User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Florida sees spike in deadly bacterial infections after Hurricane Ian
At least 4 people have died and 29 have been infected in Lee County after the hurricane, Florida health officials said in a news release.
Vibrio vulnificus bacteria is found in warm, brackish seawater, according to the Florida Department of Health. Anyone with open wounds or cuts should avoid standing water, floodwater, or seawater in the area, health officials said.
“Sewage spills in coastal waters, like those caused by Hurricane Ian, may increase bacteria levels,” the department advised in a news release. “People with open wounds, cuts, or scratches can be exposed to Vibrio vulnificus through direct contact with sea water or brackish water … Vibrio vulnificus can also cause disease in those who eat raw or undercooked oysters and shellfish.”
Infection can cause severe illness or death. Symptoms include fever, chills, decreased blood pressure, and blistering skin lesions. The bacteria does not spread person to person.
“If someone is concerned that they may have been exposed to Vibrio vulnificus and are experiencing the above symptoms, they should seek medical attention immediately,” officials said in the statement. “Individuals with wound infections should also seek care promptly.”
A version of this article first appeared on WebMD.com.
At least 4 people have died and 29 have been infected in Lee County after the hurricane, Florida health officials said in a news release.
Vibrio vulnificus bacteria is found in warm, brackish seawater, according to the Florida Department of Health. Anyone with open wounds or cuts should avoid standing water, floodwater, or seawater in the area, health officials said.
“Sewage spills in coastal waters, like those caused by Hurricane Ian, may increase bacteria levels,” the department advised in a news release. “People with open wounds, cuts, or scratches can be exposed to Vibrio vulnificus through direct contact with sea water or brackish water … Vibrio vulnificus can also cause disease in those who eat raw or undercooked oysters and shellfish.”
Infection can cause severe illness or death. Symptoms include fever, chills, decreased blood pressure, and blistering skin lesions. The bacteria does not spread person to person.
“If someone is concerned that they may have been exposed to Vibrio vulnificus and are experiencing the above symptoms, they should seek medical attention immediately,” officials said in the statement. “Individuals with wound infections should also seek care promptly.”
A version of this article first appeared on WebMD.com.
At least 4 people have died and 29 have been infected in Lee County after the hurricane, Florida health officials said in a news release.
Vibrio vulnificus bacteria is found in warm, brackish seawater, according to the Florida Department of Health. Anyone with open wounds or cuts should avoid standing water, floodwater, or seawater in the area, health officials said.
“Sewage spills in coastal waters, like those caused by Hurricane Ian, may increase bacteria levels,” the department advised in a news release. “People with open wounds, cuts, or scratches can be exposed to Vibrio vulnificus through direct contact with sea water or brackish water … Vibrio vulnificus can also cause disease in those who eat raw or undercooked oysters and shellfish.”
Infection can cause severe illness or death. Symptoms include fever, chills, decreased blood pressure, and blistering skin lesions. The bacteria does not spread person to person.
“If someone is concerned that they may have been exposed to Vibrio vulnificus and are experiencing the above symptoms, they should seek medical attention immediately,” officials said in the statement. “Individuals with wound infections should also seek care promptly.”
A version of this article first appeared on WebMD.com.
25 years of chickenpox vaccine: 91 million cases prevented
WASHINGTON – In the 25 years since the United States first launched its universal vaccinations program to protect children against chickenpox (varicella), the program has seen dramatic results, a data analysis indicates.
Results from 1995 – when universal vaccinations began – through 2019 were presented an annual scientific meeting on infectious diseases by Mona Marin, MD, a medical epidemiologist at the Centers for Disease Control and Prevention. Researchers analyzed published data and surveillance data reported to the CDC.
Deaths in under-20 group all but eliminated
Immunocompromised people or pregnant women and infants too young to be vaccinated also benefited from the children’s immunizations.
Each year, about 3.8 million cases, 10,500 hospitalizations, and 100 deaths from chickenpox are prevented in the United States thanks to the vaccination program, Dr. Marin said.
Over 25 years, 91 million cases, 238,000 hospitalizations, and 1,933 – 2,446 deaths have been prevented.
However, chickenpox is still widespread in most of the world.
U.S. first with universal program
The disease was thought to be of little consequence, Dr. Marin said, until the mid-1950s after the first cases of fatal varicella in immunocompromised children revealed the virus’ lethal potential.
The United States was the first country to introduce a universal vaccination program, Dr. Marin said. At the time, it was a one-dose vaccine. Within the first 10 years of the one-dose program, declines in chickenpox cases, hospitalization, and death rates went from 71% to 90% in comparison with previous years. But health care leaders wanted to close the remaining gap and target transmission in schools.
“It was a burden the United States considered unacceptable,” Dr. Marin said.
The leaders had seen the control of measles and polio and wanted the same for chickenpox.
Two-dose vaccines started in 2007
In 2007, the current two-dose policy was introduced. Administration of the first dose is recommended at age 12–15 months, and the second at age 4–6 years. Vaccination is required before the children enter kindergarten.
Coverage was high – at least 90% – the study authors reported; the two-dose program further reduced the number, size, and duration of outbreaks. Over the 25 years, the proportion of outbreaks with fewer than 10 cases increased from 28% to 73%.
By 2019, incidence had dropped by 97%, hospitalizations were down by 94%, and deaths had dropped by 97%.
The biggest decline was seen in those younger than 20, who were born during the vaccination program. That group saw declines of 97% to 99% in cases, hospitalizations, and incidence compared with rates before vaccinations.
Dr. Marin says one dose of the vaccine is moderately effective in preventing all varicella (82%) and is highly effective in preventing severe varicella (more than 97%).
“The second dose adds 10% or more improved protection against all varicella,” she said.
But there have been gains beyond medical advances.
Researchers calculated the economic benefit and found a net savings of $23 billion in medical costs (which also factored in lost wages from parents staying home to care for sick children).
Jaw-dropping results
Jeanne Marrazzo, MD, director of the division of infectious diseases at the University of Alabama at Birmingham, said in an interview that “as someone who is not a vaccinologist, the declines in deaths, let alone hospitalizations, were jaw-dropping. I hadn’t really seen a synthesis of the impact of one and two doses.”
She said the declines in zoster among young people were interesting. The big question, she said, is what impact this may have for shingles infections in middle-aged adults over time, since chickenpox and shingles are caused by the same virus.
Dr. Marrazzo also noted the economic savings calculations.
“It’s such a cheap intervention. It’s one of the best examples of how a simple vaccine can affect a cascade of events that are a result of chronic viral infection,” she said.
There are also messages for the current debates over COVID-19 vaccinations.
“For me, it is further evidence of the profound population-level effect safe vaccines can have,” Dr. Marrazzo said.
The authors and Dr. Marrazzo report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
WASHINGTON – In the 25 years since the United States first launched its universal vaccinations program to protect children against chickenpox (varicella), the program has seen dramatic results, a data analysis indicates.
Results from 1995 – when universal vaccinations began – through 2019 were presented an annual scientific meeting on infectious diseases by Mona Marin, MD, a medical epidemiologist at the Centers for Disease Control and Prevention. Researchers analyzed published data and surveillance data reported to the CDC.
Deaths in under-20 group all but eliminated
Immunocompromised people or pregnant women and infants too young to be vaccinated also benefited from the children’s immunizations.
Each year, about 3.8 million cases, 10,500 hospitalizations, and 100 deaths from chickenpox are prevented in the United States thanks to the vaccination program, Dr. Marin said.
Over 25 years, 91 million cases, 238,000 hospitalizations, and 1,933 – 2,446 deaths have been prevented.
However, chickenpox is still widespread in most of the world.
U.S. first with universal program
The disease was thought to be of little consequence, Dr. Marin said, until the mid-1950s after the first cases of fatal varicella in immunocompromised children revealed the virus’ lethal potential.
The United States was the first country to introduce a universal vaccination program, Dr. Marin said. At the time, it was a one-dose vaccine. Within the first 10 years of the one-dose program, declines in chickenpox cases, hospitalization, and death rates went from 71% to 90% in comparison with previous years. But health care leaders wanted to close the remaining gap and target transmission in schools.
“It was a burden the United States considered unacceptable,” Dr. Marin said.
The leaders had seen the control of measles and polio and wanted the same for chickenpox.
Two-dose vaccines started in 2007
In 2007, the current two-dose policy was introduced. Administration of the first dose is recommended at age 12–15 months, and the second at age 4–6 years. Vaccination is required before the children enter kindergarten.
Coverage was high – at least 90% – the study authors reported; the two-dose program further reduced the number, size, and duration of outbreaks. Over the 25 years, the proportion of outbreaks with fewer than 10 cases increased from 28% to 73%.
By 2019, incidence had dropped by 97%, hospitalizations were down by 94%, and deaths had dropped by 97%.
The biggest decline was seen in those younger than 20, who were born during the vaccination program. That group saw declines of 97% to 99% in cases, hospitalizations, and incidence compared with rates before vaccinations.
Dr. Marin says one dose of the vaccine is moderately effective in preventing all varicella (82%) and is highly effective in preventing severe varicella (more than 97%).
“The second dose adds 10% or more improved protection against all varicella,” she said.
But there have been gains beyond medical advances.
Researchers calculated the economic benefit and found a net savings of $23 billion in medical costs (which also factored in lost wages from parents staying home to care for sick children).
Jaw-dropping results
Jeanne Marrazzo, MD, director of the division of infectious diseases at the University of Alabama at Birmingham, said in an interview that “as someone who is not a vaccinologist, the declines in deaths, let alone hospitalizations, were jaw-dropping. I hadn’t really seen a synthesis of the impact of one and two doses.”
She said the declines in zoster among young people were interesting. The big question, she said, is what impact this may have for shingles infections in middle-aged adults over time, since chickenpox and shingles are caused by the same virus.
Dr. Marrazzo also noted the economic savings calculations.
“It’s such a cheap intervention. It’s one of the best examples of how a simple vaccine can affect a cascade of events that are a result of chronic viral infection,” she said.
There are also messages for the current debates over COVID-19 vaccinations.
“For me, it is further evidence of the profound population-level effect safe vaccines can have,” Dr. Marrazzo said.
The authors and Dr. Marrazzo report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
WASHINGTON – In the 25 years since the United States first launched its universal vaccinations program to protect children against chickenpox (varicella), the program has seen dramatic results, a data analysis indicates.
Results from 1995 – when universal vaccinations began – through 2019 were presented an annual scientific meeting on infectious diseases by Mona Marin, MD, a medical epidemiologist at the Centers for Disease Control and Prevention. Researchers analyzed published data and surveillance data reported to the CDC.
Deaths in under-20 group all but eliminated
Immunocompromised people or pregnant women and infants too young to be vaccinated also benefited from the children’s immunizations.
Each year, about 3.8 million cases, 10,500 hospitalizations, and 100 deaths from chickenpox are prevented in the United States thanks to the vaccination program, Dr. Marin said.
Over 25 years, 91 million cases, 238,000 hospitalizations, and 1,933 – 2,446 deaths have been prevented.
However, chickenpox is still widespread in most of the world.
U.S. first with universal program
The disease was thought to be of little consequence, Dr. Marin said, until the mid-1950s after the first cases of fatal varicella in immunocompromised children revealed the virus’ lethal potential.
The United States was the first country to introduce a universal vaccination program, Dr. Marin said. At the time, it was a one-dose vaccine. Within the first 10 years of the one-dose program, declines in chickenpox cases, hospitalization, and death rates went from 71% to 90% in comparison with previous years. But health care leaders wanted to close the remaining gap and target transmission in schools.
“It was a burden the United States considered unacceptable,” Dr. Marin said.
The leaders had seen the control of measles and polio and wanted the same for chickenpox.
Two-dose vaccines started in 2007
In 2007, the current two-dose policy was introduced. Administration of the first dose is recommended at age 12–15 months, and the second at age 4–6 years. Vaccination is required before the children enter kindergarten.
Coverage was high – at least 90% – the study authors reported; the two-dose program further reduced the number, size, and duration of outbreaks. Over the 25 years, the proportion of outbreaks with fewer than 10 cases increased from 28% to 73%.
By 2019, incidence had dropped by 97%, hospitalizations were down by 94%, and deaths had dropped by 97%.
The biggest decline was seen in those younger than 20, who were born during the vaccination program. That group saw declines of 97% to 99% in cases, hospitalizations, and incidence compared with rates before vaccinations.
Dr. Marin says one dose of the vaccine is moderately effective in preventing all varicella (82%) and is highly effective in preventing severe varicella (more than 97%).
“The second dose adds 10% or more improved protection against all varicella,” she said.
But there have been gains beyond medical advances.
Researchers calculated the economic benefit and found a net savings of $23 billion in medical costs (which also factored in lost wages from parents staying home to care for sick children).
Jaw-dropping results
Jeanne Marrazzo, MD, director of the division of infectious diseases at the University of Alabama at Birmingham, said in an interview that “as someone who is not a vaccinologist, the declines in deaths, let alone hospitalizations, were jaw-dropping. I hadn’t really seen a synthesis of the impact of one and two doses.”
She said the declines in zoster among young people were interesting. The big question, she said, is what impact this may have for shingles infections in middle-aged adults over time, since chickenpox and shingles are caused by the same virus.
Dr. Marrazzo also noted the economic savings calculations.
“It’s such a cheap intervention. It’s one of the best examples of how a simple vaccine can affect a cascade of events that are a result of chronic viral infection,” she said.
There are also messages for the current debates over COVID-19 vaccinations.
“For me, it is further evidence of the profound population-level effect safe vaccines can have,” Dr. Marrazzo said.
The authors and Dr. Marrazzo report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT IDWEEK 2022
In epilepsy, heart issues linked to longer disease duration
, but little is known about how they progress. A new study finds that abnormalities in electrocardiograms are linked to an earlier age of diagnosis and longer epilepsy duration.
The findings could help researchers in the search for biomarkers that could predict later problems in children with epilepsy. “In pediatric neurology I think we’re a little bit removed from some of the cardiovascular complications that can happen within epilepsy, but cardiovascular complications are well established, especially in adults that have epilepsy. Adults with epilepsy are more likely to have coronary artery disease, atherosclerosis, arrhythmias, heart attacks, and sudden cardiac death. It’s a pretty substantial difference compared with their nonepileptic peers. So knowing that, the big question is, how do these changes develop, and how do we really counsel our patients in regards to these complications?” said Brittnie Bartlett, MD, during her presentation of the research at the 2022 annual meeting of the Child Neurology Society.
Identifying factors that increase cardiac complications
Previous studies suggested that epilepsy duration might be linked to cardiovascular complications. In children with Dravet syndrome, epilepsy duration has been shown to be associated with cardiac complications. Pathological T wave alternans, which indicates ventricular instability, has been observed in adults with longstanding epilepsy but not adults with newly diagnosed epilepsy.
“So our question in this preliminary report of our data is: What factors in our general pediatric epilepsy cohort can we identify that put them at a greater risk for having EKG changes, and specifically, we wanted to verify these findings from the other studies that epilepsy duration is, in fact, a risk factor for these EKG changes in general [among children] with epilepsy aside from channelopathies,” said Dr. Bartlett, who is an assistant professor at Baylor College of Medicine and a child neurologist at Texas Children’s Hospital, both in Houston.
She presented a striking finding that cardiovascular changes appear early. “The most important thing I want you all to make note of is the fact that, in this baseline study that we got on these kids, 47% already had changes that we were seeing on their EKGs,” said Dr. Bartlett.
The researchers also looked for factors associated with EKG changes, and found that duration of epilepsy and age at diagnosis were the two salient factors. “Our kids that did have EKG changes present had an average epilepsy duration of 73 months, as opposed to [the children] that did not have EKG changes and had an average epilepsy duration of 46 months,” said Dr. Bartlett.
Other factors, such epilepsy type, etiology, refractory epilepsy, and seizure frequency had no statistically significant association with EKG changes. They also saw no associations with high-risk seizure medications, even though some antiseizure drugs have been shown to be linked to EKG changes.
“We were able to confirm our hypothesis that EKG changes were more prevalent with longer duration of epilepsy. Unfortunately, we weren’t able to find any other clues that would help us counsel our patients, but this is part of a longitudinal prospective study that we’ll be following these kids over a couple of years’ time, so maybe we’ll be able to tease out some of these differences. Ideally, we’d be able to find some kind of a biomarker for future cardiovascular complications, and right now we’re working with some multivariable models to verify some of these findings,” said Dr. Bartlett.
Implications for clinical practice
During the Q&A, Dr. Bartlett was asked if all kids with epilepsy should undergo an EKG. She recommended against it for now. “At this point, I don’t think we have enough clear data to support getting an EKG on every kid with epilepsy. I do think it’s good practice to do them on all kids with channelopathies. As a general practice, I tend to have a low threshold towards many kids with epilepsy, but a lot of these cardiovascular risk factors tend to pop up more in adulthood, so it’s more preventative,” she said.
Grace Gombolay, MD, who moderated the session where the poster was presented, was asked for comment on the study. “What’s surprising about it is that up to half of patients actually had EKG changes, different what from what we see in normal population, and it’s interesting to think about the implications. One of the things that our epilepsy patients are at risk for is SUDEP – sudden, unexplained death in epilepsy. It’s interesting to think about what these EKG changes mean for clinical care. I think it’s too early to say at this time, but this might be one of those markers for SUDEP,” said Dr. Gombolay, who is an assistant professor at Emory University, Atlanta, and director of the Pediatric Neuroimmunology and Multiple Sclerosis Clinic at Children’s Healthcare of Atlanta.
The researchers prospectively studied 213 patients who were recruited. 46% were female, 42% were white, 41% were Hispanic, and 13% were African American. The mean age at enrollment was 116 months, and mean age of seizure onset was 45 months.
The researchers found that 47% had abnormal EKG readings. None of the changes were pathologic, but they may reflect changes to cardiac electrophysiology, according to Dr. Bartlett. Those with abnormal readings were older on average (11.6 vs. 8.3 years; P < .005) and had a longer epilepsy duration (73 vs. 46 months; P = .004).
Dr. Gombolay has no relevant financial disclosures.
, but little is known about how they progress. A new study finds that abnormalities in electrocardiograms are linked to an earlier age of diagnosis and longer epilepsy duration.
The findings could help researchers in the search for biomarkers that could predict later problems in children with epilepsy. “In pediatric neurology I think we’re a little bit removed from some of the cardiovascular complications that can happen within epilepsy, but cardiovascular complications are well established, especially in adults that have epilepsy. Adults with epilepsy are more likely to have coronary artery disease, atherosclerosis, arrhythmias, heart attacks, and sudden cardiac death. It’s a pretty substantial difference compared with their nonepileptic peers. So knowing that, the big question is, how do these changes develop, and how do we really counsel our patients in regards to these complications?” said Brittnie Bartlett, MD, during her presentation of the research at the 2022 annual meeting of the Child Neurology Society.
Identifying factors that increase cardiac complications
Previous studies suggested that epilepsy duration might be linked to cardiovascular complications. In children with Dravet syndrome, epilepsy duration has been shown to be associated with cardiac complications. Pathological T wave alternans, which indicates ventricular instability, has been observed in adults with longstanding epilepsy but not adults with newly diagnosed epilepsy.
“So our question in this preliminary report of our data is: What factors in our general pediatric epilepsy cohort can we identify that put them at a greater risk for having EKG changes, and specifically, we wanted to verify these findings from the other studies that epilepsy duration is, in fact, a risk factor for these EKG changes in general [among children] with epilepsy aside from channelopathies,” said Dr. Bartlett, who is an assistant professor at Baylor College of Medicine and a child neurologist at Texas Children’s Hospital, both in Houston.
She presented a striking finding that cardiovascular changes appear early. “The most important thing I want you all to make note of is the fact that, in this baseline study that we got on these kids, 47% already had changes that we were seeing on their EKGs,” said Dr. Bartlett.
The researchers also looked for factors associated with EKG changes, and found that duration of epilepsy and age at diagnosis were the two salient factors. “Our kids that did have EKG changes present had an average epilepsy duration of 73 months, as opposed to [the children] that did not have EKG changes and had an average epilepsy duration of 46 months,” said Dr. Bartlett.
Other factors, such epilepsy type, etiology, refractory epilepsy, and seizure frequency had no statistically significant association with EKG changes. They also saw no associations with high-risk seizure medications, even though some antiseizure drugs have been shown to be linked to EKG changes.
“We were able to confirm our hypothesis that EKG changes were more prevalent with longer duration of epilepsy. Unfortunately, we weren’t able to find any other clues that would help us counsel our patients, but this is part of a longitudinal prospective study that we’ll be following these kids over a couple of years’ time, so maybe we’ll be able to tease out some of these differences. Ideally, we’d be able to find some kind of a biomarker for future cardiovascular complications, and right now we’re working with some multivariable models to verify some of these findings,” said Dr. Bartlett.
Implications for clinical practice
During the Q&A, Dr. Bartlett was asked if all kids with epilepsy should undergo an EKG. She recommended against it for now. “At this point, I don’t think we have enough clear data to support getting an EKG on every kid with epilepsy. I do think it’s good practice to do them on all kids with channelopathies. As a general practice, I tend to have a low threshold towards many kids with epilepsy, but a lot of these cardiovascular risk factors tend to pop up more in adulthood, so it’s more preventative,” she said.
Grace Gombolay, MD, who moderated the session where the poster was presented, was asked for comment on the study. “What’s surprising about it is that up to half of patients actually had EKG changes, different what from what we see in normal population, and it’s interesting to think about the implications. One of the things that our epilepsy patients are at risk for is SUDEP – sudden, unexplained death in epilepsy. It’s interesting to think about what these EKG changes mean for clinical care. I think it’s too early to say at this time, but this might be one of those markers for SUDEP,” said Dr. Gombolay, who is an assistant professor at Emory University, Atlanta, and director of the Pediatric Neuroimmunology and Multiple Sclerosis Clinic at Children’s Healthcare of Atlanta.
The researchers prospectively studied 213 patients who were recruited. 46% were female, 42% were white, 41% were Hispanic, and 13% were African American. The mean age at enrollment was 116 months, and mean age of seizure onset was 45 months.
The researchers found that 47% had abnormal EKG readings. None of the changes were pathologic, but they may reflect changes to cardiac electrophysiology, according to Dr. Bartlett. Those with abnormal readings were older on average (11.6 vs. 8.3 years; P < .005) and had a longer epilepsy duration (73 vs. 46 months; P = .004).
Dr. Gombolay has no relevant financial disclosures.
, but little is known about how they progress. A new study finds that abnormalities in electrocardiograms are linked to an earlier age of diagnosis and longer epilepsy duration.
The findings could help researchers in the search for biomarkers that could predict later problems in children with epilepsy. “In pediatric neurology I think we’re a little bit removed from some of the cardiovascular complications that can happen within epilepsy, but cardiovascular complications are well established, especially in adults that have epilepsy. Adults with epilepsy are more likely to have coronary artery disease, atherosclerosis, arrhythmias, heart attacks, and sudden cardiac death. It’s a pretty substantial difference compared with their nonepileptic peers. So knowing that, the big question is, how do these changes develop, and how do we really counsel our patients in regards to these complications?” said Brittnie Bartlett, MD, during her presentation of the research at the 2022 annual meeting of the Child Neurology Society.
Identifying factors that increase cardiac complications
Previous studies suggested that epilepsy duration might be linked to cardiovascular complications. In children with Dravet syndrome, epilepsy duration has been shown to be associated with cardiac complications. Pathological T wave alternans, which indicates ventricular instability, has been observed in adults with longstanding epilepsy but not adults with newly diagnosed epilepsy.
“So our question in this preliminary report of our data is: What factors in our general pediatric epilepsy cohort can we identify that put them at a greater risk for having EKG changes, and specifically, we wanted to verify these findings from the other studies that epilepsy duration is, in fact, a risk factor for these EKG changes in general [among children] with epilepsy aside from channelopathies,” said Dr. Bartlett, who is an assistant professor at Baylor College of Medicine and a child neurologist at Texas Children’s Hospital, both in Houston.
She presented a striking finding that cardiovascular changes appear early. “The most important thing I want you all to make note of is the fact that, in this baseline study that we got on these kids, 47% already had changes that we were seeing on their EKGs,” said Dr. Bartlett.
The researchers also looked for factors associated with EKG changes, and found that duration of epilepsy and age at diagnosis were the two salient factors. “Our kids that did have EKG changes present had an average epilepsy duration of 73 months, as opposed to [the children] that did not have EKG changes and had an average epilepsy duration of 46 months,” said Dr. Bartlett.
Other factors, such epilepsy type, etiology, refractory epilepsy, and seizure frequency had no statistically significant association with EKG changes. They also saw no associations with high-risk seizure medications, even though some antiseizure drugs have been shown to be linked to EKG changes.
“We were able to confirm our hypothesis that EKG changes were more prevalent with longer duration of epilepsy. Unfortunately, we weren’t able to find any other clues that would help us counsel our patients, but this is part of a longitudinal prospective study that we’ll be following these kids over a couple of years’ time, so maybe we’ll be able to tease out some of these differences. Ideally, we’d be able to find some kind of a biomarker for future cardiovascular complications, and right now we’re working with some multivariable models to verify some of these findings,” said Dr. Bartlett.
Implications for clinical practice
During the Q&A, Dr. Bartlett was asked if all kids with epilepsy should undergo an EKG. She recommended against it for now. “At this point, I don’t think we have enough clear data to support getting an EKG on every kid with epilepsy. I do think it’s good practice to do them on all kids with channelopathies. As a general practice, I tend to have a low threshold towards many kids with epilepsy, but a lot of these cardiovascular risk factors tend to pop up more in adulthood, so it’s more preventative,” she said.
Grace Gombolay, MD, who moderated the session where the poster was presented, was asked for comment on the study. “What’s surprising about it is that up to half of patients actually had EKG changes, different what from what we see in normal population, and it’s interesting to think about the implications. One of the things that our epilepsy patients are at risk for is SUDEP – sudden, unexplained death in epilepsy. It’s interesting to think about what these EKG changes mean for clinical care. I think it’s too early to say at this time, but this might be one of those markers for SUDEP,” said Dr. Gombolay, who is an assistant professor at Emory University, Atlanta, and director of the Pediatric Neuroimmunology and Multiple Sclerosis Clinic at Children’s Healthcare of Atlanta.
The researchers prospectively studied 213 patients who were recruited. 46% were female, 42% were white, 41% were Hispanic, and 13% were African American. The mean age at enrollment was 116 months, and mean age of seizure onset was 45 months.
The researchers found that 47% had abnormal EKG readings. None of the changes were pathologic, but they may reflect changes to cardiac electrophysiology, according to Dr. Bartlett. Those with abnormal readings were older on average (11.6 vs. 8.3 years; P < .005) and had a longer epilepsy duration (73 vs. 46 months; P = .004).
Dr. Gombolay has no relevant financial disclosures.
FROM CNS 2022
Rules for performing research with children
The road to hell is paved with good intentions – especially true in clinical research. A Food and Drug Administration press release notes, “Historically, children were not included in clinical trials because of a misperception that excluding them from research was in fact protecting them. This resulted in many FDA-approved, licensed, cleared, or authorized drugs, biological products, and medical devices lacking pediatric-specific labeling information.” In an effort to improve on this situation, the FDA published in September 2022 a proposed new draft guidance on performing research with children that is open for public comment for 3 months.

There is a long history of government attempts to promote research and development for the benefit of society. Sometimes government succeeds and sometimes not. For instance, when the U.S. federal government funded scientific research in the 1960s, it sought to increase the common good by promulgating those discoveries. The government insisted that all federally funded research be in the public domain. The funding produced a spectacular number of technological advancements that have enriched society. However, a decade later, the government concluded that too many good research ideas were never developed into beneficial products because without the ability to patent the results, the costs and risks of product development were not profitable for industry. By the late 1970s, new laws were enacted to enable universities and their faculty to patent the results of government-funded research and share in any wealth created.
Pharmaceutical research in the 1970s and 1980s was mostly performed on men in order to reduce the risk of giving treatments of unknown safety to pregnant women. The unintended consequence was that the new drugs frequently were less effective for women. This was particularly true for cardiac medications for which lifestyle risk factors differed between the sexes.
Similarly, children were often excluded from research because of the unknown risks of new drugs on growing bodies and brains. Children were also seen as a vulnerable population for whom informed consent was problematic. The result of these well-intentioned restrictions was the creation of new products that did not have pediatric dosing recommendations, pediatric safety assessments, or approval for pediatric indications. To remediate these deficiencies, in 1997 and 2007 the FDA offered a 6-month extension on patent protection as motivation for companies to develop those pediatric recommendations. Alas, those laws were primarily used to extend the profitability of blockbuster products rather than truly benefit children.
Over the past 4 decades, pediatric ethicists proposed and refined rules to govern research on children. The Common Rule used by institutional review boards (IRBs) to protect human research subjects was expanded with guidelines covering children. The new draft guidance is the latest iteration of this effort. Nothing in the 14 pages of draft regulation appears revolutionary to me. The ideas are tweaks, based on theory and experience, of principles agreed upon 30 years ago. Finding the optimal social moral contract involves some empirical assessment of praxis and effectiveness.
I am loathe to summarize this new document, which itself is a summary of a vast body of literature, that supports the Code of Federal Regulations Title 21 Part 50 and 45 CFR Part 46. The draft document is well organized and I recommend it as an excellent primer for the area of pediatric research ethics if the subject is new to you. I also recommend it as required reading for anyone serving on an IRB.
IRBs usually review and approve any research on people. Generally, the selection of people for research should be done equitably. However, children should not be enrolled unless it is necessary to answer an important question relevant to children. For the past 2 decades, there has been an emphasis on obtaining the assent of the child as well as informed consent by the parents.
An important determination is whether the research is likely to help that particular child or whether it is aimed at advancing general knowledge. If there is no prospect of direct benefit, research is still permissible but more restricted for safety and comfort reasons. Next is determining whether the research carries only minimal risk or a minor increase over minimal risk. The draft defines and provides anchor examples of these situations. For instance, oral placebos and single blood draws are typically minimal risk. Multiple injections and blood draws over a year fall into the second category. One MRI is minimal risk but a minor increase in risk if it involves sedation or contrast.
I strongly support the ideals expressed in these guidelines. They represent the best blend of intentions and practical experience. They will become the law of the land. In ethics, there is merit in striving to do things properly, orderly, and enforceably.
The cynic in me sees two weaknesses in the stated approach. First, the volume of harm to children occurring during organized clinical research is extremely small. The greater harms come from off-label use, nonsystematic research, and the ignorance resulting from a lack of research. Second, my observation in all endeavors of morality is, “Raise the bar high enough and people walk under it.”
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
The road to hell is paved with good intentions – especially true in clinical research. A Food and Drug Administration press release notes, “Historically, children were not included in clinical trials because of a misperception that excluding them from research was in fact protecting them. This resulted in many FDA-approved, licensed, cleared, or authorized drugs, biological products, and medical devices lacking pediatric-specific labeling information.” In an effort to improve on this situation, the FDA published in September 2022 a proposed new draft guidance on performing research with children that is open for public comment for 3 months.
There is a long history of government attempts to promote research and development for the benefit of society. Sometimes government succeeds and sometimes not. For instance, when the U.S. federal government funded scientific research in the 1960s, it sought to increase the common good by promulgating those discoveries. The government insisted that all federally funded research be in the public domain. The funding produced a spectacular number of technological advancements that have enriched society. However, a decade later, the government concluded that too many good research ideas were never developed into beneficial products because without the ability to patent the results, the costs and risks of product development were not profitable for industry. By the late 1970s, new laws were enacted to enable universities and their faculty to patent the results of government-funded research and share in any wealth created.
Pharmaceutical research in the 1970s and 1980s was mostly performed on men in order to reduce the risk of giving treatments of unknown safety to pregnant women. The unintended consequence was that the new drugs frequently were less effective for women. This was particularly true for cardiac medications for which lifestyle risk factors differed between the sexes.
Similarly, children were often excluded from research because of the unknown risks of new drugs on growing bodies and brains. Children were also seen as a vulnerable population for whom informed consent was problematic. The result of these well-intentioned restrictions was the creation of new products that did not have pediatric dosing recommendations, pediatric safety assessments, or approval for pediatric indications. To remediate these deficiencies, in 1997 and 2007 the FDA offered a 6-month extension on patent protection as motivation for companies to develop those pediatric recommendations. Alas, those laws were primarily used to extend the profitability of blockbuster products rather than truly benefit children.
Over the past 4 decades, pediatric ethicists proposed and refined rules to govern research on children. The Common Rule used by institutional review boards (IRBs) to protect human research subjects was expanded with guidelines covering children. The new draft guidance is the latest iteration of this effort. Nothing in the 14 pages of draft regulation appears revolutionary to me. The ideas are tweaks, based on theory and experience, of principles agreed upon 30 years ago. Finding the optimal social moral contract involves some empirical assessment of praxis and effectiveness.
I am loathe to summarize this new document, which itself is a summary of a vast body of literature, that supports the Code of Federal Regulations Title 21 Part 50 and 45 CFR Part 46. The draft document is well organized and I recommend it as an excellent primer for the area of pediatric research ethics if the subject is new to you. I also recommend it as required reading for anyone serving on an IRB.
IRBs usually review and approve any research on people. Generally, the selection of people for research should be done equitably. However, children should not be enrolled unless it is necessary to answer an important question relevant to children. For the past 2 decades, there has been an emphasis on obtaining the assent of the child as well as informed consent by the parents.
An important determination is whether the research is likely to help that particular child or whether it is aimed at advancing general knowledge. If there is no prospect of direct benefit, research is still permissible but more restricted for safety and comfort reasons. Next is determining whether the research carries only minimal risk or a minor increase over minimal risk. The draft defines and provides anchor examples of these situations. For instance, oral placebos and single blood draws are typically minimal risk. Multiple injections and blood draws over a year fall into the second category. One MRI is minimal risk but a minor increase in risk if it involves sedation or contrast.
I strongly support the ideals expressed in these guidelines. They represent the best blend of intentions and practical experience. They will become the law of the land. In ethics, there is merit in striving to do things properly, orderly, and enforceably.
The cynic in me sees two weaknesses in the stated approach. First, the volume of harm to children occurring during organized clinical research is extremely small. The greater harms come from off-label use, nonsystematic research, and the ignorance resulting from a lack of research. Second, my observation in all endeavors of morality is, “Raise the bar high enough and people walk under it.”
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
The road to hell is paved with good intentions – especially true in clinical research. A Food and Drug Administration press release notes, “Historically, children were not included in clinical trials because of a misperception that excluding them from research was in fact protecting them. This resulted in many FDA-approved, licensed, cleared, or authorized drugs, biological products, and medical devices lacking pediatric-specific labeling information.” In an effort to improve on this situation, the FDA published in September 2022 a proposed new draft guidance on performing research with children that is open for public comment for 3 months.
There is a long history of government attempts to promote research and development for the benefit of society. Sometimes government succeeds and sometimes not. For instance, when the U.S. federal government funded scientific research in the 1960s, it sought to increase the common good by promulgating those discoveries. The government insisted that all federally funded research be in the public domain. The funding produced a spectacular number of technological advancements that have enriched society. However, a decade later, the government concluded that too many good research ideas were never developed into beneficial products because without the ability to patent the results, the costs and risks of product development were not profitable for industry. By the late 1970s, new laws were enacted to enable universities and their faculty to patent the results of government-funded research and share in any wealth created.
Pharmaceutical research in the 1970s and 1980s was mostly performed on men in order to reduce the risk of giving treatments of unknown safety to pregnant women. The unintended consequence was that the new drugs frequently were less effective for women. This was particularly true for cardiac medications for which lifestyle risk factors differed between the sexes.
Similarly, children were often excluded from research because of the unknown risks of new drugs on growing bodies and brains. Children were also seen as a vulnerable population for whom informed consent was problematic. The result of these well-intentioned restrictions was the creation of new products that did not have pediatric dosing recommendations, pediatric safety assessments, or approval for pediatric indications. To remediate these deficiencies, in 1997 and 2007 the FDA offered a 6-month extension on patent protection as motivation for companies to develop those pediatric recommendations. Alas, those laws were primarily used to extend the profitability of blockbuster products rather than truly benefit children.
Over the past 4 decades, pediatric ethicists proposed and refined rules to govern research on children. The Common Rule used by institutional review boards (IRBs) to protect human research subjects was expanded with guidelines covering children. The new draft guidance is the latest iteration of this effort. Nothing in the 14 pages of draft regulation appears revolutionary to me. The ideas are tweaks, based on theory and experience, of principles agreed upon 30 years ago. Finding the optimal social moral contract involves some empirical assessment of praxis and effectiveness.
I am loathe to summarize this new document, which itself is a summary of a vast body of literature, that supports the Code of Federal Regulations Title 21 Part 50 and 45 CFR Part 46. The draft document is well organized and I recommend it as an excellent primer for the area of pediatric research ethics if the subject is new to you. I also recommend it as required reading for anyone serving on an IRB.
IRBs usually review and approve any research on people. Generally, the selection of people for research should be done equitably. However, children should not be enrolled unless it is necessary to answer an important question relevant to children. For the past 2 decades, there has been an emphasis on obtaining the assent of the child as well as informed consent by the parents.
An important determination is whether the research is likely to help that particular child or whether it is aimed at advancing general knowledge. If there is no prospect of direct benefit, research is still permissible but more restricted for safety and comfort reasons. Next is determining whether the research carries only minimal risk or a minor increase over minimal risk. The draft defines and provides anchor examples of these situations. For instance, oral placebos and single blood draws are typically minimal risk. Multiple injections and blood draws over a year fall into the second category. One MRI is minimal risk but a minor increase in risk if it involves sedation or contrast.
I strongly support the ideals expressed in these guidelines. They represent the best blend of intentions and practical experience. They will become the law of the land. In ethics, there is merit in striving to do things properly, orderly, and enforceably.
The cynic in me sees two weaknesses in the stated approach. First, the volume of harm to children occurring during organized clinical research is extremely small. The greater harms come from off-label use, nonsystematic research, and the ignorance resulting from a lack of research. Second, my observation in all endeavors of morality is, “Raise the bar high enough and people walk under it.”
Dr. Powell is a retired pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
Why the 5-day isolation period for COVID makes no sense
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
One of the more baffling decisions the CDC made during this pandemic was when they reduced the duration of isolation after a positive COVID test from 10 days to 5 days and did not require a negative antigen test to end isolation.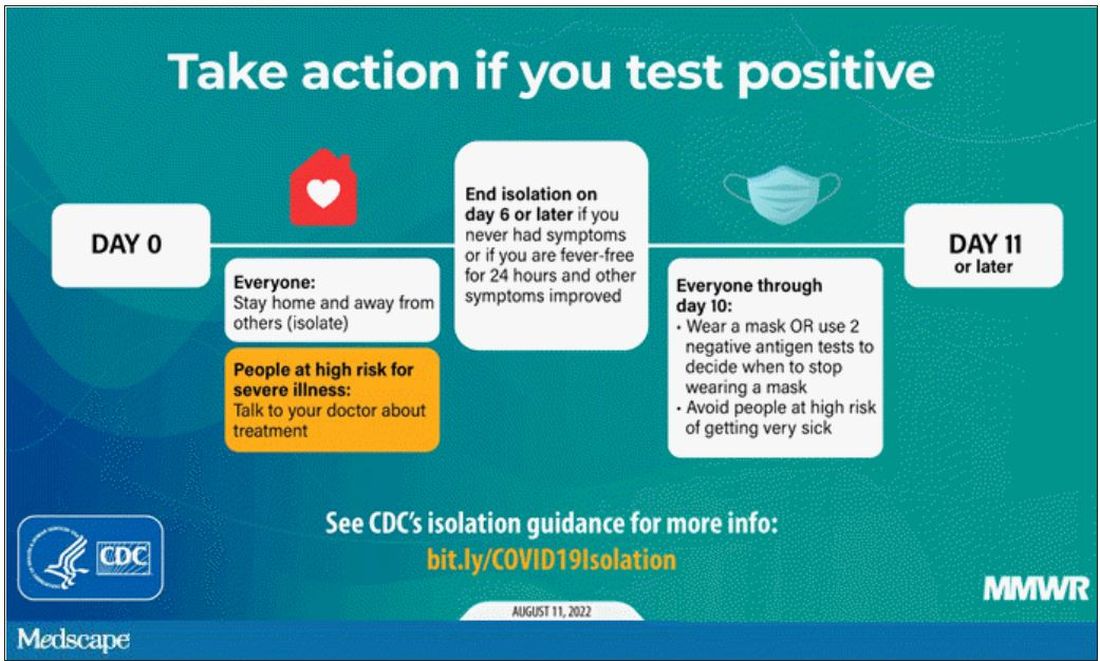
Multiple studies had suggested, after all, that positive antigen tests, while not perfect, were a decent proxy for infectivity. And if the purpose of isolation is to keep other community members safe, why not use a readily available test to know when it might be safe to go out in public again?
Also, 5 days just wasn’t that much time. Many individuals are symptomatic long after that point. Many people test positive long after that point. What exactly is the point of the 5-day isolation period?
We got some hard numbers this week to show just how good (or bad) an arbitrary-seeming 5-day isolation period is, thanks to this study from JAMA Network Open, which gives us a low-end estimate for the proportion of people who remain positive on antigen tests, which is to say infectious, after an isolation period.
This study estimates the low end of postisolation infectivity because of the study population: student athletes at an NCAA Division I school, which may or may not be Stanford. These athletes tested positive for COVID after having at least one dose of vaccine from January to May 2022. School protocol was to put the students in isolation for 7 days, at which time they could “test out” with a negative antigen test.
Put simply, these were healthy people. They were young. They were athletes. They were vaccinated. If anyone is going to have a brief, easy COVID course, it would be them. And they are doing at least a week of isolation, not 5 days.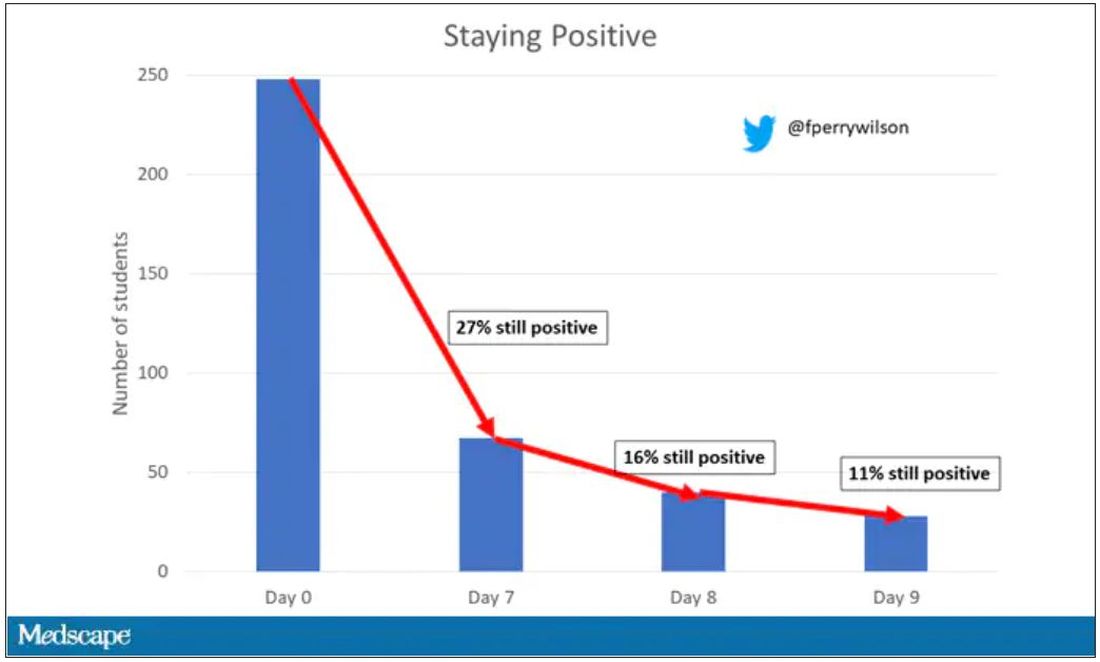
So – isolation for 7 days. Antigen testing on day 7. How many still tested positive? Of 248 individuals tested, 67 (27%) tested positive. One in four.
More than half of those positive on day 7 tested positive on day 8, and more than half of those tested positive again on day 9. By day 10, they were released from isolation without further testing.
So, right there .
There were some predictors of prolonged positivity.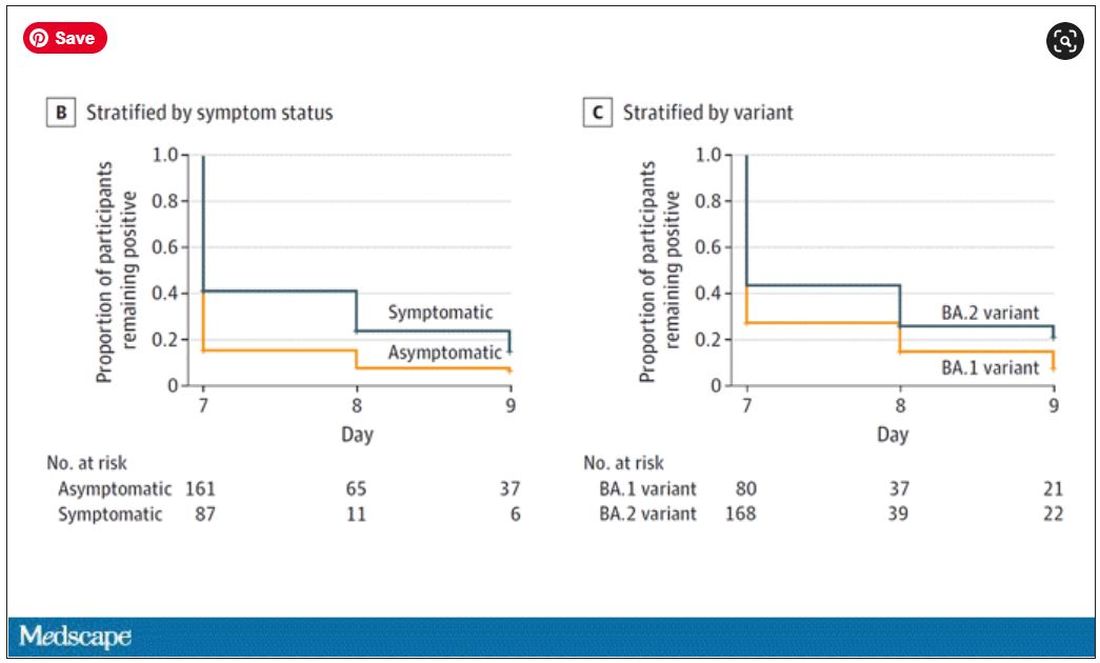
Symptomatic athletes were much more likely to test positive than asymptomatic athletes.
And the particular variant seemed to matter as well. In this time period, BA.1 and BA.2 were dominant, and it was pretty clear that BA.2 persisted longer than BA.1.
This brings me back to my original question: What is the point of the 5-day isolation period? On the basis of this study, you could imagine a guideline based on symptoms: Stay home until you feel better. You could imagine a guideline based on testing: Stay home until you test negative. A guideline based on time alone just doesn’t comport with the data. The benefit of policies based on symptoms or testing are obvious; some people would be out of isolation even before 5 days. But the downside, of course, is that some people would be stuck in isolation for much longer.
Maybe we should just say it. At this point, you could even imagine there being no recommendation at all – no isolation period. Like, you just stay home if you feel like you should stay home. I’m not entirely sure that such a policy would necessarily result in a greater number of infectious people out in the community.
In any case, as the arbitrariness of this particular 5-day isolation policy becomes more clear, the policy itself may be living on borrowed time.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and hosts a repository of his communication work at www.methodsman.com. He disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
One of the more baffling decisions the CDC made during this pandemic was when they reduced the duration of isolation after a positive COVID test from 10 days to 5 days and did not require a negative antigen test to end isolation.
Multiple studies had suggested, after all, that positive antigen tests, while not perfect, were a decent proxy for infectivity. And if the purpose of isolation is to keep other community members safe, why not use a readily available test to know when it might be safe to go out in public again?
Also, 5 days just wasn’t that much time. Many individuals are symptomatic long after that point. Many people test positive long after that point. What exactly is the point of the 5-day isolation period?
We got some hard numbers this week to show just how good (or bad) an arbitrary-seeming 5-day isolation period is, thanks to this study from JAMA Network Open, which gives us a low-end estimate for the proportion of people who remain positive on antigen tests, which is to say infectious, after an isolation period.
This study estimates the low end of postisolation infectivity because of the study population: student athletes at an NCAA Division I school, which may or may not be Stanford. These athletes tested positive for COVID after having at least one dose of vaccine from January to May 2022. School protocol was to put the students in isolation for 7 days, at which time they could “test out” with a negative antigen test.
Put simply, these were healthy people. They were young. They were athletes. They were vaccinated. If anyone is going to have a brief, easy COVID course, it would be them. And they are doing at least a week of isolation, not 5 days.
So – isolation for 7 days. Antigen testing on day 7. How many still tested positive? Of 248 individuals tested, 67 (27%) tested positive. One in four.
More than half of those positive on day 7 tested positive on day 8, and more than half of those tested positive again on day 9. By day 10, they were released from isolation without further testing.
So, right there .
There were some predictors of prolonged positivity.
Symptomatic athletes were much more likely to test positive than asymptomatic athletes.
And the particular variant seemed to matter as well. In this time period, BA.1 and BA.2 were dominant, and it was pretty clear that BA.2 persisted longer than BA.1.
This brings me back to my original question: What is the point of the 5-day isolation period? On the basis of this study, you could imagine a guideline based on symptoms: Stay home until you feel better. You could imagine a guideline based on testing: Stay home until you test negative. A guideline based on time alone just doesn’t comport with the data. The benefit of policies based on symptoms or testing are obvious; some people would be out of isolation even before 5 days. But the downside, of course, is that some people would be stuck in isolation for much longer.
Maybe we should just say it. At this point, you could even imagine there being no recommendation at all – no isolation period. Like, you just stay home if you feel like you should stay home. I’m not entirely sure that such a policy would necessarily result in a greater number of infectious people out in the community.
In any case, as the arbitrariness of this particular 5-day isolation policy becomes more clear, the policy itself may be living on borrowed time.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and hosts a repository of his communication work at www.methodsman.com. He disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
One of the more baffling decisions the CDC made during this pandemic was when they reduced the duration of isolation after a positive COVID test from 10 days to 5 days and did not require a negative antigen test to end isolation.
Multiple studies had suggested, after all, that positive antigen tests, while not perfect, were a decent proxy for infectivity. And if the purpose of isolation is to keep other community members safe, why not use a readily available test to know when it might be safe to go out in public again?
Also, 5 days just wasn’t that much time. Many individuals are symptomatic long after that point. Many people test positive long after that point. What exactly is the point of the 5-day isolation period?
We got some hard numbers this week to show just how good (or bad) an arbitrary-seeming 5-day isolation period is, thanks to this study from JAMA Network Open, which gives us a low-end estimate for the proportion of people who remain positive on antigen tests, which is to say infectious, after an isolation period.
This study estimates the low end of postisolation infectivity because of the study population: student athletes at an NCAA Division I school, which may or may not be Stanford. These athletes tested positive for COVID after having at least one dose of vaccine from January to May 2022. School protocol was to put the students in isolation for 7 days, at which time they could “test out” with a negative antigen test.
Put simply, these were healthy people. They were young. They were athletes. They were vaccinated. If anyone is going to have a brief, easy COVID course, it would be them. And they are doing at least a week of isolation, not 5 days.
So – isolation for 7 days. Antigen testing on day 7. How many still tested positive? Of 248 individuals tested, 67 (27%) tested positive. One in four.
More than half of those positive on day 7 tested positive on day 8, and more than half of those tested positive again on day 9. By day 10, they were released from isolation without further testing.
So, right there .
There were some predictors of prolonged positivity.
Symptomatic athletes were much more likely to test positive than asymptomatic athletes.
And the particular variant seemed to matter as well. In this time period, BA.1 and BA.2 were dominant, and it was pretty clear that BA.2 persisted longer than BA.1.
This brings me back to my original question: What is the point of the 5-day isolation period? On the basis of this study, you could imagine a guideline based on symptoms: Stay home until you feel better. You could imagine a guideline based on testing: Stay home until you test negative. A guideline based on time alone just doesn’t comport with the data. The benefit of policies based on symptoms or testing are obvious; some people would be out of isolation even before 5 days. But the downside, of course, is that some people would be stuck in isolation for much longer.
Maybe we should just say it. At this point, you could even imagine there being no recommendation at all – no isolation period. Like, you just stay home if you feel like you should stay home. I’m not entirely sure that such a policy would necessarily result in a greater number of infectious people out in the community.
In any case, as the arbitrariness of this particular 5-day isolation policy becomes more clear, the policy itself may be living on borrowed time.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and hosts a repository of his communication work at www.methodsman.com. He disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
NICU signs hint at cerebral palsy risk
CINCINNATI – Cerebral palsy affects about 3 in every 1,000 children, but there is usually little sign of the condition at birth. Instead, it usually shows clinical manifestation between ages 2 and 5, and a diagnosis can trigger early interventions that can improve long-term outcomes.
Physicians and patients would benefit from a screening method for cerebral palsy at birth, but that has so far eluded researchers.
At the 2022 annual meeting of the Child Neurology Society, researchers presented evidence that , with higher variability associated with increased cerebral palsy risk.
The study results were promising, according to Marc Patterson, MD, who comoderated the session. “It gives us more confidence in predicting the children at risk and making sure that they’re going to be followed closely to get the interventions they need to help them,” said Dr. Patterson, who is a professor of neurology, pediatrics, and medical genetics at Mayo Medical School in Rochester, Minn.
“By the time a child is 5 or 6, the symptoms are usually very obvious, but you really want to intervene as soon as possible before their brain’s plasticity decreases over time, so the earlier you can intervene in general, the better your results are going to be,” said Dr. Patterson.
There are tools available to diagnose cerebral palsy at an earlier age, including the Prechtl General Movements Assessment (GMA), which can be done up to 5 months of corrected age. It has 97% sensitivity and 89% specificity for cerebral palsy. The Hammersmith Infant Neurological Examination (HINE), which can be used in the same age range, and has 72-91% sensitivity and 100% specificity.
Both of the available tools are resource intensive and require trained clinicians, and may be unavailable in many areas. Despite these tools, early diagnosis of cerebral palsy is still underemployed, according to Arohi Saxena, a third-year medical student at Washington University in St. Louis, who presented the study results.
Respiratory rate variability may indicate increased risk
The researchers set out to identify objective metrics that correlated with HINE and GMA scores. They looked at kinematic data from practical assessments carried out by their physical therapists, as well as vital sign instability obtained at NICU discharge, which was based on suggestions that hemodynamic instability may be linked to later risk of cerebral palsy, according to Ms. Saxena.
They analyzed data from 31 infants with a corrected age of 8-25 weeks at a tertiary NICU follow-up clinic. Of these, 18 displayed fidgety movements on their Prechtl assessment, and 13 did not.
They used DeepLabCut software to analyze data from videos of the Prechtl assessment, with a focus on range and variance of hand and foot movements normalized to nose-to-umbilicus distance. They also analyzed pulse and respiratory data from the final 24 hours before NICU discharge.
They found that infants without fidgety movements had decreased hand and foot movement ranges (P = .04). There was no significant difference between the two groups with respect to pulse measurements. However, the respiratory rate range and variance was significantly higher in infants without fidgety movements. “Infants who are at higher risk for developing cerebral palsy had more respiratory instability early on in life,” said Ms. Saxena during her talk.
When they compared values to HINE scores, they found a correlation with less foot movement and a predisposition to develop cerebral palsy, but no correlation with hand movement. A lower HINE sore also correlated to larger respiratory rate range and variance (P < .01 for both).
“Our hypothesis to explain this link is that respiratory rate variability is likely driven by neonatal injury in the brainstem, where the respiratory centers are located. In some infants, this may correlate with more extensive cerebral injury that could predict the development of cerebral palsy,” said Ms. Saxena.
The group plans to increase its sample size as well as to conduct long-term follow-up on the infants to see how many receive formal diagnoses of cerebral palsy.
After her talk, asked by a moderator why motor assessments were not a reliable predictor in their study, Ms. Saxena pointed to the inexperience of assessors at the institution, where Prechtl testing had only recently begun.
“I think a lot of it is to do with the more subjective nature of the motor assessment. We definitely saw kind of a trend where in the earlier data that was collected, right when our institutions started doing these Prechtls, it was even less of a reliable effect. So I think possibly as clinicians continue to get more familiar with this assessment and there’s more like a validated and robust scoring system, maybe we’ll see a stronger correlation,” she said.
Ms. Saxena had no relevant disclosures. Coauthor Boomah Aravamuthan, MD, DPhil, is a consultant for Neurocrine Biosciences and has received royalties from UpToDate and funding from the National Institute of Neurological Disorders and Stroke.
CINCINNATI – Cerebral palsy affects about 3 in every 1,000 children, but there is usually little sign of the condition at birth. Instead, it usually shows clinical manifestation between ages 2 and 5, and a diagnosis can trigger early interventions that can improve long-term outcomes.
Physicians and patients would benefit from a screening method for cerebral palsy at birth, but that has so far eluded researchers.
At the 2022 annual meeting of the Child Neurology Society, researchers presented evidence that , with higher variability associated with increased cerebral palsy risk.
The study results were promising, according to Marc Patterson, MD, who comoderated the session. “It gives us more confidence in predicting the children at risk and making sure that they’re going to be followed closely to get the interventions they need to help them,” said Dr. Patterson, who is a professor of neurology, pediatrics, and medical genetics at Mayo Medical School in Rochester, Minn.
“By the time a child is 5 or 6, the symptoms are usually very obvious, but you really want to intervene as soon as possible before their brain’s plasticity decreases over time, so the earlier you can intervene in general, the better your results are going to be,” said Dr. Patterson.
There are tools available to diagnose cerebral palsy at an earlier age, including the Prechtl General Movements Assessment (GMA), which can be done up to 5 months of corrected age. It has 97% sensitivity and 89% specificity for cerebral palsy. The Hammersmith Infant Neurological Examination (HINE), which can be used in the same age range, and has 72-91% sensitivity and 100% specificity.
Both of the available tools are resource intensive and require trained clinicians, and may be unavailable in many areas. Despite these tools, early diagnosis of cerebral palsy is still underemployed, according to Arohi Saxena, a third-year medical student at Washington University in St. Louis, who presented the study results.
Respiratory rate variability may indicate increased risk
The researchers set out to identify objective metrics that correlated with HINE and GMA scores. They looked at kinematic data from practical assessments carried out by their physical therapists, as well as vital sign instability obtained at NICU discharge, which was based on suggestions that hemodynamic instability may be linked to later risk of cerebral palsy, according to Ms. Saxena.
They analyzed data from 31 infants with a corrected age of 8-25 weeks at a tertiary NICU follow-up clinic. Of these, 18 displayed fidgety movements on their Prechtl assessment, and 13 did not.
They used DeepLabCut software to analyze data from videos of the Prechtl assessment, with a focus on range and variance of hand and foot movements normalized to nose-to-umbilicus distance. They also analyzed pulse and respiratory data from the final 24 hours before NICU discharge.
They found that infants without fidgety movements had decreased hand and foot movement ranges (P = .04). There was no significant difference between the two groups with respect to pulse measurements. However, the respiratory rate range and variance was significantly higher in infants without fidgety movements. “Infants who are at higher risk for developing cerebral palsy had more respiratory instability early on in life,” said Ms. Saxena during her talk.
When they compared values to HINE scores, they found a correlation with less foot movement and a predisposition to develop cerebral palsy, but no correlation with hand movement. A lower HINE sore also correlated to larger respiratory rate range and variance (P < .01 for both).
“Our hypothesis to explain this link is that respiratory rate variability is likely driven by neonatal injury in the brainstem, where the respiratory centers are located. In some infants, this may correlate with more extensive cerebral injury that could predict the development of cerebral palsy,” said Ms. Saxena.
The group plans to increase its sample size as well as to conduct long-term follow-up on the infants to see how many receive formal diagnoses of cerebral palsy.
After her talk, asked by a moderator why motor assessments were not a reliable predictor in their study, Ms. Saxena pointed to the inexperience of assessors at the institution, where Prechtl testing had only recently begun.
“I think a lot of it is to do with the more subjective nature of the motor assessment. We definitely saw kind of a trend where in the earlier data that was collected, right when our institutions started doing these Prechtls, it was even less of a reliable effect. So I think possibly as clinicians continue to get more familiar with this assessment and there’s more like a validated and robust scoring system, maybe we’ll see a stronger correlation,” she said.
Ms. Saxena had no relevant disclosures. Coauthor Boomah Aravamuthan, MD, DPhil, is a consultant for Neurocrine Biosciences and has received royalties from UpToDate and funding from the National Institute of Neurological Disorders and Stroke.
CINCINNATI – Cerebral palsy affects about 3 in every 1,000 children, but there is usually little sign of the condition at birth. Instead, it usually shows clinical manifestation between ages 2 and 5, and a diagnosis can trigger early interventions that can improve long-term outcomes.
Physicians and patients would benefit from a screening method for cerebral palsy at birth, but that has so far eluded researchers.
At the 2022 annual meeting of the Child Neurology Society, researchers presented evidence that , with higher variability associated with increased cerebral palsy risk.
The study results were promising, according to Marc Patterson, MD, who comoderated the session. “It gives us more confidence in predicting the children at risk and making sure that they’re going to be followed closely to get the interventions they need to help them,” said Dr. Patterson, who is a professor of neurology, pediatrics, and medical genetics at Mayo Medical School in Rochester, Minn.
“By the time a child is 5 or 6, the symptoms are usually very obvious, but you really want to intervene as soon as possible before their brain’s plasticity decreases over time, so the earlier you can intervene in general, the better your results are going to be,” said Dr. Patterson.
There are tools available to diagnose cerebral palsy at an earlier age, including the Prechtl General Movements Assessment (GMA), which can be done up to 5 months of corrected age. It has 97% sensitivity and 89% specificity for cerebral palsy. The Hammersmith Infant Neurological Examination (HINE), which can be used in the same age range, and has 72-91% sensitivity and 100% specificity.
Both of the available tools are resource intensive and require trained clinicians, and may be unavailable in many areas. Despite these tools, early diagnosis of cerebral palsy is still underemployed, according to Arohi Saxena, a third-year medical student at Washington University in St. Louis, who presented the study results.
Respiratory rate variability may indicate increased risk
The researchers set out to identify objective metrics that correlated with HINE and GMA scores. They looked at kinematic data from practical assessments carried out by their physical therapists, as well as vital sign instability obtained at NICU discharge, which was based on suggestions that hemodynamic instability may be linked to later risk of cerebral palsy, according to Ms. Saxena.
They analyzed data from 31 infants with a corrected age of 8-25 weeks at a tertiary NICU follow-up clinic. Of these, 18 displayed fidgety movements on their Prechtl assessment, and 13 did not.
They used DeepLabCut software to analyze data from videos of the Prechtl assessment, with a focus on range and variance of hand and foot movements normalized to nose-to-umbilicus distance. They also analyzed pulse and respiratory data from the final 24 hours before NICU discharge.
They found that infants without fidgety movements had decreased hand and foot movement ranges (P = .04). There was no significant difference between the two groups with respect to pulse measurements. However, the respiratory rate range and variance was significantly higher in infants without fidgety movements. “Infants who are at higher risk for developing cerebral palsy had more respiratory instability early on in life,” said Ms. Saxena during her talk.
When they compared values to HINE scores, they found a correlation with less foot movement and a predisposition to develop cerebral palsy, but no correlation with hand movement. A lower HINE sore also correlated to larger respiratory rate range and variance (P < .01 for both).
“Our hypothesis to explain this link is that respiratory rate variability is likely driven by neonatal injury in the brainstem, where the respiratory centers are located. In some infants, this may correlate with more extensive cerebral injury that could predict the development of cerebral palsy,” said Ms. Saxena.
The group plans to increase its sample size as well as to conduct long-term follow-up on the infants to see how many receive formal diagnoses of cerebral palsy.
After her talk, asked by a moderator why motor assessments were not a reliable predictor in their study, Ms. Saxena pointed to the inexperience of assessors at the institution, where Prechtl testing had only recently begun.
“I think a lot of it is to do with the more subjective nature of the motor assessment. We definitely saw kind of a trend where in the earlier data that was collected, right when our institutions started doing these Prechtls, it was even less of a reliable effect. So I think possibly as clinicians continue to get more familiar with this assessment and there’s more like a validated and robust scoring system, maybe we’ll see a stronger correlation,” she said.
Ms. Saxena had no relevant disclosures. Coauthor Boomah Aravamuthan, MD, DPhil, is a consultant for Neurocrine Biosciences and has received royalties from UpToDate and funding from the National Institute of Neurological Disorders and Stroke.
FROM CNS 2022
Asthma ED visits predict failed housing inspections
, according to a new study presented at the annual meeting of the American College of Emergency Physicians.
While links between asthma and low-quality housing prone to harboring allergens have been well-documented, the current study takes the extra step of looking at housing down to the level of individual land parcels and suggests that asthma hospital visits can be used to identify hazardous housing earlier.
“Emergency department visits for asthma provide a leading indicator that can be used by health departments or housing authorities to direct housing inspections and remediation of poor housing conditions, track improvements in housing quality, measure housing department performance, support resident grievances, and inform funding allocation decisions,” said the study’s lead researcher, Elizabeth Samuels, MD, who is assistant professor of epidemiology and emergency medicine at Brown University, Providence, R.I.
Researchers retrospectively looked at cases of children and adults in the Greater New Haven area of Connecticut seen at the Yale New Haven Hospital ED for asthma-related problems between March 2013 and August 2017. The region has the fifth-highest prevalence of asthma in the United States, the researchers point out, due to its air quality, pollens, and quality of its housing. More than half of residences were built before 1,940, compared with about 13% nationally. Patient addresses were matched with HUD inspection records.
The review encompassed 11,429 ED visits by 6,366 individuals; 54% were insured by Medicaid, and 42% were Black. Controlling for patient and neighborhood data, researchers found that increased asthma ED visits at the parcel level were associated with decreased HUD inspection scores to a highly significant degree (P < .001).
They also found that there was a relationship in terms of timing between asthma ED visits and inspection scores: asthma ED visits increased more than 1 year before a failed HUD inspection. They also found that asthma ED visits were not elevated at housing units that passed inspection. Using asthma ED visits to predict failed housing inspections produced a specificity rate of 92.3% in an adjusted model, Dr. Samuels noted.
“This approach represents a novel method of early identification of dangerous housing conditions, which could aid in the prevention of asthma-related morbidity and mortality,” Dr. Samuels said.
The investigators noted that, of the parcels with the top three incidence rates of asthma ED visits, “all of them have been closed or demolished.”
In addition to limiting exposure of patients with asthma to the allergens of mold, mice and rats, and cockroaches, improving poor-quality housing earlier could help asthma by reducing stress, she said.
“There is also an increasing evidence base that psychosocial stress increases the risk of asthma attacks, and it’s therefore possible that living in poor housing conditions – often highly stressful situations – drives exacerbation risk via this pathway,” she said. “Synergistic effects between these pathways are also possible or even likely.”
Neeta Thakur, MD, associate professor of medicine at the University of California, San Francisco, who researches asthma, said the findings could lead to a strategy for improving poor-quality housing more quickly. As it is, inspections are too infrequent, often prompted by resident complaints.
“Once the complaints get to a certain threshold, then there might be an inspection that happens, and if there is a periodic review of the buildings, they often happen few and far between,” she said. “We could actually use some of the information that we’re already getting from something like ED visits and see if there is a pattern.”
An important follow-up would be to see whether asthma outcomes improve after housing deficiencies are addressed and whether the predictive capacity of ED visits occurs in other places.
“Would you then see a decline in the ED visit rates from individuals living in those buildings?” Dr. Thakur said. “It’s important to find a leading indicator, but you want to be sure that that leading indicator is useful as something that can be intervened upon.”
Dr. Samuels and Dr. Thakur have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to a new study presented at the annual meeting of the American College of Emergency Physicians.
While links between asthma and low-quality housing prone to harboring allergens have been well-documented, the current study takes the extra step of looking at housing down to the level of individual land parcels and suggests that asthma hospital visits can be used to identify hazardous housing earlier.
“Emergency department visits for asthma provide a leading indicator that can be used by health departments or housing authorities to direct housing inspections and remediation of poor housing conditions, track improvements in housing quality, measure housing department performance, support resident grievances, and inform funding allocation decisions,” said the study’s lead researcher, Elizabeth Samuels, MD, who is assistant professor of epidemiology and emergency medicine at Brown University, Providence, R.I.
Researchers retrospectively looked at cases of children and adults in the Greater New Haven area of Connecticut seen at the Yale New Haven Hospital ED for asthma-related problems between March 2013 and August 2017. The region has the fifth-highest prevalence of asthma in the United States, the researchers point out, due to its air quality, pollens, and quality of its housing. More than half of residences were built before 1,940, compared with about 13% nationally. Patient addresses were matched with HUD inspection records.
The review encompassed 11,429 ED visits by 6,366 individuals; 54% were insured by Medicaid, and 42% were Black. Controlling for patient and neighborhood data, researchers found that increased asthma ED visits at the parcel level were associated with decreased HUD inspection scores to a highly significant degree (P < .001).
They also found that there was a relationship in terms of timing between asthma ED visits and inspection scores: asthma ED visits increased more than 1 year before a failed HUD inspection. They also found that asthma ED visits were not elevated at housing units that passed inspection. Using asthma ED visits to predict failed housing inspections produced a specificity rate of 92.3% in an adjusted model, Dr. Samuels noted.
“This approach represents a novel method of early identification of dangerous housing conditions, which could aid in the prevention of asthma-related morbidity and mortality,” Dr. Samuels said.
The investigators noted that, of the parcels with the top three incidence rates of asthma ED visits, “all of them have been closed or demolished.”
In addition to limiting exposure of patients with asthma to the allergens of mold, mice and rats, and cockroaches, improving poor-quality housing earlier could help asthma by reducing stress, she said.
“There is also an increasing evidence base that psychosocial stress increases the risk of asthma attacks, and it’s therefore possible that living in poor housing conditions – often highly stressful situations – drives exacerbation risk via this pathway,” she said. “Synergistic effects between these pathways are also possible or even likely.”
Neeta Thakur, MD, associate professor of medicine at the University of California, San Francisco, who researches asthma, said the findings could lead to a strategy for improving poor-quality housing more quickly. As it is, inspections are too infrequent, often prompted by resident complaints.
“Once the complaints get to a certain threshold, then there might be an inspection that happens, and if there is a periodic review of the buildings, they often happen few and far between,” she said. “We could actually use some of the information that we’re already getting from something like ED visits and see if there is a pattern.”
An important follow-up would be to see whether asthma outcomes improve after housing deficiencies are addressed and whether the predictive capacity of ED visits occurs in other places.
“Would you then see a decline in the ED visit rates from individuals living in those buildings?” Dr. Thakur said. “It’s important to find a leading indicator, but you want to be sure that that leading indicator is useful as something that can be intervened upon.”
Dr. Samuels and Dr. Thakur have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to a new study presented at the annual meeting of the American College of Emergency Physicians.
While links between asthma and low-quality housing prone to harboring allergens have been well-documented, the current study takes the extra step of looking at housing down to the level of individual land parcels and suggests that asthma hospital visits can be used to identify hazardous housing earlier.
“Emergency department visits for asthma provide a leading indicator that can be used by health departments or housing authorities to direct housing inspections and remediation of poor housing conditions, track improvements in housing quality, measure housing department performance, support resident grievances, and inform funding allocation decisions,” said the study’s lead researcher, Elizabeth Samuels, MD, who is assistant professor of epidemiology and emergency medicine at Brown University, Providence, R.I.
Researchers retrospectively looked at cases of children and adults in the Greater New Haven area of Connecticut seen at the Yale New Haven Hospital ED for asthma-related problems between March 2013 and August 2017. The region has the fifth-highest prevalence of asthma in the United States, the researchers point out, due to its air quality, pollens, and quality of its housing. More than half of residences were built before 1,940, compared with about 13% nationally. Patient addresses were matched with HUD inspection records.
The review encompassed 11,429 ED visits by 6,366 individuals; 54% were insured by Medicaid, and 42% were Black. Controlling for patient and neighborhood data, researchers found that increased asthma ED visits at the parcel level were associated with decreased HUD inspection scores to a highly significant degree (P < .001).
They also found that there was a relationship in terms of timing between asthma ED visits and inspection scores: asthma ED visits increased more than 1 year before a failed HUD inspection. They also found that asthma ED visits were not elevated at housing units that passed inspection. Using asthma ED visits to predict failed housing inspections produced a specificity rate of 92.3% in an adjusted model, Dr. Samuels noted.
“This approach represents a novel method of early identification of dangerous housing conditions, which could aid in the prevention of asthma-related morbidity and mortality,” Dr. Samuels said.
The investigators noted that, of the parcels with the top three incidence rates of asthma ED visits, “all of them have been closed or demolished.”
In addition to limiting exposure of patients with asthma to the allergens of mold, mice and rats, and cockroaches, improving poor-quality housing earlier could help asthma by reducing stress, she said.
“There is also an increasing evidence base that psychosocial stress increases the risk of asthma attacks, and it’s therefore possible that living in poor housing conditions – often highly stressful situations – drives exacerbation risk via this pathway,” she said. “Synergistic effects between these pathways are also possible or even likely.”
Neeta Thakur, MD, associate professor of medicine at the University of California, San Francisco, who researches asthma, said the findings could lead to a strategy for improving poor-quality housing more quickly. As it is, inspections are too infrequent, often prompted by resident complaints.
“Once the complaints get to a certain threshold, then there might be an inspection that happens, and if there is a periodic review of the buildings, they often happen few and far between,” she said. “We could actually use some of the information that we’re already getting from something like ED visits and see if there is a pattern.”
An important follow-up would be to see whether asthma outcomes improve after housing deficiencies are addressed and whether the predictive capacity of ED visits occurs in other places.
“Would you then see a decline in the ED visit rates from individuals living in those buildings?” Dr. Thakur said. “It’s important to find a leading indicator, but you want to be sure that that leading indicator is useful as something that can be intervened upon.”
Dr. Samuels and Dr. Thakur have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACEP 2022
Vaccine adherence hinges on improving science communication
“I’m not getting the vaccine. Nobody knows the long-term effects, and I heard that people are getting clots.”
We were screening patients at a low-cost clinic in Philadelphia for concerns surrounding social determinants of health. During one patient visit, in addition to concerns including housing, medication affordability, and transportation, we found that she had not received the COVID-19 vaccine, and we asked if she was interested in being immunized.
News reports have endlessly covered antivaccine sentiment, but this personal encounter hit home. From simple face masks to groundbreaking vaccines, we failed as physicians to encourage widespread uptake of health-protective measures despite strong scientific backing.
Large swaths of the public deny these tools’ importance or question their safety. This is ultimately rooted in the inability of community leaders and health care professionals to communicate with the public.
Science communication is inherently difficult. Scientists use complex language, and it is hard to evaluate the lay public’s baseline knowledge. Moreover, we are trained to speak with qualifications, encourage doubt, and accept change and evolution of fact. These qualities contrast the definitive messaging necessary in public settings. COVID-19 highlighted these gaps, where regardless of novel scientific solutions, poor communication led to a resistance to accept the tested scientific solution, which ultimately was the rate-limiting factor for overcoming the virus.
As directors of Physician Executive Leadership, an organization that trains future physicians at Thomas Jefferson University to tackle emerging health care issues, we hosted Paul Offit, MD, a national media figure and vaccine advocate. Dr. Offit shared his personal growth during the pandemic, from being abruptly thrown into the spotlight to eventually honing his communication skills. Dr. Offit discussed the challenges of sharing medical knowledge with laypeople and adaptations that are necessary. We found this transformative, realizing the importance of science communication training early in medical education.
Emphasizing the humanities and building soft skills will improve outcomes and benefit broader society by producing physician-leaders in public health and policy. We hope to improve our own communication skills and work in medical education to incorporate similar training into education paradigms for future students.
As seen in our patient interaction, strong science alone will not drive patient adherence; instead, we must work at personal and system levels to induce change. Physicians have a unique opportunity to generate trust and guide evidence-based policy. We must communicate, whether one-on-one with patients, or to millions of viewers via media or policymaker settings. We hope to not only be doctors, but to be advocates, leaders, and trusted advisers for the public.
Mr. Kieran and Mr. Shah are second-year medical students at Sidney Kimmel Medical College, Philadelphia. Neither disclosed any relevant conflicts of interest. A version of this article first appeared on Medscape.com.
“I’m not getting the vaccine. Nobody knows the long-term effects, and I heard that people are getting clots.”
We were screening patients at a low-cost clinic in Philadelphia for concerns surrounding social determinants of health. During one patient visit, in addition to concerns including housing, medication affordability, and transportation, we found that she had not received the COVID-19 vaccine, and we asked if she was interested in being immunized.
News reports have endlessly covered antivaccine sentiment, but this personal encounter hit home. From simple face masks to groundbreaking vaccines, we failed as physicians to encourage widespread uptake of health-protective measures despite strong scientific backing.
Large swaths of the public deny these tools’ importance or question their safety. This is ultimately rooted in the inability of community leaders and health care professionals to communicate with the public.
Science communication is inherently difficult. Scientists use complex language, and it is hard to evaluate the lay public’s baseline knowledge. Moreover, we are trained to speak with qualifications, encourage doubt, and accept change and evolution of fact. These qualities contrast the definitive messaging necessary in public settings. COVID-19 highlighted these gaps, where regardless of novel scientific solutions, poor communication led to a resistance to accept the tested scientific solution, which ultimately was the rate-limiting factor for overcoming the virus.
As directors of Physician Executive Leadership, an organization that trains future physicians at Thomas Jefferson University to tackle emerging health care issues, we hosted Paul Offit, MD, a national media figure and vaccine advocate. Dr. Offit shared his personal growth during the pandemic, from being abruptly thrown into the spotlight to eventually honing his communication skills. Dr. Offit discussed the challenges of sharing medical knowledge with laypeople and adaptations that are necessary. We found this transformative, realizing the importance of science communication training early in medical education.
Emphasizing the humanities and building soft skills will improve outcomes and benefit broader society by producing physician-leaders in public health and policy. We hope to improve our own communication skills and work in medical education to incorporate similar training into education paradigms for future students.
As seen in our patient interaction, strong science alone will not drive patient adherence; instead, we must work at personal and system levels to induce change. Physicians have a unique opportunity to generate trust and guide evidence-based policy. We must communicate, whether one-on-one with patients, or to millions of viewers via media or policymaker settings. We hope to not only be doctors, but to be advocates, leaders, and trusted advisers for the public.
Mr. Kieran and Mr. Shah are second-year medical students at Sidney Kimmel Medical College, Philadelphia. Neither disclosed any relevant conflicts of interest. A version of this article first appeared on Medscape.com.
“I’m not getting the vaccine. Nobody knows the long-term effects, and I heard that people are getting clots.”
We were screening patients at a low-cost clinic in Philadelphia for concerns surrounding social determinants of health. During one patient visit, in addition to concerns including housing, medication affordability, and transportation, we found that she had not received the COVID-19 vaccine, and we asked if she was interested in being immunized.
News reports have endlessly covered antivaccine sentiment, but this personal encounter hit home. From simple face masks to groundbreaking vaccines, we failed as physicians to encourage widespread uptake of health-protective measures despite strong scientific backing.
Large swaths of the public deny these tools’ importance or question their safety. This is ultimately rooted in the inability of community leaders and health care professionals to communicate with the public.
Science communication is inherently difficult. Scientists use complex language, and it is hard to evaluate the lay public’s baseline knowledge. Moreover, we are trained to speak with qualifications, encourage doubt, and accept change and evolution of fact. These qualities contrast the definitive messaging necessary in public settings. COVID-19 highlighted these gaps, where regardless of novel scientific solutions, poor communication led to a resistance to accept the tested scientific solution, which ultimately was the rate-limiting factor for overcoming the virus.
As directors of Physician Executive Leadership, an organization that trains future physicians at Thomas Jefferson University to tackle emerging health care issues, we hosted Paul Offit, MD, a national media figure and vaccine advocate. Dr. Offit shared his personal growth during the pandemic, from being abruptly thrown into the spotlight to eventually honing his communication skills. Dr. Offit discussed the challenges of sharing medical knowledge with laypeople and adaptations that are necessary. We found this transformative, realizing the importance of science communication training early in medical education.
Emphasizing the humanities and building soft skills will improve outcomes and benefit broader society by producing physician-leaders in public health and policy. We hope to improve our own communication skills and work in medical education to incorporate similar training into education paradigms for future students.
As seen in our patient interaction, strong science alone will not drive patient adherence; instead, we must work at personal and system levels to induce change. Physicians have a unique opportunity to generate trust and guide evidence-based policy. We must communicate, whether one-on-one with patients, or to millions of viewers via media or policymaker settings. We hope to not only be doctors, but to be advocates, leaders, and trusted advisers for the public.
Mr. Kieran and Mr. Shah are second-year medical students at Sidney Kimmel Medical College, Philadelphia. Neither disclosed any relevant conflicts of interest. A version of this article first appeared on Medscape.com.
Children with asymptomatic celiac disease may have severe disease histology
Some pediatric patients with celiac disease whose condition is diagnosed after screening because a first-degree relative has the disease may appear asymptomatic but have severe disease histology, according to a new report.
About half of these patients had no symptoms, but disease histology was as severe as among those screened for other reasons, such as having symptomatic disease or high-risk conditions.
“This data supports current recommendations to screen all first-degree relatives of patients with celiac disease, especially pediatric patients in whom the ramifications of untreated disease may be significant,” wrote Michelle Gould, MD, and colleagues at the University of Toronto and McMaster University, Hamilton, Ont.
The study was published online in the Journal of Pediatric Gastroenterology and Nutrition.
Clinical characteristics
The incidence of celiac disease is higher among first-degree relatives of patients with the disease than among the general population, yet the clinical characteristics aren’t well described, the study authors wrote. Determining the clinical, serologic, and histologic phenotype of these patients could help clinicians determine whether continued universal screening of first-degree relatives is appropriate.
Dr. Gould and colleagues conducted a retrospective review of 227 patients diagnosed with celiac disease at McMaster Children’s Hospital between 1996 and 2014. The patients were categorized as being screened for celiac disease because a first-degree relative had the disease or because of other reasons. The other reasons included symptoms consistent with celiac disease or the presence of a high-risk clinical condition for which screening is recommended, such as type 1 diabetes or Down syndrome.
All patients were screened via tissue transglutaminase (tTG-IgA) tests. Positive serology was defined as tTG-IgA greater than the upper limit of normal in the presence of normal IgA immunoglobulin level for age.
The patients who were included in the study had biopsy-proven celiac disease in accordance with the Marsh criteria, which included Marsh III histology, Marsh II histology with positive serology, or Marsh I histology with positive serology and clinical symptoms.
The average age of the patients (144 girls and 83 boys) was 8 years at diagnosis. Among the patients, 49 (21.6%) were screened because a first-degree relative had celiac disease. Of those 49 patients, 24 (49%) were symptomatic, and 25 (51%) were asymptomatic.
By contrast, among the 178 patients who were screened for other reasons, 149 (83.7%) were symptomatic, and 29 (16.3%) were asymptomatic.
There was no significant difference between the patient groups with respect to Marsh score at biopsy and tTG-IgA levels at screening. Among the children who were screened because of family history, Marsh scores were equally severe as among other patients, whether they were symptomatic or not.
In addition, no statistically significant differences were found for other clinical characteristics, including body mass index z-score, weight z-score, height z-score, the presence of anemia, or a low mean corpuscular volume for age.
When comparing the characteristics of those screened because of family history and those screened for other high-risk conditions (type 1 diabetes and Down syndrome), the researchers found that rates of asymptomatic presentation were statistically similar between the groups, as were tissue transglutaminase values, Marsh scores, BMI z-scores, and hemoglobin levels at diagnosis. Although there was a statistical difference between the groups with respect to the mean corpuscular volume values at diagnosis, it was unlikely to be of clinical significance, the authors noted.
At 6 months, 1 year, and 2 years after diagnosis, among patients with repeat tTG-IgA measurements, 93 of 143 patients (65%), 52 of 68 patients (76.5%), and 80 of 90 patients (88.9%) had normal serum tTG-IgA levels, respectively. In comparing the proportion of patients whose tTG-IgA levels were normal, there was no difference between those screened because of family history and those screened for other reasons at any time point after diagnosis.
“This may suggest that the natural history of celiac disease is similar in these two groups following initiation of a gluten-free diet and that there are similar rates of compliance with this therapy regardless of the initial indication for screening,” the study authors wrote.
Clinical implications
Dr. Gould and colleagues noted that celiac disease was considered histologically severe – with a Marsh III score or higher – among nearly all patients whose condition was diagnosed because of family history. Histology was equally severe regardless of whether the patients were symptomatic or asymptomatic at screening – 100% of symptomatic patients had a high score, and 96% of asymptomatic patients had a high score.
“This emphasizes the importance of celiac screening in all patients with first-degree relatives with celiac disease, as symptom status does not predict diagnosis or severity of disease,” they wrote.
Previous studies have indicated that the prevalence of celiac disease is highest among siblings of patients with celiac disease, compared with other types of first-degree relatives, the authors wrote. However, they lacked this information in their records, which would be valuable for analysis in future studies.
In addition, ongoing research should investigate the optimal frequency of screening for first-degree relatives, they noted.
“One study suggests that individuals screened before 10 years of age should have repeat screening in their second decade for a small increased pick-up of diagnoses,” they wrote.
No funding for the study has been reported. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Some pediatric patients with celiac disease whose condition is diagnosed after screening because a first-degree relative has the disease may appear asymptomatic but have severe disease histology, according to a new report.
About half of these patients had no symptoms, but disease histology was as severe as among those screened for other reasons, such as having symptomatic disease or high-risk conditions.
“This data supports current recommendations to screen all first-degree relatives of patients with celiac disease, especially pediatric patients in whom the ramifications of untreated disease may be significant,” wrote Michelle Gould, MD, and colleagues at the University of Toronto and McMaster University, Hamilton, Ont.
The study was published online in the Journal of Pediatric Gastroenterology and Nutrition.
Clinical characteristics
The incidence of celiac disease is higher among first-degree relatives of patients with the disease than among the general population, yet the clinical characteristics aren’t well described, the study authors wrote. Determining the clinical, serologic, and histologic phenotype of these patients could help clinicians determine whether continued universal screening of first-degree relatives is appropriate.
Dr. Gould and colleagues conducted a retrospective review of 227 patients diagnosed with celiac disease at McMaster Children’s Hospital between 1996 and 2014. The patients were categorized as being screened for celiac disease because a first-degree relative had the disease or because of other reasons. The other reasons included symptoms consistent with celiac disease or the presence of a high-risk clinical condition for which screening is recommended, such as type 1 diabetes or Down syndrome.
All patients were screened via tissue transglutaminase (tTG-IgA) tests. Positive serology was defined as tTG-IgA greater than the upper limit of normal in the presence of normal IgA immunoglobulin level for age.
The patients who were included in the study had biopsy-proven celiac disease in accordance with the Marsh criteria, which included Marsh III histology, Marsh II histology with positive serology, or Marsh I histology with positive serology and clinical symptoms.
The average age of the patients (144 girls and 83 boys) was 8 years at diagnosis. Among the patients, 49 (21.6%) were screened because a first-degree relative had celiac disease. Of those 49 patients, 24 (49%) were symptomatic, and 25 (51%) were asymptomatic.
By contrast, among the 178 patients who were screened for other reasons, 149 (83.7%) were symptomatic, and 29 (16.3%) were asymptomatic.
There was no significant difference between the patient groups with respect to Marsh score at biopsy and tTG-IgA levels at screening. Among the children who were screened because of family history, Marsh scores were equally severe as among other patients, whether they were symptomatic or not.
In addition, no statistically significant differences were found for other clinical characteristics, including body mass index z-score, weight z-score, height z-score, the presence of anemia, or a low mean corpuscular volume for age.
When comparing the characteristics of those screened because of family history and those screened for other high-risk conditions (type 1 diabetes and Down syndrome), the researchers found that rates of asymptomatic presentation were statistically similar between the groups, as were tissue transglutaminase values, Marsh scores, BMI z-scores, and hemoglobin levels at diagnosis. Although there was a statistical difference between the groups with respect to the mean corpuscular volume values at diagnosis, it was unlikely to be of clinical significance, the authors noted.
At 6 months, 1 year, and 2 years after diagnosis, among patients with repeat tTG-IgA measurements, 93 of 143 patients (65%), 52 of 68 patients (76.5%), and 80 of 90 patients (88.9%) had normal serum tTG-IgA levels, respectively. In comparing the proportion of patients whose tTG-IgA levels were normal, there was no difference between those screened because of family history and those screened for other reasons at any time point after diagnosis.
“This may suggest that the natural history of celiac disease is similar in these two groups following initiation of a gluten-free diet and that there are similar rates of compliance with this therapy regardless of the initial indication for screening,” the study authors wrote.
Clinical implications
Dr. Gould and colleagues noted that celiac disease was considered histologically severe – with a Marsh III score or higher – among nearly all patients whose condition was diagnosed because of family history. Histology was equally severe regardless of whether the patients were symptomatic or asymptomatic at screening – 100% of symptomatic patients had a high score, and 96% of asymptomatic patients had a high score.
“This emphasizes the importance of celiac screening in all patients with first-degree relatives with celiac disease, as symptom status does not predict diagnosis or severity of disease,” they wrote.
Previous studies have indicated that the prevalence of celiac disease is highest among siblings of patients with celiac disease, compared with other types of first-degree relatives, the authors wrote. However, they lacked this information in their records, which would be valuable for analysis in future studies.
In addition, ongoing research should investigate the optimal frequency of screening for first-degree relatives, they noted.
“One study suggests that individuals screened before 10 years of age should have repeat screening in their second decade for a small increased pick-up of diagnoses,” they wrote.
No funding for the study has been reported. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Some pediatric patients with celiac disease whose condition is diagnosed after screening because a first-degree relative has the disease may appear asymptomatic but have severe disease histology, according to a new report.
About half of these patients had no symptoms, but disease histology was as severe as among those screened for other reasons, such as having symptomatic disease or high-risk conditions.
“This data supports current recommendations to screen all first-degree relatives of patients with celiac disease, especially pediatric patients in whom the ramifications of untreated disease may be significant,” wrote Michelle Gould, MD, and colleagues at the University of Toronto and McMaster University, Hamilton, Ont.
The study was published online in the Journal of Pediatric Gastroenterology and Nutrition.
Clinical characteristics
The incidence of celiac disease is higher among first-degree relatives of patients with the disease than among the general population, yet the clinical characteristics aren’t well described, the study authors wrote. Determining the clinical, serologic, and histologic phenotype of these patients could help clinicians determine whether continued universal screening of first-degree relatives is appropriate.
Dr. Gould and colleagues conducted a retrospective review of 227 patients diagnosed with celiac disease at McMaster Children’s Hospital between 1996 and 2014. The patients were categorized as being screened for celiac disease because a first-degree relative had the disease or because of other reasons. The other reasons included symptoms consistent with celiac disease or the presence of a high-risk clinical condition for which screening is recommended, such as type 1 diabetes or Down syndrome.
All patients were screened via tissue transglutaminase (tTG-IgA) tests. Positive serology was defined as tTG-IgA greater than the upper limit of normal in the presence of normal IgA immunoglobulin level for age.
The patients who were included in the study had biopsy-proven celiac disease in accordance with the Marsh criteria, which included Marsh III histology, Marsh II histology with positive serology, or Marsh I histology with positive serology and clinical symptoms.
The average age of the patients (144 girls and 83 boys) was 8 years at diagnosis. Among the patients, 49 (21.6%) were screened because a first-degree relative had celiac disease. Of those 49 patients, 24 (49%) were symptomatic, and 25 (51%) were asymptomatic.
By contrast, among the 178 patients who were screened for other reasons, 149 (83.7%) were symptomatic, and 29 (16.3%) were asymptomatic.
There was no significant difference between the patient groups with respect to Marsh score at biopsy and tTG-IgA levels at screening. Among the children who were screened because of family history, Marsh scores were equally severe as among other patients, whether they were symptomatic or not.
In addition, no statistically significant differences were found for other clinical characteristics, including body mass index z-score, weight z-score, height z-score, the presence of anemia, or a low mean corpuscular volume for age.
When comparing the characteristics of those screened because of family history and those screened for other high-risk conditions (type 1 diabetes and Down syndrome), the researchers found that rates of asymptomatic presentation were statistically similar between the groups, as were tissue transglutaminase values, Marsh scores, BMI z-scores, and hemoglobin levels at diagnosis. Although there was a statistical difference between the groups with respect to the mean corpuscular volume values at diagnosis, it was unlikely to be of clinical significance, the authors noted.
At 6 months, 1 year, and 2 years after diagnosis, among patients with repeat tTG-IgA measurements, 93 of 143 patients (65%), 52 of 68 patients (76.5%), and 80 of 90 patients (88.9%) had normal serum tTG-IgA levels, respectively. In comparing the proportion of patients whose tTG-IgA levels were normal, there was no difference between those screened because of family history and those screened for other reasons at any time point after diagnosis.
“This may suggest that the natural history of celiac disease is similar in these two groups following initiation of a gluten-free diet and that there are similar rates of compliance with this therapy regardless of the initial indication for screening,” the study authors wrote.
Clinical implications
Dr. Gould and colleagues noted that celiac disease was considered histologically severe – with a Marsh III score or higher – among nearly all patients whose condition was diagnosed because of family history. Histology was equally severe regardless of whether the patients were symptomatic or asymptomatic at screening – 100% of symptomatic patients had a high score, and 96% of asymptomatic patients had a high score.
“This emphasizes the importance of celiac screening in all patients with first-degree relatives with celiac disease, as symptom status does not predict diagnosis or severity of disease,” they wrote.
Previous studies have indicated that the prevalence of celiac disease is highest among siblings of patients with celiac disease, compared with other types of first-degree relatives, the authors wrote. However, they lacked this information in their records, which would be valuable for analysis in future studies.
In addition, ongoing research should investigate the optimal frequency of screening for first-degree relatives, they noted.
“One study suggests that individuals screened before 10 years of age should have repeat screening in their second decade for a small increased pick-up of diagnoses,” they wrote.
No funding for the study has been reported. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF PEDIATRIC GASTROENTEROLOGY AND NUTRITION
Preexisting mental illness symptoms spiked during pandemic
“Those with preexisting mental health conditions may be particularly vulnerable to these effects because they are more susceptible to experiencing high levels of stress during a crisis and are more likely to experience isolation/despair during confinement compared to the general population,” wrote Danna Ramirez of The Menninger Clinic, Houston, and colleagues.
In a study published in Psychiatry Research , the investigators compared data from 142 adolescents aged 12-17 years and 470 adults aged 18-79 years who were admitted to an inpatient psychiatric hospital in Houston. Of these, 65 adolescents and 235 adults were admitted before the pandemic, and 77 adolescents and 235 adults were admitted during the pandemic.
Clinical outcomes were scores on the Generalized Anxiety Disorder Scale (GAD-7), the Patient Health Questionnaire (PHQ-9), the Patient Health Questionnaire for Adolescents (PHQ-A), the Difficulties in Emotion Regulation Scale–Short Form (DERS-SF), the World Health Organization Disability Assessment Scale (WHODAS), the World Health Organization Alcohol, Smoking, and Substance Involvement Screening Test (WHOASSIST), the Pittsburgh Sleep Quality Index (PSQI), the Disturbing Dream and Nightmare Severity Index (DDNSI), and the Suicide Behaviors Questionnaire–Revised (SBQ-R).
Overall, adults admitted during the pandemic had significantly higher levels of anxiety, depression, emotional dysregulation, and disability (P < .001 for all) as well as nightmares (P = .013) compared to those admitted prior to the pandemic.
Among adolescents, measures of anxiety, depression, and sleep quality were significantly higher at admission during the pandemic compared to prior to the pandemic (P = .005, P = .005, and P = .011, respectively)
Reasons for the increase in symptom severity remain unclear, but include the possibility that individuals with preexisting mental illness simply became more ill; or that individuals with symptoms delayed hospital admission out of fear of exposure to COVID-19, which resulted in more severe symptoms at admission, the researchers wrote in their discussion.
The findings were limited by several factors, including the primarily White population and the reliance on self-reports, the researchers noted. Another limitation was the lack of differentiation between patients who may have had COVID-19 before hospitalization and those who did not, so the researchers could not determine whether the virus itself played a biological role in symptom severity.
However, the results support data from previous studies and identify increased psychiatry symptom severity for patients admitted for inpatient psychiatry care during the pandemic, they said. Although resources are scarce, the findings emphasize that mental health needs, especially for those with preexisting conditions, should not be overlooked, and continuity and expansion of access to mental health care for all should be prioritized, they concluded.
The study was supported by The Menninger Clinic and The Menninger Clinic Foundation. The researchers had no financial conflicts to disclose.
“Those with preexisting mental health conditions may be particularly vulnerable to these effects because they are more susceptible to experiencing high levels of stress during a crisis and are more likely to experience isolation/despair during confinement compared to the general population,” wrote Danna Ramirez of The Menninger Clinic, Houston, and colleagues.
In a study published in Psychiatry Research , the investigators compared data from 142 adolescents aged 12-17 years and 470 adults aged 18-79 years who were admitted to an inpatient psychiatric hospital in Houston. Of these, 65 adolescents and 235 adults were admitted before the pandemic, and 77 adolescents and 235 adults were admitted during the pandemic.
Clinical outcomes were scores on the Generalized Anxiety Disorder Scale (GAD-7), the Patient Health Questionnaire (PHQ-9), the Patient Health Questionnaire for Adolescents (PHQ-A), the Difficulties in Emotion Regulation Scale–Short Form (DERS-SF), the World Health Organization Disability Assessment Scale (WHODAS), the World Health Organization Alcohol, Smoking, and Substance Involvement Screening Test (WHOASSIST), the Pittsburgh Sleep Quality Index (PSQI), the Disturbing Dream and Nightmare Severity Index (DDNSI), and the Suicide Behaviors Questionnaire–Revised (SBQ-R).
Overall, adults admitted during the pandemic had significantly higher levels of anxiety, depression, emotional dysregulation, and disability (P < .001 for all) as well as nightmares (P = .013) compared to those admitted prior to the pandemic.
Among adolescents, measures of anxiety, depression, and sleep quality were significantly higher at admission during the pandemic compared to prior to the pandemic (P = .005, P = .005, and P = .011, respectively)
Reasons for the increase in symptom severity remain unclear, but include the possibility that individuals with preexisting mental illness simply became more ill; or that individuals with symptoms delayed hospital admission out of fear of exposure to COVID-19, which resulted in more severe symptoms at admission, the researchers wrote in their discussion.
The findings were limited by several factors, including the primarily White population and the reliance on self-reports, the researchers noted. Another limitation was the lack of differentiation between patients who may have had COVID-19 before hospitalization and those who did not, so the researchers could not determine whether the virus itself played a biological role in symptom severity.
However, the results support data from previous studies and identify increased psychiatry symptom severity for patients admitted for inpatient psychiatry care during the pandemic, they said. Although resources are scarce, the findings emphasize that mental health needs, especially for those with preexisting conditions, should not be overlooked, and continuity and expansion of access to mental health care for all should be prioritized, they concluded.
The study was supported by The Menninger Clinic and The Menninger Clinic Foundation. The researchers had no financial conflicts to disclose.
“Those with preexisting mental health conditions may be particularly vulnerable to these effects because they are more susceptible to experiencing high levels of stress during a crisis and are more likely to experience isolation/despair during confinement compared to the general population,” wrote Danna Ramirez of The Menninger Clinic, Houston, and colleagues.
In a study published in Psychiatry Research , the investigators compared data from 142 adolescents aged 12-17 years and 470 adults aged 18-79 years who were admitted to an inpatient psychiatric hospital in Houston. Of these, 65 adolescents and 235 adults were admitted before the pandemic, and 77 adolescents and 235 adults were admitted during the pandemic.
Clinical outcomes were scores on the Generalized Anxiety Disorder Scale (GAD-7), the Patient Health Questionnaire (PHQ-9), the Patient Health Questionnaire for Adolescents (PHQ-A), the Difficulties in Emotion Regulation Scale–Short Form (DERS-SF), the World Health Organization Disability Assessment Scale (WHODAS), the World Health Organization Alcohol, Smoking, and Substance Involvement Screening Test (WHOASSIST), the Pittsburgh Sleep Quality Index (PSQI), the Disturbing Dream and Nightmare Severity Index (DDNSI), and the Suicide Behaviors Questionnaire–Revised (SBQ-R).
Overall, adults admitted during the pandemic had significantly higher levels of anxiety, depression, emotional dysregulation, and disability (P < .001 for all) as well as nightmares (P = .013) compared to those admitted prior to the pandemic.
Among adolescents, measures of anxiety, depression, and sleep quality were significantly higher at admission during the pandemic compared to prior to the pandemic (P = .005, P = .005, and P = .011, respectively)
Reasons for the increase in symptom severity remain unclear, but include the possibility that individuals with preexisting mental illness simply became more ill; or that individuals with symptoms delayed hospital admission out of fear of exposure to COVID-19, which resulted in more severe symptoms at admission, the researchers wrote in their discussion.
The findings were limited by several factors, including the primarily White population and the reliance on self-reports, the researchers noted. Another limitation was the lack of differentiation between patients who may have had COVID-19 before hospitalization and those who did not, so the researchers could not determine whether the virus itself played a biological role in symptom severity.
However, the results support data from previous studies and identify increased psychiatry symptom severity for patients admitted for inpatient psychiatry care during the pandemic, they said. Although resources are scarce, the findings emphasize that mental health needs, especially for those with preexisting conditions, should not be overlooked, and continuity and expansion of access to mental health care for all should be prioritized, they concluded.
The study was supported by The Menninger Clinic and The Menninger Clinic Foundation. The researchers had no financial conflicts to disclose.
FROM PSYCHIATRY RESEARCH