User login
‘Sighing’ tops mindfulness for reduced stress, improved mood
In a randomized controlled study, daily breathwork – especially cyclic breathing, which emphasizes shorter inhalations and prolonged exhalations – was associated with greater improvement in mood and a slower respiratory rate than mindfulness meditation.

“We were pleased that just 5 minutes a day of the breathing exercises positively affected mood and resulted in slower respiratory rate, indicating reduced arousal,” coinvestigator David Spiegel, MD, who directs the Center for Stress and Health at Stanford (Calif.) University, told this news organization.
The findings were published online in Cell Reports Medicine.
Intentional breath control
Controlled breathwork has emerged as a potential tool to manage stress and boost well-being.
In the new study, researchers compared three different daily 5-minute breathwork exercises to an equal amount of mindfulness meditation over 1 month in 108 healthy adults recruited mostly from an undergraduate psychology class at Stanford: 33 participants practiced cyclic hyperventilation, which emphasizes robust inhalation, short retention and rapid exhalation, 30 did exhale-focused cyclic sighing, 21 performed box breathing, which emphasizes equal duration of inhalation, breath retention, and exhalation, and 24 practiced mindfulness meditation (the control group).
The primary endpoints were improvement in mood and anxiety, as well as reduced physiologic arousal (respiratory rate, heart rate, and heart rate variability). Physiological data was collected using a wearable WHOOP strap.
All four groups showed significant daily improvement in mood, as well as reduction in anxiety and negative mood, but there were significant differences between mindfulness meditation and breathwork.
Using a mixed-effects model, the researchers showed that breathwork, especially the exhale-focused cyclic sighing, produced greater improvement in mood (P < .05) and reduction in respiratory rate (P < .05), compared with mindfulness meditation.
Specific patterns vs. passive attention
The finding supports the team’s hypothesis that intentional control over breath with specific breathing patterns produces more benefit to mood than passive attention to one’s breath, as in mindfulness meditation practice.
“It turned out that the cyclic sighing was indeed most soothing,” Dr. Spiegel noted.
“We expected that because of respiratory sinus arrhythmia. Exhaling is accomplished by increasing pressure in the chest, which increases venous return to the heart, triggering parasympathetic slowing of heart rate via the sinoatrial node,” he said.
Dr. Spiegel added that, conversely, inspiration reduces venous return, triggering sympathetic activity and increased heart rate.
“The magnitude of this heart rate variability is associated with better health, including recovery from myocardial infarction and even cancer survival. So self-soothing is a good thing, and we expected an advantage for cyclic sighing,” he said.

“If you’re looking to improve sleep and reduce daytime stress, recover from intense work, life, and/or training, then interventions that facilitate autonomic control (and indeed you can control it), brief (5 minutes) structured breathwork is among the more powerful (and zero cost) tools,” tweeted senior investigator Andrew Huberman, PhD, professor of neurobiology at Stanford.
Immediate application?
Sara Lazar, PhD, Massachusetts General Hospital and Harvard Medical School, Boston, said the findings are “interesting” but cautioned that this is “just one study with a pretty small sample size,” and it only enrolled healthy college students.

Dr. Lazar, who also runs the Lazar Lab for Meditation Research at Mass General, noted that she would want to see a future study “done with working-age adults and with clinical populations.”
“It should also be noted that mindfulness had a bigger effect on negative affect, which could have implications for conditions such as depression or trauma,” said Dr. Lazar, who was not involved with the current research.
Also weighing in, Steven R. Thorp, PhD, professor at California School of Professional Psychology, Alliant International University, San Diego, said in an interview the study is “really interesting and well done.”

“Although breathing exercises and breathing retraining are commonly found in psychosocial interventions, especially for anxiety disorders, there have been few empirical studies comparing different breathing protocols,” Dr. Thorp said.
In this study, the passive observation of breaths (mindfulness) and specific breathwork interventions “all worked to decrease state anxiety; but the breathwork, particularly the cyclic sighing protocol, produced a greater overall reduction in respiratory rate and increase in positive mood,” he noted.
“These techniques can be recommended by all clinicians because all clients have access to their breath at all times – and only 5 minutes of daily practice can yield the benefits. Moreover, as the authors note, the immediate benefits may encourage clients to engage with the breathwork and potentially other aspects of treatment,” Dr. Thorp said.
The study was funded by Victor and Winnie Koo and Tianren Culture and a Stanford School of Medicine Discovery Innovation Award. WHOOP donated the wrist straps used in the study, but was not involved in the study’s design or analysis. Dr. Huberman is an advisor to WHOOP. Dr. Lazar and Dr. Thorp have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a randomized controlled study, daily breathwork – especially cyclic breathing, which emphasizes shorter inhalations and prolonged exhalations – was associated with greater improvement in mood and a slower respiratory rate than mindfulness meditation.
“We were pleased that just 5 minutes a day of the breathing exercises positively affected mood and resulted in slower respiratory rate, indicating reduced arousal,” coinvestigator David Spiegel, MD, who directs the Center for Stress and Health at Stanford (Calif.) University, told this news organization.
The findings were published online in Cell Reports Medicine.
Intentional breath control
Controlled breathwork has emerged as a potential tool to manage stress and boost well-being.
In the new study, researchers compared three different daily 5-minute breathwork exercises to an equal amount of mindfulness meditation over 1 month in 108 healthy adults recruited mostly from an undergraduate psychology class at Stanford: 33 participants practiced cyclic hyperventilation, which emphasizes robust inhalation, short retention and rapid exhalation, 30 did exhale-focused cyclic sighing, 21 performed box breathing, which emphasizes equal duration of inhalation, breath retention, and exhalation, and 24 practiced mindfulness meditation (the control group).
The primary endpoints were improvement in mood and anxiety, as well as reduced physiologic arousal (respiratory rate, heart rate, and heart rate variability). Physiological data was collected using a wearable WHOOP strap.
All four groups showed significant daily improvement in mood, as well as reduction in anxiety and negative mood, but there were significant differences between mindfulness meditation and breathwork.
Using a mixed-effects model, the researchers showed that breathwork, especially the exhale-focused cyclic sighing, produced greater improvement in mood (P < .05) and reduction in respiratory rate (P < .05), compared with mindfulness meditation.
Specific patterns vs. passive attention
The finding supports the team’s hypothesis that intentional control over breath with specific breathing patterns produces more benefit to mood than passive attention to one’s breath, as in mindfulness meditation practice.
“It turned out that the cyclic sighing was indeed most soothing,” Dr. Spiegel noted.
“We expected that because of respiratory sinus arrhythmia. Exhaling is accomplished by increasing pressure in the chest, which increases venous return to the heart, triggering parasympathetic slowing of heart rate via the sinoatrial node,” he said.
Dr. Spiegel added that, conversely, inspiration reduces venous return, triggering sympathetic activity and increased heart rate.
“The magnitude of this heart rate variability is associated with better health, including recovery from myocardial infarction and even cancer survival. So self-soothing is a good thing, and we expected an advantage for cyclic sighing,” he said.
“If you’re looking to improve sleep and reduce daytime stress, recover from intense work, life, and/or training, then interventions that facilitate autonomic control (and indeed you can control it), brief (5 minutes) structured breathwork is among the more powerful (and zero cost) tools,” tweeted senior investigator Andrew Huberman, PhD, professor of neurobiology at Stanford.
Immediate application?
Sara Lazar, PhD, Massachusetts General Hospital and Harvard Medical School, Boston, said the findings are “interesting” but cautioned that this is “just one study with a pretty small sample size,” and it only enrolled healthy college students.
Dr. Lazar, who also runs the Lazar Lab for Meditation Research at Mass General, noted that she would want to see a future study “done with working-age adults and with clinical populations.”
“It should also be noted that mindfulness had a bigger effect on negative affect, which could have implications for conditions such as depression or trauma,” said Dr. Lazar, who was not involved with the current research.
Also weighing in, Steven R. Thorp, PhD, professor at California School of Professional Psychology, Alliant International University, San Diego, said in an interview the study is “really interesting and well done.”
“Although breathing exercises and breathing retraining are commonly found in psychosocial interventions, especially for anxiety disorders, there have been few empirical studies comparing different breathing protocols,” Dr. Thorp said.
In this study, the passive observation of breaths (mindfulness) and specific breathwork interventions “all worked to decrease state anxiety; but the breathwork, particularly the cyclic sighing protocol, produced a greater overall reduction in respiratory rate and increase in positive mood,” he noted.
“These techniques can be recommended by all clinicians because all clients have access to their breath at all times – and only 5 minutes of daily practice can yield the benefits. Moreover, as the authors note, the immediate benefits may encourage clients to engage with the breathwork and potentially other aspects of treatment,” Dr. Thorp said.
The study was funded by Victor and Winnie Koo and Tianren Culture and a Stanford School of Medicine Discovery Innovation Award. WHOOP donated the wrist straps used in the study, but was not involved in the study’s design or analysis. Dr. Huberman is an advisor to WHOOP. Dr. Lazar and Dr. Thorp have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a randomized controlled study, daily breathwork – especially cyclic breathing, which emphasizes shorter inhalations and prolonged exhalations – was associated with greater improvement in mood and a slower respiratory rate than mindfulness meditation.
“We were pleased that just 5 minutes a day of the breathing exercises positively affected mood and resulted in slower respiratory rate, indicating reduced arousal,” coinvestigator David Spiegel, MD, who directs the Center for Stress and Health at Stanford (Calif.) University, told this news organization.
The findings were published online in Cell Reports Medicine.
Intentional breath control
Controlled breathwork has emerged as a potential tool to manage stress and boost well-being.
In the new study, researchers compared three different daily 5-minute breathwork exercises to an equal amount of mindfulness meditation over 1 month in 108 healthy adults recruited mostly from an undergraduate psychology class at Stanford: 33 participants practiced cyclic hyperventilation, which emphasizes robust inhalation, short retention and rapid exhalation, 30 did exhale-focused cyclic sighing, 21 performed box breathing, which emphasizes equal duration of inhalation, breath retention, and exhalation, and 24 practiced mindfulness meditation (the control group).
The primary endpoints were improvement in mood and anxiety, as well as reduced physiologic arousal (respiratory rate, heart rate, and heart rate variability). Physiological data was collected using a wearable WHOOP strap.
All four groups showed significant daily improvement in mood, as well as reduction in anxiety and negative mood, but there were significant differences between mindfulness meditation and breathwork.
Using a mixed-effects model, the researchers showed that breathwork, especially the exhale-focused cyclic sighing, produced greater improvement in mood (P < .05) and reduction in respiratory rate (P < .05), compared with mindfulness meditation.
Specific patterns vs. passive attention
The finding supports the team’s hypothesis that intentional control over breath with specific breathing patterns produces more benefit to mood than passive attention to one’s breath, as in mindfulness meditation practice.
“It turned out that the cyclic sighing was indeed most soothing,” Dr. Spiegel noted.
“We expected that because of respiratory sinus arrhythmia. Exhaling is accomplished by increasing pressure in the chest, which increases venous return to the heart, triggering parasympathetic slowing of heart rate via the sinoatrial node,” he said.
Dr. Spiegel added that, conversely, inspiration reduces venous return, triggering sympathetic activity and increased heart rate.
“The magnitude of this heart rate variability is associated with better health, including recovery from myocardial infarction and even cancer survival. So self-soothing is a good thing, and we expected an advantage for cyclic sighing,” he said.
“If you’re looking to improve sleep and reduce daytime stress, recover from intense work, life, and/or training, then interventions that facilitate autonomic control (and indeed you can control it), brief (5 minutes) structured breathwork is among the more powerful (and zero cost) tools,” tweeted senior investigator Andrew Huberman, PhD, professor of neurobiology at Stanford.
Immediate application?
Sara Lazar, PhD, Massachusetts General Hospital and Harvard Medical School, Boston, said the findings are “interesting” but cautioned that this is “just one study with a pretty small sample size,” and it only enrolled healthy college students.
Dr. Lazar, who also runs the Lazar Lab for Meditation Research at Mass General, noted that she would want to see a future study “done with working-age adults and with clinical populations.”
“It should also be noted that mindfulness had a bigger effect on negative affect, which could have implications for conditions such as depression or trauma,” said Dr. Lazar, who was not involved with the current research.
Also weighing in, Steven R. Thorp, PhD, professor at California School of Professional Psychology, Alliant International University, San Diego, said in an interview the study is “really interesting and well done.”
“Although breathing exercises and breathing retraining are commonly found in psychosocial interventions, especially for anxiety disorders, there have been few empirical studies comparing different breathing protocols,” Dr. Thorp said.
In this study, the passive observation of breaths (mindfulness) and specific breathwork interventions “all worked to decrease state anxiety; but the breathwork, particularly the cyclic sighing protocol, produced a greater overall reduction in respiratory rate and increase in positive mood,” he noted.
“These techniques can be recommended by all clinicians because all clients have access to their breath at all times – and only 5 minutes of daily practice can yield the benefits. Moreover, as the authors note, the immediate benefits may encourage clients to engage with the breathwork and potentially other aspects of treatment,” Dr. Thorp said.
The study was funded by Victor and Winnie Koo and Tianren Culture and a Stanford School of Medicine Discovery Innovation Award. WHOOP donated the wrist straps used in the study, but was not involved in the study’s design or analysis. Dr. Huberman is an advisor to WHOOP. Dr. Lazar and Dr. Thorp have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CELL REPORTS MEDICINE
Medicare ‘offers’ cancer patient a choice: Less life or more debt
We’re gonna need a bigger meth lab
In case you’ve been living under a rock for the past 15 years, the TV show “Breaking Bad” details the spiraling rise and downfall of a high school chemistry teacher who, after developing a case of terminal lung cancer, starts producing methamphetamine to provide for his family in response to the steep cost of treatment for his cancer.

Meanwhile, here in 2023 in the real world, we have Paul Davis, a retired physician in Ohio, who’s being forced to choose between an expensive cancer treatment and bankrupting his family, since Medicare’s decided it doesn’t want to cover the cost. Hey, we’ve seen this one before!
A bit of backstory: In November 2019, Dr. Davis was diagnosed with uveal melanoma, a very rare type of cancer that affects eye tissue. The news got worse in 2022 when the cancer spread to his liver, a move which typically proves fatal within a year. However, in a stroke of great news, the Food and Drug Administration approved the drug Kimmtrak earlier that year, which could be used to treat his cancer. Not cure, of course, but it would give him more time.
His initial treatments with the drug went fine and were covered, but when he transferred his care from a hospital in Columbus to one closer to home, big problem. Medicare decided it didn’t like that hospital and abruptly cut off coverage, denying the local hospital’s claims. That leaves Dr. Davis on the hook for his cancer treatment, and it’s what you might call expensive. Expensive to the tune of $50,000.
A week.
Apparently the coding the local hospital submitted was wrong, indicating that Dr. Davis was receiving Kimmtrak for a type of cancer that the FDA hadn’t approved the drug for. So until the government bureaucracy works itself out, his treatment is on hold, leaving all his faith in Medicare working quickly to rectify its mistake. If it can rectify its mistake. We’re not hopeful.
And in case you were wondering, if Dr. Davis wanted to go full Walter White, the average street price of meth is about $20-$60 per gram, so to pay for his treatment, he’d need to make at least a kilogram of meth every week. That’s, uh, quite a lot of illegal drug, or what we here at the LOTME office would call a fun Saturday night.
When you give a mouse a movie
Researchers have been successfully testing Alzheimer drugs on mice for years, but none of the drugs has proved successful in humans. Recent work, however, might have found the missing link, and it’s a combination no one ever thought of before: mice and movies.

Turns out that Orson Welles’ 1958 film noir classic “Touch of Evil” tapped a part of the mouse brain that has been overlooked: the hippocampus, which is crucial for learning and memory. Previous researchers thought it was just used as a kind of GPS system, but that’s only partially true.
Not only did the mice choose to pay attention to the movie clip, but the hippocampus responded to the visual stimuli only when the rodents saw the scenes from the clip later in the order that they were presented and not in a scrambled order. These findings represent a “major paradigm shift” in studying mouse recall, Mayank Mehta, PhD, of the University of California, Los Angeles, said in a statement from the school.
This breakthrough could run parallel to Alzheimer’s patients struggling with similar defects. “Selective and episodic activation of the mouse hippocampus using a human movie opens up the possibility of directly testing human episodic memory disorders and therapies using mouse neurons, a major step forward,” said coauthor Chinmay Purandare, PhD, who is now at the University of California, San Francisco.
Who would have thought that a classic film would help advance Alzheimer research?
A less human way to study mosquitoes
We here at LOTME have a history with mosquitoes. We know they don’t like us, and they know that we don’t like them. Trust us, they know. So when humans gain a little ground in the war against the buzzy little bloodsuckers, we want to share the joy.
To know the enemy, scientists have to study the enemy, but there is a problem. “Many mosquito experiments still rely on human volunteers and animal subjects,” bioengineering graduate student Kevin Janson, said in a statement from Rice University. Most people don’t like being bitten by mosquitoes, so that kind of testing can be expensive.
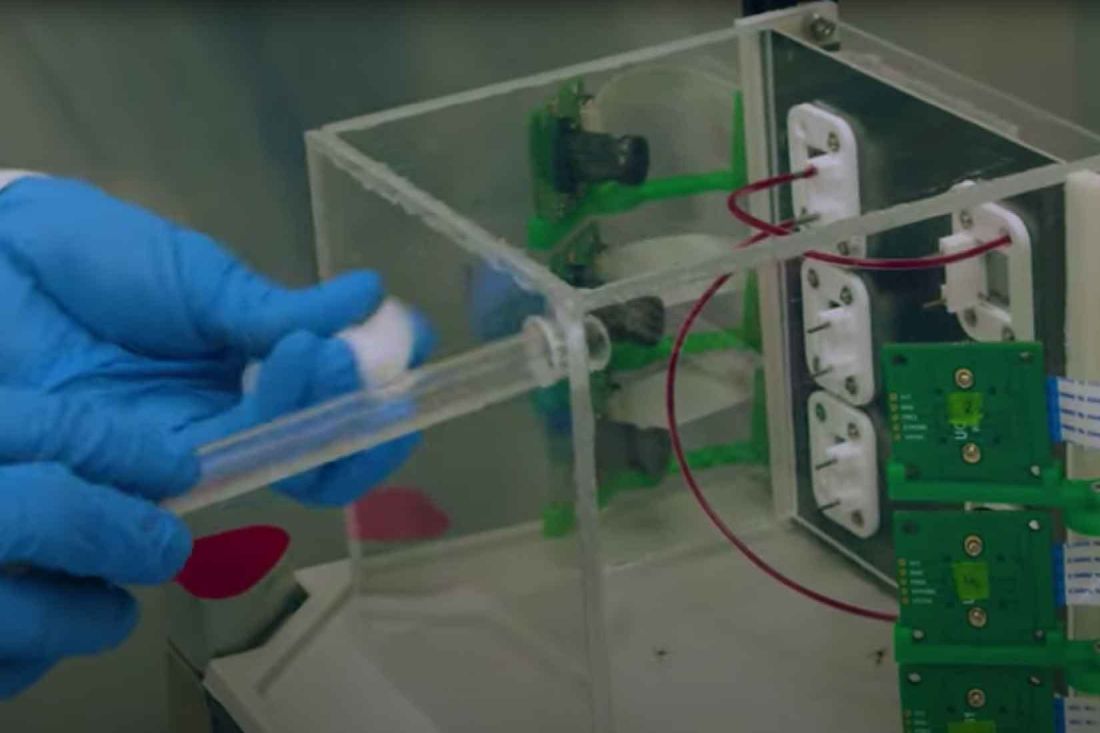
Is there a way to automate the collection and processing of mosquito behavior data using inexpensive cameras and machine-learning software? We’re glad you asked, because Mr. Janson and the research team, which includes bioengineers from Rice and tropical medicine experts from Tulane University, have managed to eliminate the need for live volunteers by using patches of synthetic skin made with a 3D printer.
“Each patch of gelatin-like hydrogel comes complete with tiny passageways that can be filled with flowing blood” from a chicken, sheep, or cow, they explained, and proof-of-concept testing showed that mosquitoes would feed on hydrogels without any repellent and stay away from those treated with a repellent.
To conduct the feeding tests, the blood-infused hydrogels are placed in a clear plastic box that is surrounded by cameras.
A bunch of mosquitoes are then tossed in the box and the cameras record all their insect activities: how often they land at each location, how long they stay, whether or not they bite, how long they feed, etc. Humans don’t have to watch and don’t have to be food sources.
Humans don’t have to be food sources, and we just pictured the future of mosquito control. Imagine a dozen Arnold Schwarzenegger–style Terminators, covered in 3D-printed skin, walking through your neighborhood in the summer while wearing sweat-soaked, brightly colored clothing. The mosquitoes wouldn’t be able to stay away, but guess what? They’re feeding off robots with nonhuman skin and nonhuman blood, so we win. It’s good to have a cerebral cortex.
Getting medieval on brain surgery
Let’s get one thing clear: The so-called “Dark Ages” were not nearly as dark as they’re made out to be. For one thing, there’s a world beyond Western Europe. The Roman Empire didn’t collapse everywhere. But even in Western Europe, the centuries between the fall of Rome and the Renaissance were hardly lacking in cultural development.

That said, we wouldn’t want to be in the position of the seventh-century noblewoman whose remains were recently uncovered in a Byzantine fortress in central Italy with multiple cross-shaped incisions in her skull. Yes, this unfortunate woman underwent at least two brain surgeries.
Then again, maybe not. Nothing like it had been discovered at the site, and while the markings – signs of a procedure called trepanation – can be surgical in nature, there are other explanations. For example, the Avar people practiced ritual trepanation during the same time period, but they were hundreds of miles away in the Carpathian mountains, and there was no evidence to support that a different form of ritualistic trepanation ever took place in Byzantine-era Italy.
The investigators then moved on to a form of judicial punishment called decalvatio, which involves mutilation by scalping. Look, the Dark Ages weren’t dark, but no one said they were fun. Anyway, this was discarded, since decalvatio was only meted out to soldiers who deserted the battlefield.
That brings us back to surgery. While one of the trepanations was fully engraved into her skull, indicating that the woman died soon after the surgery, she also bore indications of a healed trepanation. A 50% success rate isn’t terrible for our medieval surgeon. Sure, the Incas managed 80%, but even during the Civil War brain surgery only had a 50% success rate. And that’s the end of the story, nothing more to say about our medieval Italian woman.
Nope. Nothing at all.
Fine. While a surgical procedure was deemed most likely, the study investigators found no direct evidence of a medical condition. No trauma, no tumor, nothing. Just a couple of suggestions of “a systemic pathological condition,” they said. Okay, we swear, it really wasn’t that bad in the Middle [Editor’s note: Approximately 5,000 more words on medieval culture not included. This is a medical column, thank you very much.]
We’re gonna need a bigger meth lab
In case you’ve been living under a rock for the past 15 years, the TV show “Breaking Bad” details the spiraling rise and downfall of a high school chemistry teacher who, after developing a case of terminal lung cancer, starts producing methamphetamine to provide for his family in response to the steep cost of treatment for his cancer.
Meanwhile, here in 2023 in the real world, we have Paul Davis, a retired physician in Ohio, who’s being forced to choose between an expensive cancer treatment and bankrupting his family, since Medicare’s decided it doesn’t want to cover the cost. Hey, we’ve seen this one before!
A bit of backstory: In November 2019, Dr. Davis was diagnosed with uveal melanoma, a very rare type of cancer that affects eye tissue. The news got worse in 2022 when the cancer spread to his liver, a move which typically proves fatal within a year. However, in a stroke of great news, the Food and Drug Administration approved the drug Kimmtrak earlier that year, which could be used to treat his cancer. Not cure, of course, but it would give him more time.
His initial treatments with the drug went fine and were covered, but when he transferred his care from a hospital in Columbus to one closer to home, big problem. Medicare decided it didn’t like that hospital and abruptly cut off coverage, denying the local hospital’s claims. That leaves Dr. Davis on the hook for his cancer treatment, and it’s what you might call expensive. Expensive to the tune of $50,000.
A week.
Apparently the coding the local hospital submitted was wrong, indicating that Dr. Davis was receiving Kimmtrak for a type of cancer that the FDA hadn’t approved the drug for. So until the government bureaucracy works itself out, his treatment is on hold, leaving all his faith in Medicare working quickly to rectify its mistake. If it can rectify its mistake. We’re not hopeful.
And in case you were wondering, if Dr. Davis wanted to go full Walter White, the average street price of meth is about $20-$60 per gram, so to pay for his treatment, he’d need to make at least a kilogram of meth every week. That’s, uh, quite a lot of illegal drug, or what we here at the LOTME office would call a fun Saturday night.
When you give a mouse a movie
Researchers have been successfully testing Alzheimer drugs on mice for years, but none of the drugs has proved successful in humans. Recent work, however, might have found the missing link, and it’s a combination no one ever thought of before: mice and movies.
Turns out that Orson Welles’ 1958 film noir classic “Touch of Evil” tapped a part of the mouse brain that has been overlooked: the hippocampus, which is crucial for learning and memory. Previous researchers thought it was just used as a kind of GPS system, but that’s only partially true.
Not only did the mice choose to pay attention to the movie clip, but the hippocampus responded to the visual stimuli only when the rodents saw the scenes from the clip later in the order that they were presented and not in a scrambled order. These findings represent a “major paradigm shift” in studying mouse recall, Mayank Mehta, PhD, of the University of California, Los Angeles, said in a statement from the school.
This breakthrough could run parallel to Alzheimer’s patients struggling with similar defects. “Selective and episodic activation of the mouse hippocampus using a human movie opens up the possibility of directly testing human episodic memory disorders and therapies using mouse neurons, a major step forward,” said coauthor Chinmay Purandare, PhD, who is now at the University of California, San Francisco.
Who would have thought that a classic film would help advance Alzheimer research?
A less human way to study mosquitoes
We here at LOTME have a history with mosquitoes. We know they don’t like us, and they know that we don’t like them. Trust us, they know. So when humans gain a little ground in the war against the buzzy little bloodsuckers, we want to share the joy.
To know the enemy, scientists have to study the enemy, but there is a problem. “Many mosquito experiments still rely on human volunteers and animal subjects,” bioengineering graduate student Kevin Janson, said in a statement from Rice University. Most people don’t like being bitten by mosquitoes, so that kind of testing can be expensive.
Is there a way to automate the collection and processing of mosquito behavior data using inexpensive cameras and machine-learning software? We’re glad you asked, because Mr. Janson and the research team, which includes bioengineers from Rice and tropical medicine experts from Tulane University, have managed to eliminate the need for live volunteers by using patches of synthetic skin made with a 3D printer.
“Each patch of gelatin-like hydrogel comes complete with tiny passageways that can be filled with flowing blood” from a chicken, sheep, or cow, they explained, and proof-of-concept testing showed that mosquitoes would feed on hydrogels without any repellent and stay away from those treated with a repellent.
To conduct the feeding tests, the blood-infused hydrogels are placed in a clear plastic box that is surrounded by cameras.
A bunch of mosquitoes are then tossed in the box and the cameras record all their insect activities: how often they land at each location, how long they stay, whether or not they bite, how long they feed, etc. Humans don’t have to watch and don’t have to be food sources.
Humans don’t have to be food sources, and we just pictured the future of mosquito control. Imagine a dozen Arnold Schwarzenegger–style Terminators, covered in 3D-printed skin, walking through your neighborhood in the summer while wearing sweat-soaked, brightly colored clothing. The mosquitoes wouldn’t be able to stay away, but guess what? They’re feeding off robots with nonhuman skin and nonhuman blood, so we win. It’s good to have a cerebral cortex.
Getting medieval on brain surgery
Let’s get one thing clear: The so-called “Dark Ages” were not nearly as dark as they’re made out to be. For one thing, there’s a world beyond Western Europe. The Roman Empire didn’t collapse everywhere. But even in Western Europe, the centuries between the fall of Rome and the Renaissance were hardly lacking in cultural development.
That said, we wouldn’t want to be in the position of the seventh-century noblewoman whose remains were recently uncovered in a Byzantine fortress in central Italy with multiple cross-shaped incisions in her skull. Yes, this unfortunate woman underwent at least two brain surgeries.
Then again, maybe not. Nothing like it had been discovered at the site, and while the markings – signs of a procedure called trepanation – can be surgical in nature, there are other explanations. For example, the Avar people practiced ritual trepanation during the same time period, but they were hundreds of miles away in the Carpathian mountains, and there was no evidence to support that a different form of ritualistic trepanation ever took place in Byzantine-era Italy.
The investigators then moved on to a form of judicial punishment called decalvatio, which involves mutilation by scalping. Look, the Dark Ages weren’t dark, but no one said they were fun. Anyway, this was discarded, since decalvatio was only meted out to soldiers who deserted the battlefield.
That brings us back to surgery. While one of the trepanations was fully engraved into her skull, indicating that the woman died soon after the surgery, she also bore indications of a healed trepanation. A 50% success rate isn’t terrible for our medieval surgeon. Sure, the Incas managed 80%, but even during the Civil War brain surgery only had a 50% success rate. And that’s the end of the story, nothing more to say about our medieval Italian woman.
Nope. Nothing at all.
Fine. While a surgical procedure was deemed most likely, the study investigators found no direct evidence of a medical condition. No trauma, no tumor, nothing. Just a couple of suggestions of “a systemic pathological condition,” they said. Okay, we swear, it really wasn’t that bad in the Middle [Editor’s note: Approximately 5,000 more words on medieval culture not included. This is a medical column, thank you very much.]
We’re gonna need a bigger meth lab
In case you’ve been living under a rock for the past 15 years, the TV show “Breaking Bad” details the spiraling rise and downfall of a high school chemistry teacher who, after developing a case of terminal lung cancer, starts producing methamphetamine to provide for his family in response to the steep cost of treatment for his cancer.
Meanwhile, here in 2023 in the real world, we have Paul Davis, a retired physician in Ohio, who’s being forced to choose between an expensive cancer treatment and bankrupting his family, since Medicare’s decided it doesn’t want to cover the cost. Hey, we’ve seen this one before!
A bit of backstory: In November 2019, Dr. Davis was diagnosed with uveal melanoma, a very rare type of cancer that affects eye tissue. The news got worse in 2022 when the cancer spread to his liver, a move which typically proves fatal within a year. However, in a stroke of great news, the Food and Drug Administration approved the drug Kimmtrak earlier that year, which could be used to treat his cancer. Not cure, of course, but it would give him more time.
His initial treatments with the drug went fine and were covered, but when he transferred his care from a hospital in Columbus to one closer to home, big problem. Medicare decided it didn’t like that hospital and abruptly cut off coverage, denying the local hospital’s claims. That leaves Dr. Davis on the hook for his cancer treatment, and it’s what you might call expensive. Expensive to the tune of $50,000.
A week.
Apparently the coding the local hospital submitted was wrong, indicating that Dr. Davis was receiving Kimmtrak for a type of cancer that the FDA hadn’t approved the drug for. So until the government bureaucracy works itself out, his treatment is on hold, leaving all his faith in Medicare working quickly to rectify its mistake. If it can rectify its mistake. We’re not hopeful.
And in case you were wondering, if Dr. Davis wanted to go full Walter White, the average street price of meth is about $20-$60 per gram, so to pay for his treatment, he’d need to make at least a kilogram of meth every week. That’s, uh, quite a lot of illegal drug, or what we here at the LOTME office would call a fun Saturday night.
When you give a mouse a movie
Researchers have been successfully testing Alzheimer drugs on mice for years, but none of the drugs has proved successful in humans. Recent work, however, might have found the missing link, and it’s a combination no one ever thought of before: mice and movies.
Turns out that Orson Welles’ 1958 film noir classic “Touch of Evil” tapped a part of the mouse brain that has been overlooked: the hippocampus, which is crucial for learning and memory. Previous researchers thought it was just used as a kind of GPS system, but that’s only partially true.
Not only did the mice choose to pay attention to the movie clip, but the hippocampus responded to the visual stimuli only when the rodents saw the scenes from the clip later in the order that they were presented and not in a scrambled order. These findings represent a “major paradigm shift” in studying mouse recall, Mayank Mehta, PhD, of the University of California, Los Angeles, said in a statement from the school.
This breakthrough could run parallel to Alzheimer’s patients struggling with similar defects. “Selective and episodic activation of the mouse hippocampus using a human movie opens up the possibility of directly testing human episodic memory disorders and therapies using mouse neurons, a major step forward,” said coauthor Chinmay Purandare, PhD, who is now at the University of California, San Francisco.
Who would have thought that a classic film would help advance Alzheimer research?
A less human way to study mosquitoes
We here at LOTME have a history with mosquitoes. We know they don’t like us, and they know that we don’t like them. Trust us, they know. So when humans gain a little ground in the war against the buzzy little bloodsuckers, we want to share the joy.
To know the enemy, scientists have to study the enemy, but there is a problem. “Many mosquito experiments still rely on human volunteers and animal subjects,” bioengineering graduate student Kevin Janson, said in a statement from Rice University. Most people don’t like being bitten by mosquitoes, so that kind of testing can be expensive.
Is there a way to automate the collection and processing of mosquito behavior data using inexpensive cameras and machine-learning software? We’re glad you asked, because Mr. Janson and the research team, which includes bioengineers from Rice and tropical medicine experts from Tulane University, have managed to eliminate the need for live volunteers by using patches of synthetic skin made with a 3D printer.
“Each patch of gelatin-like hydrogel comes complete with tiny passageways that can be filled with flowing blood” from a chicken, sheep, or cow, they explained, and proof-of-concept testing showed that mosquitoes would feed on hydrogels without any repellent and stay away from those treated with a repellent.
To conduct the feeding tests, the blood-infused hydrogels are placed in a clear plastic box that is surrounded by cameras.
A bunch of mosquitoes are then tossed in the box and the cameras record all their insect activities: how often they land at each location, how long they stay, whether or not they bite, how long they feed, etc. Humans don’t have to watch and don’t have to be food sources.
Humans don’t have to be food sources, and we just pictured the future of mosquito control. Imagine a dozen Arnold Schwarzenegger–style Terminators, covered in 3D-printed skin, walking through your neighborhood in the summer while wearing sweat-soaked, brightly colored clothing. The mosquitoes wouldn’t be able to stay away, but guess what? They’re feeding off robots with nonhuman skin and nonhuman blood, so we win. It’s good to have a cerebral cortex.
Getting medieval on brain surgery
Let’s get one thing clear: The so-called “Dark Ages” were not nearly as dark as they’re made out to be. For one thing, there’s a world beyond Western Europe. The Roman Empire didn’t collapse everywhere. But even in Western Europe, the centuries between the fall of Rome and the Renaissance were hardly lacking in cultural development.
That said, we wouldn’t want to be in the position of the seventh-century noblewoman whose remains were recently uncovered in a Byzantine fortress in central Italy with multiple cross-shaped incisions in her skull. Yes, this unfortunate woman underwent at least two brain surgeries.
Then again, maybe not. Nothing like it had been discovered at the site, and while the markings – signs of a procedure called trepanation – can be surgical in nature, there are other explanations. For example, the Avar people practiced ritual trepanation during the same time period, but they were hundreds of miles away in the Carpathian mountains, and there was no evidence to support that a different form of ritualistic trepanation ever took place in Byzantine-era Italy.
The investigators then moved on to a form of judicial punishment called decalvatio, which involves mutilation by scalping. Look, the Dark Ages weren’t dark, but no one said they were fun. Anyway, this was discarded, since decalvatio was only meted out to soldiers who deserted the battlefield.
That brings us back to surgery. While one of the trepanations was fully engraved into her skull, indicating that the woman died soon after the surgery, she also bore indications of a healed trepanation. A 50% success rate isn’t terrible for our medieval surgeon. Sure, the Incas managed 80%, but even during the Civil War brain surgery only had a 50% success rate. And that’s the end of the story, nothing more to say about our medieval Italian woman.
Nope. Nothing at all.
Fine. While a surgical procedure was deemed most likely, the study investigators found no direct evidence of a medical condition. No trauma, no tumor, nothing. Just a couple of suggestions of “a systemic pathological condition,” they said. Okay, we swear, it really wasn’t that bad in the Middle [Editor’s note: Approximately 5,000 more words on medieval culture not included. This is a medical column, thank you very much.]
PsA prediction tool approaches clinical utility
Easily collected variables establish risk
A new tool for predicting which patients with psoriasis will develop psoriatic arthritis (PsA) is showing promise for such clinical applications as early treatment in those at risk or trials to prevent PsA, according to a summary of progress at the annual meeting of the Canadian Rheumatology Association.
Based on current levels of sensitivity and specificity, psoriasis “can be predicted with reasonable accuracy,” reported Lihi Eder, MD, PhD, director of research in the rheumatology division at the University of Toronto.

The predictive method, called PRESTO (Prediction of Psoriatic Arthritis Tool), is based on variables readily available in clinical practice, according to Dr. Eder. Once values are assigned to the risk factors, the risk of PsA over a 1-year or 5-year time frame can be estimated with a calculator.
She called PRESTO the “first clinical tool for predicting PsA among psoriasis patients.”
The work on this tool began in 2006 when the International Psoriasis and Arthritis Research Team (IPART) initiated a prospectively collected cohort of psoriasis patients. To be enrolled, patients had to be free of signs and symptoms of arthritis upon examination by a rheumatologist. They were then invited to return annually for follow-up that again included screening for joint involvement by a rheumatologist.
At baseline and at follow-up evaluations, 13 predictors were evaluated. These involved psoriasis characteristics, such as nail pitting; symptoms, such as stiffness; comorbidities, such as additional inflammatory diseases; and laboratory values, such as upregulated markers of inflammation.
Symptoms and signs used to predict PsA
Dr. Eder and her colleagues applied regression models to select an optimal combination of variables weighted for predictive value. Variables offering predictive value included higher PASI (Psoriasis Area and Severity Index), greater fatigue score as measured by FACIT (Functional Assessment of Chronic Illness Therapy) score, greater morning stiffness, and greater pain.
When applied to 635 patients in the IPART cohort, in which there were 51 incident PsA cases over 1 year and 75 incident cases over 5 years, the area under the curve (AUC) for PRESTO at the cutoffs studied was 72% for the 1-year time window and 75% for the 5-year time window.
These levels are associated with adequate accuracy, according to Dr. Eder, who explained that “an AUC greater than 70% is considered reasonable” for clinical applicability.
Moreover, the cutoffs can be adjusted for the specific purpose of the predictive tool. For example, to screen patients for risk, lower cutoffs could be employed to increase sensitivity. In order to select patients for a clinical trial to prevent PsA, higher cutoffs could be employed to increase specificity.
But sensitivities and specificities move in opposite directions when cutoffs are adjusted. Showing data from the 5-year prediction model, Dr. Eder reported that specificities climbed from about 58% to 97% as cutoffs were increased. The sensitivities with these adjustments fell from 79% to 14%.
In general, Dr. Eder said there was “excellent calibration” for the cutoffs employed when they compared the predicted and observed rates of PsA according to quintile of predictive probability. The differences were particularly minor over a 1-year time period. Over the 5-year period, observed rates were somewhat higher than predicted in the fourth and fifth quintile, but, again, this discrepancy could be modified for specific applications with cutoff adjustments.
Validation studies are planned
Even though psoriasis patients in IPART represents one of the largest cohorts of prospectively collected psoriasis patients, Dr. Eder acknowledged that the sample size would be considered “moderate” for developing a predictive model. However, the fact that the data were collected prospectively using standardized methodology strengthens the findings and provides the basis for the next step.
“Validation studies are planned with external cohorts,” said Dr. Eder, who indicated that a viable tool for identifying psoriasis patients at risk for PsA is likely. Even if it is not employed routinely in its current form at the level of individual patient care, she predicted that it will have value at a research level for understanding the relationship of psoriasis to PsA.

Christopher T. Ritchlin, MD, a professor and researcher at the University of Rochester (N.Y.), agreed that PRESTO has important potential as a clinical tool. Dr. Ritchlin has been involved in the development of PRESTO but was not involved in the presentation made at the CRA annual meeting.
“The PRESTO tool has the ability to predict the 2- and 5-year risk of developing psoriatic arthritis, which is an important advance if confirmed,” he said in an interview. He pointed out that approximately 25%-30% who develop psoriasis will go on to develop PsA but until now there has been no way to identify them.
“This tool may provide a pathway to early intervention,” he said.
Dr. Eder has financial relationships with AbbVie, Eli Lilly, Fresenius Kabi, Janssen, Novartis, Pfizer, Sandoz, and UCB. Dr. Ritchlin has financial relationships with many of the same companies.
Easily collected variables establish risk
Easily collected variables establish risk
A new tool for predicting which patients with psoriasis will develop psoriatic arthritis (PsA) is showing promise for such clinical applications as early treatment in those at risk or trials to prevent PsA, according to a summary of progress at the annual meeting of the Canadian Rheumatology Association.
Based on current levels of sensitivity and specificity, psoriasis “can be predicted with reasonable accuracy,” reported Lihi Eder, MD, PhD, director of research in the rheumatology division at the University of Toronto.
The predictive method, called PRESTO (Prediction of Psoriatic Arthritis Tool), is based on variables readily available in clinical practice, according to Dr. Eder. Once values are assigned to the risk factors, the risk of PsA over a 1-year or 5-year time frame can be estimated with a calculator.
She called PRESTO the “first clinical tool for predicting PsA among psoriasis patients.”
The work on this tool began in 2006 when the International Psoriasis and Arthritis Research Team (IPART) initiated a prospectively collected cohort of psoriasis patients. To be enrolled, patients had to be free of signs and symptoms of arthritis upon examination by a rheumatologist. They were then invited to return annually for follow-up that again included screening for joint involvement by a rheumatologist.
At baseline and at follow-up evaluations, 13 predictors were evaluated. These involved psoriasis characteristics, such as nail pitting; symptoms, such as stiffness; comorbidities, such as additional inflammatory diseases; and laboratory values, such as upregulated markers of inflammation.
Symptoms and signs used to predict PsA
Dr. Eder and her colleagues applied regression models to select an optimal combination of variables weighted for predictive value. Variables offering predictive value included higher PASI (Psoriasis Area and Severity Index), greater fatigue score as measured by FACIT (Functional Assessment of Chronic Illness Therapy) score, greater morning stiffness, and greater pain.
When applied to 635 patients in the IPART cohort, in which there were 51 incident PsA cases over 1 year and 75 incident cases over 5 years, the area under the curve (AUC) for PRESTO at the cutoffs studied was 72% for the 1-year time window and 75% for the 5-year time window.
These levels are associated with adequate accuracy, according to Dr. Eder, who explained that “an AUC greater than 70% is considered reasonable” for clinical applicability.
Moreover, the cutoffs can be adjusted for the specific purpose of the predictive tool. For example, to screen patients for risk, lower cutoffs could be employed to increase sensitivity. In order to select patients for a clinical trial to prevent PsA, higher cutoffs could be employed to increase specificity.
But sensitivities and specificities move in opposite directions when cutoffs are adjusted. Showing data from the 5-year prediction model, Dr. Eder reported that specificities climbed from about 58% to 97% as cutoffs were increased. The sensitivities with these adjustments fell from 79% to 14%.
In general, Dr. Eder said there was “excellent calibration” for the cutoffs employed when they compared the predicted and observed rates of PsA according to quintile of predictive probability. The differences were particularly minor over a 1-year time period. Over the 5-year period, observed rates were somewhat higher than predicted in the fourth and fifth quintile, but, again, this discrepancy could be modified for specific applications with cutoff adjustments.
Validation studies are planned
Even though psoriasis patients in IPART represents one of the largest cohorts of prospectively collected psoriasis patients, Dr. Eder acknowledged that the sample size would be considered “moderate” for developing a predictive model. However, the fact that the data were collected prospectively using standardized methodology strengthens the findings and provides the basis for the next step.
“Validation studies are planned with external cohorts,” said Dr. Eder, who indicated that a viable tool for identifying psoriasis patients at risk for PsA is likely. Even if it is not employed routinely in its current form at the level of individual patient care, she predicted that it will have value at a research level for understanding the relationship of psoriasis to PsA.
Christopher T. Ritchlin, MD, a professor and researcher at the University of Rochester (N.Y.), agreed that PRESTO has important potential as a clinical tool. Dr. Ritchlin has been involved in the development of PRESTO but was not involved in the presentation made at the CRA annual meeting.
“The PRESTO tool has the ability to predict the 2- and 5-year risk of developing psoriatic arthritis, which is an important advance if confirmed,” he said in an interview. He pointed out that approximately 25%-30% who develop psoriasis will go on to develop PsA but until now there has been no way to identify them.
“This tool may provide a pathway to early intervention,” he said.
Dr. Eder has financial relationships with AbbVie, Eli Lilly, Fresenius Kabi, Janssen, Novartis, Pfizer, Sandoz, and UCB. Dr. Ritchlin has financial relationships with many of the same companies.
A new tool for predicting which patients with psoriasis will develop psoriatic arthritis (PsA) is showing promise for such clinical applications as early treatment in those at risk or trials to prevent PsA, according to a summary of progress at the annual meeting of the Canadian Rheumatology Association.
Based on current levels of sensitivity and specificity, psoriasis “can be predicted with reasonable accuracy,” reported Lihi Eder, MD, PhD, director of research in the rheumatology division at the University of Toronto.
The predictive method, called PRESTO (Prediction of Psoriatic Arthritis Tool), is based on variables readily available in clinical practice, according to Dr. Eder. Once values are assigned to the risk factors, the risk of PsA over a 1-year or 5-year time frame can be estimated with a calculator.
She called PRESTO the “first clinical tool for predicting PsA among psoriasis patients.”
The work on this tool began in 2006 when the International Psoriasis and Arthritis Research Team (IPART) initiated a prospectively collected cohort of psoriasis patients. To be enrolled, patients had to be free of signs and symptoms of arthritis upon examination by a rheumatologist. They were then invited to return annually for follow-up that again included screening for joint involvement by a rheumatologist.
At baseline and at follow-up evaluations, 13 predictors were evaluated. These involved psoriasis characteristics, such as nail pitting; symptoms, such as stiffness; comorbidities, such as additional inflammatory diseases; and laboratory values, such as upregulated markers of inflammation.
Symptoms and signs used to predict PsA
Dr. Eder and her colleagues applied regression models to select an optimal combination of variables weighted for predictive value. Variables offering predictive value included higher PASI (Psoriasis Area and Severity Index), greater fatigue score as measured by FACIT (Functional Assessment of Chronic Illness Therapy) score, greater morning stiffness, and greater pain.
When applied to 635 patients in the IPART cohort, in which there were 51 incident PsA cases over 1 year and 75 incident cases over 5 years, the area under the curve (AUC) for PRESTO at the cutoffs studied was 72% for the 1-year time window and 75% for the 5-year time window.
These levels are associated with adequate accuracy, according to Dr. Eder, who explained that “an AUC greater than 70% is considered reasonable” for clinical applicability.
Moreover, the cutoffs can be adjusted for the specific purpose of the predictive tool. For example, to screen patients for risk, lower cutoffs could be employed to increase sensitivity. In order to select patients for a clinical trial to prevent PsA, higher cutoffs could be employed to increase specificity.
But sensitivities and specificities move in opposite directions when cutoffs are adjusted. Showing data from the 5-year prediction model, Dr. Eder reported that specificities climbed from about 58% to 97% as cutoffs were increased. The sensitivities with these adjustments fell from 79% to 14%.
In general, Dr. Eder said there was “excellent calibration” for the cutoffs employed when they compared the predicted and observed rates of PsA according to quintile of predictive probability. The differences were particularly minor over a 1-year time period. Over the 5-year period, observed rates were somewhat higher than predicted in the fourth and fifth quintile, but, again, this discrepancy could be modified for specific applications with cutoff adjustments.
Validation studies are planned
Even though psoriasis patients in IPART represents one of the largest cohorts of prospectively collected psoriasis patients, Dr. Eder acknowledged that the sample size would be considered “moderate” for developing a predictive model. However, the fact that the data were collected prospectively using standardized methodology strengthens the findings and provides the basis for the next step.
“Validation studies are planned with external cohorts,” said Dr. Eder, who indicated that a viable tool for identifying psoriasis patients at risk for PsA is likely. Even if it is not employed routinely in its current form at the level of individual patient care, she predicted that it will have value at a research level for understanding the relationship of psoriasis to PsA.
Christopher T. Ritchlin, MD, a professor and researcher at the University of Rochester (N.Y.), agreed that PRESTO has important potential as a clinical tool. Dr. Ritchlin has been involved in the development of PRESTO but was not involved in the presentation made at the CRA annual meeting.
“The PRESTO tool has the ability to predict the 2- and 5-year risk of developing psoriatic arthritis, which is an important advance if confirmed,” he said in an interview. He pointed out that approximately 25%-30% who develop psoriasis will go on to develop PsA but until now there has been no way to identify them.
“This tool may provide a pathway to early intervention,” he said.
Dr. Eder has financial relationships with AbbVie, Eli Lilly, Fresenius Kabi, Janssen, Novartis, Pfizer, Sandoz, and UCB. Dr. Ritchlin has financial relationships with many of the same companies.
FROM CRA 2023
Appendicitis more often missed in patients who are Black
This phenomenon, first described in children, occurs in adults as well, according to a study published in JAMA Surgery.
Some hospitals fare better than others: Those with more diverse patient populations were less likely to have missed the diagnosis, the researchers found.
“We don’t think the amount of melanin in your skin predicts how you present with appendicitis,” said Jonathan Carter, MD, professor of surgery at the University of California, San Francisco. “There’s no biological explanation,” Dr. Carter, who wrote an invited commentary on the research, said in an interview. “It’s really what’s going on in the social environment of those emergency rooms.”
For the study, Anne Stey, MD, assistant professor of surgery at Northwestern University in Chicago and her colleagues analyzed data from more than 80,000 men and women in four states – Florida, Maryland, New York, and Wisconsin – who underwent appendectomy in 2016-2017.
They identified those who had been seen for abdominal complaints at a hospital in the week before surgery but did not receive a diagnosis of appendicitis at that time, indicating a missed opportunity to intervene sooner.
Among Black patients, the proportion who had experienced this type of delay was 3.6%, whereas for White patients, it was 2.5%. For Hispanic patients, the share was 2.4%, while for Asian or Pacific Islander patients, the figure was 1.5%.
An analysis that controlled for patient and hospital variables found that among non-Hispanic Black patients, the rate of delayed diagnosis was 1.41 times higher than for non-Hispanic White patients (95% confidence interval, 1.21-1.63).
Other patient factors associated with delayed diagnosis included female sex, comorbidities, and living in a low-income zip code.
A key factor was where patients sought care. A delayed diagnosis of appendicitis was 3.51 times more likely for patients who went to hospitals where most patients are insured by Medicaid. Prior research has shown that “safety-net hospitals have fewer resources and may provide lower-quality care than hospitals with a larger private payer population,” Dr. Stey’s group writes.
On the other hand, going to a hospital with a more diverse patient population reduced the odds of a delayed diagnosis.
“Patients presenting to hospitals with a greater than 50% Black and Hispanic population were 0.73 (95% CI, 0.59-0.91) times less likely to have a delayed diagnosis, compared with patients presenting to hospitals with a less than 25% Black and Hispanic population,” the researchers report.
In the 30 days after discharge following appendectomy, Black patients returned to the hospital at a higher rate than White patients did (17.5% vs. 11.4%), indicating worse outcomes.
“Delayed diagnosis may account for some of the racial and ethnic disparities observed in outcomes after appendicitis,” according to the authors.
“It may be hospitals that are more used to serving racial-ethnic minority patients are better at diagnosing them, because they’re more culturally informed and have a better understanding of these patients,” Dr. Stey said in a news release about their findings.
Great masquerader
Diagnosing appendicitis can be challenging, Dr. Carter said. The early signs can be subtle, and the condition is sometimes called the great masquerader. It is not uncommon for patients to be diagnosed with gastroenteritis or pain associated with their menstrual period, for example, and sent home.
Scoring systems based on patients’ symptoms and liberal use of imaging have improved detection of appendicitis, but “no physician or health care system is perfect in the diagnosis,” he said.
The increased odds of delayed diagnosis for Black patients remained when the researchers focused on healthier patients who had fewer comorbidities, and it also held when they considered patients with private insurance in high-income areas, Dr. Carter noted.
“Once again, with this study we see the association of structural and systematic racism with access to health care, especially for Black patients, in emergency departments and hospitals,” he wrote. “We must redouble our efforts to become anti-racist in ourselves, our institutions, and our profession.”
‘Our health care system itself’
Elizabeth Garner, MD, MPH, a pharmaceutical executive who was not involved in the study, commented on Twitter that the study points to an underlying issue that has existed in medicine “for quite some time.”
“Minority populations are not taken as seriously as their white counterparts,” she wrote. “This needs to change.”
Measures of hospital quality need to be tied to health equity, according to Mofya Diallo, MD, MPH, of the department of anesthesiology at the Children’s Hospital Los Angeles and the University of Southern California, Los Angeles.
“Top hospitals should take pride in outcomes that do not vary based on race, income or literacy,” she tweeted in response to the study.
To better understand possible reasons for delayed diagnosis, future researchers could assess whether patients who are Black are less likely to receive a surgical consultation, imaging studies, or lab work, Dr. Carter told this news organization. He pointed to a recent analysis of patients insured by Medicare that found that Black patients were less likely than White patients to receive a surgical consultation after they were admitted with colorectal, general abdominal, hepatopancreatobiliary, intestinal obstruction, or upper gastrointestinal diagnoses.
While social determinants of health, such as income, education, housing, early childhood development, employment, and social inclusion, may account for a substantial portion of health outcomes, “Our health care system itself can be viewed as another social determinant of health,” Dr. Carter wrote. “Insurance coverage, health care professional availability, health care professional linguistic and cultural competency, and quality of care all have an effect on health outcomes.”
Dr. Stey was supported by grants from the American College of Surgeons and the National Institutes of Health.
A version of this article originally appeared on Medscape.com.
This phenomenon, first described in children, occurs in adults as well, according to a study published in JAMA Surgery.
Some hospitals fare better than others: Those with more diverse patient populations were less likely to have missed the diagnosis, the researchers found.
“We don’t think the amount of melanin in your skin predicts how you present with appendicitis,” said Jonathan Carter, MD, professor of surgery at the University of California, San Francisco. “There’s no biological explanation,” Dr. Carter, who wrote an invited commentary on the research, said in an interview. “It’s really what’s going on in the social environment of those emergency rooms.”
For the study, Anne Stey, MD, assistant professor of surgery at Northwestern University in Chicago and her colleagues analyzed data from more than 80,000 men and women in four states – Florida, Maryland, New York, and Wisconsin – who underwent appendectomy in 2016-2017.
They identified those who had been seen for abdominal complaints at a hospital in the week before surgery but did not receive a diagnosis of appendicitis at that time, indicating a missed opportunity to intervene sooner.
Among Black patients, the proportion who had experienced this type of delay was 3.6%, whereas for White patients, it was 2.5%. For Hispanic patients, the share was 2.4%, while for Asian or Pacific Islander patients, the figure was 1.5%.
An analysis that controlled for patient and hospital variables found that among non-Hispanic Black patients, the rate of delayed diagnosis was 1.41 times higher than for non-Hispanic White patients (95% confidence interval, 1.21-1.63).
Other patient factors associated with delayed diagnosis included female sex, comorbidities, and living in a low-income zip code.
A key factor was where patients sought care. A delayed diagnosis of appendicitis was 3.51 times more likely for patients who went to hospitals where most patients are insured by Medicaid. Prior research has shown that “safety-net hospitals have fewer resources and may provide lower-quality care than hospitals with a larger private payer population,” Dr. Stey’s group writes.
On the other hand, going to a hospital with a more diverse patient population reduced the odds of a delayed diagnosis.
“Patients presenting to hospitals with a greater than 50% Black and Hispanic population were 0.73 (95% CI, 0.59-0.91) times less likely to have a delayed diagnosis, compared with patients presenting to hospitals with a less than 25% Black and Hispanic population,” the researchers report.
In the 30 days after discharge following appendectomy, Black patients returned to the hospital at a higher rate than White patients did (17.5% vs. 11.4%), indicating worse outcomes.
“Delayed diagnosis may account for some of the racial and ethnic disparities observed in outcomes after appendicitis,” according to the authors.
“It may be hospitals that are more used to serving racial-ethnic minority patients are better at diagnosing them, because they’re more culturally informed and have a better understanding of these patients,” Dr. Stey said in a news release about their findings.
Great masquerader
Diagnosing appendicitis can be challenging, Dr. Carter said. The early signs can be subtle, and the condition is sometimes called the great masquerader. It is not uncommon for patients to be diagnosed with gastroenteritis or pain associated with their menstrual period, for example, and sent home.
Scoring systems based on patients’ symptoms and liberal use of imaging have improved detection of appendicitis, but “no physician or health care system is perfect in the diagnosis,” he said.
The increased odds of delayed diagnosis for Black patients remained when the researchers focused on healthier patients who had fewer comorbidities, and it also held when they considered patients with private insurance in high-income areas, Dr. Carter noted.
“Once again, with this study we see the association of structural and systematic racism with access to health care, especially for Black patients, in emergency departments and hospitals,” he wrote. “We must redouble our efforts to become anti-racist in ourselves, our institutions, and our profession.”
‘Our health care system itself’
Elizabeth Garner, MD, MPH, a pharmaceutical executive who was not involved in the study, commented on Twitter that the study points to an underlying issue that has existed in medicine “for quite some time.”
“Minority populations are not taken as seriously as their white counterparts,” she wrote. “This needs to change.”
Measures of hospital quality need to be tied to health equity, according to Mofya Diallo, MD, MPH, of the department of anesthesiology at the Children’s Hospital Los Angeles and the University of Southern California, Los Angeles.
“Top hospitals should take pride in outcomes that do not vary based on race, income or literacy,” she tweeted in response to the study.
To better understand possible reasons for delayed diagnosis, future researchers could assess whether patients who are Black are less likely to receive a surgical consultation, imaging studies, or lab work, Dr. Carter told this news organization. He pointed to a recent analysis of patients insured by Medicare that found that Black patients were less likely than White patients to receive a surgical consultation after they were admitted with colorectal, general abdominal, hepatopancreatobiliary, intestinal obstruction, or upper gastrointestinal diagnoses.
While social determinants of health, such as income, education, housing, early childhood development, employment, and social inclusion, may account for a substantial portion of health outcomes, “Our health care system itself can be viewed as another social determinant of health,” Dr. Carter wrote. “Insurance coverage, health care professional availability, health care professional linguistic and cultural competency, and quality of care all have an effect on health outcomes.”
Dr. Stey was supported by grants from the American College of Surgeons and the National Institutes of Health.
A version of this article originally appeared on Medscape.com.
This phenomenon, first described in children, occurs in adults as well, according to a study published in JAMA Surgery.
Some hospitals fare better than others: Those with more diverse patient populations were less likely to have missed the diagnosis, the researchers found.
“We don’t think the amount of melanin in your skin predicts how you present with appendicitis,” said Jonathan Carter, MD, professor of surgery at the University of California, San Francisco. “There’s no biological explanation,” Dr. Carter, who wrote an invited commentary on the research, said in an interview. “It’s really what’s going on in the social environment of those emergency rooms.”
For the study, Anne Stey, MD, assistant professor of surgery at Northwestern University in Chicago and her colleagues analyzed data from more than 80,000 men and women in four states – Florida, Maryland, New York, and Wisconsin – who underwent appendectomy in 2016-2017.
They identified those who had been seen for abdominal complaints at a hospital in the week before surgery but did not receive a diagnosis of appendicitis at that time, indicating a missed opportunity to intervene sooner.
Among Black patients, the proportion who had experienced this type of delay was 3.6%, whereas for White patients, it was 2.5%. For Hispanic patients, the share was 2.4%, while for Asian or Pacific Islander patients, the figure was 1.5%.
An analysis that controlled for patient and hospital variables found that among non-Hispanic Black patients, the rate of delayed diagnosis was 1.41 times higher than for non-Hispanic White patients (95% confidence interval, 1.21-1.63).
Other patient factors associated with delayed diagnosis included female sex, comorbidities, and living in a low-income zip code.
A key factor was where patients sought care. A delayed diagnosis of appendicitis was 3.51 times more likely for patients who went to hospitals where most patients are insured by Medicaid. Prior research has shown that “safety-net hospitals have fewer resources and may provide lower-quality care than hospitals with a larger private payer population,” Dr. Stey’s group writes.
On the other hand, going to a hospital with a more diverse patient population reduced the odds of a delayed diagnosis.
“Patients presenting to hospitals with a greater than 50% Black and Hispanic population were 0.73 (95% CI, 0.59-0.91) times less likely to have a delayed diagnosis, compared with patients presenting to hospitals with a less than 25% Black and Hispanic population,” the researchers report.
In the 30 days after discharge following appendectomy, Black patients returned to the hospital at a higher rate than White patients did (17.5% vs. 11.4%), indicating worse outcomes.
“Delayed diagnosis may account for some of the racial and ethnic disparities observed in outcomes after appendicitis,” according to the authors.
“It may be hospitals that are more used to serving racial-ethnic minority patients are better at diagnosing them, because they’re more culturally informed and have a better understanding of these patients,” Dr. Stey said in a news release about their findings.
Great masquerader
Diagnosing appendicitis can be challenging, Dr. Carter said. The early signs can be subtle, and the condition is sometimes called the great masquerader. It is not uncommon for patients to be diagnosed with gastroenteritis or pain associated with their menstrual period, for example, and sent home.
Scoring systems based on patients’ symptoms and liberal use of imaging have improved detection of appendicitis, but “no physician or health care system is perfect in the diagnosis,” he said.
The increased odds of delayed diagnosis for Black patients remained when the researchers focused on healthier patients who had fewer comorbidities, and it also held when they considered patients with private insurance in high-income areas, Dr. Carter noted.
“Once again, with this study we see the association of structural and systematic racism with access to health care, especially for Black patients, in emergency departments and hospitals,” he wrote. “We must redouble our efforts to become anti-racist in ourselves, our institutions, and our profession.”
‘Our health care system itself’
Elizabeth Garner, MD, MPH, a pharmaceutical executive who was not involved in the study, commented on Twitter that the study points to an underlying issue that has existed in medicine “for quite some time.”
“Minority populations are not taken as seriously as their white counterparts,” she wrote. “This needs to change.”
Measures of hospital quality need to be tied to health equity, according to Mofya Diallo, MD, MPH, of the department of anesthesiology at the Children’s Hospital Los Angeles and the University of Southern California, Los Angeles.
“Top hospitals should take pride in outcomes that do not vary based on race, income or literacy,” she tweeted in response to the study.
To better understand possible reasons for delayed diagnosis, future researchers could assess whether patients who are Black are less likely to receive a surgical consultation, imaging studies, or lab work, Dr. Carter told this news organization. He pointed to a recent analysis of patients insured by Medicare that found that Black patients were less likely than White patients to receive a surgical consultation after they were admitted with colorectal, general abdominal, hepatopancreatobiliary, intestinal obstruction, or upper gastrointestinal diagnoses.
While social determinants of health, such as income, education, housing, early childhood development, employment, and social inclusion, may account for a substantial portion of health outcomes, “Our health care system itself can be viewed as another social determinant of health,” Dr. Carter wrote. “Insurance coverage, health care professional availability, health care professional linguistic and cultural competency, and quality of care all have an effect on health outcomes.”
Dr. Stey was supported by grants from the American College of Surgeons and the National Institutes of Health.
A version of this article originally appeared on Medscape.com.
FROM JAMA SURGERY
Obstetric violence: How it’s defined and how we face it
In a recent, tragic case, a newborn died from being crushed by its mother, who fell asleep from the fatigue of numerous hours of labor. The case has brought the issue of obstetric violence (OV) to the attention of the Italian media. OV is defined as neglect, physical abuse, or disrespect during childbirth, according to the World Health Organization. The WHO outlined fundamental actions to be taken at various levels for its prevention, especially by health care systems, in a 2014 position paper.
Gender-based abuse
Considered a form of gender-based abuse, OV was first described in Latin America in the early 2000s. It is widespread and is increasing in European countries.
From the scientific literature on the subject, OV seems to be strongly associated with a lack of communication between health care personnel and pregnant women. It appears to have more to do with authoritarian and paternalistic behavior than actual real-life medical issues. Actively involving women in decision-making regarding childbirth and postpartum care seems to reduce the incidence of OV. Pregnant women who are more involved appear to trust health care professionals more and are therefore less likely to report disrespectful and abusive behavior.
Estimates of the prevalence of OV vary, depending on the country, the childbirth facility, and its definition. In Italy, inspired by the web campaign “#Bastatacere: le madri hanno voce [#EnoughSilence: mothers have a voice],” in 2017, the Obstetric Violence Database (OVO) investigated perceptions of having been a victim of OV in a representative sample of Italian women aged 18-54 years who had at least one child.
In 2017, just over 20% of the women interviewed considered themselves victims of OV; 33% felt they had not received adequate care; and around 35% reported serious problems concerning privacy or trust. Following the treatment received, approximately 15% of the women decided not to return to the same health care facility, and 6% did not want to proceed with further pregnancies.
At the time of publication, the results sparked a debate among relevant medical associations (the Association of Obstetricians and Gynecologists of Italian Hospitals, the Italian Society of Gynecology and Obstetrics, and the Association of Italian University Gynecologists), which immediately recognized the importance of the topic and accepted an invitation for further discussion on physician-patient relationships. They expressed reservations concerning the methodologies used by the OVO for data collection, especially regarding the representativeness of the sample.
Lack of communication
“In general, women who claim to have suffered from obstetric violence do not do so because they have been denied an aspect of care but because they have had an overall experience that, for whatever reason, did not conform with their expectations,” said Irene Cetin, MD, PhD, professor of obstetrics and gynecology at the University of Milan and director of the obstetrics and gynecology unit of the Buzzi Hospital in Milan. “Following the OVO’s exposé, the Italian Society of Gynecology and Obstetrics also conducted a large-scale study throughout Italy on all women who had given birth within a 3-month period. That investigation painted a very different picture. It wasn’t the case that no instances of obstetric violence were found, but the results were more contained. This is a very delicate subject, given that every report that we receive in hospital is always valued and looked into in detail, and women come to speak to us about errors and things that were missed.”
She added, “Experience leads me to say that complaints about what happens in the delivery room are extremely rare. What we hear more of, but still not often, are problems experienced during days spent in hospital immediately after childbirth.” There are never enough resources, which is the reason behind most problems. “The real hardships are found in the wards,” continued Dr. Cetin, “where the midwife-to-bed ratio is one or two to 30, and therefore this is where it is more difficult to feel like you’re being listened to. With COVID-19, the situation has gotten even worse, even though in my hospital we have always guaranteed, not without struggle, the presence of the partner in the delivery room.”
Only relatively recently have women’s partners been allowed into the hospital. In addition, a number of services, such as having the right beds and giving the correct explanations and information on how to establish a relationship with the child, are now being offered. These steps are necessary to guarantee what is referred to as a “humanizing birth,” a process in which the woman is at the center of the experience and is the main protagonist of the birth.
Lack of resources
This trend also is observed at the systemic level, where there is a lack of organization and resources. Few staff members are in the ward, even fewer specialists are in the psychological field, and contact is almost nonexistent after discharge from many hospitals and in many regions across Italy. There are, however, some positive aspects and hope for the future. “Just think,” said Dr. Cetin, “of how degree courses in obstetrics have changed over time, with a large part of teaching and training now being centered around the emotional aspects of birth.” From the gynecologist’s side, “most of the problems have been inherited from the past,” said Dr. Cetin. “Let’s not forget that we have only recently been giving birth in hospital. The so-called medicalization of childbirth has been responsible for a decline in the death rate and morbidity rate of pregnant women, but initially, there was little interest or care in how women felt in this situation, including with regard to physical pain. Since the 1970s, with Leboyer from France and Miraglia from Italy [promoters of so-called sweet birth], a path was cleared for a different line of thought. For this reason, I believe that the situation will improve over time.
“To continuously improve physician-patient communication,” concluded Dr. Cetin, “it would perhaps be appropriate to make sure that, even in the preparatory phase, women are well aware of possible complications and of the necessary and rapid emergency procedures that must be implemented by health care personnel. This way, a trusting relationship could be maintained, and the perception of having suffered abuse due to not being involved in strictly medical decisions could be stemmed.”
This article was translated from Univadis Italy. A version of this article appeared on Medscape.com.
In a recent, tragic case, a newborn died from being crushed by its mother, who fell asleep from the fatigue of numerous hours of labor. The case has brought the issue of obstetric violence (OV) to the attention of the Italian media. OV is defined as neglect, physical abuse, or disrespect during childbirth, according to the World Health Organization. The WHO outlined fundamental actions to be taken at various levels for its prevention, especially by health care systems, in a 2014 position paper.
Gender-based abuse
Considered a form of gender-based abuse, OV was first described in Latin America in the early 2000s. It is widespread and is increasing in European countries.
From the scientific literature on the subject, OV seems to be strongly associated with a lack of communication between health care personnel and pregnant women. It appears to have more to do with authoritarian and paternalistic behavior than actual real-life medical issues. Actively involving women in decision-making regarding childbirth and postpartum care seems to reduce the incidence of OV. Pregnant women who are more involved appear to trust health care professionals more and are therefore less likely to report disrespectful and abusive behavior.
Estimates of the prevalence of OV vary, depending on the country, the childbirth facility, and its definition. In Italy, inspired by the web campaign “#Bastatacere: le madri hanno voce [#EnoughSilence: mothers have a voice],” in 2017, the Obstetric Violence Database (OVO) investigated perceptions of having been a victim of OV in a representative sample of Italian women aged 18-54 years who had at least one child.
In 2017, just over 20% of the women interviewed considered themselves victims of OV; 33% felt they had not received adequate care; and around 35% reported serious problems concerning privacy or trust. Following the treatment received, approximately 15% of the women decided not to return to the same health care facility, and 6% did not want to proceed with further pregnancies.
At the time of publication, the results sparked a debate among relevant medical associations (the Association of Obstetricians and Gynecologists of Italian Hospitals, the Italian Society of Gynecology and Obstetrics, and the Association of Italian University Gynecologists), which immediately recognized the importance of the topic and accepted an invitation for further discussion on physician-patient relationships. They expressed reservations concerning the methodologies used by the OVO for data collection, especially regarding the representativeness of the sample.
Lack of communication
“In general, women who claim to have suffered from obstetric violence do not do so because they have been denied an aspect of care but because they have had an overall experience that, for whatever reason, did not conform with their expectations,” said Irene Cetin, MD, PhD, professor of obstetrics and gynecology at the University of Milan and director of the obstetrics and gynecology unit of the Buzzi Hospital in Milan. “Following the OVO’s exposé, the Italian Society of Gynecology and Obstetrics also conducted a large-scale study throughout Italy on all women who had given birth within a 3-month period. That investigation painted a very different picture. It wasn’t the case that no instances of obstetric violence were found, but the results were more contained. This is a very delicate subject, given that every report that we receive in hospital is always valued and looked into in detail, and women come to speak to us about errors and things that were missed.”
She added, “Experience leads me to say that complaints about what happens in the delivery room are extremely rare. What we hear more of, but still not often, are problems experienced during days spent in hospital immediately after childbirth.” There are never enough resources, which is the reason behind most problems. “The real hardships are found in the wards,” continued Dr. Cetin, “where the midwife-to-bed ratio is one or two to 30, and therefore this is where it is more difficult to feel like you’re being listened to. With COVID-19, the situation has gotten even worse, even though in my hospital we have always guaranteed, not without struggle, the presence of the partner in the delivery room.”
Only relatively recently have women’s partners been allowed into the hospital. In addition, a number of services, such as having the right beds and giving the correct explanations and information on how to establish a relationship with the child, are now being offered. These steps are necessary to guarantee what is referred to as a “humanizing birth,” a process in which the woman is at the center of the experience and is the main protagonist of the birth.
Lack of resources
This trend also is observed at the systemic level, where there is a lack of organization and resources. Few staff members are in the ward, even fewer specialists are in the psychological field, and contact is almost nonexistent after discharge from many hospitals and in many regions across Italy. There are, however, some positive aspects and hope for the future. “Just think,” said Dr. Cetin, “of how degree courses in obstetrics have changed over time, with a large part of teaching and training now being centered around the emotional aspects of birth.” From the gynecologist’s side, “most of the problems have been inherited from the past,” said Dr. Cetin. “Let’s not forget that we have only recently been giving birth in hospital. The so-called medicalization of childbirth has been responsible for a decline in the death rate and morbidity rate of pregnant women, but initially, there was little interest or care in how women felt in this situation, including with regard to physical pain. Since the 1970s, with Leboyer from France and Miraglia from Italy [promoters of so-called sweet birth], a path was cleared for a different line of thought. For this reason, I believe that the situation will improve over time.
“To continuously improve physician-patient communication,” concluded Dr. Cetin, “it would perhaps be appropriate to make sure that, even in the preparatory phase, women are well aware of possible complications and of the necessary and rapid emergency procedures that must be implemented by health care personnel. This way, a trusting relationship could be maintained, and the perception of having suffered abuse due to not being involved in strictly medical decisions could be stemmed.”
This article was translated from Univadis Italy. A version of this article appeared on Medscape.com.
In a recent, tragic case, a newborn died from being crushed by its mother, who fell asleep from the fatigue of numerous hours of labor. The case has brought the issue of obstetric violence (OV) to the attention of the Italian media. OV is defined as neglect, physical abuse, or disrespect during childbirth, according to the World Health Organization. The WHO outlined fundamental actions to be taken at various levels for its prevention, especially by health care systems, in a 2014 position paper.
Gender-based abuse
Considered a form of gender-based abuse, OV was first described in Latin America in the early 2000s. It is widespread and is increasing in European countries.
From the scientific literature on the subject, OV seems to be strongly associated with a lack of communication between health care personnel and pregnant women. It appears to have more to do with authoritarian and paternalistic behavior than actual real-life medical issues. Actively involving women in decision-making regarding childbirth and postpartum care seems to reduce the incidence of OV. Pregnant women who are more involved appear to trust health care professionals more and are therefore less likely to report disrespectful and abusive behavior.
Estimates of the prevalence of OV vary, depending on the country, the childbirth facility, and its definition. In Italy, inspired by the web campaign “#Bastatacere: le madri hanno voce [#EnoughSilence: mothers have a voice],” in 2017, the Obstetric Violence Database (OVO) investigated perceptions of having been a victim of OV in a representative sample of Italian women aged 18-54 years who had at least one child.
In 2017, just over 20% of the women interviewed considered themselves victims of OV; 33% felt they had not received adequate care; and around 35% reported serious problems concerning privacy or trust. Following the treatment received, approximately 15% of the women decided not to return to the same health care facility, and 6% did not want to proceed with further pregnancies.
At the time of publication, the results sparked a debate among relevant medical associations (the Association of Obstetricians and Gynecologists of Italian Hospitals, the Italian Society of Gynecology and Obstetrics, and the Association of Italian University Gynecologists), which immediately recognized the importance of the topic and accepted an invitation for further discussion on physician-patient relationships. They expressed reservations concerning the methodologies used by the OVO for data collection, especially regarding the representativeness of the sample.
Lack of communication
“In general, women who claim to have suffered from obstetric violence do not do so because they have been denied an aspect of care but because they have had an overall experience that, for whatever reason, did not conform with their expectations,” said Irene Cetin, MD, PhD, professor of obstetrics and gynecology at the University of Milan and director of the obstetrics and gynecology unit of the Buzzi Hospital in Milan. “Following the OVO’s exposé, the Italian Society of Gynecology and Obstetrics also conducted a large-scale study throughout Italy on all women who had given birth within a 3-month period. That investigation painted a very different picture. It wasn’t the case that no instances of obstetric violence were found, but the results were more contained. This is a very delicate subject, given that every report that we receive in hospital is always valued and looked into in detail, and women come to speak to us about errors and things that were missed.”
She added, “Experience leads me to say that complaints about what happens in the delivery room are extremely rare. What we hear more of, but still not often, are problems experienced during days spent in hospital immediately after childbirth.” There are never enough resources, which is the reason behind most problems. “The real hardships are found in the wards,” continued Dr. Cetin, “where the midwife-to-bed ratio is one or two to 30, and therefore this is where it is more difficult to feel like you’re being listened to. With COVID-19, the situation has gotten even worse, even though in my hospital we have always guaranteed, not without struggle, the presence of the partner in the delivery room.”
Only relatively recently have women’s partners been allowed into the hospital. In addition, a number of services, such as having the right beds and giving the correct explanations and information on how to establish a relationship with the child, are now being offered. These steps are necessary to guarantee what is referred to as a “humanizing birth,” a process in which the woman is at the center of the experience and is the main protagonist of the birth.
Lack of resources
This trend also is observed at the systemic level, where there is a lack of organization and resources. Few staff members are in the ward, even fewer specialists are in the psychological field, and contact is almost nonexistent after discharge from many hospitals and in many regions across Italy. There are, however, some positive aspects and hope for the future. “Just think,” said Dr. Cetin, “of how degree courses in obstetrics have changed over time, with a large part of teaching and training now being centered around the emotional aspects of birth.” From the gynecologist’s side, “most of the problems have been inherited from the past,” said Dr. Cetin. “Let’s not forget that we have only recently been giving birth in hospital. The so-called medicalization of childbirth has been responsible for a decline in the death rate and morbidity rate of pregnant women, but initially, there was little interest or care in how women felt in this situation, including with regard to physical pain. Since the 1970s, with Leboyer from France and Miraglia from Italy [promoters of so-called sweet birth], a path was cleared for a different line of thought. For this reason, I believe that the situation will improve over time.
“To continuously improve physician-patient communication,” concluded Dr. Cetin, “it would perhaps be appropriate to make sure that, even in the preparatory phase, women are well aware of possible complications and of the necessary and rapid emergency procedures that must be implemented by health care personnel. This way, a trusting relationship could be maintained, and the perception of having suffered abuse due to not being involved in strictly medical decisions could be stemmed.”
This article was translated from Univadis Italy. A version of this article appeared on Medscape.com.
Eye drops delay, may even prevent, nearsightedness
Dilating eye drops may delay – and perhaps even prevent – the onset of myopia in children, according to findings from a study published in JAMA. The study was conducted by researchers in Hong Kong.
Myopia is irreversible once it takes root and can contribute to other vision problems, such as macular degeneration, retinal detachment, glaucoma, and cataracts. The incidence of nearsightedness has nearly doubled since the 1970s, rising from 25% of the U.S. population to nearly 42%. Children have been particularly affected by the increase; reasons may include spending more time indoors looking at screens, experts say.
“Myopia is an ongoing and growing worldwide concern. This is of particular importance because of the change in children’s lifestyle, such as decreased outdoor time and increased screen time during and after the COVID-19 pandemic,” Jason C. Yam, MPH, of the department of ophthalmology and visual services at the Chinese University of Hong Kong, said in an interview.
Mr. Yam said that, while encouraging children to engage more in outdoor activity and spend less time using screens would help delay myopia, pharmaceutical interventions are needed, given myopia’s potential lifelong effects.
Putting eye drops to the test
In 2020, Mr. Yam and colleagues reported results of the Low-Concentration Atropine for Myopia Progression (LAMP) study, which showed that eye drops containing a solution of 0.05% atropine worked best at slowing the progression of myopia in 4- to 12-year-olds who already had the condition. Atropine relaxes eye muscles, causing dilation.
In that study, Mr. Yam and colleagues measured the rate of change in the eye’s ability to see at a great distance using a unit of measure known as the diopter. The higher the diopter, the more myopic a person’s vision. The 0.05% atropine solution was better at slowing this decline than placebo or solutions that contained a lower concentration of the substance.
The new study enrolled 474 children who were evenly divided by sex. None of the children had myopia when the trial began. Of that starting group, 353 children (age, 4-9 years) completed the study, which involved receiving eye drops once nightly in both eyes for 2 years.
Some children (n = 116) received 0.05% atropine, others (n = 122) received 0.01% atropine, and the rest (n = 115) received placebo drops. Mr. Yam and colleagues assessed how many children in each group had myopia after 2 years, as measured by a decline of at least a half diopter in one eye.
At the 2-year mark, more than half of children who received the placebo drops (61/115) had developed myopia, as had nearly half of those given 0.01% atropine (56/122). But fewer than one-third of children (33/116, 28.4%) who had received the drops with 0.05% atropine developed myopia during that period, the researchers reported.
The percentage of children with myopia in the placebo group (39/128, 30.5%) was larger by the end of the first year of the study than was the share of children in the 0.05% atropine group by the end of the trial. (Between 12 months and 24 months, 13 children in the placebo group left the study.) The main adverse event, in all treatment groups, was discomfort when exposed to bright light, according to the researchers.
“We are continuing the current study with the total intended follow-up duration of at least 6years,” added Mr. Yam, who hopes to determine whether the 0.05% atropine solution not only delays myopia but also prevents it altogether. While myopia is a concern worldwide, the condition is particularly prevalent in East Asia.
Mark A. Bullimore, MCOptom, PhD, FAAO, an adjunct professor at the University of Houston, and a consultant to ophthalmologic companies, called the trial “a landmark study. Finding children who are eligible and parents who are willing to deal with 2 years of drops is no small feat.
“The 0.05% atropine, on average, delays onset of myopia by a year,” Dr. Bullimore noted. He pointed to the similar percentages of myopia with placebo at 12 months, compared with 0.05% atropine 1 year later. He added that few clinicians in the United States use higher than 0.05% atropine for control of myopia because doing so can lead to excessive dilation and difficulty focusing.
While preventing myopia altogether would be ideal, simply delaying its onset can also be of tangible benefit, Bullimore said. In an article published in January, Dr. Bullimore and Noel A. Brennan of Johnson & Johnson Vision showed that delaying the onset of myopia reduces its severity.
“Optometrists prescribe low-concentration atropine already for myopia control, and there’s no reason now – in the light of this study – that they wouldn’t also do it to delay onset,” Dr. Bullimore said.
But in an editorial accompanying the journal article David A. Berntsen, OD, PhD, and Jeffrey J. Walline, OD, PhD, both of the University of Houston, wrote that a change in practice would be premature.
“The evidence presented does not yet warrant a change in the standard care of children because we do not yet know the long-term effects of delaying the onset of myopia with low-concentration atropine,” they wrote.
Identifying which children to consider for treatment is “a challenge,” they noted, because those who are not nearsighted typically do not undergo routine examination unless they have failed a vision test.
“Ultimately, the implementation of vision screenings that include determining a child’s prescription will likely be needed to identify children most likely to become myopic who may benefit from low-concentration atropine,” Dr. Berntsen and Dr. Walline wrote.
Mr. Yam and coinvestigators have applied for a patent on a 0.05% atropine solution. Dr. Bullimore reported relationships with Alcon Research,CooperVision, CorneaGen, EssilorLuxottica, Eyenovia, Genentech, Johnson & Johnson Vision, Lentechs, Novartis, and Vyluma, and is the sole owner of Ridgevue Publishing and Ridgevue Vision.
A version of this article first appeared on Medscape.com.
Dilating eye drops may delay – and perhaps even prevent – the onset of myopia in children, according to findings from a study published in JAMA. The study was conducted by researchers in Hong Kong.
Myopia is irreversible once it takes root and can contribute to other vision problems, such as macular degeneration, retinal detachment, glaucoma, and cataracts. The incidence of nearsightedness has nearly doubled since the 1970s, rising from 25% of the U.S. population to nearly 42%. Children have been particularly affected by the increase; reasons may include spending more time indoors looking at screens, experts say.
“Myopia is an ongoing and growing worldwide concern. This is of particular importance because of the change in children’s lifestyle, such as decreased outdoor time and increased screen time during and after the COVID-19 pandemic,” Jason C. Yam, MPH, of the department of ophthalmology and visual services at the Chinese University of Hong Kong, said in an interview.
Mr. Yam said that, while encouraging children to engage more in outdoor activity and spend less time using screens would help delay myopia, pharmaceutical interventions are needed, given myopia’s potential lifelong effects.
Putting eye drops to the test
In 2020, Mr. Yam and colleagues reported results of the Low-Concentration Atropine for Myopia Progression (LAMP) study, which showed that eye drops containing a solution of 0.05% atropine worked best at slowing the progression of myopia in 4- to 12-year-olds who already had the condition. Atropine relaxes eye muscles, causing dilation.
In that study, Mr. Yam and colleagues measured the rate of change in the eye’s ability to see at a great distance using a unit of measure known as the diopter. The higher the diopter, the more myopic a person’s vision. The 0.05% atropine solution was better at slowing this decline than placebo or solutions that contained a lower concentration of the substance.
The new study enrolled 474 children who were evenly divided by sex. None of the children had myopia when the trial began. Of that starting group, 353 children (age, 4-9 years) completed the study, which involved receiving eye drops once nightly in both eyes for 2 years.
Some children (n = 116) received 0.05% atropine, others (n = 122) received 0.01% atropine, and the rest (n = 115) received placebo drops. Mr. Yam and colleagues assessed how many children in each group had myopia after 2 years, as measured by a decline of at least a half diopter in one eye.
At the 2-year mark, more than half of children who received the placebo drops (61/115) had developed myopia, as had nearly half of those given 0.01% atropine (56/122). But fewer than one-third of children (33/116, 28.4%) who had received the drops with 0.05% atropine developed myopia during that period, the researchers reported.
The percentage of children with myopia in the placebo group (39/128, 30.5%) was larger by the end of the first year of the study than was the share of children in the 0.05% atropine group by the end of the trial. (Between 12 months and 24 months, 13 children in the placebo group left the study.) The main adverse event, in all treatment groups, was discomfort when exposed to bright light, according to the researchers.
“We are continuing the current study with the total intended follow-up duration of at least 6years,” added Mr. Yam, who hopes to determine whether the 0.05% atropine solution not only delays myopia but also prevents it altogether. While myopia is a concern worldwide, the condition is particularly prevalent in East Asia.
Mark A. Bullimore, MCOptom, PhD, FAAO, an adjunct professor at the University of Houston, and a consultant to ophthalmologic companies, called the trial “a landmark study. Finding children who are eligible and parents who are willing to deal with 2 years of drops is no small feat.
“The 0.05% atropine, on average, delays onset of myopia by a year,” Dr. Bullimore noted. He pointed to the similar percentages of myopia with placebo at 12 months, compared with 0.05% atropine 1 year later. He added that few clinicians in the United States use higher than 0.05% atropine for control of myopia because doing so can lead to excessive dilation and difficulty focusing.
While preventing myopia altogether would be ideal, simply delaying its onset can also be of tangible benefit, Bullimore said. In an article published in January, Dr. Bullimore and Noel A. Brennan of Johnson & Johnson Vision showed that delaying the onset of myopia reduces its severity.
“Optometrists prescribe low-concentration atropine already for myopia control, and there’s no reason now – in the light of this study – that they wouldn’t also do it to delay onset,” Dr. Bullimore said.
But in an editorial accompanying the journal article David A. Berntsen, OD, PhD, and Jeffrey J. Walline, OD, PhD, both of the University of Houston, wrote that a change in practice would be premature.
“The evidence presented does not yet warrant a change in the standard care of children because we do not yet know the long-term effects of delaying the onset of myopia with low-concentration atropine,” they wrote.
Identifying which children to consider for treatment is “a challenge,” they noted, because those who are not nearsighted typically do not undergo routine examination unless they have failed a vision test.
“Ultimately, the implementation of vision screenings that include determining a child’s prescription will likely be needed to identify children most likely to become myopic who may benefit from low-concentration atropine,” Dr. Berntsen and Dr. Walline wrote.
Mr. Yam and coinvestigators have applied for a patent on a 0.05% atropine solution. Dr. Bullimore reported relationships with Alcon Research,CooperVision, CorneaGen, EssilorLuxottica, Eyenovia, Genentech, Johnson & Johnson Vision, Lentechs, Novartis, and Vyluma, and is the sole owner of Ridgevue Publishing and Ridgevue Vision.
A version of this article first appeared on Medscape.com.
Dilating eye drops may delay – and perhaps even prevent – the onset of myopia in children, according to findings from a study published in JAMA. The study was conducted by researchers in Hong Kong.
Myopia is irreversible once it takes root and can contribute to other vision problems, such as macular degeneration, retinal detachment, glaucoma, and cataracts. The incidence of nearsightedness has nearly doubled since the 1970s, rising from 25% of the U.S. population to nearly 42%. Children have been particularly affected by the increase; reasons may include spending more time indoors looking at screens, experts say.
“Myopia is an ongoing and growing worldwide concern. This is of particular importance because of the change in children’s lifestyle, such as decreased outdoor time and increased screen time during and after the COVID-19 pandemic,” Jason C. Yam, MPH, of the department of ophthalmology and visual services at the Chinese University of Hong Kong, said in an interview.
Mr. Yam said that, while encouraging children to engage more in outdoor activity and spend less time using screens would help delay myopia, pharmaceutical interventions are needed, given myopia’s potential lifelong effects.
Putting eye drops to the test
In 2020, Mr. Yam and colleagues reported results of the Low-Concentration Atropine for Myopia Progression (LAMP) study, which showed that eye drops containing a solution of 0.05% atropine worked best at slowing the progression of myopia in 4- to 12-year-olds who already had the condition. Atropine relaxes eye muscles, causing dilation.
In that study, Mr. Yam and colleagues measured the rate of change in the eye’s ability to see at a great distance using a unit of measure known as the diopter. The higher the diopter, the more myopic a person’s vision. The 0.05% atropine solution was better at slowing this decline than placebo or solutions that contained a lower concentration of the substance.
The new study enrolled 474 children who were evenly divided by sex. None of the children had myopia when the trial began. Of that starting group, 353 children (age, 4-9 years) completed the study, which involved receiving eye drops once nightly in both eyes for 2 years.
Some children (n = 116) received 0.05% atropine, others (n = 122) received 0.01% atropine, and the rest (n = 115) received placebo drops. Mr. Yam and colleagues assessed how many children in each group had myopia after 2 years, as measured by a decline of at least a half diopter in one eye.
At the 2-year mark, more than half of children who received the placebo drops (61/115) had developed myopia, as had nearly half of those given 0.01% atropine (56/122). But fewer than one-third of children (33/116, 28.4%) who had received the drops with 0.05% atropine developed myopia during that period, the researchers reported.
The percentage of children with myopia in the placebo group (39/128, 30.5%) was larger by the end of the first year of the study than was the share of children in the 0.05% atropine group by the end of the trial. (Between 12 months and 24 months, 13 children in the placebo group left the study.) The main adverse event, in all treatment groups, was discomfort when exposed to bright light, according to the researchers.
“We are continuing the current study with the total intended follow-up duration of at least 6years,” added Mr. Yam, who hopes to determine whether the 0.05% atropine solution not only delays myopia but also prevents it altogether. While myopia is a concern worldwide, the condition is particularly prevalent in East Asia.
Mark A. Bullimore, MCOptom, PhD, FAAO, an adjunct professor at the University of Houston, and a consultant to ophthalmologic companies, called the trial “a landmark study. Finding children who are eligible and parents who are willing to deal with 2 years of drops is no small feat.
“The 0.05% atropine, on average, delays onset of myopia by a year,” Dr. Bullimore noted. He pointed to the similar percentages of myopia with placebo at 12 months, compared with 0.05% atropine 1 year later. He added that few clinicians in the United States use higher than 0.05% atropine for control of myopia because doing so can lead to excessive dilation and difficulty focusing.
While preventing myopia altogether would be ideal, simply delaying its onset can also be of tangible benefit, Bullimore said. In an article published in January, Dr. Bullimore and Noel A. Brennan of Johnson & Johnson Vision showed that delaying the onset of myopia reduces its severity.
“Optometrists prescribe low-concentration atropine already for myopia control, and there’s no reason now – in the light of this study – that they wouldn’t also do it to delay onset,” Dr. Bullimore said.
But in an editorial accompanying the journal article David A. Berntsen, OD, PhD, and Jeffrey J. Walline, OD, PhD, both of the University of Houston, wrote that a change in practice would be premature.
“The evidence presented does not yet warrant a change in the standard care of children because we do not yet know the long-term effects of delaying the onset of myopia with low-concentration atropine,” they wrote.
Identifying which children to consider for treatment is “a challenge,” they noted, because those who are not nearsighted typically do not undergo routine examination unless they have failed a vision test.
“Ultimately, the implementation of vision screenings that include determining a child’s prescription will likely be needed to identify children most likely to become myopic who may benefit from low-concentration atropine,” Dr. Berntsen and Dr. Walline wrote.
Mr. Yam and coinvestigators have applied for a patent on a 0.05% atropine solution. Dr. Bullimore reported relationships with Alcon Research,CooperVision, CorneaGen, EssilorLuxottica, Eyenovia, Genentech, Johnson & Johnson Vision, Lentechs, Novartis, and Vyluma, and is the sole owner of Ridgevue Publishing and Ridgevue Vision.
A version of this article first appeared on Medscape.com.
FROM JAMA
Time for a national ketamine registry, experts say
The number of ketamine clinics has risen dramatically, with little to no oversight. Prescriptions are being written by providers who lack training in safe ketamine use and online startups are selling the drug for at-home use, taking advantage of a temporary federal regulation that makes it easier to prescribe controlled substances without an in-person patient assessment.
All of this comes at a time when recreational use of ketamine, known on the street as “Special K,” is rising, and reports to poison control centers and drug seizures by the U.S. Drug Enforcement Agency (DEA) are climbing.
In a scenario where enthusiasm for the drug is larger than the body of evidence supporting its clinical use, support is growing for the creation of a ketamine registry to collect data on dosage, treatment frequency, adverse events, and long-term outcomes in patients receiving the therapy for depression and other mental health conditions.
“In the past, there was this question of whether a registry was even needed,” said Gerard Sanacora, MD, PhD, a professor of psychiatry at Yale University, New Haven, Conn., who has pushed for a registry for more than 5 years.
“Now, not only are people being treated with this in large numbers, but it’s also started to push the envelope with at-home dosing,” Dr. Sanacora said in an interview. “It’s come to the point that everybody agrees we do need some way to track it.”
An idea whose time has come
Interest in ketamine’s antidepressant effects has grown since 2000, when a small study suggested the drug rapidly improved depressive symptoms. Research now suggests ketamine reduces symptoms in patients with treatment-resistant depression (TRD).
Studies linking ketamine to relief of depressive symptoms are small and mostly retrospective, and none has offered longitudinal information on long-term outcomes, including side effects and the risk of addiction.
Still, clinicians desperate to help the one-third of patients with major depression who fail to respond to first-line treatments often prescribe the drug anyway.
In 2017, Dr. Sanacora, who also is director of the Yale Depression Research Program at the Yale School of Medicine, was the lead author of a consensus statement that sought to help physicians administer ketamine safely and appropriately in patients with severe depression and other mood disorders.
In that paper, Dr. Sanacora and his coauthors advocated for the creation of a ketamine registry. Such a database, they argued, would provide much-needed data for large, long-term studies, which could be used to develop treatment guidelines, certification programs, and possibly even accreditation standards for providers. Meanwhile, researchers and clinicians in the United Kingdom were also calling for a ketamine registry.
While there seemed to be wide consensus that such a registry was needed, there was no clear path to creating one and no clear line to an agency that would take responsibility for maintaining it.
Because the registry wouldn’t be tied to a drug indication, Dr. Sanacora was told the U.S. Food and Drug Administration wouldn’t take it on. The project also fell outside the purview of the U.S. Department of Health & Human Services, the National Institute of Mental Health (NIMH), and the DEA.
“I haven’t met anybody who has said this is a terrible idea, but nobody seems to have a clear mechanism of doing it, and it doesn’t seem to fall directly under anybody’s jurisdiction,” Dr. Sanacora said.
Dr. Sanacora and other ketamine registry advocates were met with an endless stream of questions. Who would pay for it? How would they get providers to participate? Who would run it and how would the data be shared? The barriers to implementation seemed insurmountable.
A changing landscape
Five years later, these barriers remain. However, advocates note support for a registry is growing, due in large part to a series of developments over the past 6 years that they believe have altered the ketamine landscape.
Chief among these was the 2019 FDA approval of esketamine, a nasal formulation of ketamine, for the treatment of resistant depression. The drug’s indication was expanded in 2020 to include major depressive disorder and acute suicidal ideation or behavior. The drug is only available through a restricted distribution system – the Spravato Risk Evaluation and Mitigation Strategy (REMS) – because of the risk for serious adverse events, including sedation and dissociation, as well as the potential for abuse or misuse.
A sharp increase in the number of ketamine prescribers and clinics has also heightened interest in a ketamine registry. In the last year alone, membership in the American Society of Ketamine Physicians, Psychotherapists, and Practitioners (ASKP) – a nonprofit trade organization for clinicians who prescribe ketamine for mental health disorders and pain conditions – swelled from 300 individual providers to more than 500.
The number of ketamine clinics in the United States has also grown exponentially and is estimated to be anywhere from 500 to 750. A spokesperson with HHS said such clinics are not regulated by the department or any other federal agency but instead are subject to oversight by individual states.
Although recreational use of ketamine remains low overall, there are signs that illicit use is rising, including an increase in DEA seizures of illicit ketamine and reports of ketamine-related poisonings to the nation’s poison control centers. Data on recreational use is spotty, at best. The Centers for Disease Control and Prevention National Vital Statistics System – the primary source of information on drug-related mortality in the United States – does not report on ketamine.
At-home ketamine use soars
Perhaps the most significant development came in March 2020 in the early days of the pandemic. To ease access to therapeutic schedule II-V controlled substances, the DEA issued a waiver that relaxed restrictions in the Ryan Haight Act, legislation that requires that patients be seen at least once in person before receiving a prescription for this class of drugs.
Under the waiver, DEA-registered practitioners are allowed to prescribe these substances – including ketamine, a schedule III substance – via telemedicine, without an in-person exam.
Startup companies cropped up almost overnight to prescribe oral ketamine online for at-home use, with almost no oversight. A spokesperson with the DEA told this news organization that the agency is working to make these “temporary” regulations permanent.
Under the relaxed DEA guidelines, a prescriber only needs to have a DEA license to dispense a ketamine prescription. An alarming number of clinics and online startups are staffed by individuals with no training in ketamine use and, in some cases, no formal mental health training at all, said Lisa Harding, MD, vice president of ASKP and a clinical instructor of psychiatry at Yale School of Medicine.
“The biggest problem is not the ketamine itself, it’s that the majority of practitioners are not psychiatrists, so they don’t have mental health training,” Dr. Harding said. “The fact that an untrained person, any practitioner with no mental health training, can administer this treatment once they have a state license to give ketamine ... then how are you protecting the patients?”
That question prompted ASKP to create the first known program to train psychiatrists, and other qualified mental health practitioners who prescribe ketamine, how to use the drug safely and effectively. The program, scheduled for June, will also include discussion by leaders in the field about how a ketamine registry might address these and other patient safety concerns.
“Nobody is really investigating the standard to which these clinics and online companies should be held, and I think a registry would help with that,” she said in an interview.
The path forward
While ASKP leadership supports the idea of a ketamine registry, Dr. Harding said the organization would need assurances the effort would not create a barrier to treatment.
“It will take somebody bringing all of us to the table and figuring that out,” Dr. Harding said.
Conversations like that with stakeholders would be one of the first steps toward creating a registry, Dr. Sanacora said.
“The more complicated we make this registry, the less compliance we’re going to get,” Dr. Sanacora said. “Our first step is to understand the major impediments and figure out how we can make this easier for people.”
Ideally, the registry would take advantage of existing data-collection tools, such as electronic health records (EHR), and include some sort of patient data entry mechanism, Dr. Sanacora said. The effort will also require skilled biostatisticians and a database system that is easy to manage.
And, of course, the registry will need a large number of patients to gather sufficient data to conduct high-quality research to develop treatment guidelines, training, and accreditation standards. A good target would be about 10,000 patients, Dr. Sanacora said.
All of this requires funding, which is the first hurdle registry advocates must clear. Dr. Sanacora is working on identifying funding sources and said that after working on this for years, he is hopeful that progress can be made.
“I had reached a point where it felt like there was no path forward,” Dr. Sanacora said. “But now I have renewed optimism that something can be done. And something does need to be done, largely for public health reasons but also to optimize the treatment.”
A version of this article first appeared on Medscape.com.
The number of ketamine clinics has risen dramatically, with little to no oversight. Prescriptions are being written by providers who lack training in safe ketamine use and online startups are selling the drug for at-home use, taking advantage of a temporary federal regulation that makes it easier to prescribe controlled substances without an in-person patient assessment.
All of this comes at a time when recreational use of ketamine, known on the street as “Special K,” is rising, and reports to poison control centers and drug seizures by the U.S. Drug Enforcement Agency (DEA) are climbing.
In a scenario where enthusiasm for the drug is larger than the body of evidence supporting its clinical use, support is growing for the creation of a ketamine registry to collect data on dosage, treatment frequency, adverse events, and long-term outcomes in patients receiving the therapy for depression and other mental health conditions.
“In the past, there was this question of whether a registry was even needed,” said Gerard Sanacora, MD, PhD, a professor of psychiatry at Yale University, New Haven, Conn., who has pushed for a registry for more than 5 years.
“Now, not only are people being treated with this in large numbers, but it’s also started to push the envelope with at-home dosing,” Dr. Sanacora said in an interview. “It’s come to the point that everybody agrees we do need some way to track it.”
An idea whose time has come
Interest in ketamine’s antidepressant effects has grown since 2000, when a small study suggested the drug rapidly improved depressive symptoms. Research now suggests ketamine reduces symptoms in patients with treatment-resistant depression (TRD).
Studies linking ketamine to relief of depressive symptoms are small and mostly retrospective, and none has offered longitudinal information on long-term outcomes, including side effects and the risk of addiction.
Still, clinicians desperate to help the one-third of patients with major depression who fail to respond to first-line treatments often prescribe the drug anyway.
In 2017, Dr. Sanacora, who also is director of the Yale Depression Research Program at the Yale School of Medicine, was the lead author of a consensus statement that sought to help physicians administer ketamine safely and appropriately in patients with severe depression and other mood disorders.
In that paper, Dr. Sanacora and his coauthors advocated for the creation of a ketamine registry. Such a database, they argued, would provide much-needed data for large, long-term studies, which could be used to develop treatment guidelines, certification programs, and possibly even accreditation standards for providers. Meanwhile, researchers and clinicians in the United Kingdom were also calling for a ketamine registry.
While there seemed to be wide consensus that such a registry was needed, there was no clear path to creating one and no clear line to an agency that would take responsibility for maintaining it.
Because the registry wouldn’t be tied to a drug indication, Dr. Sanacora was told the U.S. Food and Drug Administration wouldn’t take it on. The project also fell outside the purview of the U.S. Department of Health & Human Services, the National Institute of Mental Health (NIMH), and the DEA.
“I haven’t met anybody who has said this is a terrible idea, but nobody seems to have a clear mechanism of doing it, and it doesn’t seem to fall directly under anybody’s jurisdiction,” Dr. Sanacora said.
Dr. Sanacora and other ketamine registry advocates were met with an endless stream of questions. Who would pay for it? How would they get providers to participate? Who would run it and how would the data be shared? The barriers to implementation seemed insurmountable.
A changing landscape
Five years later, these barriers remain. However, advocates note support for a registry is growing, due in large part to a series of developments over the past 6 years that they believe have altered the ketamine landscape.
Chief among these was the 2019 FDA approval of esketamine, a nasal formulation of ketamine, for the treatment of resistant depression. The drug’s indication was expanded in 2020 to include major depressive disorder and acute suicidal ideation or behavior. The drug is only available through a restricted distribution system – the Spravato Risk Evaluation and Mitigation Strategy (REMS) – because of the risk for serious adverse events, including sedation and dissociation, as well as the potential for abuse or misuse.
A sharp increase in the number of ketamine prescribers and clinics has also heightened interest in a ketamine registry. In the last year alone, membership in the American Society of Ketamine Physicians, Psychotherapists, and Practitioners (ASKP) – a nonprofit trade organization for clinicians who prescribe ketamine for mental health disorders and pain conditions – swelled from 300 individual providers to more than 500.
The number of ketamine clinics in the United States has also grown exponentially and is estimated to be anywhere from 500 to 750. A spokesperson with HHS said such clinics are not regulated by the department or any other federal agency but instead are subject to oversight by individual states.
Although recreational use of ketamine remains low overall, there are signs that illicit use is rising, including an increase in DEA seizures of illicit ketamine and reports of ketamine-related poisonings to the nation’s poison control centers. Data on recreational use is spotty, at best. The Centers for Disease Control and Prevention National Vital Statistics System – the primary source of information on drug-related mortality in the United States – does not report on ketamine.
At-home ketamine use soars
Perhaps the most significant development came in March 2020 in the early days of the pandemic. To ease access to therapeutic schedule II-V controlled substances, the DEA issued a waiver that relaxed restrictions in the Ryan Haight Act, legislation that requires that patients be seen at least once in person before receiving a prescription for this class of drugs.
Under the waiver, DEA-registered practitioners are allowed to prescribe these substances – including ketamine, a schedule III substance – via telemedicine, without an in-person exam.
Startup companies cropped up almost overnight to prescribe oral ketamine online for at-home use, with almost no oversight. A spokesperson with the DEA told this news organization that the agency is working to make these “temporary” regulations permanent.
Under the relaxed DEA guidelines, a prescriber only needs to have a DEA license to dispense a ketamine prescription. An alarming number of clinics and online startups are staffed by individuals with no training in ketamine use and, in some cases, no formal mental health training at all, said Lisa Harding, MD, vice president of ASKP and a clinical instructor of psychiatry at Yale School of Medicine.
“The biggest problem is not the ketamine itself, it’s that the majority of practitioners are not psychiatrists, so they don’t have mental health training,” Dr. Harding said. “The fact that an untrained person, any practitioner with no mental health training, can administer this treatment once they have a state license to give ketamine ... then how are you protecting the patients?”
That question prompted ASKP to create the first known program to train psychiatrists, and other qualified mental health practitioners who prescribe ketamine, how to use the drug safely and effectively. The program, scheduled for June, will also include discussion by leaders in the field about how a ketamine registry might address these and other patient safety concerns.
“Nobody is really investigating the standard to which these clinics and online companies should be held, and I think a registry would help with that,” she said in an interview.
The path forward
While ASKP leadership supports the idea of a ketamine registry, Dr. Harding said the organization would need assurances the effort would not create a barrier to treatment.
“It will take somebody bringing all of us to the table and figuring that out,” Dr. Harding said.
Conversations like that with stakeholders would be one of the first steps toward creating a registry, Dr. Sanacora said.
“The more complicated we make this registry, the less compliance we’re going to get,” Dr. Sanacora said. “Our first step is to understand the major impediments and figure out how we can make this easier for people.”
Ideally, the registry would take advantage of existing data-collection tools, such as electronic health records (EHR), and include some sort of patient data entry mechanism, Dr. Sanacora said. The effort will also require skilled biostatisticians and a database system that is easy to manage.
And, of course, the registry will need a large number of patients to gather sufficient data to conduct high-quality research to develop treatment guidelines, training, and accreditation standards. A good target would be about 10,000 patients, Dr. Sanacora said.
All of this requires funding, which is the first hurdle registry advocates must clear. Dr. Sanacora is working on identifying funding sources and said that after working on this for years, he is hopeful that progress can be made.
“I had reached a point where it felt like there was no path forward,” Dr. Sanacora said. “But now I have renewed optimism that something can be done. And something does need to be done, largely for public health reasons but also to optimize the treatment.”
A version of this article first appeared on Medscape.com.
The number of ketamine clinics has risen dramatically, with little to no oversight. Prescriptions are being written by providers who lack training in safe ketamine use and online startups are selling the drug for at-home use, taking advantage of a temporary federal regulation that makes it easier to prescribe controlled substances without an in-person patient assessment.
All of this comes at a time when recreational use of ketamine, known on the street as “Special K,” is rising, and reports to poison control centers and drug seizures by the U.S. Drug Enforcement Agency (DEA) are climbing.
In a scenario where enthusiasm for the drug is larger than the body of evidence supporting its clinical use, support is growing for the creation of a ketamine registry to collect data on dosage, treatment frequency, adverse events, and long-term outcomes in patients receiving the therapy for depression and other mental health conditions.
“In the past, there was this question of whether a registry was even needed,” said Gerard Sanacora, MD, PhD, a professor of psychiatry at Yale University, New Haven, Conn., who has pushed for a registry for more than 5 years.
“Now, not only are people being treated with this in large numbers, but it’s also started to push the envelope with at-home dosing,” Dr. Sanacora said in an interview. “It’s come to the point that everybody agrees we do need some way to track it.”
An idea whose time has come
Interest in ketamine’s antidepressant effects has grown since 2000, when a small study suggested the drug rapidly improved depressive symptoms. Research now suggests ketamine reduces symptoms in patients with treatment-resistant depression (TRD).
Studies linking ketamine to relief of depressive symptoms are small and mostly retrospective, and none has offered longitudinal information on long-term outcomes, including side effects and the risk of addiction.
Still, clinicians desperate to help the one-third of patients with major depression who fail to respond to first-line treatments often prescribe the drug anyway.
In 2017, Dr. Sanacora, who also is director of the Yale Depression Research Program at the Yale School of Medicine, was the lead author of a consensus statement that sought to help physicians administer ketamine safely and appropriately in patients with severe depression and other mood disorders.
In that paper, Dr. Sanacora and his coauthors advocated for the creation of a ketamine registry. Such a database, they argued, would provide much-needed data for large, long-term studies, which could be used to develop treatment guidelines, certification programs, and possibly even accreditation standards for providers. Meanwhile, researchers and clinicians in the United Kingdom were also calling for a ketamine registry.
While there seemed to be wide consensus that such a registry was needed, there was no clear path to creating one and no clear line to an agency that would take responsibility for maintaining it.
Because the registry wouldn’t be tied to a drug indication, Dr. Sanacora was told the U.S. Food and Drug Administration wouldn’t take it on. The project also fell outside the purview of the U.S. Department of Health & Human Services, the National Institute of Mental Health (NIMH), and the DEA.
“I haven’t met anybody who has said this is a terrible idea, but nobody seems to have a clear mechanism of doing it, and it doesn’t seem to fall directly under anybody’s jurisdiction,” Dr. Sanacora said.
Dr. Sanacora and other ketamine registry advocates were met with an endless stream of questions. Who would pay for it? How would they get providers to participate? Who would run it and how would the data be shared? The barriers to implementation seemed insurmountable.
A changing landscape
Five years later, these barriers remain. However, advocates note support for a registry is growing, due in large part to a series of developments over the past 6 years that they believe have altered the ketamine landscape.
Chief among these was the 2019 FDA approval of esketamine, a nasal formulation of ketamine, for the treatment of resistant depression. The drug’s indication was expanded in 2020 to include major depressive disorder and acute suicidal ideation or behavior. The drug is only available through a restricted distribution system – the Spravato Risk Evaluation and Mitigation Strategy (REMS) – because of the risk for serious adverse events, including sedation and dissociation, as well as the potential for abuse or misuse.
A sharp increase in the number of ketamine prescribers and clinics has also heightened interest in a ketamine registry. In the last year alone, membership in the American Society of Ketamine Physicians, Psychotherapists, and Practitioners (ASKP) – a nonprofit trade organization for clinicians who prescribe ketamine for mental health disorders and pain conditions – swelled from 300 individual providers to more than 500.
The number of ketamine clinics in the United States has also grown exponentially and is estimated to be anywhere from 500 to 750. A spokesperson with HHS said such clinics are not regulated by the department or any other federal agency but instead are subject to oversight by individual states.
Although recreational use of ketamine remains low overall, there are signs that illicit use is rising, including an increase in DEA seizures of illicit ketamine and reports of ketamine-related poisonings to the nation’s poison control centers. Data on recreational use is spotty, at best. The Centers for Disease Control and Prevention National Vital Statistics System – the primary source of information on drug-related mortality in the United States – does not report on ketamine.
At-home ketamine use soars
Perhaps the most significant development came in March 2020 in the early days of the pandemic. To ease access to therapeutic schedule II-V controlled substances, the DEA issued a waiver that relaxed restrictions in the Ryan Haight Act, legislation that requires that patients be seen at least once in person before receiving a prescription for this class of drugs.
Under the waiver, DEA-registered practitioners are allowed to prescribe these substances – including ketamine, a schedule III substance – via telemedicine, without an in-person exam.
Startup companies cropped up almost overnight to prescribe oral ketamine online for at-home use, with almost no oversight. A spokesperson with the DEA told this news organization that the agency is working to make these “temporary” regulations permanent.
Under the relaxed DEA guidelines, a prescriber only needs to have a DEA license to dispense a ketamine prescription. An alarming number of clinics and online startups are staffed by individuals with no training in ketamine use and, in some cases, no formal mental health training at all, said Lisa Harding, MD, vice president of ASKP and a clinical instructor of psychiatry at Yale School of Medicine.
“The biggest problem is not the ketamine itself, it’s that the majority of practitioners are not psychiatrists, so they don’t have mental health training,” Dr. Harding said. “The fact that an untrained person, any practitioner with no mental health training, can administer this treatment once they have a state license to give ketamine ... then how are you protecting the patients?”
That question prompted ASKP to create the first known program to train psychiatrists, and other qualified mental health practitioners who prescribe ketamine, how to use the drug safely and effectively. The program, scheduled for June, will also include discussion by leaders in the field about how a ketamine registry might address these and other patient safety concerns.
“Nobody is really investigating the standard to which these clinics and online companies should be held, and I think a registry would help with that,” she said in an interview.
The path forward
While ASKP leadership supports the idea of a ketamine registry, Dr. Harding said the organization would need assurances the effort would not create a barrier to treatment.
“It will take somebody bringing all of us to the table and figuring that out,” Dr. Harding said.
Conversations like that with stakeholders would be one of the first steps toward creating a registry, Dr. Sanacora said.
“The more complicated we make this registry, the less compliance we’re going to get,” Dr. Sanacora said. “Our first step is to understand the major impediments and figure out how we can make this easier for people.”
Ideally, the registry would take advantage of existing data-collection tools, such as electronic health records (EHR), and include some sort of patient data entry mechanism, Dr. Sanacora said. The effort will also require skilled biostatisticians and a database system that is easy to manage.
And, of course, the registry will need a large number of patients to gather sufficient data to conduct high-quality research to develop treatment guidelines, training, and accreditation standards. A good target would be about 10,000 patients, Dr. Sanacora said.
All of this requires funding, which is the first hurdle registry advocates must clear. Dr. Sanacora is working on identifying funding sources and said that after working on this for years, he is hopeful that progress can be made.
“I had reached a point where it felt like there was no path forward,” Dr. Sanacora said. “But now I have renewed optimism that something can be done. And something does need to be done, largely for public health reasons but also to optimize the treatment.”
A version of this article first appeared on Medscape.com.
FDA puts hold on esophagitis, H. pylori drug, owing to impurity concerns
The Food and Drug Administration
The FDA approved the company’s two vonoprazan-based treatments for H. pylori infection, Voquezna Triple Pak (vonoprazan, amoxicillin, clarithromycin) and Voquezna Dual Pak (vonoprazan, amoxicillin), last May.
The target action date of the company’s NDA for vonoprazan for the treatment of erosive esophagitis was Jan. 11, 2023.
In a news release, Phathom said it has received complete response letters from the FDA related to its erosive esophagitis NDA and H. pylori postapproval supplement.
Both letters address specifications and controls for a nitrosamine drug substance–related impurity, N-nitroso-vonoprazan (NVP), which was detected in the initial commercial launch materials of both products.
The FDA letters ask Phathom to provide “additional stability data to demonstrate that levels of the impurity previously found in vonoprazan drug product will remain at or below the daily acceptable intake throughout the proposed shelf life of the product,” Phathom said.
Phathom said it has conducted “extensive root cause investigations regarding the trace levels of the impurity since it was detected and has implemented mitigation measures to control the levels of NVP below the acceptable intake.”
The company expects to meet with the FDA before the end of March to discuss a resubmission plan and a timeline for the vonoprazan products.
Owing to the regulatory delays, Phathom said it no longer expects product launches for H. pylori or erosive esophagitis in the first quarter of 2023.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration
The FDA approved the company’s two vonoprazan-based treatments for H. pylori infection, Voquezna Triple Pak (vonoprazan, amoxicillin, clarithromycin) and Voquezna Dual Pak (vonoprazan, amoxicillin), last May.
The target action date of the company’s NDA for vonoprazan for the treatment of erosive esophagitis was Jan. 11, 2023.
In a news release, Phathom said it has received complete response letters from the FDA related to its erosive esophagitis NDA and H. pylori postapproval supplement.
Both letters address specifications and controls for a nitrosamine drug substance–related impurity, N-nitroso-vonoprazan (NVP), which was detected in the initial commercial launch materials of both products.
The FDA letters ask Phathom to provide “additional stability data to demonstrate that levels of the impurity previously found in vonoprazan drug product will remain at or below the daily acceptable intake throughout the proposed shelf life of the product,” Phathom said.
Phathom said it has conducted “extensive root cause investigations regarding the trace levels of the impurity since it was detected and has implemented mitigation measures to control the levels of NVP below the acceptable intake.”
The company expects to meet with the FDA before the end of March to discuss a resubmission plan and a timeline for the vonoprazan products.
Owing to the regulatory delays, Phathom said it no longer expects product launches for H. pylori or erosive esophagitis in the first quarter of 2023.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration
The FDA approved the company’s two vonoprazan-based treatments for H. pylori infection, Voquezna Triple Pak (vonoprazan, amoxicillin, clarithromycin) and Voquezna Dual Pak (vonoprazan, amoxicillin), last May.
The target action date of the company’s NDA for vonoprazan for the treatment of erosive esophagitis was Jan. 11, 2023.
In a news release, Phathom said it has received complete response letters from the FDA related to its erosive esophagitis NDA and H. pylori postapproval supplement.
Both letters address specifications and controls for a nitrosamine drug substance–related impurity, N-nitroso-vonoprazan (NVP), which was detected in the initial commercial launch materials of both products.
The FDA letters ask Phathom to provide “additional stability data to demonstrate that levels of the impurity previously found in vonoprazan drug product will remain at or below the daily acceptable intake throughout the proposed shelf life of the product,” Phathom said.
Phathom said it has conducted “extensive root cause investigations regarding the trace levels of the impurity since it was detected and has implemented mitigation measures to control the levels of NVP below the acceptable intake.”
The company expects to meet with the FDA before the end of March to discuss a resubmission plan and a timeline for the vonoprazan products.
Owing to the regulatory delays, Phathom said it no longer expects product launches for H. pylori or erosive esophagitis in the first quarter of 2023.
A version of this article first appeared on Medscape.com.
Oncologist files whistleblower lawsuit against Roswell Park
An oncologist who says she was fired for whistleblower retaliation and gender discrimination has now filed a lawsuit against her former employer.
Anne Grand’Maison, MD, was employed at Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., for 5 years and was the first medical oncologist specifically trained in sarcoma to join the center since it was founded more than 130 years ago.
The lawsuit, filed on Jan. 31, alleges that she was pushed out of her job after raising numerous concerns about egregious medical misconduct and lack of patient safety at the facility.
Roswell Park Cancer Center “denies these unfounded claims, and will vigorously defend itself in this matter,” the organization said in a statement issued to this news organization.
The 75-page complaint alleges that Dr. Grand’Maison observed unacceptable conduct and treatment of patients, including sarcoma pathology reports replete with diagnostic errors, physicians who were not well educated in the latest sarcoma research, and senior doctors refusing to seek out second opinions even in difficult cases.
All of these issues put patient safety and lives at serious risk, according to the lawsuit, and Dr. Grand’Maison raised her concerns internally and attempted to create the necessary changes.
Of specific concern to Dr. Grand’Maison was the competence of Carl Morrison, MD, DVM, Roswell Park’s lead sarcoma pathologist and chair of pathology, whom she had questioned on many occasions and voiced concerns about to other senior staff. But once she made it known that she had gathered up medical records to prove that he had made numerous specific misdiagnoses that led to mistreatments, Dr. Grand’Maison was forced out of her job and the hospital, she said.
“Roswell failed the cancer patients who entrusted their lives to the hospital by ignoring risks to their safety,” Dr. Grand’Maison said in an interview. “The heart of my practice as an oncologist is the well-being of my patients and that is why I could not stay silent.
“I hope that by coming forward, Roswell will be held accountable for putting lives at risk,” she said.
Not up to date with best practices
Before joining Roswell, Dr. Grand’Maison had worked at the University of Texas MD Anderson Cancer Center, which is the top cancer center in the nation, noted David E. Gottlieb, a partner at Wigdor, the law firm that is representing her.
MD Anderson has set the standard for sarcoma care, as they treat the highest volume of sarcoma cases of any hospital in North America and they have the best survival outcomes for sarcoma patients, he said in an interview.
“She was bringing this knowledge and background to Roswell Park,” Mr. Gottlieb said. “She felt that Dr. Morrison was not up to date with best practices as far as diagnosing and treating sarcoma, and she raised numerous issues.
“He was not open to being critiqued and even rejected her request to send something out for a second opinion,” Mr. Gottlieb said. “Second opinions are routine in medicine, and it’s the standard of care. We are dealing with a person’s life and it’s not a personal attack – you could be wrong, and getting another opinion can save a patient’s life.”
But Dr. Morrison has been at Roswell Park for many years, is a good friend of Roswell’s president and CEO Candace Johnson, PhD, and is part of the “old guard,” and “really at the top of the organization,” Mr. Gottlieb said “Whereas Dr. Grand’Maison was relatively new, and her opinions were not popular.”
The complaint was filed against defendants Roswell Park Comprehensive Care Center; Health Research Inc. Roswell Park Division; Candace Johnson, PhD; Carl Morrison, MD, DVM; Renier Brentjens, MD, PhD, deputy director and chair of medicine; and two other senior physicians.
Denial of ‘unfounded claims’
In its statement, Roswell Park pointed out that it is one of few centers in the nation recognized by the Sarcoma Alliance as a hospital with specialized expertise and resources for patients with sarcoma. “Our physician experts not only adhere strictly to national best practices in the diagnosis and care of patients with sarcoma, they determine and disseminate the standards of appropriate medical care as lead authors of national guidelines,” the center stated.
“The facts demonstrate that Roswell Park is a richly diverse and inclusive organization committed to optimizing cancer care by incorporating the expertise of teams of specialists from many subspecialties and disciplines,” according to the statement.
Resistance and male egos
Dr. Grand’Maison has been a licensed physician for more than 30 years, and received her MD in 1988 after graduating from Sherbrooke University in Quebec. Over the next few decades she worked in clinical medicine and research, both in Canada and the United States. In 2014, she became certified in medical oncology and then secured a clinical and research fellowship focusing on sarcoma at MD Anderson.
Two years later, after completing her fellowship, she accepted a full-time position as an assistant professor of oncology in the department of medical oncology’s sarcoma division at Roswell Park. She became the first medical oncologist with a subspecialty in sarcoma, and also brought with her the advanced techniques and aggressive treatment that had been pioneered by MD Anderson, and which had never been used at Roswell Park, according to the complaint.
However, Dr. Grand’Maison said that she began to encounter some resistance from those more familiar with Roswell’s previous standard operating procedures. For example, her practice of seeing patients on days when chemotherapy was administered was viewed by some of the advanced practice clinicians as a lack of confidence in their abilities.
According to the complaint, Dr. Grand’Maison found the sarcoma tumor board at Roswell to be “male-dominated, ego-driven, fraught with defensiveness, and rife with a lack of collegiality almost from the very beginning,” which was very different from her experience at MD Anderson.
Less than 6 months after joining Roswell, she said that Dr. Morrison began treating her in a condescending manner at the tumor board meetings when she asked him questions pertaining to a diagnosis. She viewed his “physically intimidating and aggressive conduct toward her as sexist, and it was a pattern of conduct that would persist in the years that followed.” Dr. Grand’Maison observed that Dr. Morrison never behaved that way toward the men when discussing a case.
Over time, Dr. Grand’Maison made numerous and near endless efforts to raise her concerns about patient safety and gender discrimination at Roswell Park and had reached out to her supervisor and to others in upper management, the complaint alleges. All of this appeared to fall on completely deaf ears as hospital “politics” and doctor egos took precedence. Dr. Morrison continued to try to intimidate her into “silence” and block her attempts to refine diagnoses to ensure proper treatment, and several other senior physicians enabled his behavior and ignored the risk it posed to patient safety, the complaint alleges.
“While she raised complaints about gender discrimination, the crux of her complaint was patient safety,” Mr. Gottlieb emphasized.
Another issue was that Dr. Grand’Maison never received the proper clinical support she repeatedly requested and that was urgently needed. Thus, her patients faced other elevated safety risks as a result of the underresourced sarcoma clinic, she said.
Fired or resigned?
Dr. Grand’Maison left Roswell Park Cancer center last May, and has not worked since.
Although Dr. Grand’Maison stated that she was fired in retaliation for raising serious concerns, Roswell Park insists that she voluntarily resigned. Dr. Grand’Maison acknowledged that she wrote an email in January 2022 to the clinical practice plan coordinator in which she mentioned that her husband was planning to relocate back to Canada and that her last date at Roswell Park would be May 1, 2022. The coordinator never responded to that email. In the interim, her husband, also a physician with privileges at Roswell Park, made it known that he was not moving to Canada.
Dr. Grand’Maison said that, as she had not resigned, and everyone knew her husband wasn’t moving, she did not follow up on that January 2022 email, and then forgot about it.
“That email was used as the basis to force her out,”said her lawyer, Mr. Gottlieb. “The day after she put together a summary and extensively documented serious patient safety concerns, she got an email that her resignation had been accepted.”
None of the standard protocols for resignation had been completed, either by human resources or by her supervisors, Mr. Gottlieb contended. “The law says that they can’t take adverse action against her for filing a complaint, so they fired her under the guise of a resignation,” he said.
Roswell Park refused to rescind Dr. Grand’Maison’s resignation, despite multiple attempts on her part. She even contacted the CEO and stated that her January 2022 email was being used a pretext to push her out in retaliation, but she received no response, only that the matter had been referred to someone else.
“I am speaking out because time and again female doctors are unable to deliver on the promise of their medical training because of discrimination,” said Dr. Grand’Maison. “Roswell dismissed my expertise and diminished my value. While I worry that coming forward may affect my career, I am taking that risk to make the path easier for the women who will come behind me.”
A version of this article first appeared on Medscape.com.
An oncologist who says she was fired for whistleblower retaliation and gender discrimination has now filed a lawsuit against her former employer.
Anne Grand’Maison, MD, was employed at Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., for 5 years and was the first medical oncologist specifically trained in sarcoma to join the center since it was founded more than 130 years ago.
The lawsuit, filed on Jan. 31, alleges that she was pushed out of her job after raising numerous concerns about egregious medical misconduct and lack of patient safety at the facility.
Roswell Park Cancer Center “denies these unfounded claims, and will vigorously defend itself in this matter,” the organization said in a statement issued to this news organization.
The 75-page complaint alleges that Dr. Grand’Maison observed unacceptable conduct and treatment of patients, including sarcoma pathology reports replete with diagnostic errors, physicians who were not well educated in the latest sarcoma research, and senior doctors refusing to seek out second opinions even in difficult cases.
All of these issues put patient safety and lives at serious risk, according to the lawsuit, and Dr. Grand’Maison raised her concerns internally and attempted to create the necessary changes.
Of specific concern to Dr. Grand’Maison was the competence of Carl Morrison, MD, DVM, Roswell Park’s lead sarcoma pathologist and chair of pathology, whom she had questioned on many occasions and voiced concerns about to other senior staff. But once she made it known that she had gathered up medical records to prove that he had made numerous specific misdiagnoses that led to mistreatments, Dr. Grand’Maison was forced out of her job and the hospital, she said.
“Roswell failed the cancer patients who entrusted their lives to the hospital by ignoring risks to their safety,” Dr. Grand’Maison said in an interview. “The heart of my practice as an oncologist is the well-being of my patients and that is why I could not stay silent.
“I hope that by coming forward, Roswell will be held accountable for putting lives at risk,” she said.
Not up to date with best practices
Before joining Roswell, Dr. Grand’Maison had worked at the University of Texas MD Anderson Cancer Center, which is the top cancer center in the nation, noted David E. Gottlieb, a partner at Wigdor, the law firm that is representing her.
MD Anderson has set the standard for sarcoma care, as they treat the highest volume of sarcoma cases of any hospital in North America and they have the best survival outcomes for sarcoma patients, he said in an interview.
“She was bringing this knowledge and background to Roswell Park,” Mr. Gottlieb said. “She felt that Dr. Morrison was not up to date with best practices as far as diagnosing and treating sarcoma, and she raised numerous issues.
“He was not open to being critiqued and even rejected her request to send something out for a second opinion,” Mr. Gottlieb said. “Second opinions are routine in medicine, and it’s the standard of care. We are dealing with a person’s life and it’s not a personal attack – you could be wrong, and getting another opinion can save a patient’s life.”
But Dr. Morrison has been at Roswell Park for many years, is a good friend of Roswell’s president and CEO Candace Johnson, PhD, and is part of the “old guard,” and “really at the top of the organization,” Mr. Gottlieb said “Whereas Dr. Grand’Maison was relatively new, and her opinions were not popular.”
The complaint was filed against defendants Roswell Park Comprehensive Care Center; Health Research Inc. Roswell Park Division; Candace Johnson, PhD; Carl Morrison, MD, DVM; Renier Brentjens, MD, PhD, deputy director and chair of medicine; and two other senior physicians.
Denial of ‘unfounded claims’
In its statement, Roswell Park pointed out that it is one of few centers in the nation recognized by the Sarcoma Alliance as a hospital with specialized expertise and resources for patients with sarcoma. “Our physician experts not only adhere strictly to national best practices in the diagnosis and care of patients with sarcoma, they determine and disseminate the standards of appropriate medical care as lead authors of national guidelines,” the center stated.
“The facts demonstrate that Roswell Park is a richly diverse and inclusive organization committed to optimizing cancer care by incorporating the expertise of teams of specialists from many subspecialties and disciplines,” according to the statement.
Resistance and male egos
Dr. Grand’Maison has been a licensed physician for more than 30 years, and received her MD in 1988 after graduating from Sherbrooke University in Quebec. Over the next few decades she worked in clinical medicine and research, both in Canada and the United States. In 2014, she became certified in medical oncology and then secured a clinical and research fellowship focusing on sarcoma at MD Anderson.
Two years later, after completing her fellowship, she accepted a full-time position as an assistant professor of oncology in the department of medical oncology’s sarcoma division at Roswell Park. She became the first medical oncologist with a subspecialty in sarcoma, and also brought with her the advanced techniques and aggressive treatment that had been pioneered by MD Anderson, and which had never been used at Roswell Park, according to the complaint.
However, Dr. Grand’Maison said that she began to encounter some resistance from those more familiar with Roswell’s previous standard operating procedures. For example, her practice of seeing patients on days when chemotherapy was administered was viewed by some of the advanced practice clinicians as a lack of confidence in their abilities.
According to the complaint, Dr. Grand’Maison found the sarcoma tumor board at Roswell to be “male-dominated, ego-driven, fraught with defensiveness, and rife with a lack of collegiality almost from the very beginning,” which was very different from her experience at MD Anderson.
Less than 6 months after joining Roswell, she said that Dr. Morrison began treating her in a condescending manner at the tumor board meetings when she asked him questions pertaining to a diagnosis. She viewed his “physically intimidating and aggressive conduct toward her as sexist, and it was a pattern of conduct that would persist in the years that followed.” Dr. Grand’Maison observed that Dr. Morrison never behaved that way toward the men when discussing a case.
Over time, Dr. Grand’Maison made numerous and near endless efforts to raise her concerns about patient safety and gender discrimination at Roswell Park and had reached out to her supervisor and to others in upper management, the complaint alleges. All of this appeared to fall on completely deaf ears as hospital “politics” and doctor egos took precedence. Dr. Morrison continued to try to intimidate her into “silence” and block her attempts to refine diagnoses to ensure proper treatment, and several other senior physicians enabled his behavior and ignored the risk it posed to patient safety, the complaint alleges.
“While she raised complaints about gender discrimination, the crux of her complaint was patient safety,” Mr. Gottlieb emphasized.
Another issue was that Dr. Grand’Maison never received the proper clinical support she repeatedly requested and that was urgently needed. Thus, her patients faced other elevated safety risks as a result of the underresourced sarcoma clinic, she said.
Fired or resigned?
Dr. Grand’Maison left Roswell Park Cancer center last May, and has not worked since.
Although Dr. Grand’Maison stated that she was fired in retaliation for raising serious concerns, Roswell Park insists that she voluntarily resigned. Dr. Grand’Maison acknowledged that she wrote an email in January 2022 to the clinical practice plan coordinator in which she mentioned that her husband was planning to relocate back to Canada and that her last date at Roswell Park would be May 1, 2022. The coordinator never responded to that email. In the interim, her husband, also a physician with privileges at Roswell Park, made it known that he was not moving to Canada.
Dr. Grand’Maison said that, as she had not resigned, and everyone knew her husband wasn’t moving, she did not follow up on that January 2022 email, and then forgot about it.
“That email was used as the basis to force her out,”said her lawyer, Mr. Gottlieb. “The day after she put together a summary and extensively documented serious patient safety concerns, she got an email that her resignation had been accepted.”
None of the standard protocols for resignation had been completed, either by human resources or by her supervisors, Mr. Gottlieb contended. “The law says that they can’t take adverse action against her for filing a complaint, so they fired her under the guise of a resignation,” he said.
Roswell Park refused to rescind Dr. Grand’Maison’s resignation, despite multiple attempts on her part. She even contacted the CEO and stated that her January 2022 email was being used a pretext to push her out in retaliation, but she received no response, only that the matter had been referred to someone else.
“I am speaking out because time and again female doctors are unable to deliver on the promise of their medical training because of discrimination,” said Dr. Grand’Maison. “Roswell dismissed my expertise and diminished my value. While I worry that coming forward may affect my career, I am taking that risk to make the path easier for the women who will come behind me.”
A version of this article first appeared on Medscape.com.
An oncologist who says she was fired for whistleblower retaliation and gender discrimination has now filed a lawsuit against her former employer.
Anne Grand’Maison, MD, was employed at Roswell Park Comprehensive Cancer Center in Buffalo, N.Y., for 5 years and was the first medical oncologist specifically trained in sarcoma to join the center since it was founded more than 130 years ago.
The lawsuit, filed on Jan. 31, alleges that she was pushed out of her job after raising numerous concerns about egregious medical misconduct and lack of patient safety at the facility.
Roswell Park Cancer Center “denies these unfounded claims, and will vigorously defend itself in this matter,” the organization said in a statement issued to this news organization.
The 75-page complaint alleges that Dr. Grand’Maison observed unacceptable conduct and treatment of patients, including sarcoma pathology reports replete with diagnostic errors, physicians who were not well educated in the latest sarcoma research, and senior doctors refusing to seek out second opinions even in difficult cases.
All of these issues put patient safety and lives at serious risk, according to the lawsuit, and Dr. Grand’Maison raised her concerns internally and attempted to create the necessary changes.
Of specific concern to Dr. Grand’Maison was the competence of Carl Morrison, MD, DVM, Roswell Park’s lead sarcoma pathologist and chair of pathology, whom she had questioned on many occasions and voiced concerns about to other senior staff. But once she made it known that she had gathered up medical records to prove that he had made numerous specific misdiagnoses that led to mistreatments, Dr. Grand’Maison was forced out of her job and the hospital, she said.
“Roswell failed the cancer patients who entrusted their lives to the hospital by ignoring risks to their safety,” Dr. Grand’Maison said in an interview. “The heart of my practice as an oncologist is the well-being of my patients and that is why I could not stay silent.
“I hope that by coming forward, Roswell will be held accountable for putting lives at risk,” she said.
Not up to date with best practices
Before joining Roswell, Dr. Grand’Maison had worked at the University of Texas MD Anderson Cancer Center, which is the top cancer center in the nation, noted David E. Gottlieb, a partner at Wigdor, the law firm that is representing her.
MD Anderson has set the standard for sarcoma care, as they treat the highest volume of sarcoma cases of any hospital in North America and they have the best survival outcomes for sarcoma patients, he said in an interview.
“She was bringing this knowledge and background to Roswell Park,” Mr. Gottlieb said. “She felt that Dr. Morrison was not up to date with best practices as far as diagnosing and treating sarcoma, and she raised numerous issues.
“He was not open to being critiqued and even rejected her request to send something out for a second opinion,” Mr. Gottlieb said. “Second opinions are routine in medicine, and it’s the standard of care. We are dealing with a person’s life and it’s not a personal attack – you could be wrong, and getting another opinion can save a patient’s life.”
But Dr. Morrison has been at Roswell Park for many years, is a good friend of Roswell’s president and CEO Candace Johnson, PhD, and is part of the “old guard,” and “really at the top of the organization,” Mr. Gottlieb said “Whereas Dr. Grand’Maison was relatively new, and her opinions were not popular.”
The complaint was filed against defendants Roswell Park Comprehensive Care Center; Health Research Inc. Roswell Park Division; Candace Johnson, PhD; Carl Morrison, MD, DVM; Renier Brentjens, MD, PhD, deputy director and chair of medicine; and two other senior physicians.
Denial of ‘unfounded claims’
In its statement, Roswell Park pointed out that it is one of few centers in the nation recognized by the Sarcoma Alliance as a hospital with specialized expertise and resources for patients with sarcoma. “Our physician experts not only adhere strictly to national best practices in the diagnosis and care of patients with sarcoma, they determine and disseminate the standards of appropriate medical care as lead authors of national guidelines,” the center stated.
“The facts demonstrate that Roswell Park is a richly diverse and inclusive organization committed to optimizing cancer care by incorporating the expertise of teams of specialists from many subspecialties and disciplines,” according to the statement.
Resistance and male egos
Dr. Grand’Maison has been a licensed physician for more than 30 years, and received her MD in 1988 after graduating from Sherbrooke University in Quebec. Over the next few decades she worked in clinical medicine and research, both in Canada and the United States. In 2014, she became certified in medical oncology and then secured a clinical and research fellowship focusing on sarcoma at MD Anderson.
Two years later, after completing her fellowship, she accepted a full-time position as an assistant professor of oncology in the department of medical oncology’s sarcoma division at Roswell Park. She became the first medical oncologist with a subspecialty in sarcoma, and also brought with her the advanced techniques and aggressive treatment that had been pioneered by MD Anderson, and which had never been used at Roswell Park, according to the complaint.
However, Dr. Grand’Maison said that she began to encounter some resistance from those more familiar with Roswell’s previous standard operating procedures. For example, her practice of seeing patients on days when chemotherapy was administered was viewed by some of the advanced practice clinicians as a lack of confidence in their abilities.
According to the complaint, Dr. Grand’Maison found the sarcoma tumor board at Roswell to be “male-dominated, ego-driven, fraught with defensiveness, and rife with a lack of collegiality almost from the very beginning,” which was very different from her experience at MD Anderson.
Less than 6 months after joining Roswell, she said that Dr. Morrison began treating her in a condescending manner at the tumor board meetings when she asked him questions pertaining to a diagnosis. She viewed his “physically intimidating and aggressive conduct toward her as sexist, and it was a pattern of conduct that would persist in the years that followed.” Dr. Grand’Maison observed that Dr. Morrison never behaved that way toward the men when discussing a case.
Over time, Dr. Grand’Maison made numerous and near endless efforts to raise her concerns about patient safety and gender discrimination at Roswell Park and had reached out to her supervisor and to others in upper management, the complaint alleges. All of this appeared to fall on completely deaf ears as hospital “politics” and doctor egos took precedence. Dr. Morrison continued to try to intimidate her into “silence” and block her attempts to refine diagnoses to ensure proper treatment, and several other senior physicians enabled his behavior and ignored the risk it posed to patient safety, the complaint alleges.
“While she raised complaints about gender discrimination, the crux of her complaint was patient safety,” Mr. Gottlieb emphasized.
Another issue was that Dr. Grand’Maison never received the proper clinical support she repeatedly requested and that was urgently needed. Thus, her patients faced other elevated safety risks as a result of the underresourced sarcoma clinic, she said.
Fired or resigned?
Dr. Grand’Maison left Roswell Park Cancer center last May, and has not worked since.
Although Dr. Grand’Maison stated that she was fired in retaliation for raising serious concerns, Roswell Park insists that she voluntarily resigned. Dr. Grand’Maison acknowledged that she wrote an email in January 2022 to the clinical practice plan coordinator in which she mentioned that her husband was planning to relocate back to Canada and that her last date at Roswell Park would be May 1, 2022. The coordinator never responded to that email. In the interim, her husband, also a physician with privileges at Roswell Park, made it known that he was not moving to Canada.
Dr. Grand’Maison said that, as she had not resigned, and everyone knew her husband wasn’t moving, she did not follow up on that January 2022 email, and then forgot about it.
“That email was used as the basis to force her out,”said her lawyer, Mr. Gottlieb. “The day after she put together a summary and extensively documented serious patient safety concerns, she got an email that her resignation had been accepted.”
None of the standard protocols for resignation had been completed, either by human resources or by her supervisors, Mr. Gottlieb contended. “The law says that they can’t take adverse action against her for filing a complaint, so they fired her under the guise of a resignation,” he said.
Roswell Park refused to rescind Dr. Grand’Maison’s resignation, despite multiple attempts on her part. She even contacted the CEO and stated that her January 2022 email was being used a pretext to push her out in retaliation, but she received no response, only that the matter had been referred to someone else.
“I am speaking out because time and again female doctors are unable to deliver on the promise of their medical training because of discrimination,” said Dr. Grand’Maison. “Roswell dismissed my expertise and diminished my value. While I worry that coming forward may affect my career, I am taking that risk to make the path easier for the women who will come behind me.”
A version of this article first appeared on Medscape.com.
Docetaxel as alternative to cisplatin for H&N radiotherapy
say researchers reporting a phase 3 trial from India.
“This is the first randomized study demonstrating the benefit of an alternate radiosensitizing agent in cisplatin-ineligible patients,” they wrote.
“We found that the use of docetaxel as a radiosensitizer in cisplatin-ineligible patients,” compared with the use of radiation alone, “led to an improvement in disease-free survival, locoregional control, and overall survival without affecting the quality of life of the patients,” the team reported.
The investigators, led by Vijay Maruti Patil, MD, DM, a medical oncologist at Tata Memorial Hospital, Mumbai, noted that they stopped the trial early after the benefit from adding docetaxel became clear.
Cisplatin is the general standard of care to sensitize locally advanced head and neck tumors to radiation treatment, but up to a third of patients are ineligible because of age, diminished kidney function, hearing loss, and other problems, they wrote.
Many alternatives to cisplatin are used in such settings, but until now, there hasn’t been any level 1, phase 3 evidence to guide the selection.
Cetuximab is the alternative used most often in the United States, but evidence supporting it was generated in trials involving cisplatin-eligible patients, the investigators pointed out. There is also a high incidence of skin and other toxicities and, in some studies, nonideal survival outcomes, they noted.
The new study was published online in the Journal of Clinical Oncology.
It “demonstrates what could be presumed but was not known to be true in the cisplatin-ineligible context: Radiosensitizers improve outcomes over radiotherapy alone,” commented the authors of an accompanying editorial (J Clin Oncol. 2023 Feb 1. doi: 10.1200/JCO.22.02350).
“Docetaxel belongs in the armamentarium of go-to regimens,” wrote radiation oncologist Loren Mell, MD, of the University of California, San Diego, and medical oncologist Stuart Wong, MD, of the Medical College of Wisconsin, Milwaukee.
This study “fills an important gap in the head and neck cancer literature, but “since [docetaxel] was not compared head-to-head against” other radiosensitizing alternatives, it “should not be declared the lone standard. ... It is high time to shift the conversation from whether radiosensitizers are beneficial to which regimen (if any) provides the most benefit and should define the standard of care,” they added.
The trial randomly assigned 356 cisplatin-ineligible adults equally to either radiation alone or radiation with concurrent docetaxel 15 mg/m2 once weekly for a maximum of seven cycles. The investigators planned to enroll 600 patients but stopped the trial early when the survival benefit with docetaxel became clear.
The addition of docetaxel improved 2-year disease-free survival (42% vs. 30.3%; hazard ratio, 0.673; P = .002); 2-year overall survival (50.8% vs. 41.7%; HR, 0.747; P = .035), and the 2-year locoregional failure rate (41.8% vs. 54.7%; HR, 0.661; P = .002).
Median overall survival was 25.5 months with docetaxel versus 15.3 months with radiation alone (P = .035).
Docetaxel’s benefits were most pronounced in patients with hypopharyngeal primary sites and among the 61% of patients treated definitively. There was “possibly” a benefit in the adjuvant setting, but “further study would be required to show definitive applicability,” the investigators said.
There was a higher incidence of grade 3 or greater mucositis (49.7% vs. 22.2%), odynophagia (52.5% vs. 33.5%), and dysphagia (33%), but the “complications were manageable and did not affect the compliance” with either radiation or docetaxel, the team reported. Overall, 86% of patients received five or more cycles docetaxel.
In their editorial, Dr. Mell and Dr. Wong noted that the “majority of patients did not receive intensity-modulated radiotherapy, the standard in higher-income countries,” but added that “we do not expect the use of conventional radiotherapy would reduce the effectiveness of docetaxel.”
The trial was funded by Tata Memorial Hospital, where it was conducted. Several investigators had industry ties, including Dr. Patil, who reported research funding from Johnson & Johnson/Janssen, AstraZeneca, Intas, NATCO Pharma, Eisai Germany, and Novartis. Dr. Mell is an advisor for Cel-Sci and reported research funding from Merck and AstraZeneca. Dr. Wong disclosed research funding from Novartis and Merck.
A version of this article first appeared on Medscape.com.
say researchers reporting a phase 3 trial from India.
“This is the first randomized study demonstrating the benefit of an alternate radiosensitizing agent in cisplatin-ineligible patients,” they wrote.
“We found that the use of docetaxel as a radiosensitizer in cisplatin-ineligible patients,” compared with the use of radiation alone, “led to an improvement in disease-free survival, locoregional control, and overall survival without affecting the quality of life of the patients,” the team reported.
The investigators, led by Vijay Maruti Patil, MD, DM, a medical oncologist at Tata Memorial Hospital, Mumbai, noted that they stopped the trial early after the benefit from adding docetaxel became clear.
Cisplatin is the general standard of care to sensitize locally advanced head and neck tumors to radiation treatment, but up to a third of patients are ineligible because of age, diminished kidney function, hearing loss, and other problems, they wrote.
Many alternatives to cisplatin are used in such settings, but until now, there hasn’t been any level 1, phase 3 evidence to guide the selection.
Cetuximab is the alternative used most often in the United States, but evidence supporting it was generated in trials involving cisplatin-eligible patients, the investigators pointed out. There is also a high incidence of skin and other toxicities and, in some studies, nonideal survival outcomes, they noted.
The new study was published online in the Journal of Clinical Oncology.
It “demonstrates what could be presumed but was not known to be true in the cisplatin-ineligible context: Radiosensitizers improve outcomes over radiotherapy alone,” commented the authors of an accompanying editorial (J Clin Oncol. 2023 Feb 1. doi: 10.1200/JCO.22.02350).
“Docetaxel belongs in the armamentarium of go-to regimens,” wrote radiation oncologist Loren Mell, MD, of the University of California, San Diego, and medical oncologist Stuart Wong, MD, of the Medical College of Wisconsin, Milwaukee.
This study “fills an important gap in the head and neck cancer literature, but “since [docetaxel] was not compared head-to-head against” other radiosensitizing alternatives, it “should not be declared the lone standard. ... It is high time to shift the conversation from whether radiosensitizers are beneficial to which regimen (if any) provides the most benefit and should define the standard of care,” they added.
The trial randomly assigned 356 cisplatin-ineligible adults equally to either radiation alone or radiation with concurrent docetaxel 15 mg/m2 once weekly for a maximum of seven cycles. The investigators planned to enroll 600 patients but stopped the trial early when the survival benefit with docetaxel became clear.
The addition of docetaxel improved 2-year disease-free survival (42% vs. 30.3%; hazard ratio, 0.673; P = .002); 2-year overall survival (50.8% vs. 41.7%; HR, 0.747; P = .035), and the 2-year locoregional failure rate (41.8% vs. 54.7%; HR, 0.661; P = .002).
Median overall survival was 25.5 months with docetaxel versus 15.3 months with radiation alone (P = .035).
Docetaxel’s benefits were most pronounced in patients with hypopharyngeal primary sites and among the 61% of patients treated definitively. There was “possibly” a benefit in the adjuvant setting, but “further study would be required to show definitive applicability,” the investigators said.
There was a higher incidence of grade 3 or greater mucositis (49.7% vs. 22.2%), odynophagia (52.5% vs. 33.5%), and dysphagia (33%), but the “complications were manageable and did not affect the compliance” with either radiation or docetaxel, the team reported. Overall, 86% of patients received five or more cycles docetaxel.
In their editorial, Dr. Mell and Dr. Wong noted that the “majority of patients did not receive intensity-modulated radiotherapy, the standard in higher-income countries,” but added that “we do not expect the use of conventional radiotherapy would reduce the effectiveness of docetaxel.”
The trial was funded by Tata Memorial Hospital, where it was conducted. Several investigators had industry ties, including Dr. Patil, who reported research funding from Johnson & Johnson/Janssen, AstraZeneca, Intas, NATCO Pharma, Eisai Germany, and Novartis. Dr. Mell is an advisor for Cel-Sci and reported research funding from Merck and AstraZeneca. Dr. Wong disclosed research funding from Novartis and Merck.
A version of this article first appeared on Medscape.com.
say researchers reporting a phase 3 trial from India.
“This is the first randomized study demonstrating the benefit of an alternate radiosensitizing agent in cisplatin-ineligible patients,” they wrote.
“We found that the use of docetaxel as a radiosensitizer in cisplatin-ineligible patients,” compared with the use of radiation alone, “led to an improvement in disease-free survival, locoregional control, and overall survival without affecting the quality of life of the patients,” the team reported.
The investigators, led by Vijay Maruti Patil, MD, DM, a medical oncologist at Tata Memorial Hospital, Mumbai, noted that they stopped the trial early after the benefit from adding docetaxel became clear.
Cisplatin is the general standard of care to sensitize locally advanced head and neck tumors to radiation treatment, but up to a third of patients are ineligible because of age, diminished kidney function, hearing loss, and other problems, they wrote.
Many alternatives to cisplatin are used in such settings, but until now, there hasn’t been any level 1, phase 3 evidence to guide the selection.
Cetuximab is the alternative used most often in the United States, but evidence supporting it was generated in trials involving cisplatin-eligible patients, the investigators pointed out. There is also a high incidence of skin and other toxicities and, in some studies, nonideal survival outcomes, they noted.
The new study was published online in the Journal of Clinical Oncology.
It “demonstrates what could be presumed but was not known to be true in the cisplatin-ineligible context: Radiosensitizers improve outcomes over radiotherapy alone,” commented the authors of an accompanying editorial (J Clin Oncol. 2023 Feb 1. doi: 10.1200/JCO.22.02350).
“Docetaxel belongs in the armamentarium of go-to regimens,” wrote radiation oncologist Loren Mell, MD, of the University of California, San Diego, and medical oncologist Stuart Wong, MD, of the Medical College of Wisconsin, Milwaukee.
This study “fills an important gap in the head and neck cancer literature, but “since [docetaxel] was not compared head-to-head against” other radiosensitizing alternatives, it “should not be declared the lone standard. ... It is high time to shift the conversation from whether radiosensitizers are beneficial to which regimen (if any) provides the most benefit and should define the standard of care,” they added.
The trial randomly assigned 356 cisplatin-ineligible adults equally to either radiation alone or radiation with concurrent docetaxel 15 mg/m2 once weekly for a maximum of seven cycles. The investigators planned to enroll 600 patients but stopped the trial early when the survival benefit with docetaxel became clear.
The addition of docetaxel improved 2-year disease-free survival (42% vs. 30.3%; hazard ratio, 0.673; P = .002); 2-year overall survival (50.8% vs. 41.7%; HR, 0.747; P = .035), and the 2-year locoregional failure rate (41.8% vs. 54.7%; HR, 0.661; P = .002).
Median overall survival was 25.5 months with docetaxel versus 15.3 months with radiation alone (P = .035).
Docetaxel’s benefits were most pronounced in patients with hypopharyngeal primary sites and among the 61% of patients treated definitively. There was “possibly” a benefit in the adjuvant setting, but “further study would be required to show definitive applicability,” the investigators said.
There was a higher incidence of grade 3 or greater mucositis (49.7% vs. 22.2%), odynophagia (52.5% vs. 33.5%), and dysphagia (33%), but the “complications were manageable and did not affect the compliance” with either radiation or docetaxel, the team reported. Overall, 86% of patients received five or more cycles docetaxel.
In their editorial, Dr. Mell and Dr. Wong noted that the “majority of patients did not receive intensity-modulated radiotherapy, the standard in higher-income countries,” but added that “we do not expect the use of conventional radiotherapy would reduce the effectiveness of docetaxel.”
The trial was funded by Tata Memorial Hospital, where it was conducted. Several investigators had industry ties, including Dr. Patil, who reported research funding from Johnson & Johnson/Janssen, AstraZeneca, Intas, NATCO Pharma, Eisai Germany, and Novartis. Dr. Mell is an advisor for Cel-Sci and reported research funding from Merck and AstraZeneca. Dr. Wong disclosed research funding from Novartis and Merck.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL ONCOLOGY