User login
Low extent and incidence of radiographic spinal damage in PsA vs spondyloarthritis
Key clinical point: The occurrence of radiographic spinal damage was overall low among patients with psoriatic arthritis (PsA) and spondyloarthritis; however, severe spinal damage and the extent of syndesmophytes led spinal damage were more observed in spondyloarthritis vs PsA.
Major finding: Proportion of patients with PsA vs spondyloarthritis experiencing spinal damage was comparable (10.6% vs 7.9%; P = .320). However, patients with spondyloarthritis and spinal damage vs PsA had higher modified Stoke Ankylosing Spondylitis Spine Scores, indicating severe spinal damage (P < .05). Syndesmophytes were significantly higher in the total spine of patients with spondyloarthritis vs PsA (P < .05).
Study details: This study evaluated patients with PsA (n = 312) and spondyloarthritis (n = 213) who had undergone radiographic imaging assessment in the Belgian Epidemiological Psoriatic Arthritis Study (BEPAS) and observational Ghent and Belgian Inflammatory Arthritis and Spondylitis (Be-GIANT) study, respectively.
Disclosures: The BEPAS and Be-GIANT studies were funded by Merck Sharp Dohme Belgium and AbbVie, respectively. Several authors reported ties with various companies, including AbbVie or Merck Sharp Dohme.
Source: de Hooge M et al. Extent of axial damage in psoriatic arthritis and spondyloarthritis: Comparative data from the BEPAS and (Be-)GIANT multicentre cohorts. RMD Open. 2023;9(2):e002994 (May 3). Doi: 10.1136/rmdopen-2023-002994
Key clinical point: The occurrence of radiographic spinal damage was overall low among patients with psoriatic arthritis (PsA) and spondyloarthritis; however, severe spinal damage and the extent of syndesmophytes led spinal damage were more observed in spondyloarthritis vs PsA.
Major finding: Proportion of patients with PsA vs spondyloarthritis experiencing spinal damage was comparable (10.6% vs 7.9%; P = .320). However, patients with spondyloarthritis and spinal damage vs PsA had higher modified Stoke Ankylosing Spondylitis Spine Scores, indicating severe spinal damage (P < .05). Syndesmophytes were significantly higher in the total spine of patients with spondyloarthritis vs PsA (P < .05).
Study details: This study evaluated patients with PsA (n = 312) and spondyloarthritis (n = 213) who had undergone radiographic imaging assessment in the Belgian Epidemiological Psoriatic Arthritis Study (BEPAS) and observational Ghent and Belgian Inflammatory Arthritis and Spondylitis (Be-GIANT) study, respectively.
Disclosures: The BEPAS and Be-GIANT studies were funded by Merck Sharp Dohme Belgium and AbbVie, respectively. Several authors reported ties with various companies, including AbbVie or Merck Sharp Dohme.
Source: de Hooge M et al. Extent of axial damage in psoriatic arthritis and spondyloarthritis: Comparative data from the BEPAS and (Be-)GIANT multicentre cohorts. RMD Open. 2023;9(2):e002994 (May 3). Doi: 10.1136/rmdopen-2023-002994
Key clinical point: The occurrence of radiographic spinal damage was overall low among patients with psoriatic arthritis (PsA) and spondyloarthritis; however, severe spinal damage and the extent of syndesmophytes led spinal damage were more observed in spondyloarthritis vs PsA.
Major finding: Proportion of patients with PsA vs spondyloarthritis experiencing spinal damage was comparable (10.6% vs 7.9%; P = .320). However, patients with spondyloarthritis and spinal damage vs PsA had higher modified Stoke Ankylosing Spondylitis Spine Scores, indicating severe spinal damage (P < .05). Syndesmophytes were significantly higher in the total spine of patients with spondyloarthritis vs PsA (P < .05).
Study details: This study evaluated patients with PsA (n = 312) and spondyloarthritis (n = 213) who had undergone radiographic imaging assessment in the Belgian Epidemiological Psoriatic Arthritis Study (BEPAS) and observational Ghent and Belgian Inflammatory Arthritis and Spondylitis (Be-GIANT) study, respectively.
Disclosures: The BEPAS and Be-GIANT studies were funded by Merck Sharp Dohme Belgium and AbbVie, respectively. Several authors reported ties with various companies, including AbbVie or Merck Sharp Dohme.
Source: de Hooge M et al. Extent of axial damage in psoriatic arthritis and spondyloarthritis: Comparative data from the BEPAS and (Be-)GIANT multicentre cohorts. RMD Open. 2023;9(2):e002994 (May 3). Doi: 10.1136/rmdopen-2023-002994
Interleukin-17A inhibitor secukinumab safe and effective in oligoarticular PsA
Key clinical point: Secukinumab reduced disease activity at week 12, which sustained or improved by week 52, and demonstrated a consistent safety profile in patients with oligoarticular psoriatic arthritis (PsA).
Major finding: At week 12, 50% improvement in Disease Activity Index for Psoriatic Arthritis (DAPSA50) was achieved by a higher proportion of patients treated with 300 mg or 150 mg secukinumab vs placebo-treated patients (65.2% and 44.4% vs 30.0%, respectively). DAPSA50 responses further improved with 300 mg and 150 mg secukinumab at week 52 (74.2% and 71.8%; respectively). The safety profile of secukinumab was consistent with that reported in the original trials.
Study details: This post hoc analysis of the phase 3/3b FUTURE 2-5 and MAXIMISE trials included 84 patients with oligoarticular PsA who were randomly assigned to receive 150 or 300 mg secukinumab or placebo until week 12 and 150 or 300 mg `secukinumab from week 12 to 52.
Disclosures: This study was funded by Novartis Pharmaceuticals Corporation. Some authors declared being employees and holding stocks or shares or having other ties with Novartis or others.
Source: Ogdie A et al. Inhibition of interleukin-17 in patients with oligoarticular psoriatic arthritis. Rheumatol Ther. 2023 (May 6). Doi: 10.1007/s40744-023-00548-y
Key clinical point: Secukinumab reduced disease activity at week 12, which sustained or improved by week 52, and demonstrated a consistent safety profile in patients with oligoarticular psoriatic arthritis (PsA).
Major finding: At week 12, 50% improvement in Disease Activity Index for Psoriatic Arthritis (DAPSA50) was achieved by a higher proportion of patients treated with 300 mg or 150 mg secukinumab vs placebo-treated patients (65.2% and 44.4% vs 30.0%, respectively). DAPSA50 responses further improved with 300 mg and 150 mg secukinumab at week 52 (74.2% and 71.8%; respectively). The safety profile of secukinumab was consistent with that reported in the original trials.
Study details: This post hoc analysis of the phase 3/3b FUTURE 2-5 and MAXIMISE trials included 84 patients with oligoarticular PsA who were randomly assigned to receive 150 or 300 mg secukinumab or placebo until week 12 and 150 or 300 mg `secukinumab from week 12 to 52.
Disclosures: This study was funded by Novartis Pharmaceuticals Corporation. Some authors declared being employees and holding stocks or shares or having other ties with Novartis or others.
Source: Ogdie A et al. Inhibition of interleukin-17 in patients with oligoarticular psoriatic arthritis. Rheumatol Ther. 2023 (May 6). Doi: 10.1007/s40744-023-00548-y
Key clinical point: Secukinumab reduced disease activity at week 12, which sustained or improved by week 52, and demonstrated a consistent safety profile in patients with oligoarticular psoriatic arthritis (PsA).
Major finding: At week 12, 50% improvement in Disease Activity Index for Psoriatic Arthritis (DAPSA50) was achieved by a higher proportion of patients treated with 300 mg or 150 mg secukinumab vs placebo-treated patients (65.2% and 44.4% vs 30.0%, respectively). DAPSA50 responses further improved with 300 mg and 150 mg secukinumab at week 52 (74.2% and 71.8%; respectively). The safety profile of secukinumab was consistent with that reported in the original trials.
Study details: This post hoc analysis of the phase 3/3b FUTURE 2-5 and MAXIMISE trials included 84 patients with oligoarticular PsA who were randomly assigned to receive 150 or 300 mg secukinumab or placebo until week 12 and 150 or 300 mg `secukinumab from week 12 to 52.
Disclosures: This study was funded by Novartis Pharmaceuticals Corporation. Some authors declared being employees and holding stocks or shares or having other ties with Novartis or others.
Source: Ogdie A et al. Inhibition of interleukin-17 in patients with oligoarticular psoriatic arthritis. Rheumatol Ther. 2023 (May 6). Doi: 10.1007/s40744-023-00548-y
Pretreatment systemic inflammatory markers may guide therapeutic approach in PsA
Key clinical point: Patients with higher platelet lymphocyte ratio (PLR) or C-reactive protein (CRP) levels were more likely to be diagnosed with psoriatic arthritis (PsA) than psoriasis vulgaris (PsV), with patients having higher pretreatment systemic inflammatory marker scores showing lower treatment persistence with conventional therapies.
Major finding: PLR (odds ratio [OR] 7.027; P = .040) or CRP levels (OR 3.179; P = .022) at the time of initial presentation were associated with a higher probability of PsA vs PsV diagnosis, with patients having higher pretreatment platelet or neutrophil counts, PLR, and systemic immune/inflammation index scores exhibiting lower treatment continuation rates for conventional systemic agents (all P < .05).
Study details: Findings are from a retrospective analysis including patients with PsA (n = 47) and PsV (n = 117) and control individuals with no history of allergy or skin diseases (n = 50).
Disclosures: This study did not receive any external funding. The authors declared no conflicts of interest.
Source: Sugimoto E, Matsuda H, et al. Impact of pretreatment systemic inflammatory markers on treatment persistence with biologics and conventional systemic therapy: A retrospective study of patients with psoriasis vulgaris and psoriatic arthritis. J Clin Med. 2023;12(8):3046 (Apr 21). Doi: 10.3390/jcm12083046
Key clinical point: Patients with higher platelet lymphocyte ratio (PLR) or C-reactive protein (CRP) levels were more likely to be diagnosed with psoriatic arthritis (PsA) than psoriasis vulgaris (PsV), with patients having higher pretreatment systemic inflammatory marker scores showing lower treatment persistence with conventional therapies.
Major finding: PLR (odds ratio [OR] 7.027; P = .040) or CRP levels (OR 3.179; P = .022) at the time of initial presentation were associated with a higher probability of PsA vs PsV diagnosis, with patients having higher pretreatment platelet or neutrophil counts, PLR, and systemic immune/inflammation index scores exhibiting lower treatment continuation rates for conventional systemic agents (all P < .05).
Study details: Findings are from a retrospective analysis including patients with PsA (n = 47) and PsV (n = 117) and control individuals with no history of allergy or skin diseases (n = 50).
Disclosures: This study did not receive any external funding. The authors declared no conflicts of interest.
Source: Sugimoto E, Matsuda H, et al. Impact of pretreatment systemic inflammatory markers on treatment persistence with biologics and conventional systemic therapy: A retrospective study of patients with psoriasis vulgaris and psoriatic arthritis. J Clin Med. 2023;12(8):3046 (Apr 21). Doi: 10.3390/jcm12083046
Key clinical point: Patients with higher platelet lymphocyte ratio (PLR) or C-reactive protein (CRP) levels were more likely to be diagnosed with psoriatic arthritis (PsA) than psoriasis vulgaris (PsV), with patients having higher pretreatment systemic inflammatory marker scores showing lower treatment persistence with conventional therapies.
Major finding: PLR (odds ratio [OR] 7.027; P = .040) or CRP levels (OR 3.179; P = .022) at the time of initial presentation were associated with a higher probability of PsA vs PsV diagnosis, with patients having higher pretreatment platelet or neutrophil counts, PLR, and systemic immune/inflammation index scores exhibiting lower treatment continuation rates for conventional systemic agents (all P < .05).
Study details: Findings are from a retrospective analysis including patients with PsA (n = 47) and PsV (n = 117) and control individuals with no history of allergy or skin diseases (n = 50).
Disclosures: This study did not receive any external funding. The authors declared no conflicts of interest.
Source: Sugimoto E, Matsuda H, et al. Impact of pretreatment systemic inflammatory markers on treatment persistence with biologics and conventional systemic therapy: A retrospective study of patients with psoriasis vulgaris and psoriatic arthritis. J Clin Med. 2023;12(8):3046 (Apr 21). Doi: 10.3390/jcm12083046
Concomitant methotrexate has no effect on ustekinumab immunogenicity in PsA
Key clinical point: Concomitant methotrexate had no effect on ustekimumab immunogenicity in patients with psoriatic arthritis (PsA), with the formation of antidrug antibody (ADA) not being associated with reductions in ustekinumab safety or efficacy.
Major finding: The prevalence of ADA at week 52 was not significantly different between the ustekinumab+methotrexate and ustekinumab+placebo groups, with disease activity, treatment response, dropout rates, effect of pretreatment with methotrexate, and safety outcomes not being significantly different in patients with vs without ADA (all P > .05).
Study details: This post hoc analysis of the MUST trial included 112 patients with active PsA who were naive to ustekimumab and were randomly assigned to receive ustekinumab with concomitant methotrexate or placebo.
Disclosures: This study was funded by Innovative Medicines Initiative 2 Joint Undertaking, which received support from the European Union’s Horizon 2020 Research and Innovation Program and others. F Behrens, M Koehm, and H Burkhardt declared receiving research grants from Janssen Cilag. The other authors reported no conflicts of interest.
Source: Poor SM et al. The role of antidrug antibodies in ustekinumab therapy and the impact of methotrexate. Rheumatology (Oxford). 2023 (Apr 20). Doi: 10.1093/rheumatology/kead177
Key clinical point: Concomitant methotrexate had no effect on ustekimumab immunogenicity in patients with psoriatic arthritis (PsA), with the formation of antidrug antibody (ADA) not being associated with reductions in ustekinumab safety or efficacy.
Major finding: The prevalence of ADA at week 52 was not significantly different between the ustekinumab+methotrexate and ustekinumab+placebo groups, with disease activity, treatment response, dropout rates, effect of pretreatment with methotrexate, and safety outcomes not being significantly different in patients with vs without ADA (all P > .05).
Study details: This post hoc analysis of the MUST trial included 112 patients with active PsA who were naive to ustekimumab and were randomly assigned to receive ustekinumab with concomitant methotrexate or placebo.
Disclosures: This study was funded by Innovative Medicines Initiative 2 Joint Undertaking, which received support from the European Union’s Horizon 2020 Research and Innovation Program and others. F Behrens, M Koehm, and H Burkhardt declared receiving research grants from Janssen Cilag. The other authors reported no conflicts of interest.
Source: Poor SM et al. The role of antidrug antibodies in ustekinumab therapy and the impact of methotrexate. Rheumatology (Oxford). 2023 (Apr 20). Doi: 10.1093/rheumatology/kead177
Key clinical point: Concomitant methotrexate had no effect on ustekimumab immunogenicity in patients with psoriatic arthritis (PsA), with the formation of antidrug antibody (ADA) not being associated with reductions in ustekinumab safety or efficacy.
Major finding: The prevalence of ADA at week 52 was not significantly different between the ustekinumab+methotrexate and ustekinumab+placebo groups, with disease activity, treatment response, dropout rates, effect of pretreatment with methotrexate, and safety outcomes not being significantly different in patients with vs without ADA (all P > .05).
Study details: This post hoc analysis of the MUST trial included 112 patients with active PsA who were naive to ustekimumab and were randomly assigned to receive ustekinumab with concomitant methotrexate or placebo.
Disclosures: This study was funded by Innovative Medicines Initiative 2 Joint Undertaking, which received support from the European Union’s Horizon 2020 Research and Innovation Program and others. F Behrens, M Koehm, and H Burkhardt declared receiving research grants from Janssen Cilag. The other authors reported no conflicts of interest.
Source: Poor SM et al. The role of antidrug antibodies in ustekinumab therapy and the impact of methotrexate. Rheumatology (Oxford). 2023 (Apr 20). Doi: 10.1093/rheumatology/kead177
Concomitant methotrexate has no effect on ustekinumab immunogenicity in PsA
Key clinical point: Concomitant methotrexate had no effect on ustekimumab immunogenicity in patients with psoriatic arthritis (PsA), with the formation of antidrug antibody (ADA) not being associated with reductions in ustekinumab safety or efficacy.
Major finding: The prevalence of ADA at week 52 was not significantly different between the ustekinumab+methotrexate and ustekinumab+placebo groups, with disease activity, treatment response, dropout rates, effect of pretreatment with methotrexate, and safety outcomes not being significantly different in patients with vs without ADA (all P > .05).
Study details: This post hoc analysis of the MUST trial included 112 patients with active PsA who were naive to ustekimumab and were randomly assigned to receive ustekinumab with concomitant methotrexate or placebo.
Disclosures: This study was funded by Innovative Medicines Initiative 2 Joint Undertaking, which received support from the European Union’s Horizon 2020 Research and Innovation Program and others. F Behrens, M Koehm, and H Burkhardt declared receiving research grants from Janssen Cilag. The other authors reported no conflicts of interest.
Source: Poor SM et al. The role of antidrug antibodies in ustekinumab therapy and the impact of methotrexate. Rheumatology (Oxford). 2023 (Apr 20). Doi: 10.1093/rheumatology/kead177
Key clinical point: Concomitant methotrexate had no effect on ustekimumab immunogenicity in patients with psoriatic arthritis (PsA), with the formation of antidrug antibody (ADA) not being associated with reductions in ustekinumab safety or efficacy.
Major finding: The prevalence of ADA at week 52 was not significantly different between the ustekinumab+methotrexate and ustekinumab+placebo groups, with disease activity, treatment response, dropout rates, effect of pretreatment with methotrexate, and safety outcomes not being significantly different in patients with vs without ADA (all P > .05).
Study details: This post hoc analysis of the MUST trial included 112 patients with active PsA who were naive to ustekimumab and were randomly assigned to receive ustekinumab with concomitant methotrexate or placebo.
Disclosures: This study was funded by Innovative Medicines Initiative 2 Joint Undertaking, which received support from the European Union’s Horizon 2020 Research and Innovation Program and others. F Behrens, M Koehm, and H Burkhardt declared receiving research grants from Janssen Cilag. The other authors reported no conflicts of interest.
Source: Poor SM et al. The role of antidrug antibodies in ustekinumab therapy and the impact of methotrexate. Rheumatology (Oxford). 2023 (Apr 20). Doi: 10.1093/rheumatology/kead177
Key clinical point: Concomitant methotrexate had no effect on ustekimumab immunogenicity in patients with psoriatic arthritis (PsA), with the formation of antidrug antibody (ADA) not being associated with reductions in ustekinumab safety or efficacy.
Major finding: The prevalence of ADA at week 52 was not significantly different between the ustekinumab+methotrexate and ustekinumab+placebo groups, with disease activity, treatment response, dropout rates, effect of pretreatment with methotrexate, and safety outcomes not being significantly different in patients with vs without ADA (all P > .05).
Study details: This post hoc analysis of the MUST trial included 112 patients with active PsA who were naive to ustekimumab and were randomly assigned to receive ustekinumab with concomitant methotrexate or placebo.
Disclosures: This study was funded by Innovative Medicines Initiative 2 Joint Undertaking, which received support from the European Union’s Horizon 2020 Research and Innovation Program and others. F Behrens, M Koehm, and H Burkhardt declared receiving research grants from Janssen Cilag. The other authors reported no conflicts of interest.
Source: Poor SM et al. The role of antidrug antibodies in ustekinumab therapy and the impact of methotrexate. Rheumatology (Oxford). 2023 (Apr 20). Doi: 10.1093/rheumatology/kead177
Entheseal fibrocartilage abnormalities: A potential imaging biomarker of PsA
Key clinical point: The entheseal fibrocartilage (EF) thickness assessed during power Doppler ultrasound evaluation was significantly different among patients with psoriatic arthritis (PsA) and control individuals and can be explored as an imaging biomarker for PsA.
Major finding: The median EF thickness was significantly greater in patients with PsA and athletes vs control individuals (0.035 and 0.036 vs 0.030 cm, respectively; P = .05 and P = .008, respectively), with the intra- and inter-reader reliability of the evaluation of EF thickness being excellent (intraclass correlation coefficient [ICC] 0.91) and good (ICC 0.80; both P < .001), respectively.
Study details: This cross-sectional study included patients with PsA (n = 30), athletes (n = 40), and control individuals (n = 20) who underwent power Doppler ultrasound evaluation during bilateral Achilles tendon insertions.
Disclosures: This study did not receive any external funding. The authors declared no conflicts of interest.
Source: Perrotta FM et al. Ultrasonographic evaluation of entheseal fibrocartilage in patients with psoriatic arthritis, athletes and healthy controls: A comparison study. Diagnostics (Basel). 2023;13(8):1446 (Apr 17). Doi: 10.3390/diagnostics13081446
Key clinical point: The entheseal fibrocartilage (EF) thickness assessed during power Doppler ultrasound evaluation was significantly different among patients with psoriatic arthritis (PsA) and control individuals and can be explored as an imaging biomarker for PsA.
Major finding: The median EF thickness was significantly greater in patients with PsA and athletes vs control individuals (0.035 and 0.036 vs 0.030 cm, respectively; P = .05 and P = .008, respectively), with the intra- and inter-reader reliability of the evaluation of EF thickness being excellent (intraclass correlation coefficient [ICC] 0.91) and good (ICC 0.80; both P < .001), respectively.
Study details: This cross-sectional study included patients with PsA (n = 30), athletes (n = 40), and control individuals (n = 20) who underwent power Doppler ultrasound evaluation during bilateral Achilles tendon insertions.
Disclosures: This study did not receive any external funding. The authors declared no conflicts of interest.
Source: Perrotta FM et al. Ultrasonographic evaluation of entheseal fibrocartilage in patients with psoriatic arthritis, athletes and healthy controls: A comparison study. Diagnostics (Basel). 2023;13(8):1446 (Apr 17). Doi: 10.3390/diagnostics13081446
Key clinical point: The entheseal fibrocartilage (EF) thickness assessed during power Doppler ultrasound evaluation was significantly different among patients with psoriatic arthritis (PsA) and control individuals and can be explored as an imaging biomarker for PsA.
Major finding: The median EF thickness was significantly greater in patients with PsA and athletes vs control individuals (0.035 and 0.036 vs 0.030 cm, respectively; P = .05 and P = .008, respectively), with the intra- and inter-reader reliability of the evaluation of EF thickness being excellent (intraclass correlation coefficient [ICC] 0.91) and good (ICC 0.80; both P < .001), respectively.
Study details: This cross-sectional study included patients with PsA (n = 30), athletes (n = 40), and control individuals (n = 20) who underwent power Doppler ultrasound evaluation during bilateral Achilles tendon insertions.
Disclosures: This study did not receive any external funding. The authors declared no conflicts of interest.
Source: Perrotta FM et al. Ultrasonographic evaluation of entheseal fibrocartilage in patients with psoriatic arthritis, athletes and healthy controls: A comparison study. Diagnostics (Basel). 2023;13(8):1446 (Apr 17). Doi: 10.3390/diagnostics13081446
Upadacitinib safe and effective in PsA patients with axial involvement
Key clinical point: Compared with placebo, 15 mg upadacitinib led to a greater improvement in axial symptoms with a consistent safety profile in patients with psoriatic arthritis (PsA).
Major finding: The improvement in overall Bath Ankylosing Spondylitis Disease Activity Index score at week 24 was significantly higher with 15 mg upadacitinib vs placebo in both SELECT-PsA 1 (−3.12 vs −1.70; P < .0001) and SELECT PsA 2 (−2.06 vs −0.21; P < .0001) trials. Treatment-emergent adverse events were generally similar among the sub-groups.
Study details: This post hoc analysis included patients with active PsA (n = 1,281 and n = 423, respectively) from the SELECT-PsA 1 and SELECT-PsA 2 trials who were randomly assigned to receive either 15 mg upadacitinib, placebo, or adalimumab and were categorized as those with or without axial involvement.
Disclosures: This study was funded by AbbVie. Five authors declared being employees or stockholders of AbbVie, and some authors reported ties with various sources, including AbbVie.
Source: Baraliakos X et al. Efficacy and safety of upadacitinib in patients with active psoriatic arthritis and axial involvement: Results from two phase 3 studies. Arthritis Res Ther. 2023;25:56 (Apr 10). Doi: 10.1186/s13075-023-03027-5
Key clinical point: Compared with placebo, 15 mg upadacitinib led to a greater improvement in axial symptoms with a consistent safety profile in patients with psoriatic arthritis (PsA).
Major finding: The improvement in overall Bath Ankylosing Spondylitis Disease Activity Index score at week 24 was significantly higher with 15 mg upadacitinib vs placebo in both SELECT-PsA 1 (−3.12 vs −1.70; P < .0001) and SELECT PsA 2 (−2.06 vs −0.21; P < .0001) trials. Treatment-emergent adverse events were generally similar among the sub-groups.
Study details: This post hoc analysis included patients with active PsA (n = 1,281 and n = 423, respectively) from the SELECT-PsA 1 and SELECT-PsA 2 trials who were randomly assigned to receive either 15 mg upadacitinib, placebo, or adalimumab and were categorized as those with or without axial involvement.
Disclosures: This study was funded by AbbVie. Five authors declared being employees or stockholders of AbbVie, and some authors reported ties with various sources, including AbbVie.
Source: Baraliakos X et al. Efficacy and safety of upadacitinib in patients with active psoriatic arthritis and axial involvement: Results from two phase 3 studies. Arthritis Res Ther. 2023;25:56 (Apr 10). Doi: 10.1186/s13075-023-03027-5
Key clinical point: Compared with placebo, 15 mg upadacitinib led to a greater improvement in axial symptoms with a consistent safety profile in patients with psoriatic arthritis (PsA).
Major finding: The improvement in overall Bath Ankylosing Spondylitis Disease Activity Index score at week 24 was significantly higher with 15 mg upadacitinib vs placebo in both SELECT-PsA 1 (−3.12 vs −1.70; P < .0001) and SELECT PsA 2 (−2.06 vs −0.21; P < .0001) trials. Treatment-emergent adverse events were generally similar among the sub-groups.
Study details: This post hoc analysis included patients with active PsA (n = 1,281 and n = 423, respectively) from the SELECT-PsA 1 and SELECT-PsA 2 trials who were randomly assigned to receive either 15 mg upadacitinib, placebo, or adalimumab and were categorized as those with or without axial involvement.
Disclosures: This study was funded by AbbVie. Five authors declared being employees or stockholders of AbbVie, and some authors reported ties with various sources, including AbbVie.
Source: Baraliakos X et al. Efficacy and safety of upadacitinib in patients with active psoriatic arthritis and axial involvement: Results from two phase 3 studies. Arthritis Res Ther. 2023;25:56 (Apr 10). Doi: 10.1186/s13075-023-03027-5
The antimicrobial peptide that even Pharma can love
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.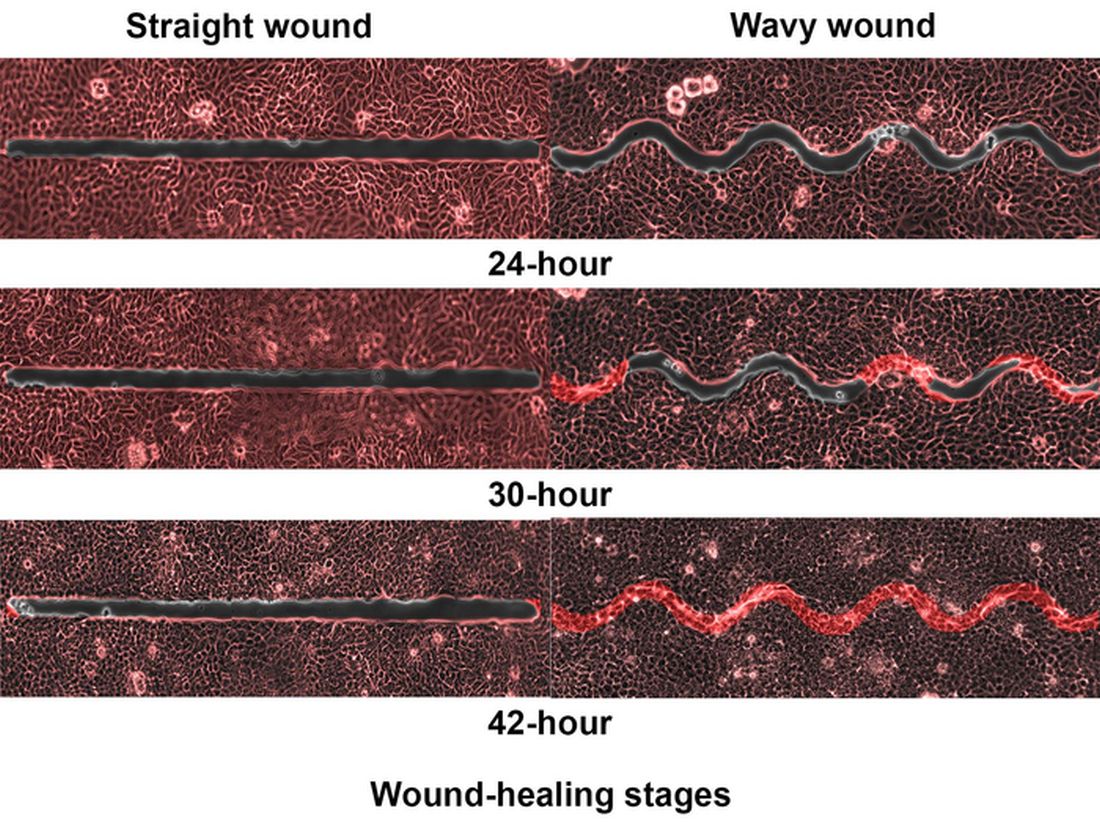
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
Sonographic enthesitis associated with sonographic synovitis and tenosynovitis in PsA
Key clinical point: Sonographic enthesitis showed strong association with sonographic synovitis and tenosynovitis in patients with psoriatic arthritis (PsA), suggesting the clinical significance of sonographic enthesitis as a potential marker for inflammation in other musculoskeletal domains.
Major finding: Sonographic enthesitis was significantly associated with sonographic synovitis (β 0.19; P = .004) and sonographic tenosynovitis (β 0.1; P = .003) and showed strong correlation with patient-reported outcomes, such as Health Assessment Questionnaire (P = .003), morning stiffness (P = .002), and others.
Study details: This study prospectively recruited 158 patients with PsA who underwent sonographic assessment of 52 joints, 40 tendons, and 14 entheses points along with clinical evaluation.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Balulu G et al. The association between sonographic enthesitis with sonographic synovitis and tenosynovitis in psoriatic arthritis patients. Rheumatology (Oxford). 2023 (May 11). Doi: 10.1093/rheumatology/kead202
Key clinical point: Sonographic enthesitis showed strong association with sonographic synovitis and tenosynovitis in patients with psoriatic arthritis (PsA), suggesting the clinical significance of sonographic enthesitis as a potential marker for inflammation in other musculoskeletal domains.
Major finding: Sonographic enthesitis was significantly associated with sonographic synovitis (β 0.19; P = .004) and sonographic tenosynovitis (β 0.1; P = .003) and showed strong correlation with patient-reported outcomes, such as Health Assessment Questionnaire (P = .003), morning stiffness (P = .002), and others.
Study details: This study prospectively recruited 158 patients with PsA who underwent sonographic assessment of 52 joints, 40 tendons, and 14 entheses points along with clinical evaluation.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Balulu G et al. The association between sonographic enthesitis with sonographic synovitis and tenosynovitis in psoriatic arthritis patients. Rheumatology (Oxford). 2023 (May 11). Doi: 10.1093/rheumatology/kead202
Key clinical point: Sonographic enthesitis showed strong association with sonographic synovitis and tenosynovitis in patients with psoriatic arthritis (PsA), suggesting the clinical significance of sonographic enthesitis as a potential marker for inflammation in other musculoskeletal domains.
Major finding: Sonographic enthesitis was significantly associated with sonographic synovitis (β 0.19; P = .004) and sonographic tenosynovitis (β 0.1; P = .003) and showed strong correlation with patient-reported outcomes, such as Health Assessment Questionnaire (P = .003), morning stiffness (P = .002), and others.
Study details: This study prospectively recruited 158 patients with PsA who underwent sonographic assessment of 52 joints, 40 tendons, and 14 entheses points along with clinical evaluation.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Balulu G et al. The association between sonographic enthesitis with sonographic synovitis and tenosynovitis in psoriatic arthritis patients. Rheumatology (Oxford). 2023 (May 11). Doi: 10.1093/rheumatology/kead202
Enthesitis resolution similar with secukinumab and adalimumab in PsA
Key clinical point: Patients with psoriatic arthritis (PsA) achieved enthesitis resolution over 52 weeks with secukinumab treatment, which was comparable to that with adalimumab treatment.
Major finding: At week 52, secukinumab vs adalimumab led to a similar proportion of patients achieving enthesitis resolution (53.2% vs 51.4%) along with site-specific resolution of lateral epicondyle enthesitis (84.6% vs 87.1%) and showing relapse after first resolution (21.0% vs 15.6%), as assessed by the Spondyloarthritis Research Consortium of Canada Enthesitis Index (SPARCC). Moreover, secukinumab vs adalimumab had a comparable response time to SPARCC enthesitis resolution (113 vs 88 days).
Study details: This post hoc analysis of the EXCEED study included 853 patients with PsA who received either secukinumab (300 mg) or adalimumab (40 mg) over 52 weeks.
Disclosures: This study was supported by Novartis Pharmaceuticals Corporation, USA. C Gaillez and B Parikh declared being current or former employees of Novartis Pharma or Novartis Pharmaceuticals Corporation, and several authors reported ties with various sources, including Novartis.
Source: Kaeley GS et al. Enthesitis in patients with psoriatic arthritis treated with secukinumab or adalimumab: A post hoc analysis of the EXCEED study. Rheumatology (Oxford). 2023 (Apr 25). Doi: 10.1093/rheumatology/kead181
Key clinical point: Patients with psoriatic arthritis (PsA) achieved enthesitis resolution over 52 weeks with secukinumab treatment, which was comparable to that with adalimumab treatment.
Major finding: At week 52, secukinumab vs adalimumab led to a similar proportion of patients achieving enthesitis resolution (53.2% vs 51.4%) along with site-specific resolution of lateral epicondyle enthesitis (84.6% vs 87.1%) and showing relapse after first resolution (21.0% vs 15.6%), as assessed by the Spondyloarthritis Research Consortium of Canada Enthesitis Index (SPARCC). Moreover, secukinumab vs adalimumab had a comparable response time to SPARCC enthesitis resolution (113 vs 88 days).
Study details: This post hoc analysis of the EXCEED study included 853 patients with PsA who received either secukinumab (300 mg) or adalimumab (40 mg) over 52 weeks.
Disclosures: This study was supported by Novartis Pharmaceuticals Corporation, USA. C Gaillez and B Parikh declared being current or former employees of Novartis Pharma or Novartis Pharmaceuticals Corporation, and several authors reported ties with various sources, including Novartis.
Source: Kaeley GS et al. Enthesitis in patients with psoriatic arthritis treated with secukinumab or adalimumab: A post hoc analysis of the EXCEED study. Rheumatology (Oxford). 2023 (Apr 25). Doi: 10.1093/rheumatology/kead181
Key clinical point: Patients with psoriatic arthritis (PsA) achieved enthesitis resolution over 52 weeks with secukinumab treatment, which was comparable to that with adalimumab treatment.
Major finding: At week 52, secukinumab vs adalimumab led to a similar proportion of patients achieving enthesitis resolution (53.2% vs 51.4%) along with site-specific resolution of lateral epicondyle enthesitis (84.6% vs 87.1%) and showing relapse after first resolution (21.0% vs 15.6%), as assessed by the Spondyloarthritis Research Consortium of Canada Enthesitis Index (SPARCC). Moreover, secukinumab vs adalimumab had a comparable response time to SPARCC enthesitis resolution (113 vs 88 days).
Study details: This post hoc analysis of the EXCEED study included 853 patients with PsA who received either secukinumab (300 mg) or adalimumab (40 mg) over 52 weeks.
Disclosures: This study was supported by Novartis Pharmaceuticals Corporation, USA. C Gaillez and B Parikh declared being current or former employees of Novartis Pharma or Novartis Pharmaceuticals Corporation, and several authors reported ties with various sources, including Novartis.
Source: Kaeley GS et al. Enthesitis in patients with psoriatic arthritis treated with secukinumab or adalimumab: A post hoc analysis of the EXCEED study. Rheumatology (Oxford). 2023 (Apr 25). Doi: 10.1093/rheumatology/kead181