groups were predominantly male and non-Hispanic.
Data on cancer incidence and mortality for these two groups were compared with data from groups of similar age in the general population through use of the Surveillance, Epidemiology, and End Results (SEER) Database of the National Cancer Institute.
For aircrew, the study found an 87% higher rate of melanoma, a 39% higher rate of thyroid cancer, a 16% higher rate of prostate cancer, and a 24% higher rate of cancer for all sites combined.
A higher rate of melanoma and prostate cancer among aircrew has been reported previously, but the increased rate of thyroid cancer is a new finding, the authors note.
The uptick in melanoma has also been reported in studies of civilian pilots and cabin crew. It has been attributed to exposure to hazardous ultraviolet and cosmic radiation.
For ground crew members, the analysis found a 19% higher rate of cancers of the brain and nervous system, a 15% higher rate of thyroid cancer, a 9% higher rate of melanoma and of kidney and renal pelvis cancers, and a 3% higher rate of cancer for all sites combined.
There is little to compare these findings with: This is the first time that cancer risk has been evaluated in such a large population of military ground crew.
Lower rates of cancer mortality
In contrast to the increase in cancer incidence, the report found a decrease in cancer mortality.
When compared with a demographically similar U.S. population, the mortality rate among aircrew was 56% lower for all cancer sites; for ground crew, the mortality rate was 35% lower.
However, the report authors emphasize that “it is important to note that the military study population was relatively young.”
The median age at the end of follow-up for the cancer incidence analysis was 41 years for aircrew and 26 years for ground crew. The median age at the end of follow-up for the cancer mortality analysis was 48 years for aircrew and 41 years for ground crew.
“Results may have differed if additional older former Service members had been included in the study, since cancer risk and mortality rates increase with age,” the authors comment.
Other studies have found an increase in deaths from melanoma as well as an increase in the incidence of melanoma. A meta-analysis published in 2019 in the British Journal of Dermatology found that airline pilots and cabin crew have about twice the risk of melanoma and other skin cancers than the general population. Pilots are also more likely to die from melanoma.
Further study underway
The findings on military air and ground crew come from phase 1 of a study that was required by Congress in the 2021 defense bill. Because the investigators found an increase in the incidence of cancer, phase 2 of the study is now necessary.
The report authors explain that phase 2 will consist of identifying the carcinogenic toxicants or hazardous materials associated with military flight operations; identifying operating environments that could be associated with increased amounts of ionizing and nonionizing radiation; identifying specific duties, dates of service, and types of aircraft flown that could have increased the risk for cancer; identifying duty locations associated with a higher incidence of cancers; identifying potential exposures through military service that are not related to aviation; and determining the appropriate age to begin screening military aircrew and ground crew for cancers.
A version of this article first appeared on Medscape.com.
Older men more at risk as dangerous falls rise for all seniors
When Senate Minority Leader Mitch McConnell (R-Ky.) fell recently at a dinner event in Washington, he unfortunately joined a large group of his senior citizen peers.
This wasn’t the first tumble the 81-year-old has taken. In 2019, he fell in his home, fracturing his shoulder. This time, he got a concussion and was recently released to an in-patient rehabilitation facility. While Sen. McConnell didn’t fracture his skull, in falling and hitting his head, he became part of an emerging statistic: One that reveals falls are more dangerous for senior men than senior women.
This new research, which appeared in the American Journal of Emergency Medicine, came as a surprise to lead researcher Scott Alter, MD, associate professor of emergency medicine at the Florida Atlantic University, Boca Raton.
“We always hear about lower bone density rates among females, so we didn’t expect to see males with more skull fractures,” he said.
Dr. Alter said that as a clinician in a southern Florida facility, his emergency department was the perfect study grounds to evaluate incoming geriatric patients due to falls. Older “patients are at higher risk of skull fractures and intercranial bleeding, and we wanted to look at any patient presenting with a head injury. Some 80% were fall related, however.”
The statistics bear out the fact that falls of all types are common among the elderly: Some 800,000 seniors wind up in the hospital each year because of falls.
The numbers show death rates from falls are on the rise in the senior citizen age group, too, up 30% from 2007 to 2016. Falls account for 70% of accidental deaths in people 75 and older. They are the leading cause of injury-related visits to emergency departments in the country, too.
Jennifer Stevens, MD, a gerontologist and executive director at Florida-based Abbey Delray South, is aware of the dire numbers and sees their consequences regularly. “The reasons seniors are at a high fall risk are many,” she said. “They include balance issues, declining strength, diseases like Parkinson’s and Alzheimer’s, side effects of their medications, and more.”
In addition, many seniors live in spaces that are not necessarily equipped for their limitations, and hazards exist all over their homes. Put together, and the risks for falls are everywhere. But there are steps seniors, their families, and even middle-aged people can take to mitigate and hopefully prevent dangerous falls.
Starting early
While in many cases the journey to lessen fall risks begins after a fall, the time to begin addressing the issue is long before you hit your senior years. Mary Therese Cole, a physical therapist and certified dementia practitioner at Manual Edge Physical Therapy in Colorado Springs, Colo., says that age 50 is a good time to start paying attention and addressing physical declines.
“This is an age where your vision might begin deteriorating,” she said. “It’s a big reason why elderly people trip and fall.”
As our brains begin to age in our middle years, the neural pathways from brain to extremities start to decline, too. The result is that many people stop picking up their feet as well as they used to do, making them more likely to trip.
“You’re not elderly yet, but you’re not a spring chicken, either,” Ms. Cole said. “Any issues you have now will only get worse if you’re not working on them.”
A good starting point in middle age, then, is to work on both strength training and balance exercises. A certified personal trainer or physical therapist can help get you on a program to ward off many of these declines.
If you’ve reached your later years, however, and are experiencing physical declines, it’s smart to check in with your primary care doctor for an assessment. “He or she can get your started on regular PT to evaluate any shortcomings and then address them,” Ms. Cole said.
She noted that when she’s working with senior patients, she’ll test their strength getting into and out of a chair, do a manual strength test to check on lower extremities, check their walking stride, and ask about conditions such as diabetes, former surgeries, and other conditions.
From there, Ms. Cole said she can write up a plan for the patient. Likewise, Dr. Stevens uses a program called Be Active that allows her to test seniors on a variety of measurements, including flexibility, balance, hand strength, and more.
“Then we match them with classes to address their shortcomings,” she said. “It’s critical that seniors have the ability to recover and not fall if they get knocked off balance.”
Beyond working on your physical limitations, taking a good look at your home is essential, too. “You can have an occupational therapist come to your home and do an evaluation,” Dr. Stevens said. “They can help you rearrange and reorganize for a safer environment.”
Big, common household fall hazards include throw rugs, lack of nightlights for middle-of-the-night visits to the bathroom, a lack of grab bars in the shower/bathtub, and furniture that blocks pathways.
For his part, Dr. Alter likes to point seniors and their doctors to the CDC’s STEADI program, which is aimed at stopping elderly accidents, deaths, and injuries.
“It includes screening for fall risk, assessing factors you can modify or improve, and more tools,” he said.
Dr. Alter also recommended seniors talk to their doctors about medications, particularly blood thinners.
“At a certain point, you need to weigh the benefits of disease prevention with the risk of injury if you fall,” he said. “The bleeding risk might be too high if the patient is at a high risk of falls.”
A version of this article originally appeared on WebMD.com.
When Senate Minority Leader Mitch McConnell (R-Ky.) fell recently at a dinner event in Washington, he unfortunately joined a large group of his senior citizen peers.
This wasn’t the first tumble the 81-year-old has taken. In 2019, he fell in his home, fracturing his shoulder. This time, he got a concussion and was recently released to an in-patient rehabilitation facility. While Sen. McConnell didn’t fracture his skull, in falling and hitting his head, he became part of an emerging statistic: One that reveals falls are more dangerous for senior men than senior women.
This new research, which appeared in the American Journal of Emergency Medicine, came as a surprise to lead researcher Scott Alter, MD, associate professor of emergency medicine at the Florida Atlantic University, Boca Raton.
“We always hear about lower bone density rates among females, so we didn’t expect to see males with more skull fractures,” he said.
Dr. Alter said that as a clinician in a southern Florida facility, his emergency department was the perfect study grounds to evaluate incoming geriatric patients due to falls. Older “patients are at higher risk of skull fractures and intercranial bleeding, and we wanted to look at any patient presenting with a head injury. Some 80% were fall related, however.”
The statistics bear out the fact that falls of all types are common among the elderly: Some 800,000 seniors wind up in the hospital each year because of falls.
The numbers show death rates from falls are on the rise in the senior citizen age group, too, up 30% from 2007 to 2016. Falls account for 70% of accidental deaths in people 75 and older. They are the leading cause of injury-related visits to emergency departments in the country, too.
Jennifer Stevens, MD, a gerontologist and executive director at Florida-based Abbey Delray South, is aware of the dire numbers and sees their consequences regularly. “The reasons seniors are at a high fall risk are many,” she said. “They include balance issues, declining strength, diseases like Parkinson’s and Alzheimer’s, side effects of their medications, and more.”
In addition, many seniors live in spaces that are not necessarily equipped for their limitations, and hazards exist all over their homes. Put together, and the risks for falls are everywhere. But there are steps seniors, their families, and even middle-aged people can take to mitigate and hopefully prevent dangerous falls.
Starting early
While in many cases the journey to lessen fall risks begins after a fall, the time to begin addressing the issue is long before you hit your senior years. Mary Therese Cole, a physical therapist and certified dementia practitioner at Manual Edge Physical Therapy in Colorado Springs, Colo., says that age 50 is a good time to start paying attention and addressing physical declines.
“This is an age where your vision might begin deteriorating,” she said. “It’s a big reason why elderly people trip and fall.”
As our brains begin to age in our middle years, the neural pathways from brain to extremities start to decline, too. The result is that many people stop picking up their feet as well as they used to do, making them more likely to trip.
“You’re not elderly yet, but you’re not a spring chicken, either,” Ms. Cole said. “Any issues you have now will only get worse if you’re not working on them.”
A good starting point in middle age, then, is to work on both strength training and balance exercises. A certified personal trainer or physical therapist can help get you on a program to ward off many of these declines.
If you’ve reached your later years, however, and are experiencing physical declines, it’s smart to check in with your primary care doctor for an assessment. “He or she can get your started on regular PT to evaluate any shortcomings and then address them,” Ms. Cole said.
She noted that when she’s working with senior patients, she’ll test their strength getting into and out of a chair, do a manual strength test to check on lower extremities, check their walking stride, and ask about conditions such as diabetes, former surgeries, and other conditions.
From there, Ms. Cole said she can write up a plan for the patient. Likewise, Dr. Stevens uses a program called Be Active that allows her to test seniors on a variety of measurements, including flexibility, balance, hand strength, and more.
“Then we match them with classes to address their shortcomings,” she said. “It’s critical that seniors have the ability to recover and not fall if they get knocked off balance.”
Beyond working on your physical limitations, taking a good look at your home is essential, too. “You can have an occupational therapist come to your home and do an evaluation,” Dr. Stevens said. “They can help you rearrange and reorganize for a safer environment.”
Big, common household fall hazards include throw rugs, lack of nightlights for middle-of-the-night visits to the bathroom, a lack of grab bars in the shower/bathtub, and furniture that blocks pathways.
For his part, Dr. Alter likes to point seniors and their doctors to the CDC’s STEADI program, which is aimed at stopping elderly accidents, deaths, and injuries.
“It includes screening for fall risk, assessing factors you can modify or improve, and more tools,” he said.
Dr. Alter also recommended seniors talk to their doctors about medications, particularly blood thinners.
“At a certain point, you need to weigh the benefits of disease prevention with the risk of injury if you fall,” he said. “The bleeding risk might be too high if the patient is at a high risk of falls.”
A version of this article originally appeared on WebMD.com.
When Senate Minority Leader Mitch McConnell (R-Ky.) fell recently at a dinner event in Washington, he unfortunately joined a large group of his senior citizen peers.
This wasn’t the first tumble the 81-year-old has taken. In 2019, he fell in his home, fracturing his shoulder. This time, he got a concussion and was recently released to an in-patient rehabilitation facility. While Sen. McConnell didn’t fracture his skull, in falling and hitting his head, he became part of an emerging statistic: One that reveals falls are more dangerous for senior men than senior women.
This new research, which appeared in the American Journal of Emergency Medicine, came as a surprise to lead researcher Scott Alter, MD, associate professor of emergency medicine at the Florida Atlantic University, Boca Raton.
“We always hear about lower bone density rates among females, so we didn’t expect to see males with more skull fractures,” he said.
Dr. Alter said that as a clinician in a southern Florida facility, his emergency department was the perfect study grounds to evaluate incoming geriatric patients due to falls. Older “patients are at higher risk of skull fractures and intercranial bleeding, and we wanted to look at any patient presenting with a head injury. Some 80% were fall related, however.”
The statistics bear out the fact that falls of all types are common among the elderly: Some 800,000 seniors wind up in the hospital each year because of falls.
The numbers show death rates from falls are on the rise in the senior citizen age group, too, up 30% from 2007 to 2016. Falls account for 70% of accidental deaths in people 75 and older. They are the leading cause of injury-related visits to emergency departments in the country, too.
Jennifer Stevens, MD, a gerontologist and executive director at Florida-based Abbey Delray South, is aware of the dire numbers and sees their consequences regularly. “The reasons seniors are at a high fall risk are many,” she said. “They include balance issues, declining strength, diseases like Parkinson’s and Alzheimer’s, side effects of their medications, and more.”
In addition, many seniors live in spaces that are not necessarily equipped for their limitations, and hazards exist all over their homes. Put together, and the risks for falls are everywhere. But there are steps seniors, their families, and even middle-aged people can take to mitigate and hopefully prevent dangerous falls.
Starting early
While in many cases the journey to lessen fall risks begins after a fall, the time to begin addressing the issue is long before you hit your senior years. Mary Therese Cole, a physical therapist and certified dementia practitioner at Manual Edge Physical Therapy in Colorado Springs, Colo., says that age 50 is a good time to start paying attention and addressing physical declines.
“This is an age where your vision might begin deteriorating,” she said. “It’s a big reason why elderly people trip and fall.”
As our brains begin to age in our middle years, the neural pathways from brain to extremities start to decline, too. The result is that many people stop picking up their feet as well as they used to do, making them more likely to trip.
“You’re not elderly yet, but you’re not a spring chicken, either,” Ms. Cole said. “Any issues you have now will only get worse if you’re not working on them.”
A good starting point in middle age, then, is to work on both strength training and balance exercises. A certified personal trainer or physical therapist can help get you on a program to ward off many of these declines.
If you’ve reached your later years, however, and are experiencing physical declines, it’s smart to check in with your primary care doctor for an assessment. “He or she can get your started on regular PT to evaluate any shortcomings and then address them,” Ms. Cole said.
She noted that when she’s working with senior patients, she’ll test their strength getting into and out of a chair, do a manual strength test to check on lower extremities, check their walking stride, and ask about conditions such as diabetes, former surgeries, and other conditions.
From there, Ms. Cole said she can write up a plan for the patient. Likewise, Dr. Stevens uses a program called Be Active that allows her to test seniors on a variety of measurements, including flexibility, balance, hand strength, and more.
“Then we match them with classes to address their shortcomings,” she said. “It’s critical that seniors have the ability to recover and not fall if they get knocked off balance.”
Beyond working on your physical limitations, taking a good look at your home is essential, too. “You can have an occupational therapist come to your home and do an evaluation,” Dr. Stevens said. “They can help you rearrange and reorganize for a safer environment.”
Big, common household fall hazards include throw rugs, lack of nightlights for middle-of-the-night visits to the bathroom, a lack of grab bars in the shower/bathtub, and furniture that blocks pathways.
For his part, Dr. Alter likes to point seniors and their doctors to the CDC’s STEADI program, which is aimed at stopping elderly accidents, deaths, and injuries.
“It includes screening for fall risk, assessing factors you can modify or improve, and more tools,” he said.
Dr. Alter also recommended seniors talk to their doctors about medications, particularly blood thinners.
“At a certain point, you need to weigh the benefits of disease prevention with the risk of injury if you fall,” he said. “The bleeding risk might be too high if the patient is at a high risk of falls.”
A version of this article originally appeared on WebMD.com.
NOVIDs: Do some have the genes to dodge COVID?
As a field service representative for a slot machine company, Ryan Alexander, 37, of Louisville, Ky., spends his working hours in casinos, covering a large territory including Norfolk, Va., Indianapolis, and Charlotte. Social distancing in the casinos is not the norm. Despite all this up-close contact with people, he said he is still COVID-free, 3 years into the pandemic.
There was one nervous night when his temperature rose to 101° F, and he figured the virus had caught up with him. “I took a test and was fine,” he said, relieved that the result was negative. The fever disappeared, and he was back to normal soon. “Maybe it was just an exhausting day.”
Mr. Alexander is one of those people who have managed – or at least think they have managed – to avoid getting COVID-19.
He is, some say, a NOVID. While some scientists cringe at the term, it’s caught on to describe these virus super-dodgers. Online entrepreneurs offer NOVID-19 T-shirts, masks, and stickers, in case these super-healthy or super-lucky folks want to publicize their good luck. On Twitter, NOVIDs share stories of how they’ve done it.
How many NOVIDs?
As of March 16, according to the CDC, almost 104 million cases of COVID – about one-third of the U.S. population – have been reported, but many cases are known to go unreported. About half of American adults surveyed said they have had COVID, according to a December report by the COVID States Project, a multiuniversity effort to supply pandemic data.
As the numbers settle over time, though, it becomes clearer that some in the U.S. have apparently managed to avoid the virus.
But some scientists bristle at the term NOVIDs. They prefer the term “resisters,” according to Elena Hsieh, MD, associate professor of pediatrics and immunology at the University of Colorado at Denver, Aurora. Currently, she said, there is much more information on who is more susceptible to contracting severe COVID than who is resistant.
Dr. Hsieh is one of the regional coordinators for the COVID Human Genetic Effort, an international consortium of more than 250 researchers and doctors dedicated to discovering the genetic and immunological bases of the forms of SARS-CoV-2 infection. These researchers and others are looking for explanations for why some people get severe COVID while others seem resistant despite repeated exposure.
Resistance research
In determining explanations for resistance to infection, “the needle in the haystack that we are looking for is a change in the genetic code that would allow for you to avoid entry of the virus into the cell,” Dr. Hsieh said. “That is what being resistant to infection is.”
Part of the reason it’s so difficult to study resistance is defining a resister, she said. While many people consider themselves among that group because they’re been exposed multiple times – even with close family members infected and sick, yet they still felt fine – that doesn’t necessarily make them a resister, she said.
Those people could have been infected but remained without symptoms. “Resistance means the virus was inside you, it was near your cell and it did not infect your cell,” Dr. Hsieh said.
“I don’t think we know a lot so far,” Dr. Hsieh said about resisters. “I do believe that, just like there are genetic defects that make someone more susceptible, there are likely to be genetic defects that make somebody less susceptible.’’
“To identify genetic variants that are protective is a really challenging thing to do,” agreed Peter K. Gregersen, MD, professor of genetics at the Feinstein Institutes for Medical Research at Northwell Health in Manhasset, N.Y. Dr. Gregersen is also a regional coordinator for the COVID Human Genetic Effort.
He suspects the number found to be truly resistant to COVID – versus dodging it so far – is going to be very small or not found at all.
“It may exist for COVID or it may not,” he said. Some people may simply have what he calls a robust immune response in the upper part of the throat, perhaps killing off the virus quickly as soon as it enters, so they don’t get a positive test.
Genetic resistance has been found for other diseases, such as HIV.
“For HIV, scientists have been able to identify a specific gene that codes for a protein that can prevent individuals from getting infected,” said Sabrina Assoumou, MD, MPH, professor of medicine at Boston University, who researches HIV.
However, she said, “we haven’t yet found a similar gene or protein that can prevent people from getting infected with SARS-CoV-2.”
What has been found “is that some people might have a mutation in a gene that encodes for what’s called human leukocyte antigen (HLA),” Dr. Assoumou said. HLA, a molecule found on the surface of most cells, has a crucial role in the immune response to foreign substances. “A mutation in HLA can make people less likely to have symptoms if they get infected. Individuals still get infected, but they are less likely to have symptoms.”
Other research has found that those with food allergies are also less likely to be infected. The researchers have speculated that the inflammation characteristic of allergic conditions may reduce levels of a protein called the ACE2 receptor on the surface of airway cells. The SARS-CoV-2 virus uses the receptor to enter the cells, so if levels are low, that could reduce the ability of the virus to infect people.
The COVID Human Genetic Effort continues to search for participants, both those who were admitted to a hospital or repeatedly seen at a hospital because of COVID, as well as those who did not get infected, even after “intense and repeated” exposure.
The number of people likely to be resistant is much smaller, Dr. Hsieh said, than the number of people susceptible to severe disease.
The testing ... or lack thereof factor
The timing of testing and a person’s “infection profile” may be factors in people incorrectly declaring themselves NOVIDs, said Anne Wyllie, PhD, a research scientist in epidemiology at the Yale School of Public Health in New Haven, Conn., and a codeveloper of a saliva PCR test for COVID.
“Infection profiles can vary between individuals,” she said. For some, the infection may start in the lower respiratory tract, others in the higher respiratory tract. “Depending on where the virus takes up residence, that can affect test results.”
Then there’s the following-instructions factor. “It’s very likely that due to tests not being done at the right time, with the right sample, or not repeated if there is ongoing evidence of symptoms, that there are individuals out there who believe they are NOVIDs but just missed catching their infection at the window of opportunity.” Dr. Wyllie said.
Susceptibility research
“The part we have proven is the genetic defect that would make you more susceptible to having severe disease,” Dr. Hsieh said.
Many published papers report that inherited and/or autoimmune deficiencies of type I interferon immunity, important for combating viral infections and modulating the immune response, can be a significant cause of life-threatening COVID pneumonia.
More recently, researchers, including Jean-Laurent Casanova, MD, PhD, professor at Rockefeller University, New York, and cofounder of the COVID Human Genome Effort, reported that deficiencies in a gene that plays a role in built-in immunity (the early response), and a gene involved in signaling within the immune cells, impair interferon production and may be the basis of severe COVID pneumonia.
NOVIDs’ habits run the gamut
As scientists continue their research, the NOVIDs have their own ideas about why they’ve dodged the pandemic bullet, and they have a variety of approaches to handling the pandemic now.
Ryan Alexander, the field rep who travels to casinos, is up to date on his vaccinations and has gotten all the recommended COVID shots. “I was wearing a mask when told to wear masks,” he said.
He still observes the social distance habit but lives life. “I’ve been to three or four concerts in the past couple of years.”
And does he worry his number will eventually be up? “Not at this point, no,” he said.
Joe Asher, 46, said he has not gotten COVID despite being in contact with about 100 people a day, on average. He works as a bartender at an Evansville, Ind., brewery.
“On a Friday night, we can get 500 people,” he said. “I feel like almost everyone at the brewery got it. There’s no way I wasn’t exposed to it all the time.”
However, he said, his coworkers who did get sick were very cautious about not infecting others, partly to help protect a coworker’s family with newborn twins, so that may have helped him stay uninfected, too.
Mr. Asher said he’s in good physical shape, and he’s worked around the public for a long time, so figures maybe that has strengthened his immune system. He’s always been careful about handwashing and said he’s perhaps a bit more conscious of germs than others might be.
Roselyn Mena, 68, a retired teacher in Richmond, Calif., about 16 miles northeast of San Francisco, said she’s managed to avoid the virus even though her husband, Jesus Mena, got infected, as did her two adult children. Now, she remains vigilant about wearing a mask. She tries not to eat inside at restaurants. “I’m super careful,” she said.
Besides her teacher training, Ms. Mena had training as a medical assistant and learned a lot about sanitizing methods. She gets an annual flu shot, washes her hands often, and uses hand sanitizer.
When she shops, she will ask salespeople not wearing masks to please mask. “Only one refused, and she got someone else [to wait on her].”
One reason she is always careful about hygiene, Ms. Mena said, is that “when I get a cold, I get really sick. It last and lasts.” Now, she does worry she might still get it, she said, with the prospect of getting long COVID driving that worry.
In the beginning of the pandemic, Rhonda Fleming, 68, of Los Angeles, lived in a “COVID bubble,” interacting with just a few close family members. As cases went down, she enlarged the bubble. Her two grown daughters got infected, but her granddaughter did not.
She has been vigilant about masking, she said, “and I do still mask in public places.” She has a mask wardrobe, including basic black as well as glittery masks for dressier occasions. “I always carry a mask because inevitably, a cougher surrounds me.”
Now, she will bypass restaurants if she doesn’t feel comfortable with the environment, choosing ones with good air flow. When she flew to Mexico recently, she masked on the plane.
At this point, she said she doesn’t worry about getting infected but remains careful.
Recently, two friends, who have been as diligent as she has about precautions, got infected, “and they don’t know how they got it.”
Bragging rights?
Until researchers separate out the true resisters from those who claim to be, some NOVIDs are simply quietly grateful for their luck, while others mention their COVID-free status to anyone who asks or who will listen, and are proud of it.
And what about those who wear a “NOVID” T-shirt?
“I would think they have a need to convey to the world they are different, perhaps special, because they beat COVID,” said Richard B. Joelson, a New York–based doctor of social work, a psychotherapist, and the author of Help Me! A Psychotherapist’s Tried-and-True Techniques for a Happier Relationship with Yourself and the People You Love. “They didn’t beat COVID, they just didn’t get it.”
Or they may be relieved they didn’t get sick, he said, because they feel defeated when they do. So “it’s a source of pride.” It might be the same people who tell anyone who will listen they never need a doctor or take no medicines, he said.
Even though science may prove many NOVIDs are inaccurate when they call themselves resisters, Dr. Hsieh understands the temptation to talk about it. “It’s kind of cool to think you are supernatural,” she said. “It’s much more attractive than being susceptible. It’s a lot sexier.” ■
A version of this article first appeared on Medscape.com.
As a field service representative for a slot machine company, Ryan Alexander, 37, of Louisville, Ky., spends his working hours in casinos, covering a large territory including Norfolk, Va., Indianapolis, and Charlotte. Social distancing in the casinos is not the norm. Despite all this up-close contact with people, he said he is still COVID-free, 3 years into the pandemic.
There was one nervous night when his temperature rose to 101° F, and he figured the virus had caught up with him. “I took a test and was fine,” he said, relieved that the result was negative. The fever disappeared, and he was back to normal soon. “Maybe it was just an exhausting day.”
Mr. Alexander is one of those people who have managed – or at least think they have managed – to avoid getting COVID-19.
He is, some say, a NOVID. While some scientists cringe at the term, it’s caught on to describe these virus super-dodgers. Online entrepreneurs offer NOVID-19 T-shirts, masks, and stickers, in case these super-healthy or super-lucky folks want to publicize their good luck. On Twitter, NOVIDs share stories of how they’ve done it.
How many NOVIDs?
As of March 16, according to the CDC, almost 104 million cases of COVID – about one-third of the U.S. population – have been reported, but many cases are known to go unreported. About half of American adults surveyed said they have had COVID, according to a December report by the COVID States Project, a multiuniversity effort to supply pandemic data.
As the numbers settle over time, though, it becomes clearer that some in the U.S. have apparently managed to avoid the virus.
But some scientists bristle at the term NOVIDs. They prefer the term “resisters,” according to Elena Hsieh, MD, associate professor of pediatrics and immunology at the University of Colorado at Denver, Aurora. Currently, she said, there is much more information on who is more susceptible to contracting severe COVID than who is resistant.
Dr. Hsieh is one of the regional coordinators for the COVID Human Genetic Effort, an international consortium of more than 250 researchers and doctors dedicated to discovering the genetic and immunological bases of the forms of SARS-CoV-2 infection. These researchers and others are looking for explanations for why some people get severe COVID while others seem resistant despite repeated exposure.
Resistance research
In determining explanations for resistance to infection, “the needle in the haystack that we are looking for is a change in the genetic code that would allow for you to avoid entry of the virus into the cell,” Dr. Hsieh said. “That is what being resistant to infection is.”
Part of the reason it’s so difficult to study resistance is defining a resister, she said. While many people consider themselves among that group because they’re been exposed multiple times – even with close family members infected and sick, yet they still felt fine – that doesn’t necessarily make them a resister, she said.
Those people could have been infected but remained without symptoms. “Resistance means the virus was inside you, it was near your cell and it did not infect your cell,” Dr. Hsieh said.
“I don’t think we know a lot so far,” Dr. Hsieh said about resisters. “I do believe that, just like there are genetic defects that make someone more susceptible, there are likely to be genetic defects that make somebody less susceptible.’’
“To identify genetic variants that are protective is a really challenging thing to do,” agreed Peter K. Gregersen, MD, professor of genetics at the Feinstein Institutes for Medical Research at Northwell Health in Manhasset, N.Y. Dr. Gregersen is also a regional coordinator for the COVID Human Genetic Effort.
He suspects the number found to be truly resistant to COVID – versus dodging it so far – is going to be very small or not found at all.
“It may exist for COVID or it may not,” he said. Some people may simply have what he calls a robust immune response in the upper part of the throat, perhaps killing off the virus quickly as soon as it enters, so they don’t get a positive test.
Genetic resistance has been found for other diseases, such as HIV.
“For HIV, scientists have been able to identify a specific gene that codes for a protein that can prevent individuals from getting infected,” said Sabrina Assoumou, MD, MPH, professor of medicine at Boston University, who researches HIV.
However, she said, “we haven’t yet found a similar gene or protein that can prevent people from getting infected with SARS-CoV-2.”
What has been found “is that some people might have a mutation in a gene that encodes for what’s called human leukocyte antigen (HLA),” Dr. Assoumou said. HLA, a molecule found on the surface of most cells, has a crucial role in the immune response to foreign substances. “A mutation in HLA can make people less likely to have symptoms if they get infected. Individuals still get infected, but they are less likely to have symptoms.”
Other research has found that those with food allergies are also less likely to be infected. The researchers have speculated that the inflammation characteristic of allergic conditions may reduce levels of a protein called the ACE2 receptor on the surface of airway cells. The SARS-CoV-2 virus uses the receptor to enter the cells, so if levels are low, that could reduce the ability of the virus to infect people.
The COVID Human Genetic Effort continues to search for participants, both those who were admitted to a hospital or repeatedly seen at a hospital because of COVID, as well as those who did not get infected, even after “intense and repeated” exposure.
The number of people likely to be resistant is much smaller, Dr. Hsieh said, than the number of people susceptible to severe disease.
The testing ... or lack thereof factor
The timing of testing and a person’s “infection profile” may be factors in people incorrectly declaring themselves NOVIDs, said Anne Wyllie, PhD, a research scientist in epidemiology at the Yale School of Public Health in New Haven, Conn., and a codeveloper of a saliva PCR test for COVID.
“Infection profiles can vary between individuals,” she said. For some, the infection may start in the lower respiratory tract, others in the higher respiratory tract. “Depending on where the virus takes up residence, that can affect test results.”
Then there’s the following-instructions factor. “It’s very likely that due to tests not being done at the right time, with the right sample, or not repeated if there is ongoing evidence of symptoms, that there are individuals out there who believe they are NOVIDs but just missed catching their infection at the window of opportunity.” Dr. Wyllie said.
Susceptibility research
“The part we have proven is the genetic defect that would make you more susceptible to having severe disease,” Dr. Hsieh said.
Many published papers report that inherited and/or autoimmune deficiencies of type I interferon immunity, important for combating viral infections and modulating the immune response, can be a significant cause of life-threatening COVID pneumonia.
More recently, researchers, including Jean-Laurent Casanova, MD, PhD, professor at Rockefeller University, New York, and cofounder of the COVID Human Genome Effort, reported that deficiencies in a gene that plays a role in built-in immunity (the early response), and a gene involved in signaling within the immune cells, impair interferon production and may be the basis of severe COVID pneumonia.
NOVIDs’ habits run the gamut
As scientists continue their research, the NOVIDs have their own ideas about why they’ve dodged the pandemic bullet, and they have a variety of approaches to handling the pandemic now.
Ryan Alexander, the field rep who travels to casinos, is up to date on his vaccinations and has gotten all the recommended COVID shots. “I was wearing a mask when told to wear masks,” he said.
He still observes the social distance habit but lives life. “I’ve been to three or four concerts in the past couple of years.”
And does he worry his number will eventually be up? “Not at this point, no,” he said.
Joe Asher, 46, said he has not gotten COVID despite being in contact with about 100 people a day, on average. He works as a bartender at an Evansville, Ind., brewery.
“On a Friday night, we can get 500 people,” he said. “I feel like almost everyone at the brewery got it. There’s no way I wasn’t exposed to it all the time.”
However, he said, his coworkers who did get sick were very cautious about not infecting others, partly to help protect a coworker’s family with newborn twins, so that may have helped him stay uninfected, too.
Mr. Asher said he’s in good physical shape, and he’s worked around the public for a long time, so figures maybe that has strengthened his immune system. He’s always been careful about handwashing and said he’s perhaps a bit more conscious of germs than others might be.
Roselyn Mena, 68, a retired teacher in Richmond, Calif., about 16 miles northeast of San Francisco, said she’s managed to avoid the virus even though her husband, Jesus Mena, got infected, as did her two adult children. Now, she remains vigilant about wearing a mask. She tries not to eat inside at restaurants. “I’m super careful,” she said.
Besides her teacher training, Ms. Mena had training as a medical assistant and learned a lot about sanitizing methods. She gets an annual flu shot, washes her hands often, and uses hand sanitizer.
When she shops, she will ask salespeople not wearing masks to please mask. “Only one refused, and she got someone else [to wait on her].”
One reason she is always careful about hygiene, Ms. Mena said, is that “when I get a cold, I get really sick. It last and lasts.” Now, she does worry she might still get it, she said, with the prospect of getting long COVID driving that worry.
In the beginning of the pandemic, Rhonda Fleming, 68, of Los Angeles, lived in a “COVID bubble,” interacting with just a few close family members. As cases went down, she enlarged the bubble. Her two grown daughters got infected, but her granddaughter did not.
She has been vigilant about masking, she said, “and I do still mask in public places.” She has a mask wardrobe, including basic black as well as glittery masks for dressier occasions. “I always carry a mask because inevitably, a cougher surrounds me.”
Now, she will bypass restaurants if she doesn’t feel comfortable with the environment, choosing ones with good air flow. When she flew to Mexico recently, she masked on the plane.
At this point, she said she doesn’t worry about getting infected but remains careful.
Recently, two friends, who have been as diligent as she has about precautions, got infected, “and they don’t know how they got it.”
Bragging rights?
Until researchers separate out the true resisters from those who claim to be, some NOVIDs are simply quietly grateful for their luck, while others mention their COVID-free status to anyone who asks or who will listen, and are proud of it.
And what about those who wear a “NOVID” T-shirt?
“I would think they have a need to convey to the world they are different, perhaps special, because they beat COVID,” said Richard B. Joelson, a New York–based doctor of social work, a psychotherapist, and the author of Help Me! A Psychotherapist’s Tried-and-True Techniques for a Happier Relationship with Yourself and the People You Love. “They didn’t beat COVID, they just didn’t get it.”
Or they may be relieved they didn’t get sick, he said, because they feel defeated when they do. So “it’s a source of pride.” It might be the same people who tell anyone who will listen they never need a doctor or take no medicines, he said.
Even though science may prove many NOVIDs are inaccurate when they call themselves resisters, Dr. Hsieh understands the temptation to talk about it. “It’s kind of cool to think you are supernatural,” she said. “It’s much more attractive than being susceptible. It’s a lot sexier.” ■
A version of this article first appeared on Medscape.com.
As a field service representative for a slot machine company, Ryan Alexander, 37, of Louisville, Ky., spends his working hours in casinos, covering a large territory including Norfolk, Va., Indianapolis, and Charlotte. Social distancing in the casinos is not the norm. Despite all this up-close contact with people, he said he is still COVID-free, 3 years into the pandemic.
There was one nervous night when his temperature rose to 101° F, and he figured the virus had caught up with him. “I took a test and was fine,” he said, relieved that the result was negative. The fever disappeared, and he was back to normal soon. “Maybe it was just an exhausting day.”
Mr. Alexander is one of those people who have managed – or at least think they have managed – to avoid getting COVID-19.
He is, some say, a NOVID. While some scientists cringe at the term, it’s caught on to describe these virus super-dodgers. Online entrepreneurs offer NOVID-19 T-shirts, masks, and stickers, in case these super-healthy or super-lucky folks want to publicize their good luck. On Twitter, NOVIDs share stories of how they’ve done it.
How many NOVIDs?
As of March 16, according to the CDC, almost 104 million cases of COVID – about one-third of the U.S. population – have been reported, but many cases are known to go unreported. About half of American adults surveyed said they have had COVID, according to a December report by the COVID States Project, a multiuniversity effort to supply pandemic data.
As the numbers settle over time, though, it becomes clearer that some in the U.S. have apparently managed to avoid the virus.
But some scientists bristle at the term NOVIDs. They prefer the term “resisters,” according to Elena Hsieh, MD, associate professor of pediatrics and immunology at the University of Colorado at Denver, Aurora. Currently, she said, there is much more information on who is more susceptible to contracting severe COVID than who is resistant.
Dr. Hsieh is one of the regional coordinators for the COVID Human Genetic Effort, an international consortium of more than 250 researchers and doctors dedicated to discovering the genetic and immunological bases of the forms of SARS-CoV-2 infection. These researchers and others are looking for explanations for why some people get severe COVID while others seem resistant despite repeated exposure.
Resistance research
In determining explanations for resistance to infection, “the needle in the haystack that we are looking for is a change in the genetic code that would allow for you to avoid entry of the virus into the cell,” Dr. Hsieh said. “That is what being resistant to infection is.”
Part of the reason it’s so difficult to study resistance is defining a resister, she said. While many people consider themselves among that group because they’re been exposed multiple times – even with close family members infected and sick, yet they still felt fine – that doesn’t necessarily make them a resister, she said.
Those people could have been infected but remained without symptoms. “Resistance means the virus was inside you, it was near your cell and it did not infect your cell,” Dr. Hsieh said.
“I don’t think we know a lot so far,” Dr. Hsieh said about resisters. “I do believe that, just like there are genetic defects that make someone more susceptible, there are likely to be genetic defects that make somebody less susceptible.’’
“To identify genetic variants that are protective is a really challenging thing to do,” agreed Peter K. Gregersen, MD, professor of genetics at the Feinstein Institutes for Medical Research at Northwell Health in Manhasset, N.Y. Dr. Gregersen is also a regional coordinator for the COVID Human Genetic Effort.
He suspects the number found to be truly resistant to COVID – versus dodging it so far – is going to be very small or not found at all.
“It may exist for COVID or it may not,” he said. Some people may simply have what he calls a robust immune response in the upper part of the throat, perhaps killing off the virus quickly as soon as it enters, so they don’t get a positive test.
Genetic resistance has been found for other diseases, such as HIV.
“For HIV, scientists have been able to identify a specific gene that codes for a protein that can prevent individuals from getting infected,” said Sabrina Assoumou, MD, MPH, professor of medicine at Boston University, who researches HIV.
However, she said, “we haven’t yet found a similar gene or protein that can prevent people from getting infected with SARS-CoV-2.”
What has been found “is that some people might have a mutation in a gene that encodes for what’s called human leukocyte antigen (HLA),” Dr. Assoumou said. HLA, a molecule found on the surface of most cells, has a crucial role in the immune response to foreign substances. “A mutation in HLA can make people less likely to have symptoms if they get infected. Individuals still get infected, but they are less likely to have symptoms.”
Other research has found that those with food allergies are also less likely to be infected. The researchers have speculated that the inflammation characteristic of allergic conditions may reduce levels of a protein called the ACE2 receptor on the surface of airway cells. The SARS-CoV-2 virus uses the receptor to enter the cells, so if levels are low, that could reduce the ability of the virus to infect people.
The COVID Human Genetic Effort continues to search for participants, both those who were admitted to a hospital or repeatedly seen at a hospital because of COVID, as well as those who did not get infected, even after “intense and repeated” exposure.
The number of people likely to be resistant is much smaller, Dr. Hsieh said, than the number of people susceptible to severe disease.
The testing ... or lack thereof factor
The timing of testing and a person’s “infection profile” may be factors in people incorrectly declaring themselves NOVIDs, said Anne Wyllie, PhD, a research scientist in epidemiology at the Yale School of Public Health in New Haven, Conn., and a codeveloper of a saliva PCR test for COVID.
“Infection profiles can vary between individuals,” she said. For some, the infection may start in the lower respiratory tract, others in the higher respiratory tract. “Depending on where the virus takes up residence, that can affect test results.”
Then there’s the following-instructions factor. “It’s very likely that due to tests not being done at the right time, with the right sample, or not repeated if there is ongoing evidence of symptoms, that there are individuals out there who believe they are NOVIDs but just missed catching their infection at the window of opportunity.” Dr. Wyllie said.
Susceptibility research
“The part we have proven is the genetic defect that would make you more susceptible to having severe disease,” Dr. Hsieh said.
Many published papers report that inherited and/or autoimmune deficiencies of type I interferon immunity, important for combating viral infections and modulating the immune response, can be a significant cause of life-threatening COVID pneumonia.
More recently, researchers, including Jean-Laurent Casanova, MD, PhD, professor at Rockefeller University, New York, and cofounder of the COVID Human Genome Effort, reported that deficiencies in a gene that plays a role in built-in immunity (the early response), and a gene involved in signaling within the immune cells, impair interferon production and may be the basis of severe COVID pneumonia.
NOVIDs’ habits run the gamut
As scientists continue their research, the NOVIDs have their own ideas about why they’ve dodged the pandemic bullet, and they have a variety of approaches to handling the pandemic now.
Ryan Alexander, the field rep who travels to casinos, is up to date on his vaccinations and has gotten all the recommended COVID shots. “I was wearing a mask when told to wear masks,” he said.
He still observes the social distance habit but lives life. “I’ve been to three or four concerts in the past couple of years.”
And does he worry his number will eventually be up? “Not at this point, no,” he said.
Joe Asher, 46, said he has not gotten COVID despite being in contact with about 100 people a day, on average. He works as a bartender at an Evansville, Ind., brewery.
“On a Friday night, we can get 500 people,” he said. “I feel like almost everyone at the brewery got it. There’s no way I wasn’t exposed to it all the time.”
However, he said, his coworkers who did get sick were very cautious about not infecting others, partly to help protect a coworker’s family with newborn twins, so that may have helped him stay uninfected, too.
Mr. Asher said he’s in good physical shape, and he’s worked around the public for a long time, so figures maybe that has strengthened his immune system. He’s always been careful about handwashing and said he’s perhaps a bit more conscious of germs than others might be.
Roselyn Mena, 68, a retired teacher in Richmond, Calif., about 16 miles northeast of San Francisco, said she’s managed to avoid the virus even though her husband, Jesus Mena, got infected, as did her two adult children. Now, she remains vigilant about wearing a mask. She tries not to eat inside at restaurants. “I’m super careful,” she said.
Besides her teacher training, Ms. Mena had training as a medical assistant and learned a lot about sanitizing methods. She gets an annual flu shot, washes her hands often, and uses hand sanitizer.
When she shops, she will ask salespeople not wearing masks to please mask. “Only one refused, and she got someone else [to wait on her].”
One reason she is always careful about hygiene, Ms. Mena said, is that “when I get a cold, I get really sick. It last and lasts.” Now, she does worry she might still get it, she said, with the prospect of getting long COVID driving that worry.
In the beginning of the pandemic, Rhonda Fleming, 68, of Los Angeles, lived in a “COVID bubble,” interacting with just a few close family members. As cases went down, she enlarged the bubble. Her two grown daughters got infected, but her granddaughter did not.
She has been vigilant about masking, she said, “and I do still mask in public places.” She has a mask wardrobe, including basic black as well as glittery masks for dressier occasions. “I always carry a mask because inevitably, a cougher surrounds me.”
Now, she will bypass restaurants if she doesn’t feel comfortable with the environment, choosing ones with good air flow. When she flew to Mexico recently, she masked on the plane.
At this point, she said she doesn’t worry about getting infected but remains careful.
Recently, two friends, who have been as diligent as she has about precautions, got infected, “and they don’t know how they got it.”
Bragging rights?
Until researchers separate out the true resisters from those who claim to be, some NOVIDs are simply quietly grateful for their luck, while others mention their COVID-free status to anyone who asks or who will listen, and are proud of it.
And what about those who wear a “NOVID” T-shirt?
“I would think they have a need to convey to the world they are different, perhaps special, because they beat COVID,” said Richard B. Joelson, a New York–based doctor of social work, a psychotherapist, and the author of Help Me! A Psychotherapist’s Tried-and-True Techniques for a Happier Relationship with Yourself and the People You Love. “They didn’t beat COVID, they just didn’t get it.”
Or they may be relieved they didn’t get sick, he said, because they feel defeated when they do. So “it’s a source of pride.” It might be the same people who tell anyone who will listen they never need a doctor or take no medicines, he said.
Even though science may prove many NOVIDs are inaccurate when they call themselves resisters, Dr. Hsieh understands the temptation to talk about it. “It’s kind of cool to think you are supernatural,” she said. “It’s much more attractive than being susceptible. It’s a lot sexier.” ■
A version of this article first appeared on Medscape.com.
Cutting social media to 1 hour a day boosts self-image in young adults
“Youth spend, on average, between 6 and 8 hours per day on screens, much of it on social media,” said senior study author Gary S. Goldfield, PhD, senior scientist at Children’s Hospital of Eastern Ontario Research Institute in Ottawa, Canada. “Social media provides exposure to so many photo-edited pictures – including those of models, celebrities, and fitness instructors – that perpetuate an unattainable beauty standard that gets internalized by impressionable youth and young adults, leading to body dissatisfaction.”
Plenty of research has linked frequent social media use with body image issues and even eating disorders. But crucial gaps in our knowledge remain, Dr. Goldfield said.
Much of that research “is correlational,” Dr. Goldfield added. And studies don’t always focus on individuals who may be more vulnerable to social media’s harmful effects, such as those with ruminative or brooding cognitive styles, affecting results.
And none have explored an obvious question: Can cutting down on social media use also diminish its potential harms?
Dr. Goldfield and his colleagues found an answer: Yes, it can.
Limiting social media use to 1 hour per day helped older teens and young adults feel much better about their weight and appearance after only 3 weeks, according to the study in Psychology of Popular Media, a journal of the American Psychological Association.
“Our randomized controlled design allowed us to show a stronger causal link between social media use and body image in youth, compared to previous research,” Dr. Goldfield said. “To our knowledge, this is the first study to show that social media use reduction leads to enhanced body image.”
Nancy Lee Zucker, PhD, professor of psychology and neuroscience at Duke University, Durham, N.C., and director of the Duke Center for Eating Disorders, said the results provide needed data that could help guide young people and parents on optimal social media use. Dr. Zucker was not involved in the study.
What the researchers did
For the study, Dr. Goldfield and colleagues recruited undergraduate psychology students aged 17-25 who averaged at least 2 hours per day of social media use on smartphones, and who had symptoms of depression or anxiety.
Participants were not told the purpose of the study, and their social media use was monitored by a screen time tracking program. At the beginning and end of the study, they answered questions such as “I’m pretty happy about the way I look,” and “I am satisfied with my weight,” on a 1 (never) to 5 (always) Likert scale.
During the first week, all 220 participants (76% female, 23% male, and 1% other) were told to use social media on their smartphones as they usually do. Over the next 3 weeks, 117 students were told to limit their social media use to 1 hour per day, while the rest were instructed to carry on as usual. In both groups, over 70% of participants were between age 17 and 19.
The first group cut their social media use by about 50%, from a mean of around 168 minutes per day during week 1 to around 78 minutes per day by the end of week 4, while the unrestricted group went from around 181 minutes per day to 189.
Cutting use by around half yielded quick, significant improvements
The students who curbed their social media use saw significant improvements in their “appearance esteem” (from 2.95 to 3.15 points; P <.001) and their “weight esteem” (from 3.16 to 3.32 points; P < .001), whereas those who used social media freely saw no such changes (from 2.72 to 2.76; P = .992 and 3.01 to 3.02; P = .654, respectively). No gender differences between the groups were found.
The researchers are now studying possible reasons for these findings.
The changes in appearance scores “represent a small- to medium-effect size,” said child psychologist Sara R. Gould, PhD, director of the Eating Disorders Center at Children’s Mercy Kansas City in Missouri, who was not associated with the research.“ As such, these are clinically meaningful results, particularly since they were achieved in only 3 weeks. Even small impacts can be added to other changes to create larger impacts or have the potential to grow over time.”
The push to limit social media
As more and more experts scrutinize the impact of social media on young people’s mental health, social media companies have responded with features designed to limit the time young users spend on their platforms.
Just this year, Instagram rolled out “quiet mode,” which lets users shut down their direct messages (DMs) for a specified amount of time. To turn on quiet mode, users can navigate to their profiles, and select the triple line icon, “settings,” “notifications,” and “quiet mode.” Another option: Tap the triple line icon, “your activity,” and “time spent” to set reminders to take breaks after 10, 20, or 30 minutes of use.
TikTok users under 18 will soon have their accounts defaulted to a 1-hour daily screen-time limit, TikTok has announced. Unlike other similar features, it will require users to turn it off rather than turn it on.
Leveraging built-in controls is “a good start to being more intentional about your screen time,” suggested lead author Helen Thai, a PhD student in clinical psychology at McGill University in Montreal. “Unfortunately, users can easily bypass these settings.”
One reason for social’s magnetic pull: “FOMO – fear of missing out – on what friends are doing can make cutting back on social media use difficult,” said Dr. Zucker. To help prevent FOMO, parents may consider talking to parents of their children’s friends about reducing usage for all the children, Dr. Zucker suggested.
Mary E. Romano, MD, MPH, associate professor of pediatrics-adolescent medicine at Vanderbilt University, Nashville, Tenn., urges parents “to have very clear rules and expectations about social media use.”
Dr. Romano, also not involved in the study, recommended the website Wait Until 8th to help parents band together to commit to delaying smartphone access until at least eighth grade.
Dr. Gould recommended the Family Media Plan, a tool from the American Academy of Pediatrics that lets users create a customized plan, complete with guidance tailored to each person’s age and the family’s goals. Sample tips: Designate a basket for holding devices during meals, and switch to audiobooks or relaxing music instead of videos to fall asleep at night.
A version of this article first appeared on Medscape.com.
“Youth spend, on average, between 6 and 8 hours per day on screens, much of it on social media,” said senior study author Gary S. Goldfield, PhD, senior scientist at Children’s Hospital of Eastern Ontario Research Institute in Ottawa, Canada. “Social media provides exposure to so many photo-edited pictures – including those of models, celebrities, and fitness instructors – that perpetuate an unattainable beauty standard that gets internalized by impressionable youth and young adults, leading to body dissatisfaction.”
Plenty of research has linked frequent social media use with body image issues and even eating disorders. But crucial gaps in our knowledge remain, Dr. Goldfield said.
Much of that research “is correlational,” Dr. Goldfield added. And studies don’t always focus on individuals who may be more vulnerable to social media’s harmful effects, such as those with ruminative or brooding cognitive styles, affecting results.
And none have explored an obvious question: Can cutting down on social media use also diminish its potential harms?
Dr. Goldfield and his colleagues found an answer: Yes, it can.
Limiting social media use to 1 hour per day helped older teens and young adults feel much better about their weight and appearance after only 3 weeks, according to the study in Psychology of Popular Media, a journal of the American Psychological Association.
“Our randomized controlled design allowed us to show a stronger causal link between social media use and body image in youth, compared to previous research,” Dr. Goldfield said. “To our knowledge, this is the first study to show that social media use reduction leads to enhanced body image.”
Nancy Lee Zucker, PhD, professor of psychology and neuroscience at Duke University, Durham, N.C., and director of the Duke Center for Eating Disorders, said the results provide needed data that could help guide young people and parents on optimal social media use. Dr. Zucker was not involved in the study.
What the researchers did
For the study, Dr. Goldfield and colleagues recruited undergraduate psychology students aged 17-25 who averaged at least 2 hours per day of social media use on smartphones, and who had symptoms of depression or anxiety.
Participants were not told the purpose of the study, and their social media use was monitored by a screen time tracking program. At the beginning and end of the study, they answered questions such as “I’m pretty happy about the way I look,” and “I am satisfied with my weight,” on a 1 (never) to 5 (always) Likert scale.
During the first week, all 220 participants (76% female, 23% male, and 1% other) were told to use social media on their smartphones as they usually do. Over the next 3 weeks, 117 students were told to limit their social media use to 1 hour per day, while the rest were instructed to carry on as usual. In both groups, over 70% of participants were between age 17 and 19.
The first group cut their social media use by about 50%, from a mean of around 168 minutes per day during week 1 to around 78 minutes per day by the end of week 4, while the unrestricted group went from around 181 minutes per day to 189.
Cutting use by around half yielded quick, significant improvements
The students who curbed their social media use saw significant improvements in their “appearance esteem” (from 2.95 to 3.15 points; P <.001) and their “weight esteem” (from 3.16 to 3.32 points; P < .001), whereas those who used social media freely saw no such changes (from 2.72 to 2.76; P = .992 and 3.01 to 3.02; P = .654, respectively). No gender differences between the groups were found.
The researchers are now studying possible reasons for these findings.
The changes in appearance scores “represent a small- to medium-effect size,” said child psychologist Sara R. Gould, PhD, director of the Eating Disorders Center at Children’s Mercy Kansas City in Missouri, who was not associated with the research.“ As such, these are clinically meaningful results, particularly since they were achieved in only 3 weeks. Even small impacts can be added to other changes to create larger impacts or have the potential to grow over time.”
The push to limit social media
As more and more experts scrutinize the impact of social media on young people’s mental health, social media companies have responded with features designed to limit the time young users spend on their platforms.
Just this year, Instagram rolled out “quiet mode,” which lets users shut down their direct messages (DMs) for a specified amount of time. To turn on quiet mode, users can navigate to their profiles, and select the triple line icon, “settings,” “notifications,” and “quiet mode.” Another option: Tap the triple line icon, “your activity,” and “time spent” to set reminders to take breaks after 10, 20, or 30 minutes of use.
TikTok users under 18 will soon have their accounts defaulted to a 1-hour daily screen-time limit, TikTok has announced. Unlike other similar features, it will require users to turn it off rather than turn it on.
Leveraging built-in controls is “a good start to being more intentional about your screen time,” suggested lead author Helen Thai, a PhD student in clinical psychology at McGill University in Montreal. “Unfortunately, users can easily bypass these settings.”
One reason for social’s magnetic pull: “FOMO – fear of missing out – on what friends are doing can make cutting back on social media use difficult,” said Dr. Zucker. To help prevent FOMO, parents may consider talking to parents of their children’s friends about reducing usage for all the children, Dr. Zucker suggested.
Mary E. Romano, MD, MPH, associate professor of pediatrics-adolescent medicine at Vanderbilt University, Nashville, Tenn., urges parents “to have very clear rules and expectations about social media use.”
Dr. Romano, also not involved in the study, recommended the website Wait Until 8th to help parents band together to commit to delaying smartphone access until at least eighth grade.
Dr. Gould recommended the Family Media Plan, a tool from the American Academy of Pediatrics that lets users create a customized plan, complete with guidance tailored to each person’s age and the family’s goals. Sample tips: Designate a basket for holding devices during meals, and switch to audiobooks or relaxing music instead of videos to fall asleep at night.
A version of this article first appeared on Medscape.com.
“Youth spend, on average, between 6 and 8 hours per day on screens, much of it on social media,” said senior study author Gary S. Goldfield, PhD, senior scientist at Children’s Hospital of Eastern Ontario Research Institute in Ottawa, Canada. “Social media provides exposure to so many photo-edited pictures – including those of models, celebrities, and fitness instructors – that perpetuate an unattainable beauty standard that gets internalized by impressionable youth and young adults, leading to body dissatisfaction.”
Plenty of research has linked frequent social media use with body image issues and even eating disorders. But crucial gaps in our knowledge remain, Dr. Goldfield said.
Much of that research “is correlational,” Dr. Goldfield added. And studies don’t always focus on individuals who may be more vulnerable to social media’s harmful effects, such as those with ruminative or brooding cognitive styles, affecting results.
And none have explored an obvious question: Can cutting down on social media use also diminish its potential harms?
Dr. Goldfield and his colleagues found an answer: Yes, it can.
Limiting social media use to 1 hour per day helped older teens and young adults feel much better about their weight and appearance after only 3 weeks, according to the study in Psychology of Popular Media, a journal of the American Psychological Association.
“Our randomized controlled design allowed us to show a stronger causal link between social media use and body image in youth, compared to previous research,” Dr. Goldfield said. “To our knowledge, this is the first study to show that social media use reduction leads to enhanced body image.”
Nancy Lee Zucker, PhD, professor of psychology and neuroscience at Duke University, Durham, N.C., and director of the Duke Center for Eating Disorders, said the results provide needed data that could help guide young people and parents on optimal social media use. Dr. Zucker was not involved in the study.
What the researchers did
For the study, Dr. Goldfield and colleagues recruited undergraduate psychology students aged 17-25 who averaged at least 2 hours per day of social media use on smartphones, and who had symptoms of depression or anxiety.
Participants were not told the purpose of the study, and their social media use was monitored by a screen time tracking program. At the beginning and end of the study, they answered questions such as “I’m pretty happy about the way I look,” and “I am satisfied with my weight,” on a 1 (never) to 5 (always) Likert scale.
During the first week, all 220 participants (76% female, 23% male, and 1% other) were told to use social media on their smartphones as they usually do. Over the next 3 weeks, 117 students were told to limit their social media use to 1 hour per day, while the rest were instructed to carry on as usual. In both groups, over 70% of participants were between age 17 and 19.
The first group cut their social media use by about 50%, from a mean of around 168 minutes per day during week 1 to around 78 minutes per day by the end of week 4, while the unrestricted group went from around 181 minutes per day to 189.
Cutting use by around half yielded quick, significant improvements
The students who curbed their social media use saw significant improvements in their “appearance esteem” (from 2.95 to 3.15 points; P <.001) and their “weight esteem” (from 3.16 to 3.32 points; P < .001), whereas those who used social media freely saw no such changes (from 2.72 to 2.76; P = .992 and 3.01 to 3.02; P = .654, respectively). No gender differences between the groups were found.
The researchers are now studying possible reasons for these findings.
The changes in appearance scores “represent a small- to medium-effect size,” said child psychologist Sara R. Gould, PhD, director of the Eating Disorders Center at Children’s Mercy Kansas City in Missouri, who was not associated with the research.“ As such, these are clinically meaningful results, particularly since they were achieved in only 3 weeks. Even small impacts can be added to other changes to create larger impacts or have the potential to grow over time.”
The push to limit social media
As more and more experts scrutinize the impact of social media on young people’s mental health, social media companies have responded with features designed to limit the time young users spend on their platforms.
Just this year, Instagram rolled out “quiet mode,” which lets users shut down their direct messages (DMs) for a specified amount of time. To turn on quiet mode, users can navigate to their profiles, and select the triple line icon, “settings,” “notifications,” and “quiet mode.” Another option: Tap the triple line icon, “your activity,” and “time spent” to set reminders to take breaks after 10, 20, or 30 minutes of use.
TikTok users under 18 will soon have their accounts defaulted to a 1-hour daily screen-time limit, TikTok has announced. Unlike other similar features, it will require users to turn it off rather than turn it on.
Leveraging built-in controls is “a good start to being more intentional about your screen time,” suggested lead author Helen Thai, a PhD student in clinical psychology at McGill University in Montreal. “Unfortunately, users can easily bypass these settings.”
One reason for social’s magnetic pull: “FOMO – fear of missing out – on what friends are doing can make cutting back on social media use difficult,” said Dr. Zucker. To help prevent FOMO, parents may consider talking to parents of their children’s friends about reducing usage for all the children, Dr. Zucker suggested.
Mary E. Romano, MD, MPH, associate professor of pediatrics-adolescent medicine at Vanderbilt University, Nashville, Tenn., urges parents “to have very clear rules and expectations about social media use.”
Dr. Romano, also not involved in the study, recommended the website Wait Until 8th to help parents band together to commit to delaying smartphone access until at least eighth grade.
Dr. Gould recommended the Family Media Plan, a tool from the American Academy of Pediatrics that lets users create a customized plan, complete with guidance tailored to each person’s age and the family’s goals. Sample tips: Designate a basket for holding devices during meals, and switch to audiobooks or relaxing music instead of videos to fall asleep at night.
A version of this article first appeared on Medscape.com.
FROM PSYCHOLOGY OF POPULAR MEDIA
EPA seeks to limit ‘forever’ chemicals in U.S. drinking water
The Environmental Protection Agency is proposing a new rule that would greatly limit the concentration of endocrine-disrupting “forever” chemicals in drinking water.
The EPA on Tuesday announced the proposed National Primary Drinking Water Regulation (NPDWR) for six polyfluoroalkyl substances, more commonly known as PFAS, which are human-made chemicals used as oil and water repellents and coatings for common products including cookware, carpets, and textiles. Such substances are also widely used in cosmetics and food packaging.
The Endocrine Society, which represents more than 18,000 doctors who treat hormone disorders, says it fully supports the new EPA proposal. It explains that these substances, also known as endocrine-disrupting chemicals, “do not break down when they are released into the environment, and they continue to accumulate over time. They pose health dangers at incredibly low levels and have been linked to endocrine disorders such as cancer, thyroid disruption, and reproductive difficulties.”
“This is the first time the government has regulated a new chemical in drinking water in more than 30 years,” the society notes, adding, this “will require major water treatment upgrades at utilities across the country.”
Robert F. Powelson, president and CEO of the National Association of Water Companies, says addressing the PFAS in the nation’s water supply will cost “billions of dollars.”
“It’s a burden that under the current structure will disproportionately fall on water and wastewater customers in small communities and low-income families,” Mr. Powelson says in a statement. He says the onus should instead fall on “the polluters” – those who manufacture and use PFAS chemicals, who “should be held directly responsible for the clean-up costs.”
Although the EPA is proposing a health-based maximum contaminant level goal of zero for these chemicals in drinking water, it acknowledges that this is unenforceable and so has set what it considers an enforceable level, or maximum contaminant level (MCL), of 4 parts per trillion for two of the PFAS, perfluorooctanoic acid (PFOA) and perfluorooctane sulfonic acid (PFOS).
A different standard has been proposed for the remaining four chemicals: perfluorononanoic acid (PFNA) and hexafluoropropylene oxide dimer acid (HFPO-DA) – known together as GenX chemicals – perfluorohexane sulfonic acid (PFHxS), and perfluorobutane sulfonic acid (PFBS).
Officials from the EPA told The Washington Post that these proposed limits would be as strong or stronger than limits from about a dozen states that have set their own drinking water standards in recent years.
“The experts here felt this was the level of stringency required to protect public health, and that the law would allow for us,” EPA Administrator Michael Regan told the newspaper. “This is a transformative action that we’re taking.”
The EPA is requesting public comment on the proposed regulation and will hold a public hearing on May 4, which members of the public can register to attend and comment on the rule proposal. The last day to register is April 28.
The EPA wants to finalize regulation by the end of 2023, although delays are common on new rules.
If it is fully implemented, “the rule will prevent thousands of deaths and reduce tens of thousands of serious PFAS-attributable illnesses,” the EPA statement says.
A version of this article first appeared on Medscape.com.
The Environmental Protection Agency is proposing a new rule that would greatly limit the concentration of endocrine-disrupting “forever” chemicals in drinking water.
The EPA on Tuesday announced the proposed National Primary Drinking Water Regulation (NPDWR) for six polyfluoroalkyl substances, more commonly known as PFAS, which are human-made chemicals used as oil and water repellents and coatings for common products including cookware, carpets, and textiles. Such substances are also widely used in cosmetics and food packaging.
The Endocrine Society, which represents more than 18,000 doctors who treat hormone disorders, says it fully supports the new EPA proposal. It explains that these substances, also known as endocrine-disrupting chemicals, “do not break down when they are released into the environment, and they continue to accumulate over time. They pose health dangers at incredibly low levels and have been linked to endocrine disorders such as cancer, thyroid disruption, and reproductive difficulties.”
“This is the first time the government has regulated a new chemical in drinking water in more than 30 years,” the society notes, adding, this “will require major water treatment upgrades at utilities across the country.”
Robert F. Powelson, president and CEO of the National Association of Water Companies, says addressing the PFAS in the nation’s water supply will cost “billions of dollars.”
“It’s a burden that under the current structure will disproportionately fall on water and wastewater customers in small communities and low-income families,” Mr. Powelson says in a statement. He says the onus should instead fall on “the polluters” – those who manufacture and use PFAS chemicals, who “should be held directly responsible for the clean-up costs.”
Although the EPA is proposing a health-based maximum contaminant level goal of zero for these chemicals in drinking water, it acknowledges that this is unenforceable and so has set what it considers an enforceable level, or maximum contaminant level (MCL), of 4 parts per trillion for two of the PFAS, perfluorooctanoic acid (PFOA) and perfluorooctane sulfonic acid (PFOS).
A different standard has been proposed for the remaining four chemicals: perfluorononanoic acid (PFNA) and hexafluoropropylene oxide dimer acid (HFPO-DA) – known together as GenX chemicals – perfluorohexane sulfonic acid (PFHxS), and perfluorobutane sulfonic acid (PFBS).
Officials from the EPA told The Washington Post that these proposed limits would be as strong or stronger than limits from about a dozen states that have set their own drinking water standards in recent years.
“The experts here felt this was the level of stringency required to protect public health, and that the law would allow for us,” EPA Administrator Michael Regan told the newspaper. “This is a transformative action that we’re taking.”
The EPA is requesting public comment on the proposed regulation and will hold a public hearing on May 4, which members of the public can register to attend and comment on the rule proposal. The last day to register is April 28.
The EPA wants to finalize regulation by the end of 2023, although delays are common on new rules.
If it is fully implemented, “the rule will prevent thousands of deaths and reduce tens of thousands of serious PFAS-attributable illnesses,” the EPA statement says.
A version of this article first appeared on Medscape.com.
The Environmental Protection Agency is proposing a new rule that would greatly limit the concentration of endocrine-disrupting “forever” chemicals in drinking water.
The EPA on Tuesday announced the proposed National Primary Drinking Water Regulation (NPDWR) for six polyfluoroalkyl substances, more commonly known as PFAS, which are human-made chemicals used as oil and water repellents and coatings for common products including cookware, carpets, and textiles. Such substances are also widely used in cosmetics and food packaging.
The Endocrine Society, which represents more than 18,000 doctors who treat hormone disorders, says it fully supports the new EPA proposal. It explains that these substances, also known as endocrine-disrupting chemicals, “do not break down when they are released into the environment, and they continue to accumulate over time. They pose health dangers at incredibly low levels and have been linked to endocrine disorders such as cancer, thyroid disruption, and reproductive difficulties.”
“This is the first time the government has regulated a new chemical in drinking water in more than 30 years,” the society notes, adding, this “will require major water treatment upgrades at utilities across the country.”
Robert F. Powelson, president and CEO of the National Association of Water Companies, says addressing the PFAS in the nation’s water supply will cost “billions of dollars.”
“It’s a burden that under the current structure will disproportionately fall on water and wastewater customers in small communities and low-income families,” Mr. Powelson says in a statement. He says the onus should instead fall on “the polluters” – those who manufacture and use PFAS chemicals, who “should be held directly responsible for the clean-up costs.”
Although the EPA is proposing a health-based maximum contaminant level goal of zero for these chemicals in drinking water, it acknowledges that this is unenforceable and so has set what it considers an enforceable level, or maximum contaminant level (MCL), of 4 parts per trillion for two of the PFAS, perfluorooctanoic acid (PFOA) and perfluorooctane sulfonic acid (PFOS).
A different standard has been proposed for the remaining four chemicals: perfluorononanoic acid (PFNA) and hexafluoropropylene oxide dimer acid (HFPO-DA) – known together as GenX chemicals – perfluorohexane sulfonic acid (PFHxS), and perfluorobutane sulfonic acid (PFBS).
Officials from the EPA told The Washington Post that these proposed limits would be as strong or stronger than limits from about a dozen states that have set their own drinking water standards in recent years.
“The experts here felt this was the level of stringency required to protect public health, and that the law would allow for us,” EPA Administrator Michael Regan told the newspaper. “This is a transformative action that we’re taking.”
The EPA is requesting public comment on the proposed regulation and will hold a public hearing on May 4, which members of the public can register to attend and comment on the rule proposal. The last day to register is April 28.
The EPA wants to finalize regulation by the end of 2023, although delays are common on new rules.
If it is fully implemented, “the rule will prevent thousands of deaths and reduce tens of thousands of serious PFAS-attributable illnesses,” the EPA statement says.
A version of this article first appeared on Medscape.com.
From PERT to AI, high-risk PE care evolves
In 2012, a small group of specialists, consisting of a critical care pulmonologist, cardiologist, cardiac surgeon, and vascular specialist, at Massachusetts General Hospital, Boston, met to Monday morning quarterback an acute pulmonary embolism case that didn’t go as well as they’d hoped. They came up with a concept known as the pulmonary embolism response team – PERT for short – an idea that soon took hold in other centers and served as the vanguard to other innovative approaches to managing critical care patients with PE, which is the third-leading cause of cardiovascular death in the United States (Intern Emerg Med. 2023. doi: 10.1007/s11739-022-03180-w).

Three years later the PERT Consortium came together, which today has 102 members, according to the organization’s website (www.pertconsortium.org), and members in South America, Europe, Asia, and Australia. Since then, and apps to expedite diagnosis and treatment. The PERT Consortium, meanwhile, is in the process of creating the PE Centers of Excellence program to certify centers that meet certain requirements.
“Part of the reason we recognized that a discussion across specialties was important was because there weren’t the large clinical trials that could tell us exactly what to do for any given case,” said Christopher Kabrhel, MD, MPH, director of the Center for Vascular Emergencies at Mass General and a professor at Harvard Medical School in Boston, who assembled that formative meeting. “Without a clear basis in data, it was really important to have all the different specialists weigh in and give their perspective and talk about what was the best approach for the patient’s care.”
Filling data gaps
Some of those data gaps persist today, Dr. Kabrhel said. “It’s precisely that lack of head-to-head data that existed in 2012, and to a great extent still exists today, that led us to create this system.” The American Heart Association just this January issued a scientific statement on surgical management and mechanical circulatory support in high-risk PE (Circulation. 2023;147:e628-47).
But the intervening research has been uneven. The Pulmonary Embolism Thrombolysis (PEITHO) trial in 2014 evaluated systemic thrombolysis and anticoagulation alone (N Engl J Med. 2014;370:1402-11), but head-to-head studies of catheter-directed thrombolysis (CDT), which was just emerging in 2012, and either systemic thrombolysis or anticoagulation have been lacking, Dr. Kabrhel said. The Hi-PEITHO trial in high-risk PE patients is evaluating ultrasound-guided CDT plus anticoagulation vs. anticoagulation alone (Am Heart J. 2022:251:43-54), but it isn’t complete.
“The therapeutic landscape for PE is evolving incredibly rapidly,” he said. “When we first started PERT we were just starting to see CDT. Since then, we’ve seen several new thrombolytic catheters come onto the market, but there’s also been a proliferation of suction embolectomy catheters and we’ve seen a potentially larger role for surgery and the use of ECMO [extracorporeal membrane oxygenation] or cardiac bypass to bridge patients to definitive therapy. With the rapid evolution and the seemingly daily addition of new therapeutic options, I think the need for PERT is only increasing.”
A recent study out of the University of Michigan reported that the PERT there led to a decrease in the use of advanced therapies given to acute PE patients without reducing mortality or extending hospital stays (Thromb Res. 2023;221:73-8). A study in Spain reported that patients with high-risk and intermediate high-risk PE who had PERT-coordinated care had half the 12-month mortality rate of non-PERT counterparts, 9% vs. 22.2% (P = .02) (Med Clin [Barc]. 2023;S0025-7753(23)00017-9). And a 2021 study at University Hospitals in Cleveland reported that PERT-managed PE patients had a 60% lower rate of adverse outcomes at 90 days than non–PERT-managed patients (J Invasive Cardiol. 2021;33:E173-E180).

Nelish Ardeshna, MD, MA, the lead author of the Michigan study, said the PERT there was formed in 2017. Besides the multispecialty team that can be summoned to a teleconference on short notice, the protocol includes having at least one noninvasive specialist, such as a cardiologist or hospitalist, and one interventionalist, such as a radiologist, always on call. The PERT gets activated through the paging system after a hospital or emergency department physician identifies a suspected or established high-risk PE.
“High-risk PE patients can present in all settings, including the emergency department, ICU, surgical floor, or medical floor,” said Dr. Ardeshna, an internal medicine resident. “Management for these patients is equally varied from anticoagulation to systemic thrombolytics. Not all providers may be familiar with current guidelines to select the optimal therapy for high-risk pulmonary embolism patients. PERT aims to bridge that gap by providing a multidisciplinary discussion with PE specialists that can help identify the correct therapeutic options for optimal outcomes.”

At Cleveland Clinic, where the PERT has been in place since 2012, the PERT can consist of six to eight different specialties and involve up to 15 providers on a conference call, said Leben Tefera, MD, a vascular specialist and head of the PERT team there.
“Each patient will come in and have certain comorbidities,” Dr. Tefera said. “The unfortunate thing about a majority of the PEs that we see, in particular ones [in patients] that are very sick and require inpatient treatment, is that they don’t really fit into a box; you can’t come up with one kind of generic care routine or care path that treats the majority of patients with PE.”
Evolving to follow-up care
As the PERT protocol led to better inpatient outcomes, the teams became more aware that discharged PE patients were struggling with mental health and other quality-of-life issues – symptoms that have been understudied, according to a protocol Dr. Tefera coauthored for a prospective observational study of psychological distress symptoms in PE survivors. By contrast, the protocol noted, these symptoms have been studied extensively in myocardial infarction and stroke patients (Res Pract Thromb Hemost. 2023. doi: 10.1016/j.rpth.2023.10045). Other studies have found that 35%-50% of patients reported mental health symptoms 3 months after PE (Chest. 2021;159:2428-38; Qual Life Res. 2019;28:2111-24).
“A lot of physicians have known it for quite some time, but it wasn’t really until the last couple of years that physicians started saying psychological stress is something that we need to quantify and that we need to actually treat, that we actually need to address,” Dr. Tefera said. That led Dr. Tefera and his Cleveland Clinic PERT colleagues to set up a follow-up clinic for PE patients.
At their follow-up visits, patients complete validated questionnaires about anxiety, depression, fear of recurrence, PE-specific quality of life, and posttraumatic stress disorder. “If they flag as positive, we give them a referral to an in-house psychologist,” he said. “One thing I can report is that patients absolutely, positively love this, because it’s something that they are all experiencing that a lot of physicians just aren’t addressing.”
Artificial intelligence emerges
At the University of Pittsburgh Medical Center, the PERT has started evaluating artificial intelligence to aid in PE diagnosis. Belinda Rivera-Lebron, MD, director of the acute and chronic embolism program at Pitt, explained that the AI protocol hasn’t been adopted yet, but the concept is to have a platform that’s compatible with the hospital system’s electronic medical record.

She described how AI would work once the PERT is activated. “Once the patient goes through the CT scanner, within 60 seconds of that scan being completed, the scan gets uploaded into the cloud and the app or the platform is able to tell you whether there is PE present or absent, and whether there is right ventricle dilation on that scan. This is even before you probably even think about opening up the computer to look at the scan, and even before radiology opens up the scan to read,” she said. “It’s so fast.”
The idea is to send the scans rapidly to the PERT. “It will send you a text, a notification on your phone that will tell you Mr. Smith is PE positive,” Dr. Rivera-Lebron said. “Then you open it and you are able to scroll through the CT scan in your phone. So, it’s really remarkable.”
Clinical trials worth watching
Meanwhile, a number of clinical trials have started to enroll patients, or will soon, that Dr. Rivera-Lebron said are worth paying attention to.
PEITHO-3 is a randomized, placebo-controlled trial with long-term follow-up comparing the efficacy of a reduced-dose alteplase regimen or standard heparin anticoagulation in patients with intermediate to high-risk PE (Thromb Haemost. 2022;122:867-66).
PEERLESS is a prospective randomized trial comparing mechanical thrombectomy and CDT (ClinicalTrials.gov identifier NCT05111613).
PE-Thrombus Removal with Catheter-directed Therapy (PE-TRACT) is an open-label Phase 3 trial comparing anticoagulation and CDT that’s not yet recruiting (ClinicalTrials.gov identifier NCT05591118).
FlowTriever for Acute Massive Pulmonary Embolism (FLAME) is a prospective cohort study evaluating a clot-retrieving device in high-risk PE patients (ClinicalTrials.gov identifier NCT04795167).
When completed and published, these trials could provide PERTs more evidence for their decision-making.
Dr. Ardeshna and Dr. Tefera have no relevant relationships to disclose. Dr. Rivera-Lebron disclosed relationships with INARI Catheter and Johnson & Johnson. Dr. Kabrhel disclosed relationships with Bristol Myers Squibb and Pfizer.
In 2012, a small group of specialists, consisting of a critical care pulmonologist, cardiologist, cardiac surgeon, and vascular specialist, at Massachusetts General Hospital, Boston, met to Monday morning quarterback an acute pulmonary embolism case that didn’t go as well as they’d hoped. They came up with a concept known as the pulmonary embolism response team – PERT for short – an idea that soon took hold in other centers and served as the vanguard to other innovative approaches to managing critical care patients with PE, which is the third-leading cause of cardiovascular death in the United States (Intern Emerg Med. 2023. doi: 10.1007/s11739-022-03180-w).
Three years later the PERT Consortium came together, which today has 102 members, according to the organization’s website (www.pertconsortium.org), and members in South America, Europe, Asia, and Australia. Since then, and apps to expedite diagnosis and treatment. The PERT Consortium, meanwhile, is in the process of creating the PE Centers of Excellence program to certify centers that meet certain requirements.
“Part of the reason we recognized that a discussion across specialties was important was because there weren’t the large clinical trials that could tell us exactly what to do for any given case,” said Christopher Kabrhel, MD, MPH, director of the Center for Vascular Emergencies at Mass General and a professor at Harvard Medical School in Boston, who assembled that formative meeting. “Without a clear basis in data, it was really important to have all the different specialists weigh in and give their perspective and talk about what was the best approach for the patient’s care.”
Filling data gaps
Some of those data gaps persist today, Dr. Kabrhel said. “It’s precisely that lack of head-to-head data that existed in 2012, and to a great extent still exists today, that led us to create this system.” The American Heart Association just this January issued a scientific statement on surgical management and mechanical circulatory support in high-risk PE (Circulation. 2023;147:e628-47).
But the intervening research has been uneven. The Pulmonary Embolism Thrombolysis (PEITHO) trial in 2014 evaluated systemic thrombolysis and anticoagulation alone (N Engl J Med. 2014;370:1402-11), but head-to-head studies of catheter-directed thrombolysis (CDT), which was just emerging in 2012, and either systemic thrombolysis or anticoagulation have been lacking, Dr. Kabrhel said. The Hi-PEITHO trial in high-risk PE patients is evaluating ultrasound-guided CDT plus anticoagulation vs. anticoagulation alone (Am Heart J. 2022:251:43-54), but it isn’t complete.
“The therapeutic landscape for PE is evolving incredibly rapidly,” he said. “When we first started PERT we were just starting to see CDT. Since then, we’ve seen several new thrombolytic catheters come onto the market, but there’s also been a proliferation of suction embolectomy catheters and we’ve seen a potentially larger role for surgery and the use of ECMO [extracorporeal membrane oxygenation] or cardiac bypass to bridge patients to definitive therapy. With the rapid evolution and the seemingly daily addition of new therapeutic options, I think the need for PERT is only increasing.”
A recent study out of the University of Michigan reported that the PERT there led to a decrease in the use of advanced therapies given to acute PE patients without reducing mortality or extending hospital stays (Thromb Res. 2023;221:73-8). A study in Spain reported that patients with high-risk and intermediate high-risk PE who had PERT-coordinated care had half the 12-month mortality rate of non-PERT counterparts, 9% vs. 22.2% (P = .02) (Med Clin [Barc]. 2023;S0025-7753(23)00017-9). And a 2021 study at University Hospitals in Cleveland reported that PERT-managed PE patients had a 60% lower rate of adverse outcomes at 90 days than non–PERT-managed patients (J Invasive Cardiol. 2021;33:E173-E180).
Nelish Ardeshna, MD, MA, the lead author of the Michigan study, said the PERT there was formed in 2017. Besides the multispecialty team that can be summoned to a teleconference on short notice, the protocol includes having at least one noninvasive specialist, such as a cardiologist or hospitalist, and one interventionalist, such as a radiologist, always on call. The PERT gets activated through the paging system after a hospital or emergency department physician identifies a suspected or established high-risk PE.
“High-risk PE patients can present in all settings, including the emergency department, ICU, surgical floor, or medical floor,” said Dr. Ardeshna, an internal medicine resident. “Management for these patients is equally varied from anticoagulation to systemic thrombolytics. Not all providers may be familiar with current guidelines to select the optimal therapy for high-risk pulmonary embolism patients. PERT aims to bridge that gap by providing a multidisciplinary discussion with PE specialists that can help identify the correct therapeutic options for optimal outcomes.”
At Cleveland Clinic, where the PERT has been in place since 2012, the PERT can consist of six to eight different specialties and involve up to 15 providers on a conference call, said Leben Tefera, MD, a vascular specialist and head of the PERT team there.
“Each patient will come in and have certain comorbidities,” Dr. Tefera said. “The unfortunate thing about a majority of the PEs that we see, in particular ones [in patients] that are very sick and require inpatient treatment, is that they don’t really fit into a box; you can’t come up with one kind of generic care routine or care path that treats the majority of patients with PE.”
Evolving to follow-up care
As the PERT protocol led to better inpatient outcomes, the teams became more aware that discharged PE patients were struggling with mental health and other quality-of-life issues – symptoms that have been understudied, according to a protocol Dr. Tefera coauthored for a prospective observational study of psychological distress symptoms in PE survivors. By contrast, the protocol noted, these symptoms have been studied extensively in myocardial infarction and stroke patients (Res Pract Thromb Hemost. 2023. doi: 10.1016/j.rpth.2023.10045). Other studies have found that 35%-50% of patients reported mental health symptoms 3 months after PE (Chest. 2021;159:2428-38; Qual Life Res. 2019;28:2111-24).
“A lot of physicians have known it for quite some time, but it wasn’t really until the last couple of years that physicians started saying psychological stress is something that we need to quantify and that we need to actually treat, that we actually need to address,” Dr. Tefera said. That led Dr. Tefera and his Cleveland Clinic PERT colleagues to set up a follow-up clinic for PE patients.
At their follow-up visits, patients complete validated questionnaires about anxiety, depression, fear of recurrence, PE-specific quality of life, and posttraumatic stress disorder. “If they flag as positive, we give them a referral to an in-house psychologist,” he said. “One thing I can report is that patients absolutely, positively love this, because it’s something that they are all experiencing that a lot of physicians just aren’t addressing.”
Artificial intelligence emerges
At the University of Pittsburgh Medical Center, the PERT has started evaluating artificial intelligence to aid in PE diagnosis. Belinda Rivera-Lebron, MD, director of the acute and chronic embolism program at Pitt, explained that the AI protocol hasn’t been adopted yet, but the concept is to have a platform that’s compatible with the hospital system’s electronic medical record.
She described how AI would work once the PERT is activated. “Once the patient goes through the CT scanner, within 60 seconds of that scan being completed, the scan gets uploaded into the cloud and the app or the platform is able to tell you whether there is PE present or absent, and whether there is right ventricle dilation on that scan. This is even before you probably even think about opening up the computer to look at the scan, and even before radiology opens up the scan to read,” she said. “It’s so fast.”
The idea is to send the scans rapidly to the PERT. “It will send you a text, a notification on your phone that will tell you Mr. Smith is PE positive,” Dr. Rivera-Lebron said. “Then you open it and you are able to scroll through the CT scan in your phone. So, it’s really remarkable.”
Clinical trials worth watching
Meanwhile, a number of clinical trials have started to enroll patients, or will soon, that Dr. Rivera-Lebron said are worth paying attention to.
PEITHO-3 is a randomized, placebo-controlled trial with long-term follow-up comparing the efficacy of a reduced-dose alteplase regimen or standard heparin anticoagulation in patients with intermediate to high-risk PE (Thromb Haemost. 2022;122:867-66).
PEERLESS is a prospective randomized trial comparing mechanical thrombectomy and CDT (ClinicalTrials.gov identifier NCT05111613).
PE-Thrombus Removal with Catheter-directed Therapy (PE-TRACT) is an open-label Phase 3 trial comparing anticoagulation and CDT that’s not yet recruiting (ClinicalTrials.gov identifier NCT05591118).
FlowTriever for Acute Massive Pulmonary Embolism (FLAME) is a prospective cohort study evaluating a clot-retrieving device in high-risk PE patients (ClinicalTrials.gov identifier NCT04795167).
When completed and published, these trials could provide PERTs more evidence for their decision-making.
Dr. Ardeshna and Dr. Tefera have no relevant relationships to disclose. Dr. Rivera-Lebron disclosed relationships with INARI Catheter and Johnson & Johnson. Dr. Kabrhel disclosed relationships with Bristol Myers Squibb and Pfizer.
In 2012, a small group of specialists, consisting of a critical care pulmonologist, cardiologist, cardiac surgeon, and vascular specialist, at Massachusetts General Hospital, Boston, met to Monday morning quarterback an acute pulmonary embolism case that didn’t go as well as they’d hoped. They came up with a concept known as the pulmonary embolism response team – PERT for short – an idea that soon took hold in other centers and served as the vanguard to other innovative approaches to managing critical care patients with PE, which is the third-leading cause of cardiovascular death in the United States (Intern Emerg Med. 2023. doi: 10.1007/s11739-022-03180-w).
Three years later the PERT Consortium came together, which today has 102 members, according to the organization’s website (www.pertconsortium.org), and members in South America, Europe, Asia, and Australia. Since then, and apps to expedite diagnosis and treatment. The PERT Consortium, meanwhile, is in the process of creating the PE Centers of Excellence program to certify centers that meet certain requirements.
“Part of the reason we recognized that a discussion across specialties was important was because there weren’t the large clinical trials that could tell us exactly what to do for any given case,” said Christopher Kabrhel, MD, MPH, director of the Center for Vascular Emergencies at Mass General and a professor at Harvard Medical School in Boston, who assembled that formative meeting. “Without a clear basis in data, it was really important to have all the different specialists weigh in and give their perspective and talk about what was the best approach for the patient’s care.”
Filling data gaps
Some of those data gaps persist today, Dr. Kabrhel said. “It’s precisely that lack of head-to-head data that existed in 2012, and to a great extent still exists today, that led us to create this system.” The American Heart Association just this January issued a scientific statement on surgical management and mechanical circulatory support in high-risk PE (Circulation. 2023;147:e628-47).
But the intervening research has been uneven. The Pulmonary Embolism Thrombolysis (PEITHO) trial in 2014 evaluated systemic thrombolysis and anticoagulation alone (N Engl J Med. 2014;370:1402-11), but head-to-head studies of catheter-directed thrombolysis (CDT), which was just emerging in 2012, and either systemic thrombolysis or anticoagulation have been lacking, Dr. Kabrhel said. The Hi-PEITHO trial in high-risk PE patients is evaluating ultrasound-guided CDT plus anticoagulation vs. anticoagulation alone (Am Heart J. 2022:251:43-54), but it isn’t complete.
“The therapeutic landscape for PE is evolving incredibly rapidly,” he said. “When we first started PERT we were just starting to see CDT. Since then, we’ve seen several new thrombolytic catheters come onto the market, but there’s also been a proliferation of suction embolectomy catheters and we’ve seen a potentially larger role for surgery and the use of ECMO [extracorporeal membrane oxygenation] or cardiac bypass to bridge patients to definitive therapy. With the rapid evolution and the seemingly daily addition of new therapeutic options, I think the need for PERT is only increasing.”
A recent study out of the University of Michigan reported that the PERT there led to a decrease in the use of advanced therapies given to acute PE patients without reducing mortality or extending hospital stays (Thromb Res. 2023;221:73-8). A study in Spain reported that patients with high-risk and intermediate high-risk PE who had PERT-coordinated care had half the 12-month mortality rate of non-PERT counterparts, 9% vs. 22.2% (P = .02) (Med Clin [Barc]. 2023;S0025-7753(23)00017-9). And a 2021 study at University Hospitals in Cleveland reported that PERT-managed PE patients had a 60% lower rate of adverse outcomes at 90 days than non–PERT-managed patients (J Invasive Cardiol. 2021;33:E173-E180).
Nelish Ardeshna, MD, MA, the lead author of the Michigan study, said the PERT there was formed in 2017. Besides the multispecialty team that can be summoned to a teleconference on short notice, the protocol includes having at least one noninvasive specialist, such as a cardiologist or hospitalist, and one interventionalist, such as a radiologist, always on call. The PERT gets activated through the paging system after a hospital or emergency department physician identifies a suspected or established high-risk PE.
“High-risk PE patients can present in all settings, including the emergency department, ICU, surgical floor, or medical floor,” said Dr. Ardeshna, an internal medicine resident. “Management for these patients is equally varied from anticoagulation to systemic thrombolytics. Not all providers may be familiar with current guidelines to select the optimal therapy for high-risk pulmonary embolism patients. PERT aims to bridge that gap by providing a multidisciplinary discussion with PE specialists that can help identify the correct therapeutic options for optimal outcomes.”
At Cleveland Clinic, where the PERT has been in place since 2012, the PERT can consist of six to eight different specialties and involve up to 15 providers on a conference call, said Leben Tefera, MD, a vascular specialist and head of the PERT team there.
“Each patient will come in and have certain comorbidities,” Dr. Tefera said. “The unfortunate thing about a majority of the PEs that we see, in particular ones [in patients] that are very sick and require inpatient treatment, is that they don’t really fit into a box; you can’t come up with one kind of generic care routine or care path that treats the majority of patients with PE.”
Evolving to follow-up care
As the PERT protocol led to better inpatient outcomes, the teams became more aware that discharged PE patients were struggling with mental health and other quality-of-life issues – symptoms that have been understudied, according to a protocol Dr. Tefera coauthored for a prospective observational study of psychological distress symptoms in PE survivors. By contrast, the protocol noted, these symptoms have been studied extensively in myocardial infarction and stroke patients (Res Pract Thromb Hemost. 2023. doi: 10.1016/j.rpth.2023.10045). Other studies have found that 35%-50% of patients reported mental health symptoms 3 months after PE (Chest. 2021;159:2428-38; Qual Life Res. 2019;28:2111-24).
“A lot of physicians have known it for quite some time, but it wasn’t really until the last couple of years that physicians started saying psychological stress is something that we need to quantify and that we need to actually treat, that we actually need to address,” Dr. Tefera said. That led Dr. Tefera and his Cleveland Clinic PERT colleagues to set up a follow-up clinic for PE patients.
At their follow-up visits, patients complete validated questionnaires about anxiety, depression, fear of recurrence, PE-specific quality of life, and posttraumatic stress disorder. “If they flag as positive, we give them a referral to an in-house psychologist,” he said. “One thing I can report is that patients absolutely, positively love this, because it’s something that they are all experiencing that a lot of physicians just aren’t addressing.”
Artificial intelligence emerges
At the University of Pittsburgh Medical Center, the PERT has started evaluating artificial intelligence to aid in PE diagnosis. Belinda Rivera-Lebron, MD, director of the acute and chronic embolism program at Pitt, explained that the AI protocol hasn’t been adopted yet, but the concept is to have a platform that’s compatible with the hospital system’s electronic medical record.
She described how AI would work once the PERT is activated. “Once the patient goes through the CT scanner, within 60 seconds of that scan being completed, the scan gets uploaded into the cloud and the app or the platform is able to tell you whether there is PE present or absent, and whether there is right ventricle dilation on that scan. This is even before you probably even think about opening up the computer to look at the scan, and even before radiology opens up the scan to read,” she said. “It’s so fast.”
The idea is to send the scans rapidly to the PERT. “It will send you a text, a notification on your phone that will tell you Mr. Smith is PE positive,” Dr. Rivera-Lebron said. “Then you open it and you are able to scroll through the CT scan in your phone. So, it’s really remarkable.”
Clinical trials worth watching
Meanwhile, a number of clinical trials have started to enroll patients, or will soon, that Dr. Rivera-Lebron said are worth paying attention to.
PEITHO-3 is a randomized, placebo-controlled trial with long-term follow-up comparing the efficacy of a reduced-dose alteplase regimen or standard heparin anticoagulation in patients with intermediate to high-risk PE (Thromb Haemost. 2022;122:867-66).
PEERLESS is a prospective randomized trial comparing mechanical thrombectomy and CDT (ClinicalTrials.gov identifier NCT05111613).
PE-Thrombus Removal with Catheter-directed Therapy (PE-TRACT) is an open-label Phase 3 trial comparing anticoagulation and CDT that’s not yet recruiting (ClinicalTrials.gov identifier NCT05591118).
FlowTriever for Acute Massive Pulmonary Embolism (FLAME) is a prospective cohort study evaluating a clot-retrieving device in high-risk PE patients (ClinicalTrials.gov identifier NCT04795167).
When completed and published, these trials could provide PERTs more evidence for their decision-making.
Dr. Ardeshna and Dr. Tefera have no relevant relationships to disclose. Dr. Rivera-Lebron disclosed relationships with INARI Catheter and Johnson & Johnson. Dr. Kabrhel disclosed relationships with Bristol Myers Squibb and Pfizer.