User login
Tofacitinib withdrawal not a universal option for all patients with RA in remission
Key clinical point: Blanket withdrawal of tofacitinib may not be suitable for all patients with rheumatoid arthritis (RA) who have achieved clinical remission as more than half relapsed after tofacitinib discontinuation. However, the majority regained remission after tofacitinib resumption.
Major finding: At week 104, the tofacitinib vs methotrexate discontinuation group had a numerically lower Clinical Disease Activity Index-based sustained remission rate (29.2% vs 50.0%) and higher relapse rate (58.3% vs 35.0%). However, 71.4% vs 28.6% of patients regained remission on tofacitinib vs methotrexate resumption.
Study details: This prospective randomized controlled trial included 113 patients with RA and an inadequate response to methotrexate with or without biologic disease-modifying antirheumatic drugs who received 52 weeks of tofacitinib plus methotrexate treatment and thereafter, were randomly assigned to discontinue tofacitinib or methotrexate if experiencing clinical remission.
Disclosures: This study was supported by the Japan Society for the Promotion of Science, KAKENHI. Several authors declared receiving consulting fees, speaking fees, research grants, or honoraria from various sources.
Source: Kubo S et al. Sustained remission following the discontinuation of tofacitinib in patients with rheumatoid arthritis (XANADU study): An open-label randomised study. RMD Open. 2023;9(2):e003029 (Apr 25). Doi: 10.1136/rmdopen-2023-003029
Key clinical point: Blanket withdrawal of tofacitinib may not be suitable for all patients with rheumatoid arthritis (RA) who have achieved clinical remission as more than half relapsed after tofacitinib discontinuation. However, the majority regained remission after tofacitinib resumption.
Major finding: At week 104, the tofacitinib vs methotrexate discontinuation group had a numerically lower Clinical Disease Activity Index-based sustained remission rate (29.2% vs 50.0%) and higher relapse rate (58.3% vs 35.0%). However, 71.4% vs 28.6% of patients regained remission on tofacitinib vs methotrexate resumption.
Study details: This prospective randomized controlled trial included 113 patients with RA and an inadequate response to methotrexate with or without biologic disease-modifying antirheumatic drugs who received 52 weeks of tofacitinib plus methotrexate treatment and thereafter, were randomly assigned to discontinue tofacitinib or methotrexate if experiencing clinical remission.
Disclosures: This study was supported by the Japan Society for the Promotion of Science, KAKENHI. Several authors declared receiving consulting fees, speaking fees, research grants, or honoraria from various sources.
Source: Kubo S et al. Sustained remission following the discontinuation of tofacitinib in patients with rheumatoid arthritis (XANADU study): An open-label randomised study. RMD Open. 2023;9(2):e003029 (Apr 25). Doi: 10.1136/rmdopen-2023-003029
Key clinical point: Blanket withdrawal of tofacitinib may not be suitable for all patients with rheumatoid arthritis (RA) who have achieved clinical remission as more than half relapsed after tofacitinib discontinuation. However, the majority regained remission after tofacitinib resumption.
Major finding: At week 104, the tofacitinib vs methotrexate discontinuation group had a numerically lower Clinical Disease Activity Index-based sustained remission rate (29.2% vs 50.0%) and higher relapse rate (58.3% vs 35.0%). However, 71.4% vs 28.6% of patients regained remission on tofacitinib vs methotrexate resumption.
Study details: This prospective randomized controlled trial included 113 patients with RA and an inadequate response to methotrexate with or without biologic disease-modifying antirheumatic drugs who received 52 weeks of tofacitinib plus methotrexate treatment and thereafter, were randomly assigned to discontinue tofacitinib or methotrexate if experiencing clinical remission.
Disclosures: This study was supported by the Japan Society for the Promotion of Science, KAKENHI. Several authors declared receiving consulting fees, speaking fees, research grants, or honoraria from various sources.
Source: Kubo S et al. Sustained remission following the discontinuation of tofacitinib in patients with rheumatoid arthritis (XANADU study): An open-label randomised study. RMD Open. 2023;9(2):e003029 (Apr 25). Doi: 10.1136/rmdopen-2023-003029
Joint damage repair: A rare phenomenon in early RA
Key clinical point: Repair of joint space narrowing occurred but was rare in patients with early rheumatoid arthritis (RA) who underwent 8 years of treatment to a target disease activity score (DAS) ≤ 2.4. Therefore, suppression of damage progression should be the focus of clinical care.
Major finding: Only 5.3% of patients showed repair of joint space narrowing and bone erosions after 8 years of treatment to a target of DAS ≤ 2.4. No significant association was observed between achieving repair and suppression of disease activity, duration of previous remission, or other predictors of repair.
Study details: Findings are from a subanalysis of BeSt study including 508 patients with severe early RA who were treated to a target of DAS ≤ 2.4 and followed for 8 years.
Disclosures: The BeSt study was supported by grants from the Dutch College of Health Insurances, Schering-Plough B.V., and Janssen B.V. The authors did not declare any conflicts of interest.
Source: van der Pol JA et al. Repair of joint damage in patients with rheumatoid arthritis does not relate to previous suppression of inflammation: A subanalysis after 8 years treat-to-target in the BeSt-trial. RMD Open. 2023;9(2):e002995 (Apr 25). Doi: 10.1136/rmdopen-2023-002995
Key clinical point: Repair of joint space narrowing occurred but was rare in patients with early rheumatoid arthritis (RA) who underwent 8 years of treatment to a target disease activity score (DAS) ≤ 2.4. Therefore, suppression of damage progression should be the focus of clinical care.
Major finding: Only 5.3% of patients showed repair of joint space narrowing and bone erosions after 8 years of treatment to a target of DAS ≤ 2.4. No significant association was observed between achieving repair and suppression of disease activity, duration of previous remission, or other predictors of repair.
Study details: Findings are from a subanalysis of BeSt study including 508 patients with severe early RA who were treated to a target of DAS ≤ 2.4 and followed for 8 years.
Disclosures: The BeSt study was supported by grants from the Dutch College of Health Insurances, Schering-Plough B.V., and Janssen B.V. The authors did not declare any conflicts of interest.
Source: van der Pol JA et al. Repair of joint damage in patients with rheumatoid arthritis does not relate to previous suppression of inflammation: A subanalysis after 8 years treat-to-target in the BeSt-trial. RMD Open. 2023;9(2):e002995 (Apr 25). Doi: 10.1136/rmdopen-2023-002995
Key clinical point: Repair of joint space narrowing occurred but was rare in patients with early rheumatoid arthritis (RA) who underwent 8 years of treatment to a target disease activity score (DAS) ≤ 2.4. Therefore, suppression of damage progression should be the focus of clinical care.
Major finding: Only 5.3% of patients showed repair of joint space narrowing and bone erosions after 8 years of treatment to a target of DAS ≤ 2.4. No significant association was observed between achieving repair and suppression of disease activity, duration of previous remission, or other predictors of repair.
Study details: Findings are from a subanalysis of BeSt study including 508 patients with severe early RA who were treated to a target of DAS ≤ 2.4 and followed for 8 years.
Disclosures: The BeSt study was supported by grants from the Dutch College of Health Insurances, Schering-Plough B.V., and Janssen B.V. The authors did not declare any conflicts of interest.
Source: van der Pol JA et al. Repair of joint damage in patients with rheumatoid arthritis does not relate to previous suppression of inflammation: A subanalysis after 8 years treat-to-target in the BeSt-trial. RMD Open. 2023;9(2):e002995 (Apr 25). Doi: 10.1136/rmdopen-2023-002995
Strong link between polycyclic aromatic hydrocarbons and raised rheumatoid arthritis risk
Key clinical point: Exposure to environmental polycyclic aromatic hydrocarbons (PAH) was significantly associated with an increased prevalence of rheumatoid arthritis (RA) in the US population, and PAH mediated the majority of the effects of smoking in RA.
Major finding: Risk of developing RA was significantly higher in participants in the highest vs lowest quartile of 1-hydroxynaphthalene level (adjusted odds ratio [aOR] 1.8; P = .020) and PAH body burden scores (aOR 2.2; P = .028). PAH body burden accounted for ~90% of the total effect of smoking on RA.
Study details: Findings are from a cross-sectional study including adult participants with (n = 1418) or without (n = 20,569) RA who underwent assessments for PAH, phthalate and plasticizer metabolite, and volatile organic compound body burden.
Disclosures: This study did not declare any specific funding source. The lead author declared receiving personal fees from Cleveland HeartLab, unrelated to this study, and holding a patent.
Source: Beidelschies M et al. Polycyclic aromatic hydrocarbons and risk of rheumatoid arthritis: A cross-sectional analysis of the National Health and Nutrition Examination Survey, 2007–2016. BMJ Open. 2023;13(5):e071514 (May 9). Doi: 10.1136/bmjopen-2022-071514
Key clinical point: Exposure to environmental polycyclic aromatic hydrocarbons (PAH) was significantly associated with an increased prevalence of rheumatoid arthritis (RA) in the US population, and PAH mediated the majority of the effects of smoking in RA.
Major finding: Risk of developing RA was significantly higher in participants in the highest vs lowest quartile of 1-hydroxynaphthalene level (adjusted odds ratio [aOR] 1.8; P = .020) and PAH body burden scores (aOR 2.2; P = .028). PAH body burden accounted for ~90% of the total effect of smoking on RA.
Study details: Findings are from a cross-sectional study including adult participants with (n = 1418) or without (n = 20,569) RA who underwent assessments for PAH, phthalate and plasticizer metabolite, and volatile organic compound body burden.
Disclosures: This study did not declare any specific funding source. The lead author declared receiving personal fees from Cleveland HeartLab, unrelated to this study, and holding a patent.
Source: Beidelschies M et al. Polycyclic aromatic hydrocarbons and risk of rheumatoid arthritis: A cross-sectional analysis of the National Health and Nutrition Examination Survey, 2007–2016. BMJ Open. 2023;13(5):e071514 (May 9). Doi: 10.1136/bmjopen-2022-071514
Key clinical point: Exposure to environmental polycyclic aromatic hydrocarbons (PAH) was significantly associated with an increased prevalence of rheumatoid arthritis (RA) in the US population, and PAH mediated the majority of the effects of smoking in RA.
Major finding: Risk of developing RA was significantly higher in participants in the highest vs lowest quartile of 1-hydroxynaphthalene level (adjusted odds ratio [aOR] 1.8; P = .020) and PAH body burden scores (aOR 2.2; P = .028). PAH body burden accounted for ~90% of the total effect of smoking on RA.
Study details: Findings are from a cross-sectional study including adult participants with (n = 1418) or without (n = 20,569) RA who underwent assessments for PAH, phthalate and plasticizer metabolite, and volatile organic compound body burden.
Disclosures: This study did not declare any specific funding source. The lead author declared receiving personal fees from Cleveland HeartLab, unrelated to this study, and holding a patent.
Source: Beidelschies M et al. Polycyclic aromatic hydrocarbons and risk of rheumatoid arthritis: A cross-sectional analysis of the National Health and Nutrition Examination Survey, 2007–2016. BMJ Open. 2023;13(5):e071514 (May 9). Doi: 10.1136/bmjopen-2022-071514
Half of teens drop below obesity cutoff with semaglutide
DUBLIN – according to a secondary analysis of the STEP TEENS (Semaglutide Treatment Effect in People With Obesity) trial.
By comparison, only 12.1% of adolescents with obesity taking placebo in the trial dropped below the obesity threshold.
The study also found that 74% of participants shifted down by at least one body mass index (BMI) category after receiving the GLP-1 agonist, compared with 19% of those taking placebo.

“In a practical sense, we see that semaglutide reduced weight to a level below what is defined as clinical obesity in nearly 50% of the teens in our trial, which is historically unprecedented with treatments other than bariatric surgery,” remarked Aaron S. Kelly, MD, codirector of the Center for Pediatric Obesity Medicine at the University of Minnesota, Minneapolis, who presented the latest data at this year’s European Congress on Obesity.
“There was a 22.7-higher odds of dropping below the obesity threshold if assigned to semaglutide versus odds on placebo (P < .0001), and a 23.5-fold higher odds of dropping BMI by one category if on semaglutide (P < .0001),” he reported.
This analysis follows the 2022 publication of the main results of STEP TEENS published in the New England Journal of Medicine, which showed semaglutide helped adolescents lose weight. The drug was subsequently approved by the U.S. Food and Drug Administration for the treatment of obesity in those aged 12 and over in January of this year.
The new analysis was presented at ECO and simultaneously published in Obesity.
Grace O’Malley, PhD, Child & Adolescent Obesity Service, Children’s Health Ireland, Dublin, commented on the findings, noting that adolescents’ access to comprehensive health care is essential for the proper treatment of obesity.
“Treatment requires a long-term, multidisciplinary chronic-care approach, and usually, when treatment stops, the biological mechanisms driving the obesity begin again to drive the build-up of adipose tissue,” she said. This means that “long-term treatment including nutrition therapy, exercise ... behavioral support, and sleep therapy needs to be available to families in combination with pharmacotherapy and surgical intervention where required.”
“The results of the STEP TEENS study represent a promising development for the treatment of adolescent obesity and for associated complications related to liver function,” she added. “The observed improvements in obesity category and [liver enzyme] alanine transaminase will help clinicians plan more tailored care for adolescents with obesity,” she noted.
Semaglutide shifts BMI category
In this new secondary analysis of STEP TEENS, the authors examined the effect of subcutaneous semaglutide 2.4 mg on moving adolescents from one BMI category to another, including dropping below the obesity threshold into the overweight or normal weight categories.
The study also looked at the effect of semaglutide on glucose metabolism and cardiovascular risk factors, as well as safety and tolerability. However, this particular analysis only examined adolescents with obesity (only one person had overweight, and so they were excluded), who were divided into three further subclasses: obesity class I (BMI ≥ 95th to < 20% above the 95th percentile); obesity class II (BMI ≥ 20% to < 40% above 95th percentile); and obesity class III (BMI ≥ 40% above the 95th percentile).
After a 12-week run-in period of lifestyle intervention only, a total of 200 adolescents (12-18 years) with obesity (in the top 5% of BMI) were randomized (2:1) to once-weekly subcutaneous semaglutide 2.4 mg or placebo for 68 weeks, after a 16-week titration period. All participants continued to receive counseling about healthy nutrition and were set a goal of 60 minutes per day of moderate- to high-intensity physical activity.
Dr. Kelly and colleagues determined levels of improvement in BMI category and attainment of normal weight, or overweight, BMI category by week 68.
At baseline, the percentage of participants in obesity class I, II, or III, in those taking placebo was 39.7%, 41.4%, and 19.0%, or taking semaglutide was 31.4%, 31.4%, and 37.3%, respectively.
“After 68 weeks, not a lot happened [in placebo participants]; however, 12.1% of placebo participants did drop below the obesity threshold into overweight or normal-weight categories,” reported Dr. Kelly.
Referring to participants taking semaglutide, he added that “a total of 45% of patients on semaglutide dropped below the clinical BMI cut point for obesity, such that 19.5% dropped into the overweight category and 25.4% reduced their BMI into the normal-weight category.”
Turning to obesity class, Dr. Kelly reported that of those initially with obesity class III taking placebo, 91% remained in that class and 9.1% dropped to obesity class II at week 68. For those adolescents with obesity class III taking semaglutide, 36.4% dropped to obesity class II, 18.2% dropped to obesity class I, 11% dropped below the obesity threshold, and 34.1% remained in obesity class III, he added.
For obesity class II specifically, 71% of placebo participants stayed in that category, while 12% moved up a category. “On semaglutide, over 50% (51.2%) reduced their BMI below the obesity cut point,” noted Dr. Kelly.
In obesity class I, 26% of patients taking placebo reduced their BMI below the obesity cut point. “On semaglutide, nearly 80% reduced their BMI below the obesity threshold, with 57% dropping their BMI into the normal category,” he said.
“When we looked at baseline factors that might predict the response to semaglutide or placebo, we did not find any factors that were ... significant due to small sample sizes,” he said. However, he pointed out that “females tended to respond better to semaglutide, likewise younger adolescents, and middle body weights tended to respond better to the drug, and there was a similar pattern with obesity classes.”
Commenting on the study, Jesse Bittman, MD, University of British Columbia, Vancouver, said: “Good to see more data on different populations that some semaglutide is used in and the variability in response to it. The focus on BMI was interesting because in obesity medicine we spend a lot of time telling our patients not to focus on BMIs and ‘normals’ because there are more important tools, and we see that when these become the focus of research outcomes they can become problematic.”
Asked whether rapid weight loss in adolescents might be problematic in some respects, Dr. Bittman pointed out that “one concern with these medications is whether people are going to have loss of muscle mass or malnutrition, or whether they develop eating disorders and other disturbed eating behaviors.”
Dr. Kelly has reported engaging in unpaid consulting and educational activities for Boehringer Ingelheim, Eli Lilly, Novo Nordisk, and Vivus, and receiving donated drug/placebo from Novo Nordisk and Vivus for National Institutes of Health–funded clinical trials. Dr. O’Malley has declared having received grants in the past 3 years from the Health Research Board, Department of Health, Ireland, European Association for the Study of Obesity (via a Novo Nordisk educational grant), Healthy Ireland fund, and the Royal College of Surgeons in Ireland Strategic Academic Recruitment (StAR) Programme. Dr. Bittman has reported receiving funding from Novo Nordisk, Bayer, and Bausch Health.
A version of this article first appeared on Medscape.com.
DUBLIN – according to a secondary analysis of the STEP TEENS (Semaglutide Treatment Effect in People With Obesity) trial.
By comparison, only 12.1% of adolescents with obesity taking placebo in the trial dropped below the obesity threshold.
The study also found that 74% of participants shifted down by at least one body mass index (BMI) category after receiving the GLP-1 agonist, compared with 19% of those taking placebo.
“In a practical sense, we see that semaglutide reduced weight to a level below what is defined as clinical obesity in nearly 50% of the teens in our trial, which is historically unprecedented with treatments other than bariatric surgery,” remarked Aaron S. Kelly, MD, codirector of the Center for Pediatric Obesity Medicine at the University of Minnesota, Minneapolis, who presented the latest data at this year’s European Congress on Obesity.
“There was a 22.7-higher odds of dropping below the obesity threshold if assigned to semaglutide versus odds on placebo (P < .0001), and a 23.5-fold higher odds of dropping BMI by one category if on semaglutide (P < .0001),” he reported.
This analysis follows the 2022 publication of the main results of STEP TEENS published in the New England Journal of Medicine, which showed semaglutide helped adolescents lose weight. The drug was subsequently approved by the U.S. Food and Drug Administration for the treatment of obesity in those aged 12 and over in January of this year.
The new analysis was presented at ECO and simultaneously published in Obesity.
Grace O’Malley, PhD, Child & Adolescent Obesity Service, Children’s Health Ireland, Dublin, commented on the findings, noting that adolescents’ access to comprehensive health care is essential for the proper treatment of obesity.
“Treatment requires a long-term, multidisciplinary chronic-care approach, and usually, when treatment stops, the biological mechanisms driving the obesity begin again to drive the build-up of adipose tissue,” she said. This means that “long-term treatment including nutrition therapy, exercise ... behavioral support, and sleep therapy needs to be available to families in combination with pharmacotherapy and surgical intervention where required.”
“The results of the STEP TEENS study represent a promising development for the treatment of adolescent obesity and for associated complications related to liver function,” she added. “The observed improvements in obesity category and [liver enzyme] alanine transaminase will help clinicians plan more tailored care for adolescents with obesity,” she noted.
Semaglutide shifts BMI category
In this new secondary analysis of STEP TEENS, the authors examined the effect of subcutaneous semaglutide 2.4 mg on moving adolescents from one BMI category to another, including dropping below the obesity threshold into the overweight or normal weight categories.
The study also looked at the effect of semaglutide on glucose metabolism and cardiovascular risk factors, as well as safety and tolerability. However, this particular analysis only examined adolescents with obesity (only one person had overweight, and so they were excluded), who were divided into three further subclasses: obesity class I (BMI ≥ 95th to < 20% above the 95th percentile); obesity class II (BMI ≥ 20% to < 40% above 95th percentile); and obesity class III (BMI ≥ 40% above the 95th percentile).
After a 12-week run-in period of lifestyle intervention only, a total of 200 adolescents (12-18 years) with obesity (in the top 5% of BMI) were randomized (2:1) to once-weekly subcutaneous semaglutide 2.4 mg or placebo for 68 weeks, after a 16-week titration period. All participants continued to receive counseling about healthy nutrition and were set a goal of 60 minutes per day of moderate- to high-intensity physical activity.
Dr. Kelly and colleagues determined levels of improvement in BMI category and attainment of normal weight, or overweight, BMI category by week 68.
At baseline, the percentage of participants in obesity class I, II, or III, in those taking placebo was 39.7%, 41.4%, and 19.0%, or taking semaglutide was 31.4%, 31.4%, and 37.3%, respectively.
“After 68 weeks, not a lot happened [in placebo participants]; however, 12.1% of placebo participants did drop below the obesity threshold into overweight or normal-weight categories,” reported Dr. Kelly.
Referring to participants taking semaglutide, he added that “a total of 45% of patients on semaglutide dropped below the clinical BMI cut point for obesity, such that 19.5% dropped into the overweight category and 25.4% reduced their BMI into the normal-weight category.”
Turning to obesity class, Dr. Kelly reported that of those initially with obesity class III taking placebo, 91% remained in that class and 9.1% dropped to obesity class II at week 68. For those adolescents with obesity class III taking semaglutide, 36.4% dropped to obesity class II, 18.2% dropped to obesity class I, 11% dropped below the obesity threshold, and 34.1% remained in obesity class III, he added.
For obesity class II specifically, 71% of placebo participants stayed in that category, while 12% moved up a category. “On semaglutide, over 50% (51.2%) reduced their BMI below the obesity cut point,” noted Dr. Kelly.
In obesity class I, 26% of patients taking placebo reduced their BMI below the obesity cut point. “On semaglutide, nearly 80% reduced their BMI below the obesity threshold, with 57% dropping their BMI into the normal category,” he said.
“When we looked at baseline factors that might predict the response to semaglutide or placebo, we did not find any factors that were ... significant due to small sample sizes,” he said. However, he pointed out that “females tended to respond better to semaglutide, likewise younger adolescents, and middle body weights tended to respond better to the drug, and there was a similar pattern with obesity classes.”
Commenting on the study, Jesse Bittman, MD, University of British Columbia, Vancouver, said: “Good to see more data on different populations that some semaglutide is used in and the variability in response to it. The focus on BMI was interesting because in obesity medicine we spend a lot of time telling our patients not to focus on BMIs and ‘normals’ because there are more important tools, and we see that when these become the focus of research outcomes they can become problematic.”
Asked whether rapid weight loss in adolescents might be problematic in some respects, Dr. Bittman pointed out that “one concern with these medications is whether people are going to have loss of muscle mass or malnutrition, or whether they develop eating disorders and other disturbed eating behaviors.”
Dr. Kelly has reported engaging in unpaid consulting and educational activities for Boehringer Ingelheim, Eli Lilly, Novo Nordisk, and Vivus, and receiving donated drug/placebo from Novo Nordisk and Vivus for National Institutes of Health–funded clinical trials. Dr. O’Malley has declared having received grants in the past 3 years from the Health Research Board, Department of Health, Ireland, European Association for the Study of Obesity (via a Novo Nordisk educational grant), Healthy Ireland fund, and the Royal College of Surgeons in Ireland Strategic Academic Recruitment (StAR) Programme. Dr. Bittman has reported receiving funding from Novo Nordisk, Bayer, and Bausch Health.
A version of this article first appeared on Medscape.com.
DUBLIN – according to a secondary analysis of the STEP TEENS (Semaglutide Treatment Effect in People With Obesity) trial.
By comparison, only 12.1% of adolescents with obesity taking placebo in the trial dropped below the obesity threshold.
The study also found that 74% of participants shifted down by at least one body mass index (BMI) category after receiving the GLP-1 agonist, compared with 19% of those taking placebo.
“In a practical sense, we see that semaglutide reduced weight to a level below what is defined as clinical obesity in nearly 50% of the teens in our trial, which is historically unprecedented with treatments other than bariatric surgery,” remarked Aaron S. Kelly, MD, codirector of the Center for Pediatric Obesity Medicine at the University of Minnesota, Minneapolis, who presented the latest data at this year’s European Congress on Obesity.
“There was a 22.7-higher odds of dropping below the obesity threshold if assigned to semaglutide versus odds on placebo (P < .0001), and a 23.5-fold higher odds of dropping BMI by one category if on semaglutide (P < .0001),” he reported.
This analysis follows the 2022 publication of the main results of STEP TEENS published in the New England Journal of Medicine, which showed semaglutide helped adolescents lose weight. The drug was subsequently approved by the U.S. Food and Drug Administration for the treatment of obesity in those aged 12 and over in January of this year.
The new analysis was presented at ECO and simultaneously published in Obesity.
Grace O’Malley, PhD, Child & Adolescent Obesity Service, Children’s Health Ireland, Dublin, commented on the findings, noting that adolescents’ access to comprehensive health care is essential for the proper treatment of obesity.
“Treatment requires a long-term, multidisciplinary chronic-care approach, and usually, when treatment stops, the biological mechanisms driving the obesity begin again to drive the build-up of adipose tissue,” she said. This means that “long-term treatment including nutrition therapy, exercise ... behavioral support, and sleep therapy needs to be available to families in combination with pharmacotherapy and surgical intervention where required.”
“The results of the STEP TEENS study represent a promising development for the treatment of adolescent obesity and for associated complications related to liver function,” she added. “The observed improvements in obesity category and [liver enzyme] alanine transaminase will help clinicians plan more tailored care for adolescents with obesity,” she noted.
Semaglutide shifts BMI category
In this new secondary analysis of STEP TEENS, the authors examined the effect of subcutaneous semaglutide 2.4 mg on moving adolescents from one BMI category to another, including dropping below the obesity threshold into the overweight or normal weight categories.
The study also looked at the effect of semaglutide on glucose metabolism and cardiovascular risk factors, as well as safety and tolerability. However, this particular analysis only examined adolescents with obesity (only one person had overweight, and so they were excluded), who were divided into three further subclasses: obesity class I (BMI ≥ 95th to < 20% above the 95th percentile); obesity class II (BMI ≥ 20% to < 40% above 95th percentile); and obesity class III (BMI ≥ 40% above the 95th percentile).
After a 12-week run-in period of lifestyle intervention only, a total of 200 adolescents (12-18 years) with obesity (in the top 5% of BMI) were randomized (2:1) to once-weekly subcutaneous semaglutide 2.4 mg or placebo for 68 weeks, after a 16-week titration period. All participants continued to receive counseling about healthy nutrition and were set a goal of 60 minutes per day of moderate- to high-intensity physical activity.
Dr. Kelly and colleagues determined levels of improvement in BMI category and attainment of normal weight, or overweight, BMI category by week 68.
At baseline, the percentage of participants in obesity class I, II, or III, in those taking placebo was 39.7%, 41.4%, and 19.0%, or taking semaglutide was 31.4%, 31.4%, and 37.3%, respectively.
“After 68 weeks, not a lot happened [in placebo participants]; however, 12.1% of placebo participants did drop below the obesity threshold into overweight or normal-weight categories,” reported Dr. Kelly.
Referring to participants taking semaglutide, he added that “a total of 45% of patients on semaglutide dropped below the clinical BMI cut point for obesity, such that 19.5% dropped into the overweight category and 25.4% reduced their BMI into the normal-weight category.”
Turning to obesity class, Dr. Kelly reported that of those initially with obesity class III taking placebo, 91% remained in that class and 9.1% dropped to obesity class II at week 68. For those adolescents with obesity class III taking semaglutide, 36.4% dropped to obesity class II, 18.2% dropped to obesity class I, 11% dropped below the obesity threshold, and 34.1% remained in obesity class III, he added.
For obesity class II specifically, 71% of placebo participants stayed in that category, while 12% moved up a category. “On semaglutide, over 50% (51.2%) reduced their BMI below the obesity cut point,” noted Dr. Kelly.
In obesity class I, 26% of patients taking placebo reduced their BMI below the obesity cut point. “On semaglutide, nearly 80% reduced their BMI below the obesity threshold, with 57% dropping their BMI into the normal category,” he said.
“When we looked at baseline factors that might predict the response to semaglutide or placebo, we did not find any factors that were ... significant due to small sample sizes,” he said. However, he pointed out that “females tended to respond better to semaglutide, likewise younger adolescents, and middle body weights tended to respond better to the drug, and there was a similar pattern with obesity classes.”
Commenting on the study, Jesse Bittman, MD, University of British Columbia, Vancouver, said: “Good to see more data on different populations that some semaglutide is used in and the variability in response to it. The focus on BMI was interesting because in obesity medicine we spend a lot of time telling our patients not to focus on BMIs and ‘normals’ because there are more important tools, and we see that when these become the focus of research outcomes they can become problematic.”
Asked whether rapid weight loss in adolescents might be problematic in some respects, Dr. Bittman pointed out that “one concern with these medications is whether people are going to have loss of muscle mass or malnutrition, or whether they develop eating disorders and other disturbed eating behaviors.”
Dr. Kelly has reported engaging in unpaid consulting and educational activities for Boehringer Ingelheim, Eli Lilly, Novo Nordisk, and Vivus, and receiving donated drug/placebo from Novo Nordisk and Vivus for National Institutes of Health–funded clinical trials. Dr. O’Malley has declared having received grants in the past 3 years from the Health Research Board, Department of Health, Ireland, European Association for the Study of Obesity (via a Novo Nordisk educational grant), Healthy Ireland fund, and the Royal College of Surgeons in Ireland Strategic Academic Recruitment (StAR) Programme. Dr. Bittman has reported receiving funding from Novo Nordisk, Bayer, and Bausch Health.
A version of this article first appeared on Medscape.com.
FROM ECO 2023
Obesity drug with swallowable balloon boosts weight loss
DUBLIN – A swallowable gastric balloon (Allurion Balloon, formerly known as Elipse) combined with daily subcutaneous injections of the glucagonlike peptide 1 (GLP-1) agonist liraglutide (Saxenda, Novo Nordisk), leads to a significant average total body weight loss of 19% (18 kg or 40 lb) after around 4 months in people with obesity.
said Roberta Ienca, MD, from the Clinica Nuova Villa Claudia, Rome, who presented the findings at this year’s European Congress on Obesity.
“Despite both the balloon and liraglutide working on the early satiety feeling, the introduction of liraglutide around 1 month after [swallowing the balloon] or more frequently after 3-4 months, could sustain these feelings for a longer period of time,” she said in an interview.
“The addition of the GLP-1 agonist therapy (liraglutide) to patients treated with the Allurion program [gastric balloon] is feasible, safe, and effective in those who need additional weight loss,” she emphasized.
The balloon stayed inside participants’ stomachs for an average of 16 weeks and liraglutide was continued for an average of 4 months, resulting in a mean reduction in body mass index (BMI) of 6.4 kg/m2.
The Allurion is the world’s first and only swallowable gastric balloon placed without surgery, endoscopy, or anesthesia, and is excreted naturally after around 16 weeks.
The Allurion program delivered “excellent weight loss in individuals with overweight and obesity without going under the knife, and liraglutide has the potential to further safely enhance weight loss in cases of suboptimal adherence with the program,” Dr. Ienca said. “These two treatment approaches appear to have complementary mechanisms of action in a geographically and demographically diverse population.”
Adelardo Caballero, MD, director of the Institute of Obesity, Madrid, said that he had over 6 years of experience with the Allurion balloon in around 2,500 cases. “Over the last 3 years, we have been using Allurion balloons in combination with GLP-1 agonists. In Europe, use of the swallowable gastric balloon is common, the results are good, and it is a safe tool.”
“Using liraglutide daily in subcutaneous form is authorized in Europe and is useful in overweight and mild obesity, while use in the combination [with the balloon] is also very popular,” he explained. “In the future, the combined use of semaglutide once-weekly GLP-1 agonist or the use of dual GLP-1/gastric inhibitory polypeptide agonists [such as tirzepatide] with the swallowable intragastric balloon Allurion program or endoscopic sleeve gastroplasty will improve results,” he added.
Average 40-lb weight loss with balloon and liraglutide
For the current study, data from three international multidisciplinary obesity centers (in Italy, Spain, and Egypt) were retrospectively analyzed. All 181 patients received the combination of the Allurion balloon and liraglutide, with the latter added 4-16 weeks after swallowing the balloon.
During a 20-minute outpatient visit, participants swallowed the balloon, which was filled with liquid after reaching the stomach, and placement was confirmed by x-ray. The balloon remained inserted for around 15-17 weeks (mean 16 weeks) before natural excretion. All patients received liraglutide once daily for 1-6 months (mean 4 months). After excreting the balloon, patients started the Mediterranean diet for weight maintenance and were followed for at least 6 months.
Patients were monitored for weight loss, percentage total body weight loss, percentage excess weight loss, and BMI reduction. The timing of combining drug therapy with the Allurion program, metabolic results, and adverse event data were collected. However, Dr. Ienca explained that “the study was preliminary and aimed to evaluate feasibility and results of a combined treatment, so we didn’t collect long-term data.”
Liraglutide was mostly added in cases of unsatisfactory weight loss to boost weight reduction in patients with high BMIs, to sustain weight maintenance, and to aid diabetes control in patients with satisfactory weight loss. There were no criteria for time of onset of drug therapy in terms of a time point or percentage weight loss.
Before treatment, mean weight was 94.8 ± 21 kg and mean BMI was 33.7 ± 6.2 kg/m2. After 4 months of balloon treatment, weight loss, percentage total body weight loss, percentage excess weight loss, and decrease in BMI were 13.1 ± 7 kg, 13.9% ± 7.7%, 74.3% ± 57.1%, and 4.5 ±1.4 kg/m2 respectively.
After a mean duration of 4 months of liraglutide treatment (in addition to the gastric balloon), participants lost on average 18.1 ± 12.1 kg overall and 18.7% ± 12% of their initial total body weight. They shed 99.4% ± 84.9% of excess weight and reduced BMI by 6.4 ± 5.9 kg/m2.
Dr. Ienca explained that the study did not explore the separate contributions of the balloon or drug therapy to weight loss. “However, existing literature shows that the Allurion program leads to a weight loss of approximately 14% of total body weight after 4 months, while liraglutide studies report 12% of total body weight loss at 1 year,” he noted.
When describing the mechanism of action, Dr. Ienca said the Allurion balloon induces satiety and delays gastric emptying but the feeling of satiety starts to decrease after the first month. “For a few patients, this feeling of satiety decreases more rapidly or they have more difficulty putting in place new alimentary habits. In these patients, the addition of liraglutide gives an additional boost to support this behavioral change.”
Liraglutide-related adverse events included nausea (16.5%), diarrhea (3.3%), constipation (2.2%), and headache (1.7%), as well as drug discontinuation due to tachycardia/chest pain (1.1%) and gastrointestinal symptoms (1.1%).
Balloon removal because of intolerance occurred in 1.1% of patients, gastric dilation in 0.5%, and early balloon deflation in 0.5%. Other expected balloon-related adverse events included nausea, vomiting, and abdominal cramps.
The researchers note that the Allurion program offers a more acceptable option to balloon placement by endoscopy.
“The ease of use, low rate of adverse events, and potentially lower cost of the Allurion Program could enable much wider application of this critical intervention, and ultimately, help the millions who struggle with obesity and its associated health complications.”
A version of this article originally appeared on Medscape.com.
DUBLIN – A swallowable gastric balloon (Allurion Balloon, formerly known as Elipse) combined with daily subcutaneous injections of the glucagonlike peptide 1 (GLP-1) agonist liraglutide (Saxenda, Novo Nordisk), leads to a significant average total body weight loss of 19% (18 kg or 40 lb) after around 4 months in people with obesity.
said Roberta Ienca, MD, from the Clinica Nuova Villa Claudia, Rome, who presented the findings at this year’s European Congress on Obesity.
“Despite both the balloon and liraglutide working on the early satiety feeling, the introduction of liraglutide around 1 month after [swallowing the balloon] or more frequently after 3-4 months, could sustain these feelings for a longer period of time,” she said in an interview.
“The addition of the GLP-1 agonist therapy (liraglutide) to patients treated with the Allurion program [gastric balloon] is feasible, safe, and effective in those who need additional weight loss,” she emphasized.
The balloon stayed inside participants’ stomachs for an average of 16 weeks and liraglutide was continued for an average of 4 months, resulting in a mean reduction in body mass index (BMI) of 6.4 kg/m2.
The Allurion is the world’s first and only swallowable gastric balloon placed without surgery, endoscopy, or anesthesia, and is excreted naturally after around 16 weeks.
The Allurion program delivered “excellent weight loss in individuals with overweight and obesity without going under the knife, and liraglutide has the potential to further safely enhance weight loss in cases of suboptimal adherence with the program,” Dr. Ienca said. “These two treatment approaches appear to have complementary mechanisms of action in a geographically and demographically diverse population.”
Adelardo Caballero, MD, director of the Institute of Obesity, Madrid, said that he had over 6 years of experience with the Allurion balloon in around 2,500 cases. “Over the last 3 years, we have been using Allurion balloons in combination with GLP-1 agonists. In Europe, use of the swallowable gastric balloon is common, the results are good, and it is a safe tool.”
“Using liraglutide daily in subcutaneous form is authorized in Europe and is useful in overweight and mild obesity, while use in the combination [with the balloon] is also very popular,” he explained. “In the future, the combined use of semaglutide once-weekly GLP-1 agonist or the use of dual GLP-1/gastric inhibitory polypeptide agonists [such as tirzepatide] with the swallowable intragastric balloon Allurion program or endoscopic sleeve gastroplasty will improve results,” he added.
Average 40-lb weight loss with balloon and liraglutide
For the current study, data from three international multidisciplinary obesity centers (in Italy, Spain, and Egypt) were retrospectively analyzed. All 181 patients received the combination of the Allurion balloon and liraglutide, with the latter added 4-16 weeks after swallowing the balloon.
During a 20-minute outpatient visit, participants swallowed the balloon, which was filled with liquid after reaching the stomach, and placement was confirmed by x-ray. The balloon remained inserted for around 15-17 weeks (mean 16 weeks) before natural excretion. All patients received liraglutide once daily for 1-6 months (mean 4 months). After excreting the balloon, patients started the Mediterranean diet for weight maintenance and were followed for at least 6 months.
Patients were monitored for weight loss, percentage total body weight loss, percentage excess weight loss, and BMI reduction. The timing of combining drug therapy with the Allurion program, metabolic results, and adverse event data were collected. However, Dr. Ienca explained that “the study was preliminary and aimed to evaluate feasibility and results of a combined treatment, so we didn’t collect long-term data.”
Liraglutide was mostly added in cases of unsatisfactory weight loss to boost weight reduction in patients with high BMIs, to sustain weight maintenance, and to aid diabetes control in patients with satisfactory weight loss. There were no criteria for time of onset of drug therapy in terms of a time point or percentage weight loss.
Before treatment, mean weight was 94.8 ± 21 kg and mean BMI was 33.7 ± 6.2 kg/m2. After 4 months of balloon treatment, weight loss, percentage total body weight loss, percentage excess weight loss, and decrease in BMI were 13.1 ± 7 kg, 13.9% ± 7.7%, 74.3% ± 57.1%, and 4.5 ±1.4 kg/m2 respectively.
After a mean duration of 4 months of liraglutide treatment (in addition to the gastric balloon), participants lost on average 18.1 ± 12.1 kg overall and 18.7% ± 12% of their initial total body weight. They shed 99.4% ± 84.9% of excess weight and reduced BMI by 6.4 ± 5.9 kg/m2.
Dr. Ienca explained that the study did not explore the separate contributions of the balloon or drug therapy to weight loss. “However, existing literature shows that the Allurion program leads to a weight loss of approximately 14% of total body weight after 4 months, while liraglutide studies report 12% of total body weight loss at 1 year,” he noted.
When describing the mechanism of action, Dr. Ienca said the Allurion balloon induces satiety and delays gastric emptying but the feeling of satiety starts to decrease after the first month. “For a few patients, this feeling of satiety decreases more rapidly or they have more difficulty putting in place new alimentary habits. In these patients, the addition of liraglutide gives an additional boost to support this behavioral change.”
Liraglutide-related adverse events included nausea (16.5%), diarrhea (3.3%), constipation (2.2%), and headache (1.7%), as well as drug discontinuation due to tachycardia/chest pain (1.1%) and gastrointestinal symptoms (1.1%).
Balloon removal because of intolerance occurred in 1.1% of patients, gastric dilation in 0.5%, and early balloon deflation in 0.5%. Other expected balloon-related adverse events included nausea, vomiting, and abdominal cramps.
The researchers note that the Allurion program offers a more acceptable option to balloon placement by endoscopy.
“The ease of use, low rate of adverse events, and potentially lower cost of the Allurion Program could enable much wider application of this critical intervention, and ultimately, help the millions who struggle with obesity and its associated health complications.”
A version of this article originally appeared on Medscape.com.
DUBLIN – A swallowable gastric balloon (Allurion Balloon, formerly known as Elipse) combined with daily subcutaneous injections of the glucagonlike peptide 1 (GLP-1) agonist liraglutide (Saxenda, Novo Nordisk), leads to a significant average total body weight loss of 19% (18 kg or 40 lb) after around 4 months in people with obesity.
said Roberta Ienca, MD, from the Clinica Nuova Villa Claudia, Rome, who presented the findings at this year’s European Congress on Obesity.
“Despite both the balloon and liraglutide working on the early satiety feeling, the introduction of liraglutide around 1 month after [swallowing the balloon] or more frequently after 3-4 months, could sustain these feelings for a longer period of time,” she said in an interview.
“The addition of the GLP-1 agonist therapy (liraglutide) to patients treated with the Allurion program [gastric balloon] is feasible, safe, and effective in those who need additional weight loss,” she emphasized.
The balloon stayed inside participants’ stomachs for an average of 16 weeks and liraglutide was continued for an average of 4 months, resulting in a mean reduction in body mass index (BMI) of 6.4 kg/m2.
The Allurion is the world’s first and only swallowable gastric balloon placed without surgery, endoscopy, or anesthesia, and is excreted naturally after around 16 weeks.
The Allurion program delivered “excellent weight loss in individuals with overweight and obesity without going under the knife, and liraglutide has the potential to further safely enhance weight loss in cases of suboptimal adherence with the program,” Dr. Ienca said. “These two treatment approaches appear to have complementary mechanisms of action in a geographically and demographically diverse population.”
Adelardo Caballero, MD, director of the Institute of Obesity, Madrid, said that he had over 6 years of experience with the Allurion balloon in around 2,500 cases. “Over the last 3 years, we have been using Allurion balloons in combination with GLP-1 agonists. In Europe, use of the swallowable gastric balloon is common, the results are good, and it is a safe tool.”
“Using liraglutide daily in subcutaneous form is authorized in Europe and is useful in overweight and mild obesity, while use in the combination [with the balloon] is also very popular,” he explained. “In the future, the combined use of semaglutide once-weekly GLP-1 agonist or the use of dual GLP-1/gastric inhibitory polypeptide agonists [such as tirzepatide] with the swallowable intragastric balloon Allurion program or endoscopic sleeve gastroplasty will improve results,” he added.
Average 40-lb weight loss with balloon and liraglutide
For the current study, data from three international multidisciplinary obesity centers (in Italy, Spain, and Egypt) were retrospectively analyzed. All 181 patients received the combination of the Allurion balloon and liraglutide, with the latter added 4-16 weeks after swallowing the balloon.
During a 20-minute outpatient visit, participants swallowed the balloon, which was filled with liquid after reaching the stomach, and placement was confirmed by x-ray. The balloon remained inserted for around 15-17 weeks (mean 16 weeks) before natural excretion. All patients received liraglutide once daily for 1-6 months (mean 4 months). After excreting the balloon, patients started the Mediterranean diet for weight maintenance and were followed for at least 6 months.
Patients were monitored for weight loss, percentage total body weight loss, percentage excess weight loss, and BMI reduction. The timing of combining drug therapy with the Allurion program, metabolic results, and adverse event data were collected. However, Dr. Ienca explained that “the study was preliminary and aimed to evaluate feasibility and results of a combined treatment, so we didn’t collect long-term data.”
Liraglutide was mostly added in cases of unsatisfactory weight loss to boost weight reduction in patients with high BMIs, to sustain weight maintenance, and to aid diabetes control in patients with satisfactory weight loss. There were no criteria for time of onset of drug therapy in terms of a time point or percentage weight loss.
Before treatment, mean weight was 94.8 ± 21 kg and mean BMI was 33.7 ± 6.2 kg/m2. After 4 months of balloon treatment, weight loss, percentage total body weight loss, percentage excess weight loss, and decrease in BMI were 13.1 ± 7 kg, 13.9% ± 7.7%, 74.3% ± 57.1%, and 4.5 ±1.4 kg/m2 respectively.
After a mean duration of 4 months of liraglutide treatment (in addition to the gastric balloon), participants lost on average 18.1 ± 12.1 kg overall and 18.7% ± 12% of their initial total body weight. They shed 99.4% ± 84.9% of excess weight and reduced BMI by 6.4 ± 5.9 kg/m2.
Dr. Ienca explained that the study did not explore the separate contributions of the balloon or drug therapy to weight loss. “However, existing literature shows that the Allurion program leads to a weight loss of approximately 14% of total body weight after 4 months, while liraglutide studies report 12% of total body weight loss at 1 year,” he noted.
When describing the mechanism of action, Dr. Ienca said the Allurion balloon induces satiety and delays gastric emptying but the feeling of satiety starts to decrease after the first month. “For a few patients, this feeling of satiety decreases more rapidly or they have more difficulty putting in place new alimentary habits. In these patients, the addition of liraglutide gives an additional boost to support this behavioral change.”
Liraglutide-related adverse events included nausea (16.5%), diarrhea (3.3%), constipation (2.2%), and headache (1.7%), as well as drug discontinuation due to tachycardia/chest pain (1.1%) and gastrointestinal symptoms (1.1%).
Balloon removal because of intolerance occurred in 1.1% of patients, gastric dilation in 0.5%, and early balloon deflation in 0.5%. Other expected balloon-related adverse events included nausea, vomiting, and abdominal cramps.
The researchers note that the Allurion program offers a more acceptable option to balloon placement by endoscopy.
“The ease of use, low rate of adverse events, and potentially lower cost of the Allurion Program could enable much wider application of this critical intervention, and ultimately, help the millions who struggle with obesity and its associated health complications.”
A version of this article originally appeared on Medscape.com.
AT ECO 2023
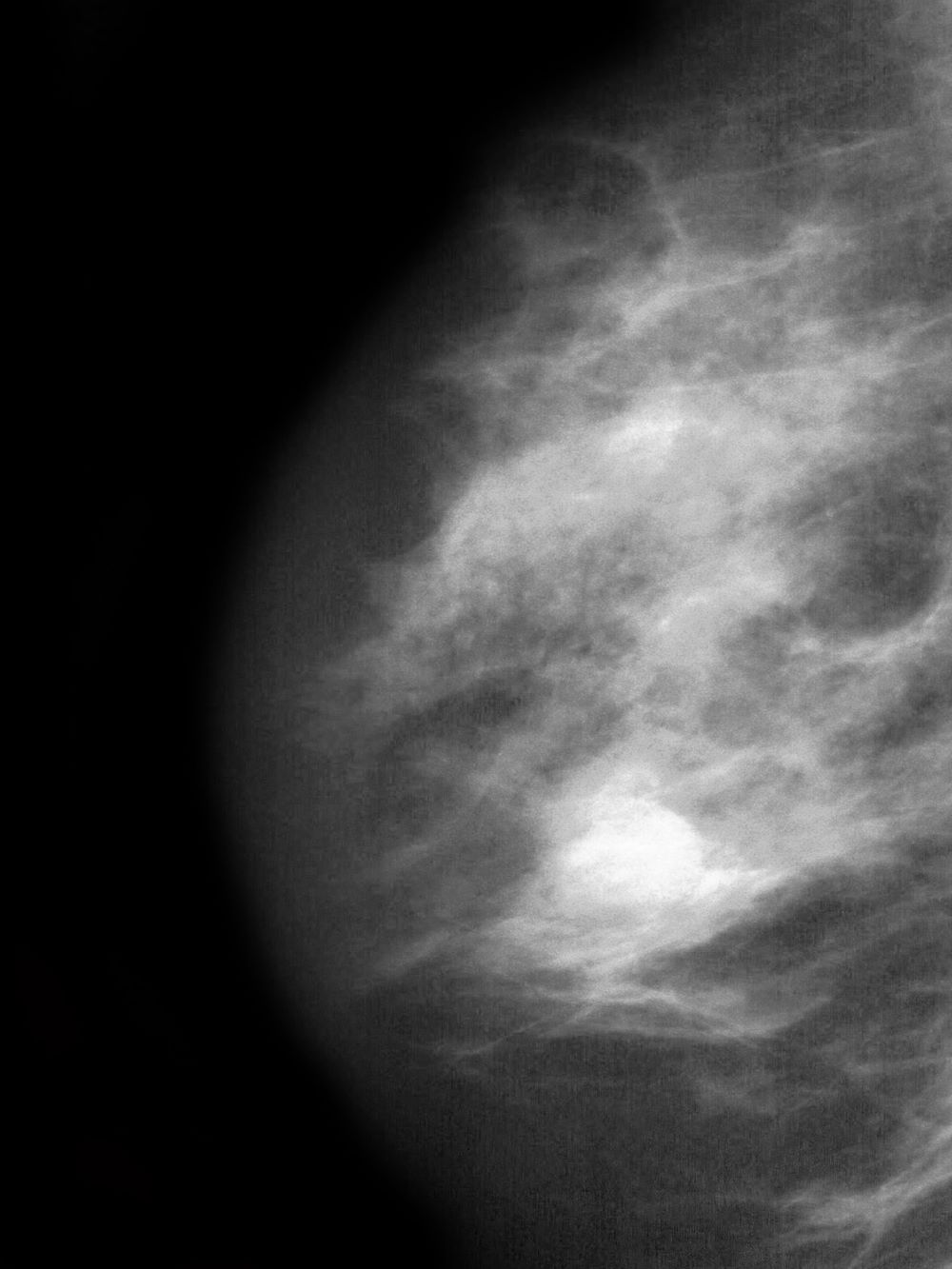
Skin changes and pain
The history and findings in this case are suggestive of inflammatory breast cancer.
Breast cancer is the leading life-threatening cancer diagnosed and the second-leading cause of cancer-related deaths in women worldwide. In the United States, estimates suggest that 287,850 new cases of invasive breast cancer were diagnosed in 2022 and 43,250 women died of the disease. Globally, approximately 2.3 million new diagnoses and 685,000 breast cancer–related deaths were reported in 2020.
Inflammatory breast cancer is a rare and highly aggressive subtype of locally advanced breast cancer. In the United States, inflammatory breast cancer accounts for approximately 2%-4% of breast cancer cases. Although its incidence is rare, 7% of breast cancer caused mortality is attributed to inflammatory breast cancer. Cases of inflammatory breast cancer tend to be diagnosed at a younger age compared with noninflammatory breast cancer cases. Risk factors include African-American race and obesity.
The symptoms of inflammatory breast cancer can vary broadly, ranging from subtle skin erythema to diffuse breast involvement with skin dimpling and nipple inversion. Diagnostic criteria include erythema occupying at least one third of the breast, edema, peau d'orange, and/or warmth, with or without an underlying mass; rapid onset (< 3 months); and pathologic confirmation of invasive breast carcinoma. Histologic findings include florid tumor emboli that obstruct dermal lymphatics, which results in swelling and inflammation of the affected breast.
Inflammatory breast cancer has been associated with a poor prognosis. However, treatment advances are helping to improve outcomes. Currently, 5-year survival rates are reported to be 40%-70%, with a median survival of 2-4 years. According to 2023 guidelines from the National Comprehensive Cancer Network (NCCN), the first-line treatment of inflammatory breast cancer involves neoadjuvant chemotherapy, modified radical mastectomy, and adjuvant radiation to the chest wall and regional nodes. Endocrine treatment should also be given to patients who are ER-positive and/or PR-positive (sequential chemotherapy followed by endocrine therapy). For patients who are HER2-positive, up to 1 year of HER2-targeted therapy should be given. HER2-targeted therapies can be administered concurrently with radiation and with endocrine therapy if indicated.
Delayed reconstruction after mastectomy remains the clinical standard for inflammatory breast cancer. This is because the need to resect involved skin negates the benefit of skin-sparing mastectomy for immediate reconstruction. Moreover, high rates of local and distant recurrence warrant comprehensive regional node irradiation in a timely fashion, which may be more challenging or subject to delay after immediate reconstruction. Rarely, the extent of skin excision at the time of mastectomy prohibits primary or local closure. In such cases, reconstruction of the chest wall defect with autologous tissue is required, and concomitant immediate reconstruction may be undertaken.
Detailed guidance on the treatment of inflammatory breast cancer, in the first line and beyond, are available from the NCCN.
Avan J. Armaghani, MD, Assistant Member, Department of Breast Oncology, Moffitt Cancer Center, University of South Florida, Tampa, FL.
Avan J. Armaghani, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The history and findings in this case are suggestive of inflammatory breast cancer.
Breast cancer is the leading life-threatening cancer diagnosed and the second-leading cause of cancer-related deaths in women worldwide. In the United States, estimates suggest that 287,850 new cases of invasive breast cancer were diagnosed in 2022 and 43,250 women died of the disease. Globally, approximately 2.3 million new diagnoses and 685,000 breast cancer–related deaths were reported in 2020.
Inflammatory breast cancer is a rare and highly aggressive subtype of locally advanced breast cancer. In the United States, inflammatory breast cancer accounts for approximately 2%-4% of breast cancer cases. Although its incidence is rare, 7% of breast cancer caused mortality is attributed to inflammatory breast cancer. Cases of inflammatory breast cancer tend to be diagnosed at a younger age compared with noninflammatory breast cancer cases. Risk factors include African-American race and obesity.
The symptoms of inflammatory breast cancer can vary broadly, ranging from subtle skin erythema to diffuse breast involvement with skin dimpling and nipple inversion. Diagnostic criteria include erythema occupying at least one third of the breast, edema, peau d'orange, and/or warmth, with or without an underlying mass; rapid onset (< 3 months); and pathologic confirmation of invasive breast carcinoma. Histologic findings include florid tumor emboli that obstruct dermal lymphatics, which results in swelling and inflammation of the affected breast.
Inflammatory breast cancer has been associated with a poor prognosis. However, treatment advances are helping to improve outcomes. Currently, 5-year survival rates are reported to be 40%-70%, with a median survival of 2-4 years. According to 2023 guidelines from the National Comprehensive Cancer Network (NCCN), the first-line treatment of inflammatory breast cancer involves neoadjuvant chemotherapy, modified radical mastectomy, and adjuvant radiation to the chest wall and regional nodes. Endocrine treatment should also be given to patients who are ER-positive and/or PR-positive (sequential chemotherapy followed by endocrine therapy). For patients who are HER2-positive, up to 1 year of HER2-targeted therapy should be given. HER2-targeted therapies can be administered concurrently with radiation and with endocrine therapy if indicated.
Delayed reconstruction after mastectomy remains the clinical standard for inflammatory breast cancer. This is because the need to resect involved skin negates the benefit of skin-sparing mastectomy for immediate reconstruction. Moreover, high rates of local and distant recurrence warrant comprehensive regional node irradiation in a timely fashion, which may be more challenging or subject to delay after immediate reconstruction. Rarely, the extent of skin excision at the time of mastectomy prohibits primary or local closure. In such cases, reconstruction of the chest wall defect with autologous tissue is required, and concomitant immediate reconstruction may be undertaken.
Detailed guidance on the treatment of inflammatory breast cancer, in the first line and beyond, are available from the NCCN.
Avan J. Armaghani, MD, Assistant Member, Department of Breast Oncology, Moffitt Cancer Center, University of South Florida, Tampa, FL.
Avan J. Armaghani, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The history and findings in this case are suggestive of inflammatory breast cancer.
Breast cancer is the leading life-threatening cancer diagnosed and the second-leading cause of cancer-related deaths in women worldwide. In the United States, estimates suggest that 287,850 new cases of invasive breast cancer were diagnosed in 2022 and 43,250 women died of the disease. Globally, approximately 2.3 million new diagnoses and 685,000 breast cancer–related deaths were reported in 2020.
Inflammatory breast cancer is a rare and highly aggressive subtype of locally advanced breast cancer. In the United States, inflammatory breast cancer accounts for approximately 2%-4% of breast cancer cases. Although its incidence is rare, 7% of breast cancer caused mortality is attributed to inflammatory breast cancer. Cases of inflammatory breast cancer tend to be diagnosed at a younger age compared with noninflammatory breast cancer cases. Risk factors include African-American race and obesity.
The symptoms of inflammatory breast cancer can vary broadly, ranging from subtle skin erythema to diffuse breast involvement with skin dimpling and nipple inversion. Diagnostic criteria include erythema occupying at least one third of the breast, edema, peau d'orange, and/or warmth, with or without an underlying mass; rapid onset (< 3 months); and pathologic confirmation of invasive breast carcinoma. Histologic findings include florid tumor emboli that obstruct dermal lymphatics, which results in swelling and inflammation of the affected breast.
Inflammatory breast cancer has been associated with a poor prognosis. However, treatment advances are helping to improve outcomes. Currently, 5-year survival rates are reported to be 40%-70%, with a median survival of 2-4 years. According to 2023 guidelines from the National Comprehensive Cancer Network (NCCN), the first-line treatment of inflammatory breast cancer involves neoadjuvant chemotherapy, modified radical mastectomy, and adjuvant radiation to the chest wall and regional nodes. Endocrine treatment should also be given to patients who are ER-positive and/or PR-positive (sequential chemotherapy followed by endocrine therapy). For patients who are HER2-positive, up to 1 year of HER2-targeted therapy should be given. HER2-targeted therapies can be administered concurrently with radiation and with endocrine therapy if indicated.
Delayed reconstruction after mastectomy remains the clinical standard for inflammatory breast cancer. This is because the need to resect involved skin negates the benefit of skin-sparing mastectomy for immediate reconstruction. Moreover, high rates of local and distant recurrence warrant comprehensive regional node irradiation in a timely fashion, which may be more challenging or subject to delay after immediate reconstruction. Rarely, the extent of skin excision at the time of mastectomy prohibits primary or local closure. In such cases, reconstruction of the chest wall defect with autologous tissue is required, and concomitant immediate reconstruction may be undertaken.
Detailed guidance on the treatment of inflammatory breast cancer, in the first line and beyond, are available from the NCCN.
Avan J. Armaghani, MD, Assistant Member, Department of Breast Oncology, Moffitt Cancer Center, University of South Florida, Tampa, FL.
Avan J. Armaghani, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
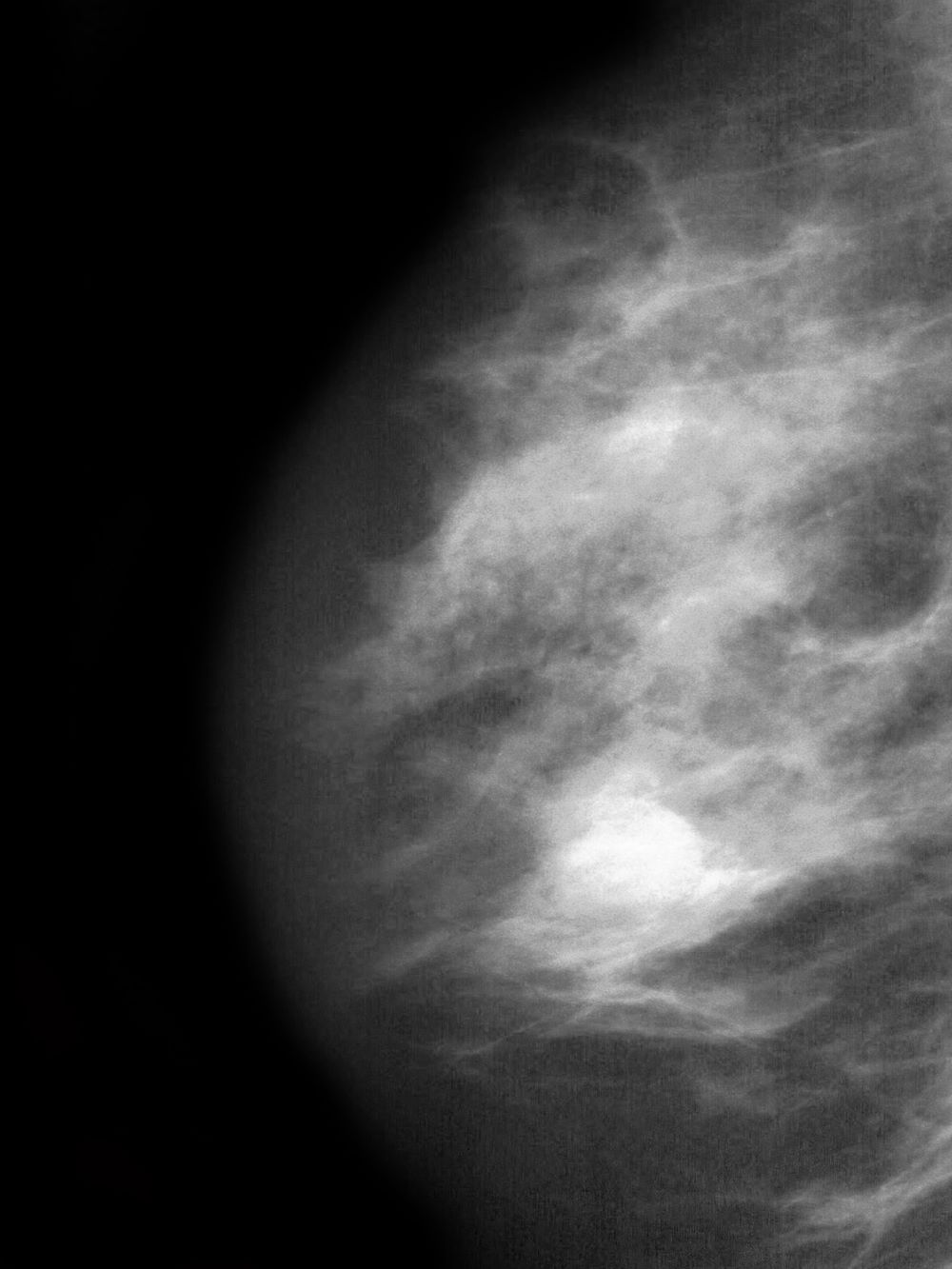
A 51-year-old nonsmoking Black woman presents with a lump in her left breast, as well as associated skin changes and pain of approximately 3 months' duration. The patient last underwent routine screening breast imaging 2 years earlier. The patient is 5 ft 7 in and weighs 200 lb (BMI 31.3). Previous medical history is unremarkable. There is a family history of breast cancer (maternal aunt) and lung cancer (maternal uncle). Physical examination reveals a palpable abnormality in the left breast with edema, skin thickening, and peau d'orange. More than one third of the breast is erythematous. A bilateral mammography reveals an irregular mass and calcifications in the upper outer quadrant of the left breast as well as numerous additional masses and focal asymmetries involving the upper outer and lower outer quadrant of the left breast that extend into the inner left breast. A 1.6-cm mass in the upper left breast is noted, with total abnormality spanning 12.7 cm. Left axillary lymphadenopathy is also observed. Skin punch biopsy of the affected breast reveals dermal lymphatic invasion by tumor cells and tumor emboli. Left axial fine-needle aspiration biopsy reveals malignant cells.
Internet use a modifiable dementia risk factor in older adults?
Investigators followed more than 18,000 older individuals and found that regular Internet use was associated with about a 50% reduction in dementia risk, compared with their counterparts who did not use the Internet regularly.
They also found that longer duration of regular Internet use was associated with a reduced risk of dementia, although excessive daily Internet usage appeared to adversely affect dementia risk.
“Online engagement can develop and maintain cognitive reserve – resiliency against physiological damage to the brain – and increased cognitive reserve can, in turn, compensate for brain aging and reduce the risk of dementia,” study investigator Gawon Cho, a doctoral candidate at New York University School of Global Public Health, said in an interview.
The study was published online in the Journal of the American Geriatrics Society.
Unexamined benefits
Prior research has shown that older adult Internet users have “better overall cognitive performance, verbal reasoning, and memory,” compared with nonusers, the authors note.
However, because this body of research consists of cross-sectional analyses and longitudinal studies with brief follow-up periods, the long-term cognitive benefits of Internet usage remain “unexamined.”
In addition, despite “extensive evidence of a disproportionately high burden of dementia in people of color, individuals without higher education, and adults who experienced other socioeconomic hardships, little is known about whether the Internet has exacerbated population-level disparities in cognitive health,” the investigators add.
Another question concerns whether excessive Internet usage may actually be detrimental to neurocognitive outcomes. However, “existing evidence on the adverse effects of Internet usage is concentrated in younger populations whose brains are still undergoing maturation.”
Ms. Cho said the motivation for the study was the lack of longitudinal studies on this topic, especially those with sufficient follow-up periods. In addition, she said, there is insufficient evidence about how changes in Internet usage in older age are associated with prospective dementia risk.
For the study, investigators turned to participants in the Health and Retirement Study, an ongoing longitudinal survey of a nationally representative sample of U.S.-based older adults (aged ≥ 50 years).
All participants (n = 18,154; 47.36% male; median age, 55.17 years) were dementia-free, community-dwelling older adults who completed a 2002 baseline cognitive assessment and were asked about Internet usage every 2 years thereafter.
Participants were followed from 2002 to 2018 for a maximum of 17.1 years (median, 7.9 years), which is the longest follow-up period to date. Of the total sample, 64.76% were regular Internet users.
The study’s primary outcome was incident dementia, based on performance on the Modified Telephone Interview for Cognitive Status (TICS-M), which was administered every 2 years.
The exposure examined in the study was cumulative Internet usage in late adulthood, defined as “the number of biennial waves where participants used the Internet regularly during the first three waves.”
In addition, participants were asked how many hours they spent using the Internet during the past week for activities other than viewing television shows or movies.
The researchers also investigated whether the link between Internet usage and dementia risk varied by educational attainment, race-ethnicity, sex, and generational cohort.
Covariates included baseline TICS-M score, health, age, household income, marital status, and region of residence.
U-shaped curve
More than half of the sample (52.96%) showed no changes in Internet use from baseline during the study period, while one-fifth (20.54%) did show changes in use.
Investigators found a robust link between Internet usage and lower dementia risk (cause-specific hazard ratio, 0.57 [95% CI, 0.46-0.71]) – a finding that remained even after adjusting for self-selection into baseline usage (csHR, 0.54 [0.41-0.72]) and signs of cognitive decline at baseline (csHR, 0.62 [0.46-0.85]).
Each additional wave of regular Internet usage was associated with a 21% decrease in the risk of dementia (95% CI, 13%-29%), wherein additional regular periods were associated with reduced dementia risk (csHR, 0.80 [95% CI, 0.68-0.95]).
“The difference in risk between regular and nonregular users did not vary by educational attainment, race-ethnicity, sex, and generation,” the investigators note.
A U-shaped association was found between daily hours of online engagement, wherein the lowest risk was observed in those with 0.1-2 hours of usage (compared with 0 hours of usage). The risk increased in a “monotonic fashion” after 2 hours, with 6.1-8 hours of usage showing the highest risk.
This finding was not considered statistically significant, but the “consistent U-shaped trend offers a preliminary suggestion that excessive online engagement may have adverse cognitive effects on older adults,” the investigators note.
“Among older adults, regular Internet users may experience a lower risk of dementia compared to nonregular users, and longer periods of regular Internet usage in late adulthood may help reduce the risks of subsequent dementia incidence,” said Ms. Cho. “Nonetheless, using the Internet excessively daily may negatively affect the risk of dementia in older adults.”
Bidirectional relationship?
Commenting for this article, Claire Sexton, DPhil, Alzheimer’s Association senior director of scientific programs and outreach, noted that some risk factors for Alzheimer’s or other dementias can’t be changed, while others are modifiable, “either at a personal or a population level.”
She called the current research “important” because it “identifies a potentially modifiable factor that may influence dementia risk.”
However, cautioned Dr. Sexton, who was not involved with the study, the findings cannot establish cause and effect. In fact, the relationship may be bidirectional.
“It may be that regular Internet usage is associated with increased cognitive stimulation, and in turn reduced risk of dementia; or it may be that individuals with lower risk of dementia are more likely to engage in regular Internet usage,” she said. Thus, “interventional studies are able to shed more light on causation.”
The Health and Retirement Study is sponsored by the National Institute on Aging and is conducted by the University of Michigan, Ann Arbor. Ms. Cho, her coauthors, and Dr. Sexton have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Investigators followed more than 18,000 older individuals and found that regular Internet use was associated with about a 50% reduction in dementia risk, compared with their counterparts who did not use the Internet regularly.
They also found that longer duration of regular Internet use was associated with a reduced risk of dementia, although excessive daily Internet usage appeared to adversely affect dementia risk.
“Online engagement can develop and maintain cognitive reserve – resiliency against physiological damage to the brain – and increased cognitive reserve can, in turn, compensate for brain aging and reduce the risk of dementia,” study investigator Gawon Cho, a doctoral candidate at New York University School of Global Public Health, said in an interview.
The study was published online in the Journal of the American Geriatrics Society.
Unexamined benefits
Prior research has shown that older adult Internet users have “better overall cognitive performance, verbal reasoning, and memory,” compared with nonusers, the authors note.
However, because this body of research consists of cross-sectional analyses and longitudinal studies with brief follow-up periods, the long-term cognitive benefits of Internet usage remain “unexamined.”
In addition, despite “extensive evidence of a disproportionately high burden of dementia in people of color, individuals without higher education, and adults who experienced other socioeconomic hardships, little is known about whether the Internet has exacerbated population-level disparities in cognitive health,” the investigators add.
Another question concerns whether excessive Internet usage may actually be detrimental to neurocognitive outcomes. However, “existing evidence on the adverse effects of Internet usage is concentrated in younger populations whose brains are still undergoing maturation.”
Ms. Cho said the motivation for the study was the lack of longitudinal studies on this topic, especially those with sufficient follow-up periods. In addition, she said, there is insufficient evidence about how changes in Internet usage in older age are associated with prospective dementia risk.
For the study, investigators turned to participants in the Health and Retirement Study, an ongoing longitudinal survey of a nationally representative sample of U.S.-based older adults (aged ≥ 50 years).
All participants (n = 18,154; 47.36% male; median age, 55.17 years) were dementia-free, community-dwelling older adults who completed a 2002 baseline cognitive assessment and were asked about Internet usage every 2 years thereafter.
Participants were followed from 2002 to 2018 for a maximum of 17.1 years (median, 7.9 years), which is the longest follow-up period to date. Of the total sample, 64.76% were regular Internet users.
The study’s primary outcome was incident dementia, based on performance on the Modified Telephone Interview for Cognitive Status (TICS-M), which was administered every 2 years.
The exposure examined in the study was cumulative Internet usage in late adulthood, defined as “the number of biennial waves where participants used the Internet regularly during the first three waves.”
In addition, participants were asked how many hours they spent using the Internet during the past week for activities other than viewing television shows or movies.
The researchers also investigated whether the link between Internet usage and dementia risk varied by educational attainment, race-ethnicity, sex, and generational cohort.
Covariates included baseline TICS-M score, health, age, household income, marital status, and region of residence.
U-shaped curve
More than half of the sample (52.96%) showed no changes in Internet use from baseline during the study period, while one-fifth (20.54%) did show changes in use.
Investigators found a robust link between Internet usage and lower dementia risk (cause-specific hazard ratio, 0.57 [95% CI, 0.46-0.71]) – a finding that remained even after adjusting for self-selection into baseline usage (csHR, 0.54 [0.41-0.72]) and signs of cognitive decline at baseline (csHR, 0.62 [0.46-0.85]).
Each additional wave of regular Internet usage was associated with a 21% decrease in the risk of dementia (95% CI, 13%-29%), wherein additional regular periods were associated with reduced dementia risk (csHR, 0.80 [95% CI, 0.68-0.95]).
“The difference in risk between regular and nonregular users did not vary by educational attainment, race-ethnicity, sex, and generation,” the investigators note.
A U-shaped association was found between daily hours of online engagement, wherein the lowest risk was observed in those with 0.1-2 hours of usage (compared with 0 hours of usage). The risk increased in a “monotonic fashion” after 2 hours, with 6.1-8 hours of usage showing the highest risk.
This finding was not considered statistically significant, but the “consistent U-shaped trend offers a preliminary suggestion that excessive online engagement may have adverse cognitive effects on older adults,” the investigators note.
“Among older adults, regular Internet users may experience a lower risk of dementia compared to nonregular users, and longer periods of regular Internet usage in late adulthood may help reduce the risks of subsequent dementia incidence,” said Ms. Cho. “Nonetheless, using the Internet excessively daily may negatively affect the risk of dementia in older adults.”
Bidirectional relationship?
Commenting for this article, Claire Sexton, DPhil, Alzheimer’s Association senior director of scientific programs and outreach, noted that some risk factors for Alzheimer’s or other dementias can’t be changed, while others are modifiable, “either at a personal or a population level.”
She called the current research “important” because it “identifies a potentially modifiable factor that may influence dementia risk.”
However, cautioned Dr. Sexton, who was not involved with the study, the findings cannot establish cause and effect. In fact, the relationship may be bidirectional.
“It may be that regular Internet usage is associated with increased cognitive stimulation, and in turn reduced risk of dementia; or it may be that individuals with lower risk of dementia are more likely to engage in regular Internet usage,” she said. Thus, “interventional studies are able to shed more light on causation.”
The Health and Retirement Study is sponsored by the National Institute on Aging and is conducted by the University of Michigan, Ann Arbor. Ms. Cho, her coauthors, and Dr. Sexton have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Investigators followed more than 18,000 older individuals and found that regular Internet use was associated with about a 50% reduction in dementia risk, compared with their counterparts who did not use the Internet regularly.
They also found that longer duration of regular Internet use was associated with a reduced risk of dementia, although excessive daily Internet usage appeared to adversely affect dementia risk.
“Online engagement can develop and maintain cognitive reserve – resiliency against physiological damage to the brain – and increased cognitive reserve can, in turn, compensate for brain aging and reduce the risk of dementia,” study investigator Gawon Cho, a doctoral candidate at New York University School of Global Public Health, said in an interview.
The study was published online in the Journal of the American Geriatrics Society.
Unexamined benefits
Prior research has shown that older adult Internet users have “better overall cognitive performance, verbal reasoning, and memory,” compared with nonusers, the authors note.
However, because this body of research consists of cross-sectional analyses and longitudinal studies with brief follow-up periods, the long-term cognitive benefits of Internet usage remain “unexamined.”
In addition, despite “extensive evidence of a disproportionately high burden of dementia in people of color, individuals without higher education, and adults who experienced other socioeconomic hardships, little is known about whether the Internet has exacerbated population-level disparities in cognitive health,” the investigators add.
Another question concerns whether excessive Internet usage may actually be detrimental to neurocognitive outcomes. However, “existing evidence on the adverse effects of Internet usage is concentrated in younger populations whose brains are still undergoing maturation.”
Ms. Cho said the motivation for the study was the lack of longitudinal studies on this topic, especially those with sufficient follow-up periods. In addition, she said, there is insufficient evidence about how changes in Internet usage in older age are associated with prospective dementia risk.
For the study, investigators turned to participants in the Health and Retirement Study, an ongoing longitudinal survey of a nationally representative sample of U.S.-based older adults (aged ≥ 50 years).
All participants (n = 18,154; 47.36% male; median age, 55.17 years) were dementia-free, community-dwelling older adults who completed a 2002 baseline cognitive assessment and were asked about Internet usage every 2 years thereafter.
Participants were followed from 2002 to 2018 for a maximum of 17.1 years (median, 7.9 years), which is the longest follow-up period to date. Of the total sample, 64.76% were regular Internet users.
The study’s primary outcome was incident dementia, based on performance on the Modified Telephone Interview for Cognitive Status (TICS-M), which was administered every 2 years.
The exposure examined in the study was cumulative Internet usage in late adulthood, defined as “the number of biennial waves where participants used the Internet regularly during the first three waves.”
In addition, participants were asked how many hours they spent using the Internet during the past week for activities other than viewing television shows or movies.
The researchers also investigated whether the link between Internet usage and dementia risk varied by educational attainment, race-ethnicity, sex, and generational cohort.
Covariates included baseline TICS-M score, health, age, household income, marital status, and region of residence.
U-shaped curve
More than half of the sample (52.96%) showed no changes in Internet use from baseline during the study period, while one-fifth (20.54%) did show changes in use.
Investigators found a robust link between Internet usage and lower dementia risk (cause-specific hazard ratio, 0.57 [95% CI, 0.46-0.71]) – a finding that remained even after adjusting for self-selection into baseline usage (csHR, 0.54 [0.41-0.72]) and signs of cognitive decline at baseline (csHR, 0.62 [0.46-0.85]).
Each additional wave of regular Internet usage was associated with a 21% decrease in the risk of dementia (95% CI, 13%-29%), wherein additional regular periods were associated with reduced dementia risk (csHR, 0.80 [95% CI, 0.68-0.95]).
“The difference in risk between regular and nonregular users did not vary by educational attainment, race-ethnicity, sex, and generation,” the investigators note.
A U-shaped association was found between daily hours of online engagement, wherein the lowest risk was observed in those with 0.1-2 hours of usage (compared with 0 hours of usage). The risk increased in a “monotonic fashion” after 2 hours, with 6.1-8 hours of usage showing the highest risk.
This finding was not considered statistically significant, but the “consistent U-shaped trend offers a preliminary suggestion that excessive online engagement may have adverse cognitive effects on older adults,” the investigators note.
“Among older adults, regular Internet users may experience a lower risk of dementia compared to nonregular users, and longer periods of regular Internet usage in late adulthood may help reduce the risks of subsequent dementia incidence,” said Ms. Cho. “Nonetheless, using the Internet excessively daily may negatively affect the risk of dementia in older adults.”
Bidirectional relationship?
Commenting for this article, Claire Sexton, DPhil, Alzheimer’s Association senior director of scientific programs and outreach, noted that some risk factors for Alzheimer’s or other dementias can’t be changed, while others are modifiable, “either at a personal or a population level.”
She called the current research “important” because it “identifies a potentially modifiable factor that may influence dementia risk.”
However, cautioned Dr. Sexton, who was not involved with the study, the findings cannot establish cause and effect. In fact, the relationship may be bidirectional.
“It may be that regular Internet usage is associated with increased cognitive stimulation, and in turn reduced risk of dementia; or it may be that individuals with lower risk of dementia are more likely to engage in regular Internet usage,” she said. Thus, “interventional studies are able to shed more light on causation.”
The Health and Retirement Study is sponsored by the National Institute on Aging and is conducted by the University of Michigan, Ann Arbor. Ms. Cho, her coauthors, and Dr. Sexton have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN GERIATRICS SOCIETY
Guidelines for children with obesity: Family and treatment are key
Douglas Lunsford’s son Samuel has struggled with obesity all his life.
Just before turning 14, Samuel, now 25, took part in a program at Ohio-based Nationwide Children’s Hospital’s Center for Healthy Weight and Nutrition. The program consisted of twice-weekly meetings with a nutritionist, including lessons in food portion size, what food does within the body, what foods can be used to supplement other foods, and similar topics, as well as physical exercise.
Although the program was designed for youngsters with weight problems, Mr. Lunsford also took part.
“They would exercise us and work us out,” he said.
Father and son did the program together for 2 years. Since then, Mr. Lunsford has advocated for youngsters with obesity.
“Samuel’s struggle spurred us into action,” he said.
Eventually, Mr. Lunsford helped create the American Academy of Pediatrics’ recently released Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity.
Helping create change
According to Sandra Hassink, MD, coauthor of the guideline and vice chair of the Clinical Practice Guideline Subcommittee on Obesity, the goal was to “help patients make changes in lifestyle, behaviors, or environment in a sustainable way and also to involve families in decision-making at every step of the way.”
Ideally, a child would receive intense behavioral and lifestyle treatment, although this approach isn’t always available and might be challenging to deliver. The most effective treatments include at least 26 hours of face-to-face, family-based treatments, consisting of many different components and lasting 3-12 months.
The guideline suggests that doctors offer adolescents 12 and older medication to assist in weight loss, along with health, behavior, and lifestyle treatment, and that teens who have severe obesity should consider metabolic and bariatric surgery as they continue intense health behavior and lifestyle treatment.
“We’re living at a time where we’ve watched obesity affect our children and adult population for 4 decades and, along with the risk of obesity, we’ve watched a rise in obesity; we’re seeing increases in illness that go along with obesity, such as type 2 diabetes, lipid diseases like high cholesterol, and nonalcoholic fatty liver disease,” Dr. Hassink said.
She explained that, as people gain weight, the cells in adipose (fatty) tissues start to malfunction and produce inflammatory chemicals that cause these illnesses.
“So having extra adipose tissue is a risk,” she said. “As pediatricians, we measure body mass index [BMI] – which is calculated based on height and weight – as a way of seeing whether the child could be at risk for developing these dysfunctioning cells. If so, we screen them for prediabetes, lipid disease, or liver disease and other obesity-related comorbidities.”
In addition, “we’re concerned about the mental health of children with obesity because of the weight bias in our culture,” said Dr. Hassink. “A child gets stigmatized, and this takes the form of bullying and teasing, and leads to low self-esteem, depression, and anxiety. So we know we have a host of physical problems we need to look out for, as well as the emotional and psychological effects of how our culture views things.”
Are parents ready for the new approach?
A new report from Harmony Healthcare IT, a data management firm that works with health data, looked at how parents regard their children’s obesity. The company surveyed more than 1,000 parents and found that one-tenth of respondents had children who were overweight or obese and over a quarter (26%) worried about their child’s weight.
Nearly 40% of parents would consider weight loss medication for their child if the child became obese at age 12, and about 16% would consider weight loss surgery. But most parents would not consider this surgery until their child was an average age of 15 rather than the AAP’s recommended age of 13.
Mr. Lunsford said that his son considered surgery and medication but was “never comfortable” with these approaches.
This isn’t unusual, Dr. Hassink said. “Not every parent will think the same way, and their view will be based on their experience and what’s going on with their child.”
The guideline wasn’t designed to encourage every child to try medication or have surgery, she said.
“But parents now know that there are potentially helpful choices here that we didn’t have years ago, and those can be discussed with the child’s pediatrician.”
Challenges to keeping healthy
It’s tough to stay healthy and not develop obesity in our modern environment, Dr. Hassink said.
“There’s a lot of processed food, a lot of sugar in our foods, a lot of sedentary behavior, and a decrease in physical activity. In many communities, it’s hard for people to get healthy foods.”
Mr. Lunsford said that when his son was in his late teens and would go out with friends, they typically went to fast-food restaurants.
“Sam would say ‘yes’ to these foods, although he knew they weren’t good for him, because he wanted to be like everyone else,” he said.
But parents now know that there are potentially helpful choices here that we didn’t have years ago, and those can be discussed with the child’s pediatrician, he said.
Harmony Health IT’s survey found that many parents say it is a struggle to get kids to eat healthy foods and get enough sleep. Although almost all respondents (83%) said they try to prepare healthy, home-cooked meals, 39% eat fast food at least once a week, mostly because parents are too tired to cook.
Dr. Hassink said the COVID-19 pandemic also played a role.
“We knew that COVID would be hard for kids with obesity, and there might be weight gain because of the extra sedentary time and fewer sporting activities, and there was a high cost of food to families who are already economically strapped,” she said.
In general, family support is essential, Dr. Hassink said. “Obesity treatment requires that the family be involved. The family is living in the same nutritional and activity environment as their child. Everyone has to be on board.”
Talking to kids about food and weight
The survey found that many parents struggle to talk about food and weight with their children. The AAP guideline notes that involving a health care professional can help.
“If a parent or caregiver is concerned about a child’s weight, he or she can take the child to their pediatrician,” Dr. Hassink said. “The first thing the pediatrician will do is ask about the child’s overall health, review the family history – because obesity tends to run in families – and see if other conditions, like diabetes, also run in the family.”
The pediatrician will do a physical examination that includes BMI and, if it’s high, other tests looking at blood sugar, lipids, and liver function may be performed.
Ideally, the child will be prescribed intense lifestyle and behavioral treatment that will take the child’s and family’s nutrition into account, as well as physical activity and the amount of sleep the child is getting, which is sometimes tied to weight gain. If the child has disordered eating, such as binge eating disorder, they can be evaluated and treated for that.
Each child is seen as an individual with a particular set of needs. “One size doesn’t fit all,” Dr. Hassink said.
Providing emotional support for children with obesity
Pediatricians can assess the child’s mental, emotional, and social well-being. “Children who are bullied or teased may need help working through that. Children experiencing depression may need treatment,” Dr. Hassink said.
Mr. Lunsford said Samuel was fortunate in that he rarely got taunted.
“Part of the reason is that, although weight was an issue, he never allowed his weight to define him,” he said. “He was always an extroverted kind of kid, athletic, very outgoing and friendly, and being overweight was never part of his identity.”
Mr. Lunsford encourages parents whose children are teased or bullied to create a “no-judgment” zone at home.
“Let your kids know that their parents love them for who they are,” he said. “Emphasize that weight is a ‘number’ and health is a ‘lifestyle.’ Try to highlight the good things in their lives and encourage them to be as active as they can in the things that interest them.”
A version of this article originally appeared on WebMD.com.
Douglas Lunsford’s son Samuel has struggled with obesity all his life.
Just before turning 14, Samuel, now 25, took part in a program at Ohio-based Nationwide Children’s Hospital’s Center for Healthy Weight and Nutrition. The program consisted of twice-weekly meetings with a nutritionist, including lessons in food portion size, what food does within the body, what foods can be used to supplement other foods, and similar topics, as well as physical exercise.
Although the program was designed for youngsters with weight problems, Mr. Lunsford also took part.
“They would exercise us and work us out,” he said.
Father and son did the program together for 2 years. Since then, Mr. Lunsford has advocated for youngsters with obesity.
“Samuel’s struggle spurred us into action,” he said.
Eventually, Mr. Lunsford helped create the American Academy of Pediatrics’ recently released Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity.
Helping create change
According to Sandra Hassink, MD, coauthor of the guideline and vice chair of the Clinical Practice Guideline Subcommittee on Obesity, the goal was to “help patients make changes in lifestyle, behaviors, or environment in a sustainable way and also to involve families in decision-making at every step of the way.”
Ideally, a child would receive intense behavioral and lifestyle treatment, although this approach isn’t always available and might be challenging to deliver. The most effective treatments include at least 26 hours of face-to-face, family-based treatments, consisting of many different components and lasting 3-12 months.
The guideline suggests that doctors offer adolescents 12 and older medication to assist in weight loss, along with health, behavior, and lifestyle treatment, and that teens who have severe obesity should consider metabolic and bariatric surgery as they continue intense health behavior and lifestyle treatment.
“We’re living at a time where we’ve watched obesity affect our children and adult population for 4 decades and, along with the risk of obesity, we’ve watched a rise in obesity; we’re seeing increases in illness that go along with obesity, such as type 2 diabetes, lipid diseases like high cholesterol, and nonalcoholic fatty liver disease,” Dr. Hassink said.
She explained that, as people gain weight, the cells in adipose (fatty) tissues start to malfunction and produce inflammatory chemicals that cause these illnesses.
“So having extra adipose tissue is a risk,” she said. “As pediatricians, we measure body mass index [BMI] – which is calculated based on height and weight – as a way of seeing whether the child could be at risk for developing these dysfunctioning cells. If so, we screen them for prediabetes, lipid disease, or liver disease and other obesity-related comorbidities.”
In addition, “we’re concerned about the mental health of children with obesity because of the weight bias in our culture,” said Dr. Hassink. “A child gets stigmatized, and this takes the form of bullying and teasing, and leads to low self-esteem, depression, and anxiety. So we know we have a host of physical problems we need to look out for, as well as the emotional and psychological effects of how our culture views things.”
Are parents ready for the new approach?
A new report from Harmony Healthcare IT, a data management firm that works with health data, looked at how parents regard their children’s obesity. The company surveyed more than 1,000 parents and found that one-tenth of respondents had children who were overweight or obese and over a quarter (26%) worried about their child’s weight.
Nearly 40% of parents would consider weight loss medication for their child if the child became obese at age 12, and about 16% would consider weight loss surgery. But most parents would not consider this surgery until their child was an average age of 15 rather than the AAP’s recommended age of 13.
Mr. Lunsford said that his son considered surgery and medication but was “never comfortable” with these approaches.
This isn’t unusual, Dr. Hassink said. “Not every parent will think the same way, and their view will be based on their experience and what’s going on with their child.”
The guideline wasn’t designed to encourage every child to try medication or have surgery, she said.
“But parents now know that there are potentially helpful choices here that we didn’t have years ago, and those can be discussed with the child’s pediatrician.”
Challenges to keeping healthy
It’s tough to stay healthy and not develop obesity in our modern environment, Dr. Hassink said.
“There’s a lot of processed food, a lot of sugar in our foods, a lot of sedentary behavior, and a decrease in physical activity. In many communities, it’s hard for people to get healthy foods.”
Mr. Lunsford said that when his son was in his late teens and would go out with friends, they typically went to fast-food restaurants.
“Sam would say ‘yes’ to these foods, although he knew they weren’t good for him, because he wanted to be like everyone else,” he said.
But parents now know that there are potentially helpful choices here that we didn’t have years ago, and those can be discussed with the child’s pediatrician, he said.
Harmony Health IT’s survey found that many parents say it is a struggle to get kids to eat healthy foods and get enough sleep. Although almost all respondents (83%) said they try to prepare healthy, home-cooked meals, 39% eat fast food at least once a week, mostly because parents are too tired to cook.
Dr. Hassink said the COVID-19 pandemic also played a role.
“We knew that COVID would be hard for kids with obesity, and there might be weight gain because of the extra sedentary time and fewer sporting activities, and there was a high cost of food to families who are already economically strapped,” she said.
In general, family support is essential, Dr. Hassink said. “Obesity treatment requires that the family be involved. The family is living in the same nutritional and activity environment as their child. Everyone has to be on board.”
Talking to kids about food and weight
The survey found that many parents struggle to talk about food and weight with their children. The AAP guideline notes that involving a health care professional can help.
“If a parent or caregiver is concerned about a child’s weight, he or she can take the child to their pediatrician,” Dr. Hassink said. “The first thing the pediatrician will do is ask about the child’s overall health, review the family history – because obesity tends to run in families – and see if other conditions, like diabetes, also run in the family.”
The pediatrician will do a physical examination that includes BMI and, if it’s high, other tests looking at blood sugar, lipids, and liver function may be performed.
Ideally, the child will be prescribed intense lifestyle and behavioral treatment that will take the child’s and family’s nutrition into account, as well as physical activity and the amount of sleep the child is getting, which is sometimes tied to weight gain. If the child has disordered eating, such as binge eating disorder, they can be evaluated and treated for that.
Each child is seen as an individual with a particular set of needs. “One size doesn’t fit all,” Dr. Hassink said.
Providing emotional support for children with obesity
Pediatricians can assess the child’s mental, emotional, and social well-being. “Children who are bullied or teased may need help working through that. Children experiencing depression may need treatment,” Dr. Hassink said.
Mr. Lunsford said Samuel was fortunate in that he rarely got taunted.
“Part of the reason is that, although weight was an issue, he never allowed his weight to define him,” he said. “He was always an extroverted kind of kid, athletic, very outgoing and friendly, and being overweight was never part of his identity.”
Mr. Lunsford encourages parents whose children are teased or bullied to create a “no-judgment” zone at home.
“Let your kids know that their parents love them for who they are,” he said. “Emphasize that weight is a ‘number’ and health is a ‘lifestyle.’ Try to highlight the good things in their lives and encourage them to be as active as they can in the things that interest them.”
A version of this article originally appeared on WebMD.com.
Douglas Lunsford’s son Samuel has struggled with obesity all his life.
Just before turning 14, Samuel, now 25, took part in a program at Ohio-based Nationwide Children’s Hospital’s Center for Healthy Weight and Nutrition. The program consisted of twice-weekly meetings with a nutritionist, including lessons in food portion size, what food does within the body, what foods can be used to supplement other foods, and similar topics, as well as physical exercise.
Although the program was designed for youngsters with weight problems, Mr. Lunsford also took part.
“They would exercise us and work us out,” he said.
Father and son did the program together for 2 years. Since then, Mr. Lunsford has advocated for youngsters with obesity.
“Samuel’s struggle spurred us into action,” he said.
Eventually, Mr. Lunsford helped create the American Academy of Pediatrics’ recently released Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity.
Helping create change
According to Sandra Hassink, MD, coauthor of the guideline and vice chair of the Clinical Practice Guideline Subcommittee on Obesity, the goal was to “help patients make changes in lifestyle, behaviors, or environment in a sustainable way and also to involve families in decision-making at every step of the way.”
Ideally, a child would receive intense behavioral and lifestyle treatment, although this approach isn’t always available and might be challenging to deliver. The most effective treatments include at least 26 hours of face-to-face, family-based treatments, consisting of many different components and lasting 3-12 months.
The guideline suggests that doctors offer adolescents 12 and older medication to assist in weight loss, along with health, behavior, and lifestyle treatment, and that teens who have severe obesity should consider metabolic and bariatric surgery as they continue intense health behavior and lifestyle treatment.
“We’re living at a time where we’ve watched obesity affect our children and adult population for 4 decades and, along with the risk of obesity, we’ve watched a rise in obesity; we’re seeing increases in illness that go along with obesity, such as type 2 diabetes, lipid diseases like high cholesterol, and nonalcoholic fatty liver disease,” Dr. Hassink said.
She explained that, as people gain weight, the cells in adipose (fatty) tissues start to malfunction and produce inflammatory chemicals that cause these illnesses.
“So having extra adipose tissue is a risk,” she said. “As pediatricians, we measure body mass index [BMI] – which is calculated based on height and weight – as a way of seeing whether the child could be at risk for developing these dysfunctioning cells. If so, we screen them for prediabetes, lipid disease, or liver disease and other obesity-related comorbidities.”
In addition, “we’re concerned about the mental health of children with obesity because of the weight bias in our culture,” said Dr. Hassink. “A child gets stigmatized, and this takes the form of bullying and teasing, and leads to low self-esteem, depression, and anxiety. So we know we have a host of physical problems we need to look out for, as well as the emotional and psychological effects of how our culture views things.”
Are parents ready for the new approach?
A new report from Harmony Healthcare IT, a data management firm that works with health data, looked at how parents regard their children’s obesity. The company surveyed more than 1,000 parents and found that one-tenth of respondents had children who were overweight or obese and over a quarter (26%) worried about their child’s weight.
Nearly 40% of parents would consider weight loss medication for their child if the child became obese at age 12, and about 16% would consider weight loss surgery. But most parents would not consider this surgery until their child was an average age of 15 rather than the AAP’s recommended age of 13.
Mr. Lunsford said that his son considered surgery and medication but was “never comfortable” with these approaches.
This isn’t unusual, Dr. Hassink said. “Not every parent will think the same way, and their view will be based on their experience and what’s going on with their child.”
The guideline wasn’t designed to encourage every child to try medication or have surgery, she said.
“But parents now know that there are potentially helpful choices here that we didn’t have years ago, and those can be discussed with the child’s pediatrician.”
Challenges to keeping healthy
It’s tough to stay healthy and not develop obesity in our modern environment, Dr. Hassink said.
“There’s a lot of processed food, a lot of sugar in our foods, a lot of sedentary behavior, and a decrease in physical activity. In many communities, it’s hard for people to get healthy foods.”
Mr. Lunsford said that when his son was in his late teens and would go out with friends, they typically went to fast-food restaurants.
“Sam would say ‘yes’ to these foods, although he knew they weren’t good for him, because he wanted to be like everyone else,” he said.
But parents now know that there are potentially helpful choices here that we didn’t have years ago, and those can be discussed with the child’s pediatrician, he said.
Harmony Health IT’s survey found that many parents say it is a struggle to get kids to eat healthy foods and get enough sleep. Although almost all respondents (83%) said they try to prepare healthy, home-cooked meals, 39% eat fast food at least once a week, mostly because parents are too tired to cook.
Dr. Hassink said the COVID-19 pandemic also played a role.
“We knew that COVID would be hard for kids with obesity, and there might be weight gain because of the extra sedentary time and fewer sporting activities, and there was a high cost of food to families who are already economically strapped,” she said.
In general, family support is essential, Dr. Hassink said. “Obesity treatment requires that the family be involved. The family is living in the same nutritional and activity environment as their child. Everyone has to be on board.”
Talking to kids about food and weight
The survey found that many parents struggle to talk about food and weight with their children. The AAP guideline notes that involving a health care professional can help.
“If a parent or caregiver is concerned about a child’s weight, he or she can take the child to their pediatrician,” Dr. Hassink said. “The first thing the pediatrician will do is ask about the child’s overall health, review the family history – because obesity tends to run in families – and see if other conditions, like diabetes, also run in the family.”
The pediatrician will do a physical examination that includes BMI and, if it’s high, other tests looking at blood sugar, lipids, and liver function may be performed.
Ideally, the child will be prescribed intense lifestyle and behavioral treatment that will take the child’s and family’s nutrition into account, as well as physical activity and the amount of sleep the child is getting, which is sometimes tied to weight gain. If the child has disordered eating, such as binge eating disorder, they can be evaluated and treated for that.
Each child is seen as an individual with a particular set of needs. “One size doesn’t fit all,” Dr. Hassink said.
Providing emotional support for children with obesity
Pediatricians can assess the child’s mental, emotional, and social well-being. “Children who are bullied or teased may need help working through that. Children experiencing depression may need treatment,” Dr. Hassink said.
Mr. Lunsford said Samuel was fortunate in that he rarely got taunted.
“Part of the reason is that, although weight was an issue, he never allowed his weight to define him,” he said. “He was always an extroverted kind of kid, athletic, very outgoing and friendly, and being overweight was never part of his identity.”
Mr. Lunsford encourages parents whose children are teased or bullied to create a “no-judgment” zone at home.
“Let your kids know that their parents love them for who they are,” he said. “Emphasize that weight is a ‘number’ and health is a ‘lifestyle.’ Try to highlight the good things in their lives and encourage them to be as active as they can in the things that interest them.”
A version of this article originally appeared on WebMD.com.
What to expect in the new concussion guidelines
This transcript has been edited for clarity.
Andrew N. Wilner, MD: I’m your host, Dr. Andrew Wilner, reporting virtually from the 2023 American Academy of Neurology meeting in Boston. It’s my pleasure today to speak with Dr. Shae Datta, codirector of the NYU Langone Concussion Center.
She’s also a clinical assistant professor of neurology at NYU School of Medicine. Dr. Datta is chair of the AAN Sports Neurology Section, and she’s leading a panel on concussion at this year’s meeting. She’s going to give us an update. Welcome, Dr. Datta.
Shae Datta, MD: Thank you so much, Andrew. I really love the fact that I’m here speaking to you about all of the new, exciting developments in the field.
Dr. Wilner: Before we get too deep, tell us how you got interested in this topic.
Dr. Datta: I initially thought, when I was in training as a resident, that I wanted to do something like neurocritical care or EEG. It also puzzled me why these seemingly smaller head injuries that didn’t end up in the hospital or ICU were bounced from neurology headache clinic to neuro-ophthalmology headache clinic to neurovestibular headache clinic, and nobody seemed to be able to put together the dots about why they’re having so many different issues — but at the same time, nobody could help them.
At that time, this field was very new. I was on a plane to Paris to a neurocritical care conference as a resident, and I saw the movie Concussion with Will Smith.
It featured one of my current mentors who taught at the fellowship that I graduated from, and it was a fascinating field. I just started looking deeply into it, and I saw that there was a new training fellowship for sports neurology and concussion management, and this is basically why we’re here today.
New concussion consensus guidelines coming
Dr. Wilner: I think this field has really exploded. It used to be that you banged your head, you did a CT scan – remember, I trained about 45 years ago – and if there was nothing on the CT scan, you were done. If you had headaches, you took Tylenol until they went away.
Now, we do MRI, and we realized that it’s really a syndrome. I understand that there are going to be some formal guidelines that have been put together. Is that correct?
Dr. Datta: That’s correct. The 6th International Consensus Conference on Concussion in Sport, in Amsterdam, where I attended and presented a poster, was really a meeting of all the best minds – clinicians and researchers in brain injury – to form a consensus on the newest guidelines that are going to direct our treatment going forward.
Dr. Wilner: I’m going to ask you a trick question because the last time I looked it up I did not get a satisfying answer. What is a concussion?
Dr. Datta: That’s a very good question, and everyone always asks. A concussion is an external force that is emitted upon the head or the neck, or the body, in general, that may cause temporary loss of function. It’s a functional problem.
We don’t see much on CT. We can do MRI. We can do SPECT or we can do these very fancy images, sometimes, of high-velocity head injuries and see small microhemorrhages.
Often, we don’t see anything, but still the patient is loopy. They can’t see straight. They are double-visioned. They have vertigo. Why is that happening? On the cellular level, we have an energy deficit in the sodium-potassium-ATPase pump of the neurons themselves.
Dr. Wilner: Suppose you do see diffuse axonal injury; does that take it out of concussion, or can you have a concussion with visible injury?
Dr. Datta: I think you can have overlap in the symptoms. The diffuse axonal injury would put it into a higher grade of head injury as opposed to a mild traumatic brain injury. Definitely, we would need to work together with our trauma doctors to ensure that patients are not on blood thinners or anything until they heal well enough. Obviously, I would pick them up as an outpatient and follow them until we resolve or rehab them as best as possible.
Concussion assessment tools
Dr. Wilner: There are many sports out there where concussions are fairly frequent, like American football and hockey, for example. Are there any statements in the new guidelines?
Dr. Datta: There are no statements for or against a particular sport because that would really make too much of a bold statement about cause and effect. There is a cause and effect in long-term, repetitive exposure, I would say, in terms of someone being able to play or sustain injury.
Right now, at least at the concussion conference I went to and in the upcoming consensus statement, they will not comment on a specific sport. Obviously, we know that the higher-impact sports are a little more dangerous.
Let’s be honest. At the high school, middle school, or even younger level, some kids are not necessarily the most athletic, right? They play because their friends are playing. If they’re repeatedly getting injured, it’s time for an astute clinician, or a coach, and a whole team to assess them to see if maybe this person is just going to continue to get hurt if they’re not taken out of the game and perhaps they should go to a lower-impact sport.
Dr. Wilner: In schools, often there’s a big size and weight difference. There are 14-year-olds who are 6 fett 2 inches and 200 pounds, and there are 14-year-olds who are 5 feet 2 inches and 110 pounds. Obviously, they’re mismatched on the football field.
You mentioned coaches. Is there anything in the guidelines about training coaches?
Dr. Datta: Specifically, there was nothing in the guidelines about that. There’s a tool for coaches at every level to use, which is called the Sports Concussion Assessment Tool, or SCAT, which is going to be updated to the SCAT6. At the NCAA level, they must receive annual training on concussion management and be given an NCAA concussion handout for coaches.
Obviously, there are more rigorous protocols for national-level coaching. As it stands now, it is not mandatory, but they are given tools to assess someone once they’ve gotten a hit to take them out of the game.
Dr. Wilner: I’ve been following the concussion research through the years. They did some neuropsychological testing on athletes who’ve had this many concussions or that many concussions, and they would find deficits here or subtle deficits there, but they had no baseline.
Then, there was a movement to start testing athletes before the season starts so that they could do a repeat test after concussion and see if there is any difference. Is that something we’re recommending?
Dr. Datta: Most of the time, NCAA-level – certainly where I trained – and national-level sports do testing, but it’s not everywhere. Prior guidelines have indicated that preseason testing is not required. That is largely because there has been no standardized neuropsychological testing established.
There are computerized testing options where the validity and reliability are questionable. Also, let’s say it’s a college student; they didn’t sleep all night and then they took this computer test. They would probably do worse than they would if they had received a head hit.
Just to be on the safe side, most places that have collegiate-level sports that are at a high level do preseason testing. If I were to speak personally, aside from the guidelines, I would say that it’s been helpful for me to look at the before and after, in general, overall, to make a decision about my treatment protocol.
Dr. Wilner: Let’s talk about the patient. You have a 20-year-old guy. He’s playing football. There’s a big play. Bonk, he gets hit on the head. He’s on the ground. He’s dazed, staggers a little bit, gets up, and you ask how he is feeling. He says he’s fine and then he wobbles off to the sideline. What do you do with that kid?
Dr. Datta: Obviously, the first thing is to remove him from the play environment to a quiet space. Second, either an athletic trainer or a coach would administer basic screening neurologic tests, such as “where are you, what’s today’s date, what is your name?” and other orientation questions.
They’ll also go through the SCAT – that’ll be SCAT6 starting in July – the SCAT5 symptom questionnaire to see what symptoms they have. Often, they’re using sideline testing software.
There are two things that can be used on a card to test eye movements, to see if they’re slower. They come out of NYU, coincidentally – the Memory Image Completion (MIC) and the Mobile Universal Lexicon Evaluation System (MULES) – and are used to determine whether eye movements are slower. That way, you can tell whether someone is, compared with before they got their head hit, slower than before.
Based on this composite information, usually the teammates and the head people on the team will know if a player looks different.
They need to be taken out, obviously, if there is nausea or vomiting, any neurologic signs and symptoms, or a neck injury that needs to be stabilized. ABCs first, right? If there’s any vomiting or seizures, they should be taken to the ER right away.
The first thing is to take them out, then do a sideline assessment. Third, see if they need to immediately go to the ED versus follow-up outpatient with me within a day or two.
Dr. Wilner: I think it’s the subtle injuries that are the tough ones. Back to our 20-year-old. He says: “Oh, I’m fine. I want to go back in the game.” Everybody can tell he’s not quite right, even though he passed all the tests. What do you do then?
Dr. Datta: You have to make a judgment call for the safety of the player. They always want to go back, right? This is also an issue when they’re competing for college scholarships and things of that nature. Sometimes they’re sandbagging, where they memorize the answers.
Everything’s on the Internet nowadays, right? We have to make a judgment call as members of the healthcare community and the sports community to keep that player safe.
Just keep them out. Don’t bring them back in the game. Keep them out for a reasonable amount of time. There’s a test called the Buffalo Concussion Treadmill Test; Dr. John Leddy from University of Buffalo has developed a way for us to put athletes through a screening protocol.
This can be part of their vestibular and ocular rehabilitation, where if they don’t have symptoms when we bring their heart rate to certain levels, then we can slowly clear them for return to play as long as they’re nonsymptomatic.
Dr. Wilner: I spoke with your colleague, Dr. Riggins, who is also on your panel, and we were talking about when they can go back. She said they can go back when they don’t have any symptoms. No more headache, no more dizziness, no more lightheadedness, no more trouble concentrating or with memory – all those things have gone away.
Sometimes these symptoms are stubborn. If you have, say, 100 patients like our 20-year-old who got bonked on the head, has some headaches, and doesn’t feel quite right, what usually happens? How many are back to play the next day, the next week, or the next month? How many are out for the season? How does that play out?
Dr. Datta: It depends on a couple of different factors. One, have they had previous head injuries? Two, do they have preexisting symptoms or signs, or diagnoses like migraines, which are likely to get worse after a head injury? Anything that’s preexisting, like a mood disorder, anxiety, depression, or trouble sleeping, is going to get worse.
If they were compensating for untreated ADD or borderline personality or bipolar, I’ve seen many people who’ve developed them. These are not the norm, but I’m saying that you have to be very careful.
Getting back to the question, you treat them. Reasonably, if they’re healthy and they don’t have preexisting signs and symptoms, I would say more than half are back in about 2 weeks.. I would say 60%-70%. It all depends. If they have preexisting issues, then it’s going to take much longer.
From SCAT to SCOAT
Dr. Wilner: This has been very informative. Before we wrap up, tell us what to expect from these guidelines in July. How are they really going to help?
Dr. Datta: We’ve been using the SCAT, which was meant for more sideline assessment because that’s all we had, and it’s worked perfectly well.
This will be better because we often see them within 24-48 hours, when the symptoms are sometimes a little bit better.
We also will see the sport and concussion group come up with added athlete perspectives, ethics discussion, power-sport athlete considerations, and development of this new SCOAT.
Dr. Wilner: Dr. Datta, this is very exciting. I look forward to reading these guidelines in July. I want to thank you for your hard work. I also look forward to talking to you at next year’s meeting. Thank you very much for giving us this update.
Dr. Datta: No problem. It’s my pleasure.
A version of this article originally appeared on Medscape.com.
This transcript has been edited for clarity.
Andrew N. Wilner, MD: I’m your host, Dr. Andrew Wilner, reporting virtually from the 2023 American Academy of Neurology meeting in Boston. It’s my pleasure today to speak with Dr. Shae Datta, codirector of the NYU Langone Concussion Center.
She’s also a clinical assistant professor of neurology at NYU School of Medicine. Dr. Datta is chair of the AAN Sports Neurology Section, and she’s leading a panel on concussion at this year’s meeting. She’s going to give us an update. Welcome, Dr. Datta.
Shae Datta, MD: Thank you so much, Andrew. I really love the fact that I’m here speaking to you about all of the new, exciting developments in the field.
Dr. Wilner: Before we get too deep, tell us how you got interested in this topic.
Dr. Datta: I initially thought, when I was in training as a resident, that I wanted to do something like neurocritical care or EEG. It also puzzled me why these seemingly smaller head injuries that didn’t end up in the hospital or ICU were bounced from neurology headache clinic to neuro-ophthalmology headache clinic to neurovestibular headache clinic, and nobody seemed to be able to put together the dots about why they’re having so many different issues — but at the same time, nobody could help them.
At that time, this field was very new. I was on a plane to Paris to a neurocritical care conference as a resident, and I saw the movie Concussion with Will Smith.
It featured one of my current mentors who taught at the fellowship that I graduated from, and it was a fascinating field. I just started looking deeply into it, and I saw that there was a new training fellowship for sports neurology and concussion management, and this is basically why we’re here today.
New concussion consensus guidelines coming
Dr. Wilner: I think this field has really exploded. It used to be that you banged your head, you did a CT scan – remember, I trained about 45 years ago – and if there was nothing on the CT scan, you were done. If you had headaches, you took Tylenol until they went away.
Now, we do MRI, and we realized that it’s really a syndrome. I understand that there are going to be some formal guidelines that have been put together. Is that correct?
Dr. Datta: That’s correct. The 6th International Consensus Conference on Concussion in Sport, in Amsterdam, where I attended and presented a poster, was really a meeting of all the best minds – clinicians and researchers in brain injury – to form a consensus on the newest guidelines that are going to direct our treatment going forward.
Dr. Wilner: I’m going to ask you a trick question because the last time I looked it up I did not get a satisfying answer. What is a concussion?
Dr. Datta: That’s a very good question, and everyone always asks. A concussion is an external force that is emitted upon the head or the neck, or the body, in general, that may cause temporary loss of function. It’s a functional problem.
We don’t see much on CT. We can do MRI. We can do SPECT or we can do these very fancy images, sometimes, of high-velocity head injuries and see small microhemorrhages.
Often, we don’t see anything, but still the patient is loopy. They can’t see straight. They are double-visioned. They have vertigo. Why is that happening? On the cellular level, we have an energy deficit in the sodium-potassium-ATPase pump of the neurons themselves.
Dr. Wilner: Suppose you do see diffuse axonal injury; does that take it out of concussion, or can you have a concussion with visible injury?
Dr. Datta: I think you can have overlap in the symptoms. The diffuse axonal injury would put it into a higher grade of head injury as opposed to a mild traumatic brain injury. Definitely, we would need to work together with our trauma doctors to ensure that patients are not on blood thinners or anything until they heal well enough. Obviously, I would pick them up as an outpatient and follow them until we resolve or rehab them as best as possible.
Concussion assessment tools
Dr. Wilner: There are many sports out there where concussions are fairly frequent, like American football and hockey, for example. Are there any statements in the new guidelines?
Dr. Datta: There are no statements for or against a particular sport because that would really make too much of a bold statement about cause and effect. There is a cause and effect in long-term, repetitive exposure, I would say, in terms of someone being able to play or sustain injury.
Right now, at least at the concussion conference I went to and in the upcoming consensus statement, they will not comment on a specific sport. Obviously, we know that the higher-impact sports are a little more dangerous.
Let’s be honest. At the high school, middle school, or even younger level, some kids are not necessarily the most athletic, right? They play because their friends are playing. If they’re repeatedly getting injured, it’s time for an astute clinician, or a coach, and a whole team to assess them to see if maybe this person is just going to continue to get hurt if they’re not taken out of the game and perhaps they should go to a lower-impact sport.
Dr. Wilner: In schools, often there’s a big size and weight difference. There are 14-year-olds who are 6 fett 2 inches and 200 pounds, and there are 14-year-olds who are 5 feet 2 inches and 110 pounds. Obviously, they’re mismatched on the football field.
You mentioned coaches. Is there anything in the guidelines about training coaches?
Dr. Datta: Specifically, there was nothing in the guidelines about that. There’s a tool for coaches at every level to use, which is called the Sports Concussion Assessment Tool, or SCAT, which is going to be updated to the SCAT6. At the NCAA level, they must receive annual training on concussion management and be given an NCAA concussion handout for coaches.
Obviously, there are more rigorous protocols for national-level coaching. As it stands now, it is not mandatory, but they are given tools to assess someone once they’ve gotten a hit to take them out of the game.
Dr. Wilner: I’ve been following the concussion research through the years. They did some neuropsychological testing on athletes who’ve had this many concussions or that many concussions, and they would find deficits here or subtle deficits there, but they had no baseline.
Then, there was a movement to start testing athletes before the season starts so that they could do a repeat test after concussion and see if there is any difference. Is that something we’re recommending?
Dr. Datta: Most of the time, NCAA-level – certainly where I trained – and national-level sports do testing, but it’s not everywhere. Prior guidelines have indicated that preseason testing is not required. That is largely because there has been no standardized neuropsychological testing established.
There are computerized testing options where the validity and reliability are questionable. Also, let’s say it’s a college student; they didn’t sleep all night and then they took this computer test. They would probably do worse than they would if they had received a head hit.
Just to be on the safe side, most places that have collegiate-level sports that are at a high level do preseason testing. If I were to speak personally, aside from the guidelines, I would say that it’s been helpful for me to look at the before and after, in general, overall, to make a decision about my treatment protocol.
Dr. Wilner: Let’s talk about the patient. You have a 20-year-old guy. He’s playing football. There’s a big play. Bonk, he gets hit on the head. He’s on the ground. He’s dazed, staggers a little bit, gets up, and you ask how he is feeling. He says he’s fine and then he wobbles off to the sideline. What do you do with that kid?
Dr. Datta: Obviously, the first thing is to remove him from the play environment to a quiet space. Second, either an athletic trainer or a coach would administer basic screening neurologic tests, such as “where are you, what’s today’s date, what is your name?” and other orientation questions.
They’ll also go through the SCAT – that’ll be SCAT6 starting in July – the SCAT5 symptom questionnaire to see what symptoms they have. Often, they’re using sideline testing software.
There are two things that can be used on a card to test eye movements, to see if they’re slower. They come out of NYU, coincidentally – the Memory Image Completion (MIC) and the Mobile Universal Lexicon Evaluation System (MULES) – and are used to determine whether eye movements are slower. That way, you can tell whether someone is, compared with before they got their head hit, slower than before.
Based on this composite information, usually the teammates and the head people on the team will know if a player looks different.
They need to be taken out, obviously, if there is nausea or vomiting, any neurologic signs and symptoms, or a neck injury that needs to be stabilized. ABCs first, right? If there’s any vomiting or seizures, they should be taken to the ER right away.
The first thing is to take them out, then do a sideline assessment. Third, see if they need to immediately go to the ED versus follow-up outpatient with me within a day or two.
Dr. Wilner: I think it’s the subtle injuries that are the tough ones. Back to our 20-year-old. He says: “Oh, I’m fine. I want to go back in the game.” Everybody can tell he’s not quite right, even though he passed all the tests. What do you do then?
Dr. Datta: You have to make a judgment call for the safety of the player. They always want to go back, right? This is also an issue when they’re competing for college scholarships and things of that nature. Sometimes they’re sandbagging, where they memorize the answers.
Everything’s on the Internet nowadays, right? We have to make a judgment call as members of the healthcare community and the sports community to keep that player safe.
Just keep them out. Don’t bring them back in the game. Keep them out for a reasonable amount of time. There’s a test called the Buffalo Concussion Treadmill Test; Dr. John Leddy from University of Buffalo has developed a way for us to put athletes through a screening protocol.
This can be part of their vestibular and ocular rehabilitation, where if they don’t have symptoms when we bring their heart rate to certain levels, then we can slowly clear them for return to play as long as they’re nonsymptomatic.
Dr. Wilner: I spoke with your colleague, Dr. Riggins, who is also on your panel, and we were talking about when they can go back. She said they can go back when they don’t have any symptoms. No more headache, no more dizziness, no more lightheadedness, no more trouble concentrating or with memory – all those things have gone away.
Sometimes these symptoms are stubborn. If you have, say, 100 patients like our 20-year-old who got bonked on the head, has some headaches, and doesn’t feel quite right, what usually happens? How many are back to play the next day, the next week, or the next month? How many are out for the season? How does that play out?
Dr. Datta: It depends on a couple of different factors. One, have they had previous head injuries? Two, do they have preexisting symptoms or signs, or diagnoses like migraines, which are likely to get worse after a head injury? Anything that’s preexisting, like a mood disorder, anxiety, depression, or trouble sleeping, is going to get worse.
If they were compensating for untreated ADD or borderline personality or bipolar, I’ve seen many people who’ve developed them. These are not the norm, but I’m saying that you have to be very careful.
Getting back to the question, you treat them. Reasonably, if they’re healthy and they don’t have preexisting signs and symptoms, I would say more than half are back in about 2 weeks.. I would say 60%-70%. It all depends. If they have preexisting issues, then it’s going to take much longer.
From SCAT to SCOAT
Dr. Wilner: This has been very informative. Before we wrap up, tell us what to expect from these guidelines in July. How are they really going to help?
Dr. Datta: We’ve been using the SCAT, which was meant for more sideline assessment because that’s all we had, and it’s worked perfectly well.
This will be better because we often see them within 24-48 hours, when the symptoms are sometimes a little bit better.
We also will see the sport and concussion group come up with added athlete perspectives, ethics discussion, power-sport athlete considerations, and development of this new SCOAT.
Dr. Wilner: Dr. Datta, this is very exciting. I look forward to reading these guidelines in July. I want to thank you for your hard work. I also look forward to talking to you at next year’s meeting. Thank you very much for giving us this update.
Dr. Datta: No problem. It’s my pleasure.
A version of this article originally appeared on Medscape.com.
This transcript has been edited for clarity.
Andrew N. Wilner, MD: I’m your host, Dr. Andrew Wilner, reporting virtually from the 2023 American Academy of Neurology meeting in Boston. It’s my pleasure today to speak with Dr. Shae Datta, codirector of the NYU Langone Concussion Center.
She’s also a clinical assistant professor of neurology at NYU School of Medicine. Dr. Datta is chair of the AAN Sports Neurology Section, and she’s leading a panel on concussion at this year’s meeting. She’s going to give us an update. Welcome, Dr. Datta.
Shae Datta, MD: Thank you so much, Andrew. I really love the fact that I’m here speaking to you about all of the new, exciting developments in the field.
Dr. Wilner: Before we get too deep, tell us how you got interested in this topic.
Dr. Datta: I initially thought, when I was in training as a resident, that I wanted to do something like neurocritical care or EEG. It also puzzled me why these seemingly smaller head injuries that didn’t end up in the hospital or ICU were bounced from neurology headache clinic to neuro-ophthalmology headache clinic to neurovestibular headache clinic, and nobody seemed to be able to put together the dots about why they’re having so many different issues — but at the same time, nobody could help them.
At that time, this field was very new. I was on a plane to Paris to a neurocritical care conference as a resident, and I saw the movie Concussion with Will Smith.
It featured one of my current mentors who taught at the fellowship that I graduated from, and it was a fascinating field. I just started looking deeply into it, and I saw that there was a new training fellowship for sports neurology and concussion management, and this is basically why we’re here today.
New concussion consensus guidelines coming
Dr. Wilner: I think this field has really exploded. It used to be that you banged your head, you did a CT scan – remember, I trained about 45 years ago – and if there was nothing on the CT scan, you were done. If you had headaches, you took Tylenol until they went away.
Now, we do MRI, and we realized that it’s really a syndrome. I understand that there are going to be some formal guidelines that have been put together. Is that correct?
Dr. Datta: That’s correct. The 6th International Consensus Conference on Concussion in Sport, in Amsterdam, where I attended and presented a poster, was really a meeting of all the best minds – clinicians and researchers in brain injury – to form a consensus on the newest guidelines that are going to direct our treatment going forward.
Dr. Wilner: I’m going to ask you a trick question because the last time I looked it up I did not get a satisfying answer. What is a concussion?
Dr. Datta: That’s a very good question, and everyone always asks. A concussion is an external force that is emitted upon the head or the neck, or the body, in general, that may cause temporary loss of function. It’s a functional problem.
We don’t see much on CT. We can do MRI. We can do SPECT or we can do these very fancy images, sometimes, of high-velocity head injuries and see small microhemorrhages.
Often, we don’t see anything, but still the patient is loopy. They can’t see straight. They are double-visioned. They have vertigo. Why is that happening? On the cellular level, we have an energy deficit in the sodium-potassium-ATPase pump of the neurons themselves.
Dr. Wilner: Suppose you do see diffuse axonal injury; does that take it out of concussion, or can you have a concussion with visible injury?
Dr. Datta: I think you can have overlap in the symptoms. The diffuse axonal injury would put it into a higher grade of head injury as opposed to a mild traumatic brain injury. Definitely, we would need to work together with our trauma doctors to ensure that patients are not on blood thinners or anything until they heal well enough. Obviously, I would pick them up as an outpatient and follow them until we resolve or rehab them as best as possible.
Concussion assessment tools
Dr. Wilner: There are many sports out there where concussions are fairly frequent, like American football and hockey, for example. Are there any statements in the new guidelines?
Dr. Datta: There are no statements for or against a particular sport because that would really make too much of a bold statement about cause and effect. There is a cause and effect in long-term, repetitive exposure, I would say, in terms of someone being able to play or sustain injury.
Right now, at least at the concussion conference I went to and in the upcoming consensus statement, they will not comment on a specific sport. Obviously, we know that the higher-impact sports are a little more dangerous.
Let’s be honest. At the high school, middle school, or even younger level, some kids are not necessarily the most athletic, right? They play because their friends are playing. If they’re repeatedly getting injured, it’s time for an astute clinician, or a coach, and a whole team to assess them to see if maybe this person is just going to continue to get hurt if they’re not taken out of the game and perhaps they should go to a lower-impact sport.
Dr. Wilner: In schools, often there’s a big size and weight difference. There are 14-year-olds who are 6 fett 2 inches and 200 pounds, and there are 14-year-olds who are 5 feet 2 inches and 110 pounds. Obviously, they’re mismatched on the football field.
You mentioned coaches. Is there anything in the guidelines about training coaches?
Dr. Datta: Specifically, there was nothing in the guidelines about that. There’s a tool for coaches at every level to use, which is called the Sports Concussion Assessment Tool, or SCAT, which is going to be updated to the SCAT6. At the NCAA level, they must receive annual training on concussion management and be given an NCAA concussion handout for coaches.
Obviously, there are more rigorous protocols for national-level coaching. As it stands now, it is not mandatory, but they are given tools to assess someone once they’ve gotten a hit to take them out of the game.
Dr. Wilner: I’ve been following the concussion research through the years. They did some neuropsychological testing on athletes who’ve had this many concussions or that many concussions, and they would find deficits here or subtle deficits there, but they had no baseline.
Then, there was a movement to start testing athletes before the season starts so that they could do a repeat test after concussion and see if there is any difference. Is that something we’re recommending?
Dr. Datta: Most of the time, NCAA-level – certainly where I trained – and national-level sports do testing, but it’s not everywhere. Prior guidelines have indicated that preseason testing is not required. That is largely because there has been no standardized neuropsychological testing established.
There are computerized testing options where the validity and reliability are questionable. Also, let’s say it’s a college student; they didn’t sleep all night and then they took this computer test. They would probably do worse than they would if they had received a head hit.
Just to be on the safe side, most places that have collegiate-level sports that are at a high level do preseason testing. If I were to speak personally, aside from the guidelines, I would say that it’s been helpful for me to look at the before and after, in general, overall, to make a decision about my treatment protocol.
Dr. Wilner: Let’s talk about the patient. You have a 20-year-old guy. He’s playing football. There’s a big play. Bonk, he gets hit on the head. He’s on the ground. He’s dazed, staggers a little bit, gets up, and you ask how he is feeling. He says he’s fine and then he wobbles off to the sideline. What do you do with that kid?
Dr. Datta: Obviously, the first thing is to remove him from the play environment to a quiet space. Second, either an athletic trainer or a coach would administer basic screening neurologic tests, such as “where are you, what’s today’s date, what is your name?” and other orientation questions.
They’ll also go through the SCAT – that’ll be SCAT6 starting in July – the SCAT5 symptom questionnaire to see what symptoms they have. Often, they’re using sideline testing software.
There are two things that can be used on a card to test eye movements, to see if they’re slower. They come out of NYU, coincidentally – the Memory Image Completion (MIC) and the Mobile Universal Lexicon Evaluation System (MULES) – and are used to determine whether eye movements are slower. That way, you can tell whether someone is, compared with before they got their head hit, slower than before.
Based on this composite information, usually the teammates and the head people on the team will know if a player looks different.
They need to be taken out, obviously, if there is nausea or vomiting, any neurologic signs and symptoms, or a neck injury that needs to be stabilized. ABCs first, right? If there’s any vomiting or seizures, they should be taken to the ER right away.
The first thing is to take them out, then do a sideline assessment. Third, see if they need to immediately go to the ED versus follow-up outpatient with me within a day or two.
Dr. Wilner: I think it’s the subtle injuries that are the tough ones. Back to our 20-year-old. He says: “Oh, I’m fine. I want to go back in the game.” Everybody can tell he’s not quite right, even though he passed all the tests. What do you do then?
Dr. Datta: You have to make a judgment call for the safety of the player. They always want to go back, right? This is also an issue when they’re competing for college scholarships and things of that nature. Sometimes they’re sandbagging, where they memorize the answers.
Everything’s on the Internet nowadays, right? We have to make a judgment call as members of the healthcare community and the sports community to keep that player safe.
Just keep them out. Don’t bring them back in the game. Keep them out for a reasonable amount of time. There’s a test called the Buffalo Concussion Treadmill Test; Dr. John Leddy from University of Buffalo has developed a way for us to put athletes through a screening protocol.
This can be part of their vestibular and ocular rehabilitation, where if they don’t have symptoms when we bring their heart rate to certain levels, then we can slowly clear them for return to play as long as they’re nonsymptomatic.
Dr. Wilner: I spoke with your colleague, Dr. Riggins, who is also on your panel, and we were talking about when they can go back. She said they can go back when they don’t have any symptoms. No more headache, no more dizziness, no more lightheadedness, no more trouble concentrating or with memory – all those things have gone away.
Sometimes these symptoms are stubborn. If you have, say, 100 patients like our 20-year-old who got bonked on the head, has some headaches, and doesn’t feel quite right, what usually happens? How many are back to play the next day, the next week, or the next month? How many are out for the season? How does that play out?
Dr. Datta: It depends on a couple of different factors. One, have they had previous head injuries? Two, do they have preexisting symptoms or signs, or diagnoses like migraines, which are likely to get worse after a head injury? Anything that’s preexisting, like a mood disorder, anxiety, depression, or trouble sleeping, is going to get worse.
If they were compensating for untreated ADD or borderline personality or bipolar, I’ve seen many people who’ve developed them. These are not the norm, but I’m saying that you have to be very careful.
Getting back to the question, you treat them. Reasonably, if they’re healthy and they don’t have preexisting signs and symptoms, I would say more than half are back in about 2 weeks.. I would say 60%-70%. It all depends. If they have preexisting issues, then it’s going to take much longer.
From SCAT to SCOAT
Dr. Wilner: This has been very informative. Before we wrap up, tell us what to expect from these guidelines in July. How are they really going to help?
Dr. Datta: We’ve been using the SCAT, which was meant for more sideline assessment because that’s all we had, and it’s worked perfectly well.
This will be better because we often see them within 24-48 hours, when the symptoms are sometimes a little bit better.
We also will see the sport and concussion group come up with added athlete perspectives, ethics discussion, power-sport athlete considerations, and development of this new SCOAT.
Dr. Wilner: Dr. Datta, this is very exciting. I look forward to reading these guidelines in July. I want to thank you for your hard work. I also look forward to talking to you at next year’s meeting. Thank you very much for giving us this update.
Dr. Datta: No problem. It’s my pleasure.
A version of this article originally appeared on Medscape.com.
Morning PT
Tuesdays and Fridays are tough. Not so much because of clinic, but rather because of the 32 minutes before clinic that I’m on the Peloton bike. They are the mornings I dedicate to training VO2max.
Training VO2max, or maximal oxygen consumption, is simple. Spin for a leisurely, easy-breathing, 4 minutes, then for 4 minutes push yourself until you see the light of heaven and wish for death to come. Then relax for 4 minutes again. Repeat this cycle four to six times. Done justly, you will dread Tuesdays and Fridays too. The punishing cycle of a 4-minute push, then 4-minute recovery is, however, an excellent way to improve cardiovascular fitness. And no, I’m not training for the Boston Marathon, so why am I working so hard? Because I’m training for marathon clinic days for the next 20 years.

Now more than ever, I feel we have to be physically fit to deal with a physicians’ day’s work. It’s exhausting. The root cause is too much work, yes, but I believe being physically fit could help.
I was talking to an 86-year-old patient about this very topic recently. He was short, with a well-manicured goatee and shiny head. He stuck his arm out to shake my hand. “Glad we’re back to handshakes again, doc.” His grip was that of a 30-year-old. “Buff” you’d likely describe him: He is noticeably muscular, not a skinny old man. He’s an old Navy Master Chief who started a business in wholesale flowers, which distributes all over the United States. And he’s still working full time. Impressed, I asked his secret for such vigor. PT, he replied.
PT, or physical training, is a foundational element of the Navy. Every sailor starts his or her day with morning PT before carrying out their duties. Some 30 years later, this guy is still getting after it. He does push-ups, sit-ups, and pull-ups nearly every morning. Morning PT is what he attributes to his success not only in health, but also business. As he sees it, he has the business savvy and experience of an old guy and the energy and stamina of a college kid. A good combination for a successful life.
I’ve always been pretty fit. Lately, I’ve been trying to take it to the next level, to not just be “physically active,” but rather “high-performance fit.” There are plenty of sources for instruction; how to stay young and healthy isn’t a new idea after all. I mean, Herodotus wrote of finding the Fountain of Youth in the 5th century BCE. A couple thousand years later, it’s still on trend. One of my favorite sages giving health span advice is Peter Attia, MD. I’ve been a fan since I met him at TEDMED in 2013 and I marvel at the astounding body of work he has created since. A Johns Hopkins–trained surgeon, he has spent his career reviewing the scientific literature about longevity and sharing it as actionable content. His book, “Outlive: The Science and Art of Longevity” (New York: Penguin Random House, 2023) is a nice summary of his work. I recommend it.
Right now I’m switching between type 2 muscle fiber work (lots of jumping like my 2-year-old) and cardiovascular training including the aforementioned VO2max work. I cannot say that my patient inbox is any cleaner, or that I’m faster in the office, but I’m not flagging by the end of the day anymore. Master Chief challenged me to match his 10 pull-ups before he returns for his follow up visit. I’ll gladly give up Peloton sprints to work on that.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
Tuesdays and Fridays are tough. Not so much because of clinic, but rather because of the 32 minutes before clinic that I’m on the Peloton bike. They are the mornings I dedicate to training VO2max.
Training VO2max, or maximal oxygen consumption, is simple. Spin for a leisurely, easy-breathing, 4 minutes, then for 4 minutes push yourself until you see the light of heaven and wish for death to come. Then relax for 4 minutes again. Repeat this cycle four to six times. Done justly, you will dread Tuesdays and Fridays too. The punishing cycle of a 4-minute push, then 4-minute recovery is, however, an excellent way to improve cardiovascular fitness. And no, I’m not training for the Boston Marathon, so why am I working so hard? Because I’m training for marathon clinic days for the next 20 years.
Now more than ever, I feel we have to be physically fit to deal with a physicians’ day’s work. It’s exhausting. The root cause is too much work, yes, but I believe being physically fit could help.
I was talking to an 86-year-old patient about this very topic recently. He was short, with a well-manicured goatee and shiny head. He stuck his arm out to shake my hand. “Glad we’re back to handshakes again, doc.” His grip was that of a 30-year-old. “Buff” you’d likely describe him: He is noticeably muscular, not a skinny old man. He’s an old Navy Master Chief who started a business in wholesale flowers, which distributes all over the United States. And he’s still working full time. Impressed, I asked his secret for such vigor. PT, he replied.
PT, or physical training, is a foundational element of the Navy. Every sailor starts his or her day with morning PT before carrying out their duties. Some 30 years later, this guy is still getting after it. He does push-ups, sit-ups, and pull-ups nearly every morning. Morning PT is what he attributes to his success not only in health, but also business. As he sees it, he has the business savvy and experience of an old guy and the energy and stamina of a college kid. A good combination for a successful life.
I’ve always been pretty fit. Lately, I’ve been trying to take it to the next level, to not just be “physically active,” but rather “high-performance fit.” There are plenty of sources for instruction; how to stay young and healthy isn’t a new idea after all. I mean, Herodotus wrote of finding the Fountain of Youth in the 5th century BCE. A couple thousand years later, it’s still on trend. One of my favorite sages giving health span advice is Peter Attia, MD. I’ve been a fan since I met him at TEDMED in 2013 and I marvel at the astounding body of work he has created since. A Johns Hopkins–trained surgeon, he has spent his career reviewing the scientific literature about longevity and sharing it as actionable content. His book, “Outlive: The Science and Art of Longevity” (New York: Penguin Random House, 2023) is a nice summary of his work. I recommend it.
Right now I’m switching between type 2 muscle fiber work (lots of jumping like my 2-year-old) and cardiovascular training including the aforementioned VO2max work. I cannot say that my patient inbox is any cleaner, or that I’m faster in the office, but I’m not flagging by the end of the day anymore. Master Chief challenged me to match his 10 pull-ups before he returns for his follow up visit. I’ll gladly give up Peloton sprints to work on that.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
Tuesdays and Fridays are tough. Not so much because of clinic, but rather because of the 32 minutes before clinic that I’m on the Peloton bike. They are the mornings I dedicate to training VO2max.
Training VO2max, or maximal oxygen consumption, is simple. Spin for a leisurely, easy-breathing, 4 minutes, then for 4 minutes push yourself until you see the light of heaven and wish for death to come. Then relax for 4 minutes again. Repeat this cycle four to six times. Done justly, you will dread Tuesdays and Fridays too. The punishing cycle of a 4-minute push, then 4-minute recovery is, however, an excellent way to improve cardiovascular fitness. And no, I’m not training for the Boston Marathon, so why am I working so hard? Because I’m training for marathon clinic days for the next 20 years.
Now more than ever, I feel we have to be physically fit to deal with a physicians’ day’s work. It’s exhausting. The root cause is too much work, yes, but I believe being physically fit could help.
I was talking to an 86-year-old patient about this very topic recently. He was short, with a well-manicured goatee and shiny head. He stuck his arm out to shake my hand. “Glad we’re back to handshakes again, doc.” His grip was that of a 30-year-old. “Buff” you’d likely describe him: He is noticeably muscular, not a skinny old man. He’s an old Navy Master Chief who started a business in wholesale flowers, which distributes all over the United States. And he’s still working full time. Impressed, I asked his secret for such vigor. PT, he replied.
PT, or physical training, is a foundational element of the Navy. Every sailor starts his or her day with morning PT before carrying out their duties. Some 30 years later, this guy is still getting after it. He does push-ups, sit-ups, and pull-ups nearly every morning. Morning PT is what he attributes to his success not only in health, but also business. As he sees it, he has the business savvy and experience of an old guy and the energy and stamina of a college kid. A good combination for a successful life.
I’ve always been pretty fit. Lately, I’ve been trying to take it to the next level, to not just be “physically active,” but rather “high-performance fit.” There are plenty of sources for instruction; how to stay young and healthy isn’t a new idea after all. I mean, Herodotus wrote of finding the Fountain of Youth in the 5th century BCE. A couple thousand years later, it’s still on trend. One of my favorite sages giving health span advice is Peter Attia, MD. I’ve been a fan since I met him at TEDMED in 2013 and I marvel at the astounding body of work he has created since. A Johns Hopkins–trained surgeon, he has spent his career reviewing the scientific literature about longevity and sharing it as actionable content. His book, “Outlive: The Science and Art of Longevity” (New York: Penguin Random House, 2023) is a nice summary of his work. I recommend it.
Right now I’m switching between type 2 muscle fiber work (lots of jumping like my 2-year-old) and cardiovascular training including the aforementioned VO2max work. I cannot say that my patient inbox is any cleaner, or that I’m faster in the office, but I’m not flagging by the end of the day anymore. Master Chief challenged me to match his 10 pull-ups before he returns for his follow up visit. I’ll gladly give up Peloton sprints to work on that.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].