User login
GLP-1 Receptor Agonists Reduce Suicidal Behavior in Adolescents With Obesity
, a large international retrospective study found.
A study published in JAMA Pediatrics suggested that GLP-1 RAs such as semaglutide, liraglutide, and tirzepatide, which are widely used to treat type 2 diabetes (T2D), have a favorable psychiatric safety profile and open up potential avenues for prospective studies of psychiatric outcomes in adolescents with obesity.
Investigators Liya Kerem, MD, MSc, and Joshua Stokar, MD, of Hadassah University Medical Center in Jerusalem, Israel, reported that the reduced risk in GLP-1 RA recipients was maintained up to 3 years follow-up compared with propensity score–matched controls treated with behavioral interventions alone.
“These findings support the notion that childhood obesity does not result from lack of willpower and shed light on underlying mechanisms that can be targeted by pharmacotherapy.” Kerem and Stokar wrote.
Other research has suggested these agents have neurobiologic effects unrelated to weight loss that positively affect mood and mental health.
Study Details
The analysis included data from December 2019 to June 2024, drawn from 120 international healthcare organizations, mainly in the United States. A total of 4052 racially and ethnically diverse adolescents with obesity (aged 12-18 years [mean age, about 15.5 years]) being treated with an anti-obesity intervention were identified for the GLP-1 RA cohort and 50,112 for the control cohort. The arms were balanced for baseline demographic characteristics, psychiatric medications and comorbidities, and diagnoses associated with socioeconomic status and healthcare access.
Propensity score matching (PSM) resulted in 3456 participants in each of two balanced cohorts.
Before PSM, intervention patients were older (mean age, 15.5 vs 14.7 years), were more likely to be female (59% vs 49%), and had a higher body mass index (41.9 vs 33.8). They also had a higher prevalence of diabetes (40% vs 4%) and treatment with antidiabetic medications.
GLP-1 RA recipients also had a history of psychiatric diagnoses (17% vs 9% for mood disorders) and psychiatric medications (18% vs 7% for antidepressants). Previous use of non–GLP-1 RA anti-obesity medications was uncommon in the cohort overall, although more common in the GLP-1 RA cohort (2.5% vs 0.2% for phentermine).
Prescription of GLP-1 RA was associated with a 33% reduced risk for suicidal ideation or attempts over 12 months of follow-up: 1.45% vs 2.26% (hazard ratio [HR], 0.67; 95% CI, 0.47-0.95; P = .02). It was also associated with a higher rate of gastrointestinal symptoms: 6.9% vs 5.4% (HR, 1.41; 95% CI, 1.12-1.78; P = .003). There was no difference in rates of upper respiratory tract infections (URTIs), although some research suggests these agents reduce URTIs.
Mechanisms
The etiology of childhood obesity is complex and multifactorial, the authors wrote, and genetic predisposition to adiposity, an obesogenic environment, and a sedentary lifestyle synergistically contribute to its development. Variants in genes active in the hypothalamic appetite-regulation neurocircuitry appear to be associated with the development of childhood and adolescent obesity.
The authors noted that adolescence carries an increased risk for psychiatric disorders and suicidal ideation. “The amelioration of obesity could indirectly improve these psychiatric comorbidities,” they wrote. In addition, preclinical studies suggested that GLP-1 RA may improve depression-related neuropathology, including neuroinflammation and neurotransmitter imbalance, and may promote neurogenesis.
A recent meta-analysis found that adults with T2D treated with GLP-1 RA showed significant reduction in depression scale scores compared with those treated with non-GLP-1 RA antidiabetic medications.
Commenting on the study but not involved in it, psychiatrist Robert H. Dicker, MD, associate director of child and adolescent psychiatry at Northwell Zucker Hillside Hospital in Glen Oaks, New York, cautioned that these are preliminary data limited by a retrospective review, not a prospective double-blind, placebo-controlled study.
“The mechanism is unknown — is it a direct effect on weight loss with an improvement of quality of life, more positive feedback by the community, enhanced ability to exercise, and a decrease in depressive symptoms?” he asked.
Dicker suggested an alternative hypothesis: Does the GLP-1 RA have a direct effect on neurotransmitters and inflammation and, thus, an impact on mood, emotional regulation, impulse control, and suicide?
“To further answer these questions, prospective studies must be conducted. It is far too early to conclude that these medications are effective in treating mood disorders in our youth,” Dicker said. “But it is promising that these treatments do not appear to increase suicidal ideas and behavior.”
Adding another outsider’s perspective on the study, Suzanne E. Cuda, MD, FOMA, FAAP, a pediatrician who treats childhood obesity in San Antonio, said that while there was no risk for increased psychiatric disease and a suggestion that GLP-1 RAs may reduce suicidal ideation or attempts, “I don’t think this translates to a treatment for depression in adolescents. Nor does this study indicate there could be a decrease in depression due specifically to the use of GLP1Rs. If the results in this study are replicated, however, it would be reassuring to know that adolescents would not be at risk for an increase in suicidal ideation or attempts.”
This study had no external funding. Kerem reported receiving personal fees from Novo Nordisk for lectures on childhood obesity outside of the submitted work. No other disclosures were reported. Dicker and Cuda had no competing interests relevant to their comments.
A version of this article appeared on Medscape.com.
, a large international retrospective study found.
A study published in JAMA Pediatrics suggested that GLP-1 RAs such as semaglutide, liraglutide, and tirzepatide, which are widely used to treat type 2 diabetes (T2D), have a favorable psychiatric safety profile and open up potential avenues for prospective studies of psychiatric outcomes in adolescents with obesity.
Investigators Liya Kerem, MD, MSc, and Joshua Stokar, MD, of Hadassah University Medical Center in Jerusalem, Israel, reported that the reduced risk in GLP-1 RA recipients was maintained up to 3 years follow-up compared with propensity score–matched controls treated with behavioral interventions alone.
“These findings support the notion that childhood obesity does not result from lack of willpower and shed light on underlying mechanisms that can be targeted by pharmacotherapy.” Kerem and Stokar wrote.
Other research has suggested these agents have neurobiologic effects unrelated to weight loss that positively affect mood and mental health.
Study Details
The analysis included data from December 2019 to June 2024, drawn from 120 international healthcare organizations, mainly in the United States. A total of 4052 racially and ethnically diverse adolescents with obesity (aged 12-18 years [mean age, about 15.5 years]) being treated with an anti-obesity intervention were identified for the GLP-1 RA cohort and 50,112 for the control cohort. The arms were balanced for baseline demographic characteristics, psychiatric medications and comorbidities, and diagnoses associated with socioeconomic status and healthcare access.
Propensity score matching (PSM) resulted in 3456 participants in each of two balanced cohorts.
Before PSM, intervention patients were older (mean age, 15.5 vs 14.7 years), were more likely to be female (59% vs 49%), and had a higher body mass index (41.9 vs 33.8). They also had a higher prevalence of diabetes (40% vs 4%) and treatment with antidiabetic medications.
GLP-1 RA recipients also had a history of psychiatric diagnoses (17% vs 9% for mood disorders) and psychiatric medications (18% vs 7% for antidepressants). Previous use of non–GLP-1 RA anti-obesity medications was uncommon in the cohort overall, although more common in the GLP-1 RA cohort (2.5% vs 0.2% for phentermine).
Prescription of GLP-1 RA was associated with a 33% reduced risk for suicidal ideation or attempts over 12 months of follow-up: 1.45% vs 2.26% (hazard ratio [HR], 0.67; 95% CI, 0.47-0.95; P = .02). It was also associated with a higher rate of gastrointestinal symptoms: 6.9% vs 5.4% (HR, 1.41; 95% CI, 1.12-1.78; P = .003). There was no difference in rates of upper respiratory tract infections (URTIs), although some research suggests these agents reduce URTIs.
Mechanisms
The etiology of childhood obesity is complex and multifactorial, the authors wrote, and genetic predisposition to adiposity, an obesogenic environment, and a sedentary lifestyle synergistically contribute to its development. Variants in genes active in the hypothalamic appetite-regulation neurocircuitry appear to be associated with the development of childhood and adolescent obesity.
The authors noted that adolescence carries an increased risk for psychiatric disorders and suicidal ideation. “The amelioration of obesity could indirectly improve these psychiatric comorbidities,” they wrote. In addition, preclinical studies suggested that GLP-1 RA may improve depression-related neuropathology, including neuroinflammation and neurotransmitter imbalance, and may promote neurogenesis.
A recent meta-analysis found that adults with T2D treated with GLP-1 RA showed significant reduction in depression scale scores compared with those treated with non-GLP-1 RA antidiabetic medications.
Commenting on the study but not involved in it, psychiatrist Robert H. Dicker, MD, associate director of child and adolescent psychiatry at Northwell Zucker Hillside Hospital in Glen Oaks, New York, cautioned that these are preliminary data limited by a retrospective review, not a prospective double-blind, placebo-controlled study.
“The mechanism is unknown — is it a direct effect on weight loss with an improvement of quality of life, more positive feedback by the community, enhanced ability to exercise, and a decrease in depressive symptoms?” he asked.
Dicker suggested an alternative hypothesis: Does the GLP-1 RA have a direct effect on neurotransmitters and inflammation and, thus, an impact on mood, emotional regulation, impulse control, and suicide?
“To further answer these questions, prospective studies must be conducted. It is far too early to conclude that these medications are effective in treating mood disorders in our youth,” Dicker said. “But it is promising that these treatments do not appear to increase suicidal ideas and behavior.”
Adding another outsider’s perspective on the study, Suzanne E. Cuda, MD, FOMA, FAAP, a pediatrician who treats childhood obesity in San Antonio, said that while there was no risk for increased psychiatric disease and a suggestion that GLP-1 RAs may reduce suicidal ideation or attempts, “I don’t think this translates to a treatment for depression in adolescents. Nor does this study indicate there could be a decrease in depression due specifically to the use of GLP1Rs. If the results in this study are replicated, however, it would be reassuring to know that adolescents would not be at risk for an increase in suicidal ideation or attempts.”
This study had no external funding. Kerem reported receiving personal fees from Novo Nordisk for lectures on childhood obesity outside of the submitted work. No other disclosures were reported. Dicker and Cuda had no competing interests relevant to their comments.
A version of this article appeared on Medscape.com.
, a large international retrospective study found.
A study published in JAMA Pediatrics suggested that GLP-1 RAs such as semaglutide, liraglutide, and tirzepatide, which are widely used to treat type 2 diabetes (T2D), have a favorable psychiatric safety profile and open up potential avenues for prospective studies of psychiatric outcomes in adolescents with obesity.
Investigators Liya Kerem, MD, MSc, and Joshua Stokar, MD, of Hadassah University Medical Center in Jerusalem, Israel, reported that the reduced risk in GLP-1 RA recipients was maintained up to 3 years follow-up compared with propensity score–matched controls treated with behavioral interventions alone.
“These findings support the notion that childhood obesity does not result from lack of willpower and shed light on underlying mechanisms that can be targeted by pharmacotherapy.” Kerem and Stokar wrote.
Other research has suggested these agents have neurobiologic effects unrelated to weight loss that positively affect mood and mental health.
Study Details
The analysis included data from December 2019 to June 2024, drawn from 120 international healthcare organizations, mainly in the United States. A total of 4052 racially and ethnically diverse adolescents with obesity (aged 12-18 years [mean age, about 15.5 years]) being treated with an anti-obesity intervention were identified for the GLP-1 RA cohort and 50,112 for the control cohort. The arms were balanced for baseline demographic characteristics, psychiatric medications and comorbidities, and diagnoses associated with socioeconomic status and healthcare access.
Propensity score matching (PSM) resulted in 3456 participants in each of two balanced cohorts.
Before PSM, intervention patients were older (mean age, 15.5 vs 14.7 years), were more likely to be female (59% vs 49%), and had a higher body mass index (41.9 vs 33.8). They also had a higher prevalence of diabetes (40% vs 4%) and treatment with antidiabetic medications.
GLP-1 RA recipients also had a history of psychiatric diagnoses (17% vs 9% for mood disorders) and psychiatric medications (18% vs 7% for antidepressants). Previous use of non–GLP-1 RA anti-obesity medications was uncommon in the cohort overall, although more common in the GLP-1 RA cohort (2.5% vs 0.2% for phentermine).
Prescription of GLP-1 RA was associated with a 33% reduced risk for suicidal ideation or attempts over 12 months of follow-up: 1.45% vs 2.26% (hazard ratio [HR], 0.67; 95% CI, 0.47-0.95; P = .02). It was also associated with a higher rate of gastrointestinal symptoms: 6.9% vs 5.4% (HR, 1.41; 95% CI, 1.12-1.78; P = .003). There was no difference in rates of upper respiratory tract infections (URTIs), although some research suggests these agents reduce URTIs.
Mechanisms
The etiology of childhood obesity is complex and multifactorial, the authors wrote, and genetic predisposition to adiposity, an obesogenic environment, and a sedentary lifestyle synergistically contribute to its development. Variants in genes active in the hypothalamic appetite-regulation neurocircuitry appear to be associated with the development of childhood and adolescent obesity.
The authors noted that adolescence carries an increased risk for psychiatric disorders and suicidal ideation. “The amelioration of obesity could indirectly improve these psychiatric comorbidities,” they wrote. In addition, preclinical studies suggested that GLP-1 RA may improve depression-related neuropathology, including neuroinflammation and neurotransmitter imbalance, and may promote neurogenesis.
A recent meta-analysis found that adults with T2D treated with GLP-1 RA showed significant reduction in depression scale scores compared with those treated with non-GLP-1 RA antidiabetic medications.
Commenting on the study but not involved in it, psychiatrist Robert H. Dicker, MD, associate director of child and adolescent psychiatry at Northwell Zucker Hillside Hospital in Glen Oaks, New York, cautioned that these are preliminary data limited by a retrospective review, not a prospective double-blind, placebo-controlled study.
“The mechanism is unknown — is it a direct effect on weight loss with an improvement of quality of life, more positive feedback by the community, enhanced ability to exercise, and a decrease in depressive symptoms?” he asked.
Dicker suggested an alternative hypothesis: Does the GLP-1 RA have a direct effect on neurotransmitters and inflammation and, thus, an impact on mood, emotional regulation, impulse control, and suicide?
“To further answer these questions, prospective studies must be conducted. It is far too early to conclude that these medications are effective in treating mood disorders in our youth,” Dicker said. “But it is promising that these treatments do not appear to increase suicidal ideas and behavior.”
Adding another outsider’s perspective on the study, Suzanne E. Cuda, MD, FOMA, FAAP, a pediatrician who treats childhood obesity in San Antonio, said that while there was no risk for increased psychiatric disease and a suggestion that GLP-1 RAs may reduce suicidal ideation or attempts, “I don’t think this translates to a treatment for depression in adolescents. Nor does this study indicate there could be a decrease in depression due specifically to the use of GLP1Rs. If the results in this study are replicated, however, it would be reassuring to know that adolescents would not be at risk for an increase in suicidal ideation or attempts.”
This study had no external funding. Kerem reported receiving personal fees from Novo Nordisk for lectures on childhood obesity outside of the submitted work. No other disclosures were reported. Dicker and Cuda had no competing interests relevant to their comments.
A version of this article appeared on Medscape.com.
From JAMA Pediatrics
Unseen Cost of Weight Loss and Aging: Tackling Sarcopenia
Losses of muscle and strength are inescapable effects of the aging process. Left unchecked, these progressive losses will start to impair physical function.
Once a certain level of impairment occurs, an individual can be diagnosed with sarcopenia, which comes from the Greek words “sarco” (flesh) and “penia” (poverty).
Muscle mass losses generally occur with weight loss, and the increasing use of glucagon-like peptide 1 (GLP-1) medications may lead to greater incidence and prevalence of sarcopenia in the years to come.
A recent meta-analysis of 56 studies (mean participant age, 50 years) found a twofold greater risk for mortality in those with sarcopenia vs those without. Despite its health consequences, sarcopenia tends to be underdiagnosed and, consequently, undertreated at a population and individual level. Part of the reason probably stems from the lack of health insurance reimbursement for individual clinicians and hospital systems to perform sarcopenia screening assessments.
In aging and obesity, it appears justified to include and emphasize a recommendation for sarcopenia screening in medical society guidelines; however, individual patients and clinicians do not need to wait for updated guidelines to implement sarcopenia screening, treatment, and prevention strategies in their own lives and/or clinical practice.
Simple Prevention and Treatment Strategy
Much can be done to help prevent sarcopenia. The primary strategy, unsurprisingly, is engaging in frequent strength training. But that doesn’t mean hours in the gym every week.
With just one session per week over 10 weeks, lean body mass (LBM), a common proxy for muscle mass, increased by 0.33 kg, according to a study which evaluated LBM improvements across different strength training frequencies. Adding a second weekly session was significantly better. In the twice-weekly group, LBM increased by 1.4 kg over 10 weeks, resulting in an increase in LBM more than four times greater than the once-a-week group. (There was no greater improvement in LBM by adding a third weekly session vs two weekly sessions.)
Although that particular study didn’t identify greater benefit at three times a week, compared with twice a week, the specific training routines and lack of a protein consumption assessment may have played a role in that finding.
Underlying the diminishing benefits, a different study found a marginally greater benefit in favor of performing ≥ five sets per major muscle group per week, compared with < five sets per week for increasing muscle in the legs, arms, back, chest, and shoulders.
Expensive gym memberships and fancy equipment are not necessary. While the use of strength training machines and free weights have been viewed by many as the optimal approach, a recent systematic review and meta-analysis found that comparable improvements to strength can be achieved with workouts using resistance bands. For those who struggle to find the time to go to a gym, or for whom gym fees are not financially affordable, resistance bands are a cheaper and more convenient alternative.
Lucas, Assistant Professor of Clinical Medicine, Comprehensive Weight Control Center, Weill Cornell Medicine, New York City, disclosed ties with Measured (Better Health Labs).
A version of this article appeared on Medscape.com.
Losses of muscle and strength are inescapable effects of the aging process. Left unchecked, these progressive losses will start to impair physical function.
Once a certain level of impairment occurs, an individual can be diagnosed with sarcopenia, which comes from the Greek words “sarco” (flesh) and “penia” (poverty).
Muscle mass losses generally occur with weight loss, and the increasing use of glucagon-like peptide 1 (GLP-1) medications may lead to greater incidence and prevalence of sarcopenia in the years to come.
A recent meta-analysis of 56 studies (mean participant age, 50 years) found a twofold greater risk for mortality in those with sarcopenia vs those without. Despite its health consequences, sarcopenia tends to be underdiagnosed and, consequently, undertreated at a population and individual level. Part of the reason probably stems from the lack of health insurance reimbursement for individual clinicians and hospital systems to perform sarcopenia screening assessments.
In aging and obesity, it appears justified to include and emphasize a recommendation for sarcopenia screening in medical society guidelines; however, individual patients and clinicians do not need to wait for updated guidelines to implement sarcopenia screening, treatment, and prevention strategies in their own lives and/or clinical practice.
Simple Prevention and Treatment Strategy
Much can be done to help prevent sarcopenia. The primary strategy, unsurprisingly, is engaging in frequent strength training. But that doesn’t mean hours in the gym every week.
With just one session per week over 10 weeks, lean body mass (LBM), a common proxy for muscle mass, increased by 0.33 kg, according to a study which evaluated LBM improvements across different strength training frequencies. Adding a second weekly session was significantly better. In the twice-weekly group, LBM increased by 1.4 kg over 10 weeks, resulting in an increase in LBM more than four times greater than the once-a-week group. (There was no greater improvement in LBM by adding a third weekly session vs two weekly sessions.)
Although that particular study didn’t identify greater benefit at three times a week, compared with twice a week, the specific training routines and lack of a protein consumption assessment may have played a role in that finding.
Underlying the diminishing benefits, a different study found a marginally greater benefit in favor of performing ≥ five sets per major muscle group per week, compared with < five sets per week for increasing muscle in the legs, arms, back, chest, and shoulders.
Expensive gym memberships and fancy equipment are not necessary. While the use of strength training machines and free weights have been viewed by many as the optimal approach, a recent systematic review and meta-analysis found that comparable improvements to strength can be achieved with workouts using resistance bands. For those who struggle to find the time to go to a gym, or for whom gym fees are not financially affordable, resistance bands are a cheaper and more convenient alternative.
Lucas, Assistant Professor of Clinical Medicine, Comprehensive Weight Control Center, Weill Cornell Medicine, New York City, disclosed ties with Measured (Better Health Labs).
A version of this article appeared on Medscape.com.
Losses of muscle and strength are inescapable effects of the aging process. Left unchecked, these progressive losses will start to impair physical function.
Once a certain level of impairment occurs, an individual can be diagnosed with sarcopenia, which comes from the Greek words “sarco” (flesh) and “penia” (poverty).
Muscle mass losses generally occur with weight loss, and the increasing use of glucagon-like peptide 1 (GLP-1) medications may lead to greater incidence and prevalence of sarcopenia in the years to come.
A recent meta-analysis of 56 studies (mean participant age, 50 years) found a twofold greater risk for mortality in those with sarcopenia vs those without. Despite its health consequences, sarcopenia tends to be underdiagnosed and, consequently, undertreated at a population and individual level. Part of the reason probably stems from the lack of health insurance reimbursement for individual clinicians and hospital systems to perform sarcopenia screening assessments.
In aging and obesity, it appears justified to include and emphasize a recommendation for sarcopenia screening in medical society guidelines; however, individual patients and clinicians do not need to wait for updated guidelines to implement sarcopenia screening, treatment, and prevention strategies in their own lives and/or clinical practice.
Simple Prevention and Treatment Strategy
Much can be done to help prevent sarcopenia. The primary strategy, unsurprisingly, is engaging in frequent strength training. But that doesn’t mean hours in the gym every week.
With just one session per week over 10 weeks, lean body mass (LBM), a common proxy for muscle mass, increased by 0.33 kg, according to a study which evaluated LBM improvements across different strength training frequencies. Adding a second weekly session was significantly better. In the twice-weekly group, LBM increased by 1.4 kg over 10 weeks, resulting in an increase in LBM more than four times greater than the once-a-week group. (There was no greater improvement in LBM by adding a third weekly session vs two weekly sessions.)
Although that particular study didn’t identify greater benefit at three times a week, compared with twice a week, the specific training routines and lack of a protein consumption assessment may have played a role in that finding.
Underlying the diminishing benefits, a different study found a marginally greater benefit in favor of performing ≥ five sets per major muscle group per week, compared with < five sets per week for increasing muscle in the legs, arms, back, chest, and shoulders.
Expensive gym memberships and fancy equipment are not necessary. While the use of strength training machines and free weights have been viewed by many as the optimal approach, a recent systematic review and meta-analysis found that comparable improvements to strength can be achieved with workouts using resistance bands. For those who struggle to find the time to go to a gym, or for whom gym fees are not financially affordable, resistance bands are a cheaper and more convenient alternative.
Lucas, Assistant Professor of Clinical Medicine, Comprehensive Weight Control Center, Weill Cornell Medicine, New York City, disclosed ties with Measured (Better Health Labs).
A version of this article appeared on Medscape.com.
Fear of Cancer Recurrence Can Persist for Childhood Survivors
TOPLINE:
About one third of adult survivors of childhood cancer experience a clinically significant or high fear that their primary cancer may recur or that they will develop a subsequent malignancy, according to a recent analysis. The study finds that several factors are associated with a higher risk of experiencing a clinically significant fear of recurrence, including being unemployed or having elevated anxiety or depression.
METHODOLOGY:
- Adult survivors of childhood cancer face a high risk of developing subsequent malignant neoplasms — about a sixfold greater risk than in the general population — and studies indicate that these cancer survivors also fear their cancer will recur. However, data on the prevalence of and risk factors associated with clinically significant fear of recurrence in this population remain limited.
- This cross-sectional study included 229 adult survivors of childhood cancer (mean age at study completion, 39.6 years), recruited from the Childhood Cancer Survivor Study, who completed online surveys between October 2018 and April 2019.
- Fear of cancer recurrence was assessed using the 9-item Fear of Cancer Recurrence Inventory–Short Form, which defines recurrence as the possibility that cancer might return to the same or a different part of the body.
- Chronic pain, symptoms of depression and anxiety, self-perceived health, and intolerance of uncertainty were also evaluated.
- Among the participants, 21 experienced a recurrence of their primary cancer and 17 were diagnosed with a subsequent malignant neoplasm.
TAKEAWAY:
- Overall, 38 (16.6%) adult survivors of childhood cancer reported clinically significant fear that their cancer would recur, and an additional 36 (15.7%) survivors experienced high levels of fear; the remaining 67.7% of participants reported minimal levels of fear.
- Survivors who were unemployed (prevalence ratio [PR], 2.5) were more likely to experience a clinically significant fear of recurrence, as were survivors who had undergone pelvic radiation (PR, 2.9) or limb-sparing or amputation surgery (PR, 2.4).
- Survivors who had elevated anxiety or depression (PR, 2.6) or both (PR, 3.2) were more likely to experience a clinically significant fear of recurrence, as were survivors who had a chronic neurologic health condition (PR, 3.3) or who perceived their health status to be poor or fair vs good to excellent (PR, 3.0).
- Among 94 participants with chronic pain, 25.5% reported clinically significant fear and 13.8% reported high levels of fear. But chronic pain (PR, 1.2; 95% CI, 0.6-2.4) was not significantly associated with a clinically significant fear of recurrence in a multivariable model.
IN PRACTICE:
“These findings underscore the substantial psychological and functional burden of FCR [fear of cancer recurrence] and suggest healthcare professionals should routinely assess FCR as a part of providing comprehensive care to long-term survivors,” the authors wrote.
SOURCE:
The study, led by Alex Pizzo, MSc, Concordia University, Montréal, Québec, Canada, was published online in JAMA Network Open.
LIMITATIONS:
The cross-sectional design limited causal inference. Self-perceived health was assessed with a single item, limiting its measurement. Internet and smartphone access eligibility could have introduced bias. The study also lacked racial and ethnic diversity.
DISCLOSURES:
The study was supported by the Childhood Cancer Survivor Study Career Development Award and a grant from the National Cancer Institute. Additional funding was provided by the Canada Research Chairs Program. Three authors reported receiving grants from various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
About one third of adult survivors of childhood cancer experience a clinically significant or high fear that their primary cancer may recur or that they will develop a subsequent malignancy, according to a recent analysis. The study finds that several factors are associated with a higher risk of experiencing a clinically significant fear of recurrence, including being unemployed or having elevated anxiety or depression.
METHODOLOGY:
- Adult survivors of childhood cancer face a high risk of developing subsequent malignant neoplasms — about a sixfold greater risk than in the general population — and studies indicate that these cancer survivors also fear their cancer will recur. However, data on the prevalence of and risk factors associated with clinically significant fear of recurrence in this population remain limited.
- This cross-sectional study included 229 adult survivors of childhood cancer (mean age at study completion, 39.6 years), recruited from the Childhood Cancer Survivor Study, who completed online surveys between October 2018 and April 2019.
- Fear of cancer recurrence was assessed using the 9-item Fear of Cancer Recurrence Inventory–Short Form, which defines recurrence as the possibility that cancer might return to the same or a different part of the body.
- Chronic pain, symptoms of depression and anxiety, self-perceived health, and intolerance of uncertainty were also evaluated.
- Among the participants, 21 experienced a recurrence of their primary cancer and 17 were diagnosed with a subsequent malignant neoplasm.
TAKEAWAY:
- Overall, 38 (16.6%) adult survivors of childhood cancer reported clinically significant fear that their cancer would recur, and an additional 36 (15.7%) survivors experienced high levels of fear; the remaining 67.7% of participants reported minimal levels of fear.
- Survivors who were unemployed (prevalence ratio [PR], 2.5) were more likely to experience a clinically significant fear of recurrence, as were survivors who had undergone pelvic radiation (PR, 2.9) or limb-sparing or amputation surgery (PR, 2.4).
- Survivors who had elevated anxiety or depression (PR, 2.6) or both (PR, 3.2) were more likely to experience a clinically significant fear of recurrence, as were survivors who had a chronic neurologic health condition (PR, 3.3) or who perceived their health status to be poor or fair vs good to excellent (PR, 3.0).
- Among 94 participants with chronic pain, 25.5% reported clinically significant fear and 13.8% reported high levels of fear. But chronic pain (PR, 1.2; 95% CI, 0.6-2.4) was not significantly associated with a clinically significant fear of recurrence in a multivariable model.
IN PRACTICE:
“These findings underscore the substantial psychological and functional burden of FCR [fear of cancer recurrence] and suggest healthcare professionals should routinely assess FCR as a part of providing comprehensive care to long-term survivors,” the authors wrote.
SOURCE:
The study, led by Alex Pizzo, MSc, Concordia University, Montréal, Québec, Canada, was published online in JAMA Network Open.
LIMITATIONS:
The cross-sectional design limited causal inference. Self-perceived health was assessed with a single item, limiting its measurement. Internet and smartphone access eligibility could have introduced bias. The study also lacked racial and ethnic diversity.
DISCLOSURES:
The study was supported by the Childhood Cancer Survivor Study Career Development Award and a grant from the National Cancer Institute. Additional funding was provided by the Canada Research Chairs Program. Three authors reported receiving grants from various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
About one third of adult survivors of childhood cancer experience a clinically significant or high fear that their primary cancer may recur or that they will develop a subsequent malignancy, according to a recent analysis. The study finds that several factors are associated with a higher risk of experiencing a clinically significant fear of recurrence, including being unemployed or having elevated anxiety or depression.
METHODOLOGY:
- Adult survivors of childhood cancer face a high risk of developing subsequent malignant neoplasms — about a sixfold greater risk than in the general population — and studies indicate that these cancer survivors also fear their cancer will recur. However, data on the prevalence of and risk factors associated with clinically significant fear of recurrence in this population remain limited.
- This cross-sectional study included 229 adult survivors of childhood cancer (mean age at study completion, 39.6 years), recruited from the Childhood Cancer Survivor Study, who completed online surveys between October 2018 and April 2019.
- Fear of cancer recurrence was assessed using the 9-item Fear of Cancer Recurrence Inventory–Short Form, which defines recurrence as the possibility that cancer might return to the same or a different part of the body.
- Chronic pain, symptoms of depression and anxiety, self-perceived health, and intolerance of uncertainty were also evaluated.
- Among the participants, 21 experienced a recurrence of their primary cancer and 17 were diagnosed with a subsequent malignant neoplasm.
TAKEAWAY:
- Overall, 38 (16.6%) adult survivors of childhood cancer reported clinically significant fear that their cancer would recur, and an additional 36 (15.7%) survivors experienced high levels of fear; the remaining 67.7% of participants reported minimal levels of fear.
- Survivors who were unemployed (prevalence ratio [PR], 2.5) were more likely to experience a clinically significant fear of recurrence, as were survivors who had undergone pelvic radiation (PR, 2.9) or limb-sparing or amputation surgery (PR, 2.4).
- Survivors who had elevated anxiety or depression (PR, 2.6) or both (PR, 3.2) were more likely to experience a clinically significant fear of recurrence, as were survivors who had a chronic neurologic health condition (PR, 3.3) or who perceived their health status to be poor or fair vs good to excellent (PR, 3.0).
- Among 94 participants with chronic pain, 25.5% reported clinically significant fear and 13.8% reported high levels of fear. But chronic pain (PR, 1.2; 95% CI, 0.6-2.4) was not significantly associated with a clinically significant fear of recurrence in a multivariable model.
IN PRACTICE:
“These findings underscore the substantial psychological and functional burden of FCR [fear of cancer recurrence] and suggest healthcare professionals should routinely assess FCR as a part of providing comprehensive care to long-term survivors,” the authors wrote.
SOURCE:
The study, led by Alex Pizzo, MSc, Concordia University, Montréal, Québec, Canada, was published online in JAMA Network Open.
LIMITATIONS:
The cross-sectional design limited causal inference. Self-perceived health was assessed with a single item, limiting its measurement. Internet and smartphone access eligibility could have introduced bias. The study also lacked racial and ethnic diversity.
DISCLOSURES:
The study was supported by the Childhood Cancer Survivor Study Career Development Award and a grant from the National Cancer Institute. Additional funding was provided by the Canada Research Chairs Program. Three authors reported receiving grants from various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
PCPs Play a Key Role in Managing and Preventing the Atopic March in Children
Primary care physicians (PCPs) play a key role in treating young patients as they progress through the “atopic march” from atopic dermatitis through food allergy, asthma, and allergic rhinitis. They can also help prevent the process from starting.
“The PCP is usually the first clinician a family with concerns about atopic conditions sees, unless they first visit urgent care or an emergency department after an allergic reaction to food. Either way, families rely on their PCP for ongoing guidance,” said Terri F. Brown-Whitehorn, MD, attending physician in the Division of Allergy and Immunology at the Center for Pediatric Eosinophilic Disorders and the Integrative Health Program at Children’s Hospital of Philadelphia.
“The most important thing PCPs can do is know that the atopic march exists, how it progresses over time, and what signs and symptoms to look for,” she told this news organization.
The Atopic March
The atopic march describes the progression of allergic diseases in a child over time, with atopic dermatitis and food allergy in infancy tending to be followed by allergic rhinitis and asthma into later childhood and adulthood.
Although the pathophysiology of the inflammation that precedes atopic dermatitis is unclear, two main hypotheses have been proposed. The first suggests a primary immune dysfunction leads to immunoglobulin E (IgE) sensitization, allergic inflammation, and a secondary disturbance of the epithelial barrier; the second starts with a primary defect in the epithelial barrier that leads to secondary immunologic dysregulation and results in inflammation.
Genetics, infection, hygiene, extreme climate, food allergens, probiotics, aeroallergens, and tobacco smoke are thought to play roles in atopic dermatitis. An estimated 10%-12% of children and 1% of adults in the United States have been reported to have the condition, and the prevalence appears to be increasing. An estimated 85% of cases occur during the first year of life and 95% before the age of 5 years.
“Atopy often, though not always, runs in families, so PCPs should inquire about the history of atopic dermatitis, IgE-mediated food allergies, allergic rhinitis, and asthma in the patient’s siblings, parents, and grandparents,” Brown-Whitehorn said.
Key Educators
PCPs treat the full gamut of atopic conditions and are key educators on ways families can help mitigate their children’s atopic march or stop it before it begins, said Gerald Bell Lee, MD, an allergist and immunologist at Children’s Healthcare of Atlanta and an associate professor in the Division of Allergy and Immunology at Emory University School of Medicine, Atlanta.
“Most parents who bring their infants with eczema to the PCP assume their child ate something that caused their rash. But the relationship between atopic dermatitis, a type of eczema, and food allergy is more complicated,” he added.
Lee said PCPs should explain to their patients what atopic dermatitis is, how it starts and progresses, and how families can help prevent the condition by, for example, introducing allergenic foods to infants at around 4-6 months of age.
Atopic Dermatitis
PCPs should inform parents and other caregivers to wash their hands before moisturizing their child, take care not to contaminate the moisturizer, and bathe their child only when the child is dirty.
“Soap removes protective natural skin oils and increases moisture loss, and exposure to soap and bathing is a main contributor to eczema,” said Lee. “Dry skin loses its protective barrier, allowing outside agents to penetrate and be identified by the immune system.”
“According to one hypothesis, parents may eat food, not wash their hands afterwards, then moisturize their baby. This unhygienic practice spreads food proteins from the adult’s meal, and possibly from contaminants present in the moisturizer, all over the baby’s body,” he added.
Lee said he and his colleagues discourage overbathing babies to minimize the risk for skin injury that begins the atopic march: “New parents are inundated with infant skincare messaging and products. But we need to weigh societal pressures against practicality and ask, ‘Is the child’s skin actually dirty?’ ”
Atopic dermatitis tends to appear on the extensor surfaces, face, and scalp in infants and around arm and leg creases in toddlers and older children. Severe forms of the condition can be more widely distributed on the body, said Aarti P. Pandya, MD, medical director of the Food Allergy Center at Children’s Mercy Kansas City and clinical assistant professor of pediatrics at the University of Missouri-Kansas City School of Medicine, Kansas City, Missouri.
Avoid Triggers, Minimize Flares
Triggers of eczema are varied and common. To help minimize flares, PCPs can encourage caregivers to avoid products with fragrances or dyes, minimize the use of soaps, and completely rinse laundry detergent from clothing and household items. “Advise them to keep fingernails short and control dander, pollen, mold, household chemicals, and tobacco smoke, as well as the child’s stress and anxiety, which can also be a trigger,” Lee said.
“Skin infections from organisms such as staph, herpes, or coxsackie can also exacerbate symptoms,” Brown-Whitehorn added. “PCPs can educate caregivers to avoid all known triggers and give them an ‘action plan’ to carry out when skin flares.”
Food Allergies
Parents may be unaware food allergens can travel far beyond the plate, Lee said. Researchers vacuuming household bedding, carpets, furniture, and other surfaces have detected unnoticeably tiny quantities of allergenic food proteins in ordinary house dust. Touching this dust appears to provide the main exposure to those allergens.
“According to the dual exposure to allergen hypothesis, an infant’s tolerance to antigens occurs through high-dose exposure by mouth, and allergic sensitization occurs through low-dose exposure through the skin,” he said. “As young as four to six months of age, even before eating solid food, a child develops eczema, has a leaky skin barrier, comes in contact with food, and develops a food allergy.”
IgE-mediated food allergies can begin at any age. “Symptoms occur when a food is ingested and the patient develops symptoms including but not limited to urticaria, angioedema, pruritus, flushing, vomiting, diarrhea, coughing, wheezing, difficulty breathing, presyncope, or syncope,” Pandya noted.
In the case of eosinophilic esophagitis, which may also be part of the atopic march, infants and toddlers often have challenging-to-treat symptoms of reflux, while school-age children have reflux and abdominal pain, and adolescents and adults may experience difficulty swallowing and impactions of food or pills, Brown-Whitehorn said.
To differentiate between food allergy and contact dermatitis, Lee suggested providers ask, “ ’Is the rash hives? If yes, is the rash generalized or in a limited area?’ Then consider the statistical probabilities. Skin problems after milk, egg, wheat, soy, peanut, tree nut, fish, shellfish, or sesame are likely due to IgE-mediated food allergy, but after ketchup or strawberry are probably from skin contact.”
Allergic Rhinitis and Asthma
“For asthma, ask about frequency of night cough and symptoms with exercise, laughing, or crying. For allergic rhinitis, look for runny nose, itchy eyes, or sneezing,” Brown-Whitehorn said.
Testing and Monitoring
Assessing the extent of eczema with the Eczema Area and Severity Index or the SCORing Atopic Dermatitis index takes time but may be necessary to obtain insurance coverage for treatments such as biologics.
Avoid ordering IgE food panels, which can result in false positives that can lead to loss of tolerance and nutritional deficiencies; psychological harm from bullying, anxiety, and decreased quality of life; and higher food and healthcare costs, Pandya said.
Treatments
Caregivers may be wary about treatments, and all the three experts this news organization spoke with stressed the importance of educating caregivers about how treatments work and what to expect from them.
“Early and aggressive atopic dermatitis treatment could prevent sensitization to food or aeroallergens, which could help prevent additional atopic diseases, including those on the atopic march,” Pandya said. “Topical steroids are considered first line at any age. Topical phosphodiesterase inhibitors are approved at 3 months of age and above. Topical calcineurin inhibitors are approved at 2 years of age and above. Wet wrap therapy and bleach baths can be effective. Other options include biologic therapy, allergen immunotherapy, and UV therapy.”
“Epinephrine auto-injectors can counteract food reactions. For allergic rhinitis, non-sedating antihistamines, steroidal nasal sprays, and nasal antihistamines help. Asthma treatments include various inhaled medications,” Brown-Whitehorn added.
When to Refer to Specialists
Involving an allergist, dermatologist, pulmonologist, or ear nose throat specialist to the patient’s care team is advisable in more challenging cases.
If a child is younger than 3 months and has moderate to severe atopic dermatitis, an underlying immune defect may be to blame, so an allergy and immunology assessment is warranted, Brown-Whitehorn said. “An allergist can help any child who has recurrent coughing or wheezing avoid the emergency room or hospitalization.”
“In pediatrics, we always try to find the medication, regimen, and avoidance strategies that use the least treatment to provide the best care for each patient,” Brown-Whitehorn added. “Children eat, play, learn, and sleep, and every stage of the atopic march affects each of these activities. As clinicians, we need to be sure that we are helping children make the best of all these activities.”
Brown-Whitehorn reported financial relationships with DBV Technologies and Regeneron Pharmaceuticals. Lee reported financial relationships with Novartis. Pandya reported financial relationships with DBV Technologies, Thermo Fisher Scientific, and Sanofi.
A version of this article first appeared on Medscape.com.
Primary care physicians (PCPs) play a key role in treating young patients as they progress through the “atopic march” from atopic dermatitis through food allergy, asthma, and allergic rhinitis. They can also help prevent the process from starting.
“The PCP is usually the first clinician a family with concerns about atopic conditions sees, unless they first visit urgent care or an emergency department after an allergic reaction to food. Either way, families rely on their PCP for ongoing guidance,” said Terri F. Brown-Whitehorn, MD, attending physician in the Division of Allergy and Immunology at the Center for Pediatric Eosinophilic Disorders and the Integrative Health Program at Children’s Hospital of Philadelphia.
“The most important thing PCPs can do is know that the atopic march exists, how it progresses over time, and what signs and symptoms to look for,” she told this news organization.
The Atopic March
The atopic march describes the progression of allergic diseases in a child over time, with atopic dermatitis and food allergy in infancy tending to be followed by allergic rhinitis and asthma into later childhood and adulthood.
Although the pathophysiology of the inflammation that precedes atopic dermatitis is unclear, two main hypotheses have been proposed. The first suggests a primary immune dysfunction leads to immunoglobulin E (IgE) sensitization, allergic inflammation, and a secondary disturbance of the epithelial barrier; the second starts with a primary defect in the epithelial barrier that leads to secondary immunologic dysregulation and results in inflammation.
Genetics, infection, hygiene, extreme climate, food allergens, probiotics, aeroallergens, and tobacco smoke are thought to play roles in atopic dermatitis. An estimated 10%-12% of children and 1% of adults in the United States have been reported to have the condition, and the prevalence appears to be increasing. An estimated 85% of cases occur during the first year of life and 95% before the age of 5 years.
“Atopy often, though not always, runs in families, so PCPs should inquire about the history of atopic dermatitis, IgE-mediated food allergies, allergic rhinitis, and asthma in the patient’s siblings, parents, and grandparents,” Brown-Whitehorn said.
Key Educators
PCPs treat the full gamut of atopic conditions and are key educators on ways families can help mitigate their children’s atopic march or stop it before it begins, said Gerald Bell Lee, MD, an allergist and immunologist at Children’s Healthcare of Atlanta and an associate professor in the Division of Allergy and Immunology at Emory University School of Medicine, Atlanta.
“Most parents who bring their infants with eczema to the PCP assume their child ate something that caused their rash. But the relationship between atopic dermatitis, a type of eczema, and food allergy is more complicated,” he added.
Lee said PCPs should explain to their patients what atopic dermatitis is, how it starts and progresses, and how families can help prevent the condition by, for example, introducing allergenic foods to infants at around 4-6 months of age.
Atopic Dermatitis
PCPs should inform parents and other caregivers to wash their hands before moisturizing their child, take care not to contaminate the moisturizer, and bathe their child only when the child is dirty.
“Soap removes protective natural skin oils and increases moisture loss, and exposure to soap and bathing is a main contributor to eczema,” said Lee. “Dry skin loses its protective barrier, allowing outside agents to penetrate and be identified by the immune system.”
“According to one hypothesis, parents may eat food, not wash their hands afterwards, then moisturize their baby. This unhygienic practice spreads food proteins from the adult’s meal, and possibly from contaminants present in the moisturizer, all over the baby’s body,” he added.
Lee said he and his colleagues discourage overbathing babies to minimize the risk for skin injury that begins the atopic march: “New parents are inundated with infant skincare messaging and products. But we need to weigh societal pressures against practicality and ask, ‘Is the child’s skin actually dirty?’ ”
Atopic dermatitis tends to appear on the extensor surfaces, face, and scalp in infants and around arm and leg creases in toddlers and older children. Severe forms of the condition can be more widely distributed on the body, said Aarti P. Pandya, MD, medical director of the Food Allergy Center at Children’s Mercy Kansas City and clinical assistant professor of pediatrics at the University of Missouri-Kansas City School of Medicine, Kansas City, Missouri.
Avoid Triggers, Minimize Flares
Triggers of eczema are varied and common. To help minimize flares, PCPs can encourage caregivers to avoid products with fragrances or dyes, minimize the use of soaps, and completely rinse laundry detergent from clothing and household items. “Advise them to keep fingernails short and control dander, pollen, mold, household chemicals, and tobacco smoke, as well as the child’s stress and anxiety, which can also be a trigger,” Lee said.
“Skin infections from organisms such as staph, herpes, or coxsackie can also exacerbate symptoms,” Brown-Whitehorn added. “PCPs can educate caregivers to avoid all known triggers and give them an ‘action plan’ to carry out when skin flares.”
Food Allergies
Parents may be unaware food allergens can travel far beyond the plate, Lee said. Researchers vacuuming household bedding, carpets, furniture, and other surfaces have detected unnoticeably tiny quantities of allergenic food proteins in ordinary house dust. Touching this dust appears to provide the main exposure to those allergens.
“According to the dual exposure to allergen hypothesis, an infant’s tolerance to antigens occurs through high-dose exposure by mouth, and allergic sensitization occurs through low-dose exposure through the skin,” he said. “As young as four to six months of age, even before eating solid food, a child develops eczema, has a leaky skin barrier, comes in contact with food, and develops a food allergy.”
IgE-mediated food allergies can begin at any age. “Symptoms occur when a food is ingested and the patient develops symptoms including but not limited to urticaria, angioedema, pruritus, flushing, vomiting, diarrhea, coughing, wheezing, difficulty breathing, presyncope, or syncope,” Pandya noted.
In the case of eosinophilic esophagitis, which may also be part of the atopic march, infants and toddlers often have challenging-to-treat symptoms of reflux, while school-age children have reflux and abdominal pain, and adolescents and adults may experience difficulty swallowing and impactions of food or pills, Brown-Whitehorn said.
To differentiate between food allergy and contact dermatitis, Lee suggested providers ask, “ ’Is the rash hives? If yes, is the rash generalized or in a limited area?’ Then consider the statistical probabilities. Skin problems after milk, egg, wheat, soy, peanut, tree nut, fish, shellfish, or sesame are likely due to IgE-mediated food allergy, but after ketchup or strawberry are probably from skin contact.”
Allergic Rhinitis and Asthma
“For asthma, ask about frequency of night cough and symptoms with exercise, laughing, or crying. For allergic rhinitis, look for runny nose, itchy eyes, or sneezing,” Brown-Whitehorn said.
Testing and Monitoring
Assessing the extent of eczema with the Eczema Area and Severity Index or the SCORing Atopic Dermatitis index takes time but may be necessary to obtain insurance coverage for treatments such as biologics.
Avoid ordering IgE food panels, which can result in false positives that can lead to loss of tolerance and nutritional deficiencies; psychological harm from bullying, anxiety, and decreased quality of life; and higher food and healthcare costs, Pandya said.
Treatments
Caregivers may be wary about treatments, and all the three experts this news organization spoke with stressed the importance of educating caregivers about how treatments work and what to expect from them.
“Early and aggressive atopic dermatitis treatment could prevent sensitization to food or aeroallergens, which could help prevent additional atopic diseases, including those on the atopic march,” Pandya said. “Topical steroids are considered first line at any age. Topical phosphodiesterase inhibitors are approved at 3 months of age and above. Topical calcineurin inhibitors are approved at 2 years of age and above. Wet wrap therapy and bleach baths can be effective. Other options include biologic therapy, allergen immunotherapy, and UV therapy.”
“Epinephrine auto-injectors can counteract food reactions. For allergic rhinitis, non-sedating antihistamines, steroidal nasal sprays, and nasal antihistamines help. Asthma treatments include various inhaled medications,” Brown-Whitehorn added.
When to Refer to Specialists
Involving an allergist, dermatologist, pulmonologist, or ear nose throat specialist to the patient’s care team is advisable in more challenging cases.
If a child is younger than 3 months and has moderate to severe atopic dermatitis, an underlying immune defect may be to blame, so an allergy and immunology assessment is warranted, Brown-Whitehorn said. “An allergist can help any child who has recurrent coughing or wheezing avoid the emergency room or hospitalization.”
“In pediatrics, we always try to find the medication, regimen, and avoidance strategies that use the least treatment to provide the best care for each patient,” Brown-Whitehorn added. “Children eat, play, learn, and sleep, and every stage of the atopic march affects each of these activities. As clinicians, we need to be sure that we are helping children make the best of all these activities.”
Brown-Whitehorn reported financial relationships with DBV Technologies and Regeneron Pharmaceuticals. Lee reported financial relationships with Novartis. Pandya reported financial relationships with DBV Technologies, Thermo Fisher Scientific, and Sanofi.
A version of this article first appeared on Medscape.com.
Primary care physicians (PCPs) play a key role in treating young patients as they progress through the “atopic march” from atopic dermatitis through food allergy, asthma, and allergic rhinitis. They can also help prevent the process from starting.
“The PCP is usually the first clinician a family with concerns about atopic conditions sees, unless they first visit urgent care or an emergency department after an allergic reaction to food. Either way, families rely on their PCP for ongoing guidance,” said Terri F. Brown-Whitehorn, MD, attending physician in the Division of Allergy and Immunology at the Center for Pediatric Eosinophilic Disorders and the Integrative Health Program at Children’s Hospital of Philadelphia.
“The most important thing PCPs can do is know that the atopic march exists, how it progresses over time, and what signs and symptoms to look for,” she told this news organization.
The Atopic March
The atopic march describes the progression of allergic diseases in a child over time, with atopic dermatitis and food allergy in infancy tending to be followed by allergic rhinitis and asthma into later childhood and adulthood.
Although the pathophysiology of the inflammation that precedes atopic dermatitis is unclear, two main hypotheses have been proposed. The first suggests a primary immune dysfunction leads to immunoglobulin E (IgE) sensitization, allergic inflammation, and a secondary disturbance of the epithelial barrier; the second starts with a primary defect in the epithelial barrier that leads to secondary immunologic dysregulation and results in inflammation.
Genetics, infection, hygiene, extreme climate, food allergens, probiotics, aeroallergens, and tobacco smoke are thought to play roles in atopic dermatitis. An estimated 10%-12% of children and 1% of adults in the United States have been reported to have the condition, and the prevalence appears to be increasing. An estimated 85% of cases occur during the first year of life and 95% before the age of 5 years.
“Atopy often, though not always, runs in families, so PCPs should inquire about the history of atopic dermatitis, IgE-mediated food allergies, allergic rhinitis, and asthma in the patient’s siblings, parents, and grandparents,” Brown-Whitehorn said.
Key Educators
PCPs treat the full gamut of atopic conditions and are key educators on ways families can help mitigate their children’s atopic march or stop it before it begins, said Gerald Bell Lee, MD, an allergist and immunologist at Children’s Healthcare of Atlanta and an associate professor in the Division of Allergy and Immunology at Emory University School of Medicine, Atlanta.
“Most parents who bring their infants with eczema to the PCP assume their child ate something that caused their rash. But the relationship between atopic dermatitis, a type of eczema, and food allergy is more complicated,” he added.
Lee said PCPs should explain to their patients what atopic dermatitis is, how it starts and progresses, and how families can help prevent the condition by, for example, introducing allergenic foods to infants at around 4-6 months of age.
Atopic Dermatitis
PCPs should inform parents and other caregivers to wash their hands before moisturizing their child, take care not to contaminate the moisturizer, and bathe their child only when the child is dirty.
“Soap removes protective natural skin oils and increases moisture loss, and exposure to soap and bathing is a main contributor to eczema,” said Lee. “Dry skin loses its protective barrier, allowing outside agents to penetrate and be identified by the immune system.”
“According to one hypothesis, parents may eat food, not wash their hands afterwards, then moisturize their baby. This unhygienic practice spreads food proteins from the adult’s meal, and possibly from contaminants present in the moisturizer, all over the baby’s body,” he added.
Lee said he and his colleagues discourage overbathing babies to minimize the risk for skin injury that begins the atopic march: “New parents are inundated with infant skincare messaging and products. But we need to weigh societal pressures against practicality and ask, ‘Is the child’s skin actually dirty?’ ”
Atopic dermatitis tends to appear on the extensor surfaces, face, and scalp in infants and around arm and leg creases in toddlers and older children. Severe forms of the condition can be more widely distributed on the body, said Aarti P. Pandya, MD, medical director of the Food Allergy Center at Children’s Mercy Kansas City and clinical assistant professor of pediatrics at the University of Missouri-Kansas City School of Medicine, Kansas City, Missouri.
Avoid Triggers, Minimize Flares
Triggers of eczema are varied and common. To help minimize flares, PCPs can encourage caregivers to avoid products with fragrances or dyes, minimize the use of soaps, and completely rinse laundry detergent from clothing and household items. “Advise them to keep fingernails short and control dander, pollen, mold, household chemicals, and tobacco smoke, as well as the child’s stress and anxiety, which can also be a trigger,” Lee said.
“Skin infections from organisms such as staph, herpes, or coxsackie can also exacerbate symptoms,” Brown-Whitehorn added. “PCPs can educate caregivers to avoid all known triggers and give them an ‘action plan’ to carry out when skin flares.”
Food Allergies
Parents may be unaware food allergens can travel far beyond the plate, Lee said. Researchers vacuuming household bedding, carpets, furniture, and other surfaces have detected unnoticeably tiny quantities of allergenic food proteins in ordinary house dust. Touching this dust appears to provide the main exposure to those allergens.
“According to the dual exposure to allergen hypothesis, an infant’s tolerance to antigens occurs through high-dose exposure by mouth, and allergic sensitization occurs through low-dose exposure through the skin,” he said. “As young as four to six months of age, even before eating solid food, a child develops eczema, has a leaky skin barrier, comes in contact with food, and develops a food allergy.”
IgE-mediated food allergies can begin at any age. “Symptoms occur when a food is ingested and the patient develops symptoms including but not limited to urticaria, angioedema, pruritus, flushing, vomiting, diarrhea, coughing, wheezing, difficulty breathing, presyncope, or syncope,” Pandya noted.
In the case of eosinophilic esophagitis, which may also be part of the atopic march, infants and toddlers often have challenging-to-treat symptoms of reflux, while school-age children have reflux and abdominal pain, and adolescents and adults may experience difficulty swallowing and impactions of food or pills, Brown-Whitehorn said.
To differentiate between food allergy and contact dermatitis, Lee suggested providers ask, “ ’Is the rash hives? If yes, is the rash generalized or in a limited area?’ Then consider the statistical probabilities. Skin problems after milk, egg, wheat, soy, peanut, tree nut, fish, shellfish, or sesame are likely due to IgE-mediated food allergy, but after ketchup or strawberry are probably from skin contact.”
Allergic Rhinitis and Asthma
“For asthma, ask about frequency of night cough and symptoms with exercise, laughing, or crying. For allergic rhinitis, look for runny nose, itchy eyes, or sneezing,” Brown-Whitehorn said.
Testing and Monitoring
Assessing the extent of eczema with the Eczema Area and Severity Index or the SCORing Atopic Dermatitis index takes time but may be necessary to obtain insurance coverage for treatments such as biologics.
Avoid ordering IgE food panels, which can result in false positives that can lead to loss of tolerance and nutritional deficiencies; psychological harm from bullying, anxiety, and decreased quality of life; and higher food and healthcare costs, Pandya said.
Treatments
Caregivers may be wary about treatments, and all the three experts this news organization spoke with stressed the importance of educating caregivers about how treatments work and what to expect from them.
“Early and aggressive atopic dermatitis treatment could prevent sensitization to food or aeroallergens, which could help prevent additional atopic diseases, including those on the atopic march,” Pandya said. “Topical steroids are considered first line at any age. Topical phosphodiesterase inhibitors are approved at 3 months of age and above. Topical calcineurin inhibitors are approved at 2 years of age and above. Wet wrap therapy and bleach baths can be effective. Other options include biologic therapy, allergen immunotherapy, and UV therapy.”
“Epinephrine auto-injectors can counteract food reactions. For allergic rhinitis, non-sedating antihistamines, steroidal nasal sprays, and nasal antihistamines help. Asthma treatments include various inhaled medications,” Brown-Whitehorn added.
When to Refer to Specialists
Involving an allergist, dermatologist, pulmonologist, or ear nose throat specialist to the patient’s care team is advisable in more challenging cases.
If a child is younger than 3 months and has moderate to severe atopic dermatitis, an underlying immune defect may be to blame, so an allergy and immunology assessment is warranted, Brown-Whitehorn said. “An allergist can help any child who has recurrent coughing or wheezing avoid the emergency room or hospitalization.”
“In pediatrics, we always try to find the medication, regimen, and avoidance strategies that use the least treatment to provide the best care for each patient,” Brown-Whitehorn added. “Children eat, play, learn, and sleep, and every stage of the atopic march affects each of these activities. As clinicians, we need to be sure that we are helping children make the best of all these activities.”
Brown-Whitehorn reported financial relationships with DBV Technologies and Regeneron Pharmaceuticals. Lee reported financial relationships with Novartis. Pandya reported financial relationships with DBV Technologies, Thermo Fisher Scientific, and Sanofi.
A version of this article first appeared on Medscape.com.
Obesity Therapies: What Will the Future Bring?
“Obesity only recently caught the public’s attention as a disease,” Matthias Blüher, MD, professor of medicine at the Leipzig University and director of the Helmholtz Institute for Metabolism, Obesity and Vascular Research, Leipzig, Germany, told attendees in a thought-provoking presentation at the European Association for the Study of Diabetes (EASD) 2024 Annual Meeting.
Even though the attitudes around how obesity is perceived may be relatively new, Blüher believes they are nonetheless significant. As a sign of how the cultural headwinds have shifted, he noted the 2022 film The Whale, which focuses on a character struggling with obesity. As Blüher pointed out, not only did the film’s star, Brendan Fraser, receive an Academy Award for his portrayal but he also theorized that the majority of celebrities in the audience were likely taking new weight loss medications.
“I strongly believe that in the future, obesity treatment will carry less stigma. It will be considered not as a cosmetic problem, but as a progressive disease.”
He sees several changes in the management of obesity likely to occur on the near horizon, beginning with when interventions directed at treating it will begin.
Obesity treatment should start at a young age, he said, because if you have overweight at ages 3-6 years, the likelihood of becoming an adult with obesity is approximately 90%. “Looking ahead, shouldn’t we put more emphasis on this age group?”
Furthermore, he hopes that clinical trials will move beyond body weight and body mass index (BMI) as their main outcome parameters. Instead, “we should talk about fat distribution, fat or adipose tissue function, muscle loss, body composition, and severity of disease.”
Blüher pointed to the recently published framework for the diagnosis, staging, and management of obesity in adults put forward by the European Association for the Study of Obesity. It states that obesity should be staged not based on BMI or body weight alone but also on an individual›s medical, functional, and psychological (eg, mental health and eating behavior) status.
“The causes of obesity are too complex to be individually targeted,” he continued, unlike examples such as hypercholesterolemia or smoking cessation, where clinicians may have one target to address.
“But overeating, slow metabolism, and low physical activity involve socio-cultural factors, global food marketing, and many other factors. Therefore, clinicians should be setting health targets, such as improving sleep apnea and improving physical functioning, rather than a kilogram number.”
Three Pillars of Treatment
Right now, clinicians have three pillars of treatments available, Blüher said. The first is behavioral intervention, including strategies such as counseling, diet, exercise, self-monitoring, stress management, and sleep management.
“We know that these behavioral aspects typically lack adherence and effect size, but they’re important, and for a certain group of people, they may be the best and safest treatment.”
The second pillar is pharmacotherapy, and the third is surgery.
Each pillar poses questions for future research, he explained.
“First, do we really need more evidence that behavioral interventions typically fail in the long run and are prone to rebound of body weight and health issues? No. Or which diet is best? We have hundreds of diet interventions, all of which basically show very similar outcomes. They lead to an average weight loss of 3% to 5% and do improve health conditions associated with obesity.”
When it comes to pharmacotherapies, Blüher does believe clinicians need more options.
Depending on affordability and access, glucagon-like peptide 1 (GLP-1) semaglutide will likely become the first-line therapy for most people living with obesity who want to take medications, he suggested. The dual glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 tirzepatide will be reserved for those with more severe conditions.
“But this is not the end of the story,” he said. “The pipelines for obesity pharmacotherapies are full, and they have different categories. We are optimistic that we will have more therapies not only for type 2 diabetes (T2D) but also for obesity. Combinations such as CagriSema (cagrilintide + semaglutide, currently indicated for T2D) may outperform the monotherapies. We have to see if they’re as safe, and we have to wait for phase 3 trials and long-term outcomes.”
“The field is open for many combinations, ideas and interactions among the incretin-based signaling systems, but personally, I think that the triple agonists have a very bright future,” Blüher said.
For example, retatrutide, an agonist of the GIP, GLP-1, and glucagon receptors, showed promise in a phase 2 trial. Although that was not a comparative study, “the average changes in body weight suggest that in a dose-dependent manner, you can expect even more weight loss than with tirzepatide.”
Treating the Causes
The future of obesity therapy might also be directed at the originating factors that cause it, Blüher suggested, adding that “treating the causes is a dream of mine.”
One example of treating the cause is leptin therapy, as shown in a 1999 study of recombinant leptin in a child with congenital leptin deficiency. A more recent example is setmelanotide treatment for proopiomelanocortin deficiency.
“We are at the beginning for these causative treatments of obesity, and I hope that the future will hold much more of these insights and targets, as in cancer therapy.”
“Finally,” he said, “We eat with our brain. And so in the future, we also will be better able to use our knowledge about the complex neural circuits that are obesogenic, and how to target them. In doing so, we can learn from surgeons because obesity surgery is very effective in changing the anatomy, and we also observe hormonal changes. We see that ghrelin, GLP-1, peptide YY, and many others are affected when the anatomy changes. Why can’t we use that knowledge to design drugs that resemble or mimic the effect size of bariatric surgery?”
And that goes to the third pillar of treatment and the question of whether the new weight loss drugs may replace surgery, which also was the topic of another EASD session.
Blüher doesn’t see that happening for at least a decade, given that there is still an effect-size gap between tirzepatide and surgery, especially for individuals with T2D. In addition, he noted, there will still be nonresponders to drugs, and clinicians are not treating to target yet. Looking ahead, he foresees a combination of surgery and multi-receptor agonists.
“I believe that obesity won’t be cured in the future, but we will have increasingly better lifelong management with a multidisciplinary approach, although behavioral interventions still will not be as successful as pharmacotherapy and bariatric surgery,” he concluded.
Q&A
During the question-and-answer session following his lecture, several attendees asked Blüher for his thoughts around other emerging areas in this field. One wanted to know whether microbiome changes might be a future target for obesity treatment.
“So far, we don’t really understand which bacteria, which composition, at which age, and at which part of the intestine need to be targeted,” Blüher responded. “Before we know that mechanistically, I think it would be difficult, but it could be an avenue to go for, though I’m a little less optimistic about it compared to other approaches.”
Given that obesity is not one disease, are there cluster subtypes, as for T2D — eg, the hungry brain, the hungry gut, low metabolism — that might benefit from individualized treatment, another attendee asked.
“We do try to subcluster people living with obesity,” Blüher said. “We did that based on adipose tissue expression signatures, and indeed there is large heterogeneity. But we are far from addressing the root causes and all subtypes of the disease, and that would be a requirement before we could personalize treatment in that way.”
Next, an attendee asked what is responsible for the differential weight loss in people with diabetes and people without? Blüher responded that although he doesn’t have the answer, he does have hypotheses.
“One could be that the disease process — eg, deterioration of beta cell function, of the balance of hormones such as insulin and leptin, of inflammatory parameters, of insulin resistance — is much more advanced in diseases such as T2D and sleep apnea. Maybe it then takes more to address comorbid conditions such as inflammation and insulin resistance. Therefore, combining current therapies with insulin sensitizers, for example, could produce better results.”
What about using continuous glucose monitoring to help people stick to their diet?
“That’s an important question that speaks to personalized treatment,” he said. “It applies not only to continuous glucose monitoring but also to nutrition and other modes of self-monitoring, which seem to be among the most successful tools for long-term weight maintenance.”
Blüher finished by saying, “As we look into the future, I hope that there will be better approaches for all aspects of personalized medicine, whether it is nutrition, exercise, pharmacotherapy, or even surgical procedures.”
Blüher received honoraria for lectures and/or served as a consultant to Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, Novo Nordisk, Novartis, Pfizer, and Sanofi.
A version of this article first appeared on Medscape.com.
“Obesity only recently caught the public’s attention as a disease,” Matthias Blüher, MD, professor of medicine at the Leipzig University and director of the Helmholtz Institute for Metabolism, Obesity and Vascular Research, Leipzig, Germany, told attendees in a thought-provoking presentation at the European Association for the Study of Diabetes (EASD) 2024 Annual Meeting.
Even though the attitudes around how obesity is perceived may be relatively new, Blüher believes they are nonetheless significant. As a sign of how the cultural headwinds have shifted, he noted the 2022 film The Whale, which focuses on a character struggling with obesity. As Blüher pointed out, not only did the film’s star, Brendan Fraser, receive an Academy Award for his portrayal but he also theorized that the majority of celebrities in the audience were likely taking new weight loss medications.
“I strongly believe that in the future, obesity treatment will carry less stigma. It will be considered not as a cosmetic problem, but as a progressive disease.”
He sees several changes in the management of obesity likely to occur on the near horizon, beginning with when interventions directed at treating it will begin.
Obesity treatment should start at a young age, he said, because if you have overweight at ages 3-6 years, the likelihood of becoming an adult with obesity is approximately 90%. “Looking ahead, shouldn’t we put more emphasis on this age group?”
Furthermore, he hopes that clinical trials will move beyond body weight and body mass index (BMI) as their main outcome parameters. Instead, “we should talk about fat distribution, fat or adipose tissue function, muscle loss, body composition, and severity of disease.”
Blüher pointed to the recently published framework for the diagnosis, staging, and management of obesity in adults put forward by the European Association for the Study of Obesity. It states that obesity should be staged not based on BMI or body weight alone but also on an individual›s medical, functional, and psychological (eg, mental health and eating behavior) status.
“The causes of obesity are too complex to be individually targeted,” he continued, unlike examples such as hypercholesterolemia or smoking cessation, where clinicians may have one target to address.
“But overeating, slow metabolism, and low physical activity involve socio-cultural factors, global food marketing, and many other factors. Therefore, clinicians should be setting health targets, such as improving sleep apnea and improving physical functioning, rather than a kilogram number.”
Three Pillars of Treatment
Right now, clinicians have three pillars of treatments available, Blüher said. The first is behavioral intervention, including strategies such as counseling, diet, exercise, self-monitoring, stress management, and sleep management.
“We know that these behavioral aspects typically lack adherence and effect size, but they’re important, and for a certain group of people, they may be the best and safest treatment.”
The second pillar is pharmacotherapy, and the third is surgery.
Each pillar poses questions for future research, he explained.
“First, do we really need more evidence that behavioral interventions typically fail in the long run and are prone to rebound of body weight and health issues? No. Or which diet is best? We have hundreds of diet interventions, all of which basically show very similar outcomes. They lead to an average weight loss of 3% to 5% and do improve health conditions associated with obesity.”
When it comes to pharmacotherapies, Blüher does believe clinicians need more options.
Depending on affordability and access, glucagon-like peptide 1 (GLP-1) semaglutide will likely become the first-line therapy for most people living with obesity who want to take medications, he suggested. The dual glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 tirzepatide will be reserved for those with more severe conditions.
“But this is not the end of the story,” he said. “The pipelines for obesity pharmacotherapies are full, and they have different categories. We are optimistic that we will have more therapies not only for type 2 diabetes (T2D) but also for obesity. Combinations such as CagriSema (cagrilintide + semaglutide, currently indicated for T2D) may outperform the monotherapies. We have to see if they’re as safe, and we have to wait for phase 3 trials and long-term outcomes.”
“The field is open for many combinations, ideas and interactions among the incretin-based signaling systems, but personally, I think that the triple agonists have a very bright future,” Blüher said.
For example, retatrutide, an agonist of the GIP, GLP-1, and glucagon receptors, showed promise in a phase 2 trial. Although that was not a comparative study, “the average changes in body weight suggest that in a dose-dependent manner, you can expect even more weight loss than with tirzepatide.”
Treating the Causes
The future of obesity therapy might also be directed at the originating factors that cause it, Blüher suggested, adding that “treating the causes is a dream of mine.”
One example of treating the cause is leptin therapy, as shown in a 1999 study of recombinant leptin in a child with congenital leptin deficiency. A more recent example is setmelanotide treatment for proopiomelanocortin deficiency.
“We are at the beginning for these causative treatments of obesity, and I hope that the future will hold much more of these insights and targets, as in cancer therapy.”
“Finally,” he said, “We eat with our brain. And so in the future, we also will be better able to use our knowledge about the complex neural circuits that are obesogenic, and how to target them. In doing so, we can learn from surgeons because obesity surgery is very effective in changing the anatomy, and we also observe hormonal changes. We see that ghrelin, GLP-1, peptide YY, and many others are affected when the anatomy changes. Why can’t we use that knowledge to design drugs that resemble or mimic the effect size of bariatric surgery?”
And that goes to the third pillar of treatment and the question of whether the new weight loss drugs may replace surgery, which also was the topic of another EASD session.
Blüher doesn’t see that happening for at least a decade, given that there is still an effect-size gap between tirzepatide and surgery, especially for individuals with T2D. In addition, he noted, there will still be nonresponders to drugs, and clinicians are not treating to target yet. Looking ahead, he foresees a combination of surgery and multi-receptor agonists.
“I believe that obesity won’t be cured in the future, but we will have increasingly better lifelong management with a multidisciplinary approach, although behavioral interventions still will not be as successful as pharmacotherapy and bariatric surgery,” he concluded.
Q&A
During the question-and-answer session following his lecture, several attendees asked Blüher for his thoughts around other emerging areas in this field. One wanted to know whether microbiome changes might be a future target for obesity treatment.
“So far, we don’t really understand which bacteria, which composition, at which age, and at which part of the intestine need to be targeted,” Blüher responded. “Before we know that mechanistically, I think it would be difficult, but it could be an avenue to go for, though I’m a little less optimistic about it compared to other approaches.”
Given that obesity is not one disease, are there cluster subtypes, as for T2D — eg, the hungry brain, the hungry gut, low metabolism — that might benefit from individualized treatment, another attendee asked.
“We do try to subcluster people living with obesity,” Blüher said. “We did that based on adipose tissue expression signatures, and indeed there is large heterogeneity. But we are far from addressing the root causes and all subtypes of the disease, and that would be a requirement before we could personalize treatment in that way.”
Next, an attendee asked what is responsible for the differential weight loss in people with diabetes and people without? Blüher responded that although he doesn’t have the answer, he does have hypotheses.
“One could be that the disease process — eg, deterioration of beta cell function, of the balance of hormones such as insulin and leptin, of inflammatory parameters, of insulin resistance — is much more advanced in diseases such as T2D and sleep apnea. Maybe it then takes more to address comorbid conditions such as inflammation and insulin resistance. Therefore, combining current therapies with insulin sensitizers, for example, could produce better results.”
What about using continuous glucose monitoring to help people stick to their diet?
“That’s an important question that speaks to personalized treatment,” he said. “It applies not only to continuous glucose monitoring but also to nutrition and other modes of self-monitoring, which seem to be among the most successful tools for long-term weight maintenance.”
Blüher finished by saying, “As we look into the future, I hope that there will be better approaches for all aspects of personalized medicine, whether it is nutrition, exercise, pharmacotherapy, or even surgical procedures.”
Blüher received honoraria for lectures and/or served as a consultant to Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, Novo Nordisk, Novartis, Pfizer, and Sanofi.
A version of this article first appeared on Medscape.com.
“Obesity only recently caught the public’s attention as a disease,” Matthias Blüher, MD, professor of medicine at the Leipzig University and director of the Helmholtz Institute for Metabolism, Obesity and Vascular Research, Leipzig, Germany, told attendees in a thought-provoking presentation at the European Association for the Study of Diabetes (EASD) 2024 Annual Meeting.
Even though the attitudes around how obesity is perceived may be relatively new, Blüher believes they are nonetheless significant. As a sign of how the cultural headwinds have shifted, he noted the 2022 film The Whale, which focuses on a character struggling with obesity. As Blüher pointed out, not only did the film’s star, Brendan Fraser, receive an Academy Award for his portrayal but he also theorized that the majority of celebrities in the audience were likely taking new weight loss medications.
“I strongly believe that in the future, obesity treatment will carry less stigma. It will be considered not as a cosmetic problem, but as a progressive disease.”
He sees several changes in the management of obesity likely to occur on the near horizon, beginning with when interventions directed at treating it will begin.
Obesity treatment should start at a young age, he said, because if you have overweight at ages 3-6 years, the likelihood of becoming an adult with obesity is approximately 90%. “Looking ahead, shouldn’t we put more emphasis on this age group?”
Furthermore, he hopes that clinical trials will move beyond body weight and body mass index (BMI) as their main outcome parameters. Instead, “we should talk about fat distribution, fat or adipose tissue function, muscle loss, body composition, and severity of disease.”
Blüher pointed to the recently published framework for the diagnosis, staging, and management of obesity in adults put forward by the European Association for the Study of Obesity. It states that obesity should be staged not based on BMI or body weight alone but also on an individual›s medical, functional, and psychological (eg, mental health and eating behavior) status.
“The causes of obesity are too complex to be individually targeted,” he continued, unlike examples such as hypercholesterolemia or smoking cessation, where clinicians may have one target to address.
“But overeating, slow metabolism, and low physical activity involve socio-cultural factors, global food marketing, and many other factors. Therefore, clinicians should be setting health targets, such as improving sleep apnea and improving physical functioning, rather than a kilogram number.”
Three Pillars of Treatment
Right now, clinicians have three pillars of treatments available, Blüher said. The first is behavioral intervention, including strategies such as counseling, diet, exercise, self-monitoring, stress management, and sleep management.
“We know that these behavioral aspects typically lack adherence and effect size, but they’re important, and for a certain group of people, they may be the best and safest treatment.”
The second pillar is pharmacotherapy, and the third is surgery.
Each pillar poses questions for future research, he explained.
“First, do we really need more evidence that behavioral interventions typically fail in the long run and are prone to rebound of body weight and health issues? No. Or which diet is best? We have hundreds of diet interventions, all of which basically show very similar outcomes. They lead to an average weight loss of 3% to 5% and do improve health conditions associated with obesity.”
When it comes to pharmacotherapies, Blüher does believe clinicians need more options.
Depending on affordability and access, glucagon-like peptide 1 (GLP-1) semaglutide will likely become the first-line therapy for most people living with obesity who want to take medications, he suggested. The dual glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 tirzepatide will be reserved for those with more severe conditions.
“But this is not the end of the story,” he said. “The pipelines for obesity pharmacotherapies are full, and they have different categories. We are optimistic that we will have more therapies not only for type 2 diabetes (T2D) but also for obesity. Combinations such as CagriSema (cagrilintide + semaglutide, currently indicated for T2D) may outperform the monotherapies. We have to see if they’re as safe, and we have to wait for phase 3 trials and long-term outcomes.”
“The field is open for many combinations, ideas and interactions among the incretin-based signaling systems, but personally, I think that the triple agonists have a very bright future,” Blüher said.
For example, retatrutide, an agonist of the GIP, GLP-1, and glucagon receptors, showed promise in a phase 2 trial. Although that was not a comparative study, “the average changes in body weight suggest that in a dose-dependent manner, you can expect even more weight loss than with tirzepatide.”
Treating the Causes
The future of obesity therapy might also be directed at the originating factors that cause it, Blüher suggested, adding that “treating the causes is a dream of mine.”
One example of treating the cause is leptin therapy, as shown in a 1999 study of recombinant leptin in a child with congenital leptin deficiency. A more recent example is setmelanotide treatment for proopiomelanocortin deficiency.
“We are at the beginning for these causative treatments of obesity, and I hope that the future will hold much more of these insights and targets, as in cancer therapy.”
“Finally,” he said, “We eat with our brain. And so in the future, we also will be better able to use our knowledge about the complex neural circuits that are obesogenic, and how to target them. In doing so, we can learn from surgeons because obesity surgery is very effective in changing the anatomy, and we also observe hormonal changes. We see that ghrelin, GLP-1, peptide YY, and many others are affected when the anatomy changes. Why can’t we use that knowledge to design drugs that resemble or mimic the effect size of bariatric surgery?”
And that goes to the third pillar of treatment and the question of whether the new weight loss drugs may replace surgery, which also was the topic of another EASD session.
Blüher doesn’t see that happening for at least a decade, given that there is still an effect-size gap between tirzepatide and surgery, especially for individuals with T2D. In addition, he noted, there will still be nonresponders to drugs, and clinicians are not treating to target yet. Looking ahead, he foresees a combination of surgery and multi-receptor agonists.
“I believe that obesity won’t be cured in the future, but we will have increasingly better lifelong management with a multidisciplinary approach, although behavioral interventions still will not be as successful as pharmacotherapy and bariatric surgery,” he concluded.
Q&A
During the question-and-answer session following his lecture, several attendees asked Blüher for his thoughts around other emerging areas in this field. One wanted to know whether microbiome changes might be a future target for obesity treatment.
“So far, we don’t really understand which bacteria, which composition, at which age, and at which part of the intestine need to be targeted,” Blüher responded. “Before we know that mechanistically, I think it would be difficult, but it could be an avenue to go for, though I’m a little less optimistic about it compared to other approaches.”
Given that obesity is not one disease, are there cluster subtypes, as for T2D — eg, the hungry brain, the hungry gut, low metabolism — that might benefit from individualized treatment, another attendee asked.
“We do try to subcluster people living with obesity,” Blüher said. “We did that based on adipose tissue expression signatures, and indeed there is large heterogeneity. But we are far from addressing the root causes and all subtypes of the disease, and that would be a requirement before we could personalize treatment in that way.”
Next, an attendee asked what is responsible for the differential weight loss in people with diabetes and people without? Blüher responded that although he doesn’t have the answer, he does have hypotheses.
“One could be that the disease process — eg, deterioration of beta cell function, of the balance of hormones such as insulin and leptin, of inflammatory parameters, of insulin resistance — is much more advanced in diseases such as T2D and sleep apnea. Maybe it then takes more to address comorbid conditions such as inflammation and insulin resistance. Therefore, combining current therapies with insulin sensitizers, for example, could produce better results.”
What about using continuous glucose monitoring to help people stick to their diet?
“That’s an important question that speaks to personalized treatment,” he said. “It applies not only to continuous glucose monitoring but also to nutrition and other modes of self-monitoring, which seem to be among the most successful tools for long-term weight maintenance.”
Blüher finished by saying, “As we look into the future, I hope that there will be better approaches for all aspects of personalized medicine, whether it is nutrition, exercise, pharmacotherapy, or even surgical procedures.”
Blüher received honoraria for lectures and/or served as a consultant to Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, Novo Nordisk, Novartis, Pfizer, and Sanofi.
A version of this article first appeared on Medscape.com.
FROM EASD 2024
White Matter Shows Decline After Bipolar Diagnosis
based on data from 88 individuals.
Patients with bipolar disorder demonstrate cognitive impairment and brain structure abnormalities, including global white matter loss, that have been associated with poor outcomes, but data on the stability or progression of neuroanatomical changes are limited, wrote Julian Macoveanu, PhD, of Copenhagen University Hospital, Denmark, and colleagues.
In a study published in The Journal of Affective Disorders, the researchers identified 97 adults aged 18 to 60 years with recently diagnosed bipolar disorder and matched them with 66 healthy controls. Participants were enrolled in the larger Bipolar Illness Onset (BIO) study. All participants underwent structural MRI and neuropsychological testing at baseline and were in full or partial remission based on total scores of 14 or less on the Hamilton Depression Rating Scale and the Young Mania Rating Scale. Approximately half of the participants (50 bipolar patients and 38 controls) participated in follow-up scans and testing after 6-27 months (mean 16 months), because of limited resources, according to the researchers.
The researchers compared changes in cortical gray matter volume and thickness, total cerebral white matter, hippocampal and amygdala volumes, estimated brain age, and cognitive functioning over time. In addition, they examined within-patient associations between baseline brain structure abnormalities and later mood episodes.
Overall, bipolar patients (BD) showed a significant decrease in total cerebral white matter from baseline, compared with healthy controls (HC) in mixed models (P = .006). “This effect was driven by BD patients showing a decrease in WM volume over time compared to HC who remained stable,” the researchers wrote, and the effect persisted in a post hoc analysis adjusting for subsyndromal symptoms and body mass index.
BD patients also had a larger amygdala volume at baseline and follow-up than HC, but no changes were noted between the groups. Changes in hippocampal volume also remained similar between the groups.
Analysis of cognitive data showed no significant differences in trajectories between BD patients and controls across cognitive domains or globally; although BD patients performed worse than controls at both time points.
BD patients in general experienced lower functioning and worse quality of life, compared with controls, but the trajectories of each group were similar for both functional and quality of life.
The researchers found no significant differences over time in total white matter, hippocampus, or amygdala volumes between BD patients who experienced at least one mood episode during the study period and those who remained in remission.
The findings were limited by several factors including the small sample size and limited generalizability of the findings because of the restriction to patients in full or partial remission, the researchers noted. Other limitations included the variation in follow-up time and the potential impact of psychotropic medication use.
However, the results were strengthened by the use of neuropsychiatric testing in addition to MRI to compare brain structure and cognitive function, the researchers said. The data suggest that both amygdala volume and cognitive impairment may be stable markers of BD soon after diagnosis, but that decreases in white matter may stem from disease progression.
The BIO study is funded by the Mental Health Services, Capital Region of Denmark, the Danish Council for Independent Research, Medical Sciences, Weimans Fund, Markedsmodningsfonden, Gangstedfonden, Læge Sofus Carl Emil og hustru Olga Boris Friis’ legat, Helsefonden, Innovation Fund Denmark, Copenhagen Center for Health Technology (CACHET), EU H2020 ITN, Augustinusfonden, and The Capital Region of Denmark. Macoveanu had no financial conflicts to disclose.
based on data from 88 individuals.
Patients with bipolar disorder demonstrate cognitive impairment and brain structure abnormalities, including global white matter loss, that have been associated with poor outcomes, but data on the stability or progression of neuroanatomical changes are limited, wrote Julian Macoveanu, PhD, of Copenhagen University Hospital, Denmark, and colleagues.
In a study published in The Journal of Affective Disorders, the researchers identified 97 adults aged 18 to 60 years with recently diagnosed bipolar disorder and matched them with 66 healthy controls. Participants were enrolled in the larger Bipolar Illness Onset (BIO) study. All participants underwent structural MRI and neuropsychological testing at baseline and were in full or partial remission based on total scores of 14 or less on the Hamilton Depression Rating Scale and the Young Mania Rating Scale. Approximately half of the participants (50 bipolar patients and 38 controls) participated in follow-up scans and testing after 6-27 months (mean 16 months), because of limited resources, according to the researchers.
The researchers compared changes in cortical gray matter volume and thickness, total cerebral white matter, hippocampal and amygdala volumes, estimated brain age, and cognitive functioning over time. In addition, they examined within-patient associations between baseline brain structure abnormalities and later mood episodes.
Overall, bipolar patients (BD) showed a significant decrease in total cerebral white matter from baseline, compared with healthy controls (HC) in mixed models (P = .006). “This effect was driven by BD patients showing a decrease in WM volume over time compared to HC who remained stable,” the researchers wrote, and the effect persisted in a post hoc analysis adjusting for subsyndromal symptoms and body mass index.
BD patients also had a larger amygdala volume at baseline and follow-up than HC, but no changes were noted between the groups. Changes in hippocampal volume also remained similar between the groups.
Analysis of cognitive data showed no significant differences in trajectories between BD patients and controls across cognitive domains or globally; although BD patients performed worse than controls at both time points.
BD patients in general experienced lower functioning and worse quality of life, compared with controls, but the trajectories of each group were similar for both functional and quality of life.
The researchers found no significant differences over time in total white matter, hippocampus, or amygdala volumes between BD patients who experienced at least one mood episode during the study period and those who remained in remission.
The findings were limited by several factors including the small sample size and limited generalizability of the findings because of the restriction to patients in full or partial remission, the researchers noted. Other limitations included the variation in follow-up time and the potential impact of psychotropic medication use.
However, the results were strengthened by the use of neuropsychiatric testing in addition to MRI to compare brain structure and cognitive function, the researchers said. The data suggest that both amygdala volume and cognitive impairment may be stable markers of BD soon after diagnosis, but that decreases in white matter may stem from disease progression.
The BIO study is funded by the Mental Health Services, Capital Region of Denmark, the Danish Council for Independent Research, Medical Sciences, Weimans Fund, Markedsmodningsfonden, Gangstedfonden, Læge Sofus Carl Emil og hustru Olga Boris Friis’ legat, Helsefonden, Innovation Fund Denmark, Copenhagen Center for Health Technology (CACHET), EU H2020 ITN, Augustinusfonden, and The Capital Region of Denmark. Macoveanu had no financial conflicts to disclose.
based on data from 88 individuals.
Patients with bipolar disorder demonstrate cognitive impairment and brain structure abnormalities, including global white matter loss, that have been associated with poor outcomes, but data on the stability or progression of neuroanatomical changes are limited, wrote Julian Macoveanu, PhD, of Copenhagen University Hospital, Denmark, and colleagues.
In a study published in The Journal of Affective Disorders, the researchers identified 97 adults aged 18 to 60 years with recently diagnosed bipolar disorder and matched them with 66 healthy controls. Participants were enrolled in the larger Bipolar Illness Onset (BIO) study. All participants underwent structural MRI and neuropsychological testing at baseline and were in full or partial remission based on total scores of 14 or less on the Hamilton Depression Rating Scale and the Young Mania Rating Scale. Approximately half of the participants (50 bipolar patients and 38 controls) participated in follow-up scans and testing after 6-27 months (mean 16 months), because of limited resources, according to the researchers.
The researchers compared changes in cortical gray matter volume and thickness, total cerebral white matter, hippocampal and amygdala volumes, estimated brain age, and cognitive functioning over time. In addition, they examined within-patient associations between baseline brain structure abnormalities and later mood episodes.
Overall, bipolar patients (BD) showed a significant decrease in total cerebral white matter from baseline, compared with healthy controls (HC) in mixed models (P = .006). “This effect was driven by BD patients showing a decrease in WM volume over time compared to HC who remained stable,” the researchers wrote, and the effect persisted in a post hoc analysis adjusting for subsyndromal symptoms and body mass index.
BD patients also had a larger amygdala volume at baseline and follow-up than HC, but no changes were noted between the groups. Changes in hippocampal volume also remained similar between the groups.
Analysis of cognitive data showed no significant differences in trajectories between BD patients and controls across cognitive domains or globally; although BD patients performed worse than controls at both time points.
BD patients in general experienced lower functioning and worse quality of life, compared with controls, but the trajectories of each group were similar for both functional and quality of life.
The researchers found no significant differences over time in total white matter, hippocampus, or amygdala volumes between BD patients who experienced at least one mood episode during the study period and those who remained in remission.
The findings were limited by several factors including the small sample size and limited generalizability of the findings because of the restriction to patients in full or partial remission, the researchers noted. Other limitations included the variation in follow-up time and the potential impact of psychotropic medication use.
However, the results were strengthened by the use of neuropsychiatric testing in addition to MRI to compare brain structure and cognitive function, the researchers said. The data suggest that both amygdala volume and cognitive impairment may be stable markers of BD soon after diagnosis, but that decreases in white matter may stem from disease progression.
The BIO study is funded by the Mental Health Services, Capital Region of Denmark, the Danish Council for Independent Research, Medical Sciences, Weimans Fund, Markedsmodningsfonden, Gangstedfonden, Læge Sofus Carl Emil og hustru Olga Boris Friis’ legat, Helsefonden, Innovation Fund Denmark, Copenhagen Center for Health Technology (CACHET), EU H2020 ITN, Augustinusfonden, and The Capital Region of Denmark. Macoveanu had no financial conflicts to disclose.
FROM THE JOURNAL OF AFFECTIVE DISORDERS
Heard of ApoB Testing? New Guidelines
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
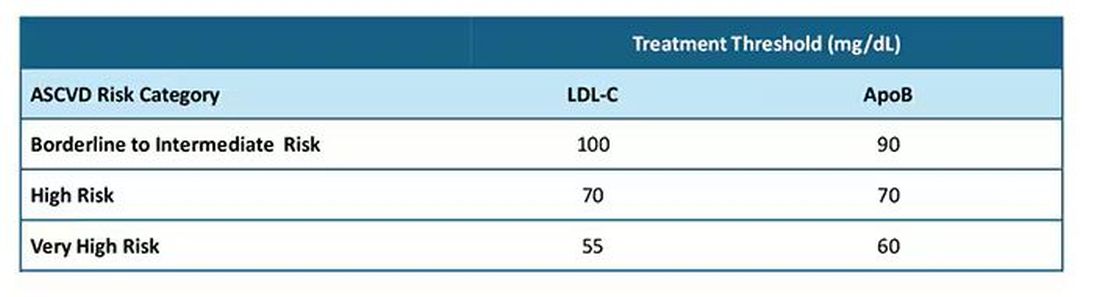
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.
Obesity Etiology
Editor's Note: This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Editor's Note: This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Editor's Note: This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Fewer Recurrent Cardiovascular Events Seen With TNF Inhibitor Use in Axial Spondyloarthritis
TOPLINE:
Tumor necrosis factor (TNF) inhibitors are associated with a reduced risk for recurrent cardiovascular events in patients with radiographic axial spondyloarthritis (axSpA) and a history of cardiovascular events.
METHODOLOGY:
- The researchers conducted a nationwide cohort study using data from the Korean National Claims Database, including 413 patients diagnosed with cardiovascular events following a radiographic axSpA diagnosis.
- Of all patients, 75 received TNF inhibitors (mean age, 51.9 years; 92% men) and 338 did not receive TNF inhibitors (mean age, 60.7 years; 74.9% men).
- Patients were followed from the date of the first cardiovascular event to the date of recurrence, the last date with claims data, or up to December 2021.
- The study outcome was recurrent cardiovascular events that occurred within 28 days of the first incidence and included myocardial infarction and stroke.
- The effect of TNF inhibitor exposure on the risk for recurrent cardiovascular events was assessed using an inverse probability weighted Cox regression analysis.
TAKEAWAY:
- The incidence of recurrent cardiovascular events in patients with radiographic axSpA was 32 per 1000 person-years.
- The incidence was 19 per 1000 person-years in the patients exposed to TNF inhibitors, whereas it was 36 per 1000 person-years in those not exposed to TNF inhibitors.
- Exposure to TNF inhibitors was associated with a 67% lower risk for recurrent cardiovascular events than non-exposure (P = .038).
IN PRACTICE:
“Our data add to previous knowledge by providing more direct evidence that TNFi [tumor necrosis factor inhibitors] could reduce the risk of recurrent cardiovascular events,” the authors wrote.
SOURCE:
The study was led by Oh Chan Kwon, MD, PhD, and Hye Sun Lee, PhD, Yonsei University College of Medicine, Seoul, South Korea. It was published online on October 4, 2024, in Arthritis Research & Therapy.
LIMITATIONS:
The lack of data on certain cardiovascular risk factors such as obesity, smoking, and lifestyle may have led to residual confounding. The patient count in the TNF inhibitor exposure group was not adequate to analyze each TNF inhibitor medication separately. The study included only Korean patients, limiting the generalizability to other ethnic populations. The number of recurrent stroke events was relatively small, making it infeasible to analyze myocardial infarction and stroke separately.
DISCLOSURES:
The study was funded by Yuhan Corporation as part of its “2023 Investigator Initiated Translation Research Program.” The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Tumor necrosis factor (TNF) inhibitors are associated with a reduced risk for recurrent cardiovascular events in patients with radiographic axial spondyloarthritis (axSpA) and a history of cardiovascular events.
METHODOLOGY:
- The researchers conducted a nationwide cohort study using data from the Korean National Claims Database, including 413 patients diagnosed with cardiovascular events following a radiographic axSpA diagnosis.
- Of all patients, 75 received TNF inhibitors (mean age, 51.9 years; 92% men) and 338 did not receive TNF inhibitors (mean age, 60.7 years; 74.9% men).
- Patients were followed from the date of the first cardiovascular event to the date of recurrence, the last date with claims data, or up to December 2021.
- The study outcome was recurrent cardiovascular events that occurred within 28 days of the first incidence and included myocardial infarction and stroke.
- The effect of TNF inhibitor exposure on the risk for recurrent cardiovascular events was assessed using an inverse probability weighted Cox regression analysis.
TAKEAWAY:
- The incidence of recurrent cardiovascular events in patients with radiographic axSpA was 32 per 1000 person-years.
- The incidence was 19 per 1000 person-years in the patients exposed to TNF inhibitors, whereas it was 36 per 1000 person-years in those not exposed to TNF inhibitors.
- Exposure to TNF inhibitors was associated with a 67% lower risk for recurrent cardiovascular events than non-exposure (P = .038).
IN PRACTICE:
“Our data add to previous knowledge by providing more direct evidence that TNFi [tumor necrosis factor inhibitors] could reduce the risk of recurrent cardiovascular events,” the authors wrote.
SOURCE:
The study was led by Oh Chan Kwon, MD, PhD, and Hye Sun Lee, PhD, Yonsei University College of Medicine, Seoul, South Korea. It was published online on October 4, 2024, in Arthritis Research & Therapy.
LIMITATIONS:
The lack of data on certain cardiovascular risk factors such as obesity, smoking, and lifestyle may have led to residual confounding. The patient count in the TNF inhibitor exposure group was not adequate to analyze each TNF inhibitor medication separately. The study included only Korean patients, limiting the generalizability to other ethnic populations. The number of recurrent stroke events was relatively small, making it infeasible to analyze myocardial infarction and stroke separately.
DISCLOSURES:
The study was funded by Yuhan Corporation as part of its “2023 Investigator Initiated Translation Research Program.” The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Tumor necrosis factor (TNF) inhibitors are associated with a reduced risk for recurrent cardiovascular events in patients with radiographic axial spondyloarthritis (axSpA) and a history of cardiovascular events.
METHODOLOGY:
- The researchers conducted a nationwide cohort study using data from the Korean National Claims Database, including 413 patients diagnosed with cardiovascular events following a radiographic axSpA diagnosis.
- Of all patients, 75 received TNF inhibitors (mean age, 51.9 years; 92% men) and 338 did not receive TNF inhibitors (mean age, 60.7 years; 74.9% men).
- Patients were followed from the date of the first cardiovascular event to the date of recurrence, the last date with claims data, or up to December 2021.
- The study outcome was recurrent cardiovascular events that occurred within 28 days of the first incidence and included myocardial infarction and stroke.
- The effect of TNF inhibitor exposure on the risk for recurrent cardiovascular events was assessed using an inverse probability weighted Cox regression analysis.
TAKEAWAY:
- The incidence of recurrent cardiovascular events in patients with radiographic axSpA was 32 per 1000 person-years.
- The incidence was 19 per 1000 person-years in the patients exposed to TNF inhibitors, whereas it was 36 per 1000 person-years in those not exposed to TNF inhibitors.
- Exposure to TNF inhibitors was associated with a 67% lower risk for recurrent cardiovascular events than non-exposure (P = .038).
IN PRACTICE:
“Our data add to previous knowledge by providing more direct evidence that TNFi [tumor necrosis factor inhibitors] could reduce the risk of recurrent cardiovascular events,” the authors wrote.
SOURCE:
The study was led by Oh Chan Kwon, MD, PhD, and Hye Sun Lee, PhD, Yonsei University College of Medicine, Seoul, South Korea. It was published online on October 4, 2024, in Arthritis Research & Therapy.
LIMITATIONS:
The lack of data on certain cardiovascular risk factors such as obesity, smoking, and lifestyle may have led to residual confounding. The patient count in the TNF inhibitor exposure group was not adequate to analyze each TNF inhibitor medication separately. The study included only Korean patients, limiting the generalizability to other ethnic populations. The number of recurrent stroke events was relatively small, making it infeasible to analyze myocardial infarction and stroke separately.
DISCLOSURES:
The study was funded by Yuhan Corporation as part of its “2023 Investigator Initiated Translation Research Program.” The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Mechanism of Action
MOA — Mechanism of action — gets bandied about a lot.
Drug reps love it. Saying your product is a “first-in-class MOA” sounds great as they hand you a glossy brochure. It also features prominently in print ads, usually with pics of smiling people.
It’s a good thing to know, too, both medically and in a cool-science-geeky way. We want to understand what we’re prescribing will do to patients. We want to explain it to them, too.

It certainly helps to know that what we’re doing when treating a disorder using rational polypharmacy.
But at the same time we face the realization that it may not mean as much as we think it should. I don’t have to go back very far in my career to find Food and Drug Administration–approved medications that worked, but we didn’t have a clear reason why. I mean, we had a vague idea on a scientific basis, but we’re still guessing.
This didn’t stop us from using them, which is nothing new. The ancients had learned certain plants reduced pain and fever long before they understood what aspirin (and its MOA) was.
At the same time we’re now using drugs, such as the anti-amyloid treatments for Alzheimer’s disease, that should be more effective than one would think. Pulling the damaged molecules out of the brain should, on paper, make a dramatic difference ... but it doesn’t. I’m not saying they don’t have some benefit, but certainly not as much as you’d think. Of course, that’s based on our understanding of the disease mechanism being correct. We find there’s a lot more going on than we know.
Like so much in science (and this aspect of medicine is a science) the answers often lead to more questions.
Observation takes the lead over understanding in most things. Our ancestors knew what fire was, and how to use it, without any idea of what rapid exothermic oxidation was. (Admittedly, I have a degree in chemistry and can’t explain it myself anymore.)
The glossy ads and scientific data about MOA doesn’t mean much in my world if they don’t work. My patients would say the same.
Clinical medicine, after all, is both an art and a science.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
MOA — Mechanism of action — gets bandied about a lot.
Drug reps love it. Saying your product is a “first-in-class MOA” sounds great as they hand you a glossy brochure. It also features prominently in print ads, usually with pics of smiling people.
It’s a good thing to know, too, both medically and in a cool-science-geeky way. We want to understand what we’re prescribing will do to patients. We want to explain it to them, too.
It certainly helps to know that what we’re doing when treating a disorder using rational polypharmacy.
But at the same time we face the realization that it may not mean as much as we think it should. I don’t have to go back very far in my career to find Food and Drug Administration–approved medications that worked, but we didn’t have a clear reason why. I mean, we had a vague idea on a scientific basis, but we’re still guessing.
This didn’t stop us from using them, which is nothing new. The ancients had learned certain plants reduced pain and fever long before they understood what aspirin (and its MOA) was.
At the same time we’re now using drugs, such as the anti-amyloid treatments for Alzheimer’s disease, that should be more effective than one would think. Pulling the damaged molecules out of the brain should, on paper, make a dramatic difference ... but it doesn’t. I’m not saying they don’t have some benefit, but certainly not as much as you’d think. Of course, that’s based on our understanding of the disease mechanism being correct. We find there’s a lot more going on than we know.
Like so much in science (and this aspect of medicine is a science) the answers often lead to more questions.
Observation takes the lead over understanding in most things. Our ancestors knew what fire was, and how to use it, without any idea of what rapid exothermic oxidation was. (Admittedly, I have a degree in chemistry and can’t explain it myself anymore.)
The glossy ads and scientific data about MOA doesn’t mean much in my world if they don’t work. My patients would say the same.
Clinical medicine, after all, is both an art and a science.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
MOA — Mechanism of action — gets bandied about a lot.
Drug reps love it. Saying your product is a “first-in-class MOA” sounds great as they hand you a glossy brochure. It also features prominently in print ads, usually with pics of smiling people.
It’s a good thing to know, too, both medically and in a cool-science-geeky way. We want to understand what we’re prescribing will do to patients. We want to explain it to them, too.
It certainly helps to know that what we’re doing when treating a disorder using rational polypharmacy.
But at the same time we face the realization that it may not mean as much as we think it should. I don’t have to go back very far in my career to find Food and Drug Administration–approved medications that worked, but we didn’t have a clear reason why. I mean, we had a vague idea on a scientific basis, but we’re still guessing.
This didn’t stop us from using them, which is nothing new. The ancients had learned certain plants reduced pain and fever long before they understood what aspirin (and its MOA) was.
At the same time we’re now using drugs, such as the anti-amyloid treatments for Alzheimer’s disease, that should be more effective than one would think. Pulling the damaged molecules out of the brain should, on paper, make a dramatic difference ... but it doesn’t. I’m not saying they don’t have some benefit, but certainly not as much as you’d think. Of course, that’s based on our understanding of the disease mechanism being correct. We find there’s a lot more going on than we know.
Like so much in science (and this aspect of medicine is a science) the answers often lead to more questions.
Observation takes the lead over understanding in most things. Our ancestors knew what fire was, and how to use it, without any idea of what rapid exothermic oxidation was. (Admittedly, I have a degree in chemistry and can’t explain it myself anymore.)
The glossy ads and scientific data about MOA doesn’t mean much in my world if they don’t work. My patients would say the same.
Clinical medicine, after all, is both an art and a science.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.